
Liver transplantation for metastatic neuroendocrine tumor disease
8
Em....E .m. -: ::m ::: ----..-::- :- ANNALS OF SURGERY Vol. 225, No. 4, 347-354 © 1997 Lippincott-Raven Publishers Liver Transplantation for Metastatic Neuroendocrine Tumors Hauke Lang, M.D.,* Karl JOrgen Oldhafer, M.D.,* Arved Weimann, M.D.,* Hans Jurgen Schlitt, M.D.,* Georg Friedrich Wilhelm Scheumann, M.D.,* Peer Flemming, M.D.,t Burkhardt Ringe, M.D.,4 and Rudolf Pichlmayr, M.D., F.R.C.S.(Hon), F.A.C.S.(Hon)* From the Klinik fOr Abdominal- und Transplantationschirurgie, * and the Institut fOr Pathologie, t Medizinische Hochschule Hannover, Hannover, Germany; and Abteilung Transplantationschirurgie,t Georg-August-Universitat, Gdttingen, Germany Objective This article describes the experience with liver transplantation in patients with irresectable neuroendocrine hepatic metastases. Summary Background Data Liver transplantation has become an established therapy in primary liver cancer. On contrast, there is little experience with liver transplantation in secondary hepatic tumors. So far, in the majority of patients being transplanted for irresectable liver metastases, long-term results have been disappointing because of early tumor recurrence. Because of their biologically less aggressive nature, the metastases of neuroendocrine tumors could represent a justified indication for liver grafting. Methods In a retrospective study, the data of 12 patients who underwent liver transplantation for irresectable neuroendocrine hepatic metastases were analyzed regarding survival, tumor recurrence, and symptomatic relief. Results Nine of 12 patients currently are alive with a median survival of 55 months (range, 1 1.0 days to 103.5 months). The operative mortality was 1 of 12, 2 patients died because of septic complications or tumor recurrences or both 6.5 months and 68.0 months after transplantation. All patients had good symptomatic relief after hepatectomy and transplantation. Four of the nine patients who are alive have no evidence of tumor with a follow-up of 2.0, 57.0, 58.0, and 103.5 months after transplantation. Conclusions In selected patients, liver transplantation for irresectable neuroendocrine hepatic metastases may provide not only long-term palliation but even cure. Regarding the shortage of donor organs, liver grafting for neuroendocrine metastases should be considered solely in patients without evidence of extrahepatic tumor manifestation and in whom all other treatment methods are no longer effective. 347
Transcript of Liver transplantation for metastatic neuroendocrine tumor disease

Em....E.m. -: ::m ::: ----..-::-:-
ANNALS OF SURGERYVol. 225, No. 4, 347-354© 1997 Lippincott-Raven Publishers
Liver Transplantation for MetastaticNeuroendocrine TumorsHauke Lang, M.D.,* Karl JOrgen Oldhafer, M.D.,* Arved Weimann, M.D.,*Hans Jurgen Schlitt, M.D.,* Georg Friedrich Wilhelm Scheumann, M.D.,*Peer Flemming, M.D.,t Burkhardt Ringe, M.D.,4 andRudolf Pichlmayr, M.D., F.R.C.S.(Hon), F.A.C.S.(Hon)*
From the Klinik fOr Abdominal- und Transplantationschirurgie, * and the Institut fOrPathologie, t Medizinische Hochschule Hannover, Hannover, Germany; and AbteilungTransplantationschirurgie,t Georg-August-Universitat, Gdttingen, Germany
ObjectiveThis article describes the experience with liver transplantation in patients with irresectableneuroendocrine hepatic metastases.
Summary Background DataLiver transplantation has become an established therapy in primary liver cancer. Oncontrast, there is little experience with liver transplantation in secondary hepatic tumors. Sofar, in the majority of patients being transplanted for irresectable liver metastases, long-termresults have been disappointing because of early tumor recurrence. Because of theirbiologically less aggressive nature, the metastases of neuroendocrine tumors couldrepresent a justified indication for liver grafting.
MethodsIn a retrospective study, the data of 12 patients who underwent liver transplantation forirresectable neuroendocrine hepatic metastases were analyzed regarding survival, tumorrecurrence, and symptomatic relief.
ResultsNine of 12 patients currently are alive with a median survival of 55 months (range, 1 1.0days to 103.5 months). The operative mortality was 1 of 12, 2 patients died because ofseptic complications or tumor recurrences or both 6.5 months and 68.0 months aftertransplantation. All patients had good symptomatic relief after hepatectomy andtransplantation. Four of the nine patients who are alive have no evidence of tumor with a
follow-up of 2.0, 57.0, 58.0, and 103.5 months after transplantation.
ConclusionsIn selected patients, liver transplantation for irresectable neuroendocrine hepatic metastasesmay provide not only long-term palliation but even cure. Regarding the shortage of donororgans, liver grafting for neuroendocrine metastases should be considered solely in patientswithout evidence of extrahepatic tumor manifestation and in whom all other treatmentmethods are no longer effective.
347

348 Lang and Others
Neuroendocrine tumors are rare neoplasms that presentdifficult and complex challenges to diagnosis and treat-ment. Even in case of metastatic spread to the liver, thepatients' course is often indolent. Initial clinical symp-toms usually are because of large tumor mass or associ-ated with hormone and peptide release rather than im-paired liver function.
Therapeutic options should consider the spontaneouscourse of the disease, the severity of clinical symptoms,as well as the relative contribution of tumor bulk andhormone release to general malaise and discomfort. Cur-rent management of metastatic neuroendocrine tumors in-cludes hepatic resection, embolization, chemotherapy, aswell as antihormonal medical treatment. In the majorityof patients, good palliation or even prolonged survival canbe achieved by these therapeutic measures.'-4 In certainconditions when these options are no longer effective,total hepatectomy and liver transplantation may offer thepatient the chance not only for relief of symptoms buteven for cure.
In this report, we describe our experience with or-thotopic liver transplantation in the treatment of unresect-able hepatic metastases of neuroendocrine tumors in 12patients.
PATIENTS AND METHODS
Between November 1982 and April 1996, 12 patients(4 men and 8 women) with a median age of 48.5 years
(range, 18 to 59 years) underwent liver transplantation(LTx) for histologically proven neuroendocrine tumorswithin the liver. The primary tumors were located in thesmall bowel (n = 5), pancreas (n = 5), stomach (n = 1),and the lung (n = 1). In only eight cases, the site of theprimary tumor had been identified before LTx. Two ofthe unknown primary tumors were detected in the stom-ach and pancreas during LTx. In two other patients, theprimaries were found in the small bowel and pancreas 2and 4 years after liver grafting.
Endocrine activity of the tumors with production ofhormones and associated clinical symptoms were notedin seven patients. Table 1 summarizes hormonal statusand clinical presentation in all 12 cases.
Before LTx, surgery for the primary tumor consistedof small bowel resection (n = 4), lobectomy of the rightlung (n = 1), left pancreatectomy and splenectomy (n =
2), and Whipple's operation (n = 1). Treatment of livermetastases before LTx had been performed in eight pa-
tients and included hepatic resection (n = 1), hepatic
resection plus application of somatostatin (n = 2), resec-tion plus chemoembolization with Gelfoam (Upjohn,Heppenheim, Germany) and epirubicin (n = 1), and so-matostatin therapy alone (n = 4).The indication for LTx was seen only in case of irres-
ectable liver tumor and when, in addition, patients weresuffering from an otherwise untreatable hormonal releaseor from massive tumor bulk resulting in disability andgeneral malaise (case report 1). In one patient, complica-tions of chemoembolization led to sclerosing cholangitisand secondary biliary cirrhosis with progressive liver in-sufficiency, which finally required transplantation (casereport 2). The median interval between first symptoms ofthe disease and LTx was 38 months (range, 3 to 90months), and the median time between detection of livertumor and LTx was 28 months (range, 3 to 62 months),respectively.The operative procedure at LTx included an extensive
lymph node dissection in the hepatic hilum in all cases.Additionally, in one patient, an intra-atrial-intracaval tu-mor thrombectomy was required. One transplantation wascombined with a gastrectomy and another with a left pan-createctomy plus splenectomy because of intraoperativelydetected primary tumors in the stomach and pancreas.
Case ReportsCase 1
In 1983, a 15-year-old girl presented with galactorrheaand exaggerated growth of the body and extremities. Se-rum hormone levels showed an increase of growth hor-mone releasing factor and prolactin. Neurosurgical partialremoval of the enlarged pituitary gland was performed,but histologic analysis only showed hyperplasia but notumor of the pituitary. Because increased serum levels ofgrowth hormone releasing factor persisted, ectopic hor-mone production was assumed. An explorative laparotomyshowed several liver metastases, and a primary neuroendo-crine tumor in the small bowel with one local lymph nodemetastasis in the mesentery was resected. After surgery,treatment with somatostatin could control tumor growthand hormone production for several months. However,after 3 years, liver metastases began to grow and hormonelevels increased again. Approximately 4 years after theexplorative laparotomy, an orthotopic LTx for irresectablemetastases was performed. Histologic examination resultsof the explanted liver showed multiple neuroendocrine me-tastases with an overall involvement of the liver of approx-imately 40%. There was no extrahepatic tumor in the dis-sected lymph nodes in the hepatic hilum. At present, thepatient is alive and in good physical condition withoutevidence of disease more than 8 years after transplantation.
Case 2
A 30-year-old man had a short history of upper abdomi-nal pain before small bowel resection and left hepatectomy
Address reprint requests to Hauke Lang, M.D., Klinik fur Abdominal-und Transplantationschirurgie, Medizinische Hochschule Hannover,Carl-Neuberg Str. 1, 30625 Hannover, Germany.
Accepted for publication July 15, 1996.
Ann. Surg. - April 1997

Liver Transplantation for Tumors 349
Table 1. ORTHOTOPIC LIVER TRANSPLANTATION (OLT) FOR METASTATICNEUROENDOCRINE TUMORS
OLT Age (yr) Site of Primary Therapy of Primary Tumor Markers Therapy of Liver MetastasisNo. Sex at LTx Tumor Clinic Tumor (elevated) Before LTx
77 F 51 Small bowel Flush254 F 59 Small bowel Small bowel
occlusion325 F 18 Small bowel Acromegaly465 F 47 Pancreas Diarrhea
521 M 49 Pancreas Abdominal pain
593 F 18 Stomach Abdominal pain,weight loss
682 M 35 Small bowel Abdominal pain
689 M 50722 F 48
762 M 58787 F 54
Pancreas Cushing syndromePancreas Recurrent peptic
ulcerLung Flush, diarrheaSmall bowel Abdominal pain
1109 F 43 Pancreas Abdominal pain,encephalopathy
Small bowel resectionSmall bowel resection
Small bowel resectionLeft pancreatectomy+ splenectomy
Pancreatectomy +subtotalgastrectomy*
Gastrectomyt
Small bowel resection
Left pancreatectomyWhipple +
gastrectomyLobectomySmall bowel resection+ leftpancreatectomyt
Left pancreatectomy+ splenectomyt
5-HIAA
GFRH, prolactinVIP, neurotensin,PTH
5-HIM
Gastnn, cortisolGastrin
5-HIM
Liver resectionSomatostatin
SomatostatinLiver resection, somatostatin
Liver resection,chemoembolization
SomatostatinSomatostatin
Liver resection, somatostatin
VIP = vasoactive intestinal polypeptide; PTH = parathyroid hormone; 5-HIM = 5-hydroxyindoleacetic acid; GFRH = growth factor releasing hormone; LTx = livertransplant.* Performed 4 years after OLT.t Performed at OLT.t Performed 2 years after OLT.
were performed for a metastatic carcinoid tumor. Aftersurgery, 5-hydroxyindoleacetic acid decreased to normalconcentrations. One year later, the patient underwent he-patic chemoembolization with Gelfoam (Upjohn) and epir-ubicin for intrahepatic tumor recurrence. As a side effect ofthat therapy, partial portal vein thrombosis and sclerosingcholangitis with subsequent secondary biliary cirrhosis oc-curred. Three years after chemoembolization, the patientunderwent orthotopic LTx for progressive chronic liverfailure in the absence of extrahepatic tumor manifestation.Histologic results of the excised liver showed biliary cir-rhosis with several vital nodules of a neuroendocrine tumor(Fig. 1). After LTx, the patient recovered fully and hasremained well without any signs of recurrence for almost5 years after transplantation.
RESULTSSurvival
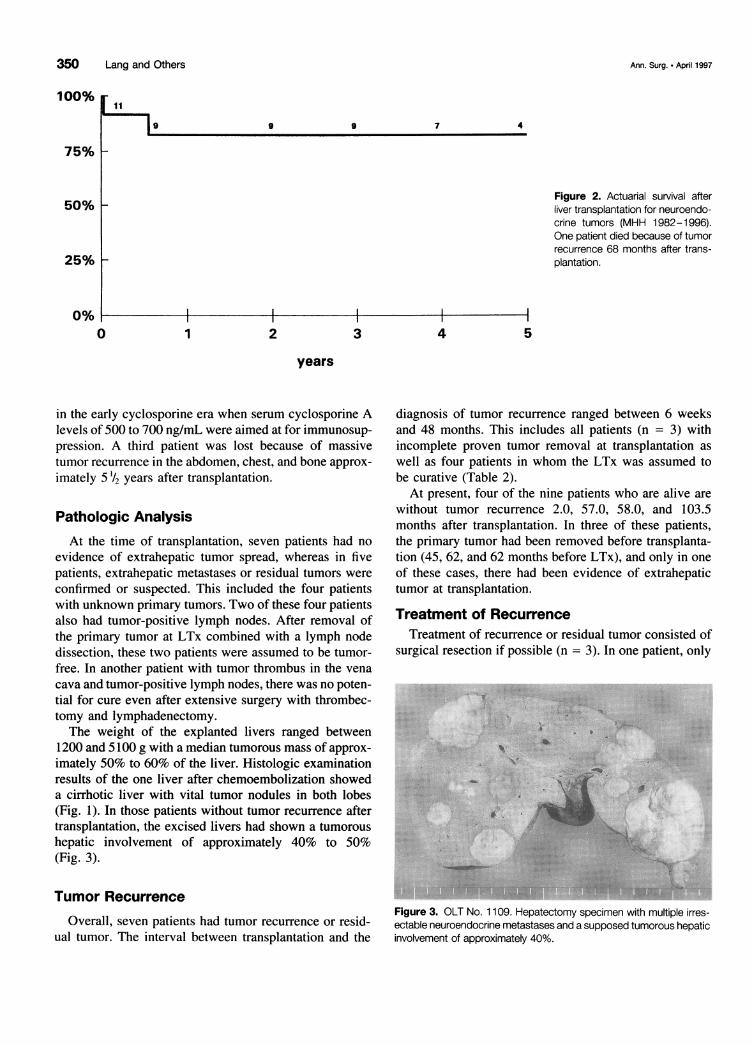
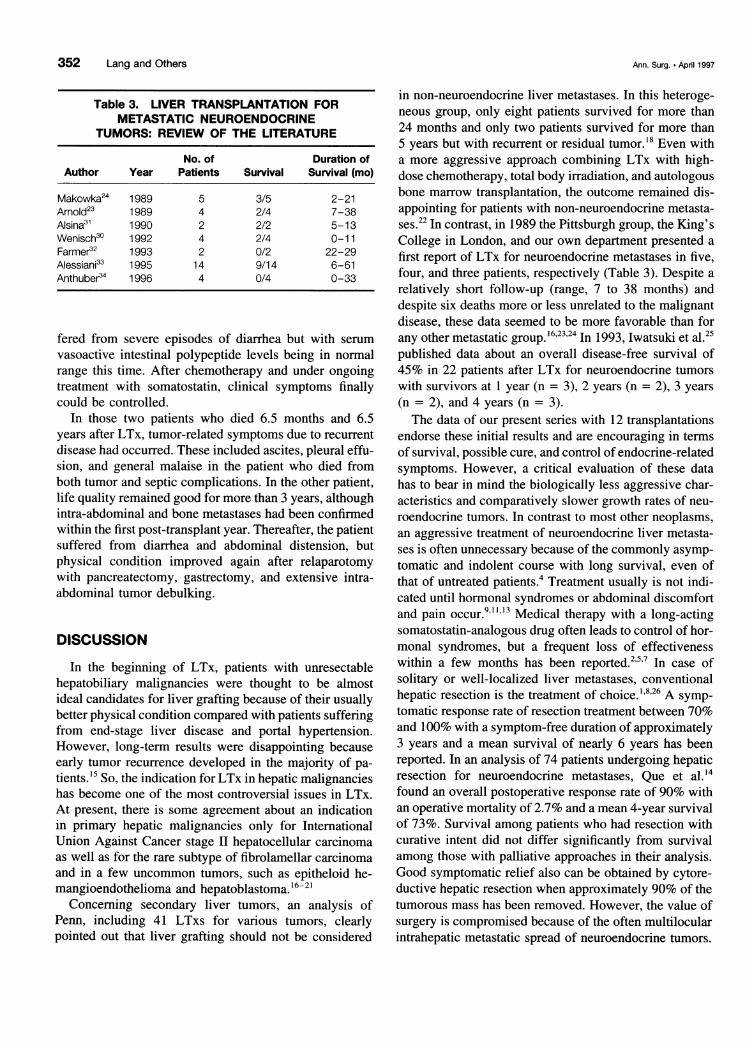
Overall, 9 of the 12 patients currently are alive with amedian survival of 55 months (range, 11.0 days to 103.5months) (Fig. 2). The operative mortality was 1 of 12(cardiopulmonary insufficiency 11 days after LTx). One
patient died because of septic complications plus tumorrecurrence 6.5 months after LTx. This patient had notbeen tumor-free after transplantation, and she was grafted
Figure 1. Case 2. The explanted liver shows a network of fibroustissue with scarning of the liver after chemoembolization (left side) andstill vital carcinoid tumor (right side). (Hematoxylin and eosin, originalmagnification x 140).
Vol. 225 - No. 4
350 Lang and Others
4
Figure 2. Actuarial survival afterliver transplantation for neuroendo-crine tumors (MHH 1982-1996).One patient died because of tumorrecurrence 68 months after trans-plantation.
5
in the early cyclosporine era when serum cyclosporine Alevels of 500 to 700 ng/mL were aimed at for immunosup-pression. A third patient was lost because of massivetumor recurrence in the abdomen, chest, and bone approx-
imately 5 '/2 years after transplantation.
Pathologic AnalysisAt the time of transplantation, seven patients had no
evidence of extrahepatic tumor spread, whereas in fivepatients, extrahepatic metastases or residual tumors were
confirmed or suspected. This included the four patientswith unknown primary tumors. Two of these four patientsalso had tumor-positive lymph nodes. After removal ofthe primary tumor at LTx combined with a lymph nodedissection, these two patients were assumed to be tumor-free. In another patient with tumor thrombus in the vena
cava and tumor-positive lymph nodes, there was no poten-tial for cure even after extensive surgery with thrombec-tomy and lymphadenectomy.The weight of the explanted livers ranged between
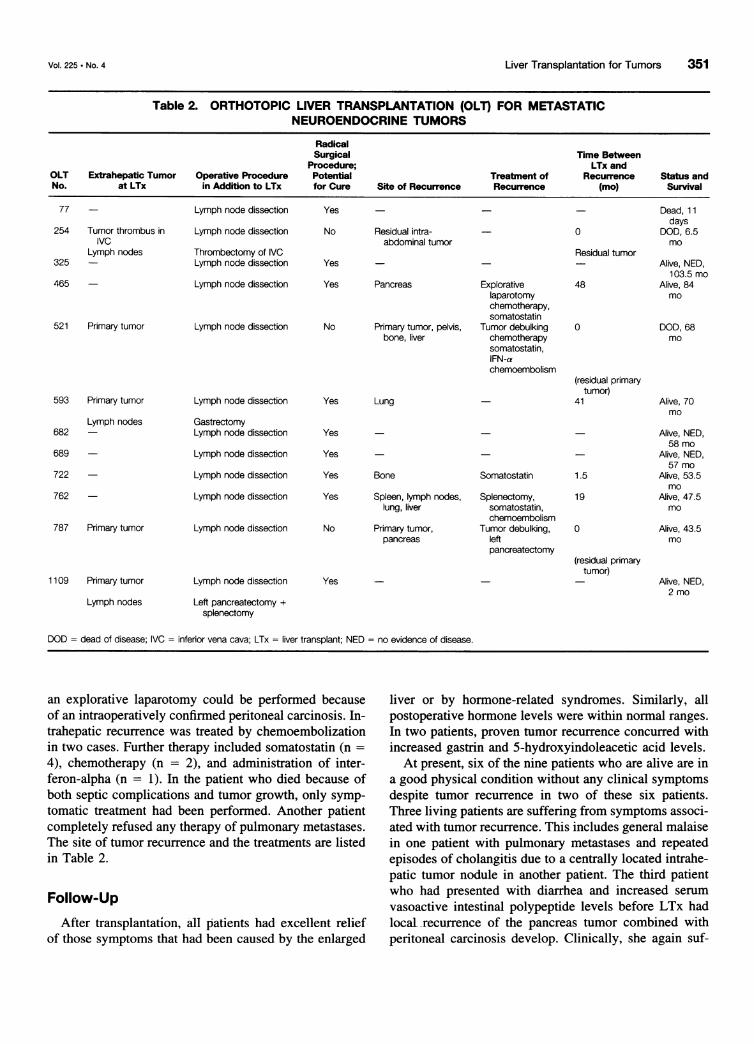
1200 and 5100 g with a median tumorous mass of approx-imately 50% to 60% of the liver. Histologic examinationresults of the one liver after chemoembolization showeda cirrhotic liver with vital tumor nodules in both lobes(Fig. 1). In those patients without tumor recurrence aftertransplantation, the excised livers had shown a tumoroushepatic involvement of approximately 40% to 50%(Fig. 3).
Tumor Recurrence
Overall, seven patients had tumor recurrence or resid-ual tumor. The interval between transplantation and the
diagnosis of tumor recurrence ranged between 6 weeksand 48 months. This includes all patients (n = 3) withincomplete proven tumor removal at transplantation as
well as four patients in whom the LTx was assumed tobe curative (Table 2).
At present, four of the nine patients who are alive are
without tumor recurrence 2.0, 57.0, 58.0, and 103.5months after transplantation. In three of these patients,the primary tumor had been removed before transplanta-tion (45, 62, and 62 months before LTx), and only in one
of these cases, there had been evidence of extrahepatictumor at transplantation.
Treatment of RecurrenceTreatment of recurrence or residual tumor consisted of
surgical resection if possible (n = 3). In one patient, only
40.
* $ ,.. .... . .;.:. .::... . ...:::.~~~~
Figure 3. OLT No. 1 109. Hepatectomy specimen with multiple irres-ectable neuroendocrine metastases and a supposed tumorous hepaticinvolvement of approximately 40%.
100%
75% F-
9 9
50% 1-
7
25% -
0%0 1 2 3
years
4
Ann. Surg. * April 1997
11
9
Liver Transplantation for Tumors
Table 2. ORTHOTOPIC LIVER TRANSPLANTATION (OLT) FOR METASTATICNEUROENDOCRINE TUMORS
RadicalSurgical Time Between
Procedure; LTx andOLT Extrahepatic Tumor Operative Procedure Potential Treatment of Recurrence Status andNo. at LTx in Addition to LTx for Cure Site of Recurrence Recurrence (mo) Survival
77 - Lymph node dissection Yes - - Dead, 11days
254 Tumor thrombus in Lymph node dissection No Residual intra- - 0 DOD, 6.5IVC abdominal tumor mo
Lymph nodes Thrombectomy of IVC Residual tumor325 - Lymph node dissection Yes - - Alive, NED,
103.5 mo465 - Lymph node dissection Yes Pancreas Explorative 48 Alive, 84
laparotomy mochemotherapy,somatostatin
521 Primary tumor Lymph node dissection No Primary tumor, pelvis, Tumor debulking 0 DOD, 68bone, liver chemotherapy mo
somatostatin,IFN-achemoembolism
(residual primarytumor)
593 Primary tumor Lymph node dissection Yes Lung - 41 Alive, 70mo
Lymph nodes Gastrectomy682 - Lymph node dissection Yes - - - Alive, NED,
58 mo689 - Lymph node dissection Yes - - - Alive, NED,
57 mo722 - Lymph node dissection Yes Bone Somatostatin 1.5 Alive, 53.5
mo762 - Lymph node dissection Yes Spleen, lymph nodes, Splenectomy, 19 AJive, 47.5
lung, liver somatostatin, mochemoembolism
787 Primary tumor Lymph node dissection No Primary tumor, Tumor debulking, 0 Alive, 43.5pancreas left mo
pancreatectomy(residual primary
tumor)1109 Primary tumor Lymph node dissection Yes - - - Alive, NED,
2 moLymph nodes Left pancreatectomy +
splenectomy
DOD = dead of disease; IVC = inferior vena cava; LTx = liver transplant; NED = no evidence of disease.
an explorative laparotomy could be performed becauseof an intraoperatively confirmed peritoneal carcinosis. In-trahepatic recurrence was treated by chemoembolizationin two cases. Further therapy included somatostatin (n =4), chemotherapy (n = 2), and administration of inter-feron-alpha (n = 1). In the patient who died because ofboth septic complications and tumor growth, only symp-tomatic treatment had been performed. Another patientcompletely refused any therapy of pulmonary metastases.The site of tumor recurrence and the treatments are listedin Table 2.
Follow-UpAfter transplantation, all patients had excellent relief
of those symptoms that had been caused by the enlarged
liver or by hormone-related syndromes. Similarly, allpostoperative hormone levels were within normal ranges.In two patients, proven tumor recurrence concurred withincreased gastrin and 5-hydroxyindoleacetic acid levels.
At present, six of the nine patients who are alive are ina good physical condition without any clinical symptomsdespite tumor recurrence in two of these six patients.Three living patients are suffering from symptoms associ-ated with tumor recurrence. This includes general malaisein one patient with pulmonary metastases and repeatedepisodes of cholangitis due to a centrally located intrahe-patic tumor nodule in another patient. The third patientwho had presented with diarrhea and increased serumvasoactive intestinal polypeptide levels before LTx hadlocal recurrence of the pancreas tumor combined withperitoneal carcinosis develop. Clinically, she again suf-
351Vol. 225 * No. 4
352 Lang and Others
Table 3. LIVER TRANSPLANTATION FORMETASTATIC NEUROENDOCRINE
TUMORS: REVIEW OF THE LITERATURE
No. of Duration ofAuthor Year Patients Survival Survival (mo)
Makowka24 1989 5 3/5 2-21Arnold23 1989 4 2/4 7-38Alsina31 1990 2 2/2 5-13Wenisch30 1992 4 2/4 0-11Farmer32 1993 2 0/2 22-29Alessiani33 1995 14 9/14 6-61Anthuber34 1996 4 0/4 0-33
fered from severe episodes of diarrhea but with serum
vasoactive intestinal polypeptide levels being in normalrange this time. After chemotherapy and under ongoingtreatment with somatostatin, clinical symptoms finallycould be controlled.
In those two patients who died 6.5 months and 6.5years after LTx, tumor-related symptoms due to recurrentdisease had occurred. These included ascites, pleural effu-sion, and general malaise in the patient who died fromboth tumor and septic complications. In the other patient,life quality remained good for more than 3 years, althoughintra-abdominal and bone metastases had been confirmedwithin the first post-transplant year. Thereafter, the patientsuffered from diarrhea and abdominal distension, butphysical condition improved again after relaparotomywith pancreatectomy, gastrectomy, and extensive intra-abdominal tumor debulking.
DISCUSSION
In the beginning of LTx, patients with unresectablehepatobiliary malignancies were thought to be almostideal candidates for liver grafting because of their usuallybetter physical condition compared with patients sufferingfrom end-stage liver disease and portal hypertension.However, long-term results were disappointing becauseearly tumor recurrence developed in the majority of pa-
tients. 15 So, the indication for LTx in hepatic malignancieshas become one of the most controversial issues in LTx.At present, there is some agreement about an indicationin primary hepatic malignancies only for InternationalUnion Against Cancer stage II hepatocellular carcinomaas well as for the rare subtype of fibrolamellar carcinomaand in a few uncommon tumors, such as epitheloid he-mangioendothelioma and hepatoblastoma.'6-21
Concerning secondary liver tumors, an analysis ofPenn, including 41 LTxs for various tumors, clearlypointed out that liver grafting should not be considered
in non-neuroendocrine liver metastases. In this heteroge-neous group, only eight patients survived for more than24 months and only two patients survived for more than5 years but with recurrent or residual tumor.'8 Even witha more aggressive approach combining LTx with high-dose chemotherapy, total body irradiation, and autologousbone marrow transplantation, the outcome remained dis-appointing for patients with non-neuroendocrine metasta-ses.22 In contrast, in 1989 the Pittsburgh group, the King'sCollege in London, and our own department presented afirst report of LTx for neuroendocrine metastases in five,four, and three patients, respectively (Table 3). Despite arelatively short follow-up (range, 7 to 38 months) anddespite six deaths more or less unrelated to the malignantdisease, these data seemed to be more favorable than forany other metastatic group.'6'23'24 In 1993, Iwatsuki et al.25published data about an overall disease-free survival of45% in 22 patients after LTx for neuroendocrine tumorswith survivors at 1 year (n = 3), 2 years (n = 2), 3 years(n = 2), and 4 years (n = 3).The data of our present series with 12 transplantations
endorse these initial results and are encouraging in termsof survival, possible cure, and control of endocrine-relatedsymptoms. However, a critical evaluation of these datahas to bear in mind the biologically less aggressive char-acteristics and comparatively slower growth rates of neu-roendocrine tumors. In contrast to most other neoplasms,an aggressive treatment of neuroendocrine liver metasta-ses is often unnecessary because of the commonly asymp-tomatic and indolent course with long survival, even ofthat of untreated patients.4 Treatment usually is not indi-cated until hormonal syndromes or abdominal discomfortand pain occur.9 1, 3 Medical therapy with a long-actingsomatostatin-analogous drug often leads to control of hor-monal syndromes, but a frequent loss of effectivenesswithin a few months has been reported.257 In case ofsolitary or well-localized liver metastases, conventionalhepatic resection is the treatment of choice." 826 A symp-tomatic response rate of resection treatment between 70%and 100% with a symptom-free duration of approximately3 years and a mean survival of nearly 6 years has beenreported. In an analysis of 74 patients undergoing hepaticresection for neuroendocrine metastases, Que et al.'4found an overall postoperative response rate of 90% withan operative mortality of 2.7% and a mean 4-year survivalof 73%. Survival among patients who had resection withcurative intent did not differ significantly from survivalamong those with palliative approaches in their analysis.Good symptomatic relief also can be obtained by cytore-ductive hepatic resection when approximately 90% of thetumorous mass has been removed. However, the value ofsurgery is compromised because of the often multilocularintrahepatic metastatic spread of neuroendocrine tumors.
Ann. Surg. - April 1997

Vol. 225 * No. 4
Therefore, only few patients are candidates for liver resec-tion.9" 3"14A variety of chemotherapeutical treatment regimens
have been introduced with response rates for islet celltumors up to 69% and a duration of response up to 20months. This treatment was significantly less effective incarcinoid tumors.6"2 Better results could be obtained bythe combination of hepatic artery occlusion and subse-quent alternating chemotherapy with doxorubicin plus de-carbazine and streptozocin plus fluorouracil. With thisapproach, Moertel et al." reported a median survival timeof 49 months for patients with advanced carcinoid tumorscompared to only 27 months for hepatic artery occlusionalone. Overall response rates were 80% for devasculariza-tion plus chemotherapy and 60% for artery occlusionalone with a duration of response of 18 months and 4months, respectively. Recently, Perry et al.'3 publisheddata about 30 patients with either carcinoid or islet celltumor metastases treated with intra-arterial application ofdoxorubicin and followed by embolization with gelatinpowder or pledgets. They described a 50% reduction oftumor size or hormone markers or both in 79% of patientswith a median survival of 24 months. A minor responserate of even 92% could be obtained, and no procedure-related death was observed.The median survival of 55 months after LTx in our
series compares favorably with all other reported treat-ment managements. Up until now, only three patientsdied, but in two of these patients, death entirely was re-lated to the transplant procedure itself or because of in-complete tumor removal combined with extremely highcyclosporin levels, which may have favored septic com-plications. So far, only one patient died because of theunderlying disease, but even in this patient, life qualityremained good for a long period despite extensive tumorrecurrence. The fact that in advanced carcinoid tumorswith liver metastases death most often results from he-patic or cardiac failure elucidates our experiences thatremoval of the diseased liver may result in significantsymptomatic relief and probably even prolong survival.24This also is reflected by the good results of cytoreductivehepatic surgery and by the even asymptomatic clinicalcourse of some of our patients with extrahepatic tumorrecurrence after LTx.9The assumption that growth of residual tumor could
be accelerated as a consequence of immunosuppressionneither can be denied nor confirmed.27 Even the late recur-rence 4 years after LTx in one of our patients does notargue against possible acceleration of tumor growth. Con-versely, most patients with extrahepatic tumor at the timeof LTx-either lymph node metastases or primary tu-mor-had tumor recurrence develop, even if all tumorshad been removed with curative intention. Consistently,the outcome in patients with extrahepatic tumor at the
Liver Transplantation for Tumors 353
time of transplantation is considerably unfavorable.Therefore, in these cases, LTx should not be applied be-cause even more aggressive surgical approaches, such asmultivisceral upper abdominal resection combined withorthotopic LTx, have not been found to provide reliablelong-term survival.28 Of three patients who underwentabdominal cluster transplantation for neuroendocrine ma-lignancies, Knechtle et al.29 reported on two deaths dueto tumor recurrence (13 and 19 months after LTx) andonly one disease-free survival (28 months after trans-plant). Similar data came from Wenisch et al.,30 who per-formed four upper abdominal exenterations combinedwith LTx for metastasizing endocrine pancreas tumors.They described two deaths within the first year and twodisease-free survivors approximately 7 and 8 months afterliver grafting.
In conclusion, although the follow-up of our series isstill too short for further evaluation, the presented resultsclearly indicate that patients without extrahepatic tumorat the time of transplantation seem to be good candidatesfor liver grafting. Additionally, the fact that in patientswithout recurrence the excised livers had shown a tumor-ous hepatic involvement of only 40% to 50% underlinesthe potency for cure of LTx when it is offered to patientsnot as an ultimate treatment. However, it remains a matterof discussion whether LTx is justified to achieve palliationwhen almost comparable or only little less effectivenesscan be obtained by chemoembolization but without therisks of surgery and immunosuppression. Regarding thecosts and capacity and particularly the inadequate re-sources of donor organs, liver grafting in neuroendocrinemetastases cannot be considered as an established indica-tion. Nevertheless, our data suggest that LTx should beconsidered in patients without evidence of extrahepatictumor and in whom all other therapeutic options, espe-cially those of cytoreductive liver resection and chem-oembolization, are no longer effective. In these selectedgroups, LTx broadens the therapeutic options in neuroen-docrine tumors metastatic to the liver and may providenot only long-term symptomatic relief but also possiblecure.
References
1. Ahlman H, Westberg G, Wangberg B, et al. Treatment of livermetastases of carcinoid tumors. World J Surg 1996; 20:196-202.
2. Arnold R. Medical treatment of metastasizing carcinoid tumors.World J Surg 1996; 20:203-207.
3. Bechstein WO, Neuhaus P. Liver transplantation for hepatic metas-tases of neuroendocrine tumors. Ann N Y Acad Sci 1994; 733:507-514.
4. Delcore R, Friesen SR. Gastrointestinal neuroendocrine tumors. JAm Coll Surg 1994; 178:187-21 1.
5. Hajarizadeh H, Ivancer K, Mueller CR, et al. Effective palliativetreatment of metastatic carcinoid tumors with intra-arterial chemo-

354 Lang and Others
therapy/chemoembolization combined with octreotide acetate. AmJ Surg 1992; 163:479-482.
6. Kvols LK, Buck M. Chemotherapy of metastatic carcinoid and isletcell tumors. Am J Med 1987; 82(Suppl 5B):77-83.
7. Kvols LK, Moertel CG, O'Connell MJ, et al. Treatment of themalignant carcinoid syndrome. Evaluation of a long-acting somato-statin analogue. N Engl J Med 1986; 315:663-666.
8. Martin K Jr, Moertel CG, Adson MA, et al. Surgical treatment offunctioning metastatic carcinoid tumors. Arch Surg 1993; 118:537-542.
9. Mc Entee GP, Nagorney DM, Kvols LK, et al. Cytoreductive he-patic surgery for neuroendocrine tumors. Surgery 1990; 108:1091 -1096.
10. Moertel CG. Karnofsky Memorial Lecture: an Odyssey in the landof small tumors. J Clin Oncol 1987; 5:1503-1522.
11. Moertel CG, Johnson M, Mc Kusick MA, et al. The managementof patients with advanced carcinoid tumors and islet cell carcino-mas. Ann Intern Med 1994; 120:302-309.
12. Moertel CG, Myrto M, Lipsitz S, et al. Streptozocin-Doxorubicin,Streptozocin-Fluorouracil, or Chlorozotocin in the treatment of ad-vanced islet-cell carcinoma. N Engl J Med 1992; 326:519-523.
13. Perry LJ, Stuart K, Stokes KR, et al. Hepatic arterial chemoemboli-zation for metastatic neuroendocrine tumors. Surgery 1994;166:1111-1117.
14. Que FG, Nagorney DM, Batts KP, et al. Hepatic resection formetastatic neuroendocrine carcinomas. Am J Surg 1995; 169:36-43.
15. Ringe B, Wittekind C, Bechstein WO, et al. The role of liver trans-plantation in hepatobiliary malignancy. A retrospective analysis of95 patients with particular regard to tumor stage and recurrence.Ann Surg 1989; 209:88-98.
16. O'Grady JG, Polson RJ, Rolles K, et al. Liver transplantation formalignant disease. Results in 93 consecutive patients. Ann Surg1989; 207:373-379.
17. Olthoff KM, Millis M, Rosove MH, et al. Is liver transplantationjustified for the treatment of hepatic malignancies? Arch Surg 1990;125:1261-1268.
18. Penn I. Hepatic transplantation for primary and metastatic cancersof the liver. Surgery 1991; 110:726-735.
19. Pichlmayr R, Weimann A, Oldhafer KJ, et al. Role of liver trans-plantation in the treatment of unresectable liver cancer. World JSurg 1995; 19:807-813.
20. Pichlmayr R, Weimann A, Ringe B. Indications for liver trans-
Ann. Surg. - April 1997
plantation in hepatobiliary malignancy. Hepatology 1994; 20:33S-40S.
21. Ringe B, Wittekind C, Weimann A, et al. Results of hepatic resec-tion and transplantation for fibrolamellar carcinoma. Surg GynecolObstet 1992; 175:299-305.
22. Margreiter R, Niederwieser D, Frommhold H, et al. Tumor recur-rence after liver transplantation followed by high-dose cyclophos-phamide, total body irradiation, and autologous bone marrow trans-plantation for treatment of metastatic liver disease. Transplant Proc1987; 19:2403-2404.
23. Arnold JC, O'Grady JG, Bird GL, et al. Liver transplantation forprimary and secondary hepatic apudomas. Br J Surg 1989; 76:248-249.
24. Makowka L, Tzakis AG, Mazzaferro V, et al. Transplantation ofthe liver for metastatic endocrine tumors of the intestine and pan-creas. Surg Gynecol Obstet 1989; 168:107-111.
25. Iwatsuki S, Tzakis A, Todo S, et al. Liver transplantation for meta-static hepatic malignancies. Hepatology 1993; 18:723.
26. Soreide 0, Berstad T, Bakka A. Surgical treatment as a principle inpatients with advanced abdominal carcinoid tumors. Surgery 1992;111:48-54.
27. Gulanikar AC, Kotylak G, Bitter-Suermann H. Does immunosup-pression alter the growth of metastatic liver carcinoid after or-thotopic liver transplantation? Transplant Proc 1991; 23:2197-2198.
28. Starzl TE, Todo S, Tzakis A, et al. Abdominal organ cluster trans-plantation for the treatment of upper abdominal malignancies. AnnSurg 1989; 210:374-386.
29. Knechtle SJ, Kalayoglu M, D'Alessandro AM, et al. Should abdom-inal cluster transplantation be abandoned? Transplant Proc 1993;25:1361-1363.
30. Wenisch HJC, Markus BH, Herrmann GH, et al. MultivisceraleOberbauchresektion und orthotope Lebertransplantation - ein chiru-rgisches Behandlungskonzept fur regionar metastasierende Tu-moren des endocrinen Pancreas. Zentralbl Chir 1992; 117:334-342.
31. Alsina AE, Bartus S, Hall D. Liver transplant for metastatic neuro-endocrine tumors. J Clin Gastroenterol 1990; 12:533-537.
32. Farmer DG, Shaked A, Colonna JO. Radical resection combinedwith liver transplantation for foregut tumors. Am J Surg 1993;59:806-812.
33. Alessiani M, Tsakis A, Todo S, et al. Assessment of five-yearexperience with abdominal organ cluster transplantation. J Am CollSurg 1995; 180:1-9.
34. Anthuber M, Jauch KW, Briegel J, et al. Results of liver transplanta-tion for gastroenteropancreatic tumor metastases. World J Surg1996; 20:73-76.




















