Pediatric and Congenital Cardiology, Cardiac Surgery and ...

Lipoprotein Management in Patients WithCardiometabolic RiskConsensus statement from the American Diabetes Association and theAmerican College of Cardiology Foundation
JOHN D. BRUNZELL, MD, FACP1
MICHAEL DAVIDSON, MD, FACC2
CURT D. FURBERG, MD, PHD3
RONALD B. GOLDBERG, MD4
BARBARA V. HOWARD, PHD5
JAMES H. STEIN, MD, FACC, FACP6
JOSEPH L. WITZTUM, MD7
R isk factors for type 2 diabetes andcardiovascular disease (CVD) oftencluster, including obesity (particu-
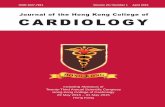
larly central), insulin resistance, hyper-glycemia, dyslipoproteinemia, andhypertension. These conditions can alsooccur in isolation, and they are exagger-ated by physical inactivity and smoking.Since each of these factors increases riskof CVD, the concept of global cardiometa-bolic risk (CMR) (Fig. 1) is of value (1).Lipoprotein abnormalities, including ele-vated triglycerides, low HDL cholesterol,and increased numbers of small denseLDL particles, are common findings in pa-tients with CMR. Clinical entities with in-creased CMR include type 2 diabetes,familial combined hyperlipidemia, famil-ial hypoalphalipoproteinemia, and poly-cystic ovary syndrome (2). Thesedisorders often share the CMR character-istics of central obesity, insulin resistance,dyslipoproteinemia, and hypertension.
There are stringent lipid treatment
goals for patients with type 2 diabetes orCVD; however, guidelines for treatmentof dyslipoproteinemia in high-risk sub-jects without diabetes or CVD are less in-tense and are based primarily on LDLcholesterol concentrations, with non-HDL concentrations a secondary consid-eration in some subjects. Numerous trialshave demonstrated that therapies (pri-marily statins) directed at LDL cholesterollowering clearly reduce risk of CVDevents in patients with diabetes and inthose without diabetes but with otherCVD risk factors; yet, a number of ques-tions remain. Even with adequate LDLcholesterol lowering, many patients onstatin therapy have significant residualCVD risk. It is unclear whether lipopro-tein parameters other than LDL or non-HDL cholesterol provide clinicallysignificant additional prognostic informa-tion regarding CVD risk, yield more infor-mation about the effectiveness of therapy,or indicate more appropriate treatment
targets. Many patients with CMR or dia-betes have relatively normal levels of LDLcholesterol but increased numbers ofsmall dense LDL particles and otheratherogenic lipoproteins. Some have ad-vocated that assessment of other lipopro-tein parameters might be more helpfulthan assessment limited to LDL or non-HDL cholesterol in these populations. Inaddition, treatment targets and the bestapproach for CVD risk reduction in thispopulation need to be better defined.
To address these issues, the AmericanDiabetes Association convened a consen-sus development conference on 18–20July 2007 focusing on lipoprotein man-agement in patients with CMR. Followingpresentations of invited speakers and in-depth discussions, a seven-member panelof experts in endocrinology and metabo-lism, cardiology, epidemiology, and pub-lic health developed a consensus position,addressing the following questions in re-lation to patients with CMR:
1. To what extent do lipoproteins con-tribute to CVD?
2. What are the clinically important li-poprotein parameters?
3. In the evaluation and treatment of pa-tients with lipoprotein abnormalities,are there other factors that should beconsidered?
4. What are the principles and objectivesof treatment of lipoprotein abnormal-ities?
5. What new information would help im-prove lipoprotein management?
TO WHAT EXTENT DOLIPOPROTEINSCONTRIBUTE TO CVD? — C V D(defined here as coronary artery disease[CAD], cerebrovascular disease, and pe-ripheral arterial disease) is the majorcause of morbidity and mortality in theWestern world. This is true despite dra-matic improvements in therapy over thelast few decades. The prevalence of CVDand its associated morbidity is high. Im-portantly, the initial presentation of CADin up to one-third of patients is sudden
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
From the 1Division of Metabolism, Endocrinology and Nutrition, Department of Medicine, and the North-west Lipid Laboratory, University of Washington, Seattle, Washington; the 2University of Chicago PritzkerSchool of Medicine, Chicago, Illinois; the 3Department of Public Health Sciences, Wake Forest University,Winston-Salem, North Carolina; the 4Division of Endocrinology, Department of Medicine, University ofMiami, Miami, Florida; the 5MedStar Research Institute, Hyattsville, Maryland; the 6Cardiovascular Medi-cine Division, Department of Medicine, University of Wisconsin School of Medicine and Public Health,Madison, Wisconsin; and the 7Department of Medicine, University of California, San Diego, La Jolla, Cali-fornia.
Address correspondence and reprint requests to M. Sue Kirkman, MD, American Diabetes Association,1701 N. Beauregard St., Alexandria, VA 22311. E-mail: [email protected].
*Simultaneous publication: this article is being simultaneously published in 2008 in Diabetes Care and theJournal of the American College of Cardiology by the American Diabetes Association and the American Collegeof Cardiology Foundation.
A complete list of the authors’ dualities of interest can be found in the APPENDIX.An American Diabetes Association/American College of Cardiology Foundation Consensus Statement
represents the authors’ collective analysis, evaluation, and opinion at the time of publication, based in parton the consensus conference proceedings, and does not represent the official position of the AmericanDiabetes Association or the American College of Cardiology Foundation.
Abbreviations: Apo, apolipoprotein; ATP III, Adult Treatment Panel III; CAD, coronary artery disease;CHD, coronary heart disease; CMR, cardiometabolic risk; CRP, C-reactive protein; CVD, cardiovasculardisease; IDL, intermediate-density lipoprotein; Lp(a), lipoprotein(a); MI, myocardial infarction; NMR, nu-clear magnetic resonance; VA-HIT, Veterans Affairs High-Density Lipoprotein Cholesterol InterventionTrial.
DOI: 10.2337/dc08-9018© 2008 by the American Diabetes Association and the American College of Cardiology Foundation.
R e v i e w s / C o m m e n t a r i e s / A D A S t a t e m e n t sC O N S E N S U S S T A T E M E N T
DIABETES CARE, VOLUME 31, NUMBER 4, APRIL 2008 811

death. Thus, a detailed knowledge of theatherosclerotic process is necessary in or-der to design interventions to prevent ath-erosclerosis or reduce its rate of progressiononce the process has been initiated.
Lipoproteins are the particles thattransport cholesterol and triglycerides, twocompounds essential to cell structure andmetabolism that are not soluble in aqueoussolutions. Lipoproteins are comprised ofproteins (apolipoproteins), phospholipids,triglycerides, and cholesterol. The classesof lipoproteins vary in the major apoli-poproteins present and the relative con-tents of all of the lipid components.
Chylomicrons are primarily triglycer-ide-bearing lipoproteins produced after ameal during the process of lipid absorp-tion. VLDLs are produced by the liverwith a primary function of supplying freefatty acids to tissues and are normally thepredominant carriers of circulating trig-lycerides. LDLs are by-products of VLDLmetabolism and, in the normal state, arethe primary carriers of plasma choles-terol. Chylomicrons, VLDL, and LDL allcarry apoB, among other apolipoproteins.HDLs carry apoAI and apoAII. NascentHDL particles are produced by the liverand intestine and then mature andbecome enriched with other apolipopro-teins and lipids by exchanges with chylo-microns and VLDL. The size and density
of the lipoprotein categories vary, from thelargest and least dense chylomicrons tothe smallest and most dense HDL. Withineach category, there is also a spectrum ofparticles that vary in size, density, and rel-ative proportions of lipid and protein.
Atherosclerosis is a form of chronicinflammation resulting from complex in-teractions between modified lipoproteins,monocyte-derived macrophages, compo-nents of innate and adaptive immunity,and the normal cellular elements of thearterial wall. This process can ultimatelylead to the development of complex le-sions or plaques that protrude into thearterial lumen, causing abnormal flowpatterns and clinical symptoms such asangina or claudication. In addition, vul-nerable areas within plaques can ruptureor erode, leading to intravascular throm-bosis resulting in the acute clinical com-plications of myocardial infarction andstroke.
Central role of LDL in atherogenesisAmong the many contributing factors, el-evated cholesterol levels play a dominantrole in both the initiation and progressionof atherosclerosis, as well as in the clinicalconsequences such as myocardial infarc-tion, stroke, peripheral vascular disease,and heart failure. Although a myriad ofdifferent genetic and environmental fac-
tors have been identified that modulatelesion formation in animal models,atherogenesis will not occur in thesemodels in the absence of greatly elevatedplasma cholesterol levels (�800 mg/dl)except by direct arterial injury. Hyper-cholesterolemia also appears to be oblig-atory for atherogenesis in humans, but inhumans, where lesion formation usuallyoccurs over many decades, the thresholdlevel of plasma total cholesterol that mustbe exceeded to produce clinically relevantdisease appears to be much lower thanthat in animal models. Atheroscleroticclinical events are uncommon in humanswith lifelong very low plasma cholesterollevels (3). In general, however, there ap-pears to be a curvilinear relationship be-tween increasing plasma cholesterol andincreasing incidence of CVD.
The dramatic success of cholesterol-lowering therapy might suggest that lowcholesterol levels would be all that is re-quired to prevent the development of ath-erosclerotic disease or halt or reverseestablished disease. This might be true ifplasma cholesterol concentration couldbe reduced to very low levels long beforethe usual time of development of clinicaldisease. However, available hypolipi-demic therapy may not lower cholesterollevels to very low values in all patients. Inaddition, drug therapy is often initiated
Figure 1—Factors contributing to cardiometabolic risk.
Consensus Statement
812 DIABETES CARE, VOLUME 31, NUMBER 4, APRIL 2008

only after clinical disease is noted, andsuch therapy may not be sufficient to pre-vent the progression of atherosclerosis.
The totality of evidence overwhelm-ingly supports the centrality of elevatedplasma cholesterol levels as a predictor ofthe development of atherosclerosis,though a complex set of genetic and envi-ronmental factors strongly influences theextent of atherogenesis and the expres-sion of clinical events at any given plasmacholesterol level. It must be recognized,however, that it is lipoproteins that inter-act with the arterial wall and set in motionthe cascade of events that leads to athero-sclerosis. Measurements of total cholesterolare indirect estimates of the lipoproteinsthat transport the bulk of cholesterol inplasma and are the most atherogenic. Inmost circumstances, these are LDLs; how-ever, in patients with CMR, VLDL andother apoB100-containing lipoproteinsalso may contribute to atherosclerosis.
Experimental studies directly supportthe central role of LDL in atherogenesis.Current concepts suggest that higherplasma levels of LDL lead to increasedtransport into the intima, where LDL be-comes bound to proteoglycans, greatlyprolonging its residence time. This makesLDL susceptible to a variety of modifica-tions, including oxidation, enzymaticmodification, nonenzymatic glycation,aggregation, and immune complex for-mation. All of these lead to enhancedmacrophage uptake, foam cell formation,and initiation of the cascade of events re-sulting in progression of the atheroscle-rotic lesion.
The LDL receptor regulates plasmaLDL levels. When human fibroblasts aregrown in cell culture, they take up mediaLDL via the LDL receptor pathway untilsufficient cholesterol is internalized tomeet cellular needs, leading to the down-regulation of LDL receptors. The amountof LDL cholesterol that is needed in suchcultures is only 2.5 mg/dl. Because thereis a 10:1 gradient between plasma and in-terstitial fluid LDL levels, this implies thata plasma level of 25 mg/dl LDL choles-terol would be sufficient to supply pe-ripheral cholesterol needs (4). Indeed,examination of plasma LDL cholesterollevels in a variety of nonhuman speciesreveals that their levels cluster around thisvalue. Human newborns have similarlylow LDL cholesterol values, in the rangeof 40–50 mg/dl. In contrast, healthy adultLDL cholesterol levels are 3– 4 timeshigher (5). People with heterozygous mu-tations in the LDL receptor have LDL cho-
lesterol levels two times normal levels atbirth and many develop CAD by age 50.Children homozygous for this disorderhave LDL cholesterol levels 10-foldhigher than normal and will, if untreated,have CAD in the first decade of life (4).These data strongly suggest that high lev-els of LDL cause atherosclerosis, as well asthe significant dose-response relationshipbetween atherogenic lipoproteins and de-velopment of disease.
Animal and human trials of dietaryand pharmacological interventions thatreduce LDL cholesterol are associatedwith stabilization and regression of ath-erosclerosis in proportion to the choles-terol lowering achieved, supporting thevalidity of “the lower the cholesterol thebetter” notion, especially in individualswith established CVD. Theoretically, allhumans should maintain “newborn” LDLcholesterol levels of about 50 mg/dl toprevent atherosclerosis, and those withexisting CVD should be treated to simi-larly low levels. The lower limit to safeand effective cholesterol lowering has notbeen established. Individuals with geneticmutations causing lifelong very low LDLcholesterol levels appear not only to avoidCVD but also to be free of other abnor-malities that might conceivably be linkedto their very low plasma cholesterol levels(6).
The role of other lipoproteins inatherosclerosisOther abnormalities in lipoprotein com-ponents have been hypothesized to be in-volved in the atherosclerotic process.There is a specific dyslipoproteinemia inindividuals with insulin resistance—andexacerbated in those with diabetes—characterized by elevated VLDL, lowerHDL cholesterol, and altered distribu-tions of particles in all lipoprotein classes.The increase in plasma VLDL, caused byboth increased hepatic production anddecreased clearance, is paired with a shiftin particle distribution such that there arehigher levels of large and intermediate-sized VLDL particles. It is not clear towhat extent these changes stimulate ath-erosclerosis or are simply a marker of amore atherogenic milieu, since largerVLDLs are usually not able to penetratethe endothelium to enter the vascularwall. Individuals with benign hypertrig-lyceridemias characterized by large VLDLdo not have increased risk of CVD. On theother hand, the smaller VLDLs and theircatabolic product, intermediate-densitylipoproteins (IDLs), can enter the suben-
dothelial space and could contribute sub-stantially to atherosclerosis. They mayalso increase prothrombotic factors, thustriggering CVD events.
Lower HDL cholesterol is consistentlyobserved in individuals with CMR or di-abetes, related in part to abnormalities inVLDL metabolism. HDL protects againstatherosclerosis, in part by virtue of itsability to promote reverse cholesteroltransport from cells in the vessel wall tothe liver for disposal. It also has anti-inflammatory properties and can protectLDL from oxidation. Population studiesand clinical trials of patients on statintherapy have demonstrated a strong in-verse association between HDL choles-terol levels and CVD risk.
Alterations in the particle distributionwithin lipoprotein classes in patients withCMR or diabetes may be pertinent to ath-erosclerosis. Of particular relevance arechanges observed in the LDL fraction,with increased numbers of small denseLDL particles. Smaller particles have in-creased endothelial permeability, aremore easily oxidized and glycated, andare more able to bind to proteoglycans inthe vessel wall.
WHAT ARE THE CLINICALLYIMPORTANT LIPOPROTEINPARAMETERS? — To intervene toprevent, halt, or reverse atherosclerosis, itis important to identify which lipopro-teins, or lipoprotein components, aremost clinically relevant. This includes thefollowing considerations: whether theycan be easily, precisely, and cost-effectively measured in a clinical setting;whether there are readily available treat-ment strategies that can alter them; andwhether the treatment strategy is effectivein reducing cardiovascular events.
LDL cholesterolA large body of research, ranging frommolecular to population studies, indi-cates that elevated LDL cholesterol is amajor predictor of CVD, including inpopulations with CMR or diabetes. MeanLDL cholesterol levels are similar in dia-betic, insulin-resistant, and nondiabeticpopulations, but levels vary widelyamong individuals within any popula-tion, due to a variety of genetic and envi-ronmental causes. In the UK ProspectiveDiabetes Study trial of patients with type2 diabetes, LDL cholesterol was the mostpowerful risk factor predicting cardiovas-
Brunzell and Associates
DIABETES CARE, VOLUME 31, NUMBER 4, APRIL 2008 813

cular risk (7). Data from several studiessuggest that elevated levels of LDL choles-terol may have even more adverse effectsin individuals with insulin resistance anddiabetes than in individuals without insu-lin resistance or diabetes (8). There do notappear to be meaningful sex differences inthe predictive value of elevated LDL cho-lesterol in individuals with diabetes orCMR. Age effects have not been thor-oughly examined in the diabetic popula-tion, although data from predominantlynondiabetic populations suggest that LDLcholesterol is not a strong predictor ofCVD in the elderly (9,10).
In addition to the robust data indicat-ing the usefulness of LDL cholesterol as apredictor of CVD in individuals with dia-betes, there are a number of large ran-domized controlled trials that haveestablished that lowering LDL cholesterolin individuals with diabetes or with mul-tiple cardiovascular risk factors lowersCVD event rates for both primary (11–14)and secondary prevention (15–21).
Despite the usefulness of LDL choles-terol for CVD prediction on a populationlevel, the measure may have limitationsfor individual risk assessment. The refer-ence method, beta quantitation, is com-plex and expensive. LDL cholesterol istypically estimated using the Friedewaldequation, but this equation progressivelyunderestimates LDL cholesterol as tri-glyceride levels increase. Available “di-rect” methods to measure LDL cholesterolare not well standardized (22). Measure-ment of LDL cholesterol (the cholesterolwithin LDL particles) has been the stan-dard approach to approximate LDL lev-els. However, the cholesterol content ofLDL particles varies from person to per-son and is influenced by metabolic abnor-malities such as insulin resistance andhyperglycemia. Hence, measurement ofLDL cholesterol may not accurately re-flect the true burden of atherogenic LDLparticles, especially in those with the typ-ical lipoprotein abnormalities of CMR: el-evated triglycerides, low HDL cholesterol,and increased numbers of small LDLparticles.
LDL particle numberA more accurate way to capture the riskposed by LDL may be to measure thenumber of LDL particles directly usingnuclear magnetic resonance (NMR) (23).Many cross-sectional (24) and prospec-tive (25–29) studies show that LDL parti-cle number is a better discriminator ofrisk than is LDL cholesterol.
The size of LDL particles can also bemeasured. As small dense LDL particlesseem to be particularly atherogenic (30),assessment of particle size has intuitiveappeal. Both LDL particle concentrationand LDL size are important predictors ofCVD (31). However, the Multi-EthnicStudy of Atherosclerosis suggested thaton multivariate analyses, both small andlarge LDL were strongly associated withcarotid intima-media thickness (24),while the Veterans Affairs High-DensityLipoprotein Cholesterol InterventionTrial (VA-HIT) showed that both weresignificantly related to coronary heart dis-ease (CHD) events (28). The associationof small LDL and CVD may simply reflectthe increased number of LDL particles inpatients with small LDL. Hence, it is un-clear whether LDL particle size measure-ments add value to measurement of LDLparticle concentration.
Limitations of the clinical utility ofNMR measurement of LDL particle num-ber or size include the facts that the tech-nique is not widely available and that it iscurrently relatively expensive. In addi-tion, there is a need for more independentdata confirming the accuracy of themethod (32) and whether its CVD predic-tive power is consistent across variousethnicities, ages, and conditions that af-fect lipid metabolism.
Lipoprotein(a)Lipoprotein(a) [Lp(a)] , an apoB-containing LDL-like particle with en-hanced binding to intimal proteoglycansand prothrombotic effect, also predictsCVD. There is little evidence that insulinresistance or diabetes influences Lp(a)concentrations. The clinical utility of rou-tine measurement of Lp(a) is unclear, al-though more aggressive control of otherlipoprotein parameters may be warrantedin those with high concentrations ofLp(a).
Non-HDL cholesterolNon-HDL cholesterol (total cholesterolminus HDL cholesterol) reflects the con-centration of cholesterol within all li-poprotein particles currently consideredatherogenic. The Adult Treatment PanelIII (ATP III) proposed that in individualswith hypertriglyceridemia (which wouldinclude many with CMR or diabetes),non-HDL cholesterol levels are a second-ary goal of therapy after targeting LDLcholesterol levels. Many studies havedemonstrated that non-HDL cholesterolis a better predictor of CVD risk than is
LDL cholesterol (33–35), and this may beespecially true of statin-treated patients(36). Additional benefits of non-HDLcholesterol measurement are its lack ofadditional expense in patients already get-ting lipid panel measurements and that itcan be calculated from nonfastingsamples.
ApoB-100ApoB is found in chylomicrons, VLDL,IDL, LDL, and Lp(a) particles. Since eachof these particles contains a single apoBmolecule, measurements of apoB repre-sent the total burden of particles consid-ered most atherogenic (37,38). ApoBmeasurements do not require a fastingsample, and the assay has been standard-ized (39,40), but is not yet widely avail-able. As with non-HDL cholesterol andNMR-based measurements of LDL parti-cle number, in several epidemiologicalstudies and in post hoc analyses of clinicaltrials, apoB has been found to be a betterpredictor of CVD risk than LDL choles-terol (41,42), particularly the on-t rea tment LDL choles te ro l l eve l(15,17,36,42). These analyses suggestthat once LDL cholesterol is lowered,apoB may be a more effective way to as-sess residual CVD risk and to determinethe need for medication adjustments.However, not all studies agree: in somestudies, apoB did not outperform LDLcholesterol and non-HDL cholesterol asrisk predictors (44–46). Discrepanciesbetween studies may be due to the inclu-sion of different proportions of subjectswith CMR. In individuals with CMR, thediscrepancies between apoB, LDL choles-terol, and non-HDL cholesterol aregreater, suggesting that apoB may be amore useful risk predictor among theseindividuals (47).
Triglyceride-rich lipoproteinsIn the fasting state, plasma triglyceridesare primarily found in VLDL, so plasmatriglyceride measurements are used as asurrogate measure of VLDL. Triglyceridesare a univariate predictor of CVD in manystudies but often not an independent pre-dictor in multivariate analyses. This maybe because triglycerides are highly linkedto abnormalities in HDL and LDL and be-cause of high biological and laboratoryvariability. Similarly, there are no clinicaltrial data establishing that lowering trig-lycerides in individuals with or withoutdiabetes independently leads to lowerCVD event rates when one adjusts forchanges in HDL cholesterol.
Consensus Statement
814 DIABETES CARE, VOLUME 31, NUMBER 4, APRIL 2008

Chylomicron remnants may beatherogenic in a manner similar to VLDLremnants. There is little population-basedevidence that chylomicron remnants arelinked to CVD, but several studies showconsistent elevations of chylomicron rem-nants in individuals with familial com-bined hyperlipidemia and diabetes,conditions associated with atherosclero-sis. Measures of chylomicron remnantsare not readily available.
HDL cholesterolHDL cholesterol levels are strong inversepredictors of CVD events in both diabeticand nondiabetic populations (48,49). Ithas been difficult to determine whetherraising HDL cholesterol independentlyreduces CVD events, because all interven-tions that raise HDL cholesterol also affectthe concentration of other lipoproteins(50). The VA-HIT was conducted in apopulation that was largely comprised ofindividuals with CAD and low HDL cho-lesterol, including 625 with diabetes.Therapy with gemfibrozil reduced CVDevents, and a post hoc analysis showed amodest association of the reduction inCVD with the extent of HDL increase(51). Strategies to raise HDL cholesterolremain a promising area of research thatmay be particularly valuable for prevent-ing CVD in individuals with CMR anddiabetes. Measurements of HDL subfrac-tions or apoA1 appear to provide littleclinical value beyond measurements ofHDL cholesterol (49).
IN THE EVALUATION ANDTREATMENT OF PATIENTSWITH LIPOPROTEINABNORMALITIES, ARETHERE OTHER FACTORSTHAT SHOULD BECONSIDERED? — In patients withlipoprotein abnormalities, good clinicalpractice calls for a comprehensive evalu-ation of their current vascular health, fac-tors contributing to the observeddyslipoproteinemia, and other factorsthat may alter the global risk of first orrecurrent CVD event. The objectives ofthe evaluation are as follows: 1) to deter-mine, to the extent possible, the magni-tude of the future risk of CVD events; 2) toidentify the presence of prognostic factorsthat may be modifiable; and 3) to estab-lish a treatment plan both in terms ofscope and intensity. An integral part ofthis process should be the active involve-ment of the patient because a better in-
formed patient is more likely to adhere tothe treatment plan.
A major objective of the risk evalua-tion is to ascertain the patient’s currentvascular health to determine whether thepatient already has CVD. Stratification bythe presence or absence of clinical CVD isimportant for decisions about the type ofintervention and its intensity. The pres-ence of so-called subclinical vascular dis-ease may be determined by measuringcoronary calcification, carotid intima-media thickness, or the ankle-brachialindex. Patients with documented subclin-ical atherosclerosis are at increased CVDrisk and may be considered candidates formore aggressive therapy (52–54).Whether such tests improve prediction orclinical decision making in patients withdiabetes or CMR is unclear.
The presence and severity of othermajor prognostic factors besides lipopro-tein abnormalities should also be ascer-tained. Modifiable risk factors includehigh blood pressure, smoking, hypergly-cemia, obesity, adverse dietary habits,and physical inactivity. The main non-modifiable prognostic factors are age, sex,ethnicity, and family history; other riskfactors such as chronic kidney diseasemay also be present. Two components ofage contribute to the risk of CVD. Theaging process per se leads to vascularchanges in a manner similar to that asso-ciated with age-related changes in otherorgans. Additionally, age is an indicator ofduration of exposure to adverse prognos-tic factors. For example, a person exposedto the toxic effects of a one pack/daysmoking habit over 30 years is more likelyto have smoking-related arterial lesionsthan another person who has smoked onepack/day for 3 years. Sex differences leadto an earlier onset of CVD in men than inwomen by about 10 years. Young menhave more CVD than premenopausalwomen; however, women’s rates catch upwith men’s after menopause. There are ra-cial differences in the prevalence of cer-tain prognostic factors, such as increasedrates of hypertension in African Ameri-cans. Family history of premature CAD,especially in siblings, also is a powerfulprognostic factor.
Additional biomarkers (e.g., C-reac-tive protein [CRP], fibrinogen, and homo-cysteine) have been evaluated todetermine their prognostic significance;however, their independent predictivepower and clinical utility are still unclear.In particular, CRP is often elevated in peo-ple with CMR, but here, too, the utility of
its measurement in individuals alreadyknown to be at high risk is unknown.
Risk assessment and strategies inprimary preventionSome global risk assessment tools esti-mate an individual’s risk of a major coro-nary heart disease event (such as fatal ornonfatal myocardial infarction) over 10years (55). There is a general consensusthat a 10-year risk of �20% requires ag-gressive intervention directed at the ab-normal prognostic factors. Those with a10-year risk �20% are given interven-tions based on the number and magni-tude of their risk factors. Although suchtools are helpful, they underestimate life-time risk, especially in youth and women.Assessments of lifetime global risk may bemore valuable guides to treatment in sub-jects at intermediate or low 10-year risk.Risk assessment models often have thelimitation that continuous prognostic fac-tors are dichotomized, which reducestheir statistical power. The American Di-abetes Association has developed a riskassessment model that addresses globalrisk over a longer time frame (30 years)and does not dichotomize continuousrisk factors (http://www.diabetes.org/diabetesphd/default.jsp).
The treatment plan for primary pre-vention may include antihypertensiveand glucose-lowering medications andlifestyle interventions directed at smokingcessation, weight loss, improved dietaryhabits, and increased physical activity.Such lifestyle interventions have majorpotential benefits on cardiovascularhealth and are often overlooked. There isstrong scientific evidence for CVD risk re-duction for antihypertensive, lipid-lowering, and smoking cessat iontherapies. An aggressive approach to pre-vent multiple comorbidities is warranted.Disappointingly, a large proportion ofhigh-risk individuals are not receiving op-timal preventive care or fail to adhere totreatment recommendations.
Risk assessment and strategies insecondary preventionThe prognostic factors for the secondaryprevention of CVD include those for pri-mary prevention but also include severalrelated to myocardial injury. For exam-ple, myocardial ischemia, left ventriculardysfunction, and ventricular arrhythmiasare powerful prognostic indicators aftermyocardial infarction (MI). Treatmentswith lipid-lowering therapy (statins), as-pirin, �-blockers, and ACE inhibitors
Brunzell and Associates
DIABETES CARE, VOLUME 31, NUMBER 4, APRIL 2008 815

have well-documented benefits in sec-ondary prevention. In addition, antihy-pertensive treatment, smoking cessationcounseling, and advice about dietarychoices and physical activity are alsobeneficial.
WHAT ARE THE PRINCIPLESAND OBJECTIVES OFTREATMENT OFLIPOPROTEINABNORMALITIES? — Dyslipopro-teinemia implies the presence of an in-creased number of atherogenic lipoproteinsand/or a reduced protective capacity ofHDL beyond what is considered optimal. Itis present when levels of triglycerides arehigh, HDL cholesterol is low, and/or there isatherogenic particle excess, such as highLDL cholesterol or an increased number ofsmall LDL particles. Cut points have beendeveloped to define values associated withincreased CVD risk. However, these cutpoints are arbitrary because the relationshipof each of these measures with cardiovascu-lar events is continuous and because the li-poprotein fractions are metabolicallyconnected in a complex fashion.
LDL cholesterolThere i s w idespread consensus(54,56,57) that for patients with elevatedCMR, the primary objective in reducingrisk for CVD events through modificationof lipid and lipoprotein risk factors is tolower LDL cholesterol values. This con-sensus is driven by the evidence that LDLis an important component of the athero-genic process and that treatments thatlower LDL cholesterol have been convinc-ingly demonstrated to reduce risk of CHDand stroke. The major issues to be consid-ered in translating this paradigm intopractice are as follows: 1) At what LDLcholesterol level should treatment be ini-tiated? 2) Through what mechanismsshould LDL cholesterol be lowered? 3) IsLDL cholesterol the best measure to assessthe response to treatment? 4) What arethe goals of treatment?Determining cut points for initiatingtherapy. Based on the curvilinear rela-tionship between LDL cholesterol andCHD in the general population, from apublic health standpoint it has been sug-gested that LDL cholesterol values �100mg/dl are optimal. Lifestyle recommenda-tions targeted at reduction of saturatedand trans unsaturated fat and cholesterolintake, lowering of excess body weight,and increasing intake of soluble fiber
should be emphasized as first-line ther-apy for those with LDL cholesterol values�100 mg/dl. It is clear that the absolutebenefit that can be achieved by LDL cho-lesterol lowering is proportional to theunderlying global risk for CVD in a givenindividual. Thus, guidelines for initiatingboth medical nutrition therapy as well aspharmacologic treatment aimed at LDLcholesterol lowering have been stratifiedby level of risk (54).
The panel agrees with the general rec-ommendations to start lifestyle and phar-macologic therapy concurrently insubjects with CVD (secondary preven-tion) and in those with diabetes and mul-tiple CVD risk factors, regardless ofbaseline LDL cholesterol. In addition, werecommend pharmacologic therapy formoderately high-risk primary preventionpatients (those with two or more CMRrisk factors and a 10-year risk �10%) ifLDL cholesterol levels remain �100mg/dl after several months of lifestylechanges.Therapeutic options for LDL choles-terol lowering. With respect to dietaryprinciples, the standard recommenda-tions for LDL cholesterol lowering havefocused on lowering saturated and transfat to �7% of calories and dietary choles-terol to �200 mg/day, lowering excessbody weight by at least 5–10%, and in-creasing soluble fiber consumption. Inaddition, increasing plant sterol andstanol intake modestly lowers LDL cho-lesterol. Weight reduction and weightmaintenance are best achieved by a com-bination of caloric reduction and in-creased physical activity.
As a result of the strong evidence basefor the benefits of statin treatment onCVD outcomes, this class of drugs pro-vides the primary pharmacologic modal-ity for LDL cholesterol lowering.Although statins’ beneficial effects arethought to be mediated predominantlythrough lowering of LDL cholesterol,their effects on HDL cholesterol and pos-sibly other lipoproteins explain some oftheir benefit, and the possibility of nonli-poprotein-mediated (pleiotropic) effectscannot be excluded. However, significantCVD benefit has been directly linked toLDL cholesterol lowering using other mo-dalities of treatment including diet, bileacid sequestrants, and ileal bypasssurgery.
For patients who cannot tolerate astatin, or in whom maximal dose statintherapy does not achieve treatment goals,other LDL cholesterol-lowering drugs in-
clude ezetimibe, bile-acid sequestrants,or niacin. As monotherapy, these drugsare less effective at lowering LDL choles-terol than statins, but each enhances theLDL-lowering effect of statins. Bile-acidbinding drugs, when used alone, can ag-gravate the dyslipidemia seen with insulinresistance by increasing triglycerides(58). Bile-acid resins in combination witha statin or nicotinic acid with a statin se-lectively decrease small dense LDL parti-cles (59).Assessing response to therapy. LDLcholesterol is the established primary tar-get of treatment. In patients with hyper-tr ig lycer idemia or the metabol icsyndrome, the ATP III (54) introducednon-HDL cholesterol as a secondary treat-ment target, recognizing that in this pa-tient population, LDL cholesterolunderestimates the burden of athero-genic, cholesterol-carrying lipoproteins.Non-HDL cholesterol adds no additionalexpense to a lipid profile and is easy tocalculate, but use of the measure has notbeen widely adopted.
Although numerous studies have af-firmed the superiority of non-HDL cho-lesterol over LDL cholesterol as a markerof CVD risk in patients with combinedhyperlipidemia (elevated triglyceridesand LDL cholesterol) or in those with apropensity for small dense LDL particles(patients with multiple CMR factors),both measures essentially focus on cho-lesterol as the agent of atherogenic risk.However, the measurement of cholesterolis a surrogate measure of atherogenic risk,given that atherosclerosis is the result of acomplex interaction between lipoproteinsand the vessel wall.
Measurements of apoB or LDL parti-cle number by NMR may more closelyquantitate the atherogenic lipoproteinload. Some studies suggest that both arebetter indices of CVD risk than LDL cho-lesterol or non-HDL cholesterol and morereliable indexes of on-treatment residualCVD risk (26,27,36,37,42,60–67). ApoBand LDL particle number also appear tobe more discriminating measures of theadequacy of LDL-lowering therapy thanare LDL cholesterol or non-HDL choles-terol. Statins lower non-HDL cholesterolmore than they lower apoB (37), and sev-eral studies have shown that reaching theapoB target usually requires more inten-sive therapy than achieving the equivalentlevel for non-HDL cholesterol (68,69).ApoB and LDL particle concentration alsoappear to be more closely associated withobesity, diabetes, insulin resistance, and
Consensus Statement
816 DIABETES CARE, VOLUME 31, NUMBER 4, APRIL 2008

other markers of CMR than are LDL cho-lesterol or non-HDL cholesterol (70–72).
When both non-HDL cholesterol andapoB are measured, the two are highlycorrelated but only moderately concor-dant (35,47,65,68,73,74). Although achange in non-HDL cholesterol is closelyrelated to a change in apoB, at any givenlevel of non-HDL cholesterol there will beconsiderable variation in apoB levels andvice versa, indicating that the correlationis of limited clinical value for assessingindividual risk. This lack of concordanceis particularly marked in patients with el-evated triglyceride levels, a common find-ing in patients with CMR.
The consensus panel concludes thatroutine calculation and use of non-HDLcholesterol constitute a better index thanLDL cholesterol for identifying high-riskpatients. That does not mean, however,that LDL cholesterol should not be mea-sured and used to guide therapy. Themany years of public and professional ed-ucation geared toward measurement ofLDL cholesterol has resulted in its suc-cessful integration into the fabric of CVDprevention and treatment, and it wouldbe a mistake to discontinue its use. On theother hand, the calculation of non-HDLcholesterol should be provided on all lab-oratory reports and should also be used toascertain risk in patients with low to mod-erate LDL cholesterol levels (i.e., LDLcholesterol �130 mg/dl). Because apoBappears to be a more sensitive index ofresidual CVD risk when LDL cholesterolor non-HDL cholesterol are �130 mg/dlor �160 mg/dl, respectively, measure-ment of apoB, using a standardized assay,is warranted in patients with CMR onpharmacologic treatment. In particular,apoB levels should be used to guide ad-
justments of therapy. While LDL particlenumber as measured by NMR appearsequally informative as apoB, the concernsexpressed above with regard to this assaylimit its widespread adoption at this time.Treatment goals for adults with CMRand lipoprotein abnormalities. By defi-nition, patients with CMR have high life-time risk for CVD. Among patients withCMR and lipoprotein abnormalities, thereare patients whom we define as at highestrisk for CVD over the short or intermedi-ate term: those with known clinical CVDand those who do not have clinical CVDbut who have diabetes and one or moreother CMR factors beyond their dyslipi-demia. We recommend that these high-est-risk individuals be treated to an LDLcholesterol goal �70 mg/dl, a non-HDLcholesterol goal �100 mg/dl, and anapoB goal �80 mg/dl.
Among patients with CMR and li-poprotein abnormalities, there are pa-tients whom we define as high (but nothighest) risk over the short or intermedi-ate term: those without diabetes or clini-cal CVD but with two or more major CVDrisk factors such as smoking, hyperten-sion, and family history of prematureCAD and those with diabetes but no otherCMR risk factors. We recommend thatthese high-risk individuals be treated toan LDL cholesterol goal �100 mg/dl, anon-HDL cholesterol goal �130 mg/dl,and an apoB goal �90 mg/dl.
These treatment goal recommenda-tions (Table 1) represent the panel’s con-sensus based on evaluation of theavailable evidence. As is the case with anytreatment recommendations, cliniciansshould recognize that individual patientfactors and preferences may reasonablylead to alteration of these goals (to higher
or lower levels) in some patients. Thesefactors might include age, life expectancy,desire for pregnancy in the near future inwomen, severity of risk factors, medica-tion interactions, and provider and pa-tient assessment of individual risks andbenefits of treatment.
Other lipids and lipoproteinsElevated triglyceride and reduced HDLcholesterol levels are the most commonabnormalities of the standard lipid profilein subjects with obesity and insulin-resistance–related CMR. Although in-creased triglycerides are modestlyassociated with increased CVD risk, espe-cially in women (75), it has been difficultto demonstrate that lowering of triglycer-ide levels is independently associatedwith a reduction in CVD events. Whilethe HDL cholesterol level is a powerfulrisk predictor, the clinical trial evidencesupporting treatment of low HDL choles-terol values is modest compared with thatfor LDL cholesterol lowering. For thesereasons, approaches directed at loweringtriglyceride-rich lipoproteins and raisingreduced HDL cholesterol levels have beenassigned secondary levels of therapeuticimportance.
For subjects with mildly or moder-ately elevated triglyceride levels (�200mg/dl), we support the ATP III recom-mendations to target LDL cholesterol firstand then use non-HDL cholesterol as asecondary target for treatment, with a goal30 mg/dl higher than the patient’s LDLcholesterol goal, but we further recom-mend that the population- equivalentapoB goal be reached. The exception tonot targeting triglycerides initially is therelatively small proportion of patientswith severe hypertriglyceridemia inwhom the initial treatment priority is toreduce the risk of pancreatitis by combin-ing dietary fat restriction with fibrate, ni-acin, or high-dose n-3 fatty acid therapy.All patients with low HDL cholesterolshould receive lifestyle counseling focus-ing on weight reduction, increased phys-ical activity, avoidance of very highcarbohydrate diets, and discontinuingsmoking.
A statin is the initial drug of choice forthe vast majority of people with CMR whohave elevated triglycerides and low HDLcholesterol. In individuals on statin ther-apy who continue to have low HDL cho-lesterol or elevated non-HDL cholesterol,especially if apoB levels remain elevated,combination therapy is recommended.
Table 1—Suggested treatment goals in patients with CMR and lipoprotein abnormalities
Goals
LDL cholesterol(mg/dl)
Non-HDL cholesterol(mg/dl)
ApoB(mg/dl)
Highest-risk patients, including those with1) known CVD or 2) diabetes plus oneor more additional major CVD riskfactor
�70 �100 �80
High-risk patients, including those with1) no diabetes or known clinical CVDbut two or more additional major CVDrisk factors or 2) diabetes but no othermajor CVD risk factors
�100 �130 �90
Other major risk factors (beyond dyslipoproteinemia) include smoking, hypertension, and family history ofpremature CAD.
Brunzell and Associates
DIABETES CARE, VOLUME 31, NUMBER 4, APRIL 2008 817

The preferred agent to use in combinationwith a statin is nicotinic acid becausethere is somewhat better evidence for re-duction in CVD events with niacin, asmonotherapy or in combination, thanthere is for fibrates. Nicotinic acid de-creased CVD in the Coronary DrugProject (76) and total mortality in ex-tended follow-up (77). Nicotinic acid incombination with a bile-acid bindingresin or a statin was associated with re-gression of atherosclerosis and reducedCVD events in several studies (78–81).Although nicotinic acid has been associ-ated with insulin resistance, in diabetesthe use of low-dose nicotinic acid (1,500mg/day) does not significantly increaseA1C levels (82,83).
Fibrates have been shown to reduceCVD events in some studies but not mor-tality. In the Fenofibrate Intervention andEvent Lowering in Diabetes (FIELD) trialof patients with type 2 diabetes, the pri-mary outcome of overall CHD events wasnot significantly reduced by the drug. Thesecondary outcome of nonfatal MI wasdecreased by 24% (P � 0.01), but fatal MIincreased by 19% (P � 0.22) (84). Similardecreases in nonfatal MI, but not fatal MIor total mortality, were seen in the WHOtrial with clofibrate (85), in the HelsinkiHeart Study with gemfibrozil (86), in theVA-HIT trial with gemfibrozil (87), and inthe Bezafibrate Infarction Prevention(BIP) trial with bezofibrate (88).
n-3 fatty acid therapy lowers plasmatriglyceride levels at high doses (�4g/day) and may be another option to con-sider to lower non-HDL cholesterol in pa-tients on statin therapy, but CVDoutcome data are lacking for hypertriglyc-eridemic patients treated with these dosesof n-3 fatty acids. In diabetic subjects, en-hanced glycemic control may improvelipid and lipoprotein abnormalities, par-ticularly hypertriglyceridemia. Specificantihyperglycemic agents may have ad-vantages in this respect. For example,metformin has modest triglyceride-lowering properties. Both peroxisomeproliferator–activated receptor-� agonistsincrease LDL particle size, but they havediffering effects on other lipoprotein frac-tions. Pioglitazone raises HDL cholesterolto a greater extent than rosiglitazone andlowers triglycerides, while rosiglitazoneleads to a modest increase in triglycerides.Furthermore, pioglitazone lowers whereasrosiglitazone increases LDL particle num-ber (89).
WHAT NEW INFORMATIONWOULD HELP IMPROVELIPOPROTEINMANAGEMENT?
Residual risk on statin therapyWhile statin therapy has proven to reducecardiovascular risk, there remains sub-stantial residual risk in treated patients.Studies are needed to determine whethervery low LDL cholesterol levels are bene-ficial and safe and to define which types ofpatients receive the most benefit. Weneed to determine whether residual riskcan be decreased by interventions thatimpact other lipoproteins, such as in-creasing HDL cholesterol or decreasingsmall dense LDL. In addition, studies areneeded to directly determine whetherapoB or other lipoproteins are better ther-apeutic targets than LDL cholesterol.
TriglyceridesAlthough patients with elevated triglycer-ides are at increased CVD risk, there is alack of data regarding the benefits of strat-egies directly targeting elevated triglycer-ide levels. Therefore, it is unclear whetheror at what level triglycerides should betreated and what should be the goal oftherapy. This will not be an easy questionto answer because of the complexities oftriglyceride and lipoprotein metabolism(90).
HDL cholesterolIn observational studies, low HDL choles-terol is a powerful risk factor for CVD andremains a risk factor even in patients withlow LDL cholesterol. Because a recent trialwith a cholesteryl ester transfer proteininhibitor to raise HDL cholesterol was ter-minated as a result of excess cardiovascu-lar events, it remains unclear whetherraising HDL cholesterol per se reducescardiovascular risk (91). It may be thatincreasing HDL cholesterol by modifyingthe reverse cholesterol pathway wouldparadoxically increase risk, while othermechanisms to increase HDL cholesterolmay lead to a reduction in risk. Strategiesto safely and effectively raise HDL choles-terol remain a promising area of researchthat is particularly relevant to CMRpatients whose dyslipoproteinemia is of-ten characterized by low levels of HDLcholesterol.
Combination therapyMonotherapy with statins, fibrates, nia-cin, and bile acid sequestrants has beenshown to reduce cardiovascular events in
clinical trials, but there is not yet robustevidence for incremental benefits or risksof combination therapy compared withthose of monotherapy. Results of ongoingand future trials of statin-niacin, statin-fibrate, and statin–n-3 fatty acids will, it ishoped, help answer these questions.
Benefits of lipoprotein managementin other high-risk subsetsAlthough statin therapy is highly effectivein reducing CVD risk in primary and sec-ondary prevention, there remain subsetsof patients regarding whom more data areneeded. These include the elderly, thosewith chronic kidney disease, and youngpatients with CMR.
Utility of biomarkersBiomarkers such as CRP have been shownto identify patients at higher risk for CVDevents. However, their additive value as aclinical tool is unclear, especially amongpatients with CMR (92). At least one on-going trial (93) is addressing the issue ofwhether prospectively selecting patientsbased on an elevated CRP will identify ahigh-risk group that will benefit from sta-tin treatment.
SUMMARY — Patients with cardiom-etabolic risk factors represent a group athigh lifetime risk for CVD. These patientsfrequently have dyslipoproteinemia (lowHDL cholesterol, increased triglycerides,and/or an increased number of small LDLparticles). We recommend an assessment ofglobal risk followed by a multifactorial riskreduction strategy for such individuals tar-geting each risk factor and emphasizingboth lifestyle and pharmacologic therapy.In terms of dyslipoproteinemia, we recom-mend the following:
● Statin therapy for the majority of dysli-poproteinemic adult patients withCMR
● For patients with CMR on statin ther-apy, guiding therapy with measure-ments of apoB and treatment to apoBgoals in addition to LDL cholesterol andnon-HDL cholesterol assessments
● Treatment goals, summarized in Table1, that address the high lifetime risk ofpatients with dyslipoproteinemia andCMR.
● Clinical trials to determine whether thepharmacologic therapy required toachieve very low levels of atherogeniclipoproteins is safe and cost-effective
● A concerted, multifaceted, publichealth effort, focused on lifestyle mod-
Consensus Statement
818 DIABETES CARE, VOLUME 31, NUMBER 4, APRIL 2008

ification, to reduce mean populationlevels of atherogenic lipoproteins tovalues well below current ones.
APPENDIX — The authors disclosethe following dualities of interest:J.D.B. NoneM.D. Consulting/speaking fees from Ab-bott Laboratories, AstraZeneca Pharma-ceuticals, Daiichi-Sankyo, diaDexus,Merck, Merck/Schering-Plough, OscientPharmaceuticals, Pfizer, Reliant Pharma-ceuticals, Roche Pharmaceuticals, Sanofi-Aventis, and Takeda Pharmaceuticals; re-search funds from Abbott Laboratories,AstraZeneca Pharmaceuticals, Daiichi-Sankyo, Merck, Merck/Schering-Plough,Pfizer, Reliant Pharmaceuticals, RochePharmaceuticals, and Takeda Pharma-ceuticals; advisory board membership forAbbott Laboratories, AstraZeneca Phar-maceuticals, Atherogenics, Daiichi-Sankyo, Merck, Merck/Schering-Plough,Oscient Pharmaceuticals, Pfizer, ReliantPharmaceuticals, Roche Pharmaceuticals,Takeda Pharmaceuticals, and XinthriaPharmaceuticals; membership of theboard of directors for Angiogen and So-nogene; and chief medical officer for Pro-fessional Evaluation, Inc.C.D.F. NoneR.B.G. Consulting/speaking fees fromLilly/Takeda, Pfizer, Merck, Merck/Schering-Plough, Kos Pharmaceuticals,AstraZeneca Pharmaceuticals, and AbbottLaboratories; and research funds fromNovo Nordisk, Merck, Kos Pharmaceuti-cals, AstraZeneca Pharmaceuticals, andDaiichi-Sankyo.B.V.H. Consulting/speaking fees fromMerck, Egg Nutrition Counsel, Unilever,and Schering-Plough.J.H.S. Consulting fees from Abbott Lab-oratories, LipoScience, Merck, Pfizer, andSchering-Plough; and research fundsfrom Bristol-Myers Squibb, Sanofi-Aventis, Takeda Pharmaceuticals, andKos Pharmaceuticals.J.L.W. Honoraria and consulting/speaking fees from Merck and researchfunds from Atherotope, Isis Pharmaceuti-cals, and Amira Pharmaceuticals.
References1. Kahn R, Buse J, Ferrannini E, Stern M:
The metabolic syndrome: time for a criti-cal appraisal. Diabetes Care 28:2289–2304, 2005
2. Carr MC, Brunzell JD: Abdominal obesityand dyslipidemia in the metabolic syn-drome: importance of type 2 diabetes andfamilial combined hyperlipidemia in cor-
onary artery disease risk. J Clin EndocriolMetab 6:2601–2607, 2004
3. Cohen JC, Boerwinkle E, Mosley TH Jr,Hobbs HH: Sequence variations inPCSK9, low LDL, and protection againstcoronary heart disease. N Engl J Med 354:1264–1272, 2006
4. Brown MS, Goldstein JL: A receptor-me-diated pathway for cholesterol homeosta-sis. Science 232:34–47, 1986
5. O’Keefe JH, Cordain L, Harris WH, MoeRM, Vogel R: Optimal low-density li-poprotein is 50 to 70 mg/dl: lower is bet-ter and physiologically normal. J Am CollCardiol 43:2142–2146, 2004
6. Young SG, Bertics SJ, Curtiss LK, DuboisBW, Witztum JL: Genetic analysis of akindred with familial hypobetalipopro-teinemia: evidence for two separate genedefects: one associated with an abnormalapolipoprotein B species, apolipoproteinB-37; and a second associated with lowplasma concentrations of apolipoproteinB-100. J Clin Invest 79:1842–1851, 1987
7. Turner RC, Millns H, Neil HA, StrattonIM, Manley SE, Matthews DR, HolmanRR: Risk factors for coronary artery dis-ease in non-insulin dependent diabetesmellitus: United Kingdom prospective di-abetes study (UKPDS: 23). BMJ 316:823–828, 1998
8. Lee ET, Howard BV, Wang W, Welty TK,Galloway JM, Best LG, Fabsitz RR, ZhangY, Yeh JL, Devereux RB: Prediction of cor-onary heart disease in a population withhigh prevalence of diabetes and albumin-uria: the Strong Heart Study. Circulation113:2897–2905, 2006
9. Pearte CA, Furberg CD, O’Meara ES,Psaty BM, Kuller L, Powe NR, Manolio T:Characteristics and baseline clinical pre-dictors of future versus nonfatal coronaryheart disease events in older adults. Cir-culation 113:2177–2185, 2006
10. Packard CJ, Ford I, Robertson M, Shep-herd J, Blauw GJ, Murphy MB, Bollen EL,Buckley BM, Cobbe SM, Gaw A, HylandM, Jukema JW, Kamper AM, MacfarlanePW, Perry JJ, Stott DJ, Sweeney BJ,Twomey C, Westendorp RG; PROSPERStudy Group: Plasma lipoproteins andapolipoproteins as predictors of cardio-vascular risk and treatment benefit in theprospective study of pravastatin in the el-derly at risk (PROSPER). Circulation 112:3058–3065, 2005
11. Heart Protection Study CollaborativeGroup: MRC/BHF Heart Protection Studyof cholesterol lowering with simvastatinin 20 536 high-risk individuals: a ran-domised placebo-controlled trial. Lancet360:7–22,2002
12. Heart Protection Study CollaborativeGroup: MRC/BHF Heart Protection Studyof cholesterol-lowering with simvastatinin 5963 people with diabetes: a random-ised placebo-controlled trial. Lancet 361:2005–2016, 2003
13. Sever PS, Dahlof B, Poulter NR, Wedel H,Beevers G, Caulfield M, Collins R, Kjeld-sen SE, Kristinsson A, McInnes GT,Mehlsen J, Nieminen M, O’Brien E, Oster-gren J, for the ASCOT Investigators: Pre-vention of coronary and stroke eventswith atorvastatin in hypertensive patientswho have average or lower-than-averagecholesterol concentrations, in the Anglo-Scandinavian cardiac outcomes trial-lipidlowering arm (ASCOT-LLA): a multicen-tre randomised controlled trial. Lancet361:1149–1158, 2003
14. Colhoun HM, Betteridge DJ, DurringtonPN, Hitman GA, Neil HA, Livingstone SJ,Thomason MJ, Mackness MI, Charlton-Menys V, Fuller JH: Primary prevention ofcardiovascular disease with atorvastatinin type 2 diabetes in the CollaborativeAtorvastatin Diabetes Study (CARDS):multicentre randomised placebo-con-trolled trial. Lancet 364:685–696, 2004
15. Pyorala K, Pedersen TR, Kjekshus J,Faergeman O, Olsson AG, ThorgeirssonG: Cholesterol lowering with simvastatinimproves prognosis of diabetic patientswith coronary heart disease: a subgroupanalysis of the Scandinavian SimvastatinSurvival Study (4S). Diabetes Care20:614–620, 1997
16. Sacks FM, Pfeffer MA, Moye LA, RouleauJL, Rutherford JD, Cole TG, Brown L,Warnica JW, Arnold JM, Wun CC, DavisBR, Braunwald E: The effect of pravastatinon coronary events after myocardial in-farction in patients with average choles-terol levels: Cholesterol and RecurrentEvents Trial Investigators. N Engl J Med335:1001–1009, 1996
17. The Long-Term Intervention with Prava-statin in Ischaemic Disease (LIPID) StudyGroup: Prevention of cardiovascularevents and death with pravastatin in pa-tients with coronary heart disease and abroad range of initial cholesterol levels.N Engl J Med 339:1349–1357, 1998
18. Serruys P: WJ, de Feyter P, Macaya C,Kokott N, Puel J, Vrolix M, Branzi A, Ber-tolami MC, Jackson G, Strauss B, Meier B,the Lescol Intervention Prevention Study(LIPS) Investigators: Fluvastatin for pre-vention of cardiac events following suc-cessful first percutaneous coronaryintervention: a randomized controlledtrial. JAMA 287:3215–3222, 2002
19. The Post Coronary Artery Bypass GraftTrial Investigators: The effect of aggres-sive lowering of low-density lipoproteincholesterol levels and low-dose anticoag-ulation on obstructive changes in saphe-nous-vein coronary-artery bypass grafts.NEJM 336:153–162, 1997
20. Pedersen TR, Faergeman O, Kastelein JJP,Olsson AG, Tikkanen MJ, Holme I, LarsenML: Bendiksen FS, Lindahl, C, Szarek M,Tsai J: High-dose atorvastatin vs usual-dose simvastatin for secondary preven-tion after myocardial infarction: the
Brunzell and Associates
DIABETES CARE, VOLUME 31, NUMBER 4, APRIL 2008 819

IDEAL Study: a randomized controlledtrial. JAMA 294:2437–2445, 2005
21. Shepherd J, Barter P, Carmena R, Deed-wania P, Fruchart JC, Haffner S, Hsia J,Breazna A, LaRosa J, Grundy S, Waters D,the Treating to New Targets Investigators:Effect of lowering LDL cholesterol sub-stantially below currently recommendedlevels in patients with coronary heart dis-ease and diabetes. Diabetes Care29:1220–1226, 2006
22. Sniderman AD: Low-density lipoproteinlowering in type 2 diabetes mellitus: howto know how low to go. Curr Opin Endo-crinol 14:116–123, 2007
23. Cromwell WC, Otvos JD: Low-density li-poprotein particle number and risk forcardiovascular disease. Curr AtherosclerRep 6:381–387, 2004
24. Mora S, Szklo M, Otvos J, Greenland P,Psaty BM, Goff DC Jr, O’Leary DH, SaadMF, Tsai MY, Sharrett AR: LDL particlesubclasses, LDL particle size, and carotidatherosclerosis in the Multi-Ethnic Studyof Atherosclerosis (MESA) Atherosclerosis192:211–217, 2007
25. Kuller LH, Arnold A, Tracy R, Otvos J,Burke G, Psaty B, Siscovick D, FreedmanDS, Kronmal R: Nuclear magnetic reso-nance spectroscopy of lipoproteins andrisk of coronary heart disease in the Car-diovascular Health Study. ArteriosclerThromb Vasc Biol 22:1175–1180, 2002
26. Rosenson RS, Otvos JD, Freedman DS:Relations of lipoprotein subclass levelsand low-density lipoprotein size to pro-gression of coronary artery disease in thePravastatin Limitation of Atherosclerosisin the Coronary Arteries (PLAC-I) Trial.Am J Cardiol 90:89–94, 2002
27. Blake GJ, Otvos JD, Rifai N, Ridker PM:Low-density lipoprotein particle concen-tration and size as determined by nuclearmagnetic resonance spectroscopy aspredictors of cardiovascular disease inwomen. Circulation 106:1930–1937,2002
28. Otvos JD, Collins D, Freedman DS, Sha-laurova I, Schaefer EJ, McNamara JR,Bloomfield HE, Rovins SJ: Low-density li-poprotein and high-density lipoproteinparticle subclasses predict coronaryevents and are favorably changed by gem-fibrozil therapy in the Veterans AffairsHigh-Density Lipoprotein InterventionTrial. Circulation 113:1556–1563, 2006
29. El Harchaoui K, van der Steeg WA, StroesES, Kuivenhoven JA, Otvos JD, WarehamNJ, Hutten BA, Kastelein JJ, Khaw KT,Boekholdt SM: Value of low-density li-poprotein particle number and size aspredictors of coronary artery disease inapparently healthy men and women: theEPIC Norfolk prospective populationstudy. J Am Coll Cardiol 49:547–553,2007
30. Sacks FM, Campos, H: Low-density li-poprotein size and cardiovascular disease:
a reappraisal. JCEM 88:4525–4532, 200331. Lamarche B, Tchernof A, Moorjani S,
Cantin B, Dagenais GR, Lupien PJ, De-spres JP: Small, dense low-density li-poprotein particles as a predictor of therisk of ischemic heart disease in men: pro-spective results from the Quebec Cardio-vascular Study: Circulation 95:69–75,1997
32. Ala-Korpela M, Lankinen N, Salminen A,Suna T, Soininen P, Laatikainen R, Ing-man P, Jauhiainen M, Taskinen MR, He-berger K, Kaski K: The inherent accuracyof 1H NMR spectroscopy to quantifyplasma lipoproteins is subclass depen-dent. Atherosclerosis 190:352–358, 2007
33. Lu W, Resnick HE, Jablonski KA, JonesKL, Jain AK, Howard WJ, Robbins DC,Howard BV: Non-HDL cholesterol as apredictor of cardiovascular disease in type2 diabetes: the Strong Heart Study. Diabe-tes Care 26:16–23, 2003
34. Liu J, Sempos C, Donahue R, Dorn J, Tre-visan M, Grundy SM: Joint distribution ofnon-HDL and LDL cholesterol and coro-nary heart disease risk prediction amongindividuals with and without diabetes.Diabetes Care 28:1916–1921, 2005
35. Pischon T, Girman CJ, Sacks FM, Rifai N,Stampfer MJ, Rimm EB: Non-high densitylipoprotein cholesterol and apolipopro-tein B in the prediction of coronary heartdisease in men. Circulation 112:3375–3383, 2005
36. Gotto AM Jr, Whitney E, Stein EA, Sha-piro DR, Clearfield M, Weis S, Jou JY, Lan-gendorfer A, Beere PA, Watson DJ, DownsJR, de Cani JS: Relation between baselineand on-treatment lipid parameters andfirst acute major coronary events in theAir Force/Texas Coronary AtherosclerosisPrevention Study (AFCAPS/TexCAPS).Circulation 101:477–484, 2000
37. Sniderman AD, Furberg CD, Keech A,Roeters Van Lennep JE, Frohlich J, Jung-ner I, Walldius G: Apolipoproteins versuslipids as indices of coronary risk and astargets for statin treatment. Lancet 361:777–780, 2003
38. Sacks FM: The apolipoprotein story. Ath-eroscler 7 (Suppl.):23–27, 2006
39. Marcovina SM, Albers JJ, Dati F, LedueTB, Ritchie RF: International Federationof Clin Chem standardization project formeasurements of apolipoproteins A-I andB. Clin Chem 37:1676–1682, 1991
40. Marcovina SM, Albers JJ, Kennedy H, MeiJV, Henderson LO, Hannon WH: Interna-tional Federation of Clin Chem standard-ization project for measurements ofapolipoproteins A-I and B. IV. Compara-bility of apolipoprotein B values by use ofinternational reference material. ClinChem 40:586–592, 1994
41. Lamarche B, Moorjani S, Lupien PJ, Can-tin B, Bernard PM, Dagenais GR, DespresJP: Apolipoprotein A-1 and B levels andthe risk of ischemic heart disease during a
five-year follow-up of men in the QuebecCardiovascularStudy.Circulation94:273–278, 1996
42. Walldius G, Jungner I, Holme I, AastveitAH, Kolar W, Steiner E: High apolipopro-tein B, low apolipoprotein A-I, and im-provement in the prediction of fatalmyocardial infarction (AMORIS study): aprospectivestudy.Lancet358:2026–2033,2001
43. Roeters van Lennep JE, Westerveld HT,Van Roeters Lennep HWO, ZwindermanAH, Erkelens DW, Van der Wall EE: Apo-lipoprotein concentrations during treat-ment and recurrent coronary arterydisease events. Arterioscler Thromb VascBiol 20:2408–2413, 2000
44. Ridker PM, Rifai N, Cook NR, Bradwin G,Buring JE: Non-HDL cholesterol, apoli-poproteins A-I and B 100, standard lipidmeasures, lipid ratios, and CRP as risk fac-tors for cardiovascular disease in women.JAMA 294:326–333, 2005
45. Inglesson E, Schaefer EJ, Contois JH, Mc-Namara JR, Sullivan L, Keyes MJ, PencinaMJ, Schoonmaker C, Wilson PWF,D’Agostino RB, Vasan RS: Clinical utilityof different lipid measurements for pre-diction of coronary heart disease in menand women. JAMA 298:776–85, 2007
46. Van der Steeg WA, Boekholdt SM, SteinEA, El-Harchaoui K, Stroes ESG, SandhuMS, Wareham NJ, Jukema JW, Luben R,Zwinderman AH, Kastelein JJP, KhawK-T: Role of the apolipoprotein B–apoli-poprotein A-I ratio in cardiovascular riskassessment: a case–control analysis in EP-IC-Norfolk.AnnInternMed146:640–648,2007
47. Sniderman AD, St-Pierre A, Cantin B, Da-genais GR, Depres J-P, Lamarche B: Con-cordance/discordance between plasmaapolipoprotein B levels and the choles-terol indexes of atherosclerotic risk. Am JCardiol 91:1173–1177, 2003
48. Castelli WP, Garrison RJ, Wilson PW, Ab-bott RD, Kalousdian S, Kannel WB: Inci-dence of coronary heart disease andlipoprotein cholesterol levels: the Fra-mingham Study. JAMA 256:2835–2838,1986
49. Sharrett AR, Ballantyne CM, Coady SA,Heiss G, Sorlie PD, Catellier D, Patsch W:Coronary heart disease prediction from li-poprotein cholesterol levels, triglycerides,lipoprotein(a), apolipoproteins A-I and B,and HDL density subfractions: the Ath-erosclerosis Risk in Communities (ARIC)Study. Circulation 104:1108–1113, 2001
50. Singh IM, Shishehbor DO, Ansell BJ:High-density lipoprotein as a therapeutictarget: a systematic review. JAMA 298:786–798, 2007
51. Robins SJ, Collins D, Wittes JT, Papadem-etriou V, Deedwania PC, Schaefer EJ, Mc-Namara JR, Kashyap ML, Hershman JM,Wexler LF, Rubins HB; VA-HIT StudyGroup. Veterans Affairs High-Density Li-
Consensus Statement
820 DIABETES CARE, VOLUME 31, NUMBER 4, APRIL 2008

poprotein Intervention Trial. Relation ofgemfibrozil treatment and lipid levelswith major coronary events: VA-HIT: arandomized controlled trial. JAMA 285:1585–1591, 2001
52. Greenland P, Abrams J, Aurigemma GP,Bond MG, Clark LT, Criqui MH, CrouseJR, Friedman L, Fuster V, Herrington DM,Kuller LH, Ridker PM, Roberts WC, Stan-ford W, Stone N, Jeremy Swan HJ, Taub-ert KA, Wexler L, the Writing Group III:Prevention Conference V: Beyond sec-ondary prevention: identifying the high-risk patient for primary prevention:noninvasive tests of atherosclerotic bur-den. Circulation 101:E16–E22, 2000
53. Taylor AJ, Merz CN, Udelson JE: 34th Be-thesda Conference: Executive summa-ry—can atherosclerosis imaging tech-niques improve the detection of patientsat risk for ischemic heart disease? J AmColl Cardiol 41:1860–1862, 2003
54. National Cholesterol Education ProgramExpert Panel on Detection, Evaluation,and Treatment of High Blood Cholesterolin Adults: Executive summary of theThird Report of the National CholesterolEducation Program (NCEP) Expert Panelon Detection, Evaluation, and Treatmentof High Blood Cholesterol in Adults(Adult Treatment Panel III). JAMA 285:2486–2497, 2001
55. Framingham Risk Assessment [articleonline]. Available from http://hp2010.nhlbihin.net/atpiii/calculator.asp. Access-ed 6 September 2007
56. American Diabetes Association: Standardsof medical care in diabetes—2008. DiabetesCare 31 (Suppl. 1):S12–S54, 2008
57. De Backer G, Ambrosioni E, Borch-Johnsen K, Brotons C, Cifkova R, Dallon-geville J, Ebrahim S, Faergeman O,Graham I, Mancia G, Manger Cats V,Orth-Gomer K, Perk J, Pyorala K, RodicioJL, Sans S, Sansoy V, Sechtem U, Silber S,Thomsen T, Wood D; Third Joint TaskForce of European and Other Societies onCardiovascular Disease and Prevention inClinical Practice: European guidelines oncardiovascular disease prevention in clin-ical practice. Eur Heart J 24:1601–1610,2003
58. Angelin B, Einarsson K, Hellstrom K,Leijd B: Effects of cholestyramine andchenodeoxycholic acid on the metabo-lism of endogenous triglyceride in hyper-lipoproteinemia. J Lipid Res 19:1017–1024, 1978
59. Zambon A, Hokanson JE, Brown BG,Brunzell JD: Evidence for a new patho-physiological mechanism for coronary ar-tery disease regression: hepatic lipase-mediated changes in LDL density.Circulation 99:1959–1964, 1999
60. Yusuf S, Hawken S, Ounpuu S, Dans T,Avezum A, Lanas F, McQueen M, BudaiA, Pais P, Varigos J, Lisheng L, the INTER-HEART Study Investigators: Effect of po-
tentially modifiable risk factors associatedwith myocardial infarction in 52 coun-tries (the INTERHEART study). Lancet364:937–952, 2004
61. Barter PJ, Ballantyne CM, Carmena R,Castro Cabezas M, Chapman MJ, CoutureP, De Graaf J, Durrington PN, FaergemanO, Frohlich J, Furberg CD, Gagne C,Haffner SM, Humphries SE, Jungner I,Krauss RM, Kwiterovich P, Marcovina S,Packard CJ, Pearson TA, Srinath Reddy K,Rosenson R, Sarrafzadegan N, SnidermanAD, Stalenhoef AF, Stein E, Talmud PJ,Tonkin AM Walldius G, Williams, KMS:Apo B versus cholesterol in estimatingcardiovascular risk and in guiding ther-apy: report of the thirty-person/ten-coun-try panel. J Int Med 259:247–258, 2006
62. Pedersen TR, Olsson AG, Faergeman O,Kjekshus J, Wedel H, Berg K, WilhelmsenL, Haghfelt T, Thorgeirsson G, Pyorala K,Miettinen T, Christophersen B, TolbertJA, Musliner TA, Cook TJ: Lipoproteinchanges and reduction in the incidence ofmajor coronary heart disease events in theScandinavian Simvastatin Survival Study(4S). Circulation 97:1453–1460, 1998
63. Jiang R, Schulze MB, Li T, Rifai N,Stampfer MJ, Rimm EB, Hu FB: Non-HDLcholesterol and apolipoprotein B predictcardiovascular disease events among menwith type 2 diabetes. Diabetes Care 27:1991–1997, 2004
64. Shai I, Rimm EB, Hankinson SE, CurhanG, Manson JE, Rifai N, Stampfer MJ, Ma J:Multivariate assessment of lipid parame-ters as predictors of coronary heart dis-ease among postmenopausal women:potential implications for clinical guide-lines. Circulation 110:2824–2830, 2004
65. Wagner AM, Perez A, Zapico E, Ordonez-Llanos J: Non-HDL cholesterol and apoli-poprotein B in the dyslipidemic clas-sification of type 2 diabetic patients. Dia-betes Care 26:2048–2051, 2003
66. Simes RJ, Marschner IC, Hunt D,Colquhoun D, Sullivan D, Stewart RA,Hague W, Keech A, Thompson P, White H,Shaw J, Tonkin A, the Lipid Study Investi-gators: Relationship between lipid levelsand clinical outcomes in the Long-termIntervention with Pravastatin in the Isch-emic Disease (LIPID) Trial: to what extent isthe reduction in coronary events with prav-astatin explained by on-study lipid levels?Circulation 105:1162–1169, 2002
67. Chien K-L, Hsu H-C, Su T-C, Chen M-F,Lee Y-T, Hu, FB: Apolipoprotein B andnon-high-density lipoprotein cholesteroland risk of coronary heart disease in Chi-nese. J Lipid Res 48:2499–2505, 2007
68. Stein EA, Sniderman A, Laskarzewski P:Assessment of reaching goal in patientswith combined hyperlipidemia: low-density lipoprotein cholesterol, non-high-density lipoprotein cholesterol, orapolipoprotein B. Am J Cardiol 96:36–43,2005
69. Ballantyne CM, Bertolami M, HernandezGarcia HR, Nul D, Stein EA, Theroux P,Weiss R, Cain VA, Raichlen JS: AchievingLDL cholesterol, non-HDL cholesterol,and apolipoprotein B target levels in high-risk patients: Measuring Effective Reduc-tions in Cholesterol Using RosuvastatintherapY (MERCURY) II. Am Heart J 151:975–983, 2006
70. Sattar N, Williams K, Sniderman AD,D’Agostino R Jr, Haffner SM: Comparisonof the associations of apoB and non-HDL cholesterol with other cardiovascu-lar risk factors in patients with the meta-bolic syndrome in the Insulin ResistanceStudy (IRAS). Circulation 110:2687–2693, 2004
71. Garvey WT, Kwon S, Zheng D, Shaugh-nessy S, Wallace P, Hutto A, Pugh K, Jen-kins AJ, Klein RL, Liao Y: Effects of insulinresistance and type 2 diabetes on lipopro-tein subclass particle size and concentra-tion determined by nuclear magneticresonance. Diabetes 52:453–462, 2003
72. Kathiresan S, Otvos JD, Sullivan LM,Keyes MJ, Schaefer EJ, Wilson PW,D’Agostino RB, Vasan RS, Robins SJ: In-creased small low-density lipoproteinparticle number: a prominent feature ofthe metabolic syndrome in the Framing-ham Heart Study. Circulation 113:20–29,2006
73. Cromwell WC, Otvos JD, Keyes MJ, Pen-cina MJ, Sullivan L, Ramachandran VS,Wilson PWF, D’agostino RB: LDL particlenumber and risk of future cardiovasculardisease in the Framingham OffspringStudy: implications for LDL management.J Clin Lipidol. In press
74. Cromwell WC, Otvos JD: Heterogeneityof low-density lipoprotein particle num-ber in patients with type 2 diabetes mel-litus and low-density lipoproteincholesterol �100mg/dL. Am J Cardiol 98:1599–1602, 2006
75. Sarwar N, Danesh J, Eiriksdottir G, Sig-urdsson G, Wareham N, Bingham S,Boekholdt SM, Khaw KT, Gudnason V:Triglycerides and the risk of coronaryheart disease: 10,158 incident casesamong 262,525 participants in 29 west-ern prospective studies. Circulation 115:450–458, 2007
76. The Coronary Drug Project Group: Clofi-brate and niacin in coronary heart disease.JAMA 231:360–381, 1975
77. Canner PL, Berge KG, Wenger NK, Stam-ler J, Friedman L, Prineas RJ, FriedewaldW: Fifteen year mortality in coronarydrug project patients: long-term benefitwith niacin. J Am Coll Cardiol 8:1245–1255, 1986
78. Brown G, Albers JJ, Fisher LD, SchaeferSM, Lin JT, Kaplan C, Zhao XQ, BissonBD, Fitzpatrick VF, Dodge HT: Regres-sion of coronary artery disease as a resultof intensive lipid-lowering in men withhigh levels of apolipoprotein B. N Engl
Brunzell and Associates
DIABETES CARE, VOLUME 31, NUMBER 4, APRIL 2008 821

J Med 323:1289–1298, 199079. Brown BG, Zhao XQ, Chait A, Fisher LD,
Cheung MC, Morse JS, Dowdy AA,Marino EK, Bolson EL, Alaupovic P,Frohlich J, Albers JJ: Simvastatin and nia-cin, antioxidant vitamins, or the combina-tion for the prevention of coronarydisease. N Engl J Med 345:1583–1592,2001
80. Taylor AJ, Sullenberger LE, Lee HJ, LeeJK, Grace KA: Arterial Biology for the In-vestigation of the Treatment Effects of Re-ducing Cholesterol (ARBITER) 2: Adouble-blind, placebo-controlled studyof extended-release niacin on atheroscle-rosis progression in secondary preventionpatients treated with statins. Circulation110:3512–3517, 2004
81. Blankenhorn DH, Nessim SA, JohnsonRL, Sanmarco ME, Azen SP, Cashin-Hemphill L: Beneficial effects of com-bined colestipol-niacin therapy oncoronary atherosclerosis and coronaryvenous bypass grafts. JAMA 257:3233–3240, 1987
82. Grundy SM, Vega GL, McGovern ME,Tulloch BR, Kendall DM, Fitz-Patrick D,Ganda OP, Rosenson RS, Buse JB, Robert-son DD, Sheehan JP: Efficacy, safety, andtolerability of once-daily niacin for thetreatment of dyslipidemia associated withtype 2 diabetes: results of the Assessmentof Diabetes Control and Evaluation of theEfficacy of Niaspan Trial. Arch Intern Med162:1568–1576, 2002
83. Elam MB, Hunninghake DB, Davis KB,Garg R, Johnson C, Egan D, Kostis JB,Sheps DS, Brinton EA: Effect of niacin onlipid and lipoprotein levels and glycemic
control in patients with diabetes and pe-ripheral arterial disease: the ADMITStudy: a randomized trial: Arterial DiseaseMultiple Intervention Trial. JAMA 284:1263–1270, 2000
84. The FIELD Study Investigators: Effects oflong-term fenofibrate therapy on cardio-vascular events in 9,795 people with type2 diabetes mellitus (the FIELD study):randomised controlled trial. Lancet 366:1849–1861, 2005
85. World Health Organization EuropeanCollaborative Group: European collabo-rative trial of multifactorial prevention ofcoronary heart disease: final report on the6-year results. Lancet 1:869–872, 1986
86. Frick MH, Elo O, Haapa K, Heinonen OP,Heinsalmi P, Helo P, Huttunen JK, Kaita-niemi P, Koskinen P, Manninen V, et al.:Helsinki Heart Study: primary-preven-tion trial with gemfibrozil in middle-agedmen with dyslipidemia: safety of treat-ment, changes in risk factors, and inci-dence of coronary heart disease. N EnglJ Med 317:1237–1245, 1987
87. Rubins HB, Robins SJ, Collins D, Fye CL,Anderson JW, Elam MB, Faas FH, LinaresE, Schaefer EJ, Schectman G, Wilt TJ,Wittes J, the Veterans Affairs High-Den-sity Lipoprotein Cholesterol InterventionTrial Study Group: Gemfibrozil for thesecondary prevention of coronary heartdisease in men with low levels of high-density lipoprotein cholesterol. N EnglJ Med 341:410–418, 1999
88. The BIP Study Group: Secondary preven-tion by raising HDL cholesterol and re-ducing triglycerides in patients withcoronary artery disease: the Bezafibrate
Infarction Prevention (BIP) study. Circu-lation 102:21–27, 2000
89. Goldberg RB, Kendall DM, Deeg MA,Buse JB, Zagar AJ, Pinaire JA, Tan MH,Khan MA, Perez, AT, Jacober SJ, the GLAIStudy Investigators: A comparison of lipidand glycemic effects of pioglitazone androsiglitazone in patients with type 2 dia-betes and dyslipidemia. Diabetes Care 28:1547–1554, 2005
90. Brunzell JD: Hypertriglyceridemia. N EnglJ Med 357:1009–1017, 2007
91. Barter PJ, Caulfield M, Eriksson M,Grundy SM, Kastelin JJP, Komajda M,Lopez-Sendon J, Mosca L, Tardif J-C, Wa-ters DD, Shear CL, Revkin JH, Buhr KA,Fisher MR, Tall AR, Brewer B: Effects oftorcetrapib in patients at high risk for cor-onary events. N Engl J Med 357:2109–2122, 2007
92. Pearson TA, Mensah GA, Alexander RW,Anderson JL, Cannon RO, Criqui M, FadlYY, Fortmann SP, Hong Y, Myers GL, RifaiN, Smith SC, Taubert K, Tracy RP, Vini-cor F: Markers of inflammation and car-diovascular disease: application to clinicaland public health practice: a statement forhealthcare professionals from the Centersfor Disease Control and Prevention andthe American Heart Association. Circula-tion 107:499–511, 2003
93. Ridker PM, the JUPITER Study Group:Rosuvastatin in the primary prevention ofcardiovascular disease among patientswith low levels of low-density lipoproteincholesterol and elevated high-sensitivityC-reactive protein: rationale and design ofthe JUPITER Trial. Circulation 108:2292–2297, 2003
Consensus Statement
822 DIABETES CARE, VOLUME 31, NUMBER 4, APRIL 2008
Copyright © 2022 FDOKUMEN