“Choose your language!” Categorisation and control in cyberspace.
Upload
independentCategory
view
3download
0
Controversies in Experimental Dermatology
Section Editor : Ralf Paus, Hamburg
Leukocyte extravasation as a target foranti-inflammatory therapy – Whichmolecule to choose?
W.-H. Boehncke, M.P. Schon,
G. Giromolomi, J.D. Bos,
K. Thestrup-Pedersen, A. Cavani,
F. Nestle, B.K. Bonish, J.J. Campbell
and B. Nickoloff
Boehncke W-H, Schon MP, Giromolomi G, Bos JD, Thestrup-Pedersen K, Cavani A,Nestle F, Bonish BK, Campbell JJ, Nickoloff B. Leukocyte extravasation as a target foranti-inflammatory therapy – Which molecule to choose?
Exp Dermatol 2005: 14: 70–80. # Blackwell Munksgaard, 2005
Abstract: In view of the central pathogenic importance of leukocyte extravasation ininflammatory skin diseases, therapeutic interference with this – surprisingly complex –process is clearly a promising new approach for treating these dermatoses. Despitesome disappointments during the clinical use of these agents and despite their cripplingprice tag, the recent incorporation of biologicals that target defined molecular controlsof leukocyte extravasation into dermatological and rheumatological practise,consequently, has greatly enriched our therapeutic options for battling major, chronic,inflammatory dermatoses such as psoriasis. However, the – as yet unresolved and stillrather controversially discussed – critical question is: Which of the multiple steps thatcontrol leukocyte extravasation in the human system really offer the most promising,most pragmatic, and safest molecular targets for therapeutic intervention for whichdisease entity? The current debate intends to stimulate public and rational debate of thiscrucial issue, beyond the evident commercial interests that are touched by whateverstand one takes.
Viewpoint 1
Rubor, calor, dolor, tumor, and functio laesa – this is whatgenerations of patients complained since the times of theRoman Empire (mankind had similar symptoms before, butcalled them differently, I suppose). As reader of the journal, youlook beyond these symptoms and understand their roots: it is thecollateral damage of leukocyte activation and extravasation intotissues, key processes of inflammation as the body’s standarddefense mechanism (1). The causal correlation between leukocyteactivation and extravasation on one hand and development ofinflammation on the other hand has convincingly been demon-strated in a multitude of diseases. In psoriasis, for example, directexperimental evidence has been generated that bacterial super-antigens activate T lymphocytes which then invade the skin com-partment and trigger the complex phenotype characteristic for thisdisease (2,3); a hugebodyof literature points towards the existence ofan epidermally located antigen as the primummovens (4–6) (Fig. 1a).
The principles of both fundamental processes, namely T-lym-phocyte activation and extravasation, are clear by now: T-cellactivation requires two signals. Signal 1 comes from the T-cellreceptor upon antigen recognition in the context of an antigen-
presenting molecule. Numerous pathways are available to pro-vide the so-called ‘co-stimulatory’ signal 2 (Fig. 1b). These includeCD2 and leukocyte function-associated antigen (LFA)-1 at theT-cell membranes and their respective ligands LFA-3 and inter-cellular adhesionmolecule (ICAM)-1 (7,8).T-cell extravasation (9)(Fig. 1c) is initiated by short-lived interactions with blood-vesselwalls via selectins, resulting in a rolling motion. Chemokines andother stimulatory signals then activate leukocyte integrins whichbind more persistently to members of the immunoglobulin super-family (e.g. ICAM-1) on the endothelial cell surface. The resultingfirm adhesion is a prerequisite for diapedesis and subsequentmigration along chemotactic gradients to the targeted tissue.
Given the relevance of T-cell activation and extravasation inpsoriasis, interference with these processes should turn out to bean effectivemeans of treating it. Indeed, therapeutic molecules havebeen generated from living cells capable of specifically interferingwith disease-relevantmediators or cell–cell interactions; twoof theseso-called ‘biologics’ are already approved for treating psoriasis.Amevive1 is a fusion protein comprising LFA-3 and the constantregion of an IgG1 antibody. Its LFA-3 portion binds to the
Experimental Dermatology 2005: 14: 70–80 Copyright # Blackwell Munksgaard 2005Blackwell Munksgaard . Printed in Denmark
EXPERIMENTAL DERMATOLOGY
ISSN 0906-6705
70

co-stimulatory CD2 receptor on T cells, thus inhibiting T-cell acti-vation (see above) (10,11); the antibody portion attracts naturalkiller cells and induces programmed cell death thereby eliminatingputative effectorT cells. Bothmechanisms are believed to contributeto its clinical effectiveness (12). And the monoclonal antibody Rap-tiva1 recognizes LFA-1, which provides co-stimulation for T-cellactivation aswell as firm adhesion in the process of T-cell extravasa-tion (13–15). Although both compounds combine two reasonablemodes of action, only one-third of the patients treated experienceda pronounced clinical benefit (16). This outcome leaves us withtwo questions (at least): Are T-cell activation and extravasationreally good targets? And are biologics suitable therapeutic tools?Amevive1 and Raptiva1 undoubtedly have an impact on T-
cell activation by blocking co-stimulatory molecules. As immu-nologic tools they exhibit an exquisite specificity too. On theother hand, numerous molecules are capable of delivering thesecond signal crucial for T-cell activation. Therefore, immunolo-gists might have outsmarted themselves by being too selective,thus leaving all alternative pathways uncovered. Proof for thefeasibility of this approach comes from the good old cyclosporineA, who’s convincing efficacy was one of the reasons why psoriasiswas considered to be a T-cell mediated disease in the first place(17). The take-home message from these clinical experiences is thatyou need a really substantial T-cell suppression in order to achievea good clinical response. This in turn raises safety concerns, giventhe increased risk of malignancies observed in patients receivingcyclosporine for longer periods of time (18).So, if sufficient T-cell suppression goes hand in handwith such a
threat, what about interferingwith lymphocyte extravasation? Theanswer, at first glance, is a clear-cut: noway!And there seems to beat least three good reasons for this reaction. First, the complexityof interactions and the multitude of molecules involved are some-what overwhelming. Which target should one go for? Second,Raptiva1does interferewith extravasation, but fails to be impress-ively effective. Worse than this, an antibody blocking one of theselectins involved in the initiation of lymphocyte rolling – CDP850recognizing E-selectin – failed badly in clinical trials (19)! Finally:Would not the blockade of lymphocyte extravasation into the skinbe at least as risky as T-cell suppression?You guess already that I totally disagree. And here is why. Let
us first consider consequences of the skin becoming inaccessiblefor T cells: imagine a mouse without selectins, which also lacks theenzyme needed to generate the lymphocyte-homing receptor forthe skin. And now imagine you challenge this mouse with viruses
or tumor cells. What do you expect to happen? This mouse ishistory, right? Wrong! This catastrophically deficient mouse elim-inates viruses and tumor cells as effectively as a normal mousefrom a range of organs. Only cutaneous inflammatory reactions,e.g. contact hypersensitivity, are reduced (20), which is good newswhen it comes to identifying a strategy to treat exactly that.Why then is interference with leukocytic firm adhesion at the level
of LFA-1 by Raptiva1 only moderately effective, and an antiE-selectin antibody does not do anything at all? I think that LFA-1is a target that comes into play quite late in the game. The early birdcatches the worm! There is good evidence that interference withlymphocyte rolling rather than firm adhesion exhibits strong anti-inflammatory efficacy (21). And my answer to the anti E-selectinantibody argument is that life is too smart to rely on just onemechanismwhen it comes to fundamental processes such as inflam-mation. If you block E-selectin only, you will find out about therelevanceof the other selectinswhich aremore than capableofdoingthe job too. So, as in the case of blocking co-stimulation, immunol-ogists might simply be too smart to develop effective drugs.This brings me to the question whether you should go with
biologics in the first place. Although these compounds providerational tools to physicians, efficacy is usually quite moderate.Their major advantage may be that most contraindications for theuse of conventional systemic therapies do not apply (22). Becausenumerous molecular targets have been identified so far, one couldaim for them using small-molecule inhibitors. Besides practicaladvantages – oral availability, inexpensive production, to namebut two– onemight choose tomake themnot too specific. Encoura-ging observations come from a relatively unselective small-moleculeselectin inhibitor which compares favorably to cyclosporine A orsystemic steroids in two pre-clinical in vivo models for T-cellmediated cutaneous inflammation and psoriasis, respectively (23).This approach obeys two criteria I consider crucial in the develop-ment of anti-inflammatory drugs: first, the compound is relativelyselective, but not over-specific, thus shutting down potentialbypasses along with knocking out the prime target. Second, it inter-feres with leukocyte rolling as the initial step of extravasation ratherthan trying to prevent downstream events.So, anyone for a good advise? I got three of them for those who
care: first, the early bird catches the worm. Therefore, leukocyteextravasation is a great target for anti-inflammatory therapiesbecause this occurs before the formation of an inflammatoryinfiltrate. Second, the early bird catches the worm (again). Ifyou go for leukocyte extravasation, do it right and block rolling
Non-lesional skinLesional skin
Epi
derm
isD
erm
is
Epiderm
isD
ermis
Antigen APC
Cytokinesecretion
Migrationto afferentlymph node
Antigenpresentation
CD45RA+
CLA– CD45RO+
CLA+
Clonal expansion
CD45RO+
CLA+
Migration
Re-activation Cytokine secretion
Keratinocyteactivation
Chemokinesecretion
Lymphocyticinfiltrate
Lymph node Blood
CD28
CD80/CD86
CD4TCR
CD3
MHC
AgCD2
LFA3
CD45RO
ICAM1
LFA1
ICAM1LFA1
Selectins
CLA
Keratinocytederivedchemokines
a b
c
Figure 1 . T-ce l l ac t iva t ion andextravasation are crucial processesinvolved in elicitation of psoriasis (a).Similar to allergic contact dermatitis, theputative antigen is taken up by dendriticcells and transported to the lymph nodeswhere naive T cells are activated tobecome effector cells (b). These cellsleave the lymph nodes and circulatethrough the body to extravasate at thesite of inflammation (c). Subsequently,they migrate along chemotactic gradientsinto the skin where they are re-activatedand perform their effector functions viasecretion of cytokines [adapted from(25)].
Controversies
71

rather than later steps during that process. Third (not this time),the enemy of the good is the better. There are reasons to usebiologics, although perhaps only in a subgroup of patients (24).But now that the targets are known, one may choose to designsmall-molecule inhibitors towards the very same targets;these could well prove superior when the lessons learnedfrom the current generation of biologics are incorporated(Do not outsmart yourselves again!). Happy research anddevelopment!
Wolf-Henning BoehnckeDepartment of Dermatology
Johann Wolfgang Goethe-UniversityD-60590 Frankfurt am Main
GermanyE-mail: [email protected]
References
1. von Andrian U, Mackay C R. N Engl J Med 2000: 343:1020–1034.
2. Boehncke W-H et al. Nature 1996: 379: 777.3. Wrone-Smith T, Nickoloff B J. J Clin Invest 1996: 98:
1878–1887.4. Chang J C C et al. Proc Natl Acad Sci USA 1994: 91:
9282–9286.
5. Prinz J et al. Eur J Immunol 1999: 29: 3360–3368.6. Nickoloff B J et al. Exp Dermatol 2000: 9: 359–375.7. June C H et al. J Immunol 1990: 144: 1591–1599.8. Danielian S et al. Eur J Immunol 1991: 21: 1967–1970.9. Springer T A. Cell 1994: 76: 301–314.
10. Miller G T et al. J Exp Med 1993: 178: 211–222.11. Majeau G R et al. 1994: 152: 2753–2767.12. Ellis C N, Krueger G G. N Engl J Med 2001: 345:
248–255.13. Krensky A M et al. J Immunol 1983: 131: 611–616.14. Wawryk S O et al. Immunol Rev 1989: 108: 135–161.15. Gottlieb A B et al. Arch Dermatol 2002: 138: 591–600.16. Boehncke W-H et al. J Dtsch Dermatol Ges 2003: 1:
620–628.17. Greaves M W, Weinstein G D. N Engl J Med 1995: 332:
581–588.18. Paul C F et al. J Invest Dermatol 2003: 120: 211–216.19. Bushan M et al. Br J Dermatol 2002: 146: 824–831.20. Erdmann I et al. J Immunol 2002: 168: 2139–2146.21. Boehncke W-H, Schon M P. Trends Pharmacol Sci 2003:
24: 49–52.22. Boehncke W-H. BMJ 2003: 327: 634–635.23. Schon M P et al. Nat Med 2002: 8: 366–372.24. Dubin D B et al. Nat Rev Drug Discov 2003: 2:
855–856.25. Grabbe S, Schwarz T. Immunol Today 1998: 19: 37–44.
Viewpoint 2
Normal human skin is endowed with a confederacy of bonemarrow-derived cells, which complements the other cell typesderived from ectodermal and endodermal precursors. Bone mar-row-derived cells include Langerhans cells and T lymphocytes inthe epidermis; and dermal dendritic cells, T cells, macrophages,and mast cells in the dermis. To maintain a constant state ofvigilance, continuous leukocyte migration involving lymphoidrecirculation is required to monitor skin for presence of invadingpathogenic organisms or other destructive stimuli. This vital anddynamic process involves trafficking of leukocytes from thebloodstream into tissue sites such as skin and then to organizedlymphoid tissue (i.e. lymph nodes and spleen), followed by returnto the blood via lymphatic vessels. This immunosurveillance pro-cess mediated by immunocytes is governed by a series of mole-cular regulators that influence three distinct phases of leukocytetrafficking; namely recruitment, retention, and return to recircu-lation (1). Besides a role for trafficking of leukocytes to maintainskin integrity, the aforementioned resident immunocytes areaccompanied by additional leukocytes recruited during theonset of acute and chronic inflammatory skin diseases. Theseadditional cells include neutrophils, T cells, monocytes, eosino-phils, and plasma cells.
Given that leukocyte trafficking is important for both normaltissue homeostasis, as well as for pathological tissue reactions,ideal targets for anti-inflammatory therapy are those molecularmediators that do not participate in the normal physiology of thetissue but are only up-regulated during the onset or maintenanceof cutaneous inflammation. During the past decade, investigativeskin biologists have uncovered key roles for a number of adhesionmolecules, cytokines, and chemotactic polypeptides that caninfluence the migration patterns of leukocytes in normal anddiseased skin (2).
Despite impressive progress in this area, our knowledge is stillincomplete, as we do not fully understand the complexity of themolecules that govern trafficking of leukocyte subsets in normalskin vs. those molecular mediators of leukocyte trafficking invarious inflammatory skin diseases. To properly address the
question posed as to the best target molecule, we will have tobetter understand the hierarchical relationships amongst poten-tial targets, as well as the nature of the redundancy and interac-tions amongst those mediators of leukocyte extravasation thatoperate to maintain tissue homeostasis, and those molecules up-regulated during inflammation. With these caveats in mind, wecan provide a brief review of the field, and highlight those mole-cules that appear to us to represent our best guess as to relevanttargets for leukocyte extravasation.
In our opinion, the best target molecule will not include thosemediators of leukocyte trafficking that contribute to normalhomeostasis. Thus, we would avoid targeting CD40 because thismay perturb the number and distribution of intraepidermal Lan-gerhans cells (3). Because Langerhans cells possess ATPase(CD39), they can actually reduce inflammation once it is presentby degrading free ATP, which is highly pro-inflammatory (4–6).Skin with absent or diminished Langerhans cells is characterizedby excessive inflammation and provides a compelling case formaking an informed decision, based on experimental results,when selecting potential anti-inflammatory targets, taking intoconsideration the potential adverse effects on resident cells.
As regards candidates for best target molecule that can pro-duce decreased inflammation, we suggest the following and pro-vide the rationale for these three selections – CD11a, VLA-4 (verylate antigen-4), and VLA-1 (Figure 1). The recommendation totarget CD11a [i.e. leukocyte function-associated antigen (LFA)-1],is based on both experimental data and emerging clinicalresponses in patients with psoriasis. From the experimentalside we, and others, established over a decade ago that adhesionof leukocytes to keratinocytes was mediated by LFA-1 expressedby T cells (7,8) such as LFA-1-bearing T cells, which could onlybind to keratinocytes that had been previously exposed to cyto-kines such as tumor necrosis factor (TNF)-a or -g interferon thatup-regulated surface expression of the ligand for LFA-1; namelyintercellular adhesion molecule (ICAM)-1 (7,8). Because ICAM-1 is only expressed by keratinocytes during inflammation, whenrequisite cytokines are present, it is likely that minimal effects on
Maurer et al.
72
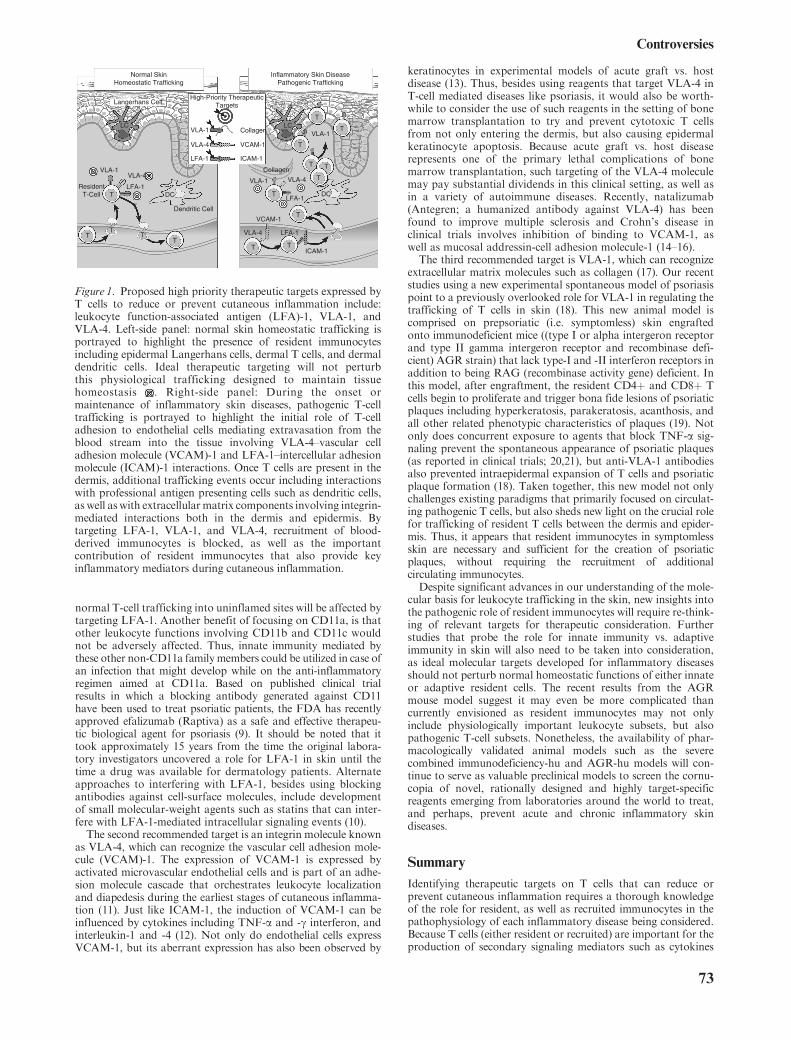
normal T-cell trafficking into uninflamed sites will be affected bytargeting LFA-1. Another benefit of focusing on CD11a, is thatother leukocyte functions involving CD11b and CD11c wouldnot be adversely affected. Thus, innate immunity mediated bythese other non-CD11a familymembers could be utilized in case ofan infection that might develop while on the anti-inflammatoryregimen aimed at CD11a. Based on published clinical trialresults in which a blocking antibody generated against CD11have been used to treat psoriatic patients, the FDA has recentlyapproved efalizumab (Raptiva) as a safe and effective therapeu-tic biological agent for psoriasis (9). It should be noted that ittook approximately 15 years from the time the original labora-tory investigators uncovered a role for LFA-1 in skin until thetime a drug was available for dermatology patients. Alternateapproaches to interfering with LFA-1, besides using blockingantibodies against cell-surface molecules, include developmentof small molecular-weight agents such as statins that can inter-fere with LFA-1-mediated intracellular signaling events (10).The second recommended target is an integrin molecule known
as VLA-4, which can recognize the vascular cell adhesion mole-cule (VCAM)-1. The expression of VCAM-1 is expressed byactivated microvascular endothelial cells and is part of an adhe-sion molecule cascade that orchestrates leukocyte localizationand diapedesis during the earliest stages of cutaneous inflamma-tion (11). Just like ICAM-1, the induction of VCAM-1 can beinfluenced by cytokines including TNF-a and -g interferon, andinterleukin-1 and -4 (12). Not only do endothelial cells expressVCAM-1, but its aberrant expression has also been observed by
keratinocytes in experimental models of acute graft vs. hostdisease (13). Thus, besides using reagents that target VLA-4 inT-cell mediated diseases like psoriasis, it would also be worth-while to consider the use of such reagents in the setting of bonemarrow transplantation to try and prevent cytotoxic T cellsfrom not only entering the dermis, but also causing epidermalkeratinocyte apoptosis. Because acute graft vs. host diseaserepresents one of the primary lethal complications of bonemarrow transplantation, such targeting of the VLA-4 moleculemay pay substantial dividends in this clinical setting, as well asin a variety of autoimmune diseases. Recently, natalizumab(Antegren; a humanized antibody against VLA-4) has beenfound to improve multiple sclerosis and Crohn’s disease inclinical trials involves inhibition of binding to VCAM-1, aswell as mucosal addressin-cell adhesion molecule-1 (14–16).The third recommended target is VLA-1, which can recognize
extracellular matrix molecules such as collagen (17). Our recentstudies using a new experimental spontaneous model of psoriasispoint to a previously overlooked role for VLA-1 in regulating thetrafficking of T cells in skin (18). This new animal model iscomprised on prepsoriatic (i.e. symptomless) skin engraftedonto immunodeficient mice ((type I or alpha intergeron receptorand type II gamma intergeron receptor and recombinase defi-cient) AGR strain) that lack type-I and -II interferon receptors inaddition to being RAG (recombinase activity gene) deficient. Inthis model, after engraftment, the resident CD4þ and CD8þ Tcells begin to proliferate and trigger bona fide lesions of psoriaticplaques including hyperkeratosis, parakeratosis, acanthosis, andall other related phenotypic characteristics of plaques (19). Notonly does concurrent exposure to agents that block TNF-a sig-naling prevent the spontaneous appearance of psoriatic plaques(as reported in clinical trials; 20,21), but anti-VLA-1 antibodiesalso prevented intraepidermal expansion of T cells and psoriaticplaque formation (18). Taken together, this new model not onlychallenges existing paradigms that primarily focused on circulat-ing pathogenic T cells, but also sheds new light on the crucial rolefor trafficking of resident T cells between the dermis and epider-mis. Thus, it appears that resident immunocytes in symptomlessskin are necessary and sufficient for the creation of psoriaticplaques, without requiring the recruitment of additionalcirculating immunocytes.Despite significant advances in our understanding of the mole-
cular basis for leukocyte trafficking in the skin, new insights intothe pathogenic role of resident immunocytes will require re-think-ing of relevant targets for therapeutic consideration. Furtherstudies that probe the role for innate immunity vs. adaptiveimmunity in skin will also need to be taken into consideration,as ideal molecular targets developed for inflammatory diseasesshould not perturb normal homeostatic functions of either innateor adaptive resident cells. The recent results from the AGRmouse model suggest it may even be more complicated thancurrently envisioned as resident immunocytes may not onlyinclude physiologically important leukocyte subsets, but alsopathogenic T-cell subsets. Nonetheless, the availability of phar-macologically validated animal models such as the severecombined immunodeficiency-hu and AGR-hu models will con-tinue to serve as valuable preclinical models to screen the cornu-copia of novel, rationally designed and highly target-specificreagents emerging from laboratories around the world to treat,and perhaps, prevent acute and chronic inflammatory skindiseases.
Summary
Identifying therapeutic targets on T cells that can reduce orprevent cutaneous inflammation requires a thorough knowledgeof the role for resident, as well as recruited immunocytes in thepathophysiology of each inflammatory disease being considered.Because T cells (either resident or recruited) are important for theproduction of secondary signaling mediators such as cytokines
Dendritic Cell
ResidentT-Cell
VLA-1VLA-4
LFA-1
Normal SkinHomeostatic Trafficking
VLA-1
VLA-4 LFA-1
VLA-4
VLA-1
Inflammatory Skin DiseasePathogenic Trafficking
VCAM-1
Langerhans Cell
ICAM-1
LFA-1
Collagen
LCVLA-1
VLA-4
LFA-1
Collagen
VCAM-1
ICAM-1
High-Priority TherapeuticTargets
T
TT
T
T
T
T
T
T T
TT
T
T
T
T
LC
DCDC
Figure 1. Proposed high priority therapeutic targets expressed byT cells to reduce or prevent cutaneous inflammation include:leukocyte function-associated antigen (LFA)-1, VLA-1, andVLA-4. Left-side panel: normal skin homeostatic trafficking isportrayed to highlight the presence of resident immunocytesincluding epidermal Langerhans cells, dermal T cells, and dermaldendritic cells. Ideal therapeutic targeting will not perturbthis physiological trafficking designed to maintain tissuehomeostasis . Right-side panel: During the onset ormaintenance of inflammatory skin diseases, pathogenic T-celltrafficking is portrayed to highlight the initial role of T-celladhesion to endothelial cells mediating extravasation from theblood stream into the tissue involving VLA-4–vascular celladhesion molecule (VCAM)-1 and LFA-1–intercellular adhesionmolecule (ICAM)-1 interactions. Once T cells are present in thedermis, additional trafficking events occur including interactionswith professional antigen presenting cells such as dendritic cells,as well as with extracellular matrix components involving integrin-mediated interactions both in the dermis and epidermis. Bytargeting LFA-1, VLA-1, and VLA-4, recruitment of blood-derived immunocytes is blocked, as well as the importantcontribution of resident immunocytes that also provide keyinflammatory mediators during cutaneous inflammation.
Controversies
73

and chemotactic polypeptides, targeting T cells will also impactother inflammatory cell types such as neutrophils. Looking intothe future, we believe the greatest opportunity exists in the devel-opment of small molecule inhibitors that can be ingested orallytargeting the three aforementioned surface molecules (LFA-1,VLA-1, and VLA-4). Such orally available inhibitors will enhancepatient acceptance, compliance, and may provide a method toregulate tissue levels so as to avoid undesirable side effects asso-ciated with immunological generation of systemically deliveredantibodies, that may lead to treatment resistance when used in achronic setting.
Brian J. NickoloffDepartment of Pathology
Oncology Institute, Loyola University Medical CenterChicago, IL, USA
E-mail: [email protected] K. Bonish
Department of Internal MedicineOncology Institute, Loyola University Medical Center
Chicago, IL, USAFrank O. Nestle
Department of DermatologyUniversity of Zurich
ZurichSwitzerland
References
1. Foreman K E, Nickoloff B J. Cell Adhesion and Migrationin Skin Disease. Vol. 8. UK: Harwood Academic PublishersLondon, UK, 1990; 251–263.
2. Nickoloff B J, Griffiths C E M, Barker J N W N. J InvestDermatol 1990: 94: 151–157.
3. Jolles S et al. Clin Exp Immunol 2002: 129: 519–526.4. Grabbe S et al. J Immunol 1995: 155: 4207–4217.5. Mehling A et al. J Exp Med 2001: 194: 615–628.6. Mizumoto N et al. Nat Med 2002: 8: 358–365.7. Nickoloff B J et al. J Invest Dermatol 1988: 90: 17–22.8. Dustin M L et al. J Exp Med 1988: 167: 1323–1340.9. Lebwohl M et al. N Engl J Med 2003: 349: 2004–2013.
10. Weitz-Schmidt G et al. Nat Med 2001: 7: 687–692.11. Elices M J et al. Cell 1990: 60: 577–584.12. McHale J F et al. J Immunol 1999: 162: 1648–1655.13. Kim J C et al. Am J Pathol 2002: 161: 763–770.14. Miller D H et al. N Engl J Med 2003: 348: 15–23.15. Ghosh S et al. N Engl J Med 2003: 348: 24–32.16. vonAndrianWH,EngelhardtB.NEngl JMed2003: 348: 68–72.17. Goldstein I et al. J Clin Invest 2003: 112: 1444–1454.18. Conrad C et al. J Invest Dermatol 2004: 122: A14.19. Boyman O et al. J Exp Med 2004: 199: 731–736.20. Mehlis S L, Gordon K B. J Am Acad Dermatol 2003: 49:
s44–s50.21. Krueger J G . J Am Acad Dermatol 2002: 46: 1–23.
Viewpoint 3
Few fields in translational science reflect not only the excitementand enthusiasm, but also quite a few disappointments associatedwith new developments as brightly as receptor-selective anti-inflammatory strategies targeting leukocyte extravasation.Indeed, as they appear to meet the desire for a mechanistic basisof diseases, and consecutively, rational therapeutic strategies (1,2)(Fig. 1), receptors involved in tissue-specific leukocyte recruit-ment are exceptionally appealing target structures. However, acloser look at the complex and intertwined molecular crosstalkunderlying leukocyte recruitment may dampen some illusions ordishearten overenthusiastic approaches. In addition, extravasa-tion is tightly connected with other cellular functions as exempli-fied by integrin-directed compounds which also affect leukocyteactivation. As a consequence, inflammatory diseases encounteredby clinicians are rarely predictable from single molecular pathways,and the design or selection of compounds targeting specific mole-cules involved in the inflammatory cascade is often a treacherouspath and may face considerable immanent problems.
Perhaps most important for the limited predictability of anti-inflammatory approaches through targeting leukocyte extravasa-tion is functional redundancy, i.e. key molecules may have over-lapping functions compensating for each other in case of loss offunction of one of the players. Prominent examples have beenreported in the selectin field (3–5) as well as the chemokine/chemokine receptor system (6,7). In case of selectins, endothelialE- and P-selectin have considerable functional overlaps (3–5). Itwas long believed that cutaneous lymphocyte antigen expressedby skin-homing T cells is predominantly an E-selectin ligand(8,9). However, the carbohydrate moieties mediating tetheringand rolling of leukocytes along the endothelial lining also bindto P- and L-selectin (3–5). L-selectin is not expressed by endothe-lia, but activated endothelial cells in inflamed tissues may expressPNAd (Peripheral Node Addressin), a ligand for lymphocyte-expressed L-selectin. This mechanism may compensate for leuko-cyte rolling when E- and P-selectin are selectively blocked, e.g. bysmall-molecule or antibody-based therapeutics (10,11). In add-ition, E-selectin-negative T cells may roll along the vessel wall
through cluster formation with activated platelets (12–14), andeven in the complete absence of selectins and their ligands rollingof some leukocytes may occur through interactions of endothelialvascular cell adhesion molecule-1 with the lymphocyte-expressedVLA-4 (Very Late Activation Antigen) integrin (4). Similar pro-blems may be encountered when glycosylation of selectin ligandsis targeted, e.g. by proteasome inhibitors (15).
Given that the functions of chemokines (approximately20 receptors and more than 45 ligands are known) overlapsubstantially, it is not surprising that redundancy and promiscu-ity may also be a major problem within the chemokine system(6,7). Hence, the initially oversimplified view of chemokine func-tions has become increasingly complex in inflammatory disorders(16,17). Another level of complexity is added by the fact thatsome chemokines may exert either agonistic or antagonisticeffects, e.g. I-TAC, Mig, and IP10 may act as agonists onCXCR3 (CXC-Chemokine Receptor-3), thereby stimulatingTh1-type immune responses, and at the same time these medi-ators are antagonists of CCR3 (CC-chemokine receptor-3),which is thought to mediate Th2-driven immune responses(18,19). Rational drug design of compounds modeled afterfunctionally relevant groups, or HTS (high throughput screen-ing) assessing the functions of single molecules as readout para-meters might therefore confront the aforesaid problems.
Recent examples for approaches which may have been toospecific (thus neglecting functional redundancy) include the fail-ure of an E-selectin-directed antibody (CDP-850) to alleviatepsoriasis in a clinical trial (20) or the limited clinical response torhPSGL-1 (recombinant human P-selectin glycoprotein ligand-1)Ig (21). In that respect, concepts interfering with a group ofmolecules with overlapping functions involved in a given step ofleukocyte extravasation may bear some advantages, such asefomycine M or the TBC-1269 compound blocking severalselectins (22,23). However, the success of such broader strategiesis not guaranteed, as exemplified by the insufficient response tothe pan-selectin inhibitor OJ-R9188 in clinical phase I/II studies(24).
Maurer et al.
74

Another group of potential problems relates to unexpectedeffects, i.e. targeting of certain molecules may result in unexpectedor even paradoxical outcomes. One possible example is based onthe structural similarity of chemokine receptors to other class A-G-protein-coupled receptor (GPCR) members, resulting in poten-tial cross reaction of small-molecule antagonists of chemokinereceptors with other GPCRs such as biogenic amine receptors.Several such examples have been reported (7,25–28). In addition, aregulatory effect of chemokines on leukocyte rolling has recentlybeen identified, inasmuch as chemokines may exert (paradoxical)anti-adhesive effects through G-protein-independent destabiliza-tion of L-selectin (29). Thus, although some preclinical evidencesupports a potential role of targets within the chemokine system(30), only few of the many reported chemokine/receptor antago-nists have progressed to clinical trial (7,31–33).It is possible, in a clinical setting, that interfering with later
steps of leukocyte extravasation, i.e. firm adhesion and transmi-gration, may elicit more pronounced anti-inflammatory effects ascompared to approaches targeting early steps, i.e. tethering androlling. Evidence to support this hypothesis includes promisingreports on some integrin-directed compounds (34–37).Ultimately, however, examination of the effect(s) of small-mole-
cule compounds or biologicals in vivo, rather than theory-basedapproaches, will provide the required evidence for target validation.Bearing the above-mentioned (selected) limitations in mind,
there is no easy answer to the question raised in the title. It appearsthat at least two levels of complex interactions influence the successof therapeutic strategies aimed at leukocyte extravasation: let usterm them here ‘a vertical and a horizontal axis of evil’, i.e. distinctplayers mediating consecutive pathogenic steps (‘vertical’, e.g. che-mokine receptor activation followed by integrin-mediated firmarrest) vs. synchronous action of several molecules mediating
a given event (‘horizontal’, e.g. selectins and chemokine recep-tors simultaneously orchestrating leukocyte rolling). It mightprove beneficial to simultaneously target two or more playersfrom one or both axes to achieve the desired therapeuticeffect(s): thus, with all due caution prudent even in a speculativearticle like this, I hypothesize that targeting a set of moleculesinvolved in either one or both axes might ultimately prevail inclinical routine. Such approaches may overcome the problemof functional redundancy, but the price to pay is reducedselectivity, and possibly, unwanted side effects.My personal favorite? I would welcome an effort combining a
chemokine receptor antagonist (e.g. against CCR4 and/or CCR10)with a selectin- or integrin-directed compound (e.g. efomycineMorefalizumab) to treat an inflammatory skin disorder.
Acknowledgements
This work was supported by a research grant (Scho 565/5–1) and aRudolf-VirchowAward from theDeutsche Forschungsgemeinschaft.
Michael P. SchonRudolf Virchow CenterDFG Research Center
for Experimental Biomedicineand Department of Dermatology
and VenereologyUniversity of Wurzburg
GermanyE-mail: [email protected]
Figure 1. Schematic representation of molecules and interactions thought to be involved in leukocyte extravasation. The flash symbolsindicate potential therapeutic target structures and/or functions to interfere with leukocyte extravasation.
Controversies
75

References
1. BoehnckeW-H,SchonMP.TrendsPharmacolSci2003:24:49–52.2. Schon M P, Zollner T M, Boehncke W H. J Invest
Dermatol 2003: 121: 951–962.3. Labow M A et al. Immunity 1994: 1: 709–720.4. Jung U, Ley K. J Immunol 1999: 162: 6755–6762.5. Collins R G et al. Blood 2001: 98: 727–735.6. Zlotnik A, Yoshie O. Immunity 2000: 12: 121–127.7. Onuffer J J,HorukR.TrendsPharmacol Sci 2002: 23: 459–467.8. Berg E L et al. J Exp Med 1991: 174: 1461–1466.9. Rossiter H F et al. Eur J Immunol 1994: 24: 205–210.
10. Alon R, Feigelson S. Semin Immunol 2002: 14: 93–104.11. Dwir O et al. J Biol Chem 2002: 277: 21130–21139.12. Ludwig R J, Schultz J E, Weber C, Kaufmann R, Podda
M, Zollner T M. J Invest Dermatol 2001: 117: 766.13. Diacovo T G, Puri K D, Warnock R A, Springer T A, von
Andrian U H. Science 1996: 273: 252–255.14. Diacovo T G, Catalina M D, Siegelman M H, von
Andrian U H. J Exp Med 1998: 187: 197–204.15. Zollner T M, Podda M, Pien C, Elliott P J, Kaufmann R,
Boehncke W-H. J Clin Invest 2002: 109: 671–679.16. Moser B, Loetscher P. Nat Immunol 2001: 2: 123–128.17. Schon M P, Ruzicka T. Nat Immunol 2001: 2: 91.18. Loetscher P et al. J Biol Chem 2001: 276: 2986–2991.19. Loetscher P, Clark-Lewis I. J Leukoc Biol 2001: 69: 881–884.20. Bhushan M et al. Br J Dermatol 2002: 146: 824–831.
21. Khor S P, McCarthy K, DuPont M, Murray K, TimonyG. J Pharmacol Exp Ther 2000: 293: 618–624.
22. Abraham W M A et al. Am J Respir Crit Care Med 1999:159: 1205–1214.
23. Schon M P et al. Nat Med 2002: 8: 366–372.24. Ikegami-Kuzuhara A, Yoshinaka T, Ohmoto H, Inoue Y,
Saito T. Br J Pharmacol 2001: 134: 1498–1504.25. Hesselgesser J et al. J Biol Chem 1998: 273: 15687–15692.26. Forbes I T et al. Bioorg Med Chem Lett 2000: 10:
1803–1806.27. Tagat J R et al. Bioorg Med Chem Lett 2001: 11:
2143–2146.28. Mirzadegan T et al. J Biol Chem 2000: 275: 25562–25571.29. Grabovsky V, Dwir O, Alon R. J Biol Chem 2002: 277:
20640–20650.30. Homey B et al. Nat Med 2002: 8: 157–165.31. Luttichau H R, Schwarz T W. Curr Opin Drug Discov
Dev 2000: 3: 610–623.32. Horuk R. Cytokine Growth Factor Rev 2001: 12: 313–335.33. Baggiolini M. J Intern Med 2001: 250: 91–104.34. Gniadecki R, Calverley M J. Expert Opin Emerg Drugs
2002: 7: 69–90.35. Gottlieb A B, Krueger J G, Wittkowski K, Dedrick R,
Walicke P A, Garovoy M. Arch Dermatol 2002: 138:591–600.
36. Shand A, Forbes A. Int J Colorectal Dis 2003: 18: 1–11.37. Krueger G G et al. J Am Acad Dermatol 2002: 47: 821–833.
Commentary 1
Animal models of chemokine/receptor involvementin cutaneous T-lymphocyte homing
Convincing arguments have been made suggesting that two dif-ferent human chemokine receptors (CR) are involved in skin-specific lymphocyte homing: CCR4 and CCR10. CCR4 isexpressed by nearly all [cutaneous lymphocyte antigen (CLA)þ]T cells in peripheral blood (1) but by very few intestinal (a4b7þ) Tcells (1). CCR4 is expressed by essentially all T cells withinnormal and inflamed human skin (1–3) but not by T cells withinintestinal tissues (1,2). CCL17 (chemokine ligand)/TARC (thy-mus and activation regulated chemokine), a chemokine ligand ofCCR4, is presented by E-selectinþ cutaneous vessels (1,4) but notby mucosal addressin-cell adhesion molecule (MAdCAM)þ
intestinal vessels (1). CCR10 is specifically expressed by a subsetof circulating CLAþ T cells (3,5). CCL27/CTACK (cutaneousT-cell-attracting chemokine), a ligand of CCR10, is stronglyexpressed by keratinocytes (6,7) and may also be presented bycutaneous vessels (7).
Although persuasive, such correlations provide only circum-stantial evidence: proof of the proposed roles for these chemo-kine/receptor pairs in cutaneous lymphocyte homing requiresfunctional confirmation in animal models.
2,4-dinitro-1-fluorobenzene (DNFB)-induced skin inflamma-tion is a widely accepted model of T-cell-dependent contacthypersensitivity (7–10). This in vivo assay is usually performedon mouse ears, where induced swelling can be easily assessed bycaliper measurements (10). The DNFBmodel has been applied toassess potential roles for these chemokine/receptor pairs in cuta-neous homing but has produced data that is somewhat contra-dictory and difficult to interpret (7,9). One group (which includedthe author) found that simultaneous elimination of both CCR4and CCR10 function (by treating CCR4-deficient micewith CCL27-blocking antibody) resulted in the reduction ofDNFB-induced cutaneous inflammation (9). No reduction ofDNFB-induced cutaneous inflammation was achieved in
CCR4-deficient mice without anti-CCL27 treatment; nor in nor-mal mice treated with CCL27-blocking antibody. These findingsled us to propose that the function of both CCR4 and CCR10were required for cutaneous T-cell homing. This explanationseemed plausible because, as mentioned above, the CCR4 ligandCCL17 is presented by cutaneous vessels (1,4), butCCL27 is directlyproduced by keratinocytes (6,7). This would invoke a scenario inwhich CCL17 might induce adhesion of circulating cutaneouslymphocytes inside cutaneous vessels, followedbyCCL27-mediatedattraction of these cells inward toward the source of CCL27.
In contrast, Homey et al. (7) performed similar experiments butconcluded that anti-CCL27 MAb treatment by itself was suffi-cient to reduce DNFB-induced inflammation in normal mice.The DNFB-induced cutaneous inflammatory models used bythe two different groups had some subtle technical differences,including the genetic backgrounds of the mice, and the quantityof blocking-antibodies injected: the studies of CCR4-deficient vs.normal mice were performed on the C57Bl/6 background (9),whereas the studies of Homey et al. (7) were performed on theBalb/c background. Further, the studies of CCR4-deficient vs.normal mice involved two injections of blocking MAb per mouse[100mg 6 h prior to challenge and 100mg at the time of challenge;a total of 200mg (9)], whereas the Homey et al. (7) studies usedvery large single doses of the blocking MAb (1mg per mouse).Either of these technical differences could potentially contributeto an explanation for the disparate findings of the two groups.However, we have been unable to reproduce the Homey et al.observation after several attempts using 1mg of the same MAb(68623, R&D systems, Minnesota, USA) on Balb/c mice in ourown facility (data not shown).
Nonetheless, these differences may be moot in light ofrecent findings: although DNFB-induced ear swelling haslong been considered a model of T-cell-dependent contacthypersensitivity (10), we demonstrate in Fig. 1 that severaltypes of T-cell-deficient mice display DNFB-induced cuta-neous inflammatory responses indistinguishable from those
Boehncke et al.
76

of WT mice. It is well known that DNFB treatment results inincreased numbers of T cells within affected cutaneous sites ofnormal mice (8,10). However, in light of the present findings, it isclear that the swelling itself is not due to the presence of T cells,because mice entirely lacking T cells (nude, severe combinedimmunodeficiency, RAG (recombinase activating gene)-1, orRAG-2 deficient) have ear-swelling responses indistinguishablefrom those of normal mice.Thus,whatever causes swelling in response toDNFB, it is clearly
not a component of the cognate immune system.The fact that anti-CCL27 can prevent this swelling demonstrates that CCL27 has
some role in cutaneous inflammation completely unrelated to theeffects ofCCL27onT-cell homing. TheHomey et al. study showedthat injection of anti-CCL27MAb also reduced skin swelling in anovalbumin-inducedmodel of atopic dermatitis (7). This model hascredibility as a T-cell dependent system but, in light of the DNFBfindings, it is unclear whether the effects of anti-CCL27 in theovalbumin model involve T-lymphocyte homing or rather involvethe poorly understood alternative T-cell-independent role ofCCL27 in cutaneous inflammation (Fig. 1).It will be very important to determine whether the in vivo effects
of anti-CCL27 MAb treatment are dependent upon CCR10function. This will be accomplished when function-blocking anti-mouse CCR10MAbs or CCR10-deficient mice become available.Thus, the strong correlations between cutaneous lymphocyte
homing and selective expression of CCR4, CCR10, and theirligands in human tissues remain convincing, but proof of theirpotential functional roles in selective cutaneous lymphocyte hom-ing will require extensive refinements to the present versions ofthese animal models.
James J. CampbellJoint Program in Transfusion Medicine
Children’s HospitalDepartment of PathologyHarvard Medical School
Boston, MA 02115USA
References
1. Campbell J J et al. Nature 1999: 400: 776–780.2. Kunkel E J et al. Am J Pathol 2002: 160: 347–355.3. Soler D, Humphreys T L, Spinola S M, Campbell J J.
Blood 2003: 101: 1677–1682.4. Chong B F, Murphy J E, Kupper T S, Fuhlbrigge R C.
J Immunol 2004: 172: 1575–1581.5. Hudak S et al. J Immunol 2002: 169: 1189–1196.6. Morales J et al. ProcNatlAcad SciUSA1999: 96: 14470–14475.7. Homey B et al. Nat Med 2002: 8: 157–165.8. Tietz W, Hamann A. Eur J Immunol 1997: 27: 2225–2232.9. Reiss Y, Proudfoot A E, Power C A, Campbell J J,
Butcher E C. J Exp Med 2001: 194: 1541–1547.10. Gaspari A A, Katz S I. Unit 4.2, Contact Hypersensitiv-
ity. Current Protocols in Immunology. XXXX: JohnWiley and Sons Inc., 2004, Hoboken, NJ.
Commentary 2
Leukocyte extravasation as a target for anti-inflammatory therapies in dermatology: Whichmolecular target is best?
The detailed knowledge on the mechanisms leading to leukocyterecruitment into the skin has led to the identification of new poten-tial targets for the therapy of chronic inflammatory skin diseasessuch as psoriasis and atopic dermatitis (1). Many compounds withantagonistic properties on leukocyte–endothelial cell interactionshave been developed. Compared to conventional immuno-suppressive therapies, strategies aimed to interfere specifically withleukocyte extravasation may have several relevant advantages. Infact, this approach could block the recruitment of leukocytesselectively into the skin, thus allowing efficient immune responsesin other districts and preserving protection to new antigens. Ideally,this therapy should block exclusively the recruitment of pathogenic
T cells. In contrast, the entrance into the skin of T-cell subsets withregulatory activity should not be inhibited as they functionas natural suppressant of immune responses (2,3). A majorlimitation of targeting leukocyte accumulation in the skin isthe high complexity of the molecules involved in this process.This means that blocking a single molecule may not besufficient for effective reduction of inflammation and that multiplemolecules should be inhibited to obtain a clinically relevant effect.Major targets proposed so far include selectins, chemokine-
chemokine receptor pairs, as well as integrins (Fig. 1). Potentialstrategies to interfere with selectin functions include blockingAbs, transcriptional regulation of selectin expression, and mod-ulation of the post-trascriptional glycosylation of selectin ligands,such as the administration of fluorinated antagonists, whichinterfere with the synthesis of the cutaneous lymphocyteantigen (CLA) (4,5). Although effective in murine models of
RAG-2 def.
RAG-1 def.
Nude
SCID
WT
0 100 200 300 400
Right ear thickness minus left ear thickness in µm
(mean and SD of 3 mice each)
Unchallenged
DNFB challenged
T cell deficient mice and WT mice respond similarlyin DNFB-induced model of contact hypersensitivity
Figure 1. Mice were sensitized with 2,4-dinitro-1-fluorobenzene(DNFB) on shaved bellies six or more days prior to challenge asdescribed (8,10). Eighteen to twenty-four hours before thicknessmeasurement, the right ears were challenged on both sides withDNFBas described (8,10) (DNFB challenged) or with vehicle only(unchallenged). Thickness was measured at three points on eachear, and the thickness of the untreated left ear was subtracted fromthe treated right ear at each corresponding measurement point.Each data point represents mean and SD for three independentanimals. All mice shown are on the Balb/c background.Mice wereobtained from Harlan (Indianapolis, IN, USA), Taconic(Germantown, NY, USA), or Jackson (Bar Harbor, ME, USA)and quarantined in our facility until determined to meet SPFcriteria. Mice were killed after ear-thickness measurements andspleen lymphocytes analyzed by flow cytometry to ensure theabsence of T cells within T-deficient strains (data not shown).
Controversies
77

inflammation, the therapeutic activity of compounds blockingonly one selectin in humans has been disappointing (6). Indeed,many small-molecule inhibitors of the selectin family have beenabandoned because of their ineffectiveness in phase I-II clinicaltrials (1). Therapeutic failure appears as a consequence of the highlevel of promiscuity and redundancy of the selectin system, withmost of the functions of either E- or P-selectins largely overlapping,and L-selectin-mediated rolling taking over when the others areinhibited. For this reason, new molecules, such as Efomycine M,which blocks multiple selectins may have a higher chance of success(7). Finally, T-regulatory cells (both T-regulatory cells 1and CD4þCD25þ T cells) homing to the skin are invariablyCLAþ (2,3).
Among chemokine receptors, two candidates for skin-specificleukocyte extravasation have been identified: CCR4 and CCR10(8,9). CCR4 is expressed on most CD4þCLAþ T cells, independ-ently from the cytokine polarization and represents a suitabletarget for skin recruitment blockade with small-moleculecompounds. However, CCR4 expression is not exclusive for
skin-homing lymphocytes, with T-lymphocytes homing in therespiratory tract enriched for CCR4þ cells. Moreover, CCR4 ispoorly expressed on CD8þ T cells, which have a major effectorfunction in allergic contact dermatitis and possibly in psoriasis(10). CCR10 is certainly more specific for T cells engaged inthe skin, being virtually absent from T cells migrating inother districts. However, only a minor portion of CLAþCCR4þ
T cells coexpress the CCR10 (11). Indeed, it has been shownin mouse that inhibition of CCL27 (CC-chemokine ligand)blocked skin homing of T cells in CCR4–/–, but not in wild-typemice (12).
Approaches aimed at targeting integrins appear so far the mostpromising. Experimental data indicate that blocking the CD18(b2 chain of leukocyte function-associated antigen-1) is stronglyeffective in reducing the expression of contact hypersensiti-vity in mice (13), and other compounds, such as efalizumab(anti-CD11a), alicaforsen (intercellular adhesion molecule-1 anti-sense oligodeoxynucleotide), and natalizumab (anti-VLA-4 (verylate antigen)), have already entered clinical trials for psoriasisand other autoimmune diseases with satisfactory results (14–16).In addition to their capacity to reduce T-cell adhesion to endo-thelium, most of integrin antagonists affect T-cell activation to acertain degree, thus augmenting the chance of therapeutic effec-tiveness in immune-mediated disorders.
Giampiero GirolomoniAndrea Cavani
Laboratory of ImmunologyIstituto Dermopatico dell’Immacolata
IRCCSI-00167 Rome
ItalyE-mail: [email protected]
References
1. Schon M P et al. J Invest Dermatol 2003: 121: 951–962.2. Cavani A et al. J Immunol 2003: 171: 5760–5768.3. Sebastiani S et al. J Immunol 2001: 166: 996–1002.4. Biedermann T et al. Eur J Immunol 2002: 32: 3171–3180.5. Dimitroff C J et al. J Clin Invest 2003: 112: 1008–1018.6. Bhushan M et al. Br J Dermatol 2002: 146: 824–831.7. Schon M P et al. Nat Med 2002: 8: 366–372.8. Campbell J J et al. Nature 1999: 400: 776–780.9. Homey B et al. Nat Med 2002: 8: 157–165.
10. Sebastiani S et al. J Invest Dermatol 2002: 118: 1052–1058.11. Soler D et al. Blood 2003: 101: 1677–1683.12. Reiss Y et al. J Exp Med 2001: 194: 1541–1547.13. Grabbe S et al. J Clin Invest 2002: 109: 183–192.14. Gordon K B et al. JAMA 2003: 290: 3073–3080.15. Maksymowych W P et al. J Rheumatol 2002: 29:
447–453.16. Ghosh S et al. N Engl J Med 2003: 348: 24–32.
Commentary 3
Solutions for failure of therapies aimed at T-cellhoming: increasing depletion or evading ligandredundancy
The skin immune system (SIS) differs from other organ immunesystems in many ways (1), one of them being that for enabling skinpercolation by immune cells, a large number of skin-specificmolecules evolved during evolution. Paired combinations of adhe-
sion molecules on white blood cells and their counterstructureswithin human skin and of chemokine receptors and subsets ofchemokines produced by SIS cells, are responsible for the in andoutflow of skin-specific leukocytes, most notably T lymphocytes (2).
It is logical then that targeted therapies, directed at indivi-dual members of these molecule pairs, are in various stagesof clinical development (3). They primarily aim to inhibitadhesion or migration by a diversity of approaches, from
12
3
Dermis
Epidermis
Chemokinegradient
shear flow
Postcapillaryvenule
Figure 1. Molecules implicated in leukocyte recruitment in theskin and potential targets of therapeutic intervention inchronic inflammatory skin diseases: 1. endothelial cellselectins, which mediate tethering and rolling of leukocytes;2. chemokine receptors on leukocytes (e.g. CCR4 andCCR10), whose engagement induces integrin activation; and3. integrins, which are responsible for firm adhesion thatprecedes leukocyte extravasation. Leukocytes are thenattracted into the dermal and epidermal compartments bygradients of chemokines produced by resident andimmigrated cells and maintained in situ by adhesionmolecules. Integrins are also involved in T-cell activationand retention in the epidermis.
Boehncke et al.
78

injections with humanized monoclonal antibodies againstadhesion receptors, to the oral application of xenobioticcompounds that inhibit the expression of a skin-specific che-mokine or its receptor.A major obstacle for the development of such targeted thera-
pies is the typical redundancy of the many ligand receptor pairsinvolved. For example, one of the first recognized combinationsof molecules involved in cutaneous T-cell homing is that ofcutaneous lymphocyte antigen (CLA) and E-selectin, expressedon T lymphocytes and endothelial cells, respectively. However,CLA is detectable on only approximately half of T cells in normalhuman skin (4) and is not unambiguously present on T cells infil-trating lesions of atopic dermatitis and psoriasis (5). This indi-cates that different sets of molecules must be simultaneouslyinvolved in skin T-cell homing.Many other pairs of molecules have been identified, including
integrin a4b1 (VLA-4)/vascular cell adhesion molecule (VCAM)-1, leukocyte function-associated antigen (LFA)-1/intercellularadhesion molecule (ICAM), PECAM/PECAM homophilic inter-action, and integrin aEb7/E-cadherin. Preliminary studies usingthe single molecule approach have been disappointing. TargetingE-selectin alone with CDP850 has shown to be ineffective inpsoriasis (6). Use of natalizumab, a fully humanized antibodyagainst integrin a4b1 (VLA-4), was also of no help in this inflam-matory skin disease.In addition, targeting single chemokines has proved to be of
limited, marginal benefit in the treatment of psoriasis. For example,interleukin (IL)-8 is an important chemokine, involved in leukocytetrafficking into the skin, mainly produced by keratinocytes. The useof a fully humanized monoclonal antibody to IL-8 (also known asCXCL8) with ABX-IL8 had no effect in an initial psoriasis study.It seems rational to conclude that the redundancy of functional
molecules that direct immune functions prevent the development ofsingle target directed therapies. One must beat the immune systemby using another and relevant phenomenon, being that single pairsof molecules are involved in multiple immune functions. For exam-ple, targeting the LFA-1a subunit with efalizumab (Raptiva1), afully humanized antiCD11a monoclonal antibody, may have tripleaction. It inhibits T-cell adhesion to ICAM-1 on endothelial cells,but it also interferes with their adhesion to dendritic cells, as well asto keratinocytes. Treating psoriasis with this biological has shownefficacy, relatively limited despite its presumable triple action, butenough to have it registered for that indication.
Thus, in the development of new therapies for inflammatoryskin diseases, one has to find single molecular targets that havemultiple roles in immune functions, enabling synergistic effectsat different sites of the inflammatory process. By doing this,one avoids encountering the phenomenon of redundancy that ischaracteristic for the migration-related molecules of the humanSIS.In addition, only negligible attention has been given to another
approach, that of stimulating departure of the T cells from theinflammatory lesions. We know that eliminating them, such as byultraviolet irradiation, is very effective in various inflammatoryskin diseases. Interest thus far has been primarily on the pairs ofmolecules involved in influx of T cells to sites of inflammation. AsT cells are thought to be percolating, attention to moleculesinvolved in outflow may probably result in completely new andinnovative targets of therapy.
Jan D. BosDepartment of Dermatology
Academic Medical Center A0-235University of Amsterdam
PO Box 227001100 DE Amsterdam
the NetherlandsE-mail: [email protected]
Conflict of interest statement: The author is an irregular, inci-dental consultant to pharmaceutical companies in this field.
References
1. Bos J D, ed. Skin Immune System (SIS): Cutaneous Immu-nology and Clinical Immunodermatology, 3rd edn. BocaRaton: CRC Press, 2004.
2. Schon M P, Zollner T H M, Boehncke W-H. J InvestDermatol 2003: 121: 951–962.
3. Gottlieb A B, Bos J D. Clin Immunol 2002: 105: 105–116.4. Bos J D, De Boer O J, Tibosch E, Das P K, Pals S T. Arch
Dermatol Res 1993: 285: 179–183.5. De Boer O J, Wakelkamp I M M J, Pals S T,
Claessen N, Bos J D, Das P K. Arch Dermatol Res 1994:286: 304–311.
6. Bhushan M et al. Br J Dermatol 2002: 146: 824–831.
Commentary 4
Leukocyte extravasation as a target for anti-inflammatory therapies in dermatology: Whichmolecular target is best?
Skin attracts haematopoietic cells – from leukocytes (pustulardermatosis), mast cells (mastocytosis), eosinophils (atopiceczema), to T lymphocytes (eczema, lichen planus, etc.). Why?Personally I believe T cells are attracted because epidermis andthymic epithelium/skin is important for a proper maturation andmaintenance of the peripheral immune system, where the T cell is‘the conductor’ – the generator of diversity – of the immuneorchestra (1).Imagine your ‘congress hotel’. Everyone gets an encoded
plastic card so you can: 1. enter the hotel (not a custom yet);2. enter the elevators (not so uncommon); 3. get off at yourfloor (more and more common); and 4. enter your room(a requirement), i.e. four steps. This is called compartmentali-zation (2).
Neutrophil granulocytes migrate in vitro with a speed �70that of lymphocytes. So, how come skin diseases are not full ofneutrophil granulocytes? Because of the selective access to theskin compartment. I will concentrate on lymphocytes. Weknow that normal skin contains 55.000 cells/mm3, whichroughly equals their number in blood (3). An adult patientwith atopic eczema affecting 30% of his/her body surfacehas double the amount of T lymphocytes in skin comparedwith blood (3). We also know that all T alpha/beta-receptorlymphocytes have access to the skin (4), which is not the casefor T-gamma/delta cells, which home to the gastrointestinaltract.The major players in getting T lymphocytes into the skin
are cutaneous lymphocyte antigen (CLA) (5), chemokinereceptors on T cells, adhesion molecule expression, and themany skin-derived chemokines such as interleukin (IL)-8,TARC (T cell activating and regulatory chemokine), etc.We observed that certain cytokines like IL-10 attracts
Controversies
79

CD8þ T cells, but inhibits CD4þ cells, whereas psoriasindoes the opposite (6,7) – at least in vitro. The responsivenessof subsets of lymphocytes is linked to their expression ofchemokine receptors (8). For example, interferon-g andother cytokines augment chemokine receptors on T cells asthey augment adhesion-molecule expression (9,10). However,these receptors are down-regulated by IL-2 and IL-4. Thismeans that when a T cell is attracted and then meetscytokines from activated T cells – further migration stops.We have called this migration and focusing – illustratingthe plasticity of T-cell chemotaxis regulated within hoursaccording to the cytokine environment (9,10).
So, which target to select? Thinking of our ‘congress hotelmodel’, we would like to focus on the culprits for skindiseases, i.e. denying access of the pathogenic T cell to itsspecific room. But we are far from being able to do so.Today, topical steroids are effective as they stop T cells atthe entrance through switching-off chemotaxins, down-regulate adhesion molecules etc. The new topical immuno-modulators are more specific in aiming at the activatedT cells. Ciclosporin may be specific in its inhibition ofentrance of CD8þ T cells (4). A recent study elegantlyshows how manipulation of the sugars involved in CLAcan lead to a significant reduction of inflammation ina mouse model (11). Another study showed how the poly-phenol epigallocatechin from green tea down-regulatesCD4þ expression on T cells thereby inhibiting gp120 bindingof HIV (12).
There are many aspects of leukocyte extravasation, which wenow know about. But likely more we do not know of yet. So, cellmigration into skin still belongs to the Holy Grail. Youngresearchers – be aware of the major pitfall: redundancy.
Kristian Thestrup-PedersenProfessor of Dermatology
University of AarhusDenmark
King Faisal Specialist Hospitaland Research Centre
RiyadhSaudi Arabia
E-mail: [email protected]
References
1. Thestrup-Pedersen K, Ellingsen A R, Olesen A B, KaltoftK. Acta Derm Venereol (Stockh) 1997: 77: 20–21.
2. Speiser D E, Lees R K, Hengartner H, Zinkernagel R M,MacDonald H R. J Exp Med 1989: 170: 2165–2170.
3. Ellingsen A R, Soerensen F B, Larsen J O, Deleuran M S,Thestrup-Pedersen K. Acta Derm Venereol (Stockh) 2001:81: 258–262.
4. Bang K, Lund M, Mogensen S C, Thestrup-Pedersen K.Exp Dermatol (in press).
5. Robert C, Kupper T S. N Engl J Med 1999: 341: 1817–1828.6. Jinquan T, Larsen C G, Gesser B, Matsushima K,
Thestrup-Pedersen K. J Immunol 1993: 151: 4545–4551.7. Jinquan T et al. J Invest Dermatol 1996: 107: 5–10.8. Jinquan T et al. J Immunol 1997: 158: 475–484.9. Jinquan T et al. J Immunol 1995: 154: 3742–3752.
10. Jinquan T et al. J Immunol 1995: 155: 5359–5368.11. Dimitroff C J, Kupper T S, Sackstein R. J Clin Invest
2003: 112: 1008–1018.12. Kawai K et al. J Allergy Clin Immunol 2003: 112: 951–957.
Boehncke et al.
80
Copyright © 2022 FDOKUMEN