LETTERS TO THE EDITOR - Journal of Neurology ...
26
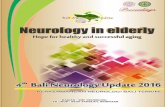
LETTERS TO THE EDITOR Postictal psychosis related regional cerebral hyperperfusion Postictal psychosis is a known complication of complex partial seizure in particular temporal lobe epilepsy. It usually runs a benign and self limiting course. A postictal phenomenon with focal cerebral hypofunc- tion (similar to Todd’s palsy), rather than ongoing seizure activity, has been postulated. 12 Surface EEG is either normal or showing non-specific slow waves. 3 Hence, antipsychotic medications are prescribed instead of antiepileptic drugs. Until recently, the pathogenic mechanisms have remained unknown. In this communication, we report on two patients with postictal psychosis, dur- ing which a cerebral SPECT study showed a hyperperfusion signal over the right temporal lobe and contralateral basal ganglion. As hyperperfusion in ictal cerebral SPECT is closely linked to epileptic activities, 4 our find- ings support a contrary explanation for postictal psychosis. Prolonged video-EEG telemetry study was performed in patients who underwent presur- gical evaluation for epilepsy surgery. Antiepi- leptic drugs were withdrawn to facilitate seizure recording. A diagnosis of temporal lobe epilepsy was based on analysis of the electroclinical events and, if applicable, post- operative outcome after anterior temporal lobectomy. Psychosis was diagnosed accord- ing to the fourth edition of the diagnostics and statistical manual of mental disorders (DSM-IV) criteria of brief psychotic disorders without marked stressor. HMPAO-SPECT was performed during the psychotic period, which ranged from 2–4 days after the last sei- zure. Interictal cerebral SPECT, brain MRI, and a Wada test were performed as part of presurgical evaluation. Patient 1 was a 34 year old Chinese woman with complex partial seizures since the age of 18. Her seizure control was suboptimal on a combination of antiepileptic drugs. Brain MRI showed a small hippocampus on the right. Interictal EEG showed bilateral tempo- ral sharp waves and ictal recordings con- firmed a right temporal epileptogenic focus. A Wada test confirmed right hippocampal memory dysfunction. Six hours after her last secondary generalised tonic-clonic seizure after video-EEG telemetry, she began to develop emotional lability, talking nonsense, motor restlessness, and auditory hallucina- tion. A cerebral SPECT study was performed at day 4 after her last seizure. Her psychotic features persisted although she was taking antipsychotic medication (pimozide). Cer- ebral SPECT showed a clear hyperperfusion signal over the right lateral temporal neocor- tex and contralateral basal ganglion. An interictal cerebral SPECT study was repeated at 4 weeks after postictal psychosis which showed a complete resolution of hyperper- fusion signal in the right temporal lobe and basal ganglia. Anterior temporal lobectomy was performed and she became seizure free after surgery. Patient 2 was a 44 year old man with intractable complex partial seizures since the age of 30. His seizures were intractable to multiple antiepileptic drugs. Brain MRI showed left hippocampal sclerosis. Interictal cerebral SPECT showed a relative hypoper- fusion area over the left hemisphere. Interic- tal surface EEG was non-lateralising but ictal EEG disclosed a right hemispheric onset. On withdrawal of antiepileptic drugs, seven complex partial seizures with secondary gen- eralised tonic clonic seizures were recorded within a period of 72 hours. His usual antiepileptic drugs were then restarted. Thirty hours after his last secondary general- ised tonic-clonic seizure; he began to develop emotional lability, talking nonsense, restless- ness, auditory hallucination, persecutory delusion, and delusion of superstition. Cer- ebral SPECT study, performed 2 days later while his psychotic features persisted, showed two relative hyperperfused areas over the right temporal neocortex and contralat- eral basal ganglion in addition to the original hypoperfused area over the left hemisphere. An antipsychotic agent (thioridazine) was Interictal SPECT and SPECT performed during postictal psychosis. (Top) A SPECT study of patient 1 showing areas of relative hyperperfusion over the right temporal neocortex (red arrows) and the left basal ganglia (blue and yellow arrows) during postictal psychosis. (Bottom) SPECT study of patient 2 showing areas of hyperperfusion over the right temporal neocortex and the left basal ganglia. Arrows indicate areas of hyperperfusion. J Neurol Neurosurg Psychiatry 2000;68:100–126 100 on February 15, 2022 by guest. Protected by copyright. http://jnnp.bmj.com/ J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.68.1.123g on 1 January 2000. Downloaded from
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of LETTERS TO THE EDITOR - Journal of Neurology ...
LETTERS TOTHE EDITOR
Postictal psychosis related regionalcerebral hyperperfusion
Postictal psychosis is a known complicationof complex partial seizure in particulartemporal lobe epilepsy. It usually runs abenign and self limiting course. A postictalphenomenon with focal cerebral hypofunc-tion (similar to Todd’s palsy), rather thanongoing seizure activity, has beenpostulated.1 2 Surface EEG is either normalor showing non-specific slow waves.3 Hence,antipsychotic medications are prescribedinstead of antiepileptic drugs. Until recently,the pathogenic mechanisms have remainedunknown. In this communication, we reporton two patients with postictal psychosis, dur-ing which a cerebral SPECT study showed ahyperperfusion signal over the right temporallobe and contralateral basal ganglion. Ashyperperfusion in ictal cerebral SPECT isclosely linked to epileptic activities,4 our find-ings support a contrary explanation forpostictal psychosis.
Prolonged video-EEG telemetry study wasperformed in patients who underwent presur-
gical evaluation for epilepsy surgery. Antiepi-leptic drugs were withdrawn to facilitateseizure recording. A diagnosis of temporallobe epilepsy was based on analysis of theelectroclinical events and, if applicable, post-operative outcome after anterior temporallobectomy. Psychosis was diagnosed accord-ing to the fourth edition of the diagnosticsand statistical manual of mental disorders(DSM-IV) criteria of brief psychotic disorderswithout marked stressor. HMPAO-SPECT wasperformed during the psychotic period,which ranged from 2–4 days after the last sei-zure. Interictal cerebral SPECT, brain MRI,and a Wada test were performed as part ofpresurgical evaluation.
Patient 1 was a 34 year old Chinese womanwith complex partial seizures since the age of18. Her seizure control was suboptimal on acombination of antiepileptic drugs. BrainMRI showed a small hippocampus on theright. Interictal EEG showed bilateral tempo-ral sharp waves and ictal recordings con-firmed a right temporal epileptogenic focus.A Wada test confirmed right hippocampalmemory dysfunction. Six hours after her lastsecondary generalised tonic-clonic seizureafter video-EEG telemetry, she began todevelop emotional lability, talking nonsense,motor restlessness, and auditory hallucina-tion. A cerebral SPECT study was performedat day 4 after her last seizure. Her psychoticfeatures persisted although she was takingantipsychotic medication (pimozide). Cer-ebral SPECT showed a clear hyperperfusion
signal over the right lateral temporal neocor-tex and contralateral basal ganglion. Aninterictal cerebral SPECT study was repeatedat 4 weeks after postictal psychosis whichshowed a complete resolution of hyperper-fusion signal in the right temporal lobe andbasal ganglia. Anterior temporal lobectomywas performed and she became seizure freeafter surgery.
Patient 2 was a 44 year old man withintractable complex partial seizures since theage of 30. His seizures were intractable tomultiple antiepileptic drugs. Brain MRIshowed left hippocampal sclerosis. Interictalcerebral SPECT showed a relative hypoper-fusion area over the left hemisphere. Interic-tal surface EEG was non-lateralising but ictalEEG disclosed a right hemispheric onset. Onwithdrawal of antiepileptic drugs, sevencomplex partial seizures with secondary gen-eralised tonic clonic seizures were recordedwithin a period of 72 hours. His usualantiepileptic drugs were then restarted.Thirty hours after his last secondary general-ised tonic-clonic seizure; he began to developemotional lability, talking nonsense, restless-ness, auditory hallucination, persecutorydelusion, and delusion of superstition. Cer-ebral SPECT study, performed 2 days laterwhile his psychotic features persisted,showed two relative hyperperfused areas overthe right temporal neocortex and contralat-eral basal ganglion in addition to the originalhypoperfused area over the left hemisphere.An antipsychotic agent (thioridazine) was
Interictal SPECT and SPECT performed during postictal psychosis. (Top) A SPECT study of patient 1 showing areas of relative hyperperfusion over theright temporal neocortex (red arrows) and the left basal ganglia (blue and yellow arrows) during postictal psychosis. (Bottom) SPECT study of patient 2showing areas of hyperperfusion over the right temporal neocortex and the left basal ganglia. Arrows indicate areas of hyperperfusion.
J Neurol Neurosurg Psychiatry 2000;68:100–126100
on February 15, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.68.1.123g on 1 January 2000. D
ownloaded from

started after the cerebral SPECT. Hispsychotic symptoms resolved 2 weeks laterwith full recovery.
Cerebral SPECT performed during theinterictal period (IP) and during postictalpsychosis (PP) were analysed visually andareas of hyperperfusion were identified.Quantitaive data at regions of interest (ROIs)were measured on coronal and axial slidescontaining basal ganglia (BG), mesial (MT),and lateral (LT) temporal lobe structures.Asymmetry index (ASI) was calculated as((ROI focus−ROI contralateral)/ROIfocus+ROI contralateral))×200%. We set anarbitrary change of ASI >100% to be signifi-cant. As there were only two patients, statisti-cal testing was not performed.
Both patients showed postictal psychosisand had a regional increase in rCBF over theright temporal neocortex and the left basalganglion compared with their interictal study(figure). Quantitative analysis for patient 1showed changes of ASI during IP and PPover right MT was +75% (-6.64476 to-1.65289); over the right LT was +1167.8%(1.07527 to 12.55764); and over the left BGwas +206.8% (-2.07373 to 2.21574). Quan-titative analysis for patient 2 showed changesof ASI during IP and PP over right MT was−3.8% (13.14217 to 12.64158); over rightLT was +178.6% (10.4696 to 18.70027);and over left BG was +155.9% (−5.85556 to3.27522).
Postictal psychosis is a distinct clinicalevent associated with temporal lobe epilepsy.1
The diagnosis of postictal psychosis requiresa close temporal relation between bouts ofcomplex partial seizures and the onset of psy-chosis. The psychosis usually develops after acluster of complex partial seizures precipi-tated by abrupt withdrawal of antiepilepticdrugs.1 The cluster occurs in patients withpoor drug compliance or during video EEGtelemetry studies when antiepileptic drugsare withdrawn purposefully. The clinicalcourse of postictal psychosis is usually benignand predictable.1 5 In our patients, theduration of psychotic disturbances lastedfrom 10 to 14 days, which is in keeping withthe good prognosis. Antipsychotic drugs,such as haloperidol and fluphenazin are usu-ally prescribed.1
The underlying mechanism of postictalpsychosis is unknown. Postictal cerebralhypofunction has been postulated as an ana-logue to Todd’s paralysis after seizure.1 2
However, the presence of increased rCBFduring postictal psychosis, may suggest analternative explanation as ictal SPECT hasbeen shown to be highly sensitive and specificin demonstrating seizure foci.4
To conclude, our results are contradictoryto the hypofunction theory of Todd’s paraly-sis in postictal psychosis. We think that thesehyperperfusion areas are responsible for thepostictal psychosis. Further serial studies
with cerebral SPECT or PET may enhanceour understanding on the mechanism of pos-tictal psychosis.
G C Y FONGK Y FONG
W MAKK L TSANGK H CHAN
R T F CHEUNGS L HO
Division of Neurology, University Department ofMedicine, The University of Hong Kong
W Y HODepartment of Nuclear Medicine, Queen Mary
Hospital, Hong Kong
Correspondence to: Dr G C Y Fong, Departmentof Medicine, Queen Mary Hospital, Pokfulam Road,Hong Kong email cyfong.medicine @graduate.hku.hk
1 Savard G, Andermann F, Olivier A, et al. Postic-tal psychosis after partial complex seizures: amultiple case study. Epilepsia 1991;32:225–31.
2 Morell F. Memory loss as a Todd’s paresis.Epilpesia 1980;21:185.
3 Kanner AM, Stagno S, Kotagal P, et al. Postictalpsychiatric events during prolonged video-electro-encephalographic monitoring studies.Arch Neurol 1996;53:258–63.
4 Ho SS, Berkovic SF, Newton MR, et al. Parietallobe epilepsy: clinical features and seizurelocalization by ictal SPECT. Neurology 1994;44:2277–84.
5 Toone B. Psychoses and epilepsy. In: ReynoldsEH, Trimble MR, eds. Epilepsy and psychiatry.London: Churchill Livingstone, 1981:113–7.
Oncofetal matrix glycoproteins incerebral arteriovenous malformationsand neighbouring vessels
Cerebral arteriovenous malformations(AVMs) are thought to be congenital lesionsexhibiting features of either mature vascularwalls or embryonal anastomotic plexuses. It isgenerally assumed that changes in size aredependent on enlargement of the venouscompartment, organisation in the setting ofmicrohaemorrhages, and gliosis. However,recent findings are consistent with thehypothesis of ongoing angiogenesis.1 2
Previous research from this laboratorydisclosed that peculiar isoforms of fibronectin(FN) and tenascin (TN) typically occur infetal and neoplastic tissues.3–5 These isoformsare a blend of structurally diVerent glycopro-teins that result from alternative splicing of theprimary transcript and are mainly expressedin the extracellular matrix. Their expression isundetectable in normal adult tissues, with theexception of the vessels in the regeneratingendometrium. To gain further insight into thepathobiology of the AVMs the present reportsought to ascertain whether these lesions alsoexpress oncofetal FN and TN isoforms.
Tissue samples were obtained after neuro-surgical excisions of ruptured AVMs. All 10patients had experienced an intracerebralhaemorrhage as the first clinical manifesta-
tion of their disease. There was no drughistory before bleeding. Control specimensfrom two right gyri recti and one cerebellartonsil were obtained, respectively, from op-erations for ruptured aneurysms of the ante-rior communicating artery or for ArnoldChiari disease.
Immunohistochemical evaluations wereperformed on 5 µm thick cryostat sectionsusing a protocol reported previously.5 Owingto the limited amount of available material,only in a few cases was some fresh tissueretained to allow western blots. Distributionof FN and TN isoforms was investigatedusing three monoclonal antibodies (mAbs) ortwo Ab fragments, obtained by phage displaytechnology, respectively. These Abs, preparedin our laboratory, were found to work on freshfrozen material. According to the previouscharacterisations the BC-1 mAb and theTN-11 Ab fragments are specific for isoformsoccurring almost exclusively in fetal tissuesand in tumours, with the recognised TN iso-form being typically associated with anaplas-tic gliomas (table).
Control sections were processed identicallyto the other specimens, but the primaryantibody was substituted with a specificimmunoglobulin of recombinant antibodies.The antibodies were blocked using the specificantigens. The antigens were recombinant pro-tein containing the epitope produced in E Coli.For the mAb BC-1 we used the recombinantprotein containing the type-III repeats 7B-8–9.For the mAb IST-4 we used the recombinantprotein containing the type-III repeats 2–8.For the recombinant antibodies TN-11 andTN-12 the recombinant type-III repeat C andthe recombinant fragment containing theEGF-like repeats were used, respectively.
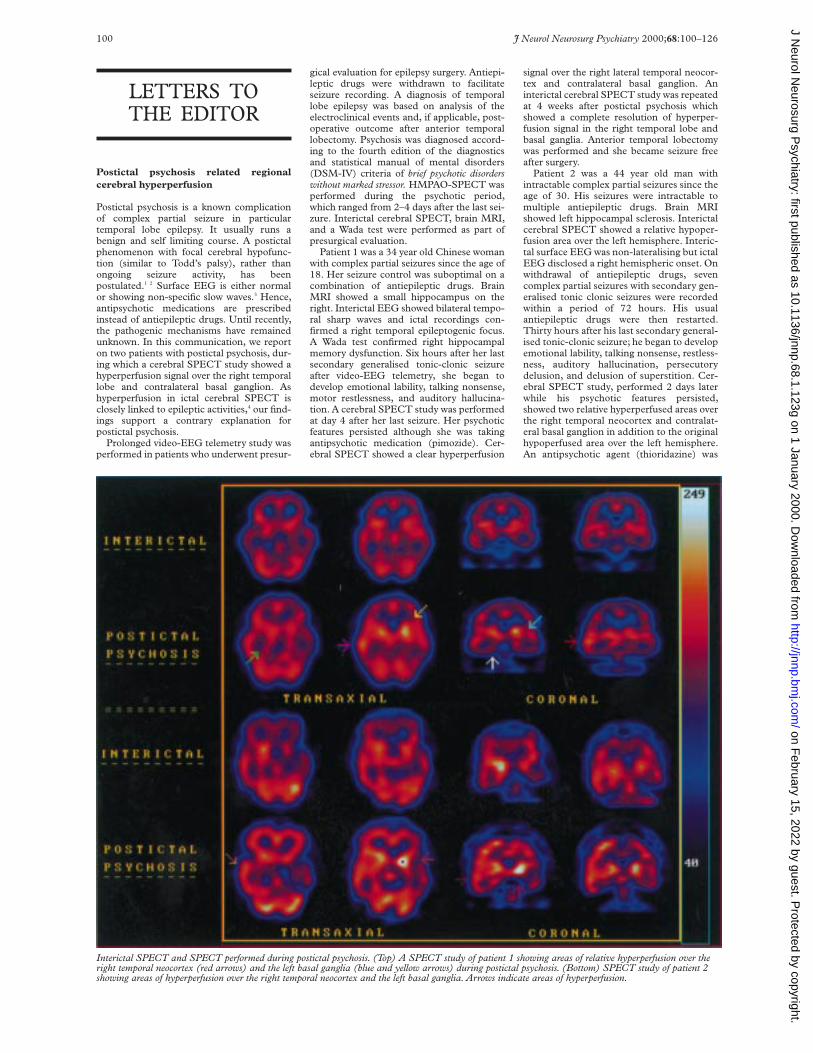
All 10 AVMs were found to contain largeamounts of FN and TN, as shown by intenseimmunostaining with the use of the IST-9 /IST-4 mAbs and the TN-12 Ab fragment.The staining was localised either in theendothelium or the subendothelial layer. Apositive response was found in several artery-like vessels and in a few vessels with thinnerwalls using the mAb BC-1. Staining with theTN-11 Ab fragment showed occurrence oftype III repeat C TN isoform in the innerlayers of the vascular components of thenidus, irrespective of their morphology.
Six out of the 10 examined specimens werefound to contain portions of cerebral tissuesurrounding the angiomatous nidus. In allthese cases the wall of several vesselsexhibited intense staining with the use of theTN-11 Ab fragment. Using the BC-1 mAbsome of these vessels exhibited some staining(figure). In the control specimens (brain andcerebellum) both the FN isoform containingthe ED-B sequence (ED-B+FN), and thetype III repeat C TN isoform were absent,despite the widespread distribution of totalFN and TN in the vascular walls.
Characterisation of the employed Abs and distribution of the recognized isoforms.
Anti-FN mAbs4 5 Anti-TN Ab fragments3
IST-4 IST-9 BC-1 TN-12 TN-11
Recognised isoforms Total FN Isoforms containingthe ED-A sequence
Isoform containing the ED-Bsequence
Total TN Type III repeat C Isoform
Distribution of the isoform (s) Widespread Widespread Absent in adult tissues (with theexception of the regeneratingendometrium)
Widespread Absent in adult tissues
Present in fetal tissues
Present in the vascular wall and thematrix of fetal tissues and tumours
Absent in several types ofmalignancies
Present in the vascular wallof anaplastic gliomas
J Neurol Neurosurg Psychiatry 2000;68:100–126 101
on February 15, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.68.1.123g on 1 January 2000. D
ownloaded from

Previous findings showed that ED-B+FNpresents with conformational modifications inits central part and results from deregulation ofFN pre-mRNA.4 The distribution of thisisoform was found to be highly restricted innormal adult tissues. By contrast, ED-B+ FNexhibited widespread distribution in the vascu-lature of fetal tissues, including brain, and ofseveral types of malignancies. It was thereforeregarded as a marker of angiogenesis.5
Similarly, the type III repeat C TNisoform, recognised by the Ab fragmentTN-11, was found to occur in the vascularwalls of anaplastic gliomas. Northern blotanalysis showed that the mRNA of thisisoform was undetectable in normal tissuesand some malignancies, but was present inlarge amounts in fetal tissues, includingbrain, and in glioblastomas3
Recent advances in the pathology of cerebralAVMs suggest that these lesions might not bestatic. Tyrosine kinase, an endothelial cell spe-cific receptor upregulated in glioblastomas,was found to be highly expressed in bothAVMs and in the vessels of cerebral tissue bor-dering the malformations, by contrast with thedown regulation occurring in the vasculatureof the normal brain.1The pattern of distribu-tion of structural proteins was consistent withthe hypothesis of diVuse activation of angio-genesis, without specific relation to individualvessel types.2
Furthermore, use of the cell proliferationmarker MIB-1 showed endothelial prolifera-tion in arterioles, venules, and capillaries ofthe cerebral tissue neighbouring AVMs.1
The present findings indicate that aparticular FN isoform, mainly expressed bythe vasculature of fetal and tumorous tissues,as well as a TN isoform typically detected inthe walls of vessels in anaplastic gliomas, alsooccur in AVMs and in vessels of adjacent cer-ebral tissue, but that both isoforms are absentin normal brain. This evidence providesfurther support to the hypothesis of ongoingangiogenesis in and around these lesions.
The presence of angiogenic features inAVMs might result from maintenance of pro-liferating and remodelling potentials, or froma specific response to haemodynamic stress invascular structures subjected to increasedblood flow and pressure. Occurrence of thesefeatures also in vessels lying in areas periph-eral to the nidus might be related torecruitment of the neighbouring vasculature,possibly dependent on focal ischaemia in thesetting of arteriovenous shunting.1 2 However,the presence in apparently normal vascula-ture of molecules typically occurring in fetaltissues and malignancies indicate that cer-ebral AVMs may not be static lesions. Furtherstudies are needed to ascertain whether thisphenomenon results merely from haemody-namic stress or actually reflects an intrinsicgrowth potential. Should this second be thecase, current therapeutic strategies wouldpossibly require revision.
This study was partially supported by theNational Research Council (CNR), AIRCand the Ministry of University and ScientificResearch (MURST). We thank Sergio De-seri, EE, for his technical help and Mr. Tho-mas Wiley for manuscript revision.
ANTONIO PAUA DORCARATTO
G L VIALEDI S C A T Departement of Surgery, Division of
Neurosurgery, University of Genoa Medical School, SMartino Hospital, Pad 2, Largo Rosanna Benzi 10,
16132 Genova, Italy
P CASTELLANIA SIRI
L ZARDILaboratory of Cell Biology National Cancer Institute,
Genoa, Italy
Correspondence to: Dr A Pau
1 Hatva E, Jääskeläinen J, Hirvonen H, et al. Tieendothelial cell-specific receptor tyrosine ki-nase is upregulated in the vasculature of arter-ovenous malformations. J Neuropathol ExpNeurol 1996;55:1124–33.
2 Rothbart D, Awad IA, Jiyon L, et al. Expressionof angiogenic factors and structural proteins incentral nervous system vascular malforma-tions. Neurosurgery 1996;38:915–25.
3 Carnemolla B, Castellani P, Borsi L, et al. Iden-tification of a glioblastoma associated tn-c iso-form by a high aYnity recombinant antibody.Am J Pathol 1999;154:1345–52.
4 Carnemolla B, Leprini A, Allemanni G, et al.The Inclusion of type III repeat ED-B in thefibronectin molecule generates conformationalmodifications that unmask a cryptic sequence.J Biol Chem 1992;267:24689–92.
5 Castellani P, Viale G, Dorcaratto A, et al. Thefibronectin isoform containing the ED-B on-cofetal domain: a marker of angiogenesis. Int JCancer 1994;59:612–18.
Hashimoto’s encephalopathy presentingas “myxoedematous madness”
The neuropsychiatric sequelae of hypo-thyroidism range from lethargy and mentalslowing to the florid psychotic illness referredto as “myxoedematous madness”. The lastcondition is characterised by frank hypo-thyroidism accompanied by psychosis, andmay respond completely to thyroxine.1 Morerecently described is a syndrome of subacuteencephalopathy, associated with high titres ofthyroid autoantibodies, raised CSF protein,EEG abnormalities, and perfusion deficits inthe presence of normal structural neuro-imaging.2–4 In most cases, the encephalopathyoccurs without any gross change in circulat-ing concentrations of thyroid hormones, sug-gesting that an inflammatory process isresponsible for the cerebral dysfunction. Inthe absence of pathological data, the evidencefor a specific pathogenetic mechanism islargely circumstantial: a small vessel vasculitisand immune complex deposition have bothbeen suggested.3 4
Although none of the published cases ofHashimoto’s encephalopathy has describedpsychosis as a primary feature, it is possiblethat “myxoedematous madness”, a conditionfirst described in detail by Asher in 19491 liesin a range of encephalopathic phenomenamediated by autoimmune mechanisms. Thissuggestion would certainly be consistent withthe range of clinical presentations of otherautoimmune cerebral vasculitides.5 As au-toimmune thyroiditis is the commonest causeof thyroid failure in this country,6 it is likely tohave been present in at least some of Asher’soriginal 14 cases. Although most had floridmyxoedematous features at psychiatric pres-entation, this may simply reflect the diYcultyof diagnosing subclinical thyroid diseasebefore rapid laboratory assays became widelyavailable. Many features of the present case,however, favoured an endocrine rather thanan inflammatory mechanism, suggesting thatthe condition of “myxoedematous madness”,though rare, remains a valid diagnostic entity.
A 63 year old market stallholder withoutmedical or psychiatric history was brought toa local psychiatric hospital by the police. Hisbusiness had been in decline for severalmonths, and his family had noticed uncharac-teristic emotional lability. In the weekspreceding admission he had experienceddelusions and hallucinations, and exhibiteduncharacteristic behaviour. He had reporteda vision of the crucifixion, and hearing thevoice of his dead mother. He claimed that hishouse was occupied by the devil, drovearound aimlessly in his car, and appearedconstantly fearful and withdrawn. On the dayof admission he had made a bonfire in thegarden and burned his wife’s clothes, familyphotographs, furniture, and business papers.When his wife and son tried to intervene he
Immunostaining with the TN-11 Ab fragment or the BC-1 mAb shows the presence of the type IIIrepeat C TN-(A) and ED-B+ FN-(B) isoforms in angiomatous vessels. These isoforms are alsopresent in the wall of vessels of the cerebral tissue adjacent to the angiomatous nidus (TN: C; FN: D).Bar=10 µm.
102 J Neurol Neurosurg Psychiatry 2000;68:100–126
on February 15, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.68.1.123g on 1 January 2000. D
ownloaded from

became aggressive and threatened them witha saw. The general practitioner was called andsuspected either an acute psychosis or asevere depressive illness. Police assistance wasrequested because of the patient’s continuingviolent behaviour.
On admission he was unkempt but coop-erative and apparently euthymic. He denieddepression, but displayed no insight into theirregularity of his behaviour. No psychoticfeatures were seen, although during theadmission he consistently rationalised allreported psychotic phenomena. He wasaggressive towards staV and made repeatedattempts to abscond. General physical exam-ination was unremarkable. Neurological ex-amination was normal except for spokenlanguage, which was fluent and grammatical,but contained word finding pauses, circum-locutions, and occasional semantic errors(for example, “I just want to get my feet backon the table”). Formal neuropsychologicaltesting, and a screen of laboratory tests forreversible causes of encephalopathy, wereperformed on admission, and results are pre-sented below (column A). Attention is drawnto his mild naming deficit, and poorperformance on the Rey figure, which wasdue to planning rather than visuospatialerrors, suggesting a predominantly “dysex-ecutive” pattern. CT and EEG were bothnormal, and SPECT disclosed widespreadbut mild cortical hypoperfusion. Trifluop-erazine (2 mg twice daily) was started onadmission, and thyroxine (75 µg once daily)added 1 week later. His mental state andbehaviour stabilised, leading to dischargeafter 2 months.
At 6 month follow up the patient hadstopped neuroleptic drugs, but continuedtaking thyroxine. He reported feeling “backto normal”, had bought a new house, and wasworking as a part time shop assistant. He stillhad subtle word finding diYculties, and wasreferred to the regional memory clinic forfurther evaluation, which took place 6months later. Behavioural assessment showedpersisting deficits in delayed recall of verbalmaterial, verbal fluency, and visuospatialfunction. Formal psychometric testing, bloodtests, and SPECT were repeated, 1 year afterthe original examinations. Laboratory andneuropsychological results are presented inthe table. It is of note that, whereas his nam-ing ability had improved, performance onfrontal executive tasks remained impaired.The appearance of the follow up SPECT dif-
fered minimally, if at all, from the first exam-ination.
In summary, therefore, this patient pre-sented in clear consciousness with a firstepisode of acute psychosis, and evidence ofsubtle executive and linguistic neuro-psychological disturbance, on the backgroundof gradual behavioural and aVective change.He was profoundly hypothyroid due to anautoimmune thyroiditis, but there was noclinical evidence of thyroid failure other thanthe abnormal mental state. The psychiatriccomponent of his illness recovered fully, andthe antithyroid microsomal antibody titre fellmarkedly after thyroxine replacement, al-though his mild neuropsychological deficitsremained unchanged. Corticosteroids werenot used at any stage.
The response to thyroxine does not, initself, imply that the cerebral illness had anendocrine origin; a recent report described apatient with a subacute encephalopathicillness and compensated hypothyroidism inthe presence of increased antimicrosomalantibodies, all of which responded to thyrox-ine replacement alone.4 In that case, however,both EEG and SPECT were abnormal, theSPECT showing multiple areas of severelyreduced perfusion, which normalised withtreatment. By contrast, in the present case theEEG was normal and the SPECT abnormal-ity was marginal and changed little, if at all,with treatment. The evidence for a significantvasculitic component to the illness is, there-fore, unconvincing.
The mild and relatively circumscribedneuropsychological deficits coupled withflorid psychotic phenomena, also contrastwith the profound global disturbance of cog-nition usually associated with Hashimoto’sencephalopathy.3 This distinction suggeststhat microvascular disruption and thyroidhormone depletion may emphasise diVerentaspects of the clinical range in Hashimoto’sencephalopathy. Although the present casewould support Asher’s conclusion that thepsychiatric features of Hashimoto’s encepha-litis typically respond to thyroid replacement,it additionally suggests that subtle neuro-psychological deficits may be apparent evenin the absence of obvious cerebral perfusiondeficits, and that these may not be fullyreversible.
P GARRARDJ R HODGES
University of Cambridge Neurology unit,Addenbrooke’s Hospital, Cambridge CB2 2QQ, UK
P J DE VRIESN HUNT
University of Cambridge Department of Psychiatry,Addenbrooke’s Hospital, Cambridge CB2 2QQ, UK
A CRAWFORDJ R HODGES
MRC Cognition and Brain Sciences Unit, 15 ChaucerRoad, Cambridge CB2 2EF, UK
K BALANDepartment of Nuclear Medicine, Addenbrooke’s
Hospital, Cambridge CB2 2QQ, UK
Correspondence to: Dr P Garrard, University ofCambridge Neurology Unit, Box 165, Adden-brooke’s Hospital, Cambridge CB2 2QQ, UKemail [email protected]
1 Asher R. Myxoedematous madness. BMJ1949;555–62.
2 Thrush DC, Boddie HG. Episodic encepha-lopathy associated with thyroid disorders. JNeurol Neurosurg Psychiatry 1974;37:696–700.
3 Shaw PJ, Walls TJ, Newman PK, et al.Hashimoto’s encephalopathy: a steroid respon-sive disorder associated with high anti-thyroidantibody titers: report of 5 cases. Neurology1991;41:228–33.
4 Forchetti CM, Katsamakis G, Garron DC.Autoimmune thyroiditis and a rapidly progres-sive dementia: global hypoperfusion onSPECT scanning suggests a possible mech-anism. Neurology 1997;49:623–6.
5 Scolding NJ, Jayne DR, Zajicek J, et al. Cerebralvasculitis: recognition, diagnosis and manage-ment. Q J Med 1997;90:61–73.
6 Dayan CM, Daniels GH. Chronic autoimmunethyroiditis. N Engl J Med 1996;335:99–107.
Alien hand sign in Creutzfeldt-Jakobdisease
The clinical picture of Creutzfeldt-Jakob dis-ease (CJD) includes various movement disor-ders such as myoclonus, parkinsonism,hemiballism, and dystonia. We report on apatient with CJD who manifested the alienhand sign. We suggest that CJD should beincluded in the diVerential diagnosis ofdiseases which present with an alien hand.
Creutztfeldt-Jakob disease, one of thehuman prion diseases, is characterised byrapidly progressive mental and motordeterioration.1 Involuntary movements occurin above 90% of the patients in the course ofthe disease, the most common beingmyoclonus.1 Other movement disordersrange from tremor to chorea, athetosis,dystonia, and hemiballism.1 We report on apatient with CJD who presented with an alienhand.
Alien hand is a rare and striking phenom-enon defined as “a patient’s failure to recog-nise the action of one of his hands as his own”.2
One of the patient’s hands acts as a stranger tothe body and is uncooperative. Thus, there isloss of feeling of ownership but not loss of sen-sation in the aVected hand. Originally de-scribed in callosal tumours,3 the aetiology ofalien hand also includes surgical callosotomy,4
infarction of the medial frontal cortex, occipi-totemporal lobe, and thalamus,1 5 infection,6
and corticobasal degeneration.5 7
A 70 year old, right handed Jewish manborn in Argentina, living in Israel for the past20 years, was admitted to the NeurologyDepartment. Until a month before hisadmission, he was apparently healthy andhelped in the accounting oYce of the villagewhere he lived. His neurological illness hadpresented insidiously during the past monthwith unsteadiness of gait and frequent falls.He also manifested behavioural changes,became aggressive, and had visual hallucina-tions, perceiving insects and mice movingthrough his visual field. Often, he expressedhis fear from seeing that the “ceiling was
Table 1 Laboratory and neuropsychological results at presentation (A) and at 12 month follow up (B)
Laboratory (units) A B
Full blood count Normal NormalErythocyte sedimentation rate 12 6Urea and electrolytes Normal NormalLiver function tests Normal NormalAntinuclear antibody Negative NegativeB12 and folate Normal Not testedVDRL Negative Not testedThyroid stimulating hormone (mU/l) 58.4 0.87Free T4 (pmol/l) 7.4 Not testedAntithyroid microsomal antibody titres 1:25600 1:1600Psychometric (normal/predicted range):
Folstein MMSE (>24) 25/30 25NART IQ 10th percentile 18th percentileWAIS-R (verbal) 13th percentile Not testedWAIS-R (performance) 27th percentile Not testedFAS verbal fluency (>30) 25 23Cognitive estimates test (<6) 10 11Graded naming test (>15) 10/30 16/30Digit span forwards (>5) 7 6Rey-Osterreith complex figure (copy) (36) 25.5 24Rey-Osterreith complex figure (recall) ( 30%) Not tested 75%
J Neurol Neurosurg Psychiatry 2000;68:100–126 103
on February 15, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.68.1.123g on 1 January 2000. D
ownloaded from

falling over him”. His wife mentioned bizarre,useless movements of his left hand whichwere present from the beginning of thedisease.
On admission, he was awake, brady-phrenic, and partially collaborative. His con-versation was often disrupted by hallucina-tions. The aVect was sad and he had partialinsight for his mental dysfunction. He wasdisoriented for time, place, and situation. Hecould understand speech and was able to fol-low oral instructions involving two consecu-tive components. Naming was preserved.Prominent dysgraphia and dyscalculia werenoticed. Immediate recall and short termmemory were severely disturbed, whereaslong term memory, especially for personal lifeevents, was relatively spared. Abstract think-ing was severely aVected. Bimanual move-ments, such as clapping, were extremely diY-cult.
The cranial nerves were normal as wereocular fundi. The motor examination showednormal force. Deep reflexes were symmetricand plantar responses were flexor. The rightarm had a dystonic posture. His gait wasataxic on a wide base.
At times, the left arm would spontaneouslyrise in front of the patient during speaking orwhile using his right hand. He was unaware ofthese movements until they were brought tohis attention. When questioned about theirpurpose, the patient denied that they werevoluntary. No grasping of either hand or footwas found. The patient had no corticalsensory loss.
The laboratory data including blood chem-istry, haematology, and sedimentation ratewere normal, as were folic acid, vitamin B12
concentrations, and thyroid function.Vene-real disease research laboratory and HIV testswere negative. The cerebrospinal fluid hadnormal content. Brain CT showed mildcerebral atrophy. An EEG showed severe dif-fuse slowing at admission. Within a week,repeated EEGs showed triphasic waves with aperiodic pattern of 1- 1.5 Hz.
During the next 2 weeks, the patient devel-oped myoclonic jerks. Severe dysphasia andcognitive decline were accompanied by con-fusion and aggression. He became grosslyataxic, and unable to walk and perform any ofhis daily activities even with help. Transferredto a chronic care hospital, he died few weekslater. Postmortem examination was not al-lowed.
This short fatal neurological disease mani-fested by fulminant dementia, myoclonicjerks, and extrapyramidal and cerebellar dys-function was strongly suggestive of CJD. Theperiodic EEG pattern reinforced this diagno-sis. Our patient’s alien hand was part of theotherwise characteristic clinical picture ofCJD, but it occurred early in the diseasecourse when no myoclonic jerks werepresent. We are aware of only one report ofalien hand in CJD. MacGowan et al8
described two patients with CJD with amyoclonic alien hand syndrome. In onepatient the left arm “was noted to havespontaneous movements which appearedpurposeful...wandered out of her view”. Inthe second, the alien limb performed com-plex actions such as unbuttoning her blouseand removing a hair pin. Although ourpatient had no myoclonus or pyramidal signswhen the alien hand appeared, in theirpatients it was associated with spontaneousor stimulus sensitive myoclonus, spastichemiparesis, and cortical sensory loss.
The literature seems to describe distinctforms of alien hand. All share the occurrenceof involuntary movements contrary to thepatient’s stated intent, but the types of move-ment diVer. In the callosal form, there arepurposeful movements of the non-dominanthand.9 In the frontal form, there is graspingand utilisation behaviour of the dominanthand.9 In the corticobasal degeneration, thereare aimless movements of either hand.5 7
When a consequence of tumorous or vascularpathology,9 alien hands can perform complexacts such as trying to tear clothes or undoingbuttons. The description by MacGowan et al8
has characteristics of the callosal form (espe-cially in patient 2). However, our casesuggests that the alien hand sign in CJD mayappear in a diVerent type, performing lesscomplex movements which resemble thosereported by Riley et al in corticobasaldegeneration.7 These authors described thealien limb as “ involuntarily rising and touch-ing the mouth and eyes” (patient 1). Thepatient thought that she “was powerless tostop this movement” and when directed tostop responded that “she can’t”. Anotherpatient’s left arm was at times “elevated infront of him”, while he was “unaware of thissituation until his attention was called to it”(patient 10).
Another related phenomenon coined as“arm levitation” was reported in progressivesupranuclear palsy. In these patients the arminvoluntarily raised and performed semi-purposeful movements.10
One common denominator between CJD,corticobasal degeneration, and progressivemultifocal leukoencephalopathy,6 in which analien hand sign has also been described, ismultifocality. In corticobasal degeneration, itwas proposed that more than one site isaVected or that a “release” phenomenonoccurs accounting for the aetiology of alienhand.7 In CJD, bilateral cortical damage tomotor areas might be the origin of their sub-sequent isolation and disconnection.
We suggest that CJD should be added tothe diVerential diagnosis of diseases present-ing with an alien hand with or without myo-clonus.
We are indebted to Professor Eran Zardel, Depart-ment of Physiology, University of California, LosAngeles, USA.
R INZELBERGP NISIPEANUS C BLUMENR L CARASSO
Department of Neurology, Hillel YaVe Medical Center,Hadera, Israel
Correspondence to: Dr Dr R Inzelberg, Depart-ment of Neurology, Hillel YaVe MedicalCenter, Hadera, 38100, Israelemail [email protected]
1 Brown P, Gibbs CJ, Rodgers-Johnson P, et al.Human spongiform encephalopathy: the Na-tional Institutes of Health series of 300 cases ofexperimentally transmitted disease. Ann Neurol1994;35:513–29.
2 Levine DN. The alien hand. In: Joseph AB,Young RR, eds. Movement disorders in neurologyand neuropsychiatry. Oxford: Blackwell, 1999:645–9.
3 Brion S, Jedynak CP. Troubles du transfertinterhemispherique. A propos de trois observa-tions de tumeurs du corps calleux. Le signe dela main etrangere. Rev Neurol 1972;126:257–66.
4 Bogen JE. The callosal syndromes. In: HeilmanKM, Valenstein E, eds. Clinical neuropsychology.2nd ed. New York: Oxford University Press,1985:295–338.
5 Doody RS, Jankovic J. The alien hand andrelated signs. J Neurol Neurosurg Psychiatry1992;55:806–10.
6 Berger JR, Concha M. Progressive multifocalleukoencephalopathy: the evolution of a diseaseonce considered rare. Journal of Neurovirology1995;1:5–18.
7 Riley DE, Lang AE, Lewis A, et al. Cortical-basal ganglionic degeneration. Neurology 1990;40:1203–12.
8 MacGowan DJL, Delanty N, Petito F, et al. Iso-lated myoclonic alien hand as the sole presen-tation of pathologically established Creutzfeldt-Jakob disease: a report of two patients. J NeurolNeurosurg Psychiatry 1997;63:404–7.
9 Feinberg TE, Schindler RJ, Gilson Flanagan N,et al. Two alien hand syndromes. Neurology1992;42:19–24.
10 Barclay CL, Bergeron C, Lang AE. Arm levita-tion in progressive supranuclear palsy. Neurol-ogy 1999;52:879–82.
Recurrent peripheral neuropathy in agirl with celiac disease
The involvement of the peripheral nervoussystem (PNS) in children with celiac diseaseis particularly rare. Furthermore, in bothchildren and adults with celiac disease,neurological complications are chronic andprogressive.1
We report on a 12 year old girl aVected byceliac disease, who on two separate occasionspresented with an acute peripheral neurologi-cal syndrome after accidental reintroductionof gluten in her diet.
This patient was born uneventfully tohealthy non-consanguineous parents with nofamily history of neurological or metabolicdiseases. At the age of 6 months she wasdiagnosed as having celiac disease accordingto the European Society of Paediatric Gastro-enterology and Nutrition (ESPGAN) crite-ria. Since then she was on a strict gluten freediet and was asymptomatic until the age of 10years when severe diarrhoea, vomiting, andabdominal pain manifested 6 days after theintake of corn flakes erroneously thought tobe gluten free. No previous infections hadbeen noticed. One week after the onset ofthese symptoms she experienced acute weak-ness and pins and needles sensation confinedto her legs. At that time her parents stoppedher intake of corn flakes on the suspicion thatthese were responsible for the symptoms.Despite this, symptoms worsened during thenext 2 days, confining her to bed.
At hospital admission, she was alert andmentally stable. Results of general physicalexamination were unremarkable. Neurologi-cal examination disclosed symmetric, pre-dominantly distal, weakness of the legs; theknee jerks and ankle reflexes were depressed;plantar reflexes were flexor. Distal stockingglove decreased in pin prick and temperaturewith sparing of propioception and lighttouch. Coordination tests were normal.
Laboratory investigations showed a whitecell count of 9300/mm3. The results of thefollowing investigations were within thenormal limits: haemogram, erythrocyte sedi-mentation rate, serum urea, nitrogen, electro-lytes, creatinine, glucose, transaminase, bi-lirubin, immunoglobulins (Igs), lead, iron,copper, urinalysis, urinary porphyrin, folicacid, and vitamins A, B1, B6, B12, and E. Anti-bodies to Campylobacter jejuni, neurotropicantivirus antibodies, specific and non-specificorgan autoantibodies, IgA and IgG antiglia-din antibodies (AGAs), IgA antiendomesiumantibodies (EMAs), and IgA antireticulumantibodies (ARA), assayed by enzyme linkedimmunoadsorbent assay (ELISA) and im-munofluorescence (IF) were also negative.Lumbar puncture was not performed. Anti-bodies against gangliosides GM1 and GQ1b,myelin associated glycoprotein and myelin
104 J Neurol Neurosurg Psychiatry 2000;68:100–126
on February 15, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.68.1.123g on 1 January 2000. D
ownloaded from

basic protein were not tested. Nerve conduc-tion studies were consistent with a predomi-nately motor demyelinating peripheral neu-ropathy (table). Her symptoms improvedspontaneously and she was discharged homeafter 2 weeks. For 2 years she was asympto-matic on a gluten free diet.
At the age of 12 she presented acutely withsevere abdominal pain 8 days after a weeklyintake of bread meant to be gluten free. Twoweeks later, due to persisting gastrointestinalsymptoms, her parents excluded the breadfrom her diet. After 2 further weeks, while theabdominal pain was gradually improving, shehad a new episode of acute weakness in thelower limbs and sensory abnormalities in-cluding burning paraesthesiae. On neurologi-cal examination the legs showed markeddiminution in muscle power; absent deeptendon reflexes, and a reduction in pain andtemperature; light touch, perception of posi-tion, and vibration were preserved. Walkingwas impaired and the patient was bedridden.Otherwise the examination was normal.
A haemogram showed white cell counts of9700/mm3. Laboratory investigations werewithin normal values as in the past. IgA andIgG AGA, IgA EMA, and IgA ARA assayedby ELISA and IF were again negative. Nerveconduction studies confirmed the presence ofa predominantly motor demyelinating neu-ropathy (table). The parents refused consentfor a lumbar puncture or nerve biopsy.
Over the next 2 weeks her neurological dis-abilities spontaneously improved until fullrecovery was complete. After 4 weeks, AGA,EMA, and ARA were still negative.
On her most recent admission, 1 year afterthe onset of her first neurological symptoms,she is still on a strict gluten free diet and hasno residual symptoms or signs.
The natural history of celiac disease is wellknown and the typical celiac enteropathy isoften associated with several other disorders.However, as celiac disease is a relatively com-mon and lifelong condition, it is likely thatsome of these associations may occur bychance.
This patient, who was diagnosed as havingfrank celiac disease at the age of 6 months,experienced two episodes of acute peripheralneuropathy, at the age of 10 and 12 years,respectively. Two major pieces of evidencestrongly support the assumption of a glutenderived disease: (1) the episodes occurred onboth occasions when gluten was accidentallyreintroduced in the diet; and (2) the responseto a gluten free diet was reasonably rapid,occurring within weeks.
The present case, however, diVers clinicallyfrom those with neurological involvement pre-viously reported. In the paediatric age group,
in fact, neurological complications of celiacdisease are rarely encountered and are mostlyconfined to the CNS2: to the best of ourknowledge, there are only two previouslyreported cases of PNS involvement in childrenwith celiac disease. In both cases, however,these were chronic axonal polyneuropathiespresenting during a gluten free diet.3 4
In both episodes in the present case neuro-physiology was strongly supportive of ademyelinating peripheral neuropathy, whichis most commonly attributed to a directimmune mediated attack to the myelin. Bycontrast, wallerian and axonal degenerationmay be caused by vasculitis, and nutritional,metabolic, and toxic factors.
An autoimmune pathogenesis in associ-ation with strong evidence of a geneticsusceptibility has been proposed for celiacdisease. Although it is well established thatAGA, EMA, and ARA are reliable indicatorsof sensitisation to gluten at least at the time ofdiagnosis, in the clinical practice at follow up,during a gluten challenge, pathological valuesof these antibodies may not be detected.5 Inthe present case the time course of the diseasemight be suggestive of an antibody mediatedresponse. However, we could not detectpathological concentrations of AGA, EMA,or ARA antibodies either during the course ofthe disease or at follow up.
It is known that in celiac disease manyimmunological perturbations can occur out-side the gastrointestinal tract. Crossing of theantigens through a damaged small intestinalmucosa, deposition of immune complexes intarget organs, a reduction in immune surveil-lance, mechanism of molecular mimicry, andactivated T cell response may contribute tothe pathogenesis of the diseases associatedwith celiac disease. Direct toxic eVects ofgliadin and vitamin deficiency are other pos-sible pathogenic mechanisms of damage tothe nervous system. Although we ruled out avitamin deficiency it is still questionablewhether a toxic neuropathy can be the case.
In conclusion, this case shows two majorissues: an acute polyneuropathy can be acomplication of celiac disease in childhoodand its benign course could help in theunderstanding of the underlying pathogenicmechanisms.
We are grateful to Professor Angela Vincent(Oxford) for her helpful suggestions in reviewing themanuscript.
AGATA POLIZZIMARIA FINOCCHIARO
ENRICO PARANOPIERO PAVONE
Division of Paediatric Neurology, Department ofPaediatrics, University of Catania
Catania, Italy
SALVATORE MUSUMECIDepartment of Paediatrics, University of Sassari,
Sassari, Italy
AGATA POLIZZINeurosciences Group, Institute of Molecular Medicine,
Department of Clinical Neurology, University ofOxford, Oxford, UK
Correspondence to: Dr Agata Polizzi, Division ofPaediatric Neurology, Department of Paediatrics,University of Catania, Viale A Doria 6, 95125Catania, Italy email: [email protected]
1 Cooke WT, Thomas Smith W. Neurologicaldisorders associated with adult coeliac disease.Brain 1966;89:683–722
2 Gobbi G, Bouquet F, Greco L, et al. Coeliacdisease, epilepsy and cerebral calcifications.Lancet 1992;340:439–43
3 Papadatou B, Di Capua M, Gambarara M, et al.Nervous system involvement in paediatric coe-liac patients. In: Mearin ML, Mulder CJJ, eds.Coeliac disease. Dordrecht: Kluwer Academic,1991:199–203.
4 Simonati A, Battistella PA, Guariso G, et al.Coeliac disease associated with peripheral neu-ropathy in a child: a case report. Neuropediatrics1998;29:155–8
5 Bottaro G, Sciacca A, Failla P, et al. Antigliadinantibodies in the various stages of coeliacdisease in children. Pediatr Med Chir 1988;10:409–13
Frontal release signs in older peoplewith peripheral vascular disease
A growing body of research examiningneurological aspects of clinically “silent” cer-ebrovascular disease suggests that neurologi-cal signs indicative of generalised organicbrain damage may occur in the absence ofcompleted stroke.1 These soft signs includeprimitive reflexes (frontal release signs), rep-resenting an anatomical and functional deaf-ferentation of cortical from subcortical struc-tures. Primitive reflexes are known to occur ina wide variety of dementias, includingAlzheimer’s disease2 and vascular dementia.3
It is likely that the presence of undetectedcerebrovascular disease accompanying pe-ripheral vascular disease is underestimated,as peripheral vascular disease is known to bea risk factor for transient ischaemic attacks. Astudy assessing 373 older patients withperipheral vascular disease found that 72 ofthe 144 patients who had not experienced atransient ischaemic attack or stroke werefound to have a degree of carotid stenosis ofbetween 60% and 99%.4
In the present study, the prevalence ofprimitive reflexes was examined in older peo-ple with peripheral vascular disease and anon-vascular control group. Independentpredictors of these reflexes were also exam-ined in peripheral vascular disease. Bothgroups were drawn from the same geographi-cal area. All were interviewed and examinedoutside hospital by myself. Interviewees werecommunity residents from the catchmentarea of an inner city London teaching hospi-tal.
Twenty five consecutive non-amputees onthe waiting list for femoropopliteal bypassoperation were compared with 25 postopera-tive patients who had undergone elective hipor knee replacement and a period of inpatientrehabilitation. All participants were aged 65and over at the time of interview. Patientswith peripheral vascular disease all had clini-cal and Doppler proved evidence of periph-eral ischaemia. Controls were interviewedbetween 6 months and 1 year after theiroperation. Both groups had no history ofstroke or transient ischaemic attack.
A more detailed description of instrumentsis provided elsewhere.1 All subjects were
Electrophysiological study suggestive in both episodes of an acute demyelinating peripheral neuropathyconfined to the lower limbs. Values were within normal limits in the upper limbs
1st Episode 2nd Episode
Peroneal LR Tibial L
R Peroneal LR Tibial L
R
MCV (ms) 26 27 22 2424 28 20 23
DL (ms) 7.3 8.0 7.2 8.87.5 8.4 7.0 9.0
F wave latency (ms) 70 72 83 84CMAP (µV) 3 2.7
Sural LR Sural L
R
SCV (ms) 38 4042 41
AMP (µV) 16.2 17.416.8 18
MVC=motor conduction velocity; DL=distal latency; CMAP=compound motor action potential;SCV=sensory conduction velocity; AMP=amplitude; L=left; R=right.
J Neurol Neurosurg Psychiatry 2000;68:100–126 105
on February 15, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.68.1.123g on 1 January 2000. D
ownloaded from

examined using a rating scale for theexamination of frontal release signs (FRSS),with nine operationally defined items, eachon a seven point semiquantitative scale. Thenine reflexes were paratonia and palmomen-tal, hand grasp, foot grasp, glabellar, rooting,snout, and visual/tactile sucking reflexes.Neuropsychological measures included theassessment of frontal lobe function (trailmak-ing tests A and B, behavioural dyscontrolscale, and the controlled word associationtest) and generalised cognitive impairment(CAMCOG). Depression was assessed usingthe Hamilton rating scale for depression, 15item geriatric depression scale, and diagnos-tic criteria for DSM IV major depressive dis-order. Family history of depression, wish todie, and suicidal ideation within the past yearwere also recorded, as were blood pressureand a checklist for chronic physical illness.
Total FRSS scores and scores on FRSSsubscales were compared between groupsusing the Mann-Whitney U test for inde-pendent samples. In the peripheral vasculardisease group, a correlation matrix for totalFRSS score against DSMIV depression,CAMCOG score, behavioural dyscontrolscale score, verbal fluency score (totalnumber of words beginning with F, A, and S)and trailmaking test times was examinedusing the Spearman correlation coeYcient,controlling for age, sex, blood pressure, andchronic physical illness. Behavioural dyscon-trol scale scores, trailmaking A/B test times,and verbal fluency scores were first convertedinto binary variables according to whetherthey were at/above or below the median valuefor the group. CAMCOG score was dividedinto subjects scoring 69 or above or less than69. Those associations with a two tailedsignificance of 0.1 or less were then enteredinto a linear regression equation using thestepwise method.
Patients with peripheral vascular diseasehad a higher mean score on the frontal releasesigns scale than controls (5.8 (SD 4.6) v 1.7(SD 1.9)) (Mann-Whitney U=144.500,Z=−3.33, two tailed p=001), as well as onglabellar and rooting reflexes (table). Onlyone variable (trailmaking B test time) wasentered into the equation; this accounted for23% of the variance in FRSS score (B=4.6,95% confidence interval (95% CI) (B)1.3–8.0, p=0.01).
In peripheral vascular disease, there is lim-ited information available concerning theintellectual and neurological sequelae ofcoexisting cerebrovascular disease. Phillips etal found greater impairment in psychomotorspeed and abstract reasoning in patients withperipheral vascular disease than age/sexmatched controls, with less significant diVer-ences between the groups in verbal fluency,concentration, abstract thought, perception,and constructional skills.5 Another study bythe same group found poorer performance inpatients with peripheral vascular disease thancontrols on visual memory, trailmaking Btest, and visuospatial skills. Patients withperipheral vascular disease were also equallyimpaired in these areas compared with amatched group of stroke patients.6
Small numbers of patients, which may alsohave obscured other significant findingsbetween the two groups, limit the presentstudy. However, there is some evidence thatclinically relevant cerebrovascular diseasemay accompany peripheral vascular diseaseand that concomitant disruption of frontal/subcortical brain function may not presentwith hard neurological signs. As it is possiblethat silent brain infarction was present inpatients with peripheral vascular disease, fur-ther studies incorporating brain imaging arerequired before there can be a clearer under-standing of the relation between peripheraland central vascular pathology.
I thank Dr Robert Howard for supervision of thisstudy and Professor Stephen Jackson and Mr PaulBaskerville for allowing me to interview patientsunder their care. The study was carried out as partof a University of London MD thesis.
RAHUL RAODepartment of Old Age Psychiatry, Maudsley Hospital
and Institute of Psychiatry, London
Correspondence to: Dr Rahul Rao, Department ofOld Age Psychiatry, Guy’s, King’s, and St ThomasMedical School, Job Ward, Thomas Guy House,Guy’s Hospital, St Thomas Street, London SE19RT, UK email [email protected]
1 Rao R, Jackson S, Howard R. Primitive reflexesin cerebrovascular disease: a community studyof older people with stroke and carotid stenosis.International Journal of Geriatric Psychiatry (inpress).
2 Burns A, Jacoby R, Levy R. Neurological signsin Alzheimer’s disease. Age Ageing 1991;20:45–51.
3 Vreeling FW, Houx PJ, Jolles J, et al. Primitivereflexes in Alzheimer’s disease and vasculardementia. Journal of Geriatric Psychiatry andNeurology 1995;8:111–17.
4 Alexandrova NA, Gibson WC, Norris JW, et al.Carotid artery stenosis in peripheral vasculardisease. J Vasc Surg 1996;23:645–9.
5 Phillips NA, Mate-Kole CC, Kirby RL. Neuro-psychological function in peripheral vasculardisease amputee patients. Arch Phys Med Reha-bil 1993;74:1309–14.
6 Phillips NA, Mate-Kole C. Cognitive deficits inperipheral vascular disease. A comparison ofmild stroke patients and normal controlsubjects. Stroke 1997;28:777–84.
Factitious clock drawing andconstructional apraxia
A 45 year old man presented with a 1 dayhistory of headache, possible seizures, andleft sided weakness. On the day of presenta-tion the patient’s wife had twice found him,inexplicably, on the floor. After the secondsuch episode she brought him to hospital forevaluation. Examination disclosed a com-plete left hemiplegia and hemianaesthesia,although muscle tone was documented to benormal and the plantar responses downgoingbilaterally. Brain CT was normal and routineblood examination was unremarkable. Therewere no further seizure-like episodes andthe patient was transferred to this hospital10 days later, hemiplegia unchanged, forpossible angiography and further investiga-tions.
He was an exsmoker with hypercholestero-laemia and peripheral vascular disease whichhad been treated by a left femoral angioplasty
5 years earlier. The angioplasty was compli-cated by the occurrence of a seizure, thoughtto be related to dye injection, and phenytoinhad been prescribed for a short time thereaf-ter. There was a remote history of heavy alco-hol use, but he had been abstinent for severalyears. His father had had a stroke at the age of65.
Six months earlier the patient had also col-lapsed at home and been taken to hospitalwith a left hemiplegia. Brain CT at that timewas normal, as were carotid Doppler studiesand an echocardiogram. During that admis-sion to hospital, several generalised seizure-like episodes were seen, some with retainedconsciousness, and he had again been startedon phenytoin therapy. A follow up outpatientbrain MRI was normal and it was concludedthat the hemiplegia was non-organic inorigin. He was described to have made agradual, near complete, recovery from thisfirst hemiplegic episode and was scheduledfor an imminent return to work at the time ofhis relapse.
On transfer to this hospital the patient wasalert, oriented, and cooperative. Although upto date on current aVairs and able to describethe investigations performed at the transfer-ring hospital, he scored only 23/30 on a minimental state examination, with absent threeword recall, impaired registration, and poorcopying of a two dimensional line drawing.Further bedside neuropsychological testingshowed other findings indicative of construc-tional apraxia and left hemineglect. Specifi-cally, when asked to draw a clock with thetime at 10 minutes to 2 o’clock, all the num-bers, and the clockhands, were placed on theright hand side of the clock outline (figure A).Copying of three dimensional line drawingswas also significantly impaired (figure B).When asked to bisect a line, however, thepatient did so only minimally to the right ofthe midpoint (58% of the distance from theleft side).
Cranial nerve examination suggested anincongruent and inconsistent left hemianop-sia to confrontation testing but was otherwisenormal, including bilaterally symmetric op-tokinetic nystagmus. Motor examinationshowed paralysis of the left arm and leg, withbilaterally symmetric bulk, tone, and deeptendon reflexes. The plantar response wasflexor bilaterally. Sensory examinationshowed decreased pinprick and absent lighttouch, joint position sense, and vibrationsense on the entire left side. There was alsoimpaired perception of a tuning fork’svibration on the left side of the forehead, witha distinct demarcation in the midline. Therest of the physical examination was unre-markable.
Brain CT and MRI, CSF examination, androutine EEG were normal. Routine haemato-logical and metabolic analyses plus erythro-cyte sedimentation rate, serum lactate, pro-thrombin time/partial thromboplastin time,fasting serum glucose, HbA1c, serum Ig sur-vey, and thyroid stimulating hormone were allwithin normal limits. A hypercoagulabilityprofile was negative. A lipid profile showedmild hyperlipidaemia with increased low
Table 1 Primitive reflexes in patients with peripheral vascular disease (n=25) and controls (n=25)
Hand grasp Foot grasp Glabellar Palmomental Paratonia Rooting Snout Sucking (tactile) Sucking (visual)
U 274.0 312.5 199.5 287.5 287.0 235.5 287.5 261.0 287.5pValue 0.15 1.0 0.001* 0.15 0.29 0.01* 0.44 0.08 0.30
*Higher mean score in people with peripheral vascular disease.
106 J Neurol Neurosurg Psychiatry 2000;68:100–126
on February 15, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.68.1.123g on 1 January 2000. D
ownloaded from

density lipoprotein (3.92 mmol/l) and triglyc-erides (4.30 mmol/l) and low high densitylipoprotein (0.73 mmol/l). Serum phenytoinconcentration was therapeutic at 74 µmol/l.An ECG was normal.
Ophthalmological consultation and formalvisual field testing demonstrated a concentri-cally constricted field of mild degree in theright eye and tunnel vision in the left eye.
The patient consented to overnight video-EEG monitoring and was seen on multipleoccasions to move his left arm and/or leg in anormal fashion, at one point using the leftarm to readjust his bed covers shortly afterarousal from sleep, before glancing briefly atthe video camera and completing the taskwith his right arm. The prolonged EEG wasnormal.
A formal neuropsychological assessmentperformed in hospital documented impairedattention, concentration, and workingmemory, as well as several atypical calcula-tion and spelling errors, the second involvingunusual “near miss” letter substitutions orreversals (for example, “anixety”, “excecu-tive”). The formal testing identified noconsistent evidence of visuospatial deficits orconstructional apraxia. The findings wereinterpreted as inconsistent with the patient’shistory but the possibility of a factitious aeti-ology was not specifically addressed—that is,tests designed to detect malingering duringneuropsychological testing1 2 were not admin-istered by the examiner, who had not beeninformed at the time of consultation of thepresumptive neurological diagnosis of malin-gering or factitious disorder.
No further investigations were performedand the patient was transferred via the origi-nal hospital to a rehabilitation facility andsubsequently discharged to home. Con-fronted with the findings of the videomonitoring the patient appeared sanguineand accepting of the evidence that he shouldbe able to move his left side. Six months laterhe was ambulatory but otherwise not signifi-cantly improved. He had been assessed by apsychiatrist but had refused psychiatric fol-low up, electing instead to be followed up bya psychologist. He understood his diagnosisto be “conversion disorder” and reported thathe was actively collecting information on thesubject via the internet.
Outpatient brain SPECT and visual andsomatosensory evoked potentials performed1 year after discharge demonstrated no hemi-spheric abnormalities. The patient remained
oV work and was receiving disability funding.He walked with a limp favouring his left sideand complained of persistent decreasedsensation on the left side. Forced choice sen-sory testing of finger and arm movement onthe left3 demonstrated performance to beworse than chance (68% wrong choices).Motor bulk, tone, and reflexes were symmet-ric and plantar responses downgoing. Hedrew a clock normally at the 1 year follow up.
The clinical and laboratory findings de-scribed above indicate beyond any doubt thenon-organic nature of this patient’s lefthemiplegia/hemianaesthesia. His seizure-likeepisodes at presentation are presumed tohave been non-epileptic in origin (as hadbeen suspected during his previous admissionto hospital) although this cannot be defini-tively proved.
The inability to copy line drawings or todraw a clock is, from a neurologist’s perspec-tive, typically associated with parietal lobedysfunction, usually of the non-dominanthemisphere, especially if associated with lefthemispatial neglect.4 To our knowledge, thisis the first reported case of factitious clockdrawing and constructional apraxia. Bedsidemental status testing also demonstrated themore common simulated deficits of impairedattention and absent three word recall.1 Inretrospect, the severe neglect on clockdrawing was perhaps “too good to be true”,especially in the light of the near normal linebisection demonstrated on the same day. Themirror image distortion of the house was alsovery unusual and, furthermore, the mirrorreversal itself is evidence of lack of clinicalneglect. The distortion of the cube, however,could easily be misinterpreted as evidence oforganic constructional impairment if seen inthe absence of the other relevent clinical andlaboratory information.
During follow up, the patient admitted tofeeling tremendous occupation relatedstresses, and described how he had come toboth fear and detest his job. Given the clearbenefit to the patient of removal from hiswork environment, the relapse of his symp-tomatology just as he was scheduled forreturn to work after his first non-organichemiplegic episode, and the intentionalityrequired to feign poor clock drawing andconstructional apraxia, there is much to sup-port a diagnosis of malingering.5
Nevertheless, classification as a factitious dis-order is at least as justifiable in view of the
patient’s willingness to undergo medicalinvestigations, including video monitoring.
It is unclear how or when the patientacquired the information needed to mimic aconstructional apraxia. Previous bedsideneuropsychological evaluations may haveserved to familiarise him with the format ofsuch testing, acting as an impetus to researchthe issue of stroke and focal brain deficits(which might also have occurred after hisfather’s stroke), much in the same way he isnow researching conversion disorder, therebydiscovering what expected answers shouldlook like. Despite repeated questioning, how-ever, no evidence could be gathered from thepatient to support this speculation.
I KHANI FAYAZ
Division of Neurology
J RIDGLEYDivision of Neuropsychology
R WENNBERGDepartment of Medicine, Division of Neurology, TheToronto Hospital, University of Toronto, Toronto, ON,
Canada
Correspondence to: Dr R Wennberg, EC8–022,The Toronto Hospital, 399 Bathurst Street, To-ronto, Ontario, Canada M5T 2S8. Telephone 001416 603 5402; fax 001 416 603 5768.
1 Bernard L, Houston W, Natoli L. Malingeringon neuropsychological memory tests: potentialobjective indicators. J Clin Psychol 1993;49:45–53.
2 Prigatano G, Amin K. Digit memory test:unequivocal cerebral dysfunction and sus-pected malingering. J Clin Exp Neuropsychol1993;15:537–46.
3 Pankratz L, Binder L, Wilcox L. Evaluation ofan exaggerated somatosensory deficit withsymptom validity testing. Arch Neurol 1987;44:798.
4 Strub R, Black W. Constructional ability. In:Strub R, Black W. The mental status examinationin neurology. Philadelphia: FA Davis, 1985:101–23.
5 American Psychiatric Association. Diagnosticand statistical manual of mental disorders. 4th ed,revised. Washington: American PsychiatricAssociation, 1994.
Anosognosia and mania associated withright thalamic haemorrhage
Both anosognosia and secondary mania areassociated with right hemispheric lesions.These two non-dominant syndromes, how-ever, are rarely described as occurringtogether. We present a patient with a rightthalamic haemorrhage giving rise to pro-found denial of hemiplegia and elated mood.This case suggests mechanisms for thecommon production of mania and anosogno-sia.
A 53 year old, right handed, black man,with a history of alcohol misuse and depend-ence and untreated hypertension, wasbrought to the emergency room a few hoursafter developing an intense headache and leftsided numbness and weakness.
On admission he was described as “bellig-erent,” “agitated,” and “confused.” Bloodpressure was 240/160. Neurological exam-ination disclosed left lower facial droop,decreased left corneal and gag reflexes, andleft hemiparesis with dense sensory deficits.With increasing obtundation, the patient wastransferred to the intensive care unit andintubated. Brain MRI showed a large, rightsided, hyperacute thalamic bleed with masseVect and oedema. The patient was extu-bated 2 days later and 4 days after the strokehe was described as being drowsy andinattentive, but was able to answer questions
(A) Asked to: “put all the numbers on a clock and make the time ten to two”. (B) Patient’s copies (atright) of three dimensional line drawings. Top: common constructional distortion of cube. Bottom:unusual mirror image representation of house.
A B
J Neurol Neurosurg Psychiatry 2000;68:100–126 107
on February 15, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.68.1.123g on 1 January 2000. D
ownloaded from

appropriately. Neurological examinationshowed contralateral gaze preference, supra-nuclear vertical gaze palsy, diYculty converg-ing, left sided flaccid hemiparesis, and dense,left sided hemianaesthesia. Deep tendonreflexes were absent on the left and Babinski’sreflex was present on the left. In addition,visual extinction and neglect were present.
At the time of onset of right sided weaknessthe patient insisted that he was “fine,” and anambulance was called over his objections.After being extubated, the patient acknowl-edged that he had had a stroke, but, despitehis hemiparesis, insisted that he was ready togo home and go back to work. His belief in hisability to walk led to near falls, and he wasmoved to a room nearer to the nurses’ stationfor closer observation. He told the nurses thatsomeone else’s arm was in his bed. On oneoccasion, holding up his left arm with hisright, he told the nurse to, “take it away; itkeeps scratching me.” That the left arm“smelled funny” was another reason hewanted the nurses to take it away.
Four weeks after the stroke he firstacknowledged that his left arm belonged tohim. He spontaneously recalled believingotherwise. By this time he had a moderatehemiplegia and recognised “a little weak-ness,” but continued to insist that he was welland able to return to work. By the 6th weekafter stroke the patient more consistentlyacknowledged that he was weak on the leftside of his body. A request for disabled hous-ing “so that I won’t be a burden to my family”seemed to indicate an appreciation of hisimpairment, but this insight was fleeting;within an hour of making such statements thepatient might insist that after a week’sexercise he would be ready to return to work.His awareness of his hemiplegia fluctuatedfor 8 weeks after stroke before becomingfixed, but remained shallow after 12 weeks; heno longer planned to return to work andapplied for social security disability insurance“because they say I’m disabled.”
The patient’s mood was remarkably cheer-ful and optimistic. A week after the stroke hewas noted to praise extravagantly the hospitalfood, and the nurses found him “talkative.”When he arrived on our ward 11 days afterthe stroke he was flirtatious with female staVand boasted of having fathered 64 children.His girlfriend was surprised when he kissedher in front of the staV because he had neverpublicly displayed aVection before. He re-ported excellent energy and expansivelyinvited all of the staV to his home for thanks-giving. Sleep was not disrupted or reducedand he had a good appetite. When beginningto acknowledge his left sided weakness, heremained blissfully unconcerned. He scored31 points on a mania rating scale,1 which waswell in the manic range. The mania resolvedgradually over a 10 week period after stroke.
Other than alcoholism, the patient had nohistory of psychiatric illness and there was nofamily history of psychiatric illness. Thepatient had not seen an physician in manyyears. Visual acuity was found to be reducedto 20/800 in both eyes on the basis of hyper-tensive retinopathy.
Evaluation 1 month after stroke showedmany deficits and a few strengths. Inattentionto the left hemispace was marked. By 2months after stroke he no longer extinguishedto double simultaneous stimulation, but,although he could see to the left, was stillmissing targets in his left visual hemifield.Visual integration, both with and without therequirement of construction, was severely
impaired. He was able to correctly recogniseand produce facial emotional information.Simple attention was intact, but attentionalcontrol (backward span and mental control)was impaired. Visuomotor tracking was slowand he had significant problems with concep-tual shifting (both auditory and visual). Lan-guage processing diYculties included verypoor reading ability, impaired confrontationnaming, and impaired performance on a ver-bal task of fluency and initiation. Auditorycomprehension was mildly impaired. Vo-cabulary scored formally in the borderlineimpaired range, as did abstract verbal reason-ing. On tests of praxis he demonstrated a ten-dency to use the hand as object. Memoryperformances were relatively intact. Hisinitial recall of two paragraphs scored for-mally within the low average range and after a30 minute delay, he was able to recall most ofthe information initially encoded, scoringformally within the average range.
Structural brain MRI on admission to theemergency room showed a large right tha-lamic hemorrhage with mass eVect andoedema, with oedema extending into the cer-ebral peduncle with internal susceptibilityconsistent with deoxyhaemoglobin. Alsopresent was increased T2 signal bilaterally infrontal areas consistent with ischaemicchanges. Brain CT 30 days after strokeshowed, in addition to the thalamic lesion,moderate cerebellar atrophy and mild tomoderate prominence of the frontal corticalsulci compatible with cerebral atrophy.
Structural MRI performed 44 days afterthe stroke showed a 2 cm right thalamic hae-matoma. Functional MRI2 performed thesame day demonstrated a 2 cm area of absentcerebral blood volume at the posteriormargin of the right thalamus without any evi-dence of decreased cerebral blood volumewithin the right parietal, frontal, or temporalcortex.
This is a case of anosognosia of hemiplegiaand mania co-occurring in a patient with alarge right thalamic haemorrhage. Althoughanosognosia and mania are not generallythought of as occurring together, whenBabinski3 introduced the term anosognosiahe used as one of his examples a case in whichthe patient, though not confused, was “a littleoverexcited,” and in a later paper he pre-sented a case4 in which there was “a certainagitation, which expresses itself by exagger-ated loquacity, a decrease in attention, and atendency to erotic ideas.” Weinstein andKahn5 noted that euphoria was common inpatients with anosognosia. Moreover, al-though Cutting6 emphasised that apathy isthe mood more usually associated withanosognosia, 10% of his patients with ano-sognosia were described as having “euphoricmood.”
Right sided thalamic lesions are known toproduce both anosognosia and mania, but therelation of each to the pathology is unclear.Only some of the patients with right hemi-spheric lesions are manic or agnosic. Thesetwo syndromes may be related to dysfunctionof diVerent neural networks and only occurtogether when a disease process aVects bothnetworks.
Another possibility is that these syndromesare aetiologically related. Could anosognosiabe a manifestation of mania? Although it iseasy to conceive how elevated mood mightfacilitate anosognosia of hemiplegia (or othertypes of anosognosia), it is diYcult to explainthe presence of denial of ownership anddislike of the left arm (other anosognosic
phenomena) on the basis of euphoria.Moreover, Starkstein et al,7 finding that simi-lar frequencies and severities of major andminor depression were present in patientswith and without anosognosia, suggest that aparticular mood state may not necessarilyinfluence insight.
Several explanations have been proposedto explain the phenomenon of anosognosia.8 9
All the models invoke dysfunction of the cer-ebral cortex, especially the parietal cortex. Itis interesting that in this case functional MRIfailed to demonstrate decreased CBV in theparietal lobe.
In summary, we present a case of maniaaccompanying anosognosia in a patient with aright thalamic haemorrhage. The coexistenceof mania and anosognosia may be more com-mon than previously appreciated. The associ-ation with anosognosia implies that themechanisms implicated in the pathogenesisof secondary mania may be similar to those ofanosognosia. The absence of evidence ofabnormal parietal, temporal, or frontal lobefunction by functional MRI in this case isintriguing.
ELIZABETH LIEBSONDepartment of Psychiatry, Tufts, New England
Medical Center, 750 Washington Street, Box 1007,Boston, MA 02111, USA. Telephone 001 617 636
1633; email [email protected]
1 Bech P, Kastrup M, Rafaelsen OJ. Mini-compendium of rating scales for states of anxi-ety, depression, mania, schizophrenia, withcorresponding DSM-III syndromes: maniascale. Acta Psychiatr Scand 1986;73(suppl236):29–31.
2 Belliveau J. Functional cerebral imaging by sus-ceptibility contrast NMR. Magn Reson Med1990;14:538–546.
3 Babinski J. Contribution a l’etude des troublesmentaux dans l’hemeplegie organique cereb-rale. Rev Neurol 1914;22:845–8.
4 Joltrain E. Un nouveau cas d’anosognosie. RevNeurol 1924:638–40.
5 Weinstein EA, Kahn RL. The syndrome of ano-sognosia. Arch Neurol Psychiatry 1950;64:772–91.
6 Cutting J. Study of anosognosia. J Neurol Neuro-surg Psychiatry 1978;41:548–55.
7 Starkstein SE, FedoroV JP, Price TR, et al. Ano-sognosia in patients with cerebrovascularlesions: a study of causative factors. Stroke1992;23:1446–53.
8 Ellis SJ, Small M. Denial of illness in stroke.Stroke 1993;24:757–9.
9 Heilman KM. Anosognosia: possible neuro-psychological mechanisms. In: Prigatano GP,Schacter DL, eds. Awareness of deficit after braininjury. New York: Oxford University Press,1991:53–62.
Epileptic cardiac asystole
A patient is reported on with habitualepisodes of collapse and loss of consciousnessassociated with EEG evidence of focalepileptiform discharges. Simultaneous ECGrecordings disclosed 25 seconds of cardiacventricular asystole occurring 24 secondsafter the onset of electrical seizure activity.After changes to antiepileptic medication andthe insertion of a permanent cardiac pace-maker he has had no further episodes. Incases of epileptic cardiac dysrhythmia, iso-lated EEG or ECG recording may proveinsuYcient and prolonged simultaneousEEG/ECG monitoring may be required.
Cardiac arrhythmias subsequent to epilep-tic seizures have been recognised for morethan 90 years. They provoke diagnosticconfusion and may be a mechanism ofsudden unexplained death in epilepsy.Whereas sinus tachycardia was noted toaccompany more than 90% of epilepticseizures, isolated bradycardia was seen much
108 J Neurol Neurosurg Psychiatry 2000;68:100–126
on February 15, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.68.1.123g on 1 January 2000. D
ownloaded from

less commonly (only 1 of 74 seizuresrecorded).1 A review in 1996 of the “ictalbradycardia syndrome” showed only 15documented cases in the literature of eitherbradycardia or asystole associated withseizures.2 Most patients had temporal lobeseizures. The longest duration of asystolepreviously reported is in a 17 year old manwith temporal lobe epilepsy who sustained a22 second pause in cardiac output. More
typically the asystolic periods in documentedcases are in the region of 5–10 seconds.2
Shorter duration asystole may not compro-mise cerebral function suYciently to causeloss of consciousness. Implantation of acardiac pacemaker is advocated but does notensure that lapses of consciousness are elimi-nated if these are directly related to theseizure rather than to the secondary asystole.We report on a patient with epileptic cardiac
asystole of 25 seconds duration demonstratedby prolonged simultaneous EEG/ECG moni-toring which responded well to pacemakerinsertion.
A previously well 34 year old right handedbuilder was referred with a 1 year history offortnightly episodes of loss of consciousness.There was no associated warning, aura, chestpain, or palpitations and the patient was onlyaware of the episode once consciousness was
16 Channel ictal EEG (eight channels illustrated with ECG) showing electrographic seizure onset and subsequent bradycardia and asystole.
Gain
Paper speed : 1.34 cm/s
Filter setting : Lf : 35 Hz
3
4
T5 T6
2
1
A
F8-T4
T4-T6
F7-T3
T3-T5
T4-C4
C4-Cz
Cz-C3
C3-T3
EKG
Time : 07:04:34
BF8-T4
T4-T6
F7-T3
T3-T5
T4-C4
C4-Cz
Cz-C3
C3-T3
EKG
Time : 07:04:58
C
F8-T4
T4-T6
F7-T3
T3-T5
T4-C4
C4-Cz
Cz-C3
C3-T3
EKG
Time : 07:05:21
T4C4CZC3T3
8 7 6 5
F8F7
J Neurol Neurosurg Psychiatry 2000;68:100–126 109
on February 15, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.68.1.123g on 1 January 2000. D
ownloaded from

restored and he found himself lying on thefloor. On recovery there was no confusion,drowsiness, dysphasia, or diuresis. Often,however, he sustained soft tissue injuries tohis face and scalp.
Witnesses reported that the patient would,without warning, suddenly collapse to theground where he would remain unrousable,inaccessible, and motionless for 90 to 120seconds. On two occasions he appeared con-fused and disorientated immediately before acollapse. During the period of unconscious-ness he would demonstrate no involuntarymovements, orofacial automatisms, or cyano-sis but he would become pale and “ashen”while staring straight ahead with a glazedlook. On resolution of the episode his colourwould return to normal and within 2 minuteshe would have fully recovered. Unusuallyduring one reported episode of unconscious-ness he was seen to briefly extend the fingersof both hands.
He was admitted to his local hospital andCT, MRI, interictal EEG, and 24 hour ECGwere normal. No episodes were witnessedwhile he was an inpatient but they werethought to be epileptic in origin and thereforehe was started on phenytoin, with no benefit.Carbamazepine was added, again with mini-mal eVect.
The patient was then referred to theEpilepsy Assessment Centre of The NationalSociety for Epilepsy and National Hospitalfor Neurology and Neurosurgery for furtherinvestigation and management.
Cardiovascular and neurological examina-tion was normal, as were MRI and routineinterictal EEG. Sixteen channel ambulatoryEEG using an Oxford Instruments digitalEEG receiver was performed continuously for340 hours before an episode was captured.Interictally rare spikes were seen over the rightfrontocentrotemporal region during sleep. Theonset of the episode was not witnessed and thepatient was found lying on the floor, regainingconsciousness at about 07:06. The event EEGshowed a short run of bilateral semirhythmic2–3 Hz activity at 07:04:34 (figure A), persist-ing for 8 seconds before being obscured bymuscle and movement artefact. Twenty fourseconds after the first EEG change, at07:04:58, the ECG changed from sinusrhythm at 90 bpm to a brief period of sinusbradycardia, followed by a period of asystolewith only very occasional ventricular com-plexes lasting 25–30 seconds (figure B). After afew seconds of bradycardia then tachycardia,sinus rhythm was restored. Throughout theepisode the QT interval on the ECG remainedwithin normal limits. The EEG became visibleagain 16 seconds into the asystolic period, atwhich time it was dominated by diVuse lowamplitude slow activity at <1–2 Hz which per-sisted for 10 seconds (figure C). This was fol-lowed by marked attenuation of the EEGactivity over the next 10 seconds before largeamplitude generalised rhythmic <1Hz activitybecame apparent. DiVuse theta activity wasseen for a further 15 seconds before the EEGreturned to its resting state.
A VVI permanent pacemaker was inserted.The phenytoin was withdrawn and replacedby lamotrigine. Carbamazepine was leftunchanged. The patient was discharged, hismedication left unaltered, and at follow up 9months later reported no further episodes.
Cardiac dysrhythmias are an uncommonbut serious consequence of partial seizures.Our case is unusual because of the durationof the asystole. In a series of 26 patients with74 temporal lobe seizures in which simulta-
neous EEG and ECG recordings wereacquired, ictal arrhythmias occurred in 52%of seizures, the commonest being irregularabrupt changes in heart rate, (both accelera-tion and deceleration) occurring towards theend of the period of EEG abnormality.1
Interictally, patients with epilepsy seem nomore likely than age and sex matched healthysubjects to experience arrhythmias althoughin one study patients with epilepsy had afaster ventricular rate and a longer QT inter-val than control subjects.3
It has been hypothesised that there is later-alisation with respect to central autonomiccardiac control with an increase in heart rateseen after an intracarotid injection of amo-barbital and inactivation of the left hemi-sphere and a decrease in heart rate on righthemispheric inactivation. Experimentalstimulation of the rostral posterior insularcortex in anaesthetised rats has been shownto induce tachycardia and more caudal regionstimulation to cause bradycardia.4 Addition-ally, prolonged stimulation resulted in ven-tricular ectopics, heart block, QT prolonga-tion, and death. In presurgical temporallobectomy patients stimulation of the leftinsular cortex (particularly posteriorly) pro-duced bradycardia and a depressor responsesignificantly more often than tachycardia anda pressor eVect.5 It was suggested that an epi-leptic discharge in the insular cortex mayresult in cardiac arrhythmias.
Recurrent episodes of loss of consciousnessare a common clinical problem. An accuratediagnosis relies principally on the patient’sand witnesses’ accounts of events. Furtherinvestigations are frequently required whichare often normal unless an episode iscaptured during monitoring. Recordingsolely the EEG or the ECG may result inerroneous conclusions being drawn andinsuYcient or inappropriate therapy beinginstituted. Distinction between a primarycardiac arrhythmia and a secondary centralarrhythmia is possible only with simultaneousEEG/ECG recordings.
FERGUS J RUGG-GUNNJOHN S DUNCAN
SHELAGH J M SMITHEpilepsy Research Group, University Department of
Clinical Neurology, Institute of Neurology, TheNational Hospital for Neurology and Neurosurgery,
Queen Square, London WC1N 3BG, UK
Correspondence to: Professor John S Duncan,National Society for Epilepsy, Chalfont St Peter,Gerrards Cross, Bucks SL9 0RJ, UKemail [email protected]
1 Blumhardt LD, Smith PEM, Owen L. Electro-cardiographic accompaniments of temporallobe epileptic seizures. Lancet 1986;i:1052–5.
2 Reeves AL, Nollet KE, Klass DW, et al. The ictalbradycardia syndrome. Epilepsia 1996;37:983–7.
3 Drake M, Reider C, Kay A. Electrocardiographyin epileptic patients without cardiac symptoms.Seizure 1993;2:63–5.
4 Oppenheimer SM, Hachinski VC, CechettoDF. Cardiac chronotropic organization of therat insular cortex. Society of NeurosciencesAbstracts 1989;15:595.
5 Oppenheimer S, Gelb A, Girvin J, et al. Cardio-vascular eVect of human insular cortex stimu-lation. Neurology 1992;42:1727–32.
Respiratory insuYciency in a patientwith hereditary neuropathy withliability to pressure palsy
Hereditary neuropathy with liability to pres-sure palsies (HNPP) is an autosomal domi-nant disorder, the molecular basis of which isa 1.5 mb deletion in chromosome 17p11.2including the peripheral myelin protein-22
(PMP-22) gene.1 HNPP typically presentsrecurrent pressure palsies of peripheralnerves, such as the axillary, median, radial,ulnar, or peroneal nerves, at common entrap-ment sites. Respiratory muscle weakness hasnot been previously reported in HNPP. Wedescribe a patient with HNPP in whomrespiratory failure and proximal muscleweakness were prominent features.
The patient started to have dyspnoea onexertion at the age of 44. At the age of 47, henoticed a slowly progressive weakness of thepelvic girdle and lower limbs. At the age of57, he experienced diYculty in going upstairs. However, he was almost independentin daily life At the age of 60, he was admittedto Narita Red Cross Hospital as an emer-gency patient with a coma due to CO2 narco-sis (PCO2 117.6, PO2 64.0). Responding tomechanical ventilatory support, he com-pletely recovered consciousness within a day.His respiratory condition in the daytimeimproved to that previously. However, heneeded mechanical ventilation during sleepbecause of nocturnal hypoventilation.
The patient had no history of diabetesmellitus, pulmonary disease, or other medicalproblems. There was no familial history ofneurological disorder, including entrapmentneuropathies. After a few months, he notedthat in his teens he had experienced someepisodes of right peroneal and right axillarynerve palsies which resolved themselves overa few months.
In a neurological examination, the patient’smental state and cranial nerves were normal.Evidence of muscular atrophy and lumbarlordosis was found. The muscular atrophywas prominent in the shoulder girdle, inter-costal muscles, paravertebral muscles, andpelvic girdle, and moderate atrophy waspresent in all four limbs (figure). There wasmoderate weakness of the shoulder and pelvicgirdle and mild weakness of the distal limbs.The thorax showed poor respiratory move-ment, and the patient showed paradoxicalmovement of the abdomen in the supineposition. Tendon reflexes were hypoactive inall limbs. The patient’s sensations of touchand pain were mildly impaired in the fourdistal limbs. His position sensation wasnormal. His vital capacity was 1.9 l (55% ofthe normal mean) in the sitting position, but1.3 l (38%) in the supine position. Thepercentage of forced expiratory volume in 1second was normal (99%). Chest radio-graphy at inspiration and expiration showedpoor movement of the diaphragm but noabnormality in the lung field. Routinehaematological and serological studies gavenormal results. No monoclonal or polyclonalproteins were detected. IgG and IgM anti-bodies to gangliosides GM1 and GD1b werenegative. Analysis of CSF showed 1lymphocyte/mm3 and 25 mg/dl protein.Motor nerve conduction studies showed pro-longed distal latencies in the right median(8.8 m/s (normal value in our laboratory<4.6)) and ulnar (6.2 ms (normal<3.6))nerves, and moderate decreased conductionvelocities in the right median (40 m/s(normal>45)), ulnar (45 m/s (normal>49)),tibial (35 m/s (normal>38)), and peroneal(29 m/s (normal>41)) nerves. There weremoderate decreases in the amplitude of com-pound action potentials in all the nervestested, and an amplitude reduction of 50%was detected across the cubital tunnel of theright ulnar nerve. Minimum F wave latencieswere prolonged in all the nerves tested. Thelatency in the right phrenic nerve was slightly
110 J Neurol Neurosurg Psychiatry 2000;68:100–126
on February 15, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.68.1.123g on 1 January 2000. D
ownloaded from

delayed (8.7 ms (normal<8.0)). Sensorynerve conduction studies showed a reducedamplitude of sensory nerve action potentialsand conduction slowing in all the nervestested. Electromyography carried out in thesupraspinatus, deltoid, biceps, flexor carpiulnaris, brachioradialis, quadriceps femoris,biceps femoris, tibialis anterior, and gastroc-nemius muscles showed polyphasic motorunit potentials of long duration, but denerva-tion potentials were rare. A left sural nervebiopsy showed scattered tomaculous thicken-ing of the myelin sheath and some abnor-mally thin axonal myelin sheaths. The densityof myelinated fibres was reduced (5726/mm2).A gene analysis disclosed a 53% gene dose ofPMP-22 related to normal controls, usingSouthern blots of DNA digested with EcoRI.
Given the possibility of superimposingdemyelinating neuropathy, especially chronicinflammatory demyelinating polyneuropathy,oral prednisolone (60 mg/day) was given for 1month. However, the patient’s clinical condi-tion did not respond to this treatment.Pulmonary dysfunction and proximal muscleweakness were almost steady during the next3 years.
We examined the patient’s elder sister (64years old), elder brother (62 years old), andyounger sister (58 years old), although theyhad no neurological complaints. All of themhad experienced generalised hyporeflexia orareflexia but no weakness or sensory loss, andnerve conduction studies showed moderateconduction slowing with accentuation at thecommon entrapment sites, suggesting demy-elinating neuropathy.
Our patient recalled experiencing recur-rent episodes of transit entrapment monone-uropathies, and the familial occurrence ofasymptomatic entrapment neuropathy wasdetected by nerve conduction studies. The
presence of tomacula, and genetic analysisconfirmed a diagnosis of HNPP. However,the patient’s dominant clinical features—respiratory failure and proximal muscleweakness—were atypical for HNPP. Al-though respiratory muscle weakness has beenreported in hereditary motor and sensoryneuropathy (HMSN),2–4 there has been noreport of respiratory insuYciency associatedwith HNPP to our knowledge.
The weakness of the truncal muscles,including the respiratory accessory muscle, isa possible cause of respiratory failure in ourpatient. On the other hand, he had experi-enced hypoventilation in the supine postureand paradoxical movement of the abdomen,which suggested diaphragmatic weakness.2
Also, chest radiography showed poor move-ment of the diaphragm. Although the prolon-gation of distal latency in the phrenic nervewas mild considering the severity of respira-tory failure, assessment of axonal loss is notpossible with phrenic nerve stimulation. Infact, phrenic nerve latency is not necessarilyassociated with pulmonary dysfunction inHMSN.4
DiVuse proximal weakness in our patient isan uncommon finding as for HNPP. Mancardiet al5 reported on three patients with progres-sive sensory-motor polyneuropathy associatedwith 17p11.2 deletion, and the initial symptomof one patient was proximal weakness in onearm. We propose that our patient represents aclinical phenotypic variability among HNPP. Itmay be necessary to pay attention to respira-tory function in HNPP.
We thank Dr T Yamamoto from the University ofOccupational and Environmental Health for thegene analysis and Mr T Nagase from Chiba Univer-sity for his technical help with the sural nervebiopsy.
MASATO ASAHINASATOSHI KUWABARA
TAKAMICHI HATTORIDepartment of Neurology, School of Medicine,Chiba University, 1–8–1 Inohana, Chuo-ku,
Chiba 260–8670, Japan
MASATO ASAHINAKAORU KATAYAMA
Department of Neurology, Narita Red Cross Hospital,90–1 Iida-cho, Narita-shi, Chiba 286–0041, Japan
Correspondence to: Dr Masato Asahina, 1–8–1Inohana, Chuo-ku, Chiba-shi, Chiba 260–8670,Japan. Telephone 0081 43 222 7171 ext 5414; fax0081 43 226 2160;email: [email protected]
1 Chance PF, Alderson MK, Lepping KA, et al.DNA deletion associated with hereditary neu-ropathy with liability to pressure palsies. Cell1993;72:143–51
2 Eichacker PQ, Spiro A, Sherman M, et al. Res-piratory muscle dysfunction in hereditarymotor sensory neuropathy, type I. Arch InternMed 1988;148:1739–40.
3 Hardie R, Harding AE, Hirsch N, et al.Diaphragmatic weakness in hereditary motorand sensory neuropathy. J Neurol NeurosurgPsychiatry 1990;53:348–50.
4 Carter GT, Kilmer DD, Bonekat HW, et al.Evaluation of phrenic nerve and pulmonaryfunction in hereditary motor and sensory neu-ropathy. Muscle Nerve 1992;15:459–62.
5 Mancardi GL, Mandich P, Nassani S, et al. Pro-gressive sensory-motor polyneuropathy withtomaculous changes is associated to 17p11.2deletion. J Neurol Sci 1995;131:30–4.
Spinal accessory neuropathy andinternal jugular thrombosis aftercarotid endarterectomy
Spinal accessory neuropathy is a rare compli-cation of carotid endarterectomy (CEA).1
Internal jugular venous thrombosis afterCEA has also been reported rarely, but islikely more common; as internal jugular
General muscle atrophies, which are most prominent in the trunk are shown. A tracheotomy was performed for nocturnal hypoventilation because thepatient required mechanical respiratory support during the night.
J Neurol Neurosurg Psychiatry 2000;68:100–126 111
on February 15, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.68.1.123g on 1 January 2000. D
ownloaded from

venous thrombosis is often asymptomatic, orpresents with non-specific pain, it is probablyunrecognised in many cases.2 Concurrentipsilateral spinal accessory neuropathy andinternal jugular venous thrombosis after CEAis expected to be rare, and this is underscoredby the lack of published cases. Despite thisapparent rarity, a common pathogeneticmechanism for postoperative spinal accessoryneuropathy and internal jugular venousthrombosis may well be present, at least insome cases, which may lead to the considera-tion of the possibility of both when either isdiscovered.
We report on a patient who developed rightspinal accessory neuropathy and internaljugular venous thrombosis after right CEA.
A 59 year old man underwent right CEAfor possibly symptomatic stenosis. Angio-graphy had shown 90% stenosis of the rightinternal carotid. The operation was doneunder general anaesthesia. The carotid bifur-cation was unusually distal, necessitating along dissection and high retraction. Noimmediate postoperative complications wereevident. The next day, the patient complainedof mild pain at the operative site, but he didnot notice any weakness. The pain spreadinto his right shoulder within several days; atthat time, he also noted diYculty raising hisright arm. His symptoms worsened further afew weeks later. The symptoms persisted, andhe presented for neurological evaluation 4months after CEA. At that time, he had someinduration along the incision site and apalpable cord within the right supraclavicularfossa. There was moderate atrophy of theright sternocleidomastoid and trapezius, withright shoulder drooping and minor rightscapular winging. Right arm abduction pro-duced more prominent scapular winging andwas limited to 90 degrees due to pain andweakness. Electrodiagnostic studies wereconsistent with partial right accessory neu-ropathy with minor denervation of the righttrapezius. Cervical ultrasonography and MRIdemonstrated right internal jugular venousthrombosis. The patient was treated with ashoulder support, analgesics, and low doseaspirin. There was no significant clinicalchange 1 year after CEA. Repeat electrodiag-nostic studies were consistent with severechronic right spinal accessory neuropathy,and repeat ultrasonography showed persist-ent right internal jugular venous thrombosis.
Spinal accessory neuropathy was firstreported as a complication of CEA in 1982.3
Since then, there have been several casereports and small series.1 4 A 1996 review ofreports of cranial neuropathy after CEAdisclosed only one patient with spinal acces-sory neuropathy in over 3000 cases.1 Al-though the authors did not include severalother reports3 4 which, taken together, mayseem to suggest a somewhat higher incidence,the overall small number of reported cases inproportion to the hundreds of thousands ofCEAs that have been done worldwidesuggests that clinically significant spinalaccessory neuropathy is a rare complication.Minor or transient spinal accessory neu-ropathy after CEA may be more frequent.The cause of spinal accessory neuropathyafter CEA is usually not well established, butintraoperative nerve stretching or compres-sion from retraction is most often invoked.4
Delayed onset (after 3 weeks) has been notedin some; for these patients, postoperativeinflammation and scarring seem more likelycauses. Spinal accessory nerve transection orischaemia/infarction (arterial or venous) are
other possibilities. As in our patient, highcarotid dissection and retraction have beenreported to precede spinal accessoryneuropathy.1 4
The spinal accessory nerve courses alongthe internal jugular vein and near the internalcarotid artery, typically well above the carotidbifurcation. It stands to reason that a highincision and retraction resulting from a highcarotid bifurcation would place the nerve atrisk. Whether this realisation may lead to anytechnical modification to decrease the risk ofspinal accessory neuropathy in those with ahigh bifurcation is unclear.
From our search, internal jugular venousthrombosis after CEA has been reported inonly one case.2 As Southcott et al noted,retraction of the internal jugular during CEAmay cause complete occlusion, leading tothrombosis from venous stasis or endothelialinjury. Other causes of internal jugularvenous thrombosis include jugular cannula-tion, blunt cervical trauma, and a hyperco-agulable state. Internal jugular venous throm-bosis may occur within a week after neckdissection, often with recanalisation after sev-eral months.5
The presence of induration about the inci-sion site and a palpable supraclavicular cordin our patient led us to suspect venousthrombosis. Internal jugular venous throm-bosis may often be asymptomatic. Potentialsymptoms of internal jugular venous throm-bosis include headache, dysphagia, and ante-rolateral neck pain, tenderness, and swelling.In addition to perivenous induration, feverand leukocytosis may occur.2
Common pathogenetic mechanisms forspinal accessory neuropathy and internaljugular venous thrombosis may include intra-operative traction, haematoma, and postop-erative inflammation and scarring.
Although the onset of either spinal acces-sory neuropathy or internal jugular venousthrombosis in our patient cannot be deter-mined precisely, it is likely that both devel-oped at about the same time. The delayedworsening of spinal accessory neuropathy inthis case suggests postoperative scarring orinflammation. The lack of improvement aftera year, as in some other cases of spinal acces-sory neuropathy after CEA, implies consider-able axonal injury, but does not clarify themanner of injury.
GEORGE WOODWARDRAM VENKATESH
Department of Neurology, University of Kansas, andNeurology Section, VA Eastern Kansas Health Care
System, VA, USA
Correspondence to: Dr George Woodward, Neu-rology Section (111), VA Medical Centre, Leaven-worth, Kansas 66048, USA. Telephone 001 913682 2000 extension 2441; fax 001 913 758 4225.
1 Yagnik PM, Chong PST. Spinal accessory nerveinjury: a complication of carotid endarterec-tomy. Muscle Nerve 1996;19:907–9.
2 Southcott AJ, Sandhu A, Ferguson LJ, et al.Internal jugular vein thrombosis followingcarotid endarterectomy. Aust N Z J Surg 1994;64:60–2.
3 Sarala PK. Accessory nerve palsy: an uncom-mon etiology. Arch Phys Med Rehabil 1982;63:445–6.
4 Sweeney PJ, Wilbourn AJ. Spinal accessory(11th) nerve palsy following carotid endarter-ectomy. Neurology 1992;42:674–5.
5 Quraishi HA, Wax MK, Granke K, et al.Internal jugular vein thrombosis after func-tional and selective neck dissection. ArchOtolaryngol Head Neck Surg 1997;123:969–73.
Ischaemic stroke in a sportsman whoconsumed MaHuang extract andcreatine monohydrate for body building
We report the first case of extensive cerebralinfarct in a young sportsman consuming highdoses of MaHuang extract and creatinemonohydrate. This should alert the sportcommunity to possible serious adverse effectsof energy supplements.
A 33 year old man had a severe aphasia onawakening in the morning of 23 January1999. He did not complain of headache or ofother symptoms. He was referred to ourdepartment on 26 January 1999. He had aWernicke aphasia with a slight right sidedface and arm weakness and a right Babinskisign. His blood pressure was 140/60 and hispulse 54 per minute. Brain CT showed signsof extensive left middle cerebral arteryinfarct. Cervical ultrasound duplex scanningand cerebral angiography were normal. Cer-ebral CSF examination was normal. Therewas no coagulopathy. D-dimeres were withinthe normal range (360 ng/ml, normal <500ng/ml). Creatinine was in the normal range(102 µmol/litre). Transoesophageal echo-cardiography and ECG were also normalexcept for a patent foramen ovale.
The patient had no vascular risk factors, inparticular no tobacco use, and he wasperfectly fit until his stroke. He was a sports-man with 2 hours daily intensive training forbody building. He was working as a baggagehandler in an international airline company.During a recent journey to Miami, Florida,he bought tablets of “energy pills” in a shop-ping store to enhance his athletic perform-ances. The first drug contained MaHuangextract (corresponding to 20 mg ephedraalkaloids), 200 mg caVeine, 100 mgL-carnitine, and 200 µg chromium per twocapsules. The second drug contained 6000mg creatine monohydrate, 1000 mg taurine,100 mg inosine, and 5 mg coenzyme Q10 perscoop. He consumed 40–60 mg ephedraalkaloids, 400–600 mg caVeine, and 6000 mgcreatine monohydrate daily for about 6 weeksbefore his stroke.
Although a paradoxical embolism througha patent foramen ovale in this patient cannotbe ruled out as he recently returned from atransatlantic air flight, there was no deepvenous thrombosis and D-dimeres were nor-mal. However, ephedrine has an indirectsympathomimetic action and is responsiblefor arteriolar vasoconstriction in addition toother catecholaminergic eVects. Both ischae-mic and haemorrhagic stroke associated withephedrine use have been reported.1–3 Acutemyocardial infarction and acute psychosishave also been reported after taking ephe-drine and other sympathomimetic drugs.3
Ephedrine and its metabolites are naturalproducts that are used in non-prescriptionmedicines for multiple uses. MaHuang ex-tract, which contains ephedrine, is usedamong young sportsmen and sportswomen asan energy supplement in non-prescriptiontablets in some countries.
Although no cardiovascular side eVectshave been reported with the use of creatinemonohydrate, this compound, used in associ-ation with other drugs as energy supplementmay have deleterious side eVects. This maybe particularly true when used at high dosesin combination with sympathomimetic drugsas in our patient. Renal dysfunction has alsobeen reported after oral creatinesupplements.4 Our patient had a slightincrease in creatinine concentration although
112 J Neurol Neurosurg Psychiatry 2000;68:100–126
on February 15, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.68.1.123g on 1 January 2000. D
ownloaded from

it remained in the normal range. Whether theuse of high doses of caVeine can enhance thecardiovascular eVect of ephedrine remains apossibility as stroke after taking a combina-tion of caVeine and amphetamine has beenreported.5
Drug addiction in sportsmen and sports-women is becoming a major concern in oursocieties, involving both professionals andamateurs. As energy supplements, thought toenhance performance, are easily available insome countries without the need of medicalprescription, everybody should be aware thatthese so called “benign” drugs may havemajor adverse eVects.
This first case report of an extensivecerebral infarct in a young sportsman con-suming high doses of MaHuang extract andcreatine monohydrate should alert the sportcommunity to this possible adverse eVects ofenergy supplements, particularly when usedin multiple combination.
K VAHEDIV DOMIGO
P AMARENCOM-G BOUSSER
Service de Neurologie, Hôpital Lariboisière, Paris,France
Correspondence to: Dr K Vahedi, Service de Neu-rologie, Hôpital Lariboisière, 2 Rue A Paré, 75010Paris, Franceemail [email protected]
1 Stoessl AJ, Young GB, Feasby TE. Intracerebralhemorrhage and angiographic beading follow-ing ingestion of catecholaminergics. Stroke1985;16:734–6.
2 Yin PA. Ephedrine-induced intracerebral hem-orrhage and central nervous system vasculitis.Stroke 1990;21:1641.
3 Bruno A, Nolte KB, Chapin J. Stroke associatedwith ephedrine use. Neurology 1993;43:1313–6.
4 GreenhaV P. Renal dysfunction accompanyingoral creatine supplements. Lancet 1998;352:213–4.
5 Lambrecht GL, Malbrain ML, Chew SL, et al.Intranasal caVeine and amphetamine causingstroke. Acta Neurol Belg 1993;93:146–9.
Petroclival meningioma as a cause ofipsilateral cervicofacial dyskinesias
Hyperkinetic movement disorders of facialand neck muscles such as blepharospasm,hemifacial spasm, facial myokimia, and cervi-cal dystonia have rarely been associated withunilateral brainstem or posterior fossapathologies. We report a case of unilateralcervicofacial dyskinesias due to an ipsilateralpetroclival meningioma.
A 32 year old left handed woman com-plained about left sided facial dysaesthesia ofthe upper quadrant of her face for 1 year. Inaddition she had intermittent ipsilateralheadache. A left sided facial palsy and hypo-geusia developed. When progressive hearingloss and persistent ipsilateral tinnitus oc-curred she sought medical advice. She wasreferred to our department for furthertreatment after a large tumour in the left cer-ebellopontine angle had been demonstratedby MRI. On admission, the left corneal reflexwas absent. There was marked hypoaesthesiaof the first two divisions of the left trigeminalnerve and a mild left facial palsy. There wasalso hypogeusia of the left half of the tongue.Speech was slightly dysarthric. During exam-ination dystonic and choreic movements ofthe left facial muscles were seen. Thedystonic grimacing increased when the pa-tient was being observed. There were alsointermittent jerky dystonic head movementswith turning of the head to the left, associated
with slight elevation of the left shoulder. Thefacial movement disorder was clearly diVer-ent from hemifacial spasm. There were notonic or clonic synchronous contractions offacial muscles and no signs of involuntary
coactivation. The patient barely noted thedyskinesias. Audiometry showed a hearingthreshold at 30 Db on the left side and lack ofstapedius reflex on the left side. Oculoves-tibular response to caloric stimulation was
(A) Axial T2 weighted SE MR images of a 32 year old woman with left sided cervicofacial dyskinesiasshow a large left petroclival meningioma compressing the brainstem. (B) Coronal inversion recovery MRscans demonstrate marked displacement and distorsion of the brainstem due to the petroclivalmeningioma. (C) Gadolinium enhanced axial T1 weighted SE MR scans 3 months postoperativly showcomplete removal of the tumour and normalisation of the displacement of the brain stem.
J Neurol Neurosurg Psychiatry 2000;68:100–126 113
on February 15, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.68.1.123g on 1 January 2000. D
ownloaded from

decreased on the left side. Furthermore, therewas mild left dysdiadochokinesia.
Neurography of the facial nerve wasnormal on both sides. Needle myography ofthe left frontalis and orbiculari oculis did notshow signs of denervation.
An MRI study showed a large gadoliniumenhancing tumour within the left cerebello-pontine angle extending to the cavum Meck-eli with marked displacement of the brain-stem to the contralateral side (figure A andB). Cerebral angiography showed a discreteblush of the tumour as typically seen in men-ingiomas. The tumour was totally removedby a combined transpetrosal supratentorialand infratentorial presigmoidal approach.The postoperative course was uneventful andthere were no new deficits. The facial palsyimproved slightly as well as the trigeminalhypoaesthesia. Audiometry remained un-changed. Postoperative imaging showed noresidual tumour and the displacement of thebrain stem within the posterior fossa hadresolved (figure C). Marked improvement ofthe left sided craniofacial dyskinesias oc-curred during the next weeks.
The postoperative improvement of the dys-tonic and choreic grimacing and the cervicaldystonia indicates a causal association betweenthe petroclival meningioma and the segmentalhyperkinetic movement disorder. Such a rela-tion is supported also by the absence of a fam-ily history of movement disorders and theabsence of previous exposure to neurolepticmedication. Hyperkinetic movement disordersdue to tumours of the brainstem or of the pos-terior fossa have been reported only rarely.Asymmetric blepharospasm was recentlyfound in a patient with an ipsilateral mesen-cephalic cyst.1 Hemifacial spasm was seen inpatients with acoustic neurinomas, meningi-omas, and epidermoid tumours of the cerebel-lopontine angle.2 Acoustic neurinomas andanaplastic pontocerebellar glioma can be asso-ciated with facial myokymia and spastic pareticfacial contracture.3 Also, cervical dystonia dueto tumours of the cerebellopontine angle havebeen reported recently.4
The pathophysiological mechanisms re-sponsible for dystonic movement disorderscaused by structural or functional lesions ofthe brainstem are not fully understood. Thepossibility of denervation supersensitivity ofcranial nerve nuclei has been proposed previ-ously. Alternatively, enhanced excitability ofbrainstem interneurons has been suggested.This pathophysiological mechanism is sup-ported by the findings of blink reflex studiesin patients with blepharospasm, spasmodicdysphonia, and cervical dystonia. Tolosa et alfound significantly less inhibition of the teststimulus polysynaptic late response andmarked enhancement of the recovery curve ofthe late response under such conditions com-pared with the response in healthy subjects.5
Our case provides further evidence thatfunctional impairment by compression anddistortion of the brain stem may cause hyper-kinetic cervicofacial movement disorders. Itis important to know that such movementdisorders are accessible to surgical treatmentof the underlying pathology. Therefore, pa-tients with cranial or cervical dystonia orchoreic dyskinesia should undergo MR imag-ing to rule out a surgically treatable cause.
THOMAS POHLEJOACHIM K KRAUSS
Department of Neurosurgery, Inselspital, University ofBerne, Berne, Switzerland
JEAN-MARC BURGUNDERDepartment of Neurology
Correspondence to: Dr J K Krauss, Department ofNeurosurgery, University Hospital, KlinikeemMannheim, Theodor-Kutzer-Ufer 1-3, 68167Mannheim, Germanyemail [email protected]
1 Singer C, Schatz N, Bowen B, et al. Asymmetricpredominantly ipsilateral blepharospasm andcontralateral parkinsonism in an elderly patientwith a right mesencephalic cyst. Mov Disord1998;13:135–9.
2 Sprik C, Wirtschafter JD. Hemifacial spasm dueto intracranial tumor. Ophthalmology 1988;95:1042–5.
3 Krauss JK, Wakhloo AK, Scheremet R, et al.Facial myokimia and spastic paretic facial con-tracture as the result of anaplastic pontocer-ebellar glioma. Neurosurgery 1993;32:1031–4.
4 Krauss JK, Seeger W, Jankovic J. Cervical dysto-nia associated with tumors of the posteriorfossa. Mov Disord 1997;12:443–7.
5 Tolosa E, Montserrat L, Bayes A. Blink reflexstudies in focal dystonias: enhanced excitabilityof brainstem interneurons in cranial dystoniaand spasmodic torticollis. Mov Disord 1988;3:61–9.
Acute multifocal cerebral white matterlesions during transfer factor therapy
Transfer factor is an active substance ofunknown structure present in dialysable leu-cocyte extract which is assumed to transfercell mediated immunity in an antigen specificfashion.1 The mechanisms of action of trans-fer factor are still far from clear; in vitro dia-lysable leucocyte extract increases macro-phage activation and interleukin (IL) 1production and enhances leucocyte chemo-taxis and natural killer function. Transfer fac-tor has been reported to stimulate the cellmediated antigen specific response in patientswith various infections1; therefore, treatmentwith transfer factor has been suggested inpatients with selective deficits in cell medi-ated immunity such as in some refractoryneoplasms and chronic infections. Moreover,it has been used in the treatment of uveitis.2
Administration of dialysable leucocyte ex-tract has seemed to be free of hypersensitivity,long lasting side eVects, or complications,except for transitory hyperpyrexia.1
We report on a patient in whom multiplecerebral white matter lesions developed aftertaking dialysable leucocyte extract orally foruveitis. A 28 year old man was admitted tohospital because of headache, mental confu-sion, and right hemiparesis. He had hadrecurrent bilateral uveitis from the age of 12to 14 with residual cataract of the right eye. InJanuary 1995 retinal vasculitis was diagnosedat fundoscopy and in July 1995 he startedoral transfer factor as dialysable leucocyteextract twice a week. He complained of gen-eralised weakness after the second dose andthe referring symptoms developed after thethird dose.
Neurological examination on admissionshowed mental confusion and severe rightspastic hemiparesis with right Babinski’s sign.No fever or meningismus were present.
Laboratory examinations on admissionshowed a slight increase in total serumprotein (8.4 g/l, normal 6.0–8.0 g/l, althoughthe serum protein fraction was normal),antistreptolysin titres (355 UI/ml, normal<200 UI/ml), and anticardiolipin IgG (30UI/ml, normal< 12 UI/ml). Negative resultswere obtained for routine tests and serumimmunoglobulins, venereal disease researchlaboratory test, erythrocyte sedimentationrate, fibrinogenaemia, C reactive protein,rheumatoid factor, Waaler-Rose, proteinelectrophoresis, antinuclear, anti-DNA, an-timitochondrial, anti-ENA, anti-smooth
muscle, and antineutrophil cytoplasmic anti-bodies, lupus anticoaugulants, cryoglobulins,immune complexes, complement fractions,and neoplastic markers.
Serological investigations showed IgG butnot IgM against cytomegalovirus (CMV),Herpes simplex, Varicella zoster, Epstein-Barrviruses, and Toxoplasma gondii; the Paul Bun-nel reaction, anti-HIV, and the markers ofhepatitis virus B and C infection werenegative.
Cell, protein, and glucose concentrationsin CSF were normal. No oligoclonal bands orantibody against CMV, Herpes simplex, Vari-cella zoster, Epstein-Barr virus, Coxsackie,Adenovirus, Enterovirus or Borrelia burgdorferiwere present. Polymerase chain reactionsearch for Herpes simplex 1 and 2, Varicellazoster, CMV, Epstein- Barr virus, and JC virusin the CSF was negative.
Brain MRI showed several extensive asym-metric lesions in the subcortical and periven-tricular cerebral white matter, some of whichexerted a mass eVect on the nearby CSFspaces. All lesions exhibited thick ring-likeenhancement after intravenous contrast ad-ministration (figure). The brain stem, cer-ebellum, and cervical spinal cord werespared.
The patient had a progressive spontaneousremission of symptoms and signs. Theneurological examination 20 days after onsetshowed slightly increased deep tendon re-flexes on the right side and was normal 40days later; all laboratory analyses werenormal except for antistreptolysin titres (265UI/ml). Two MR scans at 1 and 4 monthsafter onset showed progressive reduction ofthe extension of cerebral white matter lesions,which did not show contrast enhancement. Afinal MR scan 20 months after onset showedfurther regression of lesions without contrastenhancement but a new large lesion in the leftoccipital white matter, which showed moder-ate contrast enhancement. At present, after 5years, the patient is in a good state of healthand neurological examination and laboratorytests are normal.
The close temporal relation between as-sumption of dialysable leucocyte extracttherapy and appearance of cerebral whitematter lesions in our patient supports thepossibility that the association of the twoevents might not be casual. Despite theabsence of biopsy, we reasonably excluded
Axial T1 weighted image after contrastadministration showing multiple focal lesions inthe periventricular white matter and leftcentrum semiovalis exhibiting thick annularenhancement.
114 J Neurol Neurosurg Psychiatry 2000;68:100–126
on February 15, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.68.1.123g on 1 January 2000. D
ownloaded from

the diagnosis of vasculitis or neuro-Behçet’sdisease although in the absence of biopsy. Infact, the clinical, laboratory, and MRI find-ings were not typical and a low titre ofanticardiolipin antibodies is found in 2% ofhealthy subjects.3
The occurrence at diVerent time of focalcerebral white matter lesions highly supportsthe diagnosis of multiple sclerosis, but someclinical and laboratory findings in the ourpatient are not typical for this condition.Mental confusion is not common at the onsetof multiple sclerosis whereas it is often foundin acute disseminated encephalitis.4 In addi-tion, CSF without oligoclonal banding arguesagainst a diagnosis of multiple sclerosis,whereas it is commonly found in acutedisseminated encephalitis.4 On the otherhand the possibility that acute disseminatedencephalitis may recur has been accepted5
and on the basis of the patient’s clinicalpicture and CSF, we favoured such a diagno-sis.
The pathogenic mechanisms underlyingthe triggering, development, and duration ofmultiple sclerosis and acute disseminatedencephalitis are still far from clear despite theprogress made in unravelling them. Somefindings suggest that acute disseminatedencephalitis and multiple sclerosis lie at thetwo poles of an autoimmune range, in whichautoantigen reactivity is only temporary anddirect against a single antigen in acutedisseminated encephalitis and multiple anti-gens in multiple sclerosis.
Although the hypothesis that dialysableleucocyte extract had triggered an autoim-mune disorder in our patient cannot beproved, our finding is in line with the reportof multiple cerebral lesions after therapy withIL-2 in patients with malignancies or HIVinfections.6
On the other hand, the fact that acute dis-seminated encephalitis is often correlatedwith the administration of foreign proteins,such as during vaccinations or viralinfections4 led us to postulate in this patient acell mediated immunological mechanism.Therefore, an immunological cross reactionbetween viral antigens (or other foreignmaterial contained in vaccines) and variousparts of the nervous system resulting in acutedisseminated encephalitis might have oc-curred. As already noted, dialysable leucocyteextract contains a multitude of immunos-timulating or potentially activating sub-stances so it is impossible to pinpoint whichone could have been responsible for thedemyelinating eVect seen in our patient. Thisnotwithstanding, our finding indicates thatneurological surveillance is worthy in patientsassuming dialysable leucocyte extracttherapy.
FRANCESCO G FOSCHILORENZO MARSIGLI
MAURO BERNARDISemeiotica Medica, Dipartimento di Medicina Interna,Epatologia e Cardioangiologia, Università di Bologna,
Italy
FABRIZIO SALVIDipartimento di Scienze Neurologiche, Ospedale
Bellaria, Bologna, Italy
MARIO MASCALCHICattedra di Radiologia, Università di Pisa, Italy
GIOVANNI GASBARRINICattedra di Medicina Interna, Università Cattolica del
Sacro Cuore, Roma, Italy
GIUSEPPE F STEFANINIDivisione di Medicina Interna, Ospedale di Faenza
(Ravenna), Italy
Correspondence to: Dr Francesco Giuseppe Fo-schi, Semeiotica Medica, Dipartimento di MedicinaInterna, Epatologia e Cardioangiologia, Universitàdegli Studi di Bologna, Policlinico Sant’Orsola, viaG Massarentin°9, 40138 Bologna, Italy. Telephone0039 51 308943; fax 0039 51 308966; email:[email protected]
1 Fudenberg HH, Fudenberg HH. Transferfactor: past, present and future. Annu RevPharmacol Toxicol 1989;29:475–516.
2 Abramson A, Khan A, Tate GW, et al. Immuno-competence of transfer factor therapy inuveitis. Br J Ophthalmol 1980;64:332–8.
3 Lockshin MD. Answers to the antiphospholipidantibody-syndrome? N Engl J Med 1995;332:1025–7.
4 Kesselring J, Miller DH, Robb SA, et al. Acutedisseminated encephalomyelitis. Brain 1990;113:291–302.
5 Khan S, Yaqub BA, Poser CM, et al. Multipha-sic disseminated encephalomyelitis presentingalterning hemiplegia. J Neurol Neurosurg Psy-chiatry 1995;58:467–70.
6 Illowsky Karp B, Yang JC, Khorsand M, et al.Multiple cerebral lesions complicating therapywith interleukin-2. Neurology 1996;47:417–24.
Fahr’s disease and Asperger’s syndromein a patient with primary hypo-parathyroidism
Abnormal calcium phosphate metabolism hasnot previously been associated with Asperger’ssyndrome, a form of pervasive developmentaldisorder. Nor have symmetric calcifications ofthe basal ganglia, dentate nuclei and cortex, or
Fahr’s disease1—whether idiopathic or associ-ated with hypoparathyroidism—previouslybeen associated with this handicap. We presentthe case of a 24 year old man with Asperger’ssyndrome, primary hypoparathyroidism, andmultifocal brain calcifications.
According to medical history, the patient’smother had received weekly injections ofDepoprovera during pregnancy. A singlechild born after a normal term delivery, heunderwent surgery for an inguinal hernia at 3weeks. Developmental milestones were onlymoderately delayed. At 9 months, he rolledinstead of crawling. He walked at 15 months,spoke at 2 years with poor articulation, andstill speaks in short, unelaborated sentences.His social and language development laggedin grade school and he occasionally got intofights. In late adolescence, antisocial behav-iour took the form of shoplifting and repeatedlong distance calls to pornographic hot lines.As an adult, his social adaptation remainspoor: he currently lives with his mother andworks irregularly as a dishwasher in a restau-rant. He is indiVerent, isolated, and resistsnovelty. He enjoys repetitive and solitaryactivities such as slot machine games andplaying the piano.
Neurological examination showed bilateralhyperreflexia, mild imprecision of fine fingermovements, dysgraphaesthesia on sensorytesting, and a manneristic grippinghandshake. There were no extrapyramidal
Brain CT, axial section: dense calcific deposits in the basal ganglia, thalamus,and orbitofrontal cortexconsistent with Fahr’s disease.
J Neurol Neurosurg Psychiatry 2000;68:100–126 115
on February 15, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.68.1.123g on 1 January 2000. D
ownloaded from

symptoms. His IQ score was in the low range(WAIS-C=85 at the age of 13; Barbeau-Pinard=82 at the age of 17). He alsopresented an impairment on the Tower ofLondon test, which measures executive func-tion, and in a task assessing the understand-ing of other people’s intentions. These twofindings are reliably present in pervasivedevelopmental disorders, in this IQ range. Inaddition, his performance on the Tower ofToronto test disclosed impaired performancein procedural learning. Psychiatric assess-ment showed scores above the cut oV forautism according to the autism diagnosticinterview (ADI),2 a standardised interviewthat requires specific training and thoseadministering it to have a 0.90 reliability withother researchers. The subject was positivefor the diagnosis of autism, being above cutoV values in the three relevant areas of com-munication, social interactions, restrictedinterests, and repetitive behaviours.Nevertheless, he did not present delay in lan-guage acquisition or morphological atypicali-ties in language development, which corre-sponds to DSM-IV criteria for Asperger’ssyndrome.
Brain CT showed dense calcium depositsin the basal ganglia, thalamus, cerebellardentate nucleus, and orbitofrontal cortex,consistent with Fahr’s disease (figure).SPECT showed increased activity in basalganglia relative to the cerebral cortex. A finebanded karyotype was normal. Serum cal-cium was 1.55 mM/l (normal 2.15–2.55mM/l), phosphate 1.69 mM/l (normal 0.70–1.5 mM/l). Ionised calcium was 0.80 mM/l atpH 7.4 (normal 1.19–1.34 mM/l); urinarycalcium was 0.8 mM (normal 2.5–6.3 mM).Serum parathyroid hormone was below 0.6(normal 1.0–6.55 µM/l), and a nuclear scanof the parathyroid glands showed an absenceof activity. With a combination of vitaminD3-calcium supplementation and cognitive-behavioural therapy, serum calcium, andphosphate concentrations normalised and hisbehaviour improved marginally.
Asperger’s syndrome is a subtype of perva-sive developmental disorder of unknownaetiology. Evidence for involvement of spe-cific brain regions in pervasive developmentaldisorder are scarce and inconclusive.3 Al-though the temporo-occipital region is themost often involved in pervasive developmen-tal disorders4 5 abnormal functioning of thefrontal lobes is also suspected from replicatedfindings of executive function deficits andfrom occasional findings of frontal hypome-tabolism or abnormal macroscopic brainmorphology.3 Abnormal cell counts and mor-phology in the cerebellar hemispheres havealso been reported, but the relation of thesefindings to autism is controversial.3
Fahr’s disease consists of symmetric calci-fications, located mainly in the basal fore-brain and cerebellum, which are of variousaetiologies. Cognitive and behavioural abnor-malities may be present when calcificationsoccur early in development. A fortuitousassociation between pervasive developmentaldisorder and hypercalcaemia, given the pau-city of published cases, is plausible in the pre-sented patient. Nevertheless, our casesuggests that abnormal phospho-calciummetabolism could produce an autistic syn-drome when brain calcifications cause spe-cific neuropsychological deficits, due to theirlocalisation. For example, errors of socialjudgement may be related to calcifications ofthe orbitofrontal cortex, whereas dysfunctionof frontal-basal ganglia circuits may contrib-
ute to repetitive and ritualistic activities.Additionally, developmental lesions of thebasal ganglia and cerebellum may contributeto the abnormalities of sensory attention,procedural learning, and motor intention inthis patient.
The finding that the clinical picture ofautism can be found in a wide range of medi-cal conditions giving rise to organic braindysfunction is not new, but the relationbetween these conditions and autism areoften considered meaningless.3 By contrast,this case, similarly to some others4 5 suggeststhat dysfunction in key brain circuits mayresult in behavioural and cognitive abnor-malities currently indistinguishable fromidiopathic pervasive developmental disorder.This case also suggests that careful biologicalassessment of this group of patients may dis-close focal brain lesions associated with iden-tifiable cognitive deficits. Could these clinicalcoincidences be instructive for a neurodevel-opmental model of autism?
E STIPN BLACKJ M EKOÉ
L MOTTRONHopital LH Lafontaine, Départment de Psychiatrie,
Université de Montréal, 7331, rue Hochelaga,Montréal (Québec) H1N 3V2, Canada
Correspondence to: Dr Emmanuel Stip, Centre deRecherche Fernand Séguin, Hopital LH Lafontaine,Départment de Psychiatrie, Université de Montréal,7331, rue Hochelaga, Montréal (Québec) H1N 3V2,Canada. email [email protected]
1 Fahr T. Idiopatische Verkalkung der Hirngefas-se.Zentrabl Allg Pathol 1930–1931;50:129.
2 Le Couteur A, Rutter M, Lord C, et al. Autismdiagnostic interview: a standardizedinvestigator-based instrument. J Autism DevDisord 1989;19:363–87.
3 Minshew N, Sweeney JA, Bauman ML. Neuro-logical aspects of autism. In: DJ Cohen, FRVolkmar, eds. Handbook of autism and pervasivedevelopmental disorders . New York: John Wiley1997:344–69.
4 Mottron L, Mineau S, Décarie JC, et al. Visualagnosia with temporo-occipital brain lesions inan autistic child: a case study. Dev Med ChildNeurol 1997;39:699–705.
5 Jambaqué I, Mottron L, Ponsot G, et al. Autismand visual agnosia in a child with right occipi-tal lobectomy. J Neurol Neurosurg Psychiatry1998;65:555–60.
Hypertrophic atlantoaxial ligaments: anunusual cause of compression of theupper spinal cord
The craniovertebral junction can be aVectedby several pseudotumorous masses extradur-ally located, such as rheumatoid panus,hypertrophic non-union of odontoid fracture,post-traumatic cicatrix, synovial cysts, tumor-ous calcium pyrophosphate dihydrate crystaldeposition, tophaceous gout, calcification ofthe posterior longitudinal ligament, synovialdisease-like pigmented villonodular synovitis,and synovial chondromatosis.1–5 Hypertrophyof the atlantoaxial ligaments as a conse-quence of degenerative disease was recentlyrecognised as an individual entity. Only fiveprevious cases have been published.1 We addanother case to the short series available inthe literature, emphasising that as the causeof the spinal cord compression is amenable tosurgical removal, symptomatic patientsshould be diagnosed and treated withoutdelay.
A 66 year old woman presented with arapid development of progressive spastictetraparesis and an unremarkable medicalhistory. There was no osteolysis or instabilityon plain cervical radiography and CT. A bone
scan with 99Tc was unremarkable. Magneticresonance imaging showed a retro-odontoidextradural mass that was homogeneous andisointense on T1 weighted signal, demon-strated no enhancement after intravenousgadolinium contrast, and was compressingthe upper cervical spinal cord (figure). Thelaboratory tests were normal, confirming theabsence of rheumatoid arthritis, metabolicdisease, or gout. Surgical removal via a tran-soral approach with a minimal bony resectionwas direct and provided suYcient space toobtain spinal cord decompression. It was fol-lowed by a posterior C1-C2 fusion. Macro-scopically, the lesion had no capsule andresembled a hypertrophic ligamentum fla-vum. Microscopically, it was non-inflammatory, hypocellular, and ligamentarypieces found within the mass appearedfibrous and almost disintegrated. The patientregained normal neurological function. Overa 3 year follow up period there was no recur-rence.
We focus attention on hypertrophic atlan-toaxial ligamentary disease as a degenerativedisease that must be considered within thepossible causes of high spinal cord compres-sion.
ALEJANDRA TERESA RABADANDepartment of Neurosurgery, Instituto de
Investigaciones Medicas “Alfredo Lanari”, Facultad deMedicina, Universidad de Buenos Aires, and Equipo de
Neurocirugía de Buenos Aires, Argentina
GUSTAVO SEVLEVERDepartment of Pathology, Clinica Bazterrica, Buenos
Aires, and Equipo de Neurocirugía de Buenos Aires,Argentina
Correspondence to: Dr Alejandra T Rabadan, Bill-inghurst 1976 PB, 1425 Buenos Aires, Argentina.Telephone 0054 1 902 4417;fax 0054 1 9038928;email rabadan @ movi.com.ar
1 Crockard HA, Sett P, Geddes JF, et al. Damagedligaments at the craniovertebral junction pre-senting as an extradural tumour: a diVerentialdiagnosis in the elderly. J Neurol Neurosurg Psy-chiatry 1991;54:817–21.
2 Pare MC, Currier BL, Ebersold MJ. Resolutionof traumatic hypertrophic periodontoid cicatrixafter posterior cervical fusion: case report.Neurosurgery 1995;337:531–4.
3 ShaVrey CI, Muñoz EL, Sutton CL, et al.Tumoral calcium pyrophosphate dihydratedeposition disease mimicking a cervical spineneoplasm: case report. Neurosurgery 1995;37:335–9.
Preoperative sagittal T1 weighted MRI of thecervical spine with gadolinium enhancement. Aretro-odontoid and extradural mass displacingthe spinal cord is seen at the craniovertebraljunction.
116 J Neurol Neurosurg Psychiatry 2000;68:100–126
on February 15, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.68.1.123g on 1 January 2000. D
ownloaded from

4 Sze G, Brant-Zawadzki MN, Wilson CB, et al.Pseudotumour of the craniovertebral junctionassociated with chronic subluxation: MR imag-ing studies. Radiology 1986;161:391–4.
5 Tihanski DP. Unilateral hypertrophy of the cer-vical ligamentum flavum presenting as pseudo-tumor. N Y State J Med 1986;86:5368.
Selective hemihypaesthesia due to tentorialcoup injury against dorsolateral midbrain:potential cause of sensory impairmentafter closed head injury
A 63 year old woman who fell oV her bicyclehad a left temporal region head injury withevidence of initial loss of consciousness of 5minutes and scalp excoriation of that area.On arrival at our hospital 30 minutes later shewas alert and oriented. Cranial nerve func-tions, including extraocular motion and hear-ing function, were preserved. Pain andtemperature sensations of the right side,including her face, showed a 70% decreasecompared with the left side; however, positionand vibration sensations were normal. Otherneurological examinations, including motorfunction, coordination, and deep tendonreflex, were normal. The patient’s only com-plaints were left temporal headache and righthemihypaesthesia.
Brain CT on admission showed a discreteand linear high density at the left ambientcistern without other intracranial lesions. Onthe next day CT showed an obscure low den-
sity lesion at the dorsolateral midbrain inaddition to the previous lesion (figure).
Brain MRI, taken 3 days later, demon-strated an intraparenchymal lesion, at thesurface of the left dorsolateral midbrain inhigh intensity on a T2 weighted image. Thehigh intensity lesion corresponding to hae-matoma on CT was seen in the ambient cis-tern (figure). Taking both CT scans and MRIinto consideration, this case was diagnosed astraumatic midbrain contusion.
The loss of pain and temperature sensationimproved gradually and the patient wasdischarged 2 weeks later.
T2 weighted images 1 month later showeda more localised lesion in the same area. Thecoronal slices showed a high intensity lesionat the level of lower midbrain coinciding withthe tentorium level, disclosed as a low linebetween the occipital lobe and the cerebellarhemisphere (figure).
The neurological deficits almost disap-peared 6 months later.
Somatosensory impairment including painis one of the most common complaints amongpatients with craniocervical injury. Responsi-ble lesions for sensory impairment, detectableby neuroimaging studies, almost always ac-company associated neurological deficits.1 2 Toour knowledge, a selective injury at thespinothalamic or trigeminothalamic tracts dueto closed head injury has not been highlightedin the neurological literature.
The MR images in our case showed a dis-crete lesion at the left dorsolateral midbrain.Topographical study at this lower midbrainlevel showed that the lateral and ventralspinothalamic and ventral trigeminothalamictracts pass at the surface of this level bycarrying a superficial somatofacial sensoryinput.3 The lesion shown in our MR imagesseemed to be localised to these tracts. Themedial leminiscus for the deep sensation andlateral leminiscus and nucleus of inferior col-liculus associated with hearing function runventral and dorsal to these tracts, respec-tively; which were seemingly spared in ourpatient.3 The topographical anatomy seemedto correspond to the neurological manifesta-tions of our patient.
The mechanism of midbrain injury in ourpatient was speculated to be due to tentorialcoup injury based on MR images. Thelocation of contusion was at the lower dorso-lateral midbrain, coinciding with the tentorialedge level. Initiation of injury was the surfaceof the midbrain; however, due to the proxim-ity of the tentorial edge to the midbrain onthe injured side, tentorial contact to the mid-brain supposedly occurred more readily.Brain MRI findings support the anatomicalfeatures of this tentorial coup injury. Thisinjury is not rare in patients with severe headinjury, accompanied by other intracraniallesions, and is often caused by lateraldisplacement of the brain stem relative to thetentorium. It is influenced by congenital vari-ation in the size and shape of the tentorialincisura.1 2 The brain stem of the patient witha narrow incisura is more vulnerable to thedirect contusive eVects than that of a patientwith a wider incisura. Therefore, even inminor head injury, this mechanism may occurin patients preconditioned with narrow tento-rial incisura, which may have been the case inour patient.
The concept of tentorial coup injuryagainst the midbrain is not new.4 It usuallyaccompanies various degrees of consciousdisturbance and other long tract signs,sensory deficits as well as cerebellar andcranial nerve palsy due to the midbrainlesion or other associated intracraniallesions.1 2 4 5 The clinical manifestation of ourpatient may represent one of the mildestforms of the midbrain contusion. Therefore,when we see a patient with post-traumaticsensory deficit, the possibility of this tento-rial injury should be kept in mind even inminor head injury.
NAOKATSU SAEKIYOSHINORI HIGUCHI
Departments of Neurological Surgery, ChibaUniversity, School of Medicine, Chiba, Japan
KENRO SUNAMIKawatetsu Chiba Hospital, Japan
AKIRA YAMAURADepartments of Neurological Surgery, Chiba
University, School of Medicine, Chiba, Japan
Correspondence to: Dr Naokatsu Saeki, Depart-ment of Neurological Surgery, Chiba University,School of Medicine, 1–8–1 Inohana, Chuoh-kuChiba-shi, Chiba Japan 260–8670email [email protected]
1 Gean AD. Imaging of head trauma. New York:Raven, 1994:215.
2 Saeki N, Yamaura A, Sunami K. Brain stemcontusion due to tentorial coup injury: casereport and pathomechanical analysis from nor-mal cadavers. Br J Neurosurg 1998;12:151–5.
3 DeArmond SJ, Fusco MM, Dewey MM. Struc-ture of the human brain. 2nd ed. New York:Oxford University Press, 1976:84–8.
(A) CT on admission showed a discrete and linear high density at the left ambient cistern. (B) AxialT2 weighted image taken 3 days later showed an intraparenchymal lesion, at the left posterolateralmidbrain in high intensity. (arrow) The margin was rather obscure. The high and low intensity lesioncorresponding to haematoma on CT was seen in the ambient cistern in the axial image. (arrow head)Taking both CT scans and MRI, this case was diagnosed as traumatic midbrain contusion. (C) Anaxial T2 weighted image 1 month later demonstrated a more discrete lesion at the dorsolateralmidbrain tegmentum (arrow). (D) A coronal image showed a discrete high intensity lesion at the levelof the lower midbrain (arrow) coinciding with the level of the tentorium, which was shown in low linebetween the occipital lobe and cerebellar hemisphere. The distance between the tentorial margin andbrain stem was shorter on the injured side.
J Neurol Neurosurg Psychiatry 2000;68:100–126 117
on February 15, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.68.1.123g on 1 January 2000. D
ownloaded from

4 Lindenberg R. Significance of the tentorium inhead injury from the blunt forces. ClinNeurosurg 1964;12:129–42.
5 Miller N, Newman N. Walsh and Hoyt’s clinicalneuro-ophthamology, 5th ed. Vol 1. Baltimore:Williams and Wilkins, 1998:1227–34.
CORRESPONDENCE
Toluene induced postural tremor
We read with interest the article by Miyagi etal1 and comment on the medical treatment oftoluene induced tremor. Microdialysis experi-ments in rats have shown that inhalation oftoluene increases extracellular ã-aminobutyricacid (GABA) concentrations within the cer-ebellar cortex2 which probably explains whyGABA agonists including benzodiazepines(for example, clonazepam) are not very eVec-tive in toluene induced tremor and ataxia. Ratexperiments also showed a 50% reduction inbrain catecholaminergic neurons.3 Degenera-tion of certain cerebellar pathways is probablyresponsible for the loss of this dopaminergicinnervation.4 Dopamine agonists could there-fore be of potential interest in the treatment oftoluene induced tremor. This hypothesis wasexplored in a recently described case,5 whichshowed remarkable clinical and iconographicsimilarities with that described by Miyagi etal1: (a) long history of chronic toluene inhala-tion, (b) marked postural tremor, (c) progres-sive worsening of the symptoms despite absti-nence from inhalant misuse, and (d) mildcerebral atrophy and marked low signal inten-sity in globus pallidi, thalami, red nuclei, andsubstantia nigrae on T2 weighted MRI. Asour patient’s tremor was progressive, medicaltreatment with a dopamine agonist wasconsidered. One particular agent (amanta-dine) caught our attention because it hadproved successful in the treatment of posturaltremor and ataxias of heredodegenerative dis-orders in which the dentatorubro-olivary sys-tem is aVected. In addition, there is evidencethat catecholaminergic pathways are alsoinvolved in this type of ataxias, supported bylow concentrations of these neurotransmittersin the CSF of patients with heredodegenera-tive ataxias.6 In our patient, amantadinehydrochloride (100 mg twice daily) abolishedpostural tremor and ataxia completely over a 3month period.
Subsequently, the treatment was discontin-ued, which resulted in relapse of the tremorand ataxia. He was rechallenged to amanta-dine, which progressively oVered him thesame clinical improvement as in the first 3months. After 3 years the treatment was dis-continued without any sign of relapse.
Although this finding needs confirmation,amantadine treatment could form a newapproach in the medical treatment fortoluene induced tremor and ataxia. Intracta-ble cases would then justify a more aggressiveapproach such as ventrointermedius tha-lamotomy.
DIRK DELEUDepartments of Clinical Pharmacology and Neurology,
College of Medicine, Sultan Qaboos University,PO Box 35, Al Khod, Muscat-123,
Sultanate of Oman
YOLANDE HANSSENSDrug Information Services, Hospital Pharmacy
Correspondence to: Dr Dirk Deleu, College ofMedicine, PO Box 35, Sultan Qaboos University,Al-Khod, Muscat-123, Sultanate of Omanemail [email protected]
1 Miyagi Y, Shima F, Ishido K, Yasutakeet.Tremor induced by toluene misuse successfullytreated by a Vim thalamotomy. J Neurol Neuro-surg Psychiatry 1999;66:794–6.
2 Stengard K, Tham R, O’Connor WT, et al.Acute toluene exposure increases extracellularGABA in the cerebellum of rat: a microdialysisstudy. Pharmacol Toxicol 1993;15:327–34.
3 Bjornaes S, Naalsund LU. Biochemical changesin diVerent brain areas after toluene inhalation.Toxicology 1988;49:367–74.
4 Campanella G, Filla A, De Falco F, et al. Fried-reich’s ataxia in the south of Italy: a clinical andbiochemical survey of 23 patients. Can J NeurolSci 1980;7:351–7.
5 Deleu D, Hanssens Y. Cerebellar dysfunction inchronic toluene abuse: beneficial response toamantadine hydrochloride. J Toxicol Clin Toxicol(in press).
6 Deutch AY, Elsworth JD, Roth RH, et al.3-Acetylpyridine results in degeneration of theextrapyramidal and cerebellar motor systems:loss of dorsolateral striatal dopamine innerva-tion. Brain Res 1990;527:96–102.
Early diagnosis of subependymal giantcell astrocytoma in children withtuberous sclerosis
Nabbout et al1 have attempted to identify therisk factors for the progression of subependy-mal nodules into giant cell astrocytomas(SEGAs) in tuberous sclerosis complex. Inattempting to develop screening strategiesthat avoid iatrogenic morbidity, patient in-convenience, and excess cost, it is essentialthat the natural history of these lesions in thegeneral population of patients with tuberoussclerosis complex be understood well.
We think that there are two problems withthis study that should make the physician cau-tious about accepting the factors identified byNabbout et al as a basis for a screeningprogramme. The first is that this study wasperformed in a population that had beenreferred to a tertiary medical centre, and thenhad been further selected by virtue of havinghad at least 3 years tertiary centre follow upand needing two MR scans of the head. Theprevalence of astrocytomas and risk factors,and hence the positive predictive value of anyscreening test in a general population ofpatients with tuberous sclerosis complex islikely to be diVerent from those described inthe highly selected group studied in this paper.
The second point is that the authors havemade a potentially misleading decision toexclude more than half their study samplebecause they do not have lesions close to theforamen of Monroe. It is not certain that allSEGAs arise from lesions close to theforamen. They may arise in the fourth ventri-cle. Furthermore, the late presentation ofmany lesions in the lateral ventricles has, inthe past, precluded accurate determination oftheir point of origin. The study selects 24 of60 patients who had met their entry criteriabut does not state how many of the excluded36 patients had no subependymal nodules ornodules that were not “near the foramen ofMonroe”. Indeed no definition is given forwhat constitutes proximity to the foramen.The authors were apparently not blinded atthe point when they selected which patientshad lesions near to the foramen and thereforethere is an obvious issue of potential selectionbias.
The consequence of excluding these pa-tients may have been that false significance isgiven to their results. The data they presentare fragile. Consider, for example, the conse-
quence of introducing from these 36 non-selected patients a hypothetical single casethat had a family history of tuberous sclerosiscomplex and a subependymal nodule whichenhanced with gadolinium. The eVect wouldbe to remove the stated statistical significance(using Fisher’s exact tests) between theoutcome and both of these explanatory vari-ables.
Identifying the risk factors that can tell uswhich subependymal lesions will becomeinvasive is important. As subependymal nod-ules and SEGAs seem to be histologicallyidentical it is unlikely that pathologists willprovide an answer. The study of Nabbout etal suggests some new hypotheses and reiter-ates some others. However, the definitiveanswer will not be provided by studies ofselected samples but by follow up of a popu-lation based sample of patients with tuberoussclerosis complex. In the absence of such astudy we would be cautious about imple-menting screening programmes based onwhat may be misleading criteria.
FINBAR J K O’CALLAGHANANDREW LUX
JOHN OSBORNEBath Unit for Research in Paediatrics, Royal United
Hospital, Bath BA1 3NG, United Kingdom
Correspondence to: Dr Finbar J K O’Callaghan,Bath Unit for Research in Paediatrics, Royal UnitedHospital, Bath BA1 3NG, United Kingdom
1 Nabout R, Santos M, Rolland Y, et al. Earlydiagnosis of subependymal giant cell astrocy-toma in children with tuberous sclerosis. JNeurol Neurosurg Psychiatry 1999;66:370–5.
Atypical form of amyotrophic lateralsclerosis: a new term to define apreviously well known form of ALS
We read with interest the article by Sasaki etal1 concerning the atypical form of amyo-trophic lateral sclerosis (ALS). The pattern ofmuscular atrophy in these patients diVeredfrom that of typical ALS in that severe muscleinvolvement was confined to the upper limbs,predominantly the proximal portion andshoulder girdle, sparing the face and the legsuntil late in the disease’s course or until theterminal stage.
Over the past few years, we have noticed agrowing interest in the renaming of this clini-cal form of ALS, which has its origins andpredomination in the proximal muscles andupper limbs and little or no eVect of either abulbar nature or in the lower limbs.
Thus Hu et al2 coined the term flail armsyndrome, to describe a subgroup of patientsaVected by ALS that predominantly showedsigns of lower motor neuron disease in theupper limbs, without significant functionalinvolvement of other regions on clinical pres-entation. This subgroup of patients was clini-cally characterised by the display of progres-sive atrophy and weakness aVecting theproximal muscles in the upper limb musclesin a more or less symmetric manner.
Recently, along these lines, Katz et al3
described a series of patients aVected by anadult onset motor neuron disorder restrictedto the upper limbs, with severe proximal andvarying degrees of distal involvement, callingit amyotrophic brachial diplegia syndrome.
Other terms used in the past to refer to thisform of ALS have been dangling armsyndrome, suspended form, orangutan sign,dead arm sign, bibrachial palsy, rizomelicamyotrohy, and the idea of naming it adistinctive phenotype of a neurogenic
118 J Neurol Neurosurg Psychiatry 2000;68:100–126
on February 15, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.68.1.123g on 1 January 2000. D
ownloaded from

“man-in-the-barrel” syndrome has even beensuggested.
Probably all these terms used to define thisvariation of ALS are synonyms for an older,well known condition, the scapulohumeralform, or the chronic anterior poliomyelitisreported by Vulpian in 1886 and known inFranco-German literature as Vulpian-Bernhardt’s form of ALS.
At certain stages of the disease’s clinicalcourse, it is probably diYcult to diVerentiateit from progressive muscular atrophy (PMA).Some authors have said that PMA with lateonset scapulohumeral distribution (over 45years of age) generally leads to ALS as a mat-ter of course.4
Be that as it may, the truth is that thisatypical form of amyotrophic lateral sclerosisbehaves diVerently from typical ALS. Thecomparative study with the rest of the ALSgroup supplied important clinical findings,such as little or no functional impairment ofthe bulbar muscles or legs. Hu et al also madefour important statistical discoveries.
(1) The prevalence of this form of ALSconstituted 10% of the ALS group as a whole(n=395). (2) The age of onset of this formwas similar to the rest of ALS. (3) There wasa clear predominance among men (the male/female ratio was 9:1 in this form, comparedwith 1.5:1 in the total ALS group). (4) Therewas a longer median survival (a mediansurvival of 57 months compared with 39months in the ALS group).
Some of these patients have a long ALSclinical course, in that they usually preserveambulatory ability, albeit with gait disorders,for more than 5 years after the onset of symp-toms
On a personal level, we also note two find-ings characteristic of these patients. In theinitial stages of the illness, there is no eVect onthe diaphragm and the respiratory musclefailure occurs much later than in the typicalform of ALS. This can be seen in the followup of the results obtained in the respiratoryfunction tests (FVC, PImax, and PEmax).
We do not know the reason for either thecharacteristic distribution of weakness ormuscle atrophy. A meticulous study showsthat there is an atrophy of the deltoideus(especially in the pars spinata) and a loss ofstrength in the external rotation of the shoul-der (infraespinatus, supraespinatus, and teresminor). As a consequence, the upper limbsadopt a characteristic position, with theshoulders slumped, and the arms, forearms,and hands in pronation.
The atrophy and weakness of the in-fraespinatus and the supraespinatus, that actas an active ligament in scapulohumeralarticulation, would explain the presence ofsubluxation of the shoulder joints in thesepatients.
Finally, we are in complete agreement thatthe coexistence of cervical spondylosis andALS can cause diYculty in diagnosis. Theproblem lies in the fact that cervical spondy-losis is a common condition. It is found in83.5% of men and 80.7% of women over theage of 55. The faster progressive deteriora-tion of the symptoms, the appearance of bul-bar signs, and the absence of sensorysymptoms and signs would favour the diag-nosis of ALS.5
JOSEP GAMEZCARLOS CERVERAAGUSTIN CODINA
Servicio de Neurologia, Hospital Gral, UniversitariVall d‘Hebron, Passeig Vall d’Hebron 119–135, 08035
Barcelona, Spain
Correspondence to: Correspondence to: Dr JosepGamez, Servicio de Neurologia, Hospital Gral,Universitari Vall d‘Hebron, Passeig Vall d’Hebron119–135, 08035 Barcelona, Spain. email:[email protected]
1 Sasaki S, Iwata M. Atypical form of amyotrophiclateral sclerosis. J Neurol Neurosurg Psychiatry1999;66:581–5.
2 Hu MTM, Ellis CM, Al-Chalabri A, et al. Flailarm syndrome: a distinctive variant of amyo-trophic lateral sclerosis. J Neurol Neurosurg Psy-chiatry 1998;65:950–1.
3 Katz JS, Bryan WW, Andersson PB, et al. Thesyndrome of amyotrophic brachial diplegia.Neurology 1999;52(suppl 2):A83–4.
4 Erbslöh F. DiVerentialdiagnose der StoVwech-selerkrankungen des Zentralnervensystems(Degenerationen). In: Bodechtel G, ed. DiVer-entialdiagnose neurologischer Krankheitsbilder.2nd ed. Stuttgart: Georg Thieme Verlag, 1963:690–1.
5 Wilkinson M. Motor neuron disease andcervical spondylosis. In: Norris FH, Kurland L,eds. Motor neuron disease: research on amyo-trophic lateral sclerosis and related disorders. Vol II.New York: Grune and Stration, 1968:130–4.
Sasaki replies:We thank Gamez et al for their interest in ourarticle concerning the atypical form of amyo-trophic lateral sclerosis (ALS).1
Over many years, several researchers haverecognised this peculiar distribution of mus-cle atrophy in clinical practice. The clinicalmanifestations consist of the muscular atro-phy confined to the shoulder girdle and thearms (proximally dominant), absence of deeptendon reflex in the arms,almost normal deeptendon reflex in the legs, and subluxation ofthe shoulder joints. Some patients progress tobulbar involvement. As Gamez et al cite,many terms have been coined to describe thispeculiar pattern of the muscular atrophy suchas dangling arm, orang utan sign, dead armsign, suspended form, flail arm syndrome,amyotrophic brachial diplegia syndrome,bibrachial palsy and man-in-the-barrel syn-drome. Some researchers classified into acategory of motor neuron disease (ALS orspinal progressive muscular atrophy). How-ever, others could not exclude the possiblecause of cervical diseases such as dissociatedmotor loss in the upper extremity.2 In fact,these patients had cervical abnomalities suchas cervical spondylosis and ossification ofposterior longitudinal ligament disclosed bycervical radiography, MRI, or myelography.By contrast with clinical awareness of thispeculiar pattern of muscular atrophy, nopathological confirmation had been madeuntil we first reported necropsy cases in ourarticles.1 3 Now, these patients with theirpeculiar pattern of muscular atrophy are con-sidered to be ALS or a subtype of ALS. In myprivate opinion, “dangling arm syndrome” or“dead arm sign” seems to be the mostsuitable term depicting this type of motorneuron disease.
I agree with Hu et al reporting four impor-tant statistical discoveries in this form ofALS: the prevalence percentage of 10% of thewhole ALS group, the similar age onset to therest of ALS, a predominance among men (themale/female ratio was 3:1 in our study), and alonger median survival. It is clinically impor-tant to give wider publicity to the existence ofthis atypical form of ALS to avoid unneces-sary surgical intervention for cervical abnor-malities.
SHOICHI SASAKIDepartment of Neurology, Neurological Institute, Tokyo
Women’s Institute, Tokyo Women’s Medical College,8-1 Kawada-cho, Shinjuku-ku, Tokyo 162-8666,
Japan
1 Sasaki S, lwata M. Atypical form of amyotrophiclateral sclerosis. J Neurol Neurosurg Psychiatry1999;66:581–5.
2 Keegan JJ. The cause of dissociated motor lossin the upper extremity with cervicalspondylosis: a case report. J Neurosurg 1965;23:528–36.
3 Sasaki S, lwata M. Motor neuron disease withpredominantly upper extremity involvement: aclinicopathological study. Acta Neuropathol (inpress).
Isolated dysarthria
We read with interest the article by Urban etal. Using transcranial magnetic stimulation,the authors demonstrated electrophysiologi-cal evidence for a central monoparesis of thetongue in patients with isolated dysarthriafrom stroke.1 As in their patients transcranialmagnetic stimulation induced absent ordelayed corticolingual responses at thetongue, the authors ascribed isolated dysar-thria to interruption of the corticolingualpathways. On the whole, these results seemplausible, but we would like to comment onthe underlying mechanism of isolated dysar-thria.
As in the case of isolated dysarthriareported by Urban et al, all of our patientswith isolated dysarthria had lacunar infarc-tions involving the internal capsule andcorona radiata.2 Measurement of cerebralblood flow with IMP-SPECT in thesepatients disclosed frontal cortical hypoper-fusion, particularly in the anterior opercularand medial frontal regions. Anterior opercu-lar lesions produce facio-pharyngo-glosso-masticatory paresis (anterior opercular syn-drome), and damage to the medial frontalregions, including the supplementary motorarea, causes speech expression disorders.White matter lesions can disrupt aVerent andeVerent fibre connections with cerebral lan-guage areas, resulting in dysfunction of thesecortices.3 Therefore, we postulated that iso-lated dysarthria results from interruption ofcorticosubcortical networks indispensable forspeech output, involving the thalamocorticaland corticostriatal fibres as well as thecorticobulbar fibres. In fact, lacunar infarc-tions around the internal capsule-coronaradiata are likely to undercut these ascendingand descending projections.4 5
To assess corticopontocerebellar tractfunction, Urban et al investigated cerebellarblood flow in patients with isolated dysarthriausing HMPAO-SPECT. The authors con-cluded that the corticopontocerebellar tract ispreserved in isolated dysarthria because of noevidence for cerebellar diaschisis on SPECT.Their SPECT findings on cerebellar bloodflow were similar to our results. However, wewonder whether cerebral cortical blood flowwas preserved in their patients, because ourSPECT study suggested frontal cortical dys-function as an underlying mechanism of iso-lated dysarthria. Lingual paresis was clinicallyevident in three of seven patients reported byUrban et al and in two of 12 by us. This indi-cates that isolated dysarthria originates inincoordination of multiple organs necessaryfor articulation as well as a lingual monopare-sis. Although interruption of the corticolin-gual pathways is a likely cause of isolated dys-arthria, it should be borne in mind thatdamage to other descending and ascendingprojections may contribute to isolated dysar-thria.
BUNGO OKUDAHISAO TACHIBANA
Division of Neurology, Fifth Department of InternalMedicine, Hyogo College of Medicine, Nishinomiya
J Neurol Neurosurg Psychiatry 2000;68:100–126 119
on February 15, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.68.1.123g on 1 January 2000. D
ownloaded from

1 Urban PP, Wicht S, Hopf HC, et al. Isolateddysarthria due to extracerebellar lacunarstroke: a central monoparesis of the tongue. JNeurol Neurosurg Psychiatry 1999;66:495–501.
2 Okuda B, Kawabata K, Tachibana H, et al. Cer-ebral blood flow in pure dysarthria: role offrontal cortical hypoperfusion. Stroke 1999;30:109–13.
3 Okuda B, Tanaka H, Tachibana H, et al.Cerebral blood flow in subcortical globalaphasia: perisylvian cortical hypoperfusion as acrucial role. Stroke 1994;25:1495–9.
4 Ozaki I, Baba M, Narita S, et al. Pure dysarthriadue to anterior internal capsule and/or coronaradiata infarction: a report of five cases. J Neu-rol Neurosurg Psychiatry 1986;49:1435–7.
5 Rousseaux M, Lesoin F, Quint S. Unilateralpseudobulbar syndrome with limited cap-sulothalamic infarction. Eur Neurol 1987:27:227–30.
Urban et al reply:Okuda et al draw attention to their article onpure dysarthria in Stroke1 which we read withmuch interest. They refer to 12 patients withpure dysarthria, 11 of whom showed multiplebilateral infarctions involving the internalcapsule and corona radiata. The main diVer-ence to our series of seven patients is themultiple involvement of the brain. We thinkthat single lesions as collected by us2 are moreappropriate to correlate lesion topographywith impaired function. The findings ofOkuda et al are in line with our conclusionthat interruption of the corticolingual path-way is crucial in the pathogenesis of dysar-thria of extracerebellar origin. Obviously,impairment of the corticolingual tract of onehemisphere by a single small lesion is anadequate condition for dysarthria. The pa-tients of Okuda et al had more severe vasculardisorder of the brain than our patients as canbe concluded from the multiple infarctions.Thus, the bilateral frontal cortical hypoper-fusion as disclosed by SPECT in the series ofOkuda et al may be due to infarction in otherparts of the brain compared with the lesioncausing pure dysarthria.
P P URBANS WICHT
H CH HOPFDepartment of Neurology, University of Maine,
Langenbeckstrasse 1, D55101 Mainz, Germany
S FLEISCHERDepartment of Communication Disorders
O NICKELDepartment of Nuclear Medicine
1 Okuda B, Kawabata K, Tachibana H, et al. Cer-ebral blood flow in pure dysarthria: role offrontal cortical hypoperfusion. Stroke1999;30:109–13.
2 Urban PP, Wicht S, Hopf HC, et al. Isolateddysarthria due to extracerebellar lacunarstroke: a central monoparesis of the tongue. JNeurol Neurosurg Psychiatry 1999;66:495–501.
Motor cortical excitability inHuntington’s disease
We read with great interest the paper ofHanajima et al1 reporting that intracorticalinhibition of the motor cortex is normal inpatients with chorea of various origins. Atvariance with these results we previouslyfound2 a reduced intracortical inhibition in agroup of patients with genetically confirmedHuntington’s disease. Hanajima et al suggestthat the discrepancies between the two stud-ies might be due to diVerences in patientselection as they included patients with earlystage Huntington’s disease to “study thepathophysiology of chorea unaVected byother disorders movement.” They postulatedthat our cases, because of the reported corre-
lation with a dyskinesia rating scale, had amore advanced stage of the disease possiblywith coexisting dystonia or rigidity. Theseassertions deserve some comments.
The mean disease duration of our ninepatients with Huntington’s disease was 6.2(4.1) years which is actually shorter than theduration of the six patients reported byHanajima et al (8.3 (5.9) years). Most of ourpatients could be considered in an early stageof the disease, according to the UnifiedHuntington’s disease rating scale, and nonepresented dystonia, rigidity, or any otheradditional movement disorder. In this re-gard, however, it should be pointed out thatbradykinesia is often associated with choreain patients with Huntington’s disease3 andmay even precede the appearance of choreicdyskinesias.4 Chorea itself is often reduced inthe more advanced Huntington’s diseasestages.4 It is unlikely, therefore, that any neu-rophysiological approach can test purelychorea even in the early Huntington’s diseasestages. In addition, diVerent mechanisms areinvolved in Huntington’s disease and otherchoreas as suggested by the lack of impair-ment of somatosensory evoked responsesand long latency stretch reflexes in thesecond.5
We were not really surprised at the resultsof Hanajima et al as we do share their opinionthat patients with Huntington’s disease maybe characterised by large individual diVer-ences in the involvement of motor corticalareas. Actually, three patients in our studyshowed an amount of intracortical inhibitionwithin the confidence limits of the controlpopulation. We also think that the impair-ment of intracortical inhibition is likely todevelop during the disease progression as wedid not find any change in four patients, twoof them already reported,2 with positive DNAtesting but completely asymptomatic.
The discrepancies between the two studiesare more likely to be explained, at least inpart, by some methodological diVerences.For instance, the amplitude of the controlresponse was larger in our set (approximately1.0 mV compared with 0.3 mV in the study ofHanajima et al). This may induce a diVerentsensitivity of the test, and the amount ofintracortical inhibition in our normal con-trols is greater (see also6) than in the study ofHanajima et al.
When interpreting the results of studieswith paired transcranial magnetic stimulationpathophysiologically it should be kept inmind that similar changes of intracorticalinhibition have been shown in patients withvarious movement disorders (focal dystonia,myoclonus, parkinsonism, restless legs syn-drome, Tourette’s disorder), but also indiVerent diseases such as amyotrophic lateralsclerosis.7 We think, therefore, that theimpairment of intracortical inhibition cannotbe regarded as the marker of a specific patho-physiological mechanism, but is likely toreflect a non-specific imbalance of inhibitoryand facilitatory circuits within the motorcortex.
G ABBRUZZESE
R MARCHESE
C TROMPETTODepartment of Neurological Sciences and Vision,Movement Disorders Clinic, University of Genoa,
Via De Toni 5, I—16132 Genova, Italy
1 Hanajima R, Ugawa Y, Terao Y, et al. Intracorti-cal inhibition of the motor cortex is normal inchorea. J Neurol Neurosurg Psychiatry1999;66:783–6
2 Abbruzzese G, Buccolieri A, Marchese R, et al.Intracortical inhibition and facilitation areabnormal in Huntington’s disease: a pairedmagnetic stimulation study. Neurosci Lett 1997;228:87–90.
3 Thompson PD, Berardelli A, Rothwell JC, et al.The coexistence of bradykinesia and chorea inHuntington’s disease and its implication fortheories of basal ganglia control of movement.Brain 1988;111:223–44
4 Harper PS. Huntington’s disease. London: Saun-ders, 1991:37–80.
5 Berardelli A, Noth J, Thompson PD, et al.Pathophysiology of chorea and bradykinesia inHuntington’s disease. Mov Disord 1999;14:398–403.
6 Abbruzzese G, Assini A, Buccolieri A, et al.Comparison of intracortical inhibition andfacilitation in distal and proximal arm musclesin humans. J Physiol 1999;514:895–903.
7 Ziemann U, Winter M, Reimers CD, et al.Impaired motor cortex inhibition in patientswith amyotrophic lateral sclerosis. Evidencefrom paired transcranial magnetic stimulation.Neurology 1997;49:1292–8.
The authors reply:We are very grateful for the response ofAbbruzzese et al to our paper. We completelyagree with their opinions.
The discrepancy between the two studies1 2
may not be mainly due to the diVerent stageof the disease between the two groups ofpatients. Although the duration of the diseaseis one factor to judge the disease stage, theseverity of the disease (stage of the disease) isalso positively correlated with CAG repeatnumber.
We may have to take CAG repeat numberinto consideration in comparisons. Unfortu-nately, however, we have no way to do suchcomparisons between these two studies. Wecould say, at least, that the intracortical inhi-bition was normal even at the same stage ofthe disease as that of the patients of Abbruzz-ese et al, if studied with our method.
We also consider that methodological dif-ferences are very important in paired mag-netic stimulation. The results strongly dependon the intensities of both a conditioning and atest stimulus. Especially, the intensity of theconditioning stimulus is critical. We have nodiYculty in showing normal inhibition, buthave much diYculty in showing reduced orabsent inhibition because of such markeddependence of the results on the intensities ofstimuli. Therefore, we used several intensitiesof the conditioning stimulus before weconfirmed inhibition in studies of patients.3
We used an intensity of 5% less than the activethreshold as a conditioning stimulus in ourstudy of chorea.2 We did not need to changethe intensity of the conditioning stimulusbecause we always obtained a normal inhibi-tion with this intensity. We consider that this isvery important. If using a suprathreshold(active threshold) conditioning stimulus, afacilitatory eVect must often superimpose onthe intracortical inhibition. This makes theinterpretation diYcult. Was the intensity of80% of the resting threshold always below theactive threshold in their patients? In ourexperience, 80% of the resting threshold wassometimes above the active threshold. Thesefactors must be considered in interpreting theresults of paired magnetic stimulation.
Such a methodological problem is inherentin human studies because we have no directway of detecting the threshold of the motorcortex. Our two results must be true. We mayhave two completely diVerent interpretationsof these results. (1) The intracortical inhibi-tion is normal in Huntington’s disease.Abbruzzese et al showed the reduced inhibi-tion because they used a high intensity condi-tioning stimulus with which the degree of the
120 J Neurol Neurosurg Psychiatry 2000;68:100–126
on February 15, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.68.1.123g on 1 January 2000. D
ownloaded from
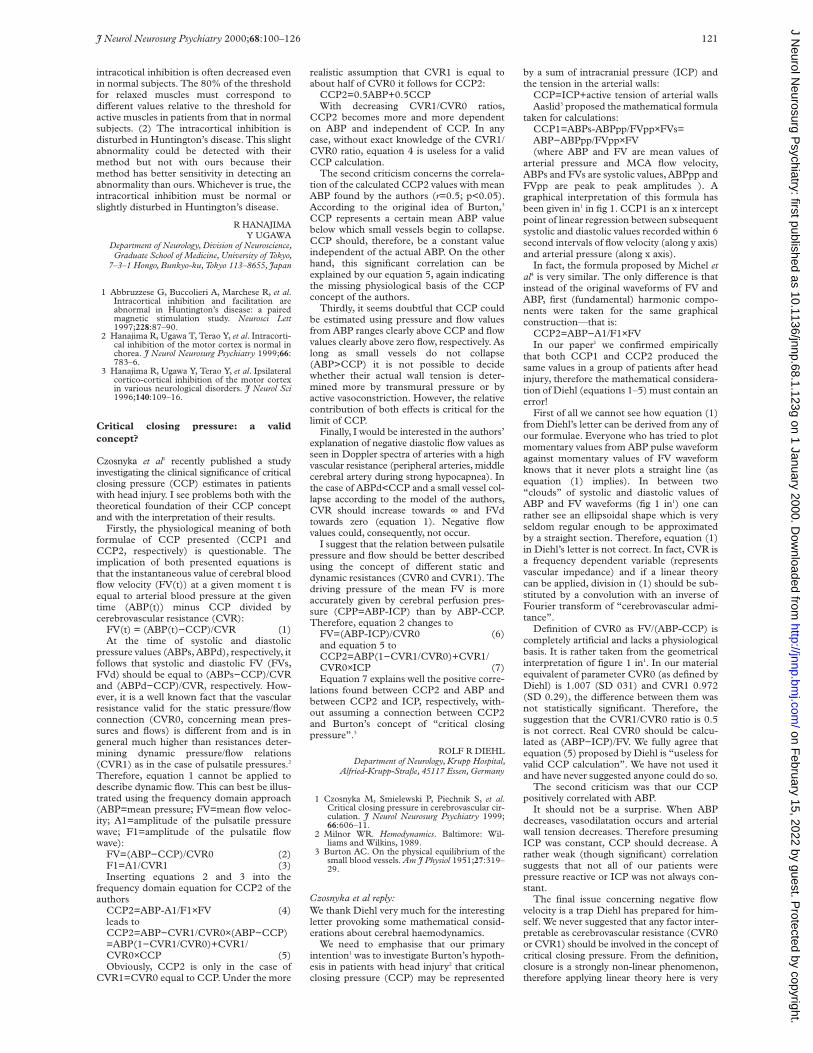
intracotical inhibition is often decreased evenin normal subjects. The 80% of the thresholdfor relaxed muscles must correspond todiVerent values relative to the threshold foractive muscles in patients from that in normalsubjects. (2) The intracortical inhibition isdisturbed in Huntington’s disease. This slightabnormality could be detected with theirmethod but not with ours because theirmethod has better sensitivity in detecting anabnormality than ours. Whichever is true, theintracortical inhibition must be normal orslightly disturbed in Huntington’s disease.
R HANAJIMAY UGAWA
Department of Neurology, Division of Neuroscience,Graduate School of Medicine, University of Tokyo,
7–3–1 Hongo, Bunkyo-ku, Tokyo 113–8655, Japan
1 Abbruzzese G, Buccolieri A, Marchese R, et al.Intracortical inhibition and facilitation areabnormal in Huntington’s disease: a pairedmagnetic stimulation study. Neurosci Lett1997;228:87–90.
2 Hanajima R, Ugawa T, Terao Y, et al. Intracorti-cal inhibition of the motor cortex is normal inchorea. J Neurol Neurosurg Psychiatry 1999;66:783–6.
3 Hanajima R, Ugawa Y, Terao Y, et al. Ipsilateralcortico-cortical inhibition of the motor cortexin various neurological disorders. J Neurol Sci1996;140:109–16.
Critical closing pressure: a validconcept?
Czosnyka et al1 recently published a studyinvestigating the clinical significance of criticalclosing pressure (CCP) estimates in patientswith head injury. I see problems both with thetheoretical foundation of their CCP conceptand with the interpretation of their results.
Firstly, the physiological meaning of bothformulae of CCP presented (CCP1 andCCP2, respectively) is questionable. Theimplication of both presented equations isthat the instantaneous value of cerebral bloodflow velocity (FV(t)) at a given moment t isequal to arterial blood pressure at the giventime (ABP(t)) minus CCP divided bycerebrovascular resistance (CVR):
FV(t) = (ABP(t)−CCP)/CVR (1)At the time of systolic and diastolic
pressure values (ABPs, ABPd), respectively, itfollows that systolic and diastolic FV (FVs,FVd) should be equal to (ABPs−CCP)/CVRand (ABPd−CCP)/CVR, respectively. How-ever, it is a well known fact that the vascularresistance valid for the static pressure/flowconnection (CVR0, concerning mean pres-sures and flows) is diVerent from and is ingeneral much higher than resistances deter-mining dynamic pressure/flow relations(CVR1) as in the case of pulsatile pressures.2
Therefore, equation 1 cannot be applied todescribe dynamic flow. This can best be illus-trated using the frequency domain approach(ABP=mean pressure; FV=mean flow veloc-ity; A1=amplitude of the pulsatile pressurewave; F1=amplitude of the pulsatile flowwave):
FV=(ABP−CCP)/CVR0 (2)F1=A1/CVR1 (3)Inserting equations 2 and 3 into the
frequency domain equation for CCP2 of theauthors
CCP2=ABP-A1/F1×FV (4)leads toCCP2=ABP−CVR1/CVR0×(ABP−CCP)=ABP(1−CVR1/CVR0)+CVR1/CVR0×CCP (5)Obviously, CCP2 is only in the case of
CVR1=CVR0 equal to CCP. Under the more
realistic assumption that CVR1 is equal toabout half of CVR0 it follows for CCP2:
CCP2=0.5ABP+0.5CCPWith decreasing CVR1/CVR0 ratios,
CCP2 becomes more and more dependenton ABP and independent of CCP. In anycase, without exact knowledge of the CVR1/CVR0 ratio, equation 4 is useless for a validCCP calculation.
The second criticism concerns the correla-tion of the calculated CCP2 values with meanABP found by the authors (r=0.5; p<0.05).According to the original idea of Burton,3
CCP represents a certain mean ABP valuebelow which small vessels begin to collapse.CCP should, therefore, be a constant valueindependent of the actual ABP. On the otherhand, this significant correlation can beexplained by our equation 5, again indicatingthe missing physiological basis of the CCPconcept of the authors.
Thirdly, it seems doubtful that CCP couldbe estimated using pressure and flow valuesfrom ABP ranges clearly above CCP and flowvalues clearly above zero flow, respectively. Aslong as small vessels do not collapse(ABP>CCP) it is not possible to decidewhether their actual wall tension is deter-mined more by transmural pressure or byactive vasoconstriction. However, the relativecontribution of both eVects is critical for thelimit of CCP.
Finally, I would be interested in the authors’explanation of negative diastolic flow values asseen in Doppler spectra of arteries with a highvascular resistance (peripheral arteries, middlecerebral artery during strong hypocapnea). Inthe case of ABPd<CCP and a small vessel col-lapse according to the model of the authors,CVR should increase towards ∞ and FVdtowards zero (equation 1). Negative flowvalues could, consequently, not occur.
I suggest that the relation between pulsatilepressure and flow should be better describedusing the concept of diVerent static anddynamic resistances (CVR0 and CVR1). Thedriving pressure of the mean FV is moreaccurately given by cerebral perfusion pres-sure (CPP=ABP-ICP) than by ABP-CCP.Therefore, equation 2 changes to
FV=(ABP-ICP)/CVR0 (6)and equation 5 toCCP2=ABP(1−CVR1/CVR0)+CVR1/CVR0×ICP (7)Equation 7 explains well the positive corre-
lations found between CCP2 and ABP andbetween CCP2 and ICP, respectively, with-out assuming a connection between CCP2and Burton’s concept of “critical closingpressure”.3
ROLF R DIEHLDepartment of Neurology, Krupp Hospital,
Alfried-Krupp-Straâe, 45117 Essen, Germany
1 Czosnyka M, Smielewski P, Piechnik S, et al.Critical closing pressure in cerebrovascular cir-culation. J Neurol Neurosurg Psychiatry 1999;66:606–11.
2 Milnor WR. Hemodynamics. Baltimore: Wil-liams and Wilkins, 1989.
3 Burton AC. On the physical equilibrium of thesmall blood vessels. Am J Physiol 1951;27:319–29.
Czosnyka et al reply:We thank Diehl very much for the interestingletter provoking some mathematical consid-erations about cerebral haemodynamics.
We need to emphasise that our primaryintention1 was to investigate Burton’s hypoth-esis in patients with head injury2 that criticalclosing pressure (CCP) may be represented
by a sum of intracranial pressure (ICP) andthe tension in the arterial walls:
CCP=ICP+active tension of arterial wallsAaslid3 proposed the mathematical formula
taken for calculations:CCP1=ABPs-ABPpp/FVpp×FVs=ABP−ABPpp/FVpp×FV(where ABP and FV are mean values of
arterial pressure and MCA flow velocity,ABPs and FVs are systolic values, ABPpp andFVpp are peak to peak amplitudes ). Agraphical interpretation of this formula hasbeen given in1 in fig 1. CCP1 is an x interceptpoint of linear regression between subsequentsystolic and diastolic values recorded within 6second intervals of flow velocity (along y axis)and arterial pressure (along x axis).
In fact, the formula proposed by Michel etal4 is very similar. The only diVerence is thatinstead of the original waveforms of FV andABP, first (fundamental) harmonic compo-nents were taken for the same graphicalconstruction—that is:
CCP2=ABP−A1/F1×FVIn our paper1 we confirmed empirically
that both CCP1 and CCP2 produced thesame values in a group of patients after headinjury, therefore the mathematical considera-tion of Diehl (equations 1–5) must contain anerror!
First of all we cannot see how equation (1)from Diehl’s letter can be derived from any ofour formulae. Everyone who has tried to plotmomentary values from ABP pulse waveformagainst momentary values of FV waveformknows that it never plots a straight line (asequation (1) implies). In between two“clouds” of systolic and diastolic values ofABP and FV waveforms (fig 1 in1) one canrather see an ellipsoidal shape which is veryseldom regular enough to be approximatedby a straight section. Therefore, equation (1)in Diehl’s letter is not correct. In fact, CVR isa frequency dependent variable (representsvascular impedance) and if a linear theorycan be applied, division in (1) should be sub-stituted by a convolution with an inverse ofFourier transform of “cerebrovascular admi-tance”.
Definition of CVR0 as FV/(ABP-CCP) iscompletely artificial and lacks a physiologicalbasis. It is rather taken from the geometricalinterpretation of figure 1 in1. In our materialequivalent of parameter CVR0 (as defined byDiehl) is 1.007 (SD 031) and CVR1 0.972(SD 0.29), the diVerence between them wasnot statistically significant. Therefore, thesuggestion that the CVR1/CVR0 ratio is 0.5is not correct. Real CVR0 should be calcu-lated as (ABP−ICP)/FV. We fully agree thatequation (5) proposed by Diehl is “useless forvalid CCP calculation”. We have not used itand have never suggested anyone could do so.
The second criticism was that our CCPpositively correlated with ABP.
It should not be a surprise. When ABPdecreases, vasodilatation occurs and arterialwall tension decreases. Therefore presumingICP was constant, CCP should decrease. Arather weak (though significant) correlationsuggests that not all of our patients werepressure reactive or ICP was not always con-stant.
The final issue concerning negative flowvelocity is a trap Diehl has prepared for him-self. We never suggested that any factor inter-pretable as cerebrovascular resistance (CVR0or CVR1) should be involved in the concept ofcritical closing pressure. From the definition,closure is a strongly non-linear phenomenon,therefore applying linear theory here is very
J Neurol Neurosurg Psychiatry 2000;68:100–126 121
on February 15, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.68.1.123g on 1 January 2000. D
ownloaded from

risky. How risky—we can see from Diehl’s let-ter. Cerebrovascular resistance certainly neverincreases to infinity, only after death.
We fully agree with the considerationsregarding equations (6) and (7). CCP can beunderstood as a combination of ABP and ICPwith coeYcients describing properties of thecerebrovascular bed. Whether it simplifies ourknowledge—we personally find it doubtful.
Finally, we are truly obliged to Diehl for anopportunity to have this interesting discus-sion.
MAREK CZOSNYKAPIOTR SMIELEWSKISTEFAN PIECHNIK
Academic Neurosurgical Unit, Box 167, Addenbrooke’sHospital, Cambridge CB2 2QQ, UK
Correspondence to: Dr Marek Czosnykaemail [email protected]
1 Czosnyka M, Smielewski P, Piechnik S, et al.Critical closing pressure in cerebrovascular cir-culation. J Neurol Neurosurg Psychiatry1999;66:606–12.
2 Burton AC. On the physical equilibrium of thesmall blood vessels. Am J Physiol 1951;164:319–29.
3 Aaslid R. Cerebral hemodynamics. In: NewellDW, Aaslid R, eds. Transcranial Doppler. NewYork: Raven Press, 1992:49–55.
4 Michel E, Hillebrand S, von Twickel J, et al.Frequency dependence of cerebrovascular im-pedance in preterm neonates: a diVerent viewon critical closing pressure. J Cereb Blood FlowMetab 1997;17:1127–31.
High frequency stimulation of thesubthalamic nucleus and levodopainduced dyskinesias in Parkinson’sdisease
Reduction in the neuronal activity of the sub-thalamic nucleus leading to diminished exci-tation of the globus pallidum internum isassociated with chorea-ballism in monkeys.1
Levodopa induced dyskinesias are currentlythought to share a similar pathophysiology2
but recent findings also suggest that abnor-mal patterns of neuronal firing in the globuspallidum internum may be as relevant.3 Datafrom both parkinsonian monkeys andpatients with Parkinson’s disease submittedto lesion4 5 or functional blockade of the sub-thalamic nucleus6 are in keeping with such ageneral principle, but the threshold to inducedyskinesias in the parkinsonian state is higherthan in intact animals.7 The case recentlydescribed by Figueiras-Mendez et al 8 isextremely interesting as it suggests that func-tional inhibition of the subthalamic nucleusby high frequency stimulation blockadeslevodopa induced dyskinesias. This is clearlyat odds with the current pathophsyiologicalmodel of the basal ganglia.9 Thus, the findingof Figueiras-Mendez et al 8 rises the intrigu-ing possibility that dyskinesias depend or aremediated by neuronal firing in a given regionof the subthalamic nucleus, which wasblocked by high frequency stimulation.Measurement of aVerent synaptic activity bythe technique of 2-deoxylucose (2-DG)uptake showed an increment in the subtha-lamic nucleus (compatible with increasedinhibition from the globus pallidum exter-num), particularly in the ventromedial tip ofthe nucleus.9 This contrasts with the findingsin monkeys with chorea induced by pharma-cological blockade of the globus pallidumexternum, in which 2-DG uptake was maxi-mal in the dorsolateral portion of the subtha-lamic nucleus, where the sensorimotor regionlies. A recent anatomical study10 also showedthat the cortical-subthalamic nucleus con-
nection is somatotopically segregated, so thatfibres from the supplementary motor areaproject to the most medial portion and fibresfrom the primary and premotor areas termi-nate in the lateral region of the subthalamicnucleus.10 All this heterogenity may havepathophysiological relevance, one aspect ofwhich could be the findings in the patientreported by Figueiras-Mendez et al.8 How-ever, before the findings of this case may beused to sustain a new hypothesis on the roleof the subthalamic nucleus in the origin oflevodopa induced dyskinesias, there is a cru-cial issue to resolve—namely, the location ofthe tip of the stimulation electrodes.
There are several points leading us toquestion the actual site of action of the elec-trode: (1) Stimulation of the subthalamicnucleus in Parkinson’s disease has been asso-ciated with the production of dyskinesias onlyrelieved by reduction in levodopa intake.6
Moreover, Benabid et al who pioneered thistechnique, consider the induction of dyskine-sias by high frequency stimulation of the sub-thalamic nucleus as a good indicator of a verypositive response. (2) Fibres travelling to thethalamus from the globus pallidum internumare placed dorsocaudally to the subthalamicnucleus and could be blocked by highfrequency stimulation. (3) When the record-ing electrode goes into a region caudally tothe subthalamic nucleus in sagittal planes 11mm or less, neuronal activity is characterisedby action potentials of large amplitudes(0.5–1 mV) with low background activity,tonically firing neurons, and absent sensori-motor responses (“driving”). All these char-acteristics seemed to be present in the patientdiscussed here. Neuronal activity in thesensorimotor region of the subthalamicnucleus is diVerent from the above but onoccasions the distinction may not be easy.
Accordingly, it is very important to docu-ment in more detail the findings in the case ofFigueiras-Mendez et al.8 Ideally we would liketo see the trajectory and length of the diVer-ent recording tracks, the eVects of micros-timulation, and the postsurgery MRI withmeasurements of the location of the tip of theelectrodes. If, as assumed, the subthalamicnucleus was indeed correctly targeted in thispatient, the pathophysiology of the basal gan-glia will need to be revisited.
J A OBESOG LINAZASORO
J GURIDIE RAMOS
Centro de Neurologia y Neurocirugia Funcional,Clinica Quiron, San Sebastian, Spain
J A OBESOM C RODRIGUEZ-OROZ
Hospiten, Tenerife, Spain
J GURIDIHospital de Navarra, Pamplona, Spain
Correspondence to: Correspondence to: ProfessorJ A Obeso, 30 Cizur Artea, Cizur Mayor, 31180Navarra, Spain.
1 Hamada I, DeLong MR. Excititoxic acid lesionsof the primate subthalamic nucleus result intransient dyskinesias in the contralateral limbs.J Neurophysiol 1992;68:1850–8.
2 Crossman AR. A hypothesis on the pathophysi-ological mechanism that underlie levodopa ordopamine agonist-induced dyskinesia in Par-kinson’s disease: implications for futurestrategies in treatment. Mov Disord 1990;5:100–8.
3 Obeso JA, Rodriguez MC, DeLong MR. Basalganglia pathophysiology. A critical review. AdvNeurol 1997;74:3–18.
4 Bergman H, Wichmann T, DeLong MR.Reversal of experimental parkinsonism bylesions of the subthalamic nucleus. Science1990;249:1436–8.
5 Guridi J, Herrero MT, Luquin MR, et al.Subthalamotomy in parkinsonian monkeys.Behavioural and biochemical analysis. Brain1996;119:1717–27.
6 Limousin P, Pollak P, HoVmann D, et al.Abnormal involuntary movements induced bysubthalamic nucleus stimulation in parkinso-nian patients. Mov Disord 1996;11:231–5.
7 Guridi J, Obeso JA. The role of the subthalamicnucleus in the origin of hemiballism andparkinsonism: new surgical perspectives. AdvNeurol 1997;74:235–47.
8 Figueiras-Mendez R, Marín F, Molina JA, et al.Subthalamic nucleus stimulation improvesdirectly levodopa-induced dyskinesias in Par-kinson’s disease. J Neurol Neurosurg Psychiatry1999;66:549–50.
9 Mitchell IJ, Jackson A, Sambrook MA, et al. Therole of the subthalamic nucleus in experimentalchorea. Evidence from 2-deoxiglucose meta-bolic mapping and horseradish peroxidasetracing studies. Brain 1989;112:1533–48.
10 Nambu A, Takada M, Inase M, et al. Dualsomatotopical representations in the primatesubthalamic nucleus: evidence for ordered butreversed body-map transformations from theprimary motor cortex and the supplementarymotor area. J Neurosci 1996;16:2671–83.
Figueiras-Méndez et al reply:We thank Obeso et al for their commentsregarding our recent report.1 In summary,they raised some interesting points whichneed further clarification.
Recognition of the electrical activity of thesubthalamic nucleus was based on the follow-ing criteria: (a) high frequency discharge (25Hz or higher) within the nucleus2 3; (b) a tonic(regular), phasic (irregular) or a rhythmic pat-tern of discharge2; (c) response to voluntary/passive movements.2 4 When rhythmic dis-charges were recorded irregular passivemanipulations were performed or the patientsasked to moved the limbs irregularly; (d)response to tremor activity. Positive cells wereso considered based on the correlated activitywith the EMG and the accelerometer re-corded simultaneously. Artificial manual stop-ping by one experimenter (confirmed byvisual inspection, silence in the EMG, andstoppage in the oscillating accelerometer)and/or spontaneous arrest in the tremormodified the firing frequency and dischargepattern or rhythmic cells corroborating thetremor nature of the cells; (e) the activity ofthe cells above the subthalamic nucleus in thethalamus and zona incerta with propercharacteristics2; (f) a change in the back-ground basal noise when entering the subtha-lamic nucleus. A higher activity is observed2;(g) the contrary is observed when leaving thenucleus. A lower background noise level; (h)the activity of substantia nigra pars reticulatacells when further lowering the microelec-tode. These cells discharge at high frequencyat regular intervals as identified in patients2
and primates.5 All these points were fulfilledby the patient reported.
Considering the questions in the letter byObeso et al, we make the following com-ments: (a) Action potentials of large ampli-tude are easily recognised from the rest of therecording cells, and are not very common.The recordings shown in the article haveamplitudes less than 0.3 mV and could not beconsidered large amplitude potentials. Westart to record activity from 3 mm beforeentering the subthalamic nucleus, traversethe length of the subthalamic nucleus, and gofurther down several mm to encountersubstantia nigra pars reticulata cells. Changesin the background activity are clearly recog-nised and are higher when entering thesubthalamic nucleus. Enough cells are re-corded along the tracks experimented so as torecognise a large amplitude potential. The
122 J Neurol Neurosurg Psychiatry 2000;68:100–126
on February 15, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.68.1.123g on 1 January 2000. D
ownloaded from

low background activity found in our record-ings is only due to the better signal-to-noiseratio of the electrodes used. “Good recordingelectrodes” depend on many variables such astip size, tip profile, insulation material,impedance, manufacture, etc.6 The signal-to-noise ratio of the cells in question has thesame ratio as the subthalamic nucleus cellshown by Hutchinson et al.2
(b) In our report, cells discharged tonically,but also other cells fired phasically, welldiVerentiated by a profuse burst activity andidentified by statistical means (autocorrela-tion and interval histograms).
(c) Motor responses and tremorgenic cellsin line with the above mentioned criteria werefound along the trajectory of the electrode.Unfortunately, this point was not mentionedin the paper. It would surely have changed theopinion of Obeso et al.
Considering the mentioned patient, a totalof eight neurons were recognised as belong-ing to the subthalamic nucleus in the righthemisphere, with a mean frequency of 74 Hz(range 38–109 Hz). Four of them respondedto passive and/or voluntary movements andone was considered tremorgenic. The stimu-lating electrode was placed in laterality 11.One track was performed. In the lefthemisphere, two tracks were performed. Onetrack was dismissed by the poor respondingactivity of the cells recorded. In the othertrack, nine neurons were recorded in the sub-thalamic nucleus (always following the abovementioned criteria) with a mean of 69 Hz(range 17–98 Hz). Five cells responded topassive and/or voluntary movements. One ofthem was also positive to tremor. The stimu-lating electrode was placed in laterality 12.The eVect of the stimulating electrode isalways tested in the surgery before cementingit and, only when the symptoms are consid-ered of unquestionable benefit it is left in thechosen place. The final position of theelectrodes, assessed by ventriculography, wasas follows: (a) posteroanterior: 1.5 mmbehind the mean point of intercommisuralline, (b) height: 6–6.5 mm below theintercommissural line, and (c) lateral: 12 mmfor the right hemisphere, and 11.5 mm for theleft hemisphere.
ROBERTO FIGUEIRAS-MÉNDEZFERNANDO MARÍN-ZARZA
JOSÉ ANTONIO MOLINAFÉLIX JAVIER JIMÉNEZ-JIMÉNEZ
MIGUEL ORTÍ-PAREJACARLOS MAGARIÑOS
MIGUEL ANGEL LÓPEZ-PINOVICENTE MARTÍNEZ
Correspondence to: Correspondence to: Dr FJiménez-Jiménez, C/Corregidor, Jose de Pasamonte24 3°D, E 28030 Madrid, Spain
1 Figueiras-Méndez R, Marín-Zarza F, MolinaJA, et al. Subthalamic nucleus stimulationimproves directly levodopa-induced dyskine-sias in Parkinson’s disease. J Neurol NeurosurgPsychiatry 1999;66:549–50.
2 Hutchinson WD, Allan RJ, Opitz H, et al. Neu-rophysiological identification of the subtha-lamic nucleus in surgery for Parkinson’sdisease. Ann Neurol 1998;44:622–8.
3 Benabid AL, Pollak P, Benazzouz A, et al.Grenoble guidelines for deep brain stimula-tion. First European Symposium on Stimula-tion in Parkinson’s disease. 1998.
4 Limousin P, Pollak P, Benazzouz A, et al. EVectof parkinsonian and symptoms of bilateral sub-thalamic nucleus stimulation. Lancet 1995;345:91–5.
5 Magariños-Ascone C, Buño W, García-AausttE. Activity in substantia nigra neurons relatedto a simple learned movement. Exp Brain Res1992;88:283–91.
6 Lemon R, Prochazka AS. In: Smith R, ed. IBROHandbook series: method in neuroscience. NewYork: Wiley, 1985:71–98.
Nitric oxide in acute ischaemic stroke
The pivotal role of nitric oxide (NO) incerebral ischaemia has been elegantly high-lighted in the recent editorial by O’Mahonyand Kendall.1 Although studies of neuropro-tective agents have been largely disappoint-ing, pharmacological manipulation of NOmay represent a novel means of protecting thebrain from ischaemic insult. One area notdiscussed in this editorial is the neuroprotec-tive eVect of 3-hydroxy-3methylglutarylcoenzyme A reductase inhibitors or “statins”in cerebral ischaemia. Preliminary studieshave shown that statins modulate brain nitricoxide synthase (NOS) isoform activity in aneuroprotective manner. Data from a murinemodel of ischaemic stroke demonstrate thatprophylactic statin therapy reduces infarctsize by about 30%, and improves neurologi-cal outcome in normocholesterolaemicanimals.2 In this investigation, statin therapydirectly up regulated endothelial NOS in thebrain without altering expression of neuronalNOS. Recent findings also suggest that statintherapy influences the activity of inducibleNOS. Lovastatin has been shown to inhibitcytokine mediated upregulation of inducibleNOS and production of NO in rat astrocytesand macrophages,3 and this inhibition mayrepresent a novel means of suppressinginflammatory responses that accompany is-chaemia. Most interestingly, these prelimi-nary findings suggest that statin therapy maymodify the friendly and unfriendly faces ofbrain NO in a synergistically neuroprotectivemanner. These and other vascular eVects4 ofstatins in cerebral ischaemia are potentially ofgreat importance in human neuroprotectionand ongoing studies such as the TheProspective Study of Pravastatin in theElderly at Risk (PROSPER) study5 will helpclarify their role in human cerebrovasculardisease.
CARL J VAUGHANDivision of Cardiology, Department of Medicine, WeillMedical College of Cornell University, The New York
Presbyterian Hospital, Starr 4, 525 E. 68th Street, NewYork, New York 10021, USA
NORMAN DELANTYDepartment of Neurology, Hospital of the University of
Pennsylvania, Philadelphia, Pennsylvania, USA
Correspondence to: Dr Carl J Vaughanemail [email protected]
1 O’Mahony D, Kendall MJ. Nitic oxide in acuteischaemic stroke: a target for neuroprotection.J Neurol Neurosurg Psychiatry 1999;67:1–3.
2 Endres M, Laufs U, Huang Z, et al. Strokeprotection by 3-hydroxy-3-methylglutaryl(HMG)-CoA reductase inhibitors mediated byendothelial nitric oxide synthase. Proc NatlAcad Sci 1998;95:8880–5.
3 Pahan K, Sheikh FG, Namboodiri AMS, et al.Lovastatin and phenylacetate inhibit the induc-tion of nitric oxide synthase and cytokines inrat primary astrocytes, microglia, and macro-phages. J Clin Invest 1997;100:2671–9.
4 Delanty N, Vaughan CJ. Vascular eVects of stat-ins in stroke. Stroke 1997;28:2315–20.
5 Gaw A, Shepherd J, Blauw GL, et al. Pravastatinin the prevention of cerebrovascular diseaseand its consequences in the elderly-the PROS-PER design [abstract]. Stroke 1999;30:251A.
O’Mahony replies:The comments of Vaughan and Delanty drawattention to the evidence that statin therapyup regulates endothelial NOS without aVect-ing neuronal NOS. Their contention is thatstatin therapy may be neuroprotective. Stat-ins may indeed prevent strokes and reduceinfarct size when given as prophylactictherapy in at risk persons. However, our edi-torial article was not intended to discuss the
wide variety of pharmacological agents thatmay have favourable eVects on endothelialNOS as stroke preventive therapy. Rather, itis focused on the possible ways of inhibitingneuronal NOS and inducible NOS mediatednitric oxide release after the event of acutestroke. At present, there is no informationindicating that acute administration of statinsin animal models of ischaemic stroke is neu-roprotective. Their point about statins andendothelial NOS is interesting, but notrelevant to neuroprotective therapy in acutestroke.
DENIS O’MAHONYClinical Investigation Unit, Queen Elizabeth Hospital,
Edgbaston, Birmingham B15 2TH, UK
BOOK REVIEWS
Immunological and Inflammatory Disorders Ofthe Central Nervous System. Edited by NEIL
SCOLDING. (Pp264, £45.00). Published byButterworth Heinemann, Oxford, 1999. ISBN0-7506-2357-8.
That neuroimmunology has come of age isdemonstrated by the profusion of volumespublished on the subject in recent years. Thisvolume focuses on the central nervoussystem, and aims to satisfy the curiosity ofboth the clinician faced with a diagnosticconundrum and the experimental immunolo-gist inquiring into the clinical relevance of hisfindings. At first sight it seems improbablethat both of these goals might be achieved inone volume; this book however, succeedsadmirably in what it sets out to do, as much asa result of its literary style as its content.
The intrusive authorial voice fell into disfa-vour in literary circles around the turn of thecentury because it was thought that callingattention to the act of narrating might detractfrom realistic illusion, so reducing the emo-tional intensity of what was being represented.It is a device much favoured by postmodernwriters, who expose the nuts and bolts of theirfictional constructs. The intrusive medicalauthor never dropped out of fashion, althoughin these days of evidence based prejudice,authorial omniscience might be consideredsuspect. The authors of this volume are intru-sive in a guiding conversational manner thatmakes this book by far the most readable ofthe neuroimmunological texts.
The book opens with a highly accessiblechapter on immune responses in the nervoussystem. There follows a chapter that inte-grates the neurobiology of multiple sclerosiswith contemporary issues of aetiology, cellinjury, and repair. Next, a chapter on inflam-matory demyelinating diseases examines syn-dromes of isolated demyelination, acutedisseminated encephalomyelitis and alliedconditions, and some of the syndromes ofdemyelination that are now accepted as partof the range of multiple sclerosis. Thechapters on demyelinating disease are drawnto a close by a discussion of existing andexperimental therapies for multiple sclerosis.
The book continues with chapters on para-neoplastic disorders of the CNS, stiV mansyndrome, neurological complications of
J Neurol Neurosurg Psychiatry 2000;68:100–126 123
on February 15, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.68.1.123g on 1 January 2000. D
ownloaded from

connective tissue disorders, organ specificautoimmunity, sarcoidosis, and cerebral vas-culitis.
Each chapter is an appropriate length andwell referenced; the wood is always clearlyvisible between the trees. This book issuYciently readable and small to be recom-mended as holiday reading. Its only drawbackis that in making erudition so readilyavailable, one risks being outshined yet againby one’s registrar.
JON SUSSMAN
Alzheimer’s Disease—From BasicResearch to Clinical Applications. Editedby HERMANN J GERTZ and THOMAS ARENDT.(Pp315, US$99.00). Published bySpringer-Verlag, Wien, 1998. ISBN
3-211-83113-4.
As Alzheimer’s disease becomes of increasingimportance to society, basic science researchin this field needs to provide the buildingblocks for both therapeutic interventions andaccurate diagnosis. This publication is acollection of papers presented at an inter-national Alzheimer’s disease research meet-ing in Leipzig in 1997. This conference aimedto bring together both clinical and basicscience disciplines and this is reflected in thepapers selected for this book. There are 31papers included, covering topics from earlysymptomatology and cognitive features toimmunobiology and theoretical neuronaltreatment strategies. The contributors to thisbook are some of the most authoritative intheir field, predominantly based in Europe.
Covering all aspects of Alzheimer’s diseaseresearch from the correct diagnosis to basicscience approaches of treatment is ambitiousfor such a compact book (315 pages), andalthough the editors succeed in collecting aninteresting series of papers around thesethemes, they make no claims to be compre-hensive in their scope. The papers includedrange from original research reports toreviews of the current literature. The reviewpapers are generally excellent, concise, clear,well referenced, and illustrated—for example,there are excellent reviews of Alzheimer’s dis-ease with vascular pathology (Pasquier et al),and Lewy body disease (McKeith et al), greatupdates on neuropathology (Jellinger andBancher, Braak et al), and several worthyreviews of treatment strategies forAlzheimer’s disease including NSAIDS(Möller), antioxidants, and radical scavengers(Rösler et al). I found the review by Reisburget al on ontogenic models in the understand-ing of the management of Alzheimer’s diseaseparticularly interesting. However, the papersof original research are of more limited inter-est to the general reader. Although, asmentioned, the quality of illustrations isgood, there is some variability in the defini-tion of abbreviations and occasional lapsesinto other European languages.
Certainly, I think this book would be ofvalue for investigators interested in theneuropathology, immunopathology, and mo-lecular biology of Alzheimer’s disease. Itwould make an excellent addition to librariesas a reference text for many researchers ofvaried interests.
CLARE GALTON
Neurologic Complications in OrganTransplant Recipients. Edited by ELCO F M
WIJDICKS (Blue Books of PracticalNeurology). (Pp 248, £70.00). Published ByButterworth Heinemann, Oxford, 1999.ISBN 0 7506 7066 5.
Organ transplantation, once medical exotica,is now almost routine. In the UnitedKingdom each year are performed cadavericorgan transplants of about 1800 kidneys (inaddition to 160 live kidney donors), 700livers, and 450 heart/lungs (UK TransplantSupport Service Authority). The basic surgi-cal techniques were established at the begin-ning of the century in canine models. Trans-lation of these experiments to humansawaited safe and eVective immunosuppres-sion. Until the 1960s, the only forms ofimmunosuppression were radiation (totalbody or total lymphoid) and non-selectivechemical reagents (benzene and toluene).Then the antiproliferative drug6-mercaptopurine (6-MP) was introduced,shortly followed by a derivative, azathioprine,with improved oral bioavailability. Combinedwith corticosteroids, these allowed the firsthuman solid organ transplants to be per-formed: in 1963 the first lung transplant inMississippi and liver transplant in Colorado.Then in 1967 Christian Barnard captured theworld’s imagination with the first heart trans-plant. His technique has been modifiedslightly since, but the increasing success oforgan transplantation rests mainly on im-proved immunosuppression with drugs thatselectively suppress lymphocytes by inhibit-ing lymphokine generation (cyclosporin A,tacrolimus), signal transduction (sirolimus,leflunomide), or diVerentiation (15-deoxyspergualin) pathways. As a result, overthe last 10 years in the United Kingdom, the1 year survival of grafts has improved from80% to 90% (kidney), 55% to 75% (liver),and 70% to 90% (heart/lung).
Wijdicks estimates that 10% of transplan-tation patients have a significant neurologicalcomplication, the three most common beingneurotoxicity of immunosuppressive drugs,seizures, and failure to awaken. Yet this is thefirst text devoted to the neurological aspectsof organ transplantation. It is therefore atimely subject for another title in the excellentBlue Books Of Practical Neurology series.Twenty authors contribute (one Dutch, oneSwiss, the rest American) to four chapters onthe transplant procedures themselves fol-lowed by 10 chapters on neurological compli-cations of transplantation including failure toawaken, and psychiatric, neuromuscular anddemyelinating complications. Especially use-ful to the neurologist without much experi-ence of transplantation are the comprehen-sive chapters on immunosuppressive drugsand the opportunistic infections associatedwith them (most commonly Listeria monocy-togenes, Aspergillus fumigatus, and Cryptococcusneoformans). The peripheral nerve and plexusinjuries associated with transplantation arepainstakingly described; astonishingly a sig-nificant ulnar neuropathy occurs in up to40% of kidney transplants. The CincinnatiTransplant Tumour Registry has recordedinformation on 10 813 cancers arising de novoin organ allograft recipients worldwide andhere are presented the data in the 300 of thesewith CNS involvement. This is one for theshelves of any neurologist involved in organtransplantation.
ALASDAIR COLES
Stroke and Alzheimer’s Disease. Editedby DIDIER LEYS, FLORENCE PASQUIER, and PHILIP
SCHELTENS. (Current Issues in Neuro-degenerative Diseases Volume 9). (Pp 225).Published by Holland Academic Graphics,The Hague, 1998. ISBN 90-5560-061-9.
Volume nine of the Current Issues in Neurode-generative Diseases series examines the inter-play between cerebrovascular disease anddementia, particularly Alzheimer’s disease.Two hundred pages of what are essentially 20brief review articles comprise this text, sadlywithout any illustrations. Ploughing throughthe introduction to each chapter there is acertain sense of deja vu, although on thepositive side each contribution is extremelywell referenced.
The book is divided into five sections cov-ering the historical concepts of vascular andAlzheimer’s dementias, the arguments for apure vascular dementia, the role ofAlzheimer’s disease in the genesis of demen-tia after stroke, the contribution of whitematter changes on neuroimaging to demen-tia, and finally a short section examiningpractical questions such as the managementof stroke in patients with dementia.
Although common conditions in their ownright, stroke and Alzheimer’s disease doseem to cross paths more often than wouldbe expected by chance alone, and more oftenthan can be explained by the presence ofamyloid angiopathy and recurrent lobarhaemorrhages. Perhaps common geneticfactors are responsible and here the APoEalleles are discussed. The comprehensivesection on deep white matter lesions seeks toexplain the connection further—and con-vinces the reader that there is still a lot whichis not well understood. It is in this sectionparticularly that illustrations are greatlymissed. Brief mention is made of other con-ditions which may produce white matterchanges and dementia such as CADASIL,cerebral lupus, and the primary antiphos-pholipid syndrome.
Some typographical errors and mistransla-tions detract a little further from a bookwhich seems unlikely to appeal to most neu-rologists, although it will no doubt be asource of reference to those working in thefield of cognitive disorders, particularly vas-cular dementias.
PETER MARTIN
Healing Stories—Narrative in Psychiatryand Psychotherapy. Edited by GLENN
ROBERTS AND JEREMY HOLMES. (Pp 226,£47.50). Published by Oxford University,Oxford, 1999 ISBN 0-19-262827-5.
Evolutionary biologists would probably tellus that the enchantment of stories is due tosurvival having been dependent on thepassing of oral culture from one generation tothe next. Information put in narrative formnot only delights, but is easily recalled.Stories also construct meaning by interweav-ing observation, inference, motive, and con-sequence in a fashion that informs futureaction. Our experience of the world isconstructed around such narratives. Theydefine us as individuals, family members,professionals, and cultural groups.
This book is a series of essays onpsychotherapy, psychiatry, and also medicinethat sees the awareness and use of narrative inclinical practice as a construct that can both
124 J Neurol Neurosurg Psychiatry 2000;68:100–126
on February 15, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.68.1.123g on 1 January 2000. D
ownloaded from

deliver eVective care as well as act as a concep-tual bridge between the diVerent disciplines.One of the great pleasures of being a doctorhas always been listening to patient’s stories,but the editors of this book fear that this essen-tial art can be overtaken by dull scientificpragmatism. Roberts, in the most outstandingchapter, writes a lucid and well reasonedaccount of the need to search for and maintainnarrative meaning in treating psychosis. Thisavoids the dehumanising eVect to both pa-tients and professionals of identifying individu-als by their illness as in schizophrenics. Everypsychiatric library should buy this book for thispaper alone, which should be required readingfor all psychiatric trainees.
The rest of this book is of variable quality.There is a rather prosaic essay on genderissues, and there is repetition in various chap-ters concerning attachment theory, a usefulbut over worked paradigm. However, thereare two very fine accounts of narrative in psy-chotherapy by James Phillips and JeremyHolmes.
DUNCAN MCLEAN
Women and Epilepsy. By TIM BETTS andPAM CRAWFORD. (Pp 84, gratis from theBritish Epilepsy Association). Published byMartin Dunitz, London, 1998. ISBN1-85317-680-X.
In a small accessible and easily digestiblevolume, the authors address a clinically impor-tant field. Faced with slim evidence on whichto base clinical recommendations, they ac-knowledge that their very useful managementadvice “has often had to be based on practicalclinical experience rather than the results ofclinical trials or formal research . . .” This dis-claimer seems to have allowed them to mixevidence and opinion, limit references, andconfuse the reader regarding the level ofevidence. A pity, as the authors, with specialexpertise in this important area, have made agood start in putting together diVerent aspectsof the care of the woman with epilepsy in apractical book that is of direct interest and rel-evance to neurologists, obstetricians, generalpractitioners, nurse specialists, and trainees.
Moving on from the general to the particu-lar, the text, although expansive in parts,glosses over some important points. Exam-ples include (a) which oral vitamin K prepa-rations are considered safe in pregnancy(phytomenadione), (b) diVerential eYcacy ofvarious antiepileptic drugs in diVerent syn-dromes versus side eVect and teratogenicityprofile, (c) more information on the limita-tion of available evidence to support thestatement “no monotherapy human abnor-mality reported” with certain new antiepilep-tic drugs in pregnancy, (d) the need toconsider osteoporosis prevention well beforethe menopause (and not only with enzymeinducing drugs such as valproate has alsobeen implicated), (e) discussion of differences(and available formulations) between syn-thetic and natural progesterone, (f) stages ofpregnancy when various malformations aredetectable on scanning, and (g) time toclosure of the neural tube (diVerent from the21-56 days they quote as the “most sensitivetime of the fetus to the induction ofmalformations by exogenous agents.”).
Despite these comments (made with an eyeon the next edition) I would recommend thisbook to all those involved in the care ofwomen with epilepsy.
LINA NASHEF
Childhood Epilepsies and BrainDevelopment. Edited by ASTRID NEHLIG,JACQUES MOTTE, SOLOMON L MOSHE, andPERRINE PLOUIN. (Pp 311, £59.00). Publishedby John Libbey, London, 1999. ISBN 0–86196–578–7.
Childhood Epilepsies and Brain Development isthe fruit of a symposium held in 1997 to tryand bridge the chasm between those workingin the clinic or at the bedside and those in thelaboratory. Both groups must collaborate andcommunicate to improve the management ofchildren (and older patients) with epilepsy.
The book is essentially a collection ofmonographs of heterogeneous content andstyle and the result, perhaps not surprisingly,is that some of the component parts are bet-ter than the sum. The clinically oriented sec-tion will clearly be of particular interest tothose who treat children and their families.The chapters on infantile spasms andLennox-Gastaut syndrome are informativeand provide some new but speculativeinsights into the pathogenesis of spasms.However, it was surprising that severe myo-clonic epilepsy of infancy did not merit a spe-cific chapter in view of the unique electro-clinical evolution and natural history of thissyndrome. The crucial issue of the cognitiveand behavioural sequelae of early and fre-quent seizures on the immature brain, whichis probably of most concern to both cliniciansand families, is succinctly addressed in twochapters—although a clear and consistentcause and eVect relation remains to be estab-lished. The chapters covering basic neuro-physiology, neuropharmacology, and neu-ropathology, are erudite and fascinating butat times are barely comprehensible. Furtherwork is needed, including answering the fun-damental question—why does the first sei-zure occur—before the clinician and basicscientist are able to talk the same language—for the benefit of the patient with epilepsy.
The concept of Childhood Epilepsies andBrain Development is innovative and com-mendable and although some of the mono-graphs are interesting and informative, theoverall impression is that the individual parts(the chapters) are better than the whole (thebook). The lack of an index is a strange omis-sion, perhaps reflecting a prolonged editorialatypical absence, and although this militatesagainst it becoming a well thumbed referencetext, the book is an erudite addition to themossy fibre-like sprouting of the epileptologi-cal literature.
RICHARD E APPLETON
DiYcult Clinical Problems inPsychiatry. Edited by MALCOLM LADER andDIETER NABER. (Pp 246, £39.95). Publishedby Martin Dunitz, London, 1999. ISBN1-85317-550-1.
DiYcult clinical problems in psychiatry comein many forms. Diagnosis often causesdiYculty, particularly in cases which demandsome assessment of the role of physical illnessin symptom formation. Perhaps for most psy-chiatrists practising in community settingsrisk assessment comes high on their list ofconcerns.
Unsurprisingly, given the psychopharma-cological expertise of the editors, this book isparticularly interested in treatment resist-ance. The first 6 chapters give excellentreviews of the management of clinically
relevant topics—for example, refractoryschizophrenia or the diYcult panic patient.The emphasis is very much on pharmacologi-cal management.
The second half of the book is more of amixed bag, both in terms of the areas coveredand the quality of the chapters. Two excellentchapters covering all aspects of the assessmentand management of anorexia nervosa andchronic fatigue are followed by a thoroughreview of the pharmacological management ofsubstance misuse. Then come two weakchapters on behavioural disturbances in oldage and the violent patient in the community.This last chapter will be of particular interestto community psychiatrists but is not one thatI would recommend because some aspects ofthe practical management of violence aremissing—for example, a documented risk-benefit analysis, good failsafe communication,or deciding when to detain. One of the lastchapters is a very good account of themanagement of hyperactivity in childhood,with good practical advice on the use of meth-ylphenidate.
Apart from the chapters on chronic fatigueand the treatment of tardive dyskinesia thereis little in this book which is of immediateinterest to neurologists. However generalpsychiatrists wishing to improve their pre-scribing skills will find this book useful.
SIMON FLEMINGER
The Bethlem and Maudsley NHS TrustPrescribing Guidelines 1999. Edited byDAVID TAYLOR, DENISE MCCONNELL, HARRY
MCCONNELL, KATHRYN ABEL, and ROBERT
KERWIN. (Pp190, £14.95). Published byMartin Dunitz, London, 1999. ISBN1-85317-835-7.
The Maudsley prescribing guidelines areproduced each year for a local readership, butthis, the fifth edition, is the first to go public.The authors and principal contributors, amixture of pharmacists and psychiatrists withan interest and background in clinicalpsychopharmacology, are to be compli-mented on producing a guide of manageablesize and ready accessibility.
The book is divided into sections dealingwith the treatment of broad groups of clinicaldisorders—for example, psychosis—specialpatient populations—for example, elderlypeople, with further sections on the manage-ment of emergencies and the adverse eVects ofpsychotropic drugs. Much of the informationis laid out in tabular form. It could become anindispensable resource for a busy on call sen-ior house oYcer (the dimensions would fitcomfortably into the pocket of a clinical whitecoat, were they still to be worn) but more sen-ior clinicians will find plenty of use for it in theclinic. It does not aim at great erudition, butprovides a useful list of references.
There are a few cavils. The section ontreatment of anxiety is skimpy (one and a halfpages) compared with say the treatment ofaVective illness (22 pages) or psychosis (16pages). The brevity is only partly explainedby the undeveloped state of that particulararea of psychopharmacology. Sections oncontraindications to and indications for lum-bar puncture and indications for EEG seemto have been displaced from some otherprimer for busy junior doctors. There is noindex.
These quibbles apart, prescribing guide-lines can be wholeheartedly recommended.
BRIAN TOONE
J Neurol Neurosurg Psychiatry 2000;68:100–126 125
on February 15, 2022 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.68.1.123g on 1 January 2000. D
ownloaded from