
Language development in autism spectrum disorder
298
Language development in autism spectrum disorder: longitudinal comparison with a community cohort of children with language impairment and typical development Amanda Brignell Bachelor of Applied Science (Speech Pathology) Master of Public Health Submitted in total fulfilment of the requirements of the degree of Doctor of Philosophy October 2016 Department of Paediatrics Faculty of Medicine, Dentistry and Health Sciences The University of Melbourne Produced on archival quality paper
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Language development in autism spectrum disorder

Language development in autism spectrum disorder:
longitudinal comparison with a community cohort of children
with language impairment and typical development
Amanda Brignell
Bachelor of Applied Science (Speech Pathology)
Master of Public Health
Submitted in total fulfilment of the requirements of the degree of
Doctor of Philosophy
October 2016
Department of Paediatrics
Faculty of Medicine, Dentistry and Health Sciences
The University of Melbourne
Produced on archival quality paper

ii
Abstract
Background
Autism spectrum disorder (ASD) is a lifelong developmental disability that affects more
than 1 in 50 children in Australia. Language difficulties are common in ASD with up to
30% of children unable to communicate using words. Despite a substantial number of
studies examining language outcomes in individuals with ASD, it is difficult for
families and clinicians to interpret study findings. This is because many studies use;
selected clinical samples that may not generalise to the broader population,
heterogeneous methodology, and the quality of studies varies. Rarely do studies use
standardised language-specific tools. In addition, few studies have compared
development in children with ASD to children without ASD, which means it is difficult
to place differences in children with ASD within a developmental context. As a
consequence, we do not yet fully understand how language develops in children with
ASD and we are not able to accurately predict language outcomes. Parents and
clinicians need evidence about language trajectories in ASD to inform decision-making
and understand prognosis. Service providers and policy makers also require information
for appropriate resource allocation for current and future needs.
Aims
The overall aim of this thesis was to examine trajectories of language development in
individuals diagnosed with ASD. To achieve this aim, three main studies were
conducted. Study 1 systematically reviewed and synthesised the extant literature on
language outcomes in individuals with ASD. Studies 2 and 3 examined individual and
mean trajectories of language development in children with ASD from 1 to 2 years and
4 to 7 years, respectively, and compared these trajectories to large samples of children

iii
with language impairment (LI) and typical language development (TD). Study 3
described language trajectories for children with ASD and investigated predictors of
language outcomes from 4 to 7 years in children with and without ASD.
Method
Children in studies 2 and 3 were recruited from a prospective longitudinal community-
based study of 1910 children in Victoria (the Early Language in Victoria Study; ELVS).
Individual and mean trajectories were mapped from 1 to 2 years (ASD; n=41, LI:
n=119, TD: n=861) and 4 to 7 years (ASD; n=27, LI n=110, TD: n=831). In Study 2,
individual and mean communication trajectories were mapped using scores from two
parent checklists, namely the Communication Symbolic Behaviour Scales Infant
Toddler Checklist and the MacArthur Bates Communicative Development Inventories.
We compared the proportion of children who lost specific communication skills
between the three groups (ASD, LI, TD) and the spread of loss across different
communication domains. In Study 3 we used the Clinical Evaluation of Language
Fundamentals data collected in ELVS (preschool second edition and fourth edition) to
map individual and mean language trajectories from 4 to 7 years. The proportion of
children who had declined, remained stable or accelerated in language skills was
compared across groups. Putative predictors of language outcomes were also
investigated.
Results
Language ability was heterogeneous, however, mean scores for children with ASD and
LI were lower than scores for children with TD and reference norms, in all studies
included in the systematic review and Studies 2 and 3 in the community sample.

iv
From 1 to 2 years, the gap between children with ASD and TD/LI grew larger in all
communication domains except in the areas of speech and expressive vocabulary, which
was similar for children with LI and ASD.
From 4-7 years, despite having lower language ability on average compared with the
typically developing group, most children with ASD were developing language at the
same pace as the LI and TD children. A diagnosis of ASD did not predict a greater gap
between receptive and expressive language ability. The child’s early language ability
and IQ were most important in predicting language ability at a later age.
Conclusion
Systematic review and synthesis of existing studies showed that children with ASD in
all studies (with one exception) had lower scores at baseline when compared with
reference norms but children tracked in parallel to reference norms. The limited amount
of data available from studies investigating children over 9 years made it difficult to
draw accurate conclusions on trajectories beyond this age, however the few studies that
had presented data suggest rate of language progress may slow from around 10 years.
In Studies 2 and 3 that utilised the ELVS, children with ASD demonstrated
communication abilities that were not significantly different to other children at12
months of age in most areas. However, on average their language and social
communication progressed at a slower rate than other children from around 12 months
to 2 years in most areas of communication. Findings from children in the ELVS aged 4
to 7 years were consistent with the systematic review findings. In Study 3 children with
ASD who were verbal and had IQ in the normal range demonstrated lower language
scores at baseline and follow up on average, but tracked in parallel to reference norms

v
over time. The knowledge gained from this thesis will help guide prognostic
information to be provided to parents. It will also assist with planning for future support
needs of individuals with ASD.

vi
Declaration
This is to certify that
1. The thesis comprises only my original work towards the Doctor of Philosophy except
where indicated in the preface
ii. Due acknowledgement has been made in the text to all other material used
iii. This thesis is fewer than 100,000 words in length, exclusive of tables, maps,
bibliographies and appendices.
Amanda Brignell

vii
Preface
I acknowledge the contribution of the following co-authors to the published and
unpublished work in Studies 1-3 (Chapters 6, 7 &8). A description of the contribution
of each author is outlined below.
Study 1. A systematic review of language outcomes in autism spectrum disorder.
Prof Katrina Williams, A/Prof Angela Morgan, Kim Jachno, Dr Susan Woolfenden, Dr
Tamara May, Dr Felicity Klopper, Dr Vanessa Sarkozy.
Protocol development and modification: KW, SW, VS, AB; database search
development and modifications; Katy Sterling-Levis, AB; sifting articles: AB, SW, VS,
FK, TM, KW; data extraction: AB, FK; risk of bias assessments: AB, AM, TM;
statistical analysis: AB, KJ; manuscript preparation: AB; manuscript review and editing:
KW, AM, SW, TM, FK, VS, KJ.
Study 2. Parent reported patterns of loss and gain in communication in 1 to 2 year
old children are not unique to autism spectrum disorder. A/Prof Angela Morgan,
Prof Katrina Williams, Prof Margot Prior, A/Prof Susan Donath, Prof Sheena Reilly,
Prof Edith Bavin, Dr Patricia Eadie.
Study conceptualisation and design: AB; data management: AB, statistical analysis:
AB, SD; manuscript preparation and submission: AB; manuscript review, response to
reviewers and manuscript revisions: AB; editing and manuscript revision: AM, KW,
MP, SR, EB, PE, SD.

viii
Study 3. Language trajectories and predictors of language outcome from 4 to 7
years in children with and without autism spectrum disorder. A/Prof Angela
Morgan, Prof Katrina Williams, Kim Jachno, Prof Margot Prior, Prof Sheena Reilly.
Study conceptualisation and design: AB; data management: AB, statistical analysis:
AB, KJ; manuscript preparation: AB; manuscript review and editing: AM, KW, MP,
SD, SR, KJ.

ix
Publications and presentations arising from this thesis
Peer reviewed publication
Brignell, A., Prior, M., Donath, S., Reilly, S., Bavin, E.L., Eadie, P., Williams, K., Morgan, A. (2016) Parent reported patterns of loss and gain in communication in 1-2 year old children are not unique to autism spectrum disorder. Autism, DOI: 10.1177/1362361316644729
Conference presentations
Brignell, A., Williams, K., Jachno, K., Reilly, S., Prior, M., Morgan, A. Trajectories of language development in children with autism spectrum disorder. Australian Society for Autism Research (ASfAR) Conference. Perth, Australia. Oral presentation. December 2016 (accepted).
Brignell, A., Morgan, A., Woolfenden, S., Klopper, F., Jachno, K., Sarkozy, V., Williams, K. A systematic review of language outcomes in autism spectrum disorder. Oral poster presentation. Autism-Europe Congress. Edinburgh, United Kingdom. Oral poster presentation. September 2016.
Brignell, A., Williams, K., Jachno, K., Reilly, S., Prior, M., Morgan, A. Trajectories of language development in children with autism spectrum disorder. Autism-Europe Congress. Edinburgh, United Kingdom. Oral presentation. September 2016.
Brignell, A., Williams, K., Morgan, A. Language Development in Autism Spectrum Disorders. International Association for the Scientific Study of Intellectual and Developmental Disabilities (IASSIDD) World Congress. Melbourne, Australia. Oral presentation. August 2016.
Brignell, A. Language outcomes in ASD. Topics in Child and Adolescent Mental Health. Melbourne, Australia. Oral presentation. March 2016.*
Brignell, A., Morgan, A., Woolfenden, S., Sarkozy, V., Klopper, F., Williams, K. A systematic review of language outcomes in autism spectrum disorders. Victorian Autism Research Forum. Melbourne, Australia. Oral presentation. November 2015.
Brignell, A., Prior, M., Donath, S., Reilly, S., Bavin, E.L., Eadie, P., Williams, K., Morgan A. Loss of communication skills over the second year of life in children with autism spectrum disorder. Victorian Autism Research Forum. Melbourne, Australia. Poster presentation. November 2015.

x
Brignell, A., Morgan, A., Woolfenden, S., Sarkozy, V., Klopper, F., Williams, K. A systematic review of language outcomes in autism spectrum disorders. International Meeting for Autism Research. Shanghai, China. Poster presentation. November 2015.
Brignell, A., Prior, M., Donath, S., Reilly, S., Bavin, E.L., Eadie, P., Williams, K., Morgan, A. Communication trajectories for children with autism spectrum disorder, language impairment and typical language between 1 and 2 years. International Meeting for Autism Research. Shanghai, China. Poster presentation. November 2015.
Brignell, A., Prior, M., Donath, S., Reilly, S., Bavin, E.L., Eadie, P., Williams, K., Morgan, A. Loss of communication skills over the second year of life in children with autism spectrum disorder: A community-based study. Research Student Association Symposium. Melbourne, Australia. Oral presentation. September 2015.
Brignell, A., Prior, M., Donath, S., Reilly, S., Bavin, E.L., Eadie, P., Williams, K., Morgan, A. Loss of communication skills over the second year of life in children with autism spectrum disorder: A community-based study. Asia Pacific Autism Conference. Brisbane, Australia. Oral presentation. September 2015.
Other presentations
Brignell, A., Prior, M., Donath, S., Reilly, S., Bavin, E.L., Eadie, P., Williams, K., Morgan, A. Parent-reported loss and gain in communication skills from 1-2 years is not unique to autism spectrum disorder. Developmental Disability Research Group. Newcastle University, United Kingdom. Oral presentation. September 2016.*
Translation/media
Contributed to Murdoch Childrens Research Institute IMPACT blog. Language and autism spectrum disorders: common question parents ask. World Autism Day. April 2016.
Produced and presented a webinar and podcast on social communication and autism spectrum disorder. This was run through the Developmental Medicine department, Royal Children’s Hospital. Target audience: parents and clinicians. Oral presentation. One hour.
Note. All presentations were selected from abstract except those marked with a star (*)

xi
Related publications during candidature
Brignell, A., Albein-Urios, N., Woolfenden, S., Iorio, A., Williams K. The diagnostic stability of Autism Spectrum Disorder. Cochrane Exemplar Review. Protocol. Cochrane Database of Systematic Reviews (under final review).
May, T., Sciberras, E., Brignell, A., Williams, K. Autism Spectrum Disorder: Updated prevalence in a nationally representative sample. Medical Journal of Australia (under review).
Brignell, A., Dodd, B., Sykes, C., Morgan, A. Childhood apraxia of speech in autism spectrum disorder. In B Dodd & A Morgan (Eds.) Intervention Case Studies of Child Speech Impairment. Guildford, UK: J& R Press (to be published January 2017).
Brignell, A., Song, H., Zhu, J., Suo, C., Lu, D., Morgan, A. (2016). Communication intervention for autism spectrum disorders (ASD) in minimally verbal children. Protocol. Cochrane Database of Systematic Reviews. Issue 8. Art no: CD1234. DOI 10.1002/14651858.
Randall, M., Albein-Urios, N., Brignell, A., Gulenc, A., Hennel, S., Coates, C., Symeonides, C., Hiscock, H., Marraffa, C., Silove, N., Bayl, V., Woolfenden, S., Williams, K. (2015). Diagnosing autism: Australian paediatric research network surveys. Journal of Paediatrics and Child Health. DOI: 10.1111/jpc.13029
Randall, M., Sciberras, E., Brignell, A., Ihsen, E., Efron, D., Dissanayake, C., Williams, K. (2015). Autism Spectrum Disorder: Presentation and prevalence in a nationally representative Australian sample. Australian and New Zealand Journal of Psychiatry. DOI: 10.1177/0004867415595287.
Williams, K., Brignell, A., Prior, M., Bartak, L., Roberts, J. (2015). Regression in Autism Spectrum Disorders. Journal of Paediatrics and Child Health. 51 (1) 61-64.
Brignell, A., Morgan, A., Woolfenden, S., Williams, K (2014). How relevant is the framework being used in Autism Spectrum Disorders today? International Journal of Speech Language Pathology. 16(1): 43–49.
Williams, K., Brignell, A., Randall, M., Silove, N., Hazell, P. (2013). Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD). Cochrane Database of Systematic Reviews. Issue 8. Art. No.: CD004677. DOI 10.1002/14651858.CD004677.
xii
Related conference presentations during candidature
Bernie, C., Klopper, F., Brignell, A., Williams, K. Exploring Sensory Profiles of Identical Twins with Autism Spectrum Disorder. International Association for the Scientific Study of Intellectual and Developmental Disabilities (IASSIDD) World Congress. Melbourne, Australia. Oral presentation. August 2016.#
May, T., Sciberras, E., Brignell, A., Williams, K. Autism Spectrum Disorder: Updated prevalence in a nationally representative sample. Australian Institute of Family Studies Conference. Melbourne, Australia. Oral presentation. July 2016.#
Guertin, J., Brignell, A., Klopper, F., Williams, K. Understanding similarities and differences between monozygotic twins. Victorian Autism Research Forum. Melbourne, Australia. Poster presentation. November 2015.#
Randall, M., Sciberras, E., Brignell, A., Ihsen, E., Efron, D., Dissanayake, C., Williams, K. Autism Spectrum Disorder: Presentation and prevalence in a nationally representative Australian sample. Asia Pacific Autism Conference. Brisbane, Australia. Oral presentation. September 2015.
Randall, M., Albein-Urios, N., Brignell, A., Gulenc, A., Hennel, S., Coates, C., Symeonides, C., Hiscock, H., Marraffa, C., Silove, N., Bayl, V., Woolfenden, S., Williams, K. Diagnosing autism: Australian paediatric research network surveys. Journal Paediatrics and Child Health. Asia Pacific Autism Conference. Brisbane, Australia. Oral presentation. September 2015.
Randall, M., Sciberras, E., Brignell, A., Ihsen, E., Efron, D., Dissanayake, C., Williams, K. Autism Spectrum Disorder: Presentation and prevalence in a nationally representative Australian sample. Australian Society for Autism Research Conference. Melbourne, Australia. Oral presentation. December 2014.
Williams, K., Craig, J., Brignell, A., O’Sullivan, M., Stevenson, S. Autism Research. Approaches to clinical questions and future research. Campus Research and Public Health Forum. Royal Childrens Hospital. Melbourne, Australia. Joint oral presentation. October 2014.
Brignell, A., Williams, K. Autistic regression. Is it different to other neurological regression? Hopkins Symposium. Royal Children’s Hospital, Melbourne, Australia. Oral presentation. Presented jointly with Prof. Katrina Williams. March 2014.*

xiii
Brignell, A., Stevenson, S., Pereira, K., Randall, M., Brown, N., Fuller, D., Scheffer, I., Williams, K. The prevalence of autism spectrum disorders by the age of eight in a region of Victoria, Australia 2007-2011. AMAZE (Autism Victoria) ASD Research Forum. Melbourne, Australia. Oral presentation. November 2013.
Albein-Urios, N., Randall, M., Gulenc, A., Brignell, A., Stevenson, S., Williams, K. Paediatric management of children with autism spectrum disorder: An Australian Paediatric Research Network Survey. AMAZE (Autism Victoria) ASD Research Forum. Melbourne, Australia. Oral presentation. November 2013.#
Williams, K., Brignell, A., Stevenson, S., Periera, K., Randall, M., Natasha, B., Fuller, D., Scheffer, I. The Prevalence of autism spectrum disorders by the age of eight in a region of Victoria, Australia 2007-2011. International Congress of Paediatrics. Melbourne, Australia. Oral presentation. August 2013.#
Brignell, A., Stevenson, S., Periera, K., Randall, M., Natasha, B., Fuller, D., Scheffer, I., Williams, K. The Prevalence of autism spectrum disorders by the age of eight in a region of Victoria, Australia 2007-2011. Autism-Europe Congress. Budapest, Hungary. Oral presentation. September 2013.
Brignell. A., Randall. M., Pereira, K., Brown, N., Stevenson, S., Fuller, D., Scheffer, I., Williams K. Comparing Diagnostic Outcomes for Autism Spectrum Disorders between DSM IV-TR and DSM-5. International Congress of Paediatrics. Melbourne, Australia. Poster presentation. August 2013.
Williams, K., Brignell, A. Language and social communication in autism spectrum disorders. Neurodevelopmental and Behavioural Paediatric Society of Australasia Conference. Melbourne, Australia. Oral presentation. One hour. Presented jointly with Prof. Katrina Williams. August 2013.*
Brignell, A., Randall, M., Pereira, K., Brown, N., Stevenson, S., Fuller, D., Scheffer, I., Williams, K. Comparing Diagnostic Outcomes for Autism Spectrum Disorders between DSM IV-TR and DSM-5. Asia Pacific Autism Conference (APAC). Adelaide, Australia. Oral presentation. August 2013.
# Presentation was given by a co-author

xiv
Acknowledgements
First and foremost, I wish to express my heartfelt appreciation to my two supervisors
A/Prof Angela Morgan and Prof Katrina Williams. Both have expressed confidence in
my ability, provided me with invaluable guidance and facilitated opportunities I hadn’t
imagined were possible. I am very grateful for their efficient, insightful and encouraging
feedback that has enabled me to develop my academic writing and research skills.
Angela, breaking new ground in our field and an indispensable asset to the speech
pathology profession and Katrina, a marvellous ability to see both the big picture and
important details and juggler-extraordinaire of clinical and research responsibilities.
Angela and Katrina have my greatest admiration and respect as role models and mentors
and I feel privileged to have been given the opportunity to be their student.
I was very fortunate that Prof Margot Prior and Prof Melissa Wake agreed to be on my
advisory panel. Their suggestions and comments were always relevant and useful and
their academic rigor and depth of experience highly valued. Thank you also to co-
authors Dr Susan Woolfenden, Dr Vanessa Sarkozy, Dr Tricia Eadie, Prof Edith Bavin,
and Prof Sheena Reilly for their very helpful contributions to the papers (submitted or in
preparation) within this thesis.
I extend special thanks to Kim Jachno and A/Prof Susan Donath for their statistical
support. Kim has a special talent for explaining complex things in simple ways, which
has greatly strengthened my knowledge of statistics and has been much appreciated.
Thank you to Poh Chua for assistance with the search strategies for the systematic
review.

xv
I would like to express my gratitude to Prof Sheena Reilly for her great forethought in
establishing the ELVS. I was very fortunate to have been given access to such a
valuable resource. I would also like to thank the ELVS research assistants for data
collection and Sandra Novakovic, Eileen Cini, Dr Fallon Cook and Dr Kathryn Harker
for their assistance.
The past three-and-a-half years completing this thesis have been very colourful. My
experience has been made all the more enjoyable by the presence of a lively, nurturing,
supportive network of people around me. I wish to thank my extraordinary colleagues
and fellow students who have been generous listeners and always helpful: Dr Felicity
Klopper, Dr Tamara May, Francesca Lami, Charmaine Bernie, Dr Monica Cooper and
Elaine Meehan. Special thanks also to Keri Little for her infectious enthusiasm and
great company during our fabulous thesis-writing retreats. I am grateful to my friends
Adrienne, Louisa, Elanor, Liz and Mike for their interest and encouragement and to my
friends in music, Sydney and Canada for their words of support.
I am very grateful to my family; Lyn, Barry and Georgie and to Maurice for their ever
constant patience, love, kindness and support from afar.
Finally, a thank you to Guthrie and Audrey. When the PhD was challenging, simply
being in your company was like a miracle tonic.
I acknowledge the financial support I have received from an Australian Post Graduate
Award, the William Collie Trust and The University of Melbourne and Murdoch
Childrens Research Institute travelling scholarships. These scholarships allowed me to
present my work at conferences in Brisbane, Perth, Shanghai and Edinburgh.

xvi
This PhD is dedicated to all the children with ASD, and their families who participated
in the studies within this thesis. It is only through their generosity that we will continue
to develop our knowledge of ASD.

xvii
Table of Contents
Abstract ........................................................................................................................... iii
Declaration....................................................................................................................... vi
Preface ........................................................................................................................... vii
Publications and Presentations ..................................................................................... viii
Acknowledgements ........................................................................................................ xv
Table of Contents ........................................................................................................ xvii
List of Figures .............................................................................................................. xxii
List of Tables .............................................................................................................. xxiii
Abbreviations .............................................................................................................. xxiv
Glossary of Terms ........................................................................................................ xxv
Thesis Outline .............................................................................................................. xxvi
Setting ........................................................................................................................ xxvii
Methodological Issues ............................................................................................... xxvii
Chapter 1 Autism spectrum disorder ........................................................................ 1
Epidemiology of ASD .................................................................................................. 1
Diagnosis ................................................................................................................... 1
Prevalence ................................................................................................................. 2
Causes of ASD .......................................................................................................... 3
Cognitive theories of ASD ............................................................................................ 5
Onset, development and life course of ASD ................................................................. 6
Associated clinical features and comorbidities ............................................................. 7
Summary ....................................................................................................................... 9
Chapter 2 Communication development in autism spectrum disorder ................ 11
Communication difficulties in ASD ........................................................................ 11
The long-term impacts of communication disorders for children with ASD .......... 12
Neurobiological underpinnings of communication difficulties in ASD ................. 13
Overlap between children with ASD and language impairment ............................. 17
Communication phenotypes in ASD ....................................................................... 21
Links between cognitive impairment and language ................................................ 22
Regression (loss) of communication skills ............................................................. 24
Receptive-expressive language discrepancy ........................................................... 27

xviii
Children with ASD who fail to develop verbal speech ........................................... 30
Chapter 3 Communication trajectories ................................................................... 33
Social communication development in children with and without ASD .................... 33
Language development in children with and without ASD ........................................ 37
Language development in children without ASD ................................................... 37
Language development in ASD .............................................................................. 40
Predictors of language outcomes in children with and without ASD ......................... 45
Predictors of language outcomes in children without ASD .................................... 45
Predictors of language outcomes in children with ASD ......................................... 49
Chapter 4 This thesis ................................................................................................ 57
Rationale for the thesis ............................................................................................... 57
Challenges in understanding communication outcomes in ASD ............................ 57
A review of the current evidence on language outcomes is required...................... 57
Existing data from a community-based sample provide new opportunities ........... 58
Summary ..................................................................................................................... 61
Thesis aims ................................................................................................................. 62
Chapter 5 Study 1. A systematic review and meta-analysis of language outcomes in autism spectrum disorder ................................................. 66
Abstract ....................................................................................................................... 67
Introduction ................................................................................................................. 69
Methods ...................................................................................................................... 71
Inclusion/exclusion criteria ..................................................................................... 71
Types of studies ....................................................................................................... 71
Types of outcome measures .................................................................................... 72
Search strategy for identification of studies ............................................................ 72
Review of studies .................................................................................................... 73
Quality Assessment ................................................................................................. 73
Data management .................................................................................................... 74
Statistical analysis ................................................................................................... 76
Results ......................................................................................................................... 77
Search results .......................................................................................................... 77
Risk of bias assessment ........................................................................................... 81
Language outcome measures .................................................................................. 85
Characteristics of studies ......................................................................................... 87

xix
Language outcome measures in each study ............................................................ 87
Clinician-administered tools ................................................................................... 91
Parent-report tools ................................................................................................. 101
Presence or absence of verbal language and phrase language .............................. 105
Predictors of language outcomes .......................................................................... 111
Discussion ................................................................................................................. 111
Summary of findings from studies ........................................................................ 112
Considerations for interpreting data in this review ............................................... 114
Research implications ........................................................................................... 115
Clinical implications ............................................................................................. 117
Future directions .................................................................................................... 118
Chapter 6 Methodology for Studies 2 and 3.......................................................... 120
Study design .............................................................................................................. 120
Population representation ......................................................................................... 120
Measures ................................................................................................................... 120
Demographic information ..................................................................................... 121
Language measures ............................................................................................... 122
Nonverbal IQ measures ......................................................................................... 124
Social communication measures ........................................................................... 125
Change in language tool versions over different study waves .................................. 127
Participants ................................................................................................................ 127
Selection criteria .................................................................................................... 127
Loss to follow up ................................................................................................... 128
Ethical considerations ............................................................................................... 129
Statistical Analysis .................................................................................................... 129
Summary of overarching methods ............................................................................ 130
Chapter 7 Study 2. Parent reported patterns of loss and gain in communication in 1 to 2 year old children are not unique to autism spectrum disorder ..................................................................... 131
Chapter 8 Study 3. Language trajectories and predictors of language outcome from 4 to 7 years in children with and without autism spectrum disorder ................................................................................. 145
Abstract ..................................................................................................................... 146
Introduction ............................................................................................................... 147
Methods .................................................................................................................... 150

xx
Participants ............................................................................................................ 150
Measures ............................................................................................................... 150
Procedures ............................................................................................................. 151
Identification of subgroups ................................................................................... 151
Outcome measures ................................................................................................ 153
Predictor measures ................................................................................................ 153
Statistical Analysis ................................................................................................ 154
Results ....................................................................................................................... 155
Individual trajectories ............................................................................................ 155
Trajectory types ..................................................................................................... 158
Mean trajectories ................................................................................................... 160
Receptive-expressive language profiles ................................................................ 164
Predictors of receptive and expressive language outcomes at 7 years .................. 166
Discussion ................................................................................................................. 168
Chapter 9 Discussion ............................................................................................. 173
Summary of principle findings ................................................................................. 174
Communication trajectories from 1 to 2 years of age ........................................... 174
Language trajectories from 4 to 9 years of age ..................................................... 177
Language trajectories beyond 9 years of age ........................................................ 180
Predictors of language outcomes .......................................................................... 182
Expressive and receptive language discrepancy ................................................... 184
Children with ASD who are minimally verbal ..................................................... 185
Strengths and Limitations ......................................................................................... 187
Methodology ......................................................................................................... 187
Sample ................................................................................................................... 190
Measures ............................................................................................................... 191
Loss to follow up ................................................................................................... 193
Clinical implications ................................................................................................. 194
Future directions ....................................................................................................... 197
Concluding remarks .................................................................................................. 199
Bibliography ............................................................................................................ 201
Appendices ............................................................................................................. 226
Appendix A. Published article on regression in autism spectrum disorders ............ 227
Appendix B. Databases and search terms used for the systematic review ............... 232

xxi
Appendix C. Risk of bias criteria (adapted from Hayden et al., 2013)..................... 235
Appendix D. Characteristics of studies included in the systematic review. ............. 238
Appendix E. Studies reporting raw scores in the systematic review. ....................... 263
Appendix F. Scores for children not included in analyses for Study 3 .................... 266

xxii
List of Figures
Figure 1 Structure of the thesis by study, chapter and age investigated ............... xxvi
Figure 2 Simplified model of the causal pathways to ASD (adapted from, Loke, Hannan, & Craig, 2015). .............................................................................. 4
Figure 3 Model of factors that may interplay to predict language outcomes ........... 45
Figure 4 Results of the literature search and study selection. .................................. 78
Figure 5 Number of studies that used each type of language measure. ................... 85
Figure 6 Standard scores in receptive (a) and expressive syntax (b) at baseline and follow-up with 95% confidence intervals for studies using the MSEL and PLS .......................................................................................... 92
Figure 7 Random effects meta-analysis on seven studies using PLS or MSEL as a scoring system for receptive syntax outcomes. ....................................... 94
Figure 8 Random effects meta-analysis on seven studies using PLS or MSEL as a scoring system for expressive syntax outcomes. .................................... 95
Figure 9 Combined receptive/expressive syntax language and receptive vocabulary language age relative to chronological age ............................. 96
Figure 10 Standard scores on the VABS at baseline and follow-up. ....................... 101
Figure 11 Random effects meta-analysis using VABS standard scores .................. 104
Figure 12 Proportion of individuals with ASD were verbal aged ≤5 years (preschool) (a) and > 5 years (b) .............................................................. 107
Figure 13 Proportion of individuals with ASD who used phrases (and longer) at baseline and follow-up. ............................................................................ 109
Figure 14 Inclusion and exclusion criteria. .............................................................. 128
Figure 15 Individual language trajectories from 4 to 7 years of children with ASD. Standard scores on the CELF are presented. ................................. 157
Figure 16 Mean language trajectories (CELF standard scores) for male and female subgroups of children with ASD, TD, LI. ................................... 162
Figure 17 Distribution of the receptive-expressive difference scores for non-ASD and ASD children at 4 (a) and 7 years (b). .............................................. 165

xxiii
List of Tables
Table 1 Co-occurring developmental, psychiatric, medical, neurological and genetic diagnoses (adapted from Levy et al., 2010). ................................... 9
Table 2 Longitudinal studies of children 2 years and under at baseline ................. 43
Table 3 Longitudinal studies investigating predictors of language outcomes in ASD ........................................................................................................... 51
Table 4. Structure, aims and hypotheses of the thesis ............................................. 63
Table 5 Clinical information collected from included studies. ............................... 74
Table 6 Studies with two or more publications and overlapping particpants. ........ 79
Table 7 Risk of bias rating on included publications .............................................. 82
Table 8 Language outcome domains and tools ....................................................... 86
Table 9 Language outcome measures used by each study. ..................................... 88
Table 10 Key messages for clinicians ..................................................................... 118
Table 11 Language and communication measures ................................................. 122
Table 12 Nonverbal IQ measures ........................................................................... 124
Table 13 Social communication measures .............................................................. 125
Table 14 Mean scores for the CELF-P and CELF-4 at each year the tool was administered. ............................................................................................ 127
Table 15. Characteristics of those children with ASD included and not included in Study 3. ................................................................................................ 129
Table 16 Trajectory types (decline, maintain and accelerate) for children with ASD, LI and TD. ..................................................................................... 159
Table 17 Predictors of language outcomes ............................................................. 167

xxiv
Abbreviations
ASD Autism Spectrum Disorder
BPVS British Picture Vocabulary Scales
CDI MacArthur Bates Communicative Development Inventories
CELF-4 Clinical Evaluation of Language Fundamentals-Fourth Edition
CELF-P2 Clinical Evaluation of Language Preschool- Second Edition
CI Confidence interval
CSBS-ITC Communication Symbolic Behaviour Scales-Infant Toddler Checklist
ELVS Early Language in Victoria Study
EOWVT Expressive One Word Vocabulary Test
EVT Expressive Vocabulary Test
GEE Generalised estimating equations
KBIT-2 Kaufman Brief Intelligence Test-second edition
LI Language impairment
MSEL Mullen Scale of Early Learning
OR Odds ratio
Peds-QL Pediatric Quality of Life Inventory 4.0
PLS Preschool Language Scales
PPVT Peabody Picture Vocabulary Test
RDLS Reynell Developmental Language Scales
SCQ Social Communication Questionnaire
SD Standard deviation
SDQ Strengths and Difficulties Questionnaire
SEIFA Socio-Economic Indexes for Areas
SICD Sequenced Inventory of Communication Development
TD Typical development
TOLD Test of Oral Language
VABS Vineland Adaptive Behaviour Scales
WASI Wechsler Abbreviated Scale of Intelligence

xxv
Glossary of Terms
Adaptive language Communication skills used to interact functionally with the environment
Communication Expressive/receptive language and social communication (pragmatics and social interaction)
Developmental Delay Development is delayed in two or more areas (e.g., IQ and language)
Expressive syntax The ability to express structural language (e.g., using sentences, grammar and words). In the context of this thesis this term involves the expression of structural language more broadly i.e. beyond only vocabulary
Expressive vocabulary The words that can be expressed
Language Receptive and expressive vocabulary and syntax (words and sentences)
Language delay Language that is slower to progress than typical language development but is not deviant in quality
Language disorder Language that is deviant in trajectory and/or in quality compared with typical language development
Language impairment Language that on formal testing is 1.33 standard deviations below the age-expected mean
Non-specific language impairment
Language and nonverbal IQ are below the average range
Receptive syntax The ability to understand structural language (e.g., sentences, grammar and words). In the context of this thesis this term involves the understanding of structural language more broadly i.e. beyond only vocabulary
Receptive vocabulary The words that can be understood
Social communication Language that is used in social situations. Includes pragmatics and social interaction
Specific language impairment
Language is below the average range (-1.33 to -1.25 standard deviations below mean), nonverbal IQ is >85
Minimally verbal Children who use 30 words or less

xxvi
Thesis outline
This thesis is divided into three sections. The first section provides a review of the
literature on the epidemiology of ASD, communication development in children with
and without ASD and predictors of language outcome. This section also reviews the
literature on trajectories of language development (Chapters 1-3). The rationale and
aims of the thesis are outlined in Chapter 4. Section 2 describes the methods and
findings of the three main studies of the thesis, depicted in Figure 1. Study 1 is a
systematic review of language outcomes and examines individuals with ASD across all
ages (Chapter 5). Studies 2 and 3 utilise data from a community-based longitudinal
study of language development, the Early Language in Victoria Study (Chapters 7-8).
These studies examine trajectories of language development in children with and
without ASD from 1 to 2 years (Study 2) and 4 to 7 years (Study 3). The thesis
concludes with Section 3, which is a discussion of the main findings from the three
studies. This final section outlines the clinical significance and implications of the
findings from Studies 1-3 and highlights suggestions for future directions, specifically
around recommendations for filling the evidence gaps (Chapter 9).
Figure 1 Structure of the thesis by study, chapter and age investigated

xxvii
Setting
Studies 2 and 3 in this thesis included data from the Early Language in Victoria Study
(ELVS). This is a longitudinal, community-based study of children living in Victoria,
Australia. The ELVS has tracked the development of the children’s language (and
related areas) from 8 months to 7 years of age and the children have been followed up
almost yearly. A proportion of the 1910 children in the ELVS have been reported by
their parents to have a diagnosis of ASD (n=44). Further details on the ELVS are
provided in the methodology chapter (Chapter 6) and in the chapter relevant to the study
(Chapters 7-8).
Methodological issues
The methods of each study are outlined chapter by chapter, however, since Study 2 and
3 both utilised data from the same broader study (ELVS) the methods were consistent.
Rather than repeat the same methodology across several chapters, only the methods not
described in the relevant chapter are outlined in the methodology chapter (Chapter 6).

1
Chapter 1 Autism spectrum disorder
Chapter 1 provides an overview of autism spectrum disorder (ASD). This chapter
discusses the epidemiology (diagnosis, prevalence, causes) and the cognitive theories
that have been proposed to explain the condition. The onset and development of the
condition over the life course are also described, along with commonly associated co-
morbidities.
Epidemiology of ASD
Diagnosis
Autism Spectrum Disorder (ASD) is a highly heterogeneous neurodevelopmental
disability characterised by a dyad of impairments that include social communication
difficulties and repetitive and restricted interests and behaviours (American Psychiatric
Association, 2013). With each new edition of the Diagnostic Statistical Manual of
Mental Disorders (DSM), attempts have been made to improve the reliability and
validity of the diagnosis of ASD. However, ongoing debate about the validity of the
current diagnostic criteria remains (Brignell, Morgan, Woolfenden, & Williams, 2014;
Buxbaum & Baron-Cohen, 2013).
More recently there has been movement towards describing psychological and
neurodevelopmental disorders such as ASD by their dimensions or cognitive profiles
(Cuthbert, 2014; Cuthbert & Insel, 2013). For example, ASD could be described using
the dimensions of social communication and repetitive behaviours. It has been argued
that this approach will better facilitate the convergence of the genetic, environmental,

2
neurobiological, cognitive and behavioural factors involved in the development of ASD
and move research into ASD beyond its current borders (Cuthbert, 2014).
Prevalence
The estimated prevalence of ASD has increased over the past two decades, with recent
estimates from the United States being one in 68 children affected (Centers for Disease
Control and Prevention, 2014) and estimates from Australia of around one in 50
(Randall et al., 2015). These slightly higher estimates from Australia may be due to the
methods used to collect prevalence data (e.g., Randall et al., 2015 used parent-reported
ASD rather than clinically confirmed cases). Males are around 4.5 times more likely to
be identified with ASD than girls (Centers for Disease Control and Prevention, 2014). A
number of factors are likely to have contributed to the increase in prevalence, including
improved awareness of ASD, changes to the criteria used to diagnose ASD (e.g., DSM-
5), diagnostic drift (e.g., children with intellectual disability now receiving dual
diagnoses) and changes to funding specifically available for ASD in some countries
(Coo et al., 2008; Hansen, Schendel, & Parner, 2015; King & Bearman, 2009;
Lundstrom, Reichenberg, Anckarsater, Lichtenstein, & Gillberg, 2015; Polyak, Kubina,
& Girirajan, 2015).
Along with the increase in estimated prevalence, there have been changes to the types of
children diagnosed with ASD. In the 1980s it was estimated that 50% of children did
not develop spoken language, or were considered nonverbal (Kobayashi, Murata, &
Yoshinaga, 1992; Tager-Flusberg, Paul, & Lord, 2005). More recently, however, it has
been estimated between 25 to 30% of children with ASD are not able to use words to
communicate functionally (Norrelgen et al., 2014). Likewise, the proportion of children

3
with ASD and co-occurring intellectual disability has decreased over the years from
around 80% in 1990s (Fombonne, 1999) to more recent estimates of around 33%
(Connolly, Mackay, & Boyle, 2016). It has been hypothesised that greater awareness of
the heterogeneity of ASD, as well as better detection of milder cases, may have
contributed to these changes in profile (Keyes et al., 2012).
Causes of ASD
The exact cause of ASD is unknown although both genetics and the environment are
thought to play a role (Chaste & Leboyer, 2012). To date standard genetic methods have
not been able to identify autism-specific genes (Hallmayer et al., 2011; Krishnan et al.,
2016), however with the emergence of more advanced analytic techniques promising,
preliminary findings are emerging. A number of genes (e.g., SCN2A, STXBP1 TRIO,
LRP1, CNTNAP2, 16p11.2) have been identified that have conveyed susceptibility to
ASD however these genes have been implicated in other conditions such as
schizophrenia, severe intellectual disability, epileptic encephalopathies, as well as ASD
(Ciuladaite et al., 2011; Tager-Flusberg, 2015; Zhu, Need, Petrovski, & Goldstein,
2014).
Several putative environmental risk factors have been investigated during the pre- and
postnatal period of development. While some risk factors have been associated with
ASD (e.g., advanced parental age, gestational diabetes, prenatal medication use) their
individual contribution to the development of ASD has been found to be small
(Gardener, Spiegelman, & Buka, 2009). Given the complexity and heterogeneity of
ASD, it is unlikely a single causative factor at the genetic, environmental, neurological

4
or cognitive level will fully explain the behavioural symptoms of ASD. Figure 2 shows
a simplified theoretical model of the potential causes pathways to ASD.
Figure 2 Simplified model of the causal pathways to ASD (adapted from, Loke, Hannan, & Craig, 2015).

5
Cognitive theories of ASD
A range of cognitive theories has been proposed to explain how the brain systems and
pathways in individuals with ASD influence the behavioural characteristics of ASD
(Baron-Cohen et al., 2011; Brunsdon et al., 2015; Brunsdon & Happe, 2014; Happe &
Frith, 1996). Three major cognitive theories have been proposed: executive dysfunction,
weak central coherence and theory of mind difficulties. Executive functions are
cognitive processes such as attention and inhibitory control, working memory, problem
solving and planning. Central coherence refers to the ability to understand context or
‘the big picture’. Theory of mind is the ability to attribute mental states such as beliefs
and intentions to oneself and others. Around one third of individuals are reported to
have multiple cognitive atypicalities in these three areas of cognition and a higher
proportion of children with ASD experience difficulties in these areas relative to
individuals without ASD (Brunsdon et al., 2015). However, difficulties with these
cognitive functions are not a universal feature of individuals with ASD and none of the
theories, individually or together, fully explain the behavioural manifestation of ASD
(Brunsdon et al., 2015). More recently it has been suggested specific profiles of ASD
may result from different combinations of these cognitive deficits. For example, theory
of mind deficits may explain social communication behaviours, executive dysfunction
may explain restricted and repetitive behaviours and interests and weak central
coherence may explain the splintered profiles of strength and weakness that result from
being detail focused (Brunsdon et al., 2015).

6
Onset, development and life course of ASD
Up until the last decade, ASD has traditionally been described as having two patterns of
onset: regressive onset, which is a loss of previously acquired skills, and early onset,
which is symptom emergence within the first year without a clear loss of skills
(Stefanatos, 2008; K. Williams, Brignell, Prior, Bartak, & Roberts, 2015). In recent
years, with the advent of high-risk sibling studies closely monitoring early development
in younger siblings of children with ASD, more detailed descriptions of the onset of
ASD and unfolding of symptoms have emerged. This research will be discussed in more
detail in Chapter 2, under ‘Regression (loss) of communication skills’.
A systematic review of 42 studies that had investigated the average age of ASD
diagnosis found mean age of diagnosis ranged from 38 to 120 months, even though the
features of ASD may appear years prior to a diagnosis (Daniels & Mandell, 2014). In
Australia, the mean age of diagnosis in children was around four years in children aged
under seven (Bent, Dissanayake, & Barbara, 2015). ASD is described as a lifelong
disability, yet a proportion of children with ASD will experience a change in the
severity of their autism behaviours and some children may even “move off” the
spectrum altogether, no longer meeting diagnostic criteria (Fein et al., 2013; Gotham,
Pickles, & Lord, 2012; Perry et al., 2011; Sutera, 2010; Woolfenden, Sarkozy, Ridley,
& Williams, 2012). The diagnosis of ASD is less stable for children who have been
diagnosed younger and for children with fewer ASD symptoms (e.g., those with the
previous diagnostic category of pervasive developmental disorder- not otherwise
specified compared with autistic disorder) (Rondeau et al., 2011; Woolfenden et al.,
2012).

7
Our knowledge about how ASD develops across the lifespan and the outcomes of
individuals with ASD remains limited because few studies have followed children
beyond childhood (Magiati, Tay, & Howlin, 2014). A systematic review of studies that
have investigated long-term outcomes in ASD found outcomes to be highly variable
between studies (Magiati et al., 2014). There was a reduction in severity of ASD
symptoms over time in most studies included in the systematic review. However, some
studies reported relative stability in language, IQ and adaptive functioning and others
reported deterioration in ability over time (Magiati et al., 2014). Several studies of
adults diagnosed with ASD found most were dependent on their families or alternate
support services, few lived independently or had close friendships and communication
and literacy difficulties were common (Howlin, Goode, Hutton, & Rutter, 2004; Howlin
& Moss, 2012; Howlin, Moss, Savage, & Rutter, 2013). It is important to note that the
aforementioned adult studies may not reflect the outcomes of individuals being
diagnosed with ASD in more recent years. Ongoing changes to the diagnostic criteria
and better identification of milder cases may result in different adult outcomes to those
reported in currently published studies.
Associated clinical features and comorbidities
Children with ASD frequently have associated clinical features and co-occurring
conditions. The prevalence rates of these co-occurring conditions in ASD vary
according to the types of samples, with population based studies generally showing
lower rates than clinical samples. In one clinically-derived study for example, 95% of
individuals with ASD had three or more comorbid psychiatric disorders (Joshi et al.,
2010). In another population-derived study, the prevalence of having at least one co-

8
morbid psychiatric disorder was 70%, with at least 41% of individuals with ASD having
two or more co-occurring conditions (Simonoff et al., 2008).
These co-occurring conditions may impact an individual’s participation, functioning
and quality of life as significantly as the ASD symptoms. Furthermore, they may
overlap with symptoms of ASD to the extent that they delay or prevent a diagnosis of
ASD. Appropriate management of associated conditions is important and interventions
are available, however further research is required to understand how effective these
interventions are specifically for individuals with ASD (Joshi et al., 2010; Nadeau et al.,
2011).
Some comorbidities now need to be specified when making a diagnosis of ASD under
DSM-5 such as intellectual disability and language impairment (American Psychiatric
Association, 2013). In this thesis we focus on the comorbidity of language impairment,
which is one of the most common co-occurring conditions in ASD (Levy et al., 2010).
A deeper understanding of how and why conditions such as language impairment and
intellectual disability often co-occur with ASD and their genetic, neurobiological and
behavioural overlap will be important in helping us understand ASD. The table below
lists some of the co-occurring conditions associated with ASD.

9
Table 1 Co-occurring developmental, psychiatric, medical, neurological and genetic diagnoses (adapted from Levy et al., 2010).
Developmental diagnoses Language impairment, intellectual disability, sensory integration disorder, attention deficit hyperactivity disorder, learning difficulties
Psychiatric diagnoses Anxiety, oppositional defiant disorder, emotional disorder, mood disorder, visual impairment, tic disorders
Medical, neurological and genetic diagnoses
Epilepsy, encephalopathy, hearing loss, cerebral palsy, chromosome disorders, down syndrome, tuberous sclerosis, fragile X syndrome, velocardiofacial syndrome, neurofibromatosis
Summary
The diagnosis and estimated prevalence of autism spectrum disorder have changed over
the past few decades. Along with these changes, there has been an abundance of
theories around the neurobiological and neuropsychological underpinnings of ASD.
Research into ASD has increased over the past decade and this has advanced our
understanding of the condition, yet our knowledge about the causes, onset patterns and
the way ASD develops across the lifespan remains limited. Further to this, our
knowledge of how ASD interacts with co-morbid conditions such as language
impairment, including how language develops over time in children with ASD, how
different language development is to other children and what predicts which children
will have better or worse outcomes remains very limited. In this context we need to
identify opportunities for ways to improve our knowledge to facilitate important
discoveries and improved support for individuals with ASD.

10
Key points
Autism is a highly heterogeneous, lifelong condition
The cause of autism unknown but is likely to be a combination of the
environment and genetics
The estimated prevalence of ASD has increased over past decade. A
variety of factors has likely influenced this increase
An abundance of cognitive theories have tried to explain the
characteristics of ASD but none fully explain the disorder
Onset of ASD can vary between individuals.
ASD is associated with a variety of adverse outcomes in adulthood
A high proportion of individuals with ASD have comorbidities such as
language impairment and psychiatric disorders

11
Chapter 2 Communication development in autism spectrum disorder
Communication difficulties in ASD
Communication presents as one of the greatest challenges to children with ASD. It has
been estimated that up to 63% of children have some difficulties with language
development (Levy et al., 2010) and around 60% of individuals with ASD have
accessed speech and language services (Pringle, Colpe, Blumberg, Avila, & Kogan,
2012). Observed problems with language development are often the primary reason for
referral for diagnostic assessment (Chakrabarti & Fombonne, 2001; De Giacomo &
Fombonne, 1998; Herlihy, Knoch, Vibert, & Fein, 2015; Noterdaeme & Hutzelmeyer-
Nickels, 2010). Language impairment can result in a number of significant adverse
sequelae even without the additional impact of social communication difficulties that
are common in ASD. In ASD language difficulties can result in both primary effects
from the initial neurobiological disruption and secondary effects that result from the
child’s atypical ability to shape their learning experiences (Mundy & Jarrold, 2010). In
other words, the effects of ASD can be additive or interactional with cumulative or even
multiplied impact on outcomes.
To meet current ASD diagnostic criteria (DSM-5), children are required to have
impairment in three areas within the social communication domain, namely: 1) the use
of nonverbal communication, 2) developing and maintaining relationships and 3) social-
emotional reciprocity. These social communication difficulties can vary considerably in
type, severity and quality for each individual. In addition, a number of communication
behaviours that were previously categorised under qualitative impairments in
communication in DSM IV (American Psychiatric Association, 2000) have been re-

12
classified to the repetitive and restricted interests and behaviours domain. These
behaviours include stereotyped and repetitive speech, incessant questioning, echolalia,
reversal of pronouns and perseverative or tangential speech (American Psychiatric
Association, 2013).
While social communication difficulties are a defining feature in children with ASD, the
structural language skills (including vocabulary, use of grammar, syntax and
phonology) are remarkably variable. A substantial number of individuals with ASD
never develop the use of verbal (25%; Norrelgen et al., 2014) or fluent language (53%;
Wodka, Mathy, & Kalb, 2013), whilst others have well-preserved (or even superior)
language skills on formal testing (Bishop, 2003; Boucher, 2012; Kjelgaard & Tager-
Flusberg, 2001; Tager-Flusberg & Caronna, 2007). To this end, some researchers have
described this heterogeneity as a ‘structural language spectrum’ (Grzadzinski, Huerta, &
Lord, 2013).
The long-term impacts of communication disorders for children with ASD
Communication is an intrinsic human experience and an important life skill. Functional
language is a key ingredient for an individual to participate and function within his or
her family and community. There is consensus in the literature that early verbal skills
play a critical role in predicting long-term outcomes for children with ASD in areas
such as adaptive functioning, psycho-social adjustment and wellbeing (Billstedt,
Gillberg, & Gillberg, 2007; Gillespie-Lynch et al., 2012; Hofvander et al., 2009;
Howlin, Mawhood, & Rutter, 2000; Howlin & Moss, 2012; Howlin, Savage, Moss,
Tempier, & Rutter, 2014; Szatmari, Bryson, Boyle, Streiner, & Duku, 2003). Language
skills are critical to school placements and academic performance as well as the ability

13
to participate in social opportunities and have successful interactions with peers
(Thurm, Lord, Lee, & Newschaffer, 2007; Venter, Lord, & Schopler, 1992).
Social communication impairments are a hallmark of ASD and have been associated
with emotional and behavioural problems (Ketelaars, Cuperus, Jansonius, & Verhoeven,
2010), high rates of referral to educational psychology services (Mackie & Law, 2010)
and difficulties forming adult relationships (Whitehouse, Watt, Line, & Bishop, 2009).
Given social communication difficulties are central to a diagnosis of ASD, it is not
surprising that studies comparing children with ASD to other neurodevelopmental
disabilities such as specific language impairment and developmental delay, consistently
report poorer outcomes for the children with ASD in areas such as general
communicative competence, social engagement and quality of peer interactions
(Mawhood & Howlin, 2000; Sigman et al., 1999).
Whilst the real-world impacts of communication disorders are clear, there is continuing
debate over the aetiology and conceptual theoretical models of early social-
communication and language development in ASD and whether the two are connected
in some, if not all, individuals with ASD. In trying to disentangle this, it is important to
understand the neurobiological mechanisms that may underlie the social communication
and language impairments in ASD.
Neurobiological underpinnings of communication difficulties in ASD
In recent years high-risk younger siblings of children with ASD have been studied
closely to gain a better understanding of the early development of ASD. These studies
have indicated a broad range of predictors are likely to play a role in social

14
communication development in ASD. No primary theory of underlying cognitive deficit
or neurobiological account in ASD has been able to account for the breadth of the
findings (see Jones, Gliga, Bedford, Charman, & Johnson, 2014 for a review). This
presents researchers with a substantial challenge trying to identify the neurobiological
underpinnings of communication development in ASD. What follows here is an outline
of some of the key areas of neurobiological investigation over recent years.
(1) Abnormal brain growth
This theory stems from findings of abnormal brain growth in some children with ASD
within the first 2 years of life (Courchesne, Carper, & Akshoomoff, 2003). Abnormal
early brain growth, as seen by measuring head circumference, is reported to particularly
affect the frontal cortex and is associated with abnormal synaptic pruning (Courchesne
et al., 2011; Rubenstein & Merzenich, 2003). It has been theorized that these
abnormalities in brain growth may interfere with the normal progression of language,
although the exact mechanism involved remains unclear. It is important to note that the
findings have primarily come from one research group (Courchesne et al., 2003). To
date increased head circumference is only reported in a subset of children with ASD
(59%) and some healthy controls have also shown this increase in head circumference
(6%). Moreover, a systematic review of early brain overgrowth and head circumference
in ASD found inconsistent support for a subgroup of children with ASD who experience
early brain overgrowth (Raznahan et al., 2013) and studies of high-risk siblings have
found head growth to be uninformative as an ASD risk marker (Zwaigenbaum et al.,
2014).

15
(2) Over pruning hypothesis
This hypothesis is an extension of a study that developed a neurocomputational model
of the regressive subtype of ASD (M. S. Thomas, Knowland, & Karmiloff-Smith,
2011). M. S. Thomas, Davis, Karmiloff-Smith, Knowland, and Charman (2016)
broadened their original study to include a more general version of the hypothesis to
account for the heterogeneity in onset types and developmental trajectories (early onset,
regressive onset and late onset) seen in ASD. This hypothesis suggests there is over-
aggressive synaptic pruning in brain connectivity in infants with ASD, which is an
exaggeration of normal pruning that occurs in infancy. The authors argue that
trajectories of development (including language and social communication) in ASD
may be explained by this single pathological mechanism. They propose unaffected
siblings of children with ASD may inherit milder versions of the pathological
mechanism or they may inherit risk factors without the pathological mechanism. The
authors claim this hypothesis is consistent with findings from high-risk sibling studies
and may explain why children with ASD do not show overt differences to those without
ASD in the first few months of development (M. S. Thomas et al., 2016). This
hypothesis is based on theory and computational modelling, not neurobiological
findings and hence warrants further exploration and demonstration in humans.
(3) Reduced connectivity in the social brain
Findings of anomalies in the modulation of neural activity in the superior temporal
sulcus (STS) in response to social stimuli have emerged from magnetic resonance
imaging (MRI) studies in adolescents and adults (Pelphrey & Carter, 2008; Pelphrey,
Shultz, Hudac, & Wyk, 2011). Further, functional MRI studies have shown that aberrant
neural activity is associated with reduced functional connectivity between the “social

16
brain” areas (i.e. fusiform gyrus, superior temporal sulcus, prefrontal cortex) (Jann et
al., 2015; Minshew & Williams, 2007; Pitskel et al., 2011). This has led to the theory
that children with ASD may develop typically until this critical “interconnection”,
required to facilitate normal social communication development and subsequent
language development fails to progress.
(4) Reduced brain activity in response to speech
One study examined the development of language in infants aged 12-24 months by
combining neurological and behaviour markers (Lombardo et al., 2015). Of the 60
children who went on to be diagnosed with ASD, 36 went on to develop age appropriate
language and 24 were minimally verbal. Brain activity during speech tasks was assessed
in infancy using functional magnetic resonance imaging (fMRI). The children’s
development and behaviour was monitored every 6 months. This study found reduced
brain activation on fMRI in response to speech, combined with behavioural markers of
ASD, predicted later language outcomes with 80% accuracy. There was 68% accuracy
when either measure was used alone. Most of the children with ASD who did not go on
to develop language difficulties demonstrated similar patterns on the fMRI to the
controls.
Parallel to these findings, it has been demonstrated in high-risk siblings that some
children with ASD experience a heightened response to their name compared with
typically developing children in the first 6 months of life followed by an under response
to their name at around 12 months of age (Nadig et al., 2007; Yirmiya & Charman,
2010). It has been theorised that this abnormal response to name may be an early
symptom of ASD and may mark the beginning of underlying language difficulties.

17
All four of the abovementioned neurobiologically informed accounts go some way to
explain the regression in social communication development reported in a substantial
minority of children with ASD. They also go some way to explain why the detection of
clinical differences between children with ASD and those with typical development
occurs after 12 months of age (Jones et al., 2014; Landa, Holman, & Garrett-Mayer,
2007; Macari et al., 2012; Szatmari et al., 2016; Zwaigenbaum, Bryson, & Garon, 2013;
Zwaigenbaum et al., 2005).
At the present time the exact neurodevelopmental abnormality underpinning the
different social communication and language trajectories in ASD remains unclear. It
seems more likely that multiple, rather than one, mechanism will be at play and that this
will explain some, if not most, of the heterogeneity between individuals. It is generally
held that the social communication difficulties that emerge in early childhood are most
likely to be related to the interactional effects of a combination of biological (including
genetic) and environmental vulnerabilities and protective factors (Chaste & Leboyer,
2012; Krishnan et al., 2016; Rubenstein, 2010). These mechanisms may combine to
produce disruption in the normal development of multiple systems in the brain,
particularly those involved in social development and language (Happé, Ronald, &
Plomin, 2006). Developing ways to identify these differences in a way that will benefit
individuals will be the next challenge.
Overlap between children with ASD and language impairment
Language impairment terminology
There has been ongoing debate about the most appropriate terminology to use to
identify children who present with language difficulties (Bishop, Snowling, Thompson,

18
& Greenhalgh, 2016; Bishop, Snowling, Thompson, Greenhalgh, & consortium, 2016;
Reilly et al., 2014). Traditionally two main types of language impairment have been
described in the literature: specific language impairment (SLI) and non-specific
language impairment (NLI). Children with SLI are usually described as having delayed
language (e.g., 1.25-1.33 standard deviations below the mean) and a nonverbal IQ of
more than 85. Children with NLI are usually described as having delayed language
(e.g., 1.25-1.33 standard deviations below the mean) and a nonverbal IQ below 85
(Bishop, Snowling, Thompson, Greenhalgh, et al., 2016; Reilly et al., 2014; Tomblin,
Zhang, Buckwalter, & O'Brien, 2003).
More recently, the terms ‘language disorder’ and ‘developmental language disorder’
(specifically for children that have language disorder of unknown biomedical cause)
have been proposed. It has been argued these terms better encapsulate the functional
impairment of language disorder and its prognosis (Bishop, Snowling, Thompson, &
Greenhalgh, 2016).
Alongside developing agreed terminology there have been attempts to gain consensus
on the most appropriate criteria to use to identify language disorder (Bishop, Snowling,
Thompson, Greenhalgh, et al., 2016). Through use of a Delphi survey which surveyed
experts in the field, it was recommended that criteria for language disorder should
include children with low nonverbal ability and not solely those with a verbal-nonverbal
discrepancy. There were several rationales for this decision including that adaptive
behaviour is equally as important as IQ but was not included in previous descriptions of
SLI and furthermore, children with a verbal-nonverbal discrepancy do not respond
differentially to intervention and they do not have unique language profiles (Bishop,
Snowling, Thompson, Greenhalgh, et al., 2016).

19
In this thesis we use the term ‘language impairment’ to describe children with impaired
language without intellectual disability. The decision to use this terminology was based
on accepted terms at the time, before the abovementioned papers (Bishop, Snowling,
Thompson, & Greenhalgh, 2016; Bishop, Snowling, Thompson, Greenhalgh, et al.,
2016) were published.
Examining the way language develops in ASD has the potential to shed light on our
knowledge about communication in the general population. Language difficulties are
common to many neurodevelopmental disabilities and there is substantial overlap in
features for young children with ASD, language disorder/delay and developmental
delay (Ellis Weismer, Lord, & Esler, 2010; Kjelgaard & Tager-Flusberg, 2001; Lord,
1995; Paul, Chawarska, & Volkmar, 2008; Rapin, Dunn, Allen, Stevens, & Fein, 2009;
Veness et al., 2012) as well as shared risk factors such as demographic, neurobiological
and behavioural factors (Tager-Flusberg, 2016).
Language impairment in children with and without ASD
Traditionally language impairment and ASD have been considered to be aetiologically
distinct with some describing the overlap as superficial and proposing distinct
aetiological mechanisms, as evidenced by differences in cognitive and language profiles
(Norbury & Sparks, 2013; L. J. Taylor, Maybery, Grayndler, & Whitehouse, 2013;
Whitehouse, Barry, & Bishop, 2007; D. L. Williams, Botting, & Boucher, 2008).
An alternative account leading to the same conclusion, known as ‘phenomimicry’ has
also been hypothesied (Bishop, 2010). Phenomimicry is when the causal pathways for
one condition leads to an outcome resembling another condition. In ASD this would
operate with ASD risk factors leading to language impairment as the consequence. As

20
such the language impairment in ASD can be thought of as different to that in children
without ASD (Bishop, 2010).
Countering these hypotheses, some authors have argued specific language impairment is
comorbid to ASD and children with language impairment are likely to be a specific
subgroup of ASD with the two conditions sharing aetiological underpinnings (Kjelgaard
& Tager-Flusberg, 2001; Tager-Flusberg, 2015). In support of this theory, children with
ASD and co-occurring language impairment and children with specific language
impairment were found to have similar patterns of performance in non-word repetition
(a task usually difficult for children with language impairment) while children with
ASD without language impairment and children with typical language development did
not present with such difficulties (Tager-Flusberg, 2015).
Although some genetic and neurobiological evidence has suggested an overlap between
specific language impairment and autism (D. L. Williams et al., 2008), this overlap has
been challenged on the grounds that a generalized learning disability might contribute to
the poor performance of lower functioning individuals with ASD leading to language
impairment as assessed using standardized language measures (Boucher, 2012).
A notable distinction between ASD and other developmental disabilities is that social
communication difficulties are central to ASD whereas in other developmental delays
and language delays/disorders, social communication difficulties tend to be secondary,
or consequential to language problems (Rice, Warren, & Betz, 2005). Admittedly, in
both practice and research this is often hard to disentangle, especially if research is
cross-sectional in type or when longitudinal research does not include early life.

21
Communication phenotypes in ASD
There are multiple described communication phenotypes of children with ASD
emerging primarily from studies using cross-sectional methodologies (Loucas et al.,
2008; Paul, Orlovski, Marcinko, & Volkmar, 2009; Rice et al., 2005; Tager-Flusberg,
2015; Tager-Flusberg & Caronna, 2007). In the interest of space these phenotypes will
not be described in detail here, however a brief summary of the characteristics more
typical of children with ASD follows. Further attention will be given to the first two
characteristics later in this Chapter.
i. A profile where receptive language skills are more impaired than expressive
language skills (Barbaro & Dissanayake, 2012; Charman, Drew, Baird, & Baird,
2003; Ellis Weismer & Kover, 2015; Ellis Weismer et al., 2010; Kover, McDuffie,
Hagerman, & Abbeduto, 2013; Luyster, Kadlec, Carter, & Tager-Flusberg, 2008;
Paul & Roth, 2011; Pickles, Anderson, & Lord, 2014; Volden et al., 2011).
ii. Regression (loss) in social communication and/or language around the second year
of life (Baird et al., 2008; Barger, Campbell, & McDonough, 2013; Lord, Shulman,
& DiLavore, 2004; Ozonoff, Williams, & Landa, 2005).
iii. Reduced use of gestures, especially to compensate for limited language (Charman,
Drew, et al., 2003; Mundy, Sigman, & Kasari, 1990).
iv. Joint attention difficulties (initiating and responding) (Anderson et al., 2007;
Charman, Baron-Cohen, et al., 2003; Mundy & Jarrold, 2010; Mundy et al., 1990).
v. Stereotypical language including echolalia, incessant questioning, pronoun reversal,
perseverative speech (Boucher, 2012; Prizant, 1996; Tager-Flusberg, 2006; Tager-
Flusberg & Caronna, 2007; Tager-Flusberg, Edelson, & Luyster, 2011).
vi. Greater use of unusual vocalisations in infants (Paul, Fuerst, Ramsay, Chawarska, &
Klin, 2011), abnormal prosody and vocal quality (Shriberg et al., 2001; Tager-
Flusberg & Caronna, 2007).
vii. Imitation difficulties (Charman, Baron-Cohen, et al., 2003; Oberman &
Ramachandran, 2007).

22
Links between cognitive impairments and language
In addition to the above communication characteristics, cognitive impairments
(specifically weak central coherence, difficulties with theory of mind and executive
dysfunction) are reported to be more common in individuals with ASD (described in
Chapter 1). Neuroconstructivist theories of development propose that one
developmental domain can have a constraining or facilitating influence on other
developmental domains. To this end, researchers have also attempted to understand how
the cognitive impairments seen in individuals with ASD may be associated with
communication and more specifically, language development (e.g., Baron-Cohen,
Campbell, Karmiloff-Smith, Grant, & Walker, 1995; Charman et al., 2000; Pellicano,
2010a, 2010b, Tager-Flusberg & Joseph, 2005).
The topic of the link between language and theory of mind has grown substantially over
the past two decades and the amount of research is far too great to cover
comprehensively in this chapter of the thesis. Hence, a summary will be provided.
Theory of mind is understood to develop from early joint attention skills and has long
been associated with pragmatic language ability, a core deficit for those with ASD
(Tager-Flusberg & Joseph, 2003). However, some researchers have argued theory of
mind may also have an important interaction with linguistic ability (e.g. syntax,
grammar, semantics, narrative), which is often impaired in ASD. Evidence suggests the
relationship between theory of mind and lexical and structural language may be more
complex than previously thought (Tager-Flusberg, 2000, Pellicano, 2010). For example,
Tager-Flusberg (2000) argues theory of mind is a prerequisite for learning language yet
children with ASD also come to understand theory of mind by using their language

23
skills. We are also yet to fully understand how different aspects of theory of mind and
language interact during different developmental periods. In order to do this
longitudinal studies are required so relationships can be studied over time. One
longitudinal study of language, theory of mind and adaptive functioning (n=39) found
theory of mind mediated an association between language and adaptive functioning but
did not mediate social skills and adaptive functioning in children with ASD and IQ>70
(Bennett et al., 2013).
Studies have also investigated the relationship between executive dysfunction and
language in ASD. To date, despite both structural language difficulties and executive
dysfunction being common in ASD, studies are yet to find a clear and direct association
between the two domains (Robert, McGrath & Tager-Flusberg, 2005). It has been
proposed the co-occurrence of these two conditions may be related to common genetic
factors that produce the neuropathology (Robert, McGrath & Tager-Flusberg, 2005).
The link between language and central coherence (the processing of local information
compared with the whole) has been explored, mainly in relation to understanding the
cognitive differences between children with language impairment and those with ASD.
On the whole, children with language impairment and no ASD have been found to have
relatively better ability in processing the whole picture rather than detail, an opposite
pattern to children with ASD with and without language impairment (L. J. Taylor,
Maybery, Grayndler, & Whitehouse, 2013). One might expect if there was a link
between language and central coherence some differences would be seen between
children with ASD with language impairments and those without language impairments.
In studies to date these two groups of children have not performed significantly
differently on central coherence tasks (L. J. Taylor, Maybery, Grayndler, &

24
Whitehouse, 2013). Further research will be required to elucidate conclusively whether
there is a relationship between language and central coherence in ASD.
In addition to the above specific cognitive abilities, children with ASD are described as
having difficulty with tasks that involve abstract or symbolic concepts and the use of
language to infer meaning from a situation (Brunsdon et al., 2015; Happé & Frith,
2006). From these findings we may infer that language and some, perhaps particular and
specific, cognitive impairments are closely linked but the nature of this relationship is
yet to be established and the centrality of language difficulties remains unclear.
Regression (loss) of communication skills
As well as enhancing our understanding of the interrelation of early social
communication and language domains, studies that have closely monitored
development from infancy also have the potential to shed light on the phenomenon of
regression that is reported to occur in around 30% of children with ASD (Barger et al.,
2013). Regression in ASD is typically defined as the loss of skills that have been
previously established (most commonly this loss involves language and social skills).
The onset of regression has been reported to occur usually around 2 years of age in
children with ASD (Lord, Shulman, et al., 2004; Stefanatos, 2008; Thurm, Manwaring,
Luckenbaugh, Lord, & Swedo, 2014).
While not pervasive in ASD, regression has rarely been reported to occur in other types
of common neurodevelopmental disorders such as language disorder and idiopathic
developmental delay (Baird et al., 2008; Lord, Shulman, et al., 2004; Pickles et al.,
2009), although these studies have been limited by a lack of comparison groups with
25
information collected prospectively. There are some rare metabolic and neurological
conditions that involve the loss of skills with biological mechanisms that are well
understood (e.g., Landau-Kleffner syndrome, infantile spasms).
The way regression had been described in the literature has evolved over time. By far
the most common description has been by dichotomous categories (regression being
present or absent) using questions from the Autism Diagnostic Interview (ADI; Barger
et al., 2013). However, over the years other ways of describing the onset of regression
have been proposed. For example, Shumway et al. (2011) has argued that 4 categories
may be a more useful way to describe the onset of regression (plateau; delay prior to 12
months then loss; no delay prior to 12 months then loss; and early onset).
High-risk sibling studies have reported regression to be far more common and
widespread across developmental skills than originally thought (Ozonoff et al., 2010)
and some have described loss of skills as a ‘process’ rather than a single event (M. S.
Thomas et al., 2016). A continuum of onset has been proposed where some children
experience substantial, catastrophic regression and others far less loss of skills or no
skill loss at all (Chawarska, 2016; Landa, Gross, Stuart, & Faherty, 2013). Findings
from high-risk sibling studies have described the onset of regression as variable and
gradual in the majority of children with a dramatic loss of skills occurring only in a
minority (Bryson et al., 2007; Landa et al., 2007; Lord, Luyster, Guthrie, & Pickles,
2012; Ozonoff et al., 2010; Rozga et al., 2011). Very recent research has also identified
a ‘recovery group’ of children who show early signs of ASD in the first 18 months
followed by a reduction of ASD symptoms over time (Chawarska, 2016), implying
potentially protective factors in this subgroup of children or different underlying
biological mechanisms.

26
More recently studies have started to investigate loss and gain of different components
of communication skills. Loss of eye contact and gaze to faces has been reported to be
the most common social communication skill lost in a number of retrospective studies
e.g., Ozonoff et al. (2005). Eye gaze, social interest, shared positive affect, smiling and
initiating interactive games have shown declining trajectories in prospective high-risk
sibling studies (Landa et al., 2013; Landa et al., 2007; Ozonoff et al., 2010) and word
loss, although it occurs, was found to be less common than social skill loss (Landa et
al., 2013; Ozonoff et al., 2010).
One of the primary reasons for slow progress in our understanding of regression is the
limited methodologies that can be applied to study regression. The most widely
published means of studying regression has been retrospective parent report. This
method relies heavily on the accuracy of parents reporting on an event that may have
occurred several years prior the child’s diagnosis. In particular the accuracy of parent
report has been found to be quite low compared with direct observation in the area of
social communication development (Ozonoff et al., 2010) and a ‘telescoping effect’ has
been reported to occur when there has been a substantial period of time between the
event and recall of the event (Lord, Shulman, et al., 2004)
Retrospective home video footage has also been used to study regression and has the
advantage of allowing direct observation of skills. However, this method also has
limitations. For example, the footage tends to be bookended by special events and may
not represent situations that allow assessment of the full picture of ASD.
High-risk sibling studies are probably the most promising for studying regression
because they are able to closely monitor very early development in children who later

27
go on to receive a diagnosis of ASD. However, sibling studies also have a number of
methodological limitations. It has been argued, for example, that growing up with an
older sibling with ASD may create a different environment to growing up with typically
developing siblings and there is evidence the phenotypes of high-risk children are
different to other children with ASD, including those later diagnosed (Pandey et al.,
2008; Pinto et al., 2010; Sebat et al., 2007; L. J. Taylor et al., 2015). Further detail on
regression in ASD in the form of a review co-authored by the author of this thesis is
provided in Appendix A.
To date only four published studies have prospectively studied regression in ASD from
infancy (Bryson et al., 2007; Landa et al., 2007; Ozonoff et al., 2010; Rozga et al.,
2011) and the majority of participants in these studies have been high-risk siblings with
ASD.
Community-based studies where children’s social and communication development
have been monitored since infancy, and where parents can report concurrently on skills
as they are observed without yet knowing their child’s developmental outcome, offer a
useful supplement to high-risk studies on regression. Community-based studies are
likely to provide a more representative picture of children with ASD as they contain
children who are at high-risk of ASD, as well as those without a family history of ASD.
Receptive-expressive language discrepancy
There has been mixed evidence about whether children with ASD have a relative
weakness in receptive compared with expressive language. Some authors propose this
discrepancy may be a characteristic of ASD (Hudry et al., 2013) and others have

28
reasoned receptive language difficulties may more reflect the reduced overall social
responsiveness in ASD rather than specific language processing deficits (Tager-
Flusberg, 2015, 2016). Findings from previous studies on the topic have not been
definitive mainly due to heterogeneous methodology including different language
measures, age ranges and few studies using clearly-defined comparison groups within
the same cohort.
Three studies have made direct comparisons with children who have typical
development. Of these, two used parent report measures (Charman, Drew, et al., 2003;
Hudry et al., 2010) and one used measures of receptive/expressive vocabulary (Kover et
al., 2013). An additional study compared children with ASD with developmentally
delayed children (Ellis Weismer et al., 2010). To our knowledge, no studies have
compared receptive-expressive language discrepancy in children with ASD to large
groups of children with typical development and language impairment using a
comprehensive measure of language.
Studies of children with ASD under 4 years using direct assessments of language (Ellis
Weismer & Kover, 2015; Ellis Weismer et al., 2010; Luyster et al., 2008; Mitchell et
al., 2006; Volden et al., 2011) and parent report tools (Hudry et al., 2010) have
consistently reported discrepancies between mean receptive and expressive language
scores, although not all children with ASD demonstrate this characteristic (e.g., only
30% of children in Hudry et al., 2010 reported a significant gap between receptive and
expressive language).
Studies of children with ASD aged between 4-14 years have noted less consistent
differences between receptive and expressive language on vocabulary in children with
29
ASD (Kjelgaard & Tager-Flusberg, 2001; Kover et al., 2013) with the latter of these
two studies reporting 18% of children with ASD had significantly lower receptive than
expressive vocabulary scores compared with 8% of children with typical language
development showing the same profile. There has been some suggestion that the gap
between receptive and expressive vocabulary may grow larger with increasing
nonverbal IQ ability, although this finding has yet to be replicated (Kover et al., 2013).
The receptive-expressive discrepancy also appears to depend on the type of tool used to
assess language, with some studies finding a discrepancy on direct formal assessments
administered by clinicians but not on parent report measures such as the MacArthur
Communicative Development Inventories (Ellis Weismer et al., 2010; Luyster, Qiu,
Lopez, & Lord, 2007). A meta-analysis of studies investigating receptive-expressive
language studies (n=74) found that although some children demonstrated this
discrepancy there was no evidence of an expressive advantage over receptive language
in children with ASD (Kwok, Brown, Smyth, & Oram Cardy, 2015).
Relative receptive language weakness profiles have been identified in some subgroups
of children with specific language impairment (Conti-Ramsden, St Clair, Pickles, &
Durkin, 2012) suggesting this profile is not unique to ASD. Also, there have been
reports with subgroups of children with ASD, language impairment and typical
development that share common features in their language profiles (Kover et al., 2013;
Tager-Flusberg, 2006; Tomblin, 2011). Without large samples of clearly delineated
children with typical development and language impairment within the same cohort, the
specificity of the receptive-expressive discrepancy to ASD remains unclear.

30
Children with ASD who fail to develop verbal speech
A subgroup of children with ASD remain minimally verbal (use less than 30 words)
throughout childhood (Norrelgen et al., 2014; Tager-Flusberg & Kasari, 2013). Theories
that have tried to explain the phenomenon of lack of speech have included: a failure of
cognitive ability; a more specific failure of symbolic capacity; failure to understand the
value of communication or a lack of motivation to communicate; social communication
deficits that impact the ability to learn language; failure to develop affective bonds that
lead to a desire to communicate and lastly, an apraxic deficit in speech motor planning
(Anderson et al., 2007; Kasari, Brady, Lord, & Tager-Flusberg, 2013; Paul, Campbell,
Gilbert, & Tsiouri, 2013; Pickett, Pullara, O'Grady, & Gordon, 2009; Shriberg, Paul,
Black, & van Santen, 2011). Research to prove or disprove these theories has failed to
produce conclusive answers, likely due to methodological constraints in studying such
complex, highly interactive domains.
The source of the failure to develop functional verbal communication has fundamental
implications for the type of intervention approach engaged. A child with apraxia may
benefit from a speech intervention, a child with poor symbolic capacity will need
intervention focused on building these skills (e.g., Kasari, Paparella, Freeman, &
Jahromi, 2008).
While attempts are made to understand the causal underpinnings of children with ASD
who remain minimally verbal, empirical research which examines the phenotypes of
those children who benefit from certain interventions and those who don’t will also be
important (Paul et al., 2013; Trembath & Vivanti, 2014). Furthermore, elucidating the
genetic underpinnings for specific speech and language disorders and their neurological

31
bases will inform which children are more at risk of not developing speech and the most
appropriate approach for these children, whether it be specific strategies for speech or
augmentative communication options. In addition to informing intervention and
prognosis, such findings will assist us to understand the theories and mechanisms that
may be at play in preventing the development of language.
Prior to the past 5 years children who were minimally verbal were often neglected from
research, in part because there were not adequate tools to assess them and they did not
respond to interventions as other children might. The establishment of a special
workshop on the topic of minimally verbal children with ASD organised by the
National Institutes of Health (National Institute of Health, 2010) has seen a flurry of
research into language development specifically dedicated to these children (e.g., Kasari
et al., 2014; Paul et al., 2013; Tager-Flusberg & Kasari, 2013; Thurm, Manwaring,
Swineford, & Farmer, 2015).

32
Key points
Language difficulties occur in around 60% of children with ASD
There is substantial heterogeneity in language ability in ASD
It remains under debate whether language impairment is part of the
cognitive/language profile in ASD or whether it is a co-occurring
condition with ASD.
Language ability in childhood is an important predictor of long term
outcome in a range of areas such as employment, social relationships
and adaptive functioning
A range of neurobiological explanations has been proposed to explain
ASD but none have fully been able to explain the condition
It has been proposed that some aspects of communication
development appear to be more characteristic of ASD than other
conditions including relative weakness in receptive versus expressive
language and loss of communication skills in the first few years of life.
Up to 30% of children with ASD remain minimally verbal. The
reasons why some children with ASD do not develop verbal language
is yet to be explained.

33
Chapter 3 Communication trajectories
ASD is a spectrum of behaviours and to understand communication development in
ASD in its entirety it is also important to understand communication development in
children without ASD.
Social communication development in children with and without ASD
It has been known for some time that early social-communication skills play an
important role in the development of language in typically developing children (Bates,
Benigni, Bretherton, Camaioni, & Volterra, 1979; Carpenter & Nagell, 1998; Charman
et al., 2000; Mundy, Henderson, Inge, & Coman, 2007; Tomasello & Farrar, 1986).
Specifically, Bates et al. (1979) have argued that symbolic capacity may lay the
foundations for early joint attention, imitation and play to subsequent language
development. Social communication skills undergo particularly rapid development
between one and two years of life (Carpenter & Nagell, 1998; Crais, Douglas, &
Campbell, 2004).
Moreover, children who are typically developing show relatively predictable patterns of
emergence of social cognition in the early years of life. In a study by Carpenter et al.
(1998) joint engagement, communicative gestures, attention following, imitative
learning and referential learning were found to follow in sequence in the majority of
typically developing children (87%). Such patterns were also seen in the majority of
children with developmental delays (90%). The remaining children tended to have less
predictable patterns of development.

34
While social cognition appears to be an equally important predictor of language
outcomes for children with ASD (Brooks & Meltzoff, 2008; Charman, Baron-Cohen, et
al., 2003; Mundy et al., 1990), some studies have shown that the development of such
skills is highly variable in ASD and that they do not develop chronologically or
predictably in the same way that they do in typically developing children. For example,
using similar methods as those used with typically developing children, Carpenter,
Pennington, and Rogers (2002) found that only 50% of children with ASD followed the
same pattern of emergence.
Rather, the children with ASD tended to develop skills in an alternate order: imitative
learning, referential language, joint engagement, attention following and communicative
gestures. Carpenter et al. (2002) argued that such findings may go some way to explain
why some children with ASD learn language differently to typically developing
children. For instance, children with ASD may use imitation as an alternate route to
learning words (i.e. to learning via social interaction, symbolism, joint attention and
toddler equivalents of theory of mind/executive function) and this may explain why
many children have extensive vocabularies but lack an understanding of the meaning of
these words or how to use such words within a social context (Carpenter et al., 2002;
Rogers & Pennington, 1991).
It is worth noting that the Carpenter et al. (2002) study had a number of limitations,
including that: the children studied were 4 years of age on average, well beyond the age
many of the early social-communication skills are expected to develop; the study was
cross-sectional in design which makes the assumption that cross-sectional results which
represent one point in time reflect developmental patterns; there were potential
problems with the way tools were used to assess skills in children with ASD (e.g., not

35
all children were able to complete all tasks and there were ceiling and floor effects), a
broad range of ages were included and the sample size was small. While these factors
limit interpretation and generalization of the findings, the study was an important first
step towards understanding the developmental sequence of the emergence of and
interrelation of social communication in children with ASD compared with other
populations.
Since the publication of Carpenter et al.(2002) limited progress has been made
regarding our understanding of the sequence of development of early social-
communication skills in ASD relevant to language growth (Pry, Petersen, & Baghdadli,
2009; Thurm et al., 2007). Most studies that have tried to investigate early social
communication development have reported on individual skills rather than the
interrelation of multiple skills (Dereu, Roeyers, Raymaekers, & Warreyn, 2012). Some
authors have described the core early communication skills such as imitation, joint
attention and play as “interactive competencies” (Pry et al., 2009).
Other authors have speculated from their findings that joint attention and imitation may
be an important “starter set” of skills that lay the foundation for later language
development, and that representational skills such as play and deferred imitation are
important in helping children extend their language once it has started to develop (Toth,
Munson, Meltzoff, & Dawson, 2006). In infants at high and low risk for ASD, response
to joint attention at 15 months has been found to mediate the association between motor
imitation at 12 months and expressive vocabulary at 18 months (Edmunds, Ibanez,
Warren, Messinger, & Stone, 2016). A recent longitudinal study examining the
associations between social and languge pathways in preschoolers with ASD (time of
diagnosis) found a pattern where the two domains appeared strongly associated at time

36
of diagnosis but appeared to become more independent over the following 12 months
(Bennett et al., 2015).
In the past five years, a small number of longitudinal studies has begun to investigate
individual trajectories of social communication behaviours in children with ASD. This
allows the examination of how such skills may relate to each other and the sequence of
development (Dereu et al., 2012; Paparella, Goods, Freeman, & Kasari, 2011). Paparella
et al. (2011) assessed the sequence of development in a range of social communication
domains in 53 children with and without ASD aged 12 to 60 months. This study had
findings that were largely consistent with those of Carpenter et al. (2002) in that the
children with ASD were found to acquire joint attention skills in a different sequence to
typical children. For example, following eye gaze, which usually emerges mid-sequence
for typically developing children, was the last nonverbal skill to emerge in children with
ASD. The skill of showing was also found to develop later in children with ASD in this
study compared with typically developing children. Interestingly, there was no
difference between children with ASD and typical development in nonverbal requesting
gestures.
Dereu et al. (2012) studied a range of domains of development in toddlers with ASD
compared with children who were typically developing. In this study the sample size
was small (n=9) which limited the conclusions that could be drawn but in general Dereu
et al. (2012) found that there was great variability in skill development even within
individuals (i.e. different skills developed at different paces), particularly in the skill of
imitation. Likewise, several other studies have found variability in trajectory for
different aspects of social communication such as gesture compared with use of eye
contact (e.g., Lord, 2014; Thurm et al., 2014). Interestingly, Dereu et al. (2012) also

37
noted substantial variability between children with ASD with some demonstrating a
deviant trajectory and others demonstrating a delay in development. Much work is still
to be done in this area in terms of describing the development of, and interrelation of
early social communication skills and language.
Language development in children with and without ASD
Language development in children without ASD
Trajectories of language development in pre-school aged children are considerably
variable (Reilly et al., 2010; Rice, Taylor, & Zubrick, 2008; Ukoumunne et al., 2012)
and prediction of language outcome is especially difficult in children aged under 3
years. In one study around 70% of late-talking 2 year olds (without comorbid
developmental conditions) had ‘caught up’ by 4 years of age (Reilly et al., 2010). Other
studies report similar findings, estimating around 75% of late-talkers demonstrate
language within the normal range on standardised language testing by 3 years (Rice et
al., 2008; Roos & Weismer, 2008). However, there are some reports late-talkers have
weaker language than non-late-talkers throughout childhood and are at greater risk for
difficulties with literacy and high-order language tasks (Rescorla, 2005, 2009).
There has been wide variability in findings on the persistence of language outcomes
with a review of published studies reporting between 11-92% of children had ongoing
language difficulties (Tomblin et al., 2003). In a sample of 196 kindergarten children
Tomblin et al. (2003) found 66% of children with receptive-expressive delays had
persistent language impairment after 2 years and 62% after 4 years. Among children
with NLI 75% had persistent language impairment after 2 years and 67% after 4 years.

38
Another study found 92% of children with SLI at 6 years of age remained language
impaired after one year and 88.5 % remained after 4 years when children were 11 years
of age (Conti-Ramsden & Botting, 1999; Conti-Ramsden, Botting, Simkin, & Knox,
2001). In a large population-based study of younger children conducted in Norway
(n=10,587) 3%, 5% and 6.5% of the children demonstrated persistent, transient and late-
onset language impairment, respectively from 3 to 5 years (Zambrana, Pons, Eadie, &
Ystrom, 2014). A number of factors may have produced the variability in study
findings. This includes the age at which children were assessed, type of sample (e.g.
population versus clinical sample) and criteria used to define language impairment.
When language ability has been investigated in more detail, different growth trajectories
have been found for different language domains. For example, different trajectories on
specific language measures such as grammatical markers (e.g., verb tenses) have been
explored. In one study it was found children with and without SLI demonstrated similar
developmental trajectories for specific language abilities with both groups experiencing
periods of acceleration over time (Rice, Wexler, & Hershberger, 1998). In a later study
Rice, Redmond, and Hoffman (2006) found no difference in trajectories of growth in
mean length of utterance between children with and without SLI over 5 years. The
finding that language trajectories in school aged children tend to be more stable and
predictable (i.e. children retain their language status) than preschool children has been
described in several studies (Law, Tomblin, & Xuyang, 2008) and it has also be found
children with SLI follow a similar developmental pattern to typically developing
children (e.g., Beitchman et al., 1996; Johnson et al., 1999; Law et al., 2008; Rice,
2004; Rice et al., 1998; Tomblin et al., 2003).

39
Consistent with the above findings, Law et al have proposed that despite children with
SLI having lower scores than typically developing children, they tend to track in
parallel over time. In other words they maintain the same rate of progress. In their study
of 184 children with SLI followed at 3 time points (7, 8, and 11 years), children with
SLI developed at a similar pace to typically developing children over time, regardless of
subgroup (e.g., combined receptive-expressive language delay, expressive language
delay only etc.). In this study the majority of children demonstrated stability and
predictability in receptive language growth. Although some children did fall behind and
others caught up, there was an overall pattern of language growth and consistency. The
primary difference between children was not their trajectory of development but their
initial severity of language impairment (Law et al., 2008).
Finally, trajectories of language development have been examined in a large sample of
children with a history of SLI (n=242) from 7 to 17 years (Conti-Ramsden et al., 2012).
Trajectories were examined for the whole group and a multidimensional approach
involving a variety of language and cognitive measures was used to ascribe subgroups.
There was variability in language ability and seven subgroups were identified based on
language functioning. Expressive language was found to be more stable in growth than
receptive language, which accelerated from 7 to 8 years of age. On the whole, the
majority of children with SLI had stable language growth regardless of subgroup over
the 10 year period (Conti-Ramsden et al., 2012), consistent with findings from previous
studies (e.g., Law et al., 2008).
Several studies have now shown children with more severe delays and those with delays
in more than one module (e.g., combined receptive and expressive delay or lower
nonverbal IQ) have more persistent impairments than children with specific deficits

40
(Beitchman et al., 1996; Bishop & Edmundson, 1987; Cole, Schwartz, Notari, Dale, &
Mills, 1995; Tomblin et al., 2003). Other studies have reported accelerated language
development in some subgroups such as preschool aged children (Bishop &
Edmundson, 1987).
Language development in ASD
Studies that have investigated language outcomes in children with ASD are not
discussed in detail here but are presented in Chapter 5 (systematic review). The
exception to this will be studies that have examined individual trajectories and studies
that have followed children in first few years of life. This is because few studies of
children under 2 years met inclusion criteria for the systematic review due to their small
sample sizes and the methods used in studies investigating individual trajectories have
informed the methods used in this thesis.
(1) Individual language trajectories in ASD
The vast majority of studies that have examined language trajectories have attempted to
develop subgroups (or classes) of children or have presented information on the group
as a whole using mean scores (e.g., Landa, Gross, Stuart, & Bauman, 2012; Pickles et
al., 2014). While this may have been appropriate 30 years ago when children diagnosed
with ASD were, perhaps, more homogeneous, there has been increasing dissatisfaction
with this approach because it fails to capture important individual differences in
children with ASD (Dereu et al., 2012). We know that children with ASD have vastly
different trajectories of development (Baghdadli et al., 2012; Chawarska, 2016; Lord et
al., 2012). Some children regress in their development, some make gradual

41
improvements and others may demonstrate dramatic improvement (Anderson et al.,
2007).
When groups are combined to form a mean trajectory we lose the nuanced differences
in development. In fact, the individual variability in children with ASD may indeed be
the most telling and interesting aspect of development. A number of studies have been
published over recent years that have reported on individual trajectories of language and
social communication development (Anderson, Oti, Lord, & Welch, 2009; Dereu et al.,
2012; Lord et al., 2012; Paparella et al., 2011). It is hoped that by examining individual
trajectories a more detailed picture of development and the heterogeneity in ASD can be
better understood and clinically meaningful subgroups formed that may assist in
tailoring interventions and prognostication. However, reporting individual trajectories is
still new to the literature on ASD and to date no clear patterns have emerged, other than
substantial variability in language ability and direction of change.
(2) Longitudinal studies of children with ASD from infancy
Five studies have prospectively investigated communication trajectories in children
under 2 years of age (Barbaro & Dissanayake, 2012; Landa et al., 2012; Lombardo et
al., 2015; Lord et al., 2012; Paul, Chawarska, Cicchetti, & Volkmar, 2008). In all but
two of the aforementioned studies children had their ASD diagnosis confirmed at 3-5
years of age. Barbaro & Dissanayake (2012) and Lord et al., (2012) were the exceptions
and these studies provided a best estimate diagnostic status at 24 months and 30 months
respectively.
Landa et al. (2012) found that changes in development were not evenly distributed
across the time span and that children tended to have periods of accelerated growth and

42
slow growth at different periods during development. Lord et al. (2012) found the
children with ASD fitted different 4 verbal trajectories classes based on social and
language development (severe persistent (21%), worsening (21%), improving (19%)
and nonspectrum (40%)). Interestingly, in this study few children experienced actual
loss of skills (regression) although a number of children did plateau in their
development and therefore appeared to be worsening relative to age norms.
Behavioural measures were described separately for those with good and poor language
outcomes in one study. In this study the children in each language group (n=36 good
n=24 poor) demonstrated improving or declining trajectories respectively based on
standard scores over time (Lombardo et al., 2015). This study did not investigate
regression of communication skills. Lastly, standard scores on a language tool were
found to increase over time in a study of children with ASD aged 15-25 months at
baseline and followed for 2 years (Paul, Chawarska, Cicchetti, et al., 2008). Table 2
shows further detail on studies that have investigated children with ASD aged 2 years
and under at baseline. There are several limitations that apply to studies that that have
included children who have been diagnosed under 3 years. In addition to a diagnosis of
ASD being less stable and reliable in younger children (Woolfenden et al., 2012), the
autism symptoms in these children are likely to be more severe. Hence the study may
not include children who have milder symptoms and therefore may not be representative
of the broader population of children with ASD.

43
Table 2 Longitudinal studies of children 2 years and under at baseline
Author Relevance Overall findings Comments
Barbaro (2012)
Community-based study
Enrolled at 12, 18 and 24 months and measured at each time point.
Diagnosed ASD: 24 months.
Used MSEL to measure language. Mean receptive language scores found to be lower than expressive language scores at 12 and 18 and 24 months for ASD. Children with AD had lower mean scores, followed by children with ASD and children with developmental delay/language impairment at 12, 18 and 24 months. At 18 months there were significant difference between ASD, AD, DD/LI for receptive and expressive language ability.
Small sample size at lower age levels limits interpretation of change over time. Diagnosis performed when children young so may be less stable/reliable.
12 months ASD n=9; 18 months ASD/AD n=37 DD/LI n=8; 24 months AD/ASD n=79, DD/LI n=20
Landa (2012)
Assessed at 27 months, 35 mo., 41mo., 72 mo.
Enrolled <2 years
Multiple time points measured
Diagnosed ASD: 21-33 months
A significant mean increase in communication scores was found between 27 and 35 and 41 and 72 months. No difference was found between 35 and 41 mo. However, mean overall gains in communication found between 27 mo. and 72 mo. were large. Changes in trajectory were not evenly distributed across the time intervals.
Trajectories taken over a period of short-term intervention. Study unclear regarding details of this intervention.
No comparison group
Lombardo (2015)
ASD n=60, DD/LD n=19; TD n=24
Enrolled at mean age <2 years.
Diagnosed ASD: 3-4 years.
Followed every 6 mo. for one year
Divided children into ‘poor’ and ‘good’ outcome. Behaviour measures (language adaptive behaviour and ADOS) and fMRI findings taken early in development predicted language outcome with 80% accuracy. Variable trajectories seen. Children in poor group had lower standard scores at follow up and those in high group had higher standard scores. Combined mean for whole cohort showed improved standard scores but not significant ‘catch up’.
Interventions received unclear. Did not report on ‘loss of skills’. Used two comparison groups (TD/DD) but don’t describe how recruited/ language characteristics. Do not describe loss to follow up. Used MSEL at outcome, not a specific language tool.

44
Author Relevance Overall findings Comments
Lord (2012)
Assessed from 6 months every 2 months for an average of 20 months.
Used comparison group (developmental delay (DD))
Enrolled<2 years
Assessed using diagnostic instruments every visit (6 monthly)
Variety of measures taken prospectively
Investigates regression
Used MSEL to measure language. Four trajectory classes. About one third of children consistently showed clear severe and persistent deficits in social-affect from 12–36 months- slower gains in receptive and expressive language skills than the improving group. Second group improved in social-affect and improved more in verbal (both receptive and expressive language) skills compared with the severe persistent group. Early ADI-R scores didn’t differentiate between these trajectory classes. Worsening group not differentiable from severe persistent group or the improving group by change in language scores. Some children in the worsening and severe persistent group and some in the DD group made little/no progress in language over 2 years
Children in DD group may not have been representatively ‘typical’ (referred for ASD diagnosis but did not get one).
Tools repeated every two months- may have resulted in a ‘practice effect’
Children very young for ASD diagnosis-stability of diagnosis at this age?
Paul (2008)
ASD n=37
Followed for 2 years.
Enrolled between 18-25 months
Diagnosed ASD: 15-25 months.
Mean standard scores increased for whole group over the 2-year period although a better and worse expressive language groups were identified. Repetitive behaviour, higher nonverbal IQ, better receptive language, symbolic play, response to joint attention and sounds and words predicted better expressive language outcomes.
No comparison group. Used Mullen Scales of Early Learning to assess language outcomes. All retained their diagnosis at each time point.

45
Predictors of language outcomes in children with and without ASD
Language develops as a complex interaction of a broad range of factors, both genetic
and environmental (Figure 3). The factors that influence language development may be
shared across conditions such as ASD or language impairment or they may be unique to
individual conditions.
Figure 3 Model of factors that may interplay to predict language outcomes
Predictors of language outcomes in children without ASD
Predicting language outcomes in children is of key importance to inform clinical
decision-making, such as whether direct intervention or close monitoring is required.
Known risk factors include congenital conditions such as genetic disorders (e.g., Down
syndrome), metabolic disorders and severe sensory impairment (e.g., deafness,
blindness). Medical risk factors for language difficulties include foetal alcohol
syndrome, cerebral palsy and brain damage. Several environmental factors have also
been identified such as chemical poisoning and parental abuse/neglect (Paul & Roth,

46
2011). While the risk of language delay for children with the abovementioned
conditions is better understood, it has been difficult to identify reliable predictors for
children with language impairment of unknown cause, particularly for children aged
under 3 years.
Study 3 in this thesis will focus primarily on the child (intrinsic) and environmental
(extrinsic) that may influence outcome rather than exploring the full range of factors
that may influence outcome, shown in Figure 3. A range of predictors (both intrinsic
and extrinsic) has been investigated in an effort to understand which children are likely
to have persisting language impairment, which may have late-onset language
impairment and which may ‘grow out’ of their language impairment. Predictors have
been assessed at a range of ages through childhood and will be presented as two
separate sections below.
Predictors of language outcomes in preschoolers
In typically developing toddlers one of the most important predictors of later language
development has been language ability at preschool age (Chiat & Roy, 2008; Watt,
Wetherby, & Shumway, 2006). That is, if children have good language early in life they
were more likely to have good language later on. Furthermore, it has been found
receptive language is an important predictor of both expressive and receptive language
outcome (Chiat & Roy, 2008; Ellis & Thal, 2008; Watt et al., 2006). The use of gestures
has also been found to predict receptive language outcomes, and acts for joint attention
and range of consonants were found to predict expressive language (Ellis & Thal, 2008;
Watt et al., 2006). Other child factors found to predict later language ability include
delayed speech sound development (Law, Boyle, Harris, Harkness, & Nye, 2000; Rice
et al., 2008), being late to combine words (Carson, Klee, Carson, & Hime, 2003; Dale,

47
Price, Bishop, & Plomin, 2003) and having less advanced sentence structures than
expected for a child’s age (Hadley & Holt, 2006; Thal, Reilly, Seibert, Jeffries, &
Fenson, 2004).
Predictors of language outcomes in children aged 4 years and older
In a community-based study mutable-proximal factors (factors that have the potential to
be modified through parent or child interventions e.g. reading to the child) and mutable-
distal factors (factors that have the potential to be modified through indirect
interventions e.g. social policy) were examined to investigate whether they predicted
language growth and language outcome from 4 to 7 years of age. Neighbourhood
disadvantage, family income and family literacy were identified as important distal
predictors of language outcomes and proximal factors such as number of books in the
home, TV viewing, shared book reading were associated with language growth over
time (McKean et al., 2015). In another study by the same authors a ‘risk model’ was
developed using seven factors measured at 12 months (family factors, parenting
characteristics and child communication skills). This risk model predicted language
outcomes at 4 years with about the same accuracy as measures of vocabulary measured
by the CDI at 24 months (McKean et al., 2016). Examining the factors that may
influence language development has important implications for the types of
interventions that may be important at different ages. In some cases, a universal broad-
brush prevention approach (such as parent education on language development or
attendance at high quality preschool) may be most effective and in others a targeted
treatment approach may be the best approach.
A similar Australian population-based study included children around the same age (4
years at baseline) who were followed up over time (C. Taylor, Christensen, Lawrence,

48
Mitrou, & Zubrick, 2013). In this study important predictors of receptive vocabulary
delays were maternal non-English speaking background, low school readiness, child
wasn’t read to at home, four or more siblings, low family income, low birthweight, low
maternal level of education, maternal poor mental health, low maternal parenting
consistency and high reactivity in the child. These factors were important in predicting
language outcomes, however, they did not predict change in language ability over time.
Rather, socio-economic disadvantage was the only significant predictor of language
growth from 4 to 8 years with the authors suggesting the impact of social determinants
may increase with child age (C. Taylor et al., 2013).
Risk factors for language impairments
To date no single risk factor has been identified to explain language impairment in its
entirety, however, a family history of speech language delay or literacy problems,
prematurity, low birth weight or slow growth, being male, and low maternal education
appear to play some role (Law et al., 2000; Stanton-Chapman, Chapman, Bainbridge, &
Scott, 2002; Zubrick, Taylor, Rice, & Slegers, 2007). Specifically, a large population-
based study based in Norway found the odds for persistent language impairment were
doubled for boys and the odds for children with poor receptive language at 1.5 years
were tripled if there was a family history of late talking. Family history of literacy
difficulties increased the odds of late-onset and persistent language impairment and
family history of speech difficulties increased the risk of transient language impairment
(Zambrana et al., 2014).
A broad range of prognostic and risk factors, both intrinsic and extrinsic have been
examined over different developmental periods and it is likely these predictors interact
with each other in different ways to compound or protect against risk for language

49
difficulties. While some factors appear to be more important than others (e.g., family
history of language impairment, receptive vocabulary and use of gesture) currently it is
not possible reliably to predict who will have persisting or resolving language
difficulties.
Predictors of language outcomes in children with ASD
A number of studies has used cross-sectional designs to investigate social
communication predictors of language in children with ASD (e.g., Charman et al., 2000;
Charman, Drew, et al., 2003; Dawson et al., 2004; Ellis Weismer et al., 2010; Luyster et
al., 2008; Mitchell et al., 2006; Wetherby & Woods, 2006). These studies have shed
light on the interactions between social communication skills and language. However,
to better understand causal relations it is important to study how early social
communication skills impact language development over time. Longitudinal studies
investigating language outcomes of children with ASD have found some early
developmental domains to be more important predictors than others. Table 3 below
outlines 10 key predictors identified across the ASD literature: play, speech sounds,
gesture, joint attention, imitation, early language, parent-child interaction, socio-
economic disadvantage, ASD symptoms, and IQ. To our knowledge, no studies have
specifically focused on gender as a potential predictor of language outcome in ASD.
The decision-making around which predictors to include and the approach taken in this
thesis is based on social-interactionist theory. Social-interactionist theory proposes that
rather than development being modular and static (where the brain has individual
components that when impaired act independently and do not impact other functions in
development), the processes are dynamic and evolve through social experience and

50
interaction between the child’s linguistic and cognitive capacities with the child’s
social-language environment. In this view, biological organization of the brain directly
impacts thinking and experience which then shapes learning (Bishop, 1997; Greenough,
Black, & Wallace, 1987; Karmiloff-Smith, 2013).

51
Table 3 Longitudinal studies investigating predictors of language outcomes in ASD
Predictors Studies Main findings
Play Paul, Chawarska, Cicchetti, et al. (2008) n=37; age: 15-25 mo.
Symbolic play predicted language ability at 4 years but functional play did not.
Poon, Watson, Baranek, and Poe (2012) n=29; age: 4-5 yrs
Object play at 18 months predicted language ability at 7 years
Sigman et al. (1999) n=42; age: 2-6 yrs age, Sigman and McGovern (2005) n=48; age:3;11 yrs
Functional play at 4 years predicted expressive but not receptive language ability. Functional play also predicted rate of language change from 12-18 years
Early sounds Paul et al. (2011) n=48; age: 6-12 mo. Lack of diminishing of abnormal sounds predicted social communication behaviours and ASD diagnosis.
Wetherby, Watt, Morgan, and Shumway (2007) n=50; age: 30 mo.
Inventory of consonants at 18 months predicted receptive language at 3 years
Gesture Bopp and Mirenda (2011) n=44; age: 3:11 yrs No association between gesture and later language ability Charman, Baron-Cohen, et al. (2003) n=18; age: 20
mo. Mastery of gesture remained stable once child learned 20 words
Luyster et al. (2007) n=62; age: 29 mo. There was a steady increase in early and late gestures with increase in expressive vocabulary.
V. Smith, Mirenda, and Zaidman-Zait (2007) n=35; age: 20-71 mo., Sigman and McGovern (2005) n=48; age:3; 11 yrs, Shumway and Wetherby (2009) n=50; age: 18-24 mo.
Gesture ability predicted later language ability
Imitation Charman, Baron-Cohen, et al. (2003) n=18; age: 20 mo., McDuffie, Yoder, and Stone (2005) n=32; age: 18-60 mo., Poon et al. (2012) n=29; age: 4-5 yrs, V. Smith et al. (2007) n=35; age: 20-71 mo., Stone and Yoder (2001) n=35; age: 2 yrs, Thurm et al. (2007)
Imitation ability predicted later language ability

52
Predictors Studies Main findings
n=83; age: 2 yrs, Toth et al. (2006) n=60; age:34-52 mo.
Bopp and Mirenda (2011) n=44; age: 3:11 yrs; Luyster et al. (2007) n=62; age: 29 mo.
Imitation abilities did not predict later language ability
Motor imitation
Edmunds et al. (2016) 15 month response to joint attention mediated the association between 12 month motor imitation and 18 month expressive vocabulary
Joint attention Charman, Baron-Cohen, et al. (2003) n=18; age: 20 mo.,, Mundy et al. (1990) n=15; age: 45 mo., Paul, Chawarska, Cicchetti, et al. (2008) n=37; age: 15-25 mo., Poon et al. (2012) n=29; age: 4-5 yrs, Pry et al. (2009) n=132; age: 5.5yrs, Stone and Yoder (2001) n=35; age: 2 yrs, Toth et al. (2006) n=60; age:34-52 mo, Wetherby et al. (2007) n=50; age: 30 mo.
Joint attention abilities (range of definitions used in studies) predicted later language ability
Sigman and McGovern (2005) n=48; age:3;11 yrs Responding to and initiating joint attention at 4 years associated with expressive language gain one year later. Response to joint attention at 4 years resulted in greater expressive language at 12 years. Neither initiating nor responding to joint attention predicted receptive language gains.
Language Bopp and Mirenda (2011) n=44; age: 3:11 yrs, Pry et al. (2009) n=132; age: 5.5yrs, Thurm et al., 2007 n=83: age: 2 yrs, Paul, Chawarska, Cicchetti, et al., 2008 n=37; age: 15-25 mo., Mawhood and Howlin (2000) n=19; age: 24 yrs, Venter et al. (1992) n=58; age: 14.7 yrs, Ellis Weismer and Kover (2015) n=129; age: 2.5 yrs,
Early language ability predicted later language ability

53
Predictors Studies Main findings
Wetherby et al. (2007) n=50; age: 30 mo. Found language to be strongest predictor of all social communication predictors of later language outcome
Parent-child interaction
Siller and Sigman (2002) n=48; age: 3;11 yrs, Maternal behaviours, such as synchrony associated with increases in both response to joint attention and initiating joint attention and language for many of the children. Higher levels of synchronization and less demanding quality of parent language associated with superior communication skills over all time periods (1, 10, 16 years).
Parent-child interaction
Siller and Sigman (2008) n=28; age: 31-64 mo. Pre-schoolers who were more responsive to their parent’s bids for joint attention made greater gains in language development and parents who were more responsive had children with better language compared with those who had lower levels of synchrony.
McDuffie and Yoder (2010) n=32; age: 18-60 mo. At the 6 mo. follow up the number of parent utterances that followed child’s focus of attention and number of parent utterances that responded to child’s communicative acts predicted vocabulary.
Haebig, McDuffie, and Ellis Weismer (2013b) n=40; age: 24-39 months
Parent directives that followed child’s focus of attention predicted comprehension and expressive language one year later (unique variance)
IQ Ellis Weismer and Kover (2015) n=129; age: 2.5 yrs, Toth et al. (2006) n=60; age: 34-52 mo., Thurm et al. (2015) n=70; age: 1-5 yrs, Anderson et al. (2007) n=156; age: 29 mo., Thurm et al. (2007) n=83: age: 2 yrs, Wodka et al. (2013) n=535; age: 11.6 yrs, Paul, Chawarska, Cicchetti, et al., (2008) n=37; age: 15-25 mo.
Baseline nonverbal cognition/IQ predicted later language outcomes

54
Predictors Studies Main findings
Charman, Baron-Cohen, et al. (2003) n=18; age: 20 mo.
Nonverbal IQ at 20 months not associated with language outcomes at 42 months
ASD symptoms
Ellis Weismer and Kover (2015) n=129; age: 2.5 yrs, Baghdadli et al. (2012) n=152; age: 4.9 yrs, Magiati, Moss, Charman, and Howlin (2011) n=36; age: 3.4 yrs
Severity of ASD symptoms predicted language outcomes
Sigman and McGovern (2005) n=48; age: 3;11 yrs, Thurm et al. (2015) n=70; age: 1-5 yrs
Severity of ASD symptoms did not predict language outcome when other important factors (e.g., IQ) taken into account
Socio economic disadvantage
Ellis Weismer and Kover (2015) n=129; age: 2.5 yrs
Socioeconomic status predicted expressive but not receptive vocabulary

55
The extant body of literature on the predictive associations between early social
communication and language outcomes present a complex picture. While the evidence
suggests that some predictors (e.g., IQ and language) are more consistently important
than others, each study has used different tools, different time periods, a combination of
different predictors and different methods. Moreover, even those studies that have used
the same tools and methods have produced conflicting findings (Bopp & Mirenda,
2011; Charman et al., 2005; Ellis Weismer & Kover, 2015; Luyster et al., 2007).
Some studies have found different predictors to have relative importance at different
time periods. For example, Toth et al. (2006) found initiating proto-declarative joint
attention and immediate imitation to be the best predictors of language ability at age 3
to 4 years, whereas deferred imitation and toy play were found to be the best predictors
of rate of communication development from age 4 to 6.5 years. These findings highlight
the importance of studying predictors at a range of ages. To improve the accuracy of
prediction of language outcomes some studies are combining behaviour descriptions
with neurological findings (Lombardo et al., 2015). Given the complex interplay
between genetics, neurobiology and behaviour in ASD such an approach will be critical
for future research (Cuthbert & Insel, 2013).

56
Key points
Language and social communication ability appear closely linked but
the exact way they interact during development is not well understood
A large number of studies have investigated language outcomes but it
is difficult to interpret findings due to varied methods
Mean trajectories for children with ASD provide information at a
group level about language development but individual trajectories
take into account individual variation
Trajectories of language development in children without ASD are
variable in the early years but appear to become increasingly stable
and predictable as children age
Many putative predictors of language outcomes have been examined
during childhood including intrinsic (e.g., autism symptoms) and
extrinsic (e.g., parent interaction style)
To date no predictor alone has been able to fully explain different
language outcomes in children with and without ASD. It is likely
predictors of language outcome vary with age and a combination of
predictors influence outcomes
The most consistent and important predictors for later language
outcomes in ASD are language ability and IQ. There is mixed
evidence for the importance of ASD symptoms on influencing
language outcomes

57
Chapter 4 This thesis
Rationale for the thesis
Challenges in understanding communication outcomes in ASD
Despite an increase in the number of studies that have investigated communication
outcomes (see Chapter 5), clinicians are still unable to provide accurate prognostic
information to parents based on their child’s characteristics. This is because studies
have been so varied in methodology, quality, age groups included and assessment tools
used. Clinicians remain limited to very general information on outcomes. For example,
children who have an IQ of less than 50 and no speech by school age are likely to have
the least favourable prognosis (Howlin et al., 2014; Lord & Schopler, 1989; Venter et
al., 1992). Parents need timely and accurate information about the likely communication
outcomes for their child with ASD. Clinicians need evidence to inform the responses
they give parents to such questions and to inform intervention and management
planning. In addition, policy makers and service providers require information about
communication outcomes to inform decisions regarding the best possible allocation of
resources and services through childhood.
A review of the current evidence on language outcomes is required
A systematic review using emerging best methods for prognosis studies will make
optimum use of the current evidence on language outcomes and provide an important
summary for parents and clinicians that is easily accessible and immediately relevant. It
is hoped the methods developed as part of this review will assist the development of

58
future methods, and inform future prognosis studies, as well as prognostic systematic
review methods development.
Existing data from a community-based sample provide new opportunities
The Early Language in Victoria Study, described earlier in this thesis (see ‘Setting’), is
a longitudinal, community-based study that contains valuable data on language
development. Studies 2 and 3 utilised data from the ELVS and have the potential to
provide the following benefits.
An opportunity to examine trajectories in context and in depth
M. S. Thomas et al. (2009) describes trajectory approaches as “a motivation to place
development at the heart of explanations of developmental deficits” (pp339). Indeed,
Thomas explains, the phenotypes associated with neurodevelopmental disorders
(including ASD) are not set in stone when a child is born but they develop gradually
over time. It is unclear from the literature whether the pathways to outcome reflect
separate developmental pathways or whether they may be interrelated throughout
childhood. Trajectories provide a powerful description of these pathways both between
and within individuals.
At a broader level it is unknown whether the divergences in trajectories are related to
extrinsic factors (e.g., parent interaction, interventions) or intrinsic factors in the child
(e.g., social communication skills). It seems likely both protective and risk factors are
involved in outcomes and that these influence the later emergence of ASD symptoms.
Gaining a deeper understanding of trajectories of development and predictors of
outcome in ASD will assist in maximizing the efficacy of intervention as well as

59
providing some clues as to what might be done to prevent the divergence in
development in children with ASD. The ELVS is the ideal platform for studying the
trajectories of language development and related behaviours in children with ASD.
One of the challenges in studying development in ASD is the extreme heterogeneity of
the condition. Many published studies have used group means and general measures of
communication to demonstrate differences in development between ASD and other
conditions (e.g., Anderson et al., 2007; Sigman & McGovern, 2005; Thurm et al.,
2007). However, this approach only permits a global picture of pathways of
development. For example, we may know that a group of children moved from A to B
but we don’t know the different pathways by which they got there.
The limitation of such group studies is that they mask individual difference and do not
account for the rich variability in ASD. An exploration of individual trajectories using
detailed assessments of language, as is being used in this thesis, enables interesting
individual differences to be visible; it also allows for investigation of phenomena that
may be more specific to ASD such as regression in development. In other words, the
variability is accepted as important information rather than being disregarded as
inconvenient noise (Dereu et al., 2012). A nuanced description of language profiles also
has the potential to identify meaningful subgroups, which may help explain the
underlying mechanisms at play in ASD. Further, studying the natural history of the
multiple systems and dimensions that may play an important role in communication
outcomes and their course through childhood is critical to a better understanding of
prognosis.

60
It is hoped a community-based study will provide generalisable findings
With the exception of studies by Barbaro and Dissanayake (2012), Veness et al. (2012)
and Bolton, Golding, Emond, and Steer (2012), which are population or community
samples, most studies that have examined early communication development in ASD
have used high-risk infant siblings, home videos or retrospective parent report. There
are methodological limitations with these three methods, as has been discussed. The
focus of the majority of these infant studies has been on early predictors of diagnostic
outcome rather than language outcome (see Jones et al., 2014 for a review). With the
exception of one study (Bolton et al., 2012) no studies have reported on children that
have been followed from infancy to 7 years of age. Further, this study will enable both
the comparison of children with ASD to children in a large community sample as well
as to other groups of children (such as language impaired, typical development). This
will enable a greater understanding of the way in which communication difficulties
manifest and whether there are similarities between groups or features that are more
common in children with ASD. Very few published longitudinal studies have used such
comparison groups. The importance of cross-population comparisons for studies of
language development has been highlighted by several authors (Beeghly, 2006; Rice et
al., 2005; M. S. Thomas et al., 2009).
Measuring predictors of communication in a large cohort has the potential to provide
novel insights
The majority of studies that have examined predictors of language outcomes in children
with ASD have reported on associations using cross-sectional designs (e.g.,Charman et
al., 2000; Charman, Baron-Cohen, et al., 2003; Dawson et al., 2004; Ellis Weismer et
al., 2010; Luyster et al., 2008; Mitchell et al., 2006). This study will investigate

61
predictors of later language outcome in a way that will allow the importance of social
communication and ASD to be examined along with other key known predictors of
outcome such as language ability and IQ.
Summary
This thesis will synthesise current evidence on language outcomes in ASD. It will also
be the first of its kind to study communication trajectories at multiple time points in the
same cohort of children with ASD from infancy until 7 years using a community
sample. This study has several advantages over other studies. The community sample
has the potential to minimize ascertainment bias, which should enable a more
representative picture of ASD. Using multiple time points enables the mapping of
trajectories of development. It also allows the assessment of predictors at a key time
point in development facilitating an understanding of their relative importance in
language outcome. By studying individual communication trajectories this study hopes
to provide a nuanced and detailed report of the development of a range of
communication skills. Further, this study will compare children who have been
diagnosed with ASD to children with language impairment and typical development
within the same community sample thus placing ASD within a developmental context.

62
Thesis aims
The overall aim of this thesis is to examine language trajectories and outcomes in
children with ASD.
Three primary studies were conducted to address the overall aim.
• The first study consisted of a systematic review and meta-analysis of studies that
have reported on language outcomes in individuals with ASD.
• The second and third studies used data from the ELVS, a longitudinal community-
based study investigating language development in children.
The studies, chapters and corresponding aims of the thesis are detailed below in Table
4.

63
Table 4. Structure, aims and hypotheses of the thesis
Study - Chapter Title Aims and hypotheses
Study 1
(Chapter 5)
A systematic review
of language
outcomes in
individuals with
autism spectrum
disorder
1. To systematically and comprehensively search the extant literature on language outcomes in
individuals with ASD
2. To collect clinically-relevant descriptive information on included studies
3. To conduct quality assessments (risk of bias) of included studies
4. To present findings from studies that reported data on language outcomes in graphical format
5. To conduct meta-analyses where five or more studies have presented data on the same
language domain
Hypothesis: We hypothesised children with ASD would have delayed language relative to
children without ASD and slower rate of language development, with the gap between
children with and without ASD growing larger over time.\

64
Study - Chapter Title Aims and hypotheses
Study 2
(Chapter 7)
Parent reported
patterns of loss and
gain in
communication in 1
to 2 year old
children are not
unique to ASD
1. To examine trajectories of communication development from 1 to 2 years in children with
ASD and compare these trajectories to those of children with LI and TD
2. To examine trajectories of expressive vocabulary development from 1 to 2 years in children
with ASD and compare these trajectories to those of children with LI and TD
3. To compare the proportion of children in each group (ASD, LI, TD) who lost communication
skills from 1 to 2 years
4. To compare the types of communication skills that were lost for each group (ASD, LI, TD)
5. To compare the spread of loss of skills across different communication domains between
the 3 groups (ASD, LI, TD)
Hypotheses: We hypothesised there would be substantial variability in early communication
trajectories. We expected children with ASD to demonstrate a higher proportion of children
who lost skills relative to the other groups, skills would be lost across a wide range of
communicative domains for children with ASD and very few children without ASD would lose
skills from 1 to 2 years.

65
Study - Chapter Title Aims and hypotheses
Study 3
(Chapter 8)
Language
trajectories and
predictors of
language outcome
from 4 to 7 years in
children with and
without autism
spectrum disorder
1. To examine trajectories of receptive and expressive language development in children with
ASD from 4 to 7 years and to compare these trajectories to those of children with LI and TD
2. To compare the proportions of children with ASD who had declining, stable and accelerating
trajectories to children with LI and TD
3. To investigate whether children with ASD were more likely to have a greater gap between
expressive and receptive language abilities from 4 to 7 years compared with children without
ASD
4. To investigate predictors of expressive and receptive language outcomes in the whole cohort
from 4 to 7 years
Hypotheses: We hypothesised children with ASD would have lower language ability than the
typically developing children and slower language growth, with the gap between the two groups
growing over time. We expected social communication, a diagnosis of ASD, early language and
IQ to be important predictors of language outcome. Given the mixed evidence about relative
weakness in receptive language we were uncertain if children with ASD would be more likely
than the other children to have a receptive-expressive language discrepancy.

66
Chapter 5 Study 1. A systematic review and meta-analysis of
language outcomes in autism spectrum disorder
In this study we systematically reviewed the existing literature on language outcomes in
individuals with ASD. This paper is being prepared for submission to Autism Research.

67
Abstract
Background
Language difficulties are common in Autism Spectrum Disorder (ASD). Parents and
clinicians need evidence about language trajectories in ASD to inform decision-making,
evaluate interventions and understand prognosis.
Objective
To systematically review studies reporting language outcomes in individuals diagnosed
with ASD.
Method
A comprehensive search strategy with a well-established sensitive prognosis filter for
Medline, adapted for 5 other database searches, was used. Included studies observed
individuals diagnosed with ASD for ≥ 12 months and had ≥ 30 participants. Risk of bias
assessments were conducted on all included studies. Data were extracted and changes in
scores mapped over time. If 5 or more studies presented data on the same language
domain random effects meta-analysis was conducted.
Results
Fifty-four studies (N=5064) met inclusion criteria. Language outcomes were
standardised assessments (n=35), notation of presence/absence of verbal language
(n=11) or both (n=8). Age at baseline ranged from 17 months to 26 years, duration of
follow-up from 1 to 38 years. Most publications (92%) were rated medium to high risk
of bias. In all but one study children with ASD had substantially lower than average
scores at baseline and follow-up. However, in most (n=24/25; 96%) studies reporting

68
standard scores, children with ASD (aged ≤11 years at follow-up) progressed at a
comparable rate to age-expected norms across a range of language domains. Meta-
analyses conducted on three language domains (expressive and receptive syntax,
adaptive language) found mean standard scores increased over time. Between 5-32%
developed the ability to use words over the course of the study. The proportion gaining
phrases from single words ranged from 23-37%.
Conclusion
Although most studies had not met criteria for best methods for prognosis studies there
was remarkable consistency of findings despite variations in inclusion criteria, age
groups, tools used and language constructs measured. Most individuals with ASD
gained language over time. Despite having below average language scores, most
children under 11 years at follow up progressed at a comparable rate (in parallel) to age-
expected norms.

69
Introduction
To meet criteria for a diagnosis of ASD, the current Diagnostic Statistical Manual of
Mental Disorders (DSM-5) (American Psychiatric Association, 2013) requires the
presence of social communication difficulties and repetitive and restricted interests and
behaviours. While other (non-social) language difficulties are not requisite for an ASD
diagnosis, they are a common comorbidity and DSM-5 now requires specification about
whether such a language impairment is present.
Language development is often the first issue raised by parents of children later
diagnosed with autism (De Giacomo & Fombonne, 1998; Herlihy et al., 2015). Once a
diagnosis is made, around 63% of children with ASD present with language disorders
(Levy et al., 2010). There is substantial heterogeneity in the extent of language
difficulties that co-occur with ASD (Ellis Weismer & Kover, 2015; Tager-Flusberg et
al., 2005; Tek, Mesite, Fein, & Naigles, 2014). Some children have well preserved (or
even superior) language abilities on formal testing, with sophisticated vocabulary and
sentence structure (Boucher, 2012; Tager-Flusberg & Caronna, 2007), yet cross-
sectional studies have found between 14 to 50% of children with ASD never develop
the ability to use words as their primary means of communicating (Chakrabarti &
Fombonne, 2001; King & Bearman, 2009; Kjelgaard & Tager-Flusberg, 2001; Lord,
Risi, & Pickles, 2004; Rice et al., 2005). Further to the variability noted in language
skills in this group, there is also variation in the types of difficulties seen. Stereotypical
verbal behaviours are commonly described including repetitive language, idiosyncratic
phrases, difficulties with pronouns and echolalia (American Psychiatric Association,
2013; Tager-Flusberg & Caronna, 2007).

70
There is consensus in the literature that verbal skills play a critical role in predicting
long-term outcomes for children with ASD in areas such as adaptive functioning,
psycho-social adjustment and wellbeing (Gillespie-Lynch et al., 2012; Hofvander et al.,
2009; Howlin, 2003; Howlin & Moss, 2012; Mawhood & Howlin, 2000; Szatmari et al.,
2003). Language skills are also critical to school placements and academic performance,
as well as the ability to participate in successful social interactions (Thurm et al., 2007).
Despite recognition of the importance of this domain to children with ASD, language
outcomes remain poorly understood.
Parents of children with ASD commonly ask health professionals whether their child
will talk, and if so, to what extent and how their language development will progress
compared with their peers. High quality evidence is required about the likely language
outcomes for children so clinicians can provide well-informed answers. Understanding
the language development in children with ASD is also important so the effectiveness of
communication interventions can be evaluated within a developmental context. A
substantial number of studies have investigated language outcomes in children with
ASD. Due to significant variation in methodologies across studies however (e.g.,
different length of follow-up, ages and developmental profiles of the children,
interventions, tools used to measure language), it is difficult to interpret study findings
in a clinically meaningful way. The aim of this review is to synthesise current evidence
for verbal language outcomes in individuals with ASD with a view to inform parents,
clinicians, service providers and policy makers.

71
Methods
Inclusion/exclusion criteria
Children and adults of all ages with a diagnosis of autism spectrum disorder, autism,
autistic disorder, childhood autism, pervasive developmental disorder (PDD), PDD-not
otherwise specified (PDD-NOS), atypical autism, PDD-unspecified, or Asperger’s
disorder/syndrome were included in the review.
Studies were included only if the diagnosis was made at the beginning of the study
using a standardised diagnostic instrument including the Autism Diagnostic Interview-
Revised (ADI-R; Le Couteur, Lord, & Rutter, 2003), Autism Diagnostic Observation
Schedule (ADOS; Lord et al., 2000), Diagnostic Interview for Social and
Communication Disorders (DISCO; Wing, Leekam, Libby, Gould, & Larcombe, 2002),
Childhood Autism Rating Scale (CARS; Schopler, Reichler, DeVellis, & Daly, 1980),
Gillian Autism Rating Scale (GARS; Gilliam, 1995)and/or by using established
diagnostic criteria of an accepted classification system at the time, such as DSM III-IV-
IV TR, 5 (American Psychiatric Association, 1980, 2000, 2013) or ICD 9-10 (World
Health Organisation, 2010). A dual diagnosis (e.g., Asperger disorder and attention
deficit hyperactivity disorder, or autism and Fragile X) did not prevent inclusion.
Types of studies
Intervention and observation studies were eligible for inclusion if initially defined
participants (diagnosed with ASD) were followed up for a period of 12 months or more.
Retrospective and prospective cohorts were included. Studies had at least 30
participants to differentiate case series from a cohort study. Randomised control trials

72
presenting data separately for the comparison/control and intervention groups were only
included if the comparison/control arm had more than 30 participants. Studies published
in languages other than English were also included.
Types of outcome measures
Studies were included if language outcomes were measured by standardised
assessments or where the study reported on the presence/absence of verbal language
(e.g., no words, use of single words, phrases). Studies were also required to have a
baseline and follow-up measure of language. Standardised parent report and direct
assessment of language tools were included, along with broader tools such as the
Vineland Adaptive Behavior Scales (Sparrow, Cicchetti, & Balla, 2005), if expressive
and/or receptive communication subdomains were assessed. The general term ‘language
outcomes’ is used to refer to the outcomes used by all included tools. Studies of
nonverbal language (e.g., augmentative/alternative communication such as use of signs
or symbols to communicate) were excluded.
Search strategy for identification of studies
Databases were searched using the search filter “prognosis sensitive” devised for the
Medline database by Wilczynski and Haynes (2004). The filter was adapted for other
databases that did not systematically offer this same filter. PsycINFO, Embase,
CINAHL, Cochrane Database of Systematic Reviews (CDSR) and the Database of
Reviews of Effectiveness (DARE) were used. Appendix B lists database specific search
terms. Conference proceedings and thesis dissertation abstracts were searched. The
73
reference lists of included articles were reviewed and experts in the field were
contacted.
Review of studies
Titles and abstracts of all references identified were screened by at least two authors
(AB, FK, VS, SW, KW, KL) assessing every title and abstract. Studies failing to meet
inclusion criteria were excluded. The full text of potentially relevant articles was
obtained and again assessed by at least two authors. Disagreement between the two
authors was resolved by consensus or referred to a third author for arbitration. Articles
not fulfilling inclusion criteria were excluded.
Quality Assessment
Risk of bias was assessed using a modified Quality in Prognosis Studies (QUIPS) tool
(Hayden, van der Windt, Cartwright, Côté, & Bombardier, 2013). The modification was
required because the current study did not analyse confounders or prognostic factors and
therefore these assessment categories did not apply. Three authors (Amanda Brignell
and either Angela Morgan or Tamara May) assessed risk of bias in all included studies
and any differences in ratings were resolved through consensus. Studies were assessed
using the domains: study participation, study attrition and outcome measurement. If
information required for assessment was not available in studies published after 2000,
authors were emailed for further information. This was because it would have been
difficult to track down authors of studies published more than 16 years ago. Appendix C
lists subcategories of each domain and specific criteria used to rate each item as unclear,
low, medium or high.

74
Data management
Data extraction was independently completed via a standardised template, by a
minimum of two authors (AB and either FK or TM). Important clinical information
likely to influence applicability and interpretation of findings (and necessary to allow
assessment of homogeneity of studies) was extracted (Table 10).
Table 5 Clinical information collected from included studies.
Clinical information collected from included studies
Type of sample (population-based or clinical) Age at baseline
Type of recruitment (prospective or retrospective) Age at follow-up
Type of diagnosis (e.g., autistic disorder, Asperger’s Syndrome)
Language measured used (e.g., Preschool Language Scales)
Type of study (intervention or observational) Mean IQ or DQ for group (<70 or >70)
Proportion lost to follow-up Length of follow-up
Tools used for measuring outcomes were categorised by five language domains:
receptive and expressive vocabulary, receptive and expressive syntax, parent-rated
adaptive language, parent-rated vocabulary and proportion verbal/nonverbal or using
phrases. For the purposes of this review, if individuals used ‘no or few words
consistently on a daily basis’ or were described as ‘minimally verbal,’ we grouped them
as ‘nonverbal’. We acknowledge, as have other authors (Kasari et al., 2013; Norrelgen
et al., 2014; Rose, Trembath, Keen, & Paynter, 2016; Tager-Flusberg & Kasari, 2013;
Tager-Flusberg et al., 2016) there is a difference between an individual being
completely nonverbal compared with using some words, however, such level of detail

75
was not often provided by studies and it was beyond the scope of this review to
subdivide groups further.
Studies were also grouped based on developmental or cognitive level measured by
either a standardised intelligence (IQ) or developmental quotient (DQ). These were
identified by whether the mean IQ or DQ for the cohort was (1) less than or equal to 70
or more than 70, or (2) if more than 70%, or less than 30%, of the sample achieved an
IQ/DQ of less than or equal to 70. Where a mental age was given we converted this to a
DQ by dividing mental age by chronological age. If only nonverbal subtests (e.g., visual
perception) of cognitive assessments were reported we used those to estimate DQ or IQ.
For tools such as the Mullen Scale of Early Learning (Mullen, 1995) a standard T score
(e.g., for the nonverbal subtests) of 30 which is 2 standard deviations below the mean
score of 50, was considered the ‘cut point’ or equivalent to <70 on an IQ test.
If a median/mean was not provided for duration of follow-up, baseline and/or follow-up
age, a mean duration or age was imputed by taking the average of the lower and upper
end points of the range given. Where available, we collected information on any
intervention. Where participants had been described as receiving a range of
interventions in the community, they were grouped as ‘treatment in the community’
(TIC), otherwise the treatment is described as a specific intervention. Descriptive
information was also collected on whether the study analysed predictors of language
outcomes although this information was not analysed because this study did not aim to
review predictors of outcome. In cases where the same participants were included in
more than one publication (also with use of the same outcome measures) data was taken
from the publication with the largest sample size and/or where data on language

76
outcomes could most easily be extracted. Publications using the same participants were
provided with an overall study identifier label (Table 6).
Statistical analysis
Outcomes were presented for relevant studies in graphical format where possible.
Studies were graphed when data describing mean/median standard scores or age
equivalent scores could be extracted, or when the proportion of children who were
verbal or used phrases at two time points was reported. This allowed comparison of
trajectories from baseline to follow-up. Standard scores allow comparison to a ‘typically
developing’ reference score. For most tools this is a score of 100. If development
progresses at a rate expected for an individual’s age, standard scores should remain the
same over time (e.g., 100 at Time 1 and 100 at Time 2).
Age equivalent scores allow comparison of an individual’s language age (age-
equivalent) to their chronological age. In typical development one would expect
chronological age to roughly match language age at any time point. If available, or able
to be calculated, confidence intervals were added to scores. A number of studies
reported raw scores. It was not possible to track change relative to age-expected levels
for raw scores, instead they were interpreted with reference to direction of change (gain,
plateau or loss of language skills) over time. Studies that did not report scores on the
same tool at two time points are described in the text.
Due to variability in study findings we were not able to present summary statistics for
all language measures. However if five or more studies reported on the same language
outcome at two time points a meta-analysis was conducted followed by meta-regression

77
co-varying for age at baseline, language level at baseline, length of follow-up and IQ. A
fixed effects meta-analysis was conducted in the first instance but if there was
substantial heterogeneity observed between studies, a random effects meta-analysis was
conducted using the DerSimonian and Laird method. This method takes the
heterogeneity into account in the final calculation of the effect size and the confidence
interval around that effect size.
Results
Search results
The literature search was completed at five time points (2006, 2007, 2010, 2013, 2016).
The final search was completed at the end of Week 2 in January 2016. Figure 4 shows a
flow diagram of the literature search, the number of studies that were excluded or met
inclusion criteria.

78
Figure 4 Results of the literature search and study selection.
The combined search yielded 19,410 studies. Review of 319 full text articles, identified
92 publications that met inclusion criteria and measured language as an outcome (see
Appendix D for the full list of publications and their characteristics). Sixteen studies
had two or more publications and overlapping participants. A total of 54 studies
(n=5064) met inclusion criteria once duplicate publications were removed. Duplicate
studies (Table 6) were grouped as one study and labelled with a study identifier.

79
Table 6 Studies with two or more publications and overlapping particpants.
Study identifier Publications
Anderson-Lord cohorta Anderson 2007*, Anderson 2009, Thurm 2007, Anderson 2014, Bal 2015, Bedford 2015, Pickles 2015*
Baghdadli-Darrou cohort Bagdadhli 2012*, Darrou 2010c
Ben Itzchak cohort Ben Itzchak 2009, Ben Itzchak 2011c, Ben Itzchak 2014*
Bennett-Starr Bennett 2008, Bennett 2013, Starr 2003*
Berry-Kleinman cohorta Berry 2009*, Kleinman 2008*
Bopp cohorta Bopp 2006*, Bopp 2009, Bopp 2011*
Chawarska-Klintwall cohort Chawarska 2009, Klintwall 2015
Freeman cohort Freeman 1985*, Freeman 1999
Howlin cohortb Howlin 2013, Howlin 2014*
Magiati-Mossa Magiati 2011*, Moss 2008*
Mazurek-Wodka Wodka 2013*, Mazurek 2012
Munson-Totha Munson 2008*, Toth 2006*

80
Study identifier Publications
Ontario cohort Freeman 2010*, Perry 2008, Perry 2011, Perry 2013
Pathways study Georgiades 2014, Bennett 2013, Bennett 2014, Flanagan 2015, Szatmari 2015
Pelicano cohort Pelicano 2010, Pelicano 2012*
Stockholm cohort Eriksson 2013, Fernell 2010, Hedvall 2015, Norrelgen 2014*
Wisconsin cohort Haebig 2013a, Haebig 2013b, Davidson 2014*, Ellis Weismer 2015, Venker 2014, Ray-Subramanian 2012
Woynarski-Yoder Woynarski 2015, Yoder 2015*
* Data were extracted from this publication.
a. Anderson-Lord, Berry-Kleinman, Bopp, Munson-Toth and Magiati-Moss and Ben Itzchak cohorts reported on the same participants butused different measures so data were included from both studies.
b. Twenty nine participants from Howlin 2004 were also included in Howlin 2014.
Note. Flanagan 2010 was an intervention trial and participants receiving the intervention overlapped with participants in the Ontario cohort, however, data were only extracted from participants in the control group. Blacklock 2014 recruited participants from the Ontario cohort but of a different age group to Freeman 2010 so data were extracted from both studies.

81
Risk of bias assessment
Risk of bias ratings are included in Table 7. We (AB, AM, TM) assessed all included
publications (n=92) of the included studies (n=54) for risk of bias because factors linked
to risk of bias varied for publications based on the same participants. For example, loss
to follow-up at one time point could be much higher than another time point. Only one
publication was at low risk of bias for study participation, study attrition and outcome
measure risk of bias categories. A further eight were at low risk of bias for two of these
three categories (Table 7). Thirty-three (36%) were at a high risk of bias for two or
more categories. Sixty-seven publications (73%) collected information prospectively
and the remainder were retrospective. Only nine publications derived their sample from
a population source and the rest were derived from clinical samples. In all publications,
individuals were diagnosed using DSM or ICD criteria or accepted standardised
diagnostic instruments. Nine publications reported blinding the outcome assessor to the
child’s baseline status. Percent followed up ranged from 24% to 100% with 46 of the 67
prospective publications (70%) reporting less than 20% of participants lost to follow-up.

82 82
Table 7 Risk of bias rating on included publications
Author Study participation
Study attrition
Outcome measures
Howlin et al. (2004) L L L
Bennett et al. (2014), Davidson and Ellis Weismer (2014), Knorring and Hägglöf (1993)
L L M
Anderson et al. (2009), Landa and Kalb (2012) L M L
Berry (2010), B. J. Freeman, Ritvo, Needleman, and Yokota (1985) L H L
Bennett et al. (2013), Eriksson et al. (2013) L M M
Flanagan et al. (2015), Hedvall et al. (2015), Szatmari et al. (2015) L H M
Siller, Hutman, and Sigman (2013) M L L
Klintwall, Macari, Eikeseth, and Chawarska (2015) M L M
Anderson et al. (2007), Ray-Subramanian and Ellis Weismer (2012) M M L
Stone and Yoder (2001), Chawarska, Klin, Paul, Macari, and Volkmar (2009) M H L
Anderson, Liang, and Lord (2014), Green and Carter (2014), Magiati et al. (2011), Oosterling et al. (2010), Pellicano (2010b, 2012), Zierhut (2002), Moss, Magiati, Charman, and Howlin (2008), Howlin et al. (2013) Howlin et al. (2014), Cederlund, Hagberg, Billstedt, Gillberg, and Gillberg (2008)
M M M
I. M. Smith, Flanagan, Garon, and Bryson (2015) M M H
Bedford, Pickles, and Lord (2015), Ben-Itzchak, Watson, and Zachor (2014), Ellis Weismer and Kover (2015), Georgiades et al. (2014), Hellendoorn et al. (2015),
M H M

83 83
Author Study participation
Study attrition
Outcome measures
Lombardo et al. (2015), Miniscalco, Rudling, Rastam, Gillberg, and Johnels (2014), T. Smith, Klorman, and Mruzek (2015), Thurm et al. (2015), Venker, Ray-Subramanian, Bolt, and Weismer (2014), Vivanti, Barbaro, Hudry, Dissanayake, and Prior (2013), Eaves and Ho (1996), Flanagan, Perry, and Freeman (2012), Kleinman et al. (2008), Steele, Joseph, and Tager-Flusberg (2003), C. J. Thomas (2009), Thurm et al. (2007), Fernell et al. (2011), Szatmari et al. (2009), Toth et al. (2006), Norrelgen et al. (2014)
Meyer (2002) M H L
Blacklock, Perry, and Dunn Geier (2014), Perry et al. (2008) Perry, Blacklock, and Dunn Geier (2013); Perry et al. (2011), Pickles et al. (2014), Sullivan (2010)
M H H
Bennett et al. (2013) H M L
Starr, Szatmari, Bryson, and Zwaigenbaum (2003) H L M
Bennett et al. (2008), Bopp (2006); Bopp, Mirenda, and Zumbo (2009), Bopp and Mirenda (2011), , Eaves and Ho (2004), Haebig, McDuffie, and Ellis Weismer (2013a); Haebig et al. (2013b)
H H L
B. J. Freeman et al. (1991), Jónsdóttir et al. (2007), Sigman and McGovern (2005), Wolf and Goldberg (1986)
H M M
Bal, Kim, Cheong, and Lord (2015), Pugliese et al. (2015), Woynaroski et al. (2015), Baghdadli et al. (2012); Bagley and McGeein (1989), Ben Itzchak and Zachor (2009), Ben Itzchak and Zachor (2011), Carbonnel-Chabas and Gepner (2009), Darrou et al. (2010), Mosconi, Steven Reznick, Mesibov, and Piven (2009), Munson, Faja, Meltzoff, Abbott, and Dawson (2008), Paul et al. (2008), Pry, Petersen, and Baghdadli (2011), Takeda, Koyama, Kanai, and Kurita (2005), Wodka et al. (2013)
H H M
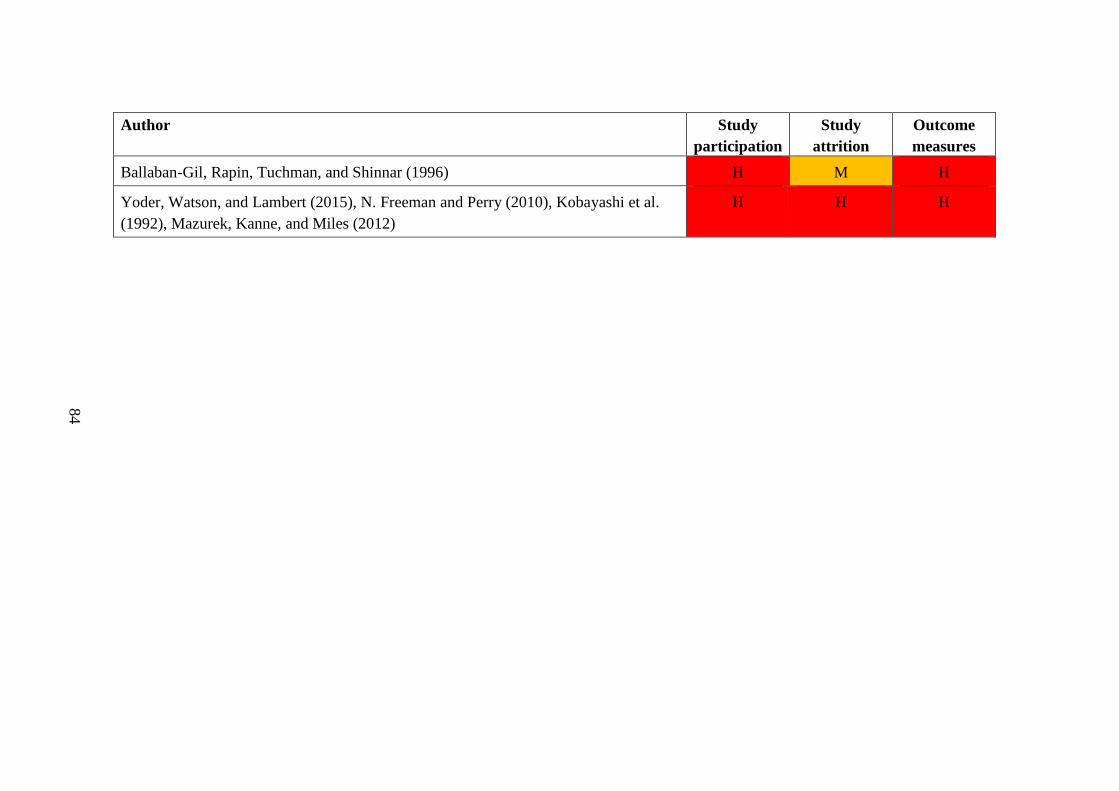
84 84
Author Study participation
Study attrition
Outcome measures
Ballaban-Gil, Rapin, Tuchman, and Shinnar (1996) H M H
Yoder, Watson, and Lambert (2015), N. Freeman and Perry (2010), Kobayashi et al. (1992), Mazurek, Kanne, and Miles (2012)
H H H

85
Language outcome measures
Of the 54 included studies, standardised parent-completed tools were reported in 29
studies, standardised clinician-completed tools in 30 and the presence/absence of verbal
language in 19 studies (Figure 5). Twenty-one studies reported language outcomes
using two or more measures at each time point. Language tools were grouped into 5
broad domains (Table 8).
Figure 5 Number of studies that used each type of language measure.

86 86
Table 8 Language outcome domains and tools
Language outcome Domain Description Tools
Standardized clinician-completed
Receptive and expressive syntax
Measures receptive or expressive language more broadly (i.e. range of language domains assessed)
Clinical Evaluation of Language Fundamentals (CELF) Mullen Scales of Early Learning (MSEL) Preschool Language Scales (PLS) Reynell Developmental Language Scales (RDLS) Sequenced Inventory of Communication Development (SICD) Test of Auditory Comprehension of Language (TACL) Test of Oral Language Development (TOLD)
Receptive and expressive vocabulary
Measures receptive or expressive vocabulary only
Expressive One Word Vocabulary Test (EOWVT) Expressive Vocabulary Test (EVT) Peabody Picture Vocabulary Test (PPVT) British Picture Vocabulary Scales (BPVS)
Standardized parent-completed
Adaptive language Measures adaptive communication skills
Vineland Adaptive Behaviour Scales (VABS)
Expressive and receptive vocabulary
Measures number of words understood or expressed
MacArthur Bates Communicative Inventories (CDI)
Presence/absence of verbal language
Verbal or phrase language
Measures whether individual had verbal language/were nonverbal or using phrases
ADI-R questions ADOS module Categorical descriptions/rating scales developed by the study e.g., <10 words used functionally on a daily basis or the use of phrases.

87
Characteristics of studies
The number of participants ranged from 32 to 1433 with 74% (n=40) having more than
50 participants. Study duration ranged from 1 to 38 years. Age at baseline ranged from
17 months to 26 years and at follow-up 35 months to 59 years. Eleven studies included
children classified with autistic disorder or autism only, two did not specify the type of
diagnosis and the remaining 40 (74%) included children from the autism spectrum. In
25 studies (46%) the majority of children had a cognitive impairment (as defined by
70% or more children having an IQ or DQ <70 or mean IQ or DQ of 70 or less). Fifteen
studies (28%) included children with mean IQ/DQ over 70 or >70% of the sample had
an IQ>70 and 14 studies did not present data on IQ or it was not possible to extract the
required information. Ten studies (19%) involved administration of a specific
intervention where outcomes had been followed up over time. The remaining studies
(81%) were observational and included children who had received a broad range of
interventions in the community (Appendix D).
Language outcome measures in each study
The 54 studies used 14 different tools to assess language (Table 9). The measures used
by the most studies were the VABS (n=25), MSEL (n=14), notation of
presence/absence of verbal language (n=19) and the PPVT (n=6). The most commonly
used standardised assessment of expressive and receptive language was the PLS (n=6).
For a variety of reasons (e.g., study did not use same measure at each time point or
could not be grouped with others) some studies could not be represented graphically and
are presented in the text.

88 88
Table 9 Language outcome measures used by each study.
Author, year Verbal or phrase speech
Parent completed tool VABS +/or CDI
Syntax PLS +/or CELF +/or RDLS +/or MSEL +/or TOLD +/- SICD
Vocabulary PPVT +/or BPVS +/or EOVWT +/or EVT
Anderson-Lord cohort x MSEL & SICD
Baghdadli-Darrou cohort, Stockholm cohort x VABS
Bagley 1999, Ballaban-Gil 1996, Carbonnel-Chabas 2009, Eaves 1996, Jonsdottir 2007, Knorring 1993, Kobayashi 1992, Mazurek-Wodka cohort, Pry 2011, Takeda 2005, Wolf 1986
x
Ben Itzchak cohort, Berry-Kleinman cohort, Chawarska-Klintwall cohort, Lombardo 2015, Mosconi 2009, Paul 2008, Smith T 2015
VABS MSEL
Bennett-Starr cohort x VABS TOLD
Bopp cohort CDI PLS PPVT & EOWVT
Eaves 2004, Wisconsin cohort VABS PLS
Ontario cohort, Flanagan 2012, Landa 2012, Meyer 2002, Munson-Toth cohort, Pugliese 2016, Sullivan 2010, Cederland 2008, Blacklock 2014
VABS
Freeman cohort x VABS TOLD & TACL PPVT

89 89
Author, year Verbal or phrase speech
Parent completed tool VABS +/or CDI
Syntax PLS +/or CELF +/or RDLS +/or MSEL +/or TOLD +/- SICD
Vocabulary PPVT +/or BPVS +/or EOVWT +/or EVT
Green 2014, Hellendoorn 2015, Siller 2013, Vivanti 2013 MSEL
Howlin 2004 PPVT & BPVS
Howlin cohort x BPVS & EOWVT
Magiati-Moss cohort x VABS BPVS & EOWVT
Miniscalco 2014, Oosterling 2010 CDI
Pathways cohort, Smith, I 2015 VABS CELF & PLS
Pelicano cohort, Thomas 2010 PPVT
Sigman 2005 CELF & RDLS
Steele 2003 PPVT & EVT
Stone 2003 SICD

90 90
Author, year Verbal or phrase speech
Parent completed tool VABS +/or CDI
Syntax PLS +/or CELF +/or RDLS +/or MSEL +/or TOLD +/- SICD
Vocabulary PPVT +/or BPVS +/or EOVWT +/or EVT
Thurm 2015 x MSEL
Yoder-Woynaroski 2015 CDI MSEL
Ziehurt 2002 RDLS
Abbreviations: BPVS: British Picture Vocabulary Scales; CDI: MacArthur Bates Communicative Inventories; CELF: Clinical Evaluation of Language Fundamentals; EVT: Expressive Vocabulary Test; EOWVT: Expressive One Word Vocabulary Test; MSEL: Mullen Scales of Early Learning; PLS: Preschool Language Scales; PPVT: Peabody Picture Vocabulary Test; RDLS: Reynell Developmental Language Scales; SICD: Sequenced Inventory of Communication Development; TACL: Test for Auditory Comprehension of Language; TOLD: Test of Language Development; VABS: Vineland Adaptive Behaviour Scales; V/PS: verbal or phrase speech measure.

91
Clinician-administered tools
Receptive and expressive syntax
Change in standard scores
Seven studies measured receptive (Ben Itzchak cohort, Berry-Kleinman cohort,
Wisconsin cohort, Lombardo 2015, Paul 2008, Smith T 2015, Vivanti 2015) and
expressive syntax respectively (Ben Itzchak cohort, Berry-Kleinman cohort, Wisconsin
cohort 2014, Lombardo 2015, Paul 2008, Smith T 2015, Vivanti 2015). In all
aforementioned studies, mean language scores for children with ASD were below age-
expected levels.
All 7 studies that measured receptive syntax reported an increase in mean standard
scores for children with ASD (i.e. more gain than expected relative to age-matched
peers) (Figure 6a). Fifty-seven percent (n=4/7) of these studies showed a statistically
significant (p<0.05) increase in scores over time (Paul 2008, Berry-Kleinman cohort,
Wisconsin cohort, Vivanti 2015) indicating some language ‘catch up’ to reference
norms. All 7 expressive syntax studies reported an increase in mean standard scores
with 43% (n=3/7) reporting a statistically significant (p<0.05) increase (Paul 2008,
Wisconsin cohort, Vivanti 2015) (Figure 6b). Participants in Ben Itzchak cohort and
Smith I (2015) received intensive behavioural interventions. Participants in the
remaining studies received a variety of interventions in the community.

92 92
Figure 6 Standard scores in receptive (a) and expressive syntax (b) at baseline and follow-up with 95% confidence intervals for studies using the MSEL and PLS
(a)

93 93
(b)
Note. Mean standard score on MSEL: 50 (upper horizontal grey line); mean standard score on PLS: 100 (lower horizontal grey line). PLS: Wisconsin cohort (2014). MSEL: Ben Itzchak cohort, Berry-Kleinman cohort, Lombardo (2015), Paul (2008), Smith I (2015), Vivanti (2013). Means for the ‘poor and good’ outcome groups were combined from Lombardo (2015).

94
Combining the results of seven studies in a random effects meta-analysis, there was an
estimated overall increase of 9.4 units (95% CI: 4.9-13.8; I2 86.6%, df 0.6, p<0.001) on
receptive syntax scales observed in a study over time, Figure 7. Substantial
heterogeneity was found between studies. In the meta-analysis a score of 0 indicates
children are progressing at rate expected for their age (i.e. norm references). A score
over 0 indicates some ‘catch up’ or acceleration.
Figure 7 Random effects meta-analysis on seven studies using PLS or MSEL as a scoring system for receptive syntax outcomes.

95
Figure 8 Random effects meta-analysis on seven studies using PLS or MSEL as a scoring system for expressive syntax outcomes.
For expressive syntax, combining the results of seven studies in a random effects meta-
analysis, there was an estimated overall increase of 5.1 units (95% CI: 3.3-7.0; I2 39.0%,
df 0.6, p=0.132) on expressive syntax scales observed in a study over time, Figure 8.
Change in age equivalent scores
Four studies provided age equivalent scores on combined expressive and receptive
syntax (Bopp cohort, Chawarska-Klintwall cohort, Stone 2003, Ziehurt 2012) and one
study provided separate scores for expressive/receptive syntax in children aged under 5
years at baseline. There was divergence away from the expected trajectory for
chronological age and the participant’s language age over time in 2 of the 4 studies in
studies reporting on combined receptive/expressive syntax (Figure 9a).

96 96
Figure 9 Combined receptive/expressive syntax language and receptive vocabulary language age relative to chronological age
(a)

97 97
(b)
Note. The grey line represents a chronological age equivalent to language age, the line of ‘average’ development. Stone (2003) only reported expressive syntax age-equivalents. Smith I (2015) reported receptive language (RL) and expressive language (EL) age equivalent scores separately.PPVT: Freeman cohort, Bopp cohort, Steele (2003); RDLS: Ziehurt (2002); MSEL: Smith I (2015), Klintwall (2015); SICD: Stone (2003); PLS: Bopp cohort.

98
In the studies of children who were under 5 years at baseline the mean language age was
substantially below chronological age at baseline, ranging from 11 months behind at 4.1
years to 2.8 years delay at 4.2 years of age. At follow-up, mean language age ranged
from 1.8 years behind at 5.2 years to 3.3 years behind at 6.2 years. A study of older
children from 12 (middle childhood) to 19 years (adolescence) showed a much lower
mean language age based on the RDLS/CELF tool than chronological age at baseline
with a substantially increasing gap between the two metrics over time. This was
reflected in quite flat language trajectories with a 1.4 month language gain over 6 years
for children with an IQ<70 and a 2.5 year gain in language over a 6-7 year period for
children with an IQ>70 (Sigman 2003). One study (Howlin 2004) provided only age-
equivalents at study end. Participants had an average language age of 8.26 (SD 6.21) at
a mean chronological age of 29.33 years. One study provided only log adjusted scores
which showed an increase in language age for participants over time (Siller 2013).
Change in raw scores
Three studies provided raw scores on clinician-administered tools (Bopp cohort,
Hellendoorn 2015, Ray Subramanian 2012), detailed in Appendix E. In receptive
syntax, mean scores increased from 13.39 to 29.19 over 2 years (Bopp cohort), 16.04 to
37.22 over 1.5 years (Hellendoorn 2015) and 20.35 to 28.44 over 1 year (Ray
Subramanian 2012). In expressive syntax mean scores increased from 14.38 to 26.05
over 2 years (Bopp cohort), 17.02 to 36.49 over 1.5 years (Hellendoorn 2015) and 24.96
to 32.25 over 1 year (Ray Subramanian 2012). This indicates improvement in language
ability over time in all studies however assessment of progress relative to what is
expected is not possible with raw scores.

99
Expressive and receptive vocabulary
Change in standard scores
Three studies reported data on receptive vocabulary (Pelicano cohort, Magiati-Moss
cohort, Thomas 2009) and one on expressive vocabulary (Magiati-Moss cohort). In all
but one study (Pelicano cohort), that only included children with verbal IQ>80, baseline
scores were substantially lower than age-expected levels.
Two of three studies (Thomas 2009, Magiati-Moss cohort) reported an increase in
standard scores over time, from 48.6 (95% confidence interval (CI) 43.1-54.1) to 55.6
(CI 48.4-62.6) over 6.9 years in one study (Magiati-Moss cohort) and from 70.9 (CI
64.4-77.3) to 77.5 (CI 71.3-83.7) over 5 years in another (Thomas 2009). The third
study demonstrated a decrease in standard scores over 2.7 years (Pelicano cohort). In
this study scores decreased from 97.1 (CI 93.7-100.5) to 93.9 (CI 88.7 to 99.1). In the
study reporting data on expressive vocabulary standard scores, the mean standard score
decreased from 69.3 (CI: 65.1-73.4) to 65.49 (CI: 59.7-71.3) (Magiati-Moss cohort).
No studies that reported on receptive and expressive vocabulary demonstrated
significant catch up or loss relative to age-matched peers. Despite having lower scores
at baseline and follow-up, on average, the children with ASD progressed at a
comparable rate to reference norms. In all studies there was greater variability in
standard scores over time, evidenced by wider confidence intervals at follow-up
compared with baseline, indicating substantial heterogeneity in language trajectories.
One study could not be presented graphically because it only reported standard scores
on the PLS at follow-up (Eaves 2004). In this study, children with autistic disorder
(n=36) achieved mean scores of 52.9 (SD 16.2) in expressive and 54.9 (SD 17.3) in

100
receptive language at follow-up and those with PDD-NOS achieved mean scores of 63.0
(SD 27.8) in expressive and 64.3 (SD 26.7) receptive language. It was not possible to
comment on change over time in this study because age-equivalents were used at
baseline and language measures varied across time points.
Change in age equivalent scores
All studies that provided data on age-equivalents reported gains in mean receptive
vocabulary language age over time (Bopp cohort, Freeman cohort, Steele 2003). Of
these three studies, one demonstrated some “catch up” to chronological age with a gap
between chronological and language age of 2.2 years at baseline and 1.8 years at follow-
up (Steele 2003). The other two studies reported a widening gap between language and
chronological age from a gap of 3.31 years at baseline to 3.8 years at follow-up in one
study (Bopp cohort) and 2.6 years at baseline to 3.7 years at follow-up (Freeman
cohort), Figure 9 (b). Participants in all studies received a variety of interventions in the
community rather than the study being an intervention trial.
Change in raw scores
Two studies provided raw scores on expressive and receptive vocabulary (Bopp cohort,
Steele 2003), detailed in Appendix E. In both studies mean raw scores increased. This
indicates improvement in language ability over time however assessment of progress
relative to what is expected is not possible with raw scores.

101
Parent-report tools
Adaptive language
Change in standard scores
Thirteen studies had data on standard scores that could be extracted on the VABS and
displayed graphically (Figure 10).
Figure 10 Standard scores on the VABS at baseline and follow-up.
Note. Smith I-A and Smith I-B are two cohorts from the same study grouped into IQ< 70 and IQ> 70 (Smith I 2015). Participants in the Flanagan (2012) study had substantially lower IQs (Time 2 IQ 39.50 (SD 18.93) than the participants in other studies. One study presented data by poor and good language groups, here we provide a combined mean (Lombardo 2015).

102
A higher score on the VABS communication domain is an indication of better
functioning and the mean standard score on the VABS is 100. All of these studies
reported mean baseline standard scores below the average range. Eighty-five percent of
studies (n=11/13) reported higher standard scores at follow-up than baseline and 31%
(n=4/13) of these studies reported a statistically significant (p<0.05) improvement in
scores from baseline to follow-up (Sullivan 2010, Landa 2012, Smith I-B 2015,
Blacklock 2013).
Two studies (Eaves 2004, Magiati-Moss cohort) reported a decline in scores from
baseline to follow-up and one of these reported a statistically significant (p<0.05)
decline (Magiati-Moss cohort). There were no substantial differences between Magiati-
Moss cohort and the other studies in participant characteristics (e.g., IQ levels) or
methodology to explain the different trajectories, however the Magiati-Moss study did
have a longer follow-up period and individuals were older at follow-up compared with
the other studies. In addition, the Magiati-Moss cohort recruited children to the study in
the late 1990s, which was substantially earlier than some of the other studies. The other
three studies where participants showed the least amount of language gain recruited
participants at the three next earliest time points (i.e. in the 1990s/early 2000s) relative
to the other studies (Berry-Kleinman cohort, Eaves 2004, Meyer 2002). It was not
possible to investigate whether type, dose or frequency of intervention may have
explained differences in study findings because descriptions of interventions were not
detailed within all papers.
In all but two studies (Meyer 2002, Smith I-B 2015) there was greater variability in
standard scores between participants at follow-up than at baseline, evidenced by wider
confidence intervals around the mean at outcome. Participants in Freeman 2010, Ben

103
Itzchak cohort, Sullivan 2010, Landa 2012, Smith T 2015, Flanagan 2012 and
Blacklock 2013 received an intensive behaviour intervention.
One study of children with IQ>70 (mean: 107.03) was unable to be presented
graphically. This study reported a mean standard score of 86.44 (SD 16.53) at 8.3 years.
At 12.9 years 12% of children improved in their standard scores, 68% remained
unchanged, 20% decreased (Pugliese 2016).
Combining the results of the fourteen studies in a random effects meta-analysis, there
was an estimated overall increase of 4.0 units on the VABS scale observed in a study
over time (95% CI 0.8, 7.4; I2 82.1%; df 13; p=0.016), Figure 11. There was substantial
heterogeneity between studies. Length of follow up was the only covariate which
explained some of the observed between-study variance with each year of follow up
resulting in an estimated decrease of 3.4 (95% CI -6.1, -0.7; I2 64%; df 12; p=0.001) in
the observed VABS score when the Magiati-Moss study was included in the analysis.
When the Magiati-Moss study was removed from the meta-regression, none of the
study-level covariates VABS score at baseline, average age at baseline, average length
of follow up and reported average IQ (<70 or >=70) provided any insight into the
observed heterogeneity.

104
Figure 11 Random effects meta-analysis using VABS standard scores
Change in age equivalent scores
One study presented age-equivalents on the VABS for the communication scale.
Children were followed from 3.6 years of age for 2 years and gained 0.73 age-
equivalence points per month (Munson-Toth). Two studies provided age-equivalents on
the VABS split into receptive and expressive communication. In one study, children
were aged 1.8 years at baseline and gained 1.85 years in expressive communication and
1.92 years in receptive communication over 2.5 years (Paul 2008). In the other study
that contained some children without ASD, children gained 6.9 years in receptive
communication and 6.7 years in expressive communication over 17 years (Pickles
2014).

105
There were five studies where data could not be extracted because they did not provide
communication subscale scores from the VABS (Mosconi 2009, Green 2014,
Stockholm cohort, Pathways cohort). In cases where data appeared to have been
collected but not presented we contacted authors but were not successful in receiving
such data.
Expressive vocabulary
Change in raw scores
Three studies reported raw data on parent-reported expressive vocabulary using the CDI
(Oosterling 2010, Bopp cohort, Woynaroski-Yoder cohort). The number of words
gained from baseline to follow-up ranged from 35 to 76 over 1.25 years in one study
(Oosterling 2010). In one study an average of 58 words was gained over 4.41 years
(Bopp cohort) and in study another (Yoder-Woynaroski cohort) 73 words were gained
over 1.3 years (Appendix E). Authors of one study were contacted but were not able to
provide results from both time points although this information had been collected
(Miniscalco 2014).
Presence or absence of verbal language and phrase language
Verbal language
Seventeen studies reported on the presence of verbal language (nonverbal or verbal) at
outcome (Bagley 1989, Ballaban-Gil 1996, Eaves 1996, Freeman cohort; Howlin 2004,
Kobayashi 1992, Sigman 2005, Bennett-Starr cohort, Takeda 2005, Anderson-Lord
cohort, Wolf 1986, Carbonnel-Chabas 2009, Baghdadli-Darrou cohort, Mazurek-Wodka
cohort, Pry 2011, Stockholm cohort, Jonsdottir 2006). As before, we included studies
reporting on ‘minimally verbal’ and ‘nonverbal’ children. We have graphed studies
106
(n=12) that report both baseline and follow-up data. Seven studies included children
aged 5 years and under at baseline and 5 studies children over 5 years at baseline
(Figure 12 a,b). The proportion of children who were verbal at baseline ranged from
40% to 70% and at follow-up 66% to 91%. For children over 5 years, the proportion of
children verbal at baseline ranged from 23% to 80% and at follow-up 55% to 88%.
Nineteen % to 30% of children aged 5 years and under gained verbal language. For
children aged over 5 years 5% to 32% gained verbal language over the course of study.

107
Figure 12 Proportion of individuals with ASD were verbal aged ≤5 years (preschool) (a) and > 5 years (b)
(a)

108
(b)

109
Figure 13 Proportion of individuals with ASD who used phrases (and longer) at baseline and follow-up.

110
The Howlin cohort followed individuals with an IQ of ≥70 from 6.75 years (SD 2.8) to
44.2 years (SD 9.3). In this study 75% (45/60) of children were verbal and by adulthood
95% (57/60) were verbal. Five studies provided only follow-up data that could be
extracted on the proportion of individuals who were verbal (Ballaban-Gil 1996 (93/99;
94%), Howlin 2004 (61/67; 91%), Knorring 1993 (25/34; 74%), Freeman cohort (44/53;
83%). One study grouped by those who were nonverbal (25/165; 15%) and minimally-
verbal (17/165; 10%) at outcome (Stockholm cohort). In addition, Anderson-Lord
cohort reported 58% (N=74) of children who were nonverbal at 2 years were verbal at 9
years.
Phrase and/or functional language
Eleven studies reported on participants who gained the ability to use phrases (Anderson-
Lord cohort, Jonsdottir 2007, Kobayashi 1992, Magiati-Moss cohort, Pry 2011, Wolf
1986, Howlin cohort, Sigman 2005, Baghdadli-Darrou cohort, Stockholm cohort,
Thurm 2015) and those studies with both baseline and follow-up are presented in Figure
13. The percentage of participants at the end of the study who were able to use phrases
ranged between 17% (mean age 7.8 years at follow-up) to 85% (mean age 9 years at
follow-up and for children with PDD only (i.e. excluded autistic disorder)). For those
children aged over 8 years at baseline, 20% of non-phrase speaking children in one
study gained the ability to use phrases over a period of 10 years (Wolf 1986).
Four studies provided only follow-up data that could be extracted on the proportion of
individuals using phrases (Howlin cohort 33/68 (49%), Sigman 2005 25/48 (52%),
Stockholm cohort 123/165 (75%), Anderson-Lord cohort (Autistic Disorder 48% and
PDD-NOS 85%)). One study reported on children who used functional language at
baseline (20%) and at follow-up (47%) (Baghdadli-Darrou cohort).

111
Combining the findings from all studies, the proportion of participants at the end of the
study duration who were verbal ranged between 55% (median age 20 years at follow-
up) to 95% (mean age 44.2 years at follow-up). The proportion of participants using
phrases ranged from 33% (mean age at follow-up 17 years) to 85% (mean age at follow-
up 9 years).
Predictors of language outcomes
Twenty-three studies (43%) investigated one or more predictors of language outcomes
including child factors (baseline language levels, adaptive behaviour, IQ, autism
symptomology, theory of mind, acting out behaviours, inattentive behaviour, rate of
change in language, age, play, joint attention, motor imitation and fine and gross motor
ability), parent factors (parent language styles and maternal responsiveness) and
external factors (intervention). Appendix D provides more information on the predictors
assessed in each study but as this review was not designed to assess predictors of
outcome no further information is presented.
Discussion
Language development in individuals with ASD is complex and heterogeneous. Not all
children with ASD experience language difficulties, but the majority do (Levy et al.,
2010). A substantial number of studies (n=54) collectively including a large number of
children (N=5064) has been published that have provided valuable longitudinal
information on language outcomes in ASD. To date however, it has been challenging
for clinicians and parents to interpret these findings. This is because there is
inconsistency and variability in study methods and participant characteristics.
112
Moreover, the quality of the studies varies, which may contribute to difficulty weighing
the significance of the findings from each study.
Summary of findings from studies
We synthesised available information on verbal language outcomes and assessed the
quality of included studies. Substantial variability was seen in mean language scores
and slopes of the language trajectories across studies. Yet, studies reported generally
similar overall findings in that mean baseline and outcome scores on standardised
language tests were consistently lower for children with ASD than reference norms,
with one exception that included only children with IQ>80 (Pellicano cohort).
Moreover, in all included studies the majority of children with ASD continued to make
positive language gains, including children aged over 5 years at baseline. Language
gains occurred across multiple domains, including syntax (receptive and expressive),
vocabulary (receptive and expressive), adaptive language and the acquisition of verbal
language. Children under 9 years progressed at a rate comparable to reference norms
based on receptive and expressive syntax and receptive vocabulary standard scores, with
some studies showing a significantly faster rate of progress or ‘catch up’ compared with
reference norms in receptive (n=4; 57%) and expressive syntax (n=3; 43%). Findings
from studies that reported age-equivalent scores for syntax and receptive vocabulary
were less consistent, with evidence of some divergence from an age expected rate of
progress in some studies but not others. The vast majority of studies (n=12/13; 92%)
reporting data on adaptive language in children aged under 11 years demonstrated a rate
of progress comparable to age expected norms with 31% of studies reporting some
‘catch up’ to age expected norms, based on standard scores. Gains in these studies
(n=12) were observed both in children with and without intellectual disability, across

113
different ASD subgroups and across studies where participants accessed intensive
behavioural interventions or intervention in the community.
The findings from studies of individuals followed from middle childhood to adulthood
are less consistent than for younger children but suggest the same rate of progress
experienced during childhood may not be maintained beyond 9 years of age. Language
trajectories reported in the few studies conducted during adolescence were flatter for
children from middle childhood to adolescence with a growing gap between language
ability in children with ASD and reference norms (Pickles et al., 2014; Sigman &
McGovern, 2005). Similar findings were reported in studies of adults (Howlin et al.,
2004). There are a number of potential explanations for slowing of language trajectories
into adulthood. There is some evidence of a ‘second wave of deficit’ or ‘second hit’ that
emerges in the second decade of life that may impact trajectories of development
(Minshew & Williams, 2007; Picci & Scherf, 2015). It may also be that individuals with
ASD have difficulty managing the increasing complexity of language required during
adolescence and adulthood.
Alternatively, it is possible more recently published studies including younger cohorts
have included individuals diagnosed using broader criteria than previous studies. As
such, more recent studies may include individuals with less severe phenotypes and a
smaller proportion of children with intellectual disabilities (Keyes et al., 2012). This
was evidenced by the studies demonstrating faster rates of development being those
more recently published. Finally, interventions, particularly intensive interventions, are
more readily available in more recent years and this may have an impact on outcomes
on children under 8 years. Many funding programs are also focused on early rather than
life course interventions, and it is possible that as interventions are reduced progress

114
also decreases. Further research on language trajectories into and throughout adulthood
is vital if we are to understand the communication support needs of adults with ASD in
the future (Magiati et al., 2014).
Considerations for interpreting data in this review
In the current review we have reported findings at a group level (group means) as this is
how included studies reported their findings, yet substantial variability was seen within
cohorts for individual baseline and outcome scores, evidenced by large standard
deviations. Some children with ASD may make dramatic progress, while others may
make limited progress. Future studies should examine individual variation and present
data for important subgroups so we can refine predictions of prognosis. Furthermore, a
review specifically designed to analyse predictors of language outcome will aid our
understanding of important factors that may impact language trajectory.
Although we have used standard scores cross-sectionally to report trajectories here to
increase clinical utility the shape of trajectories between time points is not known. The
potential for regression to the mean when plotting trajectories has been underscored by
some authors (Tomblin et al., 2003) and consideration should be given to the
heterogeneity between studies when interpreting the meta-analysis findings.
Furthermore, we used reference norms for comparison and did not require studies to
include typically developing children. It is known that some variability in scores over
time is not unique to ASD (Conti-Ramsden et al., 2012; McKean et al., 2015;
Ukoumunne et al., 2012) so ideally studies would include other groups of children so
language development in ASD can be placed within a developmental context.
115
There is some evidence from this review that studies that used age-equivalent scores
reported slower rates of development than those studies reporting standard scores and
there may be some bias in the way data is presented by studies. Studies of children who
are more severely affected may be more likely to report age-equivalents as children may
not reach the basal levels required for reporting standard scores and there may be floor
effects. A related consideration is that it can be challenging (and inappropriate) to assess
some children (e.g., minimally verbal children) using standardised tools as the children
may not have the ability to complete the tasks and/or may not reach the basal level for
scoring (Kasari et al., 2013). In addition, there may be a proportion of children with
ASD who are not represented here because of severe language impairment and their
lack of inclusion in studies may have resulted in an over-estimate of language gain in
summary scores. Finally, the VABS is an important parent-reported measure of adaptive
communication but it is susceptible to reporting bias and is not a measure of structural
language ability so caution should be taken when interpreting the findings from this tool
regarding a child’s structural language abilities.
Research implications
Improvements are needed in both the methodology and reporting of language outcome
studies for ASD cohorts. Recommendations and guidelines have been developed for
designing high-quality prognosis studies and for assessing the quality of studies
(Hayden et al., 2013). These best practice guidelines were used here to assess risk of
bias in included studies. The majority of included studies were rated medium to high
risk of bias, with less than 5% at low risk of bias. While the high risk of bias in some
studies may be because they were not intentionally planned prognosis studies, best
practice methodological approaches for prognosis are crucial for interpreting and

116
weighting the findings of individual studies. It is important that information be collected
prospectively on a sample of children diagnosed according to best practice at study
commencement. Inclusion criteria for this review stated all children required a
diagnostic assessment using established diagnostic criteria at baseline (e.g., DSM, ICD),
however a substantial number (33%) of studies were retrospective and did not report on
the children who were not available at follow-up. This may have the potential to bias
toward a positive outcome.
Ideally, studies should recruit from a population-based sample or from clinical services
that provide services for the broad population of children with ASD, so the individuals
are representative of individuals in the general population with ASD. Only five studies
derived their samples from a population source, with the rest being selected clinical
samples. Clinical samples have been reported to be skewed toward more severely
affected individuals and as such the findings may be less transferrable to the full range
of individuals with ASD. Data from such studies can still be useful, but application is
limited to children or adults with the same types of strengths and difficulties.
Studies should attempt to ensure high retention of participants over time and it is
important to report on differences between participants that were lost to follow-up and
those who were not. Of the studies in this review that were prospective, 53% retained
more than 80% of participants at follow-up. Few studies provided detailed descriptions
of the individuals who were lost to follow-up. Finally, clinicians completing the
assessments should be blind to individual’s baseline characteristics and diagnosis to
avoid bias. In this review only 10% of studies provided information about blinding of
clinicians. Individuals in studies reporting age-equivalent scores had slower trajectories
than in studies reporting standard scores. This may reflect bias as it is possible studies

117
may choose to report age-equivalents when they contain participants who are lower
functioning or less able to complete standardised tools or obtain standard scores.
Clinical implications
Despite methodological variations there was a general pattern in overall findings, which
although not fine-tuned for individuals, will be useful for clinicians and those caring for
people with ASD. Key messages are highlighted below. Table 10.

118
Table 10 Key messages for clinicians
Key messages for clinicians
55-95% of individuals who were minimally verbal became verbal at follow up
In all but one study children with ASD had mean scores below average at baseline and follow up
96% of studies showed that children aged under 11 with ASD tracked at comparable rate of language development to age-expected rates, based on standard scores. This occurred in children with and without intellectual disability and in children who received intensive behavioural interventions and those who received intervention in the community.
In 40% of studies reporting standard scores children under 11 years demonstrated some ‘catch up’ to peers (i.e. faster rate of progress than age-expected norms)
There was some evidence language development began to slow down in later years.
There is a high need for research on adolescent and adult language outcomes.
Future directions
It is clear much needs to be done to refine the accuracy of predictions of language
outcomes. Understanding how language trajectories may change across the lifespan and
the developmental periods where individuals may be more ‘vulnerable’ to slower
progress (e.g., before 2 years and after 10 years) is highly relevant for policy makers
and service providers so they can accurately plan future funding, support and service
needs for individuals with ASD across the lifespan. Moreover, families and clinicians

119
need clear and accurate information on the likely communication outcomes for their
children ASD based on their child’s characteristics so they can better anticipate ongoing
needs. A more fine-tuned understanding of language trajectories should also enable
more tailored interventions.
Very few studies reported individual trajectories or clinical subgroups of ASD. Few
studies assessed individuals beyond the age of 11 years using language specific tools.
We need information to apply the findings from the studies to individuals of different
ages and with a broad range of clinical characteristics. This study has also highlighted
an important subgroup with ASD who fail to develop the ability to speak by 24 years of
age (5-45%). The implications of being unable to speak are substantial in terms of the
impact on participation and function and the likely support needs of these individuals.
Evidence-based interventions are sorely lacking for this population but are crucial if we
are to prevent the adverse sequelae that are likely to accompany poor language
outcomes (Kasari et al., 2014; Paul et al., 2013; Tager-Flusberg et al., 2016).

120
Chapter 6 Methodology for Studies 2 and 3
The methods for each study in this thesis will be described in the relevant chapter:
Study 2 in Chapter 7 and Study 3 in Chapter 8. This Chapter provides further detail
about overarching methods used in Study 2 and 3 that have not been described in the
subsequent chapters.
Study design
The participants in Study 2 and 3 were drawn from the Early Language in Victoria
Study (ELVS). This is a prospective, longitudinal community-based study of language
development in children living in Victoria. The overarching aim of the ELVS was to
study the epidemiology and natural history of language development in children from
infancy to 7 years (for more detail see Reilly et al., 2006; Reilly et al., 2007)
Population representation
At study inception (2003-2004) 1910 participants were recruited to the ELVS. In 2011
when participants were 7 years of age there were 1189 participants, which represented
62% of the original sample. The participants in the ELVS have been followed up until
13 years but in Study 2 and 3 we used data up until Wave 8, when participants were 7
years old.
Measures
Participants were initially enrolled in the ELVS at 7.5-10 months of age and were
assessed almost yearly using direct assessments and/or parent-completed questionnaires

121
focused on language development. Direct assessments occurred at 4, 5 and 7 years.
Information was also collected on areas related to language and communication (child,
family and environmental factors) such as general development, health, parent-child
interaction, literacy, temperament, child behaviour and demographic factors.
The specific measures used by Study 2 and 3 are described below in Tables 11-13.
Demographic information
Demographic data was collected by questionnaire when participants were 8-12 months
for the following: gender, date of birth, number of children in the home, English as
main language spoken at home, Indigenous status, married/de facto, Socio-Economic
Index for Areas (SEIFA) score, maternal age at birth and primary caregiver completed
high school

122 122
Language measures
Table 11 Language and communication measures
Study Purpose of measure
Measure Brief description Age administered
Study 2 Trajectories MacArthur Bates Communicative Development Inventories -Words and Gestures form and Words and Sentences form (CDI; Fenson, 1993). Only expressive vocabulary raw scores were used.
Parent-completed questionnaire of early communication. The CDI has been validated in the general population and in children with developmental difficulties and has frequently been applied in ASD studies (e.g., Bopp & Mirenda, 2011; Charman, Drew, et al., 2003; Luyster et al., 2007; Mitchell et al., 2006).
1 year (CDI: Words and Gestures) 2 years (CDI: Words and Sentences)
Study 2 Trajectories Communication Symbolic Behaviours Scales-Infant Toddler Checklist (CSBS-ITC; Wetherby & Prizant, 2002). Raw scores used.
Parent-completed questionnaire on early communication, social and symbolic development. Validated as a broadband screener for ASD (Wetherby, Brosnan-Maddox, Peace, & Newton, 2008). There are seven clusters: emotion and eye gaze (0-8 possible points), communication (0-8), gestures (0-10), sounds (0-8), words (0-6), understanding (0-6) and object use (0-11). The cluster scores are collapsed into 3 composite scores: social (emotion, eye gaze, communication, gesture) (0-26), speech (words and sounds) (0-14),
1 & 2 years

123 123
Study Purpose of measure
Measure Brief description Age administered
symbolic (understanding and us of objects) (0-17). A total score (0-57) can be calculated.
Study 2 & 3 Determining comparison groups Trajectories and predictor analysis (Study 3)
The Clinical Evaluation of Language Fundamentals (Fourth Edition and Preschool 2 version)(CELF-4, CELF-P2; Semel, Wiig, & Secord, 2003; Wiig, Secord, & Semel, 2006)
This is a comprehensive standardised tool that measures receptive and expressive language. Language domains including morphology (grammar), syntax (sentence structure), semantics (word meanings) and vocabulary are assessed. The CELF P2 is for children aged 3 to 6 years and the CELF 4 is for individuals aged 5 to 21 years. Test-retest reliability on the CELF-4 is high (r=0.71 to 0.86 for subtests and r=0.88 to 0.92 for composite scores). Internal consistency range from 0.87 to 0.95 for subtests and 0.97 to 0.95 for composite scores. The CELF-4 has sensitivity of 1 and specificity of 0.82 at -1 standard deviation (Semel et al., 2003).
CELF-P2 at 4 years CELF-4 at 5 and 7 years
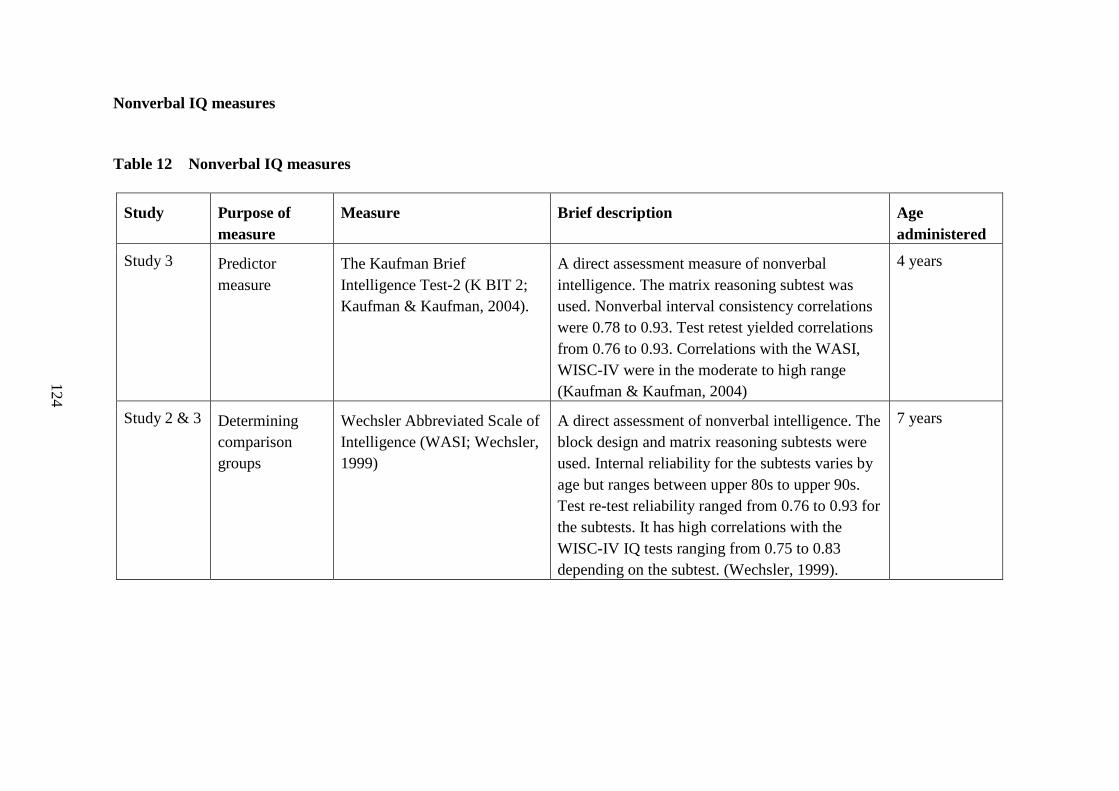
124 124
Nonverbal IQ measures
Table 12 Nonverbal IQ measures
Study Purpose of measure
Measure Brief description Age administered
Study 3 Predictor measure
The Kaufman Brief Intelligence Test-2 (K BIT 2; Kaufman & Kaufman, 2004).
A direct assessment measure of nonverbal intelligence. The matrix reasoning subtest was used. Nonverbal interval consistency correlations were 0.78 to 0.93. Test retest yielded correlations from 0.76 to 0.93. Correlations with the WASI, WISC-IV were in the moderate to high range (Kaufman & Kaufman, 2004)
4 years
Study 2 & 3 Determining comparison groups
Wechsler Abbreviated Scale of Intelligence (WASI; Wechsler, 1999)
A direct assessment of nonverbal intelligence. The block design and matrix reasoning subtests were used. Internal reliability for the subtests varies by age but ranges between upper 80s to upper 90s. Test re-test reliability ranged from 0.76 to 0.93 for the subtests. It has high correlations with the WISC-IV IQ tests ranging from 0.75 to 0.83 depending on the subtest. (Wechsler, 1999).
7 years

125 125
Social communication measures
Table 13 Social communication measures
Study Purpose of measure Measure Brief description Age administered
Study 2 & 3 Determining comparison groups
Social Communication Questionnaire (SCQ; Rutter, Bailey, & Lord, 2003)
The SCQ is a 40 item parent-report questionnaire based on the ADI-R. In a study comparing the SCQ with other screening tools this tool performed the most highly with sensitivity at 0.86 and specificity at 0.78 (Charman et al., 2007).
7 years
Study 3 Predictor measure The Pediatric Quality of Life Inventory 4.0: parent report form (Peds QL;Varni, Seid, & Kurtin, 2001)
A parent-completed questionnaire that assesses a child’s quality of life. The social functioning subscale was used from the Peds QL. Examples of social items include: ‘I have trouble getting along with other children’; ‘other kids do not want to be my friend’. A critical review reported the Peds QL was the most frequently used tool and the only tool in which reliability and validity had been established for ASD (Ikeda, Hinckson, & Krageloh, 2014). Significant correlations were found between the Peds QL and measures of ASD symptoms and functional impairments.
4 years
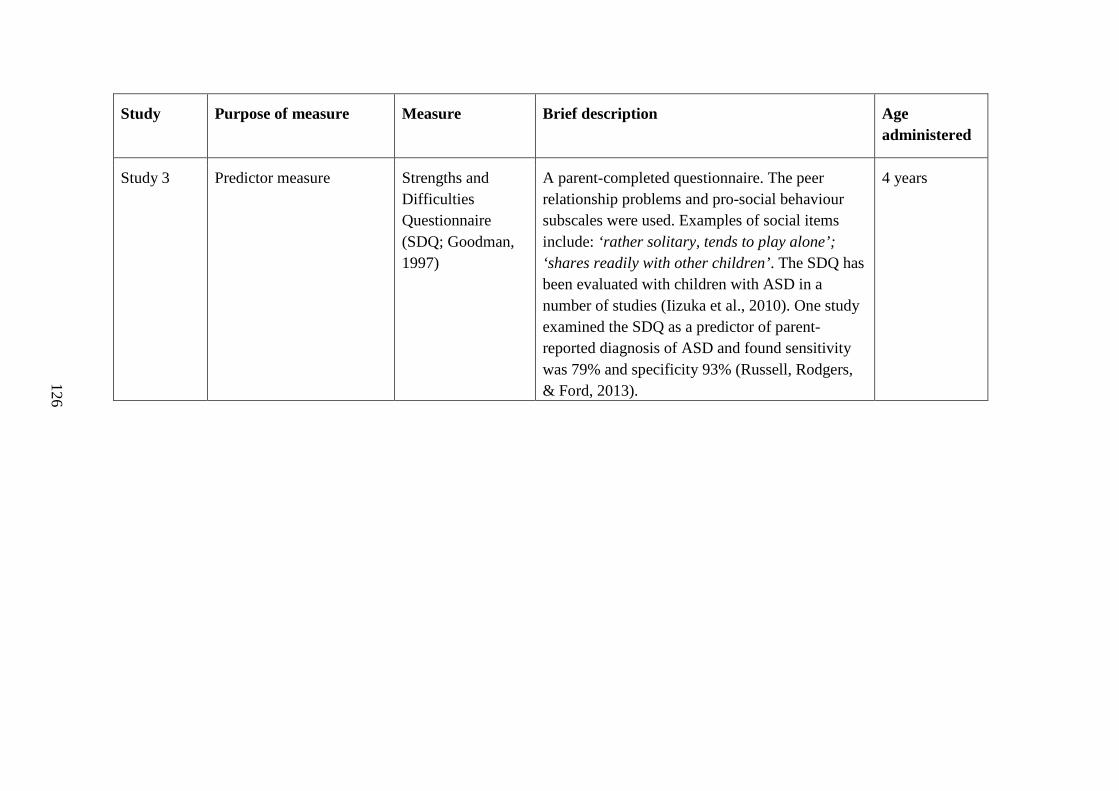
126 126
Study Purpose of measure Measure Brief description Age administered
Study 3 Predictor measure Strengths and Difficulties Questionnaire (SDQ; Goodman, 1997)
A parent-completed questionnaire. The peer relationship problems and pro-social behaviour subscales were used. Examples of social items include: ‘rather solitary, tends to play alone’; ‘shares readily with other children’. The SDQ has been evaluated with children with ASD in a number of studies (Iizuka et al., 2010). One study examined the SDQ as a predictor of parent-reported diagnosis of ASD and found sensitivity was 79% and specificity 93% (Russell, Rodgers, & Ford, 2013).
4 years

127
Change in language tool versions over different study waves
A different version of the CELF was used at 4 years (CELF-P2; n=1560) compared with
5 and 7 years (CELF-4; n=982 at 5 years and n=1204 at 7 years). To check consistency
between the measures we compared means and ranges for the sample on each wave
(Table 14). The scores were comparable across versions.
Table 14 Mean scores for the CELF-P and CELF-4 at each year the tool was administered.
Tool (age administered) Mean (SD; range)
CELF-P2 (4 years) 99.62 (15.1; 50-140)
CELF-4 (5 years) 100.6 (13.9; 55-144)
CELF-4 (7 years) 98.8 (13.6; 45-136)
Participants
Selection criteria
Inclusion and exclusion criteria varied for each study and are detailed in the flow chart
below (Figure 14).

128
Figure 14 Inclusion and exclusion criteria.
Loss to follow up
In Study 2 only 7% (3/44) of the children with ASD were lost to follow up. In Study 3 a
larger number of children with ASD (36%, n=16/44) were lost to follow up or excluded
from the study based on selection criteria. To ensure our study did not have systematic
bias due to loss to follow up we tested whether there were important differences
between characteristics of children with ASD who remained in the study and those who
did not. Children lost to follow up or excluded from the study had lower mean
nonverbal IQ and expressive vocabulary scores however the differences between the
groups were not significant (p>0.05). There were also no significant differences in any
of the demographic characteristics collected (Table 15).

129
Table 15. Characteristics of those children with ASD included and not included in Study 3.
Not included Included P
N 16 27
Male (%) 75 85.7 0.375
No. children at home M(SD) 1.56 (0.62) 1.75 (0.7) 0.381
English as main language spoken at home (%)
93.8 100 0.181
Married/defacto (%) 100 96.4 0.444
Socio-economic index (SEIFA) M (SD)
1043 (61.74) 1021 (63.99) 0.284
Maternal age at birth M (SD) 32.9 (6.40) 33.07 (4.96) 0.910
Primary caregiver has completed high school (%)
80 75 0.712
CDI score at 2 years M (SD) 104.67 (140.97) 178.48 (161.21) 0.146
Nonverbal IQ M (SD) 82.71 (21.06) 99.71 (14.35) 0.08
Ethical considerations
Ethical approval was obtained from the Human Research Ethics Committee at the Royal
Children’s Hospital (no. 23018) and La Trobe Health Sciences Human Ethics
Committee (no. 03-32).
Statistical Analysis
All statistical analyses were conducted using Stata version 13.1 and version 14.0.
Details regarding the statistical analysis relative to identified aims for the three main
studies is provided in the relevant chapter.

130
Summary of overarching methods
Studies 2 and 3 in this thesis use data from a large longitudinal community-based study.
The findings from these studies are combined with a systematic review to examine
trajectories of language development in children with and without ASD. The systematic
review (Study 1) predominantly included studies that used clinical samples and Studies
2 and 3 (utilising the ELVS data) extend the current literature to investigate language
trajectories using a community sample.

131
Chapter 7 Study 2. Parent reported patterns of loss and gain in
communication in 1 to 2 year old children are not unique
to autism spectrum disorder
The following paper examined trajectories of communication from 1 to 2 years in
children with ASD compared with children with LI and TD. It also compared the
proportion of children who lost skills, the types of skills lost and the extent of skill loss
across different communication domains between the three groups (ASD, LI, TD). This
paper was published in Autism in May 2016.

Autism 1 –13© The Author(s) 2016Reprints and permissions: sagepub.co.uk/journalsPermissions.navDOI: 10.1177/1362361316644729aut.sagepub.com
Introduction
Autism spectrum disorder (ASD) is one of the most com-mon neurodevelopmental disorders and is known to be heterogeneous. In addition to phenotypic heterogeneity, children with ASD demonstrate heterogeneous patterns of onset and trajectories of development (Kim et al., 2015; Landa et al., 2013; Ozonoff et al., 2010; Shumway et al., 2011). There has been a substantial focus on early social communication development in ASD because a deeper understanding of the loss and gain in skills in the first few years of life has the potential to build knowledge of how ASD unfolds. It may also assist identification, help deline-ate potential subgroups of children with ASD and shed light on the neurobiological mechanisms that underpin the disorder. However, one of the challenges in studying early
social communication development in ASD is that chil-dren are not typically diagnosed before 3 years of age (Bent et al., 2015).
Parent-reported patterns of loss and gain in communication in 1- to 2-year-old children are not unique to autism spectrum disorder
Amanda Brignell1,2, Katrina Williams1,2,3, Margot Prior1, Susan Donath1,2, Sheena Reilly2,4, Edith L Bavin5, Patricia Eadie1 and Angela T Morgan1,2
AbstractWe compared loss and gain in communication from 1 to 2 years in children later diagnosed with autism spectrum disorder (n = 41), language impairment (n = 110) and in children with typical language development at 7 years (n = 831). Participants were selected from a prospective population cohort study of child language (the Early Language in Victoria Study). Parent-completed communication tools were used. As a group, children with autism spectrum disorder demonstrated slower median skill gain, with an increasing gap between trajectories compared to children with typical development and language impairment. A proportion from all groups lost skills in at least one domain (autism spectrum disorder (41%), language impairment (30%), typical development (26%)), with more children with autism spectrum disorder losing skills in more than one domain (autism spectrum disorder (47%), language impairment (15%, p = 0.0003), typical development (16%, p < 0.001)). Loss was most common for all groups in the domain of ‘emotion and eye gaze’ but with a higher proportion for children with autism spectrum disorder (27%; language impairment (12%, p = 0.03), typical development (14%, p = 0.03)). A higher proportion of children with autism spectrum disorder also lost skills in gesture (p = 0.01), sounds (p = 0.009) and understanding (p = 0.004) compared to children with typical development but not with language impairment. These findings add to our understanding of early communication development and highlight that loss is not unique to autism spectrum disorder.
Keywordsautism spectrum disorder, communication, language, regression, skill loss, trajectory
1The University of Melbourne, Australia2Murdoch Childrens Research Institute, Australia3The Royal Children’s Hospital, Australia4Menzies Health Institute Queensland, Australia5La Trobe University, Australia
Corresponding author:Amanda Brignell, Department of Paediatrics, University of Melbourne, Level 2 West, Royal Children’s Hospital, 50 Flemington rd., Parkville, VIC 3052, Australia. Email: [email protected]
644729 AUT0010.1177/1362361316644729AutismBrignell et al.research-article2016
Original Article
at The Royal Childrens Hospital on May 16, 2016aut.sagepub.comDownloaded from

2 Autism
Retrospective studies have traditionally described two distinct patterns of onset in ASD: early onset ASD and regressive ASD. Early onset ASD is the gradual unfolding of symptoms over the course of the first few years of life. Regressive onset is a pattern of normal or near normal development followed by an abrupt or gradual loss of skills (Stefanatos, 2008), primarily involving the loss of words and/or social communication skills (Lord et al., 2004). Approaches to defining and measuring regression are varied in the literature. The vast majority of retrospec-tive studies have used the Autism Diagnostic Interview–Revised (ADI-R; Lord et al., 1994) to measure regression. This tool defines loss of skill as being ‘communicative use of at least five different words (other than “mama” and “dada”) on a daily basis for at least 3 months’ and requires that there has been a loss of the skill for at least 3 months (quoted from a test booklet of an assessment tool; Lord et al., 1994). A small number of retrospective studies have used the Regression Validation Interview (Luyster et al., 2005; Thurm et al., 2014). This is a detailed semi-structured parent interview that obtains more comprehensive infor-mation on skill attainment and loss. Prospective studies have generally taken a repeated measures approach by examining change in social communication skills and lan-guage across frequent time intervals (Brian et al., 2014; Landa et al., 2013; Ozonoff et al., 2010).
A systematic review of 85 studies (n = 29,035) of which 98% were retrospective, and the remainder high-risk sib-ling studies, included data on regression in ASD (Barger et al., 2013). The prevalence of regression in ASD was reported to be approximately 32% (95% confidence inter-val (CI) 30–35). The average age at which regression occurred was 20 months (95% CI 1.7–1.9; Barger et al., 2013). In children with typical development (TD), lan-guage impairment (LI) or developmental delay, regression has been reported as less common, ranging from 0% to 24% (Baird et al., 2008; Landa et al., 2013; Lord et al., 2004; Pickles et al., 2009; Thurm et al., 2014).
Retrospective studies of children with ASD carry a number of methodological limitations that substantially increase risk of bias and limit detailed assessment of devel-opment (Ozonoff et al., 2008, 2011). By contrast, high-risk sibling studies have been developed to prospectively mon-itor development on the pathway to ASD, recruiting sib-lings of children with ASD during pregnancy or soon after birth (Chawarska et al., 2014; Messinger et al., 2013; Ozonoff et al., 2010; see Jones et al., 2014 for a review). The findings from high-risk studies have challenged the way early social communication development in ASD has traditionally been understood, suggesting that dichoto-mous categories of regression do not adequately capture the many ways ASD can emerge (Kalb et al., 2010; Landa et al., 2013; Landa and Garrett-Mayer, 2006; Ozonoff et al., 2010; Shumway et al., 2011; Siperstein and Volkmar, 2004). Some studies, for example, have proposed a range of onset patterns including early onset (early delays, no
loss), delay and regression (some early delays before loss), plateau (no early delays, no loss) and regression (no delays before a clear loss of skills; Kalb et al., 2010; Ozonoff et al., 2008; Shumway et al., 2011). Whereas two high-risk sibling studies grouped children by different developmen-tal trajectory types or classes such as accelerated develop-ment, normative development, delay in some areas of development (e.g. fine/gross motor and language) and widespread delay with declining trajectories (Brian et al., 2014; Landa et al., 2012). These studies have highlighted the importance of placing loss of different types of skills within the context of trajectories of development.
Different elements of development have been reported to be lost by different studies. Specifically, loss of eye contact and gaze to faces has been reported to be the most common social communication skill lost by a number of retrospec-tive studies (e.g. Ozonoff et al., 2005; Thurm et al., 2014). Eye gaze, shared positive affect, social interest, smiling and initiating interactive games have been reported to show declining trajectories in prospective high-risk sibling stud-ies (Landa et al., 2007, 2013; Ozonoff et al., 2010) with word loss less common (Landa et al., 2013).
There has been debate about whether children in high-risk sibling studies are representative of children without a family history of ASD. For example, high-risk siblings may have different phenotypes to children without a fam-ily history of ASD (Mitchell et al., 2006; Pandey et al., 2008; Sebat et al., 2007) and may be more at risk of other developmental difficulties, including LI and learning dif-ficulties (Landa et al., 2013; Szatmari et al., 2000).
To our knowledge no longitudinal population-based studies have been published that have investigated loss and gain in communication skills prior to the child’s ASD diag-nosis. Nor have any studies used large samples of children without ASD as comparison groups. This study uses data from a prospective population-based study investigating language development collected at 1 and 2 years to describe early communication trajectories.
The aim of this study was to describe loss and gain of communication skills from 1 to 2 years in children later diagnosed with ASD, LI and in children with typical lan-guage development. Specifically, we wanted to investigate the proportion of children in each group who lost skills, the type of skills that were lost and the spread of loss across communication domains.
Methods
Study design
Participants were drawn from the Early Language in Victoria Study (ELVS), a prospective, longitudinal, popu-lation-based study in Victoria, Australia (Reilly et al., 2006, 2007). Children (n = 1910) were recruited from 6 of 31 geographical areas in Melbourne, 8–10 months of age and followed up almost annually. The Socio-Economic
at The Royal Childrens Hospital on May 16, 2016aut.sagepub.comDownloaded from

Brignell et al. 3
Index for Areas (SEIFA) from the 2001 census data was used (based on income, educational attainment and unem-ployment from the Census of Population and Housing) to stratify 31 local government areas (LGAs) into three levels (high, medium and low). Two LGAs from each level were then approached for recruiting participants. Participants were recruited via Maternal Child Health nurses, at univer-sal hearing screening appointments, and through public notices. Exclusion criteria included cerebral palsy, known developmental delays or other significant intellectual or physical disability. Participants were also excluded if par-ents did not speak or read English to a satisfactory level to complete the questionnaires. Demographic information was collected from the primary caregiver when the child was 8 months of age. Parent questionnaires were com-pleted annually, providing information about communica-tion and behaviour development, family factors and the child’s environment. Direct assessments (Clinical Evaluation of Language Fundamentals (CELF)–fourth edition (Semel et al., 2003), and/or Preschool–second edi-tion (Wiig et al., 2006) and the Wechsler Abbreviated Scale of Intelligence (WASI; block design and matrix rea-soning subtests; Wechsler, 1999)) were completed by trained psychology graduates or speech pathologists in the child’s home or school, depending on the wave of the study and caregiver preference. The CELF was adminis-tered at 4, 5 and 7 years and the WASI at 7 years. Further details on the ELVS study design and sampling methods can be found in Reilly et al. (2006, 2007).
Ethical considerations
Ethical approval was obtained from the Human Research Ethics Committee at the Royal Children’s Hospital, Melbourne (#23018) and La Trobe University, Human Ethics Committee (#03–32).
Outcome measures
Two parent-completed questionnaires, the Communication Symbolic Behaviours Scales–Infant Toddler Checklist (CSBS-ITC; Wetherby and Prizant, 2002) and the MacArthur-Bates Communicative Development Inventories (CDI; Fenson, 1993) were used to assess early communication at 1 and 2 years. The CDI (Words and Gestures form and Words and Sentences form) is a widely used parent-completed measure of early communication. Only the expressive vocabulary data were used here. The CDI has been validated in the general population and in children with developmental difficulties and has frequently been applied in ASD studies (e.g. Bopp and Mirenda, 2011; Charman et al., 2003; Luyster et al., 2007; Mitchell et al., 2006). The CSBS-ITC is a parent-completed questionnaire on early communication, social and symbolic development. It has been validated as a broadband screener for ASD (Wetherby et al., 2008). There are seven clusters: emotion
and eye gaze (0–8 possible points), communication (0–8), gestures (0–10), sounds (0–8), words (0–6), understanding (0–6) and object use (0–11). The cluster scores are col-lapsed into three composite scores: social (emotion, eye gaze, communication, gesture; 0–26), speech (words and sounds; 0–14) and symbolic (understanding and use of objects; 0–17). A total score (0–57) can also be calculated. We used raw scores from the CSBS-ITC and CDI in this study because we were specifically interested in examining loss of skills.
Group allocation
ASD. From 4 years of age, all participating parents (n = 1623 at 4 years) were asked via the annual questionnaire whether their child had ever received a diagnosis of ASD. If yes, parents were telephoned by a clinical psychologist or speech pathologist (M.P., P.E.) experienced in the diagno-sis of ASD during which information was obtained about how the diagnosis was made, the name and professions of the individuals making the diagnosis, child age at diagnosis and type of diagnosis (e.g. Asperger’s syndrome, autistic disorder) as allocated using classification systems of the time, like the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psy-chiatric Association (APA), 2000). Information about the child’s behaviour and co-morbidities was also obtained. The majority (93%) of children were given a clinical diag-nosis by a multidisciplinary team that involved at least two professionals (typically a paediatrician and psychologist and/or speech pathologist). The other children were given a diagnosis by a paediatrician only. When the children were aged 7 years parents were asked to complete the Social Communication Questionnaire (SCQ), a widely used screening questionnaire derived from the ADI-R (Rutter et al., 2003). Mean scores on the SCQ were 14.53 (standard deviation (SD): 4.66; range 5–26; Veness et al., 2014). By 7 years, 44 children had been diagnosed with ASD with a mean age of reported diagnosis of 4 years 8 months (range 2–7 years). Further details on the children with ASD in this sample can be found in Veness et al. (2012, 2014).
LI and typical language development. Children were allo-cated to these categories following review of their perfor-mance on the CELF (Preschool–second edition and/or fourth edition) and the WASI. None of the children in the LI and TD groups were reported to have ASD. Figure 1 shows the tools used for this study, the ages they were administered and their role in group allocation and meas-uring outcomes of interest. Allocation to groups was com-pleted when children were 7 years.
Exclusion criteria
A total of 743 children were excluded because (1) there were incomplete or missing data at both time points (1 and
at The Royal Childrens Hospital on May 16, 2016aut.sagepub.comDownloaded from

4 Autism
2 years), (2) they were not assessed or did not complete the CELF at 7 years and at one other time point and (3) they did not complete a non-verbal IQ measure at 7 years. They were also excluded if they did not fit into the pre-specified groups (ASD, LI and TD), for example, if the child was delayed on both the CELF-4 and the WASI and was not diagnosed as ASD. The total sample in this study consisted of 982 children (ASD: n = 41; LI: n = 110; and TD: n = 831).
Statistical procedures/data analysis
All analyses were conducted using Stata version 13.1. The ELVS sample is skewed towards families who are more advantaged and thus SEIFA quintiles, based on the Australian Bureau of Statistics reference, were used for adjusted data analysis where appropriate.
Trajectories
On inspection prior to analysis, it was clear that the data distribution was asymmetric for the children with ASD for the CSBS-ITC and CDI scores at each wave. Hence, non-parametric analyses were conducted and medians (inter-quartile ranges) were reported instead of means (SDs). Raw scores on the CSBS-ITC (social, speech and sym-bolic composites and total score) were plotted for each individual with ASD at 1 and 2 years. Classification into
trajectory types was done as follows: acceleration: higher gradient than the mean gradient for TD children, improv-ing: higher score at 2 than 1 year but no acceleration, pla-teau: same score at 1 and 2 years and loss: lower score at 2 than 1 year. Median CDI scores (number of words pro-duced) for each group were plotted at 1 and 2 years. Comparison was made between median scores on CSBS-ITC and CDI for children with ASD, TD and LI at 1 and 2 years using the Wilcoxon rank sum test, corrected for multiple comparisons using Bonferroni correction with p < 0.002 required to reach statistical significance. Box plots were graphed to show the differences in medians (interquartile ranges) and the rate and direction of change on the CSBS-ITC composites and total scores from 1 to 2 years. Questionnaires at both 1 and 2 years were all com-pleted within 2 months either side of the child’s birthday.
Definition of loss of skills
The period between 1 and 2 years is typically a period of great growth in communication skills (Fenson and Dale, 1994; Goldfield and Reznick, 1990) and it would be con-sidered unusual for a child to lose skills previously obtained over this 1-year period, either by not using a previously acquired skill or by changing from being able to use a skill ‘always’ to only using the skill ‘sometimes’. Hence, chil-dren were classified as having lost skills if they achieved a
Figure 1. Tools and ages at which they were used in this study to measure outcomes and to allocate groups.CDI: MacArthur-Bates Communicative Development Inventories; CSBS: Communication Symbolic Behaviour Scales–Infant Toddler Checklist; CELF-P: Clinical Evaluation of Language Fundamentals–Preschool; CELF-4: Clinical Evaluation of Language Fundamentals–fourth edition; WASI: Wechsler Abbreviated Scale of Intelligence.
at The Royal Childrens Hospital on May 16, 2016aut.sagepub.comDownloaded from

Brignell et al. 5
lower raw score at 2 than 1 year on the CSBS-ITC and/or if they had fewer words on the CDI at 2 years compared to 1 year. The definition of ‘loss of skills’ for the CDI was developed because to our knowledge there is no published, standardised definition of how ‘loss of skills’ should be defined. Our definition is conservative because between 1 and 2 years of age children often have rapid word acquisi-tion, and gain of only a single word or no word gain could also be considered atypical. In the absence of agreement, we decided a conservative approach was ideal.
CSBS-ITC. Differences in scores were calculated for clus-ter, composite and total scores. Average magnitude of loss (and range) was calculated for each group. The number of children per group who lost skills in one or more clusters was calculated and graphed. Odds ratios (with CIs and p values) were used to compare loss of skills in the cluster, composite and total scores across the different groups (ASD vs LI; ASD vs TD). Odds ratios were adjusted for gender and socio-economic status.
CDI. The difference between scores at 1 and 2 years was calculated using the total expressive vocabulary score on the Words and Gestures and Words and Sentences forms. We used the full vocabulary from the latter form to provide a more conservative estimate. This ensured that substitu-tion of early words with more complex words was not counted as a loss.
Results
There was a higher proportion of males in the ASD group compared to the TD and LI groups (p < 0.01), see Table 1 for descriptive characteristics. No significant difference was found in the ASD group compared to the TD and LI groups on any other feature.
Trajectories
Individual trajectories of raw scores from the CSBS-ITC were plotted for children with ASD (Figure 2). Substantial variation between children with ASD is shown, with four main trajectory types seen on both the CSBS-ITC and the CDI: worsening, plateau, improving and accelerating (Figure 3). The majority of children fell into the ‘improved’ trajectory type for both tools. The median composite and total scores at 1 year for the children in all three groups who lost skills were within the average range (see Figure 2, for example).
Median raw scores for all three groups increased over time for both the CDI and CSBS-ITC (Figures 4 and 5 and Table 2). At 1 year, no significant difference was seen in scores on the CDI between the children with TD, LI and ASD groups. However, there was a widening gap between the TD and ASD/LI groups over the next 12 months, which reached significance (p < 0.0001) at 2 years for the differ-ence between the ASD and the TD group but not between the children with ASD and LI.
On the CSBS-ITC, there was a statistically significant difference between the median scores for children with ASD and children with TD at 1 year in the social composite (p < 0.002) and the total score (p < 0.002). At 2 years, a sta-tistically significant difference between medians was found for all the composites and total score for the ASD group compared to the LI and TD groups (p < 0.002), except in the speech composite where there was not a statistically significant difference between the LI and ASD children.
Differences in proportions of children who lost communication skills across groups
Only two children in the study sample had a smaller vocabulary at 2 than 1 year on the CDI. One child diag-nosed with ASD used five words at 1 year (grandma, baa,
Table 1. Sample characteristics for children with ASD, language impairment and typical development.
ASD (n = 41) LI (n = 110) TD (n = 831) p
Male (%) 83 55 45 ASD > TD (<0.001)ASD > LI (=0.002)
Number of children at home (mean (SD; range))
1.7 (0.7; 1–3) 1.9 (0.9; 1–5) 1.7 (0.8; 1–5) LI > TD (=0.0007)
English as main language spoken at home (%) 97.6 94.6 97.5 –Indigenous (%) 0 0 0.12 –Married or de facto (%) 97.6 91.8 96.9 TD > LI (=0.008)SEIFA score (mean (SD; range)) 1029.8 (65.5;
855.5−1104.1)1012.4 (68.1; 834.4−1107.6)
1046.7 (51.8; 834.4−1147.0)
TD > LI (<0.001)
Maternal age at birth (mean (SD; range)) 32.9 (5.4; 21−46) 32.2 (4.8; 19−43) 32.4 (4.2; 19−44) –Primary caregiver has completed high school (grade 12; %)
77.5 63.3 82.2 TD > LI (<0.001)
ASD: autism spectrum disorder; LI: language impairment; TD: typical development; SD: standard deviation; SEIFA: Socio-Economic Index for Areas.Socio-economic status was measured using the SEIFA Disadvantage Index. SEIFA has a mean of 1000 and a SD of 100 with higher scores indicating greater advantage. Only the p values that reached significance (p < 0.01) for the group comparisons are reported.
at The Royal Childrens Hospital on May 16, 2016aut.sagepub.comDownloaded from

6 Autism
grr, mummy and daddy) and only 2 words at 2 years (mummy and daddy). The other child in the LI group used 3 words at 1 year (mummy, daddy and grandma) and only 1 word at 2 years (here).
A proportion of children in all three groups had lower scores on the CSBS-ITC at 2 than 1 year. Percentages are reported for CSBS-ITC cluster scores within each com-posite on the CSBS-ITC. The ASD group had a higher per-centage of children who lost skills compared to the LI and TD groups in all clusters except ‘use of objects’ (Table 3). In total, 41% of children with ASD lost skills in at least one cluster compared to LI (30%) and TD (26%). The cluster with the greatest loss for all groups was ‘emotion and use of eye gaze’, with the ASD group having around double the percentage of children who lost skills compared to the other two groups (27% ASD, 12% LI and 14% TD). Few females in the ASD group demonstrated loss of skills, while the number who lost skills in the LI and TD groups were more evenly split by gender (Table 3).
Odds ratios were calculated to investigate whether children with ASD had greater odds of losing skills than the other two groups (Table 4). In the cluster of ‘emotion and use of eye gaze’, the odds of losing skills for the children with ASD were 2.3 to 3 times higher than those for children with TD (p < 0.05) and LI (p < 0.05) respec-tively. Loss of skills was also significantly higher for
Figure 2. Individual trajectories of communication development (social, speech, symbolic composites and total raw scores, CSBS-ITC) from 1 to 2 years for children with ASD (n = 41).
Figure 3. Trajectory types for children with ASD (loss, plateau, improve and accelerate) for the CSBS-ITC and the CDI.Bars for each composite or CDI score are in order of appearance in the legend.
at The Royal Childrens Hospital on May 16, 2016aut.sagepub.comDownloaded from

Brignell et al. 7
Figure 4. Trajectory of median number of words produced for children with ASD, LI and TD at 1 and 2 years.
Figure 5. Median and interquartile range for raw scores on the CSBS-ITC (total score and composite scores) from 1 to 2 years for children with ASD, LI and TD.Groups are presented left to right as TD, LI and ASD at each age.
at The Royal Childrens Hospital on May 16, 2016aut.sagepub.comDownloaded from
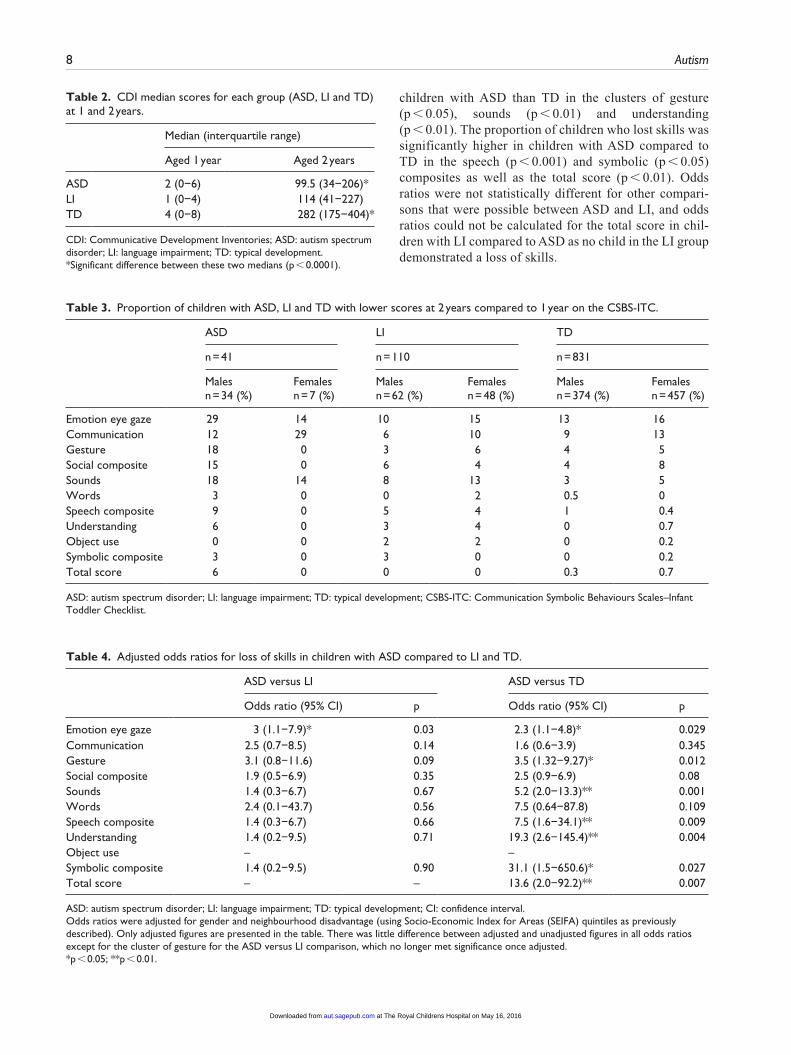
8 Autism
children with ASD than TD in the clusters of gesture (p < 0.05), sounds (p < 0.01) and understanding (p < 0.01). The proportion of children who lost skills was significantly higher in children with ASD compared to TD in the speech (p < 0.001) and symbolic (p < 0.05) composites as well as the total score (p < 0.01). Odds ratios were not statistically different for other compari-sons that were possible between ASD and LI, and odds ratios could not be calculated for the total score in chil-dren with LI compared to ASD as no child in the LI group demonstrated a loss of skills.
Table 2. CDI median scores for each group (ASD, LI and TD) at 1 and 2 years.
Median (interquartile range)
Aged 1 year Aged 2 years
ASD 2 (0−6) 99.5 (34−206)*LI 1 (0−4) 114 (41−227)TD 4 (0−8) 282 (175−404)*
CDI: Communicative Development Inventories; ASD: autism spectrum disorder; LI: language impairment; TD: typical development.*Significant difference between these two medians (p < 0.0001).
Table 3. Proportion of children with ASD, LI and TD with lower scores at 2 years compared to 1 year on the CSBS-ITC.
ASD LI TD
n = 41 n = 110 n = 831
Males n = 34 (%)
Females n = 7 (%)
Males n = 62 (%)
Females n = 48 (%)
Males n = 374 (%)
Females n = 457 (%)
Emotion eye gaze 29 14 10 15 13 16Communication 12 29 6 10 9 13Gesture 18 0 3 6 4 5Social composite 15 0 6 4 4 8Sounds 18 14 8 13 3 5Words 3 0 0 2 0.5 0Speech composite 9 0 5 4 1 0.4Understanding 6 0 3 4 0 0.7Object use 0 0 2 2 0 0.2Symbolic composite 3 0 3 0 0 0.2Total score 6 0 0 0 0.3 0.7
ASD: autism spectrum disorder; LI: language impairment; TD: typical development; CSBS-ITC: Communication Symbolic Behaviours Scales–Infant Toddler Checklist.
Table 4. Adjusted odds ratios for loss of skills in children with ASD compared to LI and TD.
ASD versus LI ASD versus TD
Odds ratio (95% CI) p Odds ratio (95% CI) p
Emotion eye gaze 3 (1.1−7.9)* 0.03 2.3 (1.1−4.8)* 0.029Communication 2.5 (0.7−8.5) 0.14 1.6 (0.6−3.9) 0.345Gesture 3.1 (0.8−11.6) 0.09 3.5 (1.32−9.27)* 0.012Social composite 1.9 (0.5−6.9) 0.35 2.5 (0.9−6.9) 0.08Sounds 1.4 (0.3−6.7) 0.67 5.2 (2.0−13.3)** 0.001Words 2.4 (0.1−43.7) 0.56 7.5 (0.64−87.8) 0.109Speech composite 1.4 (0.3−6.7) 0.66 7.5 (1.6−34.1)** 0.009Understanding 1.4 (0.2−9.5) 0.71 19.3 (2.6−145.4)** 0.004Object use – – Symbolic composite 1.4 (0.2−9.5) 0.90 31.1 (1.5−650.6)* 0.027Total score – – 13.6 (2.0−92.2)** 0.007
ASD: autism spectrum disorder; LI: language impairment; TD: typical development; CI: confidence interval.Odds ratios were adjusted for gender and neighbourhood disadvantage (using Socio-Economic Index for Areas (SEIFA) quintiles as previously described). Only adjusted figures are presented in the table. There was little difference between adjusted and unadjusted figures in all odds ratios except for the cluster of gesture for the ASD versus LI comparison, which no longer met significance once adjusted.*p < 0.05; **p < 0.01.
at The Royal Childrens Hospital on May 16, 2016aut.sagepub.comDownloaded from

Brignell et al. 9
Range of loss of communication skills
The children in the ASD group were comparable to the other groups for magnitude of loss (mean and range) on the CSBS-ITC, with amount of loss ranging from −6 to −1 in the ASD group, −6 to −1 in the LI group and −7 to −1 in the TD group.
Number of children who lost communication skills in one or more cluster
A proportion of children from all groups lost skills in at least one domain (Figure 6). A higher proportion of chil-dren with ASD lost skills in more than one area compared to the other two groups (ASD > TD: p < 0.001; ASD > LI: p < 0.01). For those children who lost skills in more than one cluster, they were more likely to lose in the ‘eye con-tact and emotion’ and ‘communication’ domains.
Discussion
Trajectories
Children in all three groups demonstrated an overall median gain in all areas of communication from 1 to 2 years. However, individual trajectories were variable and there were differences between the groups in the rate of gain of skills. Our findings are consistent with those of other pro-spective studies reporting slower developmental trajecto-ries from 1 to 2 years for children with ASD relative to their peers on language (Landa et al., 2007, 2012; Mitchell et al., 2006; Ozonoff et al., 2010) and social communication (Bryson et al., 2007; Landa et al., 2007, 2012; Ozonoff et al., 2010; Rozga et al., 2011; Veness et al., 2014; Young et al., 2009; Zwaigenbaum et al., 2005). The finding that there was no significant difference between children with ASD and LI at 1 and 2 years on both the CDI and the speech cluster on the CSBS-ITC has implications for differential diagnosis for these two groups at this young age. The CSBS-ITC speech composite includes ques-tions about both speech (e.g. number of sounds used) and
language (e.g. number of words produced or word combina-tions used). Prospective studies have found mixed evidence on whether there are differences in early language and speech between high-risk siblings who develop ASD and those who do not (see Jones et al., 2014 for a review). Very few of these prospective studies have compared speech and language development in children with ASD to a defined group of children later diagnosed with LI. Two studies with a comparison group of children with LI have produced sim-ilar findings to this study (Landa and Garrett-Mayer, 2006; Paul et al., 2008). One prospective community-based study did not find a significant difference between the language-impaired/developmentally delayed children (n = 20) and those with ASD (n = 42) on an expressive language measure at 24 months (Barbaro and Dissanayake, 2012). However, there was a significant difference between the children with LI and the children with autistic disorder. A study focused on speech found children with ASD had a higher proportion of atypical vocalisations (e.g. squeal, growl), compared to age and language matched peers but there were no sig-nificant differences in the proportion of correct consonants produced (Schoen et al., 2011). It seems likely that if there are differences between the groups in speech sound devel-opment they are unlikely to be detected by a parent-rated tool such as the CSBS-ITC. Given the similarities in trajec-tories for language-impaired and ASD groups, it would seem using speech and language ability for differential diagnosis may not be useful but, instead, contributes to an understanding of their ability to communicate and partici-pate, that may impact other behaviours.
Loss of skills
Loss of social communication skills. A minority of children lost skills, either completely or with a decrease in their fre-quency of use, in all three groups but with a greater risk of skill loss and more pervasive skill loss in children with ASD. Of those children with ASD who lost skills, the majority lost skills in the ‘use of emotion and eye gaze’ cluster. This is in keeping with findings from past retro-spective (Ozonoff et al., 2005; Thurm et al., 2014) and prospective studies (Landa et al., 2007, 2013; Ozonoff et al., 2011) investigating skill loss in ASD. Children in our study did not regress significantly more than other groups in the ‘communication’ cluster. This finding was unexpected given communication is considered a key diagnostic feature of ASD. One possible explanation for this finding is that a child’s ‘vulnerability’ to losing skills may occur at different stages of development for different skills. In support of this hypothesis, one study found some skills typically problematic in ASD (e.g. response to joint attention, amount of requesting and use of gesture) had improving trajectories between 1 and 2 years whereas other skills (e.g. eye contact and overall quality of rapport) had declining trajectories (Lord, 2014).
Figure 6. Proportion of children who lost skills in one or more clusters for each group (ASD, LI and TD).Bars for each group are in order of appearance in the legend.
at The Royal Childrens Hospital on May 16, 2016aut.sagepub.comDownloaded from

10 Autism
In general, the children in this study lost more in social communication skills than in other skills such as use of words. However, loss of skills was not as common as has been reported in other prospective studies (e.g. Ozonoff et al., 2010). There are several possible explanations for this. Our study assessed children at only two time points so may not have captured some of the subtle losses and variability that may have occurred in communication. Because several questions have been combined into clus-ters and composites, children may experience a loss in some areas and gain in others and this may counterbalance their overall score and underestimate loss of skills. It may also be argued that social communication skills are more challenging for parents to assess compared to direct clinical observations of behaviour such has been used in some pro-spective studies (Landa et al., 2007; Ozonoff et al., 2010).
Loss of words. Very few children in this study lost words on the CDI. This was perhaps unsurprising given children may have few words to lose at 1 year of age. Two children (one each from the ASD and LI group) lost words. Both had a small number of words at 1 year of age (3 and 5 words). The ages children were assessed in this study were limited to the waves data collected in the broader study and consequently may have underestimated loss as children may lose and regain words within the 1- to 2-year period.
Loss across multiple skill domains
A majority of children lost skills in one cluster; yet, many also made gains in other clusters over the same time period. This suggests loss of skills, when it does occur, is not typi-cally pervasive across all areas of communication (Meilleur and Fombonne, 2009; Thurm et al., 2014). Of those chil-dren who lost skills in more than one area, the majority had ASD. Only one child (of n = 41) in this study represented the more ‘classic’ description of regression with substan-tial loss of skills across multiple clusters. Consistent with this finding there has been increasing consensus in the lit-erature that dramatic, catastrophic loss of skills in ASD is quite rare (Lord, 2014; Ozonoff et al., 2010; Siperstein and Volkmar, 2004; Thurm et al., 2014).
Loss of skills in children without ASD
Unexpectedly, a proportion of non-ASD children in this study were reported by parents to have a loss of communi-cation skills from 1 to 2 years. One prospective study also found skill loss in children without ASD (Brian et al., 2014). In this study, 7.5% of the total sample (n = 29/389) plateaued or had a lower raw score on a subsequent devel-opmental assessment. Here, 2.8% of low-risk infants, 5.2% of high-risk infants without ASD and 21% of high-risk infants with ASD demonstrated a reduction in raw scores, thus, suggesting loss of skills is not unique to ASD.
To date, all studies investigating loss in non-ASD children have been retrospective (Baird et al., 2008; Lord et al., 2004; Pickles et al., 2009; but see Landa et al., 2013 and Brian et al., 2014 for exception). Few high-risk studies have compared developmental trajectories of the non-ASD children in detail and to our knowledge no prospective study has included a sample of TD and LI children as large as this study (Landa et al., 2007, 2013; Mitchell et al., 2006; Ozonoff et al., 2010). It is possible the smaller sam-ples of non-ASD children in high-risk samples may not have captured the broad range of developmental trajecto-ries that may occur in TD children. No prospective studies have compared ASD to a defined group of language-impaired children. In addition, they have not included chil-dren with ASD who were being diagnosed as late as middle childhood. As a result, our study may include a higher pro-portion of children with milder phenotypes and later diagnoses.
Another important difference between this study and others is the tools used to determine loss of skills. The questions in the CSBS-ITC and CDI are quite specific and based on skills being used at the current time in multiple natural contexts. In contrast, the majority of retrospective studies (such as Baird et al., 2008; Pickles et al., 2009) have relied on general questions about regression from tools that were not specifically designed to study regres-sion. One prospective study of regression that investigated development of specific social communication behaviours reported a mean decrease in some communicative behav-iours over discrete time periods in children with TD. This included gaze to faces between 6 to 18 months and directed vocalisation from 24 to 36 months (Ozonoff et al., 2010). It is likely that a proportion of TD and LI children experience some natural wax and wane in the development of specific communication skills, and loss of skills may be a natural part of development for some children. This suggestion is supported by other studies of communication development in children, which have reported a lack of stability in lan-guage skills measured over time (Lord et al., 2012; Ukoumunne et al., 2012). Our knowledge of loss of skills in children who have LI or TD remains limited, as there are very few studies that have specifically investigated loss of communication skills at an individual level.
Study limitations include that the ASD diagnostic assessments were not completed within the study but in the community and therefore were not uniform. The study may be prone to selection bias since we only included those children that had completed specific waves of the study. However, a high proportion of children were retained in the ASD group (93%). Our classification and cut-off points for loss of skills, plateau, improving and accelerating were quite narrowly defined. We are not aware of any published, consistently used guidelines or definitions of loss and trajectory classifications that have been used in longitudinal studies. Given there is
at The Royal Childrens Hospital on May 16, 2016aut.sagepub.comDownloaded from

Brignell et al. 11
substantial instability in these early years and our cut-offs required just one point difference, it is possible some chil-dren were misclassified. We have made our definitions as clear as possible in the article, so the reader can interpret the findings along with their limitations. Measurement error and classification bias can occur in parent-reported tools such as the CDI and CSBS-ITC. This may have influ-enced the number of children who had a reduction in scores and may have impacted the study findings. The use of other groups (TD and LI) for comparison in this study, however, may mitigate the effect of classification bias to some extent. One would not expect between group differ-ences for data collected prior to problems being identified, unless there are characteristics of parents of children with ASD that are in some way different to parents of non-ASD children that influence the way they score.
Clinical implications
This study demonstrated that children have variable path-ways to ASD, TD or LI and these pathways may or may not include some loss of skills. The variability and overlap in trajectories between the groups highlights the challenge in making differential diagnoses at this young age (Lord et al., 2012; Veness et al., 2014). Consistent with the findings of other prospective studies, children in this study demon-strated more loss in social communication domains than in words. Change in social communication may be subtle, and it may be that tools have not yet been adequately developed to capture these changes over time. Children who experi-ence dramatic loss of skills were rare in our sample, but these children warrant special investigation and attention. A deeper understanding of the rate of change, patterns of derailment and individual variation in trajectories will help inform the development of targeted, developmentally sen-sitive intervention, the most effective and efficient resource allocation as well as inform prognosis. This is highly rele-vant for families, clinicians and policymakers.
Funding
Amanda Brignell is supported by an Australian Postgraduate Award scholarship. Infrastructure support was provided by the Victorian Government’s Operational Infrastructure Support Program. We wish to thank the William Collie Trust Fund for their financial support. This funding organization was not involved in the development, design, analysis, or interpretation of the study.
References
American Psychiatric Association (APA) (2000) Diagnostic Statistical Manual of Mental Disorders (DSM-IV-TR). 4th ed. Text revision. Washington, DC: APA.
Baird G, Charman T, Pickles A, et al. (2008) Regression, devel-opmental trajectory and associated problems in disorders in the autism spectrum: the SNAP study. Journal of Autism and Developmental Disorders 38: 1827–1836.
Barbaro J and Dissanayake C (2012) Developmental profiles of infants and toddlers with autism spectrum disorders identi-fied prospectively in a community-based setting. Journal of Autism and Developmental Disorders 42: 1939–1948.
Barger BD, Campbell JM and McDonough JD (2013) Prevalence and onset of regression within autism spectrum disorders: a meta-analytic review. Journal of Autism and Developmental Disorders 43: 817–828.
Bent CA, Dissanayake C and Barbara J (2015) Mapping the diag-nosis of autism spectrum disorders in children aged under 7 years in Australia, 2010–2012. Medical Journal of Australia 202: 317–320.
Bopp KD and Mirenda P (2011) Prelinguistic predictors of lan-guage development in children with autism spectrum dis-orders over four-five years. Journal of Child Language 38: 485–503.
Brian AJ, Roncadin C, Duku E, et al. (2014) Emerging cognitive profiles in high-risk infants with and without autism spec-trum disorder. Research in Autism Spectrum Disorders 8: 1557–1566.
Bryson SE, Zwaigenbaum L, Brian J, et al. (2007) A pro-spective case series of high-risk infants who developed autism. Journal of Autism and Developmental Disorders 37: 12–24.
Charman T, Drew A, Baird C, et al. (2003) Measuring early language development in preschool children with autism spectrum disorder using the MacArthur Communicative Development Inventory (Infant Form). Journal of Child Language 30: 213–236.
Chawarska K, Shic F, Macari S, et al. (2014) 18-month predic-tors of later outcomes in younger siblings of children with autism spectrum disorder: a baby siblings research consor-tium study. Journal of the American Academy of Child and Adolescent Psychiatry 53: 1317–1327.
Fenson L (1993) MacArthur Communicative Development Inventories: User’s Guide and Technical Manual. San Diego, CA: Singular Publishing Group.
Fenson L and Dale PS (1994) Variability in early communicative development. Monographs of the Society for Research in Child Development 59: 1–173.
Goldfield BA and Reznick JS (1990) Early lexical acquisition: rate, content, and the vocabulary spurt. Journal of Child Language 17: 171–183.
Jones EJ, Gliga T, Bedford R, et al. (2014) Developmental path-ways to autism: a review of prospective studies of infants at risk. Neuroscience and Biobehavioural Reviews 39: 1–33.
Kalb LG, Law JK, Landa R, et al. (2010) Onset patterns prior to 36 months in autism spectrum disorders. Journal of Autism and Developmental Disorders 40: 1389–1402.
Kim SH, Macari S, Koller J, et al. (2015) Examining the pheno-typic heterogeneity of early autism spectrum disorder: sub-types and short-term outcomes. Journal of Child Psychology and Psychiatry and Allied Disciplines. Epub ahead of print 12 August. DOI: 10.1111/jcpp.12448.
Landa R and Garrett-Mayer E (2006) Development in infants with autism spectrum disorders: a prospective study. Journal of Child Psychology and Psychiatry and Allied Disciplines 47: 629–638.
Landa RJ, Gross AL, Stuart EA, et al. (2012) Latent class anal-ysis of early developmental trajectory in baby siblings of
at The Royal Childrens Hospital on May 16, 2016aut.sagepub.comDownloaded from

12 Autism
children with autism. Journal of Child Psychology and Psychiatry 53: 986–996.
Landa RJ, Gross AL, Stuart EA, et al. (2013) Developmental trajectories in children with and without autism spec-trum disorders: the first 3 years. Child Development 84: 429–442.
Landa RJ, Holman KC and Garrett-Mayer E (2007) Social and communication development in toddlers with early and later diagnosis of autism spectrum disorders. Archives of General Psychiatry 64: 853–864.
Lord C (2014) Early regression and worsening in autism spec-trum disorders. In: Australasian society for autism research conference, Melbourne, VIC, Australia, 4–5 August.
Lord C, Luyster R, Guthrie W, et al. (2012) Patterns of devel-opmental trajectories in toddlers with autism spectrum dis-order. Journal of Consulting and Clinical Psychology 80: 477–489.
Lord C, Rutter M and Le Couteur A (1994) The Autism Diagnostic Interview-Revised: a revised version of a diag-nostic interview for caregivers of individuals with possible pervasive developmental disorders. Journal of Autism and Developmental Disorders 24: 659–685.
Lord C, Shulman C and DiLavore P (2004) Regression and word loss in autistic spectrum disorders. Journal of Child Psychology and Psychiatry and Allied Disciplines 45: 936–955.
Luyster R, Qiu S, Lopez K, et al. (2007) Predicting outcomes of children referred for autism using the MacArthur-Bates Communicative Development Inventory. Journal of Speech Language and Hearing Research 50: 667–681.
Luyster R, Richler J, Risi S, et al. (2005) Early regression in social communication in autism spectrum disorders: ACPEA study. Developmental Neuropsychology 27: 311–336.
Meilleur AA and Fombonne E (2009) Regression of language and non-language skills in pervasive developmental disorders. Journal of Intellectual Disability Research 53: 115–124.
Messinger D, Young GS, Ozonoff S, et al. (2013) Beyond autism: a baby siblings research consortium study of high-risk chil-dren at three years of age. Journal of the American Academy of Child and Adolescent Psychiatry 52: 300–308.
Mitchell S, Brian J, Zwaigenbaum L, et al. (2006) Early language and communication development of infants later diagnosed with autism spectrum disorder. Journal of Developmental and Behavioral Pediatrics 27: S69–S78.
Ozonoff S, Heung K, Byrd R, et al. (2008) The onset of autism: patterns of symptom emergence in the first years of life. Autism Research 1: 320–328.
Ozonoff S, Iosif A-M, Baguio F, et al. (2010) A prospective study of the emergence of early behavioral signs of autism. Journal of the American Academy of Child and Adolescent Psychiatry 49: 256–266.
Ozonoff S, Iosif A-M, Young GS, et al. (2011) Onset patterns in autism: correspondence between home video and par-ent report. Journal of the American Academy of Child and Adolescent Psychiatry 50: 796–806.
Ozonoff S, Williams BJ and Landa R (2005) Parental report of the early development of children with regressive autism: the delays-plus-regression phenotype. Autism 9: 461–486.
Pandey J, Verbalis A, Robins DL, et al. (2008) Screening for autism in older and younger toddlers with the Modified Checklist for Autism in Toddlers. Autism 12: 513–535.
Paul R, Chawarska K and Volkmar F (2008) Differentiating ASD From DLD in Toddlers. Perspectives on Language Learning and Education 15: 101–111.
Pickles A, Simonoff E, Conti-Ramsden G, et al. (2009) Loss of language in early development of autism and specific language impairment. Journal of Child Psychology and Psychiatry 50: 843–852.
Reilly S, Eadie P, Bavin EL, et al. (2006) Growth of infant com-munication between 8 and 12 months: a population study. Journal of Paediatrics and Child Health 42: 764–770.
Reilly S, Wake M, Bavin EL, et al. (2007) Predicting language at 2 years of age: a prospective community study. Pediatrics 120: e1441–1449.
Rozga A, Hutman T, Young GS, et al. (2011) Behavioral pro-files of affected and unaffected siblings of children with autism: contribution of measures of mother-infant interac-tion and nonverbal communication. Journal of Autism and Developmental Disorders 41: 287–301.
Rutter M, Bailey A and Lord C (2003) The Social Communication Questionnaire. Los Angeles, CA: Western Psychological Services.
Schoen E, Paul R and Chawarska K (2011) Phonology and vocal behavior in toddlers with autism spectrum disorders. Autism Research 4: 177–188.
Sebat J, Lakshmi B, Malhotra D, et al. (2007) Strong associa-tion of de novo copy number mutations with autism. Science 316: 445–449.
Semel E, Wiig E and Secord WA (2003) Clinical Evaluation of Language Fundamentals, Australian Version. 4th ed. San Antonio, TX: The Psychological Corporation.
Shumway S, Thurm A, Swedo SE, et al. (2011) Brief report: symptom onset patterns and functional outcomes in young children with autism spectrum disorders. Journal of Autism and Developmental Disorders 41: 1727–1732.
Siperstein R and Volkmar F (2004) Brief report: parental report-ing of regression in children with pervasive developmental disorders. Journal of Autism and Developmental Disorders 34: 731–734.
Stefanatos GA (2008) Regression in autistic spectrum disorders. Neuropsychology Review 18: 305–319.
Szatmari P, MacLean JE, Jones MB, et al. (2000) The familial aggregation of the lesser variant in biological and non-biological relatives of PDD probands: a family history study. Journal of Child Psychology and Psychiatry 41: 579–586.
Thurm A, Manwaring SS, Luckenbaugh DA, et al. (2014) Patterns of skill attainment and loss in young children with autism. Development and Psychopathology 26: 203–214.
Ukoumunne OC, Wake M, Carlin J, et al. (2012) Profiles of language development in pre-school children: a longitudi-nal latent class analysis of data from the Early Language in Victoria Study. Child: Care, Health and Development 38: 341–349.
Veness C, Prior M, Bavin E, et al. (2012) Early indicators of autism spectrum disorders at 12 and 24 months of age: a prospective, longitudinal comparative study. Autism 16: 163–177.
Veness C, Prior M, Eadie P, et al. (2014) Predicting autism diag-nosis by 7 years of age using parent report of infant social
at The Royal Childrens Hospital on May 16, 2016aut.sagepub.comDownloaded from

Brignell et al. 13
communication skills. Journal of Paediatrics and Child Health 50: 693–700.
Wechsler D (1999) Wechsler Abbreviated Scale of Intelligence. New York: The Psychological Corporation.
Wetherby AM and Prizant BM (2002) CSBS DP Manual: Communication and Symbolic Behavior Scales: Developmental Profile. Baltimore, MD: Paul H. Brookes.
Wetherby AM, Brosnan-Maddox S, Peace V, et al. (2008) Validation of the Infant – Toddler Checklist as a broadband screener for autism spectrum disorders from 9 to 24 months of age. Autism 12: 487–511.
Wiig EH, Secord W and Semel E (2006) Clinical Evaluation of Language Fundamentals Preschool (Australian Edition). 2nd ed. Marrickville, NSW, Australia: Harcourt Assessment.
Young GS, Merin N, Rogers S, et al. (2009) Gaze behavior and affect at 6 months: predicting clinical outcomes and language development in typically developing infants and infants at risk for autism. Developmental Science 12: 798–814.
Zwaigenbaum L, Bryson S, Rogers T, et al. (2005) Behavioral manifestations of autism in the first year of life. International Journal of Developmental Neuroscience 23: 143–152.
at The Royal Childrens Hospital on May 16, 2016aut.sagepub.comDownloaded from

145
Chapter 8 Study 3. Language trajectories and predictors of language
outcome from 4 to 7 years in children with and without autism
spectrum disorder
In this chapter we examined trajectories of language development in children with ASD
from 4 to 7 years compared with children with LI and TD. We explored whether
children with ASD had a greater gap between expressive and receptive language
compared with children without ASD. Nine predictors of language outcomes for all
children (n=1004) were examined. We hypothesised that ASD and social
communication would be important predictors of later language outcome. This paper is
being prepared for submission to the Journal of Pediatrics.
146
Abstract
Objective
To describe trajectories and predictors of language development from 4 to 7 years in
children with autism spectrum disorder (ASD) compared with children with typical
language (TD) and language impairment (LI).
Study design
In a prospective, community-based study (the Early Language in Victoria Study,
n=1910) children completed standardised language assessments at 4, 5 and 7 years.
Individual trajectories for the children with ASD were plotted. Mean trajectories and
proportions of children who had declining, increasing and stable trajectories for ASD
(n=26-27), TD (n=858-861) and LI (n=119) groups, were compared. We analysed the
following predictors of receptive and expressive language outcome: gender, IQ, baseline
receptive and expressive language ability, social ability, diagnosis of ASD and
socioeconomic disadvantage.
Results
Similar proportions of children with ASD had decreasing, accelerating and stable
trajectory types as seen in the TD and LI groups. Mean trajectories for children with
ASD showed stable development, again comparable to LI and TD groups. Language
level and IQ at four years predicted language outcomes at 7 years but not social abilities
or diagnosis of ASD.

147
Conclusion
Children with ASD and LI had similar language scores at baseline that were lower on
average than those who had TD. Language progressed at a similar rate for all groups,
with progress influenced by IQ and language ability at four years rather than a diagnosis
of ASD.
Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental disorder that affects more
than one in 70 individuals (Centers for Disease Control and Prevention, 2014). Social
communication difficulties and restricted, repetitive behaviours are defining features of
ASD (American Psychiatric Association, 2013).
Structural language skills (including vocabulary, use of grammar, syntax and
phonology) in children with ASD vary widely. Some children with ASD never develop
the ability to speak while others demonstrate superior language ability (Tager-Flusberg
et al., 2011). In addition, children with ASD may show atypical language presentation
such as stronger expressive compared with receptive language ability (Ellis Weismer &
Kover, 2015; Pickles et al., 2014), regression in communication skills in the first few
years of life (see Barger et al., 2013 for a review) and persistent or unusual repetitive,
stereotyped language (Tager-Flusberg et al., 2011). Verbal skills in childhood play an
important role in predicting long-term outcome in children with ASD in wellbeing,
adaptive functioning and mental health (Billstedt, Gillberg, & Gillberg, 2011; Gillespie-
Lynch et al., 2012; Howlin & Moss, 2012; Howlin et al., 2013).
148
Children with ASD have differing trajectories of language development, which include
loss of skills, plateau, improvement and acceleration (Anderson et al., 2007; Ellis
Weismer & Kover, 2015). Children with ASD and higher verbal skills have been
reported to have trajectories comparable to those with typically developing language on
most measures while children with low verbal skills have made slower progress (Tek et
al., 2014). Substantial variability in communication trajectories has also been reported
in the first few years of life in ASD (Brignell et al., 2016; Landa et al., 2013), with more
stable and predictable patterns of development reported from 6 to 19 years (Pickles et
al., 2014).
Variability in trajectories seen in ASD may not be unique to the condition. Studies of
language trajectories in children with specific language impairment, have also reported
greater variability in trajectories before 6 years and relative consistency from 6 years of
age onwards (Conti-Ramsden et al., 2012). Variability has also been found in
population studies of children under 8 years (McKean et al., 2015; C. Taylor et al.,
2013) and in children under 9 years with non-spectrum developmental disabilities
(Anderson et al., 2007; Ellis Weismer & Kover, 2015). However, clearly-defined
comparison groups of the same age within the same study cohort are needed to test
whether this pattern of language trajectory is indeed unique to ASD.
Language trajectories may differ according to the severity of the child’s language
problems and the time period being studied (Tek et al., 2014; Toth et al., 2006). Studies
of children with ASD have examined a range of factors that may impact on later
language outcome, focusing both on environmental (e.g., parent interaction style, socio-
economic status and intervention (Ellis Weismer & Kover, 2015; McDuffie & Yoder,
2010; Siller et al., 2013) and child factors (e.g., play, gesture, joint attention, imitation,

149
IQ, language ability and ASD symptoms) (Baghdadli et al., 2012; Ellis Weismer &
Kover, 2015; Luyster et al., 2007; Toth et al., 2006). Nonverbal IQ is the most
consistently reported significant predictor of later language outcome (Thurm et al.,
2015; Wodka et al., 2013). Earlier language ability has also been found to be important
(Ellis Weismer & Kover, 2015; Turner, Stone, Pozdol, & Coonrod, 2006). To our
knowledge, no studies have specifically investigated gender as a potential predictor of
language outcomes. There have been inconsistent findings around the importance of
ASD symptoms in predicting language outcomes. Severity of ASD symptoms are
reported as significant by some (Baghdadli et al., 2012; Ellis Weismer & Kover, 2015;
Magiati et al., 2011), whereas others have noted they are less important after factors
such as nonverbal IQ are taken into account (Sigman & McGovern, 2005; Thurm et al.,
2015).
Despite an increase in the number of studies that have investigated language trajectories
and predictors of language outcome in ASD, clinicians are still unable to provide
timely, accurate prognostic information about language outcomes to parents based on
their child’s individual skill profile. Policy makers and service providers also require
information about communication outcomes to inform decisions regarding allocation of
resources and services. The aim of this study was to (a) examine trajectories of
receptive and expressive language development in children with ASD from 4 to 7 years
and to compare the trajectories of children with ASD over time to children with
language impairment (LI) and typical development (TD); b) compare the proportions of
children with ASD who had declining, stable and accelerating trajectories and
development over time to children with TD and LI; (c) investigate whether children
with ASD have relative weakness in receptive compared with expressive language (d)

150
investigate predictors of language outcomes from 4 to 7 years, in a representative
community sample.
Methods
Participants
Participants were drawn from the Early Language in Victoria Study (ELVS), a
longitudinal, community-based study of language development in children (n=1910).
Participants were recruited from 6 of 31 local government areas around metropolitan
Melbourne to represent a range of social economic advantage and disadvantage. Infants
were enrolled in the ELVS at 7.5-10 months of age and were assessed almost yearly
using direct assessments of language and/or parent-completed questionnaires and
related areas. Exclusion criteria included a diagnosis of developmental delay, cerebral
palsy and if parents had inadequate English to complete questionnaires (see Reilly et al.,
2006; Reilly et al., 2007 for further details). Several groups were selected from the
ELVS for comparison.
Measures
Demographic details were collected when participants were aged 8-12 months. The
Clinical Evaluation of Language Fundamentals-Preschool Edition (CELF-P2; Wiig et
al., 2006) was administered to participants at 4 years and the CELF-Fourth Edition
(CELF-4; Semel et al., 2003) at 5 and 7 years. This comprehensive standardised tool
measures receptive and expressive language. Language domains including morphology
(grammar), syntax (sentence structure), semantics (word meanings) and vocabulary are
assessed. The Kaufman Brief Intelligence Test-2 (KBIT-2; Kaufman & Kaufman, 2004)

151
and Wechsler Abbreviated Scale of Intelligence (WASI; Wechsler, 1999) were
administered at 4 and 7 years, respectively. The Pediatric Quality of Life Inventory 4.0:
parent report form (Peds-QL; Varni et al., 2001) and the Strengths and Difficulties
Questionnaire (SDQ; Goodman, 1997) were completed by parents when participants
were aged 4 years.
Procedures
Trained psychology graduates and speech pathologists administered direct language
assessments in the child’s school or home. All children were seen within two months
either side of their birthday at each time point.
Identification of subgroups
Identification of participants with autism spectrum disorder. From 4 years of age all
parents were asked if their child had received a diagnosis of ASD. Following parent
report a psychologist (MP), experienced in the diagnosis of ASD, conducted a telephone
interview to verify the diagnosis, collect information on age of diagnosis and
comorbidities, and determine who made the diagnosis. The majority of children (n=
41/44; 93%) received a diagnosis of ASD from a multidisciplinary team that involved at
least two professionals (typically a paediatrician, psychologist, speech pathologist). The
remaining children (n=3) were diagnosed by a paediatrician. Forty-four children in the
sample were diagnosed with ASD but in the present study only those children who had
completed the CELF at 4 or 5 and 7 years (n=26-27) were included in the analysis.
Families of children with ASD also completed the Social Communication Questionnaire

152
(SCQ; Rutter et al., 2003) at 7 years of age. Mean scores on the SCQ for the children in
this study were 13.3 (standard deviation 4.08; range 5-20).
Identification of language impaired and typical language development. Children were
allocated to the language impaired (LI) and typical language (TD) groups based on their
performance on the CELF and the WASI. Group allocation was conducted at 7 years.
Children in the LI group had a WASI score greater or equal to 70 and a CELF score at
two time points (at 7 years and at 4 or 5 years) more than or equal to 1.25 standard
deviations below the mean. For the TD group children were required to have a WASI
score of greater or equal to 85 and a CELF score at 7 years and 4 or 5 years of greater
than 1.25 standard deviations below the mean. Children were excluded from these
groups if they were reported to have ASD. Children were only included in the current
study if their language skills were measured on the CELF at 4 or 5 and 7 years. This
produced 119 children in the LI group and 861 children in the TD group.
Sixteen children were excluded from the predictor and trajectory analysis because they
were missing data from either the nine predictor measures or the two CELF time points.
Reasons for missing data included: withdrew from the ELVS (n=4), verbal ability too
limited to complete CELF (n=2), unable to schedule (n=3), child non-compliant to
testing (n=4) and parents too busy with other interventions to find time to schedule
assessment (n=3). We tested whether there were differences between the characteristics
of children with ASD who were lost to follow up and those who were included in the
study. For children with ASD there were no significant differences (p>0.05) between
those children who remained in the study (n=27) and those with ASD that were lost to
follow up or were missing data (n=16) in any of the 8 demographic factors (Chapter 6,
Table 15). While scores on language and IQ measures were lower for the children with

153
ASD who were not included in the analysis, there were also no significant differences
(p>0.05) between the two groups in language and communication ability at 2 years of
age as measured by the MacArthur Bates Communicative Development
Inventories (CDI: Fenson, 1993) and the Communication Symbolic Behaviour Scales-
Infant Toddler Checklist (CSBS-ITC: Wetherby & Prizant, 2002). See Chapter 6, Table
15. Information was not consistently collected on the receptive and expressive language
skills of the children who were not able to complete the CELF due to their limited
verbal ability. We have noted the language ability of these children in the text but were
not able to include these children in the trajectory analysis, as we could not provide
valid comparison scores.
Outcome measures
Language was measured with the CELF-4 at 7 years. Receptive and expressive indexes
from the CELF-4 were reported.
Predictor measures
Nine predictors were used in this study. Social communication skills were measured
using the social subscales from the Peds-QL and the SDQ. The social functioning
subscale was used from the Peds-QL. The peer relationship problems and prosocial
behaviour subscales were used from the SDQ. Autism was assigned as described above.
Nonverbal IQ was measured using the KBIT-2 matrices subtest. Baseline receptive and
expressive language ability was based on a child’s standard score at 4 or 5 years on the
CELF-P or the CELF-4. The ELVS sample at 7 years is skewed toward families who
are more socio-economically advantaged (McKean et al., 2015), thus Socio-Economic

154
Indexes for Areas (SEIFA) quintiles were used based on the Australian Bureau of
Statistics reference.
Ethical approval was obtained from the Royal Children’s Hospital (#23018) and La
Trobe University, Human Ethics Committee (#03–32). All parents provided written,
informed consent.
Statistical Analysis
All analyses were conducted using Stata version 13.1. Individual trajectories from 4 to 7
years were plotted for the children with ASD. Proportions of children with ASD who
had declining, increasing and stable trajectories were compared with children with LI
and TD using the Chi square statistic. We defined declining and increasing trajectories
as more than one standard deviation change (+/- 15 points) in standard scores between 4
and 7 years on the CELF. Data were also analysed using the Generalised Estimating
Equations (GEE) method for fitting the marginal models. An exchangeable correlation
structure was used and “robust” standard errors from the sandwich estimator, which
takes the dependence of the responses into account. GEE was used to plot mean
trajectories from 4 to 7 years for each group. To assess whether a diagnosis of ASD
predicted a greater gap between receptive and expressive language at 4 and 7 years of
age we used linear regression with autism diagnosis the explanatory variable and CELF
scores at 4 and 7 years the outcome variables.
We also used linear regression to analyse predictors of language outcome. Predictors
were included in the model if they were found to be significant univariate predictors of
language outcome. Multicolinearity between the social communication measures (i.e.

155
subscales of the SDQ, Peds-QL) was assessed to prioritise the measures. A variance
inflation factor of 1.2 indicated low correlation so all three social communication
measures were kept in the model.
Results
There was no significant difference between any of the three groups in number of
indigenous children, families where English was the main language spoken at home and
maternal age at birth. A higher proportion of children with ASD were male compared
with the other groups (p=0.004). Children with LI were more likely to have a greater
number of children living in the home and parents who had not completed high school
and who were not married/defacto compared with the TD group (p=0.001). The LI
group was more socially disadvantaged than both the TD and ASD groups (p<0.012).
Mean IQ was 99.71 (SD 14.35) for children included in the trajectory and predictor
analysis with no child having an IQ<70. Appendix F and Table 15 (Chapter 6) of this
thesis provides further detail on the demographic, IQ and language scores of children
with ASD in the ELVS whose data was not included in the analysis.
Individual trajectories
Individual trajectories are shown in Figure 15. Three main trajectory types: declining,
accelerating and stable were found for receptive and expressive language in children
with ASD from 4 to 7 years. The majority of children with ASD had stable trajectories
with scores remaining within 1 standard deviation of their previous standard score from
4 to 7 years. Three children with ASD could not be tested on the CELF at all three time
points due to limited language abilities. One child was minimally verbal (≤ 10 words) at

156
4 years and continued to have limited receptive and expressive language at 7 years.
Another child was verbal but did not have adequate language to complete testing at 4
and 7 years. The third child could only use a limited number of phrases and
communicated primarily using sign at 4 and 5 years. This child was verbal by 7 years
and able to complete the CELF-4.

157
Figure 15 Individual language trajectories from 4 to 7 years of children with ASD. Standard scores on the CELF are presented.
Note. One child in Figure 15 demonstrated a steep decline in his receptive language ability with very low scores on 2 of 3 subtests in the receptive language index at 7 years. His score on the third receptive language subtest was age appropriate. We completed sensitivity analyses by removing this child’s scores from the analyses and the overall summary findings remained the same.

158
Trajectory types
Trajectories were described using standard scores for children who were able to
complete the CELF (n=27). Three children who did not complete the CELF are
described separately and are not included in the sample of 27. Declining trajectory was
defined a decrease of more than one standard deviation (15 points) in standard score on
the CELF from 4 to 7 years. A stable trajectory was defined as a standard score that
remained within one standard deviation (within 15 points in either direction) from 4 to 7
years. An accelerating trajectory was one that improved by more than one standard
deviation (15 points) on the CELF from 4 to 7 years. Overall there were no significant
differences between the three groups (ASD, LI, TD) in the proportions of children who
demonstrated declining, stable and accelerating trajectories in receptive language (chi
square statistic 4.0932; p= 0.394) and expressive language (chi square statistic 5.9358;
p= 0.204) (Table 16). Eighty-one and eighty-five percent of children with ASD had
relatively stable standard scores in receptive and expressive language respectively from
4 to 7 years. Eight and eleven percent of children had increasing and 7 and 8 %
declining trajectories, in receptive and expressive language respectively.
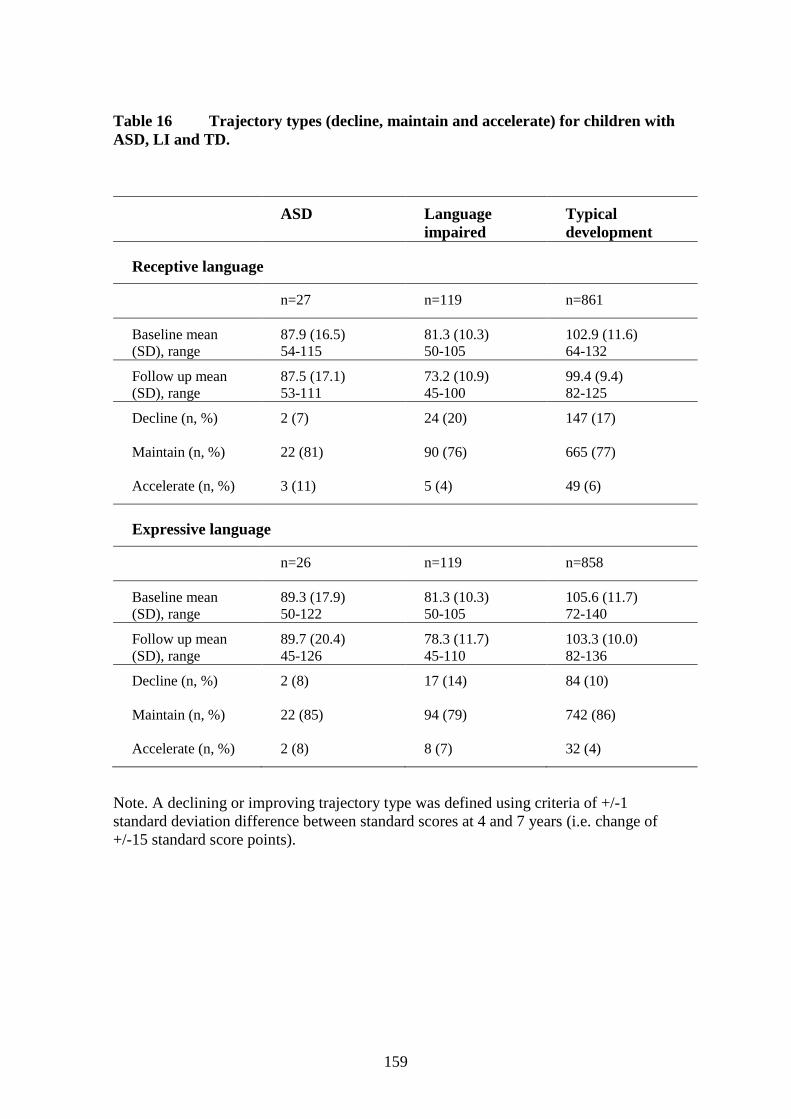
159
Table 16 Trajectory types (decline, maintain and accelerate) for children with ASD, LI and TD.
Note. A declining or improving trajectory type was defined using criteria of +/-1 standard deviation difference between standard scores at 4 and 7 years (i.e. change of +/-15 standard score points).
ASD Language impaired
Typical development
Receptive language
n=27 n=119 n=861
Baseline mean (SD), range
87.9 (16.5) 54-115
81.3 (10.3) 50-105
102.9 (11.6) 64-132
Follow up mean (SD), range
87.5 (17.1) 53-111
73.2 (10.9) 45-100
99.4 (9.4) 82-125
Decline (n, %) 2 (7) 24 (20) 147 (17)
Maintain (n, %) 22 (81) 90 (76) 665 (77)
Accelerate (n, %) 3 (11) 5 (4) 49 (6)
Expressive language
n=26 n=119 n=858
Baseline mean (SD), range
89.3 (17.9) 50-122
81.3 (10.3) 50-105
105.6 (11.7) 72-140
Follow up mean (SD), range
89.7 (20.4) 45-126
78.3 (11.7) 45-110
103.3 (10.0) 82-136
Decline (n, %) 2 (8) 17 (14) 84 (10)
Maintain (n, %) 22 (85) 94 (79) 742 (86)
Accelerate (n, %) 2 (8) 8 (7) 32 (4)

160
Mean trajectories
Receptive language
The estimated mean standard scores for the LI group were 24.6 units lower than the TD
group across the three waves of data collection (p<0.001; 95% CI -26.1, -23.1). The
estimated mean standard scores for the ASD group were 18.0 units lower than the TD
group across the three waves of data collection (p<0.001; 95% CI -23.2,-12.7). There
was a small effect of gender in the whole cohort (ASD, LI and TD) with girls having a
mean standard score 1.6 units higher than boys (p=0.005; 95% CI 0.5, 2.8). There was
no evidence of an interaction between gender and grouping (i.e. ASD, LI, TD).
Expressive language
Estimated mean standard scores were 24.4 units lower for the LI than the TD group
across the three waves of data collection (p<0.001; 95% CI -26.1, -22.6). Estimated
mean standard scores were 18.1 units lower for the ASD than the TD group across the
three waves of data collection (p<0.001; 95% CI -24.0, -12.2). There was no evidence
of an effect of gender on the mean standard scores for the whole cohort nor was there
any evidence of an interaction between gender and grouping.
Mean trajectories from four to seven years for children with ASD, LI and TD are
presented in Figure 16 (a,b). While language ability varied between the three groups, the
slopes of the trajectories in each group were generally flat, indicating the development
of language was generally at a comparable rate. Exceptions to this were girls with ASD
who demonstrated variable trajectories and the LI group who demonstrated a decrease
of approximately 7 standard score points from 5 to 7 years in expressive language. Of

161
note, girls with ASD achieved lowest scores of all three groups in receptive language.
Upon inspection of the graphs mean standard scores for expressive language were
higher than receptive language for all three groups.

162
Figure 16 Mean language trajectories (CELF standard scores) for male and female subgroups of children with ASD, TD, LI.
(a)

163
(b)
Note. Figure (a) represents receptive language and Figure (b) expressive language. Solid line is the smoothed mean from 4 to 7 years and dashed lines show actual mean scores at 4,5 and 7 years. LI and TD groups were pre-defined by the authors based on inclusion/exclusion criteria (see Participants above). For standard scores, a declining trajectory indicates progress at a slower rate but this does not necessarily indicate a loss of skills.

164
Receptive-expressive language profiles
There was a wide range of receptive/expressive difference scores observed in children
with and without ASD at 4 years (-30 to 36), 5 years (-43 to 43) and 7 years (-35 to 51).
(Figure 17). There was no evidence that having a diagnosis of ASD resulted in any
difference in receptive/expressive difference scores at 4 years, 5 years or 7 years of age
(ASD n=30, whole cohort n=1560 at 4 years; ASD n=23, whole cohort n=982 at 5
years; ASD n=30, whole cohort n=1204 at 7 years). Children with ASD aged 4 years
had on average a 0.45 unit lower difference between expressive and receptive language
than children without ASD (95% CI -4.0, 3.1, p=0.81). At 5 years children with ASD
had on average a mean difference 2.0 units higher than children without ASD (95% CI -
2.9, 6.8; p=0.43) and at 7 years children with ASD had on average a mean difference
1.7 units lower than children without ASD (95% CI -5.8, 2.3, p=0.40).

165
Figure 17 Distribution of the receptive-expressive difference scores for non-ASD and ASD children at 4 (a) and 7 years (b).
(a) (b)

166
Predictors of receptive and expressive language outcomes at 7 years
Five of nine predictors examined using multivariate analysis made a statistically
significant independent contribution to variance in receptive language outcome. These
included receptive and expressive baseline scores, gender, socio-economic disadvantage
and IQ. For expressive language only receptive and expressive baseline scores and IQ
were significant. A diagnosis of autism and social ability at 4 years were not significant
predictors of either receptive or expressive language ability at 7 years once gender,
baseline receptive language skills, baseline expressive language skills and IQ at 4 years
of age were taken into account. The model explained 44% of the variance in receptive
language outcome (p<0.001) and 58% of the variance in expressive language outcome
(p<0.001). See Table 17.

167
Table 17 Predictors of language outcomes
a lower score in this subscale indicates more difficulties in this domain
Note. Baseline receptive and expressive language at 4 or 5 years was measured using the CELF-P or CELF-4. Outcome expressive and receptive language was measured at 7 years using the CELF-4. Social communication was measured at 4 years using the pro-social and peer problems subscales from the SDQ and the social subscale from the Peds-QL. Nonverbal IQ was measured at 4 years using the KBIT-2. Socio-Economic Indexes for Areas (SEIFA) quintiles were used based on the Australian Bureau of Statistics reference.
Variable Coefficient 95% CI P value
Receptive language outcome
Baseline receptive 0.38 0.32 to 0.44 <0.000
Baseline expressive 0.23 0.17 to 0.29 <0.000
Peds-QL social 0.01 -0.05 to 0.06 0.794
SDQ pro-sociala -0.12 -0.47 to 0.22 0.497
SDQ peer problems -0.22 -0.68 to 0.23 0.334
Autism 3.66 -0.67 to 8.0 0.098
Female gender 1.63 0.38 to 2.88 0.01
Nonverbal IQ 0.17 0.12 to 0.22 <0.000
SEIFA disadvantage 0.63 0.09 to 1.18 0.022
Expressive language outcome
Baseline receptive 0.19 0.14 to 0.24 <0.000
Baseline expressive 0.56 0.50 to 0.61 <0.000
Peds-QL social -0.03 -0.08 to 0.02 0.240
SDQ pro-sociala 0.04 -0.25 to 0.34 0.773
SDQ peer problems -0.01 -0.40 to 0.38 0.953
Autism -0.75 -4.41 to 2.92 0.689
Female gender -0.80 -1.85 to 0.26 0.139
Nonverbal IQ 0.07 0.03 to 0.11 0.002
SEIFA disadvantage 0.31 -0.16 to 0.77 0.194

168
Discussion
To our knowledge this study is the first to report on children with ASD using clinician
administered, comprehensive, standardised language assessments in a longitudinal
community sample that includes and has used the same measures for children with LI
and TD. The community sample minimizes ascertainment bias, maximises external
validity and enables a broader picture of ASD as well as important comparisons.
Children with ASD demonstrated some heterogeneity in trajectory types but most
demonstrated rates of language development comparable to those with LI and TD with
parallel trajectories. In other words, progress over time for the ASD group was similar
to LI groups, and the TD group, albeit with the ASD and LI groups starting from a
lower baseline. This finding is consistent with the ‘tracking’ hypothesis proposed by
other researchers. This hypothesis suggests that despite children with LI having lower
mean scores than TD children, on average they track in parallel to TD children with
stable growth in expressive and receptive language ability over time (Law et al., 2008).
Some evidence of acceleration in receptive language ability from 7 to 8 years of age has
also been reported (Conti-Ramsden et al., 2012).
The three groups were also comparable in the proportions of children with declining,
maintaining and accelerating trajectory types. Criteria used to assess trajectory variation
(i.e. decline, maintain, accelerate) has differed from study to study and the threshold
used in the current study (more than one standard deviation difference between time
points) may be wider and less likely to find a difference compared with other studies.
Our finding that trajectories were relatively stable for many children with ASD is,
however, consistent with a previous study (Pickles et al., 2014).
169
Children with minimal verbal ability did make progress in their communication skills,
however it was not possible to assess their rate of development and they may not
maintain the same pace of development as other children. To date evidence points to
children with ASD who had relatively lower expressive language ability at baseline
experiencing a slower rate of language growth compared with children with typical
language development (Ellis Weismer & Kover, 2015; Tek et al., 2014).
A strength of this study is that we were able to report on receptive and expressive
language separately. This study did not find a significant mean difference between the
two language domains for children with ASD at any of the time points measured. Our
finding regarding children with ASD is consistent with a meta-analytic review of
studies investigating the receptive-expressive discrepancy in ASD (Kwok et al., 2015).
Receptive and expressive language ability and nonverbal IQ at 4 years were found to be
important predictors of later language at 7 years, convergent with previous research
using clinical samples of children with ASD (Ellis Weismer & Kover, 2015; Luyster et
al., 2007). Of interest, a diagnosis of ASD and social communication ability were not
significant predictors of later language outcome when other factors were controlled for.
Methods used here differ from previous studies examining predictors of language
outcomes in ASD. A categorical diagnosis of ASD rather than ASD symptom severity
was used and comparison between children with and without ASD (n=1086) was
possible.
Socio-economic disadvantage (specifically being in the most disadvantaged quintile),
and gender were predictors of receptive but not expressive language in the current
study. This finding is consistent with a study of children with ASD which found

170
maternal education discriminated higher versus low verbal outcomes (Ellis Weismer &
Kover, 2015). Low maternal education and low family income were also found to be a
risk factor of receptive vocabulary at 7 years in another large cohort longitudinal
population-based study, although expressive vocabulary was not measured (C. Taylor et
al., 2013). Low maternal education and socioeconomic status also predicted adverse
receptive and expressive language outcomes at 4 years in another study that used data
from the same cohort as the current study (Reilly et al., 2010). At this time it remains
unclear why socioeconomic disadvantage/advantage predicted receptive but not
expressive language at 7 years in this study.
Diagnosis of ASD and parent-reported social ability at 4-5 years of age were not
predictors of expressive or receptive language at 7 years once factors such as IQ and
baseline language ability were taken into account. The methodology used in this study
was unique in being able to test diagnosis of ASD as a predictor of language outcomes
in a large cohort of children with and without ASD. However, direct comparison to the
findings of previous studies is therefore not possible. Our sample of children with ASD
was small and we were not able to classify children into different levels of severity of
ASD symptoms so results should be viewed with caution and await replication.
Despite the lack of receptive-expressive gap our study did find some differences in the
types of predictors relevant to each language domain. Other studies have found ASD
symptom severity to be an important predictor of growth in expressive and receptive
language while cognition predicted growth in expressive language (Ellis Weismer &
Kover, 2015).

171
Limitations
The analysis in this study was limited to children who could complete the CELF, with
qualitative information provided about three children with ASD who were not able to
complete the CELF at two time points due to limited language and/or cognitive ability
and floor effects on tools (i.e. children were not able to achieve basal scores). Therefore,
findings are only relevant to those children who had verbal language and children with
IQ>70. The exclusion of children who were minimally verbal is likely to skew our
findings and have implications for generalising to the general population of children
with ASD. Our sample size of children with ASD (n=27) is quite small which reduces
statistical power. The substantial difference in sample size between the children with
ASD relative to those without ASD also needs to be considered when interpreting our
findings. Given this was a community-based study, the children in the study were not
diagnosed with ASD uniformly using the same methods and we relied on parent report
of ASD, with verification through interview. Different versions of the CELF were used
at 4 years compared with 5 and 7 years, however mean scores, standard deviations and
ranges for the whole sample were very similar each version of the CELF (4 years: mean
99.62 (SD 15.1; 50-140); 5 years: mean 100.6 (SD 13.9; 55-144); 7 years: mean 98.8
(SD 13.6; 45-136)).
Clinical implications
Our findings contribute new knowledge to our current understanding of language
development in children with ASD. While limited by a small sample size and
inconsistent diagnostic methods, the findings provide preliminary information that for
verbal children with ASD aged 4 to 7 years who do not have an intellectual disability, a
diagnosis of ASD in itself does not necessarily mean a child will fall further behind

172
their peers in language development, and that other factors may be more relevant to
later language ability such as nonverbal IQ and earlier language level than a diagnosis
of ASD. This is important information for clinicians to consider when parents ask them
about their child’s likely language outcome.
The age at which this study investigated predictors (4 years) of later outcomes is
consistent with the mean age children are typically diagnosed with ASD in Australia
before 7 years of age (Bent et al., 2015) and the factors found to be predictive of
language outcomes should be readily available to clinicians who diagnose children with
ASD, as part of recommended best practice assessment.
This study was not able to provide clinicians with useful prognostic information on
language development in children with ASD who have intellectual disability and/or
those children who do not have adequate language ability to complete formal testing.
Such information would be highly valuable for parents and for clinicians who are
working with this subgroup of children and needs to be a research priority. Further
research is also needed to bring together the multiple factors that interact and impact
language outcomes more personalised prognostic information can be provided to
families about the likely outcomes for their particular child.

173
Chapter 9 Discussion
This thesis has investigated trajectories of language development in children with ASD
in three studies. First, a systematic review and meta-analysis (Study 1) synthesised
existing literature on language outcomes in individuals with ASD and assessed the
quality of included studies. An important priority of the systematic review was to
present findings in a clinically meaningful way so they were relevant and useful to
clinicians and families. The review identified a large number of studies had measured
language outcomes, however, most were of medium and high risk of bias and there was
substantial heterogeneity in study methodology. Gaps in our knowledge were identified
in existing literature and with reference to best practice methods for prognosis studies.
Key suggestions were made for future research.
Second, Study 2 and 3 utilised data from a prospective, longitudinal, community-based
study. Study 2 described individual and group trajectories of communication
development from 1 to 2 years in children with ASD and investigated loss of
communication skills over the same period. Study 3 described individual and group
trajectories of language development in children with ASD from 4 to 7 years and
examined predictors of language outcomes in the whole cohort. This study also
investigated whether children with ASD were more likely to have weakness in receptive
relative to expressive language than children without ASD at several time points. In
Study 2 and 3 language trajectories in children with ASD were compared with large
cohorts of children with LI and TD, thus placing language trajectories of children with
ASD within a broad developmental context.

174
Summary of principle findings
Language ability was found to be highly heterogeneous for children with ASD in all
three studies, with some children achieving scores on standardised testing that were well
above average and others demonstrating severe delays. Mean scores on standardised
language tools for children with ASD in communication, expressive vocabulary and
receptive/expressive language domains were lower than typically developing children at
two years of age and from four to seven years of age (Study 2 and 3) and in all but one
study included in the systematic review compared with reference norms (Study 1).
Communication trajectories from 1 to 2 years of age
From 1 to 2 years of age individual communication trajectories for children with ASD
were highly variable (Study 2). Some children demonstrated accelerated development,
some improved, some plateaued and others lost skills over the one-year period. These
trajectory types were not consistent across each type of skill in each child. Some
children gained skills in some communication domains and lost skills in others. The rate
of communication development from 1 to 2 years was slower for children with ASD
relative to children with LI and TD in all areas of communication except between
children with ASD and LI in expressive vocabulary and use of sounds. As such, the gap
between the children with and without ASD grew over the one-year period. This is
convergent with the findings from other studies that have investigated language
development through repeated behaviour observations in younger, high-risk siblings of
children with ASD (Landa et al., 2013; Ozonoff et al., 2010) with authors from one
study describing a ‘derailment’ of skills for some children during the first few years
(Landa et al., 2013). We found in most areas of language and social communication

175
there were no significant differences between children with ASD and those with LI or
TD at 12 months of age. These findings gain cautious support from studies of high-risk
siblings that have found a lack of reliable behavioural markers for ASD prior to 12
months of age (Jones et al., 2014), as well as theories of abnormal neurodevelopment in
ASD that have proposed differences in early brain development and subsequent
unfolding of the expression of ASD symptoms that centre around social communication
(Courchesne et al., 2011; Lombardo et al., 2015).
Contrary to findings in previous studies, the majority of which have been retrospective
(Baird et al., 2008; Ozonoff et al., 2005; Pickles et al., 2009; Thurm et al., 2014), a
proportion of children in all three groups (ASD, LI and TD) in our study demonstrated
loss of some communication skills. Specific types of communication skills were more
likely to be lost by children with ASD relative to the other two groups. Compared with
both the LI and TD groups, children with ASD had higher odds of losing skills in the
area of ‘use emotion and eye contact’.
Use of eye contact has also been identified as an important domain regarding loss of
skills in 2 high-risk sibling studies (Landa & Garrett-Mayer, 2006; Ozonoff et al., 2010)
and one retrospective study (Thurm et al., 2014). Children with ASD had higher odds of
losing skills in the areas of gesture, sounds, speech and understanding relative to
children with TD but not LI. This has important implications for differential diagnosis
and for our understanding of common features that cut across neurodevelopmental
disorders such as ASD and LI. To some extent these findings are not surprising given
the neurodevelopmental and genetic overlap between such conditions (Zhu et al., 2014).

176
A further aim in this study was to assess spread of loss of skills across different
communication domains. Here a higher proportion of children with ASD lost skills
across two or more communication domains relative to children without ASD. Only one
child (2.4% of the sample of children with ASD) demonstrated a dramatic, widespread
loss of communication ability. This child went on to have a poor language outcome and
did not have adequate language to complete the CELF-4 at 4 or 7 years.
One explanation for the contrast in findings between this study and past studies
regarding loss of skills in non-ASD populations is differing methodology. This study
was the first of its kind to compare large groups of clearly defined children without
ASD across a wide spectrum of ability and demographic characteristics. Moreover, our
study used parent report collected prospectively at the time the child was exhibiting
their behaviour.
Our findings regarding loss of skills occurring in all three groups in our study could
indicate synaptic pruning during early brain development. It has been reported babies
have been found to be able to identify sounds from multiple languages between 6-8
months of age but enter a critical period from 10-12 months where they tune in to the
sounds of their own language and become less sensitive to the sounds in non-native
languages (Kuhl, 2004). There may be a degree of ‘normal’ pruning and wax and wane
in development for children without ASD, which may in part explain loss of skills in
children without ASD (Karmiloff-Smith, 2016; M. S. Thomas et al., 2016). It has been
hypothesised that children with ASD may experience over-aggressive pruning in the
first few years of life and this may go some way to explain the heterogeneity and timing
of the onset in ASD (M. S. Thomas et al., 2016; M. S. Thomas et al., 2011). This
hypothesis is convergent with findings from high-risk sibling studies that have reported

177
few behavioural markers for ASD in the first 12 months (Jones et al., 2014;.
Zwaigenbaum et al., 2013). If this is the case, it could be proposed there is a continuum
of synaptic pruning (atypical mechanism) with the more extreme forms, perhaps both
extreme over and under pruning resulting in loss of skills seen in ASD, less extreme
forms resulting in developmental variation that results in ‘good enough’ developmental
outcome or milder neurodisability and ‘normal’ levels resulting in optimal
developmental progress. Much is still to be learned regarding synaptic pruning and early
brain development. Considering this, monitoring the specific skills children with ASD
are vulnerable to losing may provide important information for diagnosis of ASD.
Furthermore, information about loss of skills may help delineate subgroups of children
with ASD. Our study provided unique insight into how ASD may differ from other
conditions. While some high-risk sibling studies include small groups of non-ASD
children they have not included clearly defined cohorts of children with LI or TD who
have retained their language profile/classification at several time points over time.
Language trajectories from 4 to 9 years of age
Receptive and expressive syntax and vocabulary
The individual trajectories of receptive and expressive language development for
children with ASD from 4 to 7 years (Study 3) were variable, but there appeared to be
more consistency and stability or consistency in the trajectories than between 1-2 years
of age (Study 2). The proportions of children who demonstrated declining, improving
and plateauing trajectories were not significantly different for children with ASD
compared with children with LI and TD. The majority of children with ASD, TD and LI
maintained the same rate of progress (within 1 standard deviation) over time in
receptive (ASD 81%, LI 76%, TD 77%) and expressive (ASD 85%, LI 79%, TD 86%)

178
language. This is consistent with other studies investigating language trajectories in
children with ASD (Ellis Weismer & Kover, 2015; Pickles et al., 2014), LI (Conti-
Ramsden et al., 2012; Law et al., 2008) and TD (Ukoumunne et al., 2012) that have
reported increasingly stable trajectories with age. This finding is also supported by the
mean receptive and expressive trajectories that were mapped from 4 to 7 years for
children with ASD, LI and TD (Study 3). Here children with ASD and LI had lower
mean scores on a comprehensive, standardised language assessment compared with the
TD group but the majority of children with ASD who had verbal language developed
language at a comparable rate to the children with TD and the gap between the groups
did not grow over time.
In the systematic review across all four language domains trajectories were parallel (or
in some studies accelerated) to reference norms. This occurred in studies where children
had received specific intensive intervention or more general intervention in the
community, and in studies that included children with and without intellectual
disability. Our community-based sample (Study 3) mapped mean trajectories over time
using a comprehensive measure of receptive and expressive language. Findings from
this study were consistent with the majority of findings from studies that had used
selected clinical samples and that had reported on receptive and expressive syntax and
vocabulary in the systematic review (Study 1). However, children in Study 3 did not
demonstrate the ‘catch up’ to reference norms demonstrated in 43-57% of studies in the
systematic review.
There are several possible explanations for this difference. First, the community sample
may have less study bias in regard to sample selection. All but one study (Vivanti et al.,
2013) that demonstrated ‘catch up’ in the systematic review used clinical samples.

179
These children may have different characteristics to population-based samples, for
example they may have more significant ASD symptoms and lower language ability
(Constantino & Todd, 2003; Posserud, Lundervold, & Gillberg, 2006). This may
produce a greater likelihood of regression to the mean or acceleration in language skills
(Tomblin et al., 2003).
Second, it has been reported that social communication ability (i.e. ASD symptoms)
may have a greater association with language ability in the early period (around time of
diagnosis) relative to a year after diagnosis (Bennett et al., 2015). It is possible children
in the clinical sample have more significant ASD symptoms at baseline and that over
time there is an ‘unyoking’ or ‘decoupling’ of the two domains that allows language to
develop in a more typical way or to ‘catch up’. In other words, social communication
difficulties have less influence on language development as children grow older.
Finally, it is also possible the children from clinical samples were accessing more
intensive interventions than children access in the general population. Study 3 did not
collect detailed information on amount of intervention received by children with ASD
so the impact of intervention could not be assessed.
Females with ASD had lower mean receptive and expressive language ability than
males in the study with less stable language trajectories. The small sample of females
(n=4) in our study, however, limits the conclusions that can be drawn about language
trajectories for females with ASD.
Adaptive language
Of the studies in the systematic review reporting on adaptive language standard scores
in children with ASD under 11 years, the vast majority demonstrated progress at an age-

180
expected rate, with one study demonstrating a significant decline in standard scores and
30% reporting some ‘catch up’ to reference norms. Overall there was a 4 unit increase
in adaptive language standard scores based on the meta-analysis. Adaptive language in
this study refers to parent report measures of communication. Adaptive language
measures do not provide the same level of detail on language ability as formal
standardised tests, however they provide an important indication of an individual’s
communicative functioning related to activity and participation. Measuring an
individual’s ability to communicate ‘enough’ to participate, even if language is
imperfect, is highly relevant and important and consistent with the International
Classification of Functioning model (de Schipper et al., 2015; World Health
Organisation, 2001). Other fields of neurodisability including lifelong conditions such
as cerebral palsy have begun re-orienting their thinking about disability toward a
strengths-based approach, emphasising the importance of factors such as function,
family, fitness, fun, friends and future, relative to the child’s ability to ‘perform’ on a
standardised test (Rosenbaum, 2015; Rosenbaum & Gorter, 2012). This will also be an
important way forward in ASD research.
Language trajectories beyond 9 years of age
Study 3 only followed children until 7 years, and the systematic review identified few
studies that investigated language development beyond 9 years of age. Studies that
follow children beyond 9 years are needed to build our knowledge of language
development across the lifespan, so we can fully understand the natural history of
language development in ASD and better predict future support needs of individuals
with ASD. This is especially important given the biggest proportion of one’s life is
spent in adulthood.

181
Our knowledge of language trajectories in children with ASD beyond nine years of age
remains limited due to the small number of studies focused on this age group. Of the
few studies (n=3) included in the review that reported findings using standardised direct
or parent-report measures at two time points after nine years, all have reported slower
rates of development relative to studies reporting on children’s development prior to
nine years, with more shallow trajectories and a widening gap between language age
relative to chronological age (Magiati et al., 2011; Pickles et al., 2014; Sigman &
McGovern, 2005).
In interpreting the findings of these studies several considerations are needed. All three
of these studies recruited participants in the late 1990s and earlier. A number of factors
have changed over time that may have influenced the characteristics of children with
ASD diagnosed today such as changes to the diagnostic criteria, improved access to
early intervention and better identification of milder cases. Whether this pattern of
slowed rate of development will occur in more recently recruited cohorts of children is
not yet known.
A number of possible explanations for the slowing of development through middle
childhood to adolescence have been proposed. One hypothesis based on evidence from
observing adaptive behaviour changes over time in children with ASD, describes a
‘two-hit’ model of ASD (Picci & Scherf, 2015). This theory describes early
perturbations in neural development in the very early years (i.e. prior to age 3) are the
first hit and suggests following this earlier disruption to neural development the system
is built to fail when children reach puberty and the ‘second hit’ occurs. Around 30% of
individuals with ASD demonstrated a marked decline in adaptive behaviour in this
study (Picci & Scherf, 2015). It is relevant to note two of the three above-mentioned

182
included studies conducted during adolescence measured adaptive communication
rather than direct assessments of receptive/expressive language. This may converge
with the findings of other studies investigating more general adaptive behaviour
trajectories (Picci & Scherf, 2015).
Slowed rates of development after 9 years of age could be also explained by several
other factors. Alternative explanations include: a reduction in the amount of support
services at this age, the complexity of language and social demands may increase during
puberty and children with ASD may struggle to cope with these additional demands,
major hormonal and brain changes that occur during puberty have the potential to
impact affective brain function and mental health (Whittle et al., 2015), there is
increased risk for depression and other mental disorders and antisocial behaviours and a
discrepancy between biological and social maturation (Patton & Viner, 2007) and these
may impact children with ASD more than children without ASD and lastly, an increase
in the onset of epilepsy has been reported during adolescence in some studies and
epilepsy is associated with brain changes (Viscidi et al., 2013).
Predictors of language outcomes
The systematic review presented in Study 1 was not designed to study predictors of
language outcomes with analysis of predictors requiring a different systematic review
and methodological approach. A substantial number of studies included in the
systematic review reported one or more predictors of language outcomes (43% of
studies), however, for a number of reasons it is difficult to integrate and interpret the
findings from these studies. A broad variety of predictors were analysed including child
characteristics, parent factors and external factors. These predictors were measured at

183
different ages, using a variety of language outcomes and analysis conducted in different
ways between studies.
Despite these differences, the most consistent finding across studies is that IQ and early
language are important predictors of later language outcome in ASD (Ellis Weismer &
Kover, 2015; Thurm et al., 2015; Toth et al., 2006). There is mixed evidence for
whether the severity of ASD symptoms is an important predictor of language outcomes
(Ellis Weismer & Kover, 2015; Thurm et al., 2007).
Rather than investigating predictors of language outcomes in children with ASD, as
described above, Study 3 in this thesis adopted a unique approach. Utilising the whole
community sample, Study 3 was able to assess the impact of a diagnosis of ASD and
social communication difficulties on receptive and expressive language outcomes for
children in a whole community cohort with and without ASD. While the samples and
methods differ between Study 3 and the aforementioned studies, the findings were
generally consistent. In Study 3 nonverbal IQ and language ability at baseline were
important predictors of language outcome. While social communication ability and
diagnosis of ASD were both univariate predictors of later language outcome, when
nonverbal IQ and language ability were included in the regression model, they were no
longer significant.
All children in Study 3 were verbal with IQ>70. This is an important consideration for
interpreting findings. Some authors have suggested different predictors may be
differentially important at specific ages and language ability levels (Toth et al., 2006). It
would be reasonable to hypothesise that social communication abilities (e.g., joint
attention) at age 4 may be more relevant as a predictor for future language for children

184
who have intellectual disability, limited language ability or more significant social
communication difficulties. This is supported by another study, which found weaker
associations between language and social communication in children with ASD with
age (Bennett et al., 2015).
Prediction studies don’t always assist in assessing risk for individuals unless large
sample sizes are used and there is a clear understanding of expected progress with and
without risk factors. A future systematic review with a focus on already identified
predictors of language outcome will now be possible. A better understanding of how
predictors of outcomes may influence outcome and interact will inform the type and
timing of intervention as well as refine prognostic predictions.
Expressive and receptive language discrepancy
In Study 3 we investigated whether a diagnosis of ASD predicted a larger receptive-
expressive gap relative to children without ASD. There was substantial variability in the
difference between receptive-expressive language scores in both directions for children
with and without ASD but children with ASD were no more likely than other children
to have a gap between these language domains. A diagnosis of ASD did not predict a
larger gap between receptive and expressive language for verbal children.
There has been mixed evidence about whether having weaker receptive relative to
expressive language may be hallmark of ASD with some authors finding a discrepancy
(Ellis Weismer & Kover, 2015; Hudry et al., 2010; Pickles et al., 2014) and others not
finding a discrepancy, once other factors such as IQ are taken into account, although
slower progression in receptive relative to expressive vocabulary over time was noted

185
(Kover et al., 2013). A systematic review did not find children with ASD were more
likely to demonstrate a discrepancy between receptive and expressive language (Kwok
et al., 2015).
A limitation of previous studies in this area is a lack of large, well characterised samples
of children without ASD for comparison. Furthermore, most studies have used parent
report tools (Hudry et al., 2010) or subscales of more general developmental assessment
tools (Barbaro & Dissanayake, 2012). To our knowledge only one study prior to ours
used a standardised comprehensive language assessment of children with ASD over
multiple time points (Ellis Weismer & Kover, 2015).
Children with ASD who are minimally verbal
The systematic review (Study 1) included studies that reported on the proportion of
children who were nonverbal or verbal at baseline and outcome. There was substantial
variability in outcomes but all studies reported the proportion of children who were
verbal increased over time. Approximately 19-30% of those who were under 6 years
and nonverbal gained verbal language and 5-32% of those who were over 6 years and
nonverbal gained verbal language. Adult studies reported between 91-95% were verbal
at outcome, although most of these studies included individuals with IQ>70.
In study 3 we found (n=3) 10% of children with ASD at 4 years and 6% (n=2) at 7 years
of age did not have adequate language ability to complete direct assessments of
language on the CELF. One of the children who was minimally verbal at 7 years had
intellectual disability (nonverbal (NV) IQ 55) and one did not (NVIQ 77). Language
ability and IQ can be closely linked and nonverbal IQ can assist with understanding a

186
child’s developmental profile but the limited description of language ability in these
children prevents us from drawing conclusions about their language development.
Ideally, these children would be tested using an assessment tool that is more appropriate
for their language ability so a clear picture of change in language over time could be
described (Kasari et al., 2013; Tager-Flusberg et al., 2016)
It has been hypothesised that rate of language development may be slower in children
with poorer language ability than those with better verbal ability (Ellis Weismer &
Kover, 2015; Tek et al., 2014). Our study did not contain adequate sample sizes or
appropriate measures to test this hypothesis and add further clarity. Children with ASD
who are minimally verbal have long been a group of children neglected in the literature
and are often excluded from studies (Tager-Flusberg & Kasari, 2013). Language
measures for these children have traditionally been very broad (e.g., whether an
individual can use words) and this prevents us from gaining a nuanced account of how
language changes over time in these children. Crucially, children with severe language
impairments are the most likely to have the poorest outcomes in a range of areas
(Billstedt et al., 2007; Howlin, 2011)
A focus on children who are minimally verbal has been pursued in the past five years
with the development of the National Institutes of Health special workshop for school-
aged children with ASD who are minimally verbal (National Institute of Health, 2010).
Evidence-based recommendations regarding assessment and conducting research for
this group of children have now been published (Kasari et al., 2014; Plesa Skwerer,
Jordan, Brukilacchio, & Tager-Flusberg, 2016; Tager-Flusberg et al., 2016). Further
detail on these children will allow more accurate prognostication and may guide the
development of novel and alternative approaches for intervention.

187
Strengths and Limitations
Methodology
The methodology used in Study 2 and 3 of this thesis is distinct and adds to the current
literature in several ways. First, it used very early measures of communication
development collected prospectively in a representative community sample prior to a
diagnosis of ASD. The vast majority of studies that have investigated early language
development in ASD include high-risk younger siblings of children with ASD or are
retrospective in design. In comparison to high-risk sibling studies, the current study
included children with and without a family history of ASD. As such the study is not
prone to the same sampling bias as high-risk sibling studies.
The limitations of the high-risk sibling study design have been highlighted by several
authors (Barbaro & Dissanayake, 2012; Zwaigenbaum et al., 2007) for example, it has
been argued the phenotypes of children with and without a family history of ASD may
differ (L. J. Taylor et al., 2015). Second, previous studies (with one exception, Thurm et
al., 2014) have typically described regression or loss of skills categorically (e.g.,
regression/no regression, late onset/early onset/plateau; (Baird et al., 2008; Landa et al.,
2013; Ozonoff et al., 2011; Shumway et al., 2011).
Our study was able to investigate loss and gain of skills at an individual skill level. As
such, it compared types of communication skills lost relative to others over the one-year
period. Third, large samples of clearly defined children with LI and TD allowed us to
examine whether loss of skills was unique to children with ASD and to place language
development in ASD within a developmental context. Finally, the vast majority of

188
studies of children with ASD have used selected clinical samples. These studies
typically provide detailed descriptions of children with ASD, however there is evidence
that they tend to recruit children at the more severe end of the spectrum. Our
community-based study recruited children with ASD across a range of ability as
evidenced by the individual trajectory plots in Study 2 and 3.
The current study had large well-defined samples of children without ASD within the
same cohort for comparison. This enabled a better understanding of what was unique to
language development in ASD and what was common across two other populations (LI
and TD). To our knowledge, no other study of language development in ASD has
compared children with ASD to such large samples of children without ASD. The large
cohort of children in the ELVS with the same language measures allowed us to examine
whether a diagnosis of ASD itself predicts language ability and whether children with
ASD are more likely to have a receptive-expressive language discrepancy.
A major strength of Study 1 is that we conducted risk of bias assessments of studies so
study quality could be assessed along with findings. We also combined findings from
language domains that contained five or more studies into meta-analyses and presented
data to show change over time. This allows for an overall summary of findings and is
clinically meaningful and interpretable to clinicians and families. Information on IQ was
described. This will assist clinicians and parents tailor prognostic information for
individuals based on these broad characteristics and their age.
Limitations of the systematic review (Study 1) include the potential for reporting bias as
we were not able to extract data from all included studies. To aid clinical interpretation
of the highly variable methodology used in studies we compared the children’s

189
development to that expected based on standard scores from the normed population
(reference norms) or age-equivalents. Ideally studies would include non-ASD
populations in same cohort followed over time for comparison, as done in Study 2 and
3.
The definition of ‘nonverbal’ or ‘minimally verbal’ in the systematic review was quite
blunt due to the wide variety of ways in which studies reported verbal abilities in
children. The difference between a child who is completely nonverbal and one who uses
10 words may be clinically significant both in terms of the child’s functioning and
prognosis and may dictate an alternate intervention approach. The complexity in finding
consensus for the terminology used to describe minimally verbal individuals has been
emphasized by several authors (Norrelgen et al., 2014; Rose et al., 2016; Tager-
Flusberg & Kasari, 2013).
The systematic review was only able to report mean scores for a whole cohort and mean
scores do not provide the full picture of individual variation in language trajectories.
Due to the way data were provided by studies (cohort rather than individual participant
data) we could only report mean scores and confidence intervals (when able to be
calculated). Data were presented as mean scores in graphical form as trajectories to aid
clinical translation. These were not actual trajectories provided by studies but cross
sectional time points at baseline and follow up. As a result, we do not know the actual
shape of trajectories between these two time points. Furthermore, we have used meta-
analysis when more than 5 or more studies reported data. There was substantial
heterogeneity in studies, which limits the robustness and validity of the meta-analysis
findings.

190
There is potential for reporting bias in the systematic review around the ways studies
presented data. Studies of children who have more severe disabilities may be more
likely to report age-equivalents or raw scores because it can be challenging to obtain
valid standard scores for these children due to floor effects of tools. It was difficult to
compare the results from studies presenting data in these alternate forms to what is
expected for age, as we cannot establish with certainty whether children demonstrated
significant change or a variation that was within the normal range. It is possible that by
focusing more heavily on standard scores we are including a higher proportion of
studies where children had more positive outcomes.
Sample
Studies 2 and 3 drew participants from a broad community base, systematically
designed to include a range of socioeconomic advantage/disadvantage. The prevalence
of ASD in the ELVS sample (2.3%) and proportion of males to females (82%) is
consistent with prevalence estimates from another population-based study in Victoria
(prevalence: 1.5-2.5% and males: 81.2-83.6%) (Randall et al., 2015) and does appear to
representative of the broader population of children with ASD aged under 7 years of age
in Victoria. A future aim would be to update our findings for children diagnosed with
ASD by 11 years, the next planned wave of the ELVS.
This community-based approach brings methodological strengths, such as being more
easily generalizable and providing insight into the history of ASD across a broad
spectrum of severity. There are however, limitations to the approach that need to be
acknowledged.

191
One of the exclusion criteria for entry to the ELVS was a known developmental
disorder or medical condition. Although the likely number of such children identifiable
during infancy would be small, ELVS data may not be representative of all children
with ASD, particularly those with intellectual disability or genetic conditions known to
be associated with ASD.
Furthermore, the language trajectories described in Study 3 did not include any children
with intellectual disability. All children had an IQ>70. There were a small number of
children in our sample who did not have the required level of language to complete the
CELF assessment so we cannot comment definitively on how language changed over
time for these children. The small sample of children with ASD in the trajectory
analysis from 4 to 7 years (n=26-27 for all analyses) limits statistical power to detect
differences and our ability to create meaningful subgroups based on trajectory type or
language phenotype. The limitations of our sample need be acknowledged when
generalising to minimally verbal children, as well as to those children with
comorbidities such as intellectual disability (specifically, nonverbal IQ that is 2 standard
deviations below the mean) and known genetic disorders.
Lastly, Study 3 followed children until 7 years of age. Although we expect the number
of children to be diagnosed after the age of 7 to be small, some individuals identified as
TD or LI may later receive an ASD diagnosis.
Measures
The measures used in Study 2 and 3 and information collected on the phenotypes of
children with ASD may be less detailed and standardised than a study specifically
192
designed to follow children diagnosed with ASD. For example, although 93% of the
children in our study were diagnosed with ASD by a multidisciplinary team (i.e.
including two or more relevant health professionals), children in the study did not have
uniform diagnostic assessments.
Two of our measures to assess early communication skills in Study 2 were parent
report. Although parent-report can have advantages such as being able to capture the
children’s communication ability across natural environments by those who know the
child best, this method may add misclassification bias if parents are not accurate
reporters.
Our definition of ‘loss of skills’ as lower raw scores at 24 than 12 months and one
standard deviation on standard scores for declining, improving or stable trajectories
from 4 to 7 years was informed by the current literature but was necessarily arbitrary.
To date there is no well-recognised gold standard ways of measuring loss or gain in
skills or what a ‘clinically significant’ increase or decrease in standard score might be.
We hope clear definitions used for loss of skills will be useful for future studies and
allow replication and/or comparison.
Another consequence of using a community-based study is that measures were limited
to predetermined study waves rather than time periods that may be more relevant to
ASD. More frequent assessments in early toddlerhood using the CDI and CSBS-ITC
measures (e.g., at 18 months) would have provided valuable information regarding the
loss and gain in language during this sensitive period when loss of skills is most likely
to occur.

193
A strength of Study 3 was that we had direct assessments of language using a detailed,
comprehensive, standardised language tool. The vast majority of studies that have
assessed language ability over time in children with ASD have used parent-completed
checklists about communication more generally (e.g., the Vineland Adaptive Behaviour
Scales) or subscales within more general assessment tools (e.g., language subscales
within the Mullen Scale of Early Learning). By using the CELF we were also able to
investigate receptive and expressive language separately over time. This is especially
important given the debate about relative weakness in receptive language for children
with ASD in the literature. A potential limitation was that the trajectories from 4 to 7
years were mapped using different versions of the CELF (CELF P2 and CELF 4). It is
possible that each version taps into different aspects of language ability and this may
affect our interpretation of change over time. However, to test this theory we compared
mean scores for the sample at 4, 5, 7 years (see Chapter 6). Mean scores and standard
deviations were commensurate across versions of the tool for the whole cohort.
Loss to follow up
We assessed whether children with more severe forms of ASD or intellectual disability
were more likely to be lost to follow up. This could occur if assessments are challenging
or unsuitable for them. Similarly, there may be demographic characteristics of children
who do not complete all assessments that are different to children who do complete
them. We compared the children included in the mapped trajectories (n=28) to those
who remained in the study but whose trajectories were not mapped (n=12). There were
no significant differences in any of the demographic factors measured or expressive
vocabulary when children were 2 years old (see Chapter 6). The included children
achieved a higher mean nonverbal IQ score at 7 years (M 99.71; SD 14.35; CI 94.39-

194
105.03) than the children who did not have their trajectories mapped (M 82.71; SD
21.06; CI 67.11-98.31) but the difference in scores did not reach statistical significance
(p=0.08). We provided a detailed description of demographics, cognitive and language
levels for each group to allow comparison to the findings of future studies.
Clinical implications
Understanding how language develops throughout childhood in ASD is important for
several reasons. First, parents understandably want to know what their child’s likely
future will look like and what to expect over the coming years. This will help them plan
and prioritise interventions and the services needed to assist them. Service providers and
policy makers require information on language prognosis so they can allocate
intervention and support resources in the most efficient way. Second, a better
understanding of the factors that contribute to better or worse language outcomes will
help tailor and focus interventions. Knowledge about natural development in ASD
could also provide clues as to the impact of interventions. Lastly, it is well established
that language ability in childhood is one of the most important predictors of later
outcomes in a range of areas such as employment, relationships, mental health and
quality of life (Howlin et al., 2004; Mawhood & Howlin, 2000) Importantly, restricted
language skills impact one’s ability to function and participate fully in the community.
The findings from this thesis have immediate clinical utility and will better inform the
answers clinicians provide parents when they ask about their child’s likely language
future. We can inform parents and clinicians that based on the findings from the
systematic review, while there is substantial variability in language trajectories, on
average children with ASD have delayed language relative to typically developing

195
children. On average, most children with ASD improve in their language abilities and
track at a similar pace to children without ASD between 2 to 9 years with a proportion
of those children (around 30-50%) demonstrating accelerated language development.
This has been reported to occur across a range of language domains such as receptive
and expressive syntax and vocabulary and adaptive language. Based on the findings of
this thesis and previous literature, language ability and IQ at age 4 are more important
in predicting a child’s language outcome than factors such as social communication
ability and a diagnosis of ASD. This has important implications of for the timing and
type of intervention for children at 4 years, which is the average age of ASD diagnosis
in Australia for those children under 7 diagnosed (Bent et al., 2015).
For families of children who are minimally verbal, we can provide parents with specific
information regarding the proportion of children who do develop verbal language over
time. For example, in children who are minimally verbal and under 6 years, 19-30%
will gain verbal language and for those aged over 6 years 5-32% will gain verbal
language if over 6 years. Around 91-95% of adults are reported to be verbal. This is
highly relevant and meaningful information for parents.
Communication trajectories from one to two years were highly variable for children
with and without ASD. This is important information to consider if making a diagnosis
of ASD at an early age. The slowing of development from 1 to 2 years of age and loss
of skills will not always indicate a child has ASD since a proportion of children without
ASD also experienced loss of skills. Providing inaccurate diagnoses of ASD for
children who are demonstrating an atypical developmental pathways can have important
social and economic costs and these costs need to be considered when making a
diagnosis at a very young age. However, atypical development does indicate the need

196
for close monitoring of development. Children with ASD who present with catastrophic
loss of skills across a range of communication areas, although rare in our study, are
likely to warrant an alternate care pathway and medical investigations. These children
may be a subgroup of ASD or a distinct neurodevelopmental group.
Our study highlighted convergence and difference in communicative development in
children with and without ASD. This has implications for the differential diagnosis. For
example, it was found that expressive language and speech sound development were
comparable for children with LI and ASD but different to children with TD. We also
found children with ASD were no more likely to have weakness in receptive language
relative to expressive language. The findings from our study and others (e.g., Kwok et
al., 2015) were not consistent with previous reports (Ellis Weismer & Kover, 2015;
Hudry et al., 2010) and suggest receptive-expressive language discrepancy may not be a
reliable or important behavioural marker for differential diagnosis of ASD, as has
previously been suggested. Understanding differences between clinical groups and
typically developing children informs our knowledge about how language develops and
may contribute to a greater understanding of some of the neurobiological mechanisms
and pathways at play that may influence development.

197
Future directions
Improved methods for prognosis studies
Most studies on language outcomes identified by the systematic review were of medium
to high risk of bias. Well-designed prognosis studies that use consistent methods and
tools and are based on best practice methods for prognosis studies guidelines are needed
(Hayden et al., 2013).
Gaps in the literature
Study 1 identified four gaps in the literature. First, there was a dearth of studies
identified by the review that followed children from nine years of age into adulthood.
As a result, our knowledge of how language develops over this period is limited. The
studies focused on this age group included children who were diagnosed up to 20 years
ago and these children may not be representative of the children diagnosed with ASD
today. Studies that monitor change in language after 9 years of age are needed.
Comprehensive standardised tools also need to be developed that allow language
change to be monitored over broad periods of time and that are appropriate for a wide
range of ability and ages so trajectories of all children across the spectrum of language
ability can be well described.
Second, most studies in the systematic review provide only categorical descriptions of
children with ASD who are minimally verbal (i.e. they change from being nonverbal to
verbal or remain nonverbal). Little detail has been provided about the communication
ability of these children, including their functional communication and use of
augmentative or alternative communication. We do not yet fully understand how

198
communication develops in these children or why they seem to be less responsive to
mainstream ASD interventions than verbal children (Kasari et al., 2014; Paul et al.,
2013).
Several authors have underlined the challenge of accurately assessing and characterising
communication development in children who are minimally verbal (Norrelgen et al.,
2014; Rose et al., 2016; Tager-Flusberg & Kasari, 2013), however, encouragingly
guidelines are now being developed for the assessment of minimally verbal children
with ASD (Kasari et al., 2013; Plesa Skwerer et al., 2016). High quality assessments
tailored to the child’s language ability are crucial if we are to develop accurate,
personalised prognostic information about these children. Subgrouping children by
language profile is similarly important given preliminary evidence children with poorer
verbal ability may have different trajectories to those with relatively stronger language
ability (Ellis Weismer & Kover, 2015; Tek et al., 2014).
Third, although almost half of the studies included in the systematic review analysed
predictors of language there was methodological variability including; age groups
studied, types of children included, types of predictors and outcome measures. A
systematic review of studies investigating predictors of language outcome would
complement the trajectory findings in this thesis and provide valuable information about
intervention targets. Such information will also help move us toward the ultimate goal
which is more accurate, personalised prognostication based on an individual’s specific
characteristics.
Fourth, our study identified a lack of studies that used groups of children without ASD
from the same cohort for comparison. In order for us to place language development in

199
ASD within the context of language development more generally and to identify what is
unique to ASD and what is common across conditions such groups are vital.
New frontiers
Given the pivotal interactions between genes, the brain, and behaviour throughout early
development it is not surprising neurodevelopmental disabilities such as ASD are so
heterogeneous. A complete explanatory framework of ASD, especially its onset,
subsequent trajectories of development and co-occurring conditions such as language
impairment will need to cross disciplines as well as cut across populations (e.g.,
conditions with similar features and children with typical development). Ongoing work
that monitors and tests current theories about early development in ASD, including loss
of skills language development in ASD are needed but we must also be prepared to
approach ASD in novel ways. This will require pushing away from diagnostic
constraints toward a dimensional approach of the types of difficulties and behaviours
seen in ASD (Cuthbert & Insel, 2013).
Concluding remarks
This thesis provides a unique contribution to our understanding of how language
develops in ASD. It is the first work, to our knowledge, to use large samples of children
with LI and TD for comparison and the first to use a community sample to study
language development using comprehensive standardised tools. In this study,
divergence in trajectory was noted between children with ASD and other children in
most areas of communication between 1 to 2 years. From 2 years even though the
children with ASD had lower scores than expected for their age they appear to develop

200
at a similar pace to reference norms. From 9 years of age there are some preliminary
indications that children experience another divergence in trajectory and rate of
development slows. Characterising relative strengths and weaknesses in language
development will help delineate the neurocognitive phenotype in ASD. It will also assist
with subgrouping. Ultimately it will contribute towards our knowledge of how genes,
the brain and other factors interact to influence development and behaviour in early and
later life.

201
Bibliography
American Psychiatric Association. (1980). Diagnostic and Statistical Manual of Mental Disorders (3rd edition-text revision). Washington, DC: American Psychiatric Publishing.
American Psychiatric Association. (2000). Diagnostic and Statistical Manual of Mental Disorders (4th edition-text revision). Washington, DC: American Psychiatric Publishing.
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (edition 5). Arlington, VA: American Psychiatric Association.
Anderson, D. K., Liang, J. W., & Lord, C. (2014). Predicting young adult outcome among more and less cognitively able individuals with autism spectrum disorders. Journal of Child Psychology and Psychiatry and Allied Disciplines, 55(5), 485-494. doi: http://dx.doi.org/10.1111/jcpp.12178
Anderson, D. K., Lord, C., Risi, S., DiLavore, P. S., Shulman, C., Thurm, A., . . . Pickles, A. (2007). Patterns of growth in verbal abilities among children with autism spectrum disorder. Journal of Consulting and Clinical Psychology, 75(4), 594-604.
Anderson, D. K., Oti, R. S., Lord, C., & Welch, K. (2009). Patterns of growth in adaptive social abilities among children with autism spectrum disorders. Journal of Abnormal Child Psychology, 37(7), 1019-1034.
Baghdadli, A., Assouline, B., Sonie, S., Pernon, E., Darrou, C., Michelon, C., . . . Pry, R. (2012). Developmental trajectories of adaptive behaviors from early childhood to adolescence in a cohort of 152 children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 42(7), 1314-1325. doi: http://dx.doi.org/10.1007/s10803-011-1357-z
Bagley, C., & McGeein, V. (1989). The taxonomy and course of childhood autism. Perceptual & Motor Skills, 69(3 Pt 2), 1264-1266.
Baird, G., Charman, T., Pickles, A., Chandler, S., Loucas, T., Meldrum, D., . . . Simonoff, E. (2008). Regression, developmental trajectory and associated problems in disorders in the autism spectrum: The SNAP study. Journal of Autism and Developmental Disorders, 38(10), 1827-1836. doi: 10.1007/s10803-008-0571-9
Bal, V. H., Kim, S. H., Cheong, D., & Lord, C. (2015). Daily living skills in individuals with autism spectrum disorder from 2 to 21 years of age. Autism, 19(7), 774-784. doi: http://dx.doi.org/10.1177/1362361315575840
Ballaban-Gil, K., Rapin, I., Tuchman, R., & Shinnar, S. (1996). Longitudinal examination of the behavioral, language, and social changes in a population of adolescents and young adults with autistic disorder. Pediatric Neurology, 15(3), 217-223.
Barbaro, J., & Dissanayake, C. (2012). Developmental profiles of infants and toddlers with autism spectrum disorders identified prospectively in a community-based setting. Journal of Autism and Developmental Disorders, 42(9), 1939-1948. doi: http://dx.doi.org/10.1007/s10803-012-1441-z
Barger, B. D., Campbell, J. M., & McDonough, J. D. (2013). Prevalence and onset of regression within autism spectrum disorders: A meta-analytic review. Journal of Autism and Developmental Disorders, 43(4), 817-828.

202
Baron-Cohen, S., Campbell, R., Karmiloff-Smith, A., Grant, J., & Walker, J. (1995). Are children with autism blind to the mentalistic significance of the eyes? British Journal of Developmental Psychology, 13(4), 379-398. doi: 10.1111/j.2044-835X.1995.tb00687.x
Baron-Cohen, S., Lombardo, M. V., Auyeung, B., Ashwin, E., Chakrabarti, B., & Knickmeyer, R. (2011). Why are autism spectrum conditions more prevalent in males? PLoS Biol, 9(6), e1001081. doi: 10.1371/journal.pbio.1001081
Bates, E., Benigni, L., Bretherton, I., Camaioni, L., & Volterra, V. (1979). The Emergence of Symbols: Cognition and Communication in Infancy. New York, NY: Academic Press Inc.
Bedford, R., Pickles, A., & Lord, C. (2015). Early gross motor skills predict the subsequent development of language in children with autism spectrum disorder. Autism Research, 9(9), 993-1001.
Beeghly, M. (2006). Translational research on early language development: current challenges and future directions. Development and Psychopathology, 18(03), 737-757.
Beitchman, J., Brownlie, E., Inglis, A., Wild, J., Ferguson, B., Schachter, D., . . . Mathews, R. (1996). Seven‐year follow‐up of speech/language impaired and control children: psychiatric outcome. Journal of Child Psychology and Psychiatry, 37(8), 961-970.
Ben-Itzchak, E., Watson, L., & Zachor, D. (2014). Cognitive ability is associated with different outcome trajectories in autism spectrum disorders. Journal of Autism and Developmental Disorders, 44(9), 2221-2229. doi: 10.1007/s10803-014-2091-0
Ben Itzchak, E., & Zachor, D. A. (2009). Change in autism classification with early intervention: predictors and outcomes. Research in Autism Spectrum Disorders, 3(4), 967-976. doi: http://dx.doi.org/10.1016/j.rasd.2009.05.001
Ben Itzchak, E., & Zachor, D. A. (2011). Who benefits from early intervention in autism spectrum disorders? Research in Autism Spectrum Disorders, 5(1), 345-350. doi: 10.1016/j.rasd.2010.04.018
Bennett, T. A., Szatmari, P., Bryson, S., Duku, E., Vaccarella, L., & Tuff, L. (2013). Theory of mind, language and adaptive functioning in ASD: a neuroconstructivist perspective. Journal of the Canadian Academy of Child and Adolescent Psychiatry, 22(1), 13-19.
Bennett, T. A., Szatmari, P., Bryson, S., Volden, J., Zwaigenbaum, L., Vaccarella, L., . . . Boyle, M. (2008). Differentiating autism and Asperger syndrome on the basis of language delay or impairment. Journal of Autism and Developmental Disorders, 38(4), 616-625. doi: 10.1007/s10803-007-0428-7
Bennett, T. A., Szatmari, P., Georgiades, K., Hanna, S., Janus, M., Georgiades, S., . . . Thompson, A. (2014). Language impairment and early social competence in preschoolers with autism spectrum disorders: A comparison of DSM-5 profiles. Journal of Autism & Developmental Disorders, 44(11), 2797-2808. doi: 10.1007/s10803-014-2138-2
Bennett, T. A., Szatmari, P., Georgiades, K., Hanna, S., Janus, M., Georgiades, S., . . . Thompson, A. (2015). Do reciprocal associations exist between social and language pathways in preschoolers with autism spectrum disorders? Journal of Child Psychology and Psychiatry, 56(8), 874-883. doi: 10.1111/jcpp.12356

203
Bent, C. A., Dissanayake, C., & Barbara, J. (2015). Mapping the diagnosis of autism spectrum disorders in children aged under 7 years in Australia, 2010-2012. Medical Journal of Australia, 202(6), 317-320.
Berry, L. N. (2010). Early treatments associated with optimal outcome in children with autism spectrum disorders. (Doctor of Philosophy), University of Connecticut, Storrs, Connecticut, US. Retrieved from http://search.ebscohost.com/login.aspx?direct=true&db=psyh&AN=2010-99060-184&site=ehost-live Available from EBSCOhost psyh database.
Billstedt, E., Gillberg, I. C., & Gillberg, C. (2007). Autism in adults: symptom patterns and early childhood predictors. Use of the DISCO in a community sample followed from childhood. Journal of Child Psychology and Psychiatry, 48(11), 1102-1110.
Billstedt, E., Gillberg, I. C., & Gillberg, C. (2011). Aspects of quality of life in adults diagnosed with autism in childhood: a population-based study. Autism, 15(1), 7-20.
Bishop, D. V. M. (1997). Cognitive neuropsychology and developmental disorders: Uncomfortable bedfellows. Quarterly Journal of Experimental Psychology: Section A, 50(4), 899-923. doi: 10.1080/027249897391946
Bishop, D. V. M. (2003). Autism and specific language impairment: categorical distinction or continuum? Novartis Foundation Symposium, 251, 213-234.
Bishop, D. V. M. (2010). Overlaps between autism and language impairment: phenomimicry or shared etiology? Behavior Genetics, 40(5), 618-629.
Bishop, D. V. M., & Edmundson, A. (1987). Language-impaired 4-year-olds: distinguishing transient from persistent impairment. Journal of speech and hearing disorders, 52(2), 156-173.
Bishop, D. V. M., Snowling, M. J., Thompson, P. A., & Greenhalgh, T. (2016). CATALISE: a multinational and multidisciplinary Delphi consensus study of problems with language development. Phase 2. Terminology. PeerJ Preprints, 4, e2484v2481. doi: 10.7287/peerj.preprints.2484v1
Bishop, D. V. M., Snowling, M. J., Thompson, P. A., Greenhalgh, T., & consortium, C. (2016). CATALISE: A multinational and multidisciplinary Delphi consensus study. Identifying language impairments in children. PloS one, 11(7), e0158753. doi: 10.1371/journal.pone.0158753
Blacklock, K., Perry, A., & Dunn Geier, J. (2014). Examining the effectiveness of Intensive Behavioural Intervention in children with autism aged 6 and older. Journal on Developmental Disabilities, 20(1), 37-49.
Bolton, P. F., Golding, J., Emond, A., & Steer, C. D. (2012). Autism spectrum disorder and autistic traits in the Avon Longitudinal Study of Parents and Children: Precursors and early signs. Journal of the American Academy of Child and Adolescent Psychiatry, 51(3), 249-260. doi: 10.1016/j.jaac.2011.12.009
Bopp, K. D. (2006). Behaviour predictors of child development and and parenting stress trajectories of children with autism. (Doctor of Philosophy), The Univerity of British Columbia, Vancouver, British Columbia, Canada.
Bopp, K. D., & Mirenda, P. (2011). Prelinguistic predictors of language development in children with autism spectrum disorders over four-five years. Journal of Child Language, 38(3), 485-503.
Bopp, K. D., Mirenda, P., & Zumbo, B. D. (2009). Behavior predictors of language development over 2 years in children with autism spectrum disorders. Journal of

204
Speech, Language, and Hearing Research, 52(5), 1106-1120. doi: 10.1044/1092-4388(2009/07-0262)
Boucher, J. (2012). Research Review: Structural language in autistic spectrum disorder-characteristics and causes. Journal of Child Psychology and Psychiatry, 53(3), 219-233.
Brignell, A., Morgan, A. T., Woolfenden, S., & Williams, K. (2014). How relevant is the framework being used with autism spectrum disorders today? International Journal of Speech-Language Pathology, 16(1), 43-49. doi: 10.3109/17549507.2013.861870
Brignell, A., Williams, K., Prior, M., Donath, S., Reilly, S., Bavin, E. L., . . . Morgan, A. T. (2016). Parent-reported patterns of loss and gain in communication in 1- to 2-year-old children are not unique to autism spectrum disorder. Autism. doi: 10.1177/1362361316644729
Brooks, R., & Meltzoff, A. N. (2008). Infant gaze following and pointing predict accelerated vocabulary growth through two years of age: a longitudinal, growth curve modeling study. Journal of Child Language, 35(1), 207-220. doi: http://dx.doi.org/10.1017/S030500090700829X
Brunsdon, V. E., Colvert, E., Ames, C., Garnett, T., Gillan, N., Hallett, V., . . . Happe, F. (2015). Exploring the cognitive features in children with autism spectrum disorder, their co-twins, and typically developing children within a population-based sample. Journal of Child Psychology and Psychiatry, 56(8), 893-902. doi: 10.1111/jcpp.12362
Brunsdon, V. E., & Happe, F. (2014). Exploring the 'fractionation' of autism at the cognitive level. Autism, 18(1), 17-30. doi: 10.1177/1362361313499456
Bryson, S. E., Zwaigenbaum, L., Brian, J., Roberts, W., Szatmari, P., Rombough, V., & McDermott, C. (2007). A prospective case series of high-risk infants who developed autism. Journal of Autism and Developmental Disorders, 37(1), 12-24.
Buxbaum, J. D., & Baron-Cohen, S. (2013). DSM-5: the debate continues. Molecular Autism, 4, 11-11. doi: 10.1186/2040-2392-4-11
Carbonnel-Chabas, C., & Gepner, B. (2009). The future for children affected by pervasive developmental disorders: The example of the day care unit of Aix-en-Provence. Neuropsychiatrie de l'Enfance et de l'Adolescence, 57(2), 118-127. doi: http://dx.doi.org/10.1016/j.neurenf.2008.09.008
Carpenter, M., & Nagell, K. (1998). Social cognition, joint attention, and communicative competence from 9 to 15 months of age. Monographs of the Society for Research in Child Development, 63(4), 1-143.
Carpenter, M., Pennington, B. F., & Rogers, S. J. (2002). Interrelations among social-cognitive skills in young children with autism. Journal of Autism and Developmental Disorders, 32(2), 91-106.
Carson, C. P., Klee, T., Carson, D. K., & Hime, L. K. (2003). Phonological profiles of 2-year-olds with delayed language development: predicting clinical outcomes at age 3. American Journal of Speech Language Pathology, 12(1), 28-39. doi: 10.1044/1058-0360(2003/050)
Cederlund, M., Hagberg, B., Billstedt, E., Gillberg, I. C., & Gillberg, C. (2008). Asperger syndrome and autism: a comparative longitudinal follow-up study more than 5 years after original diagnosis. Journal of Autism and Developmental Disorders, 38(1), 72-85.

205
Centers for Disease Control and Prevention. (2014). Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years — Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2010 Morbidity and Mortality Weekly Report (Vol. 63, pp. 1-21). GA: US: U.S. Department of Health and Human Service.
Chakrabarti, S., & Fombonne, E. (2001). Pervasive developmental disorders in preschool children. Journal of the American Medical Association, 285(24), 3093-3099.
Charman, T., Baird, G., Simonoff, E., Loucas, T., Chandler, S., Meldrum, D., & Pickles, A. (2007). Efficacy of three screening instruments in the identification of autistic-spectrum disorders. The British Journal of Psychiatry, 191(6), 554-559. doi: 10.1192/bjp.bp.107.040196
Charman, T., Baron-Cohen, S., Swettenham, J., Baird, G., Cox, A., & Drew, A. (2000). Testing joint attention, imitation, and play as infancy precursors to language and theory of mind. Cognitive Development, 15(4), 481-498. doi: http://dx.doi.org/10.1016/S0885-2014(01)00037-5
Charman, T., Baron-Cohen, S., Swettenham, J., Baird, G., Drew, A., & Cox, A. (2003). Predicting language outcome in infants with autism and pervasive developmental disorder. International Journal of Language and Communication Disorders, 38(3), 265-285.
Charman, T., Drew, A., Baird, C., & Baird, G. (2003). Measuring early language development in preschool children with autism spectrum disorder using the MacArthur Communicative Development Inventory (Infant Form). Journal of Child Language, 30(1), 213-236.
Charman, T., Taylor, E., Drew, A., Cockerill, H., Brown, J.-A., & Baird, G. (2005). Outcome at 7 years of children diagnosed with autism at age 2: predictive validity of assessments conducted at 2 and 3 years of age and pattern of symptom change over time. Journal of Child Psychology and Psychiatry, 46(5), 500-513. doi: 10.1111/j.1469-7610.2004.00377.x
Chaste, P., & Leboyer, M. (2012). Autism risk factors: genes, environment, and gene-environment interactions. Dialogues in Clinical Neuroscience, 14(3), 281-292.
Chawarska, K. (2016). Regression in autism spectrum disorders. Paper presented at the Loss of Skills and Onset Patterns in Neurodevelopment Disorders: Understanding the Neurobological Mechanisms Workshop, Bethesda, Maryland. https://videocast.nih.gov/Summary.asp?File=19500&bhcp=1
Chawarska, K., Klin, A., Paul, R., Macari, S., & Volkmar, F. (2009). A prospective study of toddlers with ASD: short-term diagnostic and cognitive outcomes. Journal of Child Psychology and Psychiatry and Allied Disciplines, 50(10), 1235-1245.
Chiat, S., & Roy, P. (2008). Early phonological and sociocognitive skills as predictors of later language and social communication outcomes. Journal of Child Psychology and Psychiatry, 49(6), 635-645. doi: 10.1111/j.1469-7610.2008.01881.x
Ciuladaite, Z., Kasnauskiene, J., Cimbalistiene, L., Preiksaitiene, E., Patsalis, P. C., & Kucinskas, V. (2011). Mental retardation and autism associated with recurrent 16p11.2 microdeletion: incomplete penetrance and variable expressivity. Journal of Appled Genetics, 52(4), 443-449. doi: 10.1007/s13353-011-0063-z

206
Cole, K. N., Schwartz, I. S., Notari, A. R., Dale, P. S., & Mills, P. E. (1995). Examination of the stability of two methods of defining specific language impairment. Applied Psycholinguistics, 16(01), 103-124.
Connolly, M., Mackay, T., & Boyle, J. (2016). Intellectual Disability amongst Individuals with Autism Spectrum Disorders: A Systematic Review and Meta-Analysis. Paper presented at the Autism-Europe Congress, Edinburgh, UK.
Constantino, J. N., & Todd, R. D. (2003). Autistic traits in the general population: a twin study. Archives of General Psychiatry, 60(5), 524-530. doi: 10.1001/archpsyc.60.5.524
Conti-Ramsden, G., & Botting, N. (1999). Classification of children with specific language impairment: Longitudinal considerations. Journal of Speech, Language, and Hearing Research, 42(5), 1195-1204. doi: 10.1044/jslhr.4205.1195
Conti-Ramsden, G., Botting, N., Simkin, Z., & Knox, E. (2001). Follow-up of children attending infant language units: outcomes at 11 years of age. International Journal of Language and Communication Disorders, 36(2), 207-219.
Conti-Ramsden, G (2003) Processing and linguistic markers in young children with specific language impairment (SLI). Journal of Speech, Language, and Hearing Research, 46, 1029-1037.
Conti-Ramsden, G., St Clair, M. C., Pickles, A., & Durkin, K. (2012). Developmental trajectories of verbal and nonverbal skills in individuals with a history of specific language impairment: from childhood to adolescence. Journal of Speech, Language, and Hearing Research, 55(6), 1716-1735. doi: 10.1044/1092-4388(2012/10-0182)
Coo, H., Ouellette-Kuntz, H., Lloyd, J. E., Kasmara, L., Holden, J. J., & Lewis, M. E. (2008). Trends in autism prevalence: diagnostic substitution revisited. Journal of Autism and Developmental Disorders, 38(6), 1036-1046. doi: 10.1007/s10803-007-0478-x
Courchesne, E., Carper, R., & Akshoomoff, N. (2003). Evidence of brain overgrowth in the first year of life in autism. JAMA: Journal of the American Medical Association, 290(3), 337-344.
Courchesne, E., Mouton, P. R., Calhoun, M. E., Semendeferi, K., Ahrens-Barbeau, C., Hallet, M. J., . . . Pierce, K. (2011). Neuron number and size in prefrontal cortex of children with autism. JAMA: Journal of the American Medical Association, 306(18), 2001-2010. doi: 10.1001/jama.2011.1638
Crais, E., Douglas, D. D., & Campbell, C. C. (2004). The intersection of the development of gestures and intentionality. Journal of Speech, Language and Hearing Research, 47(3), 678-694.
Cuthbert, B. N. (2014). The RDoC framework: facilitating transition from ICD/DSM to dimensional approaches that integrate neuroscience and psychopathology. World Psychiatry, 13(1), 28-35. doi: 10.1002/wps.20087
Cuthbert, B. N., & Insel, T. R. (2013). Toward the future of psychiatric diagnosis: the seven pillars of RDoC. BMC Medicine, 11, 126-126. doi: 10.1186/1741-7015-11-126
Dale, P. S., Price, T. S., Bishop, D. V., & Plomin, R. (2003). Outcomes of early language delay: I. Predicting persistent and transient language difficulties at 3 and 4 years. Journal of Speech Language, and Hearing Research, 46(3), 544-560.

207
Daniels, A. M., & Mandell, D. S. (2014). Explaining differences in age at autism spectrum disorder diagnosis: a critical review. Autism, 18(5), 583-597. doi: 10.1177/1362361313480277
Darrou, C., Pry, R., Pernon, E., Michelon, C., Aussilloux, C., & Baghdadli, A. (2010). Outcome of young children with autism: Does the amount of intervention influence developmental trajectories? Autism, 14(6), 663-677.
Davidson, M. M., & Ellis Weismer, S. (2014). Characterization and prediction of early reading abilities in children on the autism spectrum. Journal of Autism and Developmental Disorders, 44(4), 828-845. doi: http://dx.doi.org/10.1007/s10803-013-1936-2
Dawson, G., Toth, K., Abbott, R., Osterling, J., Munson, J., Estes, A., & Liaw, J. (2004). Early social attention impairments in autism: social orienting, joint attention, and attention to distress. Developmental Psychology, 40(2), 271-283.
De Giacomo, A., & Fombonne, E. (1998). Parental recognition of developmental abnormalities in autism. European Child and Adolescent Psychiatry, 7(3), 131-136.
de Schipper, E., Lundequist, A., Coghill, D., de Vries, P. J., Granlund, M., Holtmann, M., . . . Bolte, S. (2015). Ability and disability in autism spectrum disorder: A systematic literature review employing the International Classification of Functioning, Disability and Health-Children and Youth Version. Autism Research, 8(6), 782-794. doi: 10.1002/aur.1485
Dereu, M., Roeyers, H., Raymaekers, R., & Warreyn, P. (2012). Exploring individual trajectories of social communicative development in toddlers at risk for autism spectrum disorders. Research in Autism Spectrum Disorders, 6, 1038-1052. doi: 10.1016/j.rasd.2011.12.003
Eaves, L. C., & Ho, H. H. (1996). Brief report: Stability and change in cognitive and behavioral characteristics of autism through childhood. Journal of Autism and Developmental Disorders, 26(5), 557-569.
Eaves, L. C., & Ho, H. H. (2004). The very early identification of autism: outcome to age 41/2–5. Journal of Autism and Developmental Disorders, 34(4), 367-378.
Edmunds, S. R., Ibanez, L. V., Warren, Z., Messinger, D. S., & Stone, W. L. (2016). Longitudinal prediction of language emergence in infants at high and low risk for autism spectrum disorder. Development and Psychopatholgy, 1-11. doi: 10.1017/s0954579416000146
Ellis, E. M., & Thal, D. J. (2008). Early language delay and risk for language impairment. Perspectives on Language Learning and Education, 15(3), 93-100. doi: 10.1044/lle15.3.93
Ellis Weismer, S., & Kover, S. T. (2015). Preschool language variation, growth, and predictors in children on the autism spectrum. Journal of Child Psychology and Psychiatry, 56(12), 1327-1337. doi: 10.1111/jcpp.12406
Ellis Weismer, S., Lord, C., & Esler, A. (2010). Early language patterns of toddlers on the autism spectrum compared to toddlers with developmental delay. Journal of Autism and Developmental Disorders, 40(10), 1259-1273. doi: 10.1007/s10803-010-0983-1
Eriksson, M., Westerlund, J., Hedvall, Å., Åmark, P., Gillberg, C., & Fernell, E. (2013). Medical conditions affect the outcome of early intervention in preschool children with autism spectrum disorders. European Child and Adolescent Psychiatry, 22(1), 23-33. doi: 10.1007/s00787-012-0312-7

208
Fein, D., Barton, M., Eigsti, I. M., Kelley, E., Naigles, L., Schultz, R. T., . . . Rosenthal, M. (2013). Optimal outcome in individuals with a history of autism. Journal of Child Psychology and Psychiatry, 54(2), 195-205.
Fenson, L. (1993). MacArthur Communicative Development Inventories: User's guide and technical manual. San Diego, CA: Singular Publishing Group.
Fernell, E., Hedvall, A., Westerlund, J., Höglund Carlsson, L., Eriksson, M., Barnevik Olsson, M., . . . Gillberg, C. (2011). Early intervention in 208 Swedish preschoolers with autism spectrum disorder. A prospective naturalistic study. Research in Developmental Disabilities, 32(6), 2092-2101.
Flanagan, H. E., Perry, A., & Freeman, N. L. (2012). Effectiveness of large-scale community-based Intensive Behavioral Intervention: A waitlist comparison study exploring outcomes and predictors. Research in Autism Spectrum Disorders, 6(2), 673-682. doi: 10.1016/j.rasd.2011.09.011
Flanagan, H. E., Smith, I. M., Vaillancourt, T., Duku, E., Szatmari, P., Bryson, S., . . . Georgiades, S. (2015). Stability and change in the cognitive and adaptive behaviour scores of preschoolers with autism spectrum disorder. Journal of Autism and Developmental Disorders, 45(9), 2691-2703. doi: 10.1007/s10803-015-2433-6
Fombonne, E. (1999). The epidemiology of autism: a review. Psychological Medicine, 29(4), 769-786.
Freeman, B. J., Rahbar, B., Ritvo, E. R., Bice, T. L., Yokota, A., & Ritvo, R. (1991). The stability of cognitive and behavioral parameters in autism: a twelve-year prospective study. Journal of the American Academy of Child and Adolescent Psychiatry, 30(3), 479-482. doi: http://dx.doi.org/10.1097/00004583-199105000-00020
Freeman, B. J., Ritvo, E. R., Needleman, R., & Yokota, A. (1985). The stability of cognitive and linguistic parameters in autism: a five-year prospective study. Journal of the American Academy of Child Psychiatry, 24(4), 459-464. doi: http://dx.doi.org/10.1016/S0002-7138(09)60565-3
Freeman, N., & Perry, A. (2010). Outcomes of intensive behavioural intervention in the Toronto Preschool Autism Service. Journal on Developmental Disabilities, 16(2), 17-32.
Gardener, H., Spiegelman, D., & Buka, S. L. (2009). Prenatal risk factors for autism: a comprehensive meta-analysis. The British Journal of Psychiatry: The Journal of Mental Science, 195(1), 7-14. doi: 10.1192/bjp.bp.108.051672
Georgiades, S., Boyle, M., Szatmari, P., Hanna, S., Duku, E., Zwaigenbaum, L., . . . Thompson, A. (2014). Modeling the phenotypic architecture of autism symptoms from time of diagnosis to age 6. Journal of Autism and Developmental Disorders, 44(12), 3045-3055 3011p. doi: 10.1007/s10803-014-2167-x
Gillespie-Lynch, K., Sepeta, L., Wang, Y., Marshall, S., Gomez, L., Sigman, M., & Hutman, T. (2012). Early childhood predictors of the social competence of adults with autism. Journal of Autism and Developmental Disorders, 42(2), 161-174. doi: 10.1007/s10803-011-1222-0
Gilliam, J. (1995). Gilliam Autism Rating Scale Examiner's Manual. Austin, TX: Pro-Ed.
Goodman, R. (1997). The Strengths and Difficulties Questionnaire: a research note. Journal of Child Psychology and Psychiatry, 38(5), 581-586.

209
Gotham, K., Pickles, A., & Lord, C. (2012). Trajectories of autism severity in children using standardized ADOS scores. Pediatrics, 130(5), e1278-1284. doi: http://dx.doi.org/10.1542/peds.2011-3668
Green, S. A., & Carter, A. S. (2014). Predictors and course of daily living skills development in toddlers with autism spectrum disorders. Journal of Autism and Developmental Disorders, 44(2), 256-263. doi: http://dx.doi.org/10.1007/s10803-011-1275-0
Greenough, W. T., Black, J. E., & Wallace, C. S. (1987). Experience and brain development. Child Development, 539-559.
Grzadzinski, R., Huerta, M., & Lord, C. (2013). DSM-5 and autism spectrum disorders (ASDs): an opportunity for identifying ASD subtypes. Molecular Autism, 4(1), 1-6.
Hadley, P. A., & Holt, J. K. (2006). Individual differences in the onset of tense marking: a growth-curve analysis. Journal of Speech, Language, and Hearing Research, 49(5), 984-1000. doi: 10.1044/1092-4388(2006/071)
Haebig, E., McDuffie, A., & Ellis Weismer, S. (2013a). Brief report: Parent verbal responsiveness and language development in toddlers on the autism spectrum. Journal of Autism and Developmental Disorders. doi: 10.1007/s10803-013-1763-5
Haebig, E., McDuffie, A., & Ellis Weismer, S. (2013b). The contribution of two categories of parent verbal responsiveness to later language for toddlers and preschoolers on the autism spectrum. American Journal of Speech-Language Pathology, 22(1), 57-70. doi: 10.1044/1058-0360(2012/11-0004)
Hallmayer, J., Cleveland, S., Torres, A., Phillips, J., Cohen, B., Torigoe, T., . . . Risch, N. (2011). Genetic heritability and shared environmental factors among twin pairs with autism. Archives of General Psychiatry, 68(11), 1095-1102. doi: 10.1001/archgenpsychiatry.2011.76
Hansen, S. N., Schendel, D. E., & Parner, E. T. (2015). Explaining the increase in the prevalence of autism spectrum disorders: the proportion attributable to changes in reporting practices. JAMA Pediatrics, 169(1), 56-62. doi: 10.1001/jamapediatrics.2014.1893
Happe, F., & Frith, U. (1996). The neuropsychology of autism. Brain, 119 ( Pt 4), 1377-1400.
Happé, F., & Frith, U. (2006). The Weak Coherence Account: Detail-focused cognitive style in autism spectrum disorders. Journal of Autism and Developmental Disorders, 36(1), 5-25. doi: 10.1007/s10803-005-0039-0
Happé, F., Ronald, A., & Plomin, R. (2006). Time to give up on a single explanation for autism. Nature Neuroscience, 9(10), 1218-1220. doi: 10.1038/nn1770
Hayden, J. A., van der Windt, D. A., Cartwright, J. L., Côté, P., & Bombardier, C. (2013). Assessing bias in studies of prognostic factors. Annals of Internal Medicine, 158(4), 280-286. doi: 10.7326/0003-4819-158-4-201302190-00009
Hedvall, A., Westerlund, J., Fernell, E., Norrelgen, F., Kjellmer, L., Olsson, M. B., . . . Gillberg, C. (2015). Preschoolers with autism spectrum disorder followed for 2 years: Those who gained and those who lost the most in terms of adaptive functioning outcome. Journal of Autism and Developmental Disorders, 45(11), 3624-3633.
Hellendoorn, A., Wijnroks, L., van Daalen, E., Dietz, C., Buitelaar, J. K., & Leseman, P. (2015). Motor functioning, exploration, visuospatial cognition and language

210
development in preschool children with autism. Research in Developmental Disabilities, 39, 32-42. doi: http://dx.doi.org/10.1016/j.ridd.2014.12.033
Herlihy, L., Knoch, K., Vibert, B., & Fein, D. (2015). Parents’ first concerns about toddlers with autism spectrum disorder: effect of sibling status. Autism, 19(1), 20-28. doi: 10.1177/1362361313509731
Hofvander, B., Delorme, R., Chaste, P., Nydén, A., Wentz, E., Ståhlberg, O., . . . Leboyer, M. (2009). Psychiatric and psychosocial problems in adults with normal-intelligence autism spectrum disorders. BMC Psychiatry, 9, 35-35. doi: 10.1186/1471-244X-9-35
Howlin, P. (2003). Outcome in high-functioning adults with autism with and without early language delays: Implications for the differentiation between autism and Asperger syndrome. Journal of Autism and Developmental Disorders, 33(1), 3-13.
Howlin, P. (2011). Which factors can predict outcome of ASC in adulthood? In S. Bölte & J. Hallmayer (Eds.), Autism spectrum conditions: FAQs on autism, Asperger syndrome, and atypical autism answered by international experts. (pp. 87-89). Cambridge, MA US: Hogrefe Publishing.
Howlin, P., Goode, S., Hutton, J., & Rutter, M. (2004). Adult outcome for children with autism. Journal of Child Psychology and Psychiatry and Allied Disciplines, 45(2), 212-229.
Howlin, P., Mawhood, L., & Rutter, M. (2000). Autism and developmental receptive language disorder--a follow-up comparison in early adult life. II: Social, behavioural, and psychiatric outcomes. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 41(5), 561-578.
Howlin, P., & Moss, P. (2012). Adults with autism spectrum disorders. Canadian Journal of Psychiatry, 57(5), 275-283.
Howlin, P., Moss, P., Savage, S., & Rutter, M. (2013). Social outcomes in mid- to later adulthood among individuals diagnosed with autism and average nonverbal IQ as children. Journal of the American Academy of Child and Adolescent Psychiatry, 52(6), 572-581.e571. doi: http://dx.doi.org/10.1016/j.jaac.2013.02.017
Howlin, P., Savage, S., Moss, P., Tempier, A., & Rutter, M. (2014). Cognitive and language skills in adults with autism: a 40-year follow-up. Journal of Child Psychology and Psychiatry, 55(1), 49-58. doi: 10.1111/jcpp.12115
Hudry, K., Chandler, S., Bedford, R., Pasco, G., Gliga, T., Elsabbagh, M., . . . Charman, T. (2013). Early language profiles in infants at high-risk for autism spectrum disorders. Journal of Autism and Developmental Disorders, 1-14. doi: 10.1007/s10803-013-1861-4
Hudry, K., Leadbitter, K., Temple, K., Slonims, V., McConachie, H., Aldred, C., . . . Charman, T. (2010). Preschoolers with autism show greater impairment in receptive compared with expressive language abilities. International Journal of Language and Communication Disorders, 45(6), 681-690. doi: 10.3109/13682820903461493
Iizuka, C., Yamashita, Y., Nagamitsu, S., Yamashita, T., Araki, Y., Ohya, T., . . . Matsuishi, T. (2010). Comparison of the Strengths and Difficulties Questionnaire (SDQ) scores between children with high-functioning autism spectrum disorder (HFASD) and attention-deficit/hyperactivity disorder (AD/HD). Brain and Development, 32(8), 609-612. doi: 10.1016/j.braindev.2009.09.009

211
Ikeda, E., Hinckson, E., & Krageloh, C. (2014). Assessment of quality of life in children and youth with autism spectrum disorder: a critical review. Quality of Life Research, 23(4), 1069-1085. doi: 10.1007/s11136-013-0591-6
Jann, K., Hernandez, L. M., Beck-Pancer, D., McCarron, R., Smith, R. X., Dapretto, M., & Wang, D. J. (2015). Altered resting perfusion and functional connectivity of default mode network in youth with autism spectrum disorder. Brain and Behavior, 5(9), e00358. doi: 10.1002/brb3.358
Johnson, C. J., Beitchman, J. H., Young, A., Escobar, M., Atkinson, L., Wilson, B., . . . Wang, M. (1999). Fourteen-year follow-up of children with and without speech/language impairments: speech/language stability and outcomes. Journal of Speech, Language, and Hearing Research, 42(3), 744-760.
Jones, E. J., Gliga, T., Bedford, R., Charman, T., & Johnson, M. H. (2014). Developmental pathways to autism: A review of prospective studies of infants at risk. Neuroscience and Biobehavioral Reviews, 39, 1-33. doi: 10.1016/j.neubiorev.2013.12.001
Jónsdóttir, S. L., Saemundsen, E., Asmundsdóttir, G., Hjartardóttir, S., Asgeirsdóttir, B. B., Smáradóttir, H. H., . . . Smári, J. (2007). Follow-up of children diagnosed with pervasive developmental disorders: stability and change during the preschool years. Journal of Autism and Developmental Disorders, 37(7), 1361-1374.
Joshi, G., Petty, C., Wozniak, J., Henin, A., Fried, R., Galdo, M., . . . Biederman, J. (2010). The heavy burden of psychiatric comorbidity in youth with autism spectrum disorders: A large comparative study of a psychiatrically referred population. Journal of Autism and Developmental Disorders, 40(11), 1361-1370. doi: 10.1007/s10803-010-0996-9
Karmiloff-Smith, A. (2013). Challenging the use of adult neuropsychological models for explaining neurodevelopmental disorders: developed versus developing brains. Quarterly Journal of Experimental Psychology, 66(1), 1-14. doi: 10.1080/17470218.2012.744424
Karmiloff-Smith, A. (2016). Regression (NT and NDDs), the importance of timing and cross-syndrome comparisons. Paper presented at the Loss of Skills and Onset Patterns in Neurodevelopment Disorders: Understanding the Neurobological Mechanisms Workshop, Bethesda, Maryland. https://videocast.nih.gov/Summary.asp?File=19500&bhcp=1
Kasari, C., Brady, N., Lord, C., & Tager-Flusberg, H. (2013). Assessing the minimally verbal school-aged child with autism spectrum disorder. Autism Research, 6(6), 479-493. doi: 10.1002/aur.1334
Kasari, C., Kaiser, A., Goods, K., Nietfeld, J., Mathy, P., Landa, R., . . . Almirall, D. (2014). Communication interventions for minimally verbal children with autism: A sequential multiple assignment randomized trial. Journal of the American Academy of Child and Adolescent Psychiatry, 53(6), 635-646. doi: 10.1016/j.jaac.2014.01.019
Kasari, C., Paparella, T., Freeman, S., & Jahromi, L. B. (2008). Language outcome in autism: randomized comparison of joint attention and play interventions. Journal of Consulting and Clinical Psychology, 76(1), 125-137.
Kaufman, A. S., & Kaufman, N. L. (2004). Kaufman Brief Intelligence Test (second edition). Circle Pines, MN: Wiley Online Library.
Ketelaars, M. P., Cuperus, J., Jansonius, K., & Verhoeven, L. (2010). Pragmatic language impairment and associated behavioural problems. International

212
Journal of Language and Communication Disorders, 45(2), 204-214. doi: 10.3109/13682820902863090
Keyes, K. M., Susser, E., Cheslack-Postava, K., Fountain, C., Liu, K., & Bearman, P. S. (2012). Cohort effects explain the increase in autism diagnosis among children born from 1992 to 2003 in California. International Journal of Epidemiology, 41(2), 495-503. doi: 10.1093/ije/dyr193
King, M., & Bearman, P. (2009). Diagnostic change and the increased prevalence of autism. International Journal of Epidemiology, 38(5), 1224-1234.
Kjelgaard, M. M., & Tager-Flusberg, H. (2001). An investigation of language impairment in autism: implications for genetic subgroups. Language and Cognitive Processes, 16(2-3), 287-308.
Kleinman, J. M., Ventola, P. E., Pandey, J., Verbalis, A. D., Barton, M., Hodgson, S., . . . Fein, D. (2008). Diagnostic stability in very young children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 38(4), 606-615. doi: 10.1007/s10803-007-0427-8
Klintwall, L., Macari, S., Eikeseth, S., & Chawarska, K. (2015). Interest level in 2-year-olds with autism spectrum disorder predicts rate of verbal, nonverbal, and adaptive skill acquisition. Autism, 19(8), 925-933. doi: http://dx.doi.org/10.1177/1362361314555376
Knorring, A.-L., & Hägglöf, B. (1993). Autism in northern Sweden. A population based follow-up study: Psychopathology. European Child and Adolescent Psychiatry, 2(2), 91-97. doi: 10.1007/BF02098864
Kobayashi, R., Murata, T., & Yoshinaga, K. (1992). A follow-up study of 201 children with autism in Kyushu and Yamaguchi areas, Japan. Journal of Autism and Developmental Disorders, 22(3), 395-411. doi: 10.1007/BF01048242
Kover, S., McDuffie, A., Hagerman, R., & Abbeduto, L. (2013). Receptive vocabulary in boys with autism spectrum disorder: Cross-Sectional developmental trajectories. Journal of Autism and Developmental Disorders, 1-14. doi: 10.1007/s10803-013-1823-x
Krishnan, A., Zhang, R., Yao, V., Theesfeld, C. L., Wong, A. K., Tadych, A., . . . Troyanskaya, O. G. (2016). Genome-wide prediction and functional characterization of the genetic basis of autism spectrum disorder. Nature Neuroscience. doi: 10.1038/nn.4353
Kuhl, P. K. (2004). Early language acquisition: cracking the speech code. Nature Reviews Neuroscience, 5(11), 831-843.
Kwok, E. Y. L., Brown, H. M., Smyth, R. E., & Oram Cardy, J. (2015). Meta-analysis of receptive and expressive language skills in autism spectrum disorder. Research in Autism Spectrum Disorders, 9, 202-222. doi: 10.1016/j.rasd.2014.10.008
Landa, R., & Garrett-Mayer, E. (2006). Development in infants with autism spectrum disorders: a prospective study. Journal of Child Psychology & Psychiatry, 47(6), 629-638. doi: 10.1111/j.1469-7610.2006.01531.x
Landa, R., Gross, A. L., Stuart, E. A., & Bauman, M. (2012). Latent class analysis of early developmental trajectory in baby siblings of children with autism. Journal of Child Psychology and Psychiatry, 53(9), 986-996. doi: 10.1111/j.1469-7610.2012.02558.x
Landa, R., Gross, A. L., Stuart, E. A., & Faherty, A. (2013). Developmental trajectories in children with and without autism spectrum disorders: the first 3 years. Child Development, 84(2), 429-442. doi: 10.1111/j.1467-8624.2012.01870.x

213
Landa, R., Holman, K. C., & Garrett-Mayer, E. (2007). Social and communication development in toddlers with early and later diagnosis of autism spectrum disorders. Archives of General Psychiatry, 64(7), 853-864.
Landa, R., & Kalb, L. G. (2012). Long-term outcomes of toddlers with autism spectrum disorders exposed to short-term intervention. Pediatrics, 130, 186-190. doi: 10.1542/peds.2012-0900Q
Law, J., Boyle, J., Harris, F., Harkness, A., & Nye, C. (2000). Prevalence and natural history of primary speech and language delay: findings from a systematic review of the literature. International Journal of Language and Communication Disorders, 35(2), 165-188.
Law, J., Tomblin, J. B., & Xuyang, Z. (2008). Characterizing the growth trajectories of language-impaired children between 7 and 11 years of age. Journal of Speech, Language, and Hearing Research, 51(3), 739-749.
Le Couteur, A., Lord, C., & Rutter, M. (2003). Autism Diagnostic Interview-Revised. Los Angeles, CA: Western Psychological Services.
Levy, S. E., Giarelli, E., Lee, L.-C., Schieve, L. A., Kirby, R. S., Cunniff, C., . . . Rice, C. E. (2010). Autism spectrum disorder and co-occurring developmental, psychiatric, and medical conditions among children in multiple populations of the United States. Journal of Developmental and Behavioral Pediatrics, 31(4), 267-275.
Loke, Y. J., Hannan, A. J., & Craig, J. M. (2015). The role of epigenetic change in autism spectrum disorders. Frontiers in Neurology, 6, 107. doi: 10.3389/fneur.2015.00107
Lombardo, M. V., Pierce, K., Eyler, L. T., Carter Barnes, C., Ahrens-Barbeau, C., Solso, S., . . . Courchesne, E. (2015). Different functional neural substrates for good and poor language outcome in autism. Neuron, 86(2), 567-577. doi: 10.1016/j.neuron.2015.03.023
Lord, C. (1995). Follow-up of two-year-olds referred for possible autism. Journal of Child Psychology and Psychiatry and Allied Disciplines, 36(8), 1365-1382.
Lord, C. (2014). Early regression and worsening in autism spectrum disorders. Paper presented at the Australasian Society for Autism Research Conference, Melbourne, Australia.
Lord, C., Luyster, R., Guthrie, W., & Pickles, A. (2012). Patterns of developmental trajectories in toddlers with autism spectrum disorder. Journal of Consulting and Clinical Psychology, 80(3), 477-489. doi: http://dx.doi.org/10.1037/a0027214
Lord, C., Risi, S., Lambrecht, L., Cook, E. H., Jr., Leventhal, B. L., DiLavore, P. C., . . . Rutter, M. (2000). The Autism Diagnostic Observation Schedule-Generic: a standard measure of social and communication deficits associated with the spectrum of autism. Journal of Autism and Developmental Disorders, 30(3), 205-223.
Lord, C., Risi, S., & Pickles, A. (2004). Trajectory of Language Development in Autistic Spectrum Disorders. In M. L. Rice & S. F. Warren (Eds.), Developmental Language Disorders: From phenotypes to etiologies. (pp. 7-29). Mahwah, NJ US: Lawrence Erlbaum Associates Publishers.
Lord, C., & Schopler, E. (1989). Stability of assessment results of autistic and non-autistic language-impaired children from preschool years to early school age. Journal of Child Psychology and Psychiatry and Allied Disciplines, 30(4), 575-590.

214
Lord, C., Shulman, C., & DiLavore, P. (2004). Regression and word loss in autistic spectrum disorders. Journal of Child Psychology and Psychiatry and Allied Disciplines, 45(5), 936-955.
Loucas, T., Charman, T., Pickles, A., Simonoff, E., Chandler, S., Meldrum, D., & Baird, G. (2008). Autistic symptomatology and language ability in autism spectrum disorder and specific language impairment. Journal of Child Psychology and Psychiatry, 49(11), 1184-1192. doi: 10.1111/j.1469-7610.2008.01951.x
Lundstrom, S., Reichenberg, A., Anckarsater, H., Lichtenstein, P., & Gillberg, C. (2015). Autism phenotype versus registered diagnosis in Swedish children: prevalence trends over 10 years in general population samples. British Medical Journal, 350, h1961. doi: 10.1136/bmj.h1961
Luyster, R., Kadlec, M. B., Carter, A., & Tager-Flusberg, H. (2008). Language assessment and development in toddlers with autism spectrum disorders. Journal of Autism and Developmental Disorders, 38(8), 1426-1438.
Luyster, R., Qiu, S., Lopez, K., & Lord, C. (2007). Predicting outcomes of children referred for autism using the MacArthur-Bates Communicative Development Inventory. Journal of Speech Language, and Hearing Research, 50(3), 667-681.
Macari, S., Campbell, D., Gengoux, G., Saulnier, C., Klin, A., & Chawarska, K. (2012). Predicting developmental status from 12 to 24 months in infants at risk for autism spectrum disorder: A preliminary report. Journal of Autism and Developmental Disorders, 42(12), 2636-2647. doi: 10.1007/s10803-012-1521-0
Mackie, L., & Law, J. (2010). Pragmatic language and the child with emotional/behavioural difficulties (EBD): a pilot study exploring the interaction between behaviour and communication disability. International Journal of Language and Communication Disorders, 45(4), 397-410. doi: 10.3109/13682820903105137
Magiati, I., Moss, J., Charman, T., & Howlin, P. (2011). Patterns of change in children with autism spectrum disorders who received community based comprehensive interventions in their pre-school years: A seven year follow-up study. Research in Autism Spectrum Disorders, 5(3), 1016-1027. doi: 10.1016/j.rasd.2010.11.007
Magiati, I., Tay, X. W., & Howlin, P. (2014). Cognitive, language, social and behavioural outcomes in adults with autism spectrum disorders: A systematic review of longitudinal follow-up studies in adulthood. Clinical Psychology Review, 34(1), 73-86. doi: 10.1016/j.cpr.2013.11.002
Mawhood, L., & Howlin, P. (2000). Autism and developmental receptive language disorder--a comparative follow-up in early adult life. I: cognitive and language outcomes. Journal of Child Psychology and Psychiatry and Allied Disciplines, 41(5), 547.
Mazurek, M. O., Kanne, S. M., & Miles, J. H. (2012). Predicting improvement in social–communication symptoms of autism spectrum disorders using retrospective treatment data. Research in Autism Spectrum Disorders, 6(1), 535-545. doi: http://dx.doi.org/10.1016/j.rasd.2011.07.014
McDuffie, A., & Yoder, P. (2010). Types of parent verbal responsiveness that predict language in young children with autism spectrum disorder. Journal of Speech Language and Hearing Research, 53(4), 1026-1039.
McDuffie, A., Yoder, P., & Stone, W. (2005). Prelinguistic predictors of vocabulary in young children with autism spectrum disorders. Journal of Speech Language & Hearing Research, 48(5), 1080-1097.

215
McKean, C., Law, J., Mensah, F., Cini, E., Eadie, P., Frazer, K., & Reilly, S. (2016). Predicting Meaningful Differences in School-Entry Language Skills from Child and Family Factors Measured at 12 months of Age. International Journal of Early Childhood, 1-23. doi: 10.1007/s13158-016-0174-0
McKean, C., Mensah, F. K., Eadie, P., Bavin, E. L., Bretherton, L., Cini, E., & Reilly, S. (2015). Levers for language growth: Characteristics and predictors of language trajectories between 4 and 7 years. PloS one, 10(8), e0134251. doi: 10.1371/journal.pone.0134251
Meyer, E. (2002). Variability in the development of social behavior among children with autism. (Doctor of Philosophy), Univeristy of Massachusetts, Univeristy of Massachusetts, Boston, Massachusetts, US.
Miniscalco, C., Rudling, M., Rastam, M., Gillberg, C., & Johnels, J. A. (2014). Imitation (rather than core language) predicts pragmatic development in young children with ASD: a preliminary longitudinal study using CDI parental reports. International Journal of Language and Communication Disorders, 49(3), 369-375. doi: 10.1111/1460-6984.12085
Minshew, N. J., & Williams, D. L. (2007). The new neurobiology of autism - Cortex, connectivity, and neuronal organization. Archives of Neurology, 64(7), 945-950.
Mitchell, S., Brian, J., Zwaigenbaum, L., Roberts, W., Szatmari, P., Smith, I., & Bryson, S. (2006). Early language and communication development of infants later diagnosed with autism spectrum disorder. Journal of Developmental and Behavioral Pediatrics, 27(2 Suppl), S69-S78.
Mosconi, M. W., Steven Reznick, J., Mesibov, G., & Piven, J. (2009). The Social Orienting Continuum and Response Scale (SOC-RS): a dimensional measure for preschool-aged children. Journal of Autism and Developmental Disorders, 39(2), 242-250.
Moss, J., Magiati, I., Charman, T., & Howlin, P. (2008). Stability of the autism diagnostic interview-revised from pre-school to elementary school age in children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 38(6), 1081-1091.
Mullen, E. (1995). Mullen Scale of Early Learning Circle Pines, MN: American Guidance Service inc.
Mundy, P., Henderson, H., Inge, A. P., & Coman, D. (2007). The modifier model of autism and social development in higher functioning children. Research and Practice for Persons with Severe Disabilities: the Journal of TASH, 32(2), 124.
Mundy, P., & Jarrold, W. (2010). Infant joint attention, neural networks and social cognition. Neural Networks, 23(8–9), 985-997. doi: http://dx.doi.org/10.1016/j.neunet.2010.08.009
Mundy, P., Sigman, M., & Kasari, C. (1990). A longitudinal study of joint attention and language development in autistic children. Journal of Autism and Developmental Disorders, 20(1), 115-128.
Munson, J., Faja, S., Meltzoff, A., Abbott, R., & Dawson, G. (2008). Neurocognitive predictors of social and communicative developmental trajectories in preschoolers with autism spectrum disorders. Journal of the International Neuropsychological Society : JINS, 14(6), 956-966. doi: http://dx.doi.org/10.1017/S1355617708081393
Nadeau, J., Sulkowski, M. L., Ung, D., Wood, J. J., Lewin, A. B., Murphy, T. K., . . . Storch, E. A. (2011). Treatment of comorbid anxiety and autism spectrum disorders. Neuropsychiatry (London), 1(6), 567-578.
216
Nadig, A. S., Ozonoff, S., Young, G. S., Rozga, A., Sigman, M., & Rogers, S. J. (2007). A prospective study of response to name in infants at risk for autism. Archives of Pediatrics and Adolescent Medicine, 161(4), 378-383. doi: 10.1001/archpedi.161.4.378
National Institute of Health. (2010). NIH workshop on nonverbal school-aged children with autism. Retrieved 20 November 2016, from www.nidcd.nih.gov/funding/programs/10autism/pages/default.aspx
Norbury, C. F., & Sparks, A. (2013). Difference or disorder? Cultural issues in understanding neurodevelopmental disorders. Developmental Psychology, 49(1), 45-58. doi: 10.1037/a0027446
Norrelgen, F., Fernell, E., Eriksson, M., Hedvall, Å., Persson, C., Sjölin, M., . . . Kjellmer, L. (2014). Children with autism spectrum disorders who do not develop phrase speech in the preschool years. Autism. doi: 10.1177/1362361314556782
Noterdaeme, M., & Hutzelmeyer-Nickels, A. (2010). Early symptoms and recognition of pervasive developmental disorders in Germany. Autism, 14(6), 575-588. doi: 10.1177/1362361310371951
Oberman, L. M., & Ramachandran, V. S. (2007). The simulating social mind: the role of the mirror neuron system and simulation in the social and communicative deficits of autism spectrum disorders. Psychological Bulletin, 133(2), 310-327.
Oosterling, I., Visser, J., Swinkels, S., Rommelse, N., Donders, R., Woudenberg, T., . . . Buitelaar, J. (2010). Randomized controlled trial of the Focus Parent Training for toddlers with autism: 1-year outcome. Journal of Autism and Developmental Disorders, 40(12), 1447-1458. doi: 10.1007/s10803-010-1004-0
Ozonoff, S., Iosif, A.-M., Baguio, F., Cook, I. C., Hill, M. M., Hutman, T., . . . Sigman, M. (2010). A prospective study of the emergence of early behavioral signs of autism. Journal of the American Academy of Child and Adolescent Psychiatry, 49(3), 256-266.
Ozonoff, S., Iosif, A.-M., Young, G. S., Hepburn, S., Thompson, M., Colombi, C., . . . Rogers, S. J. (2011). Onset patterns in autism: Correspondence between home video and parent report. Journal of the American Academy of Child and Adolescent Psychiatry, 50(8), 796-806. doi: 10.1016/j.jaac.2011.03.012
Ozonoff, S., Williams, B. J., & Landa, R. (2005). Parental report of the early development of children with regressive autism: The delays-plus-regression phenotype. Autism, 9(5), 461-486. doi: 10.1177/1362361305057880
Pandey, J., Verbalis, A., Robins, D. L., Boorstein, H., Klin, A., Babitz, T., . . . Fein, D. (2008). Screening for autism in older and younger toddlers with the Modified Checklist for Autism in Toddlers. Autism, 12(5), 513-535. doi: 10.1177/1362361308094503
Paparella, T., Goods, K. S., Freeman, S., & Kasari, C. (2011). The emergence of nonverbal joint attention and requesting skills in young children with autism. Journal of Communication Disorders, 44(6), 569-583. doi: 10.1016/j.jcomdis.2011.08.002
Patton, G. C., & Viner, R. (2007). Pubertal transitions in health. Lancet, 369(9567), 1130-1139. doi: 10.1016/s0140-6736(07)60366-3
Paul, R., Campbell, D., Gilbert, K., & Tsiouri, I. (2013). Comparing spoken language treatments for minimally verbal preschoolers with autism spectrum disorders. Journal of Autism and Developmental Disorders, 43(2), 418-431. doi: 10.1007/s10803-012-1583-z

217
Paul, R., Chawarska, K., Cicchetti, D., & Volkmar, F. (2008). Language outcomes of toddlers with autism spectrum disorders: a two year follow-up. Autism Research, 1(2), 97-107.
Paul, R., Chawarska, K., & Volkmar, F. (2008). Differentiating ASD from DLD in toddlers. Perspectives on Language Learning and Education, 15(3), 101-111. doi: 10.1044/lle15.3.101
Paul, R., Fuerst, Y., Ramsay, G., Chawarska, K., & Klin, A. (2011). Out of the mouths of babes: Vocal production in infant siblings of children with ASD. Journal of Child Psychology and Psychiatry and Allied Disciplines, 52(5), 588-598.
Paul, R., Orlovski, S., Marcinko, H., & Volkmar, F. (2009). Conversational behaviors in youth with high-functioning ASD and Asperger syndrome. Journal of Autism and Developmental Disorders, 39(1), 115-125. doi: 10.1007/s10803-008-0607-1
Paul, R., & Roth, F. P. (2011). Characterizing and predicting outcomes of communication delays in infants and toddlers: Implications for clinical practice. Language, Speech, and Hearing Services in Schools, 42(3), 331-340.
Pellicano, E. (2010a). The development of core cognitive skills in autism: a 3-year prospective study. Child Development, 81(5), 1400-1416. doi: http://dx.doi.org/10.1111/j.1467-8624.2010.01481.x
Pellicano, E. (2010b). Individual differences in executive function and central coherence predict developmental changes in theory of mind in autism. Developmental Psychology, 46(2), 530-544. doi: 10.1037/a0018287
Pellicano, E. (2012). Do autistic symptoms persist across time? Evidence of substantial change in symptomatology over a 3-year period in cognitively able children with autism. American Journal on Intellectual and Developmental Disabilities, 117(2), 156-166. doi: http://dx.doi.org/10.1352/1944-7558-117.2.156
Pelphrey, K. A., & Carter, E. J. (2008). Brain mechanisms for social perception lessons from autism and typical development. Learning, Skill Acquisition, Reading and Dyslexia, 1145, 283-299.
Pelphrey, K. A., Shultz, S., Hudac, C. M., & Wyk, B. C. V. (2011). Constraining heterogeneity: The social brain and its development in autism spectrum disorder. Journal of Child Psychology and Psychiatry and Allied Disciplines, 52(6), 631-644. doi: 10.1111/j.1469-7610.2010.02349.x
Perry, A., Blacklock, K., & Dunn Geier, J. (2013). The relative importance of age and IQ as predictors of outcomes in Intensive Behavioral Intervention. Research in Autism Spectrum Disorders, 7(9), 1142-1150. doi: http://dx.doi.org/10.1016/j.rasd.2013.06.004
Perry, A., Cummings, A., Dunn Geier, J., Freeman, N. L., Hughes, S., LaRose, L., . . . Williams, J. (2008). Effectiveness of Intensive Behavioral Intervention in a large, community-based program. Research in Autism Spectrum Disorders, 2(4), 621-642. doi: http://dx.doi.org/10.1016/j.rasd.2008.01.002
Perry, A., Cummings, A., Geier, J. D., Freeman, N. L., Hughes, S., Managhan, T., . . . Williams, J. (2011). Predictors of outcome for children receiving intensive behavioral intervention in a large, community-based program. Research in Autism Spectrum Disorders, 5(1), 592-603. doi: 10.1016/j.rasd.2010.07.003
Picci, G., & Scherf, K. S. (2015). A two-hit model of autism: adolescence as the second hit. Clinical Psychological Science, 3(3), 349-371. doi: 10.1177/2167702614540646
Pickett, E., Pullara, O., O'Grady, J., & Gordon, B. (2009). Speech acquisition in older nonverbal individuals with autism: a review of features, methods, and prognosis.

218
Cognitive And Behavioral Neurology, 22(1), 1-21. doi: 10.1097/WNN.0b013e318190d185
Pickles, A., Anderson, D. K., & Lord, C. (2014). Heterogeneity and plasticity in the development of language: a 17-year follow-up of children referred early for possible autism. Journal of Child Psychology and Psychiatry, and Allied Disciplines. doi: 10.1111/jcpp.12269
Pickles, A., Simonoff, E., Conti-Ramsden, G., Falcaro, M., Simkin, Z., Charman, T., . . . Baird, G. (2009). Loss of language in early development of autism and specific language impairment. Journal of Child Psychology and Psychiatry, 50(7), 843-852. doi: 10.1111/j.1469-7610.2008.02032.x
Pinto, D., Pagnamenta, A. T., Klei, L., Anney, R., Merico, D., Regan, R., . . . Abrahams, B. S. (2010). Functional impact of global rare copy number variation in autism spectrum disorders. Nature, 466(7304), 368-372.
Pitskel, N. B., Bolling, D. Z., Hudac, C. M., Lantz, S. D., Minshew, N. J., Vander Wyk, B. C., & Pelphrey, K. A. (2011). Brain mechanisms for processing direct and averted gaze in individuals with autism. Journal of Autism and Developmental Disorders, 41(12), 1686-1693. doi: 10.1007/s10803-011-1197-x
Plesa Skwerer, D., Jordan, S. E., Brukilacchio, B. H., & Tager-Flusberg, H. (2016). Comparing methods for assessing receptive language skills in minimally verbal children and adolescents with autism spectrum disorders. Autism, 20(5), 591-604. doi: 10.1177/1362361315600146
Polyak, A., Kubina, R. M., & Girirajan, S. (2015). Comorbidity of intellectual disability confounds ascertainment of autism: implications for genetic diagnosis. American Journal of Medical Genetics. Part B Neuropsychiatric Genetics, 168(7), 600-608. doi: 10.1002/ajmg.b.32338
Poon, K., Watson, L., Baranek, G., & Poe, M. (2012). To what extent do joint attention, imitation, and object play behaviors in infancy predict later communication and intellectual functioning in ASD? Journal of Autism and Developmental Disorders, 42(6), 1064-1074. doi: 10.1007/s10803-011-1349-z
Posserud, M. B., Lundervold, A. J., & Gillberg, C. (2006). Autistic features in a total population of 7-9-year-old children assessed by the ASSQ (Autism Spectrum Screening Questionnaire). Journal of Child and Psychology and Psychiatry, 47(2), 167-175. doi: 10.1111/j.1469-7610.2005.01462.x
Pringle, B., Colpe, L. J., Blumberg, S. J., Avila, R. M., & Kogan, M. D. (2012). Diagnostic history and treatment of school-aged children with autism spectrum disorder and special health care needs. NCHS Data Brief(97), 1-8.
Prizant, B. M. (1996). Communication, language, social, and emotional development. Journal of Autism and Developmental Disorders, 26(2), 173-178.
Pry, R., Petersen, A. F., & Baghdadli, A. (2009). Developmental changes of expressive language and interactive competences in children with autism. Research in Autism Spectrum Disorders, 3(1), 98-112. doi: http://dx.doi.org/10.1016/j.rasd.2008.04.005
Pry, R., Petersen, A. F., & Baghdadli, A. M. (2011). On general and specific markers of lexical development in children with autism from 5 to 8 years of age. Research in Autism Spectrum Disorders, 5(3), 1243-1252. doi: 10.1016/j.rasd.2011.01.014
Pugliese, C. E., Anthony, L. G., Strang, J. F., Dudley, K., Wallace, G. L., Naiman, D. Q., & Kenworthy, L. (2015). Longitudinal examination of adaptive behavior in autism spectrum disorders: Influence of executive function. Journal of Autism

219
and Developmental Disorders, No Pagination Specified. doi: http://dx.doi.org/10.1007/s10803-015-2584-5
Randall, M., Sciberras, E., Brignell, A., Ihsen, E., Efron, D., Dissanayake, C., & Williams, K. (2015). Autism spectrum disorder: Presentation and prevalence in a nationally representative Australian sample. The Australian and New Zealand Journal of Psychiatry. doi: 10.1177/0004867415595287
Rapin, I., Dunn, M. A., Allen, D. A., Stevens, M. C., & Fein, D. (2009). Subtypes of language disorders in school-age children with autism. Developmental Neuropsychology, 34(1), 66-84.
Ray-Subramanian, C. E., & Ellis Weismer, S. (2012). Receptive and expressive language as predictors of restricted and repetitive behaviors in young children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 42(10), 2113-2120. doi: 10.1007/s10803-012-1463-6
Raznahan, A., Wallace, G. L., Antezana, L., Greenstein, D., Lenroot, R., Thurm, A., . . . Giedd, J. N. (2013). Compared to what? Early brain overgrowth in autism and the perils of population norms. Biological Psychiatry, 74(8), 563-575. doi: 10.1016/j.biopsych.2013.03.022
Reilly, S., Eadie, P., Bavin, E. L., Wake, M., Prior, M., Williams, J., . . . Ukoumunne, O. C. (2006). Growth of infant communication between 8 and 12 months: a population study. Journal of Paediatrics and Child Health, 42(12), 764-770.
Reilly, S., Tomblin, B., Law, J., McKean, C., Mensah, F. K., Morgan, A., . . . Wake, M. (2014). Specific language impairment: a convenient label for whom? International Journal of Language and Communication Disorders, 49(4), 416-451. doi: 10.1111/1460-6984.12102
Reilly, S., Wake, M., Bavin, E. L., Prior, M., Williams, J., Bretherton, L., . . . Ukoumunne, O. C. (2007). Predicting language at 2 years of age: a prospective community study. Pediatrics, 120(6), e1441-1449.
Reilly, S., Wake, M., Ukoumunne, O. C., Bavin, E., Prior, M., Cini, E., . . . Bretherton, L. (2010). Predicting language outcomes at 4 years of age: findings from Early Language in Victoria Study. Pediatrics, 126(6), e1530-e1537. doi: 10.1542/peds.2010-0254
Rescorla, L. (2005). Age 13 language and reading outcomes in late-talking toddlers. Journal of Speech, Language, and Hearing Research, 48(2), 459-472. doi: 10.1044/1092-4388(2005/031)
Rescorla, L. (2009). Age 17 language and reading outcomes in late-talking toddlers: support for a dimensional perspective on language delay. Journal of Speech, Language, and Hearing Research, 52(1), 16-30. doi: 10.1044/1092-4388(2008/07-0171)
Rice, M. L. (2004). Growth models of developmental language disorders. In M. L. R. a. S. F. Warren (Ed.), Developmental Language Disorders: from phenotypes to etiologies. Mahwah, NJ: Lawrence Erlbaum.
Rice, M. L., Redmond, S. M., & Hoffman, L. (2006). Mean length of utterance in children with specific language impairment and in younger control children shows concurrent validity and stable and parallel growth trajectories. Journal of Speech, Language, and Hearing Research, 49(4), 793-808. doi: 10.1044/1092-4388(2006/056)
Rice, M. L., Taylor, C. L., & Zubrick, S. R. (2008). Language outcomes of 7-year-old children with or without a history of late language emergence at 24 months.
220
Journal of Speech, Language, and Hearing Research, 51(2), 394-407. doi: 10.1044/1092-4388(2008/029)
Rice, M. L., Warren, S. F., & Betz, S. K. (2005). Language symptoms of developmental language disorders: An overview of autism, Down syndrome, fragile X, specific language impairment, and Williams syndrome. Applied Psycholinguistics, 26(01), 7-27.
Rice, M. L., Wexler, K., & Hershberger, S. (1998). Tense over time: The longitudinal course of tense acquisition in children with specific language impairment. Journal of Speech, Language, and Hearing Research, 41(6), 1412-1431.
Robert, J. M., McGrath L. M., & Tager-Flusberg H. (2005). Executive dysfunction and its relation to language ability in verbal school age children with ASD. Developmental Neuropsychology, 27(3), 361-378.
Rogers, S. J., & Pennington, B. F. (1991). A theoretical approach to the deficits in infantile autism. Development and Psychopathology, 3(02), 137-162.
Rondeau, E., Klein, L. S., Masse, A., Bodeau, N., Cohen, D., & Guilé, J.-M. (2011). Is pervasive developmental disorder not otherwise specified less stable than autistic disorder? A meta-analysis. Journal of Autism and Developmental Disorders, 41(9), 1267-1276. doi: 10.1007/s10803-010-1155-z
Roos, E. M., & Weismer, S. E. (2008). Language outcomes of late talking toddlers at preschool and beyond. Perspectives on Language Learning and Education, 15(3), 119-126. doi: 10.1044/lle15.3.119
Rose, V., Trembath, D., Keen, D., & Paynter, J. (2016). The proportion of minimally verbal children with autism spectrum disorder in a community-based early intervention programme. Journal of Intellectual Disability Research, 60(5), 464-477. doi: 10.1111/jir.12284
Rosenbaum, P. (2015). Developmental disability in the 21st century: New ideas for a new millennium. Indian Journal of Cerebral Palsy, 1(1), 4-8. doi: 10.4103/2395-4264.153555
Rosenbaum, P., & Gorter, J. W. (2012). The ‘F-words’ in childhood disability: I swear this is how we should think! Child: Care, Health and Development, 38(4), 457-463. doi: 10.1111/j.1365-2214.2011.01338.x
Rozga, A., Hutman, T., Young, G. S., Rogers, S. J., Ozonoff, S., Dapretto, M., & Sigman, M. (2011). Behavioral profiles of affected and unaffected siblings of children with autism: Contribution of measures of mother-infant interaction and nonverbal communication. Journal of Autism and Developmental Disorders, 41(3), 287-301.
Rubenstein, J. L. R. (2010). Three hypotheses for developmental defects that may underlie some forms of autism spectrum disorder. Current Opinion in Neurology, 23(2), 118-123 110.1097/WCO.1090b1013e328336eb328313.
Rubenstein, J. L. R., & Merzenich, M. M. (2003). Model of autism: increased ratio of excitation/inhibition in key neural systems. Genes, Brain and Behaviour, 2(5), 255-267.
Russell, G., Rodgers, L. R., & Ford, T. (2013). The strengths and difficulties questionnaire as a predictor of parent-reported diagnosis of autism spectrum disorder and attention deficit hyperactivity disorder. PloS one, 8(12), e80247. doi: 10.1371/journal.pone.0080247
Rutter, M., Bailey, A., & Lord, C. (2003). The Social Communication Questionnaire. Los Angeles CA Western Psychological Services.

221
Schopler, E., Reichler, R. J., DeVellis, R. F., & Daly, K. (1980). Toward objective classification of childhood autism: Childhood Autism Rating Scale (CARS). Journal of Autism and Developmental Disorders, 10(1), 91-103.
Sebat, J., Lakshmi, B., Malhotra, D., Troge, J., Lese-Martin, C., Walsh, T., . . . Wigler, M. (2007). Strong association of de novo copy number mutations with autism. Science, 316(5823), 445-449. doi: 10.1126/science.1138659
Semel, E., Wiig, E., & Secord, W. A. (2003). Clinical Evaluation of Language Fundamentals, Australian Version, Fourth Edition. San Antonio Tx: The Psychological Corporation.
Shriberg, L., Paul, R., Black, L. M., & van Santen, J. P. (2011). The hypothesis of apraxia of speech in children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 41(4), 405-426.
Shriberg, L., Paul, R., McSweeny, J., Klin, A., Cohen, D., & Volkmar, F. (2001). Speech and prosody characteristics of adolescents and adults with high-functioning autism and Asperger syndrome. Journal of Speech, Language and Hearing Research, 44(5), 1097-1115.
Shumway, S., Thurm, A., Swedo, S. E., Deprey, L., Barnett, L. A., Amaral, D. G., . . . Ozonoff, S. (2011). Brief report: Symptom onset patterns and functional outcomes in young children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 41(12), 1727-1732. doi: 10.1007/s10803-011-1203-3
Shumway, S., & Wetherby, A. M. (2009). Communicative acts of children with autism spectrum disorders in the second year of life. Journal of Speech, Language, and Hearing Research, 52(5), 1139-1156. doi: 10.1044/1092-4388(2009/07-0280)
Sigman, M., & McGovern, C. W. (2005). Improvement in cognitive and language skills from preschool to adolescence in autism. Journal of Autism and Developmental Disorders, 35(1), 15-23.
Sigman, M., Ruskin, E., Arbeile, S., Corona, R., Dissanayake, C., Espinosa, M., . . . Zierhut, C. (1999). Continuity and change in the social competence of children with autism, Down syndrome, and developmental delays. Monographs of the Society for Research in Child Development, 64(1), 1-114.
Siller, M., Hutman, T., & Sigman, M. (2013). A parent-mediated intervention to increase responsive parental behaviors and child communication in children with ASD: A randomized clinical trial. Journal of Autism and Developmental Disorders, 43(3), 540-555. doi: 10.1007/s10803-012-1584-y
Siller, M., & Sigman, M. (2002). The behaviors of parents of children with autism predict the subsequent development of their children's communication. Journal of Autism and Developmental Disorders, 32(2), 77-89.
Siller, M., & Sigman, M. (2008). Modeling longitudinal change in the language abilities of children with autism: parent behaviors and child characteristics as predictors of change. Developmental Psychology, 44(6), 1691-1704.
Simonoff, E., Pickles, A., Charman, T., Chandler, S., Loucas, T., & Baird, G. (2008). Psychiatric disorders in children with autism spectrum disorders: prevalence, comorbidity, and associated factors in a population-derived sample. Journal of the American Academy of Child and Adolescent Psychiatry, 47(8), 921-929. doi: 10.1097/CHI.0b013e318179964f
Smith, I. M., Flanagan, H. E., Garon, N., & Bryson, S. E. (2015). Effectiveness of community-based early intervention based on pivotal response treatment.

222
Journal of Autism and Developmental Disorders, 45(6), 1858-1872. doi: http://dx.doi.org/10.1007/s10803-014-2345-x
Smith, T., Klorman, R., & Mruzek, D. W. (2015). Predicting outcome of community-based early intensive behavioral intervention for children with autism. Journal of Abnormal Child Psychology, 43(7), 1271-1282. doi: http://dx.doi.org/10.1007/s10802-015-0002-2
Smith, V., Mirenda, P., & Zaidman-Zait, A. (2007). Predictors of expressive vocabulary growth in children with autism. Journal of Speech Language and Hearing Research, 50(1), 149-160.
Sparrow, S., Cicchetti, D., & Balla, D. (2005). Vineland Adaptive Behaviour Scales (2nd edition). Circle Pines, MN: American Guidance Service.
Stanton-Chapman, T. L., Chapman, D. A., Bainbridge, N. L., & Scott, K. G. (2002). Identification of early risk factors for language impairment. Research in Developmental Disabilities, 23(6), 390-405. doi: http://dx.doi.org/10.1016/S0891-4222(02)00141-5
Starr, E., Szatmari, P., Bryson, S., & Zwaigenbaum, L. (2003). Stability and change among high-functioning children with pervasive developmental disorders: a 2-year outcome study. Journal of Autism and Developmental Disorders, 33(1), 15-22.
Steele, S., Joseph, R. M., & Tager-Flusberg, H. (2003). Brief report: Developmental change in theory of mind abilities in children with autism. Journal of Autism and Developmental Disorders, 33(4), 461.
Stefanatos, G. A. (2008). Regression in autistic spectrum disorders. Neuropsychology Review, 18(4), 305-319. doi: 10.1007/s11065-008-9073-y
Stone, W. L., & Yoder, P. J. (2001). Predicting spoken language level in children with autism spectrum disorders. Autism, 5(4), 341-361.
Sullivan, A. (2010). Developmental trajectories of young children with autism enrolled in an intensive behaviour intervention program: What the ablls can tell us about their progress. (Doctor of Philosophy), York University, Toronto, Ontario, Canada. Retrieved from http://search.ebscohost.com/login.aspx?direct=true&db=psyh&AN=2011-99060-128&site=ehost-live Available from EBSCOhost psyh database.
Sutera, S. (2010). Predictors of optimal outcome in children with an autism spectrum disorder. (Doctor of Philosophy), University of Connecticut, Storrs, Connecticut, US. Retrieved from http://search.ebscohost.com/login.aspx?direct=true&db=psyh&AN=2010-99060-185&site=ehost-live Available from EBSCOhost psyh database.
Szatmari, P., Bryson, S., Duku, E., Vaccarella, L., Zwaigenbaum, L., Bennett, T., & Boyle, M. H. (2009). Similar developmental trajectories in autism and Asperger syndrome: from early childhood to adolescence. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 50(12), 1459-1467. doi: 10.1111/j.1469-7610.2009.02123.x
Szatmari, P., Bryson, S. E., Boyle, M. H., Streiner, D. L., & Duku, E. (2003). Predictors of outcome among high functioning children with autism and Asperger syndrome. Journal of Child Psychology and Psychiatry and Allied Disciplines, 44(4), 520-528. doi: 10.1111/1469-7610.00141
Szatmari, P., Chawarska, K., Dawson, G., Georgiades, S., Landa, R., Lord, C., . . . Halladay, A. (2016). Prospective longitudinal studies of infant siblings of children with autism: Lessons learned and future directions. Journal of the

223
American Academy of Child and Adolescent Psychiatry, 55(3), 179-187. doi: 10.1016/j.jaac.2015.12.014
Szatmari, P., Georgiades, S., Duku, E., Bennett, T. A., Bryson, S., Fombonne, E., . . . Thompson, A. (2015). Developmental trajectories of symptom severity and adaptive functioning in an inception cohort of preschool children with autism spectrum disorder. JAMA Psychiatry, 72(3), 276-283. doi: http://dx.doi.org/10.1001/jamapsychiatry.2014.2463
Tager-Flusberg H., Joseph R.M. (2005). How language facilitates the acquisition of false belief understanding in children with autism. In Astington J., Baird J. (Eds.), Why language matters for theory of mind (pp. 298–318). Oxford, UK: Oxford University Press
Tager-Flusberg, H. (2000). Language and understanding minds: connections in autism. In S. Baron-Cohen, H. Tager-Flusberg, & D. J. Cohen (Eds.), Understanding other minds: Perspectives from autism and developmental cognitive neuroscience (2nd ed., pp. 1–45). Oxford: Oxford University Press.
Tager-Flusberg, H. (2006). Defining language phenotypes in autism. Clinical Neuroscience Research (3-4), 219. doi: 10.1016/j.cnr.2006.06.007
Tager-Flusberg, H. (2015). Defining language impairments in a subgroup of children with autism spectrum disorder. Science China. Life Sciences, 58(10), 1044-1052. doi: 10.1007/s11427-012-4297-8
Tager-Flusberg, H. (2016). Risk factors associated with language in autism spectrum disorder: Clues to underlying mechanisms. Journal of Speech, Language, and Hearing Research, 59(1), 143-154. doi: 10.1044/2015_jslhr-l-15-0146
Tager-Flusberg, H., & Caronna, E. (2007). Language disorders: autism and other pervasive developmental disorders. Pediatric Clinics of North America, 54(3), 469-481.
Tager-Flusberg, H., Edelson, L., & Luyster, R. (2011). Language and communication in autism spectrum disorders. Oxford, United Kingdom: Oxford University Press.
Tager-Flusberg, H., & Kasari, C. (2013). Minimally verbal school-aged children with autism spectrum disorder: The neglected end of the spectrum. Autism Research, 6(6), 468-478. doi: 10.1002/aur.1329
Tager-Flusberg, H., Paul, R., & Lord, C. (2005). Language and Communication in Autism. In F. Volkmar, R. Paul, A. Klin, & D. Cohen (Eds.), Handbook of autism and pervasive developmental disorders (pp. 335-364). Hoboken, NJ: John Wiley & Sons, Inc.
Tager-Flusberg, H., Plesa Skwerer, D., Joseph, R. M., Brukilacchio, B., Decker, J., Eggleston, B., . . . Yoder, A. (2016). Conducting research with minimally verbal participants with autism spectrum disorder. Autism. doi: 10.1177/1362361316654605
Takeda, T., Koyama, T., Kanai, C., & Kurita, H. (2005). Clinical variables at age 2 predictive of mental retardation at age 5 in children with pervasive developmental disorder. Psychiatry and Clinical Neurosciences, 59(6), 717-722. doi: 10.1111/j.1440-1819.2005.01442.x
Taylor, C., Christensen, D., Lawrence, D., Mitrou, F., & Zubrick, S. R. (2013). Risk factors for children's receptive vocabulary development from four to eight years in the Longitudinal Study of Australian Children. PloS one, 8(9), 1-20. doi: 10.1371/journal.pone.0073046
Taylor, L. J., Maybery, M., Grayndler, L., & Whitehouse, A. J. O. (2013). Evidence for distinct cognitive profiles in autism spectrum disorders and specific language

224
impairment. Journal of Autism and Developmental Disorders, 1-12. doi: 10.1007/s10803-013-1847-2
Taylor, L. J., Maybery, M. T., Wray, J., Ravine, D., Hunt, A., & Whitehouse, A. J. O. (2015). Are there differences in the behavioural phenotypes of autism spectrum disorder probands from simplex and multiplex families? Research in Autism Spectrum Disorders, 11, 56-62. doi: http://dx.doi.org/10.1016/j.rasd.2014.12.003
Tek, S., Mesite, L., Fein, D., & Naigles, L. (2014). Longitudinal analyses of expressive language development reveal two distinct language profiles among young children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 44(1), 75-89. doi: 10.1007/s10803-013-1853-4
Thal, D. J., Reilly, J., Seibert, L., Jeffries, R., & Fenson, J. (2004). Language development in children at risk for language impairment: cross-population comparisons. Brain and Language, 88(2), 167-179. doi: 10.1016/s0093-934x(03)00096-8
Thomas, C. J. (2009). Analyses of five years of results from project data (developmentally appropriate treatment for autism), a high-quality early childhood special education program for students with autism spectrum disorders. (Doctor of Philosophy), University of Washington, Seatle, Washington, US. Retrieved from http://search.ebscohost.com/login.aspx?direct=true&db=psyh&AN=2010-99150-264&site=ehost-live Available from EBSCOhost psyh database.
Thomas, M. S., Annaz, D., Ansari, D., Scerif, G., Jarrold, C., & Karmiloff-Smith, A. (2009). Using developmental trajectories to understand developmental disorders. Journal of Speech, Language, and Hearing Research, 52(2), 336-358. doi: 10.1044/1092-4388(2009/07-0144)
Thomas, M. S., Davis, R., Karmiloff-Smith, A., Knowland, V. C., & Charman, T. (2016). The over-pruning hypothesis of autism. Developmental Science, 19(2), 284-305. doi: 10.1111/desc.12303
Thomas, M. S., Knowland, V. C., & Karmiloff-Smith, A. (2011). Mechanisms of developmental regression in autism and the broader phenotype: A neural network modeling approach. Psychological Review, 118(4), 637-654.
Thurm, A., Lord, C., Lee, L. C., & Newschaffer, C. (2007). Predictors of language acquisition in preschool children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 37(9), 1721-1734.
Thurm, A., Manwaring, S. S., Luckenbaugh, D. A., Lord, C., & Swedo, S. E. (2014). Patterns of skill attainment and loss in young children with autism. Development and Psychopathology, 26(01), 203-214.
Thurm, A., Manwaring, S. S., Swineford, L., & Farmer, C. (2015). Longitudinal study of symptom severity and language in minimally verbal children with autism. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 56(1), 97-104. doi: 10.1111/jcpp.12285
Tomasello, M., & Farrar, M. J. (1986). Joint attention and early language. Child Development, 57(6), 1454-1463.
Tomblin, J. B., Zhang, X., Buckwalter, P., & O'Brien, M. (2003). The stability of primary language disorder: four years after kindergarten diagnosis. Journal of Speech, Language, and Hearing Research, 46(6), 1283-1296.
Tomblin, B., Hafeman, L., L., & O’Brien, M. (2003) Autism and autism risk on siblings of children with specific language impairrment. International Journal of Language and Communication Disorders, 38(3), 235-250.

225
Tomblin, J. B. (2011). Co-morbidity of autism and SLI: kinds, kin and complexity. International Journal of Language and Communication Disorders, 46(2), 127-137.
Toth, K., Munson, J., Meltzoff, A. N., & Dawson, G. (2006). Early predictors of communication development in young children with autism spectrum disorder: joint attention, imitation, and toy play. Journal of Autism and Developmental Disorders, 36(8), 993-1005.
Trembath, D., & Vivanti, G. (2014). Problematic but predictive: Individual differences in children with autism spectrum disorders. International Journal of Speech-Language Pathology, 16(1), 57-60. doi: 10.3109/17549507.2013.859300
Turner, L. M., Stone, W. L., Pozdol, S. L., & Coonrod, E. E. (2006). Follow-up of children with autism spectrum disorders from age 2 to age 9. Autism, 10(3), 243-265.
Ukoumunne, O. C., Wake, M., Carlin, J., Bavin, E. L., Lum, J., Skeat, J., . . . Reilly, S. (2012). Profiles of language development in pre-school children: a longitudinal latent class analysis of data from the Early Language in Victoria Study. Child: Care, Health & Development, 38(3), 341-349. doi: 10.1111/j.1365-2214.2011.01234.x
Varni, J. W., Seid, M., & Kurtin, P. S. (2001). PedsQL™ 4.0: Reliability and validity of the Pediatric Quality of Life Inventory™ Version 4.0 Generic Core Scales in healthy and patient populations. Medical Care, 39(8), 800-812.
Veness, C., Prior, M., Bavin, E., Eadie, P., Cini, E., & Reilly, S. (2012). Early indicators of autism spectrum disorders at 12 and 24 months of age: A prospective, longitudinal comparative study. Autism, 16(2), 163-177. doi: 10.1177/1362361311399936
Venker, C., Ray-Subramanian, C., Bolt, D., & Weismer, S. (2014). Trajectories of autism severity in early childhood. Journal of Autism and Developmental Disorders, 44(3), 546-563 518p. doi: 10.1007/s10803-013-1903-y
Venter, A., Lord, C., & Schopler, E. (1992). A follow-up study of high-functioning autistic children. Journal of Child Psychology and Psychiatry and Allied Disciplines, 33(3), 489-507.
Viscidi, E. W., Triche, E. W., Pescosolido, M. F., McLean, R. L., Joseph, R. M., Spence, S. J., & Morrow, E. M. (2013). Clinical characteristics of children with autism spectrum disorder and co-occurring epilepsy. PloS one, 8(7), e67797. doi: 10.1371/journal.pone.0067797
Vivanti, G., Barbaro, J., Hudry, K., Dissanayake, C., & Prior, M. (2013). Intellectual development in autism spectrum disorders: New insights from longitudinal studies. Frontiers in Human Neuroscience Vol 7 Jul 2013, ArtID 354, 7(July 5 2003 ArtID 354).
Volden, J., Smith, I. M., Szatmari, P., Bryson, S., Fombonne, E., Mirenda, P., . . . Thompson, A. (2011). Using the Preschool Language Scale, fourth edition to characterize language in preschoolers with autism spectrum disorders. American Journal of Speech-Language Pathology, 20(3), 200-208.
Watt, N., Wetherby, A., & Shumway, S. (2006). Prelinguistic predictors of language outcome at 3 years of age. Journal of Speech, Language and Hearing Research, 49(6), 1224-1237. doi: 10.1044/1092-4388(2006/088)
Wechsler, D. (1999). Wechsler Abbreviated Scale of Intelligence. New York NY: Psychological Corporation.

226
Wetherby, A., Brosnan-Maddox, S., Peace, V., & Newton, L. (2008). Validation of the Infant—Toddler Checklist as a broadband screener for autism spectrum disorders from 9 to 24 months of age. Autism, 12(5), 487-511.
Wetherby, A., & Prizant, B. M. (2002). CSBS DP manual : Communication and Symbolic Behavior Scales : Developmental Profile. Baltimore MD: Paul H. Brookes.
Wetherby, A., Watt, N., Morgan, L., & Shumway, S. (2007). Social communication profiles of children with autism spectrum disorders late in the second year of life. Journal of Autism and Developmental Disorders, 37(5), 960-975. doi: 10.1007/s10803-006-0237-4
Wetherby, A., & Woods, J. J. (2006). Early social interaction project for children with autism spectrum disorders beginning in the second year of life a preliminary study. Topics in Early Childhood Special Education, 26(2), 67-82.
Whitehouse, A. J. O., Barry, J., & Bishop, D. (2007). The broader language phenotype of autism: a comparison with specific language impairment. Journal of Child Psychology and Psychiatry, 48(8), 822-830. doi: 10.1111/j.1469-7610.2007.01765.x
Whitehouse, A. J. O., Barry, J. G., & Bishop, D. V. M. (2008). Further defining the language impairment of autism: Is there a specific language impairment subtype? Journal of Communication Disorders, 41, 319–336.
Whitehouse, A. J. O., & Bishop, D. V. M. (2008). Cerebral dominance for language function in adults with specific language impairment and autism. Brain, 131, 3193–3200.
Whitehouse, A. J. O., Watt, H. J., Line, E. A., & Bishop, D. V. (2009). Adult psychosocial outcomes of children with specific language impairment, pragmatic language impairment and autism. International Journal of Language and Communication Disorders, 44(4), 511-528.
Whittle, S., Simmons, J. G., Byrne, M. L., Strikwerda-Brown, C., Kerestes, R., Seal, M. L., . . . Allen, N. B. (2015). Associations between early adrenarche, affective brain function and mental health in children. Social Cognitive and Affective Neuroscience, 10(9), 1282-1290. doi: 10.1093/scan/nsv014
Wiig, E. H., Secord, W., & Semel, E. (2006). Clinical Evaluation of Language Fundamentals Preschool, Australian Edition, Second Edition. Marrickville: Harcourt Assessment
Wilczynski, N. L., & Haynes, R. B. (2004). Developing optimal search strategies for detecting clinically sound prognostic studies in MEDLINE: an analytic survey. BMC Medicine, 2, 23. doi: 10.1186/1741-7015-2-23
Williams, D. L., Botting, N., & Boucher, J. (2008). Language in autism and specific language impairment: where are the links? Psychological Bulletin, 134(6), 944-963. doi: 10.1037/a0013743
Williams, K., Brignell, A., Prior, M., Bartak, L., & Roberts, J. (2015). Regression in autism spectrum disorders. Journal of Paediatrics and Child Health, 51(1), 61-64. doi: 10.1111/jpc.12805
Wing, L., Leekam, S. R., Libby, S. J., Gould, J., & Larcombe, M. (2002). The Diagnostic Interview for Social and Communication Disorders: background, inter-rater reliability and clinical use. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 43(3), 307-325.

227
Wodka, E., Mathy, P., & Kalb, L. (2013). Predictors of phrase and fluent speech in children with autism and severe language delay. Pediatrics, 1128-1134. doi: 10.1542/peds.2012-2221
Wolf, L., & Goldberg, B. (1986). Autistic children grow up: an eight to twenty-four year follow-up study. Canadian Journal of Psychiatry - Revue Canadienne de Psychiatrie, 31(6), 550-556.
Woolfenden, S., Sarkozy, V., Ridley, G., & Williams, K. (2012). A systematic review of the diagnostic stability of Autism Spectrum Disorder. Research in Autism Spectrum Disorders, 6(1), 345-354. doi: http://dx.doi.org/10.1016/j.rasd.2011.06.008
World Health Organisation. (2001). The International Classification of Functioning, Disability and Health (ICF). Geneva: WHO.
World Health Organisation. (2010). International statistical classification of diseases and related health problems (10th revision) (Vol. 2). Geneva, Switzerland: World Health Organisation.
Woynaroski, T., Watson, L., Gardner, E., Newsom, C. R., Keceli-Kaysili, B., & Yoder, P. J. (2015). Early predictors of growth in diversity of key consonants used in communication in initially preverbal children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 1013-1024.
Yirmiya, N., & Charman, T. (2010). The prodrome of autism: early behavioral and biological signs, regression, peri and postnatal development and genetics. Journal of Child Psychology and Psychiatry, 51(4), 432-458.
Yoder, P., Watson, L. R., & Lambert, W. (2015). Value-added predictors of expressive and receptive language growth in initially nonverbal preschoolers with autism spectrum disorders. Journal of Autism and Developmental Disorders, 45(5), 1254-1270. doi: http://dx.doi.org/10.1007/s10803-014-2286-4
Zablotsky, b., Black, l., Maenner, M., Schieve, l. & Blumberg, S. (2015). Estimated Prevalence of Autism and Other Developmental Disabilities Following Questionnaire Changes in the 2014 National Health Interview Survey. National Health Statistics Reports, 1-21.
Zambrana, I. M., Pons, F., Eadie, P., & Ystrom, E. (2014). Trajectories of language delay from age 3 to 5: persistence, recovery and late onset. International Journal of Language and Communication Disorders, 49(3), 304-316. doi: 10.1111/1460-6984.12073
Zhu, X., Need, A. C., Petrovski, S., & Goldstein, D. B. (2014). One gene, many neuropsychiatric disorders: lessons from Mendelian diseases. Nature Neuroscience, 17(6), 773-781. doi: 10.1038/nn.3713 http://www.nature.com/neuro/journal/v17/n6/abs/nn.3713.html#supplementary-information
Zierhut, C. (2002). Facilitative factors in the home environments of children with autism (Doctor of Philosophy), Univeristy of California, Los Angeles, Univeristy of California, Los Angeles, California, US.
Zubrick, S. R., Taylor, C. L., Rice, M. L., & Slegers, D. W. (2007). Late language emergence at 24 months: An epidemiological study of prevalence, predictors, and covariates. Journal of Speech Language and Hearing Research, 50(6), 1562-1592. doi: 10.1044/1092-4388(2007/106)
Zwaigenbaum, L., Bryson, S., & Garon, N. (2013). Early identification of autism spectrum disorders. Behavioral Brain Research, 251, 133-146. doi: 10.1016/j.bbr.2013.04.004

228
Zwaigenbaum, L., Bryson, S., Rogers, T., Roberts, W., Brian, J., & Szatmari, P. (2005). Behavioral manifestations of autism in the first year of life. International Journal of Developmental Neuroscience, 23(2-3), 143-152.
Zwaigenbaum, L., Thurm, A., Stone, W., Baranek, G., Bryson, S., Iverson, J., . . . Landa, R. (2007). Studying the emergence of autism spectrum disorders in high-risk infants: methodological and practical issues. Journal of Autism and Developmental Disorders, 37(3), 466-480.
Zwaigenbaum, L., Young, G. S., Stone, W. L., Dobkins, K., Ozonoff, S., Brian, J., . . . Messinger, D. (2014). Early head growth in infants at risk of autism: a baby siblings research consortium study. Journal of the American Academy of Child and Adolescent Psychiatry, 53(10), 1053-1062. doi: 10.1016/j.jaac.2014.07.007

226
Appendices

227
Appendix A. Published article on regression in autism spectrum disorders

REVIEW ARTICLE
Regression in autism spectrum disordersKatrina Williams,1,2,3 Amanda Brignell,2 Margot Prior,4 Lawrence Bartak5 and Jacqueline Roberts6
1Developmental Medicine, The Royal Children’s Hospital, 2Department of Paediatrics and 4Psychological Sciences, University of Melbourne, 3Murdoch Childrens
Research Institute, 5Faculty of Education, Monash University, Melbourne, Victoria, and 6Education and Professional Studies, Autism Centre of Excellence, Griffith
University, Queensland, Australia
Abstract: Since the Journal of Paediatrics and Child Health was first published, there has been substantial change in the field of autismspectrum disorders (ASDs) with an exponential increase in the amount of funded and published research. In this paper, we focus on regressionin children with ASD, a phenomenon that remains poorly understood. We discuss the implications of what we know about regression in ASD forthe way we think about ASD more broadly and for paediatric practice.
Key words: behavioural; developmental; general paediatrics; neurology.
Background
The clinical features of children who were described as ‘autistic’were published by Kanner1 in English 21 years before the Journalof Paediatrics and Child Health was launched. The recent surge ofactivity and interest in autism spectrum disorders (ASDs) isreflected in the number of articles with autism in the title inPubMed, with 90% published in 1994 or more recently (Fig. 1).Many reviews about ASD are now available including threepublished in this journal.2–4 Major changes that have occurred areshown in Box 1, with many of these contributing to the currentconcept of autism as a spectrum of strengths and difficulties.
Kanner’s original description (1943) did not report regression,rather that autism was congenital or occurred shortly afterbirth.1 However, reports emerged in the 1960s that notedbehavioural regression in children with autism5,6 and in themid-1980s, studies were published that focused specifically on
the loss of early speech in autism.7 Since that time, substantialresearch has accumulated about a subgroup of children withASD who experience some form of developmental change,plateau or regression in the first few years of life,8,9 with a recentreview of the prevalence of regression in ASD identifying 85relevant publications.10
In an attempt to disentangle the types and possible causes ofASD, a dimensional approach is being recommended and sub-types within the autism spectrum are being explored. It isthought that children displaying regression could form oneimportant subtype. There are a number of reasons why regres-sion in ASD has sparked interest: it could (i) provide clues as tocause and underlying neurobiological mechanisms; (ii) assist inthe delineation of potential subtypes in what is currently aheterogeneous condition; and (iii) inform prognosis. However,questions remain about whether the reports of loss of skills inASD is regression as we think of it for other progressiveneurodevelopmental disorders. For the remainder of this article,we will focus on what is known about this phenomenon andwhat this means for paediatric practice.
What Is Regression in ASD?
Regression is described by parents of children with ASD asapparently normal development for the first 1 to 2 years of life,followed by an abrupt or gradual loss of previously acquiredskills. The developmental skills that are typically reported toregress in ASD are language and/or social communication. Afrequently used tool to assist in characterising regression is theAutism Diagnostic Interview-Revised (ADI-R) because itincludes specific questions and guidance about regression.11 Thecharacteristics required by the ADI-R for a diagnosis of languageregression are that prior to the reported loss, ‘communicativeuse of at least five different words (other than “mama” and“dada”) on a daily basis for at least 3 months’ is established andthat there has been a loss of the skill for at least 3 months(quoted from a test booklet of an assessment tool).11 Some
Key Points
1 A focus on regression in ASD is designed to increase under-standing of ASD dimensions and heterogeneity.
2 Regression occurs in a significant subgroup of children withASD but there is little understanding of causes, underlyingneurobiology or prognosis.
3 Clinicians should obtain a detailed history and investigatepotential underlying pathophysiology, while researchersutilise a dimensional approach with new technology (geneticand epigenetic research, computer models of brain function,neuroimaging) to gain deeper understanding of onset and sub-sequent developmental trajectory for children with ASD.
Correspondence: Professor Katrina Williams, Developmental Medicine,The Royal Children’s Hospital, 50 Flemington Road, Parkville Vic. 3052,Australia. Fax: 61 3 9345 5871; email: [email protected]
Conflict of interest: None declared.
Accepted for publication 8 June 2014.
doi:10.1111/jpc.12805
bs_bs_banner
Journal of Paediatrics and Child Health 51 (2015) 61–64© 2015 The AuthorsJournal of Paediatrics and Child Health © 2015 Paediatrics and Child Health Division (Royal Australasian College of Physicians).
61

studies have suggested that the majority of children show somesubtle signs of social difficulties, perhaps unrecognisable to theirparents, prior to regression being reported.9 However, somereports based on home videos suggest at least some childrenhave advanced skills prior to regression (e.g. Ozonoff et al.12)
How Common Is Regression in ASD andOther Developmental Problems?
A recent meta-analytic review, which included 85 studies(n = 29 035), reported the overall prevalence of regression in
ASD to be 32.1% (confidence interval (CI): 29.5–34.8) and themean age of onset of regression as 1.78 years (CI: 1.69–1.89).10
Prevalence rates of regression vary according to how regressionis defined.10,13 No significant difference in the risk of regressionbetween males and females has been reported8,10,14 and regres-sion is not more common among any particular socio-economicgroup.13,15 One hypothesis is that the age of regression dependson the stage of brain maturation and developmental level of thechild rather than their chronological age.8
Regression is rare in other neurodevelopmental disabilities,apart from a select few, including seizure disorders (e.g.Landau–Kleffner syndrome, acquired epileptic aphasia), geneticdisorders (e.g. Rett syndrome) and known disorders of metabo-lism (e.g. glycogen storage disorders). In these, there is con-tinued deterioration unless the underlying cause can be treatedor there are treatments to decrease the secondary consequencesof the underlying cause. Childhood disintegrative disorder(CDD) is one other rare condition in which regression occurswith no known underlying cause. Under the Diagnostic Statis-tical Manual of Mental Disorders, Fourth Edition,16 CDD wasdefined separately as apparently normal development in thefirst 2 years after birth followed by loss of skills before the age of10, with skill loss that could extend beyond social communica-tion and language. With the release of the Diagnostic StatisticalManual of Mental Disorders, Fifth Edition,17 CDD is nowincluded under the diagnosis of ASD and is no longer a separatedisorder.
The occurrence of reported regression is higher in ASD thanother idiopathic developmental conditions. For example, only1% of children with specific language impairment regressedcompared with 15% with ASD in one study,18 and 3% of chil-dren with developmental delay were reported to regress com-pared with 38% in ASD in another.19 In both of these studies,the non-ASD children who regressed had significant medical orneurodevelopmental problems such as encephalitis, Down syn-drome with leukaemia, a stroke and epilepsy.
Cause and Underlying NeurobiologicalMechanism
To date, studies that have investigated the processes that may beinvolved in regression have been based on cross-sectional asso-ciations. Studies have examined a potential association betweenthe measles mumps and rubella vaccination,20 gastrointestinalproblems13,19 and mitochondrial diseases.21 None of these havefound differences in risk factors that are substantial enough todifferentiate subgroups of children with regressive and non-regressive ASD, nor have they been fruitful in identifying apotential cause. Studies investigating traditional risk factorssuch as pre- or post-natal complications and viral infectionshave also failed to yield a cause.13,15
There has been substantial exploration of epilepsy as a causeof regression but to date, the findings have been inconsistent. Inone study, a high proportion of children, most (90%) with an IQless than 70, who had experienced regression with ASD hadco-morbid epilepsy.22 In another, increased seizure activity wasassociated with regression.23 However, in this study, there wasno significant difference between the risks of epilepsy in chil-dren with ASD who had regressed when compared with those
2
1945
1949
1950
1954
1955
1959
1960
1964
1965
1969
1970
1974
1975
1979
1985
1989
1980
1984
1990
1994
2010
2014
1995
1999
2005
2009
2000
2004
10 21 27 47 120 146 195 344 469 689
1570
3395
6300
0
1000
2000
3000
4000
5000
6000
7000
Num
ber o
f Pub
lica
ons
Years
Fig. 1 Number of publications in PubMed with autism in the title over
time.
Box 1 Changes in the past 20 years
1. Acceptance of the spectrum concept of autism2. Emergence of many theories purporting to explain theneuropsychological underpinning of autism spectrum disor-der (ASD), like theory of mind, but with none yet achievingthis3. Acceptance that ASD is biologically (rather than psycho-dynamically) based, albeit with slow progress towards detail-ing the biological underpinnings4. Emergence of a plethora of biological theories of causa-tion, many of which have been disproven; the remainder arenot yet proven despite extensive research investment5. Widespread communication about and uptake of inter-ventions based on unproven theories of causation that havebeen harmful6. Development of systematic, expert and sophisticatedmethods for assessment and diagnosis of ASD, but variationsin diagnostic practise remain widespread and inconsistencyin diagnosis persists7. Major growth in our understanding of the cognitivestrengths and weaknesses, and preferred learning styles ofchildren with ASD, which can be applied to interventionsand educational settings8. Greater understanding of co-morbid features such asanxiety and hyperactivity, which contribute to the behav-ioural problems and which need particular treatment andmanagement, with Diagnostic Statistical Manual of MentalDisorders, Fifth Edition (DSM-5) allowing co-diagnoses
K Williams et al.Regression in autism
Journal of Paediatrics and Child Health 51 (2015) 61–64© 2015 The Authors
Journal of Paediatrics and Child Health © 2015 Paediatrics and Child Health Division (Royal Australasian College of Physicians)
62

who had not.24 Many other studies have found no associationbetween epilepsy and regression.13,14,19
A number of theories have been proposed to help explain theneurobiology of regression. It has been suggested that regressionin ASD may occur in a particular genetic subgroup. While thismay seem logical, research has so far failed to identify anygenetic differences between children who regress comparedwith those who do not.25 One study found the risk of regressionfor children with ASD in multiplex families was similar to therate of regression in singleton families.25 In the same study, laterborn children who were diagnosed with ASD were not found tobe at increased risk of regressive ASD if they had an older siblingwho has regressive ASD. Another study found similar rates ofthe broader autism phenotype in parents of children who hadboth regressive and non-regressive forms of ASD.26 To date,none of the suggested neurobiological theories, many based onneuroimaging findings, have consistently explained regressiveASD.27,28 New computer-modelled theories are emerging but arealso unproven.29
Is There a Clear Regression Subtype?
In the last 7 years, studies have looked at the onset of ASDprospectively, including population sample studies30,31 andstudies of high-risk siblings.32 In one study, around 50% ofchildren who were later diagnosed with ASD showed typicaldevelopment (apart from exhibiting fewer gaze shifts) prior to14 months but then experienced a period of developmentalchange that involved arrest, slowing and/or regression.33 A con-tinuum of impairment, where children reach a threshold fordiagnosis of ASD at different points in time in the first 3 yearsof life, was described.33 Another study reported that the symp-toms of ASD emerged over a period of time beginning aroundthe second year of life. Repeated observations of children in thisstudy found a decline in social communication skills in 86% ofchildren.9 It remains to be established whether these prospec-tive studies have captured the full range of patterns of onset ofdevelopmental problems that are later diagnosed as ASD and allthe ways regression may occur. To date, few have reported themore dramatic, rapid loss of skills, which may represent animportant subtype of regression. The methodological limita-tions of prospective studies to date (e.g. primarily high-risksiblings and small sample sizes) prevent us from forming firmconclusions.
Prognosis
There have been mixed findings in the literature about whetherchildren with ASD who experience regression have better orworse long-term outcomes than children who do not experi-ence regression. Some studies have reported no difference inoutcome for children who regressed versus those who did not(e.g. Shumway et al.34) and others have found that those whoregressed were more impaired in areas such as language,co-morbid psychopathology, adaptive function, challengingbehaviours and social skills than their counterparts.7,19,35,36 Inone study, the loss of non-specific vocalisations was associated withlower IQ and higher ASD symptomatology (as measured on theAutism Diagnostic Observation Schedule).8 However, for those
children who developed words and phrases by 5 years of age,those with word loss had similar outcomes to the childrenwithout word loss.
No Changes yet for Clinical Care
For the paediatrician, the approach to a child who presents withregression and problems of the type seen in ASD is unchanged.A thorough history to tease out the developmental trajectorywill assist with assessing if regression has occurred and whatdevelopmental dimensions are involved. When regression hasoccurred, investigation and referrals should take into accountimportant potential underlying pathophysiology, like seizuredisorders and metabolic and genetic causes. When order-ing genetic tests, like microarray, a history of suspected regres-sion should be provided along with the diagnosis of ASD.If this is done consistently, it may assist in identifying geneticunderpinnings for some children and families that are unlikelyto be found in research studies, because of sample size limita-tions. If the presence of regression is uncertain, then review tomonitor progress against baseline abilities and difficulties isneeded.
Still No Answers but Maybe Now We AreAsking the Right Questions
Research about regression in ASD, including prospective studiesof early development, has not yet provided clear answers aboutwhether there is a distinct subtype of children with autisticregression. A lack of clarity about the subtype is likely to explainwhy findings are still mixed about the possible causes and prog-nosis of children who are reported to regress. However, evi-dence from ASD research focusing on regression hascontributed to an emerging interest in the dimensions of devel-opmental difficulties for children with ASD, including timing ofonset and subsequent trajectory. This approach, rather than acategoric approach to the diagnosis of ASD, provides hope as animportant new framework from which to ask the right ques-tions about causes of and interventions for ASD, and how it isassociated with other developmental difficulties and disorders. Ifthis dimensional thinking can underpin research using newtechnology for both genetic and epigenetic research andneuroimaging and computer models of brain function, therecould be more rapid progress towards providing the sorts ofanswers we need to assist children and families in ways that aretailored to their needs. However, we do not see biologicaladvances as all that are needed to create a better life for childrenwith ASD and their families. In fact, biological advances willneed to be embedded in strong human rights and ethical frame-works to ensure they do not create more problems than theysolve.
References
1 Kanner L. Autistic disturbances of affective contact. Nerv. Child 1943;2: 217–50.
2 Williams K, Woolfenden S, Roberts J, Rodger S, Bartak L, Prior M.Autism in context 1: classification, counting and causes. J. Paediatr.Child Health 2014; 50: 335–40.
Regression in autismK Williams et al.
Journal of Paediatrics and Child Health 51 (2015) 61–64© 2015 The AuthorsJournal of Paediatrics and Child Health © 2015 Paediatrics and Child Health Division (Royal Australasian College of Physicians)
63

3 Williams K, Woolfenden S, Roberts J, Rodger S, Bartak L, Prior M.Autism in context 2: assessment, intervention and services inAustralia. J. Paediatr. Child Health 2014; 50: 341–6.
4 Tonge BJ, Dissanayake C, Brereton AV. Autism: fifty years on fromKanner. J. Paediatr. Child Health 1994; 30: 102–7.
5 Wolff S, Chess S. A behavioural study of schizophrenic children. ActaPsychiatr. Scand. 1964; 40: 438–66.
6 Lotter V. Epidemiology of autistic conditions in young children. Soc.Psychiatry 1966; 1: 124–37.
7 Kurita H. Infantile autism with speech loss before the age of thirtymonths. J. Am. Acad. Child Psychiatry 1985; 24: 191–6.
8 Lord C, Shulman C, DiLavore P. Regression and word loss in autisticspectrum disorders. J. Child Psychol. Psychiatry 2004; 45: 936–55.
9 Ozonoff S, Iosif A-M, Baguio F et al. A prospective study of theemergence of early behavioral signs of autism. J. Am. Acad. ChildAdolesc. Psychiatry 2010; 49: 256–66, e252.
10 Barger BD, Campbell JM, McDonough JD. Prevalence and onset ofregression within autism spectrum disorders: a meta-analytic review.J. Autism Dev. Disord. 2013; 43: 817–28.
11 Le Couteur A, Lord C, Rutter M. Autism Diagnostic Interview-Revised.Los Angeles, CA: Western Psychological Services, 2003.
12 Ozonoff S, Iosif A-M, Young GS et al. Onset patterns in autism:correspondence between home video and parent report. J. Am.Acad. Child Adolesc. Psychiatry 2011; 50: 796–806.
13 Hansen RL, Ozonoff S, Krakowiak P et al. Regression in autism:prevalence and associated factors in the CHARGE Study. Ambul.Pediatr. 2008; 8: 25–31.
14 Luyster R, Richler J, Risi S et al. Early regression in socialcommunication in autism spectrum disorders: a CPEA Study. Dev.Neuropsychol. 2005; 27: 311–36.
15 Christopher JA, Sears LL, Williams PG, Oliver J, Hersh J. Familial,medical and developmental patterns of children with autism and ahistory of language regression. J. Dev. Phys. Disabil. 2004; 16:163–70.
16 American Psychiatric Association. Diagnostic Statistical Manual ofMental Disorders, 4th edn, text revision ed. Washington, DC:American Psychiatric Publishing, 2000.
17 American Psychiatric Association. Diagnostic and Statistical Manualof Mental Disorders, 5th edn. Arlington, VA: American PsychiatricAssociation, 2013.
18 Pickles A, Simonoff E, Conti-Ramsden G et al. Loss of language inearly development of autism and specific language impairment. J.Child Psychol. Psychiatry 2009; 50: 843–52.
19 Baird G, Charman T, Pickles A et al. Regression, developmentaltrajectory and associated problems in disorders in the autismspectrum: the SNAP study. J. Autism Dev. Disord. 2008; 38: 1827–36.
20 Baird G, Pickles A, Simonoff E et al. Measles vaccination and antibodyresponse in autism spectrum disorders. Arch. Dis. Child. 2008; 93:832–7.
21 Shoffner J, Hyams L, Langley GN et al. Fever plus mitochondrialdisease could be risk factors for autistic regression. J. Child Neurol.2010; 25: 429–34.
22 Oslejskova H, Dusek L, Makovska Z, Pejcochova J, Autrata R, Slapak I.Complicated relationship between autism with regression andepilepsy. Neuro Endocrinol. Lett. 2008; 29: 558–70.
23 Tuchman RF, Rapin I. Regression in pervasive developmentaldisorders: seizures and epileptiform electroencephalogramcorrelates. Pediatrics 1997; 99: 560–6.
24 Tuchman R. Autism and epilepsy: what has regression got to do withit? Epilepsy Curr. 2006; 6: 107–11.
25 Parr J, Couteur A, Baird G et al. Early developmental regression inautism spectrum disorder: evidence from an international multiplexsample. J. Autism Dev. Disord. 2011; 41: 332–40.
26 Lainhart JE, Ozonoff S, Coon H et al. Autism, regression, and thebroader autism phenotype. Am. J. Med. Genet. 2002; 113: 231–7.
27 Nordahl CW, Lange N, Li DD et al. Brain enlargement is associatedwith regression in preschool-age boys with autism spectrumdisorders. PNAS 2011; 108: 20195–200.
28 Webb SJ, Nalty T, Munson J, Brock C, Abbott R, Dawson G. Rate ofhead circumference growth as a function of autism diagnosis andhistory of autistic regression. J. Child Neurol. 2007; 22: 1182–90.
29 Thomas M, Knowland VC, Karmiloff-Smith A. Mechanisms ofdevelopmental regression in autism and the broader phenotype: aneural network modeling approach. Psychol. Rev. 2011; 118: 637–54.
30 Bolton PF, Golding J, Emond A, Steer CD. Autism spectrum disorderand autistic traits in the Avon longitudinal study of parents andchildren: precursors and early signs. J. Am. Acad. Child Adolesc.Psychiatry 2012; 51: 249–60.
31 Veness C, Prior M, Bavin E, Eadie P, Cini E, Reilly S. Early indicators ofautism spectrum disorders at 12 and 24 months of age: aprospective, longitudinal comparative study. Autism 2012; 16:163–77.
32 Jones EJ, Gliga T, Bedford R, Charman T, Johnson MH. Developmentalpathways to autism: a review of prospective studies of infants at risk.Neurosci. Biobehav. Rev. 2014; 39: 1–33.
33 Landa RJ, Holman KC, Garrett-Mayer E. Social and communicationdevelopment in toddlers with early and later diagnosis of autismspectrum disorders. Arch. Gen. Psychiatry 2007; 64: 853–64.
34 Shumway S, Thurm A, Swedo SE et al. Brief report: symptom onsetpatterns and functional outcomes in young children with autismspectrum disorders. J. Autism Dev. Disord. 2011; 41: 1727–32.
35 Matson JL, Wilkins J, Fodstad JC. Children with autism spectrumdisorders: a comparison of those who regress vs. those who do not.Dev. Neurorehabil. 2010; 13: 37–45.
36 Bernabei P, Cerquiglini A, Cortesi F, D’Ardia C. Regression versus noregression in the autistic disorder: developmental trajectories. J.
Autism Dev. Disord. 2007; 37: 580–8.
K Williams et al.Regression in autism
Journal of Paediatrics and Child Health 51 (2015) 61–64© 2015 The Authors
Journal of Paediatrics and Child Health © 2015 Paediatrics and Child Health Division (Royal Australasian College of Physicians)
64

232
Appendix B. Databases and search terms used for the systematic review

233
Database Medline (1966 to 20 January 2016)
Psychinfo (1872 to 20 January 2016)
Embase (1980 to 20 January 2016)
CINAHL (1982 to 20 January 2016)*
Autism terms
1. exp child development disorders, pervasive/ or exp asperger syndrome/ or exp autistic disorder/ or exp schizophrenia, childhood/ 2. autis$.tw. 3. kanner$.tw. 4. (childhood adj3 schizophrenia).tw. 5. pervasive development$ disorder$.tw. 6. asperger$.tw. 7. (infantile adj3 psychosis).tw. 8. (childhood adj3 psychosis).tw. 9. or/1-8
1. autis$.tw. 2. kanner$.tw. 3. (childhood adj3 schizophren$).tw. 4. pervasive development$ disorder$.tw. 5. asperger$.tw. 6. (infantile adj3 psychosis).tw. 7. (childhood adj3 psychosis).tw. 8. exp EARLY INFANTILE AUTISM/ or exp AUTISM/ 9. exp Childhood Schizophrenia/ 10. exp Pervasive Developmental Disorders/ or exp Autistic Children/ 11. exp Childhood Psychosis/ 12. or/1-11
1. autis$.tw. 2. kanner$.tw. 3. (childhood adj3 schizophren$).tw. 4. pervasive development* disorder$.tw. 5. asperger$.tw. 6. (infantile adj3 psychosis).tw. 7. (childhood adj3 psychosis).tw. 8. exp Childhood Schizophrenia/ 9. exp AUTISM/ 10. exp Asperger Syndrome/ or exp pervasive developmental disorder/ 11. 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10
1. (MH “Child Development Disorders, Pervasive+”) 2. AB pervasive development* disorder* 3. AB autis* 4. AB Asperger* 5. AB Kanner* 6. AB (childhood N4 psychos*) 7. AB (childhood N4 schizophren*) 8. 1 or 2 or 3 or 4 or 5 or 6 or 7
Prognosis terms
13. epidemiology/ 14. exp "Death
11. epidemiology/ 12. sudden
9. (MH "Prospective Studies+")

234
Database Medline (1966 to 20 January 2016)
Psychinfo (1872 to 20 January 2016)
Embase (1980 to 20 January 2016)
CINAHL (1982 to 20 January 2016)*
and Dying"/ 15. sudden infant death/ 16. mortality rate/ 17. followup studies/ 18. prognos$.tw. 19. predict$.tw. 20. course.tw. 21. or/13-20
infant death/ 13. mortality/ 14. prognos$.tw. 15. predict$.tw. 16. course.tw. 17. or/11-16
10. (MH "Mortality+") 11. (MH "Incidence") 12. AB prognos* 13. AB predict* 14. AB course 15. mortalit* 16. 9 or 10 or 11 or 12 or 13 or 14 or 15
Combinations 10. limit 9 to "prognosis (sensitivity)"
22. 12 and 21 18. 11 and 17 14. 8 and 16
* when the supplier moved from OVID to EBSCO in 2009 for CINAHL the search was adapted. Search terms for EBSCO are reported here. Details on the search terms used under OVID are available upon request.

235
Appendix C. Risk of bias criteria (adapted from Hayden et al., 2013)

236
Criteria Unclear High Medium Low
1. Study participation The study sample adequately represents population of interest
Source population (described) Clinical (not community based)
Clinical but drawn from broad community base
Population-based
Description of sampling frame Not described Some description but not adequate/complete
Well described
Description of baseline study sample Not described Some description but not adequate/complete
Well described
Description of inclusion/exclusion criteria
Not described Some description but not adequate/complete
Well described
Adequacy of participation in study by all eligible
No Yes
2. Study attrition The study data available (those not lost to follow-up) adequately represents the study sample
Recruitment Retrospective Retrospective with whole cohort considered
Prospective
Loss to follow-up (LFU) (%) <80% remain ≥80% remain ≥ 85% remain
Description of attempts to collect information on those LFU
No Some information provided but not adequate
Yes
Reasons for LFU provided? No Some information provided but not adequate
Yes
Reasons for LFU linked to outcome? No Some information provided but not adequate
Yes

237
Criteria Unclear High Medium Low
Adequate description of LFU participants?
No Some information provided but not adequate
Yes
Analysis: important differences between LFU and non-LFU in study?
Important differences No important differences
3. Outcome measurement The outcomes of interest are measured in a similar way for all participants
Blinding Not blinded Blinding inadequate Blinding adequate
Clear definition of outcome provided?
No Yes
Same outcome tool for all? Not same tool for all Same for all
Valid and reliable tool? Not valid, reliable tool used Valid/reliable tool but parent rating
Standardised, reliable, valid tool used
Method and setting of outcome measurement same for all participants?
No Yes
Completeness of outcome measure Not all tools completed (>90% missing)
Not all tools completed but not >90% missing
All tools completed

238
Appendix D. Characteristics of studies included in the systematic review.
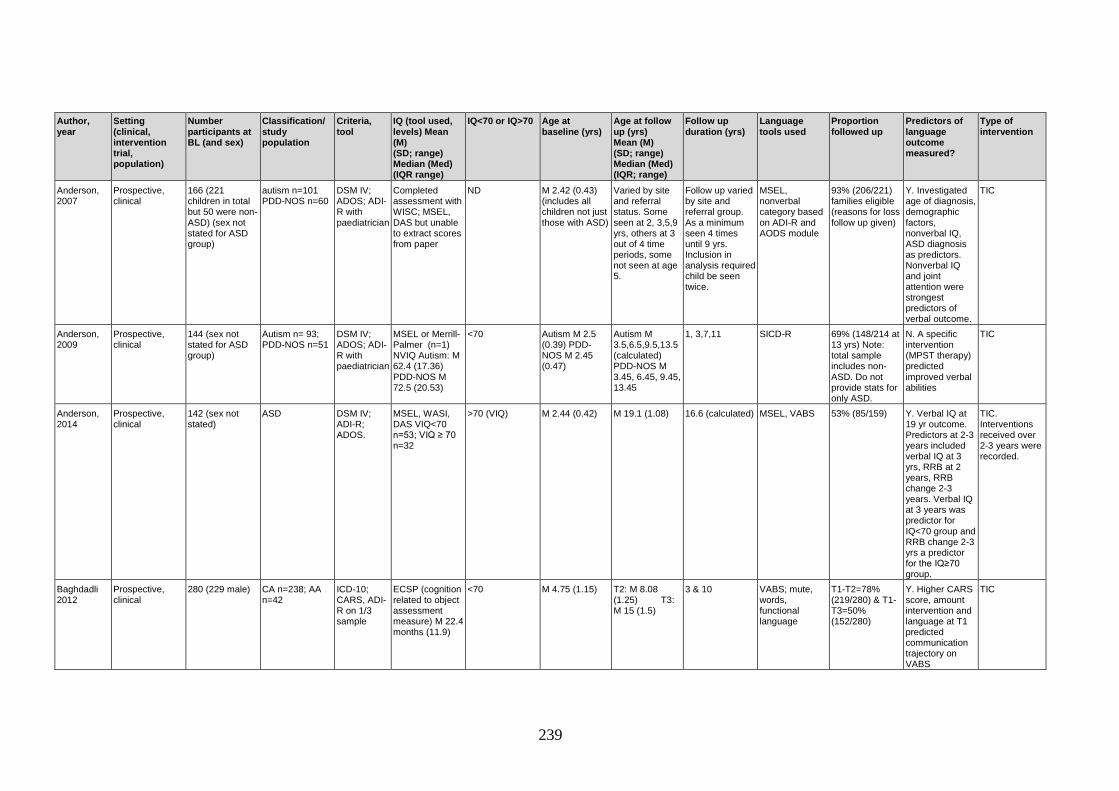
239
Author, year
Setting (clinical, intervention trial, population)
Number participants at BL (and sex)
Classification/ study population
Criteria, tool
IQ (tool used, levels) Mean (M) (SD; range) Median (Med) (IQR range)
IQ<70 or IQ>70 Age at baseline (yrs)
Age at follow up (yrs) Mean (M) (SD; range) Median (Med) (IQR; range)
Follow up duration (yrs)
Language tools used
Proportion followed up
Predictors of language outcome measured?
Type of intervention
Anderson, 2007
Prospective, clinical
166 (221 children in total but 50 were non-ASD) (sex not stated for ASD group)
autism n=101 PDD-NOS n=60
DSM IV; ADOS; ADI-R with paediatrician
Completed assessment with WISC; MSEL, DAS but unable to extract scores from paper
ND M 2.42 (0.43) (includes all children not just those with ASD)
Varied by site and referral status. Some seen at 2, 3,5,9 yrs, others at 3 out of 4 time periods, some not seen at age 5.
Follow up varied by site and referral group. As a minimum seen 4 times until 9 yrs. Inclusion in analysis required child be seen twice.
MSEL, nonverbal category based on ADI-R and AODS module
93% (206/221) families eligible (reasons for loss follow up given)
Y. Investigated age of diagnosis, demographic factors, nonverbal IQ, ASD diagnosis as predictors. Nonverbal IQ and joint attention were strongest predictors of verbal outcome.
TIC
Anderson, 2009
Prospective, clinical
144 (sex not stated for ASD group)
Autism n= 93; PDD-NOS n=51
DSM IV; ADOS; ADI-R with paediatrician
MSEL or Merrill-Palmer (n=1) NVIQ Autism: M 62.4 (17.36) PDD-NOS M 72.5 (20.53)
<70 Autism M 2.5 (0.39) PDD-NOS M 2.45 (0.47)
Autism M 3.5,6.5,9.5,13.5 (calculated) PDD-NOS M 3.45, 6.45, 9.45, 13.45
1, 3,7,11 SICD-R 69% (148/214 at 13 yrs) Note: total sample includes non-ASD. Do not provide stats for only ASD.
N. A specific intervention (MPST therapy) predicted improved verbal abilities
TIC
Anderson, 2014
Prospective, clinical
142 (sex not stated)
ASD DSM IV; ADI-R; ADOS.
MSEL, WASI, DAS VIQ<70 n=53; VIQ ≥ 70 n=32
>70 (VIQ) M 2.44 (0.42) M 19.1 (1.08) 16.6 (calculated) MSEL, VABS 53% (85/159) Y. Verbal IQ at 19 yr outcome. Predictors at 2-3 years included verbal IQ at 3 yrs, RRB at 2 years, RRB change 2-3 years. Verbal IQ at 3 years was predictor for IQ<70 group and RRB change 2-3 yrs a predictor for the IQ≥70 group.
TIC. Interventions received over 2-3 years were recorded.
Baghdadli 2012
Prospective, clinical
280 (229 male) CA n=238; AA n=42
ICD-10; CARS, ADI-R on 1/3 sample
ECSP (cognition related to object assessment measure) M 22.4 months (11.9)
<70 M 4.75 (1.15) T2: M 8.08 (1.25) T3: M 15 (1.5)
3 & 10 VABS; mute, words, functional language
T1-T2=78% (219/280) & T1-T3=50% (152/280)
Y. Higher CARS score, amount intervention and language at T1 predicted communication trajectory on VABS
TIC

240
Author, year
Setting (clinical, intervention trial, population)
Number participants at BL (and sex)
Classification/ study population
Criteria, tool
IQ (tool used, levels) Mean (M) (SD; range) Median (Med) (IQR range)
IQ<70 or IQ>70 Age at baseline (yrs)
Age at follow up (yrs) Mean (M) (SD; range) Median (Med) (IQR; range)
Follow up duration (yrs)
Language tools used
Proportion followed up
Predictors of language outcome measured?
Type of intervention
Bagley 1989 Retrospective clinical
53 (37 male) CA DSM III ND ND M 8 (4.5). M 12.8 (calculated)
M 4.8 (0.31-0.45)
Mute or full sentences.
ND. Missing data on many children.
N TIC
Bal, 2015 Prospective, clinical
152 (sex not stated)
ASD ADI-R, ADOS
MSEL, WASI, DAS NVMA M 1.62 AE (0.56) at CA of 2.44 (0.42)=66
<70 M 2.44 (0.42) 21 18.5 VABS 24% (36/152) N TIC
Ballaban-Gil 1996
Prospective, clinical
102 (93 male) (45 adults; 54 adolescents)
Autism (but appears to be range of PDD as per DSM IV)
Diagnosis made by criteria published by Rapin (1988), consistent with DSM IV
ND ND M 6.8 (0.79-20.3)
M 18.1 (12-29.5)
M 11.3 (3.2 -22.7)
Proportion verbal. Based on interview. Data per cognitive group.
61% (102/163) N TIC
Bedford 2015
Prospective, clinical
Whole gp (incl DD) n=209 (170 male) ASD only gp n=151 (139 male)
ASD or PDD-NOS
ADI-R MSEL visual reception T-score: M 31.46 (1.0) n=191 (includes non-ASD)
>70 M 2.41 (0.03) M 9.37 (0.1) 7 VABS, MSEL 95% (209/221) Includes non-ASD
Y. Early gross motor score was significant predictor of both expressive and receptive language development
TIC
Ben Itzchak 2009
Retrospective clinical, intervention.
68 (62 male) Autism (6 with ASD were excluded at baseline)
Clinical Dx by paediatrician, DSM IV, ADOS, ADI-R
Do not provide overall IQ only report individual subscales in paper
ND M 2.12 (0.33; 1.5-2.9)
M 3.12 (calculated)
1 VABS, MSEL ND. 100% (68/68). Assumed. Some missing data.
Y. Change in diagnostic classification predicted post-intervention achievement in language outcomes
Centre-based IBI
Ben Itzchak 2010
Retrospective clinical, intervention
78 (71 male) ASD Clinical Dx by paediatrician, DSM IV, ADOS, ADI-R
MSEL NV at T1 M 73.9 (23.7), T2 M 75.5 (29.2)
>70 1.25-2.9. Unclear if this is at BL or duration of study
2.25-3.92 (calculated)
1 MSEL 100% (78/78) (some missing data)
N Centre based IBI
Ben Itzchak 2014
Retrospective clinical, intervention
46 (39 male) ASD Clinical Dx by paediatrician, DSM IV, ADOS, ADI-R
Divide into high/low. High: IQ ≥70 n=22, low: IQ< 70n=24
>70 M 2.13 (0.33; 1.4-7.25)
M 3.13 (T2) 4.13 (T3) (calculated)
1 & 2 VABS, MSEL 100% (46/46) (some data missing VABS n=36)
N TIC-intervention based on ABA, provide detail

241
Author, year
Setting (clinical, intervention trial, population)
Number participants at BL (and sex)
Classification/ study population
Criteria, tool
IQ (tool used, levels) Mean (M) (SD; range) Median (Med) (IQR range)
IQ<70 or IQ>70 Age at baseline (yrs)
Age at follow up (yrs) Mean (M) (SD; range) Median (Med) (IQR; range)
Follow up duration (yrs)
Language tools used
Proportion followed up
Predictors of language outcome measured?
Type of intervention
Bennett 2008
Prospective, clinical
64 (45 HFA (42 male) and 19 AS (15 male)
HFA and AS, IQ>68
ADI HFA: M 87.24 (18.04) AS: M 99.98 (16.38) Stanford Binet >70, Leiter IQ >68
>70 HFA: M 5.41 (1) AS: M 5.77 (4.36)
HFA: M 7.41 AS: M 7.77 (calculated) *have presented data separately for SLI or no SLI groups and AD/HFA groups
2 (approximately)
TOLD, VABS 97% (62/64) Y. SLI at T1 and T2, clinical diagnosis predicted variation in communication subscales of VABS
TIC
Bennett 2013
Prospective, clinical
39 (31 male) HFA (needed IQ>68 for inclusion)
DSM III-R; ADI-R
Leiter NV IQ T1 M 86.48 (17.34; 36-127)
>70 M 7.45 (0.13; 6.08-9.33)
T2: M 15.19 (1.19; 13.17-17.58) T3: M 17.38 (1.48; 14.58-21.17)
2 yrs for TOLD and 8 yrs for VABS
VABS, TOLD 92% (36/39) Y. Theory of mind and language on adaptive communication outcomes (VABS). Language at T1 predicted communication domain on VABS and was mediated by ToM.
TIC
Bennett 2014
Prospective, clinical
330 (276 male) ASD with and without language impairment and with ID
DSM IV, ADI-R ADOS
Merrill-Palmer developmental index standard score M 58.92 (24.82)
<70 M 3.2 (0.7) M 4.2 (calculated)
1 PLS-4, CELF 4, VABS
87% (288/330) N TIC
Bennett 2015
Prospective, clinical
365 (sex not stated)
ASD DSM IV, ADI-R, ADOS
Merrill-Palmer developmental index standard score M 57.29 (24.65) 10-150
<70 M 3.2 (0.7) M 4.2 (calculated)
1 PLS-4, CELF 4, VABS
90% (330/365) N TIC
Berry, 2010
Retrospective clinical, intervention
114 (98 male) Autism n=73; PDD-NOS n=41
DSM IV-TR; CARS, ADI-R, ADOS
Scores presented separately for ASD_ASD and ASD-NON children. BL ASD IQ M 57.31 (9.74) *also have FU IQ scores. T1: Bayley’s, MSEL; T2 MSEL, DAS
<70 ASD-ASD (n=102) M 2.20 (0.36) ASD-NON (n=12) M 2.26 (0.29)
ASD-ASD M 4.44 (0.94) ASD-NON M 4.46 (0.62)
ASD-ASD M 2.23 (calculated) ASD-NON M 2.21 (calculated)
VABS, MSEL 100% (114/114) (only included those that had been measured twice)
N TIC

242
Author, year
Setting (clinical, intervention trial, population)
Number participants at BL (and sex)
Classification/ study population
Criteria, tool
IQ (tool used, levels) Mean (M) (SD; range) Median (Med) (IQR range)
IQ<70 or IQ>70 Age at baseline (yrs)
Age at follow up (yrs) Mean (M) (SD; range) Median (Med) (IQR; range)
Follow up duration (yrs)
Language tools used
Proportion followed up
Predictors of language outcome measured?
Type of intervention
Blacklock 2014
Retrospective clinical
68 (56 male) Autism/AD n=37, PDD or ASD n=26; PDD-NOS n= 5
Diagnosis completed by local diagnosticians who referred to IBI program CARS, DSM IV (see Perry 2008)
Range of IQ measures. MSEL, WISC, Stanford Binet, WPPSI
<70 M 7.40 (range 5.8-13.58)
M 9.02 (calculated)
1.62 (0.83-5.8) VABS 78% (53/68) (unclear if LFU or incomplete tools).
N Intensive IBI (publicly funded)
Bopp 2006 Retrospective clinical
70 (58 male) AD 55, PDD-NOS 15
Diagnoses done by diagnosticians in the community not involved in the study
ND ND M 4.2 (range 1.6-6)
M 5.2 (at 1 yr) M 6.2 (at 2yr) (calculated)
0.5, 1 & 2 PLS-3, EOWVT, PPVT III, CDI
90% (63/70). Y. Higher scores in acting out behaviour, inattentive behaviour and reduced stereotypic behaviour predicted greater increase in rate of change in language.
TIC
Bopp 2009 Retrospective clinical
69 (58 male) AD n=55 PDD-NOS n=14
Diagnosed in community, confirmed with CARS by blinded assessor
Estimated NVIQ using MSEL fine motor and visual subtests for 60 children (do not provide scores in table)
ND M 4.2 (1.75-6) At 1 yr M 5.2 and 2 yr M 6.2
0.5, 1 & 2 PLS-3, PPVT III, EOWVT
100 % (69/69) Y. Exploratory-child behaviour predictors (e.g., inattentiveness, acting out, social unresponsiveness, insistence on sameness, repetitive behaviours) on language outcomes. Social unresponsiveness and inattentive behaviours predictive of language outcomes
TIC

243
Author, year
Setting (clinical, intervention trial, population)
Number participants at BL (and sex)
Classification/ study population
Criteria, tool
IQ (tool used, levels) Mean (M) (SD; range) Median (Med) (IQR range)
IQ<70 or IQ>70 Age at baseline (yrs)
Age at follow up (yrs) Mean (M) (SD; range) Median (Med) (IQR; range)
Follow up duration (yrs)
Language tools used
Proportion followed up
Predictors of language outcome measured?
Type of intervention
Bopp 2011 Retrospective clinical
44 (37 male) AD n=36, PDD-NOS n=8
Diagnosed in community, confirmed with CARS by blinded assessor
MSEL at T1. NVIQ estimated for 39 children - combined visual reception and fine motor subscales from the MSEL; scores not available for other 5 children
ND M 3.9 (1.75-5.9) T6 M 9.3 (6.2-10.3)
4-5 yrs. Data collected at baseline (T1), and (on average) 6, 12, 24, 33 and 53 months later (T2–T6).
PPVT III, EOWVT, PLS-3; CDI
100% (44/44) Y. Pre-language skills investigated as predictors: initiate joint attention, conventional gestures, games-and-routines, actions with objects, pretend to be a parent, imitations of other adult actions. When all factors put in model ability to participate in games routines was the only significant predictor.
TIC
Carbonnel Chabas 2009
Prospective, clinical
32 (29 male) IA n=18, AA n=2, AS n=1, another PDD n=3 PDD-NOS n=8
ICD-10 and CFTMEA-R criteria
Very few tested- results ND
ND 3-7 yrs (at entry to program)
12-25 yrs (in 2006)
Unable to determine (assume between 9 and 18 yrs)
Questionnaire about language level (phrase, no language, only a few words, echolalic speech, generally uses correct sentences)
54% (32/59) N TIC
Cederlund 2008
Prospective, clinical
140 (140 male) Autism (n=70; n=62 with autism, n=22 with atypical autism including 2 with disintegrative disorder) or AS (n=70)
DSM-III or III-R for Autism, Gillberg & Gillberg criteria for AS. Confirmed with DISCO
Autism: < 70: n=70 ≥70: n=14 AS: VIQ 107.2 (18.6) PIQ 94.6 (18.7) NB: based on original sample.
Autism <70 and AS>70
Autism: <10 years AS: 11.3 (3.8)
Autism: 24.5 (5.4; 16.1–36.1]) AS: 21.5 (4.4; 16.0–33.0)
Autism: 14.5 (calculated) AS
VABS 76% (140/184) N TIC
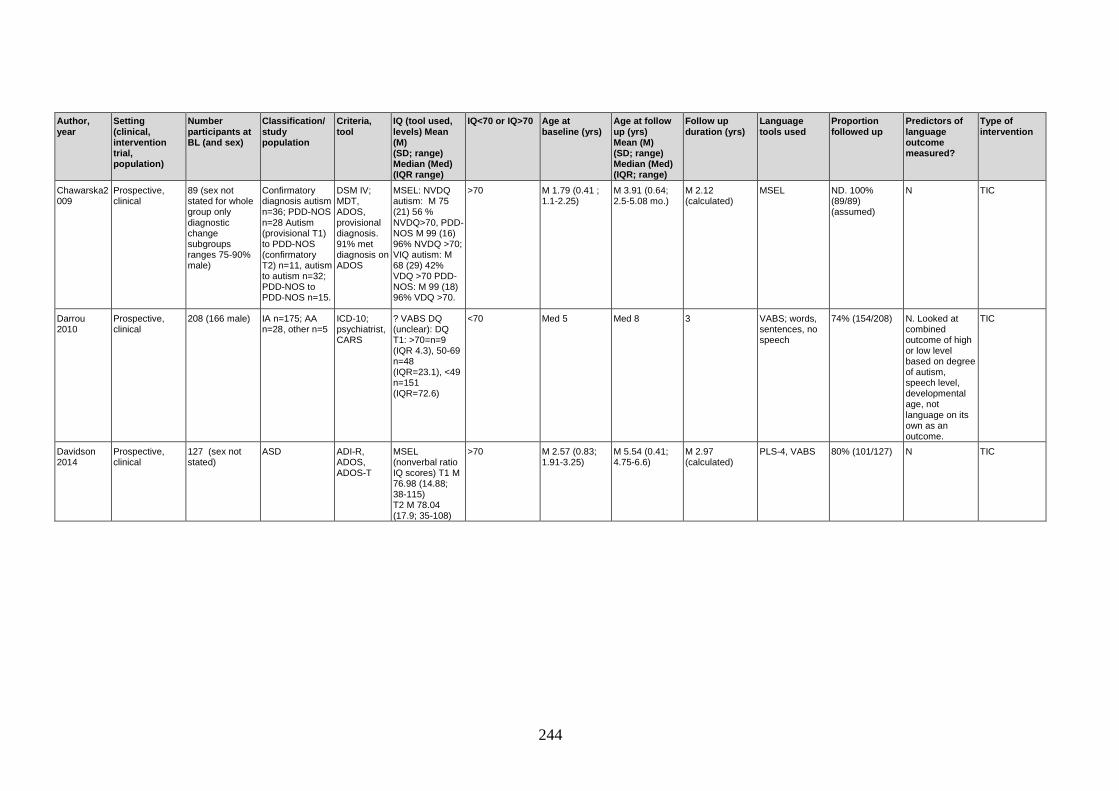
244
Author, year
Setting (clinical, intervention trial, population)
Number participants at BL (and sex)
Classification/ study population
Criteria, tool
IQ (tool used, levels) Mean (M) (SD; range) Median (Med) (IQR range)
IQ<70 or IQ>70 Age at baseline (yrs)
Age at follow up (yrs) Mean (M) (SD; range) Median (Med) (IQR; range)
Follow up duration (yrs)
Language tools used
Proportion followed up
Predictors of language outcome measured?
Type of intervention
Chawarska2009
Prospective, clinical
89 (sex not stated for whole group only diagnostic change subgroups ranges 75-90% male)
Confirmatory diagnosis autism n=36; PDD-NOS n=28 Autism (provisional T1) to PDD-NOS (confirmatory T2) n=11, autism to autism n=32; PDD-NOS to PDD-NOS n=15.
DSM IV; MDT, ADOS, provisional diagnosis. 91% met diagnosis on ADOS
MSEL: NVDQ autism: M 75 (21) 56 % NVDQ>70, PDD-NOS M 99 (16) 96% NVDQ >70; VIQ autism: M 68 (29) 42% VDQ >70 PDD-NOS: M 99 (18) 96% VDQ >70.
>70 M 1.79 (0.41 ; 1.1-2.25)
M 3.91 (0.64; 2.5-5.08 mo.)
M 2.12 (calculated)
MSEL ND. 100% (89/89) (assumed)
N TIC
Darrou 2010
Prospective, clinical
208 (166 male) IA n=175; AA n=28, other n=5
ICD-10; psychiatrist, CARS
? VABS DQ (unclear): DQ T1: >70=n=9 (IQR 4.3), 50-69 n=48 (IQR=23.1), <49 n=151 (IQR=72.6)
<70 Med 5 Med 8 3 VABS; words, sentences, no speech
74% (154/208) N. Looked at combined outcome of high or low level based on degree of autism, speech level, developmental age, not language on its own as an outcome.
TIC
Davidson 2014
Prospective, clinical
127 (sex not stated)
ASD ADI-R, ADOS, ADOS-T
MSEL (nonverbal ratio IQ scores) T1 M 76.98 (14.88; 38-115) T2 M 78.04 (17.9; 35-108)
>70 M 2.57 (0.83; 1.91-3.25)
M 5.54 (0.41; 4.75-6.6)
M 2.97 (calculated)
PLS-4, VABS
80% (101/127) N TIC

245
Author, year
Setting (clinical, intervention trial, population)
Number participants at BL (and sex)
Classification/ study population
Criteria, tool
IQ (tool used, levels) Mean (M) (SD; range) Median (Med) (IQR range)
IQ<70 or IQ>70 Age at baseline (yrs)
Age at follow up (yrs) Mean (M) (SD; range) Median (Med) (IQR; range)
Follow up duration (yrs)
Language tools used
Proportion followed up
Predictors of language outcome measured?
Type of intervention
Eaves 1996
Retrospective clinical
76 (57 male) ASD (classify at time 2 into AD and PDD)
DSM III or IIIR and CARS and clinic consensus. If seen before DSM III diagnosis based on notes and authors opinion. Some had diagnosis retrospectively applied to notes as criteria not available when patients seen.
IQ at T1; VIQ M 58 (6-135) and PIQ M 63 (6-126) WISC –R, Stanford Binet, Leiter, Bayley’s. The n, % of sample, and mean IQ score on each measure is also provided
<70 M 7.1 (3.1 to 12.7) (note: taken from Table 1, but mean age 7:6 years in text)
M 11.6 (8-17) M 4 (calculated) Proportion verbal/ nonverbal
100% (76/76) N TIC
Eaves 2004 Prospective, clinical
49 (sex not stated)
AD and PDD-NOS
CARS, DSM IV, MDT.
Bayley, WPPSI-R, Leiter, Stanford Binet
<70 M 2.75 (0.38) M 4.9 (0.62) 2.25 VABS/PLS 93% (40/43) N TIC
Ellis Weismer 2015
Prospective, clinical
129 (112 male) ASD ADI-R, ADOS, ADOS-T
Bayley cognitive scale T1: M 84.8 (12.1)
>70 M T1 2.6 (0.34) M T4 5.55 (0.4) 2.95 (calculated) PLS-4, VABS, PPVT-4 (T4 only)
80% (103/129) Y. Better receptive and expressive language at 2.5 years predicted more language growth in preschool than those with limited early language. Two variables played largest role were cognition and ASD severity.
TIC Collected amount of speech therapy and ASD therapy: total no. months and hr/month

246
Author, year
Setting (clinical, intervention trial, population)
Number participants at BL (and sex)
Classification/ study population
Criteria, tool
IQ (tool used, levels) Mean (M) (SD; range) Median (Med) (IQR range)
IQ<70 or IQ>70 Age at baseline (yrs)
Age at follow up (yrs) Mean (M) (SD; range) Median (Med) (IQR; range)
Follow up duration (yrs)
Language tools used
Proportion followed up
Predictors of language outcome measured?
Type of intervention
Eriksson 2013
Population based, prospective
208 (176 male) AD/CA n=105; AA n=58, AS n=13
MDT. Paediatrician/child psychologist examined all children with reference to DSM IV
Tool not stated for baseline data but IQ<70 n=95 & borderline IQ/low normal n=50 & average or above average IQ n=51
>70 n=64 referred before 36 months; n=83 referred between 37-48 months, n=61 referred between 49-54 months.
N=64 >60 mo.; n=83 between 61-72 mo.; n=61 between 73-78 months (calculated- note some LFU but do not describe age of ones LFU)
2 yrs
VABS 95% (198/208) N N=208 received intervention based on ABA. N=93 received intensive targeted intervention and n=105 non-intensive. See Fernell 2011 for detail.
Fernell 2011 Population based, prospective
208 (176 male) AD/CA n=105; AA n=58, AS n=13. Described in Fernell 2010.
MDT. Paediatrician/child psychologist examined all children with reference to DSM IV
Range of tools used. See Eriksson 2013 for detail.
>70 1.6-4.5 yrs months
3.6-6.5 yrs (calculated)
1.74 (0.27) VABS 95% (198/208) N TIC. High intensity n=65; other targeted interventions with ABA technique n=41; Fewer targeted interventions n=64. Detail provided.
Flanagan 2012
Retrospective clinical, intervention
122 (61 Tx (53 male), 61 WL (51 male)
PDD-NOS n=61; autism n=61. All children met diagnostic criteria for ASD towards severe end.
CARS MSEL, WPPSI-III, MA/CA. TX gp: M 55.71; WL gp M 36.46. Note measured at time 2 not baseline Tx: 18% IQ in average range (>85) WL: 3.3% IQ> 85)
<70 Tx gp: M 3.58 (0.96), WL gp: M 3.57 (0.88)
Tx gp: M 5.44; WL gp: M 4.98 (calculated)
Tx gp: M = 2.32 (0.68) WL gp: M 1.42 (0.23)
VABS 100% (122/122) N Intensive IBI intervention program (publicly funded)
Flanagan 2015
Prospective, clinical
369 (309 male) ASD ADOS, ADI-R, DSM IV
Merrill-Palmer developmental index standard score. No delay (n=23), mild-moderate (n=47) and severe (n=45) at 2 years (and also 3,4,6 years).
<70 T1 M 3.43 (0.75)
T2 M 4.54 (0.75) T3 M 6.59 (0.32)
T1-T2 M 1.11 T1-T3 M 3.16 (calculated)
VABS, PLS, CELF
ND N TIC. Provides some description of inerventions received in community.

247
Author, year
Setting (clinical, intervention trial, population)
Number participants at BL (and sex)
Classification/ study population
Criteria, tool
IQ (tool used, levels) Mean (M) (SD; range) Median (Med) (IQR range)
IQ<70 or IQ>70 Age at baseline (yrs)
Age at follow up (yrs) Mean (M) (SD; range) Median (Med) (IQR; range)
Follow up duration (yrs)
Language tools used
Proportion followed up
Predictors of language outcome measured?
Type of intervention
Freeman 1985
Prospective, clinical
62 (54 male) “Syndrome of autism”
DSM III High (VCI and PRI scores >70) =23%; medium (VCI<70, PRI>70)=29%; low (VCI and PRI <70)=48%
<70 M 3.10 (2-6) M 8.10 (calculated)
Annually for 5 yrs.
PPVT, TOLD, TACL
ND. Missing data: for cognitive and language testing.
N TIC
Freeman 1991
Prospective, clinical
62 (54 male) “Autism syndrome”
DSM III 77% had verbal IQ’s <70. High (VCI and PRI scores >70) =23%; medium (VCI<70, PRI>70)=29%; low (VCI and PRI <70)=48%
<70 M 3.8 (2.6- 5.9) M 14.6 (9-20) 12 (10-17) VABS; proportion nonverbal
85% (53/62) N TIC
Freeman 2010
Retrospective clinical, intervention
89 (73 male) AD n=55; PDD-NOS n=28; PDD or ASD n= 7
DSM IV; CARS
Tools not described.MA M 18.03 mo. (9.06; 8-55) n=31 FSIQ M 36.65 (14.83; 15-77) n=31
<70 M 4.47 (1.09; 1.67-6.92)
M 6.09 (calculated)
1.62 (0.81; 0.42-3.92)
VABS 100% (89/89) N All received IBI intervention, publicly funded program.
Georgiades 2014
Prospective, clinical
280 (241 male) ASD ADOS, ADI-R, DSM IV
MSEL ND M 3.4 (0.76; 2.0-4.9)
M 6.6 (0.3; 6.0-6.9)
3.2 (calculated) VABS 100 % (280/280) Only included participants with data at both time points.
N ND. TIC.
Green 2014 Prospective. Selected from larger longitudinal study. Unsure if clinical or population-based
161 (128 male) Autism, PDD-NOS
ADOS, ADI-R
MSEL IQ<70 Composite score: M 66.69 (16.73). Nonverbal IQ >70: M 77.15 (17.69)
<70 M 2.4 (0.35) T3 M 4.42 (0.37)
2 (calculated) VABS, MSEL T2 92% (161/175) and T3 57% (91/175)
N ND. TIC.
Haebig 2013a
Prospective, clinical
34 (28 male) autism n=14; ASD n=20
ADI-R, ADOS
MSEL: NVMA M 24.32 (4.01)
<70 M 2.61 (0.37) M 5.58 (0.48) M 2.96 PLS IV 100% (34/34) (assumed), Some missing data.
Y. Responsive verbal behaviours examined as predictors. Parent directives that followed into the child’s focus of attention predicted
TIC

248
Author, year
Setting (clinical, intervention trial, population)
Number participants at BL (and sex)
Classification/ study population
Criteria, tool
IQ (tool used, levels) Mean (M) (SD; range) Median (Med) (IQR range)
IQ<70 or IQ>70 Age at baseline (yrs)
Age at follow up (yrs) Mean (M) (SD; range) Median (Med) (IQR; range)
Follow up duration (yrs)
Language tools used
Proportion followed up
Predictors of language outcome measured?
Type of intervention
receptive language gains at 3 yr f/up. Parent comments had differential effects depending on initial language level. Minimally verbal chn at 2.5 yrs benefited from parent comments, but verbally fluent children did not.
Haebig 2013b
Prospective, clinical
40 (33 male) autism n=17; ASD n=23
ADOS, ADI-R
MSEL: NVMA M 24.24 (4.64; 17-34). Only 34 participants had valid NVMA data
<70 M 2.6 (0.36; 2-3.25)
‘on average’ 1 yr later i.e. 3.63 (3-4.25) (calculated)
1 PLS IV 100% (40/40) (assumed). Some missing data.
Y. Parent directives for language that followed into the child’s focus of attention-unique variance in predicting both receptive and expressive language 1 yr later. Parent comments predicted later receptive/expressive language for minimally verbal children at T1 (exploratory).
TIC
Hedvall 2015
Prospective, population-based
208 (176 male) AD n=128; PDD-NOS n=54; Aspergers n=9; autistic features n=17
In depth clinical assessment with ref to DSM IV
Griffith, PEP, Merrill Palmer, WPPSI
<70 (based on Fernell 2011)
T0 M 3.25 (SD 0.7) 1.7-4.42 T1 3.75 (SD 0.7) 2-5
T2 M 5.5 (SD 0.7) 3.7-6.75
2 (as reported by study)
CDI at T1, VABS at T1 and T2
95% (198/208) N ND. TIC

249
Author, year
Setting (clinical, intervention trial, population)
Number participants at BL (and sex)
Classification/ study population
Criteria, tool
IQ (tool used, levels) Mean (M) (SD; range) Median (Med) (IQR range)
IQ<70 or IQ>70 Age at baseline (yrs)
Age at follow up (yrs) Mean (M) (SD; range) Median (Med) (IQR; range)
Follow up duration (yrs)
Language tools used
Proportion followed up
Predictors of language outcome measured?
Type of intervention
Helendoorn, 2015
Prospective, population based
63 (49 male) ASD ADOS, ADI-R
MSEL- only raw scores reported
ND M 2.26 (0.73) M 3.82 (0.6) 1.56 (calculated) MSEL 73% (46/63) Y. Fine motor functioning was predictive of later receptive and expressive language
ND. TIC
Howlin 2004 Prospective, clinical
68 (61 male) CA Rutter (1966, 1972, 1978) criteria used for early cases, and then DSM-IV-TR (or ICD-10?)
NVIQ >50 Initial PIQ M 80.21 (19.28; 51-137). Initial VIQ (n=22) M 61.49 (21.26; 21-106). Used: WAIS-R, Raven, Merille Palmer and Leiter
>70 (based on NVIQ only)
M 7.24 (3.1; 3.1-15.66)
M 29.33 (7.97; 21.16-48.58)
M 22.09 (calculated)
BPVS, PPVT, used VIQ as preferred measure for final language score. ADI-R ratings of good, moderate, severe.
86% (68/79) (note: reports the 10 individuals who refused or were not contacted did not differ from study sample –unclear what happened to the extra 1 person)
N TIC
Howlin 2013 Prospective, clinical
60 (49 male) Autism NVIQ>70 Diagnosed autism, confirmed with ADI/ADI-R
WISC, WPPSI, WAIS, Merrill Palmer, Leiter:
>70 6.9 (2.9; 2.9–13)
44.2 (9.4; 29–64)
37.6 (9.2; 23-59) ADI_R rating of language (item 30). See Howlin 2014
67% (60/90) N. “Total outcome”, not specifically language outcomes.
ND. TIC
Howlin 2014 Prospective, clinical
60 (49 male) Autism
ICD-9 or 10, confirmed with ADI/ADI-R
WISC, WPPSI, WAIS, Merrill Palmer, Leiter: M 86.3
>70 6.9 (2.9; 2.9–13)
44.2 (9.4; 29–64)
37.6 (9.2) 23-59) EOWPVT, BPVS, overall level of language on ADI-R (i.e. functional use of spontaneous phrases; no phrase speech and >5 word vocab; no speech)
66% (60/91) N ND. TIC
Jonsdottir 2007
Prospective, clinical
41 (sex not stated)
PDD (CA and all other ICD 10 categories of PDD)
ICD-10 ND ND M 3.45 (0.76; 1.83-4.92)
M 5.8 (0.35, 5.1-6.6)
M 2.3 (0.78; 1-4.1), (minimum time between assessments was 1 yr)
ADIR (proportion verbal/nonverbal) and VABS at follow up
ND. Provide information on who was excluded but not loss to follow up.
N TIC

250
Author, year
Setting (clinical, intervention trial, population)
Number participants at BL (and sex)
Classification/ study population
Criteria, tool
IQ (tool used, levels) Mean (M) (SD; range) Median (Med) (IQR range)
IQ<70 or IQ>70 Age at baseline (yrs)
Age at follow up (yrs) Mean (M) (SD; range) Median (Med) (IQR; range)
Follow up duration (yrs)
Language tools used
Proportion followed up
Predictors of language outcome measured?
Type of intervention
Kleinman 2008
Prospective, clinical from population screening
46 (sex not stated)
T1: AD n=46, PDD-NOS n=15; T2 AD n=34, PDD-NOS n=12.
DSM IV, ADI-R, CARS, ADOS
FSIQ MSEL (n=35) or DAS (n=42): T1: autistic: mean IQ M 53.24 (7.34) PDD-NOS: M 62.33 (16.19).
<70 AD: M 2.26, (0.54) PDD-NOS: M 2.4 (0.24)
M 4.4 (0.67; 3.4-6.8). Note: this is data for full 77 (not only the 46 ASD)
AD: M 4.26 (0.57) PDD-NOS: M 4.44 (0.46)
VABS, MSEL 75% (46/71) N TIC
Klintwall 2015
Prospective, clinical
70 (62 male) ASD ADOS-T AODS, clinical best estimate diagnosis
MSEL T1 nonverbal DQ: T1=46.7 (SD 26.7)
<70 M 1.82 (SD 0.25)
M 3.18 (SD 0.37)
1.36 (calculated) MSEL, VABS 100% (70/70) Y. Level of interest during ADOS at 2 years predicted rate of verbal skill acquisition. Interest level predicted subsequent acquisition rate of verbal mental age.
TIC
Knorring 1993
Prospective, population-based
38 (23 male) PDD n=1; IA n=37
At baseline – Rutter and DSM III and at follow up DSM III R
ND ND Age of first symptoms M 13.7 (8.4; 2-26) Whole sample range 3-26.
M 18.9 (4.8; 10-29)
8-9 Medical Research Council Schedule of Handicaps, Behaviours and Skills. Categories: no speech, no nonverbal communication, some abnormality.
89% (34/38). Note: 39 children in original study, 1 did not meet DSM III R criteria as not symptomatic until 36 mo.
N TIC
Kobayashi 1992
Retrospective clinical
201 adults (170 male)
Autism DSM III-R applied to case notes
IQ (unclear when measured) mild or more delayed 76.4%; borderline or above (i.e., ‘normal’) 23.6%.
<70 M 6.4 (2.8) M 21.5 (3.6; 18-33)
M 15.4 (4.5; 5-28)
Categorise into very good, good, fair, poor, very poor.
98% (197/201) Some missing data.
N TIC
Landa 2012 Prospective, clinical intervention
48 (39 male) ASD or autism ADOS or expert clinician
MSEL: 81% IQ<70 and 58% VABS scores <70
<70 M 2.27 (0.23) T4: M 6.05 (1.46)
M 3.8 VABS 88% (42/48) N 6 month comprehensive intervention based on ABA/routines-based teaching and visual

251
Author, year
Setting (clinical, intervention trial, population)
Number participants at BL (and sex)
Classification/ study population
Criteria, tool
IQ (tool used, levels) Mean (M) (SD; range) Median (Med) (IQR range)
IQ<70 or IQ>70 Age at baseline (yrs)
Age at follow up (yrs) Mean (M) (SD; range) Median (Med) (IQR; range)
Follow up duration (yrs)
Language tools used
Proportion followed up
Predictors of language outcome measured?
Type of intervention
cues. 10hr/week. Detail provided.
Lombardo 2015
Prospective, clinical
60 (47 male) ASD poor language: <1 SD below norm on MSEL n=24 (19 male) and better language: >1 SD below norm n=36 (28 male) at outcome
ADOS, DSM IV
MSEL IQ Poor language IQ<70 but good language IQ >70. Poor language: ELC: 52.95 (37.08) Good language: ELC: 89.11 (17.81). Mean of means=74.6
>70 Poor: M 1.98 (SD 0.55). Good: M 1.78 (0.63)
Poor: M 3.14 (0.48). Good: M 2.8 (0.61)
Poor: 1.16; Good: 1.02 (calculated)
MSEL 100% (60/60) Y. FMRI findings (or combination of behavioural and speech-related FMRI findings) predictive of poor or good language groups. Multimodal classifier (ADOS, Vineland, Mullen and fMRI) predicted language group best.
TIC
Magiati 2011
Prospective, clinical
44 (sex not stated)
ASD 9; autism 27
ADI-R and independent diagnosis of ASD
Bayley or WPSII=T1 MA: M 26.3 mo. (13.6) 5-11 IQ: M 64.4 (30; 16-137.5) (also have T2 and T3 IQ) 26.3/40.8=64.5
<70 M 3.4 (0.05) T2: M 5.5 (0.6) T3: M 10.3 (0.8)
T2: 2 yrs post; T3: 4-5yrs post; i.e., 6-7yrs f/up period
BPVS, EOWVT T2: 100% (44/44) T3: 82% (36/44)
N. Combined outcome ranks at T3 (combination of adaptive behaviour/IQ/language). Not specifically looking at language outcomes.
TIC. All in in ‘relativelyintensive’ specialist preschool programs. Detail provided.
Mazurek 2012
Retrospective, Simons Complex database
1433 (1240 male)
ASD ADOS, ADI-R
FSIQ scores M 83.3, Med 86.0; (27.4; 7- 167)
>70 5 years (retrospective)
M 10.2 ( 3.1; 6-17)
5.2 (calculated) ADI-R question; ‘communicative’ or ‘not communicate speech’
100% (1433/1433)
Y. For those that were nonverbal at age 5 (n=402), initial severity, age, race, gender, nonverbal IQ, and treatment history predictive of presence/absence of communicative
TIC

252
Author, year
Setting (clinical, intervention trial, population)
Number participants at BL (and sex)
Classification/ study population
Criteria, tool
IQ (tool used, levels) Mean (M) (SD; range) Median (Med) (IQR range)
IQ<70 or IQ>70 Age at baseline (yrs)
Age at follow up (yrs) Mean (M) (SD; range) Median (Med) (IQR; range)
Follow up duration (yrs)
Language tools used
Proportion followed up
Predictors of language outcome measured?
Type of intervention
speech. Age, nonverbal IQ, speech therapy intensity predictive of verbal language.
Meyer 2002 Prospective, clinical
54 (45 male) Autism (AD and PDD)
ADI-R, ADOS-G, DSM IV
DAS: FSIQ: M 78.17 (20.96; 25-141). VIQ: M 78.26, (18.58; 51-118). PIQ: M 86.65 (20.31; 49-153)
>70 M 6.7 (1.25; 4-10.3)
9.7 (calculated) 3 PPVT (yr 1), VABS (yr1,3)
92% (46/50) N TIC but mainly TEACCH
Miniscalco 2014
Prospective, clinical
34 (29 male) AD n=21, PDD-NOS n=12, Asperger n=1
ADOS-G, DSM IV, multidisciplinary team
WPPPSI-R or Griffiths IQ/DQ scores M 79.5 (18.3; 46-114)
>70 M 3.42 (0.69; 27-55)
M 4.52 (calculated)
M 1.1 (0.34; 0.5-1.6)
CDI at T1 and T2
100% (34/34) Note: selected from larger sample
N ND. TIC
Mosconi 2009
Prospective, clinical
53 (sex not stated)
AD DSM IV; ADOS, ADI-R
MSEL AE (mo.) T1 M 15.1 (5.1) T2 M 27.7 (15.2) MA/CA=15.1/31.2=48
<70 M 2.6 (0.34) M 4.8 (0.46) 2 MSEL, VABS 51% (27/53) N TIC
Moss 2008 Prospective, clinical
35 (32 male) AD or ASD Needed to meet ADI-R criteria to be included
Mean IQ T1 M 68.9 (33; 16-137.5). IQ measured using: WISC, WPPSI, Bayley, Merrill-Palmer depending on CA, dev level and language ability.
<70 M 3.5 (0.6; 2.3-4.5)
M 10.5 (0.8; 9.1-12.1)
6-8 VABS, BPVS, EOWVT, presence of verbal language
47% (35/75) of original sample (75 seen at BL, 56 agreed to study and only 35 met inclusion criteria).
N TIC. Do not provide detail but see Moss above as same cohort.
Munson 2008
Prospective, clinical
70 (58 male) ASD DSM IV; ADOS, ADI-R, clinician judgement
MSEL NVDQ Visual Reception, M 27.90 ( 11.92; 20– 61); Fine Motor, M 24.77 (9.03; 20–59)
<70 M 3.63 (0.35; 2.83-4.33)
Varies per group (36-78 months)
Average of 6.6 follow up assessments from 6.63 to 10.5 (calculated)
VABS ND Y. Nonverbal problem-solving ability and the ability to learn reward associations predicted growth in communication on VABS
TIC

253
Author, year
Setting (clinical, intervention trial, population)
Number participants at BL (and sex)
Classification/ study population
Criteria, tool
IQ (tool used, levels) Mean (M) (SD; range) Median (Med) (IQR range)
IQ<70 or IQ>70 Age at baseline (yrs)
Age at follow up (yrs) Mean (M) (SD; range) Median (Med) (IQR; range)
Follow up duration (yrs)
Language tools used
Proportion followed up
Predictors of language outcome measured?
Type of intervention
Norrelgen 2014
Prospective population-based
165 (141 male) ASD autistic syndrome n=97, PDD-NOS n=56 AS n=12.
DISCO and DSM IV by MDT
WPPSI_III, Griffiths. IQ ≥70 n=81, IQ 50-69 n=27, IQ<50 n=52, IQ,70 n=5
>70 Range: 4-6.5 yrs. 4 yrs n=42, 5 yrs n=74 and 6 yrs n=49.
6-8.5 yrs (calculated)
2 yrs VABS expressive domain to classify speech as nonverbal (<3 words or expressive AE<15 months), minimally verbal (using at least 3 words but never or only sometimes/partially 2 word phrases and (expressive AE <24 months), Phrase speech: two word phrases or AE >24 months level.
63% (165/208) N TIC. All children were receiving interventions through the Autism Centre for Young Children. Intervention was based on ABA at different levels of intensity (Fernell 2011).
Oosterling 2010
Prospective, clinical intervention
75 (60 male; Tx gp 30/40 male; Co gp 30/35 male)
AD n=65 PDD-NOS n=10
ADI-R; ADOS
DQ MSEL or PEP-R=Tx gp M 58.4 (16.8); Co: DQ: M 58 (16.9)
<70 Tx gp: M 2.93 (0.46), Co gp: M 2.78 (0.53)
T gp: M 4.18; Co gp: M 4.03 (calculated)
M 1.25 (0.19) CDI 83% (62/75) Y. The intervention was not a predictor of language outcomes.
Focus Parent Training for toddlers intervention (Drew et al 2002)
Paul 2008 Prospective, clinical
37 (sex not stated)
T1 autism n=27; PDD-NOS n=10; T2 autism n=19; PDD-NOS n=18
ADOS Visual reception on MSEL (T1 M 41.5 (11.3). Fine Motor T1 M 35.6 (11.1)
>70 M 1.82 (0.24; 1.25-2.1)
M 3.91 (0.5; 3-4.83)
M 2.5 VABS, MSEL 100% (37/37) (assumed “all children had diagnosis at f/up”).
Y. Investigated NVIQ, VABS (receptive/expressive language), symbolic play, play and gestures, response to joint attention, stereotypic behaviours. Receptive language and presence of stereotypic and repetitive behaviours at the T1 predicted
TIC

254
Author, year
Setting (clinical, intervention trial, population)
Number participants at BL (and sex)
Classification/ study population
Criteria, tool
IQ (tool used, levels) Mean (M) (SD; range) Median (Med) (IQR range)
IQ<70 or IQ>70 Age at baseline (yrs)
Age at follow up (yrs) Mean (M) (SD; range) Median (Med) (IQR; range)
Follow up duration (yrs)
Language tools used
Proportion followed up
Predictors of language outcome measured?
Type of intervention
T2 expressive language outcome.
Pelicano 2010
Prospective, clinical
45 (40 male) AD n=31 PDD-NOS n=12 AS n=2
DSM IV; ADI-R
NVIQ M 113.27 (13.93; 83-141) VIQ 97.08 (11.52; 80-122
>70 M 5.67 (0.83; 4.1-7.33)
M 8.41 (0.92) 3 PPVT-III 82% (37/45). N TIC. Provides some detail.
Pelicano 2012
Prospective, clinical
45 (40 male) AD n=30 (67%); PDD-NOS n=12 (27%) AS n=3 (6%)
DSM IV; ADI-R (ADOS at follow up only) independent Dx.
VIQ or NVIQ>80 >70 M 5.63 (0.86) M 8.34 (0.95; 6.6-9.9)
M 2.74 PPVT-III 82% (37/45) N TIC. Provides some detail.
Perry 2008 Retrospective clinical, intervention
332 (276 male) AD n=194, PDD-NOS n=46, ASD/PDD n=92
Diagnosis completed by local diagnosticians who referred to IBI program CARS, DSM IV
Range of tools used. IQ: 45.5 (19.24; 11-96) n=151 MA: 22.92 (10.96; 3-60)
<70 M 4.46 (1.05; 20-86)
M 5.96 (calculated)
M 1.5 (0.7; 4-47) VABS 100% (322/322) (assumed)
N IBI intervention program, publicly funded
Perry 2011 Retrospective clinical, intervention
332 (276 male) AD, PDD-NOS, ASD
Diagnosis completed by local diagnosticians who referred to IBI program CARS, DSM IV
Range of tools used. IQ: 45.5 (19.24; 11-96) n=151 MA: 22.92 (10.96; 3-60)
<70 M 4.46 (1.05; 20-86)
M 5.96 (calculated)
M 1.5 (0.7; 4-47) VABS 100% (322/322) (assumed)
N. Composite VABS, not specifically language outcomes.
IBI intervention program, publicly funded
Perry 2013 Retrospective clinical, intervention
207 (168 male) AD, PDD-NOS, ASD
Diagnosis completed by local diagnosticians who referred to IBI program CARS
Varied based on local services/file review
<70 M 5.33 (2.01; 2.08-14.5)
M 7.01 (calculated)
M 1.68 (0.72; 10-55)
VABS 100% (207/207) N IBI intervention program, publicly funded

255
Author, year
Setting (clinical, intervention trial, population)
Number participants at BL (and sex)
Classification/ study population
Criteria, tool
IQ (tool used, levels) Mean (M) (SD; range) Median (Med) (IQR range)
IQ<70 or IQ>70 Age at baseline (yrs)
Age at follow up (yrs) Mean (M) (SD; range) Median (Med) (IQR; range)
Follow up duration (yrs)
Language tools used
Proportion followed up
Predictors of language outcome measured?
Type of intervention
Pickles 2015 Prospective, clinical
192 (162 male) Includes non-ASD children
Referred for evaluation of possible ASD (89% of group were ASD). Dx at 2 yrs: autism 53%; ASD 31%. Dx at 19 yrs: autism 66%; ASD 8%.
ADI-R, ADOS
MSEL. NVIQ 2 years M 66.9 (21.8); 19 years M 57.5 (40.9)
<70 2 19 17 (calculated) VABS 55% (106/192) N TIC. Provide detail on of hours in a range of interventions.
Pry 2011 Retrospective population-based
60 (48 male) IA (ICD-10) ICD-10; ADOS, CARS
Brunet: T1=Med 44 (25-75%iles=33-59 ; range=17-95; T2 Med= 40 (25-75%iles=28-53; range 12-89)
<70 Med 5 (IQR 4-6; 2-6)
Med 8 (IQR 7-9; 7-10)
3 ADI-R (good, intermediate, poor)
100% (60/60) (retrospective, randomly selected from epi data base)
Y. Symptom intensity (CARS) and daily living skills predicted morpheme production. Number of phonemes also predictive of lexical development. No. utterances not predictive.
TIC
Pugliese 2016
Prospective, clinical
64 (51 male) ASD without ID ADI-R (n=54); ADOS (n=56), DSM-IV
WISC, WASI, WPPSI M 107.03 (19.83; 72-154) (n=64)
>70 M 8.34 (2.29; 3-14)
12.88 (3.46; 7-23)
4.54 (calculated) VABS 100% (64/64). Data collected retrospectively.
N ND. TIC.
Ray-Subramanian 2012
Prospective, clinical
115 (97 male) AD n=106 PDD-NOS n=9
DSM IV; ADI-R ADOS or ADOS-T
MSEL: T1 (n=101) M 26.29 (5.04; 11-38; T2 (n=112) M 34.54 (8.22; 15-50). Not able to assess all children.
<70 M 2.58 (0.34) M 3.67 (0.34) M 1.12 (0.11) PLS 4 90% (based on larger study) 100% based on excluded if not both time points for RRB data
N TIC.
Sigman 2005
Prospective, clinical
48 (42 male) Autism Not specified
39/43 IQ M 52.2 (13.3).
<70 M 3.9 (1) T2 12.67 (3.75) T3 19 (3.83)
Preschool to middle years (approx. 8 yrs). Middle yrs to adolescence (approx. 6-7 yrs)
RDLS and CELF
73% (51/70) T2 and 48/70 participated in T3. Note: 3 families participated in adolescent f/up who were not
Y. Investigated IQ and early language skills as predictors of later language. Those with IQ>70 gained significantly more language
TIC

256
Author, year
Setting (clinical, intervention trial, population)
Number participants at BL (and sex)
Classification/ study population
Criteria, tool
IQ (tool used, levels) Mean (M) (SD; range) Median (Med) (IQR range)
IQ<70 or IQ>70 Age at baseline (yrs)
Age at follow up (yrs) Mean (M) (SD; range) Median (Med) (IQR; range)
Follow up duration (yrs)
Language tools used
Proportion followed up
Predictors of language outcome measured?
Type of intervention
available for mid-school f/up.
than those with IQ<70. Play skills (functional play), response to joint attention and imitation of requesting behaviours at preschool age predicted language gains from preschool to adolescence. Nonverbal communication in middle school yrs did not predict language outcomes
Siller 2013 Prospective, clinical, intervention
70 (64 male) All AD on ADI-R, AD n=64 on ADOS (5 met criteria for ASD on ADOS and 1 not administered ADOS)
ADOS; ADI-R
MSEL: visual reception Tx M 26.6 (9.4) Cx: M 24.6 (11.2)
ND Tx gp: M 4.86 (1.06), Co gp: M 4.4 (0.99)
Tx gp: M 6.02 Co gp: M 5.82 (calculated)
M 1.16 (0.39; 0.75-2.67)
MSEL- expressive language
89% (62/70) Y. Conditional effect of focused playtime intervention (FPI) on expressive language outcomes at f/up. Children with baseline language ability < 12 months most likely to benefit from FPI
FPI intervention
Smith I 2015 Retrospective clinical, intervention
118 (101 male) ASD Clinical diagnosis by specialist team based on ADOS and typically ADI-R.
Merrill-Palmer IQ>=70: n=36 M 87.44 (11.52); IQ 40-69 n=40 M 55.69 (8.94); IQ< 40 n=42 M 19.43 (10.50) Total sample: M 54.55 (29.31)
<70 4.1 (0.8) (40% 3 yrs; 39% 4 yrs; 8% 2 yrs, 14% 5 yrs)
6 months and 1.1 yrs (SD 0.12)
4.54 (calculated) VABS 100% (118/118) Y. IQ (but not age of enrolment in IBI program) was predictive of expressive and receptive language outcomes
EIBI: PRT, PECS, positive behaviour support (provide detail on amount and type of intervention)

257
Author, year
Setting (clinical, intervention trial, population)
Number participants at BL (and sex)
Classification/ study population
Criteria, tool
IQ (tool used, levels) Mean (M) (SD; range) Median (Med) (IQR range)
IQ<70 or IQ>70 Age at baseline (yrs)
Age at follow up (yrs) Mean (M) (SD; range) Median (Med) (IQR; range)
Follow up duration (yrs)
Language tools used
Proportion followed up
Predictors of language outcome measured?
Type of intervention
Smith T 2015
Prospective, clinical, intervention
71 (60 male) ASD (aged between 20-59 months)
ADI-R, ADOS
MSEL IQ <70. T1: M 58.80 (13.39; 49-20[sic]) T2: M 64.43 (18.25; 49-114); T3: M 64.93 (18.01; 49-112)
<70 T1 M 3.27 (0.65; 1.96-4.85)
T2 (n=67): M 4.46 (0.67) T3: (n=64) M 5.65 (0.81)
T2: 1.19 (calculated) T3: 2.38
VABS, MSEL, ADI-R (z scores for verbal and nonverbal algorithm).
T2: 94% (67/71) & T3 90% (64/71)
N EIBI based on Lovas UCLA model/discrete trial). ABA hours per year=866.37 (SD 243.77)
Starr 2003 Prospective, clinical
68 (51 male: AD n=38 male; AS n=13 male)
HFA n=41; AS n=17.
ICD 10 draft; ADI-R
IQ> 68 or 70 depending on test. Leiter IQ M 86.05 (17.96) for HFA gp and M 97.47 (16.19) for Asperger’s gp.
>70 M 5.82 (1.3) for those classified as having autism and M 6.2 (0.89) for those with AS
M 7.8 (calculated)
2 ADI-R question re: nonverbal
85% (58/68) N TIC
Steele 2003 Prospective, clinical
57 (sex not stated)
Autism DSM –IV Measured at baseline (DAS).
ND M 7.6 (2.3; 4.3-14.2)
M 8.8 (1.8; 5.1-15.4)
1 PPVT, EVT ND N TIC
Stone 2003 Prospective, clinical, intervention.
37 (29 male) AD and PDD-NOS
DSM III R and DSM IV depending on date seen (recruited 1993-1995)
MA M 17.1mth (3.7mths) Calculated DQ 54 (17.1/31.4)
<70 M 2.62 (0.25) M 4.88 (0.37) M 2.25 (calculated)
SICD (n=29) or PLS-3 (n=1). Scores on SICD derived from combination of parent report and behaviour observation
100% (38/38) (assumed). Note: inclusion criteria stated children had been seen at both time periods.
N TIC
Sullivan 2010
Retrospective clinical, intervention
75 (62 male) Autism 43; PDD-NOS 32
CARS used on n=70. “Diagnosed with ASD”
FSIQ on n=24 M 48.96 (15.08; 28-74)
<70 M 3.94 (1.19; 1.670-5.92)
6.12 (calculated)
M 2.18 (0.81; 1-5.25)
VABS (n=66) 100% (75/75) (retrospectively chosen)
N All in IBI intervention, publicly funded
Szatmari 2009
Prospective, clinical
55 (50 male) Autism: n=36 (31 male) AS: n=21 (19 male)
DSM III and ADI/ADI-R
Autism: M 84.5 (16.11) AS: M 101.33 (18.02)
>70 Autism M 5.46 (0.98) AS: M 5.6 (0.93)
Autism: 17.7 (1.56) AS: 17.6 (1.17) Followed up at 3 time points
Autism: M 12.24; AD: M 12
VABS 93% (53/57) Y. Investigated age, language ability/change, IQ as predictors of later communication ability (VABS.) IQ and change in language not predictive but presence of structural language impairment predictive of
ND. TIC.

258
Author, year
Setting (clinical, intervention trial, population)
Number participants at BL (and sex)
Classification/ study population
Criteria, tool
IQ (tool used, levels) Mean (M) (SD; range) Median (Med) (IQR range)
IQ<70 or IQ>70 Age at baseline (yrs)
Age at follow up (yrs) Mean (M) (SD; range) Median (Med) (IQR; range)
Follow up duration (yrs)
Language tools used
Proportion followed up
Predictors of language outcome measured?
Type of intervention
communication outcome
Szatmari 2015
Prospective, clinical
421 (355 male) ASD
ADOS, ADI-R, DSM IV
Merrill-Palmer IQ M 57.23 (26.20)
<70 3.32 (0.73) 6 years
M 2.68 (calculated)
VABS, PLS-IV 68% (285/421) N TIC. Timing and type of intervention varied by site. Offered Hanen More than Words program soon after diagnosis.
Takeda 2005
Retrospective clinical
57 adults (45 male)
ASD AD n=18 (12 males, 6 females); PDD-NOS n=38 (32 males, 6 females), AS n=1 (male)
DSM IV (used ICD 10 for atypical autism/ PDD-NOS)
Japanese version of Binet, WISC, K-test (Kyoto Scales of psychological development) At outcome evaluation: 39 had IQ/ DQ < 70 (called MR); 18 had IQ/DQ > 70 at outcome (called HFA)
<70 M 2.61 (0.3; 1.91-2.92)
M 5.5 (0.56, 5-7.5)
M 2.97 (calculated)
Categorical score: more than 3 words or less than 3 words.
ND. 100% (57/57) assumed. Enrolment requirement was 2 assessments (aged 2 and 5 or later)
N TIC
Thomas 2010
Retrospective clinical, intervention
69 (55 male) ND "Independent medical diagnosis". CARS used, but only on n=65
AEPS cog domain to assess cognition. No scores.
ND M 4.42 (3.17-5.58)
M 5.25 (3.67-6.42)
Approximately 5 yrs
PPVT-III ND (lists missing data from but not overall LFU)
Y. Cognitive ability, social skills predictive of communication outcome on PPVT III
All attended Project DATA comprehensive treatment intervention
Thurm 2007 Prospective, clinical
59 (52 male) Autism n=59; PDD-NOS n=24
DSM IV DAS, MSEL If not able to do DAS) Provide AE ratios at 2 years (0.57 in ASD gp); 0.71 in PDD-NOS group).
<70 Autism M 2.5 (0.36); PDD-NOS M 2.53 (0.39)
Autism M 4.75 (0.62); PDD M 4.76 (0.54)
Autism M 2.25; PDD-NOS M 2.2 (calculated). Authors describe it as "2 years".
MSEL (n=66) and DAS (n=52) language subtests, depending on whether reached ceiling or not. Also used 'no language' vs 'at least some
88% (97/110). Of the 131 participants, 13 children (all autism) did not receive full battery during the age 5 year testing. 118 chn with complete longitudinal data
Y. Investigated nonverbal ability, receptive & expressive communication and socialization at age 2 & 3 as predictors of receptive and expressive language age 5. Nonverbal
TIC. Many received some intervention from TEACCH.

259
Author, year
Setting (clinical, intervention trial, population)
Number participants at BL (and sex)
Classification/ study population
Criteria, tool
IQ (tool used, levels) Mean (M) (SD; range) Median (Med) (IQR range)
IQ<70 or IQ>70 Age at baseline (yrs)
Age at follow up (yrs) Mean (M) (SD; range) Median (Med) (IQR; range)
Follow up duration (yrs)
Language tools used
Proportion followed up
Predictors of language outcome measured?
Type of intervention
language' as per ADI-R.
cognitive ability at 2 yrs was the strongest predictor of language at 5 yrs, communication scores at 3 yrs were a stronger predictor of language at 5 yrs. Early joint attention and vocal and motor imitation skills more impaired in children who did not develop language by 5 yrs (but had relatively strong nonverbal cognitive skills) than in children who did develop language by 5.
Thurm 2015 Retrospective clinical
70 (53 male) AD DSM-IV, ADOS, ADI_R, best clinical judgement
MSEL T1 (also report T2). Min verbal to min verbal group IQ<70 M NVDQ=56.M 33 (12.57) MV->phrase speech grp IQ<70 NVDQ M 65.17 (15.4) PS->PS grp IQ>70 NVDQ: M 75.01 (13.92)
>70 (calculated mean IQ)
M 3.56 (0.85; 1.76-4.98)
M 5.45 (0.37; 4.62-5.98)
M 1.9 (0.81; 0.9-3.6)
MSEL 100 % (70/70) Y. VDQ and NVDQ predicted language status and VIQ on MSEL expressive language. T1 ADOS did not predict language status after controlling for NVDQ. Change in ADOS and RRB also not predictive of language status
ND. TIC.

260
Author, year
Setting (clinical, intervention trial, population)
Number participants at BL (and sex)
Classification/ study population
Criteria, tool
IQ (tool used, levels) Mean (M) (SD; range) Median (Med) (IQR range)
IQ<70 or IQ>70 Age at baseline (yrs)
Age at follow up (yrs) Mean (M) (SD; range) Median (Med) (IQR; range)
Follow up duration (yrs)
Language tools used
Proportion followed up
Predictors of language outcome measured?
Type of intervention
Toth 2006 Prospective, clinical
60 (51 male) AD n=42 (70%), PDD-NOS n=18 (30%)
DSM IV; ADOS, ADI-R, clinician judgement
MSEL composite 58.1 (19.8; 30-101)
<70 M 3.63 (0.36; 2.83-4.33)
Varies per group (seen every 6 months for VABS until 6.5 years)
2.87 (calculated) VABS ND (assume 100%)
Y. Investigated joint attention, imitation, toy play, language & communication ability on later language ability. Initiating protodeclarative joint attention and immediate imitation most strongly associated with language ability at 3-4 yrs. Toy play and deferred imitation were best predictors of rate of communication development from 4 to 6.5 years.
ND. TIC.
Venker 2014 Prospective, clinical
129 (112 male) ASD DSM IV, ADOS
MSEL M 76.39 (14.46; 38-115)
>70 M 2.6 (0.34; 23-39)
M 5.5 (0.42; 57-79)
3 years PLS-4 78% (100/129) N TIC. Intensive intervention n=71, not intensive n=36
Vivanti 2013 Prospective, clinical and surveillance samples
Clinical (S1): N=23 (22 male) Surveillance (S2) n=60 (45 male)
ASD S1: ASD diagnosis done in community and also ADOS confirmed S2: ADI-R and ADOS
MSEL MA S1: MA AE: M 21.4 (12) 8-54.5 DQ=21.4/40=53 S2: MA AE: M 16.7 (3.4) 8-26 DQ=16.7/25=67
<70 S1: M 3.33 (0.9; 1.83-5) S2: M 2.08 (0.17; 1.92-2.75)
S1: M 4.33 (calculated) S2: M 4.17
S2: 1 yr S2: 2.17 yr (calculated
MSEL S1 67% (60/89) S2 100% (23/23)
N ND. TIC.
Wodka 2013 Retrospective clinical (Simons Complex database)
535 (444 male) ASD ADOS, ADI-R
IQ<70 n=114 M 5.4 yr, IQ 70-85 n=94 M 5.3 y, IQ 86+ n=164 M 4.8yr (MSEL, DAS, WAIS). Reported for
>70 4 (based on ADI-R)
No phrase speech=11.5; phrase speech 11.7; only phrase speech=11;
No phrase speech 7.5; phrase speech 7.7; only phrase speech 7; fluent speech 8 (calculated)
ADI-R question re: nonverbal (and ADOS behaviour samples to verify)
100% (535/535) (strict inclusion criteria)
Y. Predictors examined for phrase speech: nonverbal IQ, autism symptomology. Predictors for
TIC
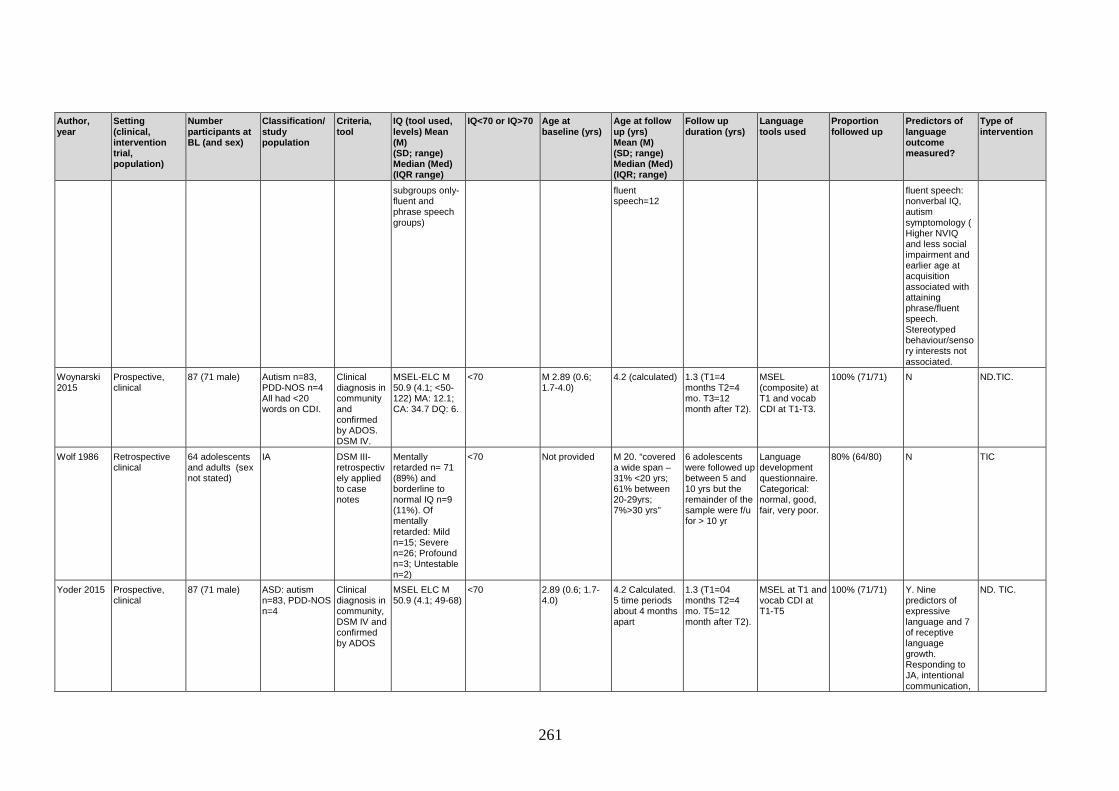
261
Author, year
Setting (clinical, intervention trial, population)
Number participants at BL (and sex)
Classification/ study population
Criteria, tool
IQ (tool used, levels) Mean (M) (SD; range) Median (Med) (IQR range)
IQ<70 or IQ>70 Age at baseline (yrs)
Age at follow up (yrs) Mean (M) (SD; range) Median (Med) (IQR; range)
Follow up duration (yrs)
Language tools used
Proportion followed up
Predictors of language outcome measured?
Type of intervention
subgroups only- fluent and phrase speech groups)
fluent speech=12
fluent speech: nonverbal IQ, autism symptomology ( Higher NVIQ and less social impairment and earlier age at acquisition associated with attaining phrase/fluent speech. Stereotyped behaviour/sensory interests not associated.
Woynarski 2015
Prospective, clinical
87 (71 male) Autism n=83, PDD-NOS n=4 All had <20 words on CDI.
Clinical diagnosis in community and confirmed by ADOS. DSM IV.
MSEL-ELC M 50.9 (4.1; <50-122) MA: 12.1; CA: 34.7 DQ: 6.
<70 M 2.89 (0.6; 1.7-4.0)
4.2 (calculated) 1.3 (T1=4 months T2=4 mo. T3=12 month after T2).
MSEL (composite) at T1 and vocab CDI at T1-T3.
100% (71/71) N ND.TIC.
Wolf 1986 Retrospective clinical
64 adolescents and adults (sex not stated)
IA DSM III-retrospectively applied to case notes
Mentally retarded n= 71 (89%) and borderline to normal IQ n=9 (11%). Of mentally retarded: Mild n=15; Severe n=26; Profound n=3; Untestable n=2)
<70 Not provided M 20. “covered a wide span – 31% <20 yrs; 61% between 20-29yrs; 7%>30 yrs”
6 adolescents were followed up between 5 and 10 yrs but the remainder of the sample were f/u for > 10 yr
Language development questionnaire. Categorical: normal, good, fair, very poor.
80% (64/80) N TIC
Yoder 2015 Prospective, clinical
87 (71 male) ASD: autism n=83, PDD-NOS n=4
Clinical diagnosis in community, DSM IV and confirmed by ADOS
MSEL ELC M 50.9 (4.1; 49-68)
<70 2.89 (0.6; 1.7-4.0)
4.2 Calculated. 5 time periods about 4 months apart
1.3 (T1=04 months T2=4 mo. T5=12 month after T2).
MSEL at T1 and vocab CDI at T1-T5
100% (71/71) Y. Nine predictors of expressive language and 7 of receptive language growth. Responding to JA, intentional communication,
ND. TIC.
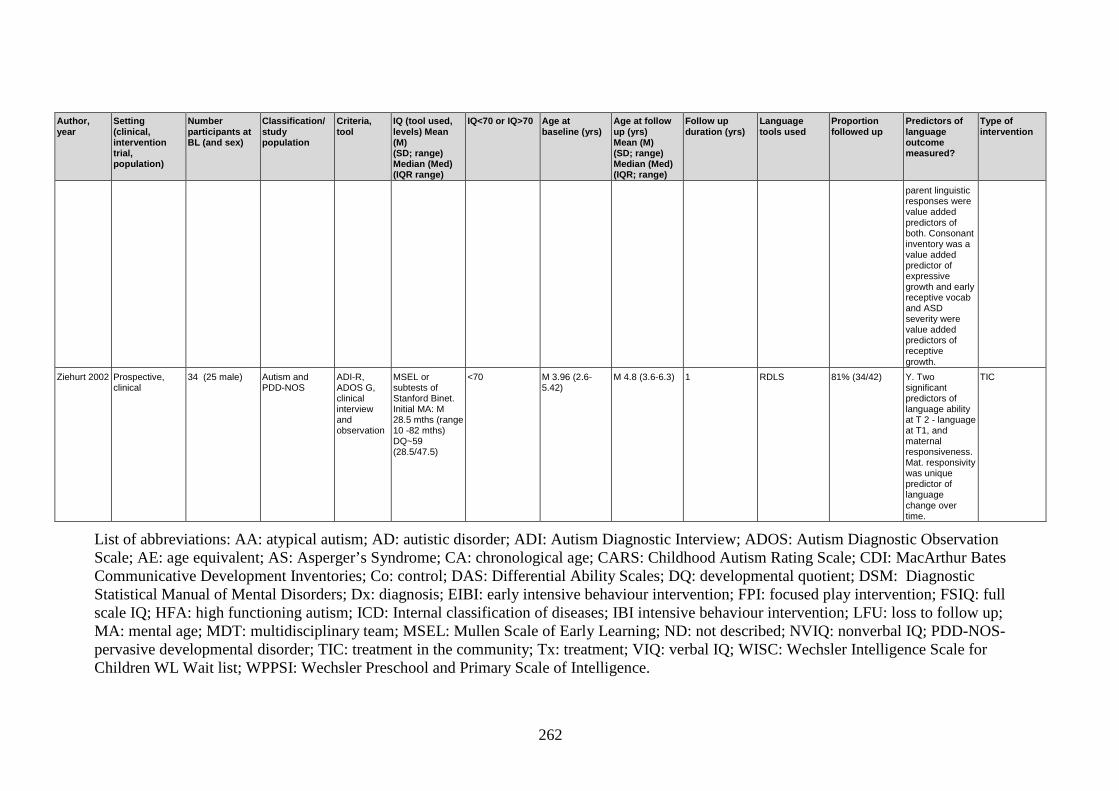
262
Author, year
Setting (clinical, intervention trial, population)
Number participants at BL (and sex)
Classification/ study population
Criteria, tool
IQ (tool used, levels) Mean (M) (SD; range) Median (Med) (IQR range)
IQ<70 or IQ>70 Age at baseline (yrs)
Age at follow up (yrs) Mean (M) (SD; range) Median (Med) (IQR; range)
Follow up duration (yrs)
Language tools used
Proportion followed up
Predictors of language outcome measured?
Type of intervention
parent linguistic responses were value added predictors of both. Consonant inventory was a value added predictor of expressive growth and early receptive vocab and ASD severity were value added predictors of receptive growth.
Ziehurt 2002 Prospective, clinical
34 (25 male) Autism and PDD-NOS
ADI-R, ADOS G, clinical interview and observation
MSEL or subtests of Stanford Binet. Initial MA: M 28.5 mths (range 10 -82 mths) DQ~59 (28.5/47.5)
<70 M 3.96 (2.6-5.42)
M 4.8 (3.6-6.3) 1 RDLS 81% (34/42) Y. Two significant predictors of language ability at T 2 - language at T1, and maternal responsiveness. Mat. responsivity was unique predictor of language change over time.
TIC
List of abbreviations: AA: atypical autism; AD: autistic disorder; ADI: Autism Diagnostic Interview; ADOS: Autism Diagnostic Observation Scale; AE: age equivalent; AS: Asperger’s Syndrome; CA: chronological age; CARS: Childhood Autism Rating Scale; CDI: MacArthur Bates Communicative Development Inventories; Co: control; DAS: Differential Ability Scales; DQ: developmental quotient; DSM: Diagnostic Statistical Manual of Mental Disorders; Dx: diagnosis; EIBI: early intensive behaviour intervention; FPI: focused play intervention; FSIQ: full scale IQ; HFA: high functioning autism; ICD: Internal classification of diseases; IBI intensive behaviour intervention; LFU: loss to follow up; MA: mental age; MDT: multidisciplinary team; MSEL: Mullen Scale of Early Learning; ND: not described; NVIQ: nonverbal IQ; PDD-NOS-pervasive developmental disorder; TIC: treatment in the community; Tx: treatment; VIQ: verbal IQ; WISC: Wechsler Intelligence Scale for Children WL Wait list; WPPSI: Wechsler Preschool and Primary Scale of Intelligence.

263
Appendix E. Studies reporting raw scores in the systematic review.

264
Author, year N Age at baseline, years.
Mean (SD; range)
Max duration of follow-up, years.
Mean (SD; range)
Raw score at baseline. Mean (SD; range)
Raw score at follow-up. Mean (SD; range)
Comments/notes
Bopp, 2006 (PPVT)
70 4;2, (1;7-6;0) 2 10.64 (18.71; 0-85) 28.80 (27.67; 0-108) Data used from the 2 year follow-up (were also followed up at 6 and 12 months)
Bopp, 2006 continued (PLS)
70 4;2, (1;7-6;0) 2 AC: 13.39 (9.78, 3-48) EC:14.38 (8.10; 4-47)
AC: 29.19 (13.37; 8-48) EC: 26.05 (12.43; 7-48)
Bopp, 2006 cont. (EOWVT)
70 4;2, (1;7-6;0) 2 25.17 (23.12; 0-86) 34.80 (26.91; 0-96)
Bopp, 2011 (CDI) 44 3:11 (1:9-5/11) 4.41 WU: 12.66 (12.60; 3-60) WS: 13.70 (11.04; 4-52)
WU: 85.56 (33.32; 17-138) WS: 72.06 (33.10; 19-123)
Followed up 4 other times too: 6,12,24,33 months.
Hellendoorn, 2015 (MSEL)
63 2.26 (0.73) 1.56 RL: 16.04 (8.45) EL: 17.02 (8.61)
RL: 37.22 (6.56) EL: 36.49 (6.89)
Oosterling, 2010 (CDI)
75 Control group: 2.78 (0.53)
1.25 (0.19) Control gp: WU: 181.5 (121.4) WS: 101.7 (109.7)
Mean difference between T1 and T2. Control gp: WU=35.2 (66.1), WS=56.1 (97.2)
Only control group means presented here.

265
Author, year N Age at baseline, years.
Mean (SD; range)
Max duration of follow-up, years.
Mean (SD; range)
Raw score at baseline. Mean (SD; range)
Raw score at follow-up. Mean (SD; range)
Comments/notes
Ray-Subramanian, 2012 (PLS)
115 2.58 (0.34) 1.1 (0.11) AC:20.35 (5.21; 10-42) EC: 24.96 (5.92; 13-42)
AC: 28.44 (11.58; 13-61) EC: 32.25 (9.27; 13-58)
Used PLS-4 subscale raw scores, controlling for chronological age
Steele, 2003 (PPVT)
57 7.6 (2.33; 4.25-14.17)
1 64.4 (32.6; 12-155) 81.7 (34.8; 26-177)
Steele, 2003 cont. (EVT)
57 7.6 (2.33; 4.25-14.17)
1 49.6 (19.2; 21-118) 60.7 (22.8) 28-137
Yoder cohort, 2015 (CDI)
87 2.89 (0.6) 1.3 WU: 75.8 (85.4; 0-385) WS: 3.7 (5.0;0-18)
WU: 169.8 (116.4; 0-396) WS: 76.4 (96.9; 0-396)
Followed up every 4 months.
Note. On the CDI, WU: words understood, WS: words spoken; PLS AC: auditory comprehension, EC: expressive communication; MSEL RL: receptive language, EL: expressive language.

266
Appendix F. Scores for children not included in analyses for Study 3

267
Language and nonverbal IQ scores for children with ASD in Study 3 who did not have language and IQ scores at required time points. Child NVIQ Rec
(4yr) Exp (4yr)
Rec (5yr) Exp (5yr) Rec (7yr)
Exp (7yr)
1 63 74 A - - - -
2 70 - - 76 79 - -
3 101 92 113 80 110 - -
4 - 50 50 55 (E) 57 (E) A 45
5 107 81 81 64 78 - -
6 - - - 64 68 - -
7 - A A - - 47 59
8 55 48 50 - - - -
9 103 - - 77 84 82 68
10 80 - - <50 (RDLS)
<50 (RDLS)
58 A
11 - - - 58 (PLS) 53 (PLS) - -
Note. RDLS: Reynell Developmental Language Scales; PLS: Preschool Language Scales, E: assessment completed externally
Total number of children with ASD by 7 years: n=44. Lost to follow up/no data at any wave: n=4. Trajectory mapped: n= 28. Unable to complete but attempted: n= 3 (receptive only in one) (IQ 55, 77, 93). Not mapped: n=11 (table above)

Minerva Access is the Institutional Repository of The University of Melbourne
Author/s:Brignell, Amanda
Title:Language development in autism spectrum disorder: longitudinal comparison with acommunity cohort of children with language impairment and typical development
Date:2016
Persistent Link:http://hdl.handle.net/11343/127483
Terms and Conditions:Terms and Conditions: Copyright in works deposited in Minerva Access is retained by thecopyright owner. The work may not be altered without permission from the copyright owner.Readers may only download, print and save electronic copies of whole works for their ownpersonal non-commercial use. Any use that exceeds these limits requires permission fromthe copyright owner. Attribution is essential when quoting or paraphrasing from these works.




















