Cortical Reconstruction Using Implicit Surface Evolution: A Landmark Validation Study
Upload
mississippimedicalCategory
view
0download
0
Landmark identification accuracy in xeroradiographic cephalometry
Robert V. V. Hurst, Bernhard Schwaninger, Robert Shaye, and J. M. Chadha New Orleans. La.
X eroradiography is the process of recording a latent radiographic image on a selenium-coated aluminum plate. The image is then transferred to a specially treated paper for visualization. The selenium coating contains a uniform positive charge which, when exposed to x-radiation, is selectively discharged according to the density of the object being radiographed. Denser areas of the skull. for example, will absorb more radiation, resulting in less discharge of the selenium coating. Less dense areas will allow more radiation to pass through, causing a greater discharge of the selenium. The charge pattern resulting from the exposure is the latent image.
In addition to the selenium-coated plates and plastic cassettes which hold them, the Xerox System 125 consists of two free-standing units-a conditioner which prepares the selenium-coated plates for exposure and a processor which develops the image and trans- fers it to the special paper. In the processor a negatively charged blue powder is misted onto the exposed plate, adhering differentially to the positively charged selenium and resulting in a visible image. The image is transferred to the paper which is then heated, making it permanent. The whole process is fully automatic, taking 90 seconds to com- plete.
The first attempts at electrostatic imaging with x-rays were made in Europe as early as 1903 by Righi,“j followed in 1905 by Gabritschewski.7 Xerography was developed by Carlson” in 1937 and applied to medical radiography upon the encouragement of the Department of the Army shortly before World War II. It was thought that silver would be in short supply for medical x-ray film and that an alternate imaging method would have to be found. Although the need did not materialize, Carlson was able to develop the xeroradiographic process. Its commercial use in the medical field began following investi- gations by Roach” in 1952. Xeroradiography was first applied to mammography by Wolfelg in 1966. Following recent advances in the processing technique, it has been used in orthopedics and angiography. Because of the size of the cassette, the dental application of this technique is limited at present to extraoral radiography. Soft tissues, bone, teeth, and air passages are clearly visible because of a large recording latitude, high resolution, and the “edge enhancement phenomenon.“‘3. I7 Edge enhancement can be defined as greater contrast between areas of different densities. It results during the developing
From the Department of Orthodontics, School of Dentistry, Louisiana State University.
568 ooO2.9416/78/0573-0568$00.70/O 0 The C. V. Mosby Co

Volume 73 Number 5
Xeroradiographic cephalometry 569
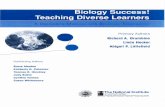
Fig. 1. Conventional cephalogram with lead markers.
process when extra powder is attracted to the edge of contiguous areas with differing amounts of electrostatic charge.
Clinical studies comparing radiographic images of bone specimens show more pro- nounced definition and contrast with xeroradiography.4 The same has been found for lateral skull radiographs. ‘2 l4 For cephalometty, Davis, and associate@ and Johnson’ conclude that xeroradiography is superior to conventional radiography. Using a standard- ized x-ray test pattern, Thunthy’* found that higher resolution was obtained with xemradiographs than with screen films. Articles relating xeroradiography to the study of the head have been mainly descriptive of the history and technical aspects of the process. Little clinical information on the application of xeroradiography to cephalometrics is available. The purpose of this study was to compare the accuracy of landmark identifica- tion between xeroradiographic cephalograms and conventional cephalograms.
Materials and methods
Spherical lead markers, 1 mm. in diameter, were used to identify fourteen landmarks on a dried skull. The skull was positioned in a Wehmer wall-mounted cephalometer. A xeroradiographic cephalogram and a conventional radiographic cephalogram were taken with a Picker KMS300 medical x-ray unit at a film-focus distance of 60 inches (Fig. 1 and 2). The xeroradiograph was developed in a Xerox 125 System processor and the con- ventional radiograph in a Kodak RP X-O-MAT automatic processor with Kodak EP chemistry.
Exposure values for the xeroradiograph were 87 kv., 100 Ma., and 0.3 second. Kodak XL-5 film was used for the conventional radiograph and was exposed at 65 kv., 100 Ma.,

570 Hurst et al
Fig. 2. Xeroradiographic cephalogram with lead markers.
and 0.1 second. The filtration was 3.5 mm. of aluminum. Following the initial exposures, the lead markers were removed without disturbing the skull position in the cephalostat. Another xeroradiograph and conventional radiograph without lead markers were made, using the previously described exposure values and processing techniques.
Ten examiners were asked to identify the fourteen landmarks on the xeroradiograph without markers and on the conventional radiograph without markers. The distances from their readings to the actual landmarks were then measured by two examiners using vernier calipers. The distances from the examiner-identified landmarks to the lead-marked land- marks were measured on like cephalograms (xeroradiographic cephalogram to xero- radiographic cephalogram with markers and conventional cephalogram to conven- tional cephalogram with markers). This avoided image magnification discrepancies resulting from differences in the thickness of the two types of cassette and corresponding differences in subject-film emulsion distance and subject-selenium coating distance.
Resutts
The measurement differentials between the marker-denoted landmarks and the land- marks identified by the examiners on the xeroradiograph and between the marker-denoted landmarks and the landmarks identified on the conventional cephalograms were subjected to statistical analysis (Table I). Four of the measurements demonstrated statistical significance for the xeroradiographs, while two were significant for the conventional cephalograms (Fig. 3).
The distances between the actual landmarks and the examiner-identified landmarks for point A, upper incisor tip, infradentale, and menton were significantly less when mea-

Volume 73 Number 5 Xeroradiographic cephalometry 571
Table I. Statistical evaluation of measured landmarks
Mean S.D. S.E.
Landmark R X R X R X 1 P
Nasion Orbitale Anterior nasal spine Point A Upper incisor tip Infradentale Point B Pogonion Menton Cusp tip maxillary molar Posterior nasal spine Ptergo-maxillary fissure Condylion Basion
1.00 .50 .62 .29 .20 .09 2.65 2.10 .29 .93 .09 .29 1.72 1.00 2.91 .26 .92 .08 2.90 1.25 2.00 .58 .63 .I8 1.47 .67 .36 .21 .11 .07 3.22 2.55 1.40 1.03 .44 .32
.57 1.80 .45 .47 .I4 .I5 4.62 4.35 .43 .50 .I4 .I6 2.00 .60 .76 .76 .24 .24
.97 1.02 .75 .61 .24 .20 2.67 3.07 2.92 1.78 .92 .56 6.92 6.35 5.87 5.92 1.86 1.87 2.90 3.92 1.70 1.23 .54 .39 1.80 1.65 .96 1.09 .30 .35
- .55 - 1.94 - .83 -2.78 -7.69 -2.49
9.71 -1.36 -6.00
.25
.42 - .67
2.56 - .46
.60
.08
.43
.02*
.oo**
.03*
.oo+t
.21
.oo**
.81
.67
.52
.03+
.66
S.D. = Standard deviation of ten numbers, each the mean of the two examiners. SE. = Standard error of the mean. R = Standard radiograph. X = Xeroradiograph. *Statistically significant; xeroradiograph closer to true landmark. **Highly significant; xeroradiograph closer to true landmark. +Statistically significant; radiograph closer to true landmark. + +Highly significant; radiograph closer to trne landmark.
sured from the xeroradiograph than when measured from the cephalogram. The distances for point B and condylion were significantly less when measured from the conventional cephalogram.
Discussion
Upon viewing a xeroradiographic cephalogram, the immediate visual impression is one of remarkable clarity and detail of both hard- and soft-tissue structures. Bony trabecu- lation, neurovascular canals, soft-tissue profile, lymphoid tissue, and even hair are clearly evident on the image. When placed side by side with a conventional cephalogram, the xeroradiograph would appear capable of yielding a much higher degree of accuracy in the standard orthodontic tracing and mensuration techniques.
The results of this investigation, however, show that only four of the fourteen land- marks studied-point A, upper incisor tip, infradentale, and menton-could be identified more accurately on the xeroradiograph than on the conventional cephalogram. Two landmarks-point B and condylion-were more accurately identified on the conventional cephalogram. A conclusion to be drawn from these findings is that, for the most part, the conventional cephalogram is as reliable as the xeroradiograph in identifying the anatomic landmarks studied. This is not too surprising since, aside from those landmarks borrowed from anthropologic craniometry, most of the current popular landmarks were employed because they could be easily visualized on the conventional cephalometric radiograph.
An obvious discrepancy was noted in the determination of pogonion. Table I shows that the mean xeroradiographic measurement as identified by the examiners was 4.35 mm.

572 Hurst et ul
Fig. 3. Landmarks demonstrating statistical significance.
from the lead-marked pogonion, while the same span on the conventional cephalogram measured 4.62 mm. These are considerable distances, given the fact that pogonion, the most anterior point on the external surface of the mandibular symphsis, is a midline structure assumed to be easily identifiable on the cephalometric image.
Upon closer examination the explanation for the large variance of the examiner mea- sured landmark from the true pogonion became apparent. With the skull in the cephalostat orientation (Frankfurt horizontal parallel to the floor), the lead marker had been placed on the most anterior aspect of the symphsis, the mental protuberance. However, when the cephalograms were exposed, the right mental tubercle, a bony prominence lateral to the mental protuberance, was projected to appear as the most anterior point (Fig. 4). In the skull used for this study, the distance from the mental protuberance to the right mental tubercle was 18 mm. If this projection phenomenon is a common occurrence in cephalometric radiography, the landmark observed by clinicians as pogonion may well be a structure a considerable distance lateral to the midline.
Much remains to be investigated in this new method of assessing craniofacial morphology. Some authors have shown that structures obscure on the conventional film could be important, useful features for determining developmental changes, treatment progress, and even growth prediction. ‘3 a, g, “3 *2 Neurovascular canals and foramina, such as mandibular canal, infraorbital canal, mandibular foramen, foramen ovale, and~foramen

Volume 73 Number 5 Xeroradiographic cephalometry 573
p t
Fig. 4. Projection of the mental tubercle anterior to the mental protuberance.
rotundum, among others, have been suggested as significant anatomic structures in the study of craniofacial growth.2, 3, s, 11, ~2, I5 Th e xeroradiographic image seems to project these structures more distinctly than the conventional radiographic image. Although this study is not directed toward soft-tissue structures, they also seem more distinct on the xeroradiograph. Subsequent articles will address these topics.
Summary
Identification accuracy of fourteen cephalometric landmarks was compared between xeroradiographic cephalograms and conventional cephalograms. Four landmarks-point A, upper incisor tip, infradentale, and menton-were more accurately determined on the xeroradiograph, while two landmarks-point B and condylion-were more accurately determined on the conventional cephalogram.
Although not conclusively demonstrated in this study, the xeroradiograph does appear to offer more clarity and detail than the conventional cephalogram. Further investigation of this new diagnostic medium will be necessary before its true significance to dentistry can be evaluated.

574 Hurst et al.
REFERENCES I. Binnie, W. H., Stacey, A. J., Davis. R.. and Cawcon. R. A.: Applications ol.xeroradiography in dentlq
J. Dent. 3: 99-104. 1975. 2. Bjork, A.: Prediction of mandibular growth rotation, AM. J. ORTHOD. 55: 585599. IYW.
3. BjGrk, A., and Skieller, V.: Facial development and tooth eruption; an implant study at the age of puberty. AM. J. ORTHOD. 62: 339-383, 1972.
4. Campbell, C. J., Roach, J. F., and Grisolia, A.: A comparative study of xeroroentgenography and routine roentgenography in the recording of mentgen images of bone specimens. J. Bone Joint Surf. 39: 577-582. 1977.
5. Carlson, C. F.: Electron photography, U.S. patent 2221776, 1938. 6. Davis, R., Binnie, W. H., Cawson, R. A., Reed, R. T.. and Stacey, A. J.: The role of xeroradiography in
cephalometric radiology, J. Dent. 5: 32-38, 1977. 7. Gabritschewski, V.: Die elektrische Radiographie, Phys. 2. 6: 33-34, 1905. 8. Johnson, N. A.: Xeroradiography for cephalometric analysis, AM. J. ORTHOD. 69: 524-527, 1976. 9. Koski, K.: Variability of the craniofacial skeleton, AM. J. ORTHOD. 64: 188-196, 1973.
10. Moss. M. L., and Greenberg, S. N.: Functional cranial analysis of the human maxillary bone. I. Basal bone, Angle Orthod. 37: 151-164, 1967.
I I. Moss, M. L., and Salentijn, L: The logarithmic growth of the human mandible, Acta Anat. 77: 341-360, 1970.
12. Moss, M. L., Moss-Salentijn, L., and Ostreicher, H. P.: The logarithmic properties of active and passive mandibular growth, AM. J. ORTHOD. 66:645-664, 1974.
13. Oliphant, W. D.: Xeroradiography. I. Apparatus and method of use, Br. J. Radiol. 28: 543-544, 1955. 14. Olson, D. J., Guralnick, W., Kalisher, L., and Donoff, R.: The application of xeroradiography in oral
surgery, J. Oral Surg. 34: 438-441, 1976. 15. Ricketts, R. M.: A principle of arcial growth of the mandible, Angle Orthod. 42: 368-386, 1972. 16. Righi, A.: Die Bewegungen der Ionen bei der elektrischen Entladung, Leipzig, Barth, Spez. S., pp. 64-70,
1907. 17. Roach, J. F.. and Hilleboe, H. E.: Xeroradiography, Am. J. Roentgenol. Radium Ther. Nucl. Med. 73:
s-9, 1955. 18. Thunthy, K.: Comparison of xeroradiographs with occlusal and screen films, ORAL SURG. (In press.) 19. Wolfe, J. N.: Mammography, Springfield, Ill., 1967, Charles C Thomas Publisher.
Copyright © 2022 FDOKUMEN