
Kirklin Early Predictors of Survival to and After Heart Transplantation in Children With Dilated
9
Kirklin, David C. Naftel and Daphne T. Hsu Larsen, R. Erik Edens, Steven D. Colan, Jeffrey A. Towbin, Steven E. Lipshultz, James K. Biagio A. Pietra, Paul F. Kantor, Heather L. Bartlett, Clifford Chin, Charles E. Canter, Ranae L. Cardiomyopathy Early Predictors of Survival to and After Heart Transplantation in Children With Dilated Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2012 American Heart Association, Inc. All rights reserved. is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Circulation doi: 10.1161/CIRCULATIONAHA.110.011999 2012;126:1079-1086; originally published online July 16, 2012; Circulation. http://circ.ahajournals.org/content/126/9/1079 World Wide Web at: The online version of this article, along with updated information and services, is located on the http://circ.ahajournals.org//subscriptions/ is online at: Circulation Information about subscribing to Subscriptions: http://www.lww.com/reprints Information about reprints can be found online at: Reprints: document. Permissions and Rights Question and Answer this process is available in the click Request Permissions in the middle column of the Web page under Services. Further information about Office. Once the online version of the published article for which permission is being requested is located, can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Circulation in Requests for permissions to reproduce figures, tables, or portions of articles originally published Permissions: by guest on July 8, 2014 http://circ.ahajournals.org/ Downloaded from by guest on July 8, 2014 http://circ.ahajournals.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Kirklin Early Predictors of Survival to and After Heart Transplantation in Children With Dilated
Kirklin, David C. Naftel and Daphne T. HsuLarsen, R. Erik Edens, Steven D. Colan, Jeffrey A. Towbin, Steven E. Lipshultz, James K.
Biagio A. Pietra, Paul F. Kantor, Heather L. Bartlett, Clifford Chin, Charles E. Canter, Ranae L.Cardiomyopathy
Early Predictors of Survival to and After Heart Transplantation in Children With Dilated
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2012 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/CIRCULATIONAHA.110.011999
2012;126:1079-1086; originally published online July 16, 2012;Circulation.
http://circ.ahajournals.org/content/126/9/1079World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on July 8, 2014http://circ.ahajournals.org/Downloaded from by guest on July 8, 2014http://circ.ahajournals.org/Downloaded from
Pediatric Cardiology
Early Predictors of Survival to and After HeartTransplantation in Children With Dilated Cardiomyopathy
Biagio A. Pietra, MD; Paul F. Kantor, MBBCh; Heather L. Bartlett, MD; Clifford Chin, MD;Charles E. Canter, MD; Ranae L. Larsen, MD; R. Erik Edens, MD, PhD; Steven D. Colan, MD;
Jeffrey A. Towbin, MD; Steven E. Lipshultz, MD; James K. Kirklin, MD;David C. Naftel, PhD; Daphne T. Hsu, MD
Background—The importance of clinical presentation and pretransplantation course on outcome in children with dilatedcardiomyopathy listed for heart transplantation is not well defined.
Methods and Results—The impact of age, duration of illness, sex, race, ventricular geometry, and diagnosis of myocarditis onoutcome in 261 children with dilated cardiomyopathy enrolled in the Pediatric Cardiomyopathy Registry and Pediatric HeartTransplant Study was studied. End points included listing as United Network for Organ Sharing status 1, death while waiting,and death after transplantation. The median age at the time of diagnosis was 3.4 years, and the mean time from diagnosis tolisting was 0.62�1.3 years. Risk factors associated with death while waiting were ventilator use and older age at listing inpatients not mechanically ventilated (P�0.0006 and P�0.03, respectively). Shorter duration of illness (P�0.04) wasassociated with listing as United Network for Organ Sharing status 1. Death after transplantation was associated withmyocarditis at presentation (P�0.009), nonwhite race (P�0.0001), and a lower left ventricular end-diastolic dimension zscore at presentation (P�0.04). In the myocarditis group, 17% (4 of 23) died of acute rejection after transplantation.
Conclusions—Mechanical ventilator use and older age at listing predicted death while waiting, whereas nonwhite race,smaller left ventricular dimension, and myocarditis were associated with death after transplantation. Although 97% ofchildren with clinically or biopsy-diagnosed myocarditis at presentation survived to transplantation, they had significantlyhigher posttransplantation mortality compared with children without myocarditis, raising the possibility that preexisting viralinfection or inflammation adversely affects graft survival. (Circulation. 2012;126:1079-1086.)
Key Words: cardiomyopathy, dilated � heart transplantation � myocarditis � pediatrics
In children, dilated cardiomyopathy (DCM) is the most com-mon form of cardiomyopathy and the most common indica-
tion for heart transplantation.1,2 The annual incidence of DCM isreported to be 0.37 per 100 000 in the United States and 0.57 to1.13 per 100 000 in Australia.3–5 In children with end-stage heartfailure secondary to DCM, heart transplantation is the onlytherapeutic option currently available. In prior studies from thePediatric Cardiomyopathy Registry (PCMR), freedom fromdeath or heart transplantation in children with DCM was 61%and 47% at 1 and 5 years, respectively.6,7 Refinements in themanagement of end-stage DCM in children over the last decadehave significantly reduced early mortality, but transplantationremains the definitive treatment.8–11 Death after listing or afterheart transplantation remains a significant problem in this groupof children, even in the era of mechanical support, and as manyas 38% of patients with DCM listed for heart transplantation
have significant complications and morbidity while waiting forheart transplantation.12 Outcomes after heart transplantation arefavorable in adults13,14 and in children with DCM.2,11,15,16 Chil-dren with DCM have a 68% to 72% 10-year survival rate aftertransplantation, higher than that for children transplanted forend-stage congenital heart disease.17,18 Improved surgical andperioperative care has led to an era of improvements in outcomesafter transplantation.19
Clinical Perspective on p 1086Studies of children with DCM requiring heart transplantation
have focused on cohorts identified at listing.18,17 The impact ofprelisting factors on outcomes both after listing and aftertransplantation has not been studied. Better outcomes in childrenwith DCM may be possible with better identification andmanagement of prelisting and pretransplantation risk factors. We
Received December 2, 2011; accepted June 22, 2012.From the University of Colorado Health Sciences, Aurora (B.A.P.); Hospital for Sick Children, Toronto, ON, Canada (P.F.K.); University of Iowa Children’s
Hospital, Iowa City (H.L.B., R.E.E.); Cincinnati Children’s Hospital Medical Center, Cincinnati, OH (C.C., J.A.T.); Washington University School of Medicine,St. Louis Children’s Hospital, St. Louis, MO (C.E.C.); Loma Linda University Medical Center, Loma Linda, CA (R.L.L.); Boston Children’s Hospital, HarvardMedical School, Boston, MA (S.D.C.); Department of Pediatrics, University of Miami Miller School of Medicine, Miami, FL (S.E.L.); University of Alabamaat Birmingham, Birmingham (J.K.K., D.C.N.); and Children’s Hospital at Montefiore, Albert Einstein College of Medicine, Bronx, NY (D.T.H.).
Guest Editor for this article was Lynn Mahony, MD.Correspondence to Biagio A. Pietra, MD, The Children’s Hospital, Denver, Division of Cardiology, 13123 E 16th Ave, B100, Aurora, CO 80045.
E-mail [email protected]© 2012 American Heart Association, Inc.
Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.110.011999
1079 by guest on July 8, 2014http://circ.ahajournals.org/Downloaded from

hypothesized that important risk factors for worse outcomesafter transplantation listing and transplantation might be identi-fied in children with DCM from their prelisting status. Toevaluate this hypothesis, we pooled longitudinal data regardingpatients with DCM from 2 large pediatric databases, the PCMRand the Pediatric Heart Transplant Study (PHTS) databases,20
and attempted to define risk factors at presentation and at listingthat were associated with worse outcomes after listing in thiscohort.
MethodsPatient PopulationPatients were identified from a merged data set that included allchildren enrolled in the PCMR who were also enrolled in thePHTS.20 The PCMR is a National Institutes of Health/NationalHeart, Lung, and Blood Institute–funded registry that enrolledchildren (�18 years of age at the time of presentation) who werediagnosed with all forms of primary cardiomyopathy from January 1,1990 (clinical trial registration, http://www.clinicaltrials.gov; uniqueidentifier, NCT00005391). Data collected include echocardiographicmeasurements and clinical and laboratory information at the time ofpresentation and at yearly follow-up visits. Patient follow-up in thePCMR is censored at heart transplantation or death.
The PHTS is an event-driven registry that has enrolled patients �18years of age listed for heart transplantation at participating institutionssince 1993. The PHTS data set includes outcome after listing, peritrans-plantation course, and posttransplantation events such as rejection,infection, graft atherosclerosis, death, malignancy, and need for retrans-plantation. The registries were merged to allow analysis of data inchildren with cardiomyopathy from the time of presentation throughtheir posttransplantation course. The merged data set included childrentransplanted in the United States and Canada. The PHTS registry iscurrently active. The PCMR is no longer enrolling new patients, butanalysis of previously enrolled patients continues. Follow-up for themerged data set was complete through December 31, 2005.
Only children who met the PCMR definition of DCM were includedin this analysis. In the PCMR data set, DCM was defined by echocar-diographic criteria that included a left ventricular (LV) end-diastolicdimension (EDD) �2 SDs for body surface area and an LV percentfractional shortening �2 SDs for age.20 The diagnosis of myocarditiswas defined in this study as it has been previously21 as either thehistological evidence of myocarditis (the presence of Dallas criteria)obtained at endomyocardial biopsy or at explantation22 or clinically bythe investigator at the submitting institution if histology was notavailable.
Risk Factors StudiedWe examined several potential diagnoses and prelisting, listing, andtransplantation risk factors for the following end points: severity ofillness as defined by the need to be listed as United Network for OrganSharing (UNOS) status 1 (highest-priority UNOS status to receive anorgan, a reflection of severity of illness at listing), death after listingwhile waiting for a heart, and death after heart transplantation. Themerged data set included 10 children transplanted in Canada, whichdoes not use UNOS listing criteria. For the variable UNOS status 1 atlisting, information was available for 3 children to be coded in theappropriate UNOS status, and the other children were excluded fromthis portion of the analysis. The potential risk factors for death afterlisting while waiting for a heart included age at listing, sex, race (whiteversus nonwhite), diagnosis of myocarditis, time from diagnosis tolisting (years), use of mechanical ventilation at the time of listing, andmultiple echocardiographic measures of cardiac performance and size,including LV fractional shortening z score and LVEDD z score atpresentation. Echocardiographic measurements were expressed as the zscore for body surface area to adjust for body size. In this analysis, olderage was defined as �10 years and younger age as �1 year; however, inthe regression analysis, age was analyzed as a continuous variable.UNOS status 1 versus 2 was also included in the analyses of death while
waiting and after transplantation. Age at transplantation, use of mechan-ical ventilation at the time of transplantation, and time spent waiting fora heart were included in the risk factor analysis for death aftertransplantation. Transplanted patients with and without the diagnosis ofmyocarditis were also analyzed.
Data CollectionInstitutional Review Board approval was obtained for each registry(PCMR and PHTS) and the merged data set at all study sites. Adata-sharing agreement was established between the data coordinat-ing centers (New England Research Institutes, Watertown, MA, andUniversity of Alabama, Birmingham) before the exchange of data.
Statistical MethodsStandard statistical methods for summarizing and displaying data wereused. Data are reported as mean and median with standard deviations.Logistic regression was used to determine which variables were asso-ciated with listing as UNOS status 1. Kaplan-Meier analysis was used toestimate the time-related probability of death. Time 0 for survivalanalysis for death while waiting was defined as the date of listing; time0 for the analysis of death after transplantation was the date oftransplantation. The log-rank test was used to compare the survival ofdesignated subgroups. Cox proportional hazard regression was used toidentify risk factors for death while waiting and death after transplan-tation; the results are reported as hazard ratios. We set � at 0.05, and alltests were 2 tailed. Forward selection was used in the multivariableanalysis. Comparison of the myocarditis and no myocarditis groups wasperformed with the unpaired t test for normally distributed data and theKruskal-Wallis test for skewed data. SAS statistical analysis software(SAS Institute, Cary, NC) was used for all analyses.
Results
PCMR and PHTS Registry MergerThe merged data set included 332 children from 16 participatingcenters, of whom 261 had a diagnosis of DCM and made up thestudy cohort (Table 1). The remaining 71 children from theoriginal merged data set (n�332) were not included in this studybecause their cardiomyopathy phenotype was not DCM. Of the261 children, 11% (n�29) died waiting for a heart. Eightypercent (209 of the 261) went on to heart transplantation, and theremaining 23 children were alive but still waiting at the time ofanalysis. Of these 209 children transplanted, 40 children (19%)died after heart transplantation.
Characteristics of Children With DCM Listedfor TransplantationDemographics of the 261 patients who were listed and the 209who were transplanted are shown in Table 1. For the childrenwho were listed, the median age at the time of diagnosis was 3.4years (range, 0–17.9 years), and 43% were diagnosed at �1 yearof age (Table 2). A third of the patients listed for transplantationpresented after 10 years of age. Thirty percent of all patientslisted were ventilator dependent at the time of listing. Data oninotropic support were not available. Of the initial 261 childrenwith DCM, 11% (n�29) were diagnosed with myocarditis eitherclinically or by biopsy at presentation.
Risk Factors Associated With Status 1 at ListingShorter duration of illness from diagnosis to listing wasassociated with listing as status 1 (odds ratio, 0.789; 95%confidence interval, 0.631–0.988; P�0.04). No other factorswere found to be associated with listing as status 1.
1080 Circulation August 28, 2012
by guest on July 8, 2014http://circ.ahajournals.org/Downloaded from

Death While Waiting for TransplantationThere were 29 deaths before transplant, 3 occurring after 2years from listing. By 2 years after listing, 11% (n�26) of thepatients had died while waiting, 11% (n�26) were still alivewaiting, and 79% (n�206) had been transplanted (Figure 1).The primary cause of death was cardiac in nature (primarycardiac failure, sudden death, or multisystem failure) in 16 ofthe 29 children (55%; Table 3). Neurological events were acommon cause of death, occurring in 6 of 29 (21%). Most ofthe risk factors analyzed did not correlate with death whilewaiting (Tables 4 and 5). The time on the wait list for childrenwho died while waiting was not significantly shorter than thetime from listing to transplantation in those who were trans-planted. Mechanical ventilation at listing (P�0.003) was asso-ciated with death while waiting by Kaplan-Meier analysis(Figure 2). Mechanical ventilation at listing had a hazard ratio of4.06 and was strongly associated with death while waiting in themultivariable analysis (P�0.0006). Age was not a risk factor for
death while waiting in the univariate analysis (Table 4). A higherproportion of younger patients were ventilated at listing com-pared with older patients; thus, when mechanical ventilation wasincluded in the analysis, multivariable analysis demonstratedthat older age at listing was a risk factor (Table 5). One childwith myocarditis died while waiting for heart transplantation. Asubgroup analysis in children with DCM without myocarditis(n�232) also showed ventilator use and older age at listing asrisk factors for death (P�0.0001 and P�0.01, respectively).
Characteristics of Children With DCM WhoSurvived to TransplantationOf the 261 patients listed for transplantation, 209 (80%) receivedheart transplants. The median age at transplantation was 4.4years. UNOS status 1 at listing did not correlate with death whilewaiting. The transplanted group had a higher proportion ofchildren who were UNOS status1 at the time of transplantationcompared with the time of listing (86% versus 79%). In themyocarditis group, 23 of 29 were transplanted (1 died waiting, 5still waiting at analysis). The proportion of children who werestatus 1 at the time of transplantation was the same in themyocarditis and nonmyocarditis groups. At the time of hearttransplantation, 22% of children were ventilator dependent.
Table 1. Demographic and Clinical Characteristics of 261Children With Dilated Cardiomyopathy Followed Up FromDiagnosis Through Heart Transplantation
CharacteristicAt Listing for
TransplantationAt
Transplantation
Age, mean (SD), y 6.5 (6.2) 7.0 (6.3)
Median 3.6 (261) 4.4 (209)
Male, % (n) 51 (261) 51 (209)
White, % (n) 66 (260) 67 (209)
Ventilator use, % (n) 30 (261) 22 (209)
UNOS status 1, % (n) 79 (254) 86 (209)
Time, diagnosis to listing, mean (SD), y 0.62 (1.3) 0.69 (1.3)
Median (n) 0.16 (261) 0.22 (209)
Time, listing to transplantation,mean (SD), y
… 0.23 (0.7)
Median (n) … (261) 0.067 (209)
Myocarditis, % (n) 11 (261) 11 (209)
LVEF, mean (SD), % 26 (9) 25 (10)
n 38 34
LVFS, mean (SD), z score �9.7 (2.4) �9.6 (2.6)
n 204 161
LVEDD, mean (SD), z score 5.2 (2.3) 5.2 (2.2)
n 185 144
UNOS indicates United Network for Organ Sharing; LVEF, left ventricularejection fraction; LVFS, left ventricular fractional shortening; and LVEDD, leftventricular end-diastolic dimension.
Table 2. Age Distributions of 261 Children WithDilated Cardiomyopathy
Age Group, yAt Diagnosis,
n (%)At Listing,
n (%)At Transplantation,
n (%)
�0.5 86 (33) 48 (18) 23 (11)
0.5–1 26 (10) 32 (12) 32 (15)
1–10 62 (24) 89 (34) 75 (36)
�10 87 (33) 92 (35) 79 (38)
Total 261 (100) 261 (100) 209 (100)
Figure 1. Kaplan-Meier survival curve for the first 2 years afterlisting (censored at transplantation) for children with dilated car-diomyopathy (n�261; 26 deaths by 2 years after listing). Errorbars represent 70% confidence limits.
Table 3. Primary Causes of Death Among 29 Children WithDilated Cardiomyopathy Who Died After Listing forCardiac Transplantation
Primary Cause of Death n %
Cardiac failure 12 41
Neurological or cerebrovascular accident 6 21
Multiorgan or system failure 2 7
Sudden cardiac death 2 7
Respiratory failure 1 4
Pulmonary hemorrhage 1 4
Other 5 17
Total 29 100
Pietra et al Outcome After Listing in Children With DCM 1081
by guest on July 8, 2014http://circ.ahajournals.org/Downloaded from

Causes of Death After TransplantationAmong the 209 children who underwent heart transplantation,40 died; 1-year survival was 92%, 5-year survival was 80%, and10-year survival was 72% (Figure 3A). The most common causeof death after transplantation was the development of graftvasculopathy and/or myocardial infarction in 11 patients (28%of deaths). Sudden cardiac death occurred in 4 children (10% ofdeaths), likely related to either vasculopathy or acute rejection.17
Rejection was the cause of death in 10 patients (9 acute, 1hyperacute rejection; 25% of deaths). There were 2 deaths fromearly graft failure and 1 from hyperacute rejection.
Risk Factors for Death After TransplantationThe results of the univariate and multivariable analyses of deathafter transplantation are shown in Tables 4 and 5, respectively.Older age at transplantation was associated with death aftertransplantation (P�0.05) by univariate analysis but not multi-variable analysis (Figure 3B). Nonwhite race was significantlyassociated with worse survival in both the univariate andmultivariable analyses (P�0.0001; Figure 3C). A diagnosis ofmyocarditis was associated with worse survival in the univariateand multivariable analyses (P�0.02 and P�0.009, respectively;Figure 4A). A lower LVEDD z score was also associated withworse posttransplantation survival by multivariable analysis(P�0.04).
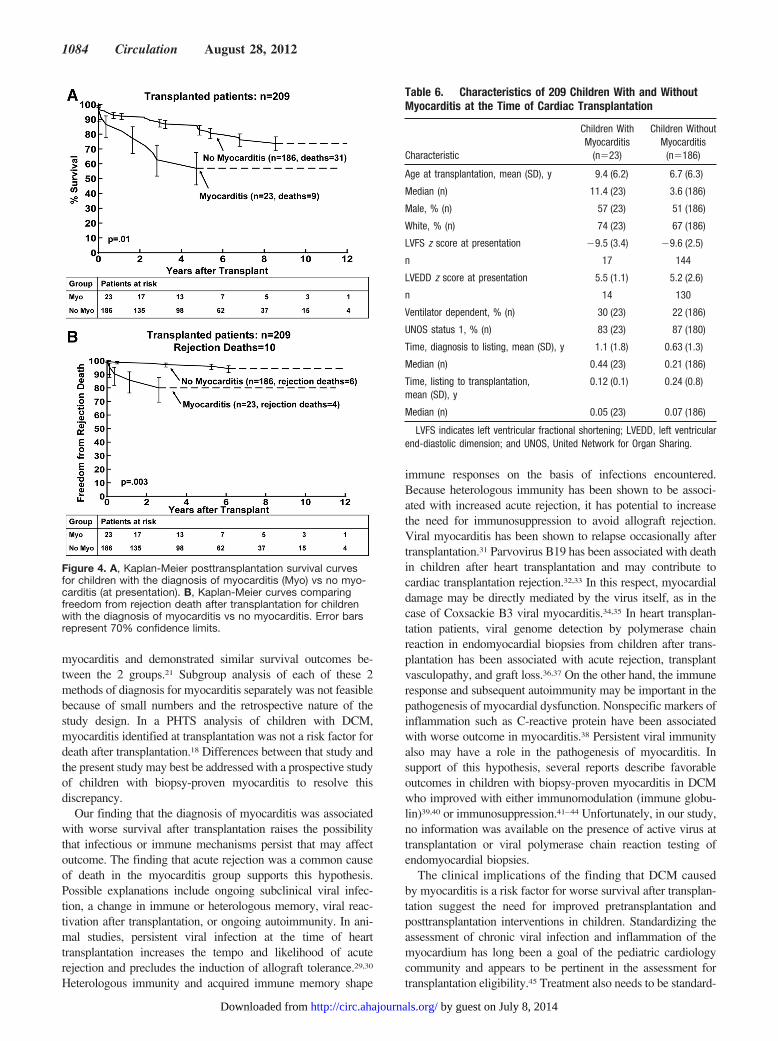
Myocarditis and OutcomesSurvival at 1 and 3 years after transplantation was 83% and65% in children with myocarditis compared with 93% and88% in the group without myocarditis (P�0.01; Figure 4A).The median age at transplantation was 11.4 years in thechildren with myocarditis at presentation and 3.6 years in thechildren who did not have myocarditis at transplantation(P�0.03; Table 6). LV fractional shortening z score was notsignificantly worse in the myocarditis group. The LVEDD zscore was similar between the 2 groups. Smaller LVEDD zscore was a risk factor for death in the nonmyocarditissubgroup (P�0.02). Because of small numbers, the LVEDDz score could not be analyzed in the myocarditis subgroup.Death resulting from acute rejection was more common in themyocarditis group compared with the nonmyocarditis group(17% versus 3%, respectively; P�0.003; Figure 4B).
DiscussionIdentification of risk factors for worse outcome after listing isan important step toward optimizing the management of childrenwith DCM. The merged data set available from the PCMR andPHTS offers a unique opportunity to follow up patients from thetime of diagnosis through the posttransplantation period. In ourstudy, mortality on the heart transplantation wait list was 11%.None of the variables measured at the time of diagnosis of DCM
Table 4. Univariate Risk Factors for Death Among ChildrenWith Dilated Cardiomyopathy
Potential Risk Factor Univariate P
Death while waiting for transplantation (29 deaths in261 children)
White race 0.12
Male sex 0.73
On ventilator at listing 0.003
Older age at listing* 0.30
UNOS status1 at listing 0.10
Time from diagnosis to listing 0.45
LVFS z score at presentation 0.52
LVEDD z score at presentation 0.89
Death after transplantation (40 deaths in 209 children)
Nonwhite race �0.0001
Male sex 0.94
On ventilator at transplantation 0.97
Older age at transplantation 0.05
UNOS status 1 at transplantation 0.48
Myocarditis at diagnosis 0.02
Time from diagnosis to listing 0.83
Time from listing to transplantation 0.47
LVFS z score at presentation 0.07
LVEDD z score at presentation (lower) 0.10
UNOS indicates United Network for Organ Sharing; LVFS, left ventricularfractional shortening; and LVEDD, left ventricular end-diastolic dimension.
*Mechanical ventilation removed from analysis.
Table 5. Multivariable Risk Factors for Death Among ChildrenWith Dilated Cardiomyopathy
Potential Risk Factor Multivariable PHazardRatio
95% ConfidenceLimits
Death while waiting fortransplantation (29deaths in 261 children)
On ventilator at listing 0.0006 4.06 1.79–9.19
Older age at listing 0.03 1.07 1.01–1.14
Death after transplantation(40 deaths in 209 children)
Nonwhite race �0.0001 4.55 2.35–8.83
Myocarditis at diagnosis 0.009 2.71 1.27–5.82
LVEDD z score atpresentation (lower)
0.04 1.19 1.01–1.42
LVEDD indicates left ventricular end-diastolic dimension.
Figure 2. Kaplan-Meier survival curves after listing (censored attransplantation) for patients who were (Yes vent) and were not(No vent) mechanically ventilated at listing. Error bars represent70% confidence limits.
1082 Circulation August 28, 2012
by guest on July 8, 2014http://circ.ahajournals.org/Downloaded from

was associated with death while waiting for heart transplantationexcept mechanical ventilation and older age, which have previ-ously been described as risk factors.23,24 Death after transplan-tation was associated with 3 factors: nonwhite race, a smallLV dimension, and a diagnosis of myocarditis at the time ofpresentation.
Other studies have identified older age and black race asrisk factors for worse survival after transplantation.2,17,18,25,26
In our study, older age was a predictor for death after transplan-tation in univariate but not multivariable analysis. Older age,particularly adolescence, is a known predictor for death aftertransplantation in children.2,17,18 This finding has been attributedto adolescent defiance, nonadherence to treatment, and risk-taking behavior. Worse outcome in this age group is not limitedto heart transplantation patients; it is also seen in other solid-organ transplantation patients27 and with other chronic diseasessuch as diabetes mellitus.28 Black race is a common finding inmany transplantation outcome studies. Higher mortality andmorbidity in blacks compared with individuals of other raceshave been attributed largely to lower socioeconomic status,lower level of education, and limited access to health care butmay also be attributed to genetic differences in drug metabolismand immunity.25 Although the black population may havegenetic as opposed to demographic causes or social characteris-
tics that predispose them to a worse outcome, this study was notpowered to address these possibilities.
In this study, the diagnosis of myocarditis was not associatedwith death while waiting for heart transplantation, but strikingly,myocarditis was associated with a worse outcome after trans-plantation compared with children without the diagnosis ofmyocarditis. In fact, 97% of the children listed who hadmyocarditis at presentation survived to heart transplantation.Efforts to be certain that these results could not be explained bymore severe cardiac dysfunction in the myocarditis group beforetransplantation were limited by the lack of complete echocar-diographic and hemodynamic data at the time of transplantation.However, the data available suggest that children with DCM,with or without myocarditis, were similar in severity of illness atthe time of transplantation. The finding that a smaller LVEDD zscore was associated with death after transplantation may rep-resent a group of children with more acute cardiomyopathy inwhom the LV has not yet dilated. However, this finding wassignificant only in multivariable analysis including the diagnosisof myocarditis, so other factors may be involved. One consid-eration as to the validity of a combined histological and clinicaldefinition of myocarditis is that this approach is supported by aPCMR-sponsored analysis that compared children with biopsy-confirmed myocarditis and those with clinically diagnosed
Figure 3. A, Kaplan-Meier posttransplantation survival curve for children with dilated cardiomyopathy (n�209). B, Kaplan-Meier post-transplantation curves for children �1, 1 to 10, and �10 years of age at transplantation. C, Kaplan-Meier posttransplantation survivalcurves for nonwhite (Non-W) vs white children. Error bars represent 70% confidence limits.
Pietra et al Outcome After Listing in Children With DCM 1083
by guest on July 8, 2014http://circ.ahajournals.org/Downloaded from
myocarditis and demonstrated similar survival outcomes be-tween the 2 groups.21 Subgroup analysis of each of these 2methods of diagnosis for myocarditis separately was not feasiblebecause of small numbers and the retrospective nature of thestudy design. In a PHTS analysis of children with DCM,myocarditis identified at transplantation was not a risk factor fordeath after transplantation.18 Differences between that study andthe present study may best be addressed with a prospective studyof children with biopsy-proven myocarditis to resolve thisdiscrepancy.
Our finding that the diagnosis of myocarditis was associatedwith worse survival after transplantation raises the possibilitythat infectious or immune mechanisms persist that may affectoutcome. The finding that acute rejection was a common causeof death in the myocarditis group supports this hypothesis.Possible explanations include ongoing subclinical viral infec-tion, a change in immune or heterologous memory, viral reac-tivation after transplantation, or ongoing autoimmunity. In ani-mal studies, persistent viral infection at the time of hearttransplantation increases the tempo and likelihood of acuterejection and precludes the induction of allograft tolerance.29,30
Heterologous immunity and acquired immune memory shape
immune responses on the basis of infections encountered.Because heterologous immunity has been shown to be associ-ated with increased acute rejection, it has potential to increasethe need for immunosuppression to avoid allograft rejection.Viral myocarditis has been shown to relapse occasionally aftertransplantation.31 Parvovirus B19 has been associated with deathin children after heart transplantation and may contribute tocardiac transplantation rejection.32,33 In this respect, myocardialdamage may be directly mediated by the virus itself, as in thecase of Coxsackie B3 viral myocarditis.34,35 In heart transplan-tation patients, viral genome detection by polymerase chainreaction in endomyocardial biopsies from children after trans-plantation has been associated with acute rejection, transplantvasculopathy, and graft loss.36,37 On the other hand, the immuneresponse and subsequent autoimmunity may be important in thepathogenesis of myocardial dysfunction. Nonspecific markers ofinflammation such as C-reactive protein have been associatedwith worse outcome in myocarditis.38 Persistent viral immunityalso may have a role in the pathogenesis of myocarditis. Insupport of this hypothesis, several reports describe favorableoutcomes in children with biopsy-proven myocarditis in DCMwho improved with either immunomodulation (immune globu-lin)39,40 or immunosuppression.41–44 Unfortunately, in our study,no information was available on the presence of active virus attransplantation or viral polymerase chain reaction testing ofendomyocardial biopsies.
The clinical implications of the finding that DCM causedby myocarditis is a risk factor for worse survival after transplan-tation suggest the need for improved pretransplantation andposttransplantation interventions in children. Standardizing theassessment of chronic viral infection and inflammation of themyocardium has long been a goal of the pediatric cardiologycommunity and appears to be pertinent in the assessment fortransplantation eligibility.45 Treatment also needs to be standard-
Figure 4. A, Kaplan-Meier posttransplantation survival curvesfor children with the diagnosis of myocarditis (Myo) vs no myo-carditis (at presentation). B, Kaplan-Meier curves comparingfreedom from rejection death after transplantation for childrenwith the diagnosis of myocarditis vs no myocarditis. Error barsrepresent 70% confidence limits.
Table 6. Characteristics of 209 Children With and WithoutMyocarditis at the Time of Cardiac Transplantation
Characteristic
Children WithMyocarditis
(n�23)
Children WithoutMyocarditis
(n�186)
Age at transplantation, mean (SD), y 9.4 (6.2) 6.7 (6.3)
Median (n) 11.4 (23) 3.6 (186)
Male, % (n) 57 (23) 51 (186)
White, % (n) 74 (23) 67 (186)
LVFS z score at presentation �9.5 (3.4) �9.6 (2.5)
n 17 144
LVEDD z score at presentation 5.5 (1.1) 5.2 (2.6)
n 14 130
Ventilator dependent, % (n) 30 (23) 22 (186)
UNOS status 1, % (n) 83 (23) 87 (180)
Time, diagnosis to listing, mean (SD), y 1.1 (1.8) 0.63 (1.3)
Median (n) 0.44 (23) 0.21 (186)
Time, listing to transplantation,mean (SD), y
0.12 (0.1) 0.24 (0.8)
Median (n) 0.05 (23) 0.07 (186)
LVFS indicates left ventricular fractional shortening; LVEDD, left ventricularend-diastolic dimension; and UNOS, United Network for Organ Sharing.
1084 Circulation August 28, 2012
by guest on July 8, 2014http://circ.ahajournals.org/Downloaded from

ized because as many as 5% of patients with DCM receiveimmunomodulatory therapy without objective evidence of myo-carditis.9 Posttransplantation immunosuppression protocols var-ied among the centers in our study. Therefore, it was not possibleto determine the impact of the type and intensity of immuno-suppression or the use of induction regimens (including theroutine use of intravenous immune globulin) on the outcome ofpatients with myocarditis.
Limitations of the Study DesignPediatric DCM is a diverse collection of diseases with bothacquired and genetic causes. As a result, registry-based studieslike ours have limitations in that heterogeneity may obscurecausal relationships. This study was limited by its retrospectivenature; despite the merger of 2 registries, there was a relativelymodest number of patients. Subgroup analysis such as that formyocarditis results in even smaller numbers in each group,which makes robust statistical statements challenging. Data werelimited to what was available and included in the databasesbefore the merger in 2005. Data were also limited to the numberof variables collected in the registries, without the possibility ofadditional collection. Despite these limitations, the informationis valuable in predicting outcome and counseling families. Theselimitations remain a reality of research into rare diseases such aspediatric cardiomyopathy and further emphasize the need forlarger and more detailed continued data collection efforts byregistries. In addition, although diagnostic evaluations and treat-ment strategies were similar at the data collection sites, standard-ized protocols were not used within the study group. Multiplephysicians initiated, manipulated, and terminated therapy forindividual patients in different ways. This limitation can beovercome only with a prospective randomized study design,which would be challenging because of the low incidence ofchildren presenting with severe heart failure and myocarditis.
ConclusionsMechanical ventilation and older age at listing in patients notmechanically ventilated were risk factors for death whilewaiting for heart transplantation, factors that allow riskstratification of patients at the time of listing. Outcomes ofchildren with DCM after transplantation are affected bynonwhite race and older age. Myocarditis is associated with ahigher mortality after transplantation and suggests a persis-tent infectious or immune mechanism.
AcknowledgmentsWe thank the participating PCMR and PHTS clinical centers forpatient recruitment; Susan Myers, BA, for statistical analysis assis-tance; Tom Lang, MA, for editorial assistance; and Dr AnneDipchand for assistance in the review and coding of data forCanadian children. T. Lang was compensated for his presubmittaleditorial review of the manuscript.
Source of FundingThis work was supported by grant RO1 HL 53392 from the NationalInstitutes of Health, National Heart, Blood, and Lung Institute.
DisclosuresNone.
References1. Alvarez JA, Wilkinson JD, Lipshultz SE, Group PCRS. Outcome pre-
dictors for pediatric dilated cardiomyopathy: a systematic review. ProgPediatr Cardiol. 2007;23:25–32.
2. Boucek MM, Aurora P, Edwards LB, Taylor DO, Trulock EP, Christie J,Dobbels F, Rahmel AO, Keck BM, Hertz MI. Registry of the InternationalSociety for Heart and Lung Transplantation: tenth official pediatric hearttransplantation report–2007. J Heart Lung Transplant. 2007;26:796–807.
3. Lipshultz SE, Sleeper LA, Towbin JA, Lowe AM, Orav EJ, Cox GF,Lurie PR, McCoy KL, McDonald MA, Messere JE, Colan SD. Theincidence of pediatric cardiomyopathy in two regions of the UnitedStates. N Engl J Med. 2003;348:1647–1655.
4. Daubeney PE, Nugent AW, Chondros P, Carlin JB, Colan SD, Cheung M,Davis AM, Chow CW, Weintraub RG. Clinical features and outcomes ofchildhood dilated cardiomyopathy: results from a nationalpopulation-based study. Circulation. 2006;114:2671–2678.
5. Wilkinson JD, Sleeper LA, Alvarez JA, Bublik N, Lipshultz SE. ThePediatric Cardiomyopathy Registry: 1995–2007. Prog Pediatr Cardiol.2008;25:31–36.
6. Towbin JA, Lowe AM, Colan SD, Sleeper LA, Orav EJ, Clunie S,Messere J, Cox GF, Lurie PR, Hsu D, Canter C, Wilkinson JD, LipshultzSE. Incidence, causes, and outcomes of dilated cardiomyopathy inchildren. JAMA. 2006;296:1867–1876.
7. Towbin JA. Cardiomyopathy and heart transplantation in children. CurrOpin Cardiol. 2002;17:274–279.
8. Kantor PF, Abraham JR, Dipchand AI, Benson LN, Redington AN. Theimpact of changing medical therapy on transplantation-free survival inpediatric dilated cardiomyopathy. J Am Coll Cardiol. 2010;55:1377–1384.
9. Harmon WG, Sleeper LA, Cuniberti L, Messere J, Colan SD, Orav EJ,Towbin JA, Wilkinson JD, Lipshultz SE. Treating children with idio-pathic dilated cardiomyopathy (from the Pediatric CardiomyopathyRegistry). Am J Cardiol. 2009;104:281–286.
10. McMahon AM, van Doorn C, Burch M, Whitmore P, Neligan S, Rees P,Radley-Smith R, Goldman A, Brown K, Cohen G, Tsang V, Elliott M, deLeval MR. Improved early outcome for end-stage dilated cardiomyopathyin children. J Thorac Cardiovasc Surg. 2003;126:1781–1787.
11. Hsu DT, Canter CE. Dilated cardiomyopathy and heart failure in children.Heart Fail Clin. 2010;6:415–432, vii.
12. Rosenthal DN, Dubin AM, Chin C, Falco D, Gamberg P, Bernstein D.Outcome while awaiting heart transplantation in children: a comparisonof congenital heart disease and cardiomyopathy. J Heart LungTransplant. 2000;19:751–755.
13. Valantine HA, Hunt SA, Fowler MB, Billingham ME, Schroeder JS.Frequency of familial nature of dilated cardiomyopathy and usefulness ofcardiac transplantation in this subset. Am J Cardiol. 1989;63:959–963.
14. Taylor DO, Edwards LB, Boucek MM, Trulock EP, Aurora P, Christie J,Dobbels F, Rahmel AO, Keck BM, Hertz MI. Registry of the InternationalSociety for Heart and Lung Transplantation: twenty-fourth official adult hearttransplant report—2007. J Heart Lung Transplant. 2007;26:769–781.
15. Adwani SS, Whitehead BF, Rees PG, Whitmore P, Fabre JW, Elliott MJ,de Leval MR. Heart transplantation for dilated cardiomyopathy. Arch DisChild. 1995;73:447–452.
16. Shaddy RE, Naftel DC, Kirklin JK, Boyle G, McGiffin DC, Towbin JA, RingWS, Pearce B, Addonizio L, Morrow WR. Outcome of cardiac transplan-tation in children: survival in a contemporary multi-institutional experience:Pediatric Heart Transplant Study. Circulation. 1996;94(suppl):II-69–II-73.
17. Dipchand AI, Naftel DC, Feingold B, Spicer R, Yung D, Kaufman B,Kirklin JK, Allain-Rooney T, Hsu D. Outcomes of children with cardio-myopathy listed for transplant: a multi-institutional study. J Heart LungTransplant. 2009;28:1312–1321.
18. Kirk R, Naftel D, Hoffman TM, Almond C, Boyle G, Caldwell RL,Kirklin JK, White K, Dipchand AI. Outcome of pediatric patients withdilated cardiomyopathy listed for transplant: a multi-institutional study.J Heart Lung Transplant. 2009;28:1322–1328.
19. Kirk R, Edwards LB, Aurora P, Taylor DO, Christie JD, Dobbels F, Kuch-eryavaya AY, Rahmel AO, Stehlik J, Hertz MI. Registry of the InternationalSociety for Heart and Lung Transplantation: twelfth official pediatric hearttransplantation report—2009. J Heart Lung Transplant. 2009;28:993–1006.
20. Grenier MA, Osganian SK, Cox GF, Towbin JA, Colan SD, Lurie PR,Sleeper LA, Orav EJ, Lipshultz SE. Design and implementation of the NorthAmerican Pediatric Cardiomyopathy Registry. Am Heart J. 2000;139:S86–S95.
21. Foerster SR, Canter CE, Cinar A, Sleeper LA, Webber SA, Pahl E, KantorPF, Alvarez JA, Colan SD, Jefferies JL, Lamour JM, Margossian R, MessereJE, Rusconi PG, Shaddy RE, Towbin JA, Wilkinson JD, Lipshultz SE.
Pietra et al Outcome After Listing in Children With DCM 1085
by guest on July 8, 2014http://circ.ahajournals.org/Downloaded from
Ventricular remodeling and survival are more favorable for myocarditis thanfor idiopathic dilated cardiomyopathy in childhood: an outcomes study fromthe Pediatric Cardiomyopathy Registry. Circ Heart Fail. 2010;3:689–697.
22. Arola A, Tuominen J, Ruuskanen O, Jokinen E. Idiopathic dilated car-diomyopathy in children: prognostic indicators and outcome. Pediatrics.1998;101:369–376.
23. McGiffin DC, Naftel DC, Kirklin JK, Morrow WR, Towbin J, Shaddy R,Alejos J, Rossi A. Predicting outcome after listing for heart transplan-tation in children: comparison of Kaplan-Meier and parametric competingrisk analysis: Pediatric Heart Transplant Study Group. J Heart LungTransplant. 1997;16:713–722.
24. Morrow WR, Frazier E, Naftel DC. Survival after listing for cardiactransplantation in children. Prog Pediatr Cardiol. 2000;11:99–105.
25. Mahle WT, Kanter KR, Vincent RN. Disparities in outcome for blackpatients after pediatric heart transplantation. J Pediatr. 2005;147:739–743.
26. Tsirka AE, Trinkaus K, Chen SC, Lipshultz SE, Towbin JA, Colan SD,Exil V, Strauss AW, Canter CE. Improved outcomes of pediatric dilatedcardiomyopathy with utilization of heart transplantation. J Am CollCardiol. 2004;44:391–397.
27. Smith JM, Stablein DM, Munoz R, Hebert D, McDonald RA. Contri-butions of the Transplant Registry: the 2006 annual report of the NorthAmerican Pediatric Renal Trials and Collaborative Studies (NAPRTCS).Pediatr Transplant. 2007;11:366–373.
28. Bryden KS, Dunger DB, Mayou RA, Peveler RC, Neil HA. Poorprognosis of young adults with type 1 diabetes: a longitudinal study.Diabetes Care. 2003;26:1052–1057.
29. Williams MA, Onami TM, Adams AB, Durham MM, Pearson TC,Ahmed R, Larsen CP. Cutting edge: persistent viral infection preventstolerance induction and escapes immune control following CD28/CD40blockade-based regimen. J Immunol. 2002;169:5387–5391.
30. Adams AB, Pearson TC, Larsen CP. Heterologous immunity: an over-looked barrier to tolerance. Immunol Rev. 2003;196:147–160.
31. Calabrese F, Rigo E, Milanesi O, Boffa GM, Angelini A, Valente M,Thiene G. Molecular diagnosis of myocarditis and dilated cardiomyopa-thy in children: clinicopathologic features and prognostic implications.Diagn Mol Pathol. 2002;11:212–221.
32. Francalanci P, Chance JL, Vatta M, Jimenez S, Li H, Towbin JA, BowlesNE. Cardiotropic viruses in the myocardium of children with end-stageheart disease. J Heart Lung Transplant. 2004;23:1046–1052.
33. Schowengerdt KO, Ni J, Denfield SW, Gajarski RJ, Bowles NE,Rosenthal G, Kearney DL, Price JK, Rogers BB, Schauer GM, ChinnockRE, Towbin JA. Association of parvovirus B19 genome in children withmyocarditis and cardiac allograft rejection: diagnosis using the poly-merase chain reaction. Circulation. 1997;96:3549–3554.
34. Badorff C, Lee GH, Lamphear BJ, Martone ME, Campbell KP, RhoadsRE, Knowlton KU. Enteroviral protease 2A cleaves dystrophin: evidenceof cytoskeletal disruption in an acquired cardiomyopathy. Nat Med.1999;5:320–326.
35. Towbin JA, Bowles KR, Bowles NE. Etiologies of cardiomyopathy andheart failure. Nat Med. 1999;5:266–267.
36. Shirali GS, Ni J, Chinnock RE, Johnston JK, Rosenthal GL, Bowles NE,Towbin JA. Association of viral genome with graft loss in children aftercardiac transplantation. N Engl J Med. 2001;344:1498–1503.
37. Moulik M, Breinholt JP, Dreyer WJ, Kearney DL, Price JF, Clunie SK,Moffett BS, Kim JJ, Rossano JW, Jefferies JL, Bowles KR, O’BrianSmith E, Bowles NE, Denfield SW, Towbin JA. Viral endomyocardialinfection is an independent predictor and potentially treatable risk factorfor graft loss and coronary vasculopathy in pediatric cardiac transplantrecipients. J Am Coll Cardiol. 2010;56:582–592.
38. Kaneko K, Kanda T, Hasegawa A, Suzuki T, Kobayashi I, Nagai R.C-reactive protein as a prognostic marker in lymphocytic myocarditis.Jpn Heart J. 2000;41:41–47.
39. Maisch B, Herzum M, Hufnagel G, Bethge C, Schonian U. Immunosup-pressive treatment for myocarditis and dilated cardiomyopathy. EurHeart J. 1995;16(suppl O):153–161.
40. McNamara DM, Rosenblum WD, Janosko KM, Trost MK, Villaneuva FS,Demetris AJ, Murali S, Feldman AM. Intravenous immune globulin in thetherapy of myocarditis and acute cardiomyopathy. Circulation. 1997;95:2476–2478.
41. Gagliardi MG, Bevilacqua M, Squitieri C, Boldrini R, Di Julio DP, Mar-celletti C. Dilated cardiomyopathy caused by acute myocarditis in pediatricpatients: evolution of myocardial damage in a group of potential hearttransplant candidates. J Heart Lung Transplant. 1993;12:S224–S229.
42. Kleinert S, Weintraub RG, Wilkinson JL, Chow CW. Myocarditis in childrenwith dilated cardiomyopathy: incidence and outcome after dual therapyimmunosuppression. J Heart Lung Transplant. 1997;16:1248–1254.
43. Gagliardi MG, Bevilacqua M, Bassano C, Leonardi B, Boldrini R,Camassei FD, Fierabracci A, Ugazio AG, Bottazzo GF. Long term followup of children with myocarditis treated by immunosuppression and ofchildren with dilated cardiomyopathy. Heart. 2004;90:1167–1171.
44. Hia CP, Yip WC, Tai BC, Quek SC. Immunosuppressive therapy in acutemyocarditis: an 18 year systematic review. Arch Dis Child. 2004;89:580–584.
45. Lipshultz SE, Wilkinson JD. Epidemiological and outcomes research inchildren with pediatric cardiomyopathy: discussions from the Interna-tional Workshop on Primary and Idiopathic Cardiomyopathies inChildren. Prog Pediatr Cardiol. 2008;25:23–25.
CLINICAL PERSPECTIVEFactors that affect outcome in pediatric heart diseases such as dilated cardiomyopathy are often difficult to define becauseof the rarity of disease. To study the potential importance of factors at presentation and at listing for heart transplantationin children with dilated cardiomyopathy on outcome, we analyzed data from 2 large pediatric registries: the PediatricCardiomyopathy Registry and the Pediatric Heart Transplant Study. In the merged data set, there were 261 children withdilated cardiomyopathy. Among the factors studied were age, duration of illness, sex, race, ventricular geometry, and theclinical or histological diagnosis of myocarditis at presentation. We found that death while waiting was associated withventilator use and older age at listing. A shorter duration of illness was associated with a more urgent listing status (UnitedNetwork for Organ Sharing status 1). Death after transplantation was associated black race and lower left ventricular end-diastolicdimension z score at presentation. We also found that death after transplantation was associated with the diagnosis of myocarditisat presentation (P�0.009). Death while waiting was not associated with the diagnosis of myocarditis, and 97% of children withmyocarditis survived to transplantation. Furthermore, the most common cause of death after transplantation in the myocarditisgroup was acute rejection (17%). This is the first study to show that children with dilated cardiomyopathy and myocarditis havesignificantly higher posttransplantation mortality compared with children without myocarditis. This finding suggests thatpreexisting viral infection or inflammation could adversely affect heart allograft survival and has implications for themanagement of these children before and after heart transplantation in the future.
1086 Circulation August 28, 2012
by guest on July 8, 2014http://circ.ahajournals.org/Downloaded from




















