Juvenile Kearns-Sayre syndrome initially misdiagnosed as a psychosomatic disorder
6
J Med Genet 1994;31:45-50 Juvenile Kearns-Sayre syndrome initially misdiagnosed as a psychosomatic disorder Soren N0rby, Patrick Lestienne, Isabelle Nelson, Inge-Merete Nielsen, Henning Schmalbruch, Ole Sjo, Mette Warburg Abstract We have investigated a 15 year old girl with progressive external ophthalmople- gia, including bilateral ptosis and retinal rod and cone cell dysfunction with atyp- ical retinal pigmentation, complicated by cerebellar ataxia, partial cardiac con- duction block, and diabetes mellitus. In infancy she had a severe crisis of bone marrow depression, and as a child she suffered from hypersensitivity to light, increasing fatigue, and vertigo, signs that were initially thought to be psychoso- matic. Histological examination showed mito- chondrial myopathy, and subsequent mitochondrial DNA (mtDNA) analysis showed a deletion of approximately 5500 base pairs in 35 to 40% of her muscle mtDNA. We therefore conclude that this patient has developed the Kearns-Sayre syndrome after a Pearson syndrome-like crisis in her first year of life. Institute of Forensic Genetics, University of Copenhagen, Frederik V's Vej 11, DK-2100 Copenhagen, Denmark S Norby INSERM U 298, CHRU, Angers, France P Lestienne I Nelson Department of Paediatrics, Sundby Hospital, Copenhagen, Denmark I-M Nielsen Institute of Neurophysiology, University of Copenhagen, Denmark H Schmalbruch Department of Ophthalmophysiology, Gentofte Hospital, Denmark O Sjo Department of Ophthalmology, Division of Paediatric Ophthalmology, Gentofte Hospital, Denmark M Warburg Correspondence to Dr N0rby Received 6 April 1993 Revised version accepted for publication 3 August 1993 (J Med Genet 1994;31:45-50) Kearns-Sayre syndrome (KSS) is a sporadic multisystem mitochondrial disorder with pro- gressive external ophthalmoplegia, retinal dys- trophy, and at least one of the following signs: heart block, cerebellar ataxia, and cerebro- spinal fluid protein levels above 1 g/1.1-3 Rag- ged red fibres in the muscles are observed histologically and imply a mitochondrial dis- order, which can be verified by electron micro- scopy and confirmed by mtDNA analysis. On- set is before 15 to 20 years of age and there is often growth retardation, delayed sexual matu- ration, and mental deterioration. The retinal dystrophy in KSS and other cases with mitochondrial ophthalmoplegia features salt and pepper pigmentation in the fundus of some patients, in others there are black pigmented clumps. Electroretinography (ERG) shows cone dystrophy or both rod and cone dystrophy.4 Pearson syndrome (PS), also a mitochon- drial disorder, presents with infantile siderob- lastic pancytopenia requiring frequent trans- fusions, insufficiency of the pancreas, and hepatic dysfunction.56 Children surviving the pancytopenic crisis have been observed to de- velop progressive symptoms of KSS.7-9 The aetiology of PS and KSS was not understood until partial deletions of mtDNA were observed in these patients.'6 104 We present here a new case of presumed PS developing into KSS and caused by an mtDNA deletion of 5491 base pairs.'5 Case report Pregnancy and delivery were unremarkable. There is no parental consanguinity and both parents and a brother are healthy. Birth weight was 3700 g. At 5-5 months of age the patient had fever, anaemia, and blood in her stools. She also had leuco- and thrombocytopenia, the bone marrow was hypoplastic, and there was slight hepatomegaly. Explorative laparotomy showed nothing pathological. A number of blood transfusions were given over the next couple of years. The cause of the condition was presumed to be a cytomegalovirus (CMV) infection, as the CMV titre was high (132 decreasing to 16) and the virus was cultured from the urine. Motor development was delayed. From the age of 3 years she was increasingly sensitive to light and preferred lying underneath the table at home. Ophthalmological examinations (elsewhere) gave no explanation and the cause of her troubles was thought to be psycholo- gical. At school she had learning as well as beha- vioural problems and was referred to a psycho- logist and later a psychiatrist; eventually at 11 years she was transferred to a special class for children with learning disabilities. She moved slowly and never ran, and complained of weak- ness in the limbs, fatigue increased by exercise, and vertigo. At 12 years she fell off her bicycle twice and had four sudden unprovoked falls with unconsciousness for a few seconds. Atonic epileptic seizures were suspected. The EEG was paroxysmal, and for a short period she was treated with antiepileptic medicine (sodium valproate), which, however, was with- drawn because of serious side effects (severe hand tremor and ataxia). Retrospectively, these attacks could have been the result of heart conduction failure. She also developed increasing hearing impairment. A cerebral CT scan showed symmetrical bilateral hypodense areas in the cerebellum. One year later a cerebral MRI scan confirmed symmetrical degeneration of the cerebellar white matter. In addition a hypodense area was seen in the left internal capsule. Ophthalmological examinations were car- ried out by one of us (MW) over the age period 13 to 15 years. Overall consideration of the clinical findings then led to the diagnosis of Kearns-Sayre syndrome, which was subse- quently supported by histological examination and eventually confirmed by mtDNA analysis. 45
Transcript of Juvenile Kearns-Sayre syndrome initially misdiagnosed as a psychosomatic disorder

J Med Genet 1994;31:45-50
Juvenile Kearns-Sayre syndrome initiallymisdiagnosed as a psychosomatic disorder
Soren N0rby, Patrick Lestienne, Isabelle Nelson, Inge-Merete Nielsen,Henning Schmalbruch, Ole Sjo, Mette Warburg
AbstractWe have investigated a 15 year old girlwith progressive external ophthalmople-gia, including bilateral ptosis and retinalrod and cone cell dysfunction with atyp-ical retinal pigmentation, complicatedby cerebellar ataxia, partial cardiac con-
duction block, and diabetes mellitus. Ininfancy she had a severe crisis of bonemarrow depression, and as a child shesuffered from hypersensitivity to light,increasing fatigue, and vertigo, signs thatwere initially thought to be psychoso-matic.Histological examination showed mito-
chondrial myopathy, and subsequentmitochondrial DNA (mtDNA) analysisshowed a deletion of approximately 5500base pairs in 35 to 40% of her musclemtDNA. We therefore conclude that thispatient has developed the Kearns-Sayresyndrome after a Pearson syndrome-likecrisis in her first year of life.
Institute of ForensicGenetics, Universityof Copenhagen,Frederik V's Vej 11,
DK-2100 Copenhagen,DenmarkS Norby
INSERM U 298,CHRU, Angers,FranceP LestienneI Nelson
Department ofPaediatrics, SundbyHospital, Copenhagen,DenmarkI-M Nielsen
Institute ofNeurophysiology,University ofCopenhagen,DenmarkH Schmalbruch
Department ofOphthalmophysiology,Gentofte Hospital,DenmarkO Sjo
Department ofOphthalmology,Division of PaediatricOphthalmology,Gentofte Hospital,DenmarkM Warburg
Correspondence toDr N0rbyReceived 6 April 1993Revised version accepted forpublication 3 August 1993
(J Med Genet 1994;31:45-50)
Kearns-Sayre syndrome (KSS) is a sporadicmultisystem mitochondrial disorder with pro-gressive external ophthalmoplegia, retinal dys-trophy, and at least one of the following signs:heart block, cerebellar ataxia, and cerebro-spinal fluid protein levels above 1 g/1.1-3 Rag-ged red fibres in the muscles are observedhistologically and imply a mitochondrial dis-order, which can be verified by electron micro-scopy and confirmed by mtDNA analysis. On-set is before 15 to 20 years of age and there isoften growth retardation, delayed sexual matu-ration, and mental deterioration.The retinal dystrophy in KSS and other
cases with mitochondrial ophthalmoplegiafeatures salt and pepper pigmentation in thefundus of some patients, in others there are
black pigmented clumps. Electroretinography(ERG) shows cone dystrophy or both rod andcone dystrophy.4
Pearson syndrome (PS), also a mitochon-drial disorder, presents with infantile siderob-lastic pancytopenia requiring frequent trans-fusions, insufficiency of the pancreas, andhepatic dysfunction.56 Children surviving thepancytopenic crisis have been observed to de-velop progressive symptoms of KSS.7-9 Theaetiology of PS and KSS was not understooduntil partial deletions of mtDNA were
observed in these patients.'6 104
We present here a new case of presumed PS
developing into KSS and caused by anmtDNA deletion of 5491 base pairs.'5
Case reportPregnancy and delivery were unremarkable.There is no parental consanguinity and bothparents and a brother are healthy. Birth weightwas 3700 g. At 5-5 months of age the patienthad fever, anaemia, and blood in her stools.She also had leuco- and thrombocytopenia, thebone marrow was hypoplastic, and there wasslight hepatomegaly. Explorative laparotomyshowed nothing pathological. A number ofblood transfusions were given over the nextcouple of years. The cause of the conditionwas presumed to be a cytomegalovirus (CMV)infection, as the CMV titre was high (132decreasing to 16) and the virus was culturedfrom the urine.Motor development was delayed. From the
age of 3 years she was increasingly sensitive tolight and preferred lying underneath thetable at home. Ophthalmological examinations(elsewhere) gave no explanation and the causeof her troubles was thought to be psycholo-gical.At school she had learning as well as beha-
vioural problems and was referred to a psycho-logist and later a psychiatrist; eventually at 11years she was transferred to a special class forchildren with learning disabilities. She movedslowly and never ran, and complained of weak-ness in the limbs, fatigue increased by exercise,and vertigo. At 12 years she fell off her bicycletwice and had four sudden unprovoked fallswith unconsciousness for a few seconds.Atonic epileptic seizures were suspected. TheEEG was paroxysmal, and for a short periodshe was treated with antiepileptic medicine(sodium valproate), which, however, was with-drawn because of serious side effects (severehand tremor and ataxia). Retrospectively,these attacks could have been the result ofheart conduction failure. She also developedincreasing hearing impairment.A cerebral CT scan showed symmetrical
bilateral hypodense areas in the cerebellum.One year later a cerebral MRI scan confirmedsymmetrical degeneration of the cerebellarwhite matter. In addition a hypodense area wasseen in the left internal capsule.
Ophthalmological examinations were car-ried out by one of us (MW) over the age period13 to 15 years. Overall consideration of theclinical findings then led to the diagnosis ofKearns-Sayre syndrome, which was subse-quently supported by histological examinationand eventually confirmed by mtDNA analysis.
45

Norby, Lestienne, Nelson, Nielsen, Schmalbruch, Sjo, Warburg
Figure 1 Facial features of the patient aged 15 years. Note the dark periorbital skin,ptosis, and hypotonia.
CLINICAL EXAMINATION FROM 13 TO 16 YEARS
OF AGE
At the first examination the facial muscles were
hypotonic with bilateral ptosis and a strikingyellow-brown discoloration of the skin of theeyelids (fig 1). When the frontalis muscle was
fixed she could raise the upper eyelids 2 mm.The excursions of the external eye muscleswere reduced: fusion horizontal -4 to + 12PD, vertical 2 PD. There was no ocular ataxia.There were no convergence movements and no
squint. Stereopsis was present. Visual acuitywas OD 6/6 +2 25-1 75X(175°), OS 6/6+2 50-2 50x (120°). Colour vision (AO-HRR) was normal.
Direct and indirect ophthalmoscopy at 13years showed parapapillary atrophy, attenu-
ated arterioles, and abnormal reticular, macu-
lar, and peripheral pigmentation. Foveolar re-
flexes were absent.A year later with fixation of the frontalis she
could not raise her eyelids and other excur-
sions were diminished. In the fundi small
Figure 2 Very early fluorescence angiogram of the left eye. The macula has a mottledpigmentation. Further peripherally, the fundus shows a granular texture. Thearterioles are narrow though not thread-like. Nasally the choroidal vessels can be seen
through the retina, indicating mild degeneration of the retinal epithelium.
clumps of dark pigmentation were beginningto appear in the inferior retina. At the latestexamination the black pigmented clumps weredispersed all over the posterior pole of thefundus. Ophthalmoscopy was hampered bythe patient's severe photoaversion.
Fluorescence angiography showed irregularatrophy of the retinal pigment epithelium (fig2). Colour vision test (AO-HRR) showed aslight tritan defect.
Electroretinography (ERG) showed conedystrophy at the age of 13 years, and one yearlater rod dystrophy was also present. Auto-matic perimetry was normal, but a Goldmannperimetry showed a concentric constriction to30°. At 14 years campimetry (3/1000, white)showed a visual field of only 10°.
Electrocardiography at 14 years showed aleft anterior hemiblock during rest with negat-ive T waves and ST depression during exer-cise. Progressive ataxia, dysarthria, and inten-tion tremor were present, and she needed awheelchair for outings with her family.
Pure tone audiometry indicated bilateralsymmetrical sensorineural hearing loss withhigh frequency dominance; the speech recep-tion threshold was 25 dB HL bilaterally. Tym-panograms were normal. There was reducedcerebellar control of the eye movements butintact peripheral vestibular function on bothsides.Menarche was absent, but breast develop-
ment had begun. Her stature was short, belowthe 3rd centile for her age. At 16 years of ageshe developed insulin dependent diabetes.
Materials and methodsHISTOLOGICAL EXAMINATIONAn open surgical biopsy was obtained undergeneral anaesthesia from the medial vastusmuscles. A sample was kept for histochemistryand frozen in a nitrogen slush. Cryostat sec-tions 8 ptm thick were stained with haematoxy-lin and eosin, Gomori's trichrome stain, vanGieson stain, and for a battery of muscleenzymes. Other fibre bundles were kept atconstant length and fixed and embedded forelectron micrscopy; thin sections were stainedwith uranyl acetate and lead citrate. The dia-meters of 590 mnuscle fibres were measured insections stained for adenosine triphosphatase.
MITOCHONDRIAL DNA ANALYSISIsolation of DNAA part of the muscle biopsy was kept frozen at-80°C in 10 mmol/l Tris-HCl, pH 80,04 mol/I NaCl, 2 mmol/l EDTA until DNAextraction. After thawing and addition of pro-teinase K and SD S (final concentrations of200 1tg/ml and 0 5% respectively), 30 to 50 mgof tissue was homogenised, incubated over-night at 37°C, and total DNA isolated byroutine methods as previously reported.'4
Southern blot analysisAliquots of 0-6 .tg total DNA were digestedovernight with 10 units of BamHI, EcoRI,
46

Jruvenile Kearns-Sayre syndrome initially misdiagnosed as a psychosomatic disorder
HindIII, PstI, PvuII, and SacI (Boehringer,Mannheim) respectively. After agarose gelelectrophoresis (0-8% BRL Ultrapure) andstaining with ethidium bromide, the DNAfragments were blotted onto a Hybond N filter(Amersham), hybridised overnight to humanmtDNA (100 ng), 32P labelled by nick transla-tion.
After washing using standard procedures16and exposure to Fuji x ray film at - 70'C usingintensifying screens, an autoradiograph of thefilter was developed. k DNA digested byEcoRI and HindIII was used as size marker.The percentage ofmtDNA harbouring a dele-tion was estimated by computerised densito-metry of the autoradiograph using the pro-gram IMAGE version 1.44.
Polymerase chain reactionWidely spaced primer (WISP) PCR'7 was per-formed as a supplement to Southern blotting,using 20mer primers (5'--3') corresponding tothe following mtDNA positions": L strand8204-.8223 (PL-1) and H strand 14 460-.14 441 (PL-17). PCR conditions and subse-quent analytical gel electrophoresis were asdescribed previously,'9 except that annealingwas at 55'C. The size marker was the same asin the Southern analysis. DNA samples frompreviously analysed patients with well charac-terised mtDNA deletions of 4977 bp2° wereincluded as controls.
DNA sequence analysisSingle stranded DNA sequence analysis wasperformed by dideoxynucleotide termination(Sequenase 2.0, US Biochemical Corpora-tion), after asymmetrical amplification using1 jg target DNA and the primers PL-1 andPL-17 in a ratio of 1:50. Sequence search andcomparisons were performed with the help ofMicrogenie (Beckman) and with the Andersonsequence'8 as reference.
ResultsHISTOLOGICAL EXAMINATIONLight microscopy showed moderately atrophicand hypertrophic fibres with diametersbetween 20 jm and 65 jim (mean diameter38 gm, SD 19%), and also an increased incid-ence of internal myonuclei. The muscle wasnot fibrotic and there was no evidence ofmuscle fibre necrosis or regeneration. Musclefibres of different types formed a normalmosaic pattern; there were no signs ofdenervation. Type 1 fibres were slightlythicker than type 2 fibres (means 41 jm v35 im).Most fibres reacted for cytochrome c oxid-
ase, but about 10% of the fibres wereunstained. Sections stained with Gomori'strichrome stain showed about 1 % of "ragged-red" fibres. The same fibres displayed heavydeposits of blue formazan when stained forlactic acid dehydrogenase or succinate dehyd-rogenase. Under the electron microscope, sub-sarcolemmal aggregations of giant mitochon-dria and of mitochondria with paracrystalline
inclusions were found (fig 3). Several intra-fusal muscle fibres contained abnormal mito-chondria as well, but the mitochondria in vas-cular smooth muscle cells were normal.
MITOCHONDRIAL DNA ANALYSISSouthern blot analysisThe autoradiograph of the Southern blot isshown in fig 4. Digestion with BamHI andPvuII (fig 4, lanes 1 and 5 respectively) showedtwo populations of mtDNA molecules, one ofwhich (AmtDNA) has a deletion of 5 to 6 kb(1 kb = 1000 base pairs) as compared to thenormal one (16-6 kb). By densitometry theAmtDNA was found to account for 35 to 40%of the total mtDNA.The presence ofAmtDNA also in the digests
with HindIII, PstI, and SacI (fig 4, lanes 3, 4,and 6) shows that only one of the normallyoccurring two (SacI and PstI) or three (Hin-dIII) sites for these enzymes remain in theAmtDNA molecule. For EcoRI (fig 4, lane 2)
@'X,}~~~~~~l
'''+;'::! t \ ~~~~~tq
Figure 3 Electron micrograph of skeletal muscleshowing ultrastructural mitochondrial changes, includingthe presence of paracrystalline bodies.
AmtDNA- --_-_-AmtDNA
am
1 2 3 4 5 6Figure 4 Autoradiograph of Southern blot of thepatient's muscle mtDNA digested with the followingenzymes: BamHI (lane 1), EcoRI (lane 2), HindIII(lane 3), PstI (lane 4), PvuII (lane 5), and SacI(lane 6). Fragments of less than 6 kb (I kb = 1000 bp)have been omittedfrom the photograph. AmtDNAindicates the deletion molecule (size approximately11 kb).
47
A.I
Norby, Lestienne, Nelson, Nielsen, Schmalbruch, Sjo, Warburg
two sites are intact in the deletion molecule,since the largest fragment in that digest isabout 1 kb smaller than AmtDNA.Taken together these results show that the
deletion which has produced the AmtDNAmolecule is 5 to 6 kb long and covers thefollowing restriction site positions: 9020(PstI), 9643 (SacI), 11 680 and 12 570 (Hin-dIII), and 12 640 (EcoRI), whereas neither ofthe flanking sites at positions 6910 (PstI) or14258 (BamHI) are included.
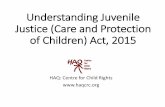
Polymerase chain reactionFig 5 shows the PCR gel using the primercombination PL-1/PL-17. The controls,heteroplasmic for mtDNA with approximately5 kb deletions, gave an amplification productof about 1-2 kb (lanes 1 and 2). Our patient'ssample, however, gave a product of only about0-8 kb (lane 3), showing that her deletion isapproximately 04 kb larger than that of thecontrols. As expected, no amplification wasobserved from the coexisting wild typemtDNA, in which the primer target sequencesare 6-2 kb apart.
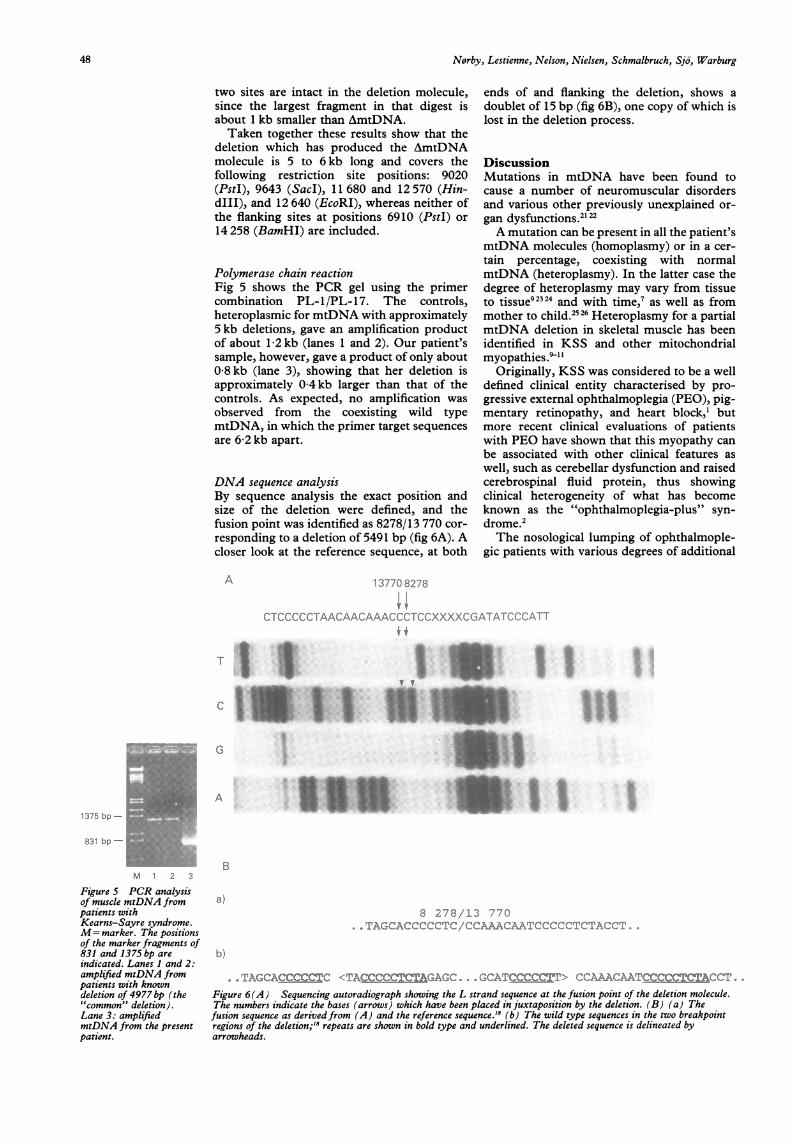
DNA sequence analysisBy sequence analysis the exact position andsize of the deletion were defined, and thefusion point was identified as 8278/13 770 cor-responding to a deletion of 5491 bp (fig 6A). Acloser look at the reference sequence, at both
ends of and flanking the deletion, shows adoublet of 15 bp (fig 6B), one copy of which islost in the deletion process.
DiscussionMutations in mtDNA have been found tocause a number of neuromuscular disordersand various other previously unexplained or-gan dysfunctions.2122A mutation can be present in all the patient's
mtDNA molecules (homoplasmy) or in a cer-tain percentage, coexisting with normalmtDNA (heteroplasmy). In the latter case thedegree of heteroplasmy may vary from tissueto tissue92324 and with time,7 as well as frommother to child.2526 Heteroplasmy for a partialmtDNA deletion in skeletal muscle has beenidentified in KSS and other mitochondrialmyopathies.?'"
Originally, KSS was considered to be a welldefined clinical entity characterised by pro-gressive external ophthalmoplegia (PEO), pig-mentary retinopathy, and heart block,' butmore recent clinical evaluations of patientswith PEO have shown that this myopathy canbe associated with other clinical features aswell, such as cerebellar dysfunction and raisedcerebrospinal fluid protein, thus showingclinical heterogeneity of what has becomeknown as the "ophthalmoplegia-plus" syn-drome.2The nosological lumping of ophthalmople-
gic patients with various degrees of additional
A
I :.. .. .-:n1 ( x, -: :'-%-.. ...r."-"CCC(-'C-i-AACAA("A -A...'I.,':(-.'-7-'- "'x".)C... )"'. -.
iff t
T. X
3V'V
..: ::~ ': .:,K e .. ...
GV: 4; r2z Y9fiO S3MLW -e.b. *.. WiE>s w:."
A
1375 bp -
831 bp -
M 1 2 3
Figure 5 PCR analysisof muscle mtDNA frompatients withKearns-Sayre syndrome.M= marker. The positionsof the marker fragments of831 and 1375 bp areindicated. Lanes 1 and 2:amplified mtDNA frompatients with knowndeletion of 4977bp (the"common" deletion).Lane 3: amplifiedmtDNA from the presentpatient.
B
-:AAACz-x..>-CfAArTi.'
b)
rTAGCACCCCC=C <TACCCCQAfAGAGC i'C(7ATC<CC Fth- -ACCCFigure 6(A) Sequencing autoradiograph showing the L strand sequence at the fusion point of the deletion molecule.The numbers indicate the bases (arrows) which have been placed in juxtaposition by the deletion. (B) (a) Thefusion sequence as derivedfrom (A) and the reference sequence.'8 (b) The wild type sequences in the two breakpointregions of the deletion;'8 repeats are shown in bold type and underlined. The deleted sequence is delineated byarrowheads.
I .'j:-x4.! ::
I
48
ill.tl 1.1,::..f.

Jtuvenile Kearns-Sayre syndrome initially misdiagnosed as a psychosomatic disorder
neuromuscular involvement has been justifiedthrough the finding of heteroplasmic mtDNAdeletions in both classical KSS and uncom-plicated ocular myopathy.""027There is no correlation between size and
location of the deletion in the mtDNA mo-lecule and the phenotype of the patient; thiscan be explained by the observed general im-pairment of translation in mitochondria withan mtDNA deletion.928 The tRNA genes are"peppered" throughout the mitochondrialgenome,'8 23 so that any sizable deletion isbound to include at least one such gene, andhence prevent translation of the remainingmitochondrial genes.However, the specific distribution of deleted
mtDNA among the cells of neuromusculartissue,29 including the degree of heteroplasmyand the possibilities for complementationbetween wild type and mutant mtDNA,'332 islikely to be decisive for the clinical manifesta-tions in a given patient.A clinical picture which is completely dif-
ferent from KSS may result when the samemtDNA deletion is predominant in other tis-sues, as in the Pearson syndrome (PS)6912 inwhich pancytopenia of the blood is associatedwith exocrine pancreatic dysfunction in earlychildhood.
Patients who recovered from a crisis of PS ininfancy and later developed neuromuscularsymptoms leading to the diagnosis of KSS at 7to 8 years of age have recently been de-scribed.89 They had heteroplasmy for anmtDNA deletion both in skeletal muscle andin leucocytes. Similarly, in another case ofKSS, progressing during early adolescenceand associated with a large deletion in a highpercentage of muscle mtDNA, a crisis of bonemarrow dysfunction had been recorded inearly childhood.7The present case is yet another example of a
patient who has developed KSS after a tran-sient crisis of bone marrow dysfunction inearly childhood, requiring blood transfusionfor survival. In such cases heteroplasmy forthe mtDNA deletion in question is probablypresent in various tissues during fetal develop-ment and infancy. The clinical manifestationsare most probably determined by the percent-age of defective mitochondria, in combinationwith tissue specific thresholds for respiratorychain insufficiency. An increase of deletedmtDNA seems to occur with time in neuro-muscular tissue, thus giving rise to KSS, aftersurvival of a possible haematological crisis inearly childhood.7 The present deletion (fig 6) isdifferent from those previously reported, but islocated in the same region of the mtDNAmolecule. 14 2032 The mechanisms underlyingmtDNA deletions are not yet understood, butaccumulated evidence stresses the involvementof direct repeats, possibly by allowing either aslippage during H strand replication or dele-tion by some kind of unequal crossing over.33-35Recently, a tandem duplication in the mtDNAD loop has been suggested to predispose tosuch deletions.'6
In the majority of cases two direct repeatsfrom 5 to 13 bp in length have been detected in
the deletion breakpoint regions, one of themalways being included in the deletion.203334The 13 bp repeats at positions 8470-8482 and13 447-13 459 seem to constitute a mutationalhotspot, being involved in the so called com-mon deletion of 4977 bp, which accounts forabout one-third of all sporadic mtDNA dele-tions."337
In the mtDNA of our patient the deletionbreakpoints are located in regions where twodirect repeats, of 6 and 9 bp, are found in thewild type molecule, the former repeat se-quence C5T also being part of the latter (fig6B). In a replication-slippage model this mightallow the formation of a structure with 15established base pairs as an intermediate in thedeletion process.A computer search shows that the 6 bp se-
quence C5T is present at 24 locations through-out the wild type mtDNA molecule. Thissequence has not been found flanking pre-viously published deletions, hence it seemsmore likely that the above mentioned 9 bprepeats or a combination of the two areinvolved in causing the present deletion.
In whites,18 as opposed to many Asians,'8 the9 bp sequence is present twice as a head to tailduplication at 8271-8288 bp (fig 6B), and onecould therefore hypothesise that in the formerpopulation this region may be more deletionprone. The fact that this 9 bp repeat is alsofound at position 8605-8613 suggests the pos-sibility of a deletion involving two of thesevery closely placed 9 bp repeats. Such a smalldeletion, comprising only about 325 bp butincluding the gene for tRNALYs, would not bedetected by routine Southern blot analysis.
It seems obvious that the search for themolecular defect in mtDNA, in cases where amajor deletion is not found, should be guidedby the accumulated evidence for the involve-ment of direct repeats and the knowledge oftheir location in wild type mtDNA.The densitometric analysis was kindly performed by Dr FinnCilius Nielsen. The present investigation was supported byThe P Carl Petersen Foundation and 0jenfonden (The EyeFoundation under the Danish Association of the Blind) (SN),The Danish Medical Research Council (HS), the VeluxFoundation (MW), and "L'Association Francaise pour la Luttecontre les Myopathies" (PL, IN). SN and PL gratefullyacknowledge collaborative grants from The Danish Ministry ofEducation and The French Ministry of Foreign Affairs.
1 Kearns TP, Sayre GP. Retinitis pigmentosa, external oph-thalmoplegia and complete heart block. Arch Ophthalmol1958;60:280-9.
2 Berenberg RA, Pellock JM, DiMauro S, et al. Lumping orsplitting? 'Ophthalmoplegia-plus' or Kearns-Sayre syn-drome? Ann Neurol 1977;1:37-54.
3 Lestienne P, Ponsot G. Kearns-Sayre syndrome withmuscle mitochondrial DNA deletion. Lancet 1988;i:885.
4 Mullie MA, Harding AE, Petty RKH, et al. The retinalmanifestations of mitochondrial myopathy. A study of 22cases. Arch Ophthalmol 1985;103:1825-30.
5 Pearson HA, Lobel JS, Kocoshis SA, et al. A new syndromeof refractory sideroblastic anemia with vacuolization ofmarrow precursors and exocrine pancreatic dysfunction.J Pediatr 1979;95:976-84.
6 Rotig A, Cormier V, Koll F, et al. Site-specific deletions ofthe mitochondrial genome in the Pearson marrow-pan-creas syndrome. Genomics 1991;10:502-4.
7 Larsson NG, Holme E, Kristiansson B, Oldfors A, TuliniusM. Progressive increase of the mutated mitochondrialDNA fraction in Kearns-Sayre syndrome. Pediatr Res1990;28:131-6.
8 McShane MA, Hammans SR, Sweeney M, et al. Pearsonsyndrome and mitochondrial encephalomyopathy in apatient with a deletion of mtDNA. Am J Hum Genet1991;48:39-42.
9 Nelson I, Bonne G, Degoul F, et al. Kearns-Sayre syn-drome with sideroblastic anemia: molecular investiga-tions. Neuropediatrics 1992;23:199-205.
10 Holt IJ, Harding AE, Morgan-Hughes JA. Deletions of
49

Norby, Lestienne, Nelson, Nielsen, Schmalbruch, Sjo, Warburg
muscle mitochondrial DNA in patients with mitochon-drial myopathies. Nature 1988;331:717-19.
11 Zeviani M, Moraes CT, DiMauro S, et al. Deletions ofmitochondrial DNA in Kearns-Sayre syndrome. Neuro-logy 1988;38:1339-46.
12 Rotig A, Colonna M, Blanche S, et al. Deletion of bloodmitochondrial DNA in pancytopenia. Lancet 1988;ii:567-8.
13 Moraes CT, DiMauro S, Zeviani M, et al. MitochondrialDNA deletions in progressive ophthalmoplegia andKeams-Sayre syndrome. N EnglJ Med 1989;320:1293-9.
14 Nelson I, Degoul F, Obermaier-Kusser B, et al. Mapping ofheteroplasmic mitochondrial DNA deletions in Kearns-Sayre syndrome. Nucleic Acids Res 1989;17:8117-24.
15 N0rby S, Lestienne P, Nelson I, Nielsen IM, Warburg M.A new deletion in mitochondrial DNA leading to theKearns-Sayre syndrome. Am J Hum Genet Suppi1991;49:207A.
16 Sambrook J, Fritsch EF, Maniatis T. Molecular cloning. Alaboratory manual. 2nd ed. New York: Cold Spring Har-bor Laboratory Press, 1989.
17 Johns DR, Hurko 0. Preferential amplification and molecu-lar characterization of junction sequences of a pathogen-etic deletion in human mitochondrial DNA. Genomics1989;5:623-8.
18 Anderson S, Banker AT, Barrell BG, et al. Sequence andorganization of the human mitochondrial genome. Nature1981;290:457-65.
19 N0rby S, Lestienne P, Nelson I, Rosenberg T. Mutationdetection in Leber's hereditary optic neuropathy by PCRwith allele-specific priming. Biochem Biophys Res Com-mun 1991;175:631-6.
20 Degoul F, Nelson I, Amselem S, et al. Different mechan-isms inferred from sequences of human mitochondrialDNA deletions in ocular myopathies. Nucleic Acids Res1991;19:493-6.
21 Lestienne P. Mitochondrial DNA mutations in humandisease: a review. Biochimie 1992;74:123-30.
22 Wallace DC. Diseases of the mitochondrial DNA. AnnuRev Biochem 1992;61:1175-212.
23 Shanske S, Moraes CT, Lombes A, et al. Widespread tissuedistribution of mitochondrial DNA deletions in Kearns-Sayre syndrome. Neurology 1990;40:24-8.
24 Lott MT, Voljavec AS, Wallace DC. Variable genotype ofLeber's hereditary optic neuropathy patients. AmJ Oph-thalmol 1990;109:625-31.
25 Vilkki J, Savontaus ML, Nikoskelainen EK. Segregation ofmitochondrial genomes in a heteroplasmic lineage withLeber hereditary optic neuroretinopathy. Am J HumGenet 1990;47:95-100.
26 Bolhuis PA, Bleeker-Wagemakers EM, Ponne NJ, et al.Rapid shift in genotype of human mitochondrial DNA in
a family with Leber's hereditary optic neuropathy. Bio-chem Biophys Res Commun 1990;170:994-7.
27 Gerbitz KD, Obermaier-Kusser B, Lestienne P, et al.Mutations of the mitochondrial DNA: the contributionof DNA techniques to the diagnosis of mitochondrialencephalomyopathies. J Clin Chem Clin Biochem1990;28:241-50.
28 Nakase H, Moraes CT, Rizzuto R, Lombes A, deMauro S,Schon EA. Transcription and translation of deleted mito-chondrial genomes in Kearns-Sayre syndrome: implica-tions for pathogenesis. AmJ7 Hum Genet 1990;46:418-27.
29 Zeviani M, Gellera C, Panacci M, et al. Tissue distributionand transmission of mitochondrial DNA deletions inmitochondrial myopathies. Ann Neurol 1990;28:94-7.
30 Lestienne P. Mitochondrial and nuclear DNA complemen-tation in the respiratory chain function and defects. Bio-chimie 1989;71:1115-23.
31 Hammans SR, Sweeney MG, Holt IJ, et al. Evidence forintramitochondrial complementation between deletedand normal mitochondrial DNA in some patients withmitochondrial myopathy. J7 Neurol Sci 1992;107:87-92.
32 Hayashi JI, Ohta S, Kikuchi A, Takemitsu M, Goto YI,Nonaka I. Introduction of disease-related mitochondrialDNA deletions into HeLa cells lacking mitochondrialDNA results in mitochondrial dysfunction. Proc NatlAcad Sci USA 1991;88:10614-18.
33 Holt IJ, Harding AE, Morgan-Hughes JA. Deletions ofmuscle mitochondrial DNA in mitochondrial myopath-ies: sequence analysis and possible mechanisms. NucleicAcids Res 1989;17:4465-9.
34 Mita S, Rizutto R, Moraes CT, et al. Recombination viaflanking direct repeats is a major cause of large-scaledeletions of human mitochondrial DNA. Nucleic AcidsRes 1990;18:561-7.
35 Schoffner JM, Lott MT, Voljavec AS, et al. SpontaneousKearns-Sayre/chronic external ophthalmoplegia plussyndrome associated with a mitochondrial DNA deletion:a slip-replication model and metabolic therapy. Proc NatlAcad Sci USA 1989;86:7952-6.
36 Brockington M, Sweeney MG, Hammans SR, Morgan-Hughes JA, Harding AE. A tandem duplication in the D-loop of human mitochondrial DNA is associated withdeletions in mitochondrial myopathies. Nature Genet1993;4:67-71.
37 Schon EA, Rizzuto R, Moraes CT, Nakase H, Zeviani M,DiMauro S. A direct repeat is a hotspot for large-scaledeletion in human mitochondrial DNA. Science1989;244:346-9.
38 Hertzberg M, Mickleson KNP, Serjeantson SW, Prior JF,Trent RJ. An Asian-specific 9-bp deletion of mitochon-drial DNA is frequently found in Polynesians. AmJ HumGenet 1989;44:504-10.
50