Isosorbide-5-mononitrate treatment prevents cyclosporin A-induced platelet hyperactivation and the...
9
Regular Article Isosorbide-5-mononitrate treatment prevents cyclosporin A-induced platelet hyperactivation and the underlying nitric oxide–cyclic guanosine-3V ,5V -monophosphate disturbances Fla ´vio Reis a , Luı ´s Almeida a , Teresa Alcobia a , Jose ´ D. Santos-Dias b , Margarida Lourenc ßo c , Aida Palmeiro c , Carlos A. Ferrer-Antunes c , Jose ´ F. Mesquita b , Fausto Pontes d , Frederico Teixeira a, * a Institute of Pharmacology and Experimental Therapeutics, Faculty of Medicine, Coimbra University, 3004-504, Coimbra, Portugal b Electronic Microscopy Laboratory, Botanic Department, Science and Technology Faculty, Coimbra University, Coimbra, Portugal c Laboratory of Haematology, Coimbra University Hospital, Coimbra, Portugal d Institute of Physiology, Medicine Faculty, Coimbra University, Coimbra, Portugal Received 13 January 2003; received in revised form 30 April 2003; accepted 26 May 2003 Abstract Introduction: The clinical use of cyclosporin A (CsA) is commonly associated with the development of hypertension and increased risk of thromboembolic events. Decreased endothelium-dependent relaxation and increased platelet activation seems to be involved on those side effects, but the underlying mechanisms are not yet elucidated. The present study aimed to evaluate the CsA effect on the platelet NO – cyclic guanosine-3V ,5V -monophosphate (cGMP) pathway and the putative benefits of concomitant isosorbide-5-mononitrate (IS-5-MN) administration on CsA-induced hypertension and on platelet hyperactivation. Materials and Methods: Blood pressures, platelet NO synthase activity and cGMP content, intracellular free calcium concentration ([Ca 2+ ] i ) and whole blood platelet aggregation were assessed in three rat groups orally treated, during 7 weeks, with the following diets: orange juice (control group), 5 mg/kg/day of CsA (CsA group) and 150 mg/kg/day, b.i.d., of IS-5-MN for 2 weeks and IS-5-MN plus 5 mg/kg/day of CsA for 7 weeks (IS-5-MN + CsA group). Results: IS-5- MN treatment has prevented hypertension development obtained in the solely CsA-treated rats. CsA treatment has inhibited NOS activity, which was reverted by the concomitant IS-5-MN and CsA administration. On the contrary, platelets from CsA-treated rats had cGMP content increased when compared with the control rats. The variation obtained when ISMN was present was less predominant. Therefore, the organic nitrate treatment has prevented platelet hyperactivation, namely, by decreasing thrombin-evoked [Ca 2+ ] i and collagen-evoked platelet aggregation, when compared with the solely CsA-treated group. The preventive effect of IS-5-MN was reinforced by electron microscopy studies of platelet activation. Conclusions: By increasing [Ca 2+ ] i and aggregation, CsA induces platelet hyperactivation and simultaneously increases cGMP content, which might represent a compensatory inhibitory mechanism. The concomitant IS-5-MN treatment prevents the above-mentioned platelet hyperreactivity and tends to normalize the NO – cGMP pathway as well as the development of hypertension. D 2003 Elsevier Ltd. All rights reserved. Keywords: Cyclosporin A; Isosorbide-5-mononitrate; Hypertension; Thromboembolic complications; Platelets; Nitric oxide; Nitric oxide synthase; cGMP 1. Introduction Despite the recent appearance of new immunosuppres- sive drugs, Cyclosporin A (CsA) is still one of the main therapeutic choices in human transplantation [1,2], particu- larly because of its selectivity and efficacy. However, the clinical use of CsA has been associated with the develop- ment of serious posttransplant side effects such as increased risk of thromboembolic complications [3–5] and drug- related hypertension [6,7]. The pathophysiological mechanisms underlying the al- tered vascular reactivity associated with CsA-induced hy- 0049-3848/03/$ - see front matter D 2003 Elsevier Ltd. All rights reserved. doi:10.1016/S0049-3848(03)00311-6 Abbreviations: CsA, cyclosporin A; IS-5-MN, isosorbide-5-mononi- trate; NO, nitric oxide; NOS, nitric oxide synthase; cGMP, cyclic guanosine-3V ,5V -monophosphate; GC, guanylate cyclase; 5-HT, 5-hydroxy- tryptamine; TXA 2 , thromboxane A 2 ; [Ca 2+ ] i , intracellular free calcium concentration; EDTA, etylene-dinitrilo-tetraacetic acid; EGTA, etylene- glycol-tetraacetic acid; PRP, platelet-rich plasma; PPP, platelet-poor plasma; ADP, adenosine 5V -diphosphate; ACD, acid citrate – dextrose solution; AAS, acethylsalicilic acid; COX, cyclooxygenase; IBMX, isobuthyl- methyl-xantine; SNP, sodium nitroprusside; IFN-g, interferon g; L-NNA, N-nitro-L-arginine; LPS, lipopolysaccharide; VSMC, vascular smooth muscle cells; SEM, standard error of mean; SBP, systolic blood pressure; DBP, diastolic blood pressure; MPV, mean platelet volume; PCT, plateletocrite; PDW, platelet deviation weight. * Corresponding author. Tel.: +351-39-857777; fax: +351-39-836200. E-mail address: [email protected] (F. Teixeira). Thrombosis Research 110 (2003) 107– 115
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Isosorbide-5-mononitrate treatment prevents cyclosporin A-induced platelet hyperactivation and the...

Thrombosis Research 110 (2003) 107–115
Regular Article
Isosorbide-5-mononitrate treatment prevents cyclosporin A-induced
platelet hyperactivation and the underlying nitric oxide–cyclic
guanosine-3V,5V-monophosphate disturbances
Flavio Reisa, Luıs Almeidaa, Teresa Alcobiaa, Jose D. Santos-Diasb, Margarida Lourenc�oc,Aida Palmeiroc, Carlos A. Ferrer-Antunesc, Jose F. Mesquitab,
Fausto Pontesd, Frederico Teixeiraa,*
a Institute of Pharmacology and Experimental Therapeutics, Faculty of Medicine, Coimbra University, 3004-504, Coimbra, PortugalbElectronic Microscopy Laboratory, Botanic Department, Science and Technology Faculty, Coimbra University, Coimbra, Portugal
cLaboratory of Haematology, Coimbra University Hospital, Coimbra, Portugald Institute of Physiology, Medicine Faculty, Coimbra University, Coimbra, Portugal
Received 13 January 2003; received in revised form 30 April 2003; accepted 26 May 2003
Abstract
Introduction: The clinical use of cyclosporin A (CsA) is commonly associated with the development of hypertension and increased risk of
thromboembolic events. Decreased endothelium-dependent relaxation and increased platelet activation seems to be involved on those side
effects, but the underlying mechanisms are not yet elucidated. The present study aimed to evaluate the CsA effect on the platelet NO–cyclic
guanosine-3V,5V-monophosphate (cGMP) pathway and the putative benefits of concomitant isosorbide-5-mononitrate (IS-5-MN)
administration on CsA-induced hypertension and on platelet hyperactivation. Materials and Methods: Blood pressures, platelet NO
synthase activity and cGMP content, intracellular free calcium concentration ([Ca2 +]i) and whole blood platelet aggregation were assessed in
three rat groups orally treated, during 7 weeks, with the following diets: orange juice (control group), 5 mg/kg/day of CsA (CsA group) and
150 mg/kg/day, b.i.d., of IS-5-MN for 2 weeks and IS-5-MN plus 5 mg/kg/day of CsA for 7 weeks (IS-5-MN+CsA group). Results: IS-5-
MN treatment has prevented hypertension development obtained in the solely CsA-treated rats. CsA treatment has inhibited NOS activity,
which was reverted by the concomitant IS-5-MN and CsA administration. On the contrary, platelets from CsA-treated rats had cGMP content
increased when compared with the control rats. The variation obtained when ISMN was present was less predominant. Therefore, the organic
nitrate treatment has prevented platelet hyperactivation, namely, by decreasing thrombin-evoked [Ca2 +]i and collagen-evoked platelet
aggregation, when compared with the solely CsA-treated group. The preventive effect of IS-5-MN was reinforced by electron microscopy
studies of platelet activation. Conclusions: By increasing [Ca2 +]i and aggregation, CsA induces platelet hyperactivation and simultaneously
increases cGMP content, which might represent a compensatory inhibitory mechanism. The concomitant IS-5-MN treatment prevents the
above-mentioned platelet hyperreactivity and tends to normalize the NO–cGMP pathway as well as the development of hypertension.
D 2003 Elsevier Ltd. All rights reserved.
Keywords: Cyclosporin A; Isosorbide-5-mononitrate; Hypertension; Thromboembolic complications; Platelets; Nitric oxide; Nitric oxide synthase; cGMP
Abbreviations: CsA, cyclosporin A; IS-5-MN, isosorbide-5-mononi-
0049-3848/03/$ - see front matter D 2003 Elsevier Ltd. All rights reserved.
doi:10.1016/S0049-3848(03)00311-6
trate; NO, nitric oxide; NOS, nitric oxide synthase; cGMP, cyclic
guanosine-3V,5V-monophosphate; GC, guanylate cyclase; 5-HT, 5-hydroxy-
tryptamine; TXA2, thromboxane A2; [Ca2+]i, intracellular free calcium
concentration; EDTA, etylene-dinitrilo-tetraacetic acid; EGTA, etylene-
glycol-tetraacetic acid; PRP, platelet-rich plasma; PPP, platelet-poor plasma;
ADP, adenosine 5V-diphosphate; ACD, acid citrate–dextrose solution;
AAS, acethylsalicilic acid; COX, cyclooxygenase; IBMX, isobuthyl-
methyl-xantine; SNP, sodium nitroprusside; IFN-g, interferon g; L-NNA,
N-nitro-L-arginine; LPS, lipopolysaccharide; VSMC, vascular smooth
muscle cells; SEM, standard error of mean; SBP, systolic blood pressure;
DBP, diastolic blood pressure; MPV, mean platelet volume; PCT,
plateletocrite; PDW, platelet deviation weight.
* Corresponding author. Tel.: +351-39-857777; fax: +351-39-836200.
E-mail address: [email protected] (F. Teixeira).
1. Introduction
Despite the recent appearance of new immunosuppres-
sive drugs, Cyclosporin A (CsA) is still one of the main
therapeutic choices in human transplantation [1,2], particu-
larly because of its selectivity and efficacy. However, the
clinical use of CsA has been associated with the develop-
ment of serious posttransplant side effects such as increased
risk of thromboembolic complications [3–5] and drug-
related hypertension [6,7].
The pathophysiological mechanisms underlying the al-
tered vascular reactivity associated with CsA-induced hy-

F. Reis et al. / Thrombosis Research 110 (2003) 107–115108
pertension are not fully enlightened, but an impaired vaso-
constrictor/vasodilator balance seems to be involved [8,9].
Several authors have reported endothelial damage and
decreased endothelium-dependent and endothelium-inde-
pendent relaxation [9–11]. Despite increasing studies, the
role of the key endothelium-derived vasodilator—nitric
oxide (NO)—is not yet fully elucidated. Conflicting results
on the vascular NO–cyclic guanosine-3V,5V-monophosphate
(cGMP) pathway disturbances underlying decreased relax-
ation are notorious because decreased, unaltered or even
increased NO production and NO synthase (NOS) activity
have been described [12–17].
Platelets are mediators of thrombotic complications and
atherosclerosis promoters [18,19]. In addition, platelets
produce, store and/or release some vasoconstricting agents,
such as 5-hydroxytryptamine (5-HT) and thromboxane A2
(TXA2), which may affect both the endothelial and the
vascular smooth muscle cells (VSMC) activity and influ-
ence vasoconstriction and peripheral vascular resistance
[20]. However, platelets also have NOS to produce NO,
which in turn activates guanylate cyclase (GC) to produce
cGMP, that it is involved on both inhibition of platelet
aggregation/adhesion and vascular regulation [21–23]. We
have previously demonstrated that CsA treatment induces
platelet hyperactivation [24–26]. However, the role of the
platelet NO–cGMP pathway is unknown.
Several authors have tested the effect of L-arginine
treatment (the NOS substratum) on the vascular disturban-
ces induced by CsA, being the results conflicting [27–29].
We have also demonstrated that L-arginine does not prevent
CsA-induced hypertension despite normalizing the vascular
and platelet NO and cGMP alterations associated with CsA
treatment [30]. Hence, this work aimed to evaluate the effect
of CsA on the platelet NO–cGMP pathway by assessing
NOS activity and cGMP content and the putative benefits of
a concomitant organic nitrate—isosorbide-5-mononitrate
(IS-5-MN)—administration on these mechanisms as well
as on CsA-induced platelet hyperactivation.
2. Materials and methods
2.1. Animals and diets
Male Wistar rats (Charles River Laboratories, Barcelona,
Spain), f 300 g, were maintained in an air-conditioned
room, subjected to 12 h dark/light cycles and given standard
laboratory rat chow and free access to tap water. Animal
experiments were conducted according to the European
Convention on Animal Care, and the research project
containing this study was approved by the Portuguese
Foundation for Science and Technology. The rats were
divided into three groups (each one with 10 rats) and treated
during 7 weeks with the following diets: control group—
receiving only orange juice; CsA-treated group—receiving
5 mg/kg/day of CsA (Sandimmun NeoralR, Novartis Farma,
Lisbon, Portugal) dissolved in orange juice; IS-5-MN+CsA-
treated group—receiving 150 mg/kg/day, b.i.d., of IS-5-MN
(MonoprontR, Ferraz-Lynce, Lisbon, Portugal) during 2
weeks and IS-5-MN+CsA for an additional period of 7
weeks. In order to have a daily nitrate-free period of about 5
h to overcome organic nitrate tolerance, IS-5-MN b.i.d.
administration was made asymmetrically at 10:00 and
17:00 h. Blood pressure values (systolic and diastolic) were
measured using a tail-cuff sphygmomanometer LE 5001
(Letica, Spain).
2.2. Blood collection and platelet preparation
Following intraperitoneal ketamine anesthesia, blood
from the control, CsA-treated and IS-5-MN+CsA-treated
rats (after 7 weeks of treatment) was withdrawn by veni-
puncture from the jugular vein and added to an anticoagu-
lant solution of acid citrate–dextrose (ACD) solution (0.1
ml/ml blood) containing citric acid (71 mmol/l), sodium
citrate (85 mmol/l) and D-glucose (111 mmol/l). The blood
was centrifuged (160� g for 10 min at 20 jC) to obtain
platelet-rich plasma (PRP), which was then incubated for 5
min with acethylsalicilic acid (AAS; 100 Amol/l) in order to
prevent endoperoxides formation and the risk of platelet
aggregation and the platelets finally recovered by a new
centrifugation at 730 g for 10 min at 20 jC. The platelet
pellet was then suspended in the appropriate buffer for each
of different protocols.
2.3. Platelet NO synthase activity
Platelet NO synthase activity was measured by moni-
toring the conversion of tritium-labeled L-arginine to triti-
um-labeled L-citrulline as previously described [31]. The
platelets from the control, the CsA-treated and the IS-5-
MN + CsA-treated group were obtained as described
above, except the AAS incubation, which was abolished
because it is known that cyclooxygenase (COX) inhibition
might result in NOS activity decrease [32]. The platelet
pellet (107 cells) was then suspended in 1 ml of NO buffer
(containing in mmol/l: HEPES, 25; NaCl, 140; KCl, 5.4;
CaCl2, 1.8; MgCl2, 1; pH 7.4) containing [3H]-L-arginine
(0.5 ACi; f 107 dpm; Amersham Pharmacia Biotech,
Buckinghamshire, UK) and incubated for 60 min at 37
jC. The reaction was terminated with 2 ml of cold buffer
(containing in mmol/l: HEPES, 25; NaCl, 118; KCl, 4.7;
CaCl2, 1.8; KH2PO4, 1.2; NaHCO3, 24.8; sodium etylene-
dinitrilo-tetraacetic acid (EDTA), 4; NN-nitro-L-arginine, 5;
pH 5.5). Each tube was centrifuged twice at 700� g for 15
min at 4 jC. The supernatant was discharged and the pellet
was disrupted by adding 1 ml of 0.3 N HClO4 and
neutralized with 65 Al of K2CO3 (3 mol/l). Aliquots of
the cell suspensions were then applied to 2 ml columns of
Dowex AG 50W-X8 (Na+ form) (Bio-Rad, Richmond,
CA) and eluted with 6 ml of distilled water. [3H]-L-
citrulline in the eluent was measured by liquid scintillation

F. Reis et al. / Thrombosis Research 110 (2003) 107–115 109
spectroscopy (Packard Tri-Carb 2000CA, Grove, USA).
NOS activity was assessed by measuring the percentage of
[3H]-L-arginine to [3H]-L-citrulline conversion, according to
the equation: 100� (Counts in the Eluent/Total Counts in
Platelet Sonicate). Platelet NO synthase activity was
assessed in the three rat groups in different experimental
conditions: (1) basal (incubation for 30 min without any
addition); (2) incubation for 30 min with iNOS inductors:
lipopolysaccharide (LPS; 10 Ag/ml) + interferon g (IFN-g;
100 U/ml); and (3) incubation for 15 min with NOS
inhibitor: N-nitro-L-arginine (L-NNA; 1 mmol/l). Incuba-
tions were performed before [3H]-L-arginine addition to
the NO buffer (calcium-free medium for iNOS induction
assays).
2.4. Platelet cGMP content
The platelet pellet obtained as described above was
suspended in modified Tyrode-HEPES buffer (pH 7.4)
containing (in mmol/l): NaCl (134), KCl (3), NaHCO3
(12), MgCl2�6H2O (1), NaH2PO4 (0.34), HEPES (5) and D-
glucose (5). Apyrase (20 Ag/ml) was added and isobuthyl-
methyl-xantine (IBMX; 10 Amol/l) was incubated for 2
min. 0.1 ml were used to platelet counts and aliquots of 0.2
ml were added to 1.8 ml of an ethanol solution (72%).
After 5 min (room temperature), the cGMP-containing
suspension was obtained by centrifugation (1200� g for
15 min at 4 jC). The final cGMP was extracted through a
drying procedure at 23 jC and further dissolved in sodium
acetate buffer (50 mmol/l, pH 6.2) and acetylated with
acetic anhidrid:triethylamine (1:2;v/v) before analysis.
Platelet GMP content was measured by using a commer-
cially available immunoassay kit (R&D Systems, McKind-
ley Place, USA). Platelet cGMP content was assessed in
the three rat groups at basal conditions (incubation for 1
min without any addition) and after 1 min incubation with
100 Amol/l of the positive control sodium nitroprusside
(SNP).
2.5. Platelet intracellular free calcium concentration
2.5.1. Preparation of fura-2-loaded platelets
The platelet pellet obtained as previously described was
suspended and incubated for 10 min in a physiological
saline solution containing (in mmol/l) NaCl (145), KCl
(5), MgSO4�7H2O (1), Hepes (10), D-glucose (10) and 20
Ag/ml apyrase [to prevent activation by residual traces of
adenosine 5V-diphosphate (ADP)]. After having been
washed and resuspended in the same buffer without apyrase,
the platelets were then loaded with 5 Amol/l fura-2/AM
(Molecular Probes, Eugene, OR) and incubated for 45 min
at 37 jC. After adding ACD (3.2%; 111 mmol/l) in order to
decrease the pH and to prevent platelet aggregation and
washing once before final suspension in the same solution,
the platelet suspension was then centrifuged (730� g, 10
min, 20 jC).
2.5.2. Fluorescence measurements
Fluorescence was measured at the emission wavelength
of 510 nm, with the excitation wavelength continuously
switched between 340 and 380 nm (FluoroMax spectroflu-
orometer, SPEX Industries, Edison, USA). Fluorescence
measurements were carried out at 37 jC with continual
agitation. The ratio of the fluorescence intensities at the two
excitation wavelengths was used to determine intracellular
free calcium concentration ([Ca2 +]i) based on the following
equation: [Ca2 +]i =Kd [(R�Rmin)/(Rmax�R)]b, accordingto Grynkiewicz et al. [33]. [Ca2 +]i calibration was achieved
by lysing the cells with 50 Amol/l digitonin in the presence
of 1 mmol/l CaCl2 or 10 mmol/l etylene-glycol-tetraacetic
acid (EGTA; pH 9.0). [Ca2 +]i was assessed after thrombin
(0.1 U/ml) addition after restoring extracellular [Ca2 +] to 1
mmol/l with CaCl2.
2.6. Whole blood platelet aggregation and haematological
parameters
Whole blood platelet aggregation was assessed by mea-
suring the electric impedance using an aggregometer
(Chrono-Log, Havertown, PA). The technique is based on
the detection of changes in electrical resistance between two
electrodes submerged in the sample. Fresh heparinized whole
blood (0.5 ml) and 0.9% NaCl (0.5 ml) were mixed using a
magnetic stirrer and allowed to balance at 37 jC for 5 min
before adding the agonist (collagen 5 Ag/ml; type I equine
native collagen fibrils from Chrono-Log). Some haemato-
logical parameters [platelet count, plateletocrit, mean platelet
volume (MPV), platelet deviation weight (PDW) and hemat-
ocrit] were also measured by using a Coulter counter.
2.7. Electron microscopy study of platelet activation
The platelet pellets from the three rat groups, collected as
previously described, were fixed with glutaraldehyde (2.5%
in phosphate buffer 0.025 mol/l, pH 6.8) for 1 h. After
several washings in the same buffer, postfixation was carried
out for 1 h in osmium tetroxide (Sigma, St. Louis, MO), 1%
in phosphate buffer 0.05 mol/l (pH 6.8). After a further
washing procedure, the platelets were preembedded in agar
(2% in distilled water). The platelet-containing agar was cut
into little pieces of 1 mm and dehydratation was achieved
through resuspension, firstly in increasing concentrations of
alcohol (20% to 100%) for at least 15 min for each concen-
tration and, finally, with increasing concentrations of pro-
pylene oxide in alcohol. The final embedding in a low-
viscosity resin EPON 812 (TAAB Laboratories Equipment,
Berkshire, UK) was carried out by progressively increasing
the concentration of the resin in propylene oxide until 100%.
After polimerization (60 jC for a day), the blocks were cut
on an LKB ultramicrotome using a diamond knife. Ultrathin
sections were picked up on uncoated copper grids and
observed under a JEM-100SX, JEOL electron microscope
(TEM) after uranyl/lead citrate staining.

F. Reis et al. / Thrombosis Research 110 (2003) 107–115110
2.8. Chemicals
Cyclosporin A (Sandimmun NeoralR) was a gift from
Novartis Farma. IS-5-MN (MonoprontR) was friendly sup-
plied by Ferraz-Lynce. [3H]-L-arginine was purchased to
Amersham Pharmacia Biotech. cGMP immunoassay kits
were obtained from R&D Systems. Dowex AG 50W-X8
resin was obtained from Bio-Rad. Fura-2/AM was pur-
chased from Molecular Probes. Collagen was obtained at
Chrono-Log. EPON 812 resin was obtained from TAAB
Laboratories Equipment. Rat thrombin, Escherichia coli
LPS and osmium tetroxide were obtained from Sigma. All
the other chemicals were of the highest analytical grade and
were also obtained from Sigma.
2.9. Statistical analysis
Data are expressed as meansF standard error of the
mean (SEM) of 10 experiments. Values were compared by
using the analysis of variance (ANOVA) and Fisher’s test
for unpaired data; p < 0.05 was considered statistically
significant. *p < 0.05 and **p < 0.01: vs. the control group;
#p < 0.05 and ## p < 0.01: vs. the CsA-treated group.
Fig. 1. Systolic (A) and diastolic (B) blood pressures from the control, CsA-
treated and IS-5-MN+CsA-treated rats before the beginning and after 7
weeks of treatment. The IS-5-MN+CsA-treated group was assessed for
blood pressures before IS-5-MN administration (week � 2), before the
concomitant IS-5-MN and CsA treatment (week 0) and at the end of IS-5-
MN+CsA treatment (week 7). Each bar represents the mean of 10 different
samples (rats)F S.E.M. **p< 0.01: vs. the control group; ##p< 0.01: vs.
the CsA-treated group.
3. Results
3.1. Blood pressures
Systolic and diastolic blood pressures (SBP and DBP,
respectively) were assessed in the three rat groups before the
beginning of each treatment and at the end (week 7). The
blood pressures of the group treated with IS-5-MN+CsA
were assessed before the IS-5-MN administration (week
� 2) and 2 weeks later, before the concomitant IS-5-MN
and CsA administration (week 0). In the beginning of each
treatment, the values of SBP and DBP were identical in the
three groups: called week 0 for the control and the CsA-
treated group and week�2 for the IS-5-MN+CsA-treated
group (Fig. 1A and B). Two weeks after solely IS-5-MN
administration (week 0) there was an increase in both the
SBP (118F 3 mm Hg) and the DBP (102F 4 mm Hg), but
not statistically significant when compared with the two
other rat groups at week 0: SBP-112F 1 mm Hg and DBP-
95F 1 mm Hg (Fig. 1A and B). After 7 weeks of treatment,
there was a significant increase in both the SBP and the
DBP in the CsA-treated group (SBP-152F 7 mm Hg and
DBP-135F 6 mm Hg; **p< 0.01 vs. control group) when
compared with the control group (SBP-107F 1 mm Hg,
DBP-94F 2 mm Hg). In opposition, the SBP for the group
treated with IS-5-MN+CsA (117F 4 mm Hg; ##p < 0.01
vs. CsA group) did not significantly increase after the
concomitant CsA treatment beginning, in opposition to what
occurred in the solely CsA-treated group vs. control. In
addition, IS-5-MN treatment also prevented the DBP in-
crease (83F 8 mm Hg; ##p < 0.01 vs. CsA group), when
compared with the CsA-treated group. In turn, a significant
decrease in DBP was observed at week 7 (Fig. 1A and B).
3.2. Platelet NO synthase activity
Platelet NO synthase activity was measured both in the
control, CsA-treated and IS-5-MN+CsA-treated rats at
basal level and after incubation with the NOS inductors
(IFN-g +LPS) or with the NOS inhibitor (L-NNA) after 7
weeks of treatment. At basal conditions, the CsA-treated
group showed less platelet NOS activity (0.80F 0.03%;
**p< 0.01) than the control group (5.10F 0.10%). The IS-
5-MN+CsA group has prevented NOS activity decrease
(5.30F 0.30%; ##p < 0.01 vs. CsA group) obtained in the
solely CsA-treated group vs. control (Fig. 2). When platelets
were incubated with the NOS inductors IFN-g +LPS, the
NOS activity for the control group increased from the basal
level to 10.9F 0.6 % (**p< 0.01), while for the CsA-treated
group, the value has changed from the basal level of

Fig. 2. Platelet NO synthase activity in control, CsA-treated and IS-5-
MN+CsA-treated rats after 7 weeks of treatment at basal level and after
incubation with IFN-g (100 U/ml) + LPS (10 Ag/ml) or L-NNA (1 mmol/l).
Each bar represents the percentage of conversion of [3H]-L-arginine in [3H]-
L-citrullineF SEM of 10 different samples (rats). **p< 0.01: vs. the control
group; ##p< 0.01: vs. the CsA-treated group.
Fig. 3. Platelet cGMP content in control, CsA-treated and IS-5-MN+CsA-
treated rats after 7 weeks of treatment at basal level and after incubation
with the positive control SNP (100 Amol/l). Each bar represents the mean of
10 different samples (rats)F S.E.M. *p< 0.05: vs. the control group.
Table 1
Basal and thrombin-evoked platelet intracellular free calcium concentration,
collagen-induced whole blood platelet aggregation and some haematolog-
ical parameters for the control, CsA-treated and IS-5-MN+CsA-treated rats
after 7 weeks of treatment
Parameter assessed Rat group
Control CsA IS-5-MN+CsA
Platelet [Ca2 +]iBasal [nM] 131F 3 139F 4 178F 6*#
Thrombin (0.1 U/ml)-
evoked [DnM]
1072F 50 1569F 77** 839F 45##
Platelet aggregation
Collagen (5 Ag/ml) [V] 10.1F 0.4 13.4F 1.0* 11.1F 0.4#
Haematology
PTC [� 103/Al] 598F 32 573F 24 623F 34
PCT [%] 0.29F 0.02 0.30F 0.02 0.32F 0.03
MPV [fl] 5.4F 0.1 5.5F 0.2 5.4F 0.2
PDW (ratio) 16.2F 0.2 16.8F 0.1 15.6F 0.2
HCT [%] 35.5F 0.4 35.1F 0.4 34.3F 0.3
Data are expressed as meansF SEM of 10 separate values (rats). CsA=
Cyclosporin A; IS-5-MN= Isosorbide-5-Mononitrate; (DnM) = Intracellular
free calcium concentration variation (above the basal level); PTC= Platelet
count; PCT= Plateletocrit; MPV=Mean platelet volume; PDW=Platelet
deviation weight; HCT=Haematocrit. *p< 0.05 and **p< 0.01: vs. the
control group; #p< 0.05 and ##p< 0.01: vs. the CsA-treated group.
F. Reis et al. / Thrombosis Research 110 (2003) 107–115 111
0.80F 0.03% to 2.60F 0.30%. In the IS-5-MN+CsA-trea-
ted group (5.10F 0.20%), the basal values have not signif-
icantly changed (Fig. 2). After the NOS inhibitor incubation
(L-NNA), the control group showed a NOS activity decrease
(1.60F 0.03%) vs. the basal level as well as the CsA-treated
group in which residual values were obtained (0.10F0.01%; **p < 0.01). In the IS-5-MN+CsA-treated group, a
significant decrease was also observed (0.60F 0.04%) vs.
the basal situation (Fig. 2).
3.3. Platelet cGMP content
Platelet cGMP content was assessed both in the control,
CsA-treated and IS-5-MN+CsA-treated groups at basal
level and after incubation with the positive control (SNP)
after 7 weeks of treatment. At basal level, there was an
cGMP content increase in the CsA-treated group (12.9F 2.6
pmol/109 plat./ml; *p < 0.05) when compared with the
control group (5.6F 1.1 pmol/109 plat./ml). In the IS-5-
MN + CsA-treated group, the cGMP content increase
(10.9F 2.2 pmol/109 plat./ml; *p< 0.05) vs. control was
less predominant (Fig. 3). When platelets where incubated
with the positive control SNP, all the groups showed higher
values of cGMP content when compared with the basal level
and in accordance with the basal tendencies despite not
statistically significant between each group and the others
(control: 23.8F 4.8 pmol/109 plat./ml; CsA-treated:
30.3F 6.1 pmol/109 plat./ml; IS-5-MN + CsA-treated:
26.2F 5.2 pmol/109 plat./ml) (Fig. 3).
3.4. Platelet intracellular free calcium concentration
The basal platelet [Ca2 +]i for the control (131F 3 nM)
and for the CsA-treated group (139F 4 nM) showed similar
values, which contrasts with higher values obtained for the
IS-5-MN+CsA group (178F 6 nM; *#p< 0.05) (Table 1).
The control group thrombin-evoked [Ca2 +]i was 1072F 50
DnM (Table 1). The CsA-treated group showed higher,
statistically significant [Ca2 +]i values (1569F 77 DnM;
**p < 0.01). This CsA-induced calcium increase vs. control
group was prevented in the IS-5-MN+CsA-treated group
(839F 45 DnM; ##p < 0.01 vs. CsA group) (Table 1).
3.5. Whole blood platelet aggregation and haemathological
parameters
Whole blood platelet aggregation induced by collagen (5
Ag/ml) was tested in the three rat groups after 7 weeks of

F. Reis et al. / Thrombosis Research 110 (2003) 107–115112
treatment. In the CsA-treated group, there was a significant
increase on collagen-induced aggregation (13.4F 1.0 V;
*p < 0.05) when compared with the control group (10.1F0.4 V). The IS-5-MN + CsA treatment has prevented
(11.4F 0.4 V; #p < 0.05 vs. CsA group) the increase on
platelet aggregation observed in the solely CsA-treated
group (Table 1).
Some haematological parameters related to the platelet
function were also tested in each of the three rat groups after
7 weeks of treatment. No statistically significant differences
were obtained between the three groups, in which platelet
count, plateletocrit, mean platelet volume, platelet deviation
weight and haematocrit concerns (Table 1).
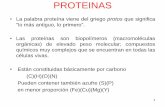
Fig. 4. Electron microscopy morphology of platelets from control (A1 and A2), Cs
weeks of treatment (original magnification � 16800).
3.6. Electron microscopy study of platelet activation
The morphological features of platelets, which are
obviously related to the platelet activation state, were
evaluated by electron microscopy studies in each of the
three groups under study after 7 weeks of treatment. In
opposition with the normal morphological structure of the
platelets from the control group, which showed regular and
well-defined shape and membrane/organelles delimitation
(Fig. 4A1), as well as a nonaggregation profile (Fig. 4A2),
the platelets from the CsA-treated group demonstrate
several signals of activation, which is a confirmation of
the above-mentioned results. Therefore, as could be seen in
A-treated (B1 and B2) and IS-5-MN+CsA-treated (C1 and C2) rats after 7

F. Reis et al. / Thrombosis Research 110 (2003) 107–115 113
Fig. 4B1 and B2, membrane structure disorganization,
pseudopodia formation and other signals of platelet acti-
vation and aggregation are clearly demonstrated by the
pictures of electron microscopy. On the contrary, the
platelets collected from the IS-5-MN+CsA-treated group
showed identical normal features and structures to those
observed for the control group (Fig. 4C1 and C2), which
also confirms the results of the biochemical–analytical
determinations of platelet activation, namely, the intracel-
lular free calcium concentration and the whole blood
platelet aggregation results.
4. Discussion
Our study has demonstrated that CsA inhibits NOS
activity, which is in accordance with other authors who
reported the same effect on the vascular cells [12,14], in
association with a decreased endothelium-dependent relax-
ation [9,11]. These effects on the NOS as well as the
decreased vascular cGMP content has been suggested by
several authors, not by all [15,17], as the main cause of
the impaired vascular reactivity associated with both CsA-
induced hypertension and nephrotoxicity [8–14,27–29].
In our study, in opposition to what was previously
obtained by those vascular studies, CsA-treated rats had
higher platelet cGMP content, which is obviously a new
and surprising data, because it is at first an unexpected
result. Therefore, CsA-induced decreased NOS activity
might result in a decreased cGMP content as a consequent
direct effect. However, the cGMP pathway has a NO-
independent mechanism, which should be affected by the
CsA treatment. We have previously shown that CsA
induces platelet hyperactivation [24,25], which was con-
firmed in this study by the increased [Ca2 +]i and collagen-
evoked aggregation. Thus, while the CsA effect on the
NOS activity might represent a net, pure, effect on the
enzyme functioning, the CsA effect on the platelet cGMP
production seems to be a compensatory effect against
CsA-induced platelet hyperactivation, putatively originated
by a calcium-induced activation of eNOS and the subse-
quent cGMP release. The molecular and cellular mecha-
nisms underlying these hypothetic counterregulation
should be further investigated, namely, by using modu-
lators of platelet [Ca2 +]i and of guanylate cyclase activity.
A similar explanation in vascular cells studies was previ-
ously suggested by others, who hypothesized that exacer-
bated vascular NO–cGMP pathway should represent a
mechanism resulting from CsA increased vasoconstriction
[15,17]. However, the majority of the works made on this
area has demonstrated a decreased vascular NO–cGMP
production and relaxation associated with CsA-induced
hypertension [8–14,27–29]. The hypothetic existence of
different mechanisms on platelets and vascular cells rec-
ommends that the use of platelets as models for the
VSMC effects in the CsA-induced hypertension should
be carefully done, at least in which NO–cGMP pathway
concerns.
One of the main steps back on these investigations are
the conflicting results about the benefits of L-arginine
treatment on the vascular and platelet activity impairment
related to CsA-induced hypertension and increased risk of
thromboembolic events [15–17,30]. This is the main reason
why we have decided to test a drug that, despite not being a
classic antihypertensive drug (it is primarily used for chron-
ic angina pectoris), might be able to prevent some of the
above-described effects, because of its NO-donor properties
[34,35]. IS-5-MN is an organic nitrate that needs intracel-
lular decomposition to release NO, in opposition to other
NO donors that are able to spontaneously release NO in
vivo. The mechanism has been suggested as one of the
putative causes of nitrate tolerance commonly associated to
organic nitrates therapy [36]. One of the strategies used to
overcome tolerance is by interrupting therapy with a daily
nitrate-free period of about 4 h [36], which was made in our
study by using asymmetric b.i.d. administrations. As a
matter of fact, in this study, concomitant IS-5-MN treatment
with CsA has prevented hypertension development during
all the treatment, which suggests tolerance overcome. This
result contrasts to what was previously shown in studies
with L-arginine supplementation [30]. Therefore, while L-
arginine is the natural NOS substratum, IS-5-MN, being
an organic nitrate, could be more effective if the NO
pathway affected by CsA it is not merely the substratum
supply but, instead of that, other mechanisms also contrib-
uting for the NO synthesis. This fact might explain the
advantage of IS-5-MN when compared with L-arginine.
However, another factor should also contribute to the
benefit of IS-5-MN on blood pressure control, i.e., the
previous treatment with IS-5-MN two weeks before starting
CsA administration. This should maintain the vascular nitric
oxide at a level that is able to impede the blood pressure rise
resulting from the NO diminishment and vascular dysfunc-
tion originated by CsA. This methodological approach
should be taken in consideration in future studies.
Besides preventing hypertension development, IS-5-MN
treatment has prevented the effect of CsA on platelet
activation. Therefore, platelets from IS-5-MN+CsA-treated
rats showed normal thrombin-evoked [Ca2 +]i and collagen-
induced aggregation when compared with the rats treated
only with CsA. The normalization of platelet function was
also demonstrated by electron microscopy studies of platelet
morphology. The effect of IS-5-MN on platelet function on
rats submitted to CsA treatment is original and no compar-
ison could be done with other CsA studies. However, an
improvement on platelet function was already demonstrated
in other studies [37–39], not with CsA-treated platelets. Our
work also demonstrated that IS-5-MN treatment has pre-
vented NOS activity decrease and, surprisingly, that cGMP
content also has decreased when compared with CsA-treated
rats. Because IS-5-MN is an organic nitrate, we should
expect a platelet cGMP content increase. However, because

F. Reis et al. / Thrombosis Research 110 (2003) 107–115114
there was a platelet function normalization, as previously
commented, the increased cGMP content which was hypo-
thetically originated to regulate platelet hyperactivation did
not occurred and it is not required when IS-5-MN is present
and [Ca2 +]i and aggregation are normal. A similar effect
was previously demonstrated by us in rats treated with L-
arginine +CsA [30], which confirms the beneficial effects of
NO supplementation on the platelet hyperreactivity of CsA-
treated rats. Thus, IS-5-MN results seems to confirm the
previous hypothesis of increased cGMP content as a com-
pensatory mechanism against platelet hyperactivation in-
duced by the CsA treatment. However, compensation seems
not to overcome hyperactivation, which might be explained
by the sequence of pathways that should occur once platelet
[Ca2 +]i is already elevated such as promotion of adhesion,
aggregation and granules content release, which will ampli-
fy the initial response, specially because of the TXA2
pathway.
Recognizing that platelet hyperactivation should be re-
sponsible for thromboembolic events and that might partic-
ipate in vascular dysfunction and atherosclerosis plaque
formation, the IS-5-MN treatment might have an important
role to prevent the above-mentioned side effects. However,
if a similar effect on the peripheral vessels is confirmed,
namely, vascular function and structure preservation or
normalization, IS-5-MN might be considered as a good
choice as preventive therapy for the CsA-induced hyperten-
sion. The classic antihypertensive drugs, despite controlling
blood pressure values in patients submitted to CsA treat-
ment, are usually unable to prevent the development of
vascular dysfunction and lesions that precedes hypertension
development and increased risk of thromboembolic events.
In conclusion, CsA induces platelet hyperactivation,
namely, by increasing [Ca2 +]i and aggregation as well as
by decreasing NOS activity. This effect seems to be com-
pensated by an increased cGMP content, whose mechanisms
should be further assessed. The concomitant IS-5-MN and
CsA treatment prevents the above-mentioned platelet hy-
perreactivity and tends to normalize the NO–cGMP path-
way as well as the development of hypertension. If a similar
benefit occurs in the vasculature, the administration of the
NO donor IS-5-MN should have an important role in
preventing CsA-induced hypertension and increased risk
of thromboembolic events.
Acknowledgements
This study had the kind collaboration of Novartis Farma
(Lisbon, Portugal) that has yielded the cyclosporin A
(Sandimmun NeoralR) and of Ferraz-Lynce (Lisbon,
Portugal), which supplied the IS-5-MN (MonoprontR).Also, our special thanks to Brystol Myers Squibb for the
financial support for this project. We also thank Paulo
Borges for his support on rat administration and blood
pressure assessment.
References
[1] Borel JF, Di Padova F, Mason J, Quesniaux V, Ryffel B, Wenger R.
Pharmacology of cyclosporine (Sandimmune): I. Introduction. Phar-
macol Rev 1989;41:239–42.
[2] Kahan BD. Cyclosporine. N Engl J Med 1989;321:1725–38.
[3] Vanrenterghem Y, Roels L, Lerut T, Gruwez L, Michielsen P, Gresele
P, et al. Thromboembolic complications and haemostatic changes in
cyclosporin-treated cadaveric kidney allograft recipients. Lancet
1985;I:999–1002.
[4] Muraki T, Sasaki Y, Gidding JC, Ishii H, Kaneko T, Yamamoto J.
Antithrombotic effects of FK506 versus prothrombotic effect of cy-
closporine in vivo. Transplantation 1995;60:308–9.
[5] Miller BW, Hmiel SP, Schnitzler MA, Brennan DC. Cyclosporine as
cause of thrombotic microangiopathy after renal transplantation. Am J
Kidney Dis 1997;29:813–4.
[6] Schachter M. Cyclosporine A and hypertension. J Hypertens 1988;6:
511–6.
[7] Sander M, Victor RG. Hypertension after cardiac transplantation:
pathophysiology and management. Curr Opin Nephrol Hypertens
1995;4:443–51.
[8] Cartier R, Dagenais F, Hollmann C, Cambron H, Buluran J. Chronic
exposure to cyclosporine affects endothelial and smooth muscle re-
activity in the rat aorta. Ann Thorac Surg 1994;58:789–94.
[9] Stephan D, Billing A, Krieger JP, Erima M, Fabre M, Hafner M, et al.
Endothelium-dependent relaxation in the isolated rat kidney: impair-
ment by cyclosporine A. J Cardiovasc Pharmacol 1995;26:859–68.
[10] Zoja C, Furci L, Ghilardi F, Zilio P, Benigni A, Remuzzi G. Cyclo-
sporin-induced endothelial cell injury. Lab Invest 1986;55:455–62.
[11] Rego A, Vargas R, Wroblewska B, Foegh ML, Ramwell PW. Attenu-
ation of vascular relaxation and cyclic GMP responses by cyclosporin
A. J Pharmacol Exp Ther 1990;252:165–70.
[12] Akita K, Dusting GJ, Hickey H. Suppression of nitric oxide produc-
tion by cyclosporin A and FK506 in rat vascular smooth muscle cells.
Clin Exp Pharmacol 1994;21:231–3.
[13] Marumo T, Nakaki T, Hishikawa K, Suzuki H, Kato R, Saruta T.
Cyclosporin A inhibits nitric oxide synthase induction in vascular
smooth muscle cells. Hypertension 1995;25(Part 2):764–8.
[14] Vaziri ND, Ni Z, Zhang YP, Ruzics EP, Maleki P, Ding Y. Depressed
renal and vascular nitric oxide synthase expression in cyclosporine-
induced hypertension. Kidney Int 1998;54(2):482–91.
[15] O’Neil GS, Chester AH, Kushwaha S, Rose M, Tadjkarimi S, Yacoub
MH. Cyclosporin treatment does not impair the release of nitric oxide
in human coronary arteries. Br Heart J 1991;66:212–6.
[16] Stroes ES, Luscher TF, Groot FG, Koomans HA, Rabelink TJ. Cyclo-
sporin A increases nitric oxide activity in vivo. Hypertension 1997;
29:570–5.
[17] Hansen JM, Johansen NJ, Mollerup HM, Anderson NF, Strandgaard
S. Effects of nitric oxide blockade and cyclosporin A on cardio-
vascular and renal function in normal man. J Hypertens 1999;17:
1707–13.
[18] Body SC. Platelet activation and interactions with the microvascula-
ture. J Cardiovasc Pharmacol 1996;27(Suppl. 1):S13–25.
[19] White JG. Platelets and atheriosclerosis. Eur J Clin Invest 1994;
24:25–9.
[20] Vanhoutte PM. Platelets, endothelium and blood vessel wall. Experi-
entia 1988;44:105–8.
[21] Radomski MW, Palmer RMJ, Moncada S. An L-arginine/nitric oxide
pathway present in human platelets regulates aggregation. Proc Natl
Acad Sci U S A 1990;87:5193–7.
[22] Bodzenta-Lukaszyk A, Gabryelewicz A, Lukaszyk A, Bielawiec M,
Konturek JW, Domschke W. Nitric oxide synthase inhibition and
platelet function. Thromb Res 1994;75(6):667–72.
[23] Berkels R, Stockklauser K, Rosen P, Rosen R. Current status of
platelet NO synthase. Thromb Res 1997;87(1):51–5.
[24] Reis F, Tavares P, Rito LC, Teixeira HM, Santos-Dias JD, Ferrer-
Antunes C, et al. Platelet activation is increased in cyclosporin

F. Reis et al. / Thrombosis Research 110 (2003) 107–115 115
A-induced hypertensive rats. J Cardiovasc Pharmacol 2000;36(1):
56–64.
[25] Reis F, Tavares P, Fontes-Ribeiro CA, Ferrer-Antunes C, Teixeira F.
The peripheral serotonergic system and platelet aggregation in
cyclosporin A-induced hypertensive rats. Thromb Res 1999;96:
365–72.
[26] Reis F, Tavares P, Teixeira F. The distribution of catecholamines
between plasma and platelets in cyclosporin A-induced hypertensive
rats. Pharmacol Res 2000;41(2):129–35.
[27] Kim HS, Kim DH, Kang SW, Choi KH, Lee HY, Han DS, et al.
L-arginine restores suppressed acetylcholine-induced endothelium-
dependent vascular relaxation in cyclosporin A-treated rats. Trans-
plant Proc 1996;28(3):1372–4.
[28] Lee J, Kim SW, Kook H, Kang DG, Kim NH, Choi KC. Effects of
L-arginine on cyclosporin-induced alterations of vascular NO/cGMP
generation. Nephrol Dial Transplant 1999;14:2634–8.
[29] Yang CW, Kim YS, Kim J, Kim YO, Min SY, Choi EJ, et al. Oral
supplementation of L-arginine prevents chronic cyclosporine nephro-
toxicity in rats. Exp Nephrol 1998;6:50–6.
[30] Santiago M, Reis F, Almeida L, Alcobia T, Dionısio J, Teixeira F.
Impaired arterial and platelet nitric oxide and cyclic guanosine-3V,5V-monophosphate content in cyclosporin A-induced hypertensive rats.
Fundam Clin Pharmacol 2003;17:43–50.
[31] Mehta JL, Chen LY, Kone BC, Mehta P, Turner P. Identification of
constitutive and inducible forms of nitric oxide synthase in human
platelets. J Lab Clin Med 1995;125:370–7.
[32] Chen L, Salafranca MN, Mehta JL. Cyclooxygenase inhibition de-
creases nitric oxide synthase activity in human platelets. Am J Physiol
1997;273:H1854–9.
[33] Grynkiewicz G, Poenie M, Tsien RY. A new generation of Ca2 +
indicators with greatly improved fluorescence properties. J Biol Chem
1985;260:3440–50.
[34] Gunasekara NS, Noble S. Isosorbide 5-mononitrate. A review of a
sustained-release formulation (IndurR) in stable pectoris angina pec-
toris. Drugs 1999;57(2):261–77.
[35] Parker JD, Parker JO. Nitrate therapy for stable angina pectoris. Drug
Ther 1998;338(8):520–31.
[36] Megson IL. Nitric oxide donor drugs. Drug Fut 2000;25(7):701–15.
[37] Wirthumer-Hoche C, Silberhauer K, Sinzinger H. Effect on nitrogly-
cerin and other organic nitrates on the in-vitro biosynthesis of arach-
idonic acid-metabolits in washed human platelets. Prostaglandins
Leukot Med 1984;15:317–23.
[38] Sinzinger H, Virgolini I, O’Grady J, Rauscha F, Fitsch P. Modification
of platelet function by isosorbide dinitrate in patients with coronary
artery disease. Thromb Res 1992;65:323–35.
[39] Gilmer JF, Moriarty LM, McCafferty DF, Clancy JM. Synthesis, hy-
drolysis kinetics and anti-platelet effects of isosorbide mononitrate
derivatives of aspirin. Eur J Pharm Sci 2001;14(3):221–7.