
The left ventricle proteome differentiates middle-aged and old left ventricles in mice
Upload
independentCategory
view
3download
0
2005;80:170-178 Ann Thorac SurgMcCarthy and Richard D. White
Leonardo Rodriguez, Michael L. Lieber, Abigail Lara, Joan A. Weaver, Patrick M. Monvadi B. Srichai, Richard A. Grimm, Arthur E. Stillman, A. Marc Gillinov, L.
Patients with Left Ventricular Systolic DysfunctionIschemic Mitral Regurgitation: Impact of the Left Ventricle and Mitral Valve in
http://ats.ctsnetjournals.org/cgi/content/full/80/1/170located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2005 by The Society of Thoracic Surgeons.
is the official journal of The Society of Thoracic Surgeons and theThe Annals of Thoracic Surgery
by on May 31, 2013 ats.ctsnetjournals.orgDownloaded from

IVVMAARCaC
cpivga(t
(cemm
pap
“
vmpw
omc[psama
A
ACE
©P
CA
RD
IOV
AS
CU
LA
R
schemic Mitral Regurgitation: Impact of the Leftentricle and Mitral Valve in Patients with Leftentricular Systolic Dysfunction
onvadi B. Srichai, MD, Richard A. Grimm, DO, Arthur E. Stillman, MD, PhD,. Marc Gillinov, MD, L. Leonardo Rodriguez, MD, Michael L. Lieber, MS,bigail Lara, MD, Joan A. Weaver, RT, (R)MR, Patrick M. McCarthy, MD, andichard D. White, MD
enter for Integrated Non-Invasive Cardiovascular Imaging of the Department of Radiology, Section of Cardiovascular Imaging,nd Departments of Cardiovascular Medicine, Thoracic and Cardiovascular Surgery, and Biostatistics and Epidemiology,
leveland Clinic Foundation, Cleveland, Ohio(srttid
gmcissgi
Background. Mitral regurgitation (MR) is a commonomplication of ischemic heart disease, and its presenceortends adverse outcomes. As the exact mechanisms of
schemic MR are not well defined, we characterized leftentricular global geometry, regional function, and re-ional myocardial scarring, in addition to mitral valvepparatus geometry, using magnetic resonance imagingMRI) of ischemic heart disease patients with left ven-ricular dysfunction and varying degrees of ischemic MR.
Methods. Sixty patients with varying degrees of MRnone, mild, moderate, and severe) determined by echo-ardiography and referred for MRI assessment of isch-mic heart disease were included. Left ventricular geo-etric, functional, and scar measurements in addition toitral valve geometric measurements were evaluated.Results. Clinical characteristics found to be significant
redictors of degree of MR included severity of coronaryrtery disease (p < 0.05), completeness of myocardial
erfusion (p < 0.005), and average systolic blood pressurehlmh
ucuaaeta
qgtrt[
ardiovascular Imaging, Desk HB6, Cleveland Clinic Foundation, 9500uclid Ave, Cleveland, OH 44195; e-mail: [email protected].
2005 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ats.ctsnetjournDownloaded from
p < 0.05). Mitral systolic tenting area (p < 0.0001) in atatistical model with scarring of the anterior-lateralegion (p < 0.05) proved to be the most powerful predic-or of MR severity (r2 � 0.31). Mitral annular dilatation inhe anterior-posterior direction (p < 0.0001) and dimin-shed LV systolic function (p < 0.005) were importanteterminants of mitral systolic tenting area (r2 � 0.57).Conclusions. Mitral tenting in combination with re-
ional left ventricular myocardial scarring are importantechanisms to the development of ischemic MR. Surgi-
al annuloplasty addresses mitral tenting, but has littlempact on the effect of regional scarring. Moderate-to-evere ischemic MR develops in patients with regionalcarring of the anterior-lateral and inferior-posterior re-ions, and new surgical developments should take thisnto account.
(Ann Thorac Surg 2005;80:170–8)
© 2005 by The Society of Thoracic SurgeonsIschemic” mitral regurgitation (MR) is functional insuffi-ciency of the mitral valve related to changes in left
entricular (LV) and mitral valve geometry and perfor-ance resulting from ischemic heart disease (IHD). The
resence of even mild degrees of ischemic MR is associatedith survival rates of less than 50% at 5 years [1, 2].The exact mechanical alterations leading to the devel-
pment of ischemic MR are not well defined. In experi-ental studies, ischemic MR was attributed to global
hanges in the LV geometry [3, 4]. More recently, in vitro5] and animal studies [6–8] have suggested that theathogenesis is more complex, related to alterations inpatial relationships between the LV and mitral valvepparatus. In human studies, LV sphericalization [9],itral annulus enlargement, increased mitral tenting
rea, and loss of systolic mitral annular contraction [10]
ccepted for publication Jan 10, 2005.
ddress reprint requests to Dr White, Center for Integrated Non-Invasive
ave been proposed as possible mechanisms. However,imitations with imaging and analysis of MR degree,
itral deformation, and global and local LV remodelingave limited these studies.Given the diversity of potential mechanisms contrib-
ting to the development of ischemic MR, current surgi-al therapy consisting of mitral annuloplasty with anndersized annular ring does not always provide predict-ble and durable repair. As a result, newer techniquesre under development based on observations fromxperimental animal models of ischemic MR. Insight intohe mechanisms causing ischemic MR is key to furtherdvancement of treatment strategies.Magnetic resonance imaging (MRI) provides high
uality images for the assessment of LV and mitral valveeometric and functional changes. With MRI, quantita-ive measurements of LV volumes and function do notely on geometric assumptions and are superior to tradi-ional two-dimensional echocardiography measurements
11]. Additionally, with the advent of delayed-enhance-0003-4975/05/$30.00doi:10.1016/j.athoracsur.2005.01.068
by on May 31, 2013 als.org

mdwohbal
M
Tvm
PTfcaeeawwpmmoau(
wspflerp
prombo
EE
dcaoosDfsaocS
Obta15g
MM
stcnhpdi
171Ann Thorac Surg SRICHAI ET AL2005;80:170–8 ISCHEMIC MITRAL REGURGITATION MECHANISMS
CA
RD
IOV
AS
CU
LA
R
ent imaging, the degree of regional and global myocar-ial scarring can be uniquely analyzed [12]. Therefore,e undertook this retrospective quantitative MRI studyf patients with IHD and LV dysfunction, with theypothesis that the degree of ischemic MR is influencedy regional and global myocardial scarring and its result-nt effects on LV geometry and function, as opposed toocal changes in the mitral valve apparatus.
aterial and Methods
he investigation was approved by the Institutional Re-iew Board of the medical center, and the followingethods were applied.
atient Populationhere were 243 patients who underwent a cardiac MRI for
unctional and anatomic evaluation of the LV and tissueharacterization of its myocardium between January 2001nd December 2002. In the subgroup of 180 patients withvidence of IHD and LV systolic dysfunction, defined as LVjection fraction of 40% or less, there were 128 patients wholso had a transthoracic echocardiography performedithin 1 week of the cardiac MRI study. Within this groupith both cardiac MRI and transthoracic echocardiographyerformed, we stratified patients by MR severity as deter-ined by echocardiography. Patients with structural abnor-alities of the mitral valve apparatus (eg, myxomatous) or
ther valves (eg, calcific aortic stenosis) were excluded. Tochieve a balanced test set, we included the first 15 consec-tive qualifying patients per group for a total of 60 patients
Fig 1).Review of each patient’s clinical data by chart reviewas performed to identify the presence or absence of
pecific risk factors potentially associated with or predis-osing to the development of ischemic MR. These risk
actors included hypertension, diabetes mellitus, hyper-ipidemia, tobacco use, severity of coronary artery dis-ase (single, double, or triple vessel), prior coronaryevascularization (coronary artery bypass graft surgery or
ercutaneous coronary intervention), and myocardial gats.ctsnetjournDownloaded from
erfusion status at time of study determined from aecent heart catheterization demonstrating either no cor-nary territories with jeopardized blood flow or one orore coronary territories with evidence of jeopardized
lood flow (significant stenoses in the coronary arteriesr bypass grafts supplying a region of myocardium).
chocardiographyCHOCARDIOGRAPHIC TECHNIQUE. Two-dimensional echocar-iography examinations were performed using commer-ially available equipment and standard techniques inccordance with the guidelines of the American Societyf Echocardiography (ASE) [13]. Examinations consistedf multiple tomographic planes including long-axis andhort-axis views with color Doppler and continuous waveoppler for detection and assessment of myocardial
unction and valvular disease. Degree of MR was as-essed semiquantitatively by jet area on color Dopplernd quantitatively by calculation of effective regurgitantrifice (ERO) area based on the proximal isovolumicontour method [14].EVERITY OF MITRAL REGURGITATION BY ECHOCARDIOGRAPHY.
verall severity of MR was graded on echocardiographyy qualitative (jet area/left atrial area ratio) and quanti-
ative (ERO) assessments into four grades: none � jetrea 0%, ERO 0 mm2; mild � jet area less than 20%, EROto 10 mm2; moderate � jet area 20% to 40%, ERO 10 to
0 mm2; and severe � jet area greater than 40%, EROreater than 50mm2.
agnetic Resonance ImagingRI TECHNIQUE. Cardiac MRI was performed on a 1.5-Tesla
canner (Symphony or Sonata; Siemens Medical Sys-ems, Erlangen, Germany) using a phased-array torsooil and standard electrocardiographic referencing tech-iques [15]. Scout imaging using an ultrafast “snapshot”alf-Fourier single-shot, turbo spin-echo sequence [15]ermitted rapid identification of the cardiac axes foriagnostic imaging. Dynamic (ie, cine) “bright-blood”
mage-loops were acquired using a segmented-k-space
Fig 1. Flow chart demonstratingpatient selection of mitral regurgi-tation (MR) severity groups. *Pa-tients with structural valvular ab-normalities were excluded. (Echo� echocardiography; LVEF � leftventricular ejection fraction; MRI� magnetic resonance imaging.)
radient-echo sequence with view-sharing for a temporal
by on May 31, 2013 als.org

rcMwwikhs
csLmicdb(vL
vc[elsaSb(L
L[tadwsgi
wbL
Tms4TotpbM
atetiavmwtl
SDdwAgceaod(uss
Fionhaa
172 SRICHAI ET AL Ann Thorac SurgISCHEMIC MITRAL REGURGITATION MECHANISMS 2005;80:170–8
CA
RD
IOV
AS
CU
LA
R
esolution of 30 to 50 msec [15]. For evaluation of myo-ardial scar, nonstress gadolinium delayed-enhancement
RI images were acquired. Delayed-enhancement MRIas based on the previously described Turbo-FLASHith inversion recovery imaging at 20 to 30 minutes after
ntravenous injection of Gadolinium-DTPA (0.2 mmol/g). Imaging was performed with or without breath-olding, based on the patient’s heart rate and ability touspend respiration.
Images were acquired in standard two-chamber, three-hamber, and four-chamber long-axis views, as well ashort-axis views at basal, middle, and apical thirds of theV. For positioning, the midpapillary muscle level (ie,iddle third) was used for reference, with the basal
mage derived from midway between it (approximately 2m above) and the mitral annulus and the apical imageerived from midway between it (approximately 2 cmelow) and the LV apex. Additionally, a short-axis series
base to apex) of cine MRI loops was acquired forolumetric analysis of the LV.EFT VENTRICULAR GLOBAL GEOMETRIC MEASUREMENTS. Leftentricular volumetric analysis was performed on theine MRI LV short-axis series using a standard approach15]. This was accomplished by manual outlining of thendocardial borders at end-diastole and end-systole at allevels with derivation of end-diastolic volume, end-ystolic volume, and ejection fraction using commerciallyvailable software (Argus Platform; Siemens Medicalystems, Erlangen, Germany). Volumes were indexed toody surface area. Additionally, the sphericity index
ratio of LV length to width) was also measured.EFT VENTRICULAR REGIONAL FUNCTIONAL MEASUREMENTS. TheV was divided according to the ASE 16-segment model
13]. Segmental wall thickening was assessed qualita-ively and graded as a wall motion score for each segments: 1 � normal, 2 � hypokinetic, and 3 � akinetic/yskinetic. Total function was assessed as the averageall motion score over the entire ventricle. Additionally,
egments adjacent to each papillary muscle wererouped together to form the anterior-lateral region and
ig 2. Cine magnetic resonancemaging three-chamber view dem-nstrating the measurement of an-ulus diameter and coaptationeight (left), and mitral tentingrea (right) of the mitral valvepparatus.
nferior-posterior region, and function of these regions a
ats.ctsnetjournDownloaded from
as taken as the average wall motion score from theasal and middle segments forming these regions.EFT VENTRICULAR REGIONAL MYOCARDIAL SCAR MEASUREMENTS.
he extent of myocardial hyperenhancement per LV seg-ent, reflecting scar, was graded using a previously de-
cribed six-level system as follows: 0%, 1% to 24%, 25% to9%, 50% to 74%, 75% to 99%, and 100% segmental scar [16].otal scarring was assessed as the average of the scar gradever the entire LV. Additionally, scarring in the vicinity ofhe papillary muscles (anterior-lateral and inferior-osterior) was assessed as the average scar grade from theasal and middle segments forming these regions.ITRAL VALVE GEOMETRIC MEASUREMENTS. Mitral annular di-meter was measured on cine MRI in two-chamber,hree-chamber, and four-chamber views (Fig 2) and av-raged at end-systole to calculate mean annular diame-er. Systolic leaflet deformation, defined as valvular tent-ng area, was measured as area enclosed between thennular plane and mitral leaflets on the three-chamberiew at early and late systole. In addition, apical displace-ent of the mitral coaptation point (coaptation height)as measured as the distance between the leaflet coap-
ation point and mitral annulus plane at early systole andate systole (Fig 1).
tatistical Analysisescriptive statistics are expressed as mean � standardeviation or as percentages. Univariate comparisonsere made using one-way analysis of variance or �2 tests.ssociations between each independent variable andrade of MR severity were assessed using Spearmanorrelation coefficients. To maintain an overall Type Irror of 0.05, a simple Bonferroni correction waspplied, and a p values less than 0.005 were required inrder to declare statistical significance. Predictors thatisplayed significant (p � 0.005) or marginally significant
0.005 � p � 0.10) relationships with degree of MR innivariate analyses were included in multivariate analy-is of variance (ANOVA) models of MR severity. Forimplification, regional (as opposed to segmental) vari-
bles of function and scarring were used in the statisticalby on May 31, 2013 als.org
asewmgitp
R
PBoomp
LTfidMtsw
LTgart
aeslo
LTtgrpMWsa
MTast(otw�s
DMtp
T
MAS
DHHPSIHS
a
r
C
173Ann Thorac Surg SRICHAI ET AL2005;80:170–8 ISCHEMIC MITRAL REGURGITATION MECHANISMS
CA
RD
IOV
AS
CU
LA
R
nalyses. Variables studied in multivariate models of MReverity included the following: LV ejection fraction, LVnd-diastolic volume index, sphericity index, averageall motion score in anterior-lateral region, average wallotion score in inferior-posterior region, average scar
rade in anterior-lateral region, average scar grade innferior-posterior region, mitral annulus diameter in an-erior-posterior dimension, mitral leaflet coaptation dis-lacement, and early systolic mitral tenting area.
esults
atient Characteristicsaseline characteristics of patients with varying degreesf MR are illustrated in Table 1. Patients with moderater severe MR were more likely to have incompleteyocardial perfusion (p � 0.005) and lower systolic blood
ressure (p � 0.05).
eft Ventricle Global Geometric Predictorshere were marginally statistically significant trends noted
or LV ejection fraction (p � 0.09, r � -0.25) and both volumendices with improved systolic function and lower end-iastolic and end-systolic volumes for the group with noR as compared with the other groups (Table 2). However,
here clearly was a statistically significant difference in thephericity index (p � 0.005, r � -0.45) among the four groupsith increasing severity of MR.
eft Ventricle Regional Functional Predictorsotal wall motion scores were similar among the fourroups of MR severity (Table 2, Fig 3). On the other hand, inn analysis by region, function in the inferior-posterioregion showed statistically significant differences among
able 1. Baseline Clinical Characteristics
No MR(n � 15)
ale 87%ge 61 � 10everity of CADa
Single-vessel 27%Double-vessel 7%Triple-vessel 67%iabetes mellitus 47%ypertension 73%yperlipidemia 73%rior revascularization 33%moking history 60%ncomplete myocardial perfusionb,c 7%eart rate 73 � 13ystolic blood pressurea 127 � 16
p � 0.05. b p � 0.005. c Incomplete myocardial perfusion � 1 corecent catheterization.
AD � coronary artery disease; MR � mitral regurgitation.
he four groups (p � 0.005, r � 0.36); this was not seen in the l
ats.ctsnetjournDownloaded from
nterior-lateral region (p � not significant; Fig 3). Whenach MR group was assessed individually, there was aignificant difference seen in the function of the anterior-ateral region compared with the inferior-posterior regionnly in the group with severe MR (p � 0.05).
eft Ventricle Regional Myocardial Scar Predictorshere was significantly increased total scarring noted in
he group with severe MR compared with the other threeroups (p � 0.005, r � 0.23; Table 2, Fig 4). In addition,egional scarring in both anterior-lateral and inferior-osterior regions was greater in the patients with severeR compared with the other groups (Table 2, Figs 4–6).ithin each group, however, there were no statistically
ignificant differences noted between scarring in thenterior-lateral and inferior-posterior regions.
itral Valve Geometric Predictorshere was no difference in the average mitral annularrea between groups (Table 2). However, despite noignificant differences in the mitral annular diameter inhe anterior-inferior (two-chamber) and septal-lateralfour-chamber) dimensions, there was increased anteri-r-posterior (three-chamber) dimension diameter in pa-ients with severe MR (Table 2). Additionally, patientsith severe MR had increased mitral coaptation height (p0.05) as well as tenting area (p � 0.005) at early and late
ystolic measurements.
eterminants of Degree of MRultivariate ANOVA modeling of MR severity pointed
o mitral systolic tenting area as the single most powerfulredictor among those studied (p � 0.0001). Anterior-
Mild MR(n � 15)
Moderate MR(n � 15)
Severe MR(n � 15)
100% 73% 73%65 � 11 63 � 8 64 � 12
0% 0% 0%7% 13% 20%
93% 87% 80%27% 53% 53%53% 73% 67%73% 80% 73%33% 33% 67%80% 73% 47%7% 7% 60%
70 � 12 74 � 9 83 � 17128 � 16 119 � 16 112 � 14
artery territory with evidence of jeopardized myocardial flow based on
onaryateral scarring also predicted more severe MR (p � 0.05;
by on May 31, 2013 als.org

Tfpdprta
DMida3asta-srs
C
Ieswm
SKMif(swctsMsrinimo
CCcmvscv
r
T
L
L
L
M
E ex;
174 SRICHAI ET AL Ann Thorac SurgISCHEMIC MITRAL REGURGITATION MECHANISMS 2005;80:170–8
CA
RD
IOV
AS
CU
LA
R
able 3). Global LV parameters including LV ejectionraction, volumes, and sphericity index, and regionalarameters of LV function and scar did not affect theeterminants of MR severity. Scarring of the inferior-osterior region, when compared directly against scar-ing of the anterior-lateral region as competing predic-ors, was found to affect a dimension of MR severity notccounted for by anterior-lateral scarring (p � 0.05).
eterminants of Mitral Systolic Tentingultivariate modeling showed that mitral systolic tent-
ng was determined predominantly by mitral annulariameter in the anterior-posterior direction (p � 0.0001),nd global LV ejection fraction (p � 0.005; r2 � 0.57; Table). In addition, regression analysis between mitral tentingrea and coaptation height showed the latter to also be atatistically significant predictor of tenting area (p � 0.0001),hough not independent of mitral annular diameter, withn r2 value of 0.83 and regression equation: Tenting area �0.465 � 2.15*(coaptation height). Global parameters of LVphericity index and end-diastolic volume, and local pa-ameters of regional LV scarring and function did notignificantly influence mitral systolic tenting.
omment
schemic MR is a frequent complication of IHD. The pres-nce of MR in patients with IHD has been shown to be atrong predictor of mortality [1, 2, 17], even when the MRas only mild to moderate in severity [2]. However, the
able 2. Results of Univariate Analyses of Magnetic Resonan
No MR
eft ventricle global geometryEjection fraction 30% � 6%ESVI 86 � 26EDVI 122 � 29Sphericity 1.94 � 0.39
eft ventricle regional functionTotal 1.87 � 0.39Anterior-lateral 1.87 � 0.53Inferior-posterior 1.75 � 0.63
eft ventricle regional myocardial scarringTotal 1.42 � 0.44Anterior-lateral 1.12 � 0.89Inferior-posterior 1.02 � 0.96itral geometryAnnulus area 11.8 � 4.5Annulus diameter 2-chamber 4.19 � 0.37Annulus diameter 3-chamber 3.39 � 0.21Annulus diameter 4-chamber 4.00 � 0.62Coaptation height 1.17 � 0.08Tenting area 1.90 � 0.31
DVI � end-diastolic volume index; ESVI � end-systolic volume ind
echanisms of ischemic MR are incompletely understood. a
ats.ctsnetjournDownloaded from
tudy Findingsey findings of this study, which employed quantitativeRI to assess the multiple different contributions to
schemic MR as graded by echocardiography, were asollows: (1) even in the setting of LV systolic dysfunctionejection fraction �40%), improved function and overallmaller LV volumes are found with no MR comparedith any degree of MR; (2) increasing severity of MR
orrelates with a more spherical LV; (3) LV function inhe inferior-posterior, but not anterior-lateral, regionhows greater impairment with increasing severity of
R; (4) increased regional and global LV myocardialcarring is seen with increasing severity of MR, and eachegion (anterior-lateral and inferior-posterior) has anndependent impact; (5) mitral annulus diameter is sig-ificantly larger with progressive increases in MR sever-
ty, but only in the anterior-posterior dimension; and (6)itral systolic tenting area is the most powerful predictor
f MR severity in multivariate analyses.
urrent Therapyurrent therapy for patients with IHD and MR remains
ontroversial. In the absence of jeopardized myocardium,edical treatment of MR has mainly been with the use of
asodilators. In the presence of jeopardized myocardium,urgical treatment of ischemic MR generally combinesoronary revascularization with correction of MR byalve repair or replacement.Valve repair for ischemic MR generally consists of
educing annular size using a significantly undersized
aging Measurements
Mild MRModerate
MRSevere
MR p Value
25% � 7% 26% � 7% 24% � 7% 0.09117 � 36 111 � 38 119 � 41 0.05154 � 36 147 � 41 157 � 46 0.07
1.80 � 0.37 1.70 � 0.19 1.52 � 0.19 �0.005
2.16 � 0.42 2.12 � 0.31 2.23 � 0.17 NS2.07 � 0.41 2.03 � 0.43 2.02 � 0.37 NS2.35 � 0.66 2.13 � 0.53 2.57 � 0.37 �0.005
1.09 � 0.58 1.10 � 0.69 1.84 � 0.56 �0.0050.92 � 0.88 0.80 � 0.58 1.77 � 0.79 �0.011.12 � 0.88 0.77 � 0.58 2.13 � 0.79 0.001
12.5 � 5.9 12.6 � 11.0 13.6 � 3.4 NS4.23 � 0.49 4.10 � 0.61 4.13 � 0.47 NS3.54 � 0.21 3.75 � 0.35 4.00 � 0.07 �0.0054.13 � 0.51 4.06 � 0.61 4.32 � 0.30 NS1.33 � 0.09 1.41 � 0.18 1.53 � 0.12 �0.052.33 � 0.57 2.55 � 0.76 3.06 � 0.62 0.001
MR � mitral regurgitation; NS � not significant.
ce Im
nnuloplasty ring. As such, repair is generally not a
by on May 31, 2013 als.org

pltipite
ambc
MImtgwmmtt
Fvg(
Fer(
175Ann Thorac Surg SRICHAI ET AL2005;80:170–8 ISCHEMIC MITRAL REGURGITATION MECHANISMS
CA
RD
IOV
AS
CU
LA
R
hysiological correction because, although restoring leaf-et coaptation via annular reduction, it does not addresshe other potential mechanisms leading to leaflet tether-ng. Additionally, LV remodeling often continues torogress and can lead to MR recurrence despite good
nitial results [18]. Therefore, new surgical techniqueshat attempt to address the primary mechanism of isch-
ig 3. Scatter plot graphs of average wall motion score for the entireentricle (top), anterior-lateral (middle), and inferior-posterior re-ion (bottom) for each mitral regurgitation (MR) severity group.Mod � moderate; NS � not significant.)
mic MR are under development using experimental v
ats.ctsnetjournDownloaded from
nimal models [19–22]. Ischemic MR in these animalodels relies on the creation of inferior-posterior infarcts
y ligation of obtuse marginal branches of the left cir-umflex artery.
echanisms of Ischemic MRn the current study, we evaluated the impact of LV
yocardial scarring and resultant geometric and func-ional changes versus changes in mitral valve apparatuseometry on the development of ischemic MR in patientsith LV dysfunction. Mitral systolic tenting area was theost powerful predictor of MR severity and significantitral annular dilatation in the anterior-posterior direc-
ion, coaptation height, and diminished LV systolic func-ion were found to be its major determinants. Mitral
ig 4. Scatter plot graphs of average myocardial scar grade for thentire ventricle (top), anterior-lateral (middle) and inferior-posterioregion (bottom) for each mitral regurgitation (MR) severity group.Mod � moderate.)
alve systolic tenting is characterized by insufficient
by on May 31, 2013 als.org
Fa4mm(aasie
Fa4mm(aamth
176 SRICHAI ET AL Ann Thorac SurgISCHEMIC MITRAL REGURGITATION MECHANISMS 2005;80:170–8
CA
RD
IOV
AS
CU
LA
R
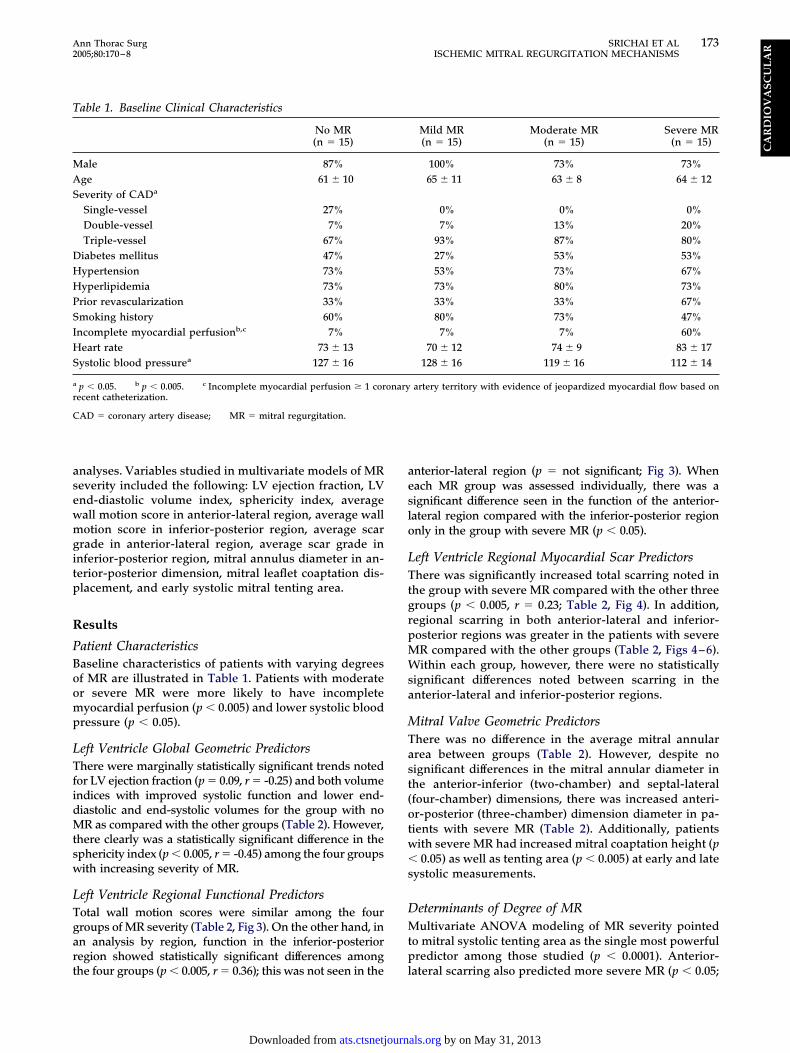
ig 5. Transthoracic color-Doppler Echo im-ges in the 2-chamber (A), 3-chamber (B) and-chamber (C) views demonstrating severeitral regurgitation. Delayed-enhancementagnetic resonance images in the 2-chamber
D), 3-chamber (E), and 4-chamber (F) long-xis views as well as basal (G), middle (H)nd apical (I) short-axis views demonstratingevere myocardial scarring localized to thenferior-posterior region as seen by the hyper-nhanced areas (arrows).
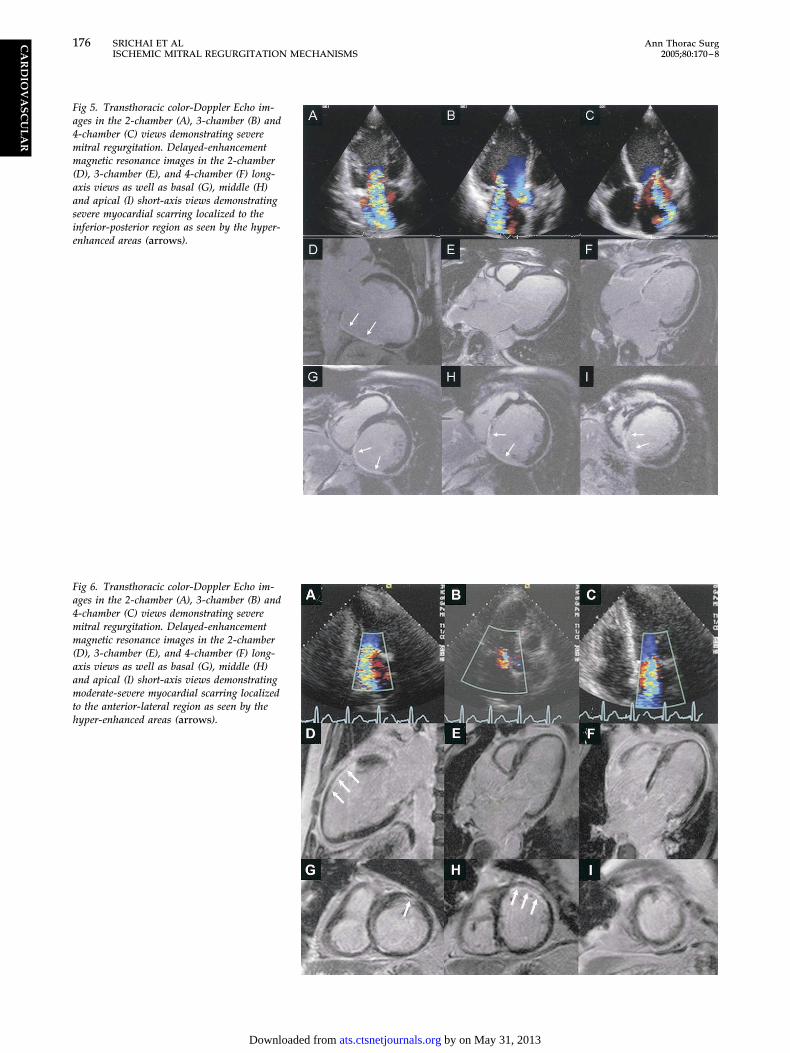
ig 6. Transthoracic color-Doppler Echo im-ges in the 2-chamber (A), 3-chamber (B) and-chamber (C) views demonstrating severeitral regurgitation. Delayed-enhancementagnetic resonance images in the 2-chamber
D), 3-chamber (E), and 4-chamber (F) long-xis views as well as basal (G), middle (H)nd apical (I) short-axis views demonstratingoderate-severe myocardial scarring localized
o the anterior-lateral region as seen by theyper-enhanced areas (arrows).
by on May 31, 2013 ats.ctsnetjournals.orgDownloaded from

swis[m
reFspr
ROhr2swtmedsmlitiaia
CCarch
tfgpedriacfitrmmrt
SAbltportbidamnfqDv
CQfstinmwnovvmMmpdnf
T
L
A
M
Mr
N
177Ann Thorac Surg SRICHAI ET AL2005;80:170–8 ISCHEMIC MITRAL REGURGITATION MECHANISMS
CA
RD
IOV
AS
CU
LA
R
ystolic leaflet body displacement toward the annulus,ith coaptation limited to the leaflet tips [23]. Interest-
ngly, LV sphericalization, which has been shown in priortudies to be important to development of ischemic MR3, 4, 9], showed significant impact on univariate, but not
ultivariate analyses.Degree of myocardial scarring in the anterior-lateral
egion was also important to the development of isch-mic MR, independent of mitral systolic tenting area.urther analyses, focusing on the interaction of regionalcarring, showed that degree of scarring in the inferior-osterior region, independent of anterior-lateral scar-ing, was important to ischemic MR severity.
elation to Prior Studiesur results differ from other studies that have shownigher incidences of ischemic MR in patients with infe-ior compared with anterior myocardial infarction [24–6]. However, diagnosis of regional scarring in thesetudies was indirect, based on regional dysfunctionhich may represent myocardial hibernation as opposed
o true myocardial scar. In the present study, regionalyocardial scarring was directly detected as hyper-
nhancement on delayed-enhancement MRI indepen-ent of regional function. Additionally, unlike earliertudies, regions were localized with regard to papillaryuscles (anterior-lateral and posteromedial). Neverthe-
ess, our findings are similar to prior studies showingmpairment of function in the inferior-posterior, but nothe anterior-lateral region, was associated with increas-ng severity of MR. However, degree of regional scarrings opposed to regional function proved to be a moremportant determinant of MR severity in multivariatenalysis.
linical Implicationsurrent surgical therapy for ischemic MR with the use ofn undersized annuloplasty ring has beneficial effects oneduction in the mitral systolic tenting area. However,linical observations suggest that this repair technique
able 3. Results of Multivariate Analyses
Model forDeterminants
of Degreeof MR
Model forDeterminants
of MitralTenting Area
p Value p Value
eft ventricular ejectionfraction
NS 0.005
nterior-lateral myocardialscarring
0.05 NS
itral annular diameter(Anterior-posteriordimension)
NS 0.0001
itral tenting area 0.0001 NA2 0.31 0.57
A � not applicable; NS � not significant.
as limited durability in selected patients [27]. m
ats.ctsnetjournDownloaded from
Surgical techniques under development for improvingreatment of ischemic MR have focused on MR resultingrom infarction or ischemia in the inferior-posterior re-ion, with resultant dysfunction and displacement of theosteromedial papillary muscle. Since in our study, mod-rate-to-severe MR was associated with regional myocar-ial scarring in the anterior-lateral or inferior-posterioregions, future surgical therapies will need to addressschemic MR in association with inferior-posterior ornterior-lateral regional scarring, or both, because clini-ally, patients may present with either type. Based on thendings in our study, we would expect that surgical
echniques that focus on the impact of LV remodelingesulting from LV myocardial scarring affecting the seg-ents adjacent to the papillary muscles, such as papillaryuscle relocation, papillary muscle sling, and infarct
estraint procedures, would have impact on improvinghe degree and recurrence of MR.
tudy Limitationsn underlying limitation of this study relates to referralias of patients with LV dysfunction and scarring in the
eft anterior descending distribution due to this institu-ion’s interest in surgical ventricular restoration forostinfarction aneurysm. Hence, the increased frequencyf ischemic MR due to anterior-lateral scarring may beeflective of referral bias and not necessarily characteris-ic of the general population with IHD. Additionally,ecause image analysis was performed retrospectively,
ncomplete imaging of the papillary muscles limitedetailed analysis of papillary muscle function, scarring,nd geometry. Finally, technical difficulties with floweasurements using the velocity phase mapping tech-
ique limited the quantification of mitral regurgitantraction by MRI for some patients (n � 19). Conse-uently, the combination of two echocardiographyoppler methods (jet area and ERO), which have been
alidated [3, 4], were used for assessment of MR severity.
onclusionuantitative MRI with delayed-enhancement imaging
or assessment of LV function, geometry and myocardialcarring is important to (1) add to our understanding ofhe diverse mechanisms involved in the development ofschemic MR; (2) aid in the design and implementation ofewer surgical and nonsurgical approaches to the treat-ent of patients with ischemic MR; (3) identify patientsith other potential mechanisms of ischemic MR,amely, primary involvement of the anterolateral aspposed to posteromedial papillary muscle and adjacententricular segments; and (4) identify patients with se-ere LV geometrical distortion who will likely requireore than a simple annuloplasty ring for treatment of theR. Mitral tenting area in combination with regional LVyocardial scarring localized to either the inferior-
osterior or anterior-lateral segments contribute to theevelopment of ischemic MR, and new surgical andonsurgical developments will need to address the ef-
ects of LV remodeling in the vicinity of both papillary
uscles for the treatment of patients with ischemic MR.by on May 31, 2013 als.org

R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
178 SRICHAI ET AL Ann Thorac SurgISCHEMIC MITRAL REGURGITATION MECHANISMS 2005;80:170–8
CA
RD
IOV
AS
CU
LA
R
eferences
1. Grigioni F, Enriquez-Sarano M, Zehr KJ, Bailey KR, Tajik AJ.Ischemic mitral regurgitation: long-term outcome and prog-nostic implications with quantitative Doppler assessment.Circulation 2001;103:1759–64.
2. Lamas GA, Mitchell GF, Flaker GC, et al. Clinical signifi-cance of mitral regurgitation after acute myocardial infarc-tion. Survival and Ventricular Enlargement Investigators.Circulation 1997;96:827–33.
3. Blumlein S, Bouchard A, Schiller NB, et al. Quantitation ofmitral regurgitation by Doppler echocardiography. Circula-tion 1986;74:306–14.
4. Rokey R, Sterling LL, Zoghbi WA, et al. Determination ofregurgitant fraction in isolated mitral or aortic regurgitationby pulsed Doppler two-dimensional echocardiography.J Am Coll Cardiol 1986;7:1273–8.
5. He S, Fontaine AA, Schwammenthal E, Yoganathan AP,Levine RA. Integrated mechanism for functional mitral re-gurgitation: leaflet restriction versus coapting force: in vitrostudies. Circulation 1997;96:1826–34.
6. Komeda M, Glasson JR, Bolger AF, et al. Geometric deter-minants of ischemic mitral regurgitation. Circulation 1997;96(9 Suppl):II128-33.
7. Gorman RC, McCaughan JS, Ratcliffe MB, et al. Pathogene-sis of acute ischemic mitral regurgitation in three dimen-sions. J Thorac Cardiovasc Surg 1995;109:684–93.
8. Otsuji Y, Handschumacher MD, Liel-Cohen N, et al. Mech-anism of ischemic mitral regurgitation with segmental leftventricular dysfunction: three-dimensional echocardio-graphic studies in models of acute and chronic progressiveregurgitation. J Am Coll Cardiol 2001;37:641–8.
9. D’Cruz IA, Shroff SG, Janicki JS, Jain A, Reddy HK, Lakier JB.Differences in the shape of the normal, cardiomyopathic,and volume overloaded human left ventricle. J Am SocEchocardiogr 1989;2:408–14.
0. Yiu SF, Enriquez-Sarano M, Tribouilloy C, Seward JB, TajikAJ. Determinants of the degree of functional mitral regurgi-tation in patients with systolic left ventricular dysfunction: aquantitative clinical study. Circulation 2000;102:1400–6.
1. Grothues F, Smith GC, Moon JC, et al. Comparison ofinterstudy reproducibility of cardiovascular magnetic reso-nance with two-dimensional echocardiography in normalsubjects and in patients with heart failure or left ventricularhypertrophy. Am J Cardiol 2002;90:29–34.
2. Simonetti OP, Kim RJ, Fieno DS, et al. An improved MRimaging technique for the visualization of myocardial infarc-tion. Radiology 2001;218:215–23.
3. Schiller NB, Shah PM, Crawford M, et al. Recommendationsfor quantitation of the left ventricle by two-dimensionalechocardiography. American Society of Echocardiography
Committee on Standards, Subcommittee on Quantitation ofats.ctsnetjournDownloaded from
Two-Dimensional Echocardiograms. J Am Soc Echocardiogr1989;2:358–67.
4. Grossmann G, Giesler M, Schmidt A, et al. Quantification ofmitral regurgitation—comparison of the proximal flow con-vergence method and the jet area method. Clin Cardiol1995;18:512–8.
5. Schvartzman PR, White RD. Magnetic resonance imaging. In:Topol EJ, ed. Textbook of cardiovascular medicine. 2nd ed.Philadelphia: Lippincott Williams & Wilkins, 2002:1213–56.
6. Schvartzman PR, Srichai MB, Grimm RA, et al. Nonstressdelayed-enhancement magnetic resonance imaging of themyocardium predicts improvement of function after revas-cularization for chronic ischemic heart disease with leftventricular dysfunction. Am Heart J 2003;146:535–41.
7. Trichon BH, Felker GM, Shaw LK, Cabell CH, O’ConnorCM. Relation of frequency and severity of mitral regurgita-tion to survival among patients with left ventricular systolicdysfunction and heart failure. Am J Cardiol 2003;91:538–43.
8. Tahta SA, Oury JH, Maxwell JM, Hiro SP, Duran CM.Outcome after mitral valve repair for functional ischemicmitral regurgitation. J Heart Valve Dis 2002;11:11–9.
9. Hung J, Guerrero JL, Handschumacher MD, Supple G, Sulli-van S, Levine RA. Reverse ventricular remodeling reducesischemic mitral regurgitation: echo-guided device applicationin the beating heart. Circulation 2002;106:2594–600.
0. Moainie SL, Guy TS, Gorman JH III, et al. Infarct restraintattenuates remodeling and reduces chronic ischemic mitralregurgitation after postero-lateral infarction. Ann ThoracSurg 2002;74:444–9.
1. Hvass U, Tapia M, Baron F, Pouzet B, Shafy A. Papillarymuscle sling: a new functional approach to mitral repair inpatients with ischemic left ventricular dysfunction and func-tional mitral regurgitation. Ann Thorac Surg 2003;75:809–11.
2. Kron IL, Green GR, Cope JT. Surgical relocation of theposterior papillary muscle in chronic ischemic mitral regur-gitation. Ann Thorac Surg 2002;74:600–1.
3. Perloff JK, Roberts WC. The mitral apparatus. Functionalanatomy of mitral regurgitation. Circulation 1972;46:227–39.
4. Kumanohoso T, Otsuji Y, Yoshifuku S, et al. Mechanism ofhigher incidence of ischemic mitral regurgitation in patientswith inferior myocardial infarction: quantitative analysis ofleft ventricular and mitral valve geometry in 103 patientswith prior myocardial infarction. J Thorac Cardiovasc Surg2003;125:135–43.
5. Heikkila J. Mitral incompetence complicating acute myocar-dial infarction. Br Heart J 1967;29:162–9.
6. Izumi S, Miyatake K, Beppu S, et al. Mechanism of mitralregurgitation in patients with myocardial infarction: a studyusing real-time two-dimensional Doppler flow imaging andechocardiography. Circulation 1987;76:777–85.
7. Liel-Cohen N, Otsuji Y, Vlahakes G. Functional ischemicmitral regurgitation can persist despite ring annuloplasty:
mechanistic insights. Circulation 1997;96(Suppl 1):540.by on May 31, 2013 als.org

2005;80:170-178 Ann Thorac SurgMcCarthy and Richard D. White
Leonardo Rodriguez, Michael L. Lieber, Abigail Lara, Joan A. Weaver, Patrick M. Monvadi B. Srichai, Richard A. Grimm, Arthur E. Stillman, A. Marc Gillinov, L.
Patients with Left Ventricular Systolic DysfunctionIschemic Mitral Regurgitation: Impact of the Left Ventricle and Mitral Valve in
& ServicesUpdated Information
http://ats.ctsnetjournals.org/cgi/content/full/80/1/170including high-resolution figures, can be found at:
References http://ats.ctsnetjournals.org/cgi/content/full/80/1/170#BIBL
This article cites 26 articles, 15 of which you can access for free at:
Citations http://ats.ctsnetjournals.org/cgi/content/full/80/1/170#otherarticles
This article has been cited by 15 HighWire-hosted articles:
Subspecialty Collections
http://ats.ctsnetjournals.org/cgi/collection/valve_disease Valve disease
following collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
[email protected]: orhttp://www.us.elsevierhealth.com/Licensing/permissions.jsp
in its entirety should be submitted to: Requests about reproducing this article in parts (figures, tables) or
Reprints [email protected]
For information about ordering reprints, please email:
by on May 31, 2013 ats.ctsnetjournals.orgDownloaded from
Copyright © 2022 FDOKUMEN




















