![[Guidelines] | Rheumatic Fever New Zealand - RHD Action |](https://static.fdokumen.com/doc/165x107/6328f1eb2dd4b030ca0c5afa/guidelines-rheumatic-fever-new-zealand-rhd-action-.jpg)
Mitral Valve Replacement With and Without Chordal Preservation in a Rheumatic Population: Serial...
10
2005;79:1926-1933 Ann Thorac Surg Subramaniam, Ram Prakash, Sandeep Seth, Rajvir Singh and Panangipalli Venugopal Ujjwal K. Chowdhury, A. Sampath Kumar, Balram Airan, Dinesh Mittal, K. Ganapathy Size and Function Rheumatic Population: Serial Echocardiographic Assessment of Left Ventricular Mitral Valve Replacement With and Without Chordal Preservation in a http://ats.ctsnetjournals.org/cgi/content/full/79/6/1926 located on the World Wide Web at: The online version of this article, along with updated information and services, is Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2005 by The Society of Thoracic Surgeons. is the official journal of The Society of Thoracic Surgeons and the The Annals of Thoracic Surgery by on June 11, 2013 ats.ctsnetjournals.org Downloaded from
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Mitral Valve Replacement With and Without Chordal Preservation in a Rheumatic Population: Serial...

2005;79:1926-1933 Ann Thorac SurgSubramaniam, Ram Prakash, Sandeep Seth, Rajvir Singh and Panangipalli Venugopal
Ujjwal K. Chowdhury, A. Sampath Kumar, Balram Airan, Dinesh Mittal, K. Ganapathy Size and Function
Rheumatic Population: Serial Echocardiographic Assessment of Left Ventricular Mitral Valve Replacement With and Without Chordal Preservation in a
http://ats.ctsnetjournals.org/cgi/content/full/79/6/1926located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2005 by The Society of Thoracic Surgeons.
is the official journal of The Society of Thoracic Surgeons and theThe Annals of Thoracic Surgery
by on June 11, 2013 ats.ctsnetjournals.orgDownloaded from
MCSVUDSDS
fcepm
dds5st2oy
sf
P(pbroscMddo
A
ArN
©P
CA
RD
IOV
AS
CU
LA
R
itral Valve Replacement With and Withouthordal Preservation in a Rheumatic Population:erial Echocardiographic Assessment of Leftentricular Size and Function
jjwal K. Chowdhury, MCh, A. Sampath Kumar, MCh, Balram Airan, MCh,inesh Mittal, MS, K. Ganapathy Subramaniam, MS, Ram Prakash, DM,andeep Seth, DM, Rajvir Singh, MSc(Stat), PhD, and Panangipalli Venugopal, MChepartments of Cardiothoracic and Vascular Surgery, Cardiology, and Biostatistics, Cardiothoracic Centre, All India Institute of Medical
ciences, Ansari Nagar, New Delhi, IndiaowI0tcTi(btp
ttpn
Background. The aim of this study is to investigate theeasibility of chordal-sparing mitral valve replacement pro-edures in a rheumatic population, and to determine thearly and late effects of different chordal preservationrocedures on the clinical outcome and left ventricularechanics.Methods. Various techniques of chordal preservation
uring mitral valve replacement for rheumatic heartisease in 451 patients between 1996 and 1999 are de-cribed. The mean age was 35.6 � 19.0 years (range, 15 to5 years). Seventy patients had complete excision of theubvalvular apparatus (group I), 124 had preservation ofhe posterior chordopapillary apparatus (group II), and57 had total chordal preservation (group III). Echocardi-graphy was performed preoperatively, at discharge, at 1ear, and at 4 years.Results. Chordal preservation groups (II and III) demon-
trated significant improvement (p < 0.05) in left ventricular
unction immediately and late postoperatively. ReductionP
AfDpaetsa
M
1
2acic and Vascular Surgery, All India Institute of Medical Sciences, Ansariagar, New Delhi 110029, India; e-mail: [email protected].
2005 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ats.ctsnetjournDownloaded from
f left ventricular end-systolic and end-diastolic volumeas significant in the chordal preservation groups (II and
II) as compared to the nonchordal group (group I; p <.005). The total chordal group demonstrated greater frac-ional change of left ventricular end-systolic volume asompared to the posterior chordal and nonchordal group.he left ventricular ejection fraction and fractional shorten-
ng continued to decline over time in the nonchordal cohortp � 0.05 and p � 0.001, respectively) and did not improvey 4 years. Statistically significant change in ejection frac-
ion occurred in the chordal preservation groups as com-ared to the nonchordal group.Conclusions. We conclude that total chordal preserva-
ion is possible in the large majority of rheumatic pa-ients and confers significant long-term advantage byreserving left ventricular function. The surgical tech-ique should be individualized.
(Ann Thorac Surg 2005;79:1926–33)
© 2005 by The Society of Thoracic Surgeonsreservation of the chordopapillary apparatus is manda-tory in patients undergoing mitral valve replacement
MVR). Between 1996 and 1999, we used different chordalreservation techniques during MVR on an individualizedasis. The possibility of prosthetic valve entrapment by theetained subvalvular apparatus, creation of left ventricularutflow tract obstruction (LVOTO), and implantation of amaller sized prosthesis for the patient have been of majoroncerns to all investigators advocating the chordal-sparing
VR [1–5]. This prospective, nonrandomized study wasesigned to evaluate the immediate and late effects ofifferent chordal preservation techniques on the clinicalutcome and left ventricular size and function.
ccepted for publication Oct 4, 2004.
ddress reprint requests to Dr Chowdhury, Department of Cardiotho-
atients and Methods
ssessment of the Mitral Valve and Selection Criteriaor Chordal Preservationecision to perform mitral valve surgery was made byhysicians and was based on clinical, echocardiographic,nd angiocardiographic criteria. Intraoperative trans-sophageal echocardiography was performed on all pa-ients using a Hewlett-Packard Sonos 1500 or 5500 ultra-ound system (Hewlett-Packard Co, Andover, MA). Wettempted valve repair whenever possible [6].The following criteria were taken into consideration forVR with or without chordal preservation.
. If the valve was heavily calcified or consideredunsuitable for valve repair due to extensive scar-ring, shortening with severe subvalvular fusion,MVR was performed.
. In patients who had undergone previous closedmitral valvotomy or mitral valve repair, MVR was
preferred.0003-4975/05/$30.00doi:10.1016/j.athoracsur.2004.10.029
by on June 11, 2013 als.org
3
4
5
Piarh
PIcfpfIigD4(f(afipppvrt
Few
T
P
NMAN
P
S
A
M
1927Ann Thorac Surg CHOWDHURY ET AL2005;79:1926–33 MVR, CHORDAL PRESERVATION, RHEUMATIC MV DISEASE, AND LV FUNCTION
CA
RD
IOV
AS
CU
LA
R
. Conventional MVR was considered when the leaf-lets and subvalvular apparatus were thick withfusion of chordae tendinae and foreshortening ofthe chordal apparatus. All tissue had to be resectedto allow the implantation of an appropriate sizedvalve for any given patient. The majority of patientsin this group had predominantly stenotic lesions.
. If the condition of the valve leaflet and subvalvulartissue was deemed worthy of preservation, everyattempt was made to ensure that the preservedchordopapillary apparatus allowed implantation ofan appropriate sized prosthesis and did not inter-fere with prosthetic valve function or createLVOTO.
. Calcified mitral leaflets with annular extensionwere dealt with by squeezing or milking out the
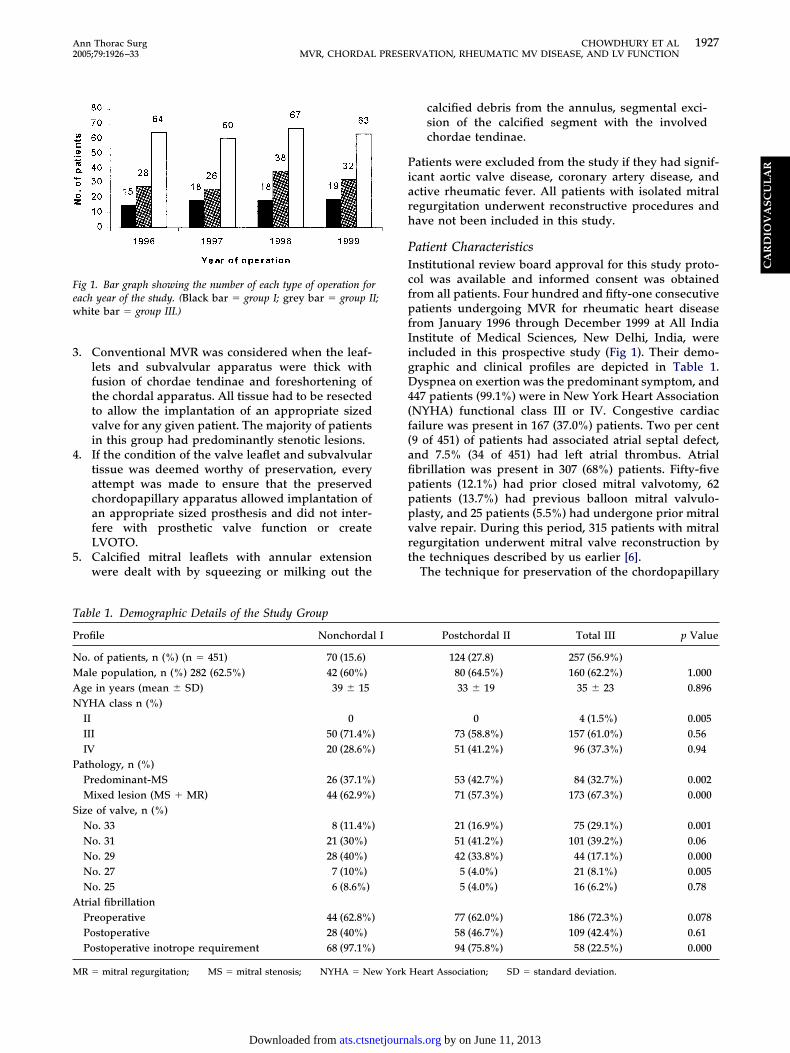
ig 1. Bar graph showing the number of each type of operation forach year of the study. (Black bar � group I; grey bar � group II;hite bar � group III.)
able 1. Demographic Details of the Study Group
rofile Nonchordal I
o. of patients, n (%) (n � 451) 70 (15.6)ale population, n (%) 282 (62.5%) 42 (60%)ge in years (mean � SD) 39 � 15YHA class n (%)II 0III 50 (71.4%)IV 20 (28.6%)
athology, n (%)Predominant-MS 26 (37.1%)Mixed lesion (MS � MR) 44 (62.9%)
ize of valve, n (%)No. 33 8 (11.4%)No. 31 21 (30%)No. 29 28 (40%)No. 27 7 (10%)No. 25 6 (8.6%)trial fibrillationPreoperative 44 (62.8%)Postoperative 28 (40%)Postoperative inotrope requirement 68 (97.1%)
R � mitral regurgitation; MS � mitral stenosis; NYHA � New York
ats.ctsnetjournDownloaded from
calcified debris from the annulus, segmental exci-sion of the calcified segment with the involvedchordae tendinae.
atients were excluded from the study if they had signif-cant aortic valve disease, coronary artery disease, andctive rheumatic fever. All patients with isolated mitralegurgitation underwent reconstructive procedures andave not been included in this study.
atient Characteristicsnstitutional review board approval for this study proto-ol was available and informed consent was obtainedrom all patients. Four hundred and fifty-one consecutiveatients undergoing MVR for rheumatic heart disease
rom January 1996 through December 1999 at All Indianstitute of Medical Sciences, New Delhi, India, werencluded in this prospective study (Fig 1). Their demo-raphic and clinical profiles are depicted in Table 1.yspnea on exertion was the predominant symptom, and
47 patients (99.1%) were in New York Heart AssociationNYHA) functional class III or IV. Congestive cardiacailure was present in 167 (37.0%) patients. Two per cent9 of 451) of patients had associated atrial septal defect,nd 7.5% (34 of 451) had left atrial thrombus. Atrialbrillation was present in 307 (68%) patients. Fifty-fiveatients (12.1%) had prior closed mitral valvotomy, 62atients (13.7%) had previous balloon mitral valvulo-lasty, and 25 patients (5.5%) had undergone prior mitralalve repair. During this period, 315 patients with mitralegurgitation underwent mitral valve reconstruction byhe techniques described by us earlier [6].
The technique for preservation of the chordopapillary
Postchordal II Total III p Value
124 (27.8) 257 (56.9%)80 (64.5%) 160 (62.2%) 1.00033 � 19 35 � 23 0.896
0 4 (1.5%) 0.00573 (58.8%) 157 (61.0%) 0.5651 (41.2%) 96 (37.3%) 0.94
53 (42.7%) 84 (32.7%) 0.00271 (57.3%) 173 (67.3%) 0.000
21 (16.9%) 75 (29.1%) 0.00151 (41.2%) 101 (39.2%) 0.0642 (33.8%) 44 (17.1%) 0.0005 (4.0%) 21 (8.1%) 0.0055 (4.0%) 16 (6.2%) 0.78
77 (62.0%) 186 (72.3%) 0.07858 (46.7%) 109 (42.4%) 0.6194 (75.8%) 58 (22.5%) 0.000
Heart Association; SD � standard deviation.
by on June 11, 2013 als.org
amteawcdgva
pst
VTbhnmTtpp
SAt(a
bfpae(
sePt(cncwc(
TT
tmabmseromc
fi
Fcflvim(aat
F
1928 CHOWDHURY ET AL Ann Thorac SurgMVR, CHORDAL PRESERVATION, RHEUMATIC MV DISEASE, AND LV FUNCTION 2005;79:1926–33
CA
RD
IOV
AS
CU
LA
R
pparatus was made after intraoperative visual assess-ent of the mitral valve. The patients were allocated to
hree groups: group I (n � 70), MVR with completexcision of the native valve including the subvalvularpparatus (nonchordal group); group II (n � 124), MVRith excision of the anterior mitral leaflet and its attached
hordae tendinae. The posterior mitral leaflet with chor-opapillary apparatus was preserved (posterior chordalroup); group III (n � 257), MVR with complete preser-ation of chordae tendinae and papillary muscles of thenterior and posterior leaflet (total chordal group).There was no statistically significant difference in the
atient population among the three groups (Table 1). Theeverity of symptoms and type and number of medica-ions given preoperatively were comparable.
alve Pathologywo hundred and eighty-eight patients (63.8%) had com-ined mitral stenosis and regurgitation, and 163 (36.1%)ad predominant mitral stenosis. All patients of theonchordal and posterior chordal group had either aixed type of lesion or predominant mitral stenosis.
otal chordal preservation was possible in 60% of pa-ients with mixed mitral valve disease and in 51.5% ofatients with mitral stenosis. Overall, 43.0% (194 of 451atients) had mitral valvular calcification.
urgical Techniquesmedian sternotomy (n � 416) or a right anterolateral
horacotomy (n � 35) was used. Moderately hypothermic28–32°C) cardiopulmonary bypass was established by
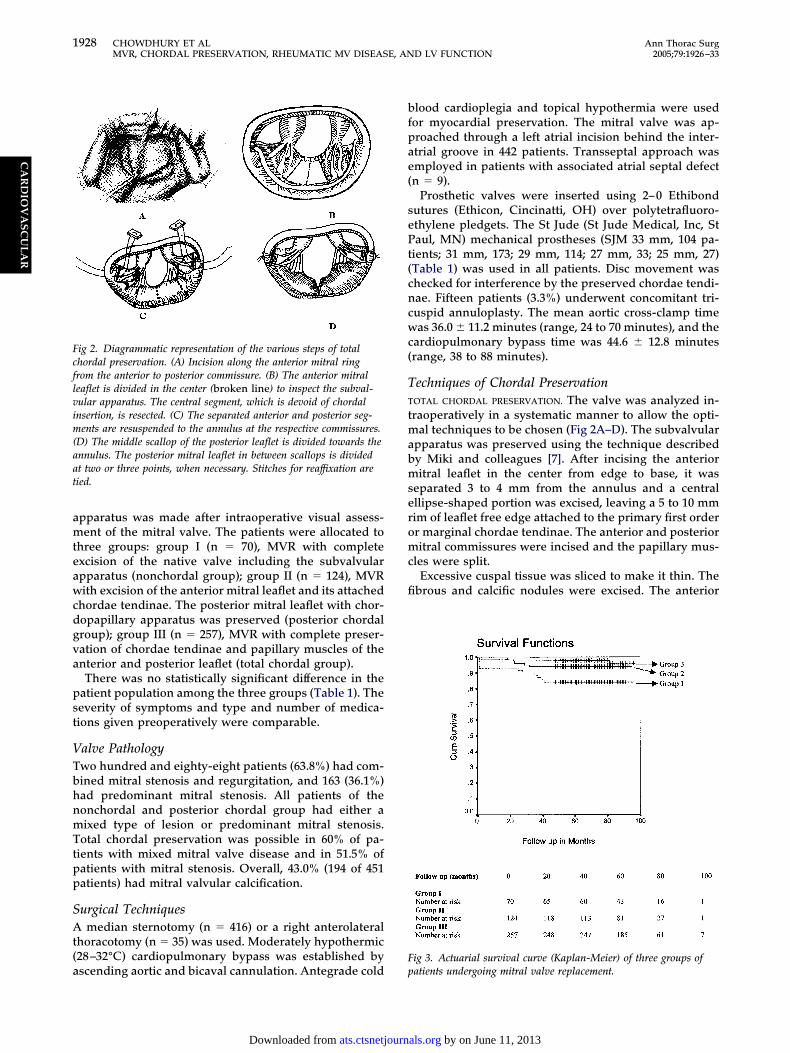
ig 2. Diagrammatic representation of the various steps of totalhordal preservation. (A) Incision along the anterior mitral ringrom the anterior to posterior commissure. (B) The anterior mitraleaflet is divided in the center (broken line) to inspect the subval-ular apparatus. The central segment, which is devoid of chordalnsertion, is resected. (C) The separated anterior and posterior seg-ents are resuspended to the annulus at the respective commissures.
D) The middle scallop of the posterior leaflet is divided towards thennulus. The posterior mitral leaflet in between scallops is dividedt two or three points, when necessary. Stitches for reaffixation areied.
scending aortic and bicaval cannulation. Antegrade cold p
ats.ctsnetjournDownloaded from
lood cardioplegia and topical hypothermia were usedor myocardial preservation. The mitral valve was ap-roached through a left atrial incision behind the inter-trial groove in 442 patients. Transseptal approach wasmployed in patients with associated atrial septal defectn � 9).
Prosthetic valves were inserted using 2–0 Ethibondutures (Ethicon, Cincinatti, OH) over polytetrafluoro-thylene pledgets. The St Jude (St Jude Medical, Inc, Staul, MN) mechanical prostheses (SJM 33 mm, 104 pa-
ients; 31 mm, 173; 29 mm, 114; 27 mm, 33; 25 mm, 27)Table 1) was used in all patients. Disc movement washecked for interference by the preserved chordae tendi-ae. Fifteen patients (3.3%) underwent concomitant tri-uspid annuloplasty. The mean aortic cross-clamp timeas 36.0 � 11.2 minutes (range, 24 to 70 minutes), and the
ardiopulmonary bypass time was 44.6 � 12.8 minutesrange, 38 to 88 minutes).
echniques of Chordal PreservationOTAL CHORDAL PRESERVATION. The valve was analyzed in-raoperatively in a systematic manner to allow the opti-
al techniques to be chosen (Fig 2A–D). The subvalvularpparatus was preserved using the technique describedy Miki and colleagues [7]. After incising the anterioritral leaflet in the center from edge to base, it was
eparated 3 to 4 mm from the annulus and a centralllipse-shaped portion was excised, leaving a 5 to 10 mmim of leaflet free edge attached to the primary first orderr marginal chordae tendinae. The anterior and posterioritral commissures were incised and the papillary mus-
les were split.Excessive cuspal tissue was sliced to make it thin. The
brous and calcific nodules were excised. The anterior
ig 3. Actuarial survival curve (Kaplan-Meier) of three groups of
atients undergoing mitral valve replacement.by on June 11, 2013 als.org

pcwtsmrswttatT
pwentwotccP
awcpi
AIcaimcsmm
aTodoafrt
NTlslp
cGAttpac
PTcenc
fim
ETDHdalwDw
blfemcc
SDSBCcugwp(ov
owgat
1929Ann Thorac Surg CHOWDHURY ET AL2005;79:1926–33 MVR, CHORDAL PRESERVATION, RHEUMATIC MV DISEASE, AND LV FUNCTION
CA
RD
IOV
AS
CU
LA
R
aramedial chorda, or anterior and posterior paramedialhordae tendinae, or paracommissural chordae tendinaeere excised along with splitting and partial shaving of
he papillary muscle tip on an individualized basis. Theeparated anterior and posterior segments of the anterioritral leaflet were shifted and reattached to the mitral
ing near the anterior and posterior commissures, re-pectively. The midportion of the posterior mitral leafletas incised in the center from free edge to base. In order
o accommodate a large size prosthesis, when necessary,he posterior mitral leaflet was incised from edge to baset two or three additional points between the scallops ofhe posterior mitral leaflet supported by “cleft chordae.”he papillary muscles were split down to their base.While securing the prosthetic valve on the annulus, the
osterior valve sutures were tied first. Excessive tissueithin these chordal “buttons” that cannot be safely
xcised was pulled out of the subvalvar area using aerve hook. The “chordopapillary buttons” were held on
he atrial side (outside the sewing ring) when the valveas seated and the sutures were tied, thus preventingutflow tract obstruction or mechanical obstruction. Ifhe posterior leaflet was excessively redundant or thehordae tendinae were elongated, the leaflet was imbri-ated into the mitral annulus using pledgeted sutures.OSTERIOR CHORDAL PRESERVATION. In this technique, thenterior mitral leaflet with its attached chordae tendinaeas completely excised. The posterior leaflet with the
hordopapillary support mechanism was retained. Theosterior mitral leaflet was incised at two or three points
n between scallops from edge to base, when necessary.
nnulus Decalcification and Reconstructionn most instances, the calcification process involved theommissures and was limited to the annulus with vari-ble extension to the posterior myocardial wall, basal andntermediary chords, and head of one or several papillary
uscles. Calcification was dealt with by excision of thealcified segment, shaving off the calcified leaflet margin,queezing or milking out the calcific debris from theitral annulus, and partial excision of the posterioritral leaflet with the involved chordae tendinae.Decalcification was done by using a knife to incise the
trial endothelium at the margin of the calcified bar.hen the base of the mural leaflet was incised at the edgef the calcium bloc and retracted. Keeping the edge of theissecting knife against the calcium, the fibrous capsuleverlying the calcium was incised. A thick hemostat andpeanut swab were used to milk out the calcific debris
rom within the capsule. No patient required “en-bloc”esection of the calcium deposit or “sliding atrioplasty” ofhe left atrium.
onchordal Grouphe mitral valve was completely excised, including the
eaflets and the subvalvular apparatus in cases of severeubvalvular fusion or calcified mitral leaflets with annu-ar extension. One or two chordal buttons-pillars of theosterior mitral leaflet were retained in some cases.
Extensive scarring, shortening, and thickening of the nats.ctsnetjournDownloaded from
hordopapillary apparatus precluded the use of artificialore-Tex sutures (WL Gore and Associates, Flagstaff,Z) to resuspend the remnant papillary muscle base to
he mitral annulus. The technique of valve insertion washe same in all groups. An everting mattress suture (ie,ledgets on the atrial side) was used in all cases. The lefttrial appendage was routinely ligated. No surgical pro-edure was performed for atrial fibrillation.
ostoperative Studieshese included six-month clinical examinations, electro-ardiograms, chest radiographs, cinefluoroscopy, andchocardiography. The functional class at follow-up wasoted. Results were reported according to prescribedriteria [8].
All patients received warfarin and aspirin (100 mg/d)or anticoagulation to maintain an international normal-zed ratio (INR) between 3.0 and 3.5. A minimum of 48
onths follow-up was mandatory for this study.
chocardiographic Studies and Measurementsransthoracic two-dimensional (2D), color flow andoppler echocardiography was performed using aewlett-Packard-Sonos-5500 with 2.7 or 3.5 MHz trans-ucer. Prosthetic valve function was assessed on 2Dpical four-chamber view, and M-mode parasternalong-axis view. Left ventricular outflow tract obstructionas assessed on an apical five-chamber view, and byoppler study. A Doppler velocity of greater than 2 m/sas considered significant for LVOTO.Preoperative studies were performed within 7 days
efore surgery. Postoperatively, all survivors were fol-owed echocardiographically at the time of dischargerom hospital, at 1 year, and at 4 year follow-up. All latechoes have been grouped into one time period (48onths) with a range no greater than 6 months. Echo-
ardiographic data were measured according to Ameri-an Society of Echocardiography criteria [9].
tatistical Analysisata were analyzed with Biomedical Data Processingtatistical Software (University of California Press,erkeley, CA) and SPSS 7.0 statistical package (SPSS Inc,hicago, IL). Descriptive statistics were calculated for
ontinuous and categorical variables. Student’s t test wassed to identify significant differences between tworoups of continuous variables. Repeated measures two-ay analysis of variance (ANOVA) with the Bonfferoniosthoc test was used to assess the influence of time
preoperatively vs postoperatively vs 4 years) for type ofperative procedure on all echocardiographically derivedariables.Percentage change between the preoperative and post-
perative values were calculated and compared by one-ay ANOVA with posthoc (LSD) analysis for the threeroups. The �2 test was used to identify associationmong the groups for categorical variables. A p value lesshan 0.05 was considered significant.
Mortality rates were calculated depending on the total
umber of years of follow-up for each patient. Actuarialby on June 11, 2013 als.org
ensgt
R
ETsvvi
v1awf
LTn�fhctf
TFTatw
PFT
aurmm�
m00og3fNptttd
PDTgemTgca
v
1
2
3
T
G
IIIB
1930 CHOWDHURY ET AL Ann Thorac SurgMVR, CHORDAL PRESERVATION, RHEUMATIC MV DISEASE, AND LV FUNCTION 2005;79:1926–33
CA
RD
IOV
AS
CU
LA
R
stimates were calculated using the Kaplan-Meier tech-ique and the log-rank test was performed to analyzetatistically the difference of survival among the threeroups [10]. Valve-related events were reported as perhe standard published criteria [8].
esults
arly Resultshere were 11 early deaths (2.4%) due to low-outputyndrome (group I: n � 5; group II: n � 2), malignantentricular arrhythmias (group III: n � 2), and cerebro-ascular accidents (group III: n � 2). Nine patients weren NYHA functional class IV preoperatively.
All patients were administered oral angiotensin con-erting enzyme (ACE) inhibitors after extubation (0.5 to.0 mg/kg; every 8 hours) before weaning from inotropicgents. Digoxin, diuretics, and ACE inhibitors wereeaned at varying time intervals. Amiodarone was used
or intractable atrial fibrillation.
ate Outcomeshere were 14 late deaths (3.1%: group I, n � 6; group II,� 5; group III, n � 3) due to ventricular arrhythmias (n2), anticoagulant hemorrhage (n � 2), congestive heart
ailure (n � 2), and viral hepatitis (n � 1). Five patientsad valve thrombosis. Two of these developed majorerebrovascular accidents after streptokinase administra-ion and subsequently died. Three patients had success-ul thrombolysis.
hromboembolic Complicationsifteen patients had thromboembolic complications.hree of them died, 6 recovered with residual weakness,nd 4 recovered completely. In 2 patients, the deficit wasransient. No single factor was found to be associatedith incidence of thromboembolism.
rosthetic Valve Endocarditisive patients developed prosthetic valve endocarditis.hey were treated conservatively and two of these died.Four hundred and twenty-six survivors (94.46%)
chieved the mandatory 48-month postoperative follow-p. Their preoperative and postoperative records wereeviewed. Follow-up was 100% complete (range, 1 to 96onths) and yielded 3327.06 patient-years of data with aean follow-up time of 93.72 months (standard error [SE
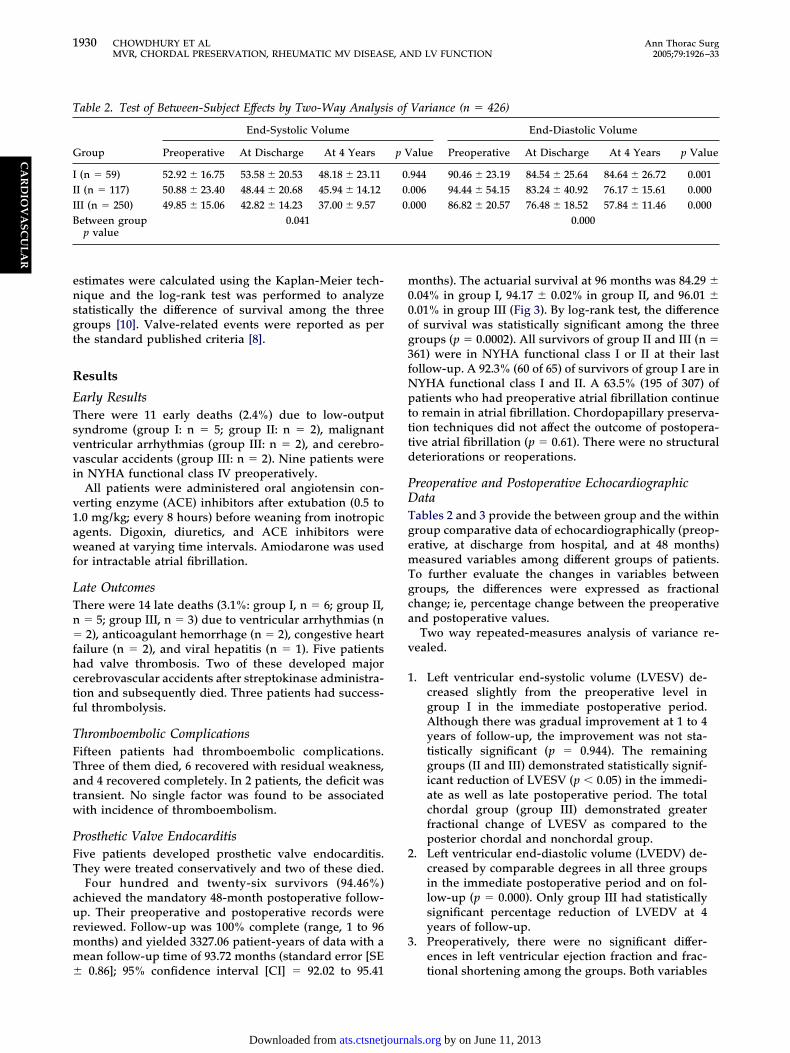
able 2. Test of Between-Subject Effects by Two-Way Analys
roup
End-Systolic Volume
Preoperative At Discharge At 4 Years
(n � 59) 52.92 � 16.75 53.58 � 20.53 48.18 � 23.11I (n � 117) 50.88 � 23.40 48.44 � 20.68 45.94 � 14.12II (n � 250) 49.85 � 15.06 42.82 � 14.23 37.00 � 9.57etween groupp value
0.041
0.86]; 95% confidence interval [CI] � 92.02 to 95.41
ats.ctsnetjournDownloaded from
onths). The actuarial survival at 96 months was 84.29 �.04% in group I, 94.17 � 0.02% in group II, and 96.01 �.01% in group III (Fig 3). By log-rank test, the differencef survival was statistically significant among the threeroups (p � 0.0002). All survivors of group II and III (n �61) were in NYHA functional class I or II at their lastollow-up. A 92.3% (60 of 65) of survivors of group I are inYHA functional class I and II. A 63.5% (195 of 307) ofatients who had preoperative atrial fibrillation continue
o remain in atrial fibrillation. Chordopapillary preserva-ion techniques did not affect the outcome of postopera-ive atrial fibrillation (p � 0.61). There were no structuraleteriorations or reoperations.
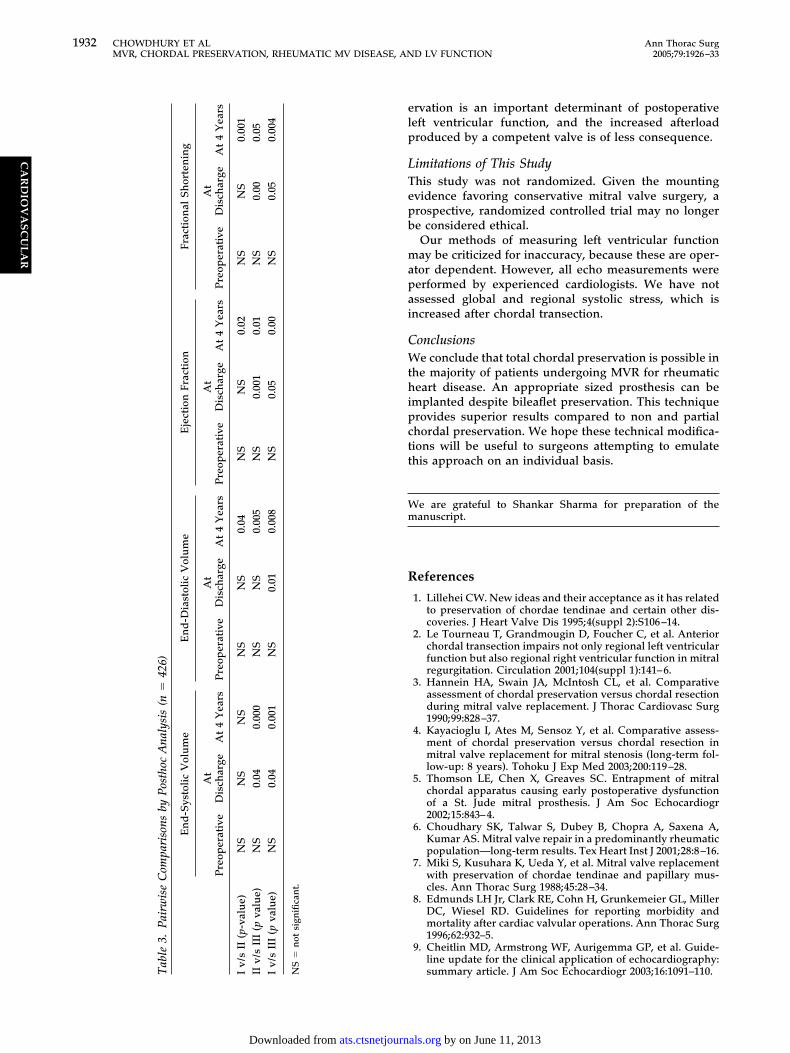
reoperative and Postoperative Echocardiographicataables 2 and 3 provide the between group and the withinroup comparative data of echocardiographically (preop-rative, at discharge from hospital, and at 48 months)easured variables among different groups of patients.
o further evaluate the changes in variables betweenroups, the differences were expressed as fractionalhange; ie, percentage change between the preoperativend postoperative values.Two way repeated-measures analysis of variance re-
ealed.
. Left ventricular end-systolic volume (LVESV) de-creased slightly from the preoperative level ingroup I in the immediate postoperative period.Although there was gradual improvement at 1 to 4years of follow-up, the improvement was not sta-tistically significant (p � 0.944). The remaininggroups (II and III) demonstrated statistically signif-icant reduction of LVESV (p � 0.05) in the immedi-ate as well as late postoperative period. The totalchordal group (group III) demonstrated greaterfractional change of LVESV as compared to theposterior chordal and nonchordal group.
. Left ventricular end-diastolic volume (LVEDV) de-creased by comparable degrees in all three groupsin the immediate postoperative period and on fol-low-up (p � 0.000). Only group III had statisticallysignificant percentage reduction of LVEDV at 4years of follow-up.
. Preoperatively, there were no significant differ-ences in left ventricular ejection fraction and frac-
Variance (n � 426)
End-Diastolic Volume
alue Preoperative At Discharge At 4 Years p Value
944 90.46 � 23.19 84.54 � 25.64 84.64 � 26.72 0.001006 94.44 � 54.15 83.24 � 40.92 76.17 � 15.61 0.000000 86.82 � 20.57 76.48 � 18.52 57.84 � 11.46 0.000
0.000
is of
p V
0.0.0.
tional shortening among the groups. Both variables
by on June 11, 2013 als.org

C
BPTd[pcttps
vTltmt(bMirmt
tetrdcchttt
sntLepcoo
limpmp
CoPruvpdc
c[Rosc
pi0Mbep
gmoS
T
G
IIIB
E
1931Ann Thorac Surg CHOWDHURY ET AL2005;79:1926–33 MVR, CHORDAL PRESERVATION, RHEUMATIC MV DISEASE, AND LV FUNCTION
CA
RD
IOV
AS
CU
LA
R
continued to decline over time in the nonchordalgroup (group I; p � 0.05 and p � 0.001, respectively)and returned to preoperative levels after the initialdecline in the chordal preservation groups. At theend of 4 years, the fractional change of ejectionfraction was statistically significant only in thechordal preservation groups (II and III).
omment
ileaflet Versus Posterior Chordal Preservation:ossibilities and Limitationshe importance of bileaflet preservation in patients un-ergoing mitral valve replacement remains controversial
1–4, 11]. Many surgeons continue to retain only theosterior leaflet with chordae tendinae because of con-erns over greater technical complexity, longer operatingime, potential interference with mechanical leaflet mo-ion, need to undersize the mitral prosthesis, and theossibility of creating left ventricular outflow tract ob-truction [1–5, 11].
To overcome the limitations of bileaflet preservation, aariety of techniques have been introduced [7, 12–14].hese differ primarily in the location where the anterior
eaflet chordae are inserted in the mitral annulus. Theension of the preserved main anterior leaflet chordae
ay act on the posterior annulus (Feike’s technique), therigonal area (Miki’s technique), on the anterior annulusKhonsari’s I and II technique), or on a point half-wayetween these locations (Hetzer’s technique) [7, 12–14].agnetic resonance studies of annulus motion have
ndicated interesting phenomena characteristic of theespective techniques, such as parallel prosthetic move-ent with Khonsari’s technique and tilting of the pros-
hesis in Feike’s technique [14].There are differences in the tension on chordae during
he cardiac cycle in various techniques but there is nostablished method for predefining chordal length at theime of prosthetic implantation, nor for determining theequired length according to the various types of mitralisease, left ventricular dimensions, or location ofhordal reattachment. The use of artificial Gore-Texhordae during MVR has been popularized by some; weave not used the same [15, 16]. There is a possibility of
hickening and hardening of the preserved chordaeendinae because of restricted physiologic movement by
able 2. Continued
Ejection Fraction
roup Preoperative At Discharge At 4 Years
(n � 59) 53.30 � 6.67 45.17 � 8.16 44.63 � 8.58I (n � 117) 52.40 � 8.10 44.33 � 8.41 51.88 � 8.72II (n � 250) 86.82 � 20.57 76.48 � 18.52 57.84 � 11.46etween groupp value
0.031
cho data: mean � standard deviation.
he prosthetic valve [13, 14]. We believe that a divided, T
ats.ctsnetjournDownloaded from
hifted, and reaffixed anterior leaflet with chordae tendi-ae may not interfere with the left ventricular outflow
ract (LVOT) [16]. No chordal structure obstructed theVOT with this technique. Doppler echocardiographicxamination did not show any evidence of LVOTO in anyatient with preserved anterior mitral leaflet. Techni-ally, total chordal preservation was feasible in 60% ofur patients with mixed mitral valve disease and in 51.5%f patients with predominant mitral stenosis.An argument against preservation of the anterior leaf-
et was that only undersized valve prosthesis could bemplanted [1–4]. However, we have implanted a 29 to 33
m prosthesis in 85.6% of patients with total chordalreservation, suggesting that preservation of the anterioritral leaflet does not preclude implantation of a large
rosthesis.
omplete Versus Partial Chordal-Sparing MVR: Effectsn Left Ventricular Volume and Functionreserving the subvalvular mitral apparatus has beenecognized as necessary for improvement of left ventric-lar systolic function, exercise capacity, and better sur-ival after MVR [1–4, 11, 16, 17]. It has been shown toreserve regional left ventricular mechanics and three-imensional contraction synergy, and may prevent myo-ardial rupture [1–4, 11, 16, 17].
Reports addressing the issue of left ventricular me-hanics with bileaflet or posterior leaflet MVR are limited2–4, 11, 17]. Although Hannein and colleagues [3] andozich and colleagues [17] demonstrated the superiorityf chordal-sparing MVR over conventional MVR, noignificant differences were noted between patients re-eiving either posterior or bileaflet chordal preservation.
Our study demonstrates that MVR with bileaflet orosterior chordal preservation is associated with a lesser
ncidence of postoperative low output syndrome (p �.000) and better long-term survival than conventionalVR (p � 0.0002; Fig 3). Also, patients undergoing
ileaflet-preserving MVR derived greater functional ben-fit than patients undergoing MVR without chordalreservation.Echocardiographically, the total chordal-preservation
roup demonstrated statistically significant improve-ent of left ventricular diastolic and systolic dimensions
ver posterior and nonchordal groups (Tables 2 and 3).imilar results were reported by others [2–4, 11, 16, 17].
Fractional Shortening
alue Preoperative At Discharge At 4 Years p Value
051 31.29 � 6.94 27.20 � 8.39 20.08 � 8.03 0.001289 29.84 � 5.80 20.43 � 39.73 27.08 � 7.59 0.480066 30.97 � 9.37 30.18 � 8.72 30.15 � 11.41 0.878
0.048
p V
0.0.0.
his supports the observation that chordopapillary pres-
by on June 11, 2013 als.org
elp
LTepb
mapai
CWthipctt
Wm
R
ble
3.Pa
irw
ise
Com
pari
sons
byPo
stho
cA
naly
sis
(n�
426)
En
d-S
ysto
licV
olu
me
En
d-D
iast
olic
Vol
um
eE
ject
ion
Frac
tion
Frac
tion
alSh
orte
nin
g
Pre
oper
ativ
eA
tD
isch
arge
At
4Y
ears
Pre
oper
ativ
eA
tD
isch
arge
At
4Y
ears
Pre
oper
ativ
eA
tD
isch
arge
At
4Y
ears
Pre
oper
ativ
eA
tD
isch
arge
At
4Y
ears
/sII
(p-v
alu
e)N
SN
SN
SN
SN
S0.
04N
SN
S0.
02N
SN
S0.
001
/sII
I(p
valu
e)N
S0.
040.
000
NS
NS
0.00
5N
S0.
001
0.01
NS
0.00
0.05
/sII
I(p
valu
e)N
S0.
040.
001
NS
0.01
0.00
8N
S0.
050.
00N
S0.
050.
004
�n
otsi
gnifi
can
t.
1932 CHOWDHURY ET AL Ann Thorac SurgMVR, CHORDAL PRESERVATION, RHEUMATIC MV DISEASE, AND LV FUNCTION 2005;79:1926–33
CA
RD
IOV
AS
CU
LA
R
rvation is an important determinant of postoperativeeft ventricular function, and the increased afterloadroduced by a competent valve is of less consequence.
imitations of This Studyhis study was not randomized. Given the mountingvidence favoring conservative mitral valve surgery, arospective, randomized controlled trial may no longere considered ethical.Our methods of measuring left ventricular functionay be criticized for inaccuracy, because these are oper-
tor dependent. However, all echo measurements wereerformed by experienced cardiologists. We have notssessed global and regional systolic stress, which isncreased after chordal transection.
onclusionse conclude that total chordal preservation is possible in
he majority of patients undergoing MVR for rheumaticeart disease. An appropriate sized prosthesis can be
mplanted despite bileaflet preservation. This techniquerovides superior results compared to non and partialhordal preservation. We hope these technical modifica-ions will be useful to surgeons attempting to emulatehis approach on an individual basis.
e are grateful to Shankar Sharma for preparation of theanuscript.
eferences
1. Lillehei CW. New ideas and their acceptance as it has relatedto preservation of chordae tendinae and certain other dis-coveries. J Heart Valve Dis 1995;4(suppl 2):S106–14.
2. Le Tourneau T, Grandmougin D, Foucher C, et al. Anteriorchordal transection impairs not only regional left ventricularfunction but also regional right ventricular function in mitralregurgitation. Circulation 2001;104(suppl 1):141–6.
3. Hannein HA, Swain JA, McIntosh CL, et al. Comparativeassessment of chordal preservation versus chordal resectionduring mitral valve replacement. J Thorac Cardiovasc Surg1990;99:828–37.
4. Kayacioglu I, Ates M, Sensoz Y, et al. Comparative assess-ment of chordal preservation versus chordal resection inmitral valve replacement for mitral stenosis (long-term fol-low-up: 8 years). Tohoku J Exp Med 2003;200:119–28.
5. Thomson LE, Chen X, Greaves SC. Entrapment of mitralchordal apparatus causing early postoperative dysfunctionof a St. Jude mitral prosthesis. J Am Soc Echocardiogr2002;15:843–4.
6. Choudhary SK, Talwar S, Dubey B, Chopra A, Saxena A,Kumar AS. Mitral valve repair in a predominantly rheumaticpopulation—long-term results. Tex Heart Inst J 2001;28:8–16.
7. Miki S, Kusuhara K, Ueda Y, et al. Mitral valve replacementwith preservation of chordae tendinae and papillary mus-cles. Ann Thorac Surg 1988;45:28–34.
8. Edmunds LH Jr, Clark RE, Cohn H, Grunkemeier GL, MillerDC, Wiesel RD. Guidelines for reporting morbidity andmortality after cardiac valvular operations. Ann Thorac Surg1996;62:932–5.
9. Cheitlin MD, Armstrong WF, Aurigemma GP, et al. Guide-
line update for the clinical application of echocardiography:summary article. J Am Soc Echocardiogr 2003;16:1091–110.Ta IvII
vI
v
NS
by on June 11, 2013 ats.ctsnetjournals.orgDownloaded from
1
1
1
1
1
1
1
1
N
TMtSre
c(
1933Ann Thorac Surg CHOWDHURY ET AL2005;79:1926–33 MVR, CHORDAL PRESERVATION, RHEUMATIC MV DISEASE, AND LV FUNCTION
©P
AR
DIO
VA
SC
UL
AR
0. Kaplan EL, Meier P. Non-parametric estimation from incom-plete observations. J Am Stat Assoc 1958;53:457–81.
1. Yun Kl, Sintek CF, Miller DC, et al. Randomized trialcomparing partial versus complete chordal-sparing mitralvalve replacement: effects on left ventricular volume andfunction. J Thorac Cardiovasc Surg 2002;123:707–14.
2. Feikes HL, Daugharthy JB, Perry JE, et al. Preservation of allchordae tendinae and papillary muscle during mitral valvereplacement with a tilting disc valve. J Cardiac Surg 1990;5:81–5.
3. Sintek CF, Pfeffer TA, Kochamba GS, Khonsari S. Mitralvalve replacement: technique to preserve the subvalvularapparatus. Ann Thorac Surg 1995;59:1027–9.
otice From the American Boar
written) examination.
ei
BC2
2005 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ats.ctsnetjournDownloaded from
Weng Y. Preservation of papillary muscles and chordaeduring mitral replacement: possibilities and limitations.J Heart Valve Dis 1995;4(suppl 2):S115–23.
5. Komeda M, DeAnda A Jr, Glasson JR, et al. Improvingmethods of chordal sparing mitral valve replacement. PartIII: Optimal direction for artificial chordae. J Heart Valve Dis1996;5:484–90.
6. Wasir H, Chaudhary SK, Airan B, et al. Mitral valve replace-ment with chordal preservation in a rheumatic population.J Heart Valve Dis 2001;10:84–9.
7. Rozich JD, Carabello BA, Usher BW, et al. Mitral valve replace-ment with and without chordal preservation in patients withchronic regurgitation: mechanism for differences in postoper-
C 4. Hetzer R, Drews T, Siniawski H, Komoda T, Hofmeister J, ative ejection performance. Circulation 1992;86:1718–26.d of Thoracic Surgery
he 2005 Part I (written) examination will be held ononday, December 5, 2005. It is planned that the examina-
ion will be given at multiple sites throughout the Unitedtates using an electronic format. The closing date foregistration is August 1, 2005. Those wishing to be consid-red for examination must apply online at www.abts.org.
To be admissible to the Part II (oral) examination, aandidate must have successfully completed the Part I
A candidate applying for admission to the certifyingxamination must fulfill all the requirements of the Boardn force at the time the application is received.
Please address all communications to the Americanoard of Thoracic Surgery, 6333 N St. Clair St, Suite 2320,hicago, IL 60611; telephone: (312) 202-5900; fax: (312)02-5960; e-mail: [email protected].
Ann Thorac Surg 2005;79:1933 • 0003-4975/05/$30.00
by on June 11, 2013 als.org

2005;79:1926-1933 Ann Thorac SurgSubramaniam, Ram Prakash, Sandeep Seth, Rajvir Singh and Panangipalli Venugopal
Ujjwal K. Chowdhury, A. Sampath Kumar, Balram Airan, Dinesh Mittal, K. Ganapathy Size and Function
Rheumatic Population: Serial Echocardiographic Assessment of Left Ventricular Mitral Valve Replacement With and Without Chordal Preservation in a
& ServicesUpdated Information
http://ats.ctsnetjournals.org/cgi/content/full/79/6/1926including high-resolution figures, can be found at:
References http://ats.ctsnetjournals.org/cgi/content/full/79/6/1926#BIBL
This article cites 17 articles, 6 of which you can access for free at:
Citations
shttp://ats.ctsnetjournals.org/cgi/content/full/79/6/1926#otherarticleThis article has been cited by 7 HighWire-hosted articles:
Subspecialty Collections
http://ats.ctsnetjournals.org/cgi/collection/valve_disease Valve disease
following collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
[email protected]: orhttp://www.us.elsevierhealth.com/Licensing/permissions.jsp
in its entirety should be submitted to: Requests about reproducing this article in parts (figures, tables) or
Reprints [email protected]
For information about ordering reprints, please email:
by on June 11, 2013 ats.ctsnetjournals.orgDownloaded from




















