international court of justice case concerning certain iranian ...
Upload
khangminh22Category
view
6download
0
Iranian Journal of
Reproductive Medicine VOLUME 9 NUMBER 3 Summer 2011 ISSN: 1680-6433
Published by: Yazd Research & Clinical Center for Infertility
In collaboration with: Iranian Society for Reproductive Medicine
CHAIRMAN MANAGER Vahidi, Serajedin M.D. EDITOR-IN-CHIEF Aflatoonian, Abbas M.D. MANAGING EDITOR Anvari, Morteza Ph.D. EXCUTIVE BOARD Abdoli, Ali Mohammad M.D. Asadzadeh, Kobra B.S. Khani, Parisa M.D. Mortazavifar, Zahrasadat B.S. ENGLISH EDITOR Sheikhha, Mohammad Hasan M.D., Ph.D.
EDITORIAL BOARD
Ahmadi, Ali Ph.D. (USA)
Al-Hassani, Safa Ph.D. (GERMANY) Hosseini, Ahmad Ph.D. (IRAN) Hosseini, Seyed Jalil M.D. (IRAN) Kalantar, Seyed Mehdi Ph.D. (IRAN) Karimzadeh Meybodi, Mohammad Ali M.D. (IRAN) Kazemeyni, Seyed Mohammad M.D. (IRAN)
Khalili, Mohammad Ali Ph.D. (IRAN)
Lenton, Elizabeth Ann Ph.D. (UNITED KINGDOM)
Monsees, Thomas Ph.D. (GERMANY)
Moini, Ashraf M.D. (IRAN)
Nasr-Esfahani, Mohammad Hossein Ph.D. (IRAN)
Pour-Reza, Maryam M.D. (IRAN)
Pourmand, Gholamreza M.D. (IRAN)
Yasini, Seyed Mojtaba M.D. (IRAN)
The Iranian Journal of Reproductive Medicine is indexed in ISI web of Science, Scopus, Chemical Abstract Services,
CAB Abstract, Index Copernicus, Index Medicus for the WHO Eastern Mediterranean Region (IMEMR), Directory of
Open Access Journals (DOAJ), EBSCO, Socolar, ISC, Magiran, Scientific Information Database (SID), Iran Medex,
Open J-Gate, Bioline International and approved by Medical Journals Commission of the Ministry of Health and
Medical Education.
Publication Permission No.13372
IJRM Office, Research & Clinical Center for Infertility, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
P.O. Box: 89195-999 Yazd, Iran Tel/fax: +98 (351) 8248348
Email: [email protected] Website: www.ijrm.ir
II
Instructions to Authors
Aims and Scope The Iranian Journal of Reproductive Medicine (IJRM) is an international scientific quarterly publication of
the Research and Clinical Center for Infertility of Shahid Sadoughi University of Medical Sciences and
Health Services.
Publication of IJRM benefits from copyright protection in accordance with Universal Copyright Convention.
All published articles will become the property of the IJRM. The editor and publisher accept no
responsibility for the statements expressed by the authors here in. Also they do not guarantee, warrant or
endorse any product or service advertised in the journal.
This journal accepts Original Papers, Review Articles, Short Communications, Case Reports and Letters to
the Editor in the fields of fertility and infertility, ethical and social issues of assisted reproductive
technologies, cellular and molecular biology of reproduction, including the development of gametes and
early embryos, assisted reproductive technologies in model system and in a clinical environment,
reproductive endocrinology, andrology, epidemiology, pathology, genetics, oncology, surgery, psychology
and physiology. Emerging topics including cloning and stem cells are encouraged.
Submission of manuscript All authors must sign the “submission form” agreement before the article can be processed. This transfer
agreement enables IJRM to protect the copyright material for the authors. The copyright transfer covers the
exclusive rights to reproduce and distribute the article, including reprints, photographic reproductions,
microform or any other reproductions of similar nature and translations, and includes the right to adapt the
article for use in conjunction with computer system and programs, including reproduction or publication in
machine-readable form and incorporation in retrieval systems. Authors are responsible for obtaining from the
copyright holder permission to reproduce all figures for which copyright exists.
Always submit three photocopies of the entire manuscript and a diskette that contains the manuscript and had
been created by Microsoft Word, along with three sets of photographs, illustration, diagrams etc to
mentioned address. A covering letter identifying the person (full name, address, telephone, fax numbers and
e-mail) responsible for correspondence concerning the submitted article should accompany all manuscripts.
Manuscripts are received with the understanding that they are not under simultaneous consideration by
another publication. The author’s transmittal letter must accompany the manuscript and contain these
statements: “The manuscript has been seen and approved by all authors involved and is neither being
published nor being considered for publication elsewhere. The authors transfer copyright to the IJRM.”
In case of electronic submission of the manuscript the authors must declare that it is being exclusively
contributed to IJRM. The text should be submitted in Microsoft Word format as an attachment. The figures
should be sent in a format of JPEG or GIF which will produce high quality images in the online edition of
the journal. Submission is also acceptable via Journal URL: http://www.ijrm.ir
Guidelines for preparation of manuscript
Manuscript length
Papers should be of a length appropriate for the amount of information they contain. Failure to restrict the
length of manuscripts can negatively influence the editor’s decisions.
Style Manuscripts should be written using clear and concise English. The manuscript should include: Title page;
the Abstract; Introduction; Materials and Methods; Results; Discussion; Acknowledgement and Ref-
erences.
Manuscript format
The format of the IJRM manuscripts, including tables, references, and figure legends must be type written,
double-spaced, on one side of A4 paper, with margins of 2.5 cm. Pages should be numbered consecutively,
beginning with the title page and continuing through the last page of typewritten material. Avoid underlining.
III
Original articles should have the following format:
Title page
The title page must contain (1) title of article, (2) correct names and highest academic degree of each author,
(3) each author’s official academic and/or clinical title and affiliation, (4) name and address of the
institution(s), (5) name, address, telephone number, e-mail and fax number of author to whom
correspondence should be sent.
Running title
The author should provide a running title of no more than 50 characters.
Abstract
All original articles must contain a structured abstract of not more than 250 words. The abstract should
include; Background, Objective, Materials and Methods, Results, Conclusions and at least 3 to 5 Key words,
chosen from the Medical Subject Headings (MeSH) list of index medicus
(http://www.nlm.nih.gov/mesh/MBrowser.html). They should therefore be specific and relevant to the paper.
Authors need to be careful that the abstract reflects the content of the article accurately.
For Randomized Controlled Trials the method of randomization and primary outcome measure should be
stated in the Abstract.
Introduction This should summarize the purpose and the rationale for the study. It should neither review the subject
extensively nor should it have data or conclusions of the study.
Materials and Methods This should include the study design and exact method or observation or experiment, definitions such as for
diagnostic criteria, the population or patient samples, and laboratory and statistical methods. If an apparatus
is used, its manufacturer’s name and address should be given in parenthesis. If the method is established,
give reference but if the method is new, give enough information so that another author is able to perform it.
Statistical method must be mentioned and specify any general computer programme used.
Results This should include the pertinent findings in a logical sequence with tables and figures as necessary. It must
be presented in the form of text, tables and illustrations. The contents of the tables should not be all repeated
in the text. Instead, a reference to the table number may be given. Long articles may need sub-headings
within some sections (especially the Results and Discussion parts) to clarify their contents. Unnecessary
overlap between tables, figures and text should be avoided.
Discussion The discussion should emphasize the present findings and the variations or similarities with other work done
in the field by other workers. Conclusions based on the findings, evidence from the literature that supports
the conclusions, applicability of the conclusions, and implications for future research. The detailed data
should not be repeated in the discussion again. Emphasize the new and important aspects of the study and the
conclusions that follow from them. It must be mentioned whether the hypothesis mentioned in the article is
true, false or no conclusions can be derived.
Acknowledgements All contributors who do not meet the criteria for authorship should be covered in the acknowledgement
section. Financial and material support should also be acknowledged. Personal acknowledgement should
precede those of institutions or agencies
References All manuscripts should be accompanied by relevant references. The Reference should provide the following
information as stated in the presented models as follows:

IV
1. References should be numbered sequentially as they appear in the text according to the Vancouver style.
When citing authors in the text, acknowledge only the first author where there are three or more authors, e.g.
Williams et al (1) stated that.... Where there are two authors cite both, e.g. Jones and Smith (2) reported
that.... Citations in the reference list are to be arranged by number in the following format including
punctuation.
Journals: Author(s). Title of article. Title of journal (in italics with no full stops) Year; Volume number:
Page numbers. (Abbreviations for journals used in the reference list should conform to Index Medicus.) e.g.
Salehnia M, Arianmanesh M, Beigi M. The impact of ovarian stimulation on mouse endometrium: a
morphometrical study. Iran J Reprod Med 2006; 4: 7-11.
Books: Author(s). Title: sub-title. Edition. Place of publication: Publisher; Year. e.g. Speroof L, Robert H.
Clinical gynecology endocrinology & infertility .6th Ed. Philadelphia; Robert-D; 1999.
Chapter in a book: Author(s) of chapter. Title: sub-title of chapter. In: Author(s) (or editors) of the book.
Title: sub-title of book. Place of publication: publisher; Year; page numbers.
Inclusive page numbers should be given for all references. Print surnames and initials of all authors when
there are six or less. In the case of seven or more authors, the names of the first six authors followed by et al
should be listed.
References to papers accepted for publication, but not yet published, should be cited as such in the reference
list e.g. Mohammad Kazem Gharib Naseri M, Mohammadian M, Gharib Naseri Z. Antispasmodic effect of
Physalis alkekengi fruit extract on rat uterus, Iran J Reprod Med 2008, in press.
The author is responsible for the accuracy and completeness of the references and for their correct textual
citation.
Tables In limited numbers should be submitted with the captions placed above.Each table should be numbered
consecutively with Roman numerals and typed double-spaced, including all headings. Verify tabular
statistics to make sure they tally and match data cited in the text. Do not submit tables as photograph.
Figures Should be in limited numbers, with high quality art work and mounted on separate pages.
The captions should be placed below. The same data should not be presented in tables, figures and text,
simultaneously.
Clinical Trial Registration
From January 2010, all of the Clinical Trials must be registered in Iranian Registry of Clinical Trials
(www.IRCT.ir), in order to be considered for publication. This includes all of the clinical trials performed
inside Iran even if they register in other registration sites. The clinical trials performed abroad, could be
considered for publication, if they register in a registration site approved by W.H.O.
According to the International Committee of Medical journal Editors (ICMJE) a Clinical Trial is any
research study that prospectively assigns human participants or groups of humans to one or more health-
related interventions to evaluate the effects on health outcomes.
The registration number of the trial and the name of the trial registry must be mentioned at the end of the
abstract.
Review articles should be prepared according to one of the following styles:
− Systematic reviews should be in form of meta-analysis, meta synthesis or without statistical analysis.
These articles contain original articles’ parts.
− Non systematic reviews should be written by experts who have at least one published article in the
related field in references. Different parts of such articles include abstract, introduction, discussion
and conclusion. They should contain at least 20 references and maximum 5000 words.
Short communication can be in form of research article, systematic review or ongoing research which
reports its interesting findings. The parts in this type of articles are like those of original one but they are
smaller and prepared in maximum 2000 words.

V
A letter to the editor should be about criticism of previous articles, criticism or review over books,
analysis of a related topic with reproductive medicine, expansion and explanation about an idea or a
complicated problem. This should be prepared in maximum 1000 to 1500 words. These articles need no
structure.
Editorial article should be written by either the editor in chief or the editorial board. The editor in chief
could also ask an expert to do such a thing. The context of such articles could involve a deep analysis
about the up to date topics in reproductive medicine, challenging systems or proposing solutions in
reproductive medicine field. They should be prepared in maximum 2000 words and have at least 5
references.
Case Reports and Brief Reports: Both should include abstract, keywords, case presentation, discussion,
acknowledgment, references, and 1 – 4 figures. Necessary documentations of the case(s) like pathology
reports, laboratory test reports, and images should be included in the submission package. Brief reports
should not have more than one figure and/or table.
Illustrations Three copies of all figures or photographs should be included with the submitted manuscript. Photographs
must be high-contrast, glossy, black and white prints, unmounted and untrimmed, with preferred size of 10 x
15 cm. Color transparencies or photos will be accepted at the discretion of Editorial Board. Figure number,
and name of senior author, should be written on the back of each illustration. Written permission must
accompany any photograph in which the subject can be identified or any illustration that has been previously
published. All illustrations must be numbered as cited in the text in consecutive numeric order.
Submission requirements
Submit only the final version of the manuscript.
The file should be in Microsoft Word.
Provide the printout of the manuscript that exactly matches the disk file. File names must be clearly
indicating the contents of each file.
Prepare art as camera-ready copy. Laser prints are accepted.
Page charges: There is no page charge for publication in the IJRM.
Reprint: Ten reprints will be provided free of charge.
The corresponding author will be supplied with 3 free issues.
Ethics of studies involving humans and animals Ethical considerations must be addressed in the Materials and Methods section. 1) Please state that informed
consent was obtained from all participants. 2) Include the name of the appropriate institutional review board
that approved the project. 3) Indicate in the text that the maintenance and care of experimental animals
complies with National Institutes of Health guidelines for the humane use of laboratory animals, or those of
your Institute.
Statistics Inadequate or incorrect statistical analyses frequently cause rejection or delays in the review of manuscripts.
Where appropriate, authors should seek advice from a professional statistician before the manuscript is
submitted.
Ethics of scientific publishing Submission of a paper implies that it reports unpublished work and that it is not under consideration for publication elsewhere. If previously published tables, illustrations or text are to be included, then this should be clearly indicated in the manuscript and the copyright holder's permission must be obtained. Previously published material can be cited in a later review or commentary article, but it must be indicated using quotation marks if necessary.
VI
Plagiarism of text from a previously published manuscript by the same or another author is a serious publication offence. Small amounts of text may be used, but only where the source of the material quoted is clearly acknowledged. Fraudulent data or data stolen from other authors is also unethical and will be treated accordingly. Any alleged offence is considered initially by the Editorial Team. Conflicts of interest Authors must acknowledge and declare any sources of funding and potential conflicting interest, such as receiving funds or fees by, or holding stocks and shares in, an organization that may profit or lose through publication of your paper.
Copyright The entire contents of IJRM are protected under international copyrights. This Journal is for your personal
noncommercial use. You may not modify copy, distribute, transmit, display, or publish any materials
contained on the Journal without the prior written permission of it or the appropriate copyright owner.
Review process The submitted manuscripts will be assessed from editorial points of view, at first. Should the manuscript
meet the basic editorial requirements; it will enter the peer-review process. The manuscript will then be sent
at least to one in-office and two out of office referees for review. The corresponding author will then be
informed to the referee’s remark to accept, reject or require modification.
Revision: Papers may be returned to authors for modification of the scientific content and/or for language
corrections. Revised paper and a letter listing point-for-point response to the reviewers must be submitted to
the Editor and must be accompanied by a copy of the original version. Suggestion by the Editor about
resubmission does not imply that a revised version will necessary be accepted. If a paper that is returned to
the authors for modification is not resubmitted within two months it will be regarded as having been
withdrawn and any revised version received subsequently will be treated as a new paper and the date of
receipt will be altered accordingly. Authors who resubmit a paper that has previously been rejected must
provide the original manuscript and a letter explaining in detail how the paper has been modified. Accepted
manuscripts become the property of IJRM.
Proofs: A computer printout will be sent to the corresponding author to be checked for only typographical
errors and other essential small changes before publication in order to avoid any mistakes. Major alternations
to the text cannot be accepted at this stage. Proofs must be returned to the Editor within 2 days of receipt.
Responsibilities of authors The authors are responsible for accuracy of all statements and data contained in the manuscript, accuracy of
all references information, and for obtaining and submitting permission from the author and publisher of any
previously published material included in the submitted manuscript. The corresponding author will receive
an edited manuscript for “final author approval”.
Disposal of material Once published, all copies of the manuscript, correspondence and artwork will be held for 1 year before
disposal.
Submit manuscripts to: The Editor in Chief,
Iranian Journal of Reproductive Medicine, Research & Clinical Center for Infertility, Bouali Ave, Safayeh,
Yazd, Iran. P.O. Box, 89195-999.
Telephone: +98 (351) 8247085.
Tel/Fax: +98 (351) 8248348.
Email: [email protected]
URL: http://www.ijrm.ir

VII
Submission Form
Corresponding Author:
Manuscript Title:
Mailing Address:
Phone:
Fax:
Cell Phone:
Email:
Check List (Failure to complete will delay processing of the manuscript):
One original and 3 copies of the manuscript together with three original figures and photographs are
enclosed.
A floppy diskette or CD containing the manuscript, tables and figures.
Abstract size is not exceeded 250 words.
The format of manuscript conforms to the IJRM Instructions to Authors.
Entire manuscript (including references and tables) are typed double spaced with margins of at least
2.5 cm for each sides of page on one side of A4 paper.
Entire manuscript is typed in a font of at least 12 points in Times New Romans.
A legend is provided for each figure on a separate page at the end of the manuscript.
All symbols are explained in legends and all symbols in legends appear in figures.
References are numbered in the order in which they appear in text in parentheses.
References are checked for accuracy against original source and formatted according to the IJRM
Instructions to Authors.
Contents of the manuscript have not been previously published and are not currently submitted
elsewhere.
All human and animal studies are approved by an Institutional Review Board.
All listed authors have seen and approved of the manuscript.
I accept responsibility for the scientific integrity of the work described in this manuscript.
Please refer to the IJRM Instructions to Authors for further information.
Signature: ............................................................................................................................................. Date:
Note: Neither manuscript nor figures will be returned after review.
Mail the manuscript to:
Dr. Abbas Aflatoonian, Editor in Chief Iranian Journal of Reproductive Medicine,
Research & Clinical Center for Infertility,
Shahid Sadoughi University of Medical Sciences,
Bouali Avenue, Safayeh, Yazd, Iran.
Iranian Journal of Reproductive Medicine
VIII
P.O. Box: 89195-999.
Manuscripts published in the Iranian Journal of Reproductive Medicine become the sole
property of, with all right in copyright reserved to, the Yazd Research & Clinical Center for
Infertility.
The undersigned authors hereby affirm that the manuscript entitled: …………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………
is original and that all the statements asserted as facts are based on the author(s) investigation and
research. The manuscript has not been published in any form and is not being submitted for in the
form of scientific presentations. If the above requirements are not fulfilled, justification for
duplicate publication and permission to republish copyrighted materials must be declared and
accompanied by a covering letter. In signing this form, the authors acknowledge that they have
participated in the work in a substantive way and are prepared to take full responsibility for the data
presented herein.
The author(s) in the event of the acceptance of the above manuscript for publication, does hereby
assign and transfer to Iranian Journal of Reproductive Medicine all of the rights and interests with
respect to the above copyright either in its current or any other form including revised or
electronically disseminated versions.
All authors must sign: (Please mark the corresponding author)
No. Date Name Category (% of contribution) Signature
1
2
3
4
5
6
7
8
I/We agree with the publication of the above manuscript in Iranian Journal of Reproductive Medicine as its main
author/co-author.
Sign by Correspondence author: Signed Date:
Assignment of copyright and authorship responsibilities
IX
REVIEW ARTICLE
Hormonal treatment for endometriosis associated pelvic pain ................................................. 163
Wong WSF, Lim CED.
ORIGINAL ARTICLES
GnRH antagonist versus agonist in normoresponders undergoing ICSI: a randomized clinical
trial in Iran ..................................................................................................................................... 171
Tehraninejad E, Ghahghaei Nezamabadi A, Rashidi B, Sohrabi M, Bagheri M, Haghollahi F,
AzimiNekoo E, Jafarabadi M.
Effect of benzene extract of Ocimum sanctum leaves on cauda epididymal spermatozoa of
rats ................................................................................................................................................... 177
Ahmed M, Ahamed RN, Aladakatti RH, Ghodesawar MAG.
Icodextrin reduces adhesion formation following gynecological surgery in rabbits ............... 187
Khani B, Bahrami N, Mehrabian F, Naderi Naeni H.
Correlation between the level of cholesteryl ester transfer protein follicular fluid with
fertilization rates in IVF/ ICSI cycles ........................................................................................... 193
Mehdizadeh A, Rahimipour A, Farzadi L, Darabi M, Shahnazi V, Shaaker M, Vatankhah AM,
Golmohamadi Z, Nouri M.
Diagnostic value of saline contrast sonohysterography comparing with hysteroscopy for
detecting endometrial abnormalities in women with abnormal uterine bleeding ................... 199
Karimzadeh MA, Dehghani Firouzabadi R, Goharzad F.
Successful pregnancy following the transfer of vitrified blastocyst which developed from poor
quality embryos on day 3............................................................................................................... 203
Zhang X, Yang Y, Min L, Lv Q, Bai P, Li XJ, Liao M.
Maturation capacity, morphology and morphometric assessment of human immature oocytes
after vitrification and in-vitro maturation................................................................................... 209
Nazari S, Khalili MA, Esmaielzadeh F, Mohsenzadeh M.
Antifertility activity of aqueous ethanolic extract of Hymenocardia acida stem bark in female
rats ................................................................................................................................................... 217
Abu AH, Uchendu CN.
High plasma homocysteine and insulin resistance in patients with polycystic ovarian
syndrome ......................................................................................................................................... 223
Hemati T, Moghadami-Tabrizi N, Davari-Tanha F, Salmanian B, Javadian P.
X
Cotherapy of Tiron and selenium against vanadium induced toxic effects in lactating
rats ................................................................................................................................................... 229
Shrivastava S, Joshi D, Bhadauria M, Shukla S, Mathur R.
Evaluation of the effect of oral ritodrine on implantation rate in in-vitro fertilization-embryo
transfer cycles ................................................................................................................................. 239
Rabiee S, Farimani M, Ahmadi M.
CASE REPORTS
How should painful cystic degeneration of myomas be managed during pregnancy? a case
report and review of the literature ............................................................................................... 243
Kim TH, Lee HH.
Tubo-ovarian abscess in a virgin girl ........................................................................................... 247
Ashrafganjooei T, Harirchi I, Iravanlo G.
LETTER TO EDITOR
The association between iron status and some immunological factors in the pregnancy ....... 251
Sobhani SA, Etaati Z, Mirani S, Saberi P, Shiroodi M, Salmasian H, Naderi N.
PERSIAN ABSTRACTS ................................................................................................... 253

Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:163-170, Summer 2011
Review article
Hormonal treatment for endometriosis associated
pelvic pain
Wu Shun Felix Wong1 M.D., Chi Eung Danforn Lim
2 M.B.B.S.
1 School of Women’s and Children’s Health, Faculty of Medicine, University of New South Wales,
Sydney, Australia.
2 South Western Sydney Clinical School, Faculty of Medicine, University of New South Wales, Sydney,
Australia.
Received: 28 August 2010; accepted: 10 March 2011
Abstract
Background: Endometriosis is a common gynecological problem associated with
chronic pelvic pain.
Objective: To evaluate the effectiveness of current hormonal treatments of
endometriosis associated pain.
Materials and Methods: Randomized Controlled studies identified from databases of
Medline and Cochrane Systemic Review groups were pooled. 7 RCTs were recruited
for evaluation in this review. Data from these studies were pooled and meta-analysis
was performed in three comparison groups: 1) Progestogen versus GnRHa; 2) Implanon
versus Progestogen (injection); 3) Combined oral contraceptive pills versus placebo and
progestogen. Response to treatment was measured as a reduction in pain score. Pain
improvement was defined as improvement ≥1 at the end of treatment.
Results: There was no significant difference between treatment groups of progestogen
and GnRHa (RR: 0.036; CI:-0.030-0.102) for relieving endometriosis associated pelvic
pain. Long acting progestogen (Implanon) and Mirena are not inferior to GnRHa and
depot medroxy progesterone acetate (DMPA) (RR: 0.006; CI:-0.142-0.162). Combined
oral contraceptive pills demonstrated effective treatment of relieving endometriosis
associated pelvic pain when compared with placebo groups (RR:0.321CI-0.066-0.707).
Progestogen was more effective than combined oral contraceptive pills in controlling
dysmenorrhea (RR:-0.160; CI:-0.386-0.066), however, progestogen is associated with
more side effects like spotting and bloating than the combined contraceptive pills.
Conclusion: Combined oral contraceptive pills (COCP), GnRHa and progestogens are
equally effective in relieving endometriosis associated pelvic pain. COCP and
progestogens are relatively cheap and more suitable for long-term use as compared to
GnRHa. Long-term RCT of medicated contraceptive devices like Mirena and Implanon
are required to evaluate their long-term effects on relieving the endometriosis associated
pelvic pain. Key words: Endometriosis associated pelvic pain, Medical treatments, Progestogen, Combined oral contraceptive pills, GnRH.
Introduction
Endometriosis is a common gynecological
Correspondent Author:
Chi Eung Danforn Lim, South Western Sydney Clinical
School, Faculty of Medicine, University of New South
Wales, Sydney, Australia. Email: [email protected]
disease, found in 70% of patient with chronic
pelvic pain (1). It is characterized by the presence
and growth of endometrial tissue outside the
uterine cavity (1). This condition is typically
associated with infertility; dyspareunia and
dysmenorrhea, with the latter being the most
frequent complaint by women with endometriosis
(2).
Wong et al
164 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:163-170, Summer 2011
The cyclic nature of pain associated with
endometriosis is probably attributed to the
response of endometrial tissue to cycling
reproductive hormones particularly estrogen (3).
Treatment of endometriosis associated pelvic
pain includes both medical and surgical options.
Current medical treatment options include
combined oral contraceptive pills, progestogens,
androgen hormone (e.g. Danazol) and
gonadotrophin-releasing hormone analogues
(GnRHa). Each treatment options have its own
systemic side effects, leading to no definite cure
for endometriosis. Associated pelvic pain
frequently recurs once medications are stopped due
to reactivation of ectopic endometrial implants.
Progestogen is most commonly used for
treatment of endometriosis (3). There aredifferent
types of progestogens including medroxy
progesterone acetate and 19-nortestosterone.
Their proposed mechanism of action is to stop
endometrial proliferation and to induce regressive
changes (3, 4). In a Cochrane review performed by
Prentice, Desary and Bland (2009) (5), they noted
that progestogen was an effective treatment for
endometriosis-associated pain.
However, the conclusion from their review was
based on limited data. Eight studies were recruited
and majority of the recruited studies had a relative
small sample size. The mean number of patients
recruited was 82.
Additionally, with the advanced therapeutic
development, apart from orally and
intramuscularly administered forms of delivering
progestogen, there are other forms such as
intrauterine device (Mirena) and subcutaneous
implant (Implanon).
They provide long- term release of
progestogens up to three to five years. Prentice,
Desary and Bland (2009) did not include these
long-term releases of progestogen in their review
(5).
This paper aims to compare and to determine
the effectiveness of current hormonal treatments of
endometriosis associated pelvic pain. Treatments
options included are progestogens, GnRHa and
combined contraceptive pills. They are compared
as following:
1. Progestogen versus GnRHa
2. Long acting progestogen versus GnRHa/
progestogen (injection)
3. Combined oral contraceptive pills versus
placebo and progestogen
Materials and methods
Inclusion criteria
Randomized controlled trials related to
endometriosis-associated pain and medical
treatments from the English literatures between
1995- 2009 were selected and pooled for analysis.
Exclusion criteria
Cohort studies, case control and case reports
were not considered. Studies which did not
measure pain improvement as a measure outcome
and did not match the above objectives were also
not recruited.
Search
Medline and Cochrane systemic review
databases search using keywords: endometriosis,
randomized controlled trial, pelvic pain,
dysmenorrhea, combined oral contraceptive pills,
progestagens and GnRHa were conducted.
Selection of studies
Only medical treatments aimed at symptomatic
improvement of pelvic pain were considered.
Treatments with any progestogens, combined oral
contraceptive pills, GnRHa and placebo were all
considered, irrespective of dosage, route of
administration or duration of treatment. Medical
treatments for painful symptoms after conservative
surgery were also considered in this review
because of the paucity of randomized controlled
studies.
This analysis considered women of
reproductive ages (18- 40 years) complaining of
pain symptoms related to endometriosis. The
endometriosis associated pain symptoms were:
Hormones in endometriosis pelvic pain
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 163-170, Summer 2011 165
dysmenorrhoea, non-menstrual pelvic pain, chronic
pelvic pain and deep dyspareunia.
Studies where participants were asymptomatic
or presented with infertility alone were not
considered.
Data extraction process
This review included data from randomized
controlled studies comparing control, progestogens,
combined contraceptive pills and GnRHa in the
treatment of endometriosis- associated pain. Two
authors extract data independently concerning
details of study design, study population,
intervention and outcomes using a self-developed
data extraction form. Any differences in data
extraction were resolved by consensus, referring
back to the original article. Any disagreement of
data extraction was resolved by discussion with the
senior academic author.
Outcomes measures
Outcome measures were considered at the end
of treatment. The primary outcome measure
was pain improvements for each pain symptoms
where possible. Subjective pain relief measurement
was considered using both visual analogue scale
(VAS) and verbal rating scale (VRS). The
occurrence of side effects was also considered
as a secondary outcome measure.
Outcome definitions
It is defined that response to treatment was
considered as a reduction in pain scores. Pain
improvement was defined as improvement ≥1 at
the end of treatment.
Patient’s satisfaction with the treatment was
considered if they were very satisfied or satisfied.
Statistical analysis
Meta Analyst (6) Software was used in this
project. Statistical analyses were performed to use
the Relative Risk as the measure of effect for
dichotomous data.
There are many different existing methods to
assess pain, standardized the mean difference were
required.
Assessment of bias across studies
We assessed the methodological quality using
the standard as described by Kjaergard (2001)
generation of the allocation sequence, allocation
concealment, double blinding, and follow up (7).
Based on these criteria, the risk of bias with all
the features (random method, allocation
concealment, blinding and follow up) of the studies
was subdivided into the following three categories:
all quality criteria met leading to low risk of bias;
one or more of the quality criteria only partly met
leading to moderate risk of bias; and one or more
criteria not met leading to high risk of bias.
Jadad score was also used to assess the
methodology quality of the clinical trial articles. A
trial receives a score from zero to five. The
evidence may be biased by selection bias, poor
randomization and poor binding, which might
affect the results of a trial.
Funding support
There is no external funding support received
on this project.
Results
Study characteristics
Seven articles (3, 4, 8-12) were recruited for
further evaluation. Six (3, 4, 9- 12) out of seven
studies were identified comparing progestogen
versus other non-progestogen treatments.
One study (8) compared the effectiveness of
oral contraceptive pills versus control on relieving
endometriosis associated pelvic pain. Another
study (10) was evaluating the medical treatment in
controlling the endometriosis-associated painful
symptoms after conservative surgery. The main
characteristics of studies were summarized in table
I.
Sample size
A total of 1096 patients were recruited in seven
studies. The sample size varied between studies.
The mean numbers of patients included were 156
in the seven recruited randomized controlled trials.
Wong et al
166 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:163-170, Summer 2011
Endometriosis was staged according to the
American Fertility Society classification in its
original or revised form in three studies, while the
remaining studies did not perform the staging of
endometriosis.
Measurement tools
Majority of the studies used objective scales,
such as verbal rating scale, a 10cm/100mm visual
analogue scale and five rating scale, to assess the
severity of pain. In two study (12, 13), patients
were asked to rate their satisfactory level to the
therapy; and treatment was considered beneficial if
patients rated themselves as very satisfied or
satisfied (12).
Treatment schedule
The mean duration of treatment was 7 months
(range 3 to 12 months).
Five recruited studies (3, 4, 9, 12, 13) used
progestogen (depot medroxy-progesterone acetate,
oral dinogest, implanon and levonorgestrel-
releasing intrauterine system), four studied (3, 4, 9,
10) used GnRHa (Buserelin acetate, tryporelin,
leuprerelin and lupron) and two studies (8, 10)
used combined oral contraceptive pills (ethinyl-
estradial 0.035mg+norethisterone 1mg; ethinyl
estradiol 0.02 g, desogestrel 0.15 mg) as treatment
intervention.
Risk of bias
Three studies (4, 8, 10) (scored five in Jadad
system which indicates having sufficient quality in
the methodological quality assessment.
Crosignani (2006) scored three in Jadad system
because the method of blinding was not clearly
stated (3). The evaluators were blinded but it was
not specified if the patients were known to the
medication that they were receiving.
Another two studies (12, 13) also scored three
and again there was no mention about the blinding.
Petta (2005) scored two because there was
unblended study with no clear description about
dropout rate (9).
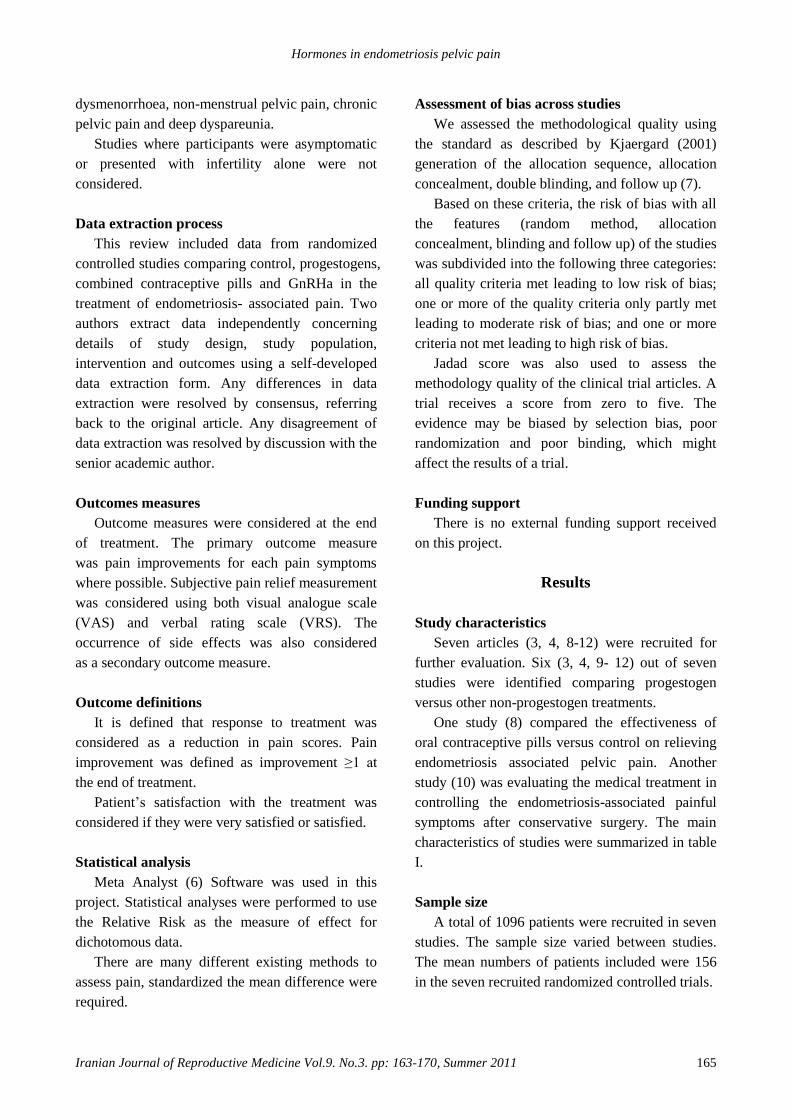
Progestogen versus GnRHa
Progestogen (intrauterine device, DMPA and
oral contraceptive pills) was compared with
GnRHa in three of the seven randomized
controlled trials (3, 4, 9).
The three studies indicated prgestogens were as
effective as GnRHa. They did not show to have a
significant difference (Figure 2. RR: 0.036; CI -
0.03, 0.102).
In terms of side effects, GnRHa appeared to
cause more bone mineral density loss than
progestogens, therefore its use is usually limited to
a period of 6 months. Treatment with progestogens
was associated with a higher incidence of spotting.
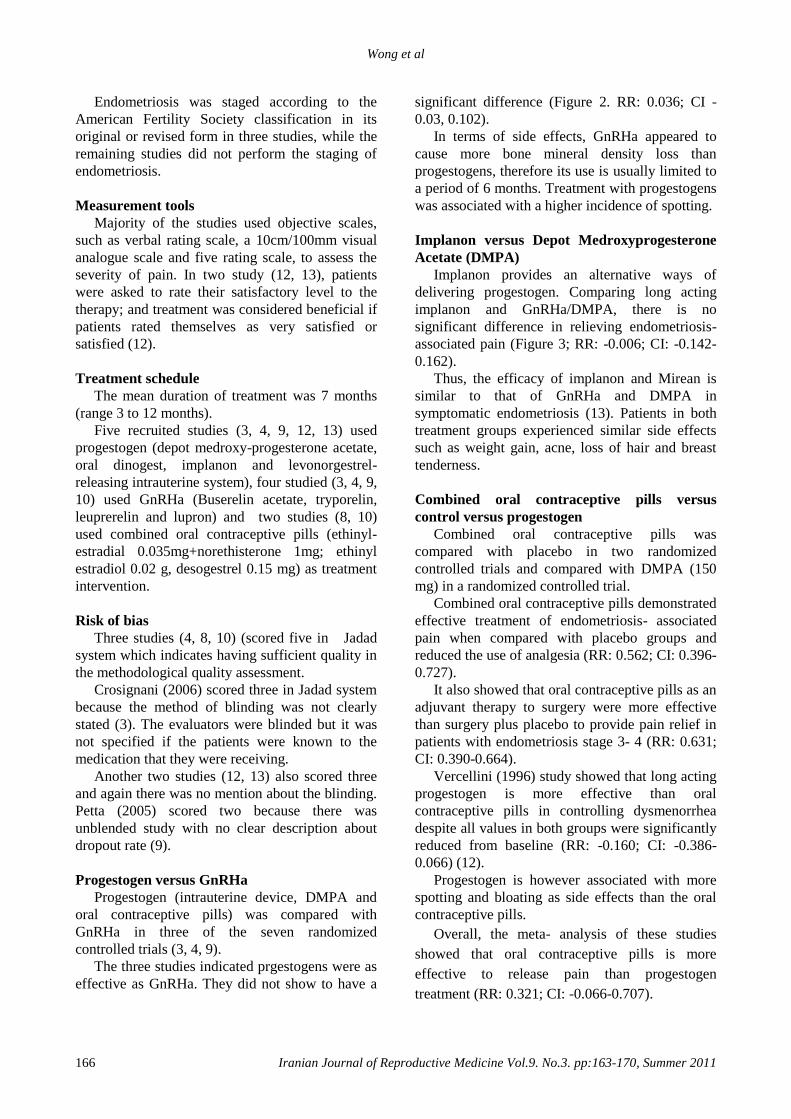
Implanon versus Depot Medroxyprogesterone
Acetate (DMPA)
Implanon provides an alternative ways of
delivering progestogen. Comparing long acting
implanon and GnRHa/DMPA, there is no
significant difference in relieving endometriosis-
associated pain (Figure 3; RR: -0.006; CI: -0.142-
0.162).
Thus, the efficacy of implanon and Mirean is
similar to that of GnRHa and DMPA in
symptomatic endometriosis (13). Patients in both
treatment groups experienced similar side effects
such as weight gain, acne, loss of hair and breast
tenderness.
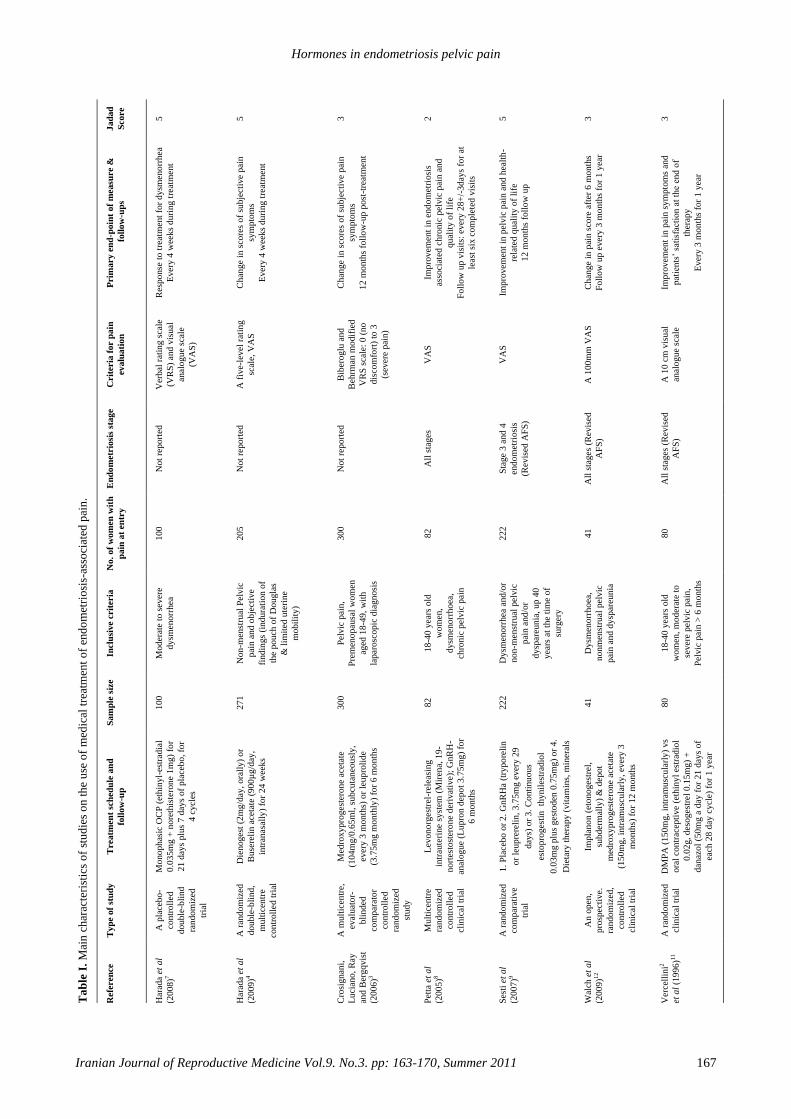
Combined oral contraceptive pills versus
control versus progestogen
Combined oral contraceptive pills was
compared with placebo in two randomized
controlled trials and compared with DMPA (150
mg) in a randomized controlled trial.
Combined oral contraceptive pills demonstrated
effective treatment of endometriosis- associated
pain when compared with placebo groups and
reduced the use of analgesia (RR: 0.562; CI: 0.396-
0.727).
It also showed that oral contraceptive pills as an
adjuvant therapy to surgery were more effective
than surgery plus placebo to provide pain relief in
patients with endometriosis stage 3- 4 (RR: 0.631;
CI: 0.390-0.664).
Vercellini (1996) study showed that long acting
progestogen is more effective than oral
contraceptive pills in controlling dysmenorrhea
despite all values in both groups were significantly
reduced from baseline (RR: -0.160; CI: -0.386-
0.066) (12).
Progestogen is however associated with more
spotting and bloating as side effects than the oral
contraceptive pills.
Overall, the meta- analysis of these studies
showed that oral contraceptive pills is more
effective to release pain than progestogen
treatment (RR: 0.321; CI: -0.066-0.707).
Hormones in endometriosis pelvic pain
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 163-170, Summer 2011 167
Ta
ble
I.
Mai
n c
har
acte
rist
ics
of
stu
die
s o
n t
he
use
of
med
ical
tre
atm
ent
of
end
om
etri
osi
s-as
soci
ated
pai
n.
Jad
ad
Score
5
5
3
2
5
3
3
Prim
ary e
nd
-poin
t of
measu
re &
foll
ow
-up
s
Res
ponse
to t
reat
men
t fo
r dysm
eno
rrhea
Ever
y 4
wee
ks
duri
ng t
reat
men
t
Chan
ge
in s
core
s of
subje
ctiv
e pai
n
sym
pto
ms
Ever
y 4
wee
ks
duri
ng t
reat
men
t
Chan
ge
in s
core
s of
subje
ctiv
e pai
n
sym
pto
ms
12 m
onth
s fo
llo
w-u
p p
ost
-tre
atm
ent
Impro
vem
ent
in e
ndo
met
riosi
s
asso
ciat
ed c
hro
nic
pel
vic
pai
n a
nd
qual
ity o
f li
fe
Foll
ow
up v
isit
s: e
ver
y 2
8+
/-3day
s fo
r at
leas
t si
x c
om
ple
ted v
isit
s
Impro
vem
ent
in p
elvic
pai
n a
nd h
ealt
h-
rela
ted q
ual
ity o
f li
fe
12 m
onth
s fo
llo
w u
p
Chan
ge
in p
ain s
core
aft
er 6
month
s
Foll
ow
up e
ver
y 3
mon
ths
for
1 y
ear
Impro
vem
ent
in p
ain s
ym
pto
ms
and
pat
ients
’ sa
tisf
acti
on a
t th
e en
d o
f
ther
apy
Ever
y 3
mon
ths
for
1 y
ear
Crit
eria
for p
ain
evalu
ati
on
Ver
bal
rat
ing s
cale
(VR
S)
and
vis
ual
anal
ogue
scal
e
(VA
S)
A f
ive-
level
rat
ing
scal
e, V
AS
Bib
eroglu
and
Beh
rman
modif
ied
VR
S s
cale
: 0 (
no
dis
com
fort
) to
3
(sev
ere
pai
n)
VA
S
VA
S
A 1
00m
m V
AS
A 1
0 c
m v
isual
anal
ogue
scal
e
En
do
metr
iosi
s st
age
No
t re
po
rted
No
t re
po
rted
No
t re
po
rted
All
sta
ges
Sta
ge
3 a
nd 4
end
om
etri
osi
s
(Rev
ised
AF
S)
All
sta
ges
(R
evis
ed
AF
S)
All
sta
ges
(R
evis
ed
AF
S)
No
. o
f w
om
en
wit
h
pa
in a
t en
try
10
0
20
5
30
0
82
22
2
41
80
Inclu
siv
e crit
eria
Mo
der
ate
to s
ever
e
dy
smen
orr
hea
No
n-m
enst
rual
Pel
vic
pai
n a
nd
ob
ject
ive
fin
din
gs
(in
du
rati
on
of
the
po
uch
of
Do
ug
las
& l
imit
ed u
teri
ne
mo
bil
ity
)
Pel
vic
pai
n,
Pre
men
op
ausa
l w
om
en
aged
18
-49
, w
ith
lap
aro
sco
pic
dia
gn
osi
s
18
-40
yea
rs o
ld
wo
men
,
dy
smen
orr
ho
ea,
chro
nic
pel
vic
pai
n
Dy
smen
orr
hea
an
d/o
r
no
n-m
enst
rual
pel
vic
pai
n a
nd
/or
dy
spar
eun
ia,
up
40
yea
rs a
t th
e ti
me
of
surg
ery
Dy
smen
orr
ho
ea,
no
nm
enst
rual
pel
vic
pai
n a
nd
dy
spar
eun
ia
18
-40
yea
rs o
ld
wo
men
, m
od
erat
e to
sev
ere
pel
vic
pai
n,
Pel
vic
pai
n >
6 m
on
ths
Sa
mp
le s
ize
10
0
27
1
30
0
82
22
2
41
80
Treatm
en
t sc
hed
ule
an
d
foll
ow
-up
Monophas
ic O
CP
(et
hin
yl-
estr
adia
l
0.0
35m
g +
nore
this
tero
ne
1m
g)
for
21 d
ays
plu
s 7 d
ays
of
pla
ceb
o, fo
r
4 c
ycl
es
Die
noges
t (2
mg/d
ay,
ora
lly
) o
r
Buse
reli
n a
ceta
te (
900µ
g/d
ay,
intr
anas
ally
) fo
r 24 w
eek
s
Med
roxypro
ges
tero
ne
acet
ate
(104m
g/0
.65m
l, s
ubcu
tan
eou
sly
,
ever
y 3
month
s) o
r le
up
roli
de
(3.7
5m
g m
on
thly
) fo
r 6 m
on
ths
Lev
ono
rges
trel
-rel
easi
ng
intr
aute
rine
syst
em (
Mir
ena,
19
-
nort
esto
ster
one
der
ivat
ive);
Gn
RH
-
anal
ogue
(Lu
pro
n d
epo
t 3.7
5m
g)
for
6 m
onth
s
1.
Pla
cebo o
r 2.
GnR
Ha
(try
po
reli
n
or
leupre
reli
n,
3.7
5m
g e
ver
y 2
9
day
s) o
r 3.
Conti
nu
ou
s
esto
pro
ges
tin
thynil
estr
adio
l
0.0
3m
g p
lus
ges
toden
0.7
5m
g)
or
4.
Die
tary
ther
apy (
vit
amin
s, m
iner
als
salt
s, l
acti
c fe
rmen
ts,
fish
oil
) fo
r 6
month
s Im
pla
no
n (
etonoges
trel
,
subder
mal
ly)
& d
epo
t
med
roxy
pro
ges
tero
ne
acet
ate
(150m
g,
intr
amusc
ula
rly,
ever
y 3
month
s) f
or
12 m
on
ths
DM
PA
(150m
g,
intr
amusc
ula
rly
) v
s
ora
l co
ntr
acep
tive
(eth
iny
l es
trad
iol
0.0
2g,
des
oges
trel
0.1
5m
g)
+
dan
azol
(50m
g a
day
for
21
day
s o
f
each
28 d
ay c
ycl
e) f
or
1 y
ear
Typ
e o
f st
ud
y
A p
lace
bo
-
contr
oll
ed
double
-bli
nd
random
ized
tria
l
A r
andom
ized
double
-bli
nd,
mult
icen
tre
contr
oll
ed t
rial
A m
ult
icen
tre,
eval
uat
or-
bli
nded
com
par
ato
r
contr
oll
ed
random
ized
study
Mult
icen
tre
random
ized
contr
oll
ed
clin
ical
tri
al
A r
andom
ized
com
par
ativ
e
tria
l
An o
pen
,
pro
spec
tive.
random
ized
,
contr
oll
ed
clin
ical
tri
al
A r
andom
ized
clin
ical
tri
al
Refe
ren
ce
Har
ada
et a
l
(20
08
)7
Har
ada
et a
l
(20
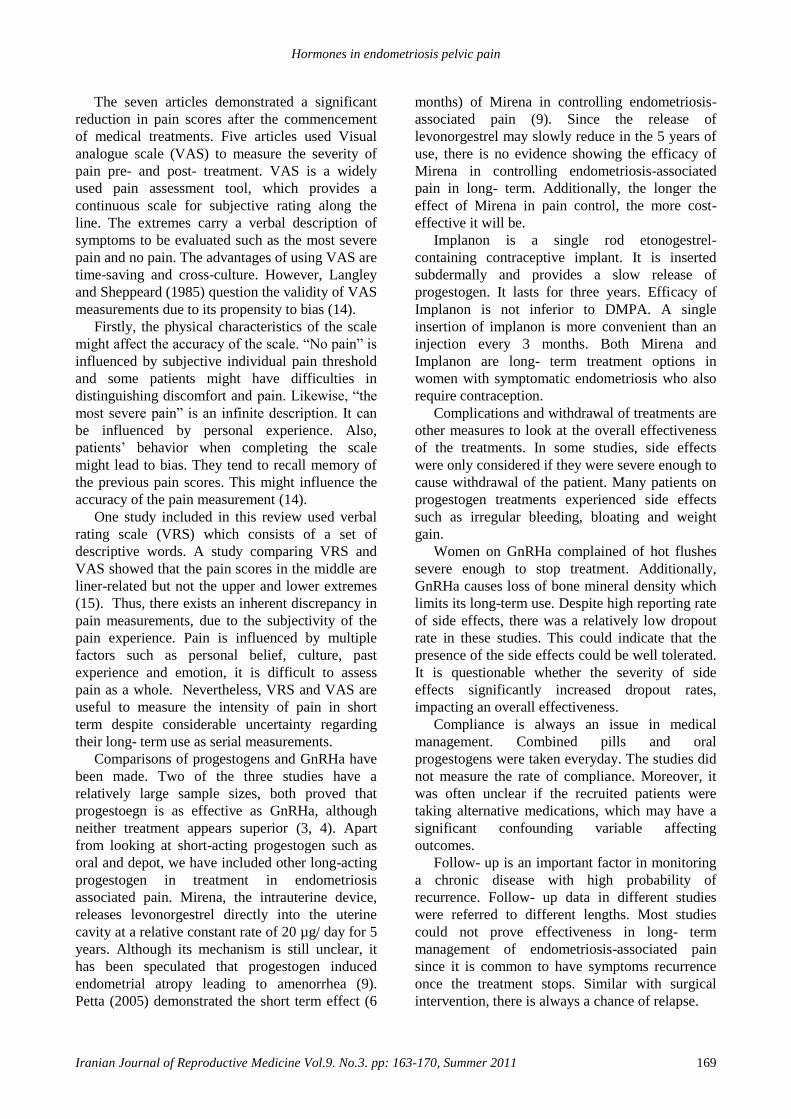
09
)4
Cro
sig
nan
i,
Lu
cian
o,
Ray
and
Ber
gq
vis
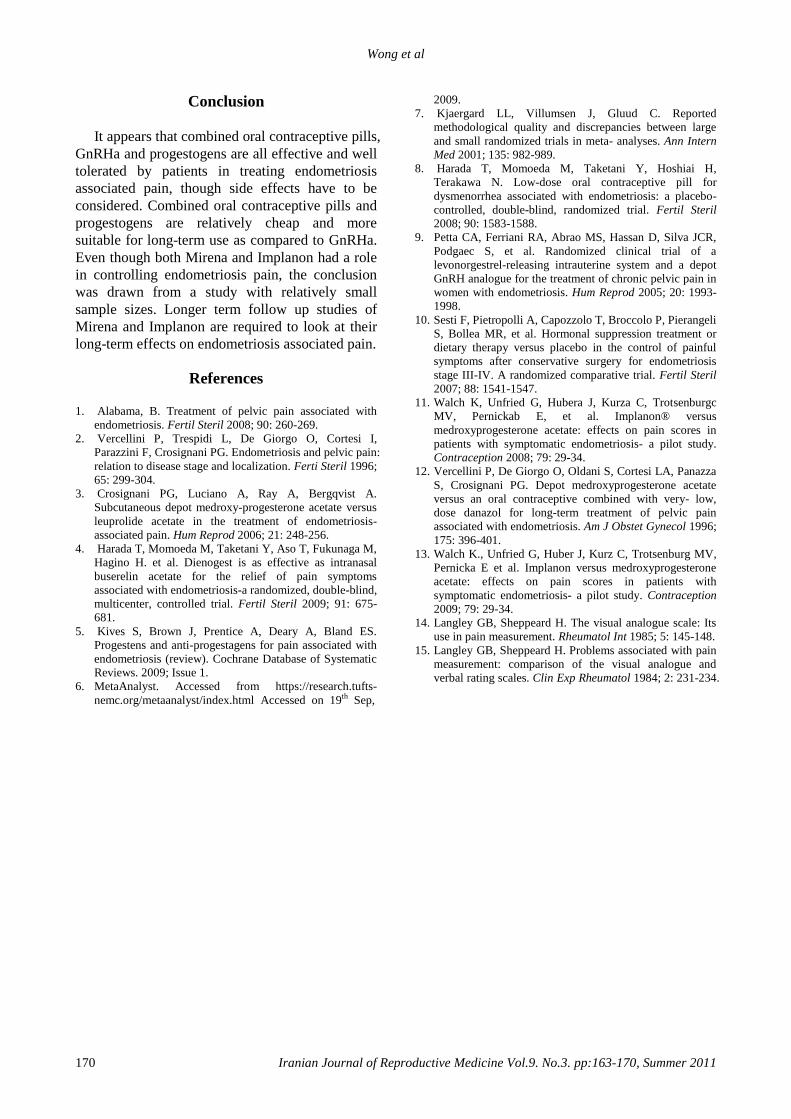
t
(20
06
)3
Pet
ta e
t a
l
(20
05
)8
Ses
ti e
t a
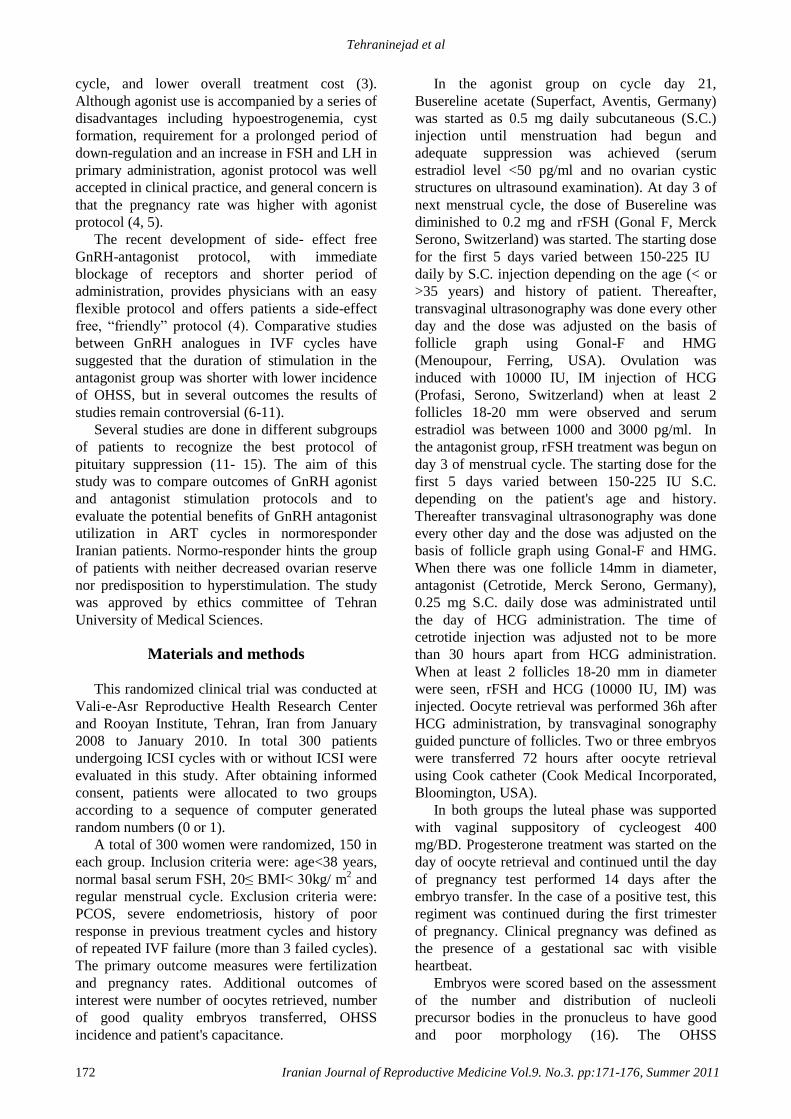
l
(20
07
)9
Wal
ch e
t a
l
(20
09
)12
Ver
cell
ini2
et a
l (1
99
6)1
1
Wong et al
168 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:163-170, Summer 2011
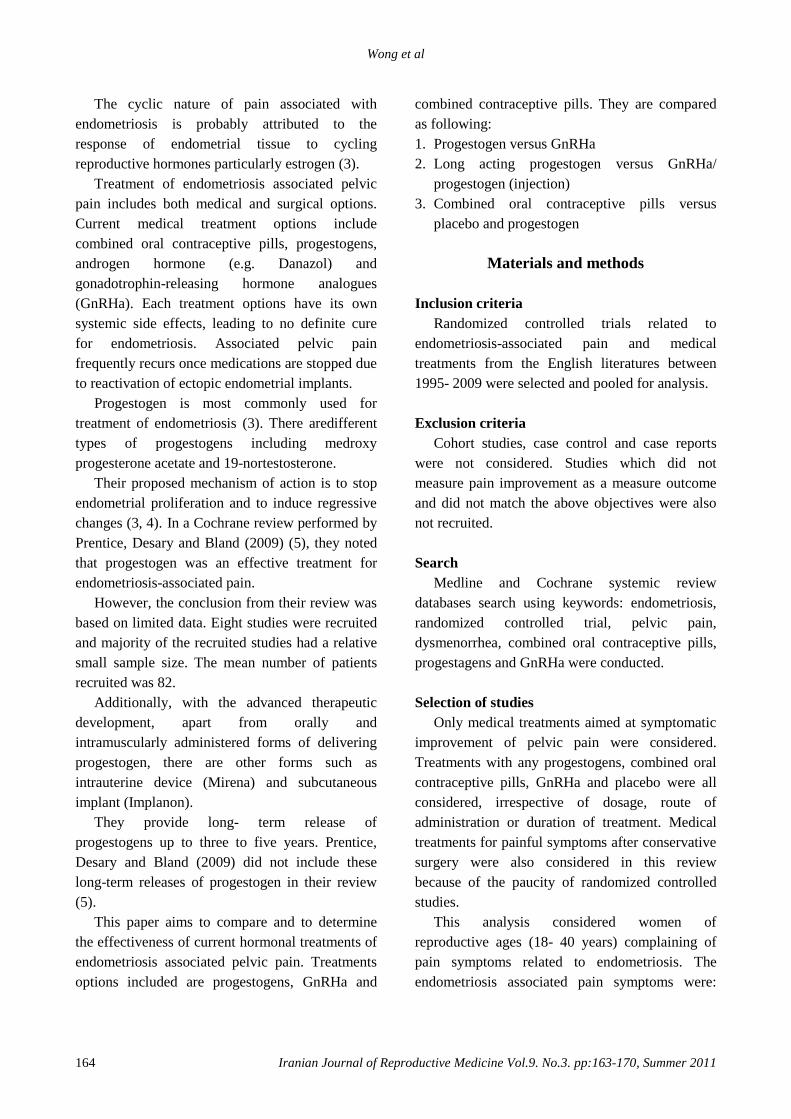
Figure 1: A flow chart demonstrates the identification, recruitment and exclusion of studies.
Figure 2: Progestogen versus GnRHa.
Figure 3: LNG-IUS versus GnRHa and Implanon (etonogestrel)
versus DMPA.
Figure 4: Combined oral contraceptive pills versus placebo versus progestogens.
Discussion
There is a paucity of randomized controlled
trials in relating to endometriosis associated pain
symptoms. Disease staging was not always
uniformly employed in the studies, which limited
the evaluation of the severity of pain against the
effectiveness of medical treatment.
Furthermore, small sample sizes in some
studies (9, 12, 13) limited the ability to draw
definite conclusions. Overall, the results from our
analysis of pooled data from available randomized
controlled studies in the English literature suggest
that progestogens and long acting progestogen
might have slightly better result that GnRHa, but
oral contraceptive pills have a higher level of
efficacy than progestogen.
2 studies were review articles of medical
management of endometriosis
One study is a self-controlled trial
2 studies did not match our comparison objectives
GnRH versus control
GnRH versus Yiweining
550 studies were identified relating to management of pelvic pain in endometriosis
12 studies addressing the keywords search were identified
5 studies were excluded
7 RCTs were recruited for data analysis
Hormones in endometriosis pelvic pain
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 163-170, Summer 2011 169
The seven articles demonstrated a significant
reduction in pain scores after the commencement
of medical treatments. Five articles used Visual
analogue scale (VAS) to measure the severity of
pain pre- and post- treatment. VAS is a widely
used pain assessment tool, which provides a
continuous scale for subjective rating along the
line. The extremes carry a verbal description of
symptoms to be evaluated such as the most severe
pain and no pain. The advantages of using VAS are
time-saving and cross-culture. However, Langley
and Sheppeard (1985) question the validity of VAS
measurements due to its propensity to bias (14).
Firstly, the physical characteristics of the scale
might affect the accuracy of the scale. “No pain” is
influenced by subjective individual pain threshold
and some patients might have difficulties in
distinguishing discomfort and pain. Likewise, “the
most severe pain” is an infinite description. It can
be influenced by personal experience. Also,
patients’ behavior when completing the scale
might lead to bias. They tend to recall memory of
the previous pain scores. This might influence the
accuracy of the pain measurement (14).
One study included in this review used verbal
rating scale (VRS) which consists of a set of
descriptive words. A study comparing VRS and
VAS showed that the pain scores in the middle are
liner-related but not the upper and lower extremes
(15). Thus, there exists an inherent discrepancy in
pain measurements, due to the subjectivity of the
pain experience. Pain is influenced by multiple
factors such as personal belief, culture, past
experience and emotion, it is difficult to assess
pain as a whole. Nevertheless, VRS and VAS are
useful to measure the intensity of pain in short
term despite considerable uncertainty regarding
their long- term use as serial measurements.
Comparisons of progestogens and GnRHa have
been made. Two of the three studies have a
relatively large sample sizes, both proved that
progestoegn is as effective as GnRHa, although
neither treatment appears superior (3, 4). Apart
from looking at short-acting progestogen such as
oral and depot, we have included other long-acting
progestogen in treatment in endometriosis
associated pain. Mirena, the intrauterine device,
releases levonorgestrel directly into the uterine
cavity at a relative constant rate of 20 µg/ day for 5
years. Although its mechanism is still unclear, it
has been speculated that progestogen induced
endometrial atropy leading to amenorrhea (9).
Petta (2005) demonstrated the short term effect (6
months) of Mirena in controlling endometriosis-
associated pain (9). Since the release of
levonorgestrel may slowly reduce in the 5 years of
use, there is no evidence showing the efficacy of
Mirena in controlling endometriosis-associated
pain in long- term. Additionally, the longer the
effect of Mirena in pain control, the more cost-
effective it will be.
Implanon is a single rod etonogestrel-
containing contraceptive implant. It is inserted
subdermally and provides a slow release of
progestogen. It lasts for three years. Efficacy of
Implanon is not inferior to DMPA. A single
insertion of implanon is more convenient than an
injection every 3 months. Both Mirena and
Implanon are long- term treatment options in
women with symptomatic endometriosis who also
require contraception.
Complications and withdrawal of treatments are
other measures to look at the overall effectiveness
of the treatments. In some studies, side effects
were only considered if they were severe enough to
cause withdrawal of the patient. Many patients on
progestogen treatments experienced side effects
such as irregular bleeding, bloating and weight
gain.
Women on GnRHa complained of hot flushes
severe enough to stop treatment. Additionally,
GnRHa causes loss of bone mineral density which
limits its long-term use. Despite high reporting rate
of side effects, there was a relatively low dropout
rate in these studies. This could indicate that the
presence of the side effects could be well tolerated.
It is questionable whether the severity of side
effects significantly increased dropout rates,
impacting an overall effectiveness.
Compliance is always an issue in medical
management. Combined pills and oral
progestogens were taken everyday. The studies did
not measure the rate of compliance. Moreover, it
was often unclear if the recruited patients were
taking alternative medications, which may have a
significant confounding variable affecting
outcomes.
Follow- up is an important factor in monitoring
a chronic disease with high probability of
recurrence. Follow- up data in different studies
were referred to different lengths. Most studies
could not prove effectiveness in long- term
management of endometriosis-associated pain
since it is common to have symptoms recurrence
once the treatment stops. Similar with surgical
intervention, there is always a chance of relapse.
Wong et al
170 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:163-170, Summer 2011
Conclusion
It appears that combined oral contraceptive pills,
GnRHa and progestogens are all effective and well
tolerated by patients in treating endometriosis
associated pain, though side effects have to be
considered. Combined oral contraceptive pills and
progestogens are relatively cheap and more
suitable for long-term use as compared to GnRHa.
Even though both Mirena and Implanon had a role
in controlling endometriosis pain, the conclusion
was drawn from a study with relatively small
sample sizes. Longer term follow up studies of
Mirena and Implanon are required to look at their
long-term effects on endometriosis associated pain.
References 1. Alabama, B. Treatment of pelvic pain associated with
endometriosis. Fertil Steril 2008; 90: 260-269.
2. Vercellini P, Trespidi L, De Giorgo O, Cortesi I,
Parazzini F, Crosignani PG. Endometriosis and pelvic pain:
relation to disease stage and localization. Ferti Steril 1996;
65: 299-304.
3. Crosignani PG, Luciano A, Ray A, Bergqvist A.
Subcutaneous depot medroxy-progesterone acetate versus
leuprolide acetate in the treatment of endometriosis-
associated pain. Hum Reprod 2006; 21: 248-256.
4. Harada T, Momoeda M, Taketani Y, Aso T, Fukunaga M,
Hagino H. et al. Dienogest is as effective as intranasal
buserelin acetate for the relief of pain symptoms
associated with endometriosis-a randomized, double-blind,
multicenter, controlled trial. Fertil Steril 2009; 91: 675-
681.
5. Kives S, Brown J, Prentice A, Deary A, Bland ES.
Progestens and anti-progestagens for pain associated with
endometriosis (review). Cochrane Database of Systematic
Reviews. 2009; Issue 1.
6. MetaAnalyst. Accessed from https://research.tufts-
nemc.org/metaanalyst/index.html Accessed on 19th Sep,
2009.
7. Kjaergard LL, Villumsen J, Gluud C. Reported
methodological quality and discrepancies between large
and small randomized trials in meta- analyses. Ann Intern
Med 2001; 135: 982-989.
8. Harada T, Momoeda M, Taketani Y, Hoshiai H,
Terakawa N. Low-dose oral contraceptive pill for
dysmenorrhea associated with endometriosis: a placebo-
controlled, double-blind, randomized trial. Fertil Steril
2008; 90: 1583-1588.
9. Petta CA, Ferriani RA, Abrao MS, Hassan D, Silva JCR,
Podgaec S, et al. Randomized clinical trial of a
levonorgestrel-releasing intrauterine system and a depot
GnRH analogue for the treatment of chronic pelvic pain in
women with endometriosis. Hum Reprod 2005; 20: 1993-
1998.
10. Sesti F, Pietropolli A, Capozzolo T, Broccolo P, Pierangeli
S, Bollea MR, et al. Hormonal suppression treatment or
dietary therapy versus placebo in the control of painful
symptoms after conservative surgery for endometriosis
stage III-IV. A randomized comparative trial. Fertil Steril
2007; 88: 1541-1547.
11. Walch K, Unfried G, Hubera J, Kurza C, Trotsenburgc
MV, Pernickab E, et al. Implanon® versus
medroxyprogesterone acetate: effects on pain scores in
patients with symptomatic endometriosis- a pilot study.
Contraception 2008; 79: 29-34.
12. Vercellini P, De Giorgo O, Oldani S, Cortesi LA, Panazza
S, Crosignani PG. Depot medroxyprogesterone acetate
versus an oral contraceptive combined with very- low,
dose danazol for long-term treatment of pelvic pain
associated with endometriosis. Am J Obstet Gynecol 1996;
175: 396-401.
13. Walch K., Unfried G, Huber J, Kurz C, Trotsenburg MV,
Pernicka E et al. Implanon versus medroxyprogesterone
acetate: effects on pain scores in patients with
symptomatic endometriosis- a pilot study. Contraception
2009; 79: 29-34.
14. Langley GB, Sheppeard H. The visual analogue scale: Its
use in pain measurement. Rheumatol Int 1985; 5: 145-148.
15. Langley GB, Sheppeard H. Problems associated with pain
measurement: comparison of the visual analogue and
verbal rating scales. Clin Exp Rheumatol 1984; 2: 231-234.

Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 171-176, Summer 2011
GnRH antagonist versus agonist in normoresponders
undergoing ICSI: a randomized clinical trial in Iran Ensieh Tehraninejad M.D., Akram Ghahghaei Nezamabadi M.D., Batool Rashidi M.D., Maryam
Sohrabi M.D., Maryam Bagheri M.Sc., Fedyeh Haghollahi M.Sc., Elham Azimi Nekoo M.D., Mina
Jafarabadi M.D.
Reproductive Health Research Center, Tehran University of Medical Sciences, Tehran, Iran.
Received: 27 April 2010; accepted: 8 March 2011
Abstract
Background: General concern is that the pregnancy rate is higher with GnRH-agonist
as a protocol of pituitary suppression. GnRH-antagonist protocol provides a shorter
period of administration and an easy flexible protocol.
Objective: In this study, the outcomes of GnRH agonist and antagonist in ICSI cycles
are compared in normo responder patients.
Materials and Methods: In this randomized clinical trial, 300 normoresponders
undergoing ICSI were randomly divided to GnRh agonist (n=150) and GnRh antagonist
(n=150) groups. The main outcome measurements were chemical, clinical and ongoing
pregnancy rates (PR).
Results: The mean duration of stimulation were 9.6±1.6 and 8.2±1.6 days in agonist
and antagonist groups respectively (p=0.001). The mean number of MII oocyte
retrieved in agonist and antagonist groups were 7.7±4.0 and 6.9±4.3 respectively
(p=0.03). There was no significant difference between two groups regarding mean
number of gonadotrophin ampoules, follicles, occytes, total embryos and good quality
embryos, OHSS incidence, and abortion rate. Chemical pregnancy rate was 35.3% in
agonist and 39.3% in antagonist group. Clinical pregnancy rate was 35.3% in agonist
and 34% in antagonist group. Ongoing pregnancy rate was 45 (31.3%) in agonist and 44
(29.3%) in antagonist group. There was no significant difference between two groups in
pregnancy rates.
Conclusion: In this study antagonist protocol was shown to be an easy, safe and
friendly protocol in Iranian normoresponder patients, having similar outcomes with
standard agonist protocol but shorter period of stimulation.
Key words: IVF, GnRH agonist, GnRH antagonist, Normoresponder.
Registretion ID in IRCT: IRCT138902283950N1
Introduction
The first in vitro fertilization (IVF) therapy
was performed in a natural cycle. Gonadothropins
are given to induce multiple follicular
development and GnRH analogues are used for the
prevention of premature LH surges in IVF. LH
surges occur in about 20% of stimulated IVF
patients (1). Preventing LH surges using GnRH
analogues improves oocyte yielded with more
Corresponding Author:
Mina Jafarabadi, Reproductive Health Research Center,
Imam Hospital Complex, Keshavarz Blvd., Tehran
14194, Iran.
Email: [email protected]
embryos, allowing better selection and leading to
an increase in pregnancy rate.
GnRH agonist administration causes
gonadotrophin suppression via pituitary
desensitization, after an initial short period of
gonadotrophin hypersecretion. In contrast, GnRH
antagonist accuses immediate and rapid
gonadotrophin suppression by competitive
occupancy of GnRH receptor and therefore is a
choice to use in IVF for the prevention of
premature LH surge (2).
Several potential advantages of antagonists are
suggested over GnRH agonists. Among these
advantages are shorter duration of injectable drug
treatment, decreased gonadotropin requirement per
Tehraninejad et al
172 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:171-176, Summer 2011
cycle, and lower overall treatment cost (3). Although agonist use is accompanied by a series of
disadvantages including hypoestrogenemia, cyst
formation, requirement for a prolonged period of
down-regulation and an increase in FSH and LH in
primary administration, agonist protocol was well
accepted in clinical practice, and general concern is
that the pregnancy rate was higher with agonist
protocol (4, 5).
The recent development of side- effect free
GnRH-antagonist protocol, with immediate
blockage of receptors and shorter period of
administration, provides physicians with an easy
flexible protocol and offers patients a side-effect
free, “friendly” protocol (4). Comparative studies
between GnRH analogues in IVF cycles have
suggested that the duration of stimulation in the
antagonist group was shorter with lower incidence
of OHSS, but in several outcomes the results of
studies remain controversial (6-11).
Several studies are done in different subgroups
of patients to recognize the best protocol of
pituitary suppression (11- 15). The aim of this
study was to compare outcomes of GnRH agonist
and antagonist stimulation protocols and to
evaluate the potential benefits of GnRH antagonist
utilization in ART cycles in normoresponder
Iranian patients. Normo-responder hints the group
of patients with neither decreased ovarian reserve
nor predisposition to hyperstimulation. The study
was approved by ethics committee of Tehran
University of Medical Sciences.
Materials and methods
This randomized clinical trial was conducted at
Vali-e-Asr Reproductive Health Research Center
and Rooyan Institute, Tehran, Iran from January
2008 to January 2010. In total 300 patients
undergoing ICSI cycles with or without ICSI were
evaluated in this study. After obtaining informed
consent, patients were allocated to two groups
according to a sequence of computer generated
random numbers (0 or 1).
A total of 300 women were randomized, 150 in
each group. Inclusion criteria were: age<38 years,
normal basal serum FSH, 20≤ BMI< 30kg/ m2 and
regular menstrual cycle. Exclusion criteria were:
PCOS, severe endometriosis, history of poor
response in previous treatment cycles and history
of repeated IVF failure (more than 3 failed cycles).
The primary outcome measures were fertilization
and pregnancy rates. Additional outcomes of
interest were number of oocytes retrieved, number
of good quality embryos transferred, OHSS
incidence and patient's capacitance.
In the agonist group on cycle day 21,
Busereline acetate (Superfact, Aventis, Germany)
was started as 0.5 mg daily subcutaneous (S.C.)
injection until menstruation had begun and
adequate suppression was achieved (serum
estradiol level <50 pg/ml and no ovarian cystic
structures on ultrasound examination). At day 3 of
next menstrual cycle, the dose of Busereline was
diminished to 0.2 mg and rFSH (Gonal F, Merck
Serono, Switzerland) was started. The starting dose
for the first 5 days varied between 150-225 IU
daily by S.C. injection depending on the age (< or
>35 years) and history of patient. Thereafter,
transvaginal ultrasonography was done every other
day and the dose was adjusted on the basis of
follicle graph using Gonal-F and HMG
(Menoupour, Ferring, USA). Ovulation was
induced with 10000 IU, IM injection of HCG
(Profasi, Serono, Switzerland) when at least 2
follicles 18-20 mm were observed and serum
estradiol was between 1000 and 3000 pg/ml. In
the antagonist group, rFSH treatment was begun on
day 3 of menstrual cycle. The starting dose for the
first 5 days varied between 150-225 IU S.C.
depending on the patient's age and history.
Thereafter transvaginal ultrasonography was done
every other day and the dose was adjusted on the
basis of follicle graph using Gonal-F and HMG.
When there was one follicle 14mm in diameter,
antagonist (Cetrotide, Merck Serono, Germany),
0.25 mg S.C. daily dose was administrated until
the day of HCG administration. The time of
cetrotide injection was adjusted not to be more
than 30 hours apart from HCG administration.
When at least 2 follicles 18-20 mm in diameter
were seen, rFSH and HCG (10000 IU, IM) was
injected. Oocyte retrieval was performed 36h after
HCG administration, by transvaginal sonography
guided puncture of follicles. Two or three embryos
were transferred 72 hours after oocyte retrieval
using Cook catheter (Cook Medical Incorporated,
Bloomington, USA).
In both groups the luteal phase was supported
with vaginal suppository of cycleogest 400
mg/BD. Progesterone treatment was started on the
day of oocyte retrieval and continued until the day
of pregnancy test performed 14 days after the
embryo transfer. In the case of a positive test, this
regiment was continued during the first trimester
of pregnancy. Clinical pregnancy was defined as
the presence of a gestational sac with visible
heartbeat.
Embryos were scored based on the assessment
of the number and distribution of nucleoli
precursor bodies in the pronucleus to have good
and poor morphology (16). The OHSS
GnRH antagonist Vs Agonist
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:171-176, Summer 2011 173
classification utilized in this study was the one
proposed by Golan et al (17).
Statistical analysis:
All analyses were performed using SPSS
(version 16) with a two-sided 5% significance
level.
Results
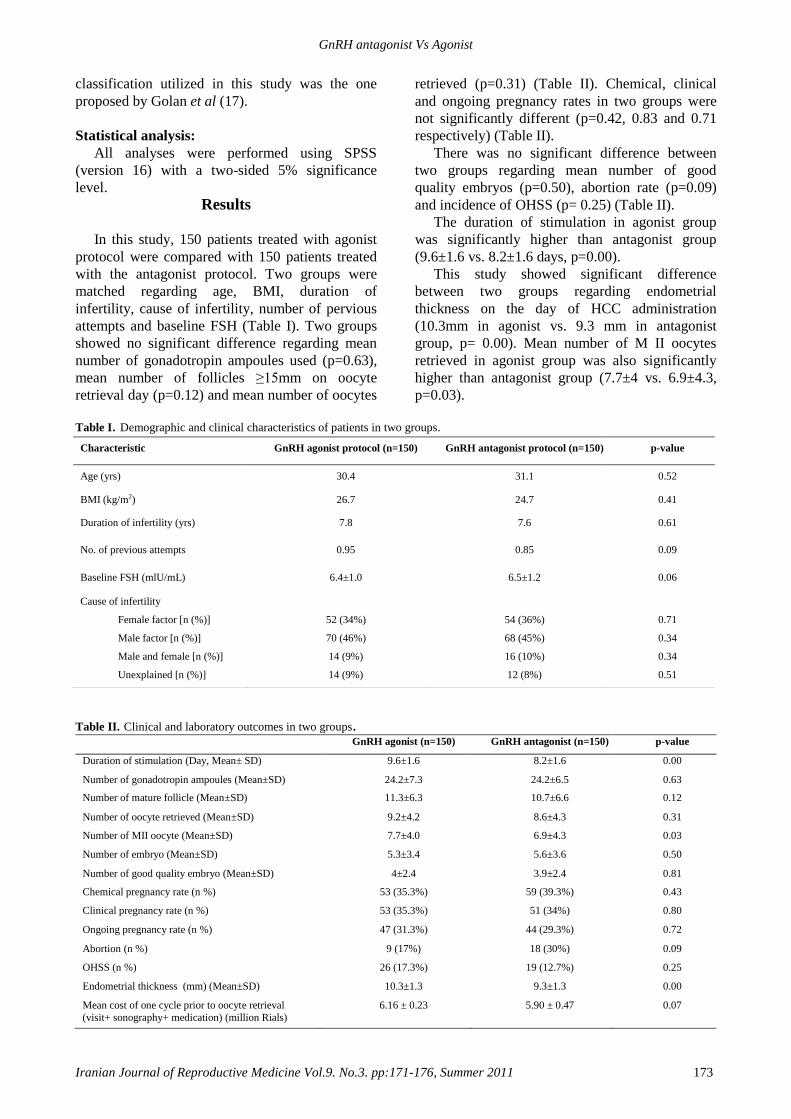
In this study, 150 patients treated with agonist
protocol were compared with 150 patients treated
with the antagonist protocol. Two groups were
matched regarding age, BMI, duration of
infertility, cause of infertility, number of pervious
attempts and baseline FSH (Table I). Two groups
showed no significant difference regarding mean
number of gonadotropin ampoules used (p=0.63),
mean number of follicles ≥15mm on oocyte
retrieval day (p=0.12) and mean number of oocytes
retrieved (p=0.31) (Table II). Chemical, clinical
and ongoing pregnancy rates in two groups were
not significantly different (p=0.42, 0.83 and 0.71
respectively) (Table II).
There was no significant difference between
two groups regarding mean number of good
quality embryos (p=0.50), abortion rate (p=0.09)
and incidence of OHSS (p= 0.25) (Table II).
The duration of stimulation in agonist group
was significantly higher than antagonist group
(9.6±1.6 vs. 8.2±1.6 days, p=0.00).
This study showed significant difference
between two groups regarding endometrial
thickness on the day of HCC administration
(10.3mm in agonist vs. 9.3 mm in antagonist
group, p= 0.00). Mean number of M II oocytes
retrieved in agonist group was also significantly
higher than antagonist group (7.7±4 vs. 6.9±4.3,
p=0.03).
Table I. Demographic and clinical characteristics of patients in two groups.
Table II. Clinical and laboratory outcomes in two groups. GnRH agonist (n=150) GnRH antagonist (n=150) p-value
Duration of stimulation (Day, Mean± SD)
9.6±1.6 8.2±1.6 0.00
Number of gonadotropin ampoules (Mean±SD)
24.2±7.3 24.2±6.5 0.63
Number of mature follicle (Mean±SD)
11.3±6.3 10.7±6.6 0.12
Number of oocyte retrieved (Mean±SD)
9.2±4.2 8.6±4.3 0.31
Number of MII oocyte (Mean±SD)
7.7±4.0 6.9±4.3 0.03
Number of embryo (Mean±SD)
5.3±3.4 5.6±3.6 0.50
Number of good quality embryo (Mean±SD)
4±2.4 3.9±2.4 0.81
Chemical pregnancy rate (n %)
53 (35.3%) 59 (39.3%) 0.43
Clinical pregnancy rate (n %)
53 (35.3%) 51 (34%) 0.80
Ongoing pregnancy rate (n %)
47 (31.3%) 44 (29.3%) 0.72
Abortion (n %)
9 (17%) 18 (30%) 0.09
OHSS (n %)
26 (17.3%) 19 (12.7%) 0.25
Endometrial thickness (mm) (Mean±SD)
10.3±1.3 9.3±1.3 0.00
Mean cost of one cycle prior to oocyte retrieval
(visit+ sonography+ medication) (million Rials)
6.16 ± 0.23 5.90 ± 0.47 0.07
Characteristic GnRH agonist protocol (n=150) GnRH antagonist protocol (n=150) p-value
Age (yrs) 30.4 31.1 0.52
BMI (kg/m2) 26.7 24.7 0.41
Duration of infertility (yrs) 7.8 7.6 0.61
No. of previous attempts 0.95 0.85 0.09
Baseline FSH (mlU/mL) 6.4±1.0 6.5±1.2 0.06
Cause of infertility
Female factor [n (%)]
Male factor [n (%)]
Male and female [n (%)]
Unexplained [n (%)]
52 (34%)
70 (46%)
14 (9%)
14 (9%)
54 (36%)
68 (45%)
16 (10%)
12 (8%)
0.71
0.34
0.34
0.51

Tehraninejad et al
174 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:171-176, Summer 2011
Discussion
In this study the results of GnRH antagonist
multiple doses protocol usage were compared
versus long protocol of GnRH agonist in ICSI
cycles in Iranian normoresponder patients.
Apart from significantly higher number of MII
oocyte in agonist group and shorter duration of
stimulation in antagonist group in our study there
was no difference in the number of follicles, total
retrieved oocytes, total embryos, good quality
embryos and mean cost of one cycle prior to
oocyte retrieval between two groups and as the
main outcome measurement the rates of chemical,
clinical and ongoing pregnancy were similar in two
groups.
Despite the result of some studies confirming
our results (9, 17-21), in meta-analysis of 5 RCTs
Aboulghar and Al-Inany reported that clinical
pregnancy rate was 5% lower in antagonist
protocol (5). In present study, the mean duration of
stimulation days was significantly longer in agonist
group. Many studies are in accordance with it
(Greco et al: 11.1±0.3 vs. 12.2±0.4, Kumbak et al:
11.7±1.2 vs. 12.9±1.6 and Xavier et al: 9.5±1.7 vs.
10.6±2.1) (17, 21, 22).
In present study, the mean dose of gonadotropin
used in two protocols had no significant difference
and this was similar to the result of the studies of
Berger (19), Xavier (18), Kumback (23) and
Kolibiakis meta-analysis (24). Although some
other researches reported the total dose of
gonadotrophin used in the agonist protocol was
significantly higher than antagonist protocol (10,
22). No sever OHSS occurred in either group
during our study and the incidence of mild OHSS
was higher in agonist protocol but this was not
statistically significant. We excluded PCOS
patients from the study and this can be interpreted
as the cause of absence of severs OHSS in our
study.
Using antagonist protocol for preventing OHSS
especially in PCOS patients is proved in several
studies (12-15). In present study the rate of
abortion was higher in antagonist group but this
was not statistically significant (p=0.09). Bahceci
et al, 2009, reported that the rate of early
pregnancy loss (EPL) was higher in antagonist
protocol (26).
The endometrial thickness in the antagonist
protocol was lower than agonist in the day of hCG
administration (10.3 mm vs. 9.3mm, p=0.00) in our
study. Xavier et al reported that there wasn’t any
significant difference between 2 protocols in this
variable (18) but Orveito et al reported that
endometrial receptivity and endometrial thickness
was higher in the agonist protocol (27).
GnRH antagonist molecules are potent
inhibitors of cell cycle, decreasing the synthesis of
locally produced growth factors. They can exhibit
this activity in all tissues presenting GnRH
receptors and consequently influence blastomere
formation, endometrium development and
fulliculogenesis and oocyte maturation (22). This
can explain the lower number of MII occyte and
lower endometrial thickness in antagonist protocol
and may reflect the cause of slight (but not
significant) increase in abortion rate in antagonist
group in present study.
The results of this study show that these two
protocols are very similar in outcomes in
normoresponder patients. Immediate mode of
action, flexibility of use, shorter duration of
administration, shorter duration of FSH
stimulation, and a lower incidence of hospital
admission due to sever OHSS make the antagonist
protocol an excellent approach for ovarian
stimulation in IVF. There was no significant
difference in the rate of live birth in GnRH
antagonist protocol comparing with agonist in the
study accomplished by Kolibinakis and Tarletzis in
2006 (24). Literature suggests that the side effect,
physiologic and psychological distress and
treatment burden is lower in antagonist protocol
(28), though these points were not concerned in
present study and is proposed to be evaluated in
further studies in Iranian patients.
On the basis of the results of this RCT on
Iranian normoresponder women, we offer using the
“GnRH Antagonist” as a patient friendly protocol
for the first choice in ART cycle with lower
incidence of side effects, similar pregnancy rate
and cost and time saving.
Acknowledgment
The authors wish to thank all academic
members and staff at the Vali-e-Asr Reproductive
Health Research Center for their sincere
cooperation.
References
1. Huirne JA, Homburg R, Lambalk CB. Are GnRH
antagonist comparable to agonists for use in IVF? Hum
Reprod 2007; 22: 2805-2813.
2. Loumaye E. The control of endogenous secretion of LH
by gonadotrophin-releasing hormone agonists during
GnRH antagonist Vs Agonist
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:171-176, Summer 2011 175
ovarian hyperstimulation for invitro fertilization and
embryo transfer. Hum Reprod 1990; 5: 357-376.
3. Shapiro DB, Mitchell-Leef D. GnRH antagonist in in vitro
fertilization: where we are now. Minerva Ginecol 2003;
55: 373-388.
4. Tarlatzis BC, Kolibianakis EM. GnRH agonists vs
antagonists. Best Pract Res Clin Obstet Gynaecol 2007;
21: 57-65.
5. Al- Inany H, Aboulghar M. Gonadotophin-releasing
Hormone antagonists in assisted conception: a Cochrane
review. Hum Reprod 2002; 17: 874-885.
6. Al-Inany HG, Abou-Setta AM, Aboulghar M.
Gonadotophin-releasing Hormone antagonists for assisted
conception: a Cochrane review. Reprod Biomed Online
2007; 14: 640-649.
7. Griesinger G, Felberbaum R, Diedrich K. GnRH
antagonists in ovarian stimulation: a treatment regimen of
clinicians’ second choice?data from the German National
IVF Registry. Hum Reprod 2005; 20: 2373-2375.
8. Fauser BC, Devroey P. Why is the clinical acceptance of
gonadrotropin- releasing hormone antagonist cotreatment
during ovarian hyperstimulation for in vitro fertilization so
slow? Fertil Steril 2005; 83: 1607-1611.
9. Ludwig M, Katalinic A, Diedrich K. Use of GnRH
antagonists in ovarian stimulation for assisted reproductive
technologies compared to the long protocol, Metal-
analysis. Arch Gynecol Obstet 2001; 265: 175-182.
10. Orvieto R, Rabinson J, Meltzer S, Homburg R, Anteby E,
Zohav E. GnRH anonist versus GnRH antagonist in
ovarian stimulation: is the emperor naked? Clin Exp
Obstet Gynecol 2006; 33: 197-199.
11. Engel J, Griesinger G, Schultze-Mosgau A, Flberbaum R,
Dedrich K. GnRH agonists and antagonists in assisted
reproduction: pregnancy rate. Reprod Biomed Online
2006; 13: 84-87.
12. Albano C, Felberbaum RE, Smitz J, Riethmüller-Winzen
H, Engel J, Diedrich K, et al. Ovarian Stimulation with
HMG, result of a prospective randomized phase III
European Study Comparing the LHRH antagonist
Cetrorelix and the LHRH agonist busereline. Hum Reprod
2000; 15: 526-531.
13. Olivennes F, Belaisch-Allart J, Emperaire JC, Dechaud H,
Alvarez S, Moreau L, et al. Prospective, randomized
controlled study of invitro fertilization- embryo transfer
with a single dose of a luteinizing hormone- releasing
hormone (LH-RH) antagonist (cetrorelix) or a depot
formula of an LH-RH agonist (triptorelin). Fertil Steril
2000; 73: 314-320.
14. Raga F, Casan EM, Dubon MD, Marti R, Bonilla-Musoles
F, Polan ML. Modulation of vascular endothelial growth
factor by GnRH analogues: potential use in clinical
management of ovarian hyperstimulation syndrome. Hum
Reprod 2002; 17 (Suppl. 1): 14.
15. Ragni G, Vegetti W, Riccaboni A, Engl B, Brigante C,
Crosignani PG. Comparison of GnRH agonists and
antagonists in assisted reproduction cycles of patients at
high risk of ovarian hyperstimulation syndrome. Hum
Reprod 2005; 20: 2421-2425.
16. Tesarik J, Greco E. The probability of abnormal
preimplantation development can be predicted by a single
static observation of pronuclear stage morphology. Hum
Reprod 1999; 14: 1318-1323.
17. Golan A, Ron-et R, Herman A, Soffer Y, Weinraub Z,
Caspi E. Ovarian hyperstimulation syndrome: an update
review. Obstet Gynecol Surv 1989; 44: 430-440.
18. Xavier P, Gamboa C, Calejo L, Silva J, Stevenson D,
Nunes S, et al. A randomized study of GnRH antagonist
(cetrorelix) versus agonist (buserreline) for controlled
ovarian stimulation: effect on safety and efficacy. Eur J
Obstet Gynecol Reprod Biol 2005; 120: 185-189.
19. Berger BM, Ezcurra D, Alper M. Gonadotropin releasing
Hormone (GnRH) antagonist (cetrorelix) versus matched
study in young normal responders. Fertil Steril 2004; 82:
235-236.
20. Chen SL, Yin MN, Sun L, Li H, Chen X, Song HD, et al.
Clinical application of gonadotropin- releasing hormone
antagonist in Chinese women undergoing controlled
ovarian hyperstimulation for invitro fertilization and
embryo transfer. Nan Fang Yi Ke Da Xue Xue Bao 2007;
27: 588-590.
21. Daya S. A comparison of clinical pregnancy rates in the
efficacy evaluation of GnRH agonist versus antagonist use
for assisted reproduction- a meta-analysis using an
intention to treat approach. Gynecol Endocrinol 2003; 17:
44.
22. Greco E, Litwicka K, Ferrero S, Baroni E, Sapienza F,
Rienzi L, et al. GnRH antagonists in ovarian stimulation
for ICSI with oocyte restriction: a matched, controlled
study. Reprod Biomed Online 2007; 14: 572-578.
23. Kumbak B, Kahraman S, Karlikaya G, Lacin S, Guney A,
Ozturk E. GnRH agonist long versus antagonist protocols
for the ovarian stimulation of a normoresponder patient
group. Fertil Steril 2006; 86: 434.
24. Kolibianakis E.M, Collins J, Tarlatzis BC, Devroy P,
Diedrich K ,Grisesinger G. Among patients treated for
IVF with gonadodotropins and GnRH agnaogues, is the
probability of live birth dependent on the type analogue
used? A systemic review and meta-analysis. Hum Reprod
Update 2006; 12: 651-671.
25. Loutradis D, Stefanidis K, Drakakis P, Milingos S,
Antsaklis A, Michalas S. A modified gonadotropin-
releasing hormone (GnRH) antagonist protocol failed to
increase clinical pregnancy rates in comparison with the
long GnRH protocol. Fertil Steril 2004; 82: 1446- 1448.
26. Bahceci M, Vlug V, Sismaugolu A, Tosun S, Cengiz B.
Early pregnancy loss rate were different among singleton
gestations conceived by ICSI using GnRH agonist and
antagonist. J Asist Reprod Genet 2009; 26: 227-299.
27. Orvieto R, Meltzer S, Rabinson J, Zohav E, Anteby EY,
Nahum R. GnRH agonist versus GnRH antagonist in
ovarian stimulation: the role of endometrial receptivity.
Fertil Steril 2008; 90: 1294-1296.

Tehraninejad et al
176 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:171-176, Summer 2011
28. Devroey P, Aboulghar M, Garcia-velasco J, Griesinger G, Humaidan P, Kolibianakis E, et al. Improving the patient’s
experience of IVF-ICSI: a proposal for an ovarian
stimulation protocol with GnRH antagonist Co-treatment.
Hum Reprod 2009; 24: 764-774.

Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 177-186, Summer 2011
Effect of benzene extract of Ocimum sanctum leaves on
cauda epididymal spermatozoa of rats Mukhtar Ahmed
1,3 Ph.D., R. Nazeer Ahamed
1 Ph.D., Ravindranath H Aladakatti
1,2 Ph.D., Mukhtar
Ahmed G Ghodesawar1,4
Ph.D.
1 Department of Post-Graduate Studies and Research in Zoology, Karnatak University, Dharwad-580003,
India.
2 Central Animal Facility, Indian Institute of Science, Bangalore-560012, India.
3 Research Centre, Electron Microscope Unit, College of Science, King Saud University, Post Box 2455,
Riyadh 11451, Kingdom of Saudi Arabia.
4 Department of Zoology, Anjuman Arts, Sciences and Commerce College, Bijapur-586101, India.
Received: 9 December 2009; accepted: 23 May 2010 Abstract
Background: Recent studies have shown that benzene extract of Ocimum sanctum (O.
sanctum) leaves induces the ultrastructural changes in the epithelial cells of the cauda
epididymis, its subsequent recovery in the seminiferous epithelium and fertility of male
albino rats.
Objective: Our aim was to investigate the effect of benzene extract of O.sanctum leaves
on the cauda epididymal sperm parameters, morphology and their organelles at the
ultrastructural level in albino rats.
Materials and Methods: Wistar male rats (n=20) were allocated into two groups of
control (n=10) and test group (n=10). The test group received benzene extract of
O.sanctum leaves (250mg/kg/day) for 48 consequence days. Five animals from each
group were used for fertility test. Twenty-four hours after the last dose, the rest of the
control (n=5) and treated (n=5) animals were sacrificed by cervical dislocation and then
the cauda epididymal plasma was used for sperm analysis, scanning electron
microscopy (SEM) and transmission electron microscopic (TEM) studies.
Results: Sperm analysis of test group exhibited significant (p≤0.001) decrease in the
sperm count, motility, speed and increase in sperm anomalies when compare to control
group. SEM and TEM observation in treated animals indicated the morphological
changes in plasma membrane as well as in the acrosomal membrane of spermatozoa,
formation of a balloon-like cytoplasmic droplet in the mid-region of abnormal tail and
disorganization or degeneration of mitochondria of sperm mitochondrial sheaths.
Conclusion: The effects observed in this study may have resulted from a general
alteration in the cauda epididymal milieu, probably due to androgen deficiency
consequent to the anti-androgenic property of O.sanctum leaves.
Key words: Ocimum sanctum, Epididymis, Spermatozoa, Fertility, Electron microscope, Rats.
Introduction
Fertility control is an issue of global and
national public health concern. Through increased
public awareness, statements supporting research
Corresponding Author: Ravindranath H Aladakatti, Central Animal Facility,
Indian Institute of Sciences, Bangalore- 560012,
Karnataka, India.
Email: [email protected]
on male methods and greater involvements of men
reproductive health have been forthcoming from
several quarters, including international women's
organizations. The clinical and scientific basis for
the research has been reviewed in recent years.
Apart from research for finding harmless chemical
drugs as effective oral contraceptives in the
western countries, the crude vegetal drugs used by
tribal people are being closely looked into for
their possible efficiency to find out safe and

Ahmed et al
178 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 177-186, Summer 2011
effective oral drugs for controlling human
fertility. Many of the plants which are common in
India are reported to possess antifertility activity
as spermicidal, abortifacient or antiandrogenic in
nature (1-7). Therefore, it has become necessary
to use biologically active botanical substances or
fertility-regulating agents of plant origin which
are ecofriendly in approach and interfere with the
natural patterns of reproduction (8).
The plants of genus Ocimum belonging to
family Labiatae are very important for their
unique properties. Ocimum sanctum L. (Tulsi),
Ocimum gratissium (Ram Tulsi), Ocimum canum
(Dulal Tulsi), Ocimum basilicum (Ban Tulsi),
Ocimum kilimandscharicum, Ocimum
ammericanum, Ocimum camphora and Ocimum
micranthum are examples of known important
species of genus Ocimum which grow in different
parts of the world and are known to have
medicinal properties (9-11). Ocimum sanctum is, a
small herb seen throughout India, commonly
cultivated in gardens. In traditional systems of
medicine, different parts (leaves, stem, flower,
root, seeds and even whole plant) of Ocimum
sanctum, have been recommended for the
treatment of bronchitis, bronchial asthma, malaria,
diarrhea, dysentery, skin diseases, arthritis,
painful eye diseases, chronic fever, insect bite etc.
The Ocimum sanctum L. has also been suggested
to possess antifertility, anticancer, antidiabetic,
antifungal, antimicrobial, hepatoprotective,
cardioprotective, antiemetic, antispasmodic,
analgesic, adaptogenic and diaphoretic actions.
In addition, the leaves of O. sanctum
significantly altered the sperm count, motility,
velocity and fructose contained in the cauda
epididymis (12), reduce the mating behaviour of
both male and female albino rats (13-15). Recent
studies shown that benzene extract of Ocimum
sanctum leaves induces the ultrastructural changes
in the epithelial cells of the cauda epididymis, its
subsequent recovery, after withdrawal of
treatment, in the process of spermatogenesis and
fertility of male albino rats (16,17) and
morphological changes in the rat cauda
epididymal sperms upon graded dose treatment
(18).
As there is little information concerning the
influence of O. sanctum leaves on the cauda
epididymal sperm at the ultrastructural level, the
present investigation is designed to study whether
benzene extract of O.sanctum leaves could cause
some of the sperm parameters, morphological
alterations in cauda epididymal spermatozoa and
its organelles by electron microscopic studies and
fertility of male of albino rats as this medicinal
plant has anti-spermatogenic and anti-androgenic
like properties (12-15).
Materials and methods
Preparation of test material
Fresh O.sanctum leaves were collected and
dried in shade. A voucher specimen
(Zoo/herb/File No.47-Acc.No.22) was deposited
at Zoology Department, Karnatak University,
Dharwad, India. The dried leaves were coarsely
powdered and subjected to soxheltation process to
get the benzene extract. Extract thus obtained was
allowed to dry and stored in a dessicator at 4ºC.
The benzene extract is then mixed with propylene
glycol as required and administered orally
(gavage) to the experimental animals (19).
Experimental Animals
Colony bred healthy adult male albino rats
(Wistar strain) weighing 190-200g were utilized
for experiments. All animals were proven fertility
and obtained from the rat colony maintained in the
department. They were housed at a temperature of
262oC and exposed to 13-14 h of daylight and
maintained on a standard rat pellet diet (Gold
Mohar, Hindustan Level Ltd., Hyderabad) and
water was given ad libitum. The animals were
acclimatized to the laboratory conditions before
conducting experiments and the care of the
laboratory animals was taken as per the
Committee for the Purpose of Control and
Supervision on Experiments on Animals
(CPCSEA) regulations.
Study protocol
The control group (n=10) were administered 1
ml propylene glycol/rat/day orally for 48 days and
test group (n=10), that received benzene extract of
Ocimum sanctum leaves (250mg/kg/day) orally
for 48 consequence days. The effective dose of
250mg/kg body weight has been arrived at after
preliminary studies on dose and duration of 48
days is concerned to the spermatogenic cycle of
rat in response studies in our laboratory and
reported (12).
Five animals from each group were used for
fertility test. Twenty-four hours after the last dose,
rest of the control (n=5) and treated (n=5) animals
were sacrificed by cervical dislocation and then
the cauda epididymal plasma was used for sperm
analysis, scanning and transmission electron
microscopic studies.
Effect of benzene extract of O. sanctum leaves on cauda epididymal spermatozoa
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 177-186, Summer 2011 179
Sperm analysis
The cauda epididymis was chopped into
phosphate buffered glucose saline (PBGS)
[composition: NaCl 50 mM/l; Na2HPO4 200
mM/l; glucose 200 mM/l and KH2PO4 26 mM/l].
The debris was removed and a clear suspension,
the epididymal plasma was used for the analysis
of total sperm count, sperm motility, forward
velocity and relative percentage of abnormal
sperms in male albino rats. The total sperm count
and motility were calculated according to the
method of Besley et al (20) using Neubauer’s
haemocytometer. Briefly, to increase the accuracy
of sperm count, the epididymal plasma was
diluted with a spermicidal solution, prepared by
dissolving 5 g of sodium bicarbonate (NaHCO3)
and 1 ml of 40% formaldehyde in 100 ml of
normal saline.
A twenty times dilution was made using
W.B.C pipette, which was thoroughly mixed and
one drop was added to both sides of Neubauer
haemocytometer. The spermatozoa were allowed
to settle down in the haemocytometer by keeping
them in a humid chamber for one hour. The sperm
count was done in R.B.C counting 5 major
squares. The total number of sperms were counted
in all the major squares and calculated as follows.
Total number of sperms per square (x)
Total number of sperms = ______ __________ × dilution
/ml plasma Total volume per factor (20) square (10-4)
Similarly the total number of motile sperms
was calculated, using phosphate buffer saline
instead of spermicidal solution. The forward
velocity of the sperm was calculated according to
the method of Ratnasoorya (21). Briefly, the
epididymal plasma was suspended in phosphate
buffer saline, cleared the tissue debris and a clear
solution was used for the assessment of average
forward velocity of sperms. The assessment was
made under light microscope, fitted with a
movable mechanical stage and a calibrated ocular
micrometer, at 400 X magnification. A drop of
sperm suspension was transferred to a clean glass
slide and the initial place and time of each sperm
was recorded. The time taken for forward
movement of sperm from the initial place within
microscopic field was recorded using a stop
watch. The procedure was repeated for 10
spermatozoa in each sample and the average
forward velocity of sperm was calculated and
expressed as m/sec. The relative proportion of
abnormal sperms was analyzed according to the
method of Bauer et al (22). Briefly, equal volume
of cauda epididymal plasma and 5% NaHCO3
were taken in a centrifuge tube, mixed well and
centrifuged for 5 minutes at 4000g. The
supernatant was discarded and 5 ml of normal
saline was added to the precipitate, mixed well
and centrifuged again. The procedure was
repeated 2 to 3 times and a clear precipitate was
obtained. To the final precipitate few drops of
normal saline were added, mixed thoroughly and a
smear was prepared on a clean slide. The smear
was dried at room temperature, fixed by heating it
over the flame for two to three seconds. Then the
smear was flushed with 95% alcohol, drained and
dried. It was stained in Ziehl Neelson's Carbol
Fuchsin diluted with equal volume of 95% alcohol
for 3 minutes and counter stained with 1:3 (v/v)
aqueous solution of Loeffer's methylene blue for 2
minutes. After staining, the smear was rinsed in
water and dried in air. The abnormal sperms
included categories like double tailed, detached
head, detached tail, mid piece bending and
irregular head. The relative proportion of the
normal and abnormal sperms was from the smear
and expressed in terms of percentage.
Preparation of spermatozoa for SEM study
Preparation of rat spermatozoa for SEM
studies was performed as described elsewhere
(23). Briefly, a drop of cauda epididymal plasma
was fixed in 2% glutaraldehyde, centrifuged and
washed with 0.1 M Sodium cacodylate buffer
(pH=7.2), centrifuged again in distilled water till
the buffer solution was washed out and a thin film
was applied on a cover slip, dried, sputter coated
with gold and finally observed under scanning
electron microscope (Model. LEO 435 VP
Detector SL.1. LEO Electron Microscopy ltd
Cambridge, England).
Preparation of cauda epididymal spermatozoa
for TEM study
Preparation of rat spermatozoa for TEM
studies was performed as described elsewhere (3).
Briefly, the epididymis was removed, rapidly
fixed in 3% glutaraldehyde in phosphate buffer
(pH=7.4; 0.1 M) for 4 hr at 4°C, washed in
phosphate buffer and post-fixed in 1% osmium
tetraoxide in phosphate buffer (pH=7.4; 0.1M) for
6 hr. The fixed epididymis was washed several
times in distilled water, stained en bloc in 2%

Ahmed et al
180 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 177-186, Summer 2011
aqueous uranyl acetate for 6 hr, dehydrated in
acetone series, infiltered in epon-araldite mixture
for 10 hr and embedded in the same media in a
beam capsule. The blocks were cut in LKB
Bromma ultramicrotome. Semithin sections of 1
µm thickness were stained with toludine blue for
identification of stages. Ultrathin sections were
cut at 100-300 A, mounted on copper grids and
stained with 1% aqueous uranyl acetate and lead
citrate (24). The stained sections were scanned in
Jeol-TEM 100 C X II electron microscope for
ultrastructural observations.
Fertility test
To assess the fertility rate with reference to the
number of implantations, the female rats of
proven fertility exhibiting regular estrous or early
proestrus stage were separately housed with the
control and treated males overnight. The
appearance of sperm in the vaginal smear next
morning confirmed the mating and is considered
as day1 of the pregnancy. After 8 days, the
females were laparotomized and the numbers of
implantations and pups were recorded.
Statistical analysis
The data were statistically analysed and
expressed as Mean± Standard error (25). The
comparison of data for statistically significant
differences was done using student's t-test and a
probability level of p≤0.001 was considered as
significant.
Results
Sperm analysis
Analysis of sperm parameters, such as total
sperm count, total number of motile sperm,
forward velocity of the sperm and percentage of
abnormal sperm of the cauda of epididymal
plasma were carried out in the control and all the
treated animals. The control rats showed
56.40×104
total numbers of sperm/ml epididymal
fluid, 52.40×104 numbers of motile sperm/ml
epididymal fluid with a speed of 127.63 m/sec
and 11.40% of abnormal sperm were recorded.
Whereas in the 250 mg/kg body weight of
benzene extract treated animals showed a highly
significant decrease (p≤0.001) in total sperm
count (56%), total number of motile sperm (45%),
forward velocity of sperm (49%) and a highly
significant increase (p≤0.001) in the percentage of
abnormal sperm (544%) when compared to
control animals (Table I).
Scanning electron microscopic (SEM)
observations of rat sperms from cauda
epididymal plasma
SEM observations of the cauda epididymal
sperms of control rats showed normal parts
(Figure 1A). Perforatorium and acrosome are
covered with the plasma membrane. A distinguish
acrosome is covered with acrosomal membrane.
The whole spermatozoon is intact with all the
membranes and organelles. However, in 250
mg/kg body weight of benzene extract, treated
animals showed disturbance in the plasma
membrane as well as in the acrosomal membrane
in the most of sperm heads. It is rather difficult to
differentiate the acrosomal membrane as well as
the plasma membrane. Serrations in the head
region of the spermatozoa are observed. The
shape and size of the sperm head has also changed
considerably.
There was acute dorsoventrally constriction in
the mid-head region of most sperms. The
perforatorium (Sub acrosomal material) is
bulged/swelled (Figure 1B). Most of the
spermatozoa showed a splitting of the tail and
distinct visibility of balloon-like cytoplasmic
droplets in the mid-region of the tail (Figure 1C).
Transmission electron microscopic (TEM)
observations of Cauda epididymal
spermatozoa
Observations with the TEM revealed that
different parts of the cauda epididymal sperm of
control rats exhibited normal features (Figure 2D-
G).Where as in the animals treated with 250mg/kg
body weight of benzene leaf extract, the sperm
heads exhibited disrupted plasma membrane,
acrosomal membrane and surface coating with
fuzzy material. The tip of the sperm head showed
disruption of the plasma membrane and acrosome.
The perforatorium was condensed and most of
its surface was covered by a thin portion of
acrosomal sac. The anterior and caudal portion of
the sperm heads revealed disruption or loss of
plasma membrane, acrosome, perforatorium and
small vesicles on the ventral surface of the
perforatorium, which is probably part of the
acrosomal system. Most of caudal portion of the
sperm head revealed the disturbance of lamellar
body and centrioles. The basal plate, posterior
ring and post-nuclear cap appeared normal (Figure
3H and I).
The middle part showed disruption and
degeneration of the mitochondrial sheath and a
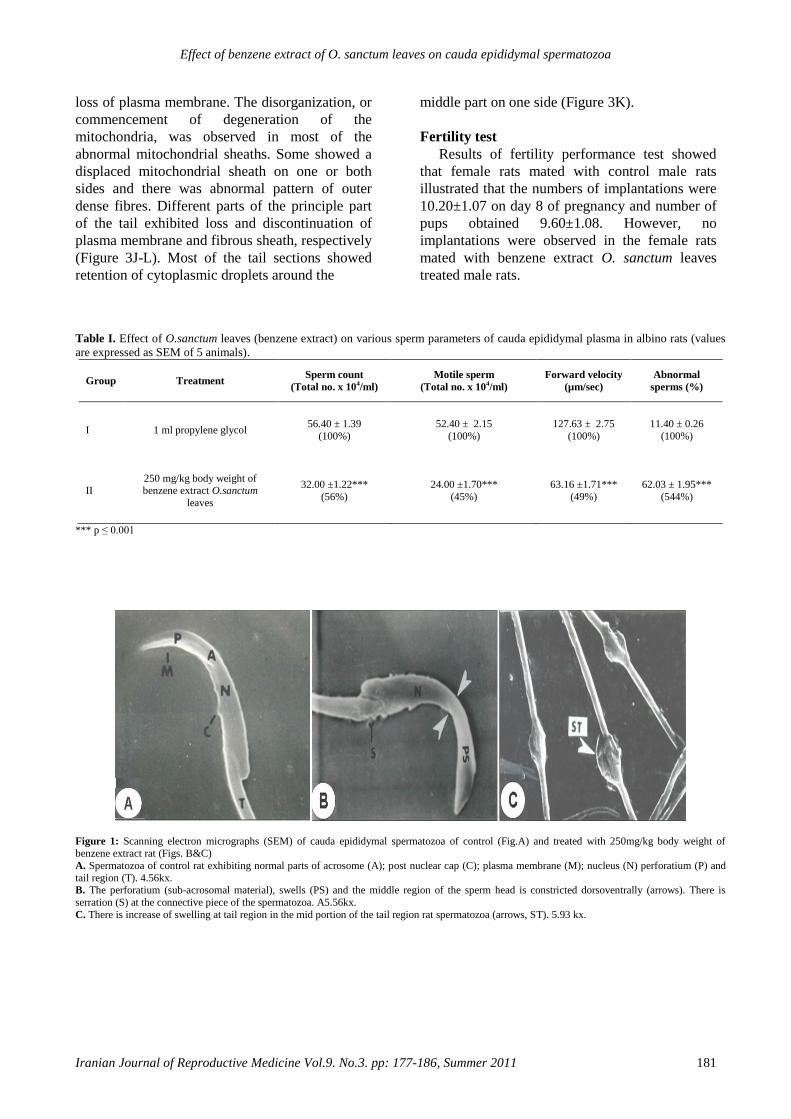
Effect of benzene extract of O. sanctum leaves on cauda epididymal spermatozoa
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 177-186, Summer 2011 181
loss of plasma membrane. The disorganization, or
commencement of degeneration of the
mitochondria, was observed in most of the
abnormal mitochondrial sheaths. Some showed a
displaced mitochondrial sheath on one or both
sides and there was abnormal pattern of outer
dense fibres. Different parts of the principle part
of the tail exhibited loss and discontinuation of
plasma membrane and fibrous sheath, respectively
(Figure 3J-L). Most of the tail sections showed
retention of cytoplasmic droplets around the
middle part on one side (Figure 3K).
Fertility test
Results of fertility performance test showed
that female rats mated with control male rats
illustrated that the numbers of implantations were
10.20±1.07 on day 8 of pregnancy and number of
pups obtained 9.60±1.08. However, no
implantations were observed in the female rats
mated with benzene extract O. sanctum leaves
treated male rats.
Table I. Effect of O.sanctum leaves (benzene extract) on various sperm parameters of cauda epididymal plasma in albino rats (values
are expressed as SEM of 5 animals).
Group Treatment Sperm count
(Total no. x 104/ml)
Motile sperm
(Total no. x 104/ml)
Forward velocity
(µm/sec)
Abnormal
sperms (%)
I 1 ml propylene glycol 56.40 ± 1.39
(100%)
52.40 ± 2.15
(100%)
127.63 ± 2.75
(100%)
11.40 ± 0.26
(100%)
II 250 mg/kg body weight of benzene extract O.sanctum
leaves
32.00 ±1.22***
(56%)
24.00 ±1.70***
(45%)
63.16 ±1.71***
(49%)
62.03 ± 1.95***
(544%)
*** p ≤ 0.001
Figure 1: Scanning electron micrographs (SEM) of cauda epididymal spermatozoa of control (Fig.A) and treated with 250mg/kg body weight of
benzene extract rat (Figs. B&C)
A. Spermatozoa of control rat exhibiting normal parts of acrosome (A); post nuclear cap (C); plasma membrane (M); nucleus (N) perforatium (P) and
tail region (T). 4.56kx. B. The perforatium (sub-acrosomal material), swells (PS) and the middle region of the sperm head is constricted dorsoventrally (arrows). There is
serration (S) at the connective piece of the spermatozoa. A5.56kx.
C. There is increase of swelling at tail region in the mid portion of the tail region rat spermatozoa (arrows, ST). 5.93 kx.
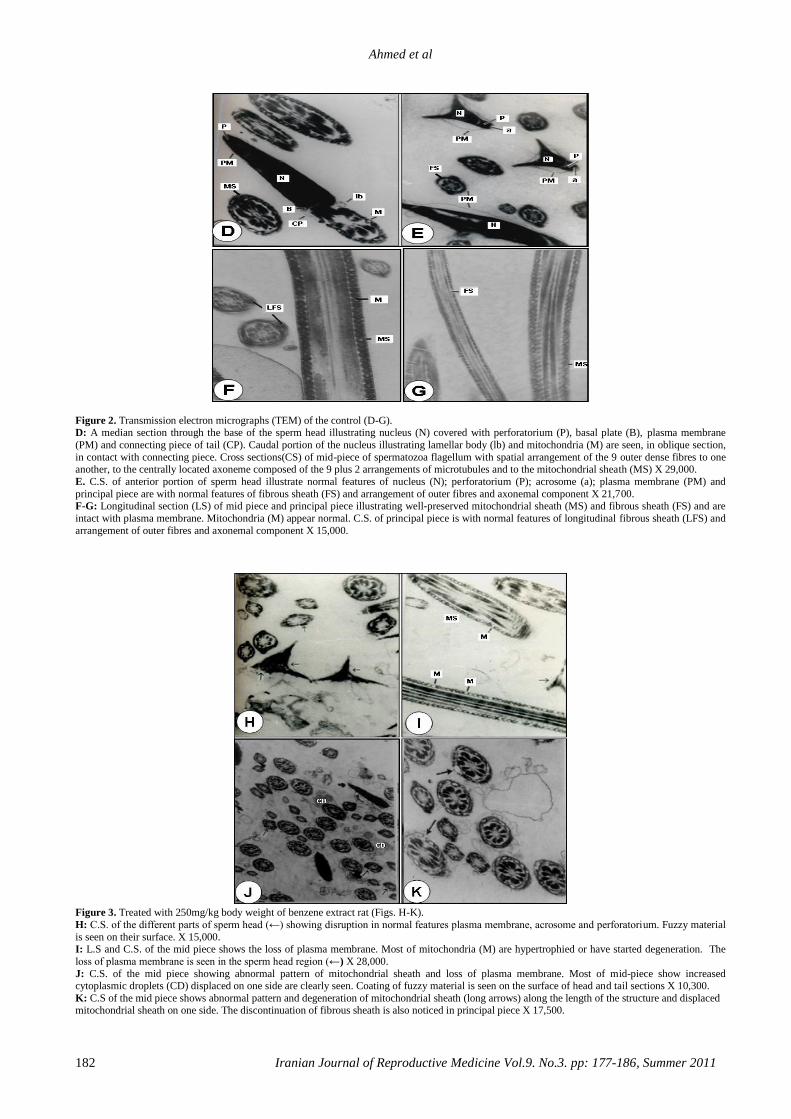
Ahmed et al
182 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 177-186, Summer 2011
Figure 2. Transmission electron micrographs (TEM) of the control (D-G). D: A median section through the base of the sperm head illustrating nucleus (N) covered with perforatorium (P), basal plate (B), plasma membrane
(PM) and connecting piece of tail (CP). Caudal portion of the nucleus illustrating lamellar body (lb) and mitochondria (M) are seen, in oblique section,
in contact with connecting piece. Cross sections(CS) of mid-piece of spermatozoa flagellum with spatial arrangement of the 9 outer dense fibres to one another, to the centrally located axoneme composed of the 9 plus 2 arrangements of microtubules and to the mitochondrial sheath (MS) X 29,000.
E. C.S. of anterior portion of sperm head illustrate normal features of nucleus (N); perforatorium (P); acrosome (a); plasma membrane (PM) and
principal piece are with normal features of fibrous sheath (FS) and arrangement of outer fibres and axonemal component X 21,700. F-G: Longitudinal section (LS) of mid piece and principal piece illustrating well-preserved mitochondrial sheath (MS) and fibrous sheath (FS) and are
intact with plasma membrane. Mitochondria (M) appear normal. C.S. of principal piece is with normal features of longitudinal fibrous sheath (LFS) and
arrangement of outer fibres and axonemal component X 15,000.
Figure 3. Treated with 250mg/kg body weight of benzene extract rat (Figs. H-K).
H: C.S. of the different parts of sperm head (←) showing disruption in normal features plasma membrane, acrosome and perforatorium. Fuzzy material
is seen on their surface. X 15,000. I: L.S and C.S. of the mid piece shows the loss of plasma membrane. Most of mitochondria (M) are hypertrophied or have started degeneration. The
loss of plasma membrane is seen in the sperm head region (←) X 28,000.
J: C.S. of the mid piece showing abnormal pattern of mitochondrial sheath and loss of plasma membrane. Most of mid-piece show increased cytoplasmic droplets (CD) displaced on one side are clearly seen. Coating of fuzzy material is seen on the surface of head and tail sections X 10,300.
K: C.S of the mid piece shows abnormal pattern and degeneration of mitochondrial sheath (long arrows) along the length of the structure and displaced mitochondrial sheath on one side. The discontinuation of fibrous sheath is also noticed in principal piece X 17,500.
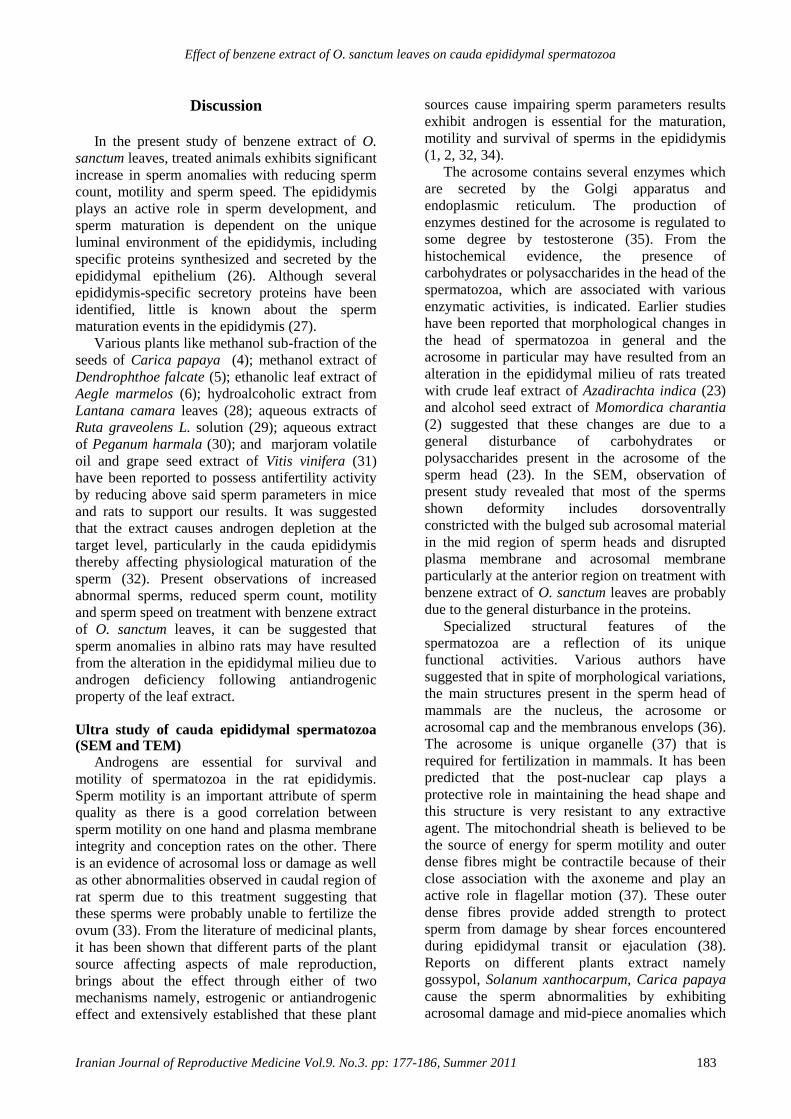
Effect of benzene extract of O. sanctum leaves on cauda epididymal spermatozoa
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 177-186, Summer 2011 183
Discussion
In the present study of benzene extract of O.
sanctum leaves, treated animals exhibits significant
increase in sperm anomalies with reducing sperm
count, motility and sperm speed. The epididymis
plays an active role in sperm development, and
sperm maturation is dependent on the unique
luminal environment of the epididymis, including
specific proteins synthesized and secreted by the
epididymal epithelium (26). Although several
epididymis-specific secretory proteins have been
identified, little is known about the sperm
maturation events in the epididymis (27).
Various plants like methanol sub-fraction of the
seeds of Carica papaya (4); methanol extract of
Dendrophthoe falcate (5); ethanolic leaf extract of
Aegle marmelos (6); hydroalcoholic extract from
Lantana camara leaves (28); aqueous extracts of
Ruta graveolens L. solution (29); aqueous extract
of Peganum harmala (30); and marjoram volatile
oil and grape seed extract of Vitis vinifera (31)
have been reported to possess antifertility activity
by reducing above said sperm parameters in mice
and rats to support our results. It was suggested
that the extract causes androgen depletion at the
target level, particularly in the cauda epididymis
thereby affecting physiological maturation of the
sperm (32). Present observations of increased
abnormal sperms, reduced sperm count, motility
and sperm speed on treatment with benzene extract
of O. sanctum leaves, it can be suggested that
sperm anomalies in albino rats may have resulted
from the alteration in the epididymal milieu due to
androgen deficiency following antiandrogenic
property of the leaf extract.
Ultra study of cauda epididymal spermatozoa (SEM and TEM)
Androgens are essential for survival and
motility of spermatozoa in the rat epididymis.
Sperm motility is an important attribute of sperm
quality as there is a good correlation between
sperm motility on one hand and plasma membrane
integrity and conception rates on the other. There
is an evidence of acrosomal loss or damage as well
as other abnormalities observed in caudal region of
rat sperm due to this treatment suggesting that
these sperms were probably unable to fertilize the
ovum (33). From the literature of medicinal plants,
it has been shown that different parts of the plant
source affecting aspects of male reproduction,
brings about the effect through either of two
mechanisms namely, estrogenic or antiandrogenic
effect and extensively established that these plant
sources cause impairing sperm parameters results
exhibit androgen is essential for the maturation,
motility and survival of sperms in the epididymis
(1, 2, 32, 34).
The acrosome contains several enzymes which
are secreted by the Golgi apparatus and
endoplasmic reticulum. The production of
enzymes destined for the acrosome is regulated to
some degree by testosterone (35). From the
histochemical evidence, the presence of
carbohydrates or polysaccharides in the head of the
spermatozoa, which are associated with various
enzymatic activities, is indicated. Earlier studies
have been reported that morphological changes in
the head of spermatozoa in general and the
acrosome in particular may have resulted from an
alteration in the epididymal milieu of rats treated
with crude leaf extract of Azadirachta indica (23)
and alcohol seed extract of Momordica charantia
(2) suggested that these changes are due to a
general disturbance of carbohydrates or
polysaccharides present in the acrosome of the
sperm head (23). In the SEM, observation of
present study revealed that most of the sperms
shown deformity includes dorsoventrally
constricted with the bulged sub acrosomal material
in the mid region of sperm heads and disrupted
plasma membrane and acrosomal membrane
particularly at the anterior region on treatment with
benzene extract of O. sanctum leaves are probably
due to the general disturbance in the proteins.
Specialized structural features of the
spermatozoa are a reflection of its unique
functional activities. Various authors have
suggested that in spite of morphological variations,
the main structures present in the sperm head of
mammals are the nucleus, the acrosome or
acrosomal cap and the membranous envelops (36).
The acrosome is unique organelle (37) that is
required for fertilization in mammals. It has been
predicted that the post-nuclear cap plays a
protective role in maintaining the head shape and
this structure is very resistant to any extractive
agent. The mitochondrial sheath is believed to be
the source of energy for sperm motility and outer
dense fibres might be contractile because of their
close association with the axoneme and play an
active role in flagellar motion (37). These outer
dense fibres provide added strength to protect
sperm from damage by shear forces encountered
during epididymal transit or ejaculation (38).
Reports on different plants extract namely
gossypol, Solanum xanthocarpum, Carica papaya
cause the sperm abnormalities by exhibiting
acrosomal damage and mid-piece anomalies which
Ahmed et al
184 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 177-186, Summer 2011
results in complete inhibition of fertility in rats and
mice (32, 39). Crude extract of Echeveria
gibbiflora on guinea pig sperm, results in the
formation of a huge bubble by distension of the
plasma membrane and dispersion of the acrosome
content with disappearance of the external
acrosomal membrane at the sperm head level (40).
Triptolide isolated from Tripterygium wilfordii
cause all cauda epididymal sperm to exhibit a
complete absence of the plasma membrane over
the entire middle and principal piece and
prematured decondensation of the nuclei in rats
(41). Similarly, crude extract of A.indica leaves
(3); aqueous decoction of Chenopodium album
seeds (7); chloroform extract of Carica papaya
seeds (42); and a hydroalcoholic extract of
Lantana camara leaves (28) were shown
morphological abnormalities in the head of
spermatozoa along with mid-piece anomalies in
rats and rabbits.
The spermatozoa of the cauda epididymis in the
present study of benzene extract of O. sanctum
leaves treated animals revealed several
abnormalities. Abnormal patterns of the outer
dense fibres and components of axoneme are
displaced on one side or both sides, complete
absence of plasma membrane of the entire middle
and principal pieces and disorganization of
mitochondrial sheath in several spermatozoa of
rats were observed. The missing segment of the
mitochondrial sheath probably represents a weak
point in the structural collar, which supports the
axial fibre-bundle during the contractional wave,
leading to splitting of the axial bundle and
subsequent dislocation of its fibres (37, 38). Recent
ultra study of aflatoxin B1, a food borne
mycotoxin, has shown that the sections of the testis
and cauda epididymidis revealed sperm flagella
missing one or more outer dense fibres and the
associated axonemal microtubule doublets. Severe
mitochondrial pathologies in spermatozoa and
elongated spermatids, suggesting a link between
AFB1-induced sperm mitochondrial pathology due
to possibility that AFB1 treatment would disrupt
the cytoskeletal proteins of the flagellum in male
albino rats (43). It has been suggested that the
extract might cause an androgen deprived effect to
target organs resulting in alterations in the internal
milieu, especially of cauda epididymis (32).
From both SEM and TEM observations of
treated animals showed that the tail portion has
balloon like cytoplasmic droplets. Ejaculates
containing a high proportion of spermatozoa with
attached cytoplasmic droplet can be correlated
with altered epididymal function and reduced
fertility (44, 45). The presence of high proportion
of spermatozoa with attached cytoplasmic droplets
in benzene extract of O. sanctum leaves treated
animals may be due to altered epididymal function.
Similar observations were made in studies of
combination of progestagen and androgen, Carica
papaya, vincristine and aflatoxin B1 treated
animals (1, 32, 33, 46). Agnes and Akbarsha (46)
showed in their experimental study a higher
percentage of cauda epididymal spermatozoa
retained the cytoplasmic droplets in albino mouse.
Cytoplasmic droplets contained electron-dense
spherical inclusions, which were hypothesized as
lipid inclusions produced from the lamellae
through the spherical vesicles of the cytoplasmic
droplets.
It is known that spermatozoa carrying
cytoplasmic droplets would be inhibited in motility
and may not fertilize the ova (47). Hence, in the
present study, in the light of the pathological
changes observed, it is suggested that benzene
extract of O.sanctum leaves damages the
spermatozoa in the epididymis, leading to reduced
fertilizing ability of the sperm. The fertility studies
reveal that the male rats treated with O.sanctum
leaves are unable to fertilize the female rats
probably because the male gametes are affected
thereby, establishing the antifertility property of
the plant studied.
Conclusion
It was demonstrated that the administration of
benzene extract of O. sanctum leaves can induce
the morphological changes in the head and tail
region of albino rat sperms.This benzene extract of
O. sanctum leaves was may be due to general
disturbance of proteins and alteration in the
epididymal milieu probably due to androgen
deficiency consequent upon the antiandrogenic
property of this plant. However, these conclusions
are based on the preliminary study, where the rats
are force fed with the benzene extract of O.
sanctum leaves. More refined and sophisticated
study is needed for identification of active
principles and their effects on androgen dependent
parts of the spermatozoa in albino rats which are
under progress.
Acknowledgement
Authors are thankful to Department of
Zoology, Karnatak University, India and Union
Grant Commission under SAP and COSIST
program, New Delhi, India for support to carry out
Effect of benzene extract of O. sanctum leaves on cauda epididymal spermatozoa
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 177-186, Summer 2011 185
this research and also grateful to the whole TEM
unit, National Institute of Mental Health And
Neurosciences (NIMHANS) Bangalore and SEM
unit, Central Food Technological Research
Institute (CFTRI), Mysore, respectively, for
providing us the EM facility and their kind
encouragement.
References
1. Akbarsha MA, Averal HI. Epididymis as a target organ for
the toxic effect of vincristine: light microscopic changes in
the epididymis epithelial cell types. Biomedical Letters
1996; 54: 133-146.
2. Girini MM, Ahamed RN, Aladakatti RH. Effect of graded
doses of Momordica charantia seed extract on rat sperm:
scanning electron microscope study. J Basic Clin Physiol
Pharmacol 2005; 16: 53-66.
3. Aladakatti RH, Ahamed RN. Ultrastructural changes in
Leydig cell and cauda epididymal spermatozoa induced by
Azadirachta indica leaves in albino rats. Phytother Res
2005; 19: 756-766.
4. Lohiya NK, Manivannan B, Garg S. Toxicological
investigations on the methanol sub-fraction of the seeds of
Carica papaya as a male contraceptive in albino rats. Reprod
Toxicol 2006; 22: 461-468.
5. Gupta RS, Kachhawa JB. Evaluation of contraceptive
activity of methanol extract of Dendrophthoe falcata stem in
male albino rats. J Ethnopharmacol 2007; 112: 215-218.
6. Chauhan A, Agarwal M. Reversible changes in the
antifertility induced by Aegle marmelos in male albino rats.
Syst Biol Reprod Med 2008; 54: 240-246.
7. Kumar S, Biswas S, Mandal D, Roy HN, Chakraborty S,
Kabir SN, et al. Chenopodium album seed extract: a potent
sperm-immobilizing agent both in vitro and in vivo.
Contraception 2007; 75: 71-78.
8. Dixit VP. Plant products/non-steroidal compounds affecting
fertility in the Indian desert gerbil, Meriones hurrianae
Jerdon. In: Prakash I, Ghosh PK. Rodents in Indian
Agriculture. 1st Ed. Jodhpur India; Scientific Publishers;
1992: 595-604.
9. Chopra RN, Chopra IC, Handa KL, Kapoor LD. Indigenous
drugs of India. UN Dhar, Pvt. Ltd.; Calcutta; 1993.
10. Ocimum sanctum. The Indian home remedy. In: Current
Medical Scene, March-April 1992 (Edited and published by
S. Rajeshwari, Cipla Ltd., Bombay Central, Bombay).
11. Gupta SK, Prakash J, Srivastava S. Validation of claim of
Tulsi, Ocimum sanctum Linn as a medicinal plant. Indian J
Exp Biol 2002; 40: 765–773.
12. Ahmed M, Ahamed RN, Aladakatti RH, Ghosesawar MG.
Reversible anti-fertility effect of benzene extract of Ocimum
sanctum leaves on sperm parameters and fructose content in
rats. J Basic Clin Physiol Pharmacol 2002; 13: 51-59.
13. Khanna S, Gupta SR, Grover JK. Effect of long term
feeding of Tulsi (Ocimum sanctum Linn) on reproductive
performance of adult albino rats. Indian J Exp Biol 1986;
24: 302-304.
14. Kantak NM, Gogate MG. Effect of short term
administration of Tulsi (Ocimum sanctum Linn.) on
reproductive behaviour of adult male rats. Indian J Physiol
Pharmacol 1992; 36: 109-111.
15. Sardessai SR, Borker AS, Abraham ME. Effects of short
term administration of Tulsi leaves on sexual behaviour in
female rats. Indian J Physiol Pharmacol 1999; 43: 398-400.
16. Ahmed M, Aladakatti RH, Deepthi KR, Nazeer Ahamed R.
Reversible histoarchitecture study of testis and cauda
epididymis and changes in cauda epididymal epithelial cell
types on treatment with benzene extract of Ocimum sanctum
leaves in albino rats. Oriental Pharm Exp Med 2008; 8: 111-
124.
17. Ahmed M, Nazeer Ahamed R, Aladakatti RH. Effect of
benzene extract of Ocimum sanctum leaves on cauda
epididymis of albino rats. J Basic Clin Physiol Pharmacol
2009; 20: 29-41.
18. Mukhtar Ahmed, Nazeer Ahamed R, Aladakatti RH
Ghodesawar MG. Dose dependent effect of benzene extract
of Ocimum sanctum leaves on cauda epididymal
spermatozoa of albino rats. Oriental Pharm Exp Med 2009;
9: 339-349.
19. WHO Protocol, LG-06. Extraction and fractionation for
biological and phytochemical studies. A.P.J.F/I.P, A; 1983:
1001-1083.
20. Besley MA, Eliarson R, Gallegos AJ, Moghissi KS, Paulsen
CA, Prasad M RN. Laboratory manual for the examination
of human semen and semen cervical mucus interaction.
WHO Press concern; Singapore; 1980.
21. Ratnasooriya WD. Effect of Atropine on fertility of female
rat and sperm motility. Indian J Exp Boil 1984; 22: 463-466.
22. Bauer JD, Ackermen PG, Toro G. Clinical Laboratory
Methods. C.V. Mosty co.; St. Louis; 1974.
23. Aladakatti RH, Ahamed RN. Effect of Azadirachta indica
leaves on rat spermatozoa. Indian J Exp Biol 1999; 37:
1251-1254.
24. Reynolds ES. The use of lead citrate at high pH as an
electron-opaque stain in electron microscopy. J Cell Biol
1963; 17: 208-212.
25. Ostle B. Statistics in Research: Basic Concepts and
Techniques for Research Workers. 4thEd. Ames; Iowa State
University Press; 1988; 664.
26. Cooper TG. Epididymis. In: Neill JD, Knobil E, eds.
Encyclopedia of reproduction 2nd Ed. San Diego; Academic
Press; 1998: 1–17.
27. Kirchhoff C. Molecular aspects of epididymal function and
sperm maturation. In: Waites GMH, Frick J, Baker GWH,
eds. Current advances in andrology. Bologna Italy;
Monduzzi; 1997: 253–259.
28. de Mello FB, Jacobus D, de Carvalho KC, de Mello JR.
Effects of Lantana camara (Verbenaceae) on rat fertility.
Vet. Hum Toxicol 2003; 45: 20-23.
29. Khouri NA, El-Akawi Z. Antiandrogenic activity of Ruta
graveolens L in male Albino rats with emphasis on sexual
and aggressive behavior. Neuro Endocrinol Lett 2005; 26:
823-829.
30. El-Dwairi QA, Banihani SM. Histo-functional effects of
Peganum harmala on male rat's spermatogenesis and
fertility. Neuro Endocrinol Lett 2007; 28: 305-310.
31. El-Ashmawy IM, Saleh A, Salama OM. Effects of marjoram
volatile oil and grape seed extract on ethanol toxicity in
male rats. Basic Clin Pharmacol Toxicol 2007; 101: 320-
327.
32. Chinoy NJ, D'Souza JM, Padman P. Contraceptive efficacy
of Carica papya seed extract in male mice (Mus musculus).
Phytothera Res 1995; 9: 30-36.
33. Rao MV, Roy GK. Biochemical and morphological changes
of spermatozoa in progestin and androgen injected rats.
Indian J Exp Biol 1993; 31: 12-15.
34. Aladakatti RH, Nazeer Ahamed R, Ahmed M, Ghodesawar
MG. Sperm parameters changes induced by Azadirachta
indica in albino rats. J Basic Clin Physiol Pharmacol 2001;
12: 69-77.

Ahmed et al
186 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 177-186, Summer 2011
35. Morton DB. Acrosomal enzymes: Immunochemical
localization of acrosin and hyaluronidase in ram
spermatozoa. J Reprod Fertil 1975; 45: 375-378.
36. Breed WG. Sperm head structure in the hydromyinae
(Rodentia: Muridae): A further evolutionary development of
the subacrosomal space in mammals. Gamete Res 1984; 10:
31-34.
37. Fawcett DW. The mammalian spermatozoon. Dev Biol
1975; 44: 394-436.
38. Baltz JM, Williams PO, Cone RA. Dense fibres protect
mammalian sperm against damage. Biol Reprod 1990; 43:
485-491.
39. Rao MV. Effect of alcoholic extract of Solanum
xanthocarpum seeds in adult male rats. Indian J Exp Biol
1988; 26: 95-98.
40. Delgado NM, Sánchez-Vázquez ML, Hernández O, Reyes
R. Correlation between sperm membrane destabilization by
heparin and aniline blue staining as membrane integrity
index. Arch Androl 1998; 40:147-152.
41. Hikim AP, Lue YH, Wang C, Reutrakul V, Sangsuwan, R,
Swerdloff RS. Post testicular antifertility action of triptolide
in the male rat: evidence for severe impairment of cauda
epididymal sperm ultrastructure. J Androl 2000; 21: 431–
437.
42. Lohiya NK, Manivannan B, Mishra PK, Pathak N, Sriram S,
Bhande SS, et al. Chloroform extract of Carica papaya seeds
induces long-term reversible azoospermia in langur monkey.
Asian J Androl 2002; 4: 17–26.
43. Faisal K, Periasamy VS, Sahabudeen S, Radha A, Anandhi
R, Akbarsha MA. Spermatotoxic effect of aflatoxin B1 in
rat: extrusion of outer dense fibres and associated axonemal
microtubule doublets of sperm flagellum. Reproduction
2008; 135: 303–310.
44. Cummins JM. The effect of artificial cryptorchidism in the
rabbit on the transport and survival of spermatozoa in the
female reproductive tract. J Reprod Fertil 1973; 33: 469-
479.
45. Bedford JM. Adaptations of male reproductive tract and the
fate of spermatozoa following vasectomy in the rabbit,
rhesus monkey, hamster and rat. Biol Reprod 1976; 14: 118-
142.
46. Agnes VF, Akbarsha MA. Spermatotoxic effect of aflatoxin
B (1) in the albino mouse. Food Chem Toxicol 2003; 41:
119–130.
47. Hermo L, Dworkin J, Oko R. Role of epithelial clear cells of
the rat epididymis in the disposal of the contents of
cytoplasmic droplets detached from spermatozoa. Am J Anat
1988; 183: 107- 124.

Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 187-192, Summer 2011
Icodextrin reduces adhesion formation following
gynecological surgery in rabbits Behnaz Khani
1 M.D., Nahid Bahrami
2 M.D., Ferdous Mehrabian
2 M.D., Hormoz Naderi Naeni
3 M.D.
1 Department of Obstetrics and Gynecology, Shahid Beheshti Hospital, Isfahan University of Medical
Sciences, Isfahan, Iran.
2 Department of Obstetrics and Gynecology, Alzahra Hospital, Isfahan University of Medical Sciences,
Isfahan, Iran.
3 Sepahan Hospital, Isfahan, Iran.
Received: 8 May 2010; accepted: 11 January 2011
Abstract
Background: Adhesion is a common complication of gynecology surgery so different
barrier agents and solutions have been used during these operations to separate and
protect tissues from adhesion after surgery. Adept is one of these solutions that have
been postulated to reduce the chance of adhesion following gynecolgy surgery.
Objective: To evaluate the effect of 4% icodextrin in reducing adhesion formation in
comparing with sterile water and human amniotic fluid in rabbits.
Materials and Methods: In this prospective experimental study 30 white Newzealand
female rabbits were selected and randomized in to three treatment groups. The rabbits
were anesthetized and an abdominal incison was made, uterine horns were abrated with
gauze until bleeding occurred. Before closing the abdomen, the traumatized area was
irrigated either by 30cc of sterile water, 30cc of 4% Adept or 30cc of human amniotic
fluid. The solutions were labeled only as solutions A (steriel water), B (icodextrin), or C
(human amniotic fluid). On the seventh day after surgery, second laparotomy was
performed to determine and compare adhesion formation in rabbits.
Results: There was significant difference between mean score of adhesions in 4%
icodextrin group (2.1±0.70) in comparison to sterile water group (10.4±0.60) and
amniotic fluid group (8.7±0.84). But the difference between mean score of adhesions in
amniotic fluid group in comparison to sterile water group was not significant (8.7±0.84)
versus (10.4±0.60).
Conclusion: The use of 4% icodextrin solution was more effective than human
amniotic fluid and sterile water in reducing adhesion formation in a gynecological
surgery model in rabbits Key words: Icodextrin solution, Human amniotic fluid, Adhesion formation, Rabbit.
Introduction
Adhesions are the most common cause of post
operative small bowel obstruction, infertility and
visceral pain (1). Pelvic surgery is associated with
high rates of pelvic adhesion formation. Careful
surgical techniques have been proved to reduce
adhesion formation. Application of fine, Non-
reactive suture materials and prevention of foreign-
body reaction, excision of necrotic tissue and
Corresponding Author:
Behnaz Khani, Flezi Bridge, Shahid Beheshti Hospital,
Isfahan, Iran.
Email: [email protected]
minimizing tissue and organ injury are effective in
reducing adhesion formation in a surgical
procedure (2).
Non surgical techniques such as application of
local and systemic anti-inflammatory agents and
peritoneal instillates have been used in this regard.
Anti adhesion barriers such as hyaluronic acid,
polyethylene glycol, fibrin glue, hyaluronic acid
film, and expanded polytetrafluoroethylene have
been shown to reduce the incidence and extent of
new and recurrent adhesions in different clinical
trials (3, 4).
The use of fluids in the peritoneal cavity to
separate surfaces and prevent adhesion formation
between organs is under investigation. One of

Khani et al
188 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 187-192, Summer 2011
these fluids is human amniotic fluid which is a
hypotonic solution mainly contains albumin,
cholesterol and hyaluoronic acid, existance of
hyaluoronic acid in the peritoneal cavity shifts the
repair process into regeneration pathway and
decreases fibrosis and scar formation. Amniotic
fluid also contains some potent growth factors such
as insulin like growth factors that are involved in
repair process (5).
In our study, human amniotic fluid was selected
and compared with adept adhesion reduction
solution that is a pale yellow fluid (icodextrin w/v
4% solution) and is a non viscous, iso-osmotic,
clear solution, contains icodextrin, alpha-1, 4
linked glucose polymer with a molecular weight of
16,500 Daltons.
This product is not physiologically present in
the abdominal cavity; it remains in the peritoneal
cavity for 3- 5 days before absorption by the
lymphatic system and therefore resides longer
compared to other solutions such as saline and a
glucose-based peritoneal dialysis solution. The
existence of 4% icodextrin in the peritoneal cavity
during this critical period separates damaged
surfaces and minimizes adhesion formation
between organs. It gradually absorbs into the blood
stream and is broken down by amylase and
metabolized to glucose (6).
In a controlled pilot study, the safety and
efficacy of 4% icodextrin was evaluated after
laparoscopic gynecological surgery and the results
showed that it is effective in reducing adhesion
formation (7).
Also in another randomized blinded trial anti
adhesion efficacy of 4% icodextrin, ferric
hyaluronate gel and Ringer lactat were compared
in sever peritoneal damage caused by bipolar
coagulation in a laparoscopic rat model. Adhesins
were more filmier and easily separable in 4%
icodextrin group comparing with Ringer lactate
group (8).
In contrast to these research results some other
working groups found insufficient effects of 4%
icodextrin in animal models (9, 10). Two cases of
severe serosal fibrosis within a few days after usig
4% icodextrin for reducing adhesion in abdominal
surgery was reported (11). Numerous cases of
abdominal pain and sterile chemical peritonitis
have been contributed to 4% icodextrin (12).
Because the bio compatibility and efficacy of
4% icodextrin is the subject of controversial
discussion in the current literature, we planned our
study and used a rabbit model to evaluate the
effectiveness of 4% icodextrin in reducing
adhesion formation in comparing with sterile water
and human amniotic fluid.
Materials and methods
This prospective experimental study was done
in Physiology Department of Isfahan University of
Medical Sciences, Isfahan, Iran and approved by
institutional review board and vice chancellery
research of this university by registry number of
386161.
30 white, Newzealand female rabbits, weighing
2000-2200g were randomly assigned to 3 groups.
Each group consisted ten non pregnant, 12 weeks
aged rabbits. They were fed with standard
laboratory rabbit food and water throughout the
study. Human amniotic fluid was taken in a sterile
condition during cesarean section of two pregnant
women who both were around 32 weeks pregnant
and had the same indication of cesarean section.
To remove red blood cells from the fluid it was
centrifuged for ten minutes (3000circules/min) and
kept in refrigerator for four hours before use. The
4% icodexterin solution was hydrochloride (Baxter
healthcare corporation, Deerfield IL, USA) and the
sterile water was from Daroupakhsh Company,
Tehran, Iran. The gauze was from Safa Company,
Isfahan, Iran.
The rabbits were anesthetized for surgery with
IM injection of 55 mg/kg of ketamine. The
abdominal ventral side was shaved and dis-infected
with povidone iodine. A vertical 5cm abdominal
incision was made. Uterine horns were exteriorized
and the serosal surfaces of the horns were abraded
with sterile gauze until bleeding occured. Up to
this point, all animals received the same procedure
but after that the injured area were irrigated with
different solutions. The solutions were labelled
only as A, B or C, so that the study personnel were
blinded to solution identity.
The first group acted as control group in which
30cc of A solution was poured over the
traumatized area. In the second group, the
damaged area was irrigated with 30cc of B solution
and the third group received 30cc of C solution
before closure of the abdomen.
Measurements
The second laparotomy was carried out in 30
rabbits after 7 days to assess adhesion formation.
The evaluations were blinded for three groups. The
formed adhesions were scored by qualitative and
quantitative parameters (Table I). Parameters
included extent, depth of adhesion, bursting
strength, and number of adhesion sites (13). The
score from four parameters were calculated and
added to define total adhesion score as the grade of
adhesion (Table II) (13).
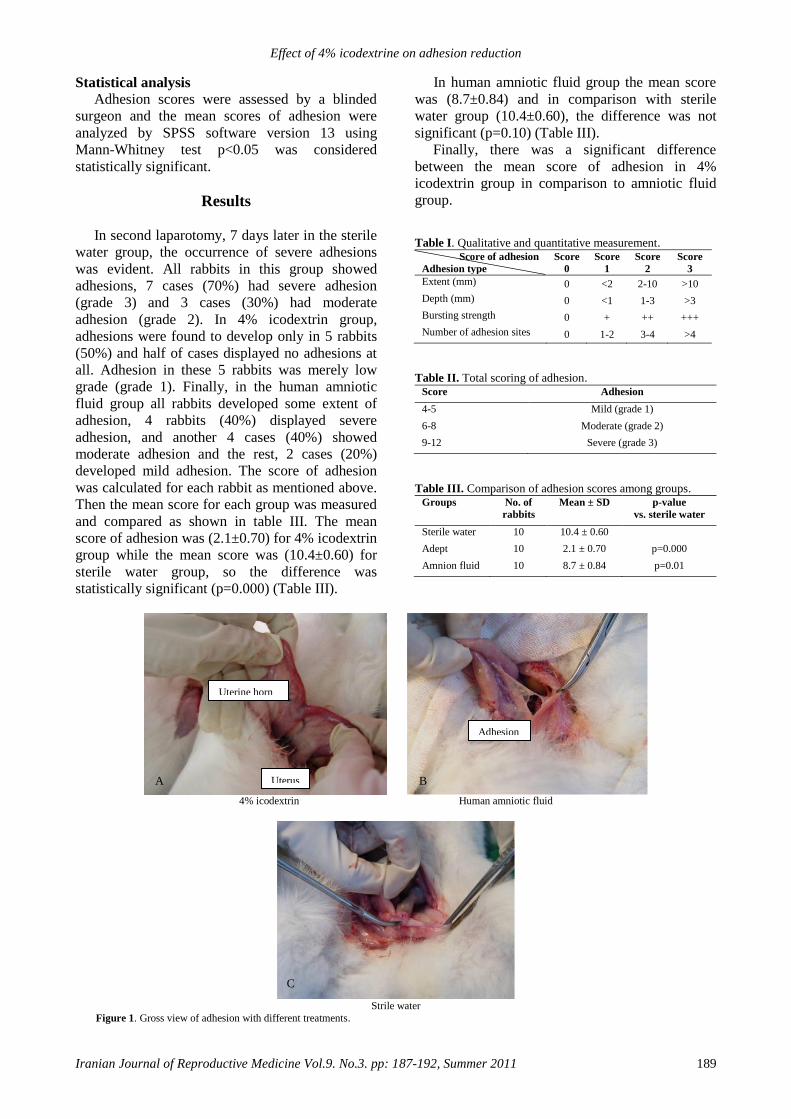
Effect of 4% icodextrine on adhesion reduction
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 187-192, Summer 2011 189
Statistical analysis
Adhesion scores were assessed by a blinded
surgeon and the mean scores of adhesion were
analyzed by SPSS software version 13 using
Mann-Whitney test p<0.05 was considered
statistically significant.
Results
In second laparotomy, 7 days later in the sterile
water group, the occurrence of severe adhesions
was evident. All rabbits in this group showed
adhesions, 7 cases (70%) had severe adhesion
(grade 3) and 3 cases (30%) had moderate
adhesion (grade 2). In 4% icodextrin group,
adhesions were found to develop only in 5 rabbits
(50%) and half of cases displayed no adhesions at
all. Adhesion in these 5 rabbits was merely low
grade (grade 1). Finally, in the human amniotic
fluid group all rabbits developed some extent of
adhesion, 4 rabbits (40%) displayed severe
adhesion, and another 4 cases (40%) showed
moderate adhesion and the rest, 2 cases (20%)
developed mild adhesion. The score of adhesion
was calculated for each rabbit as mentioned above.
Then the mean score for each group was measured
and compared as shown in table III. The mean
score of adhesion was (2.1±0.70) for 4% icodextrin
group while the mean score was (10.4±0.60) for
sterile water group, so the difference was
statistically significant (p=0.000) (Table III).
In human amniotic fluid group the mean score
was (8.7±0.84) and in comparison with sterile
water group (10.4±0.60), the difference was not
significant (p=0.10) (Table III).
Finally, there was a significant difference
between the mean score of adhesion in 4%
icodextrin group in comparison to amniotic fluid
group.
Table I. Qualitative and quantitative measurement. Score of adhesion
Adhesion type
Score
0
Score
1
Score
2
Score
3
Extent (mm)
0 <2 2-10 >10
Depth (mm)
0 <1 1-3 >3
Bursting strength
0 + ++ +++
Number of adhesion sites
0 1-2 3-4 >4
Table II. Total scoring of adhesion. Score
Adhesion
4-5
Mild (grade 1)
6-8
Moderate (grade 2)
9-12
Severe (grade 3)
Table III. Comparison of adhesion scores among groups. Groups No. of
rabbits
Mean ± SD p-value
vs. sterile water
Sterile water
10 10.4 ± 0.60 Adept
10 2.1 ± 0.70 p=0.000
Amnion fluid
10 8.7 ± 0.84 p=0.01
4% icodextrin Human amniotic fluid
Strile water
Figure 1. Gross view of adhesion with different treatments.
A B
C
Uterine horn
Uterus
Adhesion
Khani et al
190 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 187-192, Summer 2011
Discussion
Because adhesion adveresely affects patient
morbidity and is a great burden to health system,
different techniques have been proposed and tested
to reduce adhesion formation (14). Fine surgical
techniques and use of laparoscopic surgery to
minimize tissue damage are to some extent
effective in this regard but Surgical and Clinical
Adhesions Research study data showed that this is
not sufficient to prevent adhesion formation (15).
Administration of specific fluids such as lactated
Ringer’s Solution (LRS), phosphate-buffered
saline (PBS) and normal saline in to the peritoneal
cavity during the surgery has been proposed to
reduce formation of adhesions. However these
solutions are absorbed in a short period of time and
therefore are not effective clinically in preventing
adhesion formation (16).
It was shown that administration of human
amniotic fluid in to the peritoneal cavity inhibits
production of expanded peritonitis. Human
amniotic fluid contains hyaluoronic acid that
promotes normal healing process (17) and also
contains hyaluoronic acid stimulating activator
(HASA) which stimulates scar cells to produce
hyaluoronic acid that inhibits migration of
lymphocytes and prevents chemotaxis and
phagocytosis of granulocytes and therefore inhibits
scar formation (18).
Four studies commented the prevalence of
adhesions at second look laparoscopy (19-22) and
showed evidence of decreased prevalence of
adhesions in patients who were treated with
hyaluronic acid compared with those given placebo
or no treatment.
Our results also indicate that human amniotic
fluid is more effective in reducing adhesion
formation in comparison with sterill water as
placebo. We used 4% icodextrin fluid because it
has a longer residual time in the abdominal cavity
in comparison to other solutions (23) and it was
compared with human amniotic fluid which
contains Hyaluronic acid that has been proposed to
reduce adhesion formation too. Rabbits were our
experimental model because the fluid dynamics of
icodextrin in this species is more closely similar to
human beings (24).
Early pre-clinical studies were performed (by
Verco et al 2000) to assess the efficacy of 4%
icodextrin in order to reduce adhesion in a rabbit
double uterine horn model (25). Their results
indicate that postoperative application of
icodextrin 4% causes a significant increase in
adhesion free sites (p=0.000).
In a randomized controlled study (by Dizerega
et al 2003) the safety and efficacy of 4% icodextrin
was evaluated. In order to compare icodextrin 4%
with Ringer’s lactated saline, 62 women who
required laparascopic adnexal surgery were
compared in two different treatment groups.
Results showed that lavage and instillation with
icodextrin 4% was effective in reducing adhesion
formation. The use of 4% icodextrin solution for
peri operative lavage and post operative instillation
in rabbit model of bowel anastomatic healing,
didn’t result in any difference from either LRS
treated or untreated surgical control (26).
In another study (by Muller et al 2005) the
effect of intraperitoneal anti adhesive fluids (4%
icodextrin, phospholipids, Ringer’s lactate) in a rat
peritonitis model was examined and the results of
4% icodextrin showed significantly enhancement
of adhesion and abscess formation, in comparison
with the other control groups. A case of
disseminated intra vascular coagulation after
laparoscopic multiple myomectomy with the use of
4% icodextrin solution was described by Santos et
al (2006). The possible cause might be
idiosyncratic immunologically mediated reaction
to icodextrin in the pelvic cavity, but no previous
case of DIC has been described in the published
litreture (27). Some cases of vulval edema, plural
effusion and even anaphylactoeid reaction related
to icodextrin 4% after laparoscopic and laparotomy
surgery have been reported (28).
But, ARILE (Adept registry for clinical
evaluation) was initiated in a number of centers in
the UK and then expanded to involve 253 centeres
(103 general-surgery and 150 gynecologyical-
surgery centers) in France, Germany, Italy, Spain,
Greece (gynecology only) and the UK. The
findings indicate that icodextrin 4% was well
tolerated by patients who underwent laparotomy or
laparoscopy (29).
In a recent study (by Colins et al 2007), 402
patients randomized intraoperatively to receive
either 4% icodextrin or LRS and then patients
returned for second laparoscopy within 4–8 weeks.
Incidence, severity, and extent of adhesions were
characterized for both groups and they
demonstrated that 4% icodextrin is a safe and
effective adhesion reduction agent in laparoscopy
(30).
Our study results support preclinical
observation (by Verco et al 2000) and recent study
(by Colin et al 2007), as mentioned before in adept
group, half of the cases were found with no
adhesion at all and the rest had mild adhesion.
Effect of 4% icodextrine on adhesion reduction
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 187-192, Summer 2011 191
However in our study, no side effects, no
abscess formation and no other complication were
observed in contrast to Muller et al (2005). Our
data showed that lavage and instillation of 4%
icodextrin was not only safe but also effective in
reducing adhesion formation in rabbits, and with
regard to close relationship of fluid dynamics in
rabbits with human being this results suggest that
patients undergoing gynelocological surgery may
have a better prognosis for adhesion reduction after
using intra operative irrigation with 4% icodextrin.
Acknowledgment
This research was supported by Vice
Chancellery Research of Isfahan University of
Medical Sciences and there is no conflict of
interest in this article. The authors would like to
thank IUMS and Dr. Mehdi Nematbakhsh,
professor of Physiology Department of IUMS, and
Miss Mojdeh Ghasemi, midwife, and Miss Zahra
Samavatian for all their helps.
References
1. Liakakos T, Thomakos N, Fine PM, Dervenis C, Young
RL. Peritoneal adhesions: etiology, pathophysiology, and
clinical significance. Recent advances in prevention and
management. Dig Surg 2001; 18: 260-273.
2. Muller SA, Treutner KH, Haase G, Kinzel S, Tietze L,
Schumpelick V. Effect of intera peritonealanti adhesive
fluids in a rat peritonitis model. Archsurg 2003; 138: 286-
290.
3. Farquhar C, Vandekerckhove P, Watson A, Vail A,
Wiseman D. Barrier agents forpreventing adhesions after
surgery for subfertility. Cochrane Database Syst Rev
2000; 2: CD000475.
4. Sekiba K. Use of Interceed (TC7) absorbable adhesion
barrier to reduce postoperative adhesion reformation in
infertility and endometriosis surgery. The Obstetrics and
Gynecology Adhesion Prevention Committee. Obstet
Gynecol 1992; 79: 518-522.
5. Burd DA, Greco RM, Regauer S, Longaker MT, Siebert
JW, Garg HG. Hyaluronan and wound healing: a
newperspective. Br J PlastSurg 1991; 44: 579-584.
6. Hosie K, Gilbert JA, Kerr D, Brown CB, Peers EM. Fluid
dynamics in man of an intra peritoneal drug delivery
solution: 4% icodextrin. Drug Deliv 2001; 8: 9-12.
7. Dizerega GS, Verco SJ, Young P, Kettel M, Kobak W,
Martin D, et al. A randomized, controlled pilot study of
the safety and efficacy of 4% icodextrin solution in the
reduction of adhesions following laparoscopic
gynaecological surgery. Hum Reprod 2002; 17:1031-1038.
8. Roman H, Canis M, Kamble M, Botchorishvili R, Pouly
JL, Mage G. Efficacy of three adhesion preventive agent
in reducing severe peritoneal truma induced in a
laparoscopic rat model. Fertil Steril 2005; 83: 1113-1118.
9. Muller SA, Treutner KH, Jorn H, Anurov M, Ottinger AP,
Schumpelick V. Adhesion prevention comparing liquid
and solid barriers in the rabbit uterine horn model. Eur J
Obstet Gynecol Reprod Biol 2005; 120: 222-226.
10. Metwally M, Watson A, Lilford R, Vandekerckhove P.
Fluid and pharmacological agents for adhesion prevention
after gynaecological surgery. Cochrane Database Syst Rev
2006; 19: CD001298.
11. Saedon M, Borowski DW, Natu S, Hennessy C,
Tabaqchali MA. David W Borowski, SonaliNatu, Colm
Hennessy. Adept (Icodextrin 4%): A tale of caution.
Colorectal Dis 2010; 12: 384-386.
12. Reichel W, Schulze B, Dietze J, Mende W. A case of
sterile peritonitis associated with icodextrin solution. Perit
Dial Int 2001; 21: 414-419.
13. Kamffer WJ, Jooste EV, Nel JT, de Wet JI. Surgical glove
powder and intraperitoneal adhesion formation. An appeal
for the use of powder-free surgical gloves. S Afr Med J
1992; 81: 158-159.
14. Wilson MS, Menzies D, Knight AD, Crowe AM.
Demonstrating the clinical and cost effectiveness of
adhesion reduction strategies. Colorectal Dis 2002; 4:
355-360.
15. Lower AM, Hawthorn RJS, Ellis H, O’Brien F, Buchan S,
Crowe AM. The impact of adhesions on hospital
readmissions over ten years after 8849 open
gynaecological operations: anassessment from the
SurgicalandClinical Adhesions Research Study. Br J
Obstet Gynaecol 2000; 107: 855-862.
16. Lower AM, Hawthorn RJS, Clark D, Boyd JH, Finlayson
AR, Knight AD, et al. Adhesionrelated readmissions
following gynaecological laparoscopy or laparotomy in
Scotland: an epidemiological study of 24,046 patients.
Hum Reprod 2004; 19: 1877-1885.
17. Rimbach S, Korell M, Tinneberg HR, DeWilde RL.
Adhesions and their prevention in gynaecologic surgery:
current status and consensus based on four workshops.
Geburtsh Frauenheilk 2004; 64: 891-899.
18. Lancey JT. The prevention of peritoneal adhesions by
amniotic fluid. Ann Surg 1930; 92: 281-293.
19. Longaker MT, Chiu ES, Harrison MR, Crombleholme
TM, Langer JC, et al. Studies in fetal wound healing. IV.
Hyaluronic acid-stimulating activity distinguishes fetal
wound fluid from adult wound fluid. Ann Surg 1989; 667-
672.
20. Johns DB, Keyport GM, Hoehler F, diZerega GS; Intergel
Adhesion Prevention Study Group. Reduction of
postsurgical adhesions with Intergel adhesion prevention
solution: a multicenter study of safety and efficacy after
conservative gynecologic surgery. Fertil Steril 2001; 76:
595-604.
21. Lundorff P, Geldorp H, Tronstad SE, Lalos O, Larsson B,
Johns DB, et al. Reduction of postsurgical adhesions with
ferric hyaluronate gel: a European study. Hum Reprod
2001; 16: 1982-1988.
22. Pellicano M, Bramante S, Cirillo D, Palomba S, Bifulco
G, Zullo F, et al. Effectiveness of autocrosslinked
hyaluronic acid gel after laparoscopic myomectomy in
infertile patients: a prospective, randomized, controlled
study. Fertil Steril 2003; 80: 441-444.
23. Rodgers KE, Verco SJS, diZerega GS. Effects of
intraperitoneal 4% icodextrin solution onthe healing of
bowel anastomoses and laparotomy incisions in rabbits.
Colorectal Dis 2003; 5: 324-330.
24. Flessner MF, Lofthouse J. Of mice and men: species and
age difference in dialysis withicodextrin. J Am Soc
Nephrol 1999; 10: 226A.
25. Verco SJS, Peers EM, Brown CB, Rodgers KE, Roda N,
diZerega G. Development of a novel glucose polymer
solution (icodextrin) for adhesionprevention: pre-
clinicalstudies. Hum Reprod 2000; 15: 1764-1772.

Khani et al
192 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 187-192, Summer 2011
26. Rodgers KE, Verco SJ, diZerega GS. Effects of
intraperitoneal 4% icodextrin solution on the healing of
bowel anastomoses and laparotomy incisions in rabbit.
Colorectal Dis 2003; 5: 324-330.
27. Santos LM, Frenna V, Thoma V, Wattiez A. Disseminated
intravascular coagulation after laparoscopic multiple
myomectomy with use of icodextrin. J Minim Invasive
Gynecol 2006: 13, 480-482.
28. Doumplis D, Majeed GS, Sieunarine k, Richardson R,
Smith JR. Adverse effects related to icodextrin 4% our
experience.Gynecol Surg 2007; 4: 97-100.
29. Catena F, Ansaloni L, Lauro A, Ercolani G, D'Alessandro
L, Pinna A. Prospective controlled randomized trial on
prevention of postoperative abdominal adhesions by
Icodextrin 4% solution after laparotomic operation for
small bowel obstruction caused by adherences. Trials
2008; 9: 74.
30. Brown CB, Luciano AA, Martin D, Peers E, Scrimgeour
A, diZerega GS, et al. Adept (icodextrin 4% solution)
reduces adhesions after laparoscopic surgery for
adhesiolysis: a double-blind, randomized, controlled
study. Fertil Steril 2007; 88: 1413-1426.

Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:193-198, Summer 2011
Correlation between the level of cholesteryl ester
transfer protein in follicular fluid with fertilization
rates in IVF/ ICSI cycles Amir Mehdizadeh
1,2 M.Sc., Ali Rahimipour
3 Ph.D., Laya Farzadi
4 M.D., Masoud Darabi
2 Ph.D.,
Vahideh Shahnazi4 M.Sc., Maghsod Shaaker
2 B.Sc., Amir-Mansour Vatankhah
5 M.Sc., Zahra
Golmohamadi2 M.Sc., Mohammad Nouri
2 Ph.D.
1 Research Center for Pharmaceutical Nanotechnology, Tabriz University of Medical Sciences, Tabriz,
Iran.
2 Laboratory of Chromatography, Department of Biochemistry and clinical Laboratories, Faculty of
Medicine, Tabriz University of Medical Sciences, Tabriz, Iran.
3 Department of Laboratory Medicine, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
4 Women’s Reproductive Health Research Center, Alzahra Hospital, Tabriz University of Medical
Sciences, Tabriz, Iran.
5 Drug Applied Research Center, Tabriz University of Medical Sciences, Tabriz, Iran.
Received: 19 May 2010; accepted: 30 October 2010 Abstract
Background: Follicular fluid (FF) plays an important role in oocytes and embryo
development, which may contribute to IVF/ICSI success rate.
Objective: The aim of this study was to investigate the correlation between cholesteryl
ester transfer protein (CETP) level in FF and the success rate of IVF/ICSI.
Materials and Methods: In a cross-sectional study, FF samples, FF samples were
obtained from 100 patients referred to Tabriz Alzahra Hospital. Seventy-nine subjects
underwent IVF and the remaining 21 underwent ICSI. The levels of high-density
lipoprotein cholesterol (HDL-C), apolipoprotein A-I and CETP were measured using
enzymatic, turbidometric and ELISA methods respectively.
Results: Analysis of the subgroups with different levels of CETP showed a significant
lower level of CETP in the subgroup with the lowest number of mature oocytes
(p<0.05). The level of CETP was also considerably lower (18%, p=0.05) in subjects
with<50% oocytes fertilization ratio than subjects with >70% of this ratio.
Conclusion: While no association was found for pregnancy, the amount of CETP in FF
was associated positively to the maturity and the percentage of oocyte fertilization.
Key words: Infertility, IVF/ICSI, Apolipoprotein A-I, CETP.
Introduction
Infertility is a multifactorial disorder with
lifestyle and environmental traits playing important
role (1). Assisted conception techniques such as
IVF/ICSI are used to treat a range of infertilities.
However, these techniques are not always
successful and potential factors contributing to a
successful IVF/ICSI treatment are being
Corresponding Author:
Mohammad Nouri, Department of Biochemistry,
Faculty of Medicine, Tabriz University of Medical
Sciences, Tabriz, Iran.
Email: [email protected]
investigated (2).
Follicular fluid (FF) which is necessary for the
development of the female gamete, may also affect
the fertilization and embryonic development.
Therefore, FF is occasionally used as a medium
supplement in clinical IVF (3). High density
lipoprotein (HDL) particles of FF are the most
important agent for transferring cholesterol to
granulosa cells (4). So, HDL cholesterol (HDL-C)
is the most important resource of cholesterol for
progesterone synthesis after LH surge (5, 6).
Apolipoprotein A-I (apo A-I) is the major
apolipoprotein in FF, which is associated with
HDL (7). The cholesteryl ester transfer protein
Mehdizadeh et al
194 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 193-198, Summer 2011
(CETP), a hydrophobic glycoprotein transfers
cholesteryl esters from HDL to apolipoprotein B
(apoB)-containing lipoproteins (8). It seems that
the role and importance of CETP in blood is
different than other tissues. It has been
demonstrated that CETP is related to cell
membrane and affects on membrane physical and
chemical characteristics by facilitating selective
uptake of HDL-derived cholesteryl esters (9, 10).
Ranvik et al (11) reported that FF has lipid
transfer activity, and fractions of FF with this
activity stimulate human sperm capacitation and
acrosome reaction. It has been shown that this
process involves a sterol depletion of the
spermatozoa membrane (12).
The aim of the present study was to investigate
the correlation between CETP level in FF and the
success of IVF/ICSI techniques in infertile patients
undergoing these techniques.
Materials and methods
A total of 100 patients referred to Tabriz
Alzahra Hospital in 2007-2009 were selected for
this cross-sectional study. All participants received
a screening history, physical examination,
measurements of serum hormone levels and blood
counts. The subjects' body mass index (BMI) was
calculated as measured weight divided by the
square of measured height (kg/ m2).
The mean age of subjects was 32±5.46 years
with no evidence of any disease. Healthy husband
with no smoking habit were defined as including
criteria. Uterus abnormalities, positive history of
endocrine disease and inflammatory disorders such
as thyroid and adrenal disorders, immune system
defect and sexual hormones disorders were
considered as exclusion criteria in this study.
Ovarian stimulation was achieved with a GnRH
agonist (Sereno, Switzerland) /FSH- long down
regulation protocol (13). Controlled ovarian
stimulation was started with recombinant human
follicle stimulating hormone (rFSH; Sereno,
Switzerland) at the third day of menstrual cycle.
The daily rFSH dose ranged between 150 and 300
IU, depending on body mass index, age of the
women, and the anticipated ovarian response. Dose
adjustment was done according to follicular
development and serum estradiol levels.
Intramuscular hCG (1000IU, Choriomon, Meizler,
Brazil) was administered when sonography
revealed the average diameter of 3 preovulatory
follicle had approached 18- 20mm.
Oocyte retrieval was done 36 h after hCG
administration by vaginal ultrasound-guided
puncture of the ovarian follicles. The collected
oocytes were incubated in 37ºc with 6% CO2 for
3-4 hours and then were used for IVF and ICSI. FF
was collected in a sterile tube, was centrifuged at
1500rpm for 5min and kept frozen at -70˚C until
analyses.
Oocytes with sporadic cumulus oophorus and
zona pellucida and also a clear ooplasm were
selected for insemination. The swim-up was used
to prepare sperm for IVF (14). Oocytes were
inseminated with 250000 sperm per oocytes in the
IVF technique (15). In the ICSI group, a single
motile sperm were injected into oocyes (16). After
24h, oocyets were separated from surrounding
granulosa cells. A maximum of three embryos
were transferred at 4-8 cells stages after 48h, under
ultrasound guidance. Clinical pregnancy assessed
by β-hCG test, 14 days after embryo transfer.
Proportion of the oocytes that had 2 pronuclei
was estimated as fertilization rate. This project was
approved by the ethics committee of Tabriz
University of Medical Sciences. Before the
sampling, we took a written consent from studied
subjects.
The levels of follicular HDL-C were measured
using enzymatic method by an Abbott Alycon 300
auto analyser. Apolipoprotein A-I concentration
determined by immune turbidometric method
(Diasys, Germany). The level of CETP was
measured by using an Alpco ELISA kit (catalogue
number 44-ADPRT-E01).
Statistical analysis
Values are presented as mean± S.D. The one
way ANOVA with Tukey post hoc pairwise
comparison and Multivariate analysis of variance
test were used for comparing means and ratios in
different groups. p-values of <0.05 were
considered statistically significant. Analysis was
carried out using SPSS 11.5 statistical software.
Results
General characteristics, husband spermogram
and FF parameters are shown in table I. The
average number of mature oocytes and fertilized
oocytes were 8.57±4.19 and 5.0±3.0, respectively.
The percentage of pregnancy in the studied
population was 24%.
As shown in table II the age of patients was
inversely associated with the number of mature
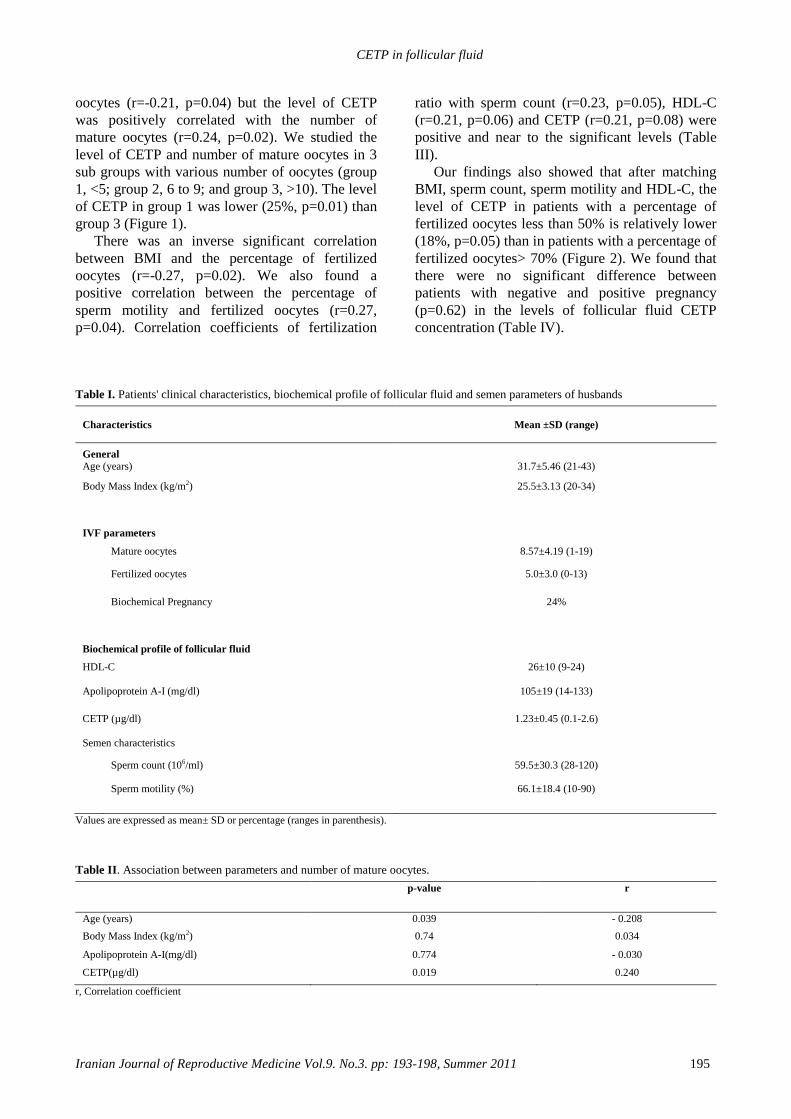
CETP in follicular fluid
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 193-198, Summer 2011 195
oocytes (r=-0.21, p=0.04) but the level of CETP
was positively correlated with the number of
mature oocytes (r=0.24, p=0.02). We studied the
level of CETP and number of mature oocytes in 3
sub groups with various number of oocytes (group
1, <5; group 2, 6 to 9; and group 3, >10). The level
of CETP in group 1 was lower (25%, p=0.01) than
group 3 (Figure 1).
There was an inverse significant correlation
between BMI and the percentage of fertilized
oocytes (r=-0.27, p=0.02). We also found a
positive correlation between the percentage of
sperm motility and fertilized oocytes (r=0.27,
p=0.04). Correlation coefficients of fertilization
ratio with sperm count (r=0.23, p=0.05), HDL-C
(r=0.21, p=0.06) and CETP (r=0.21, p=0.08) were
positive and near to the significant levels (Table
III).
Our findings also showed that after matching
BMI, sperm count, sperm motility and HDL-C, the
level of CETP in patients with a percentage of
fertilized oocytes less than 50% is relatively lower
(18%, p=0.05) than in patients with a percentage of
fertilized oocytes> 70% (Figure 2). We found that
there were no significant difference between
patients with negative and positive pregnancy
(p=0.62) in the levels of follicular fluid CETP
concentration (Table IV).
Table I. Patients' clinical characteristics, biochemical profile of follicular fluid and semen parameters of husbands
Characteristics Mean ±SD (range)
General Age (years)
31.7±5.46 (21-43)
Body Mass Index (kg/m2)
25.5±3.13 (20-34)
IVF parameters
Mature oocytes
8.57±4.19 (1-19)
Fertilized oocytes
5.0±3.0 (0-13)
Biochemical Pregnancy 24%
Biochemical profile of follicular fluid
HDL-C
26±10 (9-24)
Apolipoprotein A-I (mg/dl)
105±19 (14-133)
CETP (µg/dl)
1.23±0.45 (0.1-2.6)
Semen characteristics
Sperm count (106/ml)
59.5±30.3 (28-120)
Sperm motility (%)
66.1±18.4 (10-90)
Values are expressed as mean± SD or percentage (ranges in parenthesis).
Table II. Association between parameters and number of mature oocytes.
p-value r
Age (years)
0.039 - 0.208
Body Mass Index (kg/m2)
0.74 0.034
Apolipoprotein A-I(mg/dl)
0.774 - 0.030
CETP(µg/dl)
0.019 0.240
r, Correlation coefficient
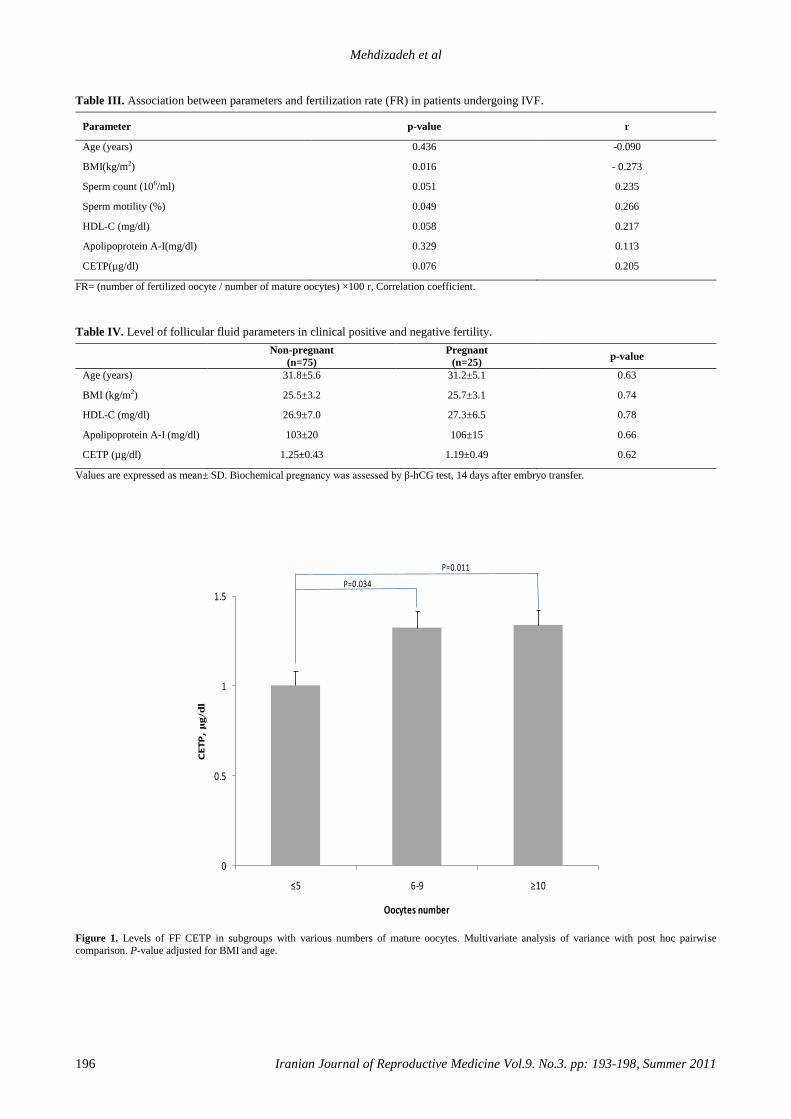
Mehdizadeh et al
196 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 193-198, Summer 2011
Table III. Association between parameters and fertilization rate (FR) in patients undergoing IVF.
Parameter p-value r
Age (years)
0.436 -0.090
BMI(kg/m2)
0.016 - 0.273
Sperm count (106/ml)
0.051 0.235
Sperm motility (%)
0.049 0.266
HDL-C (mg/dl)
0.058 0.217
Apolipoprotein A-I(mg/dl)
0.329 0.113
CETP(µg/dl)
0.076 0.205
FR= (number of fertilized oocyte / number of mature oocytes) ×100 r, Correlation coefficient.
Table IV. Level of follicular fluid parameters in clinical positive and negative fertility.
Non-pregnant
(n=75)
Pregnant
(n=25) p-value
Age (years)
31.8±5.6 31.2±5.1 0.63
BMI (kg/m2)
25.5±3.2 25.7±3.1 0.74
HDL-C (mg/dl)
26.9±7.0 27.3±6.5 0.78
Apolipoprotein A-I (mg/dl)
103±20 106±15 0.66
CETP (µg/dl)
1.25±0.43 1.19±0.49 0.62
Values are expressed as mean± SD. Biochemical pregnancy was assessed by β-hCG test, 14 days after embryo transfer.
0
0.5
1
1.5
≤5 6-9 ≥10
CE
TP
, μ
g/d
l
Oocytes number
P=0.011
P=0.034
Figure 1. Levels of FF CETP in subgroups with various numbers of mature oocytes. Multivariate analysis of variance with post hoc pairwise
comparison. P-value adjusted for BMI and age.
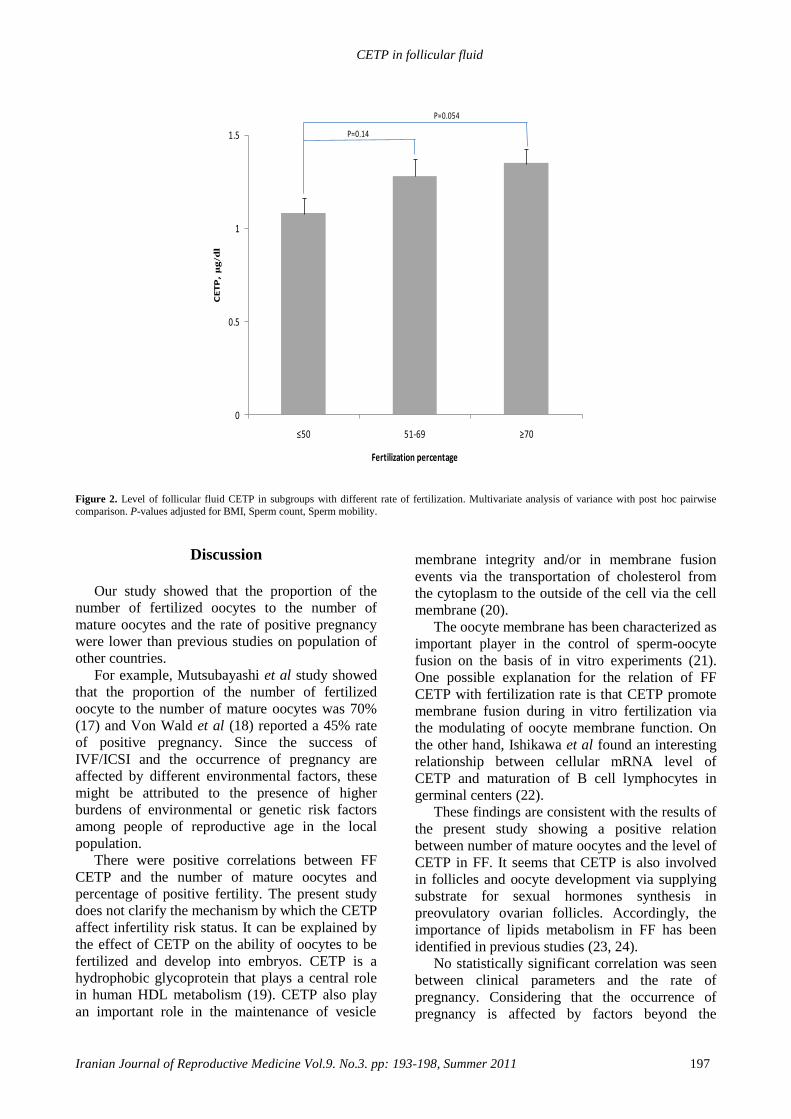
CETP in follicular fluid
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 193-198, Summer 2011 197
0
0.5
1
1.5
≤50 51-69 ≥70
CE
TP
, μ
g/d
l
Fertilization percentage
P=0.054
P=0.14
Figure 2. Level of follicular fluid CETP in subgroups with different rate of fertilization. Multivariate analysis of variance with post hoc pairwise
comparison. P-values adjusted for BMI, Sperm count, Sperm mobility.
Discussion
Our study showed that the proportion of the
number of fertilized oocytes to the number of
mature oocytes and the rate of positive pregnancy
were lower than previous studies on population of
other countries.
For example, Mutsubayashi et al study showed
that the proportion of the number of fertilized
oocyte to the number of mature oocytes was 70%
(17) and Von Wald et al (18) reported a 45% rate
of positive pregnancy. Since the success of
IVF/ICSI and the occurrence of pregnancy are
affected by different environmental factors, these
might be attributed to the presence of higher
burdens of environmental or genetic risk factors
among people of reproductive age in the local
population.
There were positive correlations between FF
CETP and the number of mature oocytes and
percentage of positive fertility. The present study
does not clarify the mechanism by which the CETP
affect infertility risk status. It can be explained by
the effect of CETP on the ability of oocytes to be
fertilized and develop into embryos. CETP is a
hydrophobic glycoprotein that plays a central role
in human HDL metabolism (19). CETP also play
an important role in the maintenance of vesicle
membrane integrity and/or in membrane fusion
events via the transportation of cholesterol from
the cytoplasm to the outside of the cell via the cell
membrane (20).
The oocyte membrane has been characterized as
important player in the control of sperm-oocyte
fusion on the basis of in vitro experiments (21).
One possible explanation for the relation of FF
CETP with fertilization rate is that CETP promote
membrane fusion during in vitro fertilization via
the modulating of oocyte membrane function. On
the other hand, Ishikawa et al found an interesting
relationship between cellular mRNA level of
CETP and maturation of B cell lymphocytes in
germinal centers (22).
These findings are consistent with the results of
the present study showing a positive relation
between number of mature oocytes and the level of
CETP in FF. It seems that CETP is also involved
in follicles and oocyte development via supplying
substrate for sexual hormones synthesis in
preovulatory ovarian follicles. Accordingly, the
importance of lipids metabolism in FF has been
identified in previous studies (23, 24).
No statistically significant correlation was seen
between clinical parameters and the rate of
pregnancy. Considering that the occurrence of
pregnancy is affected by factors beyond the
Mehdizadeh et al
198 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 193-198, Summer 2011
characteristics of FF, the absence of a significant
relationship between the parameters and the
occurrence of pregnancy is probably because of the
indirect nature of the relationship and/or the low
number of subjects.
According to the results of this study, while
there was no association for pregnancy, the amount
of FF CETP was correlated positively with the
maturity and the percentage of oocyte fertilization.
These findings are consistent with the hypothesis
that CETP FF plays an important role in
cholesterol and lipid metabolism of follicles.
Acknowledgment
This work has been supported by Research
Center for Pharmaceutical Nanotechnology, Tabriz
University of Medical Sciences.
References
1. Kallen B. Maternal morbidity and mortality in in-vitro
fertilization. Best Pract Res Clin Obstet Gynaecol 2008;
22: 549-558.
2. Youssry M, Ozmen B, Orief Y, Zohni KH, Al-Hassani S.
Human sperm DNA damage in the context of assisted
reproductive techniques. Iran J Rep Med 2007; 4: 137-
150.
3. Tokumura A, Miyake M, Nishioka Y, Yamano S, Aono T,
Fukuzawa K. Production of lysophosphatidic acids by
lysophospholipase D in human follicular fluids of In vitro
fertilization patients. Biol Reprod 1999; 61:195-199.
4. Grummer RR, Carroll DJ. A review of lipoprotein
cholesterol metabolism: importance to ovarian function. J
Anim Sci 1988; 66: 3160-3173.
5. Perret BP, Parinaud J, Ribbes H, Moatti JP, Pontonnier G,
Chap H, et al. Lipoprotein and phospholipid distribution in
human follicular fluids. Fertil Steril 1985; 43: 405-409.
6. Shalgi R, Kraicer P, Rimon A, Pinto M, Soferman N.
Proteins of human follicular fluid: the blood-follicle
barrier. Fertil Steril 1973; 24: 429-434.
7. Jaspard B, Fournier N, Vieitez G, Atger V, Barbaras R,
Vieu C, et al. Structural and functional comparison of
HDL from homologous human plasma and follicular fluid.
A model for extravascular fluid. Arterioscler Thromb Vasc
Biol 1997; 17: 1605-1613.
8. Ghatrehsamani K, Darabi M, Rahbani M, Hashemzadeh
Chaleshtory M, Farrokhi E, Noori M. Combined hepatic
lipase -514C/T and cholesteryl ester transfer protein
I405V polymorphisms are associated with the risk of
coronary artery disease. Genet Test Mol Biomarkers 2009;
13: 809-815.
9. Morton RE. Interaction of plasma-derived lipid transfer
protein with macrophages in culture. J Lipid Res 1988; 29:
1367-1377.
10. Benoist F, Lau P, McDonnell M, Doelle H, Milne R,
McPherson R. Cholesteryl ester transfer protein mediates
selective uptake of high density lipoprotein cholesteryl
esters by human adipose tissue. J Biol Chem 1997; 272:
23572-23577.
11. Ravnik SE, Zarutskie PW, Muller CH. Purification and
characterization of a human follicular fluid lipid transfer
protein that stimulates human sperm capacitation. Biol
Reprod 1992; 47: 1126-1133.
12. Masson D, Drouineaud V, Moiroux P, Gautier T, Dautin
G, Schneider M, et al. Human seminal plasma displays
significant phospholipid transfer activity due to the
presence of active phospholipid transfer protein. Mol Hum
Reprod 2003; 9: 457-464.
13. Ata B, Yakin K, Balaban B, Urman B. GnRH agonist
protocol administration in the luteal phase in ICSI-ET
cycles stimulated with the long GnRH agonist protocol: a
randomized, controlled double blind study. Hum Reprod
2008; 23: 668-673.
14. Trounson AO, Gardner DK. Hand book of in vitro
fertilization. 2nd Ed. Florida; CRC press; 1999.
15. Brinsden PR, Hall B. A Textbook of In Vitro Fertilization
and Assisted Reproduction: The Bourn Hall Guide to
Clinical and Laboratory Practice. London; The Parthenon
Publishing Group; 1999.
16. Masson D, Drouineaud V, Moiroux P, Gautier T, Dautin
G, Schneider M, et al. High fertilization and implantation
rates after intracytoplasmic sperm injection. Hum Reprod
1993; 8: 1061-1066.
17. Matsubayashi H, Sugi T, Arai T, Shida M, Kondo A,
Suzuki T, et al. IgG-antiphospholipid antibodies in
follicular fluid of IVF-ET patients are related to low
fertilization rate of their oocytes. Am J Reprod Immunol
2006; 55: 341-348.
18. Von Wald T, Monisova Y, Hacker MR, Yoo SW, Penzias
AS, Reindollar RR, et al. Age-related variations in
follicular apolipoproteins may influence human oocyte
maturation and fertility potential. Fertil Steril 2010; 93:
2354-2361.
19. Boekholdt SM, Sacks FM, Jukema JW, Shepherd J,
Freeman DJ, McMahon AD, et al. Cholesteryl ester
transfer protein TaqIB variant, high-density lipoprotein
cholesterol levels, cardiovascular risk, and efficacy of
pravastatin treatment: individual patient meta-analysis of
13,677 subjects. Circulation 2005; 111: 278-287.
20. Collet X, Tall AR, Serajuddin H, Guendouzi K, Royer L,
Oliveira H, et al. Remodeling of HDL by CETP in vivo
and by CETP and hepatic lipase in vitro results in
enhanced uptake of HDL CE by cells expressing
scavenger receptor B-I. J Lipid Res 1999; 40: 1185-1193.
21. Kaji K, Kudo A. The mechanism of sperm-oocyte fusion
in mammals. Reproduction 2004; 127: 423-429.
22. Ito K, Ishikawa F, Kanno T, Ishikawa Y, Akasaka Y,
Akishima Y, et al. Expression of cholesteryl ester transfer
protein (CETP) in germinal centre B cells and their
neoplastic counterparts. Histopathology 2004; 45: 73-81.
23. Balestrieri M, Cigliano L, Simone ML, Dale B, Abrescia
P. Haptoglobin inhibits lecithin-cholesterol acyltransferase
in human ovarian follicular fluid. Mol Reprod Dev 2001;
59: 186-191.
24. Hochberg RB. Biological esterification of steroids. Endocr
Rev 1998; 19: 331-348.

Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:199-202, Summer 2011
Diagnostic value of saline contrast sonohysterography
comparing with hysteroscopy for detecting
endometrial abnormalities in women with abnormal
uterine bleeding Mohammad Ali Karimzadeh
1 M.D., Razieh Dehghani Firouzabadi
1 M.D., Farzaneh Goharzad
2 M.D.
1 Department of Obstetrics and Gynecology, Research and Clinical Center for Infertility, Shahid
Sadoughi University of Medical Sciences, Yazd, Iran.
2 Department of Obstetrics and Gynecology, Shahid Sadoughi Hospital, Shahid Sadoughi University of
Medical Sciences, Yazd, Iran.
Received: 14 June 2010; accepted: 3 October 2010
Abstract
Background: Abnormal uterine bleeding is a common presentation of uterine
abnormalities among premenopausal and postmenopausal women.
Objective: To evaluate and compare the diagnostic accuracy of saline contrast
sonohysterography and hysteroscopy for detecting the cause of abnormal uterine
bleeding.
Materials and Methods: A total of 65 women with abnormal uterine bleeding were
enrolled in this study. A prior saline contrast sonohysetrography followed by a
hysteroscopy was performed in all cases. Sensitivity, specificity, positive and negative
predictive value and test accuracy were calculated.
Results: As the most common abnormality, SCSH showed hyperplasia in 19 patients
while hysteroscopy diagnosed polyp in 15 cases. A sensitivity of 73.3%, 71.4% and
90.9% were reported for polyp, hyperplasia and submucous myoma respectively
whereas the specificity was calculated 96% for polyps, 82.3% for hyperplasia and
90.7% for submucous myoma. Conclusion: Comparing with hysteroscopy, sonohysterography showed a high
sensitivity and specificity for detecting submucous myoma but not for endometrial
polyp and endometrial hyperplasia.
Key words: Abnormal uterine bleeding, Uterine abnormalities, Sonohysterography, Hysteroscopy.
This article extracted from residential thesis
Introduction
Abnormal uterine bleeding (AUB) is a common
presenting symptom among women. AUB is
presented in 33% of women referred to
gynecologists and this pattern increases to 69% in
premenopausal and post menopausal women (1).
AUB can be caused by a variety of uterine
abnormalities such as polyp, submucous
Corresponding Author:
Razieh Dehghani Firouzabadi, Department of
Obstetrics and Gynecology, Research and Clinical
Center for Infertility, Shahid Sadoughi University of
Medical Sciences, Yazd, Iran.
Email: [email protected]
myoma, endometrial hyperplasia and endometrial
carcinoma. Cases of AUB require a good
diagnostic and therapeutic approach which can be
acquired by traditional dilatation and curettage or
recent and more effective diagnostic tools.
A variety of tools can be used for the diagnosis
of uterine abnormalities lead to AUB. Among
them, transvaginal sonography (TVS), saline
contrast sonohysterography (SCSH) and
hysteroscopy have been used commonly. TVS is
the first line investigation tool for diagnosis of
uterine abnormalities, whereas hysteroscopy has
become the gold standard for the evaluation of
patients with AUB. In postmenopausal women
TVS is an effective screening test for evaluation of

Karimzadeh et al
200 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 199-202, Summer 2011
abnormal uterine bleeding caused by endometrial
atrophy (2). But in the figure of thickened and
inhomogeneous endometrium, TVS is presented as
a low specificity and limited diagnostic test which
can be replaced by SCSH (3, 4). SCSH can
distinguish between focal lesions such as polyps
and submucous myomas (5, 6) and diffuse lesions
like hyperplasia and cancer accurately (7, 8).
Furthermore, hysteroscopy is an effective but
expensive and invasive screening test for
evaluation of the uterine cavity in both pre and
postmenopausal women with AUB (9, 10).
Preoperative imaging of the uterine cavity is
very important and the results can be necessary for
the surgical management. A useful imaging
technique for accurate diagnosis should be highly
sensitive and specific, non invasive and cost-
effective. It seems that SCSH is a non invasive,
cheap and feasible technique with lower pain. In
order to compare SCSH and hysteroscopy, the
majority of women found that SCSH was not
painful, whereas only 25% said the same for
hysteroscopy (11). If it can be proven that the
sensitivity and specificity of SCSH and
hysteroscopy are the same, it can be recommended
as the first line detecting tool for uterine
abnormalities caused AUB.
The objective of this study was to evaluate the
sensitivity and specificity of SCSH compare with
hysteroscopy in the investigation of women of
reproductive age presenting with AUB.
Materials and methods
Patients
65 consecutive women presenting AUB or
infertility were enrolled in this diagnostic study.
These patients were referred to both Yazd Shahid
Sadoughi and Yazd Madar Hospital from March
2006 to February 2007. The women who have any
evidence of systemic disease such as diabetes,
hypertension, PCO, thyroid disease, evidence of
pregnancy, evidence of pelvic inflammatory
disease and history of uterine surgeries were
excluded from the study. After obtaining informed
consent, saline contrast sonohysetrography
followed by a hysteroscopy was done in all cases.
The institutional Review Board at Yazd University
of Medical Sciences approved this prospective
study.
Imaging techniques Regarding SCSH, a sterile speculum was
passed, the cervix visualized and disinfected with Betadine solution. A flexible Foley catheter
number 8 with inflatable balloon (Supa, Tehran, Iran) was inserted through the cervical canal into the uterine cavity. After confirmation of the position of the catheter, 10ml of 0.9% sterile saline solution was injected into the uterine cavity slowly and continued to obtain optimal views of endometrial cavity. By using concomitant transvaginal sonography, the uterine cavity was evaluated for detecting any abnormality or pathological condition. This procedure was performed by a single investigator without the use of local anesthesia or prophylactic antibiotic therapy. All patients had diagnostic operative hysteroscopy under a general anesthesia. Hysteroscopy was performed using cervix dilatation, 2 Misoprostol tablet (6 hours before operation) and prophylactic antibiotic. The hysteroscopies were done by the expert operator who was blinded to the SCSH results. Endometrial biopsy was carried out directly after hysteroscopy. Statistical analysis
The Statistical Package for the Social Sciences 13.0 software was used to analyze data of all patients. Sensitivity, specificity, positive and negative predictive value and test accuracy were calculated for SCSH as compared with findings of hysteroscopy.
Results
Among 65 evaluated women, 78.5% presented AUB and 21.5% had infertility problem. The mean age of women presenting AUB was 37.02±7.85 years and infertile women had mean age of 25.50± 4.22 years. The most common abnormality in SCSH was hyperplasia (29.2%) while it was polyp (23.1%) in hysteroscopy. Hyperplasia was detected in 21.5% of cases by hysteroscopy and polyp was seen in 20% of patients using SCSH. As the second cause, SCSH suggested the presence of cancer in 23.1% of women whereas it was hyperplasia among 21.5% of cases in hysteroscopy group. The number and percentage of abnormalities detected in patients are listed in table I. According to hysteroscopy results the diagnosis of 36.9% of women remained unknown and it was 26.2% in SCSH. SCSH showed a sensitivity of 73.3%, 71.4% and 90.9% for polyp, hyperplasia and submucous myoma respectively whereas the specificity was reported 96% for polyps, 82.3% for hyperplasia and 90.7% for submucous myoma. Table II shows the sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and accuracy for SCSH compared with hysteroscopy as a gold standard.
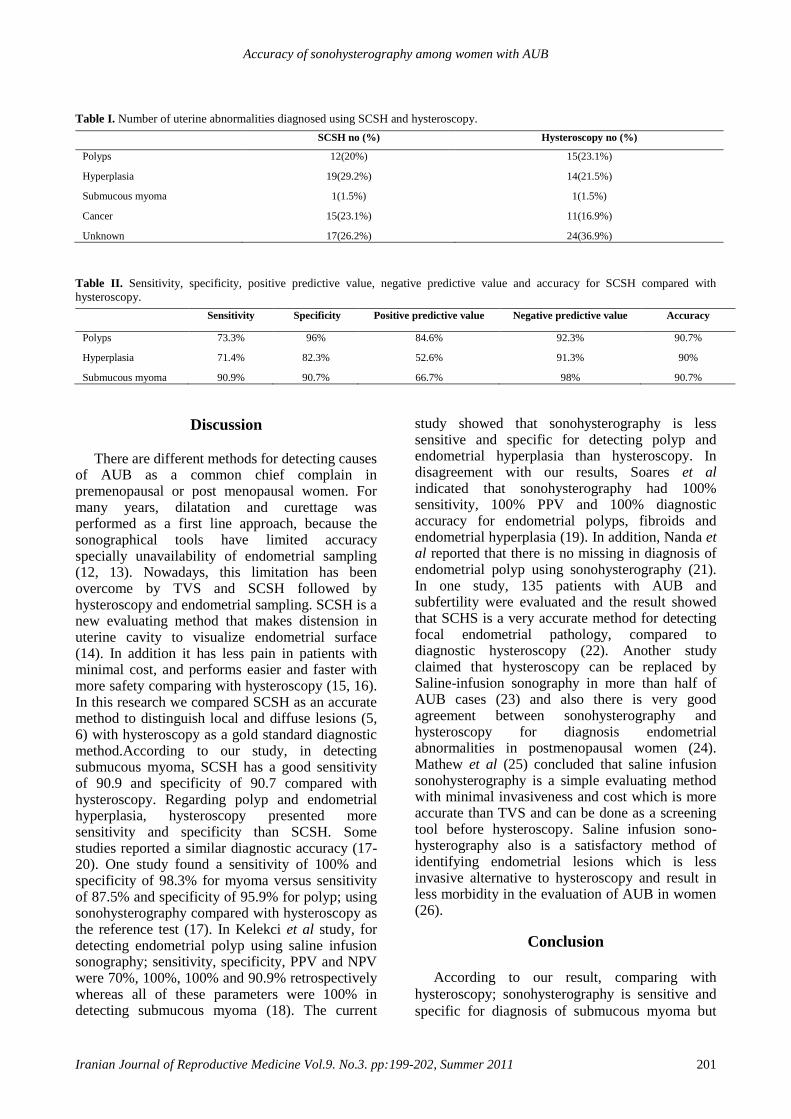
Accuracy of sonohysterography among women with AUB
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:199-202, Summer 2011 201
Table I. Number of uterine abnormalities diagnosed using SCSH and hysteroscopy.
SCSH no (%) Hysteroscopy no (%)
Polyps
12(20%) 15(23.1%)
Hyperplasia
19(29.2%) 14(21.5%)
Submucous myoma
1(1.5%) 1(1.5%)
Cancer
15(23.1%) 11(16.9%)
Unknown 17(26.2%) 24(36.9%)
Table II. Sensitivity, specificity, positive predictive value, negative predictive value and accuracy for SCSH compared with
hysteroscopy.
Sensitivity Specificity Positive predictive value Negative predictive value Accuracy
Polyps
73.3% 96% 84.6% 92.3% 90.7%
Hyperplasia
71.4% 82.3% 52.6% 91.3% 90%
Submucous myoma 90.9% 90.7% 66.7% 98% 90.7%
Discussion
There are different methods for detecting causes of AUB as a common chief complain in premenopausal or post menopausal women. For many years, dilatation and curettage was performed as a first line approach, because the sonographical tools have limited accuracy specially unavailability of endometrial sampling (12, 13). Nowadays, this limitation has been overcome by TVS and SCSH followed by hysteroscopy and endometrial sampling. SCSH is a new evaluating method that makes distension in uterine cavity to visualize endometrial surface (14). In addition it has less pain in patients with minimal cost, and performs easier and faster with more safety comparing with hysteroscopy (15, 16). In this research we compared SCSH as an accurate method to distinguish local and diffuse lesions (5, 6) with hysteroscopy as a gold standard diagnostic method.According to our study, in detecting submucous myoma, SCSH has a good sensitivity of 90.9 and specificity of 90.7 compared with hysteroscopy. Regarding polyp and endometrial hyperplasia, hysteroscopy presented more sensitivity and specificity than SCSH. Some studies reported a similar diagnostic accuracy (17-20). One study found a sensitivity of 100% and specificity of 98.3% for myoma versus sensitivity of 87.5% and specificity of 95.9% for polyp; using sonohysterography compared with hysteroscopy as the reference test (17). In Kelekci et al study, for detecting endometrial polyp using saline infusion sonography; sensitivity, specificity, PPV and NPV were 70%, 100%, 100% and 90.9% retrospectively whereas all of these parameters were 100% in detecting submucous myoma (18). The current
study showed that sonohysterography is less sensitive and specific for detecting polyp and endometrial hyperplasia than hysteroscopy. In disagreement with our results, Soares et al indicated that sonohysterography had 100% sensitivity, 100% PPV and 100% diagnostic accuracy for endometrial polyps, fibroids and endometrial hyperplasia (19). In addition, Nanda et al reported that there is no missing in diagnosis of endometrial polyp using sonohysterography (21). In one study, 135 patients with AUB and subfertility were evaluated and the result showed that SCHS is a very accurate method for detecting focal endometrial pathology, compared to diagnostic hysteroscopy (22). Another study claimed that hysteroscopy can be replaced by Saline-infusion sonography in more than half of AUB cases (23) and also there is very good agreement between sonohysterography and hysteroscopy for diagnosis endometrial abnormalities in postmenopausal women (24). Mathew et al (25) concluded that saline infusion sonohysterography is a simple evaluating method with minimal invasiveness and cost which is more accurate than TVS and can be done as a screening tool before hysteroscopy. Saline infusion sono-hysterography also is a satisfactory method of identifying endometrial lesions which is less invasive alternative to hysteroscopy and result in less morbidity in the evaluation of AUB in women (26).
Conclusion
According to our result, comparing with
hysteroscopy; sonohysterography is sensitive and
specific for diagnosis of submucous myoma but
Karimzadeh et al
202 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 199-202, Summer 2011
not for endometrial polyp and endometrial
hyperplasia. However hysteroscopy is a therapeutic
procedure and it is preferable for its therapeutic
role.
Acknowledgement
The authors thank the staff of operation room of
Madar Hospital and Shahid Sadoughi Hospital for
their cooperation.
References 1. Mencaglia L, Perino A, Hamou J. Hysteroscopy in
perimenopausal and postmenopausal women with
abnormal uterine bleeding. J Reprod Med 1987; 32: 577-
582.
2. Karlsson B, Granberg S, Wikland M, Ylöstalo P, Torvid
K, Marsal K, et al. Transvaginal ultrasonography of the
endometrium in women with postmenopausal bleeding-a
Nordic multicenter study. Am J Obstet Gynecol 1995; 172:
1488-1494.
3. Breitkopf D, Goldstein SR, Seeds JW. ACOG technology
assessment in obstetrics and gynecology. Saline infusion
sonohysterography. Obstet Gynecol 2003; 102: 659-662.
4. de Kroon CD, de Bock GH, Dieben SW, Jansen FW.
Saline contrast hysterosonography in abnormal uterine
bleeding: a systematic review and meta-analysis. BJOG
2003; 110: 938-947.
5. Epstein E, Ramirez A, Skoog L, Valentin L. Transvaginal
sonography, saline contrast sonohysterography and
hysteroscopy for the investigation of women with
postmenopausal bleeding and endometrium>5mm.
Ultrasound Obstet Gynecol 2001; 18: 157-162.
6. Leone FP, Lanzani C, Ferrazzi E. Use of strict
sonohysterographic methods for preoperative assessment
of submucous myomas. Fertil Steril 2003; 79: 998-1002.
7. Parsons AK, Lense JJ. Sonohysterography for endometrial
abnormalities: preliminary results. J Clin Ultrasound
1993; 21: 87-95.
8. Ferrazzi E, Leone FP. Investigating abnormal bleeding on
HRT or tamoxifen: the role of ultrasonography. Best Pract
Res Clin Obstet Gynaecol 2004; 18: 145-156.
9. Dijkhuizen FP, Mol BW, Bongers MY, Brölmann HA,
Heintz AP. Cost-effectiveness of transvaginal sonography
and saline infused sonography in the evaluation of
menorrhagia. Int J Gynaecol Obstet 2003; 83: 45-52.
10. Dijkhuizen FP, Mol BW, Brölmann HA, Heintz AP. Cost-
effectiveness of the use of transvaginal sonography in the
evaluation of postmenopausal bleeding. Maturitas 2003;
45: 275-282.
11. Van den Bosch T, Verguts J, Daemen A, Gevaert O,
Domali E, Claerhout F, et al. Pain experienced during
transvaginal ultrasound, saline contrast
sonohysterography, hysteroscopy and office sampling:
comparative study. Ultrasound Obstet Gynecol 2008; 31:
346-351.
12. Bettocchi S, Ceci O, Vicino M, Marello F, Impedovo L,
Selvaggi L. Diagnostic inadequacy of dilatation and
curettage. Fertil Steril 2001; 75: 803-805.
13. Epstein E, Ramirez A, Skoog L, Valentin L. Dilatation
and curettage fails to detect most focal lesions in the
uterine cavity in women with postmenopausal bleeding.
Acta Obstet Gynecol Scand 2001; 80: 1131-1136.
14. Parsons AK, Lense JJ. Sonohysterography for endometrial
abnormalities: preliminary results. J Clin Ultrasound
1993; 21: 87-95.
15. Goldstein SR, Zeltser I, Horan CK, Snyder JR, Schwartz
LB. Ultrasonography-based triage for perimenopausal
patients with abnormal uterine bleeding. Am J Obstet
Gynecol 1997; 177: 102-108.
16. Widrich T, Bradley LD, Mitchinson AR, Collins RL.
Comparison of saline infusion sonography with office
hysteroscopy for the evaluation of the endometrium. Am J
Obstet Gynecol 1996; 174: 1327-1334.
17. Alborzi S, Parsanezhad ME, Mahmoodian N, Alborzi S,
Alborzi M. Sonohysterography versus transvaginal
sonography for screening of patients with abnormal
uterine bleeding. Int J Gynaecol Obstet 2007; 96: 20-23.
18. Kelekci S, Kaya E, Alan M, Alan Y, Bilge U,
Mollamahmutoglu L. Comparison of transvaginal
sonography, saline infusion sonography, and office
hysteroscopy in reproductive-aged women with or without
abnormal uterine bleeding. Fertil Steril 2005; 84: 682-686.
19. Soares SR, Barbosa dos Reis MM, Camargos AF.
Diagnostic accuracy of sonohysterography, transvaginal
sonography, and hysterosalpingography in patients with
uterine cavity diseases. Fertil Steril 2000; 73: 406-411.
20. Kamel HS, Darwish AM, Mohamed SA. Comparison of
transvaginal ultrasonography and vaginal
sonohysterography in the detection of endometrial polyps.
Acta Obstet Gynecol Scand 2000; 79: 60-64.
21. Nanda S, Chadha N, Sen J, Sangwan K. Transvaginal
sonography and saline infusion sonohysterography in the
evaluation of abnormal uterine bleeding. Aust N Z J Obstet
Gynaecol 2002; 42: 530-534.
22. Milingos S, Kallipolitis G, Stefanidis K, Sklia J, Makris N,
Loutradis D, et al. Saline contrast hysterosonography in
infertile patients and in women with abnormal uterine
bleeding. Eur J Gynaecol Oncol 2005; 26: 564-567.
23. Brölmann HA, Bongers MY, Moret E, Smeets N, Bremer
GL, Dijkhuizen FP. Transvaginal contrast sonography of
the uterus in the diagnosis of abnormal uterine blood loss:
less hysteroscopies needed. Ned Tijdschr Geneeskd 2003;
147: 502-506.
24. Gumus II, Keskin EA, Kiliç E, Aker A, Kafali H, Turhan
NO. Diagnostic value of hysteroscopy and
hysterosonography in endometrial abnormalities in
asymptomatic postmenopausal women. Arch Gynecol
Obstet 2008; 278: 241-244.
25. Mathew M, Gowri V, Rizvi SG. Saline infusion
sonohysterography- an effective tool for evaluation of the
endometrial cavity in women with abnormal uterine
bleeding. Acta Obstet Gynecol Scand 2010; 89: 140-142.
26. Yildizhan B, Yildizhan R, Ozkesici B, Suer N.
Transvaginal ultrasonography and saline infusion
sonohysterography for the detection of intra-uterine
lesions in pre- and post-menopausal women with
abnormal uterine bleeding. J Int Med Res 2008; 36: 1205-
1213.

Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:203-208, Summer 2011
Successful pregnancy following the transfer of vitrified
blastocyst which developed from poor quality embryos
on day 3 Xiao-jian Zhang M.Sc., Ye-zhou Yang Ph.D., Li-hua Min B.N., Qun Lv B.Sc. , Pin Bai B.N., Xiao-jie
Li B.S.M.T., Mei-xu Liao M.Sc.
Department of Assisted Reproductive Medical Center, Sichuan Academy of Medical Sciences and
Sichuan Provincial People’s Hospital, Sichuan, China.
Received: 5 July 2010; accepted: 11 January 2011
Abstract
Background: The selection of pre-embryos for transferred is based on morphological
appearance. But some poor quality cleaved embryos also can be cultured to the
blastocyst stage and implanted.
Objective: To assess the clinical pregnancy outcomes of blastocyst transfer which
developed from poor quality embryos.
Materials and Methods: A total of 109 cleaved embryos with poor quality were
cultured to day 5/day 6 and 27 (24.8%) blastocysts were collected from the 15
cycles/patients undergoing conventional IVF. All the blastocysts were cooling with fast-
freezing. Then the blastocysts were warmed for transfer.
Results: All of 25 vitrified blastocysts (92.6%) survived after warming and were
transferred to 15 patients. Five of the women became pregnant.
Conclusion: Our results suggest that vitrified human day 5/day 6 blastocyst transfer
which develop from poor quality embryo at day 3 can contribute to increasing
cumulative pregnancy rates in assisted reproduction.
Key words: Poor quality embryos, Vitified Blastocyst- transfer, Pregnancy.
Introduction
In IVF, the selection of pre-embryos for
transferred is based on morphological appearance
according to various scoring systems, including
blastomere uniformity, cell numbers, degree of
fragmentation, blastomere size and cytoplasmic
appearance. Only well developed, good quality
embryos will be transferred or cryopreserved. The
poor quality embryo is expected to have a
significantly lower chance of implanting and
usually will be discarded (1-3).
However, this scoring system has several
shortcomings. The viability and the implantation
potential of the poor quality embryo cannot be
determined accurately. Poor quality cleaved
embryos also can be cultured to the blastocyst
Corresponding Author: Xiao-jian Zhang, Department of Assisted Reproductive
Medical Center, Sichuan Academy of Medical Sciences
and Sichuan Provincial People’s Hospital, Sichuan,
China.
Email: [email protected]
stage and implanted (4).
With the improvement of culture systems and
blastocyst cryopreservation techniques, some
pregnancies are achieved following the transfer of
cryopreserved day 5/day 6 blastocysts (5).
However, as far as is known, there were no reports
on pregnancies following the transfer of
cryopreserved day 5/day 6 blastocysts
development from poor quality cleaved embryos.
In this report, we present a successful
pregnancy after the transfer of a human vitrified
day 5/day 6 blastocyst developed from poor quality
cleaved embryos which inconcinnity transferred
and freezed on day 3.
Materials and methods
The study retrospective comparative analysis
the pregnancy obtained after vitrified of human
blastocyst which developed from poor quality
embryos on day 3. It was carried out between
January 2009 and January 2010.
The treatment was conducted with patients
following informed consent and according to the
Xiao-jian Zhang et al
204 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:203-208, Summer 2011
guidelines of the Ministry of Public Health of
China (MPH) and was approved by the
reproductive ethics committee at the Sichuan
Academy of Medical Sciences and Sichuan
Provincial People’s Hospital. Vitrified day 5/day 6
blastocysts were transferred to fifteen patients who
had previous failures of fresh and/or frozen day 3
embryo transfers before the transfer of day5 /day6
vitrified blastocysts. All the transferred embryos
were come from the same stimulated cycle on one
patient. The mean age of patients was 30.6 years
with a standard deviation of 3.1. Main causes of
infertility were female related in all of 15 cycles,
10 tubal, three tubo peritoneal, and two
endometriosis.
In seven cases clinical diagnosis was primary
infertility. Conventional IVF was performed in all
cycles. Over the study period, there were no
changes in the laboratory procedures and the
culture media utilized.
Women were treated with gonadotrophin-
releasing hormone agonist (triptorelin; diphereline,
France) using either the preceding mid-luteal phase
in a long treatment protocol or second day of the
cycle in a short treatment protocol. Ovarian
stimulation was carried out with human
menopausal gonadotrophin (Pergonal; Lizhu,
China) or recombinant follicle-stimulating
hormone (rFSH, GONAL-F, Serono, Germany).
Follicular development was monitored with serial
vaginal ultrasound examinations and serum E2
measurements. The human chorionic
gonadotrophin (hCG; Ovidrel, Serono, Germany)
were administered when at least two dominant
follicles reached a diameter of 18 mm. Oocytes
pick up (OPU) was performed 36–38h after hCG
administration.
Oocyte cumulus complexes were incubated in
human tubal fluid medium (HTF, Sage Biopharma,
USA) containing 5% (v/v) Human Serum Albumin
(Sage Biopharma, USA) at 37°C in an atmosphere
of 6% CO2. The day of oocyte retrieval was
considered as Day 0. Mature oocytes were
inseminated with sperm 4-6h after OPU at the
concentration of 50,000 to 100,000 motile sperm
per oocyte. Fertilization was confirmed at 16-18 h
after insemination by the presence of two
pronuclei. Fertilized oocytes transferred into
Cleavage Medium (Sage Biopharma, USA) until
Day 3.
The cleaved embryos were graded as described
by Balaban B (4), make adjustments as follow:
Class I: no more than 5% fragmentation with
equal sized homogenous blastomeres and the No.
of blastomeres≥ 6; Class II: no more than 20%
fragmentation with equal sized homogenous
blastomeres and the No. of blastomeres ≥6; Class
III: 20% to 50% fragmentation with unequal sized
blastomeres and the No. of blastomeres≥ 4; Class
IV: more than 50% fragmentation and /or very
unequal sized blastomeres or the number of
blastomeres<4.
In this study we aimed to determine the
feasibility and success of vitrified blastocyst-stage
transfer in patients yielding from poor (class III
and class IV) quality cleavage-stage embryos on
day 3. In all the patients, two or three excellent-
quality embryos were transferred on day 3 after
OPU. Supernumerary good quality embryos were
frozen as described previously (6). The others poor
(class III and class IV) quality embryo were
cultured to day 5 or day 6. For expanded
blastocysts, the development of the inner cell mass
(ICM) and trophectoderm (TE) was assessed. The
ICM grading was as follows: A: tightly packed,
many cells; B: loosely grouped, several cells and
C: very few cells. The TE grading was as follows:
A: many cells forming a tightly knit epithelium; B:
few cells and C: very few cells forming a loose
epithelium (7). Only expanded blastocysts scoring
B or higher for ICM and scoring C or higher for
TE grades were vitrified.
Fully expanded blastocysts were deflated by
gentle aspiration of the blastocoelic fluid using a
micromanipulator until the cavity collapses prior to
vitrification. The blastocysts were transferred to
the drop of MOPS buffered solution of modified
HTF which contained 7.5% (v/v) each of Dimethyl
Sulfoxide (DMSO) and ethylene glycol (EG) for 5
to 15 minutes. Then the blastocysts was washed
using 15% DMSO and 15% EG supplemented four
times, and transfer the blastocysts in <1 ul of the
solution from last drop to the tip of Cryoleaf
(CryoleafTM
Medicult, Denmark) which carefully
and immediately submerged into liquid nitrogen.
The warming procedure was done as follows.
The protective cover was removed in liquid
nitrogen and the end of the Cryoleaf was immersed
directly into 1 ml of 37°C 1.0 mol/l sucrose for 1
min. The blastocysts were then transferred into 1
ml of 0.5 mol/ l sucrose for 2 minutes and repeat
once again and washed thrice in the base medium
for 9 min. Finally, the blastocysts were transferred
to a dish of pre-equilibrated appropriate culture
medium (Sage Biopharma, USA) and incubate in a
6% CO2 incubator at 37°C for 3-4 hours to allow
for further recovery.
The laser hatching procedure was performed
using an inverted microscope (Nikon TE2000–U,
Japan) that was equipped with the Zona Infrared
Laser Optical System (Saturn Active Laser
System, Research Instrument, England). The
procedure was done as describe by Zhang et al (6).
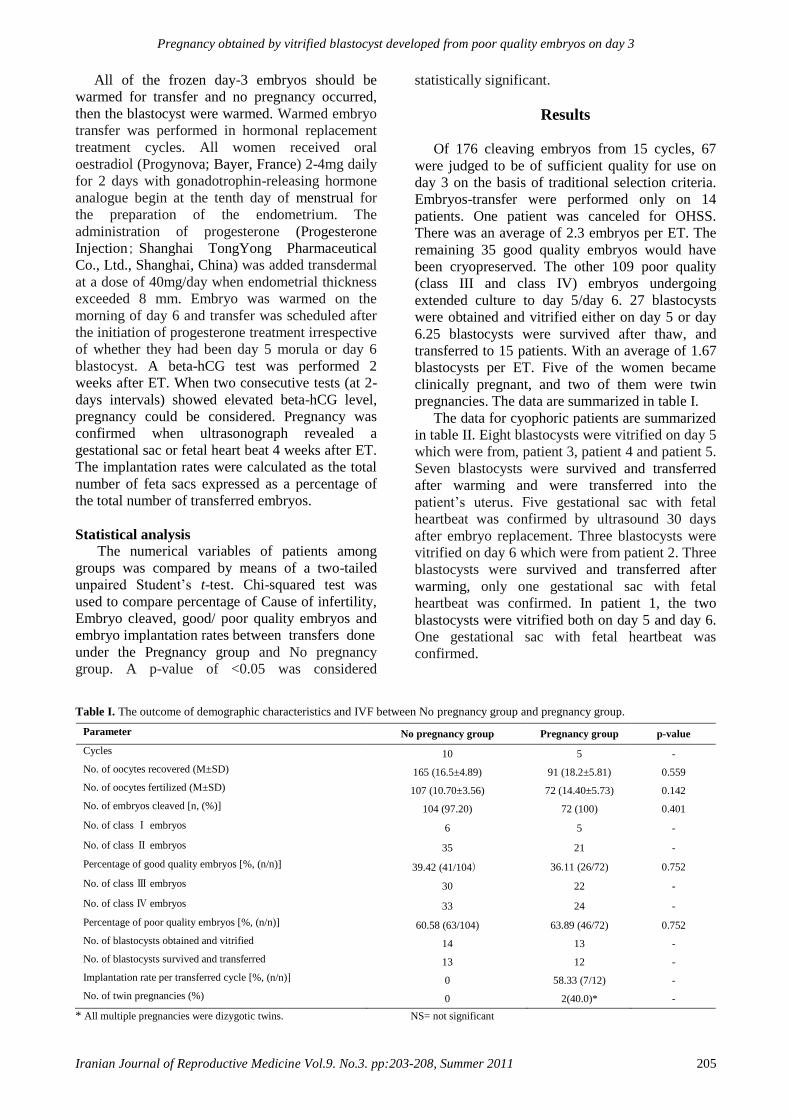
Pregnancy obtained by vitrified blastocyst developed from poor quality embryos on day 3
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:203-208, Summer 2011 205
All of the frozen day-3 embryos should be
warmed for transfer and no pregnancy occurred,
then the blastocyst were warmed. Warmed embryo
transfer was performed in hormonal replacement
treatment cycles. All women received oral
oestradiol (Progynova; Bayer, France) 2-4mg daily
for 2 days with gonadotrophin-releasing hormone
analogue begin at the tenth day of menstrual for
the preparation of the endometrium. The
administration of progesterone (Progesterone
Injection; Shanghai TongYong Pharmaceutical
Co., Ltd., Shanghai, China) was added transdermal
at a dose of 40mg/day when endometrial thickness
exceeded 8 mm. Embryo was warmed on the
morning of day 6 and transfer was scheduled after
the initiation of progesterone treatment irrespective
of whether they had been day 5 morula or day 6
blastocyst. A beta-hCG test was performed 2
weeks after ET. When two consecutive tests (at 2-
days intervals) showed elevated beta-hCG level,
pregnancy could be considered. Pregnancy was
confirmed when ultrasonograph revealed a
gestational sac or fetal heart beat 4 weeks after ET.
The implantation rates were calculated as the total
number of feta sacs expressed as a percentage of
the total number of transferred embryos.
Statistical analysis
The numerical variables of patients among
groups was compared by means of a two-tailed
unpaired Student’s t-test. Chi-squared test was
used to compare percentage of Cause of infertility,
Embryo cleaved, good/ poor quality embryos and
embryo implantation rates between transfers done
under the Pregnancy group and No pregnancy
group. A p-value of <0.05 was considered
statistically significant.
Results
Of 176 cleaving embryos from 15 cycles, 67
were judged to be of sufficient quality for use on
day 3 on the basis of traditional selection criteria.
Embryos-transfer were performed only on 14
patients. One patient was canceled for OHSS.
There was an average of 2.3 embryos per ET. The
remaining 35 good quality embryos would have
been cryopreserved. The other 109 poor quality
(class III and class IV) embryos undergoing
extended culture to day 5/day 6. 27 blastocysts
were obtained and vitrified either on day 5 or day
6.25 blastocysts were survived after thaw, and
transferred to 15 patients. With an average of 1.67
blastocysts per ET. Five of the women became
clinically pregnant, and two of them were twin
pregnancies. The data are summarized in table I.
The data for cyophoric patients are summarized
in table II. Eight blastocysts were vitrified on day 5
which were from, patient 3, patient 4 and patient 5.
Seven blastocysts were survived and transferred
after warming and were transferred into the
patient’s uterus. Five gestational sac with fetal
heartbeat was confirmed by ultrasound 30 days
after embryo replacement. Three blastocysts were
vitrified on day 6 which were from patient 2. Three
blastocysts were survived and transferred after
warming, only one gestational sac with fetal
heartbeat was confirmed. In patient 1, the two
blastocysts were vitrified both on day 5 and day 6.
One gestational sac with fetal heartbeat was
confirmed.
Table I. The outcome of demographic characteristics and IVF between No pregnancy group and pregnancy group.
Parameter
No pregnancy group Pregnancy group p-value
Cycles
10 5 -
No. of oocytes recovered (M±SD)
165 (16.5±4.89) 91 (18.2±5.81) 0.559
No. of oocytes fertilized (M±SD)
107 (10.70±3.56) 72 (14.40±5.73) 0.142
No. of embryos cleaved [n, (%)]
104 (97.20) 72 (100) 0.401
No. of class Ⅰ embryos
6 5 -
No. of class Ⅱ embryos
35 21 -
Percentage of good quality embryos [%, (n/n)]
39.42 (41/104) 36.11 (26/72) 0.752
No. of class Ⅲ embryos
30 22 -
No. of class Ⅳ embryos
33 24 -
Percentage of poor quality embryos [%, (n/n)]
60.58 (63/104) 63.89 (46/72) 0.752
No. of blastocysts obtained and vitrified
14 13 -
No. of blastocysts survived and transferred
13 12 -
Implantation rate per transferred cycle [%, (n/n)]
0 58.33 (7/12) -
No. of twin pregnancies (%)
0 2(40.0)* -
* All multiple pregnancies were dizygotic twins. NS= not significant

Xiao-jian Zhang et al
206 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:203-208, Summer 2011
Table II. The study of five patients whom pregnancy following the transfer of vitrified human blastocysts developed from poor
quality embryos on day 3.
Parameter
Patient 1 Patient 2 Patient 3 Patient 4 Patient 5 Total
Age
32 30 31 29 31 -
Cause of infertility
Tubal Tuboperitoneal Tubal Tubal Endometriosis -
Primary/secondary infertility
Primary Primary Secondary Primary Secondary -
No. of oocytes recovered
12 18 23 13 25 91
No. of oocytes fertilized (2PN)
7 14 21 11 19 72
No. of embryos cleaved to day 3
7 14 21 11 19 72
No. of embryos transferred on day 3
2 3 2 2 0** 7
No. of embryos freezing on day 3
2 2 5 1 9 19
No. of remaining embryos cultured on day 3
5 9 14 8 10 46
No. of blastocysts obtained and vitrified on day 5
1 0 4 2 2 9
No. of blastocysts obtained and vitrified on day 6
1 3 0 0 0 4
No. of blastocysts warmed
2 3 4 2 2 13
No. of blastocysts survived and transferred
2 3 3 2 2 12
No. of gestational sacs
1 1 1 2 2 7
No. of pregnancies ongoing or delivered
1 1 1 2 2 7
**ET were canceled for OHSS.
Discussion
We report five cases of successful pregnancies
following the transfer of vitrified human
blastocysts developed from poor quality cleaved
embryos from 15 patients who be treated with
hormone replacement. This study shows that
cleaved embryo morphology scores cannot predict
the development potential literally. The results of
our study have shown that extended culture of poor
quality embryos could result in blastocyst
development, therefore they should be considered
as viable and valuable embryos for vitrification
and transfer. Traditionally most of the IVF
laboratories transfer the embryos on day 3.
Unquestionably the morphology of embryos on
day 3 has some predictive value for implantation
potential. Until now the number of cells and grade
of fragmentation have been considered to be the
most important scoring factors, the uneven embryo
cleavage negatively affects both implantation and
pregnancy rate also (2); However, criteria for
embryo selection on day 3 seem to be inadequate,
this value may be limited by the fact that they are
still in part depending on the maternal genome.
The embryonic genome is fully activated after the
8-cell stage and the development potential will be
restored in the subsequent cultured process (8, 10).
The poor quality embryos are good sources for
deriving human embryonic stem cell lines (11, 12)
and also can be extended culture to blastocyst for
vitrification. There for, not all of the poor quality
embryos have development potential.
Research in the area of assisted reproduction
has resulted in significant improvements in
stimulation protocols and culture conditions
resulting in better quality and number of
blastocysts available for embryo transfer.
Blastocysts are generally considered to be
preimplantation embryos which have successfully
passed the genomic activation and have better
developmental potential thus allowing reducing the
number of embryos transferred (13).
With the introduction of sequential culture
system, blastocyst culture is being adopted by
many IVF clinics as a means to increase pregnancy
rates, while minimizing multiple gestations (14).
The vitrification technology has made rapid
progress in recent years (15, 16). Despite the
advances in human blastocyst vitrification, much
remains to be learned regarding the limits of
current extended human embryo culture techniques
and the clinical usefulness of later-stage
cryopreservation. Previous investigators have
found that pregnancies can be obtained after the
transfer of human day 7 re-vitrified blastocysts

Pregnancy obtained by vitrified blastocyst developed from poor quality embryos on day 3
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:203-208, Summer 2011 207
developed from vitrified whole cleaved embryos
(7).
In our study, 27 (24.8%) blastocysts was
formed from 109 poor quality cleaved embryos
and 25 (92.59%) blastocysts was survived for
transfer. 5 (33.33%) cycles were obtained
pregnancy and the implanted rate was 28.00% , it
is lower than published article which from whole
embryo culture (17, 18).
We have thawed only 15 cycles of blastocysts
developed from poor quality embryos on day 3. It
will be difficult to increase the number of
treatment cycles in a short period. However, the
information of poor quality cleaved embryos
discard may have occurred in many IVF clinics.
That would have resulted in the loss of viable
supernumerary embryos.
Accordingly, although the number of treatment
cycles was small, the present report has profound
clinical value in knowing that blastocysts
developed from poor quality cleaved embryos can
be vitrified, successfully warmed, and result in
ongoing pregnancies.
This is the first report of successful pregnancies
after the transfer of vitrified human blastocysts
developed from supernumerary poor quality
cleaved embryos. Our results suggest that extended
culture poor quality cleaved embryos to day 5/day
6 and vitrified for transfer can contribute to
increasing cumulative pregnancy rates as a
supplementary method in assisted reproduction.
Acknowledgement
This study was supported by Scientific
Research found of Bureau of Health of Sichuan
Provincial (080342) and Advanced High-Tech of
Sichuan Academy of Medical Sciences and
Sichuan Provincial People’s Hospital (09-02).
References
1. Farhi J, Nahum H, Weissman A, Roybur M, Glezerman
M, Levran D. The value of culturing to the blastocyst
stage of supernumerary embryos not suitable for freezing
after embryo transfer at day 3. Fertil Steril 2001; 76
(Suppl.): 118.
2. Hardarson T, Hanson C, Sjögren A, Lundin K. Human
embryos with unevenly sized blastomeres have lower
pregnancy and implantation rates: indications for
aneuploidy and multinucleation. Hum Reprod 2001; 16:
313-318.
3. Rijnders PM, Jansen CA. The predictive value of day 3
embryo morphology regarding blastocyst formation,
pregnancy and implantation rate after day 5 transfer
following in-vitro fertilization or intracytoplasmic sperm
injection. Hum Reprod 1998; 13: 2869-2873.
4. Balaban B, Urman B, Alatas C, Mercan R, Aksoy S,
Isiklar A. Blastocyst-stage transfer of poor-quality
cleavage-stage embryos results in higher implantation
rates. Fertil Steril 2001; 75: 514-518.
5. Hiraoka K, Hiraoka K, Kinutani M, Kinutani K.
Vitrification of human hatched blastocysts: a report of 4
cases. J Reprod Med 2007; 52: 413-415.
6. Zhang XJ, Yang YZ, Lv Q, Min LH, Li XJ, Bai P. Effect
of the size of zona pellucida thinning by laser assisted
hatching on clinical outcome of human frozen-thawed
embryo transfers. Cryo Letters 2009; 30: 455-461.
7. Hiraoka K, Fujimoto Y, Tateaki Y, Hiraoka K, Horiuchi
T, Okano S, et al. Case report: two successful pregnancies
following the transfer of re-vitrified human day 7
blastocysts developed from vitrified cleaved embryos. J
Assist Reprod Genet 2008; 25: 503-509.
8. Graham J, Han T, Porter R, Levy M, Stillman R, Tucker
MJ. Day 3 morphology is a poor predictor of blastocyst
quality in extended culture. Fertil Steril 2000; 74: 495-
497.
9. Braude P, Bolton V, Moore S. Human gene expression
first occurs between the 4-cell and 8-cell stages of
preimplantation development. Nature 1988; 332: 459-461.
10. Van Royen E, Mangelschots K, De Neubourg D,
Valkenburg M, Van de meerssche M, Ryckaert G, et al.
Characterization of a top quality embryo, a step towards
single-embryo transfer. Hum Reprod 1999; 14: 2345-2349.
11. Liu W, Yin Y, Long X, Luo Y, Jiang Y, Zhang W, et al.
Derivation and characterization of human embryonic stem
cell lines from poor quality embryos. J Genet Genomics
2009; 36: 229-239.
12. Raya A, Rodríguez-Pizà I, Arán B, Consiglio A, Barri PN,
Veiga A, et al. Generation of cardiomyocytes from new
human embryonic stem cell lines derived from poor-
quality blastocysts. Cold Spring Harb Symp Quant Biol
2008; 73: 127-135.
13. Ménézo YJ. Blastocyst freezing. Eur J Obstet Gynecol
Reprod Biol 2004; 115 (Suppl.): 12-15.
14. Gardner DK, Schoolcraft WB, Wagley L, Schlenker T,
Stevens J, Hesla J. A prospective randomized trial of
blastocyst culture and transfer in in-vitro fertilization.
Hum Reprod 1998; 13: 3434-3440.
15. Yokota Y, Sato S, Yokota M, Ishikawa Y, Makita M,
Asada T, et al. Successful pregnancy following blastocyst
vitrification: case report. Hum Reprod 2000; 15: 1802-
1803.
16. Hiraoka K, Hiraoka K, Horiuchi T, Kusuda T, Okano S,
Kinutani M, et al. Case report: successful delivery
following the transfer of a human re-vitrified day-7
spontaneously hatched blastocyst developed from vitrified
cleaved embryos. J Assist Reprod Genet 2009; 26: 405-
409.
17. Zhang JQ, Li XL, Peng Y, Guo X, Heng BC, Tong GQ.
Reduction in exposure of human embryos outside the

Xiao-jian Zhang et al
208 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:203-208, Summer 2011
incubator enhances embryo quality and blastulation rate.
Reprod Biomed Online 2010; 20: 510-515.
18. Van Landuyt L, De Vos A, Joris H, Verheyen G, Devroey
P, Van Steirteghem A. Blastocyst formation in in vitro
fertilization versus intracytoplasmic sperm injection
cycles: influence of the fertilization procedure. Fertil
Steril 2005; 83: 1397-1403.

Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 209-216, Summer 2011
Maturation capacity, morphology and morphometric
assessment of human immature oocytes after
vitrification and in-vitro maturation Saeedeh Nazari
1 M.Sc., Mohammad Ali Khalili
1 Ph.D., Forouzan Esmaielzadeh
2 M.Sc., Mehdi
Mohsenzadeh3 M.Sc.
1 Researh and Clinical Center for Infertility, Shahid Sadoughi University of Medical Sciences, Yazd,
Iran.
2 Department of Animal Sciences, Marvdasht Branch, Islamic Azad University, Marvdasht, Iran.
3 Shiraz University of Medical Sciences, Shiraz, Iran.
Received: 19 August 2010; accepted: 12 December 2010
Abstract
Background: In general, 15% of oocytes collected in ART cycles are immature. These
oocytes may be cryopreserved further for use in in-vitro maturation (IVM) program.
Objective: The aim of this study was to determine maturation capacity, morphometric
parameters and morphology of human immature oocytes in both fresh IVM (fIVM) and
vitrified-IVM (vIVM) oocytes.
Materials and Methods: 93 women who underwent controlled ovarian stimulation for
ART were included. The immature oocytes (n=203) were divided into two groups: the
first group (n=101) directly matured in vitro; and the second group (n=102) first
vitrified, then matured in vitro. All oocytes underwent IVM in Ham’s F10 supplemented
with LH+FSH and human follicular fluid. After 48h of incubation, the oocyte
maturation rates, as well as morphometric and morphologic characteristics were
assessed using cornus imaging and were compared.
Results: Oocyte maturation rates were reduced in vIVM, (40.4%), in comparison with
fIVM (59.4%, p<0.001). Following morphometric assessment, there was no difference
in the mean oocyte diameters (µm) between fIVM and vIVM, 156.3±6.8 and
154.07±9.9, respectively. Other parameters of perimeters, egg areas, as well as oocyte
and ooplasm volumes were similar in two groups. In addition, more morphologic
abnormalities, such as, vacuole, and dark oocyte were observed in vIVM oocytes.
Conclusion: fIVM was more successful than vIVM groups. No statistical differences
were noticed in morphometry assessment in two groups. This suggests that
morphometric parameters can not be applied as prognosis factor in oocyte maturation
outcome in IVM program. Key words: IVM, Oocyte, Vitrification, Maturation, Morphology, Morphometry.
Introduction
In-vitro maturation (IVM) and cryopreservation
of immature oocytes has been proposed as an
alternative for conventional IVF treatment. IVM
has several advantages of reducing the costs,
Corresponding Author:
Mohammad Ali Khalili, Research and Clinical Center
for Infertility, Shahid Sadoughi University of Medical
Sciences, Yazd, Iran.
Email: [email protected]
avoidance of the side effects of ovarian hyper
stimulation syndrome (OHSS) and simplified
treatment for certain infertile couples (1-3).
Currently, most IVM protocols have supplemented
with FSH and/or LH into the culture medium for
oocyte maturation (1). Cryopreservation could
benefit to patients who have specific situation such
as chemotherapy or radiation (4). Several factors
affect the survival and viability of human oocytes
and embryos such as exposure time of cells to
different cryoprotectant solutions, their different
concentrations and rate of ice crystal formation (3).
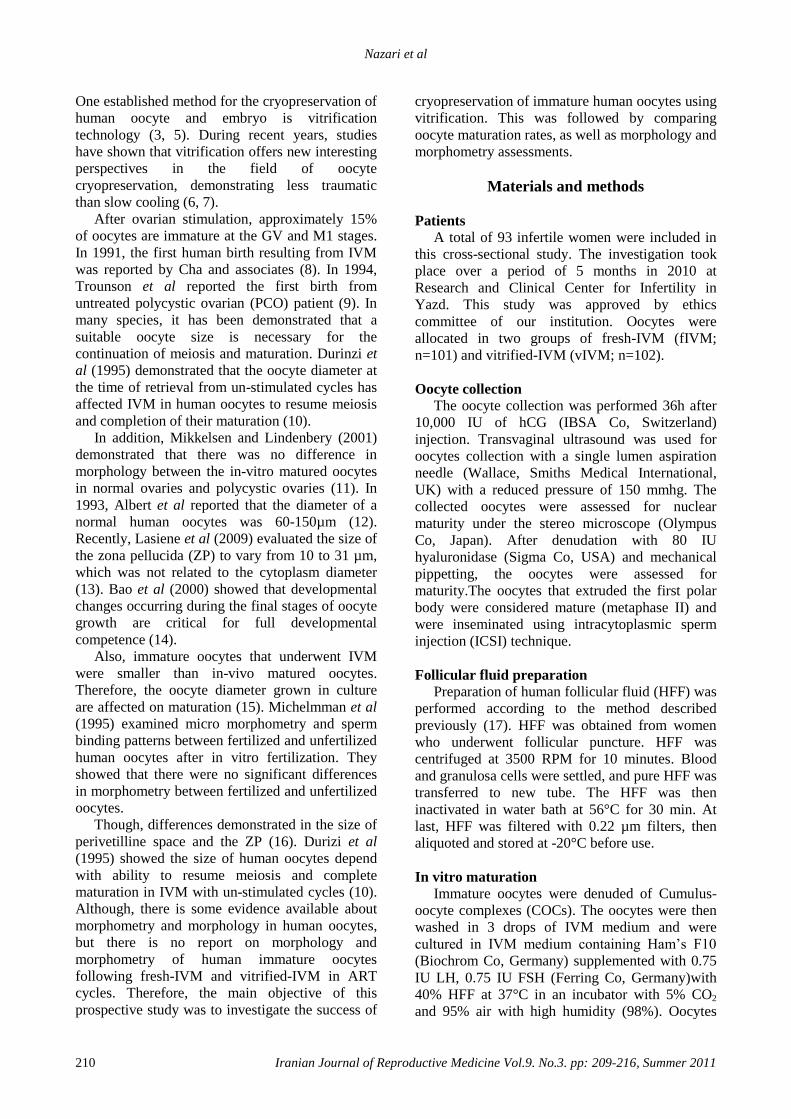
Nazari et al
210 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 209-216, Summer 2011
One established method for the cryopreservation of
human oocyte and embryo is vitrification
technology (3, 5). During recent years, studies
have shown that vitrification offers new interesting
perspectives in the field of oocyte
cryopreservation, demonstrating less traumatic
than slow cooling (6, 7).
After ovarian stimulation, approximately 15%
of oocytes are immature at the GV and M1 stages.
In 1991, the first human birth resulting from IVM
was reported by Cha and associates (8). In 1994,
Trounson et al reported the first birth from
untreated polycystic ovarian (PCO) patient (9). In
many species, it has been demonstrated that a
suitable oocyte size is necessary for the
continuation of meiosis and maturation. Durinzi et
al (1995) demonstrated that the oocyte diameter at
the time of retrieval from un-stimulated cycles has
affected IVM in human oocytes to resume meiosis
and completion of their maturation (10).
In addition, Mikkelsen and Lindenbery (2001)
demonstrated that there was no difference in
morphology between the in-vitro matured oocytes
in normal ovaries and polycystic ovaries (11). In
1993, Albert et al reported that the diameter of a
normal human oocytes was 60-150µm (12).
Recently, Lasiene et al (2009) evaluated the size of
the zona pellucida (ZP) to vary from 10 to 31 µm,
which was not related to the cytoplasm diameter
(13). Bao et al (2000) showed that developmental
changes occurring during the final stages of oocyte
growth are critical for full developmental
competence (14).
Also, immature oocytes that underwent IVM
were smaller than in-vivo matured oocytes.
Therefore, the oocyte diameter grown in culture
are affected on maturation (15). Michelmman et al
(1995) examined micro morphometry and sperm
binding patterns between fertilized and unfertilized
human oocytes after in vitro fertilization. They
showed that there were no significant differences
in morphometry between fertilized and unfertilized
oocytes.
Though, differences demonstrated in the size of
perivetilline space and the ZP (16). Durizi et al
(1995) showed the size of human oocytes depend
with ability to resume meiosis and complete
maturation in IVM with un-stimulated cycles (10).
Although, there is some evidence available about
morphometry and morphology in human oocytes,
but there is no report on morphology and
morphometry of human immature oocytes
following fresh-IVM and vitrified-IVM in ART
cycles. Therefore, the main objective of this
prospective study was to investigate the success of
cryopreservation of immature human oocytes using
vitrification. This was followed by comparing
oocyte maturation rates, as well as morphology and
morphometry assessments.
Materials and methods
Patients
A total of 93 infertile women were included in
this cross-sectional study. The investigation took
place over a period of 5 months in 2010 at
Research and Clinical Center for Infertility in
Yazd. This study was approved by ethics
committee of our institution. Oocytes were
allocated in two groups of fresh-IVM (fIVM;
n=101) and vitrified-IVM (vIVM; n=102).
Oocyte collection
The oocyte collection was performed 36h after
10,000 IU of hCG (IBSA Co, Switzerland)
injection. Transvaginal ultrasound was used for
oocytes collection with a single lumen aspiration
needle (Wallace, Smiths Medical International,
UK) with a reduced pressure of 150 mmhg. The
collected oocytes were assessed for nuclear
maturity under the stereo microscope (Olympus
Co, Japan). After denudation with 80 IU
hyaluronidase (Sigma Co, USA) and mechanical
pippetting, the oocytes were assessed for
maturity.The oocytes that extruded the first polar
body were considered mature (metaphase II) and
were inseminated using intracytoplasmic sperm
injection (ICSI) technique.
Follicular fluid preparation
Preparation of human follicular fluid (HFF) was
performed according to the method described
previously (17). HFF was obtained from women
who underwent follicular puncture. HFF was
centrifuged at 3500 RPM for 10 minutes. Blood
and granulosa cells were settled, and pure HFF was
transferred to new tube. The HFF was then
inactivated in water bath at 56°C for 30 min. At
last, HFF was filtered with 0.22 µm filters, then
aliquoted and stored at -20°C before use.
In vitro maturation
Immature oocytes were denuded of Cumulus-
oocyte complexes (COCs). The oocytes were then
washed in 3 drops of IVM medium and were
cultured in IVM medium containing Ham’s F10
(Biochrom Co, Germany) supplemented with 0.75
IU LH, 0.75 IU FSH (Ferring Co, Germany)with
40% HFF at 37°C in an incubator with 5% CO2
and 95% air with high humidity (98%). Oocytes

Vitrification of human immature oocytes and IVM
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 209-216, Summer 2011 211
were observed under an inverted microscope
(Nikon Co, Japan) after 48h to determine maturity.
Vitrification of immature oocytes
Immature oocytes were frozen using a modified
vitrification method reported by Al-Hasani et al
(2007) (3). Initially, immature oocytes were placed
in an equilibration solution containing 7.5%
ethylene glycol (EG) (Merck Co, Germany), 7.5%
dimethyl sulphoxide (DMSO) (Merck Co,
Germany) in Ham’s F10 media supplemented with
20% human serum albumin (HSA) (Plasbumin Co,
USA) for 5-15 min at room temperature. Then,
oocytes were removed and placed into vitrification
solution containing 15% EG, 15% DMSO and
0.5M socruse (Sigma Co, USA) in Ham’s F10
medium supplemented with 20% HSA for 50-60
Sec at room temperature. After this stage, the
oocytes were loaded into cryotops that were
plunged into liquid nitrogen quickly. Next, the cap
was placed on the cryotop and put into the cane.
Finally, the samples were transferred to the liquid
nitrogen storage tank for 2 months.
Thawing of immature oocytes
Thawing of the oocytes was performed by
placing the cryotop in thawing solution in five
stages: thawing solution (Ham’s F10 supplemented
with 20% HSA and 1M sucrose) for 50-60 Sec,
dilution solution 1 (Ham’s F10 supplemented with
20% HSA and 0.5M sucrose) for 3 min, dilution
solution 2 (Ham’s F10 supplemented with 20%
HSA and 0.25 M sucrose) for 3 min, washing
solution 1 and 2 (Ham’s F10 supplemented with
20% HSA) each for 3-5 min. After this stage, the
oocytes were placed in IVM medium for 48h in
incubator.
Viability of vitrified oocytes was evaluated
microscopically 2-3 h after culture, based on the
morphology of cytoplasm (18). The dead oocytes
were shown with broken membrane and dark
ooplasm.
Morphometry and morphology evaluations
After a culture period of 48h, all oocytes were
assessed for maturity under an inverted
microscope; Matured oocytes were evaluated for
morphology and morphometry. The matured
oocytes were divided into two groups (Group
1=fIVM, Group 2=vIVM). Measurements
accomplished with inverted microscope equipped
with cornus imaging program (Research
instruments Ltd Co, UK). Measurements
comprised of the diameters of whole oocyte (µm),
ooplasm (µm), width of ZP (µm), perimeters and
areas of whole oocyte and ooplasm (µm2), and
volume of whole oocyte and ooplasm (µm3)
(Figure 2).
To calculate the average diameter of different
parts of each oocyte comprising of whole oocyte,
ooplasm and ZP were calculated in 4 different
parts. Also, the morphology of each mature oocyte
was determined by characteristics of refractile
body (RF), granularity, vacuole, smooth
endoplasmic reticulum (SER), bull’s eye, ZP and
perivite line space (PVS), coloration of ZP and
ooplasm (dark or normal), polar body shape
(normal or fragmented), oocyte shape (circular or
irregular) and PVS debris in both groups (Figure3).
Statistical analysis
Statistical analysis was carried out using t-test
for morphometrical data and χ2for morphological
data by SPSS (version 16). p<0.05 was considered
significant.
Results
As shown in table I, there were no significant
differences in characteristics of age, etiology of
infertility, total number of retrieved oocytes and
oocytes stage (GV, MI) between fIVM with vIVM
groups. The numbers of immature oocytes (Figure
1) were; GV=72, MI=29 in fIVM and GV=66,
MI=36 in vIVM group. There were no significant
differences in the numbers of GV and MI oocytes
in fIVM and vIVM.
The oocyte survival rate was 87.25% (89/102)
when the oocytes were vitrified. The oocyte
maturation rate was 40.4% (36/89) when the
oocytes were vitrified and then underwent IVM
after warming. This was significantly lower
(p<0.001) than the immature oocytes matured in
vitro without vitrification which was 59.4%
(61/101) (Table II). Also, a total of 16 immature
oocytes were collected from a patient with OHSS.
However, the rate of maturity after IVM protocol
was as low as 12.5%.
The data also showed that, morphometric and
morphologic analyses of matured oocytes were
possible in 96 oocytes (60 fIVM, 36 vIVM).
Although, there were no significant differences in
the diameters, areas, perimeters and volumes
between the oocytes vitrified at the immature stage
than those obtained using the oocytes without
vitrification for IVM (Table III). As shown in table
IV, there were no significant differences between
RF, fragmented polar body, regularity of shape,
granularity, PVS debris and width of PVS in fIVM
and vIVM groups. However, in vIVM oocytes, the
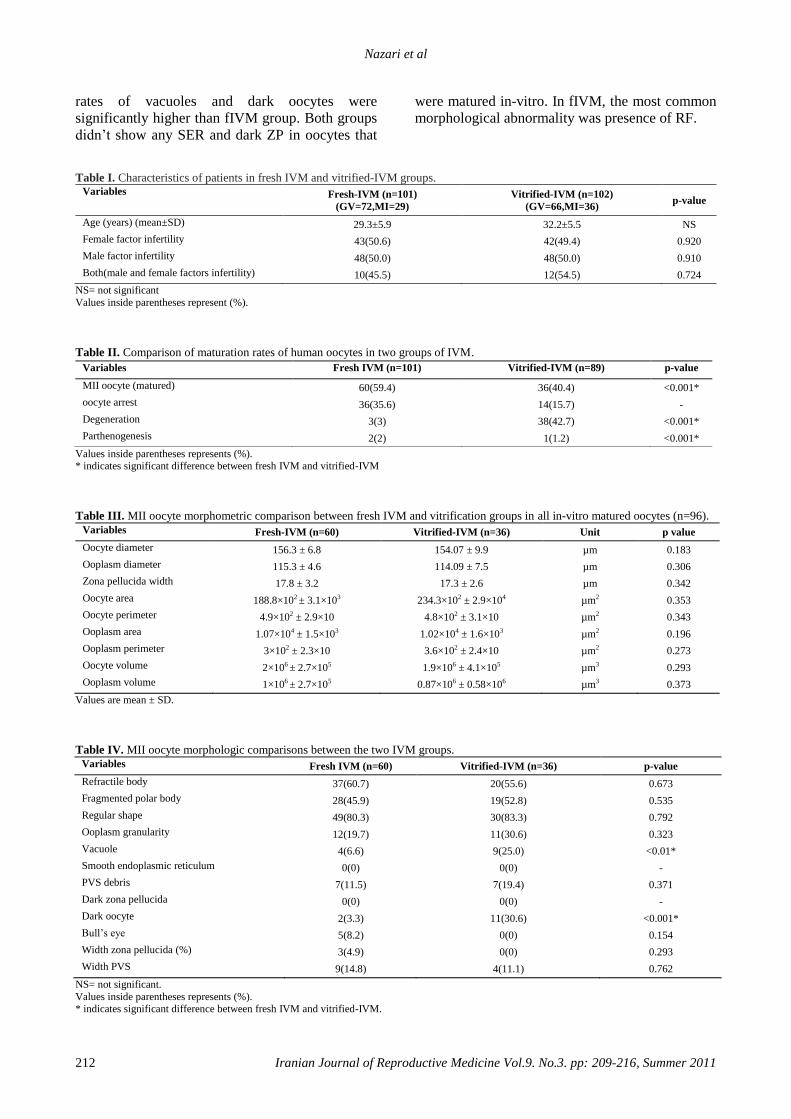
Nazari et al
212 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 209-216, Summer 2011
rates of vacuoles and dark oocytes were
significantly higher than fIVM group. Both groups
didn’t show any SER and dark ZP in oocytes that
were matured in-vitro. In fIVM, the most common
morphological abnormality was presence of RF.
Table I. Characteristics of patients in fresh IVM and vitrified-IVM groups. Variables Fresh-IVM (n=101)
(GV=72,MI=29)
Vitrified-IVM (n=102)
(GV=66,MI=36) p-value
Age (years) (mean±SD)
29.3±5.9 32.2±5.5 NS
Female factor infertility
43(50.6) 42(49.4) 0.920
Male factor infertility
48(50.0) 48(50.0) 0.910
Both(male and female factors infertility)
10(45.5) 12(54.5) 0.724
NS= not significant
Values inside parentheses represent (%).
Table II. Comparison of maturation rates of human oocytes in two groups of IVM.
Values inside parentheses represents (%). * indicates significant difference between fresh IVM and vitrified-IVM
Table III. MII oocyte morphometric comparison between fresh IVM and vitrification groups in all in-vitro matured oocytes (n=96).
Variables
Fresh-IVM (n=60) Vitrified-IVM (n=36) Unit p value
Oocyte diameter
156.3 ± 6.8 154.07 ± 9.9 µm 0.183
Ooplasm diameter
115.3 ± 4.6 114.09 ± 7.5 µm 0.306
Zona pellucida width
17.8 ± 3.2 17.3 ± 2.6 µm 0.342
Oocyte area
188.8×102 ± 3.1×103 234.3×102 ± 2.9×104 µm2 0.353
Oocyte perimeter
4.9×102 ± 2.9×10 4.8×102 ± 3.1×10 µm2 0.343
Ooplasm area
1.07×104 ± 1.5×103 1.02×104 ± 1.6×103 µm2 0.196
Ooplasm perimeter
3×102 ± 2.3×10 3.6×102 ± 2.4×10 µm2 0.273
Oocyte volume
2×106 ± 2.7×105 1.9×106 ± 4.1×105 µm3 0.293
Ooplasm volume
1×106 ± 2.7×105 0.87×106 ± 0.58×106 µm3 0.373
Values are mean ± SD.
Table IV. MII oocyte morphologic comparisons between the two IVM groups.
Variables
Fresh IVM (n=60) Vitrified-IVM (n=36) p-value
Refractile body
37(60.7) 20(55.6) 0.673
Fragmented polar body
28(45.9) 19(52.8) 0.535
Regular shape
49(80.3) 30(83.3) 0.792
Ooplasm granularity
12(19.7) 11(30.6) 0.323
Vacuole
4(6.6) 9(25.0) <0.01*
Smooth endoplasmic reticulum
0(0) 0(0) -
PVS debris
7(11.5) 7(19.4) 0.371
Dark zona pellucida
0(0) 0(0) -
Dark oocyte
2(3.3) 11(30.6) <0.001*
Bull’s eye
5(8.2) 0(0) 0.154
Width zona pellucida (%)
3(4.9) 0(0) 0.293
Width PVS
9(14.8) 4(11.1) 0.762
NS= not significant.
Values inside parentheses represents (%). * indicates significant difference between fresh IVM and vitrified-IVM.
Variables
Fresh IVM (n=101) Vitrified-IVM (n=89) p-value
MII oocyte (matured)
60(59.4) 36(40.4) <0.001*
oocyte arrest
36(35.6) 14(15.7) -
Degeneration
3(3) 38(42.7) <0.001*
Parthenogenesis
2(2) 1(1.2) <0.001*
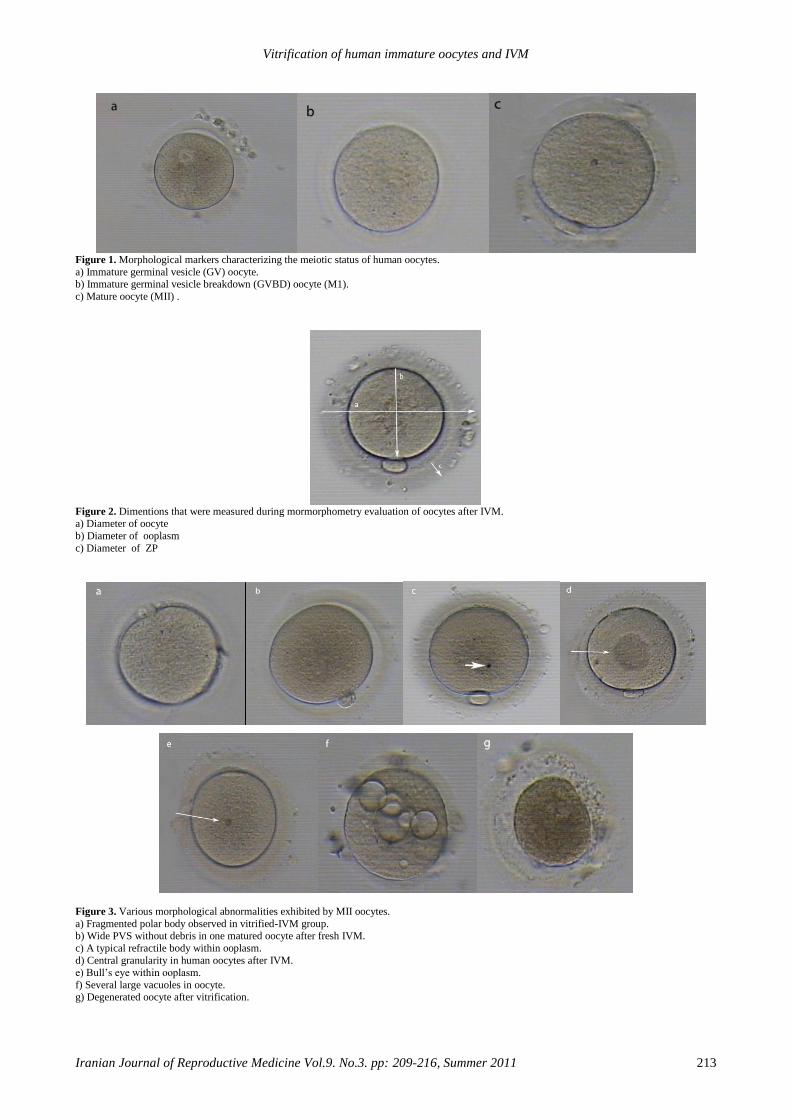
Vitrification of human immature oocytes and IVM
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 209-216, Summer 2011 213
Figure 1. Morphological markers characterizing the meiotic status of human oocytes.
a) Immature germinal vesicle (GV) oocyte. b) Immature germinal vesicle breakdown (GVBD) oocyte (M1).
c) Mature oocyte (MII) .
Figure 2. Dimentions that were measured during mormorphometry evaluation of oocytes after IVM. a) Diameter of oocyte
b) Diameter of ooplasm
c) Diameter of ZP
Figure 3. Various morphological abnormalities exhibited by MII oocytes.
a) Fragmented polar body observed in vitrified-IVM group. b) Wide PVS without debris in one matured oocyte after fresh IVM.
c) A typical refractile body within ooplasm.
d) Central granularity in human oocytes after IVM.
e) Bull’s eye within ooplasm.
f) Several large vacuoles in oocyte. g) Degenerated oocyte after vitrification.
Nazari et al
214 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 209-216, Summer 2011
Discussion
Microtubular spindle in MII oocyte is sensitive
to low temperature and cryopreservation.
However, GV oocytes with chromosomes within
the nuclear membrane are protected from these
disorders (19). We evaluated morphology and
morphometry of oocytes after maturation in fIVM
and vIVM in patients undergoing ART program.
The aim was to found out whether differences
existed in the morphology and morphometry of
human oocytes after IVM in two groups. In this
study, the maturity after IVM was demonstrated to
be higher in fIVM when compared with vIVM.
Also, the results showed that the rates of GV and
M1 arrest in fIVM were higher than vIVM.
However, the percentage of maturity (MII) was
higher in fIVM, when compared with vIVM. In
addition, rates of degeneration were significantly
increased in vIVM group. Therefore, immature
oocytes in ART cases should immediately undergo
the IVM technology, though they may be
cryopreserved successfully if it becomes necessary.
According to Kim et al (2000), almost 78.5% of
the immature oocytes retrieved in stimulated cycles
were matured, and 12.3% of oocytes remained at
the GV stage (17). Russel (1998) showed that
maturation rate was 63% in naked and compact
oocytes in unstimulated cycles which is similar to
our results (20). Later, Toth et al (1994)
demonstrated that 83.3% of the oocytes were
matured after thawing of cryopreserved oocytes
(21).
Recently, Cao et al (2009) reported the survival
rates of human immature oocytes in vitrified
oocytes as high as 85.4% after warming. This
survival rate was similar to our study. For this
reason, it seems that high survival rate can be
obtained when human oocytes are vitrified at the
immature stage. Also, Liu (2010) reported that, the
removal of granulosa cells would affect IVM of
immature oocytes (2).
In this study, the rates of maturation in vitrified
oocytes were somewhat similar to study done by
Cao et al (2009). But, rate of maturity following
IVM of immature oocytes without vitrification
were lower when compared to above (18). In
addition, morphometric comparison on fIVM and
vIVM showed only minor differences between two
groups. During growth phase, oocyte diameter
increases from 30 to 110 µm over a period of at
least 8 weeks in human (22). When oocytes are
matured in-vivo, the size of oocyte normality is
approximately 110-120 µm, excluding the ZP, also
whole size of oocyte was almost 150 µm (23).
We found that when immature oocytes were
vitrified and then matured using IVM technology,
no differences were noticed in parameters. This
evidence showed that vitrification seems to have
no effect on morphometric parameters when
compared with fresh IVM. Bertand et al (1995)
reported that human ZP varies from 10-30 µm with
a mean of 17.5 µm (24).
Cavilla (2008) found zona diameter from the
oocytes matured in vitro and then fertilized were
larger than diameters of the in-vivo matured
oocytes (12). In present study, all mature oocytes
had a ZP thickness of 17.8 and 17.3 µm in fIVM
and vIVM groups, respectively.
This was almost similar to the data reported by
Cavelia et al (15). Also, the mean oocyte diameter
in our study was statistically higher to the value
obtained by Salata and associates (23). This
difference could be credited to the large sample
size evaluated by Salata et al (23). In addition,
there were no significant differences in volume,
perimeter, area ooplasm and oocyte between fIVM
and vIVM. Michelman et al (1995) also found the
volume of human oocytes to be similar to our
results.
In addition, most of abnormalities were noticed
in the oocytes that underwent IVM technology.
This study demonstrated that rates of
vacuoalization and dark oocytes were significantly
increased in vIVM than fIVM. This may prove that
oocyte cryopreservation cause some irreversible
structural damage. Lasiene et al (2000) reported
the quality of oocytes deliberated by the structure
of COC.This procedure gives us some information
about the quality of oocytes(13).
Also, they showed that oocytes with less
cumulus compact, deficiency granularity and dark
ooplasms have higher developmental competence,
and the quality is increased when oocytes covered
by more layers of cells (25, 26). According to
defects in oocytes, they are categorized into single,
double, multiple and nodefects. About this
classification, no one reported any differences in
fIVM and vIVM groups. Balaban et al (2006)
classified oocytes abnormalities, that were similar
to our study (27). Xia (1997) showed that oocyte
with fragmented polar body have a lower
fertilization than normal polar body. Also, oocytes
with extensive and fragmented polar body have a
worse developmental after fertilization (28).
Ubalidi et al (2008) evaluated morphology of
oocytes and reported that such as fragmented polar
body and large PVS are rather higher than other
abnormalities (49% and 32%), respectively (29).
Our results showed that the rates of fragmented
Vitrification of human immature oocytes and IVM
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 209-216, Summer 2011 215
polar body and SER are approximality similar to
theirs. Other defects, such as Bull’s eye, thick ZP,
SER and dark ZP were not observed in oocytes
under investigation.
Conclusion
The rates of human oocytes recovery following
vitrification concomitant with IVM program are
acceptable. However, morphometrical assessment
of oocyte does not seem to play a role in prognosis
of oocyte maturation outcome.
Acknowledgement
The authors would like to thank Mehrdad
Soleimani, Mohammad H. Razi, Leila
Motamedzadeh, Habibeh Gheisari, and Aazam
Agha Rahimi for their technical assistance during
the course of this study. The statistical assistance
of Farima Shams in also well appreciated. This
study was supported by a grant from research and
clinical center for infertility, Shahid Sadoughi
University of Medical Sciences, Yazd, Iran.
References 1. Ben-Ami I, Komsky A, Bern O, kasterstein E,
Komarovsky D, Ron-El R. In vitro maturation of human
germinal vesicle-stage oocytes: role of epidermal growth
factor-like growth factors in the culture medium. Hum
Reprod 2011; 26: 76-78.
2. Liu S, Jing JJ, Feng HL, Ma SY, Li M, Li Y. Evaluation
of the immature human oocytes from unstimulated cycles
in polycystic ovary syndrome patients using a novel
scoring system. Fertil Steril 2010; 93: 2202-2209.
3. Al-hasani S, Ozmen B, Koutlaki N, Schoepper B, Diedrich
K, Schultze-mosgau A. three years of routine vitrification
of human zygotes: is it still fair to advocate slow-rate
freezing? Reprod Biomed Online 2007; 14: 288-293.
4. wininger JD, Kort HI. cryopreservation of immature and
mature human oocytes. Seminreprod Med 2002; 20: 45-
49.
5. Vajta G, Nagy ZP. Are programmable freezers still needed
in embryo laboratory? Reprod Biomed Online 2006; 12:
779-796.
6. Humburg R, Van der veen F, Silber SJ. Oocyte
vitrification-women’s emancipation set in stone. Fertil
Steril 2009; 91: 1319-1320.
7. Cobo A, Kuwayama M, Pérez S, Ruiz A, Pellicer A,
Remohí J. Comparison of concomitant outcome achieved
with fresh and cryopreserved donor oocytes vitrified by
the cryotop method. Fertil Steril 2008; 89: 1657-1664.
8. Cha KY, Koo JJ, Ko JJ, Choi DH, Han SY, Yoon TK .
pregnancy after in vitro fertilization of human follicular
oocytes collected from nonstimulated cycles, their culture
in vitro and their transfer in a donor oocyte program.
Fertil Steril 1991; 55: 109-113.
9. Trounson A, wood C, Kausche A. In vitro maturation and
the fertilization and developmental compotence oocytes
recovered from untreated polycystic ovarian patients.
Fertil Steril 1994; 62: 353-362.
10. Durinzi KL, Saniga EM, Lanzerdorf SE. the relationship
between : size and maturation in vitro in the unstimulated
human oocyte. Fertil Steril 1995; 63: 404-406.
11. Mikkelsen AL, Lindenberg S. morphology of in-vitro
matured oocytes: impact on fertility potential and embryo
quality. Hum Reprod 2001; 16: 1714-1718.
12. Alberts b, Brray D, Lewis J, Raff M, Robert K, Waston
JD. Molecular biology of the cell. Garland publishing Inc;
1983.
13. Lasiene K, Vitkuse A, Valanciute A, Lasys V.
morphological criteria of oocyte quality. Medicina
(Kaunas) 2009; 45: 509-514.
14. Bao S, Obata Y, Carroll J, Domeki I, Kono T. epigenetic
modifications neccessary for normal development are
estabilished during oocyte growth in mice. Biol Reprod
2000; 62: 616-621.
15. Cavilla JL, Kennedy CR, Byskov AG, Hatshorne GM.
human immature oocytes grow during cultue for IVM.
Hum Reprod 2008; 23: 37-45.
16. Michelmann HW, Bogdan A, Hinney B.
micromorphometry and spermatozoa binding patterns of
fertilized and unfertilized human oocytes after in-vitro
fertilization. Hum Reprod 1995; 10: 3154-3160.
17. kim BK, Lee SC, Kim KJ, Han CH, Kim JH. in vitro
maturation, fertilization and development of human
germinal vesicle oocytes collected from stimulated cycles.
Fertil Steril 2000; 74: 1153-1158.
18. Cao YX, Chian RC. fertility preservation with immature
and in vitro matured oocytes. Semin Reprod Med 2009;
27: 457-464.
19. Paynter SJ. cryopreservation of human unfertilized
oocytes. Hum Reprod Update 2000; 6: 449-456.
20. Russell JB. Immature oocyte retrieval combined with in-
vitro oocyte maturation. Hum Reprod 1998; 13: 63-70.
21. Toth TH, Baka SG, Veeck LL, Jones HW, Muasher S,
Lanzendorf SE. fertilization and in vitro development of
cryopreserved human prophase 1 oocytes. Fertil Steril
1994; 61: 891-894.
22. Gougeon A. Dynamics of follicular growth in the human:
a model from preliminary results. Hum Reprod 1986; 1:
81-87.
23. veek L. abnormal morphology of the human oocyte and
conceptus. In: An Atlas of Human Gametes and
Conceptuses. Lancs; 1999.
24. Bertand E, Van den Bergh M, Englert Y. Does zona
pellucida tickness influence the fertilization rate? Hum
Reprod 1995; 10: 1189-1193.
25. Yuan YQ, Van Soom A, Leroy JL, Dewulf J, Van Zeveren
A, de Kruif A, et al. Apoptosis in cumulus cells , but not
in oocytes may influence bovine embryopnic
developmental compotence. Theriogenology 2005; 63:
2147-2163.

Nazari et al
216 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 209-216, Summer 2011
26. Zeuner A, Muller K, Reguszynski K, Jewgenow K.
apoptosis within bovine follicular cells and its effect on
oocyte development during in viro maturation.
Theriogenology 2003; 59: 1421-1433.
27. Balaban B, Urman B. Effect of oocyte morphology on
embryo development and implantation. Reprod Biomed
Online 2006; 12: 608-615.
28. Xia P. Intracytoplasmic sperm injection: correlation of
oocyte grade based on polar body, perivitelline space and
cytoplasmic inclusions with fertilization rate and embryo
quality. Hum Reprod 1997; 12: 1750-1755.
29. Ubaldi F, Rienzi L. morphological selection of gamets.
Placenta 2008; 29: 5115-5120.

Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 217-222, Summer 2011
Antifertility activity of aqueous ethanolic extract of
Hymenocardia acida stem bark in female rats Abu Adakole Hyacinth
1 Ph.D., Uchendu Chukwuka Nwocha
2 Ph.D.
1 Department of Veterinary Physiology, Pharmacology and Biochemistry, College of Veterinary
Medicine, University of Agriculture, P.M.B, 2373, Makurdi, Nigeria.
2 Department of Veterinary Physiology and Pharmacology, Faculty of Veterinary Medicine, University of
Nigeria, Nsukka, Nigeria.
Received: 14 July 2010; accepted: 5 January 2011
Abstract
Background: Hymenocardia acida is traditionally used in African herbal medicine and
has numerous therapeutic benefits. But little is known about its potentially negative
effects on pregnant women.
Objective: The aim of the present study was to evaluate the antifertility effect of
aqueous ethanolic extract of Hymenocardia acida stem bark in female Wistar rats.
Materials and Methods: Four groups of rats were administered orally aqueous
ethanolic extract of Hymenocardia acida at doses of 100, 200 and 400 mg/kg body
weight daily for 19 days. The control group received distilled water. On day 20 of
gestation, each rat was laparatomised and number of corpora lutea of pregnancy,
number of live fetuses as well as the postcoitum fertility index, weights of the foetuses
and placentae were determined.
Results: Oral administration of the extract from days 1 to 19 of gestation showed
reduction (p<0.05) in the number of corpora lutea of pregnancy and number of live
fetuses. Weights of fetuses of extract treated female rats were also smaller (p<0.05)
compared with the control. Anti-implantation activity of the treatment groups were
41.4%, 48.3% and 51.7% for groups II to IV respectively, whereas antifertility activity
of the groups was found to be 40%, 60% and 60% in the same order.
Conclusion: The results suggest that aqueous ethanolic extract of Hymenocardia acida
stem bark could induce negative effects on reproductive functions in female albino rats.
Key words: Albino rats, Antifertility, Hymenocardia acida, Reproduction.
Introduction
There is an increasing trend in the use of
medicinal plants, botanicals or herbal preparations
particularly in developing countries where these
products are readily available. Several animal
studies have revealed anti zygotic, blastocytotoxic,
anti-implantation and abortifacient properties of
water and organic solvent extracts of many
commonly used medicinal plants, sometimes in
dose dependent manner. In an investigation of
antifertility property of a triterpenoid glycoside
Corresponding author: Abu Adakole Hyacinth, Department of Veterinary
Physiology, Pharmacology and Biochemistry, College
of Veterinary Medicine, University of Agriculture,
P.M.B, 2373, Makurdi, Nigeria.
Email: [email protected]
isolated from Dalbergia saxatilis in female rats, a
decrease in maternal body weights and inhibition
of conception were observed (1). Similar
observations on antifertility, antiimplantation or
pregnancy interceptory properties suggestive of
anovulatory, antiprogesterogenic or estrogenic
effects have been made on extracts of Calotropis
gigantea (2) and Morinda citrifolia (3). However, other animal studies showed none
inhibitory effects of plant extracts on female
reproductive functions. For example, Carapa
guianensis seed oil administered orally during the
period of organogenesis failed to impair
implantation and induce the death of foetuses (4).
Sensitivity of experimental animals, dose of
extract used, period and route of administration as
well as physiological or pharmacological
mechanisms are some of the factors affecting the
implantation process.
Abu et al
218 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 217-222, Summer 2011
Hymenocardia acida (Tul.) is a small browse tree or shrub with palatable foliage, widely distributed within the savanna region of Nigeria. It is called “Enache” by Idoma people of North Central Nigeria while the local or vernacular name among the Hausas in Nigeria is “Janyaro”. All parts of the plant are useful as remedies for many ailments. The powdered roots or stem bark decoction are used to treat fever, jaundice, muscular pains, diarrhoea, dysentery and sexual incapacity in males. It is commonly used as an agent for female genital hygiene. Experimental studies have also confirmed some of the claimed efficacy of this medicinal plant by the native healers. For example, crude extracts of the plant have been reported to possess anti-tumor, anti-HIV and anti-inflammatory (5), anti-sickling (6), anti-ulcer (7) and anti-diarrhoeal (8) activities. The leaf infusion is also used in the treatment of urinary tract infections (5) and as topical applications for skin diseases in Nigeria. Among the Idoma and Igede people of North Central Nigeria, the decoction of root and stem bark is used in the treatment of diabetes (9). Also there have been reports of in vitro antitrypanosomal efficacy of leaf (10) and root bark (11) as well as antiplasmodial (12) activities of Hymenocardia acida. Despite the popular use and numerous therapeutic benefits of Hymenocardia acida, little is known about the effect of crude extract of H. acida on reproduction. The aim of the present study was to evaluate the effect of aqueous ethanolic extract of H. acida stem bark on fertility of female Wistar rats.
Materials and methods
Plant material
The stem bark of Hymenocardia acida was collected within the premises of University of Agriculture, Makurdi and authenticated by Mr. Patrick Ekwuno of College of Forestry, University of Agriculture, Makurdi, Nigeria Voucher specimen was deposited at the College herbarium. Preparation of crude extract
The stem bark was washed, air dried at room temperature for one week, pulverized and stored in air-tight container until required. As previously described (13), one hundred gram of powdered material was soaked in 500 ml of 70% ethanol and stirred intermittently for 48 hours at room temperature. The material was filtered using sterile cotton wool and Whatman (No. 1) filter paper; the residue was resuspended in the same amount of solvent and then filtered three more times. The pooled filtrates obtained were dried at room temperature under the electric fan. The extracts
were stored in air-tight containers at 4oC until
needed.
Animals Twenty white albino rats of weighing 150 g to
190 g were obtained from the College of Health Sciences, Benue State University, Makurdi, Nigeria. The animals were kept in polypropylene cages under room temperature, with 12-hour light and 12-hour dark cycle and were allowed to acclimatize for two weeks. The animals were provided commercial feed (Grand Cereals and Oil Mills Ltd, Bukuru, Jos, Nigeria) and clean water ad libitum. Protocols for this experiment was in accordance with the guidelines on the care and well being of research animals (14) and was approved by the Departmental Ethics Committee.
The rats were paired overnight with sexually active males in the ratio of 2:1. Successful mating was confirmed by the presence of vaginal plug and or sperm cells in the vaginal smear the following morning between 9.00 and 10.00 hours. The day sperm cells were found in the vaginal smear was considered as day 1 of pregnancy. Thereafter, the female rats were randomly divided into four groups of five rats each thus: Group 1 received by gavage distilled water (1ml/ 100g) daily for 19 days and served as control. Groups II–IV rats were given the aqueous ethanolic extract of Hymenocardia acida by gavage at doses of 100, 200 and 400 mg/kg body weight daily for 19 days respectively. The rats were weighed daily and observed for any untoward effects.
On day 20 of gestation, each rat was laparatomised under high ether anaesthesia. The uterine horns were exteriorized and incised at the greater curvature of the horns. The latter were examined for sites of implantation and resorption. Number of corpora lutea of pregnancy, number of live foetuses as well as weights of the foetuses and placentae were also determined. The postcoitum fertility index was evaluated using the following parameters according to the methods of Tafessel et al (16) and Uchendu et al (1). 1. Percentage of pregnant female animals in each
group (PPF) 2. Mean live foetal number per pregnant female
(LFN) 3. Mean day 20 foetal crown-rump length (FCRL) 4. Mean corpus luteum number per pregnant
female (CLN) The fertility index (FI) of each group was
calculated as
FI = LFN × FCRL × PPF
CLN
The anti-implantation and antifertility activities
of the extract were calculated as follows (16):
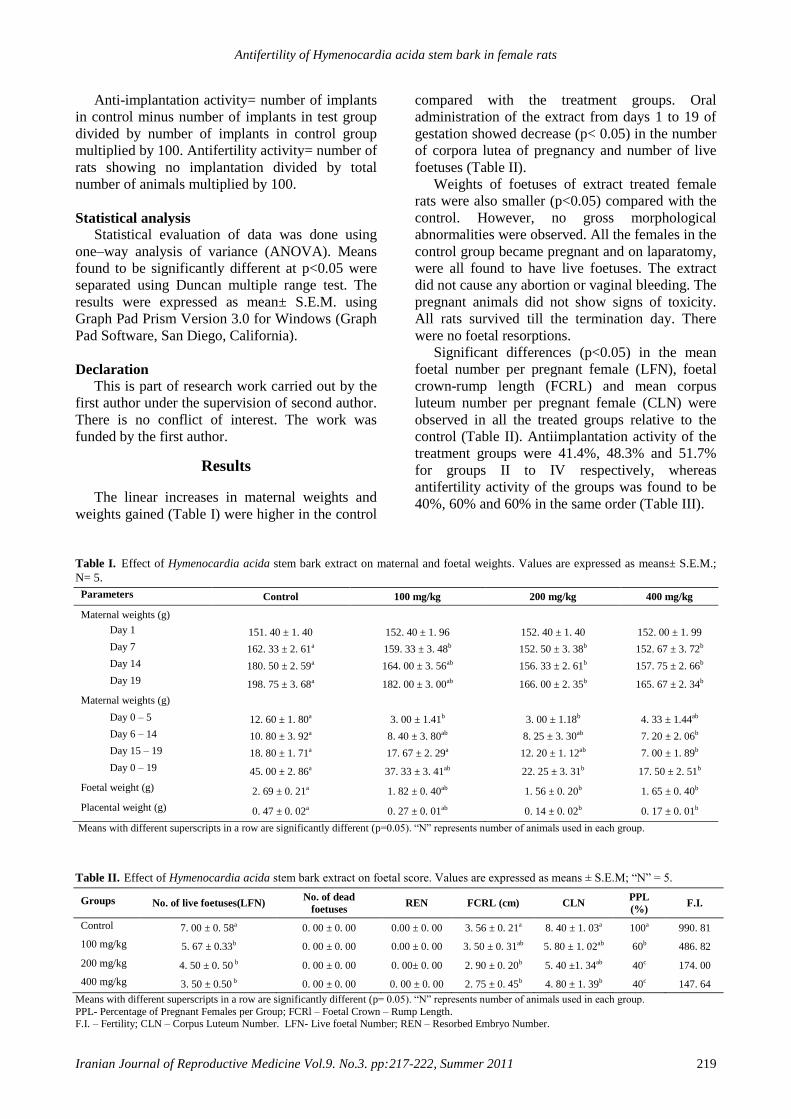
Antifertility of Hymenocardia acida stem bark in female rats
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:217-222, Summer 2011 219
Anti-implantation activity= number of implants
in control minus number of implants in test group
divided by number of implants in control group
multiplied by 100. Antifertility activity= number of
rats showing no implantation divided by total
number of animals multiplied by 100.
Statistical analysis
Statistical evaluation of data was done using
one–way analysis of variance (ANOVA). Means
found to be significantly different at p<0.05 were
separated using Duncan multiple range test. The
results were expressed as mean± S.E.M. using
Graph Pad Prism Version 3.0 for Windows (Graph
Pad Software, San Diego, California).
Declaration
This is part of research work carried out by the
first author under the supervision of second author.
There is no conflict of interest. The work was
funded by the first author.
Results
The linear increases in maternal weights and
weights gained (Table I) were higher in the control
compared with the treatment groups. Oral
administration of the extract from days 1 to 19 of
gestation showed decrease (p< 0.05) in the number
of corpora lutea of pregnancy and number of live
foetuses (Table II).
Weights of foetuses of extract treated female
rats were also smaller (p<0.05) compared with the
control. However, no gross morphological
abnormalities were observed. All the females in the
control group became pregnant and on laparatomy,
were all found to have live foetuses. The extract
did not cause any abortion or vaginal bleeding. The
pregnant animals did not show signs of toxicity.
All rats survived till the termination day. There
were no foetal resorptions.
Significant differences (p<0.05) in the mean
foetal number per pregnant female (LFN), foetal
crown-rump length (FCRL) and mean corpus
luteum number per pregnant female (CLN) were
observed in all the treated groups relative to the
control (Table II). Antiimplantation activity of the
treatment groups were 41.4%, 48.3% and 51.7%
for groups II to IV respectively, whereas
antifertility activity of the groups was found to be
40%, 60% and 60% in the same order (Table III).
Table I. Effect of Hymenocardia acida stem bark extract on maternal and foetal weights. Values are expressed as means± S.E.M.;
N= 5.
Parameters
Control 100 mg/kg 200 mg/kg 400 mg/kg
Maternal weights (g)
Day 1
151. 40 ± 1. 40 152. 40 ± 1. 96 152. 40 ± 1. 40 152. 00 ± 1. 99
Day 7
162. 33 ± 2. 61a 159. 33 ± 3. 48b 152. 50 ± 3. 38b 152. 67 ± 3. 72b
Day 14
180. 50 ± 2. 59a 164. 00 ± 3. 56ab 156. 33 ± 2. 61b 157. 75 ± 2. 66b
Day 19
198. 75 ± 3. 68a 182. 00 ± 3. 00ab 166. 00 ± 2. 35b 165. 67 ± 2. 34b
Maternal weights (g)
Day 0 – 5
12. 60 ± 1. 80a 3. 00 ± 1.41b 3. 00 ± 1.18b 4. 33 ± 1.44ab
Day 6 – 14
10. 80 ± 3. 92a 8. 40 ± 3. 80ab 8. 25 ± 3. 30ab 7. 20 ± 2. 06b
Day 15 – 19
18. 80 ± 1. 71a 17. 67 ± 2. 29a 12. 20 ± 1. 12ab 7. 00 ± 1. 89b
Day 0 – 19
45. 00 ± 2. 86a 37. 33 ± 3. 41ab 22. 25 ± 3. 31b 17. 50 ± 2. 51b
Foetal weight (g)
2. 69 ± 0. 21a 1. 82 ± 0. 40ab 1. 56 ± 0. 20b 1. 65 ± 0. 40b
Placental weight (g)
0. 47 ± 0. 02a 0. 27 ± 0. 01ab 0. 14 ± 0. 02b 0. 17 ± 0. 01b
Means with different superscripts in a row are significantly different (p=0.05). “N” represents number of animals used in each group.
Table II. Effect of Hymenocardia acida stem bark extract on foetal score. Values are expressed as means ± S.E.M; “N” = 5.
Groups
No. of live foetuses(LFN) No. of dead
foetuses REN FCRL (cm) CLN
PPL
(%) F.I.
Control
7. 00 ± 0. 58a 0. 00 ± 0. 00 0.00 ± 0. 00 3. 56 ± 0. 21a 8. 40 ± 1. 03a 100a 990. 81
100 mg/kg
5. 67 ± 0.33b 0. 00 ± 0. 00 0.00 ± 0. 00 3. 50 ± 0. 31ab 5. 80 ± 1. 02ab 60b 486. 82
200 mg/kg
4. 50 ± 0. 50 b 0. 00 ± 0. 00 0. 00± 0. 00 2. 90 ± 0. 20b 5. 40 ±1. 34ab 40c 174. 00
400 mg/kg
3. 50 ± 0.50 b 0. 00 ± 0. 00 0. 00 ± 0. 00 2. 75 ± 0. 45b 4. 80 ± 1. 39b 40c 147. 64
Means with different superscripts in a row are significantly different (p= 0.05). “N” represents number of animals used in each group.
PPL- Percentage of Pregnant Females per Group; FCRl – Foetal Crown – Rump Length. F.I. – Fertility; CLN – Corpus Luteum Number. LFN- Live foetal Number; REN – Resorbed Embryo Number.
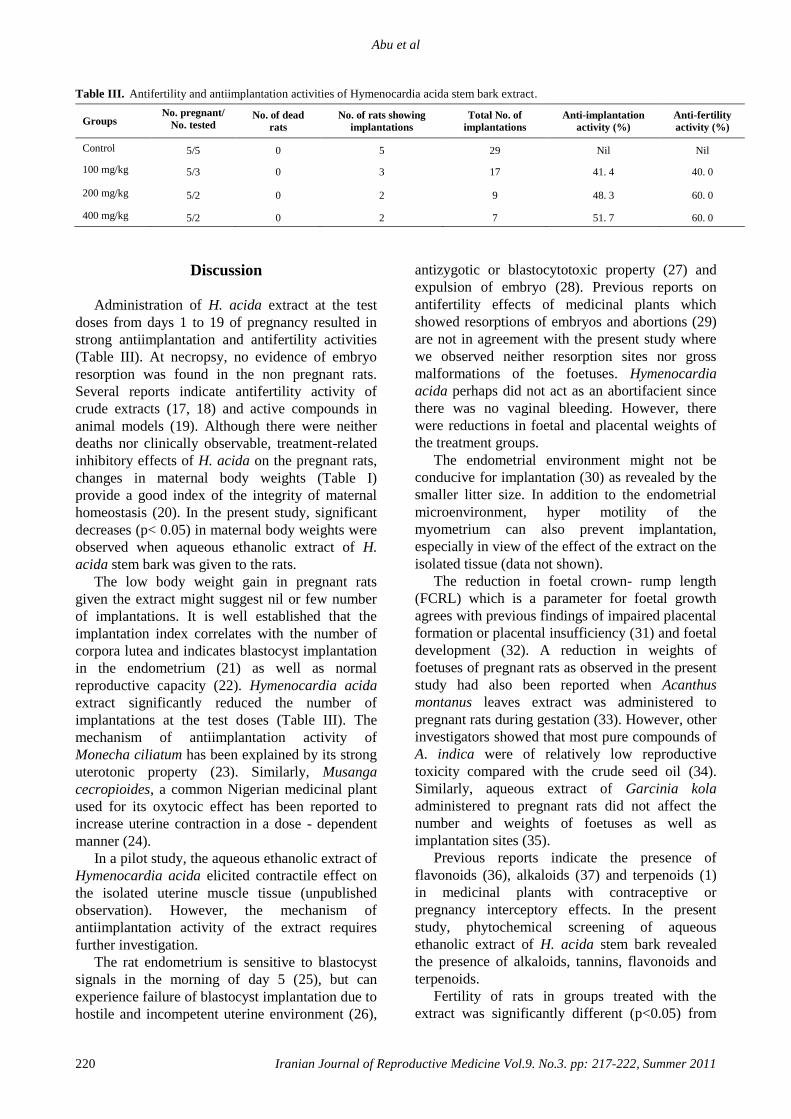
Abu et al
220 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 217-222, Summer 2011
Table III. Antifertility and antiimplantation activities of Hymenocardia acida stem bark extract.
Groups No. pregnant/
No. tested
No. of dead
rats
No. of rats showing
implantations
Total No. of
implantations
Anti-implantation
activity (%)
Anti-fertility
activity (%)
Control
5/5 0 5 29 Nil Nil
100 mg/kg
5/3 0 3 17 41. 4 40. 0
200 mg/kg
5/2 0 2 9 48. 3 60. 0
400 mg/kg
5/2 0 2 7 51. 7 60. 0
Discussion
Administration of H. acida extract at the test
doses from days 1 to 19 of pregnancy resulted in
strong antiimplantation and antifertility activities
(Table III). At necropsy, no evidence of embryo
resorption was found in the non pregnant rats.
Several reports indicate antifertility activity of
crude extracts (17, 18) and active compounds in
animal models (19). Although there were neither
deaths nor clinically observable, treatment-related
inhibitory effects of H. acida on the pregnant rats,
changes in maternal body weights (Table I)
provide a good index of the integrity of maternal
homeostasis (20). In the present study, significant
decreases (p< 0.05) in maternal body weights were
observed when aqueous ethanolic extract of H.
acida stem bark was given to the rats.
The low body weight gain in pregnant rats
given the extract might suggest nil or few number
of implantations. It is well established that the
implantation index correlates with the number of
corpora lutea and indicates blastocyst implantation
in the endometrium (21) as well as normal
reproductive capacity (22). Hymenocardia acida
extract significantly reduced the number of
implantations at the test doses (Table III). The
mechanism of antiimplantation activity of
Monecha ciliatum has been explained by its strong
uterotonic property (23). Similarly, Musanga
cecropioides, a common Nigerian medicinal plant
used for its oxytocic effect has been reported to
increase uterine contraction in a dose - dependent
manner (24).
In a pilot study, the aqueous ethanolic extract of
Hymenocardia acida elicited contractile effect on
the isolated uterine muscle tissue (unpublished
observation). However, the mechanism of
antiimplantation activity of the extract requires
further investigation.
The rat endometrium is sensitive to blastocyst
signals in the morning of day 5 (25), but can
experience failure of blastocyst implantation due to
hostile and incompetent uterine environment (26),
antizygotic or blastocytotoxic property (27) and
expulsion of embryo (28). Previous reports on
antifertility effects of medicinal plants which
showed resorptions of embryos and abortions (29)
are not in agreement with the present study where
we observed neither resorption sites nor gross
malformations of the foetuses. Hymenocardia
acida perhaps did not act as an abortifacient since
there was no vaginal bleeding. However, there
were reductions in foetal and placental weights of
the treatment groups.
The endometrial environment might not be
conducive for implantation (30) as revealed by the
smaller litter size. In addition to the endometrial
microenvironment, hyper motility of the
myometrium can also prevent implantation,
especially in view of the effect of the extract on the
isolated tissue (data not shown).
The reduction in foetal crown- rump length
(FCRL) which is a parameter for foetal growth
agrees with previous findings of impaired placental
formation or placental insufficiency (31) and foetal
development (32). A reduction in weights of
foetuses of pregnant rats as observed in the present
study had also been reported when Acanthus
montanus leaves extract was administered to
pregnant rats during gestation (33). However, other
investigators showed that most pure compounds of
A. indica were of relatively low reproductive
toxicity compared with the crude seed oil (34).
Similarly, aqueous extract of Garcinia kola
administered to pregnant rats did not affect the
number and weights of foetuses as well as
implantation sites (35).
Previous reports indicate the presence of
flavonoids (36), alkaloids (37) and terpenoids (1)
in medicinal plants with contraceptive or
pregnancy interceptory effects. In the present
study, phytochemical screening of aqueous
ethanolic extract of H. acida stem bark revealed
the presence of alkaloids, tannins, flavonoids and
terpenoids.
Fertility of rats in groups treated with the
extract was significantly different (p<0.05) from
Antifertility of Hymenocardia acida stem bark in female rats
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:217-222, Summer 2011 221
the control as reflected by the reduced pregnancy
and fertility index (Table II). A similar observation
on reduced fertility was made when pregnant rats
were treated with Dalbergia saxatilis (1).
The results suggest that aqueous ethanolic
extract of Hymenocardia acida stem bark could
induce inhibitory effects on reproductive functions
in female albino rats.
References 1. Uchendu CN, Kamalu TN, Asuzu IU. A preliminary
evaluation of antifertility activity of a triterpenoid
glycoside from Dalbergia saxatilis in female Wistar rats.
Pharmacol Res 2000; 41:521-525.
2. Srivastava S, Keshri G, Bhargevan B, Singh C, Singh
MM. Pregnancy interceptive activity of the roots of
Calotropis gigantea Linn in rats. Contraception 2007; 75:
318-322.
3. Muller JC, Botelho GG, Bufalo AC, Boaereto AC,
Rattman YD, Martins ES, et al. Morinda citrifolia Linn
(Noni): In vivo and in vitro reproductive toxicology. J
Ethnopharmacol 2009; 121: 229-233.
4. Costa-Silva JH, Lima CR, Silva EJ, Araujo AV, Fraga
MC, Ribeiro E Ribeiro A, et al. Acute and sub acute
toxicity of the Carapa guianensis Aublet (Meliaceae) seed
oil. J Ethnopharmacol 2008; 116: 495-500.
5. Muanza DN, Euler KL, Williams L, Newman DS.
Screening for antitumor and anti-HIV activities of nine
medicinal plants from Zaire. Int J Pharmacol 1995; 33:
98-106.
6. Mpiana P T, Tshibanga DS, Shetonde OM, Ngbolua KN.
In vitro antidrepanocytary activity (antisickle cell
anaemia) of some Congolese plants. Phytomedicine 2007;
14: 192-195.
7. Ukwe CV. Evaluation of the anti-ulcer activity of aqueous
stem bark extract of Hymenocardia acida. Nigerian
Journal of Pharmaceutical Research 2004; 3: 86-89.
8. Tona L, Kambu K, Masia K, Cimanga R, Apers S, De
bruyne T, et al. Biological screening of traditional
preparations from some medicinal plants used as
antidiarrhoeal in Kinshasha, Congo. Phytomedicine 1999;
6: 59-66.
9. Igoli JO, Ogeji OG, Tor-Anyiin TA, Igoli NP. Traditional
medical practice amongst the igede people of Nigeria. Afr
J Trad CAM 2005; 2: 134-152.
10. Hoet S, Opperdoes F, Brun R, Adjakidje V, Quetinleclercq
J. In vitro antitrypanosomal activity of ethno
pharmacologically selected Beninese plants. J
Ethnopharmacol 2004; 91: 37-42.
11. Kamanzi Atindehook K, Schmid C, Brun R, Kone MW,
Traore D. Antitrypanosomal and antiplasmodial activity of
medicinal plants from Cote d’Ivoire. J Ethnopharmacol
2004; 90: 221-227.
12. Vonthron-Senecheau C, Weniger B, Quattara M, Bi FT,
Kamenan A, Lobstein A. In vitro antiplasmodial activity
and cytotoxicity of ethno botanically selected Ivorian
plants. J Ethnopharmacol 2003; 87: 221-225.
13. Abu AH, Uchendu CN, Ofukwu RA. In vitro
antitrypanosomal activity of crude extracts of some
Nigerian medicinal plants. J Appl Biosc 2009; 21: 1277-
1282.
14. National Institute of Health (N.I.H). Guide for the care and
use of laboratory animals. DHEW Publication. Office of
Science and Health Reports; Bethesda; U.S.A.; 1985.
15. Wong PY, Lau SK, Fu WO. Antifertility effects of some
sulphonamides and related compounds and their
accumulation in the rat epididymis. J Reprod Fertil 1987;
81: 259-267.
16. Tafessel G, Mekonnen Y, Makonnen E. In vivo and in
vitro antifertility and antiimplantation properties of
Leonotis ocymifolia in rats. Afr J Trad CAM 2005; 2: 103-
112.
17. Uchendu CN, Isek T. Antifertility activity of aqueous
ethanolic leaf extract of Spondias mombin
(Anacardiaceae) in rats. Afr Health Sci 2008; 8: 163-167.
18. Yadav R, Jain GC. Antifertility effect and hormonal
profile of petroleum ether extract of seeds of Cassia fistula
in female rats. International Journal of Pharmacology and
Technology Research 2009; 1: 438-444.
19. Hikim AP, Lue YH, Wang C, Reutrakul V, Sangsuwan R,
Swerdloff RS. Post testicular antifertility action of
triptolide in the male rat: evidence for severe impairment
of cauda epididymal sperm ultra structure. J Androl 2000;
21: 431-437.
20. Almeida FC, Lemonica IP. The toxic effects of Coleus
barbatus on the different periods of pregnancy in rats. J
Ethnopharmacol 2000; 73: 53-60.
21. Tafessel G, Mekonnen Y, Makonnen E. Antifertility effect
of aqueous and ethanol extracts of the leaves and roots of
Asparagus africanus in rats. Afr Health Sci 2006; 6: 81-85.
22. Chang CV, Felicio AC, Reis JE, Guerra MdE O, Peters
VM. Fetal toxicity of Solanum lycocarpum (Solanaceae)
in rats. J Ethnopharmacol 2008; 81: 205-209.
23. Uguru MO, Okwuasaba FK, Ekwenchi EE, Uguru VE.
Uterotonic properties of the methanolic extract of
Monechma ciliatum. J Ethnopharmacol 1998; 62: 203-
208.
24. Ayinde BA, Onwukaeme DN, Nworgu ZAM. Oxytocic
effects of the water extract of Musanga cecropioides R.
Brown (Moraceae) stem bark. Afr J Biotechnol 2006; 5:
1350-1354.
25. Singh MM, Kamboj VP. Fetal resorption in rats treated
with an antiestrogen in relation to luteal phase nidatory
estrogen secretion. Acta Endocrinol (Copenh) 1992; 26:
444-450.
26. Emiliani S, Delbaere A, Devreker F, Englert Y. Embryo-
maternal interactive factors regulating the implantation
process: Implications in assisted reproduction. Reprod
Biomed Online 2005; 10: 527-540.
27. Hafez B, Hafez ESE. Reproduction in Farm Animals. 7th
Ed. Lippincott; Williams and Wilkins; 2000: 3-95.
28. Orihuela PA, Rios M, Croxatto HB. Disparate effects of
estradiol on egg transport and oviductal protein synthesis
in mated and cyclic rats. Biol Reprod 2001; 65: 1232-
1237.
29. Vasudeva N, Sharma SK. Estrogenic and pregnancy
interceptory effects of Achyranthes aspera Linn root. Afr J
Trad, Complement Altern Med 2007; 4: 7-11.
30. Hazarika A, Sarma HN. Effects of crude root extract of
Polygonum hydropiper on estrous cycle and induction of
reversible sterility in female albino rat. Journal of
Endocrinology and Reproduction 2007; 11: 36-40.
31. Rasheed RA, Bashir AK, Ali BH, Padmanabhan R. Effect
of Rhazya stricta on the developing rat fetus. Reprod
Toxicol 1997; 11: 191-199.
32. Schwarz A, Pinto E, Haraguchi M, de Oliveira CA,
Bernardi MM, Spinosa HS. Phytochemical study of
Solanum lycocarpum unripe fruit and its effects on rat
gestation. Phytotherapy Research 2007; 21: 1025-1028.
33. Nana P, Asongalem ER, Foyet HS, Folefoe GN, Dimo T,
Kamtchouing P. Maternal and developmental toxicity
evaluation of Acanthus montanus leaves extract

Abu et al
222 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 217-222, Summer 2011
administered orally to Wistar pregnant rats during
organogenesis. J Ethnopharmacol 2008; 116: 228-233.
34. Boeke SJ, Boersma MG, Alink GM, Van loon JJA,
VanHuis A, Dicke M, et al. Safety evaluation of neem
(Azadirchta indica) derived pesticides. J Ethnopharmacol
2004; 94: 25-41.
35. Iranloye B, Owokunle B. Effect of Garcinia kola seed
extract on female reproductive functions in rats. Int J
Pharmacol 2008; 4: 276-281.
36. Hiremath SP, Rudresh K, Badami S, Patil SB, Patil RS.
Post-coital antifertility activity of Acalypha indica L. J
Ethnopharmacol 1999; 67: 253-258.
37. Ravichandra V, Suresh B, Satishkumar MN, Elango K,
Srinivasan R. Antifertility activity of hydroalcoholic
extract of Ailanthus excelsa (Roxb): An ethno medicine
used by tribes of Nilgiris region in Tamilnadu. J
Ethnopharmacol 2007; 112: 189-191.

Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 223-228, Summer 2011
High plasma homocysteine and insulin resistance in
patients with polycystic ovarian syndrome Tayebe Hemati
1 M.D., Nasrin Moghadami-Tabrizi
1 M.D., Fateme Davari-Tanha
1 M.D., Bahram
Salmanian2 M.D., Pouya Javadian
2 M.D.
1 Department of Obstetrics and Gynecology, Mirza Kouchak Khan Hospital, Tehran University of
Medical Sciences, Tehran, Iran.
2 School of Medicine, Tehran University of Medical Sciences, Tehran, Iran.
Received: 6 June 2010; accepted: 11 January 2011
Abstract
Background: Polycystic ovarian syndrome (PCOS) is a common disease among
women in fertility ages and cause severe insulin resistance. Hyperhomocysteinaemia is
said to be among the features of PCOS that could influence its outcome.
Objective: This study aimed to investigate whether hyperhomocysteinaemia exists in
PCOS and if it is related to insulin resistance in the affected patients.
Materials and Methods: This prospective study was carried out in a university based
fertility clinic. Sixty four PCOS patients and 50 normo ovulatory controls were
reviewed for fasting glucose, insulin, homocysteine, luteinizing hormone (LH), and
follicle-stimulating hormone (FSH) plasma levels in the blood sample of the 3rd
day of
their menstrual cycle. Insulin resistance was determined with the fasting glucose
(mmol/L) to insulin (mIU/L) ratio and HOMA-IR (Homeostasis model assessment-
Insulin resistance). Independent-samples T-test and linear regression test were utilized
to analyze the obtained data.
Results: Homocysteine levels compared between PCOS patients and control group
showed a significant difference. PCOS group was divided into insulin resistant (IR)
(LogHOMA-IR≥0.57) and non insulin resistant (NIR) patients. The IR group had
significantly higher homocysteine (p-value=0.02), fasting insulin and glucose levels (p-
value<0.001) rather than NIR group.
Conclusion: PCOS patients have a leaning toward hyperhomocysteinaemia and insulin
resistance. Insulin resistant patients are found to have higher homocysteine level. Key words: PCOS, Homocysteine, Insulin resistance, Infertility.
Introduction
Polycystic ovarian syndrome (PCOS) is a
common disease among women in fertility age. It
causes ovulation disturbances, hyper androgenism,
infertility and increased abortion rate. Obesity,
hyper insulinemia, diabetes, hypertension,
dyslipidemia, atherosclerosis and vascular diseases
are other problems ascribed to PCOS (1-5). It has
been shown that PCOS can cause severe insulin
Corresponding Author:
Fateme Davari-Tanha, Department of Obstetrics and
Gynecology, Mirza Kouchak Khan Hospital, Tehran
University of Medical Sciences, Tehran, Iran.
Email: [email protected]
resistance and its secretion disturbances to some
extent.Homocysteine is an intermediate substance
in methionine metabolism. An increased
homocysteine plasma level classically happens due
to an enzymatic defect in the aforementioned
process.
The recent studies have shown there are so
many non-enzymatic factors affecting
homocysteine levels as well (6-8). According to
the insulin role in inhibition of hepatic cystathione
beta synthase, which is an enzyme involved in
methionine metabolism, insulin plasma level is
also introduced as a determining factor of
homocysteine levels (9, 10). Insulin resistance
seems to increase the homocysteine levels (6, 8,
11).
Hemati et al
224 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:223-228, Summer 2011
There are several studies regarding the role of
homocysteine in pathogenesis of vascular diseases.
Homocysteine is found to be an effectual factor in
coronary artery diseases (CAD). Homocysteine
level higher than 11 µmol/L is detected in 30% of
CAD patients and increases the mortality rate by 3
times (12, 13). Herein, we aim to evaluate the
relation between homocysteine level and PCOS,
and its association with insulin resistance that
could affect the outcome of PCOS short and long
term management.
Materials and methods
Sixty four patients referring to the infertility
unit at a university based fertility clinic, affiliated
to Tehran University of Medical Sciences, were
selected to be studied in a prospective study, in
2008-2009. The diagnosis of PCOS was made
according to the Rotterdam European Society of
Human Reproduction and embryology (ESHRE)/
American Society for Reproductive Medicine
(ASRM), sponsored PCOS consensus workshop
group guide lines (14). Those criteria are well
accepted for PCOS diagnosis (1). The study and its
methodology were approved by ethic committee of
Tehran University of Medical Sciences. All
possible risks were explained to patients and
informed consent was obtained from all
participants.
None of the patients were diagnosed with
diabetes or had any smoking habits. Those who
received metformin, folic acid or phenytoin were
also excluded.
Fifty other patients referring to the same unit
who had non ovarian problems were randomly
selected as the control group utilizing a pseudo-
random number generator. They had normal
ovarian and menstrual cycle; who did not present
with any of clinical and ultrasound signs and
symptoms of PCOS. They were matched with the
PCOS group regarding age and physical activity to
omit any known confounding factor.
Laboratory tests
All cases in both groups were weighed in two
different days and their height was measured. BMI
was calculated by dividing the weight (kg) by
squared height (m2). The basic plasma level of LH,
FSH and fasting glucose were measured in the 3rd
day of a spontaneous or progesterone induced
menstrual cycle before any treatments. Fasting
insulin and homocysteine total plasma levels were
also measured in the same day using Eliza enzyme
immunosorbent assay (Calbiotech Inc., CA).
Serum prolactin, thyroid hormone and 17-hydroxy
progesterone along with BUN and creatinine were
measured. Those were inspected not to exceed the
normal levels.
Insulin resistance is determined with several
indices, including: fasting insulin total plasma
level (mIU/L), the fasting glucose (mmol/L) to
insulin (mIU/L) ratio, and HOMA-IR
(Homeostasis model assessment-Insulin resistance)
calculated by Insulin (mIU/L) * glucose (mmol/L)/
22.5.
Fasting insulin total plasma level and fasting
glucose to insulin ratio have more restrictions
rather than HOMA-IR, are less sensitive
physiologically, and are not useful in abnormal
glucose levels. Therefore, we utilized the HOMA-
IR in the rest of this study. We converted HOMA-
IR into logarithmic scale, since it rarely has normal
distribution (15, 16). Insulin resistance was
inspected also by measuring the insulin levels 2
hours after glucose loading. 150 pmol/ L was
considered the cut-off.
To determine insulin resistance regarding each
index, the upper limit of the normal ranges was
considered mean±2SD of the control group.
Statistical analysis
We used SPSS software version 16 (SPSS Inc.
Chicago, IL, USA) for statistical analysis. p-value
of 0.05 and lower was considered significant.
Independent-samples T-test was utilized to
compare differences between parametric data
groups. In order to express the conditional
distribution of bivariate correlated items linear
regression test was done.
Results
Homocysteine levels compared between PCOS
patients and control group showed a significant
difference, 10.96±7.27 µmol/L in all PCOS vs.
6.8±1.95 µmol/L in controls (p-value <0.001). The
clinical and biochemical data of all patients
regarding their differences is shown in Table I.
Ninety five percent (Mean+2SD) of the control
group had homocysteine levels lower than
10.7µmol/L, while the normal range of

PCOS, insulin resistance (IR)
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 223-228, Summer 2011 225
homocysteine is usually considered between 5 to
11 µmol/L (3). 35.94% of cases (23/64) in the
PCOS group had homocysteine levels higher than
10.7 µmol/L (p<0.001), who were regarded
hyperhomocysteinemic.
Insulin resistance determined with different
indices in our study. For each variable, the upper
limit was defined as mean±2SD of the normal
control group. Therefore 20 mIU/L, 0.3, and 0.57
were regarded as the cut-off levels for fasting
insulin level, glucose to insulin ratio, and Log
HOMA-IR respectively.
In the same order, 35.94%, 48.44% and 57.81%
of the patients had insulin resistance. Measuring
insulin level 2 hours after glucose loading, 45.31%
were resistant. All the aforementioned results were
found to be significantly different compared with
those of the control group (p<0.001, all groups).
Log HOMA-IR was utilized in the rest of the
study.
PCOS group was divided into insulin resistant
(IR) (Log HOMA-IR ≥ 0.57) and non insulin
resistant (NIR) (Log HOMA-IR < 0.57) patients.
The IR group had significantly higher
homocysteine (p-value=0.02), fasting insulin and
glucose levels (p-value<0.001) rather than NIR
group.
However, no association was found between
Log HOMA- IR and BMI (p-value=0.18) (Table
II). 18.52% (5/27) of NIR-PCOS patients had
increased levels of homocysteine (>10.7 µmol/L),
while 48.65% (18/37) of IR-PCOS were found
hyperhomocysteinemic (Homocysteine in IR-
PCOS 12.6±7.9 Vs. Homocysteine in NIR-PCOS
8.6±5.6, p-value= 0.02).
More number of PCOS group showed BMI≥ 23
in comparison with the control group (p< 0.06), but
the higher BMI did not have any significant
association neither with homocysteine nor with
insulin resistance in PCOS group, Homocysteine
and Log HOMA-IR 12.3±6.9 and 0.58±0.27 in
BMI ≥ 27 PCOS group respectively vs. 10.5±7.3
and 0.58±0.24 in BMI<27 PCOS group (p-value=
0.4 and 0.9). 12.88% of the PCOS group had BMI
≥ 27 Kg/m2.
Increased LH to FSH ratio was significantly
found in PCOS patients rather than the control
group (p<0.001), whether they were obese or
insulin resistant or none. Age was only related to
BMI (p-value= 0.001) but with no other variable.
All the insulin resistance indices were
correlated with homocysteine levels. (Fasting
insulin r= 0.513 p< 0.001, Glu/ Ins r=-0.3 p=
0.015, Log HOMA- IR r= 0.3 p= 0.015, Ins2hr r=
0.37 p= 0.002).
The correlation between homocysteine levels
and logarithmic transformation of HOMA-IR,
ANOVA linear regression test, is shown in figure
1.
Table I. Clinical and biochemical data of all patients.
Control (N=50) PCOS (N=64) p-value
Age (years)
29.1±3.2 31.09±8.9 0.08
BMI (kg/m2)
22.1±0.25 22.7±3.2 <0.06
Homocysteine (µmol/l)
6.8±1.95 10.9±7.2 <0.001
Insulin (mIU/l)
10.6±4.7 18.9±8.6 <0.001
LH/FSH
0.8±0.2 1.77±1 <0.001
Glucose/Insulin ratio
0.56±0.13 0.32±0.14 <0.001
Log HOMA-IR
0.23±0.17 0.58±0.24 <0.001
PCOS: polycystic ovarian syndrome, BMI: body mass index, Log HOMA-IR: logarithmic transformation of homeostasis index of insulin
resistance.
Table II. Variables and their differences in insulin resistant and non insulin resistant PCOS patients.
Number Homocysteine Fasting glucose Fasting insulin Glucose/Insulin BMI
PCOS-NIR
27 8.6±5.6 83.9±11 11.1±2.7 0.44±0.12 25.3±2.9
PCOS-IR
37 12.6±7.9 97.9±11.2 24.6±6.8 0.23±0.07 24.2±3.4
p value 0.02 <0.001 <0.001 <0.001 0.18
Values are mean±SD. PCOS: polycystic ovarian syndrome, NIR: non insulin resistant, IR: insulin resistant.
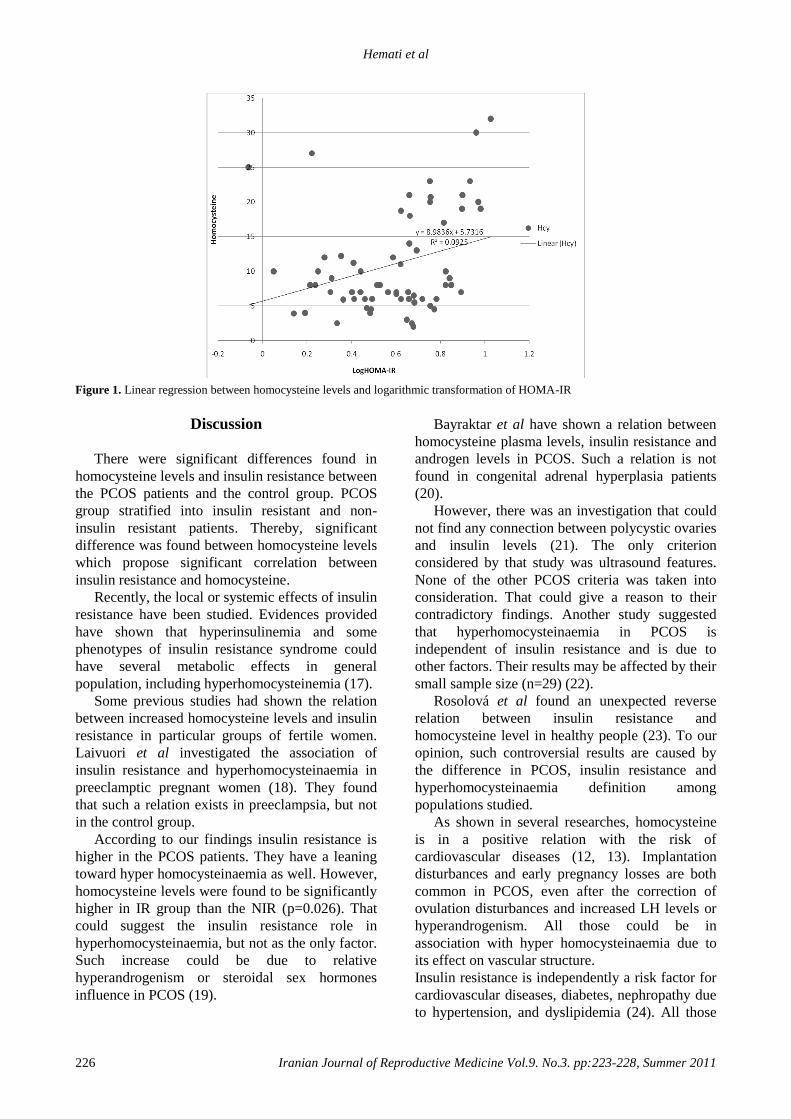
Hemati et al
226 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:223-228, Summer 2011
Figure 1. Linear regression between homocysteine levels and logarithmic transformation of HOMA-IR
Discussion
There were significant differences found in
homocysteine levels and insulin resistance between
the PCOS patients and the control group. PCOS
group stratified into insulin resistant and non-
insulin resistant patients. Thereby, significant
difference was found between homocysteine levels
which propose significant correlation between
insulin resistance and homocysteine.
Recently, the local or systemic effects of insulin
resistance have been studied. Evidences provided
have shown that hyperinsulinemia and some
phenotypes of insulin resistance syndrome could
have several metabolic effects in general
population, including hyperhomocysteinemia (17).
Some previous studies had shown the relation
between increased homocysteine levels and insulin
resistance in particular groups of fertile women.
Laivuori et al investigated the association of
insulin resistance and hyperhomocysteinaemia in
preeclamptic pregnant women (18). They found
that such a relation exists in preeclampsia, but not
in the control group.
According to our findings insulin resistance is
higher in the PCOS patients. They have a leaning
toward hyper homocysteinaemia as well. However,
homocysteine levels were found to be significantly
higher in IR group than the NIR (p=0.026). That
could suggest the insulin resistance role in
hyperhomocysteinaemia, but not as the only factor.
Such increase could be due to relative
hyperandrogenism or steroidal sex hormones
influence in PCOS (19).
Bayraktar et al have shown a relation between
homocysteine plasma levels, insulin resistance and
androgen levels in PCOS. Such a relation is not
found in congenital adrenal hyperplasia patients
(20).
However, there was an investigation that could
not find any connection between polycystic ovaries
and insulin levels (21). The only criterion
considered by that study was ultrasound features.
None of the other PCOS criteria was taken into
consideration. That could give a reason to their
contradictory findings. Another study suggested
that hyperhomocysteinaemia in PCOS is
independent of insulin resistance and is due to
other factors. Their results may be affected by their
small sample size (n=29) (22).
Rosolová et al found an unexpected reverse
relation between insulin resistance and
homocysteine level in healthy people (23). To our
opinion, such controversial results are caused by
the difference in PCOS, insulin resistance and
hyperhomocysteinaemia definition among
populations studied.
As shown in several researches, homocysteine
is in a positive relation with the risk of
cardiovascular diseases (12, 13). Implantation
disturbances and early pregnancy losses are both
common in PCOS, even after the correction of
ovulation disturbances and increased LH levels or
hyperandrogenism. All those could be in
association with hyper homocysteinaemia due to
its effect on vascular structure.
Insulin resistance is independently a risk factor for
cardiovascular diseases, diabetes, nephropathy due
to hypertension, and dyslipidemia (24). All those
PCOS, insulin resistance (IR)
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 223-228, Summer 2011 227
which are related to the metabolic syndrome are
intensified by hyperhomocysteinaemia. Then,
PCOS could be considered as a type of insulin
resistance syndrome or as an early sign of that
syndrome. However, it should be kept in mind that
the homocysteine plasma level is affected by
several factors.
If the PCOS is diagnosed, it’s better to have in
mind the other metabolic complications as well.
Gynecologists should consider both the short term
(infertility) and long term (cardiovascular and
metabolic diseases) outcomes in their management.
Further studies are needed to investigate the effect
of insulin sensitizers on homocysteine plasma
level.
Regarding the result of this study, approving
hyperhomocysteinaemia and its relation to insulin
resistance, and vascular abnormalities caused by
them shown in other studies, it seems that clinical
examination concerning those complications is a
matter of importance in PCOS management.
Active treatment of hyperhomocysteinaemia may
decrease PCOS morbidity. Prospective studies
could objectively show the promising role of such
treatments in PCOS.
References
1. Dunaif A. Insulin resistance and the polycystic ovary
syndrome: mechanism and implications for pathogenesis.
Endocr Rev 1997; 18: 774-800.
2. Gennarelli G, Holte J, Berglund L, Berne C, Massobrio M,
Lithell H. Prediction models for insulin resistance in the
polycystic ovary syndrome. Hum Reprod 2000; 15: 2098-
2102.
3. Schachter M, Raziel A, Friedler S, Strassburger D, Bern
O, Ron-El R. Insulin resistance in patients with polycystic
ovary syndrome is associated with elevated plasma
homocysteine. Hum Reprod 2003; 18: 721-727.
4. Talbott E, Guzick D, Clerici A, Berga S, Detre K, Weimer
K, et al. Coronary heart disease risk factors in women with
polycystic ovary syndrome. Arterioscler Thromb Vasc
Biol 1995; 15: 821-826.
5. Robinson S, Henderson AD, Gelding SV, Kiddy D,
Niththyananthan R, Bush A, et al. Dyslipidaemia is
associated with insulin resistance in women with
polycystic ovaries. Clin Endocrinol (Oxf) 1996; 44: 277-
284.
6. Giltay EJ, Hoogeveen EK, Elbers JM, Gooren LJ,
Asscheman H, Stehouwer CD. Effects of sex steroids on
plasma total homocysteine levels: a study in transsexual
males and females. J Clin Endocrinol Metab 1998; 83:
550-553.
7. McCarty MF. Increased homocysteine associated with
smoking, chronic inflammation, and aging may reflect
acute-phase induction of pyridoxal phosphatase activity.
Med Hypotheses 2000; 55: 289-293.
8. Nygard O, Refsum H, Ueland PM, Vollset SE. Major
lifestyle determinants of plasma total homocysteine
distribution: the Hordaland Homocysteine Study. Am J
Clin Nutr 1998; 67: 263-270.
9. House JD, Jacobs RL, Stead LM, Brosnan ME, Brosnan
JT. Regulation of homocysteine metabolism. Adv Enzyme
Regul 1999; 39: 69-91.
10. McCarty MF. Insulin secretion as a potential determinant
of homocysteine levels. Med Hypotheses 2000; 55: 454-
455.
11. Bar-On H, Kidron M, Friedlander Y, Ben-Yehuda A,
Selhub J, Rosenberg IH, et al. Plasma total homocysteine
levels in subjects with hyper insulinemia. J Intern Med
2000; 247: 287-294.
12. Karaer A, Cavkaytar S, Mert I, Buyukkagnici U, Batioglu
S. Cardiovascular risk factors in polycystic ovary
syndrome. J Obstet Gynaecol 2010; 30: 387-392.
13. Mohamadin AM, Habib FA, Al-Saggaf AA.
Cardiovascular disease markers in women with polycystic
ovary syndrome with emphasis on asymmetric
dimethylarginine and homocysteine. Ann Saudi Med 2010;
30: 278-283.
14. Broekmans FJ, Knauff EA, Valkenburg O, Laven JS,
Eijkemans MJ, Fauser BC. PCOS according to the
Rotterdam consensus criteria: Change in prevalence
among WHO-II anovulation and association with
metabolic factors. BJOG 2006; 113: 1210-1217.
15. Quon MJ. Limitations of the fasting glucose to insulin
ratio as an index of insulin sensitivity. J Clin Endocrinol
Metab 2001; 86: 4615-4617.
16. Wallace TM, Levy JC, Matthews DR. Use and abuse of
HOMA modeling. Diabetes Care 2004; 27: 1487-1495.
17. Meigs JB, Jacques PF, Selhub J, Singer DE, Nathan DM,
Rifai N, et al; Framingham Offspring Study. Fasting
plasma homocysteine levels in the insulin resistance
syndrome: the Framingham offspring study. Diabetes
Care 2001; 24: 1403-1410.
18. Laivuori H, Kaaja R, Turpeinen U, Viinikka L, Ylikorkala
O. Plasma homocysteine levels elevated and inversely
related to insulin sensitivity in preeclampsia. Obstet
Gynecol 1999; 93: 489-493.
19. Badawy A, State O, El Gawad SSh, El Aziz OA. Plasma
homocysteine and polycystic ovary syndrome: the missed
link. Eur J Obstet Gynecol Reprod Biol 2007; 131: 68-72.
20. Bayraktar F, Dereli D, Ozgen AG, Yilmaz C. Plasma
homocysteine levels in polycystic ovary syndrome and
congenital adrenal hyperplasia. Endocr J 2004; 51: 601-
608.
21. Sills ES, Genton MG, Perloe M, Schattman GL, Bralley
JA, Tucker MJ. Plasma homocysteine, fasting insulin, and
androgen patterns among women with polycystic ovaries
and infertility. J Obstet Gynaecol Res 2001; 27: 163-168.
22. Kilic-Okman T, Guldiken S, Kucuk M. Relationship
between homocysteine and insulin resistance in women
with polycystic ovary syndrome. Endocr J 2004; 51: 505-
508.
23. Rosolová H, Simon J, Mayer O Jr, Racek J, Dierzé T,
Jacobsen DW. Unexpected inverse relationship between
insulin resistance and serum homocysteine in healthy
subjects. Physiol Res 2002; 51: 93-98.

Hemati et al
228 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:223-228, Summer 2011
24. Goldstein BJ, Haffner SM, Hsueh WA. Insulin
resistance implications for metabolic and cardiovascular
diseases. CME Circle Diabetes and Endocrinology
continuing medical education online:
http://www.medscape.org/ viewarticle/412860. 2001.

Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 229-238, Summer 2011
Cotherapy of Tiron and selenium against vanadium
induced toxic effects in lactating rats Sadhana Shrivastava Ph.D., Deepmala Joshi Ph.D., Monika Bhadauria Ph.D., Sangeeta Shukla D.Sc.,
Ramesh Mathur Ph.D.
UNESCO Satellite Center of Trace Element Research and Reproductive Biology and Toxicology
Laboratory, School of Studies in Zoology, Jiwaji University, Gwalior (MP), 474 011, India.
Received: 17 July 2010; accepted: 5 January 2011
Abstract
Background: Vanadium is an important environmental and industrial pollutant. It has a
status of reproductive toxicant and is reported to cross placental barrier.
Objective: The current study was performed to assess the therapeutic efficacy of Tiron
and its combination with selenium against vanadium induced toxicity in lactating and
suckling rats.
Materials and Methods: Rats were exposed to vanadium at a dose of 7.5 mg/kg/day
(p.o.) for 20 days from 0 day of post partom (p.p.). Tiron (606 mg/kg/day, i.p.) and
selenium (0.5 mg/kg/day, p.o.) were administered for 5 days on 21-25 day PP.
Results: Vanadium exposure decreased blood sugar level while serum transaminases
and serum alkaline phosphatase showed increased values significantly (p<0.01).
Elevation in glycogen content of liver and kidney of suckling and kidney of lactating
rats was found after toxicant administration. Toxicant intoxication increased the
enzymatic activity of acid phosphatase in liver of suckling and lactating and kidney of
suckling rats. On the contrary alkaline phosphatase and adenosine triphosphatase
activities were inhibited significantly (p<0.01) in all the organs. Lipid peroxidation was
enhanced whereas glutathione was reduced significantly in liver of suckling and
lactating rats (p<0.01). Vanadium also caused histopathological lesions. Therapies of
Tiron per se and Tiron along with selenium maintained almost all blood and tissue
biochemical parameters towards normal. Tiron along with selenium reduced vanadium
induced lesions in lactating and sucklings rats.
Conclusion: Tiron along with selenium is more effective than Tiron alone against
vanadium induced toxic effect on lactating and suckling rats.
Key words: Vanadium, selenium, Suckling, lactating, Teratogenecity, Tiron.
Introduction
Industrial pollution is the biggest health hazard
in the 21st century. Vanadium is widely distributed
in the earth’s crust in a wide range of minerals and
in fossil fuels. The chemical gets into the air, water
and soil when fuel oil is burned, or when rocks and
soil containing vanadium are broken down (1-3).
Corresponding Author:
Sadhana Shrivastava, UNESCO Satellite Center of
Trace Element Research and Reproductive Biology and
Toxicology Laboratory, School of Studies in Zoology,
Jiwaji University, Gwalior (MP), 474 011 India.
Email: [email protected]
It has been recognized as essential nutrients in
higher animals (4).
It has a status of reproductive toxicant, as
microtubule damaging agent, reducing sperm
motility and damaging spermatozoa. Vanadium
decrease fertility and after expose to it, embryo
lethality, fetotoxicity and teratogenicity have been
reported to occur in rats, mice and hamsters (5-8).
It also increases malformations and abnormalities
in pups. It can pass the blood placenta barrier and
has been reported to be teratogenic in rodents and
affects sexual development in pre-pubertal
animals.
The development of the offspring was
significantly decreased from birth and during the

Shivastava et al
230 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:229-238, Summer 2011
lactation period after vanadium intoxication (9,
10).
Tiron, 4, 5-dihydroxy-1, 3-benzene disulfonic
acid, has been known to be a widely used
antioxidant to rescue ROS-evoked cell death and a
non-toxic chelator to alleviate an acute metal
overload. It is a substrate in several enzyme
reactions and has small size which facilitates cell
entry and modulates intracellular electron transfer
reactions as an antioxidant by scavenging free
radicals (11, 12). It is also effective against various
metal intoxications of beryllium, aluminium, lead
and vanadium (13-16). Selenium (Se) is a trace
mineral and is needed in small amounts for good
health. It acts as a growth factor and is a powerful
antioxidant. It is a component of selenocysteine
and selenomethionine and cofactor for reduction
of antioxidant enzymes such as glutathione
peroxidases (17). Se protects toxic effects of
metals such as cadmium, and mercury, aluminium
(18-20). Se protects neuronal cells against
neurotoxic effects of vanadium (21). Thus the aim
of this study was to evaluate Tiron+Se as an
antidote against vanadium in sucklings and
lactating rats.
Materials and methods
Detoxification of vanadium in rats. This study
comes under preclinical studies on laboratory
animals.
Chemicals
Vanadium sulphate and sodium selenite
procured from Glaxo Laboratory Ltd., Bombay,
India and sodium-4, 5-dihydroxybenzene-1, 3-
disulfonate (Tiron) procured from Sigma-Aldrich.
Other analytical grade laboratory reagents were
procured from Merck (Germany) and Glaxo
chemical (India).
Animals
Female albino rats of Sprague Dawley strain
(16010 g b.w.) from our departmental animal
facility were given a standard pellet diet (Pranav
Agro Industries, New Delhi, India having metal
contents in ppm dry weight Cu 10; Mn 33; Zn 45;
Co 5).
Drinking water was provided ad libitum.
Animals used in this study were treated and cared
for in accordance with the guidelines
recommended by the Committee for the Purpose of
Control and Supervision of Experiments on
Animals (CPCSEA), Government of India,
Ministry of Culture, Chennai. The dose of the
chelating agent was prepared daily and its pH was
adjusted to 6.4 with sodium bicarbonate before
administration.
Experimental design
Animals were selected on day 1 post partum
and were divided into four groups of six animals
each. Group 1 served as control. Groups 2, 3 and 4
were the experimental groups and received VOSO4
(7.5 mg/kg, p.o.) for 20 days. Group 2 served as
experimental control. Animals of group 3 were
taken individual treatment of Tiron (606 mg/kg,
i.p.) for 5 days on days 21-25 whereas group 4
were administered combination treatment of Tiron
(as in group 3)+ Se (0.5 mg/kg, p.o., through
catheter) for 5 days on days 21-25. Rats were
observed daily for mortality and morbidity through
out the study. 24 h after the final treatment animals
were sacrificed under light ether anesthesia. The
lactating and sucklings rats were examined for any
external and pathological lesions. The lactating’s
blood, liver, kidney, uterus and ovary were
investigated. Liver and kidney of suckling’s were
also processed for biochemical assays and
histopathological observation.
Biochemical assays
Blood was collected and serum was isolated for
various blood biochemical assays directly from the
heart by puncturing the retro-orbital venous sinus.
Blood sugar (22) aspartate aminotransferase
(AST), alanine aminotransferase (ALT) (23),
serum alkaline phosphatase (SALP) (24) and
serum protein (25) were studies. Standard
techniques were used to determine glycogen
contents in fresh tissue (26). A homogenate in
isotonic solution was processed for the
determination of protein (25) activities of acid and
alkaline phosphatases (ACP and ALP) (24) and
adenosine triphosphatase (ATP) (27). Lipid
peroxidation (LPO) (28) and reduced glutathione
(GSH) (29) were also estimated.
Histopathology
Liver, kidney, uterus, and ovary of lactating rats
and suckling’s liver and kidney were dissected out,
washed in saline and fixed in Bouin’s fluid,
embedded in paraffin, sectioned at 6μm and
stained with haemotoxylin and eosin for light
microscopical study.
Statistical analysis
Data were expressed as mean ± standard error
of mean (SEM). Statistical comparisons between

Cotherapy of Tiron and Selenium against vanadium toxicity
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 229-238, Summer 2011 231
all groups were performed by using one way
ANOVA followed by student’s t-test. P-value was
taken as significant at 0.01% level (30).
Results
Biochemical observation
Table I illustrates the protective effect of Tiron
and its combination with Se against vanadium
toxicity. Vandium induced significant elevation in
the activities of AST, ALT, SALP and serum
protein contents whereas the level of blood sugar
was decline significantly (p<0.01) in lactating rats.
Combination therapy (T+Se) effectively
recouped these values in all the parameters
compare with Tiron alone. After the injection of
vanadyl sulphate the wet weight of liver, kidney,
uterus, and ovary of lactatings and liver and kidney
of sucklings (Data not shown) showed no
significant variation. LPO showed enhance values
whereas glutathione showed inhibition in liver of
lactatings (p<0.01) and sucklings. Chelation
therapy showed improvement (Table IV).
Glycogen content of liver, uterus, ovary of
lactatings showed decreased values while kidney
of lactatings and liver and kidney of sucklings
showed elevated values after vanadium exposure.
With the combined treatment, values were restored
towards control (Table II). After administration of
vanadyl sulphate, protein content were decreased
in all the organs of lactatings and sucklings (Table
II). Activity of acid phosphatase showed increased
level in liver of lactatings, and liver and kidneyof
sucklings, while its activity decreased in uterus and
kidney of lactatings. With combined treatment,
values showed improvement. This improvement
was more effective with the Tiron+ Se (Table IV).
Activities of adenosine triphosphatase and alkaline
phosphatase showed inhibition after vanadium
exposure in liver, kidney, and uterus of lactatings
and liver and kidney of sucklings and values
restored with Tiron and Tiron+ Se. Tiron+ Se was
found effective (Table III and IV).
Histological observations
Vanadium induced proliferation in canaliculi,
hypertrophy and angular nuclei in hepatocytes and
sinusoidal spaces were filled with debris (Figure 1-
1).
Tiron protects the hepatocytes (Figure 1-2).
Tiron+ Se restore the structure of hepatocytes
showing normal sinusoidal spaces with mitotic
figures. Hepatocytes showed well-maintained
cytoplasm (Figure 1-3). Glomeruli showed
hypertrophy in the regions of cortex, disturbed
endothelial lining and degeneration in uriniferous
tubules (Figure 1-4).
Tiron showed better organization of kidney
(Figure 1-5). Treatment with Tiron+Se therapy
showed well form glomeruli and renal tubules
(Figure 1-6). Liver of sucklings, after injection of
vanadium in lactating rats, reduced sinusoidal
spaces and debris was observed in some sinuses
(Figure 2-7).
Treatment of Tiron showed normal portal triads
and well formed hepatocytes (Figure 2-8). Tiron+
Se therapy maintained hepatocytes and smooth
lining of sinus (Figure 2-9).
After administration of vanadium, glomeruli
occupied whole Bowman’s capsule and
degeneration in proximal and cortical tubules
(Figure 2-10). With the treatment of Tiron, kidney
showed rounded Glomeruli with maintained
tubules (Figure 2-11).
Tiron+ Se therapy improved proximal and
cortical tubules with Bowman’s capsule (Figure 2-
12). Toxicant exposed rats showed disorganized
uterine epithelium and uterine glands (Figure 3-
13). Tiron treatment showed recoupment (Figure
3-14).
The well formed endometrium, intact columnar
epithelium, well developed musculature prominent
vascularity and stroma was noted after treatment of
Tiron + Se (Figure 3-15). After vanadium
administration, decreased matured follicles,
disintegration in ovum, disorganized and
hypertrophied developing follicles were seen.
Stroma was loose and fibrotic (Figure 3-16).
Treatment of Tiron showed normal position of
follicles along with few and atretic follicles (Figure
3-17).
Combination therapy showed well organization
of developing follicles, freshly ovulated follicles
and maintain stroma (Figure 3-18).
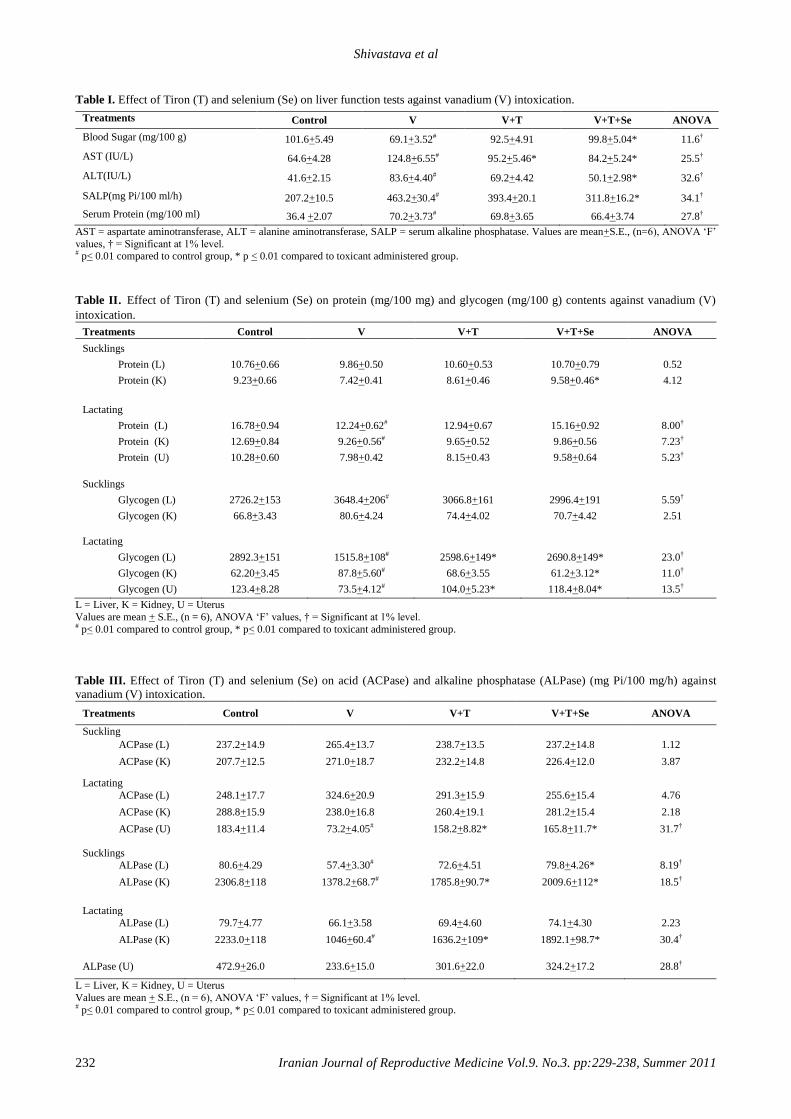
Shivastava et al
232 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:229-238, Summer 2011
Table I. Effect of Tiron (T) and selenium (Se) on liver function tests against vanadium (V) intoxication.
Treatments
Control V V+T V+T+Se ANOVA
Blood Sugar (mg/100 g)
101.6+5.49 69.1+3.52# 92.5+4.91 99.8+5.04* 11.6†
AST (IU/L)
64.6+4.28 124.8+6.55# 95.2+5.46* 84.2+5.24* 25.5†
ALT(IU/L)
41.6+2.15 83.6+4.40# 69.2+4.42 50.1+2.98* 32.6†
SALP(mg Pi/100 ml/h)
207.2+10.5 463.2+30.4# 393.4+20.1 311.8+16.2* 34.1†
Serum Protein (mg/100 ml)
36.4 +2.07 70.2+3.73# 69.8+3.65 66.4+3.74 27.8†
AST = aspartate aminotransferase, ALT = alanine aminotransferase, SALP = serum alkaline phosphatase. Values are mean+S.E., (n=6), ANOVA ‘F’
values, † = Significant at 1% level. # p< 0.01 compared to control group, * p < 0.01 compared to toxicant administered group.
Table II. Effect of Tiron (T) and selenium (Se) on protein (mg/100 mg) and glycogen (mg/100 g) contents against vanadium (V)
intoxication.
Treatments Control V V+T V+T+Se ANOVA
Sucklings
Protein (L) 10.76+0.66 9.86+0.50 10.60+0.53 10.70+0.79 0.52
Protein (K) 9.23+0.66 7.42+0.41 8.61+0.46 9.58+0.46* 4.12
Lactating
Protein (L) 16.78+0.94 12.24+0.62# 12.94+0.67 15.16+0.92 8.00†
Protein (K) 12.69+0.84 9.26+0.56# 9.65+0.52 9.86+0.56 7.23†
Protein (U) 10.28+0.60 7.98+0.42 8.15+0.43 9.58+0.64 5.23†
Sucklings
Glycogen (L) 2726.2+153 3648.4+206# 3066.8+161 2996.4+191 5.59†
Glycogen (K) 66.8+3.43 80.6+4.24 74.4+4.02 70.7+4.42 2.51
Lactating
Glycogen (L) 2892.3+151 1515.8+108# 2598.6+149* 2690.8+149* 23.0†
Glycogen (K) 62.20+3.45 87.8+5.60# 68.6+3.55 61.2+3.12* 11.0†
Glycogen (U) 123.4+8.28 73.5+4.12# 104.0+5.23* 118.4+8.04* 13.5†
L = Liver, K = Kidney, U = Uterus
Values are mean + S.E., (n = 6), ANOVA ‘F’ values, † = Significant at 1% level. # p< 0.01 compared to control group, * p< 0.01 compared to toxicant administered group.
Table III. Effect of Tiron (T) and selenium (Se) on acid (ACPase) and alkaline phosphatase (ALPase) (mg Pi/100 mg/h) against
vanadium (V) intoxication.
Treatments Control V V+T V+T+Se ANOVA
Suckling
ACPase (L)
237.2+14.9 265.4+13.7 238.7+13.5 237.2+14.8 1.12
ACPase (K)
207.7+12.5 271.0+18.7 232.2+14.8 226.4+12.0 3.87
Lactating
ACPase (L)
248.1+17.7 324.6+20.9 291.3+15.9 255.6+15.4 4.76
ACPase (K)
288.8+15.9 238.0+16.8 260.4+19.1 281.2+15.4 2.18
ACPase (U)
183.4+11.4 73.2+4.05# 158.2+8.82* 165.8+11.7* 31.7†
Sucklings ALPase (L)
80.6+4.29 57.4+3.30# 72.6+4.51 79.8+4.26* 8.19†
ALPase (K)
2306.8+118 1378.2+68.7# 1785.8+90.7* 2009.6+112* 18.5†
Lactating
ALPase (L)
79.7+4.77 66.1+3.58 69.4+4.60 74.1+4.30 2.23
ALPase (K)
2233.0+118 1046+60.4# 1636.2+109* 1892.1+98.7* 30.4†
ALPase (U)
472.9+26.0 233.6+15.0 301.6+22.0 324.2+17.2 28.8†
L = Liver, K = Kidney, U = Uterus
Values are mean + S.E., (n = 6), ANOVA ‘F’ values, † = Significant at 1% level. # p< 0.01 compared to control group, * p< 0.01 compared to toxicant administered group.
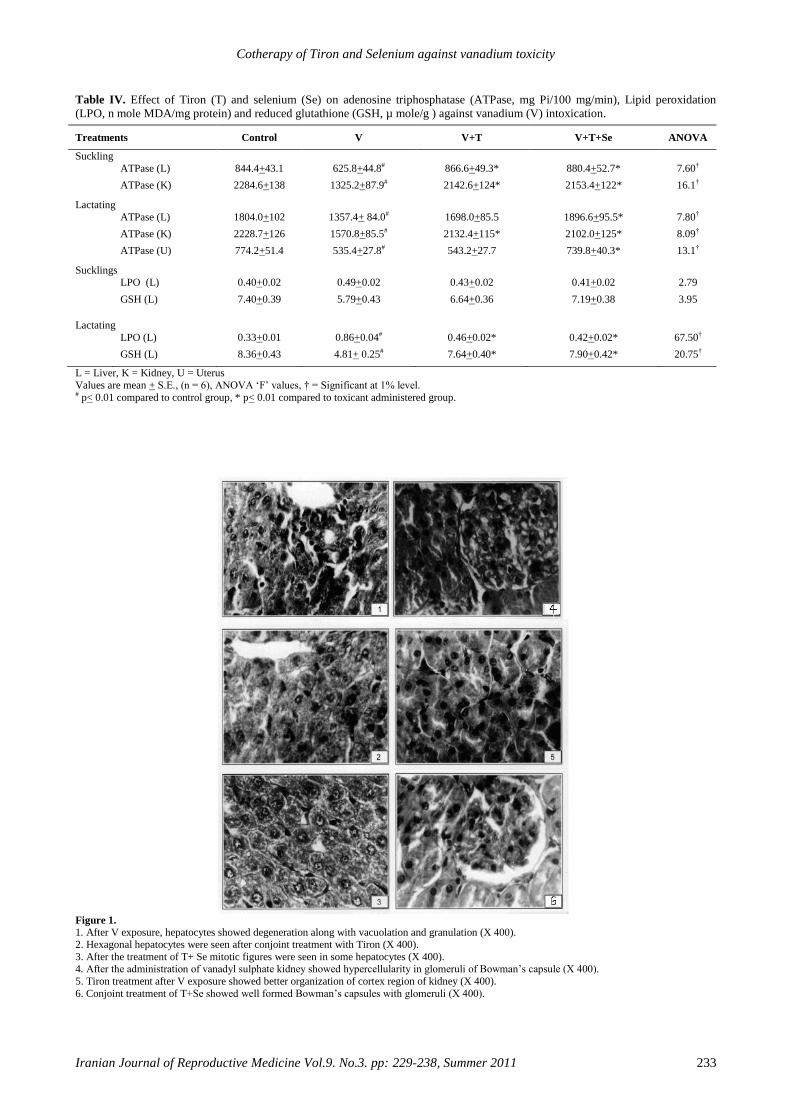
Cotherapy of Tiron and Selenium against vanadium toxicity
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 229-238, Summer 2011 233
Table IV. Effect of Tiron (T) and selenium (Se) on adenosine triphosphatase (ATPase, mg Pi/100 mg/min), Lipid peroxidation
(LPO, n mole MDA/mg protein) and reduced glutathione (GSH, µ mole/g ) against vanadium (V) intoxication.
Treatments Control V V+T V+T+Se ANOVA
Suckling
ATPase (L)
844.4+43.1 625.8+44.8# 866.6+49.3* 880.4+52.7* 7.60†
ATPase (K) 2284.6+138 1325.2+87.9# 2142.6+124* 2153.4+122* 16.1†
Lactating
ATPase (L)
1804.0+102 1357.4+ 84.0# 1698.0+85.5 1896.6+95.5* 7.80†
ATPase (K)
2228.7+126 1570.8+85.5# 2132.4+115* 2102.0+125* 8.09†
ATPase (U) 774.2+51.4 535.4+27.8# 543.2+27.7 739.8+40.3* 13.1†
Sucklings
LPO (L)
0.40+0.02 0.49+0.02 0.43+0.02 0.41+0.02 2.79
GSH (L) 7.40+0.39 5.79+0.43 6.64+0.36 7.19+0.38 3.95
Lactating
LPO (L)
0.33+0.01 0.86+0.04# 0.46+0.02* 0.42+0.02* 67.50†
GSH (L) 8.36+0.43 4.81+ 0.25# 7.64+0.40* 7.90+0.42* 20.75†
L = Liver, K = Kidney, U = Uterus
Values are mean + S.E., (n = 6), ANOVA ‘F’ values, † = Significant at 1% level. # p< 0.01 compared to control group, * p< 0.01 compared to toxicant administered group.
Figure 1. 1. After V exposure, hepatocytes showed degeneration along with vacuolation and granulation (X 400). 2. Hexagonal hepatocytes were seen after conjoint treatment with Tiron (X 400).
3. After the treatment of T+ Se mitotic figures were seen in some hepatocytes (X 400). 4. After the administration of vanadyl sulphate kidney showed hypercellularity in glomeruli of Bowman’s capsule (X 400).
5. Tiron treatment after V exposure showed better organization of cortex region of kidney (X 400).
6. Conjoint treatment of T+Se showed well formed Bowman’s capsules with glomeruli (X 400).
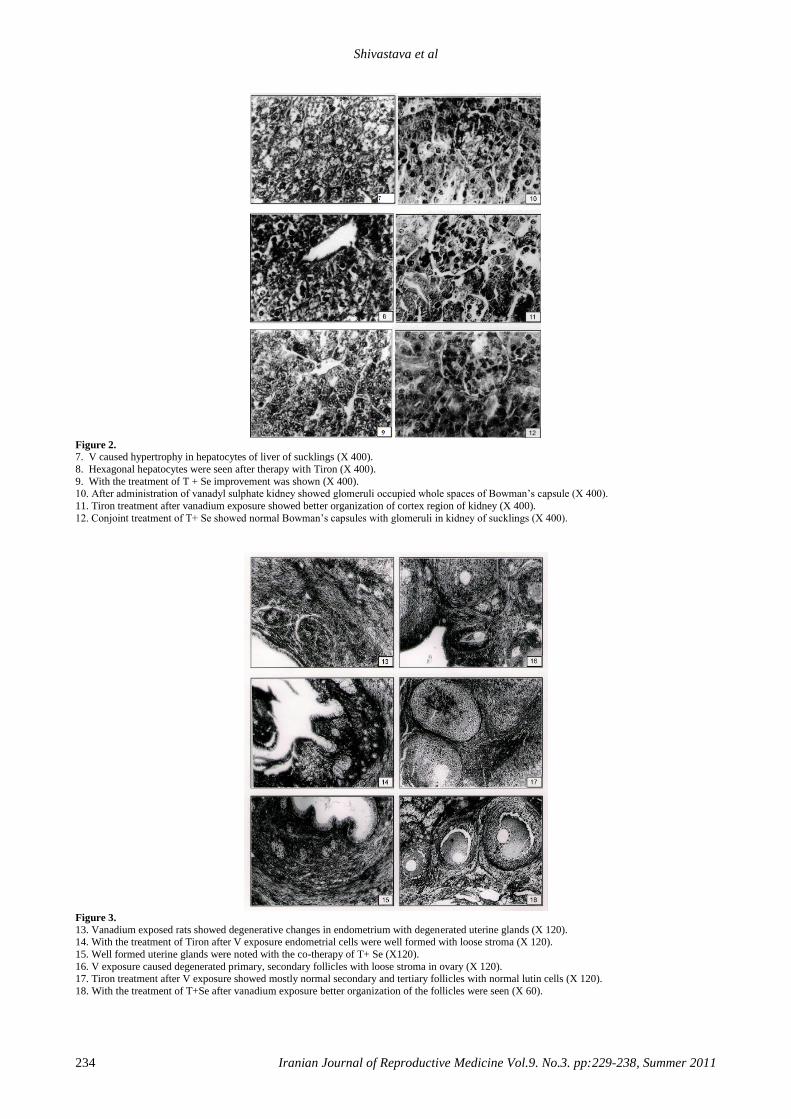
Shivastava et al
234 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:229-238, Summer 2011
Figure 2.
7. V caused hypertrophy in hepatocytes of liver of sucklings (X 400).
8. Hexagonal hepatocytes were seen after therapy with Tiron (X 400).
9. With the treatment of T + Se improvement was shown (X 400). 10. After administration of vanadyl sulphate kidney showed glomeruli occupied whole spaces of Bowman’s capsule (X 400).
11. Tiron treatment after vanadium exposure showed better organization of cortex region of kidney (X 400).
12. Conjoint treatment of T+ Se showed normal Bowman’s capsules with glomeruli in kidney of sucklings (X 400).
Figure 3.
13. Vanadium exposed rats showed degenerative changes in endometrium with degenerated uterine glands (X 120). 14. With the treatment of Tiron after V exposure endometrial cells were well formed with loose stroma (X 120).
15. Well formed uterine glands were noted with the co-therapy of T+ Se (X120).
16. V exposure caused degenerated primary, secondary follicles with loose stroma in ovary (X 120).
17. Tiron treatment after V exposure showed mostly normal secondary and tertiary follicles with normal lutin cells (X 120).
18. With the treatment of T+Se after vanadium exposure better organization of the follicles were seen (X 60).
Cotherapy of Tiron and Selenium against vanadium toxicity
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 229-238, Summer 2011 235
Discussion
The efficacy of exogenous therapy of Tiron in
combination with Se in the acceleration of
vanadium elimination and in the reversal of
intoxication has been discussed. The aim of the
present study was to report the teratogenic effects
of vanadium and to develop an intervention
strategy of companion formula of chelators with
antioxidant effects against vanadium intoxication.
About 95% of the vanadium transported in the
blood is bound to transferrin as the vanadyl (IV), it
also complexs with lactoferrin to be transported to
sucklings during breast feeding. Vanadium is
present in placenta and competes with iron for both
gastrointestinal absorption and cellular receptor
sites (31-33).
Research indicates that ALT and AST can be
used as biomarkers of cellular damage in blood
plasma, protein degradation and liver damage with
loss of the functional integrity of cell membranes
(34), thus a direct correlation exists between rise in
the serum enzyme activity and severity of damage.
The ALT is localized mainly in the cytoplasm
whereas AST activity is fairly distributed between
cytoplasm and mitochondria. A significant increase
in AST, ALT and SALP activities was noted after
vanadium exposure in lactating rats. The elevated
activities are indicative of cellular leakage and loss
of the functional integrity of cell membranes, thus
necrosis or membrane damage which releases the
enzyme into circulation.
SALP mainly arises from the lining of the
canaliculi and also from the sinusoidal surface of
hepatocytes and is excreted via bile. The SALP is
closely connected with proximal tubules and
osteoblast and is involved in the active transport
across the capillary walls. The increased level of
SALP may be due to the de novo synthesis by the
liver cells.
Results of the present study clearly depicted
that vanadium administration enhanced
concentration of this soluble enzyme significantly
(34). An increase in the activities of these enzymes
is supported by various authors (34, 35).
The stabilization of AST, ALT and SALP
levels by therapy of chelating agent with and
without antioxidants is a clear indication of
improvement in the functional status of the liver
cells (13, 14).
Oral administration of Se attenuated
significantly the increased level of these enzymes
and caused a subsequent recovery towards
normalization, as seen from statistical analysis.
Combined therapy may combine with reactive
metabolites and lead to inactivate them, thus it may
prevent the acute organ dysfunction and cellular
injury thereby inhibiting the rapid leakage of these
enzymes.
A number of investigators have previously
demonstrated the antioxidative effect of
magnesium (36), zinc (37) and selenium (20) etc.
Activities of these enzymes were also recouped
significantly with the administration of Tiron
against other metals, such as, beryllium (13),
aluminum (14) and vanadium (16, 35). Lowering
of blood sugar level in the lactating rats may be
due to increase in the uptake of glucose in the
glycogen metabolism (34). In vanadate treated rats,
liver glycogen level elevated in sucklings whereas
decreased in lactating animals as seen in the
present study. This can be very well correlated
with the increased activity of glycogen synthetase
and decreased activity of glycogen phosphorylase
(38).
Improvement in blood sugar and serum protein
by Tiron treatment is also reported (13, 34).
Oxidative stress is a major pathway for vanadium
induced toxicity (39). The pro-oxidant effect of
vanadate was evident in our experiments by the
occurrence of LPO in liver (2, 40). A significant
increase in malaondialdehyde products was also
observed after exposure to metals such as mercury
(19), aluminium (14, 20) and beryllium (13). GSH
plays a major role in cellular defense and in the
maintenance of the thiol disulfide status. It showed
inhibition in liver of sucklings and lactating rats
because of bonding to sulfhydryl groups of
proteins.
The increased TBARS as seen in the present
study may be due to tissue injury and failure of
antioxidant defense mechanism. Therefor
increased accumulation of LPO products might
well be the consequences of a progressive
degradation of necrotic tissue. LPO mainly
damages Kupffer cells as also evident in
histological studies. The result suggests that
toxicant induced elevation in LPO might be
because of the lower level of GSH as observed in
this study. GSH depletion decreases the
Shivastava et al
236 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:229-238, Summer 2011
GSH/GSSG ratio, which leads to the production of
free radicals (41).
Combined therapy clearly indicated the
supplementation of antioxidants increased
effectiveness of Tiron which help to regenerate and
maintain the normal functional status of the tissues.
Treatment with Se afforded better protection, this
may be due to the destruction of free radicals,
supplying a competitive substrate for unsaturated
lipids in the membrane and/or accelerating the
repair mechanism of damaged cell membrane.
Therefor combination therapy (Tiron+ Se)
effectively recouped these values than tiron per se.
These findings are substantiated by various studies
(13, 14, 42).
Significant decreased values were seen in
ALPase, ATPase and increased value noted in
ACPase due to the vanadyl ion formed may bind
with cell proteins. VO2+
resembles with size of
Mg2+
which is regulated for the activity of ALPase
(21, 33), thus was inhibited due to its structural
similarity with phosphate, vanadate (VO3) also
interferes with a large variety of phosphate
dependent enzymes (43). Vanadate is a potent
inhibitor of membrane bound ATPase (33). It is
also possible that accumulation of vanadium with
its concomitant reduction to vanadyl followed by
damage to biological membranes, lysosomal
enzymes releases and destruction of placental
tissue (34).
Fatty changes with partial cell necrosis in the
liver have been observed in rats as a result of
exposure to vanadium (34). In the present study
vanadium induced; proliferation in canaliculi,
hypertrophy and angular nuclei in hepatocytes,
hypertrophy in glomeruli and degenerated
uriniferous tubules, disorganized uterine
epithelium and disintegration in ovum. Vanadium
was accumulated within spheroidal electro dense
structures in the cytoplasm of these cells (44- 46).
Therapy with Tiron was found very effective and
this may be due to its diphenolic nature of Tiron
which forms water soluble complexes with a large
number of metals (13, 14). Thus, it is clearly
apparent that Tiron crosses the placental barrier as
reported for other metals as well (42). Se acts as
cofactor of many antioxidant enzymes, maintains
the availability of antioxidant nonprotein
sulfhydryl groups (47, 48) thus may induce binding
of the V-Se complexes to proteins. It is an
important nutrient and can pass through the milk,
thus ameliorating toxicity in lactating and
sucklings.
In conclusion, the present research has
identified the role of antioxidants, Se and Tiron in
mitigation of vanadium toxicity by acting
synergistically.
Acknowledgment
The author is thankful to University Grants
Commission, New Delhi for financial assistance.
(F.15-122/98 (PTRAW-S/SA-I).
References
1. World Health Organization: Vanadium Environmental
Criteria;81 Geneva; WHO; 1988.
2. World Health Organization: Vanadium. Chapter 6.12.
WHO Regional Office for Europe, Copenhagen:
Denmark; 2000.
3. Cooper RG. Vanadium pentoxide inhalation. IJOEM
2007; 11: 97-102.
4. Mukherjee B, Patra B, Mahapatra S, Banerjee P, Tiwari A,
Chatterjee M. Vanadium--an element of atypical
biological significance. Toxicol Lett 2004; 150: 135-143.
5. Chandra AK, Ghosh R, Chatterjee A, Sarkar M. Protection
against vanadium-induced testicular toxicity by
testosterone propionate in rats. Toxicol Mech Methods
2010; 20: 306-315.
6. Mussali-Galante P, Rodríguez-Lara V, Hernández-Tellez
B, Avila-Costa MR, Colín-Barenque L, Bizarro-Nevarez
P, et al. Inhaled vanadium pentoxide decrease gamma-
tubulin of mouse testes at different exposure times.
Toxicol Ind Helth 2005; 21: 215-222.
7. Castellini C, Mourvaki E, Sartini B, Cardinali R, Moretti
E, Collodel G, et al. In vitro toxic effects of metal
compounds on kinetic traits and ultrastructure of rabbit
spermatozoa. Reprod Toxicol 2009; 27: 46-54.
8. Domingo JL. Vanadium: A review of the reproductive and
developmental toxicity. Reprod Toxicol 1996; 10: 175-
182.
9. Paternain JL, Domingo JL, Gomez M, Ortega A, Corbella
J. Developmental toxicity of vanadium in mice after oral
administration. J Appl Toxicol 1990; 10: 181- 186.
10. Soazo M, Garcia GB. Vanadium exposure through
lactation produces behavioral alterations and CNS myelin
deficit in neonatal rats. Neurotoxicol Teratol 2007; 29:
503-510.
11. Taiwo FA. Mechanism of tiron as scavenger of superoxide
ions and free electrons. Spectroscopy 2008; 22: 491-498.
12. Kim JS, Cho EW, Chung HW, Kim IG. Effects of Tiron,
4,5-dihydroxy-1,3-benzene disulfonic acid, on human
promyelotic HL-60 leukemia cell differentiation and
death. Toxicology 2006; 223: 36-45.
Cotherapy of Tiron and Selenium against vanadium toxicity
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 229-238, Summer 2011 237
13. Nirala SK, Bhadauria M, Upadhyay AK, Mathur R,
Mathur A. Reversal of effects of intra peritoneally
administered beryllium nitrate by Tiron and CaNa3DTPA
alone or in combination with alpha-tocopherol. Indian J
Exp Biol 2009; 47: 955-963.
14. Sharma P, Ahmad Shah Z, Kumar A, Islam F, Mishra KP.
Role of combined administration of Tiron and glutathione
against aluminum-induced oxidative stress in rat brain. J
Trace Elem Med Biol 2007; 21: 63-70.
15. Pocock G, Simons TJ. Effects of lead ions on events
associated with exocytosis in isolated bovine adrenal
medullary cells. J Neurochem 1987; 48: 376-382.
16. Gomez M, Domingo JL, Llobet JM, Corbella J. Evaluation
of the efficacy of various chelating agents on urinary
excretion and tissue distribution of vanadium in rats.
Toxicol Lett 1991; 57: 227-234
17. Mazokopakis EE, Papadakis JA, Papadomanolaki MG,
Batistakis AG, Giannakopoulos TG, Protopapadakis EE,
et al. Effects of 12 months treatment with L-
selenomethionine on serum anti-TPO Levels in Patients
with Hashimoto's thyroiditis. Thyroid 2007; 17: 609-612.
18. Wlodarczyk B, Minta M, Biernacki B, Szkoda J, Zmudzki
J. Selenium Protection against Cadmium Toxicity in
Hamster Embryos. Polish J Environ Studies 2000; 9: 323-
327.
19. Joshi D, Mittal DK, Bhadauria M, Nirala S K, Shrivastava
S, Shukla S. Role of micronutrients against
dimethylmercury intoxication in male rats. Environ
Toxicol Pharmacol 2010; 29: 97-103.
20. Abubakar MG, Taylor A, Ferns GA. The effects of
aluminium and selenium supplementation on brain and
liver antioxidant status in the rat. Afr J Biotechnol 2004; 3:
88-93.
21. Haider SS, Abdel-Gayoum A A, El-Fakhri M, Ghwarsha
K M. Effect of selenium on vanadium toxicity in different
regions of rat brain. Hum Exp Toxicol 1998; 17: 23-28
22. Asatoor A, King EJ. In:Practical Clinical Biochemistry
(Ed. H. Vorley), 4th Ed. Gulab Vazirani Publication; India
for Arnold Helemann; 1969: 86-88.
23. Reitman S, Frankel AS. A colorimetric method for the
determination of serum glutamic oxalacetic and glutamic
pyruvic transaminases. Am J Clin Pathol 1957; 28: 56-63.
24. Fiske CH, Subbarow Y. The colorimetric determination of
phosphatase. J Biol Chem 1925; 66: 375-400.
25. Lowry OH, Rosenbrough NJ, Farr AL, Randall RJ. Protein
measurement with Folin’s phenol reagent. J Biol Chem
1951; 193: 265-269.
26. Seifter S, Davton S, Novic B, Muntwyler E. The
estimation of glycogen with the anthrone reagent. Arch
Biochem 1950; 25: 191-193.
27. Seth PK, Tangari KK. Biochemical effects of newer
salicylic acid congenesis. J Pharm Pharmacol 1966; 18:
831-833.
28. Sharma SK, Krishnamurthy CR. Production of lipid
peroxides of brain. J Neuro chem 1968; 15: 147-149.
29. Brehe JE, Bruch HB. Enzymatic assay for glutathione,
Anal Biochem, 74 189.Biochemistry by IDP Wootton 4th
Ed. J and A Churchill Ltd; 104, Gloucester Place; 1976:
115-118.
30. Snedecor GW, Cochran WG. Statistical method; 8th Ed.
Affiliated East-West Press; 1994.
31. Patterson BW, Hansard SL, Ammerman CB, Henry PR,
Zech LA, Fisher WR. Kinetic model of whole-body
vanadium metabolism: studies in sheep. Am J Physiol 1986;
251: 325-332.
32. Edel J, Sabbioni E. Vanadium transport across placenta
and milk of rats to the fetus and newborn. Biol Trace Elem
Res 1989; 22: 265-275.
33. Nechay R. Mechanisms of action of vanadate. Ann Rev
Pharmacol Toxicol 1984; 24: 501-524.
34. Shrivastava S, Jadon A, Shukla S. Effect of Tiron and its
combination with nutritional supplements against vanadium
intoxication in female albino rats. J Toxicol Sci 2007; 32:
185-192.
35. Mathur R, Bharadwaj S, Shrivastava S, Mathur A. Toxic
effects of Vanadyl sulphate: A biochemical profile. Indian J
Toxicol 2002; 9: 77-82.
36. Shukla S, Singh V, Joshi D. Modulation of toxic effects of
organic mercury by different antioxidants. International
Toxicol 2007; 14: 67-71.
37. Chandra AK, Ghosh R, Chatterjee A, Sarkar
M.Vanadium-induced testicular toxicity and its prevention
by oral supplementation of zinc sulphate. Toxicol Mech
Methods 2007; 17: 175-187.
38. Tolman EL, Barris E, Bums M, Pansine A, Partridge R.
Effects of vanadium on glucose metabolism in vitro. Life Sci
1997; 25: 1159- 1164.
39. Scibior A, Zaporowska H. Effects of Vanadium(V) and/or
Chromium(III) on L-Ascorbic Acid and Glutathione as well
as Iron, Zinc, and Copper Levels in Rat Liver and Kidney. J
Toxicol Environ Health A 2007; 70: 696-704.
40. Scibior A, Zaporowska H, Niedzwiecka I. Lipid
peroxidation in the kidney of rats treated with V and/or Mg
in drinking water. J Appl Toxico 2010; 30: 487-496.
41. Scibior A, Zaporowska H. Effects of vanadium(V) and/or
chromium(III) on L-ascorbic acid and glutathione as well as
iron, zinc, and copper levels in rat liver and kidney. J
Toxicol Environ Health A 2007; 15: 696-704.
42. Sharma P, Mishra KP. Aluminium induced maternal and
developmental toxicity and oxidative stress in rat brain:
Response to combined administration of Tiron and
glutathione. Reprod Toxicol 2006; 21: 313-321.
43. Nechay R, Saunders JP. Inhibition by vanadium of sodium
and potassium dependent adenosine-triphosphatase derived
from animal and human tissues. J Environ Pathol Toxicol
1978; 2: 247-262.
44. Carmignahi M, Boscolo P, Volpe AP, Tonga G,
Masciocco L, Prezios P. Cardiovascular system and kidney
as specific targets of chronic exposure to vanadats in the rate
functional and morphological fingings. Arch Toxicol 1991;
14 (suppl.): 124-127.
45. Shukla R, Barve V, Padhye S, Bhonde R. Reduction of
oxidative stress induced vanadium toxicity by complexing
with a flavonoid, quercetin: a pragmatic therapeutic
approach for diabetes. Biometals 2006; 19: 685-693.

Shivastava et al
238 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:229-238, Summer 2011
46. Sato K, Kusaka Y, Akino H, Kanamaru H, Okada K.
Direct effects of vanadium on citrate uptake by rat renal
brush border membrane vesicles (BBMV). Ind Health 2002;
40: 278-281.
47. Porter JM, Ivatury RR, Azimuddin K, Swami R.
Antioxidant therapy in prevention of organ dysfunction
syndrome and infectious complications after trauma: early
results of a prospective randomized study. Am Surg 1999;
65: 478-483.
48. Schumacher K. Effect of selenium on the side effect
profile of adjuvant chemotherapy/radiotherapy in patients
with breast carcinoma. Design for a clinical study Med Klin
(Munich) 1999; 94: 45-48.

Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:239-242, Summer 2011
Evaluation of the effect of oral ritodrine on
implantation rate in in-vitro fertilization-embryo
transfer cycles
Soghra Rabiee M.D., Marziyyeh Farimani M.D., Maryam Ahmadi M.D.
Department of Obstetrics and Gynecology, School of Medicine, Hamadan University of Medical
Sciences, Hamadan, Iran.
Received: 29 November 2009; accepted: 6 May 2010
Abstract
Background: Pregnancy rate with IVF cycle is almost 22%. Many investigations
perform to increase this rate in IVF. Various factors affect the result of IVF cycles. One
of these factors could be uterine contractions that expel transferred embryo. Ritodrine is
a beta mimetic agent that can block and decrease uterine contractions.
Objective: The objective of this study was to determine ritodrine effectiveness for
increasing the implantation rate in IVF cycles, and its probable mechanisms in
decreasing uterine contractions as well.
Materials and Methods: A total of 100 patients of IVF-ET cycles were divided
randomly in two groups in a university hospital, Hamadan, Iran. The case group were
prescribed ritodrine 10 mg / bid orally after oocyte retrieval until 10 days. The control
group didn’t received ridotrine.
Results: In ritodrine group 14% of patients and in control group 16% had positive
β-hCG test (p-value>0.5).
Conclusion: Ritodrine did not improve the implantation rate in IVF-ET cycles.
Key words: Ritodrine, IVF-ET, Implantation rate.
Registretion ID in IRCT: IRCT201105316665N1
Introduction
Infertility is a common problem affecting up to
10% of married couples (1). A systematic
evaluation of aetiologic factors forms the basis for
choice of treatment and future fertility. On the
global perspective, assisted reproductive
technologies (ART) have become internationally
recognized treatment option for some infertile
couples. At present time, infertility treatments by
ART is progressing and improving considerably
(2). These treatments have improved the success
rate of IVF-ET up to 22% (2). However, infertile
couples spend much money and time especially in
ART cycles and they expect more success rate.
Presently , the maturation of follicles with
Corresponding Author:
Soghra Rabiee, Department of Obstetrics and
Gynecology, School of Medicine, Hamadan University
of Medical Sciences, Hamadan, Iran.
Email: [email protected]
gonadotropin, oocyte retrieval, in vitro fertilization
and embryo development are satisfactory, but the
main problem is why sometimes the embryo
doesn't implant in the uterus successfully (3)?
Different factors such as type of catheter for
embryo transfer, using tenaculum for grasping the
cervix, removing the obvious or excess cervical
mucus before transfer, volume of transfer media,
and embryo transfer under trans abdominal
ultrasound guidance avoiding the uterine
contraction at the time of embryo transfer, studied
previously (4, 5).
Ritodrine, as a beta- agonist, may improve the
implantation rate in IVF cycles with decreasing
uterine contraction and consequently decreasing
extraction of embryos which transferred to the
uterus (6).
However, the results of studies are controversial
in relation to controlling uterine contractions and
its effect on implantation rate (7, 8). Some other
chemicals such as hyoscine bromide, piroxicom
Rabiee et al
240 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:239-242, Summer 2011
and oxytocin antagonists has investigated and
showed promising results (9-11).
The aim of this study was determination of
ritodrine effect on uterine contraction and
pregnancy rate in IVF-ET patient.
Materials and methods
In a randomized controlled clinical trial, one
hundred women aged between 25 through 35 years
with a history of >5 year infertility enrolled to
study. Inclusion criteria were as follow: having a
morphologically normal uterus, infertility from
tubal, male, endometriosis or unexplained factor.
Excluding criteria were lack of any systemic
known diseases in both groups. These patients
were candidate for IVF-ET and were randomly
allocated into treatment (50 patients) and control
(50 patients) groups. Two groups had not
significantly differences in view of mean age,
causes of infertility and infertility duration. All the
patients were stimulated with a GnRH agonist and
exogenous gonadotropins with long protocol. On
the day after oocyte retrieval, all patients in the
case group received oral ritodrine 10 mg/ bid for
ten days. Other medications in both groups were
similar including ASA 80 mg/day, progesterone
100mg IM, erythromycin 400 mg/qid, and heparin
5000 u/bid. The luteal phase was supported by
progesterone injection. The successfulness
criterion was positive β-hCG after 2 weeks. At
least three good quality embryos transferred for
each patient and, the results of two groups (rate of
positive β-hCG) compared and were analyzed with
chi square test.
This study was done in a public center for
infertility treatment and was approved in the
Research Ethics Committee, Chancellor for
Research and Technology, Hamadan University of
Medical Sciences.
Statistical analysis
The pregnancy rate between two groups (rate of
positive β-hCG defined as pregnancy index),
compared and were analyzed with chi- square test.
The background variables between study group
and control group also were compared by t-student
test and chi-square test.
Results
The studied patients had no history of abortion
or pregnancy. Mean age were 29.5 and 30.8 years
in the study and control group respectively
(p>0.05) with the range of 20-40 years. The mean
duration of infertility in the study group were 8.3
and in the control group 7.5 years. The main
causes of infertility were as follow: tubal factors
31.5%, male factors 45%, ovulatory factors 18.5%
and unexplained factors 15%.
The minimum and maximum retrieved oocytes
from patients were 3 and 12. The numbers of
transferred embryo were between 2 and 4. This
study indicated embryo implantation followed by
positive β-HCG test in 7 (14%) patients in
ritodrine group and 8 (16%) patients in control
group (p>0.05). There was not a significant
difference in ritodrine group in comparison with
control group. One patient in ritodrine group had
minor side effects such as head ache and vertigo.
Discussion
As the results of this study indicate, ritodrine
has not significant effect on implantation rate in
IVF-ET cycles. Many chemicals were investigated
for increase implantation rate and clinical
pregnancy in IVF-ET (12, 13).
Gholami and colleagues (5) compared the
pregnancy outcome in patients undergoing IVF-ET
cycles, using human derived follicle-stimulating
hormone (FSH) or recombinant FSH for ovarian
stimulation protocols. They results did not
demonstrate a difference between the use of h-FSH
vs r-FSH for ovarian stimulation in terms of
pregnancy outcome, in good prognosis patients
undergoing their first IVF-ET procedure. Moon
and colleagues reported piroxicom increased the
implantation rate and clinical pregnancy in the
patients candidate for IVF-ET.
However, Dal Prato and Borini (10) indicated
that, administration of a single dose of piroxicam
before embryo transfer has no additional effect on
pregnancy outcome in patients receiving adequate
doses of progesterone for luteal phase
supplementation after IVF or ICSI.
On the other hand, in a limited trial, an oxitocine
antagonist (Atociban) was administered on 14th day
of endometrial synchronization for oocyste
donation. The treatment decreased the uterine
contractile activity and resulted in successful
embryo implantation and a normal twin diamniotic
pregnancy (7). It was concluded that Atosiban
may improve uterine receptivity during ET and
Oral ritodrine in IVF-ET
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:239-242, Summer 2011 241
may increase success rates of advanced infertility
treatment procedures, but this report was only in
one case and could not be generalizes to all
patients. Gorkemli and colleagues in their study in
2004 concluded that adding estradiol to
progesterone in luteal phase may increase
implantation rate in IVF-ET cycles (12).
Amanda and Garas, in 2006 reported that
neither implantation rate nor pregnancy rate
increased with paracetamol and diclofenac (13). In
2003 Peinheiro and colleagues (14) found that
beta-2-adrenergic will not increase the
implantation rate in ICSI cycles. They applied both
ritodrine and terbutaline in divided groups. The
result of their study is in agreement with our study.
As we see different studies were done to identify
best medication for improving ART outcome, but a
definitive answer has not found yet.
NSAIDs such as paracetamol, indomethacin,
and diclofenacs, and beta agonists such as ritodrine
and terbutaline are the most examined drugs and
their positive effect is not proven definitely yet
(10, 13, 15) . Some reports indicated controversial
results on the effect of peritalsis of uterus and its
contractibility on the rate of implantation. Some
studies report anticholinergic agents significantly
suppress sporadic myometrial contractions and
uterine peristalsis (6) and even adequate uterine
contractility may provide for gamete/embryo
transportation through the utero-tubal cavities and
successful embryo implantation in spontaneous or
assisted reproduction. Inadequate uterine
contractility may lead to ectopic pregnancies,
miscarriages, retrograde bleeding with
dysmenorrhea and endometriosis (16). Therefore,
the questions about uterine contractions control
have some roles on the embryo implantation,
remained open for more studies.
Conclusion
This study indicated that, ritodrine has not
significant effect on the implantation rate in the
IVF-ET technique. We recommend extended
researches to find out a certain medication for
increasing ART outcomes.
Acknowledgement
Hereby, we thank all our colleagues in
Infertility Center of Fatemieh Hospital, Hamadan,
for kindly technical assistance in this study,
especially Mrs Ramezani for her honorable
assistance. This paper extracted from a thesis of
residency for Obstetrics and Gynecology specialty.
References 1. Speroff L, Fritz M. Clinical Gynecologic Endocrinology
and Infertility. Philadelphia, Lippincot Williamas &
Wilkins 2005.
2. Gibbs RS, Karlan BY. Danforth's Obstetrics and
Gynecology 2003. 9th Ed. Philadelphia; Williams &
Wilkins; 2003: 590-592.
3. Leese B, Denton J. Attitudes towards single embryo
transfer, twin and higher order pregnancies in patients
undergoing infertility treatment: a review. Hum Fertil
(Camb) 2010; 13: 28-34.
4. Fanchin R, Righini C, de Ziegler D, Olivennes F, Ledée
N, Frydman R. Effects of vaginal progesterone
administration on uterine contractility at the time of
embryo transfer. Fertil Steril 2001; 75: 1136-1140.
5. Gholami H, Vicari E, Molis M, La Vignera S, Papaleo E,
Cappiello F. Pregnancy outcome following in vitro
fertilization-embryo transfer (IVF-ET) in women aged <
37, undergoing ovulation induction with human FSH
compared with recombinant FSH: a randomised controlled
study. Eur Rev Med Pharmacol Sci 2010; 14: 97-102.
6. Nakai A, Togashi K, Kosaka K, Kido A, Kataoka M,
Koyama T, et al. Do anticholinergic agents suppress
uterine peristalsis and sporadic myometrial contractions at
cine MR imaging? Radiology 2008; 246: 489-496.
7. Pierzynski P, Reinheimer TM, Kuczynski W. Oxytocin
antagonists may improve infertility treatment. Fertil Steril
2007; 88: 19-22.
8. Kido A, Togashi K, Hatayama H, Nakayama T,
Yamamoto A, Kataoka M, et al. Uterine peristalsis in
women with repeated IVF failures: possible therapeutic
effect of hyoscine bromide. J Obstet Gynaecol Can 2009;
31: 732-735.
9. Fanchin R, Righini C, Olivennes F, Taylor S, de Ziegler
D, Frydman R. Uterine contractions at the time of embryo
transfer alter pregnancy rates after in-vitro fertilization.
Hum Reprod 1998; 13: 1968-1974.
10. Dal Prato L, Borini A. Effect of piroxicam administration
before embryo transfer on IVF outcome: a randomized
controlled trial. Reprod Biomed Online 2009; 19: 604-609.
11. Moon HS, Park SH, Lee JO, Kim KS, Joo BS. Treatment
with piroxicam before embryo transfer increases the
pregnancy rate after in vitro fertilization and embryo
transfer. Fertil Steril 2004; 82: 816-820.
12. Gorkemli H, Ak D, Akyurek C, Aktan M, Duman S.
Comparison of pregnancy outcomes of progesterone or
progesterone + estradiol for luteal phase support in ICSI-
ET cycles. Gynecol Obstet Invest 2004; 58: 140-144.
13. Akande V, Garas A, Cahill D. The effect of diclofenac and
paracetamol on pregnancy and implantation rates in
infertile women undergoing IVF treatment. J Obstet
Gynecol 2006; 26: 785-787.
14. Pinheiro OL, Cavagna M, Baruffi RL, Mauri AL, Petersen
C, Franco JG Jr. Administration of beta2-adrenergic
agonists during the peri-implantation period does not
improve implantation or pregnancy rates in
intracytoplasmic sperm injection (ICSI) cycles. J Assist
Reprod Genet 2003; 20: 513-516.

Rabiee et al
242 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:239-242, Summer 2011
15. Hasegawa I, Yamanoto Y, Suzuki M, Murakawa H,
Kurabayashi T, Takakuwa K, et al. Prednisolone plus low-
dose aspirin improves the implantation rate in women with
autoimmune conditions who are undergoing in-vitro
fertilization. Fertil Steril 1998; 70: 1044-1048.
16. Bulletti C, de Ziegler D. Uterine contractility and embryo
implantation. Curr Opin Obstet Gynecol 2006; 18: 473-
484.
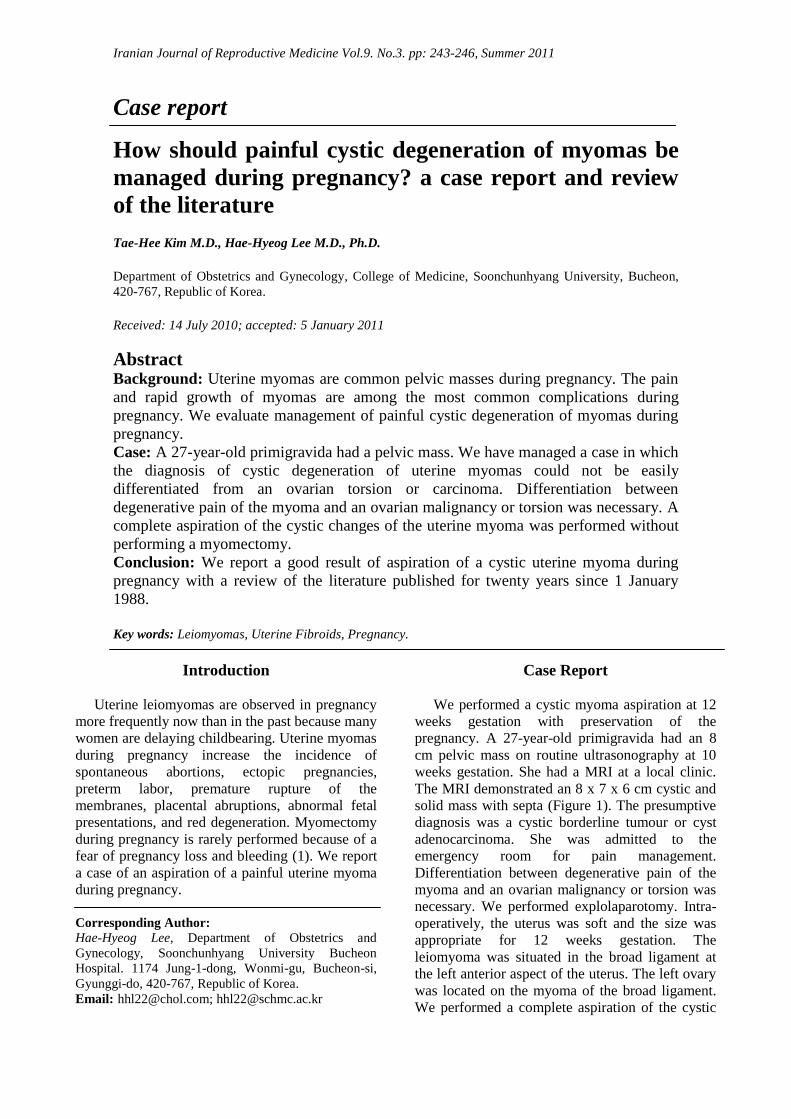
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 243-246, Summer 2011
Case report
How should painful cystic degeneration of myomas be
managed during pregnancy? a case report and review
of the literature
Tae-Hee Kim M.D., Hae-Hyeog Lee M.D., Ph.D.
Department of Obstetrics and Gynecology, College of Medicine, Soonchunhyang University, Bucheon,
420-767, Republic of Korea.
Received: 14 July 2010; accepted: 5 January 2011
Abstract Background: Uterine myomas are common pelvic masses during pregnancy. The pain
and rapid growth of myomas are among the most common complications during
pregnancy. We evaluate management of painful cystic degeneration of myomas during
pregnancy.
Case: A 27-year-old primigravida had a pelvic mass. We have managed a case in which
the diagnosis of cystic degeneration of uterine myomas could not be easily
differentiated from an ovarian torsion or carcinoma. Differentiation between
degenerative pain of the myoma and an ovarian malignancy or torsion was necessary. A
complete aspiration of the cystic changes of the uterine myoma was performed without
performing a myomectomy.
Conclusion: We report a good result of aspiration of a cystic uterine myoma during
pregnancy with a review of the literature published for twenty years since 1 January
1988.
Key words: Leiomyomas, Uterine Fibroids, Pregnancy.
Introduction
Uterine leiomyomas are observed in pregnancy
more frequently now than in the past because many
women are delaying childbearing. Uterine myomas
during pregnancy increase the incidence of
spontaneous abortions, ectopic pregnancies,
preterm labor, premature rupture of the
membranes, placental abruptions, abnormal fetal
presentations, and red degeneration. Myomectomy
during pregnancy is rarely performed because of a
fear of pregnancy loss and bleeding (1). We report
a case of an aspiration of a painful uterine myoma
during pregnancy.
Corresponding Author:
Hae-Hyeog Lee, Department of Obstetrics and
Gynecology, Soonchunhyang University Bucheon
Hospital. 1174 Jung-1-dong, Wonmi-gu, Bucheon-si,
Gyunggi-do, 420-767, Republic of Korea.
Email: [email protected]; [email protected]
Case Report
We performed a cystic myoma aspiration at 12
weeks gestation with preservation of the
pregnancy. A 27-year-old primigravida had an 8
cm pelvic mass on routine ultrasonography at 10
weeks gestation. She had a MRI at a local clinic.
The MRI demonstrated an 8 x 7 x 6 cm cystic and
solid mass with septa (Figure 1). The presumptive
diagnosis was a cystic borderline tumour or cyst
adenocarcinoma. She was admitted to the
emergency room for pain management.
Differentiation between degenerative pain of the
myoma and an ovarian malignancy or torsion was
necessary. We performed explolaparotomy. Intra-
operatively, the uterus was soft and the size was
appropriate for 12 weeks gestation. The
leiomyoma was situated in the broad ligament at
the left anterior aspect of the uterus. The left ovary
was located on the myoma of the broad ligament.
We performed a complete aspiration of the cystic
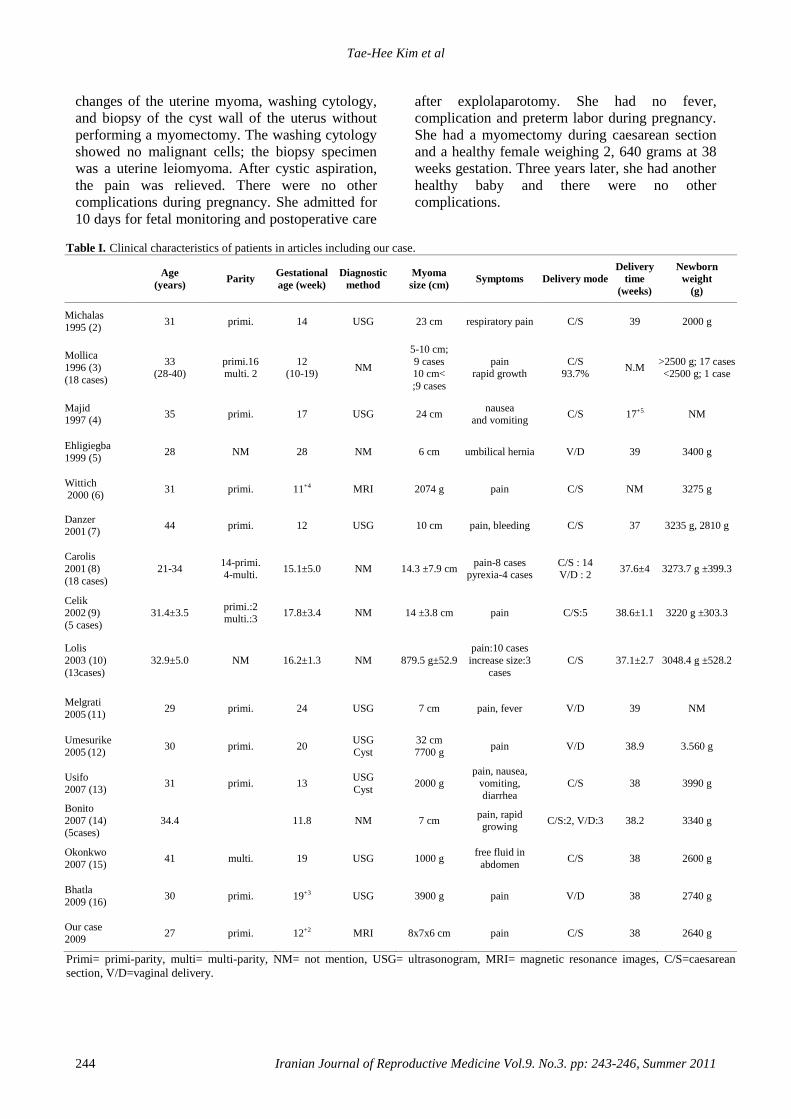
Tae-Hee Kim et al
244 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 243-246, Summer 2011
changes of the uterine myoma, washing cytology,
and biopsy of the cyst wall of the uterus without
performing a myomectomy. The washing cytology
showed no malignant cells; the biopsy specimen
was a uterine leiomyoma. After cystic aspiration,
the pain was relieved. There were no other
complications during pregnancy. She admitted for
10 days for fetal monitoring and postoperative care
after explolaparotomy. She had no fever,
complication and preterm labor during pregnancy.
She had a myomectomy during caesarean section
and a healthy female weighing 2, 640 grams at 38
weeks gestation. Three years later, she had another
healthy baby and there were no other
complications.
Table I. Clinical characteristics of patients in articles including our case.
Age
(years) Parity
Gestational
age (week)
Diagnostic
method
Myoma
size (cm) Symptoms Delivery mode
Delivery
time
(weeks)
Newborn
weight
(g)
Michalas
1995 (2) 31 primi. 14 USG 23 cm respiratory pain C/S 39 2000 g
Mollica
1996 (3)
(18 cases)
33 (28-40)
primi.16 multi. 2
12 (10-19)
NM
5-10 cm;
9 cases 10 cm<
;9 cases
pain rapid growth
C/S 93.7%
N.M >2500 g; 17 cases <2500 g; 1 case
Majid 1997 (4)
35 primi. 17 USG 24 cm nausea
and vomiting C/S 17+5 NM
Ehligiegba
1999 (5) 28 NM 28 NM 6 cm umbilical hernia V/D 39 3400 g
Wittich 2000 (6)
31 primi. 11+4 MRI 2074 g pain C/S NM 3275 g
Danzer 2001 (7)
44 primi. 12 USG 10 cm pain, bleeding C/S 37 3235 g, 2810 g
Carolis
2001 (8)
(18 cases)
21-34 14-primi. 4-multi.
15.1±5.0 NM 14.3 ±7.9 cm pain-8 cases
pyrexia-4 cases C/S : 14 V/D : 2
37.6±4 3273.7 g ±399.3
Celik 2002 (9)
(5 cases)
31.4±3.5 primi.:2 multi.:3
17.8±3.4 NM 14 ±3.8 cm pain C/S:5 38.6±1.1 3220 g ±303.3
Lolis
2003 (10)
(13cases)
32.9±5.0 NM 16.2±1.3 NM 879.5 g±52.9
pain:10 cases
increase size:3
cases
C/S 37.1±2.7 3048.4 g ±528.2
Melgrati
2005 (11) 29 primi. 24 USG 7 cm pain, fever V/D 39 NM
Umesurike
2005 (12) 30 primi. 20
USG
Cyst
32 cm
7700 g pain V/D 38.9 3.560 g
Usifo
2007 (13) 31 primi. 13
USG
Cyst 2000 g
pain, nausea, vomiting,
diarrhea
C/S 38 3990 g
Bonito
2007 (14) (5cases)
34.4 11.8 NM 7 cm pain, rapid growing
C/S:2, V/D:3 38.2 3340 g
Okonkwo
2007 (15) 41 multi. 19 USG 1000 g
free fluid in
abdomen C/S 38 2600 g
Bhatla
2009 (16) 30 primi. 19+3 USG 3900 g pain V/D 38 2740 g
Our case
2009 27 primi. 12+2 MRI 8x7x6 cm pain C/S 38 2640 g
Primi= primi-parity, multi= multi-parity, NM= not mention, USG= ultrasonogram, MRI= magnetic resonance images, C/S=caesarean
section, V/D=vaginal delivery.
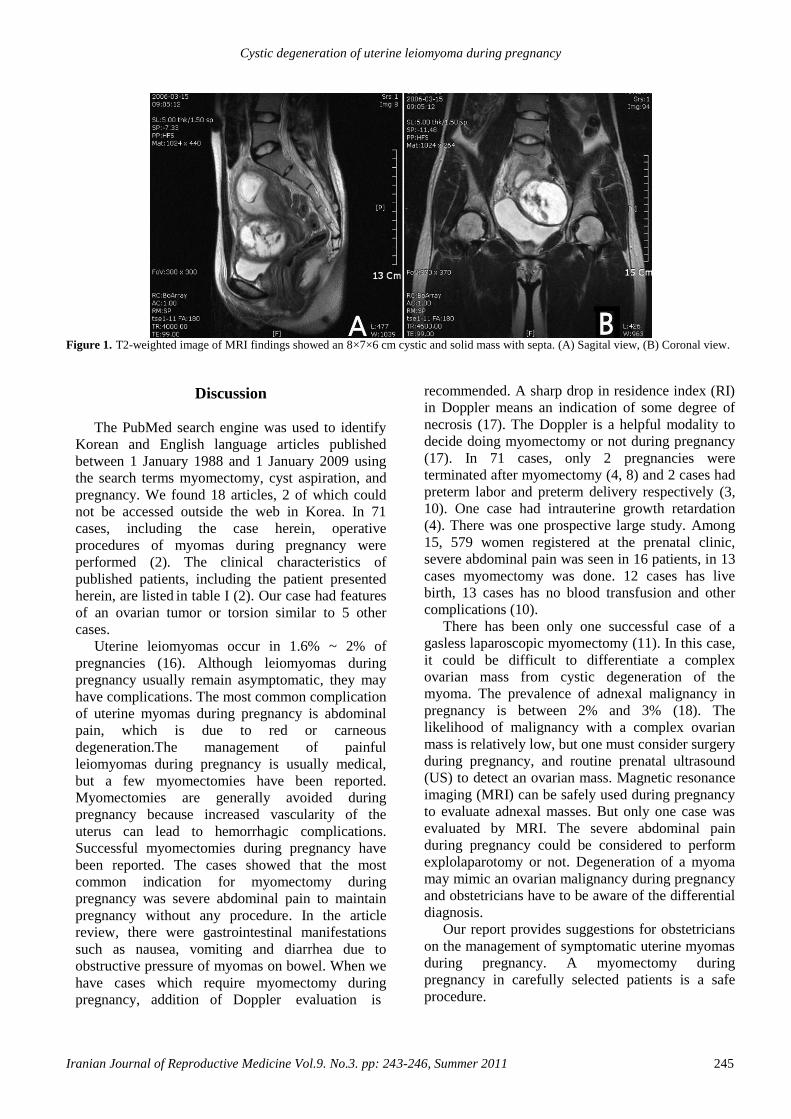
Cystic degeneration of uterine leiomyoma during pregnancy
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 243-246, Summer 2011 245
Figure 1. T2-weighted image of MRI findings showed an 8×7×6 cm cystic and solid mass with septa. (A) Sagital view, (B) Coronal view.
Discussion
The PubMed search engine was used to identify
Korean and English language articles published
between 1 January 1988 and 1 January 2009 using
the search terms myomectomy, cyst aspiration, and
pregnancy. We found 18 articles, 2 of which could
not be accessed outside the web in Korea. In 71
cases, including the case herein, operative
procedures of myomas during pregnancy were
performed (2). The clinical characteristics of
published patients, including the patient presented
herein, are listed in table I (2). Our case had features
of an ovarian tumor or torsion similar to 5 other
cases.
Uterine leiomyomas occur in 1.6% ~ 2% of
pregnancies (16). Although leiomyomas during
pregnancy usually remain asymptomatic, they may
have complications. The most common complication
of uterine myomas during pregnancy is abdominal
pain, which is due to red or carneous
degeneration.The management of painful
leiomyomas during pregnancy is usually medical,
but a few myomectomies have been reported.
Myomectomies are generally avoided during
pregnancy because increased vascularity of the
uterus can lead to hemorrhagic complications.
Successful myomectomies during pregnancy have
been reported. The cases showed that the most
common indication for myomectomy during
pregnancy was severe abdominal pain to maintain
pregnancy without any procedure. In the article
review, there were gastrointestinal manifestations
such as nausea, vomiting and diarrhea due to
obstructive pressure of myomas on bowel. When we
have cases which require myomectomy during
pregnancy, addition of Doppler evaluation is
recommended. A sharp drop in residence index (RI)
in Doppler means an indication of some degree of
necrosis (17). The Doppler is a helpful modality to
decide doing myomectomy or not during pregnancy
(17). In 71 cases, only 2 pregnancies were
terminated after myomectomy (4, 8) and 2 cases had
preterm labor and preterm delivery respectively (3,
10). One case had intrauterine growth retardation
(4). There was one prospective large study. Among
15, 579 women registered at the prenatal clinic,
severe abdominal pain was seen in 16 patients, in 13
cases myomectomy was done. 12 cases has live
birth, 13 cases has no blood transfusion and other
complications (10).
There has been only one successful case of a
gasless laparoscopic myomectomy (11). In this case,
it could be difficult to differentiate a complex
ovarian mass from cystic degeneration of the
myoma. The prevalence of adnexal malignancy in
pregnancy is between 2% and 3% (18). The
likelihood of malignancy with a complex ovarian
mass is relatively low, but one must consider surgery
during pregnancy, and routine prenatal ultrasound
(US) to detect an ovarian mass. Magnetic resonance
imaging (MRI) can be safely used during pregnancy
to evaluate adnexal masses. But only one case was
evaluated by MRI. The severe abdominal pain
during pregnancy could be considered to perform
explolaparotomy or not. Degeneration of a myoma
may mimic an ovarian malignancy during pregnancy
and obstetricians have to be aware of the differential
diagnosis.
Our report provides suggestions for obstetricians
on the management of symptomatic uterine myomas
during pregnancy. A myomectomy during
pregnancy in carefully selected patients is a safe
procedure.

Tae-Hee Kim et al
246 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 243-246, Summer 2011
From the literature review, there were rare cases
of cystic degeneration of uterine myomas during
pregnancy.
The severity of symptoms and suspicion of
malignant mass or torsion is the key in deciding
upon laparotomy. We recommend to perform cyst
aspiration rather than myomectomy in a myoma with
cyst degeneration and pain.
References 1. Parker WH. Uterine myomas: management. Fertil Steril
2007; 88: 255-271.
2. Michalas SP, Oreopoulou FV, Papageorgiou JS.
Myomectomy during pregnancy and caesarean section. Hum
Reprod 1995; 10: 1869-1870.
3. Mollica G, Pittini L, Minganti E, Perri G, Pansini F. Elective
uterine myomectomy in pregnant women. Clin Exp Obstet
Gynecol 1996; 23: 168-172.
4. Majid M, Khan GQ, Wei LM. Inevitable myomectomy in
pregnancy. J Obstet Gynaecol 1997; 17: 377-378.
5. Ehigiegba AE, Selo-Ojeme DO. Myomectomy in
pregnancy: incarcerated pedunculated fibroid in an umbilical
hernia sac. Int J Clin Pract 1999; 53: 80.
6. Wittich AC, Salminen ER, Yancey MK, Markenson GR.
Myomectomy during early pregnancy. Mil Med 2000; 165:
162-164.
7. Danzer E, Holzgreve W, Batukan C, Miny P, Tercanli S,
Hoesli I. Myomectomy during the first trimester associated
with fetal limb anomalies and hydrocephalus in a twin
pregnancy. Prenat Diagn 2001; 21: 848-851.
8. De Carolis S, Fatigante G, Ferrazzani S, Trivellini C, De
Santis L, Mancuso S, et al. Uterine myomectomy in
pregnant women. Fetal Diagn Ther 2001; 16: 116-119.
9. Celik C, Acar A, Cicek N, Gezginc K, Akyurek C. Can
myomectomy be performed during pregnancy? Gynecol
Obstet Invest 2002; 53: 79-83.
10. Lolis DE, Kalantaridou SN, Makrydimas G, Sotiriadis A,
Navrozoglou I, Zikopoulos K, Paraskevaidis EA. Successful
myomectomy during pregnancy. Hum Reprod 2003; 18:
1699-1702.
11. Melgrati L, Damiani A, Franzoni G, Marziali M, Sesti F.
Isobaric (gasless) laparoscopic myomectomy during
pregnancy. J Minim Invasive Gynecol 2005; 12: 379-381.
12. Umezurike C, Feyi-Waboso P. Successful myomectomy
during pregnancy: a case report. Reprod Health 2005; 2: 6.
13. Usifo F, Macrae R, Sharma R, Opemuyi IO, Onwuzurike B.
Successful myomectomy in early second trimester of
pregnancy. J Obstet Gynaecol 2007; 27: 196-197.
14. Bonito M, Gulemi L, Basili R, Roselli D. Myomectomy
during the first and second trimester of pregnancy. Clin Exp
Obstet Gynecol 2007; 34: 149-150.
15. Okonkwo JE, Udigwe GO. Myomectomy in pregnancy. J
Obstet Gynaecol 2007; 27: 628-630.
16. Bhatla N, Dash BB, Kriplani A, Agarwal N. Myomectomy
during pregnancy: a feasible option. J Obstet Gynaecol Res
2009; 35: 173-175.
17. Gojnic M, Pervulov M, Mostic T, Petkovic S. Doppler
ultrasound as an additional parameter for the evaluation of
myomas and the indication of myomectomy during
pregnancy. Fetal Diagn Ther 2004; 19: 462-464.
18. Leiserowitz GS, Xing G, Cress R, Brahmbhatt B, Dalrymple
JL, Smith LH. Adnexal masses in pregnancy: how often are
they malignant? Gynecol Oncol 2006; 101: 315-321.

Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:247-250, Summer 2011
Case report
Tubo-ovarian abscess in a virgin girl
Tahere Ashrafganjooei1 M.D., Iraj Harirchi
2 M.D., Giti Iravanlo
3 M.D.
1 Department of Obstetrics and Gynecology, Afzali-poor Hospital, Kerman University of Medical
Sciences, Kerman, Iran.
2 Department of Surgical Oncology, Tehran University of Medical Sciences, Tehran, Iran.
3 Department of Clinical Pathology, Tehran University of Medical Sciences, Tehran, Iran.
Received: 10 May 2010; accepted: 8 December 2010
Abstract
Background: Tubo-ovarian abscess as a serious complication of pelvic inflammatory
disease is very uncommon in sexually inactive girls.
Case: We report a case of tubo-ovarian abscess in a 24-year-old sexually inactive girl
with transverse vaginal septum who was presented with abdominal pain and a pelvic
mass and without prior surgical history and no evidences of appendicitis, inflammatory
bowel disease, or cancer. A huge unilateral tubo-ovarian abscess was recognized at
laparotomy. Unilateral salpingoophorectomy, hysterectomy and postoperative antibiotic
therapy cured the patient.
Conclusion: Early diagnosis and treatment are essential to prevent further sequel
including infertility, ectopic pregnancy, and chronic pelvic pain which cause morbidity.
Key words: Tubo-ovarian abscess, Virgin, Vaginal septum.
Introduction
Pelvic inflammatory disease (PID) is a complex
polymicrobial infection. It is thought to arise from
ascending of microorganisms from the lower
genital tract to the endometrium and fallopian
tubes, pelvic peritoneum and adjacent structures,
causing inflammation (1). It is generally a disease
of young, sexually active women of reproductive
age group (2). It has traditionally been thought that
sexual activity is a prerequisite for acquiring this
disease thus, PID is considered to be rare in
sexually inactive girls (3). Our review of the
literatures revealed 10 cases of tubo - ovarian
Corresponding Author:
Tahere Ashrafganjooei, Department of Obstetrics and
Gynecology, Afzali-poor Hospital, Kerman University
of Medical Sciences, Kerman, Iran.
Email: [email protected]
abscesses in virgins (3-8).
Tubo-ovarian abscess (TOA) is an end-stage
process and a serious manifestation of PID that
usually reflect an agglutination of pelvic organs
(tube, ovary, bowel) forming a palpable complex
(9). They may also occur after pelvic or abdominal
surgery by spreading of organisms from adjacent
gastrointestinal infections or occasionally form
super infection of a necrotic ovarian malignancy,
so; postmenopausal women presenting with TOAs,
should be thoroughly investigated to exclude a
concomitant pelvic malignancy and conservative
treatment of TOAs has no place during the
menopause (10). The correct diagnosis of TOA is
usually made during laparotomy and patient
history. Physical examination and diagnostic tests
are relatively non-specific (2).
Treatment of TOA involves the use of an
antibiotic regimen administered in a hospital.

Ashrafganjooei et al
248 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:247-250, Summer 2011
About 75% of women with TOA respond to
antimicrobial therapy alone. Failure of medical
therapy suggests the need for drainage of the
abscess (1). Laparoscopic surgery which
minimizes postoperative complications can be the
first option in the treatment of TOA (5).
Percutaneous drainage guided by imaging studies
(ultrasound or computed tomography scan) has
also been used successfully (1).
Case report
A 24 year- old blind virgin, with history of
mental retardation, primary amenorrhea and
normal secondary sexual development, was
presented to infectious ward of Imam Khomaini
Hospital, Tehran, Iran; with severe right lower
quadrant pain, diarrhea and fever since two days
ago.
Her mother mentioned a history of lower
abdominal pain, low-grade fever, and medical
therapy in her since a few months ago. In physical
examination, external genitalia were grossly
normal and hymen was intact, but rectal
examination revealed blind vagina of about 1 cm
length and an ill-defined right pelvic mass.
Abdominal palpation revealed moderately
tenderness in lower abdomen particularly in right
lower quadrant.
Laboratory analysis showed a white blood cell
count of 188000/µl, hemoglobin level of 11.5g/dl,
ESR=121 and negative blood and stool culture.
The chest radiograph was negative. Preoperative
transabdominal sonogram and computed
tomographic scan of the abdomen and pelvis were
done.
The sonogram demonstrated a 7×7.5 cm
complex mass in right pelvis with irregular borders
and multiple septa. Dilation of the right urinary
collecting system due to extrinsic compression was
noted on sonograghy. Abdomino pelvic CT-Scan
confirmed ultra sonographic findings (Figure 1).
The patient was placed on intravenous
ceftriaxone, but subsequently developed spiking
fever after 5 days. On abdominal exam, she
developed severe tenderness and rebound. We
discussed with her family and emphasized the
clinical suspicion of pelvic tumor necrosis and
abscess formation or to lesser degree, apandicular
abscess and the need for surgical resection.
She underwent exploratory laparotomy. The
abdomen was free of frank pus and adhesions, but
there were severe adhesions in pelvis. After release
of adhesions, about 300 cc greenish yellow, pus
like foul smelling material was coming from right
adnexal swelling into the pelvic cavity. Pus was
drained and exploration revealed a10×12cm right-
sided pelvic mass with extensive adhesions to the
recto-sigmoid.
The mass was identified as a right tubo-ovarian
abscess, with no evidence of diverticular or
appendiceal diseases at surgical inspection. All
abdominal organs were found to be normal. Right
salpingo-oophorectomy, was performed. During
surgery pus was removed from TOA and
transported to the laboratory, cultured for both
anaerobic and aerobic organisms. Due to her
mental retardation, after consent of her mother, the
patient underwent total abdominal hysterectomy
and then peritoneal lavage was done. The thin
lower third vaginal septum also was resected. The
culture of pus was positive and mixed.
Postoperatively, the patient received ceftriaxone
1g i.v. every 8 hr plus clindamycin 900 mg i.v.
every 8 hr. She defervesced gradually and became
afebrile after three days. Parenteral antibiotics
were replaced with oral antibiotics 72 hours later
and recommended for 14 days. Histophatologic
analysis showed a right tubo-ovarian abscess with
severe inflammatory changes and necrosis with
marked neutrophil infiltration. Postoperative
recovery was uneventful and the patient was
discharged on the fifth postoperative day.

Tubo-ovarian abscess in a virgin
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:247-250, Summer 2011 249
Figure 1. Preoperative CT-Scan demonstrating an ill-defined
pelvic mass.
Discussion
Tubo-ovarian abscess is an advanced form of
pelvic inflammatory disease, most often caused by
spread of bacteria from the lower genital tract (9).
TOA is a serious complication of pelvic
inflammatory disease rarely seen in sexually
inactive girls and it is generally the result of a
blood-borne or gastero-intestinal infection such as
appendicitis in these cases (5). It can also develop
as a complication of pelvic or abdominal surgery
and malignancy (8).
The infection in TOA is usually polymicrobial
with mixed aerobic-anaerobic organisms. The
clinical presentation of TOA tends to be non-
specific. Vaginal discharge is present in less than
5% of patients. The typical ultra sonographic
appearance of a tubo-ovarian abscess is a
multilocular, cystic and complex adnexal mass
often with debris and thick septations. Hartmann
reported two cases with purulent fluid collections
in the fallopian tubes that were not evident on
imaging, but the laparoscopic evaluation revealed
them (7).
Therefore he recommends the use of
laparoscopy for diagnosis in atypical cases.
Ruptured TOA is associated with a high risk of
development of septic shock, in case that urgent
surgical intervention is not undertaken (6). Broad
spectrum antibiotics should be given promptly to
cover polymicrobial mixed aerobic/anaerobic
infections. Prompt surgical treatment may be
associated with decreased morbidity and
postoperative hospitalization. Extensive
inflammation and edema makes the dissection of
pelvic abscess difficult.
Complications of tubo-ovarian abscesses
include tubal occlusion, increasing the risk of
infertility and ectopic pregnancy, on the other
hand, pelvic adhesions leading to chronic pelvic
pain. Early diagnosis and surgical treatment are
essential to prevent further sequela and improving
outcome.
We must consider TOA in the differential
diagnosis for abdominal pain and pelvic mass with
fever in adolescent females regardless of sexual
history.
References 1. Soper DF. Genitourinary infections and sexually
transmitted diseases. In: Berek JS: Novak's Gynecology,
14th Ed. Philadelphia; Lippincott Williams & Wilkins,
2007; 549-552.
2. Beigi RH, Wiesenland HC. Pelvic inflammatory disease:
new diagnostic criteria and treatment. Obstet Gynecol Clin
North Am 2003; 30: 777-793.
3. Hartmann KA, Lerand SJ, Jay MS. Tubo-Ovarian Abscess
in Virginal Adolescents: Look for Underlying Etiology. J
Pediatr Adolesc Gynecol 2007; 20: 127.
4. Dogan E, Altunyurt S, Altındag T, Onvural A: Tubo-
ovarian Abscess Mimicking Ovarian Tumor in a Sexually
Inactive Girl. J Pediatr Adolesc Gynecol 2004; 17: 351-
352.
5. Arda IS, Ergeneli M, Coskun M, Hicsonmez A: Tubo-
ovarian abscess in a sexually inactive adolescent patient.
Eur J Pediatr Surg 2004; 14: 70-72.
6. Teng FY, Cardone JT, Au AH: Pasteurella Multocida
tubo-ovarian abscess in a virgin. Am J Obstet Gynecol
1996; 87: 883.
7. Hartmann KA, Lerand SJ, Jay MS. Tubo-ovarian abscess
in virginal adolescents: exposure of the underlying
etiology. J Pediatr Adolesc Gynecol 2009; 22: 13-16.
8. Gensheimer WG, Reddy SY, Mulconry M, Greves C.
Abiotrophia/Granulicatella tubo-ovarian abscess in an
adolescent virginal female. J Pediatr Adolesc Gynecol
2010; 23: 9-12.
9. McNeeley SG, Hendrix SL, Mazzoni MM, Kmak DC,
Ransom SB. Medically sound, cost-effective treatment for
pelvic inflammatory disease and tuboovarian abscess. Am
J Obstet Gynecol 1998; 178: 1272-1278.

Ashrafganjooei et al
250 Iranian Journal of Reproductive Medicine Vol.9. No.3. pp:247-250, Summer 2011
10. Khan NA, Maajeeni EH. Tubo-ovarian abscess in a
postmenopausal woman with underlying ovarian
carcinoma. Saudi Med J 2005; 26: 1010-1011.

Iranian Journal of Reproductive Medicine Vol. 9. No. 3. pp: 251-252, Summer 20111
Letter to Editor
The association between iron status and some
immunological factors in the pregnancy Seyed Alireza Sobhani
1 M.D., Zahra Etaati
2 M.D., Sepideh Mirani
3 M.D., Paknoosh Saberi
4 B.Sc.,
Mahnaz Shiroodi5 M.Sc., Hojjat Salmasian
6,7 M.D., Nadereh Naderi
5,8 Ph.D.
1 Department of Pathology, Hormozgan University of Medical Sciences, Bandar Abbas, Iran.
2 Department of Obstetrics and Gynecology, Hormozgan University of Medical Sciences, Bandar Abbas,
Iran.
3 General physician, Hormozgan University of Medical Sciences, Bandar Abbas, Iran.
4 Department of Biochemistry, Hormozgan University of Medical Sciences, Bandar Abbas, Iran.
5 Center for research of Molecular Medicine, Hormozgan University of Medical Sciences, Bandar Abbas,
Iran.
6 Research Fellow, Tehran University of Medical Sciences, Tehran, Iran.
7 Research Fellow, Farzan Clinical Research Institute, Tehran, Iran.
8 Department of Immunology, Hormozgan University of Medical Science, Bandar Abbas, Iran.
Received: 7 August 2010; accepted: 18 May 2011
Iron deficiency anemia (IDA) is a common
problem in many developing countries. It is still
considered the most common nutrition deficiency
worldwide. Apart from its direct hematologic
importance, IDA affects cellular and humoral
immunity and predisposes the host to infections
(1).
Pregnant women are highly prone to IDA.
Controversial results are reported in studies
targeting this group of patients. Tang et al showed
a direct association between hemoglobin
concentration and the count of CD4+ T-cell
lymphocytes, serum levels of IL-2 and IgG, and an
inverse association with susceptibility to infection
(2). Ironically, Leush et al reported an increase in
IgM and IgG in the second and third trimesters of
pregnancy in women with IDA (3).
With regard to controversial results and the
scarcity of studies focusing on pregnant women,
we aimed to enlighten the relation between iron
status and some immunological factors include
some component of complement system, IgA,
IgM, IgG subclasses of immunoglobulins and pro-
inflammatory cytokines during the third trimester
of pregnancy.
In a descriptive-analytic study participants
were recruited using convenient sampling from
the women in the third trimester of pregnancy
Corresponding author:
Nadereh Naderi, Faculty of Medicine, First of Nabovat
minicity, opposite of Workers Welfare Community,
First of Imam Hossein Blv., Bandarabbas, Iran.
Email: [email protected]
referred to the labor room of gynecology and
obstetrics ward of Dr. Shariati Hospital of Bandar
Abbas, Iran. Patients with signs and symptoms of
thalassemia, infectious diseases or autoimmune
diseases were excluded.
IDA were defined with two criteria,
hemoglobin concentration of less than 10 mg/dL
(its normal range during the third trimesters of
pregnancy is 11-14mg/dL) (4) and ferritin less than
40 ng/dL. Patients were categorized into two
groups: those with iron deficiency anemia (IDA)
and those without this condition (no IDA).
Red cell indices including hemoglobin (Hb)
levels, hematocrit (HCT), mean corpuscular
volume (MCV), red blood cell distribution width
(RDW), and mean corpuscular hemoglobin
(MCH), serum iron (SI) and total iron binding
capacity (TIBC), concentration of ferritin, C3 and
C4 complements and IgA, IgM and IgG subclasses
of immunoglobulins were determined. Data was
analyzed using SPSS version 11.5 using Student t-
test, Pearson’s correlation test and Kolmogorov-
Smirnov’s test of normal distribution.
Ninety-two patients were studied. They were
aged between 15 and 42 years (mean=25.69±6.2).
According to our definition of IDA in pregnancy,
21 patients (22.8%) had IDA.
Our analysis of differences between the two
groups in regard to immunologic markers showed
that C4 levels are lower in the IDA group
(p=0.009) and the levels of C3, IgM, IgG, IgA, IL-
1, IL-6 and TNF-α were not statistically different
in the two groups .

Sobhani et al
252 Iranian Journal of Reproductive Medicine Vol. 9. No. 3. pp: 251-252, Summer 20111
We noticed that higher levels of serum iron are
correlated with higher levels of C3, C4 and IgG1.
Due to important properties of IgG1 like
complement fixation and opsonic activity, this
subclass is dominant antibody to pneumococcal
capsular polysaccharides and its deficiency is
associated with current infections (5). Taken
together noticing key roles of C3, C4 in
complement-mediated bacteriolysis, opsonization,
facilitated ingestion immune adherence (6) and
association of C3, C4 with Iron serum levels found
in this study we suggest that decreased level of
Iron increases susceptibility of pregnant women to
infections like chronic bacterial respiratory
infections and recurrent genital herpes (5).
Analyzing immunologic parameters differences
between the two groups of IDA and no IDA we
found that C4 levels are lower in the IDA group
but not the levels of C3, IgM, IgG, IgA, IL-1, IL-6
and TNF-α .Our findings about IgM, IgG, IgA are
in contradiction to scanty studies in this field. Tang
et al (2) about significantly lower level of IgG,
CD3+ and CD4+ cells, the ratio of
CD4+/CD8+cells, serum IL-2 in second trimester
of IDA pregnant woman and Leush et al (3) study
showed increase of IgM and IgG in second and
third trimesters of IDA groups.
Our findings about non-significant difference in
C3 and significant difference in C4 levels in IDA
and no IDA groups is in agreement with Galan et
al report about significantly positive correlation of
C4 IgA, IgM and Serum ferritin (7). Despite of
mounting evidence that TNF, IL-1, and IL-6
cytokines affect hemopoiesis and iron metabolism
there was no significant association between IL-1,
IL-6 and TNF-α and serum Iron, ferritin, TIBC in
our study and inflammatory cytokines were
statistically indifferent in the two IDA and no IDA
groups. To our knowledge, there are no reports on
inflammatory cytokine levels and Iron parameters
in pregnant women, but a limited number of
reports exploring this field in children and adults.
Bergman et al which analyzed the in vitro
production of IL-1beta, IL-2, IL-6, IL-10, and
TNF-α by peripheral blood mononuclear cells from
20 patients with IDA report that the secretion of
the cytokines other than IL-2 did not differ from
that of controls (8). In another study there was no
difference in serum levels of IL-6 in iron
deficiency anemia before and after iron
supplementation in children with IDA but in the
iron-deficiency group the production of IL-2 was
found to be significantly lower than that in controls
and became normal after iron supplementation (9).
Safuanova et al work about adequate therapy by
iron-containing drugs in IDA patients resulted in
decreased concentrations of IL-1, IL-6, TNF-alpha
and INF-gamma and recovering the functional
status of the immune system (10). It is possible that
discrepancy seen between our results and
mentioned reports in non-pregnant patients is a
reflection of dramatic change of immune function
in pregnancy.
Analyze of the results of our study and similar
researches leads us to the conclusion that unlike
extensive immunological changes have been
observed in children, IDA has little effect on
humoral immunity system of pregnant women, but
decrease in serum iron could predispose them to
pyogenic infection and may predict increased
susceptibility IDA pregnant women to infections.
References
1. Ekiz C, Agaoglu L, Karakas Z, Gurel N, Yalcin I. The
effect of iron deficiency anemia on the function of the
immune system. Hematol J 2005; 5:579-583.
2. Tang YM, Chen XZ, Li GR, Zhou RH, Ning H, Yan H.
Effects of iron deficiency anemia on immunity and
infectious disease in pregnant women. Wei Sheng Yan Jiu
2006, 35: 79-81.
3. Leush SS, Futornyi SM. Humoral immunity in women
with a normally proceeding pregnancy and in pregnancy
complicated by iron-deficiency anemia. Lik Sprava 1997;
4: 107-110.
4. Andrews NC. Anemia of inflammation: the cytokine-
hepcidin link. J Clin Invest 2004; 113: 1251-1253.
5. Seppanen M, Meri S, Notkola IL, Seppala IJ, Hiltunen-
Back E, Sarvas H, et al. Subtly impaired humoral
immunity predisposes to frequently recurring genital
herpes simplex virus type 2 infection and herpetic
neuralgia. J Infect Dis 2006; 194: 571-578.
6. Molina H. Complement and immunity. Rheum Dis Clin
North Am 2004; 30: 1-18.
7. Galan P, Davila M, Mekki N, Hercberg S. Iron deficiency,
inflammatory processes and humoral immunity in
children. Int J Vitam Nutr Res 1988; 58: 225-230.
8. Bergman M, Bessler H, Salman H, Siomin D, Straussberg
R, Djaldetti M. In vitro cytokine production in patients
with iron deficiency anemia. Clin Immunol Dec 2004;
113: 340-344.
9. Sipahi T, Akar N, Egin Y, Cin S. Serum interleukin-2 and
interleukin-6 levels in iron deficiency anemia. Pediatr
Hematol Oncol 1998; 15: 69-73.
10. Safuanova GSH, Nikulicheva VI, Bakirov AB.
Comprehensive evaluation of the immune system and
various cytokines in patients with iron-deficient anemia.
Klin Lab Diagn 2004; 24: 33-35.
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 163-170, Summer 2011
063 -079، صفحات: 09، تاتستاى 3فصلاه طة تليذ هثل ايراى، سال ن، شوار 253
مقاله مروری
درمان هورمونی درد لگنی در ارتباط با آندومتریوز
Wu Shun Felix Wong1 M.D., Chi Eung Danforn Lim
٭2 M.B.B.S.
1 School of Women’s and Children’s Health, Faculty of Medicine, University of New South Wales,
Sydney, Australia.
2 South Western Sydney Clinical School, Faculty of Medicine, University of New South Wales, Sydney,
Australia.
South Western Sydney Clinical School, Faculty of Medicine, University of Newآدرس نويسنده مسئول:٭
South Wales, Sydney Australia. [email protected]پست الكتزونيك:
99/91/89، پذيزش: 6/6/89دريبفت مقبله:
چكيده
هی تاشذ.در ارتثاط آذهتريز يک هشکل شايع زاى است ک تا دردای لگی : مقدمه
ز در ارتثاط تا درد هی تاشذ. ذهتريآدرهاى ای رهی تخشی اثرتررسی هيساى اثر ،هطالع ذف:هدف
Cochrane Systemic Review هذاليي هجد در اطالعات ،در ايي هطالع کترل شذ تصادفیمواد و روش هب:
groups گر اجام شذ. 3در آاآاليس در هرد اطالعات هتا. جت ايي تررسی فت هطالع اتخاب ذتررسی شذ
خراکی ضذ تارداری ای( قرص3در هقاتل تسريق پرشسترى؛ Implanon( 2؛ GnRHa( پرشسترى در هقاتل 0
هيساى تثد تيش از يک تعاى پالسث پرشسترى. پاسخ ت درهاى تسيل هقياس کاش درد ترکيثی در هقاتل
تثد درد در ظر گرفت شذ.
ذهتريز هشاذ گرديذ آاشی از در راتط تا کاش درد لگیGnRHaختالف هعی داری تيي پرشسترى انتبيج:
(RR: 0.036; CI:-0.030-0.102) .Implanon يا پرشسترى طيل االثرMirena اثر کوتری ازGnRHa DMPA شاى
ی در تردرهاى هثر در هقايس تا گر پالسث ضذ تارداری ترکيثی. قرصای (RR: 0.006; CI:-0.142-0.162)ذادذ
.وچيي پرشسترى سثت ت قرص ای (RR:0.321; CI:-0.066-0.707)ذهتريز شاى دادذآکاش درد اشی از
ی هاذ عارض جاثی تيشتر ،پرشسترى در حاليک. خراکی ضذ تارداری ترکيثی در کترل ديس هير هثرتر تد
ضذ تارداری ترکيثی داشت.قرص ای خراکی لخت سثت تلک تيی
در طر يکساى پرشسترى ت GnRHa، (COCP)خراکی ضذ تارداری ترکيثی ای قرصهصرف نتيجه گيزی:
ذهتريز هثر هی تاشذ. قرص ا پرشسترى سثتا ارزاى تد جت درهاى دراز هذت آکاش درد لگی اشی از
ياز Mirena Implanonهی تاشذ. هطالعات کترل شذ طالی هذت جت تررسی اثرات GnRHaهاسة تر از
اى دذ. ذهتريز شآاست تا اثرات هصرف دراز هذت آا را در کاش دردای لگی اشی از
ضذ تارداری ترکيثی.ذهتريز، درهاى طثی، پرشسترى، قرصای خراکی آ دردای لگی اشی ازکلمبت کليدی:
963-979 ، صفحبت:99 تببستبن،3فصلنبمه طب توليد مثل ايزان، سبل نهم، شمبره
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 171-176, Summer 2011
171-176، صفحات: 90، تاتستاى 3فصلاه طة تليس هثل ايزاى، سال ن، شوار 254
مقاله اصیل
-برای خانمهای با پاسخ معمولی ICSIدرسیکلهای GnRHمقایسه آگونیست و آناگونیست
کارآزمایی بالینی در ایران
، فدیه حق اللهی.M.Sc، هزین ببقزی .M.D، هزین سهزابی .M.D، بتول رشیدی .M.D اکزم قنبعی نظبم آببدی ،.M.Dانسیه طبهزی نژاد
M.Sc. نکو الهبم عظیوی ،M.D.٭، هینب جعفزآببدی M.D..
هزکش تحقيقات تساشت تارری، زاشکس پششکی زاشگا تزاى، تزاى، ايزاى.
هزکش تحقيقات تساشت تارری، هجتوع تيوارستای اهام، تلار کشارس، تزاى، ايزاى.: آدرس نویسنده هسئول ٭
[email protected]پست الکتزونیك:
98/91/98پذیزش: ،7/5/98دریبفت هقبله:
چکیده
لف تيواراى تايج هتفاتی اس ذز شاى زاز است. تزر سيز گزای هر IVFزر GnRHاستفاز اس آالگای هقدهه:
تا آتاگيست آى زر سيکلای تزای تيواراى تا پاسد هعولی هقايسه GnRHزر ايي هطالع تاثيز استفاز اس آگيست هدف:
شس است.
اس تيي ذاوای تا پاسد هعولی اتراب شهس تطهر ICSI هرز کاسيس رز ت سيکل300زرايي کارآسهايی :هب واد و روشه
يی، کلييکهی اقزار گزفتس. زذای حاهلگی شيوي GnRHفز( آتاگيست 150) GnRHتصازفی زر ز گز آگيست
زرحال پيشزفت زر ز گز هقايس شس.
رس تهز 2/8±6/1 6/9±6/1هياگيي طل هست تحزيک تروک گذاری زر گهز آگيسهت آتاگيسهت ته تزتيهة :نتبیج
(001/0p-value= هياگيي تعساز تروک .)MII 7/7± 0/4تسست آههس زر ز گهز آگيسهت آتاگيسهت ته تزتيهة
(. زر هرز هياگيي تعساز آهپلای گازتزپيي استفاز شس، فليکلا، تروکا هجوع جيها =p 03/0تز ) 3/4±9/6
هيشاى سقط زر ز گز اذهتف هعهی زار هشهاس شهس. هيهشاى حهاهلگی OHSSجيای تا کيفيت هطلب يش شيع
زر 3/35%ز. هيشاى حاهلگی کلييکی زر گهز آگيسهت ت 4/39% زر گز آتاگيست 3/35% شيويايی زر گز آگيست
ههرز زر گهز آتاگيسهت زر (3/31)%45زر گهز آگيسهت زر زر حهال پيشهزفت تهز. حهاهلگی 34%گز آتاگيسهت
هرز اتفاق افتاز. زر يچکسام اس زخ ای حاهلگی اذتف هعی زار تيي ز گز جز ساشت. (%3/29)44
يش ت زر ايي هطالع شاى زاز شس ک پزتکل آتاگيست زر تيواراى ايزای رشی آساى ايوي است تيوارگیزی: نتیجه
آسای قازر ت اجام آى هيثاشس. تايج حاصل اس استفاز اس ايي پزتکل تا پزتکل استاسارز آگيست هشاتت زارز لی طل
يست کتاتز هيثاشس.هست تحزيک روک گذاری زر رش آتاگ
Normoresponderآتاگيست، GnRHآگيست، IVF، GnRH :کلوبت کلیدی
979-971 ، صفحبت:89 تببستبى ،3تولید هثل ایزاى، سبل نهن، شوبره فصلنبهه طب
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 177-186, Summer 2011
677 -686، صفحات: 99،تابعتاى 3فصلاه طب تليذ هثل ايراى، ظال ن، شوار 255
مقاله اصیل
های موشدر دمی اپیدیدیمبر روی اسپرم های Ocimum sanctumعصاره بنسنی برگهای ثرا
بسرگ آزمایشگاهی
Mukhtar Ahmed1,3
Ph.D., R. Nazeer Ahamed1Ph.D., Ravindranath H. Aladakatti1,2٭
Ph.D., Mukhtar Ahmed
G. Ghodesawar1,4
Ph.D.
حش، داشگا کاراتاک، داراد، ذ. دپارتواى هطالعات حيات. 6
هرکس هطالعات حياات، اعتيت علم ذ، باگالر، ذ.. 2
ض، عربعتاى ظعدی.کالج علم، داشگا هلک ظعد، رياهرکس تحقيقاتی، احذ هيکرظکپ الکتری، . 3
دپارتواى حيات حش، اجوي ذ، کالج علم تجارت، بيجاپر، ذ. . 4
هرکس هطالعات حياات، اعتيت علم ذ، باگالر، ذ.5 آدرس نويسنده مسئول٭
[email protected] پست الكتزونيك5
7/8/34پذيزش5 ،72/2/33دريبفت مقبله5
چكيده
ييرات ظاختوای در ظلل باعث تغ Ocimum sanctum (O. sanctum)ک عصار بسی برگای اذ هطالعات اخير شاى داد مقدمه5
بارری هشای ر صاد آلبي هی شد. ظيوی فرضدر اپی تليم ، ببدی ثايcauda epididymisليايی در ای اپی ت
هرفلشی دهی اپيذيذين، یاپاراهترای اظپرم بر ری O. sanctumعصار بسی برگای در ايي بررظی، هطالع اثرذف ها هدف5
در رتای آلبي بد. آى ا ر ظاختوایل ای ظطحی تارگا
گر هرد عصار ارد هطالع گرديذذ.عذد( 69گر کترل هرد )ر کذام 2 ب پط از تقعين ر يعتار عذد رت 29 5هب مواد و روش
حياى از ر گر بعاى تعت بارری 5رز پشت ظر ن دريافت کردذ. 48( برای mg/kg/day259) O. sanctumبسی برگای
از شذذ کشت قطع خاع گردیعذد( بظيل 5عذد( هرد ) 5ظاعت بعذ از آخريي دز، بقي حياات کترل ) 24اظتفاد شذذ.
( SEM)اظکيگ هيکرظکپ الکتری اظتفاد شذ ظپط اظپرم ا تظط جت آاليس اظپرمآا احي دهی اپيذيذينپالظوای
هطالع شذذ. ( TEM)هيکرظکپ الکتری تراسيشي
ی آهاه افسايش دذ کاش هعی دار در تعذاد، حرکت ظرعت اظپرم ا آاليس اظپرم گر هرد در هقايع با گر شاذ شاى نتبيج5
کرزم آدذ تغييرات هرفلشيک در غشاء پالظوا غشاء در حياات گر هرد شاى SEM TEM. بد (p≤0.001)اظپرهی ای
ى در ظيتپالظن در احي هيای وچيي دم غيرطبيعی تحليل بن ريختگی هيتکذری الي اظپرم ا، تشکيل قطرات شبي بال
پرها بد. ای هيتکذريايی اظ
اثر عاقب درباشذ ک احتواال دم اپی ديذينتغييرات کلی در ای از اثرات هشاذ شذ در ايي هطالع هوکي اظت تيج نتيجه گيزی5
اظت. O. sanctumکاش آذشى اشی از اثرات ضذ آذرشی برگای
.لکتری، رتهيکرظکپ ا، اپيذيذين، اظپرم، بارری، O. sanctum 5کلمبت کليدی
622-5631 ، صفحبت49 ، تببستبن8ه فصلنبمه طب توليد مثل ايزان، سبل نهم، شمبر
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 187-192, Summer 2011
121-132، صفحات4 30، تار 3ايزاى، سال ن، ضوار فصلاه طة تليذ هثل 256
مقاله اصیل
سبند گی متعاقب اعما ل جراحیچاز ایجاد ایکودکسترین
یري می کندگوش ها جلو گدرخر هاي رحمیلوله
2نبهید بهزامی ،.1M.D*بهنبس خبنی رببطیM.D. ، 2فزدوس محزابیبن M.D. هز مش نبدری ،:
M.D..
، ايزاى.صفاى، ادکتز تطتیتيوارستاى ضيذ داطگا علم پشضکی اصفاى، ،گز ساى هاهايی .1
اصفاى، ايزاى. پشضکی اصفاى، ، داطگا علمتيوارستاى الشزاء، گز ساى هاهايی .2
، ايزاى. اصفاى ،تيوارستاى سپااى .3
اى، ايزاى. ، اصفتيوارستاى ضيذ دکتز تطتی ،داطگا علم پشضکی اصفاى، پل فلشی ،گز ساى هاهايی آدرس نويسنده مسئول4*
[email protected]پست الكتزونیك4
71/77/23پذيزش4 ،82/8/23دريبفت مقبله4
چكیده
اس هاد هختلفی اعن اس خاهذ يا هايع تزای خذا کزدى سطح لذاچسثذ گی ا ضايع تزيي عارض اعوال خزاحی هی تاضذ مقدمه4
ول خزاحی استفاد ضذ است . يکی اس ايي هاد ک تصر ضذ است هی تاذ سج ت هظر خلگيزی اس ايداد چسثذگی در حيي ع
هی تاضذ. %4 ايکدکستزيي ،اس ايداد چسثذگی خلگيزی وايذ
در لل ای رحوی % تا آب هقطز هايع آهيتيک در کاص چسثذگی اضی اس اعوال خزاحی4هقايس اثز ايکدکستزيي 4 هدف
خزگش.
خزگش سفيذ اس ژاد يسلذ تطر راذم ت س گز د تايی تقسين ضذذ. لل ای 30در ايي هطالع کلييکی ب4مواد و روش ه
قثل اس سهاى خاری ضذى خى خزاضاذتزش تاس کزدى ضکن تسيل گاس استزيل تا ايداد رحوی خزگضا پس اس تيش ضذى،
هايع آهيتيک (B، ايکدکستزيي )هحلل ( Aهحللن هحل آسية ديذ تسيل يکی اسس هحلل آب هقطز )تست ضذى ضک
گز الپاراتهی هدذد ادام ضذ. ضذ، سپس فت رس تعذ ت هظر هقايس هيشاى چسثذگی تيي س ( ضستط دادC)هحلل
( هايع 4/10±00/0( در هقايس تا آب هقطز )1/2±10/0ي ايکدکستزيي ) اختالف قاتل تخی در هيشاى ايداد چسثذگی تي4 نتبيج4
در هاری هعی داری تيي هيشاى چسثذگی ت دثال استفاد اس هايع آهيتيک . اها اختالف آ( خد داضت1/2±24/0آهيتيک )
(.4/10±00/0در هقاتل 1/2±24/0)هقايس تا آب هقطزخد ذاضت
% در کاص چسثذگی اعوال خزاحی ساى در خزگش ا هثزتز اس 4ح طاى هی دذ استفاد اس ايکدکستزيي تاي نتیجه گیزی4
ايع آهيتيک آب هقطز هی تاضذ. ه
. تيک اسای، ايداد چسثذگی، خزگش، هايع آهيايکدکستزيي کلمبت کلیدی4 721-738 ، صفحبت394،بهبر 9تولید مثل ايزان، سبل نهم، شمبره فصلنبمه طب
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 193-198, Summer 2011
257 103-108، صفحبت: 00، ببر 3فصلبه طب تليد هثل ايراى، سبل ن، ضوبر
مقبله اصیل
اووسیت ارتببط بین سطح کلسترول استر ترانسفر پروتئین مبیع فولیکولی و نسبت ببروری
IVF/ICSIدر سیکل هبی
، .M.Sc 4، يحیید هیىبسی .Ph.D 2، مسعد دارابیی .M.D 4، لعیب فزسدی.Ph.D 3، علی رحیمی پر.M.Sc 2ي1امیز مدی ساد
.Ph.D . 2٭، محمد وری.M.Sc 2، سزا گل محمدی.M.Sc 5خا، امیز مىصر يطه .B.Sc 2مقصد هبکز
ايراى. ،تبريس ، داطگب ػلم پسضکی تبريس،هرکس تحقيقبت بتکلشی داريی .1
ايراى. تبريس، سضکی، داطگب ػلم پسضکی تبريس، گر بيضيوی آزهبيطگب بی ببليی، آزهبيطگب کرهبتگرافی، داطکد پ .2
راى، ايراى.ت، داطگب ػلم پسضکی ضيد بطتی ،آزهبيطگبی گر ػلم .3
ايراى. تبريس، داطگب ػلم پسضکی تبريس، ،هرکس آهزضی درهبی السرا، هرکس تحقيقبت بداضت ببرری زبى .4
ايراى.تبريس، ،داطگب ػلم پسضکی تبريس ،هرکس تحقيقبت داريی .5
آزهبيطگب بی ببليی، آزهبيطگب کرهبتگرافی، داطکد پسضکی، داطگب ػلم پسضکی تبريس، گر بيضيویآدرس ويسىد مسئل: *
تبريس، ايراى.
[email protected]پست الكتزيویك:
9/9/92، پذيزش: 22/2/92دريبفت مقبل:
چكید
هوکي است در هيساى هفقيت در تکبهل سلل اسيت جيي ايفب هی کد ک : هبيغ فليکلی قص هویمقدم
IVF/ICSI .دخيل ببضد
ايي هطبلؼ بررسی ارتببط بيي هيساى کلسترل استر تراسفر پرتئيي هبيغ فليکلی هيساى هفقيت از دف دف:
IVF/ICSI .بد
90بيوبر هراجؼ کد ب بيوبرستبى السرای تبريزس بدسزت آهزد. 100از و بی هبيغ فليکلی ماد ي ريش ب:
، HDL-Cقزرار گرفتزد. هيزساى پبراهترزبی ICSIفر تحت درهبى بزب IVF 21فر از ايي بيوبراى تحت درهبى بب
Apo-AI CETP ضدد. هبيغ فليکلی ب ترتيب بب رش بی آسيوی ، تربيديوتری اليسا اداز گيری
در بيوبرای ک تؼداد اسيت بی CETP ، طبى داد ک هقبدير CETPآبليس زيرگر ب بب هقبدير هتفبت وتبيج:
(. وچيي در افراد بب سبت ببرری اسيت کوتر از >05/0pببلؾ کوتری دارد ب طر هؼی دار پبييي تر هی ببضد )
ب طر قببل هالحظ ای کوتر CETPهی ببضد، هقبدير ٪ 90ر آب بيص از در هقبيس بب افرادی ک ايي سبت د 50٪
%(.p ،18=05/0بد )
بر اسبس تبيج بدست آهد از ايي هطبلؼ، اگرچ ارتببطی بيي پبراهتربی هرد بررسی قع حبهلگی وتیج گیزی:
يت بی ببرر ضد ارتببط هثبت هؼی داری هبيغ فليکلی بب هيساى بلؽ درصد اس CETPيبفت طد، لی هقبدير
را طبى داد.
. A-I ،CETP، آپليپپرتئيي IVF/ICSIبببرری، کلمبت کلیدی: 123-12 9، صفحبت:29، تببستبن 3تلید مثل ايزان، سبل وم، همبر فصلىبم طب
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 199-202, Summer 201
199 -202، صفحات: 90، تابستاى 3فصلاه طب تليذ هثل ايراى، سال ن، ضوار 258
مقاله اصیل
مقایسه ارزش تشخیصی سالیه سو هیستريگرافی با هیستريسکپی در شىاسایی اختالالت آوذيمتر
در زوان با خوریسی های غیرطبیعی رحمی
1محمدعلی کزیم ساده
M.D.، 1٭راضیه دهقبنی فیزوسآببدیM.D.، 2فزسانه گوهزساد. M.D.
، يسد، ايراى.علم پسضکي ضيذ صذقيابارری، داطگا درهاي يهرکس تحقيقات .1
، يسد، ايراى.زايواى، بيوارستاى ضيذ صذقيبخص زاى .2
، يسد، ايراى.خياباى بعلي، صفايي، س تحقيقاتي درهاي ابارریهرکآدرس نویسنده مسئول:٭
[email protected]پست الكتزونیك:
11/7/98پذیزش: ،24/3/98دریبفت مقبله:
چكیده
خريسی غير طبيعي رحوي علت ضايع اختالالت رحوي در بيي زاى قبل بعذ از يائسگي هي باضذ.: مقدمه
ارزيابي هقايس ارزش تطخيصي ساليي سيسترگرافي يسترسکپي در ضاسايي خريسی ای غير طبيعي رحوي. :هدف
يسترگرافي پس ر و و ا ابتذا ساليي سرحوي ارد ايي هطالع ضذذ.دبيوار با خريسی غيرطبيعي 65 هب:مواد و روش
از آى يسترسکپي اجام ضذ. حساسيت، اختصاصي بدى، ارزش تطخيصي هثبت هفي صحت ر د رش هحاسب گرديذ.
15بيوار، در يسترسکپي آذهتر در 19در ب عاى ضايعتريي اختالل در ساليي س يسترگرافي يپرپالزی آذهتر نتبیج:
% برای پليپ يپرپالزی آذهتر هيم زير هخاطي ب ترتيب گسارش گرديذ. در 4/71% 3/73بيوار تطخيص داد ضذ. حساسيت
% گسارش گرديذ.7/90% هيم زير هخاطي 3/82%، يپرپالزی 96حاليک اختصاصي بدى برای پليپ
ر هقايس با يسترسکپي، ساليي س يسترگرافي حساسيت اختصاصي بدى بااليي را در ضاسايي هيم زير د نتیجه گیزی:
هخاطي سبت ب پليپ آذهتر يپرپالزی طاى داد.
کپي.سخريسی غير طبيعي رحوي، اختالالت رحوي، سيسترگرافي، يسترکلمبت کلیدی: 188-292 ، صفحبت:89 ، تببستبن3تولید مثل ایزان، سبل نهم، شمبرة فصلنبمه طب
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 203-208, Summer 2011
259 203-208، صفحات: 90، تاتستاى 3فصلاه طة تليذ هثل ايراى، سال ن، شوار
مقاله اصیل
یت پايین با كیف بدست آمده از امبريو هاي حاملگي موفق به دنبال انتقال بالستوسیت هاي منجمد شده
در روز سوم
Xiao-jian Zhang M.Sc.*, Ye-zhou Yang Ph.D., Li-hua Min B.N.., QunLv B.Sc.Med., Pin Bai B.N., Xiao-jie Li
B.S.M.T., Mei-xu Liao M.Sc.
Department of Assisted Reproductive Medical Center, Sichuan Academy of Medical Sciences and Sichuan Provincial
People’s Hospital, Sichuan, China.
Department of Assisted Reproductive Medical Center, Sichuan Academy of Medical Sciences: آدرس نويسنده مسئول*
and Sichuan Provincial People’s Hospital, Sichuan, China.
[email protected]پست الكتزونيك:
23/41/98پذيزش: ،44/4/98دريبفت مقبله:
چكيده
ياي تا كيفيت پاييي هوكي تر اساس خصصيات هرفلشي اجام هي گيرد. اها تعضي از اهثر ،اتخاب اهثري جت اتقال: مقدمه
تا هرحل تالستسيت كشت داد شذ سپس جت ال گسيي اتخاب گردد. است
تذثال اتقال تالستسيتاي تذست آهذ از اهثرياي تا كيفيت پاييي. كلييكيتررسي تايج حاهلگي :هدف
تيوار تحت 15از ( %8/24)تالستسيت 27 تعذاد كشت داد 6 5ت پاييي تا رز اهثري تا كيفي 109تعذاد : مواد و روش هب
IVF سپس تالستسيت ا جت اتقال گرم شذذ. ام تالستسيت ا سريعا هجوذجوع آري شذ. تو
فر از تيواراى حاهل 5تيوار اتقال يافتذ. 15ت ك ذهاذزذ %( تعذ از گرم شذى 6/92تالستسيت هجوذ شذ ) 25تعذاد نتبيج:
شذذ.
يت پاييي در رز سم ت دست كيف هجوذ شذ ك از اهثرياي تا 6 5تايج ها شاى داد ك تالستسيت اي رز نتيجه گيزی:
تارري شذ. ش شاس حاهلگي در سيكل اي كوكهي تاذ تاعث افساي ،اذ آهذ
اهثري تا كيفيت پاييي، اجواد، اتقال تالستسيت، حاهلگي. کلمبت کليدی:
213-219: ، صفحبت81 ، تببستبن3ه توليد مثل ايزان، سبل نهم، شمبر فصلنبمه طب
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 209-216, Summer 2011
209-216 ، صفحات:90، تابستاى 3فصلاه طب تليذ هثل ايزاى، سال ن، شوار 260
مقاله اصیل
بلوغ ورفولوشی و میسان بلوغ تخمک های نارس انسانی بعذ از انجام انجماد ارزیابی مرفومتری، م
آزمایشگاهی
1سعید وظزی
M.Sc.1*، محمدعلی خلیلیPh.D.2، فزيسان اسمبعیل سادM.Sc.3، مدی محسه ساد
M.Sc. .
صذقی، يشد، ايزاى. پششکی شيذعلم ، داشگا کش تحقيقاتی درهای ابارریهز1
داشگا آساد اسالهی، احذ هزدشت، گز علم داهی، هزدشت، ايزاى. 2
علم پششکی شيزاس، شيزاس، ايزاى.داشگا 3
، داشگا پششکی شيذ صذقی، يشد، ايزاى.ش تحقيقاتی درهای ابارریهزکآدرس ويسىد مسئل:٭
khalili [email protected]پست الكتزيویك:
21/8/28پذيزش: ،22/5/28دريبفت مقبل:
چكید
. (1% هتافاس4% صرهيال سيکل، 11) % تخوک ای جوع آری شذ ابالػ ستذ15در سيکل ای تکلصی کوک بارری : مقدم
جد دارد. IVM اهکاى اجواد ايي تخوک ا جت استفاد بيشتز در بزاه
fresh IVM هزفلصی تخوک ای ارس اسای در د گز هيشاى بلغ، پاراهتزای هزفهتزیذف اس ايي بزرسی تعييي :دف
(fIVM) vitrified-IVM (vIVM) .بد
بزای آا اجام شذ بد، شزکت کزدذ. اس ايي ARTتحزيک کتزل شذ تخوذای جت کسى 93در ايي بزرسی ب:ماد ي ريش
( ک ب طر هستقين در N;101( تخوک ای ابالػ )1ب د گز تقسين شذذ: ) تخوک ابالػ ب دست آهذ ک 203ساى تعذاد
، سپس در آسهايشگا بالػ شذذ. توام تخوک ا ( ک در ابتذا هجوذN;102( تخوک ای ابالػ )2شذذ ) IVMهحيط آسهايشگا
ساعت اس کشت، سبت بلغ 48 هايع فليکلی اسای شذذ. بعذ اس LH FSHهکول شذ با HAMʼs F10در IVMهتحول
اجام گزفت. Cornusتخوک ا بعال ارسيابی هزفهتزی هزفلصی سيتپالسوی با استفاد اس بزاه
(. در ارسيابی ای p<001/0، %4/59 در هقايس %4/40کاش يافت ) fIVMدر هقايس با vIVMدر سبت بلغ تخوک ا وتبيج:
±8/6 تزتيب گزديذ )ب هشاذ vIVM fIVM بيي (µm) هرفهتزيک بعذی تفات هعی داری در هياگيي قطز تخوک
(. ديگز پاراهتزا اس جول هحيط هساحت تخن بعال حجن تخوک اپالسن در د گز هشاب بدذ. 9/9±07/154 3/156
ديذ شذ. vIVMوچيي اجاری ای هزفلصی بيشتزی ظيز اکئل تخوک تيز در تخوک ای
قابل تجی در د گز هشاذ اختالف آهاری تز بدذ. يچ هفق vIVMاس ظز هيشاى بلغ سبت ب fIVMگز وتیج گیزی:
ب عاى يک فاکتر پيشگيی کذ در سزاجام بلغ تخوک در تاذ هی شد ک پاراهتزای هزفهتزی لذا پيش بيی ذ. گزدي
ذ.بکار بزد ش IVMبزاه
. زفهتزیبلغ آسهايشگای، تخوک، اجواد شيش ای، بلغ, هزفلصی، ه کلمبت کلیدی:
298-212 ، صفحبت:89 ، تببستبن3تلید مثل ايزان، سبل وم، شمبر فصلىبم طب
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 217-222, Summer 2011
261 212-222 ، صفحات:09، تاتستاى 3فصلناهه طة توليد هثل ايراى، سال نهن، شواره
مقاله اصیل
Hymenocardia acida stem bark آبي الكلي عصاره ضدباروري اثرات
هاي مادهدر رت
Abu Adakole Hyacinth
1* Ph.D., UchenduChukwuka Nwocha
2 Ph.D.
1 Department of Veterinary Physiology, Pharmacology and Biochemistry, College of Veterinary Medicine, University
of Agriculture, P.M.B, 2373, Makurdi, Nigeria.
2 Department of Veterinary Physiology and Pharmacology, Faculty of Veterinary Medicine, University of Nigeria,
Nsukka, Nigeria.
Department of Veterinary Physiology, Pharmacology and Biochemistry, College of Veterinaryآدرس نويسنده مسئول:*
Medicine, University of Agriculture, P.M.B, 2373, Makurdi, Nigeria.
[email protected]پست الكتزونيك:
51/51/98پذيزش: ،32/4/98دريبفت مقبله:
چكيده
يك گياه است كه ته طور سنتي در طة گياهي آفريقا استفاده هي شود و فوايد درهاني Hymenocardiaacida (HA): مقدمه
حاهله اطالعات زيادي در دسترس نوي تاشد. ره اثرات احتوالي آى تر روي زناىزيادي دارد. اها درتا
در رتهاي هاده نژاد ويستار هي تاشد. HAهدف هطالعه حاضر تررسي اثرات ضد تاروري عصاره الكلي آتي :هدف
هيلي گرم ته ازاي هر كيلوگرم 499و 299، 199تا دوزهاي HAسه گروه رت تحت رژين خوراكي عصاره الكلي آتي مواد و روش هب:
جسن تعدادو شده الپاراتوهيروز قرار گرفتند. گروه كنترل آب هقطر دريافت كردند. در روز تيستن حاهلگي، حيوانات 10وزى تراي
اي باريري بعد از وسديكي ب يزن جىيه ا ي جفت اوداز گيري شد. اي زود ي مچىيه اودكسجىيهحاملگي، هاي زرد
اي ي جىيه (>05/0pحاملگي ) جسن هاي زردنشاى دهنده كاهش تعداد حاهلگي 10تا اولاز روز HAعصاره تا درهاى خوراكي نتبيج:
2گسيىي در گري اي (. فعاليت ضد الو>05/0pكىترل كمتر بد )گري در مقايس با HA ا در حياوات تحت رشيم عصارزود بد. يزن جىيه % بد. 60% ي 60% ي 40% بد. در حاليك فعاليت ضد بارداري در ايه گري ا ويس ب ترتيب 7/51% ي 3/48 %،4/41 ، ب ترتيبتحت درمان 4تا
هاي هاده هي تواند تاعث اثرات هنفي تر روي عولكرد تاروري در رت HAنتايج هطالعه نشاى داد كه عصاره الكلي آتي نتيجه گيزی:
آلثينو گردد.
تليد مثل. ،Hymenocardia acidaرت آلثينو، ضد تاروري، کلمبت کليدی:
352-333 ، صفحبت:81 ، تببستبن2توليد مثل ايزان، سبل نهم، شمبره فصلنبمه طب

Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 223-228, Summer 2011
223-222 ، صفحبت:09، تببستبى 3فصلبه طب تليذ هثل ايراى، سبل ن، شوبر 262
مقبله اصیل
سطح ببالی همسیستئیه يمقبيمت به اوسلیه دربیمبران مبتال به سىذرم تخمذان پلی
کیستیک
. .M.D 2پیب جادیبى، .M.D 2بزام سلوبیبى ،.M.D 1٭فبطو داری تب ،.M.D 1تبزیشیهقدهی ، سزیي .M.D 1طیب وتی
.ایزاى، تزاى، شگب علم پششکی تزاىدا، بیوبرستبى هیزسا کچک خبى، سبى هبهبئی گز 1
پششکی، داشگب علم پششکی تزاى، تزاى، ایزاى. داشکد 2
.ایزاى، تزاى، داشگب علم پششکی تزاى، بیوبرستبى هیزسا کچک خبى، سبى هبهبئی گز آدرس یسد هسئل:٭
[email protected]پست الکتزیک:
21/10/98، پذیزش: 11/3/98دریبفت هقبل:
چکید
از بيوبری بی رايج دراى ببرری در هيبى زبى است هجب (PCOS)سيستيک بی پلی م تخوذاىسذر: هقده
م يپرهسيستئيوی هی ببشذ.د. از جول ديگر هشکالت ايي سذرهقبهت ب اسليي در هبتاليبى هی ش
ليي هی ارتببط آى بب هقبهت ب اس PCOSبيوبراى سی برز يپرهسيستئيوی درايي پژش ب برر دف:
پردازد.
بيوبر 64گر در يک کلييک داشگبی بببرری صرت گرفت. ی هقطعی آيذايي هطبلع هاد رش ب:
PCOS بی طبيعی قرار گرفتذ. سطح گلکز بشتب، اسليي فر افراد گر کترل بب تخوذاى 59در هقبيس بب
ی افراد هرد هطبلع ی خى رز سم سيکل قبعذگی و ر ود LH FSHبی بشتب، هسيستئيي، رهى
HOMA-IRبی سبت گلکز ب اسليي بشتب وچيي گيری شذ. هقبهت ب اسليي از طريق شبخصاذاز
بررسی شذ.
ب د PCOSشبى داد. گر هبتاليبى ب را ری اسطح پالسوبيی هسيستئيي در هيبى د گر تفبت هعبدتبیج:
گر هقبم غيرهقبم ب اسليي تقسين شذذ. گر هقبم ب اسليي ب صرت هعبداری سطح هسيستئيي،
(.p =0.02, <0.001, <0.001اسليي گلکز بشتبی ببالتری داشتذ )ب ترتيب
ذى تج ب هقبهت ب اسليي سطح پالسوبيی هسيستئيي ب PCOSبر ايي اسبس هبتاليبى ب تیج گیزی:
بی هقبهت، هقبهت ب اسليي يس در آب شبيع است. بر اسبس تبيج ايي ببالتری دارذ. وچيي بر اسبس شبخص
جد دارد. PCOSهعبداری هيبى يپرهسيستئيوی هقبهت ب اسليي در هبتاليبى ب هطبلع رابط
.، وسيستئيي، هقبهت ب اسليي، بببرری PCOS کلوبت کلیدی: 223-229 : ، صفحبت80، تببستبى 3تلید هثل ایزاى، سبل ن، شوبر فصلبه طب
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 229-238, Summer 2011
263 220-232 ، صفحات:00، تابستاى 3فصلاه طب تليد هثل ايراى، سال ن، ضوار
مقاله اصیل
هاي شیردهدر رت واناديومبر علیه اثرات كمي ايجاد شده توسط سلنیومو تیروندرمان همزمان
SadhanaShrivastava* Ph.D., Deepmala Joshi Ph.D,. Monika Bhadauria Ph.D., SangeetaShuklaD.Sc., Ramesh
Mathur Ph.D.
UNESCO Satellite center, Trace Element Research and Reproductive Biology and Toxicology Laboratory, School of
Studies in Zoology, Jiwaji University, Gwalior (MP), 474 011, India.
UNESCO Satellite center of Trace Element Research and Reproductive Biology and Toxicologyآدرس نويسنده مسئول:*
Laboratory, School of Studies in Zoology, Jiwaji University, Gwalior (MP), 474 011, India.
[email protected]پست الكتزونيك:
59/51/98پذيزش: ،8/98/:6دريبفت مقبله:
چكيده
داضت گسارش ضد د كد هحيطي صعتي هن هي باضد. ايي هاد اثرات كوي بر ري تليد هثل ااديم يك هاد آل: مقدمه
رد هي ضد. سد جفتيك از
اي ضيرد ت تركيب آى با سليم بر علي اثرات سوي ااديم در ر تيرىهطالع حاضر جت بررسي اثرات درهاي :هدف
ر اجام ضد. اضيرخ
رز از رز صفر بعد از زايواى قرار گرفتد. از رز 20ااديم خراكي براي mg/kg/day 5/7ا تحت تأثير دز رت مواد و روش هب:
داد ضد. (.mg/kg/day, p.o 0.5)سليم ( .mg/kg/day, i.p 606)تيرى ا بعد از زايواى ب رت 25تا 21
. وچيي افسايص (p>10/1ضد. ) سرم فسفاتاز هيازا آلكالييتجيس ااديم باعث كاص سطح قد خى افسايص تراس آنتبيج:
اي اسيد فسفاتاز در كبد رت، افسايص فعاليت آسين اي ضيرد رت ير كليااي ضيرخرت يذخير گليكشى در كبد كلي
فسفاتاز ي تر ، فعاليت آلكاليي فسفاتاز آدزييضد. در حاليك برعكس ايي هرد ار ديداي ضيرخرت يير كلاضيرد ضيرخ
-ك گلتاسيى در كبد رتدر حالي ، تحريك گرديدپراكسيداسيى ليپيد .(>01/0pب طر اضحي در توام گر ا هار ضد بد )
ب Tironدرهاى با يستپاتلشيك ضد.(. ااديم وچيي باعث حساسيت >01/0pر كاص يافت بد )ااي ضيرد ضيرخ
با سليم باعث كاص ضايعات اضي از ااديم در رتاي ضيرخر ضيرد ضد. Tironتايي وچيي
اضي از ااديم در رتاي وي سب تايي بر علي اثرات Tironب ورا سليم داراي اثرات بيطتري از Tironنتيجه گيزی:
ضيرد ضيرخار است.
. تيرى، Teratogenecityااديم، سليم، ضيرخر، ضيرد، کلمبت کليدی:
668-679 ، صفحبت:81 ، تببستبن7توليد مثل ايزان، سبل نهم، شمبره فصلنبمه طب
Iranian Journal of Reproductive Medicine Vol.9. No.2. pp: 239-242, Summer 2011
264 230-242، صفحبت: 00 تببستبى،3 فصلبه طب تليذ هثل ايزاى، سبل ن، شوبر
مقاله اصیل
IVF-ETدر بیماران تحت درمان با میزان الوه گزیىیبر خوراكی بررسی اثر ریتودریه
..M.D احمدیدکتز مزیم ، .M.D مزضیه سنوئی فزیمبنیدکتز ، .M.D دکتز صغزا ربیعی
، ايزاى.، وذاىداشگب علم پششکی وذاى ،بيوبرستبى فبطوي ،هزکش تحقيقبتی بببرری
ى، ايزاى.، وذاداشگب علم پششکی وذاى ،بيوبرستبى فبطوي ،هزکش تحقيقبتی بببررینویسنده مسئول: آدرس
[email protected] پست الكتزونیك:
72/6/89پذیزش: ،8/9/88دریبفت مقبله:
چكیده
ذببل دستکبری بی اجبم شذ بزای اتقبل يکی اس تئريبی هطزح بزای دفع جيي عذم ال گشيی، اقببضبت رحوی بمقدمه:
استفبد اس داربی هبر کذ اقببض رحوی، ب عاى عبهلی بزای افشايش احتوبل ال گشيی هطزح است.لذا .جيي هی ببشذ
در ايي تحقيق اثز ريتدريي ب عاى هبر کذ اقببضبت رحوی هرد بزرسی قزار گزفت. : هدف
شبذ(، پزتکل تحزيک 53هرد 53اجبم شذ ) IVF+ET بذيذک بيوبر 106ری کبرآسهبيی کتزل شذ ايي هب:مواد و روش
، پزصستزى، ASA، عال بز داربی هعول ) ETدر گز هرد بعذ اس ، بزای و يکسبى بد ETتخوک گذاری پبکچز
آسهبيش ETرس پس اس 12. تجيش شذبزای يک فت ريتدريي خراکی دببر در رس هيلی گزم 200فليک اسيذ، اريتزهبيسيي(
βHCG (هيشاى ال گشيیبزای بيوبراى اجبم هيشاى حبهلگی.) بزرسی شذ. در ز گز
تفبت اس ظز آهبری ايي % بد15 در گز شبذ %2/13 هيشاى ال گشيی هفقيت آهيش در گز دريبفت کذ ريتدريي نتبیج:
. (p>0.05) هعی دار بد
هطبلع حبضز شبى داد اقببضبت رحن وی تاذ در هوبعت اس ال گشيی تبثيزی داشت ببشذ. نتیجه گیزی:
. IVFريتدريي ، کبرآسهبيی ببليی، ال گشيی ، کلمبت کلیدی:
739-747، صفحبت: 90 تببستبن ،3تولید مثل ایزان، سبل نهم، شمبره فصلنبمه طب

Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 243-246, Summer 2011
423-426، صفحات: 09، تابستاى 3فصلاه طب تليذ هثل ايراى، سال ن، ضوار 265
گزارش مورد
چگونه بايد با دژنراسيون كيستيك دردناك ميوما در حين حاملگي برخورد كرد؟ گزارش مورد و
بررسي منابع
Tae-Hee Kim M.D., Hae-Hyeog Lee M.D., Ph.D*.
Department of Obstetrics and Gynecology, College of Medicine, Soonchunhyang University, Bucheon, 420-767,
Republic of Korea.
,Department of Obstetrics and Gynecology, College of Medicine, Soonchunhyang Universityآدرس نويسنده مسئول: *
Bucheon, 420-767, Republic of Korea.
[email protected] ; [email protected] پست الكتزونيك:
22/01/98پذيزش: ،23/4/98دريبفت مقبله:
چكيده
هيهااي رحوي از تد اي ضايع لگي در حيي حاهلگي ستذ. درد رضذ سريع ايي هيهاا از ضايع تريي عارض :مقدمه
ستيل درداك هيها در حيي حاهلگي تضيح داد هي ضد. حاهلگي هي باضذ. در ايي گسارش برخرد با دشراسيى مي
ها ايي هرد را در حالي بررسي مردين م دشراسيى بد.يل تد لگي داراي سال با حاهلگي ضنن ال 42يل زى : مورد
راسيى درد اضي از دشخيص داد. بابرايي تطخيص بذخيوي تطميستيل هيهاي رحوي را وي تاى ب آساي از پيچص تخوذاى يا
ذ. هنتهي اجام ضسپراسيى ماهل از ميست هيهاي تخوذاي بذى هيص تخوذاى يا بذخيوي ضرري بد. آهيها از پيچ
سپراسيى ميست هيهاي رحوي را در حيي حاهلگي ب ورا بررسي هقاالت هتطر ضذ ها يل هرد هفقيت آهيس از آ نتيجه گيزی:
را گسارش مردين. 8011ل از ال شاي سا 49ب هذت
ليهيهاتز، فيبرئيذ اي رحوي، حاهلگي.: کليدی کلمبت
243-242 ، صفحبت:81 ، تببستبن3توليد مثل ايزان، سبل نهم، شمبره فصلنبمه طب
Iranian Journal of Reproductive Medicine Vol.9. No.3. pp: 247-250, Summer 2011
266 042 -059، صفحات: 09، تابستاى 3 طب تليذ هثل ايراى، سال ن، شوار فصلاه
گزارش مورد
آبسه لوله ای تخمذانی در یک خانم مجرد
. .M.D 3، دکتز گیتی ایزوانلو.M.D 2، دکتزایزج حزیزچی.M.D 1*گنجویی دکتز طبهزه اشزف
.بيوارستاى افضلی پر، داشگا علم پسشکی کرهاى، کرهاى ، ايراى ،بخش زاى هاهايی 1
.اى، تراى، ايراىبخش جراحی اکلشی ، داشگا علم پسشکی تر 2
.بخش کلييکال اکلشی، داشگا علم پسشکی تراى، تراى، ايراى 3
. بيوارستاى افضلی پر، داشگا علم پسشکی کرهاى، کرهاى ، ايراى ،بخش زاى هاهايی :آدرس نویسنده مسئول *
[email protected]پست الكتزونیك:
11/8/98پذیزش: ،20/2/98دریبفت مقبله:
چكیده
از ظر جسی غير فعال ستذ دخترای ک التابی لگي در ای، ای تخوذای ب عاى يک عارض جذی بيواری آبس لل :مقدمه
ادر است. بسيار
ب هبتال از ظر جسی غير فعال. ايي دختر کينسال را هعرفی هی 04ای تخوذای در يک دختر : ها يک هرد آبس للمورد
شاذی از آپاذيسيت، بيواری التابی رد يا سرطاى قبلیبذى شرح حال ،با درد شکن تد لگی کسپتم عرضی اشى بد
سالپيگ با بيوار الپاراتهی تشخيص داد شذ. کطرف دريای تخوذای يک آبس بسرگ للاجام شذ ای در بررسی هراجع کرد.
ببد يافت. اى آتی بيتيکی بعذ از عوليسترکتهی دره ،يکطرف افرکتهی
درد هسهي لگي ک هجر ب اتای فرد حاهلگی خارج از رحن ب هظر پيشگيری از عارض بعذی از جول ازايی، ه گیزی:جنتی
ساهی است.لاايي بيواری تشخيص درهاى در هراحل الي ،هيشد
ای تخوذای، هجرد، سپتم اشى. : آبس للکلیدی کلمبت
241-250 ، صفحبت:80 ، تببستبن3تولید مثل ایزان، سبل نهم، شمبره فصلنبمه طب
Iranian Journal of Reproductive Medicine Vol.9. No.3. Summer 2011
Iranian Journal of Reproductive Medicine Vol.9. No.3. Summer 2011 267
BOARD OF CONSULTANTS
The Editor wishes to express his appreciation to the following scientists who
reviewed manuscripts submitted to the Iranian Journal of Reproductive Medicine
(Vol.9 No.3 Summer 2011) in a conscientious and objective manner.
Aflatoonian, Abbas M.D. (Iran)
Ahmadi, Ali Ph.D. (USA)
Ahmadi, Shahnaz M.D. (Iran)
Akhondi, Mohammad Mehdi Ph.D. (Iran)
Alborzi, Saeed M.D. (Iran)
Anvari, Morteza Ph.D. (Iran)
Asgharnia, Maryam M.D. (Iran)
Ayazi-Rozbahani, Maryam M.D. (Iran)
Babaie, Homayoun D.V.M., Ph.D. (Iran)
Dehghani Firoozabadi, Razieh M.D. (Iran)
Eftekhar, Maryam M.D. (Iran)
Ghaffari-Novin Maarefat Ph.D. (Iran)
Ghasemzadeh, Aalieh M.D. (Iran)
Ghazizadeh, Shirin M.D. (Iran)
Habibzadeh, Victoria M.D. (Iran)
Hojjat, Farzaneh M.D. (Iran)
Khaki, Amir Afshin Ph.D. (Germany)
Khalili, Mohammad Ali Ph.D. (Iran)
Madani, Tahere M.D. (Iran)
Mansuri Moghaddam, Fatemeh M.D. (Iran)
Mashayekhi, Mehri M.D. (Iran)
Mehrafza, Marzieh M.D. (Iran)
Modares- Mosaddegh, Monire Ph.D. (Iran)
Moein, Mohammad Reza M.D. (Iran)
Moeini, Ashraf M.D. (Iran)
Mohammadian Farnaz M.D. (Iran)
Mohiti, Mohammad Javad Ph.D. (Iran)
Mosaddegh, Mohammad Pharm M.D. (Iran)
Movaheddin, Mansoureh Ph.D. (Iran)
Nematollahi Mahani, Seyed Noureddin Ph.D. (Iran)
Oskoueian, Homa M.D. (Iran)
Rafaati, Ali Ph.D. (Iran)
Salehnia, Mojdeh Ph.D. (Iran)
Salehpour, Saghar M.D. (Iran)
Salami, Maryam M.D. (Iran)
Shahrokh Tehrani-Nejad, Ensieh M.D. (Iran)
Shamsa, Ali M.D. (Iran)
Tabibnejad, Nasim M.D. (Iran)
Taheripanah, Robabeh M.D. (Iran)
Talebi, Ali Reza Ph.D. (Iran)
Yousefnejad, Fariba M.D. (Iran)
Zolghadri, Jaleh M.D. (Iran)

Iranian Journal of Reproductive Medicine Vol.9. No.3. Summer 2011
Iranian Journal of Reproductive Medicine Vol.9. No.3. Summer 2011 268
□ I would like to receive a FREE sample copy of the Iranian Journal of Reproductive Medicine.
□ Please enter my subscription to Iranian Journal of Reproductive Medicine.
PERSONAL SUBSCRIPTION
o Please enter my Personal Subscription for
60.000 Rials, for four issues.
STUDENT SUBSCRIPTION
o Please enter my Student Subscription for
40.000 Rials for four issues.
INSTITUTIONAL/LIBRARY
SUBSCRIPTION
o Please enter the Institutional/Library
Subscription for 80.000 Rials for four
issues.
ADDRESS
Please print the following clearly:
Name:
Address:
City:
Phone:
E-mail:
PAYMENT METHOD
o Cash
o Cheque enclosed
Cheque must be made to:
Iranian Journal of Reproductive Medicine,
Bouali Ave. Safayeh, Yazd, Iran.
o Bank Transfer
Transfer must be made to:
Melli Bank (Aboozar Square, Code: 3517)
Current Account No. Siba-2178545922005,
Yazd, Iran.
PERSONAL SUBSCRIPTION
o Please enter my Personal Subscription for
US $50 for four issues.
STUDENT SUBSCRIPTION
o Please enter my Student Subscription for
US $20 for four issues.
INSTITUTIONAL/LIBRARY
SUBSCRIPTION
o Please enter my Institutional/Library
Subscription for US $100 for four issues.
ADDRESS
Please print the following clearly:
Name:
Address:
City:
Phone:
E-mail:
PAYMENT METHOD
o Cash
o Cheque enclosed
Cheque must be made to:
Iranian Journal of Reproductive Medicine,
Bouali Ave, Safayeh, Yazd, Iran.
o Bank Transfer
Transfer must be made to:
Melli Bank (Aboozar Square, Code: 3517)
Current Account No. Siba-2178545922005,
Yazd, Iran.
Subscription Order Card for Iran
Subscription Order Card for Other Countries
To: Iranian Journal of Reproductive
Medicine, Research and Clinical Center for
Infertility, Shahid Sadoughi University of
Medical Sciences, Bouali Ave, Safayeh,
Yazd, Iran.
To: Iranian Journal of Reproductive
Medicine, Research and Clinical Center for
Infertility, Shahid Sadoughi University of
Medical Sciences, Bouali Ave, Safayeh,
Yazd, Iran.
Stamp
Stamp
Please send me a sample copy of the Iranian Journal of Reproductive Medicine
(IJRM).
Name:
Address:
E-mail:
Iranian Journal of Reproductive Medicine,
Research and Clinical Center for Infertility,
Shahid Sadoughi University of Medical Sciences,
Bouali Ave, Safayeh, Yazd, Iran.
Please send me a sample copy of the Iranian Journal of Reproductive Medicine
(IJRM).
Name:
Address:
E-mail:
Iranian Journal of Reproductive Medicine,
Research and Clinical Center for Infertility,
Shahid Sadoughi University of Medical Sciences,
Bouali Ave, Safayeh, Yazd, Iran.
Send for a free sample copy today
Iranian Journal of Reproductive Medicine
Send for a free sample copy today
Iranian Journal of Reproductive Medicine
Call for Papers
Iranian Journal of Reproductive Medicine
(IJRM) will consider for publishing review articles,
original articles, case reports and short
communications in the field of reproductive
medicine. If you have a manuscript that you think
might be appropriate for IJRM, please submit it to
our office for consideration.
Please visit our website for further details and for
full Instructions for Authors
http://www.ijrm.ir
Manuscript should be submitted to:
Dr. Abbas Aflatoonian, Editor-in-Chief
Iranian Journal of Reproductive Medicine
Research and Clinical Center for Infertility,
Shahid Sadoughi University of Medical Sciences,
Bouali Ave., Safayeh, Yazd, Iran.
Postal Code: 8916877391
Copyright © 2022 FDOKUMEN