
Interim results of a randomized trial of mitomycin C as an adjunct to radical radiotherapy in the...
18
Interim Results of a Randomized Trial of Mitomycin C as an Adjunct to Radical Radiotherapy in the Treatment of Locally Advanced Squamous-Cell Carcinoma of the Cervix Kenneth B. Roberts, M.D. 1 * Nelson Urdaneta, M.D., 3,5 Raul Vera, M.D., 5 Andres Vera, M.D., 4,5 Enrique Gutierrez, M.D., 3,5 Yadelis Aguilar, M.D., 3 Sara Ott, M.D., 3 Ivonne Medina, M.D., 3 Pilar Sempere, M.D., 3 Sara Rockwell, Ph.D., 1,2 Alan C. Sartorelli, Ph.D., 2 Diana B. Fischer, Ph.D., M.P.H., 1 and James J. Fischer, M.D., Ph.D. 1 1 Department of Therapeutic Radiology, Yale University School of Medicine, New Haven, Connecticut, USA 2 Department of Pharmacology, Yale University School of Medicine, New Haven, Connecticut, USA 3 Therapeutic Radiology Service, Central University of Venezuela, Caracas, Venezuela 4 Domingo-Luciani Hospital, Caracas, Venezuela 5 La Floresta Medical Institute, Caracas, Venezuela SUMMARY The purpose of this study was to determine the efficacy of mitomycin C as an adjunct to radiotherapy for the treatment of locally advanced cervix cancer. Patients with squamous-cell carcinoma of the cervix, stages IB2-IVA, were randomized to receive radiotherapy alone or radiotherapy with concomitant mitomycin C. An initial cohort of 160 patients, having a mean follow-up of 46 months, is analyzed. Intravenous mitomycin C, 15 mg/M 2 , was given on the first and sixth week of radiotherapy. The 78 patients in the radiotherapy with mitomycin C group and 82 patients in the radiotherapy alone group have a comparable distribution by age and stage (mean age 47 years; stage IB 3%, IIA 11%, IIB 48%, IIIA 1%, IIIB 36%, IVA 3%). The four-year actuarial survival rates for radio- therapy with mitomycin C and radiotherapy alone were 72% and 56%, respectively (P = 0.13). The four-year actuarial disease-free survival rates for radiotherapy with mitomycin C and radiotherapy alone were 71% and 44%, respectively, a statistically significant dif- ference (P = 0.01). The four-year actuarial local recurrence-free survival rates for patients receiving radiotherapy with mitomycin C and radiotherapy alone were 78% and 63%, respectively (P = 0.11). Differences in four-year distant recurrence-free survival between radiotherapy plus mitomycin C and radiotherapy alone were significantly different at 85% vs. 61% (P = 0.01); this analysis is not adjusted for local failure. On subgroup analysis, stage III-IVA patients had a four-year actuarial disease-free survival of 75% for radiotherapy plus mitomycin C compared with 35% for radiotherapy alone (P = 0.03). There were no treatment- related deaths. Mild hematologic toxicity was seen only in the group treated with mitomycin C. No excess in non-hematologic toxicity has been observed thus far with combined mitomycin C and radiotherapy. In this open phase III trial of mitomycin C as an adjunct to radical radiotherapy for squamous-cell carcinoma of the cervix, there were Sponsor: American Cancer Society; Grant number: CRTG-97-046-01-EDT. *Correspondence to: Kenneth B. Roberts, M.D., Yale University School of Medicine, Department of Therapeutic Radi- ology, 333 Cedar Street, New Haven, CT 06520-8040. Phone: (203) 785-2957; Fax: (203) 785-4622; E-mail: kenneth.roberts@ yale.edu Received 9 December 1999; Revised 11 May 2000; Accepted 14 June 2000 Int. J. Cancer (Radiat. Oncol. Invest): 90, 206–223 (2000) © 2000 Wiley-Liss, Inc. Publication of the International Union Against Cancer
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Interim results of a randomized trial of mitomycin C as an adjunct to radical radiotherapy in the...

Interim Results of a Randomized Trial ofMitomycin C as an Adjunct to Radical
Radiotherapy in the Treatment of LocallyAdvanced Squamous-Cell Carcinoma
of the Cervix
Kenneth B. Roberts, M.D.1* Nelson Urdaneta, M.D.,3,5 Raul Vera, M.D.,5Andres Vera, M.D.,4,5 Enrique Gutierrez, M.D.,3,5 Yadelis Aguilar, M.D.,3
Sara Ott, M.D.,3 Ivonne Medina, M.D.,3 Pilar Sempere, M.D.,3Sara Rockwell, Ph.D.,1,2 Alan C. Sartorelli, Ph.D.,2
Diana B. Fischer, Ph.D., M.P.H.,1 and James J. Fischer, M.D., Ph.D.11Department of Therapeutic Radiology, Yale University School of Medicine,
New Haven, Connecticut, USA2 Department of Pharmacology, Yale University School of Medicine,
New Haven, Connecticut, USA3Therapeutic Radiology Service, Central University of Venezuela, Caracas, Venezuela
4Domingo-Luciani Hospital, Caracas, Venezuela5La Floresta Medical Institute, Caracas, Venezuela
SUMMARY The purpose of this study was to determine the efficacy of mitomycin C asan adjunct to radiotherapy for the treatment of locally advanced cervix cancer. Patientswith squamous-cell carcinoma of the cervix, stages IB2-IVA, were randomized to receiveradiotherapy alone or radiotherapy with concomitant mitomycin C. An initial cohort of160 patients, having a mean follow-up of 46 months, is analyzed. Intravenous mitomycinC, 15 mg/M2, was given on the first and sixth week of radiotherapy. The 78 patients in theradiotherapy with mitomycin C group and 82 patients in the radiotherapy alone grouphave a comparable distribution by age and stage (mean age 47 years; stage IB 3%, IIA 11%,IIB 48%, IIIA 1%, IIIB 36%, IVA 3%). The four-year actuarial survival rates for radio-therapy with mitomycin C and radiotherapy alone were 72% and 56%, respectively (P =0.13). The four-year actuarial disease-free survival rates for radiotherapy with mitomycinC and radiotherapy alone were 71% and 44%, respectively, a statistically significant dif-ference (P = 0.01). The four-year actuarial local recurrence-free survival rates for patientsreceiving radiotherapy with mitomycin C and radiotherapy alone were 78% and 63%,respectively (P = 0.11). Differences in four-year distant recurrence-free survival betweenradiotherapy plus mitomycin C and radiotherapy alone were significantly different at 85%vs. 61% (P = 0.01); this analysis is not adjusted for local failure. On subgroup analysis, stageIII-IVA patients had a four-year actuarial disease-free survival of 75% for radiotherapyplus mitomycin C compared with 35% for radiotherapy alone (P = 0.03). There were notreatment- related deaths. Mild hematologic toxicity was seen only in the group treatedwith mitomycin C. No excess in non-hematologic toxicity has been observed thus far withcombined mitomycin C and radiotherapy. In this open phase III trial of mitomycin C as anadjunct to radical radiotherapy for squamous-cell carcinoma of the cervix, there were
Sponsor: American Cancer Society; Grant number: CRTG-97-046-01-EDT.*Correspondence to: Kenneth B. Roberts, M.D., Yale University School of Medicine, Department of Therapeutic Radi-
ology, 333 Cedar Street, New Haven, CT 06520-8040. Phone: (203) 785-2957; Fax: (203) 785-4622; E-mail: [email protected]
Received 9 December 1999; Revised 11 May 2000; Accepted 14 June 2000
Int. J. Cancer (Radiat. Oncol. Invest):90, 206–223 (2000)© 2000 Wiley-Liss, Inc. Publication of the International Union Against Cancer

minimal hematologic effects and no increase in acute radiation reactions. A statisticallysignificant difference in favor of patients receiving mitomycin C is shown for disease-freesurvival. Thus far, there are trends in favor of those patients receiving mitomycin C forsurvival and local control. Patients with more advanced stage disease, predominantly stageIIIB, appear to have the most benefit. These preliminary results support the hypothesisthat targeting hypoxic cells may lead to a therapeutic enhancement in the radiotherapy ofcervix cancer. This trial continues to accrue patients and follow-up data. Int. J. Cancer(Radiat. Oncol. Invest.) 90, 206–223 (2000). © 2000 Wiley-Liss, Inc.
Key words: cervix cancer; radiotherapy; mitomycin C; combined modality therapy
INTRODUCTION
Worldwide, cervix cancer is the seventh most com-mon cancer [1]. In women, it is the third mostcommon cancer, after breast cancer and nearlyequal to colorectal cancer, representing 15% of allfemale cancers. Internationally, the estimated an-nual incidence and number of deaths are 371,200and 186,000, respectively. Seventy-eight percent ofall cervix cancer cases occur in developing coun-tries. Carcinoma of the cervix is slowly declining inincidence in the United States, with an estimatedcurrent incidence of 12,800 new cases of invasivedisease per year, causing 4,800 deaths per year [2].This translates to an age-adjusted mortality rate of2.5 per 100,000 population. Mortality rates havealso been steadily decreasing for the last severaldecades in the United States, in large part reflectingeffective screening with Pap smears. Nevertheless,of those women diagnosed with cervix cancer,roughly one-third to one-half are candidates forradical radiotherapy. Regrettably, in socioeconom-ically disadvantaged populations in the UnitedStates and around the world in developing coun-tries, the incidence of cervix cancer reaches nearepidemic proportions. In Venezuela, cancer of thecervix represents a major public health problem. Itis the most frequent malignant tumor of women inthat country, with an estimated annual incidence of3,167 cases per year in a country with a populationof 22.5 million and an incidence rate of 292 per100,000 women. Epidemiologic data suggest thata large proportion of cases have characteristicsof a sexually transmitted disease. Human papil-loma virus has been strongly linked with cervicalneoplasia.
Successful treatment of locally advanced cer-vix cancer typically includes both external beamradiotherapy and brachytherapy. Given the ana-tomic accessibility of the cervix and the toleranceof the surrounding normal tissues to the effects ofirradiation, radiotherapy of cervix cancer represents
one of the remarkable successes of oncology. Nev-ertheless, cure rates for cervical carcinoma, whichvary depending on disease stage, are low for locallyadvanced disease, and improved treatment strate-gies are needed. Five-year overall survival rates byFIGO stage reported in the medical literature are inthe range of 80%–95% for IB disease, 65%–85%for IIA disease, 40%–76% for IIB disease, 33%–50% for IIIB disease, and 20%–25% for IVA dis-ease[3–10]. Corresponding local failure rates bystage are: 5%–20% for IB, 6%–16% for IIA, 14%–31% for IIB, and 30%–49% for IIIB.
Induction and concurrent chemotherapy forlocally advanced cervical carcinoma has been un-der active investigation for several years at manycenters. Unfortunately, the limited cell kill possiblewith conventional chemotherapy in this disease hasmade the approach of induction chemotherapy lessthan satisfactory, and potentially even deleterious,for patients with cervical carcinoma [11]. Concur-rent chemotherapy and radiotherapy is a more suc-cessful approach, given the potential for supra- ad-ditive effects from the two modalities that mayachieve a true therapeutic gain. This has largelybeen the experience with combined modalitytherapy in head and neck cancer, where inductionchemotherapy usually only adds toxicity, while cer-tain concurrent chemotherapy programs do im-prove disease outcome [12–14] . Thus far, six ran-domized trials of induction chemotherapy prior toradiotherapy for locally advanced cervix cancerhave shown no benefit [15–20]. In contrast, fivetrials of cisplatinum-based concurrent chemo-therapy and radiotherapy have demonstrated a ben-efit over radiotherapy alone in terms of survivaland disease-free survival, albeit with some addedtoxicity [21–25].
There continues to be a need for significantimprovement in the treatment of patients with mod-erate and advanced stage carcinoma of the cervix.Treatment failure often reflects a lack of steriliza-tion of tumor at the primary site (cervix), in adja-
Roberts et al.: Mitomycin C and Radiotherapy for Cervix Cancer 207

cent tissues such as vagina and parametrium, and/orin lymph node areas within the pelvis. Carcinomaof the cervix is therefore well suited to the inves-tigation of approaches that are designed to improvelocal tumor control because improved local controlwould be expected to result in increased overallsurvival. Simply increasing the doses of radiationdelivered would be associated with intolerably in-creased toxicity, especially to bowel and bladder.Altered radiation fractionation schemes are notlikely to provide significant therapeutic advantage[26]. Addition of extrafascial hysterectomy forstage IB disease to radical radiotherapy increasesmorbidity without improving outcome [27–29].
A hypothesis underlying our approach is thattherapy directed at tumor hypoxia, both a source ofradioresistance and a promoter of genetic instabil-ity in tumor cells, may improve cervix cancer curerates. The evidence that hypoxic cells limit radio-curability of human tumors, including cervix can-cer, is mainly circumstantial. Almost all trans-planted animal tumor models contain hypoxic cells.In most experimental tumors, approximately 10%–20% of viable (clonogenic) tumor cells are hypoxic[30]. Cell survival curves for solid tumors showmixed populations of sensitive (aerobic) and resis-tant (hypoxic) cells [31]. The proportion of eachcan be altered using techniques that alter tissueoxygenation. Other evidence for hypoxia includeshistologic studies demonstrating areas of necrosiswithin tumors; direct measurements of oxygen ten-sions within tumors using microelectrode probes[32,33] and spectroscopic techniques[34]; and di-rect labeling of hypoxic cells using electron affiniccompounds [35].
There are several lines of evidence that tumorhypoxia may be an important source of radioresis-tance in human cervix cancer. Anemia has beenshown in several studies to be a prognostic factorpredicting for poorer outcome in patients treatedwith radiation [36,37]. In a prospective trial at thePrincess Margaret Hospital, correction of anemiawith blood transfusions in patients undergoing ra-diotherapy for cervix cancer resulted in a decreasein pelvic recurrence rates [38]. Two separate trialsof hyperbaric oxygen (HBO) as an adjunct to ra-diation therapy of cervix cancer showed significantimprovement in local tumor control for stage IIIcarcinoma of the cervix, albeit at the expense ofincreased normal tissue damage [39,40]. In addi-tion, a retrospective analysis indicated that in a sub-set of initially anemic patients, transfusion prior totreatment further improved local control.
Polarographic measurements of oxygen ten-sions in a variety of solid tumors demonstrate that
the degree of hypoxia correlates with poorer prog-nosis. For human cervix cancers, a low median in-tratumoral pO2 was found by multivariate analysisto be a statistically significant prognostic factor forpoor survival and for relapse, independent of tumorstage [41,42]. Moreover, surgically treated patientswith hypoxic tumors had a worse survival and morefrequent occult parametrial and lymph-vascularspace involvement compared with patients withnon-hypoxic tumors. This would, at least, suggestthat hypoxia is a marker for a biologically moreaggressive tumor.
Perhaps of more significance is the observa-tion that tumor microenvironmental factors, includ-ing hypoxia, may influence cell cycle checkpointsand mutational rates that may lead to progressiontowards more malignant phenotypes [43]. Of rel-evance to the influence of hypoxia on tumor pro-gression in cervix cancer is the observation thathypoxia induces p53, which then triggers apopto-sis. In cervix cancer specimens, areas of hypoxiaand areas of spontaneous apoptosis co-localize[44]. Experimentally, successive rounds of hypoxiaselect for p53 mutant cells in mixed cell popula-tions, which correlate with progressive decline inapoptotic potential [45,46]. In a small series of pa-tients treated surgically for cervix cancer, Hockel etal. reported that poor survival and disease recur-rence correlated with tumors that were both hyp-oxic and had a low apoptotic index [47]. Thiswould add to mounting evidence that suggests thatgenetic instability is induced by hypoxia; such se-lection pressures due to tumor microenvironmentmay lead to the evolution of clonal variants withincreasingly more malignant phenotypes.
A number of clinical trials have attempted toimprove the outcome of radiotherapy by circum-venting the radioprotective and tumor-promotingeffects of hypoxia. In addition to the previouslymentioned use of hyperbaric oxygen in conjunctionwith radiotherapy, these approaches have includedhigh LET irradiation [48], hypoxic cell radiationsensitizers such as misonidazole [49], perfluoro-chemical emulsions [50], and most notably, che-motherapy selectively toxic toward hypoxic cells[51]. Overgaard and Horsman have published ameta-analysis of more than 10,000 patients enteredin 83 randomized trials testing hypoxia-directed ad-junctive therapies with radiotherapy [52]. Overall,this analysis showed that hypoxia-directed adjunc-tive therapies resulted in significantly improved lo-coregional tumor control with an odds ratio of 1.21(95% confidence interval of 1.12 to 1.30). To date,these investigational strategies have been associ-ated with less striking success for cervix cancer.
208 Roberts et al.: Mitomycin C and Radiotherapy for Cervix Cancer

The concept of bioreductive alkylation as analternative approach to the problem of hypoxiccells was suggested by Sartorelli et al. in 1972 [53].These investigators have sought to develop chemo-therapeutic agents that, by virtue of their chemicaland metabolic properties, would be selectivelytoxic to hypoxic cells. It was felt that hypoxic cellswould be more likely than their normally well-oxygenated counterparts to exist in an environmentconducive to reductive reactions and that this char-acteristic could be exploited to develop prodrugsthat became cytotoxic after reductive activation.These considerations have led to an extensive in-vestigation of the properties of mitomycin C in thelaboratories of Drs. Rockwell and Sartorelli, whichultimately showed that mitomycin C was preferen-tially cytotoxic to hypoxic cells vs. well-oxygenated cells both in vitro and in animal tumormodels [51,54,55].
Simultaneously, in the clinic, mitomycin Chas been well established as an efficacious adjunctto radiotherapy in the treatment of head and neckcancer, esophageal cancer, and anal cancer [56–60]. Often times, 5-fluorouracil has been a compo-nent of these combined modality programs. Wheth-er or not mitomycin C in conjunction withradiotherapy for cervix cancer offers a therapeuticgain has come under question [61–63]. This articlepresents an early report of a randomized study de-signed to study mitomycin C alone as an adjunct toradical radiotherapy of cervix cancer.
MATERIALS AND METHODS
Location of Study
The Department of Therapeutic Radiology at theYale University School of Medicine has enjoyed along collaboration with the Radiotherapy andNuclear Medicine Service of the Central Universityof Venezuela. The high incidence of cervix cancerand the availability of high-quality radiotherapy inCaracas, Venezuela, has provided a unique oppor-tunity to conduct this ongoing randomized trial ofmitomycin C as an adjunct to radiotherapy of cer-vical carcinoma. Radiotherapeutic practices and re-sults for the past quarter-century have been com-parable in the United States and Venezuela [64–66].
The treatment protocol was reviewed and ap-proved by the Yale Human Investigation Commit-tee (IRB). Patients diagnosed with squamous-cellcarcinoma of the cervix and to be treated with stan-dard radical radiotherapy at the Departments of Ra-diotherapy and Gynecology at the University Hos-pital of Caracas, the Domingo Luciani Hospital,
and La Floresta Medical Institute were eligible forthis study. After meeting entrance criteria for en-rollment and providing informed consent, patientswere randomized by the Yale Tumor Registry andallocated to the various treatment schemes as de-scribed below. Case report forms of enrolled pa-tients with details of patient status, tumor control,and toxicities during treatment and follow-up wereforwarded to the Yale Tumor Registry and enteredinto a computerized databank at Yale, facilitatingstatistical analysis.
Patient Selection
Patients with biopsy-proven squamous-cell carci-noma of the uterine cervix were eligible for thestudy. Additional diagnostic procedures includedhistory and physical exam, including pelvic exami-nation done by two experienced physicians (oneradiation oncologist and one gynecologist). Patientsunderwent routine blood studies including com-plete blood count, platelet count, BUN, creatinineand liver function studies, as well as chest x-ray,intravenous pyelogram, cystoscopy, and transab-dominal ultrasound. Given the limitations on medi-cal resources in Venezuela, examination under an-esthesia prior to treatment was not performedroutinely. Likewise, CT scans were not routinelycarried out.
Patients were considered eligible for the studyif they fell into the FIGO stage IB2, IIA, IIB, IIIA,IIIB, or IVA categories. Patients were excludedfrom the study for any of the following reasons:
1. Histologic-type small cell, adenosquamous car-cinoma, or adenocarcinoma.
2. History of other malignancies known to be ac-tive in the past five years, other than basal cellcarcinomas of the skin outside the planned ra-diation.
3. Prior radiation therapy in areas that would nor-mally be treated for the present disease and/orany chemotherapy within the preceding fiveyears.
4. Age <20, >76.5. The presence of gastrointestinal disease such as
Crohn’s disease, ulcerative colitis, or acute di-verticulitis.
6. Hepatic or renal dysfunction defined as biliru-bin >2.0 mg/dl, transaminases >1.5 times nor-mal, history of alcoholic cirrhosis, BUN >40mg/dl, or creatinine >2.0 mg/dl.
7. Hematopoietic depression defined by hemato-crit <30%, WBC <3,000/ml, or platelet count<100,000/ml.
8. Inability to provide informed consent.
Roberts et al.: Mitomycin C and Radiotherapy for Cervix Cancer 209

Treatment
Radiation TherapyThe guidelines for radiotherapy regimens in thistrial are derived from Dr. Raul Vera’s “NationalPlan,” introduced in Venezuela in 1973 [64]. Treat-ment schedules and doses are linked to local dis-ease extent or stage:
● Stage IB2–“early” IIB: External beam radio-therapy (whole pelvis, 40 Gy in 4 weeks) fol-lowed by intracavitary radiation × 2 (2,250–2,500 mgRaeq-hr per brachytherapy).
● Stage IIB: External beam radiotherapy (wholepelvis, 40 Gy in 4 weeks) followed by intracavi-tary radiation × 2 (2,250–2,500 mgRaeq-hr), fol-lowed by parametrial boost for 10 Gy.
● Stage III–IVA, without parametrial extension:External beam radiotherapy (whole pelvis, 46Gy in 41⁄2 weeks) followed by intracavitary ra-diation × 2 (2,000–2,250 mgRaeq-hr).
● Stage III–IVA, with parametrial extension: Ex-ternal beam radiotherapy (whole pelvis, 46 Gy in41⁄2 weeks) followed by intracavitary radiation ×2 (2,000–2,250 mgRaeq-hr), followed by para-metrial boost for 8–10 Gy.
Dose per fraction was 2.0 Gy. External beamradiotherapy was performed with megavoltageequipment, using a 4-field box technique. Superiorand inferior borders were defined by the L4/L5interspace and the ischial tuberosities, respectively.Lateral fields encompassed the pubic symphysisanteriorly and the sacrum posteriorly. Brachy-therapy utilized Hensche applicators and Cs- 137sources, using standard low-dose rate techniques.
Drug TreatmentPatients randomized to receive mitomycin C weregiven the drug at a dose of 15 mg/M2 on the firstFriday during the first week of external beam ra-diation therapy. A second dose of mitomycin C,15 mg/M2 was given six weeks following the firstdose (or on the day following the removal of anintracavitary implant should the six-week intervaloverlap with an intracavitary treatment). The drugwas administered at least one-half hour followingany external beam radiation therapy treatment.
Study Parameters and Follow-upPatients were observed carefully during treatmentand follow-up for skin, mucosal, gastrointestinal,urinary tract, and hematologic reactions and for tu-mor response and recurrence. The treatment reac-tions including myelosuppression were graded us-ing standard ECOG-RTOG-EORTC scoringcriteria [67]. Clinical evaluation, which at a mini-
mum included pelvic examination and CBC, oc-curred weekly during therapy and at three-monthintervals following completion of therapy for threeyears, then every six months thereafter. Other testsand biopsies were performed as clinically indi-cated.
Modification of Treatment ProtocolPatients received a second dose of mitomycin C,with the dose modified under the following circum-stances:
● WBC 2,000–4,000/ml (granulocyte count>1,500/ml) and/or platelet count 50–75,000/ml—reduction of drug dose by 50%.
● WBC 2,000–4,000/ml (granulocyte count 1,000–1,500/ml)—reduction of drug dose by 75%.
● If > grade II hematopoietic toxicity was ob-served (i.e., WBC <2,000/ml, granulocyte count<1,000/ml, or platelets <50,000/ml), the seconddose of drug was not administered.
● If any grade III or IV toxicity was present at thetime of scheduled administration of the seconddose of drug, the drug was not administered.
Statistical Design and Methods
Initial statistical considerations indicated that asample size of 83 to 95 patients for each groupwould be required to detect a 20% difference infive-year survival using a one-tailed test with analpha4 0.05 and with a power of 0.80. With theinterim analysis presented herein not yet showing astatistically significant improvement in survival,this trial has a goal of accruing 300 patients, pend-ing our next interim analysis scheduled in mid-2000. This trial size would be sufficient to detect a15% difference in survival using an alpha4 0.05with a power of 0.80.
Prior to randomization, patients were stratifiedaccording to hospital of treatment (University Hos-pital of Caracas, Hospital Domingo-Luciani, or LaFloresta Medical Institute) as well as by treatmentscheme as dictated by stage, as previously de-scribed. Patients were then allocated by a computeralgorithm to receive either radiation alone (stan-dard therapy) or radiation with mitomycin C, usinga biased coin randomization scheme [68] to ensurebalance among strata by stage. Case report formswere kept with the patient’s chart and were updatedregularly at each treatment or follow-up visit. Pe-riodically, copies of case report forms were for-warded to the Yale Tumor Registry to allow patient
210 Roberts et al.: Mitomycin C and Radiotherapy for Cervix Cancer

baseline, treatment, and follow-up data to be en-tered into a computerized database.
Statistical tabulations and tests were per-formed using commercially available computerprograms (i.e., PRODAS—Professional DatabaseAnalysis System) and BMDP statistical software.Comparisons between treatment groups with re-spect to baseline characteristics were tested for sig-nificance with the contingency tablex2 test for cat-egorical factors and thet-test for continuousfactors. The major outcome measured was survival,however, disease-free survival as well as local anddistant recurrence-free survival were also analyzed.Survival and recurrence-free survival at one-yearintervals were estimated by standard life table ac-tuarial methods. Statistical comparisons betweenthe two treatment groups with respect to survivor-ship were made using the Mantel & Haenszelx2
test. Since baseline characteristics were wellmatched between the treatment groups, a full mul-tivariate analysis (e.g., the Cox life table regressionmethod [69]) was not performed for this interimanalysis. Future analyses, however, will use suchmultivariate statistical tests to control for stratifica-tion factors and other factors, such as age, Hgblevel, total duration of treatment, and so on, whichmay be of prognostic significance. Nevertheless, alimited multivariate analysis, not detailed in thisreport, did show that treatment hospital was not asignificant determinant in patient outcome. Strati-fication groups were consolidated to yield a sub-group analysis by radiation treatment prescription,which is linked to patient stage.
RESULTSAs of March 1999, 212 patients were enrolled inthis randomized trial. At the time of our presentinterim analysis, performed in February 1999, 174patients had at least one and one-half years of po-tential follow-up. Fourteen patients were excludedfor protocol violations, for such reasons as refusalor inability to undergo prescribed brachytherapy (n4 8), improper registration evidenced by distantmetastasis diagnosed at initiation of treatment (n44), and treatment information missing at time ofstatistical analysis (n4 2). Excluded patients num-bered eight in the radiotherapy alone group and sixin the radiotherapy plus mitomycin C group, leav-ing 82 and 78 analyzable patients in the two re-spective treatment groups. Baseline characteristicsof these 160 patients are depicted in Table 1. The78 patients in the mitomycin C group and 82 pa-tients in the radiotherapy alone group have a meanfollow-up of 46.1 months, with a comparable dis-tribution by age (mean of 48 years), by stage (stage
IB2 3%, IIA 11%, IIB 48%, IIIA 1%, IIIB 36%,IVA 3%), and by stratification factors. Table 2 liststhe mean radiation doses delivered, broken downby treatment strata. Similar radiation treatmentswere delivered to both groups.
Toxicity
There were no treatment-related deaths. Not unex-pectedly, hematologic toxicity was limited to thosepatients in the group that received mitomycin C,but was relatively low in severity, as shown inTable 3. Nine patients experienced grade 3 whiteblood cell nadirs, defined as counts between 1,000to 2,000 perml (granulocyte count 500 to 1,000/ml). There were no white blood cell count nadirsless than 1,000/ml, granulocyte counts below 500/ml, or episodes of sepsis. Grade 3 thrombocytope-nia, defined as a nadir platelet count between25,000 and 50,000/ml, occurred in two patients.One additional patient experienced a grade 4thrombocytopenia with a platelet count transientlybelow 25,000/ml, without a bleeding diathesis. All78 patients in the radiotherapy plus mitomycin Ctreatment group received two cycles of chemo-therapy six weeks apart, although 11 patients re-quired a 50% reduction in mitomycin C dosage dueto low nadir blood counts after the first cycle, asspecified in the treatment protocol.
Acute non-hematologic toxicity is summa-rized in Table 4. There were no appreciable differ-ences between the two treatment groups in terms ofcystitis, proctitis, diarrhea, or skin reactions duringradiotherapy or in the immediate follow-up period.One patient who received mitomycin C experi-enced a transient skin reaction at an intravenousaccess site due to inadvertent chemotherapy ex-
Table 1. Patient Characteristics
RT(n 4 82)
RT + mito(n 4 78)
Total(n 4 160)
StageIB2 3 (4%) 1 (1%) 4 (2.5%)IIA 7 (9%) 10 (13%) 17 (11%)IIB 41 (50%) 36 (46%) 77 (48%)IIIA 0 (0%) 1 (1%) 1 (1%)IIIB 29 (35%) 28 (34%) 57 (36%)IVA 2 (2%) 2 (3%) 4 (2.5%)
RT schedule40 Gy 12 (15%) 14 (18%) 26 (15%)40 Gy, parametrial
boost 39 (48%) 33 (42%) 72 (45%)46 Gy 0 (0%) 2 (3%) 2 (1%)46 Gy, parametrial
boost 31 (38%) 29 (37%) 60 (38%)Mean Age (years) 48.5 47.5 48.0
RT 4 radiotherapy, mito4 mitomycin C.
Roberts et al.: Mitomycin C and Radiotherapy for Cervix Cancer 211
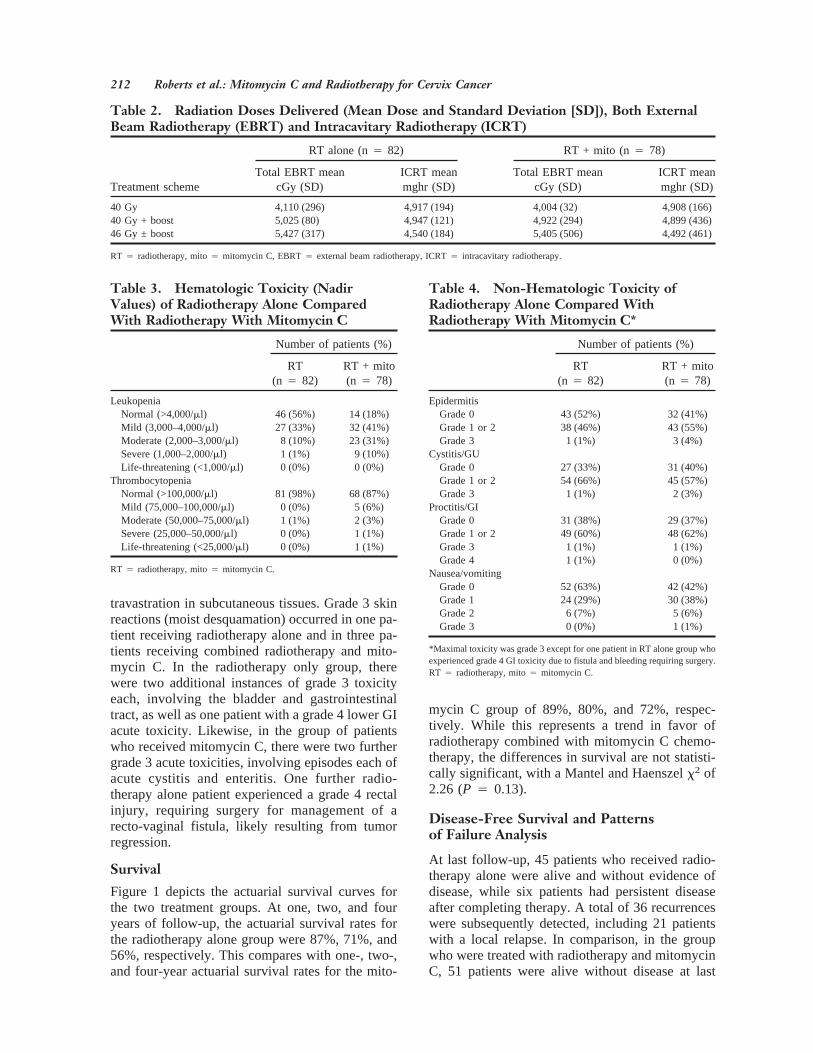
travastration in subcutaneous tissues. Grade 3 skinreactions (moist desquamation) occurred in one pa-tient receiving radiotherapy alone and in three pa-tients receiving combined radiotherapy and mito-mycin C. In the radiotherapy only group, therewere two additional instances of grade 3 toxicityeach, involving the bladder and gastrointestinaltract, as well as one patient with a grade 4 lower GIacute toxicity. Likewise, in the group of patientswho received mitomycin C, there were two furthergrade 3 acute toxicities, involving episodes each ofacute cystitis and enteritis. One further radio-therapy alone patient experienced a grade 4 rectalinjury, requiring surgery for management of arecto-vaginal fistula, likely resulting from tumorregression.
Survival
Figure 1 depicts the actuarial survival curves forthe two treatment groups. At one, two, and fouryears of follow-up, the actuarial survival rates forthe radiotherapy alone group were 87%, 71%, and56%, respectively. This compares with one-, two-,and four-year actuarial survival rates for the mito-
mycin C group of 89%, 80%, and 72%, respec-tively. While this represents a trend in favor ofradiotherapy combined with mitomycin C chemo-therapy, the differences in survival are not statisti-cally significant, with a Mantel and Haenszelx2 of2.26 (P 4 0.13).
Disease-Free Survival and Patternsof Failure Analysis
At last follow-up, 45 patients who received radio-therapy alone were alive and without evidence ofdisease, while six patients had persistent diseaseafter completing therapy. A total of 36 recurrenceswere subsequently detected, including 21 patientswith a local relapse. In comparison, in the groupwho were treated with radiotherapy and mitomycinC, 51 patients were alive without disease at last
Table 2. Radiation Doses Delivered (Mean Dose and Standard Deviation [SD]), Both ExternalBeam Radiotherapy (EBRT) and Intracavitary Radiotherapy (ICRT)
Treatment scheme
RT alone (n4 82) RT + mito (n4 78)
Total EBRT meancGy (SD)
ICRT meanmghr (SD)
Total EBRT meancGy (SD)
ICRT meanmghr (SD)
40 Gy 4,110 (296) 4,917 (194) 4,004 (32) 4,908 (166)40 Gy + boost 5,025 (80) 4,947 (121) 4,922 (294) 4,899 (436)46 Gy ± boost 5,427 (317) 4,540 (184) 5,405 (506) 4,492 (461)
RT 4 radiotherapy, mito4 mitomycin C, EBRT4 external beam radiotherapy, ICRT4 intracavitary radiotherapy.
Table 3. Hematologic Toxicity (NadirValues) of Radiotherapy Alone ComparedWith Radiotherapy With Mitomycin C
Number of patients (%)
RT(n 4 82)
RT + mito(n 4 78)
LeukopeniaNormal (>4,000/ml) 46 (56%) 14 (18%)Mild (3,000–4,000/ml) 27 (33%) 32 (41%)Moderate (2,000–3,000/ml) 8 (10%) 23 (31%)Severe (1,000–2,000/ml) 1 (1%) 9 (10%)Life-threatening (<1,000/ml) 0 (0%) 0 (0%)
ThrombocytopeniaNormal (>100,000/ml) 81 (98%) 68 (87%)Mild (75,000–100,000/ml) 0 (0%) 5 (6%)Moderate (50,000–75,000/ml) 1 (1%) 2 (3%)Severe (25,000–50,000/ml) 0 (0%) 1 (1%)Life-threatening (<25,000/ml) 0 (0%) 1 (1%)
RT 4 radiotherapy, mito4 mitomycin C.
Table 4. Non-Hematologic Toxicity ofRadiotherapy Alone Compared WithRadiotherapy With Mitomycin C*
Number of patients (%)
RT(n 4 82)
RT + mito(n 4 78)
EpidermitisGrade 0 43 (52%) 32 (41%)Grade 1 or 2 38 (46%) 43 (55%)Grade 3 1 (1%) 3 (4%)
Cystitis/GUGrade 0 27 (33%) 31 (40%)Grade 1 or 2 54 (66%) 45 (57%)Grade 3 1 (1%) 2 (3%)
Proctitis/GIGrade 0 31 (38%) 29 (37%)Grade 1 or 2 49 (60%) 48 (62%)Grade 3 1 (1%) 1 (1%)Grade 4 1 (1%) 0 (0%)
Nausea/vomitingGrade 0 52 (63%) 42 (42%)Grade 1 24 (29%) 30 (38%)Grade 2 6 (7%) 5 (6%)Grade 3 0 (0%) 1 (1%)
*Maximal toxicity was grade 3 except for one patient in RT alone group whoexperienced grade 4 GI toxicity due to fistula and bleeding requiring surgery.RT 4 radiotherapy, mito4 mitomycin C.
212 Roberts et al.: Mitomycin C and Radiotherapy for Cervix Cancer

follow-up, with eight patients having persistent lo-cal disease. An additional 16 patients experienced asubsequent recurrence, of which nine were localrelapses. Figure 2 shows the actuarial disease-freesurvival curves for the two treatment groups. Atone, two, and four years of follow-up, the actuarialdisease-free survival rates for the radiotherapyalone group were 77%, 55%, and 44%, respec-tively. This compares with one-, two-, and four-year actuarial disease-free survival rates for the mi-tomycin C group of 84%, 77%, and 70%,respectively. These differences are statistically sig-nificant, with a Mantel and Haenszelx2 of 6.72(P 4 0.01).
On follow-up, recurrence patterns were cat-egorized by either local or distant failure, allowingfor an actuarial analysis of local and distant recur-rence-free survival. At one, two, and four years of
follow-up, the actuarial local recurrence-free sur-vival rates for the radiotherapy alone group were80%, 65%, and 63%, respectively. This compareswith one-, two-, and three-year actuarial survivalrates for the mitomycin C group of 84%, 78%, and78%, respectively. While this represents a trend infavor of radiotherapy combined with mitomycin Cchemotherapy, the differences in local recurrence-free survival are not statistically significant(P 4 0.11). At one, two, and four years of follow-up, the actuarial distant recurrence-free survivalrates for the radiotherapy alone group were 91%,77%, and 61%, compared with 97%, 92%, and85%, respectively for the mitomycin C group.These differences reach statistical significance witha x2 4 6.77, P 4 0.01. Of note, this analysis ofdistant recurrence does not censor patients with lo-cal recurrences.
Fig. 1. Actuarial overall survival (±standard error), p4 0.13.
Roberts et al.: Mitomycin C and Radiotherapy for Cervix Cancer 213

Subset Analysis by RadiationPrescription and Disease Stage
With patients in this trial assigned to and stratifiedby a specific radiation prescription based on dis-ease stage, a limited subgroup analysis to assess theimpact of disease stage is possible. Patients areassigned to one of four radiation prescriptions asdescribed above. Only two patients were assigned
to the radiation prescription of 46 Gy whole pelvicexternal beam radiotherapy without a parametrialboost. This is not surprising, since it is rare forstage IIIA–IVA disease not to have significantparametrial extension that would prompt one to ad-minister a parametrial boost. Thus, these two pa-tients were combined with the other stage III–IVApatients whose teletherapy entailed 46 Gy plus apelvic sidewall boost. Table 5 details the distribu-
Table 5. Subgroup Analysis, Distribution of Patients by Stage Within Each Treatment Stratum
Strata (radiation prescription)
Stage of disease/number of patients
IB2 IIA IIB IIIA IIIB IVA
40 Gy 4 16 6 — — —40 Gy + parametrial boost — 1 71 — — —46 Gy ± parametrial boost — — — 1 57 4
Fig. 2. Actuarial disease-free survival (±standard error), p4 0.01.
214 Roberts et al.: Mitomycin C and Radiotherapy for Cervix Cancer
tion of patients in each of the three strata, sepa-rately analyzed. Strata 1 is a group of 26 stageIB–“early” IIB patients treated with 40 Gy externalbeam radiotherapy and brachytherapy, with orwithout mitomycin C. Early stage IIB is taken tomean minimal or proximal parametrial involve-ment. The 72 patients in strata 2 are essentially agroup of stage IIB patients whose radiotherapy in-cluded an appropriate parametrial boost, with orwithout mitomycin C. Strata 3 comprises 62 pa-tients predominantly with stage IIIB disease treatedwith 45 Gy external beam radiotherapy, parametrialboost (in all but two patients), and brachytherapy,with or without mitomycin C.
The disease-free survival analysis of strata 1does suggest a trend favoring treatment with mito-mycin C but without statistically significant differ-ences. At one, two, and four years, the disease-freesurvival rates for strata 1 patients treated with ra-
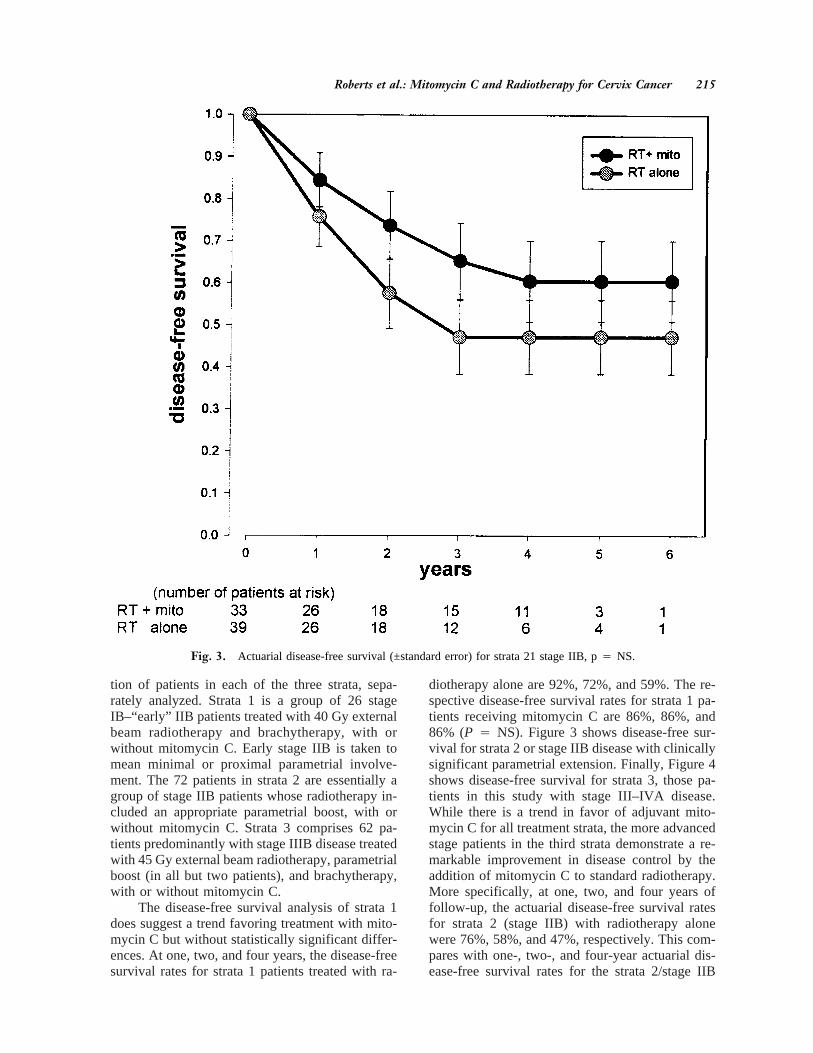
diotherapy alone are 92%, 72%, and 59%. The re-spective disease-free survival rates for strata 1 pa-tients receiving mitomycin C are 86%, 86%, and86% (P 4 NS). Figure 3 shows disease-free sur-vival for strata 2 or stage IIB disease with clinicallysignificant parametrial extension. Finally, Figure 4shows disease-free survival for strata 3, those pa-tients in this study with stage III–IVA disease.While there is a trend in favor of adjuvant mito-mycin C for all treatment strata, the more advancedstage patients in the third strata demonstrate a re-markable improvement in disease control by theaddition of mitomycin C to standard radiotherapy.More specifically, at one, two, and four years offollow-up, the actuarial disease-free survival ratesfor strata 2 (stage IIB) with radiotherapy alonewere 76%, 58%, and 47%, respectively. This com-pares with one-, two-, and four-year actuarial dis-ease-free survival rates for the strata 2/stage IIB
Fig. 3. Actuarial disease-free survival (±standard error) for strata 21 stage IIB, p4 NS.
Roberts et al.: Mitomycin C and Radiotherapy for Cervix Cancer 215

group who received mitomycin C of 84%, 74%,and 60%, respectively (P 4 NS). For strata 3/stageIII–IVA disease, the actuarial disease-free survivalrates with radiotherapy alone at one, two, and fouryears of follow-up were 73%, 46%, and 35%, re-spectively. With the addition of mitomycin C, theone-, two-, and four-year actuarial disease-free sur-vival rates for the stage III–IVA patients were sig-nificantly improved, at 83%, 75%, and 75%, re-spectively (Mantel and Haenszelx2 of 4.65,P 4 0.03).
DISCUSSION
This randomized trial of radiotherapy alone com-pared with mitomycin C with radiotherapy for lo-cally advanced cervix cancer continues to accruepatients and additional follow-up. The hypothesis
that tumor hypoxia—a significant prognostic factorin cervix cancer, a promoter of genetic instability,and a source of radioresistance—can be targetedwith bioreductive alkylating agents to achieve atherapeutic gain when administered with radio-therapy remains worthy of clinical investigation.We remain cautiously optimistic that mitomycin Cis a beneficial adjunct to radiotherapy based onthese preliminary, but strong, results.
First, the trial is successfully enrolling patientswith a high quality of patient care and follow-up.As such, this clinical study demonstrates the feasi-bility of international collaboration between aca-demic centers. Despite the significant differences inmedical resources available in the United Statesand Venezuela, this trial utilizes standard mega-voltage equipment and techniques for external
Fig. 4. Actuarial disease-free survival for strata 31 stage III–IVA, p4 0.03.
216 Roberts et al.: Mitomycin C and Radiotherapy for Cervix Cancer

beam radiotherapy. Low-dose-rate brachytherapy isdelivered in two fractions using Henschke-type ap-plicators and afterloaded Cesium-137 sources, withradiation dose prescriptions similar to practice inthe United States. Although high-dose-rate brachy-therapy is available in Caracas, we felt that it wouldbe a confounding treatment variable for the pur-poses of this trial. It needs to be emphasized thatthe published clinical results of radical radio-therapy for cervix cancer in Venezuela under itsNational Plan are as good as those reported any-where [3–10,64,66]. The differences in staging pro-cedures (with examination under anesthesia and CTscanning being infrequent in Venezuela) could cer-tainly cause some small differences in stage allo-cation relative to other published studies. One mustremember that both pelvic examination and CTscanning have their own considerable inaccuracies[70]. Any potential understaging in this trial wouldonly serve to bias against finding differences be-tween the two treatment groups, with both groupsbeing equally confounded by the inclusion of smallnumbers of patients with occult metastatic disease.Because this is a randomized study, any positiveinferences from our results would still be appli-cable to oncologic practice in the United States andelsewhere. In addition, although economic data arenot shown, this trial is demonstrating that sponsor-ship of high-quality clinical trials in oncology out-side of the United States not only is feasible butalso can be accomplished at significantly lowercost than is possible in the United States.
Second, the toxicity of combining mitomycinC at 15 mg/M2 for two doses six weeks apart withradiotherapy in the treatment of locally advancedcervix cancer thus far has been minimal. Therehave been no treatment-related deaths. Hemato-logic toxicity is mild. Most important, we haveseen no significant enhancement of either acute orlate radiation reactions. Clearly, continued follow-up will be required to definitively characterize thelate reactions in the patients in this trial.
Third, there is a trend in favor of the patientswho received mitomycin C in both survival andlocal recurrence-free survival. The differences havenot reached statistical significance, but this trial isstill ongoing and has not as yet met its accrual andfollow-up goals. Differences favoring mitomycin Cduring radiotherapy for disease-free and distant re-currence-free survival do reach statistical signifi-cance. Moreover, our trial is showing a particularbenefit for stage III–IVA patients, a subgroup in theRTOG 90-01 trial that did not seem to benefit fromthe concurrent 5-fluorouracil/cisplatinum strategy[23]. Since concurrent cisplatinum chemotherapy is
not as yet considered a standard therapy throughoutVenezuela, in part due to economic constraints, wefeel it remains ethically justified to complete thistrial.
Concomitant chemotherapy and radiotherapyis a broad strategy worthy of further investigation[11,71]. Clues of its potential impact can be seenfrom improvements in the treatment of other solidtumors, such as anal carcinoma, esophageal carci-noma, and head and neck cancers. A particularlyrelevant strategy pioneered here at Yale has beenthe combination of bioreductive alkylating agentswith radiotherapy [51]. The underlying concept isthe use of drugs such as mitomycin C to kill hyp-oxic tumor cells, which might otherwise surviveradiotherapy and be a nidus for recurrence andwhich may be biologically more aggressive thanthe original primary tumor. Mitomycin C does notsensitize cells to the effects of ionizing radiation.The mechanism of action involves an intracellularenzyme-dependent reduction of its quinone moiety,yielding reactive species capable of forming DNAcross-links and monoadducts. The enzymatic re-duction of mitomycin C and other bioreductive al-kylating agents such as porfiromycin is enhancedunder hypoxic and acidic conditions. As a result,both the number and severity of DNA lesions aregreater in hypoxic cells than in aerobic cells. Con-sequently, these drugs are more toxic to hypoxiccells than to cells under normal physiologic condi-tions. In the laboratory, murine experiments havesuggested improved tumor control by the additionof bioreductive alkylating agents to radiotherapy.
Improvements in the treatment of anal andesophageal cancer have been demonstrated by mi-tomycin C/5-fluorouracil chemotherapy with con-current radiotherapy [56–58]. Retrospective datafrom the Princess Margaret Hospital suggest thatdeletion of mitomycin C from the combined mo-dality therapy of anal carcinoma is deleterious [57].Results from an Intergroup randomized study ofanal cancer confirm the observation that the addi-tion of mitomycin C to radiotherapy and 5-fluoro-uracil is of statistically significant benefit, as evi-denced by an improvement from 51% to 73% indisease-free survival at four years as well as animprovement in colostomy- free survival rates from59% to 71% [58].
A series of randomized head and neck cancertrials at Yale has shown improved disease-free sur-vival with the addition of mitomycin C to standardradiotherapy [59,60,72]. From 1980–1992, 195 pa-tients with biopsy- proven squamous-cell carci-noma of the oral cavity, oropharynx, larynx, hypo-pharynx, and nasopharynx were randomly assigned
Roberts et al.: Mitomycin C and Radiotherapy for Cervix Cancer 217

to receive or not to receive mitomycin C. Patientswere stratified into groups for pre-operative radia-tion therapy, post-operative radiation therapy, andprimary radiation therapy. All patients randomizedto receive mitomycin C were given the drug intra-venously at a dose of 15 mg/M2 following irradia-tion on the fifth day of the radiation therapy course.Patients receiving radiation in doses in excess of5,600 cGy received a second course of mitomycinC, 15 mg/M2, six weeks later. At five years offollow-up, comparison of the 91 patients in the mi-tomycin C group with the 104 patients in the no-drug group showed a statistically significant benefitwith mitomycin C in terms of cause-specific sur-vival (74% vs. 51%,P 4 0.005), local recurrence-free survival (85% vs. 66%,P 4 0.002), and localregional recurrence-free survival (76% vs. 54%,P4 0.03). There was a trend toward improved dis-tant metastasis-free survival (88% vs. 79%) and nodifference in overall survival (48% vs. 42%), re-flecting the high rates of death due to intercurrentillness in this patient population. Hematologic tox-icities were frequent but at an acceptable level ofseverity in the mitomycin C group, with no drug-related deaths. Of equal importance, no significantdifferences were observed in acute or chronic non-hematologic radiation reactions with and withoutdrug. The International Atomic Energy Commis-sion has initiated a large, international randomizedtrial to confirm these results, comparing mitomycinC with no drug, concurrent with standard primaryradiotherapy for head and neck cancer.
Based on the successful treatment of anal can-cer with radiation, 5-fluorouracil, and mitomycinC, there have been multiple phase I/II trials pub-lished for locally advanced cervix cancer using asimilar treatment strategy [63,73–80]. With trialdesigns lacking a randomization between experi-mental and control treatments and some with smallnumbers of patients, these reports are inconclusive,although comparisons with same institution histori-cal control populations have suggested improvedlocal control and perhaps survival.
Some of these studies do raise a cautionarynote in regards to toxicity [61–63]. The series fromthe Princess Margaret Hospital in Toronto de-scribed by Thomas includes sequential modifica-tions in treatment schemes, in which radiation frac-tionation was varied; mitomycin C was droppedfrom the chemotherapy program after mid-1985.The patients receiving both mitomycin C and 5-flu-orouracil experienced an unusually high degree ofserious bowel complications, particularly of therectosigmoid colon, 22% (17/78) compared with6.6% (8/122) in patients who received 5-FU with-
out mitomycin C (P 4 0.005 by multivariate analy-sis) [62,63]. The Toronto brachytherapy techniqueemployed in this series utilizes a single tandem(linear source) delivering 40 Gy to Point A, whichmay well be associated with high doses to the rec-tum. The external beam technique for cervix cancerin Toronto, post-1986, was modified to place amidline transmission filter over the PA field to re-duce dose to rectum; as reported, this resulted in a50% reduction in bowel toxicity. The study ofChristie et al. [61] also utilizes a linear brachy-therapy source (30 Gy to Point A). Of 64 patientstreated, 23 patients (36%) developed grade 3 or 4toxicity, with seven patients (11%) developing arectovaginal fistula. However, when the clinicaloutcome of these 64 patients treated with 5- fluo-rouracil, mitomycin C, and irradiation was com-pared with 29 patients receiving 5-fluorouracil andradiotherapy and to a third group of 84 patientsreceiving radiotherapy alone were analyzed usingmultivariate analysis, there was a statistically sig-nificant improvement in survival, relapse-free sur-vival, and local control in the patients receivingmitomycin C. For those treatment regimens wherebrachytherapy source geometry (e.g., tandem andovoid-type applicator) along with robust vaginalpackings to displace the rectum results in markedlydiminished rectal doses compared with the Torontotechnique reported by Thomas and updated by Ra-kovitch as well as by Christie [61–64], one wouldnot necessarily expect to see an enhanced toxicityfrom the addition of mitomycin C to standard ra-diotherapy. Indeed, the other cited studies do notreport significantly increased bowel toxicity. It ispossible that 5-fluorouracil in these combined mo-dality studies may be contributing to toxicity with-out improving the therapeutic ratio, since 5-fluoro-uracil is known to function as a nonspecificradiosensitizer, as well as a cytotoxic drug [81].Moreover, a subsequent Princess Margaret Hospitalrandomized four-arm trial examining the additionof 5-FU and altered radiation fractionation did notconvincingly show a benefit to 5-FU as a radiosen-sitizer in cervix cancer [26].
There have been two randomized studies re-ported that are designed to evaluate mitomycinC/5-fluorouracil concurrent with radiotherapy forcervix cancer. The first, published only in abstractform, was inconclusive because 63% of the patientsreceiving combined modality therapy were un-evaluable [82]. The second is a preliminary reportfrom Thailand of a study with a double randomiza-tion, resulting in four arms: radiotherapy alone; ra-diotherapy with concurrent mitomycin C 10 mg/M2
on days 1 and 30 along with oral 5-fluorouracil
218 Roberts et al.: Mitomycin C and Radiotherapy for Cervix Cancer

300mg qd on days 1–14 and 42–56; radiotherapyand subsequent maintenance oral 5-fluorouracil200 mg qd for four weeks every six weeks for atotal of three cycles; and radiotherapy with bothconcurrent and maintenance chemotherapy pro-grams [83]. With 673 patients enrolled in this trialand a median follow-up of 25 months, there was astrong trend in disease-free survival in favor ofthose patients receiving concurrent chemotherapy.At three years of follow-up, the actuarial disease-free survival for radiotherapy alone vs. radio-therapy with concurrent mitomycin C/5-fluorouracil was 48% vs. 73%, respectively,P 40.003. Local control was more noticeably improvedin stage IIB patients compared with stage IIIB pa-tients.
Recently, several large randomized multi-institutional clinical trials of cisplatinum-basedconcurrent chemotherapy have been reported orpublished [21–25]. On February 22,1999, the Na-tional Cancer Institute issued a “Clinical Alert”strongly suggesting that outside an investigativeprotocol, cisplatinum-based chemotherapy shouldbe administered concurrently with radiotherapy forcervix cancer. An important caveat of these studiesin comparison with our mitomycin C trial was thatpatients were more extensively selected and staged,especially as to the absence of para-aortic lymphnode metastases. The Gynecologic OncologyGroup’s contributions include three noteworthystudies. Keys et al. compared radiotherapy and ad-juvant hysterectomy with or without concurrentweekly cisplatinum chemotherapy in 369 patientswith stage IB2 disease [21]. Despite a relativelylow cumulative radiation prescription dose of 75Gy to Point A and the dubious role of adjuvantextrafascial hysterectomy after radiotherapy, therewas a statistically significant improvement in three-year survival for those patients receiving chemo-therapy, 83% compared with 74% for the controlgroup. Rose et al. published the results of a three-arm randomized study of 526 patients with stageIIB–IVA disease in which all received some formof chemoirradiation [22]. The three concurrent che-motherapy programs were hydroxyurea, weeklycisplatinum, and combined 5- fluorouracil, cisplati-num, and hydroxyurea. All patients underwent sur-gical staging to exclude extra-pelvic or para-aorticmetastatic disease. Almost half the patients hadstage IIIB–IVA disease. The prescribed total radia-tion dose to Point A was 81 Gy, although 13.5% ofpatients received less than 69 Gy. Nevertheless, thepatients who received either one of the two cisplati-num-based regimens experienced a statistically sig-nificant two- year progression-free survival (67%
and 64%) over those who received hydroxyurea(47%). Whitney et al. reported a randomized trialof 368 surgically staged patients that allocated pa-tients to concurrent chemotherapy with either hy-droxyurea or combined 5-fluorouracil and cisplati-num [24]. Twelve percent of patients did notreceive brachytherapy. There were minor imbal-ances in histology (squamous-cell carcinoma vs.adenocarcinoma) and pelvic nodal metastasis be-tween the two groups favoring those receiving hy-droxyurea. Regardless, on multivariate and one-tailed univariate statistical testing, there wassignificant albeit modest improvement in survivaland progression-free survival for those patients re-ceiving 5-fluorouracil/cisplatinum. The RadiationTherapy and Oncology Group has also publishedits randomized trial of 5-fluorouracil/cisplatinumconcurrent with pelvic radiotherapy compared withextended field (pelvic plus para-aortic) radio-therapy without chemotherapy in 388 patients [23].Slightly higher doses of radiotherapy were deliv-ered than in the GOG trials, with a Point A pre-scription dose of at least 85 Gy and an actual meandose to Point A dose of 89 Gy. There was a statis-tically significant benefit in terms of overall anddisease-free survival as well as local and distantrecurrence for the combined modality group but atthe cost of increased acute toxicity. Five-year sur-vival was 73% for chemoradiotherapy comparedwith 58% for extended field radiotherapy. Of note,this trial showed a preferential survival benefit forstage IB–IIB disease treated with concurrent cis-platinum and 5-fluorouracil, while there was nosurvival or disease-free survival demonstrated forstages III–IVA. There are two other small, random-ized trials of locally advanced cervix cancer testingcisplatinum-based concurrent chemotherapy thatdo not show a benefit of chemotherapy [84,85].
Our study is of further interest given the strik-ing results for distant recurrence-free survival andthe preferential benefit to stage III–IVA diseasecompared with earlier stage disease. Our originalhypothesis was that targeting hypoxia would be im-portant because hypoxia is a tumor-specific phe-nomenon and is a cause of radioresistance. Couldenhancement in local control without appreciablyaffecting normal tissue toxicity fully explain ourpreliminary findings? Perhaps, but mitomycin Calone would not be expected to have noticeableeffects on any microscopic metastatic disease thatwas present at time of therapy. Increasing experi-mental evidence points to the role of hypoxia inperturbing cell cycle checkpoints and promotinggenetic instability [43–46]. This raises the possibil-ity that by targeting hypoxic cells, we are also tar-
Roberts et al.: Mitomycin C and Radiotherapy for Cervix Cancer 219

geting a tumor subpopulation that has a more ag-gressive and malignant phenotype.
CONCLUSION
In summary, we report an interim analysis of aphase III, randomized trial testing the toxicity andefficacy of mitomycin C as an adjunct to radicalradiotherapy for squamous-cell carcinoma of thecervix. This trial is based on extensive preclinicalwork suggesting that bioreductive alkylating agentssuch as mitomycin C would potentially producetherapeutic gain by targeting hypoxic tumor cells,as well as on our clinical trials demonstrating im-provement in patients with head and neck cancers.Thus far, the addition of mitomycin C has beenwell tolerated, with mild hematologic toxicity andno enhancement of in-field radiation reactions.There is a trend in favor of the combination ofmitomycin C with radiotherapy as compared withradiotherapy alone in terms of both survival andlocal control, but these trends have not as yetreached statistical significance. Statistically signifi-cant benefit is, however, seen for disease-free sur-vival and distant recurrence-free survival. This trialcontinues to accrue patients and to continue follow-up for future analysis.
REFERENCES1. Parkin DM, Pisani P, Ferlay J. Global Cancer Statistics.
CA 1999;49(1):33–64.2. Landis SH, Murray T, Bolden S, Wingo PA. Cancer
Statistics 1999. CA 1999;49:8–31.3. Horiot JC, Pigneux J, Pourquier H, Schraub S, Achille
E, Keiling R, Combes P, Rozan, R, Vrousos C, Daly N.Radiotherapy alone in carcinoma of the intact uterinecervix according to G.H. Fletcher Guidelines: a FrenchCooperative Study of 1383 Cases. Int J Radiat OncolBiol Phys 1988;14:605–611.
4. Eifel PJ, Morris M, Wharton JT, Oswald MJ. The in-fluence of tumor size and morphology on the outcomeof patients with FIGO stage IB squamous cell carci-noma of the uterine cervix. Int J Radiat Oncol Biol Phys1994;29:9–16.
5. Perez CA, Grigsby PW, Nene SM, Camel HM, Galaka-tos A, Kao MS, Lockett MA. Effect of tumor size onthe prognosis of carcinoma of the uterine cervix treatedwith irradiation alone. Cancer 1992;69:2796–2806.
6. Logsdon MD, Eifel PJ. FIGO stage IIIB squamous cellcarcinoma of the uterine cervix: An analysis of prog-nostic factors emphasizing the balance between exter-nal beam and intracavitary radiation therapy. Int J Ra-diat Oncol Biol Phys 1999;43:763–775.
7. Kapp DS, Fischer DB, Gutierrez E, Kohorn EI,Schwartz PE. Pretreatment prognostic factors in carci-noma of the uterine cervix: a multivariate analysis ofthe effect of age, stage, histology, and blood counts onsurvival. Int J Radiat Oncol Biol Phys 1983;9:445–455.
8. Montana GS, Fowler WC, Varia LA, Walton LA, MackY. Analysis of results of radiation therapy for Stage IIcarcinoma of the cervix. Cancer 1985;55:956–962.
9. Montana GS, Fowler WC, Varia LA, Walton LA, MackY. Analysis of results of radiation therapy for Stage IBcarcinoma of the cervix. Cancer 1987;60:2195–2200.
10. Montana GS, Fowler WC, Varia LA, Walton LA, MackY, Shemanski L. Carcinoma of the cervix Stage III.Cancer 1986;57:148-154.
11. Tannock IF. Combined modality treatment with radio-therapy and chemotherapy. Radiother Oncol 1989;16:83–101.
12. Browman GP. Evidence-based recommendationsagainst neoadjuvant chemotherapy for routine manage-ment of patients with squamous cell head and neckcancer. Cancer Invest 1994;12(6):662–671.
13. Tannock IF, Browman G. Lack of evidence for a role ofchemotherapy in the routine management of locally ad-vanced head and neck cancer. J Clin Oncol 1986;4:1121–1126.
14. Pignon JP, Bourhis J, Domenge C, Designe L. (on be-half of the MACH-NC Collaborative Group). Chemo-therapy added to locoregional treatment for head andneck squamous-cell carcinoma: three meta-analyses ofupdated individual data. Lancet 2000;355:949–955.
15. Chauvergne J, Rohart J, Heron JF, Ayme Y, Berlie J,Fargeor P, George M, Lebrun-Jezekova D, Pigneux J,Chenal C. Essai randomise´ de chimothe´rapie initialedane 151 carcinomes du col ute´ria localement e´tendus(T2b-N1, T3b, M0). Bull Cancer (Paris) 1990;77:1007–1024.
16. Souhami L, Gil RA, Allan SE, Canary PC, Araujo CM,Pinto LH, Silveira TR. A randomized trial of chemo-therapy followed by pelvic radiation therapy in stageIIIB carcinoma of the cervix. J Clin Oncol 1991;9:970–977.
17. Sundfor K, Trope CG, Hogberg T, Onsrud M, Koern J,Simonsen E, Bertelsen K, Westberg R. Radiotherapyand neoadjuvant chemotherapy in cervical carcinoma: arandomized multicenter study of sequential cisplatinand 5-fluorouracil and radiotherapy in advanced cervi-cal carcinoma stage 3B and 4A. Cancer 1996;77(11):2371–2378.
18. Tattersall MHN, Lorvidhaya V, Vootiprux V, Cheir-silpa A, Wong F, Azhar T, Lee HP, Kang SB, ManaloA, Yen MS, Kampono N, Aziz F. Randomized trial ofepirubicin and cisplatin chemotherapy followed by pel-vic radiation in locally advanced cervical cancer. J ClinOncol 1995;13:444–451.
19. Leborgne F, Leborgne JH, Doldan R, Zubjzaretta E,Ortega B, Maisonneuve J, Musetti E, Hekimian L,Mezera J. Induction chemotherapy and radiotherapy ofadvanced cancer of the cervix: a pilot study and phaseIII randomized trial. Int J Radiat Oncol Biol Phys 1997;37:343–350.
20. Tattersall MHN, Ramirez C, Coppleson M. A random-ized trial comparing platinum-based chemotherapy fol-lowed by radiotherapy alone in patients with locallyadvanced cervical cancer. Int J Gynecol Cancer 1992;2:244–251.
220 Roberts et al.: Mitomycin C and Radiotherapy for Cervix Cancer

21. Keys HM, Bundy BN, Stehman FB, Muderspach LI,Chate WE, Suggs CL 3rd, Walker JL, Gersell D. Cis-platin, radiation, and adjuvant hysterectomy comparedwith radiation and adjuvant hysterectomy for bulkystage IB cervical carcinoma. N Engl J Med 1999;340:1154–1161.
22. Rose PG, Bundy BN, Watkins EB, Thigpen JT, DeppeG, Maiman MA, Clarke- Pearson DL, Insalaco S. Con-current cisplatin-based radiotherapy and chemotherapyfor locally advanced cervical cancer. N Engl J Med1999;340:1144–1153.
23. Morris M, Eifel PJ, Lu J, Grigsby PW, Levenback C,Stevens RE, Rotman M, Gershenson DM, Mutch DG.Pelvic radiation with concurrent chemotherapy com-pared with pelvic and para-aortic radiation for high-riskcervical cancer. N Engl J Med 1999;340:1137–1143.
24. Whitney CW, Sause W, Bundy BN, Malfetano JH,Hannigan EV, Fowler WC Jr, Clarke-Pearson DL, LiaoSY. Randomized comparison of fluorouracil plus cis-platin versus hydroxyurea as an adjunct to radiationtherapy in stages IIB–IVA carcinoma of the cervix withnegative para-aortic lymph nodes: a Gynecologic On-cology Group and Southwest Oncology Group study. JClin Oncol 1999;17:1339–1348.
25. Peters WA, Liu PY, Barrett R, Gordon W Jr, Stock R,Berek J, DiSaia PJ, Souhami L, Grigsby P, Alberts DS.Cisplatin, 5-fluorouracil plus radiation therapy are su-perior to radiation therapy as adjunctive in high-risk,early-stage carcinoma of the cervix after radical hys-terectomy and pelvic lymphadenectomy: report of aphase III inter-group study. Presented at the 30th An-nual Meeting of the Society of Gynecologic Oncolo-gists, San Francisco, March 20–24, 1999. (See http://www.sgo.org/meetings/30annual/abstracts).
26. Thomas G, Dembo A, Ackerman I, Franssen E, Ba-lough J, Fyles A, Levin W. A randomized trial of stan-dard versus partially hyperfractionated radiation with orwithout concurrent 5-fluorouracil in locally advancedcervical cancer. Gyn Oncol 1998;69:137–145.
27. Perez C, Kao M. Radiation therapy alone or combinedwith surgery in the treatment of barrel-shaped carci-noma of the uterine cervix (stage IB, IIA, IIB). Int JRadiat Oncol Biol Phys 1985;11:1903–1909.
28. Rutledge F, Wharton J, Fletcher G. Clinical studieswith adjunctive surgery and irradiation therapy in thetreatment of carcinoma of the cervix. Cancer 1975;38:596–602.
29. Weems D, Mendenhall W, Bova FJ, Marcus RB Jr,Morgan LS, Million RR. Carcinoma of the intact uter-ine cervix, Stage IB-IIA-B, >6 cm in diameter: irradia-tion alone vs. preoperative irradiation and surgery. Int JRadiat Oncol Biol Phys 1985;11:1911–1914.
30. Rockwell S, Moulder JE. Hypoxic fractions of humantumors xenografted into mice: a review. Int J RadiatOncol Biol Phys 1990;19:197–202.
31. Moulder JE, Rockwell S. Tumor hypoxia: its impact oncancer therapy. Cancer Metast Rev 1987;5:313–341.
32. Bergso P, Evans JC. Oxygen tension of cervical carci-noma during the early phase of external irradiation.Scand J Clin Lab Invest 1971;27:71–82.
33. Kolstad P. Intercapillary distance, oxygen tension andlocal recurrence in cervix cancer. Scand J Clin LabInvest [Suppl] 1968;106:145–157.
34. Sostman HD, Armitage IM, Fischer JJ. NMR in Cancer.I. High resolution spectroscopy of tumors. Magn ResonImaging 1984;2:265–278.
35. Urtasun RC, Chapman JD, Raleigh JA, Franko AJ,Koch C.J. Binding of3H-misonidazole to solid humantumors as a measure of tumor hypoxia. Int J RadiatOncol Biol Phys 1986;12:1263–1267.
36. Bush RS. The significance of anemia in clinical radia-tion therapy. Int J Radiat Oncol Biol Phys 1986;12:2047–2050.
37. Girinski T, Pejovic-Lenfant MH, Bourhis J, CampanaF, Cossett JM, Petit C, Malaise EP, Haie C, Gerbault A,Chassagne D. Prognostic value of hemoglobin concen-trations and blood transfusions in advanced carcinomaof the cervix treated by radiation therapy: results of aretrospective study of 386 patients. Int J Radiat OncolBiol Phys 1989;16:37–42.
38. Bush RS, Jenkin DT, Allt WE, Beale FA, Bean H,Dembo AJ, Pringle JF. Definitive evidence for hypoxiccells influencing cure in cancer therapy. Br J Cancer1978;37[Suppl III]:302–306.
39. Dische S, Anderson PJ, Sealy R, Watson ER. Carci-noma of the cervix—anaemia, radiotherapy and hyper-baric oxygen. Br J Radiol 1983;56:251–255.
40. Watson ER, Halnan KE, Dische S, Saunders MI, CadeIS, McEwen JB, Wiernik G, Perrins DJ, Sutherland I.Hyperbaric oxygen and radiotherapy: a Medical Re-search Council trial in carcinoma of the cervix. Br JRadiol 1978;51:879–887.
41. Hockel M, Schlenger K, Aral B, Mitze M, Scha¨ffer U,Vaupel P. Association between tumor hypoxia and ma-lignant progression in advanced cancer of the uterinecervix. Cancer Res 1996;56:4509–4515.
42. Tsang RW, Fyles AW, Milosevic M, Syed A, PintilieM, Levin W, Manchal LA. Interrelationship of prolif-eration and hypoxia in carcinoma of the cervix. Int JRadiat Oncol Biol Phys 2000;46:89–95.
43. Yuan J, Glazer PM. Mutagenesis induced by the tumormicroenvironment. Mutat Res 1998;400:439–446.
44. Kim CY, Tsai MH, Osmanian C, Calkins DP, GraeberTG, Greenspan DL, Kennedy AS, Rinker LH, VariaMA, DiPaolo JA, Peehl DM, Raleigh JA, Giaccia AJ.The role of hypoxia, p53 and apoptosis in human cer-vical carcinoma pathogenesis. Int J Radiat Oncol BiolPhys 1997;39(2):206 (abstr).
45. Graeber TG, Osmanian C, Jacks T, Housman DE, KochCJ, Lowe SW, Giaccia AJ. Hypoxia-mediated selectionof cells with diminished apoptotic potential in solidtumors. Nature 1996;379:88–91.
46. Kim CY, Tsai MH, Osmanian C, Graeber TG, Lee JE,Giffard RG, DiPaolo JA, Peehl DM, Giaccia AJ. Se-lection of human cervical epithelial cells that possessreduced apoptotic potential to low-oxygen conditions.Cancer Res 1997;57:4200–4204.
47. Hockel M, Schlenger K, Ho¨ckel S, Vaupel P. Hypoxiccervical cancers with low apoptotic index are highlyaggressive. Cancer Res 1999;59:4525–4528.
Roberts et al.: Mitomycin C and Radiotherapy for Cervix Cancer 221

48. Maor MH, Gillespie BW, Peters LJ, Wambersie A,Griffin TW, Thomas FJ, Cohen L, Conner N, GardnerP. Neutron therapy in cervical cancer: results of a phaseIII RTOG study. Int J Radiat Oncol Biol Phys 1988;14:885–891.
49. Overgaard J, Bentzen SM, Kolstad P, Kjoerstad K,Davy M, Bertelsen K, Mantyla M, Frankendal B, Skry-ten A, Loftquist I, Pedersen M, Sell A, Hammer R.Misonidazole combined with radiotherapy in the treat-ment of carcinoma of the uterine cervix. Int J RadiatOncol Biol Phys 1989;16:1069–1072.
50. Evans RG, Kimler BF, Morantz RA, Vats TS, GemerLS, Liston V, Lowe N. A phase I/II study of the use ofFluosolt as an adjuvant to radiation therapy in the treat-ment of primary high-grade brain tumors. Int J RadiatOncol Biol Phys 1990;19:415–420.
51. Rockwell S. Use of hypoxia-directed drugs in thetherapy of solid tumors. Sem Onc 1992;19(4 Suppl 11):29–40.
52. Overgaard J, Horsman MR. Modification of hypoxia-induced radioresistance in tumors by the use of oxygenand sensitizers. Semin Radiat Oncol 1996;6:10–21.
53. Lin AJ, Cosby LA, Shansky CW, Sartorelli AC. Poten-tial bioreductive alkylating agents: I. Benzoquinone de-rivatives. J Med Chem 1972;15:1247–1252.
54. Sartorelli A.C. Therapeutic attack of hypoxic cells ofsolid tumors: presidential address. Cancer Res 1988;48:775–778.
55. Rockwell S, Sartorelli A.C. Mitomycin C and radiation.In Hillard BT, Bellamy AS (eds): Anti-tumor drug-radiation interactions. Boca Raton, Florida: CRC Press,Inc., pp 125–139, 1990.
56. Coia LR, Engstrom PF, Paul A. Nonsurgical manage-ment of esophageal cancer: report of a study of com-bined radiotherapy and chemotherapy. J Clin Oncol1987;5:1783–1790.
57. Cummings BJ, Keane TG, O’Sullivan B. Epidermoidanal cancer: treatment by radiation and 5-fluorouracilwith or without mitomycin C. Int J Radiat Oncol BiolPhys 1991;21:1115–1125.
58. Flam MS, John M, Pajak T, Petrelli N, Myerson R,Doggett S, Quivey J, Rotman M, Kerman H, Coia L,Murray K. Role of mitomycin in combination with flu-orouracil and radiotherapy, and of salvage chemoradia-tion in the definitive nonsurgical treatment of epider-moid carcinoma of the anal canal: results of a Phase IIIRandomized Intergroup Study. J Clin Oncol 1996;14:2527–2539.
59. Haffty BG, Son YH, Sasaki CT, Papac R, Fischer DB,Rockwell S, Sartorelli AC, Fischer JJ. Mitomycin C asan adjunct to postoperative radiation therapy in squa-mous cell carcinoma of the head and neck: results fromtwo randomized clinical trials. Int J Radiat Oncol BiolPhys 1993;27:241–250.
60. Haffty BG, Son YH, Papac R, Sasaki CT, Weissberg J,Fischer D, Rockwell S, Sartorelli AC, Fischer JJ. Che-motherapy as an adjunct to radiation in the treatment ofsquamous cell carcinoma of the head and neck: resultsof the Yale mitomycin randomized trials. J Clin Oncol1997;15:268–276.
61. Christie DRH, Bull CA, Gebski V, Langlands AO.Concurrent 5- fluorouracil, mitomycin C and irradia-tion in locally advanced cervix cancer. Radiother Oncol1995;37:181–189.
62. Rakovitch E, Fyles AW, Pintilie M, Leung PMK. Roleof mitomycin C in the development of late bowel tox-icity following chemoradiation for locally advancedcarcinoma of the cervix. Int J Radiat Oncol Biol Phys1997;38:979–987.
63. Thomas G, Dembo A, Fyles A, Gadalla T, Beale F,Bean H, Pringle J, Rawlings G, Bush R, Black B. Con-current chemoirradiation in advanced cervical cancer.Gyn Oncol 1990;38:446–451.
64. Vera R. Tratamiento radiante del cancer del cuellouterino. Plan Nacional. Acta Oncol Venezuela 1978;11:51–87.
65. Working Party on Radionuclides and AfterloadingTechniques in the Treatment of Cancer of the Uterus inDeveloping Areas. Proc. 2nd Meeting, U.S. Depart-ment of Health, Education and Welfare; March, 1974.
66. Vera R, Gutierrez E, Vera Gimon A, Turbay Perez N.Cancer del Cuello Uterino. In Urdaneta N (ed): Manualde Radioterapia Oncologica. Guilford, CT: The Pub-lishing Nexus Inc., pp 341–352, 1989.
67. John MJ. Grading of chemoradiation toxicity. In JohnMJ, Flam MS, Legha SS, Phillips TL (eds): Chemora-diation: an integrated approach to cancer treatment.Philadelphia: Lea & Febiger, pp 601–606, 1993.
68. Efron B. Forcing a sequential experiment to be bal-anced. Biometrika 1971;58:403–417.
69. Cox DR. Regression models and life tables. J R StatSoc B34:187–220.
70. Orr JW, Orr PJ. Cervical cancer—staging. In Rubin SC,Hoskins WJ (eds): Cervical Cancer and PreinvasiveNeoplasia. Philadelphia: Lippincott- Raven Publishers,pp 171–182, 1996.
71. Vokes EE, Weichselbaum RR. Concomitant chemoir-radiation: rationale and clinical experience in patientswith solid tumors. J Clin Oncol 1990;8:911–934.
72. Weissberg JB, Son YH, Papac RJ, Sasaki C, FischerDB, Lawrence R, Rockwell S, Sartorelli AC, Fischer JJ.Randomized clinical trial of Mitomycin C as an adjunctto radiotherapy in head and neck cancer. Int J RadiatOncol Biol Phys 1989;17:3–9.
73. Denehy TR, Eastman R, SanFilippo L, Gregori CA,Breen JL. Bolus mitomycin C and 5-FU with sequentialradiation for poor-prognosis locally advanced cervicalcancer. Gynecol Oncol 1996;60:64–71.
74. John M, Cooke JK, Flam M, Padmanabhan A, MowryPA. Preliminary results of concomitant radiotherapy inadvanced cervical carcinoma. Gynecol Oncol 1987;28:101–110.
75. Kersh CR, Constable WC, Spaulding CA, Hahn SS,Anderson WA, Taylor PT. A phase I-II trial of multi-modality management of bulky gynecologic malig-nancy: combined chemoradiosensitization and radio-therapy. Cancer 1990;66:30–34.
76. Khoury GG, Bulman AS, Joslin CAF, Rothwell RI.
222 Roberts et al.: Mitomycin C and Radiotherapy for Cervix Cancer

Concomitant pelvic radiotherapy, 5-fluorouracil andmitomycin C in the treatment of advanced cervical car-cinoma. Br J Radiol 1991;64:252–260.
77. Malviya VK, Deppe G, Kim Y, Gove N. Concurrentradiation therapy, cis-platinum, and mitomycin C inpatients with poor prognosis cancer of the cervix: apilot study. Am J Clin Oncol (CCT) 1989;12:434–437.
78. Nguyen PD, John B, Munoz AK, Yazigi R, Graham M,Franklin P. Mitomycin-C/5-FU and radiation therapyfor locally advanced cervical cancer. Gynecol Oncol1991;43:220–225.
79. Thomas G, Dembo A, Beale F, Bean H, Bush R, Her-man J, Pringle J, Rawlings G, Sturgeon J, Fine S, BlackB. Concurrent radiation, mitomycin C and 5-fluoroura-cil in poor prognosis carcinoma of cervix: preliminaryresults of a phase I-II study. Int J Radiat Oncol BiolPhys 1984;10:1785–1790.
80. Evans LS, Kersh CR, Constable WC, Taylor PT. Con-comitant 5- fluorouracil, mitomycin C and radiotherapyfor advanced gynecologic malignancies. Int J RadiatOncol Biol Phys 1988;15:901–906.
81. Rockwell S. Combination therapy with radiation, mito-
mycin C, and 5- fluorouracil in EMT6 tumors. Int JRadiat Oncol Biol Phys 1994;28:127–133.
82. Mickiewicz E, Roth B, Alvarez A, Rodriguez I, Espi-noza R, Brosio C, de la Torre M, Porcela H, de Dios H,Latour R, Cabalar M, Piris N, Cuevas L, Giglio R,Baurel V, Roffo AIH. Chemotherapy (CT) + Radio-therapy (RT) vs. radiotherapy alone in cervical cancerstage IIAB to IVA, a randomized study. Proceedings ofASCO 1991;10:192.
83. Lorvidhaya V, Tonusin A, Sukthomya W, ChangwiwitW, Nimmolrat A. Induction chemotherapy and irradia-tion in advanced carcinoma of the cervix. Gan ToKagaku Ryoho 1995;22 Suppl 3:244–251.
84. Tseng CJ, Chang CT, Lai CH, Soong YK, Hong JH,Tang SG, Hsueh S. A randomized trial of concurrentchemoradiotherapy versus radiotherapy in advancedcarcinoma of the uterine cervix. Gynecol Oncol 1997;66:52–58.
85. Wong LC, Choo YC, Choy D, Sham JST, Ma HK.Long-term follow-up of potentiation of radiotherapy bycisplatinum in advanced cervical cancer. Gynecol On-col 1989;35:159–163.
Roberts et al.: Mitomycin C and Radiotherapy for Cervix Cancer 223




















