Intraoperative graft flow assessment for myocardial surgical ...
Upload
independentCategory
view
6download
0
•In
Single-Clamp Technique: An ImportantAdjunct to Myocardial and Cerebral ProtectionCoronary OperationsSary F. Aranki, MD, Robert J. Rizzo, MD, David H. Adams, MD, Gregory S. Couper, MD,Nancy M. Kinchla, B5, Jennifer S. Gildea, B5, and Lawrence H. Cohn, MDDivision of Cardiac Surgery, Brigham and Women's Hospital, and the Department of Surgery, Harvard Medical School,Boston, Massachusetts
To determine the myocardial and cerebral protectiveproperties of the single cross-clamp (group I; n = 160)versus the partial occluding clamp (group II; n = 150)technique for construction of the proximal anastomoses,a retrospective analysis of 310 patients operated on by thesame surgeon was performed. Group I patients wereolder (median age, 70 versus 64 years; p :s; 0.0001), with 83(52%), versus 41 (27%) in group II, 70 years and older(p :s; 0.0001). More group I patients were in New YorkHeart Association functional class IV (42 [26%] versus 22[15%]; p = 0.008); more required preoperative ballooncounterpulsation (35 [22%] versus 16 [11%]; P = 0.006);and more required emergent operation (20 [13%] versus 3[2%]; p :s; 0.0001). Antegrade crystalloid cardioplegia wasused in both groups. The median cross-clamp time was58 minutes for group I versus 44 minutes for group II (p:s; 0.0001). However, there was no significant differencebetween the two groups in terms of the number ofbypass grafts, the use of the mammary artery, or thebypass time. The operative mortality was 2.5% (n = 4) forgroup I versus 5.3% (n = 8) for group II (p = 0.16), and theperioperative myocardial infarction/low cardiac outputstate was seen in 6 patients (3.8%) in group I versus 18
Recent advances in cardiac surgical procedures, alongwith the selection of low-risk, younger patients for
percutaneous revascularization procedures [1], have radically modified the demographic trends for patients requiring coronary artery bypass graft (CABG) procedures. Thetrend is now toward the surgical treatment of older andsicker patients who are more likely to have depressed leftventricular function and congestive heart failure, and whoare more likely to require nonelective operations [2, 3],with an attendant increased perioperative cardiac morbidity and mortality [2]. In addition, the incidence of atherosclerotic disease of the aorta is increased in older patients,as is the incidence of atheroembolic events during operation, which could be implicated in the development ofperioperative stroke and multisystem organ failure [3-5]. It
Presented at the Thirtieth Annual Meeting of The Society of ThoracicSurgeons. New Orleans, LA, Jan 3l-Feb 2, 1994.
Address reprint requests to Dr Aranki, Division of Cardiac Surgery,Brigham and Women's Hospital, 7S Francis St, Boston, MA 02llS.
© 1994 by The Society of Thoracic Surgeons
patients (12%) in group II (p = 0.006). The mediancreatine kinase MB release was 13 U/L for group I versus19 U/L for group II (p = 0.0029). A major stroke occurredin 1 patient (0.6%) in group I and in 3 patients (2%) ingroup II ip = 0.3). Multivariate logistic regression analysis for an adverse outcome (operative mortality, myocardial output/low cardiac output state, and stroke), with11 events (6.9%) occurring in 10 patients in group I and 29events (19%) occurring in 24 patients in group II ip =0.005), showed that use of the partial occluding clampwas a significant predictor for an adverse outcome ip =0.002; odds ratio, 3.6; ±95% confidence intervals, 1.6 and8.0), along with diabetes, nonelective coronary arterybypass grafting, and weight of 65 kg or less. The improved results associated with the single cross-clampmethod suggest that this technique plays an integral partin ensuring myocardial and cerebral protection, possiblydue to better cardioplegia delivery and distribution,more uniform rewarming and revascularization, and reduced manipulation of and trauma to the ascendingaorta.
(Ann Thorae Surg 1994;58:296-303)
therefore seems that adequate myocardial protection andthe prevention of atheroembolic events are probably thecornerstones of a safe and successful cardiac operation.
The conventional way of constructing CABGs, consisting of the differential application of a totally occludingclamp to construct the distal anastomoses and a partiallyoccluding clamp to construct the proximal anastomoses, isthe one widely practiced by most surgeons today. Theroutine use of an aortic partial occluding clamp has potential disadvantages that may result in adverse outcomesrelated to myocardial and cerebral protection. An alternative technique was described by Salerno [6] in 1982, inwhich the distal and proximal anastomoses are constructedduring a single period of total aortic occlusion. This techniquehas been shown to confer improved myocardial protection,even though the ischemia time is increased [7]. In addition,stroke rates secondary to atheroembolism are reduced [8].However, this technique has not been widely adopted because of concerns about the extended ischemia time.
0003-4975/94/$7.00

Ann Thorac Surg1994;58:296 -303
ARANKI ET ALSINGLE-CLAMP TECHNIQUE
297
The objective of this retrospective analysis was to determine the impact of the technique used to construct theproximal anastomoses on adverse outcome rates related tomyocardial and cerebral protection by analyzing the clinical end points of perioperative death, the myocardialinfarction/low cardiac output state, and stroke rates.
Material and Methods
Over an 18-month period, starting in September 1990, 310consecutive patients underwent a primary CABG procedure performed by the same surgeon (S.F.A.) at theBrigham and Women's Hospital. They ranged in age from31 to 87 years, with a median age of 67 years; 123 (40%)were 70 years and older; 106 (34%) were female; and 89(29%) were diabetics. The patients were retrospectivelydivided into two groups. In the group I patients, the distaland proximal anastomoses were performed during a singleperiod of ischemia by applying a total occluding clamp tothe ascending aorta (the single cross-clamp technique). Inthe group II patients, the proximal anastomoses wereperformed after removal of the total occluding clamp andby applying a tangentially placed partial occluding clamp.Patients requiring a reoperative CABG procedure andpatients requiring major concomitant cardiac procedureswere excluded from the study. The decision regarding theclamping technique to be used was nonrandomized, but aselection bias did exist in that elderly and sicker patientswere more likely to be in group I.
Data CollectionPreoperative, operative, and postoperative variables andoutcomes were retrieved from our computerized data bank(the cardiac surgery CABG registry). Data collection wasbased on the hospital charts, anesthesia records, perfusionrecords, and monthly chief resident reports on morbidityand mortality. There were 19 preoperative variables and 13operative variables that were subsequently entered into thestatistical analysis.
Operative TechniqueThrough a median sternotomy, the internal thoracic arterywas harvested before systemic heparinization. A two-stageright atrial venous cannula (Research Medical, Midvale,UT) and an ascending aortic cannula (Sarris, Ann Arbor,MI), usually placed on the left side of the upper part of theascending aorta, were used for cardiopulmonary bypass.Moderate hemodilution (hematocrit, 20% to 25%), moderate systemic hypothermia (28° to 30°C), flow rates of 1.5 to2 L . min- J
• m- z, and a mean arterial pressure of 50 to70 mm Hg were achieved in all patients. A total occludingclamp was applied, and antegrade hyperkalemic cardioplegia was infused through a cannula directly into theascending aorta. The cardioplegia apparatus had a threeway connector through which cardioplegia could be withdrawn into a syringe, and also a cardiotomy suction devicecould be connected to vent the aortic root. Local cold salinesolution (4°C) was dripped into the pericardial well toaugment myocardial cooling. An initial volume of 500 mLof crystalloid cardioplegia (30 mEq of potassium and
5 mEq of sodium bicarbonate in 1 L of dextrose 2.5% andliz normal saline) was initially given at a rate of 100mL/min. In group I patients, the proximal anastomoseswere sequentially performed after each distal anastomosisby applying suction to the cardioplegia cannula to achievea bloodless field. After the completion of each proximalanastomosis, 250 mL of crystalloid cardioplegia 00 mEqof potassium and 5 mEq of sodium bicarbonate in 1 L ofdextrose 2.5% and liz normal saline) was given at a rate of100 mL/min. The sutures were not tied until all air wasexpelled from the aortic root and the vein graft. Thisallowed cardioplegia to be distributed to newly revascularized regions of the myocardium. Grafting of the internalthoracic artery was completed last, during which rewarming was started. The cross-clamp was then removed, andspontaneous sinus rhythm was usually achieved withinfew minutes. In group II patients, all the distal anastomoses were performed first (receiving the same volume ofcardioplegia after the completion of each distal anastomoses); this was followed by removal of the cross-clamp, atwhich point rewarming was started. The proximal anastomoses were then constructed by applying a partial occluding clamp. After completion of the proximal anastomoses,the partial occluding clamp was removed, air was expelled, and the fibrillating heart was cardioverted intosinus rhythm.
DefinitionsPerioperative mortality was defined as death occurringwithin 30 days or during the same hospital stay. A myocardial infarction was defined by the presence of a new Qwave on the electrocardiogram, or an elevated creatinekinase MB isoenzyme release of 40 IU/L or greater in thepresence of a new segmental wall motion abnormality onechocardiograms, or both of these findings. The low cardiac output state was defined as the need for more thanone inotropic agent or as the need for an intraaortic balloonpump, or both. A major stroke was defined as the appearance of a permanent neurologic deficit upon recovery fromanesthesia that was likely to be related to atheroembolismbrought about by manipulation of the ascending aorta. Anadverse outcome was defined as the occurrence of any ofthe just described events-death, myocardial infarction/low cardiac output state, and stroke-that could be relatedto the technique of aortic clamping.
Statistical AnalysisUnivariate analyses were done with the K or Fisher's exacttest, and the Wilcoxon rank-sum test. Multivariate stepwise logistic regression analyses were used to identifyindependent variables that predict a perioperative adverseoutcome.
Results
Preoperative Patient CharacteristicsThe preoperative patient characteristics are summarized inTable 1. Patients in group I were significantly older; morewere in New York Heart Association functional class IV;more had had a preoperative intraaortic balloon pump;

298 ARANKI ET ALSINGLE-CLAMP TECHNIQUE
Ann Thorac Surg1994;58:296-303
Table 1. Preoperative Patient Characteristics
Group I" Group JIbCharacteristic (n = 160) (n = 150) P Value
Median age (y) 70 64 :s0.0001Patients 2-70 y 83 (52%) 41 (27%) :s0.0001No. of female patients 54 (34%) 52 (35%) 0.5No. of diabetic patients 49 (31%) 40 (27%) 0.26No. in NYHA functional 42 (26%) 2205%) 0.008
class IVNo. having emergency 2003%) 3 (2%) :s0.0001
operationNo. of hypertensive 110 (69%) 102 (68%) 0.5
patientsNo. in chronic renal failure 13 (8%) 9 (6%) 0.30No. with claudication 13 (8%) 1500%) 0.40No. having preop IABP 35 (22%) 16 (11%) 0.006No. with preop SVT 21 (13%) 9(6%) 0.03No. with three-vessel 133 (83%) 116 (77%) 0.13
diseaseNo. with left main coronary 2908%) 13(9%) 0.01
artery stenosis 2-70%
a Group in which the single cross-clamp was used. b Group in which thepartial occluding clamp was used.
IABP ~ intraaortic balloon pump; NYHA = New York Heart Associa-tion; SVT ~ supraventricular tachycardia.
more had significant left main coronary artery disease andtriple-vessel disease; more had supraventricular tachycardia preoperatively; and more were likely to require emergency surgical procedures. Based on the Cleveland Clinicpreoperative scoring system [9], the patients in group I hadsignificantly higher risk scores (Fig 1) than did the patientsin group II (29% versus 16%; p = 0.004). The distribution interms of gender, diabetes, hypertension, history of claudication, and chronic renal failure did not differ between the
Table 2. Operative Variables
Group I" Group JIb pVariable (n = 160) (n = 150) Value
No. of grafts" 3 3 0.62-Three grafts 140 (88%) 141 (87%) 0.5LIMA 140 (88%) 137 (91%) 0.14Endarterectomy 14 (9%) 21 04%) 0.1Sequential graft 65 (41%) 66 (44%) 0.3Y graft 9(6%) 4 (2.7%) 0.16Cross-clamp time" (min) 58 44 :s0.0001Bypass time" (min) 79 76 0.09Time to wean off 19 32 :s0.0001
bypass" (min)+ CEA 10(6%) 20%) 0.02
a Group in which the single cross-clamp was used. b Group in which thepartial occluding clamp was used. C Median values.
CEA = carotid endarterectomy; LIMA = left internal mammary artery.
two groupS. Based on the preoperative data, group Ipatients were older and sicker, and at the higher end of therisk stratification spectrum for increased morbidity andmortality.
Operative VariablesThe operative variables are summarized in Table 2. Thecross-clamp time was significantly longer in group I patients because the proximal anastomoses were constructedduring this period. The bypass time was similar for the twogroups. However, the time it took to wean the patients offcardiopulmonary bypass after removal of the cross-clampwas significantly shorter in the group I patients. Thenumber of bypass grafts, the use of the internal thoracicartery, and the use of sequential grafts did not differsignificantly between the two groups.
9+Clinical Risk Score
Fig 1. Distribution of high-risk patients (preoperative severity score of2-9) in each group of patients. The group treated with the singlecross-clamp technique contained twice as many patients (p = 0.0(4)at the higherend of the preoperative risk spectrum, as determined bythe Cleveland Clinic preoperative severity scoring system [91. (POC =
partial occlusion clampgroup: SCC = single cross-clamp group.!
35
30
25tilC.s 20iiia. 15?f?
10
5
OL-------
D poe• sec
Perioperative OutcomesThe perioperative outcomes are summarized in Table 3.Even though the group I patients represented a significantly higher risk group of patients, the perioperativeoutcomes in terms of death, the myocardial infarction/lowcardiac output state, and major strokes were more favorable in this group. The rate of the myocardial infarction/low cardiac output state was significantly lower (3.8%versus 12%; p = 0.006), as was the peak creatine kinase andpeak creatine kinase MB fraction release (Fig 2). The
Table 3. Postoperative Outcomes
Group I" Group lIb pVariable (n = 160) (n = 150) Value
Mortality 4 (2.5%) 8 (5.3%) 0.16
MI/ t CO 6(3.8%) 1802%) 0.006Stroke 1 (0.6%) 3 (2%) 0.3Total events/patients (%) 11/10 (6.9%) 29/2409%) 0.005
a Group in which the single cross-clamp was used. b Group in which thepartial occluding clamp was used.
Mil t CO ~ myocardial infarction/low cardiac output state.
Ann Thorac Surg1994;58:296 -303
ARANKI ET ALSINGLE-CLAMP TECHNIQUE
299
35,------------------
D poe30 • sec
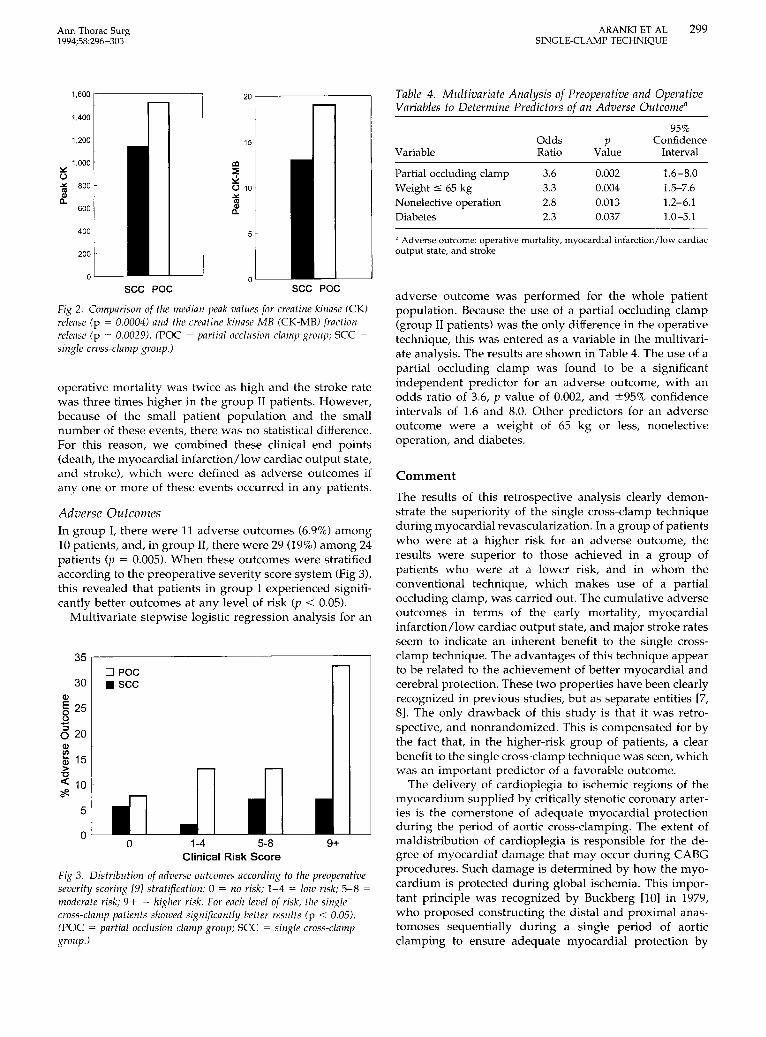
adverse outcome was performed for the whole patientpopulation. Because the use of a partial occluding clamp(group II patients) was the only difference in the operativetechnique, this was entered as a variable in the multivariate analysis. The results are shown in Table 4. The use of apartial occluding clamp was found to be a significantindependent predictor for an adverse outcome, with anodds ratio of 3.6, p value of 0.002, and ±95% confidenceintervals of 1.6 and 8.0. Other predictors for an adverseoutcome were a weight of 65 kg or less, nonelectiveoperation, and diabetes.
a Adverse outcome: operative mortality, myocardial infarction/low cardiacoutput state, and stroke.
Comment
The results of this retrospective analysis clearly demonstrate the superiority of the single cross-clamp techniqueduring myocardial revascularization. In a group of patientswho were at a higher risk for an adverse outcome, theresults were superior to those achieved in a group ofpatients who were at a lower risk, and in whom theconventional technique, which makes use of a partialoccluding clamp, was carried out. The cumulative adverseoutcomes in terms of the early mortality, myocardialinfarction/low cardiac output state, and major stroke ratesseem to indicate an inherent benefit to the single crossclamp technique. The advantages of this technique appearto be related to the achievement of better myocardial andcerebral protection. These two properties have been clearlyrecognized in previous studies, but as separate entities [7,8]. The only drawback of this study is that it was retrospective, and nonrandomized. This is compensated for bythe fact that, in the higher-risk group of patients, a clearbenefit to the single cross-clamp technique was seen, whichwas an important predictor of a favorable outcome.
The delivery of cardioplegia to ischemic regions of themyocardium supplied by critically stenotic coronary arteries is the cornerstone of adequate myocardial protectionduring the period of aortic cross-clamping. The extent ofmaldistribution of cardioplegia is responsible for the degree of myocardial damage that may occur during CABGprocedures. Such damage is determined by how the myocardium is protected during global ischemia. This important principle was recognized by Buckberg [10] in 1979,who proposed constructing the distal and proximal anastomoses sequentially during a single period of aorticclamping to ensure adequate myocardial protection by
95%Odds p Confidence
Variable Ratio Value Interval
Partial occluding clamp 3.6 0.002 1.6-8.0Weight:5 65 kg 3.3 0.004 1.5-7.6Nonelective operation 2.8 0.013 1.2-6.1Diabetes 2.3 0.037 1.0-5.1
Table 4. Multivariate Analysis of Preoperative and OperativeVariables to Determine Predictors of an Adverse Outcome"
9+
sec poe
20,---------
oo
1,600
1,400
1,200
1,000:.::o"'" 800
'"eC.600
400
200 .
0
sec poe
Q)
§ 25.8<520Q)
~ 15>
"C
<: 10?ft.
1-4 5-8Clinical Risk Score
Fig 3. Distribution of adverse outcomes according to the preoperativeseverity scoring [9] stratification: 0 = no risk; 1-4 = low risk; 5-8 =moderate risk; 9+ = higher risk. For each level of risk, the singlecross-clamp patients showed significantly better results (p < 0.05).(POC = partial occlusion clamp group; SCC = single cross-clampgroup.)
operative mortality was twice as high and the stroke ratewas three times higher in the group II patients. However,because of the small patient population and the smallnumber of these events, there was no statistical difference.For this reason, we combined these clinical end points(death, the myocardial infarction/low cardiac output state,and stroke), which were defined as adverse outcomes ifanyone or more of these events occurred in any patients.
Fig 2. Comparison of the median peak values for creatine kinase (CK)release (p = 0.0004) and the creatine kinase MB (CK-MB) fractionrelease (p = 0.0029). (POC = partial occlusion clamp group; SCC =single cross-clampgroup.)
5
Adverse OutcomesIn group I, there were 11 adverse outcomes (6.9%) among10 patients, and, in group II, there were 29 (19%) among 24patients (p = 0.005). When these outcomes were stratifiedaccording to the preoperative severity score system (Fig 3),this revealed that patients in group I experienced significantly better outcomes at any level of risk (p < 0.05).
Multivariate stepwise logistic regression analysis for an

300 ARANKI ET ALSINGLE-CLAMP TECHNIQUE
Ann Thorae Surg1994;58:296-303
achieving homogeneous cardioplegia delivery and coolingof all myocardial regions. Also in 1979, Hilton and colleagues [11] conducted experimental studies that showedmaldistribution of cardioplegia in areas of coronary arteryobstruction created in dogs, as well as nonhomogeneouscooling in these areas which resulted in localized postischemic abnormalities that were not detected when globalmyocardial function was tested. These authors proposedthat the proximal anastomoses be constructed before theinitiation of cardiopulmonary bypass, and that cardioplegia then be delivered through these grafts upon thecompletion of each distal anastomosis. Becker and associates [12] performed an experimental study in which theysimulated the construction of bypass grafts in dogs bycreating coronary occlusions that could be released immediately upon removal of the cross-clamp (which wasapplied for 60 minutes), thus simulating the single crossclamp technique, or that could be released 30 minutes afterremoval of the cross-clamp (which was applied for 30minutes), and thus simulating the conventional partialoccluding clamp technique. These investigators found thatthe myocardial temperature was lower, the reperfusionfibrillation was less, the lactate washout was less, there wasa greater recovery of compliance, and there were higherstroke work indices in the first group of animals, in whichthe single cross-clamp technique was simulated. Theyconcluded that adequate myocardial protection is relatedmore to homogeneous myocardial delivery than to theperiod of cross-clamping.
In 1982, Salerno [6] reported on 87 consecutive patientsin whom the single cross-clamp technique was used. Heobserved a low mortality and morbidity in these patients,thereby establishing the safety of the procedure in theclinical setting. Weisel and associates [7] conducted arandomized clinical trial in which the single cross-clamptechnique was used in 46 patients and the conventionaltechnique was used in 45 patients, with similar preoperative risk characteristics for both groups. Despite a significantly increased cross-clamp time, lower myocardial temperature, lower creatine kinase release, and an earlierreturn of myocardial lactate extraction was observed forthe patients treated with the single cross-clamp technique. The same group reported similar results for a smallernumber of patients who were not randomized [13]. Theadvantages of this technique appear to be related to themore homogeneous distribution of cardioplegia and the morehomogeneous cooling that occurs when distal and proximalgrafts are sequentially constructed. This allows for a reduction in the metabolic demand during ischemia and for acontinuous washout of lactic acid on repeated infusion ofcardioplegia through constructed grafts. On release of thecross-clamp, there is a maximal reactive hyperemia and animmediate maximal coronary reperfusion that results incomplete washout of the lactic acid accumulation and speedyreplenishment of the substrates needed for aerobic metabolism [14]. In contrast, when the conventional technique ofconstructing the proximal anastomoses with a partial occluding clamp is used, there is inadequate coronary hyperemiaand reperfusion, accompanied by a discordant increase inmyocardial temperature. This results in a reperfusion myo-
cardial injury stemming from the continued ischemia, theincreased production and accumulation of lactic acid [15],and the generation of oxygen free radicals [16]. This issupported by the findings of Khoury and colleagues [17],who observed a significant decline in the myocardial pH,along with an increase in the myocardial temperature, afterremoval of the cross-clamp during the period when theproximal anastomoses would be constructed. This phenomenon occurred regardless of whether crystalloid or blood(intermittent or continuous) cardioplegia was used.
Although there is a strong experimental and clinicalbasis for the superiority of the single cross-clamp technique in conferring myocardial protection, this techniquehas been eclipsed by a multitude of myocardial protectiontechniques that have evolved over the past decade. Thenumerous publications on the subject comparing crystalloid versus blood, antegrade versus retrograde, intermittent versus continuous, warm versus cold, and substrateenhanced versus non-substrate-enhanced cardioplegia areconfusing at best, with no hard evidence proving thesuperiority of one method over the other [18], especiallywhen clinical end points are analyzed [19]. However, thereare a few studies involving blood cardioplegia [8, 20-22]that show it to be superior in the clinical setting, but acommon denominator of the operative techniques is thatthey all employ a single cross-clamp [8, 21, 22] or anequivalent technique [20].
Increasing age has been shown to be a major predictor ofneurologic events after CABG procedures [5,23-26]. In thisstudy, a major stroke occurred in 0.6% of the patients ingroup I (those undergoing single cross-clamping), whosemedian age was 70 years, compared with 2% of thepatients in group II (those undergoing partial occlusionclamping), whose median age was 64 years. Although thisdifference was not statistically significant, it neverthelessrepresents a remarkably low stroke rate for a significantlyolder and higher-risk group of patients. Because the use ofa partial occluding clamp was the only difference in theoperative technique between the two groups, it is highlyimplicated as a major contributor to the occurrence ofatheroembolic events. However, because of the small number of patients in this study, and the relatively low strokerates in each group, a statistical difference was not shown.In a recent study from the Cleveland Clinic conducted byLoop and colleagues [8], the stroke rate was 0.7% forpatients undergoing CABG procedures (n = 691), in whomthe single cross-clamp technique was used. This wassignificantly lower than the stroke rate in the group ofpatients (n = 2,214) in whom the conventional techniqueemploying a partial occluding clamp was used. The authors speculated that the reduced manipulation of andtrauma to the ascending aorta achieved by a single application of the cross-clamp may have contributed to thissignificant reduction in neurologic complications.
Stefaniszyn and associates [27], in an attempt to determine the relationship between partial aortic occlusion andits effect on the ascending aorta in 5 patients who died ofnon-cardiac-related causes, applied a partial occludingclamp in a manner similar to that performed in theoperating room. Considerable atherosclerosis with calcific

Ann Thorae Surg1994;58:296-303
ARANKIET ALSINGLE-CLAMP TECHNIQUE
301
plaques of the ascending aorta was noted in most of thepatients. The clamp left indentations in the intima of allthe aortas. A partial intimal tear of 0.5 cm was observed inone specimen. The aortic lumen was reduced by 30% to50% at the clamp site. The aortic valve and the rightcoronary ostium were distorted in 1 patient with a shortaorta. Based on these observations, the authors concludedthat extreme care should be taken during application of thepartial occluding clamp to minimize any potential traumato the aorta, the risk of atheroembolism, and distortion ofthe aortic valve and the right coronary ostium in patientswith a short ascending aorta. They also suggested that itmay be safer to construct all anastomoses during a singleperiod of total aortic occlusion.
In an autopsy study, Tobler and Edwards [28] found a33% prevalence of atherosclerotic plaques exceeding 8 mmin diameter in 97 patients with coronary artery disease. Theplaques were predominantly anterior and posterior and onthe right side, with relatively fewer plaques on the left side.Further analysis of the plaque distribution revealed arelative equal distribution in terms of the anterior, right,and posterior locations in the upper half of the ascendingaorta, but, in the lower half, the plaques were concentratedpredominantly anteriorly and to the right (the site ofpartial occlusion during CABG procedures). The authorsconcluded that the findings yielded by this study mayserve as a practical guide for technical modifications thatbring about a reduction in trauma and potential atheroembolism. In another autopsy study from the ClevelandClinic [29], severe atherosclerotic disease of the ascendingaorta was found in 55.7% of the 221 patients who underwent autopsy after coronary or valvular surgical procedures. Atheroembolic disease was identified in 21.7% ofthe patients, with the brain involved in 62.5% of them.Multivariate logistic regression analysis identified increasing age and the prevalence of peripheral vascular diseaseas the major predictors for the presence of severe atherosclerotic aortic disease and atheroembolism, especially inpatients undergoing CABG procedures. This importantstudy highlighted the direct relationship between increasing age, severe aortic atherosclerosis, and atheroembolicevents, and emphasized the role of prevention (detectionand altering the operative technique) in the overall management of this difficult problem.
The severity of the atherosclerosis in the ascending aortacould be accurately determined by ultrasonic scanning inthe operating room before cannulation and cardiopulmonary bypass, with the operative technique modified asneeded based on the ultrasound findings. In extreme cases,this involved replacement of the ascending aorta undercirculatory arrest, as reported by Wareing and colleagues[30]. No strokes occurred in the 27 patients with moderateor severe atherosclerosis in whom the ascending aorta wasreplaced. However, the stroke rate was 1.1% in the 93patients with moderate or severe atherosclerosis who hadno alteration in the operative technique. These resultsshould be interpreted with caution, however, as a majorprocedure such as ascending aortic replacement performedduring circulatory arrest under urgent or emergent conditions in patients requiring a CABG may markedly increase
the surgical risk, especially in the elderly patients. We relyon digital palpation of the ascending aorta, which canreadily identify an obvious abnormality, such as a porcelain aorta, before we initiate cardiopulmonary bypass. Lesssubtle but important abnormalities can be identified withreasonable accuracy on cardiopulmonary bypass by turning the pump off and gently palpating the collapsed aorta.Under these circumstances, we tend to use the "no touch"technique described by Mills and Everson [31] and Peighand associates [32].
Application of a partial occluding clamp is probably themost traumatic manipulation of the ascending aorta, withthe total force of the clamp being distributed on a smallarea, which may increase the likelihood of an intimal tearand the dislodgement of plaque or atheromatous materialthat could embolize upon removal of the clamp. In contrast, the force of the total occluding clamp is equallydistributed along the whole circumference of the aorta. AtWake Forest Medical University, screening for embolicevents using transcarotid echography revealed that theapplication and removal of the partial occluding clampwas associated with 11% and 17% of the total embolicevents, respectively. The corresponding figures for thetotal occluding clamp were 0.1% and 9%, respectively [33].
In summary, it appears that the technique used forproximal anastomosis construction has a significant impacton the perioperative outcomes, with better results achievedin the higher-risk group of patients in whom the singleclamp technique is used. In addition, use of the partialoccluding clamp was a significant predictor for an adverseoutcome. The advantages of the single cross-clamp interms of myocardial protection may be related to the morehomogeneous cardioplegia delivery and myocardial cooling associated with its use, and to the synchronizedrewarming and maximal reperfusion that take place uponremoval of the clamp. This reduces the incidence of reperfusion injury and allows for better myocardial recovery.Eliminating the need for a partial occluding clamp avoidsadditional manipulation, trauma, and atheroembolicevents, and this may confer better cerebral protectionduring CABG procedures. Therefore, despite a significantincrease in the total ischemia time, the single cross-clampmethod is a simple and safe technique, and appears tohave better myocardial and cerebral protective propertiesthan does the conventional technique of partial aorticocclusion.
References
1. Jones EL, Craver JM, Guyton RA, Bone OK, Hatcher CR Jr.Trends in the treatment of coronary disease today. Selectiveuse of PTCA and bypass surgery. Ann Surg 1983;197:728-37.
2. Weintraub WS, Craver JM, Cohen CL, Jones EL, Guyton RA.Influence of age on results of coronary artery surgery. Circulation 1991;84(Suppl 3):226-35.
3. Cosgrove OM, Loop PO, Lytle BW, et al. Primary myocardialrevascularization: trends in surgical mortality. J Thorac Cardiovasc Surg 1984;88:673-84.
4. Jones EL, Weintraub WS, Craver JM, Guyton RA, Cohen CL.Coronary bypass surgery: is the operation different today?J Thorac Cardiovasc Surg 1991;101:108-15.
5. Gardner TJ, Horneffer PJ, Manolio TA, et al. Stroke following

302 ARANKI ET ALSINGLE-CLAMP TECHNIQUE
Ann Thorae Surg1994;58:296-303
coronary artery bypass grafting: a ten-year study. Ann ThoracSurg 1985;40:574-81.
6. Salerno TA. Single aortic cross-clamping for distal and proximal anastomoses in coronary surgery: an alternative to conventional techniques. Ann Thorac Surg 1982;33:518-20.
7. Weisel RD, Hoy FB, Baird RI, et at. Improved myocardialprotection during a prolonged cross-clamp period. Ann Thorae Surg 1983;36:664-74.
8. Loop FD, Higgins TL, Panda R, Pearce G, Estafanous FG.Myocardial protection during cardiac operations: decreasedmorbidity and lower cost with blood cardioplegia and coronary sinus perfusion. J Thorac Cardiovasc Surg 1992;104:60818.
9. Higgins TL, Estafanous FG, Loop FD, Beck GI, Blum JM,Paranandi 1. Stratification of morbidity and mortality outcome by preoperative risk factors in coronary artery bypasspatients. JAMA 1992;267:3444-8.
10. Buckberg CD. A proposed solution to the cardioplegic controversy. J Thorac Cardiovasc Surg 1979;77:803-15.
11. Hilton CJ, Teubl W, Acker M, et at. Inadequate cardioplegicprotection with obstructed coronary arteries. Ann Thorac Surg1979;28:323-34.
12. Becker H, Vinten-Iohansen I, Buckberg GD, Follette DM,Robertson JM. Critical importance of ensuring cardioplegicdelivery with coronary stenoses. J Thorac Cardiovasc Surg1981;81:507-15.
13. Weisel RD, Hoy FB, Baird RI, et at. Comparison of alternativecardioplegic techniques. J Thorac Cardiovasc Surg 1983;86:97107.
14. Buckerg GD. Myocardial temperature management duringaortic clamping for cardiac surgery. J Thorac Cardiovasc Surg1991;102:895-903.
15. Ip JH, Levin RI. Myocardial preservation during ischemia andreperfusion. Am Heart J 1988;115:1094-104.
16. McCord JM. Oxygen-derived free radicals in post ischemictissue injury. N Engl J Med 1985;312:159-62.
17. Khuri SF, Warner KC, [osa M, et at. The superiority ofcontinuous cold blood cardioplegia in the metabolic protection of the hypertrophied human heart. J Thorac CardiovascSurg 1988;95:442-54.
18. Barner HB. Blood cardioplegia: a review and comparison withcrystalloid cardioplegia. Ann Thorac Surg 1991;52:1354-67.
19. Chiu RC-J. Cardioplegia: from the bedside to the laboratoryand back again. Ann Thorac Surg 1991;52:1209-10.
20. Rosenkranz ER, Buckberg CD, Laks H, Mulder DG. Warminduction of cardioplegia with glutamate-enriched blood in
DISCUSSION
DR ELLIS 1. JONES (Atlanta, GA): I had the opportunity andgood fortune of being able to review the manuscript, and I wouldlike to compliment Dr Aranki on the conception of an excellentpaper and project. I think that trying to offer some constructivecriticism is in order here, because I think it is such an importantsubject and because the single cross-clamp technique tends tobring into question very accepted techniques, that is, the partialocclusion clamp, in the performance of coronary artery bypassgrafting. It also requires the total modification of an operation thathas become pretty standard. I would like to say, first of all, in mycriticism that the basis of this report is a retrospective, and not aprospective, randomized study. I think that the subject is worthyof a prospective study, as I would like to elaborate upon in thecomments that follow.
I am personally convinced of the worthiness of the singlecross-clamp technique, because that is what I use for reoperativecoronary artery bypass graft operations, for many other reasons.
coronary patients with cardiogenic shock who are dependenton inotropic drugs and intra-aortic balloon support. J ThoracCardiovasc Surg 1983;86:507-18.
21. Lichtenstein SV, Abel JG, Panos A. Slutsky AS, Salerno TA.Warm heart surgery: experience with long cross-clamp times.Ann Thorac Surg 1991;52:1009-13.
22. Menasche P, Subayi JB, Veyssie L, LeDref 0, Chevret 5,Piwnica A. Efficacy of coronary sinus cardioplegia in patientswith complete coronary artery occlusions. Ann Thorac Surg1991;51:418-23.
23. Faro RS, Golden MD, [avid H, et at. Coronary revascularization in septuagenarian. J Thorac Cardiovasc Surg 1983;86:61620.
24. Gersh BI, Kronmal RA, Frye RL, et at. Coronary arteriographyand coronary artery bypass surgery: morbidity and mortalityin patients ages 65 years or older. Circulation 1983;67:483-91.
25. Tuman KI, McCarthy RI, Pharm D, Najafi H, Ivankovich AD.Differential effects of advanced age on neurologic and cardiacrisks of coronary artery operations. J Thorac Cardiovasc Surg1992;104:1510-7.
26. Lynn GM, Stefanko K, Reed JF, Gee W, Nicholas G. Riskfactors for stroke after coronary artery bypass. J ThoracCardiovasc Surg 1992;104:1518-23.
27. Stefaniszyn HJ, Novick RI, Sheldon H, Sniderman AD, SalernoTA. Anatomical observations in cadavers during applicationof a partial exclusion clamp to the ascending aorta. Curr Surg1984:184-7.
28. Tobler HG, Edwards JE. Frequency and location of atherosclerotic plaques in the ascending aorta. J Thorac Cardiovasc Surg1988;96:304-6.
29. Blauth CI, Cosgrove DM, Webb BW, et at. Atheroembolismfrom the ascending aorta. An emerging problem in cardiacsurgery. J Thorac Cardiovasc Surg 1992;103:1104-12.
30. Wareing TH, Davila-Roman VG, Daily BB, et at. Strategy forthe reduction of stroke incidence in cardiac surgical patients.Ann Thorac Surg 1993;55:1400-8.
31. Mills NL, Everson CT. Atherosclerosis of the ascending aortaand coronary artery bypass: pathology, clinical correlates, andoperative management. J Thorac Cardiovasc Surg 1991;102:546-53.
32. Peigh PS, DiSesa VI, Collins JJ [r, Cohn LH. Coronary arterybypass grafting with totally calcified or acutely dissectedascending aorta. Ann Thorac Surg 1991;51:102-4.
33. Mills SA. Cerebral injury and cardiac operations. Ann ThoracSurg 1993;56:586-91.
But, a retrospective analysis always invites the possibility thatunsatisfactory results in the partial occlusion group of patients isa stimulus to change multiple factors in the conduct of theoperation, and sometimes these factors are changed without eventhe primary surgeon being aware of it.
Now, the prevention of atheroembolism, which is the majortheoretic advantage of the single cross-clamp technique, would beexpected to have its greatest effect in the prevention of perioperative stroke. However, the problem they have gotten into is that thecohort of only 150 patients in each group is not statisticallysufficiently large enough to yield answers to this importantquestion. Our statisticians tell us we need about 2,000 patients tobe able to answer questions about an event with an incidence ofaround 2% to 5%.
Now, the way they have attempted to deal with this is byincluding what they have termed the adverse outcome, and theyinclude myocardial infarction and decreased cardiac output as one

Ann Thorae Surg1994;58:296-303
ARANKI ET ALSINGLE-CLAMP TECHNIQUE
303
of the components of adverse outcome, or stroke as a second, anddeath of the patient, a third. Now, this introduces additionalproblems when trying to get specific answers.
The retrospective analysis identified that 22% of all the patientsin the single cross-clamp group required preoperative intraaorticballoon pumping, and this was 11% for the partial occlusion clampgroup. Now, this is a consecutive series, and this figure seemsmuch too high for a consecutive series.
So, my first question to Dr Aranki is, can you explain thisterrible group of patients that you are asked to operate upon withyour favorite technique. The definition of a low cardiac outputstate postoperatively is an important definition, because you havebeen very strict. The definition of the low cardiac output state isthe requirement for balloon pumping or for more than oneinotropic agent, or for both, and that may be too strict, because itmay obfuscate the data and the conclusions. Could you pleasecomment on that definition?
You also state that the elderly, sicker patients were selected forthe single cross-clamp technique. Now, when you say this, hadyou already established that this was the superior technique? Is itpossible that other subtle changes were made in the conduct of theoperative procedure?
I think my final comment is, then, that you need to begin doingyour prospective randomized study now if you truly believe thatthis technique is superior.
DR AGUSTIN ARBULU (Detroit, MI): I congratulate Dr Arankiand I predict that, as was suggested, when the randomized studyis done, the technique they recommend in this presentation willbecome a winner. Our experience in over 3,000 cases using thistechnique corroborates the results of this presentation. So, I haveno problems with your randomized study, and I think that itshould be done.
DR R. VA RICK BERNSTEIN (Fargo, ND): I am just wonderingwhether the problems with myocardial dysfunction after theoperations might have been due not to the partial occluding
clamp, but rather to the use of only antegrade cardioplegia inpatients who had multiple-vessel disease with proximal occlusions.
DR STEVEN W. GUYTON (Seattle, WA): One question I have forDr Aranki is, you did not mention whether the grafts in the partialoccluding group were perfused before being anastomosed to theaorta, and I would just question whether that was done.
DR ARANKI: Doctor Jones, thank you very much for your kindremarks. I agree with you that the shortfalls of the study were thatit is nonrandomized. and retrospective; however, we think thatthis is compensated for by the fact that, in the group that was at amuch higher risk, we were able to achieve better perioperativeoutcomes.
As far as the intraaortic balloon pump use preoperatively, as Imentioned, there was a selection bias in the use of the singlecross-clamp technique for older and sicker patients. This has notcaused a change in the rest of the operative technique or themanagement of the patients in any way. I agree with you that a22% incidence of intraaortic balloon pump use preoperatively isvery high, but I think we have this high number because of theselection bias.
We defined the low cardiac output state to be the use of morethan one inotropic agent or the use of an intraaortic balloon pumppostoperatively. This does not include patients who had a preoperative intraaortic balloon pump, unless they needed more thanone inotropic agent postoperatively.
Doctor Bernstein, I think your question was related to inadequate protection with antegrade cardioplegia. In this study, onlyantegrade cardioplegia was used. It did not compare differentcardioplegia techniques. It compared an operative technique thatmayor may not have an influence on the cardioplegia or myocardial protection.
Doctor Guyton, we have not perfused the grafts before theproximal anastomosis, and we do not use this technique at ourinstitution.
Copyright © 2022 FDOKUMEN