Animal Models of Myocardial and Vascular Injury
11
RESEARCH REVIEW Animal Models of Myocardial and Vascular Injury Aaron M. Abarbanell, M.D.,† Jeremy L. Herrmann, M.D.,† Brent R. Weil, M.D.,† Yue Wang, Ph.D.,† Jiangning Tan, M.D., Ph.D.,† Steven P. Moberly, B. S.,† Jeremy W. Fiege,† and Daniel R. Meldrum, M.D.* , † , ‡ , § ,1 *Clarian Cardiovascular Surgery, Methodist Hospital; †Department of Surgery; ‡Department of Cellular and Integrative Physiology; and §Center for Immunobiology, Indiana University School of Medicine, Indianapolis, Indiana Over the past century, numerous animal models have been developed in an attempt to understand myocardial and vascular injury. However, the success- ful translation of results observed in animals to human therapy remains low. To understand this problem, we present several animal models of cardiac and vascular injury that are of particular relevance to the cardiac or vascular surgeon. We also explore the potential clinical implications and limitations of each model with respect to the human disease state. Our results underscore the concept that animal research requires an in-depth understanding of the model, animal physi- ology, and the potential confounding factors. Future outcome analyses with standardized animal models may improve translation of animal research from the bench to the bedside. Ó 2010 Elsevier Inc. All rights reserved. Key Words: ischemia/reperfusion; myocardial infarc- tion; heart failure; atherosclerosis; endothelial damage; animal models; comparative physiology. INTRODUCTION Coronary artery disease and peripheral vascular disease are leading causes of morbidity and mortality [1–4]. As with all potential therapies, the efficacy of new treatments needs to be proven in clinical trials prior to widespread use. However, human studies involving interventions for acute injury (e.g., myocar- dial infarction [MI], aneurysm rupture, thromboembo- lus) are hampered by the inability to assess efficacy until an event occurs. Potentially, animal models that replicate myocardial and peripheral vascular disease/injury can lead to the development of novel treatment strategies. However, the costs of animal research, especially new model development, are sig- nificant from both a monetary and animal mortality perspective [5, 6]. This has led some investigators to advocate that animal models are inappropriately used for research. Several systematic reviews have been conducted in an attempt to define the exact role of animal models as plat- forms for future human therapy [7, 8]. One review of 76 animal studies found that only 37% (28) of the studies were replicated in humans, while 45% remained untested in humans [9]. In addition, only eight of the 28 studies were eventually approved for human use. Fur- ther supporting this low statistic was a recent report from a National Heart, Lung and Blood Institute working group specifically investigating the failure to translate therapies for myocardial ischemia/reperfusion injury (I/R) from the bench to the clinical world. The working group concluded that inappropriately chosen animal models, as well as a lack of reproducibility, standardized models, and blinding of the investigators hindered the success of translational research [3]. To understand the difficulties inherent in animal models of myocardial and vascular injury, this review (1) describes several current models of myocardial injury, heart failure, and vascular injury; (2) presents selected new research findings based on these models; and (3) details the challenges inherent in the models and the limitations across species. MYOCARDIAL ISCHEMIA/INFARCT MODELS The incidence of MI is estimated at 770,000 Ameri- cans/year with an additional 430,000/year having a recurrent MI [1]. Given this high incidence, signifi- cant emphasis has been placed on the use of animal models to understand the pathophysiology of acute MI 1 To whom correspondence and reprint requests should be addressed at Indiana University School of Medicine, 2017 Van Nuys Medical Science Building, 635 Barnhill Drive, Indianapolis, IN 46202. E-mail: [email protected]. 0022-4804/$36.00 Ó 2010 Elsevier Inc. All rights reserved. 239 Journal of Surgical Research 162, 239–249 (2010) doi:10.1016/j.jss.2009.06.021
Transcript of Animal Models of Myocardial and Vascular Injury

Journal of Surgical Research 162, 239–249 (2010)doi:10.1016/j.jss.2009.06.021
RESEARCH REVIEW
Animal Models of Myocardial and Vascular Injury
Aaron M. Abarbanell, M.D.,† Jeremy L. Herrmann, M.D.,† Brent R. Weil, M.D.,† Yue Wang, Ph.D.,†Jiangning Tan, M.D., Ph.D.,† Steven P. Moberly, B. S.,† Jeremy W. Fiege,†
and Daniel R. Meldrum, M.D.*,†,‡,§,1
*Clarian Cardiovascular Surgery, Methodist Hospital; †Department of Surgery; ‡Department of Cellular and Integrative Physiology;and §Center for Immunobiology, Indiana University School of Medicine, Indianapolis, Indiana
Over the past century, numerous animal modelshave been developed in an attempt to understandmyocardial and vascular injury. However, the success-ful translation of results observed in animals to humantherapy remains low. To understand this problem, wepresent several animal models of cardiac and vascularinjury that are of particular relevance to the cardiac orvascular surgeon. We also explore the potentialclinical implications and limitations of each modelwith respect to the human disease state. Our resultsunderscore the concept that animal research requiresan in-depth understanding of the model, animal physi-ology, and the potential confounding factors. Futureoutcome analyses with standardized animal modelsmay improve translation of animal research from thebench to the bedside. � 2010 Elsevier Inc. All rights reserved.
Key Words: ischemia/reperfusion; myocardial infarc-tion; heart failure; atherosclerosis; endothelial damage;animal models; comparative physiology.
INTRODUCTION
Coronary artery disease and peripheral vasculardisease are leading causes of morbidity and mortality[1–4]. As with all potential therapies, the efficacy ofnew treatments needs to be proven in clinical trialsprior to widespread use. However, human studiesinvolving interventions for acute injury (e.g., myocar-dial infarction [MI], aneurysm rupture, thromboembo-lus) are hampered by the inability to assess efficacyuntil an event occurs. Potentially, animal modelsthat replicate myocardial and peripheral vasculardisease/injury can lead to the development of novel
1 To whom correspondence and reprint requests should beaddressed at Indiana University School of Medicine, 2017 Van NuysMedical Science Building, 635 Barnhill Drive, Indianapolis,IN 46202. E-mail: [email protected].
239
treatment strategies. However, the costs of animalresearch, especially new model development, are sig-nificant from both a monetary and animal mortalityperspective [5, 6]. This has led some investigators toadvocate that animal models are inappropriatelyused for research.
Several systematic reviews have been conducted in anattempt to define the exact role of animal models as plat-forms for future human therapy [7, 8]. One review of 76animal studies found that only 37% (28) of the studieswere replicated in humans, while 45% remaineduntested in humans [9]. In addition, only eight of the 28studies were eventually approved for human use. Fur-ther supporting this low statistic was a recent reportfroma National Heart,Lungand BloodInstitute workinggroup specifically investigating the failure to translatetherapies for myocardial ischemia/reperfusion injury(I/R) from the bench to the clinical world. The workinggroup concluded that inappropriately chosen animalmodels, as well as a lack of reproducibility, standardizedmodels, and blinding of the investigators hindered thesuccess of translational research [3].
To understand the difficulties inherent in animalmodels of myocardial and vascular injury, this review(1) describes several current models of myocardialinjury, heart failure, and vascular injury; (2) presentsselected new research findings based on these models;and (3) details the challenges inherent in the modelsand the limitations across species.
MYOCARDIAL ISCHEMIA/INFARCT MODELS
The incidence of MI is estimated at 770,000 Ameri-cans/year with an additional 430,000/year havinga recurrent MI [1]. Given this high incidence, signifi-cant emphasis has been placed on the use of animalmodels to understand the pathophysiology of acute MI
0022-4804/$36.00� 2010 Elsevier Inc. All rights reserved.

JOURNAL OF SURGICAL RESEARCH: VOL. 162, NO. 2, AUGUST 2010240
and I/R (Table 1). The Langendorff, the isolatedworking heart, and the left anterior descendingcoronary artery (LAD) occlusion models are threepredominant models of myocardial ischemia/infarction.
Langendorff (Isolated Heart Perfusion System)
The Langendorff is an ex vivo model used to studycardiac physiology, acute global or regional I/R, andthe efficacy of drug or cell therapy on the heart [10].While large mammalian hearts can be studied withthe Langendorff, small animals are predominantlyused due to low cost and the ease of small animal care.Rodents in particular have short breeding cycles. Inaddition, the availability of genetically modified micefacilitates the investigation of myocardial cytokinesand signaling despite the technical challenges of usingthe small mouse heart on the Langendorff.
Elias Cyon developed the precursor model for isolatedheart perfusion using an explanted frog heart in 1866[11, 12]. Oscar Langendorff modified Cyon’s design tostudy mammalian hearts in 1895 [13]. Langendorffused a retrograde aortic cannula to supply whole bloodto the aorta under constant pressure. This retrogradeflow closed the aortic valve, sending the blood into thecoronary arteries and, subsequently, into the coronarysinus and right atrium. Right atrial coronary effluentwas measured as well as the muscular shortening ofthe heart via a pulley system connected to the apex ofthe heart [11, 12]. However, the model did not measureventricular stroke work (the product of the ejectedvolume and the pressure required to move the fluid)as the left ventricle (LV) had no preload and did noteject volume.
The modern Langendorff only retains the retrogradeperfusion of the aorta. A physiologic solution describedby Krebs and Hensleit (KH solution) replaces the blood.The KH solution is delivered at either constantpressure or constant flow [12]. To evaluate the function
TABL
Select Models of Cardi
Myocardial injury models Injury or conditionIsolated heart (Langendorff) Acute global or reIsolated working heart (Neely) Acute global or reLAD occlusion I/R, MI (acute or c
Heart failure modelsIschemia HF associated witPressure overload Left ventricular hVolume overload Dilated cardiomyo
Vascular injury modelsAAA Aneurysm formatHind limb ischemia Acute and chronicBalloon angioplasty/wire Endothelial injuryCarotid artery ligation Neointimal lesionPerivascular injury Neointimal lesion
of the heart, the left atrial appendage is excised, anda balloon attached to a pressure transducer is placedthrough the left atrium into the LV [14]. The balloonis inflated to maintain a constant pressure. Contractionof the LV against the inflated balloon generatesa continuous pressure reading that is converted intomeasurements of heart rate, LV developed pressure(LVDP), end diastolic pressure (EDP), the rate ofcontraction (þdP/dt), and the rate of relaxation (�dP/dt). Using the above parameters, the Langendorffgenerates reproducible data regarding ex vivo heartfunction.
One of the Langendorff’s strengths is the ability toassess the impact of acute regional or global I/R injuryon the heart. Regional I/R injury can be induced viatransient ligation of the LAD [15] or via a dual lumencatheter that selectively provides perfusion to one ofthe coronary ostia [16]. Regional ischemia is arrhyth-mogenic and is often used to study the effects of drugson arrhythmias. However, global I/R is of particularinterest to the cardiac surgeon as it reproduces the ef-fects of I/R on the heart when the heart is arrestedand restarted for cardiac surgery. To induce globalischemia on the Langendorff, the coronary perfusionis stopped, and the heart is immersed in a warm waterbath to induce injury for a set time prior to reperfusion.There are four key differences between this model of I/Rand the human heart undergoing arrest for cardiacsurgery. First, cold cardioplegia is given to arrest theheart in humans. Secondly, the animal prior to cardiec-tomy receives intraperitoneal heparin and not intrave-nous heparin. Thirdly, warm ischemia induces injury inthe Langendorff versus cold ischemia in the human.Finally, the isolated heart on the Langendorff is freeof any systemic factors (e.g., autonomic signaling,whole blood).
Despite the differences between the animal model ofI/R and human I/R, the Langendorff continues toprovide new insights into myocardial I/R at the
E 1
ac and Vascular Injury
s studied with the model Selected referencesgional I/R, normal physiology 10, 11, 14, 15gional I/R, LV work 20, 21hronic injury) 13, 25, 26
h ischemic injury 30, 31ypertrophy 31, 35, 36pathy 39–41, 42
ion and rupture 60–61, 67limb ischemia 54, 55, plaque formation 65, 67, 68
s 71, 76, 77s 78, 81

ABARBANELL ET AL.: MYOCARDIAL AND VASCULAR INJURY MODELS 241
molecular and genomic level. Recent representativestudies include (1) the importance of the Toll-like recep-tor 4 to myocardial dysfunction after I/R [17]; (2) theessential role of ferritin in ischemic preconditioning ofthe heart [18]; (3) the interaction between the reperfu-sion injury salvage kinase and Janus kinase-signaltransducers and activators of transcription pathwaysin post-conditioning of the heart [19]; and (4) the roleof embryonic stem cells in myocardial recovery afterI/R [20]. These developments would not have beenpossible without the use of animal hearts on theLangendorff. This knowledge may be the foundationof novel strategies that improve myocardial recoveryin patients after acute I/R.
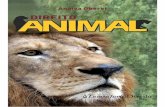
FIG. 1. Isolated working heart model. Neely’s modification of theisolated heart perfusion model (Langendorff), which allows measure-ment of LV work. Unlike the contemporary Langendorff, perfusate issupplied by the left atrial cannula instead of the aortic cannula. Theaortic cannula in the Neely model is attached to a pressure chamberwhich the LV ejects against. The change in pressure created by theLV contracting can then be converted into work. (Reprinted withpermission from Neely et al. Am. J Physiol 1967 [21] as reproducedin Zimmer News Physiol Sci 1998 [11]).
The Isolated Working Heart Model
Neely and colleagues modified the Langendorff toovercome its inability to quantify left ventricularwork [21] and developed the isolated working heartmodel (Fig. 1). In this model, the KH solution is deliv-ered into the left atrium via a cannula attached toa peristaltic pump. The LV ejects this volume againsta constant pressure head created by a hydrostaticcolumn connected to the aorta. By providing volumefor the LV to eject, the work of the LV can be can calcu-lated as mentioned previously.
Others have taken Neely’s modification one stepfurther with a four chamber working model where allfour chambers of the heart are filled and eject [22].This last modification has even been applied to humanhearts that were deemed unsuitable for transplanta-tion after explantation [23]. However, the majority ofexperiments using the isolated working heart involvesmall animals due to short breeding cycles and cost.The working heart model offers the advantage of study-ing cardiac function under variable loading conditions[24]. Recently, this model was combined with trans-genic mice and microarray data to elucidate the roleof vascular endothelial growth factor (VEGF) receptor2 in myocardial protection after I/R [25]. While theisolated working heart is technically difficult, suchresults will likely ensure the place of this model in im-proving our understanding of myocardial injury in anex vivo setting.
LAD Occlusion Models
Unlike the Langendorff and the working heartmodel, which study the heart outside the systemicinfluences from the body [12, 24], the LAD occlusionmodel provides insight into the systemic influences onthe heart after myocardial I/R or MI. Occlusion of theLAD is generally performed through a left thoracotomy.After exposing the LAD, a suture or occlusion device is
used to either temporarily occlude or permanentlyligate the LAD or a branch of the LAD [14].
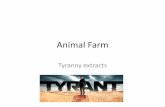
Transient LAD occlusion can also be achieved via‘‘closed chest’’ methods (Fig. 2) [26]. One closed chestmodel still involves a thoracotomy to implant an occlu-sive device, however, I/R injury is not induced untilseveral days post-operatively, when the acute inflam-matory response from surgery has resolved [26, 27].A second closed chest model utilizes catheter-basedocclusion without thoracotomy [6].
Using the LAD occlusion model, in vivo myocardialfunction as well as infarct size can be measured follow-ing injury. Two-dimensional echo and MRI are themainstays of assessing in vivo heart function. To quan-tify infarct size, triphenyltetrazolium chloride (TTC)can be infused into the LAD distal to the occlusion priorto explanation of the heart. TTC will stain the viable

FIG. 2. ‘‘Closed chest’’ model of myocardial ischemia/reperfusion.Nossuli and colleagues developed a murine model of I/R thatsurgically implants a suture snare around the LAD (A). This snareis exteriorized and the chest is closed (B). After sufficient time haselapsed to allow the inflammation of the surgery to resolve, the snareis tightened to induce myocardial ischemia (C). (Reprinted withpermission from Nossuli et al. Am J Physiol 2000 [26]).
JOURNAL OF SURGICAL RESEARCH: VOL. 162, NO. 2, AUGUST 2010242
heart tissue delineating the at-risk and infarct regions.Explanted myocardial tissue can also be analyzed forprotein expression and gene translation.
While any species can be used with the LAD occlusionmodel, small animals, such as mice, are technicallydifficult [5, 14]. Nevertheless, the short breeding cycleof the mouse, and the ability to design transgenicanimals, make the use of mice more compelling [28].Two recent examples include (1) Vidavalur andcolleagues, who using the murine LAD occlusion modeldemonstrated the potential of Sildenafil (a phosphodi-esterase inhibitor) to increase transcription of myocar-dial protective genes 24 hours after LAD occlusion [29],and (2) Aleshin and associates, who correlated the recep-tor for advanced glycation end-products (RAGE) withmyocardial damage following I/R in mice [30]. Althoughmany new pathways such as these are still to be corrob-orated in humans, these new developments based on
animal models have the potential to identify proteinsassociated with myocardial I/R. Potentially, blockadeof injurious proteins or exogenous delivery of beneficialproteins may attenuate the effects of an acute MI.
HEART FAILURE MODELS
Heart failure (HF) is a common occurrence followingMI or I/R. While HF is often considered a medicaldisease, there are aspects of the disease that requiresurgical intervention. Models of HF can be inducedvia ischemia, genetic modification, volume or pressureoverload, sustained tachycardia, or toxic drugs [31, 32].Similar to models mentioned previously, measurementof myocardial function can be performed in vivo with 2-D echo or MRI while ex vivo function can be measuredwith the Langendorff or the working heart model.Three models of heart failure of particular interest tothe surgeon are the ischemia induced HF model, thepressure overload HF (aortic banding) model, and thevolume overload HF (shunt) model.
Ischemia Induced Models of HF
Ligation of the LAD or a branch of the LAD has beenused to induce regional injury and subsequent heartfailure in multiple animal models [32]. While the proce-dures used are the same as the LAD occlusion modelsfor acute MI, a significant amount of time is requiredfor the animals to develop HF. In addition, not allanimals will progress to HF during the time frame ofthe experiment. Nonetheless, these models haveincreased our understanding of cellular and molecularevents related to ischemia-induced HF. For instance,Murray et al. examined the role of mitochondrialdysfunction in decreased efficiency of chronicallyinfarcted rat heart [33].
Clinically, ischemic models of HF have been used tostudy heart failure associated conditions, such as ische-mia related mitral regurgitation (MR). To characterizethe role of MR with respect to ischemic HF, Beeri et al.induced apical MI in sheep via LAD ligation, and useda LV to left atrial shunt to overload the left side of theheart resulting in MR [34]. This model was used todispute the clinical hypothesis that a mitral valvulo-plasty for MR after an ischemia event did not influenceremodeling of the heart [35].
Aortic Banding (Pressure Overload) Models of HF
Aortic banding models create a pressure overloadphysiology such as that which may be found in aorticstenosis, systemic hypertension, and coarctation ofthe aorta (Fig. 3) [32, 36–38]. Continued pressure over-load causes the LV to hypertrophy and eventually leads

FIG. 3. Latex casts of aortic banding model. Hu and associatesdeveloped a minimally invasive transverse aortic banding model inmice. Latex casts of the mouse heart and aorta clearly denote thestenotic area of the aorta (arrow) created by a suture ligature (leftheart) as compared to the sham (right heart). (Reprinted withpermission from Hu et al. Am. J Physiol 2003 [36]).
TABLE 2
ABARBANELL ET AL.: MYOCARDIAL AND VASCULAR INJURY MODELS 243
to HF. The aorta may be banded in several locations toproduce these results. In adult guinea pigs, banding ofthe descending thoracic aorta has led to HF [37]. Band-ing of the ascending aorta in rats has also been used toinduce LV hypertrophy (LVH) and HF [39]. Recently,Stansfield et al. described a minimally invasive murinemodel of transverse aortic banding that may yield clin-ical insights [40]. They banded the transverse arch ofthe aorta with a suture slip knot placed between theinnominate and left carotid arteries. The operationwas performed through a small incision at the supra-sternal notch, which allowed subsequent removal ofthe band up to 4 wk later through the same incision.This technique creates a reversible model of LVH,which may lead to an understanding of the molecularsignaling associated with LVH.
Benefits and Challenges of Animal Modelsfor Myocardial and Vascular Injury Research
BenefitsAbility to study injury in the acute settingPlatform for drug or cell therapiesAvailability of transgenic or knock-out/in animalsAbility to study individual protein expression and function
ChallengesPhysiologic and anatomical differences between different animalspeciesInjury or lesion does not completely replicate the human state andcomorbid conditionsFew studies in animals have been translated to human therapyLack of model standardizationCost of animal husbandry, model development, and transgenic orknock-out/ in animalsPublic perception of animal research
Volume Overload Models of HF
Arteriovenous shunts are used to create volume over-load leading to dilated cardiomyopathy and subsequentHF. Carotid artery to jugular vein shunts have beensuccessfully performed in large animal models, suchas dogs and goats [41–43]. However, these models oftenrequire doxorubicin administration to develop HF.Others have used femoral artery to femoral vein fistu-las in rodents, and demonstrated HF without the needfor doxorubicin [44]. The reported mortality, however,in all these prior studies exceeds 25%. While the priorstudies were performed to avoid a laparotomy, the
creation of an aortocaval shunt may be a viable alterna-tive. Garcia et al. reported successful aortocaval shunt-ing in rodents with 10 of 11 rats alive at postoperativeweek 4 [45]. It should be noted that this study didnot perform any hemodynamic monitoring but wasintended to improve on the high mortality of prior stud-ies of rodent aortocaval induced HF. In support ofaortocaval fistula induced HF for research, a recentstudy using this model correlated the inhibitory effectsof angiotensin converting enzyme inhibitors on matrixmetalloprotease activity to better postoperative cardiacfunction in rats [46]. The authors did not comment onmortality, but their groups appeared to be intact at8 wk post-fistula creation. Taken together, the mortal-ity of arteriovenous shunts may be high, however, theshunt model appears to be a viable method of studyingvolume overload induced HF.
SPECIES LIMITATIONS OF MYOCARDIAL INJURY ANDHEART FAILURE MODELS
While the models previously described continue toimprove our understanding of myocardial injury, inter-species differences limit the reproducibility of infarctsize and the induction of HF across animal models(Table 2). Two noteworthy differences are the presenceof collateral circulation and variable inflammatoryreactions. Dogs and guinea pigs have a well-developedcollateral circulation compared with other animals,such as rat, pig, and baboon [47, 48]. The effect of collat-eral circulation is most apparent in the guinea pig,where I/R or MI cannot be induced due to extensivecollaterals [10, 48]. Interspecies variation is alsoevident by the fact that rats tolerate a significantlygreater infarct area (>46%) than dogs, that developfatal arrhythmias with infarcts of 30% or more [49].With respect to the variable species inflammatory

JOURNAL OF SURGICAL RESEARCH: VOL. 162, NO. 2, AUGUST 2010244
responses to myocardial injury, Dewald et al. studiedthe differences between dogs and mice after closedchest I/R injury [27]. Compared with dogs, mice hada more rapid inflammatory course, less capillarydensity in the infarct region, and very transient macro-phage infiltration. These differences in the coronarycirculation and the inflammatory process likely contrib-ute to extreme variability of published results.
The history of the LAD occlusion model developmentfurther underscores the challenges of interspeciesreproducibility in animal models. In the 1950s, dogswere predominantly used to study human coronaryartery occlusion because the canine coronary circula-tion was thought to closely approximate the human.However, the canine occlusion model was plagued byhighly variable infarct sizes and a mortality exceeding50% [5]. Other models, such as the porcine model,which more closely approximated the human coronarycirculation, were equally difficult in generating consis-tent ischemic injury due to arrhythmias. As recently as2005, despite the use of angiography in a closed chestmodel, Krombach et al. induced MI in only 34 of 44swine with a high intraoperative rate of ventricularfibrillation [6]. Given the numerous challenges of largeanimal models, many investigators have focused on thedevelopment of small animal models, which haveshorter breeding cycles, require less animal husbandry[5, 50], and permit the use of transgenic or knock-outanimals.
In an attempt to avoid some challenges of the LADligation model, others have developed a spontaneousmodel of MI. Shiomi et al. bred hyperlipidemic rabbitsthat have a greater than 90% incidence of spontaneousMI associated with complex intracoronary plaques [51].However, this model requires almost 11 mo before spon-taneous MIs develop. In addition, while these rabbitsdevelop complex plaques similar to humans, theseplaques do not rupture like human plaques.
Given all the preceding data, it is no surprise that ata molecular level interspecies variation also exists.Known differences include intracellular calcium han-dling, myocardial force-frequency relationships, andthe a and b myosin chain composition of the myocar-dium [31]. These data, and the concepts they entail,must be considered when attempting to apply animalexperimental observations of myocardial injury andHF to humans.
VASCULAR INJURY MODELS
Vascular injury is associated with hyperlipidemia,hypertension, infectious microorganisms, and smoking.Injury to the arterial intima results in the formationof atherosclerotic plaques and smooth muscle cell
activation associated with neointimal hyperplasia[52, 53]. This injurious cascade leads to the develop-ment abdominal aortic aneurysms (AAA), limb ische-mia, in-stent stenosis, and restenosis of vessels afterangioplasty. As a result, animal models have beenused in an attempt to improve our understanding ofthe inflammatory and immune responses involvedwith vascular injury [54, 55]. Subsequently, clinicaltherapies, such as drug eluting stents [56, 57] and endo-vascular repair of AAAs [58, 59] have been developed orundergone clinical trials as a result of animal models.Five groups of models exemplify current approachesto study vascular injury—AAA, hind limb ischemia,balloon angioplasty/wire induced injury, carotid arteryligation, and perivascular injury models.
Abdominal Aortic Aneurysm Models
AAA models predominantly involve mice, rats, ordogs [60, 61]. Numerous methods have been used toinduce aneurysms in animals. In broadest terms, theycan be classified as genetic or metabolic manipulation;direct chemical treatment or surgical alteration of theaorta; or elastase infusion. Initial animal models ofaneurysms in the 1950s and 1960s involved systematicmetabolic changes by dietary manipulation, directchemical toxicity to the aorta, or surgical alteration ofthe aorta. One group noted that rats fed a diet of 50%sweet peas developed skeletal deformities and aorticaneurysms [62]. Another group injected nitrogenmustard into the aortic adventitia of dogs to createaneurysms [63]. Surgical excision of the adventitiaand chemical treatment of the aorta was also attempted[64]. However, the size of the aneurysms could not bereliably reproduced in these models. More recently,the use of genetically altered mice appears to bea more viable option. For instance, mice lacking tissueinhibitors of matrix metalloproteinases (TIMP) wereused to study the role of matrix metalloproteinases(MMPs) in AAA formation [65]. Others have used trans-genic mice overexpressing renin and angiotensin lead-ing to hypertension and aneurysm formation [66].One of the more often cited models of AAAs involveselastase. Elastase is a pancreatic enzyme that degradesthe elastin in the aorta, leading to subsequent aneu-rysm formation. This model has been used to furtherexplore the role of MMPs, hypertension, and variousdrugs on AAA formation [67].
While this review covers a select subset of AAAmodels, other genetic modifications and chemicalagents have been used to induce AAAs. These arecovered more extensively elsewhere [60, 61, 68]. Modelsof AAA are certainly still evolving, but the insightsgained from the current models have been significantto date.

ABARBANELL ET AL.: MYOCARDIAL AND VASCULAR INJURY MODELS 245
Hind Limb Ischemia Model
The hind limb ischemia model is a model of periph-eral arterial disease initially developed in rabbits andmice [69]. This model creates unilateral hind limbischemia with the contralateral limb serving as a con-trol (Fig. 4) [70]. Severe limb ischemia may be inducedby proximal ligation of the femoral artery and its sidebranches. To mimic chronic ischemia, distal ligation ofthe femoral artery may be performed while leavingthe arterial side branches intact. This latter methodproduces a model of mild chronic ischemia at rest andreduced blood flow reserve with exercise [71]. Thesetwo models have helped researchers identify molecularand gene transcription processes of ischemia, with theaim of developing future therapies [72–75]. Addition-ally, the hind limb model has elucidated aspects ofangiogenesis following ischemia [69, 76]. The hindlimb model can also be used to study I/R by use ofa temporary tourniquet.
Balloon Angioplasty and Wire Induced Injury Models
The balloon angioplasty model simulates the effectson the endothelium of percutaneous angioplasty. Stud-ies document that repeated endothelial injury viaballoon angioplasty causes similar lesions to that of hu-man atherosclerosis [77–80]. The balloon angioplastymodel is suggested to be superior to other vascularinjury models, which study smooth muscle prolifera-tion. This model is also used to investigate the inflam-matory and bone marrow responses to vascular injury[55, 81, 82].
The wire injury model is similar to the balloon angio-plasty model, and is mostly used in mice. This techniqueinvolves exposing the carotid artery and passing a flexi-ble wire into the common carotid artery to completelydenude the endothelium [83–85]. This technique canalso be used in the femoral artery [86]. The wire injurymodel is criticized for its inability to produce consistentinjury. In addition, endothelial injury only producesa small proliferative response, which usually does notexceed two to three cell layers [83].
FIG. 4. Hind limb ischemia model. Scanning laser Doppler perfusiofemoral artery. Immediately after ligation of the femoral artery, signifi(Reprinted with permission from Chalothorn et al. Am J Physiol 2005 [7
Carotid Artery Ligation Model
The carotid artery ligation model was developed byKumar and Lindner in the mouse [87]. The rationalefor this model is that alterations in blood flow areknown to increase intimal lesion formation in vasculargrafts and balloon injured vessels [88–90]. In thismodel, the common carotid artery is ligated near thebifurcation. Two to 4 wk following ligation, neointimallesions form. While this model is relatively simple toperform, abrupt total occlusion of the carotid arterydoes not replicate a physiological situation [84]. None-theless, investigators have used this model to clarifythe role of lipid lowering agents, such as statins, inmodulating the inflammatory cascade [91]. Severalexcellent review articles detail the potential uses forthis method, which are beyond the scope of this review[92, 93].
Perivascular Electrical Injury and Occlusion Models
Perivascular electric stimulation can be used toinjure the endothelium [94]. This model destroys themedial smooth muscle cells, denudes the endotheliumof the associated arterial segment, and transientlyinduces platelet-rich mural thrombosis. However, thistechnique is seldom used due to the extensive damageto the vessel. Alternatively, perivascular collars havebeen used to reduce blood flow and promote neointimalformation in the carotid artery. A hollow silastic band isplaced around the carotid artery, which induces macro-phage infiltration into the subendothelium, smoothmuscle cell proliferation, and deposition of extracellu-lar lipid. The collar is thought to cause obstruction ofthe adventitial vasa vasorum [95]. A similar modeldescribed in mice uses the femoral artery [96]. Unlikethe other vascular injury models described, the endo-thelial cells are not directly manipulated or removed.This permits the study of individual endothelial factors,such as endothelium-derived nitric oxide [52]. Theperivascular collar model is easy to reproduce andeasily quantified.
n images of a mouse hind limb before and after ligation of the rightcant collateral flow is seen as compared to the left control hind limb.0]). (Color version of figure is available online.)

JOURNAL OF SURGICAL RESEARCH: VOL. 162, NO. 2, AUGUST 2010246
SPECIES LIMITATIONS OF VASCULAR ANIMAL MODELS
Similar to the myocardial injury models, animalmodels of vascular disease/injury can be difficult toreproduce across species primarily due to differencesin atherosclerosis formation. Ignatowski and Anitsch-kow are credited with the discovery of the first animalmodel of atherosclerosis in 1908 and 1912, respectively[97, 98]. Their research was among the first to demon-strate that cholesterol induced atherosclerotic lesionsdiffer among species. For instance, while rabbits fedcholesterol-enriched diets form lesions similar tohuman atherosclerotic plaques, rabbits requireextremely high plasma cholesterol levels to developatherosclerotic plaques. In addition, rabbit plaquesform in the aortic arch and thoracic aorta, whereasthe abdominal aorta is the more likely site in humans[85]. Later research demonstrated that certain strainsof mice (e.g., Balb and common wild type) do not developspontaneous atherosclerosis secondary to high intake ofcholesterol [87, 90]. This has been attributed to highlevels of anti-atherosclerotic high-density lipoprotein(HDL), low levels of low-density lipoprotein (LDL),and very low-density lipoprotein (VLDL). Nonetheless,the ability to create transgenic or knock-out mice hasbeen useful in developing atherosclerotic models[99–101]. Some of the more commonly used mousemodels are the apolipoprotein E deficient (Apo E–/–),LDL receptor deficient (LDLr–/–), or Apo E3 Leiden(E3L) mice. Knockout of the ApoE or LDLr gene leadto severe hypercholesterolemia and spontaneous ather-oma formation [101]. The E3L mouse expressesa mutated form of the human ApoE3 gene, which cre-ates a hyperlipidemic phenotype. However, there aremany differences between these genetically alteredmice and humans. In mice, the disease course prog-resses rapidly, which leads to shorter induction time,unlike the more indolent course in the human. Addi-tionally, mice do not present with end-stage ischemiclesions, such as occlusive coronary artery disease orlimb ischemia [90]. Additional species differences areevident in wild type rats, which in general do notdevelop atheromas as they lack plasma cholesterylester transfer protein, unlike humans, and thus HDLis the major carrier of plasma cholesterol [98]. Hyper-lipidemia and atherosclerosis can be induced in ratswith a high cholesterol/high fat diet containing cholicacid and thiouracil. Thiouracil induces hypothyroidism,which leads to decreased LDL receptor activity andhypercholesterolemia. There are also strains of ratswith heritable hyperlipidemia and associated athero-genesis [102, 103]. Other animals have also been usedto model atherosclerosis, such as quail and chickens.Certain strains of quail can develop advanced athero-sclerotic lesions and myocardial infarction. The short
induction time of 2 wk makes chickens an attractiveatherosclerotic animal model. However, atheroscleroticlesions in chickens are not the complex plaques seen inhumans, and rarely result in complications such asmyocardial infarction [97, 104–107].
With respect to angioplasty induced injury, the por-cine model produces similar responses to humans afterangioplasty [108]. However in order to produce plaquerich in lipids, the pigs must be maintained on a highfat/cholesterol diet [109]. There are naturally occurringpigs with defective mutations in cholesterol metabo-lism. However, atherosclerosis develops in these pigsafter 7 mo of age, which leads to significant animalhusbandry costs [110].
Despite the inherent challenges of vascular injurymodels, recent research using these models has pointedto novel potential treatments of atherosclerosis andvascular injury with nitric oxide [111, 112] and genemediated therapies [113–115].
CONCLUSIONS
Animal models can provide novel mechanisticinsights into myocardial and vascular disease. Themodels described point to potential clinical therapies.However, the translation rate from the bench to thebedside remains low, likely due to differences in physi-ology and molecular pathways. A clinical understand-ing of the disease process of interest combined within-depth knowledge of the model and animal to beused may increase the predictive value of the animalmodels. Whether or not the institution of an animalmodel screening research consortium or randomizedcontrol trials, as some have proposed, will lead to thesuccessful translation of animal research is unclear inthe literature. Further outcomes analysis with stan-dardized animal models would be needed to draw thatconclusion. At the very minimum, careful scrutinyand stringent self-oversight are required to fulfill theethical, financial, and social responsibilities requiredof animal research.
ACKNOWLEDGMENTS
This work was supported in part by NIH R01GM070628 (DRM),NIH R01HL085595 (DRM), NIH 1F32HL092718 (AMA), and NIH1F32HL092719 (JLH).
REFERENCES
1. Rosamond W, Flegal K, Furie K, et al. Heart disease and strokestatistics—2008 update: A report from the American Heart As-sociation Statistics Committee and Stroke Statistics Subcom-mittee. Circulation 2008;117:e25.
2. Cohn JN, Bristow MR, Chien KR, et al. Report of the NationalHeart, Lung, and Blood Institute Special Emphasis Panel onHeart Failure Research. Circulation 1997;95:766.

ABARBANELL ET AL.: MYOCARDIAL AND VASCULAR INJURY MODELS 247
3. Bolli R, Becker L, Gross G, et al. Myocardial protection ata crossroads: The need for translation into clinical therapy.Circ Res 2004;95:125.
4. Selvin E, Erlinger TP. Prevalence of and risk factors forperipheral arterial disease in the United States: Results fromthe National Health and Nutrition Examination Survey,1999-2000. Circulation 2004;110:738.
5. Johns TN, Olson BJ. Experimental myocardial infarction. I. Amethod of coronary occlusion in small animals. Ann Surg1954;140:675.
6. Krombach GA, Kinzel S, Mahnken AH, et al. Minimally inva-sive close-chest method for creating reperfused or occlusivemyocardial infarction in swine. Invest Radiol 2005;40:14.
7. Rademaker MT, Cameron VA, Charles CJ, et al. Neurohor-mones in an ovine model of compensated postinfarction left ven-tricular dysfunction. Am J Physiol Heart Circ Physiol 2000;278:H731.
8. Knight A. Systematic reviews of animal experiments demon-strate poor human clinical and toxicological utility. AlternLab Anim 2007;35:641.
9. Hackam DG, Redelmeier DA. Translation of research evidencefrom animals to humans. JAMA 2006;296:1731.
10. Verdouw PD, van den Doel MA, de Zeeuw S, et al. Animalmodels in the study of myocardial ischemia and ischemicsyndromes. Cardiovasc Res 1998;39:121.
11. Zimmer HG. The isolated perfused heart and its pioneers. NewsPhysiol Sci 1998;13:203.
12. Skrzypiec-Spring M, Grotthus B, Szelag A, et al. Isolated heartperfusion according to Langendorff–-still viable in the newmillennium. J Pharmacol Toxicol Methods 2007;55:113.
13. Iaizzo P, Ed. Animal models for cardiac research. New Jersey:Humana Press, 2005.
14. Klocke R, Tian W, Kuhlmann MT, et al. Surgical animal modelsof heart failure related to coronary heart disease. CardiovascRes 2007;74:29.
15. Ytrehus K. The ischemic heart–experimental models. Pharma-col Res 2000;42:193.
16. Avkiran M, Curtis MJ. Independent dual perfusion of left andright coronary arteries in isolated rat hearts. Am J Physiol1991;261:H2082.
17. Cha J, Wang Z, Ao L, et al. Cytokines link Toll-like receptor 4signaling to cardiac dysfunction after global myocardial ische-mia. Ann Thorac Surg 2008;85:1678.
18. Chevion M, Leibowitz S, Aye NN, et al. Heart protection byischemic preconditioning: A novel pathway initiated by ironand mediated by ferritin. J Mol Cell Cardiol 2008.
19. Goodman MD, Koch SE, Fuller-Bicer GA, et al. Regulating risk:A role for jak-stat signaling in postconditioning? Am J PhysiolHeart Circ Physiol 2008.
20. Crisostomo PR, Abarbanell AM, Wang M, et al. Embryonicstem cells attenuate myocardial dysfunction and inflammationafter surgical global ischemia via paracrine actions. Am JPhysiol Heart Circ Physiol 2008;295:H1726.
21. Neely JR, Liebermeister H, Battersby EJ, et al. Effect ofpressure development on oxygen consumption by isolated ratheart. Am J Physiol 1967;212:804.
22. Chinchoy E, Soule CL, Houlton AJ, et al. Isolated four-chamberworking swine heart model. Ann Thorac Surg 2000;70:1607.
23. Hill AJ, Laske TG, Coles JA Jr., et al. In vitro studies ofhuman hearts. Ann Thorac Surg 2005;79:168.
24. Gauthier NS, Matherne GP, Morrison RR, et al. Determinationof function in the isolated working mouse heart: Issues inexperimental design. J Mol Cell Cardiol 1998;30:453.
25. Thirunavukkarasu M, Addya S, Juhasz B, et al. Heterozygousdisruption of Flk-1 receptor leads to myocardial ischemia reper-fusion injury in mice: Application of affymetrix gene chipanalysis. J Cell Mol Med 2008;12:1284.
26. Nossuli TO, Lakshminarayanan V, Baumgarten G, et al. Achronic mouse model of myocardial ischemia-reperfusion:Essential in cytokine studies. Am J Physiol Heart Circ Physiol2000;278:H1049.
27. Dewald O, Ren G, Duerr GD, et al. Of mice and dogs: Species-specific differences in the inflammatory response followingmyocardial infarction. Am J Pathol 2004;164:665.
28. Madeddu P, Emanueli C, Spillmann F, et al. Murine models ofmyocardial and limb ischemia: Diagnostic end-points andrelevance to clinical problems. Vascul Pharmacol 2006;45:281.
29. Vidavalur R, Penumathsa SV, Thirunavukkarasu M, et al.Sildenafil augments early protective transcriptional changesafter ischemia in mouse myocardium. Gene 2008;430:30.
30. Aleshin A, Ananthakrishnan R, Li Q, et al. RAGE modulatesmyocardial injury consequent to LAD infarction via impact onJNK and STAT signaling in a murine model. Am J PhysiolHeart Circ Physiol 2008;294:H1823.
31. Hasenfuss G. Animal models of human cardiovascular disease,heart failure and hypertrophy. Cardiovasc Res 1998;39:60.
32. Monnet E, Chachques JC. Animal models of heart failure: Whatis new? Ann Thorac Surg 2005;79:1445.
33. Murray AJ, Cole MA, Lygate CA, et al. Increased mitochondrialuncoupling proteins, respiratory uncoupling and decreased ef-ficiency in the chronically infarcted rat heart. J Mol Cell Car-diol 2008;44:694.
34. Beeri R, Yosefy C, Guerrero JL, et al. Mitral regurgitationaugments post-myocardial infarction remodeling failure ofhypertrophic compensation. J Am Coll Cardiol 2008;51:476.
35. TSt Guy, Moainie SL, Gorman JH III, et al. Prevention ofischemic mitral regurgitation does not influence the outcomeof remodeling after posterolateral myocardial infarction.J Am Coll Cardiol 2004;43:377.
36. Hu P, Zhang D, Swenson L, et al. Minimally invasive aorticbanding in mice: Effects of altered cardiomyocyte insulinsignaling during pressure overload. Am J Physiol Heart CircPhysiol 2003;285:H1261.
37. Kiss E, Ball NA, Kranias EG, et al. Differential changes incardiac phospholamban and sarcoplasmic reticular Ca(2þ)-ATPase protein levels. Effects on Ca2þ transport and mechanicsin compensated pressure-overload hypertrophy and congestiveheart failure. Circ Res 1995;77:759.
38. Stock JH, Reller MD, Sharma S, et al. Transballoon intravascu-lar ultrasound imaging during balloon angioplasty in animalmodels with coarctation and branch pulmonary stenosis.Circulation 1997;95:2354.
39. Feldman AM, Weinberg EO, Ray PE, et al. Selective changes incardiac gene expression during compensated hypertrophy andthe transition to cardiac decompensation in rats with chronicaortic banding. Circ Res 1993;73:184.
40. Stansfield WE, Rojas M, Corn D, et al. Characterization ofa model to independently study regression of ventricularhypertrophy. J Surg Res 2007;142:387.
41. Chekanov VS. A stable model of chronic bilateral ventricularinsufficiency (dilated cardiomyopathy) induced by arteriove-nous anastomosis and doxorubicin administration in sheep.J Thorac Cardiovasc Surg 1999;117:198.
42. Djelmami-Hani M, Kazemi S, Hare J, et al. Induction of heartfailure: Hemodynamic comparison of three different caninemodels. Lab Anim 2007;41:63.

JOURNAL OF SURGICAL RESEARCH: VOL. 162, NO. 2, AUGUST 2010248
43. Tessier D, Lajos P, Braunberger E, et al. Induction of chroniccardiac insufficiency by arteriovenous fistula and doxorubicinadministration. J Card Surg 2003;18:307.
44. Ozek C, Zhang F, Lineaweaver WC, et al. A new heart failuremodel in rat by an end-to-side femoral vessel anastomosis.Cardiovasc Res 1998;37:236.
45. Garcia R, Diebold S. Simple, rapid, and effective method ofproducing aortocaval shunts in the rat. Cardiovasc Res 1990;24:430.
46. Brower GL, Levick SP, Janicki JS. Inhibition of matrix metal-loproteinase activity by ACE inhibitors prevents left ventricu-lar remodeling in a rat model of heart failure. Am J PhysiolHeart Circ Physiol 2007;292:H3057.
47. Shen YT, Fallon JT, Iwase M, et al. Innate protection of baboonmyocardium: Effects of coronary artery occlusion and reperfu-sion. Am J Physiol 1996;270:H1812.
48. Maxwell MP, Hearse DJ, Yellon DM. Species variation in thecoronary collateral circulation during regional myocardialischemia: A critical determinant of the rate of evolution andextent of myocardial infarction. Cardiovasc Res 1987;21:737.
49. Pfeffer MA, Pfeffer JM, Fishbein MC, et al. Myocardial infarctsize and ventricular function in rats. Circ Res 1979;44:503.
50. Fishbein MC, Maclean D, Maroko PR. Experimental myocar-dial infarction in the rat: Qualitative and quantitative changesduring pathologic evolution. Am J Pathol 1978;90:57.
51. Shiomi M, Ito T, Yamada S, et al. Development of an animalmodel for spontaneous myocardial infarction (WHHLMIrabbit). Arterioscler Thromb Vasc Biol 2003;23:1239.
52. Hui DY. Intimal hyperplasia in murine models. Curr DrugTargets 2008;9:251.
53. Ross R. Atherosclerosis–an inflammatory disease. N Engl JMed 1999;340:115.
54. Li JM, Eslami MH, Rohrer MJ, et al. Interleukin 18 bindingprotein (IL18-BP) inhibits neointimal hyperplasia after ballooninjury in an atherosclerotic rabbit model. J Vasc Surg 2008;47:1048.
55. Tanaka K, Sata M. Contribution of circulating vascular progen-itors in lesion formation and vascular healing: Lessons fromanimal models. Curr Opin Lipidol 2008;19:498.
56. Malenka DJ, Kaplan AV, Lucas FL, et al. Outcomes followingcoronary stenting in the era of bare-metal versus the era ofdrug-eluting stents. JAMA 2008;299:2868.
57. Klugherz BD, Llanos G, Lieuallen W, et al. Twenty-eight-dayefficacy and phamacokinetics of the sirolimus-eluting stent.Coron Artery Dis 2002;13:183.
58. EVAR trial participants. Endovascular aneurysm repair versusopen repair in patients with abdominal aortic aneurysm (EVARtrial 1): Randomized controlled trial. Lancet 2005;365:2179.
59. Prinssen M, Verhoeven EL, Buth J, et al. A randomized trialcomparing conventional and endovascular repair of abdominalaortic aneurysms. N Engl J Med 2004;351:1607.
60. Cowan JA Jr., Dimick JB, Henke PK, et al. Epidemiology ofaortic aneurysm repair in the United States from 1993 to2003. Ann N Y Acad Sci 2006;1085:1.
61. Heller JA, Weinberg A, Arons R, et al. Two decades of abdomi-nal aortic aneurysm repair: Have we made any progress? J VascSurg 2000;32:1091.
62. Ponseti IV, Baird WA. Scoliosis and dissecting aneurysm of theaorta in rats fed with Lathyrus odoratus seeds. Am J Pathol1952;28:1059.
63. McCune WS, Samadi A, Blades B. Experimental aneurysms.Ann Surg 1953;138:216.
64. Economou SG, Taylor CB, Beattie EJ Jr., et al. Persistentexperimental aortic aneurysms in dogs. Surgery 1960;47:21.
65. Eskandari MK, Vijungco JD, Flores A, et al. Enhanced abdom-inal aortic aneurysm in TIMP-1-deficient mice. J Surg Res2005;123:289.
66. Nishijo N, Sugiyama F, Kimoto K, et al. Salt-sensitive aorticaneurysm and rupture in hypertensive transgenic mice thatoverproduce angiotensin II. Lab Invest 1998;78:1059.
67. Paraskevas KI, Mikhailidis DP, Perrea D. Experimentalmodels of abdominal aortic aneurysms: An overview.Curr Pharm Des 2008;14:325.
68. Daugherty A, Cassis LA. Mouse models of abdominal aorticaneurysms. Arterioscler Thromb Vasc Biol 2004;24:429.
69. Couffinhal T, Silver M, Zheng LP, et al. Mouse model of angio-genesis. Am J Pathol 1998;152:1667.
70. Chalothorn D, Zhang H, Clayton JA, et al. Catecholaminesaugment collateral vessel growth and angiogenesis in hindlimb ischemia. Am J Physiol Heart Circ Physiol 2005;289:H947.
71. Silvestre JS, Mallat Z, Duriez M, et al. Antiangiogenic effect ofinterleukin-10 in ischemia-induced angiogenesis in mice hindlimb. Circ Res 2000;87:448.
72. Hoefer IE, van Royen N, Rectenwald JE, et al. Arteriogenesisproceeds via ICAM-1/Mac-1- mediated mechanisms. Circ Res2004;94:1179.
73. Heil M, Schaper W. Influence of mechanical, cellular, andmolecular factors on collateral artery growth (arteriogenesis).Circ Res 2004;95:449.
74. Clayton JA, Chalothorn D, Faber JE. Vascular endothelialgrowth factor-A specifies formation of native collaterals andregulates collateral growth in ischemia. Circ Res 2008.
75. Shiba Y, Takahashi M, Hata T, et al. Bone marrow CXCR4induction by cultivation enhances therapeutic angiogenesis.Cardiovasc Res 2008.
76. Jacobi J, Tam BY, Wu G, et al. Adenoviral gene transfer withsoluble vascular endothelial growth factor receptors impairsangiogenesis and perfusion in a murine model of hind limbischemia. Circulation 2004;110:2424.
77. Moore S, Belbeck LW, Richardson M, et al. Lipid accumulationin the neointima formed in normally fed rabbits in response toone or six removals of the aortic endothelium. Lab Invest 1982;47:37.
78. Strauss BH, Chisholm RJ, Keeley FW, et al. Extracellularmatrix remodeling after balloon angioplasty injury in a rabbitmodel of restenosis. Circ Res 1994;75:650.
79. Richardson M, Hatton MW, Buchanan MR, et al. Wound heal-ing in the media of the normolipemic rabbit carotid arteryinjured by air drying or by balloon catheter de-endothelializa-tion. Am J Pathol 1990;137:1453.
80. Clowes AW, Breslow JL, Karnovsky MJ. Regression of myointi-mal thickening following carotid endothelial injury anddevelopment of aortic foam cell lesions in long-term hypercho-lesterolemic rats. Lab Invest 1977;36:73.
81. Rodriguez-Menocal L, St Pierre M, Wei Y, et al. The origin ofpost-injury neointimal cells in the rat balloon injury model.Cardiovasc Res 2008.
82. Plekhanova O, Berk BC, Bashtrykov P, et al. Oligonucleotidemicroarrays reveal regulated genes related to inward arterialremodeling induced by urokinase plasminogen activator.J Vasc Res 2008;46:177.
83. Lindner V, Fingerle J, Reidy MA. Mouse model of arterialinjury. Circ Res 1993;73:792.
84. Xu Q. Mouse models of arteriosclerosis: From arterial injuriesto vascular grafts. Am J Pathol 2004;165:1.
85. Zimmerman MA, Selzman CH, Reznikov LL, et al. Lack ofTNF-alpha attenuates intimal hyperplasia after mouse carotidartery injury. Am J Physiol Regul Integr Comp Physiol 2002;283:R505.

ABARBANELL ET AL.: MYOCARDIAL AND VASCULAR INJURY MODELS 249
86. Sata M, Maejima Y, Adachi F, et al. A mouse model of vascularinjury that induces rapid onset of medial cell apoptosis followedby reproducible neointimal hyperplasia. J Mol Cell Cardiol2000;32:2097.
87. Kumar A, Lindner V. Remodeling with neointima formation inthe mouse carotid artery after cessation of blood flow. Arterios-cler Thromb Vasc Biol 1997;17:2238.
88. Bassiouny HS, White S, Glagov S, et al. Anastomotic intimalhyperplasia: Mechanical injury or flow induced. J Vasc Surg1992;15:708.
89. Geary RL, Kohler TR, Vergel S, et al. Time course of flow-in-duced smooth muscle cell proliferation and intimal thickeningin endothelialized baboon vascular grafts. Circ Res 1994;74:14.
90. Kohler TR, Kirkman TR, Kraiss LW, et al. Increased blood flowinhibits neointimal hyperplasia in endothelialized vasculargrafts. Circ Res 1991;69:1557.
91. Nakamura K, Sasaki T, Cheng XW, et al. Statin preventsplaque disruption in apoE-knockout mouse model throughpleiotropic effect on acute inflammation. Atherosclerosis 2009(in press).
92. Zhang LN, Parkinson JF, Haskell C, et al. Mechanisms of inti-mal hyperplasia learned from a murine carotid artery ligationmodel. Curr Vasc Pharmacol 2008;6:37.
93. Wang X, Chai H, Lin PH, et al. Mouse models of neointimalhyperplasia: Techniques and applications. Med Sci Monit2006;12:RA177.
94. Carmeliet P, Moons L, Stassen JM, et al. Vascular woundhealing and neointima formation induced by perivascularelectric injury in mice. Am J Pathol 1997;150:761.
95. Booth RF, Martin JF, Honey AC, et al. Rapid development ofatherosclerotic lesions in the rabbit carotid artery induced byperivascular manipulation. Atherosclerosis 1989;76:257.
96. Moroi M, Zhang L, Yasuda T, et al. Interaction of genetic defi-ciency of endothelial nitric oxide, gender, and pregnancy in vas-cular response to injury in mice. J Clin Invest 1998;101:1225.
97. Moghadasian MH. Experimental atherosclerosis: A historicaloverview. Life Sci 2002;70:855.
98. Finking G, Hanke H. Nikolaj Nikolajewitsch Anitschkow(1885-1964) established the cholesterol-fed rabbit as a modelfor atherosclerosis research. Atherosclerosis 1997;135:1.
99. Getz GS, Reardon CA. Diet and murine atherosclerosis.Arterioscler Thromb Vasc Biol 2006;26:242.
100. Meir KS, Leitersdorf E. Atherosclerosis in the apolipoprotein-E-deficient mouse: A decade of progress. Arterioscler ThrombVasc Biol 2004;24:1006.
101. Zadelaar S, Kleemann R, Verschuren L, et al. Mouse models foratherosclerosis and pharmaceutical modifiers. ArteriosclerThromb Vasc Biol 2007;27:1706.
102. St John LC, Bell FP. Arterial lipid biochemistry in the sponta-neously hyperlipidemic Zucker rat and its similarity to earlyatherogenesis. Atherosclerosis 1991;86:139.
103. Chinellato A, Ragazzi E, Petrelli L, et al. Effect of cholesterol-supplemented diet in heritable hyperlipidemic Yoshida rats:Functional and morphological characterization of thoracicaorta. Atherosclerosis 1994;106:51.
104. Shih JC, Pullman EP, Kao KJ. Genetic selection, generalcharacterization, and histology of atherosclerosis-susceptibleand -resistant Japanese quail. Atherosclerosis 1983;49:41.
105. Yancey PG, St Clair RW. Cholesterol efflux is defective inmacrophages from atherosclerosis-susceptible White Carneaupigeons relative to resistant show racer pigeons. ArteriosclerThromb 1992;12:1291.
106. St Clair RW. Metabolic changes in the arterial wall associatedwith atherosclerosis in the pigeon. Fed Proc 1983;42:2480.
107. Wang R, Xu M, Marcel R, et al. Selective neointimal genetransfer in an avian model of vascular injury. Atherosclerosis1999;146:71.
108. Okamoto E, Couse T, De Leon H, et al. Perivascular inflamma-tion after balloon angioplasty of porcine coronary arteries.Circulation 2001;104:2228.
109. Mihaylov D, van Luyn MJ, Rakhorst G. Development of ananimal model of selective coronary atherosclerosis. CoronArtery Dis 2000;11:145.
110. Rapacz J, Hasler-Rapacz J, Taylor KM, et al. Lipoproteinmutations in pigs are associated with elevated plasma choles-terol and atherosclerosis. Science 1986;234:1573.
111. Ahanchi SS, Tsihlis ND, Kibbe MR. The role of nitric oxide inthe pathophysiology of intimal hyperplasia. J Vasc Surg 2007;45(Suppl A):A64.
112. Jagadeesha DK, Miller FJ Jr., Bhalla RC. Inhibition ofapoptotic signaling and neointimal hyperplasia by tempol andnitric oxide synthase following vascular injury. J Vasc Res2008;46:109.
113. Kritz AB, Yu J, Wright PL, et al. In vivo modulation of nogo-Battenuates neointima formation. Mol Ther 2008;16:1798.
114. Cooney R, Hynes SO, Sharif F, et al. Effect of gene delivery ofNOS isoforms on intimal hyperplasia and endothelial regener-ation after balloon injury. Gene Ther 2007;14:396.
115. Sharif F, Hynes SO, Cooney R, et al. Gene-eluting stents:Adenovirus-mediated delivery of eNOS to the blood vesselwall accelerates re-endothelialization and inhibits restenosis.Mol Ther 2008;16:1674.