Inpatient Compared with Home-Based Rehabilitation Following Primary Unilateral Total Hip or Knee...
8
Inpatient Compared with Home-Based Rehabilitation Following Primary Unilateral Total Hip or Knee Replacement: A Randomized Controlled Trial By Nizar N. Mahomed, MD, ScD, FRCSC, Aileen M. Davis, PhD, Gillian Hawker, MD, FRCPC, Elizabeth Badley, PhD, J. Rod Davey, MD, FRCSC, Khalid A. Syed, MD, FRCSC, Peter C. Coyte, PhD, Rajiv Gandhi, MD, FRCSC, and James G. Wright, MD, MPH, FRCSC Investigation performed at Toronto Western Hospital, University of Toronto, and North York General Hospital, Toronto, Ontario, Canada Background: Home-based rehabilitation is increasingly utilized to reduce health-care costs; however, with a shorter hospital stay, the possibility arises for an increase in adverse clinical outcomes. We evaluated the effectiveness and cost of care of home-based compared with inpatient rehabilitation following primary total hip or knee joint replacement. Methods: We randomized 234 patients, using block randomization techniques, to either home-based or inpatient rehabilitation following total joint replacement. All patients followed standardized care pathways and were evaluated, with use of validated outcome measures (Western Ontario and McMaster Universities Osteoarthritis Index [WOMAC], Short Form-36, and patient satisfaction), prior to surgery and at three and twelve months following surgery. The primary outcome was the WOMAC function score at three months after surgery. Results: The mean length of stay (and standard deviation) in the acute care hospital was 6.3 ± 2.5 days for the group designated for inpatient rehabilitation prior to transfer to that facility compared with 7.0 ± 3.0 days for the home-based rehabilitation group prior to discharge home (p = 0.06). The mean length of stay in inpatient rehabilitation was 17.7 ± 8.6 days. The mean number of postoperative home-based rehabilitation visits was eight. The prevalence of postoperative complications up to twelve months postoperatively was similar in both groups, which each had a 2% rate of dislocation and a 3% rate of clinically important deep venous thrombosis. The prevalence of infection was 0% in the home-based group and 2% in the inpatient group. None of these differences was clinically important. Both groups showed substantial improvements at three and twelve months, with no significant differences between the groups with respect to WOMAC, Short Form-36, or patient satisfaction scores (p > 0.05). The total episode-of-care costs (in Canadian dollars) for the inpatient rehabilitation and home-based rehabilitation arms were $14,532 and $11,082, respectively (p < 0.01). Conclusions: Despite concerns about early hospital discharge, there was no difference in pain, functional outcomes, or patient satisfaction between the group that received home-based rehabilitation and the group that had inpatient rehabilitation. On the basis of our findings, we recommend the use of a home-based rehabilitation protocol following elective primary total hip or knee replacement as it is the more cost-effective strategy. Level of Evidence: Therapeutic Level I. See Instructions to Authors for a complete description of levels of evidence. L imited health-care resources have created a demand for a more efficient delivery of care for patients undergoing total joint replacement. In Canada, the most notable recent change has been a substantial reduction in the lengths of stay in acute care hospitals following both total hip and knee replacements 1 . The average length of stay in a Canadian hos- Disclosure: In support of their research for or preparation of this work, one or more of the authors received, in any one year, outside funding or grants in excess of $10,000 from Physicians’ Services Incorporated. Neither they nor a member of their immediate families received payments or other benefits or a commitment or agreement to provide such benefits from a commercial entity. No commercial entity paid or directed, or agreed to pay or direct, any benefits to any research fund, foundation, division, center, clinical practice, or other charitable or nonprofit organization with which the authors, or a member of their immediate families, are affiliated or associated. A commentary is available with the electronic versions of this article, on our web site (www.jbjs.org) and on our quarterly CD-ROM (call our subscription department, at 781-449-9780, to order the CD-ROM). 1673 COPYRIGHT Ó 2008 BY THE J OURNAL OF BONE AND J OINT SURGERY,INCORPORATED J Bone Joint Surg Am. 2008;90:1673-80 d doi:10.2106/JBJS.G.01108
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Inpatient Compared with Home-Based Rehabilitation Following Primary Unilateral Total Hip or Knee...
Inpatient Compared with Home-Based RehabilitationFollowing Primary Unilateral Total Hip or KneeReplacement: A Randomized Controlled Trial
By Nizar N. Mahomed, MD, ScD, FRCSC, Aileen M. Davis, PhD, Gillian Hawker, MD, FRCPC, Elizabeth Badley, PhD,J. Rod Davey, MD, FRCSC, Khalid A. Syed, MD, FRCSC, Peter C. Coyte, PhD, Rajiv Gandhi, MD, FRCSC,
and James G. Wright, MD, MPH, FRCSC
Investigation performed at Toronto Western Hospital, University of Toronto, and North York General Hospital, Toronto, Ontario, Canada
Background: Home-based rehabilitation is increasingly utilized to reduce health-care costs; however, with a shorterhospital stay, the possibility arises for an increase in adverse clinical outcomes. We evaluated the effectiveness andcost of care of home-based compared with inpatient rehabilitation following primary total hip or knee joint replacement.
Methods: We randomized 234 patients, using block randomization techniques, to either home-based or inpatientrehabilitation following total joint replacement. All patients followed standardized care pathways and were evaluated,with use of validated outcome measures (Western Ontario and McMaster Universities Osteoarthritis Index [WOMAC],Short Form-36, and patient satisfaction), prior to surgery and at three and twelve months following surgery. The primaryoutcome was the WOMAC function score at three months after surgery.
Results: The mean length of stay (and standard deviation) in the acute care hospital was 6.3 ± 2.5 days for the groupdesignated for inpatient rehabilitation prior to transfer to that facility compared with 7.0 ± 3.0 days for the home-basedrehabilitation group prior to discharge home (p = 0.06). The mean length of stay in inpatient rehabilitation was 17.7 ±8.6 days. The mean number of postoperative home-based rehabilitation visits was eight. The prevalence of postoperativecomplications up to twelve months postoperatively was similar in both groups, which each had a 2% rate of dislocationand a 3% rate of clinically important deep venous thrombosis. The prevalence of infection was 0% in the home-basedgroup and 2% in the inpatient group. None of these differences was clinically important. Both groups showed substantialimprovements at three and twelve months, with no significant differences between the groups with respect to WOMAC,Short Form-36, or patient satisfaction scores (p > 0.05). The total episode-of-care costs (in Canadian dollars) for theinpatient rehabilitation and home-based rehabilitation arms were $14,532 and $11,082, respectively (p < 0.01).
Conclusions: Despite concerns about early hospital discharge, there was no difference in pain, functional outcomes,or patient satisfaction between the group that received home-based rehabilitation and the group that had inpatientrehabilitation. On the basis of our findings, we recommend the use of a home-based rehabilitation protocol followingelective primary total hip or knee replacement as it is the more cost-effective strategy.
Level of Evidence: Therapeutic Level I. See Instructions to Authors for a complete description of levels of evidence.
Limited health-care resources have created a demand for amore efficient delivery of care for patients undergoingtotal joint replacement. In Canada, the most notable
recent change has been a substantial reduction in the lengths ofstay in acute care hospitals following both total hip and kneereplacements1. The average length of stay in a Canadian hos-
Disclosure: In support of their research for or preparation of this work, one or more of the authors received, in any one year, outside funding or grants inexcess of $10,000 from Physicians’ Services Incorporated. Neither they nor a member of their immediate families received payments or other benefitsor a commitment or agreement to provide such benefits from a commercial entity. No commercial entity paid or directed, or agreed to pay or direct, anybenefits to any research fund, foundation, division, center, clinical practice, or other charitable or nonprofit organization with which the authors, or amember of their immediate families, are affiliated or associated.
A commentary is available with the electronic versions of this article, on our web site (www.jbjs.org) and on our quarterly CD-ROM (call oursubscription department, at 781-449-9780, to order the CD-ROM).
1673
COPYRIGHT � 2008 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED
J Bone Joint Surg Am. 2008;90:1673-80 d doi:10.2106/JBJS.G.01108

pital for total hip replacement has declined by 36%, fromfourteen days in 1994 to 1995 to nine days in 2004 to 2005. Fortotal knee replacement, the hospital length of stay over thesame period declined by 42%, from twelve days to seven days1.This reduced length of stay has resulted in an increased de-mand for both inpatient and home-based rehabilitation ser-vices2. In 2005, in the United States, the average length of staywas 3.8 days for total knee replacement and 4.9 days for totalhip replacement, which was less than that in Canada3. Lengthof stay is declining even more with the advent of minimallyinvasive total hip arthroplasty4; however, early clinical findingshave shown no significant differences in functional outcomescores between the shorter length of stay associated with theminimally invasive technique and the longer length of stayassociated with the conventional technique4,5.
Traditionally in Canada after total joint replacement,patients were routinely sent to inpatient facilities for rehabil-itation6-10. More recently, there has been an increased trend tosend patients directly home after total joint replacement withsupporting home-care services11. However, large variationsexist in current practice patterns with regard to where patientsreceive postoperative rehabilitation12,13. For example, in theprovince of Ontario, the rate of utilization for inpatient re-habilitation following total joint replacement has been re-ported to range from 3% to 79%14.
Unfortunately, to date, there is limited informationabout the effectiveness and costs of home-based rehabilitationcompared with inpatient rehabilitation for total joint re-placement9,10,15. Tribe et al.16 compared the functional out-comes for patients who were managed with either home-basedor inpatient rehabilitation after undergoing total hip and kneereplacements for primary osteoarthritis. In that nonran-domized Australian trial, there were no differences in func-tional outcomes between the two groups at the one-yearfollow-up evaluation. The authors of that study emphasized aneed for randomized trials to explore which patients are mostsuitable for the two types of rehabilitation.
Clinical trials to date have suggested that patient pref-erence and institutional factors rather than clinical parametersprimarily influence the decision regarding the type of reha-bilitation6,17. Following total joint replacement, it is unclearwhich method of rehabilitation is superior in terms of patient-related outcomes and cost of care. We evaluated the efficacyand cost of home-based compared with inpatient rehabilita-tion in a randomized controlled trial following primary totalhip and knee replacement. To our knowledge, this study pres-ents the longest follow-up to date (twelve months) and in-cludes a per diem cost analysis.
Materials and Methods
This randomized controlled trial enrolled patients under-going primary total hip or knee replacement from two
institutions: a tertiary-care referral center and a communityhospital in the same city. Patients were deemed eligible for thestudy if they were over the age of eighteen years; were un-dergoing unilateral hip or knee replacement for osteoarthritis,
inflammatory arthritis, or osteonecrosis; were residents of thecity where the two institutions were located; were fluent inEnglish; and provided informed consent to participate. Pa-tients requiring total joint replacement for a fracture, malig-nant tumor, revision of a total joint replacement, or bilateraltotal joint replacement were excluded. Eligible patients wereidentified by participating surgeons and were then approachedto participate in the trial by a study coordinator. Patientsproviding informed consent were then enrolled in the trial.The study protocol and patient consent forms were reviewedand approved by the Human Subject Review Committee.
The primary outcome of the trial was to evaluate theefficacy of inpatient compared with home-based rehabilitationat three months after surgery (the time at which both inter-ventions were discontinued), with use of the function subscaleof the Western Ontario and McMaster Universities Osteoar-thritis Index (WOMAC)18. Secondary outcomes included themeasurement of health status with use of the Short Form-36(SF-36)19 and patient satisfaction with use of the Hip and KneeSatisfaction Scale20.
At baseline and at the three and twelve-month follow-upvisits, the study subjects completed the WOMAC, SF-36, andHip and Knee Satisfaction Scale questionnaires. The WOMACis a self-administered, disease-specific questionnaire with a5-point Likert scale used to assess pain, function, and stiffnessof the hip and knee18. The descriptors range from no difficultywith respect to pain, functional activities, and stiffness (a scoreof 1 point) to extreme pain, difficulty, and stiffness (5 points).The SF-36 is a thirty-six-item questionnaire that includes eightscales measuring physical function, role limitations related tophysical health problems, bodily pain, perceptions of generalhealth, vitality, social functioning, role limitations related toemotional problems, and mental health. Mental and physicalcomponent summary scores are also calculated with use ofthese items19. In this study, the physical function, physicalcomponent score, and mental component score measures ofthe SF-36 were assessed. The Hip and Knee Satisfaction Scaleis a simple, reliable, and validated instrument that evaluatespatient satisfaction with the outcome of total joint arthroplastyin terms of improvement in pain and function20. It consists offour questions with scores ranging between 0 and 100, wherehigher scores represent greater satisfaction.
All subjects were evaluated approximately two weeksprior to surgery during a preadmission hospital visit. Thisbaseline evaluation included data on demographics, height,weight, primary diagnosis, medical comorbidities, and socialsupports as well as completion of the selected outcome mea-sures, WOMAC, SF-36, and Hip and Knee Satisfaction Scale.
One week prior to surgery, the subjects were random-ized, with use of block randomization, and were informed oftheir treatment allocation to either home-based or inpatientrehabilitation. The inpatient rehabilitation facility is a separate,independent facility wherein patient care is supervised by arehabilitation doctor. The subjects were informed of theirrandomization prior to surgery in order to allow sufficienttime to prepare their home settings if they were allocated to
1674
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 90-A d NU M B E R 8 d AU G U S T 2008IN PAT I E N T CO M PA R E D W I T H HO M E -BA S E D RE H A B I L I TAT I O N
AF T E R UN I L AT E R A L HI P O R KN E E RE P L AC E M E N T

home-based rehabilitation. All subjects were admitted to theacute care hospital on the day of surgery and were managedpostoperatively according to previously established and stan-dardized care guidelines for total joint replacement. All pa-tients received prophylactic antibiotics and prophylaxis againstdeep-vein thrombosis. Patients were excluded from the trial ifthey had development of serious postoperative complicationsthat precluded participation in the rehabilitation protocol.These included myocardial infarction, cerebrovascular acci-dent, intraoperative fracture, neurovascular injury, deep in-fection, or a return to the operating room for any reason.
The target length of stay at the acute care hospital forboth treatment groups was five days. All patients received thesame physiotherapy protocol during their stay (see Appendix).This included deep breathing and coughing, active and active-assisted bed and chair exercises, and gait training beginningwith assisted walking. On postoperative day 1, the physio-therapy goals were to transfer from lying to sitting and fromsitting to standing with minimal assistance, to stand with awalker, and to sit in a chair for one hour. On postoperative day2, physiotherapy goals were independent transfers and walkingfrom bed to bathroom with assistance. From postoperativeday 3 until discharge, the goals were to achieve independentwalking, including climbing stairs. For the home-based reha-bilitation group, subjects were deemed safe for discharge fromthe acute hospital when they had achieved four key functionalmilestones, as described by Zavadak et al.21, including theability to independently transfer from the supine position tositting and from sitting to standing, walking a distance of 30 m,and climbing stairs if necessary.
The subjects who were randomized to inpatient reha-bilitation were transferred to one of two independent inpatientrehabilitation institutions depending on the availability of re-habilitation beds. There they were managed along previouslyestablished care pathways with a target of a fourteen-day lengthof stay (see Appendix). The subjects who were randomized tohome-based rehabilitation were referred to their respectiveCommunity Care Access Centre (a provincially funded home-care agency that includes nursing, rehabilitation, and homesupport as necessary for the client) (see Appendix). The Com-munity Care Access Centre provided an early interventionprogram that ensured that each subject was seen at home by aphysiotherapist within forty-eight hours of discharge. Eachsubject was managed along a multidisciplinary clinical pathwayfor home-based rehabilitation that was developed for this trial.The subjects were discharged from the home-based programwhen the physiotherapist thought that they had achieved suf-ficient functional improvement to either attend an outpatientphysiotherapy clinic or maintain a self-directed program. Allsubjects returned to their respective acute care hospital at threeand twelve months postoperatively for a follow-up evaluationby their treating surgeon.
Cost analysis was conducted from a health system per-spective; therefore, only direct health-care costs were evaluatedfor acute care hospitals, inpatient rehabilitation hospitals, andhome-based rehabilitation services. These data did not include
physician fees, medications, or indirect costs to the patients orsecondary caregivers. We used per diem costs from the respectiveinstitutions and calculated the costs by multiplying per diem costby the actual length of stay for the patient. We were able to obtainpatient-level costs for services provided by home care using thecentralized data system. All costs were measured in Canadiandollars and were adjusted for inflation over the study period(with use of the Consumer Price Index) to the base year 200622.
Statistical MethodsThe primary analysis was on an intention-to-treat basis. Wecompared the two treatment groups at baseline (prior to sur-gery) to ensure they were equivalent on all measured variables.This was done to ensure that our randomization strategy wassuccessful and to identify any potential variables we needed toadjust for in our final analysis. Univariate analyses for differ-ences between groups were conducted with use of the Student ttest, chi-square test, or Fisher exact test as appropriate, withthe level of significance set at 0.05. Since there were no sig-nificant differences in the baseline parameters, we used ananalysis of variance to evaluate differences between groups inthe two treatment arms, adjusting for baseline severity of therespective dependent variable and the number of medical co-morbidities. Similar strategies were used for analysis of ourprimary outcome (the WOMAC function score at threemonths) as well as all secondary outcomes. For ease of pre-sentation, the WOMAC scores were rescaled from 0 to 100,with high scores representing better function and pain relief.Differences between groups in satisfaction scores were evalu-ated with use of Wilcoxon rank-sum tests. Twenty subjectsrequested a crossover from their assigned treatment groupof home rehabilitation to inpatient rehabilitation (primarilybecause of patient preference). Therefore, we replicated theanalysis on the basis of the actual discharge destination. Theresults were identical to those based on an intention-to-treatanalysis; therefore, we elected to present the results of theintention-to-treat analysis for clarity of presentation.
Power CalculationThe sample size was calculated to detect a minimal clinicallyimportant difference in the WOMAC function score at twelveweeks after total joint arthroplasty between the home-based andinpatient rehabilitation groups. We defined the minimal clini-cally important change according to criteria suggested by Bellamyet al.23: a standard deviation of 14 for calculating sample size withuse of this scale, and a change of 7.4 points following a weakintervention, such as a low dose of Voltaren (diclofenac sodium).The effect size (the mean difference divided by the standarddeviation) associated with such a change was approximately 0.5(7.4/14). Therefore, we calculated the sample size to detect aneffect size of 0.5, with a type-I error of 5% and 95% power.
Results
From 2000 to 2002, 234 subjects were entered into the trial;119 of them were randomized to the inpatient rehabilita-
tion arm and 115 to the home-based rehabilitation arm (Fig.
1675
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 90-A d NU M B E R 8 d AU G U S T 2008IN PAT I E N T CO M PA R E D W I T H HO M E -BA S E D RE H A B I L I TAT I O N
AF T E R UN I L AT E R A L HI P O R KN E E RE P L AC E M E N T

1). Our study ended in the middle of a randomization block,and thus there was some imbalance between the numbersassigned to the home-based rehabilitation and inpatient re-habilitation groups. The mean age of the subjects was sixty-eight years, and approximately two-thirds were women (seeAppendix). None of the patients randomized to the trial waslost to follow-up. The mean body mass index was 28 kg/m2.Osteoarthritis was the primary diagnosis in the vast majority ofpatients, and most had two or more medical comorbidities.Nearly two-thirds were white, and about 50% had postsec-
ondary education. Nearly 25% lived alone, and 20% wereworking at the time of surgery. There were nearly equal pro-portions of hip and knee replacements. There was no signif-icant difference between the treatment groups in any of themeasured baseline variables (see Appendix).
Preoperative baseline functional outcomes are outlinedin Table I. At baseline, both treatment arms had substantialpain and functional disability on the basis of the WOMAC painand physical function scores; however, no preoperative dif-ferences were noted between the two groups.
Fig. 1
Schematic diagram showing the number of study participants in each group who participated,
crossed over, or were lost to follow-up. The statistical analysis for this study was conducted with
use of the intention-to-treat group of 115 patients who received home-based rehabilitation and
119 patients who had inpatient rehabilitation.
1676
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 90-A d NU M B E R 8 d AU G U S T 2008IN PAT I E N T CO M PA R E D W I T H HO M E -BA S E D RE H A B I L I TAT I O N
AF T E R UN I L AT E R A L HI P O R KN E E RE P L AC E M E N T
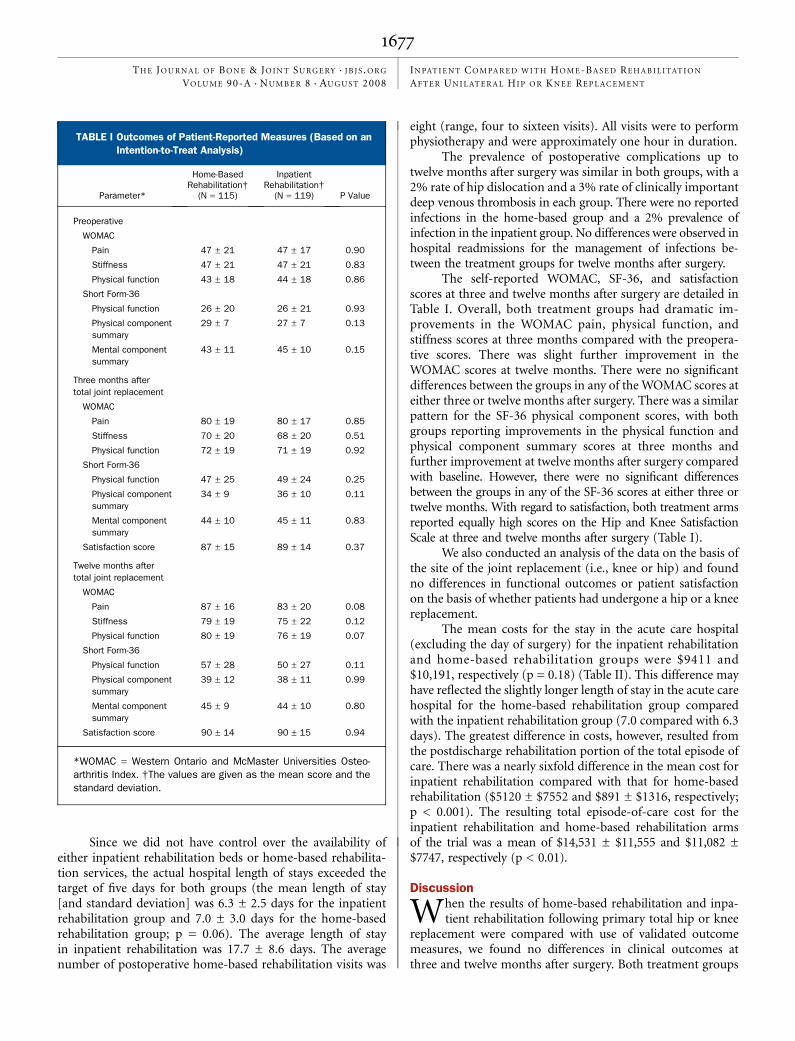
Since we did not have control over the availability ofeither inpatient rehabilitation beds or home-based rehabilita-tion services, the actual hospital length of stays exceeded thetarget of five days for both groups (the mean length of stay[and standard deviation] was 6.3 ± 2.5 days for the inpatientrehabilitation group and 7.0 ± 3.0 days for the home-basedrehabilitation group; p = 0.06). The average length of stayin inpatient rehabilitation was 17.7 ± 8.6 days. The averagenumber of postoperative home-based rehabilitation visits was
eight (range, four to sixteen visits). All visits were to performphysiotherapy and were approximately one hour in duration.
The prevalence of postoperative complications up totwelve months after surgery was similar in both groups, with a2% rate of hip dislocation and a 3% rate of clinically importantdeep venous thrombosis in each group. There were no reportedinfections in the home-based group and a 2% prevalence ofinfection in the inpatient group. No differences were observed inhospital readmissions for the management of infections be-tween the treatment groups for twelve months after surgery.
The self-reported WOMAC, SF-36, and satisfactionscores at three and twelve months after surgery are detailed inTable I. Overall, both treatment groups had dramatic im-provements in the WOMAC pain, physical function, andstiffness scores at three months compared with the preopera-tive scores. There was slight further improvement in theWOMAC scores at twelve months. There were no significantdifferences between the groups in any of the WOMAC scores ateither three or twelve months after surgery. There was a similarpattern for the SF-36 physical component scores, with bothgroups reporting improvements in the physical function andphysical component summary scores at three months andfurther improvement at twelve months after surgery comparedwith baseline. However, there were no significant differencesbetween the groups in any of the SF-36 scores at either three ortwelve months. With regard to satisfaction, both treatment armsreported equally high scores on the Hip and Knee SatisfactionScale at three and twelve months after surgery (Table I).
We also conducted an analysis of the data on the basis ofthe site of the joint replacement (i.e., knee or hip) and foundno differences in functional outcomes or patient satisfactionon the basis of whether patients had undergone a hip or a kneereplacement.
The mean costs for the stay in the acute care hospital(excluding the day of surgery) for the inpatient rehabilitationand home-based rehabilitation groups were $9411 and$10,191, respectively (p = 0.18) (Table II). This difference mayhave reflected the slightly longer length of stay in the acute carehospital for the home-based rehabilitation group comparedwith the inpatient rehabilitation group (7.0 compared with 6.3days). The greatest difference in costs, however, resulted fromthe postdischarge rehabilitation portion of the total episode ofcare. There was a nearly sixfold difference in the mean cost forinpatient rehabilitation compared with that for home-basedrehabilitation ($5120 ± $7552 and $891 ± $1316, respectively;p < 0.001). The resulting total episode-of-care cost for theinpatient rehabilitation and home-based rehabilitation armsof the trial was a mean of $14,531 ± $11,555 and $11,082 ±$7747, respectively (p < 0.01).
Discussion
When the results of home-based rehabilitation and inpa-tient rehabilitation following primary total hip or knee
replacement were compared with use of validated outcomemeasures, we found no differences in clinical outcomes atthree and twelve months after surgery. Both treatment groups
TABLE I Outcomes of Patient-Reported Measures (Based on an
Intention-to-Treat Analysis)
Parameter*
Home-BasedRehabilitation†
(N = 115)
InpatientRehabilitation†
(N = 119) P Value
Preoperative
WOMAC
Pain 47 ± 21 47 ± 17 0.90
Stiffness 47 ± 21 47 ± 21 0.83
Physical function 43 ± 18 44 ± 18 0.86
Short Form-36
Physical function 26 ± 20 26 ± 21 0.93
Physical componentsummary
29 ± 7 27 ± 7 0.13
Mental componentsummary
43 ± 11 45 ± 10 0.15
Three months aftertotal joint replacement
WOMAC
Pain 80 ± 19 80 ± 17 0.85
Stiffness 70 ± 20 68 ± 20 0.51
Physical function 72 ± 19 71 ± 19 0.92
Short Form-36
Physical function 47 ± 25 49 ± 24 0.25
Physical componentsummary
34 ± 9 36 ± 10 0.11
Mental componentsummary
44 ± 10 45 ± 11 0.83
Satisfaction score 87 ± 15 89 ± 14 0.37
Twelve months aftertotal joint replacement
WOMAC
Pain 87 ± 16 83 ± 20 0.08
Stiffness 79 ± 19 75 ± 22 0.12
Physical function 80 ± 19 76 ± 19 0.07
Short Form-36
Physical function 57 ± 28 50 ± 27 0.11
Physical componentsummary
39 ± 12 38 ± 11 0.99
Mental componentsummary
45 ± 9 44 ± 10 0.80
Satisfaction score 90 ± 14 90 ± 15 0.94
*WOMAC = Western Ontario and McMaster Universities Osteo-arthritis Index. †The values are given as the mean score and thestandard deviation.
1677
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 90-A d NU M B E R 8 d AU G U S T 2008IN PAT I E N T CO M PA R E D W I T H HO M E -BA S E D RE H A B I L I TAT I O N
AF T E R UN I L AT E R A L HI P O R KN E E RE P L AC E M E N T

achieved similar improvements in pain and function, and thecomplication rates were comparable with other studies24-26. Thestudy had sufficient sample size to detect a clinically mean-ingful difference if it existed. In fact, the two groups weresimilar on all measured outcomes except for health systemcosts, which were significantly higher in the inpatient reha-bilitation arm. The relative cost of inpatient rehabilitation was5.7 times the total cost of care for home-based rehabilitation.This difference is comparable with that in the United States,where inpatient rehabilitation costs are approximately 10.5times greater than home-based rehabilitation costs27. However,at the time of this trial, it was more difficult to organize atimely transfer to home-based rehabilitation services than toan inpatient rehabilitation facility, and this resulted in a slightlylonger length of stay in the acute care hospital for the home-based rehabilitation group.
With the increasing number of total joint replacementsbeing performed worldwide, there is an increasing emphasison cost-effective delivery of care28,29. In recent years, the as-sumption that postoperative inpatient rehabilitation results inimproved outcomes for patients receiving a total joint re-placement has been challenged, and there has been an in-creasing trend toward discharging patients who have had atotal joint replacement directly to home from the acute carefacility with home-based rehabilitation support. Decreasingcosts and improving efficiency of care are important goals inenhancing any health-care delivery system; however, thesemust not come at the cost of reduced quality of care. Onequestion that has not been clearly answered in the literatureuntil now is whether home-based rehabilitation leads to apoorer outcome for the patient. The findings from this studycertainly support the concept of home-based rehabilitationfollowing uncomplicated primary total hip or knee jointreplacement.
One randomized study has compared the effectiveness ofhome-based and inpatient rehabilitation following total jointreplacement in the lower extremity. Shepperd et al.7 used theSF-36, Oxford hip score, and Bristol knee score to measurefunctional outcome among eighty-six patients who had a hipreplacement and eighty-six patients who had a knee replace-ment. The patients in the home-based rehabilitation group hadsubstantially greater improvements in quality of life. Whetherthis difference would have been maintained in the long termwas not clear as that study had a follow-up of only three
months. The Oxford hip score did not demonstrate any sig-nificant differences in the hip replacement group, and nosignificant differences were detected in the knee replacementgroup between home-based and inpatient rehabilitation withregard to any of the outcome measures used. In another ran-domized study, Siggeirsdottir et al.30 used the Oxford hip scoreand the Nottingham health profile to compare inpatient andhome-based rehabilitation among fifty patients who had had atotal hip replacement. The Oxford hip score was not signifi-cantly different between the groups prior to surgery, but it wassignificantly better in the home-based rehabilitation group attwo months (p = 0.03) and six months (p = 0.001) postop-eratively. The better outcomes in the home-based group wereattributed to a preoperative education program conducted bya physiotherapist and/or occupational therapist about onemonth prior to surgery; this educational program was notoffered to the inpatient group.
Our study, along with other randomized trials in theliterature7,30,31, is part of a growing body of evidence that showshome-based rehabilitation programs are at least as good asinpatient postoperative rehabilitation programs in terms ofachieving functional outcomes for the patients. As patientsreceiving a total joint replacement are typically older, withcomorbidities and the potential for postoperative complica-tions, surgeons may be reluctant to prescribe home-basedrehabilitation programs31. However, our findings on the ef-fectiveness of home-based rehabilitation following total jointreplacement indicate that it is as effective as inpatient reha-bilitation with the added benefit of a lower cost of care. In-patient rehabilitation remains the optimal treatment pathwayfor patients with an increased likelihood of having postoper-ative complications develop and for those with preexistingcomplicating medical conditions that may require regular mon-itoring by health-care providers.
It is important to note that, despite the lower cost of carerelated to home-based rehabilitation programs, there is still aneed to ensure that the appropriate home-care rehabilitationstrategies are in place to contain costs while maintaining qualityof care32. In the province of Ontario in Canada, the Commu-nity Care Access Centres providing home-care services have alarge degree of variation in rehabilitation strategies, primarilyin terms of the number of rehabilitation visits allotted fol-lowing total joint replacements and the duration of treatmentin terms of weeks. By standardizing home-based rehabilitation
TABLE II Cost Comparison Between Home-Based and Inpatient Rehabilitation
Parameter Home-Based Rehabilitation* Inpatient Rehabilitation* P Value
Acute hospital costs $10,191 ± $7635 $9411 ± $8770 0.18
Rehabilitation costs $891 ± $1316 $5120 ± $7522 <0.001
Total episode-of-care costs $11,082 ± $7747 $14,531 ± $11,555 <0.01
*The values are given (in 2006 Canadian dollars) as the mean cumulative cost and the standard deviation.
1678
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 90-A d NU M B E R 8 d AU G U S T 2008IN PAT I E N T CO M PA R E D W I T H HO M E -BA S E D RE H A B I L I TAT I O N
AF T E R UN I L AT E R A L HI P O R KN E E RE P L AC E M E N T

protocols (see Appendix) and using standardized critical carepathways for total joint replacement, the efficiency of home-care services will be enhanced.
This study has a number of strengths including its ran-domized controlled design, use of validated patient-centeredoutcomes, and standardized care pathways. However, there arealso some limitations. Although the eligibility criteria werefairly broad, we had to restrict the trial to patients undergoingunilateral primary total joint replacement. Therefore, our re-sults cannot be directly extrapolated to those undergoing eitherbilateral or revision total joint replacement. Furthermore, werestricted this study to patients who were able to read and writein English. Consequently, the results may not be fully appli-cable to ethnically diverse populations who may have diffi-culties in accessing the full spectrum of the health-care system.
In summary, this study has shown that the cost of de-livery of care following total hip or knee replacement can besignificantly reduced by using home-based rehabilitation pro-grams without compromising the quality of care as evidencedby comparable functional outcomes and patient satisfactionrates for up to one year after surgery.
AppendixA description of our standardized care guidelines foracute care, inpatient, and home physiotherapy provided
by a Community Care Access Centre and a table depictingpatient demographics are available with the electronic versionsof this article, on our web site at jbjs.org (go to the articlecitation and click on ‘‘Supplementary Material’’) and on ourquarterly CD-ROM (call our subscription department, at 781-449-9780, to order the CD-ROM). n
NOTE: The authors thank all of the health-care providers who participated in this study, in particularDr. Edward Rumble and Dr. Maurice Bent.
Nizar N. Mahomed, MD, ScD, FRCSCToronto Western Hospital, University Health Network, 399 BathurstStreet, East Wing 1-435, Toronto, ON M5T 2S8, Canada. E-mail address:[email protected]
Aileen M. Davis, PhDElizabeth Badley, PhDDivision of Health Care and Outcomes Research and ArthritisCommunity Research and Evaluation Unit, Toronto Western ResearchInstitute, 399 Bathurst Street, MP 11-322, Toronto,ON M5T 2S8, Canada
Gillian Hawker, MD, FRCPCDepartment of Medicine, Sunnybrook and Women’s College HealthSciences Centre, 76 Grenville Street, 10th Floor, East Room 1010, Toronto,ON M5S 1B6, Canada
J. Rod Davey, MD, FRCSCKhalid A. Syed, MD, FRCSCRajiv Gandhi, MD, FRCSCDepartment of Surgery, Toronto Western Hospital, 399 Bathurst Street,1-011 East Wing, Toronto, ON M5T 2S8, Canada
Peter C. Coyte, PhDDepartment of Health Policy, Management and Evaluation, McMurrichBuilding, University of Toronto, Toronto, ON M5S 1A8, Canada
James G. Wright, MD, MPH, FRCSCDepartment of Surgery, The Hospital for Sick Children, 1218-555University Avenue, Toronto, ON M5G 1X8, Canada
References
1. Canadian Institute of Health Information. Canadian Joint Replacement Registry(CJRR) 2006 report. Hip and knee replacements in Canada. http://secure.cihi.ca/cihiweb/products/CJRR_Annual_Report_Hip_Knee_Replacements_2006_e.pdf.Accessed 2008 June 18.
2. Naylor CD, DeBoer DP. Variations in selected surgical procedures and medicaldiagnoses by year and region: total hip and knee replacement. In: Goel V, WilliamsJI, Anderson GM, Blackstein-Hirsch P, Fooks C, Naylor CD, editors. Patterns ofhealth care in Ontario. The ICES practice atlas. 2nd ed. Ottawa: Canadian MedicalAssociation; 1996. p 54-64.
3. HCUPnet. Healthcare Cost and Utilization Project, Agency for Healthcare Re-search and Quality, United States Department of Health and Human Services.http://www.hcupnet.ahrq.gov/. Accessed 2007 Mar 15.
4. Dorr LD, Maheshwari AV, Long WT, Wan Z, Sirianni LE. Early pain relief andfunction after posterior minimally invasive and conventional total hip arthroplasty.J Bone Joint Surg Am. 2007;89:1153-60.
5. Ogonda L, Wilson R, Archbold P, Lawlor M, Humphreys P, O’Brien S, BeverlandD. A minimal-incision technique in total hip arthroplasty does not improve earlypostoperative outcomes. A prospective, randomized, controlled trial. J Bone JointSurg Am. 2005;87:701-10.
6. Munin MC, Rudy TE, Glynn NW, Crossett LS, Rubash HE. Early inpatient reha-bilitation after elective hip and knee arthroplasty. JAMA. 1998;279:847-52.
7. Shepperd S, Harwood D, Jenkinson C, Gray A, Vessey M, Morgan P. Rando-mised controlled trial comparing hospital at home care with inpatient hospital care.I: three month follow up of health outcomes. BMJ. 1998;316:1786-91.
8. Shepperd S, Harwood D, Gray A, Vessey M, Morgan P. Randomised controlledtrial comparing hospital at home care with inpatient hospital care. II: cost mini-misation analysis. BMJ. 1998;316:1791-6.
9. Shepperd S, Iliffe S. Hospital at home compared with inpatient hospital care. In:Bero L, Grilli R, Grinshaw J, Oxman A, editors. The Cochrane library. Vol 1. Oxford:Cochrane Collaboration; 1998.
10. Shepperd S, Iliffe S. Hospital at home versus in-patient hospital care. Co-chrane Database Syst Rev. 2005; 3:CD000356.
11. Zuckerman JD. Inpatient rehabilitation after total joint replacement. JAMA.1998;279:880.
12. Coyte PC, Young W. Costs, outcomes, and potential cost savings associatedwith alternative discharge strategies [workshop]. Presented at the InternationalHealth Economics Association Meeting; 1996 May 19-22; Vancouver, BC.
13. Coyte P, Hawker G, Wright J. Variations in knee replacement utilization ratesand the supply of health professionals in Ontario, Canada. J Rheumatol.1996;23:1214-20.
14. McGlasson R. Regional clinical pathways are successful in improving thehealthcare system for total joint replacements. Canadian Agency for Drugs andTechnologies in Health Symposium. 2006 Apr 3.
15. Shepperd S, Iliffe S. The effectiveness of hospital at home compared withinpatient hospital care: a systematic review. J Public Health Med. 1998;20:344-50.
16. Tribe KL, Lapsley HM, Cross MJ, Courtney BG, Brooks PM, March LM. Se-lection of patients for inpatient rehabilitation or direct home discharge followingtotal joint replacement surgery: a comparison of health status and out-of-pocketexpenditure of patients undergoing hip and knee arthroplasty for osteoarthritis.Chronic Illn. 2005;1:289-302.
17. Mahomed NN, Koo Seen Lin MJ, Levesque J, Lan S, Bogoch ER. Determinantsand outcomes of inpatient versus home based rehabilitation following elective hipand knee replacement. J Rheumatol. 2000;27:1753-8.
1679
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 90-A d NU M B E R 8 d AU G U S T 2008IN PAT I E N T CO M PA R E D W I T H HO M E -BA S E D RE H A B I L I TAT I O N
AF T E R UN I L AT E R A L HI P O R KN E E RE P L AC E M E N T

18. Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validationstudy of WOMAC: a health status instrument for measuring clinically importantpatient relevant outcomes to antirheumatic drug therapy in patients with osteoar-thritis of the hip or knee. J Rheumatol. 1988;15:1833-40.
19. Ware JH, Snow KK, Kosinski M, Gandek B. SF-36 health survey: manual andinterpretation guide. Boston: The Health Institute; 1993.
20. Mahomed NN, Sledge CB, Daltroy L, Fossel AH, Katz JN. Self-administeredsatisfaction scale for joint replacement arthroplasty. J Bone Joint Surg Br.1998;80(1 Suppl):9.
21. Zavadak KH, Gibson KR, Whitley DM, Britz P, Kwoh CK. Variability in theattainment of functional milestones during the acute care admission after totaljoint replacement. J Rheumatol. 1995;22:482-7.
22. Bank of Canada. Inflation calculator. Data source: Statistics Canada, Con-sumer price indexes for Canada, monthly, 1914-2006. www.bankofcanada.ca/en/rates/inflation_calc.html. Accessed 2007 Feb 12.
23. Bellamy N, Kean WF, Buchanan WW, Gerecz-Simon E, Campbell J. Doubleblind randomized controlled trial of sodium meclofenamate (Meclomen) and di-clofenac sodium (Voltaren): post validation reapplication of the WOMAC Osteoar-thritis Index. J Rheumatol. 1992;19:153-9.
24. Mahomed NN, Barrett JA, Katz JN, Phillips CB, Losina E, Lew RA, GuadagnoliE, Harris WH, Poss R, Baron JA. Rates and outcomes of primary and revision totalhip replacement in the United States Medicare population. J Bone Joint Surg Am.2003;85:27-32.
25. Mahomed NN, Barrett J, Katz JN, Baron JA, Wright J, Losina E. Epidemiology oftotal knee replacement in the United States Medicare population. J Bone Joint SurgAm. 2005;87:1222-8.
26. Phillips CB, Barrett JB, Losina E, Mahomed NN, Lingard EA, Guadagnoli E,Baron JA, Harris WH, Poss R, Katz JN. Incidence rates of dislocation, pulmonaryembolism, and deep infection during the first six months after elective total hipreplacement. J Bone Joint Surg Am. 2003;85:20-6.
27. Weaver FM, Hughes SL, Almagor O, Wixson R, Mannheim L, Fulton B, Singer R.Comparison of two home care protocols for total joint replacement. J Am GeriatrSoc. 2003;51:523-8.
28. Paterson JM, DeBoer DP, Williams J, Bourne RB, Hawker G, Kreder H,Laupacis A, Mahomed N, Warner S. Total hip and knee replacement. In: Tu JV,Pinfold SP, McColgan P, Laupacis A, editors. Access to health services inOntario. ICES atlas. 2nd ed. Toronto, ON: Institute for Clinical EvaluativeSciences; 2006. p 117-48. http://www.ices.on.ca/file/chp5_v5.pd Accessed2007 Jan 12.
29. DeFrances CJ, Podgornik MN. 2004 National Hospital Discharge Survey. Ad-vance data from vital and health statistics. Hyattsville, MD: National Center forHealth Statistics; 2006.
30. Siggeirsdottir K, Olafsson O, Jonsson H, Iwarsson S, Gudnason V, Jonsson B.Short hospital stay augmented with education and home-based rehabilitation im-proves function and quality of life after hip replacement: randomized study of 50patients with 6 months of follow-up. Acta Orthop. 2005;76:555-62.
31. Kramer JF, Speechley M, Bourne R, Rorabeck C, Vaz M. Comparison of clinic-and home-based rehabilitation programs after total knee arthroplasty. Clin OrthopRelat Res. 2003;410:225-34.
32. Mahomed NN, Lau JT, Lin MK, Zdero R, Davey JR. Significant variation existsin home care services following total joint arthroplasty. J Rheumatol. 2004;31:973-5.
1680
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 90-A d NU M B E R 8 d AU G U S T 2008IN PAT I E N T CO M PA R E D W I T H HO M E -BA S E D RE H A B I L I TAT I O N
AF T E R UN I L AT E R A L HI P O R KN E E RE P L AC E M E N T