Clinical Results of Lateral Unicompartmental Knee Arthroplasty
Upload
independentCategory
view
1download
0
ELSEVIER
Clinical Eiomechanics Vol. 13, No. 3, pp. 176-M. 199X 0 1997 Elsevier Science Ltd. All rights reserved
Printed in Great Britain 0268-0033198 $19.00 +O.oO
PII: SO268-0033(97)00039-9
Rising from chair after total knee arthroplasty
F. C. Sul, K. A. Lai,2 W. H. Hong’
‘Institute of Biomedical Engineering, National Cheng Kung University, Tainan, Taiwan 2Department of Orthopaedic Surgery, National Cheng Kung University, Tainan, Taiwan
Abstract
Objective. This study was performed to determine the biomechanics of chair rising by patients after successful total knee arthroplasty (TKA). Design. Relative full body joint positions and ground reaction forces were measured by a motion analysis system and two force plates. Background. Chair-rise produces increased joint forces and moments compared with level walking, and it is difficult to rise from a chair for most patients with neurological or musculoskeletal abnormalities. Previous motion studies of patients after TKA had focused on gait analysis and stair climbing. Methods. Twelve patients after successful TKA were studied while performing sit-to-stand transfer from a chair at four chair heights without the use of arm rests. The results of this group were compared with those of 12 healthy elderly subjects and 14 osteoarthritic patients before TKA. Results. Compared with the healthy elderly group during chair rising, the patients after TKA had increased horizontal mass center velocity, increased vertical hip joint forces, the maximum sound-side hip extension moment, but decreased vertical mass center velocity. Conclusion. Compensatory mechanisms of chair rising were adopted by the arthritic patients before and after TKA. The mechanisms include increased forward body bending and more weight shift on the sound side.
Relevance
Osteoatthritic patients after successful TKA had nearly normal biomechanics in rising from a higher chair. Therefore, they are better advised to use chairs of at least the same height as their lower leg segment. 0 1998 Elsevier Science Ltd. All rights reserved
Key words: Chair rise, biomechanics, total knee arthroplasty, osteoarthritis, joint moment
C/in. Biomech. Vol 13, No. 3, 176-181, 1998
Introduction
The ability to rise from a sitting position is important for an elderly person to maintain an independent life. Rising from a sitting position includes forward bending of the trunk and extension of the back and lower limbs1,2. This maneuver can be impeded by diseases of the back and the lower extremities. Arthrosis of the knee is one of the most common illnesses of the elderly that compromises their ability to rise from a sitting position. There have been studies concerning the influences of chair heightle4,
Received: 26 February 1997; Accepted: 11 June 1997 Correspondence and reprint requests to: Fong-Chin Su, Institute Of Biomedical Engineering National Cheng Kung University Tainan, 701 Taiwan. E-mail: [email protected]
the arm res@, the speed of rising’ and age3,8 related factors concerning chair rising activities. Gait study, stair climbing, and other functional assessments of patients after total knee arthroplasty (TKA) have also been reported’-“. Jevsevar et a1.12 studied knee kinematics and kinetics during locomotor activities of daily living which included level of walking, rising from a chair, stair ascent and stair descent in patients after knee arthroplasty. In their study, the chair height was chosen to be the height of the lower leg segment of the healthy controlled subjects.
Compared with level walking, rising from a chair produces greater joint forces and moments. It is diffi- cult to rise from a chair for most patients with neuro- logical or musculoskeletal abnormalities. The primary goal of TKA is to eliminate pain and restore function by replacing the articulating surface in place of the
Su et al: Rising from chair after total knee arthroplasty 177
worn cartilaginous surface of the knee joint. It is important to maintain the normal anatomical and biomechanical interaction between the shapes of the replaced articular surfaces and soft tissues (ligaments and muscles) which remain. Previous motion studies of patients after TKA had focused on gait analysis and stair climbing. This study was performed to understand the biomechanics and compensatory mechanisms of chair-rise in patients after successful TKA. Kinematics and kinetics of chair-rise of patients after TKA were compared with those of the healthy elderly and osteoarthritic (OA) patients.
Methods
Subjects and experimental protocol
Twelve patients, 2 to 6 years (mean 3.1 years) after successful TKAs, were studied in performing sit-to- stand transfer from an armless chair. They were four males and eight females aged from 57 to 75 years (mean 64.8 years; SD 8.7 years). Body height ranged from 151 to 168 cm (mean 157 cm; SD 5.7 cm) and body weight ranged from 49 to 103 kg (mean 73.3 kg; SD 14.9 kg). All patients were originally diagnosed with osteoarthritis and had varus deformity of the knee before surgery. Eight patients had unilateral (five left and three right) and four bilateral TKAs. Back problems were excluded in these patients. The knee scores (Hospital for Special Surgery, New York, NY) ranged from 68 to 94 (mean 83.9) at the time of study.
In addition, 12 normal subjects (five males and seven females, aged from 54 to 75 years with mean 61.7years) and 14 patients with OA knees without knee arthroplasty and back problems (12 females and two males) were recruited for study. Ten of the 14 OA patients had bilateral and four had unilateral involvements. The diseased knee had varus deformity from 3 to 7” (mean 4.7”). The knee scores ranged from 76 to 88 (mean 82.2).
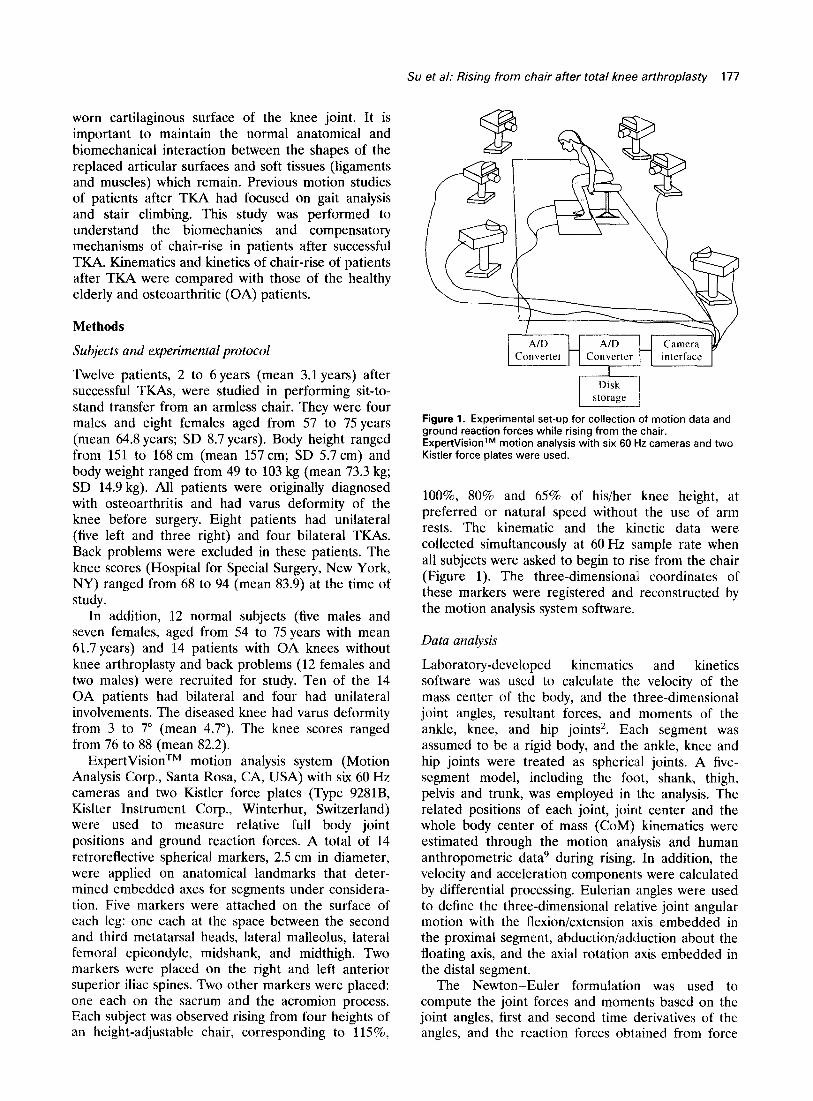
ExpertVisionTM motion analysis system (Motion Analysis Corp., Santa Rosa, CA, USA) with six 60 Hz cameras and two Kistler force plates (Type 9281B, Kislter Instrument Corp., Winterhur, Switzerland) were used to measure relative full body joint positions and ground reaction forces. A total of 14 retroreflective spherical markers, 2.5 cm in diameter, were applied on anatomical landmarks that deter- mined embedded axes for segments under considera- tion. Five markers were attached on the surface of each leg: one each at the space between the second and third metatarsal heads, lateral malleolus, lateral femoral epicondyle, midshank, and midthigh. Two markers were placed on the right and left anterior superior iliac spines. Two other markers were placed: one each on the sacrum and the acromion process. Each subject was observed rising from four heights of an height-adjustable chair, corresponding to 115%,
Figure 1. Experimental set-up for collection of motion data and grbund reaction forces while rising from the chair. ExpertVisionTM motion analysis with six 60 Hz cameras and two Kistler force plates were used.
lOO%, 80% and 65% of his/her knee height, at preferred or natural speed without the use of arm rests. The kinematic and the kinetic data were collected simultaneously at 60 Hz sample rate when all subjects were asked to begin to rise from the chair (Figure 1). The three-dimensional coordinates of these markers were registered and reconstructed by the motion analysis system software.
Data analysis
Laboratory-developed kinematics and kinetics software was used to calculate the velocity of the mass center of the body, and the three-dimensional joint angles, resultant forces, and moments of the ankle, knee, and hip joints2. Each segment was assumed to be a rigid body, and the ankle, knee and hip joints were treated as spherical joints. A five- segment model, including the foot, shank, thigh, pelvis and trunk, was employed in the analysis. The related positions of each joint, joint center and the whole body center of mass (CoM) kinematics were estimated through the motion analysis and human anthropometric data9 during rising. In addition, the velocity and acceleration components were calculated by differential processing. Eulerian angles were used to define the three-dimensional relative joint angular motion with the flexioniextension axis embedded in the proximal segment, abduction/adduction about the floating axis, and the axial rotation axis embedded in the distal segment.
The Newton-Euler formulation was used to compute the joint forces and moments based on the joint angles, first and second time derivatives of the angles, and the reaction forces obtained from force

178 Clin. Biomech. Vol. 13, No. 3, 1998
platforms with respect to the reference coordinate system3. This type of analysis is known as the ‘inverse dynamic problem’ for which the motion is known and the forces and moments required to produce the motion are calculated.
Statistical analysis
SYSTAT 3.0 software was used for the statistical analysis. The results of the TKA group were compared with those of 12 healthy elderly subjects and 14 OA patients without knee arthroplasty. Repeated measures ANOVA was conducted to evaluate differences between groups and chair heights.
Results
Phases of rising f;om chair
Chair rising was divided into three phases: flexion momentum phase (forward leaning phase), momentum transfer phase, and extension phase’,2. The total duration for the rising maneuver in normal subjects was similar for all heights of chair. Both the OA group and patients with TKA increased the duration of sit-to-stand movement with increasing chair height and required more time than the normal subjects during rising from all chair heights (Figure 2). In all subjects, the forward displacement of the CoM increased when the chair height was decreased. Both the OA and TKA patient groups showed more forward displacements of the CoM than normal subjects (Figure 3). The maximal extension momentum was not significantly different among the three groups. However, the normal subjects had
115% lOOI 80% 65%
Chair height as % of knee-heel height *: P < 0.05
#: P < 0.005
Normal old n OA q TKA Figure 2. Mean and standard deviation of the total duration of the sit-to-stand movement from four seat heights, i.e. 115% lOO%, 80%, and 65% of the subject’s knee height at preferred or natural speed without the use of arm rests. These tests were performed by 12 healthy elderly adults, 14 OA patients without knee arthroplasty, and 12 OA patients after TKA. (* value significantly greater, PiO.05, than that of normal group; # value significant greater, P<O.O05, than that of normal group.)
80% I
65%
Chair height as % of knee-heel height *: P < 0.001
Normal old n OA Cl TKA Figure 3. Mean and standard deviation of the horizontal displacement of the CoM of the body while rising from the chair at four seat heights, i.e. 115% lOO%, 80%, and 65% of the subject’s knee height at preferred or natural speed without the use of arm rests. They were performed by 12 healthy elderly adults, 14 OA patients without knee arthroplasty, and 12 OA patients after TKA. (* value significantly less, P<O.OOl, than that of normal group.)
higher extension speed than the other two groups and the extension speed differences among all three groups increased with decreasing chair height (Figure 4).
Angular changes
The range of motion of the hip, knee, and ankle joints increased as the chair height decreased in all groups of subjects. The hip joint reached the maximal flexion angle at the end of the forward leaning phase. This maximal flexion angle of the hip was the largest
0.8
c 0.7
z h 0.6
.‘;I 8 z 0.5 z
z .$
0.4
z z 0.3
-2
.!j 0.2
2 0.1
80% 65%
Chair height as % of knee-heel height *: P < 0.00 I
HNormal old HOA q TKA Figure 4. Mean and standard deviation of the maximal vertical velocity of the CoM of the body while rising from the chair at four seat heights, i.e. 115%, lOO%, 80%, and 65% of the subject’s knee height at preferred or natural speed without the use of arm rests. They were performed by 12 healthy elderly adults, 14 OA patients without knee arthroplasty, and 12 OA patients after TKA. (* value significantly less, P<O.OOl, than that of normal group.)

Su et al: Rising from chair after total knee nrthroplasty 179
80
60
115% 100% 80% 65%
Chair height as % of knee-heel height *: P < 0.001
Normal old n OA q TKA side q Sound side of TKA patient
Figure 5. Mean and standard deviation of the maximal flexion angle of the hip while rising from the chair at four seat heights, i.e. 115%, lOO%, 80%, and 65% of the subject’s knee height at preferred or natural speed without the use of arm rests. They were performed by 12 healthy elderly adults, 14 OA patients without knee arthroplasty, and 12 OA patients after TKA. (* value significantly greater, P~O.001, than that of OA group.)
in the sound side of the TKA patients while rising from the lowest chair (Figure 5). The between-group differences and between-leg (sound side-TKA side) differences in the TKA group were only identified at the lowest chair level (65% knee height).
The maximal flexion angle of the knee also occurred at the end of the forward leaning phase. While rising from the chair height of 65% of knee- heel height, the maximal flexion angles of the knee of the sound side of TKA patients were the largest for all groups (Figure 6). The between-group differences were not significant for all chair heights except for 65% knee height. The maximal flexion angle of the ankle was not significantly different among the three groups.
Joint flexion moments
Maximal flexion moments of the hip, the knee and maximal dorsiflexion moment of the ankle occurred at the beginning of the extension phase. The sound side of the TKA patient groups had higher maximal flexion moment of the hip than normal subjects for all chair heights (Figure 7). The differences of maximal hip flexion moment were not significant among the normal subjects, TKA, and OA patients. Both the OA and TKA patient groups had lower maximal flexion moment of the knees than the normal subjects. Such differences were significant in 65% and 80% of knee-heel height chairs (Figure 8). For the ankle, the sound side of the TKA patients had the highest dorsiflexion moment, wherkas the OA patients had the lowest maximal dorsiflexion moment (Figure 9).
80
60
0 115% 100% 80% 65%
Chair height as o/c of kneeheel height *: P c 0.01
0 Normal old n OA u TKA side q Sound side of TKA patient
Figure 6. Mean and standard deviation of the maximal flexion angle of the knee while rising from the chair at four seat heights, i.e. 115%. lOO%, 80%. and 65% of the subiect’s knee heioht at preferred-or natural speed without the use bf arm rests. Tiey were performed by 12 healthy elderly adults, 14 OA patients without knee arthroplasty, and 12 OA patients after TKA. (* value significantly greater, P<O.Ol, than that of OA group.)
Discussion
Using the same method to study different age groups during rising from a chair, Liao found that the time interval for elderly subjects to rise from all heights of
9 I *
115% 100% 80% 65%
Chair height as % of knee-heel height *: P < 0.01
•! Normal old m OA 0 TKA q Sound side of TKA patient
Figure 7. Mean and standard deviation of the maximal flexion moment of the hip while rising from the chair at four seat heights, i.e. 115%. 100%. 80%, and 65% of the subject’s knee height at preferred or natural soeed without the use of arm rests. They were performed b; 12 healthy elderly adults, 14 OA patients without knee at-throplasty, and 12 OA patients after TKA. (* value significantly greater. P~0.01, than that of normal wxw.)

180 Clin. Biomech. Vol. 13, No. 3, 1998
115% 100% 80% 65%
Chair height as % of knee-heel height *: P < 0.01; #: P < 0.001
q Normal old n OA 0 TKA side q Sound side of TKA patient
Figure 8. Mean and standard deviation of the maximal flexion moment of the knee while rising from the chair at four seat heights, i.e. 115%, lOO%, 80%, and 65% of the subject’s knee height at preferred or natural speed without the use of arm rests. They were performed by 12 healthy elderly adults, 14 OA patients without knee arthroplasty, and 12 OA patients after TKA. (* value significantly less, P<O.Ol, than that of normal group; # value significantly less, P ~0.001, than that of normal group.)
a chair was longer than that of younger subjects3. In this study, the time interval for both the OA and TKA patient groups to rise from the chair was longer than that for the normal elderly subjects. This incre- ment of time became more significant for shorter
Chair height as % of knee-heel height
q Normal old n OA q TKA q Sound side of TKA patient
Figure 9. Mean and standard deviation of the maximal dorsiflexion moment of the ankle while rising from the chair at four seat heights, i.e. 115%, lOO%, 80% and 65% of the subject’s knee height at preferred or natural speed without the use of arm rests. They were performed by 12 healthy elderly adults, 14 OA patients withoutknee arthroplasty, and 12 OA patients after TKA.
chair heights. This may mean that the OA and TKA patients had greater difficulties in rising from lower chairs. These patients leaned more forward during the rising maneuver. This forward leaning was more obvious for the TKA patients than OA patients. This maneuver brought the CoM to above the knee as well as anterior to the hip and ankle instead of above the hip, ankle and behind the knee at the beginning of the extension phase, as demonstrated by the normal subjects. This maneuver helped decrease the flexion angle, reaction force and flexion moment of the diseased knee where quadriceps strength might be weaker than normal. In this compensatory maneuver, the flexion angles of the hip and dorsiflexion angle of the ankle increased, and the flexion moment of the hip and dorsiflexion moment of the ankle increased. in the unilateral OA or TKA cases, the subjects tended to shift the CoM to the sound side which further increased the hip flexion angle and hip flexion moment of the sound side. This compensatory mechanism was more obvious as the chair height decreased. Jevsevar et al.r2 studied chair-rise of the TKA patients from 100% knee-heel height and compared the results with that of normal subjects whose average age was 16years younger than the TKA patients. Lower flexion angle and flexion moment of the knee was found in the TKA patients. By studying different age groups during rising from a chair, Liao3 found that younger subjects had higher flexion moments of the knee than the older subjects during chair rising. In this study, by comparing the patients with the age-matched normal subjects and OA patients, the difference of flexion angle of the knee was significant only between the sound side of TKA patients and the OA patients for the 65% knee-heel height chair. The difference of flexion moment of the knee was significant only between the OA and normal subjects as well as between the TKA side and normal subjects for the 65% knee-heel height chair.
In conclusion, the rising mechanism of OA patients after TKA did not match that of the normal subjects of the same age group. However, it was similar or slightly better than that of mild OA patients who did not need surgical intervention. The rising mechanism of TKA patients was similar to the healthy controls while rising from chairs of 100 and 115% knee-heel height, whereas the rising mechanism of OA patients was similar to the controls only for the 115% knee-heel height chair. This suggested that the OA and TKA patients were better advised to use chairs of at least the same height as their lower leg segment.
Acknowledgements
The authors are grateful to Dr Y. L. Chou and Dr S. C. Chen for their invaluable comments and assistance

Su et al: Rising from chair after total knee arthroplasty 181
with experiments. This investigation was supported by the National Science Council, NSC82-0420-E- 7 006-158, Taiwan.
References 8. 1.
2.
3.
4.
5.
6.
Rodosky, M. W. and Andriacchi, T. P. The influence of chair height on lower limb mechanics during rising. J Orthop Res, 1989,7,266-271. Lai, K. A., Su, F. C., Liao, T. Y., Wang, S. C. and Chou, Y. L. Biomechanics of chair rising. Chinese J Med Biolog Eng, 1992,12, 343-353. Liao, T. Y. Biomechanics of chair rising for patients with gonarthrosis of the knee. Master thesis, National Cheng Kung University, Tainan, Taiwan, 1993. Burdete, R. G. and Habaservich, R. Biomechanical comparison of rising from two types of chairs. Physical Therapy, 1985, 65, 1177-1183. Seedhom, B. B. and Terayama, K. Knee forces during
the activity of getting out of a chair with and without the use of arms. Biomedical Eng, 1976,11, 278-282. Ellis, M., Seedhom, B. B. and Wright, V. Forces in the
9.
10.
11.
12.
knee joint whilst rising from a seated position. J Biomedical Eng, 1984,6, 113-120. Pai, Y. C. and Rogers, M. W. Speed variation and resultant joint torques during sit-to-stand. Arch Phys Med Rehabil, 1991, 72,881-884. Ikeda, E. R. and Schenkman, M. L. Influence of age on dynamics of rising from a chair. Physical Therapy, 1991, 71,473-481. Chen, P. Q., Cheng, C. K. and Shang, H. C. Gait analysis after total knee replacement for degenerative arthritis. J Formosan Med Assoc, 1991, 90, 160-166. Andriacchi, T. P. Biomechanics and gait analysis in total knee replacement. Orthop Rev, 1988, 17,470-475. Simon, S. R., Trieshmann, H. W. and Burdete, R. G. Quantitative gait analysis after total knee arthroplasty for monoarticular degenerative arthritis. J Bone Joint kg, 1983,65, (A), 605. Jevsevar, D. S., Riley, P. O., Hodge, W. A. and Krebs, D. E. Knee kinematics and kinetics during locomotor activities of daily living in subjects with knee arthroplasty and in healthy control subjects. Physical Therapy, 1993,73,229-242.
Copyright © 2022 FDOKUMEN