Influencing Prescribing for Urinary Tract Infection and Asthma in Primary Care in Sweden
12
J Clin Epidemiol Vol. 52, No. 8, pp. 801–812, 1999 Copyright © 1999 Elsevier Science Inc. All rights reserved. 0895-4356/99/$–see front matter PII S0895-4356(99)00036-0 Influencing Prescribing for Urinary Tract Infection and Asthma in Primary Care in Sweden: A Randomized Controlled Trial of an Interactive Educational Intervention C. Stålsby Lundborg, 1, * R. Wahlström, 1 T. Oke, 1,2 G. Tomson, 1 and V. K. Diwan, 1,3 1 Department of Public Health Sciences, Division of International Health Care Research (IHCAR), Karolinska Institutet, SE-171 76 Stockholm, Sweden; 2 Department of Statistics, Uppsala University, Uppsala, Sweden; 3 The Nordic School of Public Health, Gothenburg, Sweden ABSTRACT. Our aim was to evaluate effects on prescribing for urinary tract infection (UTI) and asthma, of an education with messages based on national guidelines, aimed at improving prescribing in primary care in Sweden. The study is part of the European Drug Education Project. A randomized controlled trial, with groups of general practitioners (GPs) allocated to education on UTI (18 groups, 104 GPs) or asthma (18 groups, 100 GPs), the two parallel intervention arms being controls for each other. Feedback was provided on the GP’s judgments of simulated cases and prescribing. Prescribing indicators were developed and measured before and after the intervention. Analysis was performed by multi-level technique. Prescribing of first choice UTI drugs increased in the intervention arm from 52% to 70% and remained constant in the control arm (P , 0.001). The proportion of patients receiving an inhaled corticosteroid increased insignificantly in both study arms. The educational model can be used to improve prescribing. Further studies are needed to define when the model is effective. J CLIN EPIDEMIOL 52;8:801–812, 1999. © 1999 Elsevier Science Inc. KEY WORDS. Educational outreach, primary care, cluster randomization, urinary tract infection, asthma, prescribing INTRODUCTION In Sweden, about 85% of all drugs are prescribed in out- patient care, out of which about 60% in primary care [1]. A general practitioner (GP) prescribes drugs for, on average, almost SEK 2 million ($250,000) per year. To ensure that this money is spent wisely, continuous medical education (CME) on drug treatment is required. CME for GPs on drug use has largely been provided by drug manufacturers. How- ever, when asked, GPs also express a need for drug informa- tion/education that is academic and not promotional [2]. Review articles have suggested that multifaceted noncom- mercial educational activities using face-to-face or peer group discussions on feedback material is likely to be effec- tive in influencing prescribing practices [3–5]. Examples are available of development and implementation of noncom- mercial drug information/education for GPs in Sweden [6– 9]. Prescribing practices more in line with national guide- line recommendations were shown in a randomized con- trolled educational trial with outreach visits [10,11]. For this study, an educational model was developed based on outreach visits and using feedback as a learning tool in peer groups. Two common clinical conditions were identi- fied where improvements in drug prescribing in primary care in Sweden were considered desirable: urinary tract in- fections (UTI) and asthma [12]. National treatment guide- lines had been issued both for UTI [13] and asthma [14], and sent to all prescribers by the Medical Products Agency in 1990 and 1992, respectively. For uncomplicated UTI, several first-line antibiotics (trimethoprim, pivmecillinam, nitrofurantoin, and some cephalosporins) were recom- mended; however, individual physicians were allowed to re- strict the choice. The recommended treatment length was 3–7 days. The recommendations on drug choice have re- cently been reinforced [15]. For maintenance treatment of asthma, five treatment steps were specified (Fig. 1), indicat- ing that each individual patient may move upwards as well as downwards. Diagnosis and therapy surveys [1] indicated that nonrecommended drugs were highly used in UTI, and *Address for correspondence: Dr. Cecilia Stålsby Lundborg, Department of Public Health Sciences, Division of International Health Care Research (IHCAR), Karolinska Institutet, SE - 171 76 Stockholm, Sweden Accepted for publiction on 8 March 1999.
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Influencing Prescribing for Urinary Tract Infection and Asthma in Primary Care in Sweden

J Clin Epidemiol Vol. 52, No. 8, pp. 801–812, 1999Copyright © 1999 Elsevier Science Inc. All rights reserved.
0895-4356/99/$–see front matterPII S0895-4356(99)00036-0
Influencing Prescribing for Urinary Tract Infection and Asthma in Primary Care in Sweden: A Randomized
Controlled Trial of an Interactive Educational Intervention
C. Stålsby Lundborg,
1,
*
R. Wahlström,
1
T. Oke,
1,2
G. Tomson,
1
and V. K. Diwan,
1,3
1
Department of Public Health Sciences, Division of International Health Care Research (IHCAR), Karolinska Institutet, SE-
171 76
Stockholm, Sweden;
2
Department of Statistics, Uppsala University, Uppsala, Sweden;
3
The Nordic School of Public Health, Gothenburg, Sweden
ABSTRACT.
Our aim was to evaluate effects on prescribing for urinary tract infection (UTI) and asthma, of aneducation with messages based on national guidelines, aimed at improving prescribing in primary care in Sweden.The study is part of the European Drug Education Project. A randomized controlled trial, with groups of generalpractitioners (GPs) allocated to education on UTI (18 groups, 104 GPs) or asthma (18 groups, 100 GPs), the twoparallel intervention arms being controls for each other. Feedback was provided on the GP’s judgments ofsimulated cases and prescribing. Prescribing indicators were developed and measured before and after theintervention. Analysis was performed by multi-level technique. Prescribing of first choice UTI drugs increased inthe intervention arm from 52% to 70% and remained constant in the control arm (P
,
0.001). The proportionof patients receiving an inhaled corticosteroid increased insignificantly in both study arms. The educationalmodel can be used to improve prescribing. Further studies are needed to define when the model is effective.
J
CLIN
EPIDEMIOL
52;8:801–812, 1999. © 1999 Elsevier Science Inc.
KEY WORDS.
Educational outreach, primary care, cluster randomization, urinary tract infection, asthma,prescribing
INTRODUCTION
In Sweden, about 85% of all drugs are prescribed in out-patient care, out of which about 60% in primary care [1]. Ageneral practitioner (GP) prescribes drugs for, on average,almost SEK 2 million ($250,000) per year. To ensure thatthis money is spent wisely, continuous medical education(CME) on drug treatment is required. CME for GPs on druguse has largely been provided by drug manufacturers. How-ever, when asked, GPs also express a need for drug informa-tion/education that is academic and not promotional [2].Review articles have suggested that multifaceted noncom-mercial educational activities using face-to-face or peergroup discussions on feedback material is likely to be effec-tive in influencing prescribing practices [3–5]. Examples areavailable of development and implementation of noncom-mercial drug information/education for GPs in Sweden [6–
9]. Prescribing practices more in line with national guide-line recommendations were shown in a randomized con-trolled educational trial with outreach visits [10,11].
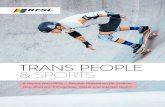
For this study, an educational model was developed basedon outreach visits and using feedback as a learning tool inpeer groups. Two common clinical conditions were identi-fied where improvements in drug prescribing in primarycare in Sweden were considered desirable: urinary tract in-fections (UTI) and asthma [12]. National treatment guide-lines had been issued both for UTI [13] and asthma [14],and sent to all prescribers by the Medical Products Agencyin 1990 and 1992, respectively. For uncomplicated UTI,several first-line antibiotics (trimethoprim, pivmecillinam,nitrofurantoin, and some cephalosporins) were recom-mended; however, individual physicians were allowed to re-strict the choice. The recommended treatment length was3–7 days. The recommendations on drug choice have re-cently been reinforced [15]. For maintenance treatment ofasthma, five treatment steps were specified (Fig. 1), indicat-ing that each individual patient may move upwards as wellas downwards. Diagnosis and therapy surveys [1] indicatedthat nonrecommended drugs were highly used in UTI, and
*Address for correspondence: Dr. Cecilia Stålsby Lundborg, Departmentof Public Health Sciences, Division of International Health Care Research(IHCAR), Karolinska Institutet, SE - 171 76 Stockholm, Sweden
Accepted for publiction on 8 March 1999.

802
C. S. Lundborg
et al.
that inhaled corticosteroids were probably not prescribedaccording to the guideline recommendations.
The aim of the study was to develop, implement, andevaluate the new educational model, with messages basedon available national guidelines aimed at improving pre-scribing in primary care. The study is part of the EuropeanDrug Education Project (DEP). The design, the educationalprogram, and the instruments used were developed jointlyby the members of this international project. In this articlewe present the results of the educational intervention inSweden, expressed as effects on prescribing for uncompli-cated UTI in adult women and asthma for adults 18–49years old.
METHODS
The study design, including the educational method, hasbeen described in detail elsewhere [16], and is summarizedbelow. The study was approved by the Ethics Committeesat Karolinska Institutet and Uppsala University Hospital.
Study Population
Participating GPs were recruited as groups made up of atleast 3 GPs. Of 112 eligible groups, 39 groups (204 GPs)agreed to participate. For practical reasons, 5 of thesegroups were merged to 2, yielding 36 GP groups (3–10 par-ticipants in each group). Written consent was obtainedfrom each participating GP in which s/he allowed us to col-lect her/his prescriptions from the pharmacies and to analyzethem for feedback and outcome. The participants were notoffered any extra incentives, except for the education itself.
Design
The study was a randomized controlled trial using two par-allel interventions (Fig. 2) designed to control for the at-tention (Hawthorne) effect, an intrinsic part of educationalactivities [9]. The GP groups were randomized to educationon either UTI (18 groups, 104 GPs) or asthma (18 groups,100 GPs), the two study arms being controls for each other.
FIGURE 1. A summary of the Swedish guidelines for maintenance treatment of asthma, the so-called “asthma stairs”.

Influencing Prescribing for Urinary Tract Infection and Asthma in Primary Care
803
The randomization was performed at group level (clusterrandomization) after stratification for group size (3–4, 5–6,and 7–10 GPs, respectively), ensuring an even participa-tion of groups with different group sizes in the two inter-
vention arms. In order to detect a prescribing difference of10% between the intervention and the control arm with apower of 90% at a significance level of 5%, at least 15groups of 3–5 GPs, were required in each study arm [17,18].
FIGURE 2. Study design.

804
C. S. Lundborg
et al.
Educational Intervention
In each participating GP group, two tailor-made educa-tional sessions were held on UTI or asthma, depending onthe intervention arm to which the GP group belonged.Certain pre-determined messages, based on the content ofthe guidelines for the respective condition, were empha-sized during the educational sessions (see below). The ses-sions were facilitated by an external team of one GP andone pharmacist (one of the researchers, CSL). During thefirst session, individual feedback on written simulated caseswas given and discussed in the GP group. Three series ofwritten simulated cases were used, one series on UTI, re-garding choice of an antibiotic and treatment length, andtwo series on asthma, regarding treatment of an exacerba-tion and dose adjustment for a patient on maintenancetherapy. Feedback was given on (1) actual decisions—forUTI, decision to prescribe a first- or second-choice drug,and for asthma, decision to prescribe, for example, a shortcourse oral steroid; and (2) factors taken into account whenthese decisions were made—so-called cognitive feedback—in our case, clinical judgment analysis (CJA) [19,20]. Dur-ing the second session, feedback on individual prescribing(dispensed prescriptions) was presented and discussed inthe GP groups: For UTI, the number and relative percent-age of prescriptions for each defined UTI drug (see below)per GP were shown; for asthma, each GP’s patients werecategorized using the “asthma stairs” (Fig. 1). The recordsof a number of actual patients were reviewed during the ses-sion in each group. The average duration of each of the twomeetings was 1.4 hours. The intervention period wasMarch to May 1995 (meetings on prescribing feedback infive GP groups were conducted in August).
Prescribing Data
Data regarding all prescriptions from the participants werecollected through 70 pharmacies and sent to the centralstatistics division of Apoteksbolaget AB (Apoteket ABfrom 1997), the owner of all pharmacies in Sweden. Datafor the analyses performed in this study were selected andsent to the research team. These data included the follow-ing drug groups (ATC code within parentheses):
2
urinaryantiseptics and anti-infectives (G04A); glucocorticoids forsystemic use (H02AB); antibacterials for systemic use(J01); and anti-asthmatics (R03). Data were collected fortwo 6-month periods one year apart, the pre-interventionperiod (September 1, 1994 to February 28, 1995) and thepost-intervention period (September 1, 1995 to February29, 1996). Data from these periods were compared to esti-mate the intervention effect. Pre-intervention data were
used to prepare the individual prescribing feedback for theeducational session in each group.
For UTI, prescriptions were selected for defined UTIdrugs (a drug with the main indication UTI; see Appendix)for women aged 18–75.
3
The main drugs were trimethoprim(J01EA01); pivmecillinam (J01CA08); nitrofurantoin (G04-AC01); and the fluoroquinolones: norfloxacin (J01MA06),ciprofloxacin (J01MA02), and ofloxacin (J01MA01). Forasthma, prescriptions were selected for both men and womenaged 18–49 who had received an anti-asthmatic drug(R03). These patients were defined as asthma patients. Fordefined asthma patients, prescriptions for antibacterials forsystemic use (J01)
4
and glucocorticoids for systemic use(H02AB) were also selected. The age limit was set to mini-mize inclusion of patients with chronic obstructive pulmo-nary disease.
Prescribing Indicators
Prescribing indicators were developed (see Appendix fordetails) to measure prescribing in relation to the messagesconveyed during the educational sessions. The messagesand the related indicators were, for UTI: (1) prescribe firstchoice drugs for uncomplicated UTI (indicator UI); and(2) prescribe short courses (3–7 days) for uncomplicatedUTI (indicator UII); for asthma: (1) start/increase inhaledcorticosteroids when bronchodilator use is “too high” (indi-cators AI, AIa, AIb); (2) treat asthma exacerbations withanti-inflammatory treatment and not routinely with antibi-otics (indicators AII, AIIa); and (3) do not start inhaledlong-acting beta-agonists when the patient is on a sub-opti-mal level of inhaled corticosteroids (indicator AIII). ForUTI, the prescribing indicators were based on the numberof prescriptions—as this is a short term treatment—witheach prescription usually referring to one treatment period.For a chronic disease such as asthma, it was found more ap-propriate to use the patient as level for analysis, as there is avariation, for example, in the time period for which medica-tion written on one prescription is supposed to last. Changeis thus measured here as change at patient level, that is, inour case not within a specific patient, but in regard to num-bers of patients fulfilling certain criteria. The prescribingindicators were developed in order to detect changes in pre-scribing behavior relevant to the messages advocated dur-ing the educational intervention. The messages with the re-lated indicators are presented in Appendix 1.
2
ATC
5
Anatomical, Therapeutic, Chemical classification according toWorld Health Organization Collaborating Centre on Drug Statistics,Oslo, Norway, 1996.
3
Cephalosporins were included in the data collection, but not in the effectanalysis, as they are mainly used for other indications than UTI.
4
Only those commonly used for respiratory tract infections. Included aretetracyclines (J01AA); penicillins (J01C) excluding pivmecillinam orcombination with pivmecillinam; cefalosporins (J01DA); and macrolides(J01FA).

Influencing Prescribing for Urinary Tract Infection and Asthma in Primary Care
805
Other Collected Data
Before and after the intervention, the participating GPscompleted (1) a knowledge and attitudes questionnaire onasthma and UTI, and (2) three series of written simulatedcases. GPs in both study arms completed the cases on bothconditions. The results of the intervention on knowledgeand attitudes and judgments of the written simulated caseswill be reported separately. The participant’s evaluations ofthe educational model were collected after the educationalintervention through a specifically designed evaluationquestionnaire and are reported elsewhere [16].
Data Analysis
Descriptive statistics of the collected prescriptions were an-alyzed and are presented as number of prescriptions per druggroup, or per individual drug, as appropriate. The number ofdefined asthma patients was calculated.
A multilevel analysis [21–23] was performed for the pre-scribing indicators. Multilevel analysis is a regression modelfor the situation in which a hierarchical (or nesting) struc-ture in the data can be seen. In our data, the following hier-archical levels can be defined: Prescriptions are nestedwithin patients, patients are nested within GPs, and GPsare nested within groups of GPs. Data were grouped per pa-tient for asthma and per prescription for UTI. Multilevelanalysis is especially suitable when an unbalanced block de-sign, as in this study, is present [24]. To study the effect ofthe intervention on the prescribing indicators, we haveused the pre-test/post-test model [25]. In testing the inter-vention effect (or the time trend effect, that is, change inthe control group from pre- to post-intervention period),the estimated coefficient is divided by its standard error.The resulting quotient is evaluated against a critical valueof the standard normal distribution (or a t-distribution). Asa comparison, we have also used a pair-wise t-test to com-pare changes in the intervention group before and after theintervention with changes in the control group before andafter the intervention for one indicator.
RESULTS
All groups completed the educational intervention, with anaverage participation rate in the two meetings of 77% (nodifference between the two study arms). For GPs not partic-ipating in the group-session, the feedback material was leftwith a colleague to be delivered later. The prescribing data,collected as dispensed prescriptions, were available for allbut one of the participating GPs.
Descriptive Statistics
In total, 424,088 prescriptions were collected in the pre-intervention period and 397,509 in the post-interventionperiod. In the pre-intervention period, the range of total
number of prescriptions for the participating doctors were35–4900 and in the post-intervention period 9–4919. Thetwo extreme values are in both cases generated by the sametwo doctors. Of the participating doctors, 14% had less thana total of 1000 prescriptions in either of the two collectionperiods, due mainly to sick-leave or leave of absence.
In the pre- and post-intervention periods, 4535 and 3737prescriptions, respectively, were dispensed for defined UTIdrugs for women aged 18–75. Of these prescriptions, 8114fulfilled inclusion criteria for the analysis. The range perGP group in the pre-intervention period was 52–203 (me-dian 129 and 123 in the UTI and control arm, respectively)and in the post-intervention period 49–169 (median 94and 91.5 in the UTI and control arm, respectively).
5
In total, 7850 prescriptions were dispensed for 2454 de-fined asthma patients in the pre-intervention period, and7844 prescriptions for 2267 defined asthma patients in thepost-intervention period. The range of defined asthma pa-tients per GP group was 14–137 (median 57.5 and 65.5 inthe asthma and control arm, respectively) in the pre-inter-vention period, and 11–119 (median 52.5 and 66 in theasthma and control arm, respectively) in the post-interven-tion period. Information per study arm is found in Table 1.
In Table 2, the distribution of main UTI drugs used inthe analysis of the UTI prescribing indicators is presentedper study arm and time period. The absolute number of pre-scriptions of the main fluoroquinolones decreased to one-half the pre-intervention value in the post-intervention pe-riod in the UTI intervention arm. No such dramatic changewas seen in the control arm. However, there is a marginalincrease in the absolute number of first choice drugs in theintervention arm and a decrease in the control arm, resultingin a total decrease, in both study arms, in numbers of UTIprescriptions from the pre- to the post-intervention period.
The distribution of prescriptions used in the analysis ofthe prescribing indicators for asthma is seen in Table 3. Themain drug groups were inhaled selective short-acting beta-agonists and inhaled glucocorticoids. For inhaled short-act-ing beta-agonists, there was a 1% increase in number ofprescriptions in the asthma intervention arm, and a 26%decrease in the control arm. For inhaled corticosteroids,there was a 16% increase in number of prescriptions in theintervention arm compared to 8% in the control arm.Other anti-asthmatic drugs had a marginal use. The use ofantibiotics for defined asthma patients decreased by 21% inthe intervention arm and by 35% in the control arm.
Prescribing Indicators
The proportion of first choice UTI drugs showed a highlysignificant intervention effect in the desired direction, sta-tistically, with a change in the intervention arm from 52%
5
In the following text, the expression “control arm” will be used for thearm not receiving educational intervention on the topic discussed.

806
C. S. Lundborg
et al.
to 70%, whereas in the control arm there was no change(57 and 58%, respectively) (UI). For the indicator on dura-tion of treatment (UII), there was a decrease in treatmenttime in both the intervention and control arms, a signifi-cant period effect (t
5
3.97, P
,
0.001) (Table 4).For asthma, the three indicators dealing with inhaled
corticosteroids and bronchdilators (AI, AIa, AIb) all changed
in the desired direction. However, also in the control arm,changes were seen giving an insignificant intervention ef-fect. For indicator AIa, a significant period effect waspresent (t
5
4.6, P
,
0.001) (Table 5). If we had used amore commonly used method—the pair-wise t-test—forboth the intervention arms separately, there is a statisticallysignificant change (P
,
0.05) from the pre- to the post-
TABLE 1.
Collected prescriptions for participating GPs. Presented as the total number ofprescriptions and number of prescriptions in the intervention arms, for pre
a
-
and post
b
-
intervention periods, respectively
Number of prescriptions
Both interventionarms
(36 GP groups)
UTI interventionarm
c
(18 GP groups)
Asthma intervention arm
d
(18 GP groups)
Pre-intervention periodAll ATC-codes, all age groups 424,088 218,971 205,117Defined UTI-prescription 4,535 2,353 2,182For defined asthma patients
e
7,850 (2454) 4,409 (1,333) 3,441 (1,121)Post-intervention period
All ATC-codes, all age groups 397,509 205,836 191,673Defined UTI-prescription 3,737 1,857 1,880For defined asthma patients
e
7,844 (2,267) 4,314 (1,243) 3,530 (1,024)
a
September 1, 1994–February 28, 1995.
b
September 1, 1995–February 29, 1996.
c
18 GP groups (104 GPs) were included.
d
18 GP groups (100 GPs) were included.
e
In brackets, number of defined asthma patients.
TABLE 2.
Prescriptions for drugs
a
included in the analysis of the UTI prescribing indica-tors. The total number of prescriptions, the group median and the ranges between groupsare presented, for pre
b
- and post
c
-intervention period
Number of prescriptions
UTI intervention arm (18 GP groups)
d
Control arm(18 GP groups)
e
Total
GP group median (range) Total
GP group median(range)
Pre-intervention periodTrimethoprim (J01EA01) 896 48.5 (13–93) 963 56 (20–86)Nitrofurantion (G04AC01) 68 2 (0–14) 32 1 (0–10)Pivmecillinam (J01CA08) 253 11 (3–59) 209 11 (0–37)Fluoroquinolones (J01MA) 1098 53 (29–107) 933 47 (15–109)
Ciprofloxacin (J01MA02) 94 2.5 (0–33) 38 0 (0–22)Norfloxacin (J01MA06) 1002 50.5 (26–106) 894 45 (15–109)
Post-intervention periodTrimethoprim (J01EA01) 939 49 (18–98) 803 40 (9–124)Nitrofurantion (G04AC01 56 2 (0–13) 51 2 (0–11)Pivmecillinam (J01CA08) 232 9.5 (4–37) 164 9 (0–23)Fluoroquinolones (J01MA) 590 31 (13–93) 829 34 (8–117)
Ciprofloxacin (J01MA02) 51 1.5 (0–15) 41 1 (0–16)Norfloxacin (J01MA06) 539 24 (13–78) 786 34 (8–116)
a
A few drugs with a very low number of prescriptions are not included in the table.
b
September 1, 1994–February 28, 1995.
c
September 1, 1995–February 29, 1996.
d
18 GP groups (104 GPs) were included.
e
18 GP groups (100 GPs) were included.

Influencing Prescribing for Urinary Tract Infection and Asthma in Primary Care
807
intervention period regarding the prescribing indicator AIin the asthma intervention arm, but not in the control arm.
For the prescribing indicators AI, AIa, AIb, AII, andAIIa, the number of patients both in the numerators anddenominators were reasonably high for most GP groups. Forindicator AI the range of patients in the numerator in thepre-intervention period were 8–64 in the asthma arm and14–67 in the control arm, and in the post-intervention pe-riod 7–72 and 8–69, respectively. In the denominator therewere 14–73 patients in the asthma arm and 38–122 in thecontrol arm in the pre-intervention period, and in the post-intervention period, 19–116 and 26–119, respectively. Forindicator AIII (regarding inhaled long-acting beta-ago-nists), the number of patients was low, with usually fewerthan 10 patients per GP group in the denominator.
DISCUSSION
The developed educational model significantly influencedprescribing, in line with treatment recommendations re-garding choice of UTI drugs. For asthma treatment, de-sired—although not statistically significant—trends were
recorded. As have been reported elsewhere, the educationwas appreciated by the participants, and 87% wanted to takepart in similar CME activities for other conditions [16].
This is one of few studies examining effects of outreachvisits or effects of feedback in a randomized controlled way,using the proper unit of analysis and appropriate statisticalmethods. In the Cochrane review on educational outreach[4], 18 studies fulfilled the inclusion criteria. One of thesestudies had a design similar to ours, using two educational ar-eas as controls for each other [26]. That study group consistedof only 39 physicians in 24 UK inner city practices, and therewas no baseline data collection. Another of the studies ful-filling the inclusion criteria compared outreach visits withaudit and feedback [27]. This study had a limited number ofparticipants as well. Thirty-four hospital physicians were in-cluded. In the Cochrane review on audit and feedback [5], 37studies in total were included. Effects of outreach visits onprescribing for UTI have previously been shown in a non-randomized controlled trial from Tasmania [28].
It is important to point out the difference for the doctor be-tween changing the way of deciding on treatment forasthma—a chronic disorder, or a short-term treatment for
TABLE 3.
Prescriptions for asthma patients
a
for drugs included in the analysis of theasthma indicators. The total number of prescriptions, the group median and the rangesbetween groups are presented, for pre-
b
and post-
c
intervention period
Number of prescriptions
Asthma intervention arm (18 GP groups)
Control arm(18 GP groups)
Total
GP groupmedian(range) Total
GP groupmedian(range)
Pre-intervention periodSelective
b
-2 agonists, inhaled (R03AC) 1809 105.5 (20–213) 3174 168.5 (83–300)Glucocorticoids, inhaled (R03BA) 862 42(15–104) 1152 51 (27–129)Ipratropium (R03BB) 67 2 (0–15) 67 2 (0–14)Sodiumcromoglycate (R03BC) 45 1 (0–14) 47 1.5 (0–15)Selective
b
-2 agonists, oral (R03CC) 84 4 (0–21) 101 5.5 (1–12)Xantines (R03DA) 41 2 (0–6) 45 1 (0–14)Glucocorticoids, oral (H02AB) 86 1 (1–15) 105 5 (2–16)Antibiotics for systemic use (J01) 433 27 (4–43) 597 26.5 (11–72)
Post-intervention periodSelective
b
-2 agonists, inhaled (R03AC) 1830 88.5 (24–188) 2343 123 (59–221)Glucocorticoids, inhaled (R03BA) 1002 52 (17–120) 1247 61 (29–140)Ipratropium (R03BB) 81 2.5 (0–15) 72 2 (0–28)Sodiumcromoglycate (R03BC) 29 1 (0–8) 58 1 (0–17)Selective
b
-2 agonists, oral (R03CC) 68 2.5 (0–24) 66 3 (1–9)Xantines (R03DA) 22 0 (0–7) 38 2 (0–9)Glucocorticoids, oral (H02AB) 95 3.5 (0–16) 89 4.5 (0–12)Antibiotics for systemic use (J01) 384 15.5 (3–67) 390 17 (8–57)
a
An asthma patients was definied as a person in the age-group 18
–
49 who had a prescription dispensed for ananti-asthmatic drug.
b
September 1, 1994
–
February 28, 1995.
c
September 1, 1995
–
February 29, 1996.
d
18 GP groups (100 GPs) were included.
e
18 GP groups (104 GPs) were included.

808
C. S. Lundborg
et al.
UTI—an acute disorder. We would expect the decision tochange the choice of a drug for a single short-term treatmentto be easier, than to change a patient’s established regimen.The difference in our results could, however, have at least twoother explanations: (1) that asthma is a special case amongchronic diseases, where the patient’s ideas and own choices ontreatment are especially pronounced, or (2) that our methodwas not suitable to detect actual differences for asthma. Re-garding the first explanations, it can be added that the patientis likely to have more interest in influencing a potentially life-long treatment affecting daily life, than a short treatment.There is support in the literature that the patient chooses howto treat asthma by him/herself [29]. This is not a decision takenby the doctor. Patient compliance with prescribed asthma reg-imens has been reported to vary between 20 and 80% [29]. Re-garding the third explanation, a longer prescription registra-tion period might have facilitated showing a change intreatment for asthma. Prescriptions in Sweden are valid forone year after the date of issue. Most asthma patients visit theirdoctor only once or twice a year, implying that many patientsdid not even visit their doctor between the intervention andthe end of the prescription registration period.
It is possible that the groups were influenced by complet-ing the questionnaire on knowledge and attitudes, and thewritten simulated cases for the control condition as well.An explanation for a larger effect in the control group forasthma than in the control group for UTI could be thatthere were two asthma series, compared to one series re-garding UTI, and that the knowledge and attitudes ques-tionnaire contained more items on asthma than on UTI.
The data were collected as dispensed prescriptions andwere not diagnosis-linked. Receiving an asthma drug andbeing between certain age limits was used as a proxy for thediagnosis. This procedure has been used previously [30,31].In our study focusing on the GP’s prescribing practices, us-ing dispensed drugs rather than prescribed ones can partlybe seen as a weakness. In most pharmacoepidemiologicalstudies it could, however, be regarded as an advantage,since the most interesting issue is not what the doctor pre-scribes, but what the patient buys and eventually uses. Ithas previously been shown, that about 20% of prescribed
asthma medications are not dispensed [32]. In this study, itwas observed during the second intervention meeting,when patient records were compared with dispensed drugs,that a number of patients who had been prescribed inhaledcorticosteroids had not had these prescriptions dispensedduring the study period. However, collecting our data at thepharmacies had advantages, the crucial one being that thedata could be delivered in time to prepare the feedback forthe intervention through the use of the pharmacies’ com-mon computer system. Collection through health centerswas not judged feasible.
In our study, the percentage of defined asthma patientsreceiving an inhalation corticosteroid was 46% in the age-group 18–49 before the intervention, rising to 53% and49%, respectively, in the intervention and control groupsafter the intervention. These percentages are in line withwhat has been found in other studies [30,33,34].
Use of prescribing indicators has been reported in two re-cent studies [35,36]. Indicators at three levels were identi-fied [35]: (1) purely descriptive, (2) based on unnecessary orpotentially harmful prescribing, and (3) assessing the ap-propriateness of prescribing specific drugs or combinations.Our indicators were designed to assess appropriateness ofprescribing in accordance with guidelines. The indicatorsthus fall into the third category.
The clinical significance of the indicators in this studycan be summarized as follows: The advantages of using therecommended drugs for uncomplicated UTI (indicator UI)are, in short, (1) the recommended drugs have a narrow an-tibacterial spectrum, which is of importance for individualpatients and for ecological reasons; and (2) the fluoroqui-nolones, which are the most common second choice drugs,are effective and important drugs needed in more compli-cated diseases; a too-widespread use of them is likely to in-crease potential resistance problems. To minimize resis-tance problems with the recommended drugs, it is advisableto change between them, both for recurrent episodes in onepatient and when choosing a drug for a single episode indifferent patients [14]. The adherence to the last recom-mendation has not been monitored through the indicators.The high use of the non-recommended fluoroquinolones
TABLE 4.
Effects of the educational programme on the prescribing indicators for UTI
UTI intervention arm (
n
5
18)
a
PeriodControl arm (
n
5
18)
b
Period
Pre-intervention Post-intervention Pre-intervention Post-intervention Intervention effect
Per cent first choice drugs (UI) 52 70 57 58 t
5
6.85
c
P
,
0.001Average duration of treatment
for first-choice drugs
d
(UII) 7.51 7.41 7.60 7.44 t
5
1.14 P
.
0.2
a
In total 104 GPs.
b
In total 100 GPs.
c
D.f.
5
32, critical t-value
5
2.03 for 0.05-level two-sided test.
d
Based on advised daily dose, set individually for each prescription from the dosage text.

Influencing Prescribing for Urinary Tract Infection and Asthma in Primary Care
809
could be due to a reliance on the argument from the pro-ducer that resistance almost certainly would not develop,and a simultaneous awareness of the potential problems re-garding both pivmecillinam (carnitin deficiency) [37] andnitrofurantoin (risk of developing pulmonary fibrosis in eld-erly women) [38]. The risk of developing resistance towardstrimethoprim in in-patient care, had also been discussed[39]. As doctors are trained for a substantial period in hospi-tals, they do not become acquainted with using trimetho-prim, but rather with using fluoroquinolones. There is ex-perience that this skepticism towards trimethoprim followsthe doctor when s/he starts working in primary care. InSweden, nitrofurantoin has been more or less reserved forpregnant women, but could well be utilized as short-termtreatment in younger non-pregnant women, as well [14].
For the asthma indicators on the use of inhaled cortico-steroids when appropriate (AI, AIa and AIb), there werechanges towards prescribing more, in line with the recom-mendations. These changes were present in both the inter-vention and the control arm, which might be a reflection ofthe promotion of the guideline recommendations both bypharmaceutical companies and professional and officialbodies. For indicator AI, we hypothesized that there was anundertreatment with inhaled corticosteroids. However, (1)the proportion of patients that should be treated with in-haled corticosteroids has not been defined, and (2) our def-inition probably includes patients without verified asthma,as an asthma patient in this study was defined as a patientin the chosen age groups who has been dispensed an anti-asthmatic drug. However, in 1994–1996, 92% of inhaledbeta-2-agonists prescribed by GPs for the age group 18–50years were prescribed for asthma, as defined by the prescrib-
ers themselves (Diagnosis and Therapy survey, ApoteketAB, personal communication).
The indicator showing nonprescribing of inhaled corti-costeroids when needed (indicator AIa), has an ideal valueof zero. The same is true for indicator AIb, which measuresthe proportion of patients on a too-low dose of inhaled cor-ticosteroids, although their use of bronchodilators is high.
For the indicator on use of antibiotics (AII) for asthmapatients, the hypothesis was a general overuse of antibiot-ics. The desired outcome would be a reduction, which wasnot the case. To estimate the appropriate level of antibiotictreatment for patients using anti-asthmatics, which is un-known, every single antibiotic course would need evalua-tion, a procedure that was not an aim of this study. Indica-tor AIIa focuses on the use of short-term courses of oralcorticosteroids. As the prescribing of an oral corticosteroidcould not be related directly to a defined exacerbation, asurrogate was defined as a situation where either an antibi-otic or an oral corticosteroid course was prescribed. Theprerequisite is that antibiotics commonly used for respira-tory infections are usually prescribed to patients withasthma in case of exacerbations. The hypothesis was thatthe use of oral corticosteroids generally was too low, imply-ing that this indicator should increase as an interventioneffect. This was not shown. However, the number of shortterm courses of oral steroids was low, only up to a maximumof 11 courses in each GP group, indicating that interven-tion results based on this indicator are quite uncertain.
Indicator AIII related to the appropriate use of long-act-ing beta-agonists, and should ideally be zero. The numberof observations for each health center was low, usually lessthan ten patients in the denominator. Regardless of the low
TABLE 5.
Effects of the educational programme on the prescribing indicators for asthma
Asthma intervention arm(
n
5
18)
a
Control arm(
n
5
18)
b
Interventioneffect
c
Pre-intervention Post-intervention Pre-intervention Post-intervention
Patients (%) on inhaled corticosteriods (AI) 46 53 46 49 t
5
0.92, P
.
0.2Patients (%), high level mono
use, bronchodilators (AIa) 45 36 50 39 t
5
0.53, P
.
0.2Patients (%), suboptimal inhaled
corticosteroids and high level bronchodilator (AIb) 11 7 15 13 t
5
2
0.91, P
.
0.2Number of antibiotic courses per
asthma patient (AII) 0.26 0.32 0.27 0.26 t 5 1.44, P . 0.2Number of oral steroid courses
divided by the sum of steroid and antibiotic courses (AIIa) .15 0.16 0.11 0.15 t 5 1.03, P . 0.2
Patients (%) on a suboptimal level inhaled corticosteroids using inhaled long-acting beta agonists (AIII) 54 54 48 51 t 5 0.17, P . 0.2
aIn total 100 GPs.bIn total 104 GPs.cD.f. 5 32, critical t-value 5 2.03 for 0.05-level two-sided test.

810 C. S. Lundborg et al.
number of patients, the result could indicate that patientsmight favor inhaled long-acting beta-agonists to inhaledcortocosteroids. It has been reported that patients mightstop their treatment with inhaled corticosteroids when get-ting a long-acting inhaled beta-agonist [40]. The resultsshow quite high proportions for both study arms, with nochange in the desired direction.
The generalization of the findings has two aspects, toother populations and to other conditions. Regarding otherpopulations, the results are probably more or less valid forother Swedish GPs. The participation in the study was vol-untary, which could be a limitation. The age and sex distri-bution of the participants was, however, approximatelysimilar to the general population of Swedish GPs and theparticipating GPs worked in ordinary health centers. Theeducational model seems promising for other conditions aswell, especially for acute conditions where there is a clearmessage that is easy to implement. For chronic conditions,there is a need to study whether the absence of significantintervention effects was an effect of the study design (a toolimited outcome period, more attention on asthma in thecontrol arm than vice-versa) or if this is something specificfor asthma. In other countries participating in the DEPproject, where prescriptions are valid for a more limitedtime, preliminary results show effects on the asthma pre-scribing (personal communication). Further studies areneeded to define under what circumstances this educa-tional model is most effective. In further studies the cost-effectiveness of the model should also be studied.
The project was financially supported by The Fund for Studies in SocialPharmacy and Health Economics, Apoteket AB, the EU BIOMED IProgramme (contract BMH1-CT93-1377), and PECO-NIS Pro-gramme (contract ERB-CIPD-CT940231). We thank the core mem-bers of the European Drug Education Project in the other participatingcountries for their input: FM Haaijer-Ruskamp (international co-ordina-tor), P. Denig, and C. C. M. Veninga (The Netherlands); M. Andrew,the late I. Matheson, M. Loeb, and P. Lagerløv (Norway); M. M.Kochen and E. Hummers-Pradier (Germany); M. Muskova and Z.Kopernicka (Slovak Republic).
We owe a special thanks to the pharmacies involved in the collectionof the prescribing data and to Göran Lindén for making the data readyfor analysis. Olle Staf was the GP facilitator during the educational ses-sions. The model for the multilevel analysis of the prescribing indicatorswas developed in co-operation with Hans Berkhof and Ronald Zwaag-stra, Department of Statistics and Measurement Theory, University ofGroningen, The Netherlands.
APPENDIX 1. PRESCRIBING INDICATORSUTI message I: Prescribe first choice drugs for uncomplicated UTI
General indicator UI: UI 5 (Total number of prescriptionsfor first-choice UTI drugs (trimethoprim, nitrofurantoin, piv-mecillinam) for defined patients)/(Total number of prescrip-tions for all UTI drugs (see below) for defined patients).
Included as UTI-drugs are drugs used for urinary tract in-fections, (excluding those commonly used for other indica-tions): Trimethoprim (J01EA01), pivmecillinam (J01CA08),combinations with pivmecillinam(J01CA20), fluoroquino-lones (J01MA) restricted to products and dosage forms in-dicated for UTI (see below), urinary antiseptives and anti-infectives (G04A).
Included fluoroquinolones are: Ofloxacin (J01MA01)200mg, ciprofloxacin (J01MA02) 100mg, norfloxacin (J01-MA06) 200 and 400mg.
UTI-message II: Prescribe short courses for uncomplicated UTI
General indicator U II: UII 5 Average duration of coursesfor first-choice UTI drugs based on advised daily doses. Theadvised daily dose is set individually for each prescriptionusing the dosage text. A course is defined as a prescriptionfor up to 14 days.
Asthma message I: Start/increase inhaled corticosteroids when bronchodilator use is too high
General indicator AI: AI 5 [Total number of defined pa-tients prescribed inhaled steroids (R03BA)]/[Total numberof defined patients (R03)].
Specific indicator AIa: AIa 5 [Total number of patientsprescribed high level mono-use of short-acting inhaledbronchodilator (beta-2-agonists [R03AC02-04], ipratro-pium [R03BB01])]/(Total number of patients prescribedany short-acting inhaled bronchodilators). High level is de-fined as an average daily use during 6 months, i.e. .1/4DDD6 per day.
Specific indicator AIb: AIb 5 [Total number of patientson suboptimal level inhaled corticosteroids AND very highlevel inhaled short acting bronchodilator without using anyinhaled long-acting beta-agonists (R03AC12-13)]/[Totalnumber of patients on inhaled corticosteroids and inhaledshort-acting bronchodilators]. Suboptimal level inhaledcorticosteroids is defined as #1/2 DDD per day during 6months. Very high level bronchodilators is defined as .1/2DDD per day during 6 months.
Asthma message II: Treat asthma exacerbation with antiinflammatory treatment and not routinelywith antibiotics
General indicator AII: AII 5 [Total number of oralantibiotic7 courses for defined patients]/[Total number ofdefined patients].
6DDD 5 Defined Daily Dose defined as follows: The DDD is the assumedaverage maintenance dose per day for a drug used on its main indicationsin adults.
7Antibiotics included are: tetracyclines (J01AA), penicillins (J01C)(excluding pivmecillinam or combination with pivmecillinam), cefa-losporins (J01DA ), macrolides (J01FA).

Influencing Prescribing for Urinary Tract Infection and Asthma in Primary Care 811
Specific indicator AIIa: AIIa 5 [Total number of oralcorticosteroid (H02AB) courses for defined patient]/[Totalnumber of oral corticosteroid 1 total number of oral antibi-otic courses for defined patients]. A course is defined as aprescription for up to 14 days or for a maximum of 30 DDD.If it is clear from the dosage text that one prescription is in-dicated for more than one course, each course is countedseparately.
Asthma message III: Do not start inhaled long-acting beta-agonists when the patient is on a suboptimal level of inhaled corticosteroids
Indicator AIII: AIII 5 [Total number of patients on subop-timal level inhaled corticosteroids AND inhaled long-act-ing beta-agonists]/[Total number of patients on inhaledlong-acting beta-agonists]. Suboptimal level inhaled corti-costeroids is defined as less than 1/2 DDD (including 0DDD and excluding 1/2 DDD) per day during 6 months.
References1. Nordenstam I, Wennberg M, Kristoferson K. Drug Statistics
(Svensk Läkemedelsstatistik 1993). Stockholm: Apoteksbo-laget AB; 1994.
2. Stålsby Lundborg C, Hensjö L-O, Gustafsson LL. Drug infor-mation sources: Reported preferences by general practitioners.Drug Inf J 1998; 32: 777–785.
3. Davis DA, Thomson MA, Oxman AD, Haynes RB. Changingphysician performance. A systematic review of the effect of con-tinuing medical education strategies. JAMA 1995; 274: 700–705.
4. Thomson MA, Oxman AD, Davis DA, Haynes RB, Freeman-tle N, Harvey EL. Outreach visits to improve health profes-sional practice and health care outcomes. In: Bero L, Grilli R,Grimshaw J, Oxman A, Eds. Collaboration on Effective Pro-fessional Practice Module of the Cochrane Database Sys-tematic Reviews. Oxford: Update Software; 1998.
5. Thomson MA, Oxman AD, Davis DA, Haynes RB, Freeman-tle N, Harvey EL. Audit and feedback (Part I). In: Bero L,Grilli R, Grimshaw J, Oxman A, Eds. Collaboration on Effec-tive Professional Practice Module of the Cochrane DatabaseSystematic Reviews. Oxford: Update Software; 1998.
6. Ekedahl A, Andersson SI, Hovelius B, Mölstad S, LiedholmH, Melander A. Drug prescription attitudes and behaviour ofgeneral practitioners. Effects of a problem oriented educa-tional programme. Eur J Clin Pharmacol 1995; 47: 381–387.
7. Stålsby Lundborg C, Hensjö L-O, Gustafsson LL. “Academicdrug-detailing” – From project to practice in a Swedish urbanarea. Eur J Clin Pharmacol 1997; 52: 167–172.
8. Tomson Y, Wessling A, Tomson G. General practitioners forrational use of drugs. Examples from Sweden. Eur J ClinPharmacol 1994; 47: 213–219.
9. Wahlström R, Tomson G, Diwan VK, Beerman B, Sterky G.Hyperlipidaemia in primary care. A randomized controlledtrial on treatment information in Sweden: Design and meth-odology. Pharmacoepidem Drug Safety 1995; 4: 75–90.
10. Diwan VK, Wahlström R, Tomson G, Beerman B, Sterky G,Eriksson B. Effects of “Group detailing” on the prescribing oflipid-lowering drugs: A randomized controlled trial in Swedishprimary care. J Clin Epidemiol 1995; 48: 705–711.
11. Wahlström R, Diwan VK, Oke T, Tomson G, Beermann B.An educational experiment in primary care in Sweden—
improving the treatment of hypercholesterolaemic patients atrisk. Euro J Gen Pract 1997; 3: 96–102.
12. Socialdepartementet. Network for pharmacoepidemiology –NEPI (in Swedish). Stockholm: Socialdepartementet; Ds1992; 104: 51.
13. Strandberg K, Beermann B, Lönnerholm G, Eds. Treatmentof Urinary Tract Infections. Uppsala: Medical ProductsAgency; 1990.
14. Strandberg K, Beermann B, Lönnerholm G, Eds. Pharmaco-logical Treatment of Bronchial Asthma II. Uppsala: MedicalProducts Agency; 1993.
15. Cars O, Sandberg T. Restrict the use of fluoroquinolones inUTI (in Swedish). Information Uppsala: Läkemedelsverket;1996; 7: 3–4.
16. Stålsby Lundborg C, Wahlström R, Diwan VK, Oke T,Mårtenson D, Tomson G. Combining feedback from simu-lated cases and prescribing, design and implementation of aneducational intervention in primary care in Sweden. J Tech-nology Assessment in Health Care. (In Press)
17. Diwan VK, Eriksson B, Sterky G, Tomson G. Randomizationby group in studying the effect of drug information in primarycare. Int J Epidem 1992; 21: 124–30.
18. Diwan VK. Epidemiology in context. Effectiveness of healthcare interventions (dissertation). Stockholm: Karolinska In-stitutet; 1992.
19. Kirwan JR, Chaput de Saintonge M, Joyce CRB. Clinicaljudgement analysis Quart J Med 1990; 76: 935–949.
20. Cocksey RW. Judgment Analysis. Theory, Methods and Ap-plications. London: Academic Press; 1996.
21. Bryk AS, Raudenbush SW. Hierarchical Linear Models. Ap-plications and Data Analysis Methods. London: Sage Publi-cations; 1992.
22. Goldstein H. Multilevel Statistical Models. London: Arnold;1995.
23. Longford NT. Random Coefficient Models. Oxford: Claren-don Press; 1993.
24. Rice N, Leyland A. Multilevel models: Application to healthdata. J Health Serv Res Policy 1996; 1: 154–164.
25. Huck SW, McLean RA. Using repeated measures ANOVA toanalyze the data from pretest-posttest design: A potentiallyconfusing task. Psychological Bull 1975; 82: 511–518.
26. Feder G, Griffiths C, Highton C, Eldridge S, Spence M,Southgate L. Do clinical guidelines introduced with practicebased education improve care of asthmatic and diabetic pa-tients. A randomised controlled trial in general practices ineast London. BMJ 1995; 311: 1473–1478.
27. Steele MA, Bess DT, Franse VL, Graber SE. Cost effective-ness of two interventions for reducing outpatient prescribingcosts. DICP 1989; 23: 497–500.
28. Peterson GM, Stanton LA, Bergin JK, Chapman GA. Im-proving the prescribing of antibiotics for urinary tract infec-tion. J Clin Pharm Ther 1997; 22: 147–53.
29. Cochrane GM. Therapeutic compliance in asthma: its magni-tude and implications. Eur Respir J1992; 5: 122–124.
30. Gaist D, Hallas J, Hansen NC, Gram LF. Are young adultswith asthma treated sufficiently with inhaled steroids? A pop-ulation-based study of prescription data from 1991 and 1994.Br J Clin Pharmacol 1996; 41: 285–289.
31. Gerdtham UG, Hertzman P, Jonsson B, Boman G. Impact ofinhaled corticosteroids on acute asthma hospitalization inSweden 1978 to 1991. Med Care 1996; 34: 1188–1198.
32. Nilsson JLG, Johansson H, Wennberg M. Large differencesbetween prescribed and dispensed medicines could indicateundertreatment. Drug Inf J 1995; 29: 1243–1246.
33. Larsson L, Boethius G. Differences in utilization of asthmadrugs between two neighbouring Swedish provinces: Relation

812 C. S. Lundborg et al.
to treatment in individuals with airway disease. J Intern Med1995; 238: 307–316.
34. Gislason T, Olafsson O, Sigvaldason A. Users of antiasthmadrugs in Iceland: A drug utilization study. Eur Respir J 1997;10: 1230–1234.
35. Oborne CA, Batty GM, Maskrey V, Swift CG, Jackson SH.Development of prescribing indicators for elderly medical in-patients. Br J Clin Pharmacol 1997; 43: 91–97.
36. Braybrook S, Walker R. Influencing prescribing in primarycare: A comparison of two different prescribing feedbackmethods. J Clin Pharm Ther 1996; 21: 247–54.
37. Holme E, Greter J, Jacobson CE, Lindstedt S, Nordin I, Kris-tiansson B, et al. Carnitine deficiency induced by pivampicil-lin and pivmecillinam therapy. Lancet 1989; 334: 69–473.
38. Hainer BL, White AA. Nitrofurantoin pulmonary toxicity. JFam Pract 1981; 13: 817–823.
39. Huovinen P, Mantyjarvi R, Toivanen P. Trimethoprim resis-tance in hospitals. BMJ 1982; 284: 782–784.
40. Ekedahl A. Cross-sectional studies on dispensed drugs couldgive information on what drug combinations are used (inSwedish). Allmänmedicin 1996; 17: 198–200.