Prescribing, Ordering and Administering Controlled Substances
Upload
independentCategory
view
2download
0
ORIGINAL RESEARCH
Nurse prescribing roles in acute care: an evaluative case study
Kathryn Jones, Margaret Edwards & Alison While
Accepted for publication 3 September 2010
Correspondence to K. Jones:
e-mail: [email protected]
Kathryn Jones DHC RGN PGCE
Programme Director Modernising Nursing
Careers
NHS London, UK
Margaret Edwards PhD RN PGCE
Senior Lecturer
Florence Nightingale School of Nursing and
Midwifery, King’s College London, UK
Alison While PhD RGN CertEd
Professor of Community Nursing
Florence Nightingale School of Nursing and
Midwifery, King’s College London, UK
JONES K. , EDWARDS M. & WHILE A. (2011)JONES K. , EDWARDS M. & WHILE A. (2011) Nurse prescribing roles in acute
care: an evaluative case study. Journal of Advanced Nursing 67(1), 117–126.
doi: 10.1111/j.1365-2648.2010.05490.x
AbstractAim. This paper is a report of an evaluation of the implementation of nurse pre-
scribing in an acute care hospital in England.
Background. At the time of the study, evaluation of nurse prescribing had taken
place in community settings, but little was known about its impact and effectiveness
in acute care. Although nurse prescribing has permitted doctor–nurse substitution in
acute episodic care, some doctors have expressed concerns about patient safety in
relation to nurse prescribing.
Methods. A mixed methods single-case study was conducted in 2005–06, using
purposive sampling. Semi-structured interviews were carried out with 18 hospital
staff, non-participant observation of two nurses and two doctors undertaking 52
patient-prescriber consultations with 47 patients, and a questionnaire survey with
122 patients (response rate 61%: n = 74).
Results. Nurse prescribing was found to benefit patients through service delivery
improvement and using staff skills differently. Nurse prescribers and their colleagues
were positive about role and service changes and their impact on patient care. No
differences were found between the ways in which nurses and doctors performed
prescribing roles, but there was a statistically significant difference between the
medication-related information satisfaction ratings of patients who had seen a nurse
prescriber, compared to those seen by a doctor.
Conclusion. Nurses and doctors were found to provide equivalent care. Shared
vision, local champions, action learning and peer support were the enabling factors
that helped to embed the new prescribing roles within the study site.
Keywords: acute care, case study, new roles, nurses, prescribing, doctor–nurse
substitution
Introduction
Nursing work is changing to meet the needs of healthcare
systems as they adjust to the rising prevalence of chronic
disease and growing numbers of older people within new cost
constraints (WHO 2006). Escalating healthcare costs due to
new technologies, new drugs and increasing public expecta-
tions, together with population changes, are drivers to deliver
health care with improved efficiency and cost-effectiveness
(Buchan & Calman 2004). Prescribing by nurses reflects the
desire to maximize the capacity of the nursing workforce to
improve both the speed of access to and the quality of care
(Department of Health 2006) and has been implemented in a
number of countries, including Botswana, South Africa,
� 2010 The Authors
Journal of Advanced Nursing � 2010 Blackwell Publishing Ltd 117
J A N JOURNAL OF ADVANCED NURSING

Sweden, Australia, New Zealand, the United States of
America (USA) and Canada (Calman & Buchan 2004). In
the USA, it is associated with advanced nurse practitioners
across 50 states, where it is reported to improve patient
outcomes, reduce healthcare costs and be well-received by
patients (Brooten et al. 2002).
Background
Prescribing by community nurses in the United Kingdom
(UK), which began in the early 1990s, has been extended to
suitably qualified nurses in all settings (Department of Health
2002). While independent prescribers assume sole responsi-
bility for the prescriptions that they write, including single
accountability for patient assessment and any clinical deci-
sions made, supplementary prescribers share responsibility
for their prescribing with an independent prescriber, most
frequently a doctor (Department of Health 2006). Latter
et al. (2005), in a national evaluation of independent nurse
prescribers (n = 246) in England, found that the majority of
nurse prescribers felt strongly that their prescribing had had a
positive impact on both patient care and patients’ access to
their medicines, and had also enabled staff to use their skills
better. Although a number of professional concerns were
initially raised about the preparation of nurse prescribers and
their competence to act (Avery & Pringle 2005, Chief
Medical Officer 2005, Connelly 2005, Crown & Miller
2005, Siriwardena 2006), a national evaluation of supple-
mentary prescribing confirmed its safety (Bissell et al. 2008).
Indeed, non-medical prescribing has been shown to improve
clinical decision-making across healthcare teams (Bradley &
Nolan 2007) and enable reassessment of roles within multi-
professional teams (Avery et al. 2007).
At the time of the study reported here, evaluation of nurse
prescribing in the UK had focused on primary care (Luker
et al. 1997, Latter & Courtenay 2004), with only two
published evaluations in acute care settings (James 2004,
Latter et al. 2005). Three studies had shown the positive
views of patients, prescribers and their colleagues about nurse
prescribing (Luker et al. 1997, James 2004, Latter et al.
2005), with only one study focusing solely on the views of
patients (Brooks et al. 2001). The majority of the studies,
both in primary and secondary care, had only reported nurse
prescribers’ views of their own prescribing roles (Rodden
2001, Luker & McHugh 2002, Lewis-Evans & Jester 2004,
While & Biggs 2004) to the neglect of other stakeholders. In
the light of the existing research there was a need for further
exploration of the nurse prescriber role, in particular an
understanding of the settings in which the nurse prescribers
worked, the differences that their new prescribing roles made
to established ways of team working, and the views of nurse
peers and healthcare colleagues across varied practice set-
tings. Further exploration of the differences in the roles of
medical and nurse prescribers was also needed to understand
better the ways in which each prescriber worked, and the
potential impact on patient outcomes, including satisfaction.
The study
Aim
The aim of the study was to evaluate the implementation of
nurse prescribing in an acute care hospital setting in England.
Design
An embedded single-case design with three units of analysis
(Yin 2003) was used (see Figure 1). The case study method
was selected so that a clear set of propositions about the
evolving phenomenon of nurse prescribing could be tested in
a new context of new roles and ways of working in acute care
(after Yin 2003). The units of analysis were chosen as
examples of where the phenomenon could be studied at an
operational level embedded within the case, and were used
both as sources of data collection and units of analysis. We
used multiple data collection methods, including semi-struc-
tured interviews, non-participant observation of patient-
prescriber consultations and a patient survey using validated
New roles and ways of working for patientbenefit with better use of staff skills
Implementation of nurseprescribing in an acute care
hospital
Renal out-patients clinic
(embedded unit ofanalysis 2)
Hypertensionclinic
(embedded unit ofanalysis 1)
Renal satelliteunit
(embedded unit ofanalysis 3)
Figure 1 The selected case.
K. Jones et al.
� 2010 The Authors
118 Journal of Advanced Nursing � 2010 Blackwell Publishing Ltd

rating scales, to investigate the experiences of multiple
stakeholders in relation to the implementation of nurse
prescribing. The triangulation of data from multiple data
sources can confirm or refute the evidence found (Hutchinson
1990). The main stakeholders were patients, prescribers and
their colleagues (as recommended by Brooks et al. 2001,
Latter & Courtenay 2004, Latter et al. 2005), and other
hospital staff who held senior strategic positions. Proposi-
tions derived from practice knowledge were developed
through discussions with staff and from an analysis of policy
and professional literature, and were used to direct the study
(see Table 1). An element within the case was a quasi-
experiment to test the null hypotheses that there were
no differences between the roles of medical and nurse
prescribers.
Setting
One acute care hospital in England was selected as a case
study. The hospital was located in a densely populated
metropolitan borough with an ethnically diverse population
[in 2001, 27% of the local population were from black and
minority ethnic (BME) groups and 44% were born outside
the UK], had 630 beds and employed 3500 staff to deliver
general and specialist services. There were nine nurses who
had undertaken preparation for prescribing, of whom seven
(78%) were actively prescribing.
Participants
Three clinical departments were purposively selected as units
of analysis because the doctors and nurses were early imple-
menters of nurse prescribing and had been involved in the study
design. These were the hypertension clinic, renal clinic and
renal satellite unit. A purposive sample of staff was interviewed
(n = 18) to explore the background and intended purpose of
the new roles and the experiences of the nurse prescribers and
their teams. Staff members were selected because they were
prescribers (n = 3), mentors or colleagues (n = 7), or senior
hospital staff (n = 8) who had influenced the implementation
of new roles and ways of working within the organization,
including the Directors of Medicine, Nursing, Human
Resources and the Chief Pharmacist. The sample was not
extended further because data saturation was achieved. Two
nurses and two doctors from the hypertension and renal clinics
were purposively selected for the observed opportunistic
patient-prescriber consultations, through discussion with the
lead clinicians for each service, as being exemplars of the new
service delivery arrangements. A convenience sample of
patients (n = 122) who attended the hypertension and renal
clinics were invited to complete a questionnaire if they met the
principal inclusion criteria of understanding an oral explana-
tion of the study in English and were able to complete the
questionnaire in English. Statistical advice was sought about
the patient sample. Although the sampling strategy yielded a
Table 1 Propositions derived from prac-
tice knowledge, with links to relevant liter-
ature
Proposition Evidence for proposition
Nurses spend more time with patients
than doctors
Luker et al. (1997),
Horrocks et al. (2002),
Buchan and Calman (2004),
Latter et al. (2005),
Laurant et al. (2005)
Nurses give patients more information about
their medicines than doctors
Luker et al. (1997),
Brooks et al. (2001),
Rodden (2001)
Patients who have medicines prescribed by
nurses are more knowledgeable about their
medicines than those who have medicines
prescribed by doctors
Wilson-Barnett and Beech (1994)
Patients who have medicines prescribed by
nurses are more compliant with their
treatment than those who have medicines
prescribed by doctors
Brown and Grimes (1995),
Berry et al. (2006)
Patients who have medicines prescribed by
nurses experience fewer side effects than
those who have medicines prescribed by
doctors
Taylor et al. (1997)
Prescribing is a risky activity irrespective of
the professional background of the
prescriber
Crown and Miller (2005)
JAN: ORIGINAL RESEARCH Nurse prescribing roles in acute care
� 2010 The Authors
Journal of Advanced Nursing � 2010 Blackwell Publishing Ltd 119

non-probability sample, the participants were chosen because
of the likelihood that they would give information relevant to
the study aim and would be most likely to confirm or refute the
propositions held (Flyvbjerg 2001).
Data collection
Data were collected from July 2005 to September 2006 using
semi-structured interviews with staff (n = 18) (July 2005–
September 2006), structured non-participant observation of
doctors (n = 2) and nurses (n = 2) conducting patient consul-
tations (n = 52) (November 2005–January 2006), and a
patient survey (n = 122) (November 2005–April 2006). In
the semi-structured interviews we investigated both the back-
ground and intended purpose of the nurse prescribing roles and
the experiences of the prescribers and of their colleagues, and
were guided by questions formulated from the policy literature.
Nurse prescribers were each interviewed on two occasions,
once at the beginning of the study and then again 9 months
later in a follow-up interview, when their colleagues were also
interviewed. Senior staff were interviewed at the beginning of
the study. Non-participant observation and a patient survey
were used to investigate the null hypothesis. A structured
observation sheet (15 items) was devised to assess prescriber
competence (demonstrated/not demonstrated), in particular
the ability to manage the patients’ medicine needs, based on a
tool that had been used in a national evaluation (Latter et al.
2005) and an Observed Structured Clinical Examination
(King’s College London 2004) tool in frequent use. The
researcher (KJ) was an established practitioner who was
familiar with structured observation for the assessment of
clinical practice competence. Consultations were observed
with patient consent at opportunistically selected clinics. Dual
observation of consultations was not undertaken because it
would have compromised the professional consultations, and
this approach precluded an estimate of inter-rater reliability.
The patient data were collected using a structured question-
naire (40 items) which included validated rating scales to assess
respondents’ beliefs about their medicines (10 items) [Beliefs
about Medicines Questionnaire (BMQ): Horne et al. 1999]
and their satisfaction with the information they received from
the prescriber (17 items) [Satisfaction with Information about
Medicines Scale (SIMS): Horne et al. 2001].
Ethical considerations
The study was approved by the appropriate research ethics
and governance committees. Four potential ethical issues
were considered during the design and development of the
study: the relationship between the researcher and the
prescribers; a risk that the findings might suggest that nurse
prescribers were either ‘not as good as’ or ‘better at’
prescribing than medical prescribers; a risk that patient
consultations might be compromised by the presence of a
researcher; and a risk that patients might not like the service
provided. Participants in all components of the study were
given study information sheets and time to consider partic-
ipation, with the assurance for patients that their participa-
tion was entirely voluntary and would not jeopardize their
care or treatment in any way.
Data analysis
The qualitative data were analysed using Ritchie and Spencer’s
(1994) data analysis framework, which is a deductive
approach that enabled the systematic sifting, charting and
organization of the data according to key issues and themes.
Quantitative data were analysed using the Statistical Package
for Social Sciences Version 14 (SPSS Inc., Chicago, IL, USA).
Numerical data were summarized using descriptive statistics.
Non-parametric techniques were used to analyse categorical
data and those that were not normally distributed.
Validity and reliability
In accordance with recommendations for case study rigour
(Yin 2003), the study was guided by propositions. The
interview schedule was guided by a literature review to
enhance content validity, and the observation schedule was
developed from tools that had been tested and used previously
to measure the performance of nurse prescribers (King’s
College London 2004, Latter et al. 2005). The patient survey
questionnaire included items taken from validated rating
scales designed to assess patients’ attitudes to and knowledge
about their medicines (Horne et al. 1999, 2001), and general
satisfaction questions taken from a national outpatient
questionnaire (Healthcare Commission 2005) that enabled
service comparison against national norms published as part
of health service monitoring. Although the potential for
researcher bias is acknowledged, a consistent approach to the
data was adopted, including member checking (Stake 1995)
by all participants at two levels: verification of interview
transcripts and credibility of the thematic analysis and
interpretation. The approaches to data analysis and interpre-
tation were regularly checked within academic supervision.
Results
The sample comprised 18 staff who participated in the
interview: nurse prescribers (n = 3), their medical, nursing
K. Jones et al.
� 2010 The Authors
120 Journal of Advanced Nursing � 2010 Blackwell Publishing Ltd

and pharmacy colleagues (n = 7) and senior hospital staff
(n = 8) (response rate 100%); of two nurses and two doctors
who were observed undertaking 52 patient-prescriber con-
sultations with 47 patients; and 122 patients who completed
the questionnaire (response rate 61%: n = 74; 51% white,
47% from BME groups).
Background and intended purpose of the prescribing roles
The staff who participated in interviews unanimously
reported that the overall intention of nurse prescribing was
for patient benefit and that it yielded improved timeliness of
care, better patient outcomes, improved team-working,
advancement of working, legitimization of practice and
increased patient and staff satisfaction:
Today it was great. I saw a … new patient today, and his blood
pressure was [states value] and he’d run out of his medication and it
would have taken him 48 hours at least to go back to his GP and get
more medication. He hadn’t had medication for a week. He was at
risk. I knew he had brought his tablets, I knew what he needed to
take and I was able to write him a prescription. (Nurse Prescriber 1)
Experiences of nurse prescribers and their teams
At the time of their initial interview the nurse who worked in
the hypertension clinic had been prescribing for 18 months,
while nurses from the renal clinic and renal satellite unit had
been prescribing for 11 months. All three nurse prescribers
considered that their prescribing practice had had a positive
impact on patient care and team-working, and had also
enabled them to make better use of their nursing skills:
I can’t split it up [the impact of nurse prescribing]. If I think about
how patients are sent to me here…our patients are very com-
plex...The doctors and I share caring for those patients totally, and
the way they use me is that they will see a patient and decide on the
way they are going to go with medication, which is their skill, and
then they will send the patient to me on a few occasions to titrate
medication, add medication. And they will have decided what format
to follow, and I will follow that format and I may discharge patients
from that. Because patients may come to me it allows the doctor to
see more patients that are more complex (that’s what their role is)
and I can – rather than sending them back to the GP, the patient stays
under our care, and I look after them in that format until they are
ready to go back to the GP. (Nurse Prescriber 1)
The themes identified in the data set were: increased
confidence to prescribe, improved patient care, increased
role fulfilment and successful implementation of nurse
prescribing. For example, all three nurse prescribers reported
that they felt confident prescribing, but acknowledged that
their confidence had developed with time. They all identified
doctor colleagues, nurse managers and peers as key to the
successful implementation of their prescribing role, and the
importance of existing, and supportive, team-working, to
their prescribing practice. They viewed the support of senior
nursing staff positively – specifically an action learning set
that had been established to provide support for novice nurse
prescribers:
We do have a culture of nurses extending roles [in the renal unit] so
then the support has already been there. Then it really, I think really,
was the support of the Trust – the action learning and being part of
the Trust, because it’s all very well doing it in renal but you do feel
very isolated. So it was very important to come outside of that and
have this opportunity to talk around the table. (Nurse Prescriber 3)
I decided to do it and was supported by the doctors because of their
research [trials] and getting nurses to increase drugs. They need
nurses who are good at it… they knew it was a safe thing for me to
do. (Nurse Prescriber 1)
The colleague sample also unanimously reported the benefits
of nurse prescribing to patient care, which was reflected in
improved timeliness of treatment, improved patient care,
improved team-work, influence on colleagues and changed
team workloads:
It’s been really positive. They [the patients] are not waiting around
for the doctors to sign prescriptions or for [names nurse prescriber] to
discuss [treatment] with the doctors. She’s able to do the whole
consultation and so it’s very positive for patients. (Nurse Colleague 5)
[She] sees patients in an individual fashion. She is extremely
experienced in what they need and when they need it and the
patients therefore get the drugs quicker. They don’t have to wait
around so long. (Doctor Colleague 1)
Differences in roles of medical and nurse prescribers
Findings from the observation data
Forty-seven patient-prescriber consultations were observed,
of which two-thirds (n = 30) took place in the renal clinic and
one-third (n = 17) in the hypertension clinic. Sixty per cent
(n = 28) of the consultations were between a patient and a
nurse, and 40% (n = 19) were between a patient and a doc-
tor. No differences were found in prescribers’ approaches to
their patients or in the ways in which they managed their
medicines. No statistically significant difference was found
between the length of the observed patient-prescriber con-
sultation and the profession of the prescriber (Chi-square
JAN: ORIGINAL RESEARCH Nurse prescribing roles in acute care
� 2010 The Authors
Journal of Advanced Nursing � 2010 Blackwell Publishing Ltd 121

test). Also, no difference was found in the prescribing practice
of the doctors and the nurses, including the number and types
of items prescribed per patient although some difference was
noted in the methods of prescription used, for example, new
or repeat medicine, but the dataset was too small to test for
statistical significance.
Findings from the survey data
Seventy-four patients returned completed questionnaires (res-
ponse rate 61%), of whom 51% (n = 38) were white and
47% (n = 35) from BME groups: Black Caribbean (n = 12);
Black African (n = 7); Asian (n = 8); Chinese (n = 4); Mixed
(n = 3); and Black other (n = 1). Seventy-two per cent
(n = 53) of the patients had attended the renal clinic and 28%
(n = 21) had attended the hypertension clinic. Three-quarters
(n = 57) had consulted a nurse and one quarter (n = 17) had
consulted a doctor, but 12 more patients reported that they
had consulted a doctor (n = 29) than had actually done so.
Patients unanimously reported confidence and trust in their
prescriber, irrespective of whom they thought that they had
consulted.
The beliefs held by patients about their prescribed med-
icines were measured using the BMQ (Horne et al. 1999).
Specific-necessity and specific-concern scores were calculated
for each of the 69 (93%) patients who had fully completed
the BMQ. In a possible range of 1–5, scores ranged from 2Æ2–
5 for specific-necessity and 1–5 for specific-concern. The
scores indicated beliefs about the necessity of medicines for
maintaining or improving health and about the potential
adverse effects of taking medicines. No statistically signif-
icant difference was found between BMQ scores and the
profession of the prescriber (Chi-square test). For example,
44% (n = 24) of patients who had consulted a nurse attained
a specific-necessity score of 5, as did 40% (n = 6) of those
who had consulted a doctor; the majority (53%, n = 8) of
those who had consulted a doctor scored 4 for specific-
necessity, as did 43% (n = 23) of those who had consulted a
nurse. These scores indicated strong beliefs in the value of
taking medicines to maintain or improve health. The
majority (74%, n = 40) of the patients who had consulted
a nurse attained a specific-concern score of 2–3, as did 73%
(n = 11) of those who had consulted a doctor. These scores
indicated low to moderate concern about the adverse effects
of taking medicines. Whilst no difference was found between
specific-necessity scores and patients’ ethnic origin, some
difference was noted relating to specific-concern scores. For
example, most patients with higher overall specific-concern
scores (indicating the greatest concerns about their medi-
cines) were from BME groups (64% n = 9), but the data set
was too small to test for statistical significance.
Patients’ satisfaction with the medication information
received from their prescribers was measured using the SIMS
(Horne et al. 2001). Total satisfaction rating scores were
calculated for each of the 64 patients (86%) who had fully
completed the SIMS tool, and were grouped by the profession
of the prescriber (Table 2). Scores ranged from 2 to 17
(possible range 0–17), with higher scores indicating a higher
degree of satisfaction. There was a statistically significant
difference between the satisfaction ratings of patients who
had seen a nurse and those who had seen a doctor, with 66%
of those (n = 33) who had consulted a nurse reporting a
satisfaction rating of 17, compared to 7% (n = 1) of those
who had consulted a doctor (v2 = 15Æ22, d.f. = 1, P <
0Æ001). Comparison of mean total satisfaction rating scores
across the professional groups was also statistically signifi-
cant, with nurses scoring a higher mean rank (36Æ56) than
doctors (18Æ0) (v2 = 12Æ82, d.f. = 1, P < 0Æ001) using the
Kruskal–Wallis test. There was also a small difference when
comparing the scores of patients from different ethnic groups;
for example, more patients from BME groups (59%, n = 20)
attained a score of 17 than white patients (41%, n = 14),
but the data set was too small to test for statistical
significance.
Discussion
Study limitations
In this small study we used a case study design in one acute
hospital as little was known about the impact and
effectiveness of nurse prescribing in the acute care setting;
therefore the findings must be considered tentative until a
larger study is conducted. Although a purposive sampling
yielded a non-probability sample, every attempt was made
to enhance validity and reliability at all stages of the
research process. The use of a single observer without inter-
Table 2 Patients’ total satisfaction rating scores grouped by pro-
fession of prescriber
Profession
Total satisfaction rating score
Total1–10 11–16 17
Nurse (n = 50) 6
(12%)
(60%)
11
(22%)
(68%)
33
(66%)
(97%)
50
(100%)
Doctor (n = 14) 4
(29%)
(40%)
9
(64%)
(32%)
1
(7%)
(3%)
14
(100%)
Total 10
(100%)
20
(100%)
34
(100%)
64
(100%)
K. Jones et al.
� 2010 The Authors
122 Journal of Advanced Nursing � 2010 Blackwell Publishing Ltd
rater observation may be a weakness; however, there were
ethical considerations which took priority, as recommended
by the research ethics committee. The use of video-recording
is an alternative means of data collection which could have
been considered in a study where the consultation process
was the focus of enquiry. Unfortunately the dataset was
limited, with fewer observed patient-doctor (n = 19) than
patient-nurse consultations (n = 28), and fewer question-
naires from patients who had seen a doctor (n = 17) than
had seen a nurse (n = 57); however, the data were sufficient
to explore the phenomenon of interest in the context of a
case study.
Benefits of nurse prescribing
Whilst the findings add to the growing body of knowledge
about nurse prescribing, they are distinctive from others to
date because we explored nurse prescribing from an organi-
zational perspective using data from multiple levels, including
senior managers and patients from a range of ethnic groups.
Nurse prescribing was reported to be of patient benefit,
echoing the findings of others (Luker et al. 1997, Latter &
Courtenay 2004, Latter et al. 2005). Similarly, the qualitative
data themes corresponding to the drivers for non-medical
prescribing identified previously in the policy literature,
namely quicker and more efficient access to medicines for
patients and better use of staff skills (Department of Health
2002, 2006). The nurse prescribers in this study reported
competence and confidence in prescribing, and considered
that their prescribing practice had had a positive impact on
both patient care and team-working and had also enabled
them to use their nursing skills better, as found by others
(Luker et al. 1997, Latter et al. 2005, Courtenay et al. 2006,
2007a, 2007b, Bradley & Nolan 2007, Carey et al. 2007,
Courtenay & Carey 2008, Stenner & Courtenay 2008a,
2008b).
Doctors, nurse managers, peers and supportive team-
working were identified as key to the successful implemen-
tation of nurse prescribing roles as reported by others (Latter
et al. 2005, Courtenay et al. 2006, Bradley & Nolan 2007,
Stenner & Courtenay 2008a, 2008b). In this study, nurse
prescribers and their colleagues also made reference to the
‘fit’ of the new roles into existing team structures as helpful to
implementation. For example, the hypertension and renal
teams had reviewed uni-professional roles and joint ways of
working in the light of the need to manage increased
caseloads. However, it was the nurses themselves who were
considered by managers, peers and colleagues to be crucial to
the project’s success, through their motivation, enthusiasm
and drive to succeed.
In contrast to Brooks et al. (2001) and Latter et al. (2005),
we surveyed the views of patients from a variety of ethnic
groups. All reported similar views about their prescribing
experience and their medicines, irrespective of their ethnic
background. No other study to date has explored the
prescribing experience of patients from different ethnic
groups. In fact, apart from an evaluation of the impact of
prescribing by a diabetes nurse specialist (Carey et al. 2008),
no other recent studies have included patients in their
samples. This is both an omission and an opportunity for
future research, given that modern healthcare systems are
increasingly focusing on patient choice and improving the
user experience (Department of Health 2008a).
Nurses and doctors were found to deliver equivalent care,
but patients who reported the highest satisfaction ratings of
medicine-related information had seen a nurse. A systematic
review of the research into doctor-nurse substitution in
Desired stateImplementation of nurse prescribing
Workforce changes
Improved service delivery
Improved patient care
Sponsors and supportersof changed practice
Advanced personal andprofessional practice
Expert care
Team engagement
Better medicine management
Enabling factors:Shared vision
Local champions Action learning
Team, peer and buddy support
Evolving infrastructure
Emerging policy
After Lewin (1951)
Driving
forces
Current
state
Resisting
forces
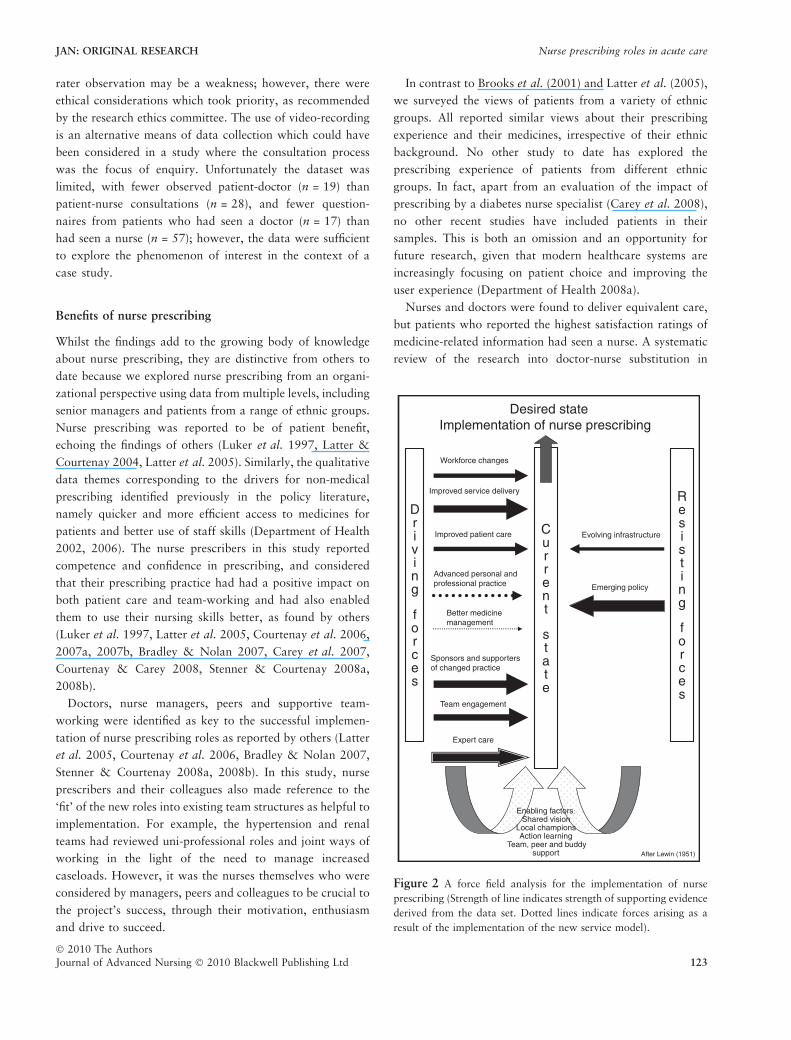
Figure 2 A force field analysis for the implementation of nurse
prescribing (Strength of line indicates strength of supporting evidence
derived from the data set. Dotted lines indicate forces arising as a
result of the implementation of the new service model).
JAN: ORIGINAL RESEARCH Nurse prescribing roles in acute care
� 2010 The Authors
Journal of Advanced Nursing � 2010 Blackwell Publishing Ltd 123
primary care has shown that the quality of care is similar for
patients seen by nurses as compared to those seen by doctors,
with no appreciable differences in health outcomes, although
higher satisfaction is reported by some patients (Horrocks
et al. 2002). Systematic reviews of the research literature
have also shown no appreciable differences in the care
delivered by doctors and nurses, although nurses spend
longer with patients (Horrocks et al. 2002, Buchan &
Calman 2004, Laurant et al. 2005). However, in the present
study the majority of the patients with the longest consulta-
tion times were seen by a doctor, which may partly be
explained by doctors seeing patients with more complex
morbidity and therefore needing longer consultations. Thus,
patients who reported higher satisfaction ratings had not
spent longer with their prescribers. This is an important
finding for healthcare professionals in England, where policy
directives focus on service improvements through changes in
delivery and role redesign (Department of Health 2008a,
2008b). The process of training team members to prescribe
has also been shown to enable reassessment of roles (Avery
et al. 2007) and improve clinical decision-making across
healthcare teams (Bradley & Nolan 2007).
A synthesis of the findings (after Lewin 1951) offers a
potential model of the driving and resisting forces identified
from the dataset which have an impact on implementation
of new nurse prescribing roles within a chosen site (see
Figure 2). These driving forces included viewing workforce
changes as an opportunity, improved patient care, better
medicine management, effective sponsorship and support of
change, team engagement, advanced practice and expert
care. The restraining forces were evolving infrastructure and
emerging policy. Thus, we recommend that employers
ensure that supportive and operational infrastructures are
in place to underpin new prescribing practices if a major
change is to be successfully implemented. Most importantly,
four variables were identified as actively enabling the
implementation of nurse prescribing roles: shared vision,
local championship, action learning and team, peer and
buddy support.
Conclusion
In the light of growing evidence of the competency of nurse
prescribers, it is now timely to focus less on behavioural and
affective measures of prescribing performance and more on
the impact that the role may have on enhancing the quality
and safety of patient care, such as identifying those interven-
tions that improve patient safety by reducing prescribing
errors. In this way, the benefits or otherwise of nurse
prescribing roles can be more comprehensively assessed,
using clearly defined performance indicators and patient
outcomes and findings compared with those derived from
preliminary reports on nurse prescribing in terms of ‘equiv-
alency to’ or ‘substitution for’ doctors only.
Acknowledgements
With acknowledgement to Jill Bunker, Wendy Brown and Jen
McDermott, the nurse prescribers who participated in this
study.
Funding
This research received no specific grant from any funding
agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
No conflict of interest has been declared by the authors.
What is already known about this topic
• Nurse prescribing works well in some primary care
settings.
• Nurse prescribing has permitted doctor–nurse
substitution in acute episodic care.
• Some doctors have expressed concerns about patient
safety and nurse prescribing.
What this paper adds
• Nurses and doctors provided equivalent care, but
patients who had seen a nurse reported higher
satisfaction ratings of medicine related information.
• Patients across ethnic groups reported similar views
about their prescribing experience and about their
medicines.
• Shared vision, local champions, action learning, team,
peer and buddy support were key to successful
implementation of nurse prescribing roles.
Implications for practice and/or policy
• Employers should ensure that supportive and
operational infrastructures are in place to underpin new
prescribing practices.
• Future research is needed to measure the impact that
nurse prescribing may have on improving patient
outcomes.
K. Jones et al.
� 2010 The Authors
124 Journal of Advanced Nursing � 2010 Blackwell Publishing Ltd

Author contributions
KJ was responsible for the study conception and design. KJ
performed the data collection. KJ performed the data
analysis. KJ was responsible for the drafting of the manu-
script. ME and AW made critical revisions to the paper for
important intellectual content. ME and AW provided statis-
tical expertise. ME and AW supervised the study.
References
Avery A.J. & Pringle M. (2005) Extended prescribing by UK
nurses and pharmacists. British Medical Journal 331, 1154–
1155.
Avery G., Todd J., Green G. & Sains K. (2007) The impact of non-
medical prescribing on practice. Nurse Prescribing, 5(11), 488–
492.
Berry D., Courtenay M. & Bersellini E. (2006) Attitudes towards,
and information needs in relation to, supplementary nurse pre-
scribing in the UK: an empirical study. Journal of Clinical Nursing
15, 22–28.
Bissell P., Cooper R., Guillaume L., Anderson C., Avery A., Hutch-
inson A., James V., Lymn J., Marsden E., Murphy E., Ratcliffe J.,
Ward P. & Woolsey I. (2008) An Evaluation of Supplementary
Prescribing in Nursing and Pharmacy. University of Sheffield,
Sheffield.
Bradley E. & Nolan P. (2007) Impact of nurse prescribing: a
qualitative study. Journal of Advanced Nursing 59(2), 120–
128.
Brooks N., Otway C., Rashid C., Kilty L. & Maggs C. (2001) The
patient’s view: the benefits and limitations of nurse prescribing.
British Journal of Community Nursing 6(7), 342–348.
Brooten D., Naylor M.D., York R., Brown L.P., Munro B.H.,
Hollingsworth A.O., Cohen S., Finkler S., Deatrick J. &
Youngblunt J.M. (2002) Lessons learned from testing the quality
cost model of Advanced Practice (APN) transitional care. Journal
of Nursing Scholarship 34(4), 369–375.
Brown S. & Grimes D. (1995) A meta-analysis of nurse practitioners
and nurse midwives in primary care. Nursing Research 44(6), 332–
339.
Buchan J. & Calman L. (2004) Skill-mix and policy change in the
health workforce: nurses in advanced roles. OECD Health working
paper 17, Organisation for Economic Co-operation and Develop-
ment, France.
Calman L. & Buchan J. (2004) Implementing Nurse Prescribing: An
Updated Review of Current Practice Internationally. International
Council of Nurses, Geneva.
Carey N., Coutenay M. & Burke J. (2007) Supplementary nurse
prescribing for patients with skin conditions: a national question-
naire survey. Journal of Clinical Nursing 16, 1230–1237.
Carey N., Coutenay M., James J., Hills M. & Roland J. (2008) An
evaluation of a Diabetes Specialist Nurse prescriber on the system
of delivering medicines to patients with diabetes. Journal of Clin-
ical Nursing 17, 1635–1644.
Chief Medical Officer Update (2005) Changes to non-medical pre-
scribing. CMO Update 43, 2.
Connelly D. (2005) Independent prescribing: pharmacists are given
flexibility of a full formulary. The Pharmaceutical Journal 275,
627–628.
Courtenay M. & Carey N. (2008) Nurse independent prescribing and
nurse supplementary prescribing practice: a national survey.
Journal of Advanced Nursing 61(3), 291–299.
Courtenay M., Carey N. & Burke J. (2006) Preparing nurses to
prescribe medicines for patients with dermatological conditions.
Journal of Advanced Nursing 55(6), 698–707.
Courtenay M., Carey N. & Burke J. (2007a) Independent extended
and supplementary nurse prescribing practice in the UK: a national
questionnaire survey. International Journal of Nursing Studies 44,
1093–1101.
Courtenay M., Carey N. & Burke J. (2007b) Independent extended
nurse prescribing for patients with skin conditions: a national
questionnaire survey. Journal of Clinical Nursing 16, 1247–1255.
Crown J. & Miller P. (2005) Access to the whole BNF: a long
awaited triumph or the wrong decision? Nurse Prescribing 3(6),
228–229.
Department of Health (2002) Extending Independent Nurse Pre-
scribing within the NHS in England. A Guide for Implementation.
Department of Health, London.
Department of Health (2006) Medicines Matters. A Guide to
Mechanisms for the Prescribing, Supply and Administration of
Medicines. Department of Health, London.
Department of Health (2008a) High Quality Care for All. NHS Next
Stage Review Final Report. Department of Health, London.
Department of Health (2008b) Framing the Nursing and Midwifery
Contribution, Driving up the Quality of Care. Department of
Health, London.
Flyvbjerg B. (2001) Making Social Science Matter. Why Social
Inquiry Fails and How it Can Succeed Again. Cambridge Univer-
sity Press, Cambridge.
Healthcare Commission (2005) National Survey Programme Out-
patient Core Questions Version 4. Retrieved from http://www.
nhssurveys.org/survey/320on 19 February 2010.
Horne R., Weinman J. & Hankins M. (1999) The beliefs about
medicines questionnaire: the development and evaluation of a new
method for assessing the cognitive representation of medication.
Psychology and Health 14, 1–24.
Horne R., Hankins M. & Jenkins J. (2001) Satisfaction with infor-
mation about medicines scale (SIMS). Quality in Health Care 10,
135–140.
Horrocks S., Anderson E. & Salisbury C. (2002) Systematic review of
whether nurse practitioners working in primary care can provide
equivalent care to doctors. British Medical Journal 324, 819–823.
Hutchinson S.A. (1990) The case study approach. In Advancing
Nursing Science Through Research, Volume 2 (Moody L.E., ed.),
Sage Publications Inc, Thousand Oaks, pp. 177–213.
James J. (2004) Supplementary prescribing by a diabetes specialist
nurse on a hospital ward. Nurse Prescribing 2(3), 112–116.
King’s College London (2004) Objective Structured Clinical Exam-
ination: Non-medical Prescribing OSCE Station 1: 24.05.05.
King’s College, London.
Latter S. & Courtenay M. (2004) Effectiveness of nurse prescribing: a
review of the literature. Journal of Clinical Nursing 13(1), 26–32.
Latter S., Maben J., Myall M., Courtenay M., Young A. & Dunn N.
(2005) An Evaluation of Extended Formulary Independent Nurse
JAN: ORIGINAL RESEARCH Nurse prescribing roles in acute care
� 2010 The Authors
Journal of Advanced Nursing � 2010 Blackwell Publishing Ltd 125

Prescribing, Executive Summary of Final Report. Policy Research
Programme at the Department of Health. University of South-
ampton, Southampton.
Laurant M., Reeves D., Hemens R., Braspenning J., Grol R. &
Sibbald B. (2005) Substitution of Doctors by Nurses in Primary
Care (Cochrane Review). John Wiley and Sons Ltd, Chichester.
Lewin K. (1951) Theory in Social Science: Selected Theoretical
Papers (Cartwright D., ed.), Harper and Brothers, New York.
Lewis-Evans A. & Jester R. (2004) Nurse prescribers’ experiences of
prescribing. Journal of Clinical Nursing 13, 796–805.
Luker K.A. & McHugh G.A. (2002) Nurse prescribing from the
community nurses perspective. International Journal of Pharma-
ceutics Practice 10, 273–280.
Luker K., Austin L., Hogg C., Willock J., Wright K., Ferguson B.,
Jenkins-Clark S. & Smith K. (1997) Evaluation of Nurse Pre-
scribing – Final Report. University of Liverpool, Liverpool.
Ritchie J. & Spencer L. (1994) Qualitative data analysis for applied
policy research. In Analyzing Qualitative Data (Bryman A. &
Burgess R., eds), Routledge, London, pp. 173–194.
Rodden C. (2001) Nurse prescribing: views on autonomy and inde-
pendence. British Journal of Community Nursing 6(7), 350–355.
Siriwardena N.A. (2006) The rise and rise of non-medical prescrib-
ing. Quality in Primary Care 14, 1–3.
Stake R.E. (1995) The Art of Case Study Research. Sage Publications
Inc, Thousand Oaks.
Stenner K. & Courtenay C. (2008a) Benefits of nurse prescribing
for patients in pain: nurses’ views. Journal of Advanced Nursing
63(1), 27–35.
Stenner K. & Courtenay C. (2008b) The role of inter-professional
relationships and support for nurse prescribing in acute and
chronic pain. Journal of Advanced Nursing 63(3), 276–283.
Taylor F., Gray A., Cohen H., Gaminara L., Ramsay M. & Miller D.
(1997) Costs and effectiveness of a nurse specialist anticoagulant
service. Journal of Clinical Pathology 50(10), 823–828.
While A. & Biggs K. (2004) Benefits and challenges of nurse pre-
scribing. Journal of Advanced Nursing 45(6), 559–567.
Wilson-Barnett J. & Beech S. (1994) Evaluating the clinical nurse
specialist. A review. International Journal of Nursing Studies
31(6), 561–571.
World Health Organisation (2006) Gaining Health. The European
Strategy for the Prevention and Control of Non-communicable
Diseases. Regional Committee for Europe. World Health Organi-
sation, Geneva.
Yin R.K. (2003) Case Study Research Design and Methods, 3rd edn
(Applied social research methods series volume 5). Sage Publica-
tions Inc, Thousand Oaks.
The Journal of Advanced Nursing (JAN) is an international, peer-reviewed, scientific journal. JAN contributes to the advancement of
evidence-based nursing, midwifery and health care by disseminating high quality research and scholarship of contemporary relevance
and with potential to advance knowledge for practice, education, management or policy. JAN publishes research reviews, original
research reports and methodological and theoretical papers.
For further information, please visit JAN on the Wiley Online Library website: http://onlinelibrary.wiley.com
Reasons to publish your work in JAN:
• High-impact forum: the world’s most cited nursing journal and with an Impact Factor of 1Æ518 – ranked 9th of 70 in the 2010
Thomson Reuters Journal Citation Report (Social Science – Nursing). JAN has been in the top ten every year for a decade.
• Most read nursing journal in the world: over 3 million articles downloaded online per year and accessible in over 7,000 libraries
worldwide (including over 4,000 in developing countries with free or low cost access).
• Fast and easy online submission: online submission at http://mc.manuscriptcentral.com/jan.
• Positive publishing experience: rapid double-blind peer review with constructive feedback.
• Early View: rapid online publication (with doi for referencing) for accepted articles in final form, and fully citable.
• Faster print publication than most competitor journals: as quickly as four months after acceptance, rarely longer than seven months.
• Online Open: the option to pay to make your article freely and openly accessible to non-subscribers upon publication on Wiley
Online Library, as well as the option to deposit the article in your own or your funding agency’s preferred archive (e.g. PubMed).
K. Jones et al.
� 2010 The Authors
126 Journal of Advanced Nursing � 2010 Blackwell Publishing Ltd
Copyright © 2022 FDOKUMEN