
infarction. The ECTIM Study Impact of apolipoprotein E polymorphism on lipoproteins and risk of...
9
Ruidavets and F Cambien G Luc, J M Bard, D Arveiler, A Evans, J P Cambou, A Bingham, P Amouyel, P Schaffer, J B The ECTIM Study. Impact of apolipoprotein E polymorphism on lipoproteins and risk of myocardial infarction. Print ISSN: 1079-5642. Online ISSN: 1524-4636 Copyright © 1994 American Heart Association, Inc. All rights reserved. Avenue, Dallas, TX 75231 is published by the American Heart Association, 7272 Greenville Arteriosclerosis, Thrombosis, and Vascular Biology doi: 10.1161/01.ATV.14.9.1412 1994;14:1412-1419 Arterioscler Thromb Vasc Biol. http://atvb.ahajournals.org/content/14/9/1412 World Wide Web at: The online version of this article, along with updated information and services, is located on the http://atvb.ahajournals.org//subscriptions/ at: is online Arteriosclerosis, Thrombosis, and Vascular Biology Information about subscribing to Subscriptions: http://www.lww.com/reprints Information about reprints can be found online at: Reprints: document. Permissions and Rights Question and Answer Further information about this process is available in the is being requested is located, click Request Permissions in the middle column of the Web page under Services. Clearance Center, not the Editorial Office. Once the online version of the published article for which permission can be obtained via RightsLink, a service of the Copyright Arteriosclerosis, Thrombosis, and Vascular Biology Requests for permissions to reproduce figures, tables, or portions of articles originally published in Permissions: by guest on October 19, 2014 http://atvb.ahajournals.org/ Downloaded from by guest on October 19, 2014 http://atvb.ahajournals.org/ Downloaded from
Transcript of infarction. The ECTIM Study Impact of apolipoprotein E polymorphism on lipoproteins and risk of...

Ruidavets and F CambienG Luc, J M Bard, D Arveiler, A Evans, J P Cambou, A Bingham, P Amouyel, P Schaffer, J B
The ECTIM Study.Impact of apolipoprotein E polymorphism on lipoproteins and risk of myocardial infarction.
Print ISSN: 1079-5642. Online ISSN: 1524-4636 Copyright © 1994 American Heart Association, Inc. All rights reserved.
Avenue, Dallas, TX 75231is published by the American Heart Association, 7272 GreenvilleArteriosclerosis, Thrombosis, and Vascular Biology
doi: 10.1161/01.ATV.14.9.14121994;14:1412-1419Arterioscler Thromb Vasc Biol.
http://atvb.ahajournals.org/content/14/9/1412World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://atvb.ahajournals.org//subscriptions/
at: is onlineArteriosclerosis, Thrombosis, and Vascular Biology Information about subscribing to Subscriptions:
http://www.lww.com/reprints
Information about reprints can be found online at: Reprints:
document.Permissions and Rights Question and AnswerFurther information about this process is available in theis being requested is located, click Request Permissions in the middle column of the Web page under Services.Clearance Center, not the Editorial Office. Once the online version of the published article for which permission
can be obtained via RightsLink, a service of the CopyrightArteriosclerosis, Thrombosis, and Vascular Biology Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on October 19, 2014http://atvb.ahajournals.org/Downloaded from by guest on October 19, 2014http://atvb.ahajournals.org/Downloaded from

1412
Impact of Apolipoprotein £ Polymorphism onLipoproteins and Risk of Myocardial Infarction
The ECTIM Study
Gerald Luc, Jean-Marie Bard, Dominique Arveiler, Alun Evans, Jean-Pierre Cambou,
Annie Bingham, Philippe Amouyel, Paul Schaffer, Jean-Bernard Ruidavets,Francois Cambien, Jean-Charles Fruchart, Pierre Ducimetiere
Abstract Human apolipoprotein (apo) E, a polymorphicprotein with three common alleles, e2, e3, and e4, plays animportant role in lipoprotein metabolism. This article de-scribes the association of this polymorphism with lipids, apo-lipoproteins, and lipoproteins with a particular regard tolipoprotein particles, as defined by their apolipoprotein con-tent, as well as the risk of myocardial infarction in a multicen-ter population-based case-control study (ECTIM study). Inthe ECTIM study, 574 male patients aged 25 to 64 wereexamined 3 to 9 months after myocardial infarction in fourregions participating in the World Health OrganizationMONICA project: Belfast (Northern Ireland) and Lille, Stras-bourg, and Toulouse (France). Control subjects (n=722) wererandomly selected from the regional populations. The distri-bution of apoE phenotypes was significantly different acrossthe four control samples (P=.O4), with a higher frequency ofthe e4 allele in Belfast (14.3%) than in Toulouse (8.2%). Theassociation of apoE polymorphism with biological measure-ments was studied in the control groups (n=640) after menwith coronary heart disease or those taking hypolipidemicdrugs were omitted, with the apoE3/3 phenotype as a refer-ence after adjustment for concomitant factors. Individualscarrying the e2 allele had lower levels of plasma cholesterol,low-density lipoprotein cholesterol (LDL-C), and apoB andhigher levels of triglycerides, very-low-density lipoprotein cho-lesterol (VLDL-C), apoC-III, apoE, lipoprotein (Lp) C-III:B,and Lp E: B. However, the effect of the e2 allele on triglycer-
A polipoprotein E (apoE) is a structural component/ \ of triglyceride-rich lipoproteins, chylomicrons
. X A - and very-low-density lipoproteins (VLDLs),and high-density lipoproteins (HDLs).1 The structuralgene locus of this apolipoprotein is polymorphic. Threecommon alleles designated e2, e3, and e4 code at asingle locus from three isoforms, E2, E3, and E4.2 Thesethree isoforms lead to six apoE phenotypes in plasma
Received August 13, 1993; revision accepted June 1, 1994.From SERLIA and INSERM U325 (G.L., J.-M.B., J.-C.F.) and
MONICA Lille (G.L., P.A.), Pasteur Institute of Lille (France);MONICA Strasbourg, Laboratoire d'Epidemiologie et de SantePublique (D.A., P.S.) (France); Belfast MONICA, Department ofEpidemiology and Public Health, The Queen University of Belfast(A.E.) (Northern Ireland); MONICA Toulouse, INSERM 326,ORSMIP (J.-P.C, J.-B.R.) (France); and INSERM U258 (A.B.,F.C., P.D.) and INSERM SC7 (F.C.), Paris, France.
Correspondence to Gerald Luc, SERLIA and INSERM U325,Pasteur Institute of Lille, 1 rue du Professeur Calmette, 59019Lille Cedex, France.
© 1994 American Heart Association, Inc.
ide, VLDL-C, apoE, and Lp E:B parameters was heteroge-neous across the populations. The magnitude of these effectswas large and statistically significant in Lille and Strasbourg,whereas only apoE was increased in Toulouse, and no effect ofthe e2 allele appeared in Belfast. The e4 allele was associatedwith increased triglyceride, VLDL-C, apoB, and Lp C-III:Blevels and a decreased LpA-I level, but apoC-III, apoE, andLp E: B levels were similar to those with the apoE3/3 pheno-type. The relative risk of myocardial infarction associated withapoE phenotypes compared with E3/3 was found to increase inthe following order: E2/2<E3/2<E3/3 (relative risk=l) <E4/3=E4/2<E4/4 (P<.05). The presence of e2 and e4 allelescarried a relative risk of 0.73 (P=.O5) and 1.33 (P=.O2), respec-tively, in a codominant logistic model, and no heterogeneitybetween centers was demonstrated. In conclusion, men carryingthe e4 allele present an atherogenic lipid and lipoprotein profilecompared with E3/3 and are at higher risk of coronary heartdisease in the populations under study. Men carrying the e2 allelehave lower apoB levels and appear to be at lower risk despitehigher triglyceride and Lp E:B levels, at least in some regions.This suggests that other genes or environmental factors play aninteractive role with the e2 allele on lipid metabolism. ApoEpolymorphism, however, seems to explain a modest proportion,12%, of myocardial infarction cases at the population level.(Arterioscler Thromb. 1994;14:1412-1419.)
Key Words • lipoproteins • apolipoproteins • myocardialinfarction • apolipoprotein E polymorphism
that can be identified by isoelectric focusing on apolyacrylamide gel.34 Numerous studies have shown arelation between the apoE phenotype and plasma lipidand lipoprotein levels, the apoE phenotype being, forexample, a determinant of interindividual differences oftotal and low-density lipoprotein cholesterol (LDL-C).56 In vivo and in vitro investigations have shownfunctional differences between apoE alleles that arethought to modulate lipid levels. Indeed, apoE plays animportant role in the metabolism of lipoproteins be-cause it can bind to the apoB,E receptor and to thehepatic remnant receptor. Therefore, the affinity of theapoE2 isoform for the LDL receptor is lower than thatof the apoE37 and results in reduced in vivo catabolismof apoE2-containing lipoproteins, whereas apoE4shows an increased in vivo catabolism compared withapoE3.8
Lipoproteins play a central role in the appearanceand development of atherosclerotic cardiovascular dis-ease in humans, so the modifications of lipid parameters
by guest on October 19, 2014http://atvb.ahajournals.org/Downloaded from

Luc et al ApoE Polymorphism 1413
related to apoE phenotypes could influence the devel-opment of atherosclerosis. Therefore, the hypothesis ofthe association of the apoE polymorphism with athero-sclerosis was tested in a number of epidemiologicalstudies.6 However, these different studies showed con-flicting results, which could be related to differences insample size; to patient and control subject selection,such as age of included subjects and definition ofcoronary heart disease (CHD) (eg, survivors of myocar-dial infarction [MI] or atherosclerosis defined by coro-nary angiography); and to the confounding effect ofmajor risk factors for atherosclerosis.6'9
The World Health Organization MONICA Project10 iscurrently studying trends in CHD incidence and mortalityin various regions. To investigate the large differences inCHD incidence between the French MONICA centers ofStrasbourg, Toulouse, and Lille and the Northern Irelandcenter of Belfast, a coordinated population-based case-control study on MI was set up in each region (the EtudeCas-Temoins sur l'lnfarctus du Myocarde [ECTIM]study). The case-control analysis of lipids, lipoproteins,and lipoprotein particles measured in the study has al-ready been published.11 In the present work we report onthe associations of apoE polymorphism with the same setof measurements as in the control population of theECTIM study. Particular emphasis is placed on the studyof lipoprotein particles. These particles are characterizedon the basis of their apolipoprotein composition. Thedevelopment of immunoassays allows the determinationof the plasma levels of several types of particles that differin their metabolic and atherogenic properties. This articlealso considers the question of whether apoE is protective(E2 carriers) or increases the risk (E4 carriers) of MI.
MethodsSubjects
The populations are those covered by the MONICA regis-ters participating in the ECTIM study: Belfast and its sur-roundings in Northern Ireland, Lille and its surroundings inthe north of France, Strasbourg and its surroundings in thenortheast of France, and Toulouse and its surroundings in thesouthwest of France. Only 25- to 64-year-old men whosefamilies had lived in the region for at least two generations andwhose four grandparents had been born in Europe wereeligible for inclusion in the study. In Belfast, the grandparentshad to have been born in the historical entity of Ulster. Thecontrol subjects were obtained from electoral rolls in Franceand from the lists of general practitioners held by the CentralServices Agency in Belfast. Among the eligible control sub-jects, 40% in Belfast, 47% in Lille, 54% in Strasbourg, and49% in Toulouse refused to participate, did not respond, orcould not be contacted. The names of MI survivors wereobtained from the MONICA registers. MI was denned asdiagnostic category 1 according to MONICA criteria,12 corre-sponding to at least two of the following: chest pain of at least20 minutes' duration, increase in cardiac enzymes, and typicalelectrocardiogram changes during the acute attack. The agedistribution of the random control samples in French centerswas chosen to match that of the MI patients as determined bythe MONICA register in each area. In Belfast, an age-matchedcontrol subject was chosen for each case. Informed consentwas obtained from the subjects and their family doctors. Eachsubject was examined by a specially trained doctor or nurse.The presence of disease, drug intake, and cigarette and alcoholconsumption were recorded. Body weight was measured to thenearest 200 g for subjects without shoes using scales that were
regularly checked and calibrated; height was determined to thenearest centimeter with a measuring tape on subjects withoutshoes standing with their backs to a wall. Epidemiological dataand blood samples from MI survivors were obtained between3 and 9 months after the event.
The total number of control subjects was 722, from whom 194were recruited in Belfast, 155 in Lille, 185 in Strasbourg, and 188in Toulouse. Among these, 648 were without CHD and were nottaking hypolipidemic drugs. An additional group of 4 subjectshad triglyceride levels higher than 800 mg/dL. Thus, 644 subjectswere included in the analysis of the association of apoE pheno-type with lipoproteins. For the second part of the study concern-ing the determination of the relative risk (RR) for MI, onlycontrol subjects with CHD were excluded. Therefore, 680 controlsubjects and 574 MI survivors were included.
MethodsVenous blood obtained from subjects was collected in
EDTA-containing tubes after an overnight fast. The blood waskept at 4°C and separated within 3 hours by centrifugation at4°C. e-Aminocaproic acid, chloramphenicol, and glutathioneat final concentrations of 0.9, 0.6, and 0.3 mmol/L, respec-tively, were added to plasma. The plasma was sent at 4°C to thecentral laboratory at the Pasteur Institute in Lille within 5days.
Cholesterol and triglyceride levels were then determined byautomated enzymatic procedures (Boehringer Mannheim)adapted to a Hitachi 705 analyzer. Cholesterol was measuredin VLDL separated by ultracentrifugation13 and in the HDL-containing supernatant after phosphotungstate/magnesiumchloride precipitation of apoB-containing lipoproteins (Boeh-ringer Mannheim). LDL-C was calculated by subtractingVLDL-C and HDL-C from total cholesterol. ApoA-I andapoB were quantified by laser immunonephelometry (Beh-ring). ApoA-II, apoC-III, and apoE were measured by non-competitive immunoassays.14 Lipoprotein particles, defined bytheir apolipoprotein composition and containing apoA-II andapoA-I (Lp A-LA-II), apoE and apoB (Lp E:B), and apoC-III and apoB (Lp C-III: B), were measured by two-site immu-noenzymatic assays as described elsewhere.1516 Particles con-taining apoA-I but free of apoA-II were quantified bydifferential electroimmunoassay on ready-to-use plates.17 TheapoE phenotype was determined from total plasma by isoelec-tric focusing followed by transfer onto a nitrocellulosesheet1819 and then by incubation with anti-mouse IgG labeledwith peroxidase.
Statistical AnalysisResults were analyzed with SAS statistical software (SAS
Institute Inc). Comparison among the four centers of allelefrequencies was tested by x2 test. The relations between eachbiological measurement and apoE phenotypes in the controlpopulation were established by multiple linear regressionmodels (GLM procedure) with the recruitment center andother variables as covariates. For that purpose, the six apoEphenotypes were coded by five (0-1) dummy variables allowingfor a direct estimation of each phenotype versus E3/3 differ-ential effect.
The e2 and e4 allelic effects with E3/3 chosen as thereference were obtained by a reduced model with two (0-1-2)dummy variables coding respectively for the number of e2 ande.4 alleles in each phenotype. This model specifies a codomi-nant additive effect of el and e4 on the level of the indepen-dent variable. The goodness of fit of the reduced model wastested by an approximate F ratio. The homogeneity of the e2and e4 effects across populations was tested by introducingspecific population effects as interaction terms in the model.For some biological measurements with a highly skeweddistribution (ie, triglycerides, VLDL-C, apoC-III, apoE, Lp
by guest on October 19, 2014http://atvb.ahajournals.org/Downloaded from
1414 Arteriosclerosis and Thrombosis Vol 14, No 9 September 1994
TABLE 1. Age, Body Mass Index, Alcohol Intake, Tobacco Consumption, and Frequencyof Apolipoprotein E Polymorphism Alleles in Control Groups of the ECTIM Study
Parameter
Age, y
Body mass index, kg/m2
Alcohol intake, g/d
Cigarettes, No. per day
Allele frequency, %
<2
e3
e4
Belfast(n=175)
54.3±7.8
25.8±3.6
35.1 ±48.1
5.0±10.4
10.3
75.4
14.3
Lille(n=139)
53.9±7.8
25.8±3.8
59.0±43.8
7.6±12.2
11.9
74.1
14.0
Region
Strasbourg(n=159)
52.7±9.3
27.4±3.6
36.0±36.8
5.4±9.6
8.5
80.8
10.7
Toulouse(n=171)
50.4+8.4
26.5±4.1
35.7±33.4
4.7±9.7
5.6
86.3
8.2
Values are mean±SD. Subjects with coronary heart disease or taking hypolipidemic drugs or thosewith triglycerides >800 mg/dL were excluded.
C-III:B, and Lp E:B), a logarithmic transformation was firstcarried out.
The associations of apoE phenotypes with MI were ana-lyzed according to the same strategy as defined above forquantitative traits but using multiple logistic regressionmodels (LOGIST procedure). Adjusted odds ratios for eachphenotype compared with E3/3 were first obtained. Thecorresponding reduced model can be interpreted as acodominant multiplicative model for the e2 and e.4 allele-specific RRs (RR associated with a given phenotype is theproduct of the respective RRs of its two alleles). Thegoodness of fit of the reduced model and the homogeneity ofthe allelic RRs across populations were tested by the likeli-hood ratio statistic.
ResultsThe distribution of apoE phenotypes in the entire
control population was compatible with Hardy-Wein-berg equilibrium (^2
3rf/=1.3).
Association of ApoE Phenotypes With LipoproteinsTable 1 shows the general characteristics of the
population included in this analysis (N=644). Globally,no large difference was apparent among the four sam-ples for any variable. However, the higher mean alcoholand tobacco consumption levels in Lille and the highermean body mass index in Strasbourg are noteworthy.The frequency of apoE alleles (Table 1) was signifi-cantly different among the four centers (6<i/=18.8,P<.01), with a higher frequency of e2 and e4 in Belfastand Lille, respectively, and e3 in Toulouse.
Table 2 shows crude mean values of plasma lipids,apolipoproteins, and lipoprotein particles in the totalpopulation according to the six apoE phenotypes afteradjustment for center, age, body mass index, cigaretteuse, and alcohol intake. The apoE phenotype signifi-cantly (P<.05) influenced the plasma lipid, lipid oflipoprotein, apolipoprotein, and lipoprotein particlelevels except for cholesterol, apoA-II, and Lp A-I:A-II.The low level of cholesterol in phenotype E2/2, E3/2,and E4/2 subsets and its high level in phenotype E4/4were mainly consequences of a variation in LDL-C. Thevariation of apoB was parallel to that of LDL-C, but ifapoE polymorphism highly modulated LDL-C, the sig-nificance level of .05 was not reached for cholesterol.
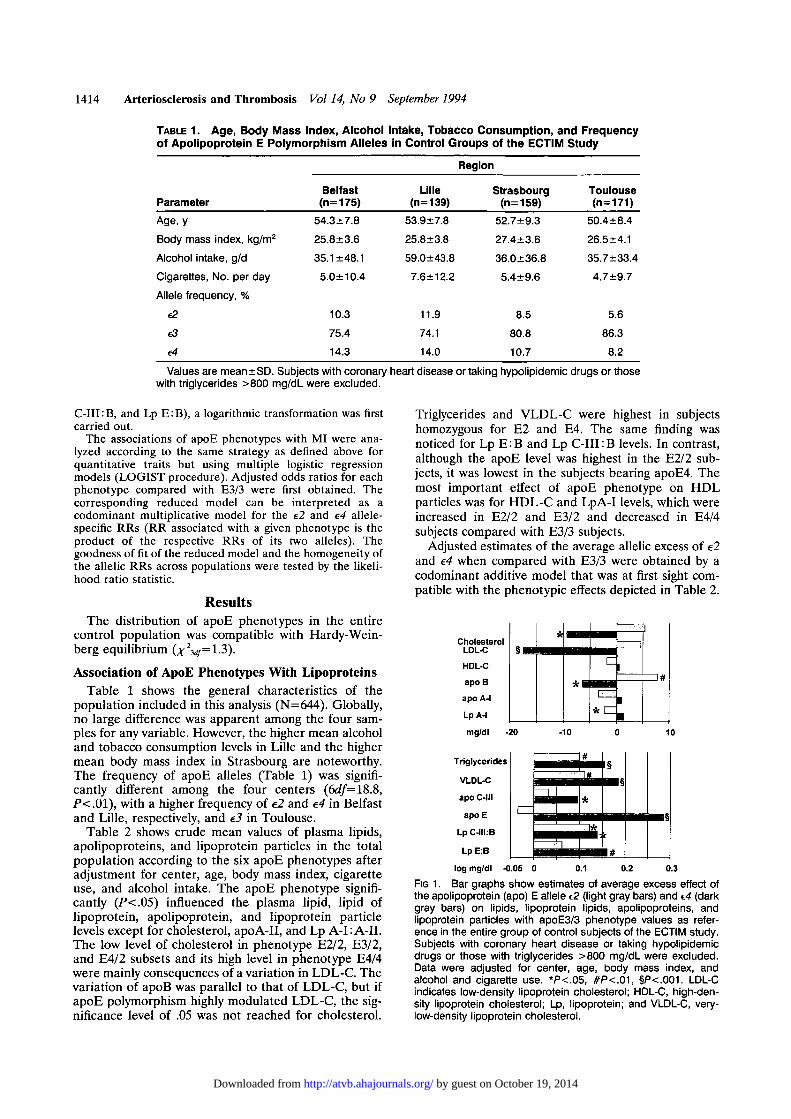
Triglycerides and VLDL-C were highest in subjectshomozygous for E2 and E4. The same finding wasnoticed for Lp E: B and Lp C-III: B levels. In contrast,although the apoE level was highest in the E2/2 sub-jects, it was lowest in the subjects bearing apoE4. Themost important effect of apoE phenotype on HDLparticles was for HDL-C and LpA-I levels, which wereincreased in E2/2 and E3/2 and decreased in E4/4subjects compared with E3/3 subjects.
Adjusted estimates of the average allelic excess of e2and e4 when compared with E3/3 were obtained by acodominant additive model that was at first sight com-patible with the phenotypic effects depicted in Table 2.
Triglycerides
VLDL-C
apo C-III
apoE
Lp C-IILB
LpE:B
- -#
*
l§
• §
l #log mg/dl -0.05 0 0.1 0.2 0.3
FIG 1. Bar graphs show estimates of average excess effect ofthe apolipoprotein (apo) E allele e2 (light gray bars) and e4 (darkgray bars) on lipids, lipoprotein lipids, apolipoproteins, andlipoprotein particles with apoE3/3 phenotype values as refer-ence in the entire group of control subjects of the ECTIM study.Subjects with coronary heart disease or taking hypolipidemicdrugs or those with triglycerides >800 mg/dL were excluded.Data were adjusted for center, age, body mass index, andalcohol and cigarette use. *P<.05, #P<.01, §P<.001. LDL-Cindicates low-density lipoprotein cholesterol; HDL-C, high-den-sity lipoprotein cholesterol; Lp, lipoprotein; and VLDL-C, very-low-density lipoprotein cholesterol.
by guest on October 19, 2014http://atvb.ahajournals.org/Downloaded from

Luc et al ApoE Polymorphism 1415
TABLE 2. Mean Levels of Lipids, Apolipoproteins, and Lipoprotein Particles According toApolipoprotein E Phenotype in the Entire Control Population of the ECTIM Study
Cholesterol
Trigiycerides
VLDL-C
LDL-C
HDL-C
ApoA-l
ApoA-ll
ApoB
ApoC-lll
ApoE
LpA-l
Lp A-UA-ll
LpC-lll:B
LpE:B
2/2
197
228
47
99
51
143
32
95
4
13
54
68
35
81
3/2
226
182
31
141
54
153
37
124
3
7
51
79
18
48
ApoE
4/2
219
154
27
143
49
131
32
122
3
5
40
78
17
40
Phenotype
3/3
230
142
24
155
52
146
35
127
3
5
48
82
15
40
4/3
238
158
26
159
54
150
36
133
3
5
48
82
17
41
4/4
244
204
32
170
41
137
34
152
3
5
42
81
22
60
P
NS
.001*
.001*
<.001
<.O5
<.O5
NS
<.01
<.O5*
•c.001*
<.O5
NS
<.O5*
<.01*
Apo indicates apolipoprotein; VLDL, very-low-density lipoprotein; -C, cholesterol; LDL, low-density lipoprotein;HDL, high-density lipoprotein; and Lp, lipoprotein. Values are expressed as milligrams per deciliter. Subjects withcoronary heart disease or taking hypolipidemic drugs or those with trigiycerides >800 mg/dL were excluded.
*Statistical signification after log modification.
The results are shown in Fig 1: for trigiycerides,VLDL-C, apoC-III, apoE, Lp C-III:B, and Lp E:Blevels that displayed a skewed distribution in the popu-lation, the regression model was applied to log-trans-formed values. For this reason the reported alleliceffects on these measurements would in fact have beenmultiplicative and not additive if they had been ex-pressed in absolute concentrations. No statistically sig-nificant departure from this codominant model forallelic effects was observed for any measurements ex-cept for apoA-I (P=.05) and log Lp C-III: B (F=.01), sothe validity of the estimated effects in these two cases isdoubtful. In this sample, e2 was associated with lowertotal cholesterol, LDL-C, and apoB and higher trigiyc-erides, VLDL-C, apoE, apoC-III, Lp C-III :B, and LpE: B. Similarly, e4 was associated with higher trigiycer-ides, VLDL-C, and Lp C-III: B but also had a positiveeffect on apoB. The e4 allele was also associated withlower LpA-I when compared with the apoE3/3 pheno-type group. Total cholesterol and LDL-C increasedwith the e4 allele, but this increase did not attainstatistical significance.
The homogeneity of the e2 and e4 effects among thefour population samples was tested using the samecodominant models. No difference in the magnitude ofthe e4 effect on the biological measurements was found.In contrast, e2 effects were significantly different amongthe samples for some measurements listed in Table 3,which gives their estimates obtained separately withineach population. No effect of the e2 allele was found onthe level of trigiycerides, VLDL-C, apoE, and Lp E: Bin Belfast and on trigiycerides, VLDL-C, and Lp E: B inToulouse. However, e2 had a significant effect of anincrease on these variables in Lille and Strasbourg andon apoE level in Toulouse.
RR of MI Associated Withthe ApoE Polymorphism
All available cases (n=574) and control subjectswithout CHD (n=680) recruited in the ECTIM studywere used in the analysis, and Table 4 shows the numberof subjects with each apoE phenotype throughout thefour centers. Fig 2 shows the RR for MI of eachphenotype, with apoE3/3 as the reference. RR increaseswith the phenotypes in the following order: E2/2<E3/2<E3/3 (RR=1) <E4/3<E4/2<E4/4, irrespective ofadjustment for age and other covariates (P=.O8) (Fig 2,left). Overall, the RR of MI differed significantly withthe apoE phenotypes after adjustment for age, center,body mass index, and alcohol and cigarette use (P=.O5)
TABLE 3. Estimates of Average Effect of c2 Allele onTriglyceride, VLDL-C, ApoE, and Lp E B Levels (AfterLog Transformation) in the Control Group of theECTIM Study
Trigiycerides
VLDL-C
ApoE
LpE:B
Belfast
.040
-.007
.037
-.003
Lille
.175*
.241*
.365*
.201*
Region
Strasbourg
.346*
.353*
.476*
.389t
Toulouse
.010
.205
.315*
.012
VLDL-C indicates very-low-density lipoprotein cholesterol;ApoE, apolipoprotein E; and Lp, lipoprotein. Values are ex-pressed as log milligrams per deciliter. Subjects with coronaryheart disease or taking hypolipidemic drugs or those withtrigiycerides >800 mg/dL were excluded. Data adjusted for age,body mass index, and alcohol and cigarette consumption.
*P<.05, fP<.01,*P<.001.
by guest on October 19, 2014http://atvb.ahajournals.org/Downloaded from

1416 Arteriosclerosis and Thrombosis Vol 14, No 9 September 1994
TABLE 4. Frequency of Apolipoprotein E Phenotypes inMyocardial Infarction Survivors and Control Subjects inthe ECTIM Study
Region and Subjects
Belfast
Ml (n=183)
C (n=176)
Lille
Ml (n=64)
C (n=150)
Strasbourg
Ml (n=187)
C (n=172)
Toulouse
Ml (n = 140)
C (n=182)
2/2
2
2
0
2
1
2
0
0
ApoE Phenotype
3/2
17
26
6
23
20
24
11
19
4/2
4
6
0
6
5
1
5
1
3/3
102
104
43
84
113
109
94
131
4/3
49
32
13
32
42
32
29
30
4/4
9
6
2
3
6
4
1
1
ApoE indicates apolipoprotein E; Ml, myocardial infarctionsurvivors; and C, control subjects. Control subjects with coro-nary heart disease were excluded.
(Fig 2, right). However, no specific risk (compared withE3/3) reached statistical significance even after adjust-ment for the covariates.
Allelic-specific risks for e2 and e4 were computed bythe codominant model for RR. The RR 95% confidenceinterval was 0.73 (0.53 to 1.00) (P=.O5) and 1.33 (1.05 to1.68) (.P=.O2) for e2 and e4, respectively, after adjust-ment for age and other covariates (Fig 2, right). Therisks were at the limit of significance (RR, 0.75 and 1.29for e2 and e4, respectively) when no adjustment otherthan for center was carried out (Fig 2, left). Thedecreased risk associated with e2 and increased risk
3
2.5
2
1.5
1
0.5
0 f +-
T
+-
3 " -
2.5 • -
1.5
0 - H - k •+--
T .
-+-
f-H-L
2/2 3/2 3/3 4/2 4/3 4/4 2/2 3/2 3/3 4/2 4/3 4/4
e2 £4
1.5
1
0.5
0a
FIG 2. Bar graphs show relative risk (mean and 95% confidenceinterval) for myocardial infarction associated with each apolipo-protein (apo) E phenotype and allele compared with apoE3/3 inthe ECTIM study. Control subjects without coronary heart dis-ease and survivors of myocardial infarction were included. Left,population-adjusted relative risk; right, covariate (center, age,body mass index, alcohol intake, and tobacco consumption)-adjusted relative risk.
associated with e.4 did not differ significantly among thefour populations (data not shown).
DiscussionApoE plays an important role in lipoprotein metab-
olism, so the possible association between the differentapoE phenotypes and a number of plasma lipoproteinparameters and the RR for MI was explored in theECTIM study, a multicenter study designed to identifygenotypes predisposing to MI. The possible biasesdisplayed by this case-control study, particularly involv-ing the selection of patients with MI and appropriatecontrol subjects, have been previously discussed indetail.11
A geographical difference appeared in the frequencyof apoE alleles among the four control populations. Ifthe allele frequency in Belfast and Lille was close to thatalready reported in Caucasian populations,6 that ofToulouse, whose ethnic background was probably dif-ferent from the other regions, was closer to the distri-bution described in the Chinese or Japanese.2021
A number of studies have demonstrated a consistentrelation between apoE phenotype and plasma lipidlevels. This relation was confirmed by Dallongeville etal5 using the powerful tool of meta-analysis. As in mostof the previous studies, we have found a lower concen-tration of cholesterol2231 and/or LDL-C2326-27.2930 forthe e2 allele. Conversely, in contrast with most previousstudies, which have shown that cholesterol and/orLDL-C levels are increased in e4 allele carriers com-pared with E3/3 subjects,2326-28-32 the estimates of thisallelic effect on these parameters were of relatively lowmagnitude and not significant, at least partly because ofthe much lower levels seen in E4/2 subjects (Table 2)and perhaps because of the exclusion of subjects takinghypolipidemic drugs and subjects having a higher fre-quency of hypercholesterolemia in relation to the effectof the e4 allele on cholesterol.
The most striking findings of this study were theinfluence of apoE alleles on triglycerides, apoE, andapoC-HI; both apolipoproteins are present at the sur-face of triglyceride-rich lipoproteins and apoB-contain-ing particles such as Lp C-III: B and Lp E: B. Indeed,triglycerides appeared elevated in subjects carrying thee2 or e4 allele compared with individuals with theapoE3/3 phenotype. A variable effect of the e2 allele ontriglyceride, apoE, and Lp E: B levels was clearly seenacross the four populations we studied, the increase oftriglycerides, VLDL-C, apoE, and Lp E:B being ob-served only in Lille and Strasbourg. Pooling all pub-lished data for a meta-analysis procedure, Dallongevilleet al5 noticed this variability for triglycerides in subsetsof subjects bearing this allele (apoE2/2, apoE3/2, orapoE4/2 phenotype). This suggests that genes or envi-ronmental factors strongly interact with the e2 alleleeffects. Among these last factors, diabetes and over-weight are candidates for this interaction.3335 Thisinteraction is also particularly obvious in hyperlipidemicindividuals bearing two e2 alleles (type III hyperlipid-emia), in whom the expression of this hyperlipidemiarequires association of the apoE2/2 phenotype withanother genetic or environmental factor.36 However, nointeraction was found to be significant in the present
by guest on October 19, 2014http://atvb.ahajournals.org/Downloaded from

Luc et al ApoE Polymorphism 1417
study between e2 effects and body mass index, alcoholintake, or tobacco use within each population.
A metabolic mechanism of the increase of thesetriglyceride-rich particles in subjects carrying the e2allele in Lille and Strasbourg could be the delayedcatabolism of remnant particles that could be repre-sented in plasma by Lp E: B and Lp C-III: B. Indeed, insubjects with type III hyperlipidemia, a disease causedby a high level of remnants in plasma, plasma Lp E: Band Lp C-III: B levels were particularly high.37
The elevated triglyceride levels were noticed in 30 of36 subsets of subjects bearing apoE4/3 included in themeta-analysis of Dallongeville et al,5 whereas theselevels were lower or higher in apoE4/4 subjects. In thepresent study the e4 allele was associated with anincrease of triglycerides and Lp C-III :B (Fig 1). Adefect in lipolysis of triglyceride-rich lipoproteins coulddelay the disappearance of these particles from theplasma. In support of this hypothesis, previous reportshave indicated that the e4 allele might be implicated inthe pathogenesis of type V hyperlipoproteinemia.3840 Itis therefore tempting to hypothesize that apoE4 inter-feres with the triglyceride-rich particle catabolism.However, only the accumulation in plasma of particulartypes of triglyceride-rich particles, such as those con-taining apoC-III and apoB but without surficial apoE,seemed to explain the increase of triglycerides (Fig 1).The absence of an increase in Lp E:B could be ex-plained by the fact that apoE4 has been shown to bepreferentially associated with VLDL.41 Therefore, thedelay of lipolysis of apoE4- and apoB-containing lipo-proteins present in the fraction of VLDL density couldbe compensated by a faster in vivo catabolism of apoE4-containing particles of VLDL or LDL density than thatof particles containing apoE3, as suggested by a rapidcatabolism of apoE4 compared with that of apoE3.8
In the present multicenter case-control study, anassociation between the apoE polymorphism and therisk of MI was evident, but despite a large number ofcases and control subjects, this association was of onlyborderline statistical significance. The presence of thee2 and e4 alleles compared with E3/3 genotype leads toa lower and higher risk of MI, respectively, but thestrength of the relation (RR 0.73 and 1.33, respectively)was relatively low. Calculation of the attributable risk42
attached to the apoE polymorphism in the four popu-lations of the ECTIM study indicated that 12% of MIcases might be attributable to this polymorphism, E3/3being the reference genotype. These results appearconsistent with most previous studies, even though theirdesign and particularly the definition of cases andcontrol subjects are highly variable. With the use of acomparable design, a comparison of MI cases andcontrol subjects in the population of Scotland43 alsoyielded a significantly higher and lower frequency of e4and e2, respectively, in both men and women with MI.The overall association was more marked in subjectsless than 60 years of age. In the present study the samephenomenon was observed with an allelic RR of 0.62(P=.O5) for e2 and 1.55 (F=.O1) for e4 in men aged lessthan 55 compared with 0.78 and 1.20, respectively, inolder men (P=NS). Several studies have compared theapoE phenotype distribution in subjects with coronaryartery disease detected by cineangiography with control
subjects. The e4 allele has been found significantly morefrequently in cases44-45 than in control subjects. Con-versely, a tendency in favor of a lower frequency of thee2 allele in subjects with coronary artery disease wasgenerally observed.43'45 In contrast, in the prospectiveMRFIT study, a statistically significant increased RR of1.5 to 1.7 compared with the phenotype E3/3 group wasobserved for E3/2, E4/3, and E4/4 subjects, (i>=.03).46
In another prospective study, the Framingham study,the risks associated with the e2, e3, and e4 alleles werenot significantly different.47 These last findings are atvariance with the present evidence in favor of a "pro-tective" effect of the e2 allele, excluding type IIIhyperlipidemia, which is uncommon at the populationlevel. However, an autopsy study in young men31 showeda differential extension of atherosclerotic lesions, par-ticularly in the aorta, according to the apoE phenotype,which indicated a lower and higher involvement, respec-tively, in e2 and e4 carriers, as expected from theestablished effects of these alleles on LDL-C and apoBconcentrations. It was suggested that the genotypiceffects on arterial lesions might not be entirely ex-plained by serum cholesterol level. In the present studythe lipoprotein and apolipoprotein profiles in the con-trol subjects with the e4 allele were consistent with theobserved risk gradient. Considering the fact that apoEpolymorphism modulates LDL-C levels and thatLDL-C represents a major risk factor for MI, it remainsquestionable as to whether LDL-C levels represent aconfounding factor when the risk for MI is calculatedaccording to apoE polymorphism. It seems impossibleto solve this problem by a case-control study because anumber of subjects, either MI or control, were takinghypolipidemic drugs, particularly in France. These sub-jects would therefore be excluded, leading to an impor-tant bias and giving doubtful results on this topic.Actually, in the ECTIM study, no significant differencein LDL-C was found between cases and control subjectsafter subjects taking hypolipidemic drugs were ex-cluded. Therefore, because in this study the e4 allelefrequency is higher in MI than in control subjects, it issuggested that the apoE polymorphism could have aninfluence on the expression of this disease indepen-dently of the effect on LDL-C levels. This seems to beconfirmed by the results of a prospective study, theMRFIT study, which demonstrated that significant dif-ferences among apoE phenotypes in CHD risk persistafter adjusting for LDL-C.46 Therefore, the apoE poly-morphism could modulate other risk factors such aslipoprotein particles, as described in the present study.
Lower LDL-C and apoB levels associated with e2were in accord with a diminished CHD risk in e2carriers. Control subjects with the e2 allele, however,had higher triglyceride, VLDL-C, and Lp E: B levels onaverage, and these parameters have been shown to behigher in control subjects living in a region (NorthernIreland) with a higher incidence of CHD (348 per100 000) than in those living in France, a country with arelatively low CHD incidence (78 to 105 per 100 000).10
These results, complicated by the finding of a heterog-enous e2 metabolic effect on VLDL particles across thecenters, are difficult to reconcile, as the numbers ofcases and control subjects in this study were too low to
by guest on October 19, 2014http://atvb.ahajournals.org/Downloaded from

1418 Arteriosclerosis and Thrombosis Vol 14, No 9 September 1994
analyze an apoE phenotype-associated risk on a re-gional basis with an acceptable power.
Finally, the present evidence, together with mostpreviously published data, is in favor of an increasingCHD risk gradient associated with apoE polymorphismin the allelic order e2<e3<e4, but the proportion of MIcases attributable to this polymorphism appears modestat the population level (12%). A more precise assess-ment of the apparently protective e2 effect would re-quire both experimental work and larger populationstudies, preferably with a prospective cohort design.
AcknowledgmentsThe Etude Cas-Temoins sur l'lnfarctus du Myocarde
(ECTIM) study is supported by grants from the Squibb andParke-Davis Laboratories, the Sanofi Clin-Midy Laboratory, theMutuelle Generate de l'Education Nationale, the British HeartFoundation, the Institut National de la Sante et de la RechercheMedicale, the Institut Pasteur de Lille, and ARCOL.
References1. Mahley RW. Apolipoprotein E: cholesterol transport protein with
expending role in cell biology. Science. 1988;240:622-630.2. Zannis VI, Breslow JL, Utermann G, Mahley RW, Weisgraber
KH, Havel RJ, Goldstein JL, Brown MS, Schonfeld G, HazzardWR, et al. Proposed nomenclature of apo E isoproteins, apo Egenotypes and phenotypes. J Lipid Res. 1982;23:911-914.
3. Pagnan A, Havel RJ, Kane JP, Kotite L. Characterization of humanvery low density lipoproteins containing two electrophoretic popu-lations: double pre-beta lipoproteinemia and primary dysbetalipopro-teinemia. / Lipid Res. 1977;18:613-622.
4. Bouthillier D, Sing CF, Davignon J. Apolipoprotein E phenotypingwith a single gel method: application to the study of informativematings. / Lipid Res. 1983;24:1060-1069.
5. Dallongeville J, Lussier-Cacan S, Davignon J. Modulation ofplasma triglycerides levels by apo E phenotype: a meta-analysis.J Lipid Res. 1992;33:447-454.
6. Davignon J, Gregg RE, Sing CF. Apolipoprotein E polymorphismand atherosclerosis. Arteriosclerosis. 1988;8:1-21.
7. Mahley RW, Innerarity TL. Lipoprotein receptors and cholesterolhomeostasis. Biochim Biophys Ada. 1983;737:197-222.
8. Gregg RG, Zech LA, Schaeffer EJ, Brewer HB. Type III hyperli-poproteinemia: defective metabolism of an abnormal apolipo-protein E. Science. 1981;211:584-585.
9. Lenzen HJ, Assmann G, Buchwalsky R, Schulte H. Association ofapo E polymorphism, low-density lipoprotein cholesterol, andcoronary artery disease. Clin Chem. 1986;32:778-781.
10. WHO Monica Project Principal Investigators. The World HealthOrganization MONICA Project (MONItoring trends and deter-minants in CArdiovascular disease): a major international collab-oration. J Clin Epidemiol. 1988;41:105-114.
11. Parra HJ, Arveiler D, Evans AE, Cambou JP, Amouyel P,Bingham A, McMaster D, Schaffer P, Douste-Blazy Ph, Luc G, etal. A case-control study of lipoprotein particles in two populationsat contrasting risk for coronary heart disease: the ECTIM study.Arterioscler Thromb. 1992;12:701-707.
12. WHO MONICA Project. WHO MONICA Project: assessing CHDmortality and morbidity. Int J Epidemiol. 1989;18:S38-S45.
13. Havel RJ, Eder HA, Bragdon JH. The distribution and chemicalcomposition of ultracentrifugally separated lipoproteins in humanserum. J Clin Invest. 1955;34:1345-1353.
14. Fruchart JC, Fievet C, Puchois P. In: Bergmeyer HU, ed. Methodsof Enzymatic Analysis: Apolipoproteins. 3rd ed. Weinheim, FRG:Verlag Chemie; 1985:126-138.
15. Fruchart JC, Kandoussi A, Parsy D, Koren E, Puchois P. Mea-surement of lipoprotein particles defined by their apolipoproteincomposition using immunosorbent assay. J Clin Chem ClinBiochem. 1985;23:619. Abstract.
16. Parra HJ, Fievet C, Boniface B, Bertrand M, Duthilleul P,Fruchart JC. Lipoproteins, apolipoproteins and coronary arterydisease assessed by coronary arteriography. In: De Gennes JL,Polonowski J, Paoletti R, eds. Latent Dyslipoproteinemia and Ath-erosclerosis. New York, NY: Raven Press, Publishers; 1984:187-197.
17. Parra HJ, Mezdour H, Ghalim N, Bard JM, Fruchart JC. Differ-ential electroimmunoassay on ready plates for human LpAI lipo-protein particles. Clin Chem. 1990;36:1431-1435.
18. Menzel HJ, Utermann G. Apolipoprotein E phenotyping fromserum Western blotting. Electrophoresis. 1986;7:492-495.
19. Leroy A, Vu-Dac N, Koffigan M, Clavey V, Fruchart JC. Character-ization of a monoclonal antibody that binds to apolipoprotein E andto lipoproteins of human plasma containing apo E. J Immunoassay.1988;9:309-334.
20. Wang K. Studies of human apolipoprotein E genetic isoforms andtheir phenotypes among the Chinese population. Ada Acad MedSinicae. 1986;8:198.
21. Gerdes LU, Klauscn IC, Sihm I, Faergeman O. Apolipoprotein Epolymorphism in a Danish population compared to findings in 45other study populations around the world. Genet Epidemiol. 1992;9:155-167.
22. Menzel HJ, Kladetzky RG, Assmann G. Apolipoprotein E poly-morphism and coronary artery disease. Arteriosclerosis. 1983;3:310-315.
23. Sing CF, Davignon J. Role of the apolipoprotein E polymorphismin determining normal plasma lipid and lipoprotein variation. AmJ Hum Genet. 1985;37:268-285.
24. Smit M, De Kniff P, Rosseneu M, Bury J, Klasen E, Frants R,Havekes L. Apolipoprotein E polymorphism in the Netherlandsand its effect on plasma lipid and apolipoprotein levels. HumGenet. 1988;80:287-292.
25. Guegen R, Visviskis S, Steinmetz J, Siest G, Boerwinkle E. Ananalysis of genotype effects and their interactions by using theapolipoprotein E polymorphism and longitudinal data. Am J HumGenet. 1989;45:793-802.
26. Eichner JE, Kuller LH, Ferrell RE, Meilahn EN, Kamboh MI.Phenotype effects of apolipoprotein. Structural variations on lipidprofiles, III: contribution of apolipoprotein E phenotype to pre-diction of total cholesterol apolipoprotein B and low density lipo-protein cholesterol in the healthy women study. Arteriosclerosis.1990;10:379-385.
27. Stuyt PMJ, Brenninkmeijer BJ, Demacker PNM, Hendriks JCM,Van Elteren P, Stalenhoef AFH, Van't Laar A. Apolipoprotein Ephenotypes, serum lipoproteins and apolipoproteins in angio-graphically assessed coronary heart disease. Scand J Clin LabInvest. 1991;51:425-435.
28. Hallman DM, Boerwinkle E, Saha N, Sandholzer C, Menzel HJ,Csazar A, Utermann G. The apolipoprotein E polymorphism: acomparison of allele frequencies and effects in nine populations.Am J Hum Genet. 1991;49:338-349.
29. Xu CF, Talmud PJ, Angelico F, Del Ben M, Savill J, HumphriesSE. Apolipoprotein E polymorphism and plasma lipid, lipoprotein,and apolipoprotein levels in Italian children. Genet Epidemiol.1991;8:389-398.
30. Xhignesse M, Lussier-Cacan S, Sing CF, Kessling AM, Davignon J.Influences of common variants of apolipoprotein E on measures oflipid metabolism in a sample selected for health. Arteriosclerosis.
31. Hixson JE, and the Pathobiological Determinants of Athero-sclerosis in Youth (PDAY) Research Group. Apolipoprotein Epolymorphisms affect atherosclerosis in young males. ArteriosclerThromb. 1991;11:1237-1244.
32. Ehnholm C, Lukka M, Kuusi T, Nikkila E, Utermann G. Apolipo-protein E polymorphism in the Finnish population: gene fre-quencies and relation to lipoprotein concentrations. J Lipid Res.1986;27:227-235.
33. Parhofer KG, Richter WO, Schwandt P. Apolipoprotein E phe-notype frequency in type II diabetic patients with different formsof hyperlipoproteinemia. Horm Metab Res. 1990;22:589-594.
34. Imari Y, Koga S, Ibayashi H. Phenotype of apolipoprotein E andabnormalities in lipid metabolism in patients with non-insulin-dependent diabetes mellitus. Metabolism. 1988;37:1134-1138.
35. Eto M, Watanabe K, Ishii K. Apolipoprotein E polymorphismand hyperlipoproteinemia in obesity. Int J Obesity. 1989;13:433-440.
36. Utermann G, Vogelberg KH, Steinmetz A, Schoenborn W, PruinN, Jaeschka M, Hees M, Canzler H. Polymorphism of apolipo-protein E, II: genetics of hyperlipoproteinemia type III. ClinGenet. 1979;15:37-62.
37. Lussier-Cacan S, Bard JM, Boulet L, Nestruck AC, Grothe AM,Fruchart JC, Davignon J. Lipoprotein composition changesinduced by fenofibrate in dysbetalipoproteinemia type III. Athero-sclerosis. 1989;78:167-182.
by guest on October 19, 2014http://atvb.ahajournals.org/Downloaded from

Luc et a1 ApoE Polymorphism 1419
38. Kuusi T, Taskinen MR, Solaviki T, Kauppinen-Makelin R. Role of apolipoproteins E and C in type V hyperlipoproteinemia. J Lipid Res. 1988;29:293-298.
39. Ghiselli G, Schaffer EJ, Zech LA, Gregg RE, Brewer HB. Increased prevalence of apolipoprotein E4 in type V hyperlipopro- teinemia. J Clin Invest. 1982;70:474-477.
40. Hegele RA, Breckenridge WC, Cox DW, Maguire GR, Little JA, Connelly PN. Interaction between variant apolipoprotein CII and E that affects plasma lipoprotein levels. Arterioscler Thromb. 1991; 11:1303-1309.
41. Steinmetz A, Jakobs C, Morzny S, Kaffarnik H. Differential distri- bution of apolipoprotein E isoforms in human plasma lipoproteins. Arteriosclerosis. 1989;9:405-411.
42. Walter SD. Calculation of attributable risks from epidemiological data. Int J Epidemiol. 1978;7:175-182.
43. Cumming AM, Robertson FW. Polymorphism of the apoprotein E locus in relation to risk of coronary disease. Clin Genet. 1984;25: 310-313.
44. Kuusi T, Nieminen MS, Ehnholm C, Yki-Jarvinen H, Valle M, Nikkila EA, Taskinen MR. Apolipoprotein E polymorphism and coronary heart disease: increased prevalence of apolipoprotein E4 in angiographically verified coronary patients. Arteriosclerosis. 1989;9:237-241.
45. Nieminen MS, Mattila KJ, Aalto-Setala K, Kuusi T, Kontula K, Kauppinen-Makelin R, Ehnholm C, Jauhiainen M, Valle M, Taskinen MR. Lipoproteins and their genetic variation in subjects with and without angiographically verified coronary artery disease. Arterioscler Thromb. 1992;12:58-69.
46. Eichner JE, Kuller LH, Orchard TJ, Grandits GA, McCallum LM, Ferrell RE, Neaton JD. Relation of apolipoprotein E phenotype to myocardial infarction and mortality from coronary artery disease. Am J Cardiol. 1993;71:160-165.
47. Wilson PWF, Larson MG, Ordovas JM, Schaefer EJ. Apolipo- protein E isoforms and CHD prevalence in the Framingham off- spring. Circulation. 1992;86(suppl 1):I-810. Abstract.
by guest on October 19, 2014http://atvb.ahajournals.org/Downloaded from




















