
Induction chemotherapy with cisplatin and gemcitabine followed by concurrent chemoradiation with...
10
Lung Cancer (2008) 62, 62—71 available at www.sciencedirect.com journal homepage: www.elsevier.com/locate/lungcan Induction chemotherapy with cisplatin and gemcitabine followed by concurrent chemoradiation with twice-weekly gemcitabine in unresectable stage III non-small cell lung cancer: Final results of a phase II study Remei Blanco a,∗ , Josep Sol´ e b,1 , Jes´ us Montesinos c,2 , Carlos Mes´ ıa d,1 , Manuel Algara e,3 , Josefa Terrassa f,4 , Monserrat Gay g,5 , Monserrat Domenech h,6 , Rom´ a Bastus i,7 , Isabel Bover j,8 , Miquel Nogu´ e g,5 , Catalina Vadell k,9 , On behalf of ACROSS (Associaci´ o Catalana per a la Recerca Oncol` ogica i les seves implicacions Sanit` aries i Socials). Barcelona, Spain a Oncology Service, Consorci Sanitari de Terrassa, Ctra. de Torrebonica sn, 08227 Terrassa, Spain b Radiation Oncology Service, Hospital Duran i Reynals, AV Granvia de l’Hospitalet sn, Km 2.7, 08908 L’Hospitalet de Llobregat, Spain c Oncology Service, Consorci Hospitalari Parc Taul´ ı, Parc Taul´ ı s/n, 08208 Sabadell, Spain d Oncology Service, Hospital Duran i Reynals, AV Granvia de l’Hospitalet sn, Km 2.7, 08908 L’Hospitalet de Llobregat, Spain e Radiation Oncology Service, Hospital de L’Esperanc ¸a, C/Sant Josep de la Muntanya 12, 08024 Barcelona, Spain f Oncology Service, Hospital Son Dureta, C/Andrea Doria 55, 07014 Palma Mallorca, Spain g Oncology Service, Hospital General de Vic, Plaza Francesc Pla El Vigat` a 1, 08500 Vic, Spain h Oncology Service, Centre Hospitalari i Cardiol` ogic de Manresa, Avda. Bases de Manresa 6-8, 08240 Manresa, Spain i Oncology Service, Hospital M´ utua de Terrassa, Plac ¸a Doctor Robert 5, 08221 Terrassa, Spain j Oncology Service, Hospital Son Llatzer, Ctra. Manacor, Km 4, 07198 Palma de Mallorca, Spain k Oncology Service, Hospital de Manacor, 07500 Manacor (Mallorca), Spain Received 26 October 2007; received in revised form 26 February 2008; accepted 26 February 2008 ∗ Corresponding author. Tel.: +34 937003612; fax: +34 937003622. E-mail addresses: [email protected] (R. Blanco), [email protected] (J. Sol´ e), [email protected] (J. Montesinos), [email protected] (C. Mes´ ıa), [email protected] (M. Algara), [email protected] (J. Terrassa), [email protected] (M. Gay), [email protected] (M. Domenech), [email protected] (R. Bastus), [email protected] (I. Bover), [email protected] (C. Vadell). 1 Tel.: +34 933357011; fax: +34 932607725. 2 Tel.: +34 937231010; fax: +34 937160646. 3 Tel.: +34 933674100; fax: +34 933674266. 4 Tel.: +34 971175000; fax: +34 971717140. 5 Tel.: +34 93889111; fax: +34 938850308. 6 Tel.: +34 938730505; fax: +34 938700015. 7 Tel.: +34 937365050; fax: +34 937365059. 8 Tel.: +34 871202000; fax: +34 871202027. 9 Tel.: +34 971847000; fax: +34 971847010. 0169-5002/$ — see front matter © 2008 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.lungcan.2008.02.024
Transcript of Induction chemotherapy with cisplatin and gemcitabine followed by concurrent chemoradiation with...
L
IgwIp
RMMM
Os
a
b
Sc
d
e
f
g
h
i
j
k
R
c2
0d
ung Cancer (2008) 62, 62—71
avai lab le at www.sc iencedi rec t .com
journa l homepage: www.e lsev ier .com/ locate / lungcan
nduction chemotherapy with cisplatin andemcitabine followed by concurrent chemoradiationith twice-weekly gemcitabine in unresectable stage
II non-small cell lung cancer: Final results of ahase II study
emei Blancoa,∗, Josep Sole b,1, Jesus Montesinosc,2, Carlos Mesıad,1,anuel Algarae,3, Josefa Terrassa f,4, Monserrat Gayg,5,onserrat Domenechh,6, Roma Bastus i,7, Isabel Bover j,8,iquel Nogue g,5, Catalina Vadell k,9,
n behalf of ACROSS (Associacio Catalana per a la Recerca Oncologica i leseves implicacions Sanitaries i Socials). Barcelona, Spain
Oncology Service, Consorci Sanitari de Terrassa, Ctra. de Torrebonica sn, 08227 Terrassa, SpainRadiation Oncology Service, Hospital Duran i Reynals, AV Granvia de l’Hospitalet sn, Km 2.7, 08908 L’Hospitalet de Llobregat,painOncology Service, Consorci Hospitalari Parc Taulı, Parc Taulı s/n, 08208 Sabadell, SpainOncology Service, Hospital Duran i Reynals, AV Granvia de l’Hospitalet sn, Km 2.7, 08908 L’Hospitalet de Llobregat, SpainRadiation Oncology Service, Hospital de L’Esperanca, C/Sant Josep de la Muntanya 12, 08024 Barcelona, SpainOncology Service, Hospital Son Dureta, C/Andrea Doria 55, 07014 Palma Mallorca, SpainOncology Service, Hospital General de Vic, Plaza Francesc Pla El Vigata 1, 08500 Vic, SpainOncology Service, Centre Hospitalari i Cardiologic de Manresa, Avda. Bases de Manresa 6-8, 08240 Manresa, SpainOncology Service, Hospital Mutua de Terrassa, Placa Doctor Robert 5, 08221 Terrassa, Spain
Oncology Service, Hospital Son Llatzer, Ctra. Manacor, Km 4, 07198 Palma de Mallorca, SpainOncology Service, Hospital de Manacor, 07500 Manacor (Mallorca), Spaineceived 26 October 2007; received in revised form 26 February 2008; accepted 26 February 2008
∗ Corresponding author. Tel.: +34 937003612; fax: +34 937003622.E-mail addresses: [email protected] (R. Blanco), [email protected] (J. Sole), [email protected] (J. Montesinos),
[email protected] (C. Mesıa), [email protected] (M. Algara), [email protected] (J. Terrassa), [email protected] (M. Gay),[email protected] (M. Domenech), [email protected] (R. Bastus), [email protected] (I. Bover), [email protected] (C. Vadell).1 Tel.: +34 933357011; fax: +34 932607725. 2Tel.: +34 937231010; fax: +34 937160646. 3Tel.: +34 933674100; fax: +34 933674266.4 Tel.: +34 971175000; fax: +34 971717140. 5Tel.: +34 93889111; fax: +34 938850308. 6Tel.: +34 938730505; fax: +34 938700015.7 Tel.: +34 937365050; fax: +34 937365059. 8Tel.: +34 871202000; fax: +34 871202027. 9Tel.: +34 971847000; fax: +34 971847010.
169-5002/$ — see front matter © 2008 Elsevier Ireland Ltd. All rights reserved.oi:10.1016/j.lungcan.2008.02.024

Final results of a phase II study 63
Summary: Concurrent chemoradiotherapy (CCR) followed or preceded by full-dose chemother-apy seems to be a standard treatment for unresectable non-small cell lung cancer (NSCLC).Gemcitabine is a strong radiosensitizer, and a phase I study confirmed the feasibility of CCR withlow-dose gemcitabine administered twice-weekly in NSCLC patients. Consequently, we designeda prospective, multicentric, phase II trial to evaluate the efficacy and toxicity of this approach,following induction chemotherapy with cisplatin and gemcitabine. We included patients withunresectable stage III NSCLC, no pleural effusion, adequate pulmonary, renal, liver and hemato-logical functions, Karnofsky index >70 and planned treated volume (PTV) <2200 cm3. Treatmentconsisted of 3 cycles of cisplatin (100 mg/m2, d1) and gemcitabine (1250 mg/m2, d1 and 8) q3w,followed by CCR (gemcitabine 50 mg/m2 on Mondays and Thursdays and radiotherapy 68.4 Gy,1.8 Gy qd). After the inclusion of 22 patients (group A), an unacceptable toxicity was detected.Thus, cisplatin dose was reduced to 70 mg/m2, and gemcitabine dose was adjusted to 35 mg/m2
during CCR. Another 34 patients (33 eligible, group B) were included. Five patients in group A and6 patients in group B discontinued the study treatment during induction. Thus, 17 and 27 patients,respectively initiated CCR. Hematological toxicity (grades III and IV) was particularly relevant ingroup A during this phase, with 35 and 23% of thrombopenia and neutropenia, respectively. Non-hematological grades III—IV toxicity of chemoradiation was significant and similar in groups A andB: esophagitis 35.2 and 33.3% and pneumonitis 23.5 and 25.9%, respectively. 40.9% of patientsin group A vs. 57.5% in group B completed treatment. Overall response (intention-to-treat anal-ysis) was 68.1% in group A and 63.5% in group B. Median survival was 17.7 months for the wholegroup with a mean follow-up of 41.2 months. 20% of patients were alive at 3 years. Long-termresults of this schedule are encouraging. However, nonhematological toxicity of chemoradiation
trate
KEYWORDSGemcitabine;Concurrentchemoradiotherapy;Non-small cell lungcancer;Locally advanced;Phase II;Toxicity
All ri
iloItcctit6gra
ctas1
aiacifi
2. Methods
is substantial and different s© 2008 Elsevier Ireland Ltd.
1. Introduction
Approximately 30% of patients with non-small cell lung can-cer (NSCLC) present with locally advanced disease. Some ofthese patients can benefit from a surgical approach [1,2],but the great majority of patients with stage IIIb, andmany with stage IIIa (e.g. N-2 bulky) are not eligible forsurgery. It is presently accepted that the best treatmentfor these patients is the combination of chemotherapy andradiotherapy. Some comparative clinical studies [3—5] showthat concurrent chemoradiotherapy (CCR) is more effec-tive than sequential treatment, though at the expense ofa major nonhematological toxicity (mainly esophagitis andpneumonitis).
Despite these new therapeutic approaches, the resultsremain poor, with 3-year survival below 20%. Two pos-sible strategies are available to improve this situation.First, the incorporation of induction or adjuvant chemother-apy to concurrent treatment, as represented in thestudies CALGB-9431 and SWOG 9504, respectively [6,7].The second strategy consists of using more radiosensitivedrugs, such as gemcitabine, in concurrent chemoradiothe-rapy.
The optimal dose for the administration of gemcitabinecombined with radiotherapy has been evaluated in variousphase I trials [8—11]. In these studies, the recommendedweekly dose of gemcitabine concurrent to radiotherapywas between 100 and 375 mg/m2, depending on the doseof radiotherapy, the type of planning (2D or 3D), andthe volume of treatment. In the first phase II trial pub-
lished, gemcitabine was administered at full weekly doses of 1 g/m2 during six consecutive weeks, combined with60 Gy of thoracic radiation [12]. High levels of toxicitywere observed, resulting in serious esophagitis and pneu-monitis, with three toxic deaths in the eight patientsTia
gies should be tested to minimize it.ghts reserved.
ncluded. Other phase II studies were subsequently pub-ished, based on the results of the phase I trials mentioned,btaining mean survival of about 15 months [13—15].n addition, we must mention the phase II randomizedrial carried out by CALGB [6], comparing three classi-al combinations of chemotherapy (cisplatin—gemcitabine,isplatin—vinorelbine and cisplatin—paclitaxel) concurrento radiotherapy. In the gemcitabine arm, after two cycles ofnduction, radiotherapy was combined with the administra-ion of cisplatin 80 mg/m2 every 3 weeks, and gemcitabine00 mg/m2 on days 1 and 8 of each cycle. Esophagitisrades III and IV was observed in 52% of cases. Overallesponse and survival were similar in the three treatmentrms.
Nevertheless, experiments in vitro showed that gem-itabine radio sensitization did not exceed 72 h. Thus,wice-weekly administration of gemcitabine would seem anttractive schedule [16]. Using this scheme, Blackstock pre-ented the preliminary results of a phase I trial in ASTRO999 [17].
On the basis of these results, the Associacio Catalana perla Recerca Oncologica i les seves implicacions SanitariesSocials (ACROSS) undertook a phase II study to evalu-
te the efficacy and toxicity of a radiotherapy treatmentoncomitant with gemcitabine administered twice-weekly,n patients with locally advanced and unresectable NSCLC,ollowing induction chemotherapy with cisplatin and gemc-tabine.
his was a multicentric, non-randomized phase II study. Thenstitutional ethics committees of each participating centerpproved the study protocol.

6
2
EtdirpdrAooa>afnoncy
ra2Cf
2
Btpcrcpit
2
Tita1rrad
ssa3B
bc
aaiwI6dma6ilciss3vcso
tacIrrs
2
Pcotg
npp3mwpo
itepc
lse
4
.1. Eligibility criteria
ligible patients had histologic or cytologic documenta-ion of NSCLC and unresectable or inoperable stage IIIisease. Patients with malignant pleural effusion wereneligible. Patients with non-extirpable locoregional recur-ence of tumors previously resected were also enrolled. Allatients presented at least one lesion measurable in two-imensions, by computed tomography (CT), or magneticesonance (MR) performed within 28 days of registration.dditional eligibility criteria included Karnofsky index equalr superior to 70%, age of 18 years or older, and absencef pregnancy. Required initial laboratory tests includedn absolute granulocyte count of ≥1500 �L−1, hemoglobin10.5 g/dL, platelet count of ≥100,000 cells/�L, and cre-tinine clearance of at least 55 mL/min. In addition, liverunction tests has to be ≤1.5 times the upper limit oformality, and the forced expiratory volume in 1 s has tover 1000 mL. Eligible patients had no serious medical ill-esses preceding treatment and no other primary invasiveancer unless they had been disease-free for at least 5ears.
All patients were visited by a radiation oncologist beforeegistration in the study. Determination of PTV was required,nd patients were only eligible if this parameter was under200 cm3, in accordance with the scheme proposed byALGB/ROTG [18]. Written informed consent was obtainedrom each patient prior to study entry.
.2. Initial evaluation
aseline evaluation was performed within 28 days beforereatment and included a complete medical history andhysical examination, complete blood cell count, bloodhemistry studies, flexible bronchoscopy, electrocardiog-aphy, pulmonary function test including lung diffusionapacity for carbon monoxide, chest radiography, and com-uted tomography of the chest and abdomen. CT or MRmaging of the brain and bone scintigraphy were not manda-ory in absence of symptoms.
.3. Study design
his was a multicentric, non-randomized phase II trial. Thenitial design of the study contemplated the administra-ion of induction chemotherapy with 3 cycles of cisplatinnd gemcitabine at a dose of 100 mg/m2 on day 1 and250 mg/m2 on days 1 and 8, respectively. Followingesponse assessment, and in the absence of progression,adiotherapy was initiated with concurrent gemcitabinedministered twice-weekly (50 mg/m2 Mondays and Thurs-ays).
The results obtained for the first 22 patients (group A)howed an excessive level of nonhematological toxicity. Sub-equently, the dose of cisplatin was reduced to 70 mg/m2,nd gemcitabine dose during concurrence was adjusted to
5 mg/m2 for the following 34 patients included (group).Concurrent radiotherapy with gemcitabine was initiatedetween the third and fourth week after the third cycle ofhemotherapy. High-energy photons (6—23 MeV) produced in
a
tvr
R. Blanco et al.
lineal accelerator were used. Planned dose was 68.4 Gy,nd fractionation was standard. Radiotherapy was deliveredn two phases. During the first phase of the treatment, 45 Gyas administered with opposed anterior and posterior fields.
n the second phase, macroscopic disease was overdosed to8.4 Gy, with a minimum of 2 entry fields. The maximumose permitted on the spinal cord was 45 Gy and efforts wereade to include less than 16 cm of esophagus. Dose fraction-
tion was according to the definitions of ICRU 50 and ICRU2 [19]. All patients received elective nodal irradiation. PTVncluded, with a margin of 1.5 cm, the primary tumor, homo-ateral hilum and mediastinum. In cases of N3 involvement,ontralateral hilum was irradiated. Homolateral supraclav-cular fossa was only treated in upper-lobe tumors or inupraclavicular N3 (in this case, both supraclavicular fos-as were treated). 3D planning system was used in 2 of thecenters where radiotherapy was administered, and dose-
olume histograms were used to calculate PTV. In the thirdentre, PTV was calculated from transversal tomographiclices every 25 mm. PTV was deduced from the interpolationf reference isodose.
Rules were established to adjust cytostatics dosehroughout induction chemotherapy, as well as during CCR,ccording to hematological toxicity. Treatment was dis-ontinued when esophagitis or pneumonitis reached gradeI or over. It was resumed when these were resolved,educing the dose of gemcitabine 50%. If toxicity was notesolved after 2 weeks, the patient was excluded from thetudy.
.4. Study evaluation and statistical methods
rimary endpoints of this phase II trial were response toomplete treatment and toxicity observed during CCR. Sec-ndary endpoints included response and toxicity to inductionreatment, time to progression, overall survival and locore-ional control rate.
Although response rate to induction chemotherapy wasot the main aim of our study, it was used to calculate sam-le size, as its assessment required the greatest number ofatients. We considered the hypothesis of obtaining at least0% response to induction chemotherapy, with a possibleaximum of 50%. Using the Fleming method, sample sizeas calculated in 60 patients, for an alpha value of 5%, aower of the study of 80%, and a possible loss of follow-upf 15%.
We reduced cisplatin dose during induction and gemc-tabine dose during concurrence, as a result of the detectedoxicity. However, the trial was not designed to compare thefficacy and toxicity of two levels of doses. Thus, a com-arative statistic analysis between the two groups was notarried out, although the results are presented separately.
The safety analysis included all patients who received ateast one dose of chemotherapy. Common Toxicity Criteriacale was used for toxicity assessment, except in lung andsophageal toxicity derived from CCR, for which the RTOG
nd RTOG/EORTC criteria were used.All eligible patients at study entry were included inhe population for efficacy, in terms of response, sur-ival and time to progression. Patients evaluable foresponse to induction and complete treatment included
Final results of a phase II study
all the patients who had received at least one cycle ofcisplatin—gemcitabine. Responses to induction and com-plete treatment were assessed separately with a CT scanafter each phase. After completion of treatment, bimonthlyfollow-up chest radiographs were performed and CT scanswere repeated every 6 months.
Overall survival and time to progression was determinedon the basis of the method of Kaplan and Meier [20].
3. Results
3.1. Patient characteristics
Fifty-six patients were included in 8 centers between April2000 and April 2003: 22 were included before the previouslydescribed dose reduction (group A), and 34 after (group B).One patient in group B was not eligible for efficacy analysisas PTV volumes obtained were above acceptable levels. Hewas nevertheless included in the toxicity analysis, as he hadreceived one cycle of induction.
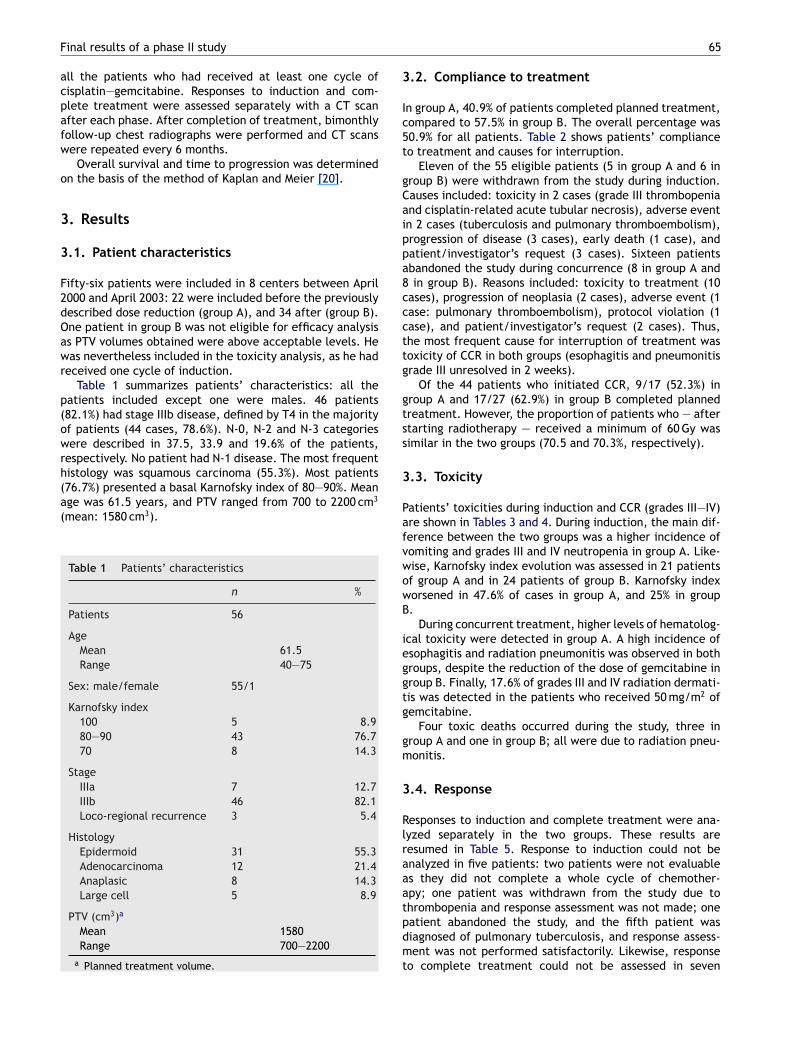
Table 1 summarizes patients’ characteristics: all thepatients included except one were males. 46 patients(82.1%) had stage IIIb disease, defined by T4 in the majorityof patients (44 cases, 78.6%). N-0, N-2 and N-3 categorieswere described in 37.5, 33.9 and 19.6% of the patients,respectively. No patient had N-1 disease. The most frequenthistology was squamous carcinoma (55.3%). Most patients(76.7%) presented a basal Karnofsky index of 80—90%. Meanage was 61.5 years, and PTV ranged from 700 to 2200 cm3
(mean: 1580 cm3).
Table 1 Patients’ characteristics
n %
Patients 56
AgeMean 61.5Range 40—75
Sex: male/female 55/1
Karnofsky index100 5 8.980—90 43 76.770 8 14.3
StageIIIa 7 12.7IIIb 46 82.1Loco-regional recurrence 3 5.4
HistologyEpidermoid 31 55.3Adenocarcinoma 12 21.4Anaplasic 8 14.3Large cell 5 8.9
PTV (cm3)a
Mean 1580Range 700—2200
a Planned treatment volume.
3
Ic5t
gCaippa8cccttg
gtss
3
PafvwowB
ieggtg
gm
3
Rlraaatpdmt
65
.2. Compliance to treatment
n group A, 40.9% of patients completed planned treatment,ompared to 57.5% in group B. The overall percentage was0.9% for all patients. Table 2 shows patients’ complianceo treatment and causes for interruption.
Eleven of the 55 eligible patients (5 in group A and 6 inroup B) were withdrawn from the study during induction.auses included: toxicity in 2 cases (grade III thrombopeniand cisplatin-related acute tubular necrosis), adverse eventn 2 cases (tuberculosis and pulmonary thromboembolism),rogression of disease (3 cases), early death (1 case), andatient/investigator’s request (3 cases). Sixteen patientsbandoned the study during concurrence (8 in group A andin group B). Reasons included: toxicity to treatment (10
ases), progression of neoplasia (2 cases), adverse event (1ase: pulmonary thromboembolism), protocol violation (1ase), and patient/investigator’s request (2 cases). Thus,he most frequent cause for interruption of treatment wasoxicity of CCR in both groups (esophagitis and pneumonitisrade III unresolved in 2 weeks).
Of the 44 patients who initiated CCR, 9/17 (52.3%) inroup A and 17/27 (62.9%) in group B completed plannedreatment. However, the proportion of patients who — aftertarting radiotherapy — received a minimum of 60 Gy wasimilar in the two groups (70.5 and 70.3%, respectively).
.3. Toxicity
atients’ toxicities during induction and CCR (grades III—IV)re shown in Tables 3 and 4. During induction, the main dif-erence between the two groups was a higher incidence ofomiting and grades III and IV neutropenia in group A. Like-ise, Karnofsky index evolution was assessed in 21 patientsf group A and in 24 patients of group B. Karnofsky indexorsened in 47.6% of cases in group A, and 25% in group.
During concurrent treatment, higher levels of hematolog-cal toxicity were detected in group A. A high incidence ofsophagitis and radiation pneumonitis was observed in bothroups, despite the reduction of the dose of gemcitabine inroup B. Finally, 17.6% of grades III and IV radiation dermati-is was detected in the patients who received 50 mg/m2 ofemcitabine.
Four toxic deaths occurred during the study, three inroup A and one in group B; all were due to radiation pneu-onitis.
.4. Response
esponses to induction and complete treatment were ana-yzed separately in the two groups. These results areesumed in Table 5. Response to induction could not benalyzed in five patients: two patients were not evaluables they did not complete a whole cycle of chemother-py; one patient was withdrawn from the study due to
hrombopenia and response assessment was not made; oneatient abandoned the study, and the fifth patient wasiagnosed of pulmonary tuberculosis, and response assess-ent was not performed satisfactorily. Likewise, responseo complete treatment could not be assessed in seven

66 R. Blanco et al.
Table 2 Compliance to treatmenta
Group A Group B Total
Patients who initiated induction 22 33 55
Interruption during induction 5 (22.7%) 6 (18.1%) 11 (20%)
CausesToxicity 1 1 2Adverse event (not toxicity) 1 1 2Death 1 0 1Patient/investigator’s request 1 2 3Progression 1 2 3
Patients who initiated concurrence 17 27 44
Interruption during concurrence 8 (47.0%) 8 (29.6%) 16 (36.3%)
CausesToxicity 4 6 10Adverse event (not toxicity) 1 0 1Death 0 0 0Patient/investigator’s request 2 0 2Progression 1 1 2Transgression of protocol 0 1 1
Treatment completed 9 (40.9%) 19 (57.5%) 28 (50.9%)a Only eligible patients.
Table 3 Toxicity of induction (only grades III and IV)
Toxicity Group A (22 patients) Group B (34 patients) Total (56 patients)
n % n % n %
Vomiting 6 30 1 3.1 7 13.5Neutropenia 6 30 6 18.8 12 23.1Thrombopenia 2 10 2 6.2 4 7.7Anaemia — — 1 3.1 1 2.3Febrile neutropenia 1 5 1 3.1 2 3.8Asthenia 1 5 1 3.1 2 3.8Anorexia — — 1 3.1 1 1.9Pruritus — — 1 3.1 1 1.9Diarrhea — — 1 3.1 1 1.9Transaminases — — 1 3.1 1 1.9
Table 4 Toxicity of concurrence (only grades III—V)
Toxicity Group A (17 patients) Group B (27 patients) Total (44 patients)
n % n % n %
Anaemia 1 5.8 — — 1 2.2Thrombopenia 6 35.2 1 3.7 7 15.9Neutropenia 4 23.5 — — 4 8.8Infection 1 5.8 — — 1 2.2Esophagitis 6 35.2 9 33.3 15 34.0Radiation pneumonitis 4 23.5 7 25.9 11 25Radiation dermatitis 3 17.6 1 3.7 4 8.8Thromboembolic accidents 2 11.7 — — 2 4.4Hemolytic-uremic syndrome 1 5.8 — — 1 2.2

Final results of a phase II study 67
Table 5 Response
Group A (22 patients) Group B (33 patients) Total (55 patients)
n % n % n %
InductionNot assessable 1 4.5 1 3 2 3.6Not available 1 4.5 2 6 3 5.4Stable disease 8 36.3 13 39.3 21 38.1Progression of disease 1 4.5 1 3 2 3.6Complete response 3 13.6 1 3 4 7.2Partial response 8 36.3 15 45.4 23 41.8Global response 11 50 16 48.4 27 49.1
Complete treatmentNot assessable 1 4.5 1 3 2 3.6Not available 2 9 3 9 5 9Stable disease 2 9 3 9 5 9Progression of disease 2 9 5 15.1 7 12.7Complete response 4 18.1 4 12 8 14.4
17 51.5 28 50.921 63.6 36 65.4
3.7. Evaluation of response and radiologicalfollow-up
A poor correlation between radiological and clinical out-come of the cases was persistent throughout the study:many patients underwent radiological assessment of diseasepersistence, or even progression, while a favorable clinicalevolution was evidenced (Fig. 3). However, this correlation
Partial response 11 50Global response 15 68.1
patients (the five aforementioned plus one patient in eachgroup who died after finalizing concurrence before responseassessment). In short, global response rate to inductiontreatment was 50 and 48.4% for groups A and B. Globalresponse rate to complete treatment was 68.1% for groupA and 63.6% for group B. Overall global response was 49.1%for induction treatment and 65.4% for complete treat-ment.
3.5. Time to progression and survival assessment
With a mean follow-up of 41.2 months, median time elapsedfrom treatment initiation to the first progression was 9.8months in group A and 10.7 months in group B.
Mean survival was 11.3 months for group A (95% CI5.7—19.0) and 21.5 months for group B (CI 95% 9.5—27.6).Overall mean survival was 17.7 months (95% CI 9.5—24.3).Three-year survival for the whole group of patients was 20%.Figs. 1 and 2 represent progression-free and global survivalin groups A and B and in the whole population.
3.6. Sites of first failure
Information about the first progression was not available in19 cases. All these patients were prematurely withdrawnfrom the study because of early death, toxicity, adverseevent or patient/investigator’s request. Progression was notobserved in 5 of the 55 patients eligible (9.1%). Informa-tion about the site of first progression was obtained inthe remaining 31 patients. Twenty-three different locationswere described, lung and bone being the most frequent.First progression was metastatic spread alone in 13 of these
31 patients. Thus, local control was achieved in 18/55patients (32.7%). In the remaining 18 patients locoregionalrelapse was demonstrated, with or without synchronousmetastasis. In five patients, first relapse was disseminationin the central nervous system.Fig. 1 (A) Progression-free survival of groups A and B. Meanprogression-free survival—–group A: 9.8 months; group B: 10.7months. (B) Overall progression-free survival. Mean progression-free survival: 10.7 months.

68
Fgs
wi
4
Iclucarner
pNbticpt
gbgio
ht
wtfat
ttwtrmrficcTtebofte2C
la[otgi
imIoofcgtrsat[lcrioiot
ig. 2 (A) Overall survival of groups A and B. Mean survival—–roup A: 11.3 months; group B: 21.5 months. (B) Global overallurvival. Mean survival: 17.7 months.
as not systematically analyzed, as it was not contemplatedn the original design of the study.
. Discussion
n our study, we analyzed the efficacy and toxicity of con-omitant radiotherapy with gemcitabine administered atow doses twice a week, in patients with locally advancednresectable NSCLC, following three cycles of inductionhemotherapy with cisplatin and gemcitabine. Our resultsre encouraging with regard to efficacy objectives: responseate and global and progression-free survival. However, theonhematological toxicity detected, though not very differ-nt from that communicated in other concurrence studies,emains excessive.
Global response rate to complete treatment (65%) is com-arable to that communicated in other larger trials [6,7].evertheless, radiological assessment of response may note a good method to assess the real efficacy of this type ofreatment, as will be discussed further. The response rate tonduction treatment (50% for group A and 48.4% for group B)onfirmed our hypothesis when designing the study. We mustoint out the similarity of these two percentages, despitehe reduction of the cisplatin dose in group B.
Overall mean survival was 17.7 months (11.3 months forroup A and 21.5 months for group B). This difference maye explained by several reasons: treatment compliance inroup B was better; investigators may have been stricter
n selection of patients of group B, because of the toxicitybserved in group A.With regard to toxicity assessment, we point out theigher incidence of grades III and IV vomiting during induc-ion in group A patients. A higher incidence of functional
s2
or
R. Blanco et al.
orsening during induction — measured by the decrease inhe Karnofsky index — was also evidenced in this group. Thisunctional worsening was considered by the investigators asn important cause of further toxicity and withdrawal fromhe study during concurrence.
Undoubtedly, the main concern of the authors duringhe trial was the toxicity detected during CCR. We ini-ially chose a gemcitabine dose of 50 mg/m2 for concurrenceith radiotherapy, based on very preliminary results of
he Blackstock study, presented in ASTRO 1999 [17]. Finalesults of this study were published in 2001 [21]. A maxi-um tolerable dose of 35 mg/m2 was then confirmed. These
eports overlapped with our own results, obtained for therst 22 patients. We did detect an excessive hematologi-al and nonhematological toxicity during CCR. Subsequently,oncurrence gemcitabine dose was adjusted to 35 mg/m2.he incidence of hematological toxicity was decreased inhe further 33 patients (group B). However, no differ-nce in esophagitis or pneumonitis incidence was observedetween the two groups, despite the reduction of the dosef gemcitabine. Esophagitis was the most frequent causeor treatment interruption. However, we must point outhe high prevalence of esophagitis in other studies thatxplore concurrence: 17% in SWOG/9504 [7]; 52, 39, and5% in the gemcitabine, paclitaxel and vinorelbine arms ofALGB/9431 [6].
The risk factors for developing esophagitis were ana-yzed in a retrospective study of 215 patients with locallydvanced lung cancer treated with CCR and 3D planning22]. In this report, the incidence of esophagitis grade IIIr IV was 20.5%. The predictive factors of developing thisoxicity were the median dose administered to the esopha-us, and the parameters related to the volume of esophagusrradiated.
Although esophagitis was the main cause for treatmentnterruption in our study, radiation pneumonitis was theost frightening toxicity. It caused four deaths in our study.
n several cases, pneumonitis did not lead to an interruptionf treatment, as it appeared during the first or second monthf follow-up. Several predictive factors have been publishedor the development of pneumonitis in patients treated withoncomitant CCR. These factors could be divided in tworoups: patient-dependent factors, and those dependent onhe technique of radiotherapy used. Amongst the patient-elated factors, Robnett et al. describe a low-performancetatus, female sex and FEV1 < 2 L [23]. Other authors havelso mentioned a higher risk in patients with chronic obstruc-ive pulmonary disease [24,25]. Likewise, a Japanese study26] relates the apparition of pneumonitis with the serumevels of KL-6, an antibody against human lung adenocar-inoma. Regarding risk factors related to the technique ofadiotherapy or dosimetric aspects, we can mention therradiation of the lower lung lobes [27,28], the mean dosef radiotherapy administered in the lungs [24,29,30], therradiation of contralateral mediastinum [31], and the V-20r percentage of pulmonary volume irradiated with morehan 20 Gy [24,32,33]. The risk of pneumonitis grade II or
uperior seems to be 8—18% in patients with a V-20 over0%.Ever-improving knowledge of these factors and continu-us progress in planning techniques and administration ofadiotherapy will allow the reduction of toxicities in CCR
Final results of a phase II study 69
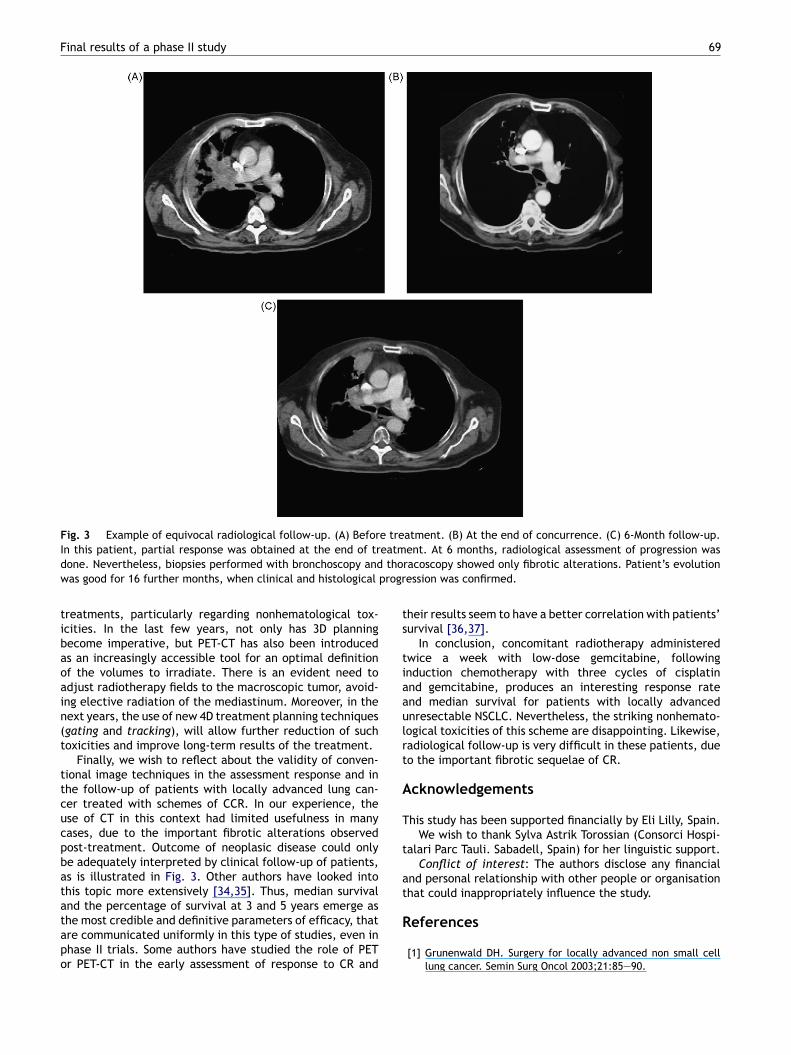
Fig. 3 Example of equivocal radiological follow-up. (A) Before treatment. (B) At the end of concurrence. (C) 6-Month follow-up.eatmtho
progr
ts
tiaaulrt
A
T
t
at
In this patient, partial response was obtained at the end of trdone. Nevertheless, biopsies performed with bronchoscopy andwas good for 16 further months, when clinical and histological
treatments, particularly regarding nonhematological tox-icities. In the last few years, not only has 3D planningbecome imperative, but PET-CT has also been introducedas an increasingly accessible tool for an optimal definitionof the volumes to irradiate. There is an evident need toadjust radiotherapy fields to the macroscopic tumor, avoid-ing elective radiation of the mediastinum. Moreover, in thenext years, the use of new 4D treatment planning techniques(gating and tracking), will allow further reduction of suchtoxicities and improve long-term results of the treatment.
Finally, we wish to reflect about the validity of conven-tional image techniques in the assessment response and inthe follow-up of patients with locally advanced lung can-cer treated with schemes of CCR. In our experience, theuse of CT in this context had limited usefulness in manycases, due to the important fibrotic alterations observedpost-treatment. Outcome of neoplasic disease could onlybe adequately interpreted by clinical follow-up of patients,as is illustrated in Fig. 3. Other authors have looked intothis topic more extensively [34,35]. Thus, median survival
and the percentage of survival at 3 and 5 years emerge asthe most credible and definitive parameters of efficacy, thatare communicated uniformly in this type of studies, even inphase II trials. Some authors have studied the role of PETor PET-CT in the early assessment of response to CR andR
ent. At 6 months, radiological assessment of progression wasracoscopy showed only fibrotic alterations. Patient’s evolutionession was confirmed.
heir results seem to have a better correlation with patients’urvival [36,37].
In conclusion, concomitant radiotherapy administeredwice a week with low-dose gemcitabine, followingnduction chemotherapy with three cycles of cisplatinnd gemcitabine, produces an interesting response ratend median survival for patients with locally advancednresectable NSCLC. Nevertheless, the striking nonhemato-ogical toxicities of this scheme are disappointing. Likewise,adiological follow-up is very difficult in these patients, dueo the important fibrotic sequelae of CR.
cknowledgements
his study has been supported financially by Eli Lilly, Spain.We wish to thank Sylva Astrik Torossian (Consorci Hospi-
alari Parc Tauli. Sabadell, Spain) for her linguistic support.Conflict of interest: The authors disclose any financial
nd personal relationship with other people or organisationhat could inappropriately influence the study.
eferences
[1] Grunenwald DH. Surgery for locally advanced non small celllung cancer. Semin Surg Oncol 2003;21:85—90.
7
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
0
[2] Naruke T. Surgery in locally advanced non-small cell lung can-cer. Lung Cancer 2003;42(Suppl. 2):S11—5 [36 ref.].
[3] Curran W, Scott C, Langer C, Komaki R, Lee JS, Hauser S, etal. Long-term benefit is observed in a phase III comparison ofsequential versus concurrent chemoradiation for patients withunresected stage III non small cell lung cancer: Radiation Ther-apy Oncology Group 9410. Proc Am Soc Clin Oncol 2003;22:621(abstract 2499).
[4] Furuse K, Fukuoka M, Kawahara M, Nishikawa H, Takada Y,Kudoh S, et al. Phase III study of concurrent versus sequentialthoracic radiotherapy in combination with misogynic, intes-tine, and cisplatin in unresectable stage III non-small-cell lungcancer. J Clin Oncol 1999;17:2692—9.
[5] Zatloukal P, Petruzelka L, Zemanova M, Havel L, Janku F, JudasL, et al. Concurrent versus sequential chemoradiotherapy withcisplatin and vinorelbine in locally advanced non-small cell lungcancer: a randomized study. Lung Cancer 2004;46:87—98.
[6] Vokes EE, Herndon II JE, Crawford J, Leopold KA, PerryMC, Miller AA, et al. Randomized phase II study of cisplatinwith gemcitabine or paclitaxel or vinorelbine as inductionchemotherapy followed by concomitant chemoradiotherapyfor stage IIIB non-small-cell lung cancer: cancer and leukemiagroup B study 9431. J Clin Oncol 2002;20:4191—8.
[7] Gandara DR, Chansky K, Albain KS, Leigh BR, Gaspar LE, Lara JrPN, et al., Southwest Oncology Group. Consolidation docetaxelafter concurrent chemoradiotherapy in stage IIIB non-small-cell lung cancer: phase II Southwest Oncology Group StudyS9504. J Clin Oncol 2003;21:2004—10.
[8] Fossella FV, Zinner RG, Komaki R, Lu R, Lee JS, Glisson BS,et al. Gemcitabine with concurrent chest radiation followedby consolidation gemcitabine plus cisplatin: a phase I trial forpatients with stage III nonsmall cell lung cancer (NSCLC). Eur JCancer 2001;37(Suppl. 6):S53—4.
[9] Gregor A, Price A, van der Leest AHD, Scalliet P, Wets M,Jungnelius U, et al. Phase I study of gemcitabine and radio-therapy in stage III non-small cell lung cancer. Proc Am SocClin Oncol 1999;18:1953a.
10] Trodella L, Granone P, Valente S, Turriziani A, Macis G, CorboGM, et al. Phase I trial of weekly gemcitabine and concurrentradiotherapy in patients with inoperable nonsmall-cell lungcancer. J Clin Oncol 2002;20(3):804—10.
11] Van Putten JWG, Price A, van der Leest AHD, Gregor A, LittleFA, Groen HJM. A Phase I study of gemcitabine with concurrentradiotherapy in stage III, locally advanced non-small cell lungcancer. Clin Cancer Res 2003;9:2472—7.
12] Goor C, Scalliet P, Van Meerbeek J, et al. A phase II study com-bining gemcitabine and radiotherapy in stage III NSCLC. Proc21st ESMO Ann Oncol 1996;7(Suppl. 5):101a.
13] Salinas J, Serna A, de la Fuente I, de las Heras M, GarcıaR, Fernandez J. Gemcitabina como radiosensibilizante en elcarcinoma no microcıtico de pulmon estadio III. Estudio faseI—II en pacientes con quimioterapia neoadyuvante. Rev Oncol2001;3(Suppl. 1):163.
14] Zajusz A, Zielonka I, Sygula D, Plewicki G, Nowicka E, BehrendtK, et al. Concurrent thoracic radiotherapy and weekly gemc-itabine in an advanced non-small cell lung cancer. RadiotherOncol 2000;56(Suppl. 1):S66.
15] Athanasiou E, Cyrgias G, Boinis K, Samantas E, Christodouli-dou M, Tamvaki F, et al. Concurrent chemoradiotherapy withgemcitabine for locally advanced non-small cell lung cancer:preliminary results of a phase II study. Proc 23rd ESMO AnnOncol 1998;9:468a.
16] Fields MT, Eisbruch A, Normolle D, Orfali A, Davis MA, Pu
AT, et al. Radiosensitization produced in vivo by once- vs.twice-weekly 2′2′-difluoro-2′-deoxycytidine (gemcitabine). IntJ Radiat Oncol Biol Phys 2000;47:785—91.17] Blackstock AW, Case LD, Richards F, White D, Petty M,Scarantino C, et al. Twice-weekly gemcitabine and concur-
[
R. Blanco et al.
rent thoracic radiotherapy. A phase I/II study in patients withadvanced non-small cell lung cancer (NSCLC). Proc 41st ASTROInt J Radiat Oncol Bio Phys 1999;45(Suppl. 3), 242.183a.
18] Armstrong JG. Target volume definition for three-dimensionalconformal radiation therapy of lung cancer. Br J Radiol1998;71:587—94.
19] ICRU. International Commission of Radiation Units and Mea-surements. Report 50 (1993) and Report 62 (1999).
20] Kaplan E, Meier P. Nonparametric estimation from incompleteobservations. J Am Stat Assoc 1958;53:457—81.
21] Blackstock AW, Lesser GJ, Fletcher-Steede J, Case LD, TuckerRW, Russo SM, et al. Phase I study of twice-weekly gemcitabineand concurrent thoracic radiation for patients with locallyadvanced non-small-cell lung cancer. Int J Radiat Oncol BiolPhys 2001;51:1281—9.
22] Wei X, Liu HH, Tucker SL, Liao Z, Hu C, Mohan R, et al.Risk factors for acute esophagitis in non-small-cell lung cancerpatients treated with concurrent chemotherapy and three-dimensional conformal radiotherapy. Int J Radiat Oncol BiolPhys 2006;66:100—7.
23] Robnett TJ, Machtay M, Vines EF, McKenna MG, Algazy KM,McKenna WG. Factors predicting severe radiation pneumonitisin patients receiving definitive chemoradiation for lung cancer.Int J Radiat Oncol Biol Phys 2000;48:89—94.
24] Rancati T, Ceresoli GL, Gagliardi G, Schipani S, Catta-neo GM. Factors predicting radiation pneumonitis in lungcancer patients: a retrospective study. Radiother Oncol2003;67:275—83.
25] Inoue A, Kunitoh H, Sekine I, Sumi M, Tokuuye K, Saijo N. Radia-tion pneumonitis in lung cancer patients: a retrospective studyof risk factors and the long-term prognosis. Int J Radiat OncolBiol Phys 2001;49:649—55.
26] Hara R, Itami J, Komiyama T, Katoh D, Kondo T. Serum levelsof KL-6 for predicting the occurrence of radiation pneumoni-tis after stereotactic radiotherapy for lung tumors. Chest2004;125:340—4.
27] Yamada M, Kudoh S, Hirata K, Nakajima T, Yoshikawa J. Riskfactors of pneumonitis following chemoradiotherapy for lungcancer. Eur J Cancer 1998;34:71—5.
28] Yorke ED, Jackson A, Rosenzweig KE, Merrick SA, Gabrys D,Venkatraman ES, et al. Dose-volume factors contributing tothe incidence of radiation pneumonitis in nonsmall-cell lungcancer patients treated with three-dimensional conformalradiation therapy. Int J Radiat Oncol Biol Phys 2002;54:329—39.
29] Kwa SLS, Lebesque JV, Theuws JC, Marks LB, Munley MT, BentelG, et al. Radiation pneumonitis as a function of mean lung dose:an analysis of pooled data of 540 patients. Int J Radiat OncolBiol Phys 1998;42:1—9.
30] Hernando ML, Marks LB, Bentel GC, Zhou SM, Hollis D, Das SK, etal. Radiation-induced pulmonary toxicity: a dose-volume his-togram analysis in 201 patients with lung cancer. Int J RadiatOncol Biol Phys 2001;51:650—9.
31] Makimoto T, Tsuchiya S, Hayakawa K, Saitoh R, Mori M. Riskfactors for severe radiation pneumonitis in lung cancer. Jpn JClin Oncol 1999;29:192—7.
32] Graham MV, Purdy JA, Emami B, Harms W, Bosch W, Lockett MA,et al. Clinical dose-volume histogram analysis for pneumonitisafter 3D treatment for non-small cell lung cancer (NSCLC). IntJ Radiat Oncol Biol Phys 1999;45:323—9.
33] Tsujino K, Hirota S, Endo M, Obayashi K, Kotani Y, SatouchiM, et al. Predictive value of dose-volume histogram param-eters for predicting radiation pneumonitis after concurrent
chemoradiation for lung cancer. Int J Radiat Oncol Biol Phys2003;55:110—5.34] Werner-Wasik M, Xiao Y, Pequignot E, Curran WJ, Hauck W.Assessment of lung cancer response after nonoperative ther-apy: tumor diameter, bidimensional product, and volume—–a

[
Final results of a phase II study
serial CT scan-based study. Int J Radiat Oncol Biol Phys2001;51:56—61.
[35] Lever AM, Henderson D, Ellis DA, Corris PA, Gilmartin JJ. Radia-
tion fibrosis mimicking local recurrence in small cell carcinomaof the bronchus. Br J Radiol 1984;57:178—80.[36] Hicks RJ, Kalff V, Mac Manus MP, Ware RE, McKenzie AF,Matthews JP, et al. The utility of 18F-FDG PET for suspectedrecurrent non-small cell lung cancer after potentially curative
71
therapy: impact on management and prognostic stratification.J Nucl Med 2001;42:1605—13.
37] Mac Manus MP, Hicks RJ, Matthews JP, McKenzie A, Rischin D,
Salminen EK, et al. Positron emission tomography is superiorto computed tomography scanning for response-assessmentafter radical radiotherapy or chemoradiotherapy in patientswith non-small-cell lung cancer. J Clin Oncol 2003;21:1285—92.



















