
In vivo efficacy of azithromycin in treatment of systemic infection and septic arthritis induced by...
10
ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, Sept. 1995, p. 1938–1947 Vol. 39, No. 9 0066-4804/95/$04.0010 Copyright q 1995, American Society for Microbiology In Vivo Efficacy of Azithromycin in Treatment of Systemic Infection and Septic Arthritis Induced by Type IV Group B Streptococcus Strains in Mice: Comparative Study with Erythromycin and Penicillin G LUCIANA TISSI, 1 * CHRISTINA VON HUNOLSTEIN, 2 PAOLO MOSCI, 1 CLAUDIA CAMPANELLI, 1 FRANCESCO BISTONI, 1 AND GRAZIELLA OREFICI 2 Microbiology Section, Department of Experimental Medicine and Biochemical Sciences, University of Perugia, 06122 Perugia, 1 and Laboratory of Bacteriology and Medical Mycology, Istituto Superiore di Sanita `, 00161 Rome, 2 Italy Received 11 November 1994/Returned for modification 13 April 1995/Accepted 15 June 1995 We compared the activities of azithromycin, erythromycin, and penicillin G in a mouse model of systemic infection and septic arthritis induced by type IV group B streptococci (GBS). The in vitro and in vivo efficacy data for these drugs were analyzed relative to the pharmacokinetics of the drugs in sera, joints, and kidneys. Adult CD-1 mice were infected intravenously with 10 7 CFU of type IV GBS. Intraperitoneal drug administra- tion was initiated with different dose regimens at different times after infection. A single dose of azithromycin (100 mg/kg) strongly reduced the incidence of articular lesions with respect to that with erythromycin or penicillin G. Treatment with azithromycin (three intraperitoneal administrations of 50 mg/kg at 12-h intervals) resulted in the complete prevention of arthritis. In contrast, erythromycin was poorly effective and penicillin G was effective only if inoculated 30 min after infection and at high doses (400,000 or 600,000 IU/kg). Furthermore, azithromycin was able to cure about 70% of the mice when administered 7, 8, and 9 days after GBS infection. Azithromycin was much more active than erythromycin and penicillin G with respect to bacterial killing in the joints and kidneys. In fact, cultures from these tissues were always negative no matter what treatment schedule was employed. The pharmacokinetics of azithromycin account for its superior in vivo efficacy against type IV GBS. A longer half-life and higher levels of this drug in serum and tissues with respect to those for erythromycin or penicillin G were achieved. The high affinity of azithromycin for the joints strongly supports its potential value for therapy of septic arthritis, which is a severe and frequent clinical manifestation of GBS infection. Streptococcus agalactiae, a group B streptococcus (GBS), is the most common cause of severe bacterial infection during the neonatal period (2, 6, 7). Invasive neonatal GBS infection has either an early (usually the first 24 h after birth) or late (7 days after birth) onset. Early-onset disease is acquired from the mother by the ascending route in the uterus during labor or by direct contact at delivery (5, 13, 20, 39). Late-onset disease may be acquired at birth from the mother or later in life from other individuals (3, 19). Common manifestations of GBS diseases include pneumonia, septicemia, meningitis, bacteremia, and bone or joint infections such as septic arthritis and osteomy- elitis (1, 7, 12, 28, 30). Although the dominance of GBS as a neonatal pathogen for nearly 2 decades has increased clinical awareness and facili- tated prompt diagnosis and aggressive therapy, permanent morbidity and mortality remain frequent outcomes. In addi- tion, treatment failure for reinfections, although rare, occurs even with optimal therapy by conventional standards (9, 25). Although penicillin G remains the drug of choice in the treat- ment of GBS infection, the clinical response is often poor (14, 31). Many reports have suggested that some strains may be penicillin tolerant (27, 35). Furthermore, infants with septic arthritis should receive at least 2 weeks of parenteral penicillin therapy, whereas those with bone involvement require 3 to 4 weeks of therapy to ensure a positive outcome (7). In vitro resistance to erythromycin, lincomycin, clindamycin, and tet- racycline has been demonstrated (10, 26). Azithromycin (CP 62-993) is a new macrolide which has been prepared semisynthetically from erythromycin. Azithro- mycin differs structurally from erythromycin by the presence of a methyl-substituted nitrogen at position 9a in the macrolide ring. This modification has produced significant advantages for azithromycin, such as better stability than erythromycin in the presence of an acidic pH (16), a longer half-life in serum, better tissue distribution with high peak levels, and a longer mean residence time (18, 21). In this study we assessed the efficacy of azithromycin in a previously described experimental mouse model of chronic infection and septic arthritis induced by type IV GBS (37). The activity of azithromycin was studied in comparison with those of erythromycin and penicillin G to determine whether the excellent pharmacokinetic profile of the drug could be bene- ficial in the treatment of GBS infections. Both prophylactic and therapeutic regimens were studied, and pharmacokinetic data were used to evaluate the possibility of low-dose admin- istration in a short schedule. MATERIALS AND METHODS Microorganism. A type IV GBS strain, reference strain GBS 1/82, was kindly supplied by J. Jelı ´nkova ´, Prague, Czechoslovakia. The microorganism was grown at 378C in Todd-Hewitt broth (Unipath Ltd., Basingstoke, Hampshire, England), and samples were stored at 2708C until used. For experimental infections, the * Corresponding author. Mailing address: Microbiology Section, Department of Experimental Medicine and Biochemical Sciences, University of Perugia, Via del Giochetto, 06122 Perugia, Italy. Phone: 39-75-585 3402. Fax: 39-75-585 3403. 1938
Transcript of In vivo efficacy of azithromycin in treatment of systemic infection and septic arthritis induced by...

ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, Sept. 1995, p. 1938–1947 Vol. 39, No. 90066-4804/95/$04.0010Copyright q 1995, American Society for Microbiology
In Vivo Efficacy of Azithromycin in Treatment of SystemicInfection and Septic Arthritis Induced by Type IV Group B
Streptococcus Strains in Mice: Comparative Studywith Erythromycin and Penicillin G
LUCIANA TISSI,1* CHRISTINA VON HUNOLSTEIN,2 PAOLO MOSCI,1 CLAUDIA CAMPANELLI,1
FRANCESCO BISTONI,1 AND GRAZIELLA OREFICI2
Microbiology Section, Department of Experimental Medicine and Biochemical Sciences, University of Perugia, 06122Perugia,1 and Laboratory of Bacteriology and Medical Mycology, Istituto Superiore di Sanita, 00161 Rome,2 Italy
Received 11 November 1994/Returned for modification 13 April 1995/Accepted 15 June 1995
We compared the activities of azithromycin, erythromycin, and penicillin G in a mouse model of systemicinfection and septic arthritis induced by type IV group B streptococci (GBS). The in vitro and in vivo efficacydata for these drugs were analyzed relative to the pharmacokinetics of the drugs in sera, joints, and kidneys.Adult CD-1 mice were infected intravenously with 107 CFU of type IV GBS. Intraperitoneal drug administra-tion was initiated with different dose regimens at different times after infection. A single dose of azithromycin(100 mg/kg) strongly reduced the incidence of articular lesions with respect to that with erythromycin orpenicillin G. Treatment with azithromycin (three intraperitoneal administrations of 50 mg/kg at 12-h intervals)resulted in the complete prevention of arthritis. In contrast, erythromycin was poorly effective and penicillinG was effective only if inoculated 30 min after infection and at high doses (400,000 or 600,000 IU/kg).Furthermore, azithromycin was able to cure about 70% of the mice when administered 7, 8, and 9 days afterGBS infection. Azithromycin was much more active than erythromycin and penicillin G with respect tobacterial killing in the joints and kidneys. In fact, cultures from these tissues were always negative no matterwhat treatment schedule was employed. The pharmacokinetics of azithromycin account for its superior in vivoefficacy against type IV GBS. A longer half-life and higher levels of this drug in serum and tissues with respectto those for erythromycin or penicillin G were achieved. The high affinity of azithromycin for the joints stronglysupports its potential value for therapy of septic arthritis, which is a severe and frequent clinical manifestationof GBS infection.
Streptococcus agalactiae, a group B streptococcus (GBS), isthe most common cause of severe bacterial infection duringthe neonatal period (2, 6, 7). Invasive neonatal GBS infectionhas either an early (usually the first 24 h after birth) or late (7days after birth) onset. Early-onset disease is acquired from themother by the ascending route in the uterus during labor or bydirect contact at delivery (5, 13, 20, 39). Late-onset disease maybe acquired at birth from the mother or later in life from otherindividuals (3, 19). Common manifestations of GBS diseasesinclude pneumonia, septicemia, meningitis, bacteremia, andbone or joint infections such as septic arthritis and osteomy-elitis (1, 7, 12, 28, 30).Although the dominance of GBS as a neonatal pathogen for
nearly 2 decades has increased clinical awareness and facili-tated prompt diagnosis and aggressive therapy, permanentmorbidity and mortality remain frequent outcomes. In addi-tion, treatment failure for reinfections, although rare, occurseven with optimal therapy by conventional standards (9, 25).Although penicillin G remains the drug of choice in the treat-ment of GBS infection, the clinical response is often poor (14,31). Many reports have suggested that some strains may bepenicillin tolerant (27, 35). Furthermore, infants with septicarthritis should receive at least 2 weeks of parenteral penicillin
therapy, whereas those with bone involvement require 3 to 4weeks of therapy to ensure a positive outcome (7). In vitroresistance to erythromycin, lincomycin, clindamycin, and tet-racycline has been demonstrated (10, 26).Azithromycin (CP 62-993) is a new macrolide which has
been prepared semisynthetically from erythromycin. Azithro-mycin differs structurally from erythromycin by the presence ofa methyl-substituted nitrogen at position 9a in the macrolidering. This modification has produced significant advantages forazithromycin, such as better stability than erythromycin in thepresence of an acidic pH (16), a longer half-life in serum,better tissue distribution with high peak levels, and a longermean residence time (18, 21).In this study we assessed the efficacy of azithromycin in a
previously described experimental mouse model of chronicinfection and septic arthritis induced by type IV GBS (37). Theactivity of azithromycin was studied in comparison with thoseof erythromycin and penicillin G to determine whether theexcellent pharmacokinetic profile of the drug could be bene-ficial in the treatment of GBS infections. Both prophylacticand therapeutic regimens were studied, and pharmacokineticdata were used to evaluate the possibility of low-dose admin-istration in a short schedule.
MATERIALS AND METHODS
Microorganism. A type IV GBS strain, reference strain GBS 1/82, was kindlysupplied by J. Jelınkova, Prague, Czechoslovakia. The microorganism was grownat 378C in Todd-Hewitt broth (Unipath Ltd., Basingstoke, Hampshire, England),and samples were stored at 2708C until used. For experimental infections, the
* Corresponding author. Mailing address: Microbiology Section,Department of Experimental Medicine and Biochemical Sciences,University of Perugia, Via del Giochetto, 06122 Perugia, Italy. Phone:39-75-585 3402. Fax: 39-75-585 3403.
1938

organism was cultured overnight in Todd-Hewitt broth and then washed anddiluted in serum-free RPMI 1640 medium (Flow Laboratories, McLean, Va.).The inoculum size was estimated turbidimetrically at 540 nm in a BeckmanDV-68 spectrophotometer (Beckman Instruments, Fullerton, Calif.). The num-ber of live bacterial cells was confirmed by enumeration of the CFU on Islamagar (Unipath Ltd.) plates containing 5% inactivated horse serum and incubatedunder anaerobic conditions. The desired number of bacteria, diluted in RPMImedium, was injected intravenously (i.v.) via the tail vein in a volume of 0.5 mlper mouse.Animals. Outbred CD-1 mice of both sexes, 8 to 10 weeks of age, were
obtained from Charles River Breeding Laboratories, Calco, Milan, Italy.Experimental GBS infection in mice. Chronic GBS infection was induced in
mice as previously described (37). Briefly, mice were challenged i.v. with 107 typeIV GBS and examined two or more times during day 1 after inoculation and thendaily for 2 months to evaluate the clinical features of the disease, in particular,the presence of joint inflammation. The time of onset, number of joints involved,incidence, duration of arthritis, and ankylosis were observed.Most of the animals were able to clear the infection from the blood, brain, and
lungs within 2 weeks and from the spleen and liver within 1 month. However, theanimals were unable to clear the microorganism from the joints and kidneysduring the 60-day observation period.About 80% of the mice challenged i.v. with type IV GBS manifested early
septic arthritis, which evolved from an active exudative synovitis to a permanentlesion characterized by irreversible joint damage and ankylosis. The joints mostinvolved were the ankle, wrist, and coxaphemoral joint and, less frequently, thetarsophalangeal, carpophalangeal, and interphalangeal joints.Antibiotics. Sodic penicillin G (Squibb, Anagni, Frosinone, Italy) was recon-
stituted in sterile distilled water and diluted to the desired concentration in salinesolution. Azithromycin (Pfizer Laboratories, Latina, Italy) and erythromycin(Sigma Chemical Co., St. Louis, Mo.) were used in a free-base form and pre-pared by homogenizing the powder in a standard diluent containing Methocel 15(0.5 g), polisorbate 80 (Tween 80) (1.0 g), carboxymethyl cellulose (low viscosity;10.0 g), sodium chloride (9.0 g), and water (984 ml). All drugs were administeredintraperitoneally (i.p.).In vitro antimicrobial susceptibility test. The GBS strain to be tested for
antimicrobial susceptibility was incubated for 18 h at 378C in Mueller-Hintonbroth (Unipath Ltd.). MICs were determined by the dilution broth method withinocula of 5 3 105 and 5 3 106 CFU/ml.The sodium salt of penicillin G (Sigma) at a potency of 1,670 IU/mg was
reconstituted to 2 mg/ml in distilled water. Azithromycin was reconstituted to 10mg/ml in absolute ethanol and then diluted in water to a final concentration of2 mg/ml. Erythromycin was reconstituted in a manner similar to that for azithro-mycin: 10 mg was solubilized in 300 ml of absolute ethanol and then diluted to 2mg/ml in distilled water.Antibiotic solutions were filter sterilized, and serial twofold dilutions were
made in Mueller-Hinton broth. Control tubes of Mueller-Hinton broth withoutantibiotics were included in each series of dilutions. Test and control tubes wereincubated at 378C for 24 h. The MIC was defined as the lowest concentration ofantibiotic at which no growth was observed upon visual inspection. MICs wereevaluated in four separate experiments.In vivo antimicrobial treatment. Different treatment schedules were em-
ployed. Each antibiotic was administered to mice in a single dose at 30 min and6, 12, and 24 h after i.v. infection with 107 type IV GBS. Penicillin G wasadministered at doses of 400,000 and 600,000 IU/kg; azithromycin and erythro-mycin were administered at 50 and 100 mg/kg. In other experiments, multipledoses of antibiotics were given at 12-h intervals starting 30 min or 6 h afterinfection. Specific treatment schedules are presented with the results. Otherstudies were performed to establish the therapeutic effects of antibiotics onrecovery from septic arthritis. In this case, all animals positive for articularlesions were treated with different drugs on days 7, 8, and 9 after infection. In allexperiments, control animals received the same volume of isotonic saline. Cu-mulative survival rates were recorded at 24-h intervals for 60 days.Histological studies.Mice, inoculated with 107 type IV GBS and treated or not
with antibiotics, were sacrificed every 2 days after infection. Specimens fromkidneys and joints were fixed in 10% formalin for 24 h. The joint specimens weresuccessively decalcified in 5% trichloroacetic acid for 7 days. All specimens weredehydrated, embedded in paraffin, sectioned at 5 to 7 mm, and stained withhematoxylin and eosin.Pharmacokinetic studies. The concentrations of azithromycin, erythromycin,
and penicillin G were examined simultaneously in healthy controls and infectedmice. Serum, kidney, and joint samples were collected from groups of 8 to 10mice at different intervals after multiple antibiotic treatments at 30 min and 1, 2,4, 8, 24, 48, 96, and 120 h after the last inoculation. Samples from antibiotic-treated mice were also collected immediately before the third administration(time zero). Blood samples were obtained by retroorbital sinus bleeding beforesacrifice, and sera were collected after centrifugation. Organs were asepticallyremoved, washed in sterile water, weighed, and then homogenized in 3 ml ofsterile RPMI medium.Joints of infected and control mice were removed, weighed, ground in a
mortar, and then resuspended in 1 ml of RPMI medium. All homogenates fromkidneys or joints were centrifuged, and supernatants were used for the assays.Antibiotic concentrations were determined by the agar well diffusion bioassay
with Micrococcus luteus ATCC 9341 as the bioassay organism (4, 21, 36). Stan-dard curves for each antibiotic were made with sera or supernatants of tissuehomogenates from control mice as described by Girard et al. (21). The sensitivityof the assay was about 0.1 mg/ml for azithromycin and erythromycin and 0.01IU/ml for penicillin G. The standard error of the assay was less than 10%. Thefollowing pharmacokinetic parameters were estimated by standard methods (24):the elimination half-life (t1/2), calculated by using linear least-squares regression;the maximal concentration observed (Cmax); the time to Cmax (Tmax); and thearea under the curve from 0 to 120 h (AUC), calculated by using the trapezoidalrule method. Furthermore, azithromycin levels in the joint homogenates weredetermined at 20, 30, and 40 days after infection.GBS recovery from organs and joints. Blood and kidney infections were
determined by CFU enumeration at 1, 5, 10, and 20 days after i.v. inoculation oftype IV GBS in mice treated or not with antibiotics. Joint samples from azithro-mycin-treated mice were also cultured 30 and 40 days postinfection. Bloodsamples were obtained by retroorbital sinus bleeding before sacrifice. The kid-neys were aseptically removed and placed in a tissue homogenizer with 3 ml ofsterile RPMI medium. After the organs were ground, appropriate 10-fold dilu-tions were made in RPMI medium and 0.2 ml of kidney suspension or blood wasplated in triplicate on Islam agar plates. The plates were then incubated underanaerobiosis at 378C for 48 h. CFU were counted, and the results were expressedas the number of CFU per milliliter of blood or per whole organ. The affectedjoints were removed, ground in a mortar, and resuspended in 1 ml of sterileRPMI medium. All samples were plated on Islam agar plates, and the resultswere expressed as the number of CFU per milliliter of homogenate and as thenumber of positive or negative cultures for the total number of animals exam-ined.Statistical analysis. Statistical analyses of the survival rate data and the inci-
dence of arthritis were performed with the models of McCullagh and Nelder (29)by estimating the probit or complementary log-log binomial models, according tothe pattern of the data. The fitted models are additive and involve the period oftreatment, the three-level factor corresponding to the three different drug treat-ments, and the two-level factor corresponding to the higher and lower dosesadministered. Differences in the effects of antibiotics, doses injected, and timesof treatment on the outcome were investigated by examining the significance ofthe corresponding parameter estimates relative to their asymptotic standarderrors associated with the fitted models. Differences in the numbers of CFU forthe treated and untreated groups were analyzed by Student’s t test. Each exper-iment was repeated three to five times.
RESULTS
In vitro antimicrobial susceptibility. A type IV GBS strainwas assayed for its susceptibility to penicillin G, erythromycin,and azithromycin. The MIC of penicillin G was 0.05 IU/ml,while that of erythromycin or azithromycin was 0.125 mg/ml.The MICs were not affected when the inoculum size was in-creased from 5 3 105 to 5 3 106 CFU/ml, and susceptibilitywas not influenced when a culture in the late exponential phaseor stationary phase was used.Protection studies. The effect of a single dose of antibiotic
on the survival of mice infected with type IV GBS was exam-ined (Table 1). The results show that no mice died whenpenicillin G was administered at a high dose (600,000 IU/kg)within the first 12 h after infection. Erythromycin was lesseffective; in fact, 100% of the mice survived only if the drug wasadministered at a dose of 50 mg/kg 30 min after GBS infectionor at a dose of 100 mg/kg 30 min or 6 h after infection. A singledose of azithromycin had a protective effect similar to thatobserved with penicillin G (Table 1).Better results were obtained with the multiple-dose treat-
ment. As shown in Table 2, no mice died with either dose ofpenicillin G when treatment was started 30 min after infection,while 400,000 IU/kg was required for 100% survival whentreatment was started 6 h after GBS inoculation.Erythromycin was effective only at the dose of 50 mg/kg.
Azithromycin was able to save 100% of the animals with alltreatment schedules and doses employed. Furthermore, allmice survived at a dose of 10 mg/kg (data not shown).Prevention of septic arthritis. Mice injected with type IV
GBS and treated with a single dose or multiple doses of anti-biotics were examined daily for 2 months to evaluate the pres-ence and the incidence of septic arthritis. As shown in Fig. 1,a single injection of penicillin G or erythromycin, given at
VOL. 39, 1995 IN VIVO EFFICACY OF AZITHROMYCIN IN GBS INFECTION 1939

different times after infection, was unable to prevent septicarthritis, even when high doses of antibiotics were employed. Asingle administration of penicillin G or erythromycin resultedin only a partial reduction of the incidence of articular lesionscompared with that in untreated controls (Fig. 1). Penicillin Gat the dose of 600,000 IU/kg and erythromycin at the dose of100 mg/kg given 30 min after GBS infection reduced the inci-dence of septic arthritis to 30 and 32.5%, respectively (Fig.1A). Better results were obtained with azithromycin; only 15%of the mice had articular lesions when this antibiotic was givenat the dose of 100 mg/kg 30 min after infection (Fig. 1B).When multiple-dose treatments were used, different re-
sponses were observed (Fig. 2). Penicillin G prevented articu-lar lesions only if inoculated at a high dose (400,000 IU/kg) notlater than 30 min after infection. Similar results were obtainedwith penicillin G at the dose of 600,000 IU/kg (data notshown). Erythromycin had a poor effect no matter what treat-ment schedule or dose was employed. In contrast, azithromy-cin totally suppressed articular lesions at the dose of 50 mg/kgand strongly reduced the incidence of arthritis at the dose of 25mg/kg.Recovery from arthritis: therapeutic regimens. Therapy was
started 7 days postinfection, when the incidence of arthritisreached the maximum level. Groups of animals with severearticular lesions were treated daily with penicillin G, erythro-mycin, or azithromycin on days 7, 8, and 9 after GBS inocula-tion, and recovery from arthritis and survival were evaluated
(Fig. 3). Azithromycin was the most effective drug, with 53.3and 70% of the animals cured at the doses of 50 and 100 mg/kg,respectively (Fig. 3A), while erythromycin cured only 16.6% ofthe mice when either dose was employed. Penicillin G also hada poor effect, with 16.6 and 26% recovery at the doses of400,000 and 600,000 IU/kg, respectively. Recovery from arthri-tis was always evaluated by clinical examination and confirmedby histopathology and negative bacterial counts. Survival rateswere enhanced by penicillin G at the dose of 600,000 IU/kg andby azithromycin at both doses used (Fig. 3B).GBS clearance from blood and kidneys.GBS clearance from
blood and kidneys in mice treated with multiple doses of an-tibiotics correlated with the survival rates (Table 3). Bloodsamples from drug-treated mice were always negative for GBSat each time point examined, while in untreated controls thenumber of CFU recovered progressively decreased from 2.1 3103 at day 2 postinfection to 0 on day 20.Remarkable differences in the numbers of CFU recovered
from the kidneys, depending on the antibiotic used, were evi-dent. GBS were undetectable in the kidneys of penicillin G-treated mice when the first dose of antibiotic was administered30 min after infection but not when treatment started 6 hpostchallenge, even if mice were able to clear the microorgan-isms within 10 days. Erythromycin treatment partially reducedthe number of CFU in the kidneys with respect to that foruntreated controls with both schedules; however, an elevatednumber of GBS was still present 20 days postinfection. Cul-tures from the kidneys of azithromycin-treated mice were al-ways negative at each time examined.Recovery of GBS from joints. Joints from antibiotic-treated
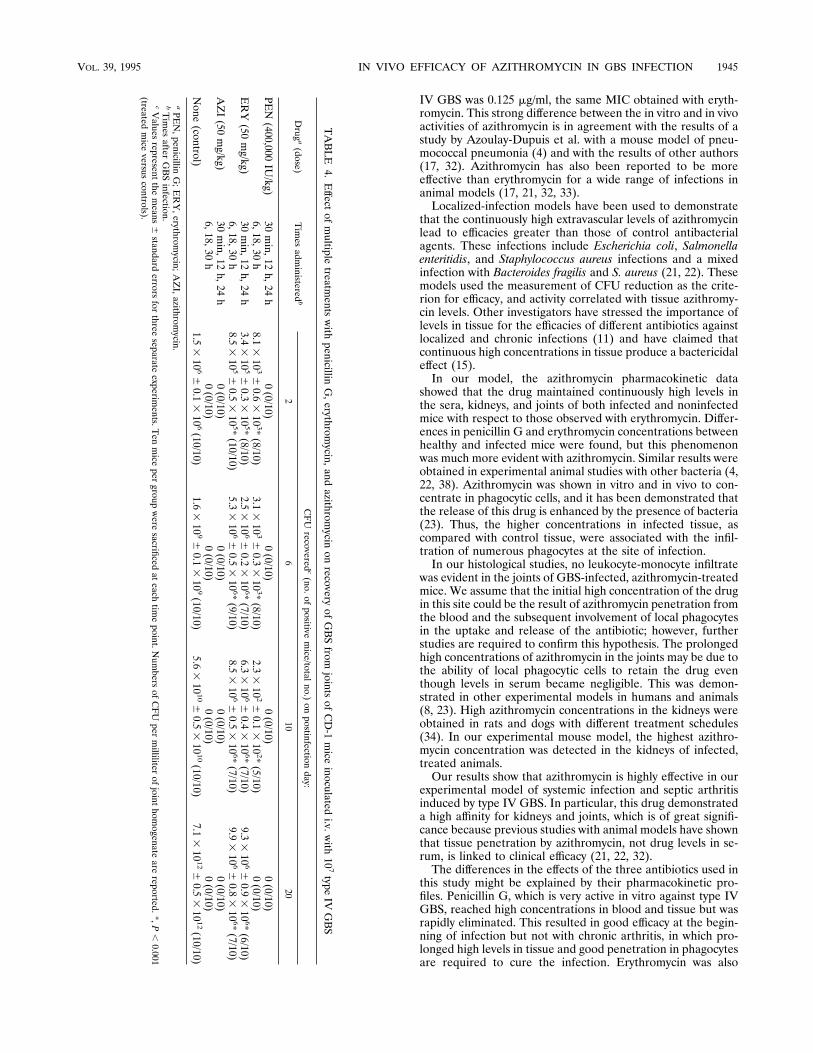
or control mice were removed, and specimens were cultured asdescribed in Materials and Methods at different times afterGBS infection (Table 4). Microorganisms were absent in jointsof animals treated with penicillin G (400,000 IU/kg) 30 minafter infection but not when treatment started 6 h later, eventhough the CFU counts were very low and the number ofpositive animals decreased progressively during the experi-mental period (Table 4).Treatment with erythromycin resulted in a reduced number
TABLE 1. Effect of single doses of penicillin G, erythromycin, andazithromycin on survival of CD-1 mice inoculated i.v. with 107 type
IV GBS
Druga Timeadministeredb Dose S/Tc
PEN 30 min 400,000 IU/kg 40/40600,000 IU/kg 40/40
6 h 400,000 IU/kg 40/40600,000 IU/kg 40/40
12 h 400,000 IU/kg 38/40600,000 IU/kg 40/40
24 h 400,000 IU/kg 36/40600,000 IU/kg 37/40
ERY 30 min 50 mg/kg 40/40100 mg/kg 40/40
6 h 50 mg/kg 37/40100 mg/kg 40/40
12 h 50 mg/kg 35/40100 mg/kg 36/40
24 h 50 mg/kg 33/40100 mg/kg 33/40
AZI 30 min 50 mg/kg 40/40100 mg/kg 40/40
6 h 50 mg/kg 40/40100 mg/kg 40/40
12 h 50 mg/kg 37/40100 mg/kg 40/40
24 h 50 mg/kg 35/40100 mg/kg 36/40
None (control) 26/40
a PEN, penicillin G; ERY, erythromycin; AZI, azithromycin.b Time after GBS infection.c S/T, number of surviving mice at 60 days/total number of animals tested.
Penicillin G treatment versus erythromycin treatment, P , 0.001; azithromycintreatment versus erythromycin treatment, P , 0.001; azithromycin treatmentversus penicillin G treatment, P . 0.1.
TABLE 2. Effect of multiple treatments with penicillin G,erythromycin, and azithromycin on survival of CD-1 mice inoculated
i.v. with 107 type IV GBS
Druga Times administeredb Dose S/Tc
PEN 30 min, 12 h, 24 h 200,000 IU/kg 40/40400,000 IU/kg 40/40
6, 18, 30 h 200,000 IU/kg 37/40400,000 IU/kg 40/40
ERY 30 min, 12 h, 24 h 25 mg/kg 36/4050 mg/kg 40/40
6, 18, 30 h 25 mg/kg 35/4050 mg/kg 40/40
AZI 30 min, 12 h, 24 h 25 mg/kg 40/4050 mg/kg 40/40
6, 18, 30 h 25 mg/kg 40/4050 mg/kg 40/40
None (control) 26/40
a PEN, penicillin G; ERY, erythromycin; AZI, azithromycin.b Times after GBS infection.c S/T, number of surviving mice at 60 days/total number of animals tested.
Penicillin G treatment versus erythromycin treatment, P , 0.001; azithromycintreatment versus erythromycin treatment, P , 0.001; azithromycin treatmentversus penicillin G treatment, P . 0.1.
1940 TISSI ET AL. ANTIMICROB. AGENTS CHEMOTHER.

of CFU with respect to that in untreated controls, but about107 microorganisms were still present in the joints in about70% of the animals 20 days after infection. In contrast, no GBSwere recovered from the joints of azithromycin-treated mice atany time point examined (Table 4). Joint cultures from azithro-mycin-treated mice were negative also at days 30 and 40postinfection. Azithromycin was never found in joint homoge-nates on days 20, 30, and 40 (data not shown).Drug concentrations in sera and organs. Erythromycin and
penicillin G were undetectable in the serum and organ samplescollected at time zero. In contrast, in the kidneys of nonin-fected mice, the azithromycin concentration was 11.6 mg/g, andin the sera, joints, and kidneys of infected mice, the azithro-mycin concentrations were 1.8 mg/ml and 11.3 and 16.1 mg/g,respectively. The antibiotic concentrations in the sera, joints,and kidneys of mice after multiple treatments are shown in Fig.4. Differences in concentrations in serum between healthy andinfected, azithromycin-treated mice were evident. In nonin-fected mice, measurable levels of drug were still present 4 hafter the last inoculation, with a t1/2 of 2.18 h, while in infectedanimals, azithromycin was detectable until 24 h, with a t1/2 of11.58 h. Furthermore, serum azithromycin concentrations in
infected mice were significantly higher than those in healthycontrols. Marked differences were also found in the elimina-tion and concentration of azithromycin in the joints and kid-neys of infected and noninfected mice. In the joints of healthycontrols, the drug was detectable up to 4 h after the lastinoculation, with a Cmax of 10.7 mg/g and a t1/2 of 1.4 h, whereasin the kidneys, azithromycin remained for 2 days, with a Cmaxof 27.4 mg/g and a t1/2 of 16.29 h. In the joints and kidneys ofinfected animals, azithromycin was detectable up to 4 daysafter the last inoculation, with a Cmax of 35.0 mg/g and a t1/2 of54.3 h for the joints and a Cmax of 80.5 mg/g and a t1/2 of 40.68h for the kidneys. Thus, the peak drug levels in the joints andkidneys of infected mice were about 3- to 3.5-fold higher thanthose in noninfected animals. The differences in the tissuepharmacokinetics of azithromycin between noninfected andinfected mice were most striking in terms of AUC. In fact, fornoninfected mice the azithromycin AUCs in sera, joints, andkidneys were 6.5 mg/ml/h, 26.0 mg/g/h, and 415.2 mg/g/h, re-spectively, while for infected mice the respective AUCs in sera,joints, and kidneys were 62.0 mg/ml/h, 1972.9 mg/g/h, and2400.9 mg/g/h (data not shown).The elimination of erythromycin from the sera and kidneys
FIG. 1. Effect of a single administration of penicillin G (h), erythromycin (z), or azithromycin (p) at 400,000 IU/kg, 50 mg/kg, and 50 mg/kg, respectively(A), or at 600,000 IU/kg, 100 mg/kg, and 100 mg/kg, respectively (B), on the incidence of articular lesions induced by i.v. inoculation of 107 type IV GBS. Mice receiveda single i.p. dose of antibiotics at different times after GBS infection. In each experiment 40 mice were used. Values are the means for three separate experiments.Standard errors which were always ,10%, have been omitted.■, controls. Penicillin G treatment versus erythromycin treatment, P , 0.05; azithromycin treatmentversus erythromycin treatment, P , 0.001; azithromycin treatment versus penicillin G treatment, P , 0.001.
VOL. 39, 1995 IN VIVO EFFICACY OF AZITHROMYCIN IN GBS INFECTION 1941

was more rapid. In both noninfected and infected mice, eryth-romycin was undetectable 2 h after the last inoculation. Drugconcentrations were slightly higher in infected animals, but thet1/2s of erythromycin in the sera and kidneys were similar innoninfected and infected mice (t1/2s ranged between 0.4 to 0.6h). Erythromycin was never found in the joints of healthy orinfected mice. The AUCs for erythromycin were very low: 7.2mg/ml/h and 10.4 mg/g/h, respectively, for sera and kidneys ofnoninfected mice and 9.4 mg/ml/h and 10.2 mg/g/h, respectively,for sera and kidneys of infected mice (data not shown).Penicillin G reached very high levels in the sera and tissues
of mice but was quickly eliminated, with t1/2s ranging between0.4 to 0.9 h. In this case also, the drug concentrations werehigher in infected mice (Fig. 4).Histopathology. As previously described (37), in control
mice the main kidney lesions detected on day 4 after infectionconsisted of isolated suppurative foci in the cortex with neu-trophilic infiltrates surrounding a central necrotic area. Oneweek after infection, many of these inflammatory foci werepresent in the cortical and medullary zones, and the suppura-tive lesions became chronic 20 days after infection. Fibroblastic
areas progressively replaced the suppurative necrotized areasuntil tissue sclerosis was observed.In the affected joints, 48 h after infection, an acute exudative
synovitis and a polymorphonuclear leukocyte-monocyte infil-trate of the subsinovium and periarticular connective tissueswere observed. One week later, the articular cavity was filledwith purulent exudate, and joint destruction progressed rapidlyuntil fibrous ankylosis was observed on day 60.In mice treated with multiple doses of antibiotics, different
results were observed. In fact, the joints and kidneys of azithro-mycin-treated and penicillin-treated mice were always negativefor lesions at each time point examined. In contrast, the lesionsin the joints and kidneys of erythromycin-treated mice weresimilar in nature and extent to those of untreated, infectedcontrol animals.With regard to therapeutic treatments, great differences in
the histological results were observed. The joints of azithro-mycin-treated mice showed complete recovery 10 days afterthe conclusion of therapy, while penicillin G- and erythromy-cin-treated mice had articular lesions similar to those of con-trols.
FIG. 2. Effect of multiple administrations of penicillin G (h), erythromycin (z), or azithromycin (p) on the incidence of articular lesions induced by i.v.inoculation of 107 type IV GBS. Mice received three i.p. doses of antibiotics at 12-h intervals starting 30 min (A) or 6 h (B) after GBS infection. In each experiment40 mice were used. Values are the means for three separate experiments. Standard errors, which were always ,10%, have been omitted.■, controls. Penicillin Gtreatment versus erythromycin treatment, P , 0.05; azithromycin treatment versus erythromycin treatment, P , 0.001; azithromycin treatment versus penicillin Gtreatment, P , 0.05.
1942 TISSI ET AL. ANTIMICROB. AGENTS CHEMOTHER.

DISCUSSION
Penicillin G is the drug of choice in the treatment of GBSinfections (7). However, despite aggressive therapy by conven-tional standards, mortality and permanent morbidity are fre-quent outcomes. Even when very high doses and a treatmentcourse of 2 to 4 weeks have been employed, relapse or recur-rence of infection has occurred (9, 19). Therefore, an appro-priate adjustment in dosage is often necessary for a positiveoutcome.In this study we assessed the efficacy of azithromycin, a new
macrolide synthesized from erythromycin, in the treatment ofsystemic infection and septic arthritis induced in mice by typeIV GBS (37) and compared its activity with those of penicillinG and erythromycin.Our study showed that all three antibiotics tested were able
to completely protect mice when administered 30 min afterinfection but that only penicillin G and azithromycin wereeffective at the lowest doses when administered 6 h after in-fection. When multiple treatments were used, only azithromy-cin was completely effective with both treatment schedulesemployed.A single dose of azithromycin, erythromycin, or penicillin G
could not prevent arthritis, but also in this case, azithromycingave the best results. In fact, fewer azithromycin-treated micethan untreated controls showed articular lesions. The arthritisincidence was significantly reduced in azithromycin-treated an-imals compared with those treated with penicillin G or eryth-romycin.Different results were obtained with multiple treatments. In
this case, azithromycin was the most effective drug. At thehighest dose (50 mg/kg), no articular lesions were observedwhether treatment was started 30 min or 6 h after infection. Incontrast, penicillin G (400,000 IU/kg) was able to completelyprevent arthritis only if the first dose was given 30 min after
infection. Treatment with erythromycin resulted in a partialreduction in the incidence of arthritis.When the antibiotics were used for the therapy of infected
mice with arthritis, both penicillin G and azithromycin slightlyenhanced the percentage of survivors, while only azithromycinsignificantly reduced the percentage of articular lesions.Data on bacterial clearance from the blood, kidneys, and
joints strongly supported the high in vivo efficacy of azithro-mycin against type IV GBS. No GBS were found in the bloodor tissues of azithromycin-treated mice at each time pointexamined during the experimental period. Penicillin G wascompletely effective when treatment was started 30 min afterGBS infection but not when the drug was administered 6 hlater. The disappearance of GBS from the kidneys and joints ofpenicillin G-treated mice 10 days after infection was probablydue to the involvement of an immune response. In fact, duringthe infection with type IV GBS, high levels of specific antibod-ies and phagocytic cells, which could be associated with thekilling of bacteria, were reached only 10 to 15 days after in-fection (37). Thus, when the number of GBS is maintained atlow levels during the first days of infection, the host immunesystem can actively react against microorganisms. In contrast,mice treated with erythromycin maintained very high levels ofbacteria in both the kidneys and joints for more than 20 daysafter infection.When penicillin G, erythromycin, and azithromycin concen-
trations in the sera and tissues of infected and noninfectedmice were determined, great differences were observed. Peni-cillin G rapidly reached very high levels in the sera, joints andkidneys, with peak concentrations 1,000 to 6,500 times higherthan the MIC (the MIC of penicillin G against type IV GBSwas 0.05 IU/ml).The in vitro activity of azithromycin does not account for its
higher in vivo efficacy. The MIC of azithromycin against type
FIG. 3. Effect of penicillin G (h), erythromycin (z), or azithromycin (p) on recovery from arthritis (A) and on survival (B) of CD-1 mice inoculated i.v.with 107 type IV GBS. Animals with articular lesions were treated with antibiotics on days 7, 8, and 9 after GBS infection. In each experiment 30 mice were used. Valuesare the means for three separate experiments. Standard errors, which were always ,10%, have been omitted. ■, controls. (A) Penicillin G treatment versuserythromycin treatment, P . 0.1; azithromycin treatment versus erythromycin treatment, P , 0.001; azithromycin treatment versus penicillin G treatment, P , 0.001.(B) Penicillin G treatment versus erythromycin treatment, P , 0.05; azithromycin treatment versus erythromycin treatment, P , 0.001; azithromycin treatment versuspenicillin G treatment, P . 0.1.
VOL. 39, 1995 IN VIVO EFFICACY OF AZITHROMYCIN IN GBS INFECTION 1943

TABLE3.EffectofmultipletreatmentswithpenicillinG,erythromycin,andazithromycinonrecoveryofGBSfrom
bloodandkidneysofCD-1miceinoculatedi.v.with107typeIVGBS
Druga
(dose)
Times
admin-
isteredb
CFUrecoveredconpostinfectionday:
26
1020
Blood
Kidneys
Blood
Kidneys
Blood
Kidneys
Blood
Kidneys
PEN (400,000
IU/kg)
30min,
12h,
24h
00
00
00
00
6,18,
30h
01.1
3105
60.1
3105 *
01.1
3104
60.2
3104 *
00
00
ERY (50mg/kg)30min,
12h,
24h
01.1
3105
60.2
3105 *
03.6
3107
60.4
3107 *
08.1
3107
60.3
3107 *
03.0
3107
60.2
3107 *
6,18,
30h
00.9
3105
60.1
3105 *
09.1
3107
60.8
3107 *
01.2
3108
60.1
3108 *
02.4
3109
60.3
3109 *
AZI (50mg/kg)30min,
12h,
24h
00
00
00
00
6,18,
30h
00
00
00
00
None
(control)
2.1
3103
60.2
31032.0
3106
60.2
31067.2
3102
60.6
31024.1
3109
60.5
31092.4
3102
60.2
31025.8
3109
60.6
3109
04.1
31010
60.4
31010
aPEN,penicillinG;ERY,erythromycin;AZI,azithromycin.
bTimesafterGBSinfection.
cValuesrepresentthemeans
6standarderrorsforthreeseparateexperiments.Eightmicepergroupweresacrificedateachtimepoint.NumbersofCFUpermilliliterofbloodorforwholeorgansarereported.*,
P,0.001(treatedmiceversuscontrols).
1944 TISSI ET AL. ANTIMICROB. AGENTS CHEMOTHER.
IV GBS was 0.125 mg/ml, the same MIC obtained with eryth-romycin. This strong difference between the in vitro and in vivoactivities of azithromycin is in agreement with the results of astudy by Azoulay-Dupuis et al. with a mouse model of pneu-mococcal pneumonia (4) and with the results of other authors(17, 32). Azithromycin has also been reported to be moreeffective than erythromycin for a wide range of infections inanimal models (17, 21, 32, 33).Localized-infection models have been used to demonstrate
that the continuously high extravascular levels of azithromycinlead to efficacies greater than those of control antibacterialagents. These infections include Escherichia coli, Salmonellaenteritidis, and Staphylococcus aureus infections and a mixedinfection with Bacteroides fragilis and S. aureus (21, 22). Thesemodels used the measurement of CFU reduction as the crite-rion for efficacy, and activity correlated with tissue azithromy-cin levels. Other investigators have stressed the importance oflevels in tissue for the efficacies of different antibiotics againstlocalized and chronic infections (11) and have claimed thatcontinuous high concentrations in tissue produce a bactericidaleffect (15).In our model, the azithromycin pharmacokinetic data
showed that the drug maintained continuously high levels inthe sera, kidneys, and joints of both infected and noninfectedmice with respect to those observed with erythromycin. Differ-ences in penicillin G and erythromycin concentrations betweenhealthy and infected mice were found, but this phenomenonwas much more evident with azithromycin. Similar results wereobtained in experimental animal studies with other bacteria (4,22, 38). Azithromycin was shown in vitro and in vivo to con-centrate in phagocytic cells, and it has been demonstrated thatthe release of this drug is enhanced by the presence of bacteria(23). Thus, the higher concentrations in infected tissue, ascompared with control tissue, were associated with the infil-tration of numerous phagocytes at the site of infection.In our histological studies, no leukocyte-monocyte infiltrate
was evident in the joints of GBS-infected, azithromycin-treatedmice. We assume that the initial high concentration of the drugin this site could be the result of azithromycin penetration fromthe blood and the subsequent involvement of local phagocytesin the uptake and release of the antibiotic; however, furtherstudies are required to confirm this hypothesis. The prolongedhigh concentrations of azithromycin in the joints may be due tothe ability of local phagocytic cells to retain the drug eventhough levels in serum became negligible. This was demon-strated in other experimental models in humans and animals(8, 23). High azithromycin concentrations in the kidneys wereobtained in rats and dogs with different treatment schedules(34). In our experimental mouse model, the highest azithro-mycin concentration was detected in the kidneys of infected,treated animals.Our results show that azithromycin is highly effective in our
experimental model of systemic infection and septic arthritisinduced by type IV GBS. In particular, this drug demonstrateda high affinity for kidneys and joints, which is of great signifi-cance because previous studies with animal models have shownthat tissue penetration by azithromycin, not drug levels in se-rum, is linked to clinical efficacy (21, 22, 32).The differences in the effects of the three antibiotics used in
this study might be explained by their pharmacokinetic pro-files. Penicillin G, which is very active in vitro against type IVGBS, reached high concentrations in blood and tissue but wasrapidly eliminated. This resulted in good efficacy at the begin-ning of infection but not with chronic arthritis, in which pro-longed high levels in tissue and good penetration in phagocytesare required to cure the infection. Erythromycin was also
TABLE4.Effect
ofmultiple
treatments
withpenicillin
G,erythrom
ycin,andazithrom
ycinonrecovery
ofGBSfrom
jointsofCD-1miceinoculated
i.v.with107type
IVGBS
Drug
a(dose)
Timesadm
inisteredb
CFUrecovered
c(no.of
positivemice/totalno.)
onpostinfection
day:
26
1020
PEN(400,000
IU/kg)
30min,12
h,24h
0(0/10)
0(0/10)
0(0/10)
0(0/10)
6,18,30h
8.13103
60.6
3103*(8/10)
3.13103
60.3
3103*(8/10)
2.33102
60.1
3102*(5/10)
0(0/10)
ERY(50
mg/kg)
30min,12
h,24h
3.43105
60.3
3105*(8/10)
2.53106
60.2
3106*(7/10)
6.33106
60.4
3106*(7/10)
9.33106
60.9
3106*(6/10)
6,18,30h
8.53105
60.5
3105*(10/10)
5.33106
60.5
3106*(9/10)
8.53106
60.5
3106*(7/10)
9.93106
60.8
3106*(7/10)
AZI(50
mg/kg)
30min,12
h,24h
0(0/10)
0(0/10)
0(0/10)
0(0/10)
6,18,30h
0(0/10)
0(0/10)
0(0/10)
0(0/10)
None
(control)1.5
3106
60.1
3106(10/10)
1.63109
60.1
3109(10/10)
5.631010
60.5
31010(10/10)
7.131012
60.5
31012(10/10)
aPEN,penicillin
G;ERY,erythrom
ycin;AZI,azithrom
ycin.bTimesafter
GBSinfection.
cValues
representthe
means
6standard
errorsforthree
separateexperim
ents.Tenmiceper
groupwere
sacrificedateach
timepoint.N
umbers
ofCFUper
milliliter
ofjoint
homogenate
arereported.*,P
,0.001
(treatedmiceversus
controls).
VOL. 39, 1995 IN VIVO EFFICACY OF AZITHROMYCIN IN GBS INFECTION 1945

cleared very rapidly; in particular, this drug was never found inthe joints and was detected in the blood and kidneys for only 1or 2 h after administration. This can explain the high incidenceof arthritis, the persistence and increase in CFU, and the pooreffect in therapeutic regimens. On the basis of these observa-tions, we conclude that in our experimental model, multipledaily administrations of penicillin G or erythromycin couldenhance survival rates without significant differences in therecovery from arthritis.Azithromycin, with its prolonged t1/2 and high concentra-
tions in tissue, seems to be a very promising drug for the cureof acute and chronic GBS infections. In our model, its efficacyseems to be similar to, and sometimes better than, that ofpenicillin G. In particular, azithromycin could be employed in
the therapy of septic arthritis, which remains a severe andfrequent clinical manifestation of GBS infections.
ACKNOWLEDGMENTS
We are grateful to Renata Siniscalchi and Eileen Zannetti for sec-retarial and editorial assistance, to Raffaella Settimi for statisticalanalysis, and to Mario De Bernardi di Valserra, Institute of Pharma-cology, University of Pavia, for pharmacokinetic analysis.This work was supported in part by a CNR Target Project on Bio-
technology and Bioinstrumentation (contract 89.00262.70), Italy.
REFERENCES
1. Ancona, R. J., J. McAuliffe, T. R. Thompson, D. P. Speert, and P. Ferrieri.1979. Group B streptococcal sepsis with osteomyelitis and septic arthritis. Itsoccurrence with acute heart failure. Am. J. Dis. Child. 133:919–920.
2. Anthony, B. F., and D. M. Okada. 1977. The emergence of group B strep-tococci in infection of the newborn infant. Annu. Rev. Med. 28:355–369.
3. Anthony, B. F., D. M. Okada, and C. J. Hobel. 1979. Epidemiology of thegroup B streptococcus: maternal and nosocomial sources for infant acquisi-tions. J. Pediatr. 95:431–436.
4. Azoulay-Dupuis, E., E. Vallee, J. P. Bedos, M. Muffat-Joly, and J. J. Po-cilado. 1991. Prophylactic and therapeutic activities of azithromycin in amouse model of pneumococcal pneumonia. Antimicrob. Agents Chemother.35:1024–1028.
5. Baker, C. J. 1978. Early onset group B streptococcal disease. J. Pediatr.93:124–125.
6. Baker, C. J., and F. F. Barret. 1974. Group B streptococcal infection ininfants: the importance of the various serotypes. JAMA 230:1158–1160.
7. Baker, C. J., and M. S. Edwards. 1990. Group B streptococcal infections, p.743–811. In J. Remington and J. O. Klein (ed.), Infectious diseases of thefetus and newborn infants. The W. B. Saunders Co., Philadelphia.
8. Baldwin, D. R., R. Wise, J. M. Andrews, J. P. Ashby, and D. Honeybourne.1990. Azithromycin concentrations at the site of pulmonary infection. Eur.Respir. J. 3:886–890.
9. Barton, L. L., and N. K. Kapoor. 1982. Recurrent group B streptococcalinfection. Clin. Pediatr. 21:100–101.
10. Berkowitz, K., J. A. Regan, and E. Greenberg. 1990. Antibiotic resistancepattern of group B streptococci in pregnant women. J. Clin. Microbiol.28:5–7.
11. Chabbert, Y., F. Boyer, M. Saviard, H. Boulingre, and J. Herve. 1957.Determination de l’action bactericide in vivo des antibiotiques dans lastaphyloccie renale de la souris. Ann. Inst. Pasteur (Paris) 92:760–777.
12. Dan, M. 1983. Neonatal septic arthritis. Isr. J. Med. Sci. 19:967–971.13. Dillon, H. C., Jr., S. Khare, and B. M. Gray. 1987. Group B streptococcal
carriage and disease: a 6-year prospective study. J. Pediatr. 110:31–36.14. Dorand, R. D., and G. Adams. 1976. Relapse during penicillin treatment of
group B streptococcal meningitis. J. Pediatr. 89:188–190.15. Eagle, H. 1948. Speculation as to therapeutic significance of penicillin blood
levels. Ann. Intern. Med. 28:260–278.16. Fiese, E. F., and S. H. Steffen. 1990. Comparison of the acid stability of
azithromycin and erythromycin A. J. Antimicrob. Chemother. 25(Suppl.A):39–47.
17. Fitzgeorge, R. B., A. S. R. Featherstone, and A. Baskerville. 1990. Efficacy ofazithromycin in the treatment of guinea pigs infected with Legionella pneu-mophila by aerosol. J. Antimicrob. Chemother. 25(Suppl. A):101–108.
18. Foulds, G., R. M. Shepard, and R. B. Johnson. 1990. The pharmacokineticsof azithromycin in human serum and tissues. J. Antimicrob. Chemother.25(Suppl. A):73–82.
19. Gardner, S. E., E. O. Mason, Jr., and M. D. Yow. 1980. Community acqui-sition of group B streptococcus by infants of colonized mothers. Pediatrics66:873–875.
20. Gerards, L. J., B. P. Cats, and J. A. A. Hoogkamp-Korstanje. 1985. Earlyneonatal group B streptococcal disease: degree of colonization as an impor-tant determinant. J. Infect. 11:119–124.
21. Girard, A. E., D. Girard, A. R. English, T. D. Gooz, C. R. Cimochowski, J. A.Faiella, S. L. Haskell, and J. A. Retsema. 1987. Pharmacokinetic and in vivostudies with azithromycin (CP-62,993), a new macrolide with an extendedhalf-life and excellent tissue distribution. Antimicrob. Agents Chemother.31:1948–1954.
22. Girard, A. E., D. Girard, and J. A. Retsema. 1990. Correlation of theextravascular pharmacokinetics of azithromycin with in vivo efficacy in mod-els of localized infection. J. Antimicrob. Chemother. 25(Suppl. A):61–71.
23. Gladue, R. P., J. M. Bright, R. E. Isaacson, and F. Newborg. 1989. In vitroand in vivo uptake of azithromycin (CP-62, 993) by phagocytic cells: possiblemechanisms of delivery and release at sites of infection. Antimicrob. AgentsChemother. 33:277–282.
24. Greenblatt, D. J., and J. Koch-Weser. 1975. Clinical pharmacokinetics. N.Engl. J. Med. 297:702–705.
25. Haque, K. N., O. Bashir, and A. M. M. Kambal. 1986. Delayed recurrence of
FIG. 4. Mean antibiotic concentrations in sera and tissues of CD-1 miceinfected or not with 107 type IV GBS. Mice received three i.p. doses of azithro-mycin (50 mg/kg), erythromycin (50 mg/kg), penicillin G (400,000 IU/kg) at 12-hintervals starting 30 min after GBS infection or saline injection. Samples werecollected at 30 min and 1, 2, 4, 8, 24, 48, 72, 96, and 120 h after the last drugadministration. Values are the means for three separate experiments. Standarderrors, which were always ,10%, have been omitted. F, sera of noninfectedmice; E, sera of infected mice; ■, joints of noninfected mice;h, joints of infectedmice; å, kidneys of noninfected mice; Ç, kidneys of infected mice. The missingtime points on the curves correspond to undetectable levels of antibiotics. Eryth-romycin was never found in the joints of noninfected or infected mice.
1946 TISSI ET AL. ANTIMICROB. AGENTS CHEMOTHER.

group B streptococcal infection in a newborn infant: a case report. Am. Trop.Pediatr. 6:219–220.
26. Kim, K. S. 1985. Antimicrobial susceptibility of GBS. Antibiot. Chemother.35:83–89.
27. Kim, K. S., and B. F. Anthony. 1981. Penicillin tolerance in group B strep-tococci isolated from infected neonates. J. Infect. Dis. 144:411–419.
28. Lai, T. K., J. Hingston, and D. Scheifele. 1980. Streptococcal neonatalosteomyelitis. Am. J. Dis. Child. 134:711.
29. McCullagh, P., and J. A. Nelder. 1989. Generalized linear models, p. 98–148.Chapman & Hall, Ltd., London.
30. Memon, I. A., N. M. Jacobs, T. F. Yeh, and L. D. Lilien. 1979. Group Bstreptococcal osteomyelitis and septic arthritis. Its occurrence in infants lessthan 2 months old. Am. J. Dis. Child. 133:921–923.
31. Paredes, A., P. Wong, and M. D. Yow. 1976. Failure of penicillin to eradicatethe carrier state of group B streptococcus in infants. J. Pediatr. 89:191–193.
32. Retsema, J. A., A. E. Girard, D. Girard, and W. B. Milisen. 1990. Relation-ship of high tissue concentrations of azithromycin to bactericidal activity andefficacy in vivo. J. Antimicrob. Chemother. 25(Suppl. A):83–89.
33. Russell, C. J., C. Kodner, M. Russell, and D. Girard. 1990. In vitro and in
vivo susceptibility of Borrellia burgdorferi to azithromycin. J. Antimicrob.Chemother. 25(Suppl. A):33–38.
34. Shepard, R. M., and F. C. Falkner. 1990. Pharmacokinetics of azithromycinin rats and dogs. J. Antimicrob. Chemother. 25(Suppl. A):49–60.
35. Siegel, J. D., K. M. Shaman, and B. M. de Passe. 1981. Recurrent infectionassociated with penicillin-tolerant group B streptococci: a report of twocases. J. Pediatr. 99:920–924.
36. Simon, H. J., and E. J. Yin. 1970. Microbioassay of antimicrobial agents.Appl. Microbiol. 19:573–579.
37. Tissi, L., P. Marconi, P. Mosci, L. Merletti, P. Cornacchione, E. Rosati, S.Recchia, C. von Hunolstein, and G. Orefici. 1990. Experimental model oftype IV Streptococcus agalactiae (group B streptococcus) infection in micewith early development of septic arthritis. Infect. Immun. 58:3093–3100.
38. Vallee, E., E. Azoulay-Dupuis, J. J. Pocilado, and E. Bergogne-Berezin. 1992.Activity and local delivery of azithromycin in a mouse model of Haemophilusinfluenzae lung infection. Antimicrob. Agents Chemother. 36:1412–1417.
39. Weisman, E., B. J. Stoll, D. F. Cruess, R. T. Hall, G. B. Mereisten, V. G.Hemming, and G. W. Fischer. 1992. Early-onset group B streptococcal sep-sis: a current assessment. J. Pediatr. 121:428–433.
VOL. 39, 1995 IN VIVO EFFICACY OF AZITHROMYCIN IN GBS INFECTION 1947




















