
Development of a transmucosal technique for erythromycin delivery to treat gastroparesis
9
Development of a Transmucosal Technique for Erythromycin Delivery to Treat Gastroparesis RYAN MCLEMORE, 1 BRIAN LUNT, 1 SARAH SALAMEH, 1 JOHN K. DIBAISE, 2 MICHAEL D. CROWELL, 2 BRENT L. VERNON 1 1 Biomaterials Laboratory, Center for Interventional Biomaterials, School of Biological and Health Systems Engineering, Arizona State University, Tempe, Arizona 85287 2 Division of Gastroenterology, Mayo Clinic, Scottsdale, Arizona 85259 Received 25 August 2009; revised 27 October 2009; accepted 31 October 2009 Published online 28 December 2009 in Wiley InterScience (www.interscience.wiley.com). DOI 10.1002/jps.22037 ABSTRACT: Gastroparesis is a serious condition that limits meal or medication emptying from the stomach, resulting in a variety of symptoms, altered nutrition, and inconsistent medication delivery. Our aim was to develop a transmucosal system to deliver erythromycin (EM), a gastric prokinetic agent, to bypass intestinal absorption. Humans and Sprague–Dawley rats were given EM by injection, gavage, or transmucosal gel with or without permeation enhancers. Pharmacokinetics were compared between subjects and across different delivery modalities. Drug concentrations in blood were measured using a bioassay. Design of Experiment techniques were used to optimize transmucosal antibiotic delivery in the Sprague–Dawley Model. Finally, we examined the scale-up of transmucosal delivery to human patients. Transmucosal delivery of EM increased with addition of ursodeoxycholate. While EM release from gels with ursodeoxycholate was significant, it was less than by injection. Scale-up to a human model indicated that delivery of EM using this transmucosal delivery system is insufficient for clinical need. The transport of EM seems limited by its solubility in water and thickness of the epithelial cell layers. Providing successful transmucosal delivery of EM and similar molecules to humans will require more aggressive techniques to disrupt the cellular layer, or pro-drug strategies to increase lipid solubility. ß 2009 Wiley-Liss, Inc. and the American Pharmacists Association J Pharm Sci 99:2905–2913, 2010 Keywords: pharmacokinetics; oral (buccal) mucosa; permeation enhancer; bioassay; Carbo- pol/Carbomer; Sprague–Dawley rat INTRODUCTION Gastrointestinal tract motility regulates the orderly movement of ingested material through the gut to ensure adequate digestion and absorption of nutri- ents, electrolytes, fluid, and medications. Many diseases can interfere with this process leading to gastrointestinal dysfunction, occasionally resulting in poor nutrition, hydration, and inconsistent med- ication absorption. Gastroparesis is an uncommon, yet serious and well recognized, disorder character- ized by symptoms related, in part, to prolonged emptying of contents from the stomach in the absence of mechanical obstruction. 1 It may occur acutely, for example, in response to surgery or medicines, or chronically, such as a result of long-standing diabetes mellitus, surgery, or in an idiopathic form. Individuals with chronic gastroparesis may present with a wide range of symptoms including bloating, abdominal pain, anorexia, early satiety, nausea, and vomiting. These symptoms may be severely disabling causing weight loss and malnutrition requiring nutritional supplementation or even gastric resection. Gastroparetic patients are frequently administered medications orally to enhance movement of ingested material through the stomach and to improve absorption of other medications necessary for treat- ment of their underlying condition. 2 The medications used to stimulate gastric motility (i.e., prokinetic agents), however, may not be absorbed consistently, thereby limiting their usefulness. A method to deliver prokinetic agents that bypasses the gastrointestinal tract could provide more consistent levels of these drugs. This would, theoretically, lead to better regulation of gastrointestinal motility and, thus, absorption. Once absorption (and serum levels) of the prokinetic agent becomes more predictable, patients who once had inconsistent motility may have more predictable absorption of medications necessary for their particular disease. Currently We have no conflicts of interest to disclose. Correspondence to: Brent L. Vernon (Telephone: 480-965-0929; Fax: 480-727-7624; E-mail: [email protected]) Journal of Pharmaceutical Sciences, Vol. 99, 2905–2913 (2010) ß 2009 Wiley-Liss, Inc. and the American Pharmacists Association JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 99, NO. 6, JUNE 2010 2905
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Development of a transmucosal technique for erythromycin delivery to treat gastroparesis

Development of a Transmucosal Technique for ErythromycinDelivery to Treat Gastroparesis
RYAN MCLEMORE,1 BRIAN LUNT,1 SARAH SALAMEH,1 JOHN K. DIBAISE,2 MICHAEL D. CROWELL,2 BRENT L. VERNON1
1Biomaterials Laboratory, Center for Interventional Biomaterials, School of Biological and Health Systems Engineering,Arizona State University, Tempe, Arizona 85287
2Division of Gastroenterology, Mayo Clinic, Scottsdale, Arizona 85259
Received 25 August 2009; revised 27 October 2009; accepted 31 October 2009
Published online 28 December 2009 in Wiley InterScience (www.interscience.wiley.com). DOI 10.1002/jps.22037
We have noCorresponde
Fax: 480-727-76
Journal of Pharm
� 2009 Wiley-Liss
ABSTRACT: Gastroparesis is a serious condition that limits meal or medication emptying fromthe stomach, resulting in a variety of symptoms, altered nutrition, and inconsistent medicationdelivery. Our aim was to develop a transmucosal system to deliver erythromycin (EM), a gastricprokinetic agent, to bypass intestinal absorption. Humans and Sprague–Dawley rats weregiven EM by injection, gavage, or transmucosal gel with or without permeation enhancers.Pharmacokinetics were compared between subjects and across different delivery modalities.Drug concentrations in blood were measured using a bioassay. Design of Experiment techniqueswere used to optimize transmucosal antibiotic delivery in the Sprague–Dawley Model.Finally, we examined the scale-up of transmucosal delivery to human patients. Transmucosaldelivery of EM increased with addition of ursodeoxycholate. While EM release from gelswith ursodeoxycholate was significant, it was less than by injection. Scale-up to a humanmodel indicated that delivery of EM using this transmucosal delivery system is insufficientfor clinical need. The transport of EM seems limited by its solubility in water and thicknessof the epithelial cell layers. Providing successful transmucosal delivery of EM and similarmolecules to humans will require more aggressive techniques to disrupt the cellular layer, orpro-drug strategies to increase lipid solubility. � 2009 Wiley-Liss, Inc. and the American Pharmacists
Association J Pharm Sci 99:2905–2913, 2010
Keywords: pharmacokinetics; oral (buccal)
mucosa; permeation enhancer; bioassay; Carbo-pol/Carbomer; Sprague–Dawley ratINTRODUCTION
Gastrointestinal tract motility regulates the orderlymovement of ingested material through the gut toensure adequate digestion and absorption of nutri-ents, electrolytes, fluid, and medications. Manydiseases can interfere with this process leading togastrointestinal dysfunction, occasionally resultingin poor nutrition, hydration, and inconsistent med-ication absorption. Gastroparesis is an uncommon,yet serious and well recognized, disorder character-ized by symptoms related, in part, to prolongedemptying of contents from the stomach in the absenceof mechanical obstruction.1 It may occur acutely, forexample, in response to surgery or medicines, orchronically, such as a result of long-standing diabetesmellitus, surgery, or in an idiopathic form. Individuals
conflicts of interest to disclose.nce to: Brent L. Vernon (Telephone: 480-965-0929;24; E-mail: [email protected])
aceutical Sciences, Vol. 99, 2905–2913 (2010)
, Inc. and the American Pharmacists Association
JOURN
with chronic gastroparesis may present with a widerange of symptoms including bloating, abdominalpain, anorexia, early satiety, nausea, and vomiting.These symptoms may be severely disabling causingweight loss and malnutrition requiring nutritionalsupplementation or even gastric resection.
Gastroparetic patients are frequently administeredmedications orally to enhance movement of ingestedmaterial through the stomach and to improveabsorption of other medications necessary for treat-ment of their underlying condition.2 The medicationsused to stimulate gastric motility (i.e., prokineticagents), however, may not be absorbed consistently,thereby limiting their usefulness. A method to deliverprokinetic agents that bypasses the gastrointestinaltract could provide more consistent levels of thesedrugs. This would, theoretically, lead to betterregulation of gastrointestinal motility and, thus,absorption. Once absorption (and serum levels) ofthe prokinetic agent becomes more predictable,patients who once had inconsistent motility mayhave more predictable absorption of medicationsnecessary for their particular disease. Currently
AL OF PHARMACEUTICAL SCIENCES, VOL. 99, NO. 6, JUNE 2010 2905

2906 MCLEMORE ET AL.
available alternatives to the oral delivery of proki-netic medications include the intravenous and sub-cutaneous injection routes. While these methods ofdrug delivery have demonstrated clinical benefits,they are not practical for long-term use in the patientwith chronic gastroparesis.
We hypothesized that transmucosal delivery wouldbe an ideal alternative to the oral or parenteraldelivery of prokinetic agents. Buccal delivery waspostulated as the route with the highest probability ofsuccess as buccal tissue is much thinner than skin,thereby increasing the ability to deliver consistentamounts of drug continuously as compared withtransdermal techniques. Several drugs have beensuccessfully delivered through the oral buccalmucosa.3 Poly(acrylic acid)s, with the trade nameCarbopol, have been available for use for transmu-cosal drug delivery for many years, in part, due totheir muco-adhesive and biocompatible propertiesand their proven safety in humans.4,5 To determinethe feasibility of buccal delivery, we performedseveral pharmacokinetic (PK) studies using erythro-mycin (EM), a macrolide antibiotic with potentprokinetic effects, in cellular, rat, and human models,and compared the various distributions. Subse-quently, we examined the effectiveness of sodiumglycodeoxycholate (SGDC), a well-recognized per-meation enhancer, and a similar clinically approveddrug, ursodeoxycholic acid, to increase the delivery ofEM across buccal tissue.
MATERIALS AND METHODS
Materials
Kirby Bauer Bioassay
Kocuria rhizophila was obtained from ATCC (Man-assas, VA) (9934). DifcoTM Nutrient Broth, AntibioticMedium 11, and bioassay dishes (REF 351040) wereobtained from Becton Dickinson (Sparks, MD).Antibiotic assay discs were obtained from WhatmanInternational Ltd (Kent, UK) (England) (CAT No.2017-006). Acetonitrile was obtained from EMDChemicals (Gibbstown, NJ) (LOT No. 47226). Imagesof each assay plate were taken with a Nikon DXcamera and analyzed using measurement tools inImageJ. Fetal bovine serum (FBS) was obtained fromGibco (Carlsbad, CA) (Cat. No. 16000-044).
Caco-2 Cell Preparation and Monolayer Growth
Caco-2 cell lines (HTB-37) and Eagle’s MinimumEssential Medium (EMEM) (Cat. No. 30-2003) wereobtained from ATCC. Penicillin/streptomycin wasobtained from Mediatech (Manassas, VA) (10,000 IU/mL/10,000mg/mL; #30-002-C1). L-glutamine wasobtained from Irvine Scientific (Santa Ana, CA)
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 99, NO. 6, JUNE 2010
(#9317). Inserts were obtained from BD Falcon(Franklin Lakes, NJ) (Cat. No. 353097). The 24-wellplates were obtained from Corning (Corning, NY)(No. 3526).
Animal Pharmacokinetic Study
Erythromycin lactobionate (EML) was obtained fromHospira (Lake Forest, IL) (LOT No. 47 767Z7).Carbomer 940 was obtained from Spectrum Chemical(Gardena, CA) Mfg. Corp. (C1477). Heparinized vialswere obtained from Sarstedt (Newton, NC) (REF41.1393.105). SGDC was obtained from Sigma (St.Louis, MO) (G9910). Preformulated erythromycinethylsuccinate (EME) (Abbott Laboratories (AbbottPark, IL) NDC 0074-6305-13) was obtained sus-pended in water (80 mg/mL). Ursodeoxycholate(Ursodiol), which is FDA approved for use in humans,was obtained from Spectrum Chemical Mfg. Corp.(Lot No. XD 1029). Plastic syringes were obtainedfrom National Scientific (Rockwood, TN) Company(S7510-1).
Methods
Kirby Bauer Bioassay: Quantification of Samples
Detection of EM in the blood samples was accom-plished via bioassay against Kocuria rhizophila in aprocedure described by Fernandes et al.6 Bacteriawere streaked across agar dishes and grown for3 days. Eighteen hours prior to the assay, a singlecompetent colony was removed from the plate andgrown in 5 mL of Nutrient Broth. Approximately50mL of the overnight culture was used to inoculate500 mL of Antibiotic Medium 11 that had beenautoclaved and cooled to 558C. Approximately 70–100 mL of inoculated agar was poured into a largebioassay dish, allowing a uniform lawn of bacteria toform on the assay plate. Upon agar/broth solidifica-tion, 25 discs were spread evenly across the top of theagar.
Blood samples were extracted with an equal volumeof acetonitrile to release bound EM. Samples werevortexed momentarily, centrifuged at 14,000 rpm for20 min, and the supernatant was removed. Twenty-five microliters of the 5 standards and 20 sampleswere pipetted on the discs in the assay plate in apredetermined fashion. The plate was inverted andallowed to incubate for 30 h at 378C. Zones ofinhibition formed around each disc based on theEM concentration of each sample. A semi-log relation-ship exists between EM concentration and zonediameter.7 The unknown concentrations were deter-mined from a standard curve created by plotting thezone diameters of inhibition against the log of theantibiotic concentration of each standard.7 Excelsoftware (Microsoft, Redmond, WA) was used to plota line of best fit, or standard curve, from the semi-log
DOI 10.1002/jps

TRANSMUCOSAL DELIVERY OF ERYTHROMYCIN 2907
plot. The correlation coefficient for the linear fit wasaccepted if it was 0.9 or higher. The standards rangedfrom 0.03 to 12mg/mL EM in DI water. The presenceof standards on each plate compensated for errorassociated with variation in agar thickness, tempera-ture, and humidity. Samples were analyzed intriplicate where volume permitted or in duplicate ifvolume was limited.
Detection of EM in the blood samples from the thirdanimal PK study occurred via bioassay as describedpreviously with minor differences. A small sterilizedglass HPLC vial, 11.3 mm in diameter, was used topunch out 25 wells into which 35mL of the extractedsamples were pipetted into. These wells were used tohouse the samples and standards instead of discs.Standards of the preformulated EM were diluted inFBS to concentrations of 5, 3, 1, 0.5, 0.25, 0.1, and0.05mg/mL. The plates were not inverted duringincubation. Each sample was analyzed only a singletime due to the minimal volume of blood collectedretro-orbitally.
Caco-2 Cell Preparation and Monolayer Growth
Caco-2 cell lines were maintained and harvested inEMEM supplemented with 20% FBS, 1% penicillin/streptomycin, and 2% L-glutamine. The cells wereincubated at 378C in a controlled atmosphere with95% relative humidity, 95% air, and 5% CO2. Prior tothe study, Caco-2 cells were seeded with 5–10,000cells per insert with 0.8mm pores and a 0.3 cm2
growth area. A monolayer was confirmed by transe-pithelial electric resistance (TEER) measurements.
Permeability across a Caco-2 monolayer was usedto correlate the permeability with the absorbedfraction in humans. Permeability coefficients werecalculated in a manner described by Khan et al.8 Oncethe monolayer was established, a release study wasperformed in cell media. Monolayers atop insertswere placed in a 24-well plate. The gels were placed ontop of the monolayer with a micro spatula. Onemilliliter of fresh growth media was placed below theinsert and 200mL of media were placed on top of thegel. The medium was collected from the well at 15, 30,45, 60, 90, 120, 150, 180, 210, and 240 min. Duringeach collection the wells were rinsed with PBS beforebeing replaced with fresh media. Between collectiontimes the 24-well plates were placed in the cell cultureincubator.
Animal Pharmacokinetic Study
Three animal PK studies were performed using maleSprague–Dawley rats. The first involved the deliveryof EM in the form of EML via intravenous bolus,gavage, and buccal delivery routes. The second studyinvolved the use of SGDC, a permeation enhancer, toimprove the buccal delivery of EML. The third
DOI 10.1002/jps
study encompassed an experiment assessing buccaldelivery of the more palatable EME with and withoutursodeoxycholate. The gels in the third study wereformulated with varied concentrations of EME,Carbomer 940, and ursodeoxycholate. The experi-mental procedures described in this report receivedprior approval from the Institutional Animal Careand Use Committee (IACUC) at Arizona StateUniversity (ASU) and were in accordance with theAnimal Welfare Act9 and NIH guidelines.10
Study #1: Bolus, Gavage, and Buccal Deliveryof EML. Initial PK experiments using male Spra-gue–Dawley rats (280–330 g) were conducted usingintravenous bolus, gavage, and buccal delivery ofEML. Rats were fasted for 12 h with access towater ad libitum. Anesthesia was induced with 5%isoflurane in a sealed chamber and maintained with2% isoflurane throughout the procedure. A 10 mg/kgbolus injection of a 10 mg/mL solution of EML insterile isotonic saline was administered for theintravenous study. The gavage was administered asa 25 mg/kg dose of the same 10 mg/mL solution. Forthe initial buccal study, a gel was formulated usingfive weight percent (wt.%) Carbomer 940 and 95 wt.%EML. The EML was solubilized in deionized water at150 mg/mL, the Carbomer was added with 0.2 MPBS, pH 7.4, and the mixture was vortexed 30 min.This produced a super-saturated gel of Carbomerwhich was placed in the cheeks (70 mg/kg) with aspatula. Gels were formulated no more than 3 h priorto use in vivo. Rat blood samples (n¼ 3 for each study)were collected in heparinized vials at 0, 5, 10, 30, 60,90, 120, 150, 180, 210, and 240 min postapplicationusing cardiac puncture (cardiocentesis) as describedby Hrapkiewicz.11 Rat cheeks were examined at theconclusion of each study for redness or swelling. Bloodwas centrifuged at 14,000 rpm for 20 min and theplasma was removed and stored at �808C to preventhydrolysis of the EML until analysis by bioassay.
Study #2: Buccal Delivery of EML with aPermeation Enhancer. An initial subset of fourrats was tested to examine whether permeationenhancers might have an effect on EM transportthrough the tissue of the rat mouth. A gel was for-mulated using 5 wt.% Carbomer 940, 5 wt.% SGDC,and 90 wt.% EML. The EML was first solubilized indeionized water at 150 mg/mL, then bile salt wasadded and vortexed. The Carbomer was added alongwith 0.2 M PBS, pH 7.4, and vortexed �30 min.
Study #3: Buccal Delivery of EME with andwithout Ursodeoxycholate. Due to the bitter tasteof EML, we also used EME for experiments involvingoral delivery. PK experiments using male Sprague–Dawley rats (274–320 g) were conducted using buccal
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 99, NO. 6, JUNE 2010
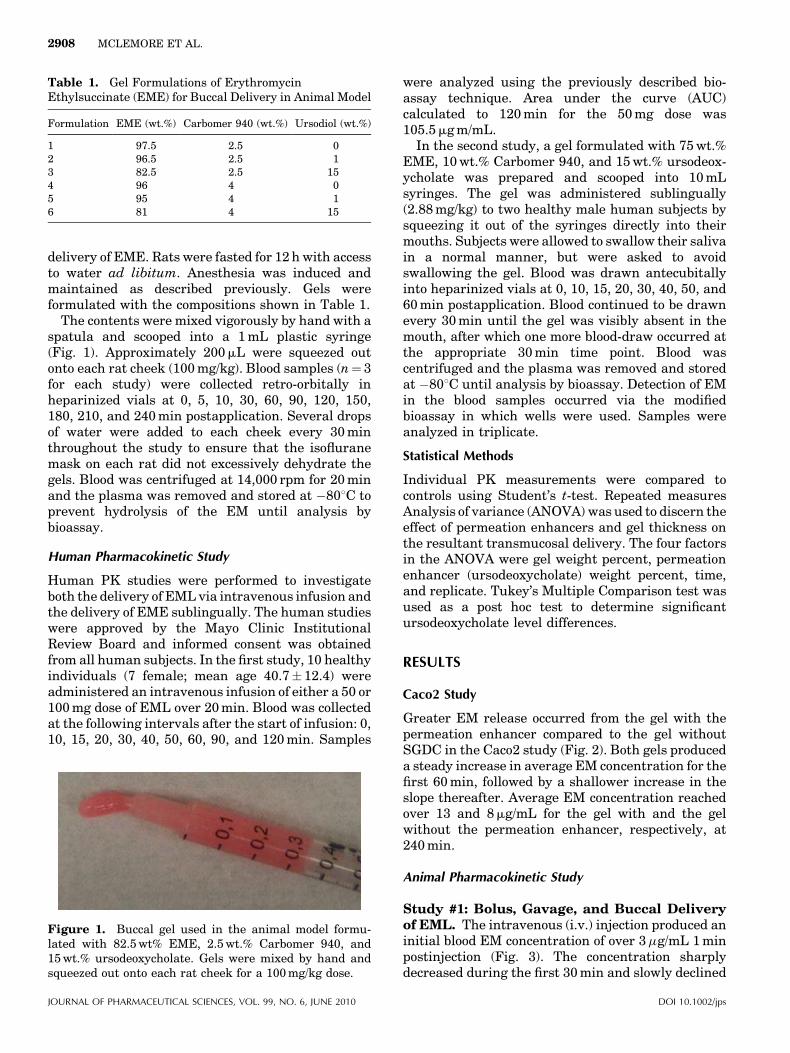
Table 1. Gel Formulations of ErythromycinEthylsuccinate (EME) for Buccal Delivery in Animal Model
Formulation EME (wt.%) Carbomer 940 (wt.%) Ursodiol (wt.%)
1 97.5 2.5 02 96.5 2.5 13 82.5 2.5 154 96 4 05 95 4 16 81 4 15
2908 MCLEMORE ET AL.
delivery of EME. Rats were fasted for 12 h with accessto water ad libitum. Anesthesia was induced andmaintained as described previously. Gels wereformulated with the compositions shown in Table 1.
The contents were mixed vigorously by hand with aspatula and scooped into a 1 mL plastic syringe(Fig. 1). Approximately 200mL were squeezed outonto each rat cheek (100 mg/kg). Blood samples (n¼ 3for each study) were collected retro-orbitally inheparinized vials at 0, 5, 10, 30, 60, 90, 120, 150,180, 210, and 240 min postapplication. Several dropsof water were added to each cheek every 30 minthroughout the study to ensure that the isofluranemask on each rat did not excessively dehydrate thegels. Blood was centrifuged at 14,000 rpm for 20 minand the plasma was removed and stored at �808C toprevent hydrolysis of the EM until analysis bybioassay.
Human Pharmacokinetic Study
Human PK studies were performed to investigateboth the delivery of EML via intravenous infusion andthe delivery of EME sublingually. The human studieswere approved by the Mayo Clinic InstitutionalReview Board and informed consent was obtainedfrom all human subjects. In the first study, 10 healthyindividuals (7 female; mean age 40.7� 12.4) wereadministered an intravenous infusion of either a 50 or100 mg dose of EML over 20 min. Blood was collectedat the following intervals after the start of infusion: 0,10, 15, 20, 30, 40, 50, 60, 90, and 120 min. Samples
Figure 1. Buccal gel used in the animal model formu-lated with 82.5 wt% EME, 2.5 wt.% Carbomer 940, and15 wt.% ursodeoxycholate. Gels were mixed by hand andsqueezed out onto each rat cheek for a 100 mg/kg dose.
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 99, NO. 6, JUNE 2010
were analyzed using the previously described bio-assay technique. Area under the curve (AUC)calculated to 120 min for the 50 mg dose was105.5mg m/mL.
In the second study, a gel formulated with 75 wt.%EME, 10 wt.% Carbomer 940, and 15 wt.% ursodeox-ycholate was prepared and scooped into 10 mLsyringes. The gel was administered sublingually(2.88 mg/kg) to two healthy male human subjects bysqueezing it out of the syringes directly into theirmouths. Subjects were allowed to swallow their salivain a normal manner, but were asked to avoidswallowing the gel. Blood was drawn antecubitallyinto heparinized vials at 0, 10, 15, 20, 30, 40, 50, and60 min postapplication. Blood continued to be drawnevery 30 min until the gel was visibly absent in themouth, after which one more blood-draw occurred atthe appropriate 30 min time point. Blood wascentrifuged and the plasma was removed and storedat �808C until analysis by bioassay. Detection of EMin the blood samples occurred via the modifiedbioassay in which wells were used. Samples wereanalyzed in triplicate.
Statistical Methods
Individual PK measurements were compared tocontrols using Student’s t-test. Repeated measuresAnalysis of variance (ANOVA) was used to discern theeffect of permeation enhancers and gel thickness onthe resultant transmucosal delivery. The four factorsin the ANOVA were gel weight percent, permeationenhancer (ursodeoxycholate) weight percent, time,and replicate. Tukey’s Multiple Comparison test wasused as a post hoc test to determine significantursodeoxycholate level differences.
RESULTS
Caco2 Study
Greater EM release occurred from the gel with thepermeation enhancer compared to the gel withoutSGDC in the Caco2 study (Fig. 2). Both gels produceda steady increase in average EM concentration for thefirst 60 min, followed by a shallower increase in theslope thereafter. Average EM concentration reachedover 13 and 8mg/mL for the gel with and the gelwithout the permeation enhancer, respectively, at240 min.
Animal Pharmacokinetic Study
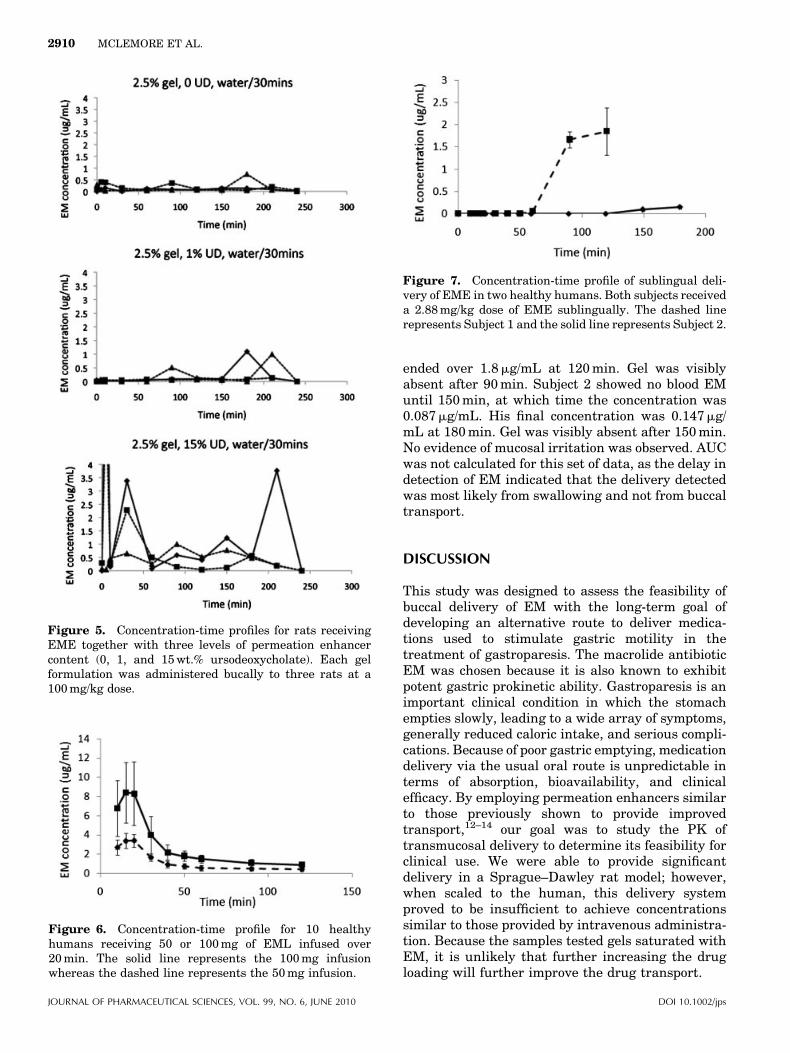
Study #1: Bolus, Gavage, and Buccal Deliveryof EML. The intravenous (i.v.) injection produced aninitial blood EM concentration of over 3mg/mL 1 minpostinjection (Fig. 3). The concentration sharplydecreased during the first 30 min and slowly declined
DOI 10.1002/jps
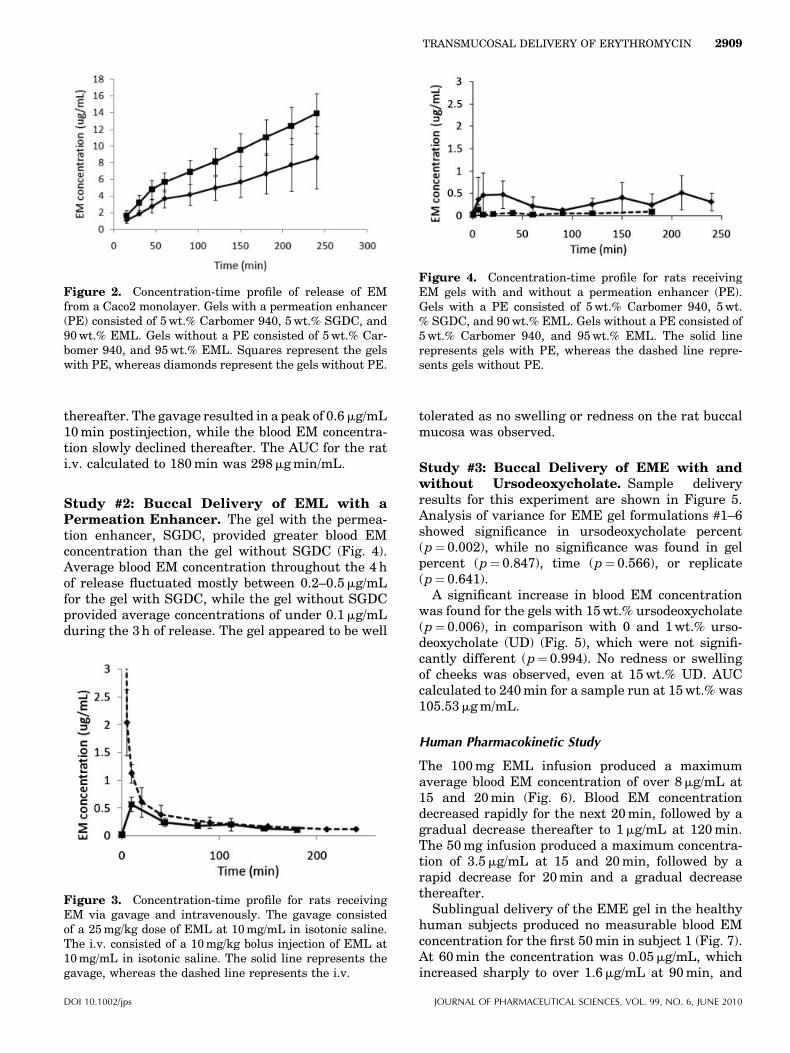
Figure 2. Concentration-time profile of release of EMfrom a Caco2 monolayer. Gels with a permeation enhancer(PE) consisted of 5 wt.% Carbomer 940, 5 wt.% SGDC, and90 wt.% EML. Gels without a PE consisted of 5 wt.% Car-bomer 940, and 95 wt.% EML. Squares represent the gelswith PE, whereas diamonds represent the gels without PE.
Figure 4. Concentration-time profile for rats receivingEM gels with and without a permeation enhancer (PE).Gels with a PE consisted of 5 wt.% Carbomer 940, 5 wt.% SGDC, and 90 wt.% EML. Gels without a PE consisted of5 wt.% Carbomer 940, and 95 wt.% EML. The solid linerepresents gels with PE, whereas the dashed line repre-sents gels without PE.
TRANSMUCOSAL DELIVERY OF ERYTHROMYCIN 2909
thereafter. The gavage resulted in a peak of 0.6mg/mL10 min postinjection, while the blood EM concentra-tion slowly declined thereafter. The AUC for the rati.v. calculated to 180 min was 298mg min/mL.
Study #2: Buccal Delivery of EML with aPermeation Enhancer. The gel with the permea-tion enhancer, SGDC, provided greater blood EMconcentration than the gel without SGDC (Fig. 4).Average blood EM concentration throughout the 4 hof release fluctuated mostly between 0.2–0.5mg/mLfor the gel with SGDC, while the gel without SGDCprovided average concentrations of under 0.1mg/mLduring the 3 h of release. The gel appeared to be well
Figure 3. Concentration-time profile for rats receivingEM via gavage and intravenously. The gavage consistedof a 25 mg/kg dose of EML at 10 mg/mL in isotonic saline.The i.v. consisted of a 10 mg/kg bolus injection of EML at10 mg/mL in isotonic saline. The solid line represents thegavage, whereas the dashed line represents the i.v.
DOI 10.1002/jps
tolerated as no swelling or redness on the rat buccalmucosa was observed.
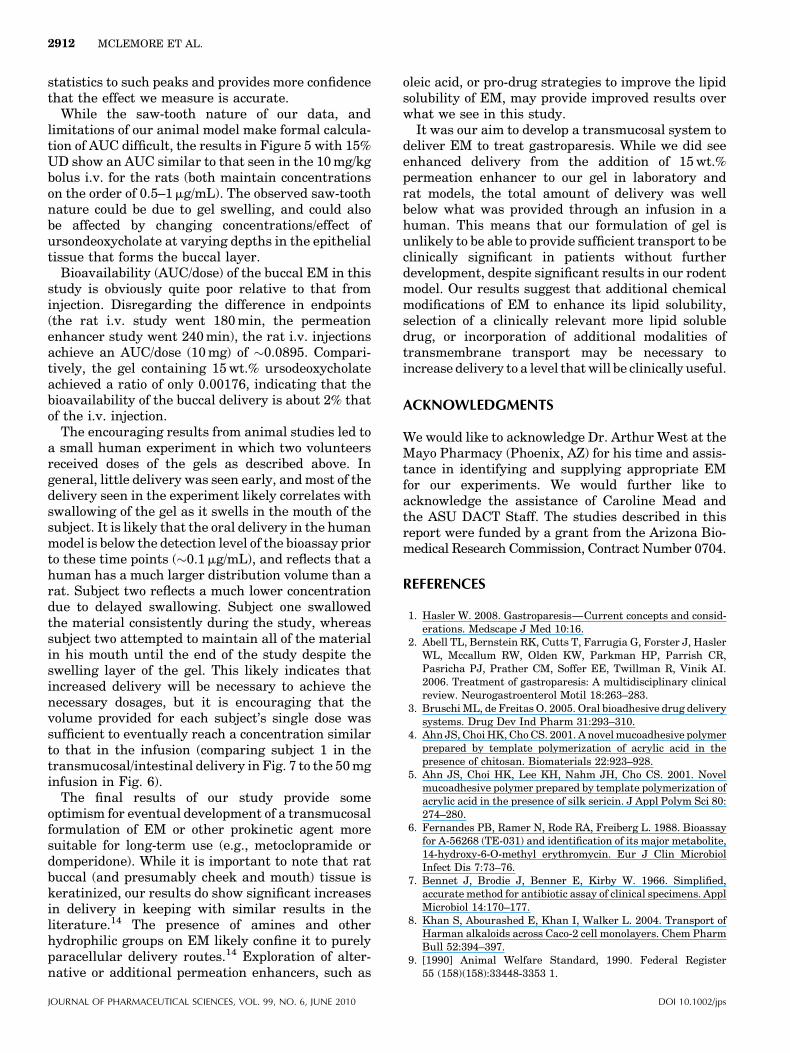
Study #3: Buccal Delivery of EME with andwithout Ursodeoxycholate. Sample deliveryresults for this experiment are shown in Figure 5.Analysis of variance for EME gel formulations #1–6showed significance in ursodeoxycholate percent(p¼ 0.002), while no significance was found in gelpercent (p¼ 0.847), time (p¼ 0.566), or replicate(p¼ 0.641).
A significant increase in blood EM concentrationwas found for the gels with 15 wt.% ursodeoxycholate(p¼ 0.006), in comparison with 0 and 1 wt.% urso-deoxycholate (UD) (Fig. 5), which were not signifi-cantly different (p¼ 0.994). No redness or swellingof cheeks was observed, even at 15 wt.% UD. AUCcalculated to 240 min for a sample run at 15 wt.% was105.53mg m/mL.
Human Pharmacokinetic Study
The 100 mg EML infusion produced a maximumaverage blood EM concentration of over 8mg/mL at15 and 20 min (Fig. 6). Blood EM concentrationdecreased rapidly for the next 20 min, followed by agradual decrease thereafter to 1mg/mL at 120 min.The 50 mg infusion produced a maximum concentra-tion of 3.5mg/mL at 15 and 20 min, followed by arapid decrease for 20 min and a gradual decreasethereafter.
Sublingual delivery of the EME gel in the healthyhuman subjects produced no measurable blood EMconcentration for the first 50 min in subject 1 (Fig. 7).At 60 min the concentration was 0.05mg/mL, whichincreased sharply to over 1.6mg/mL at 90 min, and
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 99, NO. 6, JUNE 2010
igure 6. Concentration-time profile for 10 healthyumans receiving 50 or 100 mg of EML infused over0 min. The solid line represents the 100 mg infusionhereas the dashed line represents the 50 mg infusion.
Figure 5. Concentration-time profiles for rats receivingEME together with three levels of permeation enhancercontent (0, 1, and 15 wt.% ursodeoxycholate). Each gelformulation was administered bucally to three rats at a100 mg/kg dose.
Figure 7. Concentration-time profile of sublingual deli-very of EME in two healthy humans. Both subjects receiveda 2.88 mg/kg dose of EME sublingually. The dashed linerepresents Subject 1 and the solid line represents Subject 2.
2910 MCLEMORE ET AL.
Fh2w
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 99, NO. 6, JUNE 2010
ended over 1.8mg/mL at 120 min. Gel was visiblyabsent after 90 min. Subject 2 showed no blood EMuntil 150 min, at which time the concentration was0.087mg/mL. His final concentration was 0.147mg/mL at 180 min. Gel was visibly absent after 150 min.No evidence of mucosal irritation was observed. AUCwas not calculated for this set of data, as the delay indetection of EM indicated that the delivery detectedwas most likely from swallowing and not from buccaltransport.
DISCUSSION
This study was designed to assess the feasibility ofbuccal delivery of EM with the long-term goal ofdeveloping an alternative route to deliver medica-tions used to stimulate gastric motility in thetreatment of gastroparesis. The macrolide antibioticEM was chosen because it is also known to exhibitpotent gastric prokinetic ability. Gastroparesis is animportant clinical condition in which the stomachempties slowly, leading to a wide array of symptoms,generally reduced caloric intake, and serious compli-cations. Because of poor gastric emptying, medicationdelivery via the usual oral route is unpredictable interms of absorption, bioavailability, and clinicalefficacy. By employing permeation enhancers similarto those previously shown to provide improvedtransport,12–14 our goal was to study the PK oftransmucosal delivery to determine its feasibility forclinical use. We were able to provide significantdelivery in a Sprague–Dawley rat model; however,when scaled to the human, this delivery systemproved to be insufficient to achieve concentrationssimilar to those provided by intravenous administra-tion. Because the samples tested gels saturated withEM, it is unlikely that further increasing the drugloading will further improve the drug transport.
DOI 10.1002/jps

TRANSMUCOSAL DELIVERY OF ERYTHROMYCIN 2911
Our initial experiments successfully characterizedthe i.v., gavage, and transmucosal delivery of EML ina rat model (Figs. 3–5). While the i.v. data wererelatively smooth after bioassay quantification, thetransmucosal (buccal) data frequently showed a saw-tooth pattern. Because the data are calculated byaveraging several measurements on a single animal,and then averaging across animals with similartreatment, this means that the data average fortransmucosal delivery have a larger range than wasseen for the i.v. data. We believe that the saw-toothnature of these curves arises from inconsistentdelivery due to changes in exposed surface area inthe mouth, and changes in hydration, and is not anartifact of the bioassay. Rats studied were in all casesanesthetized and placed on their stomach. While thisrenders determination of any pharmacodynamiceffects impossible due to anesthesia’s effects ongastric emptying, it does suppress the animal’sswallowing reflex, meaning that the gel is onlydisappearing through dissolution in saliva duringthe period of the experiment. This provides reason-able confidence that the absorption we see in theanimal model is through the buccal mucosa, and is notoccurring due to swallowing with subsequent intest-inal transport. This is supported by the observation ina smaller population of anesthetized rats that thestomach contents were not emptied for at least 1 h(data not shown).
Figure 6 displays the PK profile of EM seen inhealthy humans who received a 20 min infusion ofEML. The doses of EML used were chosen becausethey are commonly used in the clinical setting and areknown to result in a beneficial pharmacodynamiceffect (i.e., improvement in the rate of gastricemptying).15 The 100 mg dose peaked at around8mg/mL and declined over the 2 h the patients weremonitored. The 50 mg dose peaked at around 3–4mg/mL and declined more quickly than the 100 mg dose.These levels provided a target for the level of EMconcentration we were attempting to achieve withtransmucosal delivery in order to provide clinicalefficacy.
The gel used as a vehicle for buccal delivery in thiswork was the commercially available material,CarbopolTM. Carbopol consists of mainly acrylic acidchains, cross-linked with esters, and is of significantmolecular weight (several hundred thousand Dal-tons). This gel does not have a stable swellingequilibrium and will swell in the presence of salivauntil it has totally dissolved. As such, there is littlecontrol of the volume and surface area exposed oncethe gel is delivered, as the sample will swell and largeamounts of the formulation will be swallowedclinically over the 2–4 h, as observed in Figure 7.For our experiments, this was considered to bebeneficial since the swelling would spread the gel
DOI 10.1002/jps
over a larger surface area. Once a final formulation isidentified, exploring additional delivery vehicles withstable swelling behavior could be a useful clinicalimprovement.
Examination of initial transmucosal delivery levelswas disappointing. EML was seen to cross the buccallayer in very small quantities that were barelydetectable. After this observation and a detailedliterature search, we decided to evaluate the effects ofa permeation enhancer on the release of our drug.Initially, we used SGDC because it has been usedsuccessfully to improve penetration of a variety ofsubstances through epithelial tissue.14,16,17 SGDCwas used to evaluate the effect of permeationenhancers in a Caco monolayer cell model, and inPK studies in rats (Figs. 3 and 4). While these resultswere encouraging, SGDC is not approved for use inhumans. Because of this, we evaluated ursodeoxy-cholic acid, a related bile acid that is approved for usein humans to dissolve gallbladder stones. Addition-ally, when we began to study the permeationenhancers, a switch was made from EML to EMEbecause the EML is highly unpalatable to humans (itis very bitter), and as such is not included in oralformulations of EM.
Our rat studies on ursodeoxycholate-mediatedEME transport showed significance in ursodeoxycho-late concentration (p¼ 0.002), but not in weightpercent of gel (p¼ 0.847). Tukey’s Multiple Compar-ison Tests indicated that 15 wt.% ursodeoxycholatewas significantly different from 1% and 0% ursodeox-ycholate, but that 1% and 0% were not different fromeach other. The transmucosal delivery seen in the ratmodels at 15% ursodeoxycholate is on the same orderas the infused delivery seen in the human subjects,although the transmucosal delivery is still observablylower than that seen from the 50 mg infusion prior to40 min (Figs. 5 and 6). Due to the multiple blooddraws necessary during the course of the animalexperiment, the blood volume drawn at each timeperiod was very limited. This made multiple assays ofthese samples impractical, but still permitted statis-tical analysis through the hidden replication involvedin 2n studies. Rarely, measurements were madewhich showed highly increased, nonsustained EMdelivery (Fig. 5, 15% ursodeoxycholate). Such anom-alous measurements in single samples likely comefrom handling/contamination during blood collectionfrom the animals or are due to incomplete separationprior to assay, and probably do not reflect accuratedelivery levels. Despite the variation, these resultswere taken into account during the repeated mea-sures ANOVA, and combined with the initial saw-tooth nature of the release likely explain why ourresults do not show an effect associated with time(p¼ 0.566). The use of repeated measures ANOVAdoes, however, serve to limit the sensitivity of our
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 99, NO. 6, JUNE 2010
2912 MCLEMORE ET AL.
statistics to such peaks and provides more confidencethat the effect we measure is accurate.
While the saw-tooth nature of our data, andlimitations of our animal model make formal calcula-tion of AUC difficult, the results in Figure 5 with 15%UD show an AUC similar to that seen in the 10 mg/kgbolus i.v. for the rats (both maintain concentrationson the order of 0.5–1mg/mL). The observed saw-toothnature could be due to gel swelling, and could alsobe affected by changing concentrations/effect ofursondeoxycholate at varying depths in the epithelialtissue that forms the buccal layer.
Bioavailability (AUC/dose) of the buccal EM in thisstudy is obviously quite poor relative to that frominjection. Disregarding the difference in endpoints(the rat i.v. study went 180 min, the permeationenhancer study went 240 min), the rat i.v. injectionsachieve an AUC/dose (10 mg) of �0.0895. Compari-tively, the gel containing 15 wt.% ursodeoxycholateachieved a ratio of only 0.00176, indicating that thebioavailability of the buccal delivery is about 2% thatof the i.v. injection.
The encouraging results from animal studies led toa small human experiment in which two volunteersreceived doses of the gels as described above. Ingeneral, little delivery was seen early, and most of thedelivery seen in the experiment likely correlates withswallowing of the gel as it swells in the mouth of thesubject. It is likely that the oral delivery in the humanmodel is below the detection level of the bioassay priorto these time points (�0.1mg/mL), and reflects that ahuman has a much larger distribution volume than arat. Subject two reflects a much lower concentrationdue to delayed swallowing. Subject one swallowedthe material consistently during the study, whereassubject two attempted to maintain all of the materialin his mouth until the end of the study despite theswelling layer of the gel. This likely indicates thatincreased delivery will be necessary to achieve thenecessary dosages, but it is encouraging that thevolume provided for each subject’s single dose wassufficient to eventually reach a concentration similarto that in the infusion (comparing subject 1 in thetransmucosal/intestinal delivery in Fig. 7 to the 50 mginfusion in Fig. 6).
The final results of our study provide someoptimism for eventual development of a transmucosalformulation of EM or other prokinetic agent moresuitable for long-term use (e.g., metoclopramide ordomperidone). While it is important to note that ratbuccal (and presumably cheek and mouth) tissue iskeratinized, our results do show significant increasesin delivery in keeping with similar results in theliterature.14 The presence of amines and otherhydrophilic groups on EM likely confine it to purelyparacellular delivery routes.14 Exploration of alter-native or additional permeation enhancers, such as
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 99, NO. 6, JUNE 2010
oleic acid, or pro-drug strategies to improve the lipidsolubility of EM, may provide improved results overwhat we see in this study.
It was our aim to develop a transmucosal system todeliver EM to treat gastroparesis. While we did seeenhanced delivery from the addition of 15 wt.%permeation enhancer to our gel in laboratory andrat models, the total amount of delivery was wellbelow what was provided through an infusion in ahuman. This means that our formulation of gel isunlikely to be able to provide sufficient transport to beclinically significant in patients without furtherdevelopment, despite significant results in our rodentmodel. Our results suggest that additional chemicalmodifications of EM to enhance its lipid solubility,selection of a clinically relevant more lipid solubledrug, or incorporation of additional modalities oftransmembrane transport may be necessary toincrease delivery to a level that will be clinically useful.
ACKNOWLEDGMENTS
We would like to acknowledge Dr. Arthur West at theMayo Pharmacy (Phoenix, AZ) for his time and assis-tance in identifying and supplying appropriate EMfor our experiments. We would further like toacknowledge the assistance of Caroline Mead andthe ASU DACT Staff. The studies described in thisreport were funded by a grant from the Arizona Bio-medical Research Commission, Contract Number 0704.
REFERENCES
1. Hasler W. 2008. Gastroparesis—Current concepts and consid-erations. Medscape J Med 10:16.
2. Abell TL, Bernstein RK, Cutts T, Farrugia G, Forster J, HaslerWL, Mccallum RW, Olden KW, Parkman HP, Parrish CR,Pasricha PJ, Prather CM, Soffer EE, Twillman R, Vinik AI.2006. Treatment of gastroparesis: A multidisciplinary clinicalreview. Neurogastroenterol Motil 18:263–283.
3. Bruschi ML, de Freitas O. 2005. Oral bioadhesive drug deliverysystems. Drug Dev Ind Pharm 31:293–310.
4. Ahn JS, Choi HK, Cho CS. 2001. A novel mucoadhesive polymerprepared by template polymerization of acrylic acid in thepresence of chitosan. Biomaterials 22:923–928.
5. Ahn JS, Choi HK, Lee KH, Nahm JH, Cho CS. 2001. Novelmucoadhesive polymer prepared by template polymerization ofacrylic acid in the presence of silk sericin. J Appl Polym Sci 80:274–280.
6. Fernandes PB, Ramer N, Rode RA, Freiberg L. 1988. Bioassayfor A-56268 (TE-031) and identification of its major metabolite,14-hydroxy-6-O-methyl erythromycin. Eur J Clin MicrobiolInfect Dis 7:73–76.
7. Bennet J, Brodie J, Benner E, Kirby W. 1966. Simplified,accurate method for antibiotic assay of clinical specimens. ApplMicrobiol 14:170–177.
8. Khan S, Abourashed E, Khan I, Walker L. 2004. Transport ofHarman alkaloids across Caco-2 cell monolayers. Chem PharmBull 52:394–397.
9. [1990] Animal Welfare Standard, 1990. Federal Register55 (158)(158):33448-3353 1.
DOI 10.1002/jps

TRANSMUCOSAL DELIVERY OF ERYTHROMYCIN 2913
10. [1985] National Research Council NIH Guide for the Care andUse of Laboratory Animals, 1985. ed.: National ResearchCouncil NIH Guide for the Care and Use of Laboratory Ani-mals, PHS Publication (NIH). p 8523.
11. Hrapkiewicz K, Medina L, Holmes D. 1998. Clinical LaboratoryAnimal Medicine: An Introduction. Blackwell Publishing.
12. Sudhakar Y, Kuotsu K, Bandyopadhyay AK. 2006. Buccalbioadhesive drug delivery—A promising option for orally lessefficient drugs. J Control Release 114:15–40.
13. Senel S, Atilla Hincal A. 2001. Drug permeation enhancementvia buccal route: Possibilities and limitations. J Control Release72:133–144.
14. Nicolazzo JA, Reed BL, Finnin BC. 2005. Buccal penetrationenhancers—How do they really work? J Control Release 105:1–15.
DOI 10.1002/jps
15. DiBaise JK, Park F, Lyden E, Brand R, Brand R. 2001. Effectsof low doses of erythromycin on the 13C-spirulina platensisgastric emptying breath test and electrogastrogram: A con-trolled study in healthy volunteers. Am J Gastroenterol 96:2041–2050.
16. Senel S, Capan Y, Sargon MF, Ikinci G, Solpan D, Guven O,Bodde HE, Hincal AA. 1997. Enhancement of transbuccalpermeation of morphine sulfate by sodium glycodeoxycholatein vitro. J Control Release 45:153–162.
17. Hoogstraate AJ, Verhoef JC, Tuk B, Pijpers A, van LeengoedLAMG, Verheijden JHM, Junginger HE, Bodde HE. 1996. In-vivo buccal delivery of fluorescein isothiocyanate-dextran 4400with glycodeoxycholate as an absorption enhancer in pigs.J Pharm Sci 85:457–460.
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 99, NO. 6, JUNE 2010




















