In-Depth Thematic Analysis of AMR and National Security
52
In-Depth Thematic Analysis of Antimicrobial Resistance and National Security
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of In-Depth Thematic Analysis of AMR and National Security
In-Depth Thematic Analysis of Antimicrobial Resistance and National Security
In-Depth Thematic Analysis of AMR and National Security
October 2014
RIVM Rapport 2014-xxxxx
2 | In-Depth Thematic Analysis of AMR and National Security
Colophon
In-Depth Thematic Analysis of Antimicrobial Resistance and National Security has been produced by the Network of Analysts for National Security (ANV) for the National Steering Committee for National Safety and Security (SNV).
National Institute for Public Health and the Environment (RIVM) Research and Documentation Centre (WODC), Ministry of Security and Justice General Intelligence and Security Service of the Netherlands (AIVD) Netherlands Organisation for Applied Scientific Research (TNO) Netherlands Institute of International Relations ‘Clingendael’ International Institute of Social Studies (ISS), Erasmus University Rotterdam
© RIVM 2014 Extracts from this publication may be reproduced if cited as follows: ‘National Institute for Public Health and the Environment (RIVM), title of publication and year of publication’.
Marcel Mennen (editor)Mariken van der Lubben (editor)
Contact: [email protected]
Published by:
National Institute for Public Health and the EnvironmentP.O. Box 1 | 3720 BA BilthovenThe Netherlandswww.rivm.nl/en
In-Depth Thematic Analysis of AMR and National Securityt | 3
Contents
Summary 5
1. Introduction 7 1.1 National security and antimicrobial resistance 7 1.2 Choice of theme; assignment 8
2. Explanation of scenarios and method 11 2.1 Choice of scenarios 11 2.2 Method 13
3 Scenarios 12 3.1 Fit and healthy marines incapacitated by serious illness 15 3.1.1 Explanation and background information 15 3.1.2 Description 15 3.2 Prolonged outbreak in a nursing home 18 3.2.1 Explanation and background information 18 3.2.2 Description 18 3.3 Resistant bacteria: an unwanted souvenir 20 3.3.1 Explanation and background information 20 3.3.2 Description 20 3.4 ‘Southern European’ situations in the Netherlands 21 3.4.1 Explanation and background information 21 3.4.2 Description 22 3.5 Illegal maid spreads resistant strain of tuberculosis 22 3.5.1 Explanation and background information 22 3.5.2 Description 23 3.6 Nursing students infected with tuberculosis 24 3.6.1 Explanation and background information 24 3.6.2 Description 24 3.7 Children’s party on a farm ends in tragedy 25 3.7.1 Explanation and background information 25 3.7.2 Description 25 3.8 Cruise passengers struck down by food poisoning 27 3.8.1 Explanation and background information 27 3.8.2 Description 27
4 Assessment results 31 4.1 Likelihood 31 4.2 Vital infrastructure 32 4.3 Impact scores 32 4.4 Risk diagram 36
5 Consideration and conclusions 39
6 Future-proofing 43
Appendix 1: 47Network of Analysts for National Security (ANV) 47
Appendix 2: 49 Overview of organisations involved 49

4 | In-Depth Thematic Analysis of AMR and National Security

In-Depth Thematic Analysis of AMR and National Securityt | 5
Summary
In 2007, the Netherlands established a National Security Strategy. This strategy charted potential threats to national security and explained how these threats or the consequences of a disaster or crisis could be minimised. National security is compromised if the national security interests of the Dutch state and/or society are threatened in such a way that the breakdown of society is a potential consequence. This (potential) breakdown of society will be measured based on impact criteria relating to the following national security interests:- Territorial security (which is threatened by
encroachment upon our territory)- Economic security (uninterrupted free trade)- Ecological security (living environment and nature)- Physical safety (public health and welfare) - Social and political stability (including issues such as
social unrest, violation of freedoms/core values, etc.)
In order to chart and analyse potential threats, the Network of Analysts for National Security (ANV) was set up, a broad network of knowledge institutes and other organisations such as government services, NGOs, and companies in the business sector. In 2013, the ANV conducted an in-depth thematic analysis for the theme of antimicrobial resistance (AMR) within the framework of the National Security Strategy.
Various risks relating to AMR – with a breakdown of society at the national level as a potential consequence – were therefore analysed from the perspective of national security. Eight scenarios were created, which were then assessed by a multi-disciplinary group of experts to determine their impact and likelihood. These scenarios – descriptions of fictitious developments and events in the future – cover a wide spectrum of potential problems relating to AMR and were selected from a variety of perspectives (healthcare; environment; veterinary) and types of problem (endemic/non-endemic).
A group consisting of AMR experts (scientists, analysts, sector representatives, enforcement agencies, and NGOs) and experts on national security impact criteria (communication; socio-psychological unrest; economics) evaluated these scenarios using the NRA methodology1, a measuring
1 The NRA methodology is described in the document Guidelines for
Working with Scenarios, Risk Assessments and Capacities, Ministry of
Security & Justice’s National Security Strategy (2013).
instrument developed for the National Risk Assessment (NRA)2. A noticeable factor was that the likelihood of the scenarios was given a relatively high score compared to many other scenarios developed within the NRA, and it was noted that a number of these AMR scenarios had either already taken place in the real world or are on the verge of occurring.
The analysis provided the insight that national security is only affected if one-off incidents relating to AMR occur more frequently and at the same time. In general, unrest amongst the population can grow, and faith in governmental and other institutes is undermined. Furthermore, there is a clear division between general social consequences and consequences specific to the healthcare sector. For general social consequences, the impact is limited, although for the odd scenario, loss of income and economic damage is expected within the agricultural sector. In the field of healthcare, a significant impact is expected, particularly regarding numbers of cases of serious illness, fatalities and financial consequences.
Within the National Security Strategy, it is customary to conduct a capability analysis. However, as national and international policy visions have been developed and presented parallel to the creation of this report, this analysis was not carried out. Exploratory research was conducted relating to activities that have been or will be put in place to limit the consequences of AMR.In a variety of areas, prevention and combatting of AMR will be reinforced in the years to come. Activities will be initiated and perpetuated with regard to prevention of infectious diseases, proper use of antibiotics in human healthcare, monitoring of Highly Resistant Microorganisms (HRMOs), necessary international action, development of new antibiotics, research into resistant bacteria in the environment, further reduction of antibiotic usage/resistance as well as prevention of animal diseases in the livestock farming sector, and communication about AMR.
2 In the yearly published National Risk Assessment scenarios
describing different disasters and threats which might threatened
the Dutch state and/or society in such a way that the breakdown of
society is a potential consequence, are evaluated using the NRA
methodology. The results are used to determine capabilities,
formulate policy and establish priorities in order to prepare the
Netherlands as much as possible for various types of disaster or
threat.

6 | In-Depth Thematic Analysis of AMR and National Security
In-Depth Thematic Analysis of AMR and National Securityt | 7
1 Introduction 1.1 National security and antimicrobial resistance
The National Security Strategy identifies and analyses disasters, threats and crises that could endanger society and even potentially result in a breakdown of society. For this purpose, they are elaborated into the form of scenarios that are then assessed in accordance with an established measuring instrument: the NRA methodology3 (NRA = National Risk Assessment). Since 2008, forty-eight scenarios have been developed and published in the subsequent yearly NRA reports.The objective of this process is to give policymakers insight into the relative likelihood and impact of such scenarios. This insight is of importance in determining capabilities, formulating policy and establishing priorities in order to prepare the Netherlands as much as possible for various types of disaster or threat.
The increasing resistance to antibiotics could pose a threat to national security. The study described in
3 The NRA methodology is described in the document Guidelines for
Working with Scenarios, Risk Assessments and Capacities, Ministry of
Security & Justice’s National Security Strategy (2013).
this report is an in-depth analysis of the problem of antimicrobial resistance (AMR) viewed from the perspective of national security. For the purposes of this analysis, eight scenarios were created, and a multidisciplinary group of experts subsequently assessed the impact and likelihood of these scenarios using the NRA methodology. The goal of this in-depth thematic analysis is not only to investigate the degree to which AMR issues pose a potential threat to national security, but also to serve as input for reinforcing and supporting national and international policy with regard to this issue. This in-depth thematic analysis is not part of the regular NRA cycle, which is why the reporting is therefore conducted separately.
The eight scenarios were independently produced by the Network of Analysts for National Security (ANV). The ANV is an authoritative knowledge network that has created the annual NRA since 2011 in the name of the National Steering Committee for National Safety and Security (SNV), upon commission by the Ministry of Security & Justice. The ANV also conducts other studies and analyses within the context of national security.The ANV (see Appendix 1 for a brief description) consists of a core group of six organisations and a network of knowledge institutes, agencies and

8 | In-Depth Thematic Analysis of AMR and National Security
companies that can – depending on the knowledge required – be engaged during the production of the NRA and other products (studies, analyses, etc.) within the framework of national security. The core group consists of the National Institute for Public Health and the Environment (RIVM), the General Intelligence and Security Service of the Netherlands (AIVD), the Netherlands Organisation for Applied Scientific Research (TNO), the Netherlands Institute of International Relations ‘Clingendael’, the Research and Documentation Centre (WODC) of the Ministry of Security & Justice, and Erasmus University Rotterdam’s Institute of Social Studies (ISS). These institutes bear collective responsibility for the quality and content of the products delivered by the ANV.
This study was overseen by a committee consisting of representatives from the Ministry of Health, Welfare & Sport, the Ministry of Economic Affairs, and the National Coordinator for Counterterrorism & Security.
The report is structured as follows: In Section 1.2, the ANV’s assignment for this study is explained. Chapter 2 contains a brief summary of the scenarios developed in this study, including explanation and justification of the selected scenarios. The evaluation methodology will also be described in this chapter. The scenarios themselves are included in Chapter 3. For each scenario, an explanation, a justification and background information will be provided, followed by the description of the scenario. Chapter 4 contains the assessment results obtained using the NRA methodology in the following order: likelihood (Section 4.1), consequences for essential products and services (4.2), and impact criteria (4.3). The likelihood and total impact of each scenario as determined by the assessment are then reflected by the position of each scenario in a risk diagram. This risk diagram can be found in Section 4.4, together with a brief explanation of the results. Chapter 5 considers the results and the conclusions of this in-depth thematic analysis. The degree to which the Netherlands is future-proof in this regard is then described in Chapter 6.
Appendix 2 gives an overview of the organisations and experts involved in the development and assessment of the scenarios.
1.2 Choice of theme; assignment
The scenarios in the successive NRA cycles4 up to and including 2013 cover a large number of themes and potential threats identified previously within the framework of the National Security Strategy. One of these themes is Health and Food Safety. In the ANV’s advice document to the SNV about possible NRA subjects that require further examination5, the problem of increasing resistance to antibiotics was mentioned as a possible threat to national security. This is an insidiously growing risk that has not yet been elaborated in the NRA.
Antimicrobial medicines are essential for the treatment of infectious diseases. Use of these medicines has resulted in the development and spread of resistant microorganisms, which is a worrisome development. People can be carriers of these resistant microorganisms without falling ill (colonisation), but in some cases, the microorganisms can cause difficult-to-treat infections. Resistant and multi-resistant microorganisms frequently develop in hospitals and nursing homes due to the frequent use of antibiotics, making these institutes a potential source for further spread of these microorganisms either within the institute itself or to other institutes. In addition, resistant and multi-resistant bacteria can increasingly be found among the general population. Introduction of resistant bacteria from abroad, from the livestock farming sector, from the environment and from the general population can also play a role in the epidemiology of human infections within hospitals.
In order to gain insight into the severity and scale of these problems, the ANV was assigned the task of conducting in-depth thematic analysis of the possible risks of increasing antimicrobial resistance (AMR) using the designated system for assessing national security. The objective of the analysis is to gain insight into these risks and the potential countrywide breakdown of society that could result from them. Based on these insights, an investigation can be conducted into capabilities that could be developed or reinforced within or by the Netherlands in order to gain or improve control of
4 NRA 2007, NRA 2008-2009, NRA 2010, NRA 2011, NRA 2012, and NRA 65 Advice document: Subjects for the NRA 2013 (2012). An advice document
from the ANV’s Task Group to the IWNV and the SNV regarding the
themes and subjects being considered for inclusion in the NRA 2013.
20120176 IMG/mme, 12 September 2012, in Dutch.

In-Depth Thematic Analysis of AMR and National Securityt | 9
the AMR issue. The results of this analysis can also be used to raise national and international awareness of the problem. For the purposes of this analysis, eight scenarios were created, and the individual impact and likelihood of each was then assessed by a multidisciplinary group of experts in accordance with the NRA methodology. The scenarios were selected in such a way that they collectively paint a clear picture of the whole spectrum of (serious) types of infectious disease and the various introduction routes along which the resistance problem is manifest. The selection of scenarios was coordinated with the Supervisory Committee. The assessment will provide insight into the relative impact of each of the scenarios as well as the total potential impact on society of increasing AMR.
The fictional scenarios were developed in mid-2013. Some of the scenarios feature dates that may already have passed by the time this report is published.

10 | In-Depth Thematic Analysis of AMR and National Security
In-Depth Thematic Analysis of AMR and National Securityt | 11
2 Explanation of scenarios and methodology2.1 Choice of scenarios
The scenarios developed as part of the National Risk Assessment (NRA) are descriptions of conceivable and recognisable occurrences, incidents and processes that could play out as described in the scenario. The scenarios paint a picture of various disasters, threats and crises that the government wishes to prepare for in order to protect the following vital interests: territorial security, physical safety, economic security, ecological security, and social and political stability. The scenarios are not predictions of the future, they simply paint a fictitious – yet conceivable – picture of potential situations. They provide a basis for communicating about and getting a feel for future uncertainties relating to national security.The scenarios must have a degree of plausibility, although they do not have to be extremely likely. Collectively, they must paint a comprehensive picture of what possible threats exist and which capacities require reinforcement: essential information for deciding whether or not to invest in particular capabilities.
The eight scenarios in this in-depth thematic analysis were developed in accordance with the same guidelines used for the NRA, with the
understanding that the methodology has been slightly adjusted as described in section 2.2.
The scenarios within this theme were chosen from a variety of perspectives, namely:• The environment in which the resistance problem
is manifest• The transmission route and the source of the
infection• The microorganism and type of resistance • The consequences• Whether or not the resistance is endemic• Table 2.1 gives a brief summary of the various
scenarios.
The scenarios developed for the purposes of the National Security Strategy relate both to incidents (e.g. large-scale emission and spreading of a toxic cloud) and insidious processes (e.g. a gradual increase in the number of cases of Lyme’s disease). This study focuses exclusively on the latter type. Two scenarios are set in 2023, and the cause of these situations is a gradual increase in resistance between now and 2023 due to, amongst other factors, introduction from other countries where a large degree of resistance is already established (such as India, Pakistan, and southern Europe). The other scenarios play out in a period between now and five
12 | In-Depth Thematic Analysis of AMR and National Security
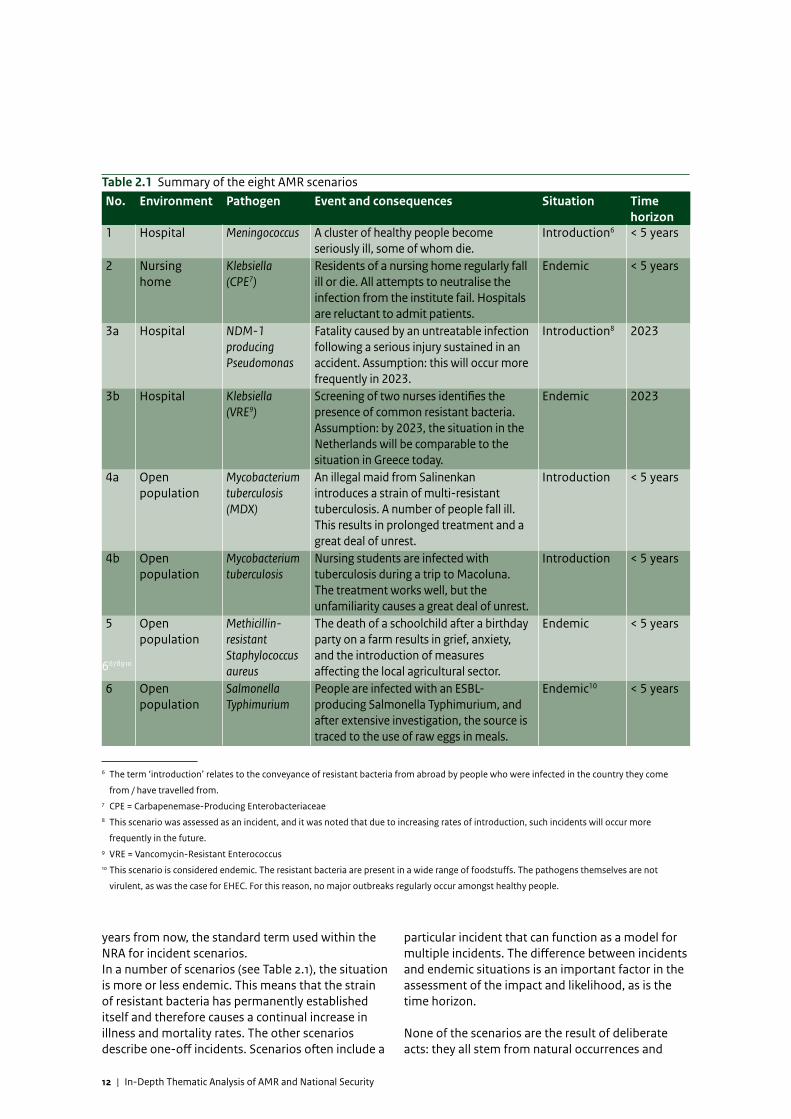
Table 2.1 Summary of the eight AMR scenarios No. Environment Pathogen Event and consequences Situation Time
horizon1 Hospital Meningococcus A cluster of healthy people become
seriously ill, some of whom die.Introduction6 < 5 years
2 Nursing home
Klebsiella (CPE7)
Residents of a nursing home regularly fall ill or die. All attempts to neutralise the infection from the institute fail. Hospitals are reluctant to admit patients.
Endemic < 5 years
3a Hospital NDM-1 producing Pseudomonas
Fatality caused by an untreatable infection following a serious injury sustained in an accident. Assumption: this will occur more frequently in 2023.
Introduction8 2023
3b Hospital Klebsiella (VRE9)
Screening of two nurses identifies the presence of common resistant bacteria. Assumption: by 2023, the situation in the Netherlands will be comparable to the situation in Greece today.
Endemic 2023
4a Open population
Mycobacterium tuberculosis (MDX)
An illegal maid from Salinenkan introduces a strain of multi-resistant tuberculosis. A number of people fall ill. This results in prolonged treatment and a great deal of unrest.
Introduction < 5 years
4b Open population
Mycobacterium tuberculosis
Nursing students are infected with tuberculosis during a trip to Macoluna. The treatment works well, but the unfamiliarity causes a great deal of unrest.
Introduction < 5 years
5 Open population
Methicillin-resistant Staphylococcus aureus
The death of a schoolchild after a birthday party on a farm results in grief, anxiety, and the introduction of measures affecting the local agricultural sector.
Endemic < 5 years
6 Open population
Salmonella Typhimurium
People are infected with an ESBL-producing Salmonella Typhimurium, and after extensive investigation, the source is traced to the use of raw eggs in meals.
Endemic10 < 5 years
6678910
6 The term ‘introduction’ relates to the conveyance of resistant bacteria from abroad by people who were infected in the country they come
from / have travelled from.7 CPE = Carbapenemase-Producing Enterobacteriaceae8 This scenario was assessed as an incident, and it was noted that due to increasing rates of introduction, such incidents will occur more
frequently in the future.9 VRE = Vancomycin-Resistant Enterococcus10 This scenario is considered endemic. The resistant bacteria are present in a wide range of foodstuffs. The pathogens themselves are not
virulent, as was the case for EHEC. For this reason, no major outbreaks regularly occur amongst healthy people.
years from now, the standard term used within the NRA for incident scenarios. In a number of scenarios (see Table 2.1), the situation is more or less endemic. This means that the strain of resistant bacteria has permanently established itself and therefore causes a continual increase in illness and mortality rates. The other scenarios describe one-off incidents. Scenarios often include a
particular incident that can function as a model for multiple incidents. The difference between incidents and endemic situations is an important factor in the assessment of the impact and likelihood, as is the time horizon.
None of the scenarios are the result of deliberate acts: they all stem from natural occurrences and

In-Depth Thematic Analysis of AMR and National Securityt | 13
developments. However, human activity does play a role in the sense that particular measures – or the lack thereof (e.g. hygiene) – can influence developments in the scenario.
2.2 Method
The scenarios in this in-depth thematic analysis were created and examined by experts from a variety of disciplines who deal with antimicrobial resistance (AMR) and various aspects of national security, under the supervision and responsibility of RIVM’s Centre for Infectious Disease Control (CIb).
The scenarios were subsequently given scores for their likelihood and their impact, in accordance with the NRA methodology. This method is described in a handbook11. The assessment was conducted by a group consisting of experts in the field of antibiotics (doctors; scientists; veterinary experts) and in the field of specific national security impact criteria (communication; socio-psychological unrest; economics). Appendix 2 contains a list of the organisations that participated in the scoring session. It was decided to evaluate all eight scenarios in a single meeting, as this enabled comparison of the scores for the various scenarios in a manner that was as fair as possible. In order to make this achievable in practice, a couple of adjustments were made to the methodology. Firstly, some impact criteria were slightly adjusted. Secondly, five of the ten impact criteria were not assessed, as it could be reasonably argued that they are not applicable or barely applicable to these scenarios.
11 Guidelines for Working with Scenarios, Risk Assessments and Capacities,
Ministry of Security & Justice’s National Security Strategy (2013).
Table 2.2 shows which criteria were assessed, which criteria were not assessed, and which criteria were simplified.
The economic damage (Criterion 3.1) was calculated and assessed by an economist from the ANV Task Group prior to the scoring session. The data, calculations and assumptions used as well as the results of these calculations were described in a memo that was sent to the experts in the scoring group prior to the scoring session. During the meeting, the scores were discussed by the experts, and based on these scores, adjustments were made to the damage assessments for a number of scenarios, as the scored numbers of fatalities and cases of serious illness (Criteria 2.1 and 2.2) turned out to be higher than was assumed during the calculations.
The scoring process was conducted with the aid of a digital Group Decision System provided by TNO. During the meeting, the experts individually gave a score for each criterion/subcriterion first. An overview of these scores (in a frequency table) was then presented to the group for discussion. After the discussion, each expert was given the opportunity to adjust their score if they felt relevant arguments had been made by other participants or if they had gained further insight during the discussion. The scores given after the discussion (displayed in Chapter 4) were used for the calculation of the total impact in accordance with the NRA methodology.
Table 2.2 Summary of impact factors including whether or not they were assessed or simplified Impact criteria Assessed? Simplified?1.1. Encroachment on the territory of the Netherlands No1.2. Infringement of the international position of the Netherlands Yes Yes2.1. Fatalities Yes No2.2. Seriously injured and chronically ill Yes No2.3. Lack of basic necessities of life No3.1. Cost and long-term impact on the economy Yes No4.1. Long-term impact on flora and fauna No5.1. Disruption of everyday life No5.2. Violation of the democratic system No5.3. Socio-psychological impact and societal unrest Yes Yes

14 | In-Depth Thematic Analysis of AMR and National Security
In-Depth Thematic Analysis of AMR and National Securityt | 15
3 ScenariosThis chapter provides a summary of the scenarios. Firstly, the context is roughly described and some background information is given on the scenario in question. A description of the scenario used for the assessment is then given.
3.1 Fit and healthy marines incapacitated by serious illness
3.1.1 Explanation and background information
For this scenario, an outbreak of Neisseria meningitidis (meningococcus) was selected. This bacterium can also cause serious illness in healthy people, such as in the following scenario involving marines. The two most common forms of meningococcal disease are as follows:1) Meningitis: symptoms include high fever, chills,
vomiting, headaches, and neck stiffness2) Sepsis: symptoms include chills, fever, drowsiness,
and a characteristic purple skin discolouration that does not fade under pressure, and that is caused by minor haemorrhaging or bruising (petechia)
The course of meningococcal sepsis can be rapid and extremely serious. The average death rate is 7.5%, although for serious cases the death rate is 20-50% within 24 hours. Permanent injury can also occur as
the infection can damage organs and tissue.
Meningococcal disease was selected for this scenario as it is one of the few bacterial infections that can cause serious illness in healthy people and is transmissible from person to person. If the bacterium is resistant to antibiotics, the consequent delay in providing effective treatment can rapidly result in serious consequences. Meningococcus is spread by intensive contact with an infected person via the air (speaking; sneezing) or via direct contact (kissing).The disease can be treated with a variety of antibiotics. If treatment is administered in time, then the chances of a cure are maximised. However, given the rapid progression of the disease, treatment is often too late and can therefore be ineffective even if the right antibiotics are administered. Resistance against regular antibiotics causes additional delay in administering the right treatment. This does not happen in this particular scenario. People who have been in close contact with a patient must take antibiotics as a precautionary measure in order to prevent them from falling ill and to minimise their infectiousness. This is known as prophylactic treatment. The antibiotics rifampicin, ceftriaxone and ciprofloxacin are suitable for prophylactic treatment of people who have been in close contact with meningococcus patients. There are many different strains of meningococcus

16 | In-Depth Thematic Analysis of AMR and National Security
(serogroups) prevalent in certain parts of the world: Group A is found mainly in developing countries, Group B mainly affects developed countries, and Group C can be found anywhere. Pilgrims to Mecca occasionally contract meningococcus serogroup W135. Vaccination is possible against the various serogroups. Since 2001, vaccination against Group-C meningococcus has been included in the National Vaccination Programme (RVP), which offers common vaccinations to all children in the Netherlands. This includes vaccines against viruses such as measles and polio, as well as bacteria such as meningococcus and Bordetella pertussis, which causes whooping cough. However, the programme does not include vaccinations against Neisseria meningitidis serotype A, which is responsible for the outbreak described in this scenario. Upon enlistment, all military personnel are given a basic package of vaccinations, including DPT, hepatitis A and B, typhoid fever, and MMR (measles/mumps/rubella). The meningococcus vaccination (A, C, W135, Y) is part of the supplementary package for military personnel sent to countries where meningococcus is endemic.
3.1.2 Description
In April 2016, a platoon of trainee marines is on an intensive two-week tactical training camp at a military training area near Lake Lauwersmeer in North Groningen. The platoon consists of fifty trainee marines and a ten-strong team of officers and NCOs. The average age of the trainees is 19 years, varying between the ages of 17 and 24.
ThursdayOn Thursday morning, the penultimate day of the training camp, one of the trainee marines wakes up ill. He is rushed to University Medical Center Groningen with symptoms of sepsis. This is very serious as this type of blood poisoning can soon prove fatal if treatment is not quickly administered. Upon arrival at the hospital, he is suffering from chills, fever, headache, petechia (skin discolouration), and extreme drowsiness. A lumbar puncture is immediately performed, and the results strongly indicate meningococcal meningitis or sepsis. Spinal fluid and blood samples are taken to confirm the diagnosis and to determine the antibiotic sensitivity of the pathogen. As meningococcal sepsis is suspected, a third-generation cephalosporin (ceftriaxone) is administered to the patient intravenously. The patient is treated in isolation. Despite prompt antibiotic treatment, the patient’s condition worsens. He lapses into a coma and is admitted to intensive care.
FridayThe remaining trainee marines have been screened for symptoms of the aforementioned illness. Thankfully, none of the marines meet the criteria. As the marines have been in constant intensive contact during the training camp (together 24 hours a day, e.g. in vehicles, sleeping close to each other, etc.) preventative (prophylactic) treatment is administered in accordance with the applicable guidelines. For practical reasons (one pill per day and immediate availability of the medication), prophylaxis with ciprofloxacin is selected as the appropriate course of treatment. Prophylaxis is provided to and taken by all marines on the Friday morning during the debriefing, and they then return home.
SaturdayOn Saturday, the blood-culture results are made available. They confirm Neisseria meningitidis as the pathogen. The results of the antibiotic sensitivity test will only be available the following day. That afternoon, it turns out that one of the other marines has been admitted to hospital in Utrecht with suspected meningococcal sepsis. This marine had displayed no symptoms on Friday and had taken his medicine as instructed.
SundayDespite receiving adequate treatment, the first patient dies in the early hours of Sunday morning. The second patient is in a stable condition and is being treated with intravenous antibiotics.
The results of the antibiotic sensitivity test are extremely surprising. The meningococcus was sensitive to penicillin, ampicillin, ceftriaxone, chloramphenicol, rifampicin, and azithromycin, but proved insensitive to ciprofloxacin, levofloxacin, and co-trimoxazol. Until this point, no cases of ciprofloxacin-resistant Neisseria meningitidis had been documented in the Netherlands. It has been documented for Group-A meningococcus isolated in patients and healthy carriers in India and in North and Central Africa. Imported cases have also been recorded in Europe and the United States. A number of the marine’s instructors have very recently returned from a mission in Central Africa.
Upon hearing of the lab results, the medical service of the Royal Netherlands Navy is trying to contact the group of marines to tell them to take a different antibiotic as prophylaxis. However, the group’s members are scattered across the Netherlands. Due to weekend leave, the medical service are unable to contact every member of the group. As timely

In-Depth Thematic Analysis of AMR and National Securityt | 17
prophylaxis is essential for maximum effectiveness of the treatment, they will continue to attempt to reach all of the marines affected.
From the conversations with the marines they did manage to contact, they learn that some of the marines travelled home by public transport. Many of them went out on Friday night to various bars and nightclubs in different parts of the country. A group of twelve marines went to a busy dance party in Noord-Holland, and some of the marines went straight home to their wives and young children.
That evening, a third marine is admitted to hospital in a critical condition with suspected meningococcal sepsis. It is one of the marines who attended the dance party. It is learned that he kissed a number of girls at the party.
MondayVia social media, the regular media has got wind of the situation. They begin reporting a highly resistant ‘superbug’ that has spread across the Netherlands and is so deadly that it can even kill super-fit marines. Many Regional Health Services (RHSs) are bombarded with phone calls from worried citizens who are afraid they have caught the dreaded ‘superbug’. Some of these people were at the dance party, some of them are worried that they shared a train carriage or bus with the marines, and some are simply afraid of getting caught up in an epidemic.
The RHS in the region where the dance party was held decides to conduct a contact investigation. This is a major challenge as the partygoers could live anywhere in the Netherlands. The RHS decides to appeal to the partygoers via popular radio stations and social media, asking them to report for screening. These messages result in a deluge of telephone calls that completely jams the RHS’s switchboard. An overwhelming number of people show up. This results in minor scuffles breaking out in the waiting room. Other RHSs are also having difficulties.
The second patient’s condition is stable and he appears to be on the mend. However, the third patient’s condition has deteriorated and he is on a respirator in the IC unit. It has also emerged that the six-month-old daughter of one of the marines has been admitted to hospital with suspected meningitis. Her father was at the training camp and had had intensive contact with the first sick marine. He had displayed no symptoms and in the late afternoon on Sunday, he had taken new, effective antibiotic prophylaxis.
By Monday evening, the highly deadly and resistant ‘superbug’ is the number one story on all news shows, as well as being the trending topic on Twitter and other social media. The third marine has since died. There is a great deal of uncertainty amongst the public about the source of the infection and about who is and isn’t at risk. Parallel to recent attacks on soldiers in Great Britain, there are even rumours of intentional infection by terrorists.
TuesdayThe shocking news coverage, which has created a great deal of unrest and uncertainty, has resulted in crisis talks in The Hague and RIVM’s headquarters in Bilthoven. According to experts, there is no reason to panic. Intensive contact is required for transmission of the disease. Brief exposure, such as sharing public transport, rarely results in infection. Conducting thorough contact investigation and providing adequate prophylaxis (e.g. rifampicin or ceftriaxone, both of which are effective against the pathogen responsible for this outbreak) to people who have had intensive contact with patients will be sufficient to manage the problem. However, contact investigation for this group is a major challenge. As it is a national problem, RIVM/CIb (Centre for Infectious Disease Control) will coordinate the contact investigation. As there has never been such a major national crisis before, an OMT12 is set up. It is the first time that such a large area of infection has been involved and also the first time resistance has played such a major role. Within the OMT, discussion takes place regarding vaccinations. The OMT concludes that there are no substantive grounds for this measure. Shortly after, an Administrative Consultative Committee (BAO)13 is set up, and as expected, the Minister complies with the decision made by the OMT/BAO.
12 Outbreak Management Team: An advisory body that can be
summoned on an ad hoc basis in order to formulate ‘best possible
professional advice’ for the administrators responsible in case of a
large-scale threat or crisis regarding an infectious disease (see the
RIVM brochure ‘Landelijke advisering bij infectieziektedreigingen en
-crises’).13 BAO: A body consisting of civil servants and representatives of
organisations. In the event of an actual or potential outbreak or
crisis, the BAO assesses the political and administrative feasibility
and desirability of the measures advised by the OMT. The BAO
formulates advice and presents it to the Minister of Health, Welfare
& Sport and/or officials from the Ministries of Health, Welfare &
Sport and Economic Affairs, who will decide whether or not to
implement the advice (see the RIVM brochure ‘Landelijke advisering
bij infectieziektedreigingen en -crises’).
18 | In-Depth Thematic Analysis of AMR and National Security
For at least one month, doctors must remain vigilant, and ciprofloxacin is to be omitted from prophylactic treatment. All confirmed and suspected cases must be reported to the CIb. Active and continual monitoring of meningococcus, and in particular, its antibiotic resistance, is of great importance in ascertaining whether the introduction and spread of this ciprofloxacin-resistant Group-A meningococcus was just a one-off event or if it will become a more regular occurrence. Information from this kind of monitoring is essential to doctors in order to enable adequate prophylactic or curative treatment of patients with meningococcal meningitis and/or sepsis.
Further course of the outbreakThe second marine and the child both recover following their treatment. The contact investigation takes an entire week, and ten or so people who probably had contact with the patients are given prophylaxis as a precautionary measure. No new primary or secondary cases are reported in the first two weeks after the first marine fell ill. Based on the DNA fingerprint, the conclusion is made that all cases were caused by the same strain of ciprofloxacin-resistant Group-A meningococcus.
Initially, this reassuring news from the government has only a limited effect, and many people, in particular a number of influential bloggers, are sceptical. During the first week, GPs, RHCs and accident & emergency departments are flooded by questions from concerned citizens. However, once people learn that the outbreak was isolated to just the first four patients, the unrest gradually dissipates. After a couple of months, the RHSs stop receiving questions about the outbreak.
3.2 Prolonged outbreak in a nursing home
3.2.1 Explanation and background information
Klebsiella is an intestinal bacterium that is generally harmless to healthy people. However, it can harm sick people as a result of their weakened immune system or when natural barriers are being penetrated (i.e. due to the use of an intravenous drip, urinary catheter or artificial respiration). Klebsiella pneumoniae is a common cause of urinary tract infections (cystitis and pyelitis) amongst patients in healthcare institutions. A particular and very serious complication of such urinary tract
infections is sepsis or bloodstream infection. Sepsis is the most feared complication of bacterial infections, as the course of the illness is very serious, and if due to a resistant strain, it can be difficult to treat. If untreated, urosepsis can quickly cause septic shock and is frequently lethal. Urinary tract infections are a frequent occurrence in nursing homes for a number of reasons. The chances of getting a urinary tract infection increase with age, especially for women. From the age of 70 onwards, 20% of women develop cystitis each year. In addition, the use of urinary catheters creates a major risk of cystitis as catheters can serve as a vehicle for bacteria to enter the bladder. Klebsiella thrives if hygiene is poor (for example, if healthcare staff do not sufficiently wash their hands), enabling it to spread quickly amongst patients of healthcare institutes. Resistance plays a major role, as treatment opportunities are seriously limited if the bacteria cannot be properly eradicated by regular antibiotics.
3.2.2 Description
DetectionIn May 2014, during a meeting of the SO-ZI/AMR (Signaling consultation for Healthcare-related Infections and Antimicrobial Resistance), a medical microbiological lab (MML) reports that a cluster of patients are suffering from serious bloodstream infection as a result of infection with a multi-resistant bacterium. The patients were admitted within days of each other and were both residents of the Rotsoord House nursing home. This nursing home accommodates some 300 residents. The infection proves to be a carbapenemase-producing Klebsiella pneumoniae, an extremely antibiotic-resistant intestinal bacterium that belongs to the group of Highly Resistant Microorganisms (HRMOs). The hospital has implemented adequate control measures. Patients are treated in isolation, active investigation of possible transmission to other patients is carried out, and these affected patients are also isolated. The outbreak is classified as ‘under control’ by the SO-ZI/AMR. However, the detection did necessitate contact with the management of the nursing home.
EvaluationFollowing the detection, the hygienist charts the problem in the nursing home. Urinary tract infections are a frequent problem in this particular home. It would seem that the number of serious infections has increased significantly in the last few months. Urinary catheters are used regularly,

In-Depth Thematic Analysis of AMR and National Securityt | 19
particularly in the neurological rehabilitation ward. Furthermore, catheter use is popular amongst the nursing staff as it makes it easier to manage patients. Catheterisation prevents the need to lift patients repeatedly, and the beds do not have to be changed as often. At the nursing home, patients with urinary tract infections are treated based on medical signs and symptoms. Microbiological diagnosis is rarely conducted due to the costs involved. A noticeable factor in recent weeks was that Augmentin, the standard antibiotic treatment given for complicated urinary tract infections (definition: patient experiences general sickness, and nitrite is detected in their urine), was no longer effective. As a result, ciprofloxacin took over as the standard treatment for complicated urinary tract infections because it was the only remaining oral antibiotic. Despite this, a number of patients have been admitted to hospital in the last few weeks with symptoms of septic shock. Also in the last few weeks, a number of patients with suspected complicated urinary tract infections died in their sleep. The nursing home has no specific policy regarding prevention of infections. It is unclear who bears final responsibility for this matter. No specific consultation takes place between doctors and nurses regarding antibiotic policy and prevention of infection. There are no fixed agreements with an MML or a microbiologist who could be regularly consulted regarding the issue of antibiotic policy or prevention of infection. No monitoring of AMR or infections (healthcare-related or otherwise) is conducted. No routine samples are taken from patients, and barrier nursing is not standard practice in the event that a patient is found to be infected with or carrying an HRMO.
Hygiene standards at the nursing home are poor. This is mainly due to the nurses’ extremely heavy workloads. The management of the nursing home has recently changed the admission policy to favour patients requiring more intensive treatment, as this earns the nursing home more money. The consequent increase in patients with greater care needs with no increase in the number of nurses results in demand for care outstripping nursing capacity. The shortfall of nursing staff is compensated by bringing in cheaper and less qualified nursing assistants.
A brief investigation of the nursing home’s residents shows that 15-20% of them are carriers of the same multi-resistant Klebsiella bacteria. The number of
carriers is highest in the wards containing patients with the highest care needs.
It is suspected that following the introduction of the multi-resistant Klebsiella pneumoniae to the nursing home, the substandard hygiene practice allowed the bacteria to spread. The frequent usage of ciprofloxacin amongst patients probably contributed to the evolution of the multi-resistant Klebsiella pneumoniae, as this also proved to be resistant to ciprofloxacin. It is no longer possible to determine how long the outbreak has been in progress due to the lack of routine diagnostics. However, a period of a month and a half is given as a minimum estimate. This is because some six weeks ago, a trainee GP who was completing her last week as an intern at the home took urine cultures from a patient with a complicated urinary tract infection who was responding poorly to standard antibiotic treatment. These cultures already revealed the presence of carbapenem-resistant Klebsiella pneumoniae bacteria. Due to the lack of clear agreements between the nursing home and the relevant MML as well as the limited structural approach to the problem of AMR, this warning went unheeded.
Consequences The discovery that many patients of Rotsoord House may be carriers of an HRMO had consequences that went far beyond official circles. For example, a number of local hospitals were reluctant to admit any patients from Rotsoord House for fear that they would cause an outbreak at the hospital. As a result, the impression is given that the nursing home has to ‘peddle’ its patients. This resulted in great anger amongst the families of the patients. Although outbreaks of such bacteria are manageable with adequate hygiene and control measures, the budgets are insufficient to fund these measures. Furthermore, if an outbreak suddenly strikes, this has an extremely negative effect on performance indicators, which causes problems when negotiating with insurers. Transferring fully recovered patients to other care homes is also increasingly a problem, as these care homes are afraid the bacteria will be passed on to their residents. This situation has enraged the children of these elderly patients.
Other nursing homesThis phenomenon can also occur in multiple nursing homes at the same time. Nursing home staff often work at multiple locations, including other nursing homes. In addition, some also work in hospitals and/or in home care. The bacteria can therefore be spread by these staff to other nursing homes or even

20 | In-Depth Thematic Analysis of AMR and National Security
to the general public, especially more vulnerable people. The trend nowadays is that people continue living at home for longer and receive care there. As a result, transmission of bacteria will become even more widespread. Hospitals are generally equipped to deal with such outbreaks, but other institutes are not yet up to speed. As the number of carriers of the bacteria increases, the risk of serious or even deadly infections is becoming ever greater.
3.3 Resistant bacteria: an unwanted souvenir
This scenario plays out in the future (the year 2023). The story addresses what happens if regular cases of serious infections occur for which treatment is no longer possible. This will create unrest as doctors will have no course of action to fight illnesses that are usually easy to treat.
3.3.1 Explanation and background information
In the first decade of the 21st century, NDM-114 -producing bacteria were predominantly found in India, but a recent publication (JAMA. 2013; 310(4): 363) shows that between 2009 and 2011, this multi-resistant pathogen was detected in eight patients in the US. It has since found its way to the Netherlands, and in some hospitals, invasive procedures such as an operation can result in infection with this bacterium. This highly resistant strain of bacteria was introduced due to an increasing number of travellers returning from countries such as India and Pakistan as carriers of the disease.As the strains are extremely resistant, treatment of infected and ill people is very difficult. As a result, the chances of fatality are high. The bacteria in the following scenario can only cause infections if the patient undergoes an invasive procedure – such as an operation or catheterisation – in a hospital where the bacteria are present.
3.3.2 Description
In August 2023, following their final secondary-school exams, a group of seven students take a summer job at a bulb farm before heading off to university later in the year. They perform all kinds of
14 New Delhi Metallo-beta-lactamase-1 or NDM-1 is an enzyme that
makes bacteria resistant to practically all known antibiotics. These
enzymes were first detected in patients from India, hence the name.
tasks during the trip. The students, four of whom are male and three female, all stay at a campsite.
AccidentOne week into the trip, a serious accident occurs. During renovation work, a falling beam causes serious injury to two of the students, one male and one female. The male student sustains a serious leg wound and a concussion, as well as losing consciousness for a short period. His leg wound requires stitches, and he must rest due to the concussion. The female student is also injured, but recovers quite quickly. She briefly develops a fever, but it is successfully treated with antibiotics. However, as resistance to antibiotics has increased in the Netherlands in recent years, the female student is required to remain in hospital. This is because there are no more antibiotics suitable for her that can be taken orally. The male student’s leg wound is stitched, but he is advised not to walk on it yet. As he also develops a fever, he remains in hospital for a few days and is treated with antibiotics. Initially, he doesn’t feel particularly ill, although he does feel weak and sweaty. However, a few days later, his condition deteriorates. As resistance is becoming increasingly frequent and hence treatment of bacteria is getting harder and harder, doctors are quicker to examine the resistance profile of the bacteria.
Tests show that the pathogen is an NDM-1-producing Pseudomonas. As a result, treatment with antibiotics is difficult, and the student undergoes emergency surgery to amputate his leg below the knee. However, he is already very sick and is admitted to intensive care, where he develops pneumonia. A couple of days later, the male student dies. He is one of the many people each year who become seriously ill or die as a result of infection with this bacteria (dozens of cases are estimated).
Screening Immediately after the male student’s death, all patients and staff at the IC unit are screened, and the other students who worked at the bulb farm are also asked to report for screening. Panic grows as it becomes ever clearer that previously easy-to-treat infections may no longer be treatable. The male student’s family approaches the press. They report the dangers of going to certain countries where bacteria were first detected. It appears that these countries are not fulfilling their responsibilities, and that they pose a threat to public health in other countries. In recent years, complex discussions have taken place in the press and the

In-Depth Thematic Analysis of AMR and National Securityt | 21
political arena about travelling to these highly endemic countries, and travellers to / visitors from these countries are blamed for a number of nasty diseases that could spread through the country. Experts indicate that screening is futile and that it is clear the bacteria have already been introduced to the Netherlands. In addition, it is not possible to distinguish between infectious diseases (such as measles) and diseases that can only be transmitted to others under exceptional circumstances. Many groups in society begin to see people from highly endemic countries as a potential threat. Travelling to such countries is seen as ‘anti-social’ as you are ‘putting healthy people at risk’.
Increase in serious infectionsIn the Netherlands and abroad, a few people each year are infected with an NDM-1-producing bacterium. These infections are barely treatable, if at all. The debate about these bacteria therefore constantly recurs. The development of new antibiotics is accelerated, but it will probably take years before new and effective antibiotics are available. Strict hygiene measures appear to help, but they cannot prevent a small number of occasional infections, which in turn can lead to untreatable or barely treatable illnesses. The medical sector appears somewhat resigned. Naturally, doctors are worried about the situation, but they have known for years that something like this was just a matter of time. From 2018 onwards, the genetic background of bacteria that cause infections are meticulously monitored, and there had already been clues that new introductions from faraway countries were a regular occurrence. Over time, the sector’s calls for attention to be paid to this problem have gotten louder and louder, but funding cuts in the healthcare sector have resulted in insufficient measures being taken. By 2023, the situation has become irreversible. Pathogens newly introduced to Europe are practically ineradicable, and new antibiotics have not yet been developed.
3.4 ‘Southern European’ situations in the Netherlands
This scenario plays out in the future (the year 2023). The basis of this scenario is that by 2023, the situation in the Netherlands is comparable to the current situation in Greece (and a number of other southern European countries). In these countries, there are major problems in IC units due to a gradual increase in AMR.
3.4.1 Explanation and background information
Greece has the highest prevalence of carbapenem-resistant Klebsiella pneumoniae15 in Europe. In 2010, it was estimated that around 49% of all Greek Klebsiella pneumoniae isolates reported to the European Centre of Disease Prevention and Control (ECDC) were carbapenem resistant (Infect Drug Resist. 2012; 5: 133-41). The percentage of bacteria with this type of resistance is also high in Italy. For other European countries, the percentage is lower, although it is not known exactly how many people are carriers of the bacteria. However, it is known that the percentage is lower in northern European countries than in southern European countries. Generally, the occurrence of carbapenem-resistant organisms in other areas of Europe is currently restricted to sporadic outbreaks in hospitals, involving one or a handful of cases in people who come from other countries (Eurosurveillance, Volume 18, Issue 28, 11 July 2013).
In order to manage/prevent the transmission of carbapenem resistance, the following measures are advised for all acute and long-term care facilities: 1) Improvement of hygiene and hand-washing
measures2) Contact and isolation measures for colonised or
infected patients 3) Cohorting of patients and staff (if applicable) 4) Minimised usage of invasive medical devices 5) Promotion of Antibiotic Stewardship 6) Screening of at-risk patients If transmission has already taken place, then two additional measures are advised: active monitoring, and the use of chlorhexidine baths or wipes.Due to the current economic situation in southern Europe, major cutbacks have been made with regard to hospital staff and resources. The above measures therefore cannot be properly implemented, which promotes further transmission. In addition, more and more unemployed young people are coming from these countries to look for work in the
15 Carbapenems are a class of β-lactam antibiotics. These are
bactericidal agents, which means that they kill bacteria.
Carbapenems are seen as a last-resort class of antibiotics as bacteria
are usually sensitive to them. Klebsiella pneumoniae is a Gram-
negative rod-shaped bacterium that is found in the mouth and
intestines and on the skin. They are opportunistic bacteria that
mostly cause infections in people with weakened immune systems.
A multi-resistant strain of the Klebsiella pneumoniae has developed
that is resistant to carbapenems. The infections it causes are
therefore practically untreatable.

22 | In-Depth Thematic Analysis of AMR and National Security
Netherlands. Travellers from highly endemic countries who have had contact with the healthcare services there increase the likelihood of these resistant microorganisms being transmitted.Because the carbapenem-resistant Klebsiella pneumoniae bacterium is also often resistant to other antibiotics, few options are available to treat infections caused by the bacteria.
3.4.2 Description
It is the year 2023, and two students in Amsterdam are involved in a scooter accident due to driving in the rain while wearing Google Glasses. They are both admitted to hospital with broken bones and possible brain injuries. Thankfully, the injuries are less severe than was feared, and they are discharged from hospital after a short two-day stay for observation. Both of them are nursing students. They recover quickly, and within one month of the accident, they resume their studies and start their internships at a hospital. One student works in the neonatology ward and the other in the IC unit. At the hospital, an outbreak of a resistant microorganism (VRE 16) has been in progress for three months.
New type of resistance?As is customary during such outbreaks, patients and staff are screened to see if they are carrying the microorganism. The screening shows that neither nurse is carrying the strain that caused the outbreak, but they are both carrying a different and – until this point – infrequently occurring KPC-positive strain of the resistant microorganism Klebsiella pneumoniae17. Around ten years ago, this microorganism was predominantly found in Greece and Italy, and there had been just one documented case of the bacteria in the Netherlands, detected in a traveller returning from one of these countries.Even if healthcare workers are carriers, infection of patients usually does not occur as long as the staff members correctly adhere to the general precautionary measures. However, budget cuts and staff shortages have resulted in a degree of laxity.
16 Vancomycin-Resistant Enterococcus (VRE) is a bacterium that has
developed resistance to the antibiotic vancomycin, which is one of
the last-resort measures used for difficult-to-treat infections. This
hospital bacterium is particularly dangerous to weakened patients.17 KPC = Klebsiella Pneumoniae Carbapenemase. KPC-producing
bacteria are resistant to carbapenems. Carbapenems are a class of
β-lactam antibiotics. These are bactericidal agents, which means
that they kill bacteria. Carbapenems are seen as a last-resort class of
antibiotics as bacteria are usually sensitive to them.
Via the interns, the bacteria are transmitted to patients and staff in the neonatology ward and the IC unit.
Klebsiella is here to stayLarge-scale screening conducted following the discovery of the two carriers shows that the prevalence of carbapenem-resistant Klebsiella pneumoniae in the Netherlands has already reached high levels, and can now be described as endemic. The bacteria are discovered not only in the hospital, but are also frequently detected in the general population. Young children, senior citizens and immunocompromised patients are most vulnerable to infection if they carry the bacteria. Treatment against infections caused by these bacteria using the available medicines is no longer effective. As a result, infected patients must either fight off the infection naturally or they will not survive. This results in social unrest and fear, particularly amongst medical practitioners. Previously, hospitals could screen patients for having visited an endemic country before they entered the hospital, but now the pathogen is endemic in the Netherlands, every member of the population is at risk of developing an untreatable infection due to this pathogen. The unrest amongst medical practitioners - resulting from the lack of treatment options - causes major variations in quality of care between different hospitals, and citizens lose their faith in both the healthcare system (as it cannot offer any treatments) and the government (that failed to prevent the situation).
3.5 Illegal maid spreads resistant strain of tuberculosis
3.5.1 Explanation and background information
Tuberculosis is a serious bacterial infection caused by the pathogen Mycobacterium tuberculosis. In recent decades, this type of bacterium has become resistant to some medicines, and cases of resistant tuberculosis are becoming ever more frequent around the globe. Tuberculosis mainly affects the lungs, although in principle, it can damage any organ in the body. The most common symptoms of pulmonary tuberculosis include persistent coughing, weight loss, night sweats, chest pain, and coughing up blood. If tuberculosis bacteria are visible in the sputum when it is coloured and viewed under a microscope, then it is referred to as ‘open pulmonary tuberculosis’. This type of pulmonary tuberculosis is infectious.

In-Depth Thematic Analysis of AMR and National Securityt | 23
Tuberculosis control is organised separately and is not part of general disease control. Due to the complexity of tuberculosis control, intensive collaboration with KNCV18 is necessary.The standard treatment for tuberculosis consists of four different medicines. If a pathogen is resistant to any two medicines, then it is referred to as multi-drug resistant (MDR). If a pathogen is resistant to even more specific medicines, then it is referred to as extensively drug resistant (XDR). Tuberculosis bacteria are transmitted via patients with open tuberculosis. The bacteria are spread when the patient coughs. Once a healthy person is infected by a patient, they can be a carrier of the bacteria for years without noticing anything. However, infection can activate decades later. About 10% of infected people become seriously ill.
Even non-resistant tuberculosis is difficult to treat and requires careful contact investigation and evaluation of infections. It is not inconceivable that the public will fail to understand the difference between tuberculosis infection and tuberculosis itself, or between resistant and non-resistant tuberculosis. This could cause unwarranted unrest in the event of non-resistant tuberculosis outbreaks, and also makes it difficult to explain existing policy. For this reason, it was decided to select two scenarios relating to tuberculosis: one with a resistant strain (Section 3.5) and one with a non-resistant strain (Section 3.6).
3.5.2 Description
Hiring a maidJan Jaap, Karina and their two daughters aged 3 and 1 live in a large villa in Hilversum. Jan Jaap is a lawyer working for a large international company, and Karina does a lot of charity work. As Karina’s work regularly requires her to travel and Jan Jaap has difficulty finding the time to help out in the house, they decide to hire a maid who can also occasionally babysit for them. One of Jan Jaap’s hockey friends tells him that maids from Salinenkan are extremely reliable and speak very good English. They are frequently available in Amsterdam and charge very reasonable prices. His friend gives Jan Jaap a telephone number. A few weeks later, Elisa comes to
18 The KNCV Tuberculosis Foundation is an internationally renowned
and authoritative knowledge and expertise centre for TB control.
This organisation has devoted itself to combatting TB in both the
Netherlands and the rest of the world for over 100 years. See www.kncvtbc.org.
work for them in Hilversum. She is a pleasant, friendly and hard-working woman in her early twenties. She is saving for her education and speaks good English. Karina regularly entrusts Elisa with the care of her children, especially as Karina is now pregnant and does not always feel up to the task. Elisa lives in Amsterdam and travels to Hilversum every day via public transport. She shares a flat with her friends.
An unknown illness?In the autumn, Elisa – like many other people – begins to cough. “The flu season’s starting early this season, isn’t it?” is a frequently uttered sentence. Elisa soldiers on, but doesn’t feel a 100%. As extra hands are called for in Hilversum due to Karina’s pregnancy, Elisa stays over at the house for the family’s Sinterklaas party. She enjoys herself that evening, but doesn’t feel well. As he does not see her very often, Jan Jaap notices that Elisa has suddenly lost a lot of weight. In the weeks to come, Elisa’s condition deteriorates further. She loses more weight, coughs a lot, and fails to perform tasks to her usual high standard. The family is worried and doesn’t know what to do. As a lawyer at a top international company, Jan Jaap cannot afford to get into trouble over an illegal maid. Jan Jaap and his wife Karina decide to give Elisa money to fly back to Salinenkan as well as $2,000 in cash to pay for treatment. Elisa accepts the money and flies back to her homeland. Jan Jaap and Karina never hear from her again and are relieved that the situation has been resolved. They have no idea what was wrong with Elisa.
About nine months later, Jan Jaap develops a serious cough and starts to lose weight rapidly. He consults his doctor, who diagnoses him with open tuberculosis. Further examination shows that it is an XDR strain. This is a cause for great concern within the Regional Health Service (RHS) concerned. Standard practice is that anyone who has had contact with somebody with open TB should be screened. If they have been infected, then the chances that they will develop the illness are roughly 10%. This can be prevented by administering preventive treatment. However, for resistant tuberculosis, this is not the case, and you simply have to wait to see if the person becomes ill.The screening discovers that 113 people have been infected. This includes five children at the nursery of one of the daughters. A national team of experts discusses whether or not these children should be treated in some way. The other infected people include several dozen of Jan Jaap’s co-workers,
24 | In-Depth Thematic Analysis of AMR and National Security
seven people at the hockey club (including two children), and three people from the Rotary, including one seriously ill woman. Investigation is also in progress to investigate contact via international relations. Only time will tell how many infections have occurred as a result of casual contact (e.g. in shops, on public transport etc.)19.
As is always the case in the event of MDR, Jan Jaap remains in hospital for a number of months. His youngest daughter is also admitted to hospital, as an X-ray clearly shows that she also has tuberculosis. A complex course of treatment follows, and Jan Jaap is quarantined. His employer offers him a golden handshake in return for his departure. The family is too drained to object.
Unrest and dissatisfaction A growing feeling of unrest develops in the city. People are afraid to go to restaurants or even their local supermarket. When a celebrity is infected, the outbreak becomes the biggest story in all news media. In the family’s neighbourhood, fierce speculation begins about the source of the infection. The link to the maid is quickly established: she often picked up the children from school, and ‘everybody’ could tell she was in poor health.Infected people demand treatment and cannot understand why they are not receiving it. People lose faith in the local RHS. Some people try to buy medication online or consult doctors abroad, and the RHS loses track of who is taking what. The discussion about ‘foreigners’ is reignited. Months pass before the unrest subsides.
Information about the treatment of tuberculosisIf left untreated, around half of the patients with tuberculosis will die. The more resistant the bacteria, the less therapy and treatment options are available to cure the illness. Resistance also hugely inflates the cost of treatment. Treatment of XDR tuberculosis in the Netherlands costs over €130,000 per patient. The treatment requires long-term admission to a sanatorium and use of medications that have numerous side effects (including deafness) and are
19 People infected with the bacteria may only fall ill at a much later
stage, making them a potential source of infection. The estimated
number of infected people is simply a rough guess. As a rule of
thumb, one in ten infected people will fall ill, with half of these
people falling ill within 1-2 years following infection. However, it can
sometimes take 10-20 years before the infected person falls ill. In
this situation, if no preventive treatment is given, a further eight or
nine new cases of TB are to be expected.
less effective at eradicating the bacteria. If a patient remains chronically sick because the illness can no longer be treated with medication, then the only chance of a cure is to let it run its course and hope that the body fights off the infection. In the past, this ‘option’ has led to patients spending years in a sanatorium, isolated from their family and friends.
3.6 Nursing students infected with tuberculosis
3.6.1 Explanation and background information
Section 3.5.1 provides general information about tuberculosis. The scenario in Section 3.5.2 concerned a resistant strain, while this scenario involves a non-resistant strain.
3.6.2 Description
Many students at Saxion University of Applied Sciences in Deventer live locally. Two such students are a couple of friends who both aspire to a career in nursing. Every day, the girls get on their mopeds and ride together from their home village to school. Nursing was a pragmatic career choice for both of them: they both enjoy taking care of people, and nurses are always in demand. They are both in their third year and have always attended the same school. They each have a boyfriend within the same group of friends, and they are both learning jazz dance. Mystery trip of a lifetime?One sunny afternoon, the school’s main entrance is surrounded by a film crew. They are here to record an episode of the TV programme ‘Destination Unknown’, in which young people are sent to a mystery location for a week to learn about life in other parts of the world. The programme makers speak to both girls and offer them this unique work experience opportunity. The girls, who have never ventured further than the Ardennes before, are understandably excited. They have no idea what they are getting themselves into, but feel confident that together, they can use their vocation to help their fellow humans in a remote corner of the globe. They hurry home and grab their video cameras. Their parents are not exactly over the moon with the girls’ choice, but they decide not to stand in their way. The girls pack their bags and head for Schiphol airport. At the airport, they are told that they are going to
In-Depth Thematic Analysis of AMR and National Securityt | 25
Macoluna. Buzzing with expectation, they board the plane. Although the time difference is not huge, the girls are extremely tired by the time their 4.5-hour journey by plane and bus finally ends at a local hospital in Macoluna. They are welcomed with open arms and are full of curiosity, although they are simply unable to stand on their feet for fatigue. Early next morning, the girls are awoken from their slumbers. The poverty-stricken conditions have a major impact on the girls. They rely on each other for support and are deeply moved by the great suffering that they witness. It is a powerful experience to see an entire community with such bleak prospects for the future and such an alarmingly high rate of HIV. The friends give as much assistance as they possibly can and have a great deal of contact with the locals. Back homeA week later, they are happy to be back home. Although their friends and family have difficulty taking everything in, the girls are happy with their experience and resolve to return in the future to complete a longer internship. Some time later, one of the girls begins to cough. The cough persists, and one of her teachers sends her to see her GP. She is quickly diagnosed with open TB, and treatment begins immediately. In compliance with standard procedure, everybody in the girl’s environment is screened. The screening is relatively simple as the girl has a structured social life and the village is pretty remote. The Regional Health Service (RHS) draws up a plan of action. As part of the plan, the girl must be quarantined at home and receive no visitors. Contact investigation is also conducted with her classmates and people she has had frequent contact with. The student accepts her situation. The treatment is effective, her condition is not serious, she has seen other people undergo much greater suffering, and she understands why the RHS has taken the measures it has. Unrest in the villageHowever, the girl’s family and the family of her now ex-boyfriend do not share this calm attitude. They are angry and afraid. They feel like they have been pilloried, fear that they could drop dead at any moment, and cast doubt on the RHS’s approach. They think the RHS simply sees this as business as usual while they are in abject panic. The girl’s brother decides to make his voice heard, writing a strongly worded article for the local newspaper. This creates unrest throughout the entire village, and a large number of people ask to be tested. The story is also buzzing around Saxion University of Applied Sciences. At first, the school thought the TV
programme was a fun idea, but once the situation developed in the way it did, the mood changed dramatically. Demands are made to the mayor of the village to offer screening to everybody, despite there not being a single medical justification to do so. The channel that broadcast the programme tries to provide nuanced coverage, but this only adds more fuel to the fire.The unrest subsides after six months, but not before over 2,000 people are screened, and numerous people with minor coughs are subjected to unnecessary additional examination.
3.7 Children’s party on a farm ends in tragedy
3.7.1 Explanation and background information
The Methicillin-Resistant Staphylococcus aureus, or MRSA for short, is a Staphylococcus bacterium. Staphylococcus bacteria are very frequently found in healthy people without them having any adverse reactions. MRSA is a special type of Staphylococcus as it is resistant to treatment with most antibiotics. MRSA is regularly found in the Netherlands. People can be carriers of MRSA without getting sick themselves. The bacteria mainly live on the skin and in the noses of carriers, although they can also be found in the throat and intestines. MRSA can cause infections, mostly skin infections such as boils. In rare cases however, it can cause blood poisoning, bone infections, or pneumonia. Fatality rates for MRSA appear to be twice as high as those of the Methicillin-Sensitive Staphylococcus aureus (MSSA), although this depends on the person’s health or underlying suffering. A specific type of MRSA occurs in farm animals, known as livestock-associated MRSA. This type of MRSA is common in the Netherlands among pigs and calves, but also occurs in dairy cows, horses, and broiler chickens. Livestock-associated MRSA can be transmitted from animals to humans, particularly via direct contact with animals.
3.7.2 Description
Party on the farmIn March 2015, a group of twelve girls in their first year at Oosterzand Grammar School attend the birthday party of their friend Lisa. It is held at a farm in Oosterzand that is available to rent for stag nights, children’s parties, and company outings. The party will involve canoeing, feeding the cows, farmyard

26 | In-Depth Thematic Analysis of AMR and National Security
golf, and a picnic in the meadow. Luckily, the weather is nice that day. The picnic includes local produce such as cheese, fresh milk, and fruit from the orchard. Because it is spring, some of the girls are even allowed to bottle-feed the lambs. There are also pigs at the farm, although these are usually reserved for stag parties. Everybody is having fun. The party ends several hours later, and the children are driven home.
Deadly infectionTwo days later, Lisa’s best friend Anne is absent from school due to illness. She is displaying flu-like symptoms and has a high fever. The next day, the GP is called for a home visit. Anne is feverish and has a cough. As the flu season is at its peak, the GP diagnoses a simple case of the flu. Paracetamol and bed rest are recommended. However, during the night, Anne has difficulty breathing, and her parents call the GP again next morning. The GP examines Anne a second time and begins to have doubts. The GP consults with a specialist, and soon an ambulance picks up Anne and takes her to the hospital where she is diagnosed with pneumonia. She is admitted to intensive care, put on a respirator, and given intravenous antibiotics. However, within 24 hours of her admission to hospital, she dies.
Further tests of samples taken just after her admission show that the girl had been infected with MRSA. The pathogen was found in a blood culture. The doctors want to perform an autopsy on the girl’s body, but the 12-year-old’s parents are extremely grief-stricken and refuse consent. Further testing of the isolated MRSA pathogen reveals it is a strain that produces an extremely dangerous toxin. Otherwise, the isolate displays all the hallmarks of livestock-associated MRSA. Unfortunately, the bacteria were also resistant to the intravenous antibiotics administered to Anne.
News of Anne’s death shocks the school, and a meeting is held to inform the children’s parents. In the intervening period, news has leaked that the cause may be livestock-associated MRSA. A great deal of unrest grows within the school. Two other children who attended the party are also at home with flu-like symptoms. Many parents fear the illness that killed Anne may be highly infectious and want to keep their children at home until more is known about the outbreak. However, the school board decides against closing the school.
Drastic measures at the sourceFollowing consultation with the parents, the
specialists at the hospital suspect a link between the MRSA infection and the children’s party at the farm. A veterinarian is contacted, and the different animals at the farm are examined. Three days later, eight of the twenty cows and four of the five pigs at the farm are confirmed as MRSA positive. Further testing of all isolates at RIVM show that the isolates from the cows and pigs are identical to that of the patient. The farm therefore appears to be harbouring a new strain of MRSA that produces dangerous toxins. All of the farm’s bookings that week (two stag parties and three company outings) are cancelled. The decision is made to cull the infected animals and to examine the ten agricultural businesses within a 2-km radius of the farm. Following the decision to investigate the surrounding area, consultation takes place between the various ministries to determine what to do next. From the public health perspective, a cull of all animals at infected businesses is recommended. This not only includes the farm, but also any other possibly infected agricultural businesses in the area. However, from an economic point of view and with the interests of the agricultural businesses involved in mind, quarantine is proposed.
Growing unrestBy now, another five children at the grammar school have fallen ill. Two of them are in Lisa’s class, the other three are not. Four of these children were not present at the birthday party. Further testing is conducted to determine whether the children have been infected with MRSA. As this test takes four to five days, uncertainty and unrest grows at the school. By now, the parents affected have set up a group and are collecting information from an acquaintance of theirs who is supposedly an MRSA expert. Based on the information they obtain and the fact that children who did not attend the party have also fallen ill, their unrest grows so much that one of the parents decides to inform the press. The next day, a story appears in the newspaper. The day after that, the story is featured in the early evening news on TV. A public debate is sparked regarding the safety of children’s farms, care farms, camping on farmland, and other farm-related activities. Various interest groups and government bodies weigh in on the debate, and questions are asked in Dutch Parliament.
Many people who attended activities at the farm shortly before it was closed to the public become very worried: shouldn’t they also be screened for the MRSA bacteria? Other people who have been to the other livestock businesses are worried, and GPs are

In-Depth Thematic Analysis of AMR and National Securityt | 27
bombarded with phone calls. Everybody wants to check that they haven’t been infected. Although the GPs sympathise with the people’s worries, they refuse further examination to people who display no symptoms and people who have had no contact with the potentially infected agricultural businesses. However, test results are the only way to put people’s minds at rest, and people who are refused tests react with anger.
Another incident Before the closure of the farm, an incident also took place during one of the stag parties. During a pig-wrestling match, one participant was bitten in the arm by a pig. Initially, the wound appeared to have been effectively treated, but a few days later, an infection set in. The pig in question turned out to be one of the infected animals. The infection spirals out of control, and eventually the young man’s right arm has to be amputated. The friends from the stag party are extremely shocked by the consequences of the seemingly innocuous party, and they decide to express their shock via various social media. In view of the intense media attention surrounding the sick children infected at the same farm, the press are quick to pounce upon this new story.
Ban on agricultural produceDue to the extensive unrest within the community, a decision must be made about screening citizens who have visited one of the businesses involved. To limit further risks to public health, it is decided to ban the sale of products from surrounding businesses until further notice and to postpone the slaughter of animals. This decision causes a great deal of inconvenience to the agricultural businesses concerned. After all, it paralyses their business operations and leads to excess stock. The only farmer who is still offering his land as a campsite has witnessed a steep decline in demand. The farmers are therefore suffering considerable economic damage.
End of the crisisEventually, it turns out that the five children were not infected with MRSA. Also, the two other children who fell ill before the group of five turn out to have had ordinary flu and are already back to full health. Examination of the surrounding area detects an infection at one other company, and the animals in question are quarantined.
Lisa misses her friend Anne terribly and feels responsible for her death. After all, it was her party that resulted in the infection. Lisa also feels like
Anne’s parents treat her differently. Her birthday will never be the same again. The young man whose arm was amputated feels a strong sense of injustice and continues to court the media. He sets up a foundation to raise awareness of MRSA and gains a lot of attention. Although the message he puts out is factually incorrect, it remains in the media due to a lack of rebuttal from the institutes concerned. The government is faced with a dilemma: should they create policy regarding animals in public places and antibiotic use in order to calm the unrest?
3.8 Cruise passengers struck down by food poisoning
3.8.1 Explanation and background information
For this scenario, an outbreak of Salmonella Typhimurium was selected. This is a strain of pathogen that can make people fairly sick. This strain of bacteria is found in chicken and eggs, and infects humans via contaminated food, in a similar way to strains of ESBL20-producing Escherichia coli which have regularly featured in the news in recent times. Salmonella bacteria can also produce ESBL, making them untreatable using regular antibiotics.
3.8.2 Description
12 January 2015: Sickness at seaOn 12 January 2015, two passengers report to the ship’s doctor with upset stomachs and diarrhoea. The two passengers are on board the luxury cruise liner ‘Maxima’, which has just embarked on a long voyage to Indonesia from its home port of Rotterdam. The passengers of the cruise liner are predominantly wealthy senior citizens from the Netherlands. In the morning of the 12th of January, a male passenger begins to feel unwell. He has an upset stomach and is soon making frequent visits to the toilet. His wife advises him to see the ship’s doctor during his surgery hours. While sat in the waiting room, the man sees a woman come in who appears to be displaying similar symptoms. The doctor examines both patients and recommends that they
20 Extended-Spectrum Beta-Lactamase (ESBL) is a collective term for a
group of enzymes created by bacteria (ESBL-producing bacteria).
These enzymes are able to hydrolyse the antibiotic groups of
cefalosporin and penicillin (the β-lactam antibiotics), which renders
them ineffective.
28 | In-Depth Thematic Analysis of AMR and National Security
drink a lot of fluids and keep eating as normal. Over the course of the day, more passengers report to the ship’s doctor with identical symptoms. In the next few days, the number of patients rises rapidly. The severity of some of the patients’ symptoms is increasing, and they are admitted to the sick bay with symptoms of dehydration. Intravenous fluids are administered via a drip. They are suffering from intense bouts of vomiting as well as headaches and high fevers.The ship’s Quality Assurance Officer is instructed to contact NVWA (the Netherlands Food and Consumer Product Safety Authority), and the ship’s doctor reports the outbreak to the Rotterdam-Rijnmond Regional Health Service (RHS).
Several days later: a major outbreak?Taking into account the symptoms and the way the illness is presenting and spreading, the ship’s doctor rules out a norovirus infection. He therefore decides to treat the patients with antibiotics. However, all of the antibiotics used (fluoroquinolones and aminoglycosides) prove ineffective. Even meropenem and imipenem fail to have the desired effect. Once again, the ship’s doctor contacts the RHS in Rotterdam. Together they conclude that the patients may have been infected with an ESBL/carbapenemase-producing strain of bacteria. Soon after, one of the patients dies. On the same day, patients with similar symptoms start reporting to GPs all over the Netherlands. A study conducted by NVWA in collaboration with RIVM shows that it is an infection caused by a carbapenemase-producing strain of Salmonella Typhimurium. Whole-genome sequencing clearly shows that the bacteria isolates from the patients on the cruise liner are identical to those of the patients on land. It is decided to turn the ship around and return to the Netherlands. Unrest amongst the passengers on the ship increases. On the way back to the port of Rotterdam, the captain and the ship’s doctor arrange an informative meeting in the dining room, but they are unable to ease the passengers’ unrest.
The outbreak goes nationalUnrest throughout the Netherlands is on the rise. The outbreak features prominently in the news and in a variety of current affairs programmes. A diverse range of ‘experts’ are approached for comment, resulting in a great deal of contradictory information being fed to the public. As the source of the outbreak has not yet been identified, a vegetarian society and a political party point the finger at the meat production and processing industry, which in turn
issues steadfast denials. Industry representatives also state that they do everything in their power to prevent Salmonella infection and that they have also halved the use of antibiotics in recent years. In consultation with RIVM, the authorities decide to set up an Outbreak Management Team (OMT), and the participants agree that simple and understandable information must be provided to the public. However, this is not enough to prevent heated discussions on internet forums and on Twitter. A percentage of the population seems to trust the opinions of people around them more than those of the government and the experts.
Mid-February 2015By this point, the outbreak has been in progress for four weeks. Since the first cases were reported, NVWA and RIVM have been extensively investigating the outbreak, but further scrutiny of the suspected sources rules them all out. Consumers are now avoiding meat products en masse, especially chicken and pork. The aforementioned vegetarian society sees its membership numbers rise by 50%. Questions are asked in Dutch Parliament, and the minister responsible is held to account. Calls for a zero-tolerance policy on salmonella in meat and the decontamination of infected carcasses get louder and louder.
Mid-March 2015Roughly eight weeks after the outbreak first originated, the number of new cases has risen to 250 per week, and the source has still not been traced. However, in the ninth week of the outbreak, it is noticed that a large number of patients are residents of the same care home. Epidemiological research shows a clear connection between the consumption of Bavarian cream (of which raw eggs are an ingredient) and the reported infections. This information is proudly announced to the media, accompanied by the advice to only consume eggs that have been cooked thoroughly. The discovery marks a turning point in the research as NVWA can now focus on large-scale analysis of eggs in order to prevent Salmonella Typhimurium. However, no infected eggs are found in the shops, and the supplier of the tainted eggs has still not been traced. This development leads to a complete consumer strike. A couple of days later, with the aid of international collaboration, NVWA is finally able to trace the source of the outbreak. It turns out the source was based outside the Netherlands. Once this becomes clear, consumer confidence is quickly restored, and the sale of eggs picks up again.

In-Depth Thematic Analysis of AMR and National Securityt | 29
The whole episode lasted for around ten weeks. During this period, 1,758 people fell ill, eleven of whom died. Both the meat and egg industries suffered major economic damage during this period.
30 | In-Depth Thematic Analysis of AMR and National Security
In-Depth Thematic Analysis of AMR and National Securityt | 31
4 Assessment resultsIn this chapter, the results of the assessment will be presented. Firstly, the likelihood scores (Section 4.1), the assessment of the effects on vital infrastructure (4.2) and the definitive scores for the separate impact criteria (4.3) will be given. In Section 4.4, a ‘risk diagram’ will be presented. As mentioned previously, the eight scenarios have been assessed by experts in compliance with the (slightly adjusted) NRA methodology, with the scoring based on the facts and incidents described in the scenarios.
4.1 Likelihood
The likelihood of NRA scenarios that involve no deliberate acts is based on factors such as failure probabilities, case histories, and historical data. If such information is unavailable, then we rely on expert judgement. In these cases, the classification as defined in the guidelines for the NRA methodology can be used as a tool for the experts to illustrate what they mean by the terms ‘Highly unlikely’, ‘Unlikely’, etc.In general, there are no solid figures for the occurrence of AMR scenarios, although there is experiential data that can be used in a manner similar to case histories (with the exception of the two scenarios that take place in 2023). For example,
it is known that incidents comparable to the one described in Scenario 4a have occurred in the past. The likelihood is assessed based on a combination of experiential data and expert judgement. The likelihood score will be expressed as one of the following categories21: A: Highly unlikely; B: Unlikely; C: Possible; D: Likely; E: Highly likely.
Table 4.1 displays the definitive scores for the eight scenarios.
Upon viewing the distribution of scores, the assembled experts clearly gave the opinion that the distribution was reasonable given all of the uncertainties involved in assessing the likelihood of these scenarios. They also agreed that Scenario 6 (widespread food poisoning) is the most likely to occur within the next five years, closely followed by Scenarios 2 (prolonged outbreak in nursing home) and 4a and 4b (tuberculosis infection). Transmission of resistant and non-resistant tuberculosis has already occurred, and situations similar to those described earlier have already affected a number of nursing homes. However, some of the occurrences in the scenarios (major unrest; intensive media attention;
21 The meaning of the various likelihood categories is described in the
guidelines of the NRA methodology (see Footnote 1 in Section 1.1).
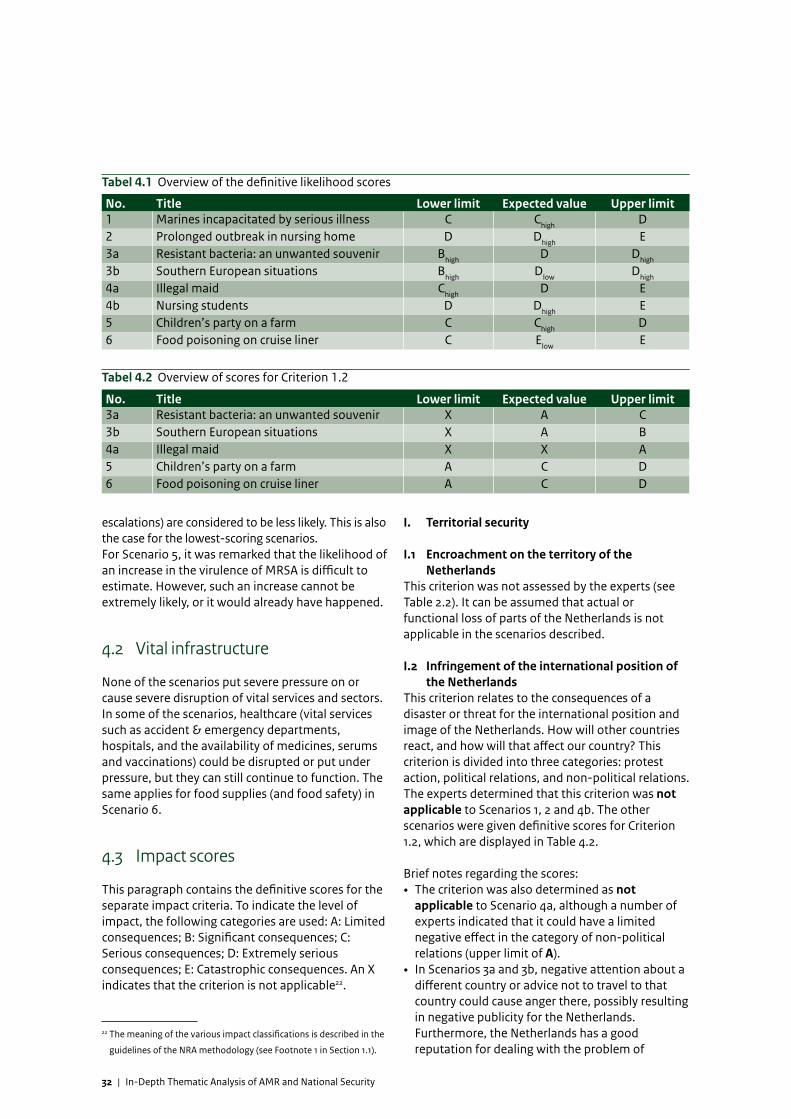
32 | In-Depth Thematic Analysis of AMR and National Security
Tabel 4.1 Overview of the definitive likelihood scores
No. Title Lower limit Expected value Upper limit1 Marines incapacitated by serious illness C Chigh D2 Prolonged outbreak in nursing home D Dhigh E3a Resistant bacteria: an unwanted souvenir Bhigh D Dhigh
3b Southern European situations Bhigh Dlow Dhigh
4a Illegal maid Chigh D E4b Nursing students D Dhigh E5 Children’s party on a farm C Chigh D6 Food poisoning on cruise liner C Elow E
Tabel 4.2 Overview of scores for Criterion 1.2
No. Title Lower limit Expected value Upper limit3a Resistant bacteria: an unwanted souvenir X A C3b Southern European situations X A B4a Illegal maid X X A5 Children’s party on a farm A C D6 Food poisoning on cruise liner A C D
escalations) are considered to be less likely. This is also the case for the lowest-scoring scenarios. For Scenario 5, it was remarked that the likelihood of an increase in the virulence of MRSA is difficult to estimate. However, such an increase cannot be extremely likely, or it would already have happened.
4.2 Vital infrastructure
None of the scenarios put severe pressure on or cause severe disruption of vital services and sectors. In some of the scenarios, healthcare (vital services such as accident & emergency departments, hospitals, and the availability of medicines, serums and vaccinations) could be disrupted or put under pressure, but they can still continue to function. The same applies for food supplies (and food safety) in Scenario 6.
4.3 Impact scores
This paragraph contains the definitive scores for the separate impact criteria. To indicate the level of impact, the following categories are used: A: Limited consequences; B: Significant consequences; C: Serious consequences; D: Extremely serious consequences; E: Catastrophic consequences. An X indicates that the criterion is not applicable22.
22 The meaning of the various impact classifications is described in the
guidelines of the NRA methodology (see Footnote 1 in Section 1.1).
I. Territorial security
I.1 Encroachment on the territory of the Netherlands
This criterion was not assessed by the experts (see Table 2.2). It can be assumed that actual or functional loss of parts of the Netherlands is not applicable in the scenarios described.
I.2 Infringement of the international position of the Netherlands
This criterion relates to the consequences of a disaster or threat for the international position and image of the Netherlands. How will other countries react, and how will that affect our country? This criterion is divided into three categories: protest action, political relations, and non-political relations.The experts determined that this criterion was not applicable to Scenarios 1, 2 and 4b. The other scenarios were given definitive scores for Criterion 1.2, which are displayed in Table 4.2.
Brief notes regarding the scores:• The criterion was also determined as not
applicable to Scenario 4a, although a number of experts indicated that it could have a limited negative effect in the category of non-political relations (upper limit of A).
• In Scenarios 3a and 3b, negative attention about a different country or advice not to travel to that country could cause anger there, possibly resulting in negative publicity for the Netherlands. Furthermore, the Netherlands has a good reputation for dealing with the problem of
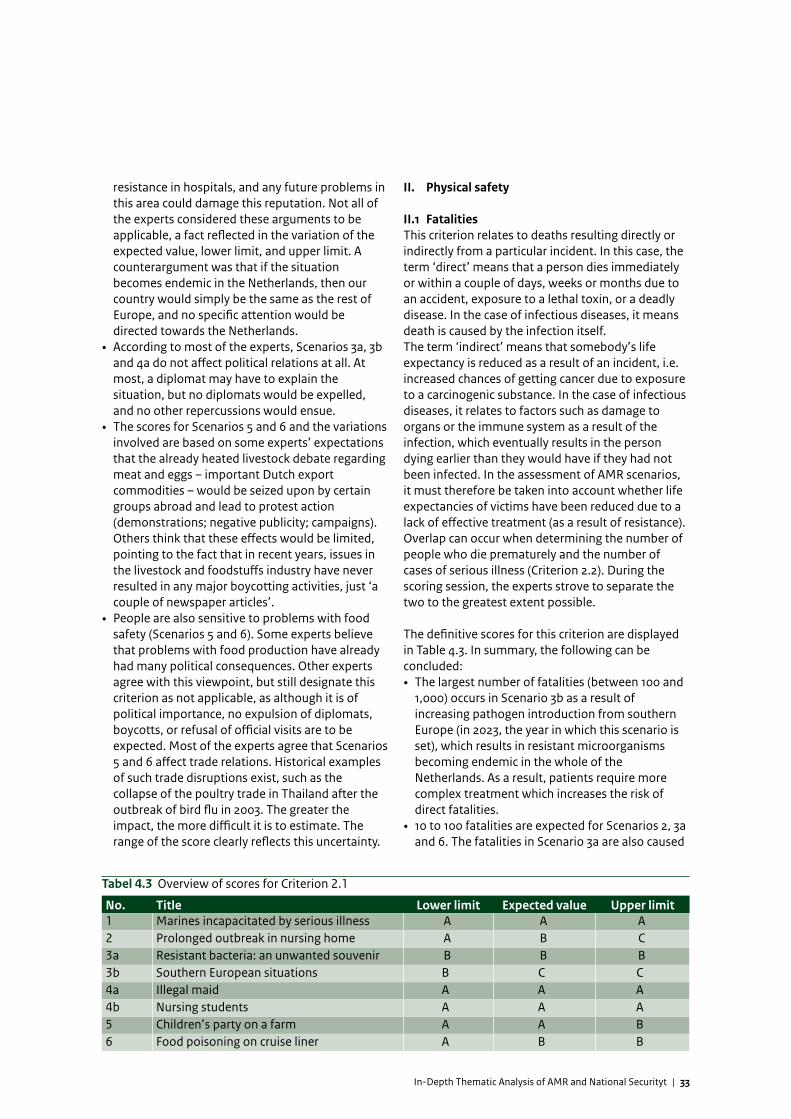
In-Depth Thematic Analysis of AMR and National Securityt | 33
resistance in hospitals, and any future problems in this area could damage this reputation. Not all of the experts considered these arguments to be applicable, a fact reflected in the variation of the expected value, lower limit, and upper limit. A counterargument was that if the situation becomes endemic in the Netherlands, then our country would simply be the same as the rest of Europe, and no specific attention would be directed towards the Netherlands.
• According to most of the experts, Scenarios 3a, 3b and 4a do not affect political relations at all. At most, a diplomat may have to explain the situation, but no diplomats would be expelled, and no other repercussions would ensue.
• The scores for Scenarios 5 and 6 and the variations involved are based on some experts’ expectations that the already heated livestock debate regarding meat and eggs – important Dutch export commodities – would be seized upon by certain groups abroad and lead to protest action (demonstrations; negative publicity; campaigns). Others think that these effects would be limited, pointing to the fact that in recent years, issues in the livestock and foodstuffs industry have never resulted in any major boycotting activities, just ‘a couple of newspaper articles’.
• People are also sensitive to problems with food safety (Scenarios 5 and 6). Some experts believe that problems with food production have already had many political consequences. Other experts agree with this viewpoint, but still designate this criterion as not applicable, as although it is of political importance, no expulsion of diplomats, boycotts, or refusal of official visits are to be expected. Most of the experts agree that Scenarios 5 and 6 affect trade relations. Historical examples of such trade disruptions exist, such as the collapse of the poultry trade in Thailand after the outbreak of bird flu in 2003. The greater the impact, the more difficult it is to estimate. The range of the score clearly reflects this uncertainty.
II. Physical safety
II.1 FatalitiesThis criterion relates to deaths resulting directly or indirectly from a particular incident. In this case, the term ‘direct’ means that a person dies immediately or within a couple of days, weeks or months due to an accident, exposure to a lethal toxin, or a deadly disease. In the case of infectious diseases, it means death is caused by the infection itself. The term ‘indirect’ means that somebody’s life expectancy is reduced as a result of an incident, i.e. increased chances of getting cancer due to exposure to a carcinogenic substance. In the case of infectious diseases, it relates to factors such as damage to organs or the immune system as a result of the infection, which eventually results in the person dying earlier than they would have if they had not been infected. In the assessment of AMR scenarios, it must therefore be taken into account whether life expectancies of victims have been reduced due to a lack of effective treatment (as a result of resistance).Overlap can occur when determining the number of people who die prematurely and the number of cases of serious illness (Criterion 2.2). During the scoring session, the experts strove to separate the two to the greatest extent possible.
The definitive scores for this criterion are displayed in Table 4.3. In summary, the following can be concluded:• The largest number of fatalities (between 100 and
1,000) occurs in Scenario 3b as a result of increasing pathogen introduction from southern Europe (in 2023, the year in which this scenario is set), which results in resistant microorganisms becoming endemic in the whole of the Netherlands. As a result, patients require more complex treatment which increases the risk of direct fatalities.
• 10 to 100 fatalities are expected for Scenarios 2, 3a and 6. The fatalities in Scenario 3a are also caused
Tabel 4.3 Overview of scores for Criterion 2.1
No. Title Lower limit Expected value Upper limit1 Marines incapacitated by serious illness A A A2 Prolonged outbreak in nursing home A B C3a Resistant bacteria: an unwanted souvenir B B B3b Southern European situations B C C4a Illegal maid A A A4b Nursing students A A A5 Children’s party on a farm A A B6 Food poisoning on cruise liner A B B
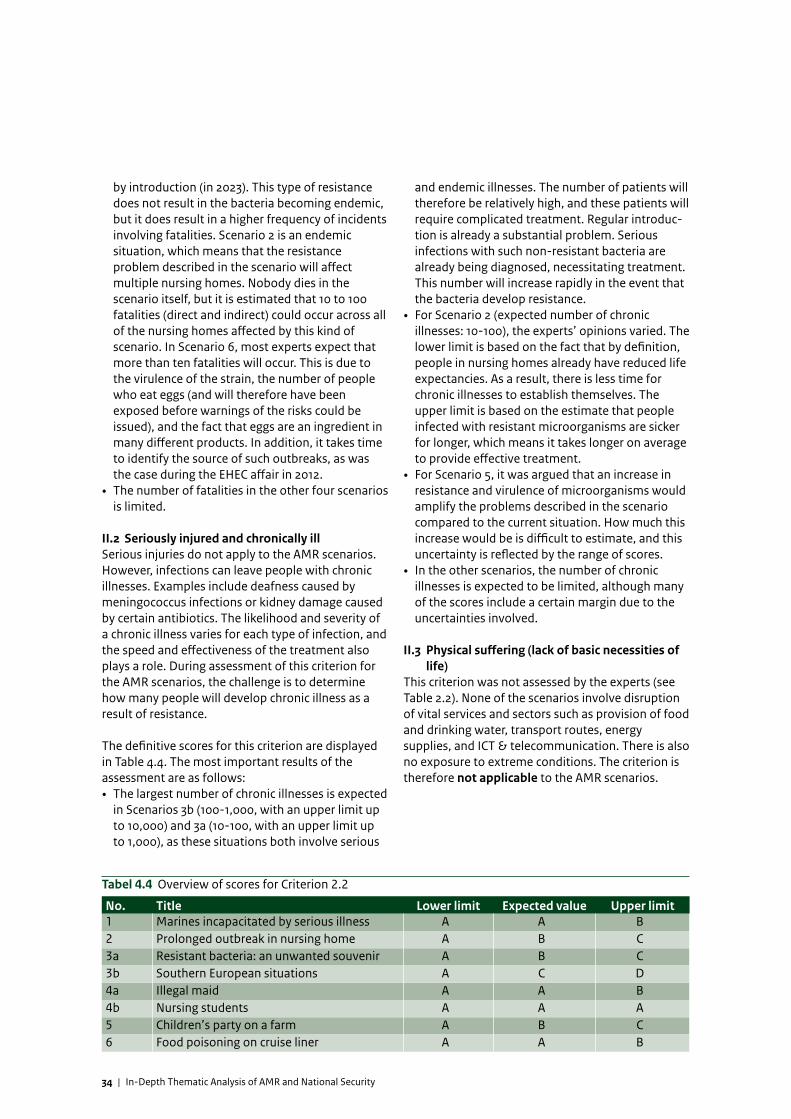
34 | In-Depth Thematic Analysis of AMR and National Security
by introduction (in 2023). This type of resistance does not result in the bacteria becoming endemic, but it does result in a higher frequency of incidents involving fatalities. Scenario 2 is an endemic situation, which means that the resistance problem described in the scenario will affect multiple nursing homes. Nobody dies in the scenario itself, but it is estimated that 10 to 100 fatalities (direct and indirect) could occur across all of the nursing homes affected by this kind of scenario. In Scenario 6, most experts expect that more than ten fatalities will occur. This is due to the virulence of the strain, the number of people who eat eggs (and will therefore have been exposed before warnings of the risks could be issued), and the fact that eggs are an ingredient in many different products. In addition, it takes time to identify the source of such outbreaks, as was the case during the EHEC affair in 2012.
• The number of fatalities in the other four scenarios is limited.
II.2 Seriously injured and chronically illSerious injuries do not apply to the AMR scenarios. However, infections can leave people with chronic illnesses. Examples include deafness caused by meningococcus infections or kidney damage caused by certain antibiotics. The likelihood and severity of a chronic illness varies for each type of infection, and the speed and effectiveness of the treatment also plays a role. During assessment of this criterion for the AMR scenarios, the challenge is to determine how many people will develop chronic illness as a result of resistance.
The definitive scores for this criterion are displayed in Table 4.4. The most important results of the assessment are as follows: • The largest number of chronic illnesses is expected
in Scenarios 3b (100-1,000, with an upper limit up to 10,000) and 3a (10-100, with an upper limit up to 1,000), as these situations both involve serious
and endemic illnesses. The number of patients will therefore be relatively high, and these patients will require complicated treatment. Regular introduc-tion is already a substantial problem. Serious infections with such non-resistant bacteria are already being diagnosed, necessitating treatment. This number will increase rapidly in the event that the bacteria develop resistance.
• For Scenario 2 (expected number of chronic illnesses: 10-100), the experts’ opinions varied. The lower limit is based on the fact that by definition, people in nursing homes already have reduced life expectancies. As a result, there is less time for chronic illnesses to establish themselves. The upper limit is based on the estimate that people infected with resistant microorganisms are sicker for longer, which means it takes longer on average to provide effective treatment.
• For Scenario 5, it was argued that an increase in resistance and virulence of microorganisms would amplify the problems described in the scenario compared to the current situation. How much this increase would be is difficult to estimate, and this uncertainty is reflected by the range of scores.
• In the other scenarios, the number of chronic illnesses is expected to be limited, although many of the scores include a certain margin due to the uncertainties involved.
II.3 Physical suffering (lack of basic necessities of life)
This criterion was not assessed by the experts (see Table 2.2). None of the scenarios involve disruption of vital services and sectors such as provision of food and drinking water, transport routes, energy supplies, and ICT & telecommunication. There is also no exposure to extreme conditions. The criterion is therefore not applicable to the AMR scenarios.
Tabel 4.4 Overview of scores for Criterion 2.2
No. Title Lower limit Expected value Upper limit1 Marines incapacitated by serious illness A A B2 Prolonged outbreak in nursing home A B C3a Resistant bacteria: an unwanted souvenir A B C3b Southern European situations A C D4a Illegal maid A A B4b Nursing students A A A5 Children’s party on a farm A B C6 Food poisoning on cruise liner A A B
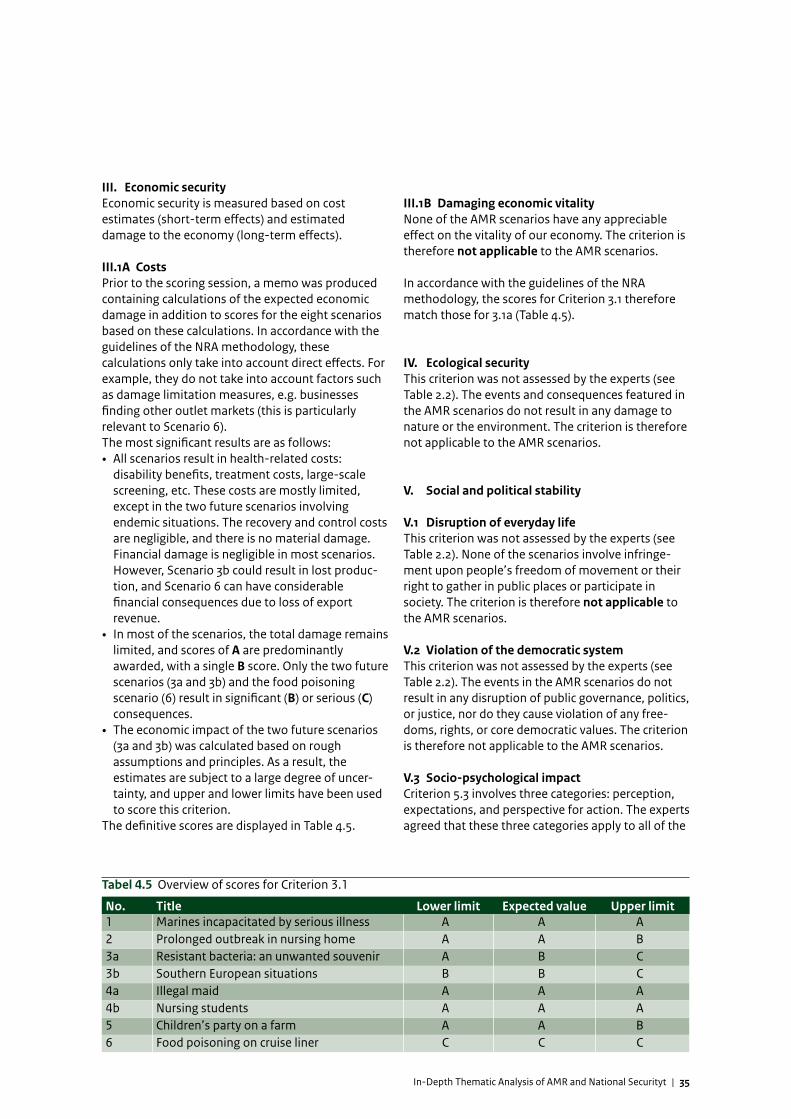
In-Depth Thematic Analysis of AMR and National Securityt | 35
III. Economic securityEconomic security is measured based on cost estimates (short-term effects) and estimated damage to the economy (long-term effects).
III.1A CostsPrior to the scoring session, a memo was produced containing calculations of the expected economic damage in addition to scores for the eight scenarios based on these calculations. In accordance with the guidelines of the NRA methodology, these calculations only take into account direct effects. For example, they do not take into account factors such as damage limitation measures, e.g. businesses finding other outlet markets (this is particularly relevant to Scenario 6).The most significant results are as follows: • All scenarios result in health-related costs:
disability benefits, treatment costs, large-scale screening, etc. These costs are mostly limited, except in the two future scenarios involving endemic situations. The recovery and control costs are negligible, and there is no material damage. Financial damage is negligible in most scenarios. However, Scenario 3b could result in lost produc-tion, and Scenario 6 can have considerable financial consequences due to loss of export revenue.
• In most of the scenarios, the total damage remains limited, and scores of A are predominantly awarded, with a single B score. Only the two future scenarios (3a and 3b) and the food poisoning scenario (6) result in significant (B) or serious (C) consequences.
• The economic impact of the two future scenarios (3a and 3b) was calculated based on rough assumptions and principles. As a result, the estimates are subject to a large degree of uncer-tainty, and upper and lower limits have been used to score this criterion.
The definitive scores are displayed in Table 4.5.
III.1B Damaging economic vitalityNone of the AMR scenarios have any appreciable effect on the vitality of our economy. The criterion is therefore not applicable to the AMR scenarios.
In accordance with the guidelines of the NRA methodology, the scores for Criterion 3.1 therefore match those for 3.1a (Table 4.5).
IV. Ecological securityThis criterion was not assessed by the experts (see Table 2.2). The events and consequences featured in the AMR scenarios do not result in any damage to nature or the environment. The criterion is therefore not applicable to the AMR scenarios.
V. Social and political stability
V.1 Disruption of everyday lifeThis criterion was not assessed by the experts (see Table 2.2). None of the scenarios involve infringe-ment upon people’s freedom of movement or their right to gather in public places or participate in society. The criterion is therefore not applicable to the AMR scenarios.
V.2 Violation of the democratic systemThis criterion was not assessed by the experts (see Table 2.2). The events in the AMR scenarios do not result in any disruption of public governance, politics, or justice, nor do they cause violation of any free-doms, rights, or core democratic values. The criterion is therefore not applicable to the AMR scenarios.
V.3 Socio-psychological impactCriterion 5.3 involves three categories: perception, expectations, and perspective for action. The experts agreed that these three categories apply to all of the
Tabel 4.5 Overview of scores for Criterion 3.1
No. Title Lower limit Expected value Upper limit1 Marines incapacitated by serious illness A A A2 Prolonged outbreak in nursing home A A B3a Resistant bacteria: an unwanted souvenir A B C3b Southern European situations B B C4a Illegal maid A A A4b Nursing students A A A5 Children’s party on a farm A A B6 Food poisoning on cruise liner C C C
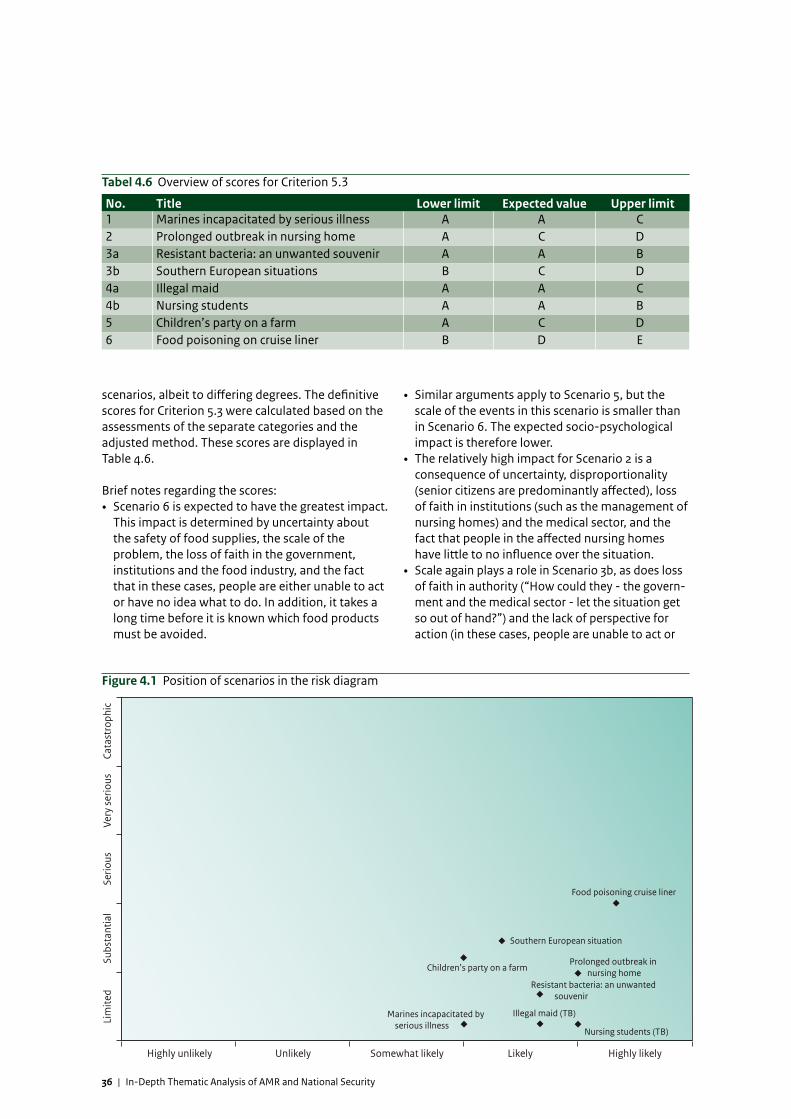
36 | In-Depth Thematic Analysis of AMR and National Security
Tabel 4.6 Overview of scores for Criterion 5.3
No. Title Lower limit Expected value Upper limit1 Marines incapacitated by serious illness A A C2 Prolonged outbreak in nursing home A C D3a Resistant bacteria: an unwanted souvenir A A B3b Southern European situations B C D4a Illegal maid A A C4b Nursing students A A B5 Children’s party on a farm A C D6 Food poisoning on cruise liner B D E
scenarios, albeit to differing degrees. The definitive scores for Criterion 5.3 were calculated based on the assessments of the separate categories and the adjusted method. These scores are displayed in Table 4.6.
Brief notes regarding the scores:• Scenario 6 is expected to have the greatest impact.
This impact is determined by uncertainty about the safety of food supplies, the scale of the problem, the loss of faith in the government, institutions and the food industry, and the fact that in these cases, people are either unable to act or have no idea what to do. In addition, it takes a long time before it is known which food products must be avoided.
• Similar arguments apply to Scenario 5, but the scale of the events in this scenario is smaller than in Scenario 6. The expected socio-psychological impact is therefore lower.
• The relatively high impact for Scenario 2 is a consequence of uncertainty, disproportionality (senior citizens are predominantly affected), loss of faith in institutions (such as the management of nursing homes) and the medical sector, and the fact that people in the affected nursing homes have little to no influence over the situation.
• Scale again plays a role in Scenario 3b, as does loss of faith in authority (“How could they - the govern-ment and the medical sector - let the situation get so out of hand?”) and the lack of perspective for action (in these cases, people are unable to act or
Figure 4.1 Position of scenarios in the risk diagram
Marines incapacitated by serious illness
Prolonged outbreak in nursing home
Resistant bacteria: an unwanted souvenir
Southern European situation
Illegal maid (TB)
Nursing students (TB)
Children’s party on a farm
Food poisoning cruise liner
Highly likelyLikelySomewhat likelyUnlikelyHighly unlikely
Cata
stro
phic
Ve
ry s
erio
us
Serio
us
Subs
tant
ial
Lim
ited
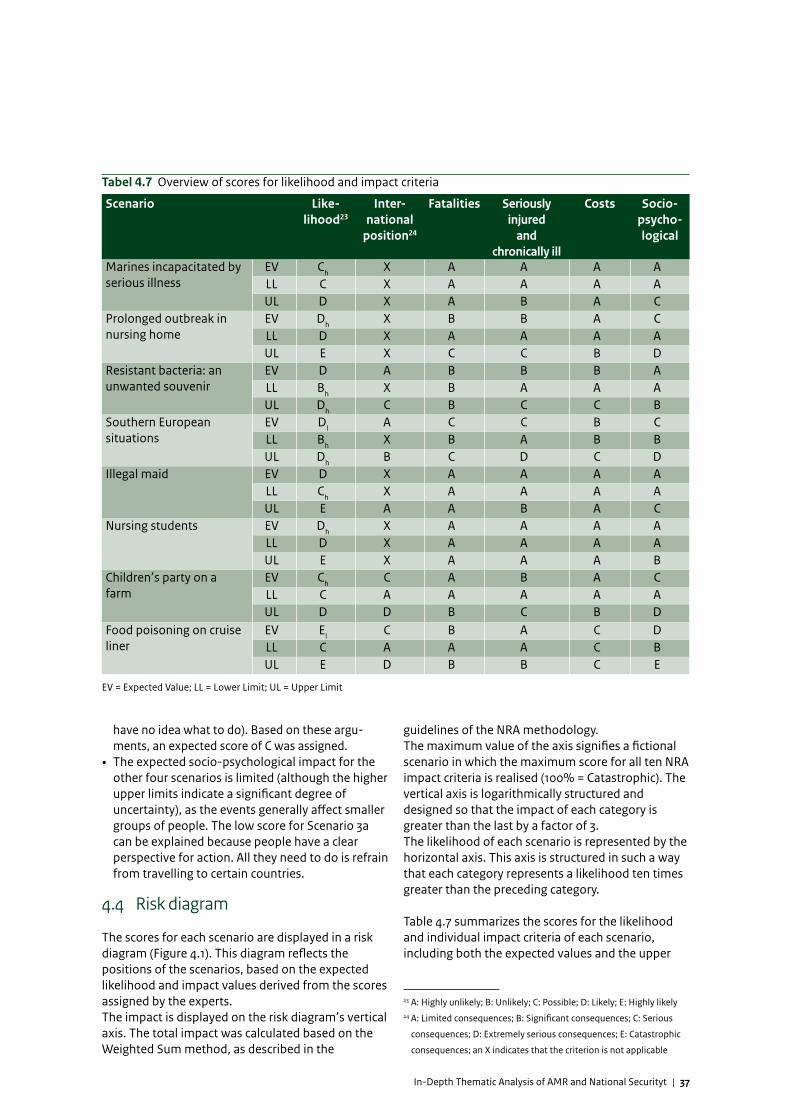
In-Depth Thematic Analysis of AMR and National Securityt | 37
Tabel 4.7 Overview of scores for likelihood and impact criteria
Scenario Like-lihood23
Inter-national
position24
Fatalities Seriously injured
and chronically ill
Costs Socio-psycho-logical
Marines incapacitated by serious illness
EV Ch X A A A ALL C X A A A AUL D X A B A C
Prolonged outbreak in nursing home
EV Dh X B B A CLL D X A A A AUL E X C C B D
Resistant bacteria: an unwanted souvenir
EV D A B B B ALL Bh X B A A AUL Dh C B C C B
Southern European situations
EV Dl A C C B CLL Bh X B A B BUL Dh B C D C D
Illegal maid EV D X A A A ALL Ch X A A A AUL E A A B A C
Nursing students EV Dh X A A A ALL D X A A A AUL E X A A A B
Children’s party on a farm
EV Ch C A B A CLL C A A A A AUL D D B C B D
Food poisoning on cruise liner
EV El C B A C DLL C A A A C BUL E D B B C E
EV = Expected Value; LL = Lower Limit; UL = Upper Limit
have no idea what to do). Based on these argu-ments, an expected score of C was assigned.
• The expected socio-psychological impact for the other four scenarios is limited (although the higher upper limits indicate a significant degree of uncertainty), as the events generally affect smaller groups of people. The low score for Scenario 3a can be explained because people have a clear perspective for action. All they need to do is refrain from travelling to certain countries.
4.4 Risk diagram
The scores for each scenario are displayed in a risk diagram (Figure 4.1). This diagram reflects the positions of the scenarios, based on the expected likelihood and impact values derived from the scores assigned by the experts. The impact is displayed on the risk diagram’s vertical axis. The total impact was calculated based on the Weighted Sum method, as described in the
guidelines of the NRA methodology. The maximum value of the axis signifies a fictional scenario in which the maximum score for all ten NRA impact criteria is realised (100% = Catastrophic). The vertical axis is logarithmically structured and designed so that the impact of each category is greater than the last by a factor of 3.The likelihood of each scenario is represented by the horizontal axis. This axis is structured in such a way that each category represents a likelihood ten times greater than the preceding category. 23 24 Table 4.7 summarizes the scores for the likelihood and individual impact criteria of each scenario, including both the expected values and the upper
23 A: Highly unlikely; B: Unlikely; C: Possible; D: Likely; E: Highly likely24 A: Limited consequences; B: Significant consequences; C: Serious
consequences; D: Extremely serious consequences; E: Catastrophic
consequences; an X indicates that the criterion is not applicable

38 | In-Depth Thematic Analysis of AMR and National Security
and lower limits. The five criteria that were considered inapplicable (see Table 2.2) have been omitted from the table.
All eight scenarios have been scored in the categories ‘Likely’ and ‘Highly likely’. This is a high score compared to many other scenarios in the NRA, which are predominantly classified in the categories ‘Highly unlikely’ to ‘Somewhat likely’. Also, during the scoring session, many of the experts remarked that the events and developments in some of the scenarios have already occurred in real life or are expected to occur within a few years. If no intervention is conducted, the chances of these situations occurring – together with their corresponding consequences – may gradually rise, which in turn increases the overall impact on society. The impact of most of the AMR scenarios is small. The total impact of five of the scenarios is limited (score: A), and two others (Children’s party on a farm and Southern European situations) are designated as having a significant impact (score: B). Only the scenario of Food poisoning on a cruise liner has an impact rating of ‘Serious’ (score: C). When compared to the impact of other NRA scenarios, it can be concluded that the AMR scenarios have a lower impact in relation to most of the scenarios for the other themes. However, due to their high probability of occurrence, the AMR scenarios could potentially strike simultaneously. This is in contrast with other scenarios, such as a flood or a terroristic attack, which are highly unlikely to occur simultaneously. If several of the described AMR scenarios occur more or less simultaneously, certain aspects of the total impact (e.g. unrest and uncertainty) may well be amplified. In Chapter 5, the assessment of the scenarios is considered in relation to the AMR issue, as well as the conclusions that can be drawn from this. Chapter 6 then discusses how future-proof the Netherlands is: what measures are already in place, and what measures will be required in the future in order to control and combat AMR?
In-Depth Thematic Analysis of AMR and National Securityt | 39
In the ANV’s advice document, antimicrobial resistance (AMR) is classified as a possible threat to the theme of Health and Food Safety. This prompted the Ministry of Security & Justice to investigate in what way, to what degree and within what time frame AMR could pose a threat to national security. An RIVM scenario analysis was used to assist this investigation.
AMR differs from most threats analysed so far within the framework of the National Risk Assessment (NRA). Firstly, AMR is a silent killer, causing a very slow increase in the number of serious illnesses and fatalities – it is an insipid process with consequences that are sometimes only discovered by chance as a result of relatively limited incidents. Secondly, the problem can occur simultaneously in different areas of society. The scale of the threat is determined by how frequently and simultaneously incidents take place rather than the scale of the incidents themselves. There are many different strains of resistant bacteria. They can cause illnesses such as pneumonia, blood poisoning, and many others. In general, vulnerable and sick people are the most likely to develop serious illnesses.
The NRA methodology enables the problem to be viewed from a variety of perspectives. In addition to experts in relevant disciplines such as AMR experts
from the medical sector, professionals such as economists, social scientists and communication advisors are also involved in the process. As the threat of AMR affects different areas and as outbreaks sometimes occur simultaneously, it was decided – following consultation with the stakeholders– to develop eight mini-scenarios instead of one big scenario. The eight scenarios take into account the different ways in which the problem of resistance to antibiotics manifests itself. For example, antibiotic resistance can be detected in a variety of sectors (healthcare; environment; livestock farming). When healthy people are infected with resistant bacteria, this does not necessarily result in illness. In such cases, the infected yet healthy person becomes a carrier of the resistant bacteria, which means they could cause it to spread. Antibiotic resistance has already caused many serious situations in foreign countries. In the above scenarios, these foreign situations have been adapted for the Netherlands. There is also an important distinction between endemic situations (in which the pathogen has permanently established itself) and incidents (one-off outbreaks of a particular bacterium).Using this approach, it is possible to gain effective insight into the likelihood and impact of the entire spectrum of AMR issues. The following paragraphs interpret the scores displayed earlier in this report.
5 Consideration and conclusions

40 | In-Depth Thematic Analysis of AMR and National Security
Interpretation of findingsIn general, the findings show that the consequences of AMR predominantly affect healthcare. For this reason, during discussion of the findings, it was decided to create two different categories: consequences for society and consequences for the healthcare sector.
Consequences for societyThe findings show that the social consequences of antibiotic resistance will remain limited. In general, AMR has a relatively low impact. The impact with regard to illness/fatalities and economic/financial damage is expected to be minor. It is also expected to have negligible impact on the integrity and the international position of the Netherlands.The only exceptions in this regard apply to infections resulting from increasing levels of MRSA in animals, illness caused by contact with livestock (Scenario 5), or food-related outbreaks (Scenario 6). As the public is generally sensitive to food-safety concerns, this can result in socio-psychological unrest and diminished trust in the function of the government and businesses. In addition, some possible consequences can be expected with regard to (political) relations with other countries. As it can be expected that people will avoid foodstuffs that are a potential source of resistant microorganisms, the number of serious illnesses and fatalities will probably be limited. With such cases of food contamination, financial impact can be expected due to loss of export revenue. Such incidents will also cause economic damage for businesses in the agricultural sector.
Consequences for the healthcare sectorDuring the scoring session, it was established that the impact of antibiotic resistance predominantly affects the healthcare sector. Outbreaks of diseases caused by or related to antibiotic-resistant bacteria can result in disruption to or strain on the healthcare sector (vital services such as accident & emergency departments, hospitals, and the availability of medicines, serums and vaccines). In all scenarios, AMR results in health-related damage, which in turn leads to disability benefits, treatment costs, large-scale screening, etc. The financial damage ensuing from this is usually limited (less than 50 million euros), except in the case of the two future scenarios involving endemic situations. In these situations, the bacterium permanently establishes itself, resulting in permanently increased mortality and illness rates (with the estimated costs ranging between 100-700 million euros).Endemic incidence of resistant microorganisms will
require more complex treatment, which will increase both the disease burden and the chances of fatality / premature death. Fatalities, chronic illnesses and serious illnesses are expected in the event that pathogenic and resistant microorganisms become endemic, for example in nursing homes or resulting from introduction of resistant microorganisms. It is estimated that this could lead to between 10 to 100 fatalities. However, this is a very rough estimate. AMR also indirectly results in deaths and illnesses as it renders treatments ineffective. Infections mostly hit people that were already ill to begin with. It is therefore difficult to determine the degree to which AMR contributes to the cause of death.The scale of the events and the number of patients determine the severity of the impact and the feeling of powerlessness among citizens in the event of, for example, an endemic spread of Highly Resistant Microorganisms (HRMOs) stemming from nursing homes or introduction from abroad.
LikelihoodThe NRA does not require the selected scenarios to be very likely, but they must be plausible and factual. During the expert meeting, the eight AMR scenarios were assigned likelihood scores ranging from ‘Likely’ to ‘Highly likely’, and a couple of them were considered to have already materialised to a certain extent. As well as some of the scenarios having already occurred, it was also remarked that other scenarios could very soon materialise. For example, transmission of resistant and non-resistant tuberculosis is already a reality, and situations similar to those described earlier have already affected a number of nursing homes. However, as any upheavals, media attention and escalations in the real world are not expected to reach the intensity described in these scenarios, they have been classified as less likely than the others. Scenario 6 (food poisoning on a cruise liner) is seen as being the most likely scenario. Scenarios 1 and 5 were designated as least likely. The likelihood score of Scenario 5 is affected by the fact that the experts consider it difficult to accurately estimate increasing virulence of MRSA as described in this scenario.
ConclusionsThe negative effects and consequences of AMR will affect society in both the short and the long term. The findings also show that the AMR issue would particularly create problems for the healthcare sector. These problems would not result in any disruption of society (social breakdown at the national level), although it would have a considerable impact with regard to the numbers of

In-Depth Thematic Analysis of AMR and National Securityt | 41
serious illnesses/fatalities, social unrest, and financial consequences. Currently, the degree of disruption to everyday life in the described scenarios appears limited due to the one-off, fragmented nature of the various problems caused by antibiotic resistance. The threat is not posed by the individual incidents themselves, but by the increasing frequency and simultaneity of such incidents. This analysis gives an overview of the consequences that AMR could have on national security. At the same time as this analysis was conducted, the WHO also established a vision with regard to AMR, and various other activities in the field of human and animal health have been announced via a number of letters to Parliament, including a letter submitted in March (TK 29683, No. 156) and one in July 2013 (124315-105291-PG). The next chapter will examine how the consequences of AMR can be limited by ongoing and proposed activities.

42 | In-Depth Thematic Analysis of AMR and National Security
In-Depth Thematic Analysis of AMR and National Securityt | 43
It is a given that antimicrobial resistance (AMR) will have an impact on the Netherlands. Research shows that vulnerable people in the Netherlands are being infected with resistant bacteria, and that this affects general well-being, the disease burden, and the chances of mortality. However, compared to other countries, the prevalence of AMR is relatively low. A comprehensive approach involving intensive monitoring in combination with adequate hospital hygiene will help to control the problem. In this chapter, we will discuss how future-proof the Dutch AMR strategy is. This approach is subdivided into the various themes. In July 2013, a letter to Parliament was submitted in which the Minister of Health, Welfare & Sport explained what was currently being done to combat AMR and what needs to be done in the future.In the years to come, AMR control measures will be stepped up, such as infection control in human healthcare, proper usage of antibiotics in human and veterinary healthcare, monitoring of Highly Resistant Microorganisms (HRMOs), necessary international action, development of new antibiotics, research into resistant bacteria in the environment, and AMR-related communication. Initiatives are mainly set up by the government, although care institutions, Regional Health Services (RHSs) and laboratories also devise initiatives. With AMR, a large proportion of control activities are conducted
within hospitals. However, the problem is no longer restricted to individual hospitals or care institutes. Transmission to other healthcare institutes is a growing problem, and in some cases, it also affects patients living in the community. Furthermore, introduction of resistant bacteria from abroad, the livestock farming sector, the environment, and the general population are playing an ever greater role in the epidemiology of human infections within healthcare institutes, and vice versa.As AMR is a complex issue in which a variety of factors play a role, a collaborative effort between professionals in the (public) human healthcare sector, the veterinary health sector and the government is essential.In this regard, the CIb (Centre for Infectious Disease Control) plays a central role as a knowledge and service centre for healthcare-related infections and AMR for the Ministry, professional institutions, and the general public. The CIb and the other involved parties collectively strive to fulfil these duties. In addition, a multidisciplinary team within the CIb conducts research in the fields of microbiology, veterinary healthcare, human healthcare, and epidemiology.
Theme 1: Monitoring and detectionIn the Netherlands, thorough investigation is conducted regarding the prevention of resistant
6 Future-proofing

44 | In-Depth Thematic Analysis of AMR and National Security
bacteria. The goal is to take the information gained and convert it into action. Based on this monitoring, guidelines for adequate treatment of patients can be drawn up, and additional hygiene measures can be put in place in specific settings where certain types of bacteria are frequently detected.In the years to come, in order to monitor trends relating to HRMOs (such as ESBL and CPE) and multi-institutional escalations, all hospitals will sign up to ISIS-AR, the monitoring system for AMR, within which the CIb, NVMM (the Netherlands Society of Medical Microbiology) and medical-microbiology labs all actively collaborate. Furthermore, work is in progress to create a flexible national network in which genetic characteristics of HRMOs can be immediately shared in order to help prevent HRMOs from spreading within/between institutes. This system will also be applied in order to achieve a better picture of transmission between humans and animals. This will further improve insight into the spread of bacteria and the sources of these pathogens. For these purposes, it is necessary to create links between epidemiological data, clinical data, and more detailed information about the pathogen itself. Faster data processing is also essential. The main threat relating to AMR are carbapenem-resistant bacteria. These bacteria possess a specific form of resistance that is still extremely rare in the Netherlands, but is spreading in the countries around us. Infections with carbapenem-resistant bacteria are barely treatable. Therefore, RIVM’s advice on carbapenem resistance is to collaborate with other parties in the field to investigate how to gain quicker and better insight into the introduction and possible spread of these bacteria. During a first meeting, hosted by RIVM, a number of representatives from laboratories and RHSs examined whether the scale of the threat justifies enabling central interpretation of all data. All of the parties in attendance recognised the importance of this, although attention was also requested for optimisation of regional collaboration, a better technical structure for sharing lab results between laboratories and with RIVM, and discussing the issue of coordinating molecular techniques to enable results from different laboratories to be accurately compared and interpreted. At the end of September 2014, a multidisciplinary group of experts has met in order to conduct the above discussion and report on it in a broader context. Improvement of monitoring is a high-priority issue in the Netherlands. However, effective future-proofing requires contributions by many different parties. Furthermore, investigation will be conducted into whether aspects such as the environment play a
major role in the spread of resistant bacteria. In 2012, the SO-ZI/AMR (Detection Council for Healthcare-related Infections and Antimicrobial Resistance) was set up by RIVM and the CIb in order to detect outbreaks of infections at healthcare institutions. The SO-ZI/AMR analyses and assesses danger signs and consequences for (other) healthcare institutes, professionals, and at-risk groups within the general public, and if necessary issues messages/warnings to the notifying institute, other institutes, specific professional groups, health services, and other professionals involved. Recently, NVZ (the Netherlands Association of Hospitals), NFU (the Netherlands Federation of University Medical Centres) and RIVM signed an agreement that establishes a simple multidisciplinary approach for monitoring and control of hospital outbreaks. This represents a mutual agreement to report outbreaks compliant with the notification criteria (see introduction to this report) to the SO-ZI/AMR. In this way, it is reasonable to assume that outbreaks in Dutch hospitals will be reported. As of 2015, nursing homes and rehabilitation centres will also sign up to the SO-ZI/AMR. In order to restrict the use of antibiotics in human healthcare, the goal is to set up an antibiotics team in every hospital from 2014 onwards. These teams, made up of various specialists, will be responsible for limiting and optimising the use of antibiotics by means of peer review.Together with WHO/Europe and ESCMID (the European Society of Clinical Microbiology and Infectious Diseases), RIVM is developing a network of national monitoring systems in all countries in the region that are not part of or affiliated with the European Union and hence are not part of the ECDC’s monitoring system (EARS-Net).
Theme 2: Infection prevention and monitoringThe methods for infection prevention are set down in guidelines. Bacteria’s ability to adjust and adapt and the fact that outbreaks in foreign countries will continue to affect the Netherlands mean that guidelines must be constantly adjusted and updated. Furthermore, the guidelines must be made available to healthcare professionals in a proper and easily-accessible manner. The CIb and the WIP (a Task Force which addresses Infection Prevention) set guidelines governing how to deal with bacteria that occur in the healthcare sector. Every healthcare institute is responsible for ensuring that local infection prevention is in order and that the guidelines in question are implemented and complied with. IGZ (the Netherlands Healthcare Inspectorate) monitors implementation and compliance.

In-Depth Thematic Analysis of AMR and National Securityt | 45
The spread of bacteria within healthcare institutes requires effective measures for hygiene and infection prevention. In order to ensure this, IGZ will conduct a second investigation in 2014, begin 2015. In addition, IGZ will define output indicators in order to clearly set out the course that the infection prevention measures must take. Subsequently, in conjunction with other parties in the field, examination will also be conducted into what makes infection prevention truly effective, how the IGZ can evaluate this, and what action hospitals can take.Responsible use of antibiotics is key to controlling AMR. In order to promote this, guidelines have been drawn up for hospitals (by SWAB – the Dutch Working Party on Antibiotic Policy) and for GPs (by NHG – the Netherlands College of General Practitioners). At the request of IGZ, SWAB has drawn up a vision document for Antibiotic Stewardship in order to further promote responsible use of antibiotics. This includes a system for monitoring limited and improved use of antibiotics by means of peer reviews. The implementation of Antibiotic Stewardship will be closely monitored. Over the past few years, in addition to responsible use of antibiotics in human healthcare, a great deal of attention has been paid to reducing antibiotic use in the veterinary sector. This has already resulted in a substantial reduction of antibiotics used in the livestock farming sector. The 57% reduction achieved in 2013 even exceeded the 50% target set by the Ministry of Health, Welfare & Sport and the Ministry of Economic Affairs.
Theme 3: Advice, knowledge transfer, and communicationThe fact that people may worry about antibiotic resistance has not been overlooked. For this purpose, the Ministry of Health, Welfare & Sport has taken a variety of actions, such as improving the provision of information via the central-government website. Here, a description is given of what is currently known about antibiotic resistance and what as yet remains unknown. These improvements are part of a communication strategy set up by the Ministry of Health, Welfare & Sport and the Ministry of Economic Affairs.Within an existing task force, the European Antibiotic Awareness Day used as an opportunity to provide information to professionals and to set a course. The task force is an initiative of KNMG (the Royal Dutch Medical Association), KNMT (the Netherlands Association of Dentists and Dental Specialists), KNMP (the Royal Dutch Society for the Advancement of Pharmacy), and KNMvD (the Royal Netherlands Veterinary Association). RIVM will
participate in and host a meeting of this task force, which will devote attention to specific subjects that are of importance to the various disciplines.It remains essential that scientists, healthcare professionals and other involved parties are encouraged and facilitated to transfer available knowledge to policymakers, and to keep considering the questions policymakers may ask. Task forces and stakeholder meetings can assist in this process. Attention to ‘grey literature’ is another important factor in this respect. Literature is sometimes disregarded if it cannot be cited as a source.
Theme 4: Care pathways and regional collaborationIn the interests of controlling resistance, improvement of the link between primary and secondary healthcare is important. This would enable quicker detection of transmission within and between healthcare institutions, enabling more effective and targeted control measures. One way to improve this link is to coordinate and exchange national findings with regional initiatives and structures. For example, the link between RHSs and healthcare professionals within institutes is not optimally organised. In order to better facilitate this aspect, a number of regional networks have been set up. A common fear is that pathogens are easily spread as a result of transferring patients from one healthcare institute to another. Such transmission can be prevented by means of effective provisioning of information at the regional level, administrative agreements regarding integrated healthcare, and regional structures. Currently, a number of regional collaborative ventures are being initiated in which attention will be paid to interpretation of guidelines and the consequences of moving patients between healthcare institutes.
Theme 5: Proportionality of measures/implementationIt is vital that measures have a wide basis of support. If there are conflicts of interests or a lack of clarity regarding costs (in terms of both money and human suffering) and benefits (actual prevention of factors such as disease burden), then this must first be resolved before national implementation and compliance can be initiated. Only then can a proper debate take place. Attention must also be paid to the proportionality of measures taken based on the precautionary principle.
Theme 6: Veterinary approachExcessive and careless use of antibiotics by livestock farmers increases the risk of antibiotic resistance.

46 | In-Depth Thematic Analysis of AMR and National Security
Over the past few years, in close collaboration with the livestock farming sector and KNMvD (the Royal Netherlands Veterinary Association), the government has developed a strategy to promote careful use of antibiotics and achieve a 70% reduction in the levels of antibiotic use by 2015 (relative to the reference year 2009). A great deal of this strategy was realised by means of self-regulation in the livestock farming sector and among veterinarians. The government made investments in enforcement measures and implemented legislation when necessary. The most important aspects of this strategy are mandatory central registration of antibiotics usage at individual livestock farming businesses, efforts to prevent animal diseases, obligations for livestock farmers to draw up farm health plans in conjunction with their local vet, and veterinary guidelines for careful use. As stated in the State Secretary of Economic Affairs’ letter dated 2 September 2014, consultation will be held with experts, SDa (the Animal Medicines Authority) and the sectors involved in order to determine the policies that will be required after 2015, with the key focus on further reducing the development and spread of resistance in the livestock farming sector. In SDa’s opinion, the time is ripe for objectives that are more specific to individual species of animal, with developments in resistance serving as the guiding principle. For this purpose, SDa will evaluate the effect of reduced antibiotic use on the prevention of resistance in farm animals. Subsequently, based on these results, it will determine the degree to which the benchmark system requires adjustment. SDa expects to be able to issue advice on this matter in 2015.
Knowledge and innovationAnother essential factor in preventing the spread of resistant bacteria is the acquisition of new knowledge about particular issues, such as how long infected people remain carriers of resistant bacteria. This requires additional research. Within the scope of the government’s policy, extra money has been made available in order to finance this.A key focus of the research is the development of new antibiotics. Currently, research in this area has practically stagnated. Due to the lack of demand from the market, the government has had to take up the task of encouraging development of new medicines. This process also needs to be adopted at the European and global level. Due in part to this factor, the Dutch government sees this as a priority issue for the next Presidency of the Council of the European Union. A variety of projects at the European level are currently in development as part
of the Innovative Medicines Initiative, which was set up by the European Commission in collaboration with the private sector.In addition to this, the Netherlands also plays an active role in the EU Joint Programming Initiative on Antimicrobial Resistance (JPIAMR). The goal of this programme is to create a European strategic research agenda, and the Netherlands is responsible for coordinating its development. It will be developed in close collaboration with the WHO in order to ensure compatibility with the global agenda. The agenda will provide an important impulse for research into all aspects of AMR, including the development of new medicines.
In-Depth Thematic Analysis of AMR and National Securityt | 47
Appendix 1: The National Network of Safety and Security AnalystsThe National Network of Safety and Security Analysts (ANV) is an authoritative knowledge network, which is tasked by the Ministry of Security and Justice with performing the annual National Risk Assessment (NRA) on behalf of the National Steering Committee for National Safety and Security (SNV).
The ANV has a permanent core of six organisations (the NRA Task Group), plus an extended network (the ‘ring’), made up of knowledge institutions, civil services, private companies, research agencies and consultancy firms, whose input is utilised for the NRA whenever a relevant topic arises. The permanent core consists of the following six organisations: • The National Institute for Public Health and the
Environment (RIVM) • The Research and Documentation Centre (WODC),
Ministry of Security and Justice • General Intelligence and Security Service of the
Netherlands (AIVD) • The Netherlands Organization for Applied
Scientific Research (TNO) • The Netherlands Institute of International
Relations ‘Clingendael’ • The International Institute of Social Studies (ISS)
of the Erasmus University Rotterdam
The core organisations possess wide-ranging, multidisciplinary expertise and thus collectively span the National Security work field. The structure ensures the NRA’s all-hazard approach, as well as methodological uniformity and cross-disciplinary analysis.
The six core organisations share responsibility for the material quality of the NRA. Specific, supplementary expertise is provided by the other organisations in the network. The organisations in the core and the ring make experts and analysts available to sit on panels, which are temporarily convened to undertake the various NRA activities. There is also a supporting secretariat (the NRA Secretariat) made up of a general secretary, panel coordinators, and project support personnel, who provide process control, progress monitoring, and support for the NRA. The NRA Secretariat acts as the fixed point of contact for the SNV, the IWNV (Interdepartmental National Security Committee), and the associated departments. The NRA Secretariat also supports the Task Group and the scenario panels in the production of the NRA, and directs and monitors the process. The NRA Secretariat is accommodated within the RIVM.
48 | In-Depth Thematic Analysis of AMR and National Security
The Methodology workgroup25 – made up of experts of a number of knowledge institutes and businesses, including several organisations belonging to the Task Group – is not part of the ANV, but operates under the responsibility of the Ministry of Security and Justice. The Methodology workgroup supports the ANV in the production of the NRA, particularly monitoring of the NRA method, answering methodi-cal questions, and preparing refinements and changes to the method. The ANV’s main tasks are: 1. To produce the annual NRA, on the basis of
themes selected by the SNV 2. To advise the SNV about appropriate themes for
the (next) NRA, taking account of incident scenarios as well as developments in the (medi-um to) long term and very gradual processes
3. To produce other scenarios and analyses and organise expert meetings regarding National Safety and Security issues, on request of the Ministry of Security and Justice
The ANV’s working methods, organisational struc-ture, tasks and responsibilities as well as the planning cycle, the production process, the arrange-ments for handling knowledge and confidential information, the communication, the transfer to the panels for capability analysis, and quality and expertise assurance are all set out in a Quality Plan.
25 This workgroup has developed the NRB methodology and has been
active since the National Safety and Security Strategy was
introduced in 2007.
In-Depth Thematic Analysis of AMR and National Securityt | 49
Appendix 2: Overview of organisations involvedThis appendix contains an overview of the organisa-tions who contributed to the creation and assess-ment of the scenarios in this NRA. The table below indicates which organisations were responsible for the content (the authors of the scenarios), which organisations contributed to the development of the scenarios (by providing essential information and calculations), and which organisations participated in the assessment (scoring) of the scenarios. A representative of the Methodology workgroup also attended the scoring session in order to answer questions and resolve problems of a methodological nature, as well as to monitor the consistency of the assessment.
Scenario authors: National Institute for Public Health and the Environment (RIVM)/ Centre for Infectious Disease Control (CIb)
Contributions made by: RIVM/CIb, International Institute of Social Studies (ISS)
Participants in the scenario assessments: RIVM/CIb, RIVM/Communication, Amphia Hospital, VU Medical Center, KNCV Tuberculosis Foundation, Netherlands Food and Consumer Product Safety Authority (NVWA), Central Veterinary Institute (CVI/Wageningen University), Erasmus University, Arq/Impact, Ministry of Health, Welfare & Sport, St Antonius Hospital, Verenso
Supervisory CommitteeThis study was supervised by a committee consisting of representatives from the ministerial departments involved.

50 | In-Depth Thematic Analysis of AMR and National Security

the Network of Analysts for National SecurityMarcel Mennen (editor)Mariken van der Lubben (editor)
0075
34
Committed to health and sustainability
This is a publication of:
National Institute for Public Health and the Environment (RIVM)
Research and Documentation Centre (WODC), Ministry of Security and Justice
General Intelligence and Security Service of the Netherlands (AIVD)
Netherlands Organisation for Applied Scientific Research (TNO)
Netherlands Institute of International Relations ‘Clingendael’
International Institute of Social Studies (ISS), Erasmus University Rotterdam
P.O. Box 1 | 3720 BA BilthovenThe Netherlandswww.rivm.nl/en
October 2014