
Impact of the hepatitis B virus genotype and genotype mixtures on the course of liver disease in...
10
Impact of the Hepatitis B Virus Genotype and Genotype Mixtures on the Course of Liver Disease in Vietnam Nguyen L. Toan, 1,3 Le H. Song, 1,2,3 Peter G. Kremsner, 3,4 Dinh N. Duy, 2 Vu Q. Binh, 5 Bernd Koeberlein, 1 Stefan Kaiser, 6 Reinhard Kandolf, 1 Joseph Torresi, 7 and C.-Thomas Bock 1 Eight genotypes (A-H) of hepatitis B virus (HBV) have been identified. However, the impact of different genotypes on the clinical course of hepatitis B infection remains controversial. We investigated the frequency and clinical outcome of HBV genotypes and genotype mixtures in HBV-infected patients from Vietnam, Europe, and Africa. In addition, we analyzed the effects of genotype mixtures on alterations in in vitro viral replication. In Asian patients, seven genotypes (A-G) were detected, with A, C, and D predominating. In European and African patients, only genotypes A, C, D, and G were identified. Genotype mixtures were more frequently encountered in African than in Asian (P .01) and European patients (P .06). In Asian patients, the predominant genotype mixtures included A/C and C/D, compared to C/D in European and A/D in African patients. Genotype A was more frequent in asymptomatic compared with symptom- atic patients (P < .0001). Genotype C was more frequent in patients with hepatocellular carci- noma (HCC; P .02). Genotype mixtures were more frequently encountered in patients with chronic hepatitis in comparison to patients with acute hepatitis B (P .015), liver cirrhosis (P .013), and HCC (P .002). Viral loads in patients infected with genotype mixtures were significantly higher in comparison to patients with a single genotype (P .019). Genotype mixtures were also associated with increased in vitro HBV replication. In conclusion, infection with mixtures of HBV genotypes is frequent in Asia, Africa, and Europe. Differences in the replication-phenotype of single genotypes compared to genotype-mixtures suggest that co-infec- tion with different HBV-genotypes is associated with altered pathogenesis and clinical outcome. (HEPATOLOGY 2006;43:1375-1384.) T he clinical course and long-term outcome of hep- atitis B virus (HBV) infection is affected by sev- eral factors including viral genotype. For instance, it has been reported that the HBV genotype C induces more severe liver disease than HBV genotype B in Asia, 1,2 whereas HBV genotype A has been more fre- quently associated with the development of chronic infec- tion than HBV genotype D in Europe. 3 Eight genotypes (A to H) of HBV have been identified based on divergence over the entire genomic sequence of more than 8%. 4-7 HBV genotypes have specific geo- graphic distributions, 8,9 with genotype A found predom- inantly in Northwest Europe, North America, central and sub-Saharan Africa; genotypes B and C in Southeast Asia, China, and Japan; genotype D in the Mediterranean, the Middle East, and India; genotype E in Africa; genotype F in American natives, Polynesia, and Central and South America; genotype G in the United States and France, 6,10 and genotype H in Central America. 7 HBV infection is endemic in Vietnam, where up to 26% of healthy individuals are seropositive for hepatitis B surface antigen (HBsAg). 11 Scant information is available about the prevalence and clinical significance of the dif- ferent genotypes of HBV in Vietnam. One previous study based on patients who had emigrated from Vietnam sug- Abbreviations: HBV, hepatitis B virus; HBsAg, hepatitis B surface antigen; HCC, hepatocellular carcinoma; RFLP, restriction fragment length polymorphism; AHB, acute hepatitis B; CHB, chronic hepatitis B; LC, liver cirrhosis; ASYM, asymptomatic hepatitis B; ALT, alanine aminotransferase; PCR, polymerase chain reaction. From the 1 Department of Molecular Pathology, Institute of Pathology, University Hospital of Tuebingen, Germany; 2 Tran Hung Dao Hospital, Hanoi, Vietnam; the 3 Department of Parasitology, Institute of Tropical Medicine, University of Tuebin- gen, Germany; the 4 Medical Research Unit, Albert Schweitzer Hospital, Lam- barene, Gabon; the 5 Institute of Prevention Medicine, Truong Dinh, Dong Da, Hanoi, Vietnam; the 6 Department of Internal Medicine I, University Hospital of Tuebingen, Germany; and the 7 Department of Medicine, Victorian Infectious Dis- eases Service, Clinical Centre for Research Excellence, Royal Melbourne Hospital, The University of Melbourne, Australia. The authors N.L. Toan and L.H. Song and J. Torresi. and C.T. Bock contrib- uted equally to this work. N.L. Toan and L.H. Song share first authorship; J. Torresi and C.T. Bock share last authorship. Received September 1, 2005; accepted March 11, 2006. Supported by grants of the Deutsche Krebshilfe, “Dr. Mildred-Scheel-Stiftung fuer Krebsforschung,” grant number 10-2142-Bo1, of the Tran Hung Dao Hospital, Hanoi, Vietnam, and by the “fortuene-program” of the University of Tuebingen, grant number 1004-0-0. Le Huu Song was supported by a scholarship from the “Deutscher Akademis- cher Austauschdienst” (DAAD). Nguyen Linh Toan was supported by a scholarship from project 322 of the Vietnam Ministry of Education and Training. Address reprint requests to: C.-Thomas Bock, Department of Molecular Pathology, Institute of Pathology, University Hospital of Tuebingen, D-72076 Tuebingen, Ger- many. E-mail: [email protected]; fax: (49) 7071-29-5334. Copyright © 2006 by the American Association for the Study of Liver Diseases. Published online in Wiley InterScience (www.interscience.wiley.com). DOI 10.1002/hep.21188 Potential conflict of interest: Nothing to report. 1375
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Impact of the hepatitis B virus genotype and genotype mixtures on the course of liver disease in...

Impact of the Hepatitis B Virus Genotype and GenotypeMixtures on the Course of Liver Disease in Vietnam
Nguyen L. Toan,1,3 Le H. Song,1,2,3 Peter G. Kremsner,3,4 Dinh N. Duy,2 Vu Q. Binh,5 Bernd Koeberlein,1 Stefan Kaiser,6
Reinhard Kandolf,1 Joseph Torresi,7 and C.-Thomas Bock1
Eight genotypes (A-H) of hepatitis B virus (HBV) have been identified. However, the impact ofdifferent genotypes on the clinical course of hepatitis B infection remains controversial. Weinvestigated the frequency and clinical outcome of HBV genotypes and genotype mixtures inHBV-infected patients from Vietnam, Europe, and Africa. In addition, we analyzed the effects ofgenotype mixtures on alterations in in vitro viral replication. In Asian patients, seven genotypes(A-G) were detected, with A, C, and D predominating. In European and African patients, onlygenotypes A, C, D, and G were identified. Genotype mixtures were more frequently encounteredin African than in Asian (P � .01) and European patients (P � .06). In Asian patients, thepredominant genotype mixtures included A/C and C/D, compared to C/D in European and A/Din African patients. Genotype A was more frequent in asymptomatic compared with symptom-atic patients (P < .0001). Genotype C was more frequent in patients with hepatocellular carci-noma (HCC; P � .02). Genotype mixtures were more frequently encountered in patients withchronic hepatitis in comparison to patients with acute hepatitis B (P � .015), liver cirrhosis (P �.013), and HCC (P � .002). Viral loads in patients infected with genotype mixtures weresignificantly higher in comparison to patients with a single genotype (P � .019). Genotypemixtures were also associated with increased in vitro HBV replication. In conclusion, infectionwith mixtures of HBV genotypes is frequent in Asia, Africa, and Europe. Differences in thereplication-phenotype of single genotypes compared to genotype-mixtures suggest that co-infec-tion with different HBV-genotypes is associated with altered pathogenesis and clinical outcome.(HEPATOLOGY 2006;43:1375-1384.)
The clinical course and long-term outcome of hep-atitis B virus (HBV) infection is affected by sev-eral factors including viral genotype. For
instance, it has been reported that the HBV genotype Cinduces more severe liver disease than HBV genotype B inAsia,1,2 whereas HBV genotype A has been more fre-quently associated with the development of chronic infec-tion than HBV genotype D in Europe.3
Eight genotypes (A to H) of HBV have been identifiedbased on divergence over the entire genomic sequence ofmore than 8%.4-7 HBV genotypes have specific geo-graphic distributions,8,9 with genotype A found predom-inantly in Northwest Europe, North America, central andsub-Saharan Africa; genotypes B and C in Southeast Asia,China, and Japan; genotype D in the Mediterranean, theMiddle East, and India; genotype E in Africa; genotype Fin American natives, Polynesia, and Central and SouthAmerica; genotype G in the United States and France,6,10
and genotype H in Central America.7
HBV infection is endemic in Vietnam, where up to26% of healthy individuals are seropositive for hepatitis Bsurface antigen (HBsAg).11 Scant information is availableabout the prevalence and clinical significance of the dif-ferent genotypes of HBV in Vietnam. One previous studybased on patients who had emigrated from Vietnam sug-
Abbreviations: HBV, hepatitis B virus; HBsAg, hepatitis B surface antigen; HCC,hepatocellular carcinoma; RFLP, restriction fragment length polymorphism; AHB,acute hepatitis B; CHB, chronic hepatitis B; LC, liver cirrhosis; ASYM, asymptomatichepatitis B; ALT, alanine aminotransferase; PCR, polymerase chain reaction.
From the 1Department of Molecular Pathology, Institute of Pathology, UniversityHospital of Tuebingen, Germany; 2Tran Hung Dao Hospital, Hanoi, Vietnam; the3Department of Parasitology, Institute of Tropical Medicine, University of Tuebin-gen, Germany; the 4Medical Research Unit, Albert Schweitzer Hospital, Lam-barene, Gabon; the 5Institute of Prevention Medicine, Truong Dinh, Dong Da,Hanoi, Vietnam; the 6Department of Internal Medicine I, University Hospital ofTuebingen, Germany; and the 7Department of Medicine, Victorian Infectious Dis-eases Service, Clinical Centre for Research Excellence, Royal Melbourne Hospital,The University of Melbourne, Australia.
The authors N.L. Toan and L.H. Song and J. Torresi. and C.T. Bock contrib-uted equally to this work. N.L. Toan and L.H. Song share first authorship; J. Torresiand C.T. Bock share last authorship.
Received September 1, 2005; accepted March 11, 2006.Supported by grants of the Deutsche Krebshilfe, “Dr. Mildred-Scheel-Stiftung fuer
Krebsforschung,” grant number 10-2142-Bo1, of the Tran Hung Dao Hospital, Hanoi,Vietnam, and by the “fortuene-program” of the University of Tuebingen, grant number1004-0-0. Le Huu Song was supported by a scholarship from the “Deutscher Akademis-cher Austauschdienst” (DAAD). Nguyen Linh Toan was supported by a scholarship fromproject 322 of the Vietnam Ministry of Education and Training.
Address reprint requests to: C.-Thomas Bock, Department of Molecular Pathology,Institute of Pathology, University Hospital of Tuebingen, D-72076 Tuebingen, Ger-many. E-mail: [email protected]; fax: (49) 7071-29-5334.
Copyright © 2006 by the American Association for the Study of Liver Diseases.Published online in Wiley InterScience (www.interscience.wiley.com).DOI 10.1002/hep.21188Potential conflict of interest: Nothing to report.
1375

gested that genotypes B and C may be the predominantviral genotypes in Vietnam.12 In addition, although HBVhas been detected in 90% of patients diagnosed with hep-atocellular carcinoma (HCC) in Vietnam,11 in contrast toTaiwan,13 China,14 and Japan,2 an association betweenHCC, severity of liver disease, and specific HBV geno-types has not been described in Vietnamese patients.
Little is also known about coinfection with differentHBV genotypes in this population. Infection with mix-tures of viral genotypes has previously been reported, al-though the presence of minor viral quasi-species may notbe detectable using standard genotyping assays or directsequencing.15 To overcome this limitation and to inves-tigate the frequency of coinfection with mixtures ofHBV-genotypes, Hannoun and colleagues16 developedan HBV core domain restriction fragment polymorphism(RFLP) assay to accurately determine the relative mix-tures of viral genotypes in patient sera. These investigatorsfound that genotypic coinfection is frequent in patientswho are chronically infected with HBV, although in gen-eral only one viral genotype predominated.16 However,little is known about potential viral–viral interactions thatoccur between mixtures of HBV genotypes and of theclinical course in coinfected patients.
We have investigated the frequency of infection withdifferent HBV genotypes, serum HBV viral loads, andclinical course in patients infected with different geno-types and mixtures of genotypes of HBV in Vietnamese(Asian) patients and compared these to European andAfrican patients. In addition, by using an in vitro trans-fection assay, we also investigated the replication pheno-type of mixtures of HBV genotypes compared toinfection with single HBV genotypes.
Patients and Methods
Patients. Three hundred seventy-five HBV-infectedVietnamese individuals were included in this study. Ofthese, 289 were symptomatic patients, 29 were on hemo-dialysis, and 86 were healthy asymptomatic chronic HBVcarriers. All patients were enrolled at Tran Hung DaoHospital, Bach Mai Hospital, 103 Military Hospital,Hanoi, Vietnam, between 2000 and 2002. The patientswere subdivided into five clinical profiles including acutehepatitis B (AHB), chronic hepatitis B (CHB), liver cir-rhosis (LC), HCC, and asymptomatic carriers (ASYM).In addition, 38 European patients with CHB infectionwere enrolled from the Department of Gastroenterology,University-Hospital of Tuebingen, Germany, and 47hepatitis B–infected Gabonese children were enrolledfrom the Medical Research Unit, Albert Schweitzer Hos-pital, Lambarene, Gabon. All Vietnamese subjects had a
positive serum HBsAg by EIA (Abbott, Chicago, IL) andwere negative for antibodies to hepatitis C virus and HIV.None of the study participants from Vietnam had a his-tory of alcohol or drug abuse, and none received antiviralfor hepatitis B infection or immunosuppressive therapybefore or during the course of this study. The clinicalcourse and severity of hepatitis infections, liver biochem-ical tests, serological markers of HBV, including diagnos-tic tests for HCC in the Vietnamese patients, have beendescribed in detail previously.17,18 With the exception ofthe ASYM group, Vietnamese patients with chronic HBVwere classified on the basis of histological examinationafter liver biopsy into those with or without evidence ofeither cirrhosis or carcinoma.18,19
European patients were classified as having active CHBwith or without cirrhosis based on clinical examination,biochemical analysis of serum liver function tests, includ-ing serum alanine (ALT) and aspartate aminotransferase,positive serum HBsAg for a period of greater than 6months, and liver biopsy.
Gabonese children admitted to hospital or treated asoutpatients for malaria were enrolled in this study. Thediagnosis for hepatitis B infection was based on clinicalcriteria and positive serum HBV-DNA(�) for a period ofgreater than 6 months. The clinical profiles of the Africanpatients have also been described elsewhere.20,21
The collection samples were performed using newequipment for every individual. Sample processing(DNA-extraction, template preparation, spinning andaliquoting, master mix preparation) and polymerasechain reaction (PCR) amplication were done in separatelaboratory rooms, which are all certified for moleculardiagnostics and especially for PCR, using standard pre-cautions to prevent assay contamination.
HBV Genotyping. The presence of HBV genotypemixtures in patient sera was determined by a modifiedRFLP PCR assay that has previously been reported byHannoun and coworkers.16 To increase the sensitivity ofthe RFLP PCR assay, we used nested PCR to amplifyHBV-DNA. Primers used for the first PCR were: HB-pre-16 5�-CACCTCTGCCTAATCATCTCT-3� andHBV-590as 5�-CTGCGAGGCGAGGGAGTT-3�. Re-actions were initially denatured at 94°C for 4 minutesfollowed by 35 cycles of 94°C for 30 seconds, 55°C for 30seconds, and 72°C for 30 seconds followed by a finalextension for 10 minutes at 72°C. The cycle conditions ofthe second-round PCR were as described elsewhere.16
The DNA amplicons were incubated with the restrictionenzyme Tsp509I, and the restriction patterns and pre-dicted fragment sizes determined (Fig. 1). In addition, toverify the RFLP-PCR results, direct DNA sequencing onboth strands using primers for nested PCR of the HBV
1376 TOAN ET AL. HEPATOLOGY, June 2006
isolates from the serum HBV-infected patients was per-formed as described previously.22 The sequences obtainedwere matched with the National Center for Biotechnol-ogy Information GenBank and compared with recentlydescribed HBV-prototypes (Accession No. for: HBV-AZ72478; HBV-B D00329; HBV-C X01587; HBV-DV01460; HBV-E X75657; HBV-F X75658; HBV-GAF160501).
Replication-Competent HBV Plasmids. The HBVreplication-competent plasmids pHBV1.28 andpHBV1.5 (genotype A), pHBV1.2 (genotype D), and
HBVpd4aI (genotype C) containing a 1.2mer, 1.28mer,1.5mer, or dimer HBV genome, respectively, have beendescribed previously.23-25
Cell Culture and Transfection Experiments.HepG2 cells were grown in Dulbecco’s modified Eaglemedium with 10% fetal calf serum as described previ-ously.26 Cells were transfected with 2 �g of plasmidHBV-DNA in a total of 20 �L Fugene-6 reaction mixture(Roche Applied Science, Mannheim, Germany) as rec-ommended by the manufacturer and harvested after 5days. All experiments were performed in triplicate.
Quantitative Real-time HBV-PCR. HBV-DNAquantification was performed with quantitative real-timePCR as previously described .17 Amplification and detec-tion was carried out using the GeneAmp 7300 sequenceanalyzer (Applied Biosystems, Perkin-Elmer, Foster City,CA). HBV-plasmid DNA (pHBV1.28) and the WHOinternational standard for HBV-DNA (NIBSC Code 97/746) in increasing dilutions (5-5 � 105 genomes per vial)were included to standardize the assay. All samples wereanalyzed in duplicates. A quantitative PCR (qPCR) of theadenosine triphosphate synthase-6 gene was also per-formed, as a control for the addition of equivalentamounts of human DNA in the qPCR, as described pre-viously.27
Isolation and Quantification of Progeny HBV-DNA. Progeny HBV-DNA was isolated from transientlytransfected HepG2 cells as previously described .28 Inbrief, transiently transfected cells were harvested 5 daysafter transfection and lysed with buffer containing 1%Igepal (Sigma-Aldrich, Munich, Germany). IntracellularHBV-core particles were immunoprecipitated with anti-HBV-core antigen antibodies (Dako, Hamburg, Ger-many). Contaminating HBV-DNA and HBV-plasmidDNA was eliminated by subsequent digestion with de-oxyribonuclease-I (Roche Biochemica, Mannheim, Ger-many) and DpnI. HBV-DNA was extracted from theHBV core particles by digestion with proteinase K and1% sodium dodecyl sulphate followed by phenol-chloro-form extraction and ethanol precipitation as de-scribed.23,28 HBV-progeny DNA was quantified usingqPCR and calculated according to genome equivalentsper microgram of isolated nucleic acid (GE/�g). Addi-tionally, to verify the quantification results of the progenyHBV-DNA assays, HBV-DNA was isolated from culturemedium supernatants as previously described and ana-lyzed using qPCR.28
Statistical Analysis. Statistical analysis were per-formed using contingency table analysis with Fisher’s ex-act test (available at www.stata.com), and the non-parametric Mann-Whitney U-test or Kruskall-Wallis test
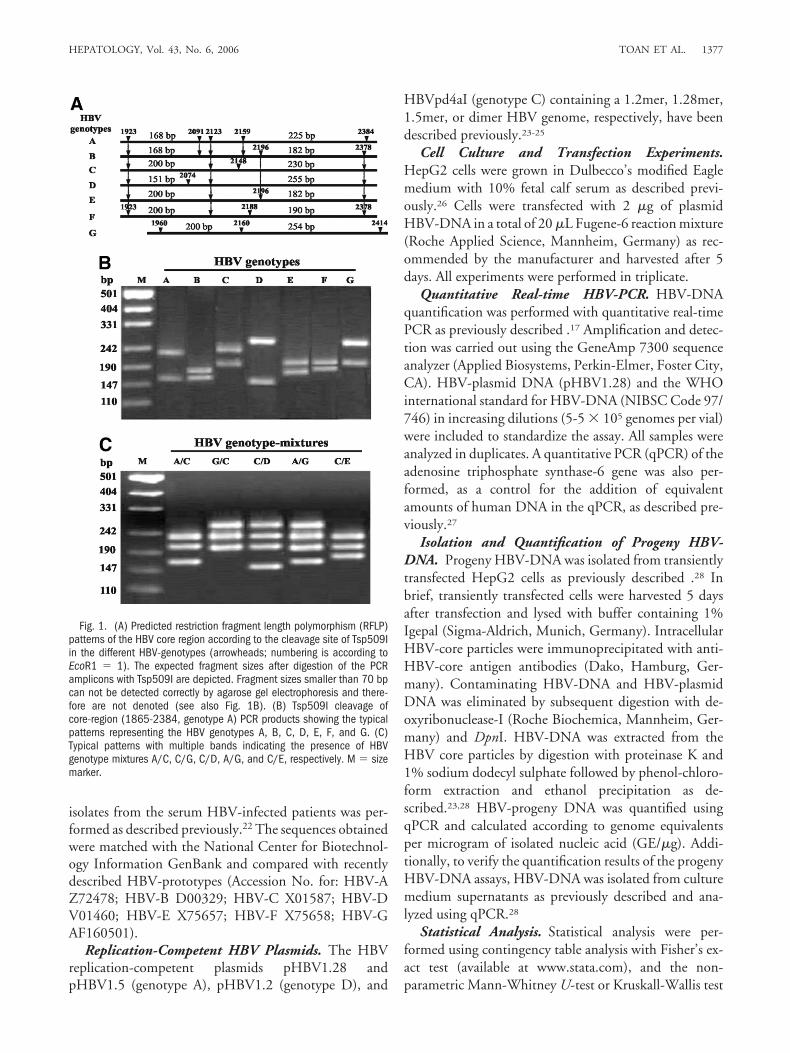
Fig. 1. (A) Predicted restriction fragment length polymorphism (RFLP)patterns of the HBV core region according to the cleavage site of Tsp509Iin the different HBV-genotypes (arrowheads; numbering is according toEcoR1 � 1). The expected fragment sizes after digestion of the PCRamplicons with Tsp509I are depicted. Fragment sizes smaller than 70 bpcan not be detected correctly by agarose gel electrophoresis and there-fore are not denoted (see also Fig. 1B). (B) Tsp509I cleavage ofcore-region (1865-2384, genotype A) PCR products showing the typicalpatterns representing the HBV genotypes A, B, C, D, E, F, and G. (C)Typical patterns with multiple bands indicating the presence of HBVgenotype mixtures A/C, C/G, C/D, A/G, and C/E, respectively. M � sizemarker.
HEPATOLOGY, Vol. 43, No. 6, 2006 TOAN ET AL. 1377

and Spearman’s rank-tests using Statview, version 4.57(available at www.statview.com).
Ethical Approval. The study was approved by theInstitutional Review Board of the Tran Hung Dao Hos-pital, Hanoi, Vietnam, by the ethics committee of theInternational Foundation for the Albert Schweitzer Hos-pital in Lambarene, Gabon, and by the ethics committeeof the University Hospital of Tuebingen.
Results
Distribution of HBV-Genotypes in Three Popula-tions: Asia, Europe, and Africa. In Vietnamese pa-tients, 7 genotypes A to G but not genotype H could bedetected. In contrast, in European and in African patientsonly the four genotypes A, C, D, and G were identified(Table 1). Fifteen different genotype mixtures were de-tected by RFLP-PCR. These included; A/B, A/C, A/D,A/E, A/F, A/G, B/C, B/F, C/D, C/E, C/F, C/G, D/G,F/G, and A/C/D. Genotype mixtures were more frequentin African (14/47; 29.8%) than Asian (59/375; 15.7%),and European (5/38; 13.2%) patients (Table 2). How-ever, with exception of the A/C (25/375; 6.66%), A/D(6/375; 1.6%), and C/D (10/375; 2.66%) combinations
in Asian patients the number of remaining genotype mix-tures was too low to permit a more detailed individualanalysis. Analysis of the geographical distribution of ge-notypes indicated that genotype A was significantly morefrequent in African patients (26/47; 55.32%), than eitherAsian (68/375; 18.13%) or European patients (6/38;15.79%) (P � .0001 and P � .0002, respectively). Incontrast, in Asian patients, genotype C predominated andwas significantly more frequent than in either African orEuropean patients (P � .011 and P � .017; respectively).Compared to Asian and African patients, genotype D wasthe predominant genotype in European patients (P �.0006 and P � .0001, respectively). Genotype B was onlyfound in Asian patients. However, genotype D was alsonot infrequent in Asian patients (76/375; 20.26%; Table 1).
Clinical Symptoms and Liver Parameters of HBV-Infected Vietnamese. The clinical profiles and serumbiochemical analyses of the different Vietnamese patientgroups are shown in Table 3. Patients with AHB weresignificantly younger than those in the other clinical cat-egories (P � .001). As expected, the serum ALT andaspartate aminotransferase levels in the AHB group weresignificantly higher compared with the other groups (P �
Table 1. Distribution of HBV Single Genotypes in Three Populations
GenotypesAsiana
n � 316/375 (%)Europeanb
n � 33/38 (%)Africanc
n � 33/47 (%)Total
N � 382/460 (%) P (�2)
A 68 (18.13) 6 (15.79) 26 (55.32) 100 (21.74) a vs. c � .0001 (33.36)b vs. c � .0002 (13.99)
B 37 (9.86) 0 0 37 (8.04) NAC 94 (25.06) 3 (7.89) 4 (8.51) 101 (21.96) a vs. b � .017 (5.66)
a vs. c � .011 (6.42)D 76 (20.26) 17 (44.73) 1 (2.12) 94 (20.43) a vs. b � .0006 (11.84)
a vs. c � .0024 (9.21)b vs. c � .0001 (22.85)
E 13 (3.47) 0 0 13 (2.83) NAF 9 (2.40) 0 0 9 (1.96) NAG 19 (5.06) 7 (18.42) 2 (4.25) 28 (6.09) a vs. b � .0012 (10.48)
b vs. c � .035 (4.45)
Abbreviation: NA, not applicable.
Table 2. Distribution of HBV Genotype Mixtures in Three Populations
Genotype MixturesAsiana
n � 59/375 (%)Europeanb
n � 5/38 (%)Africanc
n � 14/47 (%) P (�2)
A/C 25 (6.66) 0 1 (2.1) NAA/D 6 (1.6) 0 5 (10.6) NAA/G 2 (0.5) 1 (2.6) 2 (4.2) a vs. b � .05
a vs. c � 0.13 (6.16)C/D 10 (2.66) 2 (5.3) 0 NAC/G 1 (0.3) 1 (2.6) 5 (10.6) a vs. b � .045 (4.0)
a vs. c � .001 (32.0)D/G 2 (0.5) 1 (2.6) 1 (2.1) � .05Other remaining genotype mixtures 14 (3.7) 0 0 NA
Abbreviation: NA, not applicable.
1378 TOAN ET AL. HEPATOLOGY, June 2006

.001). The prothrombin time was significantly prolongedin patients with LC compared with the other clinicalgroups (P � .001, Table 3).
Distribution of HBV Genotypes in VietnamesePopulation. In Vietnamese patients, the genotypes mostfrequently detected were C (94/375; 25.06%), D (76/375; 20.26%), and A (68/375; 18.13%) (Table 4). Ge-notype A was significantly more frequent inasymptomatic carriers (P � .0001, chi-squared(1) �18.26) and patients without HCC (P � .0016, chi-squared(1) � 9.99). In contrast, genotype C was signifi-cantly more frequent in patients with HCC (P � .023,chi-squared(1) � 5.15) and asymptomatic HBV (P �.035, chi-squared (1) � 4.45). In addition, by examiningthe distribution of genotypes in the different clinicalgroups HCC occurred significantly more frequently inpatients infected with genotype C than those infectedwith genotypes B and A (P � .0005 and P � .0001;respectively). Genotype D was identified significantlymore frequently in patients with LC than other clinicalgroups (P � .0001).
Distribution of Genotype-Mixtures in HBV-In-fected Vietnamese Patients. The distribution of geno-type mixtures in the Vietnamese patients according to thedifferent clinical categories is shown in Table 5. Genotypemixtures were significantly more frequent in patients withCHB compared with patients with AHB, LC, and HCC(P � .02) and in patients with AHB, CHB, and ASYMcompared with patients with severe disease (LC andHCC, P � .028; chi-squared(1) � 4.78). No significantdifference was detected across the different clinical cate-gories in patients infected with a single genotype.
Serum Viral Load of HBV-Infected Patients. Anal-ysis of serum HBV-DNA showed significantly higher vi-ral loads in the AHB, CHB, and ASYM groups comparedwith either the LC or HCC groups (P � .05; Fig. 2A).The viral load in patients with HCC was significantlylower than in patients without HCC (P � .01; Fig. 2B).In the analysis of the relationship between viral replica-tion and genotype, we found that serum HBV-DNA lev-els in patients singly infected with HBV genotype A and Cwere significantly higher than those infected with geno-
Table 3. Characteristics of Vietnamese Patients With HBV Infection
AHBn � 43
CHB‡
n � 70LC
n � 92HCC
n � 84ASYM§
n � 86
Age (years) 35* 43 51 50 39Sex (male/female) 35/8 58/12 72/20 70/14 70/16HBsAg(�) 43/43 70/70 92/92 84/84 86/86AFP (mg/L) ND ND ND 474.5 NDTotal-bilirubin (mg/dL) 187.5 112.8 166.6 50.5 15.5*Direct-bilirubin (mg/dL) 144.6 75.8 97.1 30.1 8.9†ALT (IU/L) 1,322.2* 308.2 119.9 88.6 37.4*AST (IU/L) 1,240.1* 317.1 134.1 94.8 32.5*Prothrombin (% of standard) 84.6 73.8 48.4* 72.4 95
NOTE. Values given are medians.Abbreviations: ND, not done; IU, international units.*P � .001.†P � .05 for comparison with all other groups.‡Patients with chronic hepatitis B were defined as having a serum AST and ALT 2-fold higher than healthy controls, positive serum HBsAg for greater than 6 months,
anti-HBc-IgG(�), anti-HBc-IgM(�), no ascites, peripheral edema or splenomegaly, no clinical additional clinical evidence of cirrhosis, and liver histopathology consistentwith chronic hepatitis. §Asymptomatic, no jaundice, normal AST and ALT, HBsAg(�), but HBeAg(�).
Table 4. Distribution of HBV Genotypes in Vietnamese Patients With HBV Infection
GenotypeASYM
n � 86 (%)AHB
n � 43 (%)CHB
n � 70 (%)LC
n � 92 (%)HCC
n � 84 (%)Total
n � 375 (%)
A 29 (33.7) 6 (13.9) 15 (21.4) 10 (10.8) 8 (9.5) 68 (18.13)B 4 (4.6) 8 (18.6) 7 (10.0) 8 (8.7) 10 (11.9) 37 (9.86)C 29 (33.7) 10 (23.3) 13 (18.6) 13 (14.1) 29 (34.5) 94 (25.06)D 5 (5.8) 6 (13.9) 8 (11.4) 41 (44.6) 16 (19.0) 76 (20.26)E 2 (2.3) 3 (6.9) 2 (2.8) 2 (2.2) 4 (4.8) 13 (3.47)F 2 (2.3) 2 (4.6) 0 3(3.3) 2 (2.4) 9 (2.40)G 0 4 (9.3) 5 (7.1) 3 (3.3) 7 (8.3) 19 (5.06)A/C 2 (2.3) 2 (4.6) 9 (12.8) 7 (7.6) 5 (6.0) 25 (6.66)A/D 1 (1.2) 2 (4.6) 0 3 (3.3) 0 6 (1.6)C/D 4 (4.6) 0 3 (4.3) 1 (1.1) 2 (2.4) 10 (2.66)Other remaining genotype mixtures 8 (9.3) 0 8 (11.4) 1 (1.1) 1 (1.2) 18 (4.80)
HEPATOLOGY, Vol. 43, No. 6, 2006 TOAN ET AL. 1379

type D (P � .0002 and P � .0001, respectively, Fig. 3A).Interestingly, the viral load in patients infected with ge-notype mixtures was significant higher than those in-fected with single genotype overall (P � .019; Fig. 3B)and in LC group (P � .009; Fig. 3C). The HBV-DNAlevel in patients infected by genotype mixture C/D wassignificantly higher than in patients infected with single-genotype C and D (P � .0001; Fig. 5A).
Correlation of HBV Genotypes With HBV-DNAand Liver Disease. Multivariate analysis indicated thatgenotypes C (R � 0.38; P � .001) and D (R � 0.22; P �.001) and age (R � 0.19; P � .007) were positively cor-
related to HCC development, whereas ALT (R � �0.24;P � .001) and mixed infections (R � �0.31; P � .001)were negatively correlated to HCC. Genotype D (R �0.28; P � .001) and age (R � 0.14; P � .04) were posi-
Table 5. Distribution of Genotype Mixtures in HBV-Infected Vietnamese Patients
GenotypeASYM
n � 86 (%)AHB
n � 43 (%)CHB
n � 70 (%)LC
n � 92 (%)HCC
n � 84 (%)
Mixtures 15 (17.4) 4 (9.3) 20 (28.6)* 12 (13) 8 (9.5)Single 71 (82.6) 39 (90.7) 50 (71.4) 80 (87) 76 (90.5)
*P � .02 in comparison to AHB, LC, and HCC groups.
Fig. 2. (A) Serum viral load of HBV-infected patients demonstratinghigher HBV-DNA levels in the AHB, CHB, and ASYM groups comparedwith the LC and HCC groups. *P � .05. (B) Calculation of the serumHBV-DNA levels in HBV-infected patients without HCC indicated higherviral loads compared with the HCC group. P � .01. AHB, acute hepatitisB; CHB, chronic hepatitis B; LC, liver cirrhosis; HCC, hepatocellularcarcinoma; ASYM, asymptomatic.
Fig. 3. (A) Comparison of the viral loads of patients infected with HBVgenotypes A, C, genotype mixture A/C, A/D, and C/D demonstrate higherHBV-DNA levels than in patients infected with the genotype D. P � .0002,P � .0001, P � .0012, P � .0079, and P � .0047, respectively. Theanalysis was performed using contingency table analysis with the non-parametric Mann-Whitney U-test (*) or percentiles analysis with the unpairedcomparison t test (table on the right). (B) Calculation of the level of serumHBV-DNA in patients with genotype mixtures showed significant higher viralloads than respective single genotypes. P � .019. (C) Graph showing theserum HBV loads according to the clinical presentation of patients infectedwith either HBV genotype mixtures or with single genotypes demonstratingthat HBV genotype mixtures were associated with significantly higher viralloads than single genotypes in the LC group. P � .009. AHB, acute hepatitisB; CHB, chronic hepatitis B; LC, liver cirrhosis; HCC, hepatocellular carci-noma; ASYM, asymptomatic.
1380 TOAN ET AL. HEPATOLOGY, June 2006

tively correlated to LC. Moreover, mixed genotypes werepositively correlated with CHB (R � 0.24; P � .001) andnegatively correlated to age (R � �0.25; P � .001). Ge-notype A (R � 0.3; P � .001) was positively correlated toASYM. Genotype C (R � 0.29; P � .048) was positivelycorrelated to histological severity. Additionally, hepatitisB e antigen(�) (R � 0.41; P � .001) and ALT (R � 0.13;P � .04) were positively correlated to HBV-DNA. How-ever, using pair-wise analysis, mixed infections (R � 0.13;P � .01) were positively correlated to HBV-DNA.
In Vitro Replication Levels of Different HBV Ge-notypes. Because the serum viral loads in mixed infec-tions were significantly higher than single-genotypeinfections, we performed in vitro transfection experimentsin HepG2 cells to determine whether potential interac-tions between different viral genotypes altered HBV rep-lication. Progeny HBV-DNA and HBV-DNA in secretedvirions were extracted and used to evaluate the replicationcompetence of different HBV genotypes by real-time
PCR and reverse transcription PCR. Interestingly, consis-tent with the results of the in vivo viral loads, the in vitroexperiments demonstrated that the replication level ofHBV genotype A was significantly higher than the levelsobserved in cells transfected with genotypes C and D (P �.001; Fig. 4A-B). The results of the progeny HBV-DNAassays were in agreement with the qPCR of culture me-dium supernatants (data not shown). Moreover, the invitro experiments revealed higher levels of HBV-replica-tion in cells co-transfected with genotype mixtures com-pared to single-genotype transfections (P � .001; Fig.4C). In accordance with the results of the serum HBV-DNA, the in vitro experiments demonstrated that thelevel of HBV-DNA of genotype mixture C/D was signif-icantly higher than those transfected with single-genotypeC and D (P � .0016; Fig. 5B).
Relation Between the Different HBV Genotypes InVivo and In Vitro. To investigate the relationship be-tween the levels of replication of individual genotypes inpatients infected with genotype mixtures, we performed
Fig. 4. (A) HBV-DNA levels calculated from isolated HBV progeny DNAof transient transfected HepG2 cells. HBV plasmids representing geno-types A, C, and D included clones pHBV1.2, pHBV1.28, pHBV1.5, andpd4aI. Genotype mixtures were obtained by transient transfection ofHepG2 cells with equimolar amounts of the HBV plasmids pHBV1.2,pHBV1.28, pHBV1.5 and pd4aI, respectively. (B) Statistical analysis wasperformed using contingency table analysis with the non-parametricMann-Whitney U-test. The level of HBV replication in HepG2 cells co-transfected with genotypes A and C (A/C), A and D (A/D), and C and D(C/D) were significantly higher than those transfected with the singlegenotypes C or D (P � .0001; Kruskal-Wallis). HBV progeny DNA levelof HepG2 cells transfected with HBV genotype A and A/C were signifi-cantly higher than those observed with other genotypes (P � .0001;Kruskal-Wallis). (C) Comparison of the HBV progeny DNA levels intransiently transfected HepG2 cells demonstrated significantly higheramounts of HBV-DNA in cells co-transfected with genotype-mixturescompared with the single HBV-genotypes (P � .001). GE/�g � HBVgenome equivalents per isolated nucleic acid.
Fig. 5. (A) HBV-DNA concentrations in sera of HBV-infected patientsand (B) of cell culture progeny HBV-DNA show significantly higherconcentrations of HBV-DNA (GE/�g) of the HBV genotype mixtures C/Dcompared with infection/transfection with the single genotypes C and D((A) P � .0001, and (B) P � .0016; Kruskal-Wallis).
HEPATOLOGY, Vol. 43, No. 6, 2006 TOAN ET AL. 1381

semiquantitative PCR (sqPCR) analysis for genotypemixtures A/C, A/D, and C/D of both patient sera (Fig.6A,C) and in vitro experiments (Fig. 6B,D). sqPCR anal-ysis of genotype mixtures A/C and A/D demonstratedthat HBV-genotype A dominated over genotypes C andD (Fig. 6A-D). No difference was detected between HBVgenotypes C and D in patients or in in vitro experimentswith genotype mixture C/D (Fig. 6A-D).
DiscussionIn this study we have analyzed the distribution of HBV
genotypes and the associated clinical outcome of 460HBV-infected individuals from three geographically dis-tinct populations, Vietnam, Africa, and Europe, and theassociated clinical outcome for the Vietnamese group. Asensitive PCR-RFLP developed by Hannoun et al.16 wasadapted for our study, and this assay enabled us to detect7 HBV-genotypes (A, B, C, D, E, F, and G), with apredominance of genotypes A, C, and D, in Vietnamesepatients. In European and African patients, only HBVgenotypes A, C, D, and G were identified. In accordancewith previous studies, genotypes A and D predominatedin European and African patients.8,9 However, genotypeA was most frequently detected in Vietnamese patients;this is in contrast to previous studies, which have shown a
predominance of genotypes B and C in Asian patients.8,13
However, Hannoun and colleagues recently reported theoccurrence of recombinant HBV genotypes A and Cstrains from five Vietnamese patients,29 suggesting thatgenotype A may be more common in Vietnam than pre-viously expected. Moreover, a recent study showed thatrecombination between HBV genotypes B and C is alsofrequent in Asia, including Vietnam.30
Increasingly, evidence now supports the view that dif-ferent HBV genotypes have significant roles in determin-ing the clinical outcome of liver disease and the responseto antiviral therapies. This has been shown with geno-types A and D, which are prevalent in Europe and theUnited States, and genotypes B and C, which are preva-lent in Asia.2,3,30-32 To identify the impact of HBV geno-types on the clinical outcome of HBV infection, we havecharacterized the genotype distribution and clinical out-come of subjects with well-characterized clinical profilesof liver disease and infection. In this study, we demon-strated that in Vietnam genotypes A and C were the pre-dominant viruses in ASYM patients in comparison withsymptomatic patients and patients with HCC in whomthe predominant genotypes were C and D. This suggeststhat pathogenesis of genotype A may be different from theother viral genotypes. Multivariate analysis showed HBV
Fig. 6. (A-B) Detemination of the “dominant” HBV genotype in genotype mixtures. The semiquantitative RFLP-PCR products amplified from the HBVgenotype mixtures A/C, A/D, and C/D are shown in vivo (A) and in vitro (B). (C-D) The densitometry evaluation of the RFLP-PCR products (shownin A and B) showed a significantly higher replication competence of genotype A compared with genotypes C and D in genotype mixtures. No differencewas detected between genotype C and D in genotype mixture C/D in vivo (C) and in vitro (D). The insert letters specified the bands for theHBV-genotypes A, C, and D; respectively. M � size marker.
1382 TOAN ET AL. HEPATOLOGY, June 2006

genotypes C and D to be positively correlated to HCC,whereas genotype A was correlated to ASYM. This is fur-ther consolidated by our findings demonstrating an asso-ciation between the development of HCC and genotypeC and D but not with genotype A. This association hasalso been reported in studies from Taiwan,13 Japan,2 andChina.14 Interestingly, in our Vietnamese population, ge-notype D was also prevalent in patients with LC disease.
In addition to demonstrating an association betweenHBV-genotypes and severity of clinical disease, by usingreal-time PCR, we were able to show that the serumHBV-DNA in patients infected with HBV genotypes Cand D were significant lower compared to those infectedwith genotype A. Our in vitro cell culture findings dem-onstrating higher levels of HBV replication of genotype Acompared to genotypes C and D were consistent with theresults of the in vivo viral loads. We also found that, inaccordance with the in vivo results, HBV genotype Apredominated over the replication of genotypes C and Din genotype mixtures A/C and A/D. This, together withthe higher level of replication of genotype A, may partlyexplain the observed association between genotype A andthe more frequent progression to CHB than genotype D.3
The reasons for the differences observed in clinicalcourse of disease and viral loads is not clear, although onecould postulate that these may be the consequence ofgenotype-specific differences in viral replication, variabil-ity in the host immune response to different HBV geno-types33 possibly resulting in greater severity of liver diseaseand ultimately the development of LC and adverse effectson cell signaling events with the consequent developmentof HCC.34-36
Few studies have reported the occurrence of mixedHBV genotype infections16 or the effects of mixed infec-tions on clinical outcome or viral replication. The studyby Hannoun and coworkers16 included 30 patients whohad received treatment with interferon alpha. Using aPCR-RFLP assay, these investigators demonstrated that67% of patients were infected with more than one geno-type.16 Recently, using the DHBV model, Walters andcoworkers31 demonstrated that superinfection with a sec-ond duck HBV was not possible once the liver has becomepopulated with a single species of duck HBV supercoiledDNA.37 However, this is in contrast to our finding ofmixed HBV genotype infections in patients with CHBinfection and argues that coinfection or superinfectionwith a second species of HBV is possible in human hosts.
In our study, infection with mixed HBV genotype wasfound in 16.9% (78/460) of patients. However, in pa-tients with chronic hepatitis, the proportion of patientswith genotype mixtures was significantly higher (28.6%;Table 5), again supporting the notion that infection of the
human liver with more than a single viral population ispossible. The results of the current study are consistentwith those of previous reports, which suggest that geno-typic coinfection is not infrequent in chronic HBV infec-tion and that higher levels of HBV replication areassociated with mixed-genotype infections.16 In sum-mary, our report is the first showing an association be-tween the distribution and impact of HBV genotypes andmixed genotype infections and of viral replication on clin-ical disease severity in HBV-endemic areas. Attributingprecise roles to any given genotype or mixed genotypeinfection in the context of HBV pathogenesis or clinicalprogression is unclear. However, our findings indicatethat the clinical course of CHB and the development ofHCC is influenced by HBV genotype and by the occur-rence of mixed genotype infection and warrants furtherinvestigation to understand these effects from a virologi-cal and pathogenesis perspective.
Acknowledgment: The authors thank Don L.V., ThangH.H., Nhuong D.X., Lan D.T., Binh D.T., Thoa L.T.,Lam H.T., and Dung D.T. for their help in collectingsamples and S. Illmann, H. Kaiser, and G. Janke for ex-cellent technical assistance.
References1. Kao JH, Chen PJ, Lai MY, Chen DS. Hepatitis B genotypes correlate with
clinical outcomes in patients with chronic hepatitis B. Gastroenterology2000;118:554-559.
2. Orito E, Mizokami M, Sakugawa H, Michitaka K, Ishikawa K, Ichida T, etal. A case-control study for clinical and molecular biological differencesbetween hepatitis B viruses of genotypes B and C. Japan HBV GenotypeResearch Group. HEPATOLOGY 2001;33:218-223.
3. Mayerat C, Mantegani A, Frei PC. Does hepatitis B virus (HBV) genotypeinfluence the clinical outcome of HBV infection? J Viral Hepatol 1999;6:299-304.
4. Okamoto H, Tsuda F, Sakugawa H, Sastrosoewignjo RI, Imai M, Mi-yakawa Y, et al. Typing hepatitis B virus by homology in nucleotide se-quence: comparison of surface antigen subtypes. J Gen Virol 1988;69:2575-2583.
5. Norder H, Courouce AM, Magnius LO. Complete genomes, phylogeneticrelatedness, and structural proteins of six strains of the hepatitis B virus,four of which represent two new genotypes. Virology 1994;198:489-503.
6. Stuyver L, De Gendt S, Van Geyt C, Zoulim F, Fried M, Schinazi RF, etal. A new genotype of hepatitis B virus: complete genome and phylogeneticrelatedness. J Gen Virol 2000;81:67-74.
7. Arauz-Ruiz P, Norder H, Robertson BH, Magnius LO. Genotype H: anew Amerindian genotype of hepatitis B virus revealed in Central America.J Gen Virol 2002;83:2059-2073.
8. Lindh M, Andersson AS, Gusdal A. Genotypes, nt 1858 variants, andgeographic origin of hepatitis B virus large-scale analysis using a new geno-typing method. J Infect Dis 1997;175:1285-1293.
9. Magnius LO, Norder H. Subtypes, genotypes and molecular epidemiologyof the hepatitis B virus as reflected by sequence variability of the S-gene.Intervirology 1995;38:24-34.
10. Norder H, Hammas B, Lee SD, Bile K, Courouce AM, Mushahwar IK, etal. Genetic relatedness of hepatitis B viral strains of diverse geographicalorigin and natural variations in the primary structure of the surface antigen.J Gen Virol 1993;74:1341-1348.
HEPATOLOGY, Vol. 43, No. 6, 2006 TOAN ET AL. 1383

11. Nguyen TV, Truong XL, Nguyen TN, Phung TTY, Nguyen TN, HoangCL, et al. Hepatitis B virus infection in Vietnam. Reports of Institute ofHygien and Epidemic, Hanoi, Vietnam, 1995.
12. Alestig E, Hannoun C, Horal P, Lindh M. Phylogenetic origin of hepatitisB virus strains with precore C-1858 variant. J Clin Microbiol 2001;39:3200-3203.
13. Kao JH. Hepatitis B virus genotypes and hepatocellular carcinoma in Tai-wan. Intervirology 2003;46:400-407.
14. Ding XM, Mizokami G, Yao B, Xu E, Orito R, Ueda, et al. Hepatitis Bvirus genotype distribution among chronic hepatitis B virus carriers inShanghai, China. Intervirology 2001;44:43-47.
15. Gerner PR, Friedt M, Oettinger R, Lausch E, Wirth S. The hepatitis Bvirus seroconversion to anti-HBe is frequently associated with HBV geno-type changes and selection of preS2-defective particles in chronically in-fected children. Virology 1998;245:163-172.
16. Hannoun C, Krogsgaard K, Horal P, Lindh M, Interpred trial group.Genotype mixtures of hepatitis B virus in patients treated with interferon.J Infect Dis 2002;186:752-759.
17. Song LH, Binh VQ, Duy DN, Bock CT, Kun JFJ, Kremsner PG et al.Serum cytokine profiles associated with clinical presentation in Vietnameseinfected with hepatitis B virus. J Clin Virol 2003;28:93-103.
18. Song le H, Binh VQ, Duy DN, Bock TC, Kremsner PG, Luty AJ, et al.Variations in the serum concentrations of soluble Fas and soluble Fasligand in Vietnamese patients infected with hepatitis B virus. J Med Virol2004;73:244-249.
19. Luo JC, Hwang SJ, Lai CR, Lu CL, Li CP, Tsay SH, et al. Relationshipsbetween serum aminotransferase levels, liver histologies and virologicalstatus in patients with chronic hepatitis C in Taiwan. J GastroenterolHepatol 1998;13:685-690.
20. Kun JF, Mordmuller B, Lell B, Lehman LG, Luckner D, Kremsner PG.Polymorphism in promoter region of inducible nitric oxide synthase geneand protection against malaria. Lancet 1998;351:265-266.
21. Kun JF, Schmidt-Ott RJ, Lehman LG, Lell B, Luckner D, Greve B, et al.Merozoite surface antigen 1 and 2 genotypes and rosetting of Plasmodiumfalciparum in severe and mild malaria in Lambarene, Gabon. Trans R SocTrop Med Hyg 1998;92:110-114.
22. Song le H, Binh VQ, Duy DN, Juliger S, Bock TC, Luty AJ, KremsnerPG, et al. Mannose-binding lectin gene polymorphisms and hepatitis Bvirus infection in Vietnamese patients. Mutat Res 2003;28;522:119-125.
23. Bock CT, Malek NP, Tillmann HL, Manns MP, Trautwein C. The en-hancer I core region contributes to the replication level of hepatitis B virusin vivo and in vitro. J Virol 2000;74:2193-2202.
24. Scaglioni PP, Melegari M, Wands JR. Posttranscriptional regulation ofhepatitis B virus replication by the precore protein. J Virol 1997;71:345-353.
25. Loncarevic IF, Zentgraf H, Schroeder CH. Sequence of a replication com-petent hepatitis B virus genome with a preX open reading frame. NuclAcids Res 1990;18:4940.
26. Bock CT, Tillmann HL, Maschek HJ, Manns MP, Trautwein C. A preSmutation isolated from a patient with chronic hepatitis B infection leads tovirus retention and misassembly. Gastroenterology 1997;113:1976-1982.
27. Gerard CJ, Andrejka LM, Macina RA. Mitochondrial ATP synthase 6 asan endogenous control in the quantitative RT-PCR analysis of clinicalcancer samples. Mol Diagn 2000;5:39-46.
28. Bock CT, Tillmann HL, Torresi J, Klempnauer J, Locarnini S, MannsMP, et al. Selection of hepatitis B virus polymerase mutants with enhancedreplication by lamivudine treatment after liver transplantation. Gastroen-terology 2002;122:264-273.
29. Hannoun C, Norder H, Lindh M. An aberrant genotype revealed in re-combinant hepatitis B virus strains from Vietnam. J Gen Virol 2000;81:2267-2272.
30. Sugauchi F, Orito E, Ichida T, Kato H, Sakugawa H, Kakumu S, et al.Epidemiologic and virologic characteristics of hepatitis B virus genotype Bhaving the recombination with genotype C. Gastroenterology 2003;124:925-932.
31. Chu CJ, Hussain M, Lok AS. Hepatitis B virus genotype B is associatedwith earlier HBeAg seroconversion compared with hepatitis B virus geno-type C. Gastroenterology 2002;122:1756-1762.
32. Kao JH, Chen PJ, Lai MY, Chen DS. Genotypes and clinical phenotypesof hepatitis B virus in patients with chronic hepatitis B virus infection.J Clin Microbiol 2002;40:1207-1209.
33. Milich DR, Jones JE, McLachlan A, Bitter A, Moriarty A, Hughes JL.Importance of subtype in the immune response to the pre-S(2) region ofthe hepatitis B surface antigen. II. Synthetic Pre-S(2) immunogen. J Im-munol 1990;144:3544-3551.
34. Yoo YG, Oh SH, Park ES, Cho H, Lee N, Park H, Kim DK, et al. HepatitisB virus X protein enhances transcriptional activity of hypoxia-induciblefactor-1alpha through activation of mitogen-activated protein kinase path-way. J Biol Chem 2003;278:39076-39084.
35. Diao J, Khine AA, Sarangi F, Hsu E, Iorio C, Tibbles LA, Woodgett JR, etal. X protein of hepatitis B virus inhibits Fas-mediated apoptosis and isassociated with up-regulation of the SAPK/JNK pathway. J Biol Chem2001;276:8328-8340.
36. Tarn C, Lee S, Hu Y, Ashendel C, Andrisani OM. Hepatitis B virus Xprotein differentially activates RAS-RAF-MAPK and JNK pathways inX-transforming versus non-transforming AML12 hepatocytes. J BiolChem 2001;276:34671-34680.
37. Walters KA, Joyce MA, Addison WR, Fischer KP, Tyrrell DL. Superin-fection exclusion in duck hepatitis B virus infection is mediated by the largesurface antigen. J Virol 2004;78:7925-7937.
1384 TOAN ET AL. HEPATOLOGY, June 2006




















