Impact of CT-Guided Drainage in the Treatment of Diverticular Abscesses: Size Matters
7
680 AJR:186, March 2006 AJR 2006; 186:680–686 0361–803X/06/1863–680 © American Roentgen Ray Society M E D I C A L I M A G I N G A C E N T U R Y O F Siewert et al. CT-Guided Drainage in the Treatment of Diverticular Abscesses Gastrointestinal Imaging • Original Research Impact of CT-Guided Drainage in the Treatment of Diverticular Abscesses: Size Matters Bettina Siewert 1 Grace Tye 1 Jonathan Kruskal 1 Jacob Sosna 1 Frank Opelka 2 Siewert B, Tye G, Kruskal J, Sosna J, Opelka F Keywords: abdomen, colon, CT, gastrointestinal radiology DOI:10.2214/AJR.04.1708 Received November 4, 2004; accepted after revision February 7, 2005. 1 Department of Radiology, Beth Israel Deaconess Medical Center, 330 Brookline Ave., Boston, MA 02115. Address correspondence to B. Siewert ([email protected]) (B. Siewert and G. Tye are co-first authors). 2 Department of Surgery, Beth Israel Deaconess Medical Center, Boston, MA 02115. OBJECTIVE. Our objective was to determine whether abscess size can be used as a dis- criminating factor to guide management of patients with diverticular abscesses. MATERIALS AND METHODS. We performed a word search of our CT database be- tween July 2001 and July 2002 for the CT diagnosis of diverticulitis. CTs were retrospectively reviewed as consensus opinion of two reviewers. CTs were evaluated for presence of an ab- scess, its location, maximum diameter, and feasibility of percutaneous abscess drainage. Ab- scesses were categorized into smaller than 3 cm and larger than or equal to 3 cm, and the man- agement of these groups was compared. RESULTS. Thirty-one abscesses were noted in 30 (17%) of 181 patients with a CT diag- nosis of diverticulitis. Twenty-two (73%) of 30 patients had 23 abscesses, all of which were smaller than 3 cm and were treated and resolved with antibiotics alone (p < 0.001). Eight (36%) of 22 required surgical treatment. Eight (26%) of 31 abscesses had a maximum diameter larger than or equal to 3 cm. Four (50%) of eight patients with abscesses 3.4–4.1 cm were treated with antibiotics alone. Four (50%) of eight abscesses, all larger than 4.1 cm, were treated with CT- guided drainage and one abscess required repeat drainage. After resolution of symptoms, sur- gery was performed in five (62.5%) of eight of the larger abscesses. CONCLUSION. Patients with abscesses smaller than 3 cm in size can be treated with an- tibiotics alone and, in some cases, as outpatients, and may not uniformly require surgery. This is also likely true for patients with abscesses 3–4 cm in size, although our results in this group were limited by a small sample size. Patients with abscesses larger than or equal to 4 cm can be managed with CT-guided abscess drainage followed by referral for surgical treatment. iverticular disease is a common health problem in the Western world. Diverticulosis is noted in 33–50% of the population after age 50 and in more than 50% of the population af- ter age 80 [1]. From 10% to 20% of patients with known diverticula will develop diverticu- litis [2]. The most common complications as- sociated with acute diverticulitis are abscesses that are suspected clinically when a patient fails to improve after several days of antibiotic therapy. As many as 59% of patients with di- verticular abscesses will eventually undergo surgery [3]. Traditionally, all patients with ab- scesses were treated with multiple-stage sur- gery after a course of antibiotic therapy. Sur- gical treatment consisted of a Hartmann resection, or, when possible, a single-stage re- section with a primary anastomosis. The treat- ment of diverticular abscesses, however, dra- matically changed with the development of CT-guided percutaneous abscess drainage in the 1980s, which can serve as a temporizing measure and allows single-stage resection in the subacute period. Several authors [4–11] have reported CT-guided abscess drainage to provide definitive treatment. However, not all abscesses require an inter- ventional drainage for resolution. Abscesses smaller than 3 cm in size are often treated con- servatively with antibiotic therapy alone [12]. Furthermore, no clear guidelines exist for the optimal management of abscesses 3–5 cm in size. In addition, although elective resection has traditionally been offered after an episode of diverticulitis complicated by abscess forma- tion, it is unclear if all patients with abscesses should undergo subsequent surgical treatment. This study investigated the management and subsequent outcome of patients with di- verticular abscesses. The purpose of this study was to provide additional data and to suggest guidelines for the treatment of small diverticular abscesses. D
Transcript of Impact of CT-Guided Drainage in the Treatment of Diverticular Abscesses: Size Matters

680 AJR:186, March 2006
AJR 2006; 186:680–686
0361–803X/06/1863–680
© American Roentgen Ray Society
M E D I C A L I M A G I N G
A C E N T U R Y O F
Siewert et al.CT-Guided Drainage in the Treatment of Diverticular Abscesses
G a s t ro i n t e s t i n a l I m ag i n g • O r i g i n a l R e s e a rc h
Impact of CT-Guided Drainage in the Treatment of Diverticular Abscesses: Size Matters
Bettina Siewert1
Grace Tye1
Jonathan Kruskal1
Jacob Sosna1
Frank Opelka2
Siewert B, Tye G, Kruskal J, Sosna J, Opelka F
Keywords: abdomen, colon, CT, gastrointestinal radiology
DOI:10.2214/AJR.04.1708
Received November 4, 2004; accepted after revision February 7, 2005.
1Department of Radiology, Beth Israel Deaconess Medical Center, 330 Brookline Ave., Boston, MA 02115. Address correspondence to B. Siewert ([email protected]) (B. Siewert and G. Tye are co-first authors).
2Department of Surgery, Beth Israel Deaconess Medical Center, Boston, MA 02115.
OBJECTIVE. Our objective was to determine whether abscess size can be used as a dis-criminating factor to guide management of patients with diverticular abscesses.
MATERIALS AND METHODS. We performed a word search of our CT database be-tween July 2001 and July 2002 for the CT diagnosis of diverticulitis. CTs were retrospectivelyreviewed as consensus opinion of two reviewers. CTs were evaluated for presence of an ab-scess, its location, maximum diameter, and feasibility of percutaneous abscess drainage. Ab-scesses were categorized into smaller than 3 cm and larger than or equal to 3 cm, and the man-agement of these groups was compared.
RESULTS. Thirty-one abscesses were noted in 30 (17%) of 181 patients with a CT diag-nosis of diverticulitis. Twenty-two (73%) of 30 patients had 23 abscesses, all of which weresmaller than 3 cm and were treated and resolved with antibiotics alone (p < 0.001). Eight (36%)of 22 required surgical treatment. Eight (26%) of 31 abscesses had a maximum diameter largerthan or equal to 3 cm. Four (50%) of eight patients with abscesses 3.4–4.1 cm were treated withantibiotics alone. Four (50%) of eight abscesses, all larger than 4.1 cm, were treated with CT-guided drainage and one abscess required repeat drainage. After resolution of symptoms, sur-gery was performed in five (62.5%) of eight of the larger abscesses.
CONCLUSION. Patients with abscesses smaller than 3 cm in size can be treated with an-tibiotics alone and, in some cases, as outpatients, and may not uniformly require surgery. Thisis also likely true for patients with abscesses 3–4 cm in size, although our results in this groupwere limited by a small sample size. Patients with abscesses larger than or equal to 4 cm canbe managed with CT-guided abscess drainage followed by referral for surgical treatment.
iverticular disease is a commonhealth problem in the Westernworld. Diverticulosis is noted in33–50% of the population after age
50 and in more than 50% of the population af-ter age 80 [1]. From 10% to 20% of patientswith known diverticula will develop diverticu-litis [2]. The most common complications as-sociated with acute diverticulitis are abscessesthat are suspected clinically when a patientfails to improve after several days of antibiotictherapy. As many as 59% of patients with di-verticular abscesses will eventually undergosurgery [3]. Traditionally, all patients with ab-scesses were treated with multiple-stage sur-gery after a course of antibiotic therapy. Sur-gical treatment consisted of a Hartmannresection, or, when possible, a single-stage re-section with a primary anastomosis. The treat-ment of diverticular abscesses, however, dra-matically changed with the development ofCT-guided percutaneous abscess drainage in
the 1980s, which can serve as a temporizingmeasure and allows single-stage resection inthe subacute period. Several authors [4–11]have reported CT-guided abscess drainage toprovide definitive treatment.
However, not all abscesses require an inter-ventional drainage for resolution. Abscessessmaller than 3 cm in size are often treated con-servatively with antibiotic therapy alone [12].Furthermore, no clear guidelines exist for theoptimal management of abscesses 3–5 cm insize. In addition, although elective resectionhas traditionally been offered after an episodeof diverticulitis complicated by abscess forma-tion, it is unclear if all patients with abscessesshould undergo subsequent surgical treatment.
This study investigated the managementand subsequent outcome of patients with di-verticular abscesses. The purpose of thisstudy was to provide additional data and tosuggest guidelines for the treatment of smalldiverticular abscesses.
D

CT-Guided Drainage in the Treatment of Diverticular Abscesses
AJR:186, March 2006 681
Materials and MethodsPatient Selection
This was a retrospective study that was approvedby our institutional internal review board and in-formed consent was not necessary. We performed aword search in our comprehensive computer data-base containing all reports of CT scans of the abdo-men and pelvis performed at our institution betweenJuly 2001 and July 2002 using the keyword “diverti-culitis.” Two hundred two consecutive patients wereidentified from our patient population at a tertiarycare medical center and major teaching hospital. Thepatient population consisted of inpatients and outpa-tients. CT scans were retrospectively reviewed byconsensus opinion of two reviewers. Twenty-one(10.4%) patients were excluded from the study. Thisincluded 15 patients who did not show signs of acutediverticulitis by consensus opinion of the two re-viewers. In six (3%) patients, no follow-up informa-tion regarding outcomes was available. Thus, 181patients were included in this study.
CT ProtocolCT examinations were performed with a HiSpeed
Advantage unit (GE Healthcare) 45–60 min after theoral administration of 900 mL of a 2.1% barium sul-fate suspension (Readi-Cat 2, E-Z-EM). One hun-dred fifty milliliters of 43% iodinated contrast mate-rial (Conray, Mallinckrodt Medical) was injected IVat a rate of 2 mL/sec. Twenty-two (12.2%) of 181 pa-tients did not receive IV contrast because of elevatedcreatinine or contrast allergy. Single breath-holdscans were obtained through the entire abdomen andpelvis with a 7-mm collimation and a pitch of 1.5 af-ter a 50-sec delay. Coronal reformations were per-formed in 147 (81.2%) of 181 patients. Three (1.7%)of 181 patients received rectal contrast for better de-lineation of wall thickening.
Data AnalysisCT scans were retrospectively reviewed and in-
terpreted as consensus opinion of two radiologistswho were blinded to clinical, surgical, and patho-logic findings. CT scans were evaluated for the pres-ence, location, and maximum diameter of an ab-scess, and the feasibility of percutaneous drainagefor each abscess was noted. An abscess was diag-nosed when a fluid collection with an enhancing rimwas noted with or without air inclusion. If the CT ex-amination was performed without IV contrast, onlyfluid collections with convex borders and mass effectwere interpreted as abscesses. Abscesses were con-sidered unfeasible for imaging-guided catheterdrainage when the collection could not be reachedpercutaneously without passing traversing vitalstructures such as small- or large-bowel loops orlarge vessels. Abscesses were categorized into thosesmaller than 3 cm and those larger than or equal to 3
cm in their maximum diameter, and the managementof these two groups was compared. Treatment ofthese patients was classified as medical (antibioticsalone), radiologic (antibiotics and CT-guided percu-taneous drainage), or surgical (antibiotics and sur-gery). Statistical analysis was performed using thechi-square test. Electronic medical records were re-viewed for data regarding the patients’ initial clinicalpresentation, including symptoms (abdominal pain,nausea, vomiting, anorexia, change in bowel habits),signs (fever, abdominal tenderness, peritonealsigns), and laboratory findings (leukocytosis, leftshift, bandemia), and length of hospital stay. A min-imum follow-up of 50 days after the first presenta-tion of diverticulitis was obtained to track recurrentepisodes of diverticulitis requiring subsequent hospi-talization, imaging studies, and surgery. Pathologicfindings were analyzed when available.
The evolution of the abscesses was categorizedas resolution, persistence, or worsening. Persis-tence or recurrence of symptoms and subsequentsurgical intervention were noted. Overall outcomewas analyzed with data obtained from clinical fol-low-up, surgical reports, or both and compared be-tween the two groups.
ResultsThirty-three abscesses were diagnosed in
32 (17%) of 181 patients. Two (6%) patients
were excluded from the study because of im-aging findings on CT, such as free intraperito-neal air that necessitated immediate surgery.Thus, our study included 30 patients with 31diverticular abscesses. Thirteen (43%) of 30patients with abscesses were men and 17(57%) were women. The average age was54.2 ± 13.1 (SD) years (range, 30–91 years),with 17 (57%) of 30 patients over the age of50 (Table 1). The mean diameter of the ab-scesses was 2.3 ± 1.6 cm (range, 0.9–6.7 cm).
All patients received antibiotics, with 11(37%) of 30 treated as outpatients. The me-dian follow-up period was 393 days (range,50–758 days), during which 13 (43.3%) of 30patients underwent elective resection for di-verticulitis, six (20%) of 30 patients experi-enced mild recurrent or persistent symptomsof diverticulitis, and the remaining 10(33.3%) of 30 patients remained free ofsymptoms with full clinical resolution.
Patients with Abscesses Larger Than or Equal to 3 cm
Eight (26%) of 31 abscesses had a maxi-mum diameter larger than or equal to 3 cm.Four abscesses (50%) in eight patients weredrained within 24 hr via a CT-guided percuta-neous catheter (Table 2) (mean size, 5.9 cm;
TABLE 1: Patient Characteristics by Abscess Size
CharacteristicTotal Patients withAbscesses (n = 30)
Abscess ≥ 3 cm(n = 8)
Abscess < 3 cm(n = 22)
Men 13 3 10
Women 17 5 12
Age (years) 54.2 (30–91) 55.3 (40–74) 53.8 (30–91)
WBC (K/µL) 13.0 (6.4–28.1) 13.2 (6.4–17.9) 13.0 (6.4–28.1)
Neutrophils (%) 76.4 (41.0–93.1) 76.3 (59.7–85.1) 77.4 (59.6–91.7)
Average abscess size (cm) 2.3 (0.9–6.7) 4.9 (3.4–6.7) 1.5 (0.9–2.8)
Note—Values in parentheses indicate range. Neutrophils = percentage of WBC composed of neutrophils; average abscess size = average maximum diameter of abscess.
TABLE 2: Management of Large Abscesses (≥ 3 cm)
PatientAbscessSize (cm)
Treatment in Acute Setting Follow-Up Findings Surgery
PathologyInflammation
1 3.4 Antibiotics CT Resolution No
2 3.8 Antibiotics CT Resolution Yes Acute
3 4.0 Antibiotics Clinical Resolution No
4 4.1 Antibiotics Clinical Resolution No
5 4.9 PAD (× 2) CT Reaccumulation Yes Acute and chronic
6 5.7 PAD CT Resolution Yes Acute
7 6.5 PAD Clinical Resolution Yes Chronic
8 6.7 PAD CT Improved Yes Acute
Note—PAD = percutaneous abscess drainage.

Siewert et al.
682 AJR:186, March 2006
A B
C
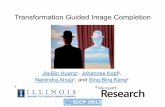
Fig. 1—57-year-old woman with large diverticular abscess.A, Axial CT image shows 4.9-cm abscess (arrow) containing air–fluid level.B, Axial CT image from CT-guided catheter drainage confirms adequate catheter position (arrow) and complete aspiration of abscess at time of examination.C, On axial CT image 22 days later, there is reaccumulation of abscess (arrow) that was again treated with CT-guided catheter drainage.
A BFig. 2—45-year-old man with large diverticular abscess.A, Axial CT image shows 3.8-cm intramural abscess (arrow) with enhancing wall. Patient was treated with antibiotics because abscess was inaccessible to percutaneous catheter drainage.B, Follow-up CT examination 21 days later shows complete resolution of abscess and inflammatory changes of colon.

CT-Guided Drainage in the Treatment of Diverticular Abscesses
AJR:186, March 2006 683
range, 4.9–6.7 cm) (Fig. 1). The remainingfour (50%) patients were treated with antibi-otics alone because the abscesses were judgednot to be amenable to drainage at the time be-cause of their location deep within the pelvis(Table 2) (Fig. 2). Abscess size in this groupranged from 3.4–4.1 cm. All four patientsshowed resolution of the abscess on follow-up CT (two patients) or on clinical evaluation(two patients). Only one patient underwentsurgery and showed acute inflammation in thesurgical specimen.
One of the four patients who underwent ra-diologic intervention required a repeat percu-taneous drainage because of reaccumulationof the abscess 10 days after the initial catheterhad been removed (Fig. 1). The initial cathe-ter had been in place for 12 days. Six (75%)of eight patients were admitted to the hospital
with an average hospital stay of 5.8 days(range, 4–8 days), whereas two (25%) ofeight patients were treated as outpatients. Six(75%) of eight patients reported a history ofdiverticulitis. Six (75%) of eight patients re-ported recurrent or persistent symptoms aftertreatment. Five (62.5%) of eight patients un-derwent surgical resection for diverticulitis ata median of 67.5 days (range, 34–644 days)after the acute episode. All surgical inter-ventions were single-stage resections withprimary anastamoses. Four (80%) of fivepatients showed acute inflammation onpathologic examination of the specimen. Theremaining patient only showed chronic in-flammatory changes, indicating response totreatment. Surgery was recommended but re-fused by one of the three patients who did notundergo eventual surgery. One patient was
not a surgical candidate. The final patient, de-spite documented episodes of recurrent diver-ticulitis, had not undergone surgical evalua-tion or intervention at 544 days’ follow-up forreasons unspecified in the clinical record.Thus, in total, interval surgery was recom-mended for seven (87.5%) of eight patientswith large diverticular abscesses.
Patients with Abscesses Smaller Than 3 cmTwenty-two (73%) of 30 patients had ab-
scesses smaller than 3 cm in greatest diame-ter, one of whom had two small abscesses. All22 patients were treated with antibioticsalone. Thirteen of 22 patients were admittedto the hospital, with an average hospital stayof 5.5 days (range, 2–16 days). The remainingnine (41%) patients were treated as outpa-tients with oral antibiotics.
A B
C
Fig. 3—55-year-old woman with diverticular abscess.A, Axial CT image shows 2.0-cm abscess (arrow) with enhancing rim containing predominantly air. Patient was treated with antibiotics.B, Axial image cranial in relation to A shows changes of diverticulitis with asymmetric wall thickening (arrow) and adjacent fat stranding.C, On follow-up CT after 25 days, abscess and inflammatory changes of colon have completely resolved.

Siewert et al.
684 AJR:186, March 2006
All 23 abscesses resolved with antibiotictreatment alone. This was documented by res-olution of abscesses on CT examination (n =8) (Fig. 3), CT examination and surgical pa-thology (n = 6), or surgical pathology (n = 2).The remaining seven patients reported clini-cal improvement at a median follow-up of341 days (range, 50–736 days), thus suggest-ing resolution of their abscesses (Fig. 4).
All patients who eventually underwent sur-gery (eight [36%] of 22 patients) had sufferedmultiple episodes of diverticulitis by the timeof surgery, with six (75%) of these eight pa-tients reporting a history of diverticulitis be-fore the index episode in the present seriesand two (25%) experiencing recurrent epi-sodes after their index presentation in thepresent series. Nine (41%) of the 22 patientsreported full resolution of symptoms after theindex episode and five (23%) had mild persis-tent or recurrent symptoms that did not war-rant surgical intervention. Short-term andlong-term treatments for small and large ab-scesses are listed in Table 3. Results were sta-tistically significant (p < 0.05).
DiscussionThe immediate treatment of diverticular
abscesses has evolved since the 1980s, withdouble- or single-stage surgical resection af-ter antibiotic treatment being gradually re-placed by CT-guided abscess drainage as atemporizing procedure to allow eventual sin-gle-stage rather than double-stage surgical re-section [4–11]. CT-guided abscess drainagehas also been shown to provide definitivetreatment for 70–90% of abdominal ab-scesses [5–8, 10, 13]. It is unclear, however, ifthat drainage is required for resolution of alldiverticular abscesses, regardless of size. Fur-thermore, eventual surgical treatment has tra-ditionally been recommended for all patientswith diverticulitis complicated by abscessformation. However, to our knowledge nostudies have evaluated the need for surgicaltreatment in patients with small diverticularabscesses. A recent survey showed a greatdeal of variation among colorectal surgeonsin their management of diverticulitis [14],thus highlighting the need for more precisedefinition of treatment recommendations.Our study was designed to evaluate retrospec-tively the differences in immediate manage-ment of large and small abscesses and theclinical outcome as indicated by the need foreventual surgical treatment. We defined asmall abscess as smaller than 3 cm in its great-est diameter because abscesses smaller than 3cm are often not considered well suited forCT-guided abscess drainage [12].
In our study, a diverticular abscess wasnoted in 17% of patients with CT evidence ofdiverticulitis (32 of 181 patients). This is con-sistent with the incidence reported in the lit-erature, ranging from 8–34% [3, 15–23]. The
Fig. 4—57-year-old man with diverticular abscess. Axial CT image shows 1.7-cm abscess (arrow) with enhancing wall. Patient was treated with antibiotics and symptoms resolved on clinical follow-up.
TABLE 3: Comparison Between Initial Treatment and Delayed Surgery in Diverticular Abscesses According to Size
Abscess No. (%) of Patients
Size No.
AcuteAntibiotics
OnlyCT
Drainage
DelayedElectiveSurgery
< 3 cm 22 22 (100) 0 (0) 8 (36)
≥ 3 cm 8 4 (50) 4 (50) 5 (62.5)
Note—p < 0.05.
mean abscess diameter was 2.3 cm, with onlyeight (26%) of 31 abscesses equal to or ex-ceeding 3 cm in diameter. Other studies havereported a mean abscess size of 3.3 to 5.4 cm[3, 15, 16]. The smaller size of the abscessesdetected in our study may represent earlier di-agnosis in our study population as a whole orless severe disease. Most patients in our studypresented to the emergency department,where a CT scan was ordered on the day ofpresentation. Thus, as a result of increasednumber of patients with suspected diverticu-litis undergoing CT early in the course of theirdisease, the abscesses detected in our studymay have been smaller in size than those pre-viously found in other studies. This trend issimilar to the one reported for the diagnosis ofappendicitis, in which an increase in CT led todiagnosis of disease in earlier stages [24].Therefore, as CT becomes increasingly im-portant in the evaluation of suspected diverti-culitis [25, 26], an increase in the detection ofsmall abscesses can be expected.
In our study, all abscesses smaller than 3cm were treated successfully with antibioticsalone and thus did not require percutaneousdrainage. In this patient population no recur-rent abscesses required secondary catheterdrainage. All patients who underwent surgeryshowed complete resolution of the inflamma-tion on surgical pathology. In addition, eventhe four large abscesses that were not amena-ble to CT-guided drainage improved on anti-biotic therapy alone. These abscesses mea-sured 3.4–4.1 cm in diameter. None of thesepatients had recurrent abscesses. Only one(25%) of these four patients underwent sur-gery and showed acute inflammation in thesurgical specimen.
These findings concur with the currentrecommendations from the American Soci-ety of Colon and Rectal Surgeons, the Amer-ican College of Gastroenterology, and theEuropean Association for Endoscopic Sur-gery, which state that small pericolic ab-scesses can initially be treated conserva-tively, with CT-guided abscess drainagereserved for those that fail to resolve [13, 27,28]. However, none of these guidelines de-fines an abscess size that does not requireCT-guided abscess drainage.
Only one study to our knowledge has at-tempted to establish a guideline for abscessesthat are likely to respond to antibiotic therapyalone. Ambrosetti et al. [3] showed that the lo-cation of the abscess was the most importantpredictor of response to conservative therapy,concluding that mesocolic abscesses were

CT-Guided Drainage in the Treatment of Diverticular Abscesses
AJR:186, March 2006 685
more likely than pelvic or intraabdominal ab-scesses to respond to antibiotics alone. How-ever, that study did not assess the effect of ab-scess size on response to medical therapy andincluded only inpatients in the study popula-tion. The abscesses encountered in their serieswere larger than in our study, ranging from 2 to15 cm, with a mean size of 5.5 cm. Detry et al.[15], who reported on treatment options inacute diverticulitis depending on staging,found resolution of abscesses with bowel restand antibiotic therapy alone in some of theirpatients, yet they also did not investigate theimpact of abscess size on treatment.
In our population, all abscesses larger thanor equal to 3 cm in diameter underwent CT-guided drainage when anatomically feasible(four [50%] of eight patients). Seventy-fivepercent of patients presenting with a large ab-scess reported persistent or recurrent symp-toms after treatment, suggesting that presen-tation with a large abscess was associatedwith a more severe course of diverticular dis-ease. This was underscored by reaccumula-tion of the abscess in one patient, requiring re-peat CT-guided drainage.
Surgical treatment is recommended for allpatients with an episode of diverticulitiscomplicated by abscess formation after theirinitial episode has resolved [13, 27, 28].Chautems et al. [29] recommended that pa-tients with evidence of a diverticular abscesson CT scan should be offered an electivecolectomy, as they are more likely to have apoor outcome as defined by episodes of re-current or persistent diverticulitis. In ourstudy, surgery was performed in 13 (43%) of30 patients: in five (62.5%) of eight patientswith an abscess larger than or equal to 3 cmand in eight (36%) of 22 patients with an ab-scess smaller than 3 cm. Antibiotic treatmentwith or without percutaneous drainage pro-vided sufficient resolution of acute inflam-mation for a single-stage resection in all pa-tients who underwent surgery. However, infour of five patients with large abscesseswho underwent surgery, acute inflammationwas seen on surgical pathology. The need forsurgical resection after resolution of an ab-scess with CT-guided drainage is under de-bate, with some authors suggesting that pa-tients who are successfully treated for anacute episode of complicated diverticulitiswith CT-guided abscess drainage may notrequire surgical resection at a later time [13].However, at our institution, all patients whowere treated with CT-guided drainage un-derwent subsequent surgical resection.
It is noteworthy that only 36% of patientswith abscesses smaller than 3 cm requiredeventual surgery. Forty-one percent reportedfull resolution of symptoms and 23% reportedimprovement with mild recurrent or persistentsymptoms that did not warrant surgery. Thesefindings suggest that the course of disease inthis population is not uniformly as severe as inpatients with large abscesses and that contraryto current guidelines, the presence of a smalldiverticular abscess does not uniformly indi-cate a need for eventual surgery.
It has been shown that patients with un-complicated diverticulitis are being treatedincreasingly as outpatients, with 65% of colo-rectal surgeons in one study reporting thatthey treat more than half of cases on an out-patient basis [14]. In our study, which in-cluded only patients with diverticular ab-scesses, nine (30%) of 30 patients with smallabscesses were treated as outpatients and allshowed clinical, radiologic, or pathologic ev-idence of resolution of their abscesses. Giventhat other patients with small diverticular ab-scesses were hospitalized for an average of5.5 days, the ability to treat some patients onan outpatient basis would allow optimal treat-ment of disease with significant improvementin quality of life and decrease in overall costs.Several factors, including the patient’s co-morbidities, functional status, and supportnetwork, must also be taken into consider-ation in determining appropriate candidatesfor outpatient treatment.
In this study, we applied CT criteria for di-agnosing abscesses as collections with an en-hancing rim with or without air inclusion.However, since none of the small and four ofthe large collections did undergo catheterdrainage, there is no proof that these collec-tions were in fact abscesses as opposed to lo-calized reactive peritoneal fluid collections,which has to be considered a limitation ofthis study. Similarly, resolution of diverticu-lar abscess formation was not documented onimaging studies in seven of 22 patients whowere followed clinically. The follow-up pe-riod was short in one patient (50 days). Alarger number of patients will need to beinvestigated to more definitively addresschanges in current treatment recommenda-tions. Another drawback of our study is usingthe somewhat arbitrary but institutionally ac-cepted size cutoff of 3 cm as a guideline forintervening on a small abscess. Although thiswas chosen because of catheter constraintsthat make percutaneous drainage much morechallenging in this population, further study
is needed to determine more precisely themaximum size at which an abscess can betreated conservatively with antibiotics alone,reserving CT-guided drainage only for largerabscesses that are unlikely to resolve on theirown. Another issue not addressed in thisstudy is that of abscess aspiration [30], as atour institution, catheter drainage is preferredin the case of a diverticular abscess.
In conclusion, our findings suggest that thesize of a diverticular abscess is of key impor-tance in determining treatment and predictingoutcome of patients with diverticulitis com-plicated by abscess formation. Patients withabscesses smaller than 3 cm can be treatedwith antibiotics alone and, in some cases, asoutpatients and may not uniformly requiresurgery. This is also likely true for patientswith abscesses 3–4 cm in size, although ourresults in this group are limited by small sam-ple size. Patients with abscesses larger than orequal to 4 cm can be managed with CT-guided abscess drainage followed by referralfor surgical treatment.
References1. Balthazar EJ. Diverticular disease of the colon. In:
Gore RM, Levine MS, eds. Textbook of gastrointes-
tinal radiology, 2nd ed. Philadelphia, PA: Saunders,
2000:915–944
2. Pemberton JH, Armstrong DN, Dietzen CD. Diver-
ticulitis. In: Yamada T, ed. Textbook of gastroenter-
ology, 2nd ed. Philadelphia, PA: JB Lippincott,
1995:1876–1890
3. Ambrosetti P, Robert J, Witzig JA, et al. Incidence,
outcome, and proposed management of isolated ab-
scesses complicating acute left-sided colonic diver-
ticulitis: a prospective study of 140 patients. Dis Co-
lon Rectum 1992; 35:1072–1076
4. Mueller PR, Saini S, Wittenburg J, et al. Sigmoid di-
verticular abscesses: percutaneous drainage as an
adjunct to surgical resection in 24 cases. Radiology
1987; 164:321–325
5. Neff CC, vanSonnenberg E, Casola G, et al. Diver-
ticular abscesses: percutaneous drainage. Radiol-
ogy 1987; 163:15–18
6. Betsch A, Wiskirchen J, Trubenbach J, et al. CT-
guided percutaneous drainage of intra-abdominal
abscesses: APACHE III score stratification of 1-
year results—Acute Physiology, Age, Chronic
Health Evaluation. Eur Radiol 2002; 12:2883–2889
7. Cinat ME, Wilson SE, Din AM. Determinants for
successful percutaneous image-guided drainage
of intra-abdominal abscess. Arch Surg 2002;
137:845–849
8. Gerzof SG, Robbins AH, Johnson WC, Birkett DH,
Nabseth DC. Percutaneous catheter drainage of ab-

Siewert et al.
686 AJR:186, March 2006
dominal abscesses: a five-year experience. N Engl
J Med 1981; 305:653–657
9. Saini S, Mueller PR, Wittenberg J, Butch RJ, Rod-
key GV, Welch CE. Percutaneous drainage of diver-
ticular abscess: an adjunct to surgical therapy. Arch
Surg 1986; 121:475–478
10. Bernini A, Spencer MP, Wong WD, Rothenberger
DA, Madoff RD. Computed tomography-guided
percutaneous abscess drainage in intestinal disease:
factors associated with outcome. Dis Colon Rectum
1997; 40:1009–1013
11. Stabile BE, Puccio E, vanSonnenberg E, Neff CC.
Preoperative percutaneous drainage of diverticular
abscesses. Am J Surg 1990; 159:99–104
12. Jeffrey RB, Federle MP, Tolentino CS. Periappen-
diceal inflammatory masses: CT-directed manage-
ment and clinical outcome in 70 patients. Radiology
1988; 167:13–16 [Erratum in Radiology 1988;
168:286]
13. Wong WD, Wexner SD, Lowry A, et al. Practice
parameters for the treatment of sigmoid diverti-
culitis—supporting documentation: The Stan-
dards Task Force—The American Society of Co-
lon and Rectal Surgeons. Dis Colon Rectum
2000; 43:290–297
14. Schechter S, Mulvey J, Eisenstat TE. Management
of uncomplicated acute diverticulitis: results of a
survey. Dis Colon Rectum 1999; 42:470–475; dis-
cussion, 475–476
15. Detry R, Jamez J, Kartheuser A, et al. Acute local-
ized diverticulitis: optimum management requires
accurate staging. Int J Colorectal Dis 1992; 7:38–42
16. Ambrosetti P, Becker C, Terrier F. Colonic diverti-
culitis: impact of imaging on surgical manage-
ment—a prospective study of 542 patients. Eur Ra-
diol 2002; 12:1145–1149
17. Shen SH, Chen JD, Tiu CM, Chang CY, Yu C. Co-
lonic diverticulitis diagnosed by computed to-
mography in the ED. Am J Emerg Med 2002;
20:551–557
18. Kircher MF, Rhea JT, Kihiczak D, Novelline RA.
Frequency, sensitivity, and specificity of individual
signs of diverticulitis on thin-section helical CT
with colonic contrast material: experience with 312
cases. AJR 2002; 178:1313–1318
19. Pradel JA, Adell J, Taourel P, Djafari M, Monnin-
Delhom E, Bruel JM. Acute colonic diverticulitis:
prospective comparative evaluation with US and
CT. Radiology 1997; 205:503–512
20. Hachigian MP, Honickman S, Eisenstat TE, Rubin
RJ, Salvati EP. Computed tomography in the initial
management of acute left-sided diverticulitis. Dis
Colon Rectum 1992; 35:1123–1129 [Erratum in Dis
Colon Rectum 1993; 36:193]
21. Schwerk WB, Schwarz S, Rothmund M, Arnold R.
Colon diverticulitis: imaging diagnosis with ultra-
sound—a prospective study [in German]. Z Gastro-
enterol 1993; 31:294–300
22. Labs JD, Sarr MG, Fishman EK, Siegelman SS,
Cameron JL. Complications of acute diverticuli-
tis of the colon: improved early diagnosis with
computerized tomography. Am J Surg 1988;
155:331–336
23. Spivak H, Weinrauch S, Harvey JC, Surick B, Fer-
stenberg H, Friedman I. Acute colonic diverticulitis
in the young. Dis Colon Rectum 1997; 40:570–574
24. Raptopoulos VR, Katsou G, Rosen MP, Siewert B,
Goldberg SN, Kruskal JB. Acute appendicitis: ef-
fect of increased use of CT on selecting patients ear-
lier. Radiology 2003; 226:521–526
25. Rao PM, Rhea JT, Novelline RA, et al. Helical CT
with only colonic contrast material for diagnosing
diverticulitis: prospective evaluation of 150 pa-
tients. AJR 1998; 170:1445–1449
26. Brengman ML, Otchy DP. Timing of computed to-
mography in acute diverticulitis. Dis Colon Rectum
1998; 41:1023–1028
27. Stollman NH, Raskin JB. Diagnosis and manage-
ment of diverticular disease of the colon in adults:
Ad Hoc Practice Parameters Committee of the
American College of Gastroenterology. Am J Gas-
troenterol 1999; 94:3110–3121
28. Köhler L, Sauerland S, Neugebauer E, et al. Di-
agnosis and treatment of diverticular disease: re-
sults of a consensus development conference—
The Scientific Committee of the European Asso-
ciation for Endoscopic Surgery. Surg Endosc
1999; 13:430–436
29. Chautems RC, Ambrosetti P, Ludwig A, Mermillod
B, Morel P, Soravia C. Long-term follow-up after
first acute episode of sigmoid diverticulitis: is sur-
gery mandatory? A prospective study of 118 pa-
tients. Dis Colon Rectum 2002; 45:962–966
30. Wroblicka JT, Kuligowska E. One-step needle as-
piration and lavage for the treatment of abdominal
and pelvic abscesses. AJR 1998; 170:1197–1203