
Functionally relevant polymorphisms in the human nuclear ...

Impact of COX-2 rs5275 an
d rs20417 and GPIIIa rs5918Polymorphisms on 90-Day Ischemic Stroke Functional Outcome:A Novel Finding
Jane Maguire, BA, BNurs(Hons),*†#†† Ammarin Thakkinstian, PhD,‡xChristopher Levi, MBBS,*†k** Lisa Lincz, PhD,†{** Linda Bisset, Masters,{Jonathan Sturm, PhD,*†† Rodney Scott, PhD,#‡‡xx Scott Whyte, PhD,††
and John Attia, PhD*†‡k**
From the *School of M
University of Newcastle
†Hunter Medical Resear
Australia; ‡Centre for Cli
sity of Newcastle, Newca
Epidemiology Unit, Facul
dol University, Bangkok,
Group, Calvary Mater Ne
Australia; kDivision of M
New South Wales, Austr
of Health, University of
Australia; **Priority Res
Research, HMRI and Stro
Research Program, Unive
ment, Gosford Hospital
Gosford, New South Wal
Information-Based Medi
134
We hypothesized that polymorphisms in 5 genes related to thrombolytic and inflam-
mation pathways will independently influence occurrence, severity, and 3-month
functional outcome in patients with ischemic stroke. This was a case-control design
with ischemic stroke patients recruited from 4 public hospitals (n 5 640) and commu-
nity controls (n 5 627). Baseline clinical data were collected, and follow-up telephone
interviews were conducted with 520 patients at 90 days postevent to determine stroke
outcome using the Barthel Index (BI), Modified Rankin Scale (mRS) and Glasgow Out-
come Scale (GOS). Blood samples were collected and genotyped for polymorphisms in
platelet glycoprotein Iba (GPIba) rs224309 and rs6065, glycoprotein IIIa (GPIIIa) rs5918, tis-
sue plasminogen activator (tPA) rs63020761, plasminogen activating inhibitor (PAI-1)
rs72578597, and cyclooxygenase-2 (COX-2) rs5275 and rs20417. COX-2 polymorphism
rs5275 demonstrated a significant association with poststroke mRS, with a dominant
genetic model demonstrating the best fit (CC 1 TC) (adjusted odds ratio [aOR] 5
1.61; P 5 .026). The COX-2 rs20417 C allele showed an association with GOS (aOR 5
1.95; P 5 .012), and again a dominant genetic model demonstrated the best fit (CC 1
GC). GPIIIa rs5918 (A1A2) was associated with poststroke BI, with a dominant model
demonstrating the best fit (A1A2 1 A2A2) (aOR 5 0.56; P 5 .014). There was a signif-
icant association between stroke severity and tPA rs63020761 TTallele (aOR 5 1.96; 95%
CI 5 1.03-3.72; P 5 .040). This is the first study to demonstrate associations between
stroke functional outcome and 2 COX-2 variants (rs20417 and rs5275) and a GPIIIa
variant (rs5918). Key Words: Genetics—functional recovery—post stroke.
� 2011 by National Stroke Association
edicine and Public Health, Faculty of Health,
, Callaghan, New South Wales, Australia;
ch Institute, Newcastle, New South Wales,
nical Epidemiology and Biostatistics, Univer-
stle, New South Wales, Australia; xClinical
ty of Medicine, Ramathibodi Hospital, Mahi-
Thailand; {Hunter Haematology Research
wcastle, Edith St Waratah, New South Wales,
edicine, John Hunter Hospital, Newcastle,
alia; #School of Biomedical Sciences, Faculty
Newcastle, Callaghan, New South Wales,
earch Centre for Brain and Mental Health
ke Research Group, Brain & Mental Health
rsity of Newcastle; ††Neurosciences Depart-
, Northern Sydney Central Coast Health,
es, Australia; ‡‡Priority Research Centre for
cine, HMRI/University of Newcastle; and
xxDivision of Genetics, Hunter Area Pathology Service, John Hunter
Hospital, Lookout Road, Newcastle, New South Wales, Australia.
Received September 22, 2009; accepted October 30, 2009.
The first author’s PhD candidature was supported by an Australian
Postgraduate Award from The University of Newcastle, Australia.
Other funding was received from the Australian National Heart
Foundation and the Northern Sydney Central Coast Health Research
Committee Fund.
The authors declare no conflicts of interest.
Address correspondence to Jane Maguire, BA, BNurs(Hons), Uni-
versity of Newcastle, Neurology Unit, John Hunter Hospital, C, The
Lodge, Lookout Road, New Lambton Heights, NSW 2305, Australia.
E-mail: [email protected].
1052-3057/$ - see front matter
� 2011 by National Stroke Association
doi:10.1016/j.jstrokecerebrovasdis.2009.10.011
Journal of Stroke and Cerebrovascular Diseases, Vol. 20, No. 2 (March-April), 2011: pp 134-144

GENETICS OF ISCHEMIC STROKE FUNCTIONAL OUTCOME 135
The influence of genetic variants on ischemic stroke
occurrence or poststroke functional outcome has come un-
der increased investigation. A major influence of genetic
factors alone on stroke occurrence is yet to be proven, al-
though evidence of genetic associations in ischemic stroke
risk from linkage analysis,1,2 case-control designs,3,4 and
genome-wide association studies5,6 has been published. In
contrast, studies examining the influence of genetic factors
on ischemic stroke outcome have been limited to examina-
tions of mortality, further vascular events,7 and poststroke
depression.8 Only one genetic study to date has examined
poststroke disability using the functional independence
measure, and it found no association with the ApoE4 allele.9
To the best of our knowledge, the present study is the
first genetic association study to examine the influence
of potentially relevant candidate genes on poststroke
functional outcome, as measured by well-validated stroke
scales. Candidate genes were chosen based on their bio-
logical role in stroke pathophysiology and, in some cases,
previously noted associations with stroke risk. In the
thrombolytic system, tissue plasminogen activator (tPA)
rs63020761 at sequence position 27351 C/T10,11 and plas-
minogen activating inhibitor (PAI-1) rs72578597, a 4G5 G
deletion/insertion variant in the promoter region,12
were selected. Similarly, variants in genes from the plate-
let glycoprotein complex involved in platelet adhesion
and aggregation (glycoprotein [GP] Iba rs22430913 and
rs606514 and GP IIb-IIIa rs591815) were chosen.
Inflammatory processes are also known to contribute to is-
chemic damage,16-18 and COX-2 inhibition has been shown
to attenuate brain injury in experimental models.19 Thus,
we examined the COX-2 gene variants recognized to have
functional significance. We found that rs20417 (sequence po-
sition 2765) plays a role in regulation of COX-2 transcription,
and that rs5275 (sequence position 6498) minor allele C is
associated with lower gene expression levels.20
We hypothesized that these recognized variations
in GPIba, GPIIIa, tPA, PAI-1, and COX-2 would have an
independent influence on incidence, severity, and the
3-month outcome in patients with ischemic stroke.
Methods
Participants
This study design has 2 components: a case control
genetic association study and a prospective 90-day
follow-up of functional disability in stroke cases. Cases
were patients with ischemic stroke admitted between
2003 and 2008 to any of 4 acute stroke units located in
principal referral hospitals in the Central Coast and
Hunter regions of New South Wales, Australia (n 5 640).
The inclusion criterion for cases was ischemic stroke pre-
senting to hospital, as defined by World Health Organiza-
tion clinical criteria.21,22 Exclusion criteria included age
,18 years, diagnosis of hemorrhagic stroke or transient
ischemic attack, and inability to undergo baseline brain
imaging. Computed tomography and/or magnetic
resonance imaging brain scans were obtained in all cases
to confirm ischemic stroke case status, and, as clinically
appropriate, other investigative tests, such as transesopha-
geal echocardiography, were conducted to define the
ischemic stroke mechanism.
The control sample (n 5 627), drawn from the Hunter
Community Study cohort,23 were healthy community-
dwelling men and women age 55-85, selected at random
from the New South Wales Electoral Roll between 2004
and 2007. Any control reporting a history of any type of
stroke was excluded.
Written informed consent was obtained from each par-
ticipant in accordance with University of Newcastle and
Hunter New England Area Health Ethics Committee
requirements.
Measures
Risk factor questionnaire interviews were conducted at
baseline by trained research staff using standardized
forms. Ethnicity was identified by self-report. Family his-
tory of stroke (defined as any first-degree family member
with stroke) and medications taken in the month before
admission were recorded. Stroke severity on hospital ad-
mission was assessed based on the National Institutes of
Health Stroke Severity Scale (NIHSS).24 The TOAST sys-
tem25 was used to determine the likely pathogenic mech-
anism of the cerebral ischemic event. The Oxfordshire
classification was used to categorize infarct topography.26
All clinical classifications were performed blind to case
genotype. Baseline clinical observations were recorded
at time of admission. Weight and height were measured
using calibrated scales, or by self-report if the patient
could not be measured. For the controls, similar demo-
graphic and clinical variables were collected by trained
research nurses at a research clinic.
Ninety-Day Assessment of Functional Outcome
in Cases
Telephone follow up was conducted following dis-
charge from hospital. Poststroke disability and handicap
were assessed using the modified Rankin Scale (mRS),27
the Glasgow Outcome Scale (GOS),28 and the Barthel In-
dex (BI).29 All of these are validated and reliable outcome
measurement tools, although the reliability of mRS via
vignette ranges from substantial to near perfect.30
In cases of loss to follow-up, an alternative means of
contact was sought through general practitioners, tele-
phone directory, and last known place of residence.
Laboratory Methods
In each subject, a venous blood sample was collected,
from which DNA was extracted as described previously.31
Genotyping was performed using formerly outlined
J. MAGUIRE ET AL.136
methods for the GPIba variants Kozak sequence variation
25 C/Trs224309332 and threonine-methionine substitution
at codon 145 rs6065,33 and for GPIIIa at position 1565
rs5918.34 Previously described methods were also used for
PAI-1 4 G/5 G rs72578597 and tPA-7351 C/T rs6302076135
and the COX-2 variants in the 30 UTR 6498 T / C region
rs5275 and promoter region 2765G / C rs20417.36,37
Statistical Methods
Baseline demographic characteristics and risk factor
profiles were compared in the case and control groups
using the t test for continuous factors and the c2 test for
categorical factors. Genotype and allele frequencies were
measured in cases and controls (Tables 1 and 2). Hardy-
Weinberg equilibrium (HWE) was assessed in the control
group using Fisher’s exact test. Univariate analysis was
performed on all covariates and genes, and those with
a P value ,.20 were included in the multiple logistic
model. Multivariate adjustment was performed for ethnic-
ity, age, sex, hypertension, heart disease (including history
of myocardial infarction), high cholesterol, renal dysfunc-
tion, atrial fibrillation, diabetes, obesity, smoking, and
alcohol use. Genes were initially entered as 3-level ordered
variables, assuming an additive genetic model. If
Table 1. Baseline characteristics of is
Risk factor Stroke
Age, years, mean 6 SD 74.9 6 13.2
Males, n (%) 334 (54.3)
NIHSS score, mean 6 SD 5.96 6 6.01
Percentile, n
25th 2
50th 4
75th 8
Ethnicity, n (%)
Caucasian 610 (99.2)
Other 5 (0.8)
BMI, n (%)
$30 128 (24.5)
,30 395 (75.5)
Risk factor history, n (%)
Hypertension 475 (77.2)
High cholesterol 301 (48.9)
Heart disease 200 (32.5)
Atrial fibrillation 163 (26.5)
Diabetes 166 (27.0)
Renal dysfunctiony 203 (69.5)
Alcohol use, n (%) 232 (48.0)
Smoking history, n (%)
Current smoker 105 (17.7)
Ex-smoker 190 (32.0)
Never smoked 298 (50.3)
*Fisher’s exact test.
yRenal dysfunction: glomerular filtration rate ,60 mL/min.
a per-genotype analysis suggested another genetic model
(ie, recessive, dominant, or additive effect), then genotypes
were combined accordingly. Stepwise forward selection
was applied for final model selection. Interaction between
gene and stroke subtype was assessed as well.
Stroke functional (BI) and disease severity (NIHSS)
scores were not normally distributed, and thus poor out-
come for BI and NIHSS was categorized by cutoffs of
,9038 and .7,39 respectively. Analyses were performed
as described earlier, using Stata version 10.0 (StataCorp,
College Station, TX). A P value ,.05 was considered
statistically significant. Possible population stratification
was addressed by adjusting for ethnicity in the model.
Results
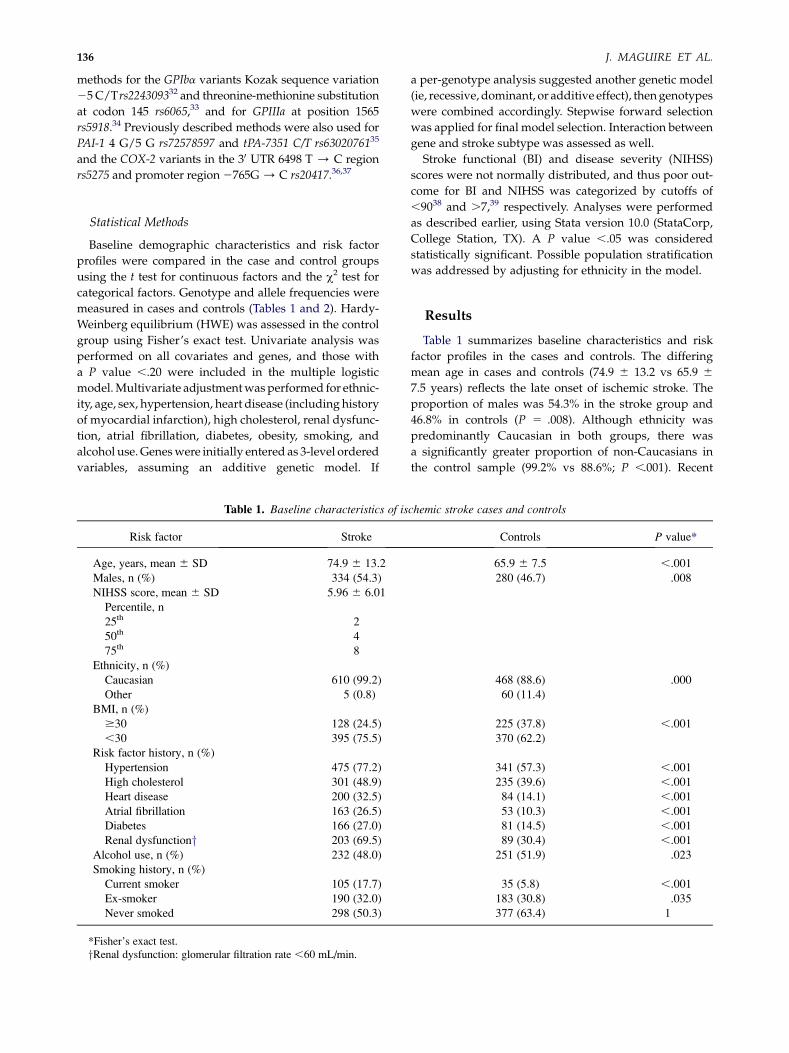
Table 1 summarizes baseline characteristics and risk
factor profiles in the cases and controls. The differing
mean age in cases and controls (74.9 6 13.2 vs 65.9 6
7.5 years) reflects the late onset of ischemic stroke. The
proportion of males was 54.3% in the stroke group and
46.8% in controls (P 5 .008). Although ethnicity was
predominantly Caucasian in both groups, there was
a significantly greater proportion of non-Caucasians in
the control sample (99.2% vs 88.6%; P ,.001). Recent
chemic stroke cases and controls
Controls P value*
65.9 6 7.5 ,.001
280 (46.7) .008
468 (88.6) .000
60 (11.4)
225 (37.8) ,.001
370 (62.2)
341 (57.3) ,.001
235 (39.6) ,.001
84 (14.1) ,.001
53 (10.3) ,.001
81 (14.5) ,.001
89 (30.4) ,.001
251 (51.9) .023
35 (5.8) ,.001
183 (30.8) .035
377 (63.4) 1

Table 2. Genes and risk factors associated with stroke occurrence
Univariate analysis Multivariate analysis
Gene/variant OR P value 95% CI Risk factor OR P value 95% CI
tPA rs63020761 Age, years
TT 1.48 .214 0.79-2.77 .75 9.97 .000 6.87-14.46
CT 0.98 .909 0.69-1.38 #75 1
CC 1
Sex
COX-2 rs5275 Male 1.46 .022 1.06-2.03
TT 1.17 .386 0.82-1.67 Female 1
TC 1.25 .228 0.87-1.79
CC 1 Hypertension
Yes 2.46 .000 1.75-3.44
COX-2 rs20417 No 1
GG 1.26 .545 0.59-2.64
GC 1.43 .364 0.66-3.06 Smoker
CC 1 Current 5.88 .000 3.55-9.71
Ex-smoker 1.04 .794 0.74-1.49
PAI-1 rs72578597 Never 1
5G5G 0.86 .335 0.63-1.17
5G4G 0.78 .072 0.61-1.02 Heart disease
4G4G 1 Yes 1.48 .048 1.00-2.17
No 1
GPIIIa rs5918A2A2 0.48 .067 0.22-1.05 Atrial fibrillation
A1A2 0.96 .789 0.73-1.26 Yes 2.23 .000 1.46-3.40
A1A1 1 No 1
GPIba rs2243093 BMI
CC 1.24 .640 0.58-1.02 $30 0.57 .001 0.41-0.81
TC 0.77 .075 0.49-3.12 ,30 1
TT 1 Diabetes
GPIba rs6065 Yes 1.84 .002 1.25-2.72
MM 0.37 .247 0.07-1.96 No 1
TM 1.03 .843 0.74-1.44
TT 1
GENETICS OF ISCHEMIC STROKE FUNCTIONAL OUTCOME 137
publications argue convincingly that population stratifi-
cation leads to a bias of ,1%;40-42 nonetheless, to adjust
for any possible bias due to population stratification, we
adjusted for ethnicity in the multivariate model.
Traditional cerebrovascular risk factors, such as a his-
tory of hypertension, high cholesterol, heart disease, atrial
fibrillation, diabetes (insulin-dependent and non–insulin-
dependent) and renal dysfunction (calculated glomerular
filtration rate ,60), were all significantly overrepresented
in the stroke group. Smoking (current, P ,.001; past, P 5
.03) and alcohol use (P 5 .023) were more prevalent in the
stroke group.
Assessment of HWE in the control group demonstrated
that all polymorphisms except GPIIIa rs5918 (P 5 .016)
and COX-2 rs5275 (P 5 .003) complied with HWE propor-
tions. We explored this deviation from HWE and
found that the allelic frequencies for these 2 polymor-
phisms in our sample were remarkably similar to those
reported in previous studies (GPIIIa, 14%-27%;43,44
COX-2, 33%20).
Stroke Occurrence and Severity
We found no evidence of a genetic association with stroke
occurrence, although there was some suggestion of a signal
for both the GPIba rs2243093 TC genotype (P 5 .08) and
GPIIIa A2A2 rs5918 (P 5 .07) (Table 2). A significant associ-
ation was found between the tPA rs63020761 TT allele and
stroke severity (odds ratio [OR] 5 2.08; 95% confidence
interval [CI] 5 1.16-3.74; P 5 .014) that persisted after
adjustment for covariates (OR 5 1.96; 95% CI 5 1.03-3.72;
P 5 .040) (Table 3).
Ninety-Day Functional Outcome
Out of the 640 stroke patients, 520 were assessed 90 days
after the acute event. GP1ba rs6065 and rs2243093, tPA
rs63020761, and PAI-1 rs72578597 demonstrated no associ-
ation with 90-day outcome scores for mRS, BI or GOS in the
univariate analysis and thus were not included in the
multivariate logistic regression model. In univariate anal-
ysis, association of COX-2 rs5275 T/C was significant for

Table 3. Associations between genes and covariates by stroke severity
Univariate analysis Multivariate analysis
Gene/variant OR P value 95% CI Gene/variant OR P value 95% CI
tPA rs63020761 tPA rs63020761
TT 2.08 .014 1.16-3.74 TT 1.96 .040 0.82-1.93
CT 1.19 .389 0.80-1.77 CT 1.26 .287 1.03-3.72
CC 1 CC 1
COX-2 rs5275 Covariate
CC 1.44 .209 0.82-2.53 Premorbid mRS score
TC 0.73 .137 0.49-1.10 .2 3.3 .001 1.67-6.73
TT 1 #2 1
COX-2 rs20417 Smoker
CC 0.57 .475 0.12-2.67 Current 0.74 .278 0.43-1.28
GC 0.97 .892 0.64-1.48 Ex-smoker 0.54 .008 0.34-0.85
GG 1 Never 1
PAI-1 rs72578597 Arthritis
5G5G 0.82 .394 0.79-1.83 Yes 0.54 .005 0.35-0.83
5G4G 1.20 .472 0.48-1.40 No 1
4G4G 1
GPIIIa rs5918A2A2 1.58 .537 0.71-1.71
A1A2 1.10 .670 0.37-6.70
A1A1 1
GPIba rs2243093CC 1.76 .384 0.49-6.37
TC 1.16 .543 0.72-1.85
TT 1
GPIba rs6065MM 0 0 0
TM 0.89 .698 0.51-1.57
TT 1
J. MAGUIRE ET AL.138
the 90-day mRS score but not for GOS or BI score (OR 5
1.54; P 5.038) (Table 4); this effect persisted after multivar-
iate logistic modeling, using both an allelic model (T/C;
OR 5 1.88; P 5 .022) and a dominant genetic model
(CC 1 TC; OR 5 1.61, P 5 .026). COX-2 rs20417 GC was
not associated with mRS or BI score, but the C allele was
highly associated with GOS score (unadjusted OR 5
1.95, P 5 .012; adjusted OR [aOR] 5 2.18, P 5 .015) (Table
4). We found an association between GPIIIa rs5918 and BI
score that followed a dominant model (A1A2 1 A2A2 vs
A1A1: unadjusted OR 5 0.57, P 5 .013; aOR 5 0.56,
P 5 .014), but this association was not significant for mRS
and GOS scores (Table 5). Table 6 reports genotype
frequencies for controls and for cases, by stroke subtype.
Table 7 reports case genotype frequencies by favourable
outcome scores.
Discussion
Three variants from 2 of the 5 genes that we examined,
COX-2 and GPIIIa, demonstrated a significant and novel
association with functional status at 90 days. Having 1
or 2 copies of the A2 allele for GPIIIa rs5918 polymor-
phism improved the likelihood of having a poor BI score,
whereas having the C allele for COX-2 rs5275 and rs20417
decreased the likelihood of having a poor functional
outcome at 90 days.
We detected a trend of association between stroke sever-
ity and the tPA gene. Carriers of the rs63020761 T allele ex-
perienced more severe stroke. Previous studies of the tPA
27351 C/T polymorphism demonstrated an increased
risk of myocardial infarction and stroke with the TT geno-
type;10,45 however, we found no association between tPA
alleles and either stroke occurrence or outcome, most
likely due to lack of statistical power.
We did not replicate any of the previously reported
significant associations with stroke occurrence. Our
previous meta-analyses provided evidence of associations
between stroke occurrence and platelet GP1ba gene vari-
ants rs2243093 and rs606546 as well as the PAI-1 4 G/4 G
polymorphism;35 however, both our results and results
reported by other groups12,47 confirm that these associa-
tions were highly heterogeneous in nature, with ORs of
.1 and ,1. We speculate that this heterogeneity might be
due to different patterns of linkage disequilibrium across
the studies, a situation termed genetic ‘‘flip-flop.’’48,49 In

Table 4. Associations between genes and 90-day favorable outcome, univariate analysis
mRS GOS BI
Gene/variant OR P value 95% CI OR P value 95% CI OR P value 95% CI
tPA rs63020761TT 1.22 .534 0.65-2.32 0.85 .642 0.43-1.68 0.98 .967 0.52-1.87
CT 1.14 .504 0.77-1.69 1.07 .752 0.69-1.67 1.09 .662 0.73-1.65
CC 1 1 1
COX-2 rs5275CC 1.09 .778 0.61-1.95 0.93 .812 0.48-1.75 1.24 .477 0.69-2.23
TC 1.54 .038 1.02-2.31 1.43 .128 0.90-2.27 1.53 .171 0.83-2.81
TT 1 1 1
COX-2 rs20417CC 3.87 .204 0.48-31.3 0 0 0 3.12 .277 0.40-24.33
GC 1.35 .178 0.87-2.07 1.81 .025 1.08-3.06 0.93 .772 0.60-1.45
GG 1 1 1
PAI-1 rs725785975G5G 1.21 .484 0.71-2.04 1.16 .630 0.64-2.08 0.89 .677 0.64-1.56
5G4G 1.00 .995 0.65-1.53 1.03 .915 0.64-1.65 1.00 .988 0.64-1.56
4G4G 1 1 1
GPIIIa rs5918A2A2 0.67 .589 0.16-2.85 0.83 .470 0.51-1.37 0.52 .355 0.13-2.06
A1A2 0.72 .138 0.46-1.11 0.43 .256 0.10-1.84 0.57 .013 0.37-0.89
A1A1 1 1 1
GPIba rs2243093CC 0.45 .260 0.11-1.81 0.43 .260 0.10-1.85 1.15 .855 0.24-5.43
TC 1.16 .557 0.71-1.89 0.84 .509 0.49-1.42 0.89 .656 0.54-1.46
TT 1 1 1
GPIba rs6065MM 0 0 0 0 0 0 0 0 0
TM 1.04 .880 0.61-1.78 0.91 .744 0.50-1.63 0.68 .168 0.40-1.17
TT 1 1 1
GENETICS OF ISCHEMIC STROKE FUNCTIONAL OUTCOME 139
this case-control analysis, no association between stroke
outcome and any of these 3 variants was seen.
The COX-2 polymorphisms demonstrated no evidence
of association with stroke occurrence. Published evidence
regarding the COX-2 rs20417 variant and ischemic stroke
risk is limited to 3 studies to date and is inconsistent.
Colaizzo et al50 found an association between the
rs20417 variant and cerebrovascular ischemia, but
Cipollone et al51 found this same variant to be associated
with a decreased risk of both myocardial infarction and
stroke. Both of these studies were conducted in Italian
populations. In the large prospective Atherosclerosis
Risk in Communities Study, rs20417 was found to in-
crease the risk of incident stroke in African-Americans
but not in other ethnic groups, including Caucasians.52
We found a significant association between the COX-2
gene and stroke outcome; carriers of either the rs5275 or
rs20417 variant had relatively lower disability and stroke
handicap scores. This finding has biological plausibility.
In general, COX-2 is known predominantly for its media-
tory function in the inflammatory pathway, through
its role in the conversion of arachidonic acid to
prostaglandin H2 and the production of macrophage
MMP-2 and MMP-9, both of which are thought to contrib-
ute to atherosclerotic plaque rupture. COX-2 also is gener-
ally considered a proinflammatory enzyme,16 although is
also known to aid in the cessation of the inflammatory
process.53
In brain ischemia, COX-2 inhibition has been shown to
attenuate brain injury and contribute to an imbalance in
prostanoid synthesis.19 Cipollone et al51 argued that a shift
in this balance between lipocalin-type prostaglandin D2
dependent synthase (anti-inflammatory) and type-1
inducible prostaglandin E2 dependent (inflammatory)
synthase could contribute to increased activation of the
inflammatory mechanisms in rupture-prone plaques. In
rat and mouse models, COX-2 has been shown to play
an active role in inflammation-related advancement of
cerebral ischemic impairment,54 and in the human brain,
evidence suggests increased expression of COX-2 con-
fined to the area of damage following ischemic stroke.18
Although there are no published in vivo studies of
COX-2 gene expression levels and their associated poly-
morphisms, there is one functional human study.20 This

Table 5. Associations between risk factors and 90-day favorable outcome, multivariate analysis*
mRS GOS BI
Risk factor OR P value 95% CI OR P value 95% CI OR P value 95% CI
Age
,70 2.73 .002 1.43-5.20 3.96 ,.001 1.83-8.56 1.61 .096 0.92-2.82
$70-#80 1.49 .097 0.93-2.40 1.62 .073 0.95-2.75 1.51 .087 0.94-2.40
.80 1 1 1
Sex
Male 1.52 .048 1.00-2.29
Female 1
Pre-mRS score
.2 0.25 ,.001 0.12-0.52 0.18 ,.001 0.08-0.38 0.24 ,.001 0.12-0.47
#2 1 1 1
Heart disease
Yes 0.50 .001 0.34-0.74
No 1
Atrial fibrillation
Yes 0.47 ,.001 0.32-0.70 0.45 .002 0.27-0.75
No 1 1
Diabetes
Yes 0.64 .035 0.38-0.96 0.44 .002 0.26-0.73
No 1 1
Renal dysfunction
Yes 1.64 .033 1.04-2.58 1.73 .026 1.07-2.79 1.92 .003 1.24-2.95
No 1 1 1
*Adjusted result shown only for covariates that were significant.
J. MAGUIRE ET AL.140
research demonstrated that both COX-2 rs5275 and
rs20417 had a significant relationship with COX-2 gene
expression. COX-2 expression levels were lower in car-
riers of the rs20417 C allele, whereas rs5275 appeared to
exert its effect through decreased mRNA stability.20
Based on the foregoing evidence, it may be speculated
that inflammation due to damage to the cerebral matter is
decreased, and thus functional recovery is potentially
enhanced, in carriers of the Cox-2 rs20417 and rs5275
variants. In the rodent model, expression of COX-2 and
mRNA was found to be up-regulated following cerebral
ischemia;55,56 thus, it would seem biologically plausible
that the presence of a variant such as rs5275 might affect
COX-2 expression and in turn reduce the degree of
inflammatory response, limiting damage to the cerebral
tissue and thus influencing poststroke outcome. This
hypothesis has yet to be tested, however.
We failed to demonstrate an association between GPIIIa
and stroke occurrence in our case-control analysis, but
did find an association with stroke outcome using the
BI. GPIIIa is a fundamental receptor site for fibrinogen,
and evidence suggests that its participation in platelet
aggregation increases thrombus formation through either
alterations in ligand binding or changes to postreceptor
inside-out signaling.57 The rs5918 T-to-C transition at nu-
cleotide 1565 results in a proline-to-leucine substitution at
amino acid 33, leading to multiple conformational
changes within the GPIIIa receptor.57 Current data are
conflicting as to whether this conformational change in-
creases or decreases binding to immobilized fibrinogen,
thereby affecting fibrin clot retraction.58 It is plausible
that the GPIIIa rs5918 C allele might play a role in stroke
etiology, given that this allele has been linked to an
increased risk of stroke.59
Our study has several limitations. We were able to deter-
mine a genetic association in patients who carried a COX-2
variant when outcome was measured by the mRS or GOS;
however, despite the fact that mRS and GOS scores were
highly correlated with BI score, we found no correspond-
ing association with BI. One possible explanation for this
is that the BI was originally designed to measure only mus-
culoskeletal causes of deficits in self-care,29 and although
this index has been shown to be a valid and reliable
measure of disability in stroke patients30 and to be highly
correlated with the mRS and GOS, it fails to measure other
aspects of disability that may contribute to stroke outcome,
such as aphasias, which severely affect the ability to
communicate, and cognition, which affects the ability to
manage one’s own affairs.
Follow-up did not occur in cases recruited at study
commencement, because this was not part of the study
protocol initially. These patients had similar risk factors
and stroke severity profiles as those patients who were
followed up. Adding follow-up data for these patients
might have increased the strength of our findings, be-
cause then we would have had a larger sample size.

Table 6. Genotype frequency for stroke TOAST subtypes and healthy community controls
Healthy
controls, n (%) Large artery, n (%) Cardioembolism, n (%) Small vessel, n (%) Determined, n (%) Undetermined, n (%)
tPA rs63020761CC 84 (45.7) 56 (20.6) 87 (31.9) 55 (20.1) 3 (1.1) 72 (26.3)
CT 86 (46.7) 70 (25.9) 76 (28.0) 52 (19.3) 8 (2.9) 65 (23.9)
TT 14 (7.6) 18 (27.3) 16 (24.2) 13 (19.7) 1 (1.5) 18 (27.3)
COX-2 rs5275CC 80 (14.1) 21 (28.8) 19 (26.0) 15 (20.5) 2 (2.7) 16 (21.9)
TC 221 (38.9) 61 (24.6) 65 (26.2) 53 (21.4) 3 (1.2) 66 (26.6)
TT 267 (47.0) 59 (20.99) 93 (33.1) 51 (18.1) 7 (2.5) 71 (25.3)
COX-2 rs20417CC 16 (2.7) 4 (33.3) 3 (25) 3 (25) 0 2 (16.7)
GC 139 (23.2) 40 (25.5) 44 (28.0) 37 (25.5) 2 (1.3) 34 (21.7)
GG 445 (74.2) 98 (22.5) 128 (29.4) 80 (18.4) 10 (2.3) 119 (27.5)
PAI-1 rs725785974G4G 169 (28.2) 48 (24.5) 63 (31.6) 27 (13.8) 4 (2.0) 56 (28.0)
5G4G 302 (50.3) 61 (21.9) 83 (29.8) 63 (22.6) 7 (2.5) 65 (23.3)
5G5G 129 (21.5) 35 (25.9) 35 (25.9) 30 (22.2) 1 (0.7) 34 (25.2)
GPIIIa rs5918A1A1 452 (75.3) 111 (23.7) 131 (27.9) 96 (20.5) 11 (2.4) 119 (25.4)
A1A2 129 (21.5) 30 (22.9) 44 (33.6) 24 (18.3) 1 (0.8) 32 (24.4)
A2A2 19 (3.2) 3 (30.0) 2 (20.0) 1 (10.0) 0 4 (40.0)
GPIba rs6065MM 5 (0.8) 0 0 0 1 (50.0) 1 (50.0)
TM 76 (12.7) 21 (26.9) 15 (19.2) 18 (23.0) 2 (2.6) 22 (28.2)
TT 519 (86.5) 123 (23.4) 163 (30.9) 102 (19.4) 9 (1.7) 129 (24.5)
GPIba rs2243093CC 8 (1.3) 2 (20.0) 4 (40.0) 2 (20.0) 0 2 (20.0)
TC 131 (21.8) 22 (20.6) 33 (30.8) 20 (18.7) 0 32 (29.9)
TT 461 (76.8) 120 (24.6) 141 (28.9) 97 (19.9) 12 (2.5) 118 (24.2)
GE
NE
TIC
SO
FIS
CH
EM
ICS
TR
OK
EF
UN
CT
ION
AL
OU
TC
OM
E1
41

Table 7. Case genotype frequencies by 90-day favorable stroke outcome score
Gene Variant Genotype GOS score .2, n (%) mRS score .2, n (%) BI score .90, n (%)
COX-2 rs5275 CC 16 (14.7) 21 (13.4) 19 (16.8)
TC 38 (34.9) 55 (35.0) 47 (32.7)
TT 55 (50.5) 81 (51.6) 63 (50.5)
COX-2 rs20417 CC 0 1 (0.6) 1 (0.8)
GC 21 (18.9) 37 (23.3) 35 (26.9)
GG 90 (81.1) 121 (76.1) 94 (72.3)
GPIIIa rs5918 A1/A1 83 (73.5) 116 (72.5) 90 (68.7)
A1/A2 27 (23.9) 41 (25.6) 38 (29.0)
A2/A2 3 (2.7) 3 (1.9) 3 (2.3)
GPIba rs6065 TT 0 0 0
TM 17 (15.1) 22 (13.8) 22 (16.8)
MM 96 (84.9) 138 (86.3) 109 (83.2)
GPIba rs2243093 TT 3 (2.7) 4 (2.5) 2 (1.5)
TC 23 (20.4) 27 (16.8) 25 (19.0)
CC 87 (76.9) 130 (80.8) 104 (79.4)
PAI-1 rs72578597 4G4G 36 (31.9) 51 (31.7) 42 (32.1)
5G4G 54 (47.8) 78 (48.5) 59 (45.0)
5G5G 23 (20.3) 32 (19.9) 30 (22.9)
tPA rs63020761 CC 51 (45.1) 76 (47.2) 60 (45.8)
CT 48 (42.5) 69 (42.9) 56 (42.8)
TT 14 (12.4) 16 (9.9) 15 (11.4)
J. MAGUIRE ET AL.142
In summary, we were unable to find an association
between stroke occurrence and the 7 genetic variants
studied. However, we did find significant associations
between stroke functional outcome at 90 days and 2
COX-2 variants (rs20417 and rs5275) and a GPIIIa variant
(rs5918), with the COX-2 variants contributing to a more
favorable stroke outcome and the GPIIIa variant contrib-
uting to an unfavorable outcome as measured by 3 well-
validated disability and handicap tools. Given the novel
nature of our results and the number of comparisons
made, these results should be considered hypothesis-
generating. More evidence is needed to determine the
robustness of the findings. This could be obtained
through independent replication in another population,
or, alternatively, an in silico model could be generated
to test the hypothesis that these genetic variations are
indeed associated with poststroke outcome.
References
1. Meschia JF, Brott TG, Brown RD Jr, et al. Phosphodiester-ase 4D and 5-lipoxygenase activating protein in ischemicstroke. Ann Neurol 2005;58:351-361.
2. Saleheen D, Bukhari S, Haider SR, et al. Association ofphosphodiesterase 4D gene with ischemic stroke ina Pakistani population. Stroke 2005;36:2275-2277.
3. Zhang L, Zhang H, Sun K, et al. The 825C/T polymor-phism of G-protein beta3 subunit gene and risk of ische-mic stroke. J Hum Hypertens 2005;19:709-714.
4. Wiklund P, Nilsson L, Ardnor S, et al. Plasminogen acti-vator inhibitor-1 4G/5G polymorphism and risk ofstroke: replicated findings in two nested case-control
studies based on independent cohorts. Stroke 2005;36:1661-1665.
5. Matarin M, Brown W, Scholz S, et al. A genome-widegenotyping study in patients with ischaemic stroke:Initial analysis and data release. Lancet Neurol 2007;6:414-420.
6. Ikram MA, Seshadri S, Bis JC, et al. Genome-wideassociation studies of stroke. N Engl J Med 2009;360:1718-1728.
7. Yeh PS, Lin HJ, Li YH, et al. Prognosis of young ischemicstroke in Taiwan: Impact of prothrombotic genetic poly-morphisms. Thromb Hemost 2004;92:583-589.
8. Kohen R, Cain K, Mitchell P, et al. Association of seroto-nin transporter gene polymorphisms with post strokedepression. Arch Gen Psychiatry 2008;65:1296-1302.
9. Treger I, Froom P, Ring H, et al. Association between apo-lipoprotein E4 and rehabilitation outcome in hospitalizedischemic stroke patients. Arch Phys Med Rehabil 2003;84:973-976.
10. Jannes J, Hamilton-Bruce MA, Pilotto L, et al. Tissueplasminogen activator -7351C/T enhancer polymor-phism is a risk factor for lacunar stroke. Stroke 2004;35:1090-1094.
11. Jood K, Ladenvall P, Tjarnlund-Wolf A, et al. Fibrinolyticgene polymorphism and ischemic stroke. Stroke 2005;36:2077-2081.
12. Catto A, Carter A, Stickland M, et al. Plasminogen acti-vating inhibitor (PAI-1) 4G5G promoter polymorphismand levels in subjects with cerebrovascular disease.Thromb Hemost 1997;77:730-734.
13. Afshar-Khargan V, Khoshnevis-Asl M. Kozak sequencepolymorphism of the glycoprotein (GP) 1Ba gene is a ma-jor determinant of plasma membrane levels of the platelet1B-IX-V complex. Blood 1999;94:186-191.
14. Corral J, Gonzalez-Conejero R, Lazano M, et al. Newalleles of the platelet glycoprotein IBalpha gene. BrJ Haematol 1998;103:997-1003.
GENETICS OF ISCHEMIC STROKE FUNCTIONAL OUTCOME 143
15. McCaslin J, Ashour H, Bhattacharya V, et al. Increasedplatelet-monocyte aggregation in male claudicants withthe PIA1A2 polymorphism of GP IIb/IIIa. Eur J EndovascSurg 2008;36:132-137.
16. Iadecola C, Alexander M. Cerebral ischemia and inflam-mation. Curr Opin Neurol 2001;14:89-94.
17. Heinel L, Rubin S, Rosenwasser R, et al. Leukocyte in-volvement in cerebral infarct generation after ischemiaand reperfusion. Brain Res Bull 1994;34:137-141.
18. Sairanen T, Ristimaki A, Karljalainen-Lindsberg M, et al.Cyclooxygenase-2 is induced globally in infarcted humanbrain. Ann Neurol 1998;43:738-747.
19. Iadecola C, Gorelick P. The Janus face of cyclooxygenase-2 in ischemic stroke shifting towards downstreamtargets. Stroke 2005;36:182-185.
20. Lee Y, Kim H, Wu T, et al. Pharmacogenetics and geno-mics genetically mediated interindividual variation inanalgesic responses to cyclooxygenase inhibitory drugs.Clin Pharmacol Ther 2006;79:407-418.
21. Hatano S. Experience from a multicenter stroke register:a preliminary report. Bull World Health Org 1976;54:541.
22. World Health Organization Task Force. Recommenda-tions on stroke prevention, diagnosis and therapy: Reportof the WHO Task Force on Stroke and Other Cerebrovas-cular Disorders. Stroke 1989;20:1407-1431.
23. Duke J, McEvoy M, Sibbritt D, et al. Vibrotactile thresholdmeasurement for detecting peripheral neuropathy:Defining variability and a normal range for clinical andresearch use. Diabetologia 2007;50:2305-2312.
24. Meyer B, Hemmen T, Jackson C, et al. Modified NationalInstitutes of Health Stroke Scale for use in stroke clinicaltrials: prospective reliability and validity. Stroke 2002;33:1261-1266.
25. Adams H, Bendixen B, Kappelle L, et al. Classification ofsubtype of acute ischemic stroke: Definitions for use ina multicenter clinical trial. Toast: Trial of Org 10172 inAcute Stroke Treatment. Stroke 1993;24:35-41.
26. Sharma J, Hasson M, Butcher C. How well does the Oxford-shire Community Stroke Project classification predict thesite and size of infarct of brain imaging [comment, letter]?J Neurol Neurosurg Psychiatry 2001;70:567.
27. Quinn T, Dawson J, Walters M, et al. Reliability of themodified Rankin scale. Stroke 2007;38:e144.
28. Jennett B. Development of Glasgow coma and outcomescales. Nepal J Neurosci 2005;2:24-28.
29. Mahoney F, Barthel D. Functional evaluation: The Barthelindex. MD State Med J 1965;14:61-65.
30. D’Olhaberriague L, Litvan I, Mitsias P, et al. A reappraisalof reliability and validity studies in stroke. Stroke 1996;27:2331-2336.
31. Miller S, Dykes D. A simple salting-out procedure forextracting DNA from human nucleated cells. NucleicAcids Res 1988;16:1215.
32. Baker RI, Eikelboom J, Lofthouse E, et al. Platelet glyco-protein IBalpha Kozak polymorphism is associatedwith an increased risk of ischemic stroke. Blood 2001;98:36-40.
33. Ishida F, Furihata K, Ishida K, et al. The largest isoform ofplatelet membrane glycoprotein 1B alpha is commonlydistributed in eastern Asian populations. Thromb Hemost1996;76:245-247.
34. Jin Y, Dietz H, Nurden A, et al. Single-strand conforma-tion polymorphism analysis is a rapid and effectivemethod for the identification of mutations and polymor-phisms in the gene for glycoprotein IIIa. Blood 1993;82:2281-2288.
35. Attia J, Thakkinstian A, Wang Y, et al. The PAI-1 4G5Ggene polymorphism and ischemic stroke: An associationstudy and meta-analysis. J Cerebrovasc Dis 2007;16:173-179.
36. Brosens L, Iacobuzio-Donahue C, Keller J, et al. Increasedcyclooxygenase-2 expression in duodenal compared withcolonic tissues in familial adenomatous polyposis and re-lationship to the -765G / C COX-2 polymorphism. ClinCancer Res 2005;11:4090-4096.
37. Institute NC. Cancer Genome Anatomy Project, SNP500Cancer Database taqman assay, PTGS2–33 (rs5275). 2008.
38. Uyttenboogaart M, Stewart R, Vroomen P, et al. Optimiz-ing cutoffs scores for the Barthel index and the modifiedRankin scale for defining outcome in acute stroke trials.Stroke 2005;36:1984-1987.
39. Greisenegger S, Endler G, Haering D, et al. The (-174) G/C polymorphism in the interleukin-6 gene is associatedwith the severity of acute cerebrovascular events.Thromb Res 2003;110:181-186.
40. Slowik A, Dziedzic T, Wojciech T, et al. A2 allele of GPIIIagene is a risk factor for stroke caused by large vesseldisease in males. Stroke 2004;35:1589-1593.
41. Casas JP, Hingorani AD, Bautista LE, et al. Meta-analysisof genetic studies in ischemic stroke: Thirty-two genes in-volving approximately 18,000 cases and 58,000 controls.Arch Neurol 2004;61:1652-1661.
42. Wacholder S, Rothman N, Caporaso N. Population strat-ification in epidemiologic studies of common geneticvariants and cancer: Quantification of bias. J Natl CancerInst 2000;92:1151-1158.
43. The Welcome Trust Case Control Consortium. Genome-wide association study of 14,000 cases of seven commondiseases and 3,000 shared controls. Nature 2007;447.
44. Khlat M, Cazes M-H, Genin E, et al. Robustness of case-control studies of genetic factors to population stratifica-tion: magnitude of bias and type I error. Cancer EpidemiolBiomarkers Prev 2004;13.
45. Ladenvall P, Wall U, Jern S, et al. Identification of eightnovel single-nucleotide polymorphisms at human tissuetype plasminogen activator (t-PA) locus: Associationwith vascular t-PA release in vivo. Thromb Hemost2000;84:150-155.
46. Maguire J, Thakkinstian A, Sturm J, et al. Polymorphismsin platelet glycoprotein 1Balpha and factor VII and riskof ischemic stroke: A meta-analysis. Stroke 2008;39:1710-1716.
47. Petrovic D, Milanez T, Kobal J, et al. Prothrombotic genepolymorphisms and atherothrombotic cerebral infarc-tion. Acta Neurol Scand 2003;108:109-113.
48. Lin P, Vance J, Pericak-Vance M, et al. No gene is anisland: the flip-flop phenomenon. Am J Hum Genet2007;80:531-538.
49. Zaykin D, Shibata K. Genetic flip flop without an accom-panying change in linkage disequilibrium. Am J HumGenet 2008;82:794-800.
50. Colaizzo D, Fofi L, Tiscia G, et al. The COX-2 G/C -765polymorphism may modulate the occurrence of cerebro-vascular ischemia. Blood Coag Fibrinol 2006;17:93-96.
51. Cipollone F, Toniato E, Martinotti S, et al. A polymor-phism in the cyclooxygenase-2 gene as an inheritedprotective factor against myocardial infarction andstroke. JAMA 2004;291:2221-2228.
52. Kohsaka S, Volcik K, Folsom A, et al. Increased risk ofincident stroke associated with the cyclooxygenase 2(COX-2) G -765C polymorphism in African-Americans:The Atherosclerosis Risk in Communities Study. Athero-sclerosis 2008;196:926-930.

J. MAGUIRE ET AL.144
53. Antman E, DeMets D, Loscalzo J. Cyclooxygenaseinhibition and cardiovascular risk. Circulation 2005;112:759-770.
54. Cipollone F, Fazia M, Iezzi A, et al. Balance between PGDsynthase and PGE synthase is a major determinant ofatheroscerotic plaque instability in humans. ArteriosclerThromb Vasc Biol 2004;24:1259-1265.
55. Miettinen S, Fusco F, Yrjanheikki J, et al. Spreading de-pression and focal brain iscahemia induce cyclooxyge-nase-2 in cortical neurons through n-methyl-d-asparticacid-receptors and phospholipase A2. Proc Natl AcadSci USA 1997;94:6500-6505.
56. Nogawa S, Fangyi Zhang M, Ross E, et al. Cyclooxy-genase-2 gene expression in neurons contributes
to ischemic brain damage. J Neurosci 1997;17:2746-2755.
57. Reiner AP, Kumar PN, Schwartz SM, et al. Genetic vari-ants of platelet glycoprotein receptors and risk of strokein young women. Stroke 2000;31:1628-1633.
58. van Goor ML, Gomez Garcia E, Brouwers GJ, et al.PLA1/A2 polymorphism of the platelet glycoproteinreceptor IIb/IIIa in young patients with cryptogenicTIA or ischemic stroke. Thromb Res 2002;108:63-65.
59. Szolnoki Z, Somogyvari F, Kondacs A, et al. Evaluation ofthe modifying effects of unfavorable genotypes on classi-cal clinical risk factors for ischemic stroke. J Neurol Neu-rosurg Psychiatry 2003;74:1615-1620.
Copyright © 2022 FDOKUMEN




















