
Newly Diagnosed Atrial Fibrillation after Acute Ischemic Stroke and Transient Ischemic Attack:...
7
Newly Diagnosed Atrial Fibrillation after Acute Ischemic Stroke and Transient Ischemic Attack: Importance of Immediate and Prolonged Continuous Cardiac Monitoring Luciano A. Sposato, MD, MBA,*† Francisco R. Klein, MD,* Agustı ´n Ja ´uregui, MD,* Marisol Ferru ´ a, MD,* Pablo Klin, MD,‡ Rafael Zamora, MD,x Patricia M. Riccio, MD,* and Alejandro Rabinstein, MD{ Atrial fibrillation (AF) is the major cause of cardioembolic stroke. It often remains occult when asymptomatic and paroxysmal. We hypothesized that the detection of AF after acute ischemic stroke (AIS) or transient ischemic attack (TIA) could be improved by using continuous cardiac monitoring (CCM) immediately after admis- sion. We sought to determine the detection rate of AF by immediate in-hospital CCM after cryptogenic and noncryptogenic AIS or TIA in patients without a previous diagnosis of AF. We retrospectively studied a cohort of 155 patients with cryptogenic and noncryptogenic AIS or TIAwithout known AF. We compared the detection rates of newly diagnosed AF (NDAF) in patients admitted to areas with CCM and those never admitted to these areas. We developed a multiple logistic regression model for identifying predictors of NDAF. We characterized NDAF episodes and analyzed how the availability of CCM data changed secondary prevention strategies. We detected NDAF in 21 patients (13.5%). Diagnostic rates of NDAF in patients who underwent CCM and those who did not undergo CCM were 18.2% and 2.2%, respec- tively (P 5 .005). The median time from admission to recognition of NDAF was 2.0 days. Most NDAFs were paroxysmal (95.2%) and lasted less than 1 hour (85.7%). Diabetes mellitus and infarct size were predictors of NDAF. Detection of NDAF prompted the initiation of anticoagulation therapy in 8.2% of the patients admitted to areas with CCM availability. Our findings suggest that immediate and prolonged CCM significantly improves the detection of NDAF after cryptogenic and noncryptogenic AIS or TIA, and that diabetes mellitus and infarct size are significantly associated with NDAF. Key Words: Strokedtransient ischemic attackdtelemetrydarrhthmyadelectrocardiographyddiagnosis. Ó 2012 by National Stroke Association Atrial fibrillation (AF) constitutes a major risk factor for ischemic stroke, and stroke patients with AF have a poorer prognosis than those without sinus rhythm [1]. The identi- fication of newly diagnosed AF (NDAF) in patients with acute ischemic stroke (AIS) or transient ischemic attack (TIA) is crucial, because oral anticoagulation significantly decreases the risk of stroke recurrence [2]. NDAF recogni- tion remains elusive, because 50% or more of cases may present with asymptomatic and intermittent patterns [3-5]. Standard electrocardiography (ECG) may be insuffi- cient for detecting NDAF. Even 24-hour ECG recording (Holter monitoring) has shown relatively poor sensitivity for the detection of NDAF, with a negative predictive From the *Stroke Center, Institute of Neurosciences, †Neurovascular Center and Vascular Research Unit at INECO. Bue- nos Aires, Argentina, ‡Telemetry Section, Cardiovascular Depart- ment, University Hospital, Favaloro Foundation, Buenos Aires, Argentina, xDepartment of Internal Medicine, Hospital de Clı ´nicas “Jose ´ de San Martı ´n,” Buenos Aires, Argentina; and {Department of Neurology, Mayo Clinic, Rochester, Minnesota. Received May 3, 2010; accepted June 27, 2010. Address correspondence to Luciano A. Sposato, MD, MBA, Stroke Center at the Institute of Neurosciences, University Hospital, Favaloro Foundation, Solı ´s 443, Piso 3, Ciudad de Buenos Aires, Argentina. E-mail: [email protected]. 1052-3057/$ - see front matter Ó 2012 by National Stroke Association doi:10.1016/j.jstrokecerebrovasdis.2010.06.010 210 Journal of Stroke and Cerebrovascular Diseases, Vol. 21, No. 3 (April), 2012: pp 210-216
Transcript of Newly Diagnosed Atrial Fibrillation after Acute Ischemic Stroke and Transient Ischemic Attack:...
NewlyDiagnosedAtrial Fibrill
ation after Acute Ischemic Strokeand Transient Ischemic Attack: Importance of Immediate andProlonged Continuous Cardiac Monitoring
Luciano A. Sposato, MD, MBA,*† Francisco R. Klein, MD,* Agustın Jauregui, MD,*
Marisol Ferrua, MD,* Pablo Klin, MD,‡ Rafael Zamora, MD,x Patricia M. Riccio, MD,*
and Alejandro Rabinstein, MD{
From the *Stroke
†Neurovascular Center a
nos Aires, Argentina, ‡
ment, University Hosp
Argentina, xDepartment
“Jose de San Martın,” B
of Neurology, Mayo Clin
Received May 3, 2010;
Address corresponden
Center at the Institute ofN
Foundation, Solıs 443, P
E-mail: lucianosposato@g
1052-3057/$ - see front
� 2012 by National Str
doi:10.1016/j.jstrokece
210
Atrial fibrillation (AF) is the major cause of cardioembolic stroke. It often remains
occult when asymptomatic and paroxysmal. We hypothesized that the detection
of AF after acute ischemic stroke (AIS) or transient ischemic attack (TIA) could be
improved by using continuous cardiac monitoring (CCM) immediately after admis-
sion.We sought to determine the detection rate of AF by immediate in-hospital CCM
after cryptogenic and noncryptogenic AIS or TIA in patients without a previous
diagnosis of AF.We retrospectively studied a cohort of 155 patients with cryptogenic
and noncryptogenic AIS or TIAwithout knownAF.We compared the detection rates
of newly diagnosed AF (NDAF) in patients admitted to areas with CCM and those
never admitted to these areas.We developed amultiple logistic regressionmodel for
identifying predictors of NDAF. We characterized NDAF episodes and analyzed
how the availability of CCM data changed secondary prevention strategies. We
detected NDAF in 21 patients (13.5%). Diagnostic rates of NDAF in patients who
underwent CCMand thosewho did not undergo CCMwere 18.2% and 2.2%, respec-
tively (P 5 .005). The median time from admission to recognition of NDAF was 2.0
days. Most NDAFs were paroxysmal (95.2%) and lasted less than 1 hour (85.7%).
Diabetes mellitus and infarct size were predictors of NDAF. Detection of NDAF
prompted the initiation of anticoagulation therapy in 8.2% of the patients
admitted to areas with CCM availability. Our findings suggest that immediate
and prolongedCCM significantly improves the detection of NDAF after cryptogenic
and noncryptogenic AIS or TIA, and that diabetes mellitus and infarct size are
significantly associated with NDAF. Key Words: Strokedtransient ischemic
attackdtelemetrydarrhthmyadelectrocardiographyddiagnosis.
� 2012 by National Stroke Association
Center, Institute of Neurosciences,
nd Vascular Research Unit at INECO. Bue-
Telemetry Section, Cardiovascular Depart-
ital, Favaloro Foundation, Buenos Aires,
of Internal Medicine, Hospital de Clınicas
uenos Aires, Argentina; and {Department
ic, Rochester, Minnesota.
accepted June 27, 2010.
ce to Luciano A. Sposato, MD, MBA, Stroke
eurosciences,UniversityHospital, Favaloro
iso 3, Ciudad de Buenos Aires, Argentina.
mail.com.
matter
oke Association
rebrovasdis.2010.06.010
Journal of Stroke and Cer
Atrial fibrillation (AF) constitutes a major risk factor for
ischemic stroke, and stroke patients with AF have a poorer
prognosis than those without sinus rhythm [1]. The identi-
fication of newly diagnosed AF (NDAF) in patients with
acute ischemic stroke (AIS) or transient ischemic attack
(TIA) is crucial, because oral anticoagulation significantly
decreases the risk of stroke recurrence [2]. NDAF recogni-
tion remains elusive, because 50% or more of cases may
present with asymptomatic and intermittent patterns [3-5].
Standard electrocardiography (ECG) may be insuffi-
cient for detecting NDAF. Even 24-hour ECG recording
(Holter monitoring) has shown relatively poor sensitivity
for the detection of NDAF, with a negative predictive
ebrovascular Diseases, Vol. 21, No. 3 (April), 2012: pp 210-216

NEWLY DIAGNOSED ATRIAL FIBRILLATION AFTER ISCHEMIC STROKE 211
value for freedom from AF of 25%-40% in paroxysmal AF
[5,6]. This means that that during a 1-year follow-upmon-
itoring period without detection of AF, only 1 in 3 patients
actually will be free of AF [7]. Furthermore, NDAF was
detected in 5.7% of patients with normal ECG and normal
Holter monitoring using a 7-day event loop recording in
the ambulatory setting [4].
To date, no clinical trial has assessed the usefulness of
immediate and prolonged in-hospital continuous cardiac
monitoring (CCM) in patients with cryptogenic and non-
cryptogenic AIS or TIA. The objective of the present study
was to determine the rate of detection of NDAF by imme-
diate and prolonged in-hospital CCM after cryptogenic
and noncryptogenic AIS or TIA.
Methods
This retrospective case series included all consecutive
patients aged.18 years admitted to our hospital with a di-
agnosis ofAIS or TIA between January 1, 2007, andDecem-
ber 31, 2008. Our study cohort comprised both cryptogenic
and noncryptogenic events. We chose to study noncrypto-
genic AIS and TIAs because more than one pathophysio-
logic mechanism can coexist in the same patient (eg,
extracranial carotiddisease andAF) [8]. Thus, evenpatients
with a defined noncardioembolic stroke could benefit from
antiarrhythmic treatment and anticoagulation if an NDAF
is identified. We defined a cryptogenic event as any AIS
or TIAwith no identifiable etiology on complete diagnostic
workup [9].
This study was conducted before publication of the
recent American Heart AssociationeAmerican Stroke
Association’s TIA Definition and Evaluation Statement
[10]. Consequently, we defined TIA as the sudden onset
of focal neurologic signs or symptoms lasting less than
24 hours with no associated ischemic lesions on neuroi-
maging studies. We defined ischemic stroke as the sud-
den onset of focal neurologic signs or symptoms lasting
longer than 24 hours.
PatientswithAIS andTIAwere admitted to the telemetry
ward unless there was no bed available, in which case
patientswithTIAandmildstrokewereadmitted to thegen-
eralward, and thosewithmore severe strokewereadmitted
to the intensive care unit (ICU) or the coronary care unit
(CCU). Most postoperative strokes were diagnosed in the
postsurgical care unit. Patients admitted to the latter critical
care area (CCA)were continuouslymonitored for thedetec-
tion of electrocardiographic abnormalities immediately
after admission, whereas patients not admitted to a CCA
did not undergo CCM. The telemetry ward is equipped
with an Infinity telemetry system (DragerMedical, Telford,
PA) for the receptors and an Infinitymultiviewworkstation
as a central monitoring device linked to portable telemetric
transmitters. In addition, 4 centrally supervised bedside
monitors (Infinity Vista XL) are available for unstable
patients requiring direct observation of cardiac rhythm.
The central monitoring workstation provides 24-hour
7-lead ECG monitoring, arrhythmia detection, and mea-
surement of ST-T segment changes. Two highly trained
nurseswatch the centralmonitors 24hours aday. If a parox-
ysmal event is noted, then the corresponding strip is
printed out for further assessment by a certified cardiolo-
gist. To decrease the risk of missing short paroxysmal
events, data are recorded and reviewed by the nurses at ev-
ery 8-hour shift. The CCU/ICU and postsurgical care unit
are equipped with Marquette Dash 4000 Pro (GE Health-
care, Chalfont St. Giles, UK), and Eagle 4000 (GE Health-
care) multilead ECG patient monitors, respectively. All
monitors are integrated into a central workstation at each
area. These systemsare configuredwith simultaneousmul-
tilead arrhythmia analysis software (including AF detec-
tion) for event notification, storage, and recall. One highly
trained nurse is exclusively available for each patient in
the CCU, ICU, and postsurgical care unit. Monitor alarms
are set to sound on any change in ECG rhythm or heart
rate$120 beats perminute. In either case, the nurse records
a rhythm strip for assessment by a certified cardiologist.
During the hospital stay, each patient with stroke or
TIA was assessed daily by one or more of the stroke
team members. On admission, each patient with AIS or
TIA underwent a neurologic examination and a 12-lead
ECG evaluation. Further ECGs were ordered only when
a patient became symptomatic while hospitalized in the
general ward (eg, palpitations, chest pain). In the patients
admitted to a CCA, ECG was performed daily and when-
ever a paroxysmal event was detected by CCM.
Our usual diagnostic workup includes an initial com-
puted tomography (CT) scan of the brain, blood tests,
neurovascular imaging studies (Doppler ultrasound, CT
angiography, or magnetic resonance angiography), and
transesophageal or transthoracic Doppler echocardiogra-
phy (TEE or TTE). During the study period, we could not
ordermagnetic resonance imaging (MRI) studies on a reg-
ular basis because of limited availability. For this reason,
we ordered an MRI only for selected patients. A second
brain CT scan was done in some patients during the
hospital stay or after discharge.
The study design and the distribution of patients into
the different monitoring groups are shown in Figure 1,
a flow diagram adapted from the Consolidated Standards
of Reporting Trials (CSRT) [11]. For the present analysis,
we excluded patients with a history of chronic AF or par-
oxysmal AF, and those with AF detected on the admission
ECG. The diagnosis of chronic and paroxysmal AF was
made on the basis of patient recall or by documentation
of the arrhythmia on a previous ECG when available.
AF was defined by the absence of P waves or evidence
of atrial flutter with irregular ventricular response.
NDAF was defined as AF diagnosed after AIS or TIA in
a patient with no history of chronic or paroxysmal AF.
We compared rates of NDAF in patients admitted to
aCCAand those not admitted to aCCA (ie, those admitted
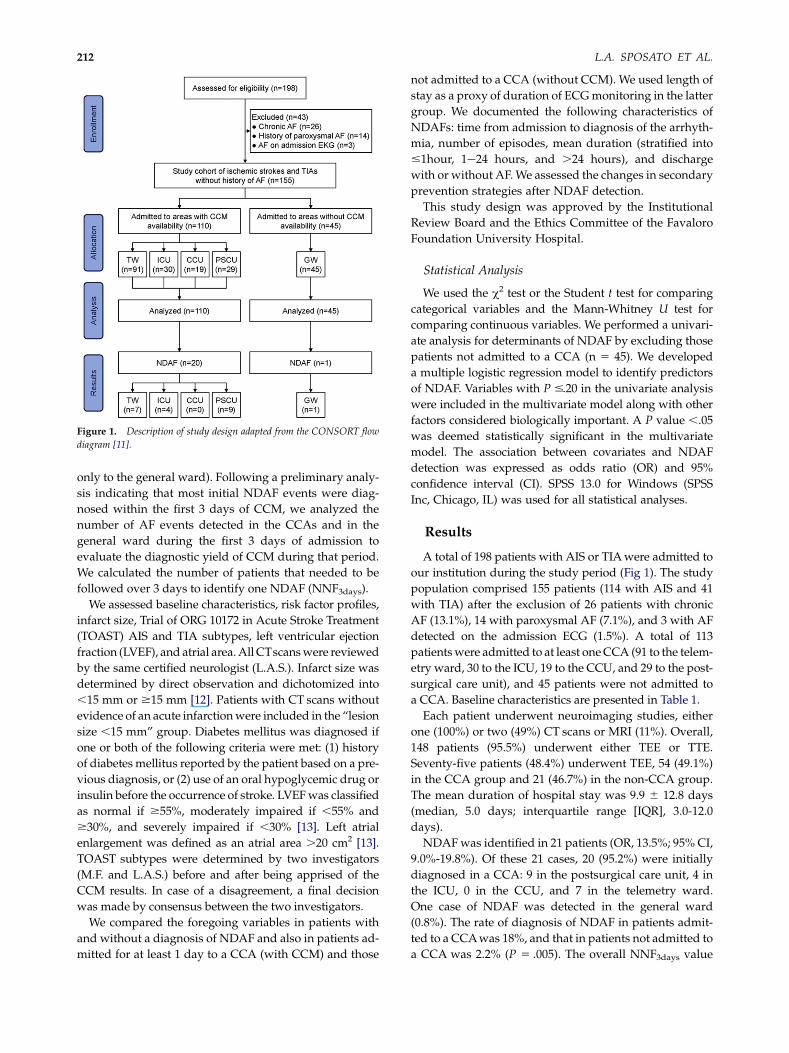
Figure 1. Description of study design adapted from the CONSORT flow
diagram [11].
L.A. SPOSATO ET AL.212
only to the general ward). Following a preliminary analy-
sis indicating that most initial NDAF events were diag-
nosed within the first 3 days of CCM, we analyzed the
number of AF events detected in the CCAs and in the
general ward during the first 3 days of admission to
evaluate the diagnostic yield of CCM during that period.
We calculated the number of patients that needed to be
followed over 3 days to identify one NDAF (NNF3days).
We assessed baseline characteristics, risk factor profiles,
infarct size, Trial of ORG 10172 in Acute Stroke Treatment
(TOAST) AIS and TIA subtypes, left ventricular ejection
fraction (LVEF), and atrial area.All CTscanswere reviewed
by the same certified neurologist (L.A.S.). Infarct size was
determined by direct observation and dichotomized into
,15 mm or $15 mm [12]. Patients with CT scans without
evidence of an acute infarctionwere included in the “lesion
size ,15 mm” group. Diabetes mellitus was diagnosed if
one or both of the following criteria were met: (1) history
of diabetes mellitus reported by the patient based on a pre-
vious diagnosis, or (2) use of an oral hypoglycemic drug or
insulin before the occurrence of stroke. LVEFwas classified
as normal if $55%, moderately impaired if ,55% and
$30%, and severely impaired if ,30% [13]. Left atrial
enlargement was defined as an atrial area .20 cm2 [13].
TOAST subtypes were determined by two investigators
(M.F. and L.A.S.) before and after being apprised of the
CCM results. In case of a disagreement, a final decision
was made by consensus between the two investigators.
We compared the foregoing variables in patients with
and without a diagnosis of NDAF and also in patients ad-
mitted for at least 1 day to a CCA (with CCM) and those
not admitted to a CCA (without CCM). We used length of
stay as a proxy of duration of ECGmonitoring in the latter
group. We documented the following characteristics of
NDAFs: time from admission to diagnosis of the arrhyth-
mia, number of episodes, mean duration (stratified into
#1hour, 1e24 hours, and .24 hours), and discharge
with or without AF.We assessed the changes in secondary
prevention strategies after NDAF detection.
This study design was approved by the Institutional
Review Board and the Ethics Committee of the Favaloro
Foundation University Hospital.
Statistical Analysis
We used the c2 test or the Student t test for comparing
categorical variables and the Mann-Whitney U test for
comparing continuous variables. We performed a univari-
ate analysis for determinants of NDAF by excluding those
patients not admitted to a CCA (n 5 45). We developed
a multiple logistic regression model to identify predictors
of NDAF. Variables with P #.20 in the univariate analysis
were included in the multivariate model along with other
factors considered biologically important. A P value ,.05
was deemed statistically significant in the multivariate
model. The association between covariates and NDAF
detection was expressed as odds ratio (OR) and 95%
confidence interval (CI). SPSS 13.0 for Windows (SPSS
Inc, Chicago, IL) was used for all statistical analyses.
Results
A total of 198 patients with AIS or TIAwere admitted to
our institution during the study period (Fig 1). The study
population comprised 155 patients (114 with AIS and 41
with TIA) after the exclusion of 26 patients with chronic
AF (13.1%), 14 with paroxysmal AF (7.1%), and 3 with AF
detected on the admission ECG (1.5%). A total of 113
patientswere admitted to at least oneCCA (91 to the telem-
etry ward, 30 to the ICU, 19 to the CCU, and 29 to the post-
surgical care unit), and 45 patients were not admitted to
a CCA. Baseline characteristics are presented in Table 1.
Each patient underwent neuroimaging studies, either
one (100%) or two (49%) CT scans or MRI (11%). Overall,
148 patients (95.5%) underwent either TEE or TTE.
Seventy-five patients (48.4%) underwent TEE, 54 (49.1%)
in the CCA group and 21 (46.7%) in the non-CCA group.
The mean duration of hospital stay was 9.9 6 12.8 days
(median, 5.0 days; interquartile range [IQR], 3.0-12.0
days).
NDAFwas identified in 21 patients (OR, 13.5%; 95% CI,
9.0%-19.8%). Of these 21 cases, 20 (95.2%) were initially
diagnosed in a CCA: 9 in the postsurgical care unit, 4 in
the ICU, 0 in the CCU, and 7 in the telemetry ward.
One case of NDAF was detected in the general ward
(0.8%). The rate of diagnosis of NDAF in patients admit-
ted to a CCAwas 18%, and that in patients not admitted to
a CCA was 2.2% (P 5 .005). The overall NNF3days value
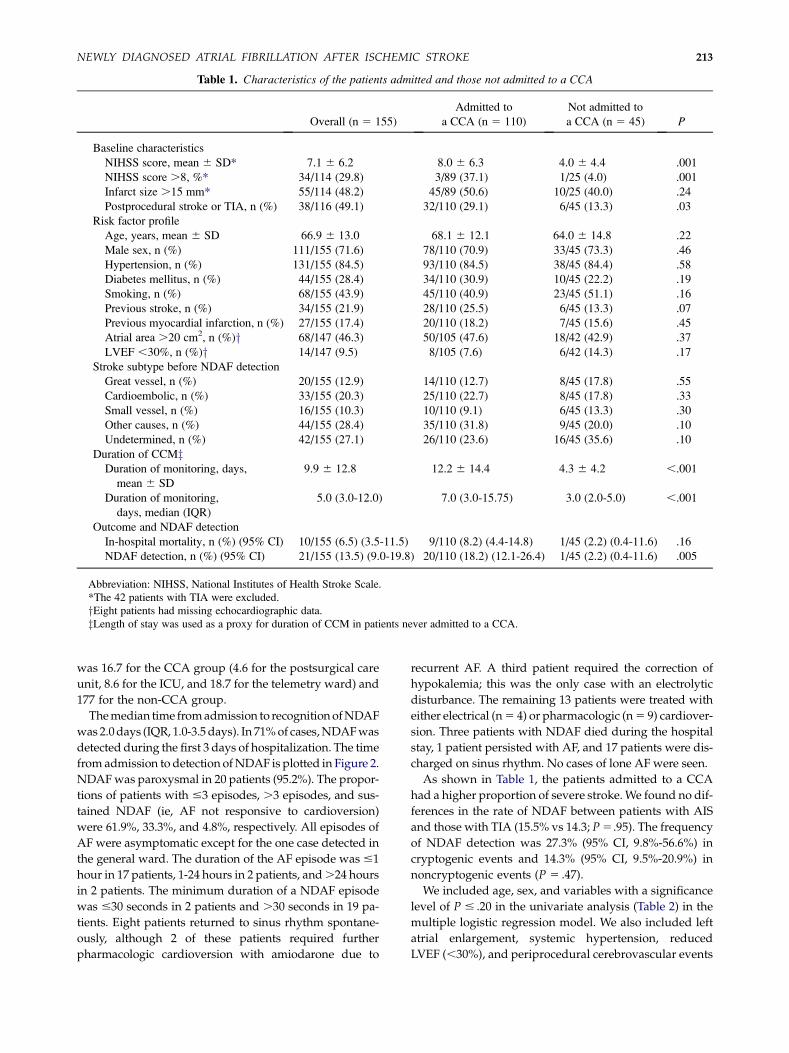
Table 1. Characteristics of the patients admitted and those not admitted to a CCA
Overall (n 5 155)
Admitted to
a CCA (n 5 110)
Not admitted to
a CCA (n 5 45) P
Baseline characteristics
NIHSS score, mean 6 SD* 7.1 6 6.2 8.0 6 6.3 4.0 6 4.4 .001
NIHSS score .8, %* 34/114 (29.8) 3/89 (37.1) 1/25 (4.0) .001
Infarct size .15 mm* 55/114 (48.2) 45/89 (50.6) 10/25 (40.0) .24
Postprocedural stroke or TIA, n (%) 38/116 (49.1) 32/110 (29.1) 6/45 (13.3) .03
Risk factor profile
Age, years, mean 6 SD 66.9 6 13.0 68.1 6 12.1 64.0 6 14.8 .22
Male sex, n (%) 111/155 (71.6) 78/110 (70.9) 33/45 (73.3) .46
Hypertension, n (%) 131/155 (84.5) 93/110 (84.5) 38/45 (84.4) .58
Diabetes mellitus, n (%) 44/155 (28.4) 34/110 (30.9) 10/45 (22.2) .19
Smoking, n (%) 68/155 (43.9) 45/110 (40.9) 23/45 (51.1) .16
Previous stroke, n (%) 34/155 (21.9) 28/110 (25.5) 6/45 (13.3) .07
Previous myocardial infarction, n (%) 27/155 (17.4) 20/110 (18.2) 7/45 (15.6) .45
Atrial area .20 cm2, n (%)y 68/147 (46.3) 50/105 (47.6) 18/42 (42.9) .37
LVEF ,30%, n (%)y 14/147 (9.5) 8/105 (7.6) 6/42 (14.3) .17
Stroke subtype before NDAF detection
Great vessel, n (%) 20/155 (12.9) 14/110 (12.7) 8/45 (17.8) .55
Cardioembolic, n (%) 33/155 (20.3) 25/110 (22.7) 8/45 (17.8) .33
Small vessel, n (%) 16/155 (10.3) 10/110 (9.1) 6/45 (13.3) .30
Other causes, n (%) 44/155 (28.4) 35/110 (31.8) 9/45 (20.0) .10
Undetermined, n (%) 42/155 (27.1) 26/110 (23.6) 16/45 (35.6) .10
Duration of CCMzDuration of monitoring, days,
mean 6 SD
9.9 6 12.8 12.2 6 14.4 4.3 6 4.2 ,.001
Duration of monitoring,
days, median (IQR)
5.0 (3.0-12.0) 7.0 (3.0-15.75) 3.0 (2.0-5.0) ,.001
Outcome and NDAF detection
In-hospital mortality, n (%) (95% CI) 10/155 (6.5) (3.5-11.5) 9/110 (8.2) (4.4-14.8) 1/45 (2.2) (0.4-11.6) .16
NDAF detection, n (%) (95% CI) 21/155 (13.5) (9.0-19.8) 20/110 (18.2) (12.1-26.4) 1/45 (2.2) (0.4-11.6) .005
Abbreviation: NIHSS, National Institutes of Health Stroke Scale.
*The 42 patients with TIA were excluded.
yEight patients had missing echocardiographic data.
zLength of stay was used as a proxy for duration of CCM in patients never admitted to a CCA.
NEWLY DIAGNOSED ATRIAL FIBRILLATION AFTER ISCHEMIC STROKE 213
was 16.7 for the CCA group (4.6 for the postsurgical care
unit, 8.6 for the ICU, and 18.7 for the telemetry ward) and
177 for the non-CCA group.
Themedian time fromadmission to recognitionofNDAF
was 2.0days (IQR, 1.0-3.5 days). In 71%of cases,NDAFwas
detected during the first 3 days of hospitalization. The time
fromadmission to detection ofNDAF is plotted in Figure 2.
NDAFwas paroxysmal in 20 patients (95.2%). The propor-
tions of patients with #3 episodes, .3 episodes, and sus-
tained NDAF (ie, AF not responsive to cardioversion)
were 61.9%, 33.3%, and 4.8%, respectively. All episodes of
AF were asymptomatic except for the one case detected in
the general ward. The duration of the AF episode was #1
hour in 17 patients, 1-24 hours in 2 patients, and.24 hours
in 2 patients. The minimum duration of a NDAF episode
was #30 seconds in 2 patients and .30 seconds in 19 pa-
tients. Eight patients returned to sinus rhythm spontane-
ously, although 2 of these patients required further
pharmacologic cardioversion with amiodarone due to
recurrent AF. A third patient required the correction of
hypokalemia; this was the only case with an electrolytic
disturbance. The remaining 13 patients were treated with
either electrical (n5 4) or pharmacologic (n5 9) cardiover-
sion. Three patients with NDAF died during the hospital
stay, 1 patient persisted with AF, and 17 patients were dis-
charged on sinus rhythm. No cases of lone AF were seen.
As shown in Table 1, the patients admitted to a CCA
had a higher proportion of severe stroke.We found no dif-
ferences in the rate of NDAF between patients with AIS
and those with TIA (15.5% vs 14.3; P5 .95). The frequency
of NDAF detection was 27.3% (95% CI, 9.8%-56.6%) in
cryptogenic events and 14.3% (95% CI, 9.5%-20.9%) in
noncryptogenic events (P 5 .47).
We included age, sex, and variables with a significance
level of P # .20 in the univariate analysis (Table 2) in the
multiple logistic regression model. We also included left
atrial enlargement, systemic hypertension, reduced
LVEF (,30%), and periprocedural cerebrovascular events
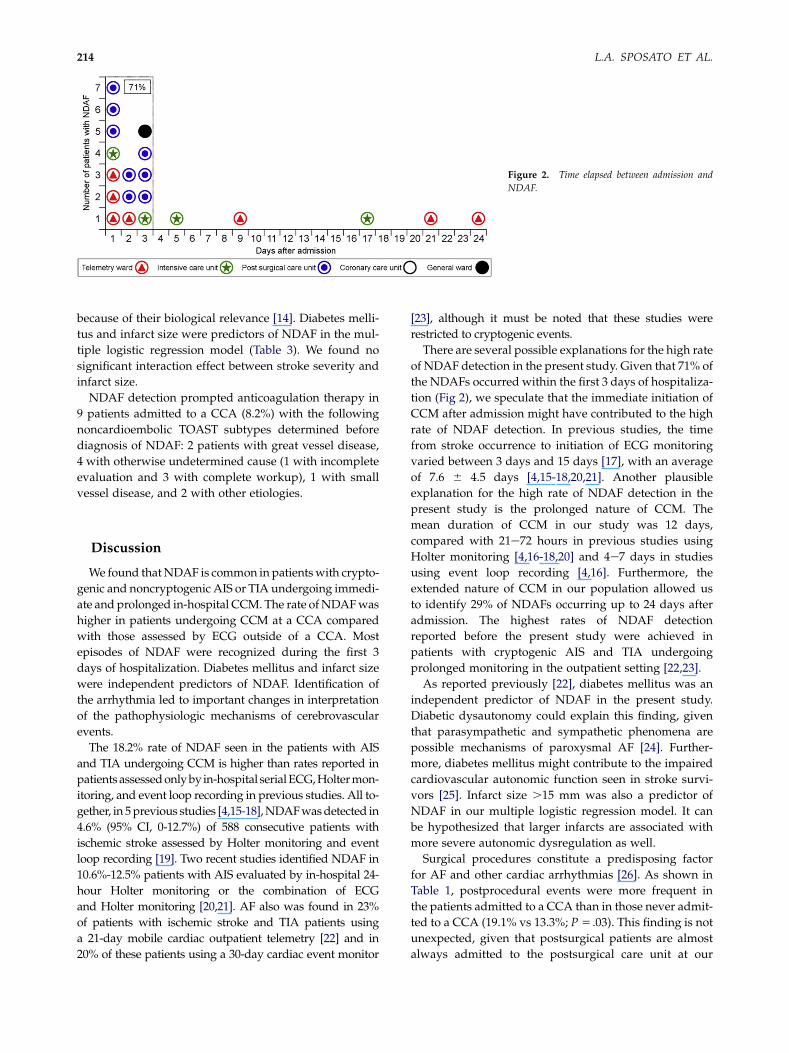
Figure 2. Time elapsed between admission and
NDAF.
L.A. SPOSATO ET AL.214
because of their biological relevance [14]. Diabetes melli-
tus and infarct size were predictors of NDAF in the mul-
tiple logistic regression model (Table 3). We found no
significant interaction effect between stroke severity and
infarct size.
NDAF detection prompted anticoagulation therapy in
9 patients admitted to a CCA (8.2%) with the following
noncardioembolic TOAST subtypes determined before
diagnosis of NDAF: 2 patients with great vessel disease,
4 with otherwise undetermined cause (1 with incomplete
evaluation and 3 with complete workup), 1 with small
vessel disease, and 2 with other etiologies.
Discussion
We found thatNDAF is common in patientswith crypto-
genic and noncryptogenic AIS or TIA undergoing immedi-
ate and prolonged in-hospital CCM. The rate ofNDAFwas
higher in patients undergoing CCM at a CCA compared
with those assessed by ECG outside of a CCA. Most
episodes of NDAF were recognized during the first 3
days of hospitalization. Diabetes mellitus and infarct size
were independent predictors of NDAF. Identification of
the arrhythmia led to important changes in interpretation
of the pathophysiologic mechanisms of cerebrovascular
events.
The 18.2% rate of NDAF seen in the patients with AIS
and TIA undergoing CCM is higher than rates reported in
patientsassessedonlyby in-hospital serialECG,Holtermon-
itoring, and event loop recording in previous studies. All to-
gether, in 5previous studies [4,15-18],NDAFwasdetected in
4.6% (95% CI, 0-12.7%) of 588 consecutive patients with
ischemic stroke assessed by Holter monitoring and event
loop recording [19]. Two recent studies identified NDAF in
10.6%-12.5% patients with AIS evaluated by in-hospital 24-
hour Holter monitoring or the combination of ECG
and Holter monitoring [20,21]. AF also was found in 23%
of patients with ischemic stroke and TIA patients using
a 21-day mobile cardiac outpatient telemetry [22] and in
20% of these patients using a 30-day cardiac event monitor
[23], although it must be noted that these studies were
restricted to cryptogenic events.
There are several possible explanations for the high rate
of NDAF detection in the present study. Given that 71% of
the NDAFs occurred within the first 3 days of hospitaliza-
tion (Fig 2), we speculate that the immediate initiation of
CCM after admission might have contributed to the high
rate of NDAF detection. In previous studies, the time
from stroke occurrence to initiation of ECG monitoring
varied between 3 days and 15 days [17], with an average
of 7.6 6 4.5 days [4,15-18,20,21]. Another plausible
explanation for the high rate of NDAF detection in the
present study is the prolonged nature of CCM. The
mean duration of CCM in our study was 12 days,
compared with 21e72 hours in previous studies using
Holter monitoring [4,16-18,20] and 4e7 days in studies
using event loop recording [4,16]. Furthermore, the
extended nature of CCM in our population allowed us
to identify 29% of NDAFs occurring up to 24 days after
admission. The highest rates of NDAF detection
reported before the present study were achieved in
patients with cryptogenic AIS and TIA undergoing
prolonged monitoring in the outpatient setting [22,23].
As reported previously [22], diabetes mellitus was an
independent predictor of NDAF in the present study.
Diabetic dysautonomy could explain this finding, given
that parasympathetic and sympathetic phenomena are
possible mechanisms of paroxysmal AF [24]. Further-
more, diabetes mellitus might contribute to the impaired
cardiovascular autonomic function seen in stroke survi-
vors [25]. Infarct size .15 mm was also a predictor of
NDAF in our multiple logistic regression model. It can
be hypothesized that larger infarcts are associated with
more severe autonomic dysregulation as well.
Surgical procedures constitute a predisposing factor
for AF and other cardiac arrhythmias [26]. As shown in
Table 1, postprocedural events were more frequent in
the patients admitted to a CCA than in those never admit-
ted to a CCA (19.1% vs 13.3%; P5 .03). This finding is not
unexpected, given that postsurgical patients are almost
always admitted to the postsurgical care unit at our
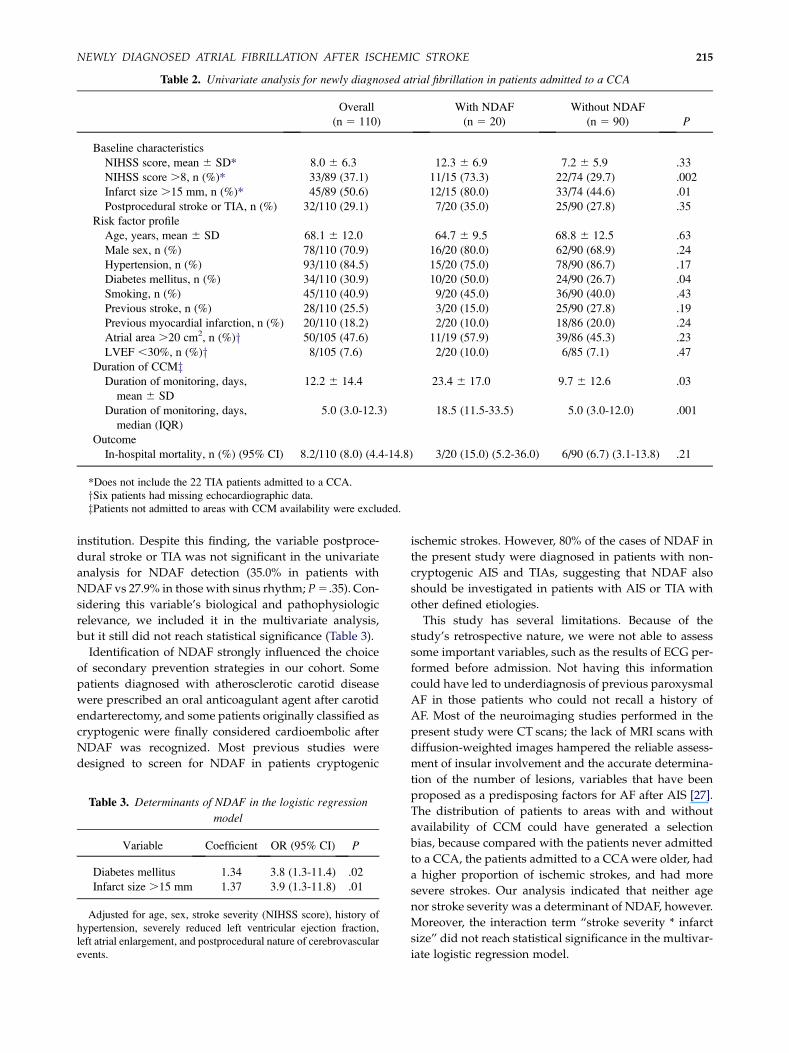
Table 2. Univariate analysis for newly diagnosed atrial fibrillation in patients admitted to a CCA
Overall
(n 5 110)
With NDAF
(n 5 20)
Without NDAF
(n 5 90) P
Baseline characteristics
NIHSS score, mean 6 SD* 8.0 6 6.3 12.3 6 6.9 7.2 6 5.9 .33
NIHSS score .8, n (%)* 33/89 (37.1) 11/15 (73.3) 22/74 (29.7) .002
Infarct size .15 mm, n (%)* 45/89 (50.6) 12/15 (80.0) 33/74 (44.6) .01
Postprocedural stroke or TIA, n (%) 32/110 (29.1) 7/20 (35.0) 25/90 (27.8) .35
Risk factor profile
Age, years, mean 6 SD 68.1 6 12.0 64.7 6 9.5 68.8 6 12.5 .63
Male sex, n (%) 78/110 (70.9) 16/20 (80.0) 62/90 (68.9) .24
Hypertension, n (%) 93/110 (84.5) 15/20 (75.0) 78/90 (86.7) .17
Diabetes mellitus, n (%) 34/110 (30.9) 10/20 (50.0) 24/90 (26.7) .04
Smoking, n (%) 45/110 (40.9) 9/20 (45.0) 36/90 (40.0) .43
Previous stroke, n (%) 28/110 (25.5) 3/20 (15.0) 25/90 (27.8) .19
Previous myocardial infarction, n (%) 20/110 (18.2) 2/20 (10.0) 18/86 (20.0) .24
Atrial area .20 cm2, n (%)y 50/105 (47.6) 11/19 (57.9) 39/86 (45.3) .23
LVEF ,30%, n (%)y 8/105 (7.6) 2/20 (10.0) 6/85 (7.1) .47
Duration of CCMzDuration of monitoring, days,
mean 6 SD
12.2 6 14.4 23.4 6 17.0 9.7 6 12.6 .03
Duration of monitoring, days,
median (IQR)
5.0 (3.0-12.3) 18.5 (11.5-33.5) 5.0 (3.0-12.0) .001
Outcome
In-hospital mortality, n (%) (95% CI) 8.2/110 (8.0) (4.4-14.8) 3/20 (15.0) (5.2-36.0) 6/90 (6.7) (3.1-13.8) .21
*Does not include the 22 TIA patients admitted to a CCA.
ySix patients had missing echocardiographic data.
zPatients not admitted to areas with CCM availability were excluded.
NEWLY DIAGNOSED ATRIAL FIBRILLATION AFTER ISCHEMIC STROKE 215
institution. Despite this finding, the variable postproce-
dural stroke or TIA was not significant in the univariate
analysis for NDAF detection (35.0% in patients with
NDAF vs 27.9% in those with sinus rhythm; P5 .35). Con-
sidering this variable’s biological and pathophysiologic
relevance, we included it in the multivariate analysis,
but it still did not reach statistical significance (Table 3).
Identification of NDAF strongly influenced the choice
of secondary prevention strategies in our cohort. Some
patients diagnosed with atherosclerotic carotid disease
were prescribed an oral anticoagulant agent after carotid
endarterectomy, and some patients originally classified as
cryptogenic were finally considered cardioembolic after
NDAF was recognized. Most previous studies were
designed to screen for NDAF in patients cryptogenic
Table 3. Determinants of NDAF in the logistic regression
model
Variable Coefficient OR (95% CI) P
Diabetes mellitus 1.34 3.8 (1.3-11.4) .02
Infarct size .15 mm 1.37 3.9 (1.3-11.8) .01
Adjusted for age, sex, stroke severity (NIHSS score), history of
hypertension, severely reduced left ventricular ejection fraction,
left atrial enlargement, and postprocedural nature of cerebrovascular
events.
ischemic strokes. However, 80% of the cases of NDAF in
the present study were diagnosed in patients with non-
cryptogenic AIS and TIAs, suggesting that NDAF also
should be investigated in patients with AIS or TIA with
other defined etiologies.
This study has several limitations. Because of the
study’s retrospective nature, we were not able to assess
some important variables, such as the results of ECG per-
formed before admission. Not having this information
could have led to underdiagnosis of previous paroxysmal
AF in those patients who could not recall a history of
AF. Most of the neuroimaging studies performed in the
present study were CT scans; the lack of MRI scans with
diffusion-weighted images hampered the reliable assess-
ment of insular involvement and the accurate determina-
tion of the number of lesions, variables that have been
proposed as a predisposing factors for AF after AIS [27].
The distribution of patients to areas with and without
availability of CCM could have generated a selection
bias, because compared with the patients never admitted
to a CCA, the patients admitted to a CCAwere older, had
a higher proportion of ischemic strokes, and had more
severe strokes. Our analysis indicated that neither age
nor stroke severity was a determinant of NDAF, however.
Moreover, the interaction term “stroke severity * infarct
size” did not reach statistical significance in the multivar-
iate logistic regression model.

L.A. SPOSATO ET AL.216
In conclusion, we found a very high rate of NDAF in
patients with cryptogenic and noncryptogenic AIS and
TIA undergoing immediate and prolonged CCM. Diabe-
tes mellitus and infarct size were associated with
NDAF. Immediate admission to a CCA for at least 3
days significantly increased the rate of NDAF detection.
These findings might have important therapeutic implica-
tions affecting a large proportion of patients with AIS and
TIA who could benefit from oral anticoagulation and
antiarrhythmic drugs. This benefit would be plausible
not only for patients with cryptogenic events, but also
for those with other defined stroke mechanisms.
Acknowledgment: We thank Professors Branco Mautner
and Gerardo Bozovich for their critical review of the manu-
script and Drs Analıa Calle, Noelia Pontello, and Francisco
Munoz Giacomelli for data collection.
References
1. Mattle HP. Long-term outcome after stroke due to atrialfibrillation. Cerebrovasc Dis 2003;16(Suppl 1):3-8.
2. EAFTStudyGroup. Secondaryprevention innon-rheumaticatrial fibrillation after transient ischaemic attack or minorstroke. Lancet 1993;342:1255-1262.
3. Lin HJ, Wolf PA, Benjamin EJ, et al. Newly diagnosedatrial fibrillation and acute stroke: The FraminghamStudy. Stroke 1995;26:1527-1530.
4. Jabaudon D, Sztajzel J, Sievert K, et al. Usefulness of am-bulatory 7-day EKG monitoring for the detection of atrialfibrillation and flutter after acute stroke and transientischemic attack. Stroke 2004;35:1647-1651.
5. Kirchhof P, Auricchio A, Bax J, et al. Recommendationsfrom a consensus conference organized by the GermanAtrial Fibrillation Competence NETwork (AFNET) andthe European Heart Rhythm Association (EHRA). EurHeart J 2007;28:2803-2817.
6. Kessler DK, Kessler KM. Is ambulatory electrocardiogra-phy useful in the evaluation of patients with recentstroke? Chest 1995;107:916-918.
7. Piorkowski C, KottkampH, TannerH, et al. Value of differ-ent follow-up strategies to assess the efficacy of circumfer-ential pulmonaryveinablation for the curative treatmentofatrial fibrillation. J Cardiovasc Electrophysiol 2005;16:1286-1292.
8. Caplan LR. Multiple potential risks for stroke. JAMA2000;283:1479-1480.
9. Sacco RL, Ellenberg JH, Mohr JP, et al. Infarcts of undeter-mined cause: The NINDS Stroke Data Bank. Ann Neurol1989;25:382-390.
10. Easton JD, Saver JL, Albers GW, et al. Definition andevaluation of transient ischemic attack. Stroke 2009;40:2276-2293.
11. Schulz KF, Altman DG, Moher D, for the CONSORTGroup. CONSORT 2010 Statement: Updated guidelinesfor reporting parallel group randomised trials. BMJ2010;340:c332.
12. Donnan GA, Norrving B, Bamford JM, et al. Subcorticalinfarction classification and terminology. CerebrovascDis 1993;3:248-251.
13. Lang RM, Bierig M, Devereux RB, et al. Recommenda-tions for chamber quantification: A report from theAmerican Society of Echocardiography’s Guidelinesand Standards Committee and the Chamber Quantifica-tion Writing Group, developed in conjunction with theEuropean Association of Echocardiography, a branch ofthe European Society of Cardiology. J Am Soc Echocar-diogr 2005;18:1440-1463.
14. Kannel WB, Wolf PA, Benjamin EJ, et al. Prevalence, inci-dence, prognosis, and predisposing conditions for atrialfibrillation: Population-based estimates. Am J Cardiol1998;82:2N-9N.
15. Rem JA, Hachinski VC, Boughner DR, et al. Value ofcardiac monitoring and echocardiography in TIA andstroke patients. Stroke 1985;16:950-956.
16. Barthelemy JC, Feasson-Gerard S, Garnier P, et al. Auto-matic cardiac event recorders reveal paroxysmal atrialfibrillation after unexplained strokes or transient ischemicattacks. Ann Noninvasive Electrocardiol 2003;8:194-199.
17. Hornig CR, Haberbosch W, Lammers C, et al. Specificcardiological evaluation after focal cerebral ischemia.Acta Neurol Scand 1996;93:297-302.
18. Schuchert A, Behrens G, Meinertz T. Impact of long-termEKG recording on the detection of paroxysmal atrialfibrillation in patients after an acute ischemic stroke.Pacing Clin Electrophysiol 1999;22:1082-1084.
19. Liao J, Khalid Z, Scallan C, et al. Noninvasive cardiacmonitoring for detecting paroxysmal atrial fibrillationor flutter after acute ischemic stroke: A systematic review.Stroke 2007;38:2935-2940.
20. Tagawa M, Takeuchi S, Chinushi M, et al. Evaluatingpatients with acute ischemic stroke with special referenceto newly developed atrial fibrillation in cerebral embo-lism. PACE 2007;30:1121-1128.
21. Douen AG, Pageau N, Medic S. Serial electrocardio-graphic assessments significantly improve detection ofatrial fibrillation 2.6-fold in patients with acute stroke.Stroke 2008;39:480-482.
22. Tayal AH, Tian M, Kelly KM, et al. Atrial fibrillationdetected by mobile cardiac outpatient telemetry in cryp-togenic TIA or stroke. Neurology 2008;71:1696-1701.
23. Elijovich L, Josephson SA, Fung GL, et al. Intermittentatrial fibrillation may account for a large proportion ofotherwise cryptogenic stroke: A study of 30-day cardiacevent monitors. J Stroke Cerebrovasc Dis 2009;18:185-189.
24. Coumel P. Neural aspects of paroxysmal atrial fibrillation.In: Falk RH, Podrid PJ, eds. Atrial Fibrillation: Mecha-nisms and Management. New York: Raven, 1992:109-125.
25. McLaren A, Kerr S, Allan L, et al. Autonomic function isimpaired in elderly stroke survivors. Stroke 2005;36:1026-1030.
26. Mariscalco G, Engstrom KG. Atrial fibrillation after car-diac surgery: Risk factors and their temporal relationshipin prophylactic drug strategy decision. Int J Cardiol 2008;129:354-362.
27. Cheshire WP, Saper CB. The insular cortex and cardiacresponse to stroke. Neurology 2006;66:1296-1297.




















