
Effects of hyperglycemia on the cerebrovascular response to rhythmic handgrip exercise
Upload
independentCategory
view
1download
0
Hyperglycemia, age and coronary mechanics 1
Impact of age and hyperglycemia on the mechanical
behavior of intact human coronary arteries: an ex-vivo
intravascular ultrasound study
Azita Tajaddini *1, Deborah L. Kilpatrick 4, Paul Schoenhagen 2, E. Murat Tuzcu 2,
Michael Lieber 3, D. Geoffrey Vince. 1
The Cleveland Clinic Foundation
1 Departments of Biomedical Engineering, 2 Cardiovascular Medicine,
and 3 Biostatistics and Epidemiology
Cleveland, OH 44195
4 Guidant Corporation, Vascular Intervention Group
Santa Clara, CA 95054
Supported by The Whitaker Foundation (97-0332, DGV-PI), The National Institute of
Health (RO1-HL64686, DGV-PI), and the Guidant Corporation
Running Head: Hyperglycemia, age and coronary mechanics
* Address for correspondence:
Azita Tajaddini, D. Eng.
Department of Biomedical Engineering/ND20
The Cleveland Clinic Foundation
9500 Euclid Avenue, Cleveland, OH 44195
Phone: (216) 445-4692, Fax: (216) 444-9198 Email: [email protected]
Articles in PresS. Am J Physiol Heart Circ Physiol (August 26, 2004). doi:10.1152/ajpheart.00646.2004
Copyright © 2004 by the American Physiological Society.

Hyperglycemia, age and coronary mechanics 2
Abstract
Background: Despite their advantages, percutaneous coronary interventional (PCI)
procedures are less effective in diabetic patients. Changes in the mechanical properties
of vascular walls secondary to long-term hyperglycemia as well as other factors such as
age may influence coronary distensibility. This investigation is aimed at deciphering the
extent of these effects on distensibility of post-mortem human coronary arteries in a
controlled manner. Methods and Results: Excised human left anterior descending
coronary arteries (LAD) were obtained within 24 hours post mortem. Using
intravascular ultrasound (IVUS), vascular deformation was analyzed at mid-regions of
51 moderate lesions. Intraluminal pressure was systematically altered using a
computerized pressure pump system, and monitored by a pressure sensing guidewire.
Distensibility, a normalized compliance term, was defined as the change in lumen area
normalized by the initial reference area, over a given pressure interval. Using
multivariate analysis, repeated measures ANOVA, coronary distensibility was
independently influenced by hyperglycemia, and age (p<0.05) through the entire
pressure range. Within physiological pressure range, distensibility was significantly
reduced with age in non-hyperglycemic coronary specimens (10.55 ± 4.41 vs. 6.99 ±
2.45, x103 kPa-1, p=0.01), while the hyperglycemic vessels were stiff even in the
younger group (7.90 ± 5.82 vs. 7.20 ± 3.36, x103 kPa-1, p=0.79). Similar results were
observed with stiffness index (β) and elastic modulus (E) of the arteries. Conclusions:
Hyperglycemia and age independently influenced the distensibility of moderately

Hyperglycemia, age and coronary mechanics 3
atherosclerotic LAD coronary arteries. The stiffening with age was overshadowed in the
hyperglycemic group by as yet undetermined factors.
Keywords: Arteriosclerosis, Coronary disease, Diabetes mellitus, Elasticity.
Introduction
Diabetes mellitus is associated with a 2-3 fold increase in the incidence of coronary
artery disease (CAD). Micro-and macrovascular complications of diabetes result in
increased cardiovascular morbidity and mortality. (7) Diabetic patients have a higher
tendency for thrombogenesis and neointimal proliferation following intervention, (20) as
well as multiple coexisting risk factors for CAD such as hypertension and age.
Additionally, atherosclerosis in diabetic patients tends to be more diffuse with more
complex lesions. (28) Despite improvements in percutaneous coronary interventional
technology, the outcome of these procedures is still less favorable for the diabetic
patients. (7, 8, 20) The underlying pathophysiologic mechanism is not completely
understood, but changes in the elastic properties of coronary arterial walls could
contribute to such increased morbidity.
The approach of this study was to quantify local coronary distensibility using diagnostic
tools such as IVUS catheters and pressure sensing guidewires. The results could
elucidate the factors affecting wall properties of moderately diseased vascular regions
that would potentially impact the rate of disease progression and the complication rates
of interventional procedures, particularly in the patients with diabetes.
Hyperglycemia, age and coronary mechanics 4
Materials and Methods
Vessels: A total of fifty-one human left anterior descending (LAD) coronary arteries
were examined within 24 hours post-mortem according to institutional regulations.
Subjects with prior history of cardiac intervention and chemotherapy were excluded. An
approximately 40 mm thick portion of myocardium, which contained the LAD from its
ostium to apex, was dissected from the heart. This extravascular tissue supported the
LAD structurally by keeping its natural boundary conditions. Blood samples were also
collected to analyze the glycohemoglobin level (HbA1c%), where a level of 6.0 and
above indicates hyperglycemia. The age of subjects was between 40 to 75 years old.
Experimental set-up: The harvested tissue was mounted in a tissue bath, cannulated
and secured at the ostium, maintaining its in-vivo orientation. The tissue bath
containing phosphate buffered saline (PBS) was kept at 37 ± 1°C to reproduce in-vivo
conditions. Luminal pressure was altered with a computer-controlled pump system, as
described previously. (30) To measure intraluminal variations accurately, a pressure
sensing guidewire (Pressurewire®, RADI medical systems, Sweden) was calibrated and
inserted proximally into the mounted vessel. The Pressurewire®, with a diameter of 360
microns, was positioned to avoid contact with the vascular wall. The input pressure,
vascular pressure, and temperature of the PBS entering the LAD were continuously
monitored and displayed.
To measure the arterial wall dimensions, a 2.9 F, 30 MHz IVUS catheter (Scimed, CA)
was inserted into the vessel over the Pressurewire®. While applying a low pressure
Hyperglycemia, age and coronary mechanics 5
(<100 mmHg), side branches were ligated until the measured lumen pressure
approached the input. When the pressure stabilized, usually in 30-45 minutes, the
catheter was manually pulled back for an overview of the vessel geometry and extent of
atherosclerosis. Vessels were excluded if they failed to reach a stable pressure due to
excessive leakage at branch sites.
Site selection: A site with concentric intimal thickening with plaque burden less than
50 % (by area) was selected from each vessel (Figure 1) to examine the properties of a
homogenous section of the arterial wall. This single site was chosen from the middle
section of the lesion to represent the behavior of that particular lesion.
Distensibility tests: Following mechanical preconditioning of the vessel, the IVUS
catheter was placed at the selected site and secured externally. The pressure
transducer was retracted a few millimeters to avoid its reflection on IVUS images. The
vessel was pressurized from 0 to 260 mm Hg in 20 mm Hg increments and held for 5
seconds each to allow the tissue to stabilize for collection of vascular images and
pressure data. For subsequent histological examination, a needle was used as an
acoustic reflector to locate the imaged site prior to marking it with a suture.
Histological Examination: Subsequent to distensibility testing, the entire vessel was
fixed with Histochoice (Amresco®, OH) at a pressure of 100-120 mm Hg for at least 8
hours in order to preserve lumen/wall structure and size. Sections from the sutured site
were prepared using H&E and Movat pentachrome stains to identify tissue components
such as collagen, elastin, smooth muscle fibers, and macrophage-derived foam cells.
Hyperglycemia, age and coronary mechanics 6
Data Analysis: The mean pressure was obtained by averaging the last five data points
from the pressure sensing guidewire for each loading step. To calculate vascular cross-
sectional area (CSA), frames of digitized IVUS images were selected (Adobe Premiere,
Adobe Systems, CA) from the mid-point in time for each pressure step. Borders were
traced using a semi-automatic segmentation software package, developed at the
Cleveland Clinic Foundation (Figure 1). (15) CSA of lumen, external elastic membrane
(EEM), and lesion (plaque plus media CSA= EEM CSA – lumen CSA) were calculated
along with plaque burden (100 * lesion CSA / EEM CSA) according to published IVUS
guidelines. (22) Various biomechanical measures of arterial behavior were calculated
as follows, which accounted for the size and structure of the arteries. The vascular
distensibility was calculated as changes in lumen CSA (∆CSA) normalized by the initial
lumen CSA (CSAi), for each pressure interval (∆P) as: D = ∆CSA / (CSAi . ∆P)
Distensibility at physiological coronary pressure, Dp, was defined for each subject at ∆P
between 60 –140 mmHg. (24) A stiffness index (β) was also calculated based on the
same pressure range as β=(ln (P2/P1)) / ((r2-r1)/r1)), where r is the radius of the vessel at
the corresponding pressure, P. (9, 11) Similar to distensibility the stiffness index
provides a normalized compliance term including a logarithmic pressure term. Elasticity
of a material can also be defined using structural independent terms of stress and strain
commonly used in engineering discipline. Circumferential Cauchy stress, σ, was
calculated in the middle of the arterial wall using the equation for thick wall cylinders.
Hyperglycemia, age and coronary mechanics 7
σ=P*(ri2/(ro
2-ri2))*(1+(ro
2/r2)), where r, ri and ro, indicate mid-wall, inner and outer radii
respectively. Circumferential strain was defined as the change in mid-wall radius within
the same pressure range as above with respect to the reference radius ε=(r2/r1)-1
The elastic modulus (E) was calculated as the slope of the stress-strain curve in the
physiological range of pressure. Elastic modulus is a material property independent of
the structure of the specimen. However calculation of stress depends on the structure
of the specimen, which in this case was assumed to be a thick walled cylinder.
Statistical Analysis: For each case, the subject’s age, plaque burden, and %HbA1c
levels were included. A statistical mixed model of repeated measures ANOVA (SAS,
release 6.12, SAS Institute Inc., NC) was used to extract the influence of fixed variables
on distensibility. Continuous variables such as age, plaque burden, and Dp were
described by mean and standard deviation. They were compared between the subject
groups using a t-test assuming an equal variance. Chi-square test was used for gender
differences. A significance level at 0.05 was used for all tests.
Results
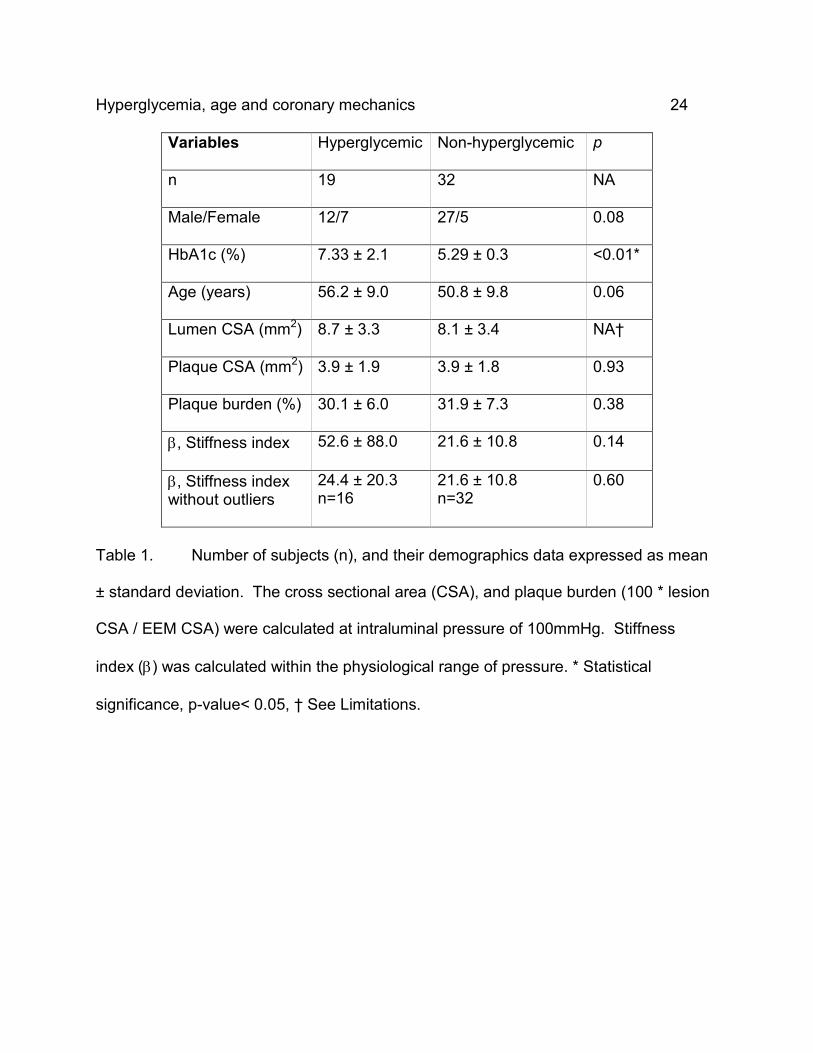
A summary of subject and vessel characteristics is shown in Table 1. Age, HbA1c, and
plaque burden ranged between 40-75 years, 4.5-14.1%, and 20-50%, respectively. The
majority of the subjects were males (n=39), some of whom were hyperglycemic (n=12).
Most of the subjects were Caucasian (n=32), mostly non-hyperglycemic.
Hyperglycemic subjects were not significantly older (p=0.06). Also there was no
difference in age between male and female subjects (51.3 ± 8.0, 53.3 ± 0.3,
Hyperglycemia, age and coronary mechanics 8
respectively, p=0.48). The LAD sections had a similar plaque burden compared to the
non-hyperglycemic group (p=0.38). The morphometric measurements of the two
groups are similar at intracoronary pressure of 100 mmHg (Table 1). The LAD sections
had similar histological profiles, including fibrous or fibrolipidic intima without
calcification.
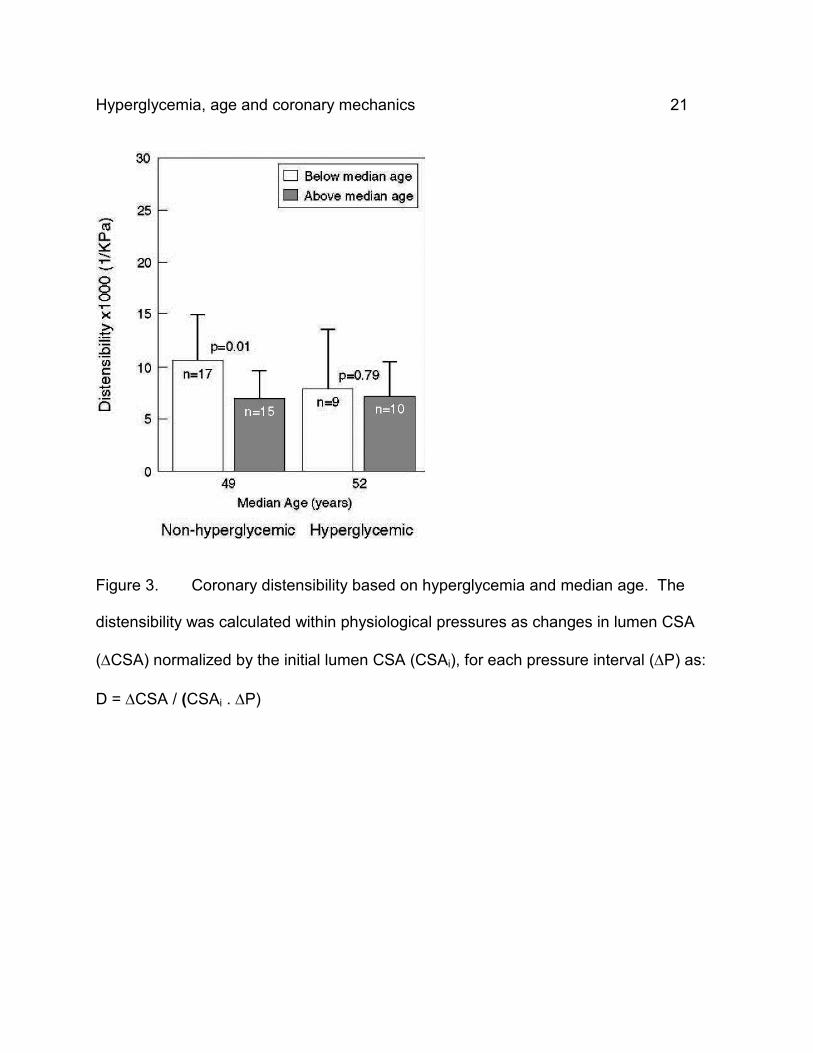
Based on multifactorial analysis, hyperglycemia influenced distensibility both
independently and significantly (p=0.02) for the entire CSA-P curve of each subject.
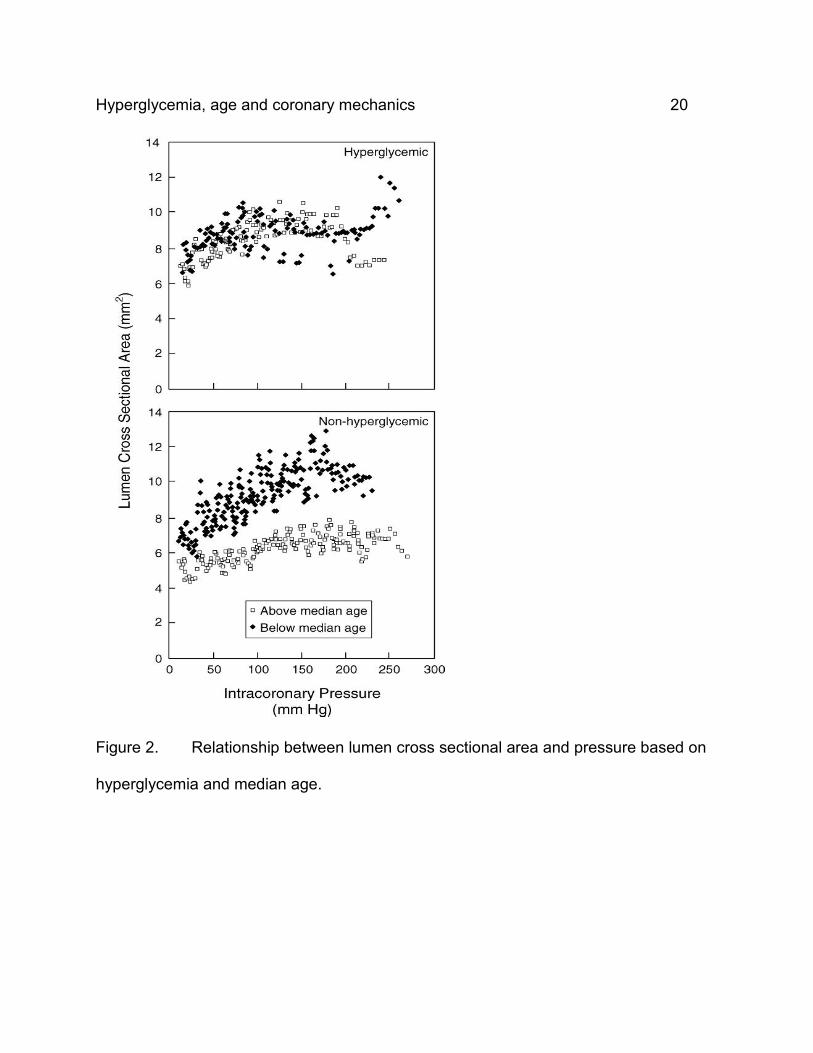
The CSA-P curves (Figure 2) for subject groups based on median age and
hyperglycemia reflect their differences. Vessels from older individuals without
hyperglycemia were significantly stiffer than the young individuals (10.55 ± 4.41 vs 6.99
± 2.45, p=0.01) within physiological coronary pressure. Such a difference was not
observed in the hyperglycemic group (7.90 ± 5.82 vs. 7.20 ± 3.36, p=0.76)(Figure 3).
Distensibility decreased with age by about 12% per year with a higher decline in the
non-hyperglycemic subjects (16% vs. 10%). The age distribution within each group is
depicted in Table 2 as well as the indices of mechanical behavior, namely, distensibility,
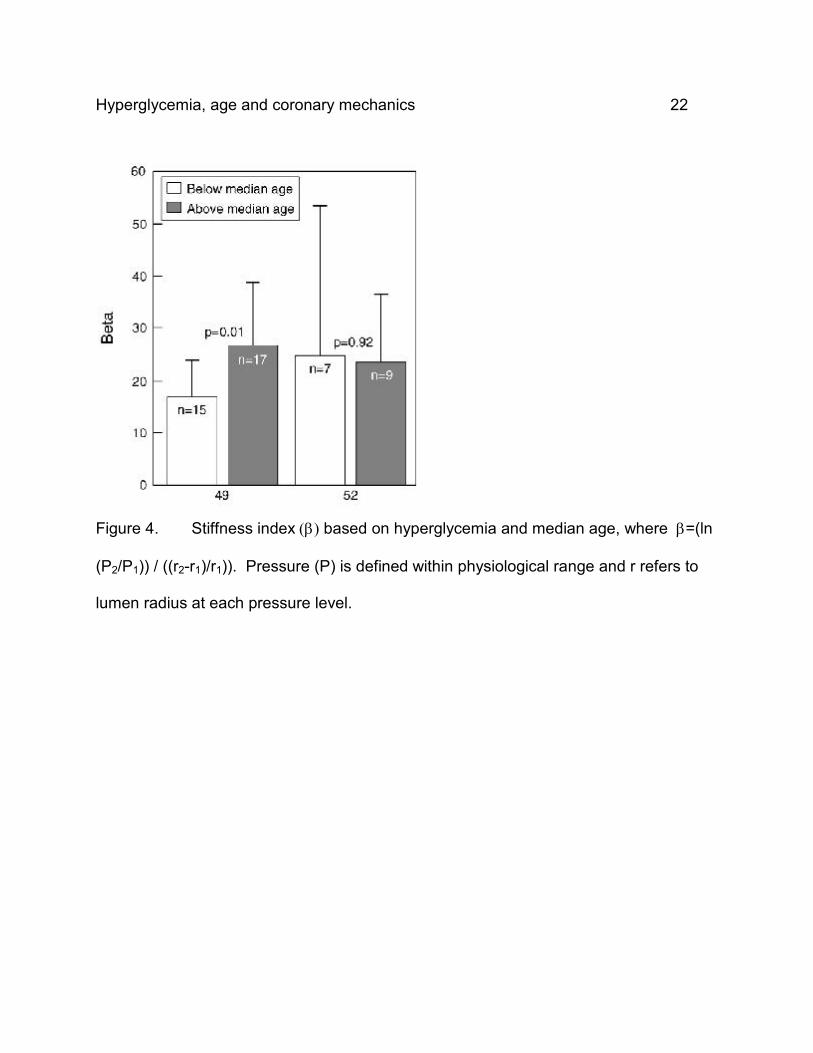
beta stiffness index and elastic modulus. Stiffness index, β, was higher but not
significantly with hyperglycemia with or without outliers, which were taken as one order
of magnitude away from the group mean (52.6 ± 88.0 vs. 21.6 ± 10.8, p=0.14, and 24.4
± 20.3 vs. 21.6 ± 10.8, p=0.6, respectively). However, when age and hyperglycemia
were considered, the influence of age on β was significant on nonhyperglycemic
subjects and lacking in hyperglycemic group (Figure 4), as seen with distensibility.
Hyperglycemia, age and coronary mechanics 9
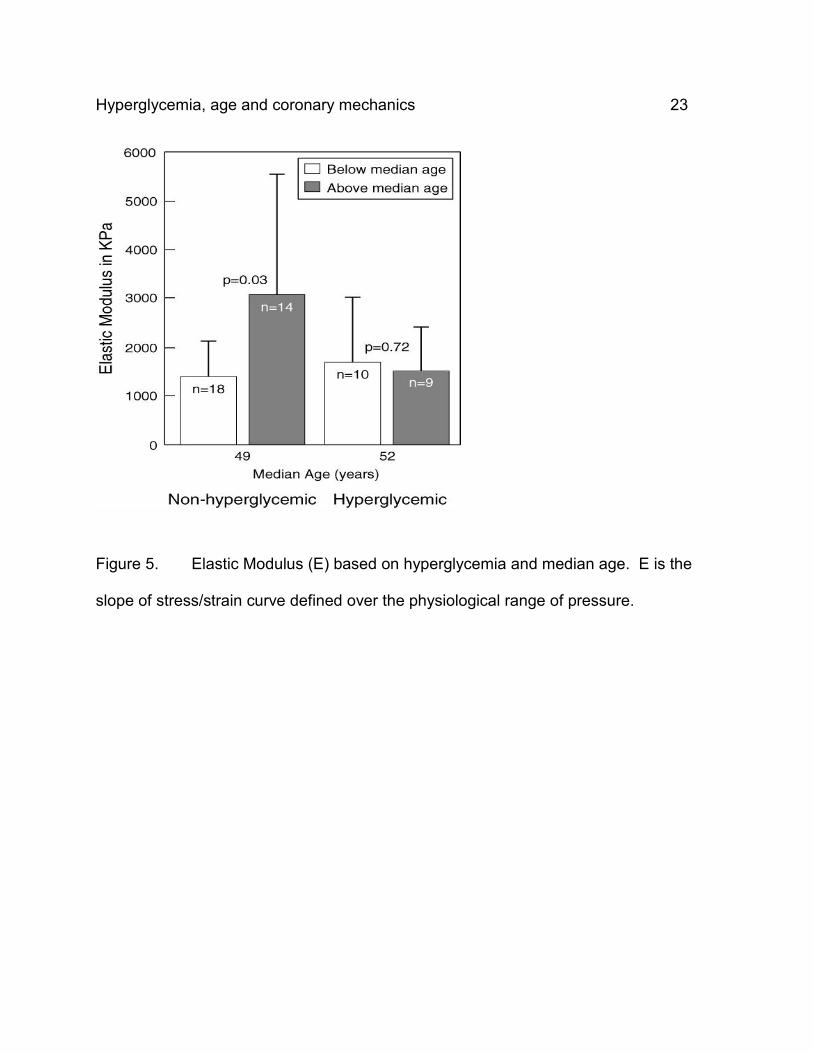
Similarly elastic modulus significantly increased with age only in the non-hyperglycemic
group (Figure 5).
Discussion
Both age and long-term glycemic state reflected by HbA1c (29) were found to
significantly influence the distensibility-pressure relationship of moderately diseased
regions of human LAD coronary arteries. A significant reduction in distensibility was
observed with age within the physiological pressure range for non-hyperglycemic
subjects. However the LAD of younger hyperglycemic subjects was as stiff as the older
non-hyperglycemic subjects, illustrating the impact of hyperglycemia on coronary
distensibility. In all biomechanical indices used, distensibility, stiffness index (β) and
elastic modulus (E), hyperglycemia masked the effect of aging clearly seen in non-
hyperglycemic group.
Fundamental biomechanical vascular changes with early metabolic dysfunction are
likely to impact the clinical complication rates in diabetic patients as suggested by these
results. Although the components of diabetic lesions do not differ greatly from those in
non-diabetic patients, (29) hyperglycemia could affect the inherent properties of
components in the vascular walls. Several molecular and cellular changes in diabetic
vessels occur in their basement membrane, (5) connective tissue matrix, (6) and
platelet function. (4) Impairment of endothelial function in NO production (31) as well as
decreased smooth muscle responsiveness influences the effective arterial capability for
vasodilation (4) and distension. (1, 23, 27) Long-term hyperglycemia leads to non-
Hyperglycemia, age and coronary mechanics 10
enzymatic glycation of proteins such as collagen fibers, and accumulation of the
byproducts, advanced glycation end products (AGEs), which may contribute to vascular
stiffness in both diabetes and aging. Recent studies have verified an increase in mean
arterial compliance of older diabetic patients after using a cross-link breaker to reduce
glycation. (14) As a result of such findings, vascular stiffness has been attracting more
attention in the study of diabetic CVD.
Due to the difficulty of testing small coronary vessels, most detailed vascular studies
have examined non-coronary/peripheral arteries as surrogates of the extent and impact
of disease in the coronary tree. Arterial compliance has been reported to change in
large arteries even prior to any evidence of complications from type I diabetes. (26)
Direct ex-vivo studies of aortic tissue in mechanical testing systems, (25) and various
non-coronary vessels in animals have shown a reduction of compliance with diabetes.
(19) Non-coronary, indirect methods, such as measuring carotid intima-media thickness
with Doppler ultrasound techniques, and pulse wave velocity methods have been used
to investigate vasculopathy in diabetic patients. Using these methods, loss of
compliance (up to 20%) of various non-coronary arteries is reported with both type I,
and II diabetes. (2, 10, 13, 18, 21, 26)Such techniques apply to large and relatively
superficial vessels with inherent limitations in studying smaller vessels, such as the
coronaries. Although all evidence point to the stiffening of vascular tissue with diabetes,
the data collected in a controlled manner from coronary arteries is scarce, underscoring
the need for a direct and accurate investigation as attempted in this study.
Hyperglycemia, age and coronary mechanics 11
The unique capability of IVUS in showing the arterial wall layers with a resolution of 125
µm axially and 250 µm laterally, (22) has been utilized in vascular elasticity testing with
few studies including diabetes vasculopathy. (1, 23, 27, 31-33) While showing the
feasibility of coronary distensibility studies in a clinical setting, selection criteria for both
subjects and lesions are varied in these studies as well as including a few diabetic
patients. (1, 23, 27, 31, 33) Coronary compliance has been shown to correlate
negatively with lesion area. Specifically the content, severity and distribution of a lesion
alter the local mechanical behavior of the artery. (3, 12) To remove the effect of lesion
distribution on the arterial wall, this study focused on the relatively homogenous
concentric sections with moderate plaque burden (<50% by area). Calcified regions
were specifically avoided to ensure a uniform distribution of material properties as
evidenced by histology.
Due to the nonlinear viscoelasticity of arteries, using isobaric settings is essential for
vascular studies, (1, 12, 21, 23, 31, 33) emphasizing the benefits of local intracoronary
pressure measurement. The aforementioned studies were based on the pulse pressure
measured in a vessel other than the one imaged. Pressure sensing guidewires used in
this study are small enough to allow measurement very close to the imaged site, with a
design easily allowing for future in-vivo studies in both animals and humans.
Employing the IVUS imaging capability in arteries with isobaric conditions measured at
the lesion site, the arterial distensibility was significantly reduced in uniform lesions from
excised coronary LADs by both aging and hyperglycemia. Similar to studies of larger,
Hyperglycemia, age and coronary mechanics 12
non-coronary arteries, the present data showed the extent of hyperglycemia to be a
significant independent factor in arterial distensibility. Within the physiological range of
coronary pressure, the influence of age was even more distinct than that of
hyperglycemia. Other indices of the arterial behavior, stiffness index (β) and elastic
modulus (E), calculated over the physiological range of pressure also showed that
hyperglycemia overshadowed the effect of age in stiffening of the arterial walls. Aging
has been associated with reduced large artery (2) and coronary compliance, (1, 27) as
well as linked to higher prevalence of both diabetes and CVD. Cross-linking of collagen
fibers, common in both aging and diabetes, may contribute to arterial stiffness and be
physically influenced by the extent of hyperglycemia, its duration, and treatment
approaches.
Beyond the biomechanical changes reported in this study, higher systolic pressure has
been reported in some diabetic patients (26) which would further compromise the
overall distensibility range of their vessels. Therefore, the combined effect of aging,
hyperglycemia and accompanying problems such as high blood pressure impact the
predisposition for CVD and treatment challenges and complications in diabetic patients.
Further combined biochemical and distensibility studies would elucidate the relationship
between local physiological factors such as coronary pressure, vascular wall
composition, and the state of the connective tissue fibers and matrix components in
arterial tissue layers, with the pathologic arterial mechanics in diabetic patients.
Limitations: The main limitation from a clinical standpoint is the lack of data from
Hyperglycemia, age and coronary mechanics 13
individual cases, which may affect the development and progression of CVD, (20)
including the duration, extent and treatment of diabetes.
From the experimental perspective, the maximum pressure obtained was variable
among the specimens, due to unpredictable remaining leakage from branches of the
post-mortem vessels. However, in this study, unlike previous ones, (16, 18, 21, 25-27,
33) local pressure was measured within millimeters of the target lesion for accurate
assessment of the true arterial pressure. The catheter was centrally placed within the
vessel and externally secured to avoid increased local pressure due to its contact with
the wall. Minor inaccuracy in plaque burden resulted due to the well-known IVUS
challenge in discerning the media-intima border in images. Therefore the reported
plaque area includes media, leading to a consistent overestimation of plaque burden
throughout the study.
Other studies have found diabetic patients to have smaller lumen CSA, larger plaque
CSA, and similar EEM CSA compared to non-diabetic patients. (17, 27) But due to the
focus on homogenous moderately diseased lesions, arterial sections in this study were
not selected based on the same anatomical reference point rather on size and
distribution. This led to the variation in mean CSA shown in Table 1, which is mostly
attributable to the site selection within the LAD. Therefore no conclusions can be drawn
regarding the arterial size and hyperglycemic status.
Hyperglycemia, age and coronary mechanics 14
Conclusions
With a systematic study, long-term hyperglycemia as indicated by HbA1c was found to
influence distensibility of moderately occluded (<50%) atherosclerotic coronary arteries.
This relationship persisted even when controlling for potential confounding factors such
as age and plaque burden. Within physiological pressures, distensibility decreased
significantly with age for non-hyperglycemic subjects. All measures of arterial stiffness
in this study indicated a significant change with age in non-hyperglycemic subjects only.
The results imply that the changes in coronary artery mechanics due to hyperglycemia
occur even prior to the processes associated with aging and with progression of
atherosclerosis in terms of increasing vascular wall thickness. These findings could
ultimately impact the use of interventional techniques and devices as applied to the
diabetic population through using clinically available diagnostic tools. Further detailed
biochemical and distensibility studies would improve our understanding of the changes
in behavior of lesions with various extent of atherosclerosis in hyperglycemic patients.
Acknowledgements
The authors are grateful to Barry Kuban, Jon Klingensmith, Anuja Nair, Misty Garcia,
and our students for their assistance with this project.
Grants
This study was supported by a grant from The Whitaker Foundation (97-0332, DGV-PI),
The National Institute of Health (RO1-HL64686, DGV-PI), and Guidant Corporation.
Disclosures
Hyperglycemia, age and coronary mechanics 15
The authors have no conflict of interest for disclosure.
References
1. Alfonso F, Macaya C, Goicolea J, Hernandez R, Segovia J, Zamorano J, Banuelos C, and Zarco P. Determinants of coronary compliance in patients with coronary artery disease: an intravascular ultrasound study. Journal of American College of Cardiology 23: 879-884, 1994. 2. Barenbrock M, Spieker C, S K, Vielnauer C, Hoeks AP, Zidek W, and Rahn KH. Different effects of hypertension, atherosclerosis and hyperlipidaemia on arterial distensibility. Journal of Hypertension 13: 1712-1717, 1995. 3. Beattie D, Xu C, Vito R, Glagov S, and Whang MC. Mechanical analysis of heterogeneous, atherosclerotic human aorta. Journal of Biomechanical Engineering 120: 602-607, 1998. 4. Creager MA and Luscher TF. Diabetes ad vascular disease pathophysiology, clinical consequences and medical therapy: part I. Circulation 108: 1527-1532, 2003. 5. Feener EP and L KG. Vascular dysfunction in diabetes mellitus. Lancet 350: 9-13, 1997. 6. Fukomoto H, Naito Z, Asano G, and Aramaki T. Immunohistochemical and morphometric evaluation of coronary atherosclerotic plaques associated with myocardial Infarction and diabetes mellitus. J Atheroscler Thromb 5: 29-35, 1998. 7. Grundy SM, Ivor JB, Burke GL, Chait A, Eckel RH, Howard BV, Mitch W, Smith SC, and Sowers JR. Diabetes and cardiovascular disease a statement for healthcare professionals from the American Heart Association. Circulation 100: 1134-1146, 1999. 8. Hammoud T, Tanguay JF, and Bourassa MG. Management of coronary artery disease: therapeutic options in patients with diabetes. Journal of American College of Cardiology 36: 355-365, 2000. 9. Hayashi K. Experimental approaches on measuring the mechanical properties and constitutive laws of arterial walls. J Biomech Eng 115: 481-488, 1993. 10. Hedblad B, Nilsson P, Janzen L, and Berglund G. Relation between insulin resistance and carotid intima-media thickness and stenosis in non-diabetic subjects. Diabetic Medicine 17: 299-307, 2000. 11. Hirai T, Sasayama S, Kawasaki T, and Yagi S. Stiffness of systemic arteries in patients with myocardial infarction. A noninvasive method to predict severity of coronary atherosclerosis. Circulation 80: 78-86, 1989. 12. Humphrey JD. Mechanics of the arterial wall: review and directions. Critical Reviews in Biomedical Engineering 23: 1-162., 1995. 13. Hunt KJ, Williams K, Rivera D, O’Leary DH, Haffner SM, Stern MP, and Villalpando CG. Elevated carotid artery intima-media thickness levels in individuals who subsequently develop type 2 diabetes. Arterioscler Thromb Vasc Bio 23: 1845-1850, 2003.
Hyperglycemia, age and coronary mechanics 16
14. Kass DA, Shapiro EP, Kawaguchi M, Capriotti A, Scuteri A, deGroof RC, and Lakatta E. Improved arterial compliance by a novel advanced glycation end-product crosslink breaker. Circulation 104: 1464-1470, 2001. 15. Klingensmith JD, Shekhar R, and Vince DG. Evaluation of three-dimensional segmentation algorithms for the identification of luminal and medial-adventitial borders in intravascular ultrasound images. IEEE Trans Med Imaging 19: 996-1011, 2000. 16. Kool MJ, Lambert J, Stehouwer CD, Hoeks AP, Struijker Boudier HA, and Van Bortel LM. Vessel wall properties of large arteries in uncomplicated IDDM. Diabetes care 18: 618-624, 1995. 17. Kornowski R, Mintz GS, Lansky AJ, Hong MK, Kent K, Pichard AD, Satler LF, Popma JJ, Bucher TA, and Leon MB. Paradoxic decrease in atherosclerotic plaque mass in insulin-treated diabetic patients. American J Cardiology 81: 1298-1304, 1998. 18. Lehman ED, Riley WA, Clarkson P, and Gosling RG. Non-invasive assessment of cardiovascular disease in diabetes mellitus. Lancet 350 ( suppl I): 14-19, 1997. 19. Liu SQ and Fung YC. Changes in the rheological properties of blood vessel tissue remodeling in the course of development of diabetes. Biorheology 29: 443-457, 1992. 20. Marso SP, Lincoff AM, Ellis SG, Bhatt DL, Tanguay JF, Kleiman NS, Hammoud T, Booth JE, Sapp SK, and Topol EJ. Optimizing the percutaneous interventional outcomes for patients with diabetes mellitus: results of the EPISTENT (Evaluation of Platelet IIb/IIIa Inhibitor for Stenting Trial) diabetic substudy. Circulation 100: 2477-2484, 1999. 21. Megnien JL, Simon A, Valensi P, Flaud P, Merli I, and Levenson J. Comparative effects of diabetes mellitus and hypertension on physical properties of human large arteries. Journal of American College of Cardiology 20: 1562-1568, 1992. 22. Mintz G, Nissen S, Anderson W, Bailey S, Erbel R, Fitzgerald P, Pinto F, Rosenfeld K, Siegel R, Tuzcu E, and Yock P. American College of Cardiology Clinical expert consensus document on standards for acquisition , measurement, reporting of intravascular ultrasound studies. Journal of American College of Cardiology 37: 1478-1492, 2001. 23. Nakatani S, Yamagishi M, Tamai J, Goto Y, Umeno T, Kawaguchi A, Yutani C, and Miyatake K. Assessment of coronary artery distensibility by intravascular ultrasound. Circulation 91: 2904-2910, 1995. 24. Olsson RA, Bunger R, and Spaan JA. Coronary circulation. In: The Heart and cardiovascular system scientific foundations (Second ed.), edited by Fozzard HA, Haber E, Jennings RB, Katz AM and Morgan HE. New York: Raven Press, 1992. 25. Oxlund H, Rasmussen LM, Andreassen T, and Heickendorff L. Increased aortic stiffness in patients with type I diabetes mellitus. Diabetologia 32: 748-752, 1989. 26. Romney JS and Lewanczuk RZ. Vascular compliance is reduced in the early stages of type I diabetes. Diabetes care 24: 2102-2106, 2001.
Hyperglycemia, age and coronary mechanics 17
27. Shaw JA, Kingwell BA, Walton AS, Cameron JD, Pillay P, Gatzka CD, and Dart AM. Determinants of coronary artery compliance in subjects with and without angiographic coronary artery disease. J Am Coll Cardiol 39: 1637-1643, 2002. 28. Silva JA, Escobar A, Collins TJ, Ramee SR, and White CJ. Unstable angina : A comparison of angioscopic findings between diabetic and nondiabetic patients. Circulation 92: 1731-1736, 1995. 29. Stout RW. Diabetes mellitus and atherosclerosis. Dordrecht, The Netherlands: Kluwer Academic Publishers, 1992. 30. Tajaddini A, Kilpatrick DL, and Vince DG. A novel experimental method to estimate stress-strain behavior of intact coronary arteries using intravascular ultrasound (IVUS). Journal of Biomechanical Engineering 125: 120-123, 2003. 31. Vauranakis M, Stefandis C, Triandaphyllidi E, Toutouzas K, and Toutouzas P. Coronary artery distensibility in diabetic patients with simultanous measurements of luminal area and intracoronary pressure. Journal of American College of Cardiology 34: 1075-1081, 1999. 32. Vonesh MA, Cho CH, Pinto JV, Kane BJ, Lee DS, Roth SI, Chandran KB, and McPherson DD. Regional vascular mechanical properties by 3-D intravascular ultrasound with finite element analysis. American Journal of Physiology 272: H425-H437, 1997. 33. Williams MJA, Stewart RAH, Low CJS, and Wilkins GT. Assessment of the mechanical properties of coronary arteries using intravascular ultrasound: an in vivo study. Int J Card Imaging 15: 287-294, 1999.
Legends
Figure 1. a) An intravascular ultrasound image of a LAD coronary artery with lumen
and external elastic membrane (EEM) borders traced. b) A histological slide of a LAD
section from a diabetic subject indicating both internal elastic membrane (IEM) and
EEM. The bar in each figure measures 1 mm.
Figure 2. Relationship between lumen cross sectional area and pressure based on
hyperglycemia and median age.
Figure 3. Coronary distensibility based on hyperglycemia and median age. The
distensibility was calculated within physiological pressures as changes in lumen CSA
Hyperglycemia, age and coronary mechanics 18
(∆CSA) normalized by the initial lumen CSA (CSAi), for each pressure interval (∆P) as:
D = ∆CSA / (CSAi . ∆P)
Figure 4. Stiffness index (β) based on hyperglycemia and median age, where β=(ln
(P2/P1)) / ((r2-r1)/r1)). Pressure (P) is defined within physiological range and r refers to
lumen radius at each pressure level.
Figure 5. Elastic Modulus (E) based on hyperglycemia and median age. E is the
slope of stress/strain curve defined over the physiological range of pressure.
List of Tables
Table 1. Number of subjects (n), and their demographics data expressed as mean
± standard deviation. The cross sectional area (CSA), and plaque burden (100 * lesion
CSA / EEM CSA) were calculated at intraluminal pressure of 100mmHg. Stiffness
index (β) was calculated within the physiological range of pressure. * Statistical
significance, p-value< 0.05, † See Limitations.
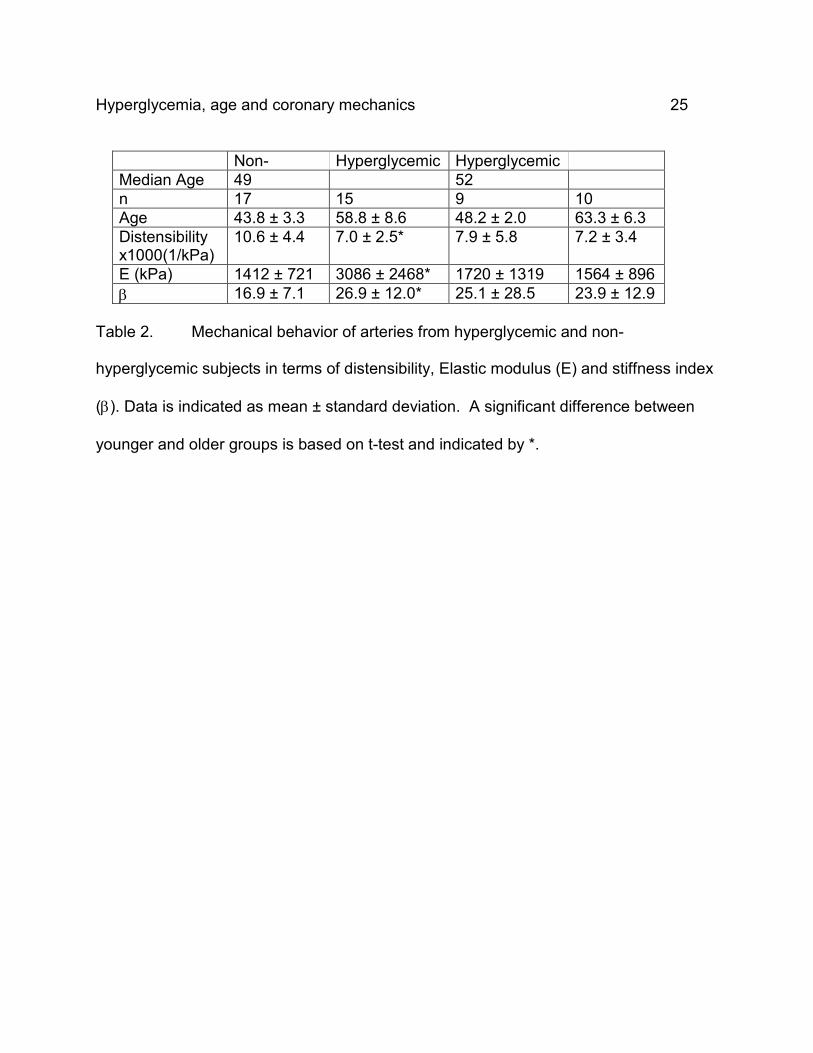
Table 2. Mechanical behavior of arteries from hyperglycemic and non-
hyperglycemic subjects in terms of distensibility, Elastic modulus (E) and stiffness index
(β). Data is indicated as mean ± standard deviation. A significant difference between
younger and older groups is based on t-test and indicated by *.

Hyperglycemia, age and coronary mechanics 19
Figure 1. a) An intravascular ultrasound image of a LAD coronary artery with lumen
and external elastic membrane (EEM) borders traced. b) A histological slide of a LAD
section from a diabetic subject indicating both internal elastic membrane (IEM) and
EEM. The bar in each figure measures 1 mm.
1mm
1mm
Hyperglycemia, age and coronary mechanics 20
Fig
hy
ure 2. Relationship between lumen cross sectional area and pressure based on
perglycemia and median age.
Hyperglycemia, age and coronary mechanics 21
Figure 3. Coronary distensibility based on hyperglycemia and median age. The
distensibility was calculated within physiological pressures as changes in lumen CSA
(∆CSA) normalized by the initial lumen CSA (CSAi), for each pressure interval (∆P) as:
D = ∆CSA / (CSAi . ∆P)
Hyperglycemia, age and coronary mechanics 22
F
(
l
igure 4. Stiffness index (β) based on hyperglycemia and median age, where β=(ln
P2/P1)) / ((r2-r1)/r1)). Pressure (P) is defined within physiological range and r refers to
umen radius at each pressure level.
Hyperglycemia, age and coronary mechanics 23
Figure 5. Elastic Modulus (E) based on hyperglycemia and median age. E is the
slope of stress/strain curve defined over the physiological range of pressure.
Hyperglycemia, age and coronary mechanics 24
Variables Hyperglycemic Non-hyperglycemic
p
n 19
32
NA
Male/Female
12/7
27/5
0.08
HbA1c (%)
7.33 ± 2.1
5.29 ± 0.3
<0.01*
Age (years)
56.2 ± 9.0
50.8 ± 9.8
0.06
Lumen CSA (mm2) 8.7 ± 3.3
8.1 ± 3.4
NA†
Plaque CSA (mm2) 3.9 ± 1.9
3.9 ± 1.8
0.93
Plaque burden (%)
30.1 ± 6.0
31.9 ± 7.3
0.38
β, Stiffness index
52.6 ± 88.0
21.6 ± 10.8
0.14
β, Stiffness index without outliers
24.4 ± 20.3 n=16
21.6 ± 10.8 n=32
0.60
Table 1. Number of subjects (n), and their demographics data expressed as mean
± standard deviation. The cross sectional area (CSA), and plaque burden (100 * lesion
CSA / EEM CSA) were calculated at intraluminal pressure of 100mmHg. Stiffness
index (β) was calculated within the physiological range of pressure. * Statistical
significance, p-value< 0.05, † See Limitations.
Hyperglycemia, age and coronary mechanics 25
Non- Hyperglycemic HyperglycemicMedian Age 49 52 n 17 15 9 10 Age 43.8 ± 3.3 58.8 ± 8.6 48.2 ± 2.0 63.3 ± 6.3 Distensibility x1000(1/kPa)
10.6 ± 4.4
7.0 ± 2.5* 7.9 ± 5.8 7.2 ± 3.4
E (kPa) 1412 ± 721 3086 ± 2468* 1720 ± 1319 1564 ± 896 β 16.9 ± 7.1 26.9 ± 12.0* 25.1 ± 28.5 23.9 ± 12.9
Table 2. Mechanical behavior of arteries from hyperglycemic and non-
hyperglycemic subjects in terms of distensibility, Elastic modulus (E) and stiffness index
(β). Data is indicated as mean ± standard deviation. A significant difference between
younger and older groups is based on t-test and indicated by *.
Copyright © 2022 FDOKUMEN




















