
Immunological Analysis in Paediatric HIV Patients at Different Stages of the Disease
10
Immunological Analysis in Paediatric HIV Patients at Different Stages of the Disease Y. C. Lian*, M. Della-Negra*, R. Rutzy, V. Ferrianiz, D. de Moraes Vasconcelos§, A. J. da Silva Duarte§, M. Kirschfinky & A. S. Grumach§ Abstract There are only few clinical studies on complement in well-defined (or characterized) paediatric HIV patients. Aim of this study was to evaluate the complement system and immunoglobulins in HIV-infected children and to correlate data to stage of disease. Blood samples of 127 HIV-infected children (11–134 months; 62 male : 65 female) were collected in order to evaluate humoral immunity. The patients were classified according to CDC clinical (N-asymptomatic; A-mild symptoms such as common recurrent infections; B-moderate symptoms such as Candidiasis and herpes infections, meningitis, sepsis and anaemia; C-severe symptoms such as opportunistic infections and neoplasia) and with respect to immunological criteria (T CD4 þ cell count). Analysis of complement system included the classical (CH50), alternative (APH50) pathway activities and plasma concentrations of mannan-binding lectin (MBL), of the C4 allotypic variants C4A and C4B. (ELISA), and of the C3 split product C3d (rocket immunoeletrophoresis). Immunodiagnosis also included CD4 þ and CD8 þ lymphocyte count and immunoglobulin concentrations. Complement activation and consumption was observed in all patients correlating with disease activity. Activated classical and alternative pathways and elevated C3d were signifi- cantly correlated with immunologic category 3. C3d levels were also significantly correlated with immunologic category 1. Undetectable CH50 and APH50 were found in two (group C) and 10 patients (n ¼ 2, A ¼ 2, B ¼ 2, C ¼ 4), respectively. Low MBL values were found in 13/127 but without correlation to disease severity. Undetectable C4B levels were observed in three patients, favouring the diagnosis of a complete deficiency. Although not related to clinical symptomatology, a strong ongoing complement activation can be observed in all stages of HIV infection. In contrast to earlier reports MBL could not be considered as a risk factor for HIV. Introduction Clinical manifestations in paediatric HIV patients differ from those observed in adults [1]. Alterations in cellular immunity are related to clinical symptomatology in adults, favouring opportunistic infections as well as Karposi’s sarcoma [2]. In HIV-infected children, respiratory and gastrointestinal infections often caused by capsulated bac- teria support the notion of an impaired humoral immune response [3]. Complement is activated by HIV particles through both the classical and the alternative pathways [4]. Glycopro- teins of the viral surface bind C1q in an antibody- independent manner. Marschang et al [5] found the gp41 sequence aa 601–620 to be the main binding site for C1q and considered this as the principal domain responsible for complement activation by HIV. These authors also sug- gested that the expression of this epitope on infected cell surface might influence the intensity of complement acti- vation with a possible impact on HIV pathogenesis [5]. Furthermore, binding of mannan-binding lectin (MBL) to the viral surface leads to activation of the lectin pathway and viral lysis may occur [6]. In vitro, binding of gp120 of the viral envelope to the CD4 molecules is prevented by MBL. This neutralizing effect can be related to comple- ment activation and to viral lysis [7]. The C4 variant C4B expresses a four times higher haemolytic activity than C4A, and its deficiency has been associated to the susceptibility to infections caused by capsulated bacteria [8], and C4 null genes have been associated with HIV disease progression [9, 10]. .................................................................................................................................................................................................. # 2004 Blackwell Publishing Ltd. Scandinavian Journal of Immunology 60, 615–624 615 *Institute of Infectology Emı ´lio Ribas, Sa ˜o Paulo; yInstitute of Immunology, University of Heidelberg, Germany; zDepartment of Pediatrics, University of Sa ˜o Paulo, Ribeira ˜o Preto; and §Laboratory of Medical Investigation (LIM56) in Allergy and Immunology, Medical School, University of Sa ˜o Paulo, Sa ˜o Paulo, Brazil Received 15 December 2003; Accepted in revised form 17 June 2004 Correspondence to: Dr A. S. Grumach, Laboratory of Medical Investigation (LIM56) in Allergy and Clinical Immunology, Medical School, University of Sa ˜o Paulo, Dr. Ene ´as de Carvalho Aguiar Avenue, 500 Building II, 3rd floor, Sa ˜o Paulo, CEP: 01246.903, Brazil. E-mail: [email protected]
Transcript of Immunological Analysis in Paediatric HIV Patients at Different Stages of the Disease

Immunological Analysis in Paediatric HIV Patients atDifferent Stages of the Disease
Y. C. Lian*, M. Della-Negra*, R. Rutzy, V. Ferrianiz, D. de Moraes Vasconcelos§, A. J. da Silva Duarte§,M. Kirschfinky & A. S. Grumach§
Abstract
There are only few clinical studies on complement in well-defined (or characterized)paediatric HIV patients. Aim of this study was to evaluate the complement systemand immunoglobulins in HIV-infected children and to correlate data to stage ofdisease. Blood samples of 127 HIV-infected children (11–134 months; 62 male : 65female) were collected in order to evaluate humoral immunity. The patients wereclassified according to CDC clinical (N-asymptomatic; A-mild symptoms such ascommon recurrent infections; B-moderate symptoms such as Candidiasis and herpesinfections, meningitis, sepsis and anaemia; C-severe symptoms such as opportunisticinfections and neoplasia) and with respect to immunological criteria (T CD4þ cellcount). Analysis of complement system included the classical (CH50), alternative(APH50) pathway activities and plasma concentrations of mannan-binding lectin(MBL), of the C4 allotypic variants C4A and C4B. (ELISA), and of the C3 splitproduct C3d (rocket immunoeletrophoresis). Immunodiagnosis also included CD4þ
and CD8þ lymphocyte count and immunoglobulin concentrations. Complementactivation and consumption was observed in all patients correlating with diseaseactivity. Activated classical and alternative pathways and elevated C3d were signifi-cantly correlated with immunologic category 3. C3d levels were also significantlycorrelated with immunologic category 1. Undetectable CH50 and APH50 werefound in two (group C) and 10 patients (n¼ 2, A¼ 2, B¼ 2, C¼ 4), respectively.Low MBL values were found in 13/127 but without correlation to disease severity.Undetectable C4B levels were observed in three patients, favouring the diagnosis of acomplete deficiency. Although not related to clinical symptomatology, a strongongoing complement activation can be observed in all stages of HIV infection. Incontrast to earlier reports MBL could not be considered as a risk factor for HIV.
Introduction
Clinical manifestations in paediatric HIV patients differfrom those observed in adults [1]. Alterations in cellularimmunity are related to clinical symptomatology in adults,favouring opportunistic infections as well as Karposi’ssarcoma [2]. In HIV-infected children, respiratory andgastrointestinal infections often caused by capsulated bac-teria support the notion of an impaired humoral immuneresponse [3].
Complement is activated by HIV particles through boththe classical and the alternative pathways [4]. Glycopro-teins of the viral surface bind C1q in an antibody-independent manner. Marschang et al [5] found the gp41sequence aa 601–620 to be the main binding site for C1qand considered this as the principal domain responsible for
complement activation by HIV. These authors also sug-gested that the expression of this epitope on infected cellsurface might influence the intensity of complement acti-vation with a possible impact on HIV pathogenesis [5].
Furthermore, binding of mannan-binding lectin (MBL)to the viral surface leads to activation of the lectin pathwayand viral lysis may occur [6]. In vitro, binding of gp120 ofthe viral envelope to the CD4 molecules is prevented byMBL. This neutralizing effect can be related to comple-ment activation and to viral lysis [7].
The C4 variant C4B expresses a four times higherhaemolytic activity than C4A, and its deficiency has beenassociated to the susceptibility to infections caused bycapsulated bacteria [8], and C4 null genes have beenassociated with HIV disease progression [9, 10].
..................................................................................................................................................................................................
# 2004 Blackwell Publishing Ltd. Scandinavian Journal of Immunology 60, 615–624 615
*Institute of Infectology Emılio Ribas, Sao Paulo;
yInstitute of Immunology, University of
Heidelberg, Germany; zDepartment of Pediatrics,
University of Sao Paulo, Ribeirao Preto; and
§Laboratory of Medical Investigation (LIM56) in
Allergy and Immunology, Medical School,
University of Sao Paulo, Sao Paulo, Brazil
Received 15 December 2003; Accepted in revisedform 17 June 2004
Correspondence to: Dr A. S. Grumach, Laboratory
of Medical Investigation (LIM56) in Allergy and
Clinical Immunology, Medical School, University
of Sao Paulo, Dr. Eneas de Carvalho Aguiar
Avenue, 500 Building II, 3rd floor, Sao Paulo,
CEP: 01246.903, Brazil. E-mail: [email protected]

Although complement activation favours a more intenseinflammatory response to HIV infection, effective immuneresponse by its opsonization capacity, could also contributeto HIV dissemination [11]. The lack of studies with HIV-infected children according to the clinical and immunolo-gical stages of the disease prompted us to analyze in moredetail, parameters of the humoural immune response suchas immunoglobulin levels (lgG, IgM and IgA), proteinlevels and function of the complement for a possiblecorrelation to clinical manifestations.
Patients and methods
One hundred and twenty-seven HIVþ children (62males : 65 females) from the second Inpatient Unit ofHospital Emilio Ribas, Sao Paulo, Brazil, with a meanage of 59.2 months (11–134 months) were included.The study protocol was developed with the permission ofthe children and/or their responsibles and was approved bythe local Ethics Committee.
All children included were vertically infected and HIVdiagnosis and classification was done according to CDC(Atlanta, GA, USA) criteria [12]. Children less than 18months old were diagnosed as HIV infected after, at least,two positive blood tests (viral culture, PCR or Antigenp24) or clinical manifestations of AIDS. Children olderthan 18 months were included if they were positive foranti-HIV enzyme-linked immunosorbent assay (ELISA),confirmed by Western blot or immunofluorescence assays.Clinical and immunological (CD4þ T cells) data contrib-uted to the classification, and the patients were grouped inclinical and immunological categories according to 1994REVISED, MMWR (Tables 1, 2 and 3) [12].
Blood samples were collected just before immunoglo-bulin infusion and serum/plasma were stored at �70 �Cfor further analysis. EDTA-blood was immediatelyanalyzed for CD4/CD8þ T-cell subpopulations by flowcytometry. CD8þ T-cell numbers were referred to valuesobtained by Erkeller-Yuksel et al [13].
Immunoglobulin concentrations were measured bynephelometer and referred to a normal range as previouslyestablished by Fujimura for Brazilian children [14].Haemolytic activity of the classical pathway (CH50) wasassessed according to Mayer [15]. Alternative pathwayactivity (APH50) was determined by a kinetic methodusing rabbit red blood cells [16]. Both haemolytic assays
were applied in a Brazilian population for normal range[17]. The C3 fragment C3d/C3dg was determined bydouble-decker rocket immunoeletrophoresis according toBrandslund et al. [17] using anti-C3c (Behring, Marburg,Germany) and anti-C3d (Fresenius, Oberursel, Germany)in the gel.
MBL concentrations were quantified by ELISA. Inbrief: Microtitre plates were coated with monoclonalmouse antihuman MBL IgG (1 mg/ml) (DPC Biermann,Bad Nauheim, Germany) overnight at 4 �C. Samples inserial dilutions were added. MBL was detected by biotini-lated mouse antihuman MBL IgG (DPC Biermann, BadNauheim, Germany), followed by streptavidin peroxidaseand substrate (OPD, Dako, Hamburg, Germany). Stand-ards were kindly provided by Dr Jens C. Jensenius(Aarhus, Denmark) and 0.3–7.5 mg/ml were consideredas normal range [18].
Quantification of C4A and C4B allotypic variants wasperformed by ELISA using isotype-specific monoclonalantibodies (Biotest, Dreieich, Germany). In brief, micro-titre plates were coated with polyclonal rabbit anti-C4 IgG(Dako) overnight at 4 �C. After blocking with PBS, 1%BSA, the samples were adjusted to 1 mg C4/ml and addedin serial dilutions. C4 variants were detected by specificmonoclonal anti-C4A and anti-C4B IgG, followed byperoxidase-conjugated F(ab0)2 goat anti-mouse IgG. Seraof individuals tested for homozygous deficiency at eitherthe C4A (C4AQ0, Q0) or C4B (C4BQ0, Q0) locus(kindly provided by Dr V. Lenhard, Biotest, Dreieich,Germany) were used as standards. Data were referred tovalues obtained from healthy volunteers (n¼ 30), pretested for normal C4 concentrations by functional andimmunochemical methods. Normal values are in agree-ment with those evaluated by a comparable ELISA [19].
Statistical evaluation was done by variance analysis(ANOVA test) to compare mean values obtained for T-cellsubsets, IgG, IgM, IgA, CH50, APH50, MBL, C4A, C4Band C3d. In order to reduce variability, results of MBL,C4A, C4B, C3d and CD8þ cells were converted to loga-rithmic data. PEARSON was applied for data correlation.It was considered to be significant for P< 0.05.
Results
There was no statistical difference in the distribution ofage and gender among the patients. Respiratory infections
Table 1 Classification of HIVþ children according to clinical symptomatology (1994 REVISED, MMWR, 1994)
N No symptoms or one condition of category A
A Mild symptoms: lymphadenopathy, hepatomegaly, splenomegaly, dermatitis, parotitis and recurrent upper airway infections
B Moderate symptoms (not included in category A and C)
C Severe symptoms: severe, recurrent or multiple bacterial infections, sepsis, pneumonia, meningitis, oesophageal
or pulmonary candidiasis, disseminated coccidioidomycosis, extra-pulmonary cryptococcosis, cytomegalovirosis,
encephalopathy, mycobacteriosis, criptosporidiasis and neoplasia as brain lymphoma or Kaposi’s sarcoma, wasting syndrome
616 Immunological Evaluation in HIVþ Children Y. C. Lian et al...................................................................................................................................................................................................
# 2004 Blackwell Publishing Ltd. Scandinavian Journal of Immunology 60, 615–624

included: bronchopneumonia (57/111; 51.4%); otitis (43/111; 38.7%); tuberculosis (40/111; 36%) and pneumocys-tosis (12/111; 10.8%). Lymphoid interstitial pneumoniawas confirmed in 19 (17.1%) of the symptomatic patients.Diarrhoea was verified in 26 (23.4%) of the children.Additional clinical symptoms included: thrombocytopae-nia in six children (5.4%), myocardiopathy in eight(7.2%), neurological disorders in 10 (9%), anaemia in11 (9.9%) and chronic hypertrophy of parotids in 19(17.1%) of the symptomatic patients. The main infectiousmanifestations are shown on Fig. 1. There was no statisti-cal correlation between each of the clinical symptoms andCD4þ cell count except for myocardiopathy, more fre-quently diagnosed in 6/8 affected patients in immunologiccategory 3 (6/127). There was no difference in T CD8þ
cell numbers among patients of the various clinical andimmunological categories.
IgG concentrations were increased in almost all patientsof both clinical (88/94; 93.6%) and immunological (88/94; 93.6%) categories. A female patient, 41 months old,presented very low IgG levels (217 mg/dl) and shebelonged to B2 category with lymphoid interstitial pneu-monia as clinical manifestation (Table 3). IgM levels wereelevated in 24/93 (25.8%) in both categories and IgAconcentrations were increased in 40/93 (43%) and 39/93(41.9%) of clinical and immunological categories, respect-ively (Fig. 2).
Classical pathway activation was not correlated withclinical categories (P¼ 0.4) and immunological categories1 (P¼ 0.89) and 2 (P¼ 0.42). Low CD4þ cell countscorrelated with low CH50 and APH50 values in patientsof category 3 (P¼ 0.03). Two patients (group C andimmunologic category 1) presented with undetectable clas-sical pathway function (CH50) (Fig. 3) but two patients ofeach of the groups N, A and B, as well as four patients ingroup C (different from those with undetectable CH50)had undetectable alternative pathway function (APH50).
With respect to immunological classification, three ofthose patients were included in group 1, five in group 2and two in group 3 (Fig. 3) (Table 4). Elevated C3dplasma levels were observed in 59 HIV-infected children,23 patients in group C (39%), 17 in group B (28.8%), 13in group A (22%) and six in group N (10.2%); 18 ingroup 1, 20 in group 2 and 21 in group 3, but withoutstatistical difference between the groups (Fig. 4). CD4þ T-cell numbers significantly correlated with C3d levels ingroups 1 (P¼ 0.035) and 3 (P¼ 0.03).
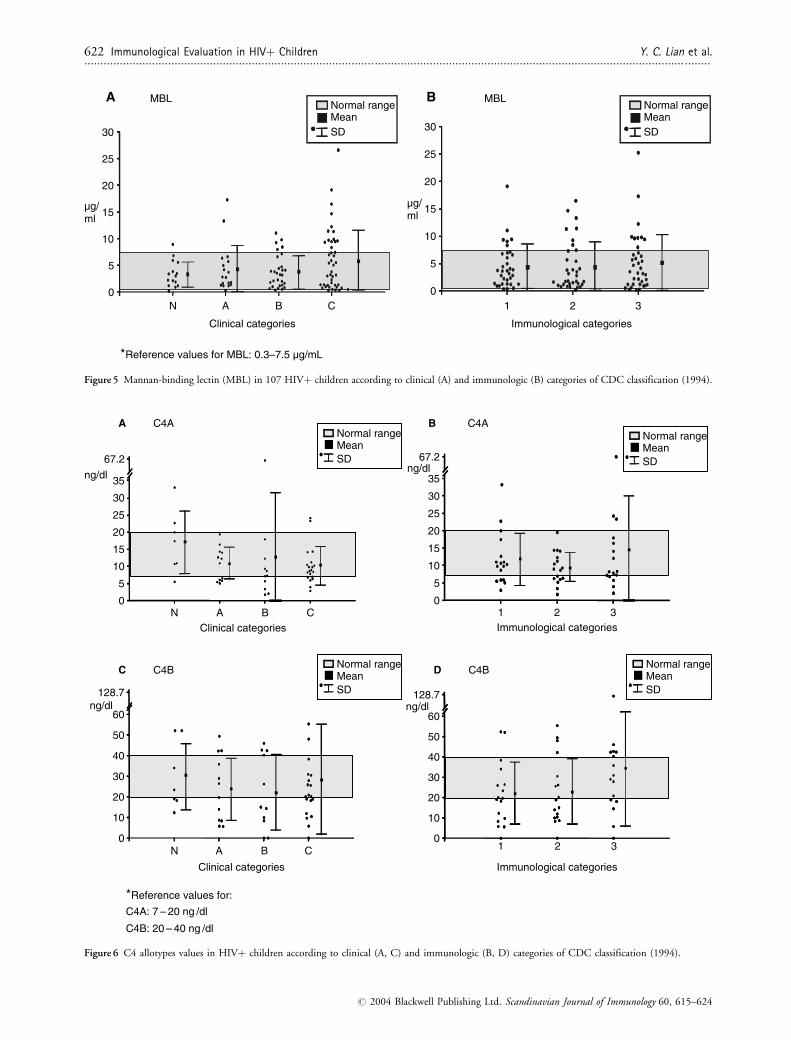
MBL plasma concentrations were increased (higher than7500 ng/ml) in more severe clinical stages of the disease:n¼ 1/15 (6.6%); A¼ 2/17 (11.8%); B¼ 5/29 (17.2%)and C¼ 14/43 (32.5%) but without statistical significance(P¼ 0.57) (Fig. 5). Low MBL levels were detected in 1/15(6.6%) patients from group N; 1/17 (5.8%) from A; 5/29from B (17.2%) and 7/43 from C (16.3%) without statis-tical significance (P¼ 0.75). Two patients had very lowMBL levels (0.21 and 0.28 ng/ml) belonging to group N2and A1, respectively. Low normal concentrations (>0.3and <0.80 ng/ml) were found in 13 patients: six in cat-egory B and thirteen in category C.
No difference in C4A (P¼ 0.44; P¼ 0.29) or C4B(P¼ 0.83; P¼ 0.20) concentrations were found betweenthe clinical and immunological groups (Fig. 6). However,undetectable C4B levels were observed in three patients,two of group B and one of group C corresponding to onepatient of each immunological group. C4B levels wereincreased in group 3 compared to other groups(P¼ 0.04) (Fig. 6). Patients with the most relevant resultswere included in Table 4.
Discussion
Although in the past years intensive research has led to aconsiderable progress in our understanding of the disease,HIV infection still represents one of the most important
Table 2 Classification of HIVþ children according to immunologic impairment (1994 REVISED, MMWR, 1994)
Immunologic Category <12 months cells/mm3 1–5 years cells/mm3 6–12 years cells/mm3
1 �1500 (�25%) �1000 (� 25%) �500 (�25%)
2 750–1499 (15–24%) 500–999 (15–24%) 200–499 (15–24%)
3 <750 (<15%) <500 (<15%) <200 (<15%)
Table 3 HIVþ children classified according to clinical and immunological groups (n¼ 127)
Clinical Immunological
Category: n (%) N A B C 1 2 3
Male 6 (37.5) 9 (42.9) 15 (41.7) 32 (59.3) 21 (51.2) 23 (52.3) 18 (42.9)
Female>/> 10 (62.5)>/> 12 (57.1) 21 (58.3) 22 (40.7) 20 (48.8) 21 (47.7) 24 (57.1)
Total 16 21 36 54 41 44 42
Y. C. Lian et al. Immunological Evaluation in HIVþ Children 617..................................................................................................................................................................................................
# 2004 Blackwell Publishing Ltd. Scandinavian Journal of Immunology 60, 615–624

health problems in the world. In Brazil, Zidovudine isavailable for all diagnosed patients, nevertheless, the num-ber of pregnant HIVþ women using this drug for preven-tion of vertical transmission is less than expected [20].
Considering the characteristics of HIV infection inpaediatric patients and the restricted knowledge aboutsome aspects of the disease and its progression in thisgroup, we evaluated humoral immunity parametersaccording to disease progression. The children presentedbetween 11 and 134 months of age, and 69/127 were lessthan 5 years old (54.3%), and 30 patients were sympto-matic with severe disease at that time (clinical category C).Latency period for the symptomatology in children isshorter than in adults. Rosenberg and Fauci [21] observedthat the mean time clinical manifestations of verticallyinfected children is 5–10 months and about 80% of thechildren develop immunologic alterations before 2 years ofage.
Several hypotheses are considered to explain the differ-ent evolutions of the disease. The period of HIV infection(pregnancy, intrapartum and neonatal), the viral pheno-type and the immunologic response to HIV have beencorrelated with the prognosis [22]. Few reports evaluatecomplement system in paediatric HIV patients and itsfunction according to clinical and immunologic HIV cate-gories. In addition, it is still unknown if complement isimportant for a successful immune response against thevirus or if it rather facilitates viral infection.
Common infections of childhood are the most frequentclinical manifestations in paediatric patients, such asbronchopneumonia, otitis and diarrhoea as observed inour population (23.2%). Almost 45% of our HIV patientspresented bronchopneumonia, 35% medium, 20% diar-rhoea. Tuberculosis, candidiasis, cryptococcosis and pneu-mocystosis are the most common infections presented inadults with HIV as the first symptoms in untreated
patients. Opportunistic infections also occur in childrenbut they are diagnosed during the follow up withouttreatment. Tuberculosis was diagnosed in 31.5% of thewhole patient population but there was no correlation withT CD4þ cell numbers as previously reported for childrenby others [23]. Atypical mycobacteriosis usually affectsseverely immunosuppressed individuals with CD4þ cellcounts below 100 cells/mm3 as it was seen in four of ourpatients. Lewis et al. [24] observed atypical mycobacteriosisin 11% of HIVþ children, although 24% of the patientshad CD4þ T-cell numbers below 100 cells/mm3.
Pulmonary infections as pneumocystosis and lymphocy-tic interstitial pneumonitis (LIP) were observed in 12(9.4%) and 19 (15%) of our patients, respectively. Thenumber of affected patients has been reported to increasewith HIV progression [25], but in contrast to earlierreports, no correlation with CD4þ cell count was foundin our children [26]. Myocardiopathy was found in eightpatients (6.3%), and low CD4þ cells (group 3) werecorrelated with this clinical manifestation.
Clinical manifestations and progression of the diseaseare not only restricted to HIVþ children with low CD4þ
numbers as previously reported [27, 28]. Pneumocystosisalso occurs in children with lymphocytes above 1000 cells/mm3 and some patients even survive long despite low TCD4þ cell counts. It is known that CD4þ T-cell functionis affected earlier than their number, and some infectionsoccur even despite high CD4þ cell count [27, 28].
Hypergammaglobulinaemia was detected in most of ourpatients irrespective of their clinical and immunologic clas-sification but IgG levels did not correlate with CD4þ T cellsas described by others [29, 30]. Hypergammaglobulinaemiais considered a consequence of hyperactivation of B cellsinduced by HIV. Chronic B-cell stimulation may result inimpaired antibody production to new antigens [30]. Onepatient presented with hypogammaglobulinaemia, which is
44.9% (n = 57)
33.9% (n=43)
31.5% (n = 40)
20.5% (n = 26)
9.4% (n = 12)
7.9% (n = 10)
6.3% (n = 8)
3.1% (n = 4)
2.4% (n = 3)
1.6% (n = 2)
1.6% (n = 2)
0.8% (n = 1)
0.8% (n = 1)
10 20 30 40 50
BronchopneumoniaOtitis
TuberculosisDiarrhoea
PneumocystosisPyodermitis
Herpes zosterAtypical mycobact
Bacterial meningitisCutaneous mycosis
MolluscusCNS tuberculosis
Toxoplasmosis
patients (%)
*Relative frequency of infections (per number of patients) among all patients (n = 127)Figure 1 Recurrent infections observed in
127 HIVþ children.
618 Immunological Evaluation in HIVþ Children Y. C. Lian et al...................................................................................................................................................................................................
# 2004 Blackwell Publishing Ltd. Scandinavian Journal of Immunology 60, 615–624

uncommon. Low IgG concentrations had been reported inpaediatric HIV children dealing to difficult serological HIVdiagnosis [31].
IgM levels were within normal range in about 70% ofour patients, but increased with disease progress, probablyrelated to more frequent infections. Four patients had lowIgM levels (4.3%), distributed in the four clinical cat-egories. Patients of category 3 had higher IgM levels(36.4%) than those of category 1 (20.7%). Elevated IgA
levels were observed in about 43%. Patients with high IgAand CD8þ cells in the initial phase of HIV infection werereported to present a faster decrease in CD4þ cells. Thiswas interpreted to reflect an elevated viral load [32].Shearer et al. [33] observed after a 5 years follow up ofpatients that high IgG levels and low IgA concentrationsare implicated with survival to HIV infection.
Following the interaction of C1q with gp41 activationof the classical complement pathway occurs already during
ABC
N
normal range
4000
5000
6000
7000
9–11 m
9–23 m 2–3 y 4–17 y
12–36 m 4–6 y 7–9 y 10–12 y
age
9–14 m 15–23 m 4–6 y2–3 y 7–9 y 10–12 y
age
9–14 m 15–23 m 4–6 y2–3 y 7–9 y 10–12 y
age
age
9–23 m 2–3 y 4–17 y
age
9–11 m 12–36 m 4–6 y 7–9 y 10–12 y
age
IgG
IgM
mg/
dlm
g/dl
mg/
dl
ABC
N
normal range
ABC
N
normal range
3
1
normal range
2
3
1
normal range
2
3
1
normal range
2
0
1000
2000
3000
300
400
500
600
0
100
200
300
400
500
600
800
700
0
100
200
300
400
500
600
800
700
0
100
200
300
400
500
600
0
100
200
4000
5000
6000
7000
mg/
dlm
g/dl
mg/
dl
0
1000
2000
3000
A IgGB
C IgMD
IgAE IgAF
* Normal range of immunoglobulin isotypes for a pediatric Brazilian population (according to Fujimuraet al., 1990).
Figure 2 IgG, IgM and IgA levels according to clinical and immunologic classification (2A, B, C, D, E, F).
Y. C. Lian et al. Immunological Evaluation in HIVþ Children 619..................................................................................................................................................................................................
# 2004 Blackwell Publishing Ltd. Scandinavian Journal of Immunology 60, 615–624

the acute phase of infection, resulting in deposition of C3fragments on the viral surface [7, 34] but only in partialvirolysis [7]. An intrinsic resistance of the virus againsthuman complement is due to the host cell-derived mem-brane-anchored complement regulators (CD55/DAF,CD46/MCP and CD59/protectin) during the buddingprocess [34]. Capturing of factor H further contributes toprotection of HIV against complement-mediated lysis [35].
Although various studies in vitro indicate an activationof complement system in HIV infection, systematic studiesin patients are still restricted and controversial. Perriconeet al. [36] observed a reduced total complement functionand low levels of C4 and C7 . They proposed an acquiredcomplement deficiency to affect the defense against HIVinfection [37]. To our knowledge, there are no previousreports investigating complement in paediatric HIV
patients of defined clinical and immunological stages ofthe disease.
Low function and increased C3d in 59/97 patients(60.8%) reflect an ongoing complement activation in ourpatients, however, without significant difference withrespect to disease progress as this had been initiallyreported by Jarvis et al. in 37 children [37], but couldnot be confirmed in later studies [38, 39]. Reduced class-ical and alternative pathway function rather correlatedwith immunological impairment as indicated by low TCD4þ cells (category 3), and C3d was markedly increasedin immunologic groups 1 and 3. These findings may pointto a more intense activation of complement with progres-sion of the disease, probably interfering with the patho-genesis of HIV infection. This finding corresponds tothose obtained in adults by Senaldi et al. [40].
020406080
100120140160180200
N B CClinical categories
%
020406080
100120140160180200
1 2Immunological categories
%
0
10
20
30
40
50
60
70
N A C
Clinical categories
0
10
20
30
40
50
60
70
1 3
Immunological categories
A
C
CH50
APH50
CH50
D
BNormal rangeMeanSD
Normal rangeMeanSD
Normal rangeMeanSD
Normal rangeMeanSD
*Reference values for:
CH50 = 80 – 120 %
APH50 = 32 – 56 U / l
A 3
B 2
APH50
Figure 3 CH50 and APH50 values in 108 HIVþ children according to clinical (3A) and immunologic (3B) categories of CDC classification (1994).
620 Immunological Evaluation in HIVþ Children Y. C. Lian et al...................................................................................................................................................................................................
# 2004 Blackwell Publishing Ltd. Scandinavian Journal of Immunology 60, 615–624
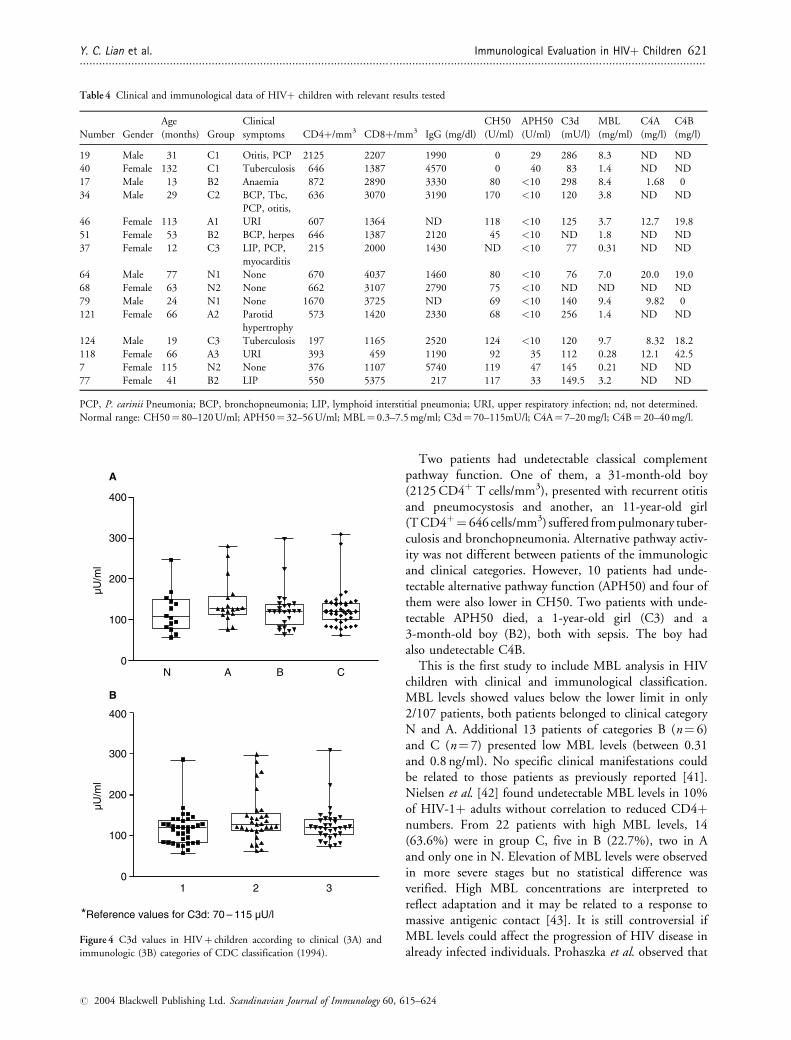
Two patients had undetectable classical complementpathway function. One of them, a 31-month-old boy(2125 CD4þ T cells/mm3), presented with recurrent otitisand pneumocystosis and another, an 11-year-old girl(T CD4þ¼ 646 cells/mm3) suffered from pulmonary tuber-culosis and bronchopneumonia. Alternative pathway activ-ity was not different between patients of the immunologicand clinical categories. However, 10 patients had unde-tectable alternative pathway function (APH50) and four ofthem were also lower in CH50. Two patients with unde-tectable APH50 died, a 1-year-old girl (C3) and a3-month-old boy (B2), both with sepsis. The boy hadalso undetectable C4B.
This is the first study to include MBL analysis in HIVchildren with clinical and immunological classification.MBL levels showed values below the lower limit in only2/107 patients, both patients belonged to clinical categoryN and A. Additional 13 patients of categories B (n¼ 6)and C (n¼ 7) presented low MBL levels (between 0.31and 0.8 ng/ml). No specific clinical manifestations couldbe related to those patients as previously reported [41].Nielsen et al. [42] found undetectable MBL levels in 10%of HIV-1þ adults without correlation to reduced CD4þnumbers. From 22 patients with high MBL levels, 14(63.6%) were in group C, five in B (22.7%), two in Aand only one in N. Elevation of MBL levels were observedin more severe stages but no statistical difference wasverified. High MBL concentrations are interpreted toreflect adaptation and it may be related to a response tomassive antigenic contact [43]. It is still controversial ifMBL levels could affect the progression of HIV disease inalready infected individuals. Prohaszka et al. observed that
Table 4 Clinical and immunological data of HIVþ children with relevant results tested
Number Gender
Age
(months) Group
Clinical
symptoms CD4þ/mm3 CD8þ/mm3 IgG (mg/dl)
CH50
(U/ml)
APH50
(U/ml)
C3d
(mU/l)
MBL
(mg/ml)
C4A
(mg/l)
C4B
(mg/l)
19 Male 31 C1 Otitis, PCP 2125 2207 1990 0 29 286 8.3 ND ND
40 Female 132 C1 Tuberculosis 646 1387 4570 0 40 83 1.4 ND ND
17 Male 13 B2 Anaemia 872 2890 3330 80 <10 298 8.4 1.68 0
34 Male 29 C2 BCP, Tbc,
PCP, otitis,
636 3070 3190 170 <10 120 3.8 ND ND
46 Female 113 A1 URI 607 1364 ND 118 <10 125 3.7 12.7 19.8
51 Female 53 B2 BCP, herpes 646 1387 2120 45 <10 ND 1.8 ND ND
37 Female 12 C3 LIP, PCP,
myocarditis
215 2000 1430 ND <10 77 0.31 ND ND
64 Male 77 N1 None 670 4037 1460 80 <10 76 7.0 20.0 19.0
68 Female 63 N2 None 662 3107 2790 75 <10 ND ND ND ND
79 Male 24 N1 None 1670 3725 ND 69 <10 140 9.4 9.82 0
121 Female 66 A2 Parotid
hypertrophy
573 1420 2330 68 <10 256 1.4 ND ND
124 Male 19 C3 Tuberculosis 197 1165 2520 124 <10 120 9.7 8.32 18.2
118 Female 66 A3 URI 393 459 1190 92 35 112 0.28 12.1 42.5
7 Female 115 N2 None 376 1107 5740 119 47 145 0.21 ND ND
77 Female 41 B2 LIP 550 5375 217 117 33 149.5 3.2 ND ND
PCP, P. carinii Pneumonia; BCP, bronchopneumonia; LIP, lymphoid interstitial pneumonia; URI, upper respiratory infection; nd, not determined.
Normal range: CH50¼ 80–120 U/ml; APH50¼ 32–56 U/ml; MBL¼ 0.3–7.5 mg/ml; C3d¼ 70–115mU/l; C4A¼ 7–20 mg/l; C4B¼ 20–40 mg/l.
*Reference values for C3d: 70 – 115 µU/l
N B0
100
200
300
400
µU/m
lµU
/ml
1 2 30
100
200
300
400
A
B
A C
Figure 4 C3d values in HIVþ children according to clinical (3A) and
immunologic (3B) categories of CDC classification (1994).
Y. C. Lian et al. Immunological Evaluation in HIVþ Children 621..................................................................................................................................................................................................
# 2004 Blackwell Publishing Ltd. Scandinavian Journal of Immunology 60, 615–624
0
5
10
15
20
25
30
N B C
µg/ml
Clinical categories
0
5
10
15
20
25
30
1 2 3
µg/ml
Immunological categories
MBL MBL
MeanSD
Normal rangeMeanSD
Normal range
*Reference values for MBL: 0.3–7.5 µg/mL
A
A B
Figure 5 Mannan-binding lectin (MBL) in 107 HIVþ children according to clinical (A) and immunologic (B) categories of CDC classification (1994).
67.2
0
5
10
15
20
25
30
35
N B C
ng/dl
Clinical categories
Clinical categories
Normal rangeMeanSD
0
5
10
15
20
25
30
35
1 3
67.2ng/dl
Immunological categories
0
10
20
30
40
50
60
128.7ng/dl
128.7
0
10
20
30
40
50
60ng/dl
C4A
C4B
C4A
Normal rangeMeanSD
Normal rangeMeanSD
Normal rangeMeanSD
*Reference values for:
C4A: 7 – 20 ng /dl
C4B: 20 – 40 ng /dl
A
N B CA
2
1 3
Immunological categories
2
A
C C4BD
B
Figure 6 C4 allotypes values in HIVþ children according to clinical (A, C) and immunologic (B, D) categories of CDC classification (1994).
622 Immunological Evaluation in HIVþ Children Y. C. Lian et al...................................................................................................................................................................................................
# 2004 Blackwell Publishing Ltd. Scandinavian Journal of Immunology 60, 615–624

serum MBL concentrations does influence survival in HIVinfection, however, in opposite direction as reported byGarred et al. [43, 44]. They referred that high serum levelsare correlated to a higher chance to die after the develop-ment of AIDS as compared to patients with low levels.The same authors propose that MBL may affect the pro-gression of HIV disease in two ways: the binding to gp120in the envelope of HIV virions activate lectin pathway, andfragments of activated complement proteins bind the vir-ions increasing their infectivity; activation of lectin path-way can be triggered by free gp120 adsorbed to CD4þlymphocytes facilitating the destruction of those cells andthe progression of HIV disease. We found very low levelsin asymptomatic children as well as in symptomaticpatients difficulting the conclusion that low MBL levelswould protect HIV progression [43, 44].
Low C4A values were detected in 16/50 cases (32%)with no difference according to categories. A heterozygousC4A deficiency is not rare and can be found in about oneof 250 healthy individuals [45]. Hentges et al. [45] havestudied C4 genotypes in HIV infected adults and observedthat patients with null C4 alleles had earlier clinical man-ifestations than other patients. Just et al. [46] found ahigher incidence of C4A gene deletion in HIVþ childrenwith encephalopathy who died before 2 years of age.
Low C4B values were seen in 23/50 children (46%) andhigh values in 12/50 (24%). Two of our patients hadundetectable C4B. The two patients with undetectableC4B had also low C4A levels and both died followingsevere bacterial infections. Several studies demonstrate theassociation of C4B deficiency and bacterial infectionscaused by Haemophylus influenzae, Streptococcus pneumo-niae and Neisseria meningitidis [47–49]. Cameron et al.[10] reported null C4B genes in 42% of HIV patientscomparing with 18% of homosexual seronegative individ-uals and 15% of seronegative individuals.
A clear difference in natural HIV progression betweenadults and children has been observed with respect totransmission, pathogenesis and clinical manifestations[1, 3]. Although not related to clinical symptomatology,a strong ongoing complement activation can be observedin all stages of HIV infection. In contrast to earlier reports,MBL could not be considered as a risk factor for HIV. Theknowledge and clinical experience with HIVþ adults can-not, therefore, be directly applied to paediatric patients.
Acknowledgments
We are grateful to Constancia L. Diogo and Lea C.Oliveira (Department of Pediatrics, Faculty of Medicine,Sao Paulo, University of Sao Paulo, Brazil), DeniseBrufato Ferraz (Faculty of Medicine, Ribeirao Preto,University of Sao Paulo, Brazil) for excellent technicalsupport.
References
1 Scott GB, Buck BE, Leterman JG, Bloom FL, Parks WP. Acquired
immunodeficiency syndrome in infants. N Engl J Med
1984;310:76–81.
2 Ebrahim SH, Peterman TA, Zaidi AA, Hamers FF. Geography of AIDS
associated Kaposi’s Sarcoma in Europe. AIDS 1997;11:1739–45.
3 Nicholas SW. Guidelines for the care of children and adolescent
with HIV infection. Management of the HIV-positive child with
fever. J Pediatr 1991;119:21–4.
4 Dierich MP, Ebenbichler CF, Marschang P, Fust G, Thielens NM,
Arlaud GJ. HIV and human complement. Mechanisms of interac-
tion and biological implication. Immunol Today 1993;14:435–40.
5 Marschang P, Ebenbichler CF, Dierich MP. HIV and complement
role of the complement system in HIV infection. Int Arch Allergy
Immunol 1994;103:113–7.
6 Haurum JS, Thiel S, Jones LM, Fischer PB, Laursen SB, Jensenius JC.
Complement activation upon binding of mannan-binding protein to
HIV envelope glycoproteins. AIDS 1993;7:1307–13.
7 Stoiber H, Clivio A, Dierich MP. Role of complement in HIV
infection. Annu Rev Immunol 1997;15:649–74.
8 Bishof NA, Welch TR, Beischel LS. C4B deficiency: a risk factor for
bacteremia with encapsulated organisms. J Infect Dis 1990;162:248–50.
9 Hentges F, Hoffman A, Oliveira De Araujo F, Hemmer R. Pro-
longed clinical asymptomatic evolution after HIV-1 infection is
marked by the absence of complement C4 null alleles at the
MHC. Clin Exp Immunol 1992;88:237–42.
10 Cameron PU, Cobain TJ, Zhang WJ, Kay PH, Dawkins RL.
Influence of C4 null genes on infection with human immunodefi-
ciency virus. BMJ 1988;296:1627–8.
11 Bouhlal H, Chomont N, Haeffner-Cavaillon N, Kazatchkine MD,
Belec L, Hocini H. Opsonization of HIV-1 by semen complement
enhances infection of human epithelial cells. J Immunol
2002;169(6):3301–6.
12 Caldwell MB, Oxtoby MJ, Simonds RJ et al. 1994 Revised classifica-
tion system for human immunodeficiency virus infection in children
less than 13 years of age. MMWR Morb Mortal Wkly Rep
1994;43:1–19.
13 Erkeller-Yuksel FM, Deneys V, Yuksel B et al. Age-related changes in
human blood lymphocyte subpopulations. J Pediatr 1992;120:216–22.
14 Fujimura MD. Niveis Sericos das Subclasses de Imunoglobulina G
em Criancas Normais e Nefroticas. Doctoral Thesis. Sao Paulo:
University of Sao Paulo Medical School, 1990: 159.
15 Mayer MM. Complement and complement fixation. In: Kabat EA,
Mayer MM eds. Experimental Immunochemistry, 2nd edn. Spring-
field: Thomas, 1991: 133–240.
16 Ferriani VPL, Barbosa JE, Carvalho IF. Complement haemolytic
activity (classical and alternative pathways), C3, C4 and factor B
titres in healthy children. Acta Paediatr 1999;88:1062–6.
17 Brandslund J, Sierted HC, Svehag SE, Teisner B. Double decker
rocket immunoelectrophoresis for direct quantitation of comple-
ment C3 split products with C3d specificities in plasma. J Immunol
Methods 1981;44:64–71.
18 Chrispeels J, Bank S, Rittner C, Bitter-Suermann D. Sandwich
enzyme-linked immunosorbent assays for the quantification of the
CD4 isotypes (C4A and C4B) in human plasma. J Immunol Meth-
ods 1989;125:5–12.20.
19 Thiel S, Holmskov U, Hviid L, Laursen SB, Jensenius JC. The
concentration of the C-type lectin, mannan-binding protein, in
human Plasma increases during an acute phase response. Clin Exp
Immunol 1992;90:31–5.
20 Vermelho LL, Silva LP, Costa AJL. Epidemiologia da Transmissao
Vertical do HIV no Brasil, National Coordenation of STD/AIDS,
Minister of Health, Brasilia. [Retrieved from http://www.aids.
gov.br/udtv/boletim_jun_ago99/trans_vertical.htm]
Y. C. Lian et al. Immunological Evaluation in HIVþ Children 623..................................................................................................................................................................................................
# 2004 Blackwell Publishing Ltd. Scandinavian Journal of Immunology 60, 615–624

21 Rosenberg ZF, Fauci AS. Immunopathogenesis of HIV infection.
FASEB J 1991;5:2382–90.
22 Pizzo PA, Wilfert CM. Markers and determinants of disease pro-
gression in children with HIV infection. J Acquir Immune Defic
Syndr Hum Retrovirol 1995;8:30–44.
23 Moss WJ, Dedyo T, Suarez M, Nicholas SW, Abrams E. Tuber-
culosis in children infected with human immunodeficiency virus a
report of five cases. Pediatr Infect Dis J 1992;11:114–6.
24 Lewis LL, Butler KM, Husson RN et al. Defining the population of
human immunodeficiency virus-infected children at risk for Myco-bacterium avium-intracellular infection. J Pediatr 1993;121:677–83.
25 Lipshultz SE, Easley KA, Orav EJ et al. Pediatric Pulmonary and
Cardiovascular Complications of Vertically Transmitted HIV infection
(P(2)C(2) HIV) Study Group. Lancet 2002;360 (9330):368–73.
26 Marks MJ, Haney PJ, Mcdermott MP, White CS, Vennos AD. Thor-
acic disease in children with AIDS. Radiographics 1996;16:1349–62.
27 Mofenson LM, Korelitz J, Meyer WA III et al. The relationship
between serum human immunodeficiency virus type 1 (HIV-1)
RNA level, CD4 lymphocyte percent, and long-term mortality risk
in HIV 1 infected children. J Infect Dis 1997;175:1029–38.
28 Chirmule N, Lesser M, Gupta A, Ravipati M, Kohn N, Pahwa S.
Immunological characteristics of HIV-infected children: relationship
to age, CD4 counts, disease progression, and survival. AIDS Res
Hum Retroviruses 1995;11:1209–19.
29 Pahwa S. Immune defects in pediatric AIDS, their pathogenesis, and
role of immunotherapy. Crit Care Med 1990;18:S138–43.
30 Schuval SJ, Bonagura VR, Ilowite NT. Rheumatologic manifesta-
tions of pediatric human immunodeficiency virus infection. J Rheu-
matol 1993;20:1578–82.
31 Simpson BJ, Andiman WA. Difficulties in assigning human immu-
nodeficiency virus-1 infection and seroreversion status in a cohort of
HIV-exposed children using serologic criteria established by the
Centers for Disease Control and Prevention. Pediatrics
1994;93:840–2.
32 Phillips AN, Sabin CA, Elford J, Bofill M, Lee CA, Janossy G. CD8
lymphocyte counts and serum immunoglobulin A levels early in
HIV infection predictors of CD4 lymphocyte depletion during 8
years of follow-up. AIDS 1993;7:975–80.
33 Shearer WT, Easley KA, Goldfarb J et al. Evaluation of immune
survival factors in pediatric HIV-1 infection. Ann N Y Acad Sci
2000;918:298–312.
34 Stoiber H, Speth C, Dierich MP. Role of complement in the control
of HIV dynamics and pathogenesis. Vaccine 2003;21 (S2):77–82.
35 Stoiber H, Pinter C, Siccardi AG, Clivio A, Dierich MP. Efficient
destruction of human immunodeficiency virus in human serum by
inhibiting the protective action of complement factor H and decay
accelerating factor (DAF, CD55). J Exp Med 1996;183:307–10.
36 Perricone R, Fontana L, De Carolis C, Carini C, Sirianni MC,
Aiuti F. Evidence for activation of complement in patients with
AIDS related complex (ARC) and/or lymphoadenopathy syndrome
(LAS). Clin Exp Immunol 1987: 70, 500–7.
37 Jarvis JN, Taylor H, Iobidze M, Dejange J, Chang S, Cohen F.
Rheumatoid factor expression and complement activation in chil-
dren congenitally infected with human immunodeficiency virus.
Clin Immunol Immunopathol 1993;67:50–4.
38 Jarvis JN, Taylor H, Iobidze M. Complement activation and
immune complexes in early congenital HIV infection. J Acquir
Immune Defic Syndr Hum Retrovirol 1995;8:480–5.
39 Fust G, Ujhelyi E, Hidvegi T et al. The complement system in HIV
disease. Immunol Invest 1991;20:231–41.
40 Senaldi G, Peakman MI, McManus T, Davies ET, Tee DEH,
Vergani D. Activation of the complement system in human
immunodeficiency virus infection relevance of the classical
pathway to pathogenesis and disease severity. J Infect Dis 1990;62:
1227–32.
41 Senaldi G, Davies ET, Mahalingam M et al. Circulating levels of
mannose binding protein in human immunodeficiency virus infec-
tion. J Infect 1995;31:145–8.
42 Nielsen SL, Andersen PL, Koch C, Jensenius JC, Thiel S. The level
of the serum opsonin, mannan-binding protein in HIV-1 antibody-
positive patients. Clin Exp Immunol 1995;100:219–22.
43 Garred P, Madsen HO, Hofmann B, Svejgaard A. Increased
frequency of homozygosity of abnormal mannan-binding-protein
alleles in patients with suspected immunodeficiency. Lancet
1995;346:941–3.
44 Prohaszka Z, Nemes J, Hidvegi T et al. Two parallel routes of the
complement mediated antibody-dependent enhancement of HIV-1
infection. AIDS 1997;11:949–58.
45 Hentges F, Hoffman A, Oliveira-de-Araujo F, Hemmer R. Pro-
longed clinical asymptomatic evolution after HIV-1 infection is
marked by the absence of complement C4 null alleles at the
MHC. Clin Exp Immunol 1992;88:237–42.
46 Just JJ, Abrams E, Loule LG et al. Influence of host genotype on
progression to acquired immunodeficiency virus type 1. J Pediatr
1995;127:544–9.
47 Goddard EA, Creemers P, Beatty DW. C4B isotype deficiency in
Haemophilus influenzae type b and meningococcal meningitis.
Pediatr Infect Dis J 1994;13:661–2.
48 Rowe PC, McLean RH, Wood RA, Leggiadro RJ, Winkelstein JA.
Association of homozygous C4B deficiency with bacterial meningi-
tis. J Infect Dis 1989;160:448–51.
49 Quinn TC, Ruff A, Halsey N. Pediatric acquired immunodeficiency
syndrome: special considerations for developing nations. Pediatr
Infect Dis J 1992;11:558–68.
624 Immunological Evaluation in HIVþ Children Y. C. Lian et al...................................................................................................................................................................................................
# 2004 Blackwell Publishing Ltd. Scandinavian Journal of Immunology 60, 615–624




















