Imaging of Acute Hematogenous Osteomyelitis and Septic ...
13
14 Imaging of Acute Hematogenous Osteomyelitis and Septic Arthritis in Children and Adults John Y. Kim and Diego Jaramillo I. What are the clinical findings that raise the suspicion for acute hematogenous osteomyelitis and septic arthritis to direct further imaging? II. What is the diagnostic performance of the different imaging studies in acute hematogenous osteomyelitis and septic arthritis? III. What is the natural history of osteomyelitis and septic arthritis, and what are the roles of medical therapy versus surgical treatment? IV. Is there a role for repeat imaging in the management? V. What is the diagnostic performance of imaging of osteomyelitis and septic arthritis in the adult? VI. What are the roles of the different imaging modalities in the evalu- ation of acute osteomyelitis and septic orthritis? 260 Issues The clinical presentation of acute osteomyelitis and septic arthritis can be nonspecific and sometimes confusing (moderate evidence). When signs and symptoms cannot be localized, bone scintigraphy is preferred over magnetic resonance imaging (MRI) (moderate evidence). When signs and symptoms can be localized, MRI is preferred (mod- erate to limited evidence). Ultrasound is the preferred imaging modality for evaluating joint effusions of the hip (moderate evidence). Magnetic resonance imaging is highly sensitive for the detection of osteomyelitis and its complications (abscess), but incurs added cost (moderate evidence). No data were found in the medical literature that evaluate the cost- effectiveness of the different imaging modalities in the evaluation of hematogenous osteomyelitis and septic joint (limited evidence). Overall, MRI is the imaging modality of choice to evaluate for oste- omyelitis and septic arthritis in the adult population, including the diabetic patient and intravenous drug users. The ability to localize Key Points
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Imaging of Acute Hematogenous Osteomyelitis and Septic ...
14Imaging of Acute HematogenousOsteomyelitis and Septic Arthritisin Children and AdultsJohn Y. Kim and Diego Jaramillo
I. What are the clinical findings that raise the suspicion for acutehematogenous osteomyelitis and septic arthritis to direct furtherimaging?
II. What is the diagnostic performance of the different imaging studiesin acute hematogenous osteomyelitis and septic arthritis?
III. What is the natural history of osteomyelitis and septic arthritis, andwhat are the roles of medical therapy versus surgical treatment?
IV. Is there a role for repeat imaging in the management?V. What is the diagnostic performance of imaging of osteomyelitis and
septic arthritis in the adult?VI. What are the roles of the different imaging modalities in the evalu-
ation of acute osteomyelitis and septic orthritis?
260
Issues
� The clinical presentation of acute osteomyelitis and septic arthritis canbe nonspecific and sometimes confusing (moderate evidence).
� When signs and symptoms cannot be localized, bone scintigraphy is preferred over magnetic resonance imaging (MRI) (moderate evidence).
� When signs and symptoms can be localized, MRI is preferred (mod-erate to limited evidence).
� Ultrasound is the preferred imaging modality for evaluating jointeffusions of the hip (moderate evidence).
� Magnetic resonance imaging is highly sensitive for the detection ofosteomyelitis and its complications (abscess), but incurs added cost(moderate evidence).
� No data were found in the medical literature that evaluate the cost-effectiveness of the different imaging modalities in the evaluation ofhematogenous osteomyelitis and septic joint (limited evidence).
� Overall, MRI is the imaging modality of choice to evaluate for oste-omyelitis and septic arthritis in the adult population, including thediabetic patient and intravenous drug users. The ability to localize
Key Points

Definition and Pathophysiology
Osteomyelitis is an infection of bone and bone marrow. Routes of infectioninclude hematogenous spread, spread by contiguity, and direct infectionby a penetrating wound (1). Hematogenous spread is the most commonroute in children, usually seeding the metaphyses of long bones due tosluggish blood flow patterns in this region (2,3). It arises in the setting ofbacteremia. In children, the capillaries in the metaphyses are the terminalbranches of the nutrient artery. The capillaries form loops that end in largevenous sinusoids where there is decreased blood flow. The inflammatoryresponse to infection leads to increased intraosseous pressure and stasis ofblood flow, causing thrombosis and eventual bone necrosis (4). In childrenless than 18 months of age, transphyseal vessels allow metaphyseal infec-tions to cross the physis and infect the epiphyses and joints. The mostcommon bones affected by acute hematogenous osteomyelitis (AHO) arethe tibia and femur (3); the most common organism is Staphylococcus aureus.
Acute septic arthritis is a bacterial infection of a joint. Most cases arise from hematogenous spread or contiguous spread from adjacentosteomyelitis in the metaphysis or epiphysis (5–7). The most commonorganism is S. aureus (3). The prognosis worsens with increasing delay oftreatment due to lytic enzymes that destroy the articular and epiphysealcartilage. In addition, increased pressure within the joint capsule reducesblood flow to the epiphyses. This can lead to long-term disability result-ing from growth disturbances, dislocations, and malalignment (8,9).
There is evidence that acute osteomyelitis and septic arthritis are a spec-trum of the same disease process (moderate evidence) (10). This hypothesisargues for a similar clinical approach and treatment for these two diseases.
The pattern of hematogenous spread of osteomyelitis and septic arthri-tis in the adult is different from the pediatric population. The unique vas-cular supply in the metaphysis normally seen in children is no longerpresent in adults, and most hematogenous infections arise in the diaphy-seal marrow space, similar in pattern to hematogenous metastatic diseaseto the bone (11). Contiguous spread of infection from adjacent soft tissuesis more prevalent in the adults than in children, although hematogenousspread is still more common (12). Contiguous infections can occur intrauma patients with open fractures, in bedridden patients with decubitusulcers, and in patients with a diabetic foot. Localizing symptoms are moreprevalent in the adult population as opposed to the pediatric population,allowing for more dedicated anatomic imaging with MRI, rather than asurvey with radionuclide bone scanning.
Epidemiology
The annual incidence of osteomyelitis in children under 13 years of age is1/5000 (13). With boys slightly more often affected than girls, fast-growinglong bones such as the tibia and femur are the most affected regions.
Chapter 14 Imaging of Acute Hematogenous Osteomyelitis and Septic Arthritis 261
symptoms and the inherent high spatial resolution allows exactanatomic detail that may be helpful for surgical planning (limited tomoderate evidence).
Approximately 25% of cases affect the flat bones including the pelvis.Although a single bone is usually affected, polyostotic involvement hasbeen reported in up to 6.8% of cases in infants and in 22% of neonates(4,14,15). The most common organisms are S. aureus, followed by b-hemolytic Streptococcus, Streptococcus pneumoniae, Escherichia coli, andPseudomonas aeruginosa (3,16). Clinical presentation can be confusing, andmany laboratory findings such as elevated sedimentation rate may be sen-sitive but not specific. Serial blood cultures are only positive in 32% to 60%of cases (1,17,18). Infections in infants and neonates are usually clinicallysilent, and toddlers may present with limping, pseudoparalysis, or pain onpassive movement (19).
Half of the cases of septic arthritis occur in children less than 3 years ofage (20). Approximately 53% are isolated cases of septic arthritis and 47%are cases of septic arthritis associated with osteomyelitis (21). Conversely,30% of patients with osteomyelitis have adjacent septic arthritis (22). Boysare slightly more affected than girls (1.2 :1), and the hip is the most affectedjoint (23). The most common symptoms are pain, fever, refusal to bearweight, and joint swelling. Most cases involve a single joint, although upto 15% of cases can affect multiple joints. Mortality rates of up to 7% havebeen reported (21). Similar organisms to those in osteomyelitis are foundin septic arthritis, including S. aureus and S. pneumoniae (21,24). The mostcommon sequelae of septic arthritis include joint instability, joint functionlimitation, and limb shortening (25).
Overall Cost to Society
No data were found in the medical literature on the overall cost to society from the diagnosis, treatment, and complications of acutehematogenous osteomyelitis or septic arthritis. Although there are severalcost-effectiveness analyses evaluating the type, extent, and route of antibi-otic administration in the treatment of osteomyelitis and septic arthritis, nocost-effectiveness data were found in the literature specifically incorporat-ing imaging strategies in the management of acute hematogenousosteomyelitis or septic arthritis.
Goals
In acute hematogenous osteomyelitis and septic arthritis, the goal is earlydiagnosis and treatment to prevent the long-term sequelae of these diseases, which include growth disturbances, joint instability, chronicinfection, malalignment, and limb deformity. The standard treatmentsinclude intravenous antibiotics and/or surgical debridement. Septic arthri-tis usually requires surgical therapy in order to decompress the intraartic-ular pressure. Surgical debridement may be necessary for osteomyelitis iffrank pus can be aspirated from the bone, if there is necrotic bone present,or if there is failure to respond to antibiotic therapy (15,26).
Methodology
The authors performed a Medline search using PubMed (National Libraryof Medicine, Bethesda, Maryland) for data relevant to the diagnostic performance and accuracy of both clinical and radiographic examination
262 J.Y. Kim and D. Jaramillo

of patients with acute hematogenous osteomyelitis and septic arthritis. The diagnostic performance of the clinical examination (history and physical exam) and surgical outcome was based on a systematic litera-ture review performed for the years 1966 to 2004. The clinical examina-tion search strategy used the following terms: (1) acute hematogenousosteomyelitis, (2) septic arthritis, (3) pediatric, (4) children, (5) clinical examina-tion, (6) epidemiology or physical examination or surgery, and (7) treatment orsurgery. The review of the diagnostic imaging literature was done for thesame years. The search strategy used the following key words: (1) acutehematogenous osteomyelitis, (2) septic arthritis, (3) magnetic resonance imagingor MRI, (4) bone scan, (5) ultrasound, and (6) imaging, as well as combina-tions of these search strings. We excluded animal studies and non–English-language articles.
I. What are the Clinical Findings that Raise the Suspicionfor Acute Hematogenous Osteomyelitis and SepticArthritis to Direct Further Imaging?
Summary of Evidence: The clinical presentation of acute hematogenousosteomyelitis and septic arthritis can be confusing and nonspecific in the pediatric population. No single clinical finding in isolation leads to the diagnosis of osteomyelitis or septic arthritis. Repeat high-resolutionimaging may be required to determine the need for surgical debridement,including extension into soft tissues or complications that are not amenableto systemic antibiotic therapy (limited evidence).
Supporting Evidence: Standard laboratory tests such as elevated sedimen-tation rate can be nonspecific or even normal (19) (limited evidence). Serialblood cultures are reported to be positive in 32% to 60% of cases (1,17,18)(moderate and limited evidence). Occasionally, direct aspiration of bonematerial may be needed for diagnosis. These aspirations can yield positivecultures in 87% of cases (27) (limited evidence).
The clinical presentation in the pediatric age group can be nonspecific.Infection in the neonate and infant is usually clinically silent. Toddlers canpresent with limping, pseudoparalysis, or pain on passive movement (4,28)(moderate to limited evidence).
Due to similarities in pathogenesis, there is also overlap in the clinicalpresentation of septic arthritis and osteomyelitis. Irritability, limping, orrefusal to bear weight, along with elevated sedimentation rate or leukocy-tosis, are the most common presentations (15,23,24,29,30) (moderate tolimited evidence). Kocher et al. (30) proposed probabilities for the presenceof septic arthritis in the hip in order to guide further imaging and jointaspiration based on four clinical variables. These four predictors wereleukocytosis greater than 12,000/mL, fever, inability to bear weight, anderythrocyte sedimentation rate (ESR) >40mm/hr. If none of these predic-tors were present, there was a 0.2% chance of septic arthritis. The predictedprobability of septic arthritis with one predictor was 3%, 40% with two pre-dictors, 93.1% with three predictors, and 99.6% with four predictors. Thisconstellation of clinical findings was most suggestive of osteomyelitis orseptic arthritis and warranted further evaluation with imaging (moderateto limited evidence).
Chapter 14 Imaging of Acute Hematogenous Osteomyelitis and Septic Arthritis 263
II. What Is the Diagnostic Performance of the DifferentImaging Studies in Acute Hematogenous Osteomyelitisand Septic Arthritis?
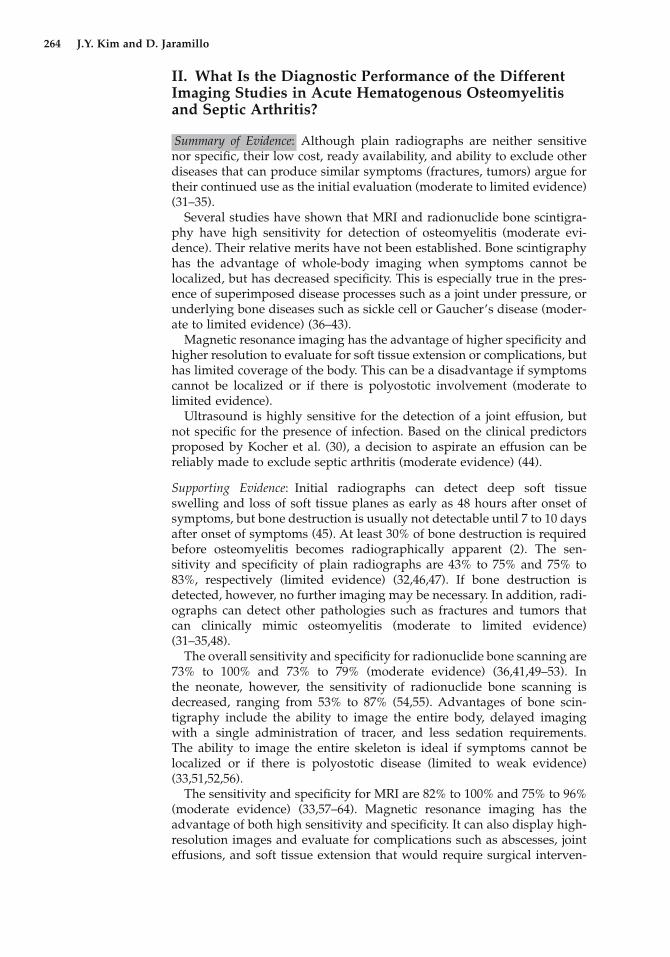
Summary of Evidence: Although plain radiographs are neither sensitive nor specific, their low cost, ready availability, and ability to exclude otherdiseases that can produce similar symptoms (fractures, tumors) argue fortheir continued use as the initial evaluation (moderate to limited evidence)(31–35).
Several studies have shown that MRI and radionuclide bone scintigra-phy have high sensitivity for detection of osteomyelitis (moderate evi-dence). Their relative merits have not been established. Bone scintigraphyhas the advantage of whole-body imaging when symptoms cannot belocalized, but has decreased specificity. This is especially true in the pres-ence of superimposed disease processes such as a joint under pressure, orunderlying bone diseases such as sickle cell or Gaucher’s disease (moder-ate to limited evidence) (36–43).
Magnetic resonance imaging has the advantage of higher specificity andhigher resolution to evaluate for soft tissue extension or complications, buthas limited coverage of the body. This can be a disadvantage if symptomscannot be localized or if there is polyostotic involvement (moderate tolimited evidence).
Ultrasound is highly sensitive for the detection of a joint effusion, butnot specific for the presence of infection. Based on the clinical predictorsproposed by Kocher et al. (30), a decision to aspirate an effusion can bereliably made to exclude septic arthritis (moderate evidence) (44).
Supporting Evidence: Initial radiographs can detect deep soft tissueswelling and loss of soft tissue planes as early as 48 hours after onset ofsymptoms, but bone destruction is usually not detectable until 7 to 10 daysafter onset of symptoms (45). At least 30% of bone destruction is requiredbefore osteomyelitis becomes radiographically apparent (2). The sen-sitivity and specificity of plain radiographs are 43% to 75% and 75% to 83%, respectively (limited evidence) (32,46,47). If bone destruction isdetected, however, no further imaging may be necessary. In addition, radi-ographs can detect other pathologies such as fractures and tumors that can clinically mimic osteomyelitis (moderate to limited evidence)(31–35,48).
The overall sensitivity and specificity for radionuclide bone scanning are73% to 100% and 73% to 79% (moderate evidence) (36,41,49–53). In the neonate, however, the sensitivity of radionuclide bone scanning isdecreased, ranging from 53% to 87% (54,55). Advantages of bone scin-tigraphy include the ability to image the entire body, delayed imaging with a single administration of tracer, and less sedation requirements. The ability to image the entire skeleton is ideal if symptoms cannot be localized or if there is polyostotic disease (limited to weak evidence)(33,51,52,56).
The sensitivity and specificity for MRI are 82% to 100% and 75% to 96%(moderate evidence) (33,57–64). Magnetic resonance imaging has theadvantage of both high sensitivity and specificity. It can also display high-resolution images and evaluate for complications such as abscesses, jointeffusions, and soft tissue extension that would require surgical interven-
264 J.Y. Kim and D. Jaramillo
tion (63,65,66). The disadvantages include slighter higher cost relative tobone scintigraphy; prolonged imaging times, which may require sedation;and limited coverage.
Ultrasound is highly sensitive for the evaluation of joint effusions andcan detect as little as 5 to 10cc of fluid within a joint (67). However, noultrasound characteristics, including complexity of the fluid, the quantityof fluid, or adjacent hyperemia on color Doppler imaging, have beenshown to be definitive in distinguishing septic arthritis from other non-infectious causes of joint effusions (68–71). Despite this limitation, theabsence of fluid by ultrasound can be very helpful as septic arthritis is veryunlikely in this setting (33,71,72). As outlined above, Kocher et al. (30) haveprovided clinical guidelines to direct joint aspiration. These include fever,the presence of elevated white count, an elevated sedimentation rate, andinability to bear weight (moderate evidence).
III. What Is the Natural History of Osteomyelitis andSeptic Arthritis, and What Are the Roles of MedicalTherapy Versus Surgical Treatment?
Summary of Evidence: Most uncomplicated cases of osteomyelitis requirehospitalization and the institution of systemic intravenous antibiotictherapy. If there is a delay of more than 4 days prior to institution oftherapy, there is increased poor outcomes and long-term sequelae (mod-erate evidence). Approximately 5% to 10% of cases require surgical inter-vention after initial antibiotic therapy, and up to 20% to 50% of all caseseventually require some form of surgery, including reconstruction andrepeat debridements.
Approximately 5% to 10% of all cases have long-term sequelae such as growth disturbance, loss of function, malalignment, and deformity.Approximately 6% of cases develop chronic osteomyelitis (73).
Supporting Evidence: Most cases of acute osteomyelitis and septic arthritisare treated with antibiotics. If frank pus is aspirated from a joint, surgicaldebridement is required immediately. Patients are admitted for initiationof systemic antibiotic therapy. Average length of stay ranges from 3 to 7days (16,24,74). Average course of systemic antibiotic therapy is approxi-mately 11 to 14 days with an additional 4 weeks of outpatient oral antibi-otic therapy (5,7,16,75). Many of the clinical signs and symptoms improvewithin 48 hours of initiation of systemic antibiotics, which is a reassuringsign. If there is no clinical improvement, further evaluation includingimaging may be required to exclude complications not amenable to antibi-otics alone, such as abscess collections, necrotic tissue, or extension intosoft tissues.
Approximately 20% to 50% of all cases eventually require surgical inter-vention (28). Up to 10% of patients eventually have long-term sequelae,including growth disturbance, loss of function, malalignment, and defor-mity (8,9,16,23,28). Up to 6% of patients eventually have chronic oste-omyelitis. There is evidence that a delay in initiation of therapy (>4 daysafter onset of symptoms), certain infecting organisms (methicillin-resistantS. aureus), and age of the patient (<6 months of age) are predictors of badoutcomes (moderate evidence) (3,7,16,73).
Chapter 14 Imaging of Acute Hematogenous Osteomyelitis and Septic Arthritis 265
IV. Is There a Role for Repeat Imaging in the Management?
Summary of Evidence: Most patients respond clinically to systemic anti-biotics within 48 hours. If there is no clinical response to therapy, repeatimaging should be performed to exclude complications that would requiresurgical intervention such as abscess collections, extensive soft tissue exten-sion, or necrotic tissue. The performance characteristics of MRI are ideal inthis setting (moderate to limited evidence).
Supporting Evidence: Approximately 95% to 98% of patients respond clini-cally to antibiotic therapy alone (76). Children usually respond quickly toantibiotics, on average within 48 hours. However, approximately 5% to 10%of patients eventually require surgical intervention (77,78). These patientsrequire high-resolution imaging to evaluate for surgical disease. The liter-ature supports the use of MRI for evaluation of necrosis, abscess collections,and soft tissue extension (63–65,79) (moderate evidence to limited evi-dence). This information can be helpful for the surgeon in planning the sur-gical approach and method of debridement. There are also some data in theliterature suggesting that MRI should be the repeat imaging modality ofchoice if the site of infection is localized to the spine or pelvis. There is ahigher incidence of abscess formation in these deep infections, whichwould require earlier surgical evaluation and treatment (33,57,63,80).
V. What Is the Diagnostic Performance of Imaging ofOsteomyelitis and Septic Arthritis in the Adult?
Summary of Evidence: Overall, MRI appears to be the imaging modality ofchoice to evaluate for osteomyelitis and septic arthritis in the adult popu-lation, including the diabetic patient and intravenous drug users. Theability to localize symptoms and inherent high spatial resolution allowsexact anatomic detail that may be helpful for surgical planning (limited tomoderate evidence).
Supporting Evidence: Osteomyelitis in the diabetic foot represents a diag-nostic challenge both clinically and by imaging. The diabetic foot is proneto infection and suboptimal healing due to the decreased blood supplyfrom diabetic vasculopathy, decreased immune response, and repetitivetrauma and abnormal mechanics from diabetic neuropathy (81). Becauseof these abnormalities, there are baseline abnormal imaging findings of thebones and joints without superimposed infection.
Radiographically, the diabetic foot has many features mimicking infec-tion, including destruction, debris, and subluxation. The diabetic foot can also have abnormal findings without osteomyelitis on three-phaseradionuclide bone scan (82). There is some evidence of using both bonescan with methylene diphosphanate (MDP) as well as a white blood cellscan to map out specific areas of infection (82–85) (limited to moderate evi-dence). Although it has excellent sensitivity and specificity (92 and 97%respectively), the technique is cumbersome and laborious (83). Its lowerresolution relative to MRI also limits the imaging of anatomic detail forsurgical planning (86,87).
Magnetic resonance imaging has both high sensitivity and specificity forevaluating osteomyelitis in the diabetic foot (88–91). Sensitivity ranges
266 J.Y. Kim and D. Jaramillo

from 88% to 92% and specificity ranges from 82% to 100% (85,90,92) (mod-erate evidence). However, the diagnosis is frequently not made based on specific imaging characteristics, but by the location of the abnormality.The neuropathic foot inherently contains signal abnormalities similar toosteomyelitis. Imaging diagnosis is made by identifying signal abnormal-ities in the bone contiguous and in direct contact with adjacent skin ulcersand known pressure points in the diabetic foot (87).
Hematogenous osteomyelitis and septic arthritis also occurs in intra-venous drug users. Many of these infections arise initially in the softtissues, such as the psoas muscle, with subsequent involvement into thespine or sacroiliac (SI) joint (93,94). Septic arthritis with osteomyelitis isslightly more common in this population than osteomyelitis alone (95). Theplain film is neither sensitive nor specific in commonly involved locations,such as the spine and SI joint. Computed tomography (CT) scan with intra-venous contrast material has been shown to be very accurate in the iden-tification of the soft tissue infections and abscesses, but not as accurate inthe evaluation of the spinal osteomyelitis/discitis or sacroiliitis (96,97)(limited to moderate evidence). Magnetic resonance imaging is superior inevaluating these structures due to its higher contrast, signal-to-noise ratio,and multiplanar imaging.
Ultrasound can still detect joint effusions, but can be technically moredifficult due to the larger amount of soft tissue in adults compared to thepediatric population (98,99). Magnetic resonance imaging is highly sensi-tive for the evaluation of septic arthritis (97,100,101). Hyperemia and syn-ovitis can also be elucidated with the use of intravenous gadolinium,increasing the accuracy of septic arthritis (102).
VI. What Are the Roles of the Difference ImagingModalities in the Evaluation of Acute Osteomyelitis andSeptic Arthritis?
The decision tree in Figure 14.1 outlines the role of each imaging modalityin the evaluation of suspected osteomyelitis. Table 14.1 summarizes thediagnostic performance of the imaging studies for osteomyelitis in childrenand adults. The plain radiograph is the initial imaging evaluation due toits relative low cost, rapid acquisition, and ready availability. If there isfrank evidence of osteomyelitis on the radiograph, immediate antibiotictherapy can be instituted and further imaging may not be necessary, as upto 80% of patients are successfully treated with antibiotics alone.
If the radiograph is negative for osteomyelitis, and there are no localiz-ing symptoms clinically, radionuclide bone scintigraphy is the next imag-ing modality, based on its ability to provide whole-body imaging.
If there are localized symptoms, MRI would be a better choice due tohigher resolution, more specificity, and ability to immediately evaluatecomplications.
Repeat imaging with MRI should be considered in all patients who donot improve clinically after 48 hours of systemic antibiotic therapy, and to direct management of those who require surgical therapy. In addition,if immediate surgical therapy is planned, such as in cases of infectionsinvolving the spine or pelvis, earlier imaging with MRI may be of use.
If symptoms are referable to the hip, an ultrasound should be performedto rapidly evaluate for the presence of an effusion, and also to provideimaging-guided joint aspiration.
Chapter 14 Imaging of Acute Hematogenous Osteomyelitis and Septic Arthritis 267
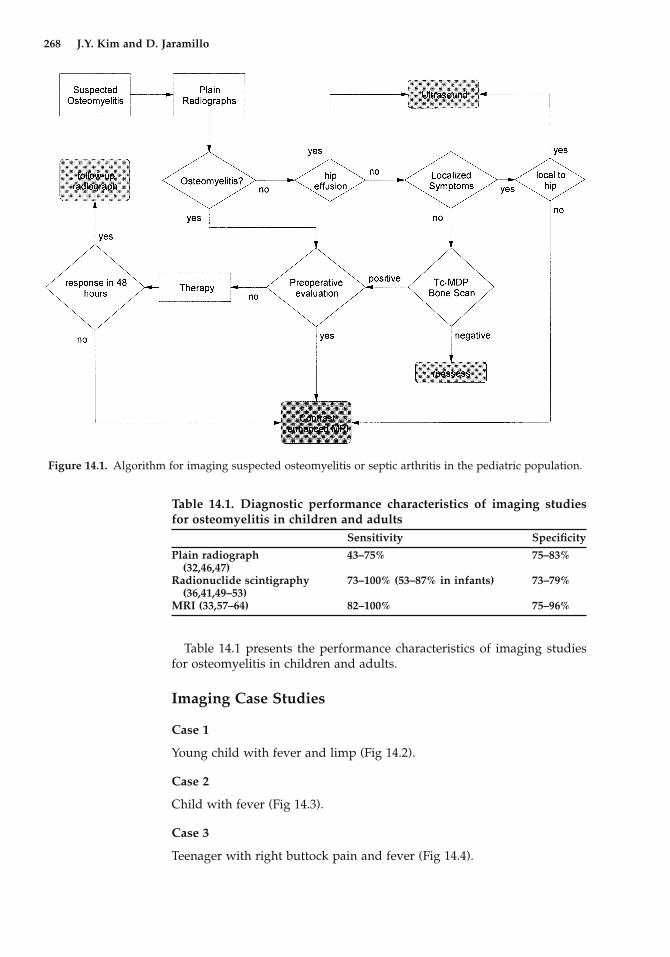
Table 14.1 presents the performance characteristics of imaging studiesfor osteomyelitis in children and adults.
Imaging Case Studies
Case 1
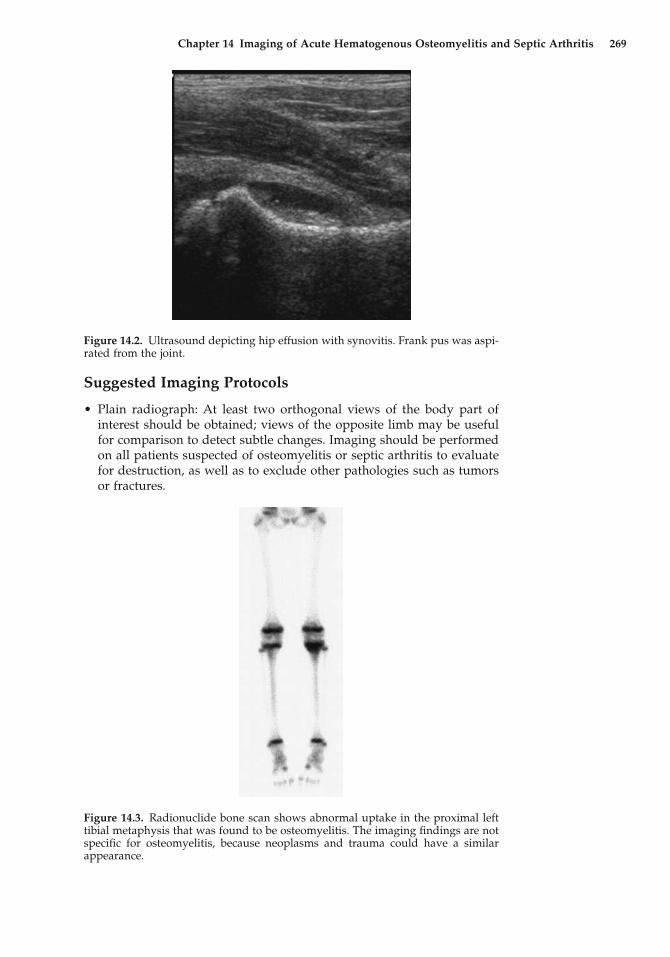
Young child with fever and limp (Fig 14.2).
Case 2
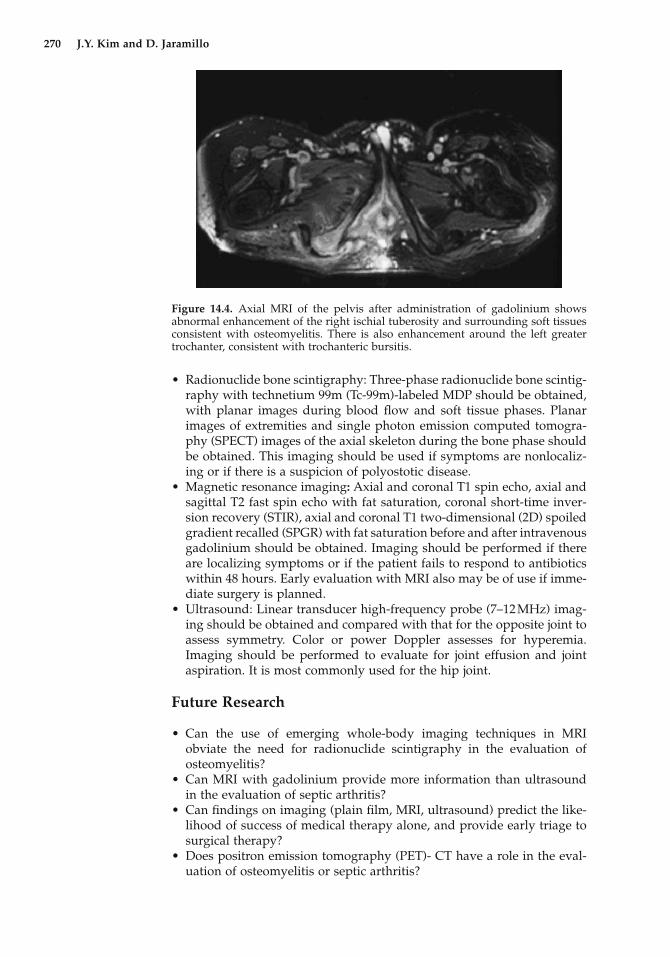
Child with fever (Fig 14.3).
Case 3
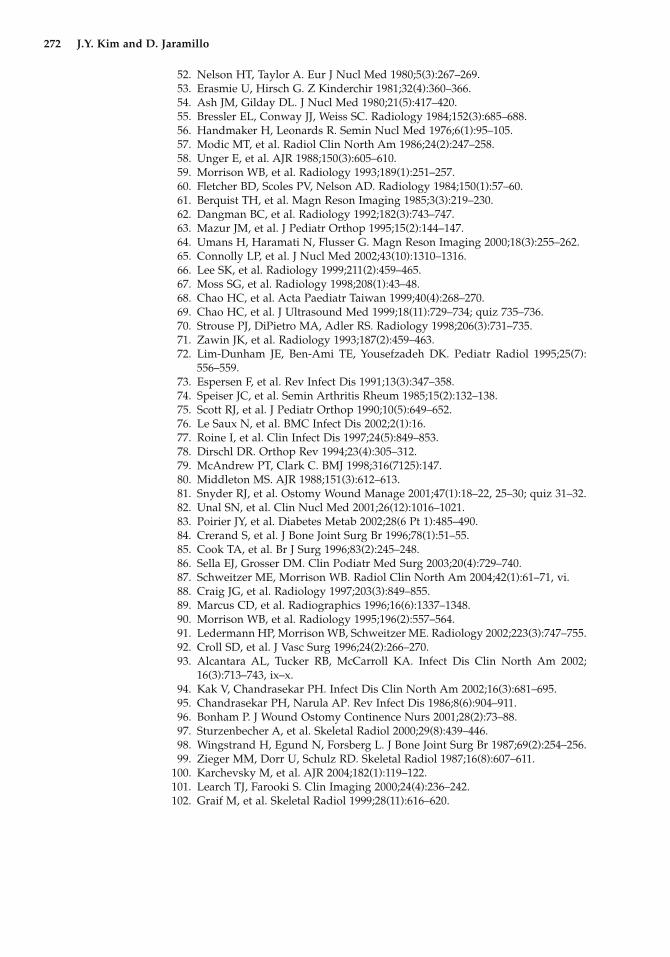
Teenager with right buttock pain and fever (Fig 14.4).
268 J.Y. Kim and D. Jaramillo
Figure 14.1. Algorithm for imaging suspected osteomyelitis or septic arthritis in the pediatric population.
Table 14.1. Diagnostic performance characteristics of imaging studiesfor osteomyelitis in children and adults
Sensitivity Specificity
Plain radiograph 43–75% 75–83%(32,46,47)
Radionuclide scintigraphy 73–100% (53–87% in infants) 73–79%(36,41,49–53)
MRI (33,57–64) 82–100% 75–96%
Chapter 14 Imaging of Acute Hematogenous Osteomyelitis and Septic Arthritis 269
Figure 14.2. Ultrasound depicting hip effusion with synovitis. Frank pus was aspi-rated from the joint.
Figure 14.3. Radionuclide bone scan shows abnormal uptake in the proximal lefttibial metaphysis that was found to be osteomyelitis. The imaging findings are notspecific for osteomyelitis, because neoplasms and trauma could have a similarappearance.
Suggested Imaging Protocols
• Plain radiograph: At least two orthogonal views of the body part ofinterest should be obtained; views of the opposite limb may be usefulfor comparison to detect subtle changes. Imaging should be performedon all patients suspected of osteomyelitis or septic arthritis to evaluatefor destruction, as well as to exclude other pathologies such as tumorsor fractures.
• Radionuclide bone scintigraphy: Three-phase radionuclide bone scintig-raphy with technetium 99m (Tc-99m)-labeled MDP should be obtained,with planar images during blood flow and soft tissue phases. Planarimages of extremities and single photon emission computed tomogra-phy (SPECT) images of the axial skeleton during the bone phase shouldbe obtained. This imaging should be used if symptoms are nonlocaliz-ing or if there is a suspicion of polyostotic disease.
• Magnetic resonance imaging: Axial and coronal T1 spin echo, axial andsagittal T2 fast spin echo with fat saturation, coronal short-time inver-sion recovery (STIR), axial and coronal T1 two-dimensional (2D) spoiledgradient recalled (SPGR) with fat saturation before and after intravenousgadolinium should be obtained. Imaging should be performed if thereare localizing symptoms or if the patient fails to respond to antibioticswithin 48 hours. Early evaluation with MRI also may be of use if imme-diate surgery is planned.
• Ultrasound: Linear transducer high-frequency probe (7–12MHz) imag-ing should be obtained and compared with that for the opposite joint toassess symmetry. Color or power Doppler assesses for hyperemia.Imaging should be performed to evaluate for joint effusion and jointaspiration. It is most commonly used for the hip joint.
Future Research
• Can the use of emerging whole-body imaging techniques in MRI obviate the need for radionuclide scintigraphy in the evaluation ofosteomyelitis?
• Can MRI with gadolinium provide more information than ultrasoundin the evaluation of septic arthritis?
• Can findings on imaging (plain film, MRI, ultrasound) predict the like-lihood of success of medical therapy alone, and provide early triage tosurgical therapy?
• Does positron emission tomography (PET)- CT have a role in the eval-uation of osteomyelitis or septic arthritis?
270 J.Y. Kim and D. Jaramillo
Figure 14.4. Axial MRI of the pelvis after administration of gadolinium showsabnormal enhancement of the right ischial tuberosity and surrounding soft tissuesconsistent with osteomyelitis. There is also enhancement around the left greatertrochanter, consistent with trochanteric bursitis.
References
1. Waldvogel FA, Medoff G, Swartz MN. N Engl J Med 1970;282(4):198–206.2. Faden H, Grossi M. Am J Dis Child 1991;145(1):65–69.3. Kao HC, et al. J Microbiol Immunol Infect 2003;36(4):260–265.4. Oudjhane K, Azouz EM. Radiol Clin North Am 2001;39(2):251–266.5. Barton LL, Dunkle LM, Habib FH. Am J Dis Child 1987;141(8):898–900.6. Azouz EM, Greenspan A, Marton D. Skeletal Radiol 1993;22(1):17–23.7. Welkon CJ, et al. Pediatr Infect Dis 1986;5(6):669–676.8. Choi IH, et al. J Bone Joint Surg Am 1990;72(8):1150–1165.9. Betz RR, et al. J Pediatr Orthop 1990;10(3):365–372.
10. Alderson M, et al. J Bone Joint Surg Br 1986;68(2):268–274.11. Tice AD, Hoaglund PA, Shoultz DA. J Antimicrob Chemother 2003;51(5):
1261–1268.12. Jensen AG, et al. J Infect 1997;34(2):113–118.13. Sonnen GM, Henry NK. Pediatr Clin North Am 1996;43(4):933–947.14. Asmar BI. Infect Dis Clin North Am 1992;6(1):117–132.15. Nelson JD. Infect Dis Clin North Am 1990;4(3):513–522.16. Karwowska A, Davies HD, Jadavji T. Pediatr Infect Dis J 1998;17(11):
1021–1026.17. Dormans JP, Drummond DS. J Am Acad Orthop Surg 1994;2(6):333–341.18. Nixon GW. AJR 1978;130(1):123–129.19. Restrepo SC, Gimenez CR, McCarthy K. Rheum Dis Clin North Am 2003;29(1):
89–109.20. Matan AJ, Smith JT. Orthopedics 1997;20(7):630–635; quiz 636–637.21. Caksen H, et al. Pediatr Int 2000;42(5):534–540.22. Perlman MH, et al. J Pediatr Orthop 2000;20(1):40–43.23. Wang CL, et al. J Microbiol Immunol Infect 2003;36(1):41–46.24. Razak M, Nasiruddin J. Med J Malaysia 1998;53(suppl A):86–94.25. Campagnaro JG, et al. Chir Organi Mov 1992;77(3):233–245.26. Dagan R. Pediatr Infect Dis J 1993;12(1):88–92.27. Howard CB, et al. J Bone Joint Surg Br 1994;76(2):311–314.28. Razak M, Ismail MM, Omar A. Med J Malaysia 1998;53(suppl A):83–85.29. Khachatourians AG, et al. Clin Orthop 2003;409:186–194.30. Kocher MS, Zurakowski D, Kasser JR. J Bone Joint Surg Am 1999;81(12):
1662–1670.31. Zucker MI, Yao L. West J Med 1992;156(3):297–298.32. Bonakdar-pour A, Gaines VD. Orthop Clin North Am 1983;14(1):21–37.33. Jaramillo D, et al. AJR 1995;165(2):399–403.34. Gold R. Pediatr Infect Dis J 1995;14(6):555.35. Fordham L, Auringer ST, Frush DP. J Pediatr 1998;132(5):906–908.36. Sullivan DC, et al. Radiology 1980;135(3):731–736.37. Wald ER, Mirro R, Gartner JC. Clin Pediatr (Phila) 1980;19(9):597–601.38. Jones DC, Cady RB. J Bone Joint Surg Br 1981;63–B(3):376–378.39. Berkowitz ID, Wenzel W. Am J Dis Child 1980;134(9):828–830.40. Handmaker H. Radiology 1980;135(3):787–789.41. Barron BJ, Dhekne RD. Clin Nucl Med 1984;9(7):392–393.42. Park HM, Rothschild PA, Kernek CB. AJR 1985;145(5):1079–1084.43. Stark JE, et al. Radiology 1991;179(3):731–733.44. Klein DM, et al. Clin Orthop 1997;338:153–159.45. Capitanio MA, Kirkpatrick JA. AJR Radium Ther Nucl Med, 1970;108(3):
488–496.46. Kaye JJ. Pediatr Ann 1976;5(1):11–31.47. Keenan AM, Tindel NL, Alavi A. Arch Intern Med 1989;149(10):2262–2266.48. Gold R. Pediatr Rev 1991;12(10):292–297.49. Duszynski DO, et al. Radiology 1975;117(2):337–340.50. Gelfand MJ, Silberstein EB. JAMA 1977;237(3):245–247.51. Hankins JH, Flowers WM Jr. J Miss State Med Assoc 1978;19(1):10–12.
Chapter 14 Imaging of Acute Hematogenous Osteomyelitis and Septic Arthritis 271
52. Nelson HT, Taylor A. Eur J Nucl Med 1980;5(3):267–269.53. Erasmie U, Hirsch G. Z Kinderchir 1981;32(4):360–366.54. Ash JM, Gilday DL. J Nucl Med 1980;21(5):417–420.55. Bressler EL, Conway JJ, Weiss SC. Radiology 1984;152(3):685–688.56. Handmaker H, Leonards R. Semin Nucl Med 1976;6(1):95–105.57. Modic MT, et al. Radiol Clin North Am 1986;24(2):247–258.58. Unger E, et al. AJR 1988;150(3):605–610.59. Morrison WB, et al. Radiology 1993;189(1):251–257.60. Fletcher BD, Scoles PV, Nelson AD. Radiology 1984;150(1):57–60.61. Berquist TH, et al. Magn Reson Imaging 1985;3(3):219–230.62. Dangman BC, et al. Radiology 1992;182(3):743–747.63. Mazur JM, et al. J Pediatr Orthop 1995;15(2):144–147.64. Umans H, Haramati N, Flusser G. Magn Reson Imaging 2000;18(3):255–262.65. Connolly LP, et al. J Nucl Med 2002;43(10):1310–1316.66. Lee SK, et al. Radiology 1999;211(2):459–465.67. Moss SG, et al. Radiology 1998;208(1):43–48.68. Chao HC, et al. Acta Paediatr Taiwan 1999;40(4):268–270.69. Chao HC, et al. J Ultrasound Med 1999;18(11):729–734; quiz 735–736.70. Strouse PJ, DiPietro MA, Adler RS. Radiology 1998;206(3):731–735.71. Zawin JK, et al. Radiology 1993;187(2):459–463.72. Lim-Dunham JE, Ben-Ami TE, Yousefzadeh DK. Pediatr Radiol 1995;25(7):
556–559.73. Espersen F, et al. Rev Infect Dis 1991;13(3):347–358.74. Speiser JC, et al. Semin Arthritis Rheum 1985;15(2):132–138.75. Scott RJ, et al. J Pediatr Orthop 1990;10(5):649–652.76. Le Saux N, et al. BMC Infect Dis 2002;2(1):16.77. Roine I, et al. Clin Infect Dis 1997;24(5):849–853.78. Dirschl DR. Orthop Rev 1994;23(4):305–312.79. McAndrew PT, Clark C. BMJ 1998;316(7125):147.80. Middleton MS. AJR 1988;151(3):612–613.81. Snyder RJ, et al. Ostomy Wound Manage 2001;47(1):18–22, 25–30; quiz 31–32.82. Unal SN, et al. Clin Nucl Med 2001;26(12):1016–1021.83. Poirier JY, et al. Diabetes Metab 2002;28(6 Pt 1):485–490.84. Crerand S, et al. J Bone Joint Surg Br 1996;78(1):51–55.85. Cook TA, et al. Br J Surg 1996;83(2):245–248.86. Sella EJ, Grosser DM. Clin Podiatr Med Surg 2003;20(4):729–740.87. Schweitzer ME, Morrison WB. Radiol Clin North Am 2004;42(1):61–71, vi.88. Craig JG, et al. Radiology 1997;203(3):849–855.89. Marcus CD, et al. Radiographics 1996;16(6):1337–1348.90. Morrison WB, et al. Radiology 1995;196(2):557–564.91. Ledermann HP, Morrison WB, Schweitzer ME. Radiology 2002;223(3):747–755.92. Croll SD, et al. J Vasc Surg 1996;24(2):266–270.93. Alcantara AL, Tucker RB, McCarroll KA. Infect Dis Clin North Am 2002;
16(3):713–743, ix–x.94. Kak V, Chandrasekar PH. Infect Dis Clin North Am 2002;16(3):681–695.95. Chandrasekar PH, Narula AP. Rev Infect Dis 1986;8(6):904–911.96. Bonham P. J Wound Ostomy Continence Nurs 2001;28(2):73–88.97. Sturzenbecher A, et al. Skeletal Radiol 2000;29(8):439–446.98. Wingstrand H, Egund N, Forsberg L. J Bone Joint Surg Br 1987;69(2):254–256.99. Zieger MM, Dorr U, Schulz RD. Skeletal Radiol 1987;16(8):607–611.
100. Karchevsky M, et al. AJR 2004;182(1):119–122.101. Learch TJ, Farooki S. Clin Imaging 2000;24(4):236–242.102. Graif M, et al. Skeletal Radiol 1999;28(11):616–620.
272 J.Y. Kim and D. Jaramillo