
Human mesenchymal stem cell-conditioned medium improves cardiac function following myocardial...
9
REGULAR ARTICLE Human mesenchymal stem cell-conditioned medium improves cardiac function following myocardial infarction Leo Timmers a , Sai Kiang Lim b , c , ⁎ , Imo E. Hoefer a , Fatih Arslan a , Ruenn Chai Lai b , d , Angelique A.M. van Oorschot e , Marie Jose Goumans e , Chaylendra Strijder a , Sui Kwan Sze f , Andree Choo g , Jan J. Piek h , Pieter A. Doevendans a , Gerard Pasterkamp a , Dominique P.V. de Kleijn a , i , ⁎⁎ a Department of Cardiology, University Medical Center Utrecht, Netherlands b Institute of Medical Biology, A*STAR, Singapore c Department of Surgery, YLL School of Medicine, NUS, Singapore d NUS Graduate School for Integrative Sciences & Engineering, NUS, Singapore e Department of Molecular Cell Biology, Leiden University Medical Center, Netherlands f Nanyang Technological University, Singapore g Biotechnology Institute, Singapore h Department of Cardiology, Academic Medical Center, Amsterdam, Netherlands i Interuniversity Cardiology Institute of the Netherlands, Utrecht, Netherlands Received 21 August 2010; received in revised form 29 December 2010; accepted 3 January 2011 Available online 28 January 2011 Abstract Recent studies suggest that the therapeutic effects of stem cell transplantation following myocardial infarction (MI) are mediated by paracrine factors. One of the main goals in the treatment of ischemic heart disease is to stimulate vascular repair mechanisms. Here, we sought to explore the therapeutic angiogenic potential of mesenchymal stem cell (MSC) secretions. Human MSC secretions were collected as conditioned medium (MSC-CM) using a clinically compliant protocol. Based on proteomic and pathway analysis of MSC-CM, an in vitro assay of HUVEC spheroids was performed identifying the angiogenic properties of MSC-CM. Subsequently, pigs were subjected to surgical left circumflex coronary artery ligation and randomized to intravenous MSC-CM treatment or non-CM (NCM) treatment for 7 days. Three weeks after MI, myocardial capillary density was higher in pigs treated with MSC-CM (645 ± 114 vs 981 ± 55 capillaries/mm 2 ; P = 0.021), which was accompanied by reduced myocardial infarct size and preserved systolic and diastolic performance. Intravenous MSC-CM treatment after myocardial infarction increases capillary density and preserves cardiac function, probably by increasing myocardial perfusion. © 2010 Elsevier B.V. All rights reserved. ⁎ Correspondence to: S.K. Lim, Institute of Medical Biology, A*STAR, Department of Surgery, YLL School of Medicine, NUS, 8A Biomedical Grove, No. 05–505 Immunos, Singapore 136648. Fax: +65 6464 2048. ⁎⁎ Correspondence to: D.P.V. de Kleijn, Laboratory of Experimental Cardiology, University Medical Center Utrecht, Room G02.523, Heidelberglaan 100, 3584 CX Utrecht, The Netherlands. Fax: +31 30 2522693. E-mail addresses: [email protected] (S.K. Lim), [email protected] (D.P.V. de Kleijn). 1873-5061/$ - see front matter © 2010 Elsevier B.V. All rights reserved. doi:10.1016/j.scr.2011.01.001 available at www.sciencedirect.com www.elsevier.com/locate/scr Stem Cell Research (2011) 6, 206–214
-
Upload
sabanciuniv -
Category
Documents
-
view
0 -
download
0
Transcript of Human mesenchymal stem cell-conditioned medium improves cardiac function following myocardial...
ava i l ab l e a t wwwsc i enced i r ec t com
wwwe l sev i e r com l oca te sc r
Stem Cell Research (2011) 6 206ndash214
REGULAR ARTICLE
Human mesenchymal stem cell-conditionedmedium improves cardiac function followingmyocardial infarctionLeo Timmers a Sai Kiang Limbc Imo E Hoefera Fatih ArslanaRuenn Chai Lai bd Angelique AM van Oorschot e Marie Jose GoumanseChaylendra Strijder a Sui Kwan Sze f Andree Choog Jan J PiekhPieter A Doevendans a Gerard Pasterkampa Dominique PV de Kleijn ai
a Department of Cardiology University Medical Center Utrecht Netherlandsb Institute of Medical Biology ASTAR Singaporec Department of Surgery YLL School of Medicine NUS Singapored NUS Graduate School for Integrative Sciences amp Engineering NUS Singaporee Department of Molecular Cell Biology Leiden University Medical Center Netherlandsf Nanyang Technological University Singaporeg Biotechnology Institute Singaporeh Department of Cardiology Academic Medical Center Amsterdam Netherlandsi Interuniversity Cardiology Institute of the Netherlands Utrecht Netherlands
Received 21 August 2010 received in revised form 29 December 2010 accepted 3 January 2011Available online 28 January 2011
Abstract Recent studies suggest that the therapeutic effects of stem cell transplantation following myocardial infarction (MI)are mediated by paracrine factors One of the main goals in the treatment of ischemic heart disease is to stimulate vascularrepair mechanisms Here we sought to explore the therapeutic angiogenic potential of mesenchymal stem cell (MSC)secretions Human MSC secretions were collected as conditioned medium (MSC-CM) using a clinically compliant protocol Basedon proteomic and pathway analysis of MSC-CM an in vitro assay of HUVEC spheroids was performed identifying the angiogenicproperties of MSC-CM Subsequently pigs were subjected to surgical left circumflex coronary artery ligation and randomized tointravenous MSC-CM treatment or non-CM (NCM) treatment for 7 days Three weeks after MI myocardial capillary density washigher in pigs treated with MSC-CM (645plusmn114 vs 981plusmn55 capillariesmm2 P=0021) which was accompanied by reducedmyocardial infarct size and preserved systolic and diastolic performance Intravenous MSC-CM treatment after myocardialinfarction increases capillary density and preserves cardiac function probably by increasing myocardial perfusion
copy 2010 Elsevier BV All rights reserved
Correspondence to SK Lim Institute of Medical Biology ASTAR Department of Surgery YLL School of Medicine NUS 8A BiomedicalGrove No 05ndash505 Immunos Singapore 136648 Fax +65 6464 2048 Correspondence to DPV de Kleijn Laboratory of Experimental Cardiology University Medical Center Utrecht Room G02523
Heidelberglaan 100 3584 CX Utrecht The Netherlands Fax +31 30 2522693E-mail addresses saikianglimimba-staredusg (SK Lim) ddekleijnumcutrechtnl (DPV de Kleijn)
1873-5061$ - see front matter copy 2010 Elsevier BV All rights reserveddoi101016jscr201101001
207
Introduction
Despite significant advances in myocardial revascularizationcoronary artery disease and subsequent myocardial infarc-tion (MI) are leading causes of morbidity and mortalityworldwide One of the main goals in the treatment ofischemic heart disease is the development of effectivestrategies to stimulate vascular repair mechanisms in orderto achieve adequate tissue perfusion
Although the potential of stem cell therapy for MI is stillheavily debated as a result of studies that failed to showimproved outcome (Moelker et al 2006 de Silva et al 2008Janssens et al 2006 Lunde et al 2006 Meyer et al 2009Menasche et al 2008) there are several preclinical andclinical studies that demonstrated the therapeutic effects ofstem cell transplantation (Hashemi et al 2008 Wolf et al2009 Assmus et al 2006 Schachinger et al 2006 Straueret al 2002 Yousef et al 2009) While robust evidence forcardiomyocyte replacement is still limited more evidence isaccumulating for vascular repair mechanisms following stemcell transplantation (van Laake et al 2009 Losordo ampDimmeler 2004 Erbs et al 2007) Among the stem cells thathave been tested for cardiac repair mesenchymal stem cells(MSCs) derived from adult bone marrow have emerged as apromising stem cell type for treating cardiovascular disease(Pittenger amp Martin 2004) Recent studies suggest that atleast some of the therapeutic effects of MSCs aremediated byparacrine factors secreted by the cells (Caplan amp Dennis2006 Gnecchi et al 2005) These paracrine factors could beexploited to extend the therapeutic possibilities of MSCs forthe treatment of a variety of diseases including MIApplication of MSC secretions rather than MSCs themselvesin order to restore tissue perfusion could enable us to avoidsome of the limiting factors associatedwith cell therapy suchas immune incompatibility tumorigenicity costs and wait-ing time for ex vivo expansion
We previously described how human MSC lines can bereproducibly generated from human embryonic stem cell(hESC) lines which constitute an invariable source ofconsistently uniform batches of MSCs (Lian et al 2007) Inaddition we established for the first time the collection ofthese MSC secretions as conditioned medium (MSC-CM) in aclinically compliant manner circumventing exposure tovirus mouse cells or serum (Sze et al 2007) Recently wedemonstrated that MSC-CM treatment following ischemiareperfusion injury reduces myocardial apoptosis and oxida-tive stress (Timmers et al 2007a) In the current paper wereveal the angiogenic potential of clinically compatible MSC-CM and demonstrate in a large animal model that it can beused to improve cardiac function following MI
Results
MSC-CM stimulates angiogenesis in vitro
Ingenuity pathway analysis of the secretory proteome ofMSC-CM revealed that within the physiological systemdevelopment and function group cardiovascular systemdevelopment and function has the highest overrepresenta-tion (Pb10-12) with 75 different focus proteins Within thegroup of cardiovascular system development and function
development of blood vessels angiogenesis proliferation ofendothelial cells neovascularization and vascularizationare the processes with the highest overrepresentation(supplementary data Table 1)
Having identified the potential involvement of MSC-CM inblood vessel formation we used an in vitro assay ofangiogenesis to further investigate this potential In anangiogenesis assay based on formation of capillary sprouts byHUVEC spheroids MSC-CM induced significantly more capil-lary sprouting compared with NCM (Fig 1A) The averagelength of the sprouts did not increase following MSC-CMtreatment compared with NCM (Fig 1B) The total length ofall sprouts however significantly increased in spheroidsincubated with MSC-CM when compared with NCM (Fig 1C)
In addition a HUVECMatrigel angiogenesis assay wasperformed which revealed a longer average tube length withCM compared with NCM (107plusmn0046 vs 099plusmn0041 mmP=0003)
MSC-CM treatment after infarction increasescapillary density and decreases collagen density
Capillary density was higher in the border areas followingMSC-CM treatment compared with NCM treatment (Figs 2Aand B) In the remote area capillary density did not differbetween MSC-CM treatment and NCM treatment (Fig 2C)We were unable to reliably quantify capillary density in theinfarct area due to the unorganized structure of the infarctgranulation tissue 3 weeks following MI
Picrosirius staining revealed that collagen density in theborder area and in the remote myocardium was lower in pigstreated with MSC-CM compared with pigs treated with NCMIn the infarct area no difference was detected between thetreatment groups (Fig 3)
MSC-CM preserves cardiac function following MI
One hour after coronary artery ligation cardiac functiondecreased similarly in both groups Fractional area shorten-ing decreased from 458plusmn19 to 323plusmn20 in the NCM groupand from 469plusmn46 to 297plusmn34 in the MSC-CM group(P=0670) Also cardiac output (280plusmn010 Lmin (NCM) vs267plusmn022 Lmin (MSC-CM) P=0596) mean aortic pressure(90plusmn83 mm Hg (NCM) vs 84plusmn54 mm Hg (MSC-CM) P=0544)and dPdtMAX (1135plusmn83 mm Hgs (NCM) vs 1096plusmn83 mm Hgs(MSC-CM) P=0741) were similar in both groups 1 h aftercoronary artery ligation
In the 3 weeks following MI the LV internal areasincreased in all pigs However the increase in LV internalarea tended to be more pronounced in NCM-treated animalspointing to reduced remodeling in MSC-CM-treated pigs(Figs 4A and B) Echocardiographic wall thickness of theinfarct area decreased in pigs treated with NCM but not inpigs treated with MSC-CM (Fig 4C) The fractional areashortening was higher following MSC-CM treatment whichreflects increased systolic cardiac performance (Fig 4D)Also other systolic functional parameters such as ejectionfraction dPdtMAX stroke volume and stroke work werehigher in animals treated with MSC-CM Improved cardiacfunction translated into improved hemodynamic parameterswith the mean arterial pressure and cardiac output being
Figure 1 HUVEC spheroid assay of angiogenesis The number of capillary sprouts (A) mean length of sprouts (pixels B) and totallength of sprouts (pixels C) after incubation of HUVEC spheroids with MSC-CM (n=12) or NCM (n=12) Representative pictures of MSC-CM and NCM are demonstrated in panels D and E respectively Pb001 vs NCM
208 L Timmers et al
higher in MSC-CM-treated pigs In addition diastolic functionimproved as assessed with dPdtMIN and diastolic chamberstiffness All functional parameters are summarized in Table 1Myocardial infarct size 3 weeks following coronary arteryligation was smaller in MSC-CM-treated pigs compared to NCM-treated pigs (116plusmn20 vs 166plusmn12 of the LV P=0050)
Two pigs died during the surgical procedure due torefractory ventricular fibrillation before treatment withMSC-CM or NCM and were therefore excluded from thestudy Two pigs (1 treated with MSC-CM and 1 treated withNCM) died in the third week following MI without signs ofheart failure or cardiac rupture probably due to ventriculartachycardiafibrillation
Discussion
Here we demonstrate that human MSC-CM treatmentenhances capillary density resulting in reduced myocardial
infarct size and preserved systolic and diastolic function in aporcine model of myocardial infarction
Recently it was demonstrated that administration of MSCsecretions improved outcome in a murine model of MI(Gnecchi et al 2005) Vascular repair mechanisms consti-tute an important means to reduce myocardial injury and toimprove cardiac function following MI Although the thera-peutic potential of stem cell transplantation is still a subjectof discussion evidence for vascular repair mechanismsfollowing stem cell transplantation is growing (van Laakeet al 2009 Losordo amp Dimmeler 2004 Erbs et al 2007) Ifvascular repair mechanisms are induced by paracrinefactors application of stem cell secretions may extend therepertoire of stem cell-based therapies with a differentdimension
An in vitro sprouting assay confirmed Ingenuity analysis ofearlier MSC-CM proteomics data and identified the angio-genic potential of MSC-CM In order to investigate thetherapeutic potential of MSC-CM to stimulate angiogenesis
Figure 2 Capillary density Representative sections of border areas after lectin staining to visualize endothelium 3 weeks after MIfrom pigs treated with NCM (A n=9) or MSC-CM (B n=9) Quantification of capillary density in remote and border area isdemonstrated in panel C Scale bars 500 μm
Figure 3 Collagen density Quantification of collaged densityin the infarct border and remote areas in pigs treated with NCMand MSC-CM
209
in vivo we used a porcine model of myocardial infarctionDuring myocardial ischemia following coronary artery liga-tion cardiomyocytes in the central infarct perish withinminutes to hours after coronary occlusion The border zoneof the ischemic area however contains injured but viablecells under hypoperfused and hypoxic conditions which mayeither be salvaged or die depending on the conditions afterischemia Restoration of myocardial perfusion by means ofangiogenesis restores the metabolic needs of cardiomyocytesin the border area and offers the cells a better chance ofsurvival which in turn could lead to reduced myocardialinjury Intracoronary delivery of bone marrow-derivedprogenitor cells has been suggested to promote vascularrepair following MI potentially via paracrine mechanisms(Erbs et al 2007) Such effect was also observed in a rodentmodel of hind limb ischemia (Kinnaird et al 2004) Asbecame evident from our histological analyses MSC-CMincreased capillary density in the border areas and myocar-dial infarct size was reduced which was accompanied bypreserved LV dimensions and cardiac function
Besides stimulation of angiogenesis it cannot be excludedthat also other mechanisms contributed to reduction of
A B
C D
WT
infa
rct
(cm
)
FAS
(
)E F
dP
dt M
AX (
mm
Hg
s)
LVE
S a
rea
(cm
2)
LVE
S a
rea
(cm
2)
dP
dt M
in (
mm
Hg
s)
Figure 4 Cardiac function Left ventricular (LV) end-diastolic internal area (A) LV end-systolic internal area (B) posterolateralmyocardial wall (infarct) thickness (C) fractional area shortening (FAS D) dPdtMAX (E) and dPdtMIN (F) before MI (baseline) 1 h postMI and 3 weeks post MI in pigs treated with MSC-CM (black dots n=9) or NCM (open dots n=9) Pb005 vs NCM
210 L Timmers et al
myocardial infarct size and preservation of myocardialfunction With preserved left ventricular dimensions andinfarct thickness inhibition of post MI cardiac remodeling is apotential contributing mechanism Collagen density in theborder area and remote myocardium was lower in pigstreated with MSC-CM Cardiac fibrosis is associated withheart failure following myocardial infarction and maycontribute to progression of systolic and diastolic dysfunc-tion (Burlew amp Weber 2002 Cleutjens et al 1999) Werecently demonstrated that intravenous and intracoronaryMSC-CM treatment reduces myocardial apoptosis and oxida-tive stress (Timmers et al 2007a) In that study cardio-myocyte death was targeted acutely following ischemia andreperfusion injury In the current study treatment wasstarted late after coronary artery ligation and a model ofpermanent coronary artery ligation was used in order toinvestigate the angiogenic potential of MSC-CM and its effecton cardiac function independent of reduction of reperfusioninjury The fact that cardiac function improved using thisprotocol shows that there may be additional benefit fromprolonged treatment with MSC secretions
For this study a permanent coronary artery ligation wasperformed in anesthetized animals and functional measure-
ments were performed with open chest In addition we havenot been able to investigate the effect of commoncomorbidities such as hypertension dyslipidemia anddiabetes which might influence the biologic effect of MSCsecretions Due to the permanent coronary artery ligationwe were not able to assess the area at risk 3 weeks post MIWe were not able to oversee the effects of human proteininjection on the immune system of the porcine host and thepotential influence on study endpoints Furthermore themolecular mechanism for the induction of angiogenesis andor arteriogenesis and an exact determination of theresponsible angiogenic factors are still lacking Severalclinical trials with potent angiogenic factors failed toimprove outcome in patients (Henry et al 2003 Simonset al 2002) It is not clear how paracrine factors in stem celltransplants or the paracrine factors alone can induce abetter effect Most likely a combination of angiogenicfactors rather than a single protein is responsible Alsoexosomes could play an important role We previouslydemonstrated exosomes in MSC-CM to contain and delivercardioprotective compounds preventing cardiomyocytedeath following ischemia and reperfusion injury (Lai et al2010) Exosomes constitute a potential delivery tool to
Table 1 Hemodynamic and Functional Parameters
Baseline 3 weeks post MI Change from baseline ()
Parameter NCM CM NCM CM NCM CM
HR bpm 66plusmn4 73plusmn6 84plusmn6 86plusmn6 28plusmn12 12plusmn11MAP mm Hg 95plusmn5 89plusmn5 66plusmn6 85plusmn5 -30plusmn5 -5plusmn8 CO Lmin 31plusmn01 30plusmn02 37plusmn06 53plusmn05 23plusmn21 78plusmn20dPdt max mm Hgs 1213plusmn77 1241plusmn56 1157plusmn162 1650plusmn124 4plusmn13 40plusmn9 dPdt min mm Hgs -1274plusmn122 -1130plusmn96 -883plusmn98 -1313plusmn95 27plusmn9 -19plusmn19 EDP mm Hg 80plusmn03 71plusmn06 133plusmn16 121plusmn11 68plusmn21 94plusmn42WT infarct cm 079plusmn004 083plusmn005 055plusmn002 079plusmn005 -27plusmn4 -5plusmn4 Lvia (ED) cm2 158plusmn05 142plusmn10 260plusmn18 218plusmn15 64plusmn12 55plusmn12Lvia (ES) cm2 85plusmn04 76plusmn09 177plusmn16 125plusmn09 104plusmn14 60plusmn14 FAS 458plusmn19 469plusmn46 326plusmn22 424plusmn33 -28plusmn6 -6plusmn8 SV ml 48plusmn3 42plusmn2 43plusmn4 62plusmn3 -4plusmn11 52plusmn10 EDV ml 134plusmn16 129plusmn9ESV ml 93plusmn15 73plusmn9EF 337plusmn44 491plusmn33 SW mm Hgmiddotml 2497plusmn333 4595plusmn361 Stiffness mm Hgml 026plusmn004 014plusmn002
Summary of cardiac functional parameters of pigs treated with NCM (n=9) and MSC-CM (n=9) determined with echocardiography andconductance catheter-based LV pressure and volumemeasurements MI indicates myocardial infarction HR heart rate MAP mean arterialpressure CO cardiac output EDP end-diastolic pressure WT wall thickness LVia left ventricular internal area SV stroke volume EDVend-diastolic volume ESV end-systolic volume EF ejection fraction SW stroke work Stiffness end-diastolic chamber stiffness Pb005vs NCM
211
effectively carry angiogenic factors into the intracellularspace of the target tissue protecting the factors fromproteases This may explain why relatively low doses canhave such profound angiogenic effects Whether exosomesand their content are also responsible for the stimulation ofangiogenesis following MI remains a subject for furtherinvestigation
Here we demonstrate that human MSC secretionsstimulate angiogenesis These data support the hypothesisthat MSC transplantation induces vascular repair mechanismsvia paracrine pathways Most importantly human MSCsecretions harvested as conditioned medium using a clini-cally compliant protocol reduced infarct size and preservedcardiac function in a large animal model of myocardialinfarction The study therefore identifies MSC-CM as a noveltherapeutic biologic in the improvement of cardiac functionafter myocardial infarction
Methods
MSC-CM preparation
The protocols for MSC generation and CM preparation havebeen described in previous papers (Lian et al 2007 Sze et al2007) In short a chemically defined serum-free culturemedium(DMEMwithoutphenol red supplementedwith insulintransferrin and selenium 5 ngml FGF2 5 ngml PDGF ABglutamine-penicillin-streptomycin and szlig-mercaptoethanol)was conditioned by MSCs derived from human embryonicstem cells (hESCs) using a clinically compliant protocol Threepolyclonal karyotypically stable and phenotypically MSC-likecultures that do not express pluripotency-associated markersbut displayed MSC-like surface antigens (CD29+ CD44+CD49a+e+ CD105+ CD166+ CD34ndash CD45ndash) and gene
expression profile were generated by trypsinization andpropagation of hESCs from either the HuES9 hESC line or theH1 hESC line in feeder- and serum-free selection media (Lianet al 2007) One of these cultures HuES9E1 can be stablyexpanded for at least 80 population doublings To harvest MSCsecretions hESC-derived MSC cultures were transferred to achemically defined serum-free culture medium to conditionthe medium for 3 days before the media containing MSCsecretions were collected clarified by centrifugation con-centrated 25 times using 10-kDa MW cutoff ultrafiltrationmembranes and sterilized by filtration through a 220-nmfilter The protein concentration after concentration was050 mgml As a negative control the above-noted serum-free culture medium was processed equally (nonconditionedmedium [NCM])
Ingenuity pathway analysis
For this analysis we used the proteomic data obtainedpreviously (Sze et al 2007) Bioinformatic analysis wasperformed using Ingenuity pathway analysis (Ingenuity IPA-2002 version 71) The 201 proteins were uploaded inIngenuity with Ingenuity Knowledge Base as a reference setand direct and indirect relationships were included Allmolecules or relationships were considered for the filtersummary In the summary the focus was on Top Bio functionsin which physiological system development and function wasanalyzed in depth
HUVEC spheroid assay
Spheroids were formed from HUVECs to determine the effectof conditioned medium on angiogenic sprout formation (Korffamp Augustin 1998) Spheroids were formed overnight in 20
212 L Timmers et al
methocel in culture medium and subsequently embedded ina collagenndashmethocel matrix Sprouting was induced over-night with MSC-CM (n=12) or non-CM (NCM) (n=12) todetermine the effect of the secreted chemotactic proteinson capillary sprouting After overnight sprouting spheroidswere fixed in 10 formaldehyde and pictures were taken andthe length and number of sprouts were quantified
Animals
All experiments were performed in accordance with theldquoGuide for the Care and Use of Laboratory Animalsrdquo preparedby the Institute of Laboratory Animal Resources andwith priorapproval by the Animal Experimentation Committee of theFaculty of Medicine Utrecht University the Netherlands
Sample size calculation
In a previous study the mean fractional area shortening(FAS) after LCx ligation was 365 (Timmers et al 2007b)With an alpha of 005 power of 080 SD of 58 anddifference of 20 considered relevant 10 animals per groupwere needed To allow for 10 mortality 11 animals pergroup were enrolled
Pig study design
Myocardial infarction was induced in 22 Dalland Landracepigs (60ndash70 kg IDDLO Lelystad the Netherlands) by surgicalleft circumflex coronary artery (LCx) ligation Two pigs diedperioperatively before randomization and were thereforeexcluded from the study The remaining 20 pigs wererandomized after surgery by using sealed envelopes tointravenous treatment with MSC-CM (20 ml MSC-CM ie10 mg protein) or 20 ml NCM initiated 4 h after coronaryartery ligation and the treatment was continued for 7 daystwice daily via a catheter inserted into the jugular vein Thepigs were sacrificed 3 weeks after MI To prevent thromboticcomplications and arrhythmias all pigs were treated withclopidogrel 75 mgday from 3 days before MI until termina-tion and amiodarone 400 mgday from 10 days before MIuntil termination
Myocardial infarction and operational procedure
Pigs were anesthetized as described previously (Timmers etal 2007b) During the entire operation electrocardiogramarterial pressure and capnogram were continuously moni-tored After median sternotomy the left ventricularpressure (LVP) was measured using a pressure tipped Millarcatheter that was inserted through the apex into the leftventricle A transonic flow probe (Transonic Systems IncIthaca NY USA) was placed around the proximal aorta tomeasure cardiac output Sutures were then tightened topermanently occlude the proximal LCx Internal defibrilla-tion with 50 J was used when VF occurred Prior to and 1 hafter induction of the infarct echocardiography wasperformed After stabilization of hemodynamic parametersand heart rhythm the thorax was closed and the animalswere allowed to recover Three weeks after induction of
myocardial infarction the animals were anesthetized oncemore and the sternum was reopened Echocardiography andconductance catheter-based pressurendashvolume (PV) looprecordings were obtained to assess cardiac function andgeometry After the functional measurements the heart wasexcised for laboratory analysis
Immunohistochemistry
Three weeks following MI myocardial biopsies were obtainedfrom the infarct area border area and remote area andfixated in 4 formalin for 24 h before being embedded inparaffin To determine capillary density a lectin stainingdelineating the endothelium was performed followingantigen retrieval by boiling in 10 mM citrate bufferEndogenous biotin was blocked using 01 avidin solution(DakoCytomation Biotin Blocking system X0590) for 15 min atroom temperature (RT) and subsequently with 001 biotinsolution (Dako) for 15 min at RT After blocking with 30 BSAin PBS the sections were incubated overnight with biotiny-lated BS-1 (Sigma L3759) in a 1300 dilution in PBS with 01BSA and subsequently with streptavidin-HRPO (11000 in PBS)for 1 h at RT Finally the sections were incubated for 30 minin 3-amino-9-ethylcarbazole (AEC) and stained with hema-toxylin before being embedded Capillary density wasexpressed as the number of capillaries per square millimetertissue Quantification of collagen density was performedusing picrosirius red staining with circularly polarized lightand digital image microscopy after conversion into gray-value images as described before (Timmers et al 2007b)
Myocardial infarct size
After excision of the heart the LV was isolated and cut into 5slices from apex to base To discriminate infarct tissue fromviable myocardium the slices were incubated in 1triphenyltetrazolium chloride (TTC Sigma-Aldrich Chemi-cals Zwijndrecht Netherlands) in 37 degC Soumlrensen buffer(136 gL KH2PO4+178 gL Na2H PO42H2O pH 74) for15 min All slices were scanned from both sides and in eachslide the infarct area was compared to total area using digitalplanimetry software After correction for the weight of theslices infarct size was calculated as a percentage of the LV
Cardiac function
Midpapillary short axis epicardial echocardiography wasperformed before coronary artery ligation 1 h after and3 weeks after coronary artery ligation (Prosound SSD-50005 MHz probe UST-5280-5 Aloka Holding Europe AG ZugSwitzerland) Wall thickness (WT) of the infarct area and leftventricular internal area (LVia) were measured at end-diastole (ED) and end-systole (ES) Systolic wall thickening(SWT) was calculated as (WT(ES) ndashWT(ED))WT(ED) 100 ()and fractional area shortening (FAS) as (LVia(ED) ndash LVia(ES))LVia(ED) 100 () Left ventricular (LV) pressurendashvolumeloops were measured using a conductance catheter asdescribed previously (Timmers et al 2009) Diastolicchamber stiffness was quantified by means of linearregression of the end-diastolic pressurendashvolume relationship(Sagawa 1981)
213
Data analysis
The data were collected and analyzed in a blinded fashionData are presented as meanplusmnSE Mortality was comparedusing Fishers exact test Capillary sprouting was comparedusing a one-way ANOVA and Bonferroni post hoc tests A two-way ANOVA with Bonferroni post hoc tests was used tocompare capillary density and collagen density in themyocardial tissue Cardiac functional parameters that werealso measured before MI (baseline) were compared using atwo-way ANOVA for repeated measures and Bonferroni posthoc tests For cardiac functional parameters that weremeasured only 3 weeks after MI Students t test was used
Acknowledgments
This work was supported by the Netherlands Heart Founda-tion [Grant 2005T022 LT] and an Internationalization grantby the University Medical Center Utrecht the Netherlands[DPVK]
Appendix A Supplementary data
Supplementary data to this article can be found online atdoi101016jscr201101001
References
Assmus B Honold J Schachinger V Britten MB Fischer-Rasokat U Lehmann R Teupe C Pistorius K Martin HAbolmaali ND Tonn T Dimmeler S Zeiher AM 2006Transcoronary transplantation of progenitor cells after myocardialinfarction N Engl J Med 355 1222ndash1232
Burlew BS Weber KT 2002 Cardiac fibrosis as a cause ofdiastolic dysfunction Herz 27 92ndash98
Caplan AI Dennis JE 2006 Mesenchymal stem cells as trophicmediators J Cell Biochem 98 1076ndash1084
Cleutjens JP Blankesteijn WM Daemen MJ Smits JF1999 The infarcted myocardium simply dead tissue or a livelytarget for therapeutic interventions Cardiovasc Res 44232ndash241
de Silva R Raval AN Hadi M Gildea KM Bonifacino ACYu ZX Yau YY Leitman SF Bacharach SL DonahueRE Read EJ Lederman RJ 2008 Intracoronary infusion ofautologous mononuclear cells from bone marrow or granulocytecolony-stimulating factor-mobilized apheresis product may notimprove remodelling contractile function perfusion or infarctsize in a swine model of large myocardial infarction Eur Heart J29 1772ndash1782
Erbs S Linke A Schachinger V Assmus B Thiele H DiederichKW Hoffmann C Dimmeler S Tonn T Hambrecht RZeiher AM Schuler G 2007 Restoration of microvascularfunction in the infarct-related artery by intracoronary transplan-tation of bone marrow progenitor cells in patients with acutemyocardial infarction the Doppler Substudy of the Reinfusion ofEnriched Progenitor Cells and Infarct Remodeling in AcuteMyocardial Infarction (REPAIR-AMI) trial Circulation 116 366ndash374
Gnecchi M He H Liang OD Melo LG Morello F Mu HNoiseux N Zhang L Pratt RE Ingwall JS Dzau VJ2005 Paracrine action accounts for marked protection ofischemic heart by Akt-modified mesenchymal stem cells NatMed 11 367ndash368
Hashemi SM Ghods S Kolodgie FD Parcham-Azad K KeaneM Hamamdzic D Young R Rippy MK Virmani R Litt HWilensky RL 2008 A placebo controlled dose-ranging safetystudy of allogenic mesenchymal stem cells injected by endo-myocardial delivery after an acute myocardial infarction EurHeart J 29 251ndash259
Henry TD Annex BH McKendall GR Azrin MA Lopez JJGiordano FJ Shah PK Willerson JT Benza RL BermanDS Gibson CM Bajamonde A Rundle AC Fine JMcCluskey ER 2003 The VIVA trial vascular endothelialgrowth factor in ischemia for vascular angiogenesis Circulation107 1359ndash1365
Janssens S Dubois C Bogaert J Theunissen K Deroose CDesmet W Kalantzi M Herbots L Sinnaeve P Dens JMaertens J Rademakers F Dymarkowski S Gheysens O VanCleemput J Bormans G Nuyts J Belmans A Mortelmans LBoogaerts M Van de Werf F 2006 Autologous bone marrow-derived stem-cell transfer in patients with ST-segment elevationmyocardial infarction double-blind randomised controlled trialLancet 367 113ndash121
Kinnaird T Stabile E Burnett MS Shou M Lee CW BarrS Fuchs S Epstein SE 2004 Local delivery of marrow-derived stromal cells augments collateral perfusion throughparacrine mechanisms Circulation 109 1543ndash1549
Korff T Augustin HG 1998 Integration of endothelial cells inmulticellular spheroids prevents apoptosis and induces differen-tiation J Cell Biol 143 1341ndash1352
Lai RC Arslan F Lee MM Sze NS Choo A Chen TSSalto-Tellez M Timmers L Lee CN El Oakley RMPasterkamp G de Kleijn DP Lim SK 2010 Exosomesecreted by MSC reduces myocardial ischemiareperfusioninjury Stem Cell Res 4 214ndash222
Lian Q Lye E Suan Yeo K KhiaWay Tan E Salto-Tellez M LiuTM PalanisamyN ElOakley RM Lee EH LimB Lim SK2007 Derivation of clinically compliant MSCs from CD105+ CD24-differentiated human ESCs Stem Cells 25 425ndash436
Losordo DW Dimmeler S 2004 Therapeutic angiogenesis andvasculogenesis for ischemic disease part II cell-based therapiesCirculation 109 2692ndash2697
Lunde K Solheim S Aakhus S Arnesen H Abdelnoor MEgeland T Endresen K Ilebekk A Mangschau A Fjeld JGSmith HJ Taraldsrud E Grogaard HK Bjornerheim RBrekke M Muller C Hopp E Ragnarsson A Brinchmann JEForfang K 2006 Intracoronary injection of mononuclear bonemarrow cells in acute myocardial infarction N Engl J Med 3551199ndash1209
Menasche P Alfieri O Janssens S McKenna W Reich-enspurner H Trinquart L Vilquin JT Marolleau JPSeymour B Larghero J Lake S Chatellier G Solomon SDesnos M Hagege AA 2008 The Myoblast AutologousGrafting in Ischemic Cardiomyopathy (MAGIC) trial first ran-domized placebo-controlled study of myoblast transplantationCirculation 117 1189ndash1200
Meyer GP Wollert KC Lotz J Pirr J Rager U Lippolt PHahn A Fichtner S Schaefer A Arseniev L Ganser ADrexler H 2009 Intracoronary bone marrow cell transfer aftermyocardial infarction 5-year follow-up from the randomized-controlled BOOST trial Eur Heart J 24 2978ndash2984
Moelker AD Baks T van den Bos EJ van Geuns RJ deFeyter PJ Duncker DJ van der Giessen WJ 2006Reduction in infarct size but no functional improvement afterbone marrow cell administration in a porcine model ofreperfused myocardial infarction Eur Heart J 27 3057ndash3064
Pittenger MF Martin BJ 2004 Mesenchymal stem cells andtheir potential as cardiac therapeutics Circ Res 95 9ndash20
Sagawa K 1981 The end-systolic pressure-volume relation of theventricle definition modifications and clinical use Circulation63 1223ndash1227
214 L Timmers et al
Schachinger V Erbs S Elsasser A Haberbosch W Ham-brecht R Holschermann H Yu J Corti R Mathey DGHamm CW Suselbeck T Assmus B Tonn T DimmelerS Zeiher AM 2006 Intracoronary bone marrow-derivedprogenitor cells in acute myocardial infarction N Engl J Med355 1210ndash1221
Simons M Annex BH Laham RJ Kleiman N Henry TDauerman H Udelson JE Gervino EV Pike M White-house MJ Moon T Chronos NA 2002 Pharmacologicaltreatment of coronary artery disease with recombinant fibroblastgrowth factor-2 double-blind randomized controlled clinicaltrial Circulation 105 788ndash793
Strauer BE Brehm M Zeus T Kostering M Hernandez ASorg RV Kogler G Wernet P 2002 Repair of infarctedmyocardium by autologous intracoronary mononuclear bonemarrow cell transplantation in humans Circulation 1061913ndash1918
Sze SK de Kleijn DP Lai RC Khia Way E 2007 Tan HZhao KS Yeo TY Low Q Lian CN Lee W Mitchell RM ElOakley SK Lim Elucidating the secretion proteome of humanembryonic stem cell-derived mesenchymal stem cells Mol CellProteomics 6 1680ndash1689
Timmers L Lim SK Arslan F Armstrong JS Hoefer IEDoevendans PA Piek JJ El Oakley RM Choo A Lee CNPasterkamp G de Kleijn DP 2007a Reduction of myocardialinfarct size by humanmesenchymal stemcell conditionedmediumStem Cell Res 1 129ndash137
Timmers L Sluijter JP Verlaan CW Steendijk P CramerMJEmons M Strijder C Grundeman PF Sze SK Hua L PiekJJ Borst C Pasterkamp G de Kleijn DP 2007b Cycloox-ygenase-2 inhibition increases mortality enhances left ventricularremodeling and impairs systolic function after myocardialinfarction in the pig Circulation 115 326ndash332
Timmers L Henriques JP de Kleijn DP Devries JHKemperman H Steendijk P Verlaan CW Kerver MPiek JJ Doevendans PA Pasterkamp G Hoefer IE2009 Exenatide reduces infarct size and improves cardiacfunction in a porcine model of ischemia and reperfusion injuryJ Am Coll Cardiol 53 501ndash510
van Laake LW Passier R denOuden K Schreurs CMonshouwer-Kloots JWard-vanOostwaard D van Echteld CJ DoevendansPA Mummery CL 2009 Improvement of mouse cardiacfunction by hESC-derived cardiomyocytes correlates with vascular-ity but not graft size Stem Cell Res 3 106ndash112
Wolf D Reinhard A Seckinger A Gross L Katus HA HansenA 2009 Regenerative capacity of intravenous autologousallogeneic and human mesenchymal stem cells in the infarctedpig myocardium-complicated by myocardial tumor formationScand Cardiovasc J 43 39ndash45
Yousef M Schannwell CM Kostering M Zeus T Brehm MStrauer BE 2009 The BALANCE Study clinical benefit andlong-term outcome after intracoronary autologous bone marrowcell transplantation in patients with acute myocardial infarctionJ Am Coll Cardiol 53 2262ndash2269

207
Introduction
Despite significant advances in myocardial revascularizationcoronary artery disease and subsequent myocardial infarc-tion (MI) are leading causes of morbidity and mortalityworldwide One of the main goals in the treatment ofischemic heart disease is the development of effectivestrategies to stimulate vascular repair mechanisms in orderto achieve adequate tissue perfusion
Although the potential of stem cell therapy for MI is stillheavily debated as a result of studies that failed to showimproved outcome (Moelker et al 2006 de Silva et al 2008Janssens et al 2006 Lunde et al 2006 Meyer et al 2009Menasche et al 2008) there are several preclinical andclinical studies that demonstrated the therapeutic effects ofstem cell transplantation (Hashemi et al 2008 Wolf et al2009 Assmus et al 2006 Schachinger et al 2006 Straueret al 2002 Yousef et al 2009) While robust evidence forcardiomyocyte replacement is still limited more evidence isaccumulating for vascular repair mechanisms following stemcell transplantation (van Laake et al 2009 Losordo ampDimmeler 2004 Erbs et al 2007) Among the stem cells thathave been tested for cardiac repair mesenchymal stem cells(MSCs) derived from adult bone marrow have emerged as apromising stem cell type for treating cardiovascular disease(Pittenger amp Martin 2004) Recent studies suggest that atleast some of the therapeutic effects of MSCs aremediated byparacrine factors secreted by the cells (Caplan amp Dennis2006 Gnecchi et al 2005) These paracrine factors could beexploited to extend the therapeutic possibilities of MSCs forthe treatment of a variety of diseases including MIApplication of MSC secretions rather than MSCs themselvesin order to restore tissue perfusion could enable us to avoidsome of the limiting factors associatedwith cell therapy suchas immune incompatibility tumorigenicity costs and wait-ing time for ex vivo expansion
We previously described how human MSC lines can bereproducibly generated from human embryonic stem cell(hESC) lines which constitute an invariable source ofconsistently uniform batches of MSCs (Lian et al 2007) Inaddition we established for the first time the collection ofthese MSC secretions as conditioned medium (MSC-CM) in aclinically compliant manner circumventing exposure tovirus mouse cells or serum (Sze et al 2007) Recently wedemonstrated that MSC-CM treatment following ischemiareperfusion injury reduces myocardial apoptosis and oxida-tive stress (Timmers et al 2007a) In the current paper wereveal the angiogenic potential of clinically compatible MSC-CM and demonstrate in a large animal model that it can beused to improve cardiac function following MI
Results
MSC-CM stimulates angiogenesis in vitro
Ingenuity pathway analysis of the secretory proteome ofMSC-CM revealed that within the physiological systemdevelopment and function group cardiovascular systemdevelopment and function has the highest overrepresenta-tion (Pb10-12) with 75 different focus proteins Within thegroup of cardiovascular system development and function
development of blood vessels angiogenesis proliferation ofendothelial cells neovascularization and vascularizationare the processes with the highest overrepresentation(supplementary data Table 1)
Having identified the potential involvement of MSC-CM inblood vessel formation we used an in vitro assay ofangiogenesis to further investigate this potential In anangiogenesis assay based on formation of capillary sprouts byHUVEC spheroids MSC-CM induced significantly more capil-lary sprouting compared with NCM (Fig 1A) The averagelength of the sprouts did not increase following MSC-CMtreatment compared with NCM (Fig 1B) The total length ofall sprouts however significantly increased in spheroidsincubated with MSC-CM when compared with NCM (Fig 1C)
In addition a HUVECMatrigel angiogenesis assay wasperformed which revealed a longer average tube length withCM compared with NCM (107plusmn0046 vs 099plusmn0041 mmP=0003)
MSC-CM treatment after infarction increasescapillary density and decreases collagen density
Capillary density was higher in the border areas followingMSC-CM treatment compared with NCM treatment (Figs 2Aand B) In the remote area capillary density did not differbetween MSC-CM treatment and NCM treatment (Fig 2C)We were unable to reliably quantify capillary density in theinfarct area due to the unorganized structure of the infarctgranulation tissue 3 weeks following MI
Picrosirius staining revealed that collagen density in theborder area and in the remote myocardium was lower in pigstreated with MSC-CM compared with pigs treated with NCMIn the infarct area no difference was detected between thetreatment groups (Fig 3)
MSC-CM preserves cardiac function following MI
One hour after coronary artery ligation cardiac functiondecreased similarly in both groups Fractional area shorten-ing decreased from 458plusmn19 to 323plusmn20 in the NCM groupand from 469plusmn46 to 297plusmn34 in the MSC-CM group(P=0670) Also cardiac output (280plusmn010 Lmin (NCM) vs267plusmn022 Lmin (MSC-CM) P=0596) mean aortic pressure(90plusmn83 mm Hg (NCM) vs 84plusmn54 mm Hg (MSC-CM) P=0544)and dPdtMAX (1135plusmn83 mm Hgs (NCM) vs 1096plusmn83 mm Hgs(MSC-CM) P=0741) were similar in both groups 1 h aftercoronary artery ligation
In the 3 weeks following MI the LV internal areasincreased in all pigs However the increase in LV internalarea tended to be more pronounced in NCM-treated animalspointing to reduced remodeling in MSC-CM-treated pigs(Figs 4A and B) Echocardiographic wall thickness of theinfarct area decreased in pigs treated with NCM but not inpigs treated with MSC-CM (Fig 4C) The fractional areashortening was higher following MSC-CM treatment whichreflects increased systolic cardiac performance (Fig 4D)Also other systolic functional parameters such as ejectionfraction dPdtMAX stroke volume and stroke work werehigher in animals treated with MSC-CM Improved cardiacfunction translated into improved hemodynamic parameterswith the mean arterial pressure and cardiac output being
Figure 1 HUVEC spheroid assay of angiogenesis The number of capillary sprouts (A) mean length of sprouts (pixels B) and totallength of sprouts (pixels C) after incubation of HUVEC spheroids with MSC-CM (n=12) or NCM (n=12) Representative pictures of MSC-CM and NCM are demonstrated in panels D and E respectively Pb001 vs NCM
208 L Timmers et al
higher in MSC-CM-treated pigs In addition diastolic functionimproved as assessed with dPdtMIN and diastolic chamberstiffness All functional parameters are summarized in Table 1Myocardial infarct size 3 weeks following coronary arteryligation was smaller in MSC-CM-treated pigs compared to NCM-treated pigs (116plusmn20 vs 166plusmn12 of the LV P=0050)
Two pigs died during the surgical procedure due torefractory ventricular fibrillation before treatment withMSC-CM or NCM and were therefore excluded from thestudy Two pigs (1 treated with MSC-CM and 1 treated withNCM) died in the third week following MI without signs ofheart failure or cardiac rupture probably due to ventriculartachycardiafibrillation
Discussion
Here we demonstrate that human MSC-CM treatmentenhances capillary density resulting in reduced myocardial
infarct size and preserved systolic and diastolic function in aporcine model of myocardial infarction
Recently it was demonstrated that administration of MSCsecretions improved outcome in a murine model of MI(Gnecchi et al 2005) Vascular repair mechanisms consti-tute an important means to reduce myocardial injury and toimprove cardiac function following MI Although the thera-peutic potential of stem cell transplantation is still a subjectof discussion evidence for vascular repair mechanismsfollowing stem cell transplantation is growing (van Laakeet al 2009 Losordo amp Dimmeler 2004 Erbs et al 2007) Ifvascular repair mechanisms are induced by paracrinefactors application of stem cell secretions may extend therepertoire of stem cell-based therapies with a differentdimension
An in vitro sprouting assay confirmed Ingenuity analysis ofearlier MSC-CM proteomics data and identified the angio-genic potential of MSC-CM In order to investigate thetherapeutic potential of MSC-CM to stimulate angiogenesis
Figure 2 Capillary density Representative sections of border areas after lectin staining to visualize endothelium 3 weeks after MIfrom pigs treated with NCM (A n=9) or MSC-CM (B n=9) Quantification of capillary density in remote and border area isdemonstrated in panel C Scale bars 500 μm
Figure 3 Collagen density Quantification of collaged densityin the infarct border and remote areas in pigs treated with NCMand MSC-CM
209
in vivo we used a porcine model of myocardial infarctionDuring myocardial ischemia following coronary artery liga-tion cardiomyocytes in the central infarct perish withinminutes to hours after coronary occlusion The border zoneof the ischemic area however contains injured but viablecells under hypoperfused and hypoxic conditions which mayeither be salvaged or die depending on the conditions afterischemia Restoration of myocardial perfusion by means ofangiogenesis restores the metabolic needs of cardiomyocytesin the border area and offers the cells a better chance ofsurvival which in turn could lead to reduced myocardialinjury Intracoronary delivery of bone marrow-derivedprogenitor cells has been suggested to promote vascularrepair following MI potentially via paracrine mechanisms(Erbs et al 2007) Such effect was also observed in a rodentmodel of hind limb ischemia (Kinnaird et al 2004) Asbecame evident from our histological analyses MSC-CMincreased capillary density in the border areas and myocar-dial infarct size was reduced which was accompanied bypreserved LV dimensions and cardiac function
Besides stimulation of angiogenesis it cannot be excludedthat also other mechanisms contributed to reduction of
A B
C D
WT
infa
rct
(cm
)
FAS
(
)E F
dP
dt M
AX (
mm
Hg
s)
LVE
S a
rea
(cm
2)
LVE
S a
rea
(cm
2)
dP
dt M
in (
mm
Hg
s)
Figure 4 Cardiac function Left ventricular (LV) end-diastolic internal area (A) LV end-systolic internal area (B) posterolateralmyocardial wall (infarct) thickness (C) fractional area shortening (FAS D) dPdtMAX (E) and dPdtMIN (F) before MI (baseline) 1 h postMI and 3 weeks post MI in pigs treated with MSC-CM (black dots n=9) or NCM (open dots n=9) Pb005 vs NCM
210 L Timmers et al
myocardial infarct size and preservation of myocardialfunction With preserved left ventricular dimensions andinfarct thickness inhibition of post MI cardiac remodeling is apotential contributing mechanism Collagen density in theborder area and remote myocardium was lower in pigstreated with MSC-CM Cardiac fibrosis is associated withheart failure following myocardial infarction and maycontribute to progression of systolic and diastolic dysfunc-tion (Burlew amp Weber 2002 Cleutjens et al 1999) Werecently demonstrated that intravenous and intracoronaryMSC-CM treatment reduces myocardial apoptosis and oxida-tive stress (Timmers et al 2007a) In that study cardio-myocyte death was targeted acutely following ischemia andreperfusion injury In the current study treatment wasstarted late after coronary artery ligation and a model ofpermanent coronary artery ligation was used in order toinvestigate the angiogenic potential of MSC-CM and its effecton cardiac function independent of reduction of reperfusioninjury The fact that cardiac function improved using thisprotocol shows that there may be additional benefit fromprolonged treatment with MSC secretions
For this study a permanent coronary artery ligation wasperformed in anesthetized animals and functional measure-
ments were performed with open chest In addition we havenot been able to investigate the effect of commoncomorbidities such as hypertension dyslipidemia anddiabetes which might influence the biologic effect of MSCsecretions Due to the permanent coronary artery ligationwe were not able to assess the area at risk 3 weeks post MIWe were not able to oversee the effects of human proteininjection on the immune system of the porcine host and thepotential influence on study endpoints Furthermore themolecular mechanism for the induction of angiogenesis andor arteriogenesis and an exact determination of theresponsible angiogenic factors are still lacking Severalclinical trials with potent angiogenic factors failed toimprove outcome in patients (Henry et al 2003 Simonset al 2002) It is not clear how paracrine factors in stem celltransplants or the paracrine factors alone can induce abetter effect Most likely a combination of angiogenicfactors rather than a single protein is responsible Alsoexosomes could play an important role We previouslydemonstrated exosomes in MSC-CM to contain and delivercardioprotective compounds preventing cardiomyocytedeath following ischemia and reperfusion injury (Lai et al2010) Exosomes constitute a potential delivery tool to
Table 1 Hemodynamic and Functional Parameters
Baseline 3 weeks post MI Change from baseline ()
Parameter NCM CM NCM CM NCM CM
HR bpm 66plusmn4 73plusmn6 84plusmn6 86plusmn6 28plusmn12 12plusmn11MAP mm Hg 95plusmn5 89plusmn5 66plusmn6 85plusmn5 -30plusmn5 -5plusmn8 CO Lmin 31plusmn01 30plusmn02 37plusmn06 53plusmn05 23plusmn21 78plusmn20dPdt max mm Hgs 1213plusmn77 1241plusmn56 1157plusmn162 1650plusmn124 4plusmn13 40plusmn9 dPdt min mm Hgs -1274plusmn122 -1130plusmn96 -883plusmn98 -1313plusmn95 27plusmn9 -19plusmn19 EDP mm Hg 80plusmn03 71plusmn06 133plusmn16 121plusmn11 68plusmn21 94plusmn42WT infarct cm 079plusmn004 083plusmn005 055plusmn002 079plusmn005 -27plusmn4 -5plusmn4 Lvia (ED) cm2 158plusmn05 142plusmn10 260plusmn18 218plusmn15 64plusmn12 55plusmn12Lvia (ES) cm2 85plusmn04 76plusmn09 177plusmn16 125plusmn09 104plusmn14 60plusmn14 FAS 458plusmn19 469plusmn46 326plusmn22 424plusmn33 -28plusmn6 -6plusmn8 SV ml 48plusmn3 42plusmn2 43plusmn4 62plusmn3 -4plusmn11 52plusmn10 EDV ml 134plusmn16 129plusmn9ESV ml 93plusmn15 73plusmn9EF 337plusmn44 491plusmn33 SW mm Hgmiddotml 2497plusmn333 4595plusmn361 Stiffness mm Hgml 026plusmn004 014plusmn002
Summary of cardiac functional parameters of pigs treated with NCM (n=9) and MSC-CM (n=9) determined with echocardiography andconductance catheter-based LV pressure and volumemeasurements MI indicates myocardial infarction HR heart rate MAP mean arterialpressure CO cardiac output EDP end-diastolic pressure WT wall thickness LVia left ventricular internal area SV stroke volume EDVend-diastolic volume ESV end-systolic volume EF ejection fraction SW stroke work Stiffness end-diastolic chamber stiffness Pb005vs NCM
211
effectively carry angiogenic factors into the intracellularspace of the target tissue protecting the factors fromproteases This may explain why relatively low doses canhave such profound angiogenic effects Whether exosomesand their content are also responsible for the stimulation ofangiogenesis following MI remains a subject for furtherinvestigation
Here we demonstrate that human MSC secretionsstimulate angiogenesis These data support the hypothesisthat MSC transplantation induces vascular repair mechanismsvia paracrine pathways Most importantly human MSCsecretions harvested as conditioned medium using a clini-cally compliant protocol reduced infarct size and preservedcardiac function in a large animal model of myocardialinfarction The study therefore identifies MSC-CM as a noveltherapeutic biologic in the improvement of cardiac functionafter myocardial infarction
Methods
MSC-CM preparation
The protocols for MSC generation and CM preparation havebeen described in previous papers (Lian et al 2007 Sze et al2007) In short a chemically defined serum-free culturemedium(DMEMwithoutphenol red supplementedwith insulintransferrin and selenium 5 ngml FGF2 5 ngml PDGF ABglutamine-penicillin-streptomycin and szlig-mercaptoethanol)was conditioned by MSCs derived from human embryonicstem cells (hESCs) using a clinically compliant protocol Threepolyclonal karyotypically stable and phenotypically MSC-likecultures that do not express pluripotency-associated markersbut displayed MSC-like surface antigens (CD29+ CD44+CD49a+e+ CD105+ CD166+ CD34ndash CD45ndash) and gene
expression profile were generated by trypsinization andpropagation of hESCs from either the HuES9 hESC line or theH1 hESC line in feeder- and serum-free selection media (Lianet al 2007) One of these cultures HuES9E1 can be stablyexpanded for at least 80 population doublings To harvest MSCsecretions hESC-derived MSC cultures were transferred to achemically defined serum-free culture medium to conditionthe medium for 3 days before the media containing MSCsecretions were collected clarified by centrifugation con-centrated 25 times using 10-kDa MW cutoff ultrafiltrationmembranes and sterilized by filtration through a 220-nmfilter The protein concentration after concentration was050 mgml As a negative control the above-noted serum-free culture medium was processed equally (nonconditionedmedium [NCM])
Ingenuity pathway analysis
For this analysis we used the proteomic data obtainedpreviously (Sze et al 2007) Bioinformatic analysis wasperformed using Ingenuity pathway analysis (Ingenuity IPA-2002 version 71) The 201 proteins were uploaded inIngenuity with Ingenuity Knowledge Base as a reference setand direct and indirect relationships were included Allmolecules or relationships were considered for the filtersummary In the summary the focus was on Top Bio functionsin which physiological system development and function wasanalyzed in depth
HUVEC spheroid assay
Spheroids were formed from HUVECs to determine the effectof conditioned medium on angiogenic sprout formation (Korffamp Augustin 1998) Spheroids were formed overnight in 20
212 L Timmers et al
methocel in culture medium and subsequently embedded ina collagenndashmethocel matrix Sprouting was induced over-night with MSC-CM (n=12) or non-CM (NCM) (n=12) todetermine the effect of the secreted chemotactic proteinson capillary sprouting After overnight sprouting spheroidswere fixed in 10 formaldehyde and pictures were taken andthe length and number of sprouts were quantified
Animals
All experiments were performed in accordance with theldquoGuide for the Care and Use of Laboratory Animalsrdquo preparedby the Institute of Laboratory Animal Resources andwith priorapproval by the Animal Experimentation Committee of theFaculty of Medicine Utrecht University the Netherlands
Sample size calculation
In a previous study the mean fractional area shortening(FAS) after LCx ligation was 365 (Timmers et al 2007b)With an alpha of 005 power of 080 SD of 58 anddifference of 20 considered relevant 10 animals per groupwere needed To allow for 10 mortality 11 animals pergroup were enrolled
Pig study design
Myocardial infarction was induced in 22 Dalland Landracepigs (60ndash70 kg IDDLO Lelystad the Netherlands) by surgicalleft circumflex coronary artery (LCx) ligation Two pigs diedperioperatively before randomization and were thereforeexcluded from the study The remaining 20 pigs wererandomized after surgery by using sealed envelopes tointravenous treatment with MSC-CM (20 ml MSC-CM ie10 mg protein) or 20 ml NCM initiated 4 h after coronaryartery ligation and the treatment was continued for 7 daystwice daily via a catheter inserted into the jugular vein Thepigs were sacrificed 3 weeks after MI To prevent thromboticcomplications and arrhythmias all pigs were treated withclopidogrel 75 mgday from 3 days before MI until termina-tion and amiodarone 400 mgday from 10 days before MIuntil termination
Myocardial infarction and operational procedure
Pigs were anesthetized as described previously (Timmers etal 2007b) During the entire operation electrocardiogramarterial pressure and capnogram were continuously moni-tored After median sternotomy the left ventricularpressure (LVP) was measured using a pressure tipped Millarcatheter that was inserted through the apex into the leftventricle A transonic flow probe (Transonic Systems IncIthaca NY USA) was placed around the proximal aorta tomeasure cardiac output Sutures were then tightened topermanently occlude the proximal LCx Internal defibrilla-tion with 50 J was used when VF occurred Prior to and 1 hafter induction of the infarct echocardiography wasperformed After stabilization of hemodynamic parametersand heart rhythm the thorax was closed and the animalswere allowed to recover Three weeks after induction of
myocardial infarction the animals were anesthetized oncemore and the sternum was reopened Echocardiography andconductance catheter-based pressurendashvolume (PV) looprecordings were obtained to assess cardiac function andgeometry After the functional measurements the heart wasexcised for laboratory analysis
Immunohistochemistry
Three weeks following MI myocardial biopsies were obtainedfrom the infarct area border area and remote area andfixated in 4 formalin for 24 h before being embedded inparaffin To determine capillary density a lectin stainingdelineating the endothelium was performed followingantigen retrieval by boiling in 10 mM citrate bufferEndogenous biotin was blocked using 01 avidin solution(DakoCytomation Biotin Blocking system X0590) for 15 min atroom temperature (RT) and subsequently with 001 biotinsolution (Dako) for 15 min at RT After blocking with 30 BSAin PBS the sections were incubated overnight with biotiny-lated BS-1 (Sigma L3759) in a 1300 dilution in PBS with 01BSA and subsequently with streptavidin-HRPO (11000 in PBS)for 1 h at RT Finally the sections were incubated for 30 minin 3-amino-9-ethylcarbazole (AEC) and stained with hema-toxylin before being embedded Capillary density wasexpressed as the number of capillaries per square millimetertissue Quantification of collagen density was performedusing picrosirius red staining with circularly polarized lightand digital image microscopy after conversion into gray-value images as described before (Timmers et al 2007b)
Myocardial infarct size
After excision of the heart the LV was isolated and cut into 5slices from apex to base To discriminate infarct tissue fromviable myocardium the slices were incubated in 1triphenyltetrazolium chloride (TTC Sigma-Aldrich Chemi-cals Zwijndrecht Netherlands) in 37 degC Soumlrensen buffer(136 gL KH2PO4+178 gL Na2H PO42H2O pH 74) for15 min All slices were scanned from both sides and in eachslide the infarct area was compared to total area using digitalplanimetry software After correction for the weight of theslices infarct size was calculated as a percentage of the LV
Cardiac function
Midpapillary short axis epicardial echocardiography wasperformed before coronary artery ligation 1 h after and3 weeks after coronary artery ligation (Prosound SSD-50005 MHz probe UST-5280-5 Aloka Holding Europe AG ZugSwitzerland) Wall thickness (WT) of the infarct area and leftventricular internal area (LVia) were measured at end-diastole (ED) and end-systole (ES) Systolic wall thickening(SWT) was calculated as (WT(ES) ndashWT(ED))WT(ED) 100 ()and fractional area shortening (FAS) as (LVia(ED) ndash LVia(ES))LVia(ED) 100 () Left ventricular (LV) pressurendashvolumeloops were measured using a conductance catheter asdescribed previously (Timmers et al 2009) Diastolicchamber stiffness was quantified by means of linearregression of the end-diastolic pressurendashvolume relationship(Sagawa 1981)
213
Data analysis
The data were collected and analyzed in a blinded fashionData are presented as meanplusmnSE Mortality was comparedusing Fishers exact test Capillary sprouting was comparedusing a one-way ANOVA and Bonferroni post hoc tests A two-way ANOVA with Bonferroni post hoc tests was used tocompare capillary density and collagen density in themyocardial tissue Cardiac functional parameters that werealso measured before MI (baseline) were compared using atwo-way ANOVA for repeated measures and Bonferroni posthoc tests For cardiac functional parameters that weremeasured only 3 weeks after MI Students t test was used
Acknowledgments
This work was supported by the Netherlands Heart Founda-tion [Grant 2005T022 LT] and an Internationalization grantby the University Medical Center Utrecht the Netherlands[DPVK]
Appendix A Supplementary data
Supplementary data to this article can be found online atdoi101016jscr201101001
References
Assmus B Honold J Schachinger V Britten MB Fischer-Rasokat U Lehmann R Teupe C Pistorius K Martin HAbolmaali ND Tonn T Dimmeler S Zeiher AM 2006Transcoronary transplantation of progenitor cells after myocardialinfarction N Engl J Med 355 1222ndash1232
Burlew BS Weber KT 2002 Cardiac fibrosis as a cause ofdiastolic dysfunction Herz 27 92ndash98
Caplan AI Dennis JE 2006 Mesenchymal stem cells as trophicmediators J Cell Biochem 98 1076ndash1084
Cleutjens JP Blankesteijn WM Daemen MJ Smits JF1999 The infarcted myocardium simply dead tissue or a livelytarget for therapeutic interventions Cardiovasc Res 44232ndash241
de Silva R Raval AN Hadi M Gildea KM Bonifacino ACYu ZX Yau YY Leitman SF Bacharach SL DonahueRE Read EJ Lederman RJ 2008 Intracoronary infusion ofautologous mononuclear cells from bone marrow or granulocytecolony-stimulating factor-mobilized apheresis product may notimprove remodelling contractile function perfusion or infarctsize in a swine model of large myocardial infarction Eur Heart J29 1772ndash1782
Erbs S Linke A Schachinger V Assmus B Thiele H DiederichKW Hoffmann C Dimmeler S Tonn T Hambrecht RZeiher AM Schuler G 2007 Restoration of microvascularfunction in the infarct-related artery by intracoronary transplan-tation of bone marrow progenitor cells in patients with acutemyocardial infarction the Doppler Substudy of the Reinfusion ofEnriched Progenitor Cells and Infarct Remodeling in AcuteMyocardial Infarction (REPAIR-AMI) trial Circulation 116 366ndash374
Gnecchi M He H Liang OD Melo LG Morello F Mu HNoiseux N Zhang L Pratt RE Ingwall JS Dzau VJ2005 Paracrine action accounts for marked protection ofischemic heart by Akt-modified mesenchymal stem cells NatMed 11 367ndash368
Hashemi SM Ghods S Kolodgie FD Parcham-Azad K KeaneM Hamamdzic D Young R Rippy MK Virmani R Litt HWilensky RL 2008 A placebo controlled dose-ranging safetystudy of allogenic mesenchymal stem cells injected by endo-myocardial delivery after an acute myocardial infarction EurHeart J 29 251ndash259
Henry TD Annex BH McKendall GR Azrin MA Lopez JJGiordano FJ Shah PK Willerson JT Benza RL BermanDS Gibson CM Bajamonde A Rundle AC Fine JMcCluskey ER 2003 The VIVA trial vascular endothelialgrowth factor in ischemia for vascular angiogenesis Circulation107 1359ndash1365
Janssens S Dubois C Bogaert J Theunissen K Deroose CDesmet W Kalantzi M Herbots L Sinnaeve P Dens JMaertens J Rademakers F Dymarkowski S Gheysens O VanCleemput J Bormans G Nuyts J Belmans A Mortelmans LBoogaerts M Van de Werf F 2006 Autologous bone marrow-derived stem-cell transfer in patients with ST-segment elevationmyocardial infarction double-blind randomised controlled trialLancet 367 113ndash121
Kinnaird T Stabile E Burnett MS Shou M Lee CW BarrS Fuchs S Epstein SE 2004 Local delivery of marrow-derived stromal cells augments collateral perfusion throughparacrine mechanisms Circulation 109 1543ndash1549
Korff T Augustin HG 1998 Integration of endothelial cells inmulticellular spheroids prevents apoptosis and induces differen-tiation J Cell Biol 143 1341ndash1352
Lai RC Arslan F Lee MM Sze NS Choo A Chen TSSalto-Tellez M Timmers L Lee CN El Oakley RMPasterkamp G de Kleijn DP Lim SK 2010 Exosomesecreted by MSC reduces myocardial ischemiareperfusioninjury Stem Cell Res 4 214ndash222
Lian Q Lye E Suan Yeo K KhiaWay Tan E Salto-Tellez M LiuTM PalanisamyN ElOakley RM Lee EH LimB Lim SK2007 Derivation of clinically compliant MSCs from CD105+ CD24-differentiated human ESCs Stem Cells 25 425ndash436
Losordo DW Dimmeler S 2004 Therapeutic angiogenesis andvasculogenesis for ischemic disease part II cell-based therapiesCirculation 109 2692ndash2697
Lunde K Solheim S Aakhus S Arnesen H Abdelnoor MEgeland T Endresen K Ilebekk A Mangschau A Fjeld JGSmith HJ Taraldsrud E Grogaard HK Bjornerheim RBrekke M Muller C Hopp E Ragnarsson A Brinchmann JEForfang K 2006 Intracoronary injection of mononuclear bonemarrow cells in acute myocardial infarction N Engl J Med 3551199ndash1209
Menasche P Alfieri O Janssens S McKenna W Reich-enspurner H Trinquart L Vilquin JT Marolleau JPSeymour B Larghero J Lake S Chatellier G Solomon SDesnos M Hagege AA 2008 The Myoblast AutologousGrafting in Ischemic Cardiomyopathy (MAGIC) trial first ran-domized placebo-controlled study of myoblast transplantationCirculation 117 1189ndash1200
Meyer GP Wollert KC Lotz J Pirr J Rager U Lippolt PHahn A Fichtner S Schaefer A Arseniev L Ganser ADrexler H 2009 Intracoronary bone marrow cell transfer aftermyocardial infarction 5-year follow-up from the randomized-controlled BOOST trial Eur Heart J 24 2978ndash2984
Moelker AD Baks T van den Bos EJ van Geuns RJ deFeyter PJ Duncker DJ van der Giessen WJ 2006Reduction in infarct size but no functional improvement afterbone marrow cell administration in a porcine model ofreperfused myocardial infarction Eur Heart J 27 3057ndash3064
Pittenger MF Martin BJ 2004 Mesenchymal stem cells andtheir potential as cardiac therapeutics Circ Res 95 9ndash20
Sagawa K 1981 The end-systolic pressure-volume relation of theventricle definition modifications and clinical use Circulation63 1223ndash1227
214 L Timmers et al
Schachinger V Erbs S Elsasser A Haberbosch W Ham-brecht R Holschermann H Yu J Corti R Mathey DGHamm CW Suselbeck T Assmus B Tonn T DimmelerS Zeiher AM 2006 Intracoronary bone marrow-derivedprogenitor cells in acute myocardial infarction N Engl J Med355 1210ndash1221
Simons M Annex BH Laham RJ Kleiman N Henry TDauerman H Udelson JE Gervino EV Pike M White-house MJ Moon T Chronos NA 2002 Pharmacologicaltreatment of coronary artery disease with recombinant fibroblastgrowth factor-2 double-blind randomized controlled clinicaltrial Circulation 105 788ndash793
Strauer BE Brehm M Zeus T Kostering M Hernandez ASorg RV Kogler G Wernet P 2002 Repair of infarctedmyocardium by autologous intracoronary mononuclear bonemarrow cell transplantation in humans Circulation 1061913ndash1918
Sze SK de Kleijn DP Lai RC Khia Way E 2007 Tan HZhao KS Yeo TY Low Q Lian CN Lee W Mitchell RM ElOakley SK Lim Elucidating the secretion proteome of humanembryonic stem cell-derived mesenchymal stem cells Mol CellProteomics 6 1680ndash1689
Timmers L Lim SK Arslan F Armstrong JS Hoefer IEDoevendans PA Piek JJ El Oakley RM Choo A Lee CNPasterkamp G de Kleijn DP 2007a Reduction of myocardialinfarct size by humanmesenchymal stemcell conditionedmediumStem Cell Res 1 129ndash137
Timmers L Sluijter JP Verlaan CW Steendijk P CramerMJEmons M Strijder C Grundeman PF Sze SK Hua L PiekJJ Borst C Pasterkamp G de Kleijn DP 2007b Cycloox-ygenase-2 inhibition increases mortality enhances left ventricularremodeling and impairs systolic function after myocardialinfarction in the pig Circulation 115 326ndash332
Timmers L Henriques JP de Kleijn DP Devries JHKemperman H Steendijk P Verlaan CW Kerver MPiek JJ Doevendans PA Pasterkamp G Hoefer IE2009 Exenatide reduces infarct size and improves cardiacfunction in a porcine model of ischemia and reperfusion injuryJ Am Coll Cardiol 53 501ndash510
van Laake LW Passier R denOuden K Schreurs CMonshouwer-Kloots JWard-vanOostwaard D van Echteld CJ DoevendansPA Mummery CL 2009 Improvement of mouse cardiacfunction by hESC-derived cardiomyocytes correlates with vascular-ity but not graft size Stem Cell Res 3 106ndash112
Wolf D Reinhard A Seckinger A Gross L Katus HA HansenA 2009 Regenerative capacity of intravenous autologousallogeneic and human mesenchymal stem cells in the infarctedpig myocardium-complicated by myocardial tumor formationScand Cardiovasc J 43 39ndash45
Yousef M Schannwell CM Kostering M Zeus T Brehm MStrauer BE 2009 The BALANCE Study clinical benefit andlong-term outcome after intracoronary autologous bone marrowcell transplantation in patients with acute myocardial infarctionJ Am Coll Cardiol 53 2262ndash2269

Figure 1 HUVEC spheroid assay of angiogenesis The number of capillary sprouts (A) mean length of sprouts (pixels B) and totallength of sprouts (pixels C) after incubation of HUVEC spheroids with MSC-CM (n=12) or NCM (n=12) Representative pictures of MSC-CM and NCM are demonstrated in panels D and E respectively Pb001 vs NCM
208 L Timmers et al
higher in MSC-CM-treated pigs In addition diastolic functionimproved as assessed with dPdtMIN and diastolic chamberstiffness All functional parameters are summarized in Table 1Myocardial infarct size 3 weeks following coronary arteryligation was smaller in MSC-CM-treated pigs compared to NCM-treated pigs (116plusmn20 vs 166plusmn12 of the LV P=0050)
Two pigs died during the surgical procedure due torefractory ventricular fibrillation before treatment withMSC-CM or NCM and were therefore excluded from thestudy Two pigs (1 treated with MSC-CM and 1 treated withNCM) died in the third week following MI without signs ofheart failure or cardiac rupture probably due to ventriculartachycardiafibrillation
Discussion
Here we demonstrate that human MSC-CM treatmentenhances capillary density resulting in reduced myocardial
infarct size and preserved systolic and diastolic function in aporcine model of myocardial infarction
Recently it was demonstrated that administration of MSCsecretions improved outcome in a murine model of MI(Gnecchi et al 2005) Vascular repair mechanisms consti-tute an important means to reduce myocardial injury and toimprove cardiac function following MI Although the thera-peutic potential of stem cell transplantation is still a subjectof discussion evidence for vascular repair mechanismsfollowing stem cell transplantation is growing (van Laakeet al 2009 Losordo amp Dimmeler 2004 Erbs et al 2007) Ifvascular repair mechanisms are induced by paracrinefactors application of stem cell secretions may extend therepertoire of stem cell-based therapies with a differentdimension
An in vitro sprouting assay confirmed Ingenuity analysis ofearlier MSC-CM proteomics data and identified the angio-genic potential of MSC-CM In order to investigate thetherapeutic potential of MSC-CM to stimulate angiogenesis
Figure 2 Capillary density Representative sections of border areas after lectin staining to visualize endothelium 3 weeks after MIfrom pigs treated with NCM (A n=9) or MSC-CM (B n=9) Quantification of capillary density in remote and border area isdemonstrated in panel C Scale bars 500 μm
Figure 3 Collagen density Quantification of collaged densityin the infarct border and remote areas in pigs treated with NCMand MSC-CM
209
in vivo we used a porcine model of myocardial infarctionDuring myocardial ischemia following coronary artery liga-tion cardiomyocytes in the central infarct perish withinminutes to hours after coronary occlusion The border zoneof the ischemic area however contains injured but viablecells under hypoperfused and hypoxic conditions which mayeither be salvaged or die depending on the conditions afterischemia Restoration of myocardial perfusion by means ofangiogenesis restores the metabolic needs of cardiomyocytesin the border area and offers the cells a better chance ofsurvival which in turn could lead to reduced myocardialinjury Intracoronary delivery of bone marrow-derivedprogenitor cells has been suggested to promote vascularrepair following MI potentially via paracrine mechanisms(Erbs et al 2007) Such effect was also observed in a rodentmodel of hind limb ischemia (Kinnaird et al 2004) Asbecame evident from our histological analyses MSC-CMincreased capillary density in the border areas and myocar-dial infarct size was reduced which was accompanied bypreserved LV dimensions and cardiac function
Besides stimulation of angiogenesis it cannot be excludedthat also other mechanisms contributed to reduction of
A B
C D
WT
infa
rct
(cm
)
FAS
(
)E F
dP
dt M
AX (
mm
Hg
s)
LVE
S a
rea
(cm
2)
LVE
S a
rea
(cm
2)
dP
dt M
in (
mm
Hg
s)
Figure 4 Cardiac function Left ventricular (LV) end-diastolic internal area (A) LV end-systolic internal area (B) posterolateralmyocardial wall (infarct) thickness (C) fractional area shortening (FAS D) dPdtMAX (E) and dPdtMIN (F) before MI (baseline) 1 h postMI and 3 weeks post MI in pigs treated with MSC-CM (black dots n=9) or NCM (open dots n=9) Pb005 vs NCM
210 L Timmers et al
myocardial infarct size and preservation of myocardialfunction With preserved left ventricular dimensions andinfarct thickness inhibition of post MI cardiac remodeling is apotential contributing mechanism Collagen density in theborder area and remote myocardium was lower in pigstreated with MSC-CM Cardiac fibrosis is associated withheart failure following myocardial infarction and maycontribute to progression of systolic and diastolic dysfunc-tion (Burlew amp Weber 2002 Cleutjens et al 1999) Werecently demonstrated that intravenous and intracoronaryMSC-CM treatment reduces myocardial apoptosis and oxida-tive stress (Timmers et al 2007a) In that study cardio-myocyte death was targeted acutely following ischemia andreperfusion injury In the current study treatment wasstarted late after coronary artery ligation and a model ofpermanent coronary artery ligation was used in order toinvestigate the angiogenic potential of MSC-CM and its effecton cardiac function independent of reduction of reperfusioninjury The fact that cardiac function improved using thisprotocol shows that there may be additional benefit fromprolonged treatment with MSC secretions
For this study a permanent coronary artery ligation wasperformed in anesthetized animals and functional measure-
ments were performed with open chest In addition we havenot been able to investigate the effect of commoncomorbidities such as hypertension dyslipidemia anddiabetes which might influence the biologic effect of MSCsecretions Due to the permanent coronary artery ligationwe were not able to assess the area at risk 3 weeks post MIWe were not able to oversee the effects of human proteininjection on the immune system of the porcine host and thepotential influence on study endpoints Furthermore themolecular mechanism for the induction of angiogenesis andor arteriogenesis and an exact determination of theresponsible angiogenic factors are still lacking Severalclinical trials with potent angiogenic factors failed toimprove outcome in patients (Henry et al 2003 Simonset al 2002) It is not clear how paracrine factors in stem celltransplants or the paracrine factors alone can induce abetter effect Most likely a combination of angiogenicfactors rather than a single protein is responsible Alsoexosomes could play an important role We previouslydemonstrated exosomes in MSC-CM to contain and delivercardioprotective compounds preventing cardiomyocytedeath following ischemia and reperfusion injury (Lai et al2010) Exosomes constitute a potential delivery tool to
Table 1 Hemodynamic and Functional Parameters
Baseline 3 weeks post MI Change from baseline ()
Parameter NCM CM NCM CM NCM CM
HR bpm 66plusmn4 73plusmn6 84plusmn6 86plusmn6 28plusmn12 12plusmn11MAP mm Hg 95plusmn5 89plusmn5 66plusmn6 85plusmn5 -30plusmn5 -5plusmn8 CO Lmin 31plusmn01 30plusmn02 37plusmn06 53plusmn05 23plusmn21 78plusmn20dPdt max mm Hgs 1213plusmn77 1241plusmn56 1157plusmn162 1650plusmn124 4plusmn13 40plusmn9 dPdt min mm Hgs -1274plusmn122 -1130plusmn96 -883plusmn98 -1313plusmn95 27plusmn9 -19plusmn19 EDP mm Hg 80plusmn03 71plusmn06 133plusmn16 121plusmn11 68plusmn21 94plusmn42WT infarct cm 079plusmn004 083plusmn005 055plusmn002 079plusmn005 -27plusmn4 -5plusmn4 Lvia (ED) cm2 158plusmn05 142plusmn10 260plusmn18 218plusmn15 64plusmn12 55plusmn12Lvia (ES) cm2 85plusmn04 76plusmn09 177plusmn16 125plusmn09 104plusmn14 60plusmn14 FAS 458plusmn19 469plusmn46 326plusmn22 424plusmn33 -28plusmn6 -6plusmn8 SV ml 48plusmn3 42plusmn2 43plusmn4 62plusmn3 -4plusmn11 52plusmn10 EDV ml 134plusmn16 129plusmn9ESV ml 93plusmn15 73plusmn9EF 337plusmn44 491plusmn33 SW mm Hgmiddotml 2497plusmn333 4595plusmn361 Stiffness mm Hgml 026plusmn004 014plusmn002
Summary of cardiac functional parameters of pigs treated with NCM (n=9) and MSC-CM (n=9) determined with echocardiography andconductance catheter-based LV pressure and volumemeasurements MI indicates myocardial infarction HR heart rate MAP mean arterialpressure CO cardiac output EDP end-diastolic pressure WT wall thickness LVia left ventricular internal area SV stroke volume EDVend-diastolic volume ESV end-systolic volume EF ejection fraction SW stroke work Stiffness end-diastolic chamber stiffness Pb005vs NCM
211
effectively carry angiogenic factors into the intracellularspace of the target tissue protecting the factors fromproteases This may explain why relatively low doses canhave such profound angiogenic effects Whether exosomesand their content are also responsible for the stimulation ofangiogenesis following MI remains a subject for furtherinvestigation
Here we demonstrate that human MSC secretionsstimulate angiogenesis These data support the hypothesisthat MSC transplantation induces vascular repair mechanismsvia paracrine pathways Most importantly human MSCsecretions harvested as conditioned medium using a clini-cally compliant protocol reduced infarct size and preservedcardiac function in a large animal model of myocardialinfarction The study therefore identifies MSC-CM as a noveltherapeutic biologic in the improvement of cardiac functionafter myocardial infarction
Methods
MSC-CM preparation
The protocols for MSC generation and CM preparation havebeen described in previous papers (Lian et al 2007 Sze et al2007) In short a chemically defined serum-free culturemedium(DMEMwithoutphenol red supplementedwith insulintransferrin and selenium 5 ngml FGF2 5 ngml PDGF ABglutamine-penicillin-streptomycin and szlig-mercaptoethanol)was conditioned by MSCs derived from human embryonicstem cells (hESCs) using a clinically compliant protocol Threepolyclonal karyotypically stable and phenotypically MSC-likecultures that do not express pluripotency-associated markersbut displayed MSC-like surface antigens (CD29+ CD44+CD49a+e+ CD105+ CD166+ CD34ndash CD45ndash) and gene
expression profile were generated by trypsinization andpropagation of hESCs from either the HuES9 hESC line or theH1 hESC line in feeder- and serum-free selection media (Lianet al 2007) One of these cultures HuES9E1 can be stablyexpanded for at least 80 population doublings To harvest MSCsecretions hESC-derived MSC cultures were transferred to achemically defined serum-free culture medium to conditionthe medium for 3 days before the media containing MSCsecretions were collected clarified by centrifugation con-centrated 25 times using 10-kDa MW cutoff ultrafiltrationmembranes and sterilized by filtration through a 220-nmfilter The protein concentration after concentration was050 mgml As a negative control the above-noted serum-free culture medium was processed equally (nonconditionedmedium [NCM])
Ingenuity pathway analysis
For this analysis we used the proteomic data obtainedpreviously (Sze et al 2007) Bioinformatic analysis wasperformed using Ingenuity pathway analysis (Ingenuity IPA-2002 version 71) The 201 proteins were uploaded inIngenuity with Ingenuity Knowledge Base as a reference setand direct and indirect relationships were included Allmolecules or relationships were considered for the filtersummary In the summary the focus was on Top Bio functionsin which physiological system development and function wasanalyzed in depth
HUVEC spheroid assay
Spheroids were formed from HUVECs to determine the effectof conditioned medium on angiogenic sprout formation (Korffamp Augustin 1998) Spheroids were formed overnight in 20
212 L Timmers et al
methocel in culture medium and subsequently embedded ina collagenndashmethocel matrix Sprouting was induced over-night with MSC-CM (n=12) or non-CM (NCM) (n=12) todetermine the effect of the secreted chemotactic proteinson capillary sprouting After overnight sprouting spheroidswere fixed in 10 formaldehyde and pictures were taken andthe length and number of sprouts were quantified
Animals
All experiments were performed in accordance with theldquoGuide for the Care and Use of Laboratory Animalsrdquo preparedby the Institute of Laboratory Animal Resources andwith priorapproval by the Animal Experimentation Committee of theFaculty of Medicine Utrecht University the Netherlands
Sample size calculation
In a previous study the mean fractional area shortening(FAS) after LCx ligation was 365 (Timmers et al 2007b)With an alpha of 005 power of 080 SD of 58 anddifference of 20 considered relevant 10 animals per groupwere needed To allow for 10 mortality 11 animals pergroup were enrolled
Pig study design
Myocardial infarction was induced in 22 Dalland Landracepigs (60ndash70 kg IDDLO Lelystad the Netherlands) by surgicalleft circumflex coronary artery (LCx) ligation Two pigs diedperioperatively before randomization and were thereforeexcluded from the study The remaining 20 pigs wererandomized after surgery by using sealed envelopes tointravenous treatment with MSC-CM (20 ml MSC-CM ie10 mg protein) or 20 ml NCM initiated 4 h after coronaryartery ligation and the treatment was continued for 7 daystwice daily via a catheter inserted into the jugular vein Thepigs were sacrificed 3 weeks after MI To prevent thromboticcomplications and arrhythmias all pigs were treated withclopidogrel 75 mgday from 3 days before MI until termina-tion and amiodarone 400 mgday from 10 days before MIuntil termination
Myocardial infarction and operational procedure
Pigs were anesthetized as described previously (Timmers etal 2007b) During the entire operation electrocardiogramarterial pressure and capnogram were continuously moni-tored After median sternotomy the left ventricularpressure (LVP) was measured using a pressure tipped Millarcatheter that was inserted through the apex into the leftventricle A transonic flow probe (Transonic Systems IncIthaca NY USA) was placed around the proximal aorta tomeasure cardiac output Sutures were then tightened topermanently occlude the proximal LCx Internal defibrilla-tion with 50 J was used when VF occurred Prior to and 1 hafter induction of the infarct echocardiography wasperformed After stabilization of hemodynamic parametersand heart rhythm the thorax was closed and the animalswere allowed to recover Three weeks after induction of
myocardial infarction the animals were anesthetized oncemore and the sternum was reopened Echocardiography andconductance catheter-based pressurendashvolume (PV) looprecordings were obtained to assess cardiac function andgeometry After the functional measurements the heart wasexcised for laboratory analysis
Immunohistochemistry
Three weeks following MI myocardial biopsies were obtainedfrom the infarct area border area and remote area andfixated in 4 formalin for 24 h before being embedded inparaffin To determine capillary density a lectin stainingdelineating the endothelium was performed followingantigen retrieval by boiling in 10 mM citrate bufferEndogenous biotin was blocked using 01 avidin solution(DakoCytomation Biotin Blocking system X0590) for 15 min atroom temperature (RT) and subsequently with 001 biotinsolution (Dako) for 15 min at RT After blocking with 30 BSAin PBS the sections were incubated overnight with biotiny-lated BS-1 (Sigma L3759) in a 1300 dilution in PBS with 01BSA and subsequently with streptavidin-HRPO (11000 in PBS)for 1 h at RT Finally the sections were incubated for 30 minin 3-amino-9-ethylcarbazole (AEC) and stained with hema-toxylin before being embedded Capillary density wasexpressed as the number of capillaries per square millimetertissue Quantification of collagen density was performedusing picrosirius red staining with circularly polarized lightand digital image microscopy after conversion into gray-value images as described before (Timmers et al 2007b)
Myocardial infarct size
After excision of the heart the LV was isolated and cut into 5slices from apex to base To discriminate infarct tissue fromviable myocardium the slices were incubated in 1triphenyltetrazolium chloride (TTC Sigma-Aldrich Chemi-cals Zwijndrecht Netherlands) in 37 degC Soumlrensen buffer(136 gL KH2PO4+178 gL Na2H PO42H2O pH 74) for15 min All slices were scanned from both sides and in eachslide the infarct area was compared to total area using digitalplanimetry software After correction for the weight of theslices infarct size was calculated as a percentage of the LV
Cardiac function
Midpapillary short axis epicardial echocardiography wasperformed before coronary artery ligation 1 h after and3 weeks after coronary artery ligation (Prosound SSD-50005 MHz probe UST-5280-5 Aloka Holding Europe AG ZugSwitzerland) Wall thickness (WT) of the infarct area and leftventricular internal area (LVia) were measured at end-diastole (ED) and end-systole (ES) Systolic wall thickening(SWT) was calculated as (WT(ES) ndashWT(ED))WT(ED) 100 ()and fractional area shortening (FAS) as (LVia(ED) ndash LVia(ES))LVia(ED) 100 () Left ventricular (LV) pressurendashvolumeloops were measured using a conductance catheter asdescribed previously (Timmers et al 2009) Diastolicchamber stiffness was quantified by means of linearregression of the end-diastolic pressurendashvolume relationship(Sagawa 1981)
213
Data analysis
The data were collected and analyzed in a blinded fashionData are presented as meanplusmnSE Mortality was comparedusing Fishers exact test Capillary sprouting was comparedusing a one-way ANOVA and Bonferroni post hoc tests A two-way ANOVA with Bonferroni post hoc tests was used tocompare capillary density and collagen density in themyocardial tissue Cardiac functional parameters that werealso measured before MI (baseline) were compared using atwo-way ANOVA for repeated measures and Bonferroni posthoc tests For cardiac functional parameters that weremeasured only 3 weeks after MI Students t test was used
Acknowledgments
This work was supported by the Netherlands Heart Founda-tion [Grant 2005T022 LT] and an Internationalization grantby the University Medical Center Utrecht the Netherlands[DPVK]
Appendix A Supplementary data
Supplementary data to this article can be found online atdoi101016jscr201101001
References
Assmus B Honold J Schachinger V Britten MB Fischer-Rasokat U Lehmann R Teupe C Pistorius K Martin HAbolmaali ND Tonn T Dimmeler S Zeiher AM 2006Transcoronary transplantation of progenitor cells after myocardialinfarction N Engl J Med 355 1222ndash1232
Burlew BS Weber KT 2002 Cardiac fibrosis as a cause ofdiastolic dysfunction Herz 27 92ndash98
Caplan AI Dennis JE 2006 Mesenchymal stem cells as trophicmediators J Cell Biochem 98 1076ndash1084
Cleutjens JP Blankesteijn WM Daemen MJ Smits JF1999 The infarcted myocardium simply dead tissue or a livelytarget for therapeutic interventions Cardiovasc Res 44232ndash241
de Silva R Raval AN Hadi M Gildea KM Bonifacino ACYu ZX Yau YY Leitman SF Bacharach SL DonahueRE Read EJ Lederman RJ 2008 Intracoronary infusion ofautologous mononuclear cells from bone marrow or granulocytecolony-stimulating factor-mobilized apheresis product may notimprove remodelling contractile function perfusion or infarctsize in a swine model of large myocardial infarction Eur Heart J29 1772ndash1782
Erbs S Linke A Schachinger V Assmus B Thiele H DiederichKW Hoffmann C Dimmeler S Tonn T Hambrecht RZeiher AM Schuler G 2007 Restoration of microvascularfunction in the infarct-related artery by intracoronary transplan-tation of bone marrow progenitor cells in patients with acutemyocardial infarction the Doppler Substudy of the Reinfusion ofEnriched Progenitor Cells and Infarct Remodeling in AcuteMyocardial Infarction (REPAIR-AMI) trial Circulation 116 366ndash374
Gnecchi M He H Liang OD Melo LG Morello F Mu HNoiseux N Zhang L Pratt RE Ingwall JS Dzau VJ2005 Paracrine action accounts for marked protection ofischemic heart by Akt-modified mesenchymal stem cells NatMed 11 367ndash368
Hashemi SM Ghods S Kolodgie FD Parcham-Azad K KeaneM Hamamdzic D Young R Rippy MK Virmani R Litt HWilensky RL 2008 A placebo controlled dose-ranging safetystudy of allogenic mesenchymal stem cells injected by endo-myocardial delivery after an acute myocardial infarction EurHeart J 29 251ndash259
Henry TD Annex BH McKendall GR Azrin MA Lopez JJGiordano FJ Shah PK Willerson JT Benza RL BermanDS Gibson CM Bajamonde A Rundle AC Fine JMcCluskey ER 2003 The VIVA trial vascular endothelialgrowth factor in ischemia for vascular angiogenesis Circulation107 1359ndash1365
Janssens S Dubois C Bogaert J Theunissen K Deroose CDesmet W Kalantzi M Herbots L Sinnaeve P Dens JMaertens J Rademakers F Dymarkowski S Gheysens O VanCleemput J Bormans G Nuyts J Belmans A Mortelmans LBoogaerts M Van de Werf F 2006 Autologous bone marrow-derived stem-cell transfer in patients with ST-segment elevationmyocardial infarction double-blind randomised controlled trialLancet 367 113ndash121
Kinnaird T Stabile E Burnett MS Shou M Lee CW BarrS Fuchs S Epstein SE 2004 Local delivery of marrow-derived stromal cells augments collateral perfusion throughparacrine mechanisms Circulation 109 1543ndash1549
Korff T Augustin HG 1998 Integration of endothelial cells inmulticellular spheroids prevents apoptosis and induces differen-tiation J Cell Biol 143 1341ndash1352
Lai RC Arslan F Lee MM Sze NS Choo A Chen TSSalto-Tellez M Timmers L Lee CN El Oakley RMPasterkamp G de Kleijn DP Lim SK 2010 Exosomesecreted by MSC reduces myocardial ischemiareperfusioninjury Stem Cell Res 4 214ndash222
Lian Q Lye E Suan Yeo K KhiaWay Tan E Salto-Tellez M LiuTM PalanisamyN ElOakley RM Lee EH LimB Lim SK2007 Derivation of clinically compliant MSCs from CD105+ CD24-differentiated human ESCs Stem Cells 25 425ndash436
Losordo DW Dimmeler S 2004 Therapeutic angiogenesis andvasculogenesis for ischemic disease part II cell-based therapiesCirculation 109 2692ndash2697
Lunde K Solheim S Aakhus S Arnesen H Abdelnoor MEgeland T Endresen K Ilebekk A Mangschau A Fjeld JGSmith HJ Taraldsrud E Grogaard HK Bjornerheim RBrekke M Muller C Hopp E Ragnarsson A Brinchmann JEForfang K 2006 Intracoronary injection of mononuclear bonemarrow cells in acute myocardial infarction N Engl J Med 3551199ndash1209
Menasche P Alfieri O Janssens S McKenna W Reich-enspurner H Trinquart L Vilquin JT Marolleau JPSeymour B Larghero J Lake S Chatellier G Solomon SDesnos M Hagege AA 2008 The Myoblast AutologousGrafting in Ischemic Cardiomyopathy (MAGIC) trial first ran-domized placebo-controlled study of myoblast transplantationCirculation 117 1189ndash1200
Meyer GP Wollert KC Lotz J Pirr J Rager U Lippolt PHahn A Fichtner S Schaefer A Arseniev L Ganser ADrexler H 2009 Intracoronary bone marrow cell transfer aftermyocardial infarction 5-year follow-up from the randomized-controlled BOOST trial Eur Heart J 24 2978ndash2984
Moelker AD Baks T van den Bos EJ van Geuns RJ deFeyter PJ Duncker DJ van der Giessen WJ 2006Reduction in infarct size but no functional improvement afterbone marrow cell administration in a porcine model ofreperfused myocardial infarction Eur Heart J 27 3057ndash3064
Pittenger MF Martin BJ 2004 Mesenchymal stem cells andtheir potential as cardiac therapeutics Circ Res 95 9ndash20
Sagawa K 1981 The end-systolic pressure-volume relation of theventricle definition modifications and clinical use Circulation63 1223ndash1227
214 L Timmers et al
Schachinger V Erbs S Elsasser A Haberbosch W Ham-brecht R Holschermann H Yu J Corti R Mathey DGHamm CW Suselbeck T Assmus B Tonn T DimmelerS Zeiher AM 2006 Intracoronary bone marrow-derivedprogenitor cells in acute myocardial infarction N Engl J Med355 1210ndash1221
Simons M Annex BH Laham RJ Kleiman N Henry TDauerman H Udelson JE Gervino EV Pike M White-house MJ Moon T Chronos NA 2002 Pharmacologicaltreatment of coronary artery disease with recombinant fibroblastgrowth factor-2 double-blind randomized controlled clinicaltrial Circulation 105 788ndash793
Strauer BE Brehm M Zeus T Kostering M Hernandez ASorg RV Kogler G Wernet P 2002 Repair of infarctedmyocardium by autologous intracoronary mononuclear bonemarrow cell transplantation in humans Circulation 1061913ndash1918
Sze SK de Kleijn DP Lai RC Khia Way E 2007 Tan HZhao KS Yeo TY Low Q Lian CN Lee W Mitchell RM ElOakley SK Lim Elucidating the secretion proteome of humanembryonic stem cell-derived mesenchymal stem cells Mol CellProteomics 6 1680ndash1689
Timmers L Lim SK Arslan F Armstrong JS Hoefer IEDoevendans PA Piek JJ El Oakley RM Choo A Lee CNPasterkamp G de Kleijn DP 2007a Reduction of myocardialinfarct size by humanmesenchymal stemcell conditionedmediumStem Cell Res 1 129ndash137
Timmers L Sluijter JP Verlaan CW Steendijk P CramerMJEmons M Strijder C Grundeman PF Sze SK Hua L PiekJJ Borst C Pasterkamp G de Kleijn DP 2007b Cycloox-ygenase-2 inhibition increases mortality enhances left ventricularremodeling and impairs systolic function after myocardialinfarction in the pig Circulation 115 326ndash332
Timmers L Henriques JP de Kleijn DP Devries JHKemperman H Steendijk P Verlaan CW Kerver MPiek JJ Doevendans PA Pasterkamp G Hoefer IE2009 Exenatide reduces infarct size and improves cardiacfunction in a porcine model of ischemia and reperfusion injuryJ Am Coll Cardiol 53 501ndash510
van Laake LW Passier R denOuden K Schreurs CMonshouwer-Kloots JWard-vanOostwaard D van Echteld CJ DoevendansPA Mummery CL 2009 Improvement of mouse cardiacfunction by hESC-derived cardiomyocytes correlates with vascular-ity but not graft size Stem Cell Res 3 106ndash112
Wolf D Reinhard A Seckinger A Gross L Katus HA HansenA 2009 Regenerative capacity of intravenous autologousallogeneic and human mesenchymal stem cells in the infarctedpig myocardium-complicated by myocardial tumor formationScand Cardiovasc J 43 39ndash45
Yousef M Schannwell CM Kostering M Zeus T Brehm MStrauer BE 2009 The BALANCE Study clinical benefit andlong-term outcome after intracoronary autologous bone marrowcell transplantation in patients with acute myocardial infarctionJ Am Coll Cardiol 53 2262ndash2269

Figure 2 Capillary density Representative sections of border areas after lectin staining to visualize endothelium 3 weeks after MIfrom pigs treated with NCM (A n=9) or MSC-CM (B n=9) Quantification of capillary density in remote and border area isdemonstrated in panel C Scale bars 500 μm
Figure 3 Collagen density Quantification of collaged densityin the infarct border and remote areas in pigs treated with NCMand MSC-CM
209
in vivo we used a porcine model of myocardial infarctionDuring myocardial ischemia following coronary artery liga-tion cardiomyocytes in the central infarct perish withinminutes to hours after coronary occlusion The border zoneof the ischemic area however contains injured but viablecells under hypoperfused and hypoxic conditions which mayeither be salvaged or die depending on the conditions afterischemia Restoration of myocardial perfusion by means ofangiogenesis restores the metabolic needs of cardiomyocytesin the border area and offers the cells a better chance ofsurvival which in turn could lead to reduced myocardialinjury Intracoronary delivery of bone marrow-derivedprogenitor cells has been suggested to promote vascularrepair following MI potentially via paracrine mechanisms(Erbs et al 2007) Such effect was also observed in a rodentmodel of hind limb ischemia (Kinnaird et al 2004) Asbecame evident from our histological analyses MSC-CMincreased capillary density in the border areas and myocar-dial infarct size was reduced which was accompanied bypreserved LV dimensions and cardiac function
Besides stimulation of angiogenesis it cannot be excludedthat also other mechanisms contributed to reduction of
A B
C D
WT
infa
rct
(cm
)
FAS
(
)E F
dP
dt M
AX (
mm
Hg
s)
LVE
S a
rea
(cm
2)
LVE
S a
rea
(cm
2)
dP
dt M
in (
mm
Hg
s)
Figure 4 Cardiac function Left ventricular (LV) end-diastolic internal area (A) LV end-systolic internal area (B) posterolateralmyocardial wall (infarct) thickness (C) fractional area shortening (FAS D) dPdtMAX (E) and dPdtMIN (F) before MI (baseline) 1 h postMI and 3 weeks post MI in pigs treated with MSC-CM (black dots n=9) or NCM (open dots n=9) Pb005 vs NCM
210 L Timmers et al
myocardial infarct size and preservation of myocardialfunction With preserved left ventricular dimensions andinfarct thickness inhibition of post MI cardiac remodeling is apotential contributing mechanism Collagen density in theborder area and remote myocardium was lower in pigstreated with MSC-CM Cardiac fibrosis is associated withheart failure following myocardial infarction and maycontribute to progression of systolic and diastolic dysfunc-tion (Burlew amp Weber 2002 Cleutjens et al 1999) Werecently demonstrated that intravenous and intracoronaryMSC-CM treatment reduces myocardial apoptosis and oxida-tive stress (Timmers et al 2007a) In that study cardio-myocyte death was targeted acutely following ischemia andreperfusion injury In the current study treatment wasstarted late after coronary artery ligation and a model ofpermanent coronary artery ligation was used in order toinvestigate the angiogenic potential of MSC-CM and its effecton cardiac function independent of reduction of reperfusioninjury The fact that cardiac function improved using thisprotocol shows that there may be additional benefit fromprolonged treatment with MSC secretions
For this study a permanent coronary artery ligation wasperformed in anesthetized animals and functional measure-
ments were performed with open chest In addition we havenot been able to investigate the effect of commoncomorbidities such as hypertension dyslipidemia anddiabetes which might influence the biologic effect of MSCsecretions Due to the permanent coronary artery ligationwe were not able to assess the area at risk 3 weeks post MIWe were not able to oversee the effects of human proteininjection on the immune system of the porcine host and thepotential influence on study endpoints Furthermore themolecular mechanism for the induction of angiogenesis andor arteriogenesis and an exact determination of theresponsible angiogenic factors are still lacking Severalclinical trials with potent angiogenic factors failed toimprove outcome in patients (Henry et al 2003 Simonset al 2002) It is not clear how paracrine factors in stem celltransplants or the paracrine factors alone can induce abetter effect Most likely a combination of angiogenicfactors rather than a single protein is responsible Alsoexosomes could play an important role We previouslydemonstrated exosomes in MSC-CM to contain and delivercardioprotective compounds preventing cardiomyocytedeath following ischemia and reperfusion injury (Lai et al2010) Exosomes constitute a potential delivery tool to
Table 1 Hemodynamic and Functional Parameters
Baseline 3 weeks post MI Change from baseline ()
Parameter NCM CM NCM CM NCM CM
HR bpm 66plusmn4 73plusmn6 84plusmn6 86plusmn6 28plusmn12 12plusmn11MAP mm Hg 95plusmn5 89plusmn5 66plusmn6 85plusmn5 -30plusmn5 -5plusmn8 CO Lmin 31plusmn01 30plusmn02 37plusmn06 53plusmn05 23plusmn21 78plusmn20dPdt max mm Hgs 1213plusmn77 1241plusmn56 1157plusmn162 1650plusmn124 4plusmn13 40plusmn9 dPdt min mm Hgs -1274plusmn122 -1130plusmn96 -883plusmn98 -1313plusmn95 27plusmn9 -19plusmn19 EDP mm Hg 80plusmn03 71plusmn06 133plusmn16 121plusmn11 68plusmn21 94plusmn42WT infarct cm 079plusmn004 083plusmn005 055plusmn002 079plusmn005 -27plusmn4 -5plusmn4 Lvia (ED) cm2 158plusmn05 142plusmn10 260plusmn18 218plusmn15 64plusmn12 55plusmn12Lvia (ES) cm2 85plusmn04 76plusmn09 177plusmn16 125plusmn09 104plusmn14 60plusmn14 FAS 458plusmn19 469plusmn46 326plusmn22 424plusmn33 -28plusmn6 -6plusmn8 SV ml 48plusmn3 42plusmn2 43plusmn4 62plusmn3 -4plusmn11 52plusmn10 EDV ml 134plusmn16 129plusmn9ESV ml 93plusmn15 73plusmn9EF 337plusmn44 491plusmn33 SW mm Hgmiddotml 2497plusmn333 4595plusmn361 Stiffness mm Hgml 026plusmn004 014plusmn002
Summary of cardiac functional parameters of pigs treated with NCM (n=9) and MSC-CM (n=9) determined with echocardiography andconductance catheter-based LV pressure and volumemeasurements MI indicates myocardial infarction HR heart rate MAP mean arterialpressure CO cardiac output EDP end-diastolic pressure WT wall thickness LVia left ventricular internal area SV stroke volume EDVend-diastolic volume ESV end-systolic volume EF ejection fraction SW stroke work Stiffness end-diastolic chamber stiffness Pb005vs NCM
211
effectively carry angiogenic factors into the intracellularspace of the target tissue protecting the factors fromproteases This may explain why relatively low doses canhave such profound angiogenic effects Whether exosomesand their content are also responsible for the stimulation ofangiogenesis following MI remains a subject for furtherinvestigation
Here we demonstrate that human MSC secretionsstimulate angiogenesis These data support the hypothesisthat MSC transplantation induces vascular repair mechanismsvia paracrine pathways Most importantly human MSCsecretions harvested as conditioned medium using a clini-cally compliant protocol reduced infarct size and preservedcardiac function in a large animal model of myocardialinfarction The study therefore identifies MSC-CM as a noveltherapeutic biologic in the improvement of cardiac functionafter myocardial infarction
Methods
MSC-CM preparation
The protocols for MSC generation and CM preparation havebeen described in previous papers (Lian et al 2007 Sze et al2007) In short a chemically defined serum-free culturemedium(DMEMwithoutphenol red supplementedwith insulintransferrin and selenium 5 ngml FGF2 5 ngml PDGF ABglutamine-penicillin-streptomycin and szlig-mercaptoethanol)was conditioned by MSCs derived from human embryonicstem cells (hESCs) using a clinically compliant protocol Threepolyclonal karyotypically stable and phenotypically MSC-likecultures that do not express pluripotency-associated markersbut displayed MSC-like surface antigens (CD29+ CD44+CD49a+e+ CD105+ CD166+ CD34ndash CD45ndash) and gene
expression profile were generated by trypsinization andpropagation of hESCs from either the HuES9 hESC line or theH1 hESC line in feeder- and serum-free selection media (Lianet al 2007) One of these cultures HuES9E1 can be stablyexpanded for at least 80 population doublings To harvest MSCsecretions hESC-derived MSC cultures were transferred to achemically defined serum-free culture medium to conditionthe medium for 3 days before the media containing MSCsecretions were collected clarified by centrifugation con-centrated 25 times using 10-kDa MW cutoff ultrafiltrationmembranes and sterilized by filtration through a 220-nmfilter The protein concentration after concentration was050 mgml As a negative control the above-noted serum-free culture medium was processed equally (nonconditionedmedium [NCM])
Ingenuity pathway analysis
For this analysis we used the proteomic data obtainedpreviously (Sze et al 2007) Bioinformatic analysis wasperformed using Ingenuity pathway analysis (Ingenuity IPA-2002 version 71) The 201 proteins were uploaded inIngenuity with Ingenuity Knowledge Base as a reference setand direct and indirect relationships were included Allmolecules or relationships were considered for the filtersummary In the summary the focus was on Top Bio functionsin which physiological system development and function wasanalyzed in depth
HUVEC spheroid assay
Spheroids were formed from HUVECs to determine the effectof conditioned medium on angiogenic sprout formation (Korffamp Augustin 1998) Spheroids were formed overnight in 20
212 L Timmers et al
methocel in culture medium and subsequently embedded ina collagenndashmethocel matrix Sprouting was induced over-night with MSC-CM (n=12) or non-CM (NCM) (n=12) todetermine the effect of the secreted chemotactic proteinson capillary sprouting After overnight sprouting spheroidswere fixed in 10 formaldehyde and pictures were taken andthe length and number of sprouts were quantified
Animals
All experiments were performed in accordance with theldquoGuide for the Care and Use of Laboratory Animalsrdquo preparedby the Institute of Laboratory Animal Resources andwith priorapproval by the Animal Experimentation Committee of theFaculty of Medicine Utrecht University the Netherlands
Sample size calculation
In a previous study the mean fractional area shortening(FAS) after LCx ligation was 365 (Timmers et al 2007b)With an alpha of 005 power of 080 SD of 58 anddifference of 20 considered relevant 10 animals per groupwere needed To allow for 10 mortality 11 animals pergroup were enrolled
Pig study design
Myocardial infarction was induced in 22 Dalland Landracepigs (60ndash70 kg IDDLO Lelystad the Netherlands) by surgicalleft circumflex coronary artery (LCx) ligation Two pigs diedperioperatively before randomization and were thereforeexcluded from the study The remaining 20 pigs wererandomized after surgery by using sealed envelopes tointravenous treatment with MSC-CM (20 ml MSC-CM ie10 mg protein) or 20 ml NCM initiated 4 h after coronaryartery ligation and the treatment was continued for 7 daystwice daily via a catheter inserted into the jugular vein Thepigs were sacrificed 3 weeks after MI To prevent thromboticcomplications and arrhythmias all pigs were treated withclopidogrel 75 mgday from 3 days before MI until termina-tion and amiodarone 400 mgday from 10 days before MIuntil termination
Myocardial infarction and operational procedure
Pigs were anesthetized as described previously (Timmers etal 2007b) During the entire operation electrocardiogramarterial pressure and capnogram were continuously moni-tored After median sternotomy the left ventricularpressure (LVP) was measured using a pressure tipped Millarcatheter that was inserted through the apex into the leftventricle A transonic flow probe (Transonic Systems IncIthaca NY USA) was placed around the proximal aorta tomeasure cardiac output Sutures were then tightened topermanently occlude the proximal LCx Internal defibrilla-tion with 50 J was used when VF occurred Prior to and 1 hafter induction of the infarct echocardiography wasperformed After stabilization of hemodynamic parametersand heart rhythm the thorax was closed and the animalswere allowed to recover Three weeks after induction of
myocardial infarction the animals were anesthetized oncemore and the sternum was reopened Echocardiography andconductance catheter-based pressurendashvolume (PV) looprecordings were obtained to assess cardiac function andgeometry After the functional measurements the heart wasexcised for laboratory analysis
Immunohistochemistry
Three weeks following MI myocardial biopsies were obtainedfrom the infarct area border area and remote area andfixated in 4 formalin for 24 h before being embedded inparaffin To determine capillary density a lectin stainingdelineating the endothelium was performed followingantigen retrieval by boiling in 10 mM citrate bufferEndogenous biotin was blocked using 01 avidin solution(DakoCytomation Biotin Blocking system X0590) for 15 min atroom temperature (RT) and subsequently with 001 biotinsolution (Dako) for 15 min at RT After blocking with 30 BSAin PBS the sections were incubated overnight with biotiny-lated BS-1 (Sigma L3759) in a 1300 dilution in PBS with 01BSA and subsequently with streptavidin-HRPO (11000 in PBS)for 1 h at RT Finally the sections were incubated for 30 minin 3-amino-9-ethylcarbazole (AEC) and stained with hema-toxylin before being embedded Capillary density wasexpressed as the number of capillaries per square millimetertissue Quantification of collagen density was performedusing picrosirius red staining with circularly polarized lightand digital image microscopy after conversion into gray-value images as described before (Timmers et al 2007b)
Myocardial infarct size
After excision of the heart the LV was isolated and cut into 5slices from apex to base To discriminate infarct tissue fromviable myocardium the slices were incubated in 1triphenyltetrazolium chloride (TTC Sigma-Aldrich Chemi-cals Zwijndrecht Netherlands) in 37 degC Soumlrensen buffer(136 gL KH2PO4+178 gL Na2H PO42H2O pH 74) for15 min All slices were scanned from both sides and in eachslide the infarct area was compared to total area using digitalplanimetry software After correction for the weight of theslices infarct size was calculated as a percentage of the LV
Cardiac function
Midpapillary short axis epicardial echocardiography wasperformed before coronary artery ligation 1 h after and3 weeks after coronary artery ligation (Prosound SSD-50005 MHz probe UST-5280-5 Aloka Holding Europe AG ZugSwitzerland) Wall thickness (WT) of the infarct area and leftventricular internal area (LVia) were measured at end-diastole (ED) and end-systole (ES) Systolic wall thickening(SWT) was calculated as (WT(ES) ndashWT(ED))WT(ED) 100 ()and fractional area shortening (FAS) as (LVia(ED) ndash LVia(ES))LVia(ED) 100 () Left ventricular (LV) pressurendashvolumeloops were measured using a conductance catheter asdescribed previously (Timmers et al 2009) Diastolicchamber stiffness was quantified by means of linearregression of the end-diastolic pressurendashvolume relationship(Sagawa 1981)
213
Data analysis
The data were collected and analyzed in a blinded fashionData are presented as meanplusmnSE Mortality was comparedusing Fishers exact test Capillary sprouting was comparedusing a one-way ANOVA and Bonferroni post hoc tests A two-way ANOVA with Bonferroni post hoc tests was used tocompare capillary density and collagen density in themyocardial tissue Cardiac functional parameters that werealso measured before MI (baseline) were compared using atwo-way ANOVA for repeated measures and Bonferroni posthoc tests For cardiac functional parameters that weremeasured only 3 weeks after MI Students t test was used
Acknowledgments
This work was supported by the Netherlands Heart Founda-tion [Grant 2005T022 LT] and an Internationalization grantby the University Medical Center Utrecht the Netherlands[DPVK]
Appendix A Supplementary data
Supplementary data to this article can be found online atdoi101016jscr201101001
References
Assmus B Honold J Schachinger V Britten MB Fischer-Rasokat U Lehmann R Teupe C Pistorius K Martin HAbolmaali ND Tonn T Dimmeler S Zeiher AM 2006Transcoronary transplantation of progenitor cells after myocardialinfarction N Engl J Med 355 1222ndash1232
Burlew BS Weber KT 2002 Cardiac fibrosis as a cause ofdiastolic dysfunction Herz 27 92ndash98
Caplan AI Dennis JE 2006 Mesenchymal stem cells as trophicmediators J Cell Biochem 98 1076ndash1084
Cleutjens JP Blankesteijn WM Daemen MJ Smits JF1999 The infarcted myocardium simply dead tissue or a livelytarget for therapeutic interventions Cardiovasc Res 44232ndash241
de Silva R Raval AN Hadi M Gildea KM Bonifacino ACYu ZX Yau YY Leitman SF Bacharach SL DonahueRE Read EJ Lederman RJ 2008 Intracoronary infusion ofautologous mononuclear cells from bone marrow or granulocytecolony-stimulating factor-mobilized apheresis product may notimprove remodelling contractile function perfusion or infarctsize in a swine model of large myocardial infarction Eur Heart J29 1772ndash1782
Erbs S Linke A Schachinger V Assmus B Thiele H DiederichKW Hoffmann C Dimmeler S Tonn T Hambrecht RZeiher AM Schuler G 2007 Restoration of microvascularfunction in the infarct-related artery by intracoronary transplan-tation of bone marrow progenitor cells in patients with acutemyocardial infarction the Doppler Substudy of the Reinfusion ofEnriched Progenitor Cells and Infarct Remodeling in AcuteMyocardial Infarction (REPAIR-AMI) trial Circulation 116 366ndash374
Gnecchi M He H Liang OD Melo LG Morello F Mu HNoiseux N Zhang L Pratt RE Ingwall JS Dzau VJ2005 Paracrine action accounts for marked protection ofischemic heart by Akt-modified mesenchymal stem cells NatMed 11 367ndash368
Hashemi SM Ghods S Kolodgie FD Parcham-Azad K KeaneM Hamamdzic D Young R Rippy MK Virmani R Litt HWilensky RL 2008 A placebo controlled dose-ranging safetystudy of allogenic mesenchymal stem cells injected by endo-myocardial delivery after an acute myocardial infarction EurHeart J 29 251ndash259
Henry TD Annex BH McKendall GR Azrin MA Lopez JJGiordano FJ Shah PK Willerson JT Benza RL BermanDS Gibson CM Bajamonde A Rundle AC Fine JMcCluskey ER 2003 The VIVA trial vascular endothelialgrowth factor in ischemia for vascular angiogenesis Circulation107 1359ndash1365
Janssens S Dubois C Bogaert J Theunissen K Deroose CDesmet W Kalantzi M Herbots L Sinnaeve P Dens JMaertens J Rademakers F Dymarkowski S Gheysens O VanCleemput J Bormans G Nuyts J Belmans A Mortelmans LBoogaerts M Van de Werf F 2006 Autologous bone marrow-derived stem-cell transfer in patients with ST-segment elevationmyocardial infarction double-blind randomised controlled trialLancet 367 113ndash121
Kinnaird T Stabile E Burnett MS Shou M Lee CW BarrS Fuchs S Epstein SE 2004 Local delivery of marrow-derived stromal cells augments collateral perfusion throughparacrine mechanisms Circulation 109 1543ndash1549
Korff T Augustin HG 1998 Integration of endothelial cells inmulticellular spheroids prevents apoptosis and induces differen-tiation J Cell Biol 143 1341ndash1352
Lai RC Arslan F Lee MM Sze NS Choo A Chen TSSalto-Tellez M Timmers L Lee CN El Oakley RMPasterkamp G de Kleijn DP Lim SK 2010 Exosomesecreted by MSC reduces myocardial ischemiareperfusioninjury Stem Cell Res 4 214ndash222
Lian Q Lye E Suan Yeo K KhiaWay Tan E Salto-Tellez M LiuTM PalanisamyN ElOakley RM Lee EH LimB Lim SK2007 Derivation of clinically compliant MSCs from CD105+ CD24-differentiated human ESCs Stem Cells 25 425ndash436
Losordo DW Dimmeler S 2004 Therapeutic angiogenesis andvasculogenesis for ischemic disease part II cell-based therapiesCirculation 109 2692ndash2697
Lunde K Solheim S Aakhus S Arnesen H Abdelnoor MEgeland T Endresen K Ilebekk A Mangschau A Fjeld JGSmith HJ Taraldsrud E Grogaard HK Bjornerheim RBrekke M Muller C Hopp E Ragnarsson A Brinchmann JEForfang K 2006 Intracoronary injection of mononuclear bonemarrow cells in acute myocardial infarction N Engl J Med 3551199ndash1209
Menasche P Alfieri O Janssens S McKenna W Reich-enspurner H Trinquart L Vilquin JT Marolleau JPSeymour B Larghero J Lake S Chatellier G Solomon SDesnos M Hagege AA 2008 The Myoblast AutologousGrafting in Ischemic Cardiomyopathy (MAGIC) trial first ran-domized placebo-controlled study of myoblast transplantationCirculation 117 1189ndash1200
Meyer GP Wollert KC Lotz J Pirr J Rager U Lippolt PHahn A Fichtner S Schaefer A Arseniev L Ganser ADrexler H 2009 Intracoronary bone marrow cell transfer aftermyocardial infarction 5-year follow-up from the randomized-controlled BOOST trial Eur Heart J 24 2978ndash2984
Moelker AD Baks T van den Bos EJ van Geuns RJ deFeyter PJ Duncker DJ van der Giessen WJ 2006Reduction in infarct size but no functional improvement afterbone marrow cell administration in a porcine model ofreperfused myocardial infarction Eur Heart J 27 3057ndash3064
Pittenger MF Martin BJ 2004 Mesenchymal stem cells andtheir potential as cardiac therapeutics Circ Res 95 9ndash20
Sagawa K 1981 The end-systolic pressure-volume relation of theventricle definition modifications and clinical use Circulation63 1223ndash1227
214 L Timmers et al
Schachinger V Erbs S Elsasser A Haberbosch W Ham-brecht R Holschermann H Yu J Corti R Mathey DGHamm CW Suselbeck T Assmus B Tonn T DimmelerS Zeiher AM 2006 Intracoronary bone marrow-derivedprogenitor cells in acute myocardial infarction N Engl J Med355 1210ndash1221
Simons M Annex BH Laham RJ Kleiman N Henry TDauerman H Udelson JE Gervino EV Pike M White-house MJ Moon T Chronos NA 2002 Pharmacologicaltreatment of coronary artery disease with recombinant fibroblastgrowth factor-2 double-blind randomized controlled clinicaltrial Circulation 105 788ndash793
Strauer BE Brehm M Zeus T Kostering M Hernandez ASorg RV Kogler G Wernet P 2002 Repair of infarctedmyocardium by autologous intracoronary mononuclear bonemarrow cell transplantation in humans Circulation 1061913ndash1918
Sze SK de Kleijn DP Lai RC Khia Way E 2007 Tan HZhao KS Yeo TY Low Q Lian CN Lee W Mitchell RM ElOakley SK Lim Elucidating the secretion proteome of humanembryonic stem cell-derived mesenchymal stem cells Mol CellProteomics 6 1680ndash1689
Timmers L Lim SK Arslan F Armstrong JS Hoefer IEDoevendans PA Piek JJ El Oakley RM Choo A Lee CNPasterkamp G de Kleijn DP 2007a Reduction of myocardialinfarct size by humanmesenchymal stemcell conditionedmediumStem Cell Res 1 129ndash137
Timmers L Sluijter JP Verlaan CW Steendijk P CramerMJEmons M Strijder C Grundeman PF Sze SK Hua L PiekJJ Borst C Pasterkamp G de Kleijn DP 2007b Cycloox-ygenase-2 inhibition increases mortality enhances left ventricularremodeling and impairs systolic function after myocardialinfarction in the pig Circulation 115 326ndash332
Timmers L Henriques JP de Kleijn DP Devries JHKemperman H Steendijk P Verlaan CW Kerver MPiek JJ Doevendans PA Pasterkamp G Hoefer IE2009 Exenatide reduces infarct size and improves cardiacfunction in a porcine model of ischemia and reperfusion injuryJ Am Coll Cardiol 53 501ndash510
van Laake LW Passier R denOuden K Schreurs CMonshouwer-Kloots JWard-vanOostwaard D van Echteld CJ DoevendansPA Mummery CL 2009 Improvement of mouse cardiacfunction by hESC-derived cardiomyocytes correlates with vascular-ity but not graft size Stem Cell Res 3 106ndash112
Wolf D Reinhard A Seckinger A Gross L Katus HA HansenA 2009 Regenerative capacity of intravenous autologousallogeneic and human mesenchymal stem cells in the infarctedpig myocardium-complicated by myocardial tumor formationScand Cardiovasc J 43 39ndash45
Yousef M Schannwell CM Kostering M Zeus T Brehm MStrauer BE 2009 The BALANCE Study clinical benefit andlong-term outcome after intracoronary autologous bone marrowcell transplantation in patients with acute myocardial infarctionJ Am Coll Cardiol 53 2262ndash2269

A B
C D
WT
infa
rct
(cm
)
FAS
(
)E F
dP
dt M
AX (
mm
Hg
s)
LVE
S a
rea
(cm
2)
LVE
S a
rea
(cm
2)
dP
dt M
in (
mm
Hg
s)
Figure 4 Cardiac function Left ventricular (LV) end-diastolic internal area (A) LV end-systolic internal area (B) posterolateralmyocardial wall (infarct) thickness (C) fractional area shortening (FAS D) dPdtMAX (E) and dPdtMIN (F) before MI (baseline) 1 h postMI and 3 weeks post MI in pigs treated with MSC-CM (black dots n=9) or NCM (open dots n=9) Pb005 vs NCM
210 L Timmers et al
myocardial infarct size and preservation of myocardialfunction With preserved left ventricular dimensions andinfarct thickness inhibition of post MI cardiac remodeling is apotential contributing mechanism Collagen density in theborder area and remote myocardium was lower in pigstreated with MSC-CM Cardiac fibrosis is associated withheart failure following myocardial infarction and maycontribute to progression of systolic and diastolic dysfunc-tion (Burlew amp Weber 2002 Cleutjens et al 1999) Werecently demonstrated that intravenous and intracoronaryMSC-CM treatment reduces myocardial apoptosis and oxida-tive stress (Timmers et al 2007a) In that study cardio-myocyte death was targeted acutely following ischemia andreperfusion injury In the current study treatment wasstarted late after coronary artery ligation and a model ofpermanent coronary artery ligation was used in order toinvestigate the angiogenic potential of MSC-CM and its effecton cardiac function independent of reduction of reperfusioninjury The fact that cardiac function improved using thisprotocol shows that there may be additional benefit fromprolonged treatment with MSC secretions
For this study a permanent coronary artery ligation wasperformed in anesthetized animals and functional measure-
ments were performed with open chest In addition we havenot been able to investigate the effect of commoncomorbidities such as hypertension dyslipidemia anddiabetes which might influence the biologic effect of MSCsecretions Due to the permanent coronary artery ligationwe were not able to assess the area at risk 3 weeks post MIWe were not able to oversee the effects of human proteininjection on the immune system of the porcine host and thepotential influence on study endpoints Furthermore themolecular mechanism for the induction of angiogenesis andor arteriogenesis and an exact determination of theresponsible angiogenic factors are still lacking Severalclinical trials with potent angiogenic factors failed toimprove outcome in patients (Henry et al 2003 Simonset al 2002) It is not clear how paracrine factors in stem celltransplants or the paracrine factors alone can induce abetter effect Most likely a combination of angiogenicfactors rather than a single protein is responsible Alsoexosomes could play an important role We previouslydemonstrated exosomes in MSC-CM to contain and delivercardioprotective compounds preventing cardiomyocytedeath following ischemia and reperfusion injury (Lai et al2010) Exosomes constitute a potential delivery tool to
Table 1 Hemodynamic and Functional Parameters
Baseline 3 weeks post MI Change from baseline ()
Parameter NCM CM NCM CM NCM CM
HR bpm 66plusmn4 73plusmn6 84plusmn6 86plusmn6 28plusmn12 12plusmn11MAP mm Hg 95plusmn5 89plusmn5 66plusmn6 85plusmn5 -30plusmn5 -5plusmn8 CO Lmin 31plusmn01 30plusmn02 37plusmn06 53plusmn05 23plusmn21 78plusmn20dPdt max mm Hgs 1213plusmn77 1241plusmn56 1157plusmn162 1650plusmn124 4plusmn13 40plusmn9 dPdt min mm Hgs -1274plusmn122 -1130plusmn96 -883plusmn98 -1313plusmn95 27plusmn9 -19plusmn19 EDP mm Hg 80plusmn03 71plusmn06 133plusmn16 121plusmn11 68plusmn21 94plusmn42WT infarct cm 079plusmn004 083plusmn005 055plusmn002 079plusmn005 -27plusmn4 -5plusmn4 Lvia (ED) cm2 158plusmn05 142plusmn10 260plusmn18 218plusmn15 64plusmn12 55plusmn12Lvia (ES) cm2 85plusmn04 76plusmn09 177plusmn16 125plusmn09 104plusmn14 60plusmn14 FAS 458plusmn19 469plusmn46 326plusmn22 424plusmn33 -28plusmn6 -6plusmn8 SV ml 48plusmn3 42plusmn2 43plusmn4 62plusmn3 -4plusmn11 52plusmn10 EDV ml 134plusmn16 129plusmn9ESV ml 93plusmn15 73plusmn9EF 337plusmn44 491plusmn33 SW mm Hgmiddotml 2497plusmn333 4595plusmn361 Stiffness mm Hgml 026plusmn004 014plusmn002
Summary of cardiac functional parameters of pigs treated with NCM (n=9) and MSC-CM (n=9) determined with echocardiography andconductance catheter-based LV pressure and volumemeasurements MI indicates myocardial infarction HR heart rate MAP mean arterialpressure CO cardiac output EDP end-diastolic pressure WT wall thickness LVia left ventricular internal area SV stroke volume EDVend-diastolic volume ESV end-systolic volume EF ejection fraction SW stroke work Stiffness end-diastolic chamber stiffness Pb005vs NCM
211
effectively carry angiogenic factors into the intracellularspace of the target tissue protecting the factors fromproteases This may explain why relatively low doses canhave such profound angiogenic effects Whether exosomesand their content are also responsible for the stimulation ofangiogenesis following MI remains a subject for furtherinvestigation
Here we demonstrate that human MSC secretionsstimulate angiogenesis These data support the hypothesisthat MSC transplantation induces vascular repair mechanismsvia paracrine pathways Most importantly human MSCsecretions harvested as conditioned medium using a clini-cally compliant protocol reduced infarct size and preservedcardiac function in a large animal model of myocardialinfarction The study therefore identifies MSC-CM as a noveltherapeutic biologic in the improvement of cardiac functionafter myocardial infarction
Methods
MSC-CM preparation
The protocols for MSC generation and CM preparation havebeen described in previous papers (Lian et al 2007 Sze et al2007) In short a chemically defined serum-free culturemedium(DMEMwithoutphenol red supplementedwith insulintransferrin and selenium 5 ngml FGF2 5 ngml PDGF ABglutamine-penicillin-streptomycin and szlig-mercaptoethanol)was conditioned by MSCs derived from human embryonicstem cells (hESCs) using a clinically compliant protocol Threepolyclonal karyotypically stable and phenotypically MSC-likecultures that do not express pluripotency-associated markersbut displayed MSC-like surface antigens (CD29+ CD44+CD49a+e+ CD105+ CD166+ CD34ndash CD45ndash) and gene
expression profile were generated by trypsinization andpropagation of hESCs from either the HuES9 hESC line or theH1 hESC line in feeder- and serum-free selection media (Lianet al 2007) One of these cultures HuES9E1 can be stablyexpanded for at least 80 population doublings To harvest MSCsecretions hESC-derived MSC cultures were transferred to achemically defined serum-free culture medium to conditionthe medium for 3 days before the media containing MSCsecretions were collected clarified by centrifugation con-centrated 25 times using 10-kDa MW cutoff ultrafiltrationmembranes and sterilized by filtration through a 220-nmfilter The protein concentration after concentration was050 mgml As a negative control the above-noted serum-free culture medium was processed equally (nonconditionedmedium [NCM])
Ingenuity pathway analysis
For this analysis we used the proteomic data obtainedpreviously (Sze et al 2007) Bioinformatic analysis wasperformed using Ingenuity pathway analysis (Ingenuity IPA-2002 version 71) The 201 proteins were uploaded inIngenuity with Ingenuity Knowledge Base as a reference setand direct and indirect relationships were included Allmolecules or relationships were considered for the filtersummary In the summary the focus was on Top Bio functionsin which physiological system development and function wasanalyzed in depth
HUVEC spheroid assay
Spheroids were formed from HUVECs to determine the effectof conditioned medium on angiogenic sprout formation (Korffamp Augustin 1998) Spheroids were formed overnight in 20
212 L Timmers et al
methocel in culture medium and subsequently embedded ina collagenndashmethocel matrix Sprouting was induced over-night with MSC-CM (n=12) or non-CM (NCM) (n=12) todetermine the effect of the secreted chemotactic proteinson capillary sprouting After overnight sprouting spheroidswere fixed in 10 formaldehyde and pictures were taken andthe length and number of sprouts were quantified
Animals
All experiments were performed in accordance with theldquoGuide for the Care and Use of Laboratory Animalsrdquo preparedby the Institute of Laboratory Animal Resources andwith priorapproval by the Animal Experimentation Committee of theFaculty of Medicine Utrecht University the Netherlands
Sample size calculation
In a previous study the mean fractional area shortening(FAS) after LCx ligation was 365 (Timmers et al 2007b)With an alpha of 005 power of 080 SD of 58 anddifference of 20 considered relevant 10 animals per groupwere needed To allow for 10 mortality 11 animals pergroup were enrolled
Pig study design
Myocardial infarction was induced in 22 Dalland Landracepigs (60ndash70 kg IDDLO Lelystad the Netherlands) by surgicalleft circumflex coronary artery (LCx) ligation Two pigs diedperioperatively before randomization and were thereforeexcluded from the study The remaining 20 pigs wererandomized after surgery by using sealed envelopes tointravenous treatment with MSC-CM (20 ml MSC-CM ie10 mg protein) or 20 ml NCM initiated 4 h after coronaryartery ligation and the treatment was continued for 7 daystwice daily via a catheter inserted into the jugular vein Thepigs were sacrificed 3 weeks after MI To prevent thromboticcomplications and arrhythmias all pigs were treated withclopidogrel 75 mgday from 3 days before MI until termina-tion and amiodarone 400 mgday from 10 days before MIuntil termination
Myocardial infarction and operational procedure
Pigs were anesthetized as described previously (Timmers etal 2007b) During the entire operation electrocardiogramarterial pressure and capnogram were continuously moni-tored After median sternotomy the left ventricularpressure (LVP) was measured using a pressure tipped Millarcatheter that was inserted through the apex into the leftventricle A transonic flow probe (Transonic Systems IncIthaca NY USA) was placed around the proximal aorta tomeasure cardiac output Sutures were then tightened topermanently occlude the proximal LCx Internal defibrilla-tion with 50 J was used when VF occurred Prior to and 1 hafter induction of the infarct echocardiography wasperformed After stabilization of hemodynamic parametersand heart rhythm the thorax was closed and the animalswere allowed to recover Three weeks after induction of
myocardial infarction the animals were anesthetized oncemore and the sternum was reopened Echocardiography andconductance catheter-based pressurendashvolume (PV) looprecordings were obtained to assess cardiac function andgeometry After the functional measurements the heart wasexcised for laboratory analysis
Immunohistochemistry
Three weeks following MI myocardial biopsies were obtainedfrom the infarct area border area and remote area andfixated in 4 formalin for 24 h before being embedded inparaffin To determine capillary density a lectin stainingdelineating the endothelium was performed followingantigen retrieval by boiling in 10 mM citrate bufferEndogenous biotin was blocked using 01 avidin solution(DakoCytomation Biotin Blocking system X0590) for 15 min atroom temperature (RT) and subsequently with 001 biotinsolution (Dako) for 15 min at RT After blocking with 30 BSAin PBS the sections were incubated overnight with biotiny-lated BS-1 (Sigma L3759) in a 1300 dilution in PBS with 01BSA and subsequently with streptavidin-HRPO (11000 in PBS)for 1 h at RT Finally the sections were incubated for 30 minin 3-amino-9-ethylcarbazole (AEC) and stained with hema-toxylin before being embedded Capillary density wasexpressed as the number of capillaries per square millimetertissue Quantification of collagen density was performedusing picrosirius red staining with circularly polarized lightand digital image microscopy after conversion into gray-value images as described before (Timmers et al 2007b)
Myocardial infarct size
After excision of the heart the LV was isolated and cut into 5slices from apex to base To discriminate infarct tissue fromviable myocardium the slices were incubated in 1triphenyltetrazolium chloride (TTC Sigma-Aldrich Chemi-cals Zwijndrecht Netherlands) in 37 degC Soumlrensen buffer(136 gL KH2PO4+178 gL Na2H PO42H2O pH 74) for15 min All slices were scanned from both sides and in eachslide the infarct area was compared to total area using digitalplanimetry software After correction for the weight of theslices infarct size was calculated as a percentage of the LV
Cardiac function
Midpapillary short axis epicardial echocardiography wasperformed before coronary artery ligation 1 h after and3 weeks after coronary artery ligation (Prosound SSD-50005 MHz probe UST-5280-5 Aloka Holding Europe AG ZugSwitzerland) Wall thickness (WT) of the infarct area and leftventricular internal area (LVia) were measured at end-diastole (ED) and end-systole (ES) Systolic wall thickening(SWT) was calculated as (WT(ES) ndashWT(ED))WT(ED) 100 ()and fractional area shortening (FAS) as (LVia(ED) ndash LVia(ES))LVia(ED) 100 () Left ventricular (LV) pressurendashvolumeloops were measured using a conductance catheter asdescribed previously (Timmers et al 2009) Diastolicchamber stiffness was quantified by means of linearregression of the end-diastolic pressurendashvolume relationship(Sagawa 1981)
213
Data analysis
The data were collected and analyzed in a blinded fashionData are presented as meanplusmnSE Mortality was comparedusing Fishers exact test Capillary sprouting was comparedusing a one-way ANOVA and Bonferroni post hoc tests A two-way ANOVA with Bonferroni post hoc tests was used tocompare capillary density and collagen density in themyocardial tissue Cardiac functional parameters that werealso measured before MI (baseline) were compared using atwo-way ANOVA for repeated measures and Bonferroni posthoc tests For cardiac functional parameters that weremeasured only 3 weeks after MI Students t test was used
Acknowledgments
This work was supported by the Netherlands Heart Founda-tion [Grant 2005T022 LT] and an Internationalization grantby the University Medical Center Utrecht the Netherlands[DPVK]
Appendix A Supplementary data
Supplementary data to this article can be found online atdoi101016jscr201101001
References
Assmus B Honold J Schachinger V Britten MB Fischer-Rasokat U Lehmann R Teupe C Pistorius K Martin HAbolmaali ND Tonn T Dimmeler S Zeiher AM 2006Transcoronary transplantation of progenitor cells after myocardialinfarction N Engl J Med 355 1222ndash1232
Burlew BS Weber KT 2002 Cardiac fibrosis as a cause ofdiastolic dysfunction Herz 27 92ndash98
Caplan AI Dennis JE 2006 Mesenchymal stem cells as trophicmediators J Cell Biochem 98 1076ndash1084
Cleutjens JP Blankesteijn WM Daemen MJ Smits JF1999 The infarcted myocardium simply dead tissue or a livelytarget for therapeutic interventions Cardiovasc Res 44232ndash241
de Silva R Raval AN Hadi M Gildea KM Bonifacino ACYu ZX Yau YY Leitman SF Bacharach SL DonahueRE Read EJ Lederman RJ 2008 Intracoronary infusion ofautologous mononuclear cells from bone marrow or granulocytecolony-stimulating factor-mobilized apheresis product may notimprove remodelling contractile function perfusion or infarctsize in a swine model of large myocardial infarction Eur Heart J29 1772ndash1782
Erbs S Linke A Schachinger V Assmus B Thiele H DiederichKW Hoffmann C Dimmeler S Tonn T Hambrecht RZeiher AM Schuler G 2007 Restoration of microvascularfunction in the infarct-related artery by intracoronary transplan-tation of bone marrow progenitor cells in patients with acutemyocardial infarction the Doppler Substudy of the Reinfusion ofEnriched Progenitor Cells and Infarct Remodeling in AcuteMyocardial Infarction (REPAIR-AMI) trial Circulation 116 366ndash374
Gnecchi M He H Liang OD Melo LG Morello F Mu HNoiseux N Zhang L Pratt RE Ingwall JS Dzau VJ2005 Paracrine action accounts for marked protection ofischemic heart by Akt-modified mesenchymal stem cells NatMed 11 367ndash368
Hashemi SM Ghods S Kolodgie FD Parcham-Azad K KeaneM Hamamdzic D Young R Rippy MK Virmani R Litt HWilensky RL 2008 A placebo controlled dose-ranging safetystudy of allogenic mesenchymal stem cells injected by endo-myocardial delivery after an acute myocardial infarction EurHeart J 29 251ndash259
Henry TD Annex BH McKendall GR Azrin MA Lopez JJGiordano FJ Shah PK Willerson JT Benza RL BermanDS Gibson CM Bajamonde A Rundle AC Fine JMcCluskey ER 2003 The VIVA trial vascular endothelialgrowth factor in ischemia for vascular angiogenesis Circulation107 1359ndash1365
Janssens S Dubois C Bogaert J Theunissen K Deroose CDesmet W Kalantzi M Herbots L Sinnaeve P Dens JMaertens J Rademakers F Dymarkowski S Gheysens O VanCleemput J Bormans G Nuyts J Belmans A Mortelmans LBoogaerts M Van de Werf F 2006 Autologous bone marrow-derived stem-cell transfer in patients with ST-segment elevationmyocardial infarction double-blind randomised controlled trialLancet 367 113ndash121
Kinnaird T Stabile E Burnett MS Shou M Lee CW BarrS Fuchs S Epstein SE 2004 Local delivery of marrow-derived stromal cells augments collateral perfusion throughparacrine mechanisms Circulation 109 1543ndash1549
Korff T Augustin HG 1998 Integration of endothelial cells inmulticellular spheroids prevents apoptosis and induces differen-tiation J Cell Biol 143 1341ndash1352
Lai RC Arslan F Lee MM Sze NS Choo A Chen TSSalto-Tellez M Timmers L Lee CN El Oakley RMPasterkamp G de Kleijn DP Lim SK 2010 Exosomesecreted by MSC reduces myocardial ischemiareperfusioninjury Stem Cell Res 4 214ndash222
Lian Q Lye E Suan Yeo K KhiaWay Tan E Salto-Tellez M LiuTM PalanisamyN ElOakley RM Lee EH LimB Lim SK2007 Derivation of clinically compliant MSCs from CD105+ CD24-differentiated human ESCs Stem Cells 25 425ndash436
Losordo DW Dimmeler S 2004 Therapeutic angiogenesis andvasculogenesis for ischemic disease part II cell-based therapiesCirculation 109 2692ndash2697
Lunde K Solheim S Aakhus S Arnesen H Abdelnoor MEgeland T Endresen K Ilebekk A Mangschau A Fjeld JGSmith HJ Taraldsrud E Grogaard HK Bjornerheim RBrekke M Muller C Hopp E Ragnarsson A Brinchmann JEForfang K 2006 Intracoronary injection of mononuclear bonemarrow cells in acute myocardial infarction N Engl J Med 3551199ndash1209
Menasche P Alfieri O Janssens S McKenna W Reich-enspurner H Trinquart L Vilquin JT Marolleau JPSeymour B Larghero J Lake S Chatellier G Solomon SDesnos M Hagege AA 2008 The Myoblast AutologousGrafting in Ischemic Cardiomyopathy (MAGIC) trial first ran-domized placebo-controlled study of myoblast transplantationCirculation 117 1189ndash1200
Meyer GP Wollert KC Lotz J Pirr J Rager U Lippolt PHahn A Fichtner S Schaefer A Arseniev L Ganser ADrexler H 2009 Intracoronary bone marrow cell transfer aftermyocardial infarction 5-year follow-up from the randomized-controlled BOOST trial Eur Heart J 24 2978ndash2984
Moelker AD Baks T van den Bos EJ van Geuns RJ deFeyter PJ Duncker DJ van der Giessen WJ 2006Reduction in infarct size but no functional improvement afterbone marrow cell administration in a porcine model ofreperfused myocardial infarction Eur Heart J 27 3057ndash3064
Pittenger MF Martin BJ 2004 Mesenchymal stem cells andtheir potential as cardiac therapeutics Circ Res 95 9ndash20
Sagawa K 1981 The end-systolic pressure-volume relation of theventricle definition modifications and clinical use Circulation63 1223ndash1227
214 L Timmers et al
Schachinger V Erbs S Elsasser A Haberbosch W Ham-brecht R Holschermann H Yu J Corti R Mathey DGHamm CW Suselbeck T Assmus B Tonn T DimmelerS Zeiher AM 2006 Intracoronary bone marrow-derivedprogenitor cells in acute myocardial infarction N Engl J Med355 1210ndash1221
Simons M Annex BH Laham RJ Kleiman N Henry TDauerman H Udelson JE Gervino EV Pike M White-house MJ Moon T Chronos NA 2002 Pharmacologicaltreatment of coronary artery disease with recombinant fibroblastgrowth factor-2 double-blind randomized controlled clinicaltrial Circulation 105 788ndash793
Strauer BE Brehm M Zeus T Kostering M Hernandez ASorg RV Kogler G Wernet P 2002 Repair of infarctedmyocardium by autologous intracoronary mononuclear bonemarrow cell transplantation in humans Circulation 1061913ndash1918
Sze SK de Kleijn DP Lai RC Khia Way E 2007 Tan HZhao KS Yeo TY Low Q Lian CN Lee W Mitchell RM ElOakley SK Lim Elucidating the secretion proteome of humanembryonic stem cell-derived mesenchymal stem cells Mol CellProteomics 6 1680ndash1689
Timmers L Lim SK Arslan F Armstrong JS Hoefer IEDoevendans PA Piek JJ El Oakley RM Choo A Lee CNPasterkamp G de Kleijn DP 2007a Reduction of myocardialinfarct size by humanmesenchymal stemcell conditionedmediumStem Cell Res 1 129ndash137
Timmers L Sluijter JP Verlaan CW Steendijk P CramerMJEmons M Strijder C Grundeman PF Sze SK Hua L PiekJJ Borst C Pasterkamp G de Kleijn DP 2007b Cycloox-ygenase-2 inhibition increases mortality enhances left ventricularremodeling and impairs systolic function after myocardialinfarction in the pig Circulation 115 326ndash332
Timmers L Henriques JP de Kleijn DP Devries JHKemperman H Steendijk P Verlaan CW Kerver MPiek JJ Doevendans PA Pasterkamp G Hoefer IE2009 Exenatide reduces infarct size and improves cardiacfunction in a porcine model of ischemia and reperfusion injuryJ Am Coll Cardiol 53 501ndash510
van Laake LW Passier R denOuden K Schreurs CMonshouwer-Kloots JWard-vanOostwaard D van Echteld CJ DoevendansPA Mummery CL 2009 Improvement of mouse cardiacfunction by hESC-derived cardiomyocytes correlates with vascular-ity but not graft size Stem Cell Res 3 106ndash112
Wolf D Reinhard A Seckinger A Gross L Katus HA HansenA 2009 Regenerative capacity of intravenous autologousallogeneic and human mesenchymal stem cells in the infarctedpig myocardium-complicated by myocardial tumor formationScand Cardiovasc J 43 39ndash45
Yousef M Schannwell CM Kostering M Zeus T Brehm MStrauer BE 2009 The BALANCE Study clinical benefit andlong-term outcome after intracoronary autologous bone marrowcell transplantation in patients with acute myocardial infarctionJ Am Coll Cardiol 53 2262ndash2269
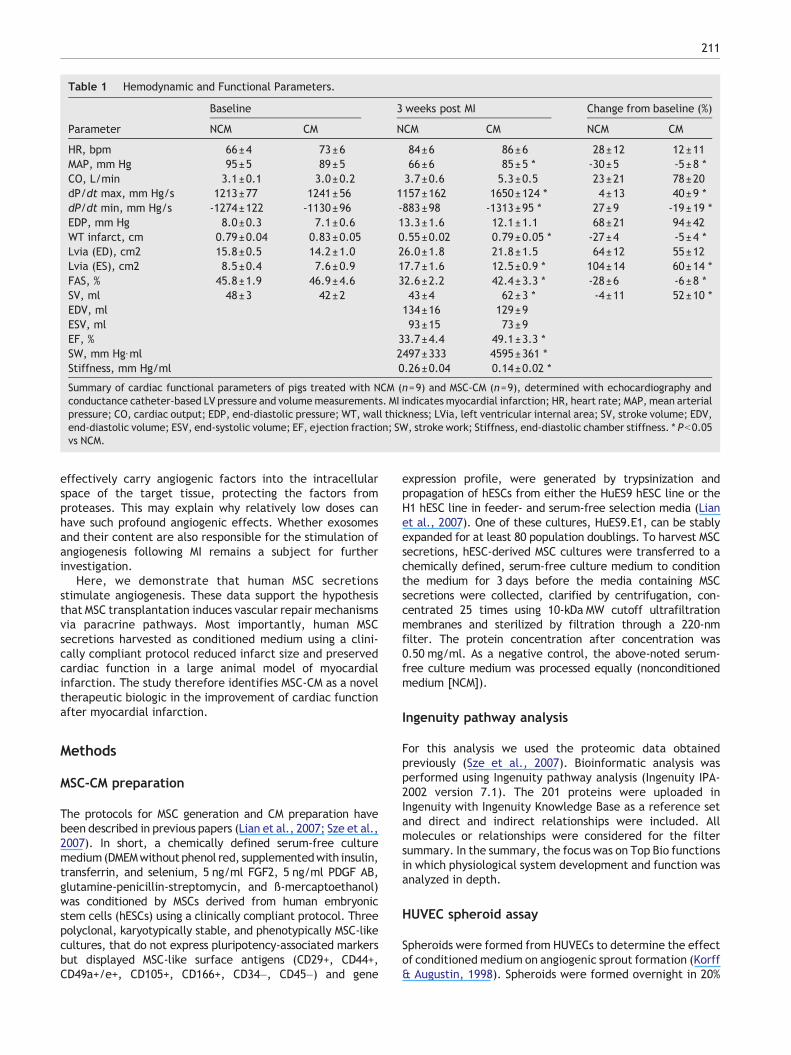
Table 1 Hemodynamic and Functional Parameters
Baseline 3 weeks post MI Change from baseline ()
Parameter NCM CM NCM CM NCM CM
HR bpm 66plusmn4 73plusmn6 84plusmn6 86plusmn6 28plusmn12 12plusmn11MAP mm Hg 95plusmn5 89plusmn5 66plusmn6 85plusmn5 -30plusmn5 -5plusmn8 CO Lmin 31plusmn01 30plusmn02 37plusmn06 53plusmn05 23plusmn21 78plusmn20dPdt max mm Hgs 1213plusmn77 1241plusmn56 1157plusmn162 1650plusmn124 4plusmn13 40plusmn9 dPdt min mm Hgs -1274plusmn122 -1130plusmn96 -883plusmn98 -1313plusmn95 27plusmn9 -19plusmn19 EDP mm Hg 80plusmn03 71plusmn06 133plusmn16 121plusmn11 68plusmn21 94plusmn42WT infarct cm 079plusmn004 083plusmn005 055plusmn002 079plusmn005 -27plusmn4 -5plusmn4 Lvia (ED) cm2 158plusmn05 142plusmn10 260plusmn18 218plusmn15 64plusmn12 55plusmn12Lvia (ES) cm2 85plusmn04 76plusmn09 177plusmn16 125plusmn09 104plusmn14 60plusmn14 FAS 458plusmn19 469plusmn46 326plusmn22 424plusmn33 -28plusmn6 -6plusmn8 SV ml 48plusmn3 42plusmn2 43plusmn4 62plusmn3 -4plusmn11 52plusmn10 EDV ml 134plusmn16 129plusmn9ESV ml 93plusmn15 73plusmn9EF 337plusmn44 491plusmn33 SW mm Hgmiddotml 2497plusmn333 4595plusmn361 Stiffness mm Hgml 026plusmn004 014plusmn002
Summary of cardiac functional parameters of pigs treated with NCM (n=9) and MSC-CM (n=9) determined with echocardiography andconductance catheter-based LV pressure and volumemeasurements MI indicates myocardial infarction HR heart rate MAP mean arterialpressure CO cardiac output EDP end-diastolic pressure WT wall thickness LVia left ventricular internal area SV stroke volume EDVend-diastolic volume ESV end-systolic volume EF ejection fraction SW stroke work Stiffness end-diastolic chamber stiffness Pb005vs NCM
211
effectively carry angiogenic factors into the intracellularspace of the target tissue protecting the factors fromproteases This may explain why relatively low doses canhave such profound angiogenic effects Whether exosomesand their content are also responsible for the stimulation ofangiogenesis following MI remains a subject for furtherinvestigation
Here we demonstrate that human MSC secretionsstimulate angiogenesis These data support the hypothesisthat MSC transplantation induces vascular repair mechanismsvia paracrine pathways Most importantly human MSCsecretions harvested as conditioned medium using a clini-cally compliant protocol reduced infarct size and preservedcardiac function in a large animal model of myocardialinfarction The study therefore identifies MSC-CM as a noveltherapeutic biologic in the improvement of cardiac functionafter myocardial infarction
Methods
MSC-CM preparation
The protocols for MSC generation and CM preparation havebeen described in previous papers (Lian et al 2007 Sze et al2007) In short a chemically defined serum-free culturemedium(DMEMwithoutphenol red supplementedwith insulintransferrin and selenium 5 ngml FGF2 5 ngml PDGF ABglutamine-penicillin-streptomycin and szlig-mercaptoethanol)was conditioned by MSCs derived from human embryonicstem cells (hESCs) using a clinically compliant protocol Threepolyclonal karyotypically stable and phenotypically MSC-likecultures that do not express pluripotency-associated markersbut displayed MSC-like surface antigens (CD29+ CD44+CD49a+e+ CD105+ CD166+ CD34ndash CD45ndash) and gene
expression profile were generated by trypsinization andpropagation of hESCs from either the HuES9 hESC line or theH1 hESC line in feeder- and serum-free selection media (Lianet al 2007) One of these cultures HuES9E1 can be stablyexpanded for at least 80 population doublings To harvest MSCsecretions hESC-derived MSC cultures were transferred to achemically defined serum-free culture medium to conditionthe medium for 3 days before the media containing MSCsecretions were collected clarified by centrifugation con-centrated 25 times using 10-kDa MW cutoff ultrafiltrationmembranes and sterilized by filtration through a 220-nmfilter The protein concentration after concentration was050 mgml As a negative control the above-noted serum-free culture medium was processed equally (nonconditionedmedium [NCM])
Ingenuity pathway analysis
For this analysis we used the proteomic data obtainedpreviously (Sze et al 2007) Bioinformatic analysis wasperformed using Ingenuity pathway analysis (Ingenuity IPA-2002 version 71) The 201 proteins were uploaded inIngenuity with Ingenuity Knowledge Base as a reference setand direct and indirect relationships were included Allmolecules or relationships were considered for the filtersummary In the summary the focus was on Top Bio functionsin which physiological system development and function wasanalyzed in depth
HUVEC spheroid assay
Spheroids were formed from HUVECs to determine the effectof conditioned medium on angiogenic sprout formation (Korffamp Augustin 1998) Spheroids were formed overnight in 20
212 L Timmers et al
methocel in culture medium and subsequently embedded ina collagenndashmethocel matrix Sprouting was induced over-night with MSC-CM (n=12) or non-CM (NCM) (n=12) todetermine the effect of the secreted chemotactic proteinson capillary sprouting After overnight sprouting spheroidswere fixed in 10 formaldehyde and pictures were taken andthe length and number of sprouts were quantified
Animals
All experiments were performed in accordance with theldquoGuide for the Care and Use of Laboratory Animalsrdquo preparedby the Institute of Laboratory Animal Resources andwith priorapproval by the Animal Experimentation Committee of theFaculty of Medicine Utrecht University the Netherlands
Sample size calculation
In a previous study the mean fractional area shortening(FAS) after LCx ligation was 365 (Timmers et al 2007b)With an alpha of 005 power of 080 SD of 58 anddifference of 20 considered relevant 10 animals per groupwere needed To allow for 10 mortality 11 animals pergroup were enrolled
Pig study design
Myocardial infarction was induced in 22 Dalland Landracepigs (60ndash70 kg IDDLO Lelystad the Netherlands) by surgicalleft circumflex coronary artery (LCx) ligation Two pigs diedperioperatively before randomization and were thereforeexcluded from the study The remaining 20 pigs wererandomized after surgery by using sealed envelopes tointravenous treatment with MSC-CM (20 ml MSC-CM ie10 mg protein) or 20 ml NCM initiated 4 h after coronaryartery ligation and the treatment was continued for 7 daystwice daily via a catheter inserted into the jugular vein Thepigs were sacrificed 3 weeks after MI To prevent thromboticcomplications and arrhythmias all pigs were treated withclopidogrel 75 mgday from 3 days before MI until termina-tion and amiodarone 400 mgday from 10 days before MIuntil termination
Myocardial infarction and operational procedure
Pigs were anesthetized as described previously (Timmers etal 2007b) During the entire operation electrocardiogramarterial pressure and capnogram were continuously moni-tored After median sternotomy the left ventricularpressure (LVP) was measured using a pressure tipped Millarcatheter that was inserted through the apex into the leftventricle A transonic flow probe (Transonic Systems IncIthaca NY USA) was placed around the proximal aorta tomeasure cardiac output Sutures were then tightened topermanently occlude the proximal LCx Internal defibrilla-tion with 50 J was used when VF occurred Prior to and 1 hafter induction of the infarct echocardiography wasperformed After stabilization of hemodynamic parametersand heart rhythm the thorax was closed and the animalswere allowed to recover Three weeks after induction of
myocardial infarction the animals were anesthetized oncemore and the sternum was reopened Echocardiography andconductance catheter-based pressurendashvolume (PV) looprecordings were obtained to assess cardiac function andgeometry After the functional measurements the heart wasexcised for laboratory analysis
Immunohistochemistry
Three weeks following MI myocardial biopsies were obtainedfrom the infarct area border area and remote area andfixated in 4 formalin for 24 h before being embedded inparaffin To determine capillary density a lectin stainingdelineating the endothelium was performed followingantigen retrieval by boiling in 10 mM citrate bufferEndogenous biotin was blocked using 01 avidin solution(DakoCytomation Biotin Blocking system X0590) for 15 min atroom temperature (RT) and subsequently with 001 biotinsolution (Dako) for 15 min at RT After blocking with 30 BSAin PBS the sections were incubated overnight with biotiny-lated BS-1 (Sigma L3759) in a 1300 dilution in PBS with 01BSA and subsequently with streptavidin-HRPO (11000 in PBS)for 1 h at RT Finally the sections were incubated for 30 minin 3-amino-9-ethylcarbazole (AEC) and stained with hema-toxylin before being embedded Capillary density wasexpressed as the number of capillaries per square millimetertissue Quantification of collagen density was performedusing picrosirius red staining with circularly polarized lightand digital image microscopy after conversion into gray-value images as described before (Timmers et al 2007b)
Myocardial infarct size
After excision of the heart the LV was isolated and cut into 5slices from apex to base To discriminate infarct tissue fromviable myocardium the slices were incubated in 1triphenyltetrazolium chloride (TTC Sigma-Aldrich Chemi-cals Zwijndrecht Netherlands) in 37 degC Soumlrensen buffer(136 gL KH2PO4+178 gL Na2H PO42H2O pH 74) for15 min All slices were scanned from both sides and in eachslide the infarct area was compared to total area using digitalplanimetry software After correction for the weight of theslices infarct size was calculated as a percentage of the LV
Cardiac function
Midpapillary short axis epicardial echocardiography wasperformed before coronary artery ligation 1 h after and3 weeks after coronary artery ligation (Prosound SSD-50005 MHz probe UST-5280-5 Aloka Holding Europe AG ZugSwitzerland) Wall thickness (WT) of the infarct area and leftventricular internal area (LVia) were measured at end-diastole (ED) and end-systole (ES) Systolic wall thickening(SWT) was calculated as (WT(ES) ndashWT(ED))WT(ED) 100 ()and fractional area shortening (FAS) as (LVia(ED) ndash LVia(ES))LVia(ED) 100 () Left ventricular (LV) pressurendashvolumeloops were measured using a conductance catheter asdescribed previously (Timmers et al 2009) Diastolicchamber stiffness was quantified by means of linearregression of the end-diastolic pressurendashvolume relationship(Sagawa 1981)
213
Data analysis
The data were collected and analyzed in a blinded fashionData are presented as meanplusmnSE Mortality was comparedusing Fishers exact test Capillary sprouting was comparedusing a one-way ANOVA and Bonferroni post hoc tests A two-way ANOVA with Bonferroni post hoc tests was used tocompare capillary density and collagen density in themyocardial tissue Cardiac functional parameters that werealso measured before MI (baseline) were compared using atwo-way ANOVA for repeated measures and Bonferroni posthoc tests For cardiac functional parameters that weremeasured only 3 weeks after MI Students t test was used
Acknowledgments
This work was supported by the Netherlands Heart Founda-tion [Grant 2005T022 LT] and an Internationalization grantby the University Medical Center Utrecht the Netherlands[DPVK]
Appendix A Supplementary data
Supplementary data to this article can be found online atdoi101016jscr201101001
References
Assmus B Honold J Schachinger V Britten MB Fischer-Rasokat U Lehmann R Teupe C Pistorius K Martin HAbolmaali ND Tonn T Dimmeler S Zeiher AM 2006Transcoronary transplantation of progenitor cells after myocardialinfarction N Engl J Med 355 1222ndash1232
Burlew BS Weber KT 2002 Cardiac fibrosis as a cause ofdiastolic dysfunction Herz 27 92ndash98
Caplan AI Dennis JE 2006 Mesenchymal stem cells as trophicmediators J Cell Biochem 98 1076ndash1084
Cleutjens JP Blankesteijn WM Daemen MJ Smits JF1999 The infarcted myocardium simply dead tissue or a livelytarget for therapeutic interventions Cardiovasc Res 44232ndash241
de Silva R Raval AN Hadi M Gildea KM Bonifacino ACYu ZX Yau YY Leitman SF Bacharach SL DonahueRE Read EJ Lederman RJ 2008 Intracoronary infusion ofautologous mononuclear cells from bone marrow or granulocytecolony-stimulating factor-mobilized apheresis product may notimprove remodelling contractile function perfusion or infarctsize in a swine model of large myocardial infarction Eur Heart J29 1772ndash1782
Erbs S Linke A Schachinger V Assmus B Thiele H DiederichKW Hoffmann C Dimmeler S Tonn T Hambrecht RZeiher AM Schuler G 2007 Restoration of microvascularfunction in the infarct-related artery by intracoronary transplan-tation of bone marrow progenitor cells in patients with acutemyocardial infarction the Doppler Substudy of the Reinfusion ofEnriched Progenitor Cells and Infarct Remodeling in AcuteMyocardial Infarction (REPAIR-AMI) trial Circulation 116 366ndash374
Gnecchi M He H Liang OD Melo LG Morello F Mu HNoiseux N Zhang L Pratt RE Ingwall JS Dzau VJ2005 Paracrine action accounts for marked protection ofischemic heart by Akt-modified mesenchymal stem cells NatMed 11 367ndash368
Hashemi SM Ghods S Kolodgie FD Parcham-Azad K KeaneM Hamamdzic D Young R Rippy MK Virmani R Litt HWilensky RL 2008 A placebo controlled dose-ranging safetystudy of allogenic mesenchymal stem cells injected by endo-myocardial delivery after an acute myocardial infarction EurHeart J 29 251ndash259
Henry TD Annex BH McKendall GR Azrin MA Lopez JJGiordano FJ Shah PK Willerson JT Benza RL BermanDS Gibson CM Bajamonde A Rundle AC Fine JMcCluskey ER 2003 The VIVA trial vascular endothelialgrowth factor in ischemia for vascular angiogenesis Circulation107 1359ndash1365
Janssens S Dubois C Bogaert J Theunissen K Deroose CDesmet W Kalantzi M Herbots L Sinnaeve P Dens JMaertens J Rademakers F Dymarkowski S Gheysens O VanCleemput J Bormans G Nuyts J Belmans A Mortelmans LBoogaerts M Van de Werf F 2006 Autologous bone marrow-derived stem-cell transfer in patients with ST-segment elevationmyocardial infarction double-blind randomised controlled trialLancet 367 113ndash121
Kinnaird T Stabile E Burnett MS Shou M Lee CW BarrS Fuchs S Epstein SE 2004 Local delivery of marrow-derived stromal cells augments collateral perfusion throughparacrine mechanisms Circulation 109 1543ndash1549
Korff T Augustin HG 1998 Integration of endothelial cells inmulticellular spheroids prevents apoptosis and induces differen-tiation J Cell Biol 143 1341ndash1352
Lai RC Arslan F Lee MM Sze NS Choo A Chen TSSalto-Tellez M Timmers L Lee CN El Oakley RMPasterkamp G de Kleijn DP Lim SK 2010 Exosomesecreted by MSC reduces myocardial ischemiareperfusioninjury Stem Cell Res 4 214ndash222
Lian Q Lye E Suan Yeo K KhiaWay Tan E Salto-Tellez M LiuTM PalanisamyN ElOakley RM Lee EH LimB Lim SK2007 Derivation of clinically compliant MSCs from CD105+ CD24-differentiated human ESCs Stem Cells 25 425ndash436
Losordo DW Dimmeler S 2004 Therapeutic angiogenesis andvasculogenesis for ischemic disease part II cell-based therapiesCirculation 109 2692ndash2697
Lunde K Solheim S Aakhus S Arnesen H Abdelnoor MEgeland T Endresen K Ilebekk A Mangschau A Fjeld JGSmith HJ Taraldsrud E Grogaard HK Bjornerheim RBrekke M Muller C Hopp E Ragnarsson A Brinchmann JEForfang K 2006 Intracoronary injection of mononuclear bonemarrow cells in acute myocardial infarction N Engl J Med 3551199ndash1209
Menasche P Alfieri O Janssens S McKenna W Reich-enspurner H Trinquart L Vilquin JT Marolleau JPSeymour B Larghero J Lake S Chatellier G Solomon SDesnos M Hagege AA 2008 The Myoblast AutologousGrafting in Ischemic Cardiomyopathy (MAGIC) trial first ran-domized placebo-controlled study of myoblast transplantationCirculation 117 1189ndash1200
Meyer GP Wollert KC Lotz J Pirr J Rager U Lippolt PHahn A Fichtner S Schaefer A Arseniev L Ganser ADrexler H 2009 Intracoronary bone marrow cell transfer aftermyocardial infarction 5-year follow-up from the randomized-controlled BOOST trial Eur Heart J 24 2978ndash2984
Moelker AD Baks T van den Bos EJ van Geuns RJ deFeyter PJ Duncker DJ van der Giessen WJ 2006Reduction in infarct size but no functional improvement afterbone marrow cell administration in a porcine model ofreperfused myocardial infarction Eur Heart J 27 3057ndash3064
Pittenger MF Martin BJ 2004 Mesenchymal stem cells andtheir potential as cardiac therapeutics Circ Res 95 9ndash20
Sagawa K 1981 The end-systolic pressure-volume relation of theventricle definition modifications and clinical use Circulation63 1223ndash1227
214 L Timmers et al
Schachinger V Erbs S Elsasser A Haberbosch W Ham-brecht R Holschermann H Yu J Corti R Mathey DGHamm CW Suselbeck T Assmus B Tonn T DimmelerS Zeiher AM 2006 Intracoronary bone marrow-derivedprogenitor cells in acute myocardial infarction N Engl J Med355 1210ndash1221
Simons M Annex BH Laham RJ Kleiman N Henry TDauerman H Udelson JE Gervino EV Pike M White-house MJ Moon T Chronos NA 2002 Pharmacologicaltreatment of coronary artery disease with recombinant fibroblastgrowth factor-2 double-blind randomized controlled clinicaltrial Circulation 105 788ndash793
Strauer BE Brehm M Zeus T Kostering M Hernandez ASorg RV Kogler G Wernet P 2002 Repair of infarctedmyocardium by autologous intracoronary mononuclear bonemarrow cell transplantation in humans Circulation 1061913ndash1918
Sze SK de Kleijn DP Lai RC Khia Way E 2007 Tan HZhao KS Yeo TY Low Q Lian CN Lee W Mitchell RM ElOakley SK Lim Elucidating the secretion proteome of humanembryonic stem cell-derived mesenchymal stem cells Mol CellProteomics 6 1680ndash1689
Timmers L Lim SK Arslan F Armstrong JS Hoefer IEDoevendans PA Piek JJ El Oakley RM Choo A Lee CNPasterkamp G de Kleijn DP 2007a Reduction of myocardialinfarct size by humanmesenchymal stemcell conditionedmediumStem Cell Res 1 129ndash137
Timmers L Sluijter JP Verlaan CW Steendijk P CramerMJEmons M Strijder C Grundeman PF Sze SK Hua L PiekJJ Borst C Pasterkamp G de Kleijn DP 2007b Cycloox-ygenase-2 inhibition increases mortality enhances left ventricularremodeling and impairs systolic function after myocardialinfarction in the pig Circulation 115 326ndash332
Timmers L Henriques JP de Kleijn DP Devries JHKemperman H Steendijk P Verlaan CW Kerver MPiek JJ Doevendans PA Pasterkamp G Hoefer IE2009 Exenatide reduces infarct size and improves cardiacfunction in a porcine model of ischemia and reperfusion injuryJ Am Coll Cardiol 53 501ndash510
van Laake LW Passier R denOuden K Schreurs CMonshouwer-Kloots JWard-vanOostwaard D van Echteld CJ DoevendansPA Mummery CL 2009 Improvement of mouse cardiacfunction by hESC-derived cardiomyocytes correlates with vascular-ity but not graft size Stem Cell Res 3 106ndash112
Wolf D Reinhard A Seckinger A Gross L Katus HA HansenA 2009 Regenerative capacity of intravenous autologousallogeneic and human mesenchymal stem cells in the infarctedpig myocardium-complicated by myocardial tumor formationScand Cardiovasc J 43 39ndash45
Yousef M Schannwell CM Kostering M Zeus T Brehm MStrauer BE 2009 The BALANCE Study clinical benefit andlong-term outcome after intracoronary autologous bone marrowcell transplantation in patients with acute myocardial infarctionJ Am Coll Cardiol 53 2262ndash2269

212 L Timmers et al
methocel in culture medium and subsequently embedded ina collagenndashmethocel matrix Sprouting was induced over-night with MSC-CM (n=12) or non-CM (NCM) (n=12) todetermine the effect of the secreted chemotactic proteinson capillary sprouting After overnight sprouting spheroidswere fixed in 10 formaldehyde and pictures were taken andthe length and number of sprouts were quantified
Animals
All experiments were performed in accordance with theldquoGuide for the Care and Use of Laboratory Animalsrdquo preparedby the Institute of Laboratory Animal Resources andwith priorapproval by the Animal Experimentation Committee of theFaculty of Medicine Utrecht University the Netherlands
Sample size calculation
In a previous study the mean fractional area shortening(FAS) after LCx ligation was 365 (Timmers et al 2007b)With an alpha of 005 power of 080 SD of 58 anddifference of 20 considered relevant 10 animals per groupwere needed To allow for 10 mortality 11 animals pergroup were enrolled
Pig study design
Myocardial infarction was induced in 22 Dalland Landracepigs (60ndash70 kg IDDLO Lelystad the Netherlands) by surgicalleft circumflex coronary artery (LCx) ligation Two pigs diedperioperatively before randomization and were thereforeexcluded from the study The remaining 20 pigs wererandomized after surgery by using sealed envelopes tointravenous treatment with MSC-CM (20 ml MSC-CM ie10 mg protein) or 20 ml NCM initiated 4 h after coronaryartery ligation and the treatment was continued for 7 daystwice daily via a catheter inserted into the jugular vein Thepigs were sacrificed 3 weeks after MI To prevent thromboticcomplications and arrhythmias all pigs were treated withclopidogrel 75 mgday from 3 days before MI until termina-tion and amiodarone 400 mgday from 10 days before MIuntil termination
Myocardial infarction and operational procedure
Pigs were anesthetized as described previously (Timmers etal 2007b) During the entire operation electrocardiogramarterial pressure and capnogram were continuously moni-tored After median sternotomy the left ventricularpressure (LVP) was measured using a pressure tipped Millarcatheter that was inserted through the apex into the leftventricle A transonic flow probe (Transonic Systems IncIthaca NY USA) was placed around the proximal aorta tomeasure cardiac output Sutures were then tightened topermanently occlude the proximal LCx Internal defibrilla-tion with 50 J was used when VF occurred Prior to and 1 hafter induction of the infarct echocardiography wasperformed After stabilization of hemodynamic parametersand heart rhythm the thorax was closed and the animalswere allowed to recover Three weeks after induction of
myocardial infarction the animals were anesthetized oncemore and the sternum was reopened Echocardiography andconductance catheter-based pressurendashvolume (PV) looprecordings were obtained to assess cardiac function andgeometry After the functional measurements the heart wasexcised for laboratory analysis
Immunohistochemistry
Three weeks following MI myocardial biopsies were obtainedfrom the infarct area border area and remote area andfixated in 4 formalin for 24 h before being embedded inparaffin To determine capillary density a lectin stainingdelineating the endothelium was performed followingantigen retrieval by boiling in 10 mM citrate bufferEndogenous biotin was blocked using 01 avidin solution(DakoCytomation Biotin Blocking system X0590) for 15 min atroom temperature (RT) and subsequently with 001 biotinsolution (Dako) for 15 min at RT After blocking with 30 BSAin PBS the sections were incubated overnight with biotiny-lated BS-1 (Sigma L3759) in a 1300 dilution in PBS with 01BSA and subsequently with streptavidin-HRPO (11000 in PBS)for 1 h at RT Finally the sections were incubated for 30 minin 3-amino-9-ethylcarbazole (AEC) and stained with hema-toxylin before being embedded Capillary density wasexpressed as the number of capillaries per square millimetertissue Quantification of collagen density was performedusing picrosirius red staining with circularly polarized lightand digital image microscopy after conversion into gray-value images as described before (Timmers et al 2007b)
Myocardial infarct size
After excision of the heart the LV was isolated and cut into 5slices from apex to base To discriminate infarct tissue fromviable myocardium the slices were incubated in 1triphenyltetrazolium chloride (TTC Sigma-Aldrich Chemi-cals Zwijndrecht Netherlands) in 37 degC Soumlrensen buffer(136 gL KH2PO4+178 gL Na2H PO42H2O pH 74) for15 min All slices were scanned from both sides and in eachslide the infarct area was compared to total area using digitalplanimetry software After correction for the weight of theslices infarct size was calculated as a percentage of the LV
Cardiac function
Midpapillary short axis epicardial echocardiography wasperformed before coronary artery ligation 1 h after and3 weeks after coronary artery ligation (Prosound SSD-50005 MHz probe UST-5280-5 Aloka Holding Europe AG ZugSwitzerland) Wall thickness (WT) of the infarct area and leftventricular internal area (LVia) were measured at end-diastole (ED) and end-systole (ES) Systolic wall thickening(SWT) was calculated as (WT(ES) ndashWT(ED))WT(ED) 100 ()and fractional area shortening (FAS) as (LVia(ED) ndash LVia(ES))LVia(ED) 100 () Left ventricular (LV) pressurendashvolumeloops were measured using a conductance catheter asdescribed previously (Timmers et al 2009) Diastolicchamber stiffness was quantified by means of linearregression of the end-diastolic pressurendashvolume relationship(Sagawa 1981)
213
Data analysis
The data were collected and analyzed in a blinded fashionData are presented as meanplusmnSE Mortality was comparedusing Fishers exact test Capillary sprouting was comparedusing a one-way ANOVA and Bonferroni post hoc tests A two-way ANOVA with Bonferroni post hoc tests was used tocompare capillary density and collagen density in themyocardial tissue Cardiac functional parameters that werealso measured before MI (baseline) were compared using atwo-way ANOVA for repeated measures and Bonferroni posthoc tests For cardiac functional parameters that weremeasured only 3 weeks after MI Students t test was used
Acknowledgments
This work was supported by the Netherlands Heart Founda-tion [Grant 2005T022 LT] and an Internationalization grantby the University Medical Center Utrecht the Netherlands[DPVK]
Appendix A Supplementary data
Supplementary data to this article can be found online atdoi101016jscr201101001
References
Assmus B Honold J Schachinger V Britten MB Fischer-Rasokat U Lehmann R Teupe C Pistorius K Martin HAbolmaali ND Tonn T Dimmeler S Zeiher AM 2006Transcoronary transplantation of progenitor cells after myocardialinfarction N Engl J Med 355 1222ndash1232
Burlew BS Weber KT 2002 Cardiac fibrosis as a cause ofdiastolic dysfunction Herz 27 92ndash98
Caplan AI Dennis JE 2006 Mesenchymal stem cells as trophicmediators J Cell Biochem 98 1076ndash1084
Cleutjens JP Blankesteijn WM Daemen MJ Smits JF1999 The infarcted myocardium simply dead tissue or a livelytarget for therapeutic interventions Cardiovasc Res 44232ndash241
de Silva R Raval AN Hadi M Gildea KM Bonifacino ACYu ZX Yau YY Leitman SF Bacharach SL DonahueRE Read EJ Lederman RJ 2008 Intracoronary infusion ofautologous mononuclear cells from bone marrow or granulocytecolony-stimulating factor-mobilized apheresis product may notimprove remodelling contractile function perfusion or infarctsize in a swine model of large myocardial infarction Eur Heart J29 1772ndash1782
Erbs S Linke A Schachinger V Assmus B Thiele H DiederichKW Hoffmann C Dimmeler S Tonn T Hambrecht RZeiher AM Schuler G 2007 Restoration of microvascularfunction in the infarct-related artery by intracoronary transplan-tation of bone marrow progenitor cells in patients with acutemyocardial infarction the Doppler Substudy of the Reinfusion ofEnriched Progenitor Cells and Infarct Remodeling in AcuteMyocardial Infarction (REPAIR-AMI) trial Circulation 116 366ndash374
Gnecchi M He H Liang OD Melo LG Morello F Mu HNoiseux N Zhang L Pratt RE Ingwall JS Dzau VJ2005 Paracrine action accounts for marked protection ofischemic heart by Akt-modified mesenchymal stem cells NatMed 11 367ndash368
Hashemi SM Ghods S Kolodgie FD Parcham-Azad K KeaneM Hamamdzic D Young R Rippy MK Virmani R Litt HWilensky RL 2008 A placebo controlled dose-ranging safetystudy of allogenic mesenchymal stem cells injected by endo-myocardial delivery after an acute myocardial infarction EurHeart J 29 251ndash259
Henry TD Annex BH McKendall GR Azrin MA Lopez JJGiordano FJ Shah PK Willerson JT Benza RL BermanDS Gibson CM Bajamonde A Rundle AC Fine JMcCluskey ER 2003 The VIVA trial vascular endothelialgrowth factor in ischemia for vascular angiogenesis Circulation107 1359ndash1365
Janssens S Dubois C Bogaert J Theunissen K Deroose CDesmet W Kalantzi M Herbots L Sinnaeve P Dens JMaertens J Rademakers F Dymarkowski S Gheysens O VanCleemput J Bormans G Nuyts J Belmans A Mortelmans LBoogaerts M Van de Werf F 2006 Autologous bone marrow-derived stem-cell transfer in patients with ST-segment elevationmyocardial infarction double-blind randomised controlled trialLancet 367 113ndash121
Kinnaird T Stabile E Burnett MS Shou M Lee CW BarrS Fuchs S Epstein SE 2004 Local delivery of marrow-derived stromal cells augments collateral perfusion throughparacrine mechanisms Circulation 109 1543ndash1549
Korff T Augustin HG 1998 Integration of endothelial cells inmulticellular spheroids prevents apoptosis and induces differen-tiation J Cell Biol 143 1341ndash1352
Lai RC Arslan F Lee MM Sze NS Choo A Chen TSSalto-Tellez M Timmers L Lee CN El Oakley RMPasterkamp G de Kleijn DP Lim SK 2010 Exosomesecreted by MSC reduces myocardial ischemiareperfusioninjury Stem Cell Res 4 214ndash222
Lian Q Lye E Suan Yeo K KhiaWay Tan E Salto-Tellez M LiuTM PalanisamyN ElOakley RM Lee EH LimB Lim SK2007 Derivation of clinically compliant MSCs from CD105+ CD24-differentiated human ESCs Stem Cells 25 425ndash436
Losordo DW Dimmeler S 2004 Therapeutic angiogenesis andvasculogenesis for ischemic disease part II cell-based therapiesCirculation 109 2692ndash2697
Lunde K Solheim S Aakhus S Arnesen H Abdelnoor MEgeland T Endresen K Ilebekk A Mangschau A Fjeld JGSmith HJ Taraldsrud E Grogaard HK Bjornerheim RBrekke M Muller C Hopp E Ragnarsson A Brinchmann JEForfang K 2006 Intracoronary injection of mononuclear bonemarrow cells in acute myocardial infarction N Engl J Med 3551199ndash1209
Menasche P Alfieri O Janssens S McKenna W Reich-enspurner H Trinquart L Vilquin JT Marolleau JPSeymour B Larghero J Lake S Chatellier G Solomon SDesnos M Hagege AA 2008 The Myoblast AutologousGrafting in Ischemic Cardiomyopathy (MAGIC) trial first ran-domized placebo-controlled study of myoblast transplantationCirculation 117 1189ndash1200
Meyer GP Wollert KC Lotz J Pirr J Rager U Lippolt PHahn A Fichtner S Schaefer A Arseniev L Ganser ADrexler H 2009 Intracoronary bone marrow cell transfer aftermyocardial infarction 5-year follow-up from the randomized-controlled BOOST trial Eur Heart J 24 2978ndash2984
Moelker AD Baks T van den Bos EJ van Geuns RJ deFeyter PJ Duncker DJ van der Giessen WJ 2006Reduction in infarct size but no functional improvement afterbone marrow cell administration in a porcine model ofreperfused myocardial infarction Eur Heart J 27 3057ndash3064
Pittenger MF Martin BJ 2004 Mesenchymal stem cells andtheir potential as cardiac therapeutics Circ Res 95 9ndash20
Sagawa K 1981 The end-systolic pressure-volume relation of theventricle definition modifications and clinical use Circulation63 1223ndash1227
214 L Timmers et al
Schachinger V Erbs S Elsasser A Haberbosch W Ham-brecht R Holschermann H Yu J Corti R Mathey DGHamm CW Suselbeck T Assmus B Tonn T DimmelerS Zeiher AM 2006 Intracoronary bone marrow-derivedprogenitor cells in acute myocardial infarction N Engl J Med355 1210ndash1221
Simons M Annex BH Laham RJ Kleiman N Henry TDauerman H Udelson JE Gervino EV Pike M White-house MJ Moon T Chronos NA 2002 Pharmacologicaltreatment of coronary artery disease with recombinant fibroblastgrowth factor-2 double-blind randomized controlled clinicaltrial Circulation 105 788ndash793
Strauer BE Brehm M Zeus T Kostering M Hernandez ASorg RV Kogler G Wernet P 2002 Repair of infarctedmyocardium by autologous intracoronary mononuclear bonemarrow cell transplantation in humans Circulation 1061913ndash1918
Sze SK de Kleijn DP Lai RC Khia Way E 2007 Tan HZhao KS Yeo TY Low Q Lian CN Lee W Mitchell RM ElOakley SK Lim Elucidating the secretion proteome of humanembryonic stem cell-derived mesenchymal stem cells Mol CellProteomics 6 1680ndash1689
Timmers L Lim SK Arslan F Armstrong JS Hoefer IEDoevendans PA Piek JJ El Oakley RM Choo A Lee CNPasterkamp G de Kleijn DP 2007a Reduction of myocardialinfarct size by humanmesenchymal stemcell conditionedmediumStem Cell Res 1 129ndash137
Timmers L Sluijter JP Verlaan CW Steendijk P CramerMJEmons M Strijder C Grundeman PF Sze SK Hua L PiekJJ Borst C Pasterkamp G de Kleijn DP 2007b Cycloox-ygenase-2 inhibition increases mortality enhances left ventricularremodeling and impairs systolic function after myocardialinfarction in the pig Circulation 115 326ndash332
Timmers L Henriques JP de Kleijn DP Devries JHKemperman H Steendijk P Verlaan CW Kerver MPiek JJ Doevendans PA Pasterkamp G Hoefer IE2009 Exenatide reduces infarct size and improves cardiacfunction in a porcine model of ischemia and reperfusion injuryJ Am Coll Cardiol 53 501ndash510
van Laake LW Passier R denOuden K Schreurs CMonshouwer-Kloots JWard-vanOostwaard D van Echteld CJ DoevendansPA Mummery CL 2009 Improvement of mouse cardiacfunction by hESC-derived cardiomyocytes correlates with vascular-ity but not graft size Stem Cell Res 3 106ndash112
Wolf D Reinhard A Seckinger A Gross L Katus HA HansenA 2009 Regenerative capacity of intravenous autologousallogeneic and human mesenchymal stem cells in the infarctedpig myocardium-complicated by myocardial tumor formationScand Cardiovasc J 43 39ndash45
Yousef M Schannwell CM Kostering M Zeus T Brehm MStrauer BE 2009 The BALANCE Study clinical benefit andlong-term outcome after intracoronary autologous bone marrowcell transplantation in patients with acute myocardial infarctionJ Am Coll Cardiol 53 2262ndash2269

213
Data analysis
The data were collected and analyzed in a blinded fashionData are presented as meanplusmnSE Mortality was comparedusing Fishers exact test Capillary sprouting was comparedusing a one-way ANOVA and Bonferroni post hoc tests A two-way ANOVA with Bonferroni post hoc tests was used tocompare capillary density and collagen density in themyocardial tissue Cardiac functional parameters that werealso measured before MI (baseline) were compared using atwo-way ANOVA for repeated measures and Bonferroni posthoc tests For cardiac functional parameters that weremeasured only 3 weeks after MI Students t test was used
Acknowledgments
This work was supported by the Netherlands Heart Founda-tion [Grant 2005T022 LT] and an Internationalization grantby the University Medical Center Utrecht the Netherlands[DPVK]
Appendix A Supplementary data
Supplementary data to this article can be found online atdoi101016jscr201101001
References
Assmus B Honold J Schachinger V Britten MB Fischer-Rasokat U Lehmann R Teupe C Pistorius K Martin HAbolmaali ND Tonn T Dimmeler S Zeiher AM 2006Transcoronary transplantation of progenitor cells after myocardialinfarction N Engl J Med 355 1222ndash1232
Burlew BS Weber KT 2002 Cardiac fibrosis as a cause ofdiastolic dysfunction Herz 27 92ndash98
Caplan AI Dennis JE 2006 Mesenchymal stem cells as trophicmediators J Cell Biochem 98 1076ndash1084
Cleutjens JP Blankesteijn WM Daemen MJ Smits JF1999 The infarcted myocardium simply dead tissue or a livelytarget for therapeutic interventions Cardiovasc Res 44232ndash241
de Silva R Raval AN Hadi M Gildea KM Bonifacino ACYu ZX Yau YY Leitman SF Bacharach SL DonahueRE Read EJ Lederman RJ 2008 Intracoronary infusion ofautologous mononuclear cells from bone marrow or granulocytecolony-stimulating factor-mobilized apheresis product may notimprove remodelling contractile function perfusion or infarctsize in a swine model of large myocardial infarction Eur Heart J29 1772ndash1782
Erbs S Linke A Schachinger V Assmus B Thiele H DiederichKW Hoffmann C Dimmeler S Tonn T Hambrecht RZeiher AM Schuler G 2007 Restoration of microvascularfunction in the infarct-related artery by intracoronary transplan-tation of bone marrow progenitor cells in patients with acutemyocardial infarction the Doppler Substudy of the Reinfusion ofEnriched Progenitor Cells and Infarct Remodeling in AcuteMyocardial Infarction (REPAIR-AMI) trial Circulation 116 366ndash374
Gnecchi M He H Liang OD Melo LG Morello F Mu HNoiseux N Zhang L Pratt RE Ingwall JS Dzau VJ2005 Paracrine action accounts for marked protection ofischemic heart by Akt-modified mesenchymal stem cells NatMed 11 367ndash368
Hashemi SM Ghods S Kolodgie FD Parcham-Azad K KeaneM Hamamdzic D Young R Rippy MK Virmani R Litt HWilensky RL 2008 A placebo controlled dose-ranging safetystudy of allogenic mesenchymal stem cells injected by endo-myocardial delivery after an acute myocardial infarction EurHeart J 29 251ndash259
Henry TD Annex BH McKendall GR Azrin MA Lopez JJGiordano FJ Shah PK Willerson JT Benza RL BermanDS Gibson CM Bajamonde A Rundle AC Fine JMcCluskey ER 2003 The VIVA trial vascular endothelialgrowth factor in ischemia for vascular angiogenesis Circulation107 1359ndash1365
Janssens S Dubois C Bogaert J Theunissen K Deroose CDesmet W Kalantzi M Herbots L Sinnaeve P Dens JMaertens J Rademakers F Dymarkowski S Gheysens O VanCleemput J Bormans G Nuyts J Belmans A Mortelmans LBoogaerts M Van de Werf F 2006 Autologous bone marrow-derived stem-cell transfer in patients with ST-segment elevationmyocardial infarction double-blind randomised controlled trialLancet 367 113ndash121
Kinnaird T Stabile E Burnett MS Shou M Lee CW BarrS Fuchs S Epstein SE 2004 Local delivery of marrow-derived stromal cells augments collateral perfusion throughparacrine mechanisms Circulation 109 1543ndash1549
Korff T Augustin HG 1998 Integration of endothelial cells inmulticellular spheroids prevents apoptosis and induces differen-tiation J Cell Biol 143 1341ndash1352
Lai RC Arslan F Lee MM Sze NS Choo A Chen TSSalto-Tellez M Timmers L Lee CN El Oakley RMPasterkamp G de Kleijn DP Lim SK 2010 Exosomesecreted by MSC reduces myocardial ischemiareperfusioninjury Stem Cell Res 4 214ndash222
Lian Q Lye E Suan Yeo K KhiaWay Tan E Salto-Tellez M LiuTM PalanisamyN ElOakley RM Lee EH LimB Lim SK2007 Derivation of clinically compliant MSCs from CD105+ CD24-differentiated human ESCs Stem Cells 25 425ndash436
Losordo DW Dimmeler S 2004 Therapeutic angiogenesis andvasculogenesis for ischemic disease part II cell-based therapiesCirculation 109 2692ndash2697
Lunde K Solheim S Aakhus S Arnesen H Abdelnoor MEgeland T Endresen K Ilebekk A Mangschau A Fjeld JGSmith HJ Taraldsrud E Grogaard HK Bjornerheim RBrekke M Muller C Hopp E Ragnarsson A Brinchmann JEForfang K 2006 Intracoronary injection of mononuclear bonemarrow cells in acute myocardial infarction N Engl J Med 3551199ndash1209
Menasche P Alfieri O Janssens S McKenna W Reich-enspurner H Trinquart L Vilquin JT Marolleau JPSeymour B Larghero J Lake S Chatellier G Solomon SDesnos M Hagege AA 2008 The Myoblast AutologousGrafting in Ischemic Cardiomyopathy (MAGIC) trial first ran-domized placebo-controlled study of myoblast transplantationCirculation 117 1189ndash1200
Meyer GP Wollert KC Lotz J Pirr J Rager U Lippolt PHahn A Fichtner S Schaefer A Arseniev L Ganser ADrexler H 2009 Intracoronary bone marrow cell transfer aftermyocardial infarction 5-year follow-up from the randomized-controlled BOOST trial Eur Heart J 24 2978ndash2984
Moelker AD Baks T van den Bos EJ van Geuns RJ deFeyter PJ Duncker DJ van der Giessen WJ 2006Reduction in infarct size but no functional improvement afterbone marrow cell administration in a porcine model ofreperfused myocardial infarction Eur Heart J 27 3057ndash3064
Pittenger MF Martin BJ 2004 Mesenchymal stem cells andtheir potential as cardiac therapeutics Circ Res 95 9ndash20
Sagawa K 1981 The end-systolic pressure-volume relation of theventricle definition modifications and clinical use Circulation63 1223ndash1227
214 L Timmers et al
Schachinger V Erbs S Elsasser A Haberbosch W Ham-brecht R Holschermann H Yu J Corti R Mathey DGHamm CW Suselbeck T Assmus B Tonn T DimmelerS Zeiher AM 2006 Intracoronary bone marrow-derivedprogenitor cells in acute myocardial infarction N Engl J Med355 1210ndash1221
Simons M Annex BH Laham RJ Kleiman N Henry TDauerman H Udelson JE Gervino EV Pike M White-house MJ Moon T Chronos NA 2002 Pharmacologicaltreatment of coronary artery disease with recombinant fibroblastgrowth factor-2 double-blind randomized controlled clinicaltrial Circulation 105 788ndash793
Strauer BE Brehm M Zeus T Kostering M Hernandez ASorg RV Kogler G Wernet P 2002 Repair of infarctedmyocardium by autologous intracoronary mononuclear bonemarrow cell transplantation in humans Circulation 1061913ndash1918
Sze SK de Kleijn DP Lai RC Khia Way E 2007 Tan HZhao KS Yeo TY Low Q Lian CN Lee W Mitchell RM ElOakley SK Lim Elucidating the secretion proteome of humanembryonic stem cell-derived mesenchymal stem cells Mol CellProteomics 6 1680ndash1689
Timmers L Lim SK Arslan F Armstrong JS Hoefer IEDoevendans PA Piek JJ El Oakley RM Choo A Lee CNPasterkamp G de Kleijn DP 2007a Reduction of myocardialinfarct size by humanmesenchymal stemcell conditionedmediumStem Cell Res 1 129ndash137
Timmers L Sluijter JP Verlaan CW Steendijk P CramerMJEmons M Strijder C Grundeman PF Sze SK Hua L PiekJJ Borst C Pasterkamp G de Kleijn DP 2007b Cycloox-ygenase-2 inhibition increases mortality enhances left ventricularremodeling and impairs systolic function after myocardialinfarction in the pig Circulation 115 326ndash332
Timmers L Henriques JP de Kleijn DP Devries JHKemperman H Steendijk P Verlaan CW Kerver MPiek JJ Doevendans PA Pasterkamp G Hoefer IE2009 Exenatide reduces infarct size and improves cardiacfunction in a porcine model of ischemia and reperfusion injuryJ Am Coll Cardiol 53 501ndash510
van Laake LW Passier R denOuden K Schreurs CMonshouwer-Kloots JWard-vanOostwaard D van Echteld CJ DoevendansPA Mummery CL 2009 Improvement of mouse cardiacfunction by hESC-derived cardiomyocytes correlates with vascular-ity but not graft size Stem Cell Res 3 106ndash112
Wolf D Reinhard A Seckinger A Gross L Katus HA HansenA 2009 Regenerative capacity of intravenous autologousallogeneic and human mesenchymal stem cells in the infarctedpig myocardium-complicated by myocardial tumor formationScand Cardiovasc J 43 39ndash45
Yousef M Schannwell CM Kostering M Zeus T Brehm MStrauer BE 2009 The BALANCE Study clinical benefit andlong-term outcome after intracoronary autologous bone marrowcell transplantation in patients with acute myocardial infarctionJ Am Coll Cardiol 53 2262ndash2269

214 L Timmers et al
Schachinger V Erbs S Elsasser A Haberbosch W Ham-brecht R Holschermann H Yu J Corti R Mathey DGHamm CW Suselbeck T Assmus B Tonn T DimmelerS Zeiher AM 2006 Intracoronary bone marrow-derivedprogenitor cells in acute myocardial infarction N Engl J Med355 1210ndash1221
Simons M Annex BH Laham RJ Kleiman N Henry TDauerman H Udelson JE Gervino EV Pike M White-house MJ Moon T Chronos NA 2002 Pharmacologicaltreatment of coronary artery disease with recombinant fibroblastgrowth factor-2 double-blind randomized controlled clinicaltrial Circulation 105 788ndash793
Strauer BE Brehm M Zeus T Kostering M Hernandez ASorg RV Kogler G Wernet P 2002 Repair of infarctedmyocardium by autologous intracoronary mononuclear bonemarrow cell transplantation in humans Circulation 1061913ndash1918
Sze SK de Kleijn DP Lai RC Khia Way E 2007 Tan HZhao KS Yeo TY Low Q Lian CN Lee W Mitchell RM ElOakley SK Lim Elucidating the secretion proteome of humanembryonic stem cell-derived mesenchymal stem cells Mol CellProteomics 6 1680ndash1689
Timmers L Lim SK Arslan F Armstrong JS Hoefer IEDoevendans PA Piek JJ El Oakley RM Choo A Lee CNPasterkamp G de Kleijn DP 2007a Reduction of myocardialinfarct size by humanmesenchymal stemcell conditionedmediumStem Cell Res 1 129ndash137
Timmers L Sluijter JP Verlaan CW Steendijk P CramerMJEmons M Strijder C Grundeman PF Sze SK Hua L PiekJJ Borst C Pasterkamp G de Kleijn DP 2007b Cycloox-ygenase-2 inhibition increases mortality enhances left ventricularremodeling and impairs systolic function after myocardialinfarction in the pig Circulation 115 326ndash332
Timmers L Henriques JP de Kleijn DP Devries JHKemperman H Steendijk P Verlaan CW Kerver MPiek JJ Doevendans PA Pasterkamp G Hoefer IE2009 Exenatide reduces infarct size and improves cardiacfunction in a porcine model of ischemia and reperfusion injuryJ Am Coll Cardiol 53 501ndash510
van Laake LW Passier R denOuden K Schreurs CMonshouwer-Kloots JWard-vanOostwaard D van Echteld CJ DoevendansPA Mummery CL 2009 Improvement of mouse cardiacfunction by hESC-derived cardiomyocytes correlates with vascular-ity but not graft size Stem Cell Res 3 106ndash112
Wolf D Reinhard A Seckinger A Gross L Katus HA HansenA 2009 Regenerative capacity of intravenous autologousallogeneic and human mesenchymal stem cells in the infarctedpig myocardium-complicated by myocardial tumor formationScand Cardiovasc J 43 39ndash45
Yousef M Schannwell CM Kostering M Zeus T Brehm MStrauer BE 2009 The BALANCE Study clinical benefit andlong-term outcome after intracoronary autologous bone marrowcell transplantation in patients with acute myocardial infarctionJ Am Coll Cardiol 53 2262ndash2269




















