
Helical Tomotherapy for treating supraclavicular and internal mammary nodal chain in breast cancer
11
World Journal of Surgical, Medical and Radiation Oncology 70 http://www.npplweb.com/wjsmro/content/2/10 Address for correspondence and reprint requests to: Moujhuri Nandi, MD, Dept. Of Radiation Oncology, Apollo Gleneagles Hospital, Kolkata, India, email: [email protected] Nandi M et al. Licensee Narain Publishers Pvt. Ltd. (NPPL) Submitted August 18, 2013; Accepted October 17, 2013; Published: October 18, 2013 Review Open Access Helical Tomotherapy for treating supraclavicular and internal mammary nodal chain in breast cancer Moujhuri Nandi 1 , Anurupa Mahato 2 , Indranil Mallick 3 , Rimpa Achari 4 and Sanjoy Chatterjee 5 1 Department of Radiation Oncology, Apollo Gleneagles Hospital, Kolkata, India, 2, 3, 4 & 5 Department of Radiation Oncology, Tata Medical Center, Kolkata, India This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited Abstract Objective- To describe one of the first clinical experiences of treating the Internal mammary chain (IMC) and supraclavicular fossa (SCF) using helical tomotherapy (HT), with brachial plexus sparing where necessary. Methods- Three breast cancer cases in whom both SCF and IMC irradiation was required were planned and treated using HT to a dose of 50Gy in 25 fractions or equivalent. In one case dose escalation to the SCF was required to treat clinically palpable node. Inverse planning dose constraints were applied to PTVs and OARs. Results- HT plans achieved adequate target coverage for all three PTVs in the three cases; mean HI of 1.09, 1.08 and 1.11 and mean CI of 0.6, 0.5 and 0.6 for chest wall, SCF and IMC were obtained respectively. The mean heart dose achieved was 11.8Gy, 18.0Gy and 6.2 Gy for the three cases respectively. The mean heart dose of the second case was higher as it involved bilateral chest wall and IMC irradiation. Mean V20Gy for ipsilateral and contralateral lung was 25.9% and 2.5% respectively. Mean dose of contralateral breast (in two cases) was 5.1Gy. Skin acute toxicity was Grade I in all three cases. At a median follow up of 1 year, all three patients are locoregionally controlled. Conclusion- Helical tomotherapy is a technique where complex volume treatment in breast cancers could be delivered with adequate homogeneity and conformity indices and high capabilities of critical organ sparing. Further long term studies are required to assess local control and late toxicity. Introduction Helical tomotherapy achieves (HT) conformal dose distributions to the planning target volume (PTV) while sparing the organs at risk (OAR) [1, 2]. In sites like the head and neck, HT has improved dose sparing effect for sensitive functional organs like the parotid glands whilst achieving good PTV coverage [3, 4]. Tangential fields still remain the standard portals for delivering radiotherapy to the breast / chest wall because it provides adequate PTV coverage with low dose to the OARs like the Lung and Heart. Inclusion of internal mammary chain or the supraclavicular fossa (SCF) in the tangential
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Helical Tomotherapy for treating supraclavicular and internal mammary nodal chain in breast cancer

World Journal of Surgical, Medical
and Radiation Oncology
70 http://www.npplweb.com/wjsmro/content/2/10
Address for correspondence and reprint requests to:
Moujhuri Nandi, MD, Dept. Of Radiation Oncology, Apollo Gleneagles Hospital, Kolkata, India, email: [email protected] Nandi M et al. Licensee Narain Publishers Pvt. Ltd. (NPPL) Submitted August 18, 2013; Accepted October 17, 2013; Published: October 18, 2013
RReevviieeww OOppeenn AAcccceessss
Helical Tomotherapy for treating supraclavicular and internal mammary nodal chain in breast cancer
Moujhuri Nandi1, Anurupa Mahato2, Indranil Mallick3, Rimpa Achari4 and Sanjoy Chatterjee5
1Department of Radiation Oncology, Apollo Gleneagles Hospital, Kolkata, India, 2, 3, 4 & 5Department of Radiation Oncology, Tata Medical Center, Kolkata, India
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Abstract Objective- To describe one of the first clinical experiences of treating the Internal mammary chain (IMC) and supraclavicular fossa (SCF) using helical tomotherapy (HT), with brachial plexus sparing where necessary. Methods- Three breast cancer cases in whom both SCF and IMC irradiation was required were planned and treated using HT to a dose of 50Gy in 25 fractions or equivalent. In one case dose escalation to the SCF was required to treat clinically palpable node. Inverse planning dose constraints were applied to PTVs and OARs. Results- HT plans achieved adequate target coverage for all three PTVs in the three cases; mean HI of 1.09, 1.08 and 1.11 and mean CI of 0.6, 0.5 and 0.6 for chest wall, SCF and IMC were obtained respectively. The mean heart dose achieved was 11.8Gy, 18.0Gy and 6.2 Gy for the three cases respectively. The mean heart dose of the second case was higher as it involved bilateral chest wall and IMC irradiation. Mean V20Gy for ipsilateral and contralateral lung was 25.9% and 2.5% respectively. Mean dose of contralateral breast (in two cases) was 5.1Gy. Skin acute toxicity was Grade I in all three cases. At a median follow up of 1 year, all three patients are locoregionally controlled. Conclusion- Helical tomotherapy is a technique where complex volume treatment in breast cancers could be delivered with adequate homogeneity and conformity indices and high capabilities of critical organ sparing. Further long term studies are required to assess local control and late toxicity.
Introduction
Helical tomotherapy achieves (HT) conformal dose distributions to the planning target volume (PTV) while sparing the organs at risk (OAR) [1, 2]. In sites like the head and neck,
HT has improved dose sparing effect for sensitive functional organs like the parotid glands whilst achieving good PTV coverage [3, 4].
Tangential fields still remain the standard portals for delivering radiotherapy to the breast / chest wall because it provides adequate PTV coverage with low dose to the OARs like the Lung and Heart. Inclusion of internal mammary chain or the supraclavicular fossa (SCF) in the tangential

World J Surg Med Radiat Oncol 2013;2:70-80 Helical Tomotherapy in Breast Cancer
71 http://www.npplweb.com/wjsmro/content/2/10
fields can be challenging, requiring the use of additional portals leading to field junctions and unsure dosimetry; which could result in overdosage or underdosage and manifest as in match line fibrosis. Use of wider tangents to include the IMC could lead to more heart or lung dose which in turn could result in increased cardiac morbidity and lung cancer [5, 6]. Two large randomized trials have evaluated the role of IMC irradiation; in women with breast cancers at high risk of loco regional recurrence. The European Organization for Research and Treatment of Cancer trial 22922 [7] included women treated by mastectomy or breast conserving surgery, while the National Cancer Institute of Canada MA20 [8] trial included women treated with breast-conserving surgery. In the Canadian trial, the usual radiation technique comprised of two partially wide tangential beams to encompass the breast and IMC nodes matched to a single anterior beam or parallel-opposed anterior and posterior beams to cover the axillary and supraclavicular regions.
CT-based radiotherapy planning has become the standard technique for breast and chest wall irradiation [9], providing more robust dose volume data. Modern radiotherapy techniques allow addition of multiple subfields to the two tangential beams, to enhance physical dose optimization, conferring improved dose homogeneity within the target. Loco regional breast IMRT has been compared with conventional forward-planned approaches in several dosimetric studies [10–15] and the results not only show improved target coverage but also lower doses to the heart and the lungs.
The use of helical tomotherapy; where radiation can be delivered from any of the 360 degree angles, has not gained universal acceptance in breast irradiation as it delivers low dose bath to unspecified areas of the body, and to the OARs; contralateral breast, lung and heart when compared to standard tangential radiation. Thus; in recent years the Tomo Direct option has been in clinical
practice in some centres to deliver static angle radiotherapy for breast cancers [16].
Nevertheless, several institutions have investigated the role of arc HT in treatment of selected breast cancers, particularly those involving complex chest wall volumes and IMC radiation whilst reducing heart dose and avoiding field junctions. Ashenafi [17] et al., did a feasibility study of post mastectomy irradiation with HT and showed a better dose conformity of chest wall and IMC PTVs. Coon et al [18] achieved a lower cardiac dose in left sided breast cancer patients with unfavourable cardiac anatomy with HT in comparison to 3DCRT. Caudrelier et al., [19] compared HT with standard 3-4 field technique in left sided breast cancer patients including nodal irradiation and concluded that compared to a standard technique; HT not only improved dose homogeneity within the PTV but also decreased the mean lung dose and spared the heart, lung and soft tissues from high dose exposure. We analysed the data from similar studies [10-15, 17-19] and clinically implemented the treatment of chest wall, supraclavicular and internal mammary nodal chain irradiation in three patients using HT with Brachial plexus sparing where necessary. This article describes the clinical implementation of such complex radiotherapy plans.
Methods
Three patients requiring irradiation of complex PTVs as adjuvant radiation were selected to have HT (Helical tomotherapy, Hi-Art II, Accuray, CA, USA). Given the unique complexities, history and radiotherapy planning processes of each one of them have been discussed separately.
Case I
56 year old female with a clinically palpable 8cm left sided breast lump underwent mastectomy with level III axillary clearance. Histopathology confirmed an infiltrating ductal carcinoma, triple negative with 6 out of

World J Surg Med Radiat Oncol 2013;2:70-80 Nandi M et al.
72 http://www.npplweb.com/wjsmro/content/1/1/5
20 axillary lymph nodes involved. 18-FDG Positron emission tomography scan (PET-CT) done for staging purpose, revealed ipsilateral metastatic internal mammary lymph nodes. She received adjuvant chemotherapy with epirubicin and carboplatin for 6 cycles prior to being referred for radiotherapy at our centre. After multidisciplinary team discussions (MDT), it was decided that she should receive chest wall, ipsilateral SCF and IMC irradiation using HT. A hypofractionated dose of 40Gy in 15 fractions was prescribed to the 95% isodose (95% of the PTV to be covered with 95% isodose) as per institutional policy.
Case II
45 year old female was diagnosed with bilateral breast cancer; right side recurrent carcinoma with skin involvement and left side new primary in March 2011. (She had been treated in 2001 with right breast conservation surgery and axillary clearance, adjuvant chemotherapy and radiotherapy for a 2.5 cm, grade III, infiltrating ductal carcinoma with 2 out of 8 axillary lymph nodes involved). 18-FDG PET-CT scan done in April 2011 for staging purpose showed high metabolic activity in bilateral breasts, left axilla and right IMC. She received 6 cycles of combination chemotherapy (Taxotere and Carboplatin), achieved complete clinical response and subsequently underwent bilateral mastectomies in Oct 2011. She was then referred to our centre for adjuvant radiotherapy. Hospital MDT recommended HT treatment to encompass bilateral chest wall, bilateral SCF and right sided IMC.
Case III
40 year old female presented with a locally advanced left breast invasive ductal carcinoma. Clinically she had palpable left axillary and supraclavicular lymph nodes for which she received neo-adjuvant chemotherapy with 4 cycles of 5 fluorouracil, Adriamycin and cyclophosphamide followed by 4 cycles of docetaxel. Subsequently she
underwent a left mastectomy and axillary clearance and her tumour histopathology was reported as residual 1.6 cm ductal carcinoma with 11 out of 18 axillary lymph nodes involved, ER/PR and Her 2 neu positive. As the tumour was in infero-medial quadrant, lack of adequate response to systemic chemotherapy, high axillary nodal burden and clinically supraclavicular lymph nodal involvement; the patient was planned for irradiation to the left chest wall along with ipsilateral SCF and IMC using HT. A dose of 40Gy in 15 fractions over 3 weeks was prescribed to the left chest wall, ipsilateral IMC and entire SCF followed by sequential boost of 10 Gy in 5 fractions to the involved SCF node.
Treatment planning
Patients were planned supine, lying on carbon fibre laminated board, arms abducted and above the head with the support of a fixed low arm rest holding a central pole. The position was marked for daily set up and reproducibility during radiotherapy treatment. 2.5mm thickness contrast enhanced CT images were acquired from the base of the skull to the umbilicus (given the SCF and IMC coverage required for the patients) on our CT scanner (Lightspeed Xtra GE CT scanner 16 slice). Radio-opaque wires were used to mark the mastectomy scar and clinical boundaries which extended superiorly to 1cm above the palpable contralateral breast tissue, inferiorly at 1 cm below inframammary fold, medially at the midline, and lateral at the midaxillary line. For Case 2 where the patient had bilateral mastectomies the superior border was marked above the level of 2nd intercostal space. The computed tomography (CT) data were then transferred to TPS system (Eclipse 3D version 10; Varian Medical Systems Inc., Palo Alto, USA) for contouring before being imported to the tomotherapy station for planning. For all cases the chest wall was contoured according to the RTOG guidelines [20]. PTV was grown by adding an isotropic margin of 1cm to CTV, edited from skin by

World J Surg Med Radiat Oncol 2013;2:70-80 Helical Tomotherapy in Breast Cancer
73 http://www.npplweb.com/wjsmro/content/2/10
3mm to prevent “dose dumping” on the skin as is common in inversed planning systems, to reduce the chances of radiation dermatitis.
Given the proximity of brachial plexus to the boost PTV in the SCF for case 3, and a hypo fractionated schedule being used in cases 1 and 3; the brachial plexus was contoured as described by Hall et al [21] in all three cases. For brachial plexus contouring, delineation of the bony vertebrae was done from C5-T2; the anterior and middle scalene muscles were identified. The nerve root was traced from the neural foramina through the path in between the muscles using a 5mm diameter brush on the Eclipse contouring station. The brachial plexus extended posterior to the subclavian neuro-vascular bundle and up to two slices below the medial head of the clavicle. Internal mammary nodes(in positive cases) or vessels were outlined as an ellipse at the level of the first to third intercostal space; a margin of 5mm given to get the IMC CTV which was grown by a further 1cm to get the IMC PTV[19]. The spinal cord, heart, bilateral lungs, contralateral breast were the other OARs contoured in all three cases.
The SCF CTV was contoured superiorly up to the cricoid cartilage, medially covering the lymphovascular bundle, laterally up to the apex of axilla and inferiorly at the lower end of the medial head of the clavicle [22].
For case 1, all three PTVs were prescribed a dose of 40Gy in 15 fractions over 3 weeks with 95% of the PTV to be covered by 95% of the prescription isodose.
In case 2 bilateral chest wall CTV and PTVs and right sided IMC PTV were contoured as described above. Given that the patient was receiving reirradiation to part of the PTV (right chest wall area), a conventional dose fractionation of 50Gy in 25fractions over 5 weeks was used, with 95% of the PTV volume being covered by 95% of the prescription dose.
Similarly, in Case 3, the left chest wall and SCF and IMC were contoured as described above. The macroscopic node in the SCF was outlined as a separate tumour volume-SCF N GTV, where a margin of 5 mm was allowed to create the SCF-N CTV, which received a 1cm isotropic margin to provide the SCF-N PTV. The chest wall, IMC and entire SCF were prescribed 40 Gy in 15 fractions over 3 weeks (95% of the PTV to receive 95% of prescribed dose) followed by a sequential boost dose of 10 Gy in 5 fractions for the clinically palpable node in SCF.
Homogeneity index was calculated by dividing the maximal PTV dose by the prescription dose; the coverage index was calculated by dividing the minimum PTV dose by the prescription dose. Both indexes were calculated according to the recommendations established for evaluating tomotherapy treatment plans [23].
The dose to the heart, both lungs and the contralateral breast was optimized using a set in-house protocol (Table 1) as described by Caudrelier et al. [19]. A mean dose constraint of 12 Gy was used for the heart in keeping with the studies by Popescu (15) and Cozzi et al [11].
The optimization was driven with a goal to deliver 95% of the prescription dose to 95% of the PTV. DVH points and penalties were adjusted throughout the optimization process to achieve adequate PTV coverage with set dose constraints to OARs.
To assist in plan optimization extra structures were contoured by the physicists in areas (not included within PTVs or OARs) to reduce “dose dumping” (unnecessary dose deposit). Such structures have been called as “dummy volumes”. Similarly, to prevent dose from splaying outside the contoured PTV and to achieve good conformity ‘ring structures’ were created by physicists allowing isotropic margins on each of the PTVs. In order to reduce dose deposition in the contralateral and ipsilateral lungs, total blocks (preventing

World J Surg Med Radiat Oncol 2013;2:70-80 Nandi M et al.
74 http://www.npplweb.com/wjsmro/content/1/1/5
Table1. Normal tissue dose-volume constraints used for plan optimization.
Normal tissue dose-volume constraints
Structures
No more than 15%
of the volume receives
dose that exceeds
(Gy)
No more than 20%
of the volume receives
dose that exceeds
(Gy)
No more than 35%
of the volume receives
dose that exceeds
(Gy)
No more than 50 % of the volume receives
dose that
exceeds (Gy)
Heart 20 15 15 15 I/P Lung 35 30 20 15 C/L Lung 15 15 12 10
C/L Breast
20 10 7 5
Table2. Target volumes, organs at risk and additional volumes contoured for Helical Tomotherapy Planning Target volumes Chest wall planning target volume, supraclavicular fossa planning target volume, internal mammary chain planning target volume. Organs at risk Brachial plexus, contralateral breast, bilateral lungs, heart, larynx, thyroid, oesophagus. Additional structures to assist planning Brachial plexus + 3mm, total contra lateral lung block, ipsilateral directional lung block, contra lateral breast block, dummy volumes, ring structures.
any entry or exit of radiation beams) were requested for areas in the contralateral lung and directional blocks (preventing entry of radiation beams from a particular area) for the contralateral breast. Table 2 lists the target volumes, OARs and dummy volumes used to treat the three cases. HT uses pitch, modulation factor and field width to achieve the prescribed inversed planned dose constraints. We used a pitch of 0.28; modulation factor of 2.5 with a field width of 2.5 to plan the three cases.
HT offers the option of daily pre treatment imaging to enable daily confirmation of adequate target positioning and coverage. Three fan beam CT modes are available namely coarse, normal or fine. In the fine mode; a pitch of 4mm/rotation is used in contrast to, 8mm/rotation in normal and 12mm/rotation in coarse modes. For the purpose of treatment we used the normal imaging mode which produced adequate image resolution to perform image guidance.
A daily image matching policy was employed; experienced therapy radiographers identified matching of the vertebral body (bony match) and then adjusted the patient position such that a balance was achieved between coverage of target volumes (soft tissue match) and sparing of OARs as intended in the original treatment plan.
Details of the doses to the PTVs and OARs for all three cases are tabulated below (Table3, 4). It is worth noting that the mean heart dose, the ipsilateral lung V20Gy, and contralateral breast mean dose achieved in all 3 cases are in comparison to the ones described in the literature (Table 5).
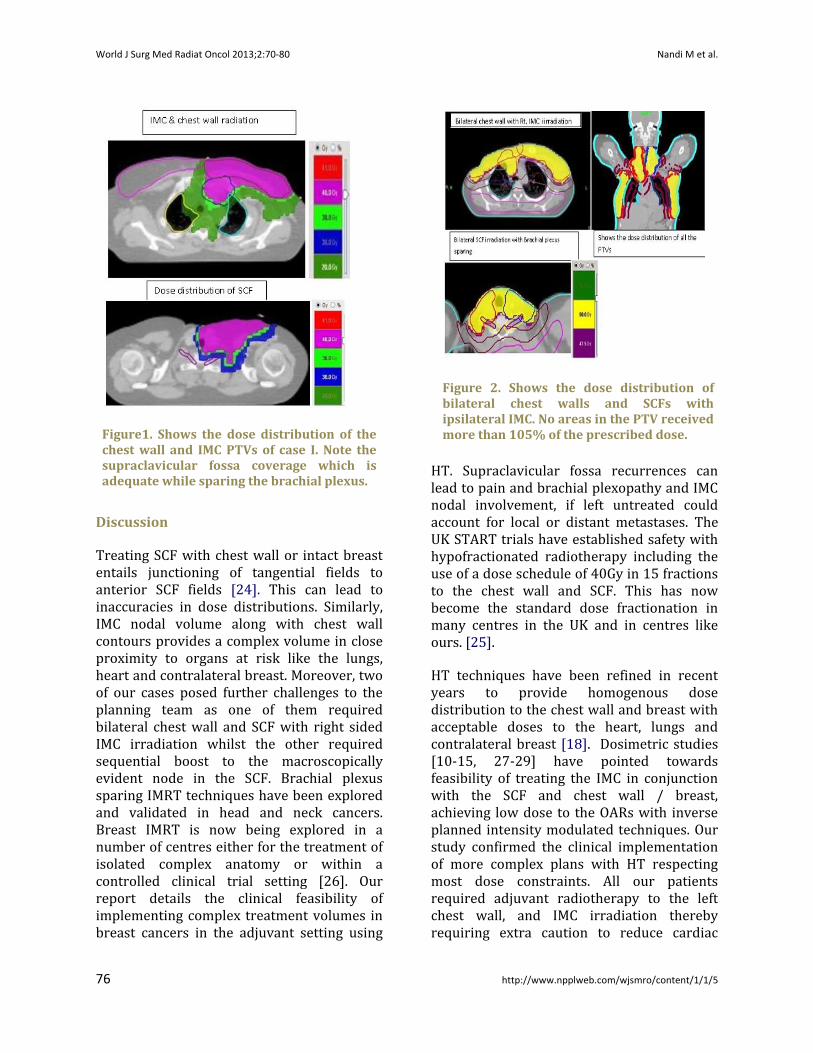
In case I, adequate dose coverage of the three PTVs was achieved (Chest wall, SCF and IMC) as is evident from Fig 1. The homogeneity indices (HI) of the three PTVs were 1.12 (chest wall PTV), 1.08 (SCF PTV) and 1.11 (PTV IMC) with conformity indices (CI) (ranging between 0.5-0.6), suggesting adequate coverage of target volumes by HT plans (Table 3).Irradiation of the IMC could be achieved with a mean dose to the heart of 11.89Gy with V15Gy and V20Gy of 20% and 16% respectively (Table 4), The V15Gy and V20Gy of the ipsilateral and contralateral lungs were 22%, 16% and 7.9% and 1.6% respectively.
In case II, there was a right sided recurrence and a second primary in the left side with node positivity. As discussed above, bilateral chest walls and SCFs and right IMC were treated. Figure 2 shows the dose distribution attained in this complex volume, using HT. Median dose to both the right and left chest wall PTV was 51.9 Gy; median dose of 51.5 Gy to the right and left SCF and 51.4 Gy to the right IMC was achieved respectively. (Table 3), similarly the HI and CI as calculated

World J Surg Med Radiat Oncol 2013;2:70-80 Helical Tomotherapy in Breast Cancer
75 http://www.npplweb.com/wjsmro/content/2/10
Table 3. Median dose, Homogeneity index and Conformity index of chest wall, IMC, SCF PTVs in all three cases with their Beam on time. PTV CHEST WALL
NO. SIDE PRESC D (Gy)
dmedian (Gy)
HI CI
Case 1
LEFT 40 42.5 1.12 0.5
Case
2
LEFT 50 51.9 1.07 0.8
RIGHT 50 51.9 1.11 0.7
Case 3
LEFT 40 40.1 1.08 0.5
PTV SCF
Case 1
LEFT 40 41.9 1.08 0.6
Case 2
LEFT 50 51.5 1.05 0.6
RIGHT 50 51.5 1.12 0.6
Case 3
LEFT 40 39.2 1.08 0.6
BOOST 10 10.5 1.07 0.9
BOT(mins)
Case 1
24.2
Case 2
18.2
Case 3
35.7(Phase 1) 17.8(Phase 2)
Table 4. The dose to the OARs in all the cases. Note only maximum dose has been shown for brachial plexus, the mean dose, V15Gy V20Gy for the heart, the mean dose, V10Gy, V15Gy and V20Gy for the ipsilateral and contralateral lungs and mean dose , V10Gy for the contralateral breast. OAR HEART Mean Dose (Gy) V 15Gy V 20Gy
Case 1 11.8 20.9 12.2 Case 2 * 18.9 39.6 30.7 Case 3 6.2 14.4 9.8
I/P LUNG Mean Dose
(Gy) V
10Gy V
15Gy V 20Gy
Case 1 11.2 29.7 23.6 17.7
Case 2* (Bilateral
Lungs)
17.5 48.0 38.0
33.3
Case 3 12.3 38.3 32.7 27.7
C/L LUNG
Mean Dose (Gy)
V 10Gy
V 15Gy
V 20Gy
Case 1 5.9 20.5 8.0 1.6 Case 3 3.6 10.3 6.1 3.3
C/L BREAST Mean Dose V 10Gy
Case 1 4.5 4.03 Case 3 5.7 14
BRACHIAL PLEXUS Dmax(Gy)
Case 1 41.7 Case 2 * 53.2 Case 3 50.9
*Disclaimer- High mean dose , high V15Gy,V20Gy to the heart and high mean dose to both lungs in case 2 as it involved bilateral chest , SCFs and Right IMC irradiation.
according to above described formulae have been enumerated in Table 3. Bilateral chest wall and ipsilateral IMC irradiation could be delivered adequately though at the expense of an increase in the mean dose to the heart, and bilateral lungs as seen in Table 4; where the dose volume constraints could not be achieved, although bilateral SCF irradiation was possible without an increase in the maximum dose to the brachial plexus. Since the aim of the treatment was to achieve maximal loco-regional control, this patient was explained the risks and benefits of treatment and penalties to achieve the set constraints for OARs were relaxed such that PTV coverage was not compromised. This patient has completed 16 months of follow up and had no evidence of disease recurrence or treatment related toxicities at last follow up.
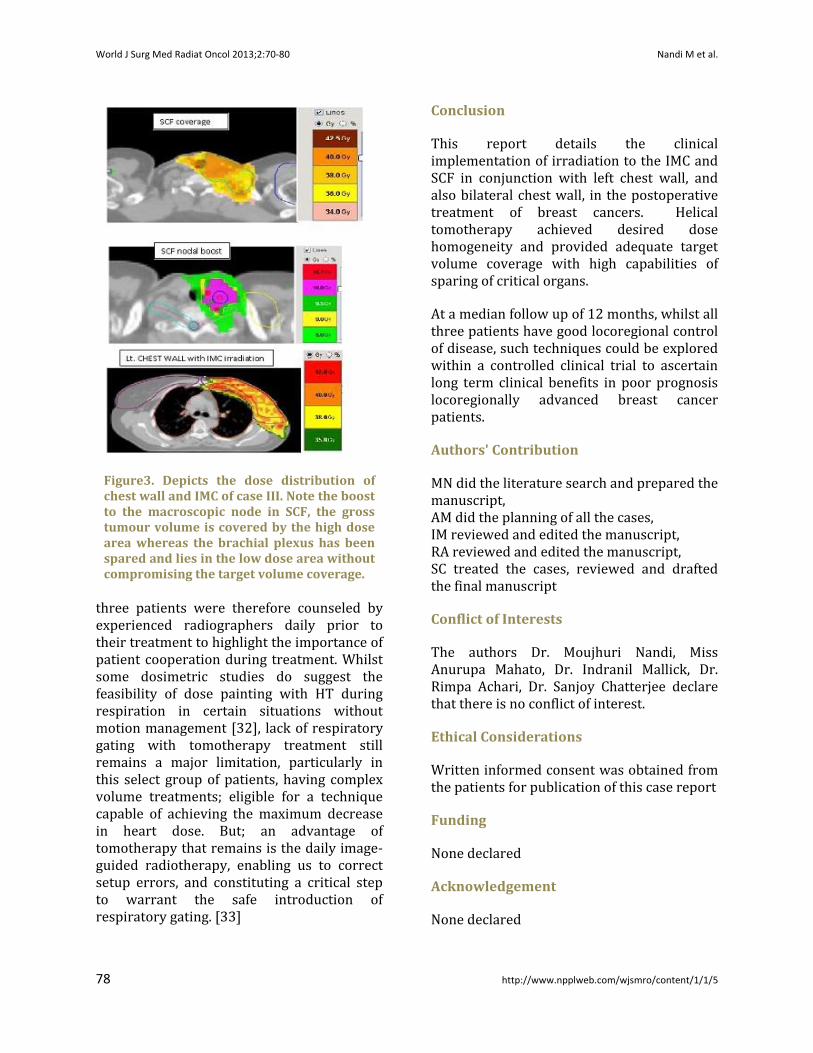
In the third case, a planned dose of 40 Gy in 15 fractions was delivered to the left chest wall, ipsilateral SCF and IMC followed by a
sequential boost to the macroscopic node in the SCF (Figure 3). We attained adequate coverage of PTV (Table 3) with a mean dose of 6.2Gy to the heart. It is worth noting that the brachial plexus was in close proximity to the SCF boost PTV but we successfully achieved sparing of the brachial plexus without compromising PTV coverage(Table 4).This patient is being followed up for 12 months and has good local control of disease without any early signs of brachial plexopathy.
World J Surg Med Radiat Oncol 2013;2:70-80 Nandi M et al.
76 http://www.npplweb.com/wjsmro/content/1/1/5
Figure1. Shows the dose distribution of the chest wall and IMC PTVs of case I. Note the supraclavicular fossa coverage which is adequate while sparing the brachial plexus.
Figure 2. Shows the dose distribution of bilateral chest walls and SCFs with ipsilateral IMC. No areas in the PTV received more than 105% of the prescribed dose.
Discussion
Treating SCF with chest wall or intact breast entails junctioning of tangential fields to anterior SCF fields [24]. This can lead to inaccuracies in dose distributions. Similarly, IMC nodal volume along with chest wall contours provides a complex volume in close proximity to organs at risk like the lungs, heart and contralateral breast. Moreover, two of our cases posed further challenges to the planning team as one of them required bilateral chest wall and SCF with right sided IMC irradiation whilst the other required sequential boost to the macroscopically evident node in the SCF. Brachial plexus sparing IMRT techniques have been explored and validated in head and neck cancers. Breast IMRT is now being explored in a number of centres either for the treatment of isolated complex anatomy or within a controlled clinical trial setting [26]. Our report details the clinical feasibility of implementing complex treatment volumes in breast cancers in the adjuvant setting using
HT. Supraclavicular fossa recurrences can lead to pain and brachial plexopathy and IMC nodal involvement, if left untreated could account for local or distant metastases. The UK START trials have established safety with hypofractionated radiotherapy including the use of a dose schedule of 40Gy in 15 fractions to the chest wall and SCF. This has now become the standard dose fractionation in many centres in the UK and in centres like ours. [25].
HT techniques have been refined in recent years to provide homogenous dose distribution to the chest wall and breast with acceptable doses to the heart, lungs and contralateral breast [18]. Dosimetric studies [10-15, 27-29] have pointed towards feasibility of treating the IMC in conjunction with the SCF and chest wall / breast, achieving low dose to the OARs with inverse planned intensity modulated techniques. Our study confirmed the clinical implementation of more complex plans with HT respecting most dose constraints. All our patients required adjuvant radiotherapy to the left chest wall, and IMC irradiation thereby requiring extra caution to reduce cardiac

World J Surg Med Radiat Oncol 2013;2:70-80 Helical Tomotherapy in Breast Cancer
77 http://www.npplweb.com/wjsmro/content/2/10
Table 5 Summary of previous IMRT treatment planning studies for locoregional breast radiation in comparison to our study
Author Patients (No.)
PTV/Fields Dose presc (Gy)
Heart I/P Lung C/L Lung Total lungs
C/L Breast
Cozzi 10 Breast/Chest wall + IMC/4-6 beams equidistant over 180
sector angle
50 Mean Dose-
12.8Gy V20Gy-
17%
V20Gy-29%
NA Mean dose-11Gy
V5Gy-34%
V10Gy-6.4%
Fogliata 5(Rt. & Lt.)
Breast + IMC/ 7 beams equidistant over 180 sector
angle
50 V20Gy- 19.6-32%
NA Mean dose-11Gy
Mean dose-5.9Gy
V10Gy-12%
Popescu 5(Lt) Breast + IMC/ 11 beams over 190 sector angle
50 Mean Dose-
12.8Gy V30Gy-
3.4%
V20Gy-15% Mean Dose
V5Gy-14%
Mean dose-8
Gy
Mean dose-4.4Gy V5Gy-32%
Johansson 11(Lt) Breast+IMC+SCF/
IMRT 6 beams over 140 sector angle
50 V30Gy-50%
V20Gy-40%
NA NA NA
Caudrelier 10(Lt) Breast+IMC+SCF/ Tomotherapy
50 Mean dose-7Gy V30Gy-
1.5% V20Gy-
6.1%
NA NA Mean dose-8Gy V20Gy-
5.8%
Mean dose-5.7Gy V5Gy-31%
V10Gy-7.3%
Nandi (Clinical study)
3(Lt+ bilateral)
Helical tomotherapy
40/50 Mean dose-
12.3Gy V20Gy-17.5%
Mean dose-
13.7Gy V20Gy-25.9%
Mean dose- 4.7Gy
V20Gy-2.5%
NA Mean dose- 5.1Gy V5Gy-34%
dose. The locally advanced stage of disease in all cases required SCF irradiation too, with one patient requiring a further 10Gy boost with brachial plexus sparing technique. HT was able to achieve comparable cardiac dose in all three patients (Table 4, 5) inspite of these complex planning requirements.
High-dose radiotherapy to the SCF has been used in patients with SCF nodal disease at presentation [30]. In that study Chatterjee et al explored the clinical possibility of dose escalation to the SCF using brachial plexus sparing HT techniques. Given the clinical feasibility of achieving longer period of local control using such techniques, one could evaluate the benefit of dose escalation in the SCF in prospective controlled trials. Also with the practical implementation of IMC, SCF and
Chest wall irradiation, we could aim to achieve longer disease free period in patients with IMC nodal involvement, as shown in our report.
For simple chest wall and SCF radiotherapy, HT techniques could provide better HI and CI as compared to conventional tangential techniques although this could come at the expense of larger low dose irradiation to OARs like the contralateral breast, heart and the lungs. With recent publications confirming long term cardiac morbidity even for low cardiac doses [31]; the use of such techniques should be limited to complex clinical challenges.
The beam on time for treatment of these complex volumes was obviously longer than required for conventional treatments. All
World J Surg Med Radiat Oncol 2013;2:70-80 Nandi M et al.
78 http://www.npplweb.com/wjsmro/content/1/1/5
Figure3. Depicts the dose distribution of chest wall and IMC of case III. Note the boost to the macroscopic node in SCF, the gross tumour volume is covered by the high dose area whereas the brachial plexus has been spared and lies in the low dose area without compromising the target volume coverage.
three patients were therefore counseled by experienced radiographers daily prior to their treatment to highlight the importance of patient cooperation during treatment. Whilst some dosimetric studies do suggest the feasibility of dose painting with HT during respiration in certain situations without motion management [32], lack of respiratory gating with tomotherapy treatment still remains a major limitation, particularly in this select group of patients, having complex volume treatments; eligible for a technique capable of achieving the maximum decrease in heart dose. But; an advantage of tomotherapy that remains is the daily image-guided radiotherapy, enabling us to correct setup errors, and constituting a critical step to warrant the safe introduction of respiratory gating. [33]
Conclusion
This report details the clinical implementation of irradiation to the IMC and SCF in conjunction with left chest wall, and also bilateral chest wall, in the postoperative treatment of breast cancers. Helical tomotherapy achieved desired dose homogeneity and provided adequate target volume coverage with high capabilities of sparing of critical organs.
At a median follow up of 12 months, whilst all three patients have good locoregional control of disease, such techniques could be explored within a controlled clinical trial to ascertain long term clinical benefits in poor prognosis locoregionally advanced breast cancer patients.
Authors' Contribution
MN did the literature search and prepared the manuscript, AM did the planning of all the cases, IM reviewed and edited the manuscript, RA reviewed and edited the manuscript, SC treated the cases, reviewed and drafted the final manuscript
Conflict of Interests
The authors Dr. Moujhuri Nandi, Miss Anurupa Mahato, Dr. Indranil Mallick, Dr. Rimpa Achari, Dr. Sanjoy Chatterjee declare that there is no conflict of interest.
Ethical Considerations
Written informed consent was obtained from the patients for publication of this case report
Funding
None declared
Acknowledgement
None declared

World J Surg Med Radiat Oncol 2013;2:70-80 Helical Tomotherapy in Breast Cancer
79 http://www.npplweb.com/wjsmro/content/2/10
References
(1) Beavis, A.W. (2004) Is tomotherapy the future of IMRT? Br J Radiol. 77, 285-295.[pubmed] (2) Mackie, T.R. (2006) History of tomotherapy. Phys Med Biol. 51, R427-R453.[pubmed] (3) Lee N, Puri, D.R., Blanco, A.I., Chao, K.S. (2007) Intensity-modulated radiation therapy in head and neck cancers: an update. Head Neck. 29, 387-400.[pubmed] (4) Ahmed M, Hansen, V.N., Harrington, K.J., Nutting, C.M. (2009) Reducing the risk of xerostomia and mandibular osteoradionecrosis: the potential benefits of intensity modulated radiotherapy in advanced oral cavity carcinoma. Med Dosim. 34, 217-224.[pubmed] (5) Darby, S.C., McGale P, Taylor, C.W., Peto R. (2005) Long-term mortality from heart disease and lung cancer after radiotherapy for early breast cancer: prospective cohort study of about 300,000 women in US SEER cancer registries. Lancet Oncol. 6, 557–65. (6) Patt, D.A., Goodwin, J.S., Kuo, Y.F., Freeman, J.L., Zhang, D.D., Buchholz, T.A., Hortobagyi, G.N., Giordano, S.H. (2005) Cardiac morbidity of adjuvant radiotherapy for breast cancer. J Clin Oncol. 23,7475–82.[pubmed] (7) Matzinger, O., Heimsoth, I., Poortmans, P., Collette, L., Struikmans, H., Van Den Bogaert, W., Fourquet, A., Bartelink, H., Ataman, F., Gulyban, A., Pierart, M., Van Tienhoven, G. (2010); EORTC Radiation Oncology Breast Cancer Groups: Toxicity at three years with and without irradiation of the internal mammary and medial supraclavicular lymph node chain in stage I to III breast cancer (EORTC trial 22922/10925). Acta Oncol. 49 (1), 24-34. (8) Whelan, T.J., Olivotto, I., Ackerman, J.W., Chapman, B. Chua., A. Nabid, K. A. Vallis, J. R. White, P. Rousseau, A. Fortin, L. J. Pierce, L. Manchul, P. Craighead, M. C. Nolan, J. Bowen, D. R. McCready, K. I. Pritchard, M. N. Levine, W. Parulekar. (2011) NCIC-CTG MA.20: an intergroup trial of regional nodal rradiation in early stage breast cancer. J Clin Oncol. 29 (18 suppl), LBA1003. (9) Nyiri, B., Macpherson, M., Szanto, J. (2002) Forward-planned dose compensation for radiotherapy of the breast sing MLC sub-fields. In: 21st Annual meeting of the European Society for Therapeutic Radiology and ncology (ESTRO), Prague, Czech Republic (September 15–19, 2002); Radiother Oncol. 64S1:S319 (Abstract). (10) Cho, B.C., Hurkmans, C.W., Damen, E.M., Zijp, L.J., Mijnheer, B.J. Intensity modulated versus non-intensity odulated radiotherapy in the treatment of the left breast and upper internal mammary lymph node chain: a comparative planning study. Radiother Oncol. 62, 127–36 (2002).[pubmed] (11) Cozzi, L., Fogliata, A., Nicolini, G., Bernier, J. Clinical experience in breast irradiation with intensity modulated photon beams. Acta Oncol. 44, 467–74 (2005).[pubmed] (12) Thilmann, C., Sroka-Perez, G., Krempien, R., Hoess, A., Wannenmacher, M., Debus, J. (2004) Inversely planned intensity modulated radiotherapy of the breast including the internal mammary chain: a plan
comparison study.Technol Cancer Res Treatment. 3, 69–75. (13) Krueger, E.A., Fraass, B.A., McShan, D.L., Marsh, R., Pierce, L.J. (2003) Potential gains for irradiation of chest wall and regional nodes with intensity modulated radiotherapy. Int J Radiat Oncol Biol Phys. 56, 1023–37.[pubmed] (14) Chui, C.S., Hong, L., McCormick, B. (2005) Intensity-modulated radiotherapy technique for three-field breast treatment. Int J Radiat Oncol Biol Phys. 62, 1217–23.[pubmed] (15) Popescu, C.C., Olivotto, I., Patenaude, V., Wai, E., Beckham, W.A. (2006) Inverse-planned, dynamic, multi-beam,intensity-modulated radiation therapy (IMRT): a promising technique when target volume is the left breast and internal mammary lymph nodes. Med Dosim. 31, 283–91. (16) Franco P, Catuzzo P, Cante D, La Porta MR, Sciacero P, Girelli G, Casanova Borca V, Pasquino M, (2011) TomoDirect: an efficient means to deliver radiation at static angles with tomotherapy.Tumori. Jul-Aug;97(4):498-502[pubmed] (17) Ashenafi, M., Boyd, R.A., Lee, T.K., Lo, K.K., Gibbons, J.P., Rosen, II., Fontenot, J.D., Hogstrom, K.R. Feasibility of postmastectomy treatment with helical tomotherapy. Int J Radiat Oncol Biol Phys Jul. 77 (3), 836-42 (2010).[pubmed] (18) Coon, A.B., Dickler, A., Kirk, M.C., Liao, Y., Shah, A.P., Strauss, J.B., Chen, S., Turian, J., Griem, K.L. (2010) Tomotherapy and multifield intensity-modulated radiotherapy planning reduce cardiac doses in left-sided breast cancer patients with unfavorable cardiac anatomy. Int J Radiat Oncol Biol Phys. Sep 1; 78 (1), 104-10. (19) Caudrelier, J.M., Morgan, S.C., Montgomery, L., Lacelle, M., Nyiri, B., Macpherson, M. (2009) Helical Tomotherapy for loco regional irradiation including the internal mammary chain in left-sided breast cancer: dosimetric evaluation. Radiother Oncol. 90 (1), 99-105. (20)Available at: http://www.rtog.org/CoreLab/ContouringAtlases/BreastCancerAtlas.aspx as reviewed on 11/3/2013 (21) Hall, W.H., Guiou, M., Lee, N.Y., Dublin, A., Narayan, S., Vijayakumar, S., Purdy, J.A., Chen, A.M. (2008) Development and validation of a standardized method for contouring the brachial plexus: preliminary dosimetric analysis among patients treated with IMRT for head-and-neck cancer. Int J Radiat Oncol Biol Phys. 72, 1362-1367.[pubmed] (22) Graham, P., Jagavkar, R., Browne, L., Millar, E. (2006) Supraclavicular radiotherapy must be limited laterally by the coracoid to avoid significant adjuvant breast nodal radiotherapy lymphoedema risk. Australas Radiol. 50(6),578-582. (23) Kantor G, Mahé MA, Giraud P, Lisbona A, Caron J, Mazal A. 2006 Helical tomotherapy: general methodology for clinical and dosimetric evaluation (national French project)]. Cancer Radiother. Nov;10(6-7):488-91. [pubmed]

World J Surg Med Radiat Oncol 2013;2:70-80 Nandi M et al.
80 http://www.npplweb.com/wjsmro/content/1/1/5
Published by Narain Publishers Pvt. Ltd. (NPPL) The Open Access publishers of peer reviewed journals. All articles are immediately published online on acceptance. All articles published by NPPL are available free online Authors retain the copyright under the Creative commons attribution license. The license permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
(24) Miles, E.A., Venables, K., Hoskin, P.J., Aird, E.G.A., (2009) on behalf of the START Trial Management Group.Dosimetry and field matching for radiotherapy to the breast and supraclavicular fossa. Radiother Oncol. 91, 42-48.[pubmed] (25) Intensity Modulated and Partial Organ Radiotherapy (IMPORT) High Trial Planning Pack. (2009) Final version. Available at: http://rttrialsqa.dnsalias.org/IMPORT%20HIGH.htm;. (26) Bentzen, S.M., Agrawal, R.K., Aird, E.G., Barrett, J.M., Barrett-Lee P.J., (2008) START Trialists’ Group. The UK Standardisation of Breast Radiotherapy (START) Trial A of radiotherapy hypofractionation for treatment of early breast cancer: a randomised trial. Lancet Oncol. 4, 331-341. (27) Goddu, S.M., Chaudhari, S., Mamalui-Hunter, M., Pechenaya, O.L., Pratt, D., Mutic, S., Zoberi, I., Jeswani, S., Powell, S.N., Low, D.A. (2009) Helical tomotherapy planning for left-sided breast cancer patients with positive lymph nodes: comparison to conventional multiport breast technique. Int J Radiat Oncol Biol Phys. 73(4), 1243-1251. (28) Gonzalez, V.J., Buchholz, D.J., Langen, K.M, Olivera, G.H., Chauhan, B., Meeks, S.L., Ruchala, K.J., Haimerl, J., Lu, W., Kupelian, P.A. (2006) Evaluation of two tomotherapy-based techniques for the delivery of whole breast intensity-modulated radiation therapy. Int J Radiat Oncol Biol Phys. 65(1), 284-290.[pubmed]
(29) O’Donnell, H., Cooke, K., Walsh, N., Plowman, P.N. (2009) Early experience of tomotherapy-based intensity-modulated radiotherapy for breast cancer treatment. Clin Oncol (R Coll Radiol). 21 (4), 294-301.[pubmed] (30) Chatterjee, S., Lee, D., Kent, N., Wintle, T., Mott, J.H., Kelly, C.G., Branson, A.N. (2011) Managing Supraclavicular disease from breast cancer with brachial plexus-sparing techniques using helical tomotherapy. Clin Oncol (R Coll Radiol). Mar. 23(2), 101-7.[pubmed] (31). Darby SC, Ewertz M, McGale P, Bennet AM, Blom-Goldman U, Brønnum D, Correa C, Cutter D, Gagliardi G, Gigante B, Jensen MB, Nisbet A, Peto R, Rahimi K, Taylor C, Hall P (2013) Risk of ischemic heart disease in women after radiotherapy for breast cancer N Engl J Med. Mar 14; 368(11):987-98. [pubmed] (32) Kissick MW, Mo X, McCall KC et al (2010) A phantom model demonstration of tomotherapy dose painting delivery, including managed respiratory motion without motion management. Phys Med Biol 55:2983–2995 43. [pubmed] (33) Korreman SS, Juhler Nøttrup T, Fredberg Persson G et al (2008) The role of image guidance in respiratory gated radiotherapy. Acta Oncol 47:1390–1396 [pubmed]
World Journal of Surgical, Medical
and Radiation Oncology




















