Health needs assessment: Syria, Iraq, Lebanon, Egypt, and ...
187
HEALTH NEEDS ASSESSMENT: SYRIA, IRAQ, LEBANON, EGYPT AND JORDAN RELIGIOUS AND ETHNIC MINORITY (REM) SEPTEMBER 10, 2020 This publication was produced for review by the United States Agency for International Development. It was prepared by Management Systems International (MSI), A Tetra Tech Company for the MENA MELS Activity.
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Health needs assessment: Syria, Iraq, Lebanon, Egypt, and ...

HEALTH NEEDS ASSESSMENT: SYRIA, IRAQ, LEBANON, EGYPT AND JORDAN RELIGIOUS AND ETHNIC MINORITY (REM)
SEPTEMBER 10, 2020 This publication was produced for review by the United States Agency for International Development. It was prepared by Management Systems International (MSI), A Tetra Tech Company for the MENA MELS Activity.

i | REM HEALTH NEEDS ASSESSMENT USAID.GOV
HEALTH NEEDS ASSESSMENT: SYRIA, IRAQ, LEBANON, EGYPT AND JORDAN Religious and Ethnic Minority (REM)
Contracted under GS00F280GA, Task Order 7200AA19M00017 Middle East & North Africa Monitoring, Evaluation, & Learning Services Activity
Report Prepared by: Dina Khaled, Heather Lorenzen, and Gwynne Zodrow (MSI) DISCLAIMER The authors’ views expressed in this report do not necessarily reflect the views of the United States Agency for International Development or the United States Government.

ii | REM HEALTH NEEDS ASSESSMENT USAID.GOV
CONTENTS ACRONYMS ............................................................................................................. 2
EXECUTIVE SUMMARY ........................................................................................ 4
INTRODUCTION .................................................................................................. 13 PURPOSE .................................................................................................................................................................. 13 FOCUS COUNTRIES AND POPULATIONS ................................................................................................. 13 ASSESSMENT QUESTIONS................................................................................................................................. 13 DATA COLLECTION AND ANALYSIS METHODS ................................................................................... 14 DATA LIMITATIONS ............................................................................................................................................ 14
NORTHEAST SYRIA ............................................................................................ 15 COUNTRY CONTEXT ....................................................................................................................................... 15 OVERVIEW OF RELIGIOUS AND ETHNIC MINORITIES IN NORTHEAST SYRIA .......................... 18
RELIGIOUS AND ETHNIC MINORITY GEOGRAPHIC FOCUS .................................................... 20 AQ 1: OVERVIEW OF HEALTH STATUS IN SYRIA ................................................................................... 20
WOMEN’S HEALTH .................................................................................................................................... 21 CHILDREN’S HEALTH ................................................................................................................................ 22 MENTAL HEALTH ........................................................................................................................................ 23 SEXUAL AND GENDER-BASED VIOLENCE ....................................................................................... 24 OUTBREAK/EPIDEMIC DATA .................................................................................................................. 25 ACCESS TO WATER, SANITATION, AND HYGIENE ..................................................................... 26 OTHER HEALTH ISSUES ............................................................................................................................ 28 CONCLUSIONS ........................................................................................................................................... 29
AQ 2: PRIMARY HEALTH CARE SYSTEM STRENGTHS AND WEAKNESSES ................................... 29 HEALTH WORKFORCE ............................................................................................................................. 30 SERVICE DELIVERY ...................................................................................................................................... 31 WOMEN’S AND CHILDREN’S HEALTH .............................................................................................. 34 MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT ..................................................................... 35 COMMUNITY HEALTH OUTREACH PROGRAMS ........................................................................... 36 HEALTH FINANCE ...................................................................................................................................... 36 ACCESS TO ESSENTIAL MEDICINES ..................................................................................................... 37 LEADERSHIP AND GOVERNANCE ....................................................................................................... 38 CONCLUSIONS ........................................................................................................................................... 38
AQ 3: CRITICAL HEALTH NEEDS AND CURRENT GAPS IN HEALTH SERVICES FOR REM COMMUNITIES ...................................................................................................................................................... 39 AQ 4: EXTERNAL STRESSES .............................................................................................................................. 40
COVID-19 ....................................................................................................................................................... 40 POLITICS AND POLICY ............................................................................................................................. 40 SECURITY AND STABILITY ...................................................................................................................... 41 FINANCIAL .................................................................................................................................................... 41 ENVIRONMENTAL ...................................................................................................................................... 42 EQUITY............................................................................................................................................................ 42 CONCLUSIONS ........................................................................................................................................... 42
USAID HEALTH AND REM PROGRAMMING ............................................................................................. 43
IRAQ ........................................................................................................................ 44

iii | REM HEALTH NEEDS ASSESSMENT USAID.GOV
COUNTRY CONTEXT ....................................................................................................................................... 44 OVERVIEW OF RELIGIOUS AND ETHNIC MINORITIES IN IRAQ ....................................................... 46
RELIGIOUS AND ETHNIC MINORITY GEOGRAPHIC FOCUS .................................................... 47 AQ 1: OVERVIEW OF HEALTH STATUS IN IRAQ .................................................................................... 48
WOMEN’S HEALTH .................................................................................................................................... 49 CHILD HEALTH ............................................................................................................................................ 49 MENTAL HEALTH ........................................................................................................................................ 51 SEXUAL AND GENDER-BASED VIOLENCE (SGBV) ........................................................................ 52 OUTBREAK/EPIDEMIC DATA .................................................................................................................. 52 ACCESS TO WASH ..................................................................................................................................... 53 CONCLUSIONS ........................................................................................................................................... 53
AQ 2: STRENGTHS AND WEAKNESSES OF THE PRIMARY HEALTH CARE SYSTEM .................. 53 HEALTH WORKFORCE ............................................................................................................................. 55 SERVICE DELIVERY ...................................................................................................................................... 55 HEALTH FINANCE ...................................................................................................................................... 58 ACCESS TO ESSENTIAL MEDICINES ..................................................................................................... 60 LEADERSHIP/GOVERNANCE .................................................................................................................. 60 CONCLUSION .............................................................................................................................................. 63
AQ 3: CRITICAL HEALTH NEEDS AND GAPS IN HEALTH SERVICES FOR THE REM COMMUNITIES ...................................................................................................................................................... 63 AQ 4: EXTERNAL STRESSES .............................................................................................................................. 64
COVID-19 ....................................................................................................................................................... 64 SECURITY AND STABILITY ...................................................................................................................... 65 POLITICS ......................................................................................................................................................... 66 FINANCIAL .................................................................................................................................................... 66
USAID HEALTH AND REM PROGRAMMING ............................................................................................. 66
LEBANON .............................................................................................................. 70 COUNTRY CONTEXT ....................................................................................................................................... 70
RELIGIOUS AND ETHNIC MINORITY POPULATION .................................................................... 72 RELIGIOUS AND ETHNIC MINORITY GEOGRAPHIC FOCUS .................................................... 73
AQ 1: OVERVIEW OF HEALTH STATUS IN LEBANON .......................................................................... 76 WOMEN’S HEALTH .................................................................................................................................... 76 CHILDREN’S HEALTH ................................................................................................................................ 78 OUTBREAK/EPIDEMIC DATA .................................................................................................................. 79 MENTAL HEALTH ........................................................................................................................................ 80 SEXUAL AND GENDER-BASED VIOLENCE ....................................................................................... 80 WATER, SANITATION, AND HYGIENE .............................................................................................. 80 CONCLUSIONS ........................................................................................................................................... 81
AQ 2: PRIMARY HEALTH CARE SYSTEM STRENGTHS AND WEAKNESSES ................................... 81 HEALTH WORKFORCE ............................................................................................................................. 82 SERVICE DELIVERY ...................................................................................................................................... 84 ACCESS TO ESSENTIAL MEDICINES ..................................................................................................... 88 HEALTH FINANCE ...................................................................................................................................... 89 LEADERSHIP AND GOVERNANCE ....................................................................................................... 91 CONCLUSIONS ........................................................................................................................................... 92

iv | REM HEALTH NEEDS ASSESSMENT USAID.GOV
AQ 3: CRITICAL HEALTH NEEDS AND CURRENT GAPS IN HEALTH SERVICES FOR REM COMMUNITIES ...................................................................................................................................................... 93
MENTAL HEALTH ........................................................................................................................................ 93 SEXUAL AND GENDER-BASED VIOLENCE ....................................................................................... 93 MATERNAL AND REPRODUCTIVE HEALTH .................................................................................... 94 CHILDREN’S HEALTH ................................................................................................................................ 94
AQ 4: EXTERNAL STRESSES .............................................................................................................................. 94 COVID-19 ....................................................................................................................................................... 94 POLITICS AND POLICY ............................................................................................................................. 95 SECURITY AND STABILITY ...................................................................................................................... 95 FINANCIAL CRISIS....................................................................................................................................... 96 ENVIRONMENT ........................................................................................................................................... 96 EQUITY............................................................................................................................................................ 96 CONCLUSIONS ........................................................................................................................................... 97
USAID HEALTH AND REM PROGRAMMING ............................................................................................. 97
JORDAN .................................................................................................................. 98 COUNTRY CONTEXT ....................................................................................................................................... 98 OVERVIEW OF RELIGIOUS AND ETHNIC MINORITIES IN JORDAN ................................................ 99
REM GEOGRAPHIC FOCUS ..................................................................................................................... 99 AQ 1: OVERVIEW OF HEALTH STATUS IN JORDAN ........................................................................... 100
WOMEN’S HEALTH .................................................................................................................................. 103 CHILD HEALTH .......................................................................................................................................... 103 MENTAL HEALTH ...................................................................................................................................... 104 SEXUAL AND GENDER-BASED VIOLENCE (SGBV) ...................................................................... 105 OUTBREAK/EPIDEMIC DATA ................................................................................................................ 106 ACCESS TO WASH ................................................................................................................................... 106 CONCLUSION ............................................................................................................................................ 106
AQ 2: STRENGTHS AND WEAKNESSES OF THE PRIMARY HEALTH CARE SYSTEM ................ 107 HEALTH WORKFORCE ........................................................................................................................... 108 SERVICE DELIVERY .................................................................................................................................... 110 HEALTH FINANCE .................................................................................................................................... 114 ACCESS TO ESSENTIAL MEDICINE ..................................................................................................... 116 LEADERSHIP/GOVERNANCE ................................................................................................................ 116 CONCLUSION ............................................................................................................................................ 117
AQ 3: CRITICAL HEALTH NEEDS AND GAPS IN HEALTH SERVICES FOR REM COMMUNITIES................................................................................................................................................................................... 117 AQ 4: EXTERNAL STRESSES ............................................................................................................................ 119
COVID-19 ..................................................................................................................................................... 119 ENVIRONMENTAL .................................................................................................................................... 119 EQUITY.......................................................................................................................................................... 120
USAID HEALTH AND REM PROGRAMMING ........................................................................................... 120
EGYPT ...................................................................................................................121 COUNTRY CONTEXT ..................................................................................................................................... 121 OVERVIEW OF RELIGIOUS AND ETHNIC MINORITIES IN EGYPT .................................................. 122
SITUATION IN GOVERNORATES WITH HIGH REM POPULATIONS IN EGYPT ............... 124 AQ 1: OVERVIEW OF HEALTH STATUS IN EGYPT ................................................................................ 125

v | REM HEALTH NEEDS ASSESSMENT USAID.GOV
WOMEN’S HEALTH .................................................................................................................................. 126 CHILD HEALTH .......................................................................................................................................... 127 MENTAL HEALTH ...................................................................................................................................... 128 SEXUAL AND GENDER-BASED VIOLENCE ..................................................................................... 128 OUTBREAK/EPIDEMIC DATA ................................................................................................................ 129 ACCESS TO WASH ................................................................................................................................... 130 CONCLUSIONS ......................................................................................................................................... 131
AQ 2: STRENGTHS AND WEAKNESSES OF THE PRIMARY HEALTH CARE SYSTEM ................ 131 HEALTH WORKFORCE ........................................................................................................................... 132 SERVICE DELIVERY .................................................................................................................................... 133 HEALTH FINANCE .................................................................................................................................... 138 ACCESS TO ESSENTIAL MEDICINES ................................................................................................... 139 LEADERSHIP/GOVERNANCE ................................................................................................................ 139 CONCLUSIONS ......................................................................................................................................... 140
AQ 3: CRITICAL HEALTH NEEDS AND GAPS IN HEALTH SERVICES FOR THE REM COMMUNITIES .................................................................................................................................................... 140
CONCLUSIONS ......................................................................................................................................... 141 AQ 4: EXTERNAL STRESSES ............................................................................................................................ 142
COVID-19 ..................................................................................................................................................... 142 POLITICAL AND POLICY ....................................................................................................................... 142 SECURITY AND STABILITY .................................................................................................................... 143 FINANCIAL .................................................................................................................................................. 143 EQUITY.......................................................................................................................................................... 143 ENVIRONMENTAL .................................................................................................................................... 144 CONCLUSIONS ......................................................................................................................................... 144
USAID HEALTH AND REM PROGRAMMING ........................................................................................... 144
AQ 5: LESSONS LEARNED FOR IMPROVING HEALTH SERVICES FOR RELIGIOUS AND ETHNIC MINORITY COMMUNITIES .............................146
LIMITED DATA AND TARGETING............................................................................................................... 146 ROLE OF PARTNERS ......................................................................................................................................... 147 COMMUNITY AWARENESS............................................................................................................................ 147 LOCAL CAPACITY BUILDING ....................................................................................................................... 147 GENDER-BASED VIOLENCE AND MENTAL HEALTH PROGRAMMING ........................................ 148 REDUCING STIGMA .......................................................................................................................................... 148 PRIORITIZING AND INTEGRATING PROGRAMMING ........................................................................ 148 MULTISECTORAL APPROACHES .................................................................................................................. 149 COVID-19 CONSIDERATIONS ...................................................................................................................... 149
RECOMMENDATIONS ......................................................................................149

2 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
ACRONYMS
ANC Antenatal Care APC Advancing Partners & Communities AQ Assessment Questions CAPMAS Central Agency for Public Mobilization and Statistics CH Child Health COVID Coronavirus Disease CFRD Center for Refugee and Disaster Response CHW Community Health Worker CSO Civil Society Organizations DFID Department for International Development DHS Demographic Health Data EPHRP Emergency Primary Healthcare Restoration Project EPI Expanded Program on Immunization EWARN Early Warning Alert and Response Network EWARS Early Warning Alert and Response System FBO Faith-Based Organizations GBV Gender-Based Violence GBVIMS GBV Information Management System GDP Gross Domestic Product HAUS Health and Utilization Survey HBV Hepatitis B Virus HCV Hepatitis C Virus HeRAMS Health Resources Availability Monitoring System HIO Health Insurance Organization HIV Human Immunodeficiency Virus HRW Human Rights Watch JD Jordanian Dinar JHAS Jordan Health Aid Society KII Key Informant Interview ICRC International Committee of the Red Cross IDP Internally Displaced Person IED Improvised Explosive Device IMC International Medical Corps IMR Infant mortality rate IOM International Organization for Migration IRC International Rescue Committee ISIS Islamic State of Iraq and Syria KRG Kurdistan Regional Government KRI Kurdistan Region of Iraq LCRP Lebanon Crisis Response Plan LSOG Lebanese Society of Obstetrics and Gynecology MDM Doctors of the World MENA MELS Middle East & North Africa Monitoring, Evaluation, & Learning Services Activity MHPSS Mental Health and Psychosocial Support MICS Multiple Indicator Cluster Survey MNCH Maternal, Newborn, and Child Health MOH Ministry of Health MOHP Ministry of Health and Population

3 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
MOPH Ministry of Public Health MOSA Ministry of Social Affairs MOSAIC MENA Organization for Services, Advocacy, Integration, and Capacity Building MSF Doctors Without Borders/Médecins Sans Frontiéres MSI Management Systems International NCD Non-Communicable Disease NES Northeast Syria NGO Non-Government Organizations NLG No Lost Generation NSSF National Social Security Fund NSVAW National Strategy for Combating Violence Against Women OCHA United Nations Office for the Coordination of Humanitarian Affairs OHCHR United Nations Human Rights Council PHC Primary Health Care PHCC Primary Health Care Center PNC Postnatal Care PPE Personal Protective Equipment PRIMASYS Primary Health Care Systems PTSD Posttraumatic Stress Disorder REM Religious and Ethnic Minorities SDG Sustainable Development Goal SGBV Sexual and Gender-Based Violence SNES Self-Administration Northeast Syria SRH Sexual and Reproductive Health TFR Total Fertility Rate UN United Nations UNHCR United Nations High Commissioner for Refugees UNICEF United Nations International Children’s Emergency Fund UNRWA United Nations Relief and Works Agency for Palestinian Refugees USAID United States Agency for International Development USCIRF United States Commission on International Religious Freedom WASH Water, sanitation, and hygiene WB World Bank WFP World Food Programme WHO World Health Organization

4 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
EXECUTIVE SUMMARY
Assessment Purpose and Context
This assessment examines the health status and needs of religious and ethnic minority (REM) communities in five countries: Egypt, Iraq, Jordan, Lebanon, and Syria. Under the Middle East and North Africa (MENA) Monitoring, Evaluation, and Learning Services Activity (MELS), Management Systems International (MSI) conducted this assessment to help inform United States Agency for International Development (USAID) health programming under the vice president’s initiative to support MENA REM communities.
The assessment focused on the following key REM populations and geographic areas within each country:
Country REM Communities
1 Northeast Syria
Christian (Assyrian, Chaldean, Syriac, Greek, and Armenian), Yazidi, Kurd, and Turkman
2 Iraq Christian (Assyrian, Chaldean, Syriac, and Armenian), Yazidi, Kurd, Kaka’I, Turkman, Shabak, Sabean-Mandaeans
3 Lebanon Christian (Maronite, Greek, Armenian, Syriac, and Chaldean), Druze, Yazidi, Palestinian, and Syrian
4 Jordan Palestinian, Christian (Greek, Maronite, Armenian, Syriac, and Chaldean), Druze, Syrian, Iraqi
5 Egypt Jewish, Christian (Coptic, Armenian, Greek, Syriac) Bahai, Berber, Bedouin, Nubian, and Refugees
Assessment Questions
This assessment addresses the following assessment questions (AQs) for each of the five selected countries and across the region.
1. What is the overall current health status of REM communities?
2. What are the primary health care system strengths and weaknesses at the community level?
3. What are the critical health needs and gaps in primary health care services for the REM communities in the region?
4. What external stresses impact the ability to provide health services and achieve outcomes?
5. What are the relevant lessons learned from other projects and donors on improving primary health care services for vulnerable populations in the region?
The assessment focused mainly on the primary health care system—including public and private health service delivery—at the local and community level as this is where most REM populations seek services.
Approach, Methods and Limitations
The team collected secondary data through a Google search of published research and studies as well as research produced by USAID, its implementing partners, and other donor or research organizations operating in the region. The assessment team also conducted group interviews with USAID staff from four missions (Iraq, Jordan, Lebanon, and Syria). The team reviewed all collected reports, data, and interview notes and extracted relevant data and information to answer each assessment question. All

5 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
extracted information was reviewed, organized, and synthesized. See more details on the assessment approach in Annex 1, Scope of Work. The assessment’s main limitation is data availability. Because the assessment relied on secondary data and focused on small subsets of the population (REM populations), the assessment team faced challenges finding data specific to REM populations. In addition, many of the countries studied published only limited current health data (i.e., in the last two to three years) and the data were not disaggregated by religion or ethnicity. Further, as many of the REM populations in these countries are refugees or internally displaced persons (IDPs), humanitarian service providers respect Do No Harm guidelines, which preclude monitoring or reporting beneficiaries’ religions or ethnicities.
Country Sections
Northeast Syria
More than 4 million people, including Christian, Yazidi, Kurd, and Turkmen REM populations, live in northeast Syria’s (NES’s) three governorates: Al-Hasakeh, Deir-ez-Zor, and Raqqa, which are governed mostly by the Self-Administration of Northeast Syria.1 Accurate estimates of the REM communities in NES are not available, but available data suggest there are 60,000 to 70,000 Christians; 3,000 to 4,000 Yazidis; and roughly 1,200 Turkmen. Kurds make up 55 percent of the population of Hasakeh and the northern areas of Raqqa.2
As a result of displacements caused by ongoing regional conflict, NES hosts approximately 790,000 IDPs, the vast majority of whom are women and children, living in overcrowded, last-resort shelters and camps. Civilians in NES are among the country’s most vulnerable, with an estimated 1.9 million people in need of humanitarian assistance.3 An estimated 83 percent of people in Syria live below the poverty line, with high levels of food insecurity.4 Despite the tremendous need, only 30 percent of NES communities can access humanitarian assistance. Access to health services is the top-ranked need among all communities, and food is the top-ranked priority among IDPs.5 The humanitarian situation in NES is further aggravated by the closure of supply lines, which exacerbates the ongoing disruption to essential services, including health and water.
Medical needs in NES are profound as the population has been exposed to repeated trauma and extreme stress.6 Chronic diseases are the most commonly reported health problem, alongside a continuing rise in maternal mortality.7 Chronic malnutrition affects all populations and is the leading cause of death among children. High rates of transmission of communicable diseases are exacerbated by low immunization rates and lack of access to water, sanitation, and hygiene (WASH) facilities. Years of exposure to conflict have led to high rates of mental health disorders and gender-based violence (GBV).
1 Maxen Gharbibah and Zaki Mehchy, "COVID-19 Pandemic: Syria’s Response and Healthcare Capacity," March 25, 2020, https://eprints.lse.ac.uk/103841/1/CRP_covid_19_in_Syria_policy_memo_published.pdf 2 Fabrice Balanche, "Rojava's Sustainability and the PKK's Regional Strategy," The Washington Institute, April 24, 2016, https://www.washingtoninstitute.org/policy-analysis/view/rojavas-sustainability-and-the-pkks-regional-strategy 3 UN Security Council, "Review of Alternative Modalities for the Border Crossing of Ya'rubiyah." 4 OCHA, "Syrian Arab Republic: COVID-19, Response Update No.6," June 19, 2020, https://reliefweb.int/sites/reliefweb.int/files/resources/covid-19_update_no.6.pdf 5 REACH, "Humanitarian Situation Overview in Syria (HSOS) Northeast Syria," April 2020, https://reliefweb.int/sites/reliefweb.int/files/resources/REACH_SYR_Factsheet_HSOS-Regional-Factsheet_Northeast-Syria_April2020.pdf 6 M. Gharbibah and Z. Mehchy, "COVID-19 Pandemic: Syria’s Response and Healthcare Capacity." 7 REACH, "Humanitarian Situation Overview in Syria (HSOS) Northeast Syria."

6 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
It is estimated that more people in Syria have died from a lack of access to health care, medicine, and nutrition than directly from the violence. Most health facilities in NES are not functioning or are only partially functioning and suffer a lack of resources, including supplies, workforce, and funding. Because of the various impediments, most health services are received at pharmacies. In addition, there is an extremely high unmet need for mental health and psychosocial support (MHPSS) and GBV services.
The ability to respond to health needs is further hindered by security concerns and border closures, which have forced a reduction in the humanitarian response and shortages in supplies, including personal protective equipment. The economic collapse and high inflation are driving up poverty rates and making these populations even more food insecure.
Further escalation of conflict, leading to increased displacement, overcrowded living conditions, and lack of WASH services, will exacerbate the many health challenges in NES. Acute food shortages that are already negatively impacting health among all populations are predicted to worsen, raising concerns of permanent disabilities among stunted children. The World Food Programme has indicated that in 2020 there is a real possibility of famine in Syria, which will be compounded by the challenges created by COVID-19.8
Iraq
Iraq’s population in 2019 was 39.3 million. The estimated Christian population in Iraq is less than 1 percent; around 97 percent of the population is Muslim. About 80 percent of the Christian population lives in the Nineveh Plains and Kurdistan Region of Iraq (KRI). This population has declined since 2002 from around 1 million to fewer than 250,000 as of June 2020. Estimates of other REM populations are as follows: 4.5 million Kurds; 3 million Turkmen; 500,000 Yazidis; 350,000 Shabak; 20,000 Kaka’I; and 10,000 Sabean-Mandaeans.9 However, precise current demographic breakdowns are not available because of political sensitivities and the absence of recent census data. Most of Iraq’s REM communities are in northern Iraq and KRI.
As of March 2020, more than 1.39 million people remained internally displaced (mainly in the north and west Iraq), with 250,000 Iraqi refugees in neighboring countries. 10 Over 300,000 Yazidis live in displacement camps or informal settlements in KRI. About 18 percent of Iraq’s IDP population is made up of REM populations, including Yazidis, Christians, Shabak, and Turkmen, but represent only 3percent of returnees.
Iraq has made progress in improving its population’s overall health status over the past decade—for example, increasing life expectancy and decreasing infant mortality—but it is still behind other countries in the region. The country exhibits disparities in health indicators among the most vulnerable, especially among IDP populations. Although over the past decade, violence has been the leading cause of death, chronic diseases now account for 43 percent of all adult deaths. Neonatal mortality accounts for 54 percent of all under-five deaths in Iraq, and most of these deaths are preventable with evidence-based interventions. Rates of underweight status, stunting, and wasting are still high, particularly in Nineveh, compared with those in KRI.
Psychosocial needs among IDP populations are reported to be extremely high, but mental health professionals and trained health staff are limited. Many Yazidis suffer from extreme psychosocial distress because of violence, displacement, and economic hardships. In 2020, an estimated 1.29 million people in
8 UN Security Council, "Senior Officials Sound Alarm over Food Insecurity, Warning of Potentially ‘Biblical’ Famine, in Briefings to Security Council," April 21, 2020, https://www.un.org/press/en/2020/sc14164.doc.htm 9 U.S. State Department, Iraq 2018 International Religious Freedom Report, accessed June 2020. https://www.state.gov/wp-content/uploads/2019/05/IRAQ-2018-INTERNATIONAL-RELIGIOUS-FREEDOM-REPORT.pdf 10 UNICEF, Iraq 2020 Internal Displacement Crisis Humanitarian Situation Report, January to March 2020.

7 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
Iraq needed SGBV services. The main reported type of SGBV in Iraq is domestic violence, followed by forced/child marriage.11
The Iraqi health system faces challenges overcoming recurring shortages of essential medicines, dealing with budget deficits, rehabilitating infrastructure, and training and deploying human resources. Access to health services is limited, geographical disparities are significant, and health data are not collected on a routine basis. The Iraqi Ministry of Health runs a network of primary health care centers and public hospitals. Charges for services are low (although they used to be free). Further, Iraq has a shortage of medical personnel, especially doctors, with a reported 7.4 physicians per 10,000 people (2018) and around 21 nurses and midwives per 10,000 people. 12 Many facilities were abandoned, destroyed, or damaged during various conflicts and need rehabilitation and upgrades.
In 2018, 5.5 million people needed but lacked access to health care services.13 In 2020, an estimated 2.8 million people need health-related humanitarian support, of which around 17 percent are children under five. In late 2019, the Government of Iraq initiated the consolidation and closure of IDP camps, which significantly reduced in-camp populations and increased out-of-camp displaced populations and returnees and movements of people between governorates.
Iraq has established a series of measures to prevent the spread of COVID-19, but the outbreak is still straining the health system by increasing equipment shortages and patient loads. Although the United Nations High Commissioner for Refugees, nongovernmental organizations, and other entities delivering humanitarian assistance are exempt from movement restrictions, the capacity to deliver support has still been affected and the overall impact on the protection of refugees, IDPs, returnees, and stateless persons has been significant.
Lebanon
Lebanon’s population is estimated as 6.8 million, of which roughly 35 percent are refugees. Displaced Syrians constitute 22 percent of the population. Approximately 21 percent of Lebanon’s population are religious or ethnic minorities, with the remainder being Sunni or Shi’a Muslims or Maronite Christians. REM populations include non-Maronite Christians, Druze, Armenians, Assyrians, Turkmen, Kurds, and Yazidis. Governorates with concentrations of REM populations are Bekaa, Mount Lebanon, and the North governorates, although Beirut also contains a significant REM population. The overflow of refugees into Lebanon, coupled with Lebanon’s economic crisis and recent civil unrest, has significantly increased the number of people living in poverty and dependent on humanitarian aid and has exacerbated development constraints, heightening social tensions and competition for livelihoods and access to services.14
Disparities in health outcomes exist across governorates and across population groups, with governorates reporting high concentrations of REM populations showing poorer health outcomes than the national average. Maternal mortality has risen in recent years, particularly among Syrian women, who have the highest percentage of maternal deaths in the three governorates that contain REM communities. Children are vulnerable to acute respiratory illnesses, high rates of diarrhea because of insufficient WASH facilities and poor hygiene practices, and outbreaks of vaccine-preventable diseases arising from inadequate vaccination coverage. Mental health challenges and SGBV are particularly high among children and adolescents and refugees.
11 Ibid. 12 World Bank, Open Data 2018, accessed June 2020. https://data.worldbank.org/indicator/SH.MED.PHYS.ZS?locations=IQ 13 EASO, Iraq Key Socioeconomic Indicators February 2019, accessed June 2020. https://www.easo.europa.eu/sites/default/files/publications/Iraq-key-socio-economic-indicators.pdf 14 UN and MOPH, "Lebanon Crisis Response Plan 2017–2020."

8 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
Public health care faces continued budget cuts alongside a vastly privatized and unregulated health care system.15 Relatively low utilization of primary care and high rates of care-seeking for curative services have substantially increased health spending on hospital-based curative care. There is a critical shortage of competent family care physicians and nurses and a severe shortage of mental health professionals.
Areas with concentrations of REM populations have substantial refugee populations with high poverty levels. Although subsidized services are available, they are still unaffordable for economically vulnerable households, which constitute more than half of the population. The limited amount of community-based services makes expanding the geographic coverage of affordable, preventive, culturally appropriate health care challenging.
COVID-19-related movement restrictions have added to the multitude of stressors that include economic decline and the ongoing instability (both locally and from the Syrian crisis) that is drastically impacting the health care system, particularly for vulnerable individuals. The situation of refugees is deteriorating sharply, increasing the number of people in need of basic humanitarian assistance and protection. The vast number of displaced persons living in Lebanon has fueled host communities’ frustration and resentment toward them.
Jordan
The majority of Jordan’s population is Muslim (97.2 percent); Christians account for 2.2 percent and other groups, including Druze, make up less than 1 percent. It is believed that half of Jordan’s population is Palestinian or of Palestinian origin from the wave of refugees arriving in Jordan between 1947 and 1967.16 Most of this population has been naturalized, however, and in 2019 there were 2.2 million registered Palestinian refugees. In addition, there are 657,068 Syrian refugees and 67,225 Iraqi refugees.17
The Jordanian health care system is considered a model for other middle-income countries in the region because of its highly educated health care workforce and emphasis on ensuring and improving the quality of care. Jordan has taken steps to improve access to health care for all populations, including vulnerable REM populations. One of the positive results was a reduction in maternal and infant mortality rates, which have declined by 54 percent and 43 percent, respectively, in the past decade. Further, access to health facilities based on location is no longer a barrier to services for Jordanians or REM populations.
Jordan’s primary health care system functions relatively well and includes both public and private service providers. It faces several challenges, however, related to the growing prevalence of noncommunicable diseases among all population groups, which places an undue burden on the health care system and the population because of the high direct costs of managing these conditions.
Jordan’s health system requires a stronger focus on ensuring coordinated care between primary and community health facilities to promote healthy lifestyles, reduce morbidity and mortality, and improve health status. The pandemic created a new set of challenges for the country, especially for vulnerable populations. In March 2020, the government instituted a nationwide lockdown that not only affected businesses but limited access to health services, especially outside the camps.
Egypt
15 Kareem Chehayed, "Lebanon Is the Experiment that Shows Neoliberalism's Failure," The Century Foundation, April 16, 2020, https://tcf.org/content/commentary/lebanon-experiment-shows-neoliberalisms-failure/?agreed=1 16 Human Rights Watch, Stateless Again Palestinian-Origin Jordanians Deprived of Their Nationality, 2010. https://www.hrw.org/report/2010/02/01/stateless-again/palestinian-origin-jordanians-deprived-their-nationality. 17 UNHCR Jordan. December 2019. https://www.unhcr.org/jo/12449-unhcr-continues-to-support-refugees-in-jordan-throughout-2019.html#:~:text=As%202019%20comes%20to%20close,total%20of%2052%20other%20nationalities.

9 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
Egypt has the largest, most densely settled population among Arab countries, with an estimated 100.5 million people. Approximately 90 percent are Sunni Muslims, fewer than 1 percent are non-Sunni Muslims, roughly 10 percent are Christians, and there are at least 2,000 Bahá’ís and fewer than 20 Jews.18 Other minority groups include Nubians, concentrated in Upper Egypt; Bedouins, who populate Sinai and parts of the Western and Eastern Deserts; and the Berber, who populate the isolated area around the Siwa Oasis in the Western Desert. Most poor and vulnerable households are in the governorates with high REM populations. The governorates of Upper Egypt have the highest poverty rates in the country, with roughly 64 percent of their populations living in poverty.19
Egypt has made significant progress in improving the health status of its population, including an increase in life expectancy, a reduction in maternal and child mortality rates, and high rates of immunization coverage. Despite these gains, wide geographic and wealth disparities exist, as seen in the higher maternal and child mortality rates in Upper Egypt, which has high concentrations of Nubians and Christians. Further, noncommunicable diseases have become more prevalent because of obesity, high cholesterol levels, hypertension, and smoking. GBV remains one of the most prevalent issues facing women and girls, with 99 percent of Egyptian women experiencing sexual harassment and 26 percent experiencing physical and/or sexual violence in their lifetimes. Despite these statistics, only 1 percent seek GBV assistance from social services because of societal stigma and lack of services.
The health system has several problems, including lack of funding, poor staffing levels, and dilapidated facilities. Further, government investment in the public health care system is just 1.7 percent of the country's GDP. Poor working conditions and salaries have led doctors to leave Egypt to work abroad or specialize in higher-income fields (e.g., plastic surgery, gynecology), which has led to a gap in health service coverage. These problems have resulted in long queues for treatment and inadequate staff training, leading to low utilization and a preference among Egyptians to use private health care facilities. This, in turn, has led to high out-of-pocket costs for health care and significant inequities based on income, gender, and geography.
Overall, the Egyptian health care system has significant inequities, which disproportionately affect the country’s most vulnerable populations. Continued support is necessary to address these inequities and disparities and improve health outcomes for the population, particularly REM populations.
Lessons Learned for Improving Health Services for REM Communities
Although specific aspects of health systems and service delivery vary across the five countries, this assessment identified several key lessons on the overall challenges facing REM populations. Awareness of these lessons can help increase access to health care and social protection services and improve health outcomes of these vulnerable populations.
All the countries are facing challenges arising from regional instability, coupled with economic impediments that are reducing government spending on health and driving up poverty levels among both host and refugee communities, adding stress to health care systems. Many IDP, refugee, returnee, and host communities are recovering from conflict and face challenges related to nutrition, livelihoods, housing, and education, further contributing to stress and poor living conditions. As vulnerable populations, many REM populations also require mental health and psychosocial services (MHPSS) and sexual and gender-based violence (SGBV) services. Many health facilities are overburdened with demand, leaving communities in need of programming and investment to address the challenges and improve access to services, as well as expand the types of services and raise service quality.
18 USCIRF, "Annual Report 2020, Egypt: Recommended for Special Watch List." 19 World Bank Group, "Understanding Poverty and Inequality in Egypt."

10 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
The following lessons draw on the research conducted for this assessment as well as an evaluation carried out concurrently by this assessment team that examines REM health programming in northern Iraq, Nineveh Plains.20
Limited Data and Targeting
• REM-specific health data are limited, and available data are outdated. • Service providers do not disaggregate data by minority populations, making it difficult to determine
whether REM populations face barriers beyond those of the wider population. • REM-specific programming might increase the vulnerability of REM populations by exacerbating
the long history of sectarian tensions in the region, increased competition for livelihoods, and strained relations between refugees and host communities.
• Efforts to address the gaps in health services for REM communities are best undertaken by implementing broad-based interventions in areas known to contain these populations.
Role of Partners
• International and national nongovernmental organizations and faith-based organizations and donors fill a critical gap by providing humanitarian services across sectors, including health service delivery and prevention, which are not otherwise available.
• Engaging and/or providing services through local organizations that have experience working in the communities and with the population subsets ensures that programming reaches the most vulnerable.
• Social cohesion and reconciliation initiatives are best received when they are embedded within the wider population and are inclusive of religion, ethnic identity, and gender.
Community Awareness
• Strengthening awareness, accessibility, availability, and affordability of services at a community level is key to improved primary care for vulnerable populations.
• Increasing funding for community health workers (CHWs) helps expand community outreach and geographical coverage of messaging, which drive demand.
• Community outreach and education help reduce the stigma surrounding GBV and MHPSS services and encourage uptake.
Local Capacity Building
• The limited number of medical professionals and low investment in the health system result in capacity challenges.
• Training and capacity building at each level of the health system (i.e., Ministry of Health, health facilities, and communities) are key to improving service provision, especially MHPSS and SGBV services.
• Training CHWs on MHPSS and SGBV services enhances the sustainability of interventions and reduces the stigma associated with accessing these services.
Gender-Based Violence and Mental Health Programming
20 Khaled, Lorenzen, and Zodrow (MSI), Evaluation Report on USAID Improving Health Services and Outcomes in the Ninewa Plains, Iraq, May 2020.

11 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
• Ensuring access to SGBV and mental health services is a critical response to the humanitarian crisis, which has generated enormous psychological stress among the conflict-affected population and has contributed to higher levels of SGBV and mental health disorders.
• It is critical to address and strategize ways to protect women and girls amid COVID-19-related restrictions.
• CHWs can help foster community dialogue to address societal perceptions that perpetuate SGBV against women and children.
Reducing Stigma
• Programming should improve acceptance and reduce stigma among potential users of these services and their communities, as well as health service providers.
• Working closely with community leaders on program implementation and decision making helps reduce stigma and empowers communities to support their members with psychosocial and mental health issues and SGBV.
• Cultural barriers and traditional practices that hinder women and girl’s ability to access health services must be addressed to ensure improved health outcomes and right to health.
Prioritizing and Integrating Programming
• Effective mental health programming and services are implemented at the community, facility, and government levels, with systems and networks developed among key actors to form a fully integrated system with comprehensive services—from awareness raising to case management and treatment—to ensure a systematic approach to improving outcomes.
• Advocacy is key for investment in these MHPSS and SGBV services, especially for development of national strategies and policies implemented in a comprehensive network of referrals.
• Mental health programming is most successful when blended into other programming to help mask stigmatized services.
COVID-19 Considerations
• As COVID-19 continues to exacerbate the many challenges experienced by vulnerable populations, including REM populations, it is important to ensure that vulnerable populations have access to services, protective equipment (e.g., masks), and education about the virus’s spread.
Recommendations
The team presents the following recommendations for future REM health programming in the five countries covered by the assessment:
1. REM health programming should not directly target REM populations but rather provide broad, area-based assistance through supporting all vulnerable groups in a community or geographic area.
2. REM health programming should use a multidisciplinary and multisectoral approach in which MHPSS and SGBV services are integrated into other sectors (e.g., primary health care, legal services, vocational skills).
3. REM health programming should actively engage and partner with local organizations on the ground to provide a more comprehensive and sustainable approach to the empowerment and well-being of REM populations.

12 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
4. Community-based health programming should explore ways to retain community health worker staff after the project has ended and over the long term.
5. REM health programming should work through and with local authorities to build their capacity and improve sustainability of health service approaches.
6. MHPSS and SGBV programming should include advocacy with national-level stakeholders to influence political buy-in, strategy, budget, policy, leadership, and human resources for improved health outcomes.
7. REM health programming in the region should support the Ministry of Health and other stakeholders to build a local resource pool of experts who can conduct continuing medical education and provide technical and supportive supervision assistance to health facilities, especially for MHPSS and GBV services.

13 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
INTRODUCTION
This assessment examines the health status and needs of religious and ethnic minority (REM) communities in five countries: Egypt, Iraq, Jordan, Lebanon, and Syria. Under the Middle East and North Africa (MENA) Monitoring, Evaluation, and Learning Services Activity (MELS), Management Systems International (MSI) conducted this assessment to help inform the United States Agency for International Development’s (USAID’s) implementation of the Office of the Vice President’s initiative to support MENA REM communities.
PURPOSE
The purpose of this assessment is to learn about the overall strengths and weaknesses in the delivery of health services to REM populations in the MENA region through focusing on the five target countries. This assessment will contribute to the understanding of the target populations’ health status as well as gaps and strengths of the health system to help identify needs to be considered for future REM health programming at USAID. Recommendations will inform future investment and programming.
FOCUS COUNTRIES AND POPULATIONS
The assessment will focus on the following key REM populations and geographic areas within each country:
Country REM Communities Geographic Areas
1 Northeast Syria
Christian (Assyrian, Chaldean, Syriac, Greek, and Armenian), Yazidi, Kurd, and Turkman
Northeast Syria (excluding regime-held areas and geographic zones part of Operation Peace Spring), including Al-Hasakeh and Raqqa governorates
2 Iraq
Christian (Assyrian, Chaldean, Syriac, and Armenian), Yazidi, Kurd, Kaka’I, Turkman, Shabak, Sabean-Mandaeans
Nineveh Governorate, Kurdistan Region of Iraq (KRI), Mosul and Baghdad
3 Lebanon Christian (Maronite, Greek, Armenian, Syriac, and Chaldean), Druze, Palestinian, and Syrian
Bekaa, Mount Lebanon, and North governorates; Beirut
4 Jordan Palestinian, Christian (Greek, Maronite, Armenian, Syriac, and Chaldean), Druze, Syrian, Iraqi
Zarqa, Amman, Irbid, Al Balqa, and Mafraq governorates
5 Egypt Jewish, Christian (Coptic, Armenian, Greek, Syriac) Bahai, Berber, Bedouin, Nubian and Refugees
Minya, Assuit, Sohag, Aswan, Matruh, North Sinai and South Sinai governorates; and Cairo and Alexandria
ASSESSMENT QUESTIONS
This assessment addresses the following assessment questions (AQs) for each of the five selected countries and across the region.
1. What is the overall current health status of REM communities?
2. What are the primary health care system strengths and weaknesses at the community level?

14 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
3. What are the critical health needs and gaps in primary health care services for the REM communities in the region?
a. Are different sets of services needed by REM communities in conflict-affected areas (e.g., sexual and gender-based violence (SGBV) services, mental health care)?
b. What are the main barriers for REM communities in accessing various types of health services?
4. What external stresses impact the ability to provide health services and achieve outcomes?
5. What are the relevant lessons learned from other projects and donors on improving primary health care services for vulnerable populations in the region?
a. Is the Advancing Partners and Communities (APC)/International Medical Corps (IMC) model as implemented in the Nineveh Plains in Iraq replicable in other REM communities across the broader region?
The assessment will focus mainly on the primary health care system—including public and private health service delivery—at the local and community level as this is where most REM populations seek services.
DATA COLLECTION AND ANALYSIS METHODS
The team collected secondary data through a Google search of published research and studies as well as research produced by USAID, its implementing partners, and other donor or research organizations. The team also searched key health information available online and reached out to USAID missions for information on their REM and health programming.
The assessment team also conducted group interviews with USAID staff from most of the relevant missions (Iraq, Jordan, Lebanon, and Syria). The team developed and used an interview guide to provide context and further understanding of the health situation in the REM communities and learn about current REM health programming. Interviews lasted one hour each; a list of interview participants is provided in Annex 2. The assessment team also requested relevant documents from USAID that could be useful in answering the questions (e.g., project documents or data).
The team reviewed all collected reports, data, and interview notes and extracted relevant data and information to answer each assessment question. All extracted information was reviewed, organized, and synthesized. The assessment team used descriptive analysis for any available secondary data to report on numbers, frequencies, or percentages of health services or statuses. See more details on the assessment approach in scope of work (SOW) Annex 1.
DATA LIMITATIONS
The assessment’s main limitation is data availability. Because the assessment relied on secondary data and focused on small subsets of the population (REM populations), the assessment team had challenges finding data specifically on REM populations. In addition, many of the countries studied had limited current health data (i.e., in the last two to three years) and did not have data disaggregated by religion, ethnicity or geographic region. In addition, many of the REM populations in these countries are refugees or internally displaced persons (IDPs) and although data are available on these groups, Do No Harm considerations among humanitarian service providers preclude monitoring or reporting beneficiaries’ religions or ethnicities. To address this limitation, the assessment team collected data based on geographic locations where REM populations are known to live, when available. The team also gathered data at multiple levels to try to understand the REM populations’ situations and contexts.

15 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
NORTHEAST SYRIA FIGURE 1: MAP OF SYRIA
COUNTRY CONTEXT
More than 4 million people, including Christian, Yazidi, Kurd and Turkmen REM populations, are living in northeast Syria’s (NES) three governorates—Raqqa, Deir-ez-Zor, and Al-Hasakeh, which are governed mostly by the Self-Administration of Northeast Syria (SNES).21 Table 1 shows population estimates per governorate.22 Since 2012, the Government of Syria has maintained control over only some pockets of this territory. ISIS was driven out of the area in 2018, enabling the region to set up an autonomous administration.23
TABLE 1: POPULATIONS BY REGION OF FOCUS
Region Population Estimate
Al-Hasakeh 1,512,000
Deir-ez-Zor 1,239,005
Raqqa 94,000
21 Maxen Gharbibah and Zaki Mehchy, "COVID-19 Pandemic: Syria’s Response and Healthcare Capacity," March 25, 2020, https://eprints.lse.ac.uk/103841/1/CRP_covid_19_in_Syria_policy_memo_published.pdf 22 OCHA, "Syrian Arab Republic: Governorates Profile," June 2014, https://reliefweb.int/sites/reliefweb.int/files/resources/Syria%20governorate%20profiles%206%20August%202014.pdf 23 ACAPS, "Syria Displacement in Northeast Briefing Note," October 21, 2019, https://www.acaps.org/sites/acaps/files/products/files/20191021_acaps_start_briefing_note_syria_displacement_in_the_northeast.pdf

16 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
On October 9, 2019, Turkey launched Operation Peace Spring. Military forces entered NES, displacing 175,000 individuals, including approximately 80,000 children.24 Most of these individuals relocated to Al-Hasakeh (Table 2).25 As a result of Operation Peace Spring, 70,000 people remain displaced in NES, adding to the 710,000 displaced civilians who had already been residing there. Additional individuals displaced by the conflict in Idlib and other areas of northwest Syria continue to arrive, particularly in Raqqa.26 Most displaced persons, 4 percent of whom are children, are in areas not under government control.27
TABLE 2: PERCENTAGE OF IDPS AND REFUGEES POPULATIONS RECEIVED OCT - NOV 2019
Governorate IDPs Returnees
Deir-ez-Zor 6% 0%
Aleppo 11% 8%
Raqqa 28% 33%
Al-Hasakeh 55% 59%
Total Number 73,859 125,772
Civilians in NES are among the country’s most vulnerable, with an estimated 1.9 million people in need of humanitarian assistance, of which 910,000 are in acute need.28 An estimated 80 percent of people in Syria live below the poverty line, with high levels of food insecurity.29 According to estimates, 9.3 million people in Syria are now considered food insecure—an increase of 1.4 million in the past six months.30 Years of conflict have depleted the country’s economy and weakened delivery of basic services. Many residents have been displaced multiple times and have experienced extreme physical and mental stress due to the conflict and uncertainty, exhausting their self-reliance and increasing their dependence on humanitarian aid.31 Despite the tremendous need for assistance, only 30 percent of communities assessed throughout the three northeast Syrian governorates could access humanitarian assistance, with insufficient assistance reported among 71 percent of communities with access and the lowest levels of humanitarian assistance reported in Deir-ez-Zor. Food was the most reported type of assistance available but remained the top-ranked priority need for internally displaced persons (IDPs).32 Figure 2 shows the barriers to accessing humanitarian assistance.33
24 OHCHR, "Report of the Independent International Commission of Inquiry on the Syrian Arab Republic," January 28, 2020, https://undocs.org/A/HRC/43/57 25 OCHA, "Northeast Syria Crisis, Humanitarian Response Within Syria," October 9 - November 30, 2019, https://www.humanitarianresponse.info/sites/www.humanitarianresponse.info/files/documents/files/nes_crisis_dashboard_humanitarian_response_within_syria_09oct-30nov2019.pdf 26 UNFPA, "North-East Syria Flash Update #13," February 1–29, 2020, https://reliefweb.int/sites/reliefweb.int/files/resources/North_East_Syria_Humanitarian_Response_Flash_update_13_-_1st_-_29th_of_February.pdf 27 UN Security Council, "Review of Alternative Modalities for the Border Crossing of Ya'rubiyah," February 21, 2020, https://undocs.org/en/S/2020/139 28 UN Security Council, "Review of Alternative Modalities for the Border Crossing of Ya'rubiyah." 29 OCHA, "Syrian Arab Republic: COVID-19, Response Update No.6," June 19, 2020, https://reliefweb.int/sites/reliefweb.int/files/resources/covid-19_update_no.6.pdf 30 OCHA, "Syrian Arab Republic: COVID-19, Response Update No.6.” 31 ACAPS, "Syria Displacement in Northeast Briefing Note." 32 REACH, "Humanitarian Situation Overview in Syria (HSOS) Northeast Syria," April 2020, https://reliefweb.int/sites/reliefweb.int/files/resources/REACH_SYR_Factsheet_HSOS-Regional-Factsheet_Northeast-Syria_April2020.pdf 33 REACH, "Humanitarian Situation Overview in Syria (HSOS) Northeast Syria."

17 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
FIGURE 2: BARRIERS REPORTED IN ACCESSING HUMANITARIAN ASSISTANCE
The repeated displacement of families has left them with no choice but to return to towns and villages where public services have collapsed. There are more than 225,000 IDPs and refugees living in last-resort sites without reliable or sufficient access to essential services such as health care; water, sanitation, and hygiene (WASH); and shelter. This includes 118,879 people in 10 formal or informal camps; 41,165 people in more than 200 collective centers, most of which are former schools; and 65,264 people in 142 informal settlements.34 Because of the recent intensification of hostilities, international humanitarian organizations have reduced their presence on the ground, further compromising access to assistance.35
The conflict has continued in 2020 in areas across northeast Syria, and ongoing shelling is affecting utility operations, including water and electricity, and disrupting supply lines.36 In January 2020, when the UN Cross-Border Resolution for Syria expired, border crossings lost authorization, cutting off key routes for aid entry.37 Economic conditions have deteriorated across Syria and the prices of basic goods have risen dramatically, due partly to the limited supply of goods and the escalation of conflict. Returnees and displaced people have been experiencing food shortages and the burden of higher prices, with civilians in rural Raqqa getting only one bag of bread every three days and paying five times as much to secure their daily family needs.38
Tremendous concern has been raised by multiple international agencies and UNHCR about the catastrophic humanitarian and health conditions inside al-Hol camp in Al-Hasakeh Governorate. 39 Originally designed to host a maximum of 10,000 people, it now holds more than 69,000, of whom 44,000 (64 percent) are children and 22,080 (32 percent) are women.40 The camp’s population is 43 percent Iraqi, 42 percent Syrian, and 15 percent third-country nationals.41 The camp hosts predominantly individuals
34 NES Forum, "COVID-19 Update No.5," April 3-16, 2020, https://drive.google.com/file/d/1fcvWcF73qlA3-W0sl-wNDTb8kGqLW2tF/view 35 OHCHR, " Report of the Independent International Commission of Inquiry on the Syrian Arab Republic." 36 OCHA Syria, "Situation Report #12: Humanitarian Impact of the Military Operation in Northeast Syria," November 1-19, 2019, https://reliefweb.int/sites/reliefweb.int/files/resources/ocha_syria_sitrep_12_nes_1-19nov_final.pdf 37 REACH, "Collective Centers and COVID-19 Vulnerability," April 2020, https://reliefweb.int/sites/reliefweb.int/files/resources/REACH_SYR_NES_Hasakeh_collective_centre_COVID-19_profiles_May20.pdf 38 ICRC, "COVID-19: Millions Dealing with Sporadic Water Shortages, Crippled Health Services in North-East Syria," May 21, 2020, https://www.icrc.org/en/document/north-east-syria-millions-dealing-sporadic-water-shortages-crippled-health-services 39 OHCHR, " Report of the Independent International Commission of Inquiry on the Syrian Arab Republic." 40 M. Gharbibah and Z. Mehchy, "COVID-19 Pandemic: Syria’s Response and Healthcare Capacity." 41 Norwegian Church Aid, GOPA-DERD, and ABAAD, "Gender-Based Violence in North-East Syria Rapid Needs Assessment," December 2019, https://www.abaadmena.org/documents/ebook.1579886028.pdf
71%
21% 18%
Assistance provided was insufficient Not aware of procedures to receiveassistance
Poor targeting of beneficiaries whoreceive assistance

18 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
with familial links to ISIS—according to documented reports, discriminatory treatment on the basis of their perceived affiliation, in violation of international humanitarian law, includes the denial of access to medical care.42 The dire living conditions due to overcrowding and prevailing insecurity pose a high risk for gender-based violence (GBV), particularly against children, and transmission of communicable diseases such as COVID-19.43 Particular concern has been raised for the large number of children who lack birth registration documents, due either to their being born as a result of rape or to an inability to register their births.44 This jeopardizes their rights to a nationality, hinders family reunification processes, and puts them at a higher risk of exploitation and abuse. This concern extends to children born in other camps in northeast Syria, as the lack of civil documentation effectively renders these children stateless.45
OVERVIEW OF RELIGIOUS AND ETHNIC MINORITIES IN NORTHEAST SYRIA
Focus REM Populations in Northeast Syria: Christian (Assyrian, Chaldean, Syriac, Greek, and Armenian), Yazidi, Kurd, and Turkmen
Geographic Area of REM Populations: Northeast Syria (excluding regime-held areas and geographic zones part of Operation Peace Spring), including El-Hasakeh Governorate and Raqqa governorate
Accurate estimates of the number of REM communities in NES are not available because before the conflict, the Syrian census did not enable citizens to declare their ethnic origin. Estimates are further weakened by the highly politicized environment and competition among political entities.46 Availability of data on REM populations’ health status and access to health services is further confounded by the fact that international organizations such as the International Organization for Migration (IOM) and the United Nations High Commissioner for Refugees (UNHCR) either do not collect information on ethnicity or religious characteristics of the populations they serve or do not readily share these data with non-protection actors, likely to support conflict-sensitive programming that does not inadvertently cause harm to minority populations.47
Research conducted by USAID in December 2019 provides the most recent estimates on REM populations in this area.48,49 This research is based on semi-structured interviews with local key informants from the NES, minority civil society organizations (CSOs), churches, and a review of open-source media. The study focused solely on five urban centers in the Al-Hasakeh governorate and is therefore not generalizable to the region.
CHRISTIANS
Before the Syrian conflict, approximately 115,000 Christians were spread across NES, primarily in Al-Hasakeh, with smaller populations in Raqqa and Deir-ez-Zor. As a result of the conflict and displacements, their numbers have fallen to an estimated 60,000 to 70,000. Current estimates indicate that 21,000 Christians reside in Al-Hasakeh City; 25,000 in Qamishli; 3,500 in Al-Malikiya and Derik and the surrounding countryside; and 1,300 in Tell Tamr and the surrounding villages. In addition, the limited data
42 OHCHR, " Report of the Independent International Commission of Inquiry on the Syrian Arab Republic." 43 UN News, Health Services for Syrian Women Caught Up in War, Foster Safety and Hope: UNFPA," January 23, 2020, https://news.un.org/en/story/2020/01/1055921 44 OHCHR, ""They Have Erased the Dreams of My Children": Children's Rights in the Syrian Arab Republic," January 13, 2020, https://www.ohchr.org/EN/HRBodies/HRC/Pages/NewsDetail.aspx?NewsID=25465&LangID=E 45 OHCHR, ""They Have Erased the Dreams of My Children": Children's Rights in the Syrian Arab Republic." 46 USAID, "Syria Essential Services II, Ad Hoc Report: Status of Vulnerable Religious and Ethnic Minority Communities in NES," December 17, 2019 47 Ibid. 48 Ibid. 49 USAID, "Syria Essential Services II, Ad Hoc Report: Status of Vulnerable Religious and Ethnic Minority Communities in NES."
19 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
available indicate that a small number of Christians, particularly Armenians, reside in Al-Raqqa City, Al-Tabqah, and Deir-ez-Zor City. Reports indicate that those residing in larger urban centers, particularly in Hasakeh, are represented by a diverse array of political parties, churches and religious bodies, and REM-affiliated CSOs and NGOs.
The main Christian groups are Assyrians, Syriacs, Chaldeans, and Armenians, with Syriac Christians representing the majority. Syriac Christians are divided among several denominations and may refer to themselves ethnically as Syriac, Assyrian, and Chaldean. The largest denomination among the Syriac Christian population in NES is Syriac Orthodox, also known as Syriacs. The Assyrian Church of the East and Chaldean Catholic denominations are also prevalent, with followers referring to themselves ethnically as Assyrian or Chaldean, respectively. Armenian Christians are primarily Armenian Orthodox Christians and make up the second-largest Christian community in NES. Smaller numbers of Armenian Catholics, Syriac Catholics, Protestants, and followers of the Ancient Church of the East are also present.
YAZIDIS
Pre-conflict estimates of the Yazidi population in NES vary dramatically, but conservative estimates are around 20,000–25,000. Yazidis were historically centered in villages around Al-Hasakeh City, Amuda, Kahtanieh, and Ras Al Ain. All Yazidis are believed to have fled Ras Al Ain in late 2012 and following Operation Peace Spring in October 2019, including the last 150 Yazidi families of Ras Al Ain. The systematic oppression of Yazidis has caused significant numbers to emigrate, even before the conflict, reducing current population estimates in NES to approximately 3,000–4,000 individuals. Sources indicate approximately 1,750 Yazidis in the villages north of Al-Hasakeh City; 1,000 in Kahtanieh; and 1,500 in 12 villages in the Amuda countryside. The Yazidi House, a SNES-affiliated body, provides humanitarian support to Yazidis in NES.50
Three thousand Yazidi women and girls kidnapped by ISIS in 2014 and sold as slaves in NES are still missing. 51 Many missing Yazidis have been found inside northern Syria, including at al-Hol camp. 52 Prospects for the estimated several hundred to 1,000 children born to Yazidi women who had been raped by members of ISIS cause concern, as the Yazidi elders in Iraq have declared that although the women and girls that had been captured by ISIS would be welcomed back into their communities, the children born of rape by ISIS would not.53
KURDS
Sunni Kurds are believed to have constituted roughly 10 percent of Syria’s prewar population (around 2 million), making up Syria’s largest minority. Estimates from 2016 indicate that Kurds make up 55 percent of the population of Hasakeh and the northern areas of Raqqa.54 Reports indicate that most Kurds are not discriminated against under the SNES. However, Kurds that oppose the Democratic Union Party, which is linked to the SNES, have reportedly been subject to political repression, increasing their
50 USAID, "Syria Essential Services II, Extended Ad Hoc Report: The Status of Minority and Vulnerable Groups in Raqqa, Deir Ez-Zor, and Hassakeh." 51 Nisan Ahmado, "Coronavirus Measures Delay Yazidi Survivor’s Reunion with Family," VOA, April 25, 2020, https://www.voanews.com/extremism-watch/coronavirus-measures-delay-yazidi-survivors-reunion-family 52 Ahmado, N., "Coronavirus Measures Delay Yazidi Survivor’s Reunion with Family." 53 Jane Arraf, "In Syria, An Orphanage Cares for Children Born to Yazidi Mothers Enslaved By ISIS," npr, June 6, 2019, https://www.npr.org/2019/06/06/729972161/in-syria-an-orphanage-cares-for-children-born-to-yazidi-mothers-enslaved-by-isis 54 Fabrice Balanche, "Rojava's Sustainability and the PKK's Regional Strategy", The Washington Institute, April 24, 2016, https://www.washingtoninstitute.org/policy-analysis/view/rojavas-sustainability-and-the-pkks-regional-strategy

20 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
vulnerability. Furthermore, the subgroup of Kurds from Al-Hasakeh are considered stateless as the Government of Syria revoked the citizenship of 300,000 Kurds in the 1960s.55
TURKMEN
Sunni Turkmen communities are located predominantly in Raqqa within areas now under Turkish control. Reliable estimates on their numbers—either current or pre-conflict—do not exist. However, reports from 2015 indicate that roughly 1,000 to 1,400 Turkmen resided close to the Turkish border and have likely fled to other areas within NES or into southern Turkey.
RELIGIOUS AND ETHNIC MINORITY GEOGRAPHIC FOCUS
Like most of Syria, NES has a majority Sunni Arab population. However, Raqqa and Hasakeh host diverse REM populations, including Sunni Kurds, various Christian denominations (predominantly Assyrians, Syriacs, Chaldeans, and Armenians), Yazidis, Circassians, Turkmen, and Alawites. In contrast, Deir-ez-Zor’s population is largely homogeneous, with only small communities of Christians and Shi‘a Arab Muslims.56 The geographic distribution of REM populations can be identified on the map found in Annex 3. The years of conflict in Syria, particularly the invasion by ISIS and other militant groups, have caused mass displacements, both internally and externally, greatly reducing ethnoreligious minority populations, especially in Raqqa and Deir-ez-Zor. The presence of Turkish-backed armed groups inside northern Syria has caused another wave of displacements, affecting the remaining Christian groups that resided in areas impacted by Operation Peace Spring. Areas within Al-Hasakeh have received the most significant numbers of displaced populations. Members of REM communities in these areas believe that gradual emigration of their populations will continue due to the region’s instability and economic challenges. REM representatives living in NES indicate that they have experienced not only safe refuge but also a substantial degree of religious freedom, gender equality, and representation in local governing bodies.57
AQ 1: OVERVIEW OF HEALTH STATUS IN SYRIA
As much of the northeast Syrian population has been displaced multiple times and experienced years of living in a conflict zone, malnutrition and poor health are common. Life expectancy at birth is 59 years for males and 69 years for females.58 Medical needs are profound, especially for pediatrics, surgery, and mental health care, as the population has been exposed to repeated trauma and extreme stress.59 Chronic diseases are the most commonly reported health problem and their treatment is the most commonly reported health need (Figures 3 and 4).60
55 Taghee Moas, "Documentary on The Stateless Kurds of Syria," Rudaw, September 29, 2011, https://web.archive.org/web/20120511094112/http:/www.rudaw.net/english/news/syria/4003.html 56 USAID, "Syria Essential Services II, Extended Ad Hoc Report: The Status of Minority and Vulnerable Groups in Raqqa, Deir Ez-Zor, and Hasakeh." 57 USCIRF, "Syria - Recommended Countries of Particular Concern," 2019, https://www.uscirf.gov/sites/default/files/Tier1_SYRIA_2019.pdf 58 https://www.who.int/countries/syr/en/ 59 M. Gharbibah and Z. Mehchy, "COVID-19 Pandemic: Syria’s Response and Healthcare Capacity." 60 REACH, "Humanitarian Situation Overview in Syria (HSOS) Northeast Syria."

21 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
FIGURE 3: MOST COMMONLY REPORTED HEALTH PROBLEMS
FIGURE 4: MOST COMMONLY REPORTED HEALTH NEEDS
WOMEN’S HEALTH
Maternal mortality, risk of miscarriage, premature labor, and undernourishment have all been exacerbated by the Syrian conflict due to the failing health care system and its shortages of medical supplies, qualified staff, and functioning facilities. Maternal mortality has risen by up to 40 percent, with increases also reported in the rate of miscarriages and undernourished mothers.61 Although the maternal mortality rate for all of Syria is 68 deaths per 100,000 live births, this number is probably much higher for women in NES
61 Human Appeal, "Risking Death to Give Birth," May 15, 2020, https://reliefweb.int/sites/reliefweb.int/files/resources/syria-report-website.pdf
83%
39% 38% 37%
Chronic Diseases Pregnancy-RelatedComplications
Diarrhea Leishmaniasis
52%
44%42%
Treatment for Chronic Diseases Skilled Care During Birth First Aid or Emergency Care

22 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
due to nutritional challenges and lack of access to health care.62 The risk of maternal mortality is also highest for adolescent girls under 15, particularly in NES given the high rate of adolescent marriages.63 Females make up 72 percent of people in need of health assistance in Syria, out of which 5.2 million women of reproductive age are in need of reproductive, maternal, and child health services. 64 Among IDP households in Al-Hasakeh, 26 percent are headed by females.65
Pregnant and lactating women are particularly vulnerable due to their specific nutritional needs and health risks. Data on nutrition screening in 2018 confirmed that moderate acute malnutrition rates among pregnant and lactating women had risen by 134 percent.66 World Health Organization (WHO) reports for 2019 highlight the enhanced vulnerabilities to acute malnutrition in Raqqa and Deir-ez-Zor due to lack of access to health services and harmful coping strategies such as meal reduction.
Among residents in Al-Hasakeh Governorate, 55 percent of IDPs residing in collective shelters report not having enough food to meet their needs.67 The highest barriers to accessing food are reported in Deir-ez-Zor, followed by Raqqa and the top barriers reported by both IDPs and residents was the inability to afford essential food items (about 75 percent) and that markets did not have all the food items available (about 30 percent).68
On feeding babies under six months of age, 78 percent of respondents indicated that there were no alternatives for non-breastfed babies and 52 percent reported breastfeeding difficulties. On feeding young children, 91 percent of respondents could not afford the prices of suitable foods and 60 percent indicated there was not enough variety of food available.69 The most commonly reported coping strategy for lack of food was to borrow money or buy food on credit, which was reported among 72 percent of respondents.70
CHILDREN’S HEALTH
Children in NES face many health challenges from years of exposure to conflict and violence, with high rates of stunting (28 percent) and infectious diseases and low rates of immunization (14 percent). The infant mortality rate is 14 deaths per 1,000 live births (Table 3). However, anecdotal evidence suggests poorer health outcomes among children in NES. In al-Hol camp, 400 children died between March and September 2019—a third of these children did not reach health facilities and died in tents. The main causes of death are severe malnutrition, diarrhea with dehydration and pneumonia. 71 In addition, children also face problems at home, with about 89 percent of children aged 1–14 years experiencing physical punishment and/or psychological aggression by caregivers. 72
62 CIA, "World Factbook: Syria," Accessed June 22, 2020, https://www.cia.gov/library/publications/the-world-factbook/geos/sy.html 63 Human Appeal, "Risking Death to Give Birth.” 64 UN, "2019 Humanitarian Response Plan," January - December 2019, https://www.humanitarianresponse.info/sites/www.humanitarianresponse.info/files/documents/files/2019_hrp_syria.pdf 65 REACH, "Rapid Needs Assessment of IDPs in Host communities, Hasakeh Governorate, Northeast Syria." 66 UN Strategic Steering Group, "2019 Humanitarian Needs Overview," March 2019, https://hno-syria.org/data/downloads/en/full_hno_2019.pdf 67 REACH, "Rapid Needs Assessment of IDPs in Host communities, Hasakeh Governorate, Northeast Syria." 68 REACH, "Humanitarian Situation Overview in Syria (HSOS) Northeast Syria." 69 Ibid. 70 REACH, "Humanitarian Situation Overview in Syria (HSOS) Northeast Syria." 71 IRC, "IRC Data Reveals Staggering Child Mortality in Al Hol Camp, Northeast Syria - Urging Repatriation of Foreign Children," September 16, 2019, https://reliefweb.int/report/syrian-arab-republic/irc-data-reveals-staggering-child-mortality-al-hol-camp-northeast-syria 72 Vernier, L., Cramond, V., Hoetjes, M. et al. “High levels of Mortality, Exposure to Violence and Psychological Distress Experienced by the Internally Displaced Population of Ein Issa Camp Prior to and During their Displacement in Northeast Syria,” November 2017. Conflict and Health 13, 33 (2019). https://doi.org/10.1186/s13031-019-0216-y

23 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
TABLE 3: INDICATORS OF CHILD HEALTH
Indicator Value
Infant mortality rate 14 deaths/1,000 live births
Under-five mortality 17 deaths/1,000 live births
Stunting (height-for-age) Children >2 years of age (2010) 28%
Children aged 24–59 months fully immunized73 14%
Historical data indicate that chronic malnutrition was a problem in Syria even before the crisis, but the proportion of the population without reliable access to food has risen by 20 percent in the last year, resulting in chronic malnourishment among half a million children across Syria.74 Due to hostilities, gaps in nutritional programming coverage, and low availability of partners implementing nutrition programs, malnutrition continues to be a challenge. According to UNICEF, given the severity of malnutrition, NES needs more nutritional humanitarian assistance than any other area in Syria.75
In areas with newly displaced populations, acute malnutrition of children under five years of age rapidly increased within six months (from 1.5 percent to 4 percent), and in hard-to-reach areas such as Raqqa, acute malnutrition nearly tripled (from 4.6 percent to 11.9 percent) in 2018. In 2019, 32 percent of children of the Tel Abiad region of northern Raqqa had “very high” stunting, according to UNICEF.76
MENTAL HEALTH
In 2020, the UN Commission of Inquiry published a report on the Syrian war’s impact on children that measured the negative effects of war, displacement, and trauma on their mental health. Among children under 15 living in Ein Issa camp in Raqqa, 20 percent have been exposed to at least one violent episode and 10 percent have witnessed atrocities (such as public floggings, executions, and public dead body displays).77 Many children described how they suffer from serious sleeping disorders, as well as feelings of insecurity, abandonment, revenge, frustration, and fear, with caregivers reporting that 20 percent of children aged 5–12 were bedwetting on at least two occasions in the two weeks prior to the survey.78 Several generations of children are accustomed to living in distress, with devastating long-term psychological and developmental consequences for them and for their caregivers.79 UNICEF reports also indicate prevalence of psychological distress among recently displaced children and women in northeast
73 Vernier, L., Cramond, V., Hoetjes, M. et al. “High levels of Mortality, Exposure to Violence and Psychological Distress Experienced by the Internally Displaced Population of Ein Issa Camp Prior to and During their Displacement in Northeast Syria,” November 2017. Conflict and Health 13, 33 (2019). https://doi.org/10.1186/s13031-019-0216-y 74 OCHA, "Syria Anniversary Press Release," March 6, 2020, https://reliefweb.int/sites/reliefweb.int/files/resources/USG%20Lowcock%20Syria%20Anniversary%20PR_%2006032020.pdf 75 UN, "2019 Humanitarian Response Plan." 76 Ibid. 77 Vernier, et al. “High levels of Mortality, Exposure to Violence and Psychological Distress Experienced by the Internally Displaced Population of Ein Issa Camp Prior to and During their Displacement in Northeast Syria.” 78 Vernier, et al. “High levels of Mortality, Exposure to Violence and Psychological Distress Experienced by the Internally Displaced Population of Ein Issa Camp Prior to and During their Displacement in Northeast Syria.” 79 OHCHR, ""They Have Erased the Dreams of My Children": Children's Rights in the Syrian Arab Republic."
ACF
Highlight
MHPSS

24 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
Syria and the great need for specialized mental health counseling services and referrals.80 Figure 5 highlights the most commonly observed behavior changes among children.81
FIGURE 5: MOST COMMONLY REPORTED TYPES OF BEHAVIOR CHANGE AMONG CHILDREN
Data available on civilians living in camps in Raqqa indicate that 38 percent of people over two years of age were so distressed/disturbed/upset in the two weeks before the survey that they were completely or almost completely inactive because of these feelings. 82 Furthermore, 32 percent of residents had experienced at least one violent episode in the previous year, with 19 percent of the population having witnessed atrocities. Sixteen percent of men over 14 had been detained/kidnapped and 11 percent had been tortured, beaten, or attacked. In the two weeks prior to interview, 14 percent of the respondents felt so hopeless that they did not want to carry on living most of the time.83 Among IDPs in host communities in Hasakeh, 56 percent reported needing psychosocial support and 43 percent reported needing psychological first aid.84
SEXUAL AND GENDER-BASED VIOLENCE
Sexual and gender-based violence (SGBV) is reported among all segments of the population, particularly in Al-Hasakeh, where many REM communities are located. According to research conducted in December 2019 covering Hasakeh and Deir-ez-Zor, 60 percent of service providers in Al-Hasakeh indicated an increase of sexual violence and rape in recent months.85 About 93 percent of key informants in Hasakeh reported women and girls with disabilities to be at the highest risk of being a victim; in Deir-ez-Zor, 84
80 UNICEF, "North East Syria Response - Situation Report," October 10-27, 2019, https://www.unicef.org/mena/media/5966/file/North%20East%20Syria%20Response#10%20-%2027%20October%202019.pdf 81 REACH, "Rapid Needs Assessment of IDPs in Host communities, Hasakeh Governorate, Northeast Syria." 82 Vernier, et al. “High Levels of Mortality, Exposure to Violence and Psychological Distress Experienced by the Internally Displaced Population of Ein Issa Camp Prior to and During their Displacement in Northeast Syria.” 83 Ibid. 84 REACH, "Rapid Needs Assessment of IDPs in Host communities, Hasakeh Governorate, Northeast Syria." 85 Norwegian Church Aid, GOPA-DERD, and ABAAD, "Gender-Based Violence in North-East Syria Rapid Needs Assessment.”
74%
60%
36%
26%20% 18%
Feeling afraid Feelings ofsadness
Feelings ofisolation
Difficultysleeping
Frequentnightmares
Violencetowards other
children
ACF
Highlight
ACF
Highlight
ACF
Highlight
ACF
Highlight

25 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
percent believed that adolescent girls were the most targeted group. Women reported feeling most vulnerable to attack when on the way to latrines.
Syria has a high rate of forced child marriage, reported at 81 percent in Al-Hasakeh; sexual violence against girls is reported at 65 percent in Al-Hasakeh and 93 percent in Deir-ez-Zor. Adolescent girls are forced into early marriage by parents to protect them against sexual violence, abuse, and exploitation and to cope with financial difficulties. Research findings indicate that early marriage often results in marital rape of adolescent girls. Commercial/survival sex to cope with financial difficulties is also reported to be increasing. Respondents reported a high tendency to blame women victims of sexual violence, which results in a low likelihood of victims reporting incidents. Fears of household imprisonment and honor killings were also reported to impede women from reporting sexual violence. Al-Hol camp has even higher levels of physical and sexual violence, in addition to reports of kidnapping for human or organ trafficking.86
In Deir-ez-Zor, 80 percent of respondents reported a risk of militarization or forced conscription of boys.87 Ninety-five percent of men in Al-Hasakeh and 81 percent of men in Deir-ez-Zor reported facing psychological violence. In Al-Hasakeh, 57 percent of men reported experiencing physical violence and 52 percent reported fears of forced conscription. Men in Al-Hasakeh and Deir-ez-Zor reported that most instances of sexual violence against men and boys involved militia.
The effects of self-isolation and quarantine, lockdown, and movement restrictions in response to COVID-19 heighten the risks of SGBV. The United Nations Population Fund (UNFPA) reports that GBV is increasing globally due to the containment measures, as evidenced by the reported 54 percent rise in harassment, violence, or abuse against women and girls in vulnerable communities in Lebanon since the COVID-19 outbreak.88
OUTBREAK/EPIDEMIC DATA
The weak health care system, combined with major gaps in the availability of safe water, has resulted in several outbreaks of infectious disease in the past few years. Poor hygiene conditions have contributed to the prevalence of diseases such as acute jaundice syndrome and acute bloody diarrhea.89 According to Early Warning Alert and Response Network (EWARN) data, the highest number of morbidities between January and May 2020 were reported in Deir-ez-Zor with 14,499 cases; 6,873 cases were reported in Al-Hasakeh and 6,508 in Raqqa (Table 4). Influenza-like illnesses and non-bloody acute diarrhea accounted for the majority of cases; acute flaccid paralysis and measles were the least commonly reported cases to EWARN, but their existence among the population causes concern and indicates poor sanitary conditions and low immunization rates.90 As testing facilities in NES are limited, epidemic surveillance monitoring is conducted through a syndromic approach. Transmission of acute flaccid paralysis is indicative of possible polio transmission, while influenza-like illnesses indicate possible COVID-19 transmission.
86 Ibid. 87 Ibid. 88 ABAAD, Care, DRC, IRC, Intersos, UNHCR, UNICEF, UNFPA and UN Women, "Impact of the COVID-19 on the SGBV Situation in Lebanon," 2020, https://data2.unhcr.org/en/documents/download/76732 89 Rojava Information Center, "The Coronavirus Crisis in North and East Syria," April 19, 2020, https://rojavainformationcenter.com/2020/04/coronavirus-crisis-in-north-and-east-syria-22-april-update/ 90 Assistance Coordination Unit, "Epidemiological Weekly Bulletin - Syria, EWARN Week 23, 2020," May 31 - June 6, 2020, https://www.acu-sy.org/en/wp-content/uploads/2015/05/EWARN-EpiBull-2020W23.pdf

26 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
TABLE 4: COMMONLY REPORTED MORBIDITIES, JANUARY 1 – MAY 9, 2020
Data reveal significant rates of morbidity from diseases preventable by vaccine or proper hygiene practices (Figure 6).91 Vaccination coverage is low at only 10 percent in Raqqa and 20 percent in Deir-ez-Zor.92 Leishmaniasis is a significant health issue, especially in Deir-ez Zor, which reported 5,566 cases between January and May 2020. Leishmaniasis is often associated with migration, displacement, poverty, and poor sanitary conditions, which facilitates disease transmission, particularly among people with weak immune systems. Reports indicate that medical organizations operating in NES are unable to provide sufficient treatment for Leishmaniasis.93
FIGURE 6: NUMBER OF REPORTED CASES, MAY 31 - JUNE 6, 2020
ACCESS TO WATER, SANITATION, AND HYGIENE
Water shortages remain one of the civilian population’s main concerns. Many families returned to heavily damaged neighborhoods where the water network had been affected by military operations. There has
91 Assistance Coordination Unit, "Epidemiological Weekly Bulletin - Syria, EWARN Week 23, 2020.” 92 UN, "2019 Humanitarian Response Plan." 93 Dejla Khalil, "500 Leishmaniasis Infections in Aleppo, Drugs Insufficient," North Press Agency, May 9, 2020, https://npasyria.com/en/blog.php?id_blog=2491&sub_blog=4%20&name_blog=500%20leishmaniasis%20infections%20in%20Aleppo,%20drugs%20insufficient
1,116
1,893
640436
2,040
748255
1,393
3,107
451 524778913
2,310
5,566
215
1,419
4,076
Acute BloodyDiarrhea
Acute JaundiceSyndrome
Leishmaniasis Meningitis Severe AcuteRespiratory Illness
Suspected TyphoidFever
Al-Hasakeh Raqqa Deir-ez-Zor
Syndrome Al-Hasakeh Raqqa Deir-ez-Zor Total
Influenza-like illness 75,861 44,022 39,172 159,055
Acute diarrhea (non-bloody) 48,102 31,922 49,960 129,984
Acute flaccid paralysis 12 14 29 55
Measles 7 14 1 22

27 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
been a huge need to support water authorities, carry out urgent repairs, provide necessary equipment for water treatment, and supply camps with clean water.94 Figure 7 shows the main WASH challenges.95,96
FIGURE 7: WASH RESTRICTIONS IN NORTHEAST SYRIA
Damages to the main water station in Al-Hasakeh (the only source for drinking water for approximately 800,000 people) and restricted access to clean drinking water have contributed to the high prevalence of infectious diseases.97 Despite repairs to the main water station, Al-Hasakeh residents have access to water for only several hours a day. Residents in rural areas, including the villages where Yazidis reside, rely on private wells for water. Local sources report that several of these wells also have serious problems with their submersible pumps, prompting residents to purchase water.
The limited access to handwashing facilities increases the challenges of reducing the spread of infectious diseases, including COVID-19. Twelve percent of households in Al-Hasakeh had no access to functioning handwashing facilities, and 8 percent did not have latrines (Figure 8).98,99 In 50 percent of collective shelters in Al-Hasakeh, not everyone had enough water to meet their daily needs, 32 percent have issues with water quality, 66 percent do not have bathing facilities, and 27 percent have access only to communal bathing facilities.100 Residents of Al-Hasakeh City and Qamishli City pay the SNES, the Government of Syria, or both depending on whether they live in a SNES or Government of Syria–held neighborhood, paying each approximately $1.25 every two months regardless of usage.101
94 ICRC, "COVID-19: Millions Dealing with Sporadic Water Shortages, Crippled Health Services in North-East Syria," May 21, 2020, https://www.icrc.org/en/document/north-east-syria-millions-dealing-sporadic-water-shortages-crippled-health-services 95 REACH, "Humanitarian Situation Overview in Syria (HSOS) Northeast Syria." 96 REACH, "Rapid Needs Assessment of IDPs in Host communities, Hasakeh Governorate, Northeast Syria." 97 ICRC, "COVID-19: Millions Dealing with Sporadic Water Shortages, Crippled Health Services in North-East Syria.” 98 REACH, "Northeast Syria: COVID-19 Multi-Sectoral Rapid Needs Assessment," April 2020, https://www.impact-repository.org/document/reach/3d6d5dfe/REACH_SYR_Factsheet_COVID-19-Rapid-needs-assessment-in-northeast-Syria_April2020.pdf 99 REACH, "Collective Centers and COVID-19 Vulnerability." 100 Ibid. 101 USAID, "Syria Essential Services II, Ad Hoc Report: Status of Vulnerable Religious and Ethnic Minority Communities in NES."
49%
70%
30%
16% 15%
Restricted access tosufficient water
No sewage system Not connected to mainwater network
IDPs with no access tosafe drinking water
IDPs with insufficientquantity of safe drinking
water

28 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
FIGURE 8: PROPORTION OF RESIDENTS IN COLLECTIVE SHELTERS IN AL-HASAKEH WITH ACCESS TO HANDWASHING FACILITIES
In Deir-ez-Zor, the destruction also extended to the water supply system, and most water treatment plants, stations, and networks have been out of service. Gaps are extensive in informal settlement coverage, where the risk of disease transmission is particularly high due to substandard sanitation and poor hygiene practices.102 Deir-ez-Zor consistently records some of the highest levels of proportionate morbidity for acute jaundice syndrome and acute diarrhea.103
Seven percent of Raqqa households reported not having access to functioning handwashing facilities.104 Raqqa residents receive water once a week from the main water station, and in rural areas families often resort to filling their own personal trucks directly from the Euphrates River to compensate for a lack of water from the main station. In most areas, even those with access to publicly supplied water services, residents must pay for water supplies. Reported barriers to accessing sufficient water, included 44 percent reported high prices of water trucks, 38 percent reported the main network was particularly or completely non-functioning and 36 percent reported insufficient pressure to pump well water.105
OTHER HEALTH ISSUES
The heavy explosive hazard contamination across Syria has driven up trauma-related health complications and disability levels. An estimated 10.2 million Syrians are at risk of being injured by explosive hazards. People on the move are exposed to high levels of this hazard, especially in areas that were retaken from ISIS, such as Raqqa. A 2019 assessment on disability among adults in Raqqa, western Aleppo, and Idlib Governorates found that 30 percent of the population was disabled.106 The assessment found that an average of 45 percent of people surveyed were expected to sustain permanent physical impairment (e.g., amputation, spinal cord injury, brain injury) as a result of hostility-related injuries.107
102 NES Forum, "COVID-19 Update No.5." 103 NES Forum, "COVID-19 Update No.5." 104 REACH, "Northeast Syria: COVID-19 Multi-Sectoral Rapid Needs Assessment." 105 REACH, "Humanitarian Situation Overview in Syria (HSOS) Northeast Syria." 106 UN Strategic Steering Group, "2019 Humanitarian Needs Overview." 107 UN, "2019 Humanitarian Response Plan."
30%
20% 20%
16%14%
Everyone Most (~75%) About half (~50%) A few (~25%) Nobody (~0%)

29 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
There are approximately 21,000 persons with disabilities in Al-Hasakeh,108 with civilian casualties due to improvised explosive devices (IEDs) occurring in the northern areas of Al-Hasakeh Governorate.109 Between December 2017 and August 2018, 581 blast injury cases were documented in Raqqa and 106 in Al-Hasakeh and Deir-ez-Zor.110 More than 60 percent of persons with disabilities interviewed in 2018 stated that their disability was exacerbated by the crisis and that a lack of access to health care and assistive devices and difficulties in meeting their basic needs were the most common reasons.111 Primary barriers for persons with disabilities to access essential health services are ancillary costs, including transportation, and distance to health care facilities.
CONCLUSIONS
The ongoing Syrian crisis has had detrimental effects on the population’s health, particularly in northeast Syria. Children have been forced to witness a brutal war and have been left acutely vulnerable to violence, abuse, and mental health challenges. Further escalation of conflict leading to increased displacement, overcrowded living conditions, and lack of WASH services will exacerbate the many health challenges. Acute food shortages are negatively impacting health among all populations, particularly mothers and children, raising concerns of permanent disabilities among stunted children. The WFP has indicated that in 2020 there is a real possibility of famine in Syria, which is further compounded by the ongoing economic crisis and the challenges created by COVID-19.112 The combination of all these factors is also contributing to a rise in SGBV.
AQ 2: PRIMARY HEALTH CARE SYSTEM STRENGTHS AND WEAKNESSES
Most health facilities in northeast Syria are not functioning or are only partially functioning. Out of 16 public hospitals, only 1 is fully functioning, 8 are partially functioning, and 7 are not functioning at all, according to the consolidated Health Resources Availability Monitoring System (HeRAMS).113 Of the 279 primary health centers across NES, only 4 are functioning at full capacity and 22 at partial capacity.114,115 None of the districts meet the emergency threshold of at least 10 hospital beds per 10,000 people, and there are only 22 ICU beds available in all of NES, including those in both public and private hospitals. Of the available ICU beds, 18 are in Al-Hasakeh and 4 are in Raqqa.116
IDP camps are putting an additional burden on the already weak health system. In the camps, where an estimated two-thirds of the population are children, the enormous medical needs include maternal and child health care, mental health care, surgery, and physical rehabilitation.117 An estimated 1.8 million people are in need of health assistance in NES (Figure 9).118 Of those in need in Deir-ez-Zor, estimates indicate that 96 percent are in critical need of health care.
108 UNFPA, "North-East Syria Flash Update #13.” 109 OCHA Syria, "Situation Report #12: Humanitarian Impact of the Military Operation in Northeast Syria," November 1-19, 2019, https://reliefweb.int/sites/reliefweb.int/files/resources/ocha_syria_sitrep_12_nes_1-19nov_final.pdf 110 UN Strategic Steering Group, "2019 Humanitarian Needs Overview." 111 Ibid. 112 UN Security Council, "Senior Officials Sound Alarm over Food Insecurity, Warning of Potentially ‘Biblical’ Famine, in Briefings to Security Council," April 21, 2020, https://www.un.org/press/en/2020/sc14164.doc.htm 113 ICRC, "COVID-19: Millions Dealing with Sporadic Water Shortages, Crippled Health Services in North-East Syria.” 114 UN Security Council, "Review of Alternative Modalities for the Border Crossing of Ya'rubiyah." 115 Rojava Information Center, "The Coronavirus Crisis in North and East Syria." 116 Gharbibah, M., and Mehchy, Z., "COVID-19 Pandemic: Syria’s Response and Healthcare Capacity." 117 ICRC, "COVID-19: Millions Dealing with Sporadic Water Shortages, Crippled Health Services in North-East Syria.” 118 UN Strategic Steering Group, "2019 Humanitarian Needs Overview."

30 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
FIGURE 9: ESTIMATED NUMBER OF PEOPLE IN NEED OF HEALTH CARE ASSISTANCE
HEALTH WORKFORCE
Roughly 70 percent of Syria’s health workers have left the country as migrants or refugees due to the ongoing crisis,119 drastically reducing the number of qualified health personnel, particularly specialized staff. Throughout Syria, there are only 0.41 psychiatrists per 100,000 people.120 Even compared with other areas of Syria, health care capacity in NES is particularly low. Of the 10 northeast Syrian districts, only 1 meets the emergency threshold of at least 22 health care workers per 10,000 people.121 Low workforce capacity also limits health service delivery,122 which therefore depends largely on humanitarian staff. Approximately 6,250 humanitarian staff work in NES, with 16 NGOs and three UN agencies operating in the health sector.123 Figure 10 shows the breakdown of staff operating at health facilities supported by the UN across all of Syria, highlighting the low level of physicians and specialized health professionals operating in Syria and the high dependence on nurses.124
119 M. Gharbibah and Z. Mehchy, "COVID-19 Pandemic: Syria’s Response and Healthcare Capacity." 120 ACAPS, "Syria Displacement in Northeast Briefing Note.” 121 NES Forum, "COVID-19 Update No.5." 122 OCHA Syria, "Situation Report #12: Humanitarian Impact of the Military Operation in Northeast Syria." 123 UN Security Council, "Review of Alternative Modalities for the Border Crossing of Ya'rubiyah." 124 Health Sector Syria, "Health Sector Bulletin," January 2020, https://reliefweb.int/sites/reliefweb.int/files/resources/Syria-Health-Sector-Bulletin-Jan-2020.pdf
614,500
501,503
644,819
Deir-ez-Zor
Raqqa
Al-Hasakeh

31 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
FIGURE 10: BREAKDOWN OF HEALTH STAFF BY ROLE
Humanitarian organizations experience serious challenges in negotiating safe access to the region and must contend with constantly changing armed actors.125 Kurdish groups report that medical personnel have been targeted throughout the Turkish operation in the area, estimating that five medical personnel were killed in the first month following Operation Peace Spring and at least seven were injured.126 Of those killed, three were abducted and executed and two died in drone strikes.
SERVICE DELIVERY
It is estimated that more people in Syria have died from a lack of access to health care, medicine, and nutrition than directly from the violence.127 The already depleted health care services in NES are further strained by the ongoing conflict. People in need of essential health care and lifesaving support experience challenges in access due to insecurity and the lack of services, as 27 percent of the health services in areas covered by the SNES are unreachable.128 Physicians for Human Rights reports that through February 2020, 595 attacks were conducted on at least 350 separate health facilities throughout Syria and 923 medical personnel were killed.129 Service delivery is impacted by frequent electricity cuts and high reliance on generators.130 There are widespread shortages of medical supplies and health workers, some of whom have also been displaced by the conflict.131
Health care access varies significantly by region, and the lowest levels of access occur in Al-Hasakeh (Figure 11).132
125 ACAPS, "Syria Displacement in Northeast Briefing Note.” 126 The Guardian, "Kurdish Medics Injured in Apparent Attack on Ambulance in Syria," November 10, 2019, https://www.theguardian.com/world/2019/nov/10/kurdish-medics-injured-in-apparent-attack-on-ambulance-in-syria 127 Human Appeal, "Risking Death to Give Birth.” 128 Humanitarian Needs Assessment Programme, "COVID-19 Rapid Assessment, Syrian Democratic Forces Controlled Areas." 129 M. Gharbibah and Z. Mehchy, "COVID-19 Pandemic: Syria’s Response and Healthcare Capacity." 130 ICRC, "COVID-19: Millions Dealing with Sporadic Water Shortages, Crippled Health Services in North-East Syria.” 131 ACAPS, "Syria Displacement in Northeast Briefing Note.” 132 REACH, "Northeast Syria: COVID-19 Multi-Sectoral Rapid Needs Assessment."
Nurses, 58%Midwives, 12%
Dentists, 10%
Laboratory, 6%
General Practitioners, 4%
Resident Doctors, 2%
Pharmacists, 1%

32 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
FIGURE 11: PROPORTION OF POPULATION WITH ACCESS TO HEALTH CARE
Although communities may have access to health care, the type of service accessed may not necessarily meet their health needs, as most health services are accessed at pharmacies (Figure 12).133
FIGURE 12: MOST COMMON TYPE OF FACILITY WHERE HEALTH CARE WAS ACCESSED
Communities in NES face multiple barriers when attempting to access health care (Figure 13).134 Only 47 percent of communities have health care services for people with disabilities, and 46 percent of people with disabilities cannot afford these services. 135 Physical access poses an additional barrier for all populations, with 21 percent of communities not having access to a health care facility within five kilometers or one-hour walking distance.136
133 REACH, "Northeast Syria: COVID-19 Multi-Sectoral Rapid Needs Assessment." 134 REACH, "Humanitarian Situation Overview in Syria (HSOS) Northeast Syria." 135 REACH, "Northeast Syria: COVID-19 Multi-Sectoral Rapid Needs Assessment." 136 REACH, "Northeast Syria: COVID-19 Multi-Sectoral Rapid Needs Assessment."
1%
56%
35%
99%
44%
65%
Deir-ez-Zor
Al-Hasakeh
Raqqa
No Access Have Access
10%
12%
32%
32%
94%
Public Hospitals
Private Hospitals
Private Clinics
Primary Care Facilities
Pharmacies

33 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
FIGURE 13: BARRIERS TO ACCESSING HEALTH CARE
Northeast Syria has a mixture of publicly and privately-owned health facilities and an array of static and mobile clinics run by SNES, the Government of Syria, national and international NGOs, UN agencies, the Syrian Arab Red Crescent, and the Kurdish Red Crescent. Some of the facilities are registered with the Government of Syria and some are overseen by the SNES. As of December 2019, Raqqa had seven hospitals, but their functionality is unclear. Five of the hospitals are privately owned and two are publicly owned facilities. Of the two publicly owned hospitals, the National Hospital is supported by the international NGOs MSF, Medical Relief, and Handicap International, and the Maternity and Pediatrics Hospital is supported by Syria Relief, a national NGO. Raqqa also has several health dispensaries supported by local and international NGOs and the Kurdish Red Crescent.137
The main cities of Al-Hasakeh that contain concentrations of REM populations have the following health facilities as of December 2019 (their degree of functionality is unclear):138
• Qamishli: There are six private hospitals and one public Government of Syria–run hospital, in addition to six community health clinics in neighborhoods where Christians are present. All six private hospitals and five community health clinics are run by NGOs and churches and are registered with the Government of Syria Ministry of Health. The only community health clinic that is not registered with the Government of Syria is operated by the SNES.
• Al-Hasakeh City: There are two public hospitals and several private hospitals, in addition to six community health clinics in neighborhoods where Christians are present. The original public hospital is now run by the SNES, and the Government of Syria has established a second public hospital in a former hotel.
• Tell Tamr: The one public hospital in Tell Tamr is overseen by the SNES. The hospital has only general practitioners and lacks sufficient medical devices and equipment; therefore, most residents seek care in Al-Hasakeh City or Qamishli City. Tell Tamr town also has one private hospital specializing in gynecology and obstetrics.
137 Assistance Coordination Unit, "Ar-Raqqa Governorate - Panoramic Report," December 2019, https://www.acu-sy.org/en/wp-content/uploads/2019/12/IMU_En-Raqqa-Panoramic____.pdf 138 USAID, "Syria Essential Services II, Ad Hoc Report: Status of Vulnerable Religious and Ethnic Minority Communities in NES."
65%
47%
38%32% 30% 30% 29%
21%
Cannot affordcost of health
services
Cannot affordcost of
transportation
Lack oftransportation
Lack ofmedicines atthe health
facility
Health facilitynot functioning
Specializedservices are
not functioning
Lack ofambulanceservices
Health facilitiesare over-crowded

34 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
• Al Malikiyah/Derik: Residents of Al-Malikiyah/Derik rely heavily on the one public and two private hospitals in the area, but reports indicate that services here are particularly inadequate. There are no public health clinics associated with local churches, as in other areas of Al-Hasakeh.
• Amuda: Yazidis in Amuda City and the surrounding area seek treatment for minor health issues in the Amuda City public hospital and Amuda community health center; both are run by the SNES. Additionally, there is one private hospital in Amuda City, which includes a center for the treatment of heart disease.
Research indicates that the private hospitals tend to provide better care than the public hospitals, but neither are capable of addressing serious conditions, so individuals requiring complex operations or advanced care must travel to Damascus or the Kurdistan Region of Iraq (KRI).139 This is due to a lack of qualified physicians and specialists and a shortage of medical devices and medications, particularly for chronic diseases. 140 As many residents cannot afford care in private hospitals, they rely heavily on community health clinics associated with local churches and affiliated organizations.
Data are not available on the uptake of services at private and public health facilities in NES, but data on services provided by UN agencies and their partners are publicly available. Between October 9, 2019, and November 30, 2019, OCHA reports that 195,331 people accessed integrated primary health care services, including medical consultations, treatment courses, and MHPSS services.141 Given the large number of people in need of health assistance, these numbers indicate a clear need to enhance service delivery. Similar limitations are noted for the number of beneficiaries reached by other types of health services. For a geographic distribution and list of health implementing partners in NES, see Annex 4.
Due to the ongoing crisis, professional development of health professionals has been limited over the past seven years, impacting the quality of health services provided. Hospital-acquired and antibiotic-resistant infections were reported across Syria, indicating low-quality infection control practices.142 The limited capacity of staff and limited resources also likely suggest poor quality of services.
WOMEN’S AND CHILDREN’S HEALTH
UNFPA is the main partner providing maternal health services in Al-Hasakeh and Raqqa through a network of 11 static reproductive health clinics and 13 mobile teams, offering antenatal care, prenatal care, family planning, treatment of reproductive tract and urinary tract infections, pediatric care, primary health care, and referral services, in addition to deliveries.143 UNICEF provides nutritional support activities through UNFPA-supported facilities. UN agencies report that reproductive health services are inadequate, particularly in camps and collective shelters, with targeted approaches needed for pregnant women, the majority of whom are under 20.144 A multitude of agencies implement child protection interventions throughout NES, but those implementing on the ground indicate insufficient access to curative and preventive nutrition services and the need for interventions to be delivered at scale, especially skilled maternal, infant, and young child nutrition support.145
139 USAID, "Syria Essential Services II, Ad Hoc Report: Status of Vulnerable Religious and Ethnic Minority Communities in NES." 140 Ibid. 141 OCHA, "Northeast Syria Crisis, Humanitarian Response Within Syria.” 142 UN Strategic Steering Group, "2019 Humanitarian Needs Overview." 143UN News, Health Services for Syrian Women Caught Up in War, Foster Safety and Hope: UNFPA.” 144 OCHA Syria, "Situation Report #12: Humanitarian Impact of the Military Operation in Northeast Syria." 145 UN Strategic Steering Group, "2019 Humanitarian Needs Overview."

35 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT
As noted earlier, there is a tremendous need for MHPSS services in the region.146 An assessment in April 2020 found that in 44 percent of the subdistricts in NES, psychosocial services in areas under the SNES were closed, 9 percent were only partially functioning, and 9 percent had no MHPSS services at all.147 The closures are due in part to restrictions put in place in response to COVID-19. Fifty-eight percent of IDPs in host communities in Al-Hasakeh reported that MHPSS services are not available, and where they were available, half the community did not know how to access them.148 Figure 14 shows the most commonly requested assistance related to MHPSS services among IDPs in host communities in Al-Hasakeh. 149 Vulnerable groups in need of assistance include female-headed households, orphans, the elderly, and the disabled.
FIGURE 14: PROTECTION NEEDS AMONG IDPS
SEXUAL AND GENDER-BASED VIOLENCE
Implementing agencies, particularly UNFPA, provide GBV services integrated into reproductive health services through protection centers such as child-friendly spaces and women’s and girls’ safe spaces. However, due to current restrictions, spaces operated by the UN and their implementing partners are now closed.150 Protection actors continue to face disproportionate imposition of restrictions on their activities, with sustained advocacy needed to explore ways of resuming activities; enhancing coverage, particularly for unaccompanied minors and GBV victims; and raising awareness about IEDs.151 Although data indicate high levels of GBV among northeast Syrian populations, there appears to be low uptake of services due to societal barriers. Figure 15 highlights barriers experienced by women and girls in accessing GBV services in December 2019 before services closed.152 UNFPA has reported that overcrowding in shelters and the lack of specialized expertise in providing GBV services continue to exacerbate the challenges faced by women and girls.153
146 UNICEF, "North East Syria Response - Situation Report." 147 Humanitarian Needs Assessment Programme, "COVID-19 Rapid Assessment, Syrian Democratic Forces Controlled Areas," April 7, 2020, https://www.humanitarianresponse.info/sites/www.humanitarianresponse.info/files/assessments/covid_rapid_assessment_2_sdf_20200407.pdf 148 REACH, "Rapid Needs Assessment of IDPs in Host communities, Hasakeh Governorate, Northeast Syria." 149 Ibid. 150 NES Forum, "COVID-19 Update No.5." 151 Ibid. 152 Norwegian Church Aid, GOPA-DERD, and ABAAD, "Gender-Based Violence in North-East Syria Rapid Needs Assessment.” 153 UN News, Health Services for Syrian Women Caught Up in War, Foster Safety and Hope: UNFPA.”
56%
43%
30%27%
17%
Psychosocial Support Psychological First Aid Information aboutProtection Services
Special Assistance forVulnerable Groups
Specialized Services forVictims of GBV
ACF
Highlight
MHPSS

36 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
FIGURE 15: BARRIERS TO WOMEN AND GIRLS ACCESSING GBV SERVICES
COMMUNITY HEALTH OUTREACH PROGRAMS
Community health-based activities appear to be a prime source of health education among populations in NES, particularly in camps and informal settlements. Recent activities to educate communities on COVID-19 prevention measures indicate that 82 percent of populations in camps and informal settlements received this information through community health workers.154 Partners on the ground indicate that CSOs and local initiatives are better placed to implement community-based activities in the SNES as, unlike in government-held areas, they are not subject to interference by nonstate armed actors.155 To enhance culturally appropriate delivery of health care services, UNFPA recruits volunteers from local communities to enhance community involvement and expand interventions’ reach to beneficiaries in need of GBV and RH services. These approaches also economically empower the health workers, who are adult and young women of working age.156
Northeast Syria health sector partners employ at least 1,735 outreach workers across Syria, 79 percent of whom have been reassigned to support COVID-specific outreach and messaging. Coverage gaps are significantly higher in Deir-ez-Zor than in Al-Hasakeh and Raqqa.157 Reports indicate that the Ministry of Health is handing over four mobile clinics to the UN and their partners in Al-Hasakeh and one in Deir-ez-Zor.158
HEALTH FINANCE
Data on public expenditures on health are not available for NES, but the WHO indicates that 4.8 percent of government expenditures are on health countrywide.159 As most of northeast Syria is under the control of the SNES, it is unclear whether health expenditures reach this level there. However, as reports indicate that public hospitals in northeast Syria are being supported by humanitarian actors, public expenditures
154 NES Forum, "COVID-19 Update No.5." 155 Gharbibah, M., and Mehchy, Z., "COVID-19 Pandemic: Syria’s Response and Healthcare Capacity." 156 UNFPA, "North-East Syria Flash Update #13.” 157 NES Forum, "COVID-19 Update No.5." 158 OCHA Syria, "Situation Report #12: Humanitarian Impact of the Military Operation in Northeast Syria." 159 WHO, "Syrian Arab Republic HeRAMS reports," Accessed June 22, 2020, http://www.emro.who.int/syr/information-resources/herams-reports.html
81% 80%70% 68% 67%
73%
59%67% 67%
35%
Stigma associated withSBGV
Restricted movementby family
Lack of privacy andconfidentiality
Lack of medications atfacility
Priority given to males
Al-Hasakeh Deir-ez-Zor

37 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
on health are likely low. Primary healthcare and some emergency services are provided free of charge at public healthcare facilities.160
In March 2020, a monthly market monitoring exercise recorded the highest Survival Minimum Expenditure Basket value since 2015, with a 41 percent increase from September 2019 alone. With prices reportedly rising and COVID-19 restrictive measures impacting livelihoods, households may not be able to afford basic commodities. A large portion of the population cannot afford health care, as was mentioned earlier—65 percent of the northeast Syrian population cannot afford the cost of health services and 47 percent cannot afford the cost of transportation to health services.161 As of April 2020, NGOs operating in northeast Syria reliant on UN funding reported a $30 million shortfall for health care, posing significant obstacles to preventing and responding to COVID-19.162
Border restrictions are also impacting costs for humanitarian partners, as many are forced to operate from KRI and the closure of border crossings has increased transportation costs as humanitarian actors must find alternative mechanisms to get supplies into northeast Syria.163 The WHO reports that since road shipments have been halted since May 2018, airlifting relief shipments has become the alternative, sometimes costing up to 20 times as much as road shipments.164
ACCESS TO ESSENTIAL MEDICINES
Restrictions on aid deliveries from Damascus and Iraq are preventing medical supplies, including medications, from entering NES due to the closure of the Yarubiyah border crossing with KRI, as was previously noted. 165 The movement of medical supplies is further hindered by Syrian authorities in Damascus that restrict aid reaching SNES areas.166 In addition, KRI authorities have banned agencies from procuring medical supplies related to the prevention of COVID-19 that are destined for NES.
Despite these restrictions, in May 2020, the WHO, with funding from the U.S. Office of Foreign Disaster Assistance and the Norwegian government, transported 55 tons of medical supplies to Qamishli for distribution throughout the three governorates of NES.167 These were the first road deliveries to reach Al-Hasakeh Governorate in the past two years. However, as previous WHO shipments into northeast Syria had been allocated only to Government of Syria–run facilities, it is unclear whether facilities operating in the SNES zones will benefit from these supplies. Medical facilities report that stockouts have already begun, and the situation will likely worsen over the coming weeks unless transportation restrictions are lifted.168
Data available on collective centers in Al-Hasakeh indicate that as of April 2020, medications for chronic illnesses were available for free in 27 percent of settlements and for a fee in 82 percent of settlements, with 16 percent having no access to these medications.169 Data from 2019 indicate that more than 70
160 USAID, "COVID-19 Prevention, Preparedness and Response in NES.” 161 REACH, "Humanitarian Situation Overview in Syria (HSOS) Northeast Syria." 162 HRW, "Syria: Aid Restrictions Hinder COVID-19 Response," April 28, 2020, https://www.hrw.org/news/2020/04/28/syria-aid-restrictions-hinder-covid-19-response 163 OCHA, "Syrian Arab Republic: COVID-19, Humanitarian Update No.7," April 25, 2020, https://reliefweb.int/sites/reliefweb.int/files/resources/Syria_COVID-19_Humanitarian%20Update%20No%207_25Apr2020_FINAL.pdf 164 WHO, "WHO Delivers Health Supplies by Road to Northeast Syria," June 1, 2020, http://www.emro.who.int/syr/syria-news/who-delivers-health-supplies-by-road-to-northeast-syria.html 165 HRW, "Syria: Aid Restrictions Hinder COVID-19 Response.” 166 Ibid. 167 WHO, "WHO Delivers Health Supplies by Road to Northeast Syria.” 168 Noah Smith, "In Northern Syria, Destruction and Displacement Confront Health Workers," Direct Relief, October 27, 2019, https://www.icrc.org/en/document/syria-life-saving-humanitarian-work-must-be-facilitated-north-east 169 REACH, "Collective Centers and COVID-19 Vulnerability."

38 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
percent of communities in NES do not have access to psychotropic medications. Despite immunization campaigns implemented by UNICEF, the Ministry of Health, and other agencies, routine Expanded Programme of Immunization coverage rates of Penta3 vaccination (diphtheria, tetanus toxoid, pertussis, hepatitis B, Hemophilus influenza type b) in children under one were only around 10–20 percent in Raqqa and Deir-ez-Zor Governorates.170 Three-quarters of the country’s suspected measles and rubella cases in 2018 occurred in Raqqa, Deir-ez-Zor, and Idlib, demonstrating the strong need to expand immunization coverage.171 Shortages of personal protective equipment and other supplies required for the COVID-19 response are also reported.172
LEADERSHIP AND GOVERNANCE
While the Government of Syria oversees health facilities in government-held areas of NES, and the Central SNES Health Commission oversees those in areas controlled by the SNES, a recent assessment indicates weak governance, dysfunctional health care systems, and limited funding and capacity among the public sector and NGOs.173 Findings of a 2020 assessment conducted by USAID in NES confirm that the SNES health authorities lack the capacity to coordinate the health response in SNES, resulting in both the public sector and humanitarian actors working in silos, with limited tracking and reporting at a central level. The lack of oversight and leadership has hindered the humanitarian response in the region and led to ad-hoc decision making at the community-level, highlighting the need to support internal reform and capacity building of SNES health authorities.
There are no standardized health information systems operating across NES, however individual facilities manage internal systems that track patients and supplies.174 Reporting on disease outbreak is complicated in SNES due to political issues hindering public health surveillance. In NES, two epidemic surveillance systems exist, the EWARS system which is linked to the Government of Syria and the EWARN system which is managed by the opposition. Each system monitors certain areas of NES, with very limited coordination between the systems and from SNES authorities, resulting in incomplete reporting and limited surveillance data in areas under the SNES, further complicating the health response in the region.
CONCLUSIONS
An exhausted health system, combined with protracted violence, extremely high poverty rates, and a tremendous number of people in need of acute health assistance, creates a significant humanitarian crisis in northeast Syria. Although the current system is already inadequate to meet the population’s health needs, multiple factors, including the economic downturn, movement restrictions affecting both access and supplies, and the challenges created by the COVID-19 response, have led many humanitarians to predict that this crisis will worsen in 2020, with a possibility of famine by winter. As many of the difficulties disproportionately affect women and children, who constitute the vast majority of the displaced population in northeast Syria, there is a dire need for targeted approaches in support of the most vulnerable populations. Barriers to accessing GBV services highlight a clear need to support community-based, culturally appropriate awareness-raising activities on societal attitudes toward GBV and the ability of victims to access care and support.
170 UN Strategic Steering Group, "2019 Humanitarian Needs Overview." 171 UN Strategic Steering Group, "2019 Humanitarian Needs Overview." 172 NES Forum, "COVID-19 Update No.5." 173 Gharbibah, M., and Mehchy, Z., "COVID-19 Pandemic: Syria’s Response and Healthcare Capacity." 174 USAID, "COVID-19 Prevention, Preparedness and Response in NES," Final Y4Q4 Quarterly Report, Amman, June 2020.

39 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
AQ 3: CRITICAL HEALTH NEEDS AND CURRENT GAPS IN HEALTH SERVICES FOR REM COMMUNITIES
Given the many challenges faced by NES communities, there are significant health needs and gaps in service provision. Although efforts to address malnutrition and the spread of infectious disease should be prioritized, sustainable, long-term improvement in health outcomes requires a comprehensive approach that will also address deficiencies in WASH, livelihoods, and shelter, as well as the large number of IDPs. As economic challenges and restrictions placed on the humanitarian response are hindering access to food, water, and health care, most IDPs and residents rank health care as their top-priority need (Figure 16).175
FIGURE 16: PRIORITY NEEDS AMONG IDPS AND RESIDENTS
Although health care is the most critical need, other priority areas are also having a negative impact on health outcomes. Inadequate livelihoods have reduced communities’ ability to pay for health care, medications, food, water, and transport and have increased the proportion of the population living in overcrowded conditions. These living conditions, coupled with inadequate WASH standards, lead to poorer health outcomes, as evidenced by the high rate of infectious disease transmission.
Health sector agencies report a lack of both basic and advanced medical supplies.176 Expanded women’s and children’s health services, along with nutritional support, are needed to address the high levels of acute malnutrition and high maternal mortality rates. The significant number of child marriages and pregnancies among women under 20 highlights the need for adolescent-friendly reproductive and maternal health services. Mental health and GBV services must be expanded to cope with the high levels of stress and violence. Furthermore, the systematic targeting of women outside their place of residence has further restricted their access to health care and WASH facilities and increased GBV levels, increasing the need to improve access and security.177 The high number of disabled persons and the risks posed by IEDs indicate a need for accessible general health services as well as specialized services such as surgery and rehabilitation.
175 REACH, "Humanitarian Situation Overview in Syria (HSOS) Northeast Syria." 176 ICRC, "COVID-19: Millions Dealing with Sporadic Water Shortages, Crippled Health Services in North-East Syria.” 177 Smith, N., "In Northern Syria, Destruction and Displacement Confront Health Workers.”
82%
71%
47% 45%
31%
10% 9%
70%63%
67%
25%
15%
24%
32%
Health Livelihoods Food WASH Education Non-Food Items Shelter
Residents IDPs

40 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
Among IDP households in host communities in Al-Hasakeh, 57 percent include vulnerable community members, mostly persons with disabilities, children at risk, and elderly persons. 178 Overcrowding in shelters was reported among 75 percent of IDPs and 51 percent of resident communities, indicating increased risk factors to the spread of communicable diseases, especially COVID-19.179 Overcrowding in health facilities was reported in 21 percent of communities.180
AQ 4: EXTERNAL STRESSES
The multiple, challenging, interrelated external stresses have hampered efforts to improve northeast Syrians’ health status. Although the restrictions arising from the response to COVID-19 are presenting challenges, other external stresses are also having a severe negative impact, necessitating a comprehensive approach.
COVID-19
As of September 18, 2020, there are 1,121 cases of COVID-19 in NES with 52 deaths. One-hundred and sixty-five of the cases were health workers. This high number is due to several factors including low levels of compliance with personal preventative measures and shortage of personal preventive equipment (PPE). Experts and doctors working across Syria fear that the pandemic will spread quickly due to overcrowding and an inability to self-isolate. Syria also is experiencing undertesting for COVID-19, a lack of capacity for contact tracing to isolate identified cases, and poor access to health facilities. Due to high poverty levels, most of the population must work daily to survive. A survey from March 2020, indicated that almost half of the population of NES lacks knowledge of COVID-19 preventive measures and only 22 percent of respondents have knowledge of COVID-19 symptoms.181
Difficulties in getting supplies into NES poses a substantial disease prevention challenge. Movement restrictions to reduce the spread of COVID-19 have reduced access to health care and humanitarian actors’ ability to support community needs. Operational delays and disruptions have already been reported among 44 percent of humanitarian organizations in Syria, and this proportion is likely higher in NES due to cross-border movement restrictions, as most international NGOs operating in NES are based in KRI and relied heavily on the now closed Yarubiyah border crossing.182
POLITICS AND POLICY
As the Syrian war has entered its 10th year, the humanitarian consequences have become tremendous, posing extreme challenges to improving health outcomes. Northeast Syria has been caught between domestic and global political decisions that have greatly affected the population’s stability and health.
The nonrenewal of the Yarubiyah border crossing in Al-Hasakeh under UN Security Council Resolution 2504 (2020) is hindering humanitarian assistance to the region, including delivery of medical supplies to improve COVID-19 prevention measures. NGOs in northeast Syria rely on multiple modes of procurement, including local procurement for basic medical items, procurement from KRI, and international procurement, which have all been recently impacted. Local supply chains have been affected by disruption to cross-border commercial activity, procurement of medical supplies has been restricted
178 REACH, "Rapid Needs Assessment of IDPs in Host communities, Hasakeh Governorate, Northeast Syria," February - March 2020, https://www.impact-repository.org/document/reach/196d01e9/REACH_SYR_HasakehRNA_Mar2020.pdf 179 REACH, "Humanitarian Situation Overview in Syria (HSOS) Northeast Syria." 180 Ibid. 181 NES Forum, "COVID-19 Update No.5." 182 OCHA, "Syrian Arab Republic: COVID-19, Humanitarian Update No.7."

41 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
in KRI, and the closure of airports in both KRI and NES have left humanitarian partners with limited procurement options, significantly adding to procurement costs and time. Reports on the movement of supplies into northeast Syria also indicate that raw materials are not entering from government-held areas, inhibiting manufacturers’ ability to locally produce personal protective equipment.183 Supplies reaching NES by road from Damascus have already been hindered due to ongoing hostilities along the route.184
SECURITY AND STABILITY
Operation Peace Spring has added to the humanitarian challenges in NES, as increased violence and targeting of health facilities and staff have led humanitarian actors to remove their staff.185 As many humanitarian organizations are based along the Turkish-Syrian border and rely on cross-border access points, concern about general humanitarian access to the region has intensified in recent months.186 Furthermore, due to ongoing hostilities in northwestern Syria, IDPs continue to arrive in northeast Syria, exacerbating humanitarian challenges.187 IED contamination has further restricted access.
FINANCIAL
The economic collapse, devaluation of the Syrian Pound, and all-time high inflation rates are devastating the Syrian population, almost 83 percent of which lives below the poverty line.188 Since March 2020, significant price increases and some shortages in basic goods have been reported across Syria, with food prices rising 40–50 percent and prices of personal sterilization items (face masks, hand sanitizers) rising up to 5,000 percent.189 The WFP reported that in the past year, the price of basic food items has risen more than 100 percent and the price of gas by 248 percent.190 The rise in food prices due to COVID-19-related factors, including panic buying, disrupted supply routes, slow replenishment of stocks, reduced shop opening hours, and movement restrictions, has already increased vulnerabilities and diminished employment opportunities.191 Food security issues are exacerbated by sharp new limits the Government of Syria has imposed on the quantities of subsidized goods available to citizens through a state-run smart card system and by corruption, which is reducing the amount of food people can access through this system.192
The economic decline has also impacted the procurement of essential medical and pharmaceutical supplies—humanitarian agencies report that quotes received from suppliers require rapid ratification as prices sometimes change multiple times each day, creating additional procurement challenges. 193 Furthermore, the Government of Syria has shut down the informal money exchange (hawala) offices through which many Syrians received remittances from relatives abroad—a crucial income source given the country’s extremely high poverty rates.194 Because of the closure of the hawala network and liquidity
183 Elizabeth Tsurkov and Qussai Jukhadar, "Ravaged by War, Syria’s Health Care System is Utterly Unprepared for a Pandemic," Middle East Institute, April 23, 2020, https://www.mei.edu/publications/ravaged-war-syrias-health-care-system-utterly-unprepared-pandemic 184 OCHA Syria, "Situation Report #12: Humanitarian Impact of the Military Operation in Northeast Syria.” 185 N. Smith, "In Northern Syria, Destruction and Displacement Confront Health Workers.” 186 ACAPS, "Syria Displacement in Northeast Briefing Note.” 187 OCHA, "Syrian Arab Republic: IDP Movements," April 2020, https://reliefweb.int/sites/reliefweb.int/files/resources/idpmovements_202004apr_final_en.pdf 188 M. Gharbibah and Z. Mehchy, "COVID-19 Pandemic: Syria’s Response and Healthcare Capacity." 189 OCHA, "Syrian Arab Republic: COVID-19, Humanitarian Update No.7." 190 Ibid. 191 Ibid. 192 Ibid. 193 Ibid. 194 Steven Heydemann, "The Caesar Act and a Pathway Out of Conflict in Syria.”

42 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
issues in KRI, humanitarian NGOs operating from KRI have been unable to transfer funds into NES, as these operations rely entirely on the hawala network due to a lack of banking services in NES.195
ENVIRONMENTAL
The lack of WASH services must be addressed to improve northeast Syrians’ health status. Intermittent water services are further disrupted by repair teams’ inability to access some of the main water stations due to IED contamination and ongoing conflict in the region’s northern areas.196 This is of particular concern in Al-Hasakeh City and Tell Tamr, where the main water station, the Allouk Station, is in a zone under Turkish control.197 Unless sewage systems are installed for the 70 percent of the northeast Syrian population that currently has no access, efforts to curb the spread of communicable disease will be severely hindered. The lack of handwashing facilities also severely hampers COVID-19 infection control measures.
EQUITY
OHCHR research indicates that children’s experiences in the Syrian conflict have been deeply gendered— females are disproportionally affected by sexual violence and the threat of rape, which has increased restrictions on their movements.198 Most women have reported that even walking to latrines puts them at a high risk of violence. Girls have been confined to their homes, removed from school, prevented from accessing health care, and forced into early marriage. Many boys, in particular those aged 12 and above, have been arrested and kept in detention facilities, targeted by armed groups and militia for recruitment, or forced to become the main breadwinner for their families. Children with disabilities encounter significant challenges with protection and assistance, especially when relocated to settlements in which access to services is severely limited. All these outcomes are highly detrimental to children’s survival and development and expose them to additional forms of violence and exploitation.
CONCLUSIONS
These external stresses will further increase the proportion of the population in critical need of assistance. The data indicate vulnerabilities among all segments of the population, particularly IDPs, women, and children. Current challenges will undoubtedly push more of the population below the poverty line, worsening food insecurity and malnutrition. The burden of infectious diseases, coupled with extremely limited access to health care, will further increase community vulnerabilities.
195 NES Forum, "COVID-19 Update No.5." 196 OCHA Syria, "Situation Report #12: Humanitarian Impact of the Military Operation in Northeast Syria.” 197 USAID, "Syria Essential Services II, Ad Hoc Report: Status of Vulnerable Religious and Ethnic Minority Communities in NES." 198 OHCHR, ""They Have Erased the Dreams of My Children: Children's Rights in the Syrian Arab Republic."

43 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
USAID HEALTH AND REM PROGRAMMING
USAID does not currently implement health programs in NES. However, under the Syria Essential Services II project, three assessments have been conducted that are extremely valuable for REM health programming in the region. They are:
• COVID-19 Prevention, Preparedness, and Response In NES: In May and June 2020, USAID conducted an assessment to provide USAID with actionable programming recommendations to support the health sector and COVID-19 response in NES. The assessment included a desk review and 31 key informant interviews with relevant stakeholders from NES, including SNES authorities, public and private health facility managers, international and national NGO representatives and public health experts.
• Status of Vulnerable Religious and Ethnic Minority Communities In NES: Conducted in December 2019, this assessment examined five communities in NES with significant concentrations of REM communities, through a desk review and 14 key informant interviews. The report provides an overview of the current demographic and displacement trends within these communities, and the distribution and status of essential services. The report also provides potential programmatic approaches.
• Status of Minority and Vulnerable Groups in Raqqa, Deir Ez-Zor, and Hasakeh: Conducted in November 2018, this assessment examined the status of the main minorities in Hasakeh, Raqqa, and Deir Ez-Zor, through a desk review and 19 key informant interviews. It compares pre-conflict to current trends and unpacks the demographic profile of the various minority groups within these governorates, their treatment by various actors, their displacement profile, and their political engagement at the local and national levels. The assessment also provides targeted recommendations to ensure the inclusion of REM populations in future programming.

44 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
IRAQ
FIGURE 17: MAP OF IRAQ
COUNTRY CONTEXT
Iraq’s population in 2019 was 39.3 million and was 75–80 percent Arab, 15–20 percent Kurdish, and 5 percent other (including Turkmen, Yazidi, Shabak, Kaka'i, Bedouin, Romani, Assyrian, Circassian, Sabaean-Mandaean, and Persian).199 Life expectancy in Iraq is 73.6 years (75.6 for women, 71.7 for men), which is about 3.6 years higher than in 2011 (69.0 years)200 About 37 percent of the population is between 0 and 14 years of age, 20 percent 15–24, 36 percent 25–54, and 7 percent older than 55.201
Iraq has faced conflict for more than 40 years. Its most recent conflict was the occupation by the Islamic State of Iraq and Syria (ISIS) from 2014 to 2017 in northern Iraq. 202 During that period, fighting forced more than 6 million people to flee their homes; many of these displaced persons ended up in the Kurdistan Region of Iraq (KRI). 203 In addition to the conflict and violence, Iraq faces political instability, corruption, and natural disasters such as earthquakes, floods, and disease outbreaks, leading to a humanitarian crisis—a reported 4.1 million people are in need of some form of humanitarian assistance. As of March 2020, more than 1.39 million people (653,000 children) remained internally displaced (mainly in the north and
199 World Bank, Iraq WB Open Data, accessed June 2020. https://data.worldbank.org/indicator/SP.DYN.LE00.IN?locations=IQ 200 UN, Iraq First National Voluntary Review on Sustainable Development Goals, 2019, accessed June 2020. https://sustainabledevelopment.un.org/content/documents/23789Iraq_VNR_2019_final_EN_HS.pdf 201 CIA Factbook, Iraq Profile, 2020, accessed June 2020. https://www.cia.gov/library/publications/the-world-factbook/geos/print_iz.html 202 OCHA, Humanitarian Needs Overview 2020, Iraq. Issued November 2019, accessed June 2020. https://reliefweb.int/sites/reliefweb.int/files/resources/iraq_hno_2020.pdf 203 IOM UN Migration, Displacement Tracking Matrix Iraq Mission, April 2020, accessed June 2020. http://iraqdtm.iom.int/
ACF
Sticky Note
IRAQ

45 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
west), with 250,000 Iraqi refugees in neighboring countries.204 In April 2020, Camp Clusters reported 277,177 internally displaced persons (IDPs) (138,758 children) living in 67 camps and 280,348 IDPs living in 938 informal sites such as abandoned, war-damaged, or unfinished buildings, farms, streets, mosques, schools, and offices. 205 Overall, the most severe and compounded needs continue to be found in governorates that witnessed direct conflict, such as Al-Anbar, Nineveh, Kirkuk, and Salah Al-Din, and in governorates that received a large number of the displaced, such as Duhok.206 About 50 percent of those in greatest need are in Nineveh and Al-Anbar. 207
Approximately 70 percent of the IDPs have been displaced for more than 3 years. In February 2019, a UN High Commission for Refugees (UNHCR) survey reported only 3 percent of the IDP displaced from Sinjar District plan to return this year. The main reasons for not wanting to return included: presence of mines (42 percent); lack of security forces (41 percent); house damaged or destroyed (33 percent); fear of discrimination (29 percent); and no financial means to return (13 percent).208
In 2019, to end the prolonged displacement, the government pushed residents of camps across northern Iraq to return. Some 31,000 families (around 186,000 people) left or were forced to leave camps in 2019, according to official data provided by the Norwegian Refugee Council. In Nineveh, 9 of the 14 camps were closed in 2019. Although nearly 4.6 million people have gone home, Iraq has no unified plan for those who cannot (Table 5).209
TABLE 5: ESTIMATED NUMBER OF IDPS AND RETURNEES BY GOVERNORATE
Governorate Number of IDPs Number of Returnees
Nineveh 328,212 1,799,628
Duhok (KRI) 319,158 768
Erbil (KRI) 237,480 52,878
Sulaymaniyah (KRI) 139,458 0
Baghdad 36,162 90,288
People are returning home, but the government is facing challenges in ensuring safety and stability, functioning infrastructure, and access to basic services and job opportunities. Most returning IDPs have found few or no economic opportunities, and some fear retaliation due to real or perceived affiliation with ISIS, which drives them to return to the camps. In March 2020, the International Organization for Migration (IOM) reported that more than 37,000 people had been re-displaced in Iraq between March
204 UNICEF, Iraq 2020 Internal Displacement Crisis Humanitarian Situation Report, January to March 2020, accessed June 2020. https://reliefweb.int/sites/reliefweb.int/files/resources/Iraq%20Humanitarian%20Situation%20Report%20%28IDP%29%20for%20January%20to%20March%202020.pdf 205 OCHA, Iraq Humanitarian Bulletin: April 2020, accessed June 2020. https://reliefweb.int/sites/reliefweb.int/files/resources/april_2020_humanitarian_bulletin_18_may_rev_1.pdf 206 OCHA, Humanitarian Needs Overview 2020, Iraq. Issued November 2019, accessed June 2020. https://reliefweb.int/sites/reliefweb.int/files/resources/iraq_hno_2020.pdf 207 Ibid. 208 UNHCR, COI Note on the Situation of Yazidi IDPs in the Kurdistan Region of Iraq, May 2019, accessed June 2020. https://www.refworld.org/pdfid/5cd156657.pdf 209 IOM UN Migration, Displacement Tracking Matrix Iraq Mission, April 2020, accessed June 2020. http://iraqdtm.iom.int/

46 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
2018 and December 2019; they tried to return home but left again. Nineveh, with 25,500 re-displacements, had the highest number. 210
As Iraq continues to try to recover, scarcity of jobs and limitations in providing basic services have prompted antigovernment protests that have been evolving since late 2019. 211 Mass protests broke out in Baghdad and across southern Iraq as thousands appealed for an overhaul of a political system they say has plundered state resources and pushed people into poverty. Poor health care is among the core grievances.212 The overall poverty rate in Iraq was 20.5 percent in 2018; northern Iraq (Nineveh, Kirkuk, Diyala, Anbar, and Salah al-Din) reported high rates of 27.5 percent, and the Kurdistan Region of Iraq (KRI) reported a much lower rate of 5.5 percent. Nineveh alone accounts for about a fifth of the poor in Iraq, and Baghdad has about 11 percent. The highest poverty rate—31.1 percent in southern Iraq—related to poor agricultural outcomes due to climate change.213
OVERVIEW OF RELIGIOUS AND ETHNIC MINORITIES IN IRAQ
Focus REM Populations in Iraq: Christian (Assyrian, Chaldean, Syriac, and Armenian), Yazidi, Kurd, Kaka’i (also known as Yarsani), Turkmen, Shabak, and Sabean-Mandaeans.
Geographic Areas of REM Populations: Nineveh Governorate, Kurdistan Region of Iraq (KRI), Mosul, and Baghdad
The estimated Christian population in Iraq is less than 1 percent; around 97 percent of the population is Muslim. About 80 percent of the Christian population lives in the Nineveh Plains and KRI. This population has declined since 2002, when estimates were between 800,000 and 1.4 million Christians. Approximately 67 percent of Christians are Chaldean Catholics (an Eastern Rite of the Roman Catholic Church), and nearly 20 percent are members of the Assyrian Church of the East. There are approximately 2,000 registered members of evangelical Christian churches in the KRI. 214 However, precise current demographic breakdowns are not available due to political sensitivities and the absence of recent census data.
Iraqi REM populations have long been discriminated against, but violence against them increased dramatically in areas under ISIS control. People were forced to flee and many (more than 2 million) ended up displaced and in refugee camps in the KRI.215 The most pressing issue still facing religious minorities in northern Iraq is the process of return for the tens of thousands of IDPs who fled the advance of ISIS in 2014.216 However, the majority of Iraqi Christians still remain displaced, and for those that have returned, their challenges have been significant.
Although ISIS targeted nearly all of Iraq’s REM components—including Turkmen, Yarsanis, and predominantly Shi’a Muslim Shabak—the most destructive violence was perpetrated against the Yazidi and
210 The New Humanitarian, Nowhere to go: Mosul residents in limbo as camps close, March 202, accessed June 2020. https://www.thenewhumanitarian.org/news-feature/2020/03/11/mosul-iraq-residents-in-limbo-camps-close 211 Ibid. 212 US Commission on International Religious Freedom, Iraq USCIRF Annual Report 2020, accessed June 2020. https://www.uscirf.gov/sites/default/files/Iraq.pdf 213 UN, Iraq First National Voluntary Review on Sustainable Development Goals, 2019, accessed June 2020. https://sustainabledevelopment.un.org/content/documents/23789Iraq_VNR_2019_final_EN_HS.pdf 214 US State Department, Iraq 2018 International Religious Freedom Report, accessed June 2020. https://www.state.gov/wp-content/uploads/2019/05/IRAQ-2018-INTERNATIONAL-RELIGIOUS-FREEDOM-REPORT.pdf 215 European Union, Minorities in Iraq: Pushed to the brink of existence, February 2015, accessed June 2020. https://www.europarl.europa.eu/RegData/etudes/BRIE/2015/548988/EPRS_BRI(2015)548988_REV1_EN.pdf 216 US Commission on International Religious Freedom, Policy Update: Protecting Religious Minorities in Northern Iraq, February 2020, accessed June 2020. https://www.uscirf.gov/sites/default/files/2020%20Iraq%20Policy%20Update_0.pdf

47 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
Christian communities. It is estimated that 30–50 percent of the population of Chaldeans, Assyrians, and other Christians have returned to their communities of origin, mostly from refuge in Erbil and other parts of the KRI,217 and Yazidis—500,000 of whom fled ISIS atrocities in 2014—still faced serious distress in 2019.218 By March 2015, 500,000 Yazidis, predominantly from Sinjar District, had been displaced, with the majority fleeing to the KRI, particularly Dohuk Governorate.219
Recognized as genocide by the UN in 2016, the ISIS attack on August 4, 2014, killed 5,000 Yazidi men. An estimated 7,000 Yazidi women and girls were enslaved and forcibly transferred to locations in Iraq and eastern Syria and held in slavery, sold, gifted, or passed around among ISIS fighters.220 The UN reported that since 2014, there was an estimated 6,417 Yazidis abducted, 3,524 have been rescued or escaped from their abductors (1,197 women, 339 men, 1,038 girls and 950 boys), and 2,893 remain missing.221
RELIGIOUS AND ETHNIC MINORITY GEOGRAPHIC FOCUS
Most of Iraq’s REM communities are in northern Iraq and KRI. Christians and Yazidis were located predominantly in the Nineveh Governorate until 2014 during ISIS occupation. Yazidis and other religious minorities were subjected to brutal attacks and forced to seek refuge; many remain in new local communities or in camps. Many Yazidis fled up Mount Sinjar were many still remain today.
Kurdish and Yazidi fighters regained control of Sinjar (Nineveh Governorate) in November 2015, but the security situation is still unstable. Landmines and booby traps cover the area, there is no reliable water or electricity supply; outside major towns, there are no schools and no hospitals and work opportunities are limited. Only a quarter of the original Yazidi inhabitants of Sinjar have tried to return to their ruined villages. About 300,000 Yazidis currently live in displacement camps or informal settlements scattered across the KRI, particularly in Duhok Governorate. 222 In addition, since 2017, Turkish airstrikes have repeatedly targeted positions of the Kurdish Workers Party (PKK) and its allies in and near Sinjar, including in November 2019 and multiple times in 2020. The threat of more such airstrikes has contributed to the fragile state of security and stability in that area.223
About 18 percent of Iraq’s IDP population are REM populations including Yazidis, Christians, Shabak, and Turkmen but represent only 2.7 percent of returnees.224 Of that 18 percent, 8 percent are Yazidi; 7 percent Turkmen; 1 percent Syriac, Chaldean, or Assyrian Christian and 2 percent Shabak Shi‘a.225 These populations cite several reasons for not returning, including targeted violence from extremist groups or militias and properties being destroyed, stolen, or occupied.226
217 US Commission on International Religious Freedom, Policy Update: Protecting Religious Minorities in Northern Iraq, February 2020, accessed June 2020. https://www.uscirf.gov/sites/default/files/2020%20Iraq%20Policy%20Update_0.pdf 218 US Commission on International Religious Freedom, Iraq USCIRF Annual Report 2020, accessed June 2020. https://www.uscirf.gov/sites/default/files/Iraq.pdf 219 UNHCR, COI Note on the Situation of Yazidi IDPs in the Kurdistan Region of Iraq, May 2019, accessed June 2020. https://www.refworld.org/pdfid/5cd156657.pdf 220 Relief Web, Five years after the genocide, Yazidis share their forgotten stories and demand justice, August 2019, accessed June 2020. https://reliefweb.int/report/iraq/five-years-after-genocide-yazidis-share-their-forgotten-stories-and-demand-justice 221 UN Office of Special Representative of the Security-General on Sexual Violence in Conflict, Iraq, June 2020, accessed June 2020. https://www.un.org/sexualviolenceinconflict/countries/iraq/ 222 US Commission on International Religious Freedom, Iraq USCIRF Annual Report 2020, accessed June 2020. https://www.uscirf.gov/sites/default/files/Iraq.pdf 223 Ibid. 224 IOM Iraq, Understanding Ethno-religious groups in Iraq: Displacement and Return, February 2019, accessed 2020. https://reliefweb.int/sites/reliefweb.int/files/resources/iom_dtm_er_singlepages_digital.pdf 225 US State Department, Iraq 2018 International Religious Freedom Report, accessed June 2020. https://www.state.gov/wp-content/uploads/2019/05/IRAQ-2018-INTERNATIONAL-RELIGIOUS-FREEDOM-REPORT.pdf 226 European Union, Country Policy and information Not Iraq: Religious minorities, October 2019, accessed June 2020. https://www.justice.gov/eoir/page/file/1215081/download

48 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
In an IOM 2019 survey, about 31 percent of IDPs and 23 percent of returnees reported being unemployed and looking for work. Unemployment levels are roughly similar among Christians, Shabak Shi‘a, and Turkmen IDPs (24 percent). However, this level is significantly higher among Yazidi IDPs, with 49.6 percent indicating that they are unemployed. Among returnee communities, Shabak Shi‘a have the highest level of unemployment (30 percent).227
TABLE 6: REM POPULATIONS IN IRAQ228,229
Population Estimated Number Geographic Area
Christian Fewer than 250,000 Baghdad, Mosul, Nineveh Plains, KRI
Yazidi 500,000 (approximately 360,000 are displaced)
Northern Iraq (disputed territories), KRI
Kurd Sunni: 4 million
Faili: 500,000
Sunni: KRI, Nineveh, Kirkuk, salah ad Din and Diyalah
Faili: Baghdad, Kirkuk, and KRI
Kaka’i 120,000 – 150,000 Nineveh Plains, Kirkuk, Diyala and Erbil
Turkmen 3 million Northern Iraq (disputed territories), southeast of Baghdad
Shabak 350,000 – 400,000 Nineveh Plains and Mosul
Sabean-Mandaeans 10,000 KRI and Baghdad; Southern Iraq
AQ 1: OVERVIEW OF HEALTH STATUS IN IRAQ
Iraq has made progress in improving the overall health status of its population over the past decade, such as in increasing life expectancy and decreasing infant mortality, however they are still behind other countries in the region. In Iraq, disparities in health indicators exist among the most vulnerable, especially among the IDP populations. Difference can be seen across different geographic areas and among sub-populations, including REM populations.
Iraq has a high death rate of 3.9 deaths per 1,000 (2020).230 The primary causes of death in 2017 were: cardiovascular diseases (28.8 percent), cancers (18.16 percent), lower respiratory infections (6.23 percent), dementia (5.44 percent), and respiratory diseases (5.39 percent).231 Although over the past decade, violence has been the leading cause of death in Iraq;201,876 people lost their lives as a result of terrorist acts.232 Chronic diseases now account for 43 percent of all adult deaths. According to WHO,
227 IOM Iraq, Understanding Ethno-religious Groups in Iraq: Displacement and Return, February 2019, access June 2020. https://reliefweb.int/sites/reliefweb.int/files/resources/iom_dtm_er_singlepages_digital.pdf 228 European Union, Minorities in Iraq: Pushed to the brink of existence, February 2015, accessed June 2020. https://www.europarl.europa.eu/RegData/etudes/BRIE/2015/548988/EPRS_BRI(2015)548988_REV1_EN.pdf 229 US State Department, Iraq 2018 International Religious Freedom Report, accessed June 2020. https://www.state.gov/wp-content/uploads/2019/05/IRAQ-2018-INTERNATIONAL-RELIGIOUS-FREEDOM-REPORT.pdf 230 CIA Factbook, Iraq Profile, 2020, accessed June 2020. https://www.cia.gov/library/publications/the-world-factbook/geos/print_iz.html 231 https://ourworldindata.org/what-does-the-world-die-from 232 UN, Iraq First National Voluntary Review on Sustainable Development Goals, 2019, accessed June 2020. https://sustainabledevelopment.un.org/content/documents/23789Iraq_VNR_2019_final_EN_HS.pdf

49 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
overweight and obesity are the leading causes of chronic diseases in Iraq and both rates are expected to rise in the next decade. However, about 80 percent of heart disease and 40 percent of cancer and diabetes cases can be prevented through behavior change (e.g. diet, exercise, not smoking).233
WOMEN’S HEALTH
Iraq’s maternal mortality rate was 79 deaths per 1,000 in 2017. 234According to the 2018 Iraq UNICEF Multiple Indicator Cluster Survey (MICS) survey, the maternal mortality ratio is 104 per 100,000 live births and about 11.2 percent of all female deaths were maternal related.235 The direct causes of maternal mortality reported by the Iraqi Ministry of Health (MOH) in 2017 included: hemorrhage (32.4 percent), pre-eclampsia/eclampsia (14.5 percent), thromboembolism (14.4 percent), rupture uterus (4.7 percent) and sepsis (4.4 percent).236
There have been increases in births attended by skilled health staff from 65 percent (2000) to 91 percent (2010) to 96 percent (2018).237 Iraq’s total fertility rate (TFR) decreased from 5.9 births per woman (1990) to 3.7 (2018). While, the adolescent fertility rate increased to 72 births per 1,000 girls ages 15-19 in 2018 from 70 in 1990. Neighboring countries reported much lower rates (2018); a TFR of 2.1 for the Islamic Republic of Iran, along with an adolescent fertility rate of 23 per 1,000; and in Jordan a TFR of 3.4 and an adolescent fertility rate of 26 per 1000.238 KRI also reported a lower total fertility rate of 3.1. Higher TFRs are reported among the poorest (4.4) and less educated women (4.7) as compared to the richest (3) and educated women (2.8). 239
Contraceptive prevalence of any method for women age 15-49 years increased from 14 percent (1990) to 53 percent (2018).240 In KRI 66.6 percent women are using contraceptive, compared to 44.4 percent in Nineveh and 54.9 percent in Baghdad. According to the 2018 MICS, 54.6 percent of married women (14-49) in Iraq and 34.6 percent in KRI have their family planning needs satisfied with modern contraceptive methods.241
CHILD HEALTH
Children under 15 years old represent about 48 percent of the population in Iraq and is one of the fastest growing populations in the region.242 and According to the MICS survey, neonatal mortality rate was 14 per 1,000 live births in Iraq, 10 in KRI, 14 in Nineveh and 12 in Baghdad.243 Neonatal mortality is 54
233 Ibid. 234 CIA Factbook, Iraq Profile, 2020, accessed June 2020. https://www.cia.gov/library/publications/the-world-factbook/geos/print_iz.html 235 UNICEF, Iraq Multiple Indicator Cluster Survey (MICS) 2018, accessed June 2020. http://mics.unicef.org/surveys 236 United Nations (WHO, UNICEF, UNFPA), Iraq Reproductive Maternal, Newborn, Child and Adolescent Health: Current Situation & Way Froward, 2017, accessed June 2020. https://www.moh.gov.iq/upload/upfile/ar/1000.pdf 237 World Bank, Country Profile, 2018, accessed June 2020. https://databank.worldbank.org/views/reports/reportwidget.aspx?Report_Name=CountryProfile&Id=b450fd57&tbar=y&dd=y&inf=n&zm=n&country=IRQ 238 United Nations (WHO, UNICEF, UNFPA), Iraq Reproductive Maternal, Newborn, Child and Adolescent Health: Current Situation & Way Froward, 2017, accessed June 2020. https://www.moh.gov.iq/upload/upfile/ar/1000.pdf 239 UNICEF, Iraq Multiple Indicator Cluster Survey (MICS) 2018, accessed June 2020. http://mics.unicef.org/surveys 240 World Bank, Country Profile, 2018, accessed June 2020. https://databank.worldbank.org/views/reports/reportwidget.aspx?Report_Name=CountryProfile&Id=b450fd57&tbar=y&dd=y&inf=n&zm=n&country=IRQ 241 UNICEF, Iraq Multiple Indicator Cluster Survey (MICS) 2018, accessed June 2020. http://mics.unicef.org/surveys 242 UNICEF, Country Office Annual report 2019, Iraq, accessed https://www.unicef.org/about/annualreport/files/Iraq-2019-COAR.pdf 243 UNICEF, Iraq Multiple Indicator Cluster Survey (MICS) 2018, accessed June 2020. http://mics.unicef.org/surveys

50 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
percent of all under-five mortality in Iraq and most are preventable with high-quality, evidence-based interventions. The Iraqi MOH reported (2017) the leading causes of neonatal mortality were; respiratory causes related to the perinatal period (39.4 percent), congenital malformations (11.1 percent), disorders related to gestational length and fetal growth (6.4 percent) and sepsis.244
Infant mortality rate (IMR) decreased to 23 per1,000 live births (2018) from 32 per 1,000 live births (2015). IMR is lower in KRI at 15 compared to Nineveh (23) and Baghdad (22). The post neonatal morality rate in Iraq is 8 per 1,000 live births; lower in KRI (4) and higher in Nineveh (10) and Baghdad (10).245
The under-five child mortality rate is 27 per1,000 live births which decreased from 44 in 2000 and 35 in 2010.246 This rate is much lower in KRI with 17 per 1,000 live births. Nineveh reported 26 per 1,000. Iraq’s under-five mortality rate is below the global rate (39 per1,000), but above neighboring countries such as Jordan (17 per 1,000), Syria (17 per1,000) and Iran (15 per1,000).247 Inequity exists between urban and rural, geographical areas, and wealth quintile, such as under-five mortality in the poorest quintile (16 per 1,000) is double than that of Richest quintile (32 per1,000).248
DIARRHEA PREVALENCE
Compared to the 48.2 percent across Iraq, in KRI, 55.8 percent of children under-five with diarrhea sought care in the last 2 weeks from a health professional. In Nineveh 53.4 percent and in Baghdad 61.3 percent of children under five sought care. While 25.4 percent of children under-five with diarrhea in the last 2 weeks received ORS in Iraq, 26.3 percent in KRI, 15 percent in Nineveh, and 39.6 percent in Baghdad. Only 5.2 percent of children received ORS and zinc. 249
MALNUTRITION RATES
In 2018 in Iraq one out of every ten children under-five was chronically malnourished (stunted). The prevalence of underweight children has decreased from 12.8 percent (2000) to 7.2 percent (2010)250 to 2.9 percent (2018).251 Stunting was nearly halved between 2011 and 2018 (9.9 percent) and wasting fell below the 5 percent Sustainable Development Goals (SDG) target (down to 2.5 percent). The overweight rates fell from 11.4 to 6.6 percent.252 In 2011, boys and girls had similar stunting rates (19 percent and 18 percent), however in 2018, 13 percent of girls and 8 percent of boys were reported as stunted. 253 The
244 United Nations (WHO, UNICEF, UNFPA), Iraq Reproductive Maternal, Newborn, Child and Adolescent Health: Current Situation & Way Froward, 2017, accessed June 2020. https://www.moh.gov.iq/upload/upfile/ar/1000.pdf 245 United Nations (WHO, UNICEF, UNFPA), Iraq Reproductive Maternal, Newborn, Child and Adolescent Health: Current Situation & Way Froward, 2017, accessed June 2020. https://www.moh.gov.iq/upload/upfile/ar/1000.pdf 246 World Bank, Country Profile, 2018, accessed June 2020. https://databank.worldbank.org/views/reports/reportwidget.aspx?Report_Name=CountryProfile&Id=b450fd57&tbar=y&dd=y&inf=n&zm=n&country=IRQ 247 UN WFP, Iraq Socio-Economic Atlas 2019, accessed 2020. https://reliefweb.int/sites/reliefweb.int/files/resources/WFP-0000110173_compressed.pdf 248 United Nations (WHO, UNICEF, UNFPA), Iraq Reproductive Maternal, Newborn, Child and Adolescent Health: Current Situation & Way Froward, 2017, accessed June 2020. https://www.moh.gov.iq/upload/upfile/ar/1000.pdf 249 UNICEF, Iraq Multiple Indicator Cluster Survey (MICS) 2018, accessed June 2020. http://mics.unicef.org/surveys 250 World Bank, Country Profile, 2018, accessed June 2020. https://databank.worldbank.org/views/reports/reportwidget.aspx?Report_Name=CountryProfile&Id=b450fd57&tbar=y&dd=y&inf=n&zm=n&country=IRQ 251 UNICEF, Iraq Multiple Indicator Cluster Survey (MICS) 2018, accessed June 2020. http://mics.unicef.org/surveys 252 UN WFP, Iraq Socio-Economic Atlas 2019, accessed 2020. https://reliefweb.int/sites/reliefweb.int/files/resources/WFP-0000110173_compressed.pdf 253 United Nations (WHO, UNICEF, UNFPA), Iraq Reproductive Maternal, Newborn, Child and Adolescent Health: Current Situation & Way Froward, 2017, accessed June 2020. https://www.moh.gov.iq/upload/upfile/ar/1000.pdf

51 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
prevalence of acute malnutrition (wasting) is 2.5 percent, with minimal difference between girls (2.8 percent) and boys (2.1 percent).
Prevalence of underweight, stunting and wasting were all higher in Iraq, particularly in Nineveh, compared to KRI. According the 2018 MICS, stunting prevalence was 13.9 percent in Baghdad and 12.7 percent in Nineveh, both are much higher than the 4.9 percent reported in KRI. Baghdad also had a higher wasting prevalence of 2.7 percent compared to Nineveh (1.6 percent) and KRI (1.8 percent). 254 (See graph 18).
FIGURE 188: MALNUTRITION RATES BY GEOGRAPHIC AREA FOR CHILDREN UNDER-FIVE255
MENTAL HEALTH
War has had an impact on the psychological and emotional well-being of people in Iraq, taking the form of Post-Traumatic Stress Syndrome (PTSD), depression, schizophrenia and severe anxiety. There is limited data available on the prevalence of these different illnesses, however, in 2019, as many as one million people in Iraq were estimated to be in need of some kind of mental health and psychosocial support services and more than 15 districts across Iraq with 30-50 percent of children showing signs of psychosocial distress (2018).256
Psychosocial needs among IDP populations are reported to be extremely high. Many Yazidis suffer from extreme psychosocial distress as a result of the serious violence they have experienced, the loss or captivity of family members, ongoing displacement and economic hardship. UNHCR reported a high number of suicides, suicide attempts and other self-destructive behavior among the displaced population in camps in Dohuk Governorate. At least 40 incidents of suicide and attempted suicide were reported in 2018. There were 10 incidents (six attempts and four committed) reported between January to April 2019 in IDP camps and non-camp locations where Yazidis reside. It is estimated that the real number is likely higher as not all cases are reported. According to the information obtained from survivors, community
254 UNICEF, Iraq Multiple Indicator Cluster Survey (MICS) 2018, accessed June 2020. https://data.unicef.org/country/irq/ 255 UNICEF, Iraq Multiple Indicator Cluster Survey (MICS) 2018, accessed June 2020. http://mics.unicef.org/surveys 256 UNICEF, Country Office Annual report 2019, Iraq, accessed https://www.unicef.org/about/annualreport/files/Iraq-2019-COAR.pdf
2.92.1
3.62.3
9.9
4.9
12.713.9
2.51.8 1.6
2.7
Iraq KRG Nineveh Baghdad
Underweight Stunting Wasting

52 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
leaders, and service providers, the main causes for attempted suicides included psycho-social distress, family disputes, domestic abuse, and poor living conditions.257
In 2018, the Iraqi National Study of Suicide conducted an analysis in 13 of Iraq’s 18 provinces. It found an increase in the rate of suicide from 1.09 per 100,000 (1.21 for males, 0.97 for females) in 2015, to 1.31 (1.54 for males, 1.07 for females) in 2016. In 24.1percent of the cases, the suicide was associated with psychiatric disorders, with a major cause being depression (53.9 percent). Other causes included psychological trauma (15.5 percent), financial problems (12.4 percent) and childhood abuse (2.2 percent).258
SEXUAL AND GENDER-BASED VIOLENCE (SGBV)
In 2020, its estimated that 1.29 million people are in need of SGBV prevention and response services in Iraq.259 Of these, an estimated 61 percent are returnees or in areas of return and 38 percent are IDPs or in areas of displacement. About 98 percent of reported SGBV survivors are women or girls. The main reported types of SGBV were domestic violence, followed by forced/child marriage.260 According to the 2018 MICS,24.8 percent of girls in Iraq married before the age of 18. The prevalence of adolescent childbearing was also high, with an adolescent pregnancy rate of 70 per 1,000 and 54 percent of married women (15-19 years) having had a live birth before the age of 15.261
A comparison of MICS responses from 2006 and 2018 shows a decrease from 59 to 37 percent of women who accepted that a man can beat his wife. These percentages were higher among poor and less educated women and women from north-west and south Iraq, where these attitudes were shared by 50 to 67 percent of women compared to 6 to10 percent in districts like Kirkuk and Sulaimaniya.262
OUTBREAK/EPIDEMIC DATA
According to the WHO, Iraq has not had an outbreak of Cholera since 2015 and no other reported outbreaks.263 However, looking at immunizations, the percentage of fully immunized264 children has not increased since 2011. In 2018 still only 58 percent of children aged 12-23 months were fully immunized. This is low compared to Jordan were 85 percent of children are fully vaccinated.265 Looking at fully immunized children in the different geographic areas, KRI reported 76.7 percent, Nineveh 38.7 percent and Baghdad 65.3 percent. About 71 percent are immunized for measles (KRI 82.7 percent, Nineveh 67 percent, and Baghdad 69.3 percent). TB immunization coverage is high across the country at 94.7 percent. Polio coverage is 73.6 percent in Iraq and 83.6 percent in KRI, 62.2 percent in Nineveh, and 78.2 percent
257 UNHCR, COI Note on the Situation of Yazidi IDPs in the Kurdistan Region of Iraq, May 2019, accessed June 2020. https://www.refworld.org/pdfid/5cd156657.pdf 258 Abbas MJ, Alhemiary N, Razaq EA, Naosh S, Appleby L. The Iraqi national study of suicide: Report on suicide data in Iraq in 2015 and 2016. J Affect Disord, accessed June 2020. https://pubmed.ncbi.nlm.nih.gov/29306693/ 259 UNICEF, Iraq 2020 Internal Displacement Crisis Humanitarian Situation Report, January to March 2020, accessed June 2020. https://reliefweb.int/sites/reliefweb.int/files/resources/Iraq%20Humanitarian%20Situation%20Report%20%28IDP%29%20for%20January%20to%20March%202020.pdf 260 OCHA, Humanitarian Needs Overview 2020, Iraq. Issued November 2019, accessed June 2020. https://reliefweb.int/sites/reliefweb.int/files/resources/iraq_hno_2020.pdf 261 UNICEF, Iraq Multiple Indicator Cluster Survey (MICS) 2018, accessed June 2020. http://mics.unicef.org/surveys 262 UN WFP, Iraq Socio-Economic Atlas 2019, accessed 2020. https://reliefweb.int/sites/reliefweb.int/files/resources/WFP-0000110173_compressed.pdf 263 WHO, Cholera – Iraq November 2015, accessed June 2020. https://www.who.int/csr/don/archive/country/irq/en/ 264 Includes: BCG, Polio 1, Polio 2, Polio 3, Hexa 1, Hexa 2, Hexa 3 and Measles 265 United Nations (WHO, UNICEF, UNFPA), Iraq Reproductive Maternal, Newborn, Child and Adolescent Health: Current Situation & Way Froward, 2017, accessed June 2020. https://www.moh.gov.iq/upload/upfile/ar/1000.pdf

53 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
in Baghdad).266 There is a disparity in vaccination coverage among Governorates, wealth quintiles and mother’s education despite the fact that vaccination is provided free of cost and from public health facilities only.267
ACCESS TO WASH
In 2020, an estimated 1.85 million people (851,000 children, 943,000 females) are in need of at least one form of humanitarian WASH support.268 This number has decreased by over 20 percent from 2019, when 2.3 million people were in need. The people in need of WASH assistance include 653,685 IDPs (283,048 reside in out-of-camp locations) and 1.06 million returnees; 14,724 people in highly vulnerable host communities; and 113,019 refugees in nine refugee camps and out-of-camp locations.269
CONCLUSIONS
Iraq’s health indicators are lower than other countries in the region. Although progress is reflected by increases in certain maternal and child indicators, others show slow or little progress. IDP populations are the most vulnerable due to lack of access to health services and poor living conditions. Until stability and the economic situation in northern Iraq improves, health indicators are not likely to improve.
In addition, although Iraq had not reported any major outbreaks of infectious diseases in recent years, in March 2020 Iraq reported its first cases of COVID 19 (see section on External Barriers for further COVID discussion). It is too early to tell the full impact of COVID-19, however testing and equipment shortages are already testing the health system.
AQ 2: STRENGTHS AND WEAKNESSES OF THE PRIMARY HEALTH CARE SYSTEM
Health status in Iraq started to improve during the 1970s when the country adopted an advanced health system and a comprehensive basic healthcare network. However, war and crises have negatively impacted the overall health system and the population’s health status. 270 The health system faces challenges overcoming recurring shortages of essential medicines, dealing with budget deficits, rehabilitating infrastructure and training, paying, and deploying human resources.271 Access to health services is limited, geographical disparities are significant, and health data is not collected on a routine basis. The country still lacks proper statistics and response plans to meet present and future health needs of its population.272
The Iraqi MoH runs 75 percent of the health system, providing services through a network of primary health care centers (PHCC) and public hospitals that charge low rates (Figure 19). The PHCCs provide
266 UNICEF, Iraq Multiple Indicator Cluster Survey (MICS) 2018, accessed June 2020. http://mics.unicef.org/surveys 267 United Nations (WHO, UNICEF, UNFPA), Iraq Reproductive Maternal, Newborn, Child and Adolescent Health: Current Situation & Way Froward, 2017, accessed June 2020. https://www.moh.gov.iq/upload/upfile/ar/1000.pdf 268 UNICEF, Iraq 2020 Internal Displacement Crisis Humanitarian Situation Report, January to March 2020, accessed June 2020. https://reliefweb.int/sites/reliefweb.int/files/resources/Iraq%20Humanitarian%20Situation%20Report%20%28IDP%29%20for%20January%20to%20March%202020.pdf 269 OCHA, Humanitarian Needs Overview 2020, Iraq. Issued November 2019, accessed June 2020. https://reliefweb.int/sites/reliefweb.int/files/resources/iraq_hno_2020.pdf 270 United Nations (WHO, UNICEF, UNFPA), Iraq Reproductive Maternal, Newborn, Child and Adolescent Health: Current Situation & Way Froward, 2017, accessed June 2020. https://www.moh.gov.iq/upload/upfile/ar/1000.pdf 271 United Nations (WHO, UNICEF, UNFPA), Iraq Reproductive Maternal, Newborn, Child and Adolescent Health: Current Situation & Way Froward, 2017, accessed June 2020. https://www.moh.gov.iq/upload/upfile/ar/1000.pdf 272 Iraqi MOH and WHO, Comprehensive Assessment of Health Information System: Iraq, 2019, accessed June 2020. https://moh.gov.iq/upload/upfile/ar/993.pdf
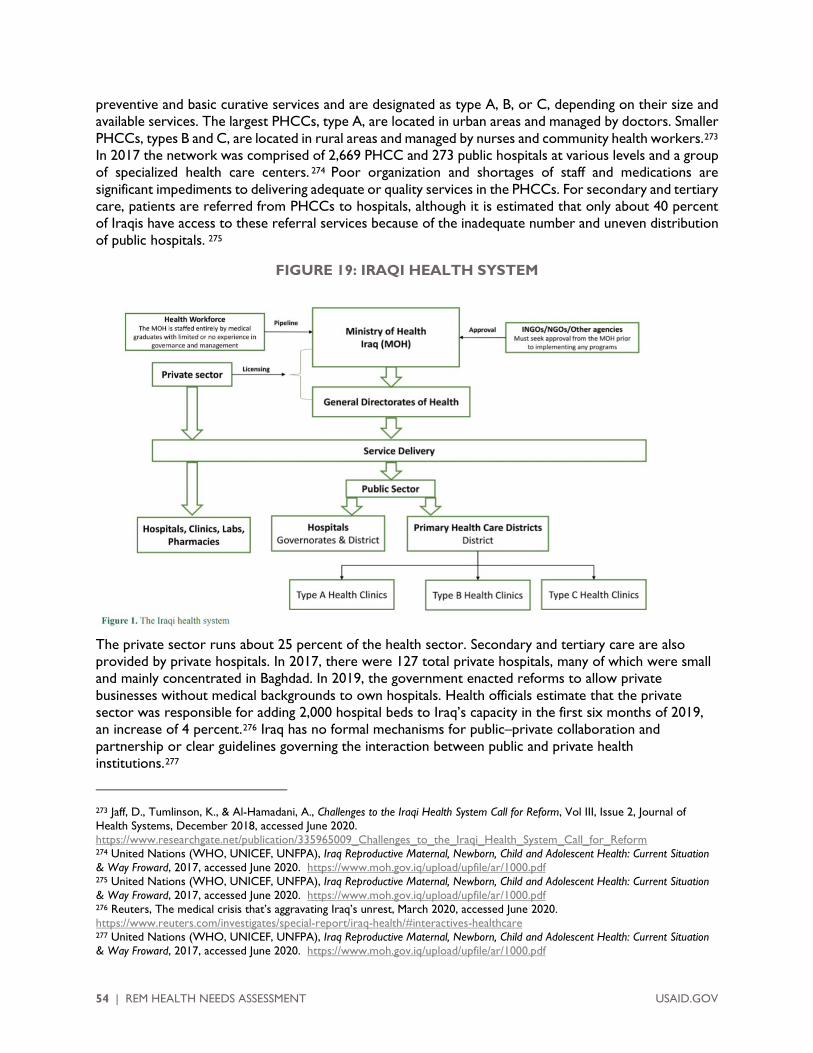
54 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
preventive and basic curative services and are designated as type A, B, or C, depending on their size and available services. The largest PHCCs, type A, are located in urban areas and managed by doctors. Smaller PHCCs, types B and C, are located in rural areas and managed by nurses and community health workers.273 In 2017 the network was comprised of 2,669 PHCC and 273 public hospitals at various levels and a group of specialized health care centers. 274 Poor organization and shortages of staff and medications are significant impediments to delivering adequate or quality services in the PHCCs. For secondary and tertiary care, patients are referred from PHCCs to hospitals, although it is estimated that only about 40 percent of Iraqis have access to these referral services because of the inadequate number and uneven distribution of public hospitals. 275
FIGURE 19: IRAQI HEALTH SYSTEM
The private sector runs about 25 percent of the health sector. Secondary and tertiary care are also provided by private hospitals. In 2017, there were 127 total private hospitals, many of which were small and mainly concentrated in Baghdad. In 2019, the government enacted reforms to allow private businesses without medical backgrounds to own hospitals. Health officials estimate that the private sector was responsible for adding 2,000 hospital beds to Iraq’s capacity in the first six months of 2019, an increase of 4 percent.276 Iraq has no formal mechanisms for public–private collaboration and partnership or clear guidelines governing the interaction between public and private health institutions.277
273 Jaff, D., Tumlinson, K., & Al-Hamadani, A., Challenges to the Iraqi Health System Call for Reform, Vol III, Issue 2, Journal of Health Systems, December 2018, accessed June 2020. https://www.researchgate.net/publication/335965009_Challenges_to_the_Iraqi_Health_System_Call_for_Reform 274 United Nations (WHO, UNICEF, UNFPA), Iraq Reproductive Maternal, Newborn, Child and Adolescent Health: Current Situation & Way Froward, 2017, accessed June 2020. https://www.moh.gov.iq/upload/upfile/ar/1000.pdf 275 United Nations (WHO, UNICEF, UNFPA), Iraq Reproductive Maternal, Newborn, Child and Adolescent Health: Current Situation & Way Froward, 2017, accessed June 2020. https://www.moh.gov.iq/upload/upfile/ar/1000.pdf 276 Reuters, The medical crisis that’s aggravating Iraq’s unrest, March 2020, accessed June 2020. https://www.reuters.com/investigates/special-report/iraq-health/#interactives-healthcare 277 United Nations (WHO, UNICEF, UNFPA), Iraq Reproductive Maternal, Newborn, Child and Adolescent Health: Current Situation & Way Froward, 2017, accessed June 2020. https://www.moh.gov.iq/upload/upfile/ar/1000.pdf

55 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
HEALTH WORKFORCE
Iraq has a shortage of medical personnel, especially doctors, with a reported 7.4 physicians per 10,000 people (2018). This is far fewer than neighboring Jordan, with 23 per 10,000. Iraq had just 21 nurses and midwives per 10,000 people, compare to 32 in Jordan and 37 in Lebanon.278
Of the total 2,669 PHCCs, 1,259 are ‘main PHCCs’ and 1,410 are health units. Currently, 119 centers apply the family medicine model. Each main PHCC is run by certified physicians and includes specialties like internal medicine, pediatrics and gynecology. These PHCC provide a wide range of services including health promotion, and preventive and curative health services. The health units are operated by a general practitioner or a medical assistant providing essential medical services and basic emergency care.
PHCC financing, shortage of trained and certified physicians, brain drain and migration due to the situation in Iraq are the main barriers to achieving quality health services.279 According to Iraq’s medical association, at least 320 doctors have been killed since 2003. Thousands more have been kidnapped or threatened. Around 20,000 doctors, a third of Iraq’s 52,000 registered physicians, have fled since the 1990s. 280 Doctors, especially young doctors, work long hours for little pay, which forces some to take second jobs in the private sector to supplement their income. It was reported that heath staff have not been paid in over 3 months. About half the PHCCs are staffed with at least one medical doctor (45.9 percent) and the remaining 54 percent are staffed by trained health workers (medical assistants and nurses). 281 In September 2019, hundreds of doctors took to the streets of Baghdad demanding better pay and conditions, joining protests over dire public services and official corruption. 282
SERVICE DELIVERY
The Iraqi health system is a mix of public and private facilities, however, the conflict and instability over the years resulted in poor-quality services and service delivery, with many facilities damaged, under-resourced and with limited skilled health workers. 283 All which has led to a breakdown in trust between doctors and patients. And although private facilities do exist, with no health insurance schemes in Iraq, the out-of-pocket costs of private health care prohibits many Iraqis, especially IDPs, from accessing them.284
In 2017, there was a reported 0.7 PHCC per 10,000 people. 285 However, many facilities were abandoned, destroyed or damaged during different conflicts and need rehabilitation and upgrades. Only half of health
278 World Bank, Open Data 2018, accessed June 2020. https://data.worldbank.org/indicator/SH.MED.PHYS.ZS?locations=IQ 279 Nagwa Nashat, et al, Primary care healthcare policy implementation in the Eastern Mediterranean region; experiences of six countries: Part II, European Journal of General Practice, 2020, accessed June 2020. https://www.tandfonline.com/doi/full/10.1080/13814788.2019.1640210 280 Reuters, The medical crisis that’s aggravating Iraq’s unrest, March 2020, accessed June 2020. https://www.reuters.com/investigates/special-report/iraq-health/#interactives-healthcare 281 United Nations (WHO, UNICEF, UNFPA), Iraq Reproductive Maternal, Newborn, Child and Adolescent Health: Current Situation & Way Froward, 2017, accessed June 2020. https://www.moh.gov.iq/upload/upfile/ar/1000.pdf 282 Reuters, The medical crisis that’s aggravating Iraq’s unrest, March 2020, accessed June 2020. https://www.reuters.com/investigates/special-report/iraq-health/#interactives-healthcare 283 Iraqi MOH and WHO, Comprehensive Assessment of Health Information System: Iraq, 2019, accessed June 2020. https://moh.gov.iq/upload/upfile/ar/993.pdf 284 European Union, Country Policy and Information Note, Iraq: Medical and Healthcare issues, 2019, access June 2020. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/800235/_external__Iraq_-_Medical_and_healthcare_-_CPIN_-_v1.0__May_2019_.pdf 285 WHO EMRO, “Framework for Health Information Systems and Core Indicators for Monitoring Health Situation and Health System Performance," 2018, https://applications.emro.who.int/docs/EMROPUB_2018_EN_20620.pdf?ua=1&ua=1

56 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
facilities in Nineveh are fully functional.286 The Iraqi MoH reported that 32 percent of hospitals and 14 percent of PHCC in Nineveh were destroyed. About 35 percent of PHCCs in Kirkuk are not functional. Water and power systems that health facilities depend on need repairs.287 A 2017 MoH survey found that less than a fifth (19.3 percent) of health facilities had regular electricity, improved water source, functioning communication equipment, computer and internet services, and functioning latrines and transportation for referrals. Only 29 percent had a full set of seven pieces of basic equipment (Adult weighing scale, uni-scale, height measuring board, thermometer, stethoscope, BP apparatus and light source).288
In 2018 UN Office for Coordination of Humanitarian Affairs (OCHA) reported 5.5 million people are in need of healthcare in Iraq but lacked access to health services. 289 Health facilities are not equally distributed across governorates or between rural and urban areas. There are also wide disparities of services between the richest and poorest areas. Even though health services in public hospitals are low cost, those that can afford it choose to receive care in the private sector to avoid long waiting times and adverse perceptions of quality in the public sector.290 A study related to child immunization reported a number of reasons why children are not being vaccinated including accessibility issues (e.g., the PHCC is too far away, no one is available to accompany the mother to the facility, and cost considerations); awareness and perceptions (e.g., myths/misinformation regarding vaccination); supply-chain management issues (e.g., stock-outs); and other quality-of-care shortcomings (e.g., attitude/interpersonal skills of vaccinators).291
In Iraq, around 2.8 million people are estimated to be in need of health-related humanitarian support in 2020, of which around 17 percent are children under five.292 Some 324,533 individuals in camps, 493,050 individuals out-of-camps, 17,455 individuals among host communities and 1,974,543 returnees need essential primary health care services, which is often provided by humanitarian partners.293 In late 2019, based on a stated goal to return IDPS home by 2020, the Government of Iraq initiated the consolidation and closure of IDP camps, which resulted in significant reductions in in-camp populations, increases in out-of-camp displaced populations and returnees, and movements of people between governorates. Although as populations return, a new challenge will be ensuring returnees have access to health services in their communities.
According to a 2019 IOM study, 60.7 percent of IDPs have at some point received health humanitarian services, 25.7 percent still receive them, and 67.4 percent of returnees used health services during displacement and 34 percent used them up until right before they returned. Yazidis received the most health services with 51.2 percent currently receiving assistance (Figure 20).294
286 United Nations (WHO, UNICEF, UNFPA), Iraq Reproductive Maternal, Newborn, Child and Adolescent Health: Current Situation & Way Froward, 2017, accessed June 2020. https://www.moh.gov.iq/upload/upfile/ar/1000.pdf 287 EASO, Iraq Key Socio-economic Indicators February 2019, accessed June 2020. https://www.easo.europa.eu/sites/default/files/publications/Iraq-key-socio-economic-indicators.pdf 288 United Nations (WHO, UNICEF, UNFPA), Iraq Reproductive Maternal, Newborn, Child and Adolescent Health: Current Situation & Way Froward, 2017, accessed June 2020. https://www.moh.gov.iq/upload/upfile/ar/1000.pdf 289 EASO, Iraq Key Socio-economic Indicators February 2019, accessed June 2020. https://www.easo.europa.eu/sites/default/files/publications/Iraq-key-socio-economic-indicators.pdf 290 United Nations (WHO, UNICEF, UNFPA), Iraq Reproductive Maternal, Newborn, Child and Adolescent Health: Current Situation & Way Froward, 2017, accessed June 2020. https://www.moh.gov.iq/upload/upfile/ar/1000.pdf 291 Ibid. 292 UNICEF, Iraq 2020 Internal Displacement Crisis Humanitarian Situation Report, January to March 2020, accessed June 2020. https://reliefweb.int/sites/reliefweb.int/files/resources/Iraq%20Humanitarian%20Situation%20Report%20%28IDP%29%20for%20January%20to%20March%202020.pdf 293 OCHA, Humanitarian Needs Overview 2020, Iraq. Issued November 2019, accessed June 2020. https://reliefweb.int/sites/reliefweb.int/files/resources/iraq_hno_2020.pdf 294 IOM Iraq, Understanding Ethno-religious groups in Iraq: Displacement and Return, February 2019, accessed 2020. https://reliefweb.int/sites/reliefweb.int/files/resources/iom_dtm_er_singlepages_digital.pdf

57 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
FIGURE 20: IDPS CURRENTLY RECEIVING HEALTH ASSISTANCE PER ETHNIC AND RELIGIOUS GROUP
MATERNAL AND CHILD HEALTH SERVICES
The 2018 MICS found that 86.6 percent of health facilities in Iraq have a place/location for delivering children. This percentage was higher in KRI (91 percent) and lower in Nineveh (83.6 percent) and Baghdad (83.4 percent). About 96 percent of women (15-49 years) who had a live birth in the last 2 years had their birth attended by a skilled health personnel. In KRI this was 97.9 percent and Baghdad 97.2 percent, and Nineveh 91.6 percent. About 70 percent of women (15-49 years) with a live birth in the last 2 years saw a provider at least 4 times during their pregnancy. This percentage was slightly higher in KRI (74.6 percent) and Baghdad (75.1 percent), but much lower in Nineveh (57.8).295 The MICS also reported that about 82 percent of mothers received a health check following the birth while in the facility or at home, but only 0.8 percent of them had a postnatal visit within two days after delivery. For newborn postnatal care, 76.7 percent of newborns received a health check following birth, as admitted by mothers, and 3.1percent of the newborns were taken for a PNC visit in the two days following birth.296
A 2017 MOH maternal and child health facility survey included 296 facilities in 19 districts (about one district per governorates) across Iraq. The most frequently provided services were child curative care and vaccination (85 percent and 84 percent), followed by ANC and PNC (73 percent) and child growth monitoring (63 percent). Family planning and delivery and new-born care services were only 40 percent and provided in 19 percent of the facilities. The overall availability of all these six basic services (child vaccination, child growth monitoring, child curative care, family planning, ANC and PNC, delivery and newborn care) was observed in only 15 percent of those facilities.297
MENTAL HEALTH AND SEXUAL AND GENDER-BASED VIOLENCE
In 2017 WHO reported, 0.34 psychiatrists working in the mental health sector per 100,000 people, 1.218 nurses per 100,000 people, 0.089 social workers per 100,000, and 0.111 psychologists 100,000.298
295 UNICEF, Iraq Multiple Indicator Cluster Survey (MICS) 2018, accessed June 2020. http://mics.unicef.org/surveys 296 https://www.moh.gov.iq/upload/upfile/ar/1000.pdf 297 United Nations (WHO, UNICEF, UNFPA), Iraq Reproductive Maternal, Newborn, Child and Adolescent Health: Current Situation & Way Froward, 2017, accessed June 2020. https://www.moh.gov.iq/upload/upfile/ar/1000.pdf 298 WHO, Human Resource data – Global Health Observatory, accessed June 2020. https://apps.who.int/gho/data/node.main.MHHR?lang=en
51%
26%
16%
8%
Yazidis Christians Shabak Shias Turkmen Shias

58 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
Mental health and psychosocial support are still a challenge in Iraq. There are very limited psychosocial support services available, and most are offered by private institutes, the cost of which is prohibitive for many families, especially IDPs. In 2017, only a reported 80 practicing psychologists in Iraq and KRI were working with a limited number of psychiatrists. All were struggling to meet overwhelming needs with limited resources. This need for psychosocial care options has pushed local and international organizations to employ health workers who lack the training to treat severe trauma and do not have the practical skills like case management, doctor-patient ethics, or emergency care for traumatized individuals.299
April 2020, the WHO Health Cluster conducted a rapid assessment looking at 48 facilities (83 percent PHCC, 12 percent hospital and 4 percent MMC) across 6 governates (Nineveh, Kirkuk, Erbil, Anbar, and Dyala, Salah Aldin). Of these, 13.5 percent were in camps and 87.5 percent outside camps. They served 14.5 percent IDPs, 72.9 percent host community residents, and 12.5 refugees. About 94 percent of facilities provided mental health and psychosocial support (MPHSS) services and 40 percent reported increases of women survivors of violence coming in for help since COVID. The most common kind of violence reported were physical, psychological, emotional, mental, sexual violence by partner/spouse and/or family member, followed by harassment by strangers, and sexual exploitation by strangers. About 47 percent were seeking MHPSS services, 33.3 percent seeking referrals to specialized GBV services and 19.4 percent clinical management of rape. Sixty-nine percent of facilities reported their staff received training on GBV, 81 percent of facilities have updated referral pathways to other services (e.g. case management, women centers, hotlines, etc.) and 95 percent of them included GBV services.300
HEALTH FINANCE
Under the 2014-2023 Iraq National Health Policy, the MOH "provides comprehensive and inclusive healthcare to all individuals and at the highest quality through the efficient use of available resources.”301 Public health expenditure increased from 1.98 percent to 3.8 percent between 2003 and 2017. The health expenditure per capita in 2015 was $36.33 and health expenditures accounts for 3.4 percent of the GDP. In contrast, the average for middle-income countries is 5.36 percent. About 60 percent of the MOH budget is dedicated to salaries with 38 percent being spent on goods and services. 302 In 2019 the government allocated just 2.5 percent of the state’s $106.5 billion budget to MOH. By comparison, security forces received 18 percent and the oil ministry 13.5 percent. Over the past decade, Iraq has spent less per capita on healthcare than its much poorer neighbors, for example $161 per citizen each year on average, compared to Jordan’s $304 and Lebanon’s $649. 303 Most health spending is allocated to emergencies and to the humanitarian crisis.304 International NGO and donor funds also account for a major source of revenue for primary care services, particularly in relation to services for IDP and refugees,
299 The European Union, Country Policy and Information Note Iraq: Medical and healthcare Issues, May 2019, access June 2020. https://www.justice.gov/eoir/page/file/1162586/download 300 WHO Health Cluster, Rapid Assessment of Health Services Response to GBV survivors during COVID, April 2020, accessed June 2020. https://www.humanitarianresponse.info/en/operations/iraq/assessment/rapid-assessment-health-services-response-gbv-survivors-during-covid-19 301 UN, Iraq First National Voluntary Review on Sustainable Development Goals, 2019, accessed June 2020. https://sustainabledevelopment.un.org/content/documents/23789Iraq_VNR_2019_final_EN_HS.pdf 302 United Nations (WHO, UNICEF, UNFPA), Iraq Reproductive Maternal, Newborn, Child and Adolescent Health: Current Situation & Way Froward, 2017, accessed June 2020. https://www.moh.gov.iq/upload/upfile/ar/1000.pdf 303 Reuters, The medical crisis that’s aggravating Iraq’s unrest, March 2020, accessed June 2020. https://www.reuters.com/investigates/special-report/iraq-health/#interactives-healthcare 304 USAID Health Finance & Governance, Trends in Health Financing and the Private Health Sector in the mIddle East and North Africa, 20181, accessed June 2020. https://www.shopsplusproject.org/sites/default/files/resources/Trends%20in%20Health%20Financing%20and%20the%20Private%20Health%20Sector%20in%20the%20Middle%20East%20and%20North%20Africa.pdf

59 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
and host communities.305 However, humanitarian funding has been decreasing over the recent years. In 2019 the humanitarian community operated under a $700 million coordinated plan to assist 1.75 million IDPs, in 2020 this budget was reported to be $520 million to continue this work.306
The Iraqi constitution states that the government is responsible for providing free health care through public facilities and hospitals to all citizens of Iraq. For example, health facilities run by the government provide MNCH services at very nominal rates or free of cost. Despite increases in health expenditures, however, there is a disproportionate rate of increase in out of pocket expenditures that further worsens the disparity between rich and poor. The absence of controls and rapid escalation of fees for private health services affects the affordability of services, even for middle-class groups.307 Recent updates from WHO (2018) indicate that out-of-pocket expenditure is 78.5 percent compared to 46.4 percent in 2012. An estimated 7.7 million people in Iraq fall into extreme poverty each year due to health expenses.308
There is no health insurance system to serve the public, so most Iraqis rely on the central government-run public health care system. In 2018, 0.4 percent of women (15 – 49 years) were covered by health insurance in Iraq, and a majority of those were in Baghdad with a reported 0.5 percent compared to 0.1 percent in KRI and 0 in Nineveh. Low numbers were reported for children as well, with 0.5 percent of both children under-five and children between 5- and 17-years old covered by health insurance.309
The Kurdistan Regional Government (KRG) is legally entitled to receive a proportion of Iraq’s overall public budget. This population-based resource allocation was previously set at 17 percent, however through recent negotiations, in 2019 KRG was allocated 12.7 percent of the budget. KRG public spending on health as a proportion of total government expenditure has been reported to be between 4.8–5.5 percent. An estimated 20 percent of the public health care budget is allocated to primary care in 2012. However, due to ongoing crises, the KRG is running high annual deficits trying to respond to the influx of refugees and IDPs. Consequently, it is estimated that per capita health expenditure decreased from $159.91 (pre-crisis) to $29 (2014).310
Historically KRG’s patient co-payments and user fees were minor and did not represent a significant source of revenue for the public health care system. However, more recently a ‘semi-private’ scheme reportedly s been applied to hospitals, which increased out-of-pocket expenditures in public hospitals to approximately 80 percent. The current economic crisis has reduced the income of the general population and shifted many patients to seek care in public facilities rather than private ones. The load on public facilities has increased as a result. 311
305 Shukor, A.R., Klazinga, N.S. & Kringos, D.S. Primary care in an unstable security, humanitarian, economic and political context: the Kurdistan Region of Iraq. BMC Health Serv Res 17, 592, 2017, accessed June 2020. https://doi.org/10.1186/s12913-017-2501-z 306 UN, UN extremely concerned about the impact of bureaucratic constraints leading to reduced humanitarian access to 2.4 million Iraqis in need of assistance, January 2020, accessed June 2020. https://reliefweb.int/report/iraq/united-nations-extremely-concerned-about-impact-bureaucratic-constraints-leading-reduced 307 United Nations (WHO, UNICEF, UNFPA), Iraq Reproductive Maternal, Newborn, Child and Adolescent Health: Current Situation & Way Froward, 2017, accessed June 2020. https://www.moh.gov.iq/upload/upfile/ar/1000.pdf 308 United Nations (WHO, UNICEF, UNFPA), Iraq Reproductive Maternal, Newborn, Child and Adolescent Health: Current Situation & Way Froward, 2017, accessed June 2020. https://www.moh.gov.iq/upload/upfile/ar/1000.pdf 309 UNICEF, Iraq Multiple Indicator Cluster Survey (MICS) 2018, accessed June 2020. http://mics.unicef.org/surveys 310 Shukor, A.R., Klazinga, N.S. & Kringos, D.S. Primary care in an unstable security, humanitarian, economic and political context: the Kurdistan Region of Iraq. BMC Health Serv Res 17, 592, 2017, accessed June 2020. https://doi.org/10.1186/s12913-017-2501-z 311 Ibid.

60 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
In 12017, the overwhelming majority of the KRG budget was dedicated to salaries. Reportedly, the public payroll includes ghost employees and salary structures bloated by allowances and lifetime pension schemes. 312
ACCESS TO ESSENTIAL MEDICINES
Kimadia is the sole government-owned public company managed by the MoH that is responsible for the importation and distribution of all pharmaceuticals, medical appliances, laboratory equipment, laboratory consumables, and medical equipment for all public health care facilities in Iraq and KRI.313 There is limited local production of medical equipment and supplies, so most are imported. There are 17 privately owned factories, which also make basic medicines with outdated technology. These firms cover less than 8 percent of market need and lack raw materials, technology and equipment to fully operate.314
There has also been erosion in cold chain maintenance and a break-down of the cold chain in some conflict affected areas risking the potency of vaccines and particular drugs.315The supply of medical services does not meet demand, particularly in areas with large numbers of IDPs.316 Local private companies are allowed to import and sell pharmaceuticals and medical equipment to the private clinics and privately owned hospitals only, not public facilities. In addition, Kimadia is only authorized to procure new equipment to be used in the public hospitals, while the private sector can buy and use refurbished equipment in their facilities. 317
The Iraqi MoH faces challenges in procuring and making available medicines and medical supplies to meet the demand due to budget cuts. In addition, Kimadia processes for procurement of medicines and medical supplies are complex and time consuming. 318 In February 2019, WHO and the MoH held a workshop to review current procurement practices and lessons learned from other countries on making the medical supply chain system more efficient.319
LEADERSHIP/GOVERNANCE
The Iraqi MOH frames the national vision, policies and strategic health planning and management. However limited funding and capacity along with ongoing conflict and instability have made it difficult for the MoH to focus on health system strengthening and implementing interventions to improve quality of care.320 The standard-setting is relatively weak in Iraq. The standards and mechanisms used for regulating health professions are complex and out of date. There is limited capacity to monitor practices at the
312 Ibid. 313 International Trade Administration (ITA), Healthcare Resource Guide: Iraq (2018), accessed June 2020. https://2016.export.gov/industry/health/healthcareresourceguide/eg_main_116238.asp 314 Reuters, The medical crisis that’s aggravating Iraq’s unrest, March 2020, accessed June 2020. https://www.reuters.com/investigates/special-report/iraq-health/#interactives-healthcare 315 United Nations (WHO, UNICEF, UNFPA), Iraq Reproductive Maternal, Newborn, Child and Adolescent Health: Current Situation & Way Froward, 2017, accessed June 2020. https://www.moh.gov.iq/upload/upfile/ar/1000.pdf 316 EASO, Iraq Key Socio-economic Indicators February 2019, accessed June 2020. https://www.easo.europa.eu/sites/default/files/publications/Iraq-key-socio-economic-indicators.pdf 317 International Trade Administration (ITA), Healthcare Resource Guide: Iraq (2018), accessed June 2020. https://2016.export.gov/industry/health/healthcareresourceguide/eg_main_116238.asp 318 WHO, Improving availability of and access to essential and life-saving medicines and medical supplies in Iraq, March 2019, accessed June 2020. http://www.emro.who.int/irq/iraq-news/improving-availability-of-and-access-to-essential-and-life-saving-medicines-and-medical-supplies-in-iraq.html 319 Ibid. 320 Jaff, D., Tumlinson, K., & Al-Hamadani, A., Challenges to the Iraqi Health System Call for Reform, Vol III, Issue 2, Journal of Health Systems, December 2018, accessed June 2020. https://www.researchgate.net/publication/335965009_Challenges_to_the_Iraqi_Health_System_Call_for_Reform

61 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
facility level and medical staff gets limited, if any, new training or professional development. Professional associations are currently delegated with the licensing authority for professional practices in both public and private sectors. Accreditation in Iraq is still being institutionalized.321
The health system is complex and difficult to manage due to decades of inefficiency and lack of accountability.322 The complexity of the health care delivery system and the increasing role of the private sector require careful planning and management of human resources in order to achieve equitable provision of health care. There is still a need for modernization of the public sector, addressing comprehensive and integrated sector governance and its implementation in terms of provision of services and effective management of the country’s resources. 323
The limited regulation and licensing of private facilities has resulted in a lack of transparency and information on the quality of services and no accountability. Clinicians working in these facilities are not held accountable to standards of practice or guidelines. The private sector is expanding with new private facilities, pharmacies, and medical warehouses nationwide, mostly unregulated. Additionally, the private sector workforce also includes public sector employees who collect full-time public-sector salaries and benefits while spending the majority of their time in private practice. 324
The KRG MoH was established in the early 1990s and generally follows the basic centralized bureaucratic organizational structure of the Iraqi MoH. The KRG MoH oversees six Directorates of Health each led by a Director General. The Directorates are comprised of Districts and Sub-Districts (Figure 21). Organizational charts exist at ministry, governorate and district levels; however, detailed descriptions of health care key roles, responsibilities and functions including primary care are lacking. Little is published about primary care governance structures, capacities and processes in either KRG or Iraq, or the interactions between them. The private health market is poorly governed and regulated.325
321 United Nations (WHO, UNICEF, UNFPA), Iraq Reproductive Maternal, Newborn, Child and Adolescent Health: Current Situation & Way Froward, 2017, accessed June 2020. https://www.moh.gov.iq/upload/upfile/ar/1000.pdf 322 Jaff, D., Tumlinson, K., & Al-Hamadani, A., Challenges to the Iraqi Health System Call for Reform, Vol III, Issue 2, Journal of Health Systems, December 2018, accessed June 2020. https://www.researchgate.net/publication/335965009_Challenges_to_the_Iraqi_Health_System_Call_for_Reform 323 United Nations (WHO, UNICEF, UNFPA), Iraq Reproductive Maternal, Newborn, Child and Adolescent Health: Current Situation & Way Froward, 2017, accessed June 2020. https://www.moh.gov.iq/upload/upfile/ar/1000.pdf 324 Jaff, D., Tumlinson, K., & Al-Hamadani, A., Challenges to the Iraqi Health System Call for Reform, Vol III, Issue 2, Journal of Health Systems, December 2018, accessed June 2020. https://www.researchgate.net/publication/335965009_Challenges_to_the_Iraqi_Health_System_Call_for_Reform 325 Shukor, A.R., Klazinga, N.S. & Kringos, D.S. Primary care in an unstable security, humanitarian, economic and political context: the Kurdistan Region of Iraq. BMC Health Serv Res 17, 592, 2017, accessed 2020. https://doi.org/10.1186/s12913-017-2501-z
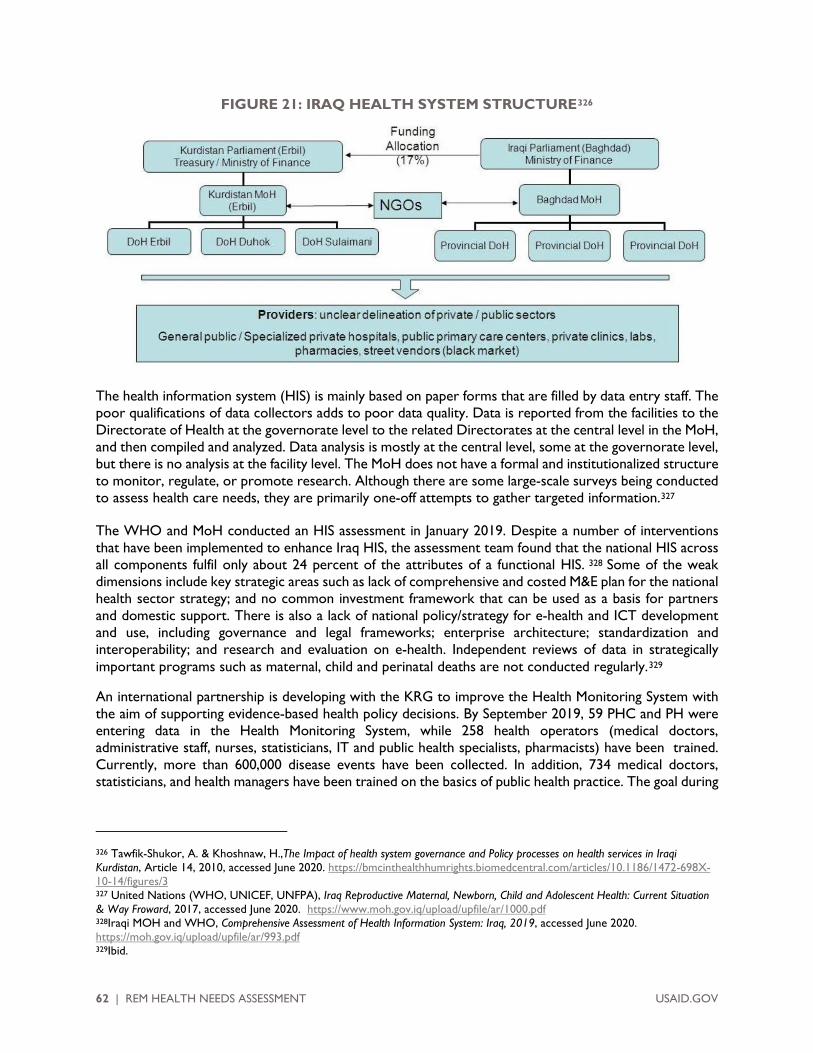
62 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
FIGURE 21: IRAQ HEALTH SYSTEM STRUCTURE326
The health information system (HIS) is mainly based on paper forms that are filled by data entry staff. The poor qualifications of data collectors adds to poor data quality. Data is reported from the facilities to the Directorate of Health at the governorate level to the related Directorates at the central level in the MoH, and then compiled and analyzed. Data analysis is mostly at the central level, some at the governorate level, but there is no analysis at the facility level. The MoH does not have a formal and institutionalized structure to monitor, regulate, or promote research. Although there are some large-scale surveys being conducted to assess health care needs, they are primarily one-off attempts to gather targeted information.327
The WHO and MoH conducted an HIS assessment in January 2019. Despite a number of interventions that have been implemented to enhance Iraq HIS, the assessment team found that the national HIS across all components fulfil only about 24 percent of the attributes of a functional HIS. 328 Some of the weak dimensions include key strategic areas such as lack of comprehensive and costed M&E plan for the national health sector strategy; and no common investment framework that can be used as a basis for partners and domestic support. There is also a lack of national policy/strategy for e-health and ICT development and use, including governance and legal frameworks; enterprise architecture; standardization and interoperability; and research and evaluation on e-health. Independent reviews of data in strategically important programs such as maternal, child and perinatal deaths are not conducted regularly.329
An international partnership is developing with the KRG to improve the Health Monitoring System with the aim of supporting evidence-based health policy decisions. By September 2019, 59 PHC and PH were entering data in the Health Monitoring System, while 258 health operators (medical doctors, administrative staff, nurses, statisticians, IT and public health specialists, pharmacists) have been trained. Currently, more than 600,000 disease events have been collected. In addition, 734 medical doctors, statisticians, and health managers have been trained on the basics of public health practice. The goal during
326 Tawfik-Shukor, A. & Khoshnaw, H.,The Impact of health system governance and Policy processes on health services in Iraqi Kurdistan, Article 14, 2010, accessed June 2020. https://bmcinthealthhumrights.biomedcentral.com/articles/10.1186/1472-698X-10-14/figures/3 327 United Nations (WHO, UNICEF, UNFPA), Iraq Reproductive Maternal, Newborn, Child and Adolescent Health: Current Situation & Way Froward, 2017, accessed June 2020. https://www.moh.gov.iq/upload/upfile/ar/1000.pdf 328Iraqi MOH and WHO, Comprehensive Assessment of Health Information System: Iraq, 2019, accessed June 2020. https://moh.gov.iq/upload/upfile/ar/993.pdf 329Ibid.

63 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
the next 3 years is to reach 120 operative centers within the region, envisaging a subsequent expansion of the system to all Iraq, but multiple stakeholder partnerships is essential.330
CONCLUSION
The deterioration of Iraq’s healthcare system ultimately leaves communities impacted by displacement and violence without the support or treatment needed to recover. Massive brain drain across the medical profession since the 1980s, compounded by infrastructure damage and targeted political violence, has left Iraq without the physicians needed to care for the populations. Shortages of medicine and limitation on funding and investment have impacted the growth, quality and coverage of health services in Iraq. Without sustained investment and capacity building the public health system is struggling and not prepared to deal with further crisis, including COVID-19.
AQ 3: CRITICAL HEALTH NEEDS AND GAPS IN HEALTH SERVICES FOR THE REM COMMUNITIES
REM communities in Iraq have faced conflict, displacement and economic hardships, which has contributed to their limited access and utilization of health services. REM populations are less than 3 percent of the overall population yet represent 18 percent of the IDP population in Iraq. In addition to the need to increase, expand and improve general public curative and prevention health services, another important gap to fill for REM communities is mental health and SGBV services.
In addition, to the general vulnerabilities, some REM communities in northern Iraq also face discrimination and violence. Although there is limited data on the prevalence of mental health needs in Iraq, the recent and continued conflict and violence negatively impacts the population’s mental health. Psychosocial needs among this IDP population are reported to be extremely high. Although the Iraqi MoH and NGOs have put more focus on mental health in the recent years, many gaps in MPHSS services exist, especially for IDPs. Referral and support systems are weak or non-existent, and services are still stigmatized or not believed to be needed or important. There is also a lack of awareness about available services. Engagement with community members is important to promote use of and decrease stigma of metal health concerns and services.331
There is also a need for more mental health service providers as well as improvements in the capacity among doctors and nurses and other frontline health works. This lack of providers limits the availability and quality of services. In addition, a strong mental health system includes prevention (e.g., community stigma reduction); case management (e.g., psychological assessment, diagnosis); treatment (e.g., counselling, psychosocial interventions, and medications); follow-up (e.g., monitoring of symptoms); and reintegration (e.g., social and economic interventions). Iraq does not have the capacity to implement all of these components across the health system and will need to continue to develop each of these elements.
Many Yazidis in northern Iraq suffer from extreme psychosocial distress as a result of the serious violence they have experienced, including the loss or captivity of family members, ongoing displacement and
330 Gialloreti, L. et al, Supporting Iraqi Kurdistan Health Authorities in Post-Conflict Recovery: The development of a Health Monitoring System, Frontiers in Public Health, Jan 2020, accessed June 2020. https://www.researchgate.net/publication/338928852_Supporting_Iraqi_Kurdistan_Health_Authorities_in_Post-conflict_Recovery_The_Development_of_a_Health_Monitoring_System 331 Protection Cluster Iraq, Psychosocial (PSS) Activities in Iraq, 2019 Achievements & 2020 Needs, accessed June 2020. https://reliefweb.int/sites/reliefweb.int/files/resources/Psychosocial%20Support%20%28PSS%29%20Activities%20in%20Iraq%20-%202019%20Achievements%20%26%202020%20Needs.pdf

64 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
economic hardship. While the humanitarian community as well as relevant institutions of the KRG are engaged in efforts to provide psychosocial support to Yazidi women and children who escaped from ISIS captivity, reports indicate that the level of support and professional capacity remains inadequate given the overwhelming and urgent needs.332
Cultural norms and traditional practices also hindered the ability of women to access services on their own, particularly SGBV and sexual and reproductive services. Women’s access was restricted both by their husbands and/or family members. The vulnerable women’s own lack of trust in the services created an additional barrier to their uptake of services. OCHA conducted a rapid assessment in 2020 to learn about the impact of COVID-19 on incidences of GBV. Lack of income, harmful social norms or traditional practices, lack of health services (including reproductive health), and lack of safe shelter for GBV survivors were among the top reported GBV risks. The assessment found that there was a 65 percent increase in reported cases of GBV during the outbreak; 94 percent of incidents were reported to be domestic violence perpetrated by a household member. Nearly three quarters of respondents reported that isolation was the main reason for an increase in domestic violence. In May 2020, there were reportedly 123 GBV-related suicide attempts or incidents reported involving women and girls, with the majority reported in Ninewa, Diyala and Kirkuk governorates since the beginning of the outbreak (March 2020).333
AQ 4: EXTERNAL STRESSES
The multiple, challenging, interrelated external stresses have hampered efforts to improve health status in northern Iraq. Iraq is in a fragile situation with recent protests, new government leadership and resurgent of conflict. This situation is exacerbated by the rapid spread of COVID-19, which the country’s healthcare system has limited capacity and limited fiscal buffers to contain and manage.334 External factors have played a large role in REM populations current situation, some of these main external stresses the effect the delivery of health services include:
COVID-19
As of September 2020, there have been over 320,000 COVID-19 cases throughout the country, with an average of 4,000 daily positive cases a day and 500 deaths a week. More than 40 percent of these cases are detected in Baghdad Governate.335 Iraq has established a series of measures to prevent the spread of the virus including strict curfew measures, closure of border crossing points, suspension of international flights, and disinfection campaigns. While UNHCR, NGOs, and other entities delivering humanitarian assistance are, in principle, excluded from these measures restricting movement, the capacity to deliver support has been slightly affected, and the overall impact on the protection environment of refugees, IDPs, returnees, and stateless persons has been significant.336
The main protection risks encountered by UNHCR include the closure of borders preventing movement of refugees, challenges to access camps and reach certain locations, lack of livelihood opportunities and its socio-economic consequences, rise in the prices of basic food items, increased risk of eviction, the rise
332 UNHCR, COI Note on the Situation of Yazidi IDPs in the Kurdistan Region of Iraq, May 2019, accessed June 2020. https://www.refworld.org/pdfid/5cd156657.pdf 333 OCHA, OCHA Iraq: Humanitarian Bulletin May 2020, accessed June 2020. https://reliefweb.int/sites/reliefweb.int/files/resources/may_2020_humanitarian_bulleti_20200614_final.pdf 334 World Bank, Iraq Country Profile, May 2020, accessed June 2020. https://www.worldbank.org/en/country/iraq/overview 335 UNHCR, Iraq UNHCR COVID-19 Update, June 23, 2020. Accessed June 2020. https://reliefweb.int/sites/reliefweb.int/files/resources/UNHCR%20Iraq%20-%20COVID-19%20Update%20XI.pdf 336 UNHCR, Iraq Fact Sheet June 2020, accessed June 2020. https://reliefweb.int/sites/reliefweb.int/files/resources/202006%20UNHCR%20Iraq%20Factsheet%20June%202020.pdf

65 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
in domestic violence, and halt of education activities, among others. Most refugees and IDPs across Iraq live on daily wages, and their inability to access job opportunities due to the current health crisis is having a profound impact on their capacity to meet their most basic needs.
Iraq is facing the same challenges as many countries and is trying to adopt a fast track mechanism to procure medical supplies, test kits, PPEs, thermal scanners, and other needed commodities through Kimadia and distribute it to all possible government sites.337 The Iraqi MoH may not have the infrastructure to deal with this outbreak since public healthcare settings are already overwhelmed dealing with many injured people from the ongoing unrest. There is also limited availability of COVID-19 tests which currently are only available in the Central Lab in Baghdad and inadequate quantity of PPE.
SECURITY AND STABILITY
In 2020, Turkey launched a wave of airstrikes against Kurdish militants in Kurdish-controlled northern Iraq, part of an ongoing campaign against the group that has been battling the Turkish army on and off for Kurdish self-rule since 1984.338 Turkish forces have hit over 500 targets in northern Iraq, including Sinjar, as an operation against the PKK. There has been one reported death and unconfirmed reports of hitting near an IDP camp.339
The Islamic State is reported to be ramping up in rural parts of Iraq since the second half of 2019, focusing on Diyala, Kirkuk and Salahaldin provinces, to the east and north of Baghdad. Both the frequency and character of the attacks have been steadily increasing, and there is data that suggests the Islamic State is moving skilled fighters to the area from Syria to stoke a new insurgency. In April 2020, the Islamic State staged 108 attacks in Iraq, including against an intelligence building in Kirkuk. A large assault targeted the paramilitary Popular Mobilization Forces on May 1 near the city of Samarra, showing that the Islamic State is willing to move beyond guerilla tactics and engage in coordinated and sustained fighting.340
Since November 2019, aid deliveries through Iraq have been slowed due to the discontinuation of previously agreed-upon access authorizations procedures. According to a January 2020 survey of NGOs, 90 percent reported the lack of national access authorization procedures has directly affected their operations. Respondents also reported that since the beginning of December 2019, more than 2,460 humanitarian missions had been cancelled or prevented from reaching their destinations. It is estimated that approximately 2.4 million people in need have been affected by the restrictions on humanitarian movements.341
337 Health Cluster Iraq Bulletin, Bulletin No. 2, February 2020, accessed 2020. https://www.humanitarianresponse.info/sites/www.humanitarianresponse.info/files/documents/files/iraq_hq_bulletin2_feb_2020.pdf 338 USCIRF, USIRF Condemns Turkish Military Operations in Northern Iraq, June 19, 20202, accessed June 2020. https://www.uscirf.gov/news-room/press-releases-statements/uscirf-condemns-turkish-military-operations-in-northern-iraq 339 Aljazeera, Turkish air strikes kill civilian in northern Iraq, June 19, 20202, accessed June 2020. https://www.aljazeera.com/news/2020/06/turkish-air-strikes-kill-civilian-northern-iraq-official-200619094440110.html 340Jiyad, S., World Political Review, With ISIS Resurgent, Can Iraq’s New Government Avoid a Repeat of the past?, June 3, 2020, accessed June 2020. https://www.worldpoliticsreview.com/articles/28806/in-iraq-isis-is-resurgent-can-the-new-government-avoid-a-repeat-of-the-past 341 UN, UN extremely concerned about the impact of bureaucratic constraints leading to reduced humanitarian access to 2.4 million Iraqis in need of assistance, January 2020, accessed June 2020. https://reliefweb.int/report/iraq/united-nations-extremely-concerned-about-impact-bureaucratic-constraints-leading-reduced

66 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
POLITICS
The Iraqi Parliament appointed Mustafa Al-Kadhimi as Prime Minister in May 2020, following six months of political uncertainty after the resignation of former Prime Minister Adel Abdul-Mahdi, and two interim appointments who were unable to obtain the necessary political support. The new Prime Minister has announced his intentions to address some of the grievances of the protestors, combat corruption and promote needed economic and security reforms. Elections were expected to take place in early 2020 but have been delayed due to the political crisis and COVID-19.342
Only time will tell how the new government will address the challenges Iraq faces, including the humanitarian crisis. Although most of the protests were in Baghdad and southern Iraq, many of the protestors’ grievances, including rampant corruption, poor public services and high employment, are aligned with the same economic burdens that effect the REM population.
FINANCIAL
Iraq is facing economic challenges with the collapse in international oil prices and other unfavorable conditions, including disruptions caused by the spread of COVID-19. In the absence of significant reforms to boost private sector participation, it will be difficult to jump-start the economy; growth is projected to gradually revert to its low-base potential of 1.9-2.7 percent in 2021–2022. Iraq is expected to face a persistent current account deficit in 2020, driven by lower oil prices and sticky imports.343
In addition, humanitarian funding has been decreasing over the recent years as donors shift money towards other causes. In 2019 the humanitarian community operated under a $700 million coordinated plan to assist 1.75 million IDPs, in 2020 this budget was reported to be $520 million to continue this work.344 There are concerns, especially with the new challenge of COVID-19, that funding will not be enough to support all those in need.
USAID HEALTH AND REM PROGRAMMING
Below is the current list of USAID programming support under the Genocide Recovery and Persecution Response initiative to help REM in northern Iraq. In total more than $350 million has been allocated for assistance in short, medium and long-term programming. See Annex 8 for list of project implementers and Annex 5 for a map of all U.S. complex emergency programming in Iraq.
342 OCHA, OCHA Iraq: Humanitarian Bulletin May 2020, accessed June 2020. https://reliefweb.int/sites/reliefweb.int/files/resources/may_2020_humanitarian_bulleti_20200614_final.pdf 343 World Bank, Iraq Country Profile, May 2020, accessed June 2020. https://www.worldbank.org/en/country/iraq/overview 344 UN, UN extremely concerned about the impact of bureaucratic constraints leading to reduced humanitarian access to 2.4 million Iraqis in need of assistance, January 2020, accessed June 2020. https://reliefweb.int/report/iraq/united-nations-extremely-concerned-about-impact-bureaucratic-constraints-leading-reduced
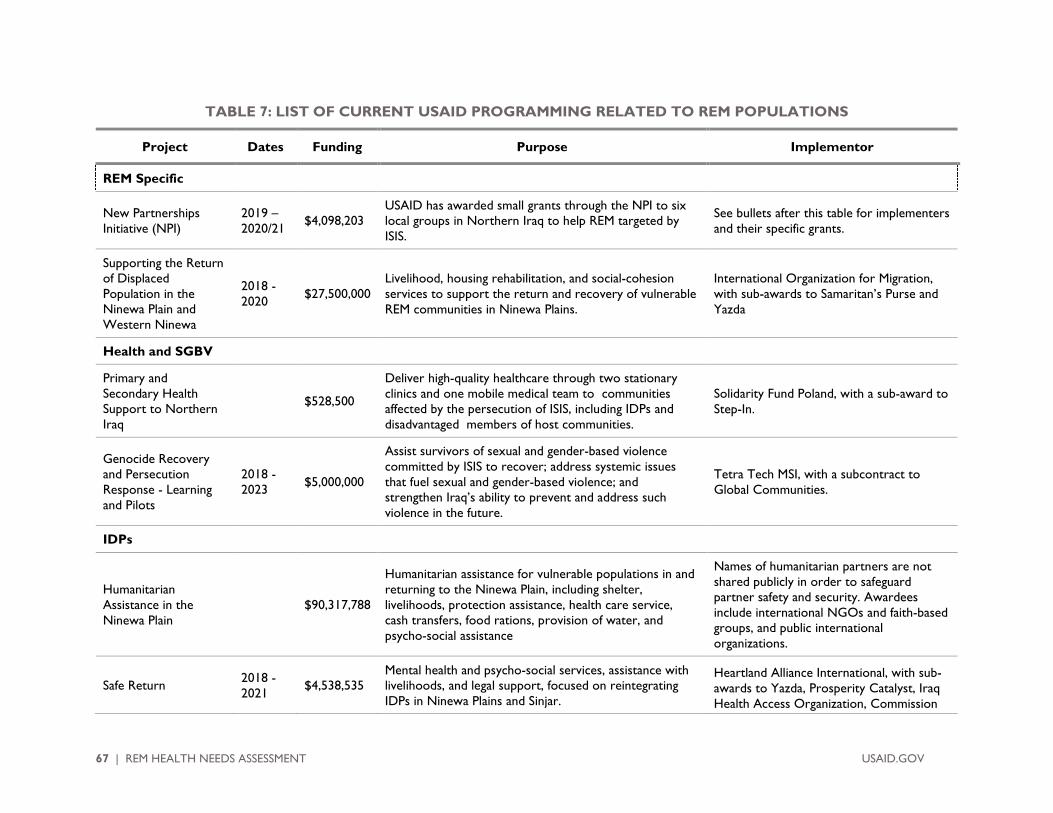
67 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
TABLE 7: LIST OF CURRENT USAID PROGRAMMING RELATED TO REM POPULATIONS
Project Dates Funding Purpose Implementor
REM Specific
New Partnerships Initiative (NPI)
2019 – 2020/21 $4,098,203
USAID has awarded small grants through the NPI to six local groups in Northern Iraq to help REM targeted by ISIS.
See bullets after this table for implementers and their specific grants.
Supporting the Return of Displaced Population in the Ninewa Plain and Western Ninewa
2018 - 2020 $27,500,000
Livelihood, housing rehabilitation, and social-cohesion services to support the return and recovery of vulnerable REM communities in Ninewa Plains.
International Organization for Migration, with sub-awards to Samaritan’s Purse and Yazda
Health and SGBV
Primary and Secondary Health Support to Northern Iraq
$528,500
Deliver high-quality healthcare through two stationary clinics and one mobile medical team to communities affected by the persecution of ISIS, including IDPs and disadvantaged members of host communities.
Solidarity Fund Poland, with a sub-award to Step-In.
Genocide Recovery and Persecution Response - Learning and Pilots
2018 - 2023 $5,000,000
Assist survivors of sexual and gender-based violence committed by ISIS to recover; address systemic issues that fuel sexual and gender-based violence; and strengthen Iraq’s ability to prevent and address such violence in the future.
Tetra Tech MSI, with a subcontract to Global Communities.
IDPs
Humanitarian Assistance in the Ninewa Plain
$90,317,788
Humanitarian assistance for vulnerable populations in and returning to the Ninewa Plain, including shelter, livelihoods, protection assistance, health care service, cash transfers, food rations, provision of water, and psycho-social assistance
Names of humanitarian partners are not shared publicly in order to safeguard partner safety and security. Awardees include international NGOs and faith-based groups, and public international organizations.
Safe Return 2018 - 2021 $4,538,535
Mental health and psycho-social services, assistance with livelihoods, and legal support, focused on reintegrating IDPs in Ninewa Plains and Sinjar.
Heartland Alliance International, with sub-awards to Yazda, Prosperity Catalyst, Iraq Health Access Organization, Commission

68 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
Project Dates Funding Purpose Implementor
for International Justice and Accountability, and Alliance of Iraqi Minorities.
Transitional Assistance to Internally Displaced Persons (IDPs) in Erbil, Iraq
2019-2020 $6,800,000
Assist vulnerable IDP families with immediate household needs, such as shelter and food, and ease their return home when possible.
Catholic Relief Services, with partner Chaldean Catholic Archdiocese of Erbil.
In REM Geographic Areas
Building Community Resilience in Ninewa Post-ISIS
2018-2021 $5,006,996
Enhance cooperation between the Government of Iraq, the Kurdistan Regional Government, local civil society, and communities from the Ninewa Plain and Western Ninewa Province to address policy actions needed to remove barriers to sustainable returns of IDPs and community resilience.
U.S. Institute for Peace, with sub-awards to Sanad for Peacebuilding, Alliance of Iraqi Minorities, Network of Iraqi Facilitators, the Middle East Research Institute, and Alliance 1325 - Supporting the Implementation of National Action Plan for
UNSCR 1325.
Iraq Community Resilience Initiative
2018 - 2022 $53,900,000
Enable recovery of communities liberated from the ISIS, including the Ninewa Plain and Western Ninewa Province, and promote community cohesion.
Chemonics, with 90 Iraqi and faith-based partners**.
Funding Facility for Stabilization (FFS) in the Ninewa Plain and Western Ninewa Province
2015 – 2020 $63,920,359
Rehabilitation of public infrastructure in liberated areas by funding water, health, education, and electricity stabilization activities. Includes support for PHCC.
United Nations Development Programme (UNDP)
Shared Future: Enabling Durable Solutions for a Cohesive and Diverse Ninewa Plain
2018- 2020 $4,969,376
Work with religious leaders and youth to build trust among communities; improve vocational and leadership skills so young people can obtain dignified employment and start their own businesses; address how competition between jobseekers for employment can inadvertently undermine trust and understanding between different religious communities in Nineveh.
Catholic Relief Services, with sub-awards to Caritas Iraq, YouthBuild International, and Iraqi al-Amal Association.
Funding Facility for Stabilization (FFS) in Mosul
2015-2020 $69,700,000
Rehabilitation of public infrastructure in liberated areas. The United States funds water, health, education, and electricity stabilization activities.
UNDP
69 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
** Iraqi and faith-based partners include: Al Diyar Center; All People Organization for Relief and Development; Assyrian Aid Society; Assyrian Christian Committee; Chaldean Catholic Archdiocese of Erbil; Chaldean Culture Society; Christian Aid Program Northern Iraq; Economic Development Organization; Eyzidi 24; Eyzidi Organization for Documentation; Friends Youth Forum; Ghasin Al-Zaiton; Hammurabi Human Rights Organization; Hope Ambassadors Volunteerism Group; Horace Organization for Development and Education; Humanitarian Ninewa Relief Organization; IRFAD; Justice Organization for Minorities Rights; Municipality for Al-Qush; Nisha for the Empowerment of Youth; Odessa; Our Lady of Assumption Catholic Church; Peace through Arts Foundation; St. Matthew’s Monastery; Tal Kayf District Office; The Bartella Sewing Factory; Wasil-Tasil; and Yazda.
New Partnerships Initiative (NPI) Implementers and Grants include:
• Philadelphia Organization for Relief and Development: Establish a community center in the town of Qaraqosh to provide services for people with disabilities, training in employment skills, child care, and a community food bank.
• Catholic University of Erbil: Provide classes in business language and computer software for windows, victims of abuse, and former captives of ISIS.
• Top Mountain: Support a business incubator and employment program for Iraqi youth, which will promote entrepreneurship, provide business training, and build commercial networks.
• Shlama Foundation: Improve job opportunities through training engineers on the installation of solar power, provide electricity for families, and install solar-powered pumps for farms and street lighting for villages.
• Beth Nahrain: Help re-establish a local, women-led organization decimated by ISIS, which will in turn provide small-business vocational training to women in the Nineveh Plains.
• Jiyan Foundation for Human Rights: Provide trauma-rehabilitation and resilience services to survivors of genocide; legal services and programs in justice/reparations; and activities to promote inter-religious and inter-ethnic dialogue.

70 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
LEBANON
FIGURE 22: MAP OF LEBANON
COUNTRY CONTEXT
Lebanon’s population is estimated at 6.8 million, 345 of which roughly 35 percent are non-Lebanese refugees.346 Population estimates vary widely because of the large number of unregistered refugees (both Palestinians and Syrians)—currently, only 30 percent of births among refugees are registered.347
Since the Syrian crisis began in 2011, Lebanon has received refugees from neighboring countries, adding to the Palestinian refugees who have been in Lebanon for more than 70 years. Displaced Syrians—80 percent of whom are women and children—constitute 22 percent of the population (Table 8).348
345 UNICEF, "Key Demographic Indicators: Lebanon," accessed June 6, 2020, https://data.unicef.org/country/lbn/ 346 Central Intelligence Agency, "The World Factbook: Lebanon" (CIA, June 2020). https://www.cia.gov/library/publications/the-world-factbook/geos/le.html 347 UN and MOPH, "Lebanon Crisis Response Plan 2017–2020.” (UN and MOPH, 2020), https://reliefweb.int/sites/reliefweb.int/files/resources/74641.pdf 348 Ibid.
ACF
Sticky Note
lebanon

71 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
TABLE 8: POPULATION BREAKDOWN
Nationality Total
Lebanese349 4,485,000
Displaced Syrians 1,500,000
Palestinian refugees from Syria350 28,800
Palestinian refugees in Lebanon351,352 180,000
Refugees from Iraq353 30,000
Roughly 60 percent of Lebanese descend from the Phoenicians/Canaanites and/or West Aramaic; 25 percent are of Arab descent; 4 percent are Armenians; and 11 percent are mainly Greeks, Assyrians, Hebrews, Kurds, and Persians. 354 The more prevalent ethnic minorities include roughly 137,500 Turkmen,355 80,000 Assyrians,356 and 25,000 Kurds.357
The overflow of refugees into Lebanon, coupled with Lebanon’s economic crisis and recent civil unrest, has significantly increased the number of people living in poverty and dependent on humanitarian aid and has exacerbated development constraints, heightening social tensions and competition for livelihood and access to services. 358 The Central Administration of Statistics reports that the cost of food and nonalcoholic beverages rose 79.5 percent between March and April 2020.359 A significant proportion of both Lebanese and refugee populations live below the poverty line ($3.84/person/day), and the numbers of those living in extreme poverty are expected to rise further in 2020. The percentage of individuals living below the poverty line are as follows: Lebanese (27–30 percent), displaced Syrians (73 percent), Palestinian refugees from Lebanon (67 percent), and Palestinian refugees from Syria (90 percent).360
349 MOPH, "Statistical Bulleting 2018," 2018. https://www.moph.gov.lb/en/DynamicPages/index/8#/en/Pages/8/327/statistical-bulletins 350 OCHA, "Lebanon Humanitarian Fund Annual Report 2019 Lebanon" (OCHA, 2019.) https://reliefweb.int/sites/reliefweb.int/files/resources/Lebanon%20HF%20Report_0.pdf 351 More than 470,000 Palestinian refugees are registered with the United Nations Relief and Works Agency for Palestinian Refugees (UNRWA) in Lebanon, but due to a lack of monitoring of those who have emigrated from Lebanon, the number reported is used for planning purposes. 352 OCHA, "Lebanon Humanitarian Fund Annual Report 2019 Lebanon." 353 U.S. Department of State, "Lebanon 2018 International Religious Freedom Report." (U.S. State Department, 2018). https://www.justice.gov/eoir/page/file/1176951/download 354 IndexMundi, "Lebanon Demographic Profile 2019" (IndexMundi, 2019). https://www.indexmundi.com/lebanon/demographics_profile.html 355 Zaman ElWasl, "Syrian Turkmen refugees face double suffering in Lebanon," October 2015, https://en.zamanalwsl.net/news/article/11837 356 Assyrian Policy Institute, "Lebanon," accessed June 6, 2020, https://www.assyrianpolicy.org/lebanon 357 Minority Rights Group International, "Lebanon," May 2020, https://minorityrights.org/country/lebanon/ 358 UN and MOPH, "Lebanon Crisis Response Plan 2017–2020." 359 Central Administration of Statistics, "Consumer Price Index for Lebanon April 2020 - CPI-COVID-19," April 2020, http://www.cas.gov.lb/images/PDFs/CPI/2020/4-CPI_APRIL2020.pdf 360 UN and MOPH, "Lebanon Crisis Response Plan 2017–2020."

72 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
RELIGIOUS AND ETHNIC MINORITY POPULATION
Focus REM Populations in Lebanon: Christians (Maronite, Greek, Armenian, Syriac, and Chaldean), Druze, Yazidis, Palestinian, and Syrian
Geographic Area of REM Populations: Bekaa governorate, Mount Lebanon governorate, North Governorate, and Beirut
Ethnic groups in Lebanon follow various religions (Figure 23). Lebanon is 60 percent Muslim, 34 percent Christian, 5 percent Druze, and 1 percent other.361 Among the Christian population, the Armenians and Assyrians are Orthodox and Catholic Christians. Catholic Assyrians are either Chaldean Catholics (20,000)362 or Syriac Catholics (32,000).363 According to the NGO Syriac League, approximately 10,000 Iraqi Christians of all denominations and 3,000 to 4,000 Coptic Christians live in Lebanon.364
FIGURE 23: RELIGIOUS BREAKDOWN
The legacy of the 15-year civil war fought along religious lines, and a political system based on confessionalism (whereby political offices are proportionately allocated to certain religious communities) create periodic friction. 365 The country officially recognizes 18 religious groups with very complex demographic patterns. Research conducted in 2019 documented increased levels of religious intolerance—currently at a rate of 20 percent, compared with 4 percent in 2010.366 Because religious balance and discrimination are sensitive political issues, accurate health data broken down by religion or ethnicity are lacking.
An estimated 15 percent of Palestinian refugees are non-Maronite Christians. Most Turkmen, Palestinian refugees, and Syrian refugees are Sunni Muslim; however, the Syrian population also includes Alawites (an offshoot of Islam), Christians, Shi’a, Druze, Isma’ilis, and Yazidis.367 Refugees and foreign migrants also
361 Minority Rights Group International, "Lebanon." 362 GC Catholic, "Chaldean Diocese of Beirut," accessed June 7, 2020, http://www.gcatholic.org/dioceses/diocese/beir4.htm 363 GC Catholic, "Syriac Diocese of Beirut," accessed June 7, 2020, http://www.gcatholic.org/dioceses/diocese/beir5.htm 364 U.S. Department of State, "Lebanon 2018 International Religious Freedom Report." 365 Amos Barshad, "The World's Most Dangerous Census," The Nation, October 17, 2019, https://www.thenation.com/article/archive/lebanon-census/ 366 U.S. Department of State, "Lebanon 2019 International Religious Freedom Report." 367 Minority Rights Group International, "Lebanon."
Sunni Muslim, 29%
Shi'a Muslim, 29%
Alawite Muslims, 2%
Druze, 5%
Maronite Christians,
21%
Greek Catholics (Melkites), 5%
Greek Orthodox, 8%
Other, 1%

73 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
include Sunni Kurds, Shi’a Muslims, Chaldeans and Yazidis from Iraq, and Coptic Christians from Egypt and Sudan.
Since the government suspended the United Nations High Commissioner for Refugees’ (UNHCR’s) ability to register refugees early in 2015, the number of illegal residents has continued to climb—for example, only 22 percent of Syrian adults have legal residency in 2019, down from 27 percent in 2018.368 And although Christians represented 10 percent of Syria’s prewar population, only 1.2 percent of Christian Syrian refugees registered with UNHCR. 369 Some believe that Syrians from religious minorities are reluctant to identify publicly as refugees in Lebanon. Interviews with service providers and Syrian minorities in Lebanon indicate multiple reasons Christian and Kurdish Syrians may not be registered with UNHCR—whereas some may have chosen not to because they are more financially stable, others may have feared that if they registered as refugees, their names would be given to Syrian security forces, thereby preventing them from returning to Syria. 370 For some refugees, the $200 registration fee was a barrier to registering. 371
Caritas, an international faith-based organization (FBO) operating in Lebanon, reports that 43 percent of the Iraqi refugees they serve in Lebanon are Christian, with 38 percent of the Christian Iraqi refugees having illegal status.372 Therefore, although data are limited on the numbers of minority groups within the refugee population, anecdotal evidence suggests that they are found among the refugees.
RELIGIOUS AND ETHNIC MINORITY GEOGRAPHIC FOCUS
Religious and ethnic minority populations are dispersed throughout the country’s eight governorates, with some areas containing larger concentrations of certain religious groups and others being relatively mixed (see Annex 6 for map distribution of religious groups in Lebanon).373 The 2018 voter registration data indicate that concentrations of minority religious groups are found predominantly in the Bekaa (mostly Zahlé) and Mount Lebanon (mostly Aley) governorates and Beirut, except for Greek Orthodox Christians, large numbers of whom reside in the North governorate in Koura, with smaller concentrations in Akkar and Matn (Mount Lebanon).374 In Zahlé, 28 percent of registered voters are Greek Catholics and 10 percent are Greek Orthodox, and in Aley 41 percent of registered voters are Druze.
368 UNICEF, UNHCR, and WFP, "Vulnerability Assessment for Syrian Refugees in Lebanon (VASyR 2019)," 2019, https://data2.unhcr.org/en/documents/download/73118 369 Marwan Kreidie, "Why Do So Few Christian Refugees Register with the United Nations High Commissioner for Refugees?," Rozenberg Quarterly, (2016), http://rozenbergquarterly.com/why-do-so-few-christian-syrian-refugees-register-with-the-united-nations-high-commissioner-for-refugees/ 370 Minority Rights Group International, "An Uncertain Future for Syrian Refugees in Lebanon: The Challenges of Life in Exile and the Barriers to Return" (Minority Rights Group International, 2019). https://minorityrights.org/wp-content/uploads/2019/02/MRG_Brief_Leb_ENG_Feb19.pdf 371 Marwan Kreidie, "Why Do So Few Christian Refugees Register with the United Nations High Commissioner for Refugees?," Rozenberg Quarterly, (2016), http://rozenbergquarterly.com/why-do-so-few-christian-syrian-refugees-register-with-the-united-nations-high-commissioner-for-refugees/ 372 Caritas Lebanon Migrant Center, "Left Behind: A Needs Assessment of Iraqi Refugees Present in Lebanon” (Caritas Lebanon Migrant Center, 2014). https://www.caritas.org/2014/10/left-behind-iraqi-refugees-lebanon/ 373 Sergey Kondrashov, "Demographic Map" Lebanon Demographics (2013). https://external-preview.redd.it/872JVWubp8BHuuHlZnXhe6cmS6dY3dgY5y_h2kqGJUI.jpg?auto=webp&s=6f365353da0f2402c46d3d8807625e141cda45c4 374 Lebanese Association for Democracy of Elections and Lamba Labs, "Lebanese Election Data," accessed June 7, 2020, http://lebanonelectiondata.org/confessions.html

74 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
Ethnic minority groups have the following geographic distribution:
• Armenians: Beirut, Mount Lebanon (Matn), and the Bekaa (Zahlé).375 • Assyrians: Beirut and the Bekaa (Zahlé).376 • Turkmen: Akkar, Bekaa, Baalbek, and Beirut.377 • Kurds: Beirut.378
UNHCR data for 2020 indicate that 38 percent of registered refugees are in the Bekaa, 27 percent in North Lebanon, and 25 percent in Beirut.379 Syrian Christian refugees have sought refuge in predominantly Christian villages and towns such as Zahlé in the Bekaa, with roughly 800 Syrian Melkite (Greek Orthodox) families in Zahlé, most of whom are not registered as refugees.380 Additional reports indicate at least 4,500 Christian families from Syria and Iraq in Beirut and the surrounding area, but it is unclear whether they are registered as refugees.381
Roughly 4,500 Palestinians, the majority of whom are Christian, live in the Dbayeh Camp in a Christian-dominated area of Mount Lebanon.382 Reports also indicate several hundred Yazidis from both Syria and Iraq in this area, but there are no accurate estimates of their numbers.383
According to the National Poverty Targeting Programme (NPTP), poor Lebanese households live mainly in the North (24 percent in Akkar and 18 percent in the North governorate) and the Bekaa (29 percent),384 which also hold concentrations of REM populations. Although the data on vulnerable communities cannot be interpreted as indicative of the status of REM communities in Lebanon, they can indicate the struggles faced by these communities’ most vulnerable members. See Figure 24 of vulnerable communities in Lebanon.385 A more detailed mapping of vulnerable communities can be found in Annex 7.
375 Lebanese Association for Democracy of Elections and Lamba Labs, "Lebanese Election Data.” 376 Assyrian Policy Institute, "Lebanon." 377 Joe Hammoura, "Turkey’s Lost Treasure: Story of a Soldier and Lebanese Turkmen Community," New Eastern Politics, May 4, 2017, https://www.neweasternpolitics.com/turkeys-lost-treasure-story-of-a-soldier-and-lebanese-turkmen-community-by-joe-hammoura/ 378 Minority Rights Group International, "Lebanon." 379 UNHCR, "Operational Portal - Refugee Situations," accessed June 6, 2020, https://data2.unhcr.org/en/situations/syria/location/71#_ga=2.67135889.1829640748.1591656668-811076588.1590871489 380 Marwan Kreidie, "Why Do So Few Christian Refugees Register with the United Nations High Commissioner for Refugees?" 381 Courtney Grogan, "Adopt a Family of Christian Refugees in Lebanon this Christmas," Catholic News Agency, December 14, 2019, https://www.catholicnewsagency.com/news/adopt-a-family-of-christian-refugees-in-lebanon-this-christmas-98450 382 UNRWA, "Where We Work," accessed June 10, 2020, https://www.unrwa.org/where-we-work/lebanon 383 Nisan Ahmado, "Uncertain Future Awaits Displaced Syrian Yazidis in Lebanon," VOA, May 12, 2019, https://www.voanews.com/extremism-watch/uncertain-future-awaits-displaced-syrian-yazidis-lebanon 384 UN and MOPH, "Lebanon Crisis Response Plan 2017–2020," 2020 update. 385 Ibid.

75 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
FIGURE 24: GEOGRAPHY OF MOST VULNERABLE CADASTRES
The influx of refugees has resulted in a large cohort of individuals in need of assistance, particularly from the health sector (Figure 25)—this number rose by roughly 9 percent among Syrian refugees in 2019.386 Data available on displaced Syrians and other refugee populations indicate greater vulnerability and poorer health outcomes than among their Lebanese counterparts. The poor health outcomes reflect the refugees’ illegal status, which restricts movement and limits access to social services, including health care.387
FIGURE 25: POPULATION IN NEED OF ASSISTANCE FROM THE HEALTH SECTOR
386 Ibid. 387 Amnesty International, "Lebanon: Wave of Hostility Exposes Hollowness of Claims that Syrian Refugee Returns are Voluntary," June 12, 2019, https://www.amnesty.org/en/latest/news/2019/06/lebanon-wave-of-hostility-exposes-hollowness-of-claims-that-syrian-refugee-returns-are-voluntary/
1,500,000
1,095,000
117,00027,700
Lebanese Displaced Syrians Palestinian Refugees inLebanon
Palestinian Refugeesfrom Syria

76 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
AQ 1: OVERVIEW OF HEALTH STATUS IN LEBANON
Although key health indicators have improved over the past decade—life expectancy has risen, and infant mortality rates have fallen—the Syrian crisis and its strain on Lebanon’s economy and public health system have reversed some of these improvements. For example, maternal mortality rates and mental health conditions, especially posttraumatic stress disorder (PTSD) and depression, have risen and outbreaks of vaccine-preventable and waterborne diseases have become more frequent. Noncommunicable diseases—caused mainly by high levels of smoking, obesity, and inactivity coupled with a lack of preventive services—account for 91 percent of all deaths (Figure 26).388
FIGURE 26: PRIMARY CAUSES OF DEATH
WOMEN’S HEALTH
Despite fertility and contraceptive prevalence rates comparable to those of many Western countries, maternal mortality rose from 9 deaths per 100,000 live births in 2014 to 26 deaths per 100,000 live births in 2017, with Syrian women accounting for the majority of this increase (Table 9).389,390 Maternal mortality rates rose in Lebanon starting in 2012, likely due to the influx of refugees, with the most significant increase observed in the Bekaa and North governorates, areas that lack large referral centers and contain high concentrations of REM populations and refugees.391 Overall, the three governorates known to contain concentrations of REM populations had among the highest percentages of maternal deaths, with 28 percent in Mount Lebanon, 24 percent in the Bekaa, and 19 percent in the North governorate.392 .
388 WHO, "Noncommunicable Diseases Country Profile: Lebanon," 2018, https://www.who.int/nmh/countries/lbn_en.pdf 389 WHO, "Country Cooperation Strategy at a Glance 2018," May 2018, https://apps.who.int/iris/bitstream/handle/10665/136909/ccsbrief_lbn_en.pdf?sequence=1 390 WHO EMRO, "Maternal and Child Health," accessed June 7, 2020, http://www.emro.who.int/fr/lbn/programmes/maternal-and-child-health.html 391 Faysal El‐Kak, Tamar Kabakian‐Khasholian, Walid Ammar, and Anwar Nassar, "A Review of Maternal Mortality Trends in Lebanon," International Journal of Gynecology & Obstetrics 148, no. 1 (October 2019). https://obgyn.onlinelibrary.wiley.com/doi/full/10.1002/ijgo.12994 392 LSOG, UNFPA, and MOPH, "Maternal Death Surveillance and Response - Annual Report 2017" (UNFPA, 2019). https://lebanon.unfpa.org/sites/default/files/pub-pdf/9.%202017%20MM%20report%20changes.pdf
Cardiovascular Diseases, 46%
Cancers, 16%
Communicable, maternal, perinatal & nutritional
conditions, 4%
Injuries, 6%
Chronic Respiratory Diseases, 4%
Diabetes, 5%
Other non-communicable diseases, 19%

77 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
TABLE 9: KEY MATERNAL HEALTH INDICATORS
Indicator Value
Maternal mortality393 26 deaths per 100,000 live births
Fertility rate394 2.1 births per woman
Women aged 15–49 pregnant in the last 12 months accessing antenatal care395 70 %
Women aged 20–24 who were first married before age 18 396, 397 6 % (Lebanese)
41% (Syrian)
Prevalence of adolescent girls aged 15–19 who have given birth398 13.3 per 1,000
Unmet need for family planning, women currently married or in union, aged 15–49 399 13 %
Lebanon provides almost universal coverage of skilled attendants at birth, and most deliveries take place in hospitals. Cesarean section rates are fairly high at 47 percent, putting mothers at higher risk of infection, blood clots, bladder damage, urogenital tract injuries, hemorrhage, and blood loss during surgery.400 Since 2016, the number of maternal deaths has been falling.401 However, maternal deaths are disproportionately higher among Syrians—only 33 percent of maternal mortality cases are among Lebanese.402 Most alarming, 35 percent of the maternal deaths among Syrians were among children and adolescents aged 10–19, reflecting the observed threefold increase in adolescent marriages among Syrian refugees since the start of the Syrian crisis.403 MOPH data indicate that 9 percent of all deliveries occurring in Lebanon were among teenagers.404
Although the majority of pregnant women access antenatal care (95 percent of Lebanese and 87 percent of refugees), WHO reports low levels of postnatal care,405 which likely contributes to the fact that 24 percent of maternal deaths are caused by postpartum hemorrhage.406 Among the 30 percent of women who did not receive antenatal care, most indicated they could not pay consultation fees or transport costs.
393 MOPH, "Vital Data Observatory Dashboard.” 394 The World Bank, "Data: Lebanon," accessed June 7, 2020, https://data.worldbank.org/country/lebanon 395 Alliance for Health Policy and Systems Research and WHO, "Primary Health Care Systems (PRIMASYS) Comprehensive Case Study from Lebanon" (AHPSR, 2017). http://origin.who.int/alliance-hpsr/projects/AHPSR-PRIMASYS-Lebanon-comprehensive.pdf 396 UNICEF, "Key Demographic Indicators: Lebanon.” 397 UNFPA, "Lebanon Scorecard on Gender-Based Violence," accessed June 6, 2020, https://arabstates.unfpa.org/sites/default/files/pub-pdf/UNFPA%20-%20Lebanon%20WEB_0.pdf 398 MOPH, "Statistical Bulleting 2018.” 399 UNICEF, "Key Demographic Indicators: Lebanon.” 400 MOPH, "Vital Data Observatory Dashboard," 2018, https://www.moph.gov.lb/userfiles/files/Programs%26Projects/Vital%20Data%20Observatory/VDO-Dashboard%202018.pdf 401 El‐Kak, Kabakian‐Khasholian, Ammar, and Nassar, "A Review of Maternal Mortality Trends in Lebanon." 402 LSOG, UNFPA, and MOPH, " Maternal Death Surveillance and Response - Annual Report 2017.” 403 LSOG, UNFPA, and MOPH, " Maternal Death Surveillance and Response - Annual Report 2017.” 404 MOPH, "Vital Data Observatory Dashboard.” 405 WHO EMRO, "Maternal and Child Health." 406 LSOG, UNFPA, and MOPH, " Maternal Death Surveillance and Response - Annual Report 2017.”

78 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
CHILDREN’S HEALTH
Refugee families also have higher rates of neonatal mortality (6.8 deaths per 1,000 live births) than the rest of the Lebanese population (4.4 deaths per 1,000 live births) (Table 10).407 The leading causes of under-five mortality are prematurity (30 percent), congenital anomalies (23 percent), intrapartum-related complications (11 percent), and acute respiratory infection (7 percent).408
TABLE 10: KEY CHILD HEALTH INDICATORS
Indicator Value
Infant mortality409 6.1 deaths per 1,000 live births
Under-five mortality 410 7.4 deaths per 1,000 live births
Neonatal mortality411 4.4 deaths per 1,000 live births (Lebanese)
6.8 deaths per 1,000 live births (non-Lebanese)
Prevalence of undernourishment412 11%
Prevalence of food insecurity413 49.3 % (total)
18.9 % (severe)
Respondents reporting prevalence of diarrhea among children 414
26 % (Lebanese)
39 % (non-Lebanese)
Reasons for seeking health care for children were similar among Lebanese and refugee populations (Figure 27), 415 but the likelihood of seeking care was higher in the host community, where 87 percent of households reported seeking medical attention the last time a child needed care, compared with 79.4 percent of Syrian refugee households, with financial constraints being the determining factor among 69 percent of host community households and 92 percent of refugee households.416 Financial constraints also contribute to high levels of food insecurity, which afflict 49 percent of the population.417
407 MOPH, "Vital Data Observatory Dashboard." 408 WHO, "Health Profile 2015 Lebanon" (WHO, 2016). https://applications.emro.who.int/dsaf/EMROPUB_2016_EN_19274.pdf?ua=1 409 UNICEF, "Key Demographic Indicators: Lebanon.” 410 Ibid. 411 MOPH, "Vital Data Observatory Dashboard.” 412 The World Bank, "Data: Lebanon.” 413 Lamis Jomaa, Farah Naja, Samer Kharroubi, and Nahla Hwalla, "Prevalence and Correlates of Food Insecurity Among Lebanese Households with Children Aged 4–18 years: Findings of a National Cross-Sectional Study." 414 UNICEF, OCHA, and REACH, "Defining Community Vulnerabilities in Lebanon" (UNHCR, 2015). https://data2.unhcr.org/fr/documents/download/44875 415 Emily Lyles, Baptiste Hanquart, the LHAS Study Team, Michael Woodman, and Shannon Doocy, "Health Service Utilization and Access to Medicines Among Syrian Refugee and Host Community Children in Lebanon." 416 Ibid. 417 Jomaa, Naja, Kharroubi, and Hwalla, "Prevalence and Correlates of Food Insecurity Among Lebanese Households with Children Aged 4–18 years: Findings of a National Cross-Sectional Study" Public Health Nutrition 22, no. 2 (2018): 1–10. https://doi.org/10.1017/S1368980018003245
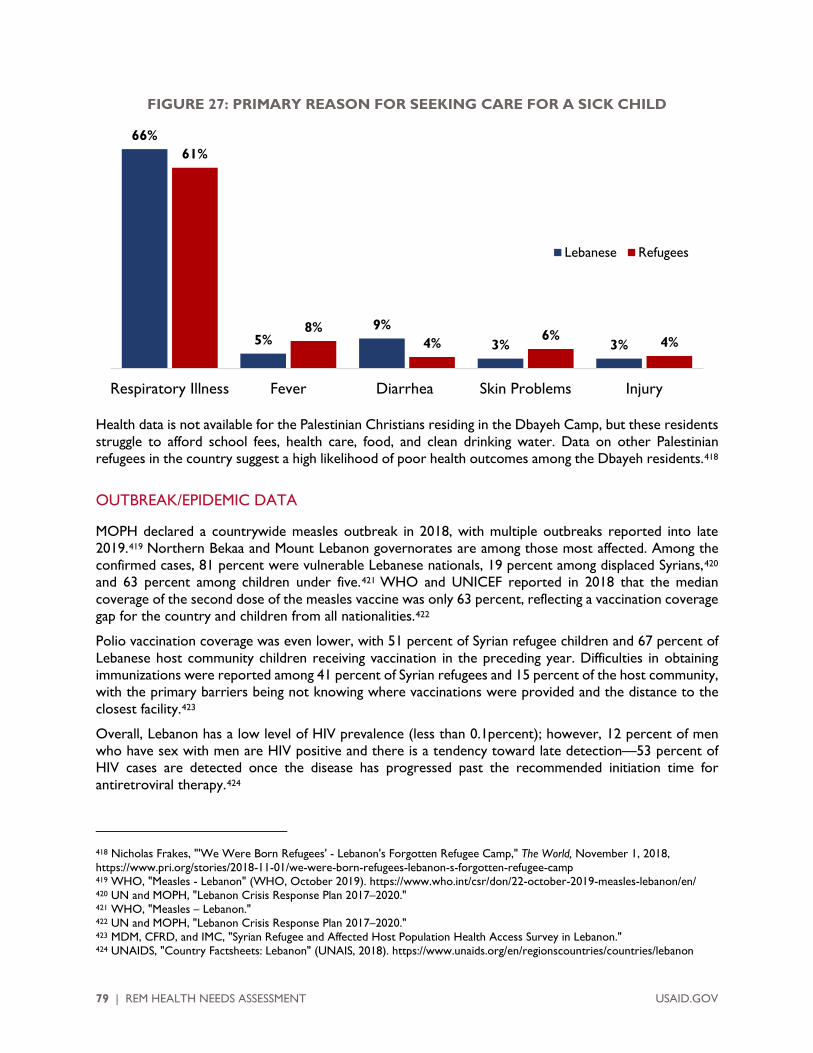
79 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
FIGURE 27: PRIMARY REASON FOR SEEKING CARE FOR A SICK CHILD
Health data is not available for the Palestinian Christians residing in the Dbayeh Camp, but these residents struggle to afford school fees, health care, food, and clean drinking water. Data on other Palestinian refugees in the country suggest a high likelihood of poor health outcomes among the Dbayeh residents.418
OUTBREAK/EPIDEMIC DATA
MOPH declared a countrywide measles outbreak in 2018, with multiple outbreaks reported into late 2019.419 Northern Bekaa and Mount Lebanon governorates are among those most affected. Among the confirmed cases, 81 percent were vulnerable Lebanese nationals, 19 percent among displaced Syrians,420 and 63 percent among children under five.421 WHO and UNICEF reported in 2018 that the median coverage of the second dose of the measles vaccine was only 63 percent, reflecting a vaccination coverage gap for the country and children from all nationalities.422
Polio vaccination coverage was even lower, with 51 percent of Syrian refugee children and 67 percent of Lebanese host community children receiving vaccination in the preceding year. Difficulties in obtaining immunizations were reported among 41 percent of Syrian refugees and 15 percent of the host community, with the primary barriers being not knowing where vaccinations were provided and the distance to the closest facility.423
Overall, Lebanon has a low level of HIV prevalence (less than 0.1percent); however, 12 percent of men who have sex with men are HIV positive and there is a tendency toward late detection—53 percent of HIV cases are detected once the disease has progressed past the recommended initiation time for antiretroviral therapy.424
418 Nicholas Frakes, "'We Were Born Refugees' - Lebanon's Forgotten Refugee Camp," The World, November 1, 2018, https://www.pri.org/stories/2018-11-01/we-were-born-refugees-lebanon-s-forgotten-refugee-camp 419 WHO, "Measles - Lebanon" (WHO, October 2019). https://www.who.int/csr/don/22-october-2019-measles-lebanon/en/ 420 UN and MOPH, "Lebanon Crisis Response Plan 2017–2020." 421 WHO, "Measles – Lebanon." 422 UN and MOPH, "Lebanon Crisis Response Plan 2017–2020." 423 MDM, CFRD, and IMC, "Syrian Refugee and Affected Host Population Health Access Survey in Lebanon." 424 UNAIDS, "Country Factsheets: Lebanon" (UNAIS, 2018). https://www.unaids.org/en/regionscountries/countries/lebanon
66%
5%9%
3% 3%
61%
8%4% 6% 4%
Respiratory Illness Fever Diarrhea Skin Problems Injury
Lebanese Refugees

80 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
MENTAL HEALTH
Diagnosed mental health conditions were reported among 4.7 percent of Lebanese and 3.1 percent of Syrian refugees; however, limited access to mental health services and stigma associated with mental health disorders likely contribute to an underestimation of prevalence.425 Mental health challenges are likely higher given that 70 percent of the Lebanese population has been exposed to one or more war events426 and 83 percent of Syrian refugees have experienced shootings or direct bombings.427 Also, more than 50 percent of Lebanese children and adolescents suffer from anxiety and 13 percent have suffered from depression—the rates among displaced Syrians are 56 percent and 17 percent, respectively. 428 Consequently, 14 percent have seriously considered attempting suicide and 10 percent have attempted suicide one or more times.429 Neuropsychiatric disorders are estimated to contribute 15 percent of the burden of diseases, and the suicide mortality rate is estimated at 0.9 per 100,000 people per year.430
SEXUAL AND GENDER-BASED VIOLENCE
Data on sexual and gender-based violence (SGBV) are limited, with no official national statistics on physical and/or sexual intimate partner violence.431 However, available data indicate that, on average, 50 percent of people report personally knowing someone who has been subjected to domestic violence.432 Twenty percent of reported SGBV cases involve children and 18 percent involve sexual violence, of which 8 percent are rape.433 Since the COVID-19 outbreak, reports of harassment, violence, or abuse against women and girls have risen by 54 percent.434 Of the observed violence, 32 percent was sexual violence, 55 percent was physical violence, and 79 percent emotional violence.
On average, 90 percent of SGBV incidents reported to specialized service providers involved women and girls, indicating that women and girls continue to be disproportionately affected, with grave consequences for their health, security, and psychosocial and socioeconomic well-being. Most of UNHCR’s partners have also raised concerns about the levels of commercial sex, particularly among young, unaccompanied refugee girls, who have limited resources and are at a higher risk for survival sex.435
WATER, SANITATION, AND HYGIENE
Lack of access to water, sanitation, and hygiene (WASH) appears to contribute to the high rates of diarrhea reported among children, with 64 percent of the population not having access to safely managed
425 Médecins du Monde (MDM), Center for Refugee and Disaster Response (CFRD), International Medical Corps (IMC), "Syrian Refugee and Affected Host Population Health Access Survey in Lebanon" (UNHCR, July 2015). https://data2.unhcr.org/en/documents/download/44869 426 MOPH, "Mental Health and Substance Use - Prevention, Promotion and Treatment - Situation Analysis and Strategy for Lebanon 2015–2020" (MOPH, 2015). https://www.mhinnovation.net/sites/default/files/downloads/resource/MH%20strategy%20LEBANON%20ENG.pdf 427 UNHCR, "Assessment of Mental Health and Psychosocial Support Services for Syrian Refugees in Lebanon" (UNHCR, December 2013). https://data2.unhcr.org/en/documents/download/39722 428 UN and MOPH, "Lebanon Crisis Response Plan 2017–2020." 429 Ministry of Education and Higher Education, MOPH, and WHO, "Global School-Based Student Health Survey: Lebanon" (UNHCR, 2017). https://data2.unhcr.org/en/documents/download/66496 430 WHO, "Health Profile 2015 Lebanon." 431 UN Women, "Lebanon: Prevalence Data on Different Forms of Violence Against Women" (UN Women, 2018). https://evaw-global-database.unwomen.org/es/countries/asia/lebanon#1 432 UNFPA, "Lebanon Scorecard on Gender-Based Violence.” 433 UN and MOPH, "Lebanon Crisis Response Plan 2017–2020." 434 Abaad, Care, DRC, IRC, Intersos, UNHCR, UNICEF, UNFPA, and UN Women, "Impact of the COVID-19 on the SGBV Situation in Lebanon" (UNHCR, 2020). https://data2.unhcr.org/en/documents/download/7673 435 UNHCR, "Assessment of Mental Health and Psychosocial Support Services for Syrian Refugees in Lebanon."
ACF
Highlight
ACF
Highlight

81 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
drinking water436 and up to 74 percent of refugee populations relying on bottled mineral water.437 Under these conditions, poor hygiene practices, particularly in relation to handling food and water, aggravate the risk of disease—food- and waterborne diseases account for up to 60 percent of notifiable communicable diseases.438 Only 22 percent of the population has access to safely managed sanitation services.439 Donor contributions to this sector have resulted in WASH improvements, but much remains to be done to improve health-related outcomes.
CONCLUSIONS
Religious and ethnic minority communities’ health status, for which data are not available, is more likely to be determined by level of financial stability than by religious or ethnic identity. However, data disaggregated by governorate reveal that some REM communities are concentrated in governorates with higher poverty levels and poorer health outcomes—such as the Bekaa and the North governorates—indicating that REM populations in those areas may have poorer outcomes than those reported in nationally representative data. The challenges faced by children and adolescents of vulnerable households cause particular concern, especially given rising poverty rates among all populations, as UNICEF reports that child labor and child marriage are increasingly used as coping mechanisms against deepening financial constraints.440
AQ 2: PRIMARY HEALTH CARE SYSTEM STRENGTHS AND WEAKNESSES
The Lebanese health system is a complex combination of public and private sector facilities with a fragmented financing system consisting of public, semipublic, and private coverage models (Figure 28).441 The private sector, including private clinics, hospitals, pharmacies, and laboratories, accounts for 82 percent of available health services and is much more widely used than the public sector.442 A range of nonstate providers, including political parties, religious charities, community-based groups, NGOs, and for-profit institutions, supply and finance health care.443 The private sector is highly decentralized and lacks regulation, which contributes to wide variations in both quality and cost of care and a limited referral system. The public sector, which comprises mostly primary health care centers (PHCCs) and dispensaries, has limited capacity compared with the private sector in terms of tertiary care infrastructure and financial resources.444 An inherent weakness of the system is the emphasis on curative rather than preventive care.445 A 2019 assessment of PHCCs across the country found that 60 percent did not meet infection control requirements and 73 percent did not meet all infrastructure requirements.446
436 UN and MOPH, "Lebanon Crisis Response Plan 2017–2020." 437 UNHCR, "Vulnerability Assessment of Refugees of Other Nationalities in Lebanon" (UNHCR, 2018). https://www.unhcr.org/lb/wp-content/uploads/sites/16/2019/10/VARON-2018.pdf 438 UN and MOPH, "Lebanon Crisis Response Plan 2017–2020." 439 UNICEF, "Key Demographic Indicators: Lebanon.’ 440 UNICEF, "Palestinian Programme," accessed June 7, 2020, https://www.unicef.org/lebanon/palestinian-programme 441 WHO, "WHO Support to the Humanitarian Response in Lebanon" (WHO, 2016). https://www.who.int/migrants/publications/WHO_Lebanon_AnnualReport.pdf?ua=1 442 MDM, CFRD, and IMC, "Syrian Refugee and Affected Host Population Health Access Survey in Lebanon." 443 Bradley Chen and Melani Cammett, "Informal Politics and Inequity of Access to Health Care in Lebanon," Int Journal Equity Health (May 2012). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3464946/ 444 MDM, CFRD, and IMC, "Syrian Refugee and Affected Host Population Health Access Survey in Lebanon." 445 Randa Hemadeh, Ola Kdouh, Rawan Hammoud, Tarek Jaber, and Lama Khalek, "The Primary Health Care Network in Lebanon: a National Facility Assessment," East Mediterranean Health Journal (March 2019): https://doi.org/10.26719/emhj.20.003 446 Hemadeh et al., "The Primary Health Care Network in Lebanon: A National Facility Assessment."

82 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
FIGURE 28: OVERVIEW OF THE HEALTH SYSTEM
HEALTH WORKFORCE
The Lebanese health care system has a surplus of specialists, a critical shortage of competent family care physicians and nurses, and a severe shortage of mental health professionals, with significant challenges in retaining employed staff, mostly due to financial constraints.447 The number of physicians exceeds the WHO-recommended ratio of 2.3 providers per 1,000 people (Figure 29).448,449,450 The majority of nurses and allied health professionals are salaried and work on a full-time basis, yet the majority of physicians work only part time, with provider salaries not standardized across centers due to the dominance of the private sector in the delivery of primary health care services. The financial constraints and challenges faced in retaining staff are aggravated by the lack of clear recruitment criteria and poor human resource planning at the central level, with evidence suggesting that PHCCs recruit less competent staff, compromising service quality.451 These factors likely contribute to the high number of health care providers who migrate to other countries.
447 Mohamad Alameddine, Shadi Saleh, Fadi El-Jardali, Hani Dimassi, and Yara Mourad, "The Retention of Health Human Resources in Primary Healthcare Centers in Lebanon: A National Survey," BMC Health Services Research, 12:419, 2012, http://www.biomedcentral.com/1472-6963/12/419 448 MOPH, "Statistical Bulleting 2018." 449 NLG, "MHPSS Programmes for Children, Youth (0-24 years) and Parents/Caregivers in Syria and from Syria and Iraq Crises Affected Countries." 450 Thomas Schellen, "A Look into Lebanon's Healthcare," Executive Magazine, August 6, 2018, https://www.executive-magazine.com/special-report/a-look-into-lebanons-healthcare 451 Alliance for Health Policy and Systems Research and WHO, "PRIMASYS Comprehensive Case Study from Lebanon."

83 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
FIGURE 29: HEALTH CARE PROVIDER RATIO PER 1,000 POPULATION
In the national network, there are significant disparities between rural and urban PHCCs and between accredited and unaccredited PHCCs. Whereas 74 percent of PHCCs in urban areas fulfill their staffing requirements, only 46 percent in rural areas are able to do so. Additionally, whereas 88 percent of accredited centers fulfill their staffing requirements, only 55 percent of unaccredited PHCCs can. Additionally, more than 20 percent of PHCCs in the national network do not employ a registered nurse as required by the national standards. Significant staff shortages are reported in areas known to contain high concentrations of REM populations, with the Bekaa suffering the most severe staffing shortages (Figure 30).452
FIGURE 30: UNFULFILLED STAFFING REQUIREMENTS (PERCENT OF HOSPITALS BY GOVERNORATE)
The number of staff employed by the MOPH has declined significantly over the last two decades, posing a serious threat to the sustainability of MOPH performance and reflecting the lack of political commitment to strengthening public administration. The current number of MOPH staff barely exceeds 1,000
452 Hemadeh et al., "The Primary Health Care Network in Lebanon: A National Facility Assessment."
3.123.4
1.98
0.24 0.23
Physicians Nurses Pharmacists Dentists Mental HealthProfessionals
57.90%
36.70%
28.60%23.60%
Bekaa North Beirut Mount Lebanon

84 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
employees.453 Although data are not available on the health workforce employed in PHCCs outside the national network, evidence suggests that employment conditions are more favorable there.454
SERVICE DELIVERY
PHCCs are divided among several operators, including the MOPH, the Ministry of Social Affairs (MOSA), NGOs, and municipalities (Figure 31).455 The national primary health care network comprises 229 PHCCs distributed across the eight governorates, of which 45 percent are in three governorates with high concentrations of REM populations (Bekaa, Mount Lebanon, and North governorates).456 The PHCCs within the national network undergo an accreditation process to ensure the quality of their services, with 52 of the 229 PHCCs currently accredited.457An additional 1,011 PHCCs provide services outside the MOPH’s network.458 The WHO reports that whereas urban areas have good coverage and quality of services, rural areas remain underserved459 even though half of the PHCCs are located in rural areas.460 There are high rates of care-seeking for curative services at secondary and tertiary levels and relatively low utilization of primary care.461
FIGURE 31: DISTRIBUTION OF ENTITIES OPERATING PHCCS
The majority of vulnerable Lebanese seek medical care at private clinics (48 percent), in stark contrast to Syrian refugees, only 18 percent of whom do. Most Syrian refugees (53 percent) seek care at PHCCs (Figure 32). 462 The reasons vulnerable Lebanese prefer to seek care at private clinics are unclear, particularly as out-of-pocket expenses, including consultation fees and medication, are significantly higher
453 MOPH, "Health Strategic Plan." 454 Ibid. 455 Alliance for Health Policy and Systems Research and WHO, "PRIMASYS Comprehensive Case Study from Lebanon.” 456 Alliance for Health Policy and Systems Research and WHO, "PRIMASYS Comprehensive Case Study from Lebanon.” 457 MOPH, "EPHRP Dashboard," January–December 2018, https://www.moph.gov.lb/userfiles/files/Programs%26Projects/Emergency%20Primary%20Health%20Care/EPHRP%202018%20Annual%20Dashboard.pdf 458 UN and MOPH, "Lebanon Crisis Response Plan 2017–2020." 459 Hemadeh et al, "The Primary Health Care Network in Lebanon: A National Facility Assessment." 460 Ibid. 461 MDM, CFRD, and IMC, "Syrian Refugee and Affected Host Population Health Access Survey in Lebanon." 462 Emily et al., "Health Service Utilization and Access to Medicines Among Syrian Refugee and Host Community Children in Lebanon.”
NGOs, 67%Governmental
(MOPH, MOSA), 13%
Municipalities, 20%
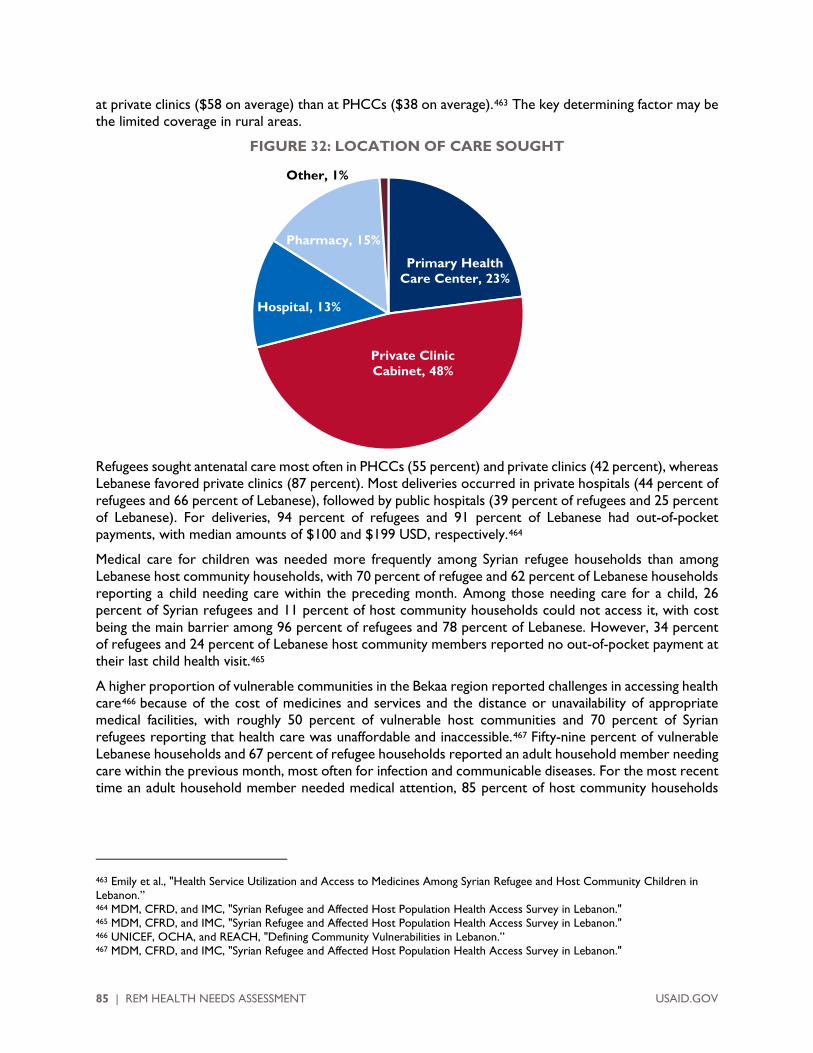
85 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
at private clinics ($58 on average) than at PHCCs ($38 on average).463 The key determining factor may be the limited coverage in rural areas.
FIGURE 32: LOCATION OF CARE SOUGHT
Refugees sought antenatal care most often in PHCCs (55 percent) and private clinics (42 percent), whereas Lebanese favored private clinics (87 percent). Most deliveries occurred in private hospitals (44 percent of refugees and 66 percent of Lebanese), followed by public hospitals (39 percent of refugees and 25 percent of Lebanese). For deliveries, 94 percent of refugees and 91 percent of Lebanese had out-of-pocket payments, with median amounts of $100 and $199 USD, respectively.464
Medical care for children was needed more frequently among Syrian refugee households than among Lebanese host community households, with 70 percent of refugee and 62 percent of Lebanese households reporting a child needing care within the preceding month. Among those needing care for a child, 26 percent of Syrian refugees and 11 percent of host community households could not access it, with cost being the main barrier among 96 percent of refugees and 78 percent of Lebanese. However, 34 percent of refugees and 24 percent of Lebanese host community members reported no out-of-pocket payment at their last child health visit.465
A higher proportion of vulnerable communities in the Bekaa region reported challenges in accessing health care466 because of the cost of medicines and services and the distance or unavailability of appropriate medical facilities, with roughly 50 percent of vulnerable host communities and 70 percent of Syrian refugees reporting that health care was unaffordable and inaccessible.467 Fifty-nine percent of vulnerable Lebanese households and 67 percent of refugee households reported an adult household member needing care within the previous month, most often for infection and communicable diseases. For the most recent time an adult household member needed medical attention, 85 percent of host community households
463 Emily et al., "Health Service Utilization and Access to Medicines Among Syrian Refugee and Host Community Children in Lebanon.” 464 MDM, CFRD, and IMC, "Syrian Refugee and Affected Host Population Health Access Survey in Lebanon." 465 MDM, CFRD, and IMC, "Syrian Refugee and Affected Host Population Health Access Survey in Lebanon." 466 UNICEF, OCHA, and REACH, "Defining Community Vulnerabilities in Lebanon.” 467 MDM, CFRD, and IMC, "Syrian Refugee and Affected Host Population Health Access Survey in Lebanon."
Primary Health Care Center, 23%
Private Clinic Cabinet, 48%
Hospital, 13%
Pharmacy, 15%
Other, 1%

86 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
and 69 percent of refugee households sought and received care; costs were the main barrier among those who did not seek care.468
To mitigate constraints on health care access among vulnerable and refugee populations, a network of 25 mobile medical units (MMUs) provides free services and referrals.469 These MMUs are funded by external donors such as UNICEF and staffed by the MOPH. Additional units are operated by local and international NGOs and faith-based organizations such as Caritas, Humedica, The Order of Malta in Lebanon, Imam Sadr Foundation, and the Lebanese Red Cross, which offer services to vulnerable Lebanese populations and displaced individuals. Some of the MMUs operate in areas with high concentrations of REM populations
The MOPH has oversight policies and practices to monitor PHCC service delivery patterns, quality of care, and performance within the national network. Immunization activities, the provision of essential drugs, and other services are regularly reported to the MOPH for analysis, evaluation, and feedback, and monitoring of PHCCs involves regular visits by government health inspectors and administration of patient satisfaction surveys.470 The MOPH also initiated an accreditation process in 2019, yet most hospitals within the national network (77 percent) remain unaccredited, with stark contrasts reported between the two on readiness to deliver services. Research indicates that unaccredited hospitals are understaffed and ill equipped and lack clinical guidelines to ensure quality of services, particularly in rural areas, where more than half of the PHCCs in the national network are located.471
Most health services are provided by the private sector, as noted above, and the lack of oversight contributes to substantial variation in service quality; with limited data. However, research findings among the most vulnerable host and refugee communities reveal a clear distinction in the quality of services depending on the type of service accessed, with respondents being satisfied with the quality of services for serious medical conditions but reporting lack of access to services for minor conditions and low-quality, unethical treatment by health care providers.472
MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT
Most mental health services are limited to the private sector, which makes it difficult for vulnerable groups to access services and contributes to documented challenges in coordination and referrals.473 Access is further exacerbated by the fact that only 37 percent of PHCCs offer mental health services,474 due to limited funding, especially in rural areas.475 A mapping of mental health services in 2020 found only five psychiatric hospitals throughout the country, 20 community-based/nonhospital mental health outpatient facilities, and only 10 facilities—mostly around Beirut— with outpatient services specifically for children and adolescents.476 Severe shortages of service are reported in the Bekaa, where REM populations are concentrated.477
468 Ibid. 469 UN and MOPH, "Lebanon Crisis Response Plan 2017–2020." 470 Alliance for Health Policy and Systems Research and WHO, "PRIMASYS Comprehensive Case Study from Lebanon.” 471 Hemadeh et al., "The Primary Health Care Network in Lebanon: A National Facility Assessment." 472 Oxfam, "Self-Protection and Coping Strategies of Refugees from Syria and Host Communities in Lebanon" (Oxfam, July 2015). https://oi-files-d8-prod.s3.eu-west-2.amazonaws.com/s3fs-public/file_attachments/rr-lebanon-refugees-protection-300616-en.pdf 473 UNHCR, "Assessment of Mental Health and Psychosocial Support Services for Syrian Refugees in Lebanon." 474 Hemadeh et al., "The Primary Health Care Network in Lebanon: A National Facility Assessment." 475 MSF, "Treating Mental Health Outside of Specialized Settings," October 17, 2019, https://www.msf.org/treating-mental-health-outside-specialised-settings-lebanon 476 No Lost Generation (NLG) MHPSS Task Force, "MHPSS Programmes for Children, Youth (0–24 years) and Parents/Caregivers in Syria and from Syria and Iraq Crises Affected Countries," January 15, 2020, https://drive.google.com/file/d/1pYgRQaZq3-Y5Sa6VHdk_-HV5tBicJ6Dh/view 477 UNHCR, "Assessment of Mental Health and Psychosocial Support Services for Syrian Refugees in Lebanon.”

87 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
Lebanon also suffers from a critical shortage of mental health professionals, with an average of three mental health professionals per 100,000 individuals, which compromises the provision of mental health services and likely contributes to the low number of diagnosed mental health conditions. PHCCs have been trying to make up for this shortage by training general practitioners and nurses to screen for mental health cases.478 To address the lack of access to mental health services, a multitude of International NGOs provide community-based mental health and psychosocial support services (MHPSS).479
SEXUAL AND GENDER-BASED VIOLENCE
Specialized services to respond to GBV and child abuse are scarce for all populations in Lebanon despite efforts of multiple partners, including the MOPH, MOSA, Ministry of Education, UNFPA, International Medical Corps (IMC), KAFA, and others.480 A referral system is in place and various agencies build service provider capacity to respond to GBV issues, including IMC and UNFPA on the clinical management of rape and clinical care for survivors of sexual abuse, but GBV reporting remains low, potentially due to the low levels of service provision.481
A survey of women and girls who had accessed GBV services indicates that only 50 percent have been able to access these services since the beginning of the COVID-19 outbreak, with 94 percent of them accessing services over the phone.482 Identifying GBV survivors may be particularly challenging because of social norms, victim-blaming culture, mobility restrictions, and economic dependence. Data on the ability of vulnerable and minority populations to access GBV services are lacking, likely due to underfunding.483 Various organizations are working with MOSA to address the very high levels of child marriage, but much remains to be done.
COMMUNITY HEALTH OUTREACH PROGRAMS
In 2016, the MOPH, with funding from the World Bank, launched the Emergency Primary Healthcare Restoration Project (EPHRP), under which PHCCs are required to carry out proactive population outreach activities to engage communities and link them to the primary health care system. It is not clear how successfully this component has been implemented, but the United Nations Development Programme (UNDP) is pilot testing an initiative in 17 municipalities to link all local partners within a certain geographical context to provide comprehensive services and ensure continuity of care at the local level.484
Multiple international and national NGOs implement health education, promotion, early detection, and referrals through community-based activities addressing a multitude of issues, such as nutrition, communicable and noncommunicable diseases, MHPSS, and SGBV, with an emphasis on women and children; however, these activities remain underfunded.485 To ensure that culturally appropriate services are delivered sustainably, IMC hires all its community health workers (CHWs) from within the communities it serves and has hired all-women outreach teams to address the needs of women and
478 UNICEF, UNHCR, and WFP, "Vulnerability Assessment for Syrian Refugees in Lebanon” (VASyR, 2019). 479 IMC, WHO, and UNICEF, "The “4Ws” in Lebanon: Who’s Doing What, Where and Until When in Mental Health and Psychosocial Support," April 2015, https://www.moph.gov.lb/en/Pages/0/9100/the-4ws-in-lebanon-whos-doing-what-where-and-until-when-in-mental-health-and-psychosocial-support- 480 UN and MOPH, "Lebanon Crisis Response Plan 2017–2020." 481 Ibid. 482 Abaad, Care, DRC, IRC, Intersos, UNHCR, UNICEF, UNFPA and UN Women, "Impact of the COVID-19 on the SGBV Situation in Lebanon," 2020, https://data2.unhcr.org/en/documents/download/76732 483 OCHA, "Assisting Survivors of Gender-Based Violence in Lebanon," December 13, 2019, https://www.unocha.org/story/assisting-survivors-gender-based-violence-lebanon 484 Alliance for Health Policy and Systems Research and WHO, "PRIMASYS Comprehensive Case Study from Lebanon.” 485 IMC et al., "The “4Ws” in Lebanon: Who’s Doing What, Where and Until When in Mental Health and Psychosocial Support.”

88 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
children, whose mobility is often restricted.486 Also, most MHPSS protection-related community outreach activities are conducted in Zahle, where multiple REM populations reside.487 The MOPH does not formally acknowledge or legally recognize CHWs’ role, which creates challenges for these workers’ legal protection and reimbursement and hinders implementing partners’ ability to hire skilled and qualified community health workers.488
ACCESS TO ESSENTIAL MEDICINES
Lebanon has been facing a severe shortage of hard currency since September 2019, restricting medical supply companies’ ability to import vital medical supplies, including masks, gloves, and other protective gear, as well as ventilators and spare parts—only 10 percent of the country’s needs are being imported.489 The impact on individuals’ ability to access medications has not yet been clearly documented, but Human Rights Watch has reported a decline in hospitals’ ability to respond to the COVID-19 outbreak. Furthermore, the government has not reimbursed public and private hospitals for bills, including from the National Social Security Fund (NSSF). This has made it harder for them to purchase medical supplies, hire additional staff to reduce the burden on hospital staff, and provide staff with necessary personal protective equipment (PPE).490
The MOPH uses three procurement mechanisms depending on the type of product being procured— vaccines and essential medicines for acute illnesses for use at primary health care level are procured through UNICEF, medications for chronic illnesses are procured and distributed through the YMCA NGO to more than 450 PHCCs (both within and outside the national network) that provide free medication to 150,000 patients annually, and medications for severe diseases such as cancer and HIV as well as some psychiatric medications are procured through a local tender mechanism. The MOPH distributes medications for severe diseases free of charge to roughly 15,000 patients annually and medications for chronic illnesses for a dispensing fee of $1 USD.491 UNHCR also provides vaccines, essential acute medicines, and family planning commodities free of charge, although it is unlikely that unregistered refugees (around 75 percent of all displaced Syrians in Lebanon) can access these benefits.492
Despite these provisions, most populations report paying some fees for medications, and the cost of medication is often higher than that of the consultation. Among the 69 percent of refugees and 78 percent of Lebanese who had out-of-pocket expenses for their last child health care visit, the average costs for medication were $17 USD for refugees and $25 USD for Lebanese, with roughly 92 percent of all communities reporting they obtained the medications and the remaining 8 percent reporting costs as the main barrier to accessing medication.493 In 2019 33 percent of Syrian refugees had to borrow money to pay for medicine (up from 23 percent in 2018).494 Stockouts also hamper access to medications—regions
486 Julie Davidson and Christina Bethke, "Integrating Community-Based Nutrition Awareness into the Syrian Refugee Response in Lebanon," Field Exchange, accessed June 11, 2020, https://www.ennonline.net/fex/48/integrating 487 IMC et al., "The “4Ws” in Lebanon: Who’s Doing What, Where and Until When in Mental Health and Psychosocial Support.” More specific data are not available on the participation of REM populations in community health outreach programs, 488 Health Europa, "Fill That Gap Supports Community Health Workers in Lebanon,” November 21, 2019, https://www.healtheuropa.eu/fill-that-gap-supports-community-health-workers-in-lebanon/95117/ 489 HRW, "Lebanon: COVID-19 Worsens Medical Supply Crisis," March 24, 2020, https://www.hrw.org/news/2020/03/24/lebanon-covid-19-worsens-medical-supply-crisis 490 Ibid. 491 Alliance for Health Policy and Systems Research and WHO, "PRIMASYS Comprehensive Case Study from Lebanon.” 492 UNHCR, " Lebanon Health Programme.” 493 MDM, CFRD, and IMC, "Syrian Refugee and Affected Host Population Health Access Survey in Lebanon." 494 UNICEF, UNHCR, and WFP, "Vulnerability Assessment for Syrian Refugees in Lebanon (VASyR 2019)."

89 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
vary, but areas containing REM populations have higher stockouts (Figure 33).495 Vaccinations are free of charge to any child under 12 years, but only 59 percent of Syrian households were aware of this benefit.496
FIGURE 33: STOCKOUTS AS REASON FOR NOT OBTAINING MEDICATION
HEALTH FINANCE
Public health care in Lebanon faces continued budget cuts, with a vastly privatized and unregulated health care system.497 Relatively low utilization of primary care and high rates of care-seeking for curative services at the secondary and tertiary levels have led to high levels of health spending primarily on hospital-based curative care.498 Less than 5 percent of the MOPH budget goes to preventive interventions.499 The Syrian crisis and the economic collapse have put tremendous pressure on the health care system, and the significant humanitarian aid funds Lebanon receives are insufficient for the crisis. As most PHCCs are operated by NGOs, they rely heavily on donor funding and regularly face funding shortages.500 The MOPH is not a direct recipient of donor funds; instead, it plays a coordinating role among donors and implementing agencies to ensure funds are allocated to priority areas and populations.501
According to the MOPH, total health care expenditures constitute 7.75 percent of GDP, with 2.73 percent of the country’s budget allocated to the MOPH.502 One-third of health care financing derives from government expenditures from tax revenues, one-third is covered by private insurance and contribution-based schemes such as the NSSF, and the remaining third derives from direct private expenditures by patients as out-of-pocket payments.503 The high out-of-pocket expenditures for households, in particular the large payments for secondary care and hospitalizations, can be catastrophic for vulnerable households
495 Emily et al., "Health Service Utilization and Access to Medicines Among Syrian Refugee and Host Community Children in Lebanon.” 496 UNICEF, UNHCR, and WFP, "Vulnerability Assessment for Syrian Refugees in Lebanon (VASyR 2019)." 497 Kareem Chehayed, "Lebanon Is the Experiment That Shows Neoliberalism's Failure," The Century Foundation, April 16, 2020, https://tcf.org/content/commentary/lebanon-experiment-shows-neoliberalisms-failure/?agreed=1 498 MDM, CFRD, and IMC, "Syrian Refugee and Affected Host Population Health Access Survey in Lebanon." 499 Hemadeh et al., "The Primary Health Care Network in Lebanon: A National Facility Assessment." 500 Alliance for Health Policy and Systems Research and WHO, "PRIMASYS Comprehensive Case Study from Lebanon.” 501 Ibid. 502 MOPH, "Statistical Bulleting 2018.” 503 Schellen, "A Look into Lebanon's Healthcare."
16.70%
13.60%
5.90%
Bekaa North Beirut/Mt. Lebanon

90 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
that are already struggling to meet basic needs, particularly due to the drastic rise in food prices beginning in early 2020.504
Whereas some donors provide subsidized services only to refugees registered with UNHCR, others include host communities within their targeted populations. Eligible beneficiaries may be further limited to certain vulnerable groups, such as children under five or pregnant women, whereas other providers may offer coverage to anyone in need. Finally, the cost of services at supported facilities also ranges from free to cost-sharing models. This combination of factors creates a confusing system that vulnerable individuals must navigate to receive the most basic health care services, such as vaccinations and antenatal care.
Subsidized health care is available to displaced Syrians and vulnerable Lebanese at around 113 PHCCs distributed across the country, but the coverage levels and the subsidized rates are insufficient to make these services fully accessible to those most in need.505 For example, in 2018, UNHCR supported only 77,580 primary health care consultations and 79,400 secondary and tertiary health care interventions.506 Registered refugees have coverage of 75–90 percent of life-saving emergency care in 56 UNHCR-supported hospitals, but many cannot afford the remaining out-of-pocket expenses.507 Palestinian refugees can access care at facilities supported by United Nations Relief and Works Agency for Palestinian Refugees (UNRWA), but budget cuts in 2018 greatly reduced the scope and scale of support, thereby intensifying the needs of this population, 99 percent of which are uninsured.508 In a positive step toward universal coverage, the MOPH, with funding from the World Bank, offers subsidized care to 150,000 vulnerable Lebanese citizens, but this number is miniscule compared with the 1.5 million Lebanese in need of health care assistance.509
Reports indicate that the MOPH has capped consultation fees at national network centers at $12 USD, while providing essential medications for acute illnesses for free and medications for chronic illnesses for a dispensing fee of less than $1 USD. UNHCR also provides subsidized care to registered refugees for a fee of $2–$3 USD at 113 PHCCs countrywide.510 However, 66 percent of refugees and 76 percent of host community households reported out-of-pocket expenditures for either the consultation or prescribed medications at the most recent visit, with refugees paying an average of $30 and host community members an average of $56.511 These findings indicate that most populations have very limited access to subsidized services. Furthermore, the differences in out-of-pocket expenses between vulnerable Lebanese and displaced Syrians add tension to an already volatile situation.512
Thirty-eight percent of non-Syrian refugees report that they pay in full for their primary health care, 28 percent benefit from assistance or subsidization, and only 5 percent benefit from free primary health care. An even higher percentage of Iraqi refugees pay the entire cost of their health care (44 percent).513 A network of mobile medical units improve access for vulnerable populations, providing consultations and medications free of charge, and refer patients to PHCCs, but medication stockouts are reported regularly.514
504 MDM, CFRD, and IMC, "Syrian Refugee and Affected Host Population Health Access Survey in Lebanon." 505 UN and MOPH, "Lebanon Crisis Response Plan 2017–2020." 506 UNHCR, " Lebanon Health Programme" (UNHCR, 2019). https://www.unhcr.org/lb/wp-content/uploads/sites/16/2019/04/Health-Factsheet.pdf 507 Health Europa, "Fill That Gap Supports Community Health Workers in Lebanon.” 508 Ibid. 509 Hemadeh et al., "The Primary Health Care Network in Lebanon: A National Facility Assessment." 510 Alliance for Health Policy and Systems Research and WHO, "PRIMASYS Comprehensive Case Study from Lebanon.” 511 Emily et al., "Health Service Utilization and Access to Medicines Among Syrian Refugee and Host Community Children in Lebanon.” 512 UN and MOPH, "Lebanon Crisis Response Plan 2017–2020." 513 UNHCR, "Vulnerability Assessment of Refugees of Other Nationalities in Lebanon.” 514 Alliance for Health Policy and Systems Research and WHO, "PRIMASYS Comprehensive Case Study from Lebanon.”

91 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
HEALTH INSURANCE COVERAGE
Despite the multiple funding mechanisms to provide health insurance to Lebanese citizens, 48 percent of the population does not have insurance coverage.515 The MOPH purchases health services from the private sector for around 52 percent of the population without health insurance, covering hospital stays and expensive medications for catastrophic illnesses. The NSSF and government employees’ funds purchase services from the private and public sectors for around 40 percent of the population, and private insurance purchases service for the remaining 8 percent.516 The NSSF restricts the coverage of its services to workers formally employed in the private sector, who represent significantly less than 50 percent of the Lebanese labor force, posing a serious challenge to female-headed households working in the informal labor sector. In addition to limited coverage, the NSSF suffers structural weaknesses limiting its capability to provide appropriate care, particularly for the elderly—upon retirement, contributors get an end-of-service lump sum, leaving them unprotected. The system’s numerous structural problems make it an inefficient mechanism for social protection.517
LEADERSHIP AND GOVERNANCE
The MOPH National Health Strategy for 2017–2020 has four main pillars: (1) modernize and strengthen sector governance, (2) improve and promote collective health across the lifecycle, (3) continue progress toward universal health coverage, and (4) develop and maintain emergency preparedness and health security.518 The MOHP Public Health Response Strategy, updated in 2016,519 emphasizes the needs of vulnerable communities, which include members of the religious and ethnic minority population. The four strategic objectives of this strategy are to increase access, strengthen health care institutions, ensure health security, and improve child survival.
The first national strategy for mental health, launched in 2015 with the support of WHO, UNICEF, and IMC a year after the establishment of the National Mental Health Program, aimed to reform mental health care in Lebanon and provide a human rights–based approach to service delivery at the community level.520
As noted earlier, the Syrian crisis led to a significant number of donors and implementing partners supporting the health sector response in Lebanon, and the MOPH coordinates the work of a multitude of these partners. Currently, work is guided by the Lebanon Crisis Response Plan (LCRP) 2017–2020, which was updated in 2020.521 The LCRP, a joint plan between the Government of Lebanon and its international and national partners, aims to respond to the current challenges in a comprehensive and integrated manner through longer-term, multiyear planning. The LCRP identifies the following strategic objectives: ensure the protection of displaced Syrians, vulnerable Lebanese, and Palestinian refugees; provide immediate assistance to vulnerable populations; support service provision through national systems; and reinforce Lebanon’s economic, social, and environmental stability.
The LCRP’s needs-based approach addresses the need to expand equitable access to health care, particularly for vulnerable populations; strengthen national institutions and capacities to respond; and boost the health system’s resilience.
515 MOPH, "Mental Health and Substance Use - Situation Analysis and Strategy for Lebanon 2015–2020." 516 WHO, "WHO Support to the Humanitarian Response in Lebanon.” 517 Lebanese Studies, "A Social Protection Emergency Response - A Bridge Toward a Comprehensive National Social Protection Plan," January 21, 2020, https://lebanesestudies.com/wp-content/uploads/2020/04/Expert-group-position-paper_final_MT.pdf 518 MOPH, "Health Strategic Plan," December 2016, https://www.moph.gov.lb/userfiles/files/%D9%90Announcement/Final-StrategicPlanHealth2017.pdf 519 Ibid. 520 MOPH, "Mental Health and Substance Use - Situation Analysis and Strategy for Lebanon 2015-2020." 521 UN and MOPH, "Lebanon Crisis Response Plan 2017–2020."

92 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
HEALTH MANAGEMENT INFORMATION SYSTEMS
Information gaps, data duplication, and inconsistent dissemination all hinder the development of an effective health information system.522 To overcome these barriers, the MOPH, with assistance from multiple donors under the EPHRP, has made concerted efforts to develop its information and communication technology systems. As of 2019, 950 health facilities, PHCCs, dispensaries, and hospitals were equipped with information technology platforms to support enhanced monitoring and reporting of both administrative and medical information at the primary health care level.523 The system includes a variety of modules for electronic medical records, personnel, appointments, drug inventory, accounting, analysis, reporting, and statistics.524 Under the EPHRP, the MOPH established a new health information system called PHENICS to register beneficiaries and to monitor health and financial indicators related to this project. This online system, currently being pilot tested at 70 facilities, links PHCCs to the Primary Health Care Department in the MOPH. 525 As of 2020, 13 PHCCs had electronic patient files for beneficiaries, along with an electronic medication monitoring system.526
The MOPH Epidemiological Surveillance Unit—currently in operation at 656 facilities across the country—oversees the country’s early warning and response system (EWARS), for monitoring infectious disease outbreaks. 527 The system also estimates the number of children not reached by routine immunization and assists this sector in understanding the potential health risks associated with environmental degradation, such as waterborne diseases, as well as the impact of poor WASH conditions on informal settlements.
Another health information system, the GBV Information Management System used by 11 agencies implementing SGBV interventions,528 captures information on incidents reported in the course of seeking SGBV services and allows partners to safely collect, store, and analyze SGBV data, including survivor and alleged perpetrator profiles, and SGBV referral services. The service-based data also help inform the organizational response to SGBV and guide interagency coordination, but it does not provide a comprehensive overview of SGBV incidents in Lebanon, as the data collected are only on reported incidents.
The MOPH lacks a human resources health information system, which hinders its ability to develop a clear understanding of the supply of, demand for, and distribution of health care providers within the national network and likely contributes to the staffing shortages noted earlier.529
CONCLUSIONS
Despite efforts to boost the health system’s resilience, much remains to be done to improve accessibility, particularly for vulnerable groups. The data indicate that areas with concentrations of REM populations have significant refugee populations and high poverty levels, highlighting the need to target interventions in those areas, especially rural areas with limited access. Subsidized services are still unaffordable for economically vulnerable households, which constitute more than half of the population. The limited amount of community-based services is a key weakness, as these approaches are more adept at providing culturally appropriate care to the many minority groups in Lebanon, including REM populations, while also creating employment opportunities for vulnerable populations. Additional community outreach and
522 Alliance for Health Policy and Systems Research and WHO, "PRIMASYS Comprehensive Case Study from Lebanon.” 523 UN and MOPH, "Lebanon Crisis Response Plan 2017–2020." 524 Alliance for Health Policy and Systems Research and WHO, "PRIMASYS Comprehensive Case Study from Lebanon.” 525 Ibid. 526 UN and MOPH, "Lebanon Crisis Response Plan 2017–2020." 527 Ibid. 528 Ibid. 529 Alliance for Health Policy and Systems Research and WHO, "PRIMASYS Comprehensive Case Study from Lebanon.”

93 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
education that focuses on appropriate homecare options and decision making on when to seek care for minor illnesses could alleviate some of the caseload at primary care facilities, and referrals for vaccinations could address the gap in vaccination coverage that is contributing to the ongoing measles outbreak.
AQ 3: CRITICAL HEALTH NEEDS AND CURRENT GAPS IN HEALTH SERVICES FOR REM COMMUNITIES
Lebanese REM populations are assimilated into the Lebanese population and therefore face the same challenges as the wider population. Although data on the geographic distribution of REM refugees are limited, these refugees likely face the same challenges as those experienced by the wider refugee population. However, the challenges refugees face are compounded by the legal barriers of registration and the consequent movement restrictions and inability to obtain formal employment. Furthermore, refugees face a higher risk of violence and abuse.530 These additional challenges likely increase their need for mental health support and their vulnerability to food insecurity, which correlates with higher rates of child labor and child marriage, lower rates of education among children, and SGBV. Therefore, these communities need the same sets of services required by the wider population, but these services should be delivered in a culturally sensitive manner to accommodate the communities’ various nationalities and religious and ethnic backgrounds.
Specific data on the challenges faced by REM communities are not available; however, these challenges are more likely to be associated with economic vulnerability and legal status than with religious or ethnic identity. For example, a study conducted among religious Druze women found that many of their medical choices were limited by the immediate context of poverty and not having access to resources to pay for medical care. 531 REM communities likely face the same challenges in health service affordability and accessibility as nonminority groups, with variations based on poverty levels and place of residence. As noted above, undocumented refugees’ movements are restricted due to their fears of coming in contact with the law, creating an additional barrier to health care access.
MENTAL HEALTH
Mental health service availability, accessibility, and affordability are inadequate, and mental health care suffers from poor integration into primary care and a critical shortage of mental health professionals. This deficiency has contributed to underdiagnosis of mental health conditions among both refugee and Lebanese populations with critical mental health needs arising from their exposure to war. Key gaps are the lack of integration of mental health care into PHCCs and the limited community-based outreach efforts concentrating on mental health. Specific interventions are needed to address women’s and children’s mental health needs.
SEXUAL AND GENDER-BASED VIOLENCE
There is a significant shortage of SGBV services despite an acute need. UNICEF reports that more than 80 percent of children in Lebanon experience violence at home.532 Reported GBV incidents have already increased tremendously since the start of the COVID-19 outbreak, further exacerbating the threat to
530 OCHA, "Assisting Survivors of Gender-Based Violence in Lebanon." 531 Nadine Yehya and Mohan Dutta, "Health, Religion, and Meaning: A Culture-Centered Study of Druze Women," Qualitative Health Research 20, no. 6 (2010): 845–858. http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.831.2120&rep=rep1&type=pdf 532 UNICEF, "A Familiar Face - Violence in the Lives of Children and Adolescents" (UNICEF, 2017). https://www.unicef.org/publications/files/Violence_in_the_lives_of_children_and_adolescents.pdf
ACF
Highlight

94 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
women and children. SGBV services also need to be integrated into other services for women at both PHCCs and clinics as integrated services help reduce the stigma faced by those accessing services. There is also a lack of community-based outreach services for women, whose movements may be restricted. Specialized services are needed to target children who are victims of violence and the high levels of child marriage, particularly among the Syrian refugee population. Additional research should be conducted to determine the extent of commercial sex among adolescent girls as a survival mechanism and provide the necessary support to address this issue. Community-based education interventions are lacking, particularly in rural areas, and should be enhanced to raise awareness of SGBV issues and facilitate open community dialogues and referrals to services. Education efforts should also address the issues of child marriage and violence against children.
MATERNAL AND REPRODUCTIVE HEALTH
Although maternal mortality rates have been falling since 2016, the rates still cause concern, particularly given the disproportionate numbers of maternal deaths among adolescents and refugees. Postnatal care is limited for all women, but the high proportion of maternal deaths in areas with high concentrations of REM and refugee populations reflects the lack of access to antenatal and postnatal care in those areas.
CHILDREN’S HEALTH
Current data on malnutrition and stunting among children are not available, but the current levels of food insecurity, which are projected to rise in 2020, highlight the need to examine this issue more closely. The proportion of measles cases among children under five and the reported gap in immunization coverage indicate low levels of awareness about the availability of free vaccination services offered countrywide. Community dialogues should be conducted to determine the constraints that prevent more expansive immunization coverage and the specific challenges faced by the vast number of undocumented children of refugee families. The frequency of waterborne diseases and diarrhea among children highlights the gap in safe WASH practices and low access to safe water and sanitation. As mentioned above, child protection measures are clearly lacking, particularly with respect to mental health and SGBV.
AQ 4: EXTERNAL STRESSES
A multitude of external stresses will significantly affect health service access, affordability, and outcomes. The current economic freefall and skyrocketing inflation, coupled with the Syrian crisis and the COVID-19 outbreak, will increase pressure on both individuals and the health system. These stresses are interrelated—the outbreak and the Syrian crisis impact the economy, which hinders the response to the outbreak and further constrains health care access for vulnerable populations.
COVID-19
Between July and September 2020, there has been a sharp rise in COVID-19 cases in Lebanon, which now records over 26,000 cases and 263 deaths. The lockdown in response to COVID-19 has accelerated the country’s economic decline, with business closures causing a spike in unemployment. Research conducted in April 2020 indicated that over 80 percent of all respondents had lost their main source of income due to the lockdown measures.533 Because of the shortage of hard currency, medical companies have been able to import only 10 percent of the country’s medical needs. The low level of imports reduces
533 PAX for Peace, "COVID-19 in Lebanon: Impact on Refugees and Host Communities," April 22, 2020, https://www.paxforpeace.nl/publications/all-publications/covid-19-in-lebanon-impact-on-refugees-and-host-communities

95 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
drug supplies and availability of personal protective equipment, hindering the country’s ability to respond effectively to the outbreak. The outbreak has already caused challenges in health care service delivery—WHO reports indicate that the nurse-to-patient ratio has fallen to one nurse for every 20 patients, compared with one nurse for every 12 patients before the outbreak. Nurses are also suffering a 50 percent salary reduction.534
UN Women highlights COVID-19’s disproportionate impact on women in terms of vulnerability to GBV, livelihood conditions, and health care access, expressing particular concern for female-headed households, which make up 29 percent of households in Lebanon; female migrant workers; and marginalized women and girls.535 As highlighted earlier, the virus’ impact has led to a 54 percent increase in harassment, violence, or abuse against women and girls. Among refugees, there has been a 71 percent increase in mental health challenges, including stress and panic536—more than 50 percent of these populations reported mental health challenges among children and adolescents.537
POLITICS AND POLICY
The ongoing Syrian war and Turkey’s incursion into Northern Syria late in 2019 reduce the likelihood that Syrian refugees in Lebanon will be able to return soon to Syria. Of concern is the decision issued by the General Director of General Security in May 2019 to deport all Syrians who entered Lebanon irregularly after April 2019. The deportations occur without any judicial investigation to ascertain that the Syrian nationals’ lives and freedom are not in danger in Syria, going against the Convention Against Torture, to which Lebanon is a signatory.538 Multiple media reports highlight the hundreds of arrests of refugees who have returned to Syria, including a Washington Post report on June 2, 2019, on the arrest and torture of more than 2,000 people who returned from Lebanon to Syria. These facts likely cause much fear among Syrian refugees who entered Lebanon illegally, as they will likely face difficulties proving whether they entered the country before or after April 2019. Other reports have surfaced of Syrian refugees being tricked into signing papers indicating that they wish to return to Syria. The fear of deportation due to this policy severely restricts Syrian refugees’ movement within Lebanon and their ability to access health care.
SECURITY AND STABILITY
Ongoing waves of antigovernment protests since October 2019, which have continued despite the COVID-19 outbreak, have in some cases led to violence, including violence between sectarian groups. The protests have concentrated on government reforms relating to widespread corruption in the public sector, the failing economy, high unemployment rates, and the government’s failure to provide basic services. Reports also highlight the sectarian tensions that have contributed to the protests, with smaller religious groups highlighting their underrepresentation and exclusion from the country’s sectarian power-sharing system and others advocating a secular, rights-based citizenship for all regardless of religion.539 The protests are affecting the country’s ability to control the outbreak and hindering individuals’ ability to
534 UNHCR, "Lebanon Crisis Monitoring Dashboard," April 28, 2020, https://data2.unhcr.org/en/documents/download/75974 535 OCHA, "Lebanon COVID-19 Emergency Appeal," May 7, 2020, https://reliefweb.int/report/lebanon/lebanon-covid-19-emergency-appeal-07-may-2020 536 Lebanon Protection Consortium, "COVID-19 Concerns and needs of Syrian refugees in Informal Tented Settlements in Lebanon," April 2020, https://www.nrc.no/globalassets/pdf/reports/covid-19-concerns-and-needs-of-syrian-refugees-in-informal-tented-settlements-in-lebanon/04072020-lpc-covid-19-concerns-and-needs-of-syrian-refugees-in-itss-in-lebanon.pdf 537 UN and MOPH, "Lebanon Crisis Response Plan 2017–2020." 538 Local Agenda, "Position Paper on the Decision to Summarily Deport Syrian Nationals who Entered Lebanon Irregularly," 2019, https://www.legal-agenda.com/uploads/Position%20Paper%20on%20the%20decision%20to%20summarily%20deport%20Syrian%20nationals%20who%20entered%20Lebanon%20irregularly.pdf 539 Central Intelligence Agency, "The World Factbook: Lebanon."

96 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
safely access health care. There is also evidence of growing tension between Lebanese and Syrian communities, rooted particularly in economic concerns such as employment.
FINANCIAL CRISIS
Business closures due to the COVID-19 outbreak response have deepened Lebanon’s financial crisis. In April 2020, the IMF projected that Lebanon’s economy will shrink 12 percent in 2020, and the Minister of Social Affairs estimated that 75 percent of the population is now in need of aid.540 The World Bank estimates that more than 40 percent of the Lebanese population will soon be living under the poverty line.541 These financial woes will be detrimental for refugee populations, 67–90 percent of whom were already living under the poverty line. The loss of purchasing power due to the devaluation of the Lebanese pound, coupled with high unemployment rates, will surely worsen food insecurity as well. These factors will make even subsidized health payments unaffordable for a large portion of the population.
The economic collapse has also hindered health care service delivery, as revealed in a statement by the prime minister in March 2020 saying that the government cannot reimburse private and public hospitals, including funds owed to the NSSF. For example, the Rafik Hariri University Hospital, the largest public hospital in Lebanon, received only 40 percent of its allocated budget in 2019 and none yet for 2020, with other hospitals reporting they received no payments in 2019.542
ENVIRONMENT
A lack of financial and human resources undermines Lebanon’s water sector, hampering service delivery effectiveness. Estimates indicate that less than half of the Lebanese population is connected to official water supplies, which provides sporadic services. 543 As a result, nearly one in three Lebanese buys alternative sources of drinking water, usually from mobile water trucks or in bottles, and those who cannot afford to purchase water rely on low-quality water for their households. Water quality is also deteriorating as a result of surface and underground water pollution caused by decades of urbanization; lack of proper waste management systems; and irregular dumping of waste of all kinds in rivers, sea outfalls, and valleys.544 Lack of safe water, poor wastewater management, hygiene and living conditions, and unsafe food all influence the incidence and spread of communicable and noncommunicable diseases, and the outbreak of COVID-19 increases the need to ensure access to safe water.
EQUITY
Equity factors likely to impede health outcomes in Lebanon are related to wealth, unemployment, gender, religion, and legal status. The country records a Gini coefficient of 86 percent, which reflects a high degree of wealth inequality, with the wealthiest 1 percent of Lebanese holding 25 percent of the nation’s wealth.545 Unemployment is particularly high in some of the country’s poorest areas, where it is nearly double the national average. The economic downturn has had a disproportionate effect on young people entering the workforce, with unemployment among youth 12 percent higher than the national average. Gender
540 Tamara Qiblawi, "75% of Lebanon Needs Aid After Coronavirus, and Hungry Protesters Are Back on the Streets," CNN, April 29, 2020, https://www.cnn.com/2020/04/28/middleeast/lebanon-hunger-aid-coronavirus-intl/index.html 541 Kareem Chehayeb, "Besides Coronavirus, Lebanon has an Equally Dangerous Outbreak on its Hands - Unemployment," The New Arab, March 29, 2020, https://english.alaraby.co.uk/english/indepth/2020/3/31/beyond-covid-19-lebanons-unemployment-outbreak 542 Chehayed, "Lebanon Is the Experiment That Shows Neoliberalism's Failure.” 543 USAID, "Water and Sanitation," Accessed June 8, 2020, https://www.usaid.gov/lebanon/water-and-sanitation 544 USAID, "Water and Sanitation.” Accessed June 8, 2020, https://www.usaid.gov/lebanon/water-and-sanitation 545 Alliance for Health Policy and Systems Research and WHO, "PRIMASYS Comprehensive Case Study from Lebanon.”

97 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
inequities are also evident in the labor market—only 22 percent of women aged 15 years and above are employed, compared with 72 percent of men. Lebanon ranks 145th out of 153 countries on the World Economic Forum Global Gender Gap Index 2020.546
The higher subsidization of primary health care services for Syrians has also raised equity concerns, with the economic crisis and competition for jobs and access to resources and services driving local tensions.547 Key informant interviews also reveal that although a form of “universal coverage” exists in Lebanon whereby any citizen is eligible for coverage of hospitalization fees and treatments, in practice, political parties and politicians use health care access as a strategy to gain and reward support from individuals and their families.548 As political affiliation in Lebanon is usually based on religion, these factors can heighten community tensions.
CONCLUSIONS
The multitude of stresses currently affecting Lebanon can drastically impact the health care system and health care access, particularly for vulnerable individuals. The situation of migrants and refugees is also deteriorating sharply, increasing the number of people in need of basic humanitarian assistance and protection. The vast number of displaced persons living in Lebanon, coupled with the economic crisis and the consequent deterioration of living conditions, has increased host communities’ frustration and resentment toward the new arrivals, whom they hold responsible for the situation.549 These tensions are further exacerbated by the perception that host communities are unfairly left out of the humanitarian response targeting refugees. Future interventions should therefore implement broad-based interventions that ensure equitable access for all vulnerable communities.
USAID HEALTH AND REM PROGRAMMING
USAID is currently not implementing health programs in Lebanon, due to limitations of working with the current Minister of Health. However, in 2020 USAID has partnered with faith-based organizations to offer online education to vulnerable Lebanese and refugee youth during COVID-19 quarantine. This program is organized by USAID’s five-year activity, BALADI CAP, which provides capacity building assistance to civil society organizations in Lebanon.
USAID also supports WASH activities, with the goal of improving water services and addressing pollution through the provision of technical assistance to the four regional water authorities that serve the entire Lebanese population, with the goal of improving their operations and the quality and reliability of service delivery. USAID also provided construction and capacity building services to the four water authorities and local municipalities. As a result, the water authorities have improved operations, financial management, planning and customer outreach.
In Lebanon, USAID also implements activities on education, agriculture and food security, democracy and governance, and various other sectors. Between 2012-2015, the United States Department of State, Bureau of Population, Refugees, and Migration implemented shelter, health, and education programs for Syrian and Iraqi refugees in Lebanon through a multitude of international NGOs and UN organizations.
546 Un Women, "Lebanon," Accessed June 12, 2020, https://arabstates.unwomen.org/en/countries/lebanon 547 OCHA, "Lebanon Humanitarian Fund Annual Report 2019 Lebanon.” 548 Chen and Cammett, "Informal Politics and Inequity of Access to Health Care in Lebanon." 549 Oxfam, "Self-Protection and Coping Strategies of Refugees from Syria and Host Communities in Lebanon.”

98 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
JORDAN
FIGURE 34. MAP OF JORDAN
COUNTRY CONTEXT
Jordan is a middle-income country with an estimated 10 million people, two-thirds of which are under the age of 30, and 47 percent are women.550 While surrounded by countries in conflict (Iraq, Syria, Israel and the Occupied Palestinian Territories), Jordan is politically stable and has not suffered from internal or external security crises in many years. Because of this relative stability and proximity to countries in crisis, Jordan experienced an increase in population due to forced migration. In 2018, Jordan was considered to have the second highest share of refugees compared to its population in the world, with 89 refugees per 1,000 inhabitants. 551 The largest group of refugees are Palestinians with an estimated 2.2 million in December 2019. In addition, there was a reported 657,068 Syrian refugees and 67,225 Iraqi refugees 552 (see table 11).
While Jordan has one of the strongest healthcare systems in the region, the influx of refugees, especially as they leave the camps and live in the urban and rural areas of Jordan, has placed increased pressure on Jordan’s infrastructure and health system.553
550 USAID Country profile. Accessed June 24, 2020. https://idea.usaid.gov/cd/jordan?comparisonGroup=region 551 UNHCR. Jordan Fact Sheet October 2018. https://reliefweb.int/report/jordan/unhcr-jordan-factsheet-october-2018 552 UNHCR Jordan. December 2019. https://www.unhcr.org/jo/12449-unhcr-continues-to-support-refugees-in-jordan-throughout-2019.html#:~:text=As%202019%20comes%20to%20close,total%20of%2052%20other%20nationalities. 553 ibid
ACF
Sticky Note
JOrdan

99 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
TABLE 8: REFUGEES IN JORDAN
Nationality Total
Palestinian Refugees 2.2 Million
Syrian Refugees 657,068
Iraqi Refugees 67,225
Yemeni Refugees 15,000
Sudanese Refugees 6,000
Other 2,500
OVERVIEW OF RELIGIOUS AND ETHNIC MINORITIES IN JORDAN
Focus REM Populations in Jordan: Christian, Druze, Syrians, Iraqis and Palestinians.
Geographic Areas of REM Populations: Zarqa, Amman, Irbid, Al Balqa, Madaba, and Mafraq Governorates
The majority of Jordan’s population is Muslim (97.2 percent), Christians account for 2.2 percent and other groups including Druze are less than 1 percent.554 The Jordanian constitution states that people have the freedom to practice one's religion. Although the government does not recognize some religious groups such as Druze, which Jordan considers to be Muslim, Jordan does not discriminate against this group and allows them to practice their beliefs.555
The Jordanian law recognizes the following Christian religious groups: Greek Orthodox, Roman Catholic, Armenian Orthodox, Melkite Catholic, Anglican, Maronite Catholic, Lutheran, Syrian Orthodox, Seventh-day Adventist, United Pentecostal, and Coptic. Heads of each of these denominations form the Council of Church Leaders (CCL), which is a government advisory.556
It is believed that half of the population in Jordan is Palestinian or of Palestinian origin that came to Jordan as refugees between 1947 and 1967.557 Most of this population has been naturalized, however, in 2019 there were 2.2 million registered Palestinian refugees.558 REM GEOGRAPHIC FOCUS
REM populations are dispersed throughout the country’s 12 governorates, in three regions (North, Central, and South). However, there are higher concentrations of REM populations in several Governorates, as shown below:
554 U.S. Department of State, 2018 Report on International Religious Freedom: Jordan, 2019. https://www.state.gov/reports/2018-report-on-international-religious-freedom/jordan/. 555U.S. Department of State, 2018 Report on International Religious Freedom: Jordan, 2019. https://www.state.gov/reports/2018-report-on-international-religious-freedom/jordan/. 556 ibid 557 Human Rights Watch, Stateless Again Palestinian-Origin Jordanians Deprived of Their Nationality, 2010. https://www.hrw.org/report/2010/02/01/stateless-again/palestinian-origin-jordanians-deprived-their-nationality. 558 UNHCR Jordan. December 2019. https://www.unhcr.org/jo/12449-unhcr-continues-to-support-refugees-in-jordan-throughout-2019.html#:~:text=As%202019%20comes%20to%20close,total%20of%2052%20other%20nationalities.

100 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
• Druze: Amman and Zarqa Governorates • Christian: Amman, Irbid, Madaba and Al Balqa Governorates559. • Palestinian refugees: Amman, Irbid, Zarqa, Balqa, Jerash
In 2011, during the uprising against the Syrian government, Syrians fled to Jordan and resided in camps (Zaatari, Azraq and Mrajeeb Al Fhood). Over the years, the number of people living in camps started to dwindle as people moved to urban and rural areas. There are currently 656,733 Syrian refugees dispersed throughout Jordan with a higher concentration living in Amman, Irbid, Zarqa and Mafraq governorates. 560
According to UNHCR there are 67,255 registered Iraqi refugees. Shia Muslims and Christians account for one third of this population and the majority are Sunni Muslims.561 As with other refugees within Jordan, this population is dispersed with the majority living in Amman, Mafraq, Zarqa and Balqa.
FIGURE 35: REM GROUPS LOCATED IN EACH GOVERNORATE562
Because there is limited information on health outcomes for REM populations, where data are not available, the focus is on the Governorates where they reside. Further, as most Palestinians in Jordan are fully naturalized and there is no official census data for how many people are Palestinians, the data focused in this report is on the UNWRA Palestinian refugee population. Lastly, it is important to recognize that the population groups discussed (Palestinians, Syrians and Iraqis) are not monolithic and may represent Christian or Druze beliefs.
AQ 1: OVERVIEW OF HEALTH STATUS IN JORDAN
Over the last decade, Jordan has made progress in improving the overall health status of its population, with an improvement in reproductive health services and maternal and child health services including vaccination rates. However, there is still a lot to be done. While life expectancy has steadily increased
559 U.S. Department of State, 2018 Report on International Religious Freedom: Jordan, 2019. https://www.state.gov/reports/2018-report-on-international-religious-freedom/jordan/. 560 UNHCR, “Operational Portal: Situation Syria Regional Refugee Response,” accessed June 2, 2020, https://data2.unhcr.org/en/situations/syria. 561 ibid 562 Wikipedia, Palestinians in Jordan, accessed June 5, 2020, https://en.wikipedia.org/wiki/Palestinians_in_Jordan,
Amman Irbid Al Mafraq Zarqa AlBalqa Madaba Al Karak Jerash
Christian
Druz
Palestinian
Iraqi
Syrian

101 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
over the years to a projected 74.60 in 2020, disparities in health indicators exist due to geographic locations, gender and nationality.563
Jordan is experiencing an epidemiological transition as non-communicable diseases (NCDs) increase. Cardiovascular disease was the leading cause of premature mortality in 2017, accounting for 1748.7 deaths per 100,000. 564 Similarly, data from urban refugee populations also revealed an increase in NCD565. As a result, Jordan is faced with an immense strain on the health system. Other significant contributors to death and disability include neonatal disorders, congenital defects, stroke and road injury (Figure 36).
FIGURE 36: TOP 10 CAUSES OF DEATH AND DISABILITY (DALYS (AGE-STANDARDIZED RATE PER 100,000) 2017
Refugee camps however had the double burden with acute care being an important need. In the first quarter of 2019, in Zaatari Camp the top acute health conditions was upper respiratory tract infections and influenza like infections and the top chronic conditions were hypertension and asthma (See Figures 37 and 38).566
563 2019 Revision of World Population Prospects. Accessed June 26, 2020. https://population.un.org/wpp/ 564 Institute for Health Metrics and Evaluation (IHME). Jordan profile. Seattle, WA: IHME, University of Washington, 2018. http://www.healthdata.org/jordan 565 UNHCR, Health Sector Humanitarian Response Strategy Jordan 2019-2020, 2019. https://reliefweb.int/sites/reliefweb.int/files/resources/68348.pdf 566 UNHCR, Public Health Profile: First quarter 2019. https://data2.unhcr.org/en/documents/download/69170
2,0321,840
1,247 1,1661,068 1,004
879
640 630 623
NeonatalDisorders
IschemicHeart
Disease
Diabetes CongenitalDefects
Stroke Low BackPain
HeadacheDisorders
RoadInjuries
Druge UseDisorders
ChronicKidneyDisease

102 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
FIGURE 37: ACUTE MORBIDITY IN ZAATARI CAMP (2019)
FIGURE 38: CHRONIC MORBIDITY IN ZAATARI CAMP (2019)
29%
16%
11%
6%4%
33%
Upper RespiratoryTract Infections
Influenza-Like Illness Dental Ear Infection Lower RespiratoryTract Infections
Other
17% 16%13%
5% 4%
45%
Hypertension Asthma Diabetes Thyroid Problems CardiovascularDisorders
Other

103 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
WOMEN’S HEALTH
Jordan has made important progress in maternal health over the years. In 2018, one of the largest successes was the reduction in maternal mortality from 59 per 100,000 births in 2010 to 29.4 in 2018. 567 UNWRA saw similar reductions with a maternal mortality rate of 15.8 per 100,000 live births in 2018.568 This reduction can be linked to the improvement in ANC visits, with over 80 percent of pregnant Jordanians attending at least 7 ANC visits and 85.7 percent of pregnant Palestinians receiving care at a UNWRA facility attending at least 4 ANC visits.569,570 There is also nearly complete coverage of skilled births and health facility deliveries (98 percent). To further improve maternal mortality, the Government of Jordan, with support from USAID, created a Maternal Mortality Surveillance and Response (JMMSR) System to identify causes and use the information to prevent future deaths.
The fertility rate in Jordan has steadily declined to 2.76 in 2018.571 Jordan’s contraception prevalence rate (CPR) decreased from 61percent in 2012 to 52 percent in 2017–2018.572 573 A cross-sectional study looking at this decline reported that the Jordanian government believed the decline was due to a decrease in the use of traditional contraceptive methods or due to the ‘influx of Syrian refugees, who tended to have lower CPR than Jordanians.’574
CHILD HEALTH
Infant and under-five mortality rates have also declined and were 13.9 and 16.2 per 1,000 respectively in 2018. However, there is a disparity of infant and under 5 mortality rates amongst the governorates (Figure 39). As an example, under-five mortality ranges from 23 in Mafraq to 11 in Balqa and infant mortality ranges from 19 in Madaba to 11 in Balqa. There is also a disparity among nationalities. The under-five mortality rates are higher among children born to Syrian women (25 deaths per 1,000) than among children born to Jordanian women or women of other nationalities (16 deaths per 1,000).575 The neonatal mortality for Syrians living in Zaatari camp has decreased from 13.8 deaths in 2017 to 9.7 in 2018.576
567 MoH, The National Maternal Mortality Report 2018, 2018. https://www.abtassociates.com/sites/default/files/files/insights/reports/2020/the-national-maternal-mortality-report-2018-for-jordan.pdf 568 This statistic is across all UNWRA country locations; Jordan specific data is not available. 569 Department of Statistics (DOS) and ICF. 2019. Jordan Population and Family and Health Survey 2017-18. Amman, Jordan, and Rockville, Maryland, USA: DOS and ICF. 570 UNWRA. Health Department Annual Report 2018, 2019. https://www.unrwa.org/resources/reports/health-department-annual-report-2018. 571 World Bank Data. Accessed June 25, 2020. https://data.worldbank.org/indicator/SP.DYN.TFRT.IN?locations=JO&display=graph--%3E 572 Department of Statistics (DOS) and ICF. 2019. Jordan Population and Family and Health Survey 2017-18. Amman, Jordan, and Rockville, Maryland, USA: DOS and ICF. 573 Komasawa, M, et. al. Demand for family planning satisfied with modern methods and its associated factors among married women of reproductive age in rural Jordan: A cross-sectional study. March 18, 2020 https://doi.org/10.1371/journal.pone.0230421 574 ibid 575 Department of Statistics (DOS) and ICF. 2019. Jordan Population and Family and Health Survey 2017-18. Amman, Jordan, and Rockville, Maryland, USA: DOS and ICF. 576 UNHCR, Health Sector Humanitarian Response Strategy Jordan 2019-2020, 2019. https://reliefweb.int/sites/reliefweb.int/files/resources/68348.pdf

104 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
FIGURE 39: INFANT AND UNDER 5 MORTALITY RATE BY GOVERNORATE
Diarrhea was the second most common illness among children under-five reported in the 2017-18 Jordan Population and Family Health Survey.577 Further, Jordanians reported a higher number of cases (9.8) than Syrians (8.8) and other nationalities (8.5). In 2017, the death rate from diarrheal diseases was 0.83 per 100,000 in Jordan.578
In 2017 the death rate from malnutrition in Jordan was 0.17 per 100,000 people, which is a decrease from previous years 579 Approximately, 3 percent of children under-five are underweight, with regional disparities between the northern and southern regions of the country. According to the Jordan Guidelines for the Management of Malnutrition, the prevalence of global acute malnutrition (GAM), among children 6-59 months, in 2012 was 5.1 percent in refugees living in host communities and 5.8 percent in Zaatari camp.580 Further, the “prevalence rates of acute malnutrition in women 15-49 years of age were 6.3 percent in the urban refugee community and in Zaatari camp 6.1 percent.” The Situation Analysis of Children in Jordan (2017) reported that 17 percent of Jordanian children 12-59 months are anemic, and the rate is 64 percent among registered Syrian refugee children 6 months to 2 years old.581 MENTAL HEALTH
In 2016 1.06 million people were diagnosed as having mental health and neurodevelopmental disorders, which was 8 percent of the total disease burden in Jordan.582 Refugees are at particular risk of mental health problems due to difficult experiences before, during and after leaving their countries. According to UNHCR, in 2018, there were more than 71,423 consultations for mental health disorders in urban refugee
577 Department of Statistics (DOS) and ICF. 2019. Jordan Population and Family and Health Survey 2017-18. Amman, Jordan, and Rockville, Maryland, USA: DOS and ICF. 578 Global Burden of Disease Collaborative Network, Global Burden of Disease Study 2017, (Seattle, 2018), Our World in Data. https://ourworldindata.org/country/jordan#search=diarrhea 579 Global Burden of Disease Collaborative Network, Global Burden of Disease Study 2017 (GBD 2017) Results. Seattle, United States: Institute for Health Metrics and Evaluation, 2018. https://ourworldindata.org/grapher/malnutrition-death-rates?tab=chart&time=2017&country=~JOR 580 MoH, Jordan Guidelines for the Management of Malnutrition, 2013. https://data2.unhcr.org/en/documents/download/40684 581 UNICEF, Situation Analysis of Children in Jordan 2017 Summary, 2017. https://www.unicef.org/jordan/media/506/file/Report%20SitAn.pdf 582 Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2016 (GBD 2016) Results. Seattle, United States: Institute for Health Metrics and Evaluation (IHME), 2017.
15
9
1819
15
17
1110
1817
16
5
1716
11
18
21
18
23
13 13
21
1718
10
17
Amman Balqa Zarqa Madaba Irbid Mafraq Jarash Karak Aljun Tafiela Ma'an Aqaba Kingdom
Infant Mortality Rate (per 1,000 Live Births) Under 5 Mortality Rate (per 1,000 Live Births)

105 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
health facilities and 13,647 consultations for mental health disorders in the refugee camps; 30.9 percent for epilepsy/seizures, 33.7 percent for depressive disorder and 14.4 percent for psychotic disorder.583 In Zaatari, men accounted for 58 percent of visits for severe emotional distress, including moderate-severe depression in the first quarter of 2019.584 Further, in the Syrian vulnerability report, more than one of every five adults sampled reported that they did not want to carry on living due to feelings of hopelessness.585
SEXUAL AND GENDER-BASED VIOLENCE (SGBV)
According to the 2017-18 Jordan Population and Family Health Survey, 20.4 percent of women and girls aged 15-49 years reported being subjected to physical, sexual or psychological abuse586 (Figure 40). The GBV Information Management System (GBVIMS) reported that single adolescent girls accounted for 3 percent of reported rape and 10 percent of sexual assault.587 Further, the report revealed the nationalities of survivors seeking help were 70 percent Syrians, 23 percent Jordanians, and 7 percent refugees of other nationalities, mainly Iraqis and Sudanese. In Zaatari Camp, in the first quarter of 2019 the incidence of rape (reported cases/10,000/yr) was 0.5.588
FIGURE 40: PROPORTION OF EVER-PARTNERED WOMEN AND GIRLS AGED 15 YEARS AND OLDER SUBJECTED TO PHYSICAL, SEXUAL OR PSYCHOLOGICAL
ABUSE (2017-2018)
583 UNHCR, Health Sector Humanitarian Response Strategy Jordan 2019-2020, 2019. https://reliefweb.int/sites/reliefweb.int/files/resources/68348.pdf 584 UNHCR, Public Health Profile: First quarter 2019. https://data2.unhcr.org/en/documents/download/69170 585 Brown, H, et al., Vulnerability Assessment Framework Population Study 2019. UNHCR. https://reliefweb.int/sites/reliefweb.int/files/resources/68856.pdf 586 DOS and ICF. Jordan Population and Family and Health Survey 2017-18. 587 GBVIMS Task Force, Jordan GBV IMS Task Force / Annual Report 2019. https://reliefweb.int/sites/reliefweb.int/files/resources/75705.pdf 588 UNHCR Public Health Profile. First quarter 2019. Available at https://data2.unhcr.org/en/documents/download/69170
20.4%
18.4%
19.8%
21.3%
15-49 15-24 25-34 35-49

106 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
OUTBREAK/EPIDEMIC DATA
In 2015 there was an outbreak of Middle East respiratory syndrome coronavirus (MERS-CoV) with 16 laboratory-confirmed cases in hospitals in Amman and Zarqa. About 44 percent of the patients diagnosed died, 69 percent of the cases were health care associated, 31percent were relatives of a known case.589
Vaccination coverage is good in Jordan. Jordanians (83 percent) had a higher vaccination rate when compared to Syrians (76 percent)590 and “immunization coverage, for both 12-month-old and 18-month-old children registered with UNRWA, continued to be above WHO target of 95 percent.”591 Further, UNWRA reported that in 2018, there were no cases of polio or other emerging diseases among Palestine refugees.
Jordan has a low HIV rate. In 2017, there were 54 new cases of HIV and a total of 525 people living with HIV in Jordan. The annual number of deaths from HIV/AIDS per 100,000 people was 0.23.592 Further, the Jordan National Strategy for Health Sector reports only “a number of AIDS cases have been reported among Syrian refugees.”
ACCESS TO WASH
Improving access to clean water and sanitation facilities is key to improving child health and the preventing the spread of infectious diseases. According to UNICEF, ‘more than 98 percent of the population has access to an improved water source, 93 percent have access to a safely-managed source and 86 percent to a piped network.593 Further, according to UNHCR, 92 percent targeted vulnerable refugees had access to an adequate quantity of safe water in late 2019.
Despite this, Jordan is a water poor country with groundwater monitoring of the country’s main aquifers revealing that water levels are declining more than ten meters annually in some aquifers.594 As the population grows, there is fear that the challenges will continue and possibly increase.
CONCLUSION
Jordan’s population, including REM populations have a good overall health status, with an increase in life expectancy and lowering of maternal and infant mortality rates. The rate of skilled deliveries, ANC visits and vaccinations have increased across all populations, while communicable diseases have decreased. NCDs have increased and are the leading causes of premature mortality in Jordan and in the refugee camps. Addressing the risk factors promoting healthy lifestyles will be key to reducing morbidity and mortality of NCDs. Vulnerable populations, including refugees, deal with the largest health burdens.
589 Payne, Daniel C et al. “Multihospital Outbreak of a Middle East Respiratory Syndrome Coronavirus Deletion Variant, Jordan: A Molecular, Serologic, and Epidemiologic Investigation.” Open forum infectious diseases vol. 5,5 ofy095. 28 Apr. 2018, doi:10.1093/ofid/ofy095 590 Department of Statistics (DOS) and ICF. 2019. Jordan Population and Family and Health Survey 2017-18. Amman, Jordan, and Rockville, Maryland, USA: DOS and ICF. 591 UNWRA. Health Department Annual Report 2018. 2019. https://www.unrwa.org/resources/reports/health-department-annual-report-2018 592 Global Burden of Disease Collaborative Network, Global Burden of Disease Study 2017, (Seattle, 2018), Our World in Data. https://ourworldindata.org/grapher/hiv-death-rates?tab=chart&time=latest&country=~JOR 593 UNICEF. Water, Sanitation and Hygiene in Jordan. https://www.unicef.org/jordan/water-sanitation-and-hygiene 594 ibid

107 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
AQ 2: STRENGTHS AND WEAKNESSES OF THE PRIMARY HEALTH CARE SYSTEM
Jordan is known for high-quality modern health services and infrastructure. The healthcare system in Jordan is mainly composed of three healthcare providers: the public sector, the private sector, and the international and charity sector (including UN, FBOs and NGOs). Jordan had 59 private hospitals, 45 public hospitals, 102 comprehensive healthcare centers and 380 primary healthcare centers in 2016.595 This includes university hospitals and specialty centers (University of Jordan Hospital, King Abdullah University hospital) and the Centre for Diabetes, Endocrinology and Genetics as well as The National Center for Woman’s Health. Within the international and charity sector, UNHCR reports 21 partners (including national, international and UN), working in the health sector for refugees in Jordan.596 This includes faith-based organizations, such as the International Orthodox Christian Charities (IOCC), Islamic Relief Worldwide. UNWRA delivers health services in 26 PHC facilities (12 inside camps, 14 outside camps), which is a ratio of 1.3 PHC facilities per 100,000 populations (2018)597. UNHCR supports health service to all registered Iraqi and Syrian refugees through implementing partners and affiliated hospitals network.
FIGURE 41: HEALTH SECTOR MAPPING
*Taken from the MoH National Health Strategy 2016-2020
595 ibid High Health Council, National Human Resources for Health Strategy for Jordan (2018-2022). 596 UNHCR. Operational Portal Refugee Situations: Number of Partners, accessed June 5, 2020. https://data2.unhcr.org/en/partners?country=36&country_1=0&text=§or=3§or_1=0&country_json=%7B%220%22%3A%2236%22%7D§or_json=%7B%220%22%3A%223%22%7D&apply=&page=2&sort=_score&direction=desc 597 UNWRA. Health Department Annual Report 2018. 2019. https://www.unrwa.org/resources/reports/health-department-annual-report-2018

108 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
HEALTH WORKFORCE
A strong and motivated health workforce is central to health care systems and advancing service delivery and quality. Jordan has highly qualified physicians, nurses, and other healthcare providers. The overall number of doctors is 23.04 per 10,000 population, which is higher than neighboring countries (Iraq 7.08 in 2018 and Lebanon 21.04 in 2018 and Syria 12.87 in 2016). Despite this, Jordan is facing shortages in some medical specialties and the female nursing workforce. See table 12 below for the breakdown of healthcare professionals by sector.
TABLE 92: HEALTH WORKFORCE IN JORDAN598
Profession Ministry of Health
Royal Medical Services
King Abdullah Hospital
Jordan University Hospital
Private Sector UNRWA Total
Average / 10,000
Population
Physicians 5,838 2,190 595 722 14,322 89 23,756 23.04
Dentists 743 411 0 111 6,161 29 7,455 7.23
Pharmacists 805 482 46 27 12,192 2 13,554 13.15
Registered Nurses 6,206 4,593 809 524 10,364 44 22,540 21.86
Midwives 1,612 410 23 18 1,222 34 3,319 3.22
Assistant Nurses 1,731 0 34 38 0 176 1,979 1.92
Associate Degree – Nursing
2,372 2,998 44 160 0 0 5,574 5.41
598 MoH. Health Indicators: Human Resources, accessed June 5, 2020. https://www.moh.gov.jo/Pages/viewpage.aspx?pageID=238

109 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
Although the number of doctors is high, the turnover of health staff (particularly nurses) is high in Jordan. Reasons for this include low job satisfaction, lack of opportunities for professional development, professional recognition and violence. It was reported that 75 percent of nurses experience verbal or physical violence. The highest turnover rates for nurses are in Amman, Zarqa and AlBalqa, Governorates with high REM populations.
There are also significant gender gaps within the health workforce (i.e. 83.1 percent of the MoH physicians are male) and disparities among urban and rural areas, since staff favor urban centers (Figure 42 and Table 13). For example, the number of midwives is lower in key governorates where REM populations live which is particularly concerning for ensuring MCH services.
FIGURE 42: HEALTH WORKER DISPARITY IN GOVERNORATES599
TABLE 10: DOCTOR/NURSE GENDER GAP IN 2018 (PERCENT)
Amman Irbid Al Mafraq Zarqa Al Balqa
Doctors 57.18 64.61 69.23 70.67 64.21
Nurses -47.77 -47.56 -23.08 -56.48 -63.64
In the pursuit of health workforce development, Jordan developed a National Human Resources for Health Strategy, which included strategies to secure funding to improve the production, employment, and capacity building for all health professionals and to attract, deploy, retain, and motivate the health workforce in both public and private sectors and especially in remote/underserved areas.600
599 Hadidi, R., The Hashemite Kingdom of Jordan National Human Resources for Health Observatory Annual Human Resources for Health Report, 2017. https://www.medicinebau.com/uploads/7/9/0/4/79048958/hrh_report_2016__1_.pdf 600 High Health Council, National Human Resources for Health Strategy for Jordan (2018-2022), 2018. https://extranet.who.int/countryplanningcycles/sites/default/files/planning_cycle_repository/jordan/national_human_resources_for_health_strategy_2018-2022_en.pdf
1,112
157 141 8416917 17 8
1,978
500341
168100 58 28 26
Amman Irbid Zarqa Mafraq
Physicians Pharmacists Nurses Midwives

110 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
SERVICE DELIVERY
The three sector (public, private and international/charity) providers play an equal and important role in health service delivery for REM populations. The 2017-2018 Jordan Population and Health Survey revealed that 48 percent of people visited a public health facility while 52 percent went to a private facility or provider. However, it was more common for people to go to public health facilities in rural than in urban areas (66 percent versus 46 percent). This implies that private sector health facilities are a more significant provider of outpatient services in urban areas than in rural areas.
FIGURE 43: PERCENTAGE OF PEOPLE RECEIVEING OUTPATIENT CARE BY SERVICE PROVIDER AND GOVERNORATE
The Health Access and Utilization Survey601 revealed that Syrians and Iraqis also prefer to seek care in private facilities. However, there was a decrease in Iraqis seeking treatment in private facilities in 2017 and an increase in utilizing the local NGO JHAS (Jordan Health Aid Society) facilities for both Syrian and Iraqis (See Figure 44). Among Palestinians who seek services in UNWRA supported facilities, there was an increase in utilization rate from 1,587,015 in 2017 to 1,570,044 in 2018.602
601 UNHCR, Health Access and Utilization Survey Access to Healthcare Services in Jordan Among Iraqi Refugees, December 2017. UNHCR, Health Access and Utilization Survey Access to Healthcare Services Among Syrian Refugees in Jordan, December 2018. 602 UNWRA. Health Department Annual Report 2018, 2019. https://www.unrwa.org/resources/reports/health-department-annual-report-2018.
38.2
54
42.6
37.9
60.5
48
71.9
81.2
89.7
73.4
71.4
59.6
61.8
46
57.4
62.1
39.5
52
28.1
18.8
10.3
25.6
28.6
40.4
Amman
Balqa
Zarqa
Madaba
Irbid
Mafraq
Jarash
Ajloun
Karak
Tafiela
Ma’an
Aqaba
Private Sector Public Sector

111 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
FIGURE 44: PERCENTAGE OF IRAQIS AND SYRIANS WHO SOUGHT TREATMENT BY PROVIDER TYPE
Further, the Health Access and Utilization Survey revealed that between 2017 and 2018, coverage of services improved in all categories for Syrians.603 This includes, an improvement in ANC and vaccination coverage and access to family planning and services for chronic conditions.
However, for Iraqi’s service accessibility and utilization worsened remarkably. For example, awareness of family planning services dropped from 43 percent in 2016 to 11 percent in 2017 and the number of people who were able to access services for chronic conditions dropped from 69 percent to 56 percent (See Figure 45).604
FIGURE 45: SELECTED SERVICES FOR SYRIAN VS IRAQI REFUGEES
603UNHCR, Health Access and Utilization Survey Access to Healthcare Services Among Syrian Refugees in Jordan, December 2018. 604 UNHCR, Health Access and Utilization Survey Access to Healthcare Services in Jordan Among Iraqi Refugees, December 2017.
37%
28%
2%
14%
5%
10%
4%
30%
13%
8%
24%
9%11%
4%
23% 22%
12%
5%
27%
1%
10%
15%
37%
7%
21%
14%
7%
Privateclinic/hospital
Private Pharmacy NGO Clinic JHAS Clinic(NGO)
Govt. Hospital Caritas Clinic Other
Iraqi 2016 Iraqi 2017 Syrian 2017 Syrian 2018
67%55%
11%
56%
97%
68%57%
78%
% that had a vaccination card >4 ANC Visits Aware of family planningservices
% of people who were able toaccess services for chronic
conditions
Iraqi 2017 Syrian 2018

112 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
Other important indicators that capture availability, access and distribution of health services are the density of hospital beds, medical facility and MCH centers. As shown in Figure 46, secondary and tertiary care is provided by private and public hospitals in all governorates with the majority of hospital beds in urban areas where the majority of the population resides and overall, 33 percent of hospital beds were in the private sector in 2013.605
FIGURE 46: MEDICAL FACILITIES AND MCH CENTERS BY GOVERNORATE PER 100,000 POPULATION (2018) 606
The rate of cesareans (CS) in Jordan is fairly high at 27 percent for Jordanians and 22 percent for Syrians607, higher than the WHO recommendation of not being above 10-15 percent. One study revealed that more CS occurred if the woman is highly educated or is over 35 years. Further it revealed that more occur in training hospitals for the purposes of training residents (45 percent of CS were in training hospitals) and due to financial gain (more occurred in private hospitals)608. As there are no national guidelines, CS are performed at the physician’s discretion.
605 High Health Council, The National Strategy for Health Sector in Jordan 2016- 2020, 2016. 606 Jordan Ministry of Health and the Department of Statistics, Indicators of Health 2018. https://www.moh.gov.jo/ 607 Department of Statistics (DOS) and ICF. 2019. Jordan Population and Family and Health Survey 2017-18. Amman, Jordan, and Rockville, Maryland, USA: DOS and ICF. 608 Baeha AM, Al-Daradkah SA, Khader YS, Basha A, Sabet F, et al. (2017) Cesarean Section: Incidence, Causes, Associated Factors and Outcomes: A Natonal Prospective Study from Jordan. Gynecol Obstet Case Rep Vol.3: No.3: 55
185
147
89 92
118
93
74
131
159
124 127 133143
313
314
614 10 16 18 20 23
12 6210
29 6 10 7 13 13 18 14 9 5
Amman Balqa Zarqa Madaba Irbid Mafraq Jarash Ajlun Karak Tafiela Ma'an Aqaba Kingdom
Hospital Beds Medical Facilities Mother and Child Health Care Centers

113 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
FIGURE 47: ANC AND CESAREAN RATES FOR JORDANIAN AND SYRIAN WOMEN (2018)
MENTAL HEALTH
Protracted crisis coupled with the ongoing stressors related to displacement, have significant impact on the mental health of refugees as well as Jordanians. An assessment conducted by IMC, revealed that 43 percent of the population assessed felt distress, including loss of interest, fear, anger, hopelessness, avoidance, and reduced functionality609. This included 38.9 percent of the host population, 57.0 percent among refugees in urban communities, and 23.0 percent among refugees in camp settings. Due to stigma, many people did not seek mental health services. Respondents reported a need for affordable mental health care (27.5 percent), affordable medications (26.1 percent), and transportation to access services (24.4 percent).
SEXUAL AND GENDER-BASED VIOLENCE
Limited livelihood opportunities coupled with displacement raises the risks of GBV, yet the stigma attached to GBV and fear of retaliation by family and the community in Jordan has kept reporting numbers low. In 2019, the majority of survivors that obtained GBV services were Syrian (70 percent), with 23 percent being Jordanians and 7 percent other (mostly Iraqi and Sudanese).610 However, it is important to note that due to outreach activities there was a 58 percent increase in Jordanians seeking services in 2019 when compared to 2018 and an 88 percent increase in other nationalities (non-Syrian) in 2019 compared to 2018.
609 IMC. Utilization of Mental and Psychosocial Support Services among Syrian Refugees and Jordanians. 2019 610 GBVIMS Task Force, Jordan GBV IMS Task Force / Annual Report 2019. https://reliefweb.int/sites/reliefweb.int/files/resources/75705.pdf
82%
62%
74%
27%22% 23%
Jordanians Syrians Other
At least seven ANC visits C-sections

114 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
HEALTH FINANCE
Costs of services, together with costs associated with accessing services, affect the affordability of health services. In 2015, national health expenditures accounted for 8.44 percent of the GDP, 60.7 percent of health expenditures were publicly financed, followed by the private sector at 34.5 percent and donors at 4.8 percent.611
Jordan has health insurance schemes for the population, which includes free health insurance for all children under the age of six. In 2015, according to WHO, 55 percent of the whole population and 68 percent of Jordanian citizens were covered by health insurance.612 The main insurers are the Health Insurance Fund of the MoH and the Military Health Insurance Fund (Figure 48). Jordan’s Health Insurance Fund is for citizens and exempts healthcare fees for the following categories: children under six years old, people classified as “poor” by the Ministry of Social Development, areas classified as least fortunate and remote areas.
FIGURE 48: POPULATION COVERED BY HEALTH INSURANCE BY INSURER
There is a disparity in health insurance coverage at the governorate level. See Figure 49, which reveals the disparity of insurance coverage by the Governorates where the majority of Syrian (Amman, Irbid, Mafraq) and Iraqi (Amman, Zarqa and Al Balqa) refugees reside. There is also a disparity in out-of-pocket expenses for health, for example the average out of pocket expense in Amman is 327JD vs. 119 JD in Mafraq Governorates (See Figure 50).
611 High Health Council, National Human Resources for Health Strategy for Jordan 612 WHO, Jordan Investing in family doctors to boost primary health care. Accessed June 5, 2020. https://extranet.who.int/countryplanningcycles/sites/default/files/planning_cycle_repository/jordan/stories_from_the_field_issue3_jordan.pdf
42%38%
12.5%
2.5% 2.5% 2.5%0.4%
Health InsuranceFund of theMinistry of
Health
Military HealthInsurance Fund
of the RoyalMedical Services
Private HealthInsurance
Health Insurancein University
Hospitals
UNRWA Other Insurances Insured Abroad

115 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
FIGURE 49: HEALTH INSURANCE DISPARITIES BY GOVERNORATE
FIGURE 50: ANNUAL HOUSEHOLD OUT OF POCKET HEALTH SPENDING BY GOVERNORATE IN 2013 JORDANIAN DINAR613
In 2019, 73 million USD was spent on health for Syrian refugees in Jordan.614 For Syrian refugees, UNHCR provides primary, secondary and tertiary health care services free of charge for people residing in Azraq and Zaatari camps, for vulnerable Syrians in urban areas and for all non-Syrians in urban areas.615 In 2019 the Government reversed a policy requiring refugees to pay 80 percent of “foreigner rates” for health services. Refugees can now once again access subsidized healthcare. Further, Syrian refugees do not have
613 UNICEF, Analysing equity in health utilization and expenditure in Jordan with focus on Maternal and Child Health Services, 2016 https://thinkwell.global/wp-content/uploads/2016/10/Thinkwell-Jordan-Report-FINAL_August31.pdf 614 Regional Refugee and Resilience Plan. 2019 Annual Report: Regional Refugee and Resilience Plan in Response to the Syria Crisis. 2020. http://www.3rpsyriacrisis.org/wp-content/uploads/2020/05/annual_report.pdf 615 UNHCR, Fact Sheet Jordan, May 2019, accessed June 5, 2020. https://reliefweb.int/sites/reliefweb.int/files/resources/69826.pdf
54%
79%84%
60%
76%
40%
66%73%
50%
65%
Amman Irbid Mafraq Zarqa Al Balqa
Jordanians Total Population
327
137119
148
119145 156 166
178
10589
72
215
Amman Irbid AlMafraq
Zarqa AlBalqa Madaba Jarash Al Karak Ma'an Ajloun Al Aqaba Tafilah Jordan
116 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
to pay fees for antenatal care, family planning, postnatal care and vaccinations provided by the MoH.616 In the UNHCR Health and Utilization Survey, Syrians spent 63.9 percent of their total income on healthcare, however, this was prior to the reversal of the requirement of refugees having to pay 80 percent of foreigner rates.
Iraqi refugees (regardless of their UNHCR registration) can access all PHC services provided to Jordanians at the same user rates as those paid by uninsured Jordanians. Preventative services are free as are ANC and family planning consultations. Iraqis who receive care at Government hospitals have to pay the foreigners rate.617 However, in contrast to Syrians, Iraqis spent on average 75 percent of their total income on healthcare.
The government of Jordan has granted citizenship to most Palestinian refugees and therefore they have the same access to health care as other Jordanian citizens. Palestinians who are not citizens are more vulnerable as they may face restrictions on their access to health care.
ACCESS TO ESSENTIAL MEDICINE
In Jordan, the pharmaceutical sector is highly regulated by the Food and Drug Administration, which ensures medicine quality assurance, registration, importation/exportation and pricing. 618 A study conducted in 2018 revealed that the lowest-price generic equivalent medicine was available 72 percent of the time in the public sector and 76 percent in the private sector.619 Further, the study found that the prices of essential medicines in private sector were high in comparison with the public sector.
As discussed above, all children in Jordan are covered with free health insurance including free access to vaccinations, this includes free child vaccinations for REM populations. However, awareness of free access is low amongst Iraqis (65 percent in 2017) when compared to Syrians (97 percent).620
LEADERSHIP/GOVERNANCE
Governance is a significant factor affecting health system performance. Good governance involves transparent, accountable, equitable, and responsive systems. The MOH provides overall leadership and guidance to health service delivery and ensures the overall functioning of the health system. In Jordan there is a national health strategy that defines the vision and direction for ensuring the health of the population. The current strategy was developed with support from WHO in 2016 and covers the years 2016-2020. It does not include specific messaging on REM populations except for mentioning UNWRA’s support for Palestinian’s and a section on the impact and challenges facing the health sector as a result of the Syrian refugees.
Health information systems are key to generating reliable and timely data to support the development of effective health policies and strategies. Jordan has several programs that support and are part of health information systems including an annual statistical report on national health statistics; a National Cancer Registry; national mortality and renal failure registry; electronic surveillance for communicable diseases;, family planning logistic information system; maternity and childhood system; general practitioners
616 UNHCR. Progress Report Regional Refugee and Resilience Plan in Response to the Syria Crisis January – June 2019. 2019. http://reporting.unhcr.org/sites/default/files/Syria%202019%203RP%20Progress%20Report%20-%20August%202019.pdf 617 UNHCR, Health Access and Utilization Survey Access to Healthcare Services in Jordan Among Iraqi Refugees, December 2017. 618 High Health Council, The National Strategy for Health Sector in Jordan 2016- 2020, 2016. 619 Alefan, Q., et al., Availability, prices and affordability of selected essential medicines in Jordan: a national survey. BMC Health Serv Res 18, 787 (2018). https://doi.org/10.1186/s12913-018-3593-9 620 UNHCR, Health Access and Utilization Survey Access to Healthcare Services in Jordan Among Iraqi Refugees, December 2017. UNHCR, Health Access and Utilization Survey Access to Healthcare Services Among Syrian Refugees in Jordan, December 2018.

117 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
database; hospitals information systems; perinatal care system; geographical information system for family planning services (GIS); medical laboratory and radiology systems; a website for the publication of studies and reports related to reproductive health (PROMISE); and an electronic health records system called " Hakeem" which is in the pilot phase621. UNHCR and UNWRA also have independent health information systems, which do not feed into the national systems. However, the data is shared with the MoH.
CONCLUSION
While services appear to be available for REM populations, it is important to look at quality. A difference in internal and external factors, such as health workforce and out of pocket expenditure, affects the quality of health services and health outcomes. Understanding the strengths and weakness of the health system building blocks and managing their interactions can achieve more equitable and sustained improvements across health services and is key to improved health for all people, especially vulnerable and REM populations. As the population continues to grow, it is important that Jordan ensures all people can access quality health care. This includes retaining and growing the health workforce, ensuring all people can afford services and strengthening current services.
AQ 3: CRITICAL HEALTH NEEDS AND GAPS IN HEALTH SERVICES FOR REM COMMUNITIES
As discussed above, services (PHC, MNCH, SRH, nutrition, GBV and mental health) are available for REM populations; however, there are gaps in affordability, awareness and quality of these services. This is especially true for GBV and MHPSS response services, which are not widely available in the national health system. This leads to difficulties with accessibility, especially for refugees outside a camp and people living rural areas.
Access to comprehensive, quality health care services is important for promoting and maintaining health and preventing and managing disease. The awareness and availability of services, geographic distance to health services and financial costs of services all define access. In Jordan, the 2016, Health Access and Quality index was 70.2 percent, which was an increase from 2000 when the percentage was 58.3 percent. While this reveals favorable signs of improvement in health care access and quality for the population as a whole, disparities exist in accessing care which can lead to unmet health needs, delays in receiving necessary care, or financial burdens. For example, In the 2017-18 Jordan Population and Family Health Survey, the top reasons adolescents had difficulty accessing health care was due to not wanting to go alone, having to take transport, no female provider and getting money for treatment. Women reported having to take transport, not wanting to go alone, getting money for treatment and distance as their top problems in accessing care.
The UNHCR Health Access and Utilization Survey revealed that more Iraqis were unaware of free access to health services in UNHCR facilities in 2017 than the year prior (38 percent compared to 35 percent in 2016). Furthermore, people were unaware of the nearest clinic when compared to 2016 (51 percent in 2017 compared to 48 percent in 2016).622 In 2017 25 percent of people reported that they were unable to receive care in the first health facility they went to and had to find a second facility for care. Top reasons for difficulty receiving vaccinations and ANC included long wait, fees and poor treatment by staff. Inability to afford fees was the top reason for not accessing medical services for chronic conditions.
621 High Health Council, The National Strategy for Health Sector in Jordan 2016- 2020, 2016. 622 UNHCR, Health Access and Utilization Survey Access to Healthcare Services in Jordan Among Iraqi Refugees, December 2017.

118 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
FIGURE 51: IRAQI REFUGEES ACCESS TO HEALTH SERVICES
In the 2018 UNHCR Health Access and Utilization Survey (HAUS), 81.5 percent of Syrians were aware of the subsidized access to governmental healthcare services and 80.5 percent were aware of free access to UNHCR facilities.623 This is a substantial increase from the previous year where only 65 percent were aware of the government services and 53 percent were aware of UNHCR services. Further the survey revealed that the first place Syrians went for a service was a Private Pharmacy (38 percent), which was followed by a JHAS clinic (21 percent). Only 7 percent went to a second facility due to the inability to be served at the initial facility. Top barriers to accessing services included the inability to afford the cost of the service fee and transport cost.
FIGURE 52: SYRIAN REFUGEE ACCESS TO HEALTH SERVICES
623 UNHCR, Health Access and Utilization Survey Access to Healthcare Services Among Syrian Refugees in Jordan, December 2018.
37%31%
7%3%
51%
44%
29%
6%
Difficulty accessing medicinefor chronic conditions
Difficulty accessing medicalservices for chronic
conditions
Difficulty accessing ANC Difficulty obtaining vaccines
2016 2017
45%
39%
17%
1%
26%22%
16%
0%
Difficulty accessing medicinefor chronic conditions
Difficulty accessing medicalservices for chronic
conditions
Difficulty accessing ANC Difficulty obtaining vaccines
2017 2018

119 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
Increase in forced migration, financial burdens and COVID-19 have placed undue stress on the health systems ability to support the various REM populations. Without additional support and a sustainable response to the stressors that accompanies mass population growth, the stability of the health systems and health outcomes of the population is as risk. Improving the awareness, availability and financial burden of services is key to decreasing the disparities in health status and improve healthcare for REM populations.
AQ 4: EXTERNAL STRESSES
The ongoing crisis in Syria and influx of refugees coupled with a static Jordanian economic growth rate and restrictions due to COVID-19, all place additional stress on the health system and ability of vulnerable populations to access health care. Therefore, this interconnectedness must be kept in mind in considering the individual stresses.
The economic growth rate (1.94 percent) has remained stable for the past 3 years and is lower than the regional average (2.28 percent). The lack of economic growth has resulted in an increase in the unemployment rate from 18.6 percent in 2018 to 19.1 percent in 2019; with women being affected the most.624 This coupled with an increase in taxes (a 42 percent increase when compared to the tax rate prior to the Syrian refugee influx), places an undue burden on the population, which could lead to a decline in health outcomes due to inability to afford services.625 COVID-19 is likely to continue the economic stagnation in Jordan, especially as Jordan enacted lockdowns and restrictions to movement in order to slow down the spread of the virus.
COVID-19
The first case of COVID-19 in Jordan was on March 2, 2020. As of September 28, 2020, there have been 8,492 confirmed cases of COVID-19 with 45 deaths.626 The COVID-19 pandemic created a new set of challenges for the country and specifically vulnerable populations. The lockdown not only affected business but also lead to difficulty in accessing health services, especially outside of camps. This was shown in the UN Woman needs assessment, which looked at the impact of COVID19 on vulnerable Syrian refugees and Jordanian women across the country.627 The assessment revealed that 71 percent of respondents were afraid that they or someone in their family would become sick, 24 percent said they cannot access their nearest health care facility and 34 percent said they cannot access medicine. Further, 62 percent said they were afraid they are at risk of violence due to the crisis and confinement. This reveals that vulnerable populations, especially women are at high risk during crisis and are unable to meet basic needs.
ENVIRONMENTAL
Jordan is among the four poorest countries in the world in terms of water availability and the shortage of water has increased due to the influx of refugees, especially in the Northern Governorates which has the
624 World Bank. Jordan Overview. https://www.worldbank.org/en/country/jordan/overview 625 Alshoubaki, W., & Harris, M. (2018).The impact of Syrian refugees on Jordan: A framework for analysis. Journal of International Studies, 11(2), 154-179. doi:10.14254/2071-8330.2018/11-2/11 626 WHO, Jordan COVID-19, accessed June 5, 2020. https://covid19.who.int/region/emro/country/jo 627 UN Woman, Rapid Needs Assessment on the Impact of COVID-19, May 2020, accessed June 5, 2020. https://data2.unhcr.org/en/documents/download/75949

120 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
highest percentage of refugees.628 Research has found that 70 percent of Jordanians and Syrian refugees are receiving less than 100 liters per person per day (national standard), and further, “62 percent of the total water vulnerability index was attributed to the presence of Syrian refugees.”
EQUITY
Religious minorities including Druze and Christians among the Syrian refugee population often do not register with UNHCR because they do not want to live within camp settings due to sectarian tensions and fears of reprisal attacks. This increases their vulnerability and may decrease their ability to access health services and humanitarian aid and assistance. 629 Due to the insecurity in the camps, these populations often go to churches for refuge and therefore may not receive the resources availed to other refugees.630
USAID HEALTH AND REM PROGRAMMING
USAID has been key supporter in strengthening Jordan’s health system including quality of care and improving maternal child health. USAIDs funding has improved family planning accessibility and has supported the reduction of maternal mortality through the development of Jordan’s Maternal Mortality Surveillance and Response (JMMSR) program. This program supports investigation of maternal deaths and actions to reduce future deaths. Further, through supporting community outreach, USAID has helped increase access to information and services including family planning, anemia prevention, and nutrition. USAID has also worked to decrease the pressure placed on the health system due to the population increase by supporting renovation of facilities and hospitals, including the Princess Rahma Pediatric Hospital, which is the only pediatric referral hospital for the four northern governorates. USAID has also worked to strengthen the national public health surveillance network and is a key actor in Jordan’s COVID-19 response.
628 Alshoubaki, W., & Harris, M. The impact of Syrian refugees on Jordan: A framework for analysis. 2018, Journal of International Studies, 11(2), 154-179. doi:10.14254/2071-8330.2018/11-2/11 629 Eghdamian,K. UCL, POLICY BRIEF Religious Minority Experiences of Displacement: Initial Lessons Learnt From Syrian Christian and Syrian Druze Refugees in Jordan, 2015, UCL Migration Research Unit. 630 Shatha, EN and Alastair A., Local faith community and civil society engagement in humanitarian response with Syrian refugees in Irbid, Jordan. 2015, Report to the Henry Luce Foundation. New York: Columbia University, Mailman School of Public Health.

121 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
EGYPT
FIGURE 53: MAP OF EGYPT
COUNTRY CONTEXT
In 2020, Egypt’s population reached 100.5 million people, making it the most populated Arab country631. Only 8 percent of Egypt’s land area is inhabited, and significant health disparities exist between urban and rural populations. While Egypt is a state founded on equal citizenship, regardless of religious or ethnic identity, long-standing grievances among minority groups indicate fundamental problems with regard to the state of pluralism in Egypt.632 The constitution identifies Islam as the state religion and while it also states that “freedom of belief is absolute,” only Muslims, Christians, and Jews can practice their religion publicly and build places of worship. 633 This has created challenges for citizens whose faith is not recognized by the state to obtain government issued ID cards, without which they are barred from education, health services, employment and even the ability to secure death certificates or legally inherit.634
Sectarian violence remains endemic in parts of rural Egypt despite a clear decline in the number of such incidents in 2019.635 Islamic state and other radical Islamist groups continue to claim responsibility for organized attacks on non-Sunni Muslims, for instance, two Christian churches and one Sufi-affiliated mosque in Sinai were bombed in 2017, which resulted in the deaths of about 50 and 305 individuals,
631 CAPMAS, "Egypt Statistics," Accessed June 28, 2020, https://www.capmas.gov.eg/HomePage.aspx 632 Nasreddine, H., "Ethnic/Religious Communities in Egypt: Grievances and Inclusive Prospects," Baker Institute for Public Policy, October 5, 2018, https://www.bakerinstitute.org/media/files/files/d762f423/bi-brief-100518-cme-carnegie-nasreddine.pdf 633 USCIRF, "Annual Report 2020, Egypt - Recommended for Special Watch List," 2020 https://www.uscirf.gov/sites/default/files/Egypt.pdf 634 Minority Rights International, "World Directory of Minorities and Indigenous Peoples - Egypt," Accessed June 21, 2020, https://minorityrights.org/country/egypt/ 635 USCIRF, "Annual Report 2020, Egypt - Recommended for Special Watch List."
ACF
Sticky Note
EGYPT

122 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
respectively.636 Late in 2018, the government formed the Supreme Committee for Confronting Sectarian Incidents to promote religious tolerance. However, Egypt’s 2020 report issued by the United States Commission on International Religious Freedom (USCIRF) indicates that religious discrimination remained pervasive, including a disparity in policies regarding places of worship, a lack of opportunities for non-Muslims to work in key areas of government service, state security harassment of former Muslims, and recurring incidents of anti-Christian violence, particularly in rural areas.637
OVERVIEW OF RELIGIOUS AND ETHNIC MINORITIES IN EGYPT
Focus REM Populations in Egypt: Christian (Coptic, Armenian, Greek, Syriac), Jewish, Baha’i, Nubians, Berber Bedouin and Refugees
Geographic Area of REM Populations: Cairo, Alexandria, Minya, Assiut, Sohag, Aswan, Matruh, North Sinai and South Sinai
Of Egypt’s estimated 100.5 million people, 638 around 90 percent are Sunni Muslims, and non-Sunni Muslims, such as Shi’a Muslims, comprise less than 1 percent. Approximately 10 percent are Christians (estimates range from 5 to 15 percent), the majority of whom belong to the Coptic Orthodox Church. There are at least 2,000 Baha’is, approximately 1,500 Jehovah’s Witnesses, and fewer than 20 Jews.639 Other minority groups found in Egypt include Nubians, mainly concentrated in Upper Egypt, Bedouins who populate Sinai and parts of the Western and Eastern Deserts and Berbers which populate the isolated area around the Siwa Oasis in the Western Desert.
Egypt also hosts over 250,000 refugees and asylum seekers that are registered with UNHCR, of which roughly 57 percent are Syrian, and 38 percent are children.640 Other nationalities of refugees and asylum seekers are broken down in Figure 54. Many refugee populations have a long-term presence in Egypt, as indicated by the fact that 72 percent are asylum seekers. Roughly 70 percent reside in Greater Cairo. A majority of the refugees from South Sudan, Eritrea and Ethiopia are non-Muslim and among them are Sudanese Christians residing in an eastern district of Cairo.641
FIGURE 54: NON-SYRIAN REFUGEES AND ASYLUM SEEKERS
636 Nasreddine, H., "Ethnic/Religious Communities in Egypt: Grievances and Inclusive Prospects." 637 USCIRF, "Annual Report 2020, Egypt - Recommended for Special Watch List." 638 CAPMAS, "Egypt Statistics," Accessed June 28, 2020, https://www.capmas.gov.eg/HomePage.aspx 639 USCIRF, "Annual Report 2020, Egypt - Recommended for Special Watch List." 640 UNHCR Egypt, "Monthly Statistical Report April 2020,” 2020, https://www.unhcr.org/eg/wp-content/uploads/sites/36/2020/05/April-2020-UNHCR-Egypt-Monthly-Statistical-Report-External.pdf 641 Miranda, P., "Getting by on the Margins," Refugees in Towns, June 2018, https://www.refugeesintowns.org/cairo
1,685
6,754
6,835
9,254
16,189
18,976
19,827
49,316
Other
Somalia
Iraq
Yemen
Ethiopia
Eritrea
South Sudan
Sudan

123 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
CHRISTIANS
Coptic Christians (also known as Orthodox Christians) are the largest minority group in Egypt and constitute the majority of the Christians in the country, accounting for approximately 10 percent of the country’s overall population.642 Other Christian communities together constitute less than 2 percent of the population and include Anglican/Episcopalian and other Protestant denominations, Armenian Apostolic, Catholic (Armenian, Chaldean, Melkite, Maronite, Latin, and Syrian), and Orthodox (Greek and Syrian).643 There are three “clusters” of Copts in Egypt: in the Minya-Assiut region (18 percent of the region’s total population), in the Assiut-Sohag region (15 percent), and in the Greater Cairo region (9 percent).644 While the proportion of Copts in each governorate is higher in Upper Egypt, Cairo has the highest actual number of Copts in the country.
BAHA’I
While most estimates indicate there are roughly 2-3,000 Baha’i in Egypt, some estimates report their numbers are over 7,000.645 Though nominally guaranteed equal rights and religious freedoms under the Constitution, Baha’i in practice suffer secondary legal status due to ongoing religious discrimination, particularly in terms of civil documentation. While some Baha’i lived in the Sohag Governorate, sectarian tensions have reduced their populations there. Data indicates they have moved to urban cities, yet exact geographic concentrations are unclear.
NUBIANS
Nubians reside in Upper Egypt, along the Nile River. Estimates put the number of Nubians around 3 to 4 million. With the drawing of country boundaries between Egypt and Sudan, Nubians became split between the two countries. Nubians were displaced when their ancestral homelands were flooded with the building of the Aswan High Dam and have never received adequate compensation for their lost land. They face many challenges in advocating for improved government services within their communities. Today, Egyptian Nubia is part of the Governorate of Aswan which also includes a large area whose residents are not Nubian. As a result, Nubians have found themselves a minority within their native province.
BERBER
The Siwa Oasis in the Matruh Governorate is about fifty kilometers from the Libyan border and home to a community of some 28,300 Berbers, an ethnic group indigenous to North Africa.646 Siwa is one of Egypt’s most isolated oasis settlements, where the local Berbers speak a distinct Berber language known as Siwi. The Berber of Siwa make up 9 percent of the population of the Matruh Governorate, however, they face particular challenges due to their isolated location. Therefore, data available on the Matruh governorate is not indicative of the challenges faced by this specific REM population.
BEDOUINS
Bedouins in Egypt are mainly located in the Sinai Peninsula, with smaller populations in the Western and Eastern deserts. Estimate indicate there are roughly 380,000 Bedouins living in the governorates of North Sinai and South Sinai.647 Since 2017, the Egyptian government has been implementing a military blockade
642 Nasreddine, H., "Ethnic/Religious Communities in Egypt: Grievances and Inclusive Prospects." 643 U.S Department of State, "International Religious Freedom Report," 2018, https://www.state.gov/report/custom/44864fb33f/ 644 Mohamoud, Y., Cuadros, D., and Abu-Raddad, L., "Characterizing the Copts in Egypt: Demographic, Socioeconomic and Health Indicators, The Jerusalem Post, May 4, 2019, https://www.jpost.com/jerusalem-report/sinais-bedouins-struggle-to-preserve-their-timeless-way-of-life-588559 645 Minority Rights International, "World Directory of Minorities and Indigenous Peoples – Egypt." 646 FAO, "Siwa Oasis Egypt," May 2016, http://www.fao.org/3/a-bp825e.pdf 647 The Guardian, "Egypt's Bedouins Begin to Demand Equal Citizenship Rights," June 17, 2020, https://www.theguardian.com/global-development/2011/jun/17/egypt-bedouin-risk-of-exclusion-citizenship-rights#:~:text=The%20name%20Bedouin%20is%20derived,currently%20estimated%20at%20about%20380%2C000.

124 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
and state of emergency in northern and central Sinai due to on-going confrontations with militants in the region.648 Bedouins in Sinai do not enjoy full citizenship rights and are treated as second class citizens. Many are much poorer than the average Egyptian.
SITUATION IN GOVERNORATES WITH HIGH REM POPULATIONS IN EGYPT
Of the 26 governorates in Egypt, significant REM populations are found in four of the governorates of Upper Egypt (Assiut, Minya, Sohag and Aswan), Sinai, Siwa (Matruh) and the urban centers of Cairo and Alexandria. Based on human development measures, certain segments of Egypt are caught in the poverty trap, often due to overpopulation. Figure 55 highlights the population (in millions) of the governorates of Egypt with concentrations of REM populations and the corresponding growth rate for each governorate. The numbers highlight notable variations in population growth between the Cairo Governorate and those of Upper Egypt, Matruh and North Sinai.649
FIGURE 55: POPULATION ESTIMATES AND GROWTH RATES FOR REM POPULATED GOVERNORATES
Despite many efforts to reduce poverty in Egypt, which saw a decline between 2012 and 2015, poverty rates in Egypt are now rising with official estimates indicating poverty has risen to 33 percent in 2019, from 28 percent in 2015.650 However, analysts indicate that the real number of poor and vulnerable households is closer to 60 percent, because the officially reported numbers are based on a poverty line set by the government at just $1.5 a day.
Most of the poor and vulnerable households are located in the governorates with high REM populations, with Assiut, Minya and Sohag having the highest rates of poverty in the country, with 60-68 percent of their populations living in poverty.651 Figure 56 highlights the regional distribution of the overall population of Egypt and the relative proportion of the population living in poverty. It highlights that while only 25
648 Marston, J.C., "Sinai’s Bedouins Struggle to Preserve Their Timeless Way of Life," The Jerusalem Post, May 4, 2019, https://www.jpost.com/jerusalem-report/sinais-bedouins-struggle-to-preserve-their-timeless-way-of-life-588559 649 World Bank Group, "Understanding Poverty and Inequality in Egypt," June 2019, http://documents1.worldbank.org/curated/en/351121575640799887/pdf/Understanding-Poverty-and-Inequality-in-Egypt.pdf 650 The Economist, "Poor on the Nile, Egypt is Reforming its Economy, But Poverty is Rising," August 8, 2019, https://www.economist.com/middle-east-and-africa/2019/08/08/egypt-is-reforming-its-economy-but-poverty-is-rising 651 World Bank Group, "Understanding Poverty and Inequality in Egypt."
9.5
4.1
1.5
4.4
5.55
0.32 0.33 0.12
1.2%
2.3% 2.2%2.5% 2.7% 2.9% 2.9% 3.0%
-1.8%
-3.0%
-2.0%
-1.0%
0.0%
1.0%
2.0%
3.0%
4.0%
0
1
2
3
4
5
6
7
8
9
10
Cairo Alexandria Aswan Assiut Minya Sohag Matruh North Sinai South Sinai
2017 Population in Millions Annual Growth Rate (%)

125 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
percent of the country’s population reside in rural Upper Egypt, residents of those regions make up 49 percent of the country’s population living in poverty.652
FIGURE 56: DISTRIBUTION OF OVERALL POPULATION AND POOR POPULATION BY REGION
AQ 1: OVERVIEW OF HEALTH STATUS IN EGYPT
Egypt's overall health status and indicators have improved over the years, yet many challenges remain, particularly due to the high prevalence of non-communicable diseases (NCD). The improvements in public health have led to an eradication of polio and almost elimination/eradication of Schistosomiasis, Filariasis and Leishmaniasis.653 However, the spread of NCDs, most notably ischemic heart disease, stroke and cirrhosis,654 are the main causes of mortality, accounting for 82 percent of all deaths and 67 percent of premature deaths in the country.655 Figure 57 highlights the top ten causes of premature mortality. The main causes of NCDs are poor prevention and control of NCD risk factors such as hypertension, obesity, high cholesterol levels, diabetes and smoking. Recent data shows that 6 percent of the adult population were diabetic, 26 percent were hypertensive, and 70 percent were overweight. In response, a Ministerial Decree was issued in September 2014 to establish an NCD unit within the Ministry of Health and Population (MOHP) to combat the risk factors of NCD.
652 World Bank Group, "Understanding Poverty and Inequality in Egypt," June 2019, http://documents1.worldbank.org/curated/en/351121575640799887/pdf/Understanding-Poverty-and-Inequality-in-Egypt.pdf 653 WHO, “Health Profile Egypt 2015,” 2015, https://applications.emro.who.int/dsaf/EMROPUB_2016_EN_19264.pdf?ua=1&ua=1 654 http://www.healthdata.org/egypt 655 World Bank, "Egypt COVID-19 Emergency Response," April 28, 2020, http://documents1.worldbank.org/curated/en/906831588109454283/pdf/Project-Information-Document-Egypt-COVID-19-Emergency-Response-P173912.pdf
19%
10%
12%
5%
32%
24%
11%
10%
25%
49%
Overall Population
Poor Population
Metropolitan Lower Urban Lower Rural Upper Urban Upper Rural

126 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
FIGURE 57: TOP 10 CAUSES OF PREMATURE MORTALITY AGE-STANDARDIZED RATE PER 100,000
WOMEN’S HEALTH
Egypt has made important progress in maternal health over the years yet has also suffered setbacks. There has been a decline in maternal mortality, yet an increase in the country’s total fertility rate (TFR). The maternal mortality ratio dropped considerably from 64 deaths per 100,000 live births in 2000 to 37 deaths per 100,000 live births in 2017, resulting in Egypt meeting the SDG-3 target for maternal mortality.656 However, there are significant geographic and wealth disparities related to health in Egypt, as exemplified by the higher maternal mortality rates in Upper Egypt (which has high concentrations of Nubians and Christians) than in Lower Egypt.657 The Assiut Governorate has the highest level of maternal mortality in Egypt at 81 deaths per 100,000 live births, a rate considerably higher than the national average of 37.658 The most common direct causes of maternal deaths are post-partum hemorrhage (24 percent), hypertensive disorders, and infection, while the most common indirect causes include anemia and cardiovascular diseases.659
Egypt’s most recent Demographic and Health Survey (DHS), conducted in 2014, reported a TFR of 3.5 children per woman, a globally unprecedented 17 percent increase in the country’s TFR since 2008, as well as a reduction in key best practices related to good maternal and child health, such as early and exclusive breastfeeding. Minya, Assiut and Sohag report the highest TFRs in the country. Some of these
656 WHO, “Maternal Mortality in 2000-2017 Egypt,” Available at https://www.who.int/gho/maternal_health/countries/egy.pdf?ua=1. Accessed 6.20.2020 657 Mahmoud, G., and Omar, A., "Women’s awareness and perceptions about maternal mortality in rural communities in Assiut and Fayoum Governorates, Egypt," Egyptian Nursing Journal, 2018, https://www.semanticscholar.org/paper/Women%E2%80%99s-awareness-and-perceptions-about-maternal-in-Mahmoud-Omar/e755f0e24c114883baad5892fe586c6fbe5a7185 658 Mahmoud, G., and Omar, A., "Women’s awareness and perceptions about maternal mortality in rural communities in Assiut and Fayoum Governorates, Egypt" Egyptian Nursing Journal, 2018, https://www.semanticscholar.org/paper/Women%E2%80%99s-awareness-and-perceptions-about-maternal-in-Mahmoud-Omar/e755f0e24c114883baad5892fe586c6fbe5a7185 659 Mahmoud, G., and Omar, A., "Women’s awareness and perceptions about maternal mortality in rural communities in Assiut and Fayoum Governorates, Egypt."
568
571
580
801
847
1447
1450
1889
2104
6521
Chronic Kidney Disease
Diarrheal Diseases
Diabetes
Neonatal Disorders
Congenital Defects
Lower Respiratory Infection
Road Injuries
Cirrhosis
Stroke
Ischemic Heart Disease

127 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
trends can be linked to low-quality health care services, poor health behaviors, and weak management of public health systems.660
CHILD HEALTH
With 37 percent of Egypt’s population under the age of 17, Egypt has achieved important progress in child wellbeing and rights over the past two decades, including a strong reduction in child mortality and high rates of immunization coverage. However, more in-depth analyses of the data also highlights striking inequalities, with under-five mortality for the poorest children at 42 deaths per 1,000 live births, versus 19 in the wealthiest quintile.661 Furthermore, child mortality is almost twice as high in rural Upper Egypt (38 deaths per 1,000 births) than in urban Lower Egypt (22 deaths per 1,000 births).662 Countrywide, the under 5-mortality rate is 20 per 1,000 live births and infant under one-year mortality rate was 15.4 per 1,000 live births. Egypt met the SDG-3 target of under-five mortality below 25 per 1,000 live births through effective interventions to prevent communicable diseases, a robust EPI system and coverage, and improved care seeking behaviors for sick children.663
According to UNICEF and the WHO World Health Report 2015, diarrhea is the second leading cause of death among children under five, with 3,500 – 4,000 under-five children dying of diarrhea every year, mainly due to dehydration. 664 Rotavirus is a prominent cause of diarrhea among Egyptian children, highlighting poor hygiene practices.665
MALNUTRITION
According to the global nutrition report, Egypt will meet its under-five stunting and under-five overweight global targets, despite the currently high rates of chronic malnutrition, with a national prevalence of 22 percent and 16 percent prevalence respectively.666 As was seen with other health related data, data on child health differs tremendously by governorate, with under-five stunting ranging from 12 percent to 85 percent across governorates.667 However, variations across wealth quintiles are minimal, with 26 percent of poor households having stunted children, compared to 21 percent among non-poor households, suggesting that social issues may be a contributing factor to the levels of stunting.668 Under-five wasting prevalence is high at 10 percent and only 39 percent of infants under six months are exclusively breastfed.
There has been some progress on adult nutrition with an improvement in anemia in women of reproductive age (28 percent). However, more needs to be done as 20 percent of adult women have
660 USAID, "Health and Population Fact Sheet," May 2019, https://www.usaid.gov/sites/default/files/documents/1883/USAIDEgypt_Health_Fact_Sheet_EN.pdf 661 USAID, "Health and Population Fact Sheet." 662 Bayoumi, S., "Health and Social Justice in Egypt: Towards a Health Equity Perspective," World Social Science Report, 2016, https://unesdoc.unesco.org/ark:/48223/pf0000245958 663 Ministry of Health and Population Egypt, Partnership for Maternal, Newborn & Child Health, WHO, World Bank and Alliance for Health Policy and Systems Research. Success factors for women’s and children’s health: Egypt. Geneva: WHO; 2014. 664 UNICEF. Accessed June 26, 2020 https://www.unicef.org/egypt/water-sanitation-and-hygiene#:~:text=In%20Egypt%2C%20diarrhea%20is%20the,die%20of%20diarrhea%20every%20year. 665 El-Shabrawi, Mortada et al. “The burden of different pathogens in acute diarrhoeal episodes among a cohort of Egyptian children less than five years old.” Przeglad gastroenterologiczny vol. 10,3 (2015): 173-80. doi:10.5114/pg.2015.51186 666 https://globalnutritionreport.org/resources/nutrition-profiles/ 667 Bayoumi, S., "Health and Social Justice in Egypt: Towards a Health Equity Perspective.” 668 World Bank Group, "Understanding Poverty and Inequality in Egypt," June 2019, http://documents1.worldbank.org/curated/en/351121575640799887/pdf/Understanding-Poverty-and-Inequality-in-Egypt.pdf

128 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
diabetes and 41 percent are obese, compared to 16 percent of men with diabetes and 3 percent are obese669.
MENTAL HEALTH
In a survey conducted by the MOHP in 2018, 25 percent of the population was found to be suffering from mental health-related problems (anxiety disorders were 43 percent and 30 percent are suffering from depression related to substance abuse).670 The same survey found that the Minya Governorate had the highest percentage of anxiety disorders and that overall, rural areas had the highest rates of both anxiety and depression. However, limited access to mental health services and stigma associated with mental health disorders likely contributes to an under estimation of prevalence rates.
SEXUAL AND GENDER-BASED VIOLENCE
Egypt is ranked at 136 out of 145 in the 2015 Global Gender Gap Index, which suggests strong disparities in in health, education, economy and politics. Women and children are exposed to high levels of violence in Egypt (Figure 58). Gender-based violence remains one of the most prevalent issues facing women and girls, with a 26 percent lifetime prevalence of physical and/or sexual violence.671 Violence against pregnant women is even higher, with 31 percent experiencing violence during pregnancy.672 Sexual harassment in public and workplaces is extremely prevalent in Egypt, with 99 percent of Egyptian women experiencing sexual harassment and 70 percent of nurses experiencing workplace harassment. 673 Children also experience high levels of violence with the 2014 DHS reporting that 93 percent of children aged one to 14 years old have been exposed to violent disciplinary practices, including psychological aggression and/or physical punishment.
FIGURE 58: VIOLENCE AGAINST WOMEN AND CHILDREN
Female genital mutilation is widespread in Egypt. In 2015, 87 percent of women age 15-49 had undergone some form of FGM with a disparity by socioeconomic status (94 percent in low wealth quintile compared
669 https://globalnutritionreport.org/resources/nutrition-profiles/ 670 https://www.egypttoday.com/Article/1/48156/25-of-Egyptians-suffer-from-mental-health-issues-survey 671 UN Woman Database Accessed 6.20.20. Available at https://evaw-global-database.unwomen.org/en/countries/africa/egypt 672 Nossier, S., "Violence Against Women in the Arab World," Journal of the Egyptian Public Health Association, September 2015, https://journals.lww.com/ephaj/pages/articleviewer.aspx?year=2015&issue=09000&article=00001&type=Fulltext 673 Nossier, S., "Violence Against Women in the Arab World."
11%
17%
26%
31%
87%
93%
99%
Teenage Pregnancies
Early Child Marriage
Lifetime Prevalence of Physical or Sexual Violence
Women Experiencing Violence during Pregnancy
FGM
Children Victims of Violent Disciplinary Measures
Women Experiencing Sexual Harrassment

129 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
to 70 percent in the highest wealth quintile).674 In 2016, FGM was criminalized, however, it is still widely practiced with an estimated four out of five genital mutilations performed by doctors in professional medical environments.675
The prevalence of early age marriage was significantly higher among governorates of upper Egypt than in lower Egypt, reaching 38 percent in rural areas of Minya, compared to the national average of 17 percent.676 Lower educational attainment (less than secondary School) had a significant association with early age marriage. Teenage pregnancies were reported among 11 percent of women aged 15-19. Results showed that early age marriage effects birth rate, with the mean number of 3.6 children per woman who married before the age of 18 years. 677 Research also indicates that women who married early had significantly higher chances of having adverse birth outcomes and infant mortality, including stillbirth.
In 2015, the National Strategy for Combating Violence Against Women (NSVAW) was launched as a step to protecting women and girls from acts of violence and to safeguard their dignity and rights.678 The pillars of the strategy include prevention, protection, intervention and legal procedures. Many ministries, agencies and groups, agreed to support the strategy, including the Orthodox Coptic Church, which agreed to include information on the necessity of rejecting violence and discrimination against women within its services.679
OUTBREAK/EPIDEMIC DATA
Egypt has one of the highest rates of Hepatitis C virus (HCV) infections in the world and high rates of Hepatitis B virus (HBV) infections, as well. About 40,000 Egyptians die of Hepatitis C every year, making it the country’s third leading cause of death, with 150,000 new infections each year.680 Overall, 7 percent of Egyptians between the ages of 15 and 59 suffer from chronic Hepatitis C, with notable geographic disparities as seen in Figure 59.681 HCV prevalence is 20 percent higher among those living in rural areas.682 Of the governorates with high REM populations, Aswan has the highest rate of HBV prevalence, while HCV prevalence is highest in Minya. Rates of HCV infection increase sharply with age, with around 17 percent of women and 25 percent of men age 50-59 with active HCV infections.683 While many Egyptians were infected with HCV as a result of the use of inadequately sterilized needles during mass campaigns to treat schistosomiasis decades ago, evidence suggests unsafe blood transfusions and improper infection control measures within healthcare facilities are the major transmission route for the on-going spread of infection.684
674 https://dhsprogram.com/pubs/pdf/CR46/CR46.pdf 675 HRW Egypt World Report 2020.. https://www.hrw.org/world-report/2020/country-chapters/egypt 676 Sos, D., El-Gaafary, M., Wahdan, M., Wassif, G., et al., "Child Marriage: A Major Risky Behavior in Developing Egyptian Governorates," Al-Azhar Medical Journal, 2020, https://amj.journals.ekb.eg/article_67556_10131.html 677 Sos, D., et al., "Child Marriage: A Major Risky Behavior in Developing Egyptian Governorates.” 678 National Strategy for Combating Violence Against Women 2015. Available at https://evaw-global-database.unwomen.org/-/media/files/un%20women/vaw/full%20text/africa/egypt%20national%20strategy%20for%20combating%20vaw%202015.pdf?vs=2221 679 ibid 680 World Bank, "Transforming Egypt's Healthcare System Project," June 6, 2018, http://documents1.worldbank.org/curated/en/796381530329773770/pdf/Egypt-PAD-06082018.pdf 681 MOHP, El-Zanaty and Associates, and ICF International, "Egypt Health Issues Survey 2015," MOHP and ICF International, 2015, https://dhsprogram.com/pubs/pdf/FR313/FR313.pdf 682 Pande, A., El Shalakani, A., and Hamed, A., "How Can We Measure Progress on Social Justice in Health Care? The Case of Egypt," Health Systems & Reform Journal, January 31, 2017, https://www.tandfonline.com/doi/full/10.1080/23288604.2016.1272981?scroll=top&needAccess=true 683 MOHP, El-Zanaty and Associates, and ICF International, "Egypt Health Issues Survey 2015." 684 MOHP, El-Zanaty and Associates, and ICF International, "Egypt Health Issues Survey 2015."

130 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
FIGURE 59: HBV AND HCV PREVALENCE BY GOVERNORATE
Gaps in vaccination coverage have contributed to occasional measles outbreaks, with over 5,000 cases reported in 2015, down to 48 in 2018. 685 Outbreaks have occurred particularly in the Matruh Governorate, in areas where the Berber minority are found. In 2015 there was an outbreak of Dengue Fever in the Assiut Governorate, with 253 infections. In response, the government sent physicians to support with medical care for the population and set up surveillance and control of the dengue vector, which has led to a decline.686 Transmission of H5N1 (avian influenza) is endemic in poultry throughout Egypt with a surge in human cases and outbreaks every year.687 WHO reported that in 2015 there were 165 cases reported in 21 out of the 29 governorates with a case fatality rate of 29 percent.688 Women comprised 60 percent of the cases and had a higher death rate (30 percent) compared to males (27 percent).
Overall, Egypt has a low HIV prevalence (<0.1 percent) and a mortality ratio of 7.57. However, Egypt is one of the few countries left where the incidence of new infections is still increasing exponentially, with newly discovered cases of HIV among the general population increasing by 25-35 percent annually.689 The prevalence of HIV is highest among men who have sex with men (6.7 percent), commercial sex workers (2.8 percent), and people who inject drugs (2.5 percent).
ACCESS TO WASH
Improving access to water, sanitation and hygiene is key to improving child health and in preventing the spread of infectious diseases. The Egypt 2014 DHS indicates that an estimated 98 percent of the Egyptian population have access to drinking water and 90 percent of the Egyptian population had access to a non-
685 Knoema, "Egypt - Measles Reported Cases," 2018, https://knoema.com/atlas/Egypt/topics/Health/Communicable-Diseases/Measles-cases 686 WHO. Dengue Fever Outbreak-Egypt. 2015. Disease Outbreak News. https://www.who.int/csr/don/12-november-2015-dengue/en/ 687 http://www.emro.who.int/egy/programmes/influenza.html 688 WHO Health Profile 2015. Accessed 6.20.2020 available at https://applications.emro.who.int/dsaf/EMROPUB_2016_EN_19264.pdf?ua=1&ua=1 689 UNAIDS. (2018). "Country Factsheets Egypt 2018," Retrieved February 27, 2020, from https://www.unaids.org/en/regionscountries/countries/egypt
11.7%
9.2%10.6%
9%9.5%
14.8%
9.1%
5.7%5%
3.6%
9%
3.5%3%
4.4%
2%3%
Cairo Alexandria Minya Assiut Sohag Aswan Luxor Matruh
HBV Prevalence HCV Prevalence

131 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
shared sanitation facility.690 Further, 90 percent of the population in Egypt had a hand washing facility with soap and water in 2017.691 However, according to UNICEF, there are still 7.3 million people who lack access to safe water and 8.4 million people who lack access to improved sanitation, mostly in rural areas.692 Disparities in access to WASH are also noted, with 15 percent of children in rural areas lacking adequate WASH facilities, compared to 1 percent in urban areas, with poor families 11 percent more likely to be deprived of access to WASH.693
Poor sanitation and hygiene not only increases the risk of parasitic infections, which are endemic in Egypt, but also is a major cause of diarrhea and respiratory infections. Estimates indicate that inadequate WASH caused 2.2 billion to 3.7 billion days lived with disease and 4,400 to 9,200 deaths in Egypt in 2017.694 Ensuring good quality drinking water, sanitation, and improved hand washing practices is key to improved health outcomes.
CONCLUSIONS
Despite long-term improvements, the rate of progress on health outcomes in Egypt is slowing, and demographic pressures are rising. While Egypt’s population has a good overall health status, with an increase in life expectancy and reduction of maternal and infant mortality rates, large geographic and wealth disparities do exist, with significant disparities in REM-populated governorates of Upper Egypt. Research has indicated that poverty plays a key role in the levels of observed disparities, with the increasing rates of poverty raising concern on the negative effects it will have on health outcomes. NCDs are a serious health burden and leading cause of death in Egypt. Continued support is necessary to address this public health problem and raise awareness about prevention and treatment. Rigorous and systemic efforts are also needed to prevent the high rates of violence affecting women and children in Egypt.
AQ 2: STRENGTHS AND WEAKNESSES OF THE PRIMARY HEALTH CARE SYSTEM
Despite improvements in several health outcomes over the years, Egypt’s aging public healthcare system suffers from low standards due to a lack of funding, poor staffing levels and dilapidated facilities. The main bodies governing Egypt’s health care system are the MOHP and the Health Insurance Organization (HIO). The health care system is highly pluralistic, with health services financed and provided by multiple different entities resulting in a fragmented health system, with no formal referral systems in the MOHP delivery system.695 The MOHP operates 3,645 health facilities, including 1,300 hospitals or 60 percent of the country’s hospital beds. Universities, the Army and the private sector constitute the other 40 percent, with roughly 600 hospitals. The private sector includes for-profit and nonprofit organizations and covers everything from traditional midwives, pharmacies, doctors, and private hospitals and clinics of all sizes. Also included in the private sector are a large number of NGOs providing services, including religiously affiliated clinics, such as those operated by the Coptic Evangelical Organization for Social Services, and
690 MOHP, El-Zanaty and Associates, and ICF International, "Egypt Demographic and Health Survey 2014," MOHP and ICF International, 2014, https://dhsprogram.com/pubs/pdf/FR302/FR302.pdf 691 Larsen, Bjorn. 2019. Egypt: Cost of Environmental Degradation: Air and Water Pollution. The World Bank. 692 https://www.unicef.org/egypt/water-sanitation-and-hygiene#_ftn3 693 MOSS and UNICEF, "Understanding Child Multidimensional Poverty in Egypt," December 2017, https://www.unicef.org/egypt/sites/unicef.org.egypt/files/2018-05/Egy_MODA_Report_Full_EN.pdf 694 Larsen, Bjorn. 2019. Egypt: Cost of Environmental Degradation: Air and Water Pollution. The World Bank. 695 DHS, "Overview of the Health System in Egypt," Accessed June 28, 2020, https://dhsprogram.com/pubs/pdf/SPA7/02Chapter02.pdf

132 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
other charitable organizations, all of which are registered with the MOHP, as well as the Ministry of Social Affairs.
Formerly the Egyptian healthcare system was predominantly controlled by the government, however in the past ten years the private sector has taken a more active role as the standard of care in the public sector declined. To improve public healthcare, the MOHP is currently undertaking an ambitious plan to build new hospitals, renovate and refurbish existing medical facilities with new technologies and up-to-date equipment, especially in the rural, under-served areas, with significant assistance from international donors.696
HEALTH WORKFORCE
The numbers of physicians, dentists, pharmacists, nursing and midwifery personnel in Egypt are below the regional average and far below the global average of 32 doctors for every 10,000 citizens, as seen in Table 15.697 Physicians in the public sector are underpaid, leading many to take on multiple jobs and contributing to estimates that 60 percent of Egyptian doctors now work outside the country.698 In the public sector, estimates are that newly graduated doctors earn only $120 per month, while specialists earn $180 per month.699 Other factors contributing to the reluctance of Egyptian doctors to remain in the country include undesirable working conditions, including poor medical facilities and a lack of supplies in government hospitals. Doctors that do remain in Egypt often choose specialties with easier working hours and higher income, such as plastic surgery, gynecology and pediatrics, leaving a critical shortage of specialists, particularly in cardiac surgery, emergency medicine and intensive care specialists.700
TABLE 115: HEALTH WORKFORCE (PERSONNEL PER 10,000 POPULATION)
Role Ratio
Physicians 8.5
Nurses and Midwives 14.5
Dentists 1.9
Pharmacists 4.1
Mental Health Professionals 0.8
Only around 35 percent of all registered doctors in Egypt work in the public sector, with 53 percent having multiple jobs, usually in the private sector.701 Reports by WHO indicate that information on human resources remains fragmented and concerns have been expressed about the relevance of the curriculum and quality of training in medical schools.702 The health workforce is further challenged by poor staff
696 International Trade Administration, "Healthcare Resources Guide: Egypt," Accessed June 24, 2020, https://2016.export.gov/industry/health/healthcareresourceguide/eg_main_108580.asp 697 WHO EMRO, “Framework for Health Information Systems and Core Indicators for Monitoring Health Situation and Health System Performance," 2018, https://applications.emro.who.int/docs/EMROPUB_2018_EN_20620.pdf?ua=1&ua=1 698 Bayoumi, S., "Health and Social Justice in Egypt: Towards a Health Equity Perspective.” 699 El-Galil, T., "Egypt’s Doctors are Fleeing, Leaving Behind a Physician Shortage," Al Fanar Media, July 29, 2019, https://www.al-fanarmedia.org/2019/07/egypts-doctors-are-fleeing-leaving-behind-a-physician-shortage/ 700 El-Galil, T., "Egypt’s Doctors are Fleeing, Leaving Behind a Physician Shortage.” 701 DHS, "Overview of the Health System in Egypt." 702 WHO, "Egypt Human Resources," Accessed June 22, 2020, http://www.emro.who.int/egy/programmes/human-resources.html

133 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
distribution and skills-mismatch, which is further compounded by the fact that health professionals in Egypt receive life-long initial or specialized licenses with no continuing medical education requirements, leading to the provision of low quality of care, particularly in the public sector.703
SERVICE DELIVERY
Even though more than 95 percent of Egypt’s population lives within 3.1 miles of a health facility, the quality of care at these facilities is often poor due to outdated equipment, long queues for treatment, inadequate staff training and poor sanitation, leading to low utilization, reduced health benefits, and a preference among Egyptians to use private healthcare facilities.704 The lowest health service utilization rates were found among the poor (Figure 60).705 Significant differences are also reported on the quality and types of services available in rural areas, compared to urban facilities, as exemplified by the fact that Berber of Siwa often travel 300 km to a health facility in the closest city, Marsa Matruh, for minor care because local health care services are inadequate. The MOHP does allow Syrian refugees to utilize public health care facilities in Egypt.
FIGURE 60: LACK OF CARE SEEKING BEHAVIORS BY ECONOMIC STATUS
Egypt has 36 university hospitals, that are regarded as secondary and tertiary care facilities and tend to be much more advanced in terms of technology and medical expertise compared to MOHP-operated facilities. These university hospitals are operated under the authority of the Ministry of Higher Education and usually charge user fees to generate income, making them inaccessible to the poor.706
The MOHP is currently the major provider of primary, preventive, and curative care in Egypt, specifically, with respect to inpatient services. 707 Under the existing primary care strategy, universal access to comprehensive primary care through the public sector has made substantial progress in recent decades. However, deficiencies do exist including in the routine provision of care to individuals and families by public providers, disparities of care across regions and socio-economic groups, and in prospects for the
703 World Bank, "Egypt COVID-19 Emergency Response.” 704 World Bank, "Transforming Egypt's Healthcare System Project." 705 World Bank, "A Roadmap to Achieve Social Justice in Health Care in Egypt," January 2015, https://www.worldbank.org/content/dam/Worldbank/Feature%20Story/mena/Egypt/Egypt-Doc/egy-roadmap-sj-health.pdf 706 DHS, "Overview of the Health System in Egypt." 707 DHS, "Overview of the Health System in Egypt."
4%
18%
0.7%
16%
Wealthiest Quintile
Poorest Quintile
Did not seek care for acute illnesss Did not seek care for chronic illness

134 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
sector to respond to emerging health challenges, such as COVID-19. As seen in Figure 60, the poorest quintile has lower uptake of services, despite having access to public healthcare facilities.708
Poor health care seeking behaviors also need to improve. Seventeen percent of the population suffers from hypertension, one of the main causes of non-communicable disease deaths in Egypt. Yet, a large portion of the population are unaware of their condition, and among those that are aware, only a small percentage are receiving adequate treatment, as seen in Figure 61.709
FIGURE 61: AWARENESS OF HYPERTENSION AND TREATMENT STATUS
Egypt has made significant progress in recent years to improve treatment for those infected with HCV, with approximately 5 million Egyptians screened and 1.6 million people treated and roughly a 96 percent cure rate.710 These screenings were largely organized through PHCs, highlighting the central role of primary care in tackling HCV infections. However, significant challenges remain; estimates indicate the need to screen 43 million people and treat 4 million infected patients in order to eliminate HCV .711 HCV screening and treatment are provided free of charge for those without health insurance.712
WOMEN AND CHILD HEALTH
The overall reduction in maternal mortality can be linked to the near universal coverage for ANC with over 90 percent of women attending one or more ANC visits.713 However, ANC coverage is lower in Upper Egypt due to distance, transportation and service fees, leaving a large number of Egypt’s Christians and Nubians who live there without access to ANC.714 Notable disparities exist across most indicators related to women and children’s health. Women and children from poor, rural communities, particularly
708 Pande, A., et al, "How Can We Measure Progress on Social Justice in Health Care? The Case of Egypt." 709 MOHP, El-Zanaty and Associates, and ICF International, "Egypt Health Issues Survey 2015." 710 World Bank, "Transforming Egypt's Healthcare System Project.” 711 MOHP and The World Bank, "Transforming Egypt's Healthcare System Project," April 2018, http://documents1.worldbank.org/curated/en/594471524601888530/pdf/ESMF.pdf 712 The National Committee for the Control of Hepatic Viruses, " Frequently Asked Questions," Accessed June 22, 2020, http://www.nccvh.org.eg/question 713 Pugliese-Garcia, M., Radovich, E., Hassanein, N. et al. Temporal and regional variations in use, equity and quality of antenatal care in Egypt: a repeat cross-sectional analysis using Demographic and Health Surveys. BMC Pregnancy Childbirth 19, 268 (2019). https://doi.org/10.1186/s12884-019-2409-1 714 ibid
47%
12%
25%
73%
24%
12%
Not aware of elevated condition Aware, treated, but not controlled Aware, treated and controlled
Women Men

135 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
those in Upper Egypt, have lower levels of access to care and poorer health outcomes, as seen in Figure 62.715
FIGURE 62: DIFFERENCES IN MCH OUTCOMES AMONG MOST AND LEAST ADVANTAGED FAMILIES
Poorer women from rural communities, are less likely to receive ANC care and less likely to have their births attended by a skilled professional. Infants born to poorer rural women are more than twice as likely to die in their first month of life than are those born to wealthier women in urban areas, and almost three times as likely to die in the first year.716 Challenges are even higher in households with more children, as is found among rural populations in Upper Egypt. Approximately 6 percent of households in Egypt are female-headed, with analysis showing that the probability of lower access to health services significantly increases for children living in female-headed households.717 Egypt has made great strides immunizing children across Egypt, with 93 percent of children in urban areas being fully immunized, however, this rate drops to 87 percent among rural children in Upper Egypt.718
The public sector is the largest provider of family planning services in Egypt, with 57 percent of users obtaining their method at a public facility.719 Egypt has nearly 6,000 governmental facilities that provide family planning services, in addition to a network of mobile family planning services in rural areas. However, continued reduction of maternal mortality faces some challenges, including the fact that the unmet need for family planning has remained steady, at around 14 percent, and has not really declined in the past 6 years. Furthermore, two-thirds of ever-married women report at least one major barrier to accessing health care for themselves, with 54 percent reporting a lack of drugs and 48 percent reporting a lack of health providers as the biggest barriers.720 Shortfalls were also noted regarding respect for privacy, choice of family planning method, access to fertility services, lack of female care providers and lack of counseling
715 Bayoumi, S., "Health and Social Justice in Egypt: Towards a Health Equity Perspective.” 716 Bayoumi, S., "Health and Social Justice in Egypt: Towards a Health Equity Perspective.” 717 MOSS and UNICEF, "Understanding Child Multidimensional Poverty in Egypt." 718 MOHP, El-Zanaty and Associates, and ICF International, "Egypt Demographic and Health Survey 2014.” 719 USAID, "Situational Analysis of the Private Sector in the Delivery of Family Planning Services in Egypt: Current Status and Potential for Increased Involvement," May 2016, https://pdf.usaid.gov/pdf_docs/PA00MGN6.pdf 720 Sos, D., et al., "Child Marriage: A Major Risky Behavior in Developing Egyptian Governorates.”
60%54%
87%96% 97% 93%
ANC Coverage Skilled Birth Attendance Child Fully Immunized
Least Advantaged Most Advantaged

136 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
on prescribed methods, reducing the ability of women to make informed reproductive decisions.721 These shortfalls are also noted for the mobile family planning units.
While breast cancer is the most common cancer among women in Egypt and is estimated to cause 22 percent of all cancer-related deaths, few women undergo screening, with notable disparities. While almost 10 percent of women in urban areas have been screened for breast cancer, only 2.4 percent of rural women in Upper Egypt have been screened. Less than 1 percent of all women have undergone a pap smear to screen for cervical cancer.722
MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT
Egypt has had a stand-alone mental health policy for health since 2015 and a specific strategy for dealing with child and adolescent mental health issues. Roughly 2 percent of government health expenditures are allocated to mental health, yet 59 percent is directed to mental health hospitals. There are 18 psychiatric hospitals in 14 governorates and 62 outpatient facilities providing mental health services, of which 6 are designated for children and adolescents.723 However, there is a lack of access in rural areas, as facilities and staffing are disproportionately allocated, with 60 percent of the psychiatric beds being in Cairo. Only 20 percent of those with severe mental disorders receive services, while treatment for opioid dependence ranges between 11-20 percent.724 High rates of societal stigma towards mental health are reported, which hinders the uptake of services. Furthermore, limited education in the medical sector regarding mental health, contributes to poor quality and unethical treatment at mental health facilities.725 Reports indicate there is one NGO providing MHPSS services in the three governorates of Upper Egypt that contain REM populations.726 Recent research by the General Secretariat of Mental Health highlights the dire need to expand mental health services in underprivileged areas, due to limited access to services and treatment.
SEXUAL AND GENDER-BASED VIOLENCE
In 2014, Egypt passed a law which criminalizes sexual harassment for the first time, however domestic violence remains de-criminalized. Despite many efforts to raise awareness regarding violence by the government, UN agencies, NGOs and other entities, including a national strategy to combat GBV by the National Council for Women, there has been a remarkable increase of violence against women and girls in recent years, yet it is grossly under-reported.727 Societal attitudes towards violence creates multiple barriers to reducing the levels of violence and improving access to services among victims. This is particularly concerning with regards to domestic violence towards married women.
Research has highlighted that 14 percent of married women in urban areas and 56 percent of married rural women in Upper Egypt believe that under certain circumstances (i.e. leaving the house without permission or refusal of sexual intercourse) a man is justified to beat his wife.728 Among the 30 percent
721 Abdel-Tawab, N., Rabie, T., Boehmova, et al., "Do public health services in Egypt help young married women exercise their reproductive rights?," International Journal of Obstetrics and Gynaecology, March 25, 2015, https://obgyn.onlinelibrary.wiley.com/doi/full/10.1016/j.ijgo.2015.03.012 722 MOHP, El-Zanaty and Associates, and ICF International, "Egypt Health Issues Survey 2015." 723 No Lost Generation (NLG) MHPSS Task Force, "MHPSS Programmes for Children, Youth (0-24 years) and Parents/Caregivers in Syria and from Syria and Iraq Crises Affected Countries," January 15, 2020, https://drive.google.com/file/d/1pYgRQaZq3-Y5Sa6VHdk_-HV5tBicJ6Dh/viewn 724 WHO EMRO, “Framework for Health Information Systems and Core Indicators for Monitoring Health Situation and Health System Performance.” 725 Loza, N., "Overview on Mental Health services in Egypt," Accessed June 22, 2020, https://www.slideserve.com/fauve/overview-on-mental-health-services-in-egypt 726 No Lost Generation (NLG) MHPSS Task Force, "MHPSS Programmes for Children, Youth (0-24 years) and Parents/Caregivers in Syria and from Syria and Iraq Crises Affected Countries." 727 UNFPA, "Gender-Based Violence in Egypt," Accessed June 23, 2020, https://egypt.unfpa.org/en/node/22540 728 MOHP, El-Zanaty and Associates, and ICF International, "Egypt Demographic and Health Survey 2014.”

137 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
of married women that have experienced abuse in their homes, 59 percent of victims of sexual violence and 37 percent of victims of physical violence sustained injuries from the abuse. In terms of care seeking behaviors among women who are victims of physical violence in the home, 48 percent in rural Upper Egypt and 39 percent in urban governorates never sought assistance nor informed anyone of their abuse. Among women that did seek assistance, less than one percent sought assistance from the police or a social service organization, while the majority sought assistance from family members.729
Care seeking behavior is further hindered by stigmatizing attitudes among care providers. Research conducted in the Assiut Governorate, found that 30 percent of physicians believed that it is not important to screen for GBV because it is a socially accepted problem and 20 percent felt screening was unnecessary because of the lack of the necessary referrals to help victims.730 GBV services in the public sector are limited, however some NGOs, including the Egyptian Red Crescent, provide services, while UNFPA has also established GBV services for Syrian refugees.
COMMUNITY HEALTH OUTREACH PROGRAMS
The MOHP supports over 14,000 CHWs (raedat refiyat) whose role is to educate and connect patients to routine care. However, the program is hindered by weak geographic coverage in certain governorates, poor skillsets among the CHWs including a lack of counseling skills, and a weak referral system. Household surveys show high community rates of uncontrolled or undiagnosed chronic conditions, as well as poor awareness of the risk of complications, highlighting the important role that should be played by CHWs.731 Routine community outreach through mass media and public health campaigns are also limited, with fewer than a quarter of married women reporting having seen information on family planning on television or in public spaces.732 In order to enhance the role played by CHWs in improving MCH and nutrition services, USAID has been providing training for all 14,000 CHWs across 23 governorates in Egypt, with a particular focus on enhancing the quality of care for rural populations.
SERVICE QUALITY
Low utilization of public health facilities is due to their poor quality of care. Unsanitary conditions at dilapidated state-run facilities, regular medication stock-outs, lack of updated and enforced clinical guidelines for managing chronic diseases and limited numbers of specialists are widely reported.733 In addition, hospitals are ill-equipped to respond to the real needs of the population in their catchment areas, particularly in rural areas. Over-worked and poorly trained staff display poor adherence to infection control measures, perpetuating the spread of hospital acquired infections and the transmission of HBV and HCV.734 Unsafe blood transfusions are also a contributing factor to the on-going spread of HCV and HBV. 735 Facilities also lack mechanisms for patients to report satisfaction with services. , Research indicates only 12 percent of facilities have a form to measure the quality of services.736 Furthermore, only 3 percent of healthcare providers felt that clients had a right to complain about the quality of services.
729 MOHP, El-Zanaty and Associates, and ICF International, "Egypt Demographic and Health Survey 2014.” 730 Aziz, M., and El-Gazzar, "Health care providers’ perceptions and practices of screening for domestic violence in Upper Egypt," Sexual and Reproductive Healthcare Journal, June 2019, https://www.sciencedirect.com/science/article/abs/pii/S1877575618302908 731 MOHP and The World Bank, "Transforming Egypt's Healthcare System Project." 732 World Bank, "Transforming Egypt's Healthcare System Project.” 733 World Bank, "Supporting Egypt’s Universal Health Insurance System." 734 Elhoseeny, T.A. and Mourad, J., "Assessment of the Safety of Injection Practices and Injection-Related Procedures in Family Health Units and Centers in Alexandria," Journal of the Egyptian Public Health Association, August 2014, https://journals.lww.com/ephaj/pages/articleviewer.aspx?year=2014&issue=08000&article=00004&type=Fulltext 735 World Bank, "Transforming Egypt's Healthcare System Project." 736 Abdel-Tawab, N., et al., "Do public health services in Egypt help young married women exercise their reproductive rights?,"

138 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
Although the government has developed quality accreditation standards for PHCCs and hospitals based on international guidelines, adoption has been patchy due to a lack of funding. Despite the lack of clear guidance on monitoring quality of services in public facilities, there is a system for supervision and monitoring NGO clinics, both at the local level and at the governorate level by the Health Directorates.737 Quality of care has also been addressed through a series of administrative decrees covering issues such as the presence of senior obstetricians during deliveries, midwife training and licensing, improvement in blood transfusion services, and use of facility-generated revenues for local service improvement.738
HEALTH FINANCE
Egypt has low levels of government health expenditures; only 1.7 percent of the GDP and 5.6 percent of the total government budget is spent on health, with public spending accounting for 38 percent of the total health expenditure.739 Although an estimated 60 percent of Egyptians have health insurance through the government’s HIO, fewer than 6 percent of households use this insurance, due in large part to their concerns about the quality of care at government facilities. Vulnerable groups, including informal sector workers, the poor, and dependents, are not covered. Despite subsidized care at public health facilities, 20 percent of services still require out-of-pocket payments. Use of private sector services is common, and out-of-pocket payments in Egypt have remained fixed at 61 percent of total health spending over the past decade, of which 90 percent is paid out of pocket by households and 10 percent by prepaid private voluntary health insurance. Other sources of healthcare financing are highlighted in Figure 63.
FIGURE 63: SOURCES OF HEALTCARE FINANCES
Payments for healthcare show significant inequities by income, gender, and geography. Families in the lowest income quintile spend 21 percent of their income on health in comparison to 13 percent among those in the highest quintile, with women spending more on all type of healthcare.740 Among women in urban governorates, 11 percent are covered by health insurance, compared to 4 percent of women in rural Upper Egypt. Nearly 7 percent of households are pushed into poverty each year due to catastrophic
737 DHS, "Overview of the Health System in Egypt." 738 DHS, "Overview of the Health System in Egypt." 739 World Bank, "Egypt COVID-19 Emergency Response.” 740 World Bank, "Egypt COVID-19 Emergency Response.”
Ministry of Finance 29%
Public Firms3%
Private Health Insurance6%
Out-of-pocket 60%
NGOs1%
Donors1%

139 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
health care expenditures, with households in rural areas and those with family members with a chronic condition more likely to suffer catastrophic health needs.741
The financial burden of health care creates a key barrier to citizens accessing services, while government funding is insufficient to support essential public health programs, including universal health insurance. Consequently, health sector reforms are largely reliant on donor funding, particularly from the World Bank and USAID. Donors have provided more than 50 percent of the funding for public-sector population program activities and almost 70 percent of the funding for these activities in the private sector.742
The 2014 Constitution has paved the way for universal health coverage with a stated target of doubling the government’s expenditure on health, bringing it to 3 percent of the GDP and with the aim of establishing a comprehensive health insurance mechanism as a way to increase access to quality health services for all citizens. Reforms are also in progress to enhance social protection, with the introduction of a cash grant program (Takaful and Karama), which specifically targets people living in extreme poverty and links them to health and education services. Data indicates that the poorest 10 percent of the population are set to receive 28 percent of the cash allocations (of Takaful and Karama programs), while the poorest 40 percent receive 70 percent of these allocations.743
ACCESS TO ESSENTIAL MEDICINES
Of the total spending on health, 28 percent is on pharmaceuticals, with over half of out-of-pocket expenditures going to medicines, underlining the challenges in affordability of and access to medicines.744 Medication stock outs at public facilities are regularly reported, due to outdated and inefficient supply chains. 745 Egypt produces 90 percent of its pharmaceuticals locally. The Expanded Program on Immunization (EPI) is probably the most accessible, available, and utilized public health program in Egypt, according to health officials, and provides free vaccinations to children aged 0-18 months. EPI in Egypt has achieved several successes in controlling vaccine preventable diseases, including strong national vaccination coverage and continuous surveillance leading to reduced illness, disability and death from diseases such as diphtheria, tetanus, whooping cough, measles and polio.746
LEADERSHIP/GOVERNANCE
In 2016, Egypt adopted and began implementing the Vision 2030 National Sustainable Development Strategy, which is aligned with the global SDGs. In working towards this vision, the government is implementing multiple health sector reforms, with significant donor funding and technical assistance, mostly from USAID, the World Bank, and the European Commission. The plan is to provide services using a family health model, where maternal, child, reproductive, and infectious disease services are offered as
741 World Bank, "Transforming Egypt's Healthcare System Project.” 742 DHS, "Overview of the Health System in Egypt." 743 Samir, N., "32.5% of Egypt Population Live in Poverty," Daily News Egypt, July 29, 2019, https://ww.dailynewssegypt.com/2019/07/29/32-5-of-egypt-population-live-in-poverty/ 744 WHO, "Health Profile 2015 Egypt, " 2015, https://applications.emro.who.int/dsaf/EMROPUB_2016_EN_19264.pdf?ua=1&ua=1 745 World Bank, "Supporting Egypt’s Universal Health Insurance System," December 13, 2019, http://documents1.worldbank.org/curated/pt/216021576393269095/pdf/Concept-Project-Information-Document-PID-Supporting-Egypt-s-Universal-Health-Insurance-System-P172426.pdf 746 DHS, "Overview of the Health System in Egypt."

140 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
a package of services in one facility, in an integrated manner.747 In addition, a Pharmaco-economics unit has been established within the MOHP to curb the disproportionately high spending on pharmaceuticals.748
In 2017, the government passed a landmark Comprehensive Health Insurance law to accelerate progress towards universal healthcare coverage. Under the law, which is funded through taxes, employer premiums, and subscription fees (with subsidies for the poorest Egyptians), the government is expanding insurance coverage to an additional 30 percent of the population, including those who are unable to pay. The law also requires public facilities to meet international accreditation standards, which were previously voluntary. Family health physicians will be utilized to support enhanced referrals to accredited facilities.749
In addition to the new law, the government has also adopted several policies targeting the country’s key disease burdens, including a strategy for the expansion of screening and treatment for HCV and another strategy to address high fertility rates and family planning needs, particularly in rural areas. Furthermore, the MOHP has launched a national strategy for incorporating CHWs within the health system. The strategy’s goal is to improve the capacity of CHWs to drive behavior change and strengthen linkages between communities and the health system.750
In Egypt, the Central Agency for Public Mobilization and Statistics (CAPMAS) is the official statistical agency that collects, processes, analyzes, and disseminates statistical data and conducts the census. Data managed by CAPMAS is closely linked to the SDGs, as highlighted by the extensive data on maternal and child mortality and immunization coverage. Egypt possesses a relatively strong public health and surveillance system at the national and local levels, yet anecdotal evidence suggests these systems are in need of improvement. As noted, medication stockouts are due to outdated and inefficient supply chains. Research on information systems within the PHCCs highlight multiple barriers to the systems utilized which have resulted in inaccurate reporting, including high workload and system complexity. A lack of referrals systems highlights the lack of information sharing across facilities. USAID has been working with the MOHP to address the on-going issue of hospital acquired infections through the implementation of a national surveillance system for hospital-acquired infections and antimicrobial resistance in intensive care units.
CONCLUSIONS
While Egypt has made significant progress over the years in terms of improving certain health outcomes, particularly with regards to those covered by the SDGs, the health system is plagued with significant disparities, which particularly affect REM populations residing in Upper Egypt and other remote areas. The low quality of services nationwide is particularly concerning, especially the inadequate infection control practices that are contributing to the on-going spread of certain communicable diseases. Continuing education and advanced certification for the workforce should be addressed as a means to improve quality. The high out-of-pocket expenditures on health continue to drive more families into poverty each year, creating a significant barrier to accessing health care.
AQ 3: CRITICAL HEALTH NEEDS AND GAPS IN HEALTH SERVICES FOR THE REM COMMUNITIES
As most REM populations in Egypt are well-integrated into society, they face the same challenges as residents in their surrounding areas, with few exceptions. Many REM populations are concentrated in
747 DHS, "Overview of the Health System in Egypt." 748 Gericke, C.A., Britain, K., Elmahdawy, M., and Elsisi G., "Health System in Egypt," Health Care Systems and Policies, May 16, 2018, https://link.springer.com/referenceworkentry/10.1007/978-1-4614-6419-8_7-2 749 World Bank, "Transforming Egypt's Healthcare System Project." 750 World Bank, "Transforming Egypt's Healthcare System Project.”

141 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
governorates and regions that face the highest disparities compared to the country as a whole, highlighting the strong need to improve their health outcomes. Poor quality of services and lack of accessibility in rural and remote areas creates many challenges for the already impoverished communities that live in those areas. Research confirms that the poorer households have poor health status and access to poorer-quality healthcare, with the governorates of Upper Egypt being most deprived.751 The high rates of poverty in Upper Egypt affects the Christians and Nubians that reside in those areas. Of particular concern are the extremely weak health services for the very remote Berber community of Siwa and Bedouin communities of Sinai and the Eastern and Western Deserts. These communities lack even basic health services, such as maternal and child health.
Upper Egypt has the highest TFR in the country, under-five mortality is twice as high as in urban areas and maternal mortality is also significantly higher. The high birth rates continue to put added pressure on already deficient health systems. Chronic diseases go undetected and untreated, contributing to the high rates of NCD-associated morbidity and mortality. These factors are further exacerbated by the lower levels of education and higher rates of poverty in those areas.
Therefore, to improve health outcomes for REM communities in Egypt, comprehensive approaches are needed to improve the accessibility and affordability of high-quality health services in the areas they reside. Quality of care should be addressed through capacity building of the workforce and improved incentives for health care providers to work in more remote and rural areas of the country. Capacity building efforts should prioritize educating health care providers on adapting to the specific needs of their catchment populations, improving infection control practices, detection and treatment of chronic diseases, and health education. Health education should seek to improve health-seeking behaviors as a preventive measure and enhance linkages and referrals to adequate health care facilities. Health education efforts should also target women of reproductive age in order to curb population growth. Research has shown that women attending family planning clinics, particularly in rural areas, are not provided with sufficient information regarding family planning methods, their effectiveness and possible side-effects, contributing to high rates of discontinuation of family planning. Social barriers to family planning should also be addressed, in addition to societal perceptions towards violence against women and children. Access to services for victims of violence also needs to be expanded and improved.
CHWs are an ideal way to enhance the geographic coverage of these interventions, while recruiting members from the community will enhance culturally appropriate interventions and serve as a means to support income generation for community members. While outdated health facilities in these regions need to properly be equipped, expansion of coverage can also be attained through the use of mobile medical units. In tandem to the government’s work towards the expansion of universal access and health insurance coverage, targeted approaches should be made to ensure the most vulnerable populations of Upper Egypt and other impoverished communities are prioritized under these mechanisms.
Specific barriers potentially exist for members of the Baha’i communities that do not have official identification cards, as this prevents them from accessing publicly available health services. Amendments to the law regarding the reporting of religion on government-issued ID cards should have removed this obstacle, yet the extent to which this is still impacting the Baha’i community is unclear and would require further research.
CONCLUSIONS
While attempts to specifically target REM populations with enhanced health services can be achieved among REM populations in remote areas, such as the Berber in Siwa and the Bedouin population, this approach is not recommended for reaching REM populations in Upper Egypt. While services may be
751 World Bank, "A Roadmap to Achieve Social Justice in Health Care in Egypt."

142 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
designed to target communities with concentrations of REM populations in Upper Egypt, a more comprehensive approach is recommended due to on-going sectarian tensions in the region, particularly in rural areas.
AQ 4: EXTERNAL STRESSES
The Egyptian health system faces multiple challenges in improving and ensuring the health and wellbeing of the Egyptian people. The system faces not only the burden of combating illnesses associated with poverty and lack of education, but a high birth rate combined with longer life expectancy is increasing the pressure on the Egyptian health system. Efforts to improve the health system are impacted by multiple variables as highlighted below.
COVID-19
As of September 28, 2020, there were 102,840 confirmed cases of COVID-19 and 5,883 deaths in Egypt752, with recent figures indicating an exponential increase in cases.753 Reports emerging from frontline doctors, the country’s Doctors Syndicate, Amnesty International and other media outlets are extremely concerning, as they highlight significant problems being faced by the health sector in response to the outbreak, particularly in terms of PPE shortages and high rates of infection among health care providers. By June, over 100 doctors have died and more than 3,000 have been infected since the outbreak of the coronavirus.754 This number does not include healthcare workers who died with COVID-19 symptoms, such as pneumonia, and those who did not undertake the PCR tests.755 As of April 2020, healthcare workers represented an alarming 13 percent of all COVID-19 cases, highlighting that due to a dual risk of exposure to infection inside health facilities, as well as in community settings, healthcare workers are seeding infections between hospitals, colleagues and patients.756 Egyptian authorities have arrested at least nine doctors and medical personnel for speaking out about the deaths of healthcare workers, the lack of PPE in hospitals, and for criticizing the government’s response to the outbreak.757
The Doctors Syndicate has released official statements accusing the MOHP of negligence in the denial of COVID-19 testing and treatment for frontline healthcare providers and the shortages of PPE. WHO has reported that healthcare staff are not trained on the proper use of PPE. Doctors from multiple hospitals have threatened mass resignations, amid extensive pressure on the healthcare system and insufficient support from the MOHP. Low levels of testing among the public and the relaxing of movement restrictions, compound the threat of increased COVID-19 transmission in Egypt.
POLITICAL AND POLICY
At a political level, Egypt has developed a multitude of strategies and reform measures with vast potential for improving the health of the population, however, questions remain regarding the capacity and
752 WHO, Egypt, 2020. https://covid19.who.int/region/emro/country/eg 753 Hassany, M., Abdel-Razak, W., Asem, N., et al., "Estimation of COVID-19 Burden in Egypt," Lancet Infectious Diseases, April 27, 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7185947/ 754 Egyptian Streets, "Egypt’s Medical Syndicate Slams PM’s Statement ‘Blaming’ Doctors for COVID-19 Deaths," June 24, 2020, https://egyptianstreets.com/2020/06/24/egypts-medical-syndicate-slams-pms-statement-blaming-doctors-for-covid-19-deaths/ 755 Amnesty International, "Egypt: Health Care Workers Forced to Make Impossible Choice Between ‘Death or Jail’," June 18, 2020, https://www.amnesty.org/en/latest/news/2020/06/egypt-health-care-workers-forced-to-make-impossible-choice-between-death-or-jail/ 756 World Bank, "Egypt COVID-19 Emergency Response - Project Information Document," April 28, 2020. 757 Malsin, J., "Egypt Is Arresting Doctors Who Raise Alarms Over Coronavirus Approach," The Wall Street Journal, June 30, 2020, https://www.wsj.com/articles/egypt-is-arresting-doctors-raising-alarms-over-coronavirus-approach-11593533638

143 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
commitment to implement these reforms. For example, while in 2016 Egypt passed a law criminalizing FGM, this practice is still extremely widespread, highlighting the need to enhance political commitment to enforce penalties associated with FGM. Furthermore, the absence of a law criminalizing domestic violence poses a severe obstacle to reducing the high rates of violence experienced by women and children. This has become of even more concern amid the COVID-19 outbreak, as the World Bank has confirmed a rise in cases of GBV.758
Arrests, arbitrary detention, and prosecution of those that voice criticism of the government have become widespread, as was seen with the arrests of frontline healthcare workers and at least 500 others, including activists and lawyers, who criticized the government’s response to the COVID-19 outbreak.759 The practice of stifling dissent has become widespread, even among regular citizens voicing their opinions on social media. Concerns exist about human rights violations committed by the state, which have been contributing to the on-going instability in the country since the 2011 uprising.
SECURITY AND STABILITY
Widespread public dissatisfaction with basic living conditions spurred the Arab Spring in 2011. Since then, the country has seen sustained political instability and slow economic growth which has hindered long-term plans for health reform.760 Furthermore, while there has been a rise in GDP and inflation is slowly declining, poverty levels are on the rise.
FINANCIAL
Socioeconomic conditions in Egypt remain challenging. Sustained inflation eroded the purchasing power and standard of living of the population. The national poverty rate is increasing, with higher rates concentrated in rural Upper Egypt, up to 68 percent in some governorates where many REM populations live. While the government is making progress on social protection measures, such as higher allocations for food subsidies through targeted cash transfers, more effort is needed to address the underlying causes of poverty in Egypt, particularly in light of the challenges created by COVID-19. Egypt has a youth bulge, with almost one-third of the population between 10-24 years of age. Moreover around 50 percent of all the unemployed in Egypt are age 15-24, with an additional 16.5 percent age 25-29.. 761 The high unemployment rate among youth must be addressed. Finally, while the government has developed reform plans, they lack crucial funding necessary to implement them and are highly reliant on donor funding.
EQUITY
While there have been improvements reported across health indicators for the country as a whole, these numbers conceal striking inequalities by gender, socio-economic status, education levels, employment status and geographical location. As has been noted, the rural areas of Upper Egypt lag the furthest behind national averages, with health challenges disproportionately affecting rural poor communities in the region.
758 World Bank, "Egypt COVID-19 Emergency Response, Appraisal Environmental and Social Review Summary," April 28, 2020, http://documents1.worldbank.org/curated/en/227361588107008681/pdf/Appraisal-Environmental-and-Social-Review-Summary-ESRS-Egypt-COVID-19-Emergency-Response-P173912.pdf 759 Reuters, "Some Medics Say They are Muzzled in Egypt’s Coronavirus Response," May 29, 2020, https://www.reuters.com/article/us-health-coronavirus-egypt-medics/some-medics-say-they-are-muzzled-in-egypts-coronavirus-response-idUSKBN2352JX 760 Gericke, C.A., et al, "Health System in Egypt." 761 UNICEF, "Health," Accessed June 28, 2020, https://www.unicef.org/egypt/health

144 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
Gender differences in disease burdens and health needs must also be acknowledged. Nearly half of Egyptian women who would prefer a female doctor are treated by a male, likely limiting their level of comfort discussing sensitive matters, such as GBV, mental health and family planning, and subsequent uptake of health services. Women in Egypt are also more likely to be uninsured, illiterate, and have risk factors for NCDs, including obesity and hypertension, raising the need for targeted outreach approaches.762 Data released by UNICEF has documented how children are disproportionately impacted by multidimensional poverty, highlighting the need to improve services targeting Egypt’s very large population of children and youth.
Long-term efforts are needed to address issues of growing inequalities in financial access to care, the low quality of public services, as well as the growing privatization of health care which furthers the existing inequalities in access to care. Efforts to improve the health of Egyptians must be done in a comprehensive manner, with equity as a guiding principle.
ENVIRONMENTAL
In Egypt, water infrastructure coverage has grown substantially over the last decade. While access to water is almost universal in urban areas, a significant number of households are still not connected with the water system in rural areas and in urban slums, resulting in 7.3 million people lacking access to safe water, of which 5.8 million live in rural areas.763 In rural areas, around 12 percent of the population live in dwellings not connected to the water system and 15 percent do not have access to adequate sanitation, while 13 percent do not have soap. Lack of access to safe water and proper sanitation facilities, as well as poor hygiene contribute to the spreading of diseases, which significantly and negatively impact health and nutrition. In Egypt, children are the most severely impacted by inadequate WASH standards, with diarrhea being the second leading cause of death among children under-five. Therefore, while it may seem impressive that over 90 percent of Egypt’s population are supplied with clean water and sanitation, almost 10 million people are not. These numbers become even more concerning, since they hinder the ability of these communities to protect themselves against COVID-19 transmission.
CONCLUSIONS
The Egyptian healthcare system faces multiple challenges to improve and protect the health and well-being of a fast-growing population. The rise in NCDs, and a high birth rate combined with a longer life expectancy, is putting additional pressure on the system and is expected to increase health care costs, against the context of limited government resources and constrained public finances. The healthcare system is further afflicted by significant inequities, which disproportionately affect the country’s most vulnerable populations. Therefore, efforts to improve the health of REM populations in Egypt, should target those that reside in vulnerable rural and remote communities, which currently face the most significant barriers to improved access to health and improved health outcomes.
USAID HEALTH AND REM PROGRAMMING
USAID programs in Egypt place particular emphasis on poor and underserved populations, including women, youth, and those in geographical areas where there are severe health disparities. USAID also works to address gender inequalities in the health sector. Below are current health projects being implemented by USAID in Egypt.
762 World Bank, "Transforming Egypt's Healthcare System Project." 763 UNICEF, "Health."

145 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
• Improving Maternal, Child Health, And Nutrition Services in Egypt (2015-2019): In coordination with the Ministry of Health and Population, this activity strengthens the nationwide CHW program through curriculum development, training for all 14,000 CHWs, and implementation of best practices to ensure quality care for rural populations.
• Family Planning Through the Private Sector (2016-2020): The activity focuses on two groups of young people as potential clients: male and female factory workers and male and female youth with secondary or university education in urban areas. Using peer educators trained through the activity, one-on-one support as well as group activities to discuss concepts such as birth spacing, and healthy mothers and babies are provided to activity participants.
• Strengthening Egypt’s Family Planning Program (2017 – 2022): USAID provides technical assistance and training for MOHP staff to improve the quality of voluntary family planning services and information, in an effort to stem the rapid total fertility rate in Egypt.
• Program to Improve Quality and Safety of Healthcare in Egypt (2014-2019): This activity supports the efforts of Egypt’s MOHP to reduce the incidence of infections originating in hospitals by instituting a national surveillance system for hospital-acquired infections and antimicrobial resistance in intensive care units. To date, 435 intensive care units at 115 hospitals (110 public and university; five private), representing 86 percent of Egypt’s total intensive care capacity, are participating in the activity.
• Supporting the Elimination of Hepatitis C in Egypt (2018 -2020): This activity contributes to Egypt’s national goal of eliminating Hepatitis C by 2023, and is in full alignment with the National Plan of Action for the Prevention, Care, and Treatment of Viral Hepatitis – Egypt’s roadmap for eliminating Hepatitis C. Implementing Partner:
• Avian Influenza Prevention and Control (2015-2019): Over the past 13 years, USAID has invested more than $40 million to support GOE efforts to prevent and control avian influenza. Although USAID/Egypt’s direct support to prevent avian influenza ended in 2015, additional support is currently provided through USAID’s Global Health Security and Development program, which seeks to reduce the risk of human exposure by reducing infections in poultry.
• COVID-19 (2020): USAID has contributed EGP 51m to the Egyptian Red Crescent (ERC) to support community outreach for COVID-19 prevention. The project supports the distribution of hygiene kits to vulnerable and rural communities, provides initial fever screenings and referral services to hospitals, as well as providing psycho-social support services to healthcare workers.

146 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
AQ 5: LESSONS LEARNED FOR IMPROVING HEALTH SERVICES FOR RELIGIOUS AND ETHNIC MINORITY COMMUNITIES
Although specific aspects of health systems and service delivery vary across these five countries, the challenges REM populations face in accessing services are similar. All five countries are addressing challenges with IDPs and refugee populations that need basic health services. REM populations, as a subset of these displaced and affected populations, also need improved access to health services, including preventive care, diagnostics, and treatment. In addition to health services provided at PHCCs and hospitals, REM populations need preventive care programming such as outreach and education on health practices (e.g., nutrition, sanitation, breastfeeding).
All of the countries are facing challenges due to the instability in the region, coupled with economic impediments that are reducing government spending on health and driving up poverty levels among both host and refugee communities, putting added stress on existing healthcare systems. Many IDP, refugee, returnee, and host communities are still recovering from conflict and face challenges related to nutrition, livelihoods, housing, and education, further contributing to stress and poor living conditions. As vulnerable populations, many REM populations also require mental health and psychosocial services (MHPSS) and sexual and gender-based violence (SGBV) services. Many health facilities are overburdened with demand, leaving communities in need of programming and investment to address the challenges and improve access to services, as well as expand the types of services and raise service quality.
The following lessons learned draw on the research conducted for this assessment as well as an evaluation conducted concurrently by this assessment team examining REM health programming in northern Iraq, Ninewa Plains.764 These lessons learned highlight key areas of consideration for future REM programming and investments.
LIMITED DATA AND TARGETING
Availability of REM-specific health data is limited. Much of the available data is old and outdated. Current service providers do not disaggregate data by minority populations, making it difficult to determine whether REM populations face barriers beyond those of the wider population. However, the long history of sectarian tensions in the region, increased competition for livelihoods and resources triggered by the influx of IDPs and refugees in certain regions, and the tensions between refugees and host communities due to the targeting of health services for refugees, make REM-targeted programming unfavorable. Such programming can make REM populations even more vulnerable by exacerbating tensions, undermining Do No Harm practices.
In addition, most REM populations are integrated into the general population, making them difficult to target directly. Therefore, efforts to address the gaps in health services for REM communities can be best accomplished by implementing broad-based interventions in areas known to contain REM concentrations; these services should be made available to all population groups, especially those most vulnerable. Several exceptions do exist where REM populations are concentrated in remote areas or villages that could be directly targeted, such as the Yazidis in villages around Amuda and Kahtanieh in NES and the Berber communities in the remote village of Siwa Egypt. However, risk assessments must be thoroughly incorporated into the design phases of all interventions to ensure conflict-sensitive programming.
764 Khaled, Lorenzen, and Zodrow (MSI), Evaluation Report on USAID Improving Health Services and Outcomes in the Ninewa Plains, Iraq, May 2020.

147 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
ROLE OF PARTNERS
International and national NGOs and FBOs, and donors are critical in providing humanitarian services across sectors, including health service delivery and prevention. IDPs, refugees, and vulnerable host community members rely on these services to access health care across these countries. Donors must continue to fund protection initiatives and services within communities and camps to fill the gaps that health systems and governments cannot. Even as IDPs and refugees return to their communities, it will be a slow return of the most vulnerable individuals inside these camps, and host communities will continue to face challenges as new populations settle back in.
These donors and international NGOs must continue to engage and/or implement through local organizations that have experience working in the communities and their various subsets of the populations. This will help ensure that programming is sensitive to the context. Social cohesion and reconciliation initiatives should be embedded within the wider population they aim to represent. They should be inclusive of religion, ethnic identity, and gender. Efforts must be augmented by a transparent and accountable justice process.
COMMUNITY AWARENESS
The key methods for improving access to primary care for vulnerable populations are to strengthen accessibility, availability, and affordability of services. Without these, vulnerable populations’ health care needs will remain unmet. Another important method for improving services for vulnerable populations, including REM populations, is to increase community awareness about service availability and importance. In USAID’s report “Strengthening Health Outcomes through the Private Sector,” funding community health workers was recommended to expand community outreach and increase demand.765 These health workers not only enhance awareness but also expand geographical coverage of messaging, especially to rural and vulnerable populations. The Ninewa Plains evaluation also found community health workers useful in educating populations; however, due to the short duration of the grant (one year), more time was needed to fully integrate the community health workers into the health system. Without this integration, the approach’s sustainability is limited.
Community outreach and education can help reduce the stigma surrounding GBV and MHPSS services and encourage utilization. Stigma is still a substantial barrier for many in seeking the limited services available. In addition, some REM populations face discrimination in their communities, which can lead to mistrust of health professionals. Community outreach can also help build trust among REM communities and encourage them to seek health services. Encouraging populations to seek preventive services is essential in order to reduce the high costs associated with curative care.
LOCAL CAPACITY BUILDING
Many of the countries studied face capacity challenges due to the limited number of medical professionals and limited investment. At each level of the health system (i.e., Ministry of Health, health facilities, and communities), there are opportunities to build health professionals’ capacities. The Ninewa Plains evaluation found that training health facility staff on basic services and on MHPSS and SGBV services filled a gap and provided staff with new knowledge and skills to improve service provision. Training members
765 MSI, Strengthening Health Outcomes through the Private Sector report, 2015, USAID, https://jordankmportal.com/resources/strengthening-health-outcomes-through-the-private-sector-shops-final-performance-evaluation

148 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
from within the community on MHPSS and SGBV services enhances the sustainability of interventions and helps providers effectively reduce the stigma associated with accessing these services.
GENDER-BASED VIOLENCE AND MENTAL HEALTH PROGRAMMING
The humanitarian crisis is generating enormous psychological stress among the conflict-affected population. Psychological stressors are a known contributor to higher levels of SGBV and mental health disorders. Furthermore, given the extensive trauma that some of these communities endured during the various crises and displacement, it would not be surprising to see significant levels of physical and psychological abuse. Recent data has indicated that SGBV is on the rise in all countries as a result of restrictive measures put into place to reduce the spread of COVID-19. This enhances the challenge women face in accessing support services, particularly those related to SGBV and mental health, and is a challenge that needs to be addressed. These services are essential for addressing the overall health of REM communities and other vulnerable populations across the region.
REDUCING STIGMA
In addition to expanding access and quality of services, programming must improve acceptance and reduce stigma among potential users of these services, their communities, and health service providers. Working closely with community leaders on program implementation and decision making and with hired and trained outreach workers from the community can help reduce stigma and empower communities to support their members with psychosocial and mental health issues, while fostering community dialogue. By acting as a bridge between the community and mental health resources, MHPSS outreach also helps improve accessibility of services.
Various cultural norms and traditional practices hinder women’s ability to access services on their own, particularly SGBV and reproductive health services. Women’s access is restricted by both their husbands and/or their family members, and they often must be accompanied by relatives to receive health services. Addressing these barriers is essential to ensure women can access services. Women’s own lack of trust in the services creates an additional barrier. Community engagement and education can help reduce these barriers.
PRIORITIZING AND INTEGRATING PROGRAMMING
Effective mental health programming and services must be implemented at the community, facility, and government levels, and key systems and networks must be developed among various actors to form a fully integrated system. Services must be comprehensive—from awareness raising to case management and treatment—to ensure a systematic approach to improving outcomes. These approaches must form part of national strategies and policies and be implemented in a comprehensive network of referrals.
Across the region, MHPSS and GBV services must be prioritized by the government. It will take time to fully integrate mental health services into the PHCCs, increase health professionals’ knowledge and practices, and reduce community stigma surrounding mental health. There is a need for advocacy for investment in these services, especially GBV, which often get overlooked.

149 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
MULTISECTORAL APPROACHES
Mental health programming has found success in blending into other programming to help mask stigmatized services. Programs have offered MHPSS along with vocational or employment training programs, especially those targeting women, allowing projects to encourage participation through other support but using the opportunity to educate and introduce participants to these services through discussions.
Coupling SGBV services with other primary and maternal health services in a comprehensive approach enhances uptake of services by women. When SGBV services are embedded within PHCCs, vulnerable women can access these services discreetly. For example, the Ninewa Plains evaluation found that while some women prefer to access these services within the PHCCs, as they could be perceived as accessing other, less-stigmatizing services at these locations, other women reported perceiving the PHCCs as being dominated by men and were therefore reluctant to access services there, highlighting the need to support both integrated and community-based services.
COVID-19 CONSIDERATIONS
In addition to the ongoing crisis in the region, including the economic crisis, COVID-19 will exacerbate the many challenges experienced by vulnerable populations, including REM populations. As countries learn more about addressing this outbreak and adjust strategies, it will be important to ensure that vulnerable populations have access to services, as well as to protective equipment (e.g., masks) and education about the virus’s spread. Because of their living conditions, many of these groups cannot social distance or practice other preventive measures. When strategies are developed and implemented, these limitations and challenges must be thought through and addressed.
RECOMMENDATIONS
The team presents the following recommendations for future REM health programming in the five countries covered by the assessment:
1. REM health programming should not directly target REM populations but rather provide broad, area-based assistance that benefit REM populations through supporting all vulnerable groups in a community or geographic area. This approach avoids adding to any existing ethnic tensions.
2. REM programming should use a multidisciplinary and multisectoral approach in which MHPSS and SGBV services are integrated with other sectors—gender, legal services, vocational skills or other educational programming, and direct service delivery. This approach will help reduce stigma, expand access, and increase beneficiary exposure to these services.
3. Programming should actively engage and partner with local organizations on the ground to support a more comprehensive and sustainable approach to the empowerment and well-being of REM populations, especially women and adolescent girls. In addition to providing local expertise, these groups can facilitate entry into the community and provide information on REM populations’ contexts, including their needs and challenges. They can also help ensure that programming is integrated with other services and sensitive to the local context.
4. Community-based health programming should explore ways to retain community health worker staff, especially after the project has ended. Given the high turnover rates often reported, additional efforts should be explored to retain trained health workers to enhance the long-term sustainability of this component.
ACF
Highlight
150 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
5. REM programming should work through and with the local authorities to help build their capacity and improve sustainability of the health service approaches. Programming can provide grants to local authorities or partner with them to deliver the needed services. This approach will help build relationships and improve government officials’ capacity.
6. MHPSS and SGBV programming should work with national-level stakeholders to influence political buy-in, strategy, budget, policy, leadership, and human resources to continue to improve health outcomes. This programming should also emphasize coordination and collaboration among the multiple ministries to enhance sustainability of interventions and support more comprehensive approaches.
7. Health programming in the region should support the Ministry of Health and other stakeholders to build a local resource pool of experts who can conduct continuing medical education and provide technical assistance to health facilities, especially for MHPSS and GBV services.

151 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
ANNEX 1: SOW
INTRODUCTION
Under the Middle East & North Africa Monitoring, Evaluation, & Learning Services Activity (MENA MELS), Management Systems International (MSI) will conduct a health needs assessment to help inform USAID in its implementation of the Office of the Vice President’s initiative to support religious and ethnic minority (REM) communities in the Middle East and North Africa (MENA). The assessment will gather data to answer key questions regarding REM health needs in five countries and will provide USAID with data-backed recommendations to inform future REM health programming in the greater region.
TARGET COUNTRIES AND POPULATIONS
Five countries have been selected to be the focus of this assessment. These include, Iraq, Syria, Lebanon, Jordan, and Egypt. In addition, the assessment will focus on key REM populations.
Country REM Communities of Focus Geographic Areas of Focus Within Country
1 Iraq Christian (Assyrian, Chaldean, Syriac, and Armenian), Yazidi, Kurd, Kaka’I, Turkman, Shabak, Sabean-Mandaeans,
Nineveh Governorate, KRG, Mosul, and Baghdad
2 Syria Christian (Assyrian, Chaldean, Syriac, Greek, and Armenian), Yazidi, Kurd, and Turkman
Northeast (NE) Syria (excluding regime-held areas and geographic zones part of Operation Peace Spring).
3 Lebanon Christian (Maronite, Greek, Armenian, Syriac, and Chaldean), Druze, Palestinian, and Syrian
All*
4 Jordan Palestinian, Christian (Greek, Maronite, Armenian, Syriac, and Chaldean), Druze, Syrian, Iraqi
All*
5 Egypt Jewish, Christian (Coptic, Armenian, Greek, Syriac) Bahai, and Nubian.
All*
*Per guidance from USAID, the evaluation team will work with key contacts in the USAID Missions in Lebanon, Jordan and Egypt to identify the specific geographic areas of focus for the REM populations identified in the table above. In addition, it is noted that the REM populations are not limited to citizens of the respective countries and refugee populations will be included as part of this assessment.
ASSESSMENT PURPOSE AND QUESTIONS
PURPOSE AND INTENDED USES
The purpose of this assessment is to assess the current status of the primary health sector and the overall strengths and weaknesses in the delivery of health services to REM populations in the MENA region, with a focus on five countries. This assessment will contribute to the understanding of the target populations’ health status as well as gaps and strengths of the health system to help identify needs in the region to be

152 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
considered for future REM health programming at USAID. Conclusions will provide an overview of status, needs, system and potential leverage points for change and improvement. Recommendations will inform future investment and programming.
ASSESSMENT QUESTIONS
This assessment will seek to answer the following assessment questions (AQ) for each of the five selected countries (Iraq, Syria, Lebanon, Jordan, and Egypt).
1. What is the overall current health status of REM communities in the region?
2. What are the overall strengths and weaknesses of the existing primary health care system in the region at the community level?
a. What are potential leverage points for supporting the strengthening of primary health care services in the region?
3. What are the critical health needs and current gaps in primary health care services for the REM communities in the region?
a. Are there different sets of services needed by REM communities in conflict- affected areas (e.g. SGBV services, mental health, etc.)?
b. What are the main barriers for REM communities in accessing different types of health services?
4. What external stresses impact the ability to provide health services and achieve outcomes?
5. What are relevant lessons learned from other projects and donors around improving primary health care services for vulnerable populations in the region?
a. Is the Advancing Partners & Communities (APC)/International Medical Corps (IMC) model as implemented in the Ninewa Plains in Iraq replicable in other REM communities across the broader region?
UNDERSTANDING THE ASSESSMENT QUESTIONS (AQ)
A description of the key information that will be collected and examined under each assessment question is provided below. It is anticipated, since this assessment is across multiple countries, that information might not be available for all countries and more specifically about the targeted REM populations of interest. In cases where data is not available for REM populations, the assessment team will rely on data at a higher level (e.g. country or district) to be able to understand the context of the situation that REM populations face. The assessment team will attempt to collect as much available data for the health indicators below and then rely on primary data through interviews to supplement.
In addition to the parameters outlined under each question, the assessment’s main focus will be on the primary health system at the local and community level since this is where the majority to REM populations will be seeking services. For this assessment, primary health care system includes both public and private health service delivery.
AQ ONE: WHAT IS THE OVERALL CURRENT HEALTH STATUS OF REM COMMUNITIES IN THE REGION?
This question will focus on the following key areas when examining the current health status in each of the five countries for the specific REM population of interest. The assessment team will review all available

153 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
data related to the health areas listed below across sub-groups of the population, including children under 5, adolescents, and women/men. For AQ1 the following data will be collected and reviewed:
Primary causes of death Infant mortality rate Maternal mortality rate Primary reasons for hospitalization Malnutrition rates Diarrhea prevalence HIV/AIDS prevalence
Malaria prevalence Mental health Sexual and gender-based violence (SGBV) Outbreak/epidemic data Sexual and reproductive health (SRH) Access to WASH and sanitation
AQ TWO: WHAT ARE THE OVERALL STRENGTHS AND WEAKNESSES OF THE EXISTING PRIMARY HEALTH CARE SYSTEM IN THE REM COMMUNITIES?
a. What are potential leverage points for supporting the strengthening of primary health care services in the region?
This question will focus on learning about the key strengths and weaknesses of the current health systems at the primary service level in the targeted REM communities. The assessment team will collect, and review data related to the relevant health system building blocks and essential components of the health system in fragile states at a community level. These areas include: health workforce, service delivery, health finance, access to essential medicines, and leadership/governance. The assessment team will look at the following key areas under each of the relevant building blocks:
Health Workforce (quality, capacity and availability) • Number of health care workers relative to population and disaggregated by cadre and sex, in REM
populated areas; if available, for both public and private institutions. • Existence of national and/or local health budget allocated to human resources development in
REM locations. • Existence of recruitment and deployment systems, or incentive schemes to ensure that primary
health-care facilities (in REM locations) meet their nationally recommended staffing norms. • REM populations’ participation in community health outreach programs.
Service Delivery • REM population has access to services (e.g. infrastructure, distance, etc.). • Breakdown of service providers: public and private organizations, including by civil society
organizations (CSO), faith-based organizations (FBO) and other non-government organizations (NGO).
• Availability and uptake of services (primary health care (PHC), maternal, newborn and child health (MNCH), SRH, mental health and psychosocial support (MHPSS), GBV, secondary and tertiary care).
• Service quality (supervisory checklists, audits of medical records, review of facility mortality causes and rates, surveillance).
• Culturally competent care.
Health Finance • Sources of funding for REM populations’ health services. • Amount of private and public spending on health care for REM populations. • Subsidized services and medicines for REM. • Health insurance coverage for REM.
Access to Essential Medicines

2 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
• Availability of key (essential) medicines and supplies in public facilities. • REM population access to essential medicines, including vaccines.
Leadership/Governance • Existence of an up-to-date national health strategy/policy linked to needs and priorities of REM. • Existence and use of an up-to-date health management information systems
AQ THREE: WHAT ARE THE CRITICAL HEALTH NEEDS AND CURRENT GAPS IN HEALTH SERVICES FOR THE REM COMMUNITIES IN THE REGION?
a. Are there different sets of services needed by REM communities in conflict- affected areas (e.g. SGBV services, mental health, etc.)?
b. What are the main barriers for REM communities in accessing different types of health services?
AQ 3 will examine what the specific health needs are in each of the five countries for the targeted REM communities. Through review of the data collected for AQ 1 and 2, the team will note what the challenges and gaps in services are specific to the REM communities, as well as if services that are needed or in demand in conflict areas are being provided. This question will also seek to answer what the barriers the REM communities are facing in being able to access services, e.g., are services not available or do REM populations not trust or know where to go to receive these services.
AQ FOUR: WHAT EXTERNAL STRESSES IMPACT THE ABILITY TO PROVIDE HEALTH SERVICES AND ACHIEVE OVERALL HEALTH OUTCOMES?
This question will examine the external stressors that affect the ability of the primary health system to provide the necessary minimum level of services and for the country to achieve overall health outcomes. This question will examine both at the community and national level the different external stressors. Different types of stressors that will be examined are: political/policy, security/stability, financial, environmental and equity.
AQ FIVE: WHAT ARE RELEVANT LESSONS LEARNED FROM OTHER PROJECTS AND DONORS AROUND IMPROVING PRIMARY HEALTH CARE SERVICES FOR VULNERABLE POPULATIONS IN THE REGION?
This question will collect relevant lessons learned from current and past USAID projects in the five focus countries. The team will also review documents describing REM programming funded by donors such as the United Nations (UN) agencies, World Bank, European Commission and Department for International Development (DFID), and non-governmental organizations (e.g. IMC, Doctors Without Borders/Médecins Sans Frontières (MSF), Save the Children, etc.).
In addition, the team will compile a list of the current CSOs, NGOs, and FBOs that are working on supporting, providing, or increasing access to health services to REM populations. A list of these organizations will be included at the end of the final assessment report.
AQ SIX: IS THE APC/IMC NINEWA PLAINS MODEL REPLICABLE IN OTHER REM COMMUNITIES ACROSS THE BROADER REGION?
This assessment question will utilize information gathered from the evaluation of “Improving Health Services and Outcomes in the Ninewa Plains, Iraq” grant implemented by IMC. Based on the evaluation findings, the assessment team will examine what lessons learned and recommendations can be useful in the broader context of the region, and the five focus countries.

3 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
ASSESSMENT METHODS AND APPROACH
The assessment will use a mixed methods approach to the extent possible, collecting and analyzing both qualitative and quantitative data. Sources of information will include secondary sources as well as primary sources, via interviews or an online survey. Although secondary data and reports will be the primary sources of data, key information interviews (KIIs) will be conducted to collect data to contextualize the secondary data analysis and fill gaps in understanding around the target population.
DATA COLLECTION METHODS
Secondary data sources will be collected through internet google search of published research and studies, as well as research being produced by USAID, their implementing partners, and other donor or research organizations. The assessment team will request any relevant documents from USAID that could be useful in answering the questions (e.g. project documents or data, etc.). The team will also search key health information online sources.
Primary data will be collected through KIIs with key stakeholders and, if needed, an online survey tool. Interviews will be conducted remotely through skype or telephone. The assessment team will develop an interview guide of questions to gather information to provide context and understanding of the health situation in the different REM communities. The team will have initial interviews with Mission staff in each country to gather information from them as well as ask for recommendation for other key respondents. Respondents will also be asked about any resources they have or are aware of that could be used by the team to answer any of the assessment questions. Interviews will last 45-60 mins and will be recorded for reference. Notes will be produced and used as part of the analysis to answer the assessment questions.
The assessment team will ask for some support from USAID in compiling a list of key USAID staff and stakeholders who could provide useful information for the assessment questions.

4 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
DATA SOURCES Below are the sources of data that will be collected and potential KIIs that can help answer each of the assessment questions. The final list of potential KIIs will depend on respondent availability and willingness to be interviewed.
TABLE 1: DATA SOURCES BY ASSESSMENT QUESTION
Assessment Question Data Sources
(e.g. Documents) Potential KIIs
What is the overall current health status of REM communities in the region?
– Demographic Health Data (e.g. DHS) – International health organization data – Assessment and evaluation reports – UN reports
– USAID Mission Staff – GBV/Health sector or
cluster lead – NGO’s/CSO’s working with
REM population
What are the overall strengths and weaknesses of the existing primary health care system in the region at the community level?
– International health organization data – Various government, donor or NGO
assessment and evaluation reports – Government reports and documents – USAID project documents
– USAID Mission Staff – GBV/Health sector or
cluster lead NGO’s/CSO’s working with REM population
What are the critical health needs and current gaps in health services for the REM communities in the region?
– Government reports and documents – USAID project documents (e.g. final
reports and evaluations) – Various donors and NGO project
documents (e.g. assessments and evaluations)
– USAID Mission Staff – GBV/Health sector or
cluster lead – NGO’s/CBO’s working with
REM population
What external stresses impact the ability to provide health services and achieve outcomes?
– USAID project documents (e.g. final reports and evaluations)
– Various donors and NGO project documents (e.g. final reports and evaluations)
– USAID Mission Staff – Health sector or cluster
lead – NGO’s/CBO’s working
with REM population
What are relevant lessons learned from other projects and donors around improving primary health care services for vulnerable populations in the region?
– USAID project documents (e.g. final reports and evaluations)
– Various donors and NGO project documents (e.g. final reports and evaluations)
– USAID Mission Staff – Health sector or cluster
lead – NGO’s/CBO’s working
with REM population
Is the APC/IMC model replicable in other rem communities across the broader region?
Evaluation report for IMC grant – IMC – Health facilities staff

5 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
Recognizing USAID Washington’s interest in latitudinal and longitudinal data, the assessment team will inquire about the availability of such data during KIIs. If any such data are obtained, they will be included in the final report.
DATA ANALYSIS
All collected documents and reports will be reviewed and relevant data and information will be extracted to answer each assessment question. All extracted information will be reviewed, organized, and synthesized. The assessment team will also use descriptive analysis for any available secondary data to report on numbers, frequencies or percentages of health services or statuses.
The assessment team will also examine qualitative data from KIIs and will identify themes and good practice, challenges, barriers and outcomes relevant to each AQ to better understand meaning and context.
PRIVACY AND CONFIDENTIALITY CONSIDERATIONS
The assessment team will obtain informed consent from respondents before carrying out any data collection. The team will pay careful attention to ensure that respondents understand that their responses will be used for research purposes and are expected to be made public. Confidentiality and/or anonymity will be available to respondents when requested.
The team will seek to audio record KIIs whenever possible, and interviewers will seek a separate consent to record. In instances where consent for audio recording is not given, notes will be taken, and these will be expanded shortly after the interviews.
ASSESSMENT LIMITATIONS
The main limitations of the assessment will be the availability of data and access to interview respondents. Since the assessment is relying mostly on secondary data and focusing on small sub-sets of the population (e.g. REM), if there is no publicity available data, there could be gaps in answering the assessment questions and in the understanding current situations of the REM population. The assessment team will do their best to gather data at multiple levels to try to understand the situation and context that the REM population are in. In addition, the team will conduct interviews with key stakeholders to further gather relevant information to answer the assessment questions and provide needed context.
In addition, there can be challenges in setting up remote interviews; however, the team will be diligent about reaching out to respondents and scheduling convenient times that people are available. In addition, the team will consider other alternatives, such as an online survey, to collect data from respondents that might be too busy for a remote interview. The team will also rely on USAID in introducing the team to key stakeholders to encourage respondents to make time for interviews or online data requests.
TEAM COMPOSITION
The assessment team is composed of two health subject matter experts (SME) and one monitoring and evaluation (M&E) expert who worked together to collect, analyze and synthesis data to answer the six assessment questions. Short summaries of team members are provided below:
Gwynne Zodrow (Team lead/M&E expert): Gwynne Zodrow is a technical manager who provides M&E support to multiple government and private sector clients in a variety of fields including health, agriculture and

6 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
food security. As a technical manager she is involved in all stages of evaluations and research studies including design, data collection and analysis and reporting. Ms. Zodrow recently worked with USAID’s Ghana Evaluate for Health project providing technical M&E assistance to the local team supporting implementing partners, the Mission, and managing multiple health evaluations and a national survey. Ms. Zodrow has a Masters of Global Public Health from George Washington University.
Dina Khaled (SME): Dina Khaled has over 19 years of experience in international health and extensive experience working with ethnic and religious minorities. In recent years, Ms. Khaled has focused on the refugee crisis, responding to emergency medical needs in Greece and Lebanon wherein she supported various clinics by offering medical translation and coordinating relief organizations. During this time, Ms. Khaled also established a medical clinic for Syrian refugees and provided direct support to over a thousand Yazidis escaping genocide in Iraq. Ms. Khaled has worked with the UN, USAID and Amnesty International to conduct research and supervise research teams for evaluations, assessments and monitoring activities. Ms. Khaled has a Masters’ of Public Health, International Health Promotion from George Washington University and is verbally fluent in Arabic.
Heather Lorenzen (SME): Heather Lorenzen is a certified nurse practitioner with nine years of experience in emergency medicine and humanitarian response. As an emergency medical coordinator, Ms. Lorenzen has coordinated medical care, conducted needs assessments, developed and implemented training programs and conducted remote monitoring in Tunisia, Libya, Lebanon, Syria, Iraq and Jordan. Ms. Lorenzen has also served as a consultant, conducting needs and quality assessments for health systems and most recently co-authoring the Sphere Standards for Assessment, Monitoring and Evaluation.
MSI Home office support also includes Carly Green (Project Manager) and Deborah Orsini (Task Technical Director).
TIMELINE AND DELIVERABLES
Based on the information gathered, the assessment team will draft a report that answers all six of the assessment questions for each country. In addition, the report will share recommendations for future programming in these areas. The final report will present findings by country with information associated with each question, followed by conclusions and recommendations for future programming. The estimated deliverable dates are as follows:
Task MSI Submit USAID Comments or Approval
1. Draft Design Document o/a March 3 April 27
2. Final Design Document o/a April 30 o/a May 7
3. Draft Assessment Report o/a June 29 o/a July 13
4. Final Assessment Report o/a July 27 o/a August 3
5. Final presentation materials o/a August 5 o/a week of August 10

7 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
ANNEX 2: USAID MISSION STAFF INTERVIEWS
The following Health and REM USAID representatives were interviewed for the assessment.
Country USAID Representatives Date
Syria Mark Kelly, Gaby Abboud, Heather Schommer, and Dana Hussein
June 24, 2020
Iraq Savannah ThomasArrigo, Violent Dancheck, Mohit Dayal, Sara Derian, Chelsea Del Grande, Alana Marsili, Jodi Rosenstein, Amy Kay
June 24, 2020
Lebanon Claude Zuilo June 22, 2020
Jordan John Spears and Dan Sinclair June 24, 2020

8 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
ANNEX 3: DISTRIBUTION OF REM POPULATIONS IN NES

9 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
ANNEX 4: HEALTH IMPLEMENTING PARTNERS IN AL-HASAKEH
Source: Health Sector Syria, "Health Projects Implementing Organizations in Al-Hasakeh," Accessed June 22, 2020, https://www.humanitarianresponse.info/sites/www.humanitarianresponse.info/files/documents/files/health_sector_agency_present_al-hasakeh.pdf

10 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
ANNEX 5: MAP OF U.S. COMPLEX EMERGENCY PROGRAMS IN IRAQ

11 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
ANNEX 6: MAP OF LEBANON - DISTRIBUTION OF RELIGIOUS GROUPS
Source: Sergey Kondrashov, "Demographic Map" Lebanon Demographics (2013). https://external-preview.redd.it/872JVWubp8BHuuHlZnXhe6cmS6dY3dgY5y_h2kqGJUI.jpg?auto=webp&s=6f365353da0f2402c46d3d8807625e141cda45c4

12 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
ANNEX 7: MAP OF VULNERABLE CADASTRES IN LEBANON

13 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
ANNEX 8: HEALTH PARTNERS IN EACH COUNTRY
Below are lists of NGOs and FBOs that are currently delivering health programming in each of the five countries. Illustrative program areas are provided but are not inclusive of all the work that each organization supports.
NORTHEAST SYRIA
Organization Name Example Types of Programming
Al Amany Charity Association Health and IDP assistance
Al Birr and Al Ihsan Ras Al Ain Health and IDP assistance
Al Mawadda Charity Association Health and IDP assistance
Armenian Catholic Charity Health and IDP assistance
Ashour Foundation for Relief and Development Health and IDP Assistance
Doctors without Borders (MSF) Health and WASH
Health Promotion Charity Organization Assistance to IDPs
International Committee of the Red Cross (ICRC) Health and Shelter
International Rescue Committee Health, MHPSS, SGBV, CH
Mercy Corps WASH and Nutrition
Monastery Saint James the Mutilated (MSJM) IDP assistance
Norwegian Red Cross Health
Save the Children WASH, Child Protection
Sham El kher Association Health
Syirac Catholic Archbishopric Health
Syria Al Yamama Association Health
Syriac Cross Health
Syrian American Medical Society Health and MHPSS
Syrian Arab Red Crescent Health
Syrian Family Planning Association (SFPA) Health and FP
Yazidi House Assistance to Yazidis
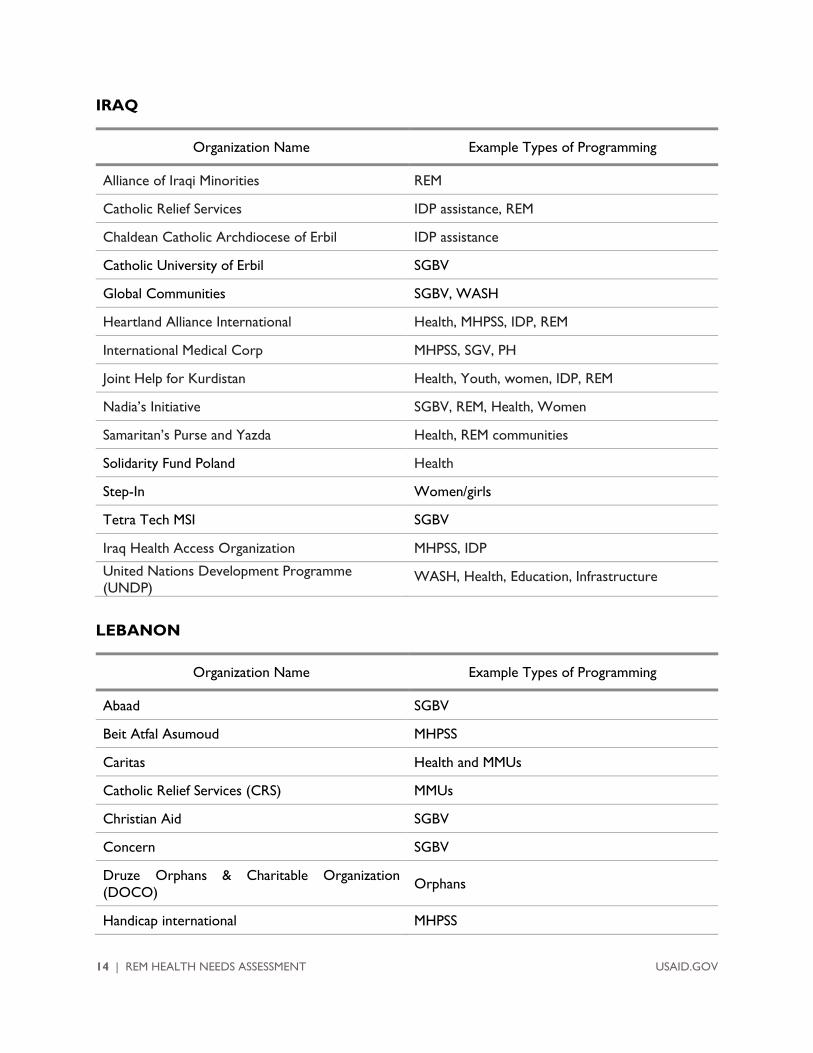
14 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
IRAQ
Organization Name Example Types of Programming
Alliance of Iraqi Minorities REM
Catholic Relief Services IDP assistance, REM
Chaldean Catholic Archdiocese of Erbil IDP assistance
Catholic University of Erbil SGBV
Global Communities SGBV, WASH
Heartland Alliance International Health, MHPSS, IDP, REM
International Medical Corp MHPSS, SGV, PH
Joint Help for Kurdistan Health, Youth, women, IDP, REM
Nadia’s Initiative SGBV, REM, Health, Women
Samaritan’s Purse and Yazda Health, REM communities
Solidarity Fund Poland Health
Step-In Women/girls
Tetra Tech MSI SGBV
Iraq Health Access Organization MHPSS, IDP
United Nations Development Programme (UNDP)
WASH, Health, Education, Infrastructure
LEBANON
Organization Name Example Types of Programming
Abaad SGBV
Beit Atfal Asumoud MHPSS
Caritas Health and MMUs
Catholic Relief Services (CRS) MMUs
Christian Aid SGBV
Concern SGBV
Druze Orphans & Charitable Organization (DOCO) Orphans
Handicap international MHPSS

15 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
Organization Name Example Types of Programming
Humedica Health and MMUs
International Orthodox Christian Charities Health and Child Health
International Rescue Committee (IRC) SGBV
KAFA (Enough Violence Against Women) SGBV
Medair Health and WASH
MENA Organization for Services, Advocacy, Integration & Capacity Building (MOSAIC) SGBV
MSF (Doctors without Borders) Health and MHPSS
Beit Atfal Assumoud (BAS) Health and Child Health
Oxfam Health and WASH
Relief International UN Focal Point Health Bekaa
JORDAN
Organization Name Example Types of Programming
CARE International Protection, SGBV
Caritas Health
Center for Victims of Torture MHPSS, Protection
Humanity & Inclusion Health
Institute for Family Health/Noor Al Hussein Foundation Health, RH, SGBV
International Medical Corps Health, RH, MHPSS, SGBV, Child Protection
International Organization for Migration Health
International Orthodox Christian Charities Health, Protection
International Relief & Development Health, Protection, Child Protection, GBV, WASH
International Rescue Committee Child Protection, SGBV, Health, RH,
Islamic Relief Worldwide Health
Jesuit Refugee Service MHPSS
Jordan Health Aid Society Health, Protection
MEDAIR Health
Medecins Du Monde Health

16 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
Organization Name Example Types of Programming
Nippon International Cooperation for Community Development Protection, MHPSS
Noor Al Hussein Foundation Child Protection, Community Services, SGBV, Health, MHPSS
Pathfinder International RH
Premiere Urgence - Aide Medicale Internationale Health
Qatar Red Crescent Health
Royal Health Awareness Society Health, WASH
Save the Children International Health
Terre Des Hommes Health, RH, Child Protection
The Eastern Mediterranean Public Health Network Health
Un Ponte Per Protection
United Nations Children's Fund Child Protection, SGBV, Health, Nutrition, WASH
United Nations High Commissioner for Refugees Child Protection, SGBV, Health, Nutrition, WASH
United Nations Populations Fund SGBV, RH
World Health Organization Health, RH, MHPSS
EGYPT
Organization Name Example Types of Programming
Association of Upper Egypt Health and Nutrition
Caritas Health and MCH
Egyptian Red Crescent Health and GBV
Health Outreach to the Middle East (HOME) Health and MHPSS
Helwan Association for Community Development (Bashayer) Health and MHPSS
John Snow, Inc. FP
Misr El-Kheir Foundation Health, MCH and Protection
Nebny Foundation Health and Education
Population Council FP
Save the Children MCH and CHWs

17 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
Organization Name Example Types of Programming
St. Andrew's Refugee Services MHPSS and Community Outreach

18 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
ANNEX 9: BIBLIOGRAPHY
ABAAD, Care, DRC, IRC, Intersos, UNHCR, UNICEF, UNFPA and UN Women, "Impact of the COVID-19 on the SGBV Situation in Lebanon," 2020.
Abdel-Tawab, N., Rabie, T., Boehmova, et al., "Do public health services in Egypt help young married women exercise their reproductive rights?," International Journal of Obstetrics and Gynaecology, March 25, 2015.
ACAPS, "Syria Displacement in Northeast Briefing Note," October 21, 2019.
AFP, "Lebanon Minister Warns Health Sector Threatened Over Dollar Shortage," Al-Arabiya, November 26, 2019.
Ahmado, N., "Coronavirus Measures Delay Yazidi Survivor’s Reunion with Family," VOA, April 25, 2020.
--- "Uncertain Future Awaits Displaced Syrian Yazidis in Lebanon," VOA, May 12, 2019.
Alameddine, M., Saleh, S., El-Jardali, F., Dimassi, H., and Mourad, Y., "The Retention of Health Human Resources in Primary Healthcare Centers in Lebanon: A National Survey," BMC Health Services Research, 12:419, 2012.
Alefan, Q., et al., Availability, prices and affordability of selected essential medicines in Jordan: a national survey. BMC Health Serv Res 18, 787 (2018).
Alliance for Health Policy and Systems Research and WHO, "Primary Health Care Systems (PRIMASYS) Comprehensive Case Study from Lebanon" (AHPSR, 2017).
Alshoubaki, W., & Harris, M. (2018).The impact of Syrian refugees on Jordan: A framework for analysis. Journal of International Studies, 11(2), 154-179. doi:10.14254/2071-8330.2018/11-2/11
Amnesty International, "Egypt: Health Care Workers Forced to Make Impossible Choice Between ‘Death or Jail’," June 18, 2020.
--- "Lebanon: Wave of Hostility Exposes Hollowness of Claims that Syrian Refugee Returns are Voluntary," June 12, 2019.
Arraf, J., "In Syria, An Orphanage Cares for Children Born to Yazidi Mothers Enslaved By ISIS," npr, June 6, 2019.
Assistance Coordination Unit, "Ar-Raqqa Governorate - Panoramic Report," December 2019.
--- "Epidemiological Weekly Bulletin - Syria, EWARN Week 23, 2020," May 31 - June 6, 2020.
Assyrian Policy Institute, "Lebanon," accessed June 6, 2020.
Aziz, M., and El-Gazzar, "Health care providers’ perceptions and practices of screening for domestic violence in Upper Egypt," Sexual and Reproductive Healthcare Journal, June 2019.

19 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
Baeha AM, Al-Daradkah SA, Khader YS, Basha A, Sabet F, et al. (2017) Cesarean Section: Incidence, Causes, Associated Factors and Outcomes: A National Prospective Study from Jordan. Gynecol Obstet Case Rep Vol.3: No.3: 55
Balanche, F., "Rojava's Sustainability and the PKK's Regional Strategy", The Washington Institute, April 24, 2016.
Barshad, A., "The World's Most Dangerous Census," The Nation, October 17, 2019.
Bayoumi, S., "Health and Social Justice in Egypt: Towards a Health Equity Perspective," World Social Science Report, 2016.
Brown, H, et al., Vulnerability Assessment Framework Population Study 2019. UNHCR.
CAPMAS, "Egypt Statistics," Accessed June 28, 2020.
Caritas Lebanon Migrant Center, "Left Behind: A Needs Assessment of Iraqi Refugees Present in Lebanon” (Caritas Lebanon Migrant Center, 2014).
Central Administration of Statistics, "Consumer Price Index for Lebanon April 2020 - CPI-COVID-19," April 2020.
Central Intelligence Agency, "The World Factbook: Lebanon" (CIA, June 2020).
Chehayeb, K. "Besides Coronavirus, Lebanon has an Equally Dangerous Outbreak on its Hands - Unemployment," The New Arab, March 29, 2020,
--- “Lebanon Is the Experiment That Shows Neoliberalism's Failure," The Century Foundation, April 16, 2020.
Chen, D. and Cammett, M."Informal Politics and Inequity of Access to Health Care in Lebanon," Int Journal Equity Health (May 2012).
CIA Factbook, Iraq Profile, 2020, accessed June 2020.
CIA, "World Factbook: Syria," Accessed June 22, 2020.
Davidson J., and Bethke, C., "Integrating Community-Based Nutrition Awareness into the Syrian Refugee Response in Lebanon," Field Exchange, accessed June 11, 2020.
Department of Statistics (DOS) and ICF. 2019. Jordan Population and Family and Health Survey 2017-18. Amman, Jordan, and Rockville, Maryland, USA: DOS and ICF.
DHS, "Overview of the Health System in Egypt," Accessed June 28, 2020.
DOS and ICF. Jordan Population and Family and Health Survey 2017-18.
EASO, Iraq Key Socio-economic Indicators February 2019, accessed June 2020.
Eghdamian,K. UCL, POLICY BRIEF Religious Minority Experiences of Displacement: Initial Lessons Learnt From Syrian Christian and Syrian Druze Refugees in Jordan, 2015, UCL Migration Research Unit.

20 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
Egyptian Streets, "Egypt’s Medical Syndicate Slams PM’s Statement ‘Blaming’ Doctors for COVID-19 Deaths," June 24, 2020.
El Wasl, Z., "Syrian Turkmen refugees face double suffering in Lebanon," October 2015.
El-Galil, T., "Egypt’s Doctors are Fleeing, Leaving Behind a Physician Shortage," Al Fanar Media, July 29, 2019.
Elhoseeny, T.A. and Mourad, J., "Assessment of the Safety of Injection Practices and Injection-Related Procedures in Family Health Units and Centers in Alexandria," Journal of the Egyptian Public Health Association, August 2014
El‐Kak, F., Kabakian‐Khasholian, T., Ammar, W., and Nassar, A., "A Review of Maternal Mortality Trends in Lebanon," International Journal of Gynecology & Obstetrics 148, no. 1 (October 2019).
El-Shabrawi, M., et al. “The burden of different pathogens in acute diarrhoeal episodes among a cohort of Egyptian children less than five years old.” Przeglad gastroenterologiczny vol. 10,3 (2015): 173-80. doi:10.5114/pg.2015.51186
European Union, Country Policy and information Not Iraq: Religious minorities, October 2019, accessed June 2020.
--- Country Policy and Information Note, Iraq: Medical and Healthcare issues, 2019, access June 2020.
--- Minorities in Iraq: Pushed to the brink of existence, February 2015, accessed June 2020.
FAO, "Siwa Oasis Egypt," May 2016.
Frakes, N., "'We Were Born Refugees' - Lebanon's Forgotten Refugee Camp," The World, November 1, 2018.
GBVIMS Task Force, Jordan GBV IMS Task Force / Annual Report 2019.
GC Catholic, "Chaldean Diocese of Beirut," accessed June 7, 2020.
--- "Syriac Diocese of Beirut," accessed June 7, 2020.
Gericke, C.A., Britain, K., Elmahdawy, M., and Elsisi G., "Health System in Egypt," Health Care Systems and Policies, May 16, 2018.
Gharbibah M. and Mehchy, Z., "COVID-19 Pandemic: Syria’s Response and Healthcare Capacity," March 25, 2020.
Global Burden of Disease Collaborative Network, Global Burden of Disease Study 2017 (GBD 2017) Results. Seattle, United States: Institute for Health Metrics and Evaluation, 2018.
--- Global Burden of Disease Study 2016 (GBD 2016) Results. Seattle, United States: Institute for Health Metrics and Evaluation (IHME), 2017.
Grogan, C., "Adopt a Family of Christian Refugees in Lebanon this Christmas," Catholic News Agency, December 14, 2019.

21 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
Hadidi, R., The Hashemite Kingdom of Jordan National Human Resources for Health Observatory Annual Human Resources for Health Report, 2017.
Hammoura, J., "Turkey’s Lost Treasure: Story of a Soldier and Lebanese Turkmen Community," New Eastern Politics, May 4, 2017.
Hassany, M., Abdel-Razak, W., Asem, N., et al., "Estimation of COVID-19 Burden in Egypt," Lancet Infectious Diseases, April 27, 2020.
HCR, Health Access and Utilization Survey Access to Healthcare Services Among Syrian Refugees in Jordan, December 2018.
Health Europa, "Fill That Gap Supports Community Health Workers in Lebanon,” November 21, 2019.
Health Sector Syria, "Health Projects Implementing Organizations in Al-Hasakeh," Accessed June 22, 2020.
--- "Health Sector Bulletin," January 2020.
Hemadeh, R., Kdouh, O., Hammoud, R., Jaber, T., and Khalek, L., "The Primary Health Care Network in Lebanon: a National Facility Assessment," East Mediterranean Health Journal (March 2019): https://doi.org/10.26719/emhj.20.003
Heydemann, S., "The Caesar Act and a Pathway Out of Conflict in Syria.”
High Health Council, National Human Resources for Health Strategy for Jordan (2018-2022), 2018.
Human Appeal, "Risking Death to Give Birth," May 15, 2020.
Human Rights Watch, Egypt World Report 2020.
--- Humanitarian Needs Assessment Programme, "COVID-19 Rapid Assessment, Syrian Democratic Forces Controlled Areas," April 7, 2020.
--- "Lebanon: COVID-19 Worsens Medical Supply Crisis," March 24, 2020.
--- Stateless Again Palestinian-Origin Jordanians Deprived of Their Nationality, 2010.
---"Syria: Aid Restrictions Hinder COVID-19 Response," April 28, 2020,
ICRC, "COVID-19: Millions Dealing with Sporadic Water Shortages, Crippled Health Services in North-East Syria," May 21, 2020.
IMC, WHO, and UNICEF, "The “4Ws” in Lebanon: Who’s Doing What, Where and Until When in Mental Health and Psychosocial Support," April 2015.
IMC. Utilization of Mental and Psychosocial Support Services among Syrian Refugees and Jordanians. 2019
IndexMundi, "Lebanon Demographic Profile 2019" (IndexMundi, 2019).

22 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
Institute for Health Metrics and Evaluation (IHME). Jordan profile. Seattle, WA: IHME, University of Washington, 2018.
International Trade Administration (ITA), Healthcare Resource Guide: Iraq (2018), accessed June 2020.
--- "Healthcare Resources Guide: Egypt," Accessed June 24, 2020.
IOM Iraq, Understanding Ethno-religious Groups in Iraq: Displacement and Return, February 2019, access June 2020.
IOM UN Migration, Displacement Tracking Matrix Iraq Mission, April 2020, accessed June 2020.
IRC, "IRC Data Reveals Staggering Child Mortality in Al Hol Camp, Northeast Syria - Urging Repatriation of Foreign Children," September 16, 2019.
Jaff, D., Tumlinson, K., & Al-Hamadani, A., Challenges to the Iraqi Health System Call for Reform, Vol III, Issue 2, Journal of Health Systems, December 2018, accessed June 2020.
Jomaa, L., Naja, F., Kharroubi, S., and Hwalla, N., "Prevalence and Correlates of Food Insecurity Among Lebanese Households with Children Aged 4–18 years: Findings of a National Cross-Sectional Study."
Jordan Ministry of Health and the Department of Statistics, Indicators of Health 2018.
Khaled, Lorenzen, and Zodrow (MSI), Evaluation Report on USAID Improving Health Services and Outcomes in the Ninewa Plains, Iraq, May 2020.
Khalil, D., "500 Leishmaniasis Infections in Aleppo, Drugs Insufficient," North Press Agency, May 9, 2020.
Knoema, "Egypt - Measles Reported Cases," 2018.
Komasawa, M, et. al. Demand for family planning satisfied with modern methods and its associated factors among married women of reproductive age in rural Jordan: A cross-sectional study. March 18, 2020.
Kondrashov, S., "Demographic Map" Lebanon Demographics (2013).
Kreidie, M., "Why Do So Few Christian Refugees Register with the United Nations High Commissioner for Refugees?," Rozenberg Quarterly, (2016).
Larsen, B., 2019. Egypt: Cost of Environmental Degradation: Air and Water
Lebanese Association for Democracy of Elections and Lamba Labs, "Lebanese Election Data," accessed June 7, 2020.
Lebanese Studies, "A Social Protection Emergency Response - A Bridge Toward a Comprehensive National Social Protection Plan," January 21, 2020.
Lebanon Protection Consortium, "COVID-19 Concerns and needs of Syrian refugees in Informal Tented Settlements in Lebanon," April 2020.

23 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
Local Agenda, "Position Paper on the Decision to Summarily Deport Syrian Nationals who Entered Lebanon Irregularly," 2019
Loza, N., "Overview on Mental Health services in Egypt," Accessed June 22, 2020.
LSOG, UNFPA, and MOPH, "Maternal Death Surveillance and Response - Annual Report 2017" (UNFPA, 2019).
Lyles, E., Hanquart, B., the LHAS Study Team, Woodman, M., and Doocy, S., "Health Service Utilization and Access to Medicines Among Syrian Refugee and Host Community Children in Lebanon."
Mahmoud, G., and Omar, A., "Women’s awareness and perceptions about maternal mortality in rural communities in Assiut and Fayoum Governorates, Egypt" Egyptian Nursing Journal, 2018.
Malsin, J., "Egypt Is Arresting Doctors Who Raise Alarms Over Coronavirus Approach," The Wall Street Journal, June 30, 2020.
Marston, J.C., "Sinai’s Bedouins Struggle to Preserve Their Timeless Way of Life," The Jerusalem Post, May 4, 2019
Médecins du Monde (MDM), Center for Refugee and Disaster Response (CFRD), International Medical Corps (IMC), "Syrian Refugee and Affected Host Population Health Access Survey in Lebanon" (UNHCR, July 2015).
Ministry of Education and Higher Education, MOPH, and WHO, "Global School-Based Student Health Survey: Lebanon" (UNHCR, 2017).
Minority Rights Group International, "An Uncertain Future for Syrian Refugees in Lebanon: The Challenges of Life in Exile and the Barriers to Return" (Minority Rights Group International, 2019).
--- "Lebanon," May 2020.
--- "World Directory of Minorities and Indigenous Peoples - Egypt," Accessed June 21, 2020.
Miranda, P., "Getting by on the Margins," Refugees in Towns, June 2018.
Moas, T., "Documentary on The Stateless Kurds of Syria," Rudaw, September 29, 2011.
MoH, Jordan Guidelines for the Management of Malnutrition, 2013.
--- The National Maternal Mortality Report 2018, 2018.
--- Health Indicators: Human Resources, accessed June 5, 2020.
Mohamoud, Y., Cuadros, D., and Abu-Raddad, L., "Characterizing the Copts in Egypt: Demographic, Socioeconomic and Health Indicators, The Jerusalem Post, May 4, 2019.
MOHP and The World Bank, "Transforming Egypt's Healthcare System Project," April 2018.
MOHP, El-Zanaty and Associates, and ICF International, "Egypt Demographic and Health Survey 2014," MOHP and ICF International, 2014.

24 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
--- "Egypt Health Issues Survey 2015," MOHP and ICF International, 2015.
MOPH, "EPHRP Dashboard," January–December 2018.
--- "Health Strategic Plan," December 2016,
--- “Mental Health and Substance Use - Prevention, Promotion and Treatment - Situation Analysis and Strategy for Lebanon 2015–2020" (MOPH, 2015).
--- "Statistical Bulleting 2018," 2018.
--- "Vital Data Observatory Dashboard," 2018.
MOSS and UNICEF, "Understanding Child Multidimensional Poverty in Egypt," December 2017.
MSF, "Treating Mental Health Outside of Specialized Settings," October 17, 2019.
MSI, Strengthening Health Outcomes through the Private Sector report, 2015, USAID.
Nashat, N. et al, Primary care healthcare policy implementation in the Eastern Mediterranean region; experiences of six countries: Part II, European Journal of General Practice, 2020, accessed June 2020.
Nasreddine, H., "Ethnic/Religious Communities in Egypt: Grievances and Inclusive Prospects," Baker Institute for Public Policy, October 5, 2018.
National Strategy for Combating Violence Against Women 2015.
NES Forum, "COVID-19 Update No.5," April 3-16, 2020.
No Lost Generation (NLG) MHPSS Task Force, "MHPSS Programmes for Children, Youth (0-24 years) and Parents/Caregivers in Syria and from Syria and Iraq Crises Affected Countries," January 15, 2020.
Norwegian Church Aid, GOPA-DERD, and ABAAD, "Gender-Based Violence in North-East Syria Rapid Needs Assessment," December 2019.
Nossier, S., "Violence Against Women in the Arab World," Journal of the Egyptian Public Health Association, September 2015.
OCHA Syria, "Situation Report #12: Humanitarian Impact of the Military Operation in Northeast Syria," November 1-19, 2019,
OCHA, "Assisting Survivors of Gender-Based Violence in Lebanon," December 13, 2019.
--- "Lebanon COVID-19 Emergency Appeal," May 7, 2020.
--- “Lebanon Humanitarian Fund Annual Report 2019 Lebanon" (OCHA, 2019.)
--- "Northeast Syria Crisis, Humanitarian Response Within Syria," October 9 - November 30, 2019,
--- "Syria Anniversary Press Release," March 6, 2020,
--- "Syrian Arab Republic: COVID-19, Humanitarian Update No.7," April 25, 2020,

25 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
--- "Syrian Arab Republic: COVID-19, Response Update No.6," June 19, 2020,
-- "Syrian Arab Republic: Governorates Profile," June 2014,
--- "Syrian Arab Republic: IDP Movements," April 2020,
--- Humanitarian Needs Overview 2020, Iraq. Issued November 2019, accessed June 2020.
--- Iraq Humanitarian Bulletin: April 2020, accessed June 2020.
OHCHR, ""They Have Erased the Dreams of My Children": Children's Rights in the Syrian Arab Republic," January 13, 2020,
--- "Report of the Independent International Commission of Inquiry on the Syrian Arab Republic," January 28, 2020
Oxfam, "Self-Protection and Coping Strategies of Refugees from Syria and Host Communities in Lebanon" (Oxfam, July 2015).
Pande, A., El Shalakani, A., and Hamed, A., "How Can We Measure Progress on Social Justice in Health Care? The Case of Egypt," Health Systems & Reform Journal, January 31, 2017,
PAX for Peace, "COVID-19 in Lebanon: Impact on Refugees and Host Communities," April 22, 2020,
Payne, D et al. “Multihospital Outbreak of a Middle East Respiratory Syndrome Coronavirus Deletion Variant, Jordan: A Molecular, Serologic, and Epidemiologic Investigation.” Open forum infectious diseases vol. 5,5 ofy095. 28 Apr. 2019
Pugliese-Garcia, M., Radovich, E., Hassanein, N. et al. Temporal and regional variations in use, equity and quality of antenatal care in Egypt: a repeat cross-sectional analysis using Demographic and Health Surveys. BMC Pregnancy Childbirth
REACH, "Collective Centers and COVID-19 Vulnerability," April 2020.
--- "Humanitarian Situation Overview in Syria (HSOS) Northeast Syria," April 2020.
--- "Northeast Syria: COVID-19 Multi-Sectoral Rapid Needs Assessment," April 2020.
--- "Rapid Needs Assessment of IDPs in Host communities, Hasakeh Governorate, Northeast Syria," February - March 2020.
Regional Refugee and Resilience Plan. 2019 Annual Report: Regional Refugee and Resilience Plan in Response to the Syria Crisis. 2020.
Relief Web, Five years after the genocide, Yazidis share their forgotten stories and demand justice, August 2019, accessed June 2020.
Reuters, "Some Medics Say They are Muzzled in Egypt’s Coronavirus Response," May 29, 2020.
--- The medical crisis that’s aggravating Iraq’s unrest, March 2020, accessed June 2020.
Rojava Information Center, "The Coronavirus Crisis in North and East Syria," April 19, 2020.

26 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
Samir, N., "32.5% of Egypt Population Live in Poverty," Daily News Egypt, July 29, 2019.
Schellen, T., "A Look into Lebanon's Healthcare," Executive Magazine, August 6, 2018.
Shatha, EN and Alastair A., Local faith community and civil society engagement in humanitarian response with Syrian refugees in Irbid, Jordan. 2015, Report to the Henry Luce Foundation. New York: Columbia University, Mailman School of Public Policy.
Shukor, A.R., Klazinga, N.S. & Kringos, D.S. Primary care in an unstable security, humanitarian, economic and political context: the Kurdistan Region of Iraq. BMC Health Serv Res 17, 592, 2017, accessed 2020.
Smith, N., "In Northern Syria, Destruction and Displacement Confront Health Workers," Direct Relief, October 27, 2019.
Sos, D., El-Gaafary, M., Wahdan, M., Wassif, G., et al., "Child Marriage: A Major Risky Behavior in Developing Egyptian Governorates," Al-Azhar Medical Journal, 2020.
Tamara Qiblawi, "75% of Lebanon Needs Aid After Coronavirus, and Hungry Protesters Are Back on the Streets," CNN, April 29, 2020.
Tawfik-Shukor, A. & Khoshnaw, H.,The Impact of health system governance and Policy processes on health services in Iraqi Kurdistan, Article 14, 2010, accessed June 2020.
The Economist, "Poor on the Nile, Egypt is Reforming its Economy, But Poverty is Rising," August 8, 2019.
The European Union, Country Policy and Information Note Iraq: Medical and healthcare Issues, May 2019, access June 2020.
The Guardian, "Egypt's Bedouins Begin to Demand Equal Citizenship Rights," June 17, 2020.
--- "Kurdish Medics Injured in Apparent Attack on Ambulance in Syria," November 10, 2019.
The National Committee for the Control of Hepatic Viruses, " Frequently Asked Questions," Accessed June 22, 2020.
The New Arab, "Lebanon Hospitals 'Discriminating Against' Undocumented Migrant Workers Seeking Vital Coronavirus Testing," March 29, 2020.
The New Humanitarian, Nowhere to go: Mosul residents in limbo as camps close, March 202, accessed June 2020.
The World Bank, "Data: Lebanon," accessed June 7, 2020.
Tsurkov E., and Jukhadar, Q., "Ravaged by War, Syria’s Health Care System is Utterly Unprepared for a Pandemic," Middle East Institute, April 23, 2020.
U.S Department of State, "International Religious Freedom Report," 2018.
--- "Lebanon 2018 International Religious Freedom Report." (U.S. State Department, 2018).

27 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
UN and MOPH, "Lebanon Crisis Response Plan 2017–2020.” (UN and MOPH, 2020),
UN News, Health Services for Syrian Women Caught Up in War, Foster Safety and Hope: UNFPA," January 23, 2020.
UN Security Council, "Review of Alternative Modalities for the Border Crossing of Ya'rubiyah," February 21, 2020.
--- Senior Officials Sound Alarm over Food Insecurity, Warning of Potentially ‘Biblical’ Famine, in Briefings to Security Council," April 21, 2020.
UN Strategic Steering Group, "2019 Humanitarian Needs Overview," March 2019.
UN WFP, Iraq Socio-Economic Atlas 2019, accessed 2020.
UN Women, Rapid Needs Assessment on the Impact of COVID-19, May 2020, accessed June 5, 2020.
--- "Lebanon: Prevalence Data on Different Forms of Violence Against Women" (UN Women, 2018).
UN, Iraq First National Voluntary Review on Sustainable Development Goals, 2019, accessed June 2020.
--- "2019 Humanitarian Response Plan," January - December 2019.
UNAIDS, "Country Factsheets: Lebanon"
--- "Country Factsheets Egypt 2018," Retrieved February 27, 2020.
UNFPA, "Gender-Based Violence in Egypt," Accessed June 23, 2020.
--- "Lebanon Scorecard on Gender-Based Violence," accessed June 6, 2020.
--- "North-East Syria Flash Update #13," February 1–29, 2020.
UNHCR Egypt, "Monthly Statistical Report April 2020,” 2020.
UNHCR Public Health Profile. First quarter 2019.
UNHCR, " Lebanon Health Programme" (UNHCR, 2019).
--- "Assessment of Mental Health and Psychosocial Support Services for Syrian Refugees in Lebanon" (UNHCR, December 2013).
--- "Lebanon Crisis Monitoring Dashboard," April 28, 2020,
--- "Operational Portal - Refugee Situations," accessed June 6, 2020,
--- "Vulnerability Assessment of Refugees of Other Nationalities in Lebanon" (UNHCR, 2018).
--- “Operational Portal: Situation Syria Regional Refugee Response,” accessed June 2, 2020,
--- COI Note on the Situation of Yazidi IDPs in the Kurdistan Region of Iraq, May 2019, accessed June 2020.

28 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
--- Fact Sheet Jordan, May 2019, accessed June 5, 2020.
--- Health Access and Utilization Survey Access to Healthcare Services Among Syrian Refugees in Jordan, December 2018.
--- Health Access and Utilization Survey Access to Healthcare Services in Jordan Among Iraqi Refugees, December 2017.
--- Health Sector Humanitarian Response Strategy Jordan 2019-2020, 2019.
--- Public Health Profile: First quarter 2019.
--- Jordan Fact Sheet October 2018.
--- Operational Portal Refugee Situations: Number of Partners, accessed June 5, 2020.
--- Progress Report Regional Refugee and Resilience Plan in Response to the Syria Crisis January – June 2019. 2019.
UNICEF, "A Familiar Face - Violence in the Lives of Children and Adolescents" (UNICEF, 2017).
--- "Health," Accessed June 28, 2020.
--- Key Demographic Indicators: Lebanon," accessed June 6, 2020.
--- "North East Syria Response - Situation Report," October 10-27, 2019.
--- “Palestinian Programme," accessed June 7, 2020.
--- Analysing equity in health utilization and expenditure in Jordan with focus on Maternal and Child Health Services, 2016.
--- Iraq 2020 Internal Displacement Crisis Humanitarian Situation Report, January to March 2020, accessed June 2020.
--- Iraq Multiple Indicator Cluster Survey (MICS) 2018, accessed June 2020.
--- "Defining Community Vulnerabilities in Lebanon" (UNHCR, 2015).
--- Situation Analysis of Children in Jordan 2017 Summary, 2017.
--- "Vulnerability Assessment for Syrian Refugees in Lebanon” (VASyR, 2019).
--- Water, Sanitation and Hygiene in Jordan. https://www.unicef.org/jordan/water-sanitation-and-hygiene
United Nations (WHO, UNICEF, UNFPA), Iraq Reproductive Maternal, Newborn, Child and Adolescent Health: Current Situation & Way Froward, 2017, accessed June 2020.
UNRWA, "Where We Work," accessed June 10, 2020.
--- Health Department Annual Report 2018, 2019.

29 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
US Commission on International Religious Freedom, Iraq USCIRF Annual Report 2020, accessed June 2020.
--- Policy Update: Protecting Religious Minorities in Northern Iraq, February 2020, accessed June 2020.
US State Department, Iraq 2018 International Religious Freedom Report, accessed June 2020.
USAID Country profile. Accessed June 24, 2020.
USAID, "Health and Population Fact Sheet," May 2019,
--- "COVID-19 Prevention, Preparedness and Response in NES," Final Y4Q4 Quarterly Report, Amman, June 2020.
--- "Situational Analysis of the Private Sector in the Delivery of Family Planning Services in Egypt: Current Status and Potential for Increased Involvement," May 2016,
--- "Syria Essential Services II, Ad Hoc Report: Status of Vulnerable Religious and Ethnic Minority Communities in NES," December 17, 2019.
--- "Syria Essential Services II, Extended Ad Hoc Report: The Status of Minority and Vulnerable Groups in Raqqa, Deir Ez-Zor, and Hasakeh," November 2018.
--- "Water and Sanitation," Accessed June 8, 2020.
USCIRF, "Annual Report 2020, Egypt - Recommended for Special Watch List," 2020.
--- "Syria - Recommended Countries of Particular Concern," 2019.
Vernier, L., Cramond, V., Hoetjes, M. et al. “High levels of Mortality, Exposure to Violence and Psychological Distress Experienced by the Internally Displaced Population of Ein Issa Camp Prior to and During their Displacement in Northeast Syria,” November 2017. Conflict and Health 13, 33 (2019).
WHO EMRO, "Maternal and Child Health," accessed June 7, 2020.
--- “Framework for Health Information Systems and Core Indicators for Monitoring Health Situation and Health System Performance," 2018.
WHO Health Cluster, Rapid Assessment of Health Services Response to GBV survivors during COVID, April 2020, accessed June 2020.
WHO Health Profile 2015. Accessed 6.20.2020.
WHO, "Country Cooperation Strategy at a Glance 2018," May 2018,
--- "Egypt Human Resources," Accessed June 22, 2020,
--- "Health Profile 2015 Egypt, " 2015,
--- “Health Profile 2015 Lebanon" (WHO, 2016).
--- “Measles - Lebanon" (WHO, October 2019).

30 | REM HEALTH NEEDS ASSESSMENT USAID.GOV
--- "Noncommunicable Diseases Country Profile: Lebanon," 2018,
--- "Syrian Arab Republic HeRAMS reports," Accessed June 22, 2020,
--- "WHO Delivers Health Supplies by Road to Northeast Syria," June 1, 2020,
--- "WHO Support to the Humanitarian Response in Lebanon" (WHO, 2016).
---“Health Profile Egypt 2015,” 2015,
--- Human Resource data – Global Health Observatory, accessed June 2020.
--- Improving availability of and access to essential and life-saving medicines and medical supplies in Iraq, March 2019, accessed June 2020.
--- Jordan COVID-19, accessed June 5, 2020.
--- Jordan Investing in family doctors to boost primary health care. Accessed June 5, 2020.
--- Dengue Fever Outbreak-Egypt. 2015. Disease Outbreak News.
Wikipedia, Palestinians in Jordan, accessed June 5, 2020.
World Bank Data. Accessed June 25, 2020.
World Bank Group, "Understanding Poverty and Inequality in Egypt," June 2019,
World Bank, "A Roadmap to Achieve Social Justice in Health Care in Egypt," January 2015,
--- "Egypt COVID-19 Emergency Response - Project Information Document," April 28, 2020,
--- "Supporting Egypt’s Universal Health Insurance System," December 13, 2019,
--- "Transforming Egypt's Healthcare System Project," June 6, 2018,
--- Iraq WB Open Data, accessed June 2020.
--- Jordan Overview.
Yehya N., and Dutta, M., "Health, Religion, and Meaning: A Culture-Centered Study of Druze Women," Qualitative Health Research 20, no. 6 (2010): 845–858.