Haemodynamical Variables Versus Endothelial Hormones in Hypertensive and Type 2 Diabetic Patients...
14
Haemodynamical Variables Versus Endothelial Hormones in Hypertensive and Type 2 Diabetic Patients With Endothelial Dysfunction Christian Fouillioux, MD, 1 * Freddy Contreras, MD, 2 Mary Lares, MgSc, 3 Luis Magaldi, MD, 2 Manuel Velasco, MD, FRCP Edin, 4 Claudia La Mayda, MD, 5 Betsy Pacheco, MD, 6 Joselyn Rojas, MD, 7 Maricarmen Chacı ´n, BSc, 7 Raquel Cano, MD, 7 Daniela Gotera, BSc, 7 and Valmore Bermu ´ dez, MD, MPH, PhD 7 Leptin is a 167 aminoacid peptidic hormone secreted by adipose tissue. It works mainly in the hypothalamus at thirst signal, but given its closed connections with inflammatory and endothelial systems, also has been postulated that it may exert a regulatory control over blood pressure (BP), interacting with nitric oxide (NO) and C reactive protein (CRP). The cold pressor test (CPT) is a simple test that indirectly determines endothelial dysfunction. In this work, biochemical indicators (CRP, leptin, and NO) and hemodynamic indicators (systolic and diastolic BP) were performed and evaluated in hypertensive, type 2 diabetic, and control subjects during a single CPT for assessment of endothelial dysfunction. A total of 43 subjects, males and females aged 25 to 60 years and divided in three groups, 15 healthy volunteers, 13 hypertensive patients, and 15 patients with type 2 diabetes, were included in the study. A complete clinical history was obtained from each subject, and a complete physical examination, including an electrocardiogram was carried out. During the assay of 30 minutes, 0.9% saline was infused intravenously. CPT was performed to assess the cardiovascular reactivity at minute 15. The cardiovascular variables (systolic and diastolic BP) were measured in minute 0, 16, and 30. In addition, serum variables were obtained at the beginning and at the end of the experiment, and statistical analysis was performed. CPT caused in all subjects a significant increase of BP and pulse. There were no significant differences to CPR and leptin in any group, although we observed significant differences for NO (P , 0.05). Sensitivity and specificity for all biochemical variables resulted in nonsignificant statistical or clinical importance as markers of endothelial dysfunction; however, a positive association was found when leptin and NO were evaluated together (sensitivity: 0.2; specificity. 0.8). CRP, leptin, and NO did not shown any direct and significant association with the hemodynamic variables in this study, although a relationship was noted between NO according to group and biochemical variables when studied altogether. Keywords: hypertension, type 2 diabetes mellitus, leptin, C reactive protein, nitric oxide 1 Clinical Imaging Department, University Hospital of Caracas, Caracas, Venezuela; 2 Medicine Faculty, Central University of Venezuela, Caracas, Venezuela; 3 Endocrinology and Metabolic Diseases Research Laboratory, Military Hospital ‘‘Dr. Carlos Arvelo,’’ Caracas, Venezuela; 4 Clinical Pharmacology Unit, Jose ´ Marı ´a Vargas School of Medicine, Central University of Venezuela, Caracas, Venezuela; 5 Department of Internal Medicine, ‘‘Victorino Santaella’’ Hospital, Los Teques, Estado Miranda, Venezuela; 6 Department of Anesthesiology, University Hospital of Caracas, Caracas, Venezuela; and 7 Endocrine and Metabolic Diseases Research Center, University of Zulia, School of Medicine, Zulia, Venezuela. This work was supported by research grant N° S1-2001000300 from the National Fund for Science, Technology and Innovation (FONACIT), Ministerio del Poder Popular para la Ciencia y la Tecnologı ´a, Repu ´blica Bolivariana de Venezuela. *Address for correspondence: Servicio de Radiologia, Hospital Universitario, Ciudad Universitaria, Los Chaguaramos Avenue, Caracas, 1040, Venezuela. E-mail: [email protected] American Journal of Therapeutics 17, 306–319 (2010) 1075-2765 Ó 2010 Lippincott Williams & Wilkins www.americantherapeutics.com
Transcript of Haemodynamical Variables Versus Endothelial Hormones in Hypertensive and Type 2 Diabetic Patients...

Haemodynamical Variables Versus Endothelial
Hormones in Hypertensive and Type 2 Diabetic
Patients With Endothelial Dysfunction
Christian Fouillioux, MD,1* Freddy Contreras, MD,2 Mary Lares, MgSc,3
Luis Magaldi, MD,2 Manuel Velasco, MD, FRCP Edin,4
Claudia La Mayda, MD,5 Betsy Pacheco, MD,6 Joselyn Rojas, MD,7
Maricarmen Chacın, BSc,7 Raquel Cano, MD,7 Daniela Gotera, BSc,7 andValmore Bermudez, MD, MPH, PhD7
Leptin is a 167 aminoacid peptidic hormone secreted by adipose tissue. It works mainly in thehypothalamus at thirst signal, but given its closed connections with inflammatory and endothelialsystems, also has been postulated that it may exert a regulatory control over blood pressure (BP),interacting with nitric oxide (NO) and C reactive protein (CRP). The cold pressor test (CPT) isa simple test that indirectly determines endothelial dysfunction. In this work, biochemical indicators(CRP, leptin, and NO) and hemodynamic indicators (systolic and diastolic BP) were performed andevaluated in hypertensive, type 2 diabetic, and control subjects during a single CPT for assessment ofendothelial dysfunction. A total of 43 subjects, males and females aged 25 to 60 years and divided inthree groups, 15 healthy volunteers, 13 hypertensive patients, and 15 patients with type 2 diabetes,were included in the study. A complete clinical history was obtained from each subject, anda complete physical examination, including an electrocardiogram was carried out. During the assayof 30 minutes, 0.9% saline was infused intravenously. CPT was performed to assess thecardiovascular reactivity at minute 15. The cardiovascular variables (systolic and diastolic BP) weremeasured in minute 0, 16, and 30. In addition, serum variables were obtained at the beginning and atthe end of the experiment, and statistical analysis was performed. CPT caused in all subjectsa significant increase of BP and pulse. There were no significant differences to CPR and leptin in anygroup, although we observed significant differences for NO (P , 0.05). Sensitivity and specificity forall biochemical variables resulted in nonsignificant statistical or clinical importance as markers ofendothelial dysfunction; however, a positive association was found when leptin and NO wereevaluated together (sensitivity: 0.2; specificity. 0.8). CRP, leptin, and NO did not shown any directand significant association with the hemodynamic variables in this study, although a relationshipwas noted between NO according to group and biochemical variables when studied altogether.
Keywords: hypertension, type 2 diabetes mellitus, leptin, C reactive protein, nitric oxide
1Clinical Imaging Department, University Hospital of Caracas, Caracas, Venezuela; 2Medicine Faculty, Central University of Venezuela,Caracas, Venezuela; 3Endocrinology and Metabolic Diseases Research Laboratory, Military Hospital ‘‘Dr. Carlos Arvelo,’’ Caracas,Venezuela; 4Clinical Pharmacology Unit, Jose Marıa Vargas School of Medicine, Central University of Venezuela, Caracas, Venezuela;5Department of Internal Medicine, ‘‘Victorino Santaella’’ Hospital, Los Teques, Estado Miranda, Venezuela; 6Department of Anesthesiology,University Hospital of Caracas, Caracas, Venezuela; and 7Endocrine and Metabolic Diseases Research Center, University of Zulia, School ofMedicine, Zulia, Venezuela.This work was supported by research grant N� S1-2001000300 from the National Fund for Science, Technology and Innovation(FONACIT), Ministerio del Poder Popular para la Ciencia y la Tecnologıa, Republica Bolivariana de Venezuela.*Address for correspondence: Servicio de Radiologia, Hospital Universitario, Ciudad Universitaria, Los Chaguaramos Avenue, Caracas,1040, Venezuela. E-mail: [email protected]
American Journal of Therapeutics 17, 306–319 (2010)
1075-2765 � 2010 Lippincott Williams & Wilkins www.americantherapeutics.com

INTRODUCTION
Recently, it has been concluded that adipocytes arenot just energy stores but also a source of metabolicallyactive substances such as tumor necrosis factor-a,angiotensinogen, prostaglandins, estrogens, and theob gene product leptin.1 Leptin is a peptidic hormonecomposed of 167 amino acids obtained from thetranscription of the ob gene, which was described forthe first time in 1994.2
This hormone is secreted primarily from the whiteadipose tissue, although it can also be found in brownadipose tissue.3 The main feature ascribed to thissubstance is the one of satiety signal acting in thehypothalamus, for which it has to go through the bloodbrain barrier,4 and it takes part in the signals related tothe regulation of ingestion of food: basically, inhibitingthe synthesis of the ‘‘Y’’ neuropeptide, which is a potentstimulator of appetite.5
Leptin achieves most of its metabolic effects inter-acting with specific receptors localized in the centralnervous system and peripheral tissues. The leptinreceptor is a class I cytokine, which are also membersthe interleukin 6 receptor, interferon receptor, and thegrowth hormone.6 It also expresses in other tissuessuch as kidneys, the cardiovascular system, hepato-cytes, haematopoyetical cells, and pancreatic islets.7
Because of the existence of peripheral receptors, leptinhas been associated with the development of obesityand arterial hypertension, it being a regulator andmetabolic integrator.8
Leptin secretion is proportional to the amount ofadipose tissue, and its plasmatic concentration increasesprofoundly in obese patients. This hyperleptinemia hasgiven rise to the ‘‘leptin resistance’’ hypothesis in obesepatients, in which a defect in the receptor or itsintracellular mediators would generate high levels ofthis hormone in plasma without achieving the prin-cipal goal completely, very much like insulin resistancesyndrome.9 It is because of this that the therapeutic useof leptin as an anti-obesity agent has not been able to beapplied because many obese patients are resistant tothis hormone.10
The relation between obesity and hypertension hasbeen widely documented for many years.11–18 It hasbeen speculated, given the strength of this relationship,that the adipose tissue acts as an important tissue inthe regulation of blood pressure, and, beyond the factthat the mechanisms involved in this theory are notcompletely understood,19 leptin has been establishedas the link between the two.20
When the sympathetic nerve terminations areremoved and leptin is administered, it produces a
vasodilatation that has been linked to the enhancedproduction of nitric oxide (NO) in a dose-dependentmanner.21 This synthesis of NO stimulated by leptintakes place in the endothelium,22,23 which is why it isalso denoted as endothelium-derived NO. In recentyears, the endothelium has been considered a paracrineorgan because it produces and secrets very largeamounts of contractile and relaxing factors.24 Nonethe-less, there is the possibility that not only is NO involvedin vasodilatation but that there is a cascade of eventsthat end in the same effect, probably with the inter-vention of factors such as endothelium-derived hyper-polarization factor.25
The chronic and continued administration of leptinin humans and animals with an intact central nervoussystem produces a sustained activity of the sympa-thetic system.26–28 The physiologic significance of thisfeature is related to metabolic and immunologic func-tions, and most importantly, it is related to regulationof arterial blood pressure (AP) because of the enhancedsympathetic activity which increases the pressurereflex.29–31
Given all this, the balance between the pressor effectof leptin, mediated by activation of the sympatheticeffect, and the hypotensive vasodilator effect willdetermine the end result of leptin over the regulationof AP.32 After the administration of leptin in healthyvolunteer subjects, when combining the vasodilatoreffect of the NO secretion and the sympathetic stim-ulation, no apparent change in AP was observed.33–35
The involvement of the adventitia in relation to leptinand arterial control has also been studied. The adven-titial layer, the outer capillary membrane, is made ofcollagen, elastic fibers, and the vasa vasorum. It wasconsidered for many years only a support layer, butrecent evidence suggest that it should be given morecredit for its functionality.36,37 These considerationsarise from the fact that many blood vessels aresurrounded by adipose tissue in variable amountsand the presence of perivascular fat diminishes theconstrictor response of the rat aorta when givennoradrenaline. This is a result of the release of theadipocyte-derived relaxing factor.38 Therefore, it hasbeen concluded that this tiny piece of tissue, which isremoved from the isolated organ preparations, not onlyhas a support function, but it also participates in thecontrol of vascular tone.36
C reactive protein (CRP) is an inflammatory marker,but in recent years it has been used as an indicatorof cardiovascular risk,39 even being considered a prog-nostic factor in stable angina and myocardial infarc-tion.40 CRP, by itself, can contribute to vascular diseaseby inhibiting NO synthetase, resulting in incrementalactivation of plasminogen inhibitor and causing direct
www.americantherapeutics.com American Journal of Therapeutics (2010) 17(3)
Hemodynamical Variables in Endothelial Dysfunction 307

proinflammatory effects over endothelial cells.41,42
CRP has been postulated as a marker for endothelialdysfunction, especially high-sensitivity CRP.43–45
CRP is synthesized primarily in the liver and isregulated by cytokines, of which the most important isinterleukin-6.46 To establish a relationship betweenCRP and leptin, because of the simple fact that both arefound in high concentrations in obesity and inflam-mation, their plasma levels have been examined inhealthy volunteer subjects, with the finding that thereis a positive association independent of factors such asbody mass index (BMI) or smoking or alcohol habits.47
Obesity is characterized by hyperleptinemia andhypothalamus resistance to its anorexic effect. Themajority of cases of obesity are also accompanied byhyperinsulinemia and insulin resistance.48 On the otherhand, insulin stimulates de production of NO, andthis effect is diminished in obesity.49 Another studydemonstrated that insulin and leptin share the samesignaling mechanism, including the activation of thephosphatidylinositol-3 kinase, which is involved in thesecretion of endothelial NO.35
In light of all the evidence relating obesity witharterial hypertension and leptin – insulin – NO, all ofthese in are encircled in the realms of endothelialfunctionalism.50–53 An indirect method of measuringthis functionalism is the cold pressor test (CPT).54–56
This test has been used since 1933 as an indicator of APchanges in subjects exposed to a standard stimulator.The procedure consists of the immersion of the handin cold water, at 4 to 6�C, for 1 to 2 minutes.57–59 Themenstrual cycle in women causes significant differ-ences in the CPT.60
The CPT, by way of the nociception pathways,activates the sympathetic system and enhances theoxygen demand from the myocardium (incrementalcardiac frequency and AP).61 When oxygen demandsare raised, a vasodilatation in the coronary arteries isproduced, and this mechanism is mediated by NOderived from the endothelium.58 This same testproduces a constriction in the atherosclerotic coronaryarteries in diabetic patients, which is an indicator ofendothelial dysfunction.62,63 Endothelial dysfunction ischaracterized by the reduction of the bioavailability ofvasodilators secreted by the endothelium, especiallyNO, and the elevation of the constrictor factors derivedfrom the same.64 This in the end leads to the existenceof a proinflammatory state65 because of the unbalanceof the regulatory forces.
The vascular endothelium is also a highly selectivepermeability barrier, which has many functions relatedto homeostasis, one being the principal regulator tissueof vascular tone.66 In response to various stimuli, itsecrets vasoactive substances, vasodilators such as
bradikinine, prostacyclin, histamine, P substance, andprincipally NO as the most powerful vasodilator, orvasoconstrictors, such as thromboxanes, araquidonicacid, prostaglandins, thrombin, nicotine, angiotensin II,and endothelin-1,67,68 the last two being the mostpowerful vasoconstrictor substances.65 All of these sub-stances participate directly or indirectly in the regula-tion of vascular tone and in homeostasis, and it isclearly observable that endothelial dysfunction is alwayspresent in arterial hypertension either as a primaryphenomenon or as a consequence of elevated AP.69
Purpose
The purpose of this study was to evaluate biochemicalmarkers (CRP, leptin, NO) and hemodynamic variablesin endothelial dysfunction (systolic and diastolicarterial pressure [SAP and DAP]) during the CPT inhypertensive and type 2 diabetic subjects.
METHODOLOGY
This study was revised and approved by CENABI(Bioethics National Center) and by the Bioethicalcommittee of FONACIT (National Found for Science,Technology and Investigation). The CENABI alsosupervised and ensured that all experiments wereperformed under good clinical practice and under thenorms set forth in the bioethics code of humanexperimentation.70
Forty-two subjects were selected, between the ages of18 and 60 years, both male and female, and distributedin the following manner: 14 healthy subjects, 13hypertensive subjects, and 15 subjects with type 2diabetic diagnoses. Hypertensive and diabetic patientshad greater than 5 years of disease evolution sinceprimary diagnosis.
The method of selection was random, using aninquiry about cardiovascular risk factors at the out-patient Diabetes Clinic in the Department of InternalMedicine of the ‘‘Victorino Santaella’’ Hospital, in thetime interval of February 2005 to April 2005. Writtenconsent was obtained from all patients, The hyperten-sive nondiabetic and control subjects were selectedthrough a preventive care program in the same clinic.The diabetic condition was defined using the AmericanDiabetes Association criteria published in 2004. Thehypertensive condition was defined following therecommendations of the VI Joint Committee on Pre-vention, Detection, Evaluation and Treatment of HighBlood Pressure, 1997, by dividing the hypertensivegroup into hypertensive class 1, subjects with a DAPbetween 90 and 105 mm Hg, and hypertensive class 2,subjects with DAP between 105 and 114 mm Hg.
American Journal of Therapeutics (2010) 17(3) www.americantherapeutics.com
308 Fouillioux et al
For the selection of patients, the following criteriawere used.
Inclusion criteria
1. Written consent from the patient to be enrolled inthe study.
2. Arterial hypertension class 1 or 2 (for the hyper-tensive group).
3. Isolated systolic arterial hypertension (for thehypertensive group).
4. Type 2 diabetes mellitus (for the diabetic group).5. No disease (for the healthy control group).
Exclusion criteria
1. Severe alcoholic habit (CAGE 3) (Ewing, 1984).2. Small size (weight # 40 Kg and/or BMI $
19 kg/m2).3. Associated diseases: thyrotoxicosis, Cushing’s
syndrome, rheumatoid arthritis, hemolytic ane-mia, hepatopathy, hyperparathyroidism, Paget’sdisease, terminal renal insufficiency, intestinalmalabsorption syndrome, type 1 diabetes melli-tus, acute ischemic cardiopathy, and arterialhypertension with recent target organ damage(last 6 mo); for this last criterion, a profile of basiclaboratory tests were performed (glycemia, bloodurea nitrogen, creatinine, urine test, electrocardio-gram [EKG], retinal examination), and a completemedical history was taken.
4. Use of medications such as levothyroxin forthyroid hormone replacement, glucocorticoids,insulin, sildenafil, labetalol, bromocriptin, adren-ergic blockers, and stimulants.
During the first part of the study, a survey asked for thefollowing details: family history, physical activity,cardiovascular risk factors, hypertension, diabetes,dyslipidemias, smoking habits, alcohol consumption,nutritional treatment, pharmacologic treatment. Thelaboratory examinations included red blood cell count,white count and formula, hemoglobin, platelets, basalglycemia, blood urea nitrogen, and creatinine.In the second part of the study, anthropometric
parameters were measured: weight, height, BMI, aswells as hemodynamic variables. Once patients wereselected, they were separated into three groups: 14control healthy volunteers, 13 hypertensive class 1 and2 subjects, and 15 diabetic subjects; the last two groupswere metabolically and hemodynamically compensated.For the execution of this controlled experimental
clinical study, which lasted 30 minutes, each subjecthad an appointment at 7:00 AM in the morning,according to a chronogram made over a period of
6 months (June–December 2005), maintaining thesebasic conditions:
� Fasting of 14 hours.� No exercise or physical activity in the day beforethe study.
� Five day stop of any hypertensive treatment.� Oral hypoglycemic medications were stoppedduring the test day only.
On the test day, the patients were examinedaccording to this protocol:
� Arterial blood pressure using a mercury sphyg-momanometer and a Dynamap.
� Heart frequency with EKG.
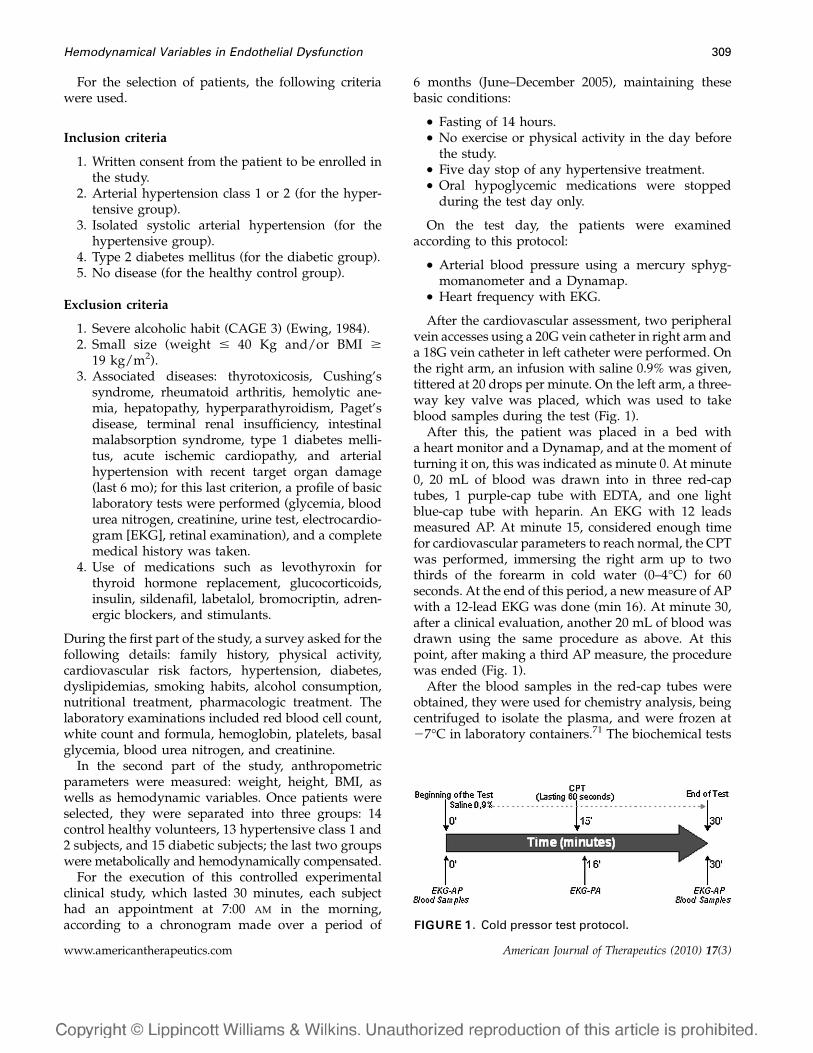
After the cardiovascular assessment, two peripheralvein accesses using a 20G vein catheter in right arm anda 18G vein catheter in left catheter were performed. Onthe right arm, an infusion with saline 0.9% was given,tittered at 20 drops per minute. On the left arm, a three-way key valve was placed, which was used to takeblood samples during the test (Fig. 1).After this, the patient was placed in a bed with
a heart monitor and a Dynamap, and at the moment ofturning it on, this was indicated as minute 0. At minute0, 20 mL of blood was drawn into in three red-captubes, 1 purple-cap tube with EDTA, and one lightblue-cap tube with heparin. An EKG with 12 leadsmeasured AP. At minute 15, considered enough timefor cardiovascular parameters to reach normal, the CPTwas performed, immersing the right arm up to twothirds of the forearm in cold water (0–4�C) for 60seconds. At the end of this period, a newmeasure of APwith a 12-lead EKG was done (min 16). At minute 30,after a clinical evaluation, another 20 mL of blood wasdrawn using the same procedure as above. At thispoint, after making a third AP measure, the procedurewas ended (Fig. 1).After the blood samples in the red-cap tubes were
obtained, they were used for chemistry analysis, beingcentrifuged to isolate the plasma, and were frozen at27�C in laboratory containers.71 The biochemical tests
FIGURE 1. Cold pressor test protocol.
www.americantherapeutics.com American Journal of Therapeutics (2010) 17(3)
Hemodynamical Variables in Endothelial Dysfunction 309
were made with this plasma, taken at minute 0 andminute 30:
a. Leptin was measured using the ‘‘Immunoradiomet-ric Assay’’ from Diagnostic Systems Laboratories(Webster, TX, USA).72
b. High-sensitivity CRP was measured by immunitur-bidimetry with a Tina-quant CRP kit obtained fromBoehringer Mannheim Systems (Mannheim,Germany).73
c. NO was measured by colorimetric analysis with a kitobtained from Cayman Chemical Company.74
After applying the CPT, the patients were groupedaccording to their reactivity (positive or negative)taking as criteria the change in AP value.58 Thedifference between SAP and DAP was calculated atminute 0 and minute 15:75
DSAP0–15: SAP0 – SAP15DDAP0–15: DAP0 – DAP15If DSAP0–15 $ 15 mmHg and/or DDAP0–15 $ 12 mm
Hg, it was considered a positive reaction, a situationexpected in those with endothelial dysfunction.56,58,76 IfDSAP0–15 , 15 mmHg and/or DDAP0–15 , 12 mmHg,it was considered a negative reaction.
Various definitions have been proposed for a reactiveCPT, including 10 mm Hg elevations in SAP58 until200 mm Hg.77 In the report of Woisetchlager,78 anincremental rise of 14.1 mm Hg in the SAP during theCPT was enough to predict preeclampsia in pregnantwomen. In this study, the cut-off was 15 mm Hg toconsider it a mean value change in pressure.
In reality, this occurred at minute 16 (the minute afterfinished the CPT), but it will be taken as minute 15 tosimplify the measure the CPT.
Statistical analysis
Descriptive tests were applied (median, standarddeviation, and percentages) to the hemodynamic andbiochemical variables. The correlations between twodifferent obtained values were based on parametriccorrelation coefficients such as ANOVA and x2 . It wasconsidered significant at P , 0.05 and highly signifi-cant at P , 0.01. For the sensitivity and specificityanalysis, the Bayes Theorem79,80 was applied:
Sensitivity = TP/(TVP + FN)Positive predictive value = TP/(TP + FP)Specificity = TN/(TN + FP)Negative predictive value = TN/(TN + FN)For all statistical analyses, SPSS 13.0 for Windows
was used (SPSS, Inc., Chicago, IL).
RESULTS
As can be observed in Table 1, there was a significantdifferences in age among the study groups, but nodifference was seen in the BMI of the participants. Of 43total eligible subjects, 53.5% were males and 46.5 %were females (Table 2). The changes observed incardiovascular clinical variables during the CPT arelisted in Table 3 and Figure 2.
There were no statistically significant differencesduring the study period for any of the biochemicalvariables in this study (Table 4), but there weredifferences among the groups for NO (P , 0.05).When a linear comparison was made between repeatedmeasures, no significant differences in time or in groupvariables were observed (Table 5).
The difference between the AP at minute 0 andminute 15 (DSAP0–15 and DDAP0–15) correlated withbiochemical parameters were graphically represented,and a linear regression was applied. The results of thesedispersions are shown in Figures 4 to 6.
In Figure 4, there is a mild negative correlation seenbetween the levels of leptin and the change in SAP and
Result of Test Pathology Present Absent PathologyPositive True positives (TP) False positives (FP)Negative False negatives (FN) True negatives (TN)
Table 1. Distribution by age and body mass index (BMI) according to each study group.
Variables Healthy Diabetic Hypertensive Total P
Age (yr) 37.8 6 6.9 47.5 6 5.5 45.6 6 4.4 43.5 6 7.1 0.001BMI (kg/m2) 28.5 6 4.2 28.2 6 4.1 29.4 6 6.5 28.7 6 4.9 0.815
Values expressed as median 6 standard deviation.
Table 2. Distribution by sex according to eachstudy group.
Variable
Healthy Diabetic Hypertensive Total
n % n % n % n %
SexMale 7 46.7 10 66.7 6 46.2 23 53.5Female 8 53.3 5 33.3 7 53.8 20 46.5
American Journal of Therapeutics (2010) 17(3) www.americantherapeutics.com
310 Fouillioux et al

DAP during the CPT. In this figure, leptin at minute0 was used because there were no significant differ-ences at the various moments samples were taken(Table 4). In Figure 5, a mild negative correlation forCRP in the regression curve is seen. The CRP at minute0 was used in this figure. Correlation between levels ofNO and the CPT is illustrated in Figure 6, showinga reduced positive association, with a regressioncoefficient value of 0.003 for SAP and 0.002 for DAP.
With use of a Bayesian model of analysis, theprevalence, specificity, and sensitivity of leptin asa marker for CPT reactivity was calculated (Table 6).The cut-off point is shown in Table 5. In Table 6, thesesindexes were calculated for CRP. By applying the same
Table 3. Linear model for general repeated measures of heart rate, SAP, DAP, and AMP according to each study group.
Groups n 0 min 15 min 30 min
HR (beat/min)*Healthy 14 71.3 6 11.2 68.1 6 9.8 68.7 6 9Diabetic 15 74.9 6 13.6 70.7 6 12.1 71 6 13.8Hypertensive 13 66.6 6 8 62.6 6 9.9 69.5 6 10.8
SAP (mm Hg)†Healthy 15 121.5 6 10.5 127.3 6 11.7 121.6 6 12.5Diabetic 15 134 6 15 141.8 6 16.3 132.2 6 16.1Hypertensive 13 149.8 6 20.1 162 6 20.5 160 6 16.5
DAP (mm Hg)‡Healthy 15 74.2 6 9.8 78.3 6 11.2 72.9 6 8Diabetic 15 80.4 6 9.1 83.9 6 11.5 79 6 9.1Hypertensive 13 88.6 6 10.5 93.7 6 12 92.7 6 10.4
MAP (mm Hg)§Healthy 15 89.8 6 10.3 96.7 6 9.4 91.9 6 9Diabetic 15 97.8 6 12.3 104.9 6 14 95.7 6 9.8Hypertensive 13 107.2 6 10.7 117.9 6 13 113.3 6 12.4
*Time: F = 1.125 (P = 0.295). Groups: F = 1.282 (P = 0.289). Time 3 Group: F = 3.133 (P = 0.054).†Time: F = 4.009 (P = 0.052). Groups: F = 18.722 (P = 0.000). Time 3 Group: F = 6.541 (P = 0.003).‡Time: F = 0.208 (P = 0.651). Groups: F = 11.663 (P = 0.000). Time 3 Group: F = 3.338 (P = 0.046).§Time: F = 2.809 (P = 0.102). Groups: F = 15.243 (P = 0.000). Time 3 Group: F = 3.703 (P = 0.033).Values expressed as median 6 standard deviation.DAP, diastolic arterial pressure; HR, heart rate; MAP, mean arterial pressure; SAP, systolic arterial pressure.
FIGURE2. Changes in AP before and after CPT, accordingto each group.
Table 4. Linear model for general measures at minute0 and 30 of nitric oxide, leptin, and C reactive protein(CRP) according to each study group.
Groups n 0 min 30 min
Nitric Oxide (uM)*Healthy 15 18.9 6 5.3 18.1 6 6.5Diabetic 15 21.4 6 6.4 23.8 6 8.8Hypertensive 13 29.3 6 17.4 30.3 6 16
Leptin (ng/mL)†Healthy 15 22.9 6 23.3 23.2 6 24.7Diabetic 15 20.3 6 19.4 20.4 6 20Hypertensive 13 13 6 12.5 13.2 6 13.1
CRP (mg/dL)‡Healthy 15 0.41 6 0.20 0.42 6 0.20Diabetic 15 0.48 6 0.25 0.44 6 0.23Hypertensive 13 0.64 6 0.65 0.68 6 0.61
*Time: F = 0.773 (P = 0.385). Groups: F = 4.195 (P = 0.022). Time 3
Group: F = 1.058 (P = 0.357).†Time: F = 0.247 (P = 0.622). Groups: F = 0.935 (P = 0.401). Time 3
Group: F = 0.079 (P = 0.924).‡Time: F = 0.172 (P = 0.680). Groups: F = 1.520 (P = 0.231). Time 3
Group: F = 4.736 (P = 0.014).Values expressed as median 6 standard deviation.
www.americantherapeutics.com American Journal of Therapeutics (2010) 17(3)
Hemodynamical Variables in Endothelial Dysfunction 311

model, the relation between CPTand NOwas analyzed(Table 6). The cut-off point was made by consideringthe values obtained as shown in Table 6.
DISCUSSION
The standard procedure used to diagnose endothelialdysfunction is the measurement of arterial diameters
using ultrasound of the brachial artery. This is achievedby provoking an hyperemia reaction using acetylcho-line and then measuring the diameter of the artery.81
Nonetheless, this test is less practical because of itscomplexity and the high price of the necessaryequipment. For some time now, the use of biochemicalparameters with the purpose of avoiding use of this testand to provide simpler and lower-cost methods toprove the existence of endothelial dysfunction andmetabolic pathways alterations have been undertaken.
Table 5. Linear model for general measures at minute0 and 30 of leptin (ng/mL), C reactive protein (CRP), andnitric oxide according to reactivity during cold pressortest (CPT) and time.
Reactivity n 0 min 30 min
Leptin (ng/mL)*CPT+ 21 15.41 6 18.5 15.73 6 20.18CPT– 22 22.89 6 19.61 22.86 6 19.91
CRP (mg/dL)†CPT+ 21 0.51 6 0.22 0.53 6 0.30CPT– 22 0.50 6 0.25 0.49 6 0.25
Nitric Oxide (uM)‡CPT+ 21 25.35 6 14.41 26.95 6 13.92CPT– 22 20.45 6 6.32 20.46 6 8.01
*Time: F = 0.284 (P = 0.621). Group: F = 1.503 (P = 0.227). Time 3
Group: F = 0.363 (P = 0.550).†Time: F = 0.037 (P = 0.847). Group: F = 0.028 (P = 0.869). Time 3
Group: F = 2.602 (P = 0.114).‡Time: F = 0.722 (P = 0.401). Group: F = 2.932 (P = 0.094). Time 3
Group: F = 0.700 (P = 0.408).Values expressed as median 6 standard deviation.
FIGURE 3. Differences in CPT proportions according toeach reactivity group.
FIGURE4. Relation between differences of AP before andafter CPT and leptin.
FIGURE 5. Relation between difference of AP before andafter CPT and levels of RCP.
American Journal of Therapeutics (2010) 17(3) www.americantherapeutics.com
312 Fouillioux et al

In this study, NO, CRP, and leptin were testedas biochemical markers for endothelial dysfunctionin a population of hypertensive and diabetic patients,using an indirect indicator for dysfunction called theCPT. The sample population studied showed charac-teristics that limited the analysis of factors such as ageand elevated BMI. The mean BMI was 28.7 kg/m2,
without significant differences among the three groups,so it can be established that all patients involved inthis study (even the healthy subjects) were overweightaccording to classification.82 Likewise, significant dif-ferences were observed in the age ranges of the groups,which makes them heterogeneous and contaminatedfor other comparisons. Even so, some valuable findingswere obtained.With respect to the hemodynamic variables, some
significant differences were observed among thevariables within the groups (P , 0.01) and for SAPand time, with a value of P = 0.05. When time andgroup are correlated, another significant difference isseen (P , 0.05) among all variables. Change in APwas more serious in hypertensive patients, as seenin Figure 2. The mean difference was positive for allgroups. These results were expected and concur withthe results observed in the literature.The distribution according to CPT (Fig. 3) shows
a steady proportion between the healthy and thediabetic and hypertensive groups; the latter had 7%patients with a reactive CPT in comparison with theother two. It was expected that the control groupwould have the most patients with a nonreactive CPT,but the small difference seen between the groups can beattributed to the limitations mentioned above. To thisdistribution, a x2 test was applied, obtaining x2 = 0.803,without any statistical significant difference seenbetween the groups (P = 0.669).In other studies, it has been determined that up to
29.7% of normal subjects can have a positive reactiveCPT.83 This is a result of the fact that normal subjectscan have endothelial dysfunction, particularly thosewith family history of hypertension, which underlinesa genetic predisposition to this disease.56,58 Thus, thebiochemical markers were compared with the hemo-dynamic indicators based on the reactivity of the CPT.In our groups, leptin and NO showed numericaldifferences in media, but had high standard deviationsand no statistical differences. For better visualization ofthe levels of leptin and NO as based on CPT reactivity,a histogram of frequencieswas constructed (Figs. 5 and 6).Leptin showed an inverse distribution to pressure
change in the CPT. In Figure 7, the normality curve isseen to move to the left in CPT+ patients in respect toCPT- patients (median approximately 15 vs. 22ng/mL). As was previously mentioned, leptin tendsto be elevated in obese patients and diminished inthose of normal weight, for which BMI was evaluatedaccording to the reactivity to CPT distribution groups(Table 7).As can be observed, there were no significant
differences in the BMI in this distribution because allpatients were overweight. The mild difference caused
FIGURE 6. Relation between difference of AP before andafter CPT and levels of NO.
Table 6. Prevalence, specificity, and sensitivity of leptin,C reactive protein (CRP), and NO + leptin as marker forcold pressor test (CPT) reactivity.
CPT+ CPT-
n = 43* Reactivity (cases)Leptin $ 23 ng/mL 5 8Leptin , 23 ng/mL 16 14
n = 43†CRP $ 0.5 mg/dL 9 12CRP , 0.5 mg/dL 13 9
n = 43‡NO $ 20 mMol 14 13NO , 20 mMol 7 9
n = 43§NO + elevated leptin 4 5NO + low leptin 17 17
*Prevalence: 0.4884. Sensitivity: 0.2381. Specificity: 0.6364. Posi-tive predictive value: 0.3846. Negative predictive value: 0.4667.†Prevalence: 0. 5116. Sensitivity: 0.4091. Specificity: 0.4286.Positive predictive value: 0.4286. Negative predictive value:0.4091.‡Prevalence: 0.4884. Sensitivity: 0.6667. Specificity: 0.4091. Posi-tive predictive value; 0.5185. Negative predictive value: 0.5625.§Prevalence: 0.4884. Sensitivity: 0.1905. Specificity: 0.7727.Positive predictive value: 0.4444. Negative predictive value: 0.5.
www.americantherapeutics.com American Journal of Therapeutics (2010) 17(3)
Hemodynamical Variables in Endothelial Dysfunction 313

the displacement of the curves in Figure 7, but otherstudies must be done to support this finding.
Correlations were made between biochemical in-dicators and changes in AP during the CPT, as can beseen in Figures 4 to 6. In none of the correlations wasa significant difference found, only mildly negativecurves for leptin and positive curves for NO (Fig. 8),which supports the previous finding of a mayorpositive change in AP, lesser are the levels of serumleptin in patients. In regard to NO, in nonreactivepatients, the values of NO were a bit lower than inthose with CPT+ tests, which concurs with otherinvestigations in which low levels were found inhealthy patients and vice versa.84–86
The application of sensitivity, specificity, positive andnegative predictive values, and prevalence of leptinversus CPT (Table 6) showed no evidence of any highcorrelation among these measures. This was also seenwith correlations of CRP and NO with CPT (Table 6).
To determine the relationship between CRP and NO,a linear regression curve was applied, separating thegroups according to their reactivity to the CRP andtaking into consideration the average weight of eachgroup during association. As seen in Figure 9, thestrongest association was seen in the CPT+ group.
All of this data indicates that there was nota significant statistical correlation between CPT andNO, but there is in fact a relation between thesemarkers. If we consider that in hypertension there isa persistent inflammatory state in the endothelial realmand that this inflammation generates some degree ofendothelial dysfunction, the observed elevated levelsof NO are not enough to produce a vasodilatorresponse. There is still some controversy over theclinical use of NO, even after the differences betweennitrate (NO3
2) and nitrite (NO22) levels have been
established. These components help to measure NO,and it has been demonstrated that levels of nitrite arethe main indicators of the functionality of theendothelial NO synthethase but not the nitrates.87
To enhance the value of our results, it would benecessary to establish the predominant type of NOand determine the quantity of oxygen reactive speciespresent because the latter are determinant in theeffectiveness of plasma NO.88 In addition, recentevidence shows that levels of NO differ dependingon the kind of sample taken, arterial or venous, withlevels being lower in the venous samples.89 A linearregression curve between leptin and NO according to
FIGURE 7. Histogram of frequencies of leptin values according to reactivity to CPT.
Table 7. Body mass index (BMI) according to coldpressor test (CPT) reactivity.
Reactivity
Reactivity (cases)
n BMI
CPT+ 21 27.44 6 4.43CPT- 22 29.91 6 5.1
Values expressed as median 6 standard deviation. Groups: F =2.880 (P = 0.097).
American Journal of Therapeutics (2010) 17(3) www.americantherapeutics.com
314 Fouillioux et al

their reactivity in the CPT and group was made (Figs.10 and 11).An inverse relation was observed between the
subjects with a negative CPT, and this difference waseven higher when subjects were separated according toexperimental groups: healthy and diabetic patients hadnegative correlations, while, the hypertensive patientshad a positive correlation.
It was previously determined that the group witha negative CPT had a slightly higher BMI than in thosewith a positive CPT. In this last group, the followingphenomena was observed: the higher the leptin, thehigher the NO. Seeing that leptin increases in a directproportion to BMI and NO increases according to thedegree of endothelial dysfunction and that hyperten-sive patients have endothelial dysfunction, it is not
FIGURE 8. Histogram of frequencies of NO values according to reactivity in CPT.
FIGURE 9. Relation between CRP and NO according to CPT reactivity.
www.americantherapeutics.com American Journal of Therapeutics (2010) 17(3)
Hemodynamical Variables in Endothelial Dysfunction 315

difficult to hypothesize that, if both indicators areelevated, this would enhance the specificity of de-termining a real endothelial dysfunction. This isbecause an elevated NO with low leptin is morereasonable in normal patients, and both are elevated inhypertensive patients. With this in mind, prevalence,specificity, and sensitivity were calculated for elevated
leptin and NO, as shown in Table 6. The problem withthis reasoning is demonstrated by the diabetic pop-ulation because, in the natural history of the disease,some degree of endothelial dysfunction is alsoencountered. It is plausible that more studies witha larger population will clarify this issue and establisha true clinical application for these indicators.
FIGURE 11. Relation between leptin and NO according to each group.
FIGURE 10. Relation between leptin and NO according to CPT reactivity.
American Journal of Therapeutics (2010) 17(3) www.americantherapeutics.com
316 Fouillioux et al

Another important point of discussion is thata positive CPT reactivity does not always result inendothelial dysfunction, as this can be seen when thereare some alterations of such pathways measured in theCPT. In this article, it was assumed that all patients hadno nervous conduction alteration, which is required fora physiologic response in the CPT, and all estimationsof sensitivity and specificity were made based on this.
CONCLUSIONS
In this study, it was demonstrated that there is animportant relation between biochemical markers andhemodynamic variables in the studied populations.The markers NO and leptin proved to be independentmarkers for endothelial dysfunction without regardto BMI or preexisting pathology, with a high specificitybut lacking any important sensitivity. Subsequentstudies are needed to shed more light on these data.The CPT has been established as a highly potent
tool for the evaluation of underlying mechanismsof cardiovascular disease development as well asendocrine diseases. This has also been proven in otherinvestigations,75,60,90–92 with CPT being used in variousapplications. The present study also demonstrates itsusefulness and recommends its application in futureresearch.
REFERENCES
1. Stenvinkel P. Leptin and blood pressure–is there a link?Nephrol Dial Transplant. 2000;15:1115–1117.
2. Zhang Y, Proenca R, Maffei M, et al. Positional cloning ofthe mouse obese gene and its human homologue. Nature.1994;372:425–432.
3. Auwerx J, Staels B. Leptin. Lancet. 1998;351:737–742.4. Banks WA, Kastin AJ, Huang W, et al. Leptin enters the
brain by a saturable system independent of insulin.Peptides. 1996;17:305–311.
5. Naveilhan P, Hassani H, Canals JM, et al. Normal feedingbehavior, body weight and leptin response require theneuropeptide Y Y2 receptor. Nat Med. 1999;5:1188–1193.
6. Tartaglia LA. The leptin receptor. J Biol Chem. 1997;272:6093–6096.
7. Margetic S, Gazzola C, Pegg GG, et al. Leptin: a reviewof its peripheral actions and interactions. Int J Obes RelatMetab Disord. 2002;26:1407–1433.
8. Friedman JM, Halaas JL. Leptin and the regulation ofbody weight in mammals. Nature. 1998;395:763–770.
9. Considine RV, Sinha MK, Heima ML, et al. Serumimmunoreactive-leptin concentrations in normal-weightand obese humans. N Engl J Med. 1996;334:292–295.
10. Cock TA, Auwerx J. Leptin: cutting the fat off the bone.Lancet. 2003;362:1572–1574.
11. Hovell MF. The experimental evidence for weight-losstreatment of essential hypertension: a critical review. Am JPublic Health. 1982;72:359–368.
12. Kannel WB, Brand N, Skinner JJ Jr, et al. The relation ofadiposity to blood pressure and development of hyper-tension. The Framingham study. Ann Intern Med. 1967;67:48–59.
13. Masuo K, Mikami H, Ogihara T, et al. Familial obesity,sympathetic activation and blood pressure level. BloodPress. 1200;10:199–204.
14. Niskanen L, Laaksonen DE, Nyyssonen K, et al. In-flammation, abdominal obesity, and smoking as predic-tors of hypertension. Hypertension. 2004;44:859–865.
15. Rahmouni K, Correia ML, Haynes WG, et al. Obesity-associated hypertension: new insights into mechanisms.Hypertension. 2005;45:9–14.
16. Sharma AM, Grassi G. Obesity and hypertension: causeor consequence? J Hypertens. 2001;19:2125–2126.
17. Thakur V, Richards R, Reisin E. Obesity, hypertension,and the heart. Am J Med Sci. 2001;321:242–248.
18. York DA, Rossner S, Caterson I, et al. PreventionConference VII: obesity, a worldwide epidemic relatedto heart disease and stroke. Group I: worldwide de-mographics of obesity. Circulation. 2004;110:E463–E470.
19. Davy KP, Hall JE. Obesity and hypertension: twoepidemics or one? Am J Physiol Regul Integr Comp Physiol.2004;286:R803–R813.
20. Aizawa-Abe M, Ogawa Y, Masuzaki H, et al. Pathophys-iological role of leptin in obesity-related hypertension.J Clin Invest. 2000;105:1243–1252.
21. Fruhbeck G. Pivotal role of nitric oxide in the control ofblood pressure after leptin administration. Diabetes. 1999;48:903–908.
22. Beltowski J, Wojcicka G, Borkowska E. Human leptinstimulates systemic nitric oxide production in the rat.Obes Res. 2002;10:939–946.
23. Winters B, Mo Z, Brooks-Asplund E, et al. Reductionof obesity, as induced by leptin, reverses endothelialdysfunction in obese (Lep(ob)) mice. J Appl Physiol. 2000;89:2382–2390.
24. Hintze TH. Prologue: nitric oxide–hormones, metabo-lism, and function. Am J Physiol Heart Circ Physiol. 2001;281:H2253–H2255.
25. Matsuda K, Teragawa H, Fukuda Y, et al. Leptin causesnitric-oxide independent coronary artery vasodilation inhumans. Hypertens Res. 2003;26:147–152.
26. Carlyle M, Jones OB, Kuo JJ, et al. Chronic cardiovascularand renal actions of leptin: role of adrenergic activity.Hypertension. 2002;39:496–501.
27. Shek EW, Brands MW, Hall JE. Chronic leptin infu-sion increases arterial pressure. Hypertension. 1998;31:409–414.
28. Mark, AL, Rahmouni K, Correia M, et al. A leptin-sympathetic-leptin feedback loop: potential implicationsfor regulation of arterial pressure and body fat. ActaPhysiol Scand. 2003;177:345–349.
www.americantherapeutics.com American Journal of Therapeutics (2010) 17(3)
Hemodynamical Variables in Endothelial Dysfunction 317

29. Eikelis N, Schlaich M, Aggarwal A, et al. Interactionsbetween leptin and the human sympathetic nervoussystem. Hypertension. 2003;41:1072–1079.
30. Haynes WG, Sivitz WI, Morgan DA, et al. Sympatheticand cardiorenal actions of leptin. Hypertension. 1997;30:619–623.
31. Lohmeier TE, Hildebrandt DA, Warren S, et al. Recentinsights into the interactions between the baroreflex andthe kidneys in hypertension. Am J Physiol Regul IntegrComp Physiol. 2005;288:R828–R836.
32. Antic V, Dullo A, Montano J. Multiple mechanismsinvolved in obesity-induced hypertension. Heart LungCirculation. 2003;12:84–93.
33. Kuo JJ, Jones OB, Hall JE. Inhibition of NO synthesisenhances chronic cardiovascular and renal actions ofleptin. Hypertension. 2001;37:670–676.
34. Mitchell JL, Morgan DA, Correia ML, et al. Does leptinstimulate nitric oxide to oppose the effects of sympatheticactivation? Hypertension. 2001;38:1081–1086.
35. Vecchione C, Aretini A, Maffei A, et al. Cooperationbetween insulin and leptin in the modulation of vasculartone. Hypertension. 2003;42:166–170.
36. Fernandez-Alfonso MS. Regulation of vascular tone: thefat connection. Hypertension. 2004;44:255–256.
37. Verlohren S, Dubrovska G, Tsang SY, et al. Visceralperiadventitial adipose tissue regulates arterial tone ofmesenteric arteries. Hypertension. 2004;44:271–276.
38. Soltis EE, Cassis LA. Influence of perivascular adiposetissue on rat aortic smooth muscle responsiveness. ClinExp Hypertens A. 1991;13:277–296.
39. Ridker PM. High-sensitivity C-reactive protein: potentialadjunct for global risk assessment in the primaryprevention of cardiovascular disease. Circulation. 2001;103:1813–1818.
40. Panteghini M. Role and importance of biochemical mark-ers in clinical cardiology. Eur Heart J. 2004;25:1187–1196.
41. Pasceri V, Willerson JT, Yeh ET, et al. Direct proinflam-matory effect of C-reactive protein on human endothelialcells. Circulation. 2000;102:2165–2168.
42. Sesso HD, Buring JE, Rifai N, et al. C-reactive protein andthe risk of developing hypertension. JAMA. 2003;290:2945–2951.
43. Soltero I. La proteına C reactiva: un marcador para elproceso aterosclerotico. In: Aterosclerosis al Dıa. 5th ed.Caracas: Asociacion Venezolana de Aterosclerosis, 2002:285–300.
44. Szmitko PE, Wang CH, Weisel RD, et al. New markersof inflammation and endothelial cell activation. Part I.Circulation. 2003;108:1917–1923.
45. Verma S, Buchanan MR, Anderson TJ. Endothelialfunction testing as a biomarker of vascular disease.Circulation. 2003;108:2054–2059.
46. Juge-Aubry CE, Meier CA. Immunomodulatory actionsof leptin. Mol Cell Endocrinol. 2002;194:1–7.
47. Shamsuzzaman AS, Winnicki M, Wolk R, et al. In-dependent association between plasma leptin andC-reactive protein in healthy humans. Circulation. 2004;109:2181–2185.
48. Moran O, Phillip M. Leptin: obesity, diabetes and otherperipheral effects–a review. Pediatr Diabetes. 2003;4:101–109.
49. Jiang ZY, Lin YW, Clemont A, et al. Characterization ofselective resistance to insulin signaling in the vasculatureof obese Zucker (fa/fa) rats. J Clin Invest. 1999;104:447–457.
50. Das UN. Is obesity an inflammatory condition? Nutrition.2001;17:953–966.
51. Niswender KD, Schwartz MW. Insulin and leptinrevisited: adiposity signals with overlapping physiolog-ical and intracellular signaling capabilities. Front Neuro-endocrinol. 2003;24:1–10.
52. Sweeney G. Leptin signalling. Cell Signal. 2002;14:655–663.
53. Triggle CR, Hollenberg M, Anderson TJ, et al. Theendothelium in health and disease–a target for therapeu-tic intervention. J Smooth Muscle Res. 2003;39:249–267.
54. Hines JE, Brown GE. The cold pressor test for measuringthe reactibility of the blood pressure: Data concerning 571normal and hypertensive subjects. Am Heart J. 1936;11:1–9.
55. McMurray G, Jaques L. Capillary resistance and bloodpressure changes associated with pain due to localcooling: cold pressor test. J Appl Physiol. 1959;14:813–816.
56. Velasco M, Urbina-Quintana A, Andrews-Figueroa P,et al. Effect of indoramin and propranolol on cardiovas-cular response to cold in hypertensive patients. ClinPharmacol Ther. 1982;32:7–11.
57. Mitchell L, MacDonald R, Brodie E. Temperature and thecold pressor test. J Pain. 2004;5:233–237.
58. Velasco M, Gomez J, Blanco M, et al. The cold pressor test:pharmacological and therapeutic aspects. Am J Ther. 1997;4:34–38.
59. Victor RG, Leimbach WN Jr, Seals DR, et al. Effects of thecold pressor test on muscle sympathetic nerve activity inhumans. Hypertension. 1987;9:429–436.
60. Kowalczyk WJ, Evans SM, Bisaga AM, et al. Sexdifferences and hormonal influences on response to coldpressor pain in humans. J Pain. 2006;7:151–160.
61. Kjaer A, Meyer C, Nielsen FS, et al. Dipyridamole, coldpressor test, and demonstration of endothelial dysfunc-tion: a PET study of myocardial perfusion in diabetes.J Nucl Med. 2003;44:19–23.
62. Nitenberg A, Paycha F, Ledoux S, et al. Coronary arteryresponses to physiological stimuli are improved bydeferoxamine but not by L-arginine in non-insulin-dependent diabetic patients with angiographically normalcoronary arteries and no other risk factors. Circulation.1998;97:736–743.
63. Nitenberg A, Valensi P, Sachs R, et al. Prognostic value ofepicardial coronary artery constriction to the cold pressortest in type 2 diabetic patients with angiographicallynormal coronary arteries and no other major coronaryrisk factors. Diabetes Care. 2004;27:208–215.
64. Perticone F, Ceravolo R, Pujia A, et al. Prognosticsignificance of endothelial dysfunction in hypertensivepatients. Circulation. 2001;104:191–196.
American Journal of Therapeutics (2010) 17(3) www.americantherapeutics.com
318 Fouillioux et al

65. Bonetti PO, Lerman LO, Lerman A. Endothelial dysfunc-tion: a marker of atherosclerotic risk. Arterioscler ThrombVasc Biol. 2003;23:168–175.
66. Endemann DH, Schiffrin EL. Endothelial dysfunction.J Am Soc Nephrol. 2004;15:1983–1992.
67. Baumgartner-Parzer SM, Waldhausl WK. The endothe-lium as a metabolic and endocrine organ: its relation withinsulin resistance. Exp Clin Endocrinol Diabetes. 2001;109(Suppl 2):S166–S179.
68. Sumpio BE, Riley JT, Dardik A. Cells in focus: endothelialcell. Int J Biochem Cell Biol. 2002;34:1508–1512.
69. DiBona GF. The sympathetic nervous system and hyper-tension: recent developments. Hypertension. 2004;43:147–150.
70. Castillo A. Bioetica. (1st ed. Caracas: Disinlimed CA, 2006.71. Seifarth CC, Miertschischk J, Hahn EG, et al. Measure-
ment of serum and plasma osmolality in healthy younghumans–influence of time and storage conditions. ClinChem Lab Med. 2004;42:927–932.
72. BlumWF, Englaro P, Hanitsch S, et al. Plasma leptin levelsin healthy children and adolescents: dependence on bodymass index, body fat mass, gender, pubertal stage, andtestosterone. J Clin Endocrinol Metab. 1997;82:2904–2910.
73. Roberts WL, Moulton L, Law TC, et al. Evaluation of nineautomated high-sensitivity C-reactive protein methods:implications for clinical and epidemiological applications.Part 2. Clin Chem. 2001;47:418–425.
74. Moshage H. Nitric oxide determinations: much ado aboutNO�-thing? Clin Chem. 1997;43:553–556.
75. Choh AC, Czerwinski SA, Lee M, et al. Quantitativegenetic analysis of blood pressure response during thecold pressor test. Am J Hypertens. 2005;18:1211–1217.
76. Seneviratne BI, Linton I, Wilkinson R, et al. Cold pressortest in diagnosis of coronary artery disease: echophono-cardiographic method. Br Med J. 1983;286:1924– 1926.
77. Greene MA, Boltax AJ, Lustig GA, et al. Circulatorydynamics during the cold pressor test. Am J Cardiol. 1965;16:54–60.
78. Woisetschlager C, Waldenhofer U, Bur A, et al. Differentblood pressure response to the cold pressor test pre-dicts preeclampsia. Am J Hypertens. 2000;13(Suppl 1):S301–S301.
79. Dawson-Saunders B, Trapp R. Cap. 5: Probabilidad ytemas relacionados. In: Bioestadıstica Medica, 2nd ed.Mexico City: Manual Moderno, 1997:77–97.
80. Medical College of Wisconsin. Online clinical calculator.Accessed August 10, 2006, Available at: http://www.intmed.mcw.edu/clincalc/bayes.html.
81. Celermajer DS, Sorensen KE, Gooch VM, et al. Non-invasive detection of endothelial dysfunction in childrenand adults at risk of atherosclerosis. Lancet. 1992;340:1111–1115.
82. Aronne LJ. Classification of obesity and assessment ofobesity-related health risks. Obesity Res. 2002;10:S105–S115.
83. Feldt RH, Wenstrand DE. The cold-pressor test in subjectswith normal blood pressure: Report of observations on350 subjects, with special reference to the family history.Am Heart J. 1942;23:766–771.
84. Heiss C, Lauer T, Dejam A, et al. Plasma nitrosocompounds are decreased in patients with endothelialdysfunction. J Am Coll Cardiol. j.jacc.2005.2006.2089.
85. Kleinbongard P, Dejam A, Lauer T, et al. Plasma nitriteconcentrations reflect the degree of endothelial dysfunc-tion in humans. Free Rad Biol Med. 2006;40:295–302.
86. Rondon S, Cluet I, Rossell M, et al. Niveles sericos deoxido nıtrico en adolescentes con antecedentes hereditar-ios de hipertension arterial sistemica. Arch Venez Puer Ped.2002;65:159–164.
87. Lauer T, Preik M, Rassaf T, et al. Plasma nitrite rather thannitrate reflects regional endothelial nitric oxide synthaseactivity but lacks intrinsic vasodilator action. PNAS. 2001;98:12814–12819.
88. Heitzer T, Schlinzig T, Krohn K, et al. Endothelialdysfunction, oxidative stress, and risk of cardiovascularevents in patients with coronary artery disease. Circula-tion. 2001;104:2673–2678.
89. Cicinelli E, Ignarro LJ, Schonauer LM, et al. Differentplasma levels of nitric oxide in arterial and venous blood.Clin Physiol. 1999;19:440–442.
90. Roatta S, Micieli G, Bosone D, et al. Effect of generalisedsympathetic activation by cold pressor test on cerebralhaemodynamics in healthy humans. J Auton Nerv Syst.1998;71:159–166.
91. Tousoulis D, Antoniades C, Charakida M, et al. Coldpressor test as a marker for the detection of early stagecoronary atherosclerosis. Int J Cardiol. 2007;115:120–122.
92. Tousoulis D, Davies G, Tentolouris C, et al. Inhibition ofnitric oxide synthesis during the cold pressor test inpatients with coronary artery disease. Am J Cardiol. 1997;79:1676–1679.
www.americantherapeutics.com American Journal of Therapeutics (2010) 17(3)
Hemodynamical Variables in Endothelial Dysfunction 319




















