Gastrostomy Tubes - Lippincott
10
485 of The Children’s Hospital of Philadelphia. The ages of those undergoing placement of gastrostomy or gastrojejunostomy tubes ranges from 2 months (weight greater than 1.50 kg) to older than 21 years. The number of gastrostomy tubes placed surgically as the sole procedure for the years 2002 and 2003 were 24 and 20, respectively. When combined with other surgical procedures (such as fundoplication), the number of gastrostomy tubes placed during surgery in 2002 and 2003 was 66 and 45, respectively. At our facility, most gastrostomy tubes are placed in the interventional radiology (IR) department with the patient under conscious sedation. Only about 30% are performed under general anesthesia. The exact number of pediatric gastrostomy and jejunos- tomy tubes placed annually in the United States is difficult to ascertain. According to the Healthcare Cost and Utiliza- tion Project (HCUP), approximately 230,000 gastrostomy and jejunostomy procedures were performed in U.S. hospi- tals in 2001. It is estimated 11,000 of these were performed in those younger than 18 years. The Role of the Gastrostomy Tube Nurse Collaboration between the Division of Gastroenterology and Interventional Radiology has led to the development of a unique role, the “G-tube nurse.” A dedicated advanced prac- tice nurse or nurse practitioner is assigned to be a liaison between the two departments. The primary purpose of this Gastrostomy Tubes Facts, Fallacies, Fistulas, and False Tracts Elizabeth Goldberg, MSN, RN, CPNP Robin Kaye, MD Jennifer Yaworski, RT Chris Liacouras, MD The first successful gastrostomy was performed 130 years ago. Although it is difficult to ascertain the exact number of gastrostomy or jejunostomy tubes placed annually in the United States, it is estimated approximately 230,000 gastrostomy procedures were performed in U.S. hospitals in 2001. Of these, 11,000 were performed in children. Despite the many years gastrostomy tubes have been in use, they are not free from complications. The purpose of this article is to review the authors’ experience with pediatric patients who have undergone radiographic placement of gastrostomy or jejunostomy tubes. Received February 22, 2005; accepted April 16, 2005. The authors declare no conflict of interest. About the authors: Elizabeth Goldberg, RN, MSN, CPNP, is Advance Prac- tice Nurse, Division of Gastroenterology & Nutrition; Robin Kaye, MD is Chief Radiologist; Jennifer Yaworski, RT, is Lead Technologist, Division of Interventional Radiology; Chris Liacouras, MD, is Attending Physician, Division of Gastroenterology & Nutrition; The Children’s Hospital of Philadelphia, Pennsylvania. Address correspondence to: Elizabeth Goldberg, RN, MSN, CPNP, Division of Gastroenterology & Nutrition, The Children’s Hospital of Philadelphia, 34th & Civic Center Boulevard, Philadelphia, PA 19104 (e-mail: [email protected]). T he first successful gastrostomy was performed by Jones of London 130 years ago (Jones, 1875). Gauderer, Ponsky, and Izant (1980) introduced the nonsurgical placement of a gas- trostomy tube by means of a percutaneous technique under endoscopic guidance. One year later, a percutaneous radio- logic gastrostomy was placed by a Canadian surgeon (Pre- shaw, 1981). Regardless of the method for placement of a gastrostomy tube, the indication for use is to provide long- term nutrition in patients who cannot orally ingest sufficient nutrition, even though the patient has a functioning gut. The purpose of this article is to review our experience with pediatric patients who have undergone radiographic place- ment of enteral feeding tubes at The Children’s Hospital of Philadelphia (CHOP). Approximately 95 gastrostomy or gastrojejonostomy tubes are placed yearly in the Interventional Radiology Department 3214-04_GN280605_Goldberg.qxd 12/16/05 3:15 PM Page 485
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of Gastrostomy Tubes - Lippincott

485
of The Children’s Hospital of Philadelphia. The ages of thoseundergoing placement of gastrostomy or gastrojejunostomytubes ranges from 2 months (weight greater than 1.50 kg) toolder than 21 years. The number of gastrostomy tubesplaced surgically as the sole procedure for the years 2002and 2003 were 24 and 20, respectively. When combinedwith other surgical procedures (such as fundoplication), thenumber of gastrostomy tubes placed during surgery in 2002and 2003 was 66 and 45, respectively. At our facility, mostgastrostomy tubes are placed in the interventional radiology(IR) department with the patient under conscious sedation.Only about 30% are performed under general anesthesia.
The exact number of pediatric gastrostomy and jejunos-tomy tubes placed annually in the United States is difficultto ascertain. According to the Healthcare Cost and Utiliza-tion Project (HCUP), approximately 230,000 gastrostomyand jejunostomy procedures were performed in U.S. hospi-tals in 2001. It is estimated 11,000 of these were performedin those younger than 18 years.
The Role of the Gastrostomy Tube Nurse
Collaboration between the Division of Gastroenterology andInterventional Radiology has led to the development of aunique role, the “G-tube nurse.” A dedicated advanced prac-tice nurse or nurse practitioner is assigned to be a liaisonbetween the two departments. The primary purpose of this
Gastrostomy TubesFacts, Fallacies, Fistulas, and False TractsElizabeth Goldberg, MSN, RN, CPNP
Robin Kaye, MD
Jennifer Yaworski, RT
Chris Liacouras, MD
The first successful gastrostomy was performed 130 years ago. Although it is difficult to ascertain the exact
number of gastrostomy or jejunostomy tubes placed annually in the United States, it is estimated
approximately 230,000 gastrostomy procedures were performed in U.S. hospitals in 2001. Of these, 11,000
were performed in children. Despite the many years gastrostomy tubes have been in use, they are not free
from complications. The purpose of this article is to review the authors’ experience with pediatric patients who
have undergone radiographic placement of gastrostomy or jejunostomy tubes.
Received February 22, 2005; accepted April 16, 2005.The authors declare no conflict of interest.About the authors: Elizabeth Goldberg, RN, MSN, CPNP, is Advance Prac-tice Nurse, Division of Gastroenterology & Nutrition; Robin Kaye, MD isChief Radiologist; Jennifer Yaworski, RT, is Lead Technologist, Division ofInterventional Radiology; Chris Liacouras, MD, is Attending Physician,Division of Gastroenterology & Nutrition; The Children’s Hospital ofPhiladelphia, Pennsylvania.Address correspondence to: Elizabeth Goldberg, RN, MSN, CPNP, Divisionof Gastroenterology & Nutrition, The Children’s Hospital of Philadelphia,34th & Civic Center Boulevard, Philadelphia, PA 19104 (e-mail: [email protected]).
The first successful gastrostomy was performedby Jones of London 130 years ago (Jones,1875). Gauderer, Ponsky, and Izant (1980)introduced the nonsurgical placement of a gas-
trostomy tube by means of a percutaneous technique underendoscopic guidance. One year later, a percutaneous radio-logic gastrostomy was placed by a Canadian surgeon (Pre-shaw, 1981). Regardless of the method for placement of agastrostomy tube, the indication for use is to provide long-term nutrition in patients who cannot orally ingest sufficientnutrition, even though the patient has a functioning gut.The purpose of this article is to review our experience withpediatric patients who have undergone radiographic place-ment of enteral feeding tubes at The Children’s Hospital ofPhiladelphia (CHOP).
Approximately 95 gastrostomy or gastrojejonostomy tubesare placed yearly in the Interventional Radiology Department
3214-04_GN280605_Goldberg.qxd 12/16/05 3:15 PM Page 485

486 GASTROENTEROLOGY NURSING
role is to facilitate and coordinate the care of the patientwith gastrostomy or gastrojejunostomy tubes, including carebefore and after tube placement. In addition to facilitatingthe care of the gastrostomy tube patient and family, the G-tube nurse has many other responsibilities. She managesand tracks complications associated with the placement ofthe tube, including problems with equipment. She participatesin the development of patient and family education materials,provides lectures on gastrostomy tube care to the nursing andmedical staff, and participates in enteral feeding research.
Preprocedural CareIt is our practice that a gastrointestinal (GI) consult beobtained for any in-patient who is in need of a gastrostomytube. At the request of the in-patient care team, the G-tubenurse meets with the patient and family to review the pro-cedure for gastrostomy tube placement and to allow thepatient and family to see and touch the gastrostomy tubebefore placement. Follow-up after the procedure is arrangedbefore discharge, and the patient and family have an ongoingresource for support via the G-tube nurse should questions orconcerns about the tube arise after discharge.
Outpatients who seek placement of a gastrostomy tube arereferred to the Pediatric Enteral Access Clinic (PEAC). Thisclinic was started in 1995 to provide specialty care to anychild who either has or is in need of a gastrostomy tube. ThePEAC clinic meets weekly and consists of an attending gas-troenterologist and the G-tube nurse. There is also access toa nutritionist. Outpatients seeking a gastrostomy tube areevaluated with regard to the indications for gastrostomy tubeplacement. A patient history, physical exam, and a nutritionalassessment are completed by the G-tube nurse.
A review of past medical and nutritional interventionsmay result in recommendations other than the need for gas-trostomy tube placement. Teaching regarding the advantagesand disadvantages of gastrostomy tube placement and theprocedure for placement also are done. Depending upon thepatient, endoscopy may be needed and timing coordinated tocoincide with placement of the gastrostomy tube. An upperGI series is mandatory before gastrostomy tube placementcan proceed. An upper GI series, an x-ray study that uses bar-ium to outline the anatomy of the upper GI tract, is done toassure patency of the esophagus, positioning of the stomach,and rule out malrotation of the intestines.
We also recommend a trial of nasogastric (N/G) feedingsbefore gastrostomy tube placement. Although many familiesare resistant to N/G feeding because they see such feedings asa traumatic intervention, we have found that with coordi-nated teaching and adequate home support, most families dowell with the N/G trial. This trial provides us with much valu-able information regarding the child’s tolerance of enteralfeedings before the more invasive procedure of gastrostomy.In some of the older children, the trial of N/G feedings provesso successful, they opt to continue N/G feedings, rather thanundergo placement of a gastrostomy tube. Once they havemastered placing the N/G tube, they are fed overnight andthus are free during the day to eat. They discover improvednutrition enhances their energy and helps in alleviating com-plications associated with their underlying disease. Alterna-tively, for many families, the trial of N/G feedings confirmsthe benefits of good nutrition while underscoring the need forgastrostomy tube placement.
In addition, N/G feedings allow us to provide nutritionbefore the scheduling of a gastrostomy tube. Some childrenwho present for gastrostomy tube placement are in a direnutritional state. Refeeding syndrome is a concern in childrenwho are malnourished. Aggressive feeding after a period ofstarvation can result in metabolic and physiologic conse-quences that include disturbances in electrolytes, vitamindeficiencies, glucose and fluid intolerance, and cardiac,pulmonary, hematologic, and neuromuscular dysfunction(Solomon & Kirby, 1990). A poor nutritional state alsocan hinder wound healing.
A slow increase in the rate of N/G tube feedings not onlydecreases the chance of refeeding syndrome but also allows usto assess for an increase in gastroesophageal reflux and theneed for feedings into the jejunum. A trial of N/G feedingsalso allows time before gastrostomy tube placement for logis-tical and technical troubleshooting. Clarification of insuranceissues and the identification of the home care company, com-pletion of pump teaching, and the need for in-home nursingcare after gastrostomy tube placement make the postproce-dural period less complicated and free the patient and familyto concentrate on learning the care of the gastrostomy. Thetrial of N/G feedings need not be lengthy, often only 1 to2 weeks. We think N/G feedings are an important part ofthe gastrostomy tube placement process.
Postprocedural CareAfter the gastrostomy tube is placed, the patient is admit-ted to the hospital (usually for about 24 hours) for intra-venous (IV) antibiotics, pain control, initiation of feedings,and patient and family teaching. A standardized format forteaching gastrostomy tube care is used at our Family Learn-ing Center, where anyone caring for a gastrostomy tube canlearn how to maintain the tube and discover other relevanthospital resources.
Within 2 weeks of gastrostomy tube placement, patientsreturn to PEAC for a wound check. After 12 weeks, thepatient may return to radiology for the placement of anappropriate low-profile device. A dye study is completed toconfirm intragastric placement after the first changing of thetube. The patient or caregiver is taught how to change bal-loon replacement gastrostomy tubes in the Family LearningCenter. If the family is uncomfortable with performing theroutine change of these tubes, they are referred to PEAC.We advise all our patients to return to PEAC at least yearlyfor remeasurement of gastrostomy tube size. Any problemsrelated to a gastrostomy tube are referred to the PEAC clinicor to the advanced practice nurse who is responsible for thegastrostomy tube pager.
Complications of Gastrostomy and Gastrojejunostomy Tubes
Despite the many years gastrostomy tubes have been in use,they are not free from complications. Complications are usu-ally reported as either early or late (2 weeks after placement)onset or as major versus minor problems. Major complica-tions include bleeding, perforation, peritonitis, and intes-tinal obstruction. Minor complications generally are listedas leakage, granulation tissue, stoma irritation, dislodgedtubes, transient superficial wound infection, and migrationof the tube. A review of the literature (Khattak, Kimber,
3214-04_GN280605_Goldberg.qxd 12/16/05 3:15 PM Page 486

Kiely, & Spitz, 1998; Kutiyanawala, Hussain, Johnstone,Everson, & Nour, 1998; Marin, Glassman, Schoen, &Caplan, 1994) reveals major complication rates range from7% to 19% and minor complications occur in 22% to 90%of pediatric patients. One study reported the overall rate ofcomplications in infants and children with gastrostomy tubesas high as 43% (Kutiyanawala et al.).
Most articles do not compare rates of complications bymethod of tube insertion or by the ages of the patients. Arecent article, however, evaluated complications associatedwith radiologic placed gastrostomy and gastrojejunostomytubes in children (Friedman, Ahmed, Connolly, Chait, &Mahany, 2004). After reviewing a convenience sample of208 charts involving children ages 7 days to 18 years, a majorcomplication rate of 5% and minor complication rate of 73%were found. The minor complications found in 73% of thechildren included tube dislodgement, tube leakage, and gas-trostomy site skin infections. The group reported higher ratesof obstruction, migration, dislodgement, leakage, and intus-susception in gastrojejunostomy tubes (Friedman et al.).
An earlier study involving a review of 453 charts ofchildren (mean age 3.8 years) found that radiologic place-ment of gastrostomy tubes was successful 99% of the time(Chait et al., 1996). An assessment of late complications was20%, but these findings were thought to be inaccuratebecause the nurses reported dealing with at least four to fivegastrostomy tube-related problems per week (Chait et al.).One study compared the different methods of placement ofgastrostomy tubes, including surgical, percutaneous endo-scopic (PEGs), and percutaneous radiologic gastrostomies(PRGs). In this study of adult patients, there were no majordifferences among the three procedures with regard to procedure-related complications (Cosentini et al., 1998).
In Wollman, D’Agostino, Walus-Wigle, Easter, & Beale’s(1995) study comparing radiologic, endo copic, and surgicalgastrostomy placement, endoscopic placement was successfulonly 95.7% of the time, which was significantly lower thanplacement with radiologic and surgical gastrostomy (99.2%and 100.0%, respectively). Surgical gastrostomy had thehighest total complication rate (29.0%), compared with radi-ologic gastrostomy (13.3%) and endoscopic gastrostomy(15.4%) (Wollman et al.). This study included 72 patients, ofwhom only 4 were younger than 16 years.
InfectionsInfections involving the gastrostomy tube tract occur mostoften in the first several weeks after placement. It has beenestimated peristomal infections occur in one-fourth to one-third of patients (Friedman et al., 2004; Gossner, Keymling,Hahn, & Ell, 1999). A review of the literature shows greatvariability in infection rates after placement of gastrostomytubes, with few studies addressing the rates of infection inchildren. In addition, we have noted that some children haverecurrent infections of their gastrostomy tube sites. Many ofthe children who undergo gastrostomy tube placement haveserious underlying medical conditions such as complex heartdisease, metabolic disorders, and impaired immunity thatincrease their risk for infections and hinder wound healing.
Several articles have evaluated the benefits of antibioticprophylaxis in the placement of percutaneous endoscopicgastrostomies (Dormann et al., 1999; Gossner et al., 1999;Kulling, Sonnenberg, Fried, & Bauerfeind, 2000). Prophylac-
tic antibiotics are thought to be cost-effective. The AmericanSociety for Gastrointestinal Endoscopy (1995) recommendsthe use of antibiotic prophylaxis before PEG placement in allpatients. Of course, the effectiveness of antibiotic prophylaxisis dependent upon the correct selection of antibiotic useful intreating the spectrum of bacteria responsible for peristomalinfections. At CHOP, we use an intravenous cephalosporin atthe time of the procedure and after the procedure.
Infections of the gastrostomy tube site can present in dif-ferent ways. Typically one expects an infected site to presentwith spreading erythema, increased tenderness or pain,induration, fever, or purulent discharge. In contrast, theoften seen yellow-brown crusty discharge noted around gas-trostomy tube sites in the absence of other signs or symp-toms suggestive of infection is not actually an infection. Thisfinding is often confusing to parents. Cellulitis of a newlyplaced gastrostomy can be either bacterial or chemical.Chemical cellulitis may result if gastric contents leak intothe surrounding subcutaneous tissues and result in aninflammatory response that is often difficult to differentiatefrom bacterial cellulitis. Because the symptoms of increasingerythema and pain are diagnostically indistinguishable,antibiotic therapy is typically employed.
Patients can present with a history of a “pimple” formingadjacent to the gastrostomy tube stoma. These lesions are fre-quently described as having rapid onset of a pustular or deepred-purple fluid-filled lesion that is tender to the touch. Whenthe pimple ruptures, a punctate opening becomes apparentand may drain for several days before closing. Warm com-presses and antibiotic therapy should be prescribed. If theinfection does not clear or repeatedly returns, options includeobtaining a wound culture, treating for longer with oralantibiotic (for 2 to 3 weeks), or obtaining a surgical opinion.Sometimes the wound must be packed for it to heal properly,and on rare occasions, the gastrostomy tube site may need tobe surgically revised.
Feeding tubes are frequently colonized with microbialorganisms as well as yeast and fungi. This can complicatethe interpretation of cultures obtained from gastrostomytubes and their placement sites. A variety of organisms havebeen found in the biofilm that surrounds gastrostomy tubes.Bacterial biofilm is defined as a “structured bacterial com-munity enclosed in a self-produced polysaccharide matrixthat prefers to surround inert surfaces” (Dautle, Wilkinson,& Gauderer, 2003). There have been more than 100 differ-ent microorganisms isolated from gastrostomy tubes. Com-monly found organisms include Candida, Pseudomonas,Escherichia coli, Enterobacter cloacae, streptococci, lacto-bacillus, Staphylococcus aureus, and Bacteroides.
There have also been reports of yeast crusts occluding large-bore feeding tubes and upon histologic examination of thesesilicone feeding tubes, 40% of the tube walls were penetratedby yeast (Gottlieb & Mobarhan, 1994). Colonization mostlikely occurs as a result of autoinoculation (spread of organ-isms from the oral cavity, the stomach, or skin onto the gas-trostomy tube) or perhaps from contaminated enteral feedings.The significance of gastrostomy tube colonization is unclear,although it has been hypothesized that biofilm organisms maybe a risk factor for infections, may contribute to tube or bal-loon deterioration, or may possibly play a role in granulationtissue formation (Dautle et al., 2003; Gottlieb & Mobarhan).
Resistance to antibiotics in the treatment of gastrostomytube-related infections might be increasing. Biofilm organisms
VOLUME 28 • NUMBER 6 487
3214-04_GN280605_Goldberg.qxd 12/16/05 3:15 PM Page 487
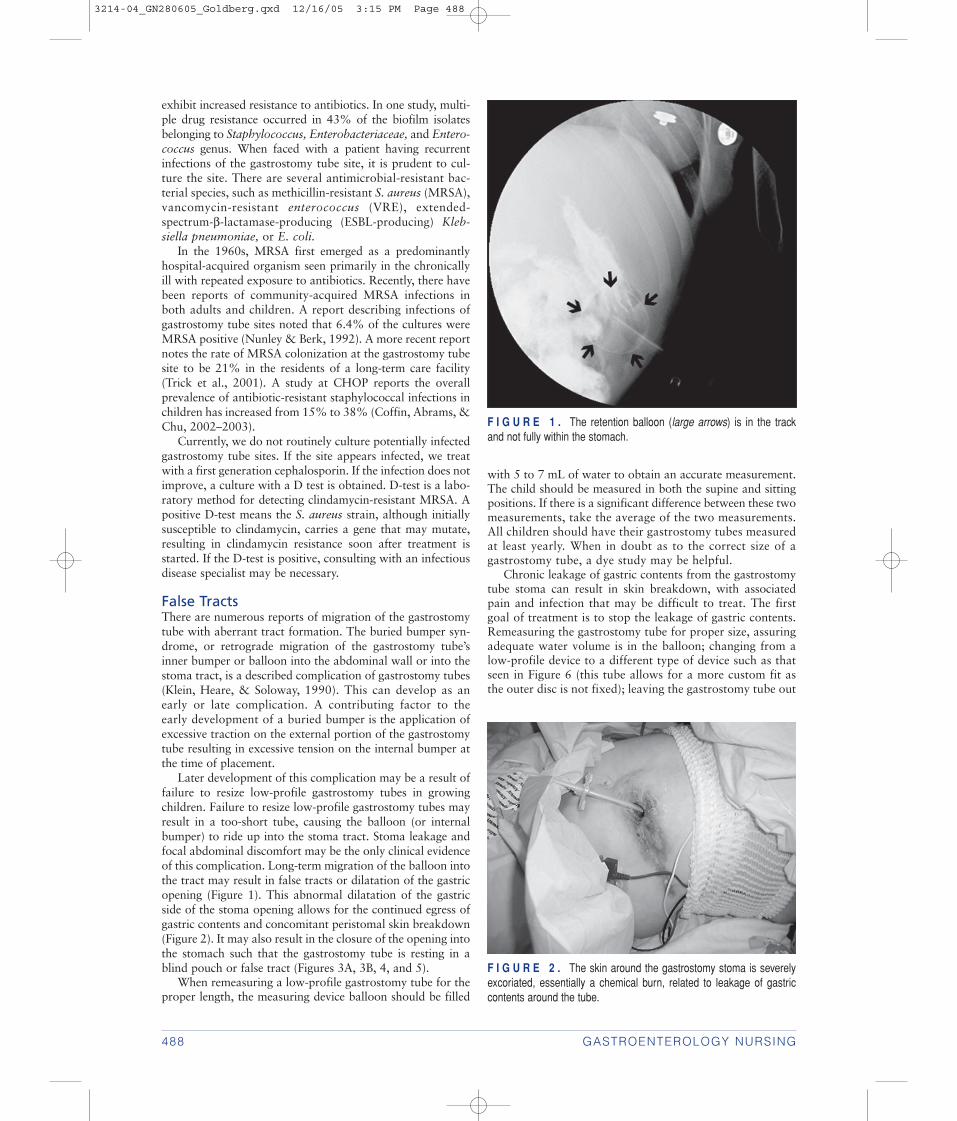
exhibit increased resistance to antibiotics. In one study, multi-ple drug resistance occurred in 43% of the biofilm isolatesbelonging to Staphylococcus, Enterobacteriaceae, and Entero-coccus genus. When faced with a patient having recurrentinfections of the gastrostomy tube site, it is prudent to cul-ture the site. There are several antimicrobial-resistant bac-terial species, such as methicillin-resistant S. aureus (MRSA),vancomycin-resistant enterococcus (VRE), extended-spectrum-β-lactamase-producing (ESBL-producing) Kleb-siella pneumoniae, or E. coli.
In the 1960s, MRSA first emerged as a predominantlyhospital-acquired organism seen primarily in the chronicallyill with repeated exposure to antibiotics. Recently, there havebeen reports of community-acquired MRSA infections inboth adults and children. A report describing infections ofgastrostomy tube sites noted that 6.4% of the cultures wereMRSA positive (Nunley & Berk, 1992). A more recent reportnotes the rate of MRSA colonization at the gastrostomy tubesite to be 21% in the residents of a long-term care facility(Trick et al., 2001). A study at CHOP reports the overallprevalence of antibiotic-resistant staphylococcal infections inchildren has increased from 15% to 38% (Coffin, Abrams, &Chu, 2002–2003).
Currently, we do not routinely culture potentially infectedgastrostomy tube sites. If the site appears infected, we treatwith a first generation cephalosporin. If the infection does notimprove, a culture with a D test is obtained. D-test is a labo-ratory method for detecting clindamycin-resistant MRSA. Apositive D-test means the S. aureus strain, although initiallysusceptible to clindamycin, carries a gene that may mutate,resulting in clindamycin resistance soon after treatment isstarted. If the D-test is positive, consulting with an infectiousdisease specialist may be necessary.
False TractsThere are numerous reports of migration of the gastrostomytube with aberrant tract formation. The buried bumper syn-drome, or retrograde migration of the gastrostomy tube’sinner bumper or balloon into the abdominal wall or into thestoma tract, is a described complication of gastrostomy tubes(Klein, Heare, & Soloway, 1990). This can develop as anearly or late complication. A contributing factor to theearly development of a buried bumper is the application ofexcessive traction on the external portion of the gastrostomytube resulting in excessive tension on the internal bumper atthe time of placement.
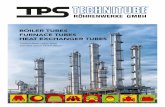
Later development of this complication may be a result offailure to resize low-profile gastrostomy tubes in growingchildren. Failure to resize low-profile gastrostomy tubes mayresult in a too-short tube, causing the balloon (or internalbumper) to ride up into the stoma tract. Stoma leakage andfocal abdominal discomfort may be the only clinical evidenceof this complication. Long-term migration of the balloon intothe tract may result in false tracts or dilatation of the gastricopening (Figure 1). This abnormal dilatation of the gastricside of the stoma opening allows for the continued egress ofgastric contents and concomitant peristomal skin breakdown(Figure 2). It may also result in the closure of the opening intothe stomach such that the gastrostomy tube is resting in ablind pouch or false tract (Figures 3A, 3B, 4, and 5).
When remeasuring a low-profile gastrostomy tube for theproper length, the measuring device balloon should be filled
488 GASTROENTEROLOGY NURSING
F I G U R E 1 . The retention balloon (large arrows) is in the trackand not fully within the stomach.
F I G U R E 2 . The skin around the gastrostomy stoma is severelyexcoriated, essentially a chemical burn, related to leakage of gastriccontents around the tube.
with 5 to 7 mL of water to obtain an accurate measurement.The child should be measured in both the supine and sittingpositions. If there is a significant difference between these twomeasurements, take the average of the two measurements.All children should have their gastrostomy tubes measuredat least yearly. When in doubt as to the correct size of agastrostomy tube, a dye study may be helpful.
Chronic leakage of gastric contents from the gastrostomytube stoma can result in skin breakdown, with associatedpain and infection that may be difficult to treat. The firstgoal of treatment is to stop the leakage of gastric contents.Remeasuring the gastrostomy tube for proper size, assuringadequate water volume is in the balloon; changing from alow-profile device to a different type of device such as thatseen in Figure 6 (this tube allows for a more custom fit asthe outer disc is not fixed); leaving the gastrostomy tube out
3214-04_GN280605_Goldberg.qxd 12/16/05 3:15 PM Page 488

VOLUME 28 • NUMBER 6 489
F I G U R E 3 . (A) This is a preliminary image of the abdomen, taken before contrast injection, showing the gastrostomy tube in what appears tobe a good position. (B) Contrast injection reveals the retention disk (white arrowheads) is not within the stomach. There is extravasation of contrast(large arrows) into the soft tissues of the abdominal wall. Contrast fills a thin track (long arrow) to the decompressed stomach (black arrowheads).
F I G U R E 4 . In this patient, contrast injection of the gastrostomytube reveals the track to the stomach has completely closed. The gas-filled stomach has no contrast (small arrows). There is a collection ofcontrast around the retention disk (white arrowheads) and extravasationof contrast (large arrows) into the soft tissues of the abdominal wall.
F I G U R E 5 . In this patient, a lateral view of the abdomen showsa filling defect surrounded by a thin rim of contrast where the retentionballoon sat in the track between the skin and the stomach (blackarrows). A thin track of contrast (white arrowheads) leads to the stom-ach (white arrows).
for several hours in hopes the tract will partially shrink(place a smaller size catheter into the stoma to prevent com-plete closure of the tract), upsizing the width (going from a14 French to a 16 French for example), using acid suppres-sion medications to reduce the pH of gastric reflux into thestoma and venting the tube during feedings are possibleoptions in the treatment of chronic leakage.
If after upsizing the width of the gastrostomy tube, thereis continued leakage from the stoma, do not continue toincrease the width of the tube as this results in progressivewidening of the stoma and continued leakage. Use of a Far-rell Valve Enteral Gastric Pressure Relief System is helpful inventing gastrostomy tubes (Viaysis Healthcare Medsystems).In cases of severe leakage, it may be necessary to place a gas-
A B
3214-04_GN280605_Goldberg.qxd 12/16/05 3:15 PM Page 489

trojejunostomy tube, use N/G suction to reduce the egress ofgastric contents from the stoma, or stop enteral feedings fora period of time (using parenteral nutrition support). Wehave had several children in whom the leakage from the gas-trostomy tube stoma was recalcitrant. Surgical revision ofthe site may be needed in such children.
Wound management of an eroded gastrostomy tube sitecan be a challenge. Skin barriers may be helpful in preventingongoing damage from gastric acid. Secondary infections witheither bacteria or yeast must be addressed using the appro-priate topical or oral antibiotic. Pain relief is an importantaspect and directly affects the patient’s quality of life. Wehave found using Maalox or Mylanta on the peristomal skin,in addition to an adequate skin barrier such as zinc oxide, isa comfort to the patient.
There are also numerous wound dressings that supportwound healing. One category of dressings is known asabsorbent hydrogels. Some of the hydrogel dressings have ahigh glycerin content that does not dry out and is highlyabsorbent. The dehydrating effects of the glycerin are thoughtto reduce wound bacteria (Oliveria-Gandia, Davis, & Mertz,1998). Some of the dressing materials do not have adhesivebackings that allow for fast, painless dressing changes. Topi-cal antibiotic ointments can be used under some of the hydro-gel dressings.
FistulasPersistent gastrocutaneous fistulas may occur after gastros-tomy tube removal. A persistent gastrocutaneous fistula isone that does not close spontaneously 1 month after removalof the gastrostomy tube. The prevalence of persistent gastro-cutaneous fistula in children who underwent endoscopicplacement of the gastrostomy tube is estimated at approxi-mately 25% (El-Rifai et al., 2004; Kobak, McClenathan, &Schurman, 2000). The longer the child has had the gastros-tomy tube, the less likely the fistula will heal spontaneously.
A variety of techniques are reported in the literature as use-ful in promoting closure of gastrocutaneous fistulas. Limited
success with conservative management has been achievedusing mechanical obstruction of the tract, drug-inducedincreases in gastric pH, or improvement in gastric emptying.Tract cauterization is thought to achieve fistula closure in53% of cases (Kobak et al., 2000). Makris and Sheiman(2002) reported successful closure of a gastrocutaneous fistulain an 87-year-old man by direct cauterization of the tract withsilver nitrate followed by tract embolization with Betadine-soaked Gelfoam pledgets (Upjohn, Kalamazoo, MI). How-ever, it is believed this approach is feasible only in tractsgreater than 2 cm in length. There have been several casereports in the literature of using biodegradable adhesives, suchas fibrin glue, in the management of gastrocutaneous fistulasin adults (Gonzalez-Ojeda et al., 2004; Shand, Pendlebury,Reading, Papachrysostomou, & Ghosh, 1997). More researchinto nonsurgical closure of gastrocutaneous fistulas in childrenis needed.
Development of gastrocolonic fistulas is reported in theliterature (Figure 7). Gastrocolonic fistulas can develop anytime after placement of the gastrostomy tube. Fecal drainagefrom the stoma, foul breath, or leakage of formula from therectum should raise the suspicion of a gastrocolonic fistula.Treatment involves surgical closure of the fistula withreplacement of the gastrostomy tube.
Granulation TissueGranulation tissue is often cited as a minor complication ofhaving a gastrostomy tube. Despite anecdotal reports of itsoccurrence, little research exists that outlines the incidence,predisposing factors, or best therapy for gastrostomy tube-induced granulation tissue. Granulation tissue is a prolifera-tion of capillaries that forms not only around the externalstoma opening, but also inside the stoma tract or within thegastric opening. This may explain why some children reportpain at the gastrostomy tube site but have no visible reasonfor the pain. Granulation tissue is often painful, bleeds, oozes,and is unsightly. There have been no published controlledstudies evaluating the various treatments currently in use formanaging gastrostomy tube-induced granulation tissue. Cur-rent treatment options include stomahesive powder, silvernitrate, or topical steroids.
The time-honored method of treatment for excessive gran-ulation tissue at the gastrostomy tube site has been either cau-terization with silver nitrate or the application of stoma-hesive powder. Stomahesive powder is primarily used as adrying agent. Unfortunately, silver nitrate treatment for gas-trostomy tube-induced granulation tissue can cause signifi-cant complications, including burns to the surrounding skinwhen the silver nitrate is improperly applied. Silver nitratecauterization can be painful and often needs to be repeated tobe effective. We usually apply a protective barrier to the peri-stomal skin before application of silver nitrate and after treat-ment. We cauterize granulation tissue two to three times aweek until resolution.
There are limited references for using steroid creams in thetreatment of gastrostomy tube-induced granulation tissue.Dermatologists have successfully used superpotent topicalcorticosteroids for the past 5 years as therapy for postopera-tive exuberant granulation tissue (Mandrea, 1998; Nordin,Hersle, Liander, & Roupe, 1999). It is hypothesized that top-ical steroids may have an antiangiogenic effect on granulationtissue much the same as systemic steroids have had in thetreatment of large capillary hemangiomas.
490 GASTROENTEROLOGY NURSING
F I G U R E 6 . Maintenance-type gastrostomy.
3214-04_GN280605_Goldberg.qxd 12/16/05 3:15 PM Page 490

There have been anecdotal reports on the successful use oftriamcinolone cream (a midpotency corticosteroid that hasbeen labeled for use in pediatric patients for the treatment ofvarious types of dermatitis and eczema) in treating gastros-tomy or jejunostomy tube-induced granulation tissue. Weuse 0.1% triamcinolone cream twice daily for no longer than2 weeks as treatment for granulation tissue with some suc-cess. Do not apply an occlusive dressing to the gastrostomytube site while using a topical steroid. There have been nocontrolled clinical trials evaluating topical steroids as therapyfor gastrostomy tube-induced granulation tissue.
Prolapse of gastric mucosa is often confused with gastros-tomy tube-induced granulation tissue (Figure 8). Gastric pro-lapse has a deeper red, more granular appearance. It does notresolve with silver nitrate therapy and may appear and thendisappear on its own.
Treatment of gastric prolapse is difficult. Placement of alarger width tube may be helpful. It is rare that a new gastros-tomy tube may need to be placed. Silver nitrate should not beused in treating gastric prolapse because it may cause bleeding.
Clogged TubesAnyone who cares for children with gastrojejunal tubes isfamiliar with the problems of clogged tubes and “J” tubemigration or dislodgment. Children undergoing jejunostomyfeedings most commonly have GI dysmotility. Jejunostomyfeeding is often attempted as an alternative to the perform-ance of fundoplication. Dysmotility contributes to the reversemigration of the tube out of the jejunum and into the stom-ach. A review of the literature failed to uncover any informa-tion or research directed at the problem of J-tube migration.
Tube occlusion of small-bore feeding tubes is reported torange from 23% to 35% (Bourgault et al., 2003). An excel-lent review article, “Restoring and Maintaining Patency ofEnteral Feeding Tubes,” is recommended (Lord, 2003). Toprevent clogging of J tubes, it is best to emphasize routine
VOLUME 28 • NUMBER 6 491
F I G U R E 7 . (A) Early in the study, contrast injection fills the colon first (arrowheads) and then slowly fills the stomach (arrows). (B) Later inthe study, the fistula from the colon to the stomach can be seen filled with contrast (arrows). The stomach (outlined by arrowheads medially and adotted line laterally) is filled with more contrast than seen in A.
F I G U R E 8 . Lobular, granular-appearing gastric mucosa is seenprolapsed through the track and out around the stoma.
flushing. Flushing should occur before and after bolus feed-ings or medication administration and every 2–4 hours dur-ing continuous feedings.
Water is the best solution for feeding tube flushes. Med-ications should not be mixed into formulas but given withwater. It has been suggested a pancreatic enzyme solutionwith an elevated pH level is effective in dissolving clottedformula in feeding tubes. Sriram, Jayanthi, Lakshmi, andGeorge (1997) used pancreatic enzyme with sodium bicar-bonate as a prophylactic lock solution after intermittententeral feeding to successfully reduce feeding tube occlusions.In another study involving adult patients receiving continu-ous enteral feedings (both gastric and jejunal), pancreatic
A B
3214-04_GN280605_Goldberg.qxd 12/16/05 3:15 PM Page 491

enzyme solution with sodium bicarbonate administered every4 hours significantly decreased the time to occlusion of small-bore feeding tubes (Bourgault et al., 2003). There is littleresearch on unclogging or preventing clogs in enteral feedingtubes in pediatric patients.
SummaryCaring for the pediatric patient with enteral access is chal-lenging. This article provides an overview of our experienceswith gastrostomy and jejunostomy tubes in pediatricpatients. Gastrostomy or jejunostomy tubes, while provid-ing an advantage in enteral feedings, are not free from com-plications. There are many aspects of gastrostomy andjejunostomy feedings that have yet to be researched. Ourpatients, however, deserve research-based care to improvethe quality of their lives.
ReferencesAmerican Society for Gastrointestinal Endoscopy (ASGE).
(1995). Antibiotic prophylaxis for gastrointestinalendoscopy. Gastrointestinal Endoscopy, 42, 630–635.
Bourgault, A. M., Heyland, D. K., Drover, J. W., Keefe, L.,Newman, P., & Day, A. G. (2003). Prophylactic pancre-atic enzymes to reduce feeding tube occlusions. Nutritionin Clinical Practice, 18, 398–401.
Chait, P. G., Weinberg, J., Connolly, B., Pencharz, P.,Richards, H., Clift, J. E., et al. (1996). Retrograde percu-taneous gastrostomy and gastrojejunostomy in 505 chil-dren: A 41/2 year experience. Radiology, 201, 691–695.
Coffin, S. E., Abrams, T. J., & Chu, J. (2004). Emergence ofcommunity-onset methicillin-resistant Staphylococcusaureus infection in children. Abstract #164. InfectiousDiseases in Children, 17.
Cosentini, E. P., Sautner, T., Gnant, M., Winkelbauer, F.,Teleky, B., & Jakesz, R. (1998). Outcomes of surgical,percutaneous endoscopic, and percutaneous radiologicgastrostomies. Archives of Surgery, 133, 1076–1083.
Dautle, M. P., Wilkinson, T. R., & Gauderer, M. W. L.(2003). Isolation and identification of biofilm microor-ganisms from silicone gastrostomy devices. Journal ofPediatric Surgery, 38, 216–220.
Dormann, A. J., Wigginghaus, B., Risius, H., Kleimann, F.,Kloppenborg, A., Grunewald, T., & Huchzermeyer, H.(1999). A single dose of ceftriaxone administered 30 min-utes before percutaneous endoscopic gastrostomy signifi-cantly reduces local and systemic infective complications.American Journal of Gastroenterology, 94, 3220–3223.
El-Rifai, N., Michaud, L., Mention, K., Guimber, D., Cal-dari, D., Turck, D., & Gottrand, F. (2004). Persistence ofgastrocutaneous fistula after removal of gastrostomytubes in children: Prevalence and associated factors.Endoscopy, 36, 700–704.
Friedman, J. N., Ahmed, S., Connolly, B., Chait, P., &Mahany, S. (2004). Complications associated withimage-guided gastrostomy and gastrojejunostomy tubesin children. Pediatrics, 114, 458–461.
Gauderer, M. W. L., Ponsky, J. L., & Izant, R. J. Jr. (1980).Gastrostomy without laparotomy: A percutaneous endo-scopic technique. Journal of Pediatric Surgery, 15,872–875.
Gonzalez-Ojeda, A., Avalos-Gonzalez, J., Mucino-Hernan-dez, M. I., Lopez-Ortega, A., Fuentes-Orozco, C.,Sanchez-Hochoa, M., et al. (2004). Fibrin glue as adju-
vant treatment for gastrocutaneous fistula after gastros-tomy tube removal. Endoscopy, 36, 337–341.
Gossner, L., Keymling, J., Hahn, E. G., & Ell, C. (1999).Antibiotic prophylaxis in percutaneous endoscopic gas-trostomy (PEG): A prospective randomized clinical trial.Endoscopy, 31, 119–124.
Gottlieb, K., & Mobarhan, S. (1994). Review: Microbiol-ogy of the gastrostomy tube. Journal of the AmericanCollege of Nutrition 13, 311–313.
Jones, S. (1875). Gastrostomy for stricture (?cancerous) ofoesophagus: Death from bronchitis forty days after oper-ation. Lancet, 1, 678–679.
Khattak, I. U., Kimber, C., Kiely, E. M., & Spitz, L. (1998).Percutaneous endoscopic gastrostomy in pediatric prac-tice: Complications and outcome. Journal of PediatricSurgery, 33, 67–72.
Klein, S., Heare, B. R., & Soloway, R. D. (1990). The‘buried bumper syndrome’: A complication of percuta-neous endoscopic gastrostomy. American Journal ofGastroenterology, 85, 448–451.
Kobak, G. E., McClenathan, D. T., & Schurman, S. J.(2000). Complications of removing percutaneous endo-scopic gastrostomy tubes in children. Journal of PediatricGastroenterology and Nutrition, 30, 404–407.
Kulling, D., Sonnenberg, A., Fried, M., & Bauerfeind, P.(2000). Cost analysis of antibiotic prophylaxis for PEG.Gastrointestinal Endoscopy, 51, 152–156.
Kutiyanawala, M. A., Hussain, A., Johnstone, J. M. S.,Everson, N. W., & Nour, S. (1998). Gastrostomy com-plications in infants and children. Annals of the RoyalCollege of Surgeons of England, 80, 240–243.
Lord, L. M. (2003). Restoring and maintaining patency ofenteral feeding tubes. Nutrition in Clinical Practice 18,422–426
Makris, J., & Sheiman, R. G. (2002). Percutaneous treat-ment of a gastrocutaneous fistula after gastrostomy tuberemoval. Journal of Vascular & Interventional Radiol-ogy, 13, 205–207.
Mandrea, E. (1998). Topical Diflorasone ointment for thetreatment of recalcitrant, excessive granulation tissue.American Society for Dermatologic Surgery, 24,1409–1410.
Marin, O. E., Glassman, M. S., Schoen, B. T., & Caplan,D. B. (1994). Safety and efficacy of percutaneous endo-scopic gastrostomy in children. American Journal ofGastroenterology, 89, 357–361.
Nordin, P. C., Hersle, K. S., Liander, W. K., & Roupe, G. A.(1999). Topical potent corticosteroids for excessive granu-lation tissue. American Society for Dermatologic Surgery,25, 517.
Nunley, D., & Berk, S. L. (1992). Percutaneous endoscopicgastrostomy as an unrecognized source of methicillin-resistant Staphylococcus aureus colonization. AmericanJournal of Gastroenterology, 87, 58–61.
Oliveria-Gandia, M., Davis, S. C., & Mertz, P. M. (1998).Can occlusive dressing composition influence prolifera-tion of bacterial wound pathogens? Wounds, 10, 4–11.
Preshaw, R. M. (1981). A percutaneous method for insert-ing a feeding-gastrostomy tube. Surgery, Gynecology, &Obstetrics, 152, 659–660.
Shand, A., Pendlebury, J., Reading, S., Papachrysostomou,M., & Ghosh, S. (1997). Endoscopic fibrin sealant injec-tion: A novel method of closing a refractory gastrocuta-neous fistula. Gastrointestinal Endoscopy, 46, 357–358.
492 GASTROENTEROLOGY NURSING
3214-04_GN280605_Goldberg.qxd 12/16/05 3:15 PM Page 492

Solomon, S. M., & Kirby, D. F. (1990). The refeeding syn-drome: A review. Journal of Parenteral & Enteral Nutri-tion, 14, 90–97.
Sriram, K., Jayanthi, V., Lakshmi, R. G., & George, V. S.(1997). Prophylactic locking of enteral feeding tubeswith pancreatic enzymes. Journal of Parenteral &Enteral Nutrition, 21, 353–356.
Trick, W. E., Weinstein, R. A., DeMarais, P. L., Kuehnert,M. J., Tomaska, W., Nathan, C., et al. (2001). Coloniza-
tion of skilled-care facility residents with antimicrobial-resistant pathogens. Journal of the American GeriatricSociety, 49, 270–276.
Wollman, B., D’Agostino, H. B., Walus-Wigle, J. R., Easter,D. W., & Beale, A. (1995). Radiologic, endoscopic andsurgical gastrostomy: An institutional evaluation andmeta-analysis of the literature. Radiology, 197, 699–704.
VOLUME 28 • NUMBER 6 493
Instructions:• Read the article on page 485.• Take the test, recording your answers in the test answers
section (Section B) of the CE enrollment form. Eachquestion has only one correct answer.
• Complete registration information (Section A) and courseevaluation (Section C).
• Mail completed test with registration fee to: LippincottWilliams & Wilkins, CE Group, 333 7th Avenue, 19thFloor, New York, NY 10001.
• Within 4-6 weeks after your CE enrollment form isreceived, you will be notified of your test results.
• If you pass, you will receive a certificate of earned con-tact hours and answer key. If you fail, you have theoption of taking the test again at no additional cost.
• A passing score for this test is 11 correct answers.• Need CE STAT? Visit www.nursingcenter.com for imme-
diate results, other CE activities, and your personalizedCE planner tool.
• No Internet access? Call 800-933-6525 for other rushservice options.
• Questions? Contact Lippincott Williams & Wilkins:646-674-6617 or 646-674-6621.
Registration Deadline: December 31, 2007.
Provider Accreditation:This Continuing Nursing Education (CNE) activity for 2.5contact hours is provided by Lippincott Williams & Wilkins,which is accredited as a provider of continuing education innursing by the American Nurses Credentialing Center’sCommission on Accreditation and by the American Associa-tion of Critical-Care Nurses (AACN 00012278, CERP Cate-gory O). This activity is also provider approved by the Cali-fornia Board of Registered Nursing, Provider Number CEP11749 for 2.5 contact hours. LWW is also an approvedprovider of CNE in Alabama, Florida, and Iowa and holdsthe following provider numbers: AL #ABNP0114, FL
#FBN2454, IA #75. All of its home study activities are classified for Texas nursing continuing education require-ments as Type I.
Your certificate is valid in all states. This means that yourcertificate of earned contact hours is valid no matter whereyou live.
Payment and Discounts:• The registration fee for this test is $20.00 for members;
$25.00 for nonmembers.• If you take two or more tests in any nursing journal pub-
lished by LWW and send in your CE enrollment formstogether, you may deduct $0.75 from the price of eachtest.
• We offer special discounts for as few as six tests andinstitutional bulk discounts for multiple tests. Call (800)933-6525, ext. 6617 or 6621 for more information.
CE TestGastrostomy Tubes: Facts, Fallacies, Fistulas, and False Tracts
CE TEST QUESTIONS
GENERAL PURPOSE: To familiarize the registered professional nurse withthe experiences of pediatric patients who have undergone radiographicplacement of enteral feeding tubes at The Children’s Hospital of Philadelphia.
LEARNING OBJECTIVES: After reading this article and taking this test,the reader will be able to:
1. Describe the pre- and postprocedural care of the patient receiving agastrostomy tube.
2. Explain the complications of gastrostomy and gastrojejunostomy tubes.
1. The primary purpose of the gastrostomy tube nurse is toa. provide outpatient and home care to the patient with a gastrojejunostomy tube.b. perform enteral feedings.c. facilitate and coordinate care of the patient before and after tube placement.d. participate in gastrostomy care research.
2. The primary purpose of the Pediatric Enteral Access Clinicis toa. provide outpatient care to the child who has or is in need of a gastrostomy
tube.b. perform outpatient research.c. provide inpatient access to enteral feedings.d. perform nutritional needs assessments related to the chronic care of patients
receiving enteral feedings.
3. Which of the following is mandatory before gastrostomytube placement can proceed?a. chest x-rayb. upper GI series
c. esophageal reflux studiesd. colonoscopy
4. If a child is malnourished the nurse should be concernedabouta. refeeding syndrome.b. dumping syndrome.c. gastroesophageal reflux disease.d. regurgitation.
5. Which of the following decreases the chance of refeedingsyndrome?a. a fast increase in the rate of nasogastric tube feedingsb. a slow increase in the rate of nasogastric tube feedingsc. a decreased volume of nasogastric tube feedingsd. an increased volume of nasogastric tube feedings
6. Which of the following is performed to confirm intragastricplacement after the first changing of the gastrostomy tube?a. a wound checkb. a lower GI studyc. a dye studyd. an abdominal flat plate x-ray
7. A patient is experiencing a major complication of gastro-stomy tubes if they havea. migration of the tube.b. a dislodged tube.c. bleeding.d. stoma irritation.
3214-04_GN280605_Goldberg.qxd 12/16/05 3:15 PM Page 493
Test Answers: Darken one for your answer to each question.B
Course Evaluation*C Two Easy Ways to Pay:D
A B C D1. ❍ ❍ ❍ ❍2. ❍ ❍ ❍ ❍3. ❍ ❍ ❍ ❍4. ❍ ❍ ❍ ❍
A B C D5. ❍ ❍ ❍ ❍6. ❍ ❍ ❍ ❍7. ❍ ❍ ❍ ❍
A B C D8. ❍ ❍ ❍ ❍9. ❍ ❍ ❍ ❍
10. ❍ ❍ ❍ ❍
A B C D11. ❍ ❍ ❍ ❍12. ❍ ❍ ❍ ❍13. ❍ ❍ ❍ ❍
A B C D14. ❍ ❍ ❍ ❍15. ❍ ❍ ❍ ❍16. ❍ ❍ ❍ ❍
A B
1. Did this CE activity’s learning objectives relate to its ❑ Yes ❑ Nogeneral purpose?
2. Was the journal home study format an effective way ❑ Yes ❑ Noto present the material?
3. Was the content relevant to your nursing practice? ❑ Yes ❑ No
4. How long did it take you to complete this CE activity?____ hours____minutes
5. Suggestion for future topics_____________________________________
❑ Check or money order enclosed
(Payable to Lippincott Williams & Wilkins)
❑ Charge my ❑ Mastercard ❑ Visa ❑ American Express
Card #_____________________________________Exp. Date_________
Signature___________________________________________________
*In accordance with the Iowa Board of Nursing Administrative rules governinggrievances, a copy of your evaluation of the CE offering may be submitteddirectly to the Iowa Board of Nursing.
Registration Information:
Last name______________________ First name____________________MI____
Address__________________________________________________________
City_______________________________State_________________Zip_______
Telephone___________________Fax______________email________________
Registration Deadline: December 31, 2007.
Contact Hours: 2.5
Fee: $20.00 for members
$25.00 for nonmembers
❑ LPN ❑ RN ❑ CNS ❑ NP ❑ CRNA ❑ CNM ❑ other______________
Job Title______________________Specialty_____________________________
Type of facility_____________________________________________________
Are you certified? ❑ Yes ❑ No
Certified by_______________________________________________________
State of License (1)__________License #________________________________
State of License (2) __________License#________________________________
A
CE Enrollment FormGastroenterology Nursing, November/December 2005
Gastrostomy Tubes: Facts, Fallacies, Fistulas, and False Tracts
Need CE STAT? Visit www.NursingCenter.com for immediate results, other CE activities, and your personalized CE planner tool!
8. The American Society of Gastrointestinal Endoscopy rec-ommends which of the following before PEG placement inall patients?a. upper GI seriesb. antibiotic prophylaxisc. enteral feeding challenged. high protein diet
9. Retrograde migration of the gastrostomy tube’s innerbumper or balloon into the abdominal wall or into thestoma tract refers to which of the following syndromes?a. retrograde balloon syndromeb. buried bumper syndromec. aberrant tract syndromed. gastrostomy fistula syndrome
10. A patient who may be suffering from buried bumpersyndrome hasa. severe abdominal pain.b. stoma leakage and focal abdominal discomfort.c. projectile vomiting and abdominal swelling.d. persistent peristomal skin breakdown.
11. To measure a low profile gastrostomy tube for the properlength, the measuring device balloon should be filled withwhich of the following to obtain an accurate measurement?a. 5 to 7 cc of waterb. 10 to 15 cc of waterc. 10 cc of normal saline solutiond. 20 cc of normal saline solution
12. The following is helpful in venting gastrostomy tubes?a. changing to a maintenance tubeb. upsizing the width of the tubec. Farrell valve setd. Heimlich valve
13. A persistent gastrocutaneous fistula does not closea. spontaneously 1 month after removal of the gastrostomy tube.b. immediately after removal of the gastrostomy tube.c. after surgical wound closure.d. gradually 3 months after removal of the gastrostomy tube.
14. Granulation tissue occursa. when the gastrostomy tube migrates upward.b. after the gastrostomy tube has been in place for 2 weeks.c. after a gastrocutaneous fistula has closed.d. around the external stoma opening, inside the stoma tract, and within the
gastric opening.
15. Which of the following should be avoided when treatinggastric prolapse?a. occlusive dressingsb. topical corticosteroidsc. Stomahesive powderd. silver nitrate cauterization
16. Clogging of “J” tubes can be prevented bya. monthly replacement of the tube.b. routine flushing with water.c. dilution of the enteral feeding formula with water.d. flushing pancreatic enzyme solution with normal saline and heparin solution.
494 GASTROENTEROLOGY NURSING
3214-04_GN280605_Goldberg.qxd 12/16/05 3:15 PM Page 494