Fourth Mission on DOTS Implementation in Tajikistan
35
Fourth Mission on DOTS Implementation in Tajikistan 22 November to 2 December 2002 Conducted by the World Health Organization, Ministry of Health of Tajikistan and Project HOPE Prepared by Drs Pierre-Yves Norval, WHO, G. Tsogt, WHO, Dennis Falzon, WHO Regional Office for Europe Tuberculosis Programme, Konrad Juszkiewicz, Project HOPE
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Fourth Mission on DOTS Implementation in Tajikistan

Fourth Mission on DOTS Implementation in Tajikistan
22 November to 2 December 2002
Conducted by the World Health Organization, Ministry of Health of Tajikistan and Project HOPE Prepared by Drs Pierre-Yves Norval, WHO, G. Tsogt, WHO,
Dennis Falzon, WHO Regional Office for Europe Tuberculosis Programme, Konrad Juszkiewicz, Project HOPE

E78552
Keywords
TUBERCULOSIS, PULMONARY – drug therapy – epidemiology ANTITUBERCULAR AGENTS – administration and dosage COMMUNICABLE DISEASE CONTROL – organization and administration NATIONAL HEALTH PROGRAMS – organization and administration VACCINES – supply and distribution HEALTH POLICY TAJIKISTAN
© World Health Organization – 2003 All rights in this document are reserved by the WHO Regional Office for Europe. The document may nevertheless be freely reviewed,abstracted, reproduced or translated into any other language (but not for sale or for use in conjunction with commercial purposes) provided that full acknowledgement is given to the source. For the use of the WHO emblem, permission must be sought from the WHORegional Office. Any translation should include the words: The translator of this document is responsible for the accuracy of the translation. The Regional Office would appreciate receiving three copies of any translation. Any views expressed by named authors aresolely the responsibility of those authors.
This document was text processed in Health Documentation Services
WHO Regional Office for Europe, Copenhagen

CONTENTS
Page
1. Recommendations...............................................................................................................................1 1.1 Policy issues..............................................................................................................................1 1.2 Technical issues ........................................................................................................................1
2. Main achievements in 2002 and remaining concerns .........................................................................3 2.1 Achievements in 2002 ..............................................................................................................3 2.2 Remaining concerns..................................................................................................................4
3. Objectives and activities .....................................................................................................................5 3.1 Objectives .................................................................................................................................5 3.2 Activities...................................................................................................................................6
4. Epidemiology of tuberculosis .............................................................................................................6 4.1 DOTS detection ........................................................................................................................8 4.2 Outcomes ..................................................................................................................................8
5. TB policy for DOTS expansion ..........................................................................................................9 5.1 Political commitment................................................................................................................9 5.2 Funding mechanism..................................................................................................................9 5.3 Partnership ..............................................................................................................................10 5.4 Main policy documents...........................................................................................................11
6. DOTS implementation and plan for expansion.................................................................................12 6.1 DOTS implementation in pilot areas and DOTS expansion...................................................12 6.2 DOTS coverage.......................................................................................................................13 6.3 Human resource ......................................................................................................................13 6.4 Training and supervision ........................................................................................................14 6.5 Diagnosis ................................................................................................................................14 6.6 TB treatment regimen .............................................................................................................15 6.7 DOTS......................................................................................................................................16 6.8 Food support ...........................................................................................................................16 6.9 Recording and reporting .........................................................................................................17 6.10 Drugs supply, storage, distribution, and monitoring...............................................................18 6.11 GDF Drugs needs in 2003 ......................................................................................................19 6.12 Laboratory supplies.................................................................................................................23 6.13 Budget 2002 and partnership (see part 5.3 and 5.4 page 12 above) .......................................23
Annex 1. Visit schedule and persons met...................................................................................................25
Annex 2. TB drugs formulation for children and adults using 2 FDCs (R150H100) ...............................27
Annex 3. Quarterly order form for TB drugs .............................................................................................28
Annex 4. Quarterly order form for laboratory supplies..............................................................................29
Annex 5. Core functions of the central TB team........................................................................................30


EUR/03/5037563 page 1
1. Recommendations
1.1 Policy issues
1. The Ministry of Health of Tajikistan should be officially constituted as a National Tuberculosis (TB) Programme team of 5–10 people with job descriptions, including 2 additional supervision staff and 2 additional central laboratory staff. The central TB team and Project HOPE should develop common working plan and identify counterparts for Project HOPE staff at central level.
2. The Ministry of Health should continue to expand DOTS strategy in phase manner in the 10 following TB centres during next 12 months: Leninsky raion – 2 zones in December 2002 and 1 zone in January 2003; Hissar TB Dispensary in March 2003; Kuliab TB Dispensary in May; Khojent TB Dispensary in July; Khorog TB Dispensary in August; Matcha TB Dispensary in September; Isfara TB Dispensary in October; and Kanibadam TB Dispensary in November.
3. In order to expand DOTS, the Ministry of Health with the central TB team should develop following steps:
�� establish ICC and hold meetings at least once a year;
�� finalize the 5 year costed DOTS expansion plan;
�� endorse and print national TB medical guidelines and distribute it;
�� establish central laboratory (rehabilitation, staff etc);
�� promote intermediate level at regional level (2 to 3 in RRS, GBAO, Khatlan, Sogd) in charge of TB control for several districts.
4. The Ministry of Health should change budget allocation system based on number of beds to more rationalized system allowing decrease of excessive number of beds in general hospital, integration of TB beds inside general hospital, ambulatory strategy on line with DOTS strategy. Ratio based on population covered/number of smear positive case diagnosed and cured, level of work (village, district, region, central, urban) should be elaborated.
1.2 Technical issues
5. Mapping and inventory: The Central TB team should identify and map in each DOTS area one TB laboratory (per 50 000–100 000 population), hospitalization location (10 to 20 beds per 100 000 population), DOTS relays for continuation phase (1 per each 5000 to 10 000 population), inventory of existing staff equipment and staff identified at each level to be trained.
6. TB drugs: a) The Ministry of Health should send during the first quarter of 2003 the next GDF
order for streptomycin and a 1 year supply + 6 month buffer stock based on blister pack of 4-FDCs (R150H75Z400E275) and 2-FDCs (R150H150) with following quantity:

EUR/03/5037563 page 2
Expected arrival date March 2003 June 2003 RHZE blister 1 355 000 RH blister 1 730 000 E 326 000 S 10 000 81 600 Water 10 000 81 600 H 536 000
Syringes and needles should be provided by the national budget or other sources. The following regimen should be adopted:
– Category I 2(RHZE)/4(RH) 3 (fully supervised)
– Category II 2S(RHZE)/(RHZE)/5(RH) 3E3 (fully supervised)
– Category III 2(RHZE)/4(RH) 3 (fully supervised)
– Prophylaxis 6H (without supervision).
b) GDF should initiate issuance of temporary registration license of donated pharmaceutical for 4-FDCs (R150H75Z400E275) and 2-FDCs (R150H150) and send in January 2003 to the Ministry of Health in Tajikistan c/o WHO:
– Application for registration of 4-FDCs (R150H75Z400E275) and 2-FDCs (R150H150) prepared by the supplier;
– Certificate on pharmaceutical product (WHO recommended form);
– Russian pharmacopoeia (European, British, United States pharmacopoeia accepted);
– License for import based on batch certificate;
– Instruction on use of medicines (if possible in Russian language);
– Certificate of quality of pharmaceutical product entering international trade;
– 50 tablets of 4-FDCs (R150H75Z400E275) and 50 tablets of 2-FDCs (R150H150) for quality control.
c) The central TB team should implement in early 2003 a new drug management system and train pharmacists from all DOTS TB centre based on: 1) quarterly order TB drugs form sent together with the quarterly report on notification and treatment outcome; 2) three months delivery supply based on the quarterly TB drugs order form and notification; and 3) Simplified TB drug register.
7. Diagnosis and treatment: a) The TB reference laboratory should be established in adequate space and design to
serve its function for the entire country.
b) The TB central team should carefully monitor use of X-ray and apply the recommended diagnosis procedure based on smear examination only. The TB central team should stop active screening with fluorography.
8. Logistics: Car transportation should be provided and strictly reserved for supervision, monitoring and drug/lab supplying. This should not be used for patient tracing, collection of sputum containers and other individual management purposes.

EUR/03/5037563 page 3
9. DOTS: The TB central team should promote ambulatory treatment during entire treatment in Dushanbe polyclinics and the prikaz revised accordingly. Existing regulations, which do not allow treatment of smear positive patient on outpatient basis, should be revised. Outside Dushanbe, continuation phase should be provided on ambulatory basis preferably by health care workers.
10. Social support: The TB team should consider food support as a social incentive to increase access and case detection and establish careful monitoring of diagnosis before food supply is provided. WFP should consider possibility to provide food for TB health worker.
11. SES should conduct control according to DOTS strategy including defaulter tracing.
2. Main achievements in 2002 and remaining concerns
2.1 Achievements in 2002
�� Government political commitment for DOTS implementation is very high, as demonstrated through the release of an important prikaz 192 on 8 July 2002 endorsing the main components of DOTS strategy and the preparation of a pricaz to expand DOTS in Leninsky raion.
�� The Ministry of Health successfully implemented DOTS in 7 TB pilot sites covering all Dushanbe city, representing 10% of the country population, and following the plan drafted last year. Initial smear conversion rates among new cases tested at month 2 reached 77%.
�� All DOTS component were successfully implemented:
– The central laboratory has been strengthened with equipment and reagent. Diagnosis of case is based on smear exam in all 7 DOTS TB pilot sites;
– Standardized treatment has been successfully applied in DOTS centres;
– DOTS is applied on full ambulatory basis for 18% of the cases and through hospitalized and ambulatory basis for the rest;
– Registration system is in place and well maintained (TB forms, Lab and medical register, PHC register);
– Drugs were correctly stored, packaged in kit form and distributed;
– Extensive amount of training and supervision activities have been conducted for TB staff.
�� All Ministry of Health and Project HOPE TB staff met during the visit were very dedicated to DOTS strategy and knowledgeable.
�� TB drugs provided by GDF is properly managed including custom clearance, registration, storage, packaging and distribution.
�� Laboratory supply for one-year consumption and binocular microscopes for DOTS areas have been secured.
�� Partnership for TB has increased with the support of GDF, Project HOPE, USAID and WFP. Additional NGOs have shown some interest to implement DOTS, such as Merlin, Aga Khan Foundation and IFRC for food distribution.

EUR/03/5037563 page 4
2.2 Remaining concerns
Policy issues �� There is insufficient staff at central level and no identified supervision team in charge of
specific DOTS areas. There is also lack of staff at central and peripheral laboratory level.
�� Policy documents need to be completed: 5-year costed plan, medical and PHC guidelines, job descriptions, detailed NTP prikaz not yet finalized.
�� Coordination mechanism led by NTP between NGOs interested in TB support and Ministry of Health is too limited. It is expected that ICC meetings will allow an increase in transparency and help identify financial and technical gaps.
�� The GFATM proposal is not technically sound (eg. extensive number of X-ray film for US $450 000 per year), with duplicate requests for TB drug support (i.e. TB drugs from GFATM and from GDF), does not demonstrate complementarity (Project HOPE budget and technical support not included).
�� Irregular distribution of TB beds throughout the country with an excessive number of TB beds in 26 places and lack of TB beds in other districts limiting decentralization of initial phase at district level. Extensive habits of specialized TB institutions and budget allocation based on number of beds constitute major obstacles to integrate and better distribute TB beds in general hospital.
�� No clear mapping of DOTS catchment areas by district and oblast available with the central TB team.
�� Lack of identified DOTS intermediate level available with the central TB team.
�� Lack of detailed working plan between the central TB team and Project HOPE for DOTS expansion. Define more precisely role and task of staff from the central TB team and Project HOPE in order to improve future DOTS expansion.
�� Lack of incentive to TB staff.
Technical issues �� Lack of clear plan to supervise continuation phase in rural area. It is not clear if the link
between TB centre and PHC will function. The following issues are not fully resolved: transfer of sputum container to upper level, communication system, transfer of TB drugs for each patient kit to the health post, registration at health post level, supervision from upper level giving lack of any transportation means.
�� Use of streptomycin in category 1 regimen (2SRZH/5R3H3) was not initially planned leading to over consumption of sptrepmycin.
�� Current TB drugs distribution is not applicable outside Dushanbe and needs to be revised. Pull system based on quarterrly order needs to be introduced.
�� Quality assurance has not started yet and there is little attraction for laboratory staff to work on TB.
�� Systematic use of X-ray for diagnosis and follow-up disregarding the recommended diagnosis procedure. There is still extensive use of fluorography
�� There is lack of means of transportation at central level and in future also anticipated at intermediate level for programme management issues (supervision, TB drug distribution).

EUR/03/5037563 page 5
Table 1. Next Steps in 2003
Action Responsible Time US $
1. Stop use of streptomycin in category 1 regimen. TB team 12.2002
2. Finalize national medical TB guidelines. Endorse the guidelines by the Ministry of Health. Print the medical and PHC TB guidelines (100 to 300 copies each) and distribute.
TB team WHO HOPE
12.2002 3000
3. Constitute TB training and monitoring team among central TB team and establish together with HOPE incentives system for trainers and supervisors.
MOH TB team HOPE
12.2002 5000
4. Prepare TB drug (and lab supply) distribution plan based on quarterly order form in Leninsky raion.
TB team HOPE 1.2003
5. Conduct training for medical-lab and PHC staff in Leninsky raion.
TB team Hope 12.2003 2000
6. Prepare 5 year costed DOTS expansion plan. TB team WHO 2.2003
7. Constitute and held ICC meeting with all partners and TB staff from raions to present status of DOTS expansion and 5 year cost DOTS expansion plan.
MOH TB team WHO
4.2003 4000
8. Conduct training workshops for next 2 raions to implement DOTS (Hissar and) based on the national TB guidelines.
TB team HOPE 2.2003 2000
9. Conduct regular on-site training for laboratory technicians from Dushanbe, Machenton and Leninsky to improve their practice.
TB central lab team, HOPE
Once per month
10. Collect and analyse quarterly TB order form from each TB centre together with case notification report during the first week after the end of each quarter.
TB team HOPE
Month 1, 4, 7,10
11. Arrange quarterly meeting with TB staff from polyclinics, Machenton and Leninsky TB centre.
TB team HOPE
Month 1, 4, 7,10 3000
12. Equip central level with cars for supervision and drug delivery.MOH WHO HOPE
2003 30 000
3. Objectives and activities
3.1 Objectives
WHO with collaboration of the Ministry of Health and project HOPE undertook a mission to Tajikistan with the following objectives:
1. To monitor DOTS implementation in pilot areas in 2002 including diagnosis and treatment guidelines, prikaz, training and supervision activities, reporting and recording, drug management, laboratory activities and quality assurance, case detection and treatment outcome;
2. To monitor GDF support and prepare drug needs for one year of GDF support;
3. To conduct one day training session on recording and reporting system;
4. To submit a report at the end of the mission.

EUR/03/5037563 page 6
3.2 Activities
From 25 November to 2 December 2002, Drs G. Tsogt, Pierre-Yves Norval (WHO consultant), Dr Dennis Falzon (WHO/EURO TB), Mr Konrad Juszkiewic and Mr Thomas Mohr (Project HOPE) participated in meetings with Mr Latipov Asomiddin (Deputy Minister, Ministry of Health of Tajikistan), discussed the state of DOTS implementation in pilot areas and future plan to expand DOTS with the team of the National TB Centre (NTC), deliver lectures to TB health staff and head doctors from Dushanbe and Leninsky and meet partners to be involved in DOTS implementation. The Mission visited Dushanbe Republic TB centre, Polyclinics 1, 2, city TB centre, Machenton hospital, Tajik Pharmacy Fabrika, Children’s TB Hospital, Leninsky raion hospital and TB dispensary. The Mission is grateful to the officials of the Ministry of Health and Professor Sirojiddinova and her team for their cooperation and generous hospitality. This report includes: (i) an analysis of TB epidemiology and notification, using data from the NTC; (ii) policy issues; (iii) DOTS implementation status and DOTS expansion plan; and (iv) GDF monitoring system.
4. Epidemiology of tuberculosis
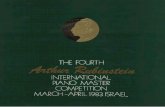
For the past decade, the notification rate of TB in Tajikistan has been the lowest in the former Soviet Central Asian Republics (CAR), and in 2001 it notified three times less cases per population than Kazakhstan (see Graph 1, 2). While there is anecdotal evidence of much TB morbidity and mortality, patient access to care has been hindered by the lack of free TB medication, diagnostic services, difficult terrain and conflict. The dip in notifications in the early 1990s coincides with the period of the civil war following independence. Since then, notifications picked up steadily and the current rate is comparable to the one in the mid-1980s. Tajikistan is the least affluent of the CARs, and it has endured the same health service reversals as its neighbours following the dismantlement of the Soviet Union. In 1998, Tajikistan ranked 108 among 174 countries in the world on the Human Development Index. Its GDP (adjusted for PPP) is less than a half of the CAR average, and over 80% of the population fall below the poverty line. The ratio of physicians to population is much higher in the cities than in the rural areas. BCG vaccination levels at childbirth are reportedly low, as many deliveries are nowadays done at home with limited medical care. Up to June 2002, only one AIDS case and 58 HIV infections have been reported. Table 2 shows the trend for TB between 1995 and 2001. Data on sputum positive notifications has been available since 1998, and although the term applies to BK+, this refers almost solely to smear positive detection since culture has not been performed in the country for some time. The quality of smear microscopy has been problematic lately, so these figures should still be treated with caution. Additionally, standardized definitions of new and retreatment have only started being applied from 2002, and only in the pilot DOTS areas in Dushanbe city. Since 1995, total TB notification rates have fluctuated around 40% of what the WHO estimates for incidence. The sharp increase of notifications in 2001 may be partly explained by improved detection of smear positive cases in the city prison in that year with the assistance of an external agency. No consistent data could be obtained for the first three quarters of 2002.

EUR/03/5037563 page 7
Table 2. TB notification 1995-2002 and estimates 2002-2005
1995 1996 1997 1998 1999 2000 2001 2002 DOTS* non DOTS
2003 2004 2005
S+ TB case 435 622 434 781 62 Relapse 28 S- TB case 1 636 1 589 1 918 2 346 23 EP TB case 376 34 427 381 37 Total TB 1 659 1 647 2 007 2 447 2 552 2 779 3508 150 TB notif.rate/100000 S+/100000
28.8 28.2 33.9 40.7 7.2
41.8 10.2
44.9 7
55.8 12.4
Detection rate % 40.8% 36.1% 39.3% 42.8% 39.9% 38.9% 39.8% Estimate numberTB 4 071 4 557 5 103 5 714 6 395 7 151 7 990 786 8 136 9 962 11 129 12 442 Estimate rate/100000h 71 78 86 95 105 115 127 140 154 170 187
Population 5 754 426 5 840 132 5 927 114 6 015 392 6 103 670 6 193 244 6 284 132 562 000 5 814 563 6 469 929 6 564 877 6 661 219 * July to November 2002
0
45
90
135
180
225
1980 1981 1982 1983 1984 1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001
Cases / 100 000
TB Notification rates, Central Asian Republics, 1980–2001Source: WHO Global TB Report, 2002 / EuroTB data
Tajikistan
Other CAR countries
0
45
90
135
180
1980 1981 1982 1983 1984 1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000
Cases / 100 000Graph2: TB Notification rates, Central Asian Republics, 1980-2001
Source: WHO Global TB Report, 2002 / EuroTB data
Tajikistan
Other CAR countries
Graph 2. TB notifications, Central Asian Republics 1980–2001 Source WHO Global TB Report, 2002/EURO TB data
Cases/100 000
Other CAR countries
Tajikistan

EUR/03/5037563 page 8
4.1 DOTS detection
Table 3 shows registrations in the 7 city polyclinics participating in the pilot phase of DOTS (population 568 500), from July to October 2002. The indices of the registered cases were within acceptable limits, i.e. 75% were pulmonary (target > 80%) and 80% of pulmonary cases were sputum smear positive (target = 65-80%). The sex ratio of these cases was nearly 1, and over 70% of new smear positives were under 35 years, most being in the 15–24 year age group. Relapse rate is 19% of notified cases (28/150) and retreatment rate is 36% of notified cases (48/150). Table 3 also shows the mean detection of all new and relapse cases by clinic for each month based on the registrations undertaken in the first four completed months. It is thus estimated that over 1000 such cases will be detected in the first year of DOTS, although this may be an overestimate since recruitment in the first months may be higher than expected and access may also drop in the winter months. On the other hand, a number of re-treated cases may also be started on treatment and these would not show up on the standard TB07 report.
Table 3. DOTS detection, Dushanbe, July–October 2002.
Clinic New SS+ New SS- New EP Relapse Total Mean cases* month Expected /12 mnths1 (+6) mid7/2002 13 6 10 5 34 9 108 2 (+5) 9/2002 13 6 6 1 26 13 156 Central PC 9/02 8 5 8 8 29 15 180 7 (+13) 9/2002 10 2 5 3 20 12 144 9 (+10) 10/2002 4 0 5 5 14 14 168 8(+12) 9/2002 3 1 0 1 5 3 36 10(+14) 10/2002 11 3 3 5 22 22 264 Total 62 23 37 28 150 88** 1056**
* clinics opened at different time during period (see Table under DOTS implementation) ** plus 20 treatment after interruption since July i.e 7 per month equivalent to 95 TB all form per month or 1140 per year.
4.2 Outcomes
Out of 37 new cases registered between July and September in DOTS areas, 30 cases had smear results for the end of the second month by 26 November, while the remaining 7 were still pending. Early conversions were achieved in 23/30 (77%), and 7 failed to convert. This is short of the 85% target although numbers are relatively small. Lower performance may be due to some previously treated cases among new cases due to inadequate enquiry before starting treatment. Five of the 12 relapses registered in the 3rd quarter also had results, with 3 of them becoming negative at 3 months and 2 remaining positive. Treatment outcomes reported for cases treated by regimen other than DOTS in 2000 are not reliable (665 new and 9 retreatment smear positives). The size of these cohorts exceed the number of cases notified to WHO/EURO TB for the same period. The success rates were claimed to be 77% in new and 67% in retreatment cases, with 15% of cases dying while on treatment. Some case histories were examined in Dushanbe republican dispensary for this period; apart from the fact that treatment was not standardized (composition, duration), the time of testing was also not fixed for these patients. A number of defaulters were noted as well although

EUR/03/5037563 page 9
none were reported in the official statistics. Hence there are reservations about concluding much on these outcomes. Active case detection performed in 2001 in Dushanbe prison with the help of Global Partner NGO has contributed to the total increase of smear positive TB case notification. Out of 421 prisoners screened for TB, about 212 smear positive cases were diagnosed and treated with 6 months regimen treatment 2RHZE/4RH. Unfortunately approximately half of the TB cases diagnosed in prison default after 2 to 3 months treatment leading to the retrieval of the NGO support in Dushanbe prison.
5. TB policy for DOTS expansion
5.1 Political commitment
Pricaz 192 dated 8 July 2002 from the Minister of Health of Tajikistan officially endorse DOTS strategy and allow to start to implement DOTS in Tajikistan. DOTS was successfully implemented in 2002 in Dushanbe capital city covering within less than 6 months nearly 10% of the population demonstrating Ministry of health political commitment for change. DOTS was implemented in all 6 polyclinics and the TB city centre and continue to demonstrate excellent results. This excellent achievement is mainly due to strong political commitment to DOTS in Tajikistan. A new pricaz has been prepared but not yet signed for expansion of DOTS in Leninsky raion. Additional regulation could be developed to facilitate rationalization of TB care through integration of TB beds in general hospital with low occupancy rate and located inside the cities and to involve PHC facilities in ambulatory treatment. However, major obstacles are due to inadequate budget allocation based on number of beds freezing any change (see below). The number of TB beds in Tajikistan is centralized in 26 TB hospitals most often located outside the city and not properly distributed throughout the country. Integration of TB control activities in general hospitals has a clear aim to better rationalize TB services and increase case detection. This ambitious change will need prior discussion with head doctor currently involved in TB training.
5.2 Funding mechanism
Thanks to the national budget, Project HOPE, GDF and WHO support, most activities and supply needed to start DOTS implementation were available in 2002. However, the Ministry of Health does not have a clear picture of available funds from external partners, budget needs and gaps. Budget coordination mechanism should be based on complementary and additionally of different funding sources. ICC meeting should address in transparent way clear budget plan from each partner. Tajikistan applied successfully to GDF and was approved for a 3-year agreement ensuring drug support for DOTS areas countrywide. GDF could also be considered as very cost-effective supplier in the future for centralized purchase for TB drugs (US $10 per treatment, i.e. 10 times

EUR/03/5037563 page 10
cheaper than TB drugs purchase locally with drug quality control insured) and soon for laboratory supply. Tajikistan also applied for GFATM appeal in September 2002 for US $7 million for 4 years support. There is limited chance that GFATM application will be approved as it is not technically sounded with extensive use of X-ray films (US $450 000 per year) and does not meet the requirement for complementarity of support at least for TB drugs already provided by GDF and for project HOPE support not included in the proposal. However, Tajikistan meets most of the economic criteria to benefit from GFATM and has large need to expand DOTS countrywide. New GFATM proposal should be prepared with clear DOTS expansion plan, budget need especially regarding transportation, rehabilitation, equipment, budget distribution and gaps. Although the national budget is insufficient to support most of the TB operational expenditure and modern equipment the current budget allocation based on number of TB beds does not allow rationalization of expenditure and integration of TB beds in general hospital as mentioned above. Better rationalization of expense could be discussed and tested to adapt the national budget to DOTS strategy needs. Criteria could be based on ratio of population covered, case notification and treatment outcome and level of work. To replace the allocation based on beds leading to excess number of unoccupied beds.
Recommendations The Ministry of Health should analyse and revise allocation of the national budget according to DOTS strategy replacing the budget allocation based on beds toward ratio composed on population covered/number of smear positive case diagnosed and cured, level of work (village, district, region, central, urban). The Ministry of Health should initiate integration of TB bed in general hospitals starting in the TB centre without TB beds. Pricaz or local agreement could be start in 2 DOTS TB centre in Leninsky raion starting DOTS without TB beds close to laboratory services. The Ministry of Health and the Central TB team should prepare a new GFATM application in based on DOTS strategy. Policy documents (5 year costed DOTS expansion plan, existing pricaz on DOTS strategy, TB guidelines) and ICC meeting demonstrating the complementarity of funding should be consider as the basis of a sound technical and financial proposal.
5.3 Partnership
WHO, WFP, USAID, Project HOPE and CDC Atlanta are currently the main external partners to support DOTS implementation in Tajikistan. Additional external partners were seeking to contribute to DOTS implementation at peripheral level in 2003, i.e. Aga Khan Foundation, Merlin, Swiss Development Agency and IFRC. The TB interagency committee has not been established in Tajikistan. The aim of such a committee is to bring together influential and interested persons, technical agencies supporting the NTP, aid agencies, national and international NGOs, associations and representatives of civil society to form a coalition against TB. Events and activities should be arranged every year to contribute to the national DOTS expansion plan and the achievement of its goals.

EUR/03/5037563 page 11
Recommendation The Ministry of Health should establish an Interagency Committee and hold at least a yearly meeting.
5.4 Main policy documents
5-year costed DOTS expansion plan Draft 5-year costed Plan to Stop TB in Tajikistan was prepared in 2000 but never officially endorsed. Updating of this plan aiming at increasing DOTS coverage, improving case detection and cure rates is on preparation and should be completed by mid December 2002. It is anticipated that this midterm plan will increase link and integration of DOTS into the primary and secondary health network by introducing TB activities in hospitals, polyclinics, and primary health care services. It also will define role of central (see Annex 5), intermediate and peripheral level and number of facilities delivering DOTS strategy (diagnosis-treatment and registration). In addition, efforts will be made to ensure the availability of DOTS on an outpatient basis since onset of treatment. The 5-year DOTS expansion plan also calls for a partnership approach to expand ownership for TB control beyond the specialized TB care network. The plan suggests collaboration between various Ministry of Health departments; namely finance, human resources, primary health care, essential drugs, HIV/AIDS programme, communicable diseases, health information, and IEC. Furthermore, the plan envisages collaboration between the many local and international partners including academic institutions, and national and international organizations (WHO, WFP, Agha Khan Foundation, Merlin, Swiss Development Agency, etc.).
TB guidelines Most components of the Primary Health Care TB guidelines have been revised during the mission. Twenty copies of the TB laboratory guidelines prepared by RIT (Research Institute of Tuberculosis, Japan) left by the mission should be used as TB laboratory guidelines. TB medical guidelines need to be completed.
Recommendations The Ministry of Health together with the central TB team should finalized and print national TB control guidelines for medical staff, and PHC staff. TB laboratory guidelines developed by RIT Japan could be used as national guidelines The Ministry of Health should complete and endorse a costed 5-year DOTS expansion plan currently at draft stage including:
�� Role of central, intermediate, TB centre, PHC level;
�� Mapping of TB services with identification of intermediate and peripheral level with following criteria one TB laboratory, 10 TB beds, 10 DOTS providers for continuation phase per 50 000–100 000 population;
�� Links with PHC (polyclinics without TB cabinet, PHC) and with secondary health care (general hospital).

EUR/03/5037563 page 12
6. DOTS implementation and plan for expansion
6.1 DOTS implementation in pilot areas and DOTS expansion
DOTS was implemented successfully since July 2002 in 6 Dushanbe polyclinics and the city centre covering the 4 raions of Dushanbe, representing 562 000 inhabitants or 9% of the country population. Although DOTS implementation started with some delay while awaiting signature of pricaz, it followed the implementation plan agreed during last mission. In 2003, the NTP plan is to expand DOTS outside the capital city as mentioned in the table below. Expected population coverage at the end of 2003 will be 1.5 million inhabitants representing 30% of the country population.
Table 4. DOTS implementation and expansion
Date District DOTS TB centre Population DOTS coverage 2002 11 July 28 August 10 September 29 September December
Dushanbe
October raion Railroad raion Frunze raion Central raion
Leninsky raion: 2
7 TB centres Polyclinics 1 Polyclinics 2, City Centre Polyclinics 7, 8 Polyclinics 9, 10 2 TB centres
54 600
125 785 222 169 136 000 181 000
Cumulative % 1 % 3 % 7 % 9 %
11 % (720 000 h)
2003 January March May July August September October November
Leninsky raion: 1 Hissar, Khorog, Khojent, Kuliab Matcha, Isfara, Kanibadam
8 TB centres 1TB centres 1TB centres 1TB centres 1TB centres 1TB centres 1TB centres 1TB centres 1TB centres
91 000
200 000 210 000 150 000 78 000 84 000 37 000 44 000
13% 16% 19% 22% 23% 24% 25%
26% (1.6 M hab) 2004 RRS (2 to 3)
GBAO Khatlan Sogd 20 to 30 raions Pashar Vosse
6 regional TB centres 20–30 TB centres
75 %
2005 20 to 30 raions 20–30 TB centres 100 % DOTS expansion in 2004 will need to upgrade 6 TB centres into 6 intermediate levels. In addition to TB activities within catchment area of the TB centre, main functions at intermediate level are similar than at central level but for limited number of TB centres i.e. supervision, training, drug and lab supplies management (storage and distribution), data collection and analysis, report to upper level and planning. Identification of regional staff, training of the intermediate level by the central team and equipment with transportation means will allow to expand DOTS in TB centres related to each intermediate level.

EUR/03/5037563 page 13
Selected TB centres to implement DOTS in 2004 and 2005 will be discussed again during the previous year of implementation. Aim is to cover the entire country with 64 TB centres including regional and central level.
6.2 DOTS coverage
DOTS population coverage based on population access to TB polyclinics is 9% in 2002. DOTS coverage for TB facilities trained was 11% at the time of the visit. DOTS TB case coverage was 10% in 2002.
Table 5. DOTS coverage in November 2002
DOTS coverage 11/2002
DOTS TB case coverage 10 % projected
DOTS TB facilities coverage (64 TB facilities)
11% (7/64)
DOTS population coverage 9%
6.3 Human resource
The current central TB team was functioning as mentioned in the last mission report. The central team has been strengthening with 2 additional supervisors. However, there is a need to better define among TB central team a supervision team in charge of specific geographical areas and to increase transportation means at NTP level. The large number of technical staff hired by Project HOPE (11 staff) raise some concerns as they might replace MOH central team leaving aside excessive number of MOH specialized staff. The main aim of additional expertise from Project HOPE is to strengthen central and future intermediate level teams during limited period of time to be defined by Project HOPE and MOH to allow transfer of knowledge and technology.
Table 6. Central TB team 11/2002
Central team Trainers Supervision Information system
TB drugs management
Laboratory Training, QC
Dr Sirojiddinova * Dr Zokirova * Dr Saidaliev * Dr Yusupova Mr Mulomalikov Dr Makhmadova Dr Kosimova Dr Maximova Dr Idrissiva Ms Pashkova * Ms Nikolaeva * Ms Firouza (secret)
X
X
X
X
X
X X
X
X X
X
X
X
X
X
X X
X
X X
X X
Total 10 staff 3 (+1) 6 3 (+1) 3 (+1) 2 (+2) *staff currently involved in the preparation of DOTS implementation at the time of the visit

EUR/03/5037563 page 14
TB specialists from the republican centre were posted in the Dushanbe polyclinics. It is planned to post TB specialist at intermediate level in 2004 to become regional TB coordinators to establish an intermediate level.
6.4 Training and supervision
Nine DOTS medical training courses have been held in 2002 in Dushanbe involving 51 TB medical staff coming from Leninsky raion, Machenton hospital, Dushanbe City Centre and the 6 Dushanbe polyclinics and 58 family doctors. Medical staff received a 3 days session based on training document prepared by the TB team in Russian language adapted from the WHO training module on “management of TB at district level”. Training documents in Russian were provided to every participant and are used as TB guidelines while awaiting the official printing of the Tajik TB guidelines. Three medical doctors have been trained at WHO Warsaw course and 4 specialist (2 from central TB unit, 1 from MOH and one from Hotlon oblast) attended the WHO/Project HOPE 2 week course for TB managers conducted in Almaty in 2002. Several laboratory courses based on the IUATLD laboratory guidelines translated in Russian have been delivered in 2002. Two laboratory staff from central level participated in the laboratory course for Central Asian Republics conducted by WHO/CDC in Almaty in 2002. Illustrative microscopy examination manual have been translated, printed and distributed among laboratory staff by WHO TB Office during the visit. Simultaneous TB laboratory missions were conducted by CDC/USAID at the time of WHO/Project HOPE monitoring mission without clear complementarity between both teams. Incomplete information was collected by WHO/Project HOPE mission. It is expected that CDC will conduct joint mission and prepare joint report in the future. Supervision was conducted together with technical advisers from Project HOPE to every DOTS centre once every alternative week. Transport is provided by Project HOPE and there was a clear need to dedicate specific transportation means for supervision at NTP level. The current pace of supervision will decrease in Dushanbe to become monthly visits in 2003 and quarterly visits in 2004. At least monthly supervision visits outside Dushanbe in DOTS expansion area need to be conducted in 2003 at the time of expansion.
6.5 Diagnosis
Case finding is officially based on systematic smear examination as the first diagnosis step for symptomatic patients. NTP adopted the WHO recommended diagnosis procedure prescribing X-ray and fluroscopy only if 3 smear examination are negative and if 10 days of non-TB specific antibiotics without clinical improvement. However the mission notes extensive use of X-ray, still performed before receiving result of smear exam. All polyclinics continued to be performed X-ray together with smear exam for diagnosis, and during follow up with no added value. Since inception of DOTS, 1675 X-ray and about 1000 smear exams were performed for 412 TB suspects during 1.5 month showing systematic use of Xray. Screening by mass miniature radiography (fluorography) continue to be extensively performed in 2002.

EUR/03/5037563 page 15
Since introduction of DOTS (11.07.2002) in Dushanbe city until 1 November, 48 new smear positive cases were detected in polyclinics. Case detection rate by microscopy examination is 8.6% (out of 599 suspected cases). 60% of positive smears and 10% of negative smears were re-checked by Project HOPE laboratory specialist (Dr. Shulgina.M). False-positive rate was 0.1%, false negative 3.9%.
Recommendation The TB central team should carefully monitor use of X-ray and applied the recommended diagnosis procedure based on smear examination only. The TB central team should stop fluorography
6.6 TB treatment regimen
The Ministry of Health adopted standardized TB treatment regimen at the time of the WHO/MSH mission in May 2001 and TB drugs were ordered accordingly through GDF. Standardized regimen in DOTS areas with DOT during entire regimen is as follows:
�� Category I 2RHZE/4R3H3 (fully supervised)
�� Category II 2SRHZE/RHZE/5R3H3E3 (fully supervised)
�� Category III 2RHZ/4R3H3 (fully supervised)
�� Prophylaxis 6H (without supervision). The mission noted that the 8 month regimen (without rifampicin in the continuation phase) agreed with Ministry of Health in November 2000 during a WHO mission was change to a 6 month regimen in 2001. This change will necessarily need establishment of DOTS providers outside TB centre during the continuation phase to ensure supervision of rifamcin intake. In November 2001, the Indian Government provided TB drugs for approximately 600 TB treatments. These TB drugs were stored in Machenton hospital and used for people living outside Dushanbe during their two-month or more hospitalization phase in Machenton hospital. The regimen used for non-DOTS area were similar than DOTS areas but continuation phase was based on TB drugs prescription without follow-up control, registration nor treatment outcome result contributing to MDR increase. All patients receiving Indian drugs have been discharged at the time of the visit as the Indian drug ran out 3 months ago and patients from non-DOTS areas were currently receiving prescription contributing to MDR increase.
Recommendation The TB central team should conduct during third quarter 2003 refresher course with representatives from all DOTS TB centre to introduce new drug regimen and formulation, (R150H75Z400E275; R150H150), quarterly order forms (annex 3) and pharmacy register:
�� Category I 2(RHZE)/4(RH) 3 (fully supervised)
�� Category II 2S(RHZE)/(RHZE)/5(RH) 3E3 (fully supervised)
�� Category III 2(RHZE)/4(RH) 3 (fully supervised)
�� Prophylaxis 6H (without supervision).

EUR/03/5037563 page 16
6.7 DOTS
Dushanbe city �� As planned last year, 24% of TB patients from Dushanbe city (30% planned in 2001)
received their treatment on fully ambulatory basis with daily visits to the polyclinic during the initial phase of 2 to 3 months treatment and thrice weekly visits to polyclinic during continuation phase of 4 to 5 months. All TB patients discharged from Machenton received ambulatory treatment during continuation phase. Identification of place of residence was strictly controlled based on identification residence paper.
�� 76% of TB patients from Dushanbe city were hospitalized in Macheton Republican TB hospitals located 20 km outside of Dushanbe during initial phase of 2 to 3 month and were on ambulatory basis from one of the 7 TB centres (6 polyclinics + 1 city Tb centre) closer to patient address during continuation phase of 4 to 5 months through thrice weekly visits to polyclinic.
Rest of the country (outside Dushanbe) �� TB patients diagnosed in Dushanbe or elsewhere coming from outside Dushanbe were
hospitalized during at least the entire initial phase and often for longer period in Machenton hospital. The initial phase was strictly observed as the continuation phase based on prescription of TB drugs was not observed.
�� Considering that any intake of rifampicin tablets should be strictly observed, it was discussed during the mission the establishment of authorized DOTS providers during the entire treatment in future DOTS pilot areas. Initial phase will be mainly based on hospitalization in TB beds as continuation phase will be provide in first stage by TB polyclinic with TB centre. DOTS provider within PHC should start in 2003 in existing … soup and …???.
�� Weekly visit during continuation phase would be acceptable for remote areas. Family members of TB case should NOT become a DOTS provider.
Recommendation The TB central team should promote ambulatory treatment during entire treatment in Dushanbe city through polyclinics and during continuation phase elsewhere through all polyclinics and health posts.
6.8 Food support
�� WFP will start in December food support for 1000 TB patients and 5000 family members during continuation phase through Project HOPE staff based on WFP/Project HOPE agreement. Patient will receive from month 2 until end of the treatment 2 months food provision based on daily ratio for 5 family members and the TB patient of 200 grams wheat, 15 grams of oil and 10 grams sugar per day representing 100 kilograms of wheat per month. WFP support food cost amounting approximately US $12 per month and per person i.e. US $400 per case (40 time the cost of TB drugs). This high level of support should be carefully monitor to avoid ghost TB cases.
�� The mission met WFP representative and he agreed to consider food support since inception of treatment in DOTS areas throughout the country. Agreement between WFP and NGOs should be signed for each TB centre to monitor drug distribution.

EUR/03/5037563 page 17
�� Food is used as an incentive for TB patients who are considered the poorest people for better access to TB services. Project HOPE will apply for food support for all TB patients and staff starting from the onset of the treatment delivered during hospitalization.
�� IFRC did not establish a soup kitchen in Dushanbe as planned last due to insufficient number of TB patient at the moment.
Recommendations The TB team should consider food support as a social incentive to increase access and case detection and establish careful monitoring of diagnosis and DOTS before food supply is provided. WFP should consider possibility to provide food for TB health worker
6.9 Recording and reporting
The conventional Soviet-styled TB registration is now in transition and has automatically phased over the WHO type reporting system in DOTS areas. Pricaz no. 192 issued on 8 July 2002 sanctions the forms used for information gathering and outcome summarization. It assigns responsibility for “proper keeping of reporting and registration documents” and half-yearly summarization of DOTS implementation results to a team of three senior workers at the MOH (Dr Bobokhodjaev, Professor Sirijiddinova and Dr Zzakirova). Dr Sadulo Saidaliev, Chief Physician at the City TB Centre, is responsible for reporting within the city precincts. He has been proactive in summarizing the first 170 cases registered from July to October, and in addition, he has produced a report on early smear conversions for the first sputum positive cases coming to term (see section on Epidemiology). Some computer spreadsheeting of patient records has been started at his office. The quarterly report on new and relapse TB cases (TB07) is of standard format. A merged version for all 7 city centres implementing DOTS for the 3rd quarter and another one for October have been produced by Dr Saidaliev. While lab activities were not looked at specifically by this mission (given a concomitant inspection visit by CDC expert), the TB04 registers seen were generally well completed. Workers seem to be familiar with the concepts of sensitivity and specificity, and they themselves generate the index of proficiency (% patient diagnostic tests which are positive, reportedly averaging 10–20%). In the Macheton lab in October, sensitivity was 100% and specificity 97%. A system for positive quality control by a reference lab in the country has yet to be instituted. Some problems noted in the centres visited include:
�� Treatment after default is only intended for use in smear negatives of patients who default any treatment regimen for an unspecified period of time.
�� The outcome “Default” is only used for those who are sputum smear negative when they interrupt treatment, while those positive would be classified as “Failure”. This leads to over-estimation of failures at the expense of defaulters.

EUR/03/5037563 page 18
Recommendations �� There should be no need to replicate the contents of the district TB register centrally. This
practice of hand-copying might create errors and difficulties to keep all records updated and the possibility of double counting.
�� Patient type “Treatment after default” should be reserved for default after DOTS regardless of the smear status at time of registration. Patients who interrupt non-standard treatments should be registered under “Other”. By limiting the use of this category to DOTS, it will provide in future a useful index of how many defaulting patients actually re-enter the system. Analogously, distinction between DOTS and non-DOTS relapses, by simply using 2 different letter codes should be indicate in the “Relapse” column.
6.10 Drugs supply, storage, distribution, and monitoring
GDF TB drug formulations were delivered in Dushanbe on 24 November 2001, transferred to the TB drug warehouse 2 days later but distributed only 7 months later awaiting for release of pricaz on DOTS implementation. All TB drugs were already registered on the Tajik Essential Drug List. There are 3 different storage places. Main storage of TB drugs was established in the children’s hospital and TB drugs are properly stored in an approximately 50 square meters room with adequate shelves and secured door fixed since last mission. Temperature taken every day is between 10 and 26 degree Celsius so far. From the children’s warehouse, TB drugs are delivered and stored in kit form in Tajik Farm Fabrika, private company preparing 18 different patient kit forms (1 kit per category, per phase/per band weight). Average cost per kit prepared is about US $3 supported by Project HOPE. Moreover, it was not clear if Project HOPE will support this additional cost for the entire country. Third storage is at the TB city centre receiving TB drug kits from the Tajik Farm Fabrika and boxes from the children warehouse. The city centre distributes on one by one basis, kits to Machenton and polyclinics when a new case is diagnosed. Kit for initial phase is distributed separately from kit for continuation phase. Regular transportation is ensured by Project HOPE from central store to Tajik Farm Fabrika and to city centre or by TB coordinator from TB city centre to Machenton hospital or to polyclinics in Dushanbe. Lastly kits are stored in facilities. The delivery system is entirely secured but complicated and costly. Hand packaging allows easier drug distribution, and conservation of TB drugs but management of numerous kits and additional box of separate drugs for extension of initial phase for positive cases at month 2 and for children is found very complicated. Distribution on one by one kit basis is found too complicated.

EUR/03/5037563 page 19
Table 7. TB drugs distribution
Machenton (S+ month2)
Machenton initial phase
Airport Central store Children hos
Tajik Farm Fabrika
City TB centre
Polyclinic initial phase
Children hospital
Polyclinic continuation
TB drugs register and individual TB drug cards at the children’s warehouse were correctly held and accurate. Transfer out and return few days later of TB drugs in the children’s warehouse occurred in September without clear explanation. Another register at the Tajik Farm Fabrika indicates the number of tablets received and equivalent to 206 patient kits, corresponding to the current number of TB case notified at the time of the visit 190 all forms and 26 patient kits on shelves at the city TB centre. Third registration is held at TB city centre and fourth registration book in each polyclinic. Register at warehouse, Tajik Pharma, and city centre is not crosschecked. Simplification will be possible with introduction of drug delivery based on quarterly order form and later at the time of receiving 4-FDCs in blister pack. Distribution of TB drugs from the children’s warehouse should be done on regular basis every quarter (April, July, October, January) with specific transport or at the time of quarterly meeting in Dushanbe Comparison between drug consumption in Dushanbe and TB notification indicates adequate TB drug use including 6000 tablets RH, 6000 Z, 6000 E and 5000 H300 used in the children’s hospital. Total consumption is equivalent to 1.7 months for all Dushanbe.
Table 8. GDF TB drugs distribution and use in Tajikistan
Received in warehouse 26/11/2001
Prepared in kit Tjk Farm Fabrika
Stock at warehouse shelves 26/11/2002
Distributed Dushanbe July–November
Stock warehouse +TJK Farm 26/11/2002
R150H100 Z400 E400 H300 S 0.75 Water
1 161 000 630 000 440 000 177 000 24 000 24 000*
313 000222 000146 00043 00014 85015 300
848 000 408 000 294 000 134 000 9 150 8 700 *
12 5000 71 000 57 000 11 000 3150 3150
1 036 000 559 000 383 000 166 000 20 850 20 850
*number of water vials labeled on boxes is not accurate presenting 3 to 5% missing vials inside boxes
6.11 GDF Drugs needs in 2003
Notification in October and average notification since July allow to build an average notification per 100 000 habitants which is used for TB drugs estimates for 2003 according to population covered by DOTS expansion.

EUR/03/5037563 page 20
Table 9. Average TB drug consumption in DOTS area per 100 000 habitants
TB notification in October in Dushanbe
Number of patient per month since July (95 TB per month see table 3 page 10)
Mean notification value per month per 538 554 habitants
Mean notification value per month per 100 000 habitants
Cat. 1 25 35 30 5.54 Cat. 2 17 (26%) 27 (28%) 22 (27%) 4.07 Cat. 3 23 33 28 5.25 Total 65 95 80 14.85
Current stock allow to cover 3 month buffer stock plus 4 months for Streptomycin (until the end of May 2003) if use of streptomycin for category 1 is stopped in December 2002, 3 month buffer stock plus 8 months for Ethambutol, RH and Z (till July2003), and for to 2 years for H. Difference in remaining stock is due to use of streptomycine in category 1 and limited use of H for chemoprophylaxis (see Tables 10 and 11)
Table 10. Projected TB notification until end July 2003 with current GDF stock during DOTS expansion, including 3 month buffer stock
Pop. Month with DOTS
Cat.1
Cat.2 Cat.3 Total
Dushanbe 538 554 8+3 328 241 311 880 Leninsky 272 000 7+3 151 111 143 404 Hissar 198 400 4+3 77 57 73 206 Khorog 210 000 2+3 58 43 55 156 Khodjent 150 000 2+3 42 31 39 111 Kuliab 78 000 1+3 17 13 16 46 Matcha 84 000 1+3 19 14 18 50
153 0954 691 508 655 1854
Table 11. Projected current TB drugs coverage till end July 2003 with current GDF stock during DOTS expansion, including 3 month buffer stock
Cat. 1 Cat. 2 Cat. 3 Total Stock end November
2003
Stock end July 2003
TB cases 691 508 655 1854 R150H100 304 108 345 305 28 8213 937 626 1 036 000 98 374Z400 165 877 182 808 157 207 505 893 559 000 53 107E400 124 408 258 979 383 387 383 000 -387H300 0 60 936 60 936 166 000 105 064S 0.75 0 30 468 30 468 20 850 -9618Water 0 30 468 30 468 20 850 -9618
Considering the need to establish a 3 month buffer stock with current regimen and later 6 month buffer stock with 4-FDCs, GDF should deliver 10 000 vials of streptomycin during first quarter 2003 and one year supply with 4-FDCs in June 2003. It is expected that DOTS expansion from July 2003 to July 2004 will cover progressively over a 2.2 million population, representing 4966 TB cases, which includes 6 month buffer stock as calculated in Table 12 below.

EUR/03/5037563 page 21
Needs for one year consumption from June 2003 to June 2004 including 6 month buffer stock and 1 prophylaxis for every 5 TB cases is estimated in Table 13.
Table 12. Projected DOTS population coverage till July 2004 and number of expected TB case from July 2003 to July 2004
Population Month with DOTS
Cat. 1 Cat. 2 Cat. 3
Dushanbe 538 554 18 537 394 509 Leninsky 272 000 18 271 199 257 Hissar 198 400 18 198 145 187 Khorog 210 000 18 209 154 198 Khodjent 150 000 18 150 110 142 Kuliab 78 000 17 73 54 70 Matcha 84 000 15 70 51 66 Isfara 37 000 14 29 21 27 Kanibadam 45 000 13 32 24 31 Jan 2004 100 000 11 61 45 58 Feb 2004 100 000 10 55 41 52 March 2004 100 000 9 50 37 47 April 2004 100 000 8 44 33 42 May 2004 100 000 7 39 28 37 June 2004 100 000 6 33 24 31
2 212 954 1851 1360 1755
Table 13. GDF order in 2003 to cover the DOTS expansion till July 2004 including 6 month buffer stock
Drug Expected date of arrivalMarch 2003
Expected date of arrival June 2003
RHZE 1 355 000 RH 1 730 000 E 326 000 S 10 000 81 600 H 536 000
Based on the “Guidance on pharmaceutical and medical donations in the Republic of Tajikistan” prepared by the Ministry of Foreign Affairs and approved by the Ministry of Health from Tajikistan, temporary license for registration of 4-FDCs (R150H75Z400E275) and 2-FDCs (R150H150) not on the Tajik Essential Drug List requires preparatory steps which can last 4 months. Following steps should be initiated early 2003:
�� Application for registration of 4-FDCs (R150H75Z400E275) and 2-FDCs (R150H150) prepared by the supplier;
�� Certificate on pharmaceutical product (WHO recommended form);
�� Russian pharmacopoeia (European, British, United States pharmacopoeia accepted);
�� License for import based on batch certificate;
�� Instruction on use of medicines (if possible in Russian language);

EUR/03/5037563 page 22
�� Certificate of quality of pharmaceutical product entering international trade;
�� 50 tablets of each drugs for quality control.
Recommendations The TB programme should stop to use category 1 regimen 2SRHZ/4R3H3 with streptomycin and apply the recommended category 1 with 2RHZE/4R3H3 to avoid shortage of streptomycin. The TB programme should establish buffer stock equivalent to 3-month consumption with current drug formulation and 6 month buffer stock latter with 4-FDCs regimen The Ministry of Health should order blister pack presentation for initial and continuation phase in the next GDF delivery and stop kit packaging. The Ministry of Health should place during first quarter 2003 next GDF order for streptomycin and for blister pack of 1 year supply + 6 month buffer stock based on 4-FDCs (R150H75Z400E275) and 2-FDCs (R150H150) with following quantity:
Expected arrival date March 2003 June 2003 RHZE blister 1 355 000 RH blister 1 730 000 E 326 000 S 10 000 81 600 Water 10 000 81 600 H 536 000
The central team should implement in early 2003 new drug management system based on:
�� quarterly order TB drugs form to be sent together with the quarterly report on notification and treatment outcome;
�� 3 months delivery supply based on the quarterly TB drugs order and TB report on notification;
�� One common TB drug register replacing the multiple registers at each level. The central team should conduct training session with representative and pharmacists from all DOTS TB centres to introduce: new drugs regimen (categories 3 and 1 will be similar next July), new drug formulation, new quarterly order on TB drugs form, and common TB register. GDF should initiate issuance of temporary registration licences of donated pharmaceutical for 4-FDCs (R150H75Z400E275) and 2-FDCs (R150H150) and send in January 2003 to the Ministry of Health in Tajikistan c/o WHO:
�� Application for registration of 4-FDCs (R150H75Z400E275) and 2-FDCs (R150H150) prepared by the supplier;
�� Certificate on pharmaceutical product (WHO recommended form);
�� Russian pharmacopoeia (European, British, United States pharmacopoeia accepted);
�� Licence for import based on batch certificate;
�� Instruction on use of medicines (if possible in Russian language);

EUR/03/5037563 page 23
�� Certificate of quality of pharmaceutical product entering international trade;
�� 50 tablets of 4-FDCs (R150H75Z400E275) and 50 tablets of 2-FDCs (R150H150) for quality control.
6.12 Laboratory supplies
A concomitant CDC/USAID laboratory mission visiting Tajikistan at the time of our visit addressed this part. A detailed report is to be provided to the Ministry of Health soon.
6.13 Budget 2002 and partnership (see part 5.3 and 5.4 page 12 above)
Table 14. Proportion of TB funding from government vs. other sources
Budget/Expenditure US $ 2001 2002 2003 A. Total TB budget from
national government (non-donor funds)
US $34 475 US $40 552 US $43 851
B. Total TB budget from donors (Specify name of donor(s) beside amount)
HOPE: unknownWHO: 10 000India: 72 931
BIF: 23 954Germany: 23 000Global P. 15 000
AKF: 7000Red Cross: 5600
HOPE: unknownWFP: 50 000WHO: 20 000
HOPE: US $1 Million (to be confirmed)
WFP: 200 000IFRC: 30 000WHO: 20 000
AKF: unknownMerlin: unknown
C. GDF grant (equivalent $) 40 000 40 000
D. Total TB budget (A + B + C + D)
US $191 980 US$ 150 552 + USAID/HOPE
US $333 851 + AKF + IFRC +Merlin + USAID/HOPE
The TB programme has no information about budget support and plan from its main donor USAID/Project HOPE. ICC meeting is expected to gather such budget information from every partner to better identify remaining gaps.

EUR/03/5037563 page 24
Table 15. Major gaps
Item Government contribution
Donors contribution Gap
1. Staff: national, technical assistance
National staff USAID HOPE team WHO consultant CDC/USAID lab consult.
2. Laboratory and X-ray supplies, equipment, maintenance and equipment, reference laboratory
WHO 1 year lab supplies USAID/HOPE reference lab (equipment) USAID/HOPE microsc.
Buffer stock lab supply Reference lab (building)
3. Drugs (incl. distribution costs) GDF for DOTS areas Transport (1 truck) TB drugs for non DOTS areas
4. Programme management: supervision, transport and maintenance, recording/reporting, case management (excluding staff costs covered in 1, laboratory covered in 2)
WHO (supervision) USAID/HOPE
Transport (2 cars at central level, 1 car in Leninsky) Staff incentive Supervision incentive
5. Training including fellowship, conference, meeting
WHO USAID/HOPE
Training incentive
6. Activities designed to raise case detection rates, and cure rates including IEC/advocacy (excluding those already identified above e.g. public/private strategy)
WFP: food for TB patients IFRC soup kitchen
7. Operating costs of dedicated TB facilities: office equipment, building, maintenance building (excluding staff included in and those indentified above)
Building Maintenance building Reference lab Central level
8. Surveillance and research including HIV/TB, MDR, prevalence and mortality surveys etc (excluding those identified above)
MDR survey
Major gaps concern transportation for central and intermediate level, building for central laboratory and central level, office equipment. One truck and 2 cars are needed for the central level and 5 cars for intermediate level. Multipurpose transport means are needed at raion level outside Dushanbe.

EUR/03/5037563 page 25
Annex 1
VISIT SCHEDULE AND PERSONS MET
24 Nov. Arrival in Dushanbe, Tajikistan
25 Nov. Briefing with Professor Asasomiddin Latipov, Deputy Minister, Ministry of Health of Tajikistan
Meeting with TB Manager – Professor U. Sirojiddinova and National TB team Briefing meeting with Dr Artykova Nazira, WHO liaison officer Visit Republican TB Centre – Dr Kurbanhon Zokirova, Director
26 Nov. Visit to Polyclinic #1, Dr A. Rakhmattulaev, Chief doctor Visit to Polyclinic #2, Dr I. Khudaidodov, Chief doctor Visit to Central Polyclinic – Dr M. Sharipov, Chief Debriefing and working on TB guidelines for PHC (Tsogt, Project HOPE)
27 Nov. Visit to Macheton TB hospital – Dr S. Rustamov, Director Visit Leninski Central Rayon Hospital – Dr T. Umurzakov, Director Leninsky TB centre – Dr S. Rakhmonov, Chief TB doctor Finalizing TB guidelines for PHC (Tsogt, Professor Sirojiddinova, Project HOPE) Visit to children’s hospital and central medical store (P.Y. Norval)
28 Nov. Training of TB Coordinators and epidemiologists (D. Falzon) Visit to Tajik Farm Fabrika (P.Y. Norval) Discussion with Directors of Polyclinics (G. Tsogt) Meeting with WFP representative (P.Y. Norval) Meeting with Professor Asasomiddin Latipov, Deputy Minister, Ministry of Health
(G. Tsogt, K. Juszkiewicz, M. Sirojiddinova, K. Zokirova) Meeting with Aga Khan Foundation (P.Y. Norval)
29 Nov. Discussion on mission report (team, Tom Mohr project HOPE manager, Ms A. Khadimova, USAID)
Debriefing with Professor Asasomiddin Latipov, Deputy Minister, Ministry of Health
Meeting with D. Zappa, Merlin (P.Y. Norval, G. Tsogt, S. Saidaliev)
30 Nov. Report writing
1 Dec. Departure to Almaty Persons met �� Asasomiddin Latipov, Deputy Minister, Ministry of Health, [email protected]
�� Umriniso Iusupovna Sirojiddinova, TB manager, Ministry of Health,
�� Kurbanhon Akramovna Zokirova, Director of the Centre, TB City Centre
�� Lidiya Phedorovna Pashkova, Head of Laboratory, Republic TB Centre, Dushanbe
�� Dr Rahmatullaer, head of polyclinic no. 1
�� Dr Mirzoev Aziz, TB coordinator, polyclinic no. 1
�� Dr T. Umurzakov, Director Leninsky raion

EUR/03/5037563 page 26
�� Dr S. Rakhmonov, TB coordinator Leninsky raion
�� Dr Jamshedov, Head, Tajik Pharma Fabrika, Dushanbe
�� World Food Programme representative
�� Ms Husniya Dorgabekova, health programme manager Aga Khan Foundation
�� Merlin
�� Dr Artykova Nazira WHO liaison officer
�� Thomas Morh Project HOPE programme manager, [email protected]
�� Ms A. Khadimova, USAID/CAR Almaty

EUR/03/5037563 page 27
Annex 2
TB DRUGS FORMULATION FOR CHILDREN AND ADULTS USING 2 FDCS (R150H100)
Recommended doses mg/kg for essential TB drugs
Recommended dose mg/kg Anti-TB drug Daily 3 x per week
Isoniazid (H) Rifampicin (R) Pyrazinamide (Z) Ethambutol (E) Streptomycin (S)
5 (4–6) 10 (8–12) 25 (20–30) 15 (15–20) 15 (12–18)
10 (8–12) 10 (8–12) 35 (30–40) 30 (25–35) 15 (12–18)
Category 1 and 3: 2 (RHZE)/4 (RH) 3, dosage schedule for adult (number of tablets)
Initial phase 2 months daily
Continuation phase 4 months, 3X per week
Patient body weight
R150H75Z400E275 R150H150 30–37 2 2 38–54 3 3 55–70 4 4 >71 5 5
Category 2: 2S(RHZE)/(RHZE)/5(RH)3E3, dosage schedule for adult (number of tablets)
Initial phase 3 months daily (except S for 2 months
daily)
Continuation phase 5 months, 3X per week
Patient body
weight S 1
2 months injection
R150H75Z400E275 3 months
R150H150 5 months
E400 5 months
30–37 0.50 2 2 2 38–54 0.75 3 3 3 55–70 0.75 4 4 4 >71 1 5 5 5
Dosage schedule for children (number of tablets)
Continuation phase 6 months
Patient body weight Initial phase 2 months
R60H30Z150 * R60H30 * Up to 7 1 1
8–9 1.5 1.5 10–14 2 2 15–19 3 3 20–24 4 4 25–29 5 5
*not available through GDF

EUR/03/5037563 page 28
Annex 3
QUARTERLY ORDER FORM FOR TB DRUGS
Republic of Tajikistan Ministry of Health
Quarterly order form for TB treatment supplies Enter the number of cases enrolled in the previous 3 months (from the quarterly report on case finding) Number of cases
enrolled in previous quarter per category
Requirement Reserve Existing Stock
ORDER
a B=a C=B D B+C-D Cat. 1 A Cat. 1 B
Cat. 2 A Cat. 2 B
Cat. 3 A Cat. 3 B
1 month A 6H Category 1 A (2RHZE) = 240 tablets R150H75Z400E275 Category 1 B (4R3H3) = 192 tablets R150H150 Category 2 A (2SRHZE/RHZE)= 360 tablets R150H75Z400E275 + 60 vials S0.75 + 60 syringes
+ 60 needles + 60 vials 5ml Category 2 B (5R3H3E3) = 240 tablets R150H150 + 240 tablets E400 Category 3 A (2RHZE) = 240 tablets R150H75Z400E275 Category 3 B (4R3H3) = 192 tablets R150H150 1 month A (1RHZE) = 120 tablets R150H75Z400E275 6H = 180 tablets H100 or (90 tablets H300) R: Rifampicine H: Isoniazide Z: Pyrazinamide E: Ethambutol S: Streptomycine Date: Name of the TB centre: Name and signature:

EUR/03/5037563 page 29
Annex 4
QUARTERLY ORDER FORM FOR LABORATORY SUPPLIES
Republic of Tajikistan Ministry of Health
Quarterly order form for laboratory supplies Enter the number of cases enrolled in the previous 3 months (from the quarterly report on case finding)
Amount for 1000 slides
No of patients
Factor 6 month requirement
A
1 year reserve Ax2 = B
Existing stock
C
ORDER
A+B-C=D Basic fuchsine 15 g 0.5 Methylene blue 15 g 0.5 Immersion oil 100 ml 3 Sulfuric acid 1250 ml 38 Phenol 250 g 7.6 Xylol 1000 ml 30 Methanol 500 ml 15 Slides 1000 33 Sputum containers
1000 33
Column 2: amounts of reagents required for 1000 slides based on the assumption that 5ml saturated fuchsin solution, 5ml 25% sulfuric acid, and 5ml methylene blue solution are needed for 1 slide Column 4: The factor is based on the assumption of requiring examination of 10 suspects for each smear positive cases (3 slides each) and 3 follow-up examinations. Date: Name of the TB centre: Name and signature:

EUR/03/5037563 page 30
Annex 5
CORE FUNCTIONS OF THE CENTRAL TB TEAM
1. Strategic planning The central team develop and update: - a costed strategic plan.
Strategic planning aims to: a) advocate for TB control as a public health priority; b) nurture a policy, financing and operating environment that will support full implementation of DOTS through the health system; c) perpetuate a needs assessment and response cycle that includes ongoing monitoring of programme performance; and d) foster collaboration between all levels of the health system and among all partners involved in TB control.
2. Normative functions
The central unit of the TB programme maintains authority for defining and ensuring compliance with normative and technical standards for: - Diagnostics procedure based on sputum smear microscopy - Standardized treatment regimen (band weight, strength, formulation) - Treatment delivery (i.e. DOTS) - Standardized reporting and recording - Elaboration of service delivery norms.
3. Financing
The central unit ensure and maintains: - Political commitment reflected in adequate funding of TB control.
4. Human resource capacity
The central unit - define role of health providers - ensure all necessary training.
5. Drug supply
The central team ensure following functions are properly done: - specification of drug formulation - quantification - drug distribution, - stock monitoring - quality of TB drugs - centralized TB drug tendering and procurement.
6. Service delivery
The central team ensure and prepare: - the DOTS strategy is an integral part of the essential services package delivered
through the primary and secondary health care network; - a mapping of the existing and future (anticipated) service delivery network; - a laboratory network not decentralized to small population in order to maintain technical
expertise (microscopist should perform 10–15 smear examinations each week).

EUR/03/5037563 page 31
As most of the TB cases are hospitalized during few days to few weeks before being transfer to primary health care system, the central team ensure particular attention is paid for smooth transition from hospital to PHC.
7. Monitoring and evaluation
The central team ensure: - Standardized TB case recording and reporting forms are adopted nationwide. - Monitoring and supervision visit are conducted several times per year and per health
facility (supplemented by potential integrated supervision activities). - Development of monitoring criteria, such as: a) the availability of TB drugs, b) access
to a laboratory with smear microscopy capacity, c) regular supervision, and d) trained health worker. These criteria could be used to prioritize interventions (ex. training) that need to be conducted to improve service delivery.
- Monitoring of epidemic and national trends in TB control. The recording and reporting system is a job-aid for health providers, ensuring that they know what medications to provide, following patient progress, highlighting problems in treatment, and confirming cure.
8. IEC, social mobilization and advocacy
The central team ensure - social mobilization techniques that build demand and ownership for DOTS among
provider, political and social communities; - IEC to decrease stigma and ensure symptomatics person seek care. Stimulating ownership for TB control by the broader health system and possibly among new or different stakeholders may require some changes in perception related to DOTS or TB in general as there may be perceptions that TB control is the responsibility of a specialized service. In addition, stigma associated with TB may act as a disincentive for general health providers and or communities considering how to prioritize TB control activities.
9. Operational research
Operational research can build the local evidence needed to appropriately guide policy decisions.
10. Delegation
The central team ensure delegation of functions are performed according to local demand and capacity for: - strategic planning, - training, - supervision - data analysis.