
Flurithromycin versus clarithromycin in upper respiratory tract infections
11
CURRENT THFXAPEUTIC RESEARCH@ VOL. 59, NO. 1, JANUARY 1998 FLURITHROMYCIN VERSUS CLARITHROMYCIN IN UPPER RESPIRATORY TRACT INFECTIONS MARCO BENAZZO,lGIUSEPPE GIACOPINI,2 CESARE OLDINI,3 ENRICO SCHEIBER, ALBERT0 TOMBOLINL6 AND EUGENIO MIRAl ‘Clinica ORL, Universitk di Pavia e IRCCS, Policlinico San Matteo, Pavia, sServizio di ORL, Ospedale di Riva de1 Garda, Trento, 3Divisione di ORL, Ospedale Maggiore di Lodi, 4Divisione di ORL, Ospedale Caduti Bollatesi, Bollate, Milan, and 5Divisione di ORL, Presidio Ospedaliero di San Remo, Imperia, Italy ABSTRACT The efficacy and tolerabillty of flurltbromyclu aud clarltbromyclu lu the treatment of bacterial upper respiratory tract infections were compared lu a multicenter, parallel-group, double-masked, double- dummy study of 320 adult patients who were randomized to two treatment groups. Flurithromyciu was administered as one 376-mg tablet twice dally and clarithromycin as one 260~mg tablet twice daily for up to 14 days. In the flurithromycin group, 3 patients were lost to observation, 1 withdrew because of poor compliance and 1 because of diarrhea, and 2 were considered clinical failures at treat- ment completion. In the clarithromycin group, 2 patients withdrew for treatment inefficacy and 12 were considered clinical failures at treatment completion. All other patients were judged to be cured or improved. Thus the intent-to-treat success rates were 163 (95.6%) of 160 patients in the flurithromycin group and 146 (91.3%) of 160 patients in the clarlthromycin group; the difference was not statis- tically significant. The eradication rate of the baseline pathogens, mostly gram-positive cocci, was 123 (90.4%) of 136 patients in the flurithromycin group and 126 (91.3%) of 138 patients in the cla- rithromycin group. Response rates did not vary appreciably by in- fection site or baseline pathogen. Adverse events, mostly mild-to- moderate gsstrointestinal disturbances, were observed in 8 patients (6.0%) in the Burithromycin group and in 11 patients (6.9%) in the clarithromycin group. These results suggest that fiurithromycln 375 mg twice daily is as effective and well tolerated as clarlthromycin 260 mg twice daily in the treatment of upper respiratory tract in- fections. Key words: clarithromycin, flurithromycin, upper resplra- tory tract infection. INTRODUCTION Infections affecting the ear, nose, and throat, broadly defined as upper respiratory tract infections, are the most frequent group of diseases en- Address correspondence to: Prof. Eugenio Mira, Policlinico S. Ma&o, Universit& degli Studi di Pavia, Piazzale C. Golgi, 2, I-27100 Pavia, Italy. Received for publication on October 15, 1997. Printed in the USA. Reproduction in whole or part is not permitted. 28 0011-393w9w$19.00
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Flurithromycin versus clarithromycin in upper respiratory tract infections

CURRENT THFXAPEUTIC RESEARCH@ VOL. 59, NO. 1, JANUARY 1998
FLURITHROMYCIN VERSUS CLARITHROMYCIN IN UPPER RESPIRATORY TRACT INFECTIONS
MARCO BENAZZO,l GIUSEPPE GIACOPINI,2 CESARE OLDINI,3 ENRICO SCHEIBER, ALBERT0 TOMBOLINL6 AND EUGENIO MIRAl
‘Clinica ORL, Universitk di Pavia e IRCCS, Policlinico San Matteo, Pavia, sServizio di ORL, Ospedale di Riva de1 Garda, Trento, 3Divisione di ORL, Ospedale Maggiore di Lodi,
4Divisione di ORL, Ospedale Caduti Bollatesi, Bollate, Milan, and 5Divisione di ORL, Presidio Ospedaliero di San Remo, Imperia, Italy
ABSTRACT
The efficacy and tolerabillty of flurltbromyclu aud clarltbromyclu lu the treatment of bacterial upper respiratory tract infections were compared lu a multicenter, parallel-group, double-masked, double- dummy study of 320 adult patients who were randomized to two treatment groups. Flurithromyciu was administered as one 376-mg tablet twice dally and clarithromycin as one 260~mg tablet twice daily for up to 14 days. In the flurithromycin group, 3 patients were lost to observation, 1 withdrew because of poor compliance and 1 because of diarrhea, and 2 were considered clinical failures at treat- ment completion. In the clarithromycin group, 2 patients withdrew for treatment inefficacy and 12 were considered clinical failures at treatment completion. All other patients were judged to be cured or improved. Thus the intent-to-treat success rates were 163 (95.6%) of 160 patients in the flurithromycin group and 146 (91.3%) of 160 patients in the clarlthromycin group; the difference was not statis- tically significant. The eradication rate of the baseline pathogens, mostly gram-positive cocci, was 123 (90.4%) of 136 patients in the flurithromycin group and 126 (91.3%) of 138 patients in the cla- rithromycin group. Response rates did not vary appreciably by in- fection site or baseline pathogen. Adverse events, mostly mild-to- moderate gsstrointestinal disturbances, were observed in 8 patients (6.0%) in the Burithromycin group and in 11 patients (6.9%) in the clarithromycin group. These results suggest that fiurithromycln 375 mg twice daily is as effective and well tolerated as clarlthromycin 260 mg twice daily in the treatment of upper respiratory tract in- fections. Key words: clarithromycin, flurithromycin, upper resplra- tory tract infection.
INTRODUCTION
Infections affecting the ear, nose, and throat, broadly defined as upper respiratory tract infections, are the most frequent group of diseases en-
Address correspondence to: Prof. Eugenio Mira, Policlinico S. Ma&o, Universit& degli Studi di Pavia, Piazzale C. Golgi, 2, I-27100 Pavia, Italy. Received for publication on October 15, 1997. Printed in the USA. Reproduction in whole or part is not permitted.
28 0011-393w9w$19.00

M. BENAZZO ET AL.
countered in medical practice. Although not life threatening, they may evolve into serious infections such as pneumonia or meningitis if not treated adequately. Upper respiratory tract infections of bacterial etiology are mainly caused by Streptococcus pneumoniae, Streptococcus pyogenes, Staphylococcus aureus, Haemophilus influenzae, Branhamella catarrhalis, and Mycoplasma pneumoniae, but the relative importance of each agent varies according to the infection site.
Penicillins (alone or combined with beta-lactamase inhibitors) and macrolides are considered the first-choice antibacterial agents in the treat- ment of upper respiratory tract infections.lm3 In particular, the use of mac- rolides has increased greatly over the past decade, following the develop- ment of several new agents.4 One of these agents, flurithromycin, is obtained by substituting a fluorine atom in the core macrolide structure.5 In the eradication of bacteria commonly involved in respiratory tract in- fections, flurithromycin is generally active against most streptococci, S aureus, B catarrhalis, Bordetella pertussis, Mpneumoniae, and, to a lesser extent, H influenzae and Clostridium and Bacteroides species; in contrast, mycobacteria are often resistant to flurithromycin.M
Like other macrolides, flurithromycin is absorbed inside polymorpho- nuclear monocytes and may act on susceptible bacteria that are able to survive phagocytosis.g Peak plasma concentration of flurithromycin is reached about 1 hour after oral administrationlOT1l; excretion occurs mainly via the bile, and only small amounts are excreted in the urine.g The pharmacokinetic profile is not appreciably affected by age and liver or renal impairment. Flurithromycin is well absorbed in tissues’; steady- state concentrations have been shown to be twice as high in tonsillary tissue as in serum.12
The aim of this study was to evaluate the efficacy and tolerability of flurithromycin in the treatment of bacterial infections of the upper respi- ratory tract. Flurithromycin was compared with another macrolide, cla- rithromycin, whose pharmacologic and clinical characteristics have been studied extensively.13
PATIENTS AND METHODS
Studg Design and Patient Selection
This multicenter study was designed as a controlled, parallel-group, double-masked, double-dummy, randomized clinical trial. The study pro- tocol was approved by the ethics committee at each institution.
Patients of both sexes, either inpatients or outpatients, aged 18 years or older, and requiring antibacterial therapy because of an acute infection or relapse of a chronic infection of the middle ear, nose, sinuses, tonsils, pharynx, larynx, or trachea were eligible for the study. Exclusion criteria
29
FLURITHROMYCIN VERSUS CLARITHROMYCIN
were any antibacterial treatment during the week preceding the screening visit, hypersensitivity to macrolides, immunodepression, neoplastic dis- ease, pregnancy or lactation, liver or renal insufficiency, malabsorption, psychiatric disease, addiction, or alcohol abuse. Patients judged to be un- cooperative or unreliable were also excluded, as were those who required treatment with any other antibacterial agent or with drugs that might interact with macrolides, such as carbamazepine and theophylline. Eli- gible patients were enrolled in the study after written informed consent was obtained.
Treatment Allocation and Treatment Regimens
Enrolled patients were randomly allocated to oral treatment with flu- rithromycin or clarithromycin. Separate computer-generated randomiza- tion lists were used for each participating center; randomization was bal- anced (1:l) within each block of four patients. Double dummies were prepared and dispensed with the active treatments to preserve masking of investigators and patients.
Flurithromycin was given as one 375mg tablet twice daily; clarithro- mycin was given at the standard dose, one 250-mg tablet twice daily. Tablets were administered every 12 hours, in the morning and in the evening, with or after meals. Treatment duration was established by the investigator according to the severity and evolution of the infection and could vary between 5 and 14 days, provided that treatment was not di.+ continued earlier because of inefficacy, adverse events, or withdrawal of patient consent.
Examinations
Patient history and demographic and clinical data were recorded dur- ing the entry visit. Physical examination was performed, and axillary tem- perature was measured. Symptoms were rated as absent, mild, moderate, or severe. Serum samples were collected for routine laboratory tests (eryth- rocyte count and sedimentation rate, hematocrit, hemoglobin, platelet and leukocyte counts, glucose, urea nitrogen, creatinine, total bilirubin, trans- aminases, and alkaline phosphatase) and culturing.
Physical examination, measurement of axillary temperature, and symptom evaluation were repeated after 3 days and at the final visit. Samples for microbiologic tests and serum samples for laboratory tests were collected again at the end of treatment. The investigator expressed a final judgment by assessing clinical outcome as cure (complete regression of all signs and symptoms of infection), improvement (complete regression of some of the signs and symptoms of infection with partial regression of the others), or failure (persistence of some of the signs and symptoms of infection, or worsening after at least 3 days of treatment). The microbio-
30

logic response was assessed as eradication, persistence of the baseline pathogen, reinfection (eradication of the baseline pathogen but infection by a new agent), or superinfection (persistence of the baseline pathogen with infection by a new agent).
Any adverse event, either spontaneously referred by the patient or observed by the investigator, was recorded. Patient compliance with the prescribed treatment was assessed by counting the tablets returned at completion of the study.
Data Analysis
The investigator’s assessment of clinical outcome was considered the primary measure of efficacy. The proportions of patients judged clinically cured or improved were compared by using Fisher’s exact test. Analyses were performed both by intent to treat (including all randomized patients) and per protocol (including only patients who either completed treatment or dropped out because of its inefficacy), with the former being the main analysis.
The microbiologic response was considered a secondary measure of efficacy. The proportions of eradications were compared by means of Fish- er’s exact test. Only patients in whom the baseline pathogen was presum- ably identified and a final assessment was performed were included in this analysis.
The incidence of adverse events was compared by using Fisher’s exact test. All randomized patients were included in this analysis. P < 0.05 (two-tailed) was considered statistically significant.
RESULTS
Baseline Characteristics
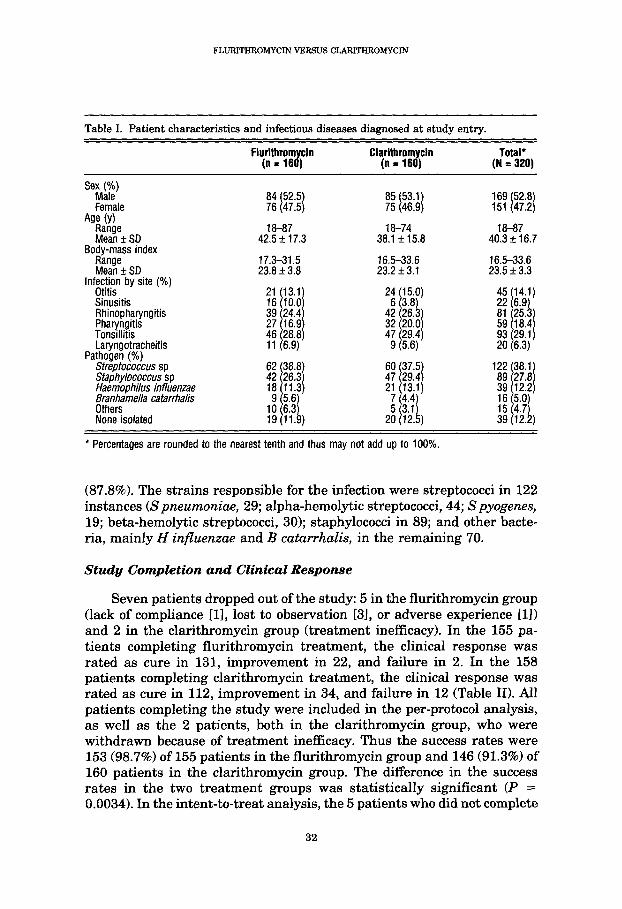
A total of 320 patients, 169 men and 151 women aged 18 to 87 years (mean age, 40 years), were enrolled in the study (Table I). Approximately 73% of all patients had rhinopharyngitis, pharyngitis, or tonsillitis, whereas about 14% had middle ear infections. Sinusitis and laryngotra- cheitis were relatively uncommon.
The demographic characteristics of the two treatment groups, each comprising 160 patients, were well balanced, as were the entry diagnoses, except for a higher frequency of sinusitis in the flurithromycin group (Table I).
Infections occurred as acute episodes in 216 patients (67.5%) and as relapses of chronic diseases in the remaining 104 patients (32.5%) and were diagnosed according to clinical symptoms (local pain, inflammation of mucous membranes, discharge of secretion, hoarseness, fever).
The bacterial pathogens were presumably identified in 281 patients
31
FLURITHROMYCIN VERSUS CLAFUTHROMYCIN
Table I. Patient characteristics and infectious diseases diagnosed at study entry.
Total* (N = 320)
Sex,g)
Female Age (Y)
ET* SD Body-mass index
?Zek SD
84 52.5 76 47.5 I 1
18-87 42.5 k 17.3
17.3-31.5 23.8 f 3.8
85 53.1 75 46.9 I 1
18-74 38.1 +_ 15.8
16.5-33.6 23.2 f 3.1
18-87 40.3 f 16.7
16.5-33.6 23.5 f 3.3
lnf;ec;n by site (%)
Sinusitis Rhinopharyngitis Pharyngitis Tonsillitis Laryngotracheitis
Pathogen (%) Streptococcus sp Staphylococcus sp Haemophilus influenzae Br$?mella catarrhahs
None isolated
* Percentages are rounded to the nearest tenth and thus may not add up to 100%.
(87.8%). The strains responsible for the infection were streptococci in 122 instances (Spneumoniae, 29; alpha-hemolytic streptococci, 44; Spyogenes, 19; beta-hemolytic streptococci, 30); staphylococci in 89; and other bacte- ria, mainly H influenzae and B catarrhalis, in the remaining 70.
Study Completion and Clinical Response
Seven patients dropped out of the study: 5 in the flurithromycin group (lack of compliance [ll, lost to observation 131, or adverse experience [l]) and 2 in the clarithromycin group (treatment inefficacy). In the 155 pa- tients completing flurithromycin treatment, the clinical response was rated as cure in 131, improvement in 22, and failure in 2. In the 158 patients completing clarithromycin treatment, the clinical response was rated as cure in 112, improvement in 34, and failure in 12 (Table II). All patients completing the study were included in the per-protocol analysis, as well as the 2 patients, both in the clarithromycin group, who were withdrawn because of treatment inefficacy. Thus the success rates were 153 (98.7%) of 155 patients in the flurithromycin group and 146 (91.3%) of 160 patients in the clarithromycin group. The difference in the success rates in the two treatment groups was statistically significant (P = 0.0034). In the intent-to-treat analysis, the 5 patients who did not complete
32

M.BENAZZOETAL.
Table II. Treatment outcome using per-protocol and intent-to-treat analyses.
Fluriihromycin Clarithromycin
Treatment completion Cure or improvement (a) 153 Failure (b) 2 ‘Z
Treatment withdrawal Inefficacy (c) Cl 2 Other reasons (d) 5 0
Per-protocol analysrs* Successes (a) and success rate (%) Failures (b t c) and failure rate (%)
intent-to-treat analysist
15; g;) I
‘$ $$I I
Successes (a) and success rate (%) Failures (b t c t d) and failure rate (%) 15f iY) I
1;: ;y’ 1
* P = 0.0034 t P = 0.174 ( L
Fisher’s exact test [two-tailed]). isher’s exact test [two-tailed]).
treatment for other reasons, all in the flurithromycin group, were added, giving a total of 7 failures; therefore, the success rate in the flurithromycin group was 153 (95.6%) of 160 patients. The difference between the success rates of the two treatment groups was not statistically significant.
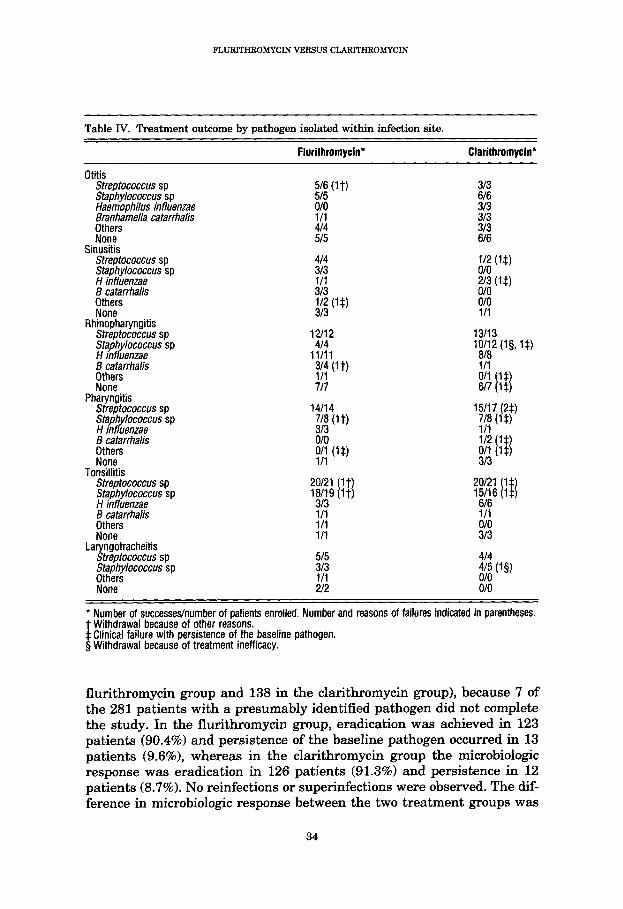
Response rates did not appear to vary appreciably according to the infection site or the baseline pathogen (Table III). A more detailed account of treatment outcome is reported in Table IV, in which data are grouped according to infection site and to baseline pathogen within a given site. All clinical failures at the end of treatment were associated with persistence of the baseline bacteria.
Microbiologic Response
The microbiologic response was assessed in 274 patients (136 in the
Table III. Treatment outcome by infection site and by pathogen isolated. (Number of suc- cesses/number of patients evaluated by intention to treat; if different, correspond- ing per-protocol figures are given in parentheses.)
Flurithromycin Clarithmmycin
fnfrggrr by site
Sinusitis Rhinopharyngitis Pharyngitis Tonsillitis Laryngotracheitis
Pathogen Streptococcus sp staphy/ococcus sp Haemophilus influenzae Branhamella catarrhalis Others None isolated
:W; (20/20) YE4 36142 27132
?Z7
56160 42147
2F rgd6l6) 315
19119 19120
33
FLURITHROMYCIN VERSUS CLARITHROMYCIN
Table IV. Treatment outcome by pathogen isolated within infection site.
Flurithromycin” Clarithromycin*
Otitis Streptococcus sp Staphylococcus sp Haemophilus infiuenzae Branhamella catarrhalis
Zree’s Sinusitis
Streptococcus sp Staphylococcus sp H influenzae B catarrhalis Others None
Rhinopharyngitis Streptococcus sp Staphylococcus sp H influenzae B catarrhalis Others None
Pharyngitis Streptococcus sp Staphylococcus sp H influenzae B catarrhalis
E-F Tonsillitis
Streptococcus sp Staphylococcus sp H influenzae ;tEzrhalis
None La ngotracheitis
5 treptococcus sp Staphylococcus sp
Kn”e’
l Number of successes/number of patients enrolled. Number and reasons of failures indicated in parentheses. t Withdrawal because of other reasons. $ Clinical failure with persistence of the baseline pathogen. 5 Withdrawal because of treatment inefficacy.
flurithromycin group and 138 in the clarithromycin group), because 7 of the 281 patients with a presumably identified pathogen did not complete the study. In the flurithromycin group, eradication was achieved in 123 patients (90.4%) and persistence of the baseline pathogen occurred in 13 patients (9.6%>, whereas in the clarithromycin group the microbiologic response was eradication in 126 patients (91.3%) and persistence in 12 patients (8.7%). No reinfections or superinfections were observed. The dif- ference in microbiologic response between the two treatment groups was
34
M. BENAZZO ET AL.
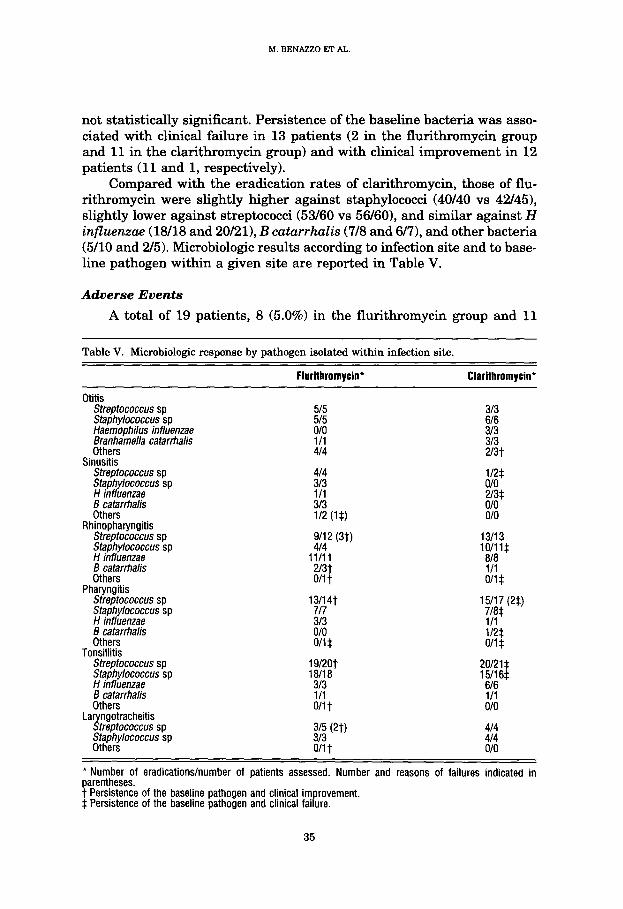
not statistically significant. Persistence of the baseline bacteria was asso- ciated with clinical failure in 13 patients (2 in the flurithromycin group and 11 in the clarithromycin group) and with clinical improvement in 12 patients (11 and 1, respectively).
Compared with the eradication rates of clarithromycin, those of flu- rithromycin were slightly higher against staphylococci (40140 vs 42/45), slightly lower against streptococci (53160 vs 56/60), and similar against H influenzae (18/18 and 20/21), B catarrhalis (7/8 and 6/7), and other bacteria (500 and 2/5). Microbiologic results according to infection site and to base- line pathogen within a given site are reported in Table V.
Adverse Events
A total of 19 patients, 8 (5.0%) in the flurithromycin group and 11
Table V. Microbiologic response by pathogen isolated within infection site.
Flurithromycin* ClarithromyciV
Otitis Sfreptococcus sp Staphylococcus sp Haemophilus influenzae Branhamella catarrhalis Others
Sinusitis Streptococcus sp Staphylococcus sp H influenzae B catarrhalis Others
Rhinopharyngitis Streptococcus sp Staphylococcus sp H influenzae B catarrhalis Others
Pharyngitis Streptococcus sp Staphylococcus sp H influenzae B catarrhalis Others
Tonsillitis Streptococcus sp Staphylococcus sp H influenzae B catarrhalis Others
La ngotracheitis !Y treptococcus sp Staphylococcus sp Others
5/5 515
z: 414
414
E 313 112 S$)
9/l 2 (3t) 414
11/11 2/3t O/l t
‘%4t 313 o/o o/i*
19/20t 18118
7;; O/l t
315 (2t) 313 O/l t
313
% 313 2/3t
i/2* o/o
:;* o/o
13113 lc$l$
l/l O/l-J
1;;;; (2*)
l/l i/2$ o/i *
:%~ 616 l/l o/o
414 414 o/o
* Number of eradications/number of patients assessed. Number and reasons of failures indicated in parentheses. t Persistence of the baseline pathogen and clinical improvement. $ Persistence of the baseline pathogen and clinical failure.
35

FLURITHROMYCIN VERSUS CLARITHROMYCIN
(6.9%) in the clarithromycin group, experienced one or more adverse events during the study (Table VI). This difference between the two treat- ment groups was not statistically significant. A total of 23 adverse events were observed: 9 in the flurithromycin group (nausea 2, gastralgia 1, me- teorism 1, diarrhea 4, headache 1) and 14 in the clarithromycin group (nausea 3, gastralgia 7, abdominal pain 1, diarrhea 2, headache 1). All adverse events were mild or moderate. Only one adverse experience, mod- erate diarrhea in a patient receiving flurithromycin, led to treatment discontinuation.
DISCUSSION AND CONCLUSION
In this clinical trial, oral flurithromycin 375 mg twice daily was compared with oral clarithromycin at the standard dose of 250 mg twice daily in the treatment of upper respiratory tract infections.
The clinical response rate by intention to treat (ie, including all ran- domized patients and considering withdrawals for any reason as failures) was higher, although not significantly different statistically, with flu- rithromycin (95.6%) than with clarithromycin (91.3%). All five patients who dropped out for reasons other than inefficacy belonged to the flurithro- mycin group; removal of these patients from analysis (per protocol) re- sulted in a larger, statistically significant difference. However, because such exclusion may appear somewhat arbitrary and is a potential source of bias, the intent-to-treat approach was considered more appropriate as the main analysis of treatment outcome. It should also be noted that the analy- sis of microbiologic response (a per-protocol analysis, because it did not include patients withdrawn from the study) did not show any significant difference between treatments. Thus it appears safer to conclude that flu- rithromycin was approximately as effective as clarithromycin and that the small advantage observed may have been due to chance.
Table VI. Number of patients having one or more adverse events.
Symptom Flurithromycin Clarithromycin
Nausea Gastralgia Gastralgia-nausea* GastralgWnauseat Abdominal pain Meteorism Diarrhea Diarrhea-gastralgia’ Headache Headache-nausea* Total
* Occurring together. t Occurring in separate episodes 3 days apart.
36
MBENAZZOETAL.
Response rates did not vary substantially, if examined according to specific infection site, pathogen isolated at baseline, or both. Larger samples, however, would be required to adequately test any correlation between these factors and treatment outcome.
Both flurithromycin and clarithromycin were well tolerated, and tol- erability results were in accordance with the known safety profile of both drugs. Adverse events occurred in 5.0% of the patients treated with flu- rithromycin and in 6.9% of those treated with clarithromycin, and con- sisted almost exclusively of mild-to-moderate gastrointestinal distur- bances. It should be noted, however, that these data were based on spontaneous reporting by the patients, a method that may considerably underestimate the incidence of adverse events obtained by eliciting re- sponses to specific questions.
The results obtained with flurithromycin in the present trial confirm the findings of a previous uncontrolled study in which flurithromycin given as 375 mg twice daily to 103 patients with bacterial upper respiratory tract infections achieved a 98% clinical response rate (complete recovery or im- provement) with few side effects.14 In view of these results, a 375mg twice-daily regimen was considered suitable to ensure a satisfactory risk/ benefit ratio and was therefore adopted in the present study. In fact, the results of this trial suggest that flurithromycin 375 mg twice daily is as effective and well tolerated as clarithromycin 250 mg twice daily in the treatment of upper respiratory tract infections.
Acknowledgments
The study was sponsored by Pharmacia-Upjohn S.p.A., Milan, Italy. The authors thank Dr. G. V. Zottino, director of GIARL S.A.S., for data
analysis, and G. Airoldi for assistance in preparing the manuscript.
References:
1. Lang SDR, Singh Ii_ The sore throat. When to investigate and when to prescribe. Drugs. 1990;40:854-862.
2. Froom J, Culpepper L, Grob P, et al. Diagnosis and antibiotic treatment of acute otitis media: Report from International Primary Care Network. BMJ. 1990;300:582-586.
3. Evans KL. Diagnosis and management of sinusitis. BMJ. 1994;309:1415-1422.
4. Kirst HA. New macrolides: Expanded horizons for an old class of antibiotics. J Antimi- crab Chemother. 1991;28:787-790.
5. Zanuso G, Toscano L, Pezzali R, Seghetti E. (8S)-Mluoroerythromycin A: A novel mac- rolide with increased acid stability: Synthesis and microbiological activity. In: Proceed- ings of the 13th International Congress of Chemotherapy, Vienna, 1983.1984:PS 4.4/l-12.
6. Gialdroni Grassi G, Alesina R, Bersani C, et al. In vitro activity of flurithromycin, a novel macrolide antibiotic. Chemioterapia. 1986;5:177-184.
37
FLURITHROMYCIN VERSUS CLARITHROMYCIN
7. Nord CE, Lindmark A, Persson I. Comparative antimicrobial activity of the new macro- lide flurithromycin against respiratory pathogens. Eur J Clin Microbial Infect Dis. 1988; 7:71-73.
8. Saverino D, Debbia EA, Pesce A, et al. Antibacterial profile of flurithromycin, a new macrolide. J Antimicrob Chemother. 1992;30:261-272.
9. Fietta A, Boeri P, Colombo ML, et al. Bioactivity of flurithromycin and other macrolides against intracellular susceptible staphylococci. Chemotherapy. 1993;39:48-54.
10. Benoni G, Cuzzolin L, Leone R, et al. Pharmacokinetics and human tissue penetration of flurithromycin. Antimicrob Agents Chemother. 1988;32:1875-1878.
11. Ferrara AM, Lepore AM, Bonfanti C, Gialdroni Grassi G. Pharmacokinetics of flurithro- mycin ethylsuccinate. In: Recent Advances in Chemotherapy. Proceedings of the 17th Znternational Congress of Chemotherapy, Berlin, 1991. Armonk, NY: Futura; 1992:2284- 2285.
12. Galioto GB, Mevio E, Galioto P, et al. Concentrations of flurithromycin in serum and tonsils. Znt J Clin Pharmucol Ther. 1989;27:126-128.
13. Peters DH, Clissold SP. Clarithromycin: A review of its antimicrobial activity, pharma- cokinetic properties and therapeutic potential. Drugs. 1992;44:117-164.
14. Galioto GB, Passali D, Catalan0 GB, et al. Oral therapy with flurithromycin in ear, nose and throat infections. Znt J Clin Pharmacol Ther. 1995;33:204-207.
38




















