Florida State University Libraries
218
Florida State University Libraries Electronic Theses, Treatises and Dissertations The Graduate School 2019 Using Telepractice to Coach Caregivers of Children with Visual Impairments to Increase the Independent Living Skills of Their Children Susan Elizabeth Yarbrough Follow this and additional works at the DigiNole: FSU's Digital Repository. For more information, please contact [email protected]
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Florida State University Libraries
Florida State UniversityLibrariesElectronic Theses, Treatises and Dissertations The Graduate School
2019
Using Telepractice to Coach Caregiversof Children with Visual Impairments toIncrease the Independent Living Skills ofTheir ChildrenSusan Elizabeth Yarbrough
Follow this and additional works at the DigiNole: FSU's Digital Repository. For more information, please contact [email protected]

FLORIDA STATE UNIVERSITY
COLLEGE OF EDUCATION
USING TELEPRACTICE TO COACH CAREGIVERS OF CHILDREN WITH
VISUAL IMPAIRMENTS TO INCREASE THE INDEPENDENT LIVING SKILLS OF
THEIR CHILDREN
By
SUSAN YARBROUGH
A Dissertation submitted to the School of Teacher Education in partial fulfillment of the
requirements for the degree of Doctor of Philosophy
2019
ii
Susan Yarbrough defended this dissertation on June 28, 2019.
The members of the supervisory committee were:
Sandra Lewis
Professor Directing Dissertation
Juliann Woods
University Representative
Amy Guerette
Committee Member
Mary Frances Hanline
Committee Member
The Graduate School has verified and approved the above-named committee members, and
certifies that the dissertation has been approved in accordance with university requirements.

iii
To the children and caregivers who participated. Your contributions helped deepen our knowledge of how to teach children with visual impairments.
iv
ACKNOWLEDGMENTS
I would first like to thank my advisor and major professor, Dr. Sandra Lewis. I am
grateful for the unending encouragement she has provided me over the years. Her support has
helped me turn opportunity into reality.
I would also like to thank previous and current members of my doctoral committee, Drs.
Juliann Woods, Amy Guerette, and Mary Frances Hanline, and Sarah Ivy. Their expertise and
support have made this project possible.
The contributions of the caregivers and children who participated in this study should
also be acknowledged. They opened their homes to me several times a week and remained
steadfastly engaged in this project, despite their many familial demands. Their participation was
essential for the completion of this endeavor. I found great joy in working with these families
and watching their children learn.
The volunteered help of Lakia Griffin and Jamie Dennis was instrumental in the
development of operational definitions and reliable measurement of variables, necessary to
establish the validity of the research findings.
My doctoral program would not have been possible without the financial support and
professional development provided by the National Leadership Consortium in Sensory
Disabilities. Additionally, I would like to thank my fellow doctoral students in NLCSD and at
Florida State University for generously sharing their encouragement and expertise.
Finally, I must thank my family and friends. Their relentless support helped me achieve
this goal. I am particularly grateful to my parents, who instilled in me a firm belief in the power
of education to improve lives.

v
TABLE OF CONTENTS
List of Tables ............................................................................................................................... viii List of Figures ................................................................................................................................ ix Abstract ............................................................................................................................................x 1. INTRODUCTION ......................................................................................................................1 Statement of the Problem ............................................................................................................1 Purpose of the Study ...................................................................................................................3 Research Questions .....................................................................................................................3 Justification of the Methods ........................................................................................................3 Delimitations ...............................................................................................................................4 Significance of the Study ............................................................................................................6 Definitions and Terms .................................................................................................................7 2. REVIEW OF THE LITERATURE ...........................................................................................10 Educational Implications of Visual Impairment .......................................................................11 Population of Children with Visual Impairments ...................................................................11 Impact of Visual Impairment on Development ......................................................................13 The Expanded Core Curriculum .............................................................................................18 Families .....................................................................................................................................24 Family Systems Framework ...................................................................................................24 Impact of Visual Impairment on Families ..............................................................................26 Family Systems of Children with Visual Impairments ...........................................................31 Caregiver Education ..................................................................................................................33 Adult Learning Principles .......................................................................................................33 Coaching .................................................................................................................................34 Telepractice .............................................................................................................................42 Promise of Telecoaching for Caregivers of Children with Visual Impairments .......................54 3. RESEARCH METHODOLOGY ..............................................................................................56 Experimental Design .................................................................................................................56 Participants ................................................................................................................................59 Demographic Characteristics ..................................................................................................61 Independent Living Skills Selection .......................................................................................65 Setting .......................................................................................................................................66 Procedures .................................................................................................................................67 Approval and Recruitment ......................................................................................................67 Baseline One ...........................................................................................................................69 Training ...................................................................................................................................71 Post-Training Baseline ............................................................................................................71 Coaching .................................................................................................................................72
vi
Maintenance ............................................................................................................................74 Materials ....................................................................................................................................75 Response Definitions and Measurement Procedure ..................................................................76 Dependent Variables ...............................................................................................................76 Measurement ...........................................................................................................................78 Reliability ...............................................................................................................................78 Procedural Fidelity ....................................................................................................................80 Social Validity ...........................................................................................................................81 Data Analysis ............................................................................................................................82 4. RESULTS .................................................................................................................................84 Procedural Administration ........................................................................................................84 Caregiver and Child Outcomes .................................................................................................86 Dyad 1 .....................................................................................................................................86 Dyad 2 .....................................................................................................................................92 Dyad 3 .....................................................................................................................................99 Social Validity Outcomes .......................................................................................................105 Goals .....................................................................................................................................106 Procedures .............................................................................................................................107 Outcomes ..............................................................................................................................108 5. DISCUSSION .........................................................................................................................110 Changes in Caregiver Instructional Strategy Use ...................................................................110 Changes in Child Independent Task Completion ...................................................................111 Social Validity .........................................................................................................................112 Limitations ..............................................................................................................................114 Implications for Teachers ........................................................................................................118 Implications for Future Research ............................................................................................120
Conclusion ..............................................................................................................................126 APPENDICES .............................................................................................................................127 A. CHILD INDEPENDENT LIVING SKILLS TASK COMPONENTS ...................................127 B. CAREGIVER INSTRUCTIONAL STRATEGIES THEORETICAL FRAMEWORK ........136 C. CAREGIVER INSTRUCTIONAL STRATEGIES OPERATIONAL DEFINITIONS .........137 D. CAREGIVER CONSENT FORM ..........................................................................................141 E. CHILD CONSENT FORM .....................................................................................................143 F. CHILD ASSENT FORM ........................................................................................................145 G. SKILLS SCREENING AND DEMOGRAPHIC DATA SCRIPT .........................................146 H. IRB APPROVAL LETTERS ..................................................................................................151 I. TEACHER RECRUITMENT MESSAGE .............................................................................153 J. CAREGIVER RECRUITMENT MESSAGE .........................................................................154 K. INCLUSION SCREENING PHONE SCRIPT .......................................................................155 L. CAREGIVER OR GUARDIAN CONSENT SCRIPT ...........................................................158
vii
M. CHILD ASSENT SCRIPT ......................................................................................................162 N. SKILLS SELECTION AND SCHEDULE DEVELOPMENT SCRIPT ................................165 O. BASELINE ONE PHASE DATA COLLECTION SCRIPT ..................................................167 P. CAREGIVER AND CHILD DATA COLLECTION FORM ................................................169 Q. TRAINING SLIDES ...............................................................................................................170 R. TRAINING SCRIPT ...............................................................................................................177 S. POST-TRAINING BASELINE PHASE DATA COLLECTION SCRIPT ...........................179 T. COACHING PHASE DATA COLLECTION SCRIPT .........................................................181 U. MAINTENANCE PHASE DATA COLLECTION SCRIPT .................................................185 V. FGRBI KEY INDICATOR CHECKLIST ..............................................................................187 W. SOCIAL VALIDITY ..............................................................................................................188 References ....................................................................................................................................191 Biographical Sketch .....................................................................................................................201
viii
LIST OF TABLES
1 Selected Participant Characteristics .........................................................................................63 2 Independent Living Skills Tasks for Each Dyad and Each Context ........................................66 3 Interobserver Agreement for Each Dyad and Each Phase .......................................................80 4 Frequency of Caregiver Correct Instructional Strategy Use and Percentage of Child Independent Task Completion for Dyad One ..........................................................................93 5 Frequency of Caregiver Correct Instructional Strategy Use and Percentage of Child Independent Task Completion for Dyad Two .......................................................................100 6 Frequency of Caregiver Correct Instructional Strategy Use and Percentage of Child Independent Task Completion for Dyad Three .....................................................................106
ix
LIST OF FIGURES
1 Caregiver instructional strategy use and child independent task completion for Dyad 1. .......88 2 Caregiver instructional strategy use and child independent task completion for Dyad 2. .......94 3 Caregiver instructional strategy use and child independent task completion for Dyad 3. .....102
x
ABSTRACT
Children with visual impairments have unique learning needs because visual impairment impacts
a child’s ability to learn incidentally though observation (Lowenfeld, 1952, 1973). Literature
suggests children with visual impairments do not perform independent living skills at the same
level as their peers with typical vision (e.g., Lewis & Iselin, 2002). Teachers of students with
visual impairments (TVIs) struggle to find time to teach independent living skills during the
school day (e.g., Lohmeier, Blankenship, & Hatlen, 2009), but caregivers may have the time and
motivation to prioritize these skills at home. Caregiver coaching has been shown to increase the
skills of caregivers of children with disabilities (e.g., Marturana & Woods, 2012); however,
coaching models have not yet been widely applied to caregivers of children with visual
impairments. Some researchers have applied teleconferencing technologies to provide access to
coaching and successfully build the capacity of caregivers of children with disabilities (e.g.,
Baharav & Reiser, 2010). As such, telepractice coaching was explored as a tool to bridge
physical distance between coaches with expertise in educating children with visual impairments
and caregivers who have the opportunity to implement instruction in independent living skills for
their children with visual impairments.
A single case, multiple baseline across contexts design was used to implement a
telepractice caregiver coaching intervention in the homes of three caregiver-child dyads for two
to three times a week over about 10 weeks. The included children were tactual learners with no
other significant disabilities aged 5 to 11 years old. The study sought to answer the questions: (a)
does telepractice coaching with the Family Guided Routines Based Intervention (FGRBI)
coaching model (e.g., Woods, 2017) increase caregiver correct use of coached instructional
strategies during independent living skills routines with their children who have visual
xi
impairments? and (b) does caregiver use of coached instructional strategies increase the child’s
independent completion of independent living skills tasks?
Because the coaching intervention was only implemented across all three contexts in one
dyad, data from that dyad only can be considered as evidence of the effectiveness of the
intervention. In that dyad, the caregiver increased her skills above baseline levels in all three
contexts and demonstrated mastery in two contexts. However, great variability in the data make
it difficult to conclude with certainty that there is a functional relation between telepractice
caregiver coaching and caregiver instructional strategy use in teaching her child with a visual
impairment. In addition, instructional skills learned in one skill context were generalized by
some caregivers to other independent living skills contexts without coaching. Challenges with
the length and duration of sessions caused concern regarding the social validity of the
intervention. However, data collected after the study from participants and an external rater as
well as maintenance data suggested high social validity of the intervention.
Findings suggest the use of telepractice to deliver interactive caregiver coaching should
be further investigated to determine its effectiveness to increase both caregiver instructional
skills and the independent living skills of children with visual impairments. If telepractice is
found to be effective, TVIs may benefit from using telepractice coaching to build relationships
and strengthen capacity within the families of their students. Further research is necessary to
examine the use of the telepractice coaching intervention to meet the needs of families and
children with diverse characteristics, explore the role of siblings as peer models, and expand the
role of the child in coaching. Further, the composition of the telepractice coaching intervention
should be investigated to determine which intervention components may be most effective for
which families, and how frequently they should be delivered for maximum efficiency.
1
CHAPTER 1
INTRODUCTION
Statement of the Problem
Children with visual impairments have unique learning needs resulting from their visual
impairments (Lowenfeld, 1952, 1973) because visual impairment reduces a child’s ability to
learn incidentally though observation. The expanded core curriculum (ECC) was developed to
delineate the disability-specific educational needs of children with visual impairments resulting
from their lack of incidental learning (Hatlen, 1996, 2004). Though children with visual
impairments are entitled to special education services to address needs related to their
disabilities, many children with visual impairments are not receiving sufficient instruction in the
ECC (Grimmett, Pogrund, & Griffin-Shirley, 2011; Lohmeier, Blankenship, & Hatlen, 2009;
Wolffe et al., 2002).
One of the nine areas of the ECC, independent living skills, has received little attention
despite consensus that children with visual impairments have specific instructional needs in
independent living skills (e.g., Bardin, 2014; Hatlen, 1996). However, TVIs spend little time
teaching independent living skills (e.g., Wolffe et al., 2002), despite the limited literature base
suggesting children with visual impairments are not able to perform independent living skills at
the same level as their peers with typical vision (Lewis & Iselin, 2002; Papadopoulos, Metsiou,
& Agaliotis, 2011).
Caregivers of children with visual impairments have unique opportunities to meet their
children’s instructional needs for independent living skills if they have regular contact with their
children and participate in routines in which the skills are taught. Family systems theory suggests
skill deficits, such as those in independent living skills, may disrupt the balance and relationships
2
within the family system (Turnbull, Turnbull, Erwin, Soodak, & Shogren, 2015). Caregivers of
children with disabilities, including those with visual impairments, may need specific strategies
and support so they may teach their children effectively and restore the balance of the family
system (e.g., Jackson & Turnbull, 2004; Nixon, 1988).
Coaching has been a widely-explored solution for building the skills and capacity of
caregivers. Coaching models support principles of adult learning: practical application,
connection to existing knowledge, and sustained interactions to build skills (Dunst, Trivette, &
Hamby, 2010). Coaching has been shown to increase the skills of caregivers of children with
disabilities (e.g., Marturana & Woods, 2012; Nunes, Araujo, Walter, Soares, & Mendonca,
2016). Coaching models have not yet been widely applied to caregivers of children with visual
impairments, as most research has focused on coaching professionals (e.g., Damen, Kef, Worm,
Janssen, & Schuengel, 2011; Probst & Walker, 2017). Existing intervention research is limited in
scope, but holds promise for the efficacy of coaching adults to teach children with visual
impairments.
Some researchers have applied teleconferencing technologies to provide access to
coaching and successfully build the capacity of caregivers of children with disabilities, like those
with developmental delays and autism spectrum disorder (ASD; e.g., Baharav & Reiser, 2010;
Boutain, 2014; McDuffie et al., 2013). Teleconferencing technologies are emerging to provide
access to medical care and rehabilitation services to people who are visually impaired (Ihrig,
2016; Pathipati & Moshfeghi, 2017). As such, telecoaching may prove effective to bridge
physical distance between coaches with expertise in educating children with visual impairments
and caregivers who have the opportunity to implement instruction in independent living skills for
their children with visual impairments.
3
Purpose of the Study
The primary purpose of this study was to investigate the impact of a telepractice coaching
intervention using the Family Guided Routines Based Intervention (FGRBI) coaching model on
the frequency with which caregivers correctly used coached instructional strategies during
independent living skills routines with their children who have visual impairments. A secondary
purpose of the study is to examine the impact of caregiver use of coached instructional strategies
on the child’s independent completion of independent living skills tasks.
Research Questions
1. Does telecoaching caregivers of children with visual impairments using the FGRBI
model increase the frequency with which coached instructional strategies are
correctly implemented during independent living skills routines?
3. Does caregiver implementation of coached instructional strategies increase the
independent completion of targeted independent living skills tasks by children with
visual impairments?
Justification of the Methods
Single case research design was selected because it allows researchers to evaluate the
effectiveness of interventions in heterogeneous, low incidence populations, like children with
visual impairments (Hatton, 2014). Because each participant acts as his or her own experimental
control in single case design, functional relations among independent and dependent variables
may be detected with experimental control and may yield high internal validity (Gast & Ledford,
2018). External validity in single case research is limited due the heterogeneity of participants
and the specificity of experimental conditions; however, external validity may be enhanced by
4
inter-subject replication within the same study and reporting of details to facilitate replication by
other research teams (Horner et al., 2005). Single case research plays a critical role in the
establishment of evidence-based practices in special education because it can rigorously evaluate
the effectiveness of interventions among populations that do not follow norms of the larger
population of children without disabilities (Horner et al., 2005; Kratochwill et al., 2010).
Of the single case research designs available, multiple baseline across contexts was
selected because it is one of the few single case designs available to measure behaviors that do
not readily return to baseline level with the removal of the intervention (i.e., non-reversible
behaviors; Ledford, Lane, & Gast, 2018). Multiple baseline across contexts (i.e., independent
living skills domains) was selected instead of multiple baseline across behaviors because the
coached instructional strategies are not functionally independent behaviors, as is necessary to use
a multiple baseline across behaviors design (Gast, Lloyd, & Ledford, 2018). Multiple baseline
across participants was not selected because of ethical considerations related to delaying access
to the intervention to a family for whom it was promised and practical concerns related to
participant attrition (Gast et al., 2018). Risks related to the use of multiple baseline across
contexts have been minimized by the selection of behaviors in functionally independent contexts
(e.g., food management and clothing management) and replication across multiple participant
dyads.
Delimitations
1. Three children with visual impairments and no other significant disabilities, aged 5 to
11 years old, and their caregivers were recruited to participate in the intervention.
Children with visual impairments were selected for inclusion if they participated in a
braille literacy program. After inclusion, data regarding visual condition and type and
5
intensity of services provided by special educators was collected to enhance
replicability. In addition, children were invited to participate based on their inclusion
in a general education classroom and a school readiness screening. Because these
screenings were not comprehensive, it is possible participating children had
additional significant disabilities that were not disclosed by their caregivers or
observed by the researcher.
2. Because of the use of teleconferencing, participants lived in two different states. The
children and their caregivers shared varied experiences with special education
services and delivery models, including amount and quality of services.
3. Caregiver coaching and application of the coached strategies took place in the context
of independent living skills in the home. Though children with visual impairments
have a variety of instructional needs, independent living skills were selected for
intervention because of their logical fit in a family-guided intervention and the need
to broaden the limited research base in this instructional area. As such, functional
relations related to coaching caregivers are bound to the domain of independent living
skills.
4. It is assumed that caregivers value independence for their children with visual
impairments, though in some families, interdependence is valued. To screen for the
value of independence, caregivers were informed of the aims of the research and
included based on their agreement to participate in an intervention that may increase
the independent living skills of their children.
5. Children selected for inclusion had a caregiver-reported deficit in independent living
skills. The coach and caregiver targeted independent living skills unlikely to be taught
6
at school (e.g., setting the table for dinner). Though not necessary, alternative
independent living skills tasks targeted for instruction could have been selected if the
child began to learn the targeted skill at school.
6. The variables of interest are caregiver coaching, caregiver use of instructional
strategies, and child independent living skills. Caregivers choose which coached
strategies to apply to increase the independent living skills of their children. Because
increased child independent living skills is a distal outcome, the researcher measured
both caregiver and child dependent variables concurrent with the implementation of
the independent variable, caregiver coaching.
Significance of the Study
This present study has the potential to make contributions to the literature bases in
telepractice, coaching, and the education of children with visual impairments. This study added
to the rapidly developing literature base related to using technology to enable the coaching
caregivers of children with disabilities, despite physical distances. In addition, this study was
among the first to apply the FGRBI model beyond its originally developed use in early
intervention to coaching caregivers of school-aged children with visual impairments. The study
advanced a model of caregiver instructional strategies, compiled from the evidence base and best
practices, that may prove useful to others who teach children with visual impairments. Coaching
caregivers of children with visual impairments using telepractice coaching changed how
caregivers used instructional strategies to teach their children, and as a result, this model of
delivering coaching may be applied to additional research with caregivers and instructional
personnel (e.g., teachers and educational assistants). The model of instruction used in this study
7
may also be applied to studies investigating instruction for children with visual impairments in
independent living skills and other areas of the ECC.
Definitions and Terms
Caregiver: An adult who regularly assumes responsibility for a child’s physical safety and
attends to a child’s needs (i.e., at least two hours a day for at least four days each week). This
relationship may be biological, adoptive, fostered, or paid care (e.g., foster parent, biological
grandparent, nanny, etc.).
Child with a Visual Impairment: A child who has reduced visual acuity, visual field restriction,
oculomotor disorder, and/or brain-based impairment so significant that it adversely impacts
educational performance (Individuals with Disabilities Education Act [IDEA] 2004; United
States Department of Education Office of Special Education and Rehabilitative Services
[USDOE USERS], 2017).
Coaching: Process used to change the behavior of a learner in which a person expert in the task
facilitates the connection of new knowledge to existing knowledge, the practical application of
the new knowledge, and ongoing and sustained interactions that support mastery of the content
(Donovan, Bransford, & Pellegrino, 1999; Dunst et al., 2010).
Family-Guided Routines Based Intervention (FGRBI): A model of family-centered coaching
practices developed for use in early intervention of children with disabilities. It features four
coaching components: setting the stage, observations and opportunities to embed, problem
solving and planning, and reflection and review (Woods, 2017).
Family Systems: A theoretical framework to guide the interactions of professionals working with
the families of children who have disabilities. It emphasizes the child as a member of his or her
family and one part of the larger family system. The model suggests interfaces among the
8
constructs of family characteristics, family functions, family life cycle, and family interactions
(Turnbull et al., 2015).
Functional Relation: May be documented when “the change in the dependent variable (behavior)
is causally (functionally) related to the implementation of the independent variable” (Gast &
Ledford, 2018, p. 4).
Independent Living Skills: Skills “necessary to take care of one’s self, family, and home and to
live as independently as possible” (Bardin, 2014, p. 283). Independent living skills are learned
through observation by children with typical vision and are one of the nine targeted areas of
instruction for children with visual impairments (Hatlen, 1996, 2004).
Independent Living Skills Task: An independent living skill selected from one of three domains
outlined in Independent Living: A Curriculum with Adaptations for Students with Visual
Impairments (hereafter: Independent Living Curriculum; Loumiet & Levack, 1993). Domains
include clothing management, food management, and housekeeping and home maintenance. The
caregiver and coach will work together to select a task in each domain that the child cannot yet
complete independently, is age appropriate, and fits into existing family routines.
Independent Living Skills Task Component: Criteria for independent completion of each
independent living skills task developed based on caregiver priorities, existing routines, and
coached guidance. See examples in Appendix A.
Caregiver Instructional Strategies: Operationalized caregiver behaviors used to teach
independent living skills to children with visual impairments, organized into three categories:
expectation, access, and contingent responding. See Appendix B for a theoretical framework and
Appendix C for operational definitions of each caregiver behavior.
9
Single Case Research Design: Experimental research methodology in which each participant acts
as his or her own experimental control (Gast & Ledford, 2018). The operationalized behavior of
a participant before the systematic introduction of an intervention is compared with the behavior
of the participant during and after the implementation of the intervention in order to establish a
functional relation between the implementation of the intervention and changes in the dependent
variables of interest.
Tactual Learner: A child with a visual impairment so significant he or she learns primarily
through tactual sensory channels. Children included in this investigation were tactual learners
who participated in a conventional braille literacy program.
Telecoaching: The use of telepractice to provide access to instructional coaching.
Telepractice: The use of a technology (e.g., Internet-enabled computers, telephones,
videoconferencing software, etc.) to enable synchronous communication to bridge the physical
distance between individuals in need of medical or educational services and the experts who
deliver that service (Boutian, 2014). Telepractice has applications in the delivery of medical care
and rehabilitation (i.e., telehealth) and instructional coaching (i.e., telecoaching).
10
CHAPTER 2
REVIEW OF THE LITERATURE
Families of children with visual impairments face unique challenges in teaching their
children independent living skills that are generally acquired by children with typical vision
through observation. Instruction in independent living skills is an identified educational need of
children with visual impairments (Hatlen, 1996, 2004; Lewis & Iselin, 2002), but many children
do not receive the instruction they need because of a variety of factors that exist within the
educational and family systems (e.g., Lohmeier et al., 2009, Wolffe et al., 2002). Family
members may require intervention from educational professionals to learn to better teach their
children how to become independent adults. Telepractice has been applied widely in medicine
and is emerging as a promising modality for coaching caregivers to better teach their children
with disabilities (e.g., McDuffie et al., 2013; Wacker et al., 2013b). As such, telepractice
coaching may provide opportunities for families to learn how to better teach their children with
visual impairments and increase their independent living skills.
In the following literature review, the author will outline what is known about the
implications of visual impairment on the development and education of children, including
disability specific instructional needs in independent living skills. In addition, the impact of
disability on the family system and the specific impact of visual impairment on the family’s
capacity to provide instruction to their children with disabilities will be described. Finally, best
practices and emerging evidence in adult learning, coaching of professional or family caregivers,
and applications with telepractice technologies will be discussed to provide a rationale for a
coaching intervention delivered through teleconferencing technologies for caregivers of children
with visual impairment to increase the independent living skills of their children.
11
Educational Implications of Visual Impairment
Population of Children with Visual Impairments
Definitions. A variety of definitions are used to document visual impairment. To be
considered blind and qualify for social security disability benefits, an individual must have a
visual acuity of less than 20/200 in the better eye with correction or a visual field of less than 20
degrees (Social Security Administration, 2017). The American Printing House for the Blind
(APH), follows similar guidelines to qualify students for educational materials. Students must
have a central visual acuity of 20/200 or less, a visual field of less than 20 degrees, or have a
doctor document blindness as a result of a brain-based visual impairment (APH, n.d.).
IDEA (2004) broadens the definition of visual impairment to include any impairment of
vision, after best correction, that has a negative educational impact. Additional policy guidance
to State Departments of Education from the USDOE OSERS (2017) supports IDEA’s broad
definition and reiterates “any impairment in vision, regardless of significance or severity” may
qualify a child with a visual impairment for special educational services if, after best possible
correction, the condition “adversely affects the child’s educational performance” (p. 2). To
comply with the USDOE’s policy guidance, the Florida Administrative Code’s Exceptional
Student Education Eligibility for Students Who Are Visually Impaired was amended in 2017 to
expand the definition of visual impairment, assessment, and eligibility criteria to reflect the
broadest federal definition of visual impairment.
Prevalence. Because definitions of visual impairment vary widely, estimates of the
number of students with visual impairments also vary. In 2016, APH recorded 62,528 students
with visual impairments receiving educational services who met their definition of visual
impairment. The USDOE’s report to Congress in 2016 further emphasizes the low incidence of
12
visual impairment. Of the six million students aged 6-21 served by IDEA (i.e., those students
with documented disabilities), only 0.4%, about 24,000 students, were reported to have a primary
disability of visual impairment. Less than 0.05%, about 3,000 students, were reported to have
deafblindness as a primary disability.
It is known, however, about two-thirds of students with visual impairments have an
additional disability (Hatton, Ivy, & Boyer, 2013). Because USDOE requires reporting under a
primary disability category, it is possible that many students with visual impairments and
additional disabilities are reported under alternative primary disability categories and are, as a
result, not reflected in the USDOE counts of students with visual impairments. For example, a
student with a visual impairment and specific learning disability may have been reported to have
a primary disability of specific learning disability and would not be counted in the USDOE data
as a student with a visual impairment. It is likely, therefore, the USDOE data underestimates the
number of students with visual impairments.
The National Plan for Training Personnel to Serve Children with Blindness and Low
Vision (NPTP; Mason & Davidson, 2000) represents a field-wide effort to document the need for
TVIs. In their synthesis, the authors documented 93,600 students with an “educationally
significant visual impairment” (p. 28). Among those students, they reported 32,700 students with
a visual impairment as their only disability, 10,800 students with deafblindness, and 50,100
students with a visual impairment and another disability, excluding those students with
deafblindness.
Though APH, USDOE, and NPTP vary in their documentation of the number of students
with visual impairments, all three sources reflect the low incidence of the population. The
variability of their findings, combined with the low prevalence of the condition, highlight the
13
heterogeneity of students with visual impairments and suggests challenges in providing
appropriate educational services.
Educational settings. Children with visual impairments are educated in a variety of
educational settings (USDOE, 2016). According to the USDOE data on children reported to have
visual impairment as their primary disability, most school-aged children with visual impairments
(66.3%) served under IDEA attend their local public schools, spending more than 80% of time in
general education classrooms, with the support of a TVI. A smaller percentage (12.3%) of
children with visual impairments spend 40-79% of their time in the general education classroom,
receiving more intensive resource support from a TVI or special education teacher. Another
group of students with visual impairments (10.3%) are educated in their local public schools, but
spend less than 20% of their time in a general education classroom and spend most of their time
with students who also have disabilities. Like all students with visual impairments, students in
self-contained classrooms are eligible to receive consultative or direct services from a TVI. Due
to the complexity of their educational needs, a final group of students with visual impairments
(11.1%), are educated outside of their local public schools in one of several settings: special
schools, residential schools, hospitals, correctional facilities, private schools, or at home.
Children with visual impairments educated in these settings may still receive assessment and
appropriate instruction related to their visual impairment (IDEA, 2004).
Impact of Visual Impairment on Development
Vision and learning. Children who have visual impairments have unique learning needs.
Little empirical evidence exists regarding the specific influence of visual impairment on
learning; however, generations of accumulated experience emphasize the impact of blindness or
low vision on the acquisition of knowledge and skills. Ferrell (2000) explained that because
14
typical vision allows the access of information beyond a child’s reach, vision allows children to
learn through “vicarious participation” or incidental learning (p. 128). Children with typical
vision can learn by simply watching the objects and people in their environments. Their vision
motivates communication with others and movement within their environments. Vision also
enhances conceptual and cognitive development because the “consistent, coordinated, and
reliable information” gained through vision is unique from information gathered by the other
senses (p. 128). Vision gives children a sense of the whole experience, gained with relatively
little effort or initiation by the child.
Developmental differences. However, when children are born with or acquire a visual
impairment early in life, incomplete or absent visual information impacts their development.
Ferrell (2011) reported on the findings of Project PRISM, which found that young children with
visual impairments may have unique developmental patterns and modalities. Among the findings
were indications of alternative sequences of developmental milestones, unique salient features
for learning, and alternative modes of sensory processing.
In 1952, Lowenfeld described the impact of visual impairment on concept development.
Children born with visual impairments develop conceptual understandings that are unique, and at
times, incomplete or inaccurate. In a child with typical vision, vision acts to create meaning from
experiences; however, without vision, it is necessary for teachers and caregivers to provide
unifying experiences to compensate for incomplete visual input.
Instructional needs. To facilitate the development of concepts and skills of children with
visual impairments, Lowenfeld (1952) noted several principles critical in learning:
individualization, concreteness, unified instruction, additional stimulation, and self-activity.
Children with visual impairments need individualized, concrete, unified instruction in which a
15
teacher or caregiver organizes and delivers experiences that the student may not have had the
opportunity to engage in otherwise. In doing so, teachers and caregivers challenge students to
learn to be as independent as possible. Key among Lowenfeld’s principles is the role of teachers
or caregivers to organize and present instruction to students with visual impairments to develop
their conceptual understandings as completely as possible.
Lowenfeld further advanced the theory of teaching children with visual impairments in
1973 when he identified three impacts of visual impairment on the cognitive development of
children with visual impairment. Visual impairment limits the “range and variety of
experiences,” “ability to get about,” and “interaction with the environment” (p. 34). As a result
of the impact of visual impairment, Lowenfeld then argued for three key principles in the
education of children with visual impairments. First, children with visual impairments need
concrete experiences with real objects to develop comprehensive conceptual understandings.
Second, Lowenfeld emphasized the need for unifying experiences to counteract the ways in
which children with visual impairments acquire information. When children are only able to
touch, hear, or smell objects, it is difficult for them to develop concepts of the whole experience,
as those senses only provide information about part of the experience. To facilitate deep
conceptual understanding, Lowenfeld suggested teachers plan opportunities for students to
participate in and master skills related to beginning-to-end, every day experiences. Finally,
Lowenfeld stressed the need for learning by doing. To address the lack of a visually-driven
motivation to learn, he suggested teachers and caregivers encourage and provide opportunities
for children with visual impairments to be engaged in routines in which they may learn to
perform tasks as independently as possible.
16
Lowenfeld’s (1952, 1973) principles continue to carry relevance in the education of
children with visual impairments. Lewis and Allman (2014b) described critical needs in the
education of children with visual impairments. They argued that to gain competence in a wide
range of skills, children with visual impairments need instruction that allows for “direct
experiences” with the materials and concepts under discussion, direct “immersion” in whole
activities to develop comprehensive concepts and to avoid isolated, splintered skills, “repeated
opportunities” to develop skill competence, and “targeted and realistic feedback” for refinement
of skills and concepts (p. 12).
Theoretical framework for instructional needs. Based on a theoretical understanding
of the developmental differences and instructional needs of children with visual impairments
(Ferrell, 2000; Lewis & Allman, 2014b; Lowenfeld, 1952, 1973), and in combination with
empirical evidence and best practices in specific instructional strategies, a theoretical framework
for providing instruction to children with visual impairments can be hypothesized (Appendix B).
The proposed framework has been cross referenced with proposed models of learning for
children without disabilities (Cambourne, 1988) and children with communication needs (Brown
& Woods, 2015, 2016).
First, adults must raise the expectation for the participation of a child with a visual
impairment. A child should be told he is expected to participate (Langley, 2006) and explicitly
invited to join (Bardin, 2014). Next, an adult should provide access to the task the child is asked
to complete, which may be accomplished though previewing the task with visual or physical
models (Bardin, 2014; Lewis, Slay, & Bischof, 2008; Loumiet & Levack, 1993), facilitated
exploration in which the adult guides the child through the task and its materials (Bardin, 2014;
17
Lewis & Allman, 2014a), and presenting the task and materials in a way to optimize visual and
tactile perception through environmental arrangement (Sticken & Kapperman, 2010).
If expectation and access strategies do not lead to independent completion, an adult
should provide contingent responses to the child’s attempts to complete the task. An adult may
use wait time (Bardin, 2014; Johnson & Parker, 2013), specific praise for successful
approximations of the components of a task (Ferrell, 2011; Langley, 2006), and realistic
feedback about attempts that are unsuccessful (Langley, 2006; Lewis & Allman, 2014a).
Some children with visual impairments will require explicit, systematic instruction to
master given skills. Adults may use task analysis to break down a skill into its component parts
and chain the skills together into a larger task (Bardin, 2014; Lewis & Allman, 2014a; Loumiet
& Levack, 1993). In addition, adults may use systematic response prompting (i.e., time delay,
system of least prompt) to enable child success while allowing for fading to naturally occurring
reinforcement (Ivy & Hatton, 2014).
Once a child nears task mastery, the adult should begin to fade support. An adult might
provide specific praise for the entire task rather than each task component (Lewis et al., 2008) or
reduce prompting so the child can successfully complete the task without being interrupted by
unnecessary prompts (Ferrell, 2011; Langley, 2006; Lewis et al., 2008). An adult can also
provide opportunities for generalizing the task by providing different materials or contexts for
the skill (Lewis et al., 2008). This model of implementing the least intensive support necessary
and fading support as the child approaches task mastery may provide teachers and caregivers of
children with visual impairments specific instructional strategies to mitigate the impact of visual
impairment on learning.
18
The Expanded Core Curriculum
Lowenfeld’s (1952, 1973) principles are also reflected in the most contemporary
understanding of the educational needs of children with visual impairments. In 1996, Hatlen
codified years of commonly accepted practitioner and researcher knowledge into what he called
the ECC. As originally described by Hatlen, the ECC is the unique set of disability-specific skills
that complement the traditional, core academic curriculum presented to all children. The ECC is
not a separate curriculum for children with visual impairments; rather, in combination with the
core academic curriculum, the ECC is integral to the provision of a comprehensive education for
all children with visual impairments. Hatlen cited Lowenfeld widely and further emphasized the
need for the ECC to complete the education of children with visual impairments. In 2004, Hatlen
wrote, “experiences and concepts casually and incidentally learned by sighted students must be
systematically and sequentially taught to the visually impaired student” (p. 26). Systematic,
sequential instruction in specific skills is critical to the implementation of the ECC.
Hatlen (1996) outlined eight areas of instruction in the ECC specific to children who are
visually impaired: compensatory access, social skills, recreation and leisure, assistive
technology, orientation and mobility (O&M), independent living skills, career education, and
visual (later sensory) efficiency. In 2004, Hatlen added a ninth area to the expanded core
curriculum (ECC), self-determination. As Hatlen wrote, the ECC is necessary for children with
visual impairments to work toward “neutralizing the effects of visual impairment on incidental
learning” (1996, p. 31). Carefully assessed and delivered instruction in the ECC allows TVIs to
provide the unifying experiences necessary to fully develop the concepts and skills of children
with visual impairments.
19
Support for instruction in the ECC is widespread among both TVIs and parents of
children with visual impairments (e.g., Grimmett et al., 2011; Lewis & McKenzie, 2010;
Lohmeier, et al., 2009). The authors of the National Agenda, a mission statement published by
leading experts in the field of educating children with visual impairments, dedicated one of only
ten goals to the ECC when they wrote, “All educational goals and instruction will address the
academic and expanded core curricula based on the assessed needs of each student with visual
impairments” (Huebner, Merk-Adam, Stryker, & Wolffe, 2004, p. 13). Most recently, direct
instruction in some areas of the ECC (i.e., orientation and mobility, social skills, and career
skills) has been linked to positive post-school outcomes, like employment, post-secondary
training, and social activities (Cmar, 2015; McDonnall, 2011; Wolffe & Kelly, 2011).
In addition to support from researchers, teachers, and caregivers, instruction in the ECC
is supported by existing law and proposed legislation. IDEA (2004) provides for free and
appropriate education (FAPE) for children with disabilities and mandates comprehensive
assessments to document the unique needs of children with visual impairments. The USDOE
OSERS further supported assessment and instruction in ECC areas (e.g. compensatory skills,
assistive technology, and orientation and mobility) through policy guidance issued in 2000. This
past year, the Alice Cogswell and Anne Sullivan Macy Act (2017) was re-introduced as House
Bill 1120 to further strengthen the support for ECC in law by explicitly outlining the need for
instruction and assessment in all nine ECC areas. Also in 2017, the Florida Administrative
Code’s Exceptional Student Education Eligibility for Students Who Are Visually Impaired was
revised to require assessment in all nine ECC areas before determination of eligibility for special
educational services for children with visual impairments.
20
Independent living skills. Like all areas of the ECC, instruction in independent living
skills is important in the education of children with visual impairments (Bardin, 2014). Though
definitions of independent living skills vary, Bardin (2014) defined them as “activities necessary
to take care of one’s self, family, and home and to live as independently as possible” (p. 283).
Those skills include a wide range of activities (e.g., clothing management, food management,
personal hygiene, money management, etc.). People who have typical vision acquire many of
their independent living skills incidentally (i.e., without systematic instruction) and at home
because of their ability to learn by watching (Bardin, 2014; Pogrund, 2002). However, because
of their lack of access to visual models and need for hands-on, concrete, unifying experiences
(Lowenfeld, 1973), children with visual impairments need direct instruction in independent
living skills at home and in school (Hatlen, 1996, 2004).
Though it is accepted that children with visual impairments have instructional needs in
independent living skills (Lohmeier et al., 2009), there is little empirical evidence documenting
differences between children with visual impairments and children with typical vision. Lewis
and Iselin (2002) surveyed parents of 20 young children with and without visual impairments
and found children with visual impairments completed fewer tasks independently (44% of tasks)
than their same-age peers with vision (84% of tasks). They also found that children with visual
impairments attempted independent living tasks less frequently than their sighted peers. Children
with visual impairments had not even attempted 41% of the surveyed tasks compared to their
sighted peers, who had not tried 14.5% of the listed tasks. Lewis and Iselin highlighted this lack
of practice among children with visual impairments as a potential reason for the delays in skill
development that many children with visual impairments experience.
21
Further differences in the independent living skills of children with visual impairments
were documented by Papadopoulos et al. in 2011. Papadopoulos et al. administered the Vineland
Adaptive Behavior Scales - Survey Form (1984 edition) and interviewed adult caregivers, who
reported the adaptive behavior skills (i.e., communication, daily living, and socialization) of
children with visual impairments. Papadopoulos et al. found that when compared to norms
including both children with and without disabilities, the children with visual impairments
assessed had moderately low adaptive behavior skills. Of the three adaptive behavior domains
measured, children with visual impairments scored lowest on daily living skills. However, when
compared to the normative group of children with visual impairments, the authors found the
daily living skills of their sampled students to be average.
Despite their importance, the findings of both studies are limited. Lewis and Iselin (2002)
examined a small volunteer sample of 10 children with visual impairments. Both Lewis and
Iselin and Papadopoulos et al. (2011) measured the independent living skills of children through
parent reports rather than direct observation of the students’ skills. Papadopoulos et al.’s findings
are further limited in two ways: (a) data on the normative group of children with visual
impairments were gathered in 1984 among children aged 6 to 13 years old who attended
residential facilities and (b) the data were gathered in Greece, through a translated instrument,
but compared to norms gathered in the United States. Despite these limitations, the findings of
both research teams are important because they contribute to the body of limited knowledge
concerning the differences in independent living skills of students with visual impairments.
Further, Papadopoulos et al.’s and Lewis and Iselin’s results share a common finding: children
with visual impairments may have delays in independent living skills behaviors compared to
their same age peers with typical vision.

22
The delays in independent living skills acquisition (Lewis & Iselin, 2002; Papadopoulos
et al., 2011) may be attributable to the learned helplessness demonstrated by many children with
visual impairments (Bardin, 2014). It is possible many children with visual impairments do not
initiate tasks because they learn others are likely to perform the task instead (Bardin, 2014). This
pattern of behavior was detected by Lewis and Iselin (2002) when they reported children with
visual impairments initiated fewer independent living skills tasks than children with typical
vision. The independent living skill deficits and lack of child-initiated learning among children
with visual impairments suggest a need for adult-directed intervention for children with visual
impairments to initiate practice of and acquire competence in independent living skills.
However, very little is known about how best to deliver instruction in independent living
skills to children with visual impairments. Lewis, Savaiano, Blankenship, and Greeley-Bennett
(2014) conducted a meta-analysis of the extant literature in independent living skills of children
with visual impairments. They found most of the existing literature to be descriptive, locating
only seven intervention studies with children. Of those seven studies, only three instructional
areas were addressed: food management, oral hygiene, and money management. In those seven
interventions, specific instructional strategies were examined for efficacy with specific students.
However, few of the studies featured experimental control or replicated results, so it is difficult
to determine if the growth in independent living skills was unique to the children included in the
studies or if the practices implemented may be effective with other children who have visual
impairments.
Instructional time. Compounding the lack of experience and skill deficits is the lack of
teacher-directed instructional time in the ECC (Grimmett et al., 2011; Lohmeier et al., 2009;
Wolffe et al., 2002). Lohmeier et al. (2009) found that despite common consensus among TVIs
23
on its importance, 57% of those teachers reported they did not have time to teach the ECC.
Correspondingly, only 35% of parents thought their children were receiving appropriate
instruction in ECC areas.
Lack of instructional time in the ECC during the school day may be an issue across
educational placements. In their observations of TVIs, Wolffe et al. (2002) found teachers in
both local public schools and residential schools spent an average of 41% of their time providing
instruction in academics or tutoring, 18% of their time supporting academics with instruction in
communication, assistive technology, and compensatory skills, leaving 32% of their time for
instruction in all other ECC areas. Independent living skills were addressed in only 7% of the
time available to TVIs. In 2005, Lohmeier surveyed schools for the blind and reported the
percentage of schools that provided instruction in the ECC during (75%), before (25%), and after
(33%) the school day. Lohmeier reported 87.5% of the surveyed schools for the blind offered
direct instruction in independent living skills. Lohmeier’s findings revealed that most, but not all,
of the schools for the blind she surveyed reported providing instruction in the ECC and
independent living skills.
Lewis and McKenzie (2010) surveyed TVIs and paraprofessionals (i.e., educational
assistants) and found both groups reported paraprofessionals providing direct instruction in the
ECC, even though the paraprofessional’s role has traditionally been limited to instructional
support. Lewis and McKenzie defined direct instruction as “the teaching of new concepts and
skills” (p. 467). Only 50.6% of local school paraprofessionals and 29.6% of residential school
paraprofessionals reported providing no direct instruction in the ECC. Among those
paraprofessionals who reported providing direct instruction in the ECC, 24.1% of those working
in local schools and 70.4% of those working in residential schools reported providing direct
24
instruction in independent living skills. The evidence suggests that instruction in the ECC
broadly, and independent living skills specifically, is second to other educational priorities and
often left to paraprofessionals or families.
Unique developmental processes of children with visual impairments produce a need for
instruction in a disability-specific curriculum, including instruction in independent living skills
(Hatlen, 1996, 2004; Lowenfeld, 1952, 1973). Though there is little empirical evidence
describing specific skill deficits or effective instructional practices for teaching independent
living skills to children with visual impairments (e.g., Lewis & Iselin, 2012, Lewis et al., 2014),
best practice suggests these children need instruction that differs from those of children with
typical vision (e.g., Bardin, 2014; Ferrell, 2011; Lewis et al., 2008). Because instruction in
independent living skills is not frequently provided in schools (e.g., Lohmeier et al., 2009;
Wolffe et al., 2002), caregivers may be left to provide instruction at home. As a result, caregivers
may need support to implement instructional strategies unique to children with visual
impairments to meet the independent living skills needs of their children.
Families
Family Systems Framework
Turnbull et al. (2015) outlined a conceptual framework of family systems to guide the
interactions of professionals working with the families of children who have disabilities. They
highlighted the child with a disability as a member of his or her family and outlined the
interactions among family characteristics, family functions, family life cycle, and family
interactions. As defined by Turnbull et al., family characteristics act as inputs in the family
systems model and feature both individual and group characteristics of members of the family
(e.g., individual personalities and shared culture). Family functions act as outputs in the model
25
and include the roles and responsibilities families perform for one another (e.g., meal
preparation, emotional support, etc.). The family life cycle component reflects the relational
changes that occur as families change over time.
The fourth construct in the Turnbull et al. (2015) model, family interactions, includes the
family subsystem and the surrounding constructs of cohesion and adaptability. The family
interactions subsystem may prove to be an area of influence for professionals seeking to work
with children who have disabilities and their families. Within the sphere of family interactions
are the relationships among all members of the immediate and extended family, including
parental, marital, and sibling relationships. Family systems theory suggests that the elements of
the system seek balance, and when one element demands more attention, the other elements
receive less attention.
Turnbull et al. (2015) proposed that the principles of adaptability and cohesion, which
surround the family subsystem, each exist on their own continuum. A family’s ability to adapt
may range from rigidity to chaos, and cohesion may range from disengagement to enmeshment.
Members of families with low cohesion may be disengaged from each other, including the child
with a disability. Similarly, a family with high cohesion may be enmeshed and provide too much
protection toward or involvement in the life of the child with a disability. Such high levels of
involvement may limit the acquisition of independence in the child with a disability. The enacted
and desired level of adaptability and cohesion are likely to vary by family because of individual
and group characteristics.
Jackson and Turnbull (2004) applied an earlier edition of Turnbull et al.’s (2015) family
systems framework to the families of children who are deaf, arguing that deafness impacts the
entire family, not just the child who is deaf. Jackson and Turnbull identified specific needs for
26
families of children who are deaf, including specific supports for parents. As a result of the
child’s deafness, Jackson and Turnbull outlined a unique need for parent support in “knowledge
in ways children learn” (p. 22). The authors argued that children who are deaf learn differently
from other children, and their parents need specific instructional strategies to best maintain the
family system. Children with visual impairments also learn differently from children who do not
have disabilities (e.g., Ferrell, 2011; Hatlen, 1996, 2004; Lowenfeld, 1952, 1973). As such, the
work of Turnbull et al. and Jackson and Turnbull may extend to children with visual impairments
and their families.
Impact of Visual Impairment on Families
Adjustment. Parents of children with visual impairments may face unique challenges in
their parenting, beginning with the acquisition of a child’s visual impairment. Herring (1996) and
Forster (2006), both parents of children with visual impairments, documented their own
adjustment processes, including similar descriptions of adjustment behaviors like grief, guilt,
fear, anxiety, shock, denial, anger, anxiety, and resentment. Forster described additional phases,
including bargaining and acceptance. The experiences of Herring and Forster are reflected in
Fazzi, Klein, Pogrund, and Salcedo’s (2002) conceptual model of emotional reactions to a child’s
visual impairment, which features feelings of shock, denial, guilt, anger, sadness, objectivity, and
resolution. Alternatively, some parents may not grieve their child’s visual impairment (Ferrell,
2011), and even if they do undergo a grieving process, each parent is likely to have unique
experiences with and feelings about his or her child’s visual impairment. As a result, skilled
practitioners must be sensitive to variable experiences of parents of children with visual
impairments (Fazzi et al., 2002).
27
Infancy and childhood. The unique challenges of parenting children with visual
impairments may extend beyond the initial adjustment period. Through a qualitative
investigation, Smyth, Spicer, and Morgese (2004) found that parents of infants and toddlers with
visual impairments experienced challenges teaching their children to feed themselves. Parents of
children who were tactual learners demonstrated less confidence in their abilities to feed their
children and their children’s abilities to learn to self-feed. Smyth et al. also found that all
children with visual impairments, regardless of visual abilities, were delayed in their use of
utensils and benefitted from routines during mealtime experiences. Smyth et al. reported that
building parental confidence through support from early interventionists may be beneficial to
improve outcomes for children with visual impairments and their families.
Though the limited evidence varies widely, mothers of children with visual impairments
may interact in different ways with their children who are visually impaired than mothers of
children with typical vision interact with their children. Dote-Kwan and Hughes (1994)
examined the home environments of 18 young children with visual impairments, including
variables related to socioeconomic status, the environment of the home, and the child’s
interactions with his or her mother. The authors found that socio-economic status did not predict
significant differences in the home environment or in the developmental outcomes of the
children with visual impairments; however, they found the home environment significantly
predicted developmental levels of young children with visual impairments in expressive
pragmatic language.
In 1995, Dote-Kwan extended her research to include an investigation of the maternal
interactions of young children with congenital visual impairments. In this investigation, Dote-
Kwan coded maternal responsiveness, (i.e., the mother’s behaviors in response to her child’s
28
behaviors), maternally initiated behaviors intended to engage her child, and each child’s
developmental level. She found that responsive behaviors from mothers, like responding to the
child’s request or engaging with the child’s vocal behaviors, were significantly and positively
correlated with developmental scores for children. She also found that mothers who sought their
children’s attention more often had children with lower vocalization skills. Other mother-
initiated behaviors had no correlation with development.
Behl, Akers, Boyce, and Taylor (1996) also examined interactions between mothers and
their children with visual impairments and compared those interactions to mothers of children
without visual impairments, but who did have developmental delays. Behl et al. assessed several
maternal characteristics (i.e., like sensitivity, directiveness, and play interaction) and found
mothers of children with more significant visual impairments had significantly higher levels of
physical involvement and control of activities.
Kekelis and Prinz (1996) observed conversations between mothers and their young
children during playtime; two of the children were blind and two had typical vision. Kekelis and
Prinz found mothers and their children with typical vision spoke for similar amounts of time, but
mothers of children who were blind spoke for almost two and a half times longer than their
children spoke. The authors also found that mothers of children who were blind asked more
factual questions of their children, while the mothers of children with typical vision asked more
critical thinking questions of their children.
Campbell (2003) used data from a longitudinal study of children with disabilities in
Australia to compare the interactions during play of mothers with their young children who have
visual impairments to the interactions of mothers and their young children with sight. Children
were around 18 months old when the data were collected about maternal interactions, though the

29
data for the two groups were collected at different times. Campbell found that there were no
significant differences overall in the number of directives given to children who were blind or
children who were sighted, but she did find a significantly higher number of directives in the
“deterrence of self-harm,” particularly eye-poking, for mothers of children who were blind (p.
361).
Adolescence and adulthood. Challenges in parenting children with visual impairments
may extend into adolescence. Chang and Schaller (2000) conducted a qualitative investigation
into the perceptions of parental support perceived by adolescents with visual impairments. Chang
and Schaller reported themes that represent the variability of the experiences of those teenagers
interviewed. They described a variety of parental roles, including emotional support,
informational support, and tangible aid. Though most respondents reported their parents met
their needs for emotional support for safety, inclusion, and emotional development, not all
children felt their parents understood their unique emotional support needs. Similarly, the
adolescents interviewed varied in their beliefs that their parents met their needs for informational
support on knowledge of visual impairment, friendships, and personal interests. Finally, these
teenagers reported their parents often attempted to provide tangible assistance to help them meet
personal or career goals or to address their educational needs. Some of the respondents, however,
felt their parents’ interventions limited their abilities to demonstrate independence.
Similar tensions have been reported among parents of young adults who are visually
impaired. In a heuristic inquiry, de Klerk and Greef (2011) reported common themes of the
process by which parents adjusted to their child’s visual impairment. Parents reported the impact
of internal family values on their adjustment, including the role of a change in attitude regarding
the child’s visual impairment, the role of faith, and an increased closeness among family
30
members. As parents adjusted to their child’s visual impairment, they were then able to allow
individuals outside of the immediate family to be involved in their lives. During this time, they
could accept and seek help from others, including extended family and educational professionals.
The final phase of adjustment described by de Klerk and Greef included a widening of
perceptions of their child beyond the visual impairment. In this phase, parents reported positive
feelings about their child, his abilities, and his potential for a happy, independent life. To reach
this final phase, de Klerk and Greef suggested families and educational professionals must work
together to “infiltrate the family boundaries” that might otherwise limit parent-professional
partnerships (p. 422).
Need for support. Nixon (1988) reported the results of a qualitative investigation of
support groups for parents of children who are blind. He reported support groups appeared to be
useful for the parents who sought and utilized them, but many parents he interviewed did not
engage in support groups because they felt support groups were not appropriate to meet their
needs. Several parents reported a need for support from professionals beyond the emotional
support they perceived a group of parents could give them. Nixon proposed the involvement of
professionals in parent support groups, but he stressed the need for professionals to be responsive
to individual families and their unique needs. In fact, Kyzar, Brady, Summers, Haines, and
Turnbull (2016) found the quality of the relationships between families of children who are
deafblind and the primary educational professionals serving those children was predictive of
family quality of life. According to the authors, relationships among parents and professionals
may be important in helping families establish a positive outlook, which facilitates positive
family relationships.
31
Beyond individual parental factors related to adjustment to a child’s visual impairment,
factors related to the individual child may impact parental priorities. In his survey of parents of
young children with visual impairments, Craig (1996) found parental instructional priorities
varied based on the presence or absence of additional disabilities. Parents of children who had a
visual impairment as their only disability had priorities for literacy instruction over functional
skills instruction. Conversely, parents of children with visual and multiple disabilities prioritized
functional skills over literacy instruction.
As a consequence of the differences inherent in raising and educating children with visual
impairments (e.g., Dote-Kwan, 1995; Smyth et al., 2004), a family-centered approach to the
education of children with visual impairments has been widely accepted as necessary to help a
child reach his or her full potential (Fazzi et al., 2002; Lewis & Allman, 2014b). Goal Two of the
National Agenda echoes the provisions for parent participation of IDEA; Huebner et al. (2004)
wrote “policies and procedures will be implemented to ensure the right of all parents to full
participation and equal partnership in the education process” (p. 8). In addressing parents of
children with visual impairments, Ferrell (2011) encouraged parents to actively engage in their
roles and rights as parents of children with visual impairments.
Family Systems of Children with Visual Impairments
The family systems approach described by Turnbull et al. (2015) may be applied to work
with families of children who have visual impairments. Of particular interest are two principles:
daily care and cohesion. Turnbull et al. identified daily care for children with disabilities as one
of the family functions in their family systems framework, including both routines related to the
whole family (e.g., preparing nightly family meals) and those specific to the child with a
disability (e.g., cutting up the food of a child who cannot do it for himself). Children with visual
32
impairments may have deficits in adaptive behaviors (Lewis & Iselin, 2002; Papadopoulos et al.,
2011), and as a result, the families of those children may be called upon to organize and provide
daily care for children with visual impairments beyond the care required for their children with
typical vision.
The polar constructs within cohesion, disengagement and enmeshment (Turnbull et al.,
2015), may also be applicable to the education of children with visual impairments. Because
children with visual impairments may have unique developmental differences and conceptual
understandings (Ferrell, 2011; Lowenfeld, 1952, 1973) and require purposefully organized direct
instruction (Hatlen, 1996, 2004; Lewis & Allman, 2014b), caregivers of children with visual
impairments may need specific instructional interventions to achieve an appropriate cohesive
balance between disengagement and enmeshment. Further, the extra effort and time involved in
teaching children with visual impairment to perform daily care skills (Bardin, 2014), combined
with the learned helplessness and lack of task initiation (Lewis & Iselin, 2002) of many children
with visual impairments, may reveal a need for instruction and intervention for families of
children with visual impairments.
Nixon (1991) proposed a model to conceptualize reactions of parents of children with
visual impairments. He proposed four patterns: denial, minimizing, protectiveness, and
disavowal or deviance. Nixon’s framework shares principles with Turnbull et al.’s (2015) family
systems construct of cohesion. For parents who fall into the categories of denial, minimizing, or
disavowal (Nixon, 1991), it is possible that family cohesion may be low, or the family members
disengaged (Turnbull et al., 2015). Similarly, families who follow a pattern of coping with
protectiveness (Nixon, 1991) may demonstrate high levels of cohesion or enmeshment (Turnbull
et al., 2015). Appropriate interaction from a professional who incorporates caregiver education
33
(Kyzar et al., 2016; Nixon, 1991) may be a strategy to restore cohesive balance to the families of
children with visual impairments.
Caregiver Education
Adult Learning Principles
In their meta-analysis of adult learning approaches, Dunst et al. (2010) described the
literature regarding the use of four methods: accelerated learning, coaching, guided design, and
just-in-time training. Dunst et al. outlined the key constructs of each learning approach.
Accelerated learning promotes a “holistic,” multisensory-based approach to relax the learner to
“promote creation (and not consumption), enhance retention, and quicken the learning process”
(p. 93). As defined by Dunst et al., coaching is a cooperative, relational, and long-term process
that aims to increase the transfer of knowledge and skills from experts to novices. Guided design
builds knowledge and skills by involving teams of participants in real life problems for which
they may consider the issues and propose solutions with feedback from both their teammates and
the instructor. Dunst et al. described just-in-time training as a method in which individuals
receive feedback from a more skilled person who provides only the necessary information or
skills to address the situation at hand. Just-in-time training does not anticipate future needs, but
rather is “tailored training in response to a request specific to an immediate concern or need” (p.
94).
Dunst et al. (2010) operationalized six characteristics in adult learning: introduction,
illustration/demonstration, practicing, evaluation, reflection, and mastery. They then defined two
to six specific practices in each characteristic (e.g., role paying simulations, instructional videos,
self-assessment, etc.). After operationalizing the characteristics and practices, Dunst et al.
conducted a meta-analysis of 49 studies with over 4,000 participants across a variety of adult

34
learning environments, including both schools and business settings. They calculated both mean
effect sizes and significance for each characteristic and strategy in impacting learner outcomes of
knowledge, skills, attitudes, and self-efficacy. Dunst et al. found all six characteristics to be
effective in adult learning, (i.e., introduce, illustrate, practice, evaluate, reflection, and mastery),
though specific practices were found to have variations in significance and effect size within the
same category. For example, within the construct of practicing, all five practices were found to
be significant, but real life application had an effect size of .94, while the authors calculated an
effect size of .35 for role playing exercises. Across all six characteristics and 22 practices, “the
more actively involved learners were in mastering new knowledge or practice, and the more
instructors or trainers supported and facilitated the learning process, the better were the learner
outcomes (p. 106).
Coaching Rationale. One method of adult learning, coaching, has been applied widely in
education. Dunst et al. (2010) defined coaching as “a cyclic process that improves knowledge
and skills, self-confidence, and collegial relationships as a result of ongoing coaching episodes”
(p. 93). Coaching aims to change the behavior of the learner, and it supports many practices in
adult learning theory because it allows for the connection of new knowledge to existing
knowledge, the practical application of the new knowledge, and ongoing and sustained
interactions that support mastery of the content (Donovan et al., 1999; Dunst et al., 2010).
Further, coaching interventions can include all six adult learning characteristics (i.e.,
introduction, illustration/demonstration, practicing, evaluation, reflection, and mastery) that
Dunst et al. found to be effective in the acquisition of new knowledge and skills by adults.
35
Implementation with teachers. Leat, Lofthouse, and Wilcock (2006) conducted a case
study in which they described an initial implementation of coaching teachers to incorporate
research-based practices in their work. Overall, Leat et al. found experiences with coaching
practices to be positive, but they found the trainings needed to be short, about one to two hours,
and include actionable elements that could be immediately applied by practitioners. Their
findings also highlighted a need for “widespread ownership of the innovation” for it to be
accepted in a school culture (p. 336). Leat et al. emphasized the importance of building trusting
relationships between coaches and teachers. Without positive relationships, Leat et al. argued,
coaching is less likely to be effective.
While Leat et al. (2006) described the impact of an outside expert coaching teachers,
other researchers have applied the coaching model to within-school experts. Briere, Simonsen,
Sugai, and Meyers (2015) used a multiple baseline, single case design to examine the efficacy of
expert teacher coaching on the use of specific praise among new teachers. Expert teachers within
the school were paired with beginning teachers, and the two participated in an intervention that
included self-monitoring, structured consultation meetings, and performance feedback. Briere et
al. found a functional relation between the expert teacher coaching model and the beginning
teachers’ use of specific praise. The authors’ findings suggest coaching may be a useful way to
support less skilled practitioners, and coaching may be especially useful when the model is
applied to the acquisition of narrowly targeted skills (i.e., appropriate use of specific praise),
rather than a broad range of skills.
Snyder, Hemmeter, and Fox (2015) outlined the theory of the practice-based coaching
(PBC) model widely used in early childhood education to increase the effectiveness of teaching
practices. PBC exists within collaborative partnerships between coaches and teachers in which
36
both parties work together to improve the practice of teachers. Within the collaborative
partnerships, the coach and teacher participate in shared goals and action planning, focused
observation, and reflection and feedback. PBC should be cyclical, in which reflection and
feedback drive new goals to improve instructional practice.
Implementation with educational assistants. Coaching has also been used with
educational assistants (i.e., paraprofessionals) serving students with disabilities. In 2013, Brock
and Carter conducted a systematic review of the literature regarding interventions delivered by
educational assistants and the support necessary for educational assistants to implement those
interventions well. They found modeling, performance feedback, and follow-up training were
frequently implemented in educational assistant professional development. In 2015, Brock and
Carter conducted a randomized control trial (RCT) in which they examined the relative
effectiveness of video modeling and coaching in the professional development of educational
assistants. Coaching took place over one session and included targeted feedback, modeling, and
guided practice. They found both practices to be effective; however, they documented a larger
effect size for coaching alone than for video modeling alone. Brock and Carter (2017) conducted
a meta-analysis of RCTs of teacher and educational assistant professional development and
found the coaching elements of modeling and performance feedback were especially effective
when used together, demonstrating larger effects than those that used either in isolation.
Implementation with caregivers. Coaching models have also been applied to caregiver
education, most frequently in early intervention for young children who have disabilities. Early
intervention specialists may coach caregivers to increase a variety of behaviors that may improve
the educational outcomes of their children. For example, Nunes et al. (2016) examined the
efficacy of coaching mothers of young children with ASD to increase the child’s communication.
37
The mothers were coached weekly by two practitioners, a teacher and a speech language
pathologist, in a university classroom setting. After each weekly session, mothers brought videos
of themselves applying the newly learned skill in routines with their children (i.e., play,
caregiving, and pre-academic skills), and those videos were used for discussion in the following
session. Interventionists helped the mothers to identify opportunities for responsiveness in their
daily interactions with their children. Though most coaching occurred in a classroom setting,
interventionists followed up with home visits at one and five months. Coaching was found to
increase maternal responsiveness to the communication attempts of their children. Though many
of the data on child communication were highly variable, implementing the new strategies
increased the communication responsiveness of each child in at least one home routine.
In 2012, Friedman, Woods, and Salisbury coded videos of early interventionists coaching
caregivers of children with disabilities and identified stages and strategies used in caregiver
coaching. Though the authors were clear the stages and strategies were not prescriptive, the
authors suggested they were features of family-centered caregiver coaching. The three stages
were identified: setting the stage, application opportunities and feedback, and mastery. Specific
strategies within each stage were also operationalized: conversation and information sharing,
observation, direct teaching, demonstrating, guided practice with feedback, caregiver practice
with feedback, joint interaction, and problem solving/reflection. The authors also operationalized
the absence of coaching (i.e., no coaching) when the interventionist provided direct services to
the child without including the caregiver.
The stages and strategies of family-centered caregiver coaching outlined by Friedman et
al. (2012) have been applied to several interventions for caregivers of young children with
disabilities. Wetherby et al. (2014) implemented a RCT in which the social communication skills
38
of toddlers with ASD showed greater increases when caregivers received individualized
coaching rather than traditional, group education. The effective coaching model featured
elements operationalized by Friedman et al. (i.e., direct teaching, guided practice, and reflection).
Brown and Woods (2015) implemented a family-centered coaching intervention for
caregivers of young children with Down syndrome, ASD, and developmental delays to increase
the communication of those children during family routines. They used a single case, non-
concurrent multiple baseline design replicated across nine caregiver-child dyads to document (a)
the impact of caregiver coaching on caregiver use of strategies and (b) how child language
targets changed as a result of caregiver use of coached strategies. Caregivers were coached to
increase communication according to the KidTalk-TaCTICS Project (KKTP), which incorporates
Enhanced Milieu Teaching (EMT) and FGRBI. The intervention model features stages (i.e.,
setting the stage/information sharing, intervention, and problem solving collection) and specific
coaching strategies (i.e., direct teaching, demonstration, guided practice with feedback, caregiver
practice with feedback, and problem solving and/or reflection) outlined by Friedman et al. in
2012. Brown and Woods found when early interventionists coached caregivers for about an hour,
once a week in specific caregiver intervention strategies (i.e., responsive interactions, modeling,
and prompting/milieu teaching), the frequency of caregivers’ use of specific strategies increased
and the children’s targeted communication skills also improved.
In 2016, Brown and Woods analyzed the data collected in their 2015 intervention and
found that caregivers were more likely to immediately apply the use of a coached strategies that
had been taught in a way that encouraged their active participation. The findings of Brown and
Woods (2015, 2016) suggest that coaching caregivers can change both caregiver and child
39
behavior and that caregiver coaching should be highly relevant and immediately applicable to the
lives of caregivers.
The principles found to be successful in coaching caregivers of young children with
disabilities are operationalized in the FGRBI Key Indicators manual (Woods, 2107). It outlines
the FGRBI caregiver coaching stages and specific indicators of effective coaching. In this model,
early interventionists follow four stages to complete each coaching session: setting the stage,
observations and opportunities to embed, problem solving and planning, and reflection and
review. In setting the stage, the coach listens to the family and child updates, asks for specific
information on use of strategies since the last visit, expands on existing knowledge with new
information related to the child’s development, and makes clear the goals for the session. In
observation and opportunities to embed, the coach watches the child and caregiver participate in
a routine without coach input. After the observation, the coach uses specific coaching strategies
to allow the caregiver to practice the skill several times with feedback. During problem solving
and planning, the coach and caregiver jointly brainstorm possible intervention strategies and plan
opportunities to implement strategies. Finally, in reflection and review, the coach prompts
caregiver reflection and helps the caregiver conceptualize successful implementation of
strategies across routines.
The empirical base for coaching educators and caregivers continues to grow, suggesting
the success of coaching models to improve the skills of adults who work with children who have
disabilities and to improve the educational outcomes for those children. Successful coaching of
both educators and caregivers features elements of rapport building, observation and/or guided
practice, collaborative problem solving, reflection, and planning for the future (e.g., Brock &
Carter, 2013, 2017; Brown & Woods, 2016; Snyder et al., 2015; Wetherby et al., 2014).
40
Implementation with people with visual impairments. Coaching models have also
been applied to support the care of people with visual impairments. Damen et al. (2011) used
several A-B designs to investigate the efficacy of coaching professional caregivers to improve
the quality of their interactions with adolescents and adults who have visual impairments and
intellectual disabilities in a residential facility in the Netherlands. Researchers investigated this
application of the Contact program, designed to increase caregiver responsiveness to signals
from individuals with disabilities. After a one day training in principles of responsive
communication, caregivers participated in coaching across nine weeks that included analyzing
video-recorded interactions with the clients and discussing how to increase responsiveness.
During those sessions, the coaches discussed specific client behaviors and helped caregivers
interpret the signals of the client. Quality of interactions were measured across three categories:
confirmation of initiation, initiation of interaction, and reaction to initiation of others. Though
there are limitations related to the selected design, Damen et al. found coaching professional
caregivers increased the quality of their interactions with their clients who had intellectual and
visual disabilities. Damen et al. did not find that coaching caregivers changed client
responsiveness across the nine weeks of the intervention. They proposed that because of the
complexity of their disabilities, detecting changes in client responsiveness may require
measurement across longer periods of time.
A similar model was applied to coach the mothers of two young boys who are deafblind.
Janssen, Riksen-Walraven, van Dijk, and Ruijssenaars (2010) used single case design to extend
the Diagnostic Intervention Model, which previously had been found to be effective to increase
the quality of interactions among children who are deafblind and their teachers. In this
application of the model, mothers were coached to interact more purposefully with their children
41
by determining and clarifying questions initiated by their children, analyzing the interaction,
applying an intervention, and evaluating its effectiveness. The duration of coaching varied for
each child’s mother. One boy’s mother was coached for a total of nine hours over five sessions in
six weeks, and the other boy’s mother was coached for eight hours total in five sessions across
eight weeks. Janssen et al. found that the coaching intervention increased maternal and child
responsiveness for both dyads across a variety of behaviors (e.g., initiations, turn giving, and
appropriate intensity). For one boy, data were also collected on responsiveness when play
materials were present. Janssen et al. found maternal and child responsiveness improved less
after coaching when materials were present than it did when materials were absent. The authors
suggested this difference may be because the presence of play materials complicated the
interaction and additional coaching to improve interactions in the more complex situation may be
required.
In 2017, Probst and Walker used a single case multiple baseline across behaviors design
to evaluate the effectiveness of an educational team coaching intervention to use a system of
least prompts to increase the personal hygiene skills of a 17-year-old with a visual impairment,
ASD, and intellectual disability. They found after a workshop and follow-up coaching sessions,
team members (i.e., one special education teacher and two educational assistants) were able to
implement the system of least prompts with high fidelity while the student increased the
percentage of steps he completed independently in three tasks: cleaning his communication
device, washing his hands, and brushing his teeth. After the workshop, each team member
provided instruction in a single student behavior while using the same system of least prompts.
Coaching sessions were delivered if fidelity of implementation of the system of least prompts fell
below 80%. The number of coaching sessions required varied across the three team members,
42
ranging from one to three sessions. Though this study makes an important contribution to the
limited research base regarding the delivery of independent living skills to students with visual
impairments, it is limited in its application to the coaching literature primarily because the
researchers did not measure fidelity of implementation of the system of least prompts during
baseline data collection. Consequentially, they were unable to establish a functional relation
between the educational team workshop and coaching and high fidelity of use of the system of
least prompts by team members. Nevertheless, they did document an increase in the student’s
personal hygiene skills resulting from the implementation of a system of least prompts.
The success of coaching interventions in increasing the skills of teachers, educational
assistants, and caregivers of children with and without disabilities (e.g., Brock & Carter, 2015;
Brown & Woods, 2015; Wetherby et al., 2014) is promising in its applications to the education
of children with unique learning needs. The limited research base suggests people who have
visual impairments may increase their skills if their educators and caregivers receive training,
which may include coaching elements, to help them deliver instructional practices with greater
fidelity (Damen et al., 2011; Janssen et al., 2010; Probst & Walker, 2017).
Telepractice
Though coaching has been found effective in delivering educational interventions to
children with disabilities and their caregivers, coaching requires sustained contact between
caregivers, individuals with disabilities, and coaches (e.g., Damen et al., 2011; Dunst et al.,
2010; Nunes et al., 2016), which may be unfeasible among populations of students with low
incidence disabilities, as the children and families who would benefit from coaching may not be
in close physical proximity to the experts providing the coaching. In recent years, one model,
telepractice (i.e., telehealth, telecoaching) has been implemented to allow access to care and
43
education for people who do not otherwise have convenient access to those services. Telepractice
typically involves the use of a technology (e.g., Internet-enabled computers, telephones,
videoconferencing software, etc.) to enable synchronous communication to bridge the physical
distance between individuals in need of medical or educational services and the experts who
deliver that service (Boutian, 2014). The low incidence and heterogeneity of the population of
children with visual impairments (Mason & Davidson, 2000; USDOE OSERS, 2017) suggests
the potential of telepractice to provide access to instructional strategies for children with visual
impairments and their families despite their physical distance from expert service providers.
Hall and Bierman (2015) conducted a comprehensive review of the literature on
technological interventions for parents of young children both with and without disabilities. In
their synthesis, they outlined several uses for technology to support the education of parents.
Websites have been used to share information or deliver sequenced content, provide discussion
boards that act as support groups, and facilitate incidental communication. Hall and Biermann
found that mobile devices were often used to provide communication to support another
technological intervention. In contrast, video conferencing applications were frequently the
mechanism through which interventions were delivered to parents. Hall and Biermann
emphasized that, though the body of literature is growing quickly, it is unclear whether
interventions that include technology are more or less effective than traditional methods of
parent education and coaching. They did note, however, that when technological elements are
paired with real-time support from professionals (as in coaching models), effects for parents and
children may be greater.
Telehealth. Telehealth is the application of telepractice to medical care and therapies. It
has been widely used to provide access to care for families of children with complex needs or
44
children who live in rural areas. Monaghan, Hilliard, Cogen, and Streisand (2011) used a
telephone-based education and support group for parents of young children with type 1 diabetes.
In their small-scale pilot, Monaghan et al. found positive effects on measures of parental stress
and social support as a result of the intervention. In Australia, Johansen et al. (2004) used digital
cameras and email to facilitate communication between parents of children with burns and burn
specialists. The authors found little training was needed for parents to learn to take and to email
pictures to the specialists for consultation. In a similar investigation, Clawson et al. (2008)
implemented a teleconferencing intervention for parents of young children with rare feeding
disorders and found the intervention both reduced the costs associated with travel to specialists
and led to high parent satisfaction. Glueckauf et al. (2002) compared the efficacy of three modes
of counseling adolescents with epilepsy and their parents who lived in rural areas without
convenient access to care. They found all three interventions (i.e., telephone counseling from
home, video counseling at home, and traditional office-based counseling) led to positive
outcomes for the teenagers. Because of a lack of providers to meet the unique needs of children
with retinal disease and their parents, Pathipati and Moshfeghi (2017) suggested telepractice
retinal imaging and consultation to diagnose retinal disease in time for medical interventions that
might preserve remaining vision in children.
Telepractice models have also been implemented to deliver behavior therapies for
children with ASD. Wacker et al. (2013b) used telepractice to train parents of young children
with ASD to conduct functional analyses of problem behavior. In this intervention, parents
traveled to one of five nearby medical clinics and participated in videoconferencing consultation
with a behavior specialist an average of 222 miles away. Across four phases, parents learned
about behavior analysis and the study purpose and methods. Parents and the behavior specialist
45
discussed each child’s problem behaviors, likely antecedents, and preferred and non-preferred
items. In the final phase, the parents conducted the functional analyses in the clinic with the
teleconferenced support of the behavior specialist and an on-site assistant. For all children who
demonstrated problem behavior during the functional analysis sessions, their parents were able to
identify functions of their behaviors. Wacker et al. found the intervention to be both time and
cost effective for parents and the behavior specialist.
Lindgren et al. (2015) compared the efficacy and efficiency of three models of behavior
therapy for children with ASD and developmental delays (i.e., therapy delivered in person at the
child’s home, telepractice therapy in a clinic, and telepractice therapy based in the child’s home).
The caregivers of 107 children were coached to complete functional behavior analyses and
functional communication training via one of the three service delivery models. The authors
found that all three models were effective in training caregivers to assess their child’s behavior
so they could better engage with their children. Despite their comparable effectiveness and
acceptability to caregivers, the clinic- and home-based telepractice models were significantly less
expensive ($3068.46 and $2145.64) than traditional therapy held in the child’s home ($5949.97).
Telecoaching. The use of telepractice has been applied beyond serving the health and
behavioral needs of families of children with medical needs and children with disabilities.
Telepractice has also been used to coach caregivers to change their behaviors to improve
outcomes of their children who have disabilities. Most telepractice coaching models involve the
principles of adult learning that Dunst et al. (2010) found to be effective in changing the
behaviors of adults, because they allow for sustained interactions with individuals expert in
particular practices while mitigating the limitations of physical distance and cost.
46
Early intervention. Telepractice has been applied to work with parents of very young
children who receive early intervention services. Cason, Behl, and Ringwalt (2012) surveyed
state education agency representatives from 26 states and one jurisdiction of the United States.
The representatives reported that 9 of the 27 educational agencies used telepractice for some
service delivery currently or planned to implement it in the next two years. Cason et al. also
reported that among the six states currently using telepractice models, a variety of professionals
are represented: early intervention developmental specialists (1 state), teachers of the deaf and
hard of hearing (2 states), speech-language pathologists (3 states), occupational therapists (1
state), physical therapists (1 state), behavior specialists (2 states), and audiologists (1 state).
Among those states that have not implemented telepractice models, about 40% percent of the
representatives reported concerns with security, privacy, and the quality of the educational
services.
Olsen, Fiechtl, and Rule (2012) described the results of a project in which they
implemented “virtual home visits” for young children with disabilities who lived in rural and
remote locations. A team of educational service providers (e.g., physical therapy, special
education, speech-language pathologists, etc.) used videoconferencing to coach parents to build
their children’s skills. Service providers interacted directly with children via teleconferencing but
generally, they watched interactions and advised parents on how to better engage their children.
Like Lindgren et al. (2015) and Wacker et al. (2013b), Olsen et al. found their telepractice
intervention to be cost effective, particularly for families who lived in rural and remote areas,
with savings per visit ranging from $14 to $112, based on the location of the family’s home.
After the implementation of the videoconferencing systems, both parents and service providers
reported comfort with the technology and its application.
47
Marturana and Woods (2012) used telepractice to provide feedback to early
interventionists who provide coaching to caregivers of young children with disabilities.
Interventionists recorded and uploaded videos of caregiver coaching sessions to cloud storage
and received remote performance feedback from mentor early interventionists via web-based
teleconferencing and telephone conference calls to increase adherence to the FGRBI coaching
model (e.g., Friedman et al., 2012; Woods, 2017). The researchers compared the first and last
coded videos for coaching behaviors and found a significant decrease in the coaches’ use of
child-focused strategies while also detecting a significant increase in specific coaching strategies
(e.g., guided caregiver practice). These findings suggest that elements of the FGRBI can be
applied effectively through telecoaching.
Children with ASD. Telepractice coaching has been applied in the education of
caregivers of children with ASD. Most literature to date has explored interventions to increase
communication and decrease problem behaviors. When examining the efficacy of telepractice
speech-language therapy in a pilot study, Baharav and Reiser (2010) used an A-B design to
examine the impact of parent-delivered speech-language therapy on the child outcomes. Two
young children with ASD first received traditional services, which included two visits per week
in the speech-language clinic. At the onset of the intervention, each child attended one traditional
session per week, but then received his or her second weekly visit via telepractice. In this model,
parents delivered the treatment but were coached during treatment via videoconferencing
software. Though their findings are limited because the authors did not attempt to reverse the
behaviors or use a design that controlled for the effects of time, Baharav and Reiser found
growth on measures of language and social behaviors for the two children. They also found that
through the telepractice model, parents increased their engagement with their children. After
48
intervention, parents offered as many opportunities to engage socially with their children as the
speech-language therapists.
Other researchers have sought to involve parents in language interventions for children
with ASD. McDuffie et al., 2013 examined the effects of an intervention package that included
face-to-face and telepractice language interventions for children with ASD. They used a single-
case, A-B design to investigate the effectiveness of the intervention across eight parent-child
dyads. Over four months, parents were coached weekly, including one face-to-face session each
month, and 12 distance, video-teleconferencing sessions in the remaining weeks. Though many
of the data points are variable, McDuffie et al. found parent coaching delivered in face-to-face
and distance methods increased the parents’ facilitation of specific communication skills in their
children. Despite the change in parent behavior, it is unclear if child communication acts were
similarly changed. The authors attributed the lack of clarity to the distal nature of child measures,
but it is also possible that more time is needed to capture changes in child behavior.
After using telepractice to coach parents to complete functional behavior analyses
(Wacker et al., 2013b), Wacker et al. (2013a) used a single case, non-concurrent multiple
baseline design to implement telepractice to coach parents to increase the communication skills
of 17 young children with ASD. Parents visited a local clinic to communicate with a behavior
specialist hundreds of miles away through teleconferencing software. The behavior specialist
observed the parent and child interact and then coached the parent on how to change his or her
behavior to reduce problematic behaviors (e.g., aggression, self-injury, screaming, etc.) in the
child with ASD. Wacker et al. (2013a) found parents could be coached through telepractice to
implement functional communication training to effectively reduce problem behaviors in their
children. In the last three treatment sessions, all 17 children demonstrated the targeted problem
49
behavior in less than 4% of intervals, and nine of the children demonstrated the problem
behaviors in none of the last three sessions.
Simacek, Dimian, and McComas (2017) also used telepractice to coach parents to
conduct functional behavior assessments and complete functional communication training in
three young children with ASD or Rett syndrome. Simacek et al. used a single case, multiple
baseline across behaviors design, which they replicated across the three children. Baseline data
were gathered and then parents were coached in functional analysis and functional
communication training. During intervention, the coaching team was situated in a university, and
the children and parents were observed and coached via teleconferencing systems in their homes.
Through coaching, all three parents facilitated an increase in communication of their children
across multiple routines. Parents reported positively on the coaching intervention and its impact,
but Simacek et al. reported the time intensiveness of the intervention may limit its applicability.
Parents may not be as involved in more traditional speech and behavior therapy, and models in
which parents deliver interventions require an additional time commitment that may be
prohibitive for families accustomed to using the time their children are in therapy for other
purposes.
Vismara, McCormick, Young, Nadhan, and Monlux (2013) combined videoconferencing
and a website with online resources to coach parents of children with ASD to increase the
communication skills of those children. They used a single case, multiple baseline design across
eight parent-child dyads. The researchers recorded 10-minute, twice-weekly baseline probes of
child and parent behavior using the videoconferencing software. As each dyad entered
intervention, parents were given full access to a self-guided website that included a variety of
resources on engaging children with ASD. The website also hosted the videoconferencing
50
application, through which parents were coached for 12 weekly, 90 minute sessions. Coaching
sessions included a review of previous materials and parent-child interactions, introduction of a
new strategy, and time to practice the new strategy and receive feedback. After the intervention,
parents also participated in three monthly follow up sessions. Across the eight dyads, parents
implemented the interventions suggested by their coaches with high fidelity and increased their
engagement with their children. Parents also reported high levels of satisfaction with the
telepractice model. Though the child behaviors were far more variable, most children
demonstrated a clear increase in communication skills during and after the intervention.
In her dissertation research, Boutain (2014) applied telepractice coaching models beyond
interventions in communication and behavior to teach parents of young children with ASD to
teach their children how to perform self-care skills (i.e., independent living skills) with a greater
level of independence. Boutain used a single case, multiple baseline across behaviors design,
replicated across three parent-child dyads. Parents were coached at home using teleconferencing
software on tablet computers and Bluetooth headphones to communicate discretely during
coaching sessions. Parents learned to complete preference assessments and to use graduated
guidance (i.e., a response prompting system) to teach their children independent living skills.
The author measured the parent’s acquisition of assessment and teaching skills as well as the
child’s performance in three independent living skills taught by his or her parent (i.e., washing
face, applying lotion, and washing hands). After coaching, all three parents not only
demonstrated an increase in their ability to complete preference assessments, but all three parents
also used graduated guidance to successfully teach their children the three independent living
skill routines.
51
Children with other disabilities. Telepractice models have been used to coach parents of
young children with traumatic brain injury (TBI; Antonini et al., 2014). The authors
implemented a RCT to compare the effectiveness of an Internet-based parenting skills program
that included both informational and coaching elements with a comparison group of parents who
were given access to Internet resources related to TBI. Families completed 14 sessions, at a pace
of about one session per week. During the first session, the therapist came to the family’s home
to build rapport, but subsequent sessions were completed online. Antonini et al. included static
elements (e.g., example videos and exercises) and dynamic, synchronous coaching sessions in
which the therapist coached the parent to apply the newly learned information within the context
of the family. Parents were also able to interact with their children while wearing a Bluetooth
headset, through which the therapist could coach the parent in his or her interaction with the
child. The authors found that coaching parents of children with TBI though telepractice changed
both parent and child behaviors. Parents were less likely to give negative statements and more
likely to give positive ones. Antonini et al. did note that family income may moderate the effect
of the intervention, as parents in both the low and high income groups were significantly more
likely to give their children more positive statements after the intervention.
Houston and Stredler-Brown (2012) proposed a model of teleconferencing to coach
parents of young children with hearing impairments. They argued that the low incidence of
children with hearing impairments and lack of qualified personnel make telepractice models
ideal to support the education of children who are deaf or hard of hearing and their families. The
authors argued that telepractice may encourage the application of coaching principles because
the service provider is not able to interact directly with the child. Because the parent is present
with the child, the service provider must teach the parent what to do, rather than interact directly
52
with the child herself. Houston and Stredler-Brown also highlighted the need to consider the
cost, access, and comfort issues related to implementing telepractice interventions with young
children who are deaf or hard of hearing.
Grisham-Brown, Degirmenci, Snyder, and Luiselli (2018) have suggested a model for
supporting the educational needs of students who are deafblind by coaching caregivers and
instructional personnel through state deafblind projects. The model features three phases: (a) in-
person visits to the student’s classroom and home to gather information on the student’s
strengths and needs while assessing practical considerations related to distance coaching, (b) an
in-person consultation with the entire educational team for goal planning, and (c) ongoing,
telecoaching of the educational team. The telecoaching element featured shared viewing of video
clips, a discussion of those clips, and instructional strategies to support student needs. Though
the model appears to be centered around educational performance within the context of school, it
does value the inclusion of caregiver participation and family priorities.
People with visual impairments. Despite the growth of telepractice coaching
interventions for caregivers of children with disabilities, at this time, there are no published
interventions exploring the efficacy of telepractice coaching for caregivers of children with
visual impairments. However, in-person coaching models have been used to increase the skills of
educators and caregivers and people who are blind or who have low vision (Damen et al., 2011;
Janssen et al., 2010; Probst & Walker, 2017). Telepractice models have been applied to the
rehabilitation of adults with visual impairments, including low vision evaluations and assessment
by a vocational rehabilitation teacher (Ihrig, 2016), and Grisham-Brown et al. (2018) proposed a
program for in-person and telecoaching caregivers and educational personnel of students who are
53
deafblind. As such, telepractice coaching models may prove effective in coaching caregivers of
children with visual impairments.
Summary of caregiver telecoaching interventions. Using telepractice to deliver
coaching models to caregivers of children with disabilities has been found to be effective both to
increase the capacity of caregivers of children with disabilities and to increase the skills of their
children (e.g., Baharav & Reiser, 2010; Boutain, 2014; McDuffie et al., 2013). Though the
practice was found to be time and cost effective when compared to clinical delivery (Clawson et
al., 2008; Lindgren et al., 2015; Wacker et al., 2013b), some caregivers reported difficulty
finding time to deliver clinical interventions at home (Simacek et al., 2017). Most research teams
applied synchronous videoconferencing software, but some teams added Bluetooth headphones
to unobtrusively coach caregivers (Antonini et al., 2012; Boutain, 2014), and other research
teams added static online resources (Antonini et al., 2012; Vismara, 2013) to enhance
synchronous coaching. Though some researchers used group designs (e.g., Lindgren et al.,
2015), many applied single case, A-B (Baharav & Reiser, 2010; McDuffie et al., 2103) or
multiple baseline designs (Boutain, 2014; Simacek et al., 2017; Vismara, et al., 2013) to monitor
growth in individual caregivers and children over time and across behaviors. Though telepractice
coaching models have not yet been applied to the education of children with visual impairments
and their families, telepractice has been used to deliver eye medical care (Pathipati & Moshfeghi,
2017), in the rehabilitation of adults with visual impairments (Ihrig, 2016), and has modeled
applications for educating children who are deaf or hard of hearing (Houston & Stredler-Brown,
2012) and who are deafblind (Grisham-Brown et al., 2018).
54
Promise of Telecoaching for Caregivers of Children with Visual Impairments
Children with visual impairments have unique educational needs because of their visual
impairments (Hatlen, 1996, 2004; Lowenfeld 1952, 1973), but because of their low incidence
and heterogeneity (Mason & Davidson, 2000; USDOE OSERS; 2017), delivering appropriate
services can be a challenge. Family-centered approaches to the education of children with visual
impairments are well accepted (Fazzi et al., 2002; Lewis & Allman, 2014b; Nixon, 1991) and
hold promise to meet the needs of the family system (Turnbull et al., 2015), not just the child
with the visual impairment. Because children with visual impairments have unique needs in
learning to complete independent living skills (Lewis & Iselin, 2002), their families may have
unique support needs related to daily care that result in an appropriate balance of child
independence and family care to prevent enmeshment (Turnbull et al., 2015).
Coaching has been shown to improve the skills of teachers, educational assistants, and
caregivers of children with and without disabilities (e.g., Brock & Carter, 2015; Brown &
Woods, 2015; Wetherby et al., 2014). Coaching has been shown to be beneficial to teach
educators and caregivers of children with visual impairments how to better teach their children
communication and independent living skills (e.g., Janssen et al., 2013, Probst & Walker, 2017).
In recent years, telepractice models have extended the availability of coaching to caregivers of
children with disabilities who might otherwise have difficulty accessing expert coaches and have
been shown to increase both caregiver and child skills (e.g., Antonini et al., 2014) and be cost
effective (e.g., Lindgren et al., 2015). As such, telepractice coaching for caregivers of children
who have visual impairments shows promise as an intervention that may increase caregiver
instructional skills, facilitate child independence, and restore balance to the family system.
However, experimental research is needed to establish the efficacy of a telecoaching intervention

55
to increase the instructional skills of caregivers and the independent living skills of their children
with visual impairments.
56
CHAPTER 3
RESEARCH METHODOLOGY
Experimental Design Single case research design is appropriate for use in special education because of its focus
on individuals, its adaptability to changing conditions, and use in natural contexts (Horner et al.,
2005). Children with visual impairments represent a low incidence, heterogeneous population
(Mason & Davidson, 2000; USDOE OSERS; 2017) with instructional needs that differ from
their peers without visual impairments (Hatlen, 1996, 2004; Lowenfeld 1952, 1973). Hatton
(2014) suggested the use of single case research to establish evidence-based practices because
single case designs can be responsive to the great diversity of abilities and needs among children
with visual impairments while allowing for true experimental control. Much of the small base of
rigorous, causal research in the education of children with visual impairments has used single
case designs (Hatton, 2014). As such, single case design was appropriate to address the purpose
of the current study (i.e., investigate the efficacy of telecoaching caregivers to use instructional
strategies to increase the independent living skills of their children with visual impairments).
Single case design allowed the researcher to implement a flexible caregiver coaching
intervention with families that include children with visual impairments, make changes mid-
intervention when caregivers or children responded uniquely to the treatment, and coach
caregivers in skills they continued to use after the intervention ends (Horner et al., 2005).
Like all experimental designs, single case research design is subject to threats to internal
and external validity. Internal validity threats are typically addressed by the establishment of
experimental control, though threats related to selection, history, maturation, regression to the
mean, attrition, testing, and instrumentation are still possible (Kratochwill et al., 2010). Due to
57
the selection of single cases, external validity is difficult to establish (Horner et al., 2005).
However, external validity of single case research may be enhanced by replication among
different participants in single studies (i.e., inter-subject), different participant behaviors or
conditions within an individual (i.e., intra-subject), and through detailed reporting of researcher
and participant attributes, procedures, and experimental conditions (Horner et al., 2005). Such
detailed reporting allows other researchers to replicate the study with fidelity and build an
evidence base for the efficacy of an intervention.
Among the single case research designs available for use, multiple baseline or multiple
probe designs are most appropriate for investigations related to non-reversible behaviors (Gast et
al., 2018). Further, multiple baseline and multiple probe designs may be used to “improve
desirable behaviors” (Gast et al., 2018, p. 249). Both dependent variables of interest, caregiver
instructional strategy use and child independent completion of independent living skills tasks
should increase with training and coaching and are unlikely to return to baseline levels after the
removal of the intervention.
Multiple probe design was originally selected over multiple baseline design because
multiple probe allows for less frequent probes prior to intervention (Gast et al., 2018). However,
because caregivers and children demonstrated variable performance of both dependent variables,
the frequency of data collection was increased to each session, resulting in a multiple baseline
design. As a result, data were collected more frequently, yielding a more complete image of
caregiver and child behavior (Gast et al., 2018). This decision did increase testing risks related to
frequent assessment (Gast et al., 2018) and may have contributed to both generalization of skills
to novel independent living skills contexts and attrition as caregivers may be have been averse to
extensive data collection (Gast et al., 2018).
58
Three types of multiple baseline designs were considered: across behaviors, across
participants, and across contexts. Multiple baseline design across behaviors (i.e., caregiver
instructional strategy) would likely lack experimental control, as the behaviors of interest are not
functionally independent (Gast et al., 2018). Multiple baseline across participants is widely used
in single case research design (Gast et al., 2018) and has been used by many researchers
investigating the impact of coaching interventions (e.g., Brown & Woods, 2015; Vismara et al.,
2012). However, implementing the intervention across participants allows only for inter-subject
replication and does not allow researchers to demonstrate the effectiveness and wide utility of an
intervention across different skills or contexts within an individual (Gast et al., 2018).
Multiple baseline across contexts was considered as an appropriate single case design for
this study. Dyad performance on both instructional strategy use and independent living skills task
completion was measured across one of three independent living skills contexts (i.e., clothing
management, food management, and housekeeping and home maintenance). Before beginning,
the researcher considered the risk of possible caregiver use of instructional strategies
generalizing across contexts, limiting the strength of the design (Gast et al., 2018). However, the
limited literature describing the independent living skills of children with visual impairments
suggests the independent living skills of children are variable across different independent living
skills tasks (Lewis & Iselin, 2002; Papadopoulos et al., 2011) and children with visual
impairments are likely to have incomprehensive and incongruent concepts and skills (Lewis &
Allman, 2014b). To limit the risk of generalization, the coach and caregiver selected independent
living skills tasks for each context that were as unique as possible. The interventionist randomly
assigned the order in which each dyad entered the new context when possible and measured both
caregiver and child behaviors as dependent variables. Doing so allowed the researcher to
59
determine that, although caregivers began to generalize instructional strategies to new contexts at
lower levels, implementation of the coaching intervention was required for the child to master
the targeted independent living skill. Though it has potential for intra-subject replication,
multiple baseline across contexts design is limited in that it does not allow for inter-subject
replication (Gast et al., 2018), thus limiting external validity.
To reduce the limited external validity inherent in the multiple baseline across contexts
design, a combination of multiple baseline across both participants and contexts design was
considered to allow for both intra- and inter-subject replication (Ledford & Gast, 2018). In such
a design, each dyad would have remained in baseline until the preceding dyad met mastery
criteria in more than one context. However, use of a combination design would delay delivery of
the intervention to subsequent dyads and be both unethical and impractical. As a result, the
researcher planned a multiple baseline across contexts design and intended to replicate it across
three dyads. In addition, pilot data prompted the introduction of a one-time training and post-
training baseline phase between the originally planned baseline and coaching phases. The three
dyads participated independently of one another, beginning baseline data collection in
November, February, and March. Collecting data for three dyads across three independent living
skills contexts enhanced external validity without risking threats to validity related to a true
combination of multiple baseline across participants and contexts designs.
Participants
Three dyads composed of caregivers and children with visual impairments were selected
for inclusion in the study. Six caregivers contacted the researcher with interest in participating in
the study. After an initial conversation about the nature of the intervention, three caregivers
60
chose to be considered for inclusion. All three caregivers and their children who expressed
interest were eligible for inclusion.
Each caregiver was selected according to the following inclusion criteria: (a) spends at
least two hours a day and four days a week with the child, (b) commitment to coaching two to
three times a week for at least ten weeks, (c) interest in implementing coached strategies to
increase child independence, and (d) reliable access to both wireless Internet in the home and a
mobile device (i.e., laptop, tablet computer, or cell phone).
Each child was selected according to the following inclusion criteria: (a) age of 5 to 11
years old, (b) eligibility in his or her home state for special educational services as a student with
visual impairment, (c) tactual learner, as demonstrated by inclusion in a conventional literacy
program that included braille instruction, (d) caregiver reported or individualized educational
program (IEP) documented need for instruction in independent living skills, and (e) no known
additional significant disabilities. The presence of no known additional significant disabilities
was indicated by both an educational placement in a general education setting greater than 80%
of the school day and a score of greater than 80% on the School Readiness Checklist from The
Oregon Project for Preschool Children Who are Blind or Visually Impaired (Anderson, Boigon,
Davis, & deWaard, 2007), a criterion-referenced assessment for children from birth through 6
years old. Though validity and reliability data do not exist for this tool, the Oregon Project is
used to assess children with visual impairments because the criteria have been adjusted to reflect
alternative developmental sequences of children with visual impairments. Using excerpts from
the School Readiness Checklist, caregivers reported the child’s skills across two academic
domains: (a) classification and (b) math and reading. Included children independently
demonstrated greater than 80% of the skills in both domains to be included in the intervention.
61
Other skill domains are addressed by the School Readiness Checklist (e.g., social, orientation
and mobility, self-help), but they were not included in the screening because they reflect
disability-specific skills known to follow unique developmental sequences in children with
visual impairments (Hatlen, 1996).
Demographic Characteristics
Once the dyads were selected and caregiver consent, child guardian consent, and child
assent were obtained (Appendices D, E, and F), additional data were reported by the caregivers
about age, gender, race, ethnicity, and socioeconomic status to increase replicability (Wolery,
Lane, & Common, 2018). Caregiver data regarding the relationship of the caregiver to child
(e.g., father, grandmother, nanny), previous experience with caregiver coaching, other caregiver
education or support related to child’s visual impairment, and the presence and age of other
children living in the household who may serve as peer models were also recorded. Child data
were collected to describe the child’s eye condition, any additional disabilities, and type and
intensity of special educational services (Appendix G). Selected participant characteristics are
summarized below in Table 1.
Dyad 1. Dyad 1 included a 51-year-old mother and her biological son who lived in
Georgia. The caregiver of Dyad 1 did not work outside the home and regularly spent most non-
school hours with her child. She expressed commitment to coaching and an interest in using new
instructional strategies. She had no previous experience with caregiver coaching but was familiar
with adult education and coaching models, as she had previously worked as a human resource
professional. She described close connections to the local center for people with visual
impairments and other families of children with visual impairments.
62
The caregiver of Dyad 1 described both her and her son’s race as black and indicated they
were of middle class socioeconomic status. The child of Dyad 1 and his brother, who was 8 years
old, lived in the home. They had two adult brothers who lived outside the family home. Both
parents were present in the home.
The child of Dyad 1 was 10 years old at the beginning of the study and turned 11 during
the intervention phase. He had both a caregiver-reported and previously IEP-documented
educational need of instruction in independent living skills. He was placed in a general education
setting greater than 80% of his school day, had no additional disabilities, and scored 100% of the
skills on the Oregon School Readiness Checklist. The child received services from both a TVI
and/or O&M specialist for an estimated total of 7 hours a week. The etiology of his eye condition
was unknown to his family, but it resulted in a significant visual impairment that caused him to
participate in a braille literacy program.
Dyad 2. Dyad 2 was also composed of a 52-year-old mother and her adoptive son. She
also cared for her child outside of school hours, was committed to coaching, and interested in
learning new instructional strategies. She reported working 20-30 hours a week for pay outside
of the work she did to care for her child. She could flexibly work from an office or home and
was present after school with her child most days. The caregiver had no previous experience with
caregiver coaching but did receive some support and training related to her son’s visual
impairment when he was adopted four years before. She reported conducting extensive Internet
research about educating her child and connecting with other families of children with visual
impairments.
The mother of Dyad 2 reported their socioeconomic status as middle class and reported
her race as white and her son’s race as Asian. Though he was the only child currently living at
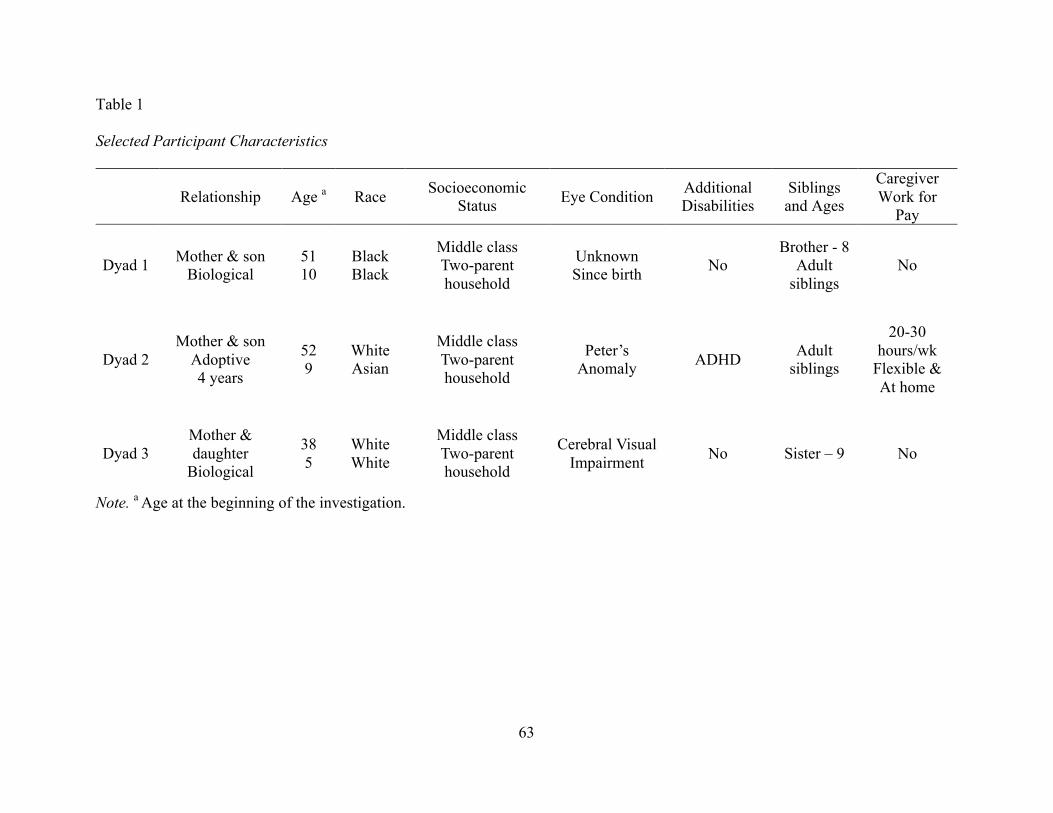
63
Table 1 Selected Participant Characteristics
Relationship Age a Race Socioeconomic
Status Eye Condition Additional Disabilities
Siblings and Ages
Caregiver Work for
Pay
Dyad 1 Mother & son Biological
51 10
Black Black
Middle class Two-parent household
Unknown Since birth No
Brother - 8 Adult
siblings No
Dyad 2 Mother & son
Adoptive 4 years
52 9
White Asian
Middle class Two-parent household
Peter’s Anomaly ADHD Adult
siblings
20-30 hours/wk
Flexible & At home
Dyad 3 Mother & daughter
Biological
38 5
White White
Middle class Two-parent household
Cerebral Visual Impairment No Sister – 9 No
Note. a Age at the beginning of the investigation.
64
home, he had three adult sisters who lived in their own homes. Both parents lived at home with
their son in Alabama.
The child of Dyad 2 was 9 years old and included in a general education placement
greater than 80% of the school day. He scored 85% on the School Readiness Checklist and was
diagnosed with attention-deficit/hyperactivity disorder (ADHD). During the study, he received
weekly services from a TVI and had previously received orientation and mobility services. He
also had a caregiver-reported need for independent living skills instruction. His visual condition,
Peter’s Anomaly, allowed for some use of functional vision, though his visual impairment was so
severe that he participated in a braille literacy program.
Dyad 3. Dyad 3 included a mother and her biological daughter. The mother of Dyad 3
was 38 years old and cared for her daughter regularly outside of the school day. She described a
commitment to regular coaching and an interest in developing her instructional skills. She had no
previous experience with caregiver coaching but described many channels of support for learning
about her child’s unique educational needs. She noted participation in parent groups, good early
intervention, and a positive relationship with her child’s current TVI. The caregiver of Dyad 3
noted she and her child were white and middle class. She did not work for pay outside of the
home. The child of Dyad 3 had a sister, aged 9, who lived in the home with the family and was
generally present for coaching sessions. Both parents lived in the family home in Alabama.
The child of Dyad 3 was 5 years old at the beginning of the study and turned 6 during the
last month. She had a caregiver-reported need for independent living skills instruction and would
soon have IEP goals related to independent living skills. She was placed in a general education
setting for greater than 80% of her school day and scored 90% on the school readiness checklist.
The child had no disabilities in addition to her visual impairment, cerebral visual impairment
65
(CVI). Her significant visual impairment led to her participation in a braille literacy program. At
the time of the study, she received regular services from her TVI/O&M specialist. She also had
an educational assistant assigned to her to help prepare educational materials.
Independent Living Skills Selection
Each child’s independent living skills and instructional needs were documented using a
checklist modified from the Independent Living Curriculum (Loumiet & Levack, 1993), which
aligns independent living skills with suggested ages for instruction. Though the Independent
Living Curriculum lacks validity and reliability data, it is one of the few comprehensive tools
available to measure the independent living skills of children with visual impairments, has been
recommended for use by TVIs (Bardin, 2014), and is easy for caregivers to administer.
Caregivers reported the child’s skills in three domains: clothing management, food management,
and housekeeping and home maintenance. The skills listed within each domain were arranged
developmentally from ages 2 to 11. Data from this report documented each child’s need for
independent living skills instruction and guided the coach and caregiver selection of age- and
developmentally-appropriate targeted independent living skills in each of the three domains.
After conversations with the caregiver, tasks were selected by mutual agreement and based on
child interests, caregiver need, complexity of task, and implementation in a non-private space in
the home (i.e., not a bathroom). Tasks for each dyad are summarized below in Table 2.
The caregiver of Dyad 1 selected wiping the counter for the housekeeping and home
maintenance task, pouring hot water as the food management task, and hanging shirts as the
clothing management task. For Dyad 2, the caregiver selected scraping food waste from a plate
into the trash for the housekeeping and home maintenance task, using an apple corer to cut an
apple for the food management task, and zipping his coat as his clothing management task. The
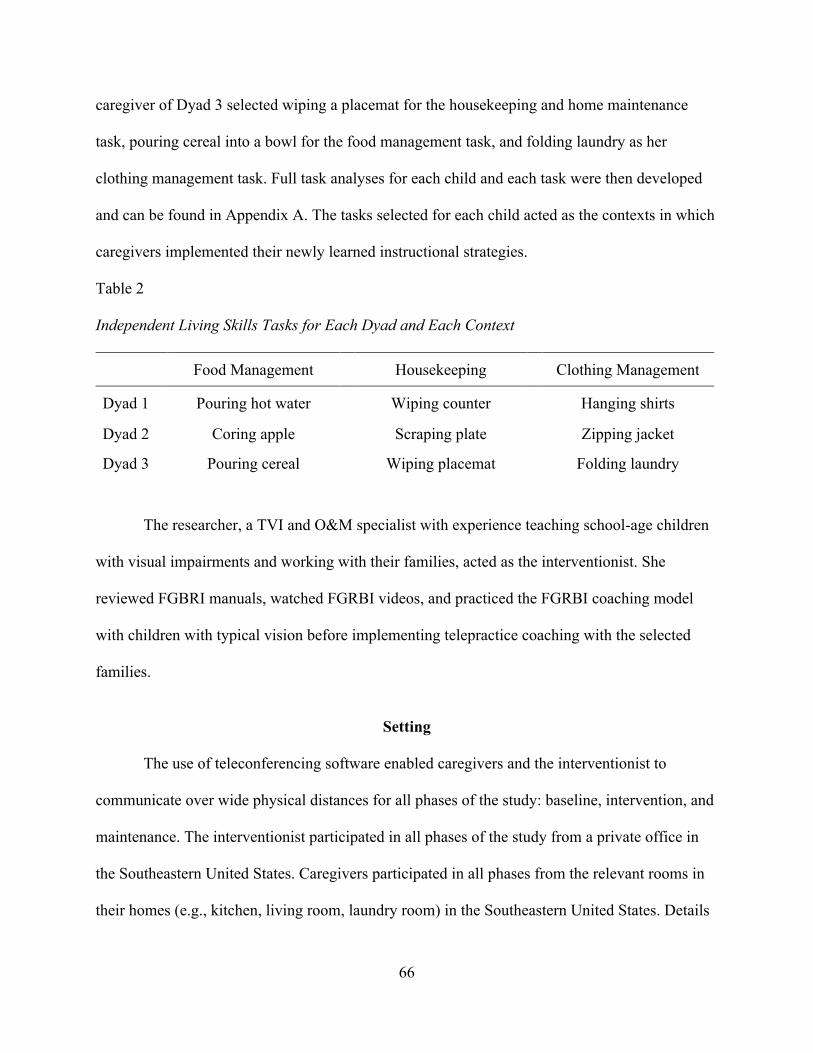
66
caregiver of Dyad 3 selected wiping a placemat for the housekeeping and home maintenance
task, pouring cereal into a bowl for the food management task, and folding laundry as her
clothing management task. Full task analyses for each child and each task were then developed
and can be found in Appendix A. The tasks selected for each child acted as the contexts in which
caregivers implemented their newly learned instructional strategies.
Table 2 Independent Living Skills Tasks for Each Dyad and Each Context
Food Management Housekeeping Clothing Management
Dyad 1 Pouring hot water Wiping counter Hanging shirts
Dyad 2 Coring apple Scraping plate Zipping jacket
Dyad 3 Pouring cereal Wiping placemat Folding laundry
The researcher, a TVI and O&M specialist with experience teaching school-age children
with visual impairments and working with their families, acted as the interventionist. She
reviewed FGBRI manuals, watched FGRBI videos, and practiced the FGRBI coaching model
with children with typical vision before implementing telepractice coaching with the selected
families.
Setting
The use of teleconferencing software enabled caregivers and the interventionist to
communicate over wide physical distances for all phases of the study: baseline, intervention, and
maintenance. The interventionist participated in all phases of the study from a private office in
the Southeastern United States. Caregivers participated in all phases from the relevant rooms in
their homes (e.g., kitchen, living room, laundry room) in the Southeastern United States. Details
67
of the physical setting in which the intervention was implemented are reported below to enhance
replicability (Wolery et al., 2018).
Dyad 1 participated from the kitchen of their home. The child of Dyad 1 wiped the island
counter, folded laundry on the same island counter, and poured hot water from a “water pouring
station” created by the caregiver on one portion of the kitchen counter. Dyad 2 also participated
from their kitchen. The child zipped his jacket while standing near the kitchen table, scraped
food into the garbage can under the sink, and cored the apple from the kitchen table. Dyad 3
participated in coaching from their kitchen, laundry room, and living room, which were all
connected in a great room. The child wiped the placement at her place at the kitchen counter,
poured cereal standing at the kitchen counter, and retrieved shirts from the laundry room
connected to the kitchen and took them to the adjoining living room for folding.
Procedures
Approval and Recruitment
Approval from Florida State University’s Institutional Review Board (IRB) was obtained
(Appendix H). Participants were first recruited through professional relationships with TVIs and
O&M specialists who served students they believed may meet the inclusion criteria (Appendix
I). Interested caregivers were advised to contacted the researcher directly. After only two
caregivers expressed interest in participating, additional permission to recruit caregivers through
listservs and organizations was obtained (Appendix J). Four more caregivers contacted the
researcher with interest. Of the six who expressed initial interest in the study, only three
caregivers followed up with the researcher, and all three met eligibility criteria and were enrolled
after a brief inclusion phone screening (Appendix K).
68
After a description of the study and its aims, caregivers gave informed consent for their
own participation. All participating caregivers were legal guardians for their children and able to
give consent for their children’s participation. Before beginning baseline data collection, the
study was also explained to each child using age appropriate language so each child could give
assent for his or her participation. The scripts used to obtain consent and assent are included in
Appendices L and M.
Once consent was obtained, the coach sent the caregiver the School Readiness Checklist
and the Independent Living Curriculum Screening for completion. The coach and caregivers met
using teleconferencing to discuss the results of the independent living skills screening and select
a targeted skill for each of the three domains (e.g., clothing management: zip jacket, food
management: pour hot water, and housekeeping and home maintenance: wipe a placemat) from
the Independent Living Curriculum. See Appendix N for the included skills selection script.
For each targeted skill, the coach and caregiver together identified component criteria for
child independent completion of the task, based on the child strengths and existing family
routines. See Appendix A for full task analyses for each dyad and each context. Caregivers were
then asked to refrain from changing anything about their regular routines during baseline and
prior to intervention. They were specifically asked not to teach the targeted independent living
skills tasks and report to the coach any instruction in the targeted tasks at home or at school prior
to intervention. During this initial meeting, the caregiver and coach clarified and reconciled
expectations regarding coaching and the potential outcomes.
Before the first baseline data collection session, the interventionist sent an email to
caregivers with the link to the online video teleconferencing room in which all sessions would
take place and directions to download the free application for their mobile devices in the
69
application store. All participants used personal mobile devices. One caregiver used her
smartphone, and two caregivers used their tablet computers. At an agreed upon time before data
collection began in the first baseline session, the researcher called the caregivers on the phone
and asked if caregivers had any issues with the online video teleconferencing application. Two
caregivers had minor challenges downloading the application, which were related to forgetting
passwords to their online application store accounts.
After the application was downloaded and the participants had it open, the caregiver and
researcher ended the phone call and continued the conversation on the teleconferencing
application with video and audio. Then, caregivers were asked to place their mobile devices in
the three locations that corresponded with the selected independent living skills tasks (e.g., by
the kitchen sink, on the ottoman in the living room) to test the sound and video. The test was
conducted by asking the caregiver to move a few feet away from the device and say “hello.”
Placement adjustments were made based on feedback from the researcher. Two caregivers
explained the use of the teleconferencing application to their children without prompting from
the researcher, explaining to the children they would talk to the researcher like they talked to
relatives on their smart phone and tablet video call applications. Occasionally during sessions,
caregivers would open the video teleconferencing application with video but forget to turn on
their microphones. In such cases, the researcher would call the caregiver to troubleshoot the
issue.
Baseline One
Data for both caregiver instructional strategy use and child targeted independent living
skills were collected during an initial baseline phase to document the need for caregiver and
child intervention. In each baseline one session (Appendix O), the correct caregiver use of
70
instructional strategies (i.e., expectation, access, and contingent responding) and child
independent completion of each independent living skills task component (e.g., hold plate with
non-dominant hand) was measured using the data collection tool in Appendix P. Caregiver
instructional strategies are operationalized in Appendix C. Task analyses for each task and each
child are in Appendix A.
The researcher planned to probe intermittently caregiver use of instructional strategies
and child independent living skills task completion in baseline across all three contexts (i.e.,
clothing management, food management, and housekeeping and home maintenance). However,
because baseline data were variable in at least one context for all three dyads, baseline data were
collected in each session for all three contexts for all three dyads (Gast et al., 2018).
It was possible the selected independent living skills tasks were not appropriate for
intervention, so variables for each caregiver and child were assessed daily for appropriateness.
All included children demonstrated independent living skills task performance below 60%
during baseline. As a result, baseline data collection did not need to begin on a different
independent living skills context. Caregivers were also monitored for consistently high
performance on coached strategies (i.e., greater than 90% for three sessions), so they could be
monitored for mastery that would preclude a need for intervention. All three caregivers
demonstrated performance below the set criteria in the first baseline phase.
The researcher sought a stable baseline in all three contexts prior to intervention. Baseline
continued for four sessions for Dyad 1. However, safety risks related to pouring hot water
prompted the delivery of the training for Dyad 1. Dyad 2 remained in baseline for four sessions,
and Dyad 2 completed three baseline sessions. For Dyads 2 and 3, a prolonged baseline was not
71
considered as both caregivers expressed an interest in learning instructional strategies as soon as
possible.
Training
After baseline one data collection was completed, each caregiver participated in a one-
time training in which she watched a 10-minute narrated PowerPoint presentation. The
presentation was narrated to limit variability in content delivery across caregivers. The slides
shared with caregivers are included in Appendix Q. During this session, the interventionist
followed a script (Appendix R) during which the training was shared via the screen sharing
feature of the online video teleconferencing application. After watching the training, the
caregiver was given an opportunity to ask questions about the strategies. All three caregivers
took notes during the training, and if requested by the caregiver, the interventionist emailed the
presentation file to the caregiver. Children were not present during the delivery of the training,
and two of the three mothers chose to complete the training session while the children were in
school.
Post-Training Baseline After the delivery of the training, each caregiver and child were again asked to practice
the same three independent living tasks. A return to baseline was necessary to document any
changes in caregiver instructional skills after the training. Because there is little literature on the
education of caregivers and teachers of children with visual impairments, it was unclear how
caregiver behaviors may be impacted by the given training. Though no experimental control was
documented because of the simultaneous introduction of the training across all three independent
living skills contexts, a return to baseline was necessary to help document a need for the time
72
intensive coaching intervention. If the less time intensive training was associated with increases
in caregiver and child skills, then caregiver telecoaching may not have been necessary. Though
the literature in caregiver education suggests ongoing, active engagement with learned content is
necessary for mastery (e.g., Dunst et al., 2010), Probst & Walker (2017) found educational
assistants needed very few (i.e., 1 to 3) follow up coaching sessions after an initial workshop on
implementing a system of least prompts in independent living skills tasks with a high school
student with a visual and multiple impairments.
Caregiver and child variables were coded in the same manner as they were in the baseline
one phase. During this post-training baseline phase, the interventionist did not provide any
feedback during sessions. The script followed by the interventionist during the post-training
baseline phase is included in Appendix S. Post-training baseline sessions continued for five
sessions in Dyad 1 and three sessions in Dyads 2 and 3 before the coaching intervention began in
the first context.
Coaching
Once each dyad demonstrated counter therapeutic, low, or stable baseline performance of
both caregiver and child variables, the FGRBI coaching sessions were implemented according to
the FGRBI Key Indicators Manual (Woods, 2017). Dyad 1 was coached in the first context,
pouring hot water, for eight sessions. They were then coached for only four sessions in the
second and third contexts, hanging shirts and wiping the counter. Dyad 2 received coaching in
the first context, coring the apple, for nine sessions. Because the caregiver began to generalize
skills and the child increased task mastery in the other two contexts, coaching did not occur in
the final contexts. The final dyad, Dyad 3, was coached for seven sessions. The caregiver

73
reached mastery, and though the child did not, the coaching intervention ended in all three
contexts due to the caregiver’s limited time available to commit to the intervention.
Caregivers met via teleconferencing two to three times a week for a live session of up to
one hour for each session. At least 24 hours passed between each session. Each coaching session
was recorded and later coded for dependent variables and interobserver agreement (IOA).
Procedural fidelity was measured to ensure consistent implementation of the intervention and
differentiation from other phases of the study. Though each dyad completed a similar number of
baseline and presentation sessions, dyads entered and participated in coaching at different times
in each context, based on their previous demonstration of skills.
During the first coaching session, the coach and caregiver followed the FGRBI coaching
model and provided an overview of the instructional strategy model (Appendix B) so caregivers
became aware of the variety of instructional strategies they would learn to use during coaching
See Appendix T for the coaching session script. During each coaching session, the
interventionist followed the Key Indicator Checklist for the FGRBI model (Woods, 2017). Exact
time spent in each component varied across session and dyad, but approximate times were:
setting the stage (2 minutes), observations and opportunities to embed (10 minutes), problem
solving and planning (8 minutes), and reflection and review (5 minutes). Across all four
coaching model components, caregivers were coached to increase their correct use of eight
instructional strategies: explanation, direction, environmental arrangement, facilitated
exploration, preview task, wait time, specific praise for component, and realistic feedback. See
Appendix C for operational definitions of instructional strategies.
In accordance with the FGRBI model, the coach used instructional strategies to teach
caregivers as they engaged with their children in the targeted independent living skills task.
74
During the observations and opportunities to embed component, the coach most frequently
watched with minimal interruption as the caregiver and child worked together. As necessary, the
coach used demonstration or direct teaching of caregiver instructional strategies. The coach
followed the lead of the caregiver, refining her use of attempted instructional strategies. The
problem solving and planning component of the FGRBI model allowed the coach to suggest
alternative instructional strategies to the caregiver as needed. Child independence and caregiver
application of coached strategies was later coded for progress on the dependent variables of
interest.
Coaching continued in the first context, and after three sessions of high (greater than
80%) caregiver instructional strategy fidelity and child independent task completion (defined by
independent completion of 80% of the task components), the dyad was determined to have
reached mastery in the given context. Then, they moved to the next independent living skills
context. The order in which the three independent living skills contexts were introduced for each
dyad during each session was randomized to increase rigor (Kratochwill et al., 2010). Though
Dyads 2 and 3 did not participate in coaching for all three contexts, the order in which the
baseline and maintenance data were collected in each session were still randomized.
Maintenance
After each dyad entered a new independent living skills context, coaching in the previous
contexts ended, and maintenance data on caregiver and child performance in previous contexts
were gathered (Reichow, Volkmar, & Cicchetti, 2007). At least two maintenance sessions were
planned for each context after mastery was reached. Sessions occurred up to once a week in
mastered contexts and were planned until both the caregiver and child demonstrated mastery in
all three contexts (Appendix U).
75
For Dyad 1, maintenance data were collected in the first two contexts as planned, but
because of the long length of the intervention (i.e., 25 sessions), maintenance data were not
collected in the final context. For Dyad 2, maintenance data were collected at least twice for all
three contexts, though the caregiver and child did not reach mastery before maintenance was
initiated because of caregiver concerns with child’s tolerance for additional intervention sessions.
In Dyad 3, a single maintenance session occurred because the family was unable to contribute
further time to the intervention.
Materials
To participate in telecoaching, caregivers used a mobile, Internet-enabled device with a
camera and microphone (e.g., laptop, tablet computer, or smart phone). Two caregivers used
tablet computers, and one used a smart phone. Participation required access to wireless Internet
in the space in which they performed the independent living skills tasks. Online video
teleconferencing software was used to conduct and record telecoaching sessions. Coaching
sessions were stored on the researcher’s computer and coded by hand with hard copy data sheets.
Data sheets were stored in the researcher’s locked office. Materials used during independent
living skills tasks were selected among items already in the home. During coaching sessions, the
coach did at times suggest alternative items in conversation with the caregiver; the caregiver
selected alternative items from those already owned.
To complete food preparation tasks, the dyads used an apple corer, a small plastic bowl, a
clothespin, an electric kettle, a ceramic mug, a large plastic tray, and an audible liquid level
indicator. When completing clothing care tasks, the families used washcloths, a variety of shirts,
a laundry basket, hangers, and a jacket. Housekeeping tasks were completed with pre-moistened
76
wipes in a plastic container, child-safe spray cleaner, paper towels, a placemat, a plate with food
waste, a table knife, and a garbage can.
Response Definitions and Measurement Procedure
Dependent Variables The researcher measured two dependent variables: correct caregiver use of coached
instructional strategies and child independent completion of independent living skills tasks. The
tool used to code data is included in Appendix P. The primary variable, caregiver use of
instructional strategies, includes a menu of three categories: expectation, access, and contingent
responding. Operational definitions and examples of each caregiver instructional strategy are
included in Appendix C. Definitions were refined as coders were trained and reached reliability
in IOA before the onset of data collection.
For each child task component attempt, the caregiver response was recorded. Whether
she attempted an instructional strategy and whether she used the strategy according to its
operational definition were noted. The child’s response to caregiver strategy use was
documented as an attempt and the child’s level of independence in the attempt was recorded. The
child’s response to the caregiver action often prompted additional caregiver instructional strategy
use.
Most research on caregiver coaching reports frequency of use, likely because most of the
research aims to increase skills like communication (e.g., Brown & Woods, 2015). However, as
children increase their ability to independently complete targeted independent living skills,
caregivers may use instructional strategies less frequently as they begin to fade their instruction.
Frequency of instructional strategy use for independent living skills is an incomplete measure.
As a result, the fidelity with which caregivers used the coached strategies was also measured.
77
Even as children approached independent completion of the target task, caregivers should still
implement their selected instructional strategies with high fidelity. Operational definitions,
examples, and non-examples of caregiver instructional strategy use have been provided in
Appendix C.
Caregiver correct use of strategies was calculated for each context in each session by
dividing the number of strategies correctly used by the total number of strategies attempted.
Though the originally developed instructional strategies model had two additional instructional
strategy categories (Appendix B), only three categories with their eight strategies were
considered together for analysis (Appendix C). This decision to reduce the number of
instructional strategies was made as a result of pilot data suggesting the low frequency of
occurrence and unreliability of coding the final two categories, systematic instruction and fading
prompting.
Because child independent completion of independent living skills task components was
dependent on caregiver use of instructional strategies, the child behavior served as a secondary
variable. In each phase and context, the researcher measured child independent completion of
three independent living skills tasks, one in each of three domains: clothing management, food
management, and housekeeping and home maintenance. Each task was selected based on child
needs assessment and criteria for independent completion of each task was developed by the
coach and caregiver before baseline data were collected. Task analyses developed for each child
and each task are included in Appendix A. Developed criteria were unique to each child and
reflect the expectations and needs of each family. For each step of the task to be coded as
independent, the child had to complete the task component correctly and with no caregiver
78
prompt. Independence was calculated by dividing the number of independent attempts into the
number of total attempts.
Measurement
Because each coaching session was recorded, both variables of interest were collected
and coded across baseline, treatment, and maintenance phases. As suggested by Ledford et al.
(2018), a system for “direct, systematic observation and recording” (p. 100) was developed and
is included in Appendix P. The measurement system allowed for event recording of trial-based
events (Ledford et al., 2018). For each child attempt of an independent living skill task
component (e.g., open the cabinet door) addressed in a coaching session, caregivers had an
opportunity to demonstrate use of a caregiver instructional strategy. A child attempt was defined
as movement toward or child-initiated discussion about the items. For each child attempt at the
task component, the caregiver strategy attempt and fidelity of strategy use was measured. In
addition, the child’s independent completion of the task component was coded. Data were
collected in sessions that took place three times a week, for up to one hour each week.
Dependent variables were recorded while caregivers and children participated in all three
targeted independent living skills routines (i.e., 15-20 minutes for reach context and each
session). Refer to session scripts that outline these processes in Appendices O, S, T and U.
Reliability
Before rating baseline, intervention, and maintenance videos, the researcher trained
secondary observers, both undergraduate students, in IOA according to guidelines in Ledford et
al. (2018). With the researcher, the secondary coders reviewed written dependent variable
definitions and the FGRBI Key Indicators Manual (Woods, 2017). Then the researcher and
79
secondary coders together coded training videos of school-age children without visual
impairments being taught by their caregiver. When discrepancies occurred, the researcher made
clarifications and added additional examples to the dependent variable operational definitions.
The coders then rated at least three additional videos independently and discussed discrepancies
with the researcher. The researcher and second coders reached 90% IOA (range: 88-100%) on
the sample videos (Ledford et al., 2018).
To establish reliability of coding, a randomly selected 30% of data from each baseline,
intervention, and maintenance condition were coded by a second observer and assessed for IOA.
The researcher and second observers sought 80% or greater IOA to meet accepted criteria
(Horner et al., 2005; Ledford et al., 2018). IOA was gathered and assessed formatively to address
any discrepancies (Ledford et al., 2018). During baseline and presentation sessions in the first
dyad, IOA dipped below 80% to near 70% for several sessions. As a result, the primary and
secondary coders retrained, and IOA increased above 90% in subsequent sessions.
IOA data were calculated with the following formula: (number of agreements/number of
agreements + number of disagreements)*100. For Dyad 1, IOA was collected in 33.33% of
sessions and was 95.89% (range: 73.91%-100%) for caregiver variables and 93.23% (range:
71.43%-100%) for child variables. In Dyad 2, IOA was completed for 33.93% of sessions. For
caregiver data, IOA was 99.18% (range: 93.1%-100%) and 97.03% (range: 88.46%-100%) for
child data. For 43.75% of sessions in Dyad 3, IOA was calculated. On caregiver strategy use, the
primary and secondary coders reached 99.66% IOA (range: 95.24%-100%), and 99.39% (range:
95.34%-100%) on child independence. IOA for each dyad and each phase are reported in Table
3.
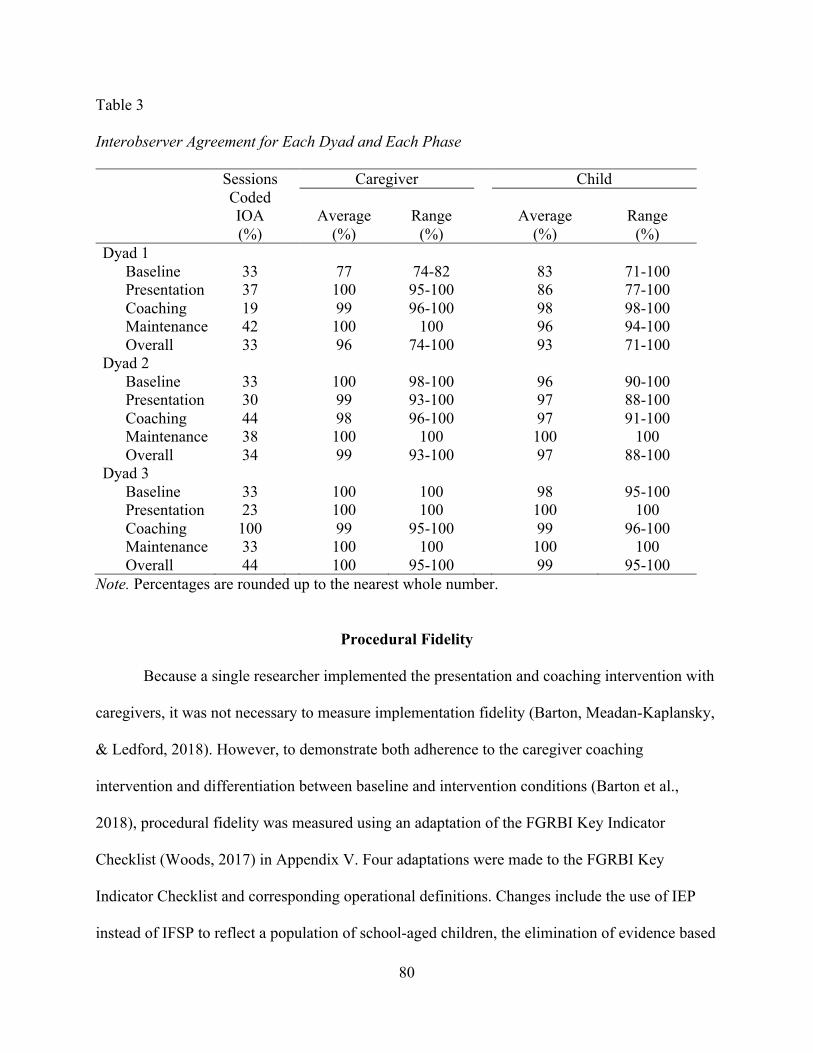
80
Table 3 Interobserver Agreement for Each Dyad and Each Phase
Sessions Coded IOA (%)
Caregiver Child
Average (%)
Range (%)
Average
(%) Range
(%) Dyad 1
Baseline 33 77 74-82 83 71-100 Presentation 37 100 95-100 86 77-100 Coaching 19 99 96-100 98 98-100 Maintenance 42 100 100 96 94-100 Overall 33 96 74-100 93 71-100
Dyad 2 Baseline 33 100 98-100 96 90-100 Presentation 30 99 93-100 97 88-100 Coaching 44 98 96-100 97 91-100 Maintenance 38 100 100 100 100 Overall 34 99 93-100 97 88-100
Dyad 3 Baseline 33 100 100 98 95-100 Presentation 23 100 100 100 100 Coaching 100 99 95-100 99 96-100 Maintenance 33 100 100 100 100 Overall 44 100 95-100 99 95-100
Note. Percentages are rounded up to the nearest whole number.
Procedural Fidelity
Because a single researcher implemented the presentation and coaching intervention with
caregivers, it was not necessary to measure implementation fidelity (Barton, Meadan-Kaplansky,
& Ledford, 2018). However, to demonstrate both adherence to the caregiver coaching
intervention and differentiation between baseline and intervention conditions (Barton et al.,
2018), procedural fidelity was measured using an adaptation of the FGRBI Key Indicator
Checklist (Woods, 2017) in Appendix V. Four adaptations were made to the FGRBI Key
Indicator Checklist and corresponding operational definitions. Changes include the use of IEP
instead of IFSP to reflect a population of school-aged children, the elimination of evidence based
81
from caregiver instructional strategies because the proposed strategies have not yet been
established in empirical research, the use of task components instead of routine categories to
correspond to the design of multiple baseline across independent living skills task contexts, and
the use of instructional strategies instead of intervention strategies to match the model of
strategies used by caregivers.
At least 33% of randomly selected sessions across conditions and participants were
observed (Barton et al., 2018) and coded by a second observer using the modified Key Indicators
Checklist (Appendix V) and the corresponding coding manual (Woods, 2017). Procedural
fidelity was calculated for 44.0% of sessions in Dyad 1, 42.11% in Dyad 2, and 35.71% in Dyad
3. Procedural fidelity was analyzed during the study and areas of low fidelity were targeted for
remediation before continuing. In baseline, presentation, and maintenance phases across all
dyads, when no coaching occurred, procedural fidelity ranged from 0% to 8.33% with an average
of 6.82%. The item often included in non-coaching phases was the first element: “gathers
updates on child and family,” as this element was naturally met in most sessions. Procedural
fidelity remained above 90% for all coaching sessions. For coaching sessions in Dyads 1 and 3,
procedural fidelity was 100% in all selected sessions. For Dyad 2, average procedural fidelity
was 97.92% (range: 91.66%-100%).
Social Validity
Social validity is highly valued in single case research design because of the focus on
applying interventions to outcomes that are valued by participants (e.g., Barton et al., 2018;
Horner et al., 2005). Wolf (1978) originally suggested the evaluation of the goals, procedures,
and effects of the intervention, and these principles continue to be valued in single case research
(Barton et al., 2018). Social validity is reflected in the aims of the current study (i.e., to meet the
82
unique needs of families of children with visual impairments). Caregiver selection of
independent living skills tasks and the flexible, caregiver- and child-centered coaching model
both strengthen the social validity of the intervention.
Accordingly, social validity was directly assessed through several methods suggested by
Barton et al. (2018). Though self-reports of participants may be subject to bias (Barton et al.,
2018), caregivers and children reported their perceptions of the social validity of the goals,
procedures, and effects of the intervention (Wolf, 1978), including practical considerations like
time-effectiveness (Reichow et al., 2007). See Appendix W for social validity questionnaires.
Randomly selected baseline, intervention, and maintenance videos were shared with a rater who
was unaware of the intervention, and that rater was asked to assess whether the goals,
procedures, and outcomes were socially valid (Appendix W). Finally, maintenance data collected
after each dyad has reached mastery criteria were evaluated. High social validity may be
suggested if caregivers continue to use instructional strategies with frequency and fidelity and
the children continue to perform the independent living skills without help even after the
coaching intervention has been completed (Barton et al., 2018).
Data Analysis
Each dyad was considered individually for data analysis. Data for both dependent
measures were measured for all three dyads in all phases. Once a flat or counter-therapeutic trend
of both caregiver and child data was detected across at least three sessions in baseline, the
intervention in the first independent living skills context began. If data were variable, additional
data were collected to establish a stable baseline.
Once a caregiver performed the coached instructional strategies with greater than 80%
fidelity and the child performed 80% of the independent living skills task for three consecutive
83
sessions, the dyad reached mastery in that context. Then, the caregiver began coaching in the
next independent living skills context. Baseline data collection were continued in the third
context. Once mastery was reached in the second context, intervention began in the third context.
Once mastery was reached in all three contexts, maintenance data collection continued for the
final context for at least two sessions.
Coders used training videos to reach 90% IOA before baseline data collection began
(Ledford, et al., 2018). Then, IOA was assessed for randomly selected sessions and remained
above 80% agreement (Horner et al., 2005; Ledford, et al., 2018) after an initial decrease in IOA
to close to 70%. When IOA decreased below 80%, the coders re-trained to 90% IOA on sample
videos. Procedural fidelity was measured by adherence to the FGRBI Key Indicators Checklist
(Appendix V) in at least 33% of randomly selected sessions (Barton et al., 2018). Procedural
fidelity remained above 90% in all coaching sessions.
Data for fidelity of caregiver instructional strategy and child independent living skill
performance were graphed for each session across all three phases. To document evidence of a
functional relation, visual analysis was used to analyze the level, trend, variability, immediacy of
change, overlap, and consistency of data throughout baseline, intervention, and maintenance
phases for each participant and each context (Kratochwill et al., 2010).
84
CHAPTER 4
RESULTS
Procedural Administration
Procedures were administered as described in the methods section with changes.
Procedures were implemented as planned for Dyad 1, with the exception of collecting
maintenance data in the final context. As a result, the design for Dyad 1 meets Institute of
Education Sciences What Works Clearinghouse (IES WWC) standards with reservations because
at least 3 data points in each phase were documented across at least 6 phases (Kratochwill et al.,
2010). Collecting 5 data points in each phase would have strengthened the design, but caregivers
and children were eager to begin the intervention and would likely not have tolerated more than
4 data points in baseline phases. However, because of time pressure and child skill increases, the
coaching intervention was not implemented in the second and third contexts for Dyads 2 and 3.
As a result, Dyads 2 and 3 lack experimental control. Though the changes in caregiver and child
behaviors of Dyads 2 and 3 are described below, the lack of experimental control makes it
impossible to conclude the changes in caregiver behavior detected in the first contexts reflect a
functional relation.
Additionally, during the first context with the first dyad, it became clear the caregiver and
child would not reach the previously set 100% caregiver and 90% child mastery criteria without
causing frustration to the dyad. As performance leveled off near 80-85% and frustration with
repeating the task with little improvement increased, the researcher chose to set mastery at 80%
for all caregivers and children in all three dyads.
The experiment was designed as a multiple probe across contexts to reduce the number of
probes necessary and reduce the risk of threats to validity from repeated testing (Gast et al.,
85
2018). However, unstable baseline data for both caregiver and child variables in all three dyads
prompted an increase in the frequency of data collection. Baseline data were collected for each
baseline session in all three contexts for all three dyads, thus reflecting a multiple baseline design
(Gast et al., 2018). Changing to a multiple baseline design did increase testing threats to internal
validity. However, the change was necessary to collect as much data as possible to determine a
stable baseline in as little time as possible, minimizing maturation threats to validity (Gast et al.,
2018).
Caregivers in all three dyads began to generalize skills from the training and coaching to
other contexts. As a result, caregivers increased skills to levels that met their own criteria for
mastery, which did not match the 80% criteria set by the researcher. The caregivers in both Dyad
1 and Dyad 3 both expressed concerns with their abilities to commit the time necessary to
complete the intervention to such high levels of mastery. The caregiver of Dyad 2 had the time
to commit to the intervention, but conveyed the child might begin to demonstrate boredom-
related acting out behaviors that would reduce his task independence.
As a result, data collection for all three dyads was truncated. With Dyad 1, all phases for
all contexts were completed with the exception of maintenance data in the final context, wiping
the counter. Due to increases in skills across all three contexts, the caregiver of Dyad 2 and the
researcher decided not to intervene in the zipping jacket and scraping plate contexts. However,
maintenance data were collected for all three contexts for Dyad 2. Dyad 3 had the most concerns
related to the time intensiveness of the intervention, perhaps because the child was the youngest
of the participants. After the first full coaching session in the first context, the caregiver and
coach decided to limit coaching to one context, folding laundry, and end data collection in the
presentation phases for wiping the placemat and pouring cereal. Doing so shortened the sessions
86
from 45-60 minutes to 15-20 minutes. A single maintenance data point was collected for all three
contexts of Dyad 3 in one longer, 60-minute session.
Though visual analysis of each dyad, phase, participant, and context (Kratochwill, 2010)
was planned for all three dyads, changes in the implementation of the intervention led to a lack
of experimental control for Dyads 2 and 3. As a result, evidence of a functional relation for Dyad
1 was examined by comparing dependent variables from the post-training baseline and coaching
phases as the training was delivered once and simultaneously across all three contexts for each
dyad. Data for caregiver correct use of instructional strategies and child task independence were
analyzed by the primary coder after each baseline, presentation, coaching, and maintenance
session for all three contexts and all three dyads. Interobserver agreement was used to establish
reliability of findings (Ledford et al., 2018). The primary and secondary observers coded both
caregiver and child variables for 33.33% to 43.75% of sessions across all three dyads. The
primary and secondary coders reported overall IOA of greater than 93% for both caregiver and
child variables in all three dyads. IOA for each dyad and each phase are reported in Table 3.
Caregiver and Child Outcomes
Dyad 1 Pouring hot water. Dyad 1 demonstrated their skills in three independent living skills
contexts: pouring hot water, hanging shirts, and wiping the counter. Graphed results are shown
for Dyad 1 in Figure 1. In the first context, pouring hot water, the caregiver began with 46%
correct strategy use, and after an initial ascent to 62%, decreased her performance to near 20%.
The child’s independent task completion demonstrated a rapid upward trend, increasing from 7%
to 75% in four sessions. However, the interventionist observed concerns with the safety of the
pouring hot water task. Although the caregiver and child increased their skills, the child spilled
87
hot water near his hand, and the caregiver expressed a need for support to safely teach her child.
As a result, the pouring hot water context became the first to receive coaching.
After the training, and during the post-training baseline phase, the caregiver demonstrated
an immediate level increase to 58% in the first session. She then increased to 88% and then
demonstrated a rapid, counter therapeutic trend over three sessions. During this same phase, the
child demonstrated a moderate upward trend in his independent task completion, and though he
continually increased his performance, he did so at a slower rate than in baseline. Despite his
increased independence in pouring hot water, the caregiver’s low rate of correct instructional
strategy use, frustration in teaching the task, and remaining safety concerns prompted the
introduction of the coaching intervention. Because the introduction of the training was not
staggered across all three contexts, the changes in caregiver and child behaviors cannot be taken
as evidence of a functional relation between the training and caregiver instructional strategy use.
During the coaching intervention in the pouring hot water context, the caregiver
demonstrated an initial increase in level from the post-training baseline phase low of 33% to
86% in the first coaching session. She maintained a high level of performance (i.e., above 79%)
except for in one session, in which she correctly used 51% of the strategies she attempted. This
was the only data point to overlap the first baseline performance. During the coaching phase, the
caregiver demonstrated an overall upward trend and reached mastery (i.e., greater than 80% for
three sessions) in the final three sessions of the phase, including 100% correct strategy use in the
final two sessions.
During this phase, the child initially demonstrated a decrease in independent task
completion from 77% to 50%. However, he then steadily increased his independent completion
of the pouring hot water task, reaching task mastery (i.e., greater than 80% performance for more
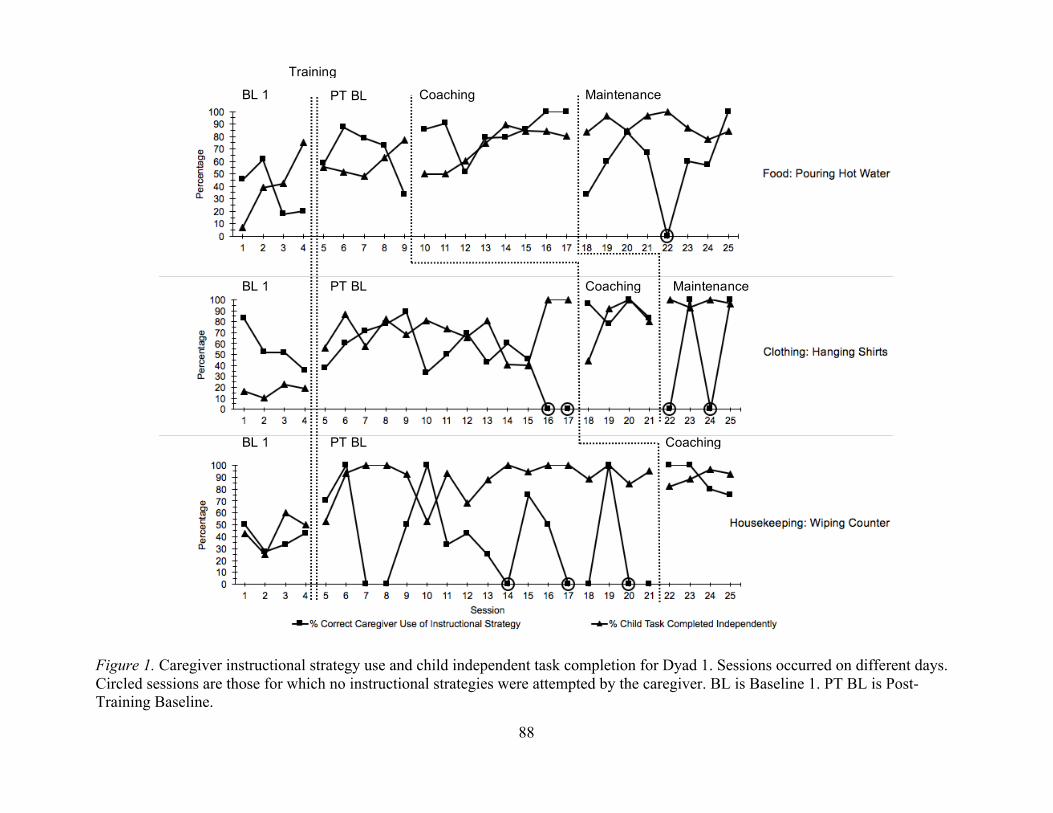
88
Figure 1. Caregiver instructional strategy use and child independent task completion for Dyad 1. Sessions occurred on different days. Circled sessions are those for which no instructional strategies were attempted by the caregiver. BL is Baseline 1. PT BL is Post-Training Baseline.
Training
BL 1
BL 1 PT BL
PT BL
Coaching
Coaching
Coaching
Maintenance
Maintenance PT BL
BL 1
89
than three sessions) after seven sessions in the coaching phase. Though he did reach mastery
criteria, his performance was never greater than 89% independent task completion. Despite the
increase of caregiver skills to mastery, her performance in the coaching phase overlapped with
many of the data points in the post-training baseline phase. In fact, only 37.5% of the data points
did not overlap. In addition, the caregiver used the strategies with great variability (i.e., 51-
100%) across 8 sessions. The variability and overlapping data limit the evidence of a functional
relation between caregiver telecoaching and caregiver instructional strategy use.
Maintenance data for pouring hot water were collected as the intervention was delivered
in the next context, hanging shirts. After the removal of the coaching intervention, the caregiver
demonstrated variable performance. Her correct use of instructional strategies varied from 33%
to 100%; during one session, she did not attempt any strategy use. During this phase, the child
maintained a high level of independent completion, ranging from 77% to 100%, with a slight
downward trend. He maintained mastery in seven of eight sessions in this phase.
Hanging shirts. During the baseline one phase of data collection for Dyad 1, data were
also collected in the second context, hanging shirts. During this phase, the caregiver
demonstrated a counter therapeutic trend, decreasing her correct use of instructional strategies
from 83% to 35% in four sessions. Her child’s performance remained low (i.e., between 10%
and 23% independent completion) and relatively stable, with a slight upward trend. These data
prompted the introduction of the presentation phase but were not considered to determine the
presence of a functional relation between telepractice coaching and caregiver instructional
strategy use.
After the training and during the post-training baseline phase, the caregiver demonstrated
an immediate reversal in trend, in which her correct use of instructional strategies began to
90
steadily increase from 38% to 89% over five sessions. During session 10, the first session in
which coaching was delivered in the pouring hot water context, her correct use of instructional
strategies decreased to 33% and then rebounded to stabilize between 43% and 69%. In the post-
training baseline phase, the child immediately increased his level of performance from 19% to
56%. He maintained a flat and stable trend, oscillating between 56% and 86% for nine sessions.
During the next two sessions, his independent completion of the task dropped to near 40% and
then increased to 100% for the last two sessions in this phase. In these last two sessions, the
caregiver did not attempt to use any instructional strategies. Nonetheless, the introduction of the
training concurrently across each phase caused a lack experimental control, so the changes in
behavior detected cannot be used as evidence of a functional relation between the training and
caregiver instructional strategy use.
Because the caregiver had not yet demonstrated mastery in the post-training baseline
phase, the coaching intervention was introduced. In the first session of coaching, the caregiver
increased her correct use of instructional strategies to 97%. Her correct instructional strategy use
remained high, with a flat trend and some variability (i.e., between 77% and 100%) during this
phase. In the first coaching session, the child decreased his independent performance to 44%
from 100% in the presentation phase. After this initial decrease, his performance increased, and
he then achieved mastery in three sessions. In this context, the caregiver demonstrated less
variability (i.e., 77-100% in four sessions) and less overlapping data (i.e., 50%). Nonetheless, the
evidence of a functional relation is limited by the large percentage of data overlapping with the
post-training baseline phase.
Maintenance data were collected for this task during coaching in the final context, wiping
the counter. The caregiver correctly used 100% of the instructional strategies she attempted;
91
however, she did not attempt any instructional strategies in two of the four maintenance sessions.
During the maintenance phase, the child maintained mastery with high and stable performance
between 93% and 100% independent task completion.
Wiping counter. Baseline one data were collected in the wiping counter context
concurrently with the other two contexts. During the four baseline one sessions, the caregiver
used instructional strategies with variability (i.e., 27%-50%), though her overall use of strategies
demonstrated a slightly decreasing trend. The child also completed the task with variable
independence, ranging from 25% to 60% with an increasing trend, though his independence
decreased to 50% in the final session of the baseline one phase.
After the training and during the post-training baseline phase, the caregiver increased her
correct use of instructional strategies to 70% in the first session, demonstrating a level increase
from baseline one performance. However, the simultaneous introduction of the presentation
across all three phases prohibits the detection of a functional relation. During the 17 presentation
phase sessions, the caregiver correctly used instructional strategies with wide variability (i.e., 0%
to 100%). In this phase, an overall decreasing trend was established for the caregiver. In this
same phase, however, her child increased his performance with an upward trend. He increased
his independent completion and achieved mastery by the fourth session of the phase. He then
demonstrated variable independence (i.e., between 53% and 93%) for four sessions. He resumed
mastery level performance of the wiping counter task for the final nine sessions of the phase.
Despite the child’s high performance, the caregiver’s highly variable and sometimes very
low use of instructional strategies prompted delivery of the coaching intervention in the final
context. With the introduction of caregiver coaching, correct caregiver use of instructional
strategies increased in level to 100% for two sessions before demonstrating a decreasing trend to
92
75% in the final of four intervention sessions. In this phase, the child maintained his mastery of
wiping the counter.
Maintenance data were not collected for this context because of caregiver concerns
related to the time intensiveness of the sessions. Despite the caregiver’s task mastery and less
variability of the caregiver data in this phase (i.e.,75-100%), she ended the coaching phase in a
counter therapeutic trend. In addition, 0% of the data points in the coaching phase do not overlap
with the post-training baseline phase. As a result, a functional relation is between caregiver
telepractice coaching and caregiver instructional strategy use is unclear.
Frequency of caregiver instructional strategy use. The caregiver of Dyad 1 generally
increased her frequency of instructional strategy use during presentation and coaching sessions
from baseline levels. Once her child neared mastery (i.e., 80% for three consecutive sessions),
she reduced the number of correct strategies attempted, sometimes to zero strategies. More
detailed data are shared in Table 4.
Dyad 2 The design used with Dyad 2 and the data described below lack experimental control
because the independent variable was not introduced in all three contexts. Because the coaching
intervention was not delivered in all three contexts, it is not possible to conclude the changes in
caregiver and child behavior detected in the first context, coring the apple, reflect a functional
relation resulting from the introduction of caregiver coaching. In addition, because the
introduction of the training was not staggered across contexts, no functional relation between the
implementation of the training and caregiver instructional strategy use can be detected.

93
Table 4 Frequency of Caregiver Correct Instructional Strategy Use and Percentage of Child Independent Task Completion for Dyad One
Pouring Hot Water Hanging Shirts Wiping Counter Session
(#) Phase Cg (#)
Ch (%)
Phase
Cg (#)
Ch (%)
Phase
Cg (#)
Ch (%)
1 B 5 7 B 5 17 B 3 43 2 B 8 39 B 13 10 B 3 25 3 B 3 42 B 14 23 B 2 60 4 B 1 75 B 11 19 B 3 50 5 P 7 56 P 6 56 P 7 53 6 P 14 51 P 3 87 P 2 93 7 P 11 48 P 15 58 P 0 100 8 P 8 63 P 7 82 P 0 100 9 P 2 77 P 8 68 P 1 92 10 C 6 50 P 2 81 P 9 53 11 C 19 50 P 2 73 P 1 93 12 C 18 60 P 9 66 P 3 68 13 C 15 75 P 6 81 P 1 88 14 C 19 89 P 12 41 P 0 100 15 C 6 85 P 11 40 P 3 94 16 C 6 84 P 0 100 P 1 100 17 C 13 80 P 0 100 P 0 100 18 M 1 83 C 28 44 P 0 88 19 M 3 96 C 7 92 P 1 100 20 M 5 84 C 1 100 P 0 84 21 M 4 97 C 5 80 P 0 95 22 M 0 100 M 0 100 C 1 82 23 M 3 87 M 1 93 C 1 88 24 M 4 78 M 0 100 C 4 97 25 M 2 84 M 2 97 C 3 93
Note. Percentages are rounded up to the nearest whole number. B – Baseline. P – Presentation. C – Coaching. M – Maintenance. Cg – Caregiver. Ch – Child.
Coring an apple. Dyad 2 demonstrated their skills in three contexts: coring an apple,
zipping his jacket, and scraping food from a plate into the trash. Graphed results are shown in
Figure 2.
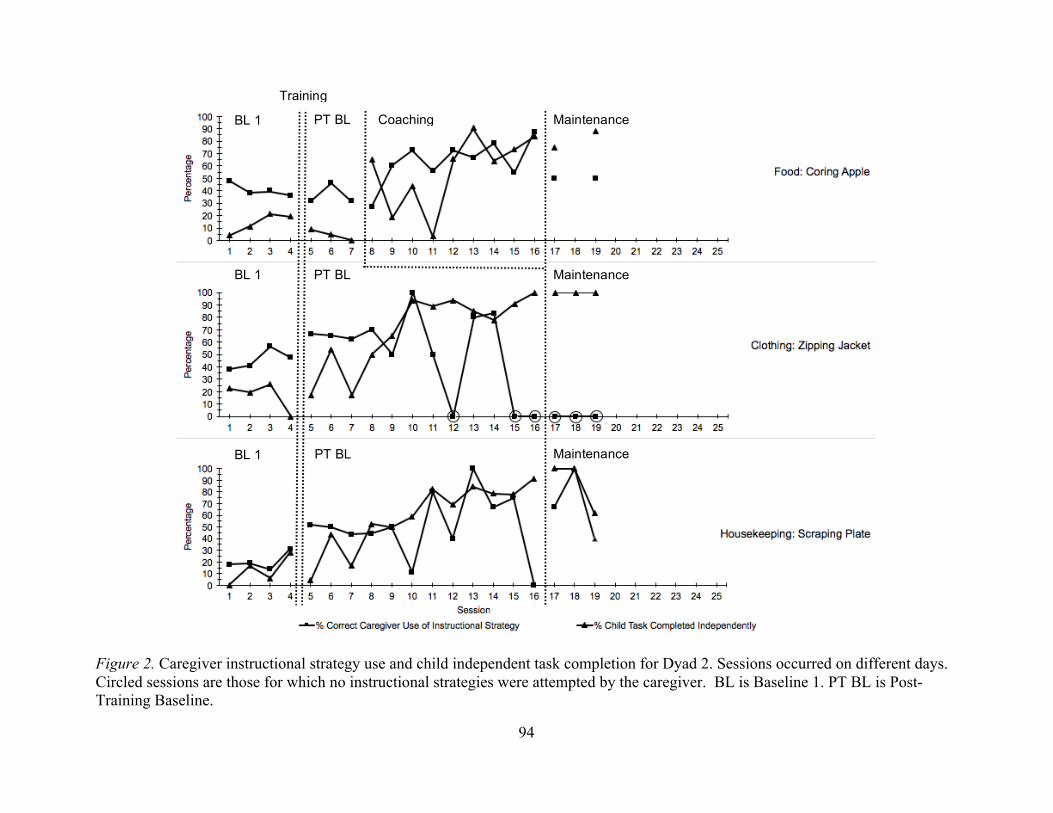
94
Figure 2. Caregiver instructional strategy use and child independent task completion for Dyad 2. Sessions occurred on different days. Circled sessions are those for which no instructional strategies were attempted by the caregiver. BL is Baseline 1. PT BL is Post-Training Baseline.
Maintenance
BL 1
BL 1
Training
PT BL
Coaching
Maintenance
Maintenance PT BL
PT BL
BL 1
95
In the baseline one sessions of the first context, coring an apple, the caregiver used
instructional strategies correctly in 48% of opportunities. In the next three sessions, she
demonstrated a stable, decreasing trend to 36%. During the same baseline phase, the child
increased his independent completion from 4% to 21% in three sessions and then stabilized at
19% for the final session of the baseline one phase.
Due to the counter-therapeutic trend in the caregiver’s instructional strategy use in the
coring apple context and high child motivation to learn the coring the apple task, the training was
given and the post-training baseline phase was introduced after four baseline one sessions.
During the three sessions of this phase, the caregiver used instructional strategies near the same
level as her baseline one performance and also demonstrated a flat trend. At the same time, the
child’s independent completion decreased from 8% to 0%. Consequentially, coaching was
delivered in the coring apple context.
After the introduction of coaching, the caregiver’s correct use of strategies increased
steadily. After the first session, which dipped below baseline performance to 27%, the caregiver
increased and maintained performance above both baseline one and post-training baseline
phases. In the final coaching session, the caregiver used instructional skills with 88% accuracy.
Despite the upward trend in performance, the caregiver demonstrated variable skills, ranging
from 55% to 72%. In the coaching phase, the child also increased his independent performance
of the coring the apple task. After an initial increase in level to 64%, far above his 20% baseline
one phase performance, the child’s independent completion decreased over three sessions to 3%.
After this low task completion, the child demonstrated a rapid increase in trend for the remaining
five sessions, ending at 83% independent task completion. Though the caregiver and child did
not reach the mastery criteria set by the interventionist (i.e., 80% performance over three
96
consecutive sessions), the caregiver expressed satisfaction with her child’s learning and her
increase in instructional skills. As a result, coaching was discontinued and maintenance data
collected.
Maintenance data were collected across all three contexts during the same three sessions.
However, prior to the second maintenance session, the apple coring tool was misplaced, so the
caregiver and child were unable to complete all three apple coring maintenance sessions. For the
two sessions in which there were data collected, the caregiver maintained her increased level of
correct use of instructional strategies above both baseline and presentation levels, though her
50% maintenance use was below her 88% correct use at the end of coaching. During the
maintenance sessions, however, the child maintained his high independent task completion at
75% and 88%. His maintenance performance was near his 83% independent task completion at
the end of coaching. The maintenance data, though not near the researcher-set mastery levels, do
reflect the caregiver-approved mastery level for the child’s independence.
Zipping jacket. In the second context, zipping the jacket, the caregiver demonstrated a
baseline one performance with an upward trend from 38% to 57%, though correct use of
instructional strategies dipped to 48% in the final session before the phase change. During this
same time, the child’s independent completion of zipping his jacket increased slowly from 23%
to 26%, but in the final session before the phase change, he completed 0% of the task
independently, demonstrating great frustration with the task.
After the training session and during post-training baseline in the zipping jacket context,
the caregiver’s correct use of instructional strategies increased in level above baseline one
performance to 67%. Her use of instructional strategies remained relatively flat for four sessions,
and as the child increased his mastery of the zipping jacket task and coaching was introduced in
97
the first context, coring an apple, the caregiver’s correct use of instructional strategies became
more variable, ranging from 50% to 100%. The caregiver did not attempt instructional strategy
use in three of the last five sessions. The child demonstrated a slower increase in trend, with the
two lowest points overlapping baseline performance. After variability in the first four sessions
(i.e., 17% to 54%), the trend of the child’s independent task completion increased rapidly from
54% to 94% in three sessions, well above the baseline high of 26%. The child then maintained
his high level of performance with independent completion ranging from 77% to 100%, with
mastery-level performance (i.e., greater than 80% over three sessions) for seven of the last eight
sessions.
Dyad 2 did not receive the coaching intervention in the second context because the
child’s skills increased to near mastery without the intervention. As with the coring apple task,
the caregiver expressed concerns with prolonging the sessions despite not meeting the
researcher-established criteria for mastery. She conveyed her satisfaction with her child’s
increase in skills and suggested the child’s independent performance might decrease, despite his
new skills, due to behavioral issues that may manifest from his boredom with the task after
perceived mastery and his anxiety over the coming separation from the interventionist.
Consequentially, coaching was not administered in the zipping jacket context.
However, maintenance data were collected for three sessions in the zipping jacket
context. In all three of the sessions, the caregiver did not attempt to use any instructional
strategies. The child, however, independently completed 100% of the steps for zipping his jacket
in all three maintenance sessions.
Scraping plate. During the first baseline data collection in the final context for Dyad 2,
scraping the plate of food waste into the garbage, the caregiver and child both demonstrated low,
98
stable, and flat performance for the first three sessions. In the fourth session, both increased their
skills to near 30% correct use or independent completion. However, because of the flat and
counter therapeutic trends in coring and zipping, the training was delivered across all three
contexts after the fourth session.
The post-training baseline phase lasted 12 sessions, during which the caregiver first
demonstrated an increase in level from 31% in baseline to 52% in the first presentation session.
After the first session, the caregiver’s performance remained relatively flat and stable for four
sessions. During the sixth presentation session, her correct use of instructional strategies became
much more variable, though her correct strategy use did demonstrate an overall upward trend for
the next six sessions. The sixth presentation session in the scraping the plate context coincided
with the child’s increase in independent completion of the scraping the plate task and coaching in
the first context, coring the apple. In the first post-training baseline session, the child’s
independent task completion decreased in level to 4% from a baseline high of 28%. After three
sessions of variable, but upward performance, the child’s independent completion steadily
increased from 4% to 92% over the remaining nine presentation sessions.
Coaching was not implemented in the scraping the plate context because the child
increased his task independence to levels that satisfied his caregiver. As with coring and zipping,
the child did not reach the researcher-established mastery criteria of 80% performance in three
consecutive sessions, but his caregiver told the researcher she was satisfied with his progress in
the last three sessions, which included 79%, 78%, and 92% independent task completion. As a
result of reaching caregiver-approved mastery and concerns about child behaviors related to
boredom and anxiety, coaching was not implemented in the final context, scraping the plate.
99
Maintenance data were collected in the scraping the plate context. Caregiver correct use
of instructional strategies remained variable and at similar levels to the end of the presentation
phase, ranging from 40% to 100% correct use. During the first two maintenance sessions, the
child maintained the upward trend from the presentation phase and reached 100% independent
task completion. In the final session, he decreased to 61% independent task completion. This
task was the first of the three completed in this session, and it was conducted after the child had
become upset about the upcoming separation from the researcher after the end of the study. The
child needed 20 minutes to calm himself before he could complete the scraping the plate task.
His distraught mood may have contributed to his relatively low independence during this session.
Frequency of caregiver instructional strategy use. The caregiver of Dyad 2 also
decreased the frequency of instructional strategy use as her child increased independent living
skill task mastery in each context. For example, in the zipping jacket context, the caregiver
correctly used instructional strategies five times when her child achieved 65% task completion,
and when he completed 91% or 100% of the task, she used no instructional strategies. See Table
5 for the number of correct caregiver instructional strategy use and the child independent task
completion for each session and context.
Dyad 3
Similar to Dyad 2, Dyad 3’s design also lacks experimental control because the coaching
intervention was not delivered in all three contexts. Therefore, though changes in caregiver and
child behaviors in the folding laundry context are present, it is not possible to attribute those
changes to the introduction of the coaching intervention. In addition, the training was
implemented across all three contexts at the same time. Because the introduction was not
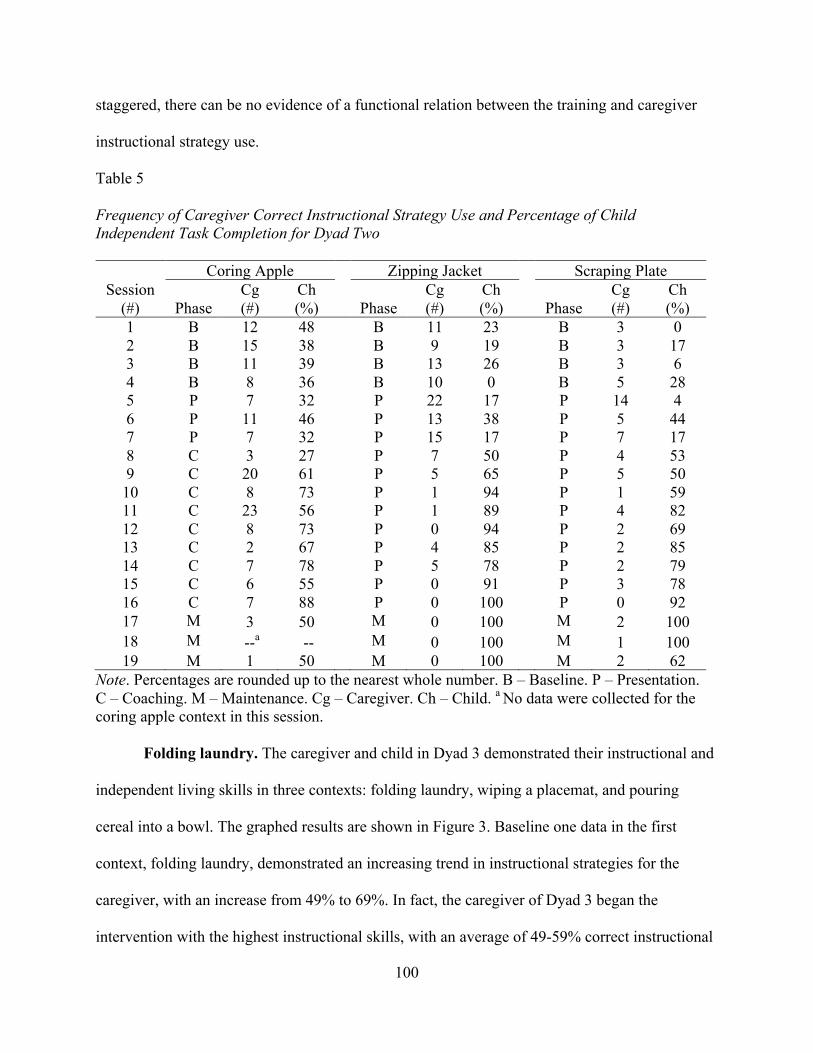
100
staggered, there can be no evidence of a functional relation between the training and caregiver
instructional strategy use.
Table 5 Frequency of Caregiver Correct Instructional Strategy Use and Percentage of Child Independent Task Completion for Dyad Two
Coring Apple Zipping Jacket Scraping Plate Session
(#) Phase Cg (#)
Ch (%)
Phase
Cg (#)
Ch (%)
Phase
Cg (#)
Ch (%)
1 B 12 48 B 11 23 B 3 0 2 B 15 38 B 9 19 B 3 17 3 B 11 39 B 13 26 B 3 6 4 B 8 36 B 10 0 B 5 28 5 P 7 32 P 22 17 P 14 4 6 P 11 46 P 13 38 P 5 44 7 P 7 32 P 15 17 P 7 17 8 C 3 27 P 7 50 P 4 53 9 C 20 61 P 5 65 P 5 50 10 C 8 73 P 1 94 P 1 59 11 C 23 56 P 1 89 P 4 82 12 C 8 73 P 0 94 P 2 69 13 C 2 67 P 4 85 P 2 85 14 C 7 78 P 5 78 P 2 79 15 C 6 55 P 0 91 P 3 78 16 C 7 88 P 0 100 P 0 92 17 M 3 50 M 0 100 M 2 100 18 M --a -- M 0 100 M 1 100 19 M 1 50 M 0 100 M 2 62
Note. Percentages are rounded up to the nearest whole number. B – Baseline. P – Presentation. C – Coaching. M – Maintenance. Cg – Caregiver. Ch – Child. a No data were collected for the coring apple context in this session. Folding laundry. The caregiver and child in Dyad 3 demonstrated their instructional and
independent living skills in three contexts: folding laundry, wiping a placemat, and pouring
cereal into a bowl. The graphed results are shown in Figure 3. Baseline one data in the first
context, folding laundry, demonstrated an increasing trend in instructional strategies for the
caregiver, with an increase from 49% to 69%. In fact, the caregiver of Dyad 3 began the
intervention with the highest instructional skills, with an average of 49-59% correct instructional
101
strategy use during baseline one sessions in each of the three contexts. Conversely, the child’s
skills remained low and with minimal variability (i.e., between 12% and 18%).
Despite the caregiver’s increase in instructional skills in the folding laundry context, her
child’s low independence and the caregiver’s counter therapeutic strategy use in the other two
contexts prompted the training and post-training baseline phase. Once the training was delivered
and the post-training baseline phase begun, caregiver use of instructional strategies continued to
increase, though the rate of increase slowed, topping at 79%. During the post-training baseline
sessions, the child’s performance remained low (6%-15%), overlapping with baseline one levels
of independent skills completion.
Despite increasing levels of caregiver correct strategy use, the coaching intervention was
implemented in this context because of the child’s low independence and caregiver readiness for
support. During the first three coaching sessions, the caregiver reached the researcher-set 80%
mastery and maintained mastery level performance for five additional coaching sessions, though
the overall trend in correct strategy use was decreasing. While the caregiver demonstrated high
levels of instructional skills, the child’s independent completion steadily increased from 16% to
30%-50% over seven intervention phase sessions. Coaching ended before child mastery; this
decision was reached after conversations between the researcher and caregiver. Because the
caregiver had reached mastery in her instructional skills and the child’s skills had increased,
though not to mastery level, the caregiver felt the child would continue to increase her skills
without coaching. The decision to discontinue coaching was also made because of concerns
related to family time available to commit to the study.
Due to time constraints, one maintenance session was collected in the folding laundry
context. The caregiver maintained her high level of performance, correctly using 91% of the
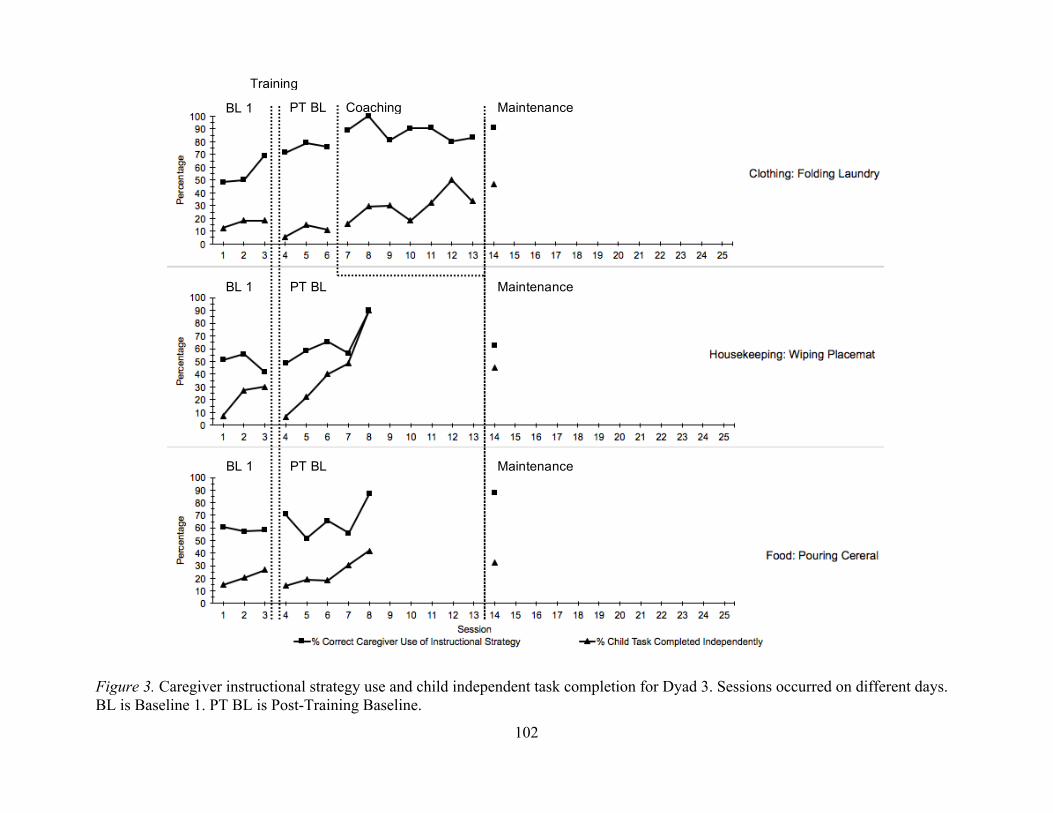
102
Figure 3. Caregiver instructional strategy use and child independent task completion for Dyad 3. Sessions occurred on different days. BL is Baseline 1. PT BL is Post-Training Baseline.
Maintenance
BL 1
BL 1
Training
PT BL
Coaching
Maintenance
Maintenance PT BL
PT BL
BL 1
103
instructional strategies she attempted. The child also remained at levels similar to the end of
coaching, which reflect a level increase from baseline one performance. She independently
completed 47% of the folding task in the maintenance session.
Wiping placemat. Three baseline one data sessions were completed in the second
context, wiping the placemat, concurrent with the other two contexts. In this context, the
caregiver demonstrated correct use of instructional strategies in 42% to 56% of opportunities.
The caregiver strategies demonstrated a slight decreasing trend. During the baseline sessions, the
child demonstrated an increase in her independent task completion from 7% to 30%. Due to her
caregiver’s decreasing performance, the presentation phase was introduced.
In the post-training baseline phase, the caregiver maintained similar levels of correct use
(i.e., 48% and 58%) in the first two sessions, but then began to increase her correct use with
some variability over five total presentation phase sessions. During the final session for which
data were recorded in the post-training baseline phase, the caregiver’s correct use of instructional
strategies increased to 90%. The caregiver’s jump in correct strategy use from 56% to 90% in
one session coincides with the first full session after coaching began in the folding laundry
context and suggests generalization of skills. The child’s independent task completions followed
a similar pattern. After an initial drop in independence from baseline levels of 30% to 7% in the
presentation phase, the child steadily increased her independent task completion to 49% in four
sessions. In the first session after the introduction of coaching in the folding context and the final
recorded session in the presentation phase, the child’s independent task completion rapidly
increased in trend to 90%. Though coaching continued in the folding laundry context for five
more sessions, data were not collected for the wiping placemat and pouring cereal contexts
because of caregiver concerns over the time commitment. Eliminating presentation phase data
104
collection in the two contexts shortened sessions from 45 to 60 minutes to 15 to 20 minutes,
which allowed Dyad 2 to continue to participate in the study.
As a result of time constraints and satisfaction with skill increases, the coaching
intervention was not introduced in the wiping placemat context. A final maintenance session was
collected after coaching ended in the first context, folding laundry. Caregiver correct use of
instructional strategies in wiping the placemat was 63%, near her correct use in later presentation
sessions, and above the baseline session performance of 56%. The child demonstrated
independence in a similar pattern. Her maintenance of independent task completion was 45%,
higher than her highest baseline task independence of 30%, and nearer later sessions in the
presentation context.
Pouring cereal. Caregiver and child behaviors in the final context, pouring cereal,
followed similar patterns as the wiping placemat context. Three baseline sessions were
completed. In those sessions, the caregiver used instructional strategies with a stable, and slightly
decreasing trend from 60% to 58%. The child demonstrated relatively low skill independence,
though the trend of task independence increased from 15% to 27%.
After the training was delivered and the post-training baseline phase begun, the caregiver
increased the trend and overall level of correct strategy use, though the data were variable (i.e.,
48% to 90%). Two post-training baseline phase caregiver data points overlapped with baseline
one performance. Like in the wiping placemats context, in the final session for which post-
training baseline phase data were collected and the first session after coaching was introduced in
the folding context, the caregiver’s correct use of instructional strategies increased to 87%,
higher than the previous session’s performance of 56% correct use. The child’s independence
also increased, though her independence in the first three post-training baseline sessions
105
overlapped with her independence in the baseline one phase. In the fourth and fifth sessions, the
child’s task independence increased to 31% and 42%. The child’s 42% independent task
completion occurred after the first full coaching session in the folding laundry context.
For the same issue of time intensiveness, coaching was not introduced in the pouring
cereal context. Maintenance data were collected six sessions after the end of presentation data
collection and after the end of coaching in the folding laundry context. Both the caregiver and
child demonstrated skills near the level of the last recorded presentation session. The caregiver
correctly used instructional strategies in 88% of opportunities, and the child independently
completed 32% of the pouring cereal task.
Frequency of caregiver instructional strategy use. Dyad 3 only completed 14 sessions,
and though the caregiver reached mastery in the first context, her child did not reach mastery.
The coaching intervention was not delivered in the second and third contexts. In the sessions in
which the child completed the task at higher levels, the caregiver correctly used fewer
instructional strategies. Table 6 outlines the number of correct strategy uses and child
independent task completion for each session and each phase.
Social Validity Outcomes
The goals, procedures, and outcomes of the research were considered to evaluate the
social validity of the intervention (Wolf, 1978). After the study concluded, caregivers were sent
two surveys (Appendix W). The first survey evaluated caregiver perceptions of the social
validity of the intervention. Caregivers were also sent surveys to evaluate child perceptions of
social validity, and the child surveys were completed with adult help. Though surveys were sent
to all three dyads, only Dyads 2 and 3 returned the surveys. Despite several attempts to contact
the caregiver of Dyad 1, she could not be reached, so social validity survey data for Dyad 1 are
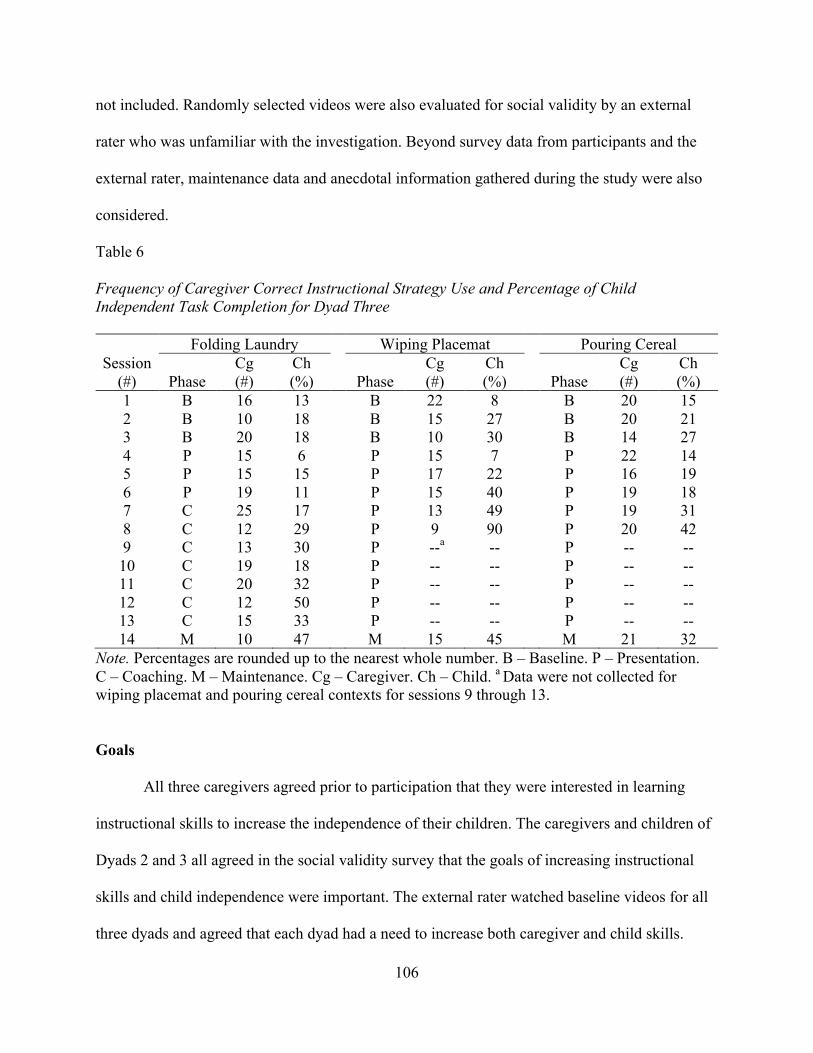
106
not included. Randomly selected videos were also evaluated for social validity by an external
rater who was unfamiliar with the investigation. Beyond survey data from participants and the
external rater, maintenance data and anecdotal information gathered during the study were also
considered.
Table 6
Frequency of Caregiver Correct Instructional Strategy Use and Percentage of Child Independent Task Completion for Dyad Three
Folding Laundry Wiping Placemat Pouring Cereal Session
(#) Phase Cg (#)
Ch (%) Phase
Cg (#)
Ch (%) Phase
Cg (#)
Ch (%)
1 B 16 13 B 22 8 B 20 15 2 B 10 18 B 15 27 B 20 21 3 B 20 18 B 10 30 B 14 27 4 P 15 6 P 15 7 P 22 14 5 P 15 15 P 17 22 P 16 19 6 P 19 11 P 15 40 P 19 18 7 C 25 17 P 13 49 P 19 31 8 C 12 29 P 9 90 P 20 42 9 C 13 30 P --a -- P -- -- 10 C 19 18 P -- -- P -- -- 11 C 20 32 P -- -- P -- -- 12 C 12 50 P -- -- P -- -- 13 C 15 33 P -- -- P -- -- 14 M 10 47 M 15 45 M 21 32
Note. Percentages are rounded up to the nearest whole number. B – Baseline. P – Presentation. C – Coaching. M – Maintenance. Cg – Caregiver. Ch – Child. a Data were not collected for wiping placemat and pouring cereal contexts for sessions 9 through 13.
Goals
All three caregivers agreed prior to participation that they were interested in learning
instructional skills to increase the independence of their children. The caregivers and children of
Dyads 2 and 3 all agreed in the social validity survey that the goals of increasing instructional
skills and child independence were important. The external rater watched baseline videos for all
three dyads and agreed that each dyad had a need to increase both caregiver and child skills.

107
Procedures
All three dyads anecdotally reported challenges with the procedures of the intervention
during the study. Dyads 1 and 3 both contacted the researcher outside of coaching sessions to
discuss the challenges with finding time to work with the coach 2-3 times a week for up to an
hour each session. The time intensiveness of the intervention led to attrition with Dyad 1 after 25
sessions. The caregiver and researcher agreed to end participation before maintenance data could
be completed in the final context, wiping the counter. The length and frequency of sessions also
led to attrition in Dyad 3. The caregiver did not feel she could dedicate more than 30 minutes per
session, and as a result, Dyad 3 did not enter intervention in the second and third contexts (i.e.,
wiping the counter and pouring cereal). The frequency and length of the sessions was not as
challenging for Dyad 2. However, the caregiver of Dyad 2 expressed that she did not think her
child would maintain his current agreeable behaviors for the extended number of sessions needed
to help him reach the researcher-determined mastery level.
When evaluating procedures after the study through the social validity survey, the
caregivers of Dyads 2 and 3 rated procedures of the intervention more positively than they
reported during the study. In the social validity survey, the children and caregivers all agreed
with the value of teleconferencing coaching. They also all agreed using telecoaching during
independent living skills contexts was useful and worth their time. The external rater also
evaluated the social validity of the procedures by watching a randomly selected coaching session
for each dyad. Like the caregivers of Dyads 2 and 3, the external rater reported the use of
teleconference coaching in independent living skills was socially acceptable.
108
Outcomes Outcomes were also evaluated for social validity directly by participants and the external
rater and indirectly through maintenance data. The caregivers and children of Dyads 2 and 3
reported several positive outcomes though the social validity survey. They reported benefits for
both caregiver and child outcomes after the intervention and a belief that both the caregivers and
children would continue to use their skills after the end of the coaching intervention. They also
reported that coaching could benefit children without disabilities by increasing caregiver and
child skills.
After watching coaching and maintenance videos for all three dyads, the external rater
also agreed that children and caregivers increased and maintained their learned skills. The
external rater agreed the intervention may benefit families of children without disabilities. After
watching maintenance videos, she was unsure the caregiver of Dyad 2 continued to use strategies
after the coaching intervention ended. This reflects the finding that the caregiver of Dyad 2 did
not reach mastery in instructional skills. Similarly, the external rater determined the changes in
behavior to be significant for Dyads 1 and 2. However, she was unsure if the changes were
significant for Dyad 3. This external rater finding also reflects the results. The caregiver of Dyad
3 began with the highest instructional skills, and her child did not reach independent living skill
mastery, perhaps because of the short duration of the intervention.
During maintenance phases for all three dyads, the children completed each of their three
tasks with more independence than they demonstrated during baseline phases. For Dyad 1,
caregiver maintenance data were variable. Except for one context, pouring hot water, both
caregiver and child showed no overlap with baseline data. Though the caregiver of Dyad 2 did
not achieve mastery, she did correctly use instructional strategies at a higher rate during
109
maintenance than she did during baseline sessions in two contexts, coring and scraping. She did
not, however, use any instructional strategies during the jacket zipping context, perhaps due to
her son’s 100% task independence during maintenance. Though only a single maintenance data
point was taken, the caregiver of Dyad 3 correctly used instructional strategies at levels above
her baseline use in all three contexts.
110
CHAPTER 5
DISCUSSION
Children with visual impairments have unique learning needs (e.g., Lowenfeld 1952,
1973) and a specific need for instruction in independent living skills (Hatlen, 1996). Families of
children with disabilities need support to sustain their family systems (Turnbull et al., 2015), and
many researchers have explored the use of caregiver coaching (e.g., Marturana & Woods, 2012;
Wetherby et al., 2014) and the use of telepractice to deliver that support (e.g., Baharav & Reiser,
2010; Boutain, 2014; McDuffie et al., 2013). Given the literature base, the purpose of this study
was to investigate the impact of telepractice caregiver coaching on the instructional skills of
caregivers and the independent living skills of their children with visual impairments. In the
following sections, changes in caregiver and child behaviors and the implications of those
findings are discussed.
Changes in the implementation of the methodology significantly limit the strength of the
findings. Because coaching was not introduced in the second and third contexts for Dyads 2 and
3, the changes in behavior cannot be used as evidence of a functional relation between
telepractice coaching and caregiver instructional strategy use for Dyads 2 and 3. However, the
design used with Dyad 1 does meet IES WWC standards with reservations (Kratochwill et al.,
2010), so these data may be considered with caution.
Changes in Caregiver Instructional Strategy Use
The caregiver of Dyad 1 increased her instructional strategy use above post-training
baseline levels in all three contexts in which she was coached. She demonstrated mastery (i.e.,
greater than 80% in three consecutive sessions) in two contexts, and in the third context, she
111
demonstrated greater than 80% performance in 3 of 4 coaching sessions. During maintenance
sessions, her correct instructional strategy use became more variable. However, the caregiver of
Dyad 1 consistently demonstrated variable use of instructional strategies. The percentage of non-
overlapping data point between post-training baseline and coaching phases was 37.5% in pouring
hot water, 50% in hanging shirts, and 0% in wiping the counter. Despite the caregiver reaching
mastery in two contexts, data variability makes it difficult to determine a clear functional relation
between the introduction of the coaching and caregiver instructional strategy use.
The variability in caregiver instructional strategy use may be related to child task
attempts. The number and type of caregiver strategies attempted varied from session to session.
For example, as the child began to learn a new skill, caregivers used strategies like ‘preview
task’ more frequently. As the child increased independence, caregivers used strategies like
‘specific praise for component’ and ‘realistic feedback’ more often. Caregivers could also decide
to have the child practice portions of the task multiple times (e.g., practice aligning the kettle
spout with the mug four times before attempting to pour hot water). As the children approached
100% independent task completion, the number of instructional strategies used by caregivers
decreased, sometime to zero strategies. (See Tables 4, 5, and 6 for more detailed information
about caregiver attempts and child mastery.) As a result, the caregiver instructional strategy use
became more variable as the child increased his or her independence.
Changes in Child Independence Task Completion
The child of Dyad 1 mastered all three independent living skills tasks. He improved
above baseline one and early post-training baseline phases. However, child independence was
considered a secondary variable to the primary variable of correct caregiver strategy use because
the primary independent variable, caregiver coaching, did not directly address child
112
independence. As the caregiver of Dyad 1 correctly used instructional strategies at higher levels,
her son became more independent in his task completion, though the strength of this finding is
impacted by internal validity threats related to testing and maturation. It is possible he increased
his task independence because he practiced in the task many times. The threat to validity may be
limited because of the immediate level increases in skills for the child of Dyads 1 after the
introduction of the training and post-training baseline phases. Additionally, in two of three
contexts, child task independence dropped as his caregiver began to provide more correct
instruction in the post-training baseline phases before child independence increased again in later
sessions.
Social Validity
Though the coaching intervention may have positively influenced caregiver instructional
skills and child independence in Dyad 1, social validity concerns were raised regarding the
procedures of the intervention. The time intensity of the intervention led to participant attrition
and may limit the participants for whom this intervention could be useful. Available family time
to commit to coaching was limited in Dyads 1 and 3. For both Dyads 2 and 3, child attention
limited the ability of the families to participate in all originally planned sessions. The combined
challenges of available family time and the child’s attention caused Dyad 3 to limit coaching and
data collection to just one context.
Despite concerns raised during the intervention, after the investigation was complete,
Dyad 2, Dyad 3, and the external rater all rated goals, procedures, and outcomes of the
investigation as socially valid. It is possible the few weeks that lapsed between ending the
intervention and completing the social validity survey allowed the participants to reconsider the
acceptability of the study procedures. However, it is also possible the researcher’s relationships
113
built through prolonged contact with the caregivers and children contributed to more positive
ratings (Hurley, 2012). Caregivers and children may have rated the intervention highly to please
the researcher. Correspondingly, the caregiver of Dyad 1 may have chosen not to respond to
requests to complete social validity surveys because she did not want to rate the intervention
badly.
In addition, though caregiver correct use of instructional strategies varied across the three
contexts, all three caregivers had relatively high skills for teaching their children during baseline
one data collection in at least one context. If the training and coaching increased caregiver
instructional skills, it helped develop pre-existing caregiver instructional skills. For caregivers
with lower instructional skills, the coaching intervention may prove to have different social
validity.
However, caregivers appeared to generalize instructional strategies across independent
living skills contexts without coaching and to other independent living skills tasks outside of the
research study. Because of increased caregiver instructional skills and increased child
independence, the caregivers of Dyad 2 and Dyad 3 chose not to implement the coaching
intervention in the final two contexts. The caregiver of Dyad 1 generalized in similar ways, but
she wanted her child to reach researcher-set mastery criteria. This difference in expectations may
be related to differences in caregiver expectations and the child’s age, 11 years old.
The caregiver of Dyad 2 regularly spoke to the coach about her generalization of
instructional strategies outside of the research study. During the first coaching session, she said,
“I’ve just noticed a difference… I’m asking him to do more.” Later, in the final coaching
session, she said, “[Coaching’s] really helped me in so many other areas with him. I’m having
him do so much more. It’s just crazy all I’m having him do.” Throughout the study, she shared
114
new activities she’d begun to teach her child, including putting away clean silverware from the
dishwasher, bathing himself, dressing himself, and cooking eggs on the stovetop. After the study
ended, she continued to send photos and videos of her child completing tasks like using a hand
mixer, baking a pie, and lighting a match for the outdoor fireplace.
Online video teleconferencing also proved to be a useful tool. For caregivers, the
application was free, easy to use after a 10-minute session, and could be used with tools already
in the home (i.e., tablet computers, smart phones, and wireless Internet). The use of basic
features is free, but the researcher opted for the enhanced recording and security features, which
cost $15 a month. Internet connection speeds caused an issue with only one dyad, who lived in a
rural area. Internet connectivity led to a few session interruptions, but it never caused sessions to
be cancelled.
Limitations
A small sample of children with visual impairments participated in the study. Because of
the heterogeneity of the population of children with visual impairments, it would be impossible
to select a representative sample of children that reflects the variability in visual and intellectual
abilities of children with visual impairments. To obtain a more homogeneous sample, each child
selected for inclusion was aged 5 to 11 years old, had no other significant disability, was
educated in a general education classroom, was a tactual learner, and had skill deficits in
independent living.
The small number of participants included in single case research design limits the
generalizability of the findings. To attempt to increase the external validity, the researcher
applied the coaching intervention in three dyads to allow for inter-subject replication. To
115
enhance intra-subject replication, each dyad demonstrated coached instructional strategies across
three independent living skills contexts.
Though families were widely recruited, the families who participated in the study shared
many similarities. All three families were middle class, and all three caregivers were mothers.
Participating caregivers committed at least two to three hours a week for at least ten consecutive
weeks to participate in the coaching intervention. As such, the intervention was limited to
caregivers who had sufficient time and resources to commit to the intervention. The caregivers of
Dyads 1 and 3 did not work outside the home for pay. The caregiver from Dyads 2 did work
outside the home for pay, but she worked less than full time (i.e., 20-30 hours a week) outside
the home. As a result, all three caregivers could spend time participating in the research study
after school, between 3:00pm and 6:00pm local time each day. Additionally, the use of
teleconferencing limited the intervention to caregivers who had access to the Internet at home
and the tools and skills necessary to use the teleconferencing application (e.g., laptop or tablet
computer with microphone and video camera). It is possible caregivers with greater resources
naturally selected themselves for participation, knowing they had more time available than most
families.
Additionally, because caregivers contacted the researcher directly to indicate interest in
participation, it is possible those caregivers with fewer resources removed themselves from
consideration before expressing interest in the intervention. They may have read the recruitment
materials, decided the intervention was too time-intensive, and chosen not to participate. As a
result, families with fewer resources may be more difficult to recruit in future investigations with
the given materials.
116
Caregivers were coached to implement instructional strategies so they could teach their
children independent living skills in their homes. Implementing interventions at home introduces
unanticipated variables (e.g., presence of a sibling, television noise). However, the natural
context of the coaching model aligns with the conceptual frameworks of both family systems and
the coaching intervention being implemented.
The children of Dyads 1 and 3 were one of two siblings in the home, and the child of
Dyad 2 was the only child at home. As such, the caregivers may have had more time to dedicate
to the independent living skills instruction of their children than caregivers with more children.
Two of the mothers, from Dyad 1 and Dyad 2, were 51 and 52 years old and had young adult
children outside of the home. Their long parenting experience may have impacted how they
learned and used the coached instructional strategies. The presence of siblings in the home for
Dyads 1 and 3 may also have impacted the time available for coaching sessions. For both
families, coaching sessions had to be scheduled around the after-school activities of the child
included in the study and his or her sibling.
All three of the children who participated in this study attended general education
classrooms with their same age peers. They had no additional significant disabilities, though the
child of Dyad 2 did have ADHD. Consequentially, caregivers were generally able to focus on
instructional strategies to address needs specific to visual impairment and not needs related to
other disabilities. The child of Dyad 2 did display some challenging behaviors related to his
ADHD, which may have led to increased prompting from his mother and variability in his task
independence. Caregivers of children without significant additional disabilities may react
differently to caregiver coaching than caregivers of children who have additional significant
disabilities.
117
Though caregivers were encouraged to place the phone or tablet used to participate in
sessions in a static location, they often chose to hold the tool to allow a better view for the
researcher. Their holding the phone or tablet may have impacted whether or how they chose to
use one instructional strategy, previewing task, as it generally required the use of hand-under-
hand or hand-over-hand physical modeling.
At least some data of all three dyads in all three contexts demonstrated variability. Some
of the variability may be attributed to the time of day in which data were collected. At least one
and sometimes two sessions were conducted after school and before dinner or after school
activities. The time constraints were less present during weekend sessions. It is possible data
collected only on weekends would have yielded more consistent results.
The model of caregiver instructional strategies (Appendix B) in which caregivers were
coached was developed for use in the current study and was based on theoretical models
identified outside of educating children with visual impairments, as the empirical evidence base
in teaching caregivers of children with visual impairments is limited. However, the specific
strategies outlined in the model are aligned with best practice and accumulated empirical
evidence in educating children with visual impairment. The content of the caregiver instructional
strategies model was validated by two individuals with doctoral degrees in special education and
specialization in educating children with visual impairments. They provided feedback that was
incorporated in the model.
The number of sessions and length of each session created challenges with family
availability. As such, the data collected were limited, particularly Dyad 3. The frequent data
collection necessary to establish stable data before the second tier of the intervention could have
introduced a testing threat. Additionally, the long length of intervention for Dyad 1, 25 sessions,
118
may reveal maturation, not the impact of the intervention. As such, it is unclear how much or if
the strength of the findings is limited.
The greatest limitation, however, is the lack of experimental control for Dyads 2 and 3.
Because the coaching intervention was not delivered in the second and third contexts for Dyads 2
and 3, the designs for Dyads 2 and 3 lack experimental control. As a result, the data, though
promising, cannot be used as evidence of a functional relation. Though Dyad 1 did complete the
intervention in all three contexts and achieved task mastery in two contexts, the high variability
of the data make it difficult to conclude the coaching intervention caused the changes in
caregiver behavior detected.
Beyond challenges with experimental control and data variability, multiple factors
introduced in this study are new to the field of teaching children with visual impairments,
including the use of coaching, telepractice, and an instructional strategy model. As a result, it is
difficult to determine which component resulted in any changes identified in the participants’
skills. Further research is necessary to determine the efficacy of telepractice caregiver coaching
with the population of caregivers of children with visual impairments.
Implications for Teachers
The use of telepractice to coach caregivers of children with visual impairments has great
implications for TVIs. This investigation provides limited evidence that coaching may increase
caregiver instructional skills. Developing an extended coaching relationship with a caregiver
may have been responsible for further increased and maintained caregiver skills for Dyad 1.
Developing prolonged, supportive relationships between caregivers and professionals is also
supported by the findings of other authors (e.g., Kyzar et at., 2016; Nixon, 1988). Further
investigation is necessary to determine whether telepractice coaching is effective to increase the
119
skills of caregivers and the appropriate intensity of contact for a wide range of children, but the
promise of telepractice to increase the skills of caregivers of children with visual impairments
should be monitored by TVIs committed seeking to increase the ECC skills of their students.
Internet-based video teleconferencing proved to be a cost-effective and easy-to-use tool
to connect families with practitioners and increase the instructional skills of caregivers. As noted
by Houston and Stredler-Brown (2012), telepractice service delivery and coaching models
decrease direct teaching from practitioners while increasing the capacity of caregivers. As
caregivers have the most prolonged contact with their children who have visual impairments,
they need skills to teach their children when teachers are not present.
Children with visual impairments also need instruction in natural contexts, and learning
independent living skills at home with natural teachers (i.e., caregivers) increases child
opportunities to learn. The caregiver selection of child skills also enhanced motivation of both
the child and caregiver. Caregivers selected tasks (e.g., pouring cereal and hanging shirts) not
only that they suspected the child would find motivating, but also that would benefit the family
system by reducing caregiver workload. Turnbull et al.’s (2015) family systems model can be
used to understand the learning of children with visual impairments. Supporting the learning of
caregivers in daily care allowed caregivers to release some daily care tasks to their children, thus
decreasing stress on family systems.
Working on learning independent living skills at home allows multiple opportunities to
practice skills. Repeated practice of unified tasks is known to be important to develop the
concepts and skills of children with visual impairments (e.g., Lowenfeld, 1973; Lewis & Allman,
2014b). As that instruction may not be possible in the time constraints of the school (Lohmeier et
al., 2009), telepractice caregiver coaching may expand instructional time available to TVIs to
120
meet IEP goals. Additionally, teachers in many school districts are prohibited from making home
visits because of the increased liability of providing instruction outside the school building. The
use of telepractice coaching may provide teachers with a tool to teach families and children
without the increased liability of a home visit. However, challenges with delivering caregiver
coaching after school and on weekends may prove challenging for teachers bound to a typical
school day schedule. The need for instruction may reveal a place for agencies and schools for the
blind to expand services outside of the typical school day.
All three caregivers noted that the regular meetings caused them to set aside time to work
on increasing independent living skills, an area they acknowledged as important but had not
previously prioritized. Finally, the caregiver of Dyad 3 noted that the use of coaching by a
professional outside of her child’s TVI and family confirmed for the child the importance of
increasing independent living skills. The coach’s confirmation of the value of independence for
the child amplified expectations set by the caregiver.
The model of instructional strategies in which caregivers were coached (Appendix B)
may also prove useful for practitioners. Though the model was developed for use in this
investigation, it reflects current best practice in educating children with visual impairments.
Though further investigation is necessary to validate the strategies in all nine ECC areas and with
all types of individuals (e.g., caregivers, TVIs, educational assistants), this model may help TVIs
organize instruction for children with visual impairments.
Implications for Future Research
The FGRBI model of caregiver coaching has been effective in increasing the capacity of
caregivers of young children with disabilities. Implementation of this intervention may have
increased and stabilized the instructional skills of one caregiver of a school-age child with a
121
visual impairment in the given study, but data variability limits the strength of the finding.
Despite its potential benefit, the model as implemented in this study was not a good fit for all
three participating families. A modified implementation of the FGRBI coaching model that
reduces the frequency and length of baseline and intervention sessions may be more readily
accepted by families and therefore reduce attrition. As delivered, the telepractice coaching model
added pressure to the family system (Turnbull et al., 2015) of at least one dyad.
In addition to challenges in overall time commitment, caregivers reported challenges with
implementing the intervention on weeknights, when after-school activities and early bedtimes
conflicted with coaching sessions. A modified intervention that makes use of weekend time may
be more acceptable. Many studies investigating caregiver coaching featured coaching once a
week (e.g., Brown & Woods, 2015; Nunes et al., 2016). It is possible that once-weekly coaching
sessions, conducted on weekends, may prove to be more acceptable to caregivers of children
with visual impairments. Correspondingly, plans made during the coaching sessions for
practicing skills between sessions were often not carried out because families reported not
having enough time to dedicate to extra activities. Some caregiver coaching models have used
the support of static online resources (Vismara et al., 2013) or analysis of previously recorded
videos (Nunes et al., 2016). Use of alternative supports for caregiver growth could be used along
with a weekly FGRBI telepractice coaching session. Lowering the frequency of data collection
sessions may prolong the overall length of the intervention, but make it easier for caregivers to
fit the activity in their lives. Changes to the experimental design may also lead to results with
greater experimental control. Reducing the frequency with which data are probed may decrease
some of the threats to validity related to maturation and attrition (Gast et al., 2018) which led to a
lack of experimental control in Dyads 2 and 3.
122
Though the children all had significant visual impairments, they did not have additional
disabilities that precluded their placements in general education classrooms. As such, their
educational needs were relatively straightforward and primarily related to their visual
impairments. Because of their overall typical development, the independent living skills the
children learned were near age appropriate (e.g., the five-year-old learned to pour dry cereal into
a bowl). The FGRBI model has been often implemented with very young children with
significant disabilities. It may be that caregivers of children who are visually impaired and have
no other disabilities need less intensive interventions to meet the relatively less intense needs of
their children.
Because caregivers appear to have generalized instructional skills from training only and
coaching to other experimental contexts and to outside tasks, it may be that less intensive
supports in one context increase caregiver and child skills to levels considered acceptable for
caregivers. For all three children, the most difficult tasks were selected for intervention first.
Caregivers spent the most time in those phases. It is possible if less difficult tasks were selected
for intervention first, the caregiver and child may have achieved mastery in that context more
quickly and generalized mastery-level skills to the other two contexts with less need for
intervention in other contexts. Though generalized increases in caregiver and child skills did
occur, they did not all increase to mastery without coaching support. However, the caregiver and
child skill increases experienced were perceived as successes by all three dyads, even if they did
not meet the researcher-set criteria for mastery.
Caregivers conveyed different expectations for mastery than the researcher. Initial
mastery was set at 100% for the caregiver and 90% for the child. Levels were lowered to 80%
for both caregiver and child in consultation with the caregiver after prolonged intervention with
123
Dyad 1. In Dyads 2 and 3, caregivers were satisfied with increases in child independence even
though they did not reach the researcher-set mastery criteria of 80%. This difference in perceived
mastery may be related to child age. The child of Dyad 1 was 10 and turned 11 during
intervention. The children of Dyads 2 and 3 were 9 and 5 years old, respectively. Caregivers may
have different expectations for skill mastery when their children are younger. Though all three
caregivers indicated independent task completion as a goal for their children during coaching
sessions, as the intervention continued, their willingness to commit additional time to reach
100% waned. Future investigations should consider parent-perceived independence and may
include direct sharing of data as it is coded and graphed by the researcher.
It may also be useful to set criteria in which coaching may begin in additional contexts
once a change in behavior is detected in the first context but before the caregiver and child reach
task mastery at high levels (e.g., 80%). Doing so may allow the coaching intervention to be
delivered in multiple contexts before children learn the tasks through practice or caregivers find
the time dedicated to the intervention to be too intensive.
The instructional strategies in which caregivers were coached should also be further
refined. Though caregiver skills in expectation, access, and contingent responding were
collected, caregiver use of two originally conceived categories, systematic instruction and fading
support, were not captured during data collection. Strategies included in fading support (i.e.,
specific praise for task, generalization, and fading prompting) should be included in future
investigations. Caregivers spontaneously exhibited instructional strategies like elaborating on
item use and rationale for task, particularly as the child approached task mastery. These
strategies were not measured in the current study and may reveal how caregivers perceive
readiness for child independence and then release children to complete tasks independently.
124
Further empirical investigation of this instructional strategies model may be useful for
identifying which strategies are useful for whom and under what conditions those strategies are
useful.
Other modifications to the FGRBI model may increase its effectiveness and acceptability
to caregivers of children with visual impairments. The children in this study were school-age and
without additional disabilities. They were interested in their learning and often, without
invitation of their caregivers or the coach, participated in phases of the coaching session like
setting the stage and problem solving and planning. These expressions of self-determination
related to learning should be encouraged in a population of children known to exhibit learned
helplessness in independent living skills (Bardin, 2014) and who need explicit instruction in self-
determination (Hatlen, 2004).
Similarly, the siblings of the children who participated in the study showed great interest
in the research sessions. The children of Dyad 1 and Dyad 2 both had siblings in the home. In
Dyad 1, the brothers were close in age, 8 and 10 years old; in Dyad 3, the sibling was 9 years old
and very interested in learning to teach her 5-year-old sister, the child of Dyad 3. Further
investigations in the efficacy of caregiver coaching of children with visual impairments may
benefit from considering the natural role of siblings as peer models. As Turnbull et al. (2015)
suggested, a child’s disability impacts the whole family system. Teaching siblings to modify the
ways in which they naturally teach their siblings may prove useful for increasing learning
opportunities and maintaining appropriate family cohesion.
The role of food related tasks should also be considered. The children were more
motivated by food-related tasks, and in two of three dyads, the food preparation task was
selected as the first for intervention. Dyad 3 did not complete coaching in the food preparation
125
task, and it is possible intervening in this context first may have changed how the family
tolerated the intervention.
Though the children and their caregivers included in this investigation shared many
characteristics (e.g., level of visual impairment, lack of additional significant disabilities,
socioeconomic status, two-parent homes), they did vary on some traits (e.g., age, race).
However, the variance among the children and their families does not fully reflect the
heterogeneity of the larger population of children with visual impairments (Mason & Davidson,
2000; USDOE OSERS, 2017). The use of telepractice caregiver coaching should be investigated
with families who represent that diversity. Families with fewer resources (i.e., time and money)
may also benefit from the use of telepractice caregiver coaching, but the time and tools necessary
to participate may not be available to all families. They may not be able to participate in
telepractice caregiver coaching, however beneficial it may be. Additionally, families of children
with more intensive needs may benefit more from coaching as their caregivers may be less able
to generalize instructional skills learned to other task contexts because of the unique needs of
their children. The caregiver of Dyad 2 reported the greatest anecdotal tolerance of the
intervention, and her child had ADHD and the greatest need for independent living skills
instruction.
The combination of telepractice, caregiver coaching, and an instructional strategies model
has not before been examined in the literature of teaching children with visual impairments. Each
element of the intervention, therefore, should be examined in isolation to determine which
component or components may result in increased caregiver instructional strategy use and
increased child independence in independent living skills tasks.
126
Conclusion Caregivers of children with visual impairments need support to increase the independent
living skills of their children. In this study, the researcher investigated the use of telepractice
caregiver coaching with the FGRBI model to increase both caregiver instructional skills and the
independent living skills of their children. The results, however, are unclear. The coaching
intervention was only implemented in multiple contexts for one dyad. Though the caregiver
increased her use of instructional strategies to mastery in two of three contexts, the variability of
her correct instructional strategy use makes it unclear whether caregiver telecoaching caused
those changes in her behavior. Though the caregivers of Dyads 2 and 3 demonstrated level and
trend increases in their instructional skills after the introduction of the coaching intervention, the
design as implemented lacked experimental control. Additionally, after coaching was introduced,
caregivers began to generalize instructional skills to other contexts.
Nonetheless, telepractice proved to be a convenient way to connect families of children
with visual impairments to a coach who could facilitate an increase in their skills. Despite the
lack of a clear functional relation, the use of telepractice caregiver coaching in the given study
shows some promise of usefulness and should be further explored to determine its effectiveness
in increasing caregiver instructional strategies. After its efficacy is determined, further
investigations in which alternative or modified models for delivering telepractice caregiver
coaching should be conducted to learn which elements are most useful, for whom, and under
what conditions.
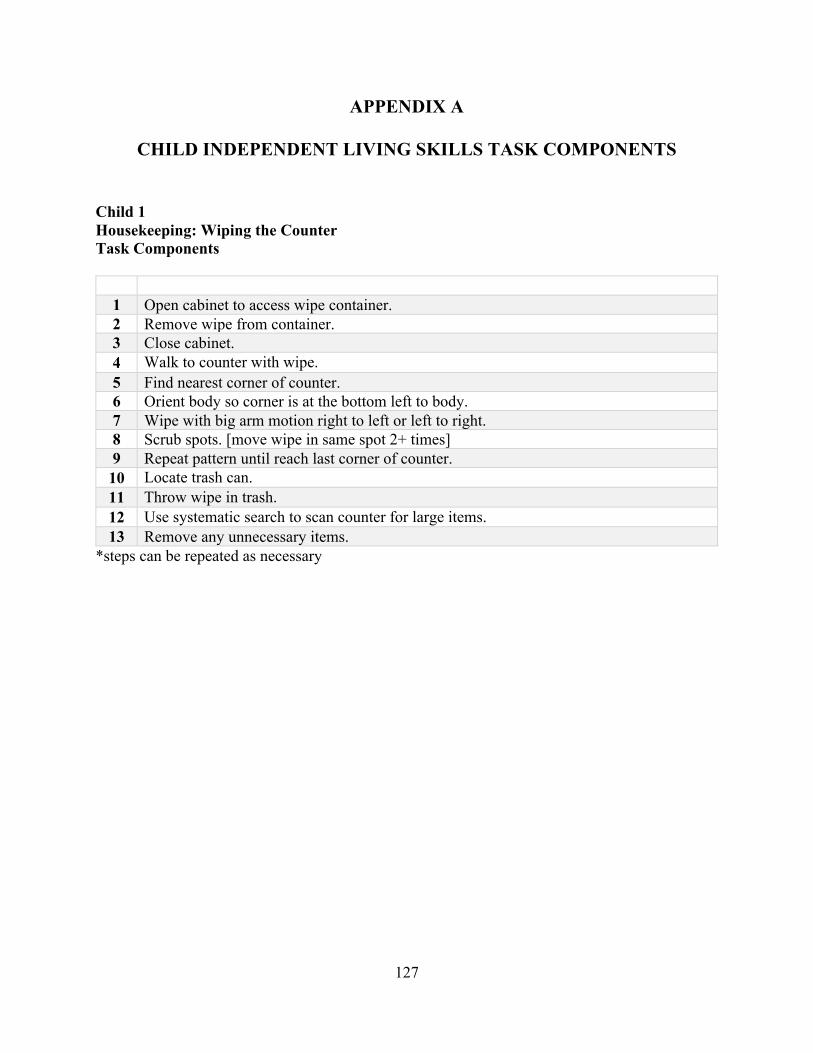
127
APPENDIX A
CHILD INDEPENDENT LIVING SKILLS TASK COMPONENTS
Child 1 Housekeeping: Wiping the Counter Task Components
1 Open cabinet to access wipe container. 2 Remove wipe from container. 3 Close cabinet. 4 Walk to counter with wipe. 5 Find nearest corner of counter. 6 Orient body so corner is at the bottom left to body. 7 Wipe with big arm motion right to left or left to right. 8 Scrub spots. [move wipe in same spot 2+ times] 9 Repeat pattern until reach last corner of counter. 10 Locate trash can. 11 Throw wipe in trash. 12 Use systematic search to scan counter for large items. 13 Remove any unnecessary items.
*steps can be repeated as necessary
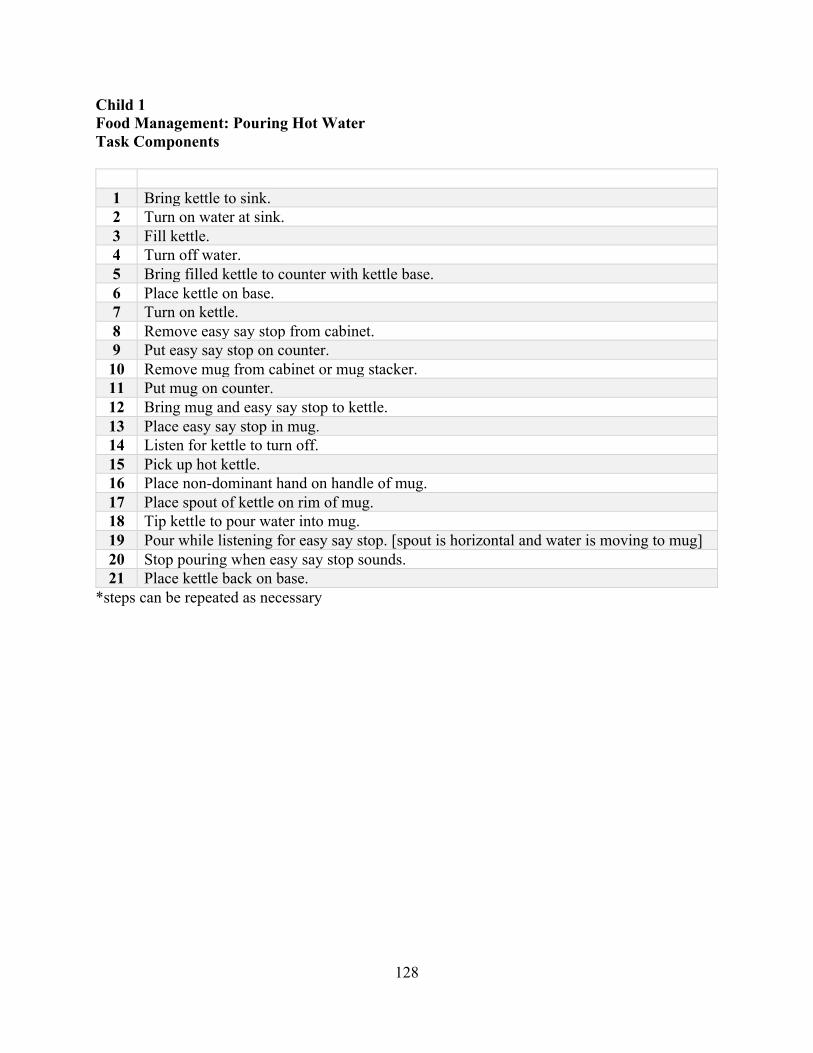
128
Child 1 Food Management: Pouring Hot Water Task Components
1 Bring kettle to sink. 2 Turn on water at sink. 3 Fill kettle. 4 Turn off water. 5 Bring filled kettle to counter with kettle base. 6 Place kettle on base. 7 Turn on kettle. 8 Remove easy say stop from cabinet. 9 Put easy say stop on counter. 10 Remove mug from cabinet or mug stacker. 11 Put mug on counter. 12 Bring mug and easy say stop to kettle. 13 Place easy say stop in mug. 14 Listen for kettle to turn off. 15 Pick up hot kettle. 16 Place non-dominant hand on handle of mug. 17 Place spout of kettle on rim of mug. 18 Tip kettle to pour water into mug. 19 Pour while listening for easy say stop. [spout is horizontal and water is moving to mug] 20 Stop pouring when easy say stop sounds. 21 Place kettle back on base.
*steps can be repeated as necessary

129
Child 1 Clothing Management: Hanging shirts Task Components
1 Locate hanger. 2 Lay shirt on table. 3 Orient shirt toward body. 4 Slip hanger inside shirt [bottom hem or neck]. 5 Slide right hand through neck of shirt. 6 Move hanger around shirt [move neck of shirt on hanger or move hand through shirt]. 7 Grab hook of hanger with hand. 8 Pull hanger by the handle up through shirt. 9 Pick up hanger and shirt off table. 10 Gently shake hanger to straighten shirt. 11 Check shirt is still on hanger. 12 Take shirt and hanger to chair/stool/table.
*steps can be repeated as necessary
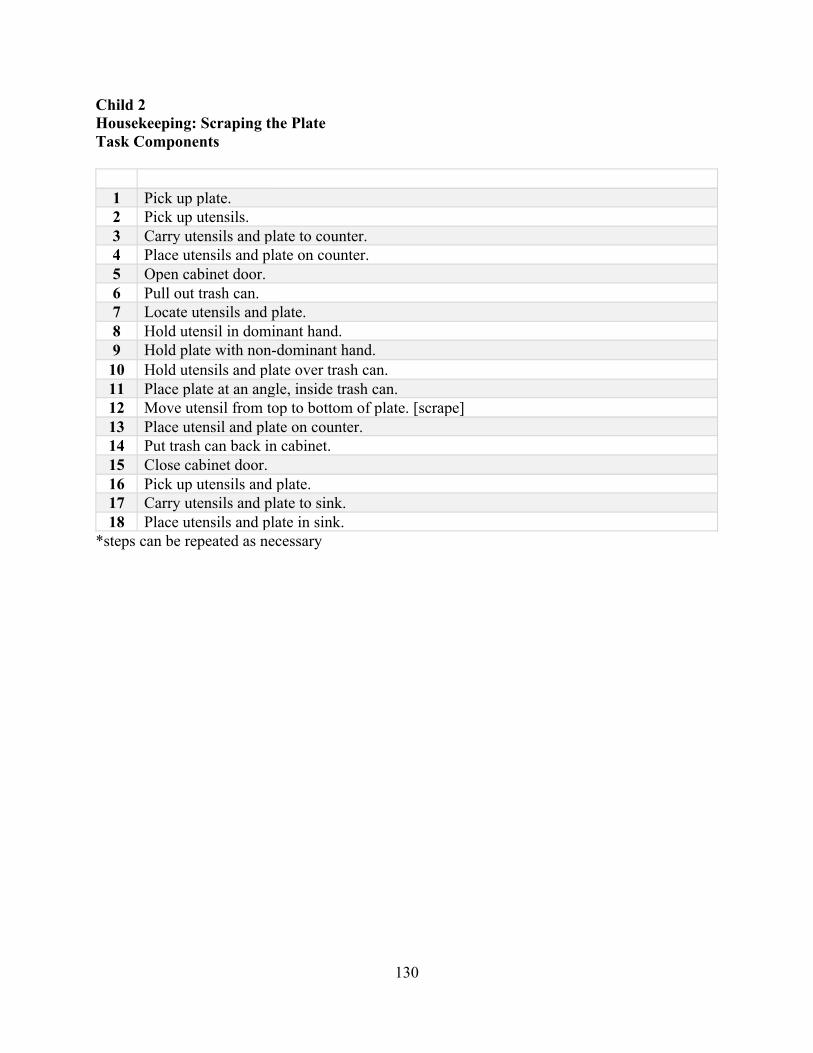
130
Child 2 Housekeeping: Scraping the Plate Task Components
1 Pick up plate. 2 Pick up utensils. 3 Carry utensils and plate to counter. 4 Place utensils and plate on counter. 5 Open cabinet door. 6 Pull out trash can. 7 Locate utensils and plate. 8 Hold utensil in dominant hand. 9 Hold plate with non-dominant hand. 10 Hold utensils and plate over trash can. 11 Place plate at an angle, inside trash can. 12 Move utensil from top to bottom of plate. [scrape] 13 Place utensil and plate on counter. 14 Put trash can back in cabinet. 15 Close cabinet door. 16 Pick up utensils and plate. 17 Carry utensils and plate to sink. 18 Place utensils and plate in sink.
*steps can be repeated as necessary
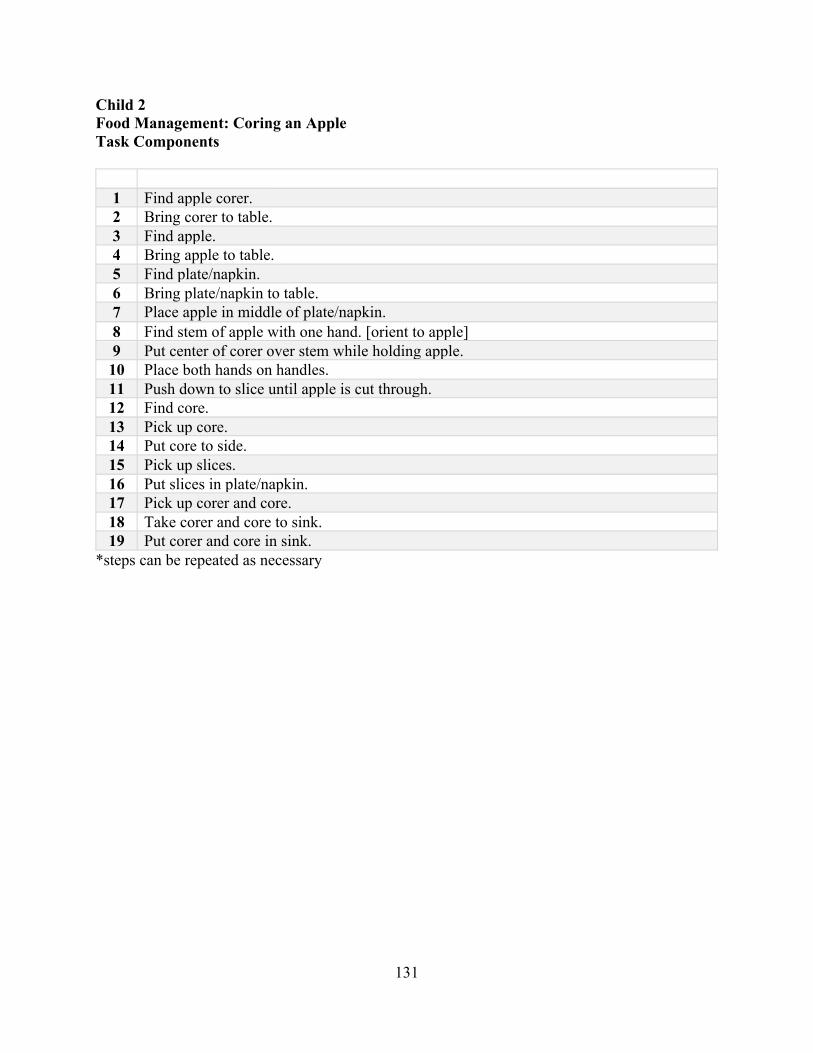
131
Child 2 Food Management: Coring an Apple Task Components
1 Find apple corer. 2 Bring corer to table. 3 Find apple. 4 Bring apple to table. 5 Find plate/napkin. 6 Bring plate/napkin to table. 7 Place apple in middle of plate/napkin. 8 Find stem of apple with one hand. [orient to apple] 9 Put center of corer over stem while holding apple. 10 Place both hands on handles. 11 Push down to slice until apple is cut through. 12 Find core. 13 Pick up core. 14 Put core to side. 15 Pick up slices. 16 Put slices in plate/napkin. 17 Pick up corer and core. 18 Take corer and core to sink. 19 Put corer and core in sink.
*steps can be repeated as necessary
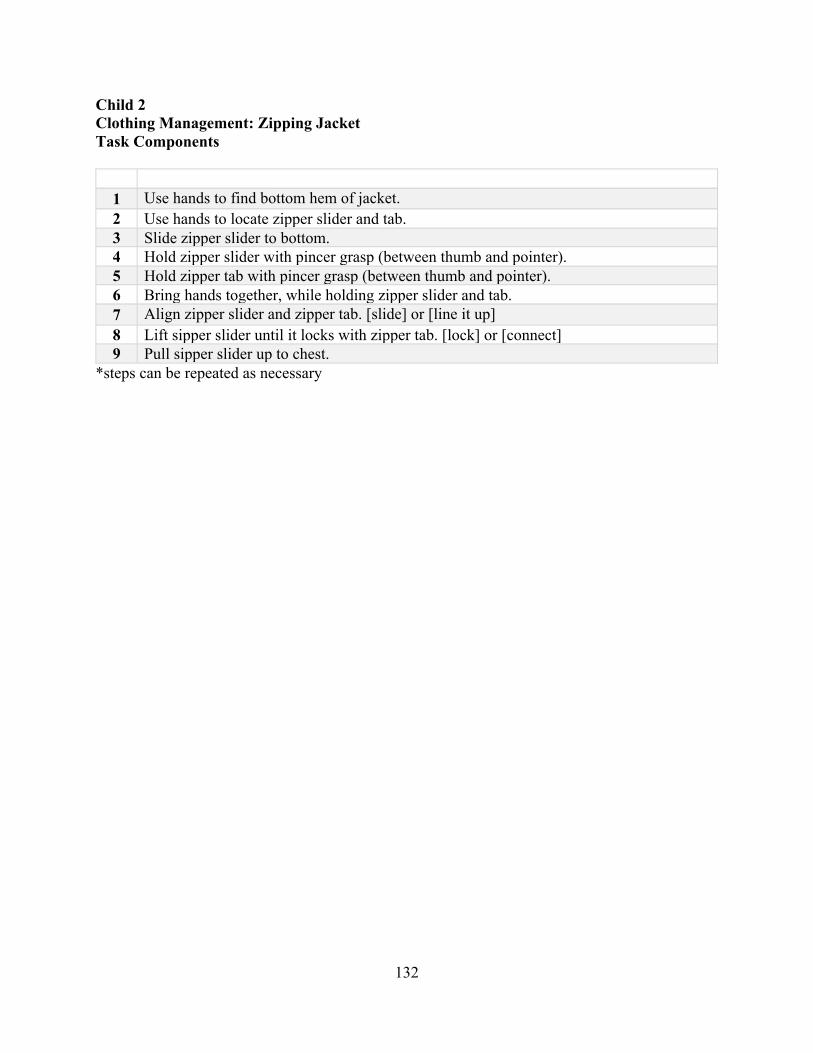
132
Child 2 Clothing Management: Zipping Jacket Task Components
1 Use hands to find bottom hem of jacket. 2 Use hands to locate zipper slider and tab. 3 Slide zipper slider to bottom. 4 Hold zipper slider with pincer grasp (between thumb and pointer). 5 Hold zipper tab with pincer grasp (between thumb and pointer). 6 Bring hands together, while holding zipper slider and tab. 7 Align zipper slider and zipper tab. [slide] or [line it up] 8 Lift sipper slider until it locks with zipper tab. [lock] or [connect] 9 Pull sipper slider up to chest.
*steps can be repeated as necessary
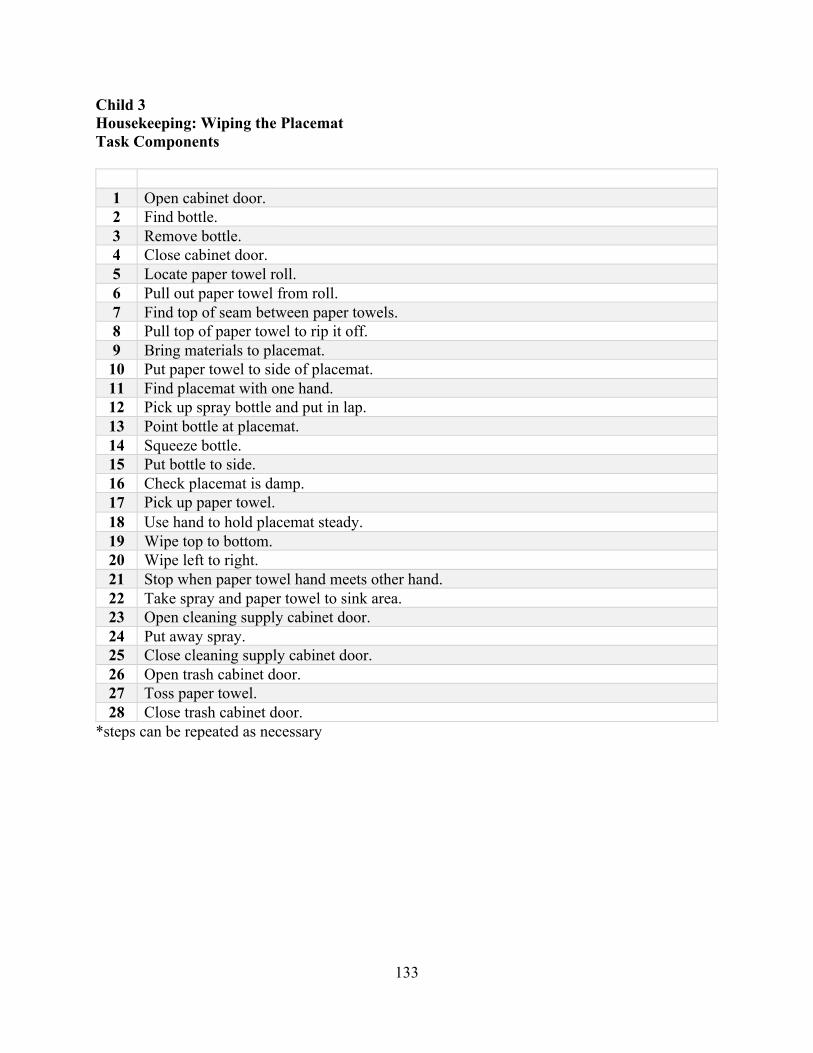
133
Child 3 Housekeeping: Wiping the Placemat Task Components
1 Open cabinet door. 2 Find bottle. 3 Remove bottle. 4 Close cabinet door. 5 Locate paper towel roll. 6 Pull out paper towel from roll. 7 Find top of seam between paper towels. 8 Pull top of paper towel to rip it off. 9 Bring materials to placemat. 10 Put paper towel to side of placemat. 11 Find placemat with one hand. 12 Pick up spray bottle and put in lap. 13 Point bottle at placemat. 14 Squeeze bottle. 15 Put bottle to side. 16 Check placemat is damp. 17 Pick up paper towel. 18 Use hand to hold placemat steady. 19 Wipe top to bottom. 20 Wipe left to right. 21 Stop when paper towel hand meets other hand. 22 Take spray and paper towel to sink area. 23 Open cleaning supply cabinet door. 24 Put away spray. 25 Close cleaning supply cabinet door. 26 Open trash cabinet door. 27 Toss paper towel. 28 Close trash cabinet door.
*steps can be repeated as necessary
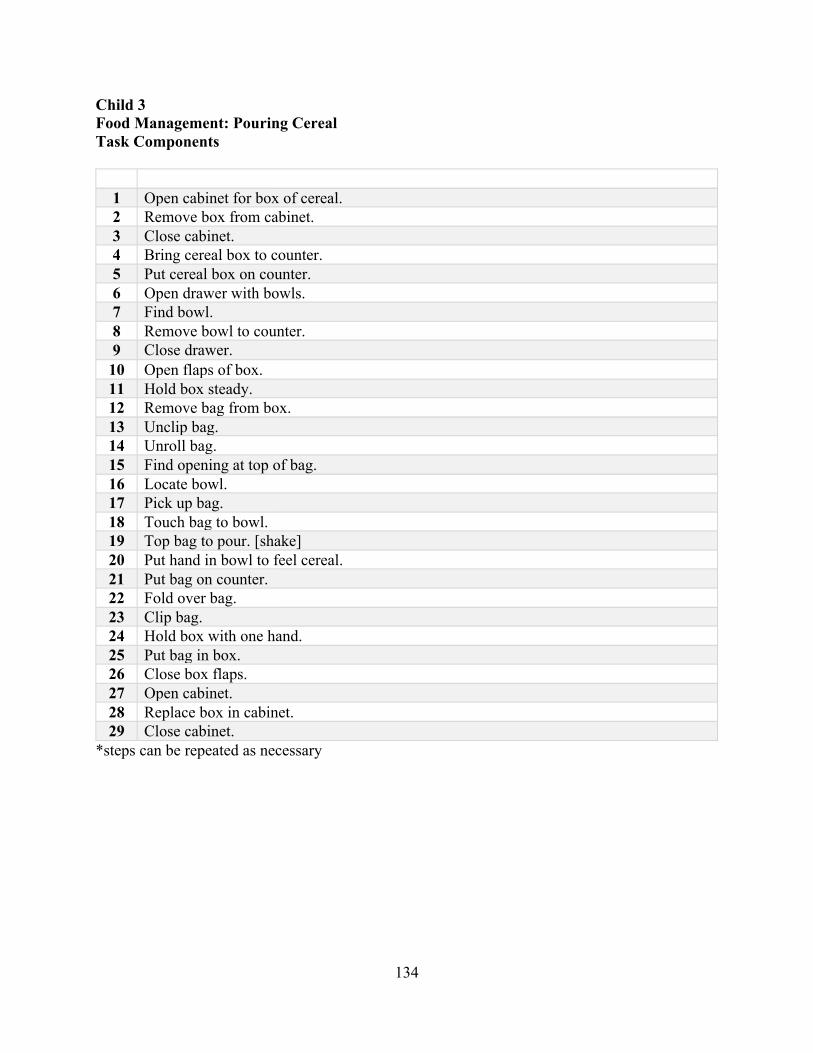
134
Child 3 Food Management: Pouring Cereal Task Components
1 Open cabinet for box of cereal. 2 Remove box from cabinet. 3 Close cabinet. 4 Bring cereal box to counter. 5 Put cereal box on counter. 6 Open drawer with bowls. 7 Find bowl. 8 Remove bowl to counter. 9 Close drawer. 10 Open flaps of box. 11 Hold box steady. 12 Remove bag from box. 13 Unclip bag. 14 Unroll bag. 15 Find opening at top of bag. 16 Locate bowl. 17 Pick up bag. 18 Touch bag to bowl. 19 Top bag to pour. [shake] 20 Put hand in bowl to feel cereal. 21 Put bag on counter. 22 Fold over bag. 23 Clip bag. 24 Hold box with one hand. 25 Put bag in box. 26 Close box flaps. 27 Open cabinet. 28 Replace box in cabinet. 29 Close cabinet.
*steps can be repeated as necessary
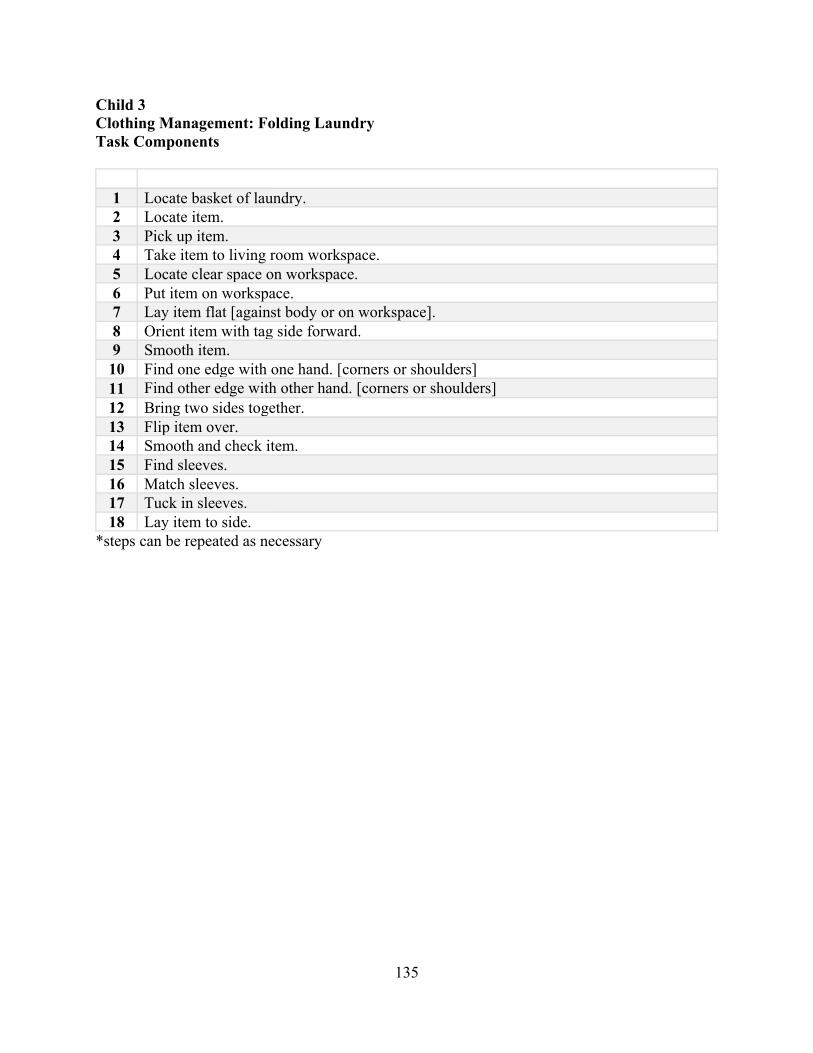
135
Child 3 Clothing Management: Folding Laundry Task Components
1 Locate basket of laundry. 2 Locate item. 3 Pick up item. 4 Take item to living room workspace. 5 Locate clear space on workspace. 6 Put item on workspace. 7 Lay item flat [against body or on workspace]. 8 Orient item with tag side forward. 9 Smooth item. 10 Find one edge with one hand. [corners or shoulders] 11 Find other edge with other hand. [corners or shoulders] 12 Bring two sides together. 13 Flip item over. 14 Smooth and check item. 15 Find sleeves. 16 Match sleeves. 17 Tuck in sleeves. 18 Lay item to side.
*steps can be repeated as necessary
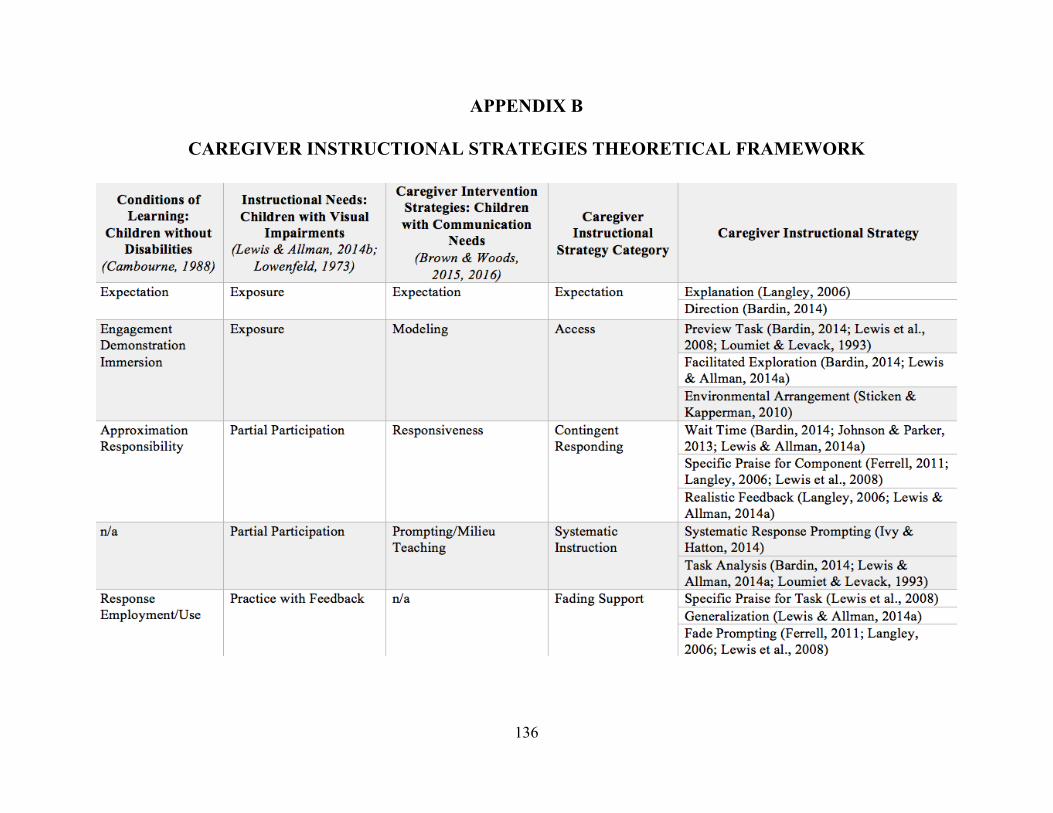
136
APPENDIX B
CAREGIVER INSTRUCTIONAL STRATEGIES THEORETICAL FRAMEWORK
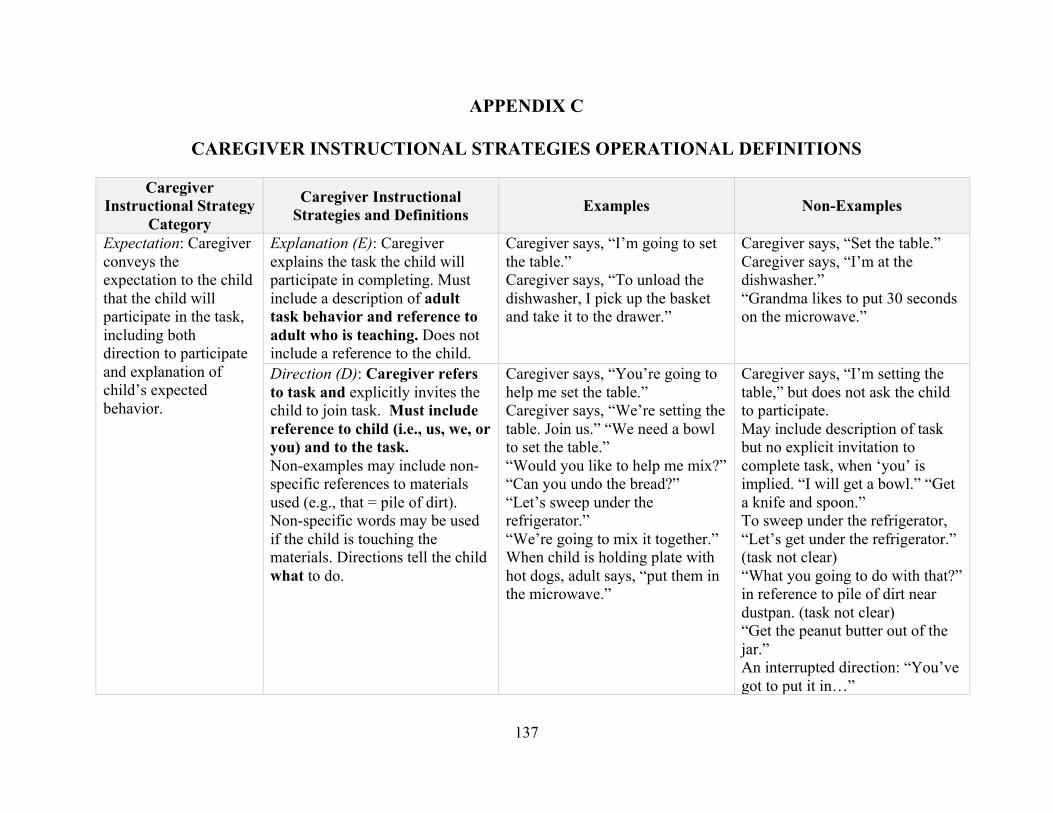
137
APPENDIX C
CAREGIVER INSTRUCTIONAL STRATEGIES OPERATIONAL DEFINITIONS
Caregiver Instructional Strategy
Category
Caregiver Instructional Strategies and Definitions Examples Non-Examples
Expectation: Caregiver conveys the expectation to the child that the child will participate in the task, including both direction to participate and explanation of child’s expected behavior.
Explanation (E): Caregiver explains the task the child will participate in completing. Must include a description of adult task behavior and reference to adult who is teaching. Does not include a reference to the child.
Caregiver says, “I’m going to set the table.” Caregiver says, “To unload the dishwasher, I pick up the basket and take it to the drawer.”
Caregiver says, “Set the table.” Caregiver says, “I’m at the dishwasher.” “Grandma likes to put 30 seconds on the microwave.”
Direction (D): Caregiver refers to task and explicitly invites the child to join task. Must include reference to child (i.e., us, we, or you) and to the task. Non-examples may include non-specific references to materials used (e.g., that = pile of dirt). Non-specific words may be used if the child is touching the materials. Directions tell the child what to do.
Caregiver says, “You’re going to help me set the table.” Caregiver says, “We’re setting the table. Join us.” “We need a bowl to set the table.” “Would you like to help me mix?” “Can you undo the bread?” “Let’s sweep under the refrigerator.” “We’re going to mix it together.” When child is holding plate with hot dogs, adult says, “put them in the microwave.”
Caregiver says, “I’m setting the table,” but does not ask the child to participate. May include description of task but no explicit invitation to complete task, when ‘you’ is implied. “I will get a bowl.” “Get a knife and spoon.” To sweep under the refrigerator, “Let’s get under the refrigerator.” (task not clear) “What you going to do with that?” in reference to pile of dirt near dustpan. (task not clear) “Get the peanut butter out of the jar.” An interrupted direction: “You’ve got to put it in…”
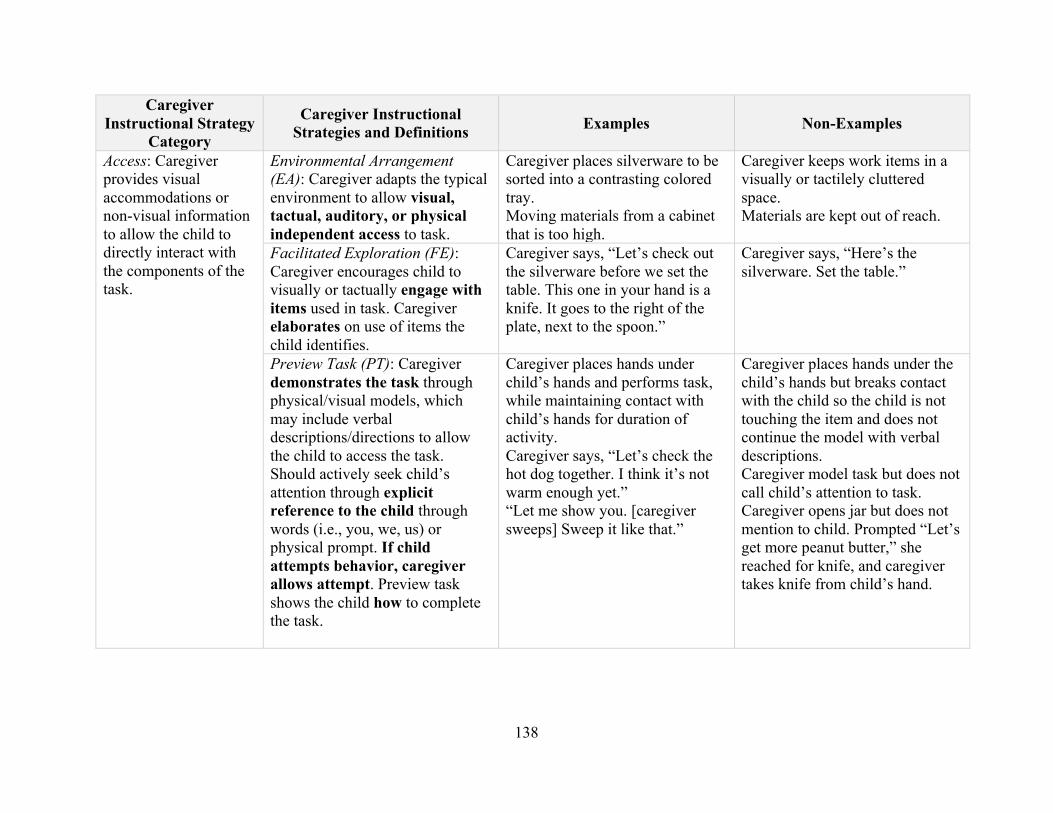
138
Caregiver Instructional Strategy
Category
Caregiver Instructional Strategies and Definitions Examples Non-Examples
Access: Caregiver provides visual accommodations or non-visual information to allow the child to directly interact with the components of the task.
Environmental Arrangement (EA): Caregiver adapts the typical environment to allow visual, tactual, auditory, or physical independent access to task.
Caregiver places silverware to be sorted into a contrasting colored tray. Moving materials from a cabinet that is too high.
Caregiver keeps work items in a visually or tactilely cluttered space. Materials are kept out of reach.
Facilitated Exploration (FE): Caregiver encourages child to visually or tactually engage with items used in task. Caregiver elaborates on use of items the child identifies.
Caregiver says, “Let’s check out the silverware before we set the table. This one in your hand is a knife. It goes to the right of the plate, next to the spoon.”
Caregiver says, “Here’s the silverware. Set the table.”
Preview Task (PT): Caregiver demonstrates the task through physical/visual models, which may include verbal descriptions/directions to allow the child to access the task. Should actively seek child’s attention through explicit reference to the child through words (i.e., you, we, us) or physical prompt. If child attempts behavior, caregiver allows attempt. Preview task shows the child how to complete the task.
Caregiver places hands under child’s hands and performs task, while maintaining contact with child’s hands for duration of activity. Caregiver says, “Let’s check the hot dog together. I think it’s not warm enough yet.” “Let me show you. [caregiver sweeps] Sweep it like that.”
Caregiver places hands under the child’s hands but breaks contact with the child so the child is not touching the item and does not continue the model with verbal descriptions. Caregiver model task but does not call child’s attention to task. Caregiver opens jar but does not mention to child. Prompted “Let’s get more peanut butter,” she reached for knife, and caregiver takes knife from child’s hand.
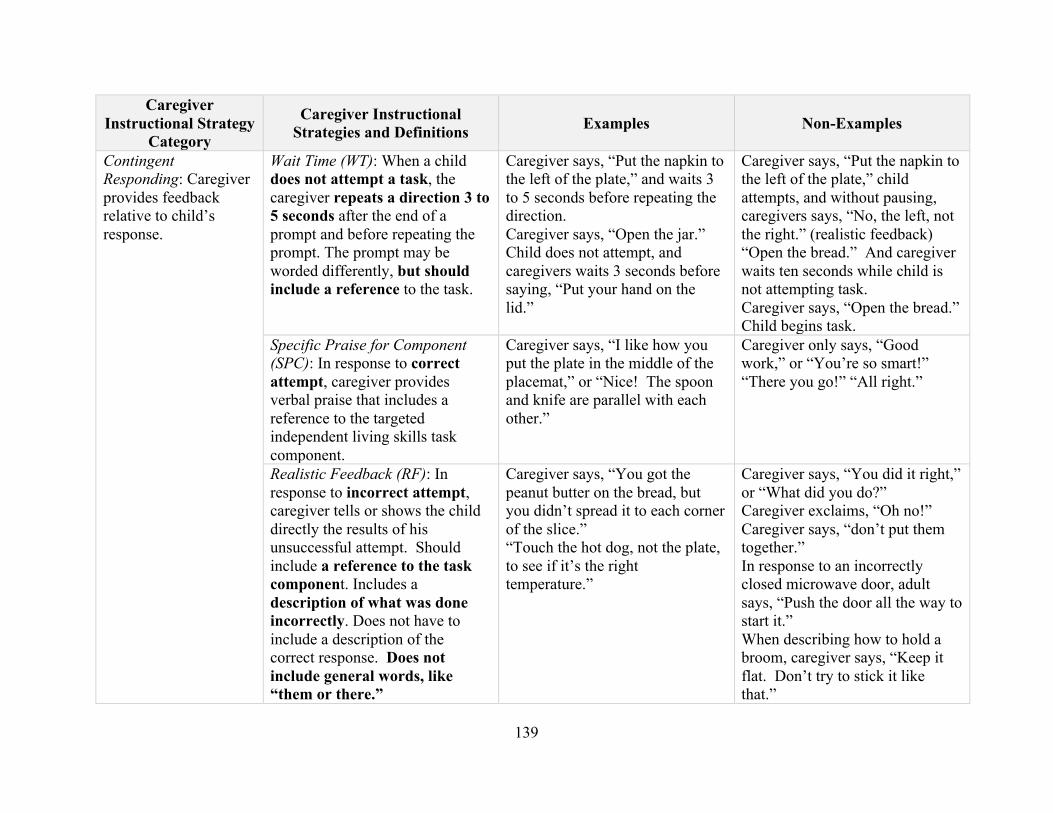
139
Caregiver Instructional Strategy
Category
Caregiver Instructional Strategies and Definitions Examples Non-Examples
Contingent Responding: Caregiver provides feedback relative to child’s response.
Wait Time (WT): When a child does not attempt a task, the caregiver repeats a direction 3 to 5 seconds after the end of a prompt and before repeating the prompt. The prompt may be worded differently, but should include a reference to the task.
Caregiver says, “Put the napkin to the left of the plate,” and waits 3 to 5 seconds before repeating the direction. Caregiver says, “Open the jar.” Child does not attempt, and caregivers waits 3 seconds before saying, “Put your hand on the lid.”
Caregiver says, “Put the napkin to the left of the plate,” child attempts, and without pausing, caregivers says, “No, the left, not the right.” (realistic feedback) “Open the bread.” And caregiver waits ten seconds while child is not attempting task. Caregiver says, “Open the bread.” Child begins task.
Specific Praise for Component (SPC): In response to correct attempt, caregiver provides verbal praise that includes a reference to the targeted independent living skills task component.
Caregiver says, “I like how you put the plate in the middle of the placemat,” or “Nice! The spoon and knife are parallel with each other.”
Caregiver only says, “Good work,” or “You’re so smart!” “There you go!” “All right.”
Realistic Feedback (RF): In response to incorrect attempt, caregiver tells or shows the child directly the results of his unsuccessful attempt. Should include a reference to the task component. Includes a description of what was done incorrectly. Does not have to include a description of the correct response. Does not include general words, like “them or there.”
Caregiver says, “You got the peanut butter on the bread, but you didn’t spread it to each corner of the slice.” “Touch the hot dog, not the plate, to see if it’s the right temperature.”
Caregiver says, “You did it right,” or “What did you do?” Caregiver exclaims, “Oh no!” Caregiver says, “don’t put them together.” In response to an incorrectly closed microwave door, adult says, “Push the door all the way to start it.” When describing how to hold a broom, caregiver says, “Keep it flat. Don’t try to stick it like that.”
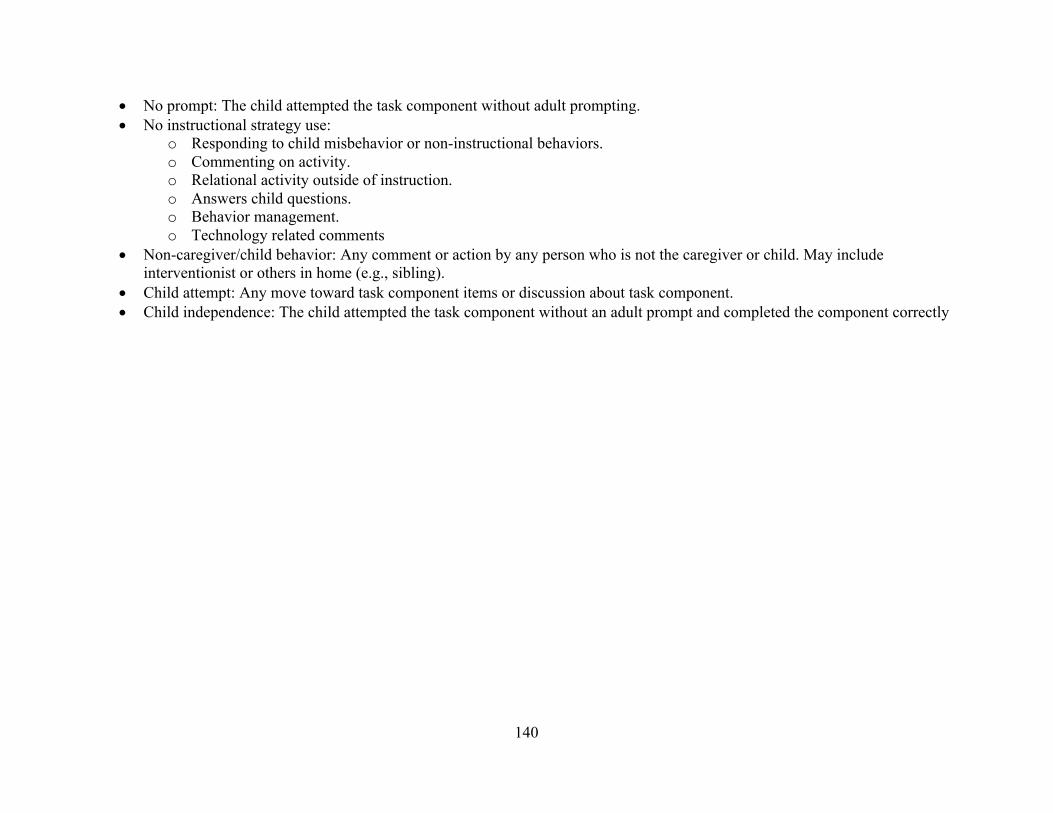
140
• No prompt: The child attempted the task component without adult prompting. • No instructional strategy use:
o Responding to child misbehavior or non-instructional behaviors. o Commenting on activity. o Relational activity outside of instruction. o Answers child questions. o Behavior management. o Technology related comments
• Non-caregiver/child behavior: Any comment or action by any person who is not the caregiver or child. May include interventionist or others in home (e.g., sibling).
• Child attempt: Any move toward task component items or discussion about task component. • Child independence: The child attempted the task component without an adult prompt and completed the component correctly
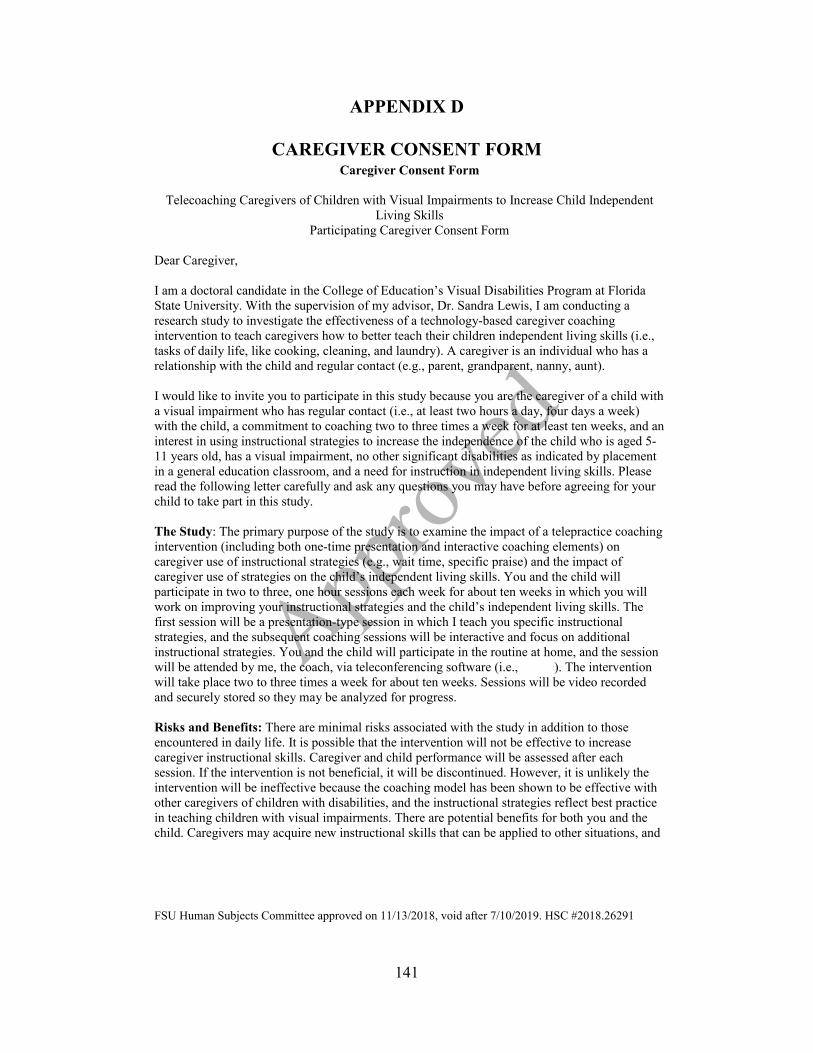
141
APPENDIX D
CAREGIVER CONSENT FORM
Caregiver Consent Form
Telecoaching Caregivers of Children with Visual Impairments to Increase Child Independent Living Skills
Participating Caregiver Consent Form Dear Caregiver, I am a doctoral candidate in the College of Education’s Visual Disabilities Program at Florida State University. With the supervision of my advisor, Dr. Sandra Lewis, I am conducting a research study to investigate the effectiveness of a technology-based caregiver coaching intervention to teach caregivers how to better teach their children independent living skills (i.e., tasks of daily life, like cooking, cleaning, and laundry). A caregiver is an individual who has a relationship with the child and regular contact (e.g., parent, grandparent, nanny, aunt). I would like to invite you to participate in this study because you are the caregiver of a child with a visual impairment who has regular contact (i.e., at least two hours a day, four days a week) with the child, a commitment to coaching two to three times a week for at least ten weeks, and an interest in using instructional strategies to increase the independence of the child who is aged 5-11 years old, has a visual impairment, no other significant disabilities as indicated by placement in a general education classroom, and a need for instruction in independent living skills. Please read the following letter carefully and ask any questions you may have before agreeing for your child to take part in this study. The Study: The primary purpose of the study is to examine the impact of a telepractice coaching intervention (including both one-time presentation and interactive coaching elements) on caregiver use of instructional strategies (e.g., wait time, specific praise) and the impact of caregiver use of strategies on the child’s independent living skills. You and the child will participate in two to three, one hour sessions each week for about ten weeks in which you will work on improving your instructional strategies and the child’s independent living skills. The first session will be a presentation-type session in which I teach you specific instructional strategies, and the subsequent coaching sessions will be interactive and focus on additional instructional strategies. You and the child will participate in the routine at home, and the session will be attended by me, the coach, via teleconferencing software (i.e., Skype). The intervention will take place two to three times a week for about ten weeks. Sessions will be video recorded and securely stored so they may be analyzed for progress. Risks and Benefits: There are minimal risks associated with the study in addition to those encountered in daily life. It is possible that the intervention will not be effective to increase caregiver instructional skills. Caregiver and child performance will be assessed after each session. If the intervention is not beneficial, it will be discontinued. However, it is unlikely the intervention will be ineffective because the coaching model has been shown to be effective with other caregivers of children with disabilities, and the instructional strategies reflect best practice in teaching children with visual impairments. There are potential benefits for both you and the child. Caregivers may acquire new instructional skills that can be applied to other situations, and
FSU Human Subjects Committee approved on 11/13/2018, void after 7/10/2019. HSC #2018.26291
Approv
ed
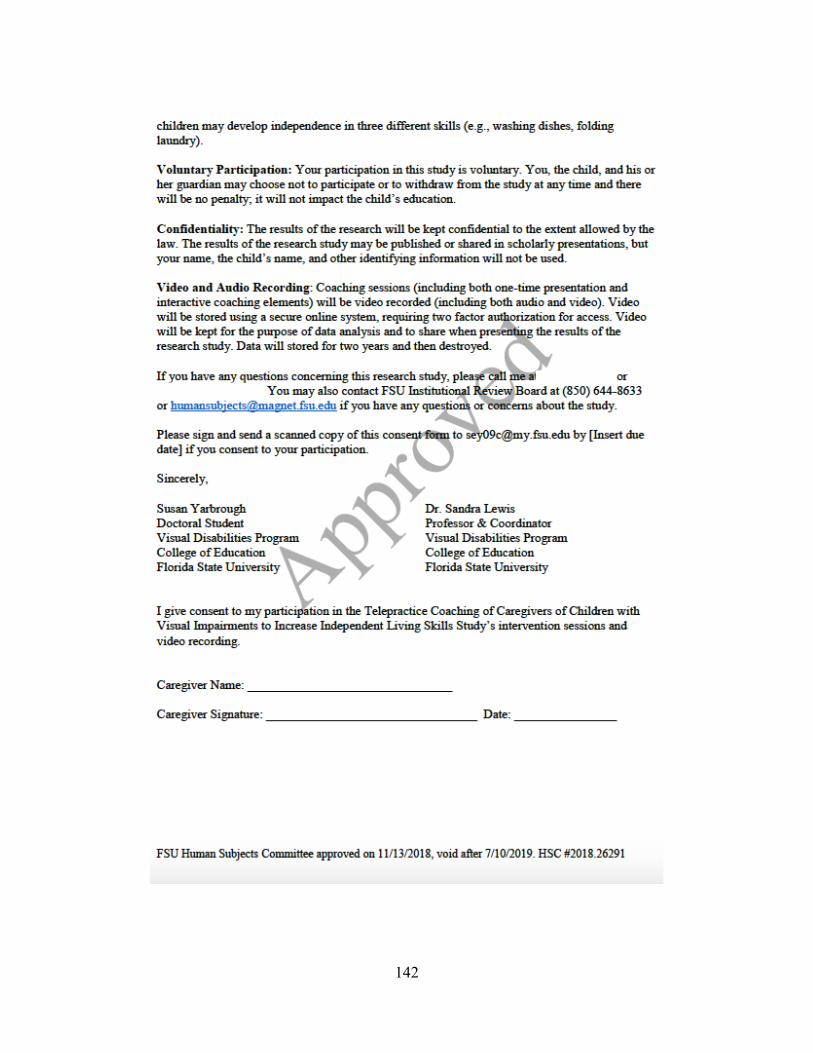
142
143
APPENDIX E
CHILD CONSENT FORM
Child Consent Form
Telecoaching Caregivers of Children with Visual Impairments to Increase Child Independent Living Skills
Guardian of Minor Child Participation Consent Form Dear Guardian, I am a doctoral candidate in the College of Education’s Visual Disabilities Program at Florida State University. With the supervision of my advisor, Dr. Sandra Lewis, I am conducting a research study to investigate the effectiveness of a technology-based caregiver coaching intervention to teach caregivers how to better teach their children independent living skills (i.e., tasks of daily life like cooking, cleaning, and laundry). I would like to invite your child to participate in the study because he or she is aged 5-11 years old, has a visual impairment, no other significant disabilities as indicated by placement in a general education classroom, and a need for instruction in independent living skills. Please read the following letter carefully and ask any questions you may have before agreeing for your child to take part in this study. The Study: The primary purpose of the study is to examine the impact of a telepractice coaching intervention (including both one-time presentation and interactive coaching elements) on caregiver use of instructional strategies (e.g., wait time, specific praise) and the impact of caregiver use of strategies on the child’s independent living skills. A caregiver and your child will participate in two to three, one hour sessions each week for about ten weeks in which they work on improving instructional strategies and independent living skills. The first session will be a presentation-type session in which I teach you specific instructional strategies, and the subsequent coaching sessions will be interactive and focus on additional instructional strategies. The caregiver and child will participate in the routine at home, and the session will be attended by me, the coach, via teleconferencing software (i.e., Skype). The intervention will take place two to three times a week for about ten weeks. Sessions will be video recorded and securely stored so they may be analyzed for progress. Risks and Benefits: There are minimal risks associated with the study in addition to those encountered in daily life. It is possible that the intervention will not be effective to increase caregiver instructional skills. Caregiver and child performance will be assessed after each session. If the intervention is not beneficial, it will be discontinued. It is unlikely the intervention will be ineffective because the coaching model has been shown to be effective with other caregivers of children with disabilities, and the instructional strategies reflect best practice in teaching children with visual impairments. There are potential benefits for both your child and the selected caregiver. Caregivers may acquire new instructional skills that can be applied to other situations, and children may develop independence in three different skills (e.g., washing dishes, folding laundry). Voluntary Participation: Your child’s participation is voluntary. You may choose to discontinue your child’s participation at any time. Your child and the caregiver may also choose to withdraw at any time. There will be no penalty. Withdrawing will not impact your child’s education.
FSU Human Subjects Committee approved on 11/13/2018, void after 7/10/2019. HSC #2018.26291
Approv
ed
144
145
APPENDIX F
CHILD ASSENT FORM
Child Assent Form
Telecoaching Caregivers of Children with Visual Impairments to Increase Child Independent Living Skills
Child Participation Assent Form
Dear Student, My name is Susan Yarbrough. I am a student Florida State University. I would like to help me with a research study about how people who take care of you, like your parents or babysitter, teach you to do more things by yourself. We call those people who help you caregivers. If you agree to be part of the study, I will teach your caregiver some tips for helping you learn, and you will get to learn how to do three new skills, like setting the table or folding your clothes. You’ll practice these skills at home, and your caregiver and I will chat on the computer two to three times a week for about ten weeks. You may not know how to do the things that your caregiver asks you to do, and that is okay. This study may help your caregiver and others learn better ways to teach you or other students who are visually impaired. Think about whether or not you want to participate in this study. Then, ask your caregiver and parents to give their permission for you to participate in the study. Even if your parents said “yes” to this study, you can still decide you do not want to participate, and that will be fine. If you do not want to be in this study, then you do not have to participate. This study is voluntary, which means that you decide whether to take part in the study. Being in this study is up to you, and no one will be upset in any way if you do not want to participate or even if you change your mind later and want to stop participating. You can ask any questions that you have about this study. If you have a question later that you did not think of now, you can ask me next time. Sincerely, Susan Yarbrough Dr. Sandra Lewis Doctoral Student Professor & Coordinator Visual Disabilities Program Visual Disabilities Program College of Education College of Education Florida State University Florida State University Continuing to participate means that you agree to help with the sessions and video recording described above. You and your parents will get a copy of this form.
FSU Human Subjects Committee approved on 11/13/2018, void after 7/10/2019. HSC #2018.26291
Approv
ed
146
APPENDIX G
SKILLS SCREENING AND DEMOGRAPHIC DATA SCRIPT
Skills Screening and Demographic Data Script
Date: ________________________________ Hello [caregiver name] How are you today? It’s Susan. Is this a good time for you to talk? � Yes (continue) � No, Please call back at ___________________________________ (Stop) Thank you for consenting to participate. Have you had a chance to complete the School Readiness Checklist and the Independent Living Skills Selection? � Yes (continue) � No, please call back after I’ve had a chance to complete it: ______________________ (Stop) Let’s start with the School Readiness Checklist: Did you have questions about how to score any of the skills? � Yes � No How many skills in both categories has your child consistently demonstrated? Remember, consistently demonstrated means he/she has done the skills at least three times without help. ___ / 20 skills If fewer than 16 skills are independently demonstrated, your child may not be a good fit for this study. Now, let’s discuss the Independent Livings Skills Selection: Did you have questions about how to score any of the skills? � Yes � No
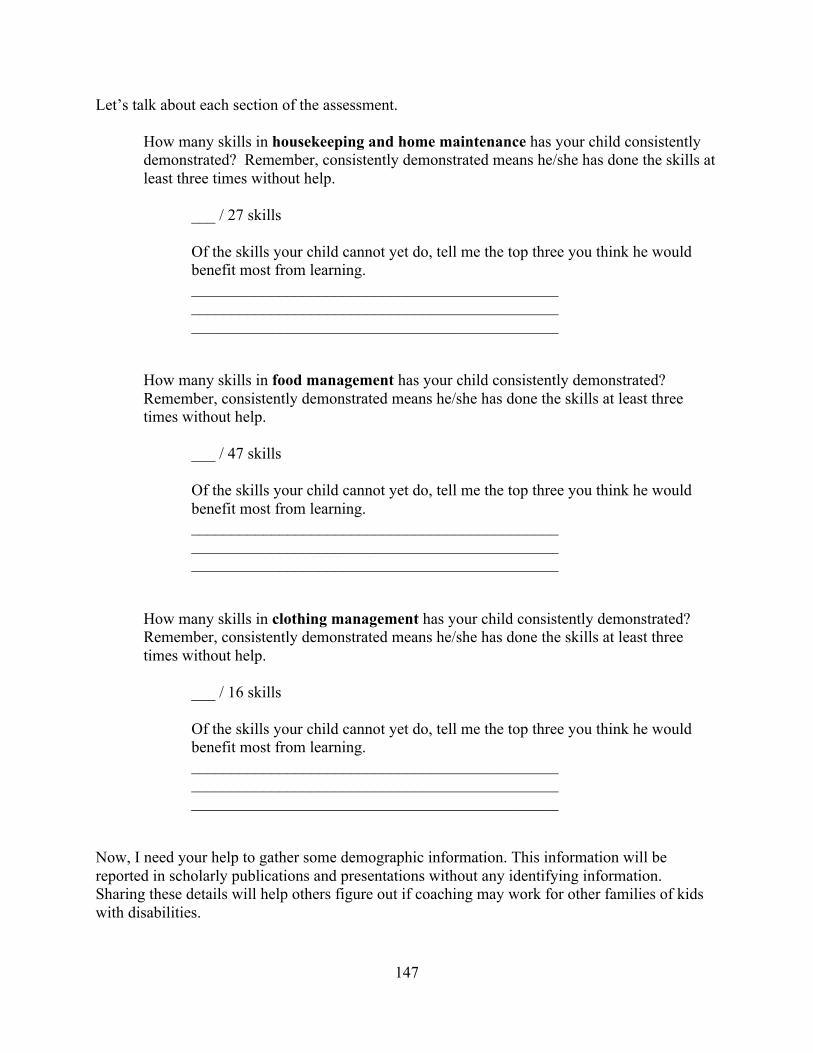
147
Let’s talk about each section of the assessment.
How many skills in housekeeping and home maintenance has your child consistently demonstrated? Remember, consistently demonstrated means he/she has done the skills at least three times without help.
___ / 27 skills Of the skills your child cannot yet do, tell me the top three you think he would benefit most from learning. ______________________________________________ ______________________________________________ ______________________________________________
How many skills in food management has your child consistently demonstrated? Remember, consistently demonstrated means he/she has done the skills at least three times without help.
___ / 47 skills Of the skills your child cannot yet do, tell me the top three you think he would benefit most from learning. ______________________________________________ ______________________________________________ ______________________________________________
How many skills in clothing management has your child consistently demonstrated? Remember, consistently demonstrated means he/she has done the skills at least three times without help.
___ / 16 skills Of the skills your child cannot yet do, tell me the top three you think he would benefit most from learning. ______________________________________________ ______________________________________________ ______________________________________________
Now, I need your help to gather some demographic information. This information will be reported in scholarly publications and presentations without any identifying information. Sharing these details will help others figure out if coaching may work for other families of kids with disabilities.
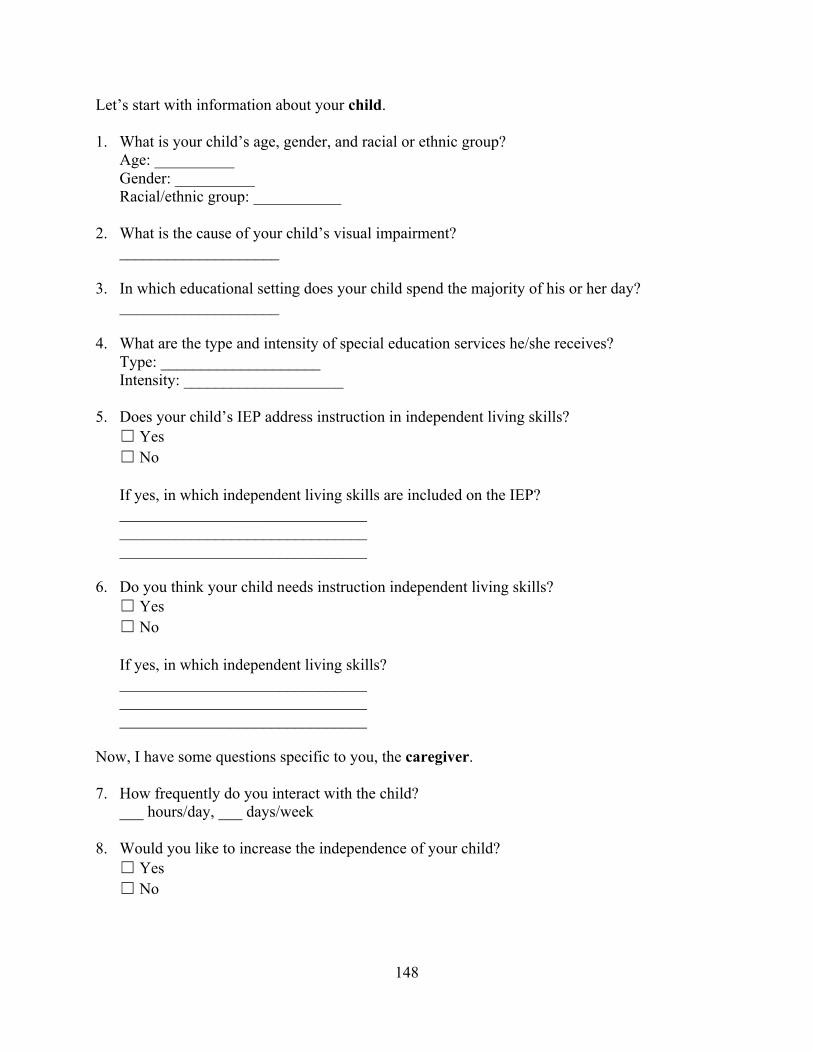
148
Let’s start with information about your child. 1. What is your child’s age, gender, and racial or ethnic group?
Age: __________ Gender: __________ Racial/ethnic group: ___________
2. What is the cause of your child’s visual impairment? ____________________
3. In which educational setting does your child spend the majority of his or her day?
____________________ 4. What are the type and intensity of special education services he/she receives?
Type: ____________________ Intensity: ____________________
5. Does your child’s IEP address instruction in independent living skills? � Yes � No If yes, in which independent living skills are included on the IEP? _______________________________ _______________________________ _______________________________
6. Do you think your child needs instruction independent living skills? � Yes � No If yes, in which independent living skills? _______________________________ _______________________________ _______________________________
Now, I have some questions specific to you, the caregiver.
7. How frequently do you interact with the child?
___ hours/day, ___ days/week
8. Would you like to increase the independence of your child? � Yes � No
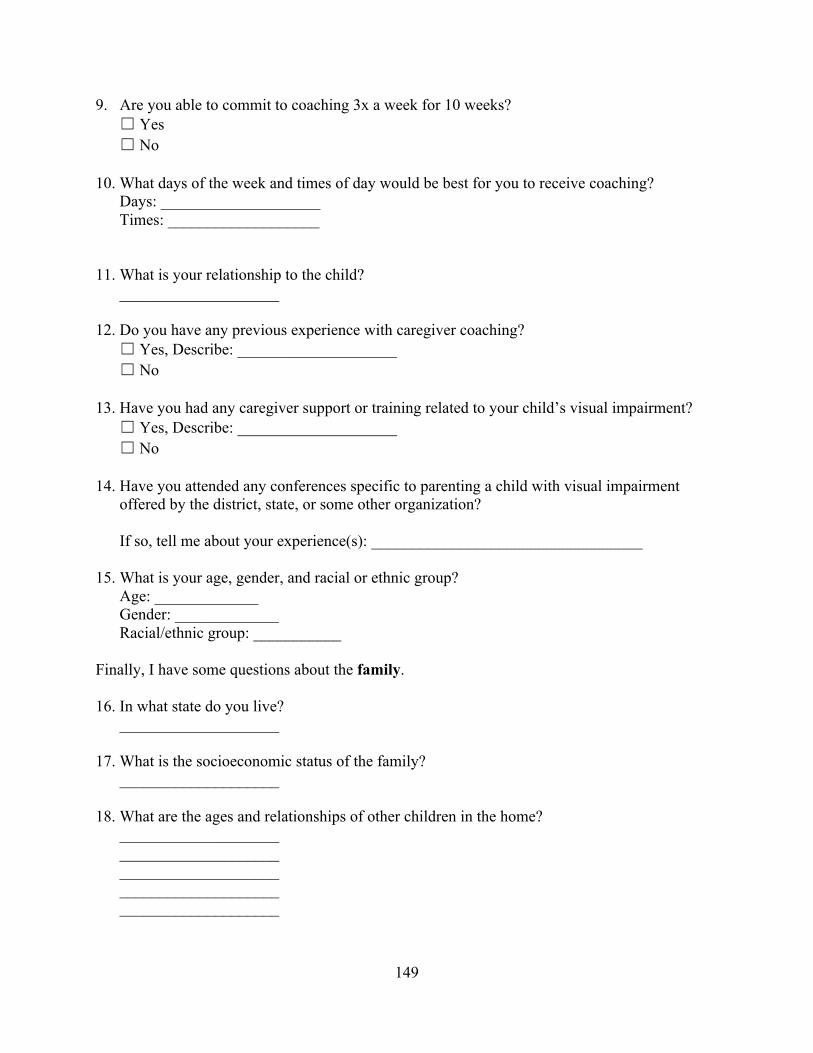
149
9. Are you able to commit to coaching 3x a week for 10 weeks? � Yes � No
10. What days of the week and times of day would be best for you to receive coaching? Days: ____________________ Times: ___________________
11. What is your relationship to the child?
____________________
12. Do you have any previous experience with caregiver coaching? � Yes, Describe: ____________________ � No
13. Have you had any caregiver support or training related to your child’s visual impairment? � Yes, Describe: ____________________ � No
14. Have you attended any conferences specific to parenting a child with visual impairment offered by the district, state, or some other organization? If so, tell me about your experience(s): __________________________________
15. What is your age, gender, and racial or ethnic group? Age: _____________ Gender: _____________ Racial/ethnic group: ___________
Finally, I have some questions about the family. 16. In what state do you live?
____________________
17. What is the socioeconomic status of the family? ____________________
18. What are the ages and relationships of other children in the home?
____________________ ____________________ ____________________ ____________________ ____________________
150
End of Script Thank you so much for your time, that’s all the questions I have today. Let’s set up a time to meet for our next session. When would you like to meet? Day: __________________ Time: ___________________ Okay, we will see you (review meeting time). Do you have any questions for me at this time? If there is an emergency and you need to reschedule, you can email me at ______________________ or call me at _________________________. Thank you so much for your time today. Have a great day! (Stop) COMPLETE DURING PHONE CALL: Person Called: Contact Number: Date /Time: Person Making Contact: Notes:
151
APPENDIX H
IRB APPROVAL LETTERS
Office of the Vice President For Research Human Subjects Committee Tallahassee, Florida 32306-2742 (850) 644-8673 · FAX (850) 644-4392 APPROVAL MEMORANDUM Date: To: Address: Dept.: From: Thomas L. Jacobson, Chair Re: Use of Human Subjects in Research The application that you submitted to this office in regard to the use of human subjects in the research proposal referenced above has been reviewed by the Human Subjects Committee at its meeting on Your project was approved by the Committee. The Human Subjects Committee has not evaluated your proposal for scientific merit, except to weigh the risk to the human participants and the aspects of the proposal related to potential risk and benefit. This approval does not replace any departmental or other approvals which may be required. If you submitted a proposed consent form with your application, the approved stamped consent form is attached to this approval notice. Only the stamped version of the consent form may be used in recruiting research subjects. If the project has not been completed by you must request a renewal of approval for continuation of the project. As a courtesy, a renewal notice will be sent to you prior to your expiration date; however, it is your responsibility as the Principal Investigator to timely request renewal of your approval from the Committee. You are advised that any change in protocol for this project must be reviewed and approved by the Committee prior to implementation of the proposed change in the protocol. A protocol change/amendment form is required to be submitted for approval by the Committee. In addition, federal regulations require that the Principal Investigator promptly report, in writing, any unanticipated problems or adverse events involving risks to research subjects or others. By copy of this memorandum, the chairman of your department and/or your major professor is reminded that he/she is responsible for being informed concerning research projects involving human subjects in the department, and should review protocols as often as needed to insure that the project is being conducted in compliance with our institution and with DHHS regulations. This institution has an Assurance on file with the Office for Human Research Protection. The Assurance Number is IRB00000446. Cc: HSC No.
Susan Yarbrough <[email protected]>
2205B Stone Building, 1114 W. Call Street, Tallahassee, FL, 32306
SPECIAL EDUCATION & REHABILITATION COUNSELING
Telecoaching Caregivers of Children with Visual Impairments to Increase Child Independent Living Skills
07/10/2019
2018.25126
08/21/2018
07/11/2018
Sandra Lewis <[email protected]>, Advisor
152
Office of the Vice President For Research Human Subjects Committee P O Box 3062742 Tallahassee, Florida 32306-2742 (850) 644-8673 · FAX (850) 644-4392 APPROVAL MEMORANDUM (for change in research protocol) Date: To: Address: Dept: From: Thomas L. Jacobson, Chair Re: Use of Human subjects in Research Project entitled: The application that you submitted to this office in regard to the requested change/amendment to your research protocol for the above-referenced project has been reviewed and approved. Please be reminded that if the project has not been completed by , you must request renewed approval for continuation of the project. By copy of this memorandum, the chairman of your department and/or your major professor is reminded that he/she is responsible for being informed concerning research projects involving human subjects in the department, and should review protocols as often as needed to insure that the project is being conducted in compliance with our institution and with DHHS regulations. This institution has an Assurance on file with the Office for Human Research Protection. The Assurance Number is IRB00000446. Cc: HSC NO.
11/13/2018
Susan Yarbrough <[email protected]>
2205B Stone Building, 1114 W. Call Street, Tallahassee, FL, 32306
SPECIAL EDUCATION & REHABILITATION COUNSELING
Telecoaching Caregivers of Children with Visual Impairments to Increase Child Independent LivingSkills
07/10/2019
2018.26291Sandra Lewis <[email protected]>, Advisor
153
APPENDIX I
TEACHER RECRUITMENT MESSAGE Dear fellow teacher, I am contacting you all because I am recruiting participants for a research study at Florida State University, and I hope you will be able to help. I will use Internet-based coaching techniques to attempt to increase the capacity of caregivers of children with visual impairments so that those caregivers will be better prepared to teach their children independent living skills at home. By the end of the intervention, I hope the caregivers will acquire new instructional skills and the children will master specific independent living skills tasks. I plan to work with a specific group of children and their caregivers. Children should:
• be 5 to 11 years old • are tactual learners who participate in a braille literacy program • have no other significant disabilities, as indicated by an educational placement in a
general education setting • need instruction in independent living skills
Caregivers should: • be biological, adoptive, fostered, or paid • have contact with the child in the home at least 4 days a week for 2 hours a day • be committed to coaching 2 to 3 times a week for at least 10 weeks • be interested in implementing coached strategies to increase child independence
Because I will use Internet-based software, like XXXX, to deliver the coaching sessions, interested participants can live anywhere in the United States. However, they should have a mobile device (laptop, tablet computer, or cell phone) and reliable access to wireless Internet in the home. If you believe you know of a caregiver and child who may benefit from this intervention, meet the criteria, and would be interested in participating, please pass along my contact information and ask caregivers and/or the child’s legal guardians to contact me directly. Thank you, Susan Yarbrough Doctoral Candidate Visual Disabilities Program Florida State University
154
APPENDIX J
CAREGIVER RECRUITMENT MESSAGE Hello, I am recruiting participants for a research study and I hope you will be able to help. I am doing a research study at Florida State University to determine if caregiver coaching conducted via the Internet can increase the teaching skills of caregivers of children with visual impairments. By the end of the intervention, I hope all the caregivers will develop new instructional skills, like using wait time or specific praise. I also hope the children will master at least three independent living skills tasks, like setting the table or making the bed. I hope to work with a specific group of children and their caregivers. Children should:
• be 5 to 11 years old • participate in a braille literacy program • have no other significant disabilities, as indicated by an educational placement in a
general education setting • need instruction in independent living skills
Caregivers should: • be biological, adoptive, fostered, or paid • have contact with the child in the home at least 4 days a week for 2 hours a day • be committed to coaching 2 to 3 times a week for at least 10 weeks • be interested in implementing coached strategies to increase child independence
Because I will use Internet-based software, like XXXX, to deliver the coaching sessions, interested participants can live anywhere in the United States. However, they should have a mobile device (laptop, tablet computer, or cell phone) and reliable access to wireless Internet in the home. I am hoping to begin soon. If you think your child and you or another caregiver may qualify, are interested, and may benefit from Internet-based coaching of instructional skills, please contact me directly. I would be glad to tell you more about the intervention and the potential benefits to you and your child. Thank you, Susan Yarbrough Doctoral Candidate Visual Disabilities Program Florida State University
155
APPENDIX K
INCLUSION SCREENING PHONE SCRIPT
Date: ________________________________ Hello _______________ (caregiver’s name). How are you today? My name is Susan Yarbrough. I hope we can talk about the research study that you indicated through email that you may be interested in. Is this a good time for you to talk? � Yes (continue) � No, Please call back at ___________________________________ (Stop) This research project is about working with caregivers using Internet-based coaching to do two things: increase the teaching skills of caregivers and the independent living skills of their children. I hope to begin this project very soon, and expect the project will take 4-5 months to complete. I would want you to participate in one hour sessions, three times a week. During those sessions, you and your child will participate in independent living skills routines. We’ll use software like XXXX to chat about strategies for teaching your child. You’ll show me how you teach, and then I’ll give you feedback to help improve your teaching. I will give you all the details before I ask if you would like to participate, but for now, I would like to know if you are interested. If you’re still interested, I have a few questions for you to see if your child will qualify for the study. Are you still interested and can I ask you a few questions? � No, I’m not interested
Well thank you very much for your time. I hope that this school year is a good one. Have a good day. (Stop)
� Yes, I’m still interested Great! If you have any questions for me, feel free to ask them at anytime. Ready? Questions 19. Is your child between the ages of 5 and 11? � Yes (continue with questions) � No (skip to the end of phone script)
20. Does your child have a visual impairment? � Yes (continue with questions) � No (skip to the end of phone script)
21. Does your child participate in a braille literacy program? � Yes (continue with questions) � No (skip to the end of phone script)
22. Does your child have any other documented disabilities (as documented by participation in general education setting? � Yes (skip to the end of phone script) � No (continue with questions)

156
23. Does your child need instruction in independent living skills? � Yes (continue with questions) � No (skip to the end of phone script)
24. Do you or another caregiver spend at least 2 hours a day and 4 days a week with the child in the home? � Yes � No (skip to the end of phone script)
25. Could you or another caregiver commit to coaching for 1 hour sessions, 3 times a week for at least 10 weeks? � Yes (continue with questions) � No (skip to the end of phone script)
26. Are you or another caregiver interested in trying coached instructional strategies to increase child independence? � Yes (continue with questions) � No (skip to the end of phone script)
27. Do you have reliable access to the Internet and a mobile device like a laptop, tablet, or phone? � Yes (end script) � No (end script)
End of Script Thank you so much for your time, that’s all the questions I have today. � Unfortunately, this study may not be a good fit for your child at this time. Reasons: ______________________________________________ Thanks again for your time! Have a good day. (Stop)
� Your child may be a good fit for this study! Are you still interested in participating? � No, I’m not interested Well thank you very much for your time. I hope that this school year is a good one. Have a good day. (Stop)
� Yes, I’m still interested Wonderful! We need to set up a time to meet and discuss the study. I can send you the forms that we will go over at this meeting, so that you can look at them before if you would like.
� Yes, send forms to: _______________________________________(continue) � No (continue) Would you like to set up a time to meet now or would you like me to call you back to set up a time? � Call back (When? _______________________________) � Now is good
When would you like to meet? Day: __________________ Time: ___________________
157
Okay, we will see you (review meeting time and location). Do you have any questions for me at this time?
If there is an emergency and you need to reschedule, you can email me at ______________________ or call me at _________________________.
Thank you so much for your time today. Have a great day! (Stop)
COMPLETE DURING PHONE CALL: Person Called: Contact Number: Date /Time: Person Making Contact:
158
APPENDIX L
CAREGIVER OR GUARDIAN CONSENT SCRIPT
Caregiver or Guardian Consent Phone Script Date: ________________________________ Hello _______________ (caregiver’s name). How are you today? It’s Susan Yarbrough. Today, I wanted to chat about consent for participation in the research study we discussed on ________. Is this a good time for you to talk? ☐ Yes (continue) � No, Please call back at ___________________________________ (Stop) The Study: First I want to describe the study in more detail, explain the risks and benefits, and give you an opportunity to ask some questions. This research project has two goals. The first is to see if telepractice (Internet-based) coaching helps caregivers like you better use instructional strategies when you teach your child. The second goal is to see if your use of those instructional strategies increases your child’s independent living skills. In this project, you and your child would participate in three, one hour sessions each week for about ten weeks. During those sessions, you and I will talk using software like XXXX. You will participate in a regular activity or routine at home, I will watch you teach, and you and I will discuss how to improve your child’s skills. We’ll do this for three different independent living skills that your child needs to learn, like making the bed, folding laundry, and pouring juice. I will video record and securely store our sessions so I and another researcher can analyze you and your child’s skills for progress. Do you have any questions about the study in general? � Yes _________________________ � No Do you have questions about the goals of the study? � Yes _________________________ � No Do you have questions about the procedures or process of the study? � Yes _________________________ � No Do you have questions about video recording? � Yes _________________________ � No
159
Risks and Benefits: There are minimal risks involved in participating in a study like this. Those risks might be greater than those you would encounter in daily life. First, it is possible the coaching will not be effective. I will analyze the data after each session, and if it isn’t effective after a while, we’ll discuss the situation and, if necessary, stop the coaching. It is unlikely the intervention won’t work at all because the coaching model has been shown to be effective with other caregivers of children with disabilities, and the instructional strategies reflect best practice in teaching children with visual impairments. There are potential benefits for both you and the child. You may acquire new instructional skills that can be applied to other situations, and children may develop independence in three different skills (e.g., washing dishes, folding laundry). Do you have any questions about potential risks? � Yes _________________________ � No Do you have questions about the potential benefits? � Yes _________________________ � No Voluntary Participation: Your participation in this study is completely voluntary. You or the child (and his/her guardian, if appropriate) may choose to stop participating and quit the study at any time. There will be no penalty or punishment. I will not tell your child’s teacher, and it will not impact your child’s education. Do you have any questions about voluntary participation and your right to quit at any time? � Yes _________________________ � No Confidentiality: The results of the research will be kept confidential to the extent allowed by the law. I may publish the results or share them in scholarly presentations, but your name, the child’s name, and other identifying information will not be used. Do you have any questions or concerns about the confidentiality of your information? � Yes _________________________ � No Video and Audio Recording: Our sessions will be video recorded (including both audio and video). The video will be stored using a secure online system, requiring two factor authorization for access. This means, those accessing the videos will have to verify their identity in two ways, like with a password and a
160
text message code. The video will be kept for only two reasons: to analyze your and your child’s progress and to present the results of the research study at professional conferences. Do you have any questions about the storage and security of video and audio recordings? � Yes _________________________ � No Do you have any questions about the use of video and audio recordings? � Yes _________________________ � No You should also know that if you have any questions, you may contact me at any time. Call at XXXXXXXXX or email XXXXXXXX. You can also contact FSU Institutional Review Board at (850) 644-8633 or [email protected] if you have any questions or concerns about the study. Do you have any other questions about any part of the research study? � Yes _________________________ � No If you’re still interested and consent to participation, you’ll need to sign and send a scanned copy of this consent form to XXXXXXXXXX by _________. Your signing the form gives consent for you and/or your child to participate in the research study and in video and audio recording. Do you consent for you and/or your child to both participate in the research study and in video and audio recording? � Yes (continue) � No (end script) Thank you so much for your time, that’s all the questions I have about consent. I’d like for us to set up a time to gather more information about you, your child, and the skills you would like to work on building.
I will send you two documents. The first is a School Readiness Checklist that will give me a broad picture of your child’s skills. The second is an Independent Living Skill Screening, and it will tell me more about the specific independent living skills your child needs help learning. What is the best email address to send these documents? ___________________
161
Would you like to set up a time to meet now or would you like me to call you back to set up a time? � Call back (When? _______________________________) � Now is good
When would you like to meet? Day: __________________ Time: ___________________
Okay, we will see you (review meeting time and location). Do you have any questions for me at this time?
If there is an emergency and you need to reschedule, you can email me at ______________________ or call me at _________________________.
Thank you so much for your time today. Have a great day! (Stop)
COMPLETE DURING PHONE CALL: Person Called: Contact Number: Date /Time: Person Making Contact:
162
APPENDIX M
CHILD ASSENT SCRIPT
Child Assent Phone or Videochat Script Date: ________________________________ Hello [child name]. How are you today? My name is Susan. I’m a teacher like [teacher name]. Today, I want to chat about a research study I’m doing. Your [caregiver name] thinks you might like to help me with the study. The Study: If you agree to help me, I’ll use a computer to chat with you and [caregiver name] a few times a week. You and [caregiver name] will work on learning new independent living skills like making a sandwich or setting the table. I’ll teach your [caregiver name] new tricks to make [him/her] a better teacher. You’ll get to learn how to do new things all by yourself. I will also take a video so I can check what you and your caregiver need to learn next. Do you have any questions about what we’ll do in the study? � Yes _________________________ � No Do you have questions about what your [caregiver name] will learn? � Yes _________________________ � No Do you have questions about what you will learn? � Yes _________________________ � No Do you have questions about the computer or the videos? � Yes _________________________ � No Risks and Benefits: You may not know how to do the things your [caregiver name] asks you to do. That will be okay. If the work is too hard, then we’ll try something that isn’t as hard for you. If you help, you might how to do learn three things all by yourself. You might also help me and other teachers learn better ways to teach you and other kids who are visually impaired. Do you have any questions about what might be too hard? � Yes _________________________ � No
163
Do you have questions about how you might help us? � Yes _________________________ � No Voluntary Participation: Think about whether or not you want to help with the study. Your [guardian name] also has to give permission. Even if [he/she] says “yes,” you can still say you don’t want to participate. You are allowed to say, “No, I don’t want to help.” You can even say, “yes” now and then change your mind later to say, “no.” No one will be mad if you change your mind. Can you say “no” even if [caregiver name] says “yes”? � Yes _________________________ � No Can you agree to help and then change your mind? � Yes _________________________ � No Will anyone be mad if you change your mind? � Yes _________________________ � No Remember you can ask me questions at any time. Do you have any other questions about what you will do to help with this study? � Yes _________________________ � No Okay, if you want to help, you’ll need to sign the form I sent your [caregiver name]. [He/she] will email it to me. When you sign, you are saying, “Yes, I want to help with the study.” Do you agree to help in the research study and be video recorded? � Yes � No Thanks for your help! End Script

164
COMPLETE DURING PHONE CALL: Person Called: Contact Number: Date /Time: Person Making Contact: Notes:
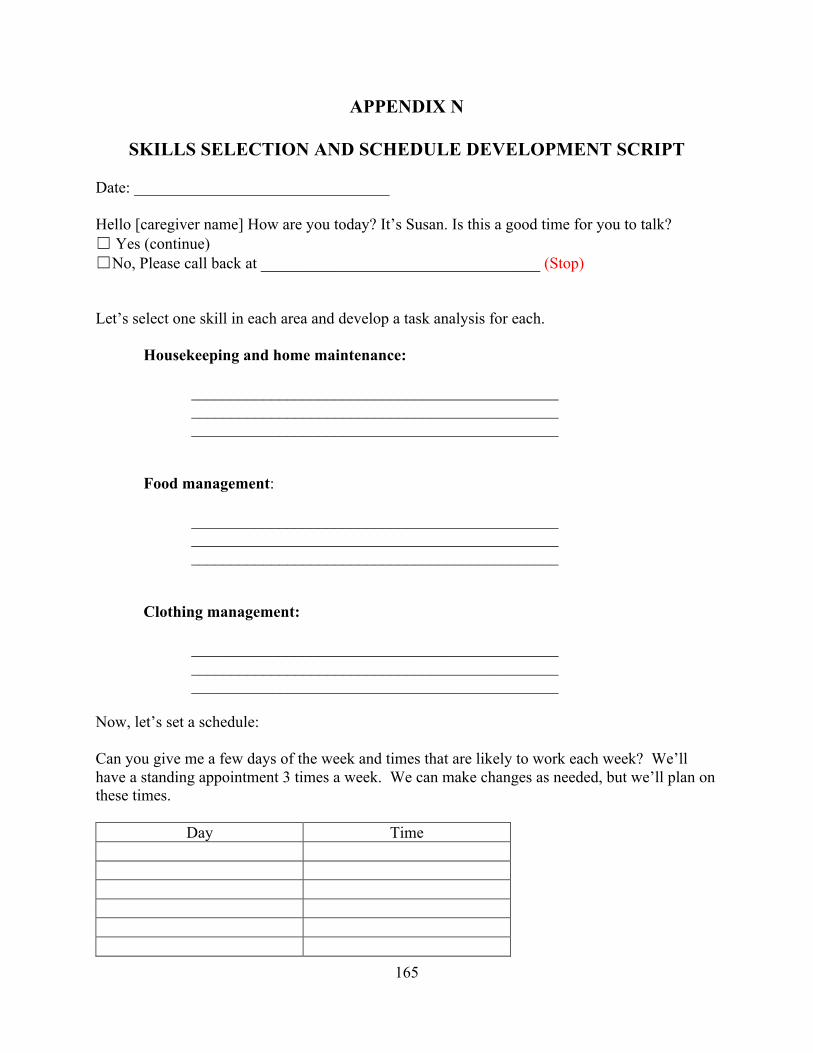
165
APPENDIX N
SKILLS SELECTION AND SCHEDULE DEVELOPMENT SCRIPT Date: ________________________________ Hello [caregiver name] How are you today? It’s Susan. Is this a good time for you to talk? � Yes (continue) � No, Please call back at ___________________________________ (Stop) Let’s select one skill in each area and develop a task analysis for each.
Housekeeping and home maintenance: ______________________________________________ ______________________________________________ ______________________________________________
Food management:
______________________________________________ ______________________________________________ ______________________________________________
Clothing management: ______________________________________________ ______________________________________________ ______________________________________________
Now, let’s set a schedule: Can you give me a few days of the week and times that are likely to work each week? We’ll have a standing appointment 3 times a week. We can make changes as needed, but we’ll plan on these times.
Day Time
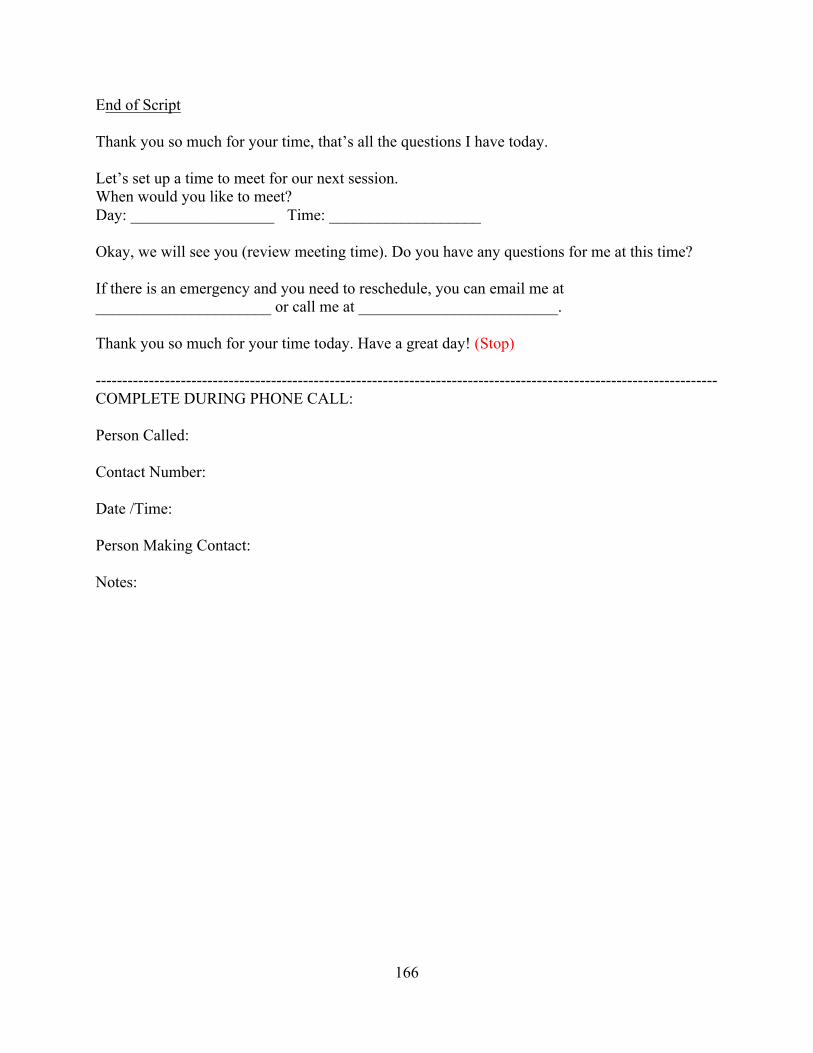
166
End of Script Thank you so much for your time, that’s all the questions I have today. Let’s set up a time to meet for our next session. When would you like to meet? Day: __________________ Time: ___________________ Okay, we will see you (review meeting time). Do you have any questions for me at this time? If there is an emergency and you need to reschedule, you can email me at ______________________ or call me at _________________________. Thank you so much for your time today. Have a great day! (Stop) --------------------------------------------------------------------------------------------------------------------- COMPLETE DURING PHONE CALL: Person Called: Contact Number: Date /Time: Person Making Contact: Notes:
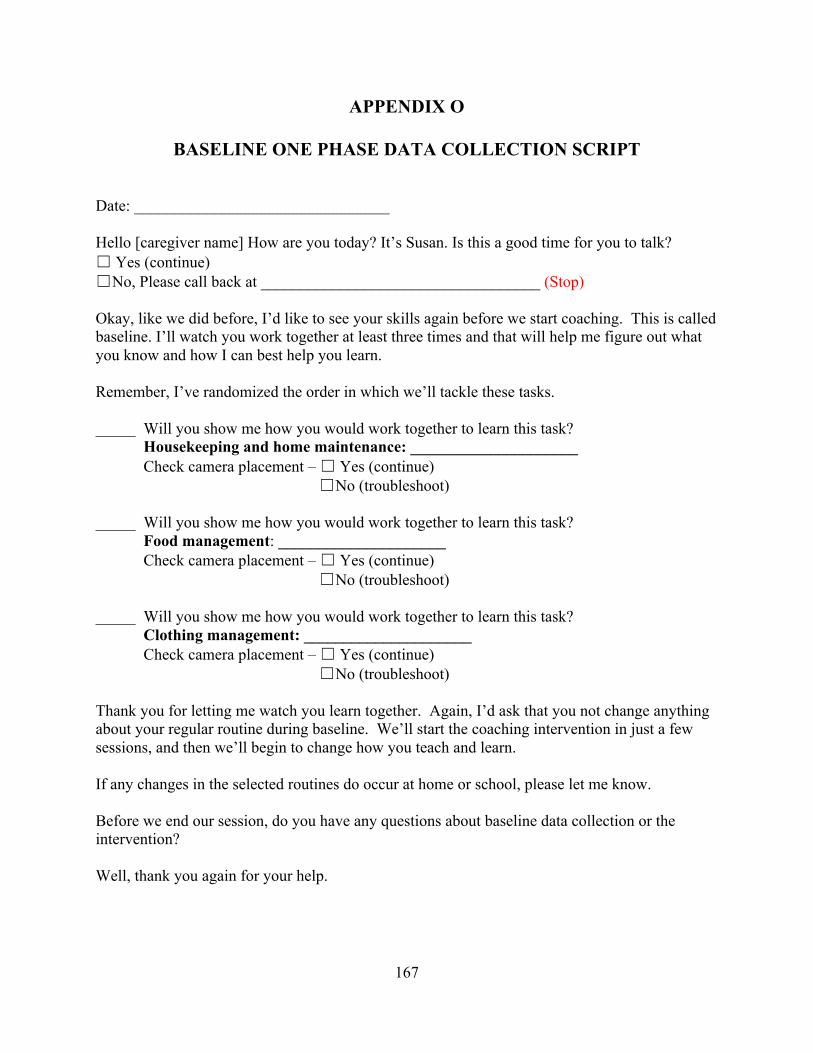
167
APPENDIX O
BASELINE ONE PHASE DATA COLLECTION SCRIPT Date: ________________________________ Hello [caregiver name] How are you today? It’s Susan. Is this a good time for you to talk? � Yes (continue) � No, Please call back at ___________________________________ (Stop) Okay, like we did before, I’d like to see your skills again before we start coaching. This is called baseline. I’ll watch you work together at least three times and that will help me figure out what you know and how I can best help you learn. Remember, I’ve randomized the order in which we’ll tackle these tasks. _____ Will you show me how you would work together to learn this task?
Housekeeping and home maintenance: _____________________ Check camera placement – � Yes (continue) � No (troubleshoot) _____ Will you show me how you would work together to learn this task?
Food management: _____________________ Check camera placement – � Yes (continue)
� No (troubleshoot) _____ Will you show me how you would work together to learn this task?
Clothing management: _____________________ Check camera placement – � Yes (continue) � No (troubleshoot) Thank you for letting me watch you learn together. Again, I’d ask that you not change anything about your regular routine during baseline. We’ll start the coaching intervention in just a few sessions, and then we’ll begin to change how you teach and learn. If any changes in the selected routines do occur at home or school, please let me know. Before we end our session, do you have any questions about baseline data collection or the intervention? Well, thank you again for your help.
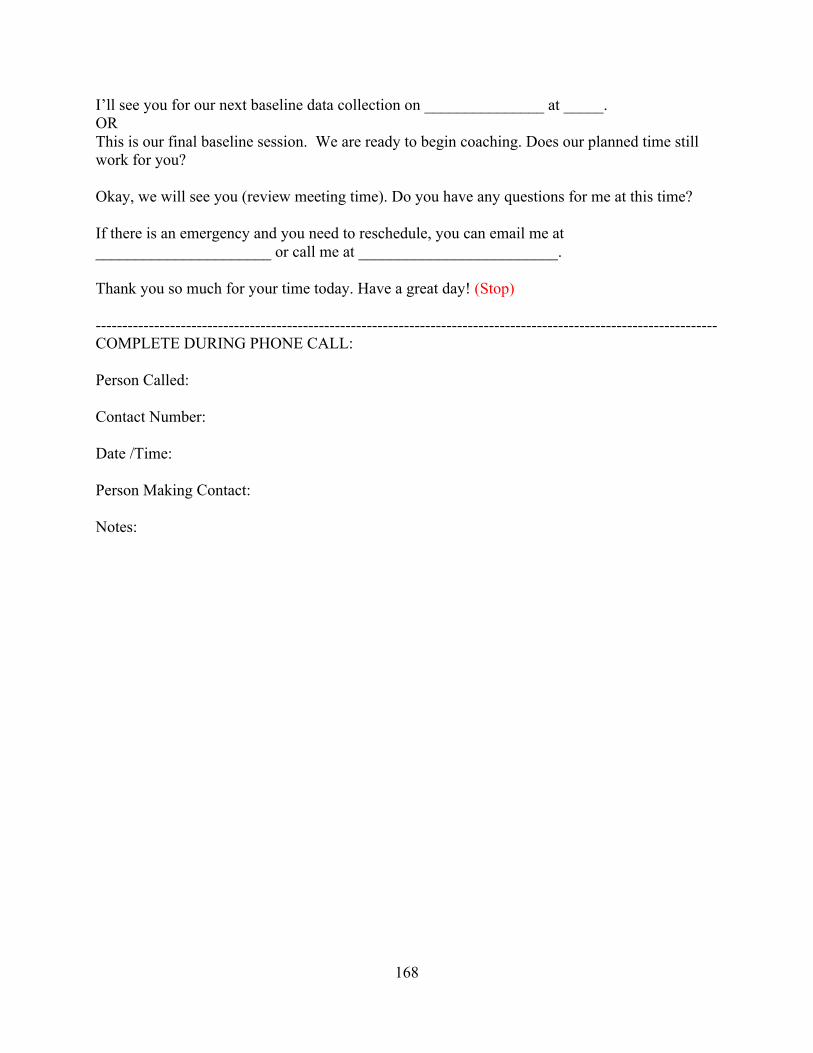
168
I’ll see you for our next baseline data collection on _______________ at _____. OR This is our final baseline session. We are ready to begin coaching. Does our planned time still work for you? Okay, we will see you (review meeting time). Do you have any questions for me at this time? If there is an emergency and you need to reschedule, you can email me at ______________________ or call me at _________________________. Thank you so much for your time today. Have a great day! (Stop) --------------------------------------------------------------------------------------------------------------------- COMPLETE DURING PHONE CALL: Person Called: Contact Number: Date /Time: Person Making Contact: Notes:
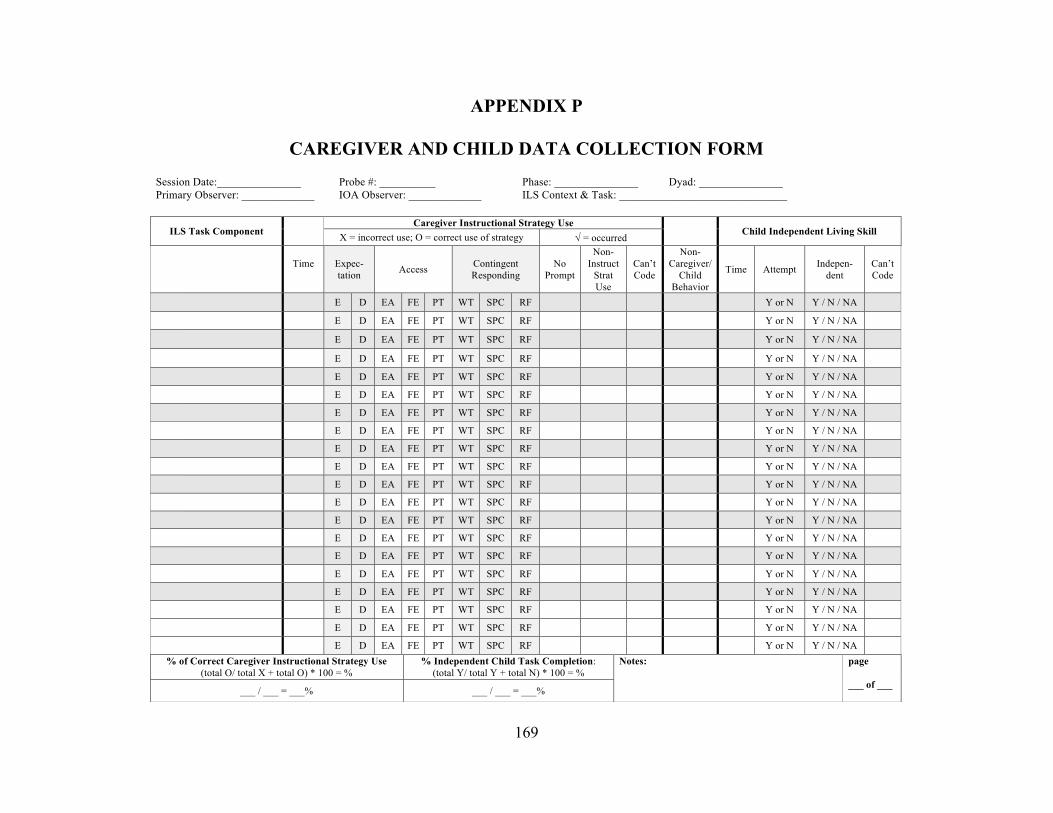
169
APPENDIX P
CAREGIVER AND CHILD DATA COLLECTION FORM
Caregiver and Child Data Collection Form Session Date:_______________ Probe #: __________ Phase: _______________ Dyad: _______________ Primary Observer: _____________ IOA Observer: _____________ ILS Context & Task: ______________________________
ILS Task Component Caregiver Instructional Strategy Use
Child Independent Living Skill X = incorrect use; O = correct use of strategy Ö = occurred
Time
Expec-tation Access Contingent
Responding No
Prompt
Non- Instruct
Strat Use
Can’t Code
Non-Caregiver/
Child Behavior
Time Attempt Indepen-dent
Can’t Code
E D EA FE PT WT SPC RF Y or N Y / N / NA E D EA FE PT WT SPC RF Y or N Y / N / NA E D EA FE PT WT SPC RF Y or N Y / N / NA E D EA FE PT WT SPC RF Y or N Y / N / NA E D EA FE PT WT SPC RF Y or N Y / N / NA E D EA FE PT WT SPC RF Y or N Y / N / NA E D EA FE PT WT SPC RF Y or N Y / N / NA E D EA FE PT WT SPC RF Y or N Y / N / NA E D EA FE PT WT SPC RF Y or N Y / N / NA E D EA FE PT WT SPC RF Y or N Y / N / NA E D EA FE PT WT SPC RF Y or N Y / N / NA E D EA FE PT WT SPC RF Y or N Y / N / NA E D EA FE PT WT SPC RF Y or N Y / N / NA E D EA FE PT WT SPC RF Y or N Y / N / NA E D EA FE PT WT SPC RF Y or N Y / N / NA E D EA FE PT WT SPC RF Y or N Y / N / NA E D EA FE PT WT SPC RF Y or N Y / N / NA E D EA FE PT WT SPC RF Y or N Y / N / NA E D EA FE PT WT SPC RF Y or N Y / N / NA E D EA FE PT WT SPC RF Y or N Y / N / NA
% of Correct Caregiver Instructional Strategy Use (total O/ total X + total O) * 100 = %
% Independent Child Task Completion: (total Y/ total Y + total N) * 100 = %
Notes: page ___ of ___ ___ / ___ = ___% ___ / ___ = ___%
170
APPENDIX Q
TRAINING SLIDES
TeachingYourChildINSTRUCTIONALSTRATEGIESFORSUCCESS
OurGoal
Improvehowyouteach(instructionalstrategies)
Improveyourchild’sindependentlivingskills
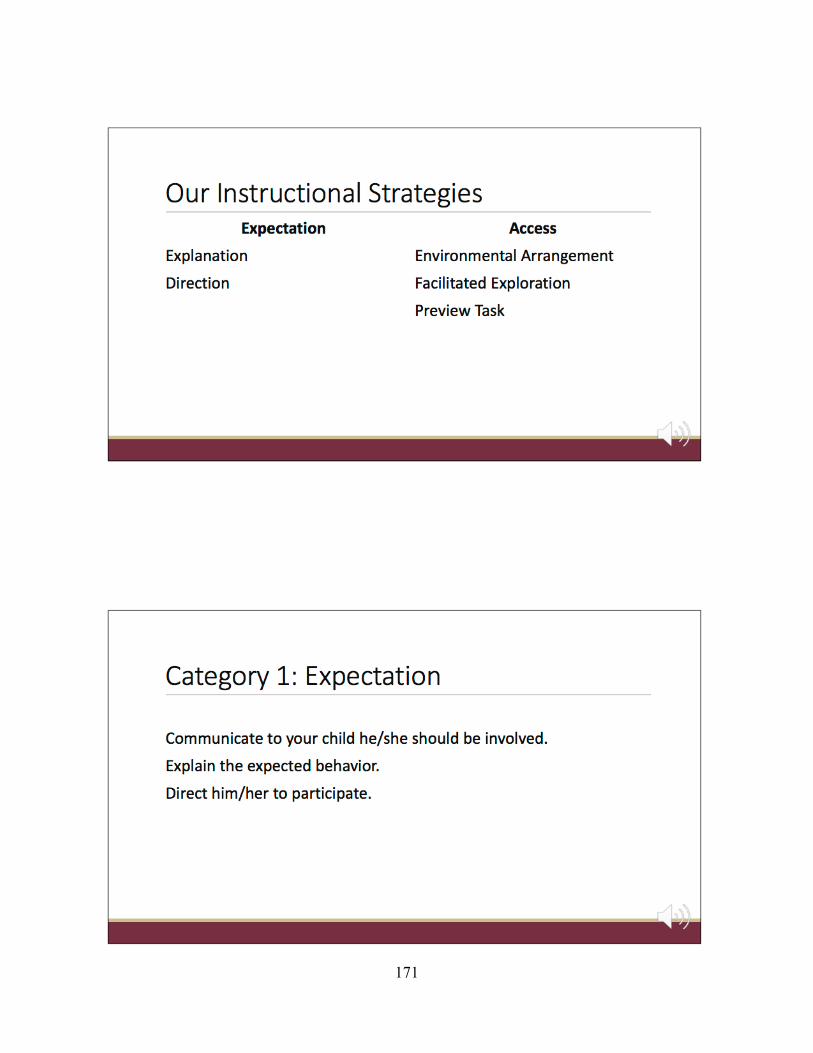
171
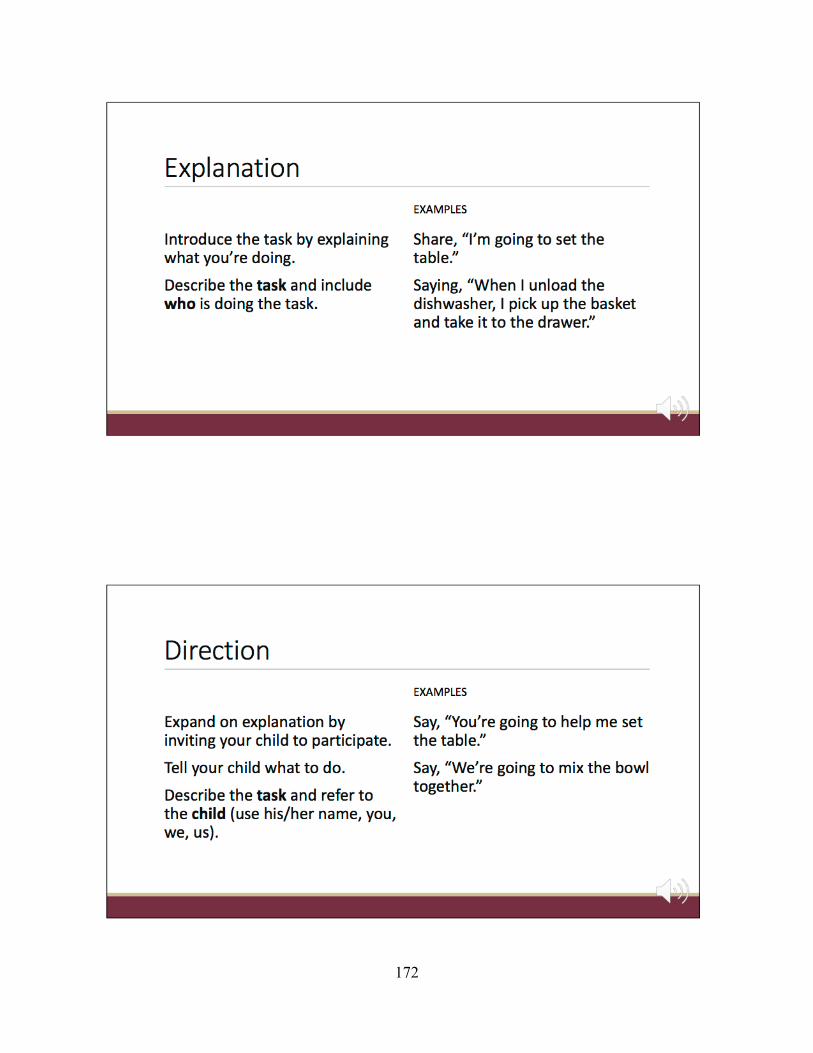
172
173
174
175
176
177
APPENDIX R
TRAINING SCRIPT Date: ________________________________ Hello [caregiver name]. How are you today? It’s Susan. Is this a good time for us to chat? � Yes (continue) � No. Please call back at ___________________________________. (Stop) Today, I’m going to teach you strategies you can use to improve how you teach your child. I have a quick presentation for you to watch. After the presentation, I can answer your questions. Now, let’s watch the presentation. [Share presentation on screen.] Do you have any questions about the instructional strategies or how to implement them? � Yes
Q: _____________________________________ A: _____________________________________ Q: _____________________________________ A: _____________________________________ Q: _____________________________________ A: _____________________________________ Q: _____________________________________ A: _____________________________________
� No Now you can begin to practice these instructional strategies when you teach your child. You can practice these strategies on the three independent living skills tasks we selected. We’ll meet again in a few days to see how you are implementing the strategies and how your child is learning the independent living skills tasks. If you and your child aren’t learning the strategies or the independent living skills after you apply the information from the presentation, we’ll begin coaching on these and other strategies. Before we end our session, do you have any questions? � Yes _________________________________ � No
178
Thank you again for your help. I’ll see you for our next session on _______________ at _____. If there is an emergency and you need to reschedule, you can email me at ______________________ or call me at _________________________. Thank you so much for your time today. Have a great day! (Stop) --------------------------------------------------------------------------------------------------------------------- COMPLETE DURING PHONE CALL: Person Called: Contact Number: Date /Time: Person Making Contact: Notes:
179
APPENDIX S
POST-TRAINING BASELINE PHASE DATA COLLECTION SCRIPT
Date: ________________________________ Hello [caregiver name]. How are you today? It’s Susan. Is this a good time for you to talk? � Yes (continue) � No, Please call back at ___________________________________ (Stop) Now that I’ve shared with you some information about instructional strategies, I’d like to see how you applied the strategies and how your child is learning the independent living skills tasks. As you work, think about the information from the presentation. For now, I won’t be able to give you any additional information while you practice. As we discussed before, if you and your child aren’t learning the strategies or the independent living skills after you apply the information from the presentation, we’ll begin coaching. During coaching, I can give you feedback while you practice. Are you ready to begin? Remember, I’ve randomized the order in which we’ll practice these tasks. _____ Will you show me how you would work together to learn this task?
Housekeeping and home maintenance: _____________________ Check camera placement – � Yes (continue) � No (troubleshoot) _____ Will you show me how you would work together to learn this task?
Food management: _____________________ Check camera placement – � Yes (continue)
� No (troubleshoot) _____ Will you show me how you would work together to learn this task?
Clothing management: _____________________ Check camera placement – � Yes (continue) � No (troubleshoot) Thank you for letting me watch you learn together. Remember, you can now practice these strategies and the independent living skills tasks between our sessions, as it fits in your routine. We’ll meet again in a few days to see how you are implementing the strategies and how your child is learning the independent living skills tasks.
180
Remember, if you and your child aren’t learning the strategies or the independent living skills after you apply the information from the presentation, we’ll begin coaching on these and other strategies in a few sessions. Before we end our session, do you have any questions? � Yes _________________________________ � No Thank you again for your help. I’ll see you for our next session on _______________ at _____. If there is an emergency and you need to reschedule, you can email me at ______________________ or call me at _________________________. Thank you so much for your time today. Have a great day! (Stop) --------------------------------------------------------------------------------------------------------------------- COMPLETE DURING PHONE CALL: Person Called: Contact Number: Date /Time: Person Making Contact: Notes:
181
APPENDIX T
COACHING PHASE DATA COLLECTION SCRIPT Date: ________________________________ Session Number: ________________ Hello [caregiver name]. How are you today? It’s Susan. Is this a good time for you to talk? � Yes (continue) � No, Please call back at ___________________________________ (Stop) Today, we’ll continue coaching. Remember, in coaching, we’ll catch up on your progress, I’ll watch you teach and give you feedback, and then we’ll work together to solve any challenges. Finally, we’ll develop a plan for moving forward. While we coach, we’ll continue to focus on instructional strategies like explanation, direction, environmental arrangement, facilitated exploration, previewing the task, wait time, specific praise, and realistic feedback. You already do many of these strategies, so we’ll build on your current skills to increase the effectiveness of your teaching and increase your child’s independent living skills. Remember, we’ll first do the tasks that will not include coaching, and then we’ll coach on the third task. Like before, I’ve randomized the order in which we’ll practice the first two tasks. Are you ready to begin? _____ Will you show me how you would work together to learn this task?
Housekeeping and home maintenance: _____________________ Check camera placement – � Yes (continue) � No (troubleshoot) _____ Will you show me how you would work together to learn this task?
Clothing management: _____________________ Check camera placement – � Yes (continue) � No (troubleshoot)
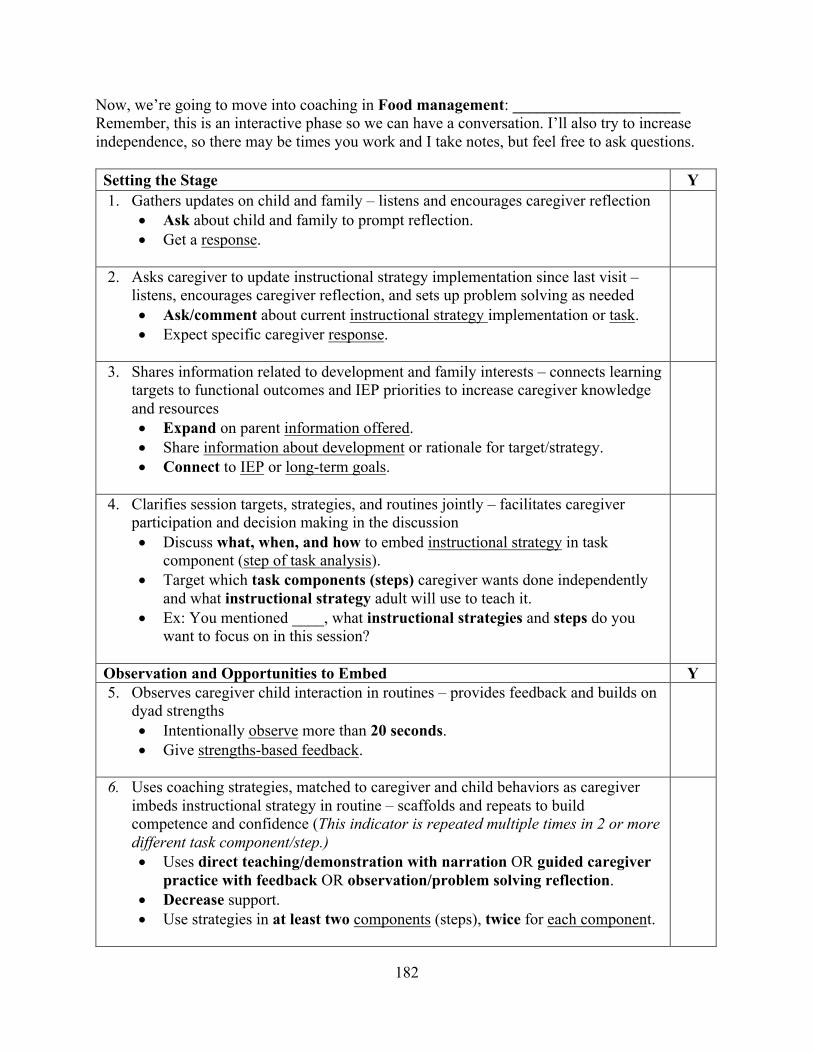
182
Now, we’re going to move into coaching in Food management: _____________________ Remember, this is an interactive phase so we can have a conversation. I’ll also try to increase independence, so there may be times you work and I take notes, but feel free to ask questions. Setting the Stage Y 1. Gathers updates on child and family – listens and encourages caregiver reflection
• Ask about child and family to prompt reflection. • Get a response.
2. Asks caregiver to update instructional strategy implementation since last visit – listens, encourages caregiver reflection, and sets up problem solving as needed • Ask/comment about current instructional strategy implementation or task. • Expect specific caregiver response.
3. Shares information related to development and family interests – connects learning targets to functional outcomes and IEP priorities to increase caregiver knowledge and resources • Expand on parent information offered. • Share information about development or rationale for target/strategy. • Connect to IEP or long-term goals.
4. Clarifies session targets, strategies, and routines jointly – facilitates caregiver participation and decision making in the discussion • Discuss what, when, and how to embed instructional strategy in task
component (step of task analysis). • Target which task components (steps) caregiver wants done independently
and what instructional strategy adult will use to teach it. • Ex: You mentioned ____, what instructional strategies and steps do you
want to focus on in this session?
Observation and Opportunities to Embed Y 5. Observes caregiver child interaction in routines – provides feedback and builds on
dyad strengths • Intentionally observe more than 20 seconds. • Give strengths-based feedback.
6. Uses coaching strategies, matched to caregiver and child behaviors as caregiver imbeds instructional strategy in routine – scaffolds and repeats to build competence and confidence (This indicator is repeated multiple times in 2 or more different task component/step.) • Uses direct teaching/demonstration with narration OR guided caregiver
practice with feedback OR observation/problem solving reflection. • Decrease support. • Use strategies in at least two components (steps), twice for each component.
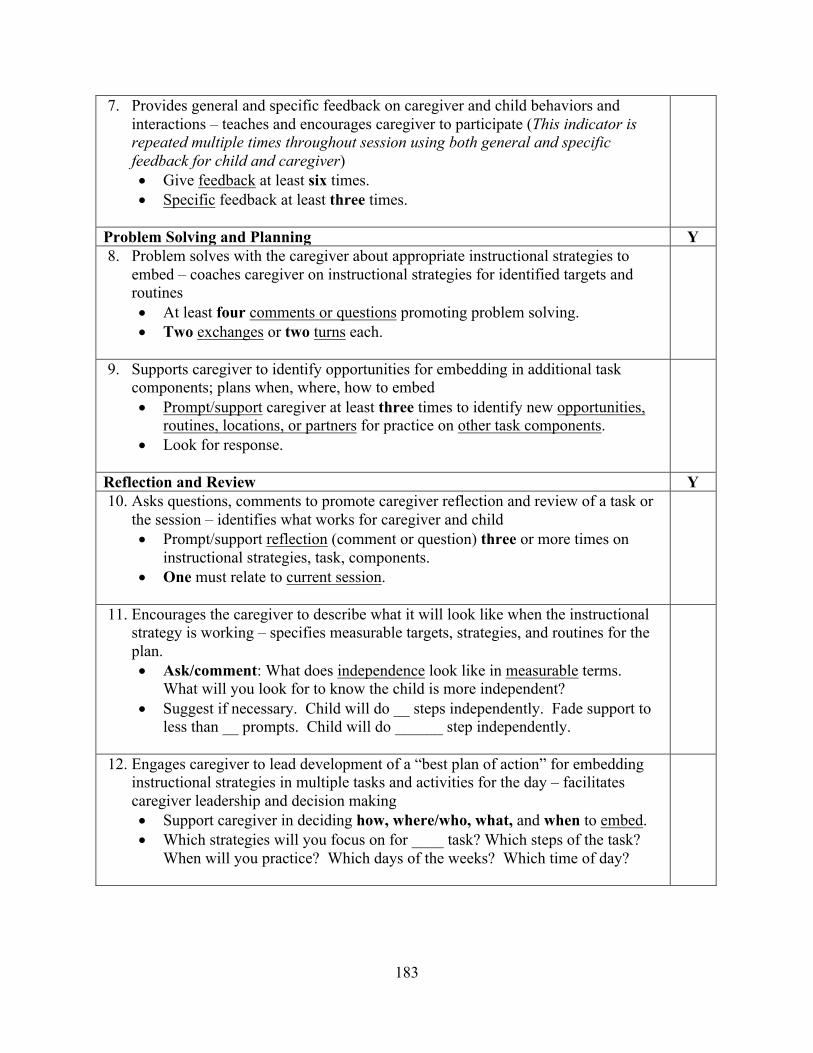
183
7. Provides general and specific feedback on caregiver and child behaviors and interactions – teaches and encourages caregiver to participate (This indicator is repeated multiple times throughout session using both general and specific feedback for child and caregiver) • Give feedback at least six times. • Specific feedback at least three times.
Problem Solving and Planning Y 8. Problem solves with the caregiver about appropriate instructional strategies to
embed – coaches caregiver on instructional strategies for identified targets and routines • At least four comments or questions promoting problem solving. • Two exchanges or two turns each.
9. Supports caregiver to identify opportunities for embedding in additional task components; plans when, where, how to embed • Prompt/support caregiver at least three times to identify new opportunities,
routines, locations, or partners for practice on other task components. • Look for response.
Reflection and Review Y 10. Asks questions, comments to promote caregiver reflection and review of a task or
the session – identifies what works for caregiver and child • Prompt/support reflection (comment or question) three or more times on
instructional strategies, task, components. • One must relate to current session.
11. Encourages the caregiver to describe what it will look like when the instructional strategy is working – specifies measurable targets, strategies, and routines for the plan. • Ask/comment: What does independence look like in measurable terms.
What will you look for to know the child is more independent? • Suggest if necessary. Child will do __ steps independently. Fade support to
less than __ prompts. Child will do ______ step independently.
12. Engages caregiver to lead development of a “best plan of action” for embedding instructional strategies in multiple tasks and activities for the day – facilitates caregiver leadership and decision making • Support caregiver in deciding how, where/who, what, and when to embed. • Which strategies will you focus on for ____ task? Which steps of the task?
When will you practice? Which days of the weeks? Which time of day?
184
Thank you again for participating in coaching. Remember, you can practice these instructional strategies and the independent living skills task: ___________ between our sessions, using the plan we developed. I’d ask that you not intentionally change how you use the instructional strategies in the other two tasks until we begin coaching on those tasks in a few sessions. Before we end our session, do you have any questions? � Yes _________________________________ � No Thank you again for your help. We’ll meet again in a few days for coaching on _______________ at _____. If there is an emergency and you need to reschedule, you can email me at ______________________ or call me at _________________________. Thank you so much for your time today. Have a great day! (Stop) --------------------------------------------------------------------------------------------------------------------- COMPLETE DURING PHONE CALL: Person Called: Contact Number: Date /Time: Person Making Contact: Notes:
185
APPENDIX U
MAINTENANCE PHASE DATA COLLECTION SCRIPT
Date: ________________________________ Session Number: _______________ Hello [caregiver name] How are you today? It’s Susan. Is this a good time for you to talk? � Yes (continue) � No, Please call back at ___________________________________ (Stop) We have finished coaching! You have both learned a lot of skills in teaching and learning. So, we’re going to see how well you use the instructional skills and practice the independent living skills tasks without coaching. Like always, I’ve randomized the order in which we’ll tackle these tasks. _____ Will you show me how you would work together to learn this task?
Housekeeping and home maintenance: _____________________ Check camera placement – � Yes (continue) � No (troubleshoot) _____ Will you show me how you would work together to learn this task?
Food management: _____________________ Check camera placement – � Yes (continue)
� No (troubleshoot) _____ Will you show me how you would work together to learn this task?
Clothing management: _____________________ Check camera placement – � Yes (continue) � No (troubleshoot) Thank you for letting me watch you learn together. Before we end our session, do you have any questions about maintenance data collection? Well, thank you again for your help. I’ll see you for our next maintenance data collection on _______________ at _____. If there is an emergency and you need to reschedule, you can email me at ______________________ or call me at _________________________. Thank you so much for your time today. Have a great day! (Stop)
186
-------------------------------------------------------------------------------------------------------------------- COMPLETE DURING PHONE CALL: Person Called: Contact Number: Date /Time: Person Making Contact: Notes:
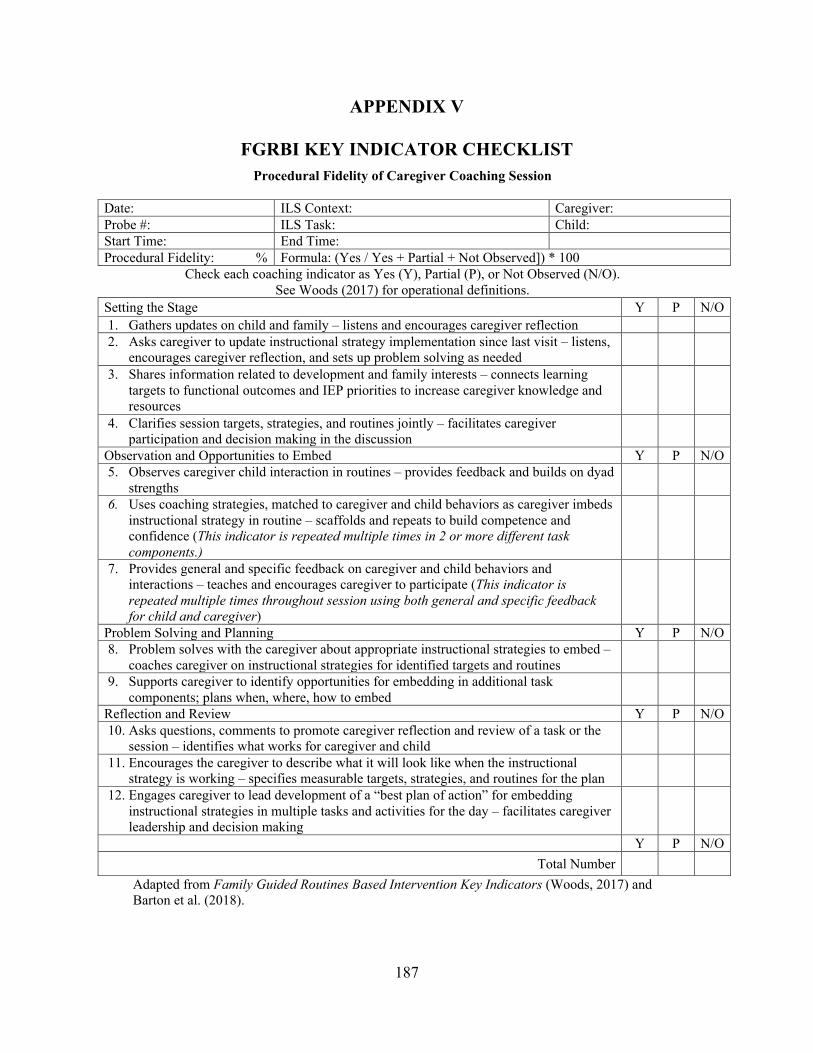
187
APPENDIX V
FGRBI KEY INDICATOR CHECKLIST
Procedural Fidelity of Caregiver Coaching Session
Date: ILS Context: Caregiver: Probe #: ILS Task: Child: Start Time: End Time: Procedural Fidelity: % Formula: (Yes / Yes + Partial + Not Observed]) * 100
Check each coaching indicator as Yes (Y), Partial (P), or Not Observed (N/O). See Woods (2017) for operational definitions.
Setting the Stage Y P N/O 1. Gathers updates on child and family – listens and encourages caregiver reflection 2. Asks caregiver to update instructional strategy implementation since last visit – listens,
encourages caregiver reflection, and sets up problem solving as needed
3. Shares information related to development and family interests – connects learning targets to functional outcomes and IEP priorities to increase caregiver knowledge and resources
4. Clarifies session targets, strategies, and routines jointly – facilitates caregiver participation and decision making in the discussion
Observation and Opportunities to Embed Y P N/O 5. Observes caregiver child interaction in routines – provides feedback and builds on dyad
strengths
6. Uses coaching strategies, matched to caregiver and child behaviors as caregiver imbeds instructional strategy in routine – scaffolds and repeats to build competence and confidence (This indicator is repeated multiple times in 2 or more different task components.)
7. Provides general and specific feedback on caregiver and child behaviors and interactions – teaches and encourages caregiver to participate (This indicator is repeated multiple times throughout session using both general and specific feedback for child and caregiver)
Problem Solving and Planning Y P N/O 8. Problem solves with the caregiver about appropriate instructional strategies to embed –
coaches caregiver on instructional strategies for identified targets and routines
9. Supports caregiver to identify opportunities for embedding in additional task components; plans when, where, how to embed
Reflection and Review Y P N/O 10. Asks questions, comments to promote caregiver reflection and review of a task or the
session – identifies what works for caregiver and child
11. Encourages the caregiver to describe what it will look like when the instructional strategy is working – specifies measurable targets, strategies, and routines for the plan
12. Engages caregiver to lead development of a “best plan of action” for embedding instructional strategies in multiple tasks and activities for the day – facilitates caregiver leadership and decision making
Y P N/O Total Number
Adapted from Family Guided Routines Based Intervention Key Indicators (Woods, 2017) and Barton et al. (2018).
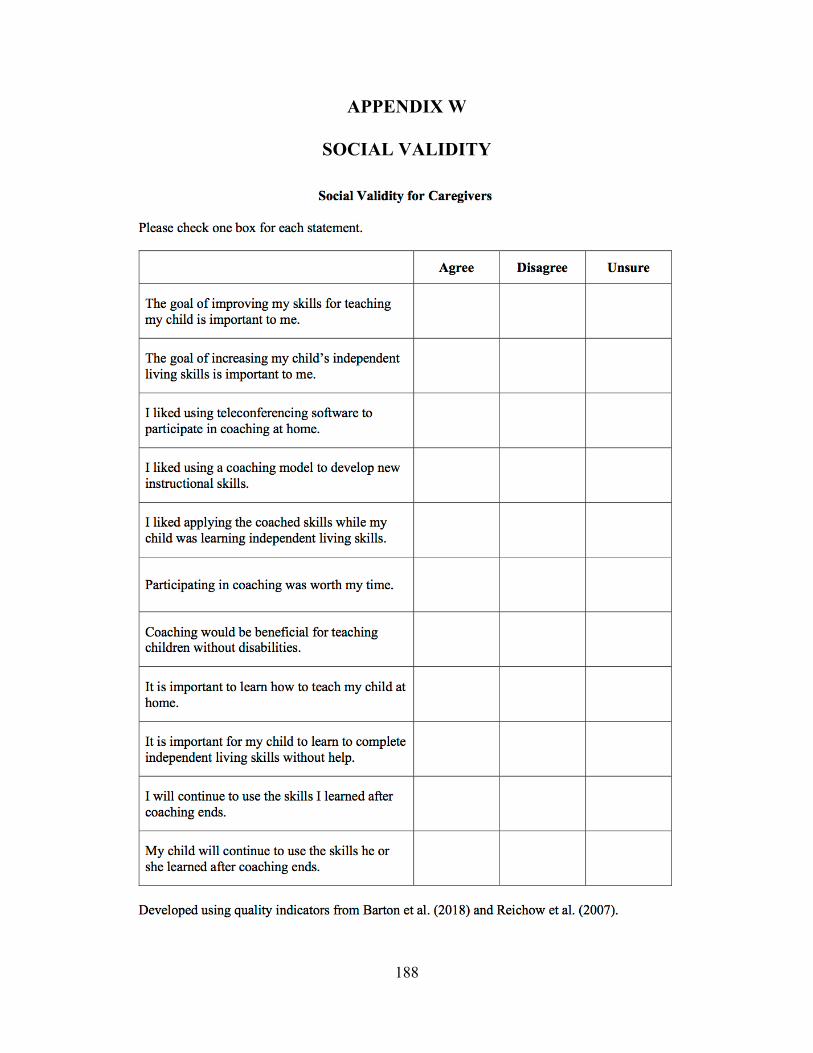
188
APPENDIX W
SOCIAL VALIDITY
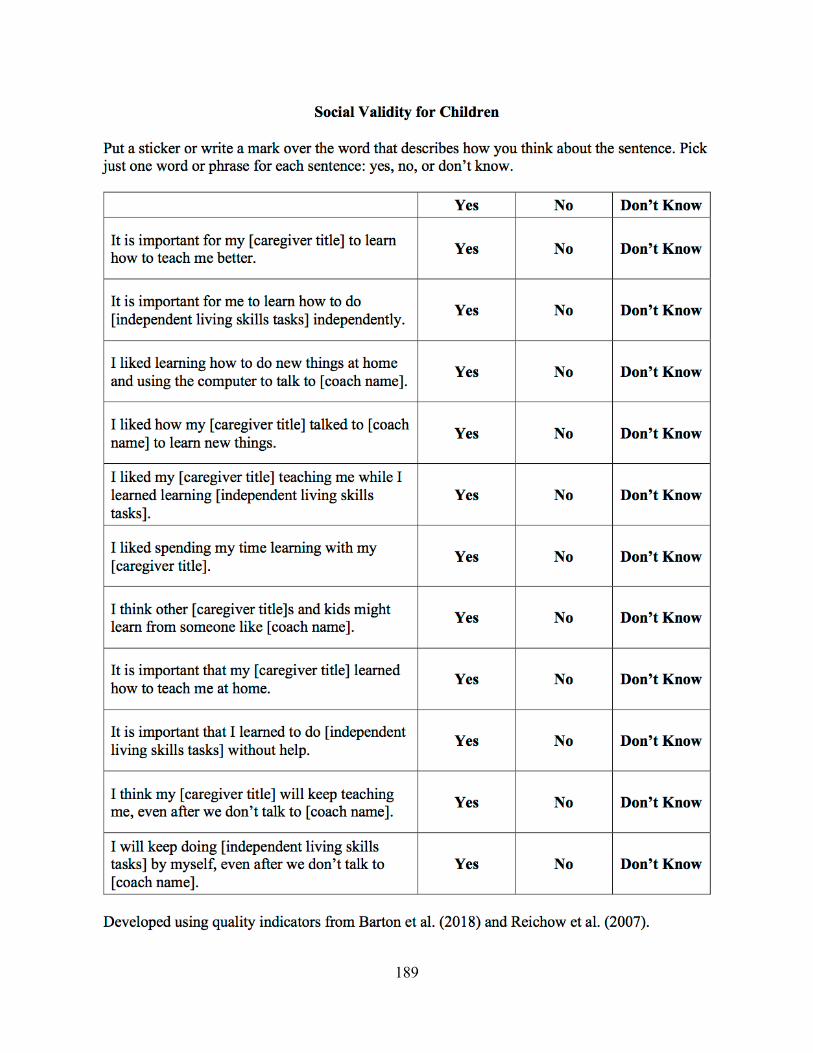
189
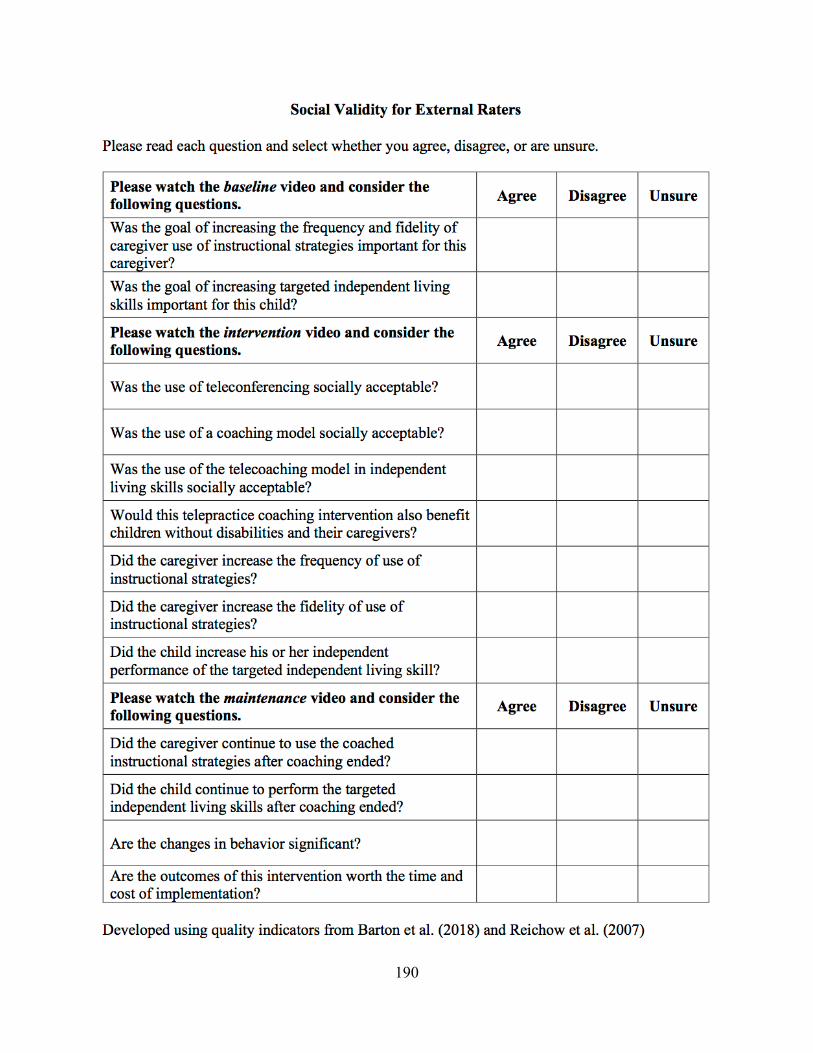
190
191
REFERENCES
Alice Cogswell and Anne Sullivan Macy Act, H. R. 1120, 115th Cong. (2017). American Printing House for the Blind. (n.d.). What is federal quota? Retrieved from
http://www.aph.org/federal-quota/what-is-federal-quota/ American Printing House for the Blind. (2016). Annual report 2016: Distribution of eligible
students based on the federal quota census of January 3, 2015 (Fiscal year 2016). Retrieved from http://www.aph.org/federal-quota/what-is-federal-quota/
Anderson, S., Boigon, S., Davis, K., & deWaard, C. (2007). The Oregon project for preschool
children who are blind or visually impaired (6th ed.). Medford, OR: Southern Oregon Educational Service District.
Antonini, T. N., Raj, S. P., Oberjohn, K., S., Cassedy, A., Makoroff, K. L., Fouladi, M., & Wade,
S. L. (2012). A pilot randomized trial of an online parenting skills program for pediatric traumatic brain injury: Improvements in parenting and child behavior. Behavior Therapy, 45, 455-468. Retrieved from https://www.sciencedirect.com/journal/behavior-therapy
Baharav, E., & Reiser, C. (2010). Using telepractice in parent training in early autism.
Telemedicine and e-Health, 16, 727-731. doi: 10.1089/tmj.2010.0029 Bardin, J. A. (2014). Independent living. In C. B. Allman & S. Lewis (Eds.), ECC essentials:
Teaching the expanded core curriculum to students with visual impairments (pp. 283-323). New York, NY: AFB Press.
Barton, E. E., Meadan-Kaplansky, H., & Ledford, J. R. (2018). Independent variables, fidelity,
and social validity. In J. R. Ledford & D. L. Gast (Eds.), Single case research methodology: Applications in special education and behavioral sciences (3rd ed., pp. 133-156). New York, NY: Routledge.
Behl, D., Akers, J., Boyce, G., & Taylor, M. (1996). Do mothers interact differently with
children who are visually impaired? Journal of Visual Impairment & Blindness, 90, 501-511. Retrieved from http://www.afb.org/afbpress/jvib.aspx
Boutain, A. R. (2014). An evaluation of a telehealth parent training program in teaching self-
care skills to children with autism (Doctoral dissertation). Retrieved from https://kuscholarworks.ku.edu
Briere, D. E., Simonsen, B., Sugai, G., & Myers, D. (2015). Increasing new teachers’ specific
praise using a within-school consultation intervention. Journal of Positive Behavior Interventions, 17, 50-60. doi: 10.1177/1098300713497098
192
Brock, M. E., & Carter, E. W. (2013). A systematic review of paraprofessional-delivered educational practices to improve outcomes for students with intellectual and developmental disabilities. Research & Practice for Persons with Severe Disabilities, 38, 211-221. doi: 10.1177/154079691303800401
Brock, M. E., & Carter, E. W. (2015). Effects of a professional development package to prepare
special education paraprofessionals to implement evidence-based practice. The Journal of Special Education, 49, 39-51. doi: 10.1177/0022466913501882
Brock, M. E., & Carter, E. W. (2017). A meta-analysis of educator training to improve
implementation of interventions for students with disabilities. Remedial and Special Education, 38, 131-144. doi: 10.1177/0741932516653477
Brown, J. A., & Woods, J. J. (2015). Effects of triadic parent-implemented home-based
communication intervention for toddlers. Journal of Early Intervention, 37, 44-68. doi: 10.1177/1053815115589350
Brown, J. A., & Woods, J. J. (2016). Parent-implemented communication intervention:
Sequential analysis of triadic relationships. Topics in Early Childhood Special Education, 36, 115-124. doi: 10.1177/0271121416628200
Cambourne, B. (1988). The whole story: Natural learning and the acquisition of literacy in the
classroom. New York, NY: Ashton Scholastic. Campbell, J. (2003). Maternal directives to young children who are blind. Journal of Visual
Impairment & Blindness, 97, 355-365. Retrieved from http://www.afb.org/afbpress/jvib.aspx
Cason, J., Behl, D., & Ringwalt, S. (2012). Overview of states’ use of telehealth for the delivery
of early intervention (IDEA Part C) services. International Journal of Telerehabilitation, 4, 39-46. doi: 10.5195/IJT.2012.6105
Chang, S. C.-H., & Schaller, J. (2000). Perspectives of adolescents with visual impairments on
social support from their parents. Journal of Visual Impairment & Blindness, 94, 69-84. Retrieved from http://www.afb.org/afbpress/jvib.aspx
Clawson, B., Selden, M., Lacks, M., Deaton, A. V., Hall, B., & Bach, R. (2008). Complex
pediatric feeding disorders: Using teleconferencing technology to improve access to a treatment program. Pediatric Nursing, 34, 213-216. Retrieved from http://www.pediatricnursing.net
Cmar, J. L. (2015). Orientation and mobility skills and outcome expectations as predictors of
employment for young adults with visual impairments. Journal of Visual Impairment & Blindness, 109, 95-106. Retrieved from http://www.afb.org/afbpress/jvib.aspx

193
Craig, C. J. (1996). Family support of the emergent literacy of children with visual impairments. Journal of Visual Impairment & Blindness, 90, 194-200. Retrieved from http://www.afb.org/afbpress/jvib.aspx
Damen, S., Kef, S., Worm, M., Janssen, M. J., & Schuengel, C. (2011). Effects of video-
feedback interaction training for professional caregivers of children and adults with visual impairments. Journal of Intellectual Disability Research, 55, 581-595. doi: 10.1111/j.1365-2788.2011.01414.x
de Klerk, H., & Greef, A. P. (2011). Resilience in parents of young adults with visual
impairments. Journal of Visual Impairment & Blindness, 105, 414-424. Retrieved from http://www.afb.org/afbpress/jvib.aspx
Donovan, M. S., Bransford, J. D., & Pellegrino, J. W. (1999). How people learn: Bridging
research and practice, Washington, DC: National Academy Press. Dote-Kwan, J. (1995). Impact of mothers’ interactions on the development of their young
visually impaired children. Journal of Visual Impairment & Blindness, 89, 46-58. Retrieved from http://www.afb.org/afbpress/jvib.aspx
Dote-Kwan, J., & Hughes, M. (1994). The home environments of young blind children. Journal
of Visual Impairment & Blindness, 88, 31-42. Retrieved from http://www.afb.org/afbpress/jvib.aspx
Dunst, C. J., Trivette, C. M., & Hamby, D. W. (2010). Meta-analysis of the effectiveness of four
adult learning methods and strategies. International Journal of Continuing Education and Lifelong Learning, 3, 91-112.
Fazzi, D. L., Klein, M. D., Pogrund, R. L., & Salcedo, P. S. (2002). Family focus. In R. L.
Pogrund & D. L. Fazzi (Eds.), Early focus: Working with young children who are blind or visually impaired and their families (2nd ed., pp. 6-51). New York, NY: AFB Press.
Ferrell, K. A. (2000). Growth and development of young children. In M. C. Holbrook & A. J.
Koenig (Eds.), Foundations of education: Vol. 1. History and theory of teaching children and youths with visual impairments (2nd ed., pp. 111-134). New York, NY: AFB Press.
Ferrell, K. A. (2011). Reach out and teach: Helping your child who is visually impaired learn
and grow (2nd ed.). New York, NY: AFB Press. Florida Administrative Code. (2017). Exceptional Student Education Eligibility for Students
Who Are Visually Impaired, 6A-6.03014. Forster, E. (2006). Adjusting to your child’s visual impairment. In M. C. Holbrook (Ed.),
Children with visual impairments: A parents’ guide (2nd ed., pp. 51-84). Bethesda, MD: Woodbine House.
194
Friedman, M., Woods, J., & Salisbury, C. (2012). Caregiver coaching strategies for early intervention providers: Moving toward operational definitions. Infants & Young Children, 25, 62-82. doi: 10.1097/IYC.0b013e31823d8f12
Gast, D. L., & Ledford, J. R. (2018). Research approaches in applied settings. In J. R. Ledford &
D. L. Gast (Eds.), Single case research methodology: Applications in special education and behavioral sciences (3rd ed., pp. 1-26). New York, NY: Routledge.
Gast, D. L., Lloyd, B. P., & Ledford, J. R. (2018). Multiple baseline and multiple probe designs.
In J. R. Ledford & D. L. Gast (Eds.), Single case research methodology: Applications in special education and behavioral sciences (3rd ed., pp. 239-283). New York, NY: Routledge.
Glueckauf, R. L., Fritz, S. P., Ecklund-Johnson, E. P., Liss, H J., Dages, P., & Carney, P. (2002).
Videoconferencing-based family counseling for rural teenagers with epilepsy: Phase 1 findings. Rehabilitation Psychology, 47, 49-72. doi: 10.1037//0090-5550.47.1.49
Grimmett, E. S., Pogrund, R. L., & Griffin-Shirley, N. (2011). A national study of parents’
perspectives on dual-certified vision professionals. Journal of Visual Impairment & Blindness, 105, 211-221. Retrieved from http://www.afb.org/afbpress/jvib.aspx
Grisham-Brown, J., Degirmenci, H. D., Snyder, D., & Luiselli, T. E. (2018). Improving practices
for learners with deaf-blindness: A consultation and coaching model. TEACHING: Exceptional Children, 50, 263-271. doi: 10.1177/0040059918763123
Hall, C. M., & Bierman, K. L. (2015). Technology-assisted interventions for parents of young
children: Emerging practices, current research, and future directions. Early Childhood Research Quarterly, 33, 21-32. doi: 10.1016/j.ecresq.2015.05.003
Hatlen, P. (1996). The core curriculum for blind and visually impaired students, including those
with additional disabilities. RE:view, 28, 25-32. Hatlen, P. (2004). The impact of literacy on the expanded core curriculum. SEE/HEAR, 9, 9-14. Hatton, D. D. (2014). Advancing the education of students with visual impairments through
evidence-based practices. International Review of Research in Developmental Disabilities, 46, 1-22. doi: 10.1016/B978-0-12-420039-5.00001-0
Hatton, D. D., Ivy, S. E., & Boyer, C. (2013). Severe visual impairments in infants and toddlers
in the United States. Journal of Visual Impairment & Blindness, 107, 325-336. Retrieved from http://www.afb.org/afbpress/jvib.aspx
Herring, J. (1996). Adjusting to your child’s visual impairment. In M. C. Holbrook (Ed.),
Children with visual impairments: A parents’ guide (pp. 49-72). Bethesda, MD: Woodbine House.
195
Horner, R. H., Carr, E. G., Halle, J., McGee, G., Odom, S., & Wolery, M. (2005). The use of single-subject research to identify evidence-based practice in special education. Exceptional Children, 71, 165-179. doi:10.1177/001440290507100203
Houston, K. T., & Stredler-Brown, A. (2012). A model of early intervention for children with
hearing loss provided through telepractice. The Volta Review, 112, 283-296. Retrieved from https://www.agbell.org/connect/publications/the-volta-review/
Hurley, J. J. (2012). Social validity assessment in social competence interventions for preschool
children: A review. Topics in Early Childhood Special Education, 32, 164-174. doi: 10.1177/0271121412440186
Huebner, K. M., Merk-Adam, B., Stryker, D., & Wolffe, K. (2004). The national agenda for the
education of children and youths with visual impairments, including those with multiple disabilities (2nd ed.). New York, NY: AFB Press.
Ihrig, C. (2016). Steps to offering low vision rehabilitation services through clinical video
telehealth. Journal of Visual Impairment & Blindness, 110, 441-447. Retrieved from http://www.afb.org/afbpress/jvib.aspx
Individuals with Disabilities Education Act, 20 U.S.C. § 1400 (2004). Ivy, S. E., & Hatton, D. D. (2014). Teaching skill acquisition to individuals with blindness: A
systematic review of response-prompting procedures. International Review of Research in Developmental Disabilities, 46, 55-100. doi: 10.1016/B978-0-12-420039-5.00001-0
Jackson, C. W., & Turnbull, A. (2004). Impact of deafness on family life: A review of the
literature. Topics in Early Childhood Special Education, 24, 15-29. Retrieved from http://journals.sagepub.com/home/tec
Janssen, M. J., Riksen-Walraven, M., van Dijk, J. P. M., & Ruijssenaars, W. A. J. J. M. (2010).
Interaction coaching with mothers of children with congenital deaf-blindness at home: Applying the Diagnostic Intervention Model. Journal of Visual Impairment & Blindness, 104, 15-29. Retrieved from http://www.afb.org/afbpress/jvib.aspx
Johansen, M. A., Wootton, R., Kimble, R., Mill, J., Smith, A., & Hockey, A. (2004). A
feasibility study of email communication between the patient’s family and the specialist burns team. Journal of Telemedicine and Telecare, 10, 53-56. Retrieved from https://us.sagepub.com/en-us/nam/journal-of-telemedicine-and-telecare/journal202189
Johnson, N., & Parker. A. T. (2013). Effects of wait time when communicating with children
who have sensory and additional disabilities. Journal of Visual Impairment & Blindness 107, 363-374. Retrieved from http://www.afb.org/afbpress/jvib.aspx
196
Kekelis, L., & Prinz, P. (1996). Blind and sighted children with their mothers. Journal of Visual Impairment & Blindness, 90, 423-436. Retrieved from http://www.afb.org/afbpress/jvib.aspx
Kratochwill, T. R., Hitchcock, J., Horner, R. H., Levin, J. R., Odom, S. L., Rindskopf, D. M., &
Shadish, W. R. (2010). Single-case designs technical documentation. Retrieved from http://ies.ed.gov/ncee/wwc_scd.pdf
Kyzar, K. B., Brady, S. E., Summers, J. A., Haines, S. J., & Turnbull, A. P. (2016). Services and
supports, partnership, and family quality of life: Focus on deaf-blindness. Exceptional Children, 83, 1-15. doi: 10.1177/0014402916655432
Langley, B. (2006). Daily life. In M. C. Holbrook (Ed.), Children with visual impairments: A
parents’ guide (2nd ed., pp. 109-151). Bethesda, MD: Woodbine House. Leat, D., Lofthouse, R., & Wilcock, A. (2006). Teacher coaching: Connecting research and
practice. Teaching Education, 17, 329-339. doi: 10.1080/10476210601017477 Ledford, J. R., & Gast, D. L. (2018). Combination and other designs. In J. R. Ledford & D. L.
Gast (Eds.), Single case research methodology: Applications in special education and behavioral sciences (3rd ed., pp. 335-364). New York, NY: Routledge.
Ledford, J. R., Lane, J. D., & Gast, D. L. (2018). Dependent variables, measurement, and
reliability. In J. R. Ledford & D. L. Gast (Eds.), Single case research methodology: Applications in special education and behavioral sciences (3rd ed., pp. 97-132). New York, NY: Routledge.
Lewis, S., & Allman, C. B. (2014a). Instruction and assessment: General principles and
strategies. In C. B. Allman & S. Lewis (Eds.), ECC essentials: Teaching the expanded core curriculum to students with visual impairments (pp. 31-58). New York, NY: AFB Press.
Lewis, S., & Allman, C. B. (2014b). Learning, development, and children with visual
impairments: The evolution of skills. In C. B. Allman & S. Lewis (Eds.), ECC essentials: Teaching the expanded core curriculum to students with visual impairments (pp. 3-14). New York, NY: AFB Press.
Lewis, S., & Iselin, S. A. (2002). A comparison of the independent living skills of primary
students with visual impairments and their sighted peers: A pilot study. Journal of Visual Impairment & Blindness, 96, 335-334. Retrieved from http://www.afb.org/afbpress/jvib.aspx
Lewis, S., & McKenzie, A. R. (2010). The competencies, roles, supervision, and training needs
of paraeducators working with students with visual impairments in local and residential schools. Journal of Visual Impairment & Blindness, 104, 464-476. Retrieved from http://www.afb.org/afbpress/jvib.aspx
197
Lewis, S., Savaiano, M. E., Blankenship, K., & Greeley-Bennett, K. (2014). Three areas of the expanded core curriculum for students with visual impairment: Research priorities for independent living skills, self-determination, and social interaction skills. International Review of Research in Developmental Disabilities, 46, 207-252. doi: 10.1016/B978-0-12-420039-5.00001-0
Lewis, S., Slay, S., Bischof, E. (2008). PATTER: Preschool attainment through typical everyday
routines. Louisville, KY: American Printing House for the Blind. Lindgren, S., Wacker, D., Suess, A., Schieitz, K., Pelzel, K., Kopelman, T. … Waldron, D.
(2015). Telehealth and autism: Treating challenging behavior at a lower cost. Pediatrics, 137, 165-175. doi: 10.1542/peds.2015-28510
Lohmeier, K. L. (2005). Implementing the expanded core curriculum in specialized schools for
the blind. RE:view, 37, 125-133. Lohmeier, K., Blankenship, K., & Hatlen, P. (2009). Expanded core curriculum: 12 years later.
Journal of Visual Impairment & Blindness, 103, 103-112. Retrieved from http://www.afb.org/afbpress/jvib.aspx
Loumiet, R., & Levack, N. (1993). Independent living: A curriculum with adaptations for
students with visual impairments. Austin: Texas School for the Blind and Visually Impaired.
Lowenfeld, B. (1952). The child who is blind. Exceptional Children, 19, 96-102. doi:
10.1177/001440295201900303 Lowenfeld, B. (1973). Psychological considerations. In B. Lowenfeld (Ed.), The visually
handicapped child in school (pp. 27-60). New York, NY: The John Day Company. Marturana, E. R., & Woods, J. J. (2012). Technology-supported performance-based feedback for
early intervention home visiting. Topics in Early Childhood Special Education, 32, 14-23. doi: 10.1177/0271121411434935
Mason, C., & Davidson, R. (2000). National plan for training personnel to serve children with
blindness and low vision. Reston, VA: Council for Exceptional Children. McDonnall, M. C. (2011). Predictors of employment for youths with visual impairments:
Findings from the Second National Longitudinal Transition Survey. Journal of Visual Impairment & Blindness, 105, 453-466. Retrieved from http://www.afb.org/afbpress/jvib.aspx
McDuffie, A., Machalicek, E., Oakes, A., Haebig, E., Weismer, S. E., & Abbeduto, L. (2013).
Distance video-teleconferencing in early intervention: pilot study of a naturalistic parent-implemented language intervention. Topics in Early Childhood Special Education, 33, 172-185. doi: 10.1177/0271121413476348
198
Monaghan, M., Hilliard, M. E., Cogen, F. R., & Streisand, R. (2011). Supporting parents of very young children with type 1 diabetes: Results from a pilot study. Patient Education and Counseling, 82, 271-274. doi: 10.1016/j.pec.2010.04.007
Nixon, H. L. (1988). Reassessing support groups for parents of visually impaired children.
Journal of Visual Impairment & Blindness, 82, 271-278. Retrieved from http://www.afb.org/afbpress/jvib.aspx
Nixon, H. L. (1991). Mainstreaming and the American dream: Sociological perspectives on
parental coping with blind and visually impaired children. New York, NY: American Foundation for the Blind.
Nunes, D. R. P., Araujo, E. R., Walter, E., Soares, R., & Mendonca, C. (2016). Augmenting
caregiver responsiveness: An intervention proposal for youngsters with autism in Brazil. Early Childhood Education Journal, 44, 39-49. doi: 10.1007/s10643-014-0677-y
Olsen, S., Fiechtl, B., & Rule, S. (2012). An evaluation of virtual home visits in early
intervention: feasibility of “virtual intervention.” The Volta Review, 112, 267-281. Retrieved from https://www.agbell.org/connect/publications/the-volta-review/
Papadopoulos, K., Metsiou, K., & Agaliotis, I. (2011). Adaptive behavior of children and
adolescents with visual impairments. Research in Developmental Disabilities, 32, 1086-1096. doi: 10.1016/j.ridd.2011.01.021
Pathipati, A. S., & Moshfeghi, D. M. (2017). Telemedicine applications in pediatric retinal
disease. Journal of Clinical Medicine, 6, 1-6. doi: 10.3390/jcm6040036 Pogrund, R L. (2002). Independence focus. In R. L. Pogrund & D. L. Fazzi (Eds.), Early focus:
Working with young children who are blind or visually impaired and their families (2nd ed., pp. 218-249). New York, NY: AFB Press.
Probst, K. M., & Walker, V. L. (2017). Using the system of least prompts to teach personal
hygiene skills to a high school student with comorbid visual impairment and autism spectrum disorder. Journal of Visual Impairment & Blindness, 111, 511-525. Retrieved from http://www.afb.org/afbpress/jvib.aspx
Reichow, B., Volkmar, F. R., & Cicchetti, D. V. (2007). Development of the evaluative method
for evaluating and determining evidence-based practices in autism. Journal of Autism and Developmental Disorders, 38, 1311-1319. doi:10.1007/s10803-0070517-7
Simacek, J., Dimian, A. F., & McComas, J. J. (2017). Communication intervention for young
children with neurodevelopmental disabilities via. Journal of Autism and Developmental Disorders, 47, 744-767. doi: 10.1007/s10803-016-3006-z
199
Smyth, C. A., Spicer, C. L., & Morgese, Z. L. (2004). Family voices at mealtime: Experiences with young children with visual impairment. Topics in Early Childhood Special Education, 34, 175-185. doi: 10.1177/0271121414536622
Snyder, P. A., Hemmeter, M. L., & Fox, L. (2015). Supporting implementation of evidence-
based practices through practice-based coaching. Topics in Early Childhood Special Education, 35, 133-143. doi: 10.1177/02711214115594925
Social Security Administration. (2017, January). If you’re blind of have low vision – How we can
help. (Publication Number: 05-10052). Retrieved from https://www.ssa.gov/pubs/EN-05-10052.pdf
Sticken, J., & Kapperman, G. (2010). Integration of visual skills for independent living. In A. L.
Corn & J. N. Erin (Eds.), Foundations of low vision: Clinical and functional perspectives (2nd ed., pp. 97-110). New York, NY: AFB Press.
Turnbull, A., Turnbull, R., Erwin, E. J., Soodak, L. C., & Shogren, K. A. (2015). Families,
professionals, and exceptionality: Positive outcomes through partnerships and trust. (7th ed.). Upper Saddle River, NJ: Pearson Education.
U.S. Department of Education, Office of Special Education and Rehabilitative Services, Office
of Special Education Programs. (2000, June). Educating blind and visually impaired students: Policy guidance. (65 Fed. Reg. 36586-36594). Retrieved from www.ed.gov/legislation/FedRegister/other/2000-2/060800a.html
U.S. Department of Education, Office of Special Education and Rehabilitative Services, Office
of Special Education Programs. (2016, October). 38th Annual Report to Congress on the Implementation of the Individuals with Disabilities Education Act, 2016. Retrieved from https://www2.ed.gov/about/reports/annual/osep/2016/parts-b-c/index.html
U.S. Department of Education, Office of Special Education and Rehabilitative Services, Office
of Special Education Programs. (2017, May). Eligibility determination for children suspected of having a visual impairment including blindness under the Individuals with Disabilities Education Act. (OSEP 17-05). Retrieved from https://www2.ed.gov/policy/speced/guid/idea/memosdcltrs/letter-on-visual-impairment-5-22-17.pdf
Vismara, L. A., McCormick, C., Young, G. S., Nadhan, A., & Monlux, K. (2013). Preliminary
findings of a telehealth approach to parent training in autism. Journal of Autism and Developmental Disorders, 43, 2953-2969. doi: 10.1007/s10803-013-1841-8
Wacker, D. P., Lee, J. F., Padilla-Dalmau, Y. C., Kopelman, T. G., Lindgren, S. D., Kuhle, J. …
Waldron, D. B. (2013a). Conducting functional communication training via telehealth to reduce the problem behavior of young children with autism. Journal of Developmental and Physical Disabilities, 25, 35-48. doi: 10.1007/s10882-012-9314-0
200
Wacker, D. P., Lee, J. F., Padilla-Dalmau, Y. C., Kopelman, T. G., Lindgren, S. D., Kuhle, J., … Waldron, D. B. (2013b). Conducting functional analyses of problem behavior via telehealth. Journal of Applied Behavior Analysis, 46, 31-46. doi: 10.1002/jaba.29
Wetherby, A. M., Guthrie, W., Woods, J., Schatschneider, C., Holland, R. D., Morgan, L., &
Lord, C. (2014). Parent-implemented social intervention for toddlers with Autism: An RCT. Pediatrics, 134, 1084-1093. doi: 10.1542/peds.2014-0757
Wolery, M., Lane, K. L., & Common, E. A. (2018). Writing tasks: Literature reviews, research
proposals, and final reports. In J. R. Ledford & D. L. Gast (Eds.), Single case research methodology: Applications in special education and behavioral sciences (3rd ed., pp. 43-76). New York, NY: Routledge.
Wolf, M. M. (1978). Social validity: The case for subjective measurement or how applied
behavior analysis is finding its heart. Journal of Applied Behavior Analysis, 11, 203-214. doi: 10.1901/jaba.1978.11-203
Wolffe, K. E., & Kelly, S. M. (2011). Instruction in areas of the expanded core curriculum linked
to transition outcomes for students with visual impairments. Journal of Visual Impairment and Blindness, 105, 340-348. Retrieved from http://www.afb.org/afbpress/jvib.aspx
Wolffe, K. E., Sacks, S. Z., Corn, A. L., Erin, J. N., Huebner, K. M., & Lewis, S. (2002).
Teachers of students with visual impairments: What are they teaching? Journal of Visual Impairment and Blindness, 96, 293-304. Retrieved from http://www.afb.org/afbpress/jvib.aspx
Woods, J. (2017). Family Guided Routines Based Intervention: Key Indicators (2nd ed.)
Unpublished manual, Communication and Early Childhood Research and Practice Center, Florida State University, Tallahassee, FL.
201
BIOGRAPHICAL SKETCH
Susan Yarbrough Curriculum Vitae
Summer 2019 Professional Preparation 2015-present Doctoral Candidate, Florida State University’s Ph.D. Program in
Curriculum and Instruction in Special Education - Visual Disabilities. Scholar, National Leadership Consortium in Sensory Disabilities
Major professor: Dr. Sandra Lewis Dissertation: Using Telepractice to Coach Caregivers of Children with Visual Impairments to Increase the Independent Living Skills of Their Children Expected graduation date: Summer 2019
2012 M.S., Florida State University, Tallahassee. Major: Special Education -
Visual Disabilities. Comprehensive Examination: The relationship between phonological awareness and braille literacy.
2009 B.S. with University Honors, Mercer University, Macon, Georgia. Major:
Elementary Education. Honors Project: A playground for the Butler Center.
Professional Credentials 2012-present Academy for the Certification of Vision Rehabilitation and Education
Professionals Certified Orientation and Mobility Specialist (COMS) 2012-present Tennessee Educator License Number 000594025 Professional License with Endorsements in: Special Education: Early Childhood, PK-3 Special Education: Modified, K-12 Special Education: Vision, PK-12 2009-2014 Georgia Educator Certificate Number 833757 Certificate Level 4 with Endorsements in: Special Education General Curriculum Consultative/ECE P-5 Special Education Subject Areas Cognitive Level P-5
202
Teaching Experience 2019, 2018 Course Instructor: EVI 4220 – Introduction to Orientation and Mobility
(O&M). Florida State University, Tallahassee, Florida. Provided instruction to undergraduate pre-service teachers related to basic concepts and skills in O&M, including collaboration and assessment. Taught and supervised peer teaching of basic O&M skills.
2018, 2017, 2016 Course Instructor: EVI 4311 - Teaching Reading and Writing Skills to
Students with Visual Impairments. Florida State University, Tallahassee, Florida. Provided instruction to undergraduate pre-service teachers in strategies for providing instruction in literacy development for children with visual impairments. Coordinated field placements. Organized and monitored peer teaching. Realigned course syllabus with state accreditation standards.
2018 Fieldwork Supervisor – Florida State University, Tallahassee, Florida.
Directed collaboration among student teacher, cooperating teacher, and university personnel to mentor exceptional student education teacher intern. Conducted observations. Completed evaluations of intern using university- and state-wide evaluation systems. Provided feedback and support to intern and cooperating teacher.
2015 Teaching Assistant: EVI 4311, Florida State University, Tallahassee,
Florida. Provided instructional support for undergraduate course in literacy development for children with visual impairments. Delivered original and prepared lectures upon request. Monitored peer teaching and provided formative feedback. Shared grading responsibilities with course instructor.
2013-2015 Orientation and Mobility Instructor, Tennessee School for the Blind,
Nashville, Tennessee. Taught orientation and mobility skills to students aged 3 to 22 with visual and additional impairments. Conducted assessments, wrote evaluation reports, and determined appropriate educational goals for IEPs. Developed IEP-based instructional plans and conducted regular formative assessments. Collaborated with teachers and educational assistants to implement appropriate instruction. Participated in piloting of new orientation and mobility program to provide orientation and mobility services to all students in school.
2012-2013 Expanded Core Curriculum Instructor, Tennessee School for the Blind,
Nashville, Tennessee. Taught a broad range of expanded core curriculum skills in a group setting to high school students with diverse skills. Differentiated instruction based on task analysis assessment and IEP requirements. Provided living skills instruction for students in on-campus
203
independent living apartments. Piloted new expanded core curriculum program and provided program development feedback to supervisors.
2012-2015 Head Cheerleading Coach, Tennessee School for the Blind, Nashville,
Tennessee. Taught complicated cheer routines, including stunting, to cheerleaders with visual impairments and/or with other physical and intellectual disabilities. Fostered teamwork, managed student behavior, and increased opportunities for appropriate social interaction. Organized practice schedules and communicated regularly with school staff. Assisted in the coordination and hosting of multi-state sports competitions.
Other Professional Experience 2018-present Contracted Editor, National Research and Training Center on Blindness
and Low Vision, Mississippi State University. Edited reading level, language, and tone of pre-existing content to be appropriate for parents and youth with visual impairments.
August 2017 Internship, California School for the Blind. Supervisor: Dr. Sharon Sacks.
Observed superintendent, state officials, administrators, and school personnel to learn daily mechanics of special school administration.
2009-2011 Graduate Research Assistant, Dr. Sandra Lewis, Florida State University.
Assisted in research projects through locating relevant research and organizing collected data. Collaborated with major professor to organize and present course content.
2003-2014 Assistant Director, Activity Leader, General Counselor, and Volunteer,
Georgia Lions Camp for the Blind, Waycross, Georgia. Planned and implemented residential camping programs for children and adults with visual and multiple impairments. Conducted staff trainings on the unique impact of visual impairments and appropriate methods of assistance. Revised policies and procedures to comply with accepted standards for residential camps. Utilized effective leadership and communication skills to supervise staff. Provided care for and instruction in daily living skills for children and adults with disabilities.
Presentations Peer Reviewed Yarbrough, S., Trotter, N., & Lewis, S. (accepted to present 2019, November). Preparing TVIs to
teach braille with peer teaching experiences. Paper presented at biennial meeting, Getting in Touch with Literacy, Seattle, WA. (International).
204
Yarbrough, S., Trotter, N., & Lewis, S. (presented 2019, January). Relationships among barriers and facilitators in the delivery of expanded core curriculum instruction for students with visual impairments. Paper presented at annual meeting, Council for Exceptional Children, Indianapolis, IN. (International).
Trotter, N., & Yarbrough, S. (presented 2018, December). Barriers and facilitators to expanded
core curriculum instruction reported by orientation and mobility specialists. Paper presented at biennial meeting, Southeast Orientation and Mobility Association, Tampa, FL. (Regional).
Trotter, N., Yarbrough, S., & Lewis, S. (presented 2018, July). Barriers and facilitators in the
delivery of expanded core curriculum instruction. Paper presented at biennial meeting, Association for Education and Rehabilitation of the Blind and Visually Impaired, Reno, NV. (International).
Yarbrough, S. (presented 2018, February). Expanded core curriculum and schools for the blind.
Poster presented at annual meeting, Council for Exceptional Children, Tampa, FL. (International).
Yarbrough, S. (presented 2017, September). Expanded core curriculum and schools for the
blind. Paper presented at biennial meeting, Association for Education and Rehabilitation of the Blind and Visually Impaired, Florida Chapter, Orlando, FL. (State).
Yarbrough, S., & Lewis, S. (presented 2016, July). Expanded core curriculum and schools for
the blind. Paper presented at biennial meeting, Association for Education and Rehabilitation of the Blind and Visually Impaired, Jacksonville, FL. (International).
Invited Yarbrough, S. (presented 2018, November). Art for children with visual impairments. Invited
lecture, Florida State University Fine Arts Program, Tallahassee, FL. (Local). Yarbrough, S. (presented 2018, January). Expanded core curriculum for parents. Invited
presentation, Florida School for the Deaf and Blind Parent Education Workshop: Northeast Florida, St. Augustine, FL. (Local).
Yarbrough, S. (presented 2017, October). Expanded core curriculum for parents. Invited
presentation, Florida School for the Deaf and Blind Parent Education Workshop: Northwest Florida, Tallahassee, FL. (Local).
Yarbrough, S. (presented 2017, July). Expanded core curriculum and schools for the blind: For
instructional staff. Invited presentation, Georgia Academy for the Blind, Macon, GA. (Local).
Yarbrough, S. (presented 2017, January). Lesson planning for pre-service teachers. Guest
lecture, Florida State University Visual Disabilities Program, Tallahassee, FL. (Local).

205
Yarbrough, S. (presented 2016, March). Multiple regression for visual disabilities research. Guest lecture, Florida State University Visual Disabilities Program, Tallahassee, FL. (Local).
Hedrick, J., & Yarbrough, S. (presented 2014, October). Orientation and mobility for the teacher
of the visually impaired. Invited presentation at annual meeting, Tennessee Unity Conference, Nashville, TN. (Local).
Conway, A., Hedrick, J., & Yarbrough, S. (presented 2013, October). Orientation and mobility
and the expended core curriculum. Mix and Mingle Session Facilitators, Tennessee Unity Conference, Nashville, TN. (Local).
Publications Yarbrough, S. (2018). The expanded core curriculum and schools for the blind: Applications for
practitioners. Visual Impairment and Deafblind Education Quarterly, 63, 49-54. Yarbrough, S. (2017). Book review: I-M-ABLE: Individualized meaning-centered approach to
braille literacy education. Visual Impairment and Deafblind Education Quarterly, 62, 9-12.
Submitted Trotter, N., Yarbrough, S., & Lewis, S. (2018). Provision and adequacy of expanded core
curriculum instruction. Manuscript submitted for publication. In Preparation Yarbrough, S., & Lewis, S. (2019). Implementation of the expanded core curriculum at schools
for the blind. Manuscript in preparation. Yarbrough, S., Trotter, N., & Lewis, S. (2019). Barriers and facilitators to expanded core
curriculum instruction. Manuscript in preparation. Honors
2019 Nominated, 2018-2019 Outstanding Teaching Assistant Award, Florida
State University 2015-present Scholar, National Leadership Consortium in Sensory Disabilities, U.S.
Office of Special Education Programs, (full tuition support, $96,000 stipend, travel awards)
2012 Delta Gamma Fellow, American Foundation for the Blind Leadership
Conference (travel award)
206
2008 McAfee Vision and Leadership Scholarship, Mercer University ($10,000) 2005-2009 Presidential Scholar, Mercer University (full tuition support) 2005-2009 Honors Program, Mercer University Professional Organizations 2016-present American Educational Research Association (AERA) 2015-present Council for Exceptional Children - Division on Visual Impairments and
Deafblindness (CEC-DVIDB) 2012-present Association for the Education and Rehabilitation of the Blind and Visually
Impaired (AERBVI) Service 2018-present Mentor, Undergraduate Research Opportunity Project, Florida State
University 2017-present International Board of Directors Student Representative, AERBVI 2017-present Membership Committee, CEC-DVIDB 2016-present Peer Reviewer, Journal of Visual Impairment & Blindness 2016-present Student Member, Enrichment Committee, National Leadership
Consortium for Sensory Disabilities 2017 Evaluator, Schools for the Blind. Prepared evaluation reports and
presented evaluation results to administrators at two schools for the blind. Reports and presentations included detailed documentation of school-specific findings, implications, and recommendations for administrators and personnel.
2011 Volunteer, Ability Beyond the Horizon, Tallahassee, Florida. Participated
in orientation and mobility training for teachers to adapt standard techniques for a non-standard environment in Bangalore, India. Developed and administered in-service presentations for parents and professionals. Assisted parents and professionals in finding solutions for problems related to unique cultural differences. Provided direct instruction in cane use to children and adults to increase functional skills. Assisted in establishing a braille book and low vision device donation program.