
Prostatic abscess with infected aneurysms and ... - BMC Urology

Feasibility of estimating regional mechanical properties of cerebralaneurysms in vivo
Simone Baloccoa� and Oscar Camarab�
Department of Information and Communication Technologies (DTIC), Centre for Computational Imagingand Simulation Technologies in Biomedicine (CISTIB), Universitat Pompeu Fabra, E08018Barcelona, Spain and Networking Research Center on Bioengineering, Biomaterials and Nanomedicine(CIBER-BBN), E08018 Barcelona, Spain
Elio Vivas, Teresa Sola, and Leopoldo GuimaraensNeuroangiografia Terapèutica J.J.Merland, Hospital General de Catalunya, 08195 Sant Cugat del Vallés,Barcelona, Spain
Hugo A. F. Gratama van Andel and Charles B. MajoieDepartment of Radiology, Academic Medical Centre, Univesity of Amsterdam, P.O. Box 22660, 1100 DD,Amsterdam, The Netherlands
José María Pozoc�
Department of Information and Communication Technologies (DTIC), Centre for Computational Imagingand Simulation Technologies in Biomedicine (CISTIB), Universitat Pompeu Fabra, E08018Barcelona, Spain and Networking Research Center on Bioengineering, Biomaterials and Nanomedicine(CIBER-BBN), E08018 Barcelona, Spain
Bart H. Bijnensd� and Alejandro F. Frangie�
Department of Information and Communication Technologies (DTIC), Centre for Computational Imagingand Simulation Technologies in Biomedicine (CISTIB), Universitat Pompeu Fabra, E08018Barcelona, Spain; Networking Research Center on Bioengineering, Biomaterials and Nanomedicine(CIBER-BBN), E08018 Barcelona, Spain; and Institució Catalana de Recerca i Estudis Avançats (ICREA),E08018 Barcelona, Spain
�Received 10 June 2009; revised 6 February 2010; accepted for publication 8 February 2010;published 22 March 2010�
Purpose: In this article, the authors studied the feasibility of estimating regional mechanical prop-erties in cerebral aneurysms, integrating information extracted from imaging and physiological datawith generic computational models of the arterial wall behavior.Methods: A data assimilation framework was developed to incorporate patient-specific geometriesinto a given biomechanical model, whereas wall motion estimates were obtained from applyingregistration techniques to a pair of simulated MR images and guided the mechanical parameterestimation. A simple incompressible linear and isotropic Hookean model coupled with computa-tional fluid-dynamics was employed as a first approximation for computational purposes. Addition-ally, an automatic clustering technique was developed to reduce the number of parameters toassimilate at the optimization stage and it considerably accelerated the convergence of the simula-tions. Several in silico experiments were designed to assess the influence of aneurysm geometricalcharacteristics and the accuracy of wall motion estimates on the mechanical property estimates.Hence, the proposed methodology was applied to six real cerebral aneurysms and tested against avarying number of regions with different elasticity, different mesh discretization, imaging reso-lution, and registration configurations.Results: Several in silico experiments were conducted to investigate the feasibility of the proposedworkflow, results found suggesting that the estimation of the mechanical properties was mainlyinfluenced by the image spatial resolution and the chosen registration configuration. According tothe in silico experiments, the minimal spatial resolution needed to extract wall pulsation measure-ments with enough accuracy to guide the proposed data assimilation framework was of 0.1 mm.Conclusions: Current routine imaging modalities do not have such a high spatial resolution andtherefore the proposed data assimilation framework cannot currently be used on in vivo data toreliably estimate regional properties in cerebral aneurysms. Besides, it was observed that the incor-poration of fluid-structure interaction in a biomechanical model with linear and isotropic materialproperties did not have a substantial influence in the final results. © 2010 American Association ofPhysicists in Medicine. �DOI: 10.1118/1.3355933�
Key words: cerebral aneurysms, patient-specific estimation of material properties, biomechanical
models, inverse problems1689 1689Med. Phys. 37 „4…, April 2010 0094-2405/2010/37„4…/1689/18/$30.00 © 2010 Am. Assoc. Phys. Med.

1690 Balocco et al.: Feasibility of regional mechanical properties of cerebral aneurysms 1690
I. INTRODUCTION
Cerebral aneurysms are pathological dilatations of the arte-rial walls that usually occur on or near the Circle of Willis.1
Cerebral aneurysms are common lesions, as it is demon-strated by autopsy studies that indicate a prevalence in theadult population between 1% and 5%,1 but fortunately, mostof them �50%–80%� do not rupture during the course of aperson’s lifetime.2 On the other hand, the catastrophic con-sequences of subarachnoid hemorrhage following rupture ofcerebral aneurysms are associated to an incidence of suddendeath of 12.4% and high rates of fatality �32%–67%� afterthe hemorrhage.1,3,4 The aneurysm formation, growth, andrupture processes are believed to be dependent on complexinteractions among multiple biological and mechanicalfactors:5 Hemodynamics, wall biomechanics, mechanobiol-ogy, and the intracranial environment. During aneurysm for-mation, arterial wall characteristics such as geometrical andmechanical properties change through a degenerative pro-cess, influenced by the hemodynamic forces resulting fromthe pulsatile blood flow.6 Ultimately, the aneurysm ruptureswhen the wall stresses exceed the strength of the tissue.
Hence, solid biomechanics biomarkers can, in combina-tion with vascular morphology and flow information, provideuseful insight into the natural history of cerebral aneurysms.As a matter of fact, changes in wall mechanical propertiescan contribute to the assessment of disease progression7,8 andhave been proposed as biomarkers of vascular structuralfragility.8 In addition, the periodical monitoring of these wallstructural changes may allow the identification of potentialrupture sites.9 A few histological experiments on the me-chanical properties of cerebral aneurysm sacs are available inthe literature, including aneurysm samples from autopsy.10
Unfortunately, patient-specific mechanical properties and thenonuniform distribution of wall thickness through the aneu-rysm cannot be measured in vivo with current noninvasivemedical imaging techniques.6 However, computational mod-els offer the possibility of integrating the limited informationavailable from medical images and, together with an appro-priate set of boundary conditions and some necessary as-sumptions on missing data, being able to estimate nonob-servable parameters such as mechanical properties. Similardata assimilation frameworks have been widely used in dif-ferent applications such as the estimation of local contractil-ity or shear behavior in myocardial tissue,11,12 elasticity inatherosclerotic plaques,13 or viscoelasticity in cartilage,14 aswell as for local brain volume change.15
In our application, the data assimilation framework willconsist of estimating the mechanical parameters of a compu-tational model of the cerebral aneurysm wall based on avail-able wall pulsation measurements. Some authors fitted ex-perimental data to computational models of different levelsof complexity �Laplace’s law,16–18 nonlinear,19–21 anisotropichyperelastic,22,23 or considering collagen fiber informa-tion24–27� to represent the mechanical behavior and/or prop-erties of the intracranial aneurysm wall. Alternatively, thedata assimilation framework can be guided by synthetic de-
formation fields representing the dynamic aneurysm pulsa-Medical Physics, Vol. 37, No. 4, April 2010
tion �i.e., wall motion� as in Kroon and Holzapfel.26 Al-though these biomechanics studies have been pivotal toimprove our knowledge on the wall mechanics of cerebralaneurysms, all of them were based on ex vivo, in vitro, orsimulated data and have been tested on idealized �sphericaland axisymmetric� aneurysm geometries. Therefore, there isa need to investigate the feasibility of the estimation of me-chanical properties of cerebral aneurysms with respect to invivo imaging characteristics as well as with different con-figurations in the data assimilation framework.
In Balocco et al.,28 we presented a first version of a dataassimilation framework for the estimation of regional me-chanical properties of cerebral aneurysms. A single patient-specific morphology was used and wall motion estimateswere given by the forward biomechanical model. In this pa-per, we present some improvements in the methodology andseveral in silico experiments were designed to study the fea-sibility of estimating regional mechanical properties of cere-bral aneurysms considering different imaging characteristicsas well as different choices in the data assimilation frame-work.
Registration techniques were applied to a pair �diastoleand systole� of simulated MR images to estimate the wallpulsation that guided the optimization of the model param-eters. In order to reduce the number of parameters to esti-mate at the optimization stage, an automatic region cluster-ing technique, furnishing a regional distribution of theelasticity, was applied on the strain maps obtained from wallmotion estimates. In this paper, we made use of a simple�incompressible linear and isotropic� biomechanical modelas a first approximation for computational cost purposes. Ad-ditionally, we coupled fluid-dynamics and solid mechanicsequations in order to assess the influence of hemodynamicson the estimation of mechanical properties of cerebral aneu-rysms.
The in silico experiments mentioned above were specifi-cally designed to study the robustness of the proposed meth-odology with respect to aneurysm characteristics derivedfrom imaging �different geometries and mesh discretizationoptions, number of regions with different mechanical prop-erties� and to investigate imaging resolution and registration/clustering configurations required to capture wall pulsationaccurately enough to guide the estimation of mechanical pa-rameters of cerebral aneurysms.
The paper is organized as follows. Section II describes thedifferent components of the data assimilation framework, in-cluding the generation of the anatomical meshes, the finite-element forward model �solid and fluid-dynamics� and theinverse problem stage with the different image processingtools needed to estimate wall motion. Section III presents thein silico experiments designed to study the feasibility of theproposed methodology. A discussion about the results is pro-vided in Sec. IV and, finally, some conclusions and futureworks are described in Sec. V.
II. MATERIALS AND METHODS
This section describes the proposed methodology to esti-
mate regional mechanical properties of cerebral aneurysms
1691 Balocco et al.: Feasibility of regional mechanical properties of cerebral aneurysms 1691
from imaging data and the optimization of the parameters ofa biomechanical model with aneurysm wall pulsation esti-mates. A scheme of the whole proposed methodology is de-picted in Fig. 1.
The parametric biomechanical model was used to gener-ate the modeled aneurysm morphology in systole from thediastolic morphology segmented from subject-specific im-ages; a given regional distribution of the elasticity param-eters; and a set of boundary conditions �pressure variationsand inflow velocity�. The segmented diastolic geometry wasincorporated into the biomechanical model in the form of avolumetric finite-element mesh. The structural mechanics be-havior of the model was controlled by regional elasticityparameters, which were initialized with values based on exvivo experiments available in the literature and optimized atthe inverse problem solving stage. A local pressure distribu-tion that was estimated with computational fluid-dynamicsand, using pressure variations and inflow velocity as inputs,was introduced into the structural mechanics as an additionalconstraint.
The inverse problem part consisted in an iterative loopaiming at estimating the mechanical �or elasticity� param-eters of computational model that minimized the differencebetween two aneurysm morphologies in systole: The onegiven by the biomechanical model, named “systolic mor-phology modeled” in Fig. 1 and the one generated from ap-plying the deformation field capturing the aneurysm wallpulsation to the diastolic morphology, named “systolic mor-phology deformed” in Fig. 1. In this manuscript, the defor-
FIG. 1. Scheme of the proposed methodology. The parametric biomechanicaflow variation, as well as an initial set of parameters describing the regioaneurysm morphology �systole� corresponding to such settings. The distancfield capturing the aneurysm pulsation was iteratively minimized in order tothe iterative loop of the parameter optimization stage.
mation field capturing aneurysm wall pulsation was obtained
Medical Physics, Vol. 37, No. 4, April 2010
applying a registration technique to a pair of simulated MRimages. Strain maps were computed from the obtained wallmotion estimates since they were well suited to distinguishbetween regions with different deformation patterns. Finally,a region clustering technique was applied to these strainmaps in order to speed up the optimization of the elasticityparameters.
II.A. Patient-specific geometrical mesh
Three-dimensional geometrical information of cerebralaneurysms can accurately be obtained by imaging modalitiessuch as 3DCTA, 3DMRA, or 3DRA. For this study, 3DRAimages corresponding to six cerebral aneurysms of patientswere available. The images were acquired within the frame-work of a multicenter study �Department of Radiology of theAcademic Medical Centre, Amsterdam, The Netherlands;Department of Therapeutic Neuroangiography JJ Merland ofthe Hospital General de Catalunya, Barcelona, Spain� usingPhilips Integris Systems �Philips Medical Systems, Best, TheNetherlands� scanners. Images were acquired with two injec-tions of contrast material, one per each internal carotid ar-tery. The projection images were transferred to a dedicatedworkstation where they were reconstructed into a 3D volumedata set with 128�128�128 or 256�256�256 voxels andcovering a field of view of 59.91, 62.58, or 96.40 mm.
The aneurysm geometries were reconstructed with thepipeline described by Cebral et al.29 for the patient-specificanalysis of cerebral aneurysm hemodynamics. A segmenta-
30
el, given the initial aneurysm morphology �diastole� and the patient’s bloodistribution of the wall elasticity, enabled the computation of the modeled
een this modeled morphology and the one obtained from the deformationate the optimal set of elasticity parameters. The dotted connectors indicate
l modnal de betwestim
tion technique developed by Hernandez and Frangi, which

1692 Balocco et al.: Feasibility of regional mechanical properties of cerebral aneurysms 1692
is based on a geometric deformable model that incorporateshigh-order multiscale features in a nonparametric statisticalframework, was employed to extract initial aneurysm geom-etries from the images. The next step consisted of the gen-eration of a surface mesh from the segmentation results usinga Marching Tetrahedra algorithm.29 The obtained surface wasthen smoothed and a truncation of vessel branches was per-formed to isolate the aneurysm. Finally, the number of meshelements was reduced �between 1712 and 2050 elements forthe six meshes� with a uniform remeshing strategy imple-mented in the freeware package REMESH
31 �REMESH v.1.2,IMATI-GE/CNR, Genova, Italy�, while guaranteeing theconservation of morphological details of the aneurysm sur-face. The sharp edges at the inlet and outlet boundaries of theaneurysm surface were preserved by detecting all mesh ele-ments in which the normals of the two incident trianglesexceeded 45°. The last meshing step provided the volumetricmesh needed for the fluid-dynamic computation, which wasautomatically generated from the surface triangulation toolavailable at the COMSOL software, which will also be used asfinite-element solver, resulting in 3D meshes with a numberof tetrahedral elements ranging from 19 299 to 41 822.
II.B. Finite-element forward model
II.B.1. Structural mechanics
In this paper, the aneurysm mechanics behavior was de-fined as an incompressible linear elastic and isotropic mate-rial, thus not capturing the nonlinear anisotropic and layer-dependent nature of the stress-strain curves at high strainsgiven by some hyperelastic constitutive models of the arte-rial wall. Nevertheless, this simplification resulted in reason-able computational costs due to the reduced number of un-known parameters to optimize at the inverse problem stage.Hence, the membrane dynamics was modeled by theHooke’s law, whose most general form for isotropic materi-als relates the stress ��ij� and strain ��kk� tensors as
�ij = 3K�1
3�kk�ij� + 2G��ij −
1
3�kk�ij� , �1�
with K being the bulk modulus, G the shear modulus, and �ij
the Kronecker delta. In this paper, the equations of the bio-mechanical model described above were solved by finite-element analysis, using the COMSOL MULTIPHYSICS
® v3.4�COMSOL Inc., Burlington, MA� software �http://www.comsol.com�.
II.B.2. Elasticity parameters
In finite-element solid mechanics, a membrane objectconsists in a three-dimensional solid element, intermediatebetween the conventional 3D tetrahedral element and a tri-angular in-plane mesh, where one of its dimensions, thethickness, is negligible compared to the two others. Suchstructure is particularly suited for modeling thin membranesbecause the three-dimensional equations governing motionare solved along the surface without the need of a volumetric
mesh. Since the aneurysm wall is usually characterized by aMedical Physics, Vol. 37, No. 4, April 2010
thin membrane,27 we modeled it as a membrane object inwhich the surface is composed by triangular elements andthe thickness is then a variable of the mesh element. As aconsequence, we used a surrogate of elasticity, the stiffnessof a membrane element E�, which was defined as the productbetween the Young’s modulus and the wall thickness, to rep-resent the mechanical properties of the arterial wall �averageover the three arterial tunicae�. Using such a surrogate ofelasticity, a membrane element with a low stiffness may cor-respond either to a region of small elasticity or small thick-ness. Furthermore, the use of membrane elements simplifiedthe stress tensor since we assumed the stresses with respectto the thin surface were zero, i.e., a state of plane stress. Thenonzero components of the Hooke’s law relating the stressand strain tensors can then be expressed as
�xx =1
E��xx − ��yy� ,
�yy =1
E��yy − ��xx� ,
�zz =1
E�− ���xx + �yy�� ,
�xy = �yx =3�xy�1 − 2��
2E, �2�
with E being the modulus of elasticity �Young’s modulus�and � the Poisson’s ratio.
Literature values of thickness and elasticity that were ob-tained from histological sampling of the communicatingartery32 were used as initial reference values for the modelparameters characterizing the mechanical properties of theaneurysm wall �Young’s modulus in Table I�. To the best ofour knowledge, no in vivo measurements of the ratio be-tween the elasticity and wall thickness of the dome and thebleb before aneurysm rupture are available in the literature.However, Kroon and Holzapfel26 theoretically predicted thatthe difference in thickness between the vessel before aneu-rysm growth and the tissue of a developed aneurysm canreach a factor of 6 or 9 at the neck and at the fundus of theaneurysm, respectively. In addition, these authors showedthat the thickness of the neck could be three times biggerthan the fundus of the dome for tissues with uniform elastic-ity. This result was in agreement with measurements ob-
10
TABLE I. Initial reference mechanical parameters.
Young’s modulus�MPa�
Thickness�mm�
Normalizedstiffness ratio
Stiffness�MPa�
Vessel 1.6 0.180 1 288.00Dome 1.6 0.045 1/4 72.00Bleb 1 0.8 0.022 1/16 18.00Bleb 2 0.8 0.011 1/32 9.00Bleb 3 0.8 0.007 1/48 6.00
tained by MacDonald et al., which showed, in an ex vivo

1693 Balocco et al.: Feasibility of regional mechanical properties of cerebral aneurysms 1693
study, that the thickness in different aneurysm regions couldvary by a factor of around 3 �from 13 to 38 �m� at themoment of critical rupture.
Hence, we assumed that the material constituting the ves-sel remodeled to develop the aneurysm, leading to a reduc-tion �1/4 in the third column of Table I� in the thickness �andsubsequently the stiffness� between the vessel and the domeregions. This reduction accounted for the degradation of theinner elastic lamina and the media.26 Furthermore, we madethe assumption that the elastic properties of the bleb werereduced by a half with respect to the vessel and the domesince blebs are usually characterized by a weaker wall.9 Inthe case of having a single bleb in the aneurysm, we set itsthickness to 1/2 of the dome, similar to MacDonald et al.,10
leading to a stiffness value for the bleb equal to 1/4 of thedome �1/16 with respect to the vessel, as shown in Table I�,similar to the 1/5 ratio used by Challa and Han.33 In the caseof multiple blebs, their thicknesses were progressively re-duced �stiffness ratio normalized with respect to the vessel of1/32 and 1/48 for the second and third bleb, respectively, asshown in Table I�, generating blebs with weaker walls. Ad-ditional details about the elastic properties set to aneurysmswith multiple blebs are given in Sec. III A. Finally, all re-gions were modeled as an almost incompressible material,thus Poisson’s ratio � was always set to 0.49.26
II.B.3. Fluid-structure interaction
Fluid-structure interaction �FSI� was used to couple fluid-dynamics equations, describing the hemodynamics inside thevessel, with structural equations, modeling the wall motionunder pulsatile flow conditions. The main reason for thiscoupling was to investigate the influence of hemodynamicsin the estimation of mechanical properties in cerebral aneu-rysms. Furthermore, the structural model was then con-strained with additional boundary conditions since the non-uniform blood pressure distribution, derived fromnonidealized geometries, was taken into account. The rela-tion between blood velocity and pressure for complex geom-etries and flow regimes was described by the Navier–Stokesnonlinear equations for a Newtonian incompressible fluid
��v�t
− ����v + ��v�T� + ���v�v + �p = 0, �3�
where v was the time-dependent flow velocity vector at apoint in 3D space, p was the hydraulic pressure, � was themass density of blood �1060 kg /m3�, and � was the dy-namic viscosity of the medium �3.2�10−3 Pa·s�.
In order to solve Eq. �3�, blood pressure �p̂� and flowvelocity �v̂� gradient information was required as boundaryconditions. In this work, we used inflow velocity information�maximum velocity range, given by systolic and diastolictime-points� at the inlet and blood pressure variations �alsobetween systolic and diastolic time-points� at the outlet ofthe vessel. Following the energy conservation principle, thehydrodynamic pressure calculated at each point of the sur-face was dynamically applied to the aneurysm surface as a
mechanical load along the cardiac cycle. The relationshipMedical Physics, Vol. 37, No. 4, April 2010
between the hydraulic pressure �p�, the wall stress tensor��ij�, the local curvature tensor �Cij�, and the wall thickness�h� was described by a generalized version of the Laplace’slaw for nonisotropic stresses �see Theorem 5.3 in Gurtin andMurdoch34�
p = hTr��Cxx Cxy
Cyx Cyy���xx �xy
�yx �yy�� , �4�
Tr being the trace of the matrix.The inflow-related boundary conditions determined the
behavior of the blood flow in the arterial vessel and consistedof pressure values that were applied to the aneurysm wall. Ifpatient-specific inflow-related boundary conditions v̂ andp̂ �velocity and pressure gradients, respectively� wereavailable, they could be included in the computational modelfor personalization purposes. In this work, velocity changesover the cardiac cycle �v̂� were noninvasively estimatedusing MR imaging of the inflow section of the artery feedingthe aneurysm, specifically in the upper part of the internalcarotid artery of a 52 yr old, normal male subject, using aMRA Q-flow technique from a 1.5 T Intera MRI scanner�Philips Medical Systems, Best, The Netherlands�, as illus-trated in Fig. 2. The mean velocity profile was automaticallyobtained from the manufacturer’s software.
As for the outlet boundary conditions, the systemic varia-tion in blood pressure �p̂� of the patient can easily be mea-sured with a brachial sphygmomanometer since it does notsignificantly change throughout the arterial tree.35
The aneurysm geometry extracted from current 3DRA im-aging systems was an average of the aneurysm shapechanges during several cardiac cycles. Since wall pulsationcan hardly be observed with the current spatiotemporal res-olution of these imaging systems, we assumed that the aneu-rysm geometries obtained from the segmentation stage cor-responded to the morphology of the vessel at rest position,i.e., under diastolic flow and pressure conditions. Thus, thegradient between the minimum and the maximum values ofthe velocity waveform �from 0.18 to 0.38 m/s� and the cor-responding pressure measurements �from 12 932 to17 731 Pa� were employed as inlet and outlet boundary con-ditions, respectively. Finally, the pressure distribution at the
FIG. 2. Mean velocity profile acquired with a MRA Q-flow technique. Peak�0.38 m/s� and rest position �0.18 m/s� velocities were set as inlet boundaryconditions.
systolic peak was computed for each element of the aneu-

1694 Balocco et al.: Feasibility of regional mechanical properties of cerebral aneurysms 1694
rysm surface solving Eq. �3�. Hence, the rest state configu-ration before wall pulsation was considered by associatingthe diastolic aneurysm geometry with rest state velocity andpressure, whereas the systolic aneurysm geometry was takenas the loaded state after wall pulsation.
II.C. Inverse problem
II.C.1. Wall motion estimates
Aneurysm wall motion can be estimated by applying reg-istration techniques to a pair of images corresponding to thediastolic and systolic phases in the cardiac cycle, where thelargest amplitude of the wall pulsation should occur. Themain goal of a registration technique is to find the geometri-cal transformation �nonrigid in our case due to the localizednature of the aneurysm pulsation� that maximizes the simi-larity between the two images to register. In our application,this geometrical transformation will subsequently be appliedto the diastolic aneurysm morphology in order to generatethe deformed systolic aneurysm geometry ssys
def, which will becompared with the modeled one, ssys
mod, given by the biome-chanical model at the parameter optimization stage �see Fig.1�.
II.C.1.a. Imaging techniques. Although noninvasive esti-mation of tissue elasticity using in vivo wall motion measure-ments in other vascular segments has been demonstrated,36
these techniques have small applicability in intracranial seg-ments due to limited imaging resolution.9 Nevertheless, itseems that visualization of cerebral aneurysm pulsation isbecoming possible with four-dimensional computer tomogra-phic angiography �4DCTA�,9,37,38 but its quantification re-mains challenging due to the presence of imaging artifactsrelated to patient motion during the acquisition.39 Dynamicbiplane digital subtraction angiography images were pro-cessed by Oubel et al.40 to extract 2D wall information andthen combine it with computational fluid-dynamics �CFD�simulations in order to improve the realism of intra-aneurysm flow patterns. Finally, Zhang et al.41 proposed amethod to estimate 3D aneurysm wall motion over one car-diac cycle from 3DRA acquisitions, but this approach wasonly evaluated with in vitro data.
The clinical condition of patients presenting symptomaticaneurysms is routinely evaluated with 3DRA images sincethe current diagnostic criterion is solely based on geometri-cal features and these images provide the best trade-off be-tween geometrical accuracy, acquisition times, availabilityand costs. Additionally, noninvasive MR images can be ac-quired if flow information is needed.
II.C.1.b. Registration techniques. There exists a vast lit-erature on nonrigid image registration techniques �seeHolden42 for a recent review�. One the most popular andwidely used in multiple clinical applications is the B-splinefree-form deformation �FFD� proposed by Rueckert et al.43
This technique deforms an image volume by manipulating anunderlying mesh of control points. Displacements are theninterpolated using the 3D cubic B-spline tensor product. Let denote a uniformly spaced grid of nx�ny �nz control
points x,y,z, with nx, ny, nz being the number of controlMedical Physics, Vol. 37, No. 4, April 2010
points in the x, y, and z axes, respectively. The nonlineartransformation at each voxel �x ,y ,z� is then expressed as
u�x,y,z� = l=0
3
m=0
3
n=0
3
�l�r��m�s��n�t��i+l,j+m,k+n, �5�
� being the 3D tensor product of the 1D cubic B-splinesbasis functions and �r ,s , t� the relative positions of �x ,y ,z� inthe grid. One of the most critical parameters to tune is thenumber of control points of the FFD grid that will guide theregistration procedure. The influence of this parameter on thefinal stiffness estimates is detailed in Sec. III B 2. The simi-larity measure of choice was the mutual information and theimplementation of the whole registration algorithm wasbased on the one available in the open-source ITK package�http://www.itk.org�.
Recently, a lot of effort has been devoted to a class ofregistration algorithms furnishing diffeomorphic mappingsthat are obtained from the integration of a smooth and regu-lar velocity field over time. The advantage of these methodslies in the smoothness of the resulting deformation fields,which is a desirable property for several applications such asthe Jacobian integration of these mappings. For that reason,we also studied the nonparametric diffeomorphic Demonstechnique proposed by Vercauteren et al.,44 which can beseen as an optimization procedure on the space of diffeomor-phic transformations. Results obtained with the different reg-istration techniques are compared and summarized in Sec.III B 2.
II.C.1.c. Strain map computation. Strain can be defined asthe amount of stretch or compression along a material line,and it corresponds to the deformation caused by the action ofstress on a physical body. For a given displacement field dwith small deformations, the Cauchy’s strain tensor, which isthe linearized version of the Lagrangian and Eulerian straintensors for finite strains, is a symmetric matrix composed bythe elements �ij =
12 ��idj +� jdi�, where �ij is the strain along
the axis i and j, and �idj is a differential of the component dj
at any point in the direction i. The eigenvalues of � j j, calledprincipal strains, correspond to the strain in the direction ofits maximum variation. Since, according to the Laplace’slaw, the aneurysm surface is a quasispherical thin-walled ob-ject always stretching in the tangential directions, one canassume that the first and the second principal strains approxi-mate the maximum deformation in the tangential directions,whereas the third corresponds to the maximum membranethickness, i.e., the radial strain. Sharp gradients correlatingwith the different region contours appeared in the strainmaps, especially in the radial one, as illustrated in Fig. 3.Considering conservation of volume and the fact that firstand second principal strains correspond to the in-plane sur-face stretching, we then decided to use the third strain mapfor regional separation purposes.
II.C.1.d. Region clustering. The estimation of the stiffnessfor each element of the mesh implies that the number ofvariables to assimilate is proportional to the number of meshelements, making the numerical problem ill-conditioned
when meshes with a large number of elements were used.
1695 Balocco et al.: Feasibility of regional mechanical properties of cerebral aneurysms 1695
For that reason, some authors such as Khalil et al.45 reducedthe number of unknown elasticity values via segmentation ofelements with similar morphology. In our work, strain mapsobtained from the wall motion estimates, given by a regis-tration technique applied to simulated MR images, were usedfor similar purposes, under the hypothesis that clusters in thehistogram of these strain maps corresponded to regions withsimilar elasticity properties. In this way, we assumed that theaneurysm membrane had a piecewise distribution of uniformstiffness, i.e., different regions were likely to present differ-ent degrees of rupture fragility. Therefore, we developed aregion clustering technique to identify these regions and itbasically consisted in applying the k-means algorithm46 tothe radial strain map computed from wall motion estimates.The optimal number of clusters was automatically estimatedwith a technique based on cluster silhouettes.47
Silhouettes estimate, for each cluster, the distance of eachpoint in one cluster to the points in the neighboring clusters.This measure ranged from +1, indicating points that were farfrom neighboring clusters; through 0, for points that were notdistinctly in one cluster or another; to 1, corresponding topoints that were probably assigned to the wrong cluster. Thehigher the average silhouette value, the more separated theclusters were. The k-means algorithm was iterated �ten itera-tions� until the number of clusters maximizing the average
FIG. 3. Strain maps obtained from a displacement field �a� corresponding toa simulated aneurysm pulsation, representing the �b� first, �c� the second,i.e., the tangential strains, and �d� the third, i.e., the radial strain, principalcomponents of the strain tensor, respectively. The color scale indicates theamplitude of the strain. Regional differences between the bleb, the dome andthe vessel are easily distinguished in these maps, especially the one corre-sponding to the radial strain.
silhouette value was reached. For instance, we computed the
Medical Physics, Vol. 37, No. 4, April 2010
silhouette distributions after applying the k-means algorithmwith a different number of clusters to a typical radial strainmap with different stiffness values for the vessel, the bleband the dome. The average silhouette values were 0.9057,0.9610, 0.8384, and 0.8024 for two, three, four, or five clus-ters, respectively, the highest value being the one corre-sponding to the correct number of clusters.
II.C.2. Optimization of elasticity parameters
In pulsatile flow conditions, the modeled aneurysm shapein systole ssys
mod can be expressed at any point of the vesselwall as a function of the regional stiffness E� and the corre-sponding blood flow according to the biomechanical modelEqs. �1� and �3�. Let � be the error function, defined as thedistance between the nodes of the modeled surface generatedby the biomechanical model and the closest nodal point ofthe surface given by deforming the diastolic morphologywith the wall motion estimates, ssys
def
� = n
ssysmod�Eest
� �,ssysdef , �6�
where , represents the Euclidian distance. Hence, the pa-rameter estimation method consisted in minimizing �, usingthe Nelder–Mead simplex method48 to solve for the stiffnessparameters of the biomechanical model.
The initialization of the algorithm with reasonable valuesof E� from the literature was required to reduce the numberof iterations needed to converge and the risk of gettingtrapped by local minima of �. Therefore, all model param-eters were initialized with the mean reference stiffness valueaveraged over the different aneurysm regions. We assumedthat the convergence of the optimization stage was reachedwhen the difference between two successive values of � waslower than a given threshold �the threshold was set to 1�10−4 in our experiments�. At the optimization stage, theconvergence of the simulations was reached after 60–150iterations and it strongly depended on the number of modelparameters to estimate �number of different stiffness regions�and on the mesh resolution. The whole process took between15 and 45 min on a Pentium 4 dual core PC.
III. RESULTS
We have several in silico experiments to evaluate inde-pendently the robustness of some of the stages of the pro-posed workflow and to test some hypotheses about the re-gional distribution of mechanical properties in realisticcerebral aneurysm geometries. The experiments can be clas-sified into two categories: The ones studying different as-pects of the aneurysm geometries used in our analysis andthe ones investigating the influence of the wall motion accu-racy on final results.
The performance of the clustering stage was quantified bycomputing the Dice’s coefficient,49 which is commonly usedfor segmentation validation. We also computed the percent-age of true positives �e.g., elements that were manually la-beled as bleb and that the clustering stage classified as bleb�,
false positives �e.g., elements that were not manually labeled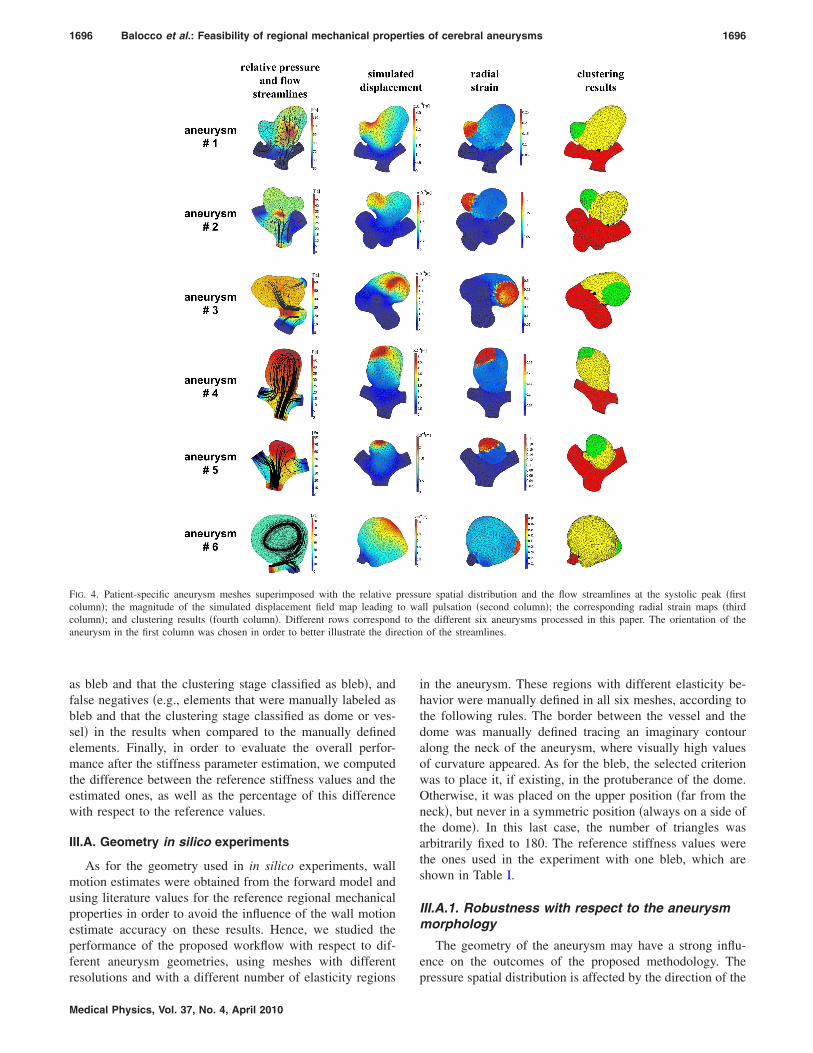
ection
1696 Balocco et al.: Feasibility of regional mechanical properties of cerebral aneurysms 1696
as bleb and that the clustering stage classified as bleb�, andfalse negatives �e.g., elements that were manually labeled asbleb and that the clustering stage classified as dome or ves-sel� in the results when compared to the manually definedelements. Finally, in order to evaluate the overall perfor-mance after the stiffness parameter estimation, we computedthe difference between the reference stiffness values and theestimated ones, as well as the percentage of this differencewith respect to the reference values.
III.A. Geometry in silico experiments
As for the geometry used in in silico experiments, wallmotion estimates were obtained from the forward model andusing literature values for the reference regional mechanicalproperties in order to avoid the influence of the wall motionestimate accuracy on these results. Hence, we studied theperformance of the proposed workflow with respect to dif-ferent aneurysm geometries, using meshes with different
FIG. 4. Patient-specific aneurysm meshes superimposed with the relative pcolumn�; the magnitude of the simulated displacement field map leadingcolumn�; and clustering results �fourth column�. Different rows correspondaneurysm in the first column was chosen in order to better illustrate the dir
resolutions and with a different number of elasticity regions
Medical Physics, Vol. 37, No. 4, April 2010
in the aneurysm. These regions with different elasticity be-havior were manually defined in all six meshes, according tothe following rules. The border between the vessel and thedome was manually defined tracing an imaginary contouralong the neck of the aneurysm, where visually high valuesof curvature appeared. As for the bleb, the selected criterionwas to place it, if existing, in the protuberance of the dome.Otherwise, it was placed on the upper position �far from theneck�, but never in a symmetric position �always on a side ofthe dome�. In this last case, the number of triangles wasarbitrarily fixed to 180. The reference stiffness values werethe ones used in the experiment with one bleb, which areshown in Table I.
III.A.1. Robustness with respect to the aneurysmmorphology
The geometry of the aneurysm may have a strong influ-ence on the outcomes of the proposed methodology. The
re spatial distribution and the flow streamlines at the systolic peak �firstll pulsation �second column�; the corresponding radial strain maps �thirdhe different six aneurysms processed in this paper. The orientation of the
of the streamlines.
ressuto wa
to t
pressure spatial distribution is affected by the direction of the

1697 Balocco et al.: Feasibility of regional mechanical properties of cerebral aneurysms 1697
flow, as mentioned in Sec. II B 2, while the tangentialstresses acting on the aneurysm surface depend on the localcurvature tensor �see Eq. �3��. The strain computation and,consequently, the clustering stage, may also be affected bythe spatial distribution of regions with different elasticity atthe surface of the aneurysm. In order to study these effects,the proposed workflow was applied to six different cerebralaneurysms, segmented with the technique detailed in Sec.II A.
Results obtained from the clustering and some intermedi-ate steps are shown in Fig. 4. The four columns of Fig. 4illustrate, from left to right, the relative �the absolute systolicpressure used for the FSI boundary conditions can be ob-tained by adding the systemic pressure �17 731 Pa� to therelative pressure� pressure spatial distribution, the magnitudeof the displacement field, the corresponding radial strainmaps, and the clustering results, respectively, for the six an-eurysm geometries processed with the proposed workflow.The triangles corresponding to elements incorrectly classi-fied by the proposed methodology are in black. The cluster-ing technique was able to recognize the different elasticityregions with high accuracy, with a percentage of true posi-tives consistently above 98.2% for all regions, which was the
TABLE II. Clustering and stiffness estimates with respect to number of regionegatives; RE�: Reference stiffness; EE�: Estimated stiffness.
Region Mesh elementsTP�%�
Three regions Vessel 264 100.00Dome 1686 99.53Bleb 1 100 100.00
Four regions Vessel 264 100.00Dome 1613 99.38Bleb 1 100 97.00Bleb 2 73 94.52
Five regions Vessel 264 100.00Dome 1543 99.22Bleb 1 100 97.00Bleb 2 73 94.52Bleb 3 70 91.43
FIG. 5. Distribution of the blebs on the aneurysm geometry �left� and twoviews of the corresponding clustering results �middle and right�. The fistbleb was placed in the protuberance of the dome on the opposite side of theneck. The second bleb was placed in the second protuberance of the aneu-rysm, and the third bleb on the opposite site of the previous two blebs andneck. Center and right images correspond to two different views of theclustering results when having three blebs, being the darker elements theones misclassified. Arrows indicate the position of some elements incor-rectly clustered.
Medical Physics, Vol. 37, No. 4, April 2010
value corresponding to the dome of patient 5. The maximumpercentage of true negatives was found for the vessel regionof patient 6, which was wrinkled and characterized by a verysmall number of elements. Moreover, as observed in Fig. 4�fourth column�, the mesh elements incorrectly clusteredwere mainly distributed along the interfaces of the differentregions, where the strain variations between two adjacentareas were smaller.
As for stiffness parameter errors, they were relatively low�less than 1%� and the highest discrepancies appeared in thevessel region in patients 5 and 6 in the estimation of thedome �8.30% and 12.94%, respectively�. In the case of pa-tient 5, this could be explained by the fact that the highestclustering errors appeared in the border between the vesseland the dome. In the case of patient 6, as discussed above,the vessel region was particularly small and wrinkled, thusthe triangles wrongly assigned along its border may highlyinfluence the estimation of the stiffness parameters.
III.A.2. Robustness with respect to the number ofdifferent elasticity regions
Cerebral aneurysms may have several regions with differ-ent mechanical properties, some of them with a weaker walland thus with a higher probability of rupture risk. The pro-posed workflow was then tested against an increasing num-ber of blebs, having different mechanical properties �seeTable I�, in the aneurysm geometry of patient 6. The differentblebs were distributed distinctly on the aneurysm dome, asillustrated in Fig. 5, placing them in the protuberance of thedome and at the upper position �far from the neck�. The sizeof this last bleb was arbitrarily fixed to 180 mesh elements.
In this in silico experiment, we considered that the ratiobetween the vessel and the dome stiffness values was un-changed with respect to the experiment including a singlebleb. As for the Young’s modulus of the different blebs, weassumed the same reduction �1/2� with respect to the domefor all blebs, as can be seen in Table I. On the other hand, thethickness of each bleb was progressively reduced �from 1/2to 1/6 of the dome’s thickness value� in order to maintain a
th different elasticity properties. TP: True positives; FP/FN: False positives/
P�
FN�%� DICE
RE�
�MPa�EE�
�MPa�Error�%�
7 0.00 98.88 288.00 325.27 12.940 0.47 99.76 72.00 71.83 0.240 0.00 99.01 18.00 17.83 0.963 0.00 98.51 288.00 313.92 9.000 0.62 99.69 72.00 72.00 0.000 3.00 95.57 18.00 18.00 0.001 5.48 95.17 9.00 8.99 0.111 0.00 98.32 288.00 266.60 7.430 0.78 99.61 72.00 70.79 1.680 3.00 94.63 18.00 17.51 2.728 5.48 94.52 9.00 9.24 2.671 8.57 92.75 6.00 4.84 19.33
ns wi
F�%
2.20.02.03.00.06.04.13.40.08.05.45.7

1698 Balocco et al.: Feasibility of regional mechanical properties of cerebral aneurysms 1698
ratio of 1/3 between the stiffest and the softest blebs, assuggested by MacDonald et al.10 The stiffness values as-signed to the different regions as well as their relative ratioswith respect to the vessel and the dome are summarized inTable I.
Table II illustrates that the performance of the clusteringstage moderately decreased when the number of regions in-creased. In particular, when comparing the result obtainedfor geometries with four and five regions, the Dice’s coeffi-cient was very similar for Bleb 1 �95.57 and 94.63� and Bleb2 �95.17 and 94.52�. The error in the vessel stiffness esti-mates was always below 13%, while for the dome and thedifferent blebs were very accurate, except in the case of thethird bleb �five regions� that reached almost 20%, being 1.16MPa the absolute error. This Bleb 3 was characterized by themaximum displacements and with abrupt changes in stiffness�since it has the lowest stiffness� at its interface with thedome, the clustering errors then having a substantial impacton the elasticity estimation phase.
III.A.3. Robustness with respect to the meshresolution
Since wall motion estimates were obtained from the bio-mechanical model, the use of meshes with different resolu-tions for the forward and inverse problem stages needed tobe considered. Therefore, the performance of the proposedmethodology was studied when having a coarser mesh in theinverse problem stage, including the region clustering andparameter estimation phases. The surface mesh correspond-ing to patient 1 was therefore progressively reduced from1712 to 1512, 1312, and 1112 elements using the uniformremeshing feature implemented in the REMESH software.31 Ateach resampling step, all mesh nodes were slightly moved,leading to some small topological changes.
Table III shows that with a coarser mesh the clusteringalgorithm was still able to accurately identify the boundariesof the regions with different mechanical properties, its per-formance slightly decreasing when reducing the number of
TABLE III. Clustering and stiffness estimates with respect to mesh resolutionEE�: Estimated stiffness.
Region Mesh elementsTP�%�
Mesh 1712 elements Vessel 785 100.00Dome 807 98.51Bleb 120 100.00
Mesh 1512 elements Vessel 615 100.00Dome 789 98.86Bleb 108 100.00
Mesh 1312 elements Vessel 490 100.00Dome 732 98.91Bleb 90 100.00
Mesh 1112 elements Vessel 397 100.00Dome 648 98.92Bleb 67 100.00
mesh elements. The same tendency can be observed for the
Medical Physics, Vol. 37, No. 4, April 2010
stiffness estimates where the error reached a maximum valueof 3.12% in the bleb region when using coarser meshes�mesh containing 65% of elements with respect to the initialgeometry�. This behavior was due to the current implemen-tation of the optimization stage, which attempted to matchpoints of the two surface meshes that did not correspond tothe same spatial position.
III.B. In silico experiments incorporating wall motion
In these experiments, we again used the forward modeland literature values for the reference regional mechanicalproperties to generate aneurysm wall pulsation, but this time,the initial and the deformed aneurysm geometries were in-troduced into a MR simulator that generated two simulatedMR images with wall pulsation between them. Registrationtechniques were then applied to these simulated MR images,thus providing an estimation of the aneurysm wall pulsation,as illustrated in Fig. 6. Finally, we also generated MR imageswith different image resolutions in order to find out the mini-mum spatial resolution required for an accurate estimation ofthe aneurysm wall mechanical properties.
III.B.1. Simulation of MR images
In this paper, the IMAGESIM MRI simulator50 was used,due to its simplicity and its ability to generate realistic simu-
True positives; FP/FN: False positives/negatives; RE�: Reference stiffness;
FP�%�
FN�%� DICE
RE�
�MPa�EE�
�MPa�Error�%�
1.53 0.00 99.24 288.00 288.00 0.000.00 1.49 99.25 72.00 72.00 0.000.00 0.00 100.00 12.00 12.01 0.081.46 0.00 99.27 288.00 292.12 1.430.00 1.14 99.43 72.00 70.82 1.640.00 0.00 100.00 12.00 11.98 0.171.63 0.00 99.19 288.00 283.71 1.490.00 1.09 99.45 72.00 71.54 0.640.00 0.00 100.00 12.00 11.84 1.331.76 0.00 99.13 288.00 283.82 1.450.00 1.08 99.46 72.00 70.68 1.830.00 0.00 100.00 12.00 11.64 3.00
FIG. 6. Registration results. �a� Original aneurysm diastolic �surface� andsystolic after simulated wall pulsation �wireframe� meshes. �b� and �c�Simulated MR image �resolution of 0.05 mm� of diastolic aneurysm super-imposed with simulated systolic aneurysm �contours� before �b� and after �c�registration with the diffeomorphic Demons algorithm. The white arrowsindicate regions of interest where the largest displacements need to be
. TP:
recovered.

1699 Balocco et al.: Feasibility of regional mechanical properties of cerebral aneurysms 1699
lated MR images of the aneurysm. A gradient echo protocolwith typical values of echo time, time to repetition, and flipangle51 �2 and 10 ms and 35°, respectively� was simulated,providing several 1.5 T MR 2D images of 256�256 pixels,which were subsequently reconstructed into a 3D MR vol-ume through a quantization step dependent on the requiredimage resolution �12, 22, 41, 80, and 159 slices for imageresolution of 0.8, 0.4, 0.2, 0.1, and 0.05 mm, respectively�.The number of excitations parameter was set to 1 since onlyone cardiac cycle simulation was needed. Binary masks ofthe aneurysm meshes in diastole �original mesh� and systole�after mesh warping using the deformation field generated bythe forward finite-element model� were used as inputs of theMR simulator. The region included within the aneurysm wasdefined as being blood liquid mixed with contrast agent,52
whereas we assumed that the surrounding tissue was whitematter. An example of a pair of simulated MR images with aspatial resolution of 0.05 mm is displayed in Fig. 6.
TABLE IV. Clustering and stiffness estimates with respect to registration constiffness; EE�: Estimated stiffness.
Region Mesh elementsTP�%�
Demons Vessel 785 90.06Dome 807 92.44Bleb 120 77.50
FFD 3 CP Vessel 785 62.17Dome 807 49.69Bleb 120 100.00 3
FFD 5 CP Vessel 785 65.22Dome 807 44.49Bleb 120 100.00 2
FFD 8 CP Vessel 785 80.38Dome 807 68.65Bleb 120 91.67 1
FIG. 7. Front �top row� and back �bottom row� views of the stiffness distriInitial reference; diffeomorphic Demons; and FFD with three, five, or eightbleb regions.
Medical Physics, Vol. 37, No. 4, April 2010
III.B.2. Robustness with respect to the registrationmethod
The main goal of this experiment was to assess the influ-ence of the registration algorithm in the stiffness estimates.For that reason, we tested one of the most popular nonrigidregistration techniques, proposed by Rueckert et al.,43 vary-ing one of the most relevant parameters of the technique, thenumber of control points �CPs� in the FFD grid �three, five,or eight control points per dimension in our experiment�. Ingeneral, the higher the number of control points, the moreaccurate and localized the resulting transformation will be, atthe expense of a higher computational cost. Furthermore, wealso tested the diffeomorphic Demons algorithm, developedby Vercauteren et al.,44 since it provides invertible deforma-tion fields with a high number of degrees of freedom andwith a reasonable computational cost.
First, we quantified the registration quality provided bythe different registration scenarios by computing the classical
tion. TP: True positives; FP/FN: False positives/negatives; RE�: Reference
FN�%� DICE
RE�
�MPa�EE�
�MPa�Error�%�
9.94 92.42 288.00 391.59 35.977.56 89.99 72.00 95.61 32.79
22.50 79.15 12.00 12.94 7.8337.83 76.55 288.00 385.95 34.0150.31 54.67 72.00 116.09 61.24
0.00 35.24 12.00 41.47 245.5834.78 72.21 288.00 256.70 10.8755.51 49.90 72.00 92.68 28.72
0.00 42.40 12.00 34.64 188.6719.62 81.89 288.00 271.11 5.8631.35 72.66 72.00 86.72 20.44
8.33 61.62 12.00 36.22 201.83
n results obtained with different registration techniques. From left to right:ol points. The different clusters correspond to the vessel, the dome, and the
figura
FP�%�
4.8413.0118.33
0.2532.0967.5015.4133.8371.6715.9220.3205.83
butiocontr

1700 Balocco et al.: Feasibility of regional mechanical properties of cerebral aneurysms 1700
Jaccard overlap measure53 of the aneurysm masks introducedat the MR simulator before and after each registration tech-nique was applied. Overlap values provided by the differentregistration cases in the 0.05 mm MR simulated images werevery similar: Before registration, 0.87; FFD three CPs=0.94; FFD five CPs, 0.95; FFD eight CPs, 0.95; diffeomor-phic Demons, 0.96.
The clustering results displayed in Fig. 7 prove that theperformance of the clustering stage considerably variedwhen different registration configurations were used for wallmotion estimation purposes. The cluster distribution obtainedby the diffeomorphic Demons technique �second column inFig. 7� was the most similar to the reference one �first col-umn of Fig. 7�. Most of the triangles in the bleb and in thevessel were correctly identified, although some false positivetriangles were located at the top part of the dome. On theother hand, when using the FFD registration technique withthree or five CPs, the percentage of false positives in thedome region was extremely high �see Table IV� and, conse-quently, the Dice’s coefficient for all three regions were sub-stantially lower. Only when eight CPs were used, results be-came comparable with the Demons-based method ones, butit can be noticed that a high number of triangles in the vesselregion were wrongly assigned to the dome �bottom right inFig. 6�, as demonstrated by the high percentage of false posi-tives of the dome region, considerably worsening the FFDeight CPs Dice’s coefficient when comparing to the Demonsresult �92.42 vs 81.89, 89.99 vs 72.66, and 79.15 vs 61.62 forvessel, dome, and bleb, respectively�. Those results can beexplained by the fact that, in the case of the Demons-basedalgorithm, the vessel and bleb regions had quite uniformstrain values leading to high strain gradients at the regionsborders, while the FFD method with three CPs presented amore blurred strain map, and the FFD with five and eightcontrol points exhibited heterogeneity of strain values in thevessel region. The Demons-based algorithm gave the lowest
FIG. 8. Stiffness distribution results obtained with different image resolutionMR simulated images. Middle and bottom rows: Front �middle� and back �vessel, the dome, and the bleb regions.
errors in the stiffness values for the bleb region, where the
Medical Physics, Vol. 37, No. 4, April 2010
largest movements occurred. It seems that the FFD tech-niques gave better results than the diffeomorphic Demons forthe vessel. This was due to the intrinsic smoothness of thediffeomorphic field that made regions with very small defor-mations such as the vessel stiffer than they really were. Nev-ertheless, this was not critical for our application since wewere mostly interested on the dome and the bleb regions andthe stiffness estimates given by all registration configurationswere good enough to identify areas with different mechanicalproperties.
III.B.3. Robustness with respect to the MR imagespatial resolution
The main goal of this experiment was to investigate theinfluence of the MR image resolution on the wall motionestimates and, in consequence, on the estimation of wall me-chanical properties and to find the minimal MR resolutionrequired to obtain accurate enough results. Hence, we ap-plied the proposed methodology to five pairs of MR simu-lated images, representing the aneurysm in diastole and sys-tole, with different spatial resolution �0.05, 0.1, 0.2, 0.4, and0.8 mm, respectively�. The diffeomorphic Demons registra-tion algorithm was applied to each pair of images to obtainthe wall motion estimates.
The first row of Fig. 8 shows a coronal slice of the MRsimulated images with different resolutions �from left toright: 0.05, 0.1, 0.2, 0.4, and 0.8 mm�, where we can observethe decrease in contour sharpness when the resolution de-creases. As can be observed in Fig. 8 �second and third row�,the performance of the clustering stage also decreased pro-gressively with the resolution increase, being most of themesh elements not assigned to the correct region for resolu-tions lower than 0.1 mm. On the other hand, clustering re-sults were similar with resolutions of 0.05 mm and 0.1 mm,as quantitatively shown in Table V. For 0.05 mm, the vessel
m left to right: Reference maps, 0.05, 0.1, 0.2, 0.4, and 0.8 mm�. Top row:m� views of the clustering results. The different clusters correspond to the
�frobotto
and the dome were identified with slightly higher accuracy

1701 Balocco et al.: Feasibility of regional mechanical properties of cerebral aneurysms 1701
than with 0.1 mm, as illustrated by the corresponding Dice’scoefficient �92.42 vs 90.94 and 89.99 vs 81.36 for vessel anddome, respectively�. As for the stiffness estimates, better re-sults were obtained with 0.05 mm images for the vessel andthe dome, while the stiffness value corresponding to the blebwas slightly more accurate using 0.1 mm images �absoluteerror of 0.94 MPa for 0.05 mm and 0.33 MPa for 0.1 mmwith a reference stiffness value of 12 MPa�. Finally, the me-chanical parameter optimization stage did not converge toreasonable values when using images with resolutions worsethan 0.1 mm.
IV. DISCUSSION
In this manuscript, we studied the feasibility of estimatingregional mechanical properties of cerebral aneurysms with amethodology based on the optimization of the parameters ofa biomechanical model guided by aneurysm wall motion es-timates. For doing so, in silico experiments were designed totest the robustness of the proposed methodology with respectto limiting factors such as aneurysm geometrical character-istics and the accuracy of wall motion estimates. This sectionpresents a discussion on results obtained in the in silico ex-periments, as well as on the employed biomechanical modeland inverse problem strategy, finishing with the clinical fea-sibility and limitations of the proposed methodology.
IV.A. Geometry in silico experiments
For the geometry in silico experiments, the proposedworkflow proved to be very robust with respect to differentinput geometries, with percentages of true positives above98.2% for all regions, including cases with wrinkled andsmall regions. The manual definition of borders between re-gions was performed by an expert operator following thesame rules for all six aneurysm geometries. In particular forthe border between the aneurysm and the parent vessel, in
TABLE V. Clustering and stiffness estimates with respect to image resolutionEE�: Estimated stiffness.
Region Mesh elementsTP�%�
FP�%�
0.05 mm Vessel 785 90.06 4.8Dome 807 92.44 13.0Bleb 120 77.50 18.3
0.1 mm Vessel 785 97.83 17.3Dome 807 71.13 3.7Bleb 120 89.17 80.0
0.2 mm Vessel 785 59.36 2.4Dome 807 43.00 39.2Bleb 120 76.67 391.6
0.4 mm Vessel 785 29.43 4.7Dome 807 48.95 63.4Bleb 120 46.67 400.0
0.8 mm Vessel 785 18.47 12.2Dome 807 62.83 65.4Bleb 120 25.00 337.5
which a visual imaginary contour along the neck of the an-
Medical Physics, Vol. 37, No. 4, April 2010
eurysm is used, this process may generate some operator biasin nonstandard geometries, such as the one of patient 6 illus-trated in Fig. 4 �last row�. Automatic, robust, and objectivetechniques for aneurysm geometrical characterization, suchas the one recently proposed by Piccinelli et al.,54 will reducethis operator dependence as well as speed up the whole pro-cedure.
We also varied the number of blebs �i.e., different elastic-ity regions� in the aneurysm and we obtained a moderatedecrease in performance �both in terms of regional locationand stiffness estimates� when the number of blebs increased,as observed in Table II. The highest errors corresponded tointerfaces between regions having very different stiffnessvalues �e.g., the bleb with the lowest stiffness value and thedome�, where abrupt changes in the radial strain map oc-curred. The third bleb introduced into the aneurysm geom-etry was associated with a very low stiffness value, thus itwas prone to undergo large deformations and to be moresensitive to clustering errors, as it was shown in the experi-ments. Nevertheless, the estimated stiffness values were ac-curate enough to distinguish between the regions with differ-ent elasticity properties.
Finally, we studied the effect of having different meshesfor the forward and inverse analysis stages in order to ruleout the possibility of a correlation between the mesh discreti-zation level and the final stiffness distribution and estimatedvalues. The obtained results, summarized in Table III, con-firmed their independence with respect to the mesh reso-lution for the vessel and dome regions, but care must betaken with very small bleb regions since they were sensitiveto discretization errors.
IV.B. In silico wall motion experiments
As for the wall motion in silico experiments, we analyzedthe influence of the registration configuration �different tech-
True positives; FP/FN: False positives/negatives; RE�: Reference stiffness;
FN�%� DICE
RE�
�MPa�EE�
�MPa�Error�%�
9.94 92.42 288.00 391.59 35.977.56 89.99 72.00 95.61 32.79
22.50 79.15 12.00 12.94 7.832.17 90.94 288.00 405.30 40.73
28.87 81.36 72.00 100.83 40.0410.83 66.25 12.00 11.67 2.7540.64 73.39 288.00 1069.26 271.2757.00 47.18 72.00 194.50 170.1423.33 26.98 12.00 61.72 414.3370.57 43.87 288.00 2.84 99.0151.05 46.09 72.00 4513.80 6169.1753.33 17.07 12.00 1349.11 11 142.5881.53 28.27 288.00 1.61�105 5.58�104
37.17 55.05 72.00 1.48�107 2.06�107
75.00 10.81 12.00 7.09�106 5.91�107
. TP:
413220287140330
niques and parameter tuning� and the spatial resolution of the

1702 Balocco et al.: Feasibility of regional mechanical properties of cerebral aneurysms 1702
images required to have wall motion estimates accurateenough to guide the estimation of regional mechanical pa-rameters of cerebral aneurysms.
IV.B.1. Registration configuration
We observed �see Table IV and Fig. 7� that the choice ofthe registration configuration had a substantial effect on therecovered stiffness distribution and estimated values. Thehigher-dimensional registration techniques provided moredegrees of freedom to cope with deformations �diffeomor-phic Demons to FFD eight CP� and they consequently out-performed simpler registration ones �FFD with three and fiveCPs� due to the localized nonlinear nature of the wall motionto recover. The regional distribution of stiffness provided bythe diffeomorphic and FFD eight CP registration methodswas similar, but the former gave less false positives in thedome and the bleb and more true positives in the vessel thanthe FFD method. These differences may be related to thehigher degree of smoothness of the deformation fields fur-nished by the diffeomorphic Demons technique compared tothe FFD ones, which could generate more homogeneous ra-dial strain maps. In terms of the stiffness estimate errors, thediffeomorphic Demons technique outperformed FFD-basedones in the bleb but gave slightly worst results �overestima-tion of the stiffness� in regions undergoing small deforma-tions such as the vessel due to the intrinsic smoothness of thediffeomorphic deformation fields. Since the bleb was themost critical region due to its theoretical correlation with therisk of rupture, we used the diffeomorphic Demons registra-tion technique for subsequent experiments. In summary, thechoice of the registration strategy can have a major impacton the wall elasticity values estimated with the proposedworkflow, but the experiment conducted in this work sug-gests that registration configurations with a considerableamount of degrees of freedom �Demons and FFD with eightCPs per dimension� could be used to distinguish betweenregions with different wall mechanical properties.
IV.B.2. Imaging spatial resolution
We found very substantial differences in the workflowperformance when using simulated MR images with differ-ent spatial resolutions, as can be observed in Fig. 8 and inTable V. We also obtained accurate stiffness values and as-sociated regional distributions on MR images with resolu-tions of 0.05 and 0.1 mm �slightly better stiffness estimateswith 0.05 mm for the vessel and the dome, and similar forthe bleb�, but results were not acceptable for lower resolu-tions. It must be pointed out that the stiffness estimates cor-responding to the bleb were more accurate than for the vesseland the dome at the best resolutions �0.05 and 0.1 mm�, thisfact having a relation with the magnitude of the displace-ments undergone by the different regions. The bleb was theregion undergoing the largest displacements, thus this regionwas more robust to noise/errors at the highest resolutions,whereas vessel and dome displacements were very small andcomparable to the image resolution, thus prone to be more
affected by noise and registration errors. Besides, the clus-Medical Physics, Vol. 37, No. 4, April 2010
tering stage globally achieved better results at the bleb regionwith 0.05 mm resolution than with 0.1 mm �79.15 vs 66.25of Dice’s coefficient� but the resulting stiffness estimateswere not substantially different. This fact indicated that theproposed methodology could cope with some of the cluster-ing errors, suggesting a relative independence of the finalstiffness estimates with respect to the clustering stage.
In summary, according to the in silico experiments pre-sented in this paper, 0.1 mm was the minimum image reso-lution required for using registration-based deformationfields to distinguish aneurysm regions with different me-chanical properties. These findings were in good agreementwith results obtained by Zhang et al.41 with 3DRA-reconstructed volumes acquired on physical phantom experi-ments, where they concluded that cerebral aneurysm wallpulsation could be recovered from registration techniques ap-plied on volumes reconstructed from projections having aspatial resolution of 0.155 mm per dimension.
Unfortunately, a resolution of 0.1 mm cannot currently beobtained with the 3DRA or MR acquisition protocols com-monly used in clinical routine. However, several researchgroups are actively developing new acquisition protocols andimaging systems to improve spatial resolution currentlyavailable in neurovascular images such as Rudin et al.55 forendovascular image guided interventions or Ganguly et al.56
for microangiography images. Finally, high-field MRI sys-tems �e.g., 7 T, 9.4 T MR scans�, which can already providethe spatial resolutions required in our application, could alsobe considered in the future to obtain in vivo wall pulsationestimates if current issues �imaging, artifacts, patient’s com-fort, and unknown risks, etc.� to its application in clinicalroutine are sorted out.
In addition, temporal resolution of the images was alsocritical to recover wall motion estimates in cerebral aneu-rysms from imaging. Ishida et al.37 needed 4DCTA imageswith 15–16 frames per cycle to extract wall motion informa-tion, while Zhang et al.57 recently showed that around 10frames per second will be enough to capture cerebral aneu-rysm pulsation from 3DRA data. Nevertheless, the inverseproblem strategy proposed in this work will be valid even ifjust two frames corresponding to systolic and diastolicphases are acquired, in order to capture the maximum gradi-ent between rest and pressurized vessel status.
IV.C. Proposed methodology
IV.C.1. Finite-element forward model
In this paper, we made use of a simple incompressiblelinear and isotropic Hookean model, as a first implementa-tion, but the proposed methodology allows a straightforwardincorporation of more complex and realistic constitutiveequations including nonlinearity, hyperelasticity, wall aniso-tropy �as demonstrated by the experiments of MacDonald etal.10 and others�, the multilayer structural nature of the arte-rial walls, and the role of collagen fibers such as the modelsproposed by Kroon and Holzapfel27 and Lu et al.58 Hence,the assumption of linearity and isotropy used in this work led
to an estimation of broad areas of the aneurysm prone to
1703 Balocco et al.: Feasibility of regional mechanical properties of cerebral aneurysms 1703
rupture, but more realistic models are required to identifymore accurate spots of risk of rupture. However, some pa-rameters of these complex models such as collagen fiber ori-entation will be quite difficult to personalize/validate sincecurrent imaging modalities cannot provide noninvasive mea-surements of aneurysm fiber orientation.
IV.C.2. Inverse problem strategy
The use of finite-element techniques to solve our numeri-cal problem required the optimization of the unknown modelparameters for each element of the mesh, which could easilylead to ill-conditioning and prohibitive computational costswhen using large meshes. This problem could become evenmore critical when using nonlinear constitutive equationssince they imply a larger number of parameters to estimate.Therefore, we proposed a region clustering method, appliedto the radial strain map derived from the displacement fieldrepresenting wall motion, in order to reduce the number ofparameters to estimate and allowing reasonable convergencetimes �between 15 and 45 min�. The number of clusters wasautomatically obtained with a silhouette-based algorithm thatgave the correct number of regions in all experiments. Nev-ertheless, due to the localized nature of the mechanical prop-erties, it could be convenient to have a higher number ofdifferent elasticity regions, as well as adding noise and agradient between different stiffness regions in order to betterevaluate the performance of the clustering stage.
Multiresolution approaches27 and genetic optimizationstrategies45 could be considered, in conjunction with the pro-posed region clustering technique, to deal with more regionsof piecewise constant elasticity and with more complex bio-mechanical models. In addition, longitudinal and circumfer-ential components of the strain may be relevant and thusneeded at the clustering stage if more complex biomechani-cal models will be used to model the aneurysm wall.
Besides, we formulated the wall mechanic behavior as afunction of a surrogate of elasticity called stiffness, whichaccounted for both the wall thickness and the elasticity �char-acterized by the Young’s modulus when using linear mod-els�. This ambiguity can be overcome by measuring the exactthickness at each point �between 16 and 212 �m, accordingto experiments of MacDonald et al.10�, which is unfeasiblenowadays with the current imaging techniques, or assuminga uniform thickness around the surface. However, the pro-posed stiffness parameter can be seen as a comprehensivebiomarker of the risk of rupture since it is directly related tochanges in thickness and/or elasticity, both considered indi-ces of early structure fragility.7,8
IV.C.3. Fluid-structure interaction
We coupled solid mechanics equations with hemodynam-ics through FSI and considering subject-specific informationon inflow-related boundary conditions �gradients of bloodvelocity and pressure� in order to study the influence of he-modynamics on the estimation of mechanical properties incerebral aneurysms. The systemic pressure �gradient between
systolic and diastolic pressures� was, in general, about twoMedical Physics, Vol. 37, No. 4, April 2010
orders of magnitude higher than the relative spatial pressurevariations, which could then be neglected for stiffness esti-mations by imposing a uniform pressure distribution tempo-rally varying along the cardiac cycle.27 These results sug-gested that the incorporation of FSI was not necessary for theestimation of mechanical properties in cerebral aneurysmswith the assumption of linear and isotropic material proper-ties, even with the different and complex patient-specific ge-ometries used in this paper �see Fig. 4�. On the other hand,nonuniform pressure distributions and FSI in general mayplay a role if more complex and anisotropic aneurysm wallstructure is incorporated.
Besides it would be very interesting to investigate corre-lations between different stiffness regions, areas with highwall shear stress and with rupture sites, in order to have acomplete clinical evaluation of the risk of rupture.
IV.C.4. Clinical feasibility and limitations
The ultimate goal of the proposed methodology was toprovide patient-specific information on the mechanical prop-erties of the aneurysm wall for the assessment of aneurysmrupture risk and support treatment decisions. However, at thetime being, there are some limiting factors that hamper theclinical feasibility of the proposed methodology, mainly thespatial resolution in the imaging systems currently availablein clinical routine.
The spatial resolution of the imaging was the most criticalissue since results given by the proposed methodology fullydepended on the ability to extract wall pulsation informationfrom imaging, requiring a spatial resolution of 0.1 mm, asconcluded from the in silico experiments presented in thiswork. As discussed above, continued developments in theimaging acquisition systems, including better image recon-struction algorithms,57 would make this type of high-resolution images possible in the future. Regarding the dif-ferent stages of the proposed methodology, the registrationconfiguration chosen to recover wall pulsation from imagingwas the most affected by the available spatial resolution.Moreover, the registration algorithm must be robust enoughto be used in clinical routine since large registration errorswould propagate to subsequent steps of the workflow andaffect the estimated mechanical properties. Even if the clus-tering stage may filter out some of these registration errors,as shown in the in silico experiments presented in Sec. III,improvements in the registration strategy such as the use ofnarrow-band regions of interest57 or better similarity metricscould reduce wall pulsation errors and then have more accu-rate stiffness estimates.
Finally, other aspects restricting the implementation of theproposed workflow in clinical routine are the validation ofthe resulting mechanical properties with in vivo data and thecomputational cost of the whole methodology. The lack of invivo information about the mechanical properties of the ce-rebral aneurysm wall limits the validation of the methodol-ogy to histological or ex vivo measurements, thus being dif-ficult to apply the proposed workflow in the large number of
different cases required for a thorough validation. In terms of
1704 Balocco et al.: Feasibility of regional mechanical properties of cerebral aneurysms 1704
computational cost of the proposed workflow, the most de-manding stage was the optimization of the stiffness param-eters of the biomechanical model, even if a simple modelwas used in this work. As discussed above, multiresolutiontechniques could be used to reduce convergence times at theoptimization stage and, in conjunction with the automaticcharacterization of the aneurysm geometries, make the com-putational time of the whole workflow be in the order ofminutes. The use of more complex and realistic biomechani-cal models, requiring the optimization of a large number ofunknown parameters, would considerably increase the com-putational cost of the workflow, making its application inclinical routine even more challenging.
V. CONCLUSIONS
In this paper, we presented a feasibility study of the esti-mation of mechanical properties of cerebral aneurysms givenby a data assimilating framework integrating imaging andcomputational models. Aneurysm geometry and wall motionestimates recovered from image postprocessing techniqueswere used in conjunction with a simple model of the wallbehavior �including flow� which was guided by a surrogateof the elasticity that also included wall thickness. Addition-ally, we developed a region clustering method aimed at re-ducing the number of parameters to estimate and allowingreasonable convergence times. Finally, we also designedsome in silico experiments to assess the robustness of theproposed workflow with respect to aneurysm geometry andwall motion factors. The main conclusion of these experi-ments were that spatial resolution of current clinical imagesis not sufficient yet to extract wall pulsation measurementswith enough accuracy to guide the estimation of mechanicalproperties in the proposed data assimilation framework. Theregistration configuration chosen to recover wall pulsationestimates from imaging was very important to assure esti-mated stiffness values accurate enough to distinguish be-tween aneurysm regions having different mechanical proper-ties. On the other hand, in agreement with the resultsreported by Oshima,59 we observed that the incorporation offluid-structure interaction in the biomechanical model did nothave a substantial influence in the final results, since theregional pressure variation obtained from CFD simulationwas minimal �of the order of tens of mmHg�, leading to theconclusion that an uniform pressure can be reasonably as-sumed in these simulations.
The proposed workflow may help to test different as-sumptions on how wall thickness and mechanical propertiesvary regionally or between different subjects, thus improvingour knowledge about cerebral aneurysms. Furthermore, thepersonalized aspect of the proposed workflow will allow fu-ture investigations on correlations between the estimated re-gional stiffness distributions, rupture sites and with patient-specific geometry-based and/or flow-based indices such aswall shear stress maps.
Future work will focus on the development of in vitroexperiments using physical phantoms to generate images
�MR, 3DRA, and 4DCTA� with sufficient resolution to en-Medical Physics, Vol. 37, No. 4, April 2010
able wall motion measurements. A further improvement inthe proposed workflow might be to use more sophisticatednonlinear models of the arterial wall behavior including an-isotropy and the role of collagen fibers such as the onesproposed by Holzapfel et al.27 and Lu et al.,60 as well asexploring the incorporation of thrombus formation in themodel.
ACKNOWLEDGMENTS
The authors would like to acknowledge G. Blasco and S.Pedraza, MD, PhD, of the Hospital Josep Trueta �Girona,Spain� for providing the MR-based flow measurements. Theauthors would also like to thank C. Zhang, M.C. Villa, M.Kim, A.G. Radaelli, C. Butakoff, E. Oubel, and M. DeCraene, all colleagues at the UPF, for providing the aneu-rysm meshes and for their support in Laplace’s law deriva-tion and the interpretation of the registration results. B.H.Bijnens is ICREA Research Professor at the CISTIB, DTIC,Universitat Pompeu Fabra, Barcelona, Spain. The work of O.Camara is supported by the Spanish Ministry of Science andInnovation �MICINN� under a Ramon y Cajal Research Fel-lowship. S. Balocco is currently at the Centre de Visió perComputador, Universitat Autònoma de Barcelona, Bellaterra,Spain, and his work is supported by the Catalan Agency forAdministration of University and Research �AGAUR� undera Beatriu de Pinós Fellowship. This research has been par-tially funded by the Industrial and Technological Develop-ment Centre �CDTI� of the Spanish Ministry of Industry un-der the CENIT Programme �CDTEAM Project� and by theEuropean Commission Sixth Framework Programme underthe Integrated Project @neurIST �Grant No. IST-2005-027703�.
a�Electronic mail: [email protected]�Electronic mail: [email protected]�Electronic mail: [email protected]�Electronic mail: [email protected]�Electronic mail: [email protected]. O. Wiebers, D. G. Piepgras, F. B. Meyer, D. F. Kallmes, and I. F.Meissner, “Pathogenesis, natural history and treatment of unruptured in-tracranial aneurysms,” Mayo Clin. Proc. 79, 1572–1583 �2004�.
2J. L. Brisman, “Cerebral aneurysms,” N. Engl. J. Med. 355, 928–939�2006�.
3J. Huang and J. M. van Gelder, “The probability of sudden death fromrupture of intracranial aneurysms: A meta-analysis,” Neurosurgery 51,1101–1107 �2002�.
4J. W. Hop, G. J. Rinkel, A. Algra, and J. van Gijn, “Case-fatality rates andfunctional outcome after subarachnoid hemorrhage: A systematic review,”Stroke 28, 660–664 �1997�.
5D. M. Sforza, C. M. Putman, and J. R. Cebral, “Hemodynamics of cere-bral aneurysms,” Annu. Rev. Fluid Mech. 41, 91–107 �2009�.
6J. C. Lasheras, “The biomechanics of arterial aneurysms,” Annu. Rev.Fluid Mech. 39, 293–319 �2007�.
7M. Tóth, G. L. Nádasy, I. Nyáry, T. Kerényi, and E. Monos, “Are theresystemic changes in the arterial biomechanics of intracranial aneurysmpatients?,” Eur. J. Phys. 439, 573–578 �2000�.
8T. Anderson, “Arterial stiffness or endothelial dysfunction as a surrogatemarker of vascular risk,” Can. J. Cardiol. 22, 72B–80B �2006�.
9M. Hayakawa, K. Katada, H. Anno, S. Imizu, J. Hayashi, K. Irie, M.Negoro, Y. Kato, T. Kanno, and H. Sano, “CT angiography with electro-cardiographically gated reconstruction for visualizing pulsation of intrac-ranial aneurysms: Identification of aneurysmal protuberance presumablyassociated with wall thinning,” AJNR Am. J. Neuroradiol. 26, 1366–1369
�2005�.
1705 Balocco et al.: Feasibility of regional mechanical properties of cerebral aneurysms 1705
10D. J. MacDonald, H. M. Finlay, and P. B. Canham, “Directional wallstrength in saccular brain aneurysms from polarized light microscopy,”Ann. Biomed. Eng. 28, 533–542 �2000�.
11M. Sermesant, P. Moireau, O. Camara, J. Sainte-Marie, R. Andriantsimi-avona, R. Cimrman, D. L. G. Hill, D. Chapelle, and R. Razavi, “Cardiacfunction estimation from MRI using a heart model and data assimilation:Advances and difficulties,” Med. Image Anal. 10, 642–656 �2006�.
12H. Schmid, P. O’Callaghan, M. P. Nash, W. Lin, I. J. LeGrice, B. H.Smaill, A. A. Young, and P. J. Hunter, “Myocardial material parameterestimation. A non-homogeneous finite element study from simple sheartests,” Biomech. Model. Mechanobiol. 7, 161–173 �2008�.
13R. Karimi, T. Zhu, B. E. Bouma, and M. R. Mofrad, “Estimation ofnonlinear mechanical properties of vascular tissues via elastography,”Cardiovasc. Eng. 8, 191–202 �2008�.
14C. Y. Huang, M. A. Soltz, M. Kopacz, V. C. Mow, and G. A. Ateshian,“Experimental verification of the roles of intrinsic matrix viscoelasticityand tension–compression nonlinearity in the biphasic response of carti-lage,” J. Biomech. Eng. 125, 84–93 �2003�.
15M. Schweiger, O. Camara-Rey, W. R. Crum, E. Lewis, J. A. Schnabel, S.R. Arridge, D. L. G. Hill, and N. C. Fox, “An inverse problem approachto the estimation of volume change,” in Proceedings of the InternationalConference on Medical Image Computing and Computer-Assisted Inter-vention (MICCAI’05), Lecture Notes in Computer Science Vol. 3750�Springer, Palm Springs, 2005�, pp. 616–623.
16S. Scott, G. G. Ferguson, and M. R. Roach, “Comparison of the elasticproperties of human intracranial arteries and aneurysms,” Can. J. Physiol.Pharmacol. 50, 328–332 �1972�.
17P. B. Canham and G. G. Ferguson, “A mathematical model for the me-chanics of saccular aneurysms,” Neurosurgery 17, 291–295 �1985�.
18G. J. Hademenos, T. Massoud, D. J. Valentino, G. Duckwiler, and F.Vinuela, “A nonlinear mathematical model for the development and rup-ture of intracranial saccular aneurysms,” Neurol. Res. 16, 376–384�1994�.
19H. J. Steiger, R. Aaslid, S. Keller, and H. J. Reulen, “Strength, elasticityand viscoelastic properties of cerebral aneurysms,” Heart Vessels 5,41–46 �1989�.
20M. Tóth, G. L. Nadasy, I. Nyary, T. Kerenyi, M. Orosz, G. Molnarka, andE. Monos, “Sterically inhomogenous viscoelastic behavior of human sac-cular cerebral aneurysms,” J. Vasc. Res. 35, 345–355 �1998�.
21F. P. K. Hsu, A. C. M. Liu, J. Downs, D. Rigamonti, and J. D. Humphrey,“A triplane video-based experimental system for studying axisymmetri-cally inflated biomembranes,” IEEE Trans. Biomed. Eng. 42, 442–450�1995�.
22S. K. Kyriacou, A. D. Shah, and J. D. Humphrey, “Inverse finite elementcharacterization of nonlinear hyperelastic membranes,” ASME J. Appl.Mech. 64, 257–262 �1997�.
23P. Seshaiyer, F. P. K. Hsu, A. D. Shah, S. K. Kyriacou, and J. D. Hum-phrey, “Multiaxial mechanical behavior of human saccular aneurysms,”Comput. Methods Biomech. Biomed. Eng. 4, 281–289 �2001�.
24S. Baek, K. R. Rajagopal, and J. D. Humphrey, “Competition betweenradial expansion and thickening in the enlargement of an intracranialsaccular aneurysm,” J. Elast. 80, 13–31 �2005�.
25S. Baek, K. R. Rajagopal, and J. D. Humphrey, “A theoretical model ofenlarging intracranial fusiform aneurysms,” J. Biomech. Eng. 128, 142–149 �2006�.
26M. Kroon and G. A. Holzapfel, “A model for saccular cerebral aneurysmgrowth by collagen fibre remodeling,” J. Theor. Biol. 247, 775–787�2007�.
27M. Kroon and G. A. Holzapfel, “Estimation of the distributions of aniso-tropic, elastic properties and wall stresses of saccular cerebral aneurysmsby inverse analysis,” Proc. R. Soc. London, Ser. A 464, 807–825 �2008�.
28S. Balocco, O. Camara, and A. F. Frangi, “Towards regional elastographyof intracranial aneurysms,” in Proceedings of the International Confer-ence on Medical Image Computing and Computer-Assisted Intervention(MICCAI’08), Lecture Notes in Computer Science Vol. 11, Pt.2 �Springer,New York, 2008�, pp. 131–138.
29J. R. Cebral, M. A. Castro, S. Appanaboyina, C. Putman, D. Millan, andA. F. Frangi, “Efficient pipeline for image-based patient-specific analysisof cerebral aneurysm hemodynamics: Technique and sensitivity,” IEEETrans. Med. Imaging 24, 457–467 �2005�.
30M. Hernandez and A. F. Frangi, “Non-parametric geodesic active regions:Method and evaluation for cerebral aneurysms segmentation in 3DRA
and CTA,” Med. Image Anal. 11, 224–241 �2007�.Medical Physics, Vol. 37, No. 4, April 2010
31M. Attene and B. Falcidieno, “ReMESH: An interactive environment toedit and repair triangle meshes,” in Proceedings of Shape Modeling In-ternational (SMI’06) �I.C.S. Press, Sendai, Japan, 2006�, pp. 271–276.
32J. Alastruey, K. Parker, J. Peiró, S. Byrd, and S. Sherwin, “Modeling thecircle of Willis to assess the effects of anatomical variations and occlu-sions on cerebral flows,” J. Biomech. 40, 1794–1805 �2007�.
33V. Challa and H. C. Han, “Spatial variations in wall thickness, materialstiffness and initial shape affect wall stress and shape of intracranial an-eurysms,” Neurol. Res. 29, 569–577 �2007�.
34M. E. Gurtin and A. Ian Murdoch, “A continuum theory of elastic mate-rial surfaces,” Arch. Ration. Mech. Anal. 57, 291–323 �1975�.
35W. Nichols and M. O’Rourke, McDonald’s Blood Flow in Arteries: The-oretical, Experimental and Clinical Principles, 3rd ed. �Arnold, Londonand Oxford University Press, New York, 1998�.
36X. Zhang, M. Fatemi, and J. Greenleaf, “Inverse method for estimatingelastic modulus of arterial walls,” Eur. J. Vasc. Endovasc. Surg. 19, 221–225 �2000�.
37F. Ishida, H. Ogawa, T. Simizu, T. Kojima, and W. Taki, “Visualizing thedynamics of cerebral aneurysms with four-dimensional computed tomog-raphic angiography,” Neurosurgery 57, 460–471 �2005�.
38Y. Kato, M. Hayakawa, H. Sano, M. V. Sunil, S. Imizu, M. Yoneda, S.Watanabe, M. Abe, and T. Kanno, “Prediction of impending rupture inaneurysms using 4D-CTA: Histopathological verification of a realtimeminimally invasive tool in unruptured aneurysms,” Minim Invasive Neu-rosurg. 47, 131–135 �2004�.
39M. Matsumoto, T. Sasaki, K. Suzuki, J. Sakuma, Y. Endo, and N.Kodama, “Visualizing the dynamics of cerebral aneurysms with four-dimensional computed tomographic angiography,” Neurosurgery 58,E1003 �2006�.
40E. Oubel, M. D. Craene, C. M. Putman, J. R. Cebral, and A. F. Frangi,“Analysis of intracranial aneurysm wall motion and its effects on hemo-dynamic patterns,” in Proceedings of SPIE Medical Imaging, 2007, Vol.6511, p. 65112A.
41C. Zhang, M. C. Villa-Uriol, M. De Craene, J. Pozo, and A. Frangi,“Morphodynamic analysis of cerebral aneurysm pulsation from time-resolved rotational angiography,” IEEE Trans. Med. Imaging 28, 1105–1116 �2009�.
42M. Holden, “A review of geometric transformations for nonrigid bodyregistration,” IEEE Trans. Med. Imaging 27, 111–128 �2008�.
43D. Rueckert, L. I. Sonoda, C. Hayes, D. L. G. Hill, M. O. Leach, and D.J. Hawkes, “Non-rigid registration using free-form deformations: Appli-cation to breast MR images,” IEEE Trans. Med. Imaging 18, 712–721�1999�.
44T. Vercauteren, X. Pennec, A. Perchant, and N. Ayache, “Non-parametricdiffeomorphic image registration with the demons algorithm,” in Pro-ceedings of the International Conference on Medical Image Computingand Computer-Assisted Intervention (MICCAI’07), Lecture Notes inComputer Science Vol. 4792, 2007, pp. 319–326.
45A. S. Khalil, B. E. Bouma, and M. R. K. Mofrad, “A combined FEM/genetic algorithm for vascular soft tissue elasticity estimation,” Cardio-vasc. Eng. 6, 93–102 �2006�.
46J. A. Hartigan, Clustering Algorithms �Wiley, New York, 1975�.47L. Kaufman and P. J. Rousseeuw, Finding Groups in Data: An Introduc-
tion to Cluster Analysis �Wiley, New York, 1990�.48J. A. Nelder and R. Mead, “A simplex method for function minimiza-
tion,” Comput. J. 7, 308–313 �1965�.49L. R. Dice, “Measures of the Amount of Ecologic Association Between
Species,” Ecology 26, 297–302 �1945�.50R. K. Kwan, A. C. Evans, and G. B. Pike, “MRI simulation-based evalu-
ation of image-processing and classification methods,” IEEE Trans. Med.Imaging 18, 1085–1097 �1999�; IMAGESIM, http://learnfmri.ucsd.edu/howto/imagesim.html
51X. Leclerc, L. Nicol, J.-Y. Gauvrit, V. L. Thuc, D. Leys, and J.-P. Pruvo,“Contrast-enhanced MR angiography of supraaortic vessels: The effect ofvoxel size on image quality,” AJNR Am. J. Neuroradiol. 21, 1021–1027�2000�.
52M. S. Wang, D. R. Haynor, G. J. Wilson, T. Leiner, and J. H. Maki,“Maximizing contrast-to-noise ratio in ultra-high resolution peripheralMR angiography using a blood pool agent and parallel imaging,” J.Magn. Reson Imaging 26, 580–588 �2007�.
53A. K. Jain and R. C. Dubes, Algorithms for Clustering Data �Prentice-Hall, Englewood Cliffs, 1988�.
54
M. Piccinelli, A. Veneziani, D. Steinman, A. Remuzzi, and L. Antiga, “A
1706 Balocco et al.: Feasibility of regional mechanical properties of cerebral aneurysms 1706
framework for geometric analysis of vascular structures: Application tocerebral aneurysms,” IEEE Trans. Med. Imaging 28, 1141–1155 �2009�.
55S. Rudin, D. R. Bednarek, and K. R. Hoffmann, “Endovascular image-guided interventions �EIGIs�,” Med. Phys. 35, 301–309 �2008�.
56A. Ganguly, S. Rudin, D. R. Bednarek, K. R. Hoffmann, and I. S. Kyp-rianou, “Micro-angiography for neuro-vascular imaging. I. Experimentalevaluation and feasibility,” Med. Phys. 30, 3018–3028 �2003�.
57C. Zhang, M. De Craene, M.-C. Villa-Uriol, J. Pozo, B. Bijnens, and A.Frangi, in Estimating Continuous 4D Wall Motion of Cerebral Aneurysmsfrom 3D Rotational Angiography, in Proceedings of the InternationalConference on Medical Image Computing and Computer-Assisted Inter-
vention �MICCAI’09�, Lecture Notes in Computer Science 5761Medical Physics, Vol. 37, No. 4, April 2010
�Springer, London, 2009�, pp. 140–147.58J. Lu, X. Zhou, and M. L. Raghavan, “Inverse method of stress analysis
for cerebral aneurysms,” Biomech. Model. Mechanobiol. 7, 477–486�2008�.
59M. Shojima, M. Oshima, K. Takagi, R. Torii, K. Nagata, I. Shirouzu, A.Morita, and T. Kirino, “Role of the bloodstream impacting force and thelocal pressure elevation in the rupture of cerebral aneurysms,” Stroke 36,1933–1938 �2005�.
60J. Lu, X. Zhou, and M. L. Raghavan, “Inverse elastostatic stress analysisin predeformed biological structures: Demonstration using abdominal aor-tic aneurysms,” J. Biomech. 40, 693–696 �2007�.
Copyright © 2022 FDOKUMEN




















