
Expression of hepatocyte growth factor (HGF) and its receptor (MET) in medullary carcinoma of the...
12
HGF and MET in Medullary Thyroid Carcinoma 19 19 Department of Biomedical Sciences and Oncology, University of Turin, Italy and *Division of Gastroenterology, Hopital Cantonal, Geneve, Switzerland Address correspondence to: M. Papotti, MD Department of Biomedical Sciences and Oncology University of Turin, Via Santena 7, I-10126 Torino, Italy Fax 663 5267 Endocrine Pathology, vol. 11, no. 1, 19–30, Spring 2000 © Copyright 2000 by Humana Press Inc. All rights of any nature whatsoever reserved. 1046–3976/00/11:19–30/ $13.00 Expression of Hepatocyte Growth Factor (HGF) and its Receptor (MET) in Medullary Carcinoma of the Thyroid Mauro Papotti, Martina Olivero, Marco Volante, Francesco Negro,* Maria Prat, Paolo M. Comoglio, and Maria Flavia DiRenzo Abstract The tyrosine kinase receptor encoded by the MET oncogene has the unusual property of mediating the invasive growth of epithelial cells upon binding with the hepatocyte growth factor (HGF). The MET/HGF receptor is known to be overexpressed in thyroid carcinomas originated from follicular cells, but has not been reported in C cell tumors. To investigate the role of HGF and of its receptor (encoded by MET oncogene] in medullary carcinoma of the thyroid (MCT), we studied the expression of HGF and MET in 20 cases by means of different techniques. By RT-PCR, HGF mRNA was found in 10/20 cases, while MET mRNA presence was demonstrated in 8/20, of which 7 also expressed HGF. Northern blot analy- sis and in situ hybridization were performed in selected cases and confirmed RT-PCR data in some cases, although the lower sensitivity of these procedures did not allow the iden- tification of all RT-PCR positive cases. By immunohistochemistry (using specific mono- clonal antibodies) HGF was demonstrated in 8/9 RT-PCR positive cases and a monoclonal to MET immunostained 5/6 RT-PCR positive cases. All receptor positive cases also expressed the ligand in the same tumor cell population. These findings demonstrate MET and HGF co-expression in a subset of MCT, in which autocrine/paracrine circuits may be active. No correlation was found between HGF/MET expression and clinico-pathological param- eters, except for the more common multifocality of HGF/MET positive MCT. Whether the potential activation of MET in MCT is responsible for local invasion and malignant evolu- tion is to be further investigated, especially in multifocal and aggressive tumors. Key Words: Thyroid; medullary carcinoma; MET oncogene; HGF; RT-PCR; immu- nohistochemistry. Introduction Several oncogenes were found to be implicated in the development of thyroid cancer. Follicular tumors, both adenomas and carcinomas, were associated with ras mutation [1]. Other authors found an overexpression of the bcl-2 gene product [2], while p53 protein was found in an altered form in poorly differentiated folli- cular or undifferentiated carcinomas [3,4]. TRK, PTC, and RET oncogenes (encod- ing thyrosine kinases) are rearranged and activated at high frequency in papillary carcinoma [5,6]. Conversely, in tumors of parafollicular origin, only RET was exten- sively studied, and point mutations were observed in both sporadic and familial medullary carcinoma [7]. The MET oncogene encodes a trans- membrane tyrosine kinase corresponding Clinical Research
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Expression of hepatocyte growth factor (HGF) and its receptor (MET) in medullary carcinoma of the...
HGF and MET in Medullary Thyroid Carcinoma 19
19
Department of BiomedicalSciences and Oncology,University of Turin, Italy and*Division of Gastroenterology,Hopital Cantonal, Geneve,Switzerland
Address correspondence to:M. Papotti, MD Departmentof Biomedical Sciences andOncologyUniversity of Turin, ViaSantena 7, I-10126 Torino, ItalyFax 663 5267
Endocrine Pathology, vol. 11,no. 1, 19–30, Spring 2000© Copyright 2000 by HumanaPress Inc. All rights of anynature whatsoever reserved.1046–3976/00/11:19–30/$13.00
Expression of Hepatocyte Growth Factor (HGF) and itsReceptor (MET) in Medullary Carcinoma of the Thyroid
Mauro Papotti, Martina Olivero, Marco Volante, Francesco Negro,*Maria Prat, Paolo M. Comoglio, and Maria Flavia DiRenzo
AbstractThe tyrosine kinase receptor encoded by the MET oncogene has the unusual property ofmediating the invasive growth of epithelial cells upon binding with the hepatocyte growthfactor (HGF). The MET/HGF receptor is known to be overexpressed in thyroid carcinomasoriginated from follicular cells, but has not been reported in C cell tumors. To investigatethe role of HGF and of its receptor (encoded by MET oncogene] in medullary carcinomaof the thyroid (MCT), we studied the expression of HGF and MET in 20 cases by means ofdifferent techniques. By RT-PCR, HGF mRNA was found in 10/20 cases, while MET mRNApresence was demonstrated in 8/20, of which 7 also expressed HGF. Northern blot analy-sis and in situ hybridization were performed in selected cases and confirmed RT-PCR datain some cases, although the lower sensitivity of these procedures did not allow the iden-tification of all RT-PCR positive cases. By immunohistochemistry (using specific mono-clonal antibodies) HGF was demonstrated in 8/9 RT-PCR positive cases and a monoclonalto MET immunostained 5/6 RT-PCR positive cases. All receptor positive cases also expressedthe ligand in the same tumor cell population. These findings demonstrate MET andHGF co-expression in a subset of MCT, in which autocrine/paracrine circuits may be active.No correlation was found between HGF/MET expression and clinico-pathological param-eters, except for the more common multifocality of HGF/MET positive MCT. Whether thepotential activation of MET in MCT is responsible for local invasion and malignant evolu-tion is to be further investigated, especially in multifocal and aggressive tumors.
Key Words: Thyroid; medullary carcinoma; MET oncogene; HGF; RT-PCR; immu-nohistochemistry.
IntroductionSeveral oncogenes were found to be
implicated in the development of thyroidcancer. Follicular tumors, both adenomasand carcinomas, were associated with rasmutation [1]. Other authors found anoverexpression of the bcl-2 gene product[2], while p53 protein was found in analtered form in poorly differentiated folli-cular or undifferentiated carcinomas [3,4].
TRK, PTC, and RET oncogenes (encod-ing thyrosine kinases) are rearranged andactivated at high frequency in papillarycarcinoma [5,6]. Conversely, in tumors ofparafollicular origin, only RET was exten-sively studied, and point mutations wereobserved in both sporadic and familialmedullary carcinoma [7].
The MET oncogene encodes a trans-membrane tyrosine kinase corresponding
Clinical Research
20 Endocrine Pathology Volume 11, Number 1 Spring 2000
to the receptor of hepatocyte growth fac-tor/scatter factor (HGF) [8]. It was origi-nally identified in rearranged form in anosteosarcoma cell line [9] and subsequentlythe proto-oncogene was found expressedin several normal and neoplastic epithelialtissues [10–14]. A direct genetic relation-ship between MET activation and humancancer has been established by the identi-fication of germline and somatic mutationsin the catalytic domain of the receptor inpapillary renal cell carcinomas [15,16]. TheHGF receptor gene (MET) was foundoverexpressed in thyroid carcinomas of fol-licular cell lineage, with special referenceto papillary carcinoma [17,18], but not inthe few cases of medullary thyroid carci-noma (MCT) previously examined byNorthern blot [19,20]. The MET geneproduct was identified in 2/3 MCT stud-ied by immunohistochemistry [21], but nocorrelations with the mRNA expressionwas made and the number of cases was toolow to allow a definite conclusion.
The purpose of the present study was toinvestigate whether HGF and MET geneswere expressed in parafollicular C celltumors. To this aim, a series of 20 MCTwas studied using different procedures toreveal the ligand and its receptor at bothgene and protein levels.
Materials and Methods
Tumors
Twenty cases of medullary carcinoma ofthe thyroid in which fresh frozen tissuefrom total thyroidectomy specimens wasavailable for RNA extraction, were selectedfrom a larger series of tumors (see ref. 22)observed at the Department of Pathologyof the University of Turin between 1989and 1998. The tumor was cut into twoparts immediately after surgery. One of
them was frozen in liquid nitrogen andstored at –80°C for a period ranging from3 mo to 5 yr, until processed for RNAextraction. The adjacent portion of thetumor was fixed in formalin and processedfor conventional histology, Congo redstaining, and immunohistochemical char-acterization. The following antibodies wereemployed: thyroglobulin (Dako, Glostrup,Denmark, diluted 1/3000), calcitonin(Ortho Diagnostic, Raritan, NJ, diluted 1/1of kit dilution), chromogranin A (Biogenex,SanRamon, USA, diluted 1/50). C-cellhyperplasia was evaluated in non-tumoralthyroid tissue immunostained for calcito-nin, according to the criteria outlined byAlbores-Saavedra et al. [23], i.e., presenceof at least 50 C-cells per low power field.
Reverse Transcriptase–PolymeraseChain Reaction (RT-PCR)
Total RNA was extracted according tothe guanidine thiocyanate cesium chloridemethod [24] and the concentration ofRNA estimated by spectrophotometry.Total RNA (1 µg) was used as a templatefor synthesis of oligodR-primed doublestrand cDNA, using M-ML-V-RT fromBRL (UK). The RT product was heated at95°C for 3 min and then cooled on ice.The suitability of the RT reaction productfor PCR amplification was first checkedby performing a PCR reaction for G6PDHcDNA (Accession number J02642)using oligonucleotide primers: senseprimer, nucleotides 527–546 5'-ACCACAGTCCATGCCATCAC-3'; antisenseprimer, nucleotides 959–978 5'-TCCACCACCCTGTTGCTGTA-3'. To amplifyMET gene expressed sequences (Accessionnumber X54559), oligonucleotide prim-ers were: sense primer, nucleotides 2908–2937 5'-TTCCTGTGGCTGAAAAAGAGAAAGCAAATT-3'; antisense primer,
HGF and MET in Medullary Thyroid Carcinoma 21
nucleotides 3322–3352 5'-TGTCCAAC A A A G T C C C AT G ATATA C A CAACC-3'. HGF sequences (Accessionnumber M29145) were amplified usingprimers: sense primer, nucleotides 49–74,5'-TTTCACCCAGGCATCTCCTCCAGAG–3'; antisense primer, nucleotides1130–1150, 5'-CGTAGGTCCTTGCACTTGAAA-3' [25]. All the bands weredirectly sequenced. Positive controls wererepresented by MET and HGF expressingcell lines, namely, GTL-16 gastric carci-noma cell line, in which the MET gene isoverexpressed and amplified, and MRC5human fibroblast cell line, which secretesHGF. Additional control tissues includedtwo papillary carcinomas of the thyroidand two samples of normal thyroid,resected in the course of parathyroidec-tomy. To investigate tyrosine kinasedomain of the MET receptor expressed inmedullary carcinomas for mutation alreadydescribed in kidney carcinomas [15,16],MET gene expressed sequences corre-sponding to exons 16–20 were also ampli-fied (nucleotides 3341–3899), and PCRproducts were directly sequenced afterbeing purified from agarose gels using aQiagen (Germany) PCR product purifica-tion kit. Automatic sequences (forward andreverse) were performed using the ABIPrism 310 (Perkin Elmer) following themanufacturer’s protocols.
Northern Blot Analysis
In selected cases, Northern blot analysiswas performed. Hybridization was car-ried out at 42°C in the presence of 50%formamide, using 32P-labeled probescorresponding to the entire HGF andMET cDNAs. Nitrocellulose sheetswere washed twice in 2× saline sodiumcitrate (SSC)–0.1% sodium dodecylsulfate (SDS) at room temperature for
15 min and once at 65°C for 20 min.Positive controls were represented byMET and HGF expressing cell lines,namely, GTL-16 gastric carcinoma cellline, in which the MET gene is over-expressed and amplified, and MRC5 hu-man fibroblast cell line, which secretesHGF.
In Situ Hybridization
In selected cases (nos. 3, 4, 5, 6), HGFmRNA was analyzed by a non-radioactivein situ hybridization (ISH) procedure,using a digoxigenin-labeled cDNA probecorresponding to nucleotides 1–785 of theHGF sequence. The procedure followedthat employed for other probes, as describedelsewhere [26]. Briefly, after dewaxingand hydration, sections were incubatedwith PBS pH 7.2 at room temperaturefor 10 min. A proteinase K digestion step(500 µg/mL PBS, pH 7.2 at 37°C for15 min) was performed. After pre-hybrid-ization for 1 hr at room temperature (thebuffer contained 4× SSC, 50% formamide,1× Denhardt’s solution, 5% dextran sul-fate, 0.5 mg/mL salmon sperm DNA, 0.25mg/mL yeast tRNA), sections were hybrid-ized in the same buffer containing HGFprobe (at a concentration of 100 pmol/mL)overnight at 37°C in a humidified cham-ber. Finally, sections were washed withdecreasing concentrations of SSC, and thehybrids revealed with a nonradioactivelabeling and detection kit (Boehringer-Mannheim). MET mRNA was also revealedby a non-radioactive ISH according to theabove described procedure, using a PCRgenerated probe at a concentration of 100pmol/mL. The RNA probe correspondedto bases 1–804 of the MET complemen-tary DNA [27] and was obtained by aPCR-generated template, containing ateach end a suitable phage RNA polymerase
22 Endocrine Pathology Volume 11, Number 1 Spring 2000
promoter [28]. Briefly, two primers (whosesequence is shown in Table 1) were used toamplify the portion of MET cDNA en-compassing positions 1–804. To facilitatethe procedure, a small amount of a plas-mid containing the MET cDNA [29] wasused as starting material. The 853 base pairPCR product contained the amplifiedMET sequence flanked by two promotersspecific for SP6 and T7 RNA polymerases,respectively. Transcribing the PCR prod-uct with the T7 RNA polymerase will yieldan RNA probe complementary to theMET mRNA, while transcribing with theSP6 RNA polymerase will yield an RNAprobe having a sense sequence. Appropri-ate controls were introduced. Hybrid-ization with a non-related probe, with senseprobes of both HGF and MET and pre-treatment with RNase were used as nega-tive controls. A papillary thyroid carcinoma(known to overexpress MET), and liver tis-sue served as positive controls for MET andHGF, respectively.
Immunohistochemistry
Sixteen cases, in which residual frozentissue was available for immunohis-tochemical stains, were tested for MET andHGF protein expression. Cryostatic sec-tions were fixed in formalin for 5 min andimmersed in 3% H
2O
2/methanol to
quench endogenous peroxidase activity.Then, an incubation in avidin blockingreagent (Avidin biotin blocking kit, Bio-genex Laboratories, San Ramon, CA) for15 min and in biotin blocking reagent (Avi-din biotin blocking kit, Biogenex) for 15
min were performed to block endogenousbiotin activity. Incubation with the pri-mary antibodies followed at room tempera-ture for 1 h. Anti-MET/HGF receptormonoclonal antibody DO-24 was directedagainst the extracellular domain of theMET protein [11]. Monoclonal antibodyagainst HGF (clone DV-14) was raisedusing recombinant HGF/SF secreted by theSpodoptera frugiperda insect cells (Sf9),which were infected with the baculovirusvector containing the full size humanHGF/SF cDNA, as immunogen. Theworking dilutions were 1:1 for anti-MET(supernatant) and 1:50 for anti-HGF(ascitic fluid). The DAKO LSAB2 peroxi-dase kit (DAKO, Golstrup, Denmark) wasused in the streptavidin procedure, with a10 min incubation with peroxidase-con-jugated streptavidin. The slides were thendeveloped in liquid H
2O
2-3,3'-diamin-
obenzidine (Sigma Chemical Co., St.Louis, MO) solution for 5'. Paraffin sec-tions of selected cases were studied in par-allel with no pretreatment using theprimary antibodies anti-MET and HGFat the same dilutions applied on cryostaticsections.
Results
Clinical data (sex, age, size of tumor,stage, metastases, and/or recurrences) andfollow-up information on the 20 cases ofMCT are summarized in Table 2. Therewere 6 males and 14 females having amedian age of 46.5 yr. The tumors mea-sured on average 2.5 cm. Nine cases were
Table 1. Sequence of the Primers Used for the Generation of the MET Template by PCRa
SP6 MET1-S5'-GATTTAGGTGACACTATAGAATAC ATGAAGGCCCCCGCTGTGCT-3'T7 MET804-AS5'-TCTAATACGACTCACTATAGGGAGA GAGTTTCCCTTTGGACCGTC -3'
aThe sequence of the promoters is in italics and the MET sequence is in bold characters.
HGF and MET in Medullary Thyroid Carcinoma 23
multifocal. Six of these cases occurredin known multiple endocrine neoplasia(5 MEN2A and 1 MEN2B) affected fami-lies and had C-cell hyperplasia in theperitumoral thyroid parenchyma. Theother three cases were apparently sporadiccases and no mutational analysis for RET hadbeen performed. Thirteen cases (65%) hadcervical lymph node metastases at the timeof operation. Nine patients (47%) devel-oped local recurrence, mediastinal lymphnode metastases, or distant spread to boneand/or lung, 1–3 yr after operation. Twoof them actually died of their disease 2 and4 yr after diagnosis. Ten patients are cur-rently free of disease 1–17 yr after diagno-sis (mean 4.5 yr) and six other patients haddisease progression. Finally, one patient waslost to follow up. Histologically, the tumorshad heterogeneous features, as commonlyobserved in MCT. The dominant growthpatterns were alveolar, trabecular, and
spindle cell bundles. One case each ofpseudopapillary, pseudo-angiosarcoma-tous, and carcinoid-like MCT were alsoincluded in this series.
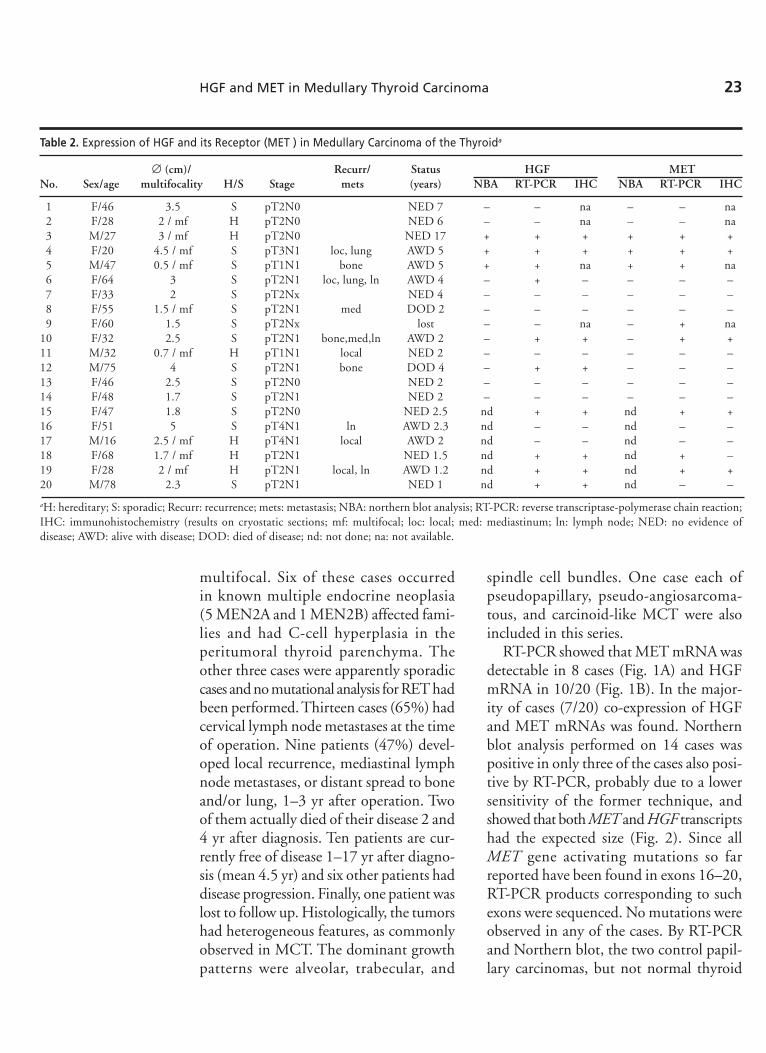
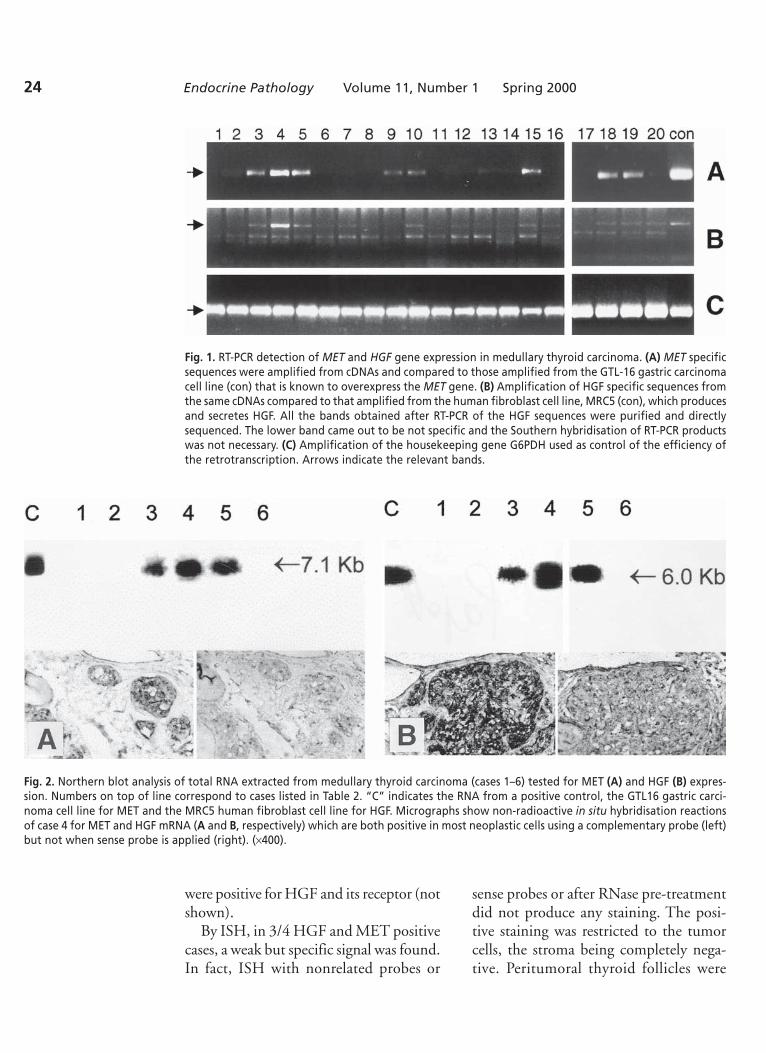
RT-PCR showed that MET mRNA wasdetectable in 8 cases (Fig. 1A) and HGFmRNA in 10/20 (Fig. 1B). In the major-ity of cases (7/20) co-expression of HGFand MET mRNAs was found. Northernblot analysis performed on 14 cases waspositive in only three of the cases also posi-tive by RT-PCR, probably due to a lowersensitivity of the former technique, andshowed that both MET and HGF transcriptshad the expected size (Fig. 2). Since allMET gene activating mutations so farreported have been found in exons 16–20,RT-PCR products corresponding to suchexons were sequenced. No mutations wereobserved in any of the cases. By RT-PCRand Northern blot, the two control papil-lary carcinomas, but not normal thyroid
Table 2. Expression of HGF and its Receptor (MET ) in Medullary Carcinoma of the Thyroida
∅ (cm)/ Recurr/ Status HGF METNo. Sex/age multifocality H/S Stage mets (years) NBA RT-PCR IHC NBA RT-PCR IHC
1 F/46 3.5 S pT2N0 NED 7 – – na – – na2 F/28 2 / mf H pT2N0 NED 6 – – na – – na3 M/27 3 / mf H pT2N0 NED 17 + + + + + +4 F/20 4.5 / mf S pT3N1 loc, lung AWD 5 + + + + + +5 M/47 0.5 / mf S pT1N1 bone AWD 5 + + na + + na6 F/64 3 S pT2N1 loc, lung, ln AWD 4 – + – – – –7 F/33 2 S pT2Nx NED 4 – – – – – –8 F/55 1.5 / mf S pT2N1 med DOD 2 – – – – – –9 F/60 1.5 S pT2Nx lost – – na – + na
10 F/32 2.5 S pT2N1 bone,med,ln AWD 2 – + + – + +11 M/32 0.7 / mf H pT1N1 local NED 2 – – – – – –12 M/75 4 S pT2N1 bone DOD 4 – + + – – –13 F/46 2.5 S pT2N0 NED 2 – – – – – –14 F/48 1.7 S pT2N1 NED 2 – – – – – –15 F/47 1.8 S pT2N0 NED 2.5 nd + + nd + +16 F/51 5 S pT4N1 ln AWD 2.3 nd – – nd – –17 M/16 2.5 / mf H pT4N1 local AWD 2 nd – – nd – –18 F/68 1.7 / mf H pT2N1 NED 1.5 nd + + nd + –19 F/28 2 / mf H pT2N1 local, ln AWD 1.2 nd + + nd + +20 M/78 2.3 S pT2N1 NED 1 nd + + nd – –
aH: hereditary; S: sporadic; Recurr: recurrence; mets: metastasis; NBA: northern blot analysis; RT-PCR: reverse transcriptase-polymerase chain reaction;IHC: immunohistochemistry (results on cryostatic sections; mf: multifocal; loc: local; med: mediastinum; ln: lymph node; NED: no evidence ofdisease; AWD: alive with disease; DOD: died of disease; nd: not done; na: not available.
24 Endocrine Pathology Volume 11, Number 1 Spring 2000
Fig. 1. RT-PCR detection of MET and HGF gene expression in medullary thyroid carcinoma. (A) MET specificsequences were amplified from cDNAs and compared to those amplified from the GTL-16 gastric carcinomacell line (con) that is known to overexpress the MET gene. (B) Amplification of HGF specific sequences fromthe same cDNAs compared to that amplified from the human fibroblast cell line, MRC5 (con), which producesand secretes HGF. All the bands obtained after RT-PCR of the HGF sequences were purified and directlysequenced. The lower band came out to be not specific and the Southern hybridisation of RT-PCR productswas not necessary. (C) Amplification of the housekeeping gene G6PDH used as control of the efficiency ofthe retrotranscription. Arrows indicate the relevant bands.
Fig. 2. Northern blot analysis of total RNA extracted from medullary thyroid carcinoma (cases 1–6) tested for MET (A) and HGF (B) expres-sion. Numbers on top of line correspond to cases listed in Table 2. “C” indicates the RNA from a positive control, the GTL16 gastric carci-noma cell line for MET and the MRC5 human fibroblast cell line for HGF. Micrographs show non-radioactive in situ hybridisation reactionsof case 4 for MET and HGF mRNA (A and B, respectively) which are both positive in most neoplastic cells using a complementary probe (left)but not when sense probe is applied (right). (×400).
were positive for HGF and its receptor (notshown).
By ISH, in 3/4 HGF and MET positivecases, a weak but specific signal was found.In fact, ISH with nonrelated probes or
sense probes or after RNase pre-treatmentdid not produce any staining. The posi-tive staining was restricted to the tumorcells, the stroma being completely nega-tive. Peritumoral thyroid follicles were
HGF and MET in Medullary Thyroid Carcinoma 25
negative. A topographical association be-tween HGF and MET positive tumor ar-eas was found, although a coexpression ofboth the receptor and its ligand by the sameneoplastic cell could have not been dem-onstrated in the available tumor tissues.
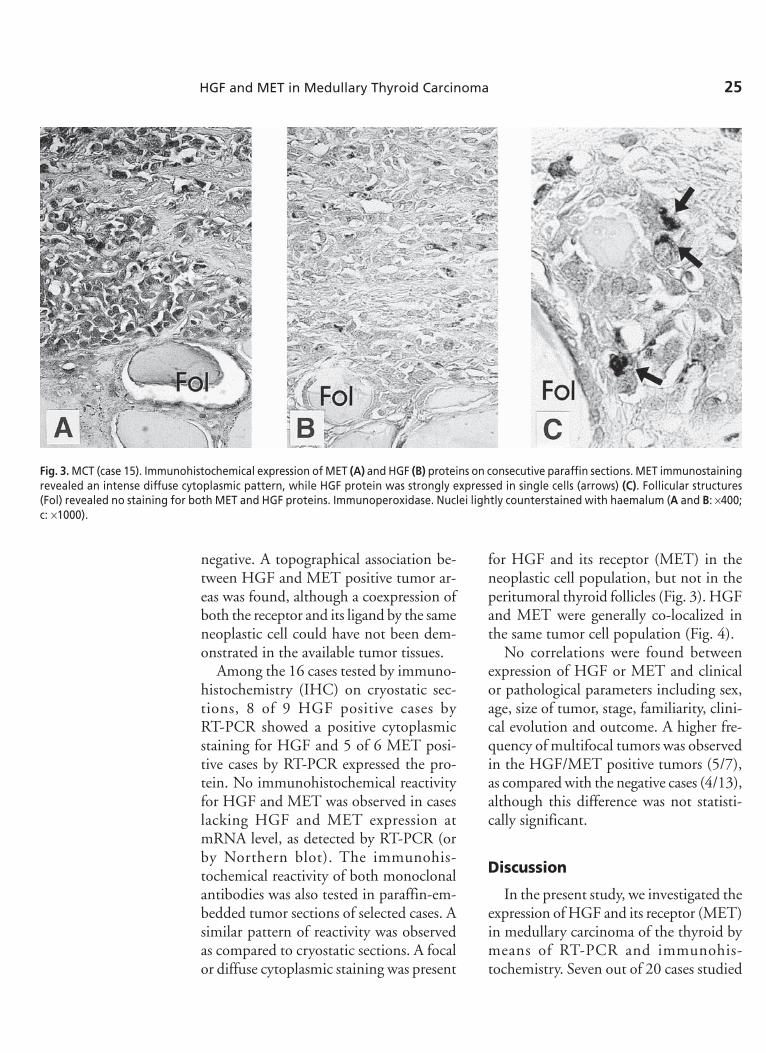
Among the 16 cases tested by immuno-histochemistry (IHC) on cryostatic sec-tions, 8 of 9 HGF positive cases byRT-PCR showed a positive cytoplasmicstaining for HGF and 5 of 6 MET posi-tive cases by RT-PCR expressed the pro-tein. No immunohistochemical reactivityfor HGF and MET was observed in caseslacking HGF and MET expression atmRNA level, as detected by RT-PCR (orby Northern blot). The immunohis-tochemical reactivity of both monoclonalantibodies was also tested in paraffin-em-bedded tumor sections of selected cases. Asimilar pattern of reactivity was observedas compared to cryostatic sections. A focalor diffuse cytoplasmic staining was present
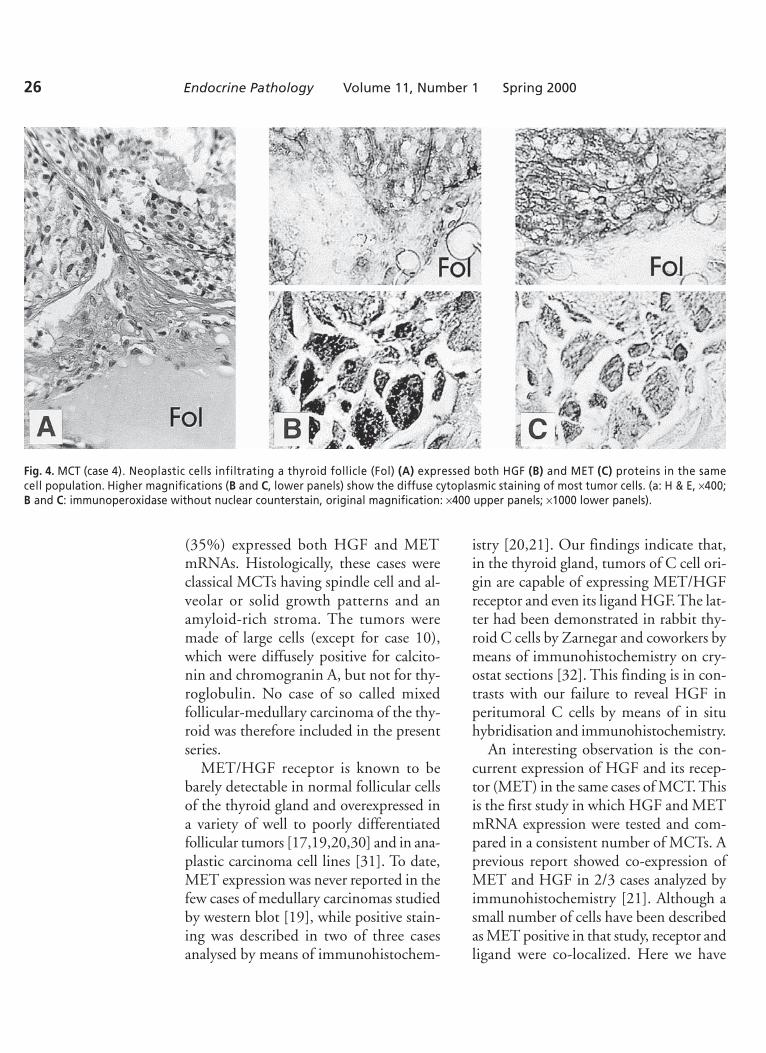
for HGF and its receptor (MET) in theneoplastic cell population, but not in theperitumoral thyroid follicles (Fig. 3). HGFand MET were generally co-localized inthe same tumor cell population (Fig. 4).
No correlations were found betweenexpression of HGF or MET and clinicalor pathological parameters including sex,age, size of tumor, stage, familiarity, clini-cal evolution and outcome. A higher fre-quency of multifocal tumors was observedin the HGF/MET positive tumors (5/7),as compared with the negative cases (4/13),although this difference was not statisti-cally significant.
Discussion
In the present study, we investigated theexpression of HGF and its receptor (MET)in medullary carcinoma of the thyroid bymeans of RT-PCR and immunohis-tochemistry. Seven out of 20 cases studied
Fig. 3. MCT (case 15). Immunohistochemical expression of MET (A) and HGF (B) proteins on consecutive paraffin sections. MET immunostainingrevealed an intense diffuse cytoplasmic pattern, while HGF protein was strongly expressed in single cells (arrows) (C). Follicular structures(Fol) revealed no staining for both MET and HGF proteins. Immunoperoxidase. Nuclei lightly counterstained with haemalum (A and B: ×400;c: ×1000).
26 Endocrine Pathology Volume 11, Number 1 Spring 2000
(35%) expressed both HGF and METmRNAs. Histologically, these cases wereclassical MCTs having spindle cell and al-veolar or solid growth patterns and anamyloid-rich stroma. The tumors weremade of large cells (except for case 10),which were diffusely positive for calcito-nin and chromogranin A, but not for thy-roglobulin. No case of so called mixedfollicular-medullary carcinoma of the thy-roid was therefore included in the presentseries.
MET/HGF receptor is known to bebarely detectable in normal follicular cellsof the thyroid gland and overexpressed ina variety of well to poorly differentiatedfollicular tumors [17,19,20,30] and in ana-plastic carcinoma cell lines [31]. To date,MET expression was never reported in thefew cases of medullary carcinomas studiedby western blot [19], while positive stain-ing was described in two of three casesanalysed by means of immunohistochem-
istry [20,21]. Our findings indicate that,in the thyroid gland, tumors of C cell ori-gin are capable of expressing MET/HGFreceptor and even its ligand HGF. The lat-ter had been demonstrated in rabbit thy-roid C cells by Zarnegar and coworkers bymeans of immunohistochemistry on cry-ostat sections [32]. This finding is in con-trasts with our failure to reveal HGF inperitumoral C cells by means of in situhybridisation and immunohistochemistry.
An interesting observation is the con-current expression of HGF and its recep-tor (MET) in the same cases of MCT. Thisis the first study in which HGF and METmRNA expression were tested and com-pared in a consistent number of MCTs. Aprevious report showed co-expression ofMET and HGF in 2/3 cases analyzed byimmunohistochemistry [21]. Although asmall number of cells have been describedas MET positive in that study, receptor andligand were co-localized. Here we have
Fig. 4. MCT (case 4). Neoplastic cells infiltrating a thyroid follicle (Fol) (A) expressed both HGF (B) and MET (C) proteins in the samecell population. Higher magnifications (B and C, lower panels) show the diffuse cytoplasmic staining of most tumor cells. (a: H & E, ×400;B and C: immunoperoxidase without nuclear counterstain, original magnification: ×400 upper panels; ×1000 lower panels).
HGF and MET in Medullary Thyroid Carcinoma 27
shown that in a consistent number of MCTcases, HGF and MET are co-expressed byMCT tumor cells. The MET/HGF recep-tor is newly expressed by MCT cells, sincethis tumor is derived from the para-folli-cular C cells, which do not express thereceptor [17]. MET neo-expression can bedriven by either one of the cytokines whichare known to influence MET gene expres-sion [33] or by an increased expression ofHGF [34]. Whatever the mechanism, theco-localisation demonstrated by ISH andIHC suggests that an autocrine circuitmight stimulate MET/HGF receptor sig-naling. A few cases expressed HGF only.This finding needs further investigationand may possibly be related to the inabil-ity of HGF to induce its receptor of to adelayed response to HGF [34] in the indi-vidual tumors.
HGF and MET overexpression hadrecently been studied in prostatic carci-noma cell lines by Northern blot analysis[35], in lung cancer by Western blot [36],in liver cell carcinoma by polymerase chainreaction and immunofluorescence [37] andin breast cancer by ISH [38]. In these caseseries, a proportion of lung and liver carci-nomas were shown to co-express HGF andMET proteins. Although HGF is knownto be produced by mesenchymal cells andto be active on epithelial cells, promotingmitogenesis and cell motility [8], probablyalternative pathways do exist which involveautocrine loops, since the same tumors andpossibly the same cells express both theligand and its receptor. Autocrine circuitshave already been reported in carcinomacells of other organs, namely lung andbreast, and in tumors of mesenchymal ori-gin [39,40], but never in physiological con-ditions, in which HGF action is mainlyparacrine.
The role of MET/HGF receptor in med-ullary carcinoma in particular, and in thy-
roid carcinomas in general, is largely un-known. The MET/HGF receptor belongsto a receptor family with the distinctiveproperty of eliciting a motogenic-invasiveresponse. MET can be converted into atransforming oncogene by differentmechanisms. In experimental models,transformation and metastasis are achievedafter the establishment of an HGF autocrinecircuit, that was found in spontaneouslyoccurring human osteosarcomas and rhab-domyosarcomas [25]. Point mutations ofthe MET gene have been found in a rareinherited and sporadic papillary renal cellcarcinoma [15]. In both experimentalmodels and in vitro, it has been shown thatall the members of the MET/HGF recep-tor family affect primarily cell motility andinvasiveness [41], and recent evidenceindicates that MET expression correlateswith the grade of malignancy [13,42]. Inthyroid carcinoma derived from follicularepithelium, MET overexpression is notassociated to an increase in cell prolifera-tion [20]. In this paper, we show that inmedullary thyroid carcinoma, HGF andits receptor are co-expressed in a subset ofmedullary carcinomas, but there was noapparent association with increased aggres-siveness or malignant evolution. The onlyinteresting correlation is with multifocality.The majority of the tumors were in factmultifocal (71% versus 31% of HGF/MET negative cases). Three cases occurredin the setting of MEN 2A syndrome, be-ing the other four positive cases apparentlysporadic forms of MCT. It is known thatthe majority of familial MCT and approx25% of sporadic forms are associated withC-cell hyperplasia, which is a precursor ofneoplastic transformation. In all hereditarycases, C-cell hyperplasia was documentedin non-tumoral thyroid parenchyma, butin situ hybridisation and immunohis-tochemical techniques failed to confirm the

28 Endocrine Pathology Volume 11, Number 1 Spring 2000
presence of MET or HGF positive cells inthe hyperplastic C-cell component.
We conclude that: (A) tyrosine kinaseencoded by MET oncogene and its ligandHGF are expressed not only in thyroidcarcinomas of follicular cell origin, but alsoin a group of medullary carcinomas; (B)an autocrine circuit is probably activein such cases, since the majority of posi-tive cases were found to express bothMET and HGF; (C) whether the activa-tion of MET/HGF receptor builds up anautocrine loop which may play a role inthe neoplastic spread and progression,needs to be further investigated, with spe-cial reference to HGF/MET positive mul-tifocal tumors.
Acknowledgments
We are grateful to Prof. G. Bussolati andDr. S. Giordano (University of Turin) fortheir suggestions; to Mrs. M. Cerrato,Mr. A. Ferraro and Mr A. Grua for skillfultechnical support and to Dr. F. Pietribiasi(Moncalieri, Torino) for providing clinicaldata of cases 13 and 14.
Work supported by grants from the Ital-ian Ministry of University (Rome, grant“60%” to MP), the Italian Association forCancer Research (Milan) and the ItalianNational Research Council (Rome, P.F.ACRo No. 96.00556.PF39 to MFD).
References
1. Suarez HG, duVillard JA, Severino M, CaillouB, Schlumberger M, Tubiana M, et al. Pres-ence of mutations of all three ras genes inhuman thyroid tumors. Oncogene 5:565–570, 1990.
2. Pilotti S, Collini P, Rilke F, Cattoretti G,Delbo R, Pierotti M. bcl-2 protein expressionin carcinomas originating from the follicularepithelium of the thyroid gland. J Pathol172:337–342, 1994.
3. Pilotti S, Collini P, Delbo R, Cattoretti G,Pierotti MA, Rilke F. A novel panel of anti-bodies that segregates immunocytochemicallypoorly differentiated carcinoma from undif-ferentiated carcinoma of the thyroid gland.Am J Surg Pathol 18:1054–1064, 1994.
4. Matias-Guiu X, Villanueva A, Cuatrecasas M,Capella G, DeLeiva A, Prat J. p53 in a thy-roid follicular carcinoma with foci of poorlydifferentiated and anaplastic carcinoma. PathRes Pract 192:1242–1249, 1996.
5. Fusco A, Grieco M, Santoro M, BerlingeriMT, Pilotti S, Pierotti MA, Della Porta G,Vecchio GC. A new oncogene in humanthyroid papillary carcinomas and theirlymphnodal metastases. Nature 328:170–172,1987.
6. Grieco M, Santoro M, Berlingeri MT, MelilloRM, Donghi R, Bongarzone I, Pierotti MA,DellaPorta G, Fusco A, Vecchio GC. PTC isa novel rearranged form of the ret proto-oncogene and is frequently detected in vivoin human thyroid papillary carcinomas. Cell60:557–563, 1990.
7. Komminoth P, Kunz EK, Matias-Guiu X,Hiort O, Christiansen G, Colomer A, RothJ, Heitz PhU. Analysis of RET protooncogenepoint mutations distinguishes heritable fromnonheritable medullary carcinomas. Cancer76:479–89, 1995.
8. Naldini L, Vigna E, Narsimhan R, , GaudinoG, Zarnegar R, Michalopoulos GK, ComoglioPM. Hepatocyte growth factor (HGF) stimu-lates the tyrosine kinase activity of the recep-tor encoded by the proto-oncogene c-met.Oncogene 6:501–504, 1991.
9. Cooper CS, Park M, Blair DG, Tainsky MA,Huebner K, Croce CM, VandeWoude G.Molecular cloning of a new transforming genefrom a chemically transformed human cellline. Nature 311:29–33, 1984.
10. Di Renzo MF, Narsimhan RP, Olivero M,Bretti S, Giordano S, Medico E, et al. Expres-sion of the met/HGF receptor in normal andneoplastic human tissues. Oncogene 6:1997–2003, 1991.
11. Prat M, Narsimhan RP, Crepaldi T, NicotraMR, Natali PG, Comoglio PM. The receptorencoded by the human c-MET oncogene isexpressed in hepatocytes, epithelial cells andsolid tumors. Int J Cancer 49:323–328, 1991.
12. Scotlandi K, Baldini N, Olivero M, DiRenzoMF, Martano M, Serra M, et al. Expression
HGF and MET in Medullary Thyroid Carcinoma 29
of MET/Hepatocyte growth factor receptorgene and malignant behavior of musculoskel-etal tumors. Am J Pathol 149:1209–1219,1996.
13. Nabeshima K, Shimao Y, Sato S, Kataoka H,Horiyama T, Kawano H, et al. Expression ofc-Met correlates with grade of malignancy inhuman astrocytic tumors: an immunohis-tochemical study. Histopathol 31:436–443,1997.
14. Naka T, Iwamoto Y, Shinohara N, UshijimaM, Chuman H, Tsuneyoshi M. Expression ofc-met proto-oncogene product (c-MET) inbenign and malignant bone tumors. ModPthol 10:832–838, 1997.
15. Schmidt L, Duh FM, Chen F, Kishida T,Glenn G, Choyke P, et al. Germline andsomatic mutations in the tyrosine kinasedomain of the MET protooncogene in papil-lary renal carcinomas. Nat Genet 16:68–73,1997.
16. Olivero M, Valente G, Bardelli A, Longati P,Ferrero N, Cracco C, et al. A novel mutationin the ATP binding site of the MET oncogenetyrosine kinase in a HPRCC family. . Int. J.Cancer:82, 640–643, 1999
17. Belfiore A, Gangemi P, Costantino A, RussoG, Santonocito GM, Ippolito O, et al. Nega-tive/low expression of the Met/hepatocytegrowth factor receptor identifies papillarythyroid carcinomas with high risk of distantmetastases. J Clin Endocrinol Metab 82:2322–2328, 1997.
18. Oyama T, Ichimura E, Sano T, KashiwabaraK, Fukuda T, Nakajiama T. c-Met expressionof thyroid tissue with special reference to pap-illary carcinoma. Pathol Int 48:763–768, 1998.
19. Di Renzo MF, Olivero M, Ferro S, Prat M,Bongarzone I, Pilotti S, et al. Overexpressionof the c-MET/HGF receptor gene in humanthyroid carcinomas. Oncogene 7:2549–2553,1992.
20. Ruco LP, Ranalli T, Marzullo A, Bianco P, PratM, Comoglio PM, Baroni C. Expression ofMet protein in thyroid tumors. J Pathol180:266–270, 1996.
21. Trovato M, Villari D, Bartolone L, SpinellaS, Simone A, Violi MA, et al. Expression ofthe hepatocyte growth factor and c-met innormal thyroid, non-neoplastic, and neoplas-tic nodules. Thyroid 8:125–131, 1998.
22. Papotti M, Sambataro D, Pecchioni C,Bussolati G. The pathology of medullary
carcinoma of the thyroid. Endocrine Pathol7:1–20, 1996.
23. Albores-Saavedra J, Monforte H, Nadji M,Morales AR. C-cell hyperplasia in thyroidtissue adjacent to follicular cell tumors. HumPathol 19:795–799, 1988.
24. Chirgwin JM, Przybyla AE, McDonald RJ,Rutter WJ. Isolation of biologically activeRNA from sourses enriched in ribonuclease.Biochemistry 18:5294–5297, 1979.
25. Ferraccini R, Di Renzo MF, Scotlandi K,Baldini N, Olivero M, Lollini P, et al. TheMet/HGF receptor is over-expressed inhuman osteosarcomas and is activated byeither a paracrine or an autocrine circuit.Oncogene 1:739–749, 1995.
26. Papotti M, Pacchioni D, Negro F, Bonino F,Bussolati G. Albumin gene expression in livertumors: diagnostic interest in fine needleaspiration biopsies. Modern Pathol 7:271–275, 1994.
27. Park M, Dean M, Kaul K, Braun MJ, GondaMA, Vande Woude G. Sequence of METprotooncogene cDNA has features character-istic of the thyrosine kinase family of growthfactor receptors. Proc Natl Acad Sci USA84:6379–6383, 1987.
28. Sitzmann JH, LeMotte PK. Rapid andefficient generation of PCR-derived riboprobetemplates for in situ hybridisation histoch-emistry. J Histochem Cytochem 41:773–776,1993.
29. DiRenzo MF, Poulson R, Olivero M, ComoglioPM, Lemoine NR. Expression of the Met/Hepatocyte growth factor receptor in humanpancreatic cancer. Cancer Res 55:1129–1138,1995.
30. Zanetti A, Stoppacciaro A, Marzullo A,Ciabatta M, Fazioli F, Prat M, et al. Expres-sion of MET protein and urokinase-type plas-minogen activator receptor (uPA-R) inpapillary carcinoma of the thyroid. J Pathol186:287–291, 1998.
31. Bergstrom JD, Hermansson A, Diaz de StahlT, Heldin NE. Non-autocrine, constitutiveactivation of Met in human anaplastic thy-roid carcinoma cells in culture. Br J Cancer80:650–656, 1999.
32. Zarnegar R, Muga S, Enghild J, MichalopulosG. Tissue distribution of hepatopoietin A:aheparin binding polypeptide growth factor forhepatocytes. Proc Natl Acad Sci USA 87:1252–1256, 1990.
30 Endocrine Pathology Volume 11, Number 1 Spring 2000
33. Zarnegar R. Regulation of HGF and HGFRgene expression. EXS 74:33–49, 1995.
34. Boccaccio C, Gaudino G, Gambarotta G,Galimi F, Comoglio PM. Hepatocyte growthfactor (HGF) receptor espression in inducibleand is part of the delayed-early response toHGF. J Biol Chem 269:12846–12851, 1994.
35. Humphrey PA, Zhu X, Zarnegar R, SwansonPE, Ratliff TL, Vollmer RT, Day ML. Hepa-tocyte growth factor and its receptor (c-MET)in prostatic carcinoma. Am J Pathol 147:386–396, 1995.
36. Olivero M, Rizzo M, Madeddu R, CasadioC, Pennecchietti S, Nicotra MR, et al.Overexpression and activation of hepatocytegrowth factor/scatter factor in human non-small-cell lung carcinomas. Br J Cancer74:1862–1868, 1996.
37. Ljubimova JY, Petrovic LM, Wilson SE, GellerSA, Demetriou AA. Expression of HGF, itsreceptor c-met, c-myc, and albumin in cir-rhotic and neoplastic human liver tissue. JHistochem Cytochem 45:79–87, 1997.
38. Tuck AB, Park M, Sterns EE, Boag A, ElliottBE. Coexpression of hepatocyte growth fac-tor and receptor (Met) in human breast car-cinoma. Am J Pathol 148:225–232, 1996.
39. Tsao MS, Zhu H, Giaid A, Viallet J, NakmuraT, Park M. Hepatocyte growth factor/scatterfactor is an autocrine factor for human bron-chial epithelial and lung carcinoma cells. CellGrowth & Differ 4:571–579, 1993.
40. Wang Y, Selden AC, Morgan N, StampGWH, Hodgson HJF. Hepatocyte growthfactor/scatter factor expression in humanmammary epithelium. Am J Pathol 144:675–682, 1994.
41. Tamagnone L, Comoglio PM. Control ofinvasive growth by hepatocyte growth factor(HGF) and related scatter factors. CytokineGrowth Factor Rev 8:129–142, 1997.
42. Rao UNM, Sonmez-Alpan E, MichalopulosGK. Hepatocyte growth factor and c-Met inbenign and malignant peripheral nervesheath tumors. Hum Pathol 28:1066–1070,1997.




















