Additive effect of RET polymorphisms on sporadic medullary thyroid carcinoma susceptibility and...
8
CLINICAL STUDY Additive effect of RET polymorphisms on sporadic medullary thyroid carcinoma susceptibility and tumor aggressiveness Lucieli Ceolin, De ´bora Rodrigues Siqueira, Carla Vaz Ferreira, Mı ´rian Romitti, Silvana Cavalcante Maia, Leonardo Leiria, Daisy Crispim, Patrı ´cia Ashton Prolla and Ana Luiza Maia Thyroid Section, Endocrine Division, Servic ¸o de Endocrinologia, Hospital de Clı ´nicas de Porto Alegre, Universidade Federal do Rio Grande do Sul, Rua Ramiro Barcelos 2350, 90035 –003 Porto Alegre, RS, Brazil (Correspondence should be addressed to A L Maia; Email: [email protected]) Abstract Objective: RET single nucleotide polymorphisms (SNPs) have been implicated in the pathogenesis and progression of medullary thyroid carcinoma (MTC). Here, we investigated the influence of multiple RET variants (G691S, L769L, S836S, and S904S) on the risk of MTC and tumor behavior. Design and methods: One hundred and seven MTC patients and 308 cancer-unaffected control individuals were included. SNPs were analyzed using Custom TaqMan Genotyping Assays. Haplotypes based on the combination of allelic variants were inferred using a Bayesian statistical method. Results: The minor allele frequencies in MTC patients were as follows: L769L: 28.0%, S836S: 8.9%, and G691S/S904S: 22.2%. The RET L769L and S836S SNPs were associated with increased risk of MTC (odds ratio (OR)Z1.95, 95% CI: 1.2–3.1, PZ0.005 and ORZ2.29, 95% CI: 1.2–4.5, PZ0.017 respectively). The adjusted OR for individuals harboring haplotypes with three or more polymorphic alleles was 3.79 (95% CI: 1.5–9.5; PZ0.004), indicating an additive effect of these variants on the risk for MTC. Among MTC patients, no significant associations were observed between RET variants and age of diagnosis or tumor size but serum calcitonin levels increased according to the number of risk alleles (PZ0.003). Remarkably, patients carrying haplotypes with three or four risk alleles had increased risk for lymph node and distant metastases at diagnosis (ORZ5.84, 95% CI: 1.1–31.2, PZ0.039). Further analysis using Kaplan–Meier model demonstrated that metastatic disease occurred earlier in individuals harboring multiple risk alleles. Conclusion: Our results demonstrated an additive effect of RET polymorphic alleles on the estimated risk of developing aggressive MTC. European Journal of Endocrinology 166 847–854 Introduction Medullary thyroid carcinoma (MTC), a malignant tumor originating in parafollicular C cells of the thyroid, represents 5–10% of all thyroid cancers (1, 2). About 75% of all MTCs are sporadic whereas the remaining patients have an inherited cancer syndrome known as multiple endocrine neoplasia type 2 (MEN2). Features of MEN2A include MTC, pheochromocytoma (PHEO), and hyperparathyroidism (HPT). MEN2B presents a specific phenotype that encompasses MTC, PHEO, ganglioneur- omas of the digestive tract, mucosal neuromas, and/or skeletal abnormalities (1, 3). In familial MTC (FMTC), MTC is the only clinical feature (3). The rearranged during transfection (RET) proto-oncogene is the suscep- tibility gene for hereditary MTC. Several germline mutations of this gene have been associated with hereditary MTC. Genotype–phenotype correlation has been reported and mutations in exon 10 (codons 609, 611, 618, and 620) or exon 11 (codon 634) occur in more than 98% of MEN2A families. MEN2B is primarily associated with a single missense mutation in exon 16 (M918T), which is found in more than 90% of all reported cases (4, 5). The RET gene encodes a tyrosine kinase receptor implicated in the neural crest tissue development and differentiation. Although much is known about hereditary MTC, the molecular mechanisms underlying sporadic MTC tumors remain to be clarified. Somatic RET point mutations in exon 16 (M918T) and gene deletions are described in 40–80% of MTC (6, 7, 8, 9). However, the mutation does not appear to be uniform among the various cell subpopulations in the same tumor or in the metastases, suggesting that MTC may be of polyclonal origin or that the mutations in the RET proto-oncogene are not initial events in MTC tumorigenesis (10, 11). In the last years, several studies have investigated whether the presence of variant sequences in the RET gene could be associated with susceptibility to develop- ment or progression of MTC (12, 13). Based on the over- representation of the RET single nucleotide polymorph- isms (SNPs) G691S (exon 11, GlyGGT/SerAGT), L769L European Journal of Endocrinology (2012) 166 847–854 ISSN 0804-4643 q 2012 European Society of Endocrinology DOI: 10.1530/EJE-11-1060 Online version via www.eje-online.org
Transcript of Additive effect of RET polymorphisms on sporadic medullary thyroid carcinoma susceptibility and...

European Journal of Endocrinology (2012) 166 847–854 ISSN 0804-4643
CLINICAL STUDY
Additive effect of RET polymorphisms on sporadic medullarythyroid carcinoma susceptibility and tumor aggressivenessLucieli Ceolin, Debora Rodrigues Siqueira, Carla Vaz Ferreira, Mırian Romitti, Silvana Cavalcante Maia,Leonardo Leiria, Daisy Crispim, Patrıcia Ashton Prolla and Ana Luiza MaiaThyroid Section, Endocrine Division, Servico de Endocrinologia, Hospital de Clınicas de Porto Alegre, Universidade Federal do Rio Grande do Sul,Rua Ramiro Barcelos 2350, 90035 –003 Porto Alegre, RS, Brazil
(Correspondence should be addressed to A L Maia; Email: [email protected])
q 2012 European Society of E
Abstract
Objective: RET single nucleotide polymorphisms (SNPs) have been implicated in the pathogenesis andprogression of medullary thyroid carcinoma (MTC). Here, we investigated the influence of multiple RETvariants (G691S, L769L, S836S, and S904S) on the risk of MTC and tumor behavior.Design and methods: One hundred and seven MTC patients and 308 cancer-unaffected controlindividuals were included. SNPs were analyzed using Custom TaqMan Genotyping Assays. Haplotypesbased on the combination of allelic variants were inferred using a Bayesian statistical method.Results: The minor allele frequencies in MTC patients were as follows: L769L: 28.0%, S836S: 8.9%,and G691S/S904S: 22.2%. The RET L769L and S836S SNPs were associated with increased risk ofMTC (odds ratio (OR)Z1.95, 95% CI: 1.2–3.1, PZ0.005 and ORZ2.29, 95% CI: 1.2–4.5, PZ0.017respectively). The adjusted OR for individuals harboring haplotypes with three or more polymorphicalleles was 3.79 (95% CI: 1.5–9.5; PZ0.004), indicating an additive effect of these variants on the riskfor MTC. Among MTC patients, no significant associations were observed between RET variants andage of diagnosis or tumor size but serum calcitonin levels increased according to the number of riskalleles (PZ0.003). Remarkably, patients carrying haplotypes with three or four risk alleles hadincreased risk for lymph node and distant metastases at diagnosis (ORZ5.84, 95% CI: 1.1–31.2,PZ0.039). Further analysis using Kaplan–Meier model demonstrated that metastatic diseaseoccurred earlier in individuals harboring multiple risk alleles.Conclusion: Our results demonstrated an additive effect of RET polymorphic alleles on the estimated riskof developing aggressive MTC.
European Journal of Endocrinology 166 847–854
Introduction
Medullary thyroid carcinoma (MTC), a malignanttumor originating in parafollicular C cells of the thyroid,represents 5–10% of all thyroid cancers (1, 2). About75% of all MTCs are sporadic whereas the remainingpatients have an inherited cancer syndrome known asmultiple endocrine neoplasia type 2 (MEN2). Features ofMEN2A include MTC, pheochromocytoma (PHEO), andhyperparathyroidism (HPT). MEN2B presents a specificphenotype that encompasses MTC, PHEO, ganglioneur-omas of the digestive tract, mucosal neuromas, and/orskeletal abnormalities (1, 3). In familial MTC (FMTC),MTC is the only clinical feature (3). The rearrangedduring transfection (RET) proto-oncogene is the suscep-tibility gene for hereditary MTC. Several germlinemutations of this gene have been associated withhereditary MTC. Genotype–phenotype correlation hasbeen reported and mutations in exon 10 (codons 609,611, 618, and 620) or exon 11 (codon 634) occur inmore than 98% of MEN2A families. MEN2B is primarily
ndocrinology
associated with a single missense mutation in exon 16(M918T), which is found in more than 90% of allreported cases (4, 5). The RET gene encodes a tyrosinekinase receptor implicated in the neural crest tissuedevelopment and differentiation.
Although much is known about hereditary MTC, themolecular mechanisms underlying sporadic MTCtumors remain to be clarified. Somatic RET pointmutations in exon 16 (M918T) and gene deletions aredescribed in 40–80% of MTC (6, 7, 8, 9). However, themutation does not appear to be uniform among thevarious cell subpopulations in the same tumor or in themetastases, suggesting that MTC may be of polyclonalorigin or that the mutations in the RET proto-oncogeneare not initial events in MTC tumorigenesis (10, 11).
In the last years, several studies have investigatedwhether the presence of variant sequences in the RETgene could be associated with susceptibility to develop-ment or progression of MTC (12, 13). Based on the over-representation of the RET single nucleotide polymorph-isms (SNPs) G691S (exon 11, GlyGGT/SerAGT), L769L
DOI: 10.1530/EJE-11-1060
Online version via www.eje-online.org

848 L Ceolin and others EUROPEAN JOURNAL OF ENDOCRINOLOGY (2012) 166
(exon 13, LeuCTT/LeuCTG), S836S (exon 14, Ser-AGC/SerAGT), and S904S (exon 15, SerTCC/SerTCG)in individuals with hereditary or sporadic MTC, a rolefor these genetic variants in the pathogenesis of thisdisease has been suggested. Nevertheless, the results onthe effect of RET polymorphic variants in the predis-position to develop MTC are still conflicting. Somestudies have demonstrated that the RET variant G691Sis more frequent in MTC patients than in the generalpopulation (14). The G691S/S904S variants were alsoassociated with a 1.5- to 2.5-fold risk for thedevelopment of MTC (15). Patients with MTC youngerthan 30 years presented a higher frequency of the RETL769L variant than those diagnosed between 31 and45 years (16). This polymorphism was also associatedwith increased risk for MTC whereas patientshomozygous for the minor allele of this variant wereyounger at the MTC diagnosis (17). Ruiz et al. (2001)(18) have demonstrated that the RET S836S variantwas associated with a two- to three-fold increase inthe risk of MTC in the Spanish population. Morerecently, the S836S variant was associated with earlyonset of the MTC and increased risk for metastaticdisease (9). Nonetheless, several other studies failed todemonstrate any effect of RET variants on the risk fordevelopment or on the natural course of MTC (19, 20,21). The reasons for these conflicting results are stillunknown and illustrate the need for additional studiesto explore the molecular mechanisms underlying MTC.Recently, two other variants of RET (IVS1K126 GOT),and (IVS8C82 AOG and 85–86 insC) have beenassociated with phenotypic variability in hereditaryMTC patients (22). It has also been described a higherfrequency of intron 14 (IVS14–24) polymorphism inMTC patients with elevated serum calcitonin concen-trations (23). On the other hand, a polymorphism inexon 2, codon 45, which encodes an alanine(AlaGCG/AlaGCA), occurred at a lower frequencyamong the cases of MTC and, according to the authors,it could confer a protective allele against the develop-ment of MTC (15).
Carcinogenesis is a multistep process that occursthrough a multifactorial interplay between manygenetic and environmental factors. In this context, theeffect of a single polymorphism is unlikely to besubstantial in studies of complex diseases. Thus, theapproach based on combining multiple polymorphismsthat interact in the same pathway may amplify the effectof single variants and enhance the predictive power ofpolymorphism analysis for multifactorial disease (24,25). Here, we have investigated the influence of multipleRET variants, isolated or in combination, in theestimated risk for MTC as well as in its clinicalpresentation. The polymorphisms G691S/S904S,L769L, and S836S were selected based on their previousassociation with increased risk for sporadic MTCdevelopment and aggressive clinical course.
www.eje-online.org
Materials and methods
Patients
Patients with a diagnosis of MTC attending theEndocrine Division at Hospital de Clınicas de PortoAlegre were invited to participate in the study. From1997, our division has been a reference center for RETmutation testing in Brazil, and therefore, patientsreferred to us by other Brazilian centers were alsoinvited to participate. All patients and/or their legalrepresentatives provided written informed consent ofthe study in accordance with the institutional ethicscommittee.
Our study included 107 consecutive patients withMTC. The diagnosis of MTC was based on histopatho-logical/immunohistochemistry findings and theabsence of known germline RET point mutations inexons 8, 10, 11, or 13–16. Clinical and laboratory datawere collected for each individual. Patients underwent acomplete clinical examination, and laboratory testswere performed as described previously (9, 26). Thecontrol group was composed of 308 unrelated cancer-unaffected volunteers attending the blood donationfacility of our Institution. A standard questionnaire wasused to collect information about age, sex, skin color,and history of neoplasias. The analyses were basedon the limited number of cases, and thus, to increasethe statistical power, we expand the control group to1:3 ratio.
Genotyping assay
RET variants G691S (rs1799939, codon 691 of exon11, GlyGGT/SerAGT), L769L (rs1800861, codon 769of exon 13, LeuCTT/LeuCTG; L769L(TOG)), S836S(rs1800862, codon 836 of exon 14, SerAGC/SerAGT;S836S(COT)), and S904S (rs1800863, codon 904 ofexon 15, SerTCC/SerTCG; S904S(COG)) were analyzed.Genomic DNA was obtained from peripheral bloodleukocytes by standardized procedures. Genotypeanalysis was performed using Human Custom TaqManSNP Genotyping Assays 40! (Applied Biosystems,Foster City, CA, USA). Primer and probe sequencesused for genotyping the RET variants were as follows:L769L (rs1800861): 5 0-GGGTGGTTGACCTGCTTCAG-3 0 (forward primer), 5 0-CTGCTCTGTGCTGCATTTCAG-3 0
(reverse primer), VIC-5 0-AGGTCTCGAAGCTCA-3 0,FAM-5 0-AGGTCTCGCAGCTCA-30; S836S (rs1800862):5 0-GCGAGAGCCGCAAAGTG-3 0 (forward primer),5 0-GTGAGGGCCCGCTCATC-3 0 (reverse primer), VIC-5 0-CAACTCCAGCTCCCTG-3 0, FAM-5 0-CAACTCCAGTT-CCCTG-3 0; S904S (rs1800863): 5 0-GCTTGTCCCGA-GATGTTTATGAAGA-3 0 (forward primer), 5 0-GGG-CACCTGGCTCCT-30 (reverse primer), VIC-50-CTTCACG-TAGGAATCC-30, FAM-50-CTTCACGTACGAATCC-30. Thetwo variants G691S and S904S were in linkage

Table 1 Clinical and oncological features of patients with medullarythyroid carcinoma.
Total patients 107Female (%) 59 (54.6)Age at diagnosis (years) 46.2G15.8a
Calcitonin (pg/ml) 870.0 (154.75–2900)b
CEA (ng/ml) 69.2 (11.65–166.8)b
Size tumor (cm) 3.0 (1.6–3.8)b
Lymph node metastases (%)N0 41.7N1 58.3
Distant metastases (%)M0 72.3M1 27.7
RET variants and MTC 849EUROPEAN JOURNAL OF ENDOCRINOLOGY (2012) 166
disequilibrium (LD); therefore, only S904S was genotypedand the results were shown as G691S/S904S.
The reactions were conducted in a 96-well plate, in atotal 5 ml reaction volume using 2 ng genomic DNA,TaqMan Genotyping Master Mix 1! (Applied Biosys-tems), and Custom TaqMan Genotyping Assay 1!. Theplates were then positioned in a real-time PCR thermalcycler (7500 Fast Real PCR System; Applied Biosystems)and heated for 10 min at 95 8C, followed by 45 cycles of95 8C for 15 s and 62 8C for 1 min. Fluorescence datafiles from each plate were analyzed using automatedallele calling software (SDS 2.1; Applied Biosystems).
aData expressed as meanGS.D.bData expressed as median (IQ 25–75).
Statistical analysisResults are expressed as meanGS.D. or median (IQ 25–75) unless otherwise specified. Hardy–Weinberg equili-brium for each polymorphism was assessed by c2 tests.Baseline characteristics were compared using c2 tests orFisher’s exact test for qualitative variables. Quantitativevariables were compared between groups using Stu-dent’s t-test, ANOVA, or Kruskal–Wallis tests.
The haplotypes were constructed based on thecombination of allelic variants and their frequencieswere inferred using the phase 2.1 program, whichimplements a Bayesian statistical method (27). We alsoused the phase 2.1 program to compare the distributionsof different RET haplotypes between MTC patients andcontrols through permutation analyses of 1000 randomreplicates (27). Between all pairs of biallelic loci, weexamined widely used measures of LD, Lewontin’s D 0 jD 0jand r2 (28). Multivariate logistic regression analysis wasperformed to evaluate the estimated risk of MTC, usingMTC as the dependent variable and age, gender, andnumber of RET polymorphic alleles in the haplotype asindependent variables. Logistic regression analysis wasalso performed with the presence of metastases as thedependent variable and age, gender, and number of RETpolymorphic alleles in the haplotype as independentvariables. Differences in cumulative lymph node and/or
Table 2 Frequency of RET polymorphic alleles in medullary thyroid c
Genotype distribution
Sequencevariant Wild type
Heterozy-gous Homozygous MTC (%
L769L(TOG) 56 42 9 28.0S836S(COT) 88 19 0 8.9G691S/S904S(COG)
63 39 4 22.2
aData compared using the c2 test or Fisher’s exact test.bReferences: 16, 17, 26, 27, 28.cPZadjusted OR, 95% CI, and P values for the comparisons between casesanalyses were age, gender, and RET polymorphic allele.
distant metastases between groups were tested byKaplan–Meier curves, and comparisons between curveswere performed using the log rank test. The StatisticalPackage for the Social Sciences 18.0 (PASW, Inc.,Chicago, IL, USA) software was used for all analyses,and P!0.05 was considered as statistically significant.
Results
Clinical and oncological features of the subjectsincluded in the study are summarized in Table 1. Thecontrol group comprises 308 cancer-unaffected indi-viduals. The mean age (46.2G15.8 vs 46.1G9.1,PZ0.91) and ethnic background (95% Caucasian)were similar between MTC patients and control group(PO0.05). However, the frequency of females washigher in MTC patients (54.6 vs 43.6%, PZ0.047).
The G691S and S904S(COG) variants were incomplete LD, and therefore, to avoid redundantinformation, the results were grouped together andreferred to as G691S/S904S(COG) (14, 22, 29). Allgenotypes were analyzed using Hardy–Weinberg equili-brium (PO0.05).
arcinoma and control groups.
) Controls (%) Pa
Prevalencein
literatureb
(%)OR
(95% CI); P c
20.8 0.03 15–26 1.95 (1.2–3.1); 0.0054.2 0.01 1.2–9.3 2.29 (1.2–4.5); 0.017
21.7 0.62 11.1–24 1.09 (0.6–1.7); 0.706
and controls. The independent variables included in the multiple regression
www.eje-online.org

Table 3 Frequency of RET haplotypes in medullary thyroid carcinoma and control groups.
Presence/absence of Haplotype (%)
Haplotypes L769L(TOG) S836S(COT) S904S(COG)Polymorphicalleles (n) MTC (nZ214)a Controls (nZ616)a
Hpt1 K K K None 49.42 57.63Hpt2 C K K 1 20.39 16.69Hpt3 K C K 1 2.0 0.41Hpt4 K K C 1 20.51 20.92Hpt5 C C K 2 6.07 3.56Hpt6 C K C 2 0.78 0.54Hpt7 K C C 2 0 0Hpt8 C C C 3 0 0
Hpt, haplotype; PZ0.08 (P value for the comparisons of haplotype frequencies between patients and controls was calculated using permutation test (1000replications).anZnumber of chromosomes.
850 L Ceolin and others EUROPEAN JOURNAL OF ENDOCRINOLOGY (2012) 166
RET polymorphisms in sporadic MTC patientsand controls
The allele frequencies in MTC patients were similar tothose reported in the literature (18, 19, 23, 30, 31).There were no differences in the frequency ofG691S/S904S(COG) polymorphisms between patientsand controls (Table 2). Nevertheless, the L769L(TOG)polymorphic allele frequency was higher in MTCpatients compared with control group (28.0 vs 20.8%,PZ0.03). Confirming previously published data (9), weobserved a higher allelic frequency of S836S(COT)variant in MTC patients (8.9 vs 4.2%, PZ0.01). Whenevaluating the effect of single RET polymorphisms onthe risk for MTC, we found an adjusted odds ratio (OR)of 1.95 (95% CI: 1.2–3.1, PZ0.005) for individualsharboring the L769L(TOG) variant while the adjustedOR for the presence of the S836S(COT) variant was2.29 (95% CI: 1.2–4.5, PZ0.017).
Table 4 Distribution of the various RET haplotype combinations inmedullary thyroid carcinoma and control groups.
Polymorphicalleles (n)
MTC,nZ107 (%)
Controls,nZ308 (%)
Hpt1/Hpt1 None 26 (24.3) 110 (35.7)Hpt1/Hpt2 1 22 (20.6) 47 (15.3)Hpt1/Hpt3 1 4 (3.7) 1 (0.3)Hpt1/Hpt4 1 22 (20.6) 75 (24.4)Hpt1/Hpt5 2 4 (3.7) 11 (3.6)Hpt2/Hpt2 2 5 (4.7) 16 (5.2)Hpt2/Hpt4 2 9 (8.4) 18 (5.8)Hpt2/Hpt5 3 3 (2.8) 6 (1.9)Hpt2/Hpt6 3 0 1 (0.3)Hpt3/Hpt4 2 0 1 (0.3)Hpt4/Hpt4 2 4 (3.7) 15 (4.9)Hpt4/Hpt5 3 7 (6.5) 7 (2.3)Hpt5/Hpt6 4 1 (0.9) 0
Hpt, haplotype (please refer to Table 3, for haplotype description). P value forthe comparisons of haplotype combinations between patients and controlswas 0.035 (data compared using Fisher’s exact test).
Additive effect of RET polymorphic alleleson MTC susceptibility
Next, we evaluated whether the presence of multipleRET variants would increase the estimated risk for MTC.We used a Bayesian statistical method to estimate thefrequency of different haplotypes produced by thecombination of the G691S/S904S(COG), L769L(TOG), and S836S(COT) polymorphisms in MTC patientsand controls. A total of six haplotypes were inferred inboth groups (Table 3). The frequency of haplotype 3 wasfivefold higher in the cases, but permutation analysesshowed that the distributions of these six haplotypeswere not significantly different between case and controlgroups (PZ0.08). Interestingly, none of the individualsstudied presented the three polymorphic variants in thesame allele (haplotype 8) or the S836S and S904Spolymorphic variants in the same allele (haplotype 7).Thirteen different combinations of the six haplotypesinferred by Phase program were found in the case andcontrol individuals (Table 4). The permutation analyses
www.eje-online.org
showed that the distributions of haplotypes werestatistically different between case and control groups(PZ0.035).
We also examined LD among G691S/S904S(COG),L769L(TOG), and S836S(COT) polymorphisms. Wedid not find LD between S836S(COT) and S904S(COG)polymorphisms (jD 0jZ0.696; r2Z0.013). However, theL769L(TOG) polymorphism was in partial LD withthe S836S(COT) and S904S(COG) polymorphisms(jD 0jZ0.875; r2Z0.192 and jD 0jZ0.871; r2Z0.084respectively).
In order to test the impact that multiple RETpolymorphisms had on the MTC susceptibility, theindividuals were grouped according to the presence ofhaplotypes constituted by i) no RET risk allele, ii) oneor two risk alleles, or iii) three or four risk alleles.The distributions of RET risk alleles in the haplotypeswere significantly different between groups (Table 5;PZ0.02). Interestingly, further analysis by multivariatelogistic regression showed that individuals harboringthree or four risk alleles in the haplotypes have increased

Table 5 Additive effect of RET polymorphic alleles on medullarythyroid carcinoma susceptibility.
Risk allelesMTC,
nZ107 (%)Controls,nZ308 (%) OR (95% CI); P
None 26 (24.3) 110 (35.7) 1One or two 70 (65.4) 184 (59.7) 1.57 (0.9–2.7); 0.10Three orfour
11 (10.3) 14 (4.5) 3.79 (1.5–9.5); 0.004
The distribution of RET risk haplotypes were significantly different betweenMTC patients and controls (PZ0.02). PZadjusted OR, 95% CI and P valuesfor the comparisons between cases and controls. The independent variablesincluded in the multiple regression analyses were age, gender, and numberof RET polymorphic alleles in the haplotype.
RET variants and MTC 851EUROPEAN JOURNAL OF ENDOCRINOLOGY (2012) 166
estimated risk of MTC development (ORZ3.79; 95%CI: 1.5–9.5; PZ0.004).
Additive effect of RET polymorphic alleleson MTC presentation at diagnosis
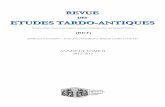
Next, we examined the additive effect of RET risk alleles(G691S/S904S(COG), L769L(TOG), and S836S(COT))on clinical and oncological features of MTC patients(Table 6). No significant difference was observed in theage at diagnosis (PO0.05) but serum calcitonin levelsincreased according to the number of RET risk alleles(PZ0.003). The same trend was observed for CEA levelsand tumor size, although they did not reach statisticalsignificance (PZ0.07 and PZ0.06 respectively).Remarkably, we found an association between numberof RET risk alleles and advanced disease at diagnosis. Allpatients with three or four risk alleles presented lymphnode metastases whereas only 50% of patients with twoor less risk alleles had this feature (PZ0.01). Patientswith three or four risk alleles also presented increasedestimated risk for distant metastases (ORZ5.84, 95%CI: 1.1–31.2, PZ0.039). Additionally, Kaplan–Meierestimates of cumulative lymph node and distantmetastases yielded distinct curves for patients withthree or four risk alleles compared with those carryingone or two risk alleles (PZ0.001 and P!0.001respectively, Fig. 1), further demonstrating that meta-static disease occurred earlier in those individualsharboring multiple RET risk alleles.
Table 6 Additive effect of RET polymorphic alleles on clinical feature
None (nZ26) One or
Age at diagnosis (years) 44.5G18.6 48.3G1Calcitonin (pg/ml) 645 (8–2331) 719 (23CEA (ng/ml) 13 (7.2–14) 113 (19Tumor size (cm) 2.7 (2.0–3.7) 2.2 (1.5Lymph node metastases (%) 52 54.8Distant metastases (%) 27.3 23
aData compared using ANOVA.bData compared using Kruskal–Wallis.cData compared using c2 tests.
Discussion
This study demonstrated that the presence of multipleRET risk alleles is associated with increased estimatedrisk for MTC development and aggressiveness, indicat-ing an additive effect of different RET variants in thepathogenesis of this rare malignant thyroid neoplasia.
SNPs are involved in gene–environment interactionand commonly associated with a large number ofsporadic cancers (32). The role of RET polymorphismsin the development or progression of MTC is stillcontroversial. Several studies have demonstrated thatRET variants may be associated with the risk of MTC aswell as MTC-aggressive behavior (9, 18, 31). However,other studies failed to demonstrate such associations(19, 20, 21). Although the reasons for the conflictingresults remain unsolved, differences in the geneticbackground of distinct population have been suggestedas a potential explanation. Here, we found no differencesin the frequency of G691S/S904S(COG) polymorph-isms between MTC patients and controls. However,similar to others, we observed that both L769L(TOG)and S836S(COT) polymorphisms were associated withincreased risk for MTC (9, 16, 17, 18, 31).
Combination of genetic variants that interact in thesame pathway may amplify the effects of a singlepolymorphism and enhance the predictive power for amultifactorial disease. Thus, we wondered whether RETpolymorphic variants could act synergistically in thedevelopment or progression of MTC. Our resultsdemonstrated that this might be the case because thepresence of three or more RET risk alleles was associatedwith a 3.79-fold increased risk for MTC development. Inagreement with findings reported by Lesueur et al., weobserved a partial LD between the L769L(TOG)polymorphism and S836S(COT) and S904S(COG)polymorphic variants. Nevertheless, contrasting withtheir data, we did not find LD between the S836S(COT)and S904S(COG) variants (33). Differences in thegenetic background of distinct populations mightpartially explain differences in LD analysis. The LDbetween L769L(TOG) and S836S(COT) polymorph-isms might also explain the positive association of boththe variants with MTC observed in this study and others(9, 13, 14, 15). Taken together, these observations
s of patients with medullary thyroid carcinoma.
two (nZ70) Three or four (nZ11) P
4.6 38.5G15.4 0.146a
6–2030) 7087 (3545–13 988) 0.003b
–161) 208 (162–255) 0.069b
–3.5) 3.8 (3.4–4.4) 0.055b
100 0.014c
72.7 0.004c
www.eje-online.org

1.0A
B
0.8
Fra
ctio
n fr
ee o
f lym
ph n
ode
met
asta
ses
0.6
0.4
0.2
0.00 20 40 60
Age at diagnosis (years)
80 100
One or two risk allelesThree or four risk alleles
1.0
0.8
Fra
ctio
n fr
ee o
f di
stan
t met
asta
ses
0.6
0.4
0.2
0.00 20 40 60
Age at diagnosis (years)
80 100
One or two risk allelesThree or four risk alleles
P=0.001
P<0.001
Figure 1 Kaplan–Meier estimates of the proportion of sporadic MTCpatients with lymph node (A) or distant metastases (B) at diagnosis.The log rank test was used to compare curves.
852 L Ceolin and others EUROPEAN JOURNAL OF ENDOCRINOLOGY (2012) 166
indicate that analysis of RET haplotypes, instead ofsingle RET polymorphisms, may be more useful indetermining the effect of RET variants on the estimatedrisk of MTC.
The additive effect of RET polymorphic variantsbecomes even more apparent in MTC disease presen-tation. The number of risk alleles was associated withincreases in serum calcitonin levels. Moreover, weobserved a nonsignificant trend toward a positivecorrelation between the number of risk alleles andCEA and tumor size. Notably, all MTC patientsharboring three or more polymorphic alleles presentedlymph node metastases at diagnosis whereas the
www.eje-online.org
estimated risk of distant metastases for those individualsharboring haplotypes with three or four variants wasalmost sixfold higher compared with those with fewerpolymorphic alleles, demonstrating a cumulative effectof these variants on phenotype of disease.
The synergistic effect of polymorphisms has beendescribed in several studies. Phillips et al. (34) showed anadditive effect of polymorphisms on the IL-6, LTA, andTNFa genes and plasma fatty acid level in modulatingthe risk for metabolic syndrome and its components. Thepresence of polymorphisms in the brain-derived neuro-tropic factor (BDNF) and RE1-silencing transcriptionfactor (REST) genes were associated with improvedgeneral cognitive ability (35). Moreover, Sfar et al. (36)have demonstrated that gene–gene interaction ofangiogenic gene polymorphisms increased the risk ofprostate cancer onset and aggressiveness. Interestingly,the authors observed a significant gene–dosage effect forincreasing number of potential high-risk genotypes.Compared with the reference group (low-risk geno-types), individuals with one, two, and three high-riskgenotypes had increasingly elevated risks of prostatecancer. Another interesting finding of the study was thatinteractions between vascular endothelial growth factor(VEGFA) and thrombospondin 1 (THBS1) polymorph-isms increase the risk of developing an aggressivephenotype disease. Patients carrying three high-riskgenotypes showed a 20-fold increased risk of high-gradetumor (36).
The molecular mechanism by which RET polymorph-isms affect the development and evolution of MTC arestill not properly understood. One of the mechanismsproposed is that the polymorphism could influence thestability of the mRNA. However, quantitative studies ofmRNA in MTC tumor tissues did not show a differencein RET expression in patients with or without theG691S/S904S, L769L, and S836S polymorphisms (14).Another hypothesis is that bases exchange in the DNAmolecule could create a new alternative splicing site,leading to the synthesis of a truncated protein,erroneous ligand binding, micro-RNA binding, changeof structure and mRNA stability as well as a number ofcopies, and also the change in the structure of proteinscaused by interference of translation (37). Bioinformaticanalysis showed differences in minimal free energy(MFE) structures in the case of exon 13. The L769L(TOG) variant reduces the energy of the wild type by17% and the mutant Y791F by 7%, leading the authorsto conclude that the L769L polymorphism reduces theMFE of small RET mRNA (17). It is also possible that thisneutral variant is in LD with an as yet unknownfunctional variant (22, 31). Besides, in the polymorph-isms that promote the substitution of amino acids, it canbe assumed that the modification has a cooperativeeffect on the dimerization of the RET protein or forms anew phosphorylation site in the tyrosine kinase domain(29). The S836S(COT) polymorphic variant failed toaffect DNA–protein binding, transcript stability, or RNA

RET variants and MTC 853EUROPEAN JOURNAL OF ENDOCRINOLOGY (2012) 166
splicing and editing (38), but it is possible that thisgenetic variant may create an unstable sequenceupstream or downstream at germline or somatic RETmutations instead of directly participating in thetumorigenic process (31). The result of these biologicalinteractions may influence the occurrence of somaticmutation or, alternatively, may indirectly reflect otherpolymorphisms that are in LD with these genotypedpolymorphisms and thus contribute to the tumorigen-esis of MTC.
In conclusion, our data indicate that the presence ofmultiple polymorphic alleles in the RET gene mayincrease the estimated risk for development andprogression of MTC and suggest that the analysis ofRET haplotypes provide higher predictive value for MTCthan single polymorphism study. Nevertheless, thesefindings need to be confirmed on sufficiently largestudies to validate or rule out a role of these variants asa cause or modifying agent in this rare disease. To thebest of our knowledge, no previous studies haveinvestigated the potential synergistic effects of RETpolymorphisms on MTC.
Declaration of interest
The authors declare that there is no conflict of interest that could beperceived as prejudicing the impartiality of the research reported.
Funding
This work was supported by Conselho Nacional de DesenvolvimentoCientıfico e Tecnologico (CNPq), Fundacao de Amparo Pesquisa doEstado do Rio Grande do Sul (FAPERGS), Fundo de Incentivo aPesquisa do Hospital de Clınicas de Porto Alegre (FIPE) and Programade Apoio a Nucleos de Excelencia (PRONEX), Brazil.
References
1 Maia AL, Gross JL & Punales MK. Multiple endocrine neoplasiatype 2. Arquivos Brasileiros de Endocrinologia e Metabologia 2005 49725–734. (doi:10.1590/S0004-27302005000500013)
2 Marsh DJ, Learoyd DL & Robinson BG. Medullary thyroidcarcinoma: recent advances and management update. Thyroid1995 5 407–424. (doi:10.1089/thy.1995.5.407)
3 Pacini F, Castagna MG, Cipri C & Schlumberger M. Medullarythyroid carcinoma. Clinical Oncology 2010 22 475–485. (doi:10.1016/j.clon.2010.05.002)
4 Eng C & Mulligan LM. Mutations of the RET proto-oncogene in themultiple endocrine neoplasia type 2 syndromes, related sporadictumours, and Hirschsprung disease. Human Mutation 19979 97–109. (doi:10.1002/(SICI)1098-1004(1997)9:2!97::AID-HUMU1O3.0.CO;2-M)
5 Punales MK, Graf H, Gross JL & Maia AL. RET codon 634mutations in multiple endocrine neoplasia type 2: variable clinicalfeatures and clinical outcome. Journal of Clinical Endocrinology andMetabolism 2003 88 2644–2649. (doi:10.1210/jc.2002-021422)
6 Donis-Keller H. The RET proto-oncogene and cancer. Journal ofInternal Medicine 1995 238 319–325. (doi:10.1111/j.1365-2796.1995.tb01205.x)
7 Marsh DJ, Learoyd DL, Andrew SD, Krishnan L, Pojer R,Richardson AL, Delbridge L, Eng C & Robinson BG. Somatic
mutations in the RET proto-oncogene in sporadic medullarythyroid carcinoma. Clinical Endocrinology 1996 44 249–257.(doi:10.1046/j.1365-2265.1996.681503.x)
8 Mulligan LM, Eng C, Healey CS, Clayton D, Kwok JB, Gardner E,Ponder MA, Frilling A, Jackson CE, Lehnert H, Neumann HPH,Thibodeau SN & Ponder BAJ. Specific mutations of the RET proto-oncogene are related to disease phenotype in MEN 2A and FMTC.Nature Genetics 1994 6 70–74. (doi:10.1038/ng0194-70)
9 Siqueira DR, Romitti M, da Rocha AP, Ceolin L, Meotti C,Estivalet A, Punales MK & Maia AL. The RET polymorphic alleleS836S is associated with early metastatic disease in patients withhereditary or sporadic medullary thyroid carcinoma. Endocrine-Related Cancer 2010 17 953–963. (doi:10.1677/ERC-09-0312)
10 Eng C, Mulligan LM, Healey CS, Houghton C, Frilling A, Raue F,Thomas GA & Ponder BA. Heterogeneous mutation of the RETproto-oncogene in subpopulations of medullary thyroid carci-noma. Cancer Research 1996 56 2167–2170.
11 Romei C, Elisei R, Pinchera A, Ceccherini I, Molinaro E, Mancusi F,Martino E, Romeo G & Pacini F. Somatic mutations of the retprotooncogene in sporadic medullary thyroid carcinoma are notrestricted to exon 16 and are associated with tumor recurrence.Journal of Clinical Endocrinology and Metabolism 1996 81 1619–1622. (doi:10.1210/jc.81.4.1619)
12 Ceolin L, Siqueira DR, Romitti M, Ferreira CV & Maia AL.Molecular basis of medullary thyroid carcinoma: the role of RETpolymorphisms. International Journal of Molecular Sciences 2012 13221–239. (doi:10.3390/ijms13010221)
13 Landa I & Robledo M. Association studies in thyroid cancersusceptibility: are we on the right track? Journal of MolecularEndocrinology 2011 47 R43–R58. (doi:10.1530/JME-11-0005)
14 Elisei R, Cosci B, Romei C, Bottici V, Sculli M, Lari R, Barale R,Pacini F & Pinchera A. RET exon 11 (G691S) polymorphism issignificantly more frequent in sporadic medullary thyroidcarcinoma than in the general population. Journal of ClinicalEndocrinology and Metabolism 2004 89 3579–3584. (doi:10.1210/jc.2003-031898)
15 Cebrian A, Lesueur F, Martin S, Leyland J, Ahmed S, Luccarini C,Smith PL, Luben R, Whittaker J, Pharoah PD, Dunning AM &Ponder BA. Polymorphisms in the initiators of RET (rearrangedduring transfection) signaling pathway and susceptibility tosporadic medullary thyroid carcinoma. Journal of Clinical Endo-crinology and Metabolism 2005 90 6268–6274. (doi:10.1210/jc.2004-2449)
16 Wiench M, Wygoda Z, Gubala E, Wloch J, Lisowska K,Krassowski J, Scieglinska D, Fiszer-Kierzkowska A, Lange D,Kula D, Zeman M, Roskosz J, Kukulska A, Krawczyk Z &Jarzab B. Estimation of risk of inherited medullary thyroidcarcinoma in apparent sporadic patients. Journal of ClinicalOncology 2001 19 1374–1380.
17 Sromek M, Czetwertynska M, Skasko E, Zielinska J, Czapczak D &Steffen J. The frequency of selected polymorphic variants of theRET gene in patients with medullary thyroid carcinoma and in thegeneral population of central Poland. Endocrine Pathology 2010 21178–185. (doi:10.1007/s12022-010-9125-8)
18 Ruiz A, Antinolo G, Fernandez RM, Eng C, Marcos I & Borrego S.Germline sequence variant S836S in the RET proto-oncogene isassociated with low level predisposition to sporadic medullarythyroid carcinoma in the Spanish population. Clinical Endo-crinology 2001 55 399–402. (doi:10.1046/j.1365-2265.2001.01328.x)
19 Berard I, Kraimps JL, Savagner F, Murat A, Renaudin K, Nicolli-Sire P, Bertrand G, Moisan JP & Bezieau S. Germline-sequencevariants S836S and L769L in the RE arranged during transfection(RET) proto-oncogene are not associated with predisposition tosporadic medullary carcinoma in the French population. ClinicalGenetics 2004 65 150–152. (doi:10.1111/j.0009-9163.2004.00172.x)
20 Gursoy A, Erdogan MF & Erdogan G. Significance of the RET proto-oncogene polymorphisms in Turkish sporadic medullary thyroidcarcinoma patients. Journal of Endocrinological Investigation 200629 858–862.
www.eje-online.org

854 L Ceolin and others EUROPEAN JOURNAL OF ENDOCRINOLOGY (2012) 166
21 Wohllk N, Soto E, Bravo M & Becker P. Polimorfismos G691S,L769L y S836S del proto-oncogen RET no se asocian a mayorriesgo de cancer medular tiroideo esporadico en pacienteschilenos. Revista Medica de Chile 2005 133 397–402.
22 Tamanaha R, Camacho CP, Pereira AC, da Silva AM, Maciel RM &Cerutti JM. Evaluation of RET polymorphisms in a six-generationfamily with G533C RET mutation: specific RET variants maymodulate age at onset and clinical presentation. ClinicalEndocrinology 2009 71 56–64. (doi:10.1111/j.1365-2265.2008.03491.x)
23 Baumgartner-Parzer SM, Lang R, Wagner L, Heinze G, Niederle B,Kaserer K, Waldhausl W & Vierhapper H. Polymorphisms in exon13 and intron 14 of the RET protooncogene: genetic modifiers ofmedullary thyroid carcinoma? Journal of Clinical Endocrinology andMetabolism 2005 90 6232–6236. (doi:10.1210/jc.2005-1278)
24 Beuten J, Gelfond JA, Franke JL, Weldon KS, Crandall AC, Johnson-Pais TL, Thompson IM & Leach RJ. Single and multigenic analysisof the association between variants in 12 steroid hormonemetabolism genes and risk of prostate cancer. Cancer Epidemiology,Biomarkers & Prevention 2009 18 1869–1880. (doi:10.1158/1055-9965.EPI-09-0076)
25 Schottenfeld D. Genetic and environmental factors in humancarcinogenesis. Journal of Chronic Diseases 1986 39 1021–1030.(doi:10.1016/0021-9681(86)90137-2)
26 Punales MK, da Rocha AP, Meotti C, Gross JL & Maia AL. Clinicaland oncological features of children and young adults withmultiple endocrine neoplasia type 2A. Thyroid 2008 18 1261–1268. (doi:10.1089/thy.2007.0414)
27 Stephens M, Smith NJ & Donnelly P. A new statistical method forhaplotype reconstruction from population data. American Journal ofHuman Genetics 2001 68 978–989. (doi:10.1086/319501)
28 Hedrick PW. Gametic disequilibrium measures: proceed withcaution. Genetics 1987 117 331–341.
29 Robledo M, Gil L, Pollan M, Cebrian A, Ruiz S, Azanedo M,Benitez J, Menarguez J & Rojas JM. Polymorphisms G691S/S904Sof RET as genetic modifiers of MEN 2A. Cancer Research 2003 631814–1817.
30 Fernandez RM, Pecina A, Antinolo G, Navarro E & Borrego S.Analysis of RET polymorphisms and haplotypes in the context ofsporadic medullary thyroid carcinoma. Thyroid 2006 16 411–417. (doi:10.1089/thy.2006.16.411)
31 Gimm O, Neuberg DS, Marsh DJ, Dahia PL, Hoang-Vu C, Raue F,Hinze R, Dralle H & Eng C. Over-representation of a germline RETsequence variant in patients with sporadic medullary thyroidcarcinoma and somatic RET codon 918 mutation. Oncogene 199918 1369–1373. (doi:10.1038/sj.onc.1202418)
www.eje-online.org
32 Song M, Lee KM & Kang D. Breast cancer prevention based ongene–environment interaction. Molecular Carcinogenesis 2011 50280–290. (doi:10.1002/mc.20639)
33 Lesueur F, Corbex M, McKay JD, Lima J, Soares P, Griseri P,Burgess J, Ceccherini I, Landolfi S, Papotti M, Amorim A,Goldgar DE & Romeo G. Specific haplotypes of the RET proto-oncogene are over-represented in patients with sporadic papillarythyroid carcinoma. Journal of Medical Genetics 2002 39 260–265.(doi:10.1136/jmg.39.4.260)
34 Phillips CM, Goumidi L, Bertrais S, Ferguson JF, Field MR, Kelly ED,Mehegan J, Peloso GM, Cupples LA, Shen J, Ordovas JM,McManus R, Hercberg S, Portugal H, Lairon D, Planells R &Roche HM. Additive effect of polymorphisms in the IL-6, LTA, andTNF-{alpha} genes and plasma fatty acid level modulate risk forthe metabolic syndrome and its components. Journal of ClinicalEndocrinology and Metabolism 2010 95 1386–1394. (doi:10.1210/jc.2009-1081)
35 Miyajima F, Quinn JP, Horan M, Pickles A, Ollier WE, Pendleton N& Payton A. Additive effect of BDNF and REST polymorphisms isassociated with improved general cognitive ability. Genes, Brain andBehavior 2008 7 714–719. (doi:10.1111/j.1601-183X.2008.00409.x)
36 Sfar S, Saad H, Mosbah F & Chouchane L. Combined effects of theangiogenic genes polymorphisms on prostate cancer susceptibilityand aggressiveness. Molecular Biology Reports 2009 36 37–45.(doi:10.1007/s11033-007-9149-4)
37 Borrego S, Saez ME, Ruiz A, Gimm O, Lopez-Alonso M, Antinolo G& Eng C. Specific polymorphisms in the RET proto-oncogene areover-represented in patients with Hirschsprung disease and mayrepresent loci modifying phenotypic expression. Journal of MedicalGenetics 1999 36 771–774.
38 Griseri P, Sancandi M, Patrone G, Bocciardi R, Hofstra R,Ravazzolo R, Devoto M, Romeo G & Ceccherini I. A single-nucleotide polymorphic variant of the RET proto-oncogene isunderrepresented in sporadic Hirschsprung disease. EuropeanJournal of Human Genetics 2000 8 721–724. (doi:10.1038/sj.ejhg.5200521)
Received 9 December 2011
Revised version received 13 February 2012
Accepted 17 February 2012