Excess mortality of schizophrenia. A meta-analysis
8
10.1192/bjp.171.6.502 Access the most recent version at DOI: 1997, 171:502-508. BJP S Brown Excess mortality of schizophrenia. A meta-analysis. References http://bjp.rcpsych.org/content/171/6/502#BIBL This article cites 0 articles, 0 of which you can access for free at: permissions Reprints/ [email protected] to To obtain reprints or permission to reproduce material from this paper, please write to this article at You can respond http://bjp.rcpsych.org/letters/submit/bjprcpsych;171/6/502 from Downloaded The Royal College of Psychiatrists Published by on October 3, 2014 http://bjp.rcpsych.org/ http://bjp.rcpsych.org/site/subscriptions/ go to: The British Journal of Psychiatry To subscribe to
Transcript of Excess mortality of schizophrenia. A meta-analysis

10.1192/bjp.171.6.502Access the most recent version at DOI: 1997, 171:502-508.BJP
S BrownExcess mortality of schizophrenia. A meta-analysis.
Referenceshttp://bjp.rcpsych.org/content/171/6/502#BIBLThis article cites 0 articles, 0 of which you can access for free at:
permissionsReprints/
[email protected] To obtain reprints or permission to reproduce material from this paper, please write
to this article atYou can respond http://bjp.rcpsych.org/letters/submit/bjprcpsych;171/6/502
from Downloaded
The Royal College of PsychiatristsPublished by on October 3, 2014http://bjp.rcpsych.org/
http://bjp.rcpsych.org/site/subscriptions/ go to: The British Journal of PsychiatryTo subscribe to

from unhygienic ways of life―.The mortalityin the asylums during the first part of thiscentury was described in three large studiesfrom the USA (Malzburg, 1934), Norway(ødegârd, 1936) and Sweden (Alström,1942). These authors used the standardisedmortality ratio (SMR), calculated by dividingthe observed mortality of a cohort by theexpected mortality of an age- and gendermatched cohort of the general population, tomeasure variations in mortality. Each founda significantly raised SMR in schizophreniaof between 2i0 and 400. Excess mortalitywas greater among females and in the acutestages of the disease, and lessened withincreasing age and length of stay. Most ofthe excess deaths were from pulmonarytuberculosis and pneumonia, consequencesof overcrowding, malnutrition and otherdeficiencies of the asylums. Suicide wasincreased but accounted for only a fewdeaths. During the First World War manyasylum patients in England and Wales diedfrom tuberculosis secondary to malnutrition(Crammer, 1992), while in Nazi Germanymany were systematically murdered by thestate (Burleigh, 1994).
The treatments of the pre-neuroleptic eraalso caused many deaths. Leucotomy had anoperative mortality of between 0.8 and 2.5%(Swayze, 1995), while the mortality of insulincoma therapy was 0.6% and that of cardiazol-induced convulsions 0. 1% (Henderson &Gillespie, 1952). Treatment-related deathsaccounted for 17% of the mortality of acohort followed at the Burgholzi Hospitalfrom 1942 to 1965 (Bleuler, 1978).
The treatment of schizophrenia changedafter the war, as a result of de-institutionalisation and the subsequent introduction ofeffective antipsychotic drugs. Most modempatients with schizophrenia, therefore, cxperience very different environmental conditions from their predecessors. It is notpossible to define a precise point at whichthese changes occurred; however, the introduction of chlorpromazine in 1952 providesa convenient starting point for the analysisof contemporary mortality.
CONTEMPORARY STUDIES OFSCHIZOPHRENIA MORTALITY
Record linkage studies
Record linkage studies, the most commonmethod of measuring mental illness mortality, use identifying characteristics (usually
name and date of birth) to link psychiatriccase records with population or death
Excessmortality of schizophrenia
A meta-analysis
STEVE BROWN
Background Thispaperpresentsastructured review ofthe published
information on the mortality of
schizophrenia.
Method A meta-analysisoftheliterature.
Results Schizophreniahasasignificantly increased mortality from
natural and unnatural causes.Twenty-eight
percentofthe excessmortalityisattributable to suicide and 2% to accidents.
Therestofthe excessmortalityisfromthe same broad range ofconditions which
cause deaths in the general population.
Further interpretation is hampered by
confounding variables, wide confidence
intervals and reservations about
generalising from individual cohorts.
Conclusions The availableevidencesuggests that schizophrenia is associated
with a large increased mortality from
suicide and a moderate increased mortality
from natural causes.A number of possible
interventions have been identified, but
we do not yet have reliable means of
detecting any changes in mortality which
might result.
Schizophrenia is associated with an increased risk of premature death (Mortensen& Juel, i990, i993). Improving the lifeexpectancy of sufferers should be a priorityof the psychiatric services. This will requirean understanding of the causes of the excessdeaths. This paper presents the first metaanalysis of the mortality of schizophrenia. Itdiscusses the methodology and limitationsof current work, places contemporary studies in a historical framework and offerssuggestions for further research.
DEVELOPMENT OFMORTALITY STUDIESIN SCHIZOPHRENIA
The first commentary on the mortality oflunacy in England and Wales dates from the17th century (Graunt, 1662). The earliestsystematic measurement was probably in184i, when William Farr reported that themortality of lunatics in England and Walesvaried between three and 14 times that ofthe general population. He concluded thatsome of the excess deaths “¿�maybe fairlyascribed to insanity―,but that most resultedfrom the conditions in the asylums. About aquarter of Victorian asylum patients wouldprobably now receive a diagnosis of schizophrenia (Turner, 1990), hence the contemporary mortality of schizophrenia wasprobably increased.
Kraepelin commented of dementia praecox, that “¿�lifeis threatened only veryslightly―.He noted that suicide occurred inthe acute and chronic stages, and speculatedthat negativism, inadequate diet and poorcooperation with treatment of concurrentmedical disorders also contributed to theincreased mortality (Kraepelin, 1919). EugenBleuler (1950) calculated that schizophreniawas associated with an excess mortality of1.4: 1. Deaths resulted from “¿�theindirectconsequences of psychosis: refusal of food,intentional or unintentional injuries, suicide,tuberculosis and other diseases resulting
502

AuthorsCountryDiagnostic
criteriaMethodSize
ofcohortLength of
follow-upObserveddeathsExpecteddeathsSMR
(95%Cl)(years)Babigian
& Odoroff(1969)USACase registerRecord linkage8080'0-654l3l075(160—l89)Weiner
& Marvit (l977)USACase registerRecord linkage6890219I 6.388(164—210)Gieleta! (1978)NetherlandsCase registerIn-patient records8142253742626 (I16—l36)Eastwood
eta! (1982)CanadaICD—8Record linkage82974.845(57—273)Haugland
eta! (l983)USADSM—lllRecord linkage3513.520I I181 (Il0—270)Herrmaneta/(1983)UKICD—8Record
linkage59245729.6l92(l46—246)Brook(l985)NetherlandsCaseregisterln-patientrecords52262486305l59(l45—l74)Wood
eta! (l985)USADSM—lllRecord linkage8779'570937987 (l74—20l)*Allebeck
& Wistedt (l986)SwedenICD—9Record linkageI 901023196.5239(209_27l)*Black(l988)USAICD—9Recordlinkage8910—10457.8260(178—358)Hassall
eta! (1988)UKCase registerRecord linkage6952—I I6839.2173(l34—2l7)Zilberetal(1989)IsraelICD—9Recordlinkage9178'58l6395207(l92_22l)*Mortensen
&Juel (l990)Denmark‘Kraepelinian
lines'Record
linkage6l520—3045693882I 18(Il4—l22)Andersonetal(l991)UKICD—9Follow-up5322—l46927.6249(l94—3l2)Newman
& Bland (1991)CanadaICD—9Record linkage36230—lO30 II l6259(23l—290)Mortensen
& Juel ( I993)DenmarkICD—8Record linkage9 I56I 0—I8I I00329334 (3 I5_354)*Amaddeoetal(l995)ItalyICD—9Recordlinkage305'0—lO23l3.ll76(lll—255)Baxter(l996)UKICD—9Record
linkagel398l0—l846229l.3l59(l44@l73)*Total66
161lO 2606788.2ISI (l48—l54)
(c) there was a stated loss to follow-up ofless than 15%.
The analysis was restricted to cohortsfrom North America, The Netherlands,Israel, Scandinavia and the UK as no otherstudies met the inclusion criteria. Wheresubjects were included in more than onestudy, the data come from the paperdescribing the largest cohort (Black, 1988;Mortensen & Juel, 1990, 1993).
Aggregate SMRs were calculated by
dividing the sum of the observed deaths by
the sum of the expected deaths, and multiplying the result by 100. Confidence intervals and significance statistics werecalculated from the Poisson distribution(Gardener & Altman, 1989), and heterogeneity of the cohorts measured as described
by Thompson (1993).
RESULTS
The aggregate mortalityof schizophrenia
Mortality was increased in every studyincluded in the meta-analysis (Table 1),though the increase was non-significant in
registers. The introduction of computeriseddatabases has allowed large cohorts to bestudied, with consequently high statisticalpower. The validity of the results dependson the accuracy of original entries on thedatabases and on the accuracy of the recordlinkage process. The size of error from thesesources varies from study to study, and israrely discussed in satisfactory detail.
Individual follow-up studies
In these studies subjects are traced personally.This is time-consuming, but provides thedetails about illness, treatment, and outcomewhich explain individual deaths. Only threeindividual follow-up studies that presentedresults in the form of SMRs have beenpublished (Martin et al, 1985; Lesage et a!,1990; Anderson et a!, 1991). These studies
analysed a total of 85 deaths, hence the
generalisability ofthe findings is questionable.
Analysis of in-patient registers
These studies use information from in-patientregisters to measure the mortality of hospitalpopulations (Giel et a!, 1978; Brook, 1985).
The data are from official records and shouldbe complete; however, patients who leavehospital are lost to follow-up. The cohorts
are therefore poorly representative of thepopulation with schizophrenia.
THE META-ANALYSIS
Papers were identified through searches of
the Medline and BIDS Gateway databasesfrom January 1986 to December 1996, usingthe key-words ‘¿�mortality',‘¿�outcome'and‘¿�follow-up'with ‘¿�schizophrenia'and ‘¿�mentalillness'. The citations in each paper werethen checked until no further references wereforthcoming. The meta-analysis was re
stricted to the English and French languages,peer-reviewed studies, of more than 100individuals with schizophrenia, recruitedsince 1952, which met the following criteria:
(a) the paper included the number ofobserved and expected deaths, or
contained sufficient details to allowthese figures to be calculated;
(b) the cohort was followed up for at leasttwo years; and
TableI All-causemortalityofschizophrenia
Variationfromexpectedvaluesignificantat5%level.I. Calculatedfrom datasuppliedinthetext.
503

ICD—9categoryMaleFemaleTotalObserved
ExpectedSMR(95%Cl)Observed ExpectedSMR(95%Cl)ObservedExpectedSMR(95%Cl)Allcauses
All natural causes (00 —¿�799)
Cardiovasculardisease
(390—429)
Cerebrovasculardisease
(430—438)
Respiratorydisease (460—519)
Neoplastic disease ( I40—SI9)
Digestivediseases(520—579)
Genito-urinarydisease(580—629)
Other diseases (I —¿�389,630—799)
Allunnaturalcauses
(E800—E999)
Accidents (E800—E949)
Suicide(E950-E959)3819
257l.5
2443 990.8
057 944
225 247.4
308 148.2
5 I3 596.0
141 67.7
98 54.5
356 204.6
715 140.6
217 02.6
650 68.0l48(144—l52)
23 (I l8_l28)*
l12(l05_l19)*
91 (79—103)
208 (185_23l)*
86 (78—93)
208(l75@@244)*
l80(l45—217)
I74 (I 56—I92)*
508(47l_546)*
2l I (l84@240)*
956(884_lO3l)*3605
2601.4
2566 2055.8
888 814
245 347.5
315 127.4
589 544
27 77.9
64 38.7
422 265.2
351 lOl.8
62 75.3
231 34.3l39(l34@l44)*
125(l20@l30)*
l09(l02_1I6)*
70(6l_79)*
247 (22l_275)*
I08 (99—I I7)
63 (l35_l92)*
165(137_208)*
I59 (I 44—I75)
345(3l0@382)*
215 (l54_286)*
673(59l_763)*10
260 6788.2
5956 4492.l
2029 835.6
490 607.6
634 280.2
I2 I3 I25 I.0
278 50.0
168 04.5
809 480.9
1160 272.6
443 204.8
896 106.9ISI
(l48_l54)*
l34 (l3l_l37)*
llo(lO5—lls)
81 (73_87)*
226 (209_244)*
97 (9 I—¿�I02)
l85(l64@208)*
161(137_l86)*
I68 (I 57—I80)
426(402—45l)
216 (l96_236)*
838(784@894)*
one small cohort (Eastwood et a!, 1982).The meta-analysis produced an aggregatecrude mortality rate (CMR) of 189 deaths/10 000 population per year, an aggregateSMR of 151 (95% CI 148—154)and a 10-
year survival of 81%.
Trends in mortality
Two Danish studies which measured thefive-year SMR in successive national cohortssuggest that the SMR is rising in the firstepisode of schizophrenia (Munk-Jørgensen& Mortensen, 1992), but falling in chronicschizophrenia (Licht et a!, 1993). This meta
analysis found a significantly higher(P<0.001) aggregate SMR from studiespublished in the 1980s (SMR 191, 95% CI183—199),than from studies published inthe 1970s (SMR 152, 95% CI 144—160),or1990s (SMR 140, 95% CI 137—143),butthe differences may be due to confoundingvariables.
Gender
The male unnatural-cause SMR was significantly higher than the female figure butthere was no gender difference in naturalcause mortality (Table 2). This resulted in asmall but significantly higher overall malemortality (aggregate male SMR 148, 95%CI 144—152;aggregate female SMR 139,95% CI 134—144).
Age
The SMR in schizophrenia appears todecrease exponentially with age (Fig. 1). Thisis largely due to a high rate of suicide in the
young (Anderson et a!, 1991; Newman &Bland, 1991; Mortensen & Juel, 1993). Thenatural-cause SMR probably also falls withage, but the slope is gradual (Newman &Bland, 1991; Mortensen & Juel, 1993).
Length of follow-up
The all-cause SMR fell incrementally overthe five years following a first episode ofschizophrenia (Munk-Jørgensen & Mortensen, 1992), and fell with length of followup in most (Black, 1988; Hassall et a!,1988; Newman & Bland, 1991), thoughnot all (Allebeck & Wistedt, 1986) cohortsrecruited later in their illness. This waslargely due to a clustering of suicides at thestart of follow-up (Black, 1988; Hassall et
a!, 1988; Newman & Bland, 1991; Mortensen & Juel, 1993). There is no directevidence that the natural-cause SMR fallswith length of follow-up; however, it wassignificantly lower in the Danish national
cohort with chronic schizophrenia than inthe equivalent first-episode cohort (Mortensen & Juel, 1990, 1993).
Diagnostic criteria and subtypesof schizophrenia
The aggregate SMR of narrowly defined(ICD—9 or DSM—III) schizophrenia wassignificantly lower (SMR 138, 95% CI
135—142) than that of broadly definedschizophrenia (SMR 193, 95% CI 186—200), but the difference may be due to
confounding variables. Mortality is prob
ably increased in all the subtypes of schizo
phrenia. Comparison of the aggregate
mortality of different subtypes was notpossible as a different classification system
was used in each study which addressed thisissue.
2o@.
1000@ .
@@ . ..@ :‘s...@. •¿�•¿�
0,@@@ -.-@@10 20 30 40 50 60 70 50 90
Mid-point of age group (years)
Fig. I Variation in schizophrenia mortality with age.
References:Gieletal (1978);Brook(1985);Black
(1988);Hassalleta!(1988);Zilberetal (l989);Andersoneta! (1991);Newman& Bland(1991);
Morensen&Juel(1993).
Table 2 Mortalityof schizophreniabyICD—9category(categoriesinwhichfewer than20 deathswere recordedhavenot beenanalysedseparately)
Variation from expected value significant at 5% level.References:Eastwood etol (1982);Hermann etal (1983):Brook (1985);Allebeck & Wistedt (1986);Black (1988);Zilber (l989): Mortensen &juel (1990);Newman & Bland (1991);Mortensen& juel (1993).
504
AuthorsMaleFemaleTotalObserved
ExpectedSMR(95%Cl)Observed ExpectedSMR(95%Cl)ObservedExpectedSMR(95%Cl)Weiner
& Marvitt, USA (I 977)
Copas & Robin, UK (1982)
Pokorny, USA (I 983)
Allebeck,Sweden(l986)
Nyman & Johnsson, Sweden
( I986)
Black, USA(1988)
Zilberetal, Israel (1989)
Mortensen & Juel, Denmark
(1990)
Andersonetal,UK (1991)
Newman&Bland,Canada
(1991)
Mortensen&Juel,Denmark
( I993)I
3 I
86 14.1
I9 0.9
l8 1.8
9 0.3
12 0.4
37 27.4
S 0.3
81 3.9
370 17.9I
300 (689—I954)*
610 (488_746)*
I980 ( I268—3I67)*
l000(59l_l5l5)*
3000 (I 360@S280)*
3000(l542_4937)*
I35 (95—I82)
l950(526_3448)*
2076(1649_2543)*
2067(186l_2283)*4
0.4
30 0
IS 0.9
I 0. I
6 0.1
I9 IS
2 0.15
16 .0
138 6.6I
000 (26 I
300 (202@4l70)*
l660(930@26l7)*
I000 (4-3920)
5450(2l59—3465)
I36 (76—I90)
l280(l040@382l)*
l600(9l2—33S4)
2091 (1757_2454)*I
7 I.4
I 16 24.l
I9 0.9
33 2.7
I0 0.4
18 0.5
IS 4.7
56 42.4
7 0.4
97 4.9
508 24.5I
2 l4 (706—I860)*
48l (398—573)
I980 ( I268—3I67)*
l230(84l_l675)*
2500 (I I90@4290)*
3600(2l30@S4S5)*
320 (l78—50l)
I36 (I 00—I70)
l660(693_3286)*
209l(1602_2393)*
2073(l897_2258)*Total650
68.09S6(884—lO3I)231 34.3673(59l_763)*896106.9838(784—894)Variation
from expected value signifcant at 5% level.
Newman & Bland, 1991). The excess ulcerdeaths were probably secondary to alcoholmisuse, while most pneumonia deaths were
of elderly institutionalised patients. Thelow aggregate male cancer mortality (Table2) is largely explained by a reduced lungcancer mortality (Mortensen & Juel, 1990;Newman & Bland, 1991). Female cancermortality is unexceptional. Deaths from
tuberculosis are now rare.
Unnatural-cause mortality
Unnatural deaths (ICD—9800—999) weresignificantly increased among both males
and females in all studies (Table 2) thatanalysed the cause of death (aggregate SMR426, 95% CI 402—451), and account forabout 41 % of the total excess mortality ofschizophrenia.
Accidents
The SMR from accidents was twice the ratein the general population (SMR 216, 95%
CI 196—236), with no significant genderdifference, and accounted for about 12%of the excess mortality. Mortensen & Juel(1990) reported that two-thirds of the excessaccidental deaths among older patients werefrom falls (SMR 166, 95% CI 138—199),andthe remainder from aspiration (SMR 3153,95% CI 2196—4385).The absolute mortalityfrom road traffic accidents is reduced;
however, significantly fewer people withschizophrenia drive, and the risk of accident
per mile driven is probably increased(Edlund et a!, 1989). The mortality fromnon-motor vehicle accidents is increased(Weiner & Marvit, 1977; Wood eta!, 1985).
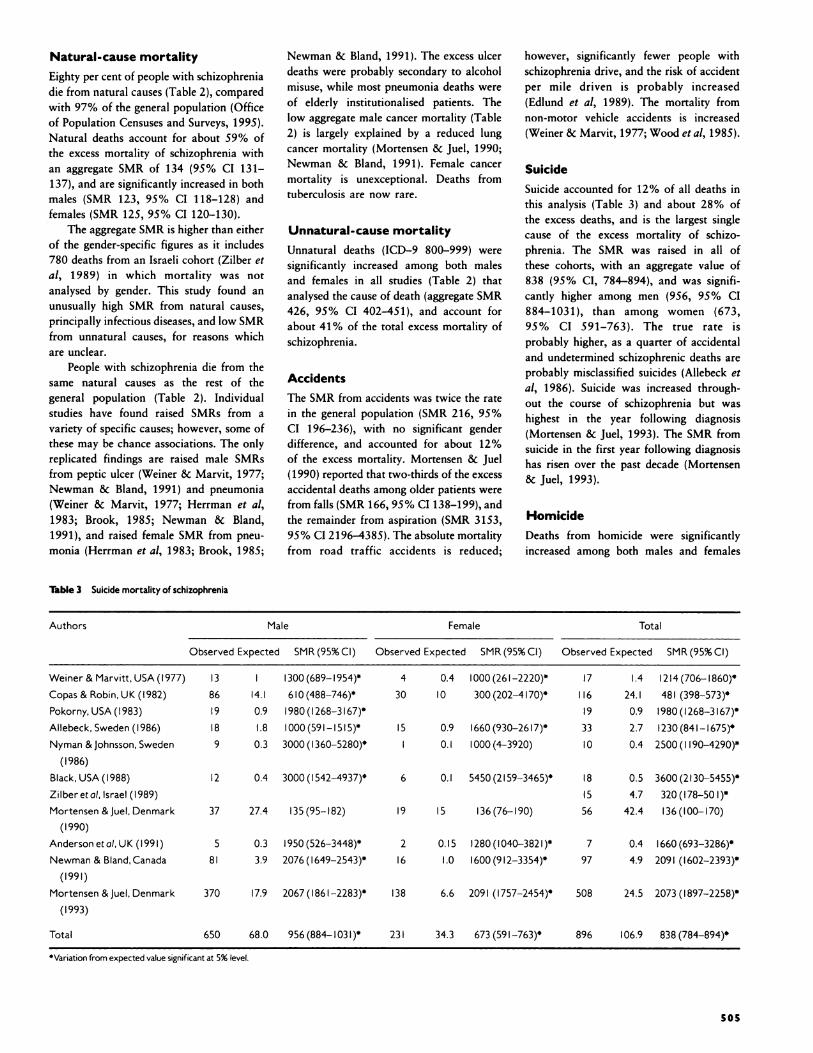
Suicide
Suicide accounted for 12% of all deaths inthis analysis (Table 3) and about 28% of
the excess deaths, and is the largest singlecause of the excess mortality of schizophrenia. The SMR was raised in all ofthese cohorts, with an aggregate value of838 (95% CI, 784—894), and was significantly higher among men (956, 95% CI884—1031), than among women (673,95% CI 591—763). The true rate isprobably higher, as a quarter of accidentaland undetermined schizophrenic deaths areprobably misclassified suicides (Allebeck eta!, 1986). Suicide was increased throughout the course of schizophrenia but washighest in the year following diagnosis
(Mortensen & Juel, 1993). The SMR fromsuicide in the first year following diagnosishas risen over the past decade (Mortensen& Juel, 1993).
Homicide
Deaths from homicide were significantlyincreased among both males and females
Natural-cause mortality
Eighty per cent of people with schizophreniadie from natural causes (Table 2), compared
with 97% of the general population (Officeof Population Censuses and Surveys, 1995).Natural deaths account for about 59% ofthe excess mortality of schizophrenia withan aggregate SMR of 134 (95% CI 131—137), and are significantly increased in both
males (SMR 123, 95% CI 118—128)andfemales (SMR 125, 95% CI 120—130).
The aggregate SMR is higher than eitherof the gender-specific figures as it includes780 deaths from an Israeli cohort (Zilber eta!, 1989) in which mortality was notanalysed by gender. This study found anunusually high SMR from natural causes,principally infectious diseases, and low SMR
from unnatural causes, for reasons whichare unclear.
People with schizophrenia die from thesame natural causes as the rest of thegeneral population (Table 2). Individualstudies have found raised SMRs from avariety of specific causes; however, some ofthese may be chance associations. The onlyreplicated findings are raised male SMRsfrom peptic ulcer (Weiner & Marvit, 1977;Newman & Bland, 1991) and pneumonia(Weiner & Marvit, 1977; Herrman et a!,1983; Brook, 1985; Newman & Bland,1991), and raised female SMR from pneumonia (Herrman et a!, 1983; Brook, 1985;
Table3 Suicidemortalityofschizophrenia
505

(SMR 733, 95% CI 363—1230), but accounted for only 1% of the excess mortality.
Undetermined deaths
Death is coded as undetermined if there isinsufficient evidence to decide the cause.The mortality from undetermined causeswas greatly increased (Allebeck & Wistedt,1986) with an SMR of 1430 (95% CI 960—2130).
DISCUSSION
Limitations and errors of thismeta-analysis
Meta-analysis weights information by thesize of the cohort from which it was derived.It has the potential to produce significantresults by aggregating individually nonsignificant studies. However, important differences between studies may be obscured,in this case differences in diagnostic criteria,hospital discharge patterns and death cciiification.
The most accurate form of metaanalysis involves the review and analysisof individua! patient data, and can includeunpublished series and data on patientsexcluded from published analysis (Stewart& Parmar, 1993). This paper describesameta-analysis of the literature. Literatureanalysis may be affected by publicationbias, in this case a preference for studiesreporting variation from expected mortality. Small cohort studies (e.g. Wilkinson,
1982; Lesage et a!, 1990) were excluded toreduce the possibility of this. Funnelanalysis (Dickersin & Berlin, 1992) suggests that publication bias was not animportant source of error. Studies of lessthan two years' duration were excludedfrom the meta-analysis to reduce bias fromthe clustering of suicide around contactwith psychiatric services (Caldwell &Gottesman, 1990).
Cohorts with a high drop-out rate (e.g.Saku et a!, 1995) were excluded as mortalityis higher among subjects lost to follow-upthan among those who are traced (Sims,1973). Some studies did not measure completeness of follow-up as they only linkedcase registers to death certificates, hencesubjects without death certificates wereassumed to be alive. These studies (Babigian& Odoroff, 1969; Eastwood et a!, 1982;Haugland et a!, 1983; Herrman et a!, 1983;Allebeck & Wistedt, 1986; Black, 1988;Hassall et a!, 1988; Zilber et a!, 1989;Newman & Bland, 1991) will have under
estimated mortality, but were included inthe meta-analysis to avoid giving undueweight to in-patient cohorts.
Analysis of heterogeneity
The results of the studies included in themeta-analysis were significantly heterogeneous (x265.9, d.f.=17, P<0.001). Analysis of the data by phase of illness of thecohort suggested that first-episode schizophrenia (Eastwood et a!, 1982; Mortensen& Juel, 1993) had a SMR of 332 (95% CI312—351) and chronic schizophrenia (Gielet a!, 1978; Brook, 1985; Mortensen &Juel, 1990) a SMR of 121 (95% CI 118—124). Cohorts of subjects at varying pointsin their illness had an SMR of 193 (95% CI187—206). Division of the cohorts intothree groups in this way, led to a substantial fall in hete,rogeneity ([email protected].=1S, P=0.S) and suggeststhat phaseof illness explains a large part of theoriginal heterogeneity.
First-episode cohort studies provide themost accurate estimate of the excess mortality of schizophrenia, as other cohorts willcontain subjects who have already survivedthe period of greatest excess mortality. Evenfirst-episode studies will underestimate thetrue mortality, as a number of people withschizophrenia die, for example from suicide,before being recognised by the mental healthservices. The aggregate figure from the twofirst-episode studies (SMR 332, 95% CI312—351)is slightly high, as the SMR wouldprobably have fallen if the cohorts had beenfollowed for longer (Munk-Jorgensen &Mortensen, 1992), but is the best figurewhich can currently be placed on the excessmortality of schizophrenia.
Comparison with the mortality ofother diseases
The SMR of schizophrenia is comparablewith that of chronic physical diseases suchas diabetes (SMR 2.2; Riley eta!, 1995). Themortality is similar to that of affective illness(Eastwood et a!, 1982; Wood et a!, 1985;Zilber et a!, 1989; Amaddeo et al, 1995;Baxter, 1996), which has a similar largeexcess of suicide deaths, but is lower thanthat of organic mental disease (Wood et a!,1985; Hassall et a!, 1988; Zilber et a!,1989).
Monitoring trends in mortality
We do not know whether or not themortality of schizophrenia was affected by
de-institutionalisation. The aggregate SMRof modern cohorts with schizophrenia islower than the SMRs of asylum cohorts(Malzburg, 1934; ødegârd,1936; Alström,1942), but the effects of confounding vanables and selection bias means that wecannot be sure whether or not this is a realchange. We do not know how manypremature deaths occur in schizophrenia inthe UK each year, or whether the mortalityis different in other Western countries, andhave no reliable way of measuring whethermortality is rising or falling.
This is surely unacceptable, as mortalityis a fundamental measure of outcome. Themortality of mental illness should be monitored nationally to measure the impact ofnational policy changes, and locally tomeasure the effect of local interventionsand the performance of individual services.Measurement should be diagnosis-specific,as case mix introduces a further source ofcontamination, and tracing should be cornplete. Cohorts should be matched forpotential confounding variables. Local measurement of schizophrenia mortality isfeasible in the UK (Hassall et a!, 1988;Baxter, 1996). However, reliable nationalmeasurement is not yet possible as there isno mechanism, such as a national psychiatnic case register, from which to identifyrepresentative cohorts.
Specific causes of death
Suicide is the single largest cause of premature death in schizophrenia, and hencethe area where there is the greatest potentialto reduce mortality. Many factors associatedwith suicide in schizophrenia are known,but attempts to identify high-risk patientshave so far produced too many false positiveresults to be clinically useful (Caldwell &Gottesman, 1990). Further work in this areashould be a priority, as the rate of suicide inschizophrenia appears to be increasing(Mortensen & Juel, 1993). Accidentaldeaths are also significantly increased, andcould probably be reduced by closer medicaland nursing supervision.
The excess natural mortality of schizophrenia also needs to be addressed. Much ofthe variation is probably determined byfactors which affect mortality in the generalpopulation. There is no explicit link betweenschizophrenia mortality and poverty, thoughBaxter (1996) found that about 20% of theexcess mortality in an undifferentiatedpopulation with mental illness disappearedwhen the rates were adjusted to take
506

the contribution of cigarette smoking andsocial factors. Individual follow-up studiesare needed to identify specific deficiencies intreatment and to suggest changes in clinicalpractice.
Health education programmes whichhave been effective in the general populationshould be evaluated in cohorts with schizophrenia. Such interventions may have to beadapted to fit the needs of people withschizophrenia, and should have explicitprotocols and goals in order that benefitsand costs can be established.
Crammer, j. L. (1992) Extraordinary deaths of asyluminpatients during the l9l4—1918war. Medical History. 36,
430—44l.
Dlck.rsln, K. & Berlin, j. A. (1992) Meta.analysis: state ofthe science.EpidemiologicRewews.l4, l54—176.
Dupont, A., Jenson, 0. M., Stromgren, E., at al (1956)Incidenceof cancerin patientsdiagnosedasschizophrenicinDenmark. In PsychiatricCaseRegistersin PublicHealth (l963)(edsG. H.TenHorn, R.Giel,W.H.Gulbinat, et al). Amsterdam:Elsevier.
Eastwood, M. R., Stiainy, S., Mel.,', H. M. R., at ci (1982)Mentalillnessand mortality. ComprehensivePsychiatry.23,377—385.
Edlund,M.J., Conrad,C. & Morris, M. (1989)Accidentsamong schizophrenic outpatients. Comprehensive Psychiatry.
30, 522—526.
Farr,W.(1841) Report on the mortality of lunatics.Journalofthe Royal Statistical Society,IV. 17—33.
Gardener, N.J. & Altman, D. G. (1989) Statistics withConfidence. London: British Medical Journal.
GISI, R., Dljk, S. 1, van Weerden Dljkstra, j. R. (1978)
Mortality in the long-staypopulationof all Dutch mentalhospitals. Acta Psychiatrica Scandinavica, 57, 361—368.
Graunt, J. (1662) Natural and political observations
mentioned in a following index, and made upon the bills of
mortality. InThreeHundredYearsof Psychiatry1538—1860(1963)(edt R.A. Hunter & I.Macalpine),p. 166.London:Oxford University Press.
Hassall,C., Prior, P. a Cross, K.W. (1988) A preliminary
study of excess mortality using a psychiatric case register.
Journal of Epidemiology and Community Health, 42, 286—289.
Haugland, G., Cralg,T.J., Goodman, A. B., .t al (1983)
Mortality in the era of deinstitutionalisation.AmericanJournalof Psychiatry,140.848—852.
Henderson, D. a GIllespie, R. D. (1952) A Textbook of
Psychiatry. London: Oxford University Press.
Herrman, H. E., BaldwIn, j.W. a ChrIstIe, D. (1983)
A record-linkagestudyof mortality andgeneralhospitaldischargein patientsdiagnosedasschizophrenic.PsychologicalMedicine, 13. @81—593.
Kraepelln, E. (1919) Dementia Praecoxand Paraphrenia.
Edinburgh:Livingstone.
Lesage, A. D.,Trapani,V. a Tans&la, M. (1990) Excessmortality by naturalcausesof Italianschizophrenicpatients.European Archives of Psychiatry and Neurological Sciences,239,
361—365.
Llcht, R.W., Mortensen, P. B., Gouliaev, G., at al (1993)
Mortality in Danishpsychiatriclong-staypatients, 972—I982.Acta Psychiatrica Scandinavica, 87, 336—341.
Malzburg, B. (1934) Mortality among Patients woh Mental
Disease. New York: Utica State Hospital Press.
Martin, R. L., Cionlng.r, R., Gus., S. B., at at (1985)Mortality in a follow-up of 500 psychiatric outpatients. II.
Cause-specificmortality. Archivesof GeneralPsychiatry,42,58—66.
Mortensen, P. B. (1989) The incidence of cancer inschizophrenicpatients.Journalof Epidemiologyand CommunityHealth, 43, 43—47.
—¿�a [email protected], K. (1990) Mortality and causesof death in
schizophrenicpatientsin Denmark. Acta PsychiatricaScandinavica. 81, 372—377.
—¿�a (l9@3) Mortality and causesofdeath in first
admittedschizophrenicpatients.BritishJournalof Psychiatry,163,183—189.
Munk.J.rgensen, R a Mortensen, P. B. (1992) Incidenceandother aspectsofthe epidemiologyof schizophreniainDenmark, 1971—¿�87.BritishJournalof Psychiatry.161,489—495.
507
ACKNOWLEDGEMENTS
Thanks to Dr Brian Barraclough and Clare Harris for
their support and advice in the preparation of this
work.
REFERENCES
AUsbeck P.,Varla, A. A Wistedt, B. (1986) Suicideandviolentdeath amongpatientswith schizophrenia.ActoPsychEatricaScandinavico, 74. 43—49.
—¿� It Wistedt, B. (1986) Mortality in schizophrenia. A ten
year follow.up basedon the Stockholmcounty inpatientregister. Archives of General Psychiatry. 43. 650—653.
Alstrom. C. H. (1942)Mortalityinmentalhospitalswithespecialregardto tuberculosis.Acta PsychiatricaandNeurolagica Scandinavica, suppi. 24.
Amaddeo, F., Bisoffi,G., Bonizato, P.. at aI(1995) Mortalityamongpatientswith psychiatricillness.A ten year caseregister study in an area with a community based system of
care. British Journal of Psychiatry. 166, 783—788.
Anderson. C.. Connally, J.. johnstone. E. C., at al (1991)Disabilities and circumstances of schizophrenic patients —¿�a
follow.up study:V.Causeof death.BritishJournalof Psychiatry.159 (suppl. 3). 30—33.
Babigian, H. M. & Odoroff. C. L (1969) The mortalityexperienceof a populationwith psychiatricillness.AmericanJournal of Psychiatry. 126. 470—480.
Buter 0. N. (1996) The mortality experience of individualson the Salford case register I. All-cause mortality. British
journal of Psychiatry, 168. 772—779.
Black, D.W. (1988) Mortality in schizophrenia —¿�The Iowa
record.linkagestudy: A comparisonwith generalpopulationmortality. Psychosomatics,29, 55—60.
Bleuler, E. (1950) Dementia Praecoxor the Group
Schizophrenias(first publishedin German,1911).New York:International Universities Press.
Bleuler, M. (1978) The SchizophrenicDisorders.New Haven:
YaleUniversity Press.
Brook, 0. H. (1985) Mortalityinthe long.stay populationofDutch mentalhospitals.Acta PsychiatricaScandinavica.71.626—635.
Burlelgh, M. (1994) Death and Deliverance —¿�Euthanasia in
Germany 1900—45.Cambridge: Cambridge University Press.
Caidwell, C. B. A Gottesman, I. I. (l990) Schizophrenicskillthemselvestoo: A review of risk factors for suicide.Schizophrenia Bulletin, 16. 57l —¿�588.
Copas, J. B. A Robin, A. (l982) Suicide in psychiatric inpatients. British Journal of Psychiatry, 141,503—SII.
account of social class. Other possibleculprits include cigarettes and alcohol (Mortensen & Juel, 1993) and unhealthy diet andlack of exercise.
The relationship between smoking andschizophrenia mortality is particularly interesting. Cancer mortality (Saku et a!, 1995)and incidence (Dupont et a!, 1986; Mortensen, 1989) is reduced at a number of sites.Some of this may be chance association, ordue to known risk factors such as theassociation between sexual activity andcervical cancer or low fertility and increasedbreast cancer. There are no specific studies ofthe mortality of smokers with schizophrenia.However, smoking provides a plausibleexplanation of the raised mortality fromrespiratory disease. The reduced male mortality from lung cancer is therefore verysurprising.
The impact of psychotropic drugs on themortality of schizophrenia is unknown.Mortensen & Juel (1990) found a raisedSMR (180, 95% CI 161—199)among olderpatients from causes such as falls, aspirationand diabetes, which were possibly related todrug side-effects. Some of the variation incerebrovascular and cardiovascular mortality (Table 2) may be due to the effects ofpsychotropic drugs, while Mortensen (1989)suggests that the reduced cancer incidencemay be secondary to their effects onprolactin secretion.
Avoidable natural deaths
Kraepelin (1919) and others have suggestedthat reluctance to seek medical attentionand poor compliance with treatment mightcontribute to the mortality of schizophrenia. Mortensen & Juel (1990, 1993) foundthat the mortality from ‘¿�treatable'conditions (Rutstein et a!, 1976), was significantly increased (SMR 135, 95% CI 109—163). It is unclear whether psychiatrists orgeneral practitioners are best equipped totreat physical disease in people with severemental illness. Until this is decided, responsibility for the physical care of each patient
should be explicitly allocated and accepted,and all doctors should be alert for signs ofphysical disease.
Further research
Further research is needed to tease out the
factors which cause the excess mortality ofschizophrenia and to provide a sound basisfor intervention studies. Further large prospective cohort studies are needed to examinc the mortality from specific causes and

Newman, S.C. a Bl@d, R. C. (1991)Mortality in a cohortof patientswith schizophrenia:A record linkagestudy.Canadian Journal of Psychiatry. 36, 239—245.
@‘¿�1yman,A. K. a Jo@sson, H. (1986) Patterns of self
destructive behaviourin schizophrenia.ActaPsychiatricaScoriciinavica,73@252—262.
Office of Population C.nsus and Sumys (1995) 1993Mortality Statistics:Cause.London:HMSO.
ød.gIrd, 0. (1936) Mortality in Norwegian mental hospitalsfrom I9I6 to 933. Acta Psychiatrica Scandinavica, II. 323—356.
Pokorny, A. 0. (1983)Predictingsuicidein psychiatricpatients.Report of a prospectivestudy.Archivesof GeneralPsychiatry,40. 249—257.
Riley, M. a, McCarty, D.J., Coup..', D@J.,.t ci (1995)The1984Tasmanianinsulintreated diabetesmellitusprevalencecohort: An eight and a half year mortality follow.up. DiabetesResearchand ClinicalPractice,29, 27—35.
Rutatsin, D. D., B.rwb.Fg,W.,Ch*Im.rI,T. C., it at (1976)Measuringthe qualityof medicalcare.A clinicalmethod.NewEnglandJournalof Medicine,294, 582—588.
Sakii, M..Tokudom., S., lk.da, M., it aI(l99S) Mortality inpsychiatricpatients,with a specificfocuson cancermortalityassociatedwith schizophrenia.InternationalJournalofEpidemiology. 24, 366—372.
STEVEBROWN, MRCPsych,Department of Psychiatry.University of Southampton,RoyalSouth Hants Hospital.BrintonsTerrace,Southampton S0I4 OYG
Correspondence: Dr Steve Brown,Wolston Park Hospital.Wacol 4076, Queensland, Australia
(First received 2l February 997, final revision 17June1997,accepted30 June1997)
Sims, A. C. P. (1973) Importance of a high tracing-rate in
long-term medicalfollow-up studies.Lancet.ii.433—435.
Stewart, L. A. & Parmar, M. K. (1993) Meta.analysis of the
literature or of individualpatientdata: isthere a difference?Lancet.341.4I8—42l.
Swayzs,V.W. (l@5) Frontal leucotomy and related
psychosurgicalproceduresin the era before antipsychotics(I935—54):A historicaloverview.AmericanJournalofPsychiatry.152,505—515.
Thompson. S. G. (1993) Controversies in meta-analysis: thecaseofthe trialsof serumcholesterolreduction.StatisticalMethodsinMedicalResearch,2, l73—I92.
flirner,T. H. (1990) Rich and mad in Victorian England:
Diagnostic analysis ofthe casebooks of Ticehurst House. In
Lectures on the History of Psychiatry (edt R, Murray & T.
Turner),p. 30.London:Gaskell.
Weiner, B. P. a Marvlt, R. C. (1977) Schizophrenia in Hawaii:
analysisof cohort mortality risk in a multi-ethnic population.British Journal of Psychiatry, 131,497-503.
Wilkinson, a G. (I@82) The suicide rate in schizophrenia.
BritishJournalof Psychiatry.140. 38—I4I.
Wood, j. B., Ev.nson, R. C., Cho, D.W., at at (1985)Mortality variations among public mental health patients. Acto
Psychiotrico Scandinovica. 72. 218—229.
Zilber, N., Schufman, N. a Lsrner,Y. (1989)Mortalityamong psychiatric patients —¿�the groups at risk. Acto
PsychiatricaScandinavica.79. 248—256.
508