EVALUATION OF THE LEVELS OF INTERLEUKIN 8 AND ...
81
I EVALUATION OF THE LEVELS OF INTERLEUKIN 8 AND INTERLEUKIN 4 AROUND MINI-IMPLANTS DURING ORTHODONTIC TOOTH MOVEMENT - A CLINICAL STUDY By Dr. BIANCA B. RODRIGUES Dissertation Submitted to the Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore In partial fulfillment of the requirements for the degree of MASTER OF DENTAL SURGERY in the speciality of ORTHODONTICS AND DENTOFACIAL ORTHOPAEDICS Under the guidance of Prof. (Dr.) SANJU SOMAIAH M.K. Professor DEPARTMENT OF ORTHODONTICS AND DENTOFACIAL ORTHOPAEDICS COORG INSTITUTE OF DENTAL SCIENCES VIRAJPET, COORG, KARNATAKA-571218. 2016– 2019
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of EVALUATION OF THE LEVELS OF INTERLEUKIN 8 AND ...
I
EVALUATION OF THE LEVELS OF INTERLEUKIN 8 AND
INTERLEUKIN 4 AROUND MINI-IMPLANTS DURING
ORTHODONTIC TOOTH MOVEMENT - A CLINICAL STUDY
By
Dr. BIANCA B. RODRIGUES
Dissertation Submitted to the
Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore
In partial fulfillment of the requirements for the degree of
MASTER OF DENTAL SURGERY
in the speciality of
ORTHODONTICS AND DENTOFACIAL ORTHOPAEDICS
Under the guidance of
Prof. (Dr.) SANJU SOMAIAH M.K.
Professor
DEPARTMENT OF ORTHODONTICS AND DENTOFACIAL
ORTHOPAEDICS
COORG INSTITUTE OF DENTAL SCIENCES
VIRAJPET, COORG, KARNATAKA-571218.
2016– 2019
VI
ACKNOWLEDGEMENT
As this dissertation draws to an end I would like to take this opportunity to express
my gratitude to several people who have been instrumental in the completion of this
study.
I thank god almighty for showering his immense blessings and providing strength
for completing this study successfully.
I express my deepest sense of gratitude to my teacher and guide,
Dr. Sanju Somaiah M.K., Professor, Department of Orthodontics and Dentofacial
Orthopaedics, Coorg Institute of Dental Sciences, for the proficient guidance, vigilant
supervision and incessant encouragement given to me throughout the study.
I am immensely obliged to Dr. Goutham B., Professor and Head, Department Of
Orthodontics and Dentofacial Orthopedics, Coorg Institute Of Dental Science for his
pricely support and constant encouragement. I have been amazingly fortunate to have
an advisor who gave me the freedom to explore on my own.
I would also like to thank Dr.Sunil Muddaiah, Dean, Professor, Department Of
Orthodontics And Dentofacial Orthopedics, for his valuable suggestions and
overwhelming support.
I take this opportunity to express my gratitude and heartfelt thanks to
Dr.Balakrishna Shetty, Professor, Department Of Orthodontics And Dentofacial
Orthopedics for timely help and encouragement.
VII
I also thank Dr. Roopa S., Dr.Vikram Susil Faculty, Department Of Orthodontics
And Dentofacial Orthopedics, Coorg Institute Of Dental Sciences for all the help,
guidance and encouragement rendered throughout the study.
I am also thankful to Dr. Bhakti Sadhu, Department of Public Health Dentistry,
Coorg Institute Of Dental Sciences for helping me with the statistical analysis of the
data for my study.
I thank Dr. K. C. Ponnapa, Principal, Coorg Institute of Dental Sciences, for his co-
operation and guidance throughout my post-graduation course.
I also thank my co post-graduates, Dr. Dixit T.P., Dr. Athul Tom, Dr. Justin Jolly,
Dr. Muhasin and Dr. Nikhil for standing by me and lending me helping hands
throughout these past years of postgraduate training. Their support and friendship were
constant during this tenure; I appreciate it from the bottom of my heart.
I take immense pleasure to thank my seniors, Dr. Jeffy, Dr. Shafeeq,
Dr. Shanahaz, Dr. Abin, Dr. Saran, Dr. Shafad for their constant advice and support.
It would be unjust on my part if I don’t extent my gratitude to my juniors
Dr. Basil, Dr. Ann, Dr. Razeen, Dr. Roni, Dr. Tripthi, Dr. Manu, Dr. Amric,
Dr. Elbin, Dr. Eric, Dr. Anna, Dr. John, Dr. Noufal for their constant help and
encouraging me out at various levels of work.
A Special thanks to my friends Dr.Manju, Dr.Anusha, Dr.Dhanya and
Dr.Nithya for their constant encouragement and support during my thesis.
I would also like to extend my gratitude to all the nonteaching staff of my
department for rendering timely support.
VIII
IX
LIST OF ABBREVIATIONS
ELISA ENZYME LINKED IMMUNOSORBANT ASSAY
GCF GINGIVAL CREVICULAR FLUID
IL- 8 INTERLUEKIN 8
IL- 4 INTERLUEKIN 4
mm MILLIMETER
MSI MINISCREW IMPLANT
OTM ORTHODONTIC TOOTH MOVEMENT
pg/μl PICOGRAMS PER MICROLITER
PMICF PERI-MINISCREW IMPLANT CREVICULAR FLUID
TAD TEMPORARY ANCHORAGE DEVICE
X
LIST OF TABLES
Table.
No.
Title Page No.
1 Comparison of Interleukin 8 levels at different intervals
among study subjects around miniscrew implants using
paired t test.
37
2 Comparison of Interleukin 8 levels at different intervals
among study subjects around miniscrew implants between
maxilla and mandible using independent t test.
38
3 Comparison of Interleukin 4 level among study subjects
around miniscrew implants using paired t test.
40
4 Comparison of Interleukin 4 levels among study subjects
around miniscrew implants between maxilla and mandible
using independent t test.
41
XI
LIST OF FIGURES
Figure
No.
Title Page No.
1 Comparison of mean Interleukin 8 levels at T1, T2, and T3. 36
2 Comparison of mean Interleukin 4 levels at T1, T2, and T3. 39
3 Eppendorf tube and microcappilary tube used for sample
collection.
64
4 Peri-miniscrew implant crevicular fluid sample collection. 64
5 Samples stored in Eppendorf tubes. 64
6 ELISA kits of IL-8 and IL-4. 65
7 Contents of ELISA kits IL-8 and IL-4. 65
8 Performing the ELISA test. 65
9 Yellow colour change after adding stop solution. 66
10 Elisa spectrometer for reading colour change 66
11 Dontrix gauge 66
XIII
EVALUATION OF THE LEVELS OF INTERLEUKIN 8 AND
INTERLEUKIN 4 AROUND MINI-IMPLANTS DURING
ORTHODONTIC TOOTH MOVEMENT - A CLINICAL STUDY
Background and objectives:
The evaluation of cytokines in the peri-miniscrew implant crevicular fluid (PMICF)
has been proposed as a non-invasive means of monitoring the healthy or diseased
status of peri-implant tissues. The objective of this study was to evaluate the levels of
interleukin 8 (IL-8) and interleukin 4 (IL-4) around miniscrew implants during
orthodontic tooth movement and to draw clinical inferences from the same.
Methodology:
The present study was done around 22 healthy miniscrew implants in subjects
within an age range between 16-25 years without any signs of peri-implantitis. The
selected subjects were in retraction stage using titanium miniscrew implants with a
force of 150g. The samples were collected over a month time period after force
application on miniscrew implants according to the following schedule: T1, T2 and
T3 at 1 hour, 7th
day and 21st day respectively. The PMICF samples were put through
ELISA test for determining the concentration of IL-8 and IL-4.
Result:
It was observed that in healthy miniscrew implants the IL- 8 levels increased from
one hour to 7th
day due to perimucositis and slightly decreased or remained the same
from 7th
to 21st day indicating that the progress of inflammation has regressed.
XIV
The IL-4 levels decreased from one hour to 7th
day due to perimucositis. It
decreased from 7th
to 21st day. This could be attributed to the persistence of
inflammation through 21st day.
Conclusion:
These findings demonstrated that the levels of IL-8 and IL- 4 in PMICF could be
considered in detecting the stability of miniscrew implants.
Keywords: Miniscrew implant, Peri-miniscrew implant crevicular fluid,
Interleukin 8, Interleukin 4.
Introduction
1
EVALUATION OF THE LEVELS OF INTERLEUKIN 8 AND
INTERLEUKIN 4 AROUND MINI-IMPLANTS DURING
ORTHODONTIC TOOTH MOVEMENT - A CLINICAL STUDY
INTRODUCTION
Anchorage is a critical issue during orthodontic treatment and if inadequate can be
the most limiting factor, no matter which technique or philosophy the clinician
follows especially when treating adults. Orthodontic tooth movement has always been
limited to action-reaction reciprocal force mechanics in anchorage control.
Although extraoral anchorage can be used to supplement tooth-borne anchorage
and deliver force in directions not possible with an intraoral anchorage, extraoral
anchorage has such limitations that it requires excellent patient cooperation. Over the
past 10 to 15 years, several techniques at a skeletally based anchorage have been
attempted clinically which include fixation wires, bone plates, fixation screws,
miniaturized dental implants in the palate and retromolar areas and palatal onplants.
The control of anchorage is one of the most crucial factors in orthodontic treatment
planning. Achieving absolute anchorage has been one of the main objectives for an
orthodontist and mini implants have become the most effective and powerful tool for
achieving this. Miniscrew implants that have increasingly been used for anchorage
control in orthodontic treatment for non-compliant patients have many advantages,
such as ease of placement and removal, small size, and low cost.1
Introduction
2
Background of the study:
Clinicians and researchers have tried to use endosseous implants as orthodontic
anchorage for over half a century. The first successful attempt to move teeth against a
stationary screw was published as early as in 1969 by Linkow, although routine
application of dental implants for orthodontic purposes in humans began 20 years
later.2
The disadvantages of dental implants became apparent during this period. The
requirement of specific surgical procedures during insertion and removal, the demand
for complicated clinical and laboratory procedures to accurately transfer the implant
position to cast models and to facilitate safe and precise implant insertion, delayed
loading resulting from the waiting period necessary for osseointegration increasing
total treatment time, possible location limited only to edentulous or retromolar areas
of the maxilla and mandible and large dimensions apparently increases the risk of
damage to the adjacent tissues or root injuries.
To overcome these problems, Kanomi in 1997 and Costa et al. in 1998 introduced
miniscrew implants as temporary anchorage devices (TADs). Their decreased
diameter facilitates insertion in almost all sites of the jaws, with no flap surgery
required. Osseointegration does not usually occur; therefore, they provide only
temporary stationary anchorage; consequently, there is no 6-month waiting period.
Immediate loading of TAD apparently decreases total treatment time.2
From this point onwards, the single most important implant used during
orthodontic treatment for an anchorage is the miniscrew implant. The clinical use of
miniscrew implants as temporary anchorage devices has been widespread. This is due
to the possibility of absolute orthodontic anchorage and the ease of installation and
Introduction
3
removal of these devices. Miniscrew implants are routinely used to anchor retraction
of the anterior segment, mesiodistal movement of the posterior teeth, asymmetrical
tooth movement, intrusive mechanics and orthopaedic corrections.
Miniscrew implants (MSI), are customarily placed without a flap or after a punch
incision under local infiltration only. It is important to realize that the potential
complications are relatively insignificant relative to major orthognathic surgical
procedures; however, tooth root damage, bony and soft tissue infection, and implant
failure are possible.
Need and significance of the study:
It was reported in a review article that the miniscrew implants have an average
survival rate of 84% (range 57–95.3%) which is largely dependent on factors
governing primary and secondary stability. The primary stability pertains to the
mechanical holding of MSI in the bone, while the secondary stability relates to
biological retention. Broadly, the factors affecting the stability can be grouped into a
host, miniscrew implant and technique-related factors. Contemporary research has
focused on the biological seal between the implant and host tissue, more so on its
surrounding peri-implant oral epithelium.3
The occurrence of screw failures has required ongoing investigation of potential
risk factors. Since peri-implantitis turned out to be the main cause of screw loosening,
assessment of factors involved in such inflammation has become crucial to increase
TAD stability in orthodontics.2 An early and reliable detection of any adverse peri-
miniscrew tissue reaction is essential for patients being treated with miniscrew.
Introduction
4
As in periodontitis and other infections, pathogens and their virulence factors
stimulate the release of several immunoinflammatory biomarkers by peri-implant
cells. Among the numerous biomarkers, proinflammatory cytokines [e.g., tumor
necrosis factor (TNF)-a, interferon-c, interleukin(IL)-1b, IL-6, IL-12, IL-17,IL-8 and
RANKL] and anti-inflammatory cytokines(e.g. IL-4, IL-10 and IL-1 receptor
antagonist) have been suggested to be important mediators of inflammation and
immunity in the pathogenesis of peri-implantitis.
Peri-implantitis accounts for about 30% of miniscrew failures.4, 5
Peri-implantitis
is a progressive peri-implant bone loss in conjunction with soft tissue inflammatory
lesion. Initially, peri-mucositis (a reversible inflammation of the soft tissues
surrounding the miniscrew) occurs, which if left untreated may progress to peri-
implantitis.4, 6
Peri-implantitis is clinically characterized by increased probing depth,
pain, and/or radiographic bone loss, which may cause implant failure. An early and
reliable detection of any adverse peri-miniscrew tissue reaction is essential for
patients being treated with miniscrew.4, 7
Orthodontic forces cause acute inflammatory reactions, vascular changes, and
migration of leucocytes. Recent studies show that in periodontal and peri miniscrew
tissues cytokines, tumour necrosis factor and transforming growth factor have
important roles in regulating and amplifying inflammatory response.4, 7, 8, 9
Cytokines
are involved in initiating, amplifying, perpetuating and resolving inflammatory
responses in periodontal and peri-implant tissues.1
Cytokines are classified as pro-inflammatory and anti-inflammatory. Pro-
inflammatory cytokines include TNF, IL-1, IL-2, IL-6 and IL-8. These are ‘alarm’
cytokines that induce vascular dilation through increased permeability and enhanced
Introduction
5
inflammatory response, whereas IL-4, IL-10, IL-13, IFN-alpha and transforming
growth factor-beta are recognized as anti-inflammatory cytokines and are involved in
the reduction of inflammatory reactions.1
Many studies on dental implants have
reported that an increase in proinflammatory cytokine levels in peri-implant crevicular
fluid causes peri-implantitis.1, 10, 11, 12
IL-8 plays a key role in recruiting and activating neutrophils during inflammation.
It is important for regulating alveolar bone resorption during tooth movement by
acting at an early stage in the inflammatory response. IL-8 is secreted mainly by
monocytes, macrophage, epithelial cells and endothelial cells and is essential in early
inflammatory response with a role in neutrophil recruitment and degranulation during
inflammation. Evidence from research studies also supports high IL-8 levels in
periodontitis and at peri-implant inflammation sites.3
The various activities of IL-8 indicate that this cytokine plays a major role in
mediating inflammatory responses. In a study conducted to analyse the levels of
interleukin-8 during tooth movement, it was found that orthodontic forces evoke
changes in IL-8 levels.13
In another study it was found that IL-8 levels were
significantly higher in patients with failing implants than in those with healthy
implants.1, 14
Interleukin-4 (IL-4) is a pleiotropic cytokine secreted by activated T lymphocytes,
mast cells, eosinophils, and basophils. It is a key regulator in humoral and adaptive
immunity that regulates the function of lymphocytes and macrophages.15
In a recent
study it was found that IL-4, secreted by T helper type 2 (TH2) cells, is a potent
inhibitor of the RANKL induced osteoclastogenic process.16
The effect of IL-4 in
osteoclastogenesis is supported by the finding from studies which revealed that
Introduction
6
over-expression of IL-4 in vivo prevents bone erosion in animal models of
inflammatory arthritis.17, 18, 19
In periodontitis sites where IL-4 levels were found to be too low, there was
persistent accumulation of activated macrophages, leading to increased destruction of
the periodontium. It has been hypothesized by researchers that localized absence of
IL-4 at the site of gingival inflammation plays a fundamental role in the progression
of gingivitis to periodontitis. In a study done in India an inverse relationship has been
reported in between gingival crevicular fluid IL-4 levels and periodontal status; IL-4
was higher in the periodontally healthy group, but very low in the periodontally
diseased group.20
It was found that the anti-inflammatory effect of IL-4 results from
its efficient inhibition of the production of proinflammatory cytokines such as tumor
necrosis factor-a (TNF-a), IL-1a, IL-1b, IL-6 and IL-8 by monocytes/ macrophages.
In a recent article it was stated that IL-4 plays an important role in the regulation of
the immunoinflammatory response.17, 20
Additionally, it was reported in two studies
that IL-4 inhibited TNF-α-mediated osteoclast formation in vitro 17, 21
and in vivo via
both TNF-α- activated stromal cells and TNF-α-activated osteoclast precursors.17, 22
Peri-miniscrew crevicular fluid (PMCF) is an osmotically mediated inflammatory
exudate originating from the vessels of the gingival plexus. Its composition is similar
to that of the gingival crevicular fluid (GCF) containing host-derived enzymes and
their inhibitors, inflammatory mediators, host response modifiers and tissue
breakdown products.23
Analysis of PMCF offers a non-invasive means of studying
host response in peri-miniscrew disease and may provide an early indication of
patients at risk for active disease.24
Introduction
7
The possible correlation of the immune response and prime instability of cortical
TADs may help to improve control of risk factors responsible for the premature loss
of orthodontic miniscrew implants essential in the sophisticated and modern treatment
of malocclusions. Therefore, the evaluation of such cytokines in the peri-miniscrew
implant crevicular fluid (PMICF) has been proposed as a noninvasive means of
monitoring the healthy or diseased status of peri-implant tissues as well as the local
response of peri-implant treatments.
Despite investigative efforts to identify the levels of several cytokines in the
PMICF, the efficacy of these parameters to predict or to contribute to the diagnosis of
peri-implantitis is still undetermined. Hence, the investigator is interested to evaluate
the levels of interleukin 8 and interleukin 4 around mini-implants during orthodontic
tooth movement and to draw clinical inferences from the same.
Aims & Objectives
8
AIM AND OBJECTIVES
The present study was conducted with the following aim and objectives:
Aim
The aim of the study was to determine whether the levels of interleukin 8 and
interleukin 4 could be considered in detecting the stability of miniscrew implants.
Objectives
1. To assess the levels of interleukin IL-8 and IL-4 in peri-miniscrew implant
crevicular fluid around miniscrew implants.
2. To analyse the levels of interleukin IL-8 and IL-4 at different intervals in
peri-miniscrew implant crevicular fluid around miniscrew implants.
3. To draw clinical inferences from the differences in the IL-8 and IL-4 at
different intervals in peri-miniscrew implant crevicular fluid around miniscrew
implants.
Review of literature
9
REVIEW OF LITERATURE
The review of literature for the present study has been organised under the
following headings.
Miniscrew implants as an effective anchorage system.
Role of cytokines as inflammatory markers.
Different cytokines around mini-implants.
Interleukin 8, a biomarker.
Interleukin 4, a biomarker.
Miniscrew implants as an effective anchorage system:
A review was done about mini-implants used in orthodontics as a temporary
anchorage device for orthodontic tooth movement. The review analysed all the
different aspects of mini implants such as classification, size and shapes, site and
method of insertion, advantages, diagnosis and treatment planning and mechanics.
Clinical implications of mini implants are closure of extraction spaces (retraction),
single tooth intrusion, and correction of canted occlusal plane, molar intrusion,
mesializaion and distalization. It was concluded that implants could be used in
minimal patient cooperation cases with absolute anchorage needs.25
The authors in a study illustrated three cases. One was treated with maxillary
microscrew implants, another with mandibular microscrew implants, and the third
with both maxillary and mandibular microscrew implants. With the maxillary
microscrew implants, the maxillary anterior teeth were retracted bodily with a slight
intrusion and all the premolar extraction space was closed without loss of anchorage.
Furthermore, the maxillary posterior teeth showed distal movement. The mandibular
Review of literature
10
microscrew implants controlled the vertical position of the mandibular posterior teeth
and played an important role in improving the facial profile. Sliding mechanics with
maxillary microscrew implants provide anchorage for bodily retraction with a slight
intrusion by making the force pass near the centre of resistance. The maxillary
posterior teeth and anterior teeth can both be retracted without anchorage loss. The
mandibular microscrew implants control the vertical mandibular molar position and
contribute to improvement of the facial profile.26
Role of cytokines as inflammatory markers:
A short review was conducted to evaluate the importance of substances as valid
biomarkers of periodontal health during orthodontic movements. The conclusion is
that GCF is a powerful vehicle for clinical diagnostics, since it contains different
biochemical and cellular arrays in relation to different clinical situations indicative of
the state of periodontal health during orthodontic treatment.The main gingival
crevicular fluid (GCF) biomarkers related to orthodontic movements and classified
them into four main groups: biomarkers of inflammation, bone metabolism, cell death
and bone deposition and mineralization. Biomarkers of inflammation were
Interleukins (IL-1𝛽, IL-6, IL-8), Tumour Necrosis factors (TNF-𝛼), Colony-
stimulating factors (M-CSF, G-CSF, GM-CSF), Prostaglandins (PGE), Vascular
endothelial growth factors (VEGF), Calcitonin gene related peptide (CGRP),
Substance P. Increased levels of these proinflammatory cytokines are demonstrated in
GCF during orthodontic tooth movement.27
The authors performed an in situ hybridization to measure the messenger RNA
expression of IL-1β, IL-6, and TNF- α at 3, 7, and 10 days after the application of
orthodontic force on the maxillary first molars of 12 rats. The contralateral side and 3
Review of literature
11
untreated rats served as controls. Measurements of the messenger RNA expression
were selected as the means to investigate the role of orthodontic force in de novo
synthesis of proinflammatory cytokines. After the application of force, the induction
of IL-1β and IL-6 was observed to reach a maximum on day 3 and to decline
thereafter. No messenger RNA induction of either cytokine was measured in the
control teeth. The messenger RNA expression of TNF-α was not detected at any time
point of this study in the experimental or contralateral sides or in the control animals.
The data support the hypothesis that these proinflammatory cytokines may play
important roles in bone resorption after the application of orthodontic force.28
The authors studied the pattern of expression of mRNA encoding several pro- and
anti-inflammatory cytokines in relation to several extracellular matrix and bone
remodeling markers, in tension (T) and compression (C) sides of the PDL of human
teeth subjected to rapid maxillary expansion, by means of real-time polymerase chain
reaction (PCR). The PDL of normal teeth was used as a control. The results showed
that both T and C sides exhibited significantly higher expression of all targets when
compared with controls, except for type I collagen (COL-I) and tissue inhibitor of
metalloproteinase-1 (TIMP-1) on the C side. Comparing C and T sides, the C side
exhibited higher expression of tumor necrosis factor-α (TNF-α), receptor activator of
nuclear factor-κB ligand (RANKL), and matrix metalloproteinase-1 (MMP-1),
whereas the T side presented higher expression of interleukin-10 (IL-10), TIMP-1,
COL-I, osteoprotegerin (OPG), and osteocalcin (OCN). The expression of
transforming growth factor-β (TGF-β) was similar in both C and T sides. The data
demonstrate a differential expression of pro- and anti-inflammatory cytokines in
compressed and stretched PDL during orthodontic tooth movement.29
Review of literature
12
The authors concluded through a review that the interaction between bacteria and
host cells are important both for the induction of responsiveness to infectious agents
and for the induction of non-responsiveness to commensal bacteria. These interactions
can result in the production of cytokines. The lipopolysaccharides (LPS) are the key
bacterial component inducing pro-inflammatory cytokine (IL-1,IL-6,IL-8 & TNF)
gene expression. In this study the authors also classified cytokines based on their
receptors: immunoglobin receptor (IL-1,IL6), haemopoietin receptor(IL-3,IL4), nerve
growth factor receptor(TNF.R I &II) , G-protein coupled receptor(IL-8), tyrosine
kinase –coupled receptor(EGF.R,IGF.R).30
Different cytokines around mini-implants:
The authors did a literature review and found six relevant studies: two on IL-1β;
one on IL-2, IL-6 and IL-8; one on TNF-α; one on chondroitin sulphate (CS); and one
on receptor activator of nuclear factor kappa-B ligand
(RANKL)/osteoprotegerin(OPG) ratio. One study showed an increase in IL-1β levels
upon miniscrew implant (MSI) loading, peak in 24 hours (h), followed by a decrease
in 21 days to reach baseline in 300 days. A 6.87% decrease in IL-2 levels was seen
before loading and a 5.97% increase post-loading. IL-8 showed a 6.31% increase after
loading and IL-6 increased by 3.08% before MSI loading and 15.06% after loading.
RANKL/OPG ratio increased in loaded compared to unloaded MSIs. It was concluded
that cytokines (mainly ILs and TNF-α) and RANKL/OPG ratio showed alteration in
PMICF levels upon loading of MSIs as direct or indirect anchorage.3
The aim of this review was to conduct an assessment of the immunological
response following application of cortical temporary anchorage devices, titanium
miniscrew implants in orthodontic patients. They reviewed studies evaluating the
Review of literature
13
immune response subsequent to insertion of dental implants. It was concluded that the
following factors are associated with dental implant rejection: (1) correlation of the
volume of gingival and peri-implant crevicular fluid and the amount of interleukin
(IL)-1b with mucosal inflammation, thus serving as a peri-implantitis evaluation
index; (2) significantly more frequent marginal bone loss around implants in patients
with IL-1B-511 2/2 genotype; (3) humoral response to Staphylococcus aureus.2
A study was conducted to describe levels of selected pro-inflammatory cytokines
in clinically healthy peri-implant and periodontal sites, and to examine whether
cytokine levels may be related to specific bacterial/viral pathogens. Eleven subjects
(mean age 56.2) participated in the study. Subgingival microbial samples were
cultured for periodontopathic bacteria. Gingival crevicular fluid samples were
analyzed by nested polymerase chain reaction for Cytomegalovirus (HCMV) and
were tested for the quantification of Interleukin (IL)-8, IL-1b, IL-6, IL-10,Tumor
Necrosis Factor (TNF)-a, and IL-12p70 using flow cytometry (FACS). Findings for
microbiota composition and cytokine levels were compared between implants and
teeth (chi square, Kruskall–Wallis, Mann–Whitney; p 2 .05). Both the frequency (%)
and levels (%) of periodontopathic bacteria were higher around teeth than implants.
The concentration (picogram per milliliter) of cytokines was more prominent around
implants than teeth, reaching nearly twofold differences in some instances. Cytokine
levels were higher when the sites analyzed were positive for any bacteriatested.
HCMV was not detected. Pro-inflammatory cytokine production was unrelated to
heavy bacterial challenge and when periodontopathic bacteria were detected by
culture, cytokine levels were increased around both implants and teeth.14
A study was done to analyse IL-1β in peri-miniscrew crevicular fluid obtained
from crevices around the miniscrews inserted in 11 patients (eight females and three
Review of literature
14
males, mean age 17.3 ± 4.64 years) with all first premolar extraction and maximum
anchorage requirement using miniscrew-supported anchorage. Miniscrews were
loaded at 3 weeks after placement by 200g nitinol closed coil springs of 9-mm length
for en masse retraction. Peri-miniscrew crevicular fluid was collected at miniscrew
placement (T1), at 3 weeks (T2/baseline) and on loading at 0 (T3) and 1 day (T4), 21
(T5), 72 (T6), 120 (T7), 180 (T8) and 300 (T9) days. IL-1β levels were estimated by
enzyme-linked immunosorbent assay (ELISA). Peri-miniscrew tissue was examined
for signs of inflammation, and also, miniscrew mobility was assessed with Periotest
and handles of two mouth mirrors. It was concluded that the changing levels of IL-1β
levels in PMCF over duration of 300 days are suggestive of the underlying
inflammatory process. IL-1β levels in PMCF show a significant rise during miniscrew
insertion and on immediate loading. The trend of gradually reducing IL-1β levels
around the miniscrew over the period after loading towards baseline is suggestive of
adaptive bone response to stimulus.4
The authors did a study to determine the peri-miniscrew implant crevicular fluid
receptor activator of nuclear factor-kB ligand (RANKL) and osteoprotegerin (OPG)
levels around loaded and unloaded miniscrew implants at different time intervals.
Twenty loaded and 16 unloaded miniscrew implants were included in this study. All
miniscrew implants were placed bilaterally between the maxillary second premolars
and first molars as anchorage units for canine distalization. Peri-miniscrew implant
crevicular fluid was taken from the mesiobuccal aspects of the loaded and unloaded
miniscrew implants before loading; at 24, 48, and 168 hours; and on day 30 after
force application. ELISA kits were used to determine RANKL and OPG levels in the
peri-miniscrew implant crevicular fluid samples. Although the total amount of OPG
was not different between the groups, the total amount of RANKL was significantly
Review of literature
15
elevated in the loaded miniscrew implant group (P<0.05) at all time periods.
Peri-miniscrew implant crevicular fluid volume was the highest at 48 hours in the
loaded group. Also, the OPG/RANKL ratio in the peri-miniscrew implant crevicular
fluid was significantly decreased in the loaded miniscrew implant group. They
concluded that OPG and RANKL levels vary around loaded and unloaded miniscrew
implants as a result of force application.31
The authors did a study to measure Tumor Necrosis Factor-α (TNF-α) levels
around miniscrews used for anchorage during a 3-month period of canine
distalization. Sixteen patients whose upper first premolars were extracted for
orthodontic treatment were included in this study. Miniscrews were used as an
anchorage unit in canine distalization. Thirty-two miniscrew implants were placed
bilaterally in the alveolar bone between the maxillary second premolars and first
molars. The treatment, miniscrew, and control groups comprised upper canines,
miniscrew implants, and upper first premolars, respectively. Peri-miniscrew implant
crevicular fluid and gingival crevicular fluid were obtained before applying force and
at 1, 24, and 48 hours, and at 7 and 21 days, and 3 months after applying force. In
conclusion during the 3-month period, the TNF-α level increased significantly at 24
hours only in the treatment group. In the miniscrew and control groups, there were no
statistically significant changes. No significant differences was observed between
groups.32
The authors did a study to monitor changes in chondroitin sulphate (CS; WF6
epitope) levels in peri-miniscrew implant crevicular fluid (PMICF) during orthodontic
loading. Ten patients (seven males and three females; aged 22.0 ± 3.4 years), who
required orthodontic treatment with extraction of all four premolar teeth, participated
in the study. Twenty miniscrew implants (used as orthodontic anchorage) were
Review of literature
16
placed, two in each patient, buccally and bilaterally in the alveolar bone between the
roots of the maxillary posterior teeth. Sentalloy closed-coil springs (50 g) were used
to load the miniscrew implants and to move the maxillary canines distally. During the
unloaded period, PMICF samples were collected on days 1, 3, 5, and 7 after
miniscrew implant placement and on days 14,21, 28, and 35 during the loaded period.
Clinical mobility assessments of the miniscrew implants were recorded at each visit.
The competitive enzyme-linked immunosorbent assay with monoclonal antibody
WF6 was used to detect CS (WF6 epitope) levels in the PMICF samples. The
differences between the CS (WF6 epitope) levels during the unloaded and loaded
periods were determined by a Mann – Whitney U -test. They concluded that CS (WF6
epitope) levels in PMICF can be detected and may be used as biomarkers for
assessing alveolar bone remodelling around miniscrew implants during orthodontic
loading.33
A study was conducted to determine whether interleukin 1(IL-1) levels are
elevated around microscrew implants that are used as anchorage for tooth movement.
Ten young adults, aged 16.3 +/- 2.5 years and with all four premolars extracted ,
comprised the study group. Twenty maxillary microscrew implants were placed
bilaterally in the alveolar bone between the maxillary second premolars and first
molars as anchorage units for distal movement of the maxillary canines. The
maxillary canines served as the treatment group, and the microscrew implants were
designated as the implant group. The mandibular canines were used as controls. Peri-
microscrew implant crevicular fluid (MICF) and gingival crevicular fluid (GCF) were
collected at the beginning of tooth movement (2 weeks after implant placement); at
24, 48, and 168 hours later; and on days 14 and 21. An automated enzyme
immunoassay was used to measure 1L-1 in the MICF and the GCF. It was found that
Review of literature
17
the mean 1L-1 level in the treatment group was significantly elevated at 24 hours ,
whereas the levels in the control and implant groups did not change significantly
during the experimental period. Also, the mean 1L-1level of the treatment group was
significantly higher than in both the control and implant groups at 24 and 48 hours.
The conclusion of the above study was that the microscrew implants did not
demonstrate increased 1L-1levels during tooth movement.9
Interleukin 8, a biomarker:
A study was conducted to identify the levels of interleukin IL-2, IL-6 and IL-8
around miniscrews used for anchorage during canine distalization. Sixteen patients
(eight males and eight females; mean age, 16.6 ± 2.4 years) who were treated with
bilateral upper first premolar extractions were included in the study. Thirty-two
maxillary miniscrew implants were placed bilaterally in the alveolar bone between the
maxillary second premolars and first molars as anchorage units for maxillary canine
distalization. Three groups were constructed. The treatment, miniscrew, and control
groups consisted of upper canines, miniscrew implants, and upper second premolars,
respectively. Peri-miniscrew implant crevicular fluid and gingival crevicular fluid
(GCF) were obtained at baseline (T1) and at 1 (T2), 24 (T3), and 48 (T4) hours, 7
(T5) and 21 (T6) days, and 3 months (T7) after force application. Paired sample t-tests
were used to determine within-group changes and Dunnett’s t and Tukey’s honestly
significant difference tests for between-group multiple comparisons. During the 3
month period, IL-2 levels significantly increased (P < 0.01) but only in the treatment
group after 24 hours. IL-6 levels were unchanged at all times points in the three
groups. IL-8 levels increased significantly at 1 (P < 0.05), 24 (P < 0.01), and 48 (P <
0.01) hours in the treatment group and at 24 (P < 0.05) and 48 (P < 0.01) hours in the

Review of literature
18
miniscrew group. It appears that miniscrews can be used for anchorage in
orthodontics when correct physiological forces are applied.1
A study was conducted to evaluate the levels of IL-8 during mechanical forces on
periodontal tissues at different stages of orthodontic therapy. Ten canine teeth of
patients having different Angle classifications were selected for the study. After the
premolars were extracted, the maxillary/mandibular canines were tipped distally.
Gingival crevicular fluid was sampled from mesial and distal gingival crevices of
each canine separately at baseline and one hour, 24 hours, six days, 10 days, and 30
days after the application of the force. An enzyme-linked immunosorbent assay for
quantitative detection of IL-8 was used. Although there was an increase in the
concentration of IL-8 at tension (mesial) sites after one hour, 24 hours, six days, and
10 days, a decrease was observed at 30 days. Pressure (distal) sites did not
demonstrate such an increase at any period except at 10 days. However, the
concentration of IL-8 at both sites showed a similar decrease and approached each
other at day 30. They concluded that local host response toward the orthodontic forces
might lead to an increase in IL-8 and neutrophil accumulation, and this may be one of
the triggers for bone remodelling processes.13
The authors measured intercellular messenger and cytokines that are regulatory for
osteoblast and osteoclast function. Production of osteocalcin, a marker for osteoblast
maturation was also estimated. Human osteoblastlike cells from osteosarcoma cell
line MG 63 were grown in wells in the presence of titanium (Ti), titanium alloy
(Ti6A14V) and stainless steel implant materials incubated at 370C. Interleukin- 1α
(IL-1α), IL-6, IL-8, IL-11 and osteocalcin were quantitated using standard enzyme
linked immunosorbant assay (ELISA) kits from the growth media extracted at specific
intervals over the critical ten day period. In all dishes, cells were seen adhering to the
Review of literature
19
base after 24 hours and to confluence at 96 hours. Both IL-1α and IL-11 were not
produced in sufficient quantities to be measured in the assay (<pg/ml).Interleukin-6
production was significantly higher for stainless steel than for titanium and the alloy.
There was a progressive rise in osteocalcin production for titanium contrasted to a
basal rate for stainless steel and alloy. Interleukin-8 levels for all metals and controls
increased markedly after two days implicating inherent cellular characteristics. A
relatively high constant range for macrophage colony stimulating factor from the first
day was seen for all metals, including the controls. In conclusion, it appears that
titanium implants activate osteocalcin production while stainless steel activates IL-6.10
A study was done to determine the distribution of IL-8 and IL-8R in gingival
tissues and cultured human gingival keratinocytes in vitro. Standard
immunohistochemical and immunocytochemical techniques were utilized in order to
localize IL-8 and its receptors CXCR-1 and CXCR-2 in archival gingival specimens
(eight periodontitis and four non-inflamed controls) and in cultured gingival
keratinocytes. It was demonstrated that, in vivo, IL-8 and IL-8R were present in
gingival epithelium, MVEC and leukocytes. It was concluded that IL-8 and IL-8
receptors are expressed in gingival epithelium both in vivo and in vitro.34
A study was done with the aim to determine levels of interleukins 2, 6, and 8
during tooth movement, and test whether they differ from each other with levelling
and distalization forces used in various treatment stages of standard orthodontic
therapy. Fifteen patients (9 female, 6 male; ages, 15-19 years; mean age, 16.7+/-2.3
year participated in this study. Each underwent a session of professional oral hygiene
and received oral hygiene instructions. Two months later, a fixed orthodontic
appliance was placed. The patients were seen at baseline, at days 7 and 21, and as the
teeth were leveled. Records of the baseline scores for the distalization forces were
Review of literature
20
taken at the sixth month. Scores of days 7 and 21 after 6 months of the distalization
treatment were also recorded. It was found that the increases were seen in the volume
of gingival crevicular fluid and the concentrations of interleukins 2, 6, and 8. From
this study it was concluded that levelling and distalization of the teeth evoke increases
in interleukins 2, 6, and 8 levels in the periodontal tissues that can be detected in
gingival crevicular fluid. Distalization forces increased IL-8 levels at the 7th day and
decreased them the 21st day.35
In an in vitro study, understand the contribution of stromal cells, such as
granulation tissue fibroblasts, to peri-implantitis with regard to (1) the secretion of
constitutive factors promoting migration/survival of infiltrates into osseointegrated
sites; and (2) the effect of exogenous infiltrate cytokines on the cells' secretion.
Fibroblasts were cultured from eight peri-implantitis sites. Multiplexed enzyme-
linked immunosorbent assay was used to quantify factors secreted by the cells either
unstimulated or stimulated with gamma interferon (lFNγ), interleukin 4 (1L4), or
tumor necrosis factor alpha (TNFα). Controls consisted of fibroblasts cultured from
healthy gingival and chronic periodontitis granulation tissues. Peri-implantitis
fibroblasts differed significantly from periodontitis fibroblasts in their reduced
secretion of the collagen inducer transforming growth factor beta-1 (TGFβ1) and
tissue inhibitor of metalloproteinase-1. The cells exhibited enhanced secretion of
angiogenic factor vascular endothelial growth factor (VEGF) and collagenolytic
matrix metalloproteinase 1 (MMP1) compared to both healthy and periodontitis
fibroblasts. Fibroblasts from both periodontitis and peri-implantitis sites exhibited a
pronounced proinflammatory profile compared to normal gingival fibroblasts with
respect to secretion of chemokines 1L6, 1L8, and monocyte chemoattractant protein 1
(MCP1). Fibroblasts stimulated with TNFα showed increased levels of 1L6, 1L8,
Review of literature
21
MCP1; neutrophil chemokine growth-related oncogene alpha stimulation with IFNγ
increased MCP1; and stimulation with 1L4 increased VEGF. The results indicate that
peri-implantitis fibroblasts represent a distinct stromal population. The cells might
participate in the pathogenesis of peri-implantitis by up-regulating both vascularity
and matrix breakdown, thus promoting migration/maintenance of infiltrates into the
site. Cytokines produced by infiltrates could enhance the inflammatory nature of the
cells in a self-feeding loop. It was concluded that the fibroblasts of the patients with
peri-implantitis and periodontitis synthesized more IL-6 and IL-8, and thus presented
a more accentuated proinflammatory profile.36
A study was done to evaluate the expression of IL-1b, IL-4, and IL-8 in the
gingival crevicular fluid (GCF) of children, adolescents, and young adults with and
without fixed orthodontic appliances. Eighty systemically healthy children and
adolescents participated in the study: 56 aged between 8 and 16 years without any
orthodontic appliance (Group A) and 24 aged between 10 and 20 years having worn
fixed orthodontic appliances for at least 12 months (Group B). Clinical examination
included presence or absence of plaque, probing depth, bleeding on probing, and
gingival overgrowth. GCF was collected by means of Durapore strips from four
randomly selected sites per subject. The contents of interleukin-1 beta (IL-1b),
interleukin-4 (IL-4), and interleukin-8 (IL-8) were detected by ELISA, measured as
total amounts (pg/30s) and expressed in log scale. Statistically significant differences
were noted for the mean log IL-1b, IL-4, and IL-8 between the two groups: Group B
showed significantly higher mean levels in log IL-1b and log IL-8 compared to Group
A. Mean levels of log IL-4 were lower in Group B, although they did not reach
statistical significance. Furthermore, mean levels of log IL-1b and log IL-8 were
associated with bleeding sites (pB0.001) and gingival overgrowth, while mean level
Review of literature
22
of log IL-4 was associated with non-bleeding sites and no gingival overgrowth
(pB0.001). It was concluded that fixed orthodontic appliances result in an increase in
the expression of IL-1b and IL-8. This may reflect biologic activity in the
periodontium during orthodontic tooth movement.41
Interleukin 4, a biomarker:
The authors did a study to investigate the effect of IL-4 on tooth movement and its
associated root resorption in a mouse model. The maxillary first molars of four male
mice for each experimental group were subjected to mesial force by a nickel titanium
coil spring for 12 days. Control mice were not given appliances and injections.
Varying doses of IL-4 were injected locally, adjacent to the first molar. Two sets of
experiments were designed. The first set was composed of three groups: the control,
treatment with phosphate-buffered saline (PBS), or 1.5 μg/day of IL-4. The second set
was composed of five groups: the control, treatment with 0 (PBS only), 0.015, 0.15,
or 1.5 μg/day of IL-4.The distance of orthodontic tooth movement (OTM) was
measured and tartrate-resistant acid phosphatase positive cells along the loaded
alveolar bone and root surface were identified. The root resorption associated with
OTM was evaluated by a scanning electron microscope. The authors found the
amount of OTM and the number of osteoclasts was significantly decreased in the IL-
4-treated mice. Moreover, IL-4 significantly suppressed force-induced odontoclasts
and root resorption. It was concluded that IL-4 inhibits tooth movement and prevents
root resorption in the mouse model. These results suggest that IL-4 could be used as a
useful adjunct to regulate the extent of OTM and also to control root resorption.17
The authors investigated the effect of IL-4 on TNF-α-mediated osteoclast
formation in vivo. TNF-α was administered with and without IL-4 into the
Review of literature
23
supracalvariae of mice. The number of osteoclasts and the levels of mRNA for
cathepsin K and tartrate-resistant acid phosphate, both osteoclast markers, in mice
administered TNF-α and IL-4 were lower than those in mice administered TNF-α
alone. The level of tartrate-resistant acid phosphatase form 5b (TRACP5b) as a
marker of bone resorption in mice administered both TNF-α and IL-4 was also lower.
It showed that IL-4 inhibited TNF-α-mediated osteoclast formation in osteoclast
precursors in vitro. It was concluded that IL-4 inhibited TNF-α-mediated osteoclast
formation by inhibiting expression of RANKL in TNF-α-activated stromal cells, and
directly inhibited TNF-α-activated osteoclast precursors in vivo via a T cell-
independent mechanism.22
A study was done to assess the relation between clinical parameters and
concentrations of IL-4 within gingival crevicular fluid from inflamed gingiva and
periodontitis sites and, subsequently, after treatment of the periodontitis sites. A total
of 60 subjects were divided into three groups based on gingival index (GI), pocket
probing depth and clinical attachment loss (CAL): healthy (group 1), gingivitis (group
2) and chronic periodontitis (group 3). A fourth group (group 4) consisted of 20
subjects from group 3, 6–8 weeks after treatment (i.e. scaling and root planing).
Gingival crevicular fluid samples collected from each patient were quantified for IL-4
using the enzymatic immunometric assay. It was concluded that the mean
concentration of IL-4 decreased from periodontal health to disease. Thus, they
suggested that type 2 helper T cell cytokine, as represented by IL-4, was associated
with the remission or improvement of periodontal disease.20
A study was done to define the molecular mechanism(s) by which interleukin(IL)-
4 reversibly inhibits formation of osteoclasts (OCs) from bone marrow macrophages
(BMMs), The authors examined the capacity of this T cell-derived cytokine to impact
Review of literature
24
signals known to modulate osteoclastogenesis, which include those initiated by
macrophage colony stimulating factor (M-CSF), receptor for activation of NF-kB
ligand (RANKL), tumor necrosis factor (TNF) and IL-1. They concluded that IL-4
reversibly arrests osteoclastogenesis in a STAT6-dependent manner by 1) preventing
IB phosphorylation and thus NF-B activation, and 2) blockade of the JNK, p38, and
ERK mitogen-activated protein kinase pathways.16
In another article the authors discussed about IL-4 receptor (IL -4R), its signalling
mechanisms and biologic functions. They gave emphasis on different pathways of IL-
4R signalling, its modulation. It was concluded that the signalling pathways that are
activated by IL-4R engagement, such as the IRS-1/2 and Jak-Stat pathways, mirror
those activated by a number of other cytokines. The activation of these pathways
results in a unique array of cellular responses to IL-4. The specific cellular responses
to IL-4 may also result from the unique character of the IL-4R.15
The study was done to determine the levels of interleukin (IL)-1b, IL-4, IL-6 and
IL-8 in gingival crevicular fluid of periodontaly healthy and diseased individuals and
to study their association to smoking, stress and clinical periodontal parameters. A
total of 80 patients were included in the study: 20 patients with early onset or
aggressive periodontitis (EOP), 20 with chronic adult periodontitis (AP), 20 with
gingivitis (G) and 20 patients with healthy periodontium (H). GCF was collected by
means of Durapore strips, from four sites per patient, randomly selected in each
quadrant. The contents of IL- 1b, IL-4, IL-6 and IL-8 were measured in 320 samples
by use of commercially available sandwich enzyme-linked immunoadsorbent assays.
In periodontally diseased subjects the total amounts of IL-1b, IL-6 and IL-8 were
significantly elevated as compared to healthy subjects, whereas IL-4 showed an
inverse relationship to periodontal status and higher amounts were found in the
Review of literature
25
healthy group. The amounts of all four cytokines were positively correlated with
probing depths. IL-4, IL-6 and IL-8 were significantly correlated to smoking while
stress was associated with IL-1b, IL-6 and IL-8 level. This study suggested that
crevicular IL-1b, IL-6 and IL-8 reflect the activity of periodontal destruction, whereas
IL-4 shows an inverse correlation to it. They also stated that the enhanced production
of inflammatory cytokines in the presence stress of smoking and stress may have
clinical consequences.37
A review was conducted in USA with the hypothesis that, in the case of Adult
periodontitis, a localized lack of the regulatory cytokine interleukin-4 (IL-4) in the
gingival tissues predisposes susceptible individuals to progress from gingivitis to
periodontitis. The authors found an analogous situation may exist in the case of
rheumatoid arthritis (RA). There are several similarities in the pathogenesis of tissue
damage in RA and periodontal disease, suggesting RA may provide a model for host
response mediated tissue destruction. The studies using the RA model in animals have
found that lL-4 injected directly into the lesion prevents the tissue destruction
observed in control sites. These results suggest several experimental treatment
protocols for periodontitis. IL-4 is biologically active in very low concentrations (3
U/ml, 29). Therefore, susceptible patients may benefit from local delivery of IL4 in a
sustained release vehicle. Such a vehicle may provide a localized source of IL-4 at the
site of inflammation. This may reduce the deleterious effects of the bacteria-host
interaction in a site specific manner, thereby reducing or preventing local periodontal
tissue destruction.38
A study was conducted to assess whether IL-1 ra and IL-4 play an important role
in the natural homeostatic mechanisms by regulating the effect of IL-1 on
inflammatory periodontal disease and whether they are present in GCF or not. GCF
Review of literature
26
samples were obtained from eight adult patients (mean age 46 years) with
periodontitis radiographic-evideoce of generalized alveolar bone loss and deep
pockets. As a negative control, GCF samples were obtained from healthy volunteers
without periodontal disease. The following clinical parameters were evaluated at the
time of sampling; gingiva) index (Gl), pocket depth, pus discharge, spontaneous pain,
and alveolar bone loss calculated from radiographs. lnterleukin-1 receptor antagonist
(IL-lra) and interleukin-4 (IL-4) were detected in gingival crevicular fluid (GCF) by
an immunochemical method. But they could not detect IL-4 in GCF from severe
inflammation sites. The cell types expressing CD 68 were identified as
monocytes/macrophages and stained positively for IL-lra. The helper T cells
identified by immunostaining for CD 4 stained positively for IL-4. These results
suggest that IL-4 is one of the mediators regulating the degree of local inflammation
in periodontal disease.39
A study was done to examine the impact of local IL-4 on bone erosion in the knee
joint of mice with collagen - induced arthritis (CIA), using gene transfer with an IL-
4–expressing adenoviral vector. They also investigated the effects of IL-4 on the
degradation and formation of collagen type I in bone samples from patients with
arthritis. It was reported that local overexpression of IL-4, introduced by a
recombinant human type 5 adenovirus vector (Ad5E1mIL-4) prevents joint damage
and bone erosion in the knees of mice with collagen arthritis (CIA). No difference
was noted in the course of CIA in the injected knee joints between Ad5E1mIL-4 and
the control vector, but radiographic analysis revealed impressive reduction of joint
erosion and more compact bone structure in the Ad5E1mIL-4 group. Although severe
inflammation persisted in treated mice, Ad5E1mIL-4 prevented bone erosion and
diminished tartrate-resistant acid phosphatase (TRAP) activity, indicating that local
Review of literature
27
IL-4 inhibits the formation of osteoclast-like cells. Messenger RNA levels of IL-17,
IL-12, and cathepsin K in the synovial tissue were suppressed, as were IL-6 and IL-12
protein production. Osteoprotegerin ligand (OPGL) expression was markedly
suppressed by local IL-4, but no loss of OPG expression was noted with Ad5E1mIL-4
treatment. Finally, in in vitro studies, bone samples of patients with arthritis revealed
consistent suppression by IL-4 of type I collagen breakdown. IL-4 also enhanced
synthesis of type I procollagen, suggesting that it promoted tissue repair.40
Materials and Methods
28
MATERIALS AND METHODS
Source of data
The study subjects were patients seeking fixed orthodontic treatment from the
Department of Orthodontics and Dentofacial Orthopaedics, Coorg Institute of Dental
Sciences, Virajpet, Karnataka. The nature and purpose of the study and the treatment
protocol was explained to the subjects included in the study and a written consent
from all patients / parents of patients under the age 18 was obtained before
commencing the study.
Inclusion criteria
Patients seeking fixed orthodontic treatment with miniscrew implants
In the age group 16 to 25.
With periodontal probing depth upto 3mm.
With no radiographic evidence of periodontal bone loss after a full–mouth
radiographic peri-apical examination.
Exclusion criteria
Patients seeking fixed orthodontic treatment with miniscrew implants
With periodontal problems.
With gingival inflammation.
With any systemic diseases.
Who have taken anti-inflammatory and antibiotic medications during the past
3 months.
Materials and Methods
29
Armamentarium:
PMICF collection-
1. Graduated capillary pipettes
2. Eppendorf tubes
Elisa analysis-
1. ELISA reader
2. Microplate
3. Micropipette
4. Disposable micropipette tips
5. ELISA kit
Procedure:
The study sample comprised of 22 miniscrew implants (12 in maxilla and 10 in
mandible) from 7 patients who are undergoing orthodontic treatment with miniscrew
implants. The selected subjects were in retraction stage using mini-implants. The
miniscrew implants were titanium implants (B K Surgicals) of the size 1.5mm
diameter, 8mm long and was placed by the same orthodontist in all the cases. A force
of 150g (measured using dontrix gauge) was applied on each miniscrew implant for
retraction.
Before commencement of study, the patients were instructed oral hygiene methods
and also were systematically checked for periodontal problems. An oral prophylaxis
was performed 1 week prior to study.
Materials and Methods
30
Sample collection:
Peri-miniscrew implant crevicular fluid (PMICF) was collected by isolating the
area with cotton rolls, drying the adjacent marginal gingiva and teeth with air and
using graduated micro capillary tubes from the mesial aspect of the miniscrew
implants.9 The samples were collected over a month time period according to the
following schedule: T1, T2 and T3 at one hour, 7th
day and 21st day after force
application on miniscrew implants respectively. The samples were stored in sterile
eppendrof tubes at -200 Celsius until the start of the experiment in Coorg Institute of
Dental Sciences.
Laboratory analysis:
Quantitative analysis of IL-8 and IL-4 in the PMICF samples was assessed using a
commercially available ELISA test (Elabscience® human interleukin 8 and
interleukin 4). A calibration curve was plotted by regression analysis and the optical
density of each sample was used to estimate the concentration of IL-8 and IL-4
(pg/μL). This was corrected for the original volume of PMICF and the result was
recorded as the concentration of interleukin-8/4 in the samples, expressed in pg/ml.
Test principle:
This ELISA kit uses the Sandwich-ELISA principle. The micro ELISA plate provided
in this kit has been pre-coated with an antibody specific to Human IL-8/IL-4.
Standards or samples are added to the micro ELISA plate wells and combined with
the specific antibody. Then a biotinylated detection antibody specific for Human IL-
8/IL -4 and Avidin-Horseradish Peroxidase (HRP) conjugate are added successively
to each micro plate well and incubated. Free components are washed away. The
Materials and Methods
31
substrate solution is added to each well. Only those wells that contain Human IL-8/
IL-4, biotinylated detection antibody and Avidin-HRP conjugate will appear blue in
color. The enzyme-substrate reaction is terminated by the addition of stop solution
and the color turns yellow. The optical density (OD) is measured
spectrophotometrically at a wavelength of 450 nm ± 2 nm. The OD value is
proportional to the concentration of Human IL-8/IL-4. The amounts of IL-8/IL-4 in
each sample were compared with standard curves for these interleukins.
Reagent preparation:
1. Bring all reagents to room temperature (18~25℃) before use. Follow the
Microplate reader manual for set-up and preheat it for 15 min before OD
measurement.
2. Wash Buffer: Dilute 30 mL of Concentrated Wash Buffer with 720 mL of
deionized or distilled water to prepare 750 mL of Wash Buffer. Note: if crystals have
formed in the concentrate, warm it in a 40℃ water bath and mix it gently until the
crystals have completely dissolved
3. Standard working solution: Centrifuge the standard at 10,000×g for 1 min. Add 1.0
mL of Reference Standard & Sample Diluent, let it stand for 10 min and invert it
gently several times. After it dissolves fully, mix it thoroughly with a pipette. This
reconstitution produces a working solution of 4000 pg/mL. Then make serial dilutions
as needed. The recommended dilution gradient is as follows: 4000, 2000, 1000, 500,
250, 125, 62.50, 0 pg/mL.
Dilution method: Take 7 EP tubes, add 500uL of Reference Standard & Sample
Diluent to each tube. Pipette 500uL of the 4000 pg/mL working solution to the first
Materials and Methods
32
tube and mix up to produce a 2000 pg/mL working solution. Pipette 500uL of the
solution from the former tube into the latter one according to these steps.
4. Biotinylated Detection Ab working solution: Calculate the required amount before
the experiment (100 μL/well).
In preparation, slightly more than calculated should be prepared. Centrifuge the stock
tube before use, dilute the 100× Concentrated Biotinylated Detection Ab to
1×working solution with Biotinylated Detection Ab Diluent.
5. Concentrated HRP Conjugate working solution: Calculate the required amount
before the experiment (100μL/well). In preparation, slightly more than calculated
should be prepared. Dilute the 100× Concentrated HRP Conjugate to 1× working
solution with Concentrated HRP Conjugate Diluent.
Assay procedure:
1. Add the Standard working solution to the first two columns: Each concentration of
the solution is added in duplicate, to one well each, side by side (100 uL for each
well). Add the samples to the other wells (100 uL for each well). Cover the plate with
the sealer provided in the kit. Incubate for 90 min at 37℃. Note: solutions should be
added to the bottom of the micro ELISA plate well, avoid touching the inside wall and
causing foaming as much as possible.
2. Remove the liquid out of each well, do not wash. Immediately add 100 μL of
Biotinylated Detection Ab working solution to each well. Cover with the Plate sealer.
Gently mix up. Incubate for 1 hour at 37°C.
Materials and Methods
33
3. Aspirate or decant the solution from each well, add 350 uL of wash buffer to each
well. Soak for 1~2 min and aspirate or decant the solution from each well and pat it
dry against clean absorbent paper. Repeat this wash step 3 times.
4. Add 100 μL of HRP Conjugate working solution to each well. Cover with the Plate
sealer. Incubate for 30 min at 37°C.
5. Aspirate or decant the solution from each well, repeat the wash process for five
times as conducted in step 3.
6. Add 90 μL of Substrate Reagent to each well. Cover with a new plate sealer.
Incubate for about 15 min at 37°C. Protect the plate from light. Note: the reaction
time can be shortened or extended according to the actual color change, but not more
than 30min.
7. Add 50 μL of Stop Solution to each well. Note: Adding the stop solution should be
done in the same order as the substrate solution.
8. Determine the optical density (OD value) of each well at once with a micro-plate
reader set to 450 nm.
Statistical Analysis :
The data were collected, coded and fed in the SPSS (IBM version 23) and are
analyzed using descriptive and inferential statistics. The inferential statistics included
paired t test and independent t test.
Sample Size Estimation
34
SAMPLE SIZE ESTIMATION
Sample size was determined using nMASTER software.
Single Mean - Paired t-test was chosen.
The following parameters were chosen from a similar study by Hamamcı N et al 1 ;
Pre-test mean = 1292.30
Post-test mean = 1845.02
Standard deviation in Pre-test= 345.80
Standard deviation in Post-test = 1425.90
Effect size = 0.6239431054919
Power (%) = 80
Alpha Error (%) = 5
sided = 2
Required sample size = 22
The sample size for the study was determined as 22.
Results
35
RESULTS
The present study was carried out to evaluate the levels of interleukin 8 and
interleukin 4 in peri-miniscrew implant crevicular fluid (PMICF) around miniscrew
implants during orthodontic tooth movement.
In this study PMICF was collected by isolating the area with cotton rolls, drying the
adjacent marginal gingiva with air and using graduated micro capillary tubes from the
mesial aspect of the miniscrew implant.
The samples were collected over a month time period according to the following
schedule: T1, T2 and T3 at one hour, 7th
day and 21st day respectively after force
application on miniscrew implants. The collected PMICF was then tested for
Interleukin 8 and Interleukin 4 using ELISA test.
The data were collected, coded and fed in the SPSS (IBM version 23) and are
analyzed using descriptive and inferential statistics. The inferential statistics included
paired t test and independent t test.
The results of the present study were evaluated as follows:
The analysis is done under two sections.
Section 1 - Levels of Interleukin 8.
Section 2 - Levels of Interleukin 4.
Results
36
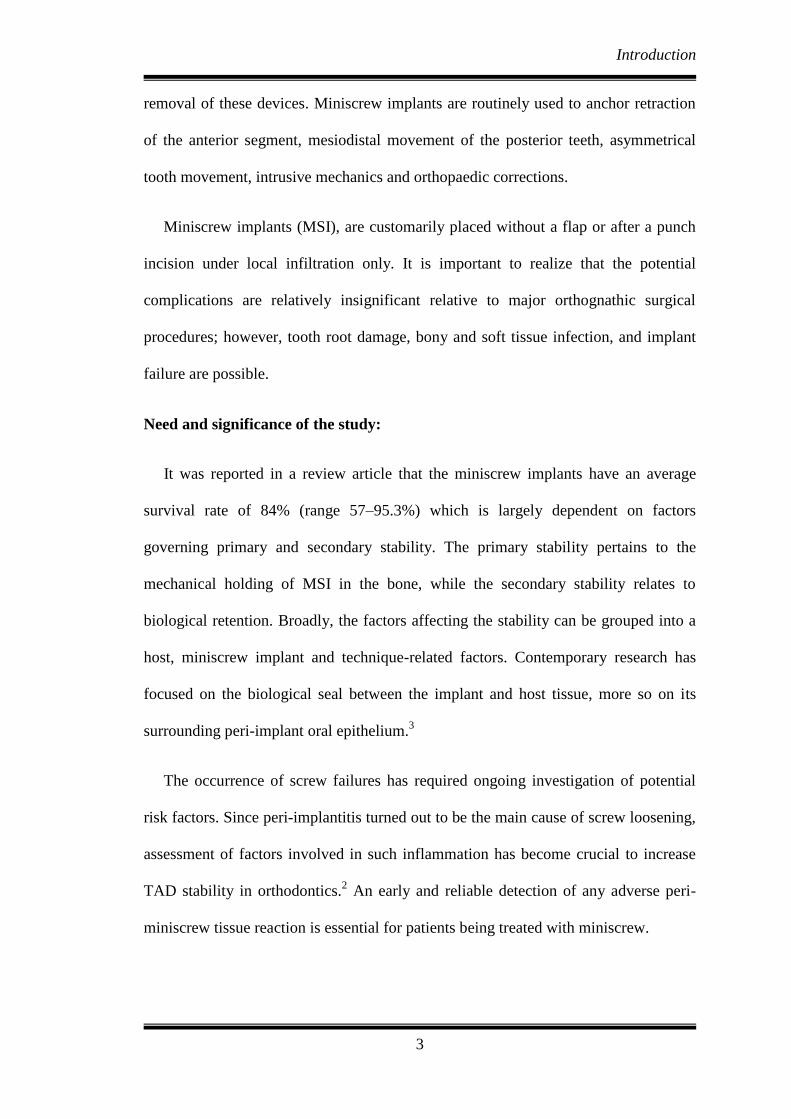
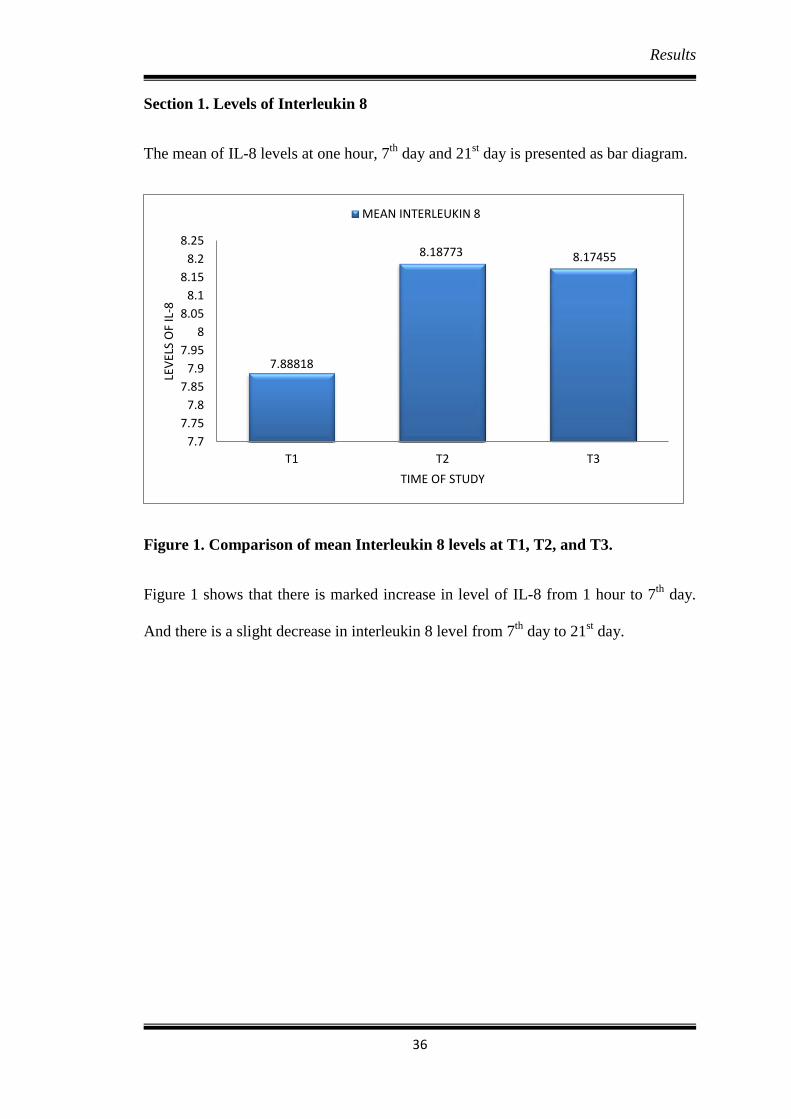
Section 1. Levels of Interleukin 8
The mean of IL-8 levels at one hour, 7th
day and 21st day is presented as bar diagram.
Figure 1. Comparison of mean Interleukin 8 levels at T1, T2, and T3.
Figure 1 shows that there is marked increase in level of IL-8 from 1 hour to 7th
day.
And there is a slight decrease in interleukin 8 level from 7th
day to 21st day.
7.88818
8.18773 8.17455
7.7
7.75
7.8
7.85
7.9
7.95
8
8.05
8.1
8.15
8.2
8.25
T1 T2 T3
LEV
ELS
OF
IL-8
TIME OF STUDY
MEAN INTERLEUKIN 8
Results
37
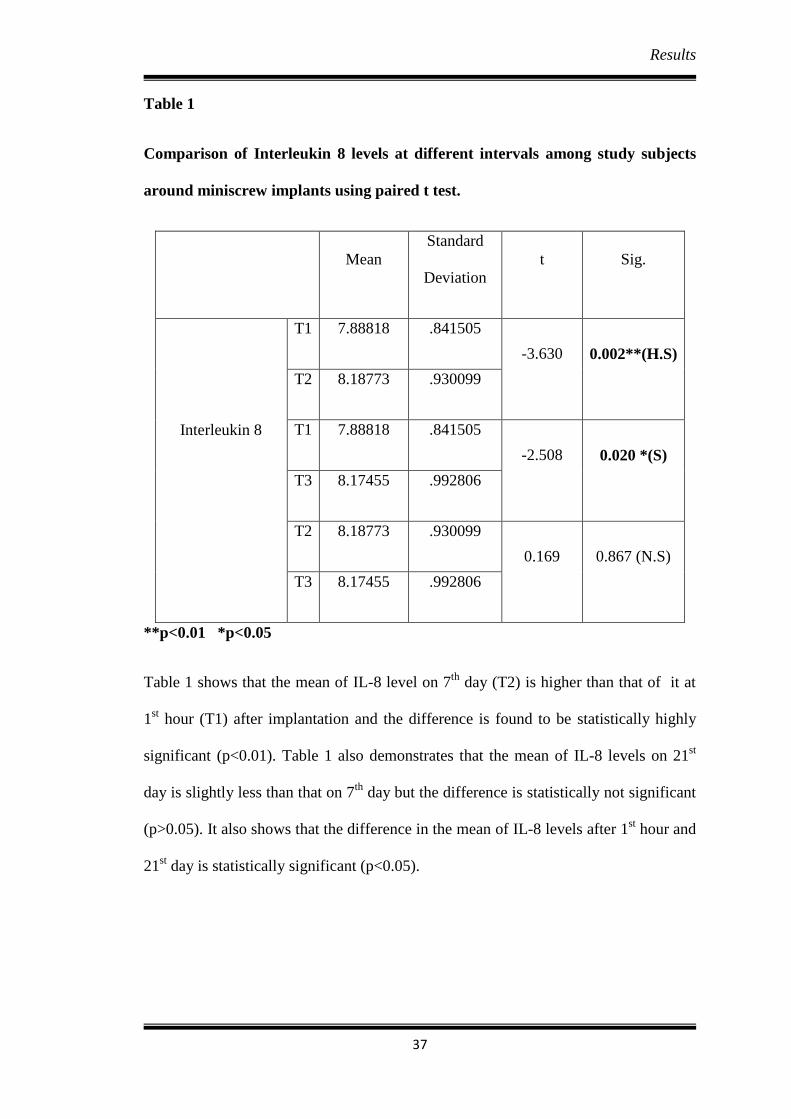
Table 1
Comparison of Interleukin 8 levels at different intervals among study subjects
around miniscrew implants using paired t test.
Mean
Standard
Deviation
t Sig.
Interleukin 8
T1 7.88818 .841505
-3.630 0.002**(H.S)
T2 8.18773 .930099
T1 7.88818 .841505
-2.508 0.020 *(S)
T3 8.17455 .992806
T2 8.18773 .930099
0.169 0.867 (N.S)
T3 8.17455 .992806
**p<0.01 *p<0.05
Table 1 shows that the mean of IL-8 level on 7th
day (T2) is higher than that of it at
1st hour (T1) after implantation and the difference is found to be statistically highly
significant (p<0.01). Table 1 also demonstrates that the mean of IL-8 levels on 21st
day is slightly less than that on 7th
day but the difference is statistically not significant
(p>0.05). It also shows that the difference in the mean of IL-8 levels after 1st hour and
21st day is statistically significant (p<0.05).
Results
38
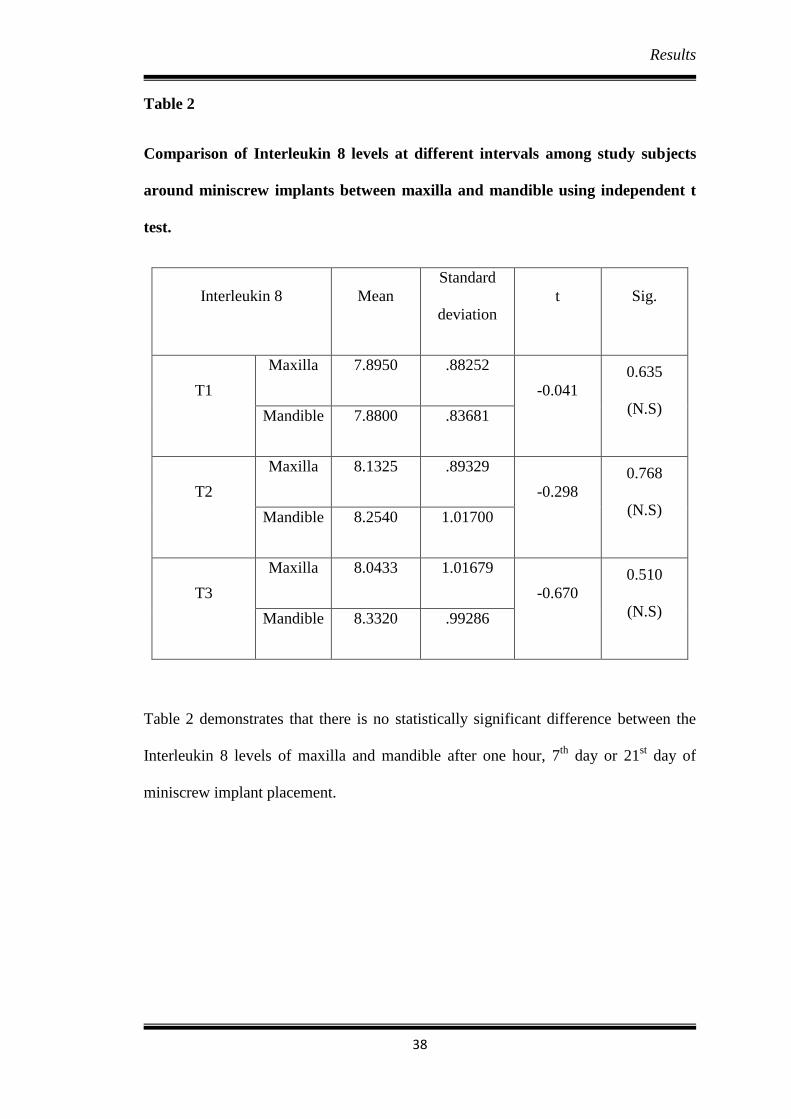
Table 2
Comparison of Interleukin 8 levels at different intervals among study subjects
around miniscrew implants between maxilla and mandible using independent t
test.
Interleukin 8 Mean
Standard
deviation
t Sig.
T1
Maxilla 7.8950 .88252
-0.041
0.635
(N.S) Mandible 7.8800 .83681
T2
Maxilla 8.1325 .89329
-0.298
0.768
(N.S) Mandible 8.2540 1.01700
T3
Maxilla 8.0433 1.01679
-0.670
0.510
(N.S) Mandible 8.3320 .99286
Table 2 demonstrates that there is no statistically significant difference between the
Interleukin 8 levels of maxilla and mandible after one hour, 7th
day or 21st day of
miniscrew implant placement.

Results
39
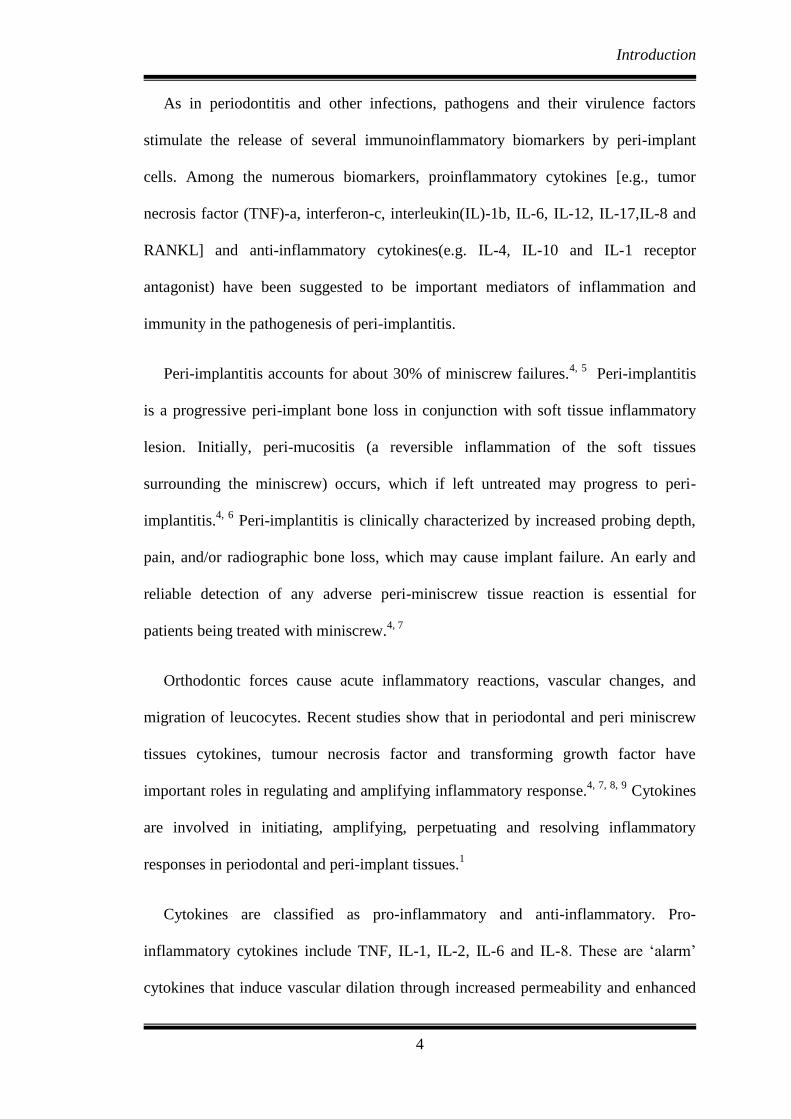
Section 2. Levels of Interleukin 4
The mean of IL-4 at one hour, 7th
day and 21st day is presented as bar diagram.
Figure 2. Comparison of mean Interleukin 4 levels at T1, T2, and T3.
Figure 2 shows that there is a decrease in IL-4 level from 1 hour to 7th
day. And also
there is a decrease in interleukin 4 levels from 7th
day to 21st day.
1.2
1.22
1.24
1.26
1.28
1.3
1.32
1.34
1.36
T1 T2 T3
1.35545
1.30136
1.25818
LEV
ELS
OF
IL-4
TIME OF STUDY
MEAN INTERLEUKIN 4
Results
40
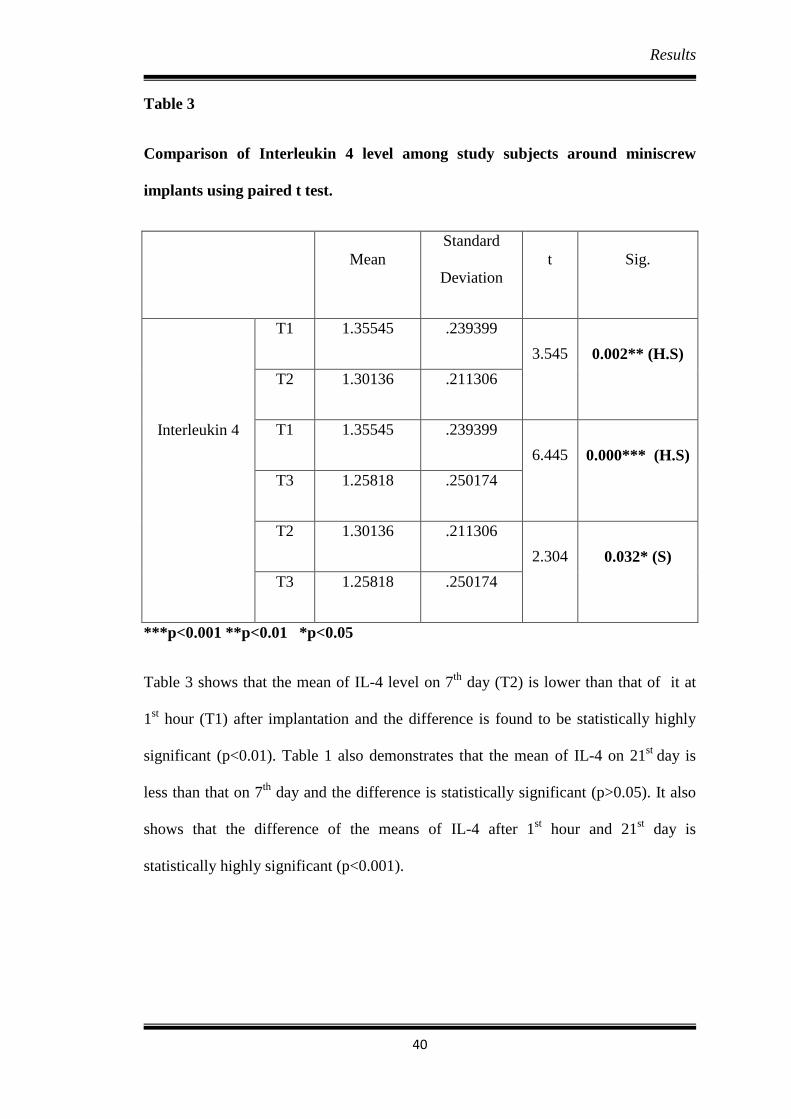
Table 3
Comparison of Interleukin 4 level among study subjects around miniscrew
implants using paired t test.
Mean
Standard
Deviation
t Sig.
Interleukin 4
T1 1.35545 .239399
3.545 0.002** (H.S)
T2 1.30136 .211306
T1 1.35545 .239399
6.445 0.000*** (H.S)
T3 1.25818 .250174
T2 1.30136 .211306
2.304 0.032* (S)
T3 1.25818 .250174
***p<0.001 **p<0.01 *p<0.05
Table 3 shows that the mean of IL-4 level on 7th
day (T2) is lower than that of it at
1st hour (T1) after implantation and the difference is found to be statistically highly
significant (p<0.01). Table 1 also demonstrates that the mean of IL-4 on 21st
day is
less than that on 7th
day and the difference is statistically significant (p>0.05). It also
shows that the difference of the means of IL-4 after 1st hour and 21
st day is
statistically highly significant (p<0.001).
Results
41
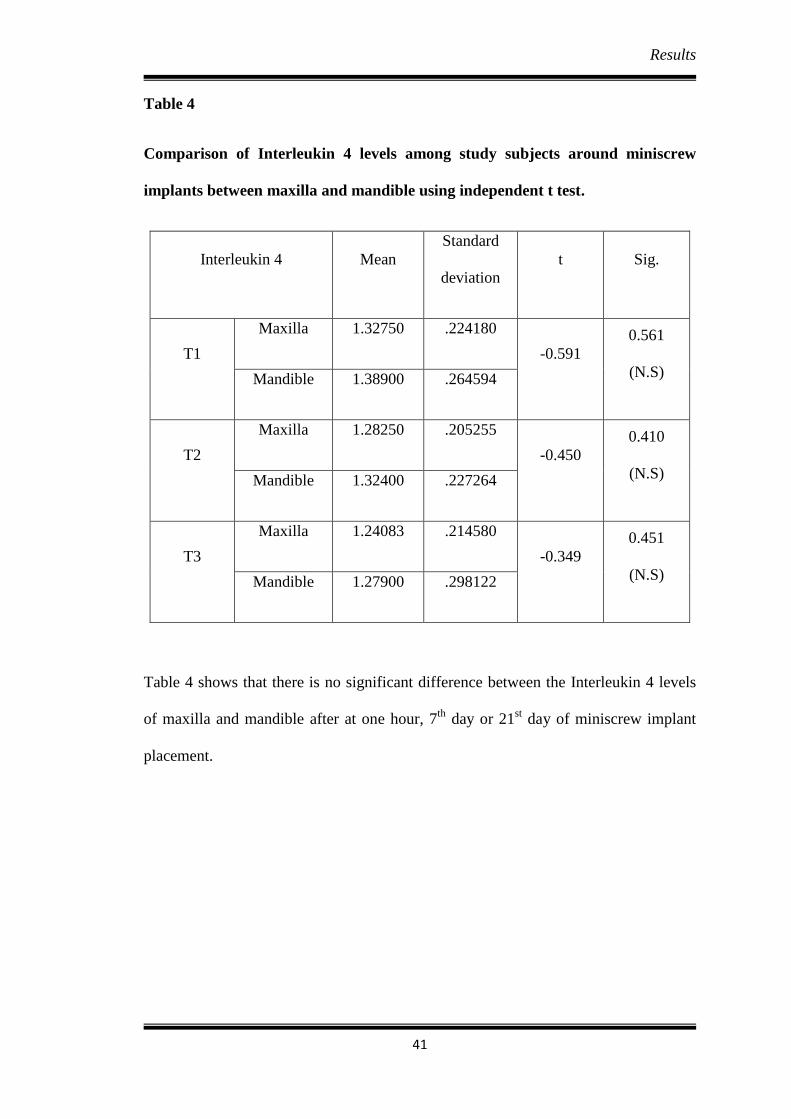
Table 4
Comparison of Interleukin 4 levels among study subjects around miniscrew
implants between maxilla and mandible using independent t test.
Interleukin 4 Mean
Standard
deviation
t Sig.
T1
Maxilla 1.32750 .224180
-0.591
0.561
(N.S) Mandible 1.38900 .264594
T2
Maxilla 1.28250 .205255
-0.450
0.410
(N.S) Mandible 1.32400 .227264
T3
Maxilla 1.24083 .214580
-0.349
0.451
(N.S) Mandible 1.27900 .298122
Table 4 shows that there is no significant difference between the Interleukin 4 levels
of maxilla and mandible after at one hour, 7th
day or 21st day of miniscrew implant
placement.

Results
42
The results obtained from the study were;
Section1. Levels of Interleukin 8.
Interleukin 8 level increased from 1 hour (7.8882 +/-0.8415) to 7th
day
(8.1877+/-0.9301) which is statistically highly significant with p value < 0.01.
There is a slight decrease in interleukin 8 levels from 7th
day (8.1877+/-
0.9301) to 21st day (8.1745+/-0.9928) which is statistically not significant with
p value > 0.050.
The difference between 1 hour and 21st day is significant with p value < 0.05.
No statistically significant difference (p value >0.05) were observed in levels
of interleukin 8 between maxilla and mandible at one hour, 7th
day or 21st day
of miniscrew implant placement.
From the above findings, it is concluded that in healthy miniscrew implants the
Interleukin 8 levels significantly increases from one hour to 7th
day. Eventhough there
is a slight decrease in levels of IL-8 from 7th
day to 21st day, it was not statistically
significant.
Section 2. Levels of Interleukin 4.
Interleukin 4 level decreased from 1 hour (1.3554+/-0.2394) to 7th
day
(1.3014+/-0.2113) which is statistically highly significant with p value < 0.01.
There is a decrease in interleukin 4 levels from 7th
day (1.3014+/-0.2113) to
21st day (1.2582+/-0.2502) which is statistically significant with
p value < 0.05.
The difference between IL-4 levels at 1st hour and 21
st day is highly significant
with p value < 0.01.

Results
43
No statistically significant difference (p value > 0.05) were observed in levels
of IL-4 between maxilla and mandible at one hour, 7th
day or 21st day of
miniscrew implant placement.
From the above findings, it is concluded that in healthy miniscrew implants the
Interleukin 4 levels decreases from one hour to 7th
day and from 7th
to 21st day.
Discussion
44
DISCUSSION
An early and reliable detection of any adverse peri-miniscrew implant tissue
reaction is essential for patients being treated with miniscrew implants. The
evaluation of cytokines in the peri-miniscrew implant crevicular fluid (PMICF) has
been proposed as a noninvasive means of monitoring the healthy or diseased status of
peri-implant tissues as well as the local response of peri-implant treatments. In this
scenario, the present study was done to evaluate the levels of interleukin 8 and
interleukin 4 in PMICF around healthy mini-implants.
The present study was conducted in 22 healthy miniscrew implants from 7 patients
(6 females and 1 male) within an age range between 16-25 years with 12 miniscrew
implants in the maxilla and 10 in the mandible without any signs of peri-implantitis.
The selected subjects were in retraction stage using miniscrew implants. The
miniscrew implants were titanium implants (B K Surgicals) of the size 1.5mm
diameter, 8mm long and was inserted by the same orthodontist in all the cases. A
force of 150g (measured using dontrix gauge) was applied on each miniscrew implant
for retraction.
The samples were collected over a month time period according to the following
schedule: T1, T2 and T3 at 1 hour, 7th
day and 21st day after force application on
miniscrew implants respectively. The samples were stored in sterile eppendorf tubes
at -200 Celsius until the start of the experiment. The PMICF samples were put through
Elisa test (Elabscience® human interleukin 8 and interleukin 4) for determining the
concentration of IL-8 and IL-4. This was corrected for the original volume of PMICF
and the results were recorded as the concentration of interleukin-8/4 in the samples,
expressed in pg/ml.
Discussion
45
In the present study, Interleukin 8 level was used to assess the peri-miniscrew
implant tissue inflammation because the various activities of IL-8 indicate that this
cytokine plays a major role in mediating inflammatory responses.1 Sfakianakis et al
reported the precise localization of IL-8 receptors in periodontitis and noninflamed
human gingivae and suggested that IL-8 plays a multifunctional role in the
pathogenesis of periodontal disease.34
In a previous study, it was demonstrated that
orthodontic forces evoked changes in the levels of IL-8.13
In the present study, Interleukin 4 level was used to assess the peri miniscrew
implant tissue inflammation because Interleukin-4 plays an important role in the
regulation of the immunoinflammatory response.20
The anti-inflammatory effect of
IL-4 results from its efficient inhibition of the production of proinflammatory
cytokines such as tumor necrosis factor-a (TNF-a), IL-1a, IL-1b, IL-6 and IL-8 by
monocytes/ macrophages.17
In the present study the IL-8 levels in healthy implants increases from one hour to
7th
day. It could be related to the perimucositis due to the injury during insertion of
miniscrew implant.
These findings agree with the study by Shaama where the author measured
intercellular messenger and cytokines that are regulatory for osteoblast and osteoclast
function. Human osteoblast like cells from osteosarcoma cell line MG 63 were grown
in wells in the presence of titanium (Ti), titanium alloy (Ti6A14V) and stainless steel
implant materials incubated at 370C. Interleukin- 1α (IL-1α), IL-6, IL-8, IL-11 and
osteocalcin were quantitated using standard enzyme linked immunosorbant assay
(ELISA) kits from the growth media extracted at specific intervals over the critical ten
Discussion
46
day period. It was reported that IL-8 levels in implant crevicular fluid increased from
day 1 but decreased by day 10.10
In the present study, there was a slight decrease in interleukin 8 levels from 7th
day to 21st day. But it was statistically not significant with p value 0.867.
The present study is also supported by Hamamcı N et al who aimed to identify the
levels of interleukin IL-2, IL-6 and IL-8 around miniscrews used for anchorage during
canine distalization. Peri-miniscrew implant crevicular fluid and gingival crevicular
fluid (GCF) were obtained at baseline (T1) and at 1 (T2), 24 (T3), and 48 (T4) hours,
7 (T5) and 21 (T6) days, and 3 months (T7) after force application. IL-8 levels
increased significantly in both the miniscrew and the canine groups at 24 and 48
hours. No statistically significant difference in the levels of IL-8 was noted on 7th
and
21st day from baseline in this study.
1
The present study finding is also supported by a study done with the aim to
determine levels of interleukins 2, 6, and 8 during tooth movement and test whether
they differ from each other with levelling and distalization forces used in various
treatment stages of standard orthodontic therapy. Fifteen patients (9 female, 6 male;
ages, 15-19 years; mean age, 16.7+/-2.3 year participated in this study. The patients
were seen at baseline, at days 7 and 21, and as the teeth were levelled. Records of the
baseline scores for the distalization forces were taken at the sixth month. Scores of
days 7 and 21 after 6 months of the distalization treatment were also recorded. From
this study it was concluded that levelling and distalization of the teeth evoke increases
in IL-8 levels in the periodontal tissues that can be detected in gingival crevicular
fluid and distalization forces increased IL-8 levels at the 7th
day and decreased on the
21st day.
35

Discussion
47
In the present study, the IL-8 level decrease from 7th
to 21st day but it was not
statistically significant (p value>0.05). It indicates that the progress of inflammation is
slightly reduced or regressed. This can be attributed to fact that there is no progression
towards peri-implantitis.
This could be stated in accordance with an in vitro study by Bordin et al. The
authors evaluated the fibroblasts of patients with peri-implantitis, patients with
periodontitis, and healthy subjects. They found that the fibroblasts of the patients with
peri-implantitis and periodontitis synthesized more IL-8 and thus presented a more
accentuated proinflammatory profile.36
In the present study, it was concluded that in healthy implants the IL-4 levels
decreases from one hour to 7th
day. From this it can be inferred that there is some
amount of perimucositis around the implant due to the tissue injury during insertion of
the miniscrew implants. In the present study, the decrease in IL-4 from 7th to 21st day
could be attributed to the persistence of inflammation through 21st day.
The present study findings is consistent with a study conducted in India aimed to
assess the relation between clinical parameters and concentrations of IL-4 within
gingival crevicular fluid from inflamed gingiva and periodontitis sites and,
subsequently, after treatment of the periodontitis sites. A total of 60 subjects were
divided into three groups based on gingival index (GI), pocket probing depth and
clinical attachment loss (CAL): healthy (group 1), gingivitis (group 2) and chronic
periodontitis (group 3). A fourth group (group 4) consisted of 20 subjects from group
3, 6–8 weeks after treatment (i.e. scaling and root planing). Gingival crevicular fluid
samples collected from each patient were quantified for IL-4 using the enzymatic
immunometric assay. It was concluded that the mean concentration of IL-4 decreased
Discussion
48
from periodontal health to disease. Thus, they suggested that type 2 helper T cell
cytokine, as represented by IL-4 was associated with the remission or improvement of
periodontal disease.20
The findings of the present study is congruent with the findings of another study
conducted to determine the levels of interleukin (IL)-1b, IL-4, IL-6 and IL-8 in
gingival crevicular fluid of periodontally healthy and diseased individuals and to
study their association to smoking, stress and clinical periodontal parameters. A total
of 80 patients were included in the study: 20 patients with early onset or aggressive
periodontitis (EOP), 20 with chronic adult periodontitis (AP), 20 with gingivitis (G)
and 20 patients with healthy periodontium (H). In periodontally diseased subjects the
total amounts of IL-8 were significantly elevated as compared to healthy subjects,
whereas IL-4 showed an inverse relationship to periodontal status and higher amounts
were found in the healthy group.37
This study was also supported by the previous
studies by Shapira et al and Kabashima et al who reported lack of IL-4 in gingival
crevicular fluid from severe inflammatory sites.38, 39
In conclusion, the present findings demonstrate that the levels of IL-8 and IL-4
could be considered in detecting the stability of miniscrew implants.
LIMITATION:
The study is done in a smaller sample size.
SCOPE FOR FUTURE STUDY:
1. A study can also be done on a larger scale with a higher sample size to get
more accurate and authentic results.
Discussion
49
2. A longitudinal study can be conducted to assess the levels of IL-8 and IL- 4
with clinical correlation of implants.
3. Further studies are required to elaborate on the levels of interleukins in
different condition such as in health, in progression to peri-implantitis and
during peri-implantitis.
4. A study can be conducted to compare the levels of other cytokines like IL-2,
IL-6 as these also haven been associated with peri-implantitis or bone
turnover.

Conclusion
50
CONCLUSION
Within the limitations of the present study, it was observed that:
In the present study the IL-8 levels in healthy implants increases from one hour to
7th
day. It could be related to the perimucositis due to the injury during insertion of
miniscrew implant. The IL-8 level decreases or remains the same from 7th
to 21st day
indicating that the progress of inflammation is reduced or regressed. This can
attributed to fact that there is no progression towards peri-implantitis.
In the present study, the IL-4 levels in healthy implants decreases from one hour to
7th
day. From this it can be inferred that there is some amount of perimucositis around
the implant due to the tissue injury during insertion of the miniscrew implants. In the
present study, IL-4 levels the decreases from 7th
to 21st day. This could be attributed
to the persistence of inflammation through 21st day.
These findings demonstrate that the levels of Interleukin 8 and Interleukin 4 could
be considered in detecting the stability of miniscrew implants.
Summary
51
SUMMARY
The study was carried out in the Department of Orthodontics and Dentofacial
Orthopaedics, Coorg Institutes of Dental Sciences, Virajpet, Karnataka.
The purpose of this study was to evaluate the levels of interleukin 8 and interleukin
4 around mini-implants during orthodontic tooth movement and to draw clinical
inferences from the same.
The study was done around 22 healthy miniscrew implants from 7 patients (6
females and 1 male) within an age range between 16-25 years with 12 mini-implants
in the maxilla and 10 in the mandible without any signs of peri-implantitis were taken
into consideration. The selected subjects were in retraction stage using miniscrew
implants. The miniscrew implants were titanium implants (B K Surgicals) of the size
1.5mm diameter, 8mm long and was inserted by the same orthodontist in all the cases.
A force of 150g (measured using dontrix gauge) was applied on each miniscrew
implant for retraction.
The samples were collected over a month time period after force application on
mini-implants according to the following schedule: T1, T2 and T3 at 1 hour, 7th
day
and 21st day respectively, after force application on miniscrew implant. The samples
were stored in sterile eppendorf tubes at -200 Celsius until the start of the experiment.
The GCF samples were put through Elisa test (Elabscience® human interleukin 8
and interleukin 4) for determining the concentration of IL-8 and IL-4. The results
were analysed using descriptive and inferential statistics.
Within the limitations of the study, it was observed that in healthy miniscrew
implants the Interleukin 8 levels increased from one hour to 7th
day. It could be related
Summary
52
to the perimucositis due to the injury during insertion of miniscrew implant. The IL-8
level slightly decreased or remained the same from 7th
to 21st day indicating that the
progress of inflammation is reduced or regressed. This can attributed to fact that there
is no progression towards peri-implantitis.
In this study, the IL-4 levels in healthy implants decreased from one hour to 7th
day. From this it can be inferred that there is some amount of perimucositis around the
implant due to the tissue injury during insertion of the miniscrew implants. The IL-4
levels the decreased from 7th
to 21st day .This could be attributed to the persistence of
inflammation through 21st day.
These findings demonstrated that the levels of Interleukin 8 and Interleukin 4 in
PMICF around could be considered in detecting the stability of miniscrew implants.
Bibliography
53
BIBLIOGRAPHY
1) Hamamcı N, Acun Kaya F, Uysal E, Yokuş B. Identification of interleukin 2, 6,
and 8 levels around miniscrews during orthodontic tooth movement. The
European Journal of Orthodontics. 2011 Apr 7;34(3):357-61
2) Antoszewska J, Raftowicz-Wójcik K, Kawala B, Matthews-Brzozowska T.
Biological factors involved in implant-anchored orthodontics and in prosthetic-
implant therapy: a literature review. Archivum immunologiae et therapiae
experimentalis. 2010 Oct 1;58(5):379-83.
3) Kaur A, Kharbanda OP, Kapoor P, Kalyanasundaram D. A review of biomarkers in
peri-miniscrew implant crevicular fluid (PMICF). Progress in orthodontics. 2017
Dec 1; 18(1):42.
4) Monga N, Chaurasia S, Kharbanda OP, Duggal R, Rajeswari MR. A study of
interleukin 1β levels in peri-miniscrew crevicular fluid (PMCF). Progress in
orthodontics. 2014 Dec 1;15(1):30.
5) Miyawaki S, Koyama I, Inoue M, Mishima K, Sugahara T, Takano-Yamamoto T.
Factors associated with the stability of titanium screws placed in theposterior
region for orthodontic anchorage. Am J Orthod Dentofacial Orthop.2003;
124:373–8.
6) Mombelli A, Lang NP. The diagnosis and treatment of peri-implantitis.
Periodontol 2000. 1998; 17:63–76.
7) Javed F, Al-Hezaimi K, Salameh Z, Almas K, Romanos GE. Proinflammatory
cytokines in the crevicular fluid of patients with peri-implantitis. Cytokine.2011;
53:8–12.
8) Graves DT, Cochran D. The contribution of interleukin-1 and tumor necrosis
factor to periodontal tissue destruction. J Periodontol. 2003;74(3):391–401.
Bibliography
54
9) Sari E, Uçar C. Interleukin 1beta levels around microscrew implants during
orthodontic tooth movement. Angle Orthod. 2007; 77:1073–8.
10) Shaama FA. An in vitro comparison of implant materials, cell attachment,
cytokine and osteocalcin production. West indian medical journal. 2005
Sep;54(4):250-6.
11) Aboyoussef H, Carter C, Jandinski JJ, Panagakos FS. Detection of Prostaglandin
E 2 and Matrix Metalloproteinases in Implant Crevicular Fluid. International
journal of oral & maxillofacial implants. 1998 Sep 1;13(5).
12) Kao RT, Curtis DA, Richards DW, Preble J. Increased Interleukin-1β in the
Crevicular Fluid of Diseased Implants. International journal of oral &
maxillofacial implants. 1995 Nov 1;10(6).
13) Tuncer BB, Özmeriç N, Tuncer C, Teoman İ, Çakılcı B, Yücel A, Alpar R, Baloş
K. Levels of interleukin-8 during tooth movement. The Angle Orthodontist. 2005
Jul;75(4):631-6.
14) Nowzari H, Botero JE, DeGiacomo M, Villacres MC, Rich SK. Microbiology
and cytokine levels around healthy dental implants and teeth. Clinical implant
dentistry and related research. 2008 Sep;10(3):166-73.
15) Nelms K, Keegan AD, Zamorano J, Ryan JJ, Paul WE. The IL-4 receptor:
signaling mechanisms and biologic functions. Annual review of immunology.
1999 Apr;17(1):701-38.
16) Wei S, Wang MW, Teitelbaum SL, Ross FP. Interleukin-4 reversibly inhibits
osteoclastogenesis via inhibition of NF-κB and mitogen-activated protein kinase
signaling. Journal of Biological Chemistry. 2002 Feb 22;277(8):6622-30.
17) Hakami Z, Kitaura H, Kimura K, Ishida M, Sugisawa H, Ida H, Jafari S, Takano-
Yamamoto T. Effect of interleukin-4 on orthodontic tooth movement and

Bibliography
55
associated root resorption. European journal of orthodontics. 2014 Jul
29;37(1):87-94.
18) Lubberts E, Joosten LA, Chabaud M, van den Bersselaar L, Oppers B, Coenen-de
Roo CJ, Richards CD, Miossec P, van den Berg WB. IL-4 gene therapy for
collagen arthritis suppresses synovial IL-17 and osteoprotegerin ligand and
prevents bone erosion. The Journal of clinical investigation. 2000 Jun
15;105(12):1697-710.
19) Woods JM, Katschke KJ, Volin MV, Ruth JH, Woodruff DC, Amin MA, Connors
MA, Kurata H, Arai KI, Haines GK, Kumar P. IL-4 adenoviral gene therapy
reduces inflammation, proinflammatory cytokines, vascularization, and bony
destruction in rat adjuvant-induced arthritis. The Journal of Immunology. 2001
Jan 15;166(2):1214-22.
20) Pradeep AR, Roopa Y, Swati PP. Interleukin‐4, a T‐helper 2 cell cytokine, is
associated with the remission of periodontal disease. Journal of periodontal
research. 2008 Dec;43(6):712-6.
21) Kitaura H, Nagata N, Fujimura Y, Hotokezaka H, Tatamiya M, Nakao N, Yoshida
N, Nakayama K. Interleukin-4 directly inhibits tumor necrosis factor-α-mediated
osteoclast formation in mouse bone marrow macrophages. Immunology letters.
2003 Sep 8;88(3):193-8.
22) Fujii T, Kitaura H, Kimura K, Hakami ZW, Takano-Yamamoto T. IL-4 inhibits
TNF-α-mediated osteoclast formation by inhibition of RANKL expression in
TNF-α-activated stromal cells and direct inhibition of TNF-α-activated osteoclast
precursors via a T-cell-independent mechanism in vivo. Bone. 2012 Oct
31;51(4):771-80.
Bibliography
56
23) Wennstrom JL, Ekestubbe A, Grondahl K, Karlsson S, Lindhe J. Oral
rehabilitation with implant-supported fixed partial dentures in periodontitis
susceptible subjects. J Clin Periodontol. 2004; 31:713–24
24) Severino VO, Napimoga MH, de Lima Pereira SA. Expression of IL-6, IL-10,IL-
17 and IL-8 in the peri-implant crevicular fluid of patients with peri-implantitis.
Arch Oral Biol. 2011; 56:823–8
25) Rastogi N, Kumar D, Bansal A. The role of implants in orthodontics. Journal of
Dental Implants. 2011 Jul 1;1(2):86
26) Park HS, Kwon TG. Sliding mechanics with microscrew implant anchorage. The
Angle Orthodontist. 2004 Oct;74(5):703-10.
27) Lauritano D, Avantaggiato A, Cura F, Girardi A, Carinci F. Biomarkers of
periodontl tissue in gingival crevicular fluid during orthodontic movement: An
overview. OA Dent. 2014;2013:105873
28) Alhashimi N, Frithiof L, Brudvik P, Bakhiet M. Orthodontic tooth movement and
de novo synthesis of proinflammatory cytokines. American Journal of
Orthodontics and Dentofacial Orthopedics. 2001 Mar 1;119(3):307-12.
29) Garlet TP, Coelho U, Silva JS, Garlet GP. Cytokine expression pattern in
compression and tension sides of the periodontal ligament during orthodontic
tooth movement in humans. European journal of oral sciences. 2007
Oct;115(5):355-62
30) Wilson M, Reddi K, Henderson B. Cytokine‐inducing components of
periodontopathogenic bacteria. Journal of periodontal research. 1996
Aug;31(6):393-407.
Bibliography
57
31) Enhos S, Veli I, Cakmak O, Ucar FI, Alkan A, Uysal T. OPG and RANKL levels
around miniscrew implants during orthodontic tooth movement. American Journal
of Orthodontics and Dentofacial Orthopedics. 2013 Aug 1;144(2):203-9.
32) Kaya FA, Hamamcı N, Uysal E, Yokuş B. Identification of tumor necrosis factor-
α levels around miniscrews during canine distalization. Korean Journal of
Orthodontics. 2011 Feb 1;41(1):36-41.
33) Intachai I, Krisanaprakornkit S, Kongtawelert P, Ong-chai S, Buranastidporn B,
Suzuki EY, Jotikasthira D. Chondroitin sulphate (WF6 epitope) levels in peri-
miniscrew implant crevicular fluid during orthodontic loading. The European
Journal of Orthodontics. 2009 Sep 13;32(1):60-5.
34) Sfakianakis A, Barr CE, Kreutzer DL. Localization of the chemokine interleukin‐
8 and interleukin‐8 receptors in human gingiva and cultured gingival
keratinocytes. Journal of periodontal research. 2002 Apr;37(2):154-60.
35) Başaran G, Özer T, Kaya FA, Hamamci O. Interleukins 2, 6, and 8 levels in
human gingival sulcus during orthodontic treatment. American Journal of
Orthodontics and Dentofacial Orthopedics. 2006 Jul 1;130(1):7-e1.
36) Bordin S, Flemmig TF, Verardi S. Role of fibroblast populations in peri-
implantitis. Int J Oral Maxillofac Implants. 2009;24:197-204.
37) Giannopoulou C, Kamma JJ, MombelliA. Effect of inflammation, smoking
andstress on gingival crevicular fluid cytokine level. J Clin Periodontol
2003;30:145–153
38) Shapira L, Van Dyke TE, Hart TC. A localized absence of interleukin-4 triggers
periodontal disease activity: a novel hypothesis. Medical hypotheses. 1992 Dec
1;39(4):319-22.
Bibliography
58
39) Kabashima H, Nagata K, Hashiguchi I, Toriya Y, Iijima T, Maki K, Maeda K.
Interleukin‐1 receptor antagonist and interleukin‐4 in gingival crevicular fluid of
patients with inflammatory periodontal disease. Journal of oral pathology &
medicine. 1996 Sep;25(8):449-55.
40) Lubberts E, Joosten LA, Chabaud M, van den Bersselaar L, Oppers B, Coenen-de
Roo CJ, Richards CD, Miossec P, van den Berg WB. IL-4 gene therapy for
collagen arthritis suppresses synovial IL-17 and osteoprotegerin ligand and
prevents bone erosion. The Journal of clinical investigation. 2000 Jun
15;105(12):1697-710.
41) Giannopoulou C, Mombelli A, Tsinidou K, Vasdekis V, Kamma J. Detection of
gingival crevicular fluid cytokines in children and adolescents with and without
fixed orthodontic appliances. Acta Odontologica Scandinavica. 2008 Jan
1;66(3):169-73.
Consent form
60
CONSENT FORM
This Informed Consent form is for the Participant.
TITLE OF RESEARCH:
EVALUATION OF THE LEVELS OF INTERLEUKIN 8 AND INTERLEUKIN 4
AROUND MINI-IMPLANTS DURING ORTHODONTIC TOOTH MOVEMENT - A
CLINICAL STUDY.
I am Dr. Bianca B. Rodrigues, Post Graduate Student, Coorg Institute of Dental Sciences,
Virajpet. Under the guidance of Dr. Sanju Somaiah, Professor, Department of Orthodontics
and Dentofacial Orthopaedics, I am doing a “EVALUATION OF THE LEVELS OF
INTERLEUKIN 8 AND INTERLEUKIN 4 AROUND MINI-IMPLANTS DURING
ORTHODONTIC TOOTH MOVEMENT - A CLINICAL STUDY”. This research
includes an oral examination and collection of peri mini-implant crevicular fluid. I am going
to give you information and invite you to be a part of this research. Before you decide, you
can talk to anyone if you feel comfortable with, about the research. There may be some words
that you do not understand. Please ask me to stop as we go through this information sheet and
I will take time to explain. If you have questions later, you can ask them to me.
Your participation in this research is entirely voluntary. It is your choice whether to
participate or not. There may not be any benefits for you at this stage of the research, but your
participation is likely to help us find the answer to the research question. By participating in
this research you will not be at any risk. The information that we collect from this research
project will be kept confidential. You are entitled to withdraw from the study at any point of
time. The procedure will be of free of cost.
If you have any questions you may ask them now or later, even after the study has started.
If you wish to ask questions later, you may contact me as follows:
Investigator:
DR.BIANCA B. RODRIGUES
POST GRADUATE STUDENT
Contact no. – 9481665642
Email id: [email protected]
Guided by:
DR. SANJU SOMAIAH
PROFESSOR
DEPARTMENT OF ORTHODONTICS
COORG INSTITUTE OF DENTAL SCIENCES, VIRAJPET
Contact no. 9945527999
Email id:[email protected]
This proposal has been reviewed and approved by Institutional Review Board of Coorg
Institute of Dental Sciences, Virajpet, which is a committee whose task is to make sure that
research participants are protected from harm. By signing on the consent form you will be
waving off all legal liabilities against the institution and staff.
Consent form
61
CERTIFICATE OF CONSENT
I have read the foregoing information or it has been read to me. I have had the opportunity
to ask questions about it and any questions that I have asked have been answered to my
satisfaction.
I consent voluntarily to participate as a participant in this research. I understand that I have
the right to withdraw from the study at any time before the publication of the data. I have
been assured that the data will be kept confidential and anonymous. I also give consent for
my data to be published or presented if the above conditions are met.
Name of Participant
Signature of Participant
Date
If illiterate
I have witnessed the accurate reading of the consent form to the potential participant and
the individual has had the opportunity to ask questions. I confirm that the individual has
given consent freely.
Name of witness Thumb print of participant
Signature of witness
Date
Statement by the researcher/person taking consent
I have accurately read out the information sheet to the potential participant, and to the best
of my ability and made sure that the participant understands that the following will be done.
1. Oral examination.
2. Collection of peri mini-implant crevicular fluid
I confirm that the participant was given an opportunity to ask questions about the study,
and all questions asked by the participant have been answered correctly and to the best of my
ability.
I confirm that the individual has not been forced into giving consent and the consent has
been given freely and voluntarily. A copy of informed consent form has been provided to the
participant.
Name of Researcher/person taking consent
Signature of Researcher/person taking consent
Date
Consent form
62
INFORMED CONSENT FROM PARENT/GUARDIAN
I, Dr. BIANCA B RODRIGUES, post graduate student, Department of Orthodontics and
Dentofacial Orthopedics, Coorg institute of Dental Sciences, Virajpet certify that all the
elements including the nature, purpose risks of the above study and described in this consent
document have been fully explained to the subjects. In my judgment the guardian/parents
possess the legal capacity to give informed consent to participate in this research and are
voluntarily and knowingly giving informed consent to participate.
Name of investigator: Dr. Bianca B Rodrigues
Signature of investigator:
CONSENT
I……………………the undersigned, parent/ guardian of …………….. agree to give the
voluntary consent for the participation of my ward in the study. I …………have read the
information in this form (or it has been read to me). I was free to ask any questions and they
have been answered.
1. I have read and understood this consent form and the information provided to me.
2. I have had the consent document explained to me
3. I have been explained about the nature of the study.
4. My ward’s rights and responsibilities have been explained to me by the investigator.
5. I have been advised about the risks associated with my ward’s participation in the study.
6. I agree to cooperate with the investigator and I will inform him/ her immediately if any
ward’s suffer unusual symptoms.
7. My ward has not participated in any research study within the past months.
8. I am aware of the fact that I can opt of the study at any time without having to
give any reason and this will not affect my future treatment in the dental hospital.
9. I am also aware that the investigator may terminate my participation in the study at any
time, for any reason, without my consent.
10. If, despite following the instructions, my ward is physically harmed because of any
substance or any procedure as stipulated in the study plan.
11. I have had my questions answered to my satisfaction.
Date: Signature of the Parent/guardian
Ethical Committee Clearance Certificate
59
ETHICAL COMMITTEE CLEARANCE CERTIFICATE
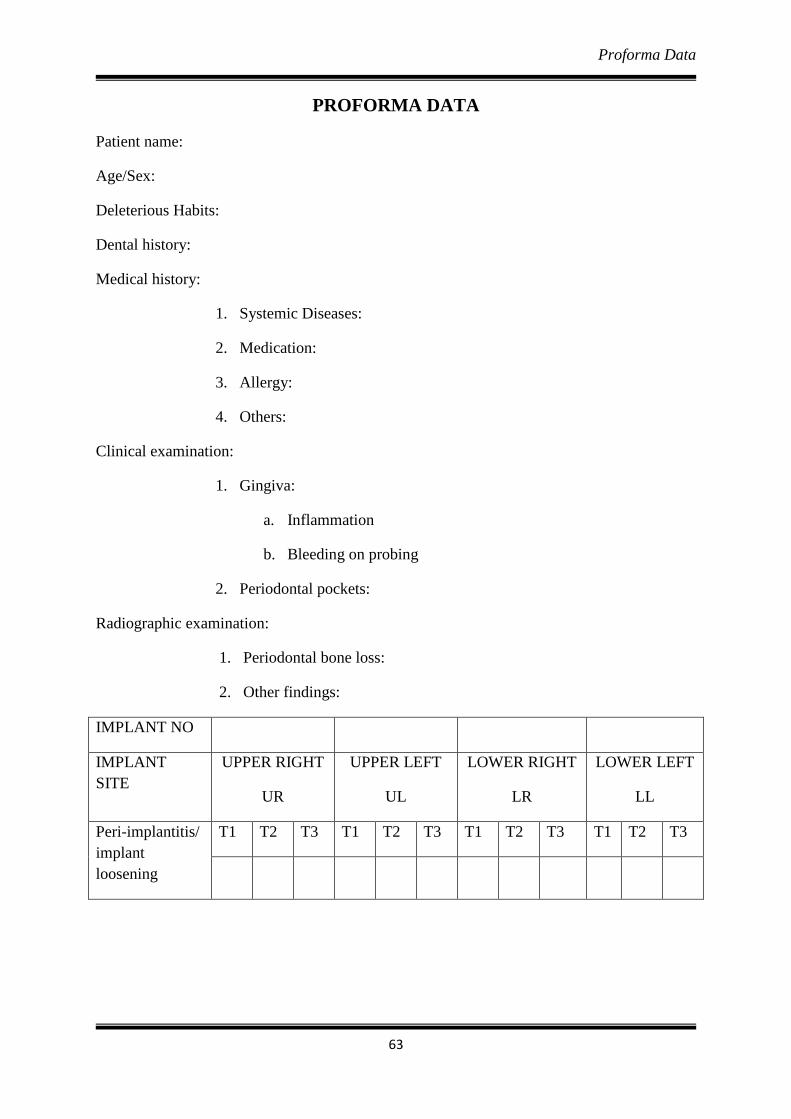
Proforma Data
63
PROFORMA DATA
Patient name:
Age/Sex:
Deleterious Habits:
Dental history:
Medical history:
1. Systemic Diseases:
2. Medication:
3. Allergy:
4. Others:
Clinical examination:
1. Gingiva:
a. Inflammation
b. Bleeding on probing
2. Periodontal pockets:
Radiographic examination:
1. Periodontal bone loss:
2. Other findings:
IMPLANT NO
IMPLANT
SITE
UPPER RIGHT
UR
UPPER LEFT
UL
LOWER RIGHT
LR
LOWER LEFT
LL
Peri-implantitis/
implant
loosening
T1 T2 T3 T1 T2 T3 T1 T2 T3 T1 T2 T3
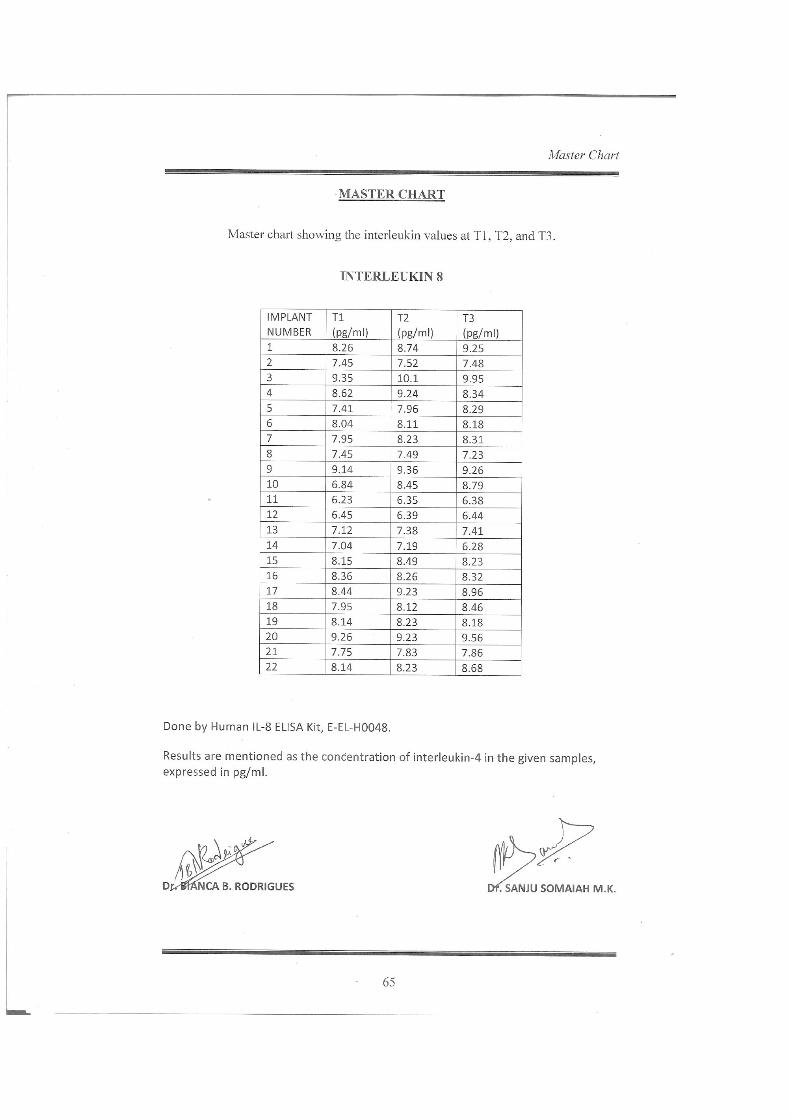
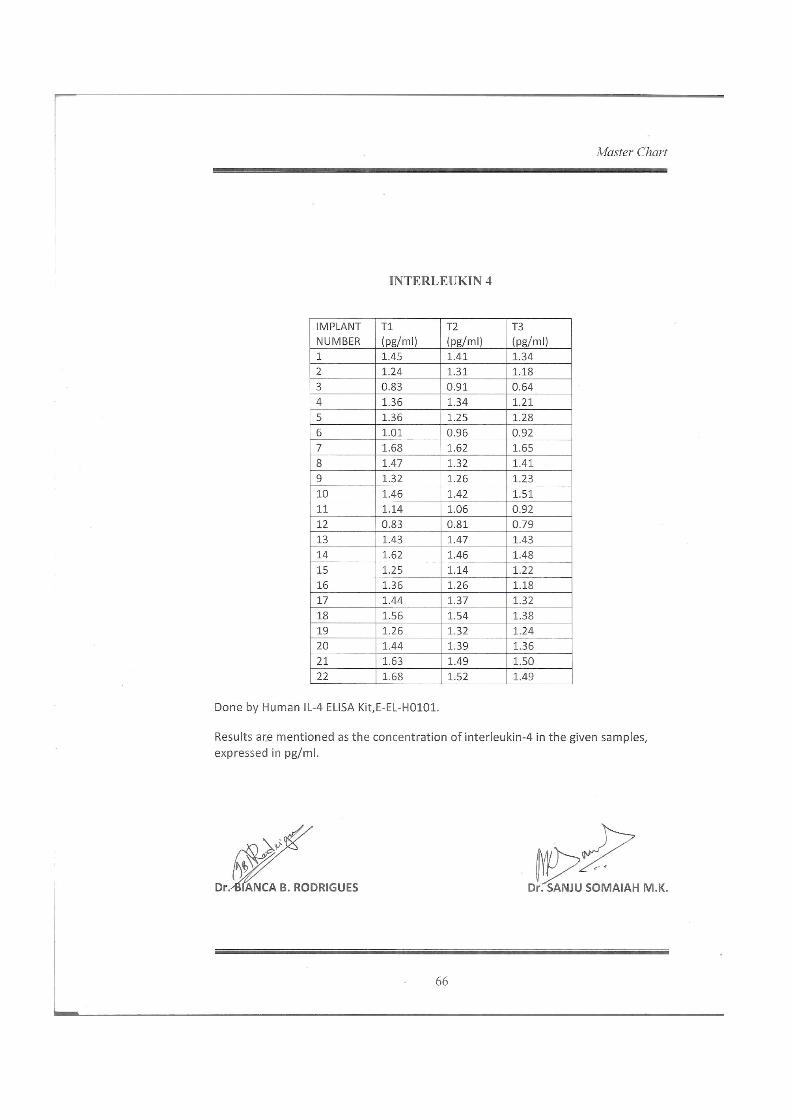

Figures
64
FIGURES
Figure 3. Eppendorf tube and microcappilary tube used for sample collection.
Figure 4. Peri-miniscrew implant crevicular fluid sample collection.
Figure 5. Samples stored in Eppendorf tubes.
Figures
65
Figure 6. ELISA kits of IL-8 and IL-4.
Figure 7. Contents of ELISA kits IL-8 and IL-4.
Figure 8. Performing the ELISA test.
Figures
66
Figure 9. Yellow color change after adding stop solution.
Figure 10. Elisa spectrometer for reading colour change.
Figure 11. Dontrix gauge