Interleukin (IL)-22, IL-17, IL-23, IL-8, vascular endothelial growth factor and tumour necrosis...
10
PHOTOBIOLOGY BJD British Journal of Dermatology Interleukin (IL)-22, IL-17, IL-23, IL-8, vascular endothelial growth factor and tumour necrosis factor-a levels in patients with psoriasis before, during and after psoralen–ultraviolet A and narrowband ultraviolet B therapy S. Coimbra,* à H. Oliveira,§ F. Reis,– L. Belo,* S. Rocha,* A. Quintanilha, ** A. Figueiredo,§ F. Teixeira,– E. Castro,* P. Rocha-Pereira , and A. Santos-Silva* *Servic ¸o de Bioquı ´mica, Faculdade de Farma ´cia, Universidade do Porto, 4050-047 Porto, Portugal Instituto de Biologia Molecular e Celular, Universidade do Porto, Porto, Portugal àCentro de Investigac ¸a ˜o das Tecnologias da Sau ´de, Instituto Polite ´cnico da Sau ´de Norte, CESPU, Gandra-Paredes, Portugal §Servic ¸o de Dermatologia, Hospitais da Universidade de Coimbra, Coimbra, Portugal –Faculdade de Medicina, Instituto de Farmacologia e Terape ˆutica Experimental, IBILI, Universidade de Coimbra, Coimbra, Portugal **Instituto de Cie ˆncias Biome ´dicas Abel Salazar, Universidade do Porto, Porto, Portugal Centro de Investigac ¸a ˜o em Cie ˆncias Sau ´de, Universidade da Beira Interior, Covilha ˜, Portugal Correspondence Susana Coimbra. E-mail: [email protected] Accepted for publication 9 August 2010 Key words cytokines, growth factors, narrowband ultraviolet B, psoralen–ultraviolet A, psoriasis therapy, psoriasis vulgaris Conflicts of interest None declared. DOI 10.1111/j.1365-2133.2010.09992.x Summary Background Several cross-sectional studies have shown that different cytokines and growth factors are enhanced in psoriasis. Objectives We aimed to understand the role ⁄ relation of interleukin (IL)-22, IL-17, IL-23, IL-8, vascular endothelial growth factor (VEGF) and tumour necrosis fac- tor (TNF)-a in psoriasis vulgaris, addressing their levels and changes before, during and after psoralen–ultraviolet A (PUVA) and narrowband ultraviolet B (NB-UVB) treatment. Methods A cross-sectional and a longitudinal study (n = 34) – before (T0) and at 3 (T3), 6 (T6) and 12 (T12) weeks of NB-UVB and PUVA therapy – were per- formed; 17 patients started NB-UVB and 17 PUVA, and IL-22, IL-17, IL-23, IL-8, TNF-a and VEGF levels were evaluated. Results At T0, compared with controls (n = 20), all the parameters were signifi- cantly higher in patients, except for TNF-a. Both NB-UVB and PUVA treatment gave, at T3, a significant decrease in TNF-a and IL-23; IL-22 and IL-17 decreased significantly at T6; all parameters and Psoriasis Area and Severity Index decreased significantly at T12. However, in both groups, at T12, VEGF was still signifi- cantly higher than control. Conclusions Psoriasis seems to be a complex disease in which the cytokine network is disturbed, namely in levels of IL-22, IL-17, IL-23, IL-8, TNF-a and VEGF. NB-UVB and PUVA follow-up studies suggested that the reduction in the IL-23 ⁄ Th17 axis might be important in the pathogenic mechanisms of psoriasis. Further follow-up studies of patients with psoriasis treated with these and other therapies could be very helpful for the understanding of the disturbance in the cytokine network in psoriasis and indirectly in its pathogenesis. Psoriasis vulgaris is a chronic relapsing hyperproliferative skin disease, characterized histologically by acanthosis, parakeratosis and dermal infiltration of mononuclear cells such as T cells, dendritic cells (DCs) and monocytes ⁄ macrophages; neutrophilic infiltrates and the development of elongated ⁄ hyperplastic blood vessels in the papillary dermal region can also be observed. 1–3 All these cells, given their ability to link the innate and acquired immune systems and to regulate cytokine Ó 2010 The Authors 1282 BJD Ó 2010 British Association of Dermatologists 2010 163, pp1282–1290
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Interleukin (IL)-22, IL-17, IL-23, IL-8, vascular endothelial growth factor and tumour necrosis...

PHOTOBIOLOGY
BJD
British Journal of Dermatology
Interleukin (IL)-22, IL-17, IL-23, IL-8, vascular endothelialgrowth factor and tumour necrosis factor-a levels inpatients with psoriasis before, during and afterpsoralen–ultraviolet A and narrowband ultraviolet BtherapyS. Coimbra,*�� H. Oliveira,§ F. Reis,– L. Belo,*� S. Rocha,*� A. Quintanilha,�** A. Figueiredo,§ F. Teixeira,–E. Castro,*� P. Rocha-Pereira�,�� and A. Santos-Silva*�
*Servico de Bioquımica, Faculdade de Farmacia, Universidade do Porto, 4050-047 Porto, Portugal
�Instituto de Biologia Molecular e Celular, Universidade do Porto, Porto, Portugal
�Centro de Investigacao das Tecnologias da Saude, Instituto Politecnico da Saude Norte, CESPU, Gandra-Paredes, Portugal
§Servico de Dermatologia, Hospitais da Universidade de Coimbra, Coimbra, Portugal
–Faculdade de Medicina, Instituto de Farmacologia e Terapeutica Experimental, IBILI, Universidade de Coimbra, Coimbra, Portugal
**Instituto de Ciencias Biomedicas Abel Salazar, Universidade do Porto, Porto, Portugal
��Centro de Investigacao em Ciencias Saude, Universidade da Beira Interior, Covilha, Portugal
CorrespondenceSusana Coimbra.
E-mail: [email protected]
Accepted for publication9 August 2010
Key wordscytokines, growth factors, narrowband ultraviolet
B, psoralen–ultraviolet A, psoriasis therapy,
psoriasis vulgaris
Conflicts of interestNone declared.
DOI 10.1111/j.1365-2133.2010.09992.x
Summary
Background Several cross-sectional studies have shown that different cytokines andgrowth factors are enhanced in psoriasis.Objectives We aimed to understand the role ⁄relation of interleukin (IL)-22, IL-17,IL-23, IL-8, vascular endothelial growth factor (VEGF) and tumour necrosis fac-tor (TNF)-a in psoriasis vulgaris, addressing their levels and changes before,during and after psoralen–ultraviolet A (PUVA) and narrowband ultraviolet B(NB-UVB) treatment.Methods A cross-sectional and a longitudinal study (n = 34) – before (T0) and at3 (T3), 6 (T6) and 12 (T12) weeks of NB-UVB and PUVA therapy – were per-formed; 17 patients started NB-UVB and 17 PUVA, and IL-22, IL-17, IL-23, IL-8,TNF-a and VEGF levels were evaluated.Results At T0, compared with controls (n = 20), all the parameters were signifi-cantly higher in patients, except for TNF-a. Both NB-UVB and PUVA treatmentgave, at T3, a significant decrease in TNF-a and IL-23; IL-22 and IL-17 decreasedsignificantly at T6; all parameters and Psoriasis Area and Severity Index decreasedsignificantly at T12. However, in both groups, at T12, VEGF was still signifi-cantly higher than control.Conclusions Psoriasis seems to be a complex disease in which the cytokine networkis disturbed, namely in levels of IL-22, IL-17, IL-23, IL-8, TNF-a and VEGF.NB-UVB and PUVA follow-up studies suggested that the reduction in theIL-23 ⁄Th17 axis might be important in the pathogenic mechanisms of psoriasis.Further follow-up studies of patients with psoriasis treated with these and othertherapies could be very helpful for the understanding of the disturbance in thecytokine network in psoriasis and indirectly in its pathogenesis.
Psoriasis vulgaris is a chronic relapsing hyperproliferative skin
disease, characterized histologically by acanthosis, parakeratosis
and dermal infiltration of mononuclear cells such as T cells,
dendritic cells (DCs) and monocytes ⁄macrophages; neutrophilic
infiltrates and the development of elongated ⁄hyperplastic
blood vessels in the papillary dermal region can also be
observed.1–3 All these cells, given their ability to link the
innate and acquired immune systems and to regulate cytokine
� 2010 The Authors
1282 BJD � 2010 British Association of Dermatologists 2010 163, pp1282–1290

production, seem to contribute to establish the psoriatic le-
sions.
Psoriasis is currently accepted as a T-helper (Th) 1 ⁄Th17
inflammatory disease, and it is therefore associated with an
increase of Th1 and Th17 cytokines.2,3 Interleukin (IL)-23,
produced by DCs and by macrophages, has the potential to
activate T cells, stimulating survival and proliferation of Th17
cells.4 It seems also to induce dermal infiltration by mixed
inflammatory cells and acanthosis.5 As IL-23 stimulates
tumour necrosis factor (TNF)-a and IL-22 expression, its
deregulation has been proposed as a causative factor in psoria-
sis onset.6
Th17 cells are characterized by the production of IL-22 and
IL-17.7 IL-22 induces epidermal hyperplasia and hypogranulo-
sis; it also induces proinflammatory responses such as the
production of cytokines, chemokines and acute-phase proteins
from many cell types, and it regulates the differentiation and
migration of keratinocytes. The production of IL-22 is directly
induced by IL-23, and IL-22 can mediate IL-23-induced acan-
thosis and dermal inflammation.8,9 The production of IL-22 is
upregulated in psoriatic skin,7 and high blood levels of IL-22
are correlated with psoriasis severity.10 IL-17 is a critical com-
ponent in the establishment and perpetuation of inflammation,
inducing the production of proinflammatory cytokines, mainly
by endothelial cells and macrophages.11 It also activates kerati-
nocytes to produce ILs such as IL-8.12 Increased levels of IL-17
have been found in skin lesions and in blood of patients with
psoriasis, and they were correlated with psoriasis severity.13–16
TNF-a is involved in the regulation of keratinocyte prolifer-
ation. It also influences the activation, proliferation and differ-
entiation of many other cells, and enhances the synthesis of
several cytokines.12 TNF-a seems to increase the expression of
IL-8.1,2 Dermal macrophages in the papillary dermis could be
the main source of TNF-a in psoriatic skin, although it might
also be produced by DCs, T cells and keratinocytes.3,17,18
IL-8, produced by keratinocytes,19 induces neutrophil
mobilization and degranulation.12,20 A significant rise in IL-8
levels has been observed in psoriasis.15,21,22
The vascular endothelial growth factor (VEGF) released
from keratinocytes appears to contribute to the vascularization
of the lesions in psoriasis.23 It can stimulate epidermal hyper-
plasia, vascular growth, and leucocyte infiltration in the
skin,24 and can induce proliferation, sprouting, migration and
tube formation of endothelial cells. Moreover, it increases the
permeability of the endothelium and causes vasodilatation.25
In psoriasis, VEGF levels are significantly higher in skin
lesions, its plasma concentrations are raised during the active
stage,26–29 and both skin and plasma levels have been posi-
tively correlated with Psoriasis Area and Severity Index
(PASI).23,29 As angiogenesis is particularly dependent on
VEGF,30 its role in psoriasis seems to be a key factor in the
link between inflammation and angiogenesis.31 All data about
VEGF in psoriasis suggest that it might be a central growth
factor in psoriasis pathology, and that the manipulation of
VEGF levels could be another promising therapeutic approach
for inflammatory diseases such as psoriasis.
Several cross-sectional studies have shown that different
cytokines and growth factors are enhanced in psoriasis. How-
ever, few longitudinal studies have been performed, address-
ing the levels and changes in those cytokines and growth
factors before, during and after treatment. These studies could
contribute to a better understanding of psoriasis pathogenesis
and on the efficacy of the therapies used.
Psoriatic lesions seem to be the result of the interaction of
several different cell types, and there seems to be a close inter-
dependence between these cells and their activation products.
The aim of the present work was to understand the role and the
cross-talk between some inflammatory cytokines and growth
factors (IL-22, IL-17, IL-23, IL-8, TNF-a and VEGF) that are
produced or that induce the different cell types (macrophages,
DCs, lymphocytes, neutrophils, keratinocytes) present in the
psoriatic lesions. With that perspective, we evaluated their
blood levels during psoralen–ultraviolet (UV) A (PUVA) and
narrowband UVB (NB-UVB) treatment ⁄ improvement. We per-
formed a cross-sectional and a longitudinal study – before, and
3, 6 and 12 weeks after commencing therapy – in Portuguese
patients with psoriasis vulgaris.
Materials and methods
Subjects
The protocol used was approved by the Committee on Ethics
of the University Hospital of Coimbra; all the 34 patients pre-
sented chronic psoriasis vulgaris and gave informed consent to
participate in the study. Psoriasis severity was evaluated by
PASI.32 To diminish subjectivity, PASI was evaluated by the
same dermatologist. Psoriasis was diagnosed between 2
months and 55 years before the present study. All patients
were studied clinically and analytically in an active phase of
the disease (T0), meaning exacerbation of psoriatic lesions,
and 3 (T3), 6 (T6) and 12 (T12) weeks after commencing
treatment. Of the 34 patients, 17 received PUVA therapy and
17 were treated with NB-UVB radiation. The type of treatment
was decided by the patient’s dermatologist, according to sever-
ity of the disease presentation and to the clinical and therapeu-
tic history. Afterwards, patients were invited to participate in
the study. Patients in the NB-UVB and PUVA groups presented
similar characteristics regarding age (mean ± SD 41 ± 16 vs. 48
± 15 years, respectively; P = 0Æ131), duration of the disease
(mean ± SD 16 ± 11 vs. 23 ± 13 years, respectively; P =
0Æ099), gender (11 women ⁄six men and nine women ⁄eight men, respectively), body mass index [median (interquar-
tile range, IQR) 28Æ6 (21Æ9–29Æ9) vs. 27Æ7 (26Æ1–29Æ6),
respectively; P = 0Æ540] and PASI [median (IQR) 17Æ2 (12Æ6–
25Æ0) vs. 26Æ5 (13Æ7–34Æ8), respectively; P = 0Æ057].
NB-UVB irradiation (311 ± 2 nm) was administered using
a Waldmann 7001K cabinet (UVA ⁄UVB–TL-01; Waldmann
Medizintechnik, Villigen-Schwenningen, Germany); the initial
dose, dependent on the phototype of the patient, was 0Æ1–0Æ3J cm)2, and an increasing dose schedule based on an increase
of 0Æ1 J cm)2 was used at each session (thrice weekly), until a
� 2010 The Authors
BJD � 2010 British Association of Dermatologists 2010 163, pp1282–1290
Psoriasis vulgaris cytokines and PUVA ⁄NB-UVB therapy, S. Coimbra et al. 1283
maximum dose of 2Æ5 J cm)2 was reached. UVA irradiation
(320–400 nm) was administered using the same cabinet, and
8-methoxypsoralen (0Æ6 mg kg)1) was administered 2 h
before. The initial dose was 2–3 J cm)2, according to the
phototype; an increasing dose schedule based on an increase
of 0Æ5 J cm)2 was used at each session (thrice weekly), until a
maximum dose of 12 J cm)2 was reached. Eyes and genitals
were shielded during the irradiation procedures.
The control group included 20 healthy volunteers without
psoriasis or other skin disease and with normal haematological
and biochemical values. Patients and controls were cross-
matched for age (mean ± SD 45 ± 16 vs. 44 ± 14 years,
respectively; P = 0Æ821), gender (20 women ⁄14 men and 11
women ⁄nine men, respectively) and body mass index [med-
ian (IQR) 28Æ1 (23Æ6–29Æ7) vs. 25Æ6 (23Æ5–29Æ6), respectively;
P = 0Æ329].
Patients and controls presenting other skin diseases, diabetes
mellitus, inflammatory or infectious diseases, or cardiovascular,
liver or kidney diseases were excluded from the study. None of
the patients received any treatment for at least 1 month prior
to inclusion.
Collection and preparation of blood samples
Blood from nonfasted subjects was collected in order to obtain
plasma (anticoagulant used: heparin lithium) and serum. None
of the collected samples was icteric or haemolysed.
Assays
The IL-22, IL-23, IL-8, TNF-a and VEGF plasma levels and the
IL-17 serum levels were evaluated by enzyme immunoassays:
Human IL-22 Immunoassay (R&D Systems, Minneapolis, MN,
U.S.A.), Human IL-23 enzyme-linked immunosorbent assay
(ELISA), Human IL-8 ⁄NAP-1 ELISA, Human TNF-a ELISA and
Human VEGF-A ELISA (Bender MedSystems, Vienna, Austria)
and Human IL-17 Immunoassay (R&D Systems), respectively.
Statistical analysis
The statistical analysis was performed using the Statistical
Package for Social Sciences version 16 for Windows (SPSS,
Chicago, IL, U.S.A.). To evaluate the differences between
groups we used the Mann–Whitney test. To evaluate the dif-
ferences between active stage of disease and the end of treat-
ment, we used the Wilcoxon test. Measurements are expressed
as median (IQR). P < 0Æ05 was considered as statistically
significant. The correlation analysis was performed by calculat-
ing the Spearman correlation coefficient.
Results
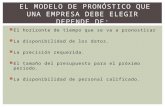
Before starting a therapy, in the active stage of the disease,
our studied patients presented moderate to severe forms of
psoriasis vulgaris as shown by a median (IQR) PASI33 of 22Æ6(12Æ7–29Æ9).
Patients with psoriasis presented several significant disturb-
ances, as compared with controls, namely higher levels of
IL-22, IL-17, IL-23, IL-8 and VEGF, and a trend towards
higher TNF-a values (Table 1). We also observed, in the
active stage of the disease, a significant positive correlation
between PASI and TNF-a (r = 0Æ441; P = 0Æ009), between
PASI and IL-8 (r = 0Æ345; P = 0Æ046) and between TNF-a and
VEGF (r = 0Æ418; P = 0Æ014).
When comparing the NB-UVB and PUVA groups, before
starting the treatment, we found that patients who underwent
PUVA therapy showed significantly higher values of IL-8 (P =
0Æ041). At T3, IL-8 levels were still significantly higher in
patients treated with PUVA (P = 0Æ031); at T6, PUVA patients
presented significantly higher levels of IL-22 (P = 0Æ045). No
other differences were observed.
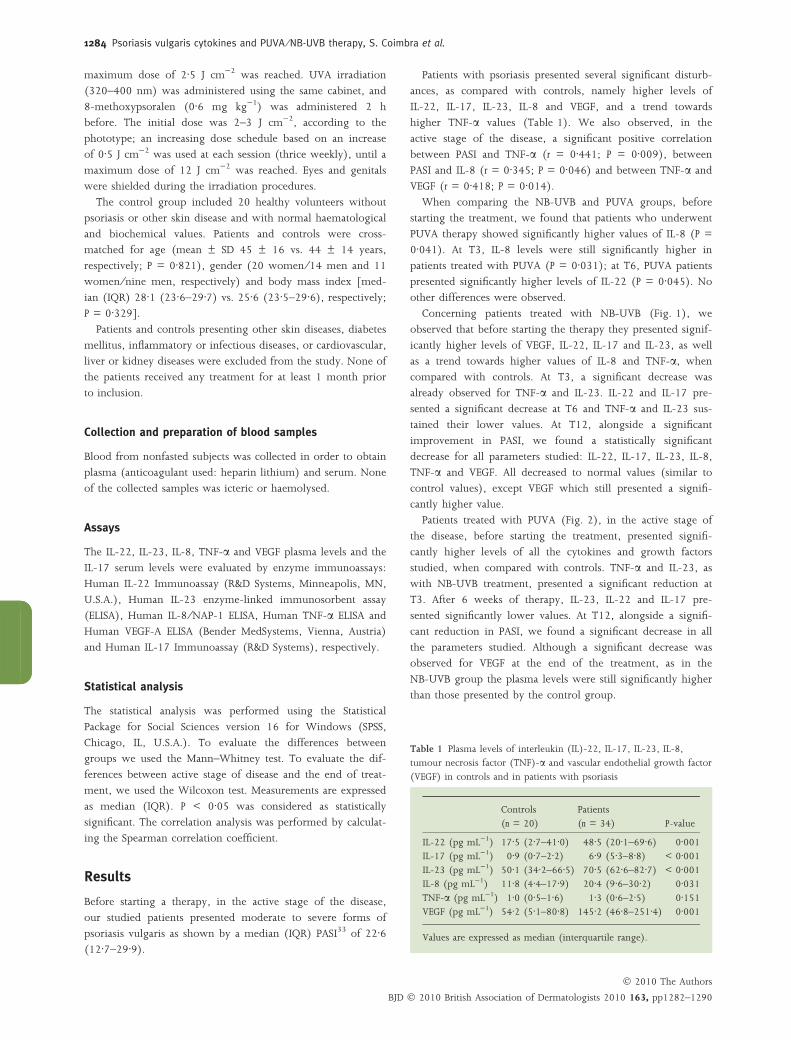
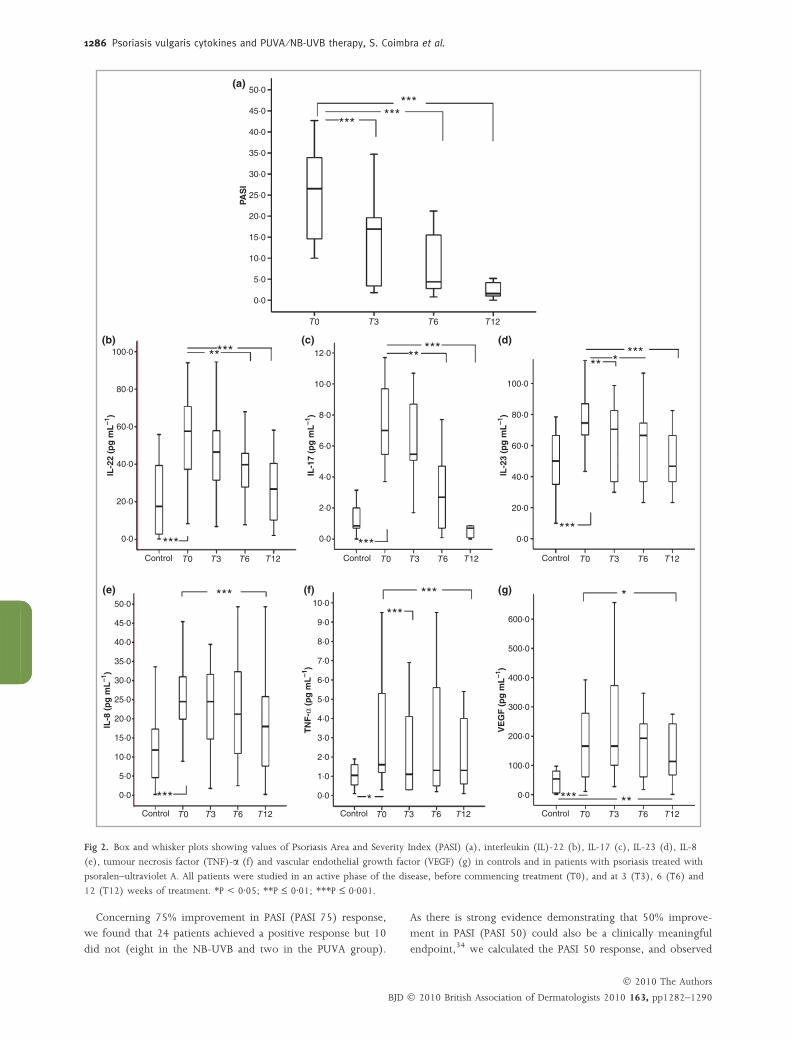
Concerning patients treated with NB-UVB (Fig. 1), we
observed that before starting the therapy they presented signif-
icantly higher levels of VEGF, IL-22, IL-17 and IL-23, as well
as a trend towards higher values of IL-8 and TNF-a, when
compared with controls. At T3, a significant decrease was
already observed for TNF-a and IL-23. IL-22 and IL-17 pre-
sented a significant decrease at T6 and TNF-a and IL-23 sus-
tained their lower values. At T12, alongside a significant
improvement in PASI, we found a statistically significant
decrease for all parameters studied: IL-22, IL-17, IL-23, IL-8,
TNF-a and VEGF. All decreased to normal values (similar to
control values), except VEGF which still presented a signifi-
cantly higher value.
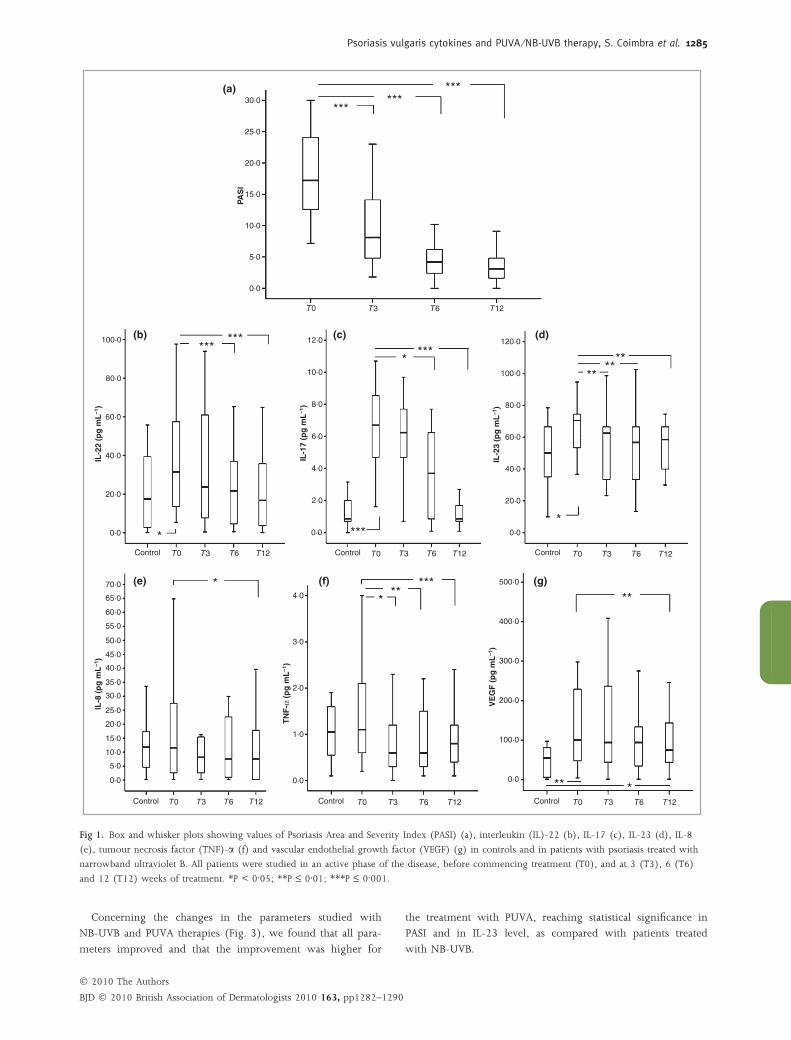
Patients treated with PUVA (Fig. 2), in the active stage of
the disease, before starting the treatment, presented signifi-
cantly higher levels of all the cytokines and growth factors
studied, when compared with controls. TNF-a and IL-23, as
with NB-UVB treatment, presented a significant reduction at
T3. After 6 weeks of therapy, IL-23, IL-22 and IL-17 pre-
sented significantly lower values. At T12, alongside a signifi-
cant reduction in PASI, we found a significant decrease in all
the parameters studied. Although a significant decrease was
observed for VEGF at the end of the treatment, as in the
NB-UVB group the plasma levels were still significantly higher
than those presented by the control group.
Table 1 Plasma levels of interleukin (IL)-22, IL-17, IL-23, IL-8,tumour necrosis factor (TNF)-a and vascular endothelial growth factor
(VEGF) in controls and in patients with psoriasis
Controls
(n = 20)
Patients
(n = 34) P-value
IL-22 (pg mL)1) 17Æ5 (2Æ7–41Æ0) 48Æ5 (20Æ1–69Æ6) 0Æ001IL-17 (pg mL)1) 0Æ9 (0Æ7–2Æ2) 6Æ9 (5Æ3–8Æ8) < 0Æ001
IL-23 (pg mL)1) 50Æ1 (34Æ2–66Æ5) 70Æ5 (62Æ6–82Æ7) < 0Æ001IL-8 (pg mL)1) 11Æ8 (4Æ4–17Æ9) 20Æ4 (9Æ6–30Æ2) 0Æ031
TNF-a (pg mL)1) 1Æ0 (0Æ5–1Æ6) 1Æ3 (0Æ6–2Æ5) 0Æ151VEGF (pg mL)1) 54Æ2 (5Æ1–80Æ8) 145Æ2 (46Æ8–251Æ4) 0Æ001
Values are expressed as median (interquartile range).
� 2010 The Authors
BJD � 2010 British Association of Dermatologists 2010 163, pp1282–1290
1284 Psoriasis vulgaris cytokines and PUVA ⁄NB-UVB therapy, S. Coimbra et al.
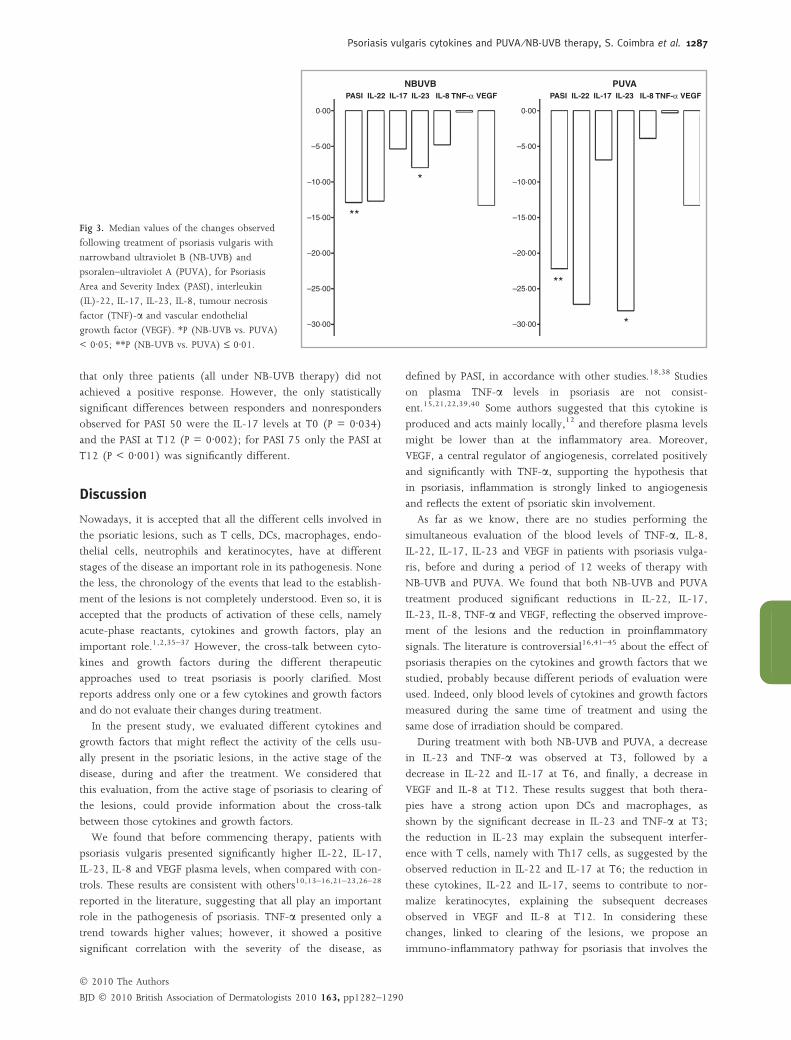
Concerning the changes in the parameters studied with
NB-UVB and PUVA therapies (Fig. 3), we found that all para-
meters improved and that the improvement was higher for
the treatment with PUVA, reaching statistical significance in
PASI and in IL-23 level, as compared with patients treated
with NB-UVB.
(a)
(b)
(e) (f) (g)
(c) (d)
30·0
******
***
***
** **
***
* ****
**
*
**
***
*
******
***
25·0
20·0
15·0
10·0
5·0
0·0
12·0 120·0
100·0
80·0
60·0
40·0
20·0
0·0
500·0
400·0
300·0
200·0
100·0
0·0
10·0
8·0
6·0
4·0
2·0
0·0
4·0
3·0
2·0
1·0
0·0
100·0
80·0
60·0
40·0
20·0
0·0
70·0
65·0
60·0
55·0
50·0
45·0
40·0
35·0
30·0
25·0
20·0
15·0
10·0
5·0
0·0
T0 T3 T6 T12 T0 T3 T6 T12 T0 T3 T6 T12
T0 T3 T6 T12T0 T3 T6 T12
T0
PAS
I
IL-1
7 (p
g m
L–1
)
IL-2
2 (p
g m
L–1
)
IL-2
3 (p
g m
L–1
)
TN
F-α
(p
g m
L–1
)
IL-8
(p
g m
L–1
)
VE
GF
(p
g m
L–1
)
ControlControl
Control Control
Control
Control
T3 T6 T12
T0 T3 T6 T12
Fig 1. Box and whisker plots showing values of Psoriasis Area and Severity Index (PASI) (a), interleukin (IL)-22 (b), IL-17 (c), IL-23 (d), IL-8
(e), tumour necrosis factor (TNF)-a (f) and vascular endothelial growth factor (VEGF) (g) in controls and in patients with psoriasis treated with
narrowband ultraviolet B. All patients were studied in an active phase of the disease, before commencing treatment (T0), and at 3 (T3), 6 (T6)
and 12 (T12) weeks of treatment. *P < 0Æ05; **P £ 0Æ01; ***P £ 0Æ001.
� 2010 The Authors
BJD � 2010 British Association of Dermatologists 2010 163, pp1282–1290
Psoriasis vulgaris cytokines and PUVA ⁄NB-UVB therapy, S. Coimbra et al. 1285
Concerning 75% improvement in PASI (PASI 75) response,
we found that 24 patients achieved a positive response but 10
did not (eight in the NB-UVB and two in the PUVA group).
As there is strong evidence demonstrating that 50% improve-
ment in PASI (PASI 50) could also be a clinically meaningful
endpoint,34 we calculated the PASI 50 response, and observed
T0 T3 T6 T12Control T0 T3 T6 T12Control T0 T3 T6 T12Control
T0 T3 T6 T12Control
0·0
50·0
45·0
40·0
35·0
30·0
25·0
20·0
15·0
10·0
5·0
0·0
50·0(a)
(b) (c) (d)
(e) (f) (g)
******
***
***
***
***
*** *
***
***
******
*
*** **
*** ******
****
45·0
40·0
35·0
30·0
25·0
PAS
I
IL-2
2 (p
g m
L–1
)
IL-1
7 (p
g m
L–1
)
IL-2
3 (p
g m
L–1
)
IL-8
(p
g m
L–1
)
TN
F-α
(p
g m
L–1
)
VE
GF
(p
g m
L–1
)
20·0
15·0
10·0
5·0
0·0
20·02·0
4·0
6·0
8·0
10·0
12·0
0·0
2·0
4·0
6·0
8·0
10·0
0·0 0·0
100·0
200·0
300·0
400·0
500·0
600·0
3·0
5·0
7·0
9·0
1·0
40·0
60·0
80·0
100·0
0·0
20·0
40·0
60·0
80·0
100·0
T0 T3 T6 T12
T0 T3 T6 T12Control T0 T3 T6 T12Control
Fig 2. Box and whisker plots showing values of Psoriasis Area and Severity Index (PASI) (a), interleukin (IL)-22 (b), IL-17 (c), IL-23 (d), IL-8
(e), tumour necrosis factor (TNF)-a (f) and vascular endothelial growth factor (VEGF) (g) in controls and in patients with psoriasis treated with
psoralen–ultraviolet A. All patients were studied in an active phase of the disease, before commencing treatment (T0), and at 3 (T3), 6 (T6) and
12 (T12) weeks of treatment. *P < 0Æ05; **P £ 0Æ01; ***P £ 0Æ001.
� 2010 The Authors
BJD � 2010 British Association of Dermatologists 2010 163, pp1282–1290
1286 Psoriasis vulgaris cytokines and PUVA ⁄NB-UVB therapy, S. Coimbra et al.
that only three patients (all under NB-UVB therapy) did not
achieved a positive response. However, the only statistically
significant differences between responders and nonresponders
observed for PASI 50 were the IL-17 levels at T0 (P = 0Æ034)
and the PASI at T12 (P = 0Æ002); for PASI 75 only the PASI at
T12 (P < 0Æ001) was significantly different.
Discussion
Nowadays, it is accepted that all the different cells involved in
the psoriatic lesions, such as T cells, DCs, macrophages, endo-
thelial cells, neutrophils and keratinocytes, have at different
stages of the disease an important role in its pathogenesis. None
the less, the chronology of the events that lead to the establish-
ment of the lesions is not completely understood. Even so, it is
accepted that the products of activation of these cells, namely
acute-phase reactants, cytokines and growth factors, play an
important role.1,2,35–37 However, the cross-talk between cyto-
kines and growth factors during the different therapeutic
approaches used to treat psoriasis is poorly clarified. Most
reports address only one or a few cytokines and growth factors
and do not evaluate their changes during treatment.
In the present study, we evaluated different cytokines and
growth factors that might reflect the activity of the cells usu-
ally present in the psoriatic lesions, in the active stage of the
disease, during and after the treatment. We considered that
this evaluation, from the active stage of psoriasis to clearing of
the lesions, could provide information about the cross-talk
between those cytokines and growth factors.
We found that before commencing therapy, patients with
psoriasis vulgaris presented significantly higher IL-22, IL-17,
IL-23, IL-8 and VEGF plasma levels, when compared with con-
trols. These results are consistent with others10,13–16,21–23,26–28
reported in the literature, suggesting that all play an important
role in the pathogenesis of psoriasis. TNF-a presented only a
trend towards higher values; however, it showed a positive
significant correlation with the severity of the disease, as
defined by PASI, in accordance with other studies.18,38 Studies
on plasma TNF-a levels in psoriasis are not consist-
ent.15,21,22,39,40 Some authors suggested that this cytokine is
produced and acts mainly locally,12 and therefore plasma levels
might be lower than at the inflammatory area. Moreover,
VEGF, a central regulator of angiogenesis, correlated positively
and significantly with TNF-a, supporting the hypothesis that
in psoriasis, inflammation is strongly linked to angiogenesis
and reflects the extent of psoriatic skin involvement.
As far as we know, there are no studies performing the
simultaneous evaluation of the blood levels of TNF-a, IL-8,
IL-22, IL-17, IL-23 and VEGF in patients with psoriasis vulga-
ris, before and during a period of 12 weeks of therapy with
NB-UVB and PUVA. We found that both NB-UVB and PUVA
treatment produced significant reductions in IL-22, IL-17,
IL-23, IL-8, TNF-a and VEGF, reflecting the observed improve-
ment of the lesions and the reduction in proinflammatory
signals. The literature is controversial16,41–45 about the effect of
psoriasis therapies on the cytokines and growth factors that we
studied, probably because different periods of evaluation were
used. Indeed, only blood levels of cytokines and growth factors
measured during the same time of treatment and using the
same dose of irradiation should be compared.
During treatment with both NB-UVB and PUVA, a decrease
in IL-23 and TNF-a was observed at T3, followed by a
decrease in IL-22 and IL-17 at T6, and finally, a decrease in
VEGF and IL-8 at T12. These results suggest that both thera-
pies have a strong action upon DCs and macrophages, as
shown by the significant decrease in IL-23 and TNF-a at T3;
the reduction in IL-23 may explain the subsequent interfer-
ence with T cells, namely with Th17 cells, as suggested by the
observed reduction in IL-22 and IL-17 at T6; the reduction in
these cytokines, IL-22 and IL-17, seems to contribute to nor-
malize keratinocytes, explaining the subsequent decreases
observed in VEGF and IL-8 at T12. In considering these
changes, linked to clearing of the lesions, we propose an
immuno-inflammatory pathway for psoriasis that involves the
PASI
0·00
–5·00
–10·00
–15·00 **
**
*
*
–20·00
–25·00
–30·00
0·00
–5·00
–10·00
–15·00
–20·00
–25·00
–30·00
IL-22 IL-17 IL-23
NBUVBIL-8 TNF-α VEGF PASI IL-22 IL-17 IL-23
PUVAIL-8 TNF-α VEGF
Fig 3. Median values of the changes observed
following treatment of psoriasis vulgaris with
narrowband ultraviolet B (NB-UVB) and
psoralen–ultraviolet A (PUVA), for Psoriasis
Area and Severity Index (PASI), interleukin
(IL)-22, IL-17, IL-23, IL-8, tumour necrosis
factor (TNF)-a and vascular endothelial
growth factor (VEGF). *P (NB-UVB vs. PUVA)
< 0Æ05; **P (NB-UVB vs. PUVA) £ 0Æ01.
� 2010 The Authors
BJD � 2010 British Association of Dermatologists 2010 163, pp1282–1290
Psoriasis vulgaris cytokines and PUVA ⁄NB-UVB therapy, S. Coimbra et al. 1287
production of IL-23, as well as TNF-a, from DCs, which cause
activation and proliferation of Th17 cells. Subsequently, Th17
cells induce the expression of IL-22 and IL-17. IL-22 induces
keratinocyte hyperplasia and mediates IL-23-induced dermal
inflammation and acanthosis. On the other hand, IL-17
induces keratinocyte activation to produce several ILs such as
IL-8. Indeed, IL-8 secretion appears to be stimulated not only
by TNF-a but also by IL-17.12 IL-8 induces neutrophil mobili-
zation and activation, characteristic of active psoriatic
lesions.46,47 Activation of keratinocytes also leads to an
increase in their own proliferation with altered maturation
and to the production of several inflammatory mediators that
might cause further recruitment of immune cells and activa-
tion of stromal cells. Furthermore, as a result of keratinocyte
activation, VEGF is produced, contributing to induction of
angiogenesis, characteristic of psoriasis lesions. Therefore, the
involvement of the IL-23 ⁄Th17 axis in psoriasis seems to be a
key event in its pathogenesis, explaining some of the typical
histological characteristics of the psoriatic lesions, such as
hyperplasia of keratinocytes (by IL-22) and the neutrophil
infiltration (IL-8 production induced by IL-17). The release of
activation products occurs as a consequence of neutrophil acti-
vation, as we reported previously.48 TNF-a is known to
induce the production of IL-6, and both cytokines are able to
trigger the synthesis and release of C-reactive protein (CRP);49
indeed, the rise in blood levels of CRP and a correlation
between CRP and the severity of psoriasis vulgaris, as defined
by PASI, was reported recently in patients with psoriasis,48
confirming psoriasis as a condition in which systemic inflam-
matory response is marked.
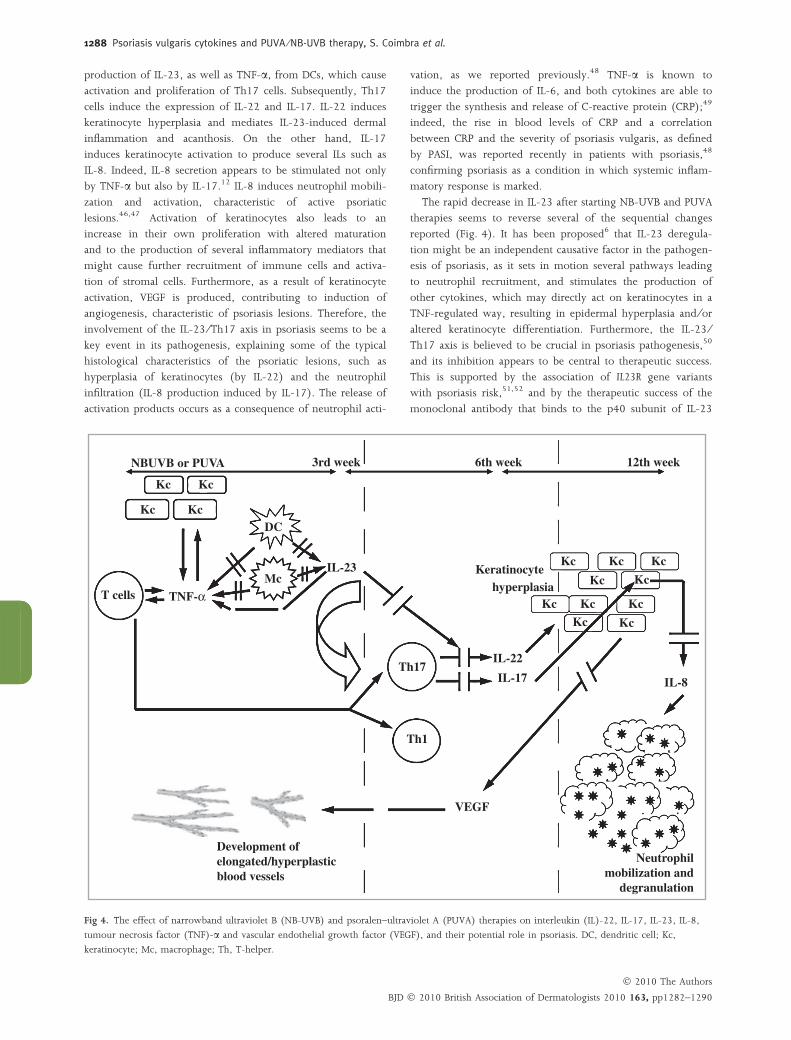
The rapid decrease in IL-23 after starting NB-UVB and PUVA
therapies seems to reverse several of the sequential changes
reported (Fig. 4). It has been proposed6 that IL-23 deregula-
tion might be an independent causative factor in the pathogen-
esis of psoriasis, as it sets in motion several pathways leading
to neutrophil recruitment, and stimulates the production of
other cytokines, which may directly act on keratinocytes in a
TNF-regulated way, resulting in epidermal hyperplasia and ⁄or
altered keratinocyte differentiation. Furthermore, the IL-23 ⁄Th17 axis is believed to be crucial in psoriasis pathogenesis,50
and its inhibition appears to be central to therapeutic success.
This is supported by the association of IL23R gene variants
with psoriasis risk,51,52 and by the therapeutic success of the
monoclonal antibody that binds to the p40 subunit of IL-23
NBUVB or PUVA
Kc Kc
3rd week 6th week 12th week
KcDC
McKc
Keratinocytehyperplasia
VEGF
Development ofelongated/hyperplasticblood vessels
Neutrophilmobilization and
degranulation
Kc Kc
KcKc
Kc KcKc
Kc Kc
IL-23
TNF-α
Th17
Th1
IL-17
IL-22
IL-8
T cells
Kc
Fig 4. The effect of narrowband ultraviolet B (NB-UVB) and psoralen–ultraviolet A (PUVA) therapies on interleukin (IL)-22, IL-17, IL-23, IL-8,
tumour necrosis factor (TNF)-a and vascular endothelial growth factor (VEGF), and their potential role in psoriasis. DC, dendritic cell; Kc,
keratinocyte; Mc, macrophage; Th, T-helper.
� 2010 The Authors
BJD � 2010 British Association of Dermatologists 2010 163, pp1282–1290
1288 Psoriasis vulgaris cytokines and PUVA ⁄NB-UVB therapy, S. Coimbra et al.

and IL-12.53 Our results support this hypothesis, as the reduc-
tion in IL-23 (the first change observed with treatment of the
disease) seems to be crucial for the subsequent changes
observed for the other cytokines. Our data are consistent with
the concept54 that the response to psoriasis therapy is depen-
dent on the inactivation of DC products, and inactivation of,
besides the Th1, the Th17 immune response.
Despite the similar final changes observed for both thera-
pies, the improvements were higher in patients treated with
PUVA, which may explain its higher remission rate, as com-
pared with NB-UVB.55
After both types of therapies, all cytokines returned to values
similar to those presented by the control; only VEGF was still
significantly higher than the control. NB-UVB irradiation is
known to upregulate VEGF;56 however, similar results were
found for patients treated with PUVA. Sustained high levels of
VEGF, even at remission, as defined by PASI, suggest that VEGF
might be important in defining the time of remission, as VEGF
is known to promote vascular permeability that enhances leuco-
cyte traffic into the skin and alters the dermal capillaries to
express leucocyte chemoattractant molecules.57 Moreover, we
found48 that a residual inflammation persists after treatment with
PUVA and NB-UVB, as CRP was still higher than the control.
We wonder if this residual inflammatory stimulus, along with
higher VEGF levels, could favour infiltration of inflammatory
cells into the skin and, therefore, the development of lesions.
In summary, psoriasis seems to be a complex disease in
which the cytokine network is disturbed, namely in blood
levels of IL-22, IL-17, IL-23, IL-8, TNF-a and VEGF. Our fol-
low-up studies of patients with psoriasis treated with NB-UVB
and PUVA suggest that the reduction in the IL-23 ⁄Th17 axis
might be important in the pathogenic mechanisms of psoria-
sis. Further follow-up studies of patients with psoriasis treated
with these and other therapies could be very helpful for the
understanding of the disturbance in the cytokine network in
psoriasis and indirectly in its pathogenesis.
What’s already known about this topic?
• Cross-sectional studies have shown that different cyto-
kines and growth factors are enhanced in psoriasis.
What does this study add?
• This is a cross-sectional ⁄ longitudinal study that aims to
elucidate the role ⁄relation of some inflammatory cyto-
kines and growth factors [interleukin (IL)-22, IL-17,
IL-23, IL-8, tumour necrosis factor-a and vascular endo-
thelial growth factor] in psoriasis vulgaris before, during
and after psoralen–ultraviolet A and narrowband ultra-
violet B treatment of Portuguese patients. This study is
intended to contribute to a better understanding of pso-
riasis pathogenesis and the efficacy of therapies used.
Acknowledgments
This study was supported by Fundacao para a Ciencia e Tecno-
logia (FCT: POCI ⁄SAU – OBS ⁄58600 ⁄2004) and Fundo Euro-
peu de Desenvolvimento Regional (FEDER).
References
1 Lowes MA, Bowcock AM, Krueger JG. Pathogenesis and therapy ofpsoriasis. Nature 2007; 445:866–73.
2 Sabat R, Philipp S, Hoflich C et al. Immunopathogenesis of psoria-sis. Exp Dermatol 2007; 16:779–98.
3 Ghoreschi K, Weigert C, Rocken M. Immunopathogenesis and roleof T cells in psoriasis. Clin Dermatol 2007; 25:574–80.
4 Blauvelt A. T-helper 17 cells in psoriatic plaques and additionalgenetic links between IL-23 and psoriasis. J Invest Dermatol 2008;
128:1064–7.5 Torti DC, Feldman SR. Interleukin-12, interleukin-23, and psoria-
sis: current prospects. J Am Acad Dermatol 2007; 57:1059–68.6 Chan JR, Blumenschein W, Murphy E et al. IL-23 stimulates epidermal
hyperplasia via TNF and IL-20R2-dependent mechanisms with impli-cations for psoriasis pathogenesis. J Exp Med 2006; 203:2577–87.
7 Ouyang W, Kolls JK, Zheng Y. The biological functions of T helper
17 cell effector cytokines in inflammation. Immunity 2008; 28:454–67.8 Zheng Y, Danilenko DM, Valdez P et al. Interleukin-22, a T(H)17
cytokine, mediates IL-23-induced dermal inflammation and acan-thosis. Nature 2007; 445:648–51.
9 Fitch E, Harper E, Skorcheva I et al. Pathophysiology of psoriasis:recent advances on IL-23 and Th17 cytokines. Curr Rheumatol Rep
2007; 9:461–7.10 Wolk K, Witte E, Wallace E et al. IL-22 regulates the expression of
genes responsible for antimicrobial defense, cellular differentiation,and mobility in keratinocytes: a potential role in psoriasis. Eur J
Immunol 2006; 36:1309–23.11 Hunter CA. New IL-12-family members: IL-23 and IL-27, cyto-
kines with divergent functions. Nat Rev Immunol 2005; 5:521–31.12 Pietrzak AT, Zalewska A, Chodorowska G et al. Cytokines and anti-
cytokines in psoriasis. Clin Chim Acta 2008; 394:7–21.13 Takahashi H, Tsuji H, Hashimoto Y et al. Serum cytokines and
growth factor levels in Japanese patients with psoriasis. Clin Exp Der-matol 2010; 35:645–9.
14 Caproni M, Antiga E, Melani L et al. Serum levels of IL-17 and IL-22are reduced by etanercept, but not by acitretin, in patients with pso-
riasis: a randomized-controlled trial. J Clin Immunol 2009; 29:210–14.15 Arican O, Aral M, Sasmaz S, Ciragil P. Serum levels of TNF-alpha,
IFN-gamma, IL-6, IL-8, IL-12, IL-17, and IL-18 in patients withactive psoriasis and correlation with disease severity. Mediators In-
flamm 2005; 2005:273–9.16 Vahavihu K, Ala-Houhala M, Peric M et al. Narrowband ultraviolet
B treatment improves vitamin D balance and alters antimicrobialpeptide expression in skin lesions of psoriasis and atopic derma-
titis. Br J Dermatol 2010; 163:321–8.17 Toebak MJ, de Rooij J, Moed H et al. Differential suppression of
dendritic cell cytokine production by anti-inflammatory drugs. Br JDermatol 2008; 158:225–33.
18 Kastelan D, Kastelan M, Massari LP et al. Possible association of
psoriasis and reduced bone mineral density due to increased TNF-alpha and IL-6 concentrations. Med Hypotheses 2006; 67:1403–5.
19 Asadullah K, Docke WD, Volk HD et al. The pathophysiological roleof cytokines in psoriasis. Drugs Today (Barc) 1999; 35:913–24.
� 2010 The Authors
BJD � 2010 British Association of Dermatologists 2010 163, pp1282–1290
Psoriasis vulgaris cytokines and PUVA ⁄NB-UVB therapy, S. Coimbra et al. 1289

20 Narbutt J, Lesiak A, Skibinska M et al. Repeated doses of UVR causeminor alteration in cytokine serum levels in humans. Mediators
Inflamm 2005; 2005:298–303.21 Jacob SE, Nassiri M, Kerdel FA et al. Simultaneous measurement of
multiple Th1 and Th2 serum cytokines in psoriasis and correlationwith disease severity. Mediators Inflamm 2003; 12:309–13.
22 Abanmi A, Al Harthi F, Al Agla R et al. Serum levels of pro-inflammatory cytokines in psoriasis patients from Saudi Arabia. Int
J Dermatol 2005; 44:82–3.23 Bhushan M, McLaughlin B, Weiss JB et al. Levels of endothelial cell
stimulating angiogenesis factor and vascular endothelial growth
factor are elevated in psoriasis. Br J Dermatol 1999; 141:1054–60.24 Guttman-Yassky E, Krueger JG. Psoriasis: evolution of pathogenic
concepts and new therapies through phases of translationalresearch. Br J Dermatol 2007; 157:1103–15.
25 Tammela T, Enholm B, Alitalo K et al. The biology of vascularendothelial growth factors. Cardiovasc Res 2005; 65:550–63.
26 Young HS, Summers AM, Read IR et al. Interaction between geneticcontrol of vascular endothelial growth factor production and reti-
noid responsiveness in psoriasis. J Invest Dermatol 2006; 126:453–9.27 Creamer D, Allen M, Jaggar R et al. Mediation of systemic vascular
hyperpermeability in severe psoriasis by circulating vascular endo-thelial growth factor. Arch Dermatol 2002; 138:791–6.
28 Nielsen HJ, Christensen IJ, Svendsen MN et al. Elevated plasma lev-els of vascular endothelial growth factor and plasminogen activator
inhibitor-1 decrease during improvement of psoriasis. Inflamm Res2002; 51:563–7.
29 Nofal A, Al-Makhzangy I, Attwa E et al. Vascular endothelial growthfactor in psoriasis: an indicator of disease severity and control.
J Eur Acad Dermatol Venereol 2009; 23:803–6.30 Zhang Y, Matsuo H, Morita E. Vascular endothelial growth factor
121 is the predominant isoform in psoriatic scales. Exp Dermatol2005; 14:758–64.
31 Simonetti O, Lucarini G, Goteri G et al. VEGF is likely a key factorin the link between inflammation and angiogenesis in psoriasis:
results of an immunohistochemical study. Int J Immunopathol Pharmacol2006; 19:751–60.
32 Fredriksson T, Pettersson U. Severe psoriasis – oral therapy with anew retinoid. Dermatologica 1978; 157:238–44.
33 Naldi L, Gambini D. The clinical spectrum of psoriasis. Clin Dermatol2007; 25:510–18.
34 Carlin CS, Feldman SR, Krueger JG et al. A 50% reduction in thePsoriasis Area and Severity Index (PASI 50) is a clinically significant
endpoint in the assessment of psoriasis. J Am Acad Dermatol 2004;
50:859–66.35 Sabat R, Sterry W, Philipp S et al. Three decades of psoriasis
research: where has it led us? Clin Dermatol 2007; 25:504–9.36 Strober B, Teller C, Yamauchi P et al. Effects of etanercept on
C-reactive protein levels in psoriasis and psoriatic arthritis. Br JDermatol 2008; 159:322–30.
37 Coimbra S, Oliveira H, Reis F et al. Circulating levels of adiponec-tin, oxidized LDL and C-reactive protein in Portuguese patients
with psoriasis vulgaris, according to body mass index, severity andduration of the disease. J Dermatol Sci 2009; 55:202–4.
38 Qiu S, Tan S, Zhang J et al. Effect of liangxue huoxue xiaoyin tangon serum levels of TNF-alpha, IFN-gamma and IL-6 in psoriasis of
blood-heat type. J Tradit Chin Med 2005; 25:292–5.39 Roussaki-Schulze AV, Kouskoukis C, Petinaki E et al. Evaluation of
cytokine serum levels in patients with plaque-type psoriasis. Int JClin Pharmacol Res 2005; 25:169–73.
40 Chodorowska G, Juszkiewicz-Borowiec M, Czelej D et al. Activity oftumor necrosis factor-alfa (TNF-alpha) and selected acute phase
proteins in plasma of psoriatic patients receiving local treatment.Ann Univ Mariae Curie Sklodowska [Med] 2001; 56:165–9.
41 Akman A, Dicle O, Yilmaz F et al. Discrepant levels of vascularendothelial growth factor in psoriasis patients treated with PUVA,
re-PUVA and narrow-band UVB. Photodermatol Photoimmunol Photomed2008; 24:123–7.
42 Andrys C, Borska L, Pohl D et al. Angiogenic activity in patientswith psoriasis is significantly decreased by Goeckerman’s therapy.
Arch Dermatol Res 2007; 298:479–83.
43 McLoone P, Man I, Yule S et al. Whole-body UVB (TL-01) orUVA-1 irradiation does not alter the levels of immunomodulatory
cytokines in the serum of human volunteers. Photodermatol Photoimmu-nol Photomed 2004; 20:76–80.
44 Sigmundsdottir H, Johnston A, Gudjonsson JE et al. Narrowband-UVB irradiation decreases the production of pro-inflammatory
cytokines by stimulated T cells. Arch Dermatol Res 2005; 297:39–42.
45 Piskin G, Tursen U, Sylva-Steenland RM et al. Clinical improvementin chronic plaque-type psoriasis lesions after narrow-band UVB
therapy is accompanied by a decrease in the expression of IFN-gamma inducers – IL-12, IL-18 and IL-23. Exp Dermatol 2004;
13:764–72.46 Krueger G, Ellis CN. Psoriasis – recent advances in understanding
its pathogenesis and treatment. J Am Acad Dermatol 2005; 53:S94–100.
47 Krueger JG, Bowcock A. Psoriasis pathophysiology: current con-cepts of pathogenesis. Ann Rheum Dis 2005; 64 (Suppl. 2):ii30–6.
48 Coimbra S, Oliveira H, Reis F et al. C-reactive protein and leucocyteactivation in psoriasis vulgaris according to severity and therapy.
J Eur Acad Dermatol Venereol 2010; 24:789–96.49 McBride JD, Cooper MA. A high sensitivity assay for the inflamma-
tory marker C-reactive protein employing acoustic biosensing.J Nanobiotechnology 2008; 6:5.
50 Di Cesare A, Di Meglio P, Nestle FO. The IL-23 ⁄Th17 axis in theimmunopathogenesis of psoriasis. J Invest Dermatol 2009; 129:1339–
50.51 Capon F, Di Meglio P, Szaub J et al. Sequence variants in the genes
for the interleukin-23 receptor (IL23R) and its ligand (IL12B) con-fer protection against psoriasis. Hum Genet 2007; 122:201–6.
52 Cargill M, Schrodi SJ, Chang M et al. A large-scale genetic associa-tion study confirms IL12B and leads to the identification of IL23R as
psoriasis-risk genes. Am J Hum Genet 2007; 80:273–90.
53 Farhi D. Ustekinumab for the treatment of psoriasis. Drugs Today(Barc) 2010; 46:259–64.
54 Zaba LC, Suarez-Farinas M, Fuentes-Duculan J et al. Effective treat-ment of psoriasis with etanercept is linked to suppression of IL-17
signaling, not immediate response TNF genes. J Allergy Clin Immunol2009; 124:1022–10.e1-395.
55 Karrer S, Eholzer C, Ackermann G et al. Phototherapy of psoriasis:comparative experience of different phototherapeutic approaches.
Dermatology 2001; 202:108–15.56 Yano K, Kadoya K, Kajiya K et al. Ultraviolet B irradiation of human
skin induces an angiogenic switch that is mediated by upregulationof vascular endothelial growth factor and by downregulation of
thrombospondin-1. Br J Dermatol 2005; 152:115–21.57 Guenther LC, Ortonne JP. Pathophysiology of psoriasis: science
behind therapy. J Cutan Med Surg 2002; 6:2–7.
� 2010 The Authors
BJD � 2010 British Association of Dermatologists 2010 163, pp1282–1290
1290 Psoriasis vulgaris cytokines and PUVA ⁄NB-UVB therapy, S. Coimbra et al.

This document is a scanned copy of a printed document. No warranty is given about the accuracy of the copy.
Users should refer to the original published version of the material.