Evaluation of serum biomarkers of fibrosis and injury in Egyptian patients with chronic hepatitis C
8
Evaluation of serum biomarkers of fibrosis and injury in Egyptian patients with chronic hepatitis C q Gamal Esmat 1,2 , Mohamed Metwally 1,3 , Khalid R. Zalata 4 , Shahinaz Gadalla 8 , Mohamed Abdel-Hamid 1,5,8 , Amr Abouzied 1 , Abdel-Aziz Shaheen 1 , Maissa El-Raziky 2 , Hani Khatab 2 , Sherif El-Kafrawy 1,6 , Nabiel Mikhail 1,7 , Laurence S. Magder 8 , Nezam H. Afdhal 9 , G. Thomas Strickland 8, * 1 National Hepatology and Tropical Medicine Research Institute, Cairo, Egypt 2 Faculty of Medicine, Cairo University, Egypt 3 Faculty of Medicine, Benha University, Egypt 4 Faculty of Medicine, Mansoura University, Egypt 5 Faculty of Medicine, Minya University, Egypt 6 Faculty of Medicine, Menoufiya University, Egypt 7 Faculty of Medicine, Assiut University, Egypt 8 Department of Epidemiology and Preventive Medicine, University of Maryland School of Medicine, Room 102 D, Howard Hall, 606 West Redwood Street, Baltimore, MD 21201, USA 9 Beth Israel Deaconess Medical Center, Boston, MA, USA Background/ Aims: We evaluated whether surrogate serum biomarkers for liver injury are comparable to liver biopsy in Egyptian patients with hepatitis C virus (HCV) infection. Subjects: Two hundred and twenty Egyptian patients, 91% infected with genotype-4 HCV, undergoing liver biopsy dur- ing evaluation for interferon /ribavirin therapy. Methods: Liver biopsy scored by the Ishak method was compared to biochemical tests, platelet count and two fibrosis biomarkers: hyaluronic acid (HA) and YKL-40. Univariate and logistic regression analyses determined independent pre- dictors of fibrotic, inflammatory, and fatty changes. Biomarkers were evaluated for ability to differentiate between severe fibrosis / cirrhosis and no/mild fibrosis. Results: Although increasing age, HA, YKL-40, AST, reduced platelet count, and AST and HA/ platelet count ratios were associated with fibrosis by univariate analysis, the other variables were not significant after controlling for HA (p = 0.0001) and age (p = 0.004). Although age and some biomarkers were associated with inflammation, none remained significant after controlling for fibrosis. YKL-40 (p = 0.04) and aspartate aminotransferase (p = 0.05) remained associated with steatosis after controlling for fibrosis. Conclusions: In Egyptians with chronic HCV, young patients with low levels of HA are at very low risk of fibrosis. This can limit the number of liver biopsies to those whose clinical findings conflict with the biomarker results. Ó 2007 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved. Keywords: Hepatitis C virus; HCV; Fibrosis; Cirrhosis; Morbidity assessment; Liver biopsy; Serum hepatic fibrosis markers; Hyaluronic acid; YKL-40 0168-8278/$32.00 Ó 2007 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.jhep.2006.12.010 Received 30 May 2006; received in revised form 5 December 2006; accepted 13 December 2006; available online 24 January 2007 q The authors who have taken part in this study declared that they have no relationship with the manufacturers of the drugs involved either in the past or present and received funding from WellcomeTrust and Schering-Plough. * Corresponding author. Tel.: +1 410 706 7550; fax: +1 410 706 8013. E-mail address: [email protected] (G.T. Strickland). www.elsevier.com/locate/jhep Journal of Hepatology 46 (2007) 620–627
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Evaluation of serum biomarkers of fibrosis and injury in Egyptian patients with chronic hepatitis C

www.elsevier.com/locate/jhep
Journal of Hepatology 46 (2007) 620–627
Evaluation of serum biomarkers of fibrosis and injuryin Egyptian patients with chronic hepatitis Cq
Gamal Esmat1,2, Mohamed Metwally1,3, Khalid R. Zalata4, Shahinaz Gadalla8,Mohamed Abdel-Hamid1,5,8, Amr Abouzied1, Abdel-Aziz Shaheen1, Maissa El-Raziky2,
Hani Khatab2, Sherif El-Kafrawy1,6, Nabiel Mikhail1,7, Laurence S. Magder8,Nezam H. Afdhal9, G. Thomas Strickland8,*
1National Hepatology and Tropical Medicine Research Institute, Cairo, Egypt2Faculty of Medicine, Cairo University, Egypt3Faculty of Medicine, Benha University, Egypt
4Faculty of Medicine, Mansoura University, Egypt5Faculty of Medicine, Minya University, Egypt
6Faculty of Medicine, Menoufiya University, Egypt7Faculty of Medicine, Assiut University, Egypt
8Department of Epidemiology and Preventive Medicine, University of Maryland School of Medicine, Room 102 D, Howard Hall,
606 West Redwood Street, Baltimore, MD 21201, USA9Beth Israel Deaconess Medical Center, Boston, MA, USA
Background/Aims: We evaluated whether surrogate serum biomarkers for liver injury are comparable to liver biopsy inEgyptian patients with hepatitis C virus (HCV) infection.
Subjects: Two hundred and twenty Egyptian patients, 91% infected with genotype-4 HCV, undergoing liver biopsy dur-
ing evaluation for interferon/ribavirin therapy.
Methods: Liver biopsy scored by the Ishak method was compared to biochemical tests, platelet count and two fibrosis
biomarkers: hyaluronic acid (HA) and YKL-40. Univariate and logistic regression analyses determined independent pre-
dictors of fibrotic, inflammatory, and fatty changes. Biomarkers were evaluated for ability to differentiate between severe
fibrosis/cirrhosis and no/mild fibrosis.
Results: Although increasing age, HA, YKL-40, AST, reduced platelet count, and AST and HA/ platelet count ratioswere associated with fibrosis by univariate analysis, the other variables were not significant after controlling for HA
(p = 0.0001) and age (p = 0.004). Although age and some biomarkers were associated with inflammation, none remained
significant after controlling for fibrosis. YKL-40 (p = 0.04) and aspartate aminotransferase (p = 0.05) remained associated
with steatosis after controlling for fibrosis.
Conclusions: In Egyptians with chronic HCV, young patients with low levels of HA are at very low risk of fibrosis. This
can limit the number of liver biopsies to those whose clinical findings conflict with the biomarker results.
� 2007 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved.
Keywords: Hepatitis C virus; HCV; Fibrosis; Cirrhosis; Morbidity assessment; Liver biopsy; Serum hepatic fibrosis
markers; Hyaluronic acid; YKL-40
0168-8278/$32.00 � 2007 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved.
doi:10.1016/j.jhep.2006.12.010
Received 30 May 2006; received in revised form 5 December 2006; accepted 13 December 2006; available online 24 January 2007q The authors who have taken part in this study declared that they have no relationship with the manufacturers of the drugs involved either in the
past or present and received funding from WellcomeTrust and Schering-Plough.* Corresponding author. Tel.: +1 410 706 7550; fax: +1 410 706 8013.
E-mail address: [email protected] (G.T. Strickland).

G. Esmat et al. / Journal of Hepatology 46 (2007) 620–627 621
1. Introduction
We rely on repeated liver biopsies with their associat-ed risks, cost, and sampling errors to detect, grade, andmonitor hepatic pathology in hepatitis C (HCV) infec-tions and other chronic liver diseases [1–6]. It is difficultto justify serial liver biopsies to diagnose and monitorpatients with chronic HCV when there are limitedoptions for managing their disease, as is the usual casein Egypt [7].
Noninvasive reliable biomarkers for diagnosing andgrading hepatic fibrosis and to monitor outcome oftreatment and the course of HCV infection are an activearea of clinical interest [3,4,8–22]. This study’s objectivewas to evaluate individually and in combination theability of routine laboratory tests and two serum bio-markers of extracellular matrix to predict hepatic fibro-sis, inflammation and steatosis and compare them withliver biopsy findings in Egyptian patients being evaluat-ed for a clinical trial comparing antiviral therapy forgenotype-4 HCV.
2. Methods
2.1. Patients
This cross-sectional study included 220 adults with chronic HCVinfections being evaluated for a randomized clinical trial to comparetwo interferon and ribavirin regimens at the National Hepatologyand Tropical Medicine Research Institute in Cairo, Egypt. All gavetheir informed consent, which included undergoing a pretreatment liv-er biopsy. The study protocol conformed to the ethical guidelines ofthe 1975 Declaration of Helsinki, and was reviewed and approved bythe Egyptian Ministry of Health and Population’s, University ofMaryland-Baltimore’s, and Walter Reed Army Medical Center’s Insti-tutional Review Boards. Prior to acceptance in the treatment trial, allsubjects were screened for schistosomiasis and treated with praziquan-tel if they had ova in their stools or urine. Four individuals had schis-tosoma granuloma, evidence of previous infection with Schistosomamansoni, detected on their liver biopsies.
Diagnosis of chronic HCV was established by elevated alanine ami-notransferase enzyme (ALT) levels in persons having HCV antibody(anti-HCV) by a third generation enzyme immunoassay (EIA) andHCV-RNA using an in-house direct reverse transcriptase polymerasechain reaction (RT-PCR) assay [23]. Patients were excluded if theyhad other causes of chronic liver diseases, including chronic hepatitisB, or previously received interferon therapy. All patients denied intra-venous drug abuse and four patients reported they consumed aboutone alcoholic drink per week.
Study subjects included the 200 patients enrolled in the treatmenttrial and 20 others screened but not enrolled having stage 1, 2, 5 and6 Ishak fibrosis scores. We included a second control population of88 HCV patients at Beth Israel Deaconess Medical Center in Bostonfor validation of our findings.
2.2. Survey and laboratory data
A previously validated questionnaire was used to collect demo-graphic and medical information. Laboratory test results used in thisreport, serum ALT, aspartate aminotransferase (AST), alkaline phos-phatase (ALP), total and direct bilirubin, and blood platelet counts,were all performed using standard methods. Serum hyaluronic acid(HA; Corgenix, Denver, CO) and YKL-40 (Metra, Biosystems, Moun-
tain View, CA) were measured using commercially available bioassays.The ALT and AST indexes were calculated by dividing the patient’stest result by the upper limit of normal for the test. The AST/plateletcount ratio index (APRI) was calculated as AST index/platelet countdivided by 103 times 100. The HA/platelet count ratio was calculatedas the HA level/platelet count divided by 103 times 100.
2.3. Liver biopsy
These were examined by a hepatopathologist (KRZ) blinded topatient characteristics. All biopsy cores were at least 1 cm in lengthand encompassed at least three portal areas. The scoring system ofIshak et al. (modified HAI and staging) was used to assess fibrosisstage and necroinflammatory injury [24]. Necroinflammatory activitywas classified into mild (score 1–5), moderate (score 6–8), and severe(score 9–18). Fibrosis was staged separately on a scale of 0–6. Stages0–1 indicated no or mild fibrosis, stages 2- and -3 moderate fibrosis,and 4–6 more severe fibrosis or cirrhosis. Macrovesicular steatosiswas classified into grades: 0 (no fatty infiltration), I (up to 33% of hepa-tocytes affected), II (greater than 33–66% of hepatocytes), and III(greater than 66% of hepatocytes) [25].
2.4. Statistical analysis
Patients were classified according to their stage of fibrosis, inflam-mation, or steatosis as noted on liver biopsy. Box plots were used toshow distribution of different biomarkers in relation to stages of fibro-sis. Univariate logistic regression was used to assess the associationbetween biomarker levels and severe fibrosis or cirrhosis, inflammationor steatosis. Multiple logistic regression was used to assess the associ-ation between biomarkers and outcomes, while controlling for othervariables.
Sensitivity, specificity, positive (PPV) and negative (NPV) predic-tive values were calculated for predicting severe fibrosis and cirrhosis(stages 4–6), moderate or severe inflammatory changes (grade 6 ormore), and grade II or III fatty infiltration. Receiver operating charac-teristic curves (ROC) were constructed to assess the power of the bio-markers in predicting severe and mild hepatic fibrosis by calculatingthe area under the curve.
3. Results
The 220 subjects were predominately (79%) male witha mean age of 39.3 years; 91% were infected with geno-type 4 HCV (Table 1). Severe hepatic fibrosis was pres-ent in 23%; 59% had mild-to-moderate fibrosis, while18% had mild or no fibrosis; 49% of biopsies were readas moderate grades of necroinflammatory changes; 29%had minimal inflammation; while 22% had severeinflammation. No steatosis was present in 43%; 39%had minimal steatosis (grade I); and 18% had grade IIand III steatosis (Table 1). There was a strong relation-ship (p < 0.001) between stage of fibrosis and necroin-flammatory changes, but not between fibrosis andsteatosis; 77.5% of biopsies with mild or no fibrosishad Ishak grade 1–5 inflammatory changes while 57%of biopsies with moderate-to-severe fibrosis or cirrhosishad Ishak grade 9–18 inflammatory changes (Table 2).
3.1. Association of the biomarkers with hepatic fibrosis
Univariate analysis showed that older age, but notgender, was associated with stage of fibrosis (Table 2).

Table 1
Age, gender, HCV genotype, demographics, laboratory test results, and liver biopsy findings in the Egyptian and American subjects
Egyptian N (%) American N (%) p-value
Age (mean ± SD) 39.3 ± 8.7 50.4 ± 7.4 <0.0001Male gender 173 (78.6) 59 (65.6) 0.016BMI (mean ± SD) 27.9 ± 4.0 26.8 ± 4.4 0.052HCV genotype 4a 175 (90.7) 2 (3.5) <0.0001ALT ratio above upper limits normal (mean ± SD) 1.76 ± 1.05 2.05 ± 1.85 0.16AST ratio above upper limits normal (mean ± SD) 1.74 ± 1.2 1.58 ± 1.56 0.37Alkaline phosphatase (ALP) 101.3 ± 39.6Platelet count (mean ± SD) 219.8 ± 66.5 224 ± 74.5 0.64Fibrosis
Stages 0–1 40 (18.2) 27 (30.7)Stages 2–3 129 (58.6) 39 (44.3) 0.03Stages 4–6 51 (23.2) 22 (25.0)
NecroinflammationGrades 1–5 64 (29.1)Grades 6–8 107 (48.6)Grades 9–12 49 (22.3)
Steatosisb
Grade 0 93 (42.9)Grade I 84 (38.7)Grades II and III 40 (18.4)
a Data from 27 Egyptians missing.b Data from 3 Egyptians missing.
622 G. Esmat et al. / Journal of Hepatology 46 (2007) 620–627
Comparisons with demographic and laboratory param-eters showed increase in age (p < 0.0001), HA(p < 0.0001), HA/platelet count ratio (p < 0.0001),YKL-40 (p < 0.0001), APRI (p = 0.0007) and AST(p = 0.009) was all associated with the level of fibrosis.In addition, the platelet count was inversely related(p = 0.0004) to fibrosis. Neither the ALT (p = 0.063),ALP (p = 0.17), nor total (p = 0.22) or direct(p = 0.089) bilirubin levels were associated with hepaticfibrosis. In addition, combinations of test results, otherthan APRI, did not improve the predictive value of indi-vidual tests.
When age and the biomarkers were included in a for-ward stepwise logistic regression model, only age(p = 0.004) and HA (p < 0.0001) were significantly asso-ciated with severe fibrosis or cirrhosis. Table 3 shows thesensitivity, specificity, and PPV and NPV of the bio-
Table 2
Comparison of hepatic fibrosis with age, gender, HCV genotype and necroinfla
Fibrosis stages Stages 0–1 number (%) Stages 2
Total 40 (18.2) 129 (58.Age (mean ± SD) 36.4 ± 7.4 38.4 ± 8Male gender 31 (77.5) 100 (77.HCV Genotype 4 18/20 (90) 113/125
Inflammatory changesGrades 1–5 31 (77.5) 30 (23.3Grades 6–8 8 (20.0) 80 (62)Grades 9–12 1 (2.5) 19 (14.7
SteatosisGrade 0 12 (30) 56 (44.1Grade I 20 (50) 48 (37.8Grades II and III 8 (20) 23 (18.1
markers for predicting stage 4–6 fibrosis using conve-nient cut-off levels in which 23% of biopsies weregraded as stages 4–6. HA levels of 20 ng/ml or greaterhad a sensitivity of 88%, a specificity of 68%, and PPVand NPV of 45% and 95%, respectively. These resultsare slightly superior to those of the YKL-40 and theAPRI, and are about the same as those for the HA/platelet count ratio with a cut-off of 10.
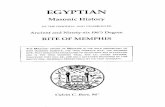
Fig. 1 shows the median 50th percentile (in the box)and 25th and 75th percentile (in the whiskers) for sixbiomarkers as they relate to hepatic fibrosis. Althoughthere was considerable overlap, in the case of HA,YKL-40, AST, HA/platelet count ratio, and APRI,the median and 50th percentile of each group increasedprogressively with increasing stages of fibrosis and themedian and 50th percentile of the platelet countdecreased with increasing fibrosis. Despite overlap with
mmatory and fatty changes in liver biopsies
–3 number (%) Stages 4–6 number (%) p-value
6) 51 (23.2).7 43.9 ± 7.9 <0.0015) 42 (82.4) 0.76(90.4) 44/48 (91.7) 0.96
) 3 (5.9) <0.00119 (37.3)
) 29 (56.9)
) 25 (50) 0.38) 16 (32)) 9 (18)

Table 3
Sensitivity, specificity and positive (PPV) and negative (NPV) predictive
values of different biomarkers to diagnose severe fibrosis or cirrhosis
(stages 4–6) based on its observed prevalence of 23%
Cut-off value for biomarkers Sensitivity Specificity PPV NPV
Hyaluronic acid (HA)5 0.98 0.39 0.33 0.9920 0.88 0.68 0.45 0.95140 0.22 0.96 0.65 0.80
YKL- 4020 1.00 0.08 0.25 1.00100 0.82 0.57 0.37 0.92400 0.20 0.96 0.63 0.80
AST index/platelet count ratio0.2 1.00 0.04 0.24 1.000.6 0.86 0.53 0.36 0.932.0 0.17 0.95 0.56 0.80
HA/platelet count ratio2.0 0.98 0.37 0.32 0.9810.0 0.84 0.69 0.45 0.9475.0 0.29 0.95 0.65 0.82
G. Esmat et al. / Journal of Hepatology 46 (2007) 620–627 623
the group having moderate fibrosis, these box chartsclearly show that patients with severe fibrosis and cir-rhosis had different values for the biomarkers than thegroup having no/mild fibrosis.
We also analyzed the data comparing the differentbiomarkers to hepatic fibrosis using ROC. The resultsconfirmed that HA, HA/platelet count ratio, YKL-40and APRI were predictive of level of hepatic fibrosis.When predicting more severe fibrosis or cirrhosis (stages4–6), the areas under the curves were 0.84 for HA/plate-let count ratio, 0.83 for HA, 0.74 for APRI, and 0.74 forYKL-40. When ROC was used to differentiate no/mildfibrosis (stage 0–1) from stage 2 to 6 fibrosis the areasunder the curve were 0.73 for HA/platelet count ratio,0.73 for HA, 0.62 for YKL-40 and 0.59 for APRI.
3.2. Association of biomarkers with hepatic inflammation
HA (p = 0.007), YKL-40 (p = 0.009), and HA/plate-let count (p = 0.02) and APRI (p = 0.03) ratios predict-ed the levels of necroinflammatory changes in hepaticbiopsies using univariant analyses. However, whenadjusted for fibrosis (Table 2), none were significantlyassociated with inflammatory changes.
3.3. Association of biomarkers with hepatic steatosis
YKL-40 and AST were associated with grades of ste-atosis by univariant analyses; and they remained signif-icant after adjusting for fibrosis (p = 0.036 andp = 0.046, respectively). The odds of presence of stageII or III fatty infiltration doubled when YKL-40 levelwas 100 or more (OR = 2.0, 95% CI = 0.95–4.25,p = 0.06). Table 4 shows the sensitivity, specificity andpredictive values of different levels of YKL-40, AST
index and YKL/AST index ratio in predicting grade IIor III steatosis. HA levels were not associated(p = 0.30) with hepatic steatosis.
3.4. Clinical utilization of serum biomarkers for assessing
hepatic injury in Egyptian patients
Only 5 (4.5%; 95% CI = 1.5–10.2%) of 111 patientsunder age 45 with HA levels less than 30 had severefibrosis or cirrhosis. Thus, such patients could be viewedat low risk for chronic complications and the cliniciancould follow them at intervals without performing a liv-er biopsy. On the other hand, 17/25 (68%; 95% CI = 46–86%) among those with HA of 100 or greater who were40 or older had severe fibrosis or cirrhosis. Such patientsshould be considered at high risk for cirrhosis and itscomplications and candidates for further diagnosticand therapeutic interventions, with or without a confir-matory liver biopsy. Eighty-three (37.7%) patients couldnot be classified by our algorithm using HA and age.They would require additional studies, including a liverbiopsy if clinically indicated.
3.5. American patients
We analyzed results in a cohort of 88 Americanpatients having biopsies and serum biomarker data.These patients were somewhat older, less likely to bemale, had a slightly lower BMI, more likely to have mildthan moderate fibrosis, and as expected, only two hadgenotype-4 infections (Table 1). Generally similar, butless strong, associations were found between the bio-markers and fibrosis in the Americans. For example,of those with an HA less than 30, 6/46 (13%) had severefibrosis or cirrhosis, whereas, 12/23 (52%) of those withan HA over 100 had severe fibrosis or cirrhosis. The bio-markers with the strongest associations with fibrosiswere decreased in platelets (p = 0.0003) and increasedin the HA level (p = 0.01).
4. Discussion
Noninvasive methods to measure severity of liverinjury are clinically important in Egypt whereadvanced liver disease from HCV is common andaccess to liver biopsy is limited [7,26,27]. In addition,reliability of the biopsy to detect and measure hepaticpathology is not ideal [3,5,6,28]. For instance, in a mul-ticenter study validating biochemical markers for pre-dicting liver fibrosis in patients with chronic HCV,the authors proposed discordance caused by interpreta-tion of the biopsy (4%) as frequent as in the Fibrotest(5%) being evaluated [4]. Many of the reports evaluat-ing biomarkers for detecting hepatic fibrosis have usedscoring systems encompassing combinations of results

4-6 2-3 0-1
IN
OR
ULAYH
ICA
CD
400
350
300
250
200
150
100
50
0 4-6 2-3 0-1
STN
UO
CTELETALP
400
300
200
100
0
4-62-30-1
/AH
ITAR
ETALETALPO
200
150
100
50
0 4-62-3 0-1
TSA
10
8
6
4
2
0
4-6 2-3 0-1
IRPA
I/TSA(
XED
NITA
RTELE TALP
)O 6
5
4
3
2
1
0 4-62-3 0-1
04LKY
700
600
500
400
300
200
100
0
Stage of fibrosis
a b
dc
fe
Fig. 1. Box plot of: (a) hyaluronic acid (HA); (b) platelet count; (c) HA/platelet count ratio; (d) AST; (e) APRI (AST/platelet count ratio); and (f) YKL-
40 in relation to Ishak fibrosis score (stages 0–1 represent no or mild fibrosis, stages 2–3 represent moderate fibrosis, while stages 4–6 represent severe
fibrosis or cirrhosis).
624 G. Esmat et al. / Journal of Hepatology 46 (2007) 620–627
from several blood tests and demographic data[4,9,12,13,17,20,22,29].
Most of the indexes proposed in these studies wouldnot be practical in Egypt and other developing countriesbecause of cost and unavailability of some tests. For thisreason we evaluated a few blood tests routinely per-formed on patients with chronic HCV in Egypt in addi-tion to two commercially available tests for measuringhepatic fibrosis. Predictability of hepatic injury was
not significantly improved when we evaluated combina-tions of results from two or more tests. Thus, we believethat we present a useful, practical and cost-effectiveapproach for using serum biomarkers of hepatic fibrosis,inflammation and steatosis in Egypt and other areaswith limited resources.
Prior studies of serum biomarkers for HCV in devel-oped countries have arbitrarily chosen to stratify for noor mild fibrosis (Metavir F0/1 or Ishak F0-2) compared

Table 4
Sensitivity, specificity and predictive values of different biomarkers to
diagnose stage II and III fatty infiltration (steatosis) based on its
observed prevalence of 18.4%
Cut-off of different biomarkers Sensitivity Specificity PPV NPV
YKL- 4020 0.95 0.07 0.19 0.86100 0.63 0.49 0.22 0.86400 0.13 0.94 0.33 0.83
AST index1 0.70 0.26 0.18 0.792 0.13 0.72 0.09 0.784 0.03 0.96 0.13 0.81
YKL/AST20 0.95 0.12 0.20 0.91100 0.58 0.65 0.27 0.87400 0.05 0.98 0.33 0.82
G. Esmat et al. / Journal of Hepatology 46 (2007) 620–627 625
to moderate/advanced disease (Metavir F2-4 or IshakF3-6) since F2 is the point at which interferon therapyis usually offered. Other experts state that biomarkershave a greater role, and higher sensitivity in diagnosingadvanced disease, and particularly cirrhosis (MetavirF3/4 or Ishak F4-6). This is particularly important inEgypt where there is a heavy chronic liver disease bur-den since diagnosing severe fibrosis or cirrhosis couldinitiate strategies for treatment of HCV and screeningfor hepatocellular carcinoma. Time of exposure toHCV is known only in a few of our patients. Their meanage of 39 years suggests that as many as half were infect-ed as children during treatment campaigns for schistoso-miasis 20–40 years earlier [7,30].
In a multicenter study in 486 patients with chronicHCV undergoing liver biopsy, the clinical value of HAmeasurement was its ability to exclude cirrhosis [14]. AHA value of less than 60 ng/L excluded cirrhosis or sig-nificant fibrosis in their patients with a NPV of 99% and93%, respectively. Oberti et al. evaluated markers offibrosis in 243 patients [16]. HA performed the best ofthe four being evaluated having a diagnostic accuracyof 86% for detecting cirrhosis in subpopulations havingviral or combined viral and alcoholic etiologies. Wonget al. showed that HA had 85% sensitivity and 88% spec-ificity for predicting stage 4 and 5 fibrosis [8]. Morerecently, Kelleher et al. developed the SHASTA index,using HA, age and albumin, to differentiate mild fromadvanced fibrosis in patients co-infected with HCVand HIV [13]. Patel and colleagues reported a panel ofHA, TIMP-1, and alpha2-macroglobulin had about a75% PPV and NPV in differentiating moderate/severefibrosis from no/mild fibrosis in almost 700 patients withchronic HCV infection [22]. Furthermore, HIV co-infec-tion did not reduce the value of noninvasive biomarkersto detect and measure fibrosis in HCV infected patients[31].
HA was our optimal single test for predicting fibrosis.A HA level of less than 30 ng/ml among those under 45
years of age excluded severe fibrosis or cirrhosis with aNPV of 95%. Using HA would have saved performingliver biopsies in more than half of our patients. Onecaveat regarding this calculation is that the NPV willvary depending on the prevalence of fibrosis in thepatient population.
We have focused on presenting a practical noninva-sive and inexpensive alternative to liver biopsy forassessing hepatic injury in Egyptian patients with chron-ic HCV infections. However, it is customary to validatethe conclusion from studies such as this in a secondgroup of patients. Results from a cohort of Americanpatients with chronic HCV show that our conclusionsare valid, albeit with less reliability.
In addition to diagnosing cirrhosis, biomarkers havevalue if they also detect severe inflammation or steatosis.The risk of disease progression has been shown to bedependent on the grade of inflammation on biopsy[32]. Most previous studies reported HA levels couldnot predict grade of hepatic inflammation. However,Ishibashi et al. reported HA levels correlated withinflammatory changes in their patients’ biopsies [10].Our initial analysis also showed that HA and YKL-40levels could predict hepatic inflammation, but afteradjusting for fibrosis, these associations were not statis-tically significant. Serum ALT has long been a surrogatefor inflammation and until better markers are deter-mined it will probably remain the most widely used test.Although our study did not show a relationship betweenALT values and the necroinflammatory grades, an ALTlevel of 200 IU/L or greater may be associated withincreased risk of HCV disease progression [33].
The prevalence of steatosis in our Egyptian patientsinfected with genotype 4 HCV, 57%, is close to the aver-age of 55.5% reported in chronic HCV [34]. Unlike ourfindings, steatosis has correlated with fibrosis in othercross-sectional studies of patients with HCV. The verylittle consumption of alcohol among our almost exclu-sively Muslim population may explain this differencesince alcohol is believed to increase steatosis in patientswith chronic HCV[35], or the relationship between fibro-sis and steatosis is less in patients infected with genotype4 than those infected with other genotypes. Steatosis hasbeen reported to reduce therapeutic response to antiviraltherapy in patients with chronic HCV [34,36]. There wasa significant reduction in sustained viral clearanceamong our 200 patients having grade II and III hepaticsteatosis who were treated with interferon and ribavirin(unpublished, Esmat G). Our finding that both YKL-40and AST remained predictive for grade II and III stea-tosis, even after adjusting for hepatic fibrosis, shouldbe further evaluated.
In addition to reliability issues, routine liver biopsyfor following HCV infected patients in a country likeEgypt is expensive and impractical. Therefore, aneffective surrogate test to stage hepatic fibrosis that

626 G. Esmat et al. / Journal of Hepatology 46 (2007) 620–627
is inexpensive, reproducible and simple to perform ishighly desired. The combination of HA, YKL-40,platelet count, and transaminases appeared adequateto achieve this cost-effectively, and also providedinformation about the amount of hepatic inflamma-tion and steatosis in our Egyptian patients. In Egypt,with limited resources but almost twice the number ofpeople with chronic HCV infections as in the USA[7,30], these serum biomarkers, particularly HA, canassist the clinician in making prognostic and therapeu-tic decisions. They can provide guidance as to whetherthe patient has minimal hepatic fibrosis or more severelesions, and in many cases replace the need for a liverbiopsy with a simple blood test. However, they mustbe evaluated in cohorts of HCV patients being pro-spectively followed to determine whether HA or otherserum biomarkers can predict hepatic disease progres-sion and its clinical outcome.
Acknowledgements
We thank Dr. Maria Sjogren of Walter Reed ArmyMedical Center in Washington, DC, who arrangedfunding from Schering-Plough Corporation and provid-ed advice for the randomized clinical trial for which theliver biopsies were performed. Professor Alaa Ismail,Dean of the National Hepatology and Tropical Medi-cine Research Institute, provided support and advice.Financial support: This work was partially funded bySchering-Plough Corporation and Wellcome Trust-Bur-roughs Wellcome Fund Infectious Diseases InitiativeGrants 059113/Z/99/A and 059113/13/Z/99/Z.
References
[1] Andriulli A, Persico M, Iacobellis A, Maio G, Di Salvo D,Spadaccini A, et al. Treatment of patients with HCVinfection with or without liver biopsy. J Viral Hepat2004;11:536–542.
[2] Perrault J, McGill DB, Ott BJ, Taylor WF. Liver biopsy:complications in 1000 inpatients and outpatients. Gastroenterol-ogy 1978;74:103–106.
[3] Afdhal NH, Nunes D. Evaluation of liver fibrosis: a concisereview. Am J Gastroenterol 2004;99:1160–1174.
[4] Halfon P, Bourliere M, Deydier R, Botta-Fridlund D, Renou C,Tran A, et al. Independent prospective multicenter validation ofbiochemical markers (fibrotest-actitest) for the prediction of liverfibrosis and activity in patients with chronic hepatitis C: thefibropaca study. Am J Gastroenterol 2006;101:547–555.
[5] Regev A, Berho M, Jeffers LJ, Milikowski C, Molina EG,Pyrsopoulos NT, et al. Sampling error and intraobserver varia-tion in liver biopsy in patients with chronic HCV infection. Am JGastroenterol 2002;97:2614–2618.
[6] Colloredo G, Guido M, Sonzogni A, Leandro G. Impact of liverbiopsy size on histological evaluation of chronic viral hepatitis: thesmaller the sample, the milder the disease. J Hepatol2003;39:239–244.
[7] Strickland GT. Liver disease in Egypt: Hepatitis C supersededschistosomiasis as a result of iatrogenic and biological factors.Hepatology 2006;43:915–922.
[8] Wong VS, Hughes V, Trull A, Wight DG, Petrik J, AlexanderGJ. Serum hyaluronic acid is a useful marker of liver fibrosisin chronic hepatitis C virus infection. J Viral Hepat1998;5:187–192.
[9] Poynard T, Imbert-Bismut F, Munteanu M, Messous D, MyersRP, Thabut D, et al. Overview of the diagnostic value ofbiochemical markers of liver fibrosis (FibroTest, HCV FibroSure)and necrosis (ActiTest) in patients with chronic hepatitis C. CompHepatol 2004;3:8.
[10] Ishibashi K, Kashiwagi T, Ito A, Tanaka Y, Nagasawa M,Toyama T, et al. Changes in serum fibrogenesis markers duringinterferon therapy for chronic hepatitis type C. Hepatology1996;24:27–31.
[11] Afdhal NH. The natural history of hepatitis C. Semin Liver Dis2004;24:3–8.
[12] Imbert-Bismut F, Ratziu V, Pieroni L, Charlotte F, Benhamou Y,Poynard T. Biochemical markers of liver fibrosis in patients withhepatitis C virus infection: a prospective study. Lancet2001;357:1069–1075.
[13] Kelleher TB, Mehta SH, Bhaskar R, Sulkowski M, AstemborskiJ, Thomas DL, et al. Prediction of hepatic fibrosis in HIV/HCVco-infected patients using serum fibrosis markers: the SHASTAindex. J Hepatol 2005;43:78–84.
[14] McHutchison JG, Blatt LM, de Medina M, Craig JR, Conrad A,Schiff ER, et al. Measurement of serum hyaluronic acid inpatients with chronic hepatitis C and its relationship to liverhistology. Consensus Interferon Study Group. J GastroenterolHepatol 2000;15:945–951.
[15] Myers RP, Ratziu V, Imbert-Bismut F, Charlotte F, Poynard T.Biochemical markers of liver fibrosis: a comparison with historicalfeatures in patients with chronic hepatitis C. Am J Gastroenterol2002;97:2419–2425.
[16] Oberti F, Valsesia E, Pilette C, Rousselet MC, Bedossa P, Aube C,et al. Noninvasive diagnosis of hepatic fibrosis or cirrhosis.Gastroenterology 1997;113:1609–1616.
[17] Poynard T, McHutchison J, Manns M, Myers RP, Albrecht J.Biochemical surrogate markers of liver fibrosis and activity in arandomized trial of peginterferon alfa-2b and ribavirin. Hepatol-ogy 2003;38:481–492.
[18] Rosenberg WM, Voelker M, Thiel R, Becka M, Burt A, SchuppanD, et al. Serum markers detect the presence of liver fibrosis: acohort study. Gastroenterology 2004;127:1704–1713.
[19] Wai CT, Greenson JK, Fontana RJ, Kalbfleisch JD, Marrero JA,Conjeevaram HS, et al. A simple noninvasive index can predictboth significant fibrosis and cirrhosis in patients with chronichepatitis C. Hepatology 2003;38:518–526.
[20] Poynard T, Munteanu M, Imbert-Bismut F, Charlotte F, ThabutD, Le Calvez S, et al. Prospective analysis of discordant resultsbetween biochemical markers and biopsy in patients with chronichepatitis C. Clin Chem 2004;50:1344–1355.
[21] Fontana RJ, Lok AS. Noninvasive monitoring of patients withchronic hepatitis C. Hepatology 2002;36:S57–S64.
[22] Patel K, Gordon SC, Jacobson I, Hezode C, Oh E, Smith KM,et al. Evaluation of a panel of non-invasive serum markers todifferentiate mild from moderate-to-advanced liver fibrosis inchronic hepatitis C patients. J Hepatol 2004;41:935–942.
[23] Abdel-Hamid M, Edelman DC, Highsmith WE, Constantine NT.Optimization, assessment, and proposed use of a direct nestedreverse transcription-polymerase chain reaction protocol for thedetection of hepatitis C virus. J Hum Virol 1997;1:58–65.
[24] Ishak K, Baptista A, Bianchi L, Callea F, De Groote J, Gudat F,et al. Histological grading and staging of chronic hepatitis. JHepatol 1995;22:696–699.
[25] Brunt EM, Janney CG, Di Bisceglie AM, Neuschwander-TetriBA, Bacon BR. Nonalcoholic steatohepatitis: a proposal forgrading and staging the histological lesions. Am J Gastroenterol1999;94:2467–2474.

G. Esmat et al. / Journal of Hepatology 46 (2007) 620–627 627
[26] Waked IA, Saleh SM, Moustafa MS, Raouf AA, Thomas DL,Strickland GT. High prevalence of hepatitis C in Egyptianpatients with chronic liver disease. Gut 1995;37:105–107.
[27] Strickland GT, Elhefni H, Salman T, Waked I, Abdel-Hamid M,Mikhail NN, et al. Role of hepatitis C infection in chronic liverdisease in Egypt. Am J Trop Med Hyg 2002;67:436–442.
[28] Perrillo RP. The role of liver biopsy in hepatitis C. Hepatology1997;26:57S–61S.
[29] Islam S, Antonsson L, Westin J, Lagging M. Cirrhosis in hepatitisC virus-infected patients can be excluded using an index ofstandard biochemical serum markers. Scand J Gastroenterol2005;40:867–872.
[30] Frank C, Mohamed MK, Strickland GT, Lavanchy D, ArthurRR, Magder LS, et al. The role of parenteral antischistosomaltherapy in the spread of hepatitis C virus in Egypt. Lancet2000;355:887–891.
[31] Nunes D, Fleming C, Offner G, O’Brien M, Tumilty S, Fix O,et al. HIV infection does not affect the performance of noninva-sive markers of fibrosis for the diagnosis of hepatitis C virus-
related liver disease. J Acquir Immune Defic Syndr2005;40:538–544.
[32] Kage M, Shimamatu K, Nakashima E, Kojiro M, Inoue O, YanoM. Long-term evolution of fibrosis from chronic hepatitis tocirrhosis in patients with hepatitis C: morphometric analysis ofrepeated biopsies. Hepatology 1997;25:1028–1031.
[33] Ghany MG, Kleiner DE, Alter H, Doo E, Khokar F, Promrat K,et al. Progression of fibrosis in chronic hepatitis C. Gastroenter-ology 2003;124:97–104.
[34] Lonardo A, Loria P, Adinolfi LE, Carulli N, Ruggiero G. HepatitisC and steatosis: a reappraisal. J Viral Hepat 2006;13:73–80.
[35] Serfaty L, Poujol-Robert A, Carbonell N, Chazouilleres O,Poupon RE, Poupon R. Effect of the interaction between steatosisand alcohol intake on liver fibrosis progression in chronic hepatitisC. Am J Gastroenterol 2002;97:1807–1812.
[36] Poynard T, Ratziu V, McHutchison J, Manns M, Goodman Z,Zeuzem S, et al. Effect of treatment with peginterferon orinterferon alfa-2b and ribavirin on steatosis in patients infectedwith hepatitis C. Hepatology 2003;38:75–85.