Evaluation of Pathologists (Histopathology) and Radiologists (Cone Beam Computed Tomography)...
6
Evaluation of Pathologists (Histopathology) and Radiologists (Cone Beam Computed Tomography) Differentiating Radicular Cysts from Granulomas Paul A. Rosenberg, DDS, Jared Frisbie, DDS, Jaehoon Lee, DDS, Kyung Lee, DS, Herbert Frommer, DDS, Shailesh Kottal, DDS, Joan Phelan, DDS, Louis Lin, BDS, DMD, PhD, and Gene Fisch, PhD Abstract Introduction: This study investigated the differentiation of radicular cysts from granulomas. Cone beam computed tomography (CBCT) imaging was compared with the ex- isting standard, biopsy and histopathology. Methods: Forty-five patients scheduled for an apicoectomy received a CBCT scan of the involved arch. Two oral and maxillofacial radiologists, working independently and using the same criteria, categorized the CBCT images as one of the following: cyst, likely cyst, likely granuloma, granuloma, or other. After apicoectomies, two oral pathologists, working independently and using the same criteria, diagnosed the surgical specimens as one of the following: radicular cyst, granuloma, or other. We examined the following: (1) interrater agreement between pathologists as to the biopsy diagnosis, (2) in- terrater agreement between radiologists as to the CBCT diagnosis, and (3) accuracy of radiologists’ diagnostic assessments using histopathology as the standard. Results: Findings showed strong interrater reliability between pathologists (k = 0.79, z = 5.46, p < 0.0001) and weak interrater reliability between radiologists (k = 0.14, p = not significant). Accuracy (true-positives plus true-negatives) for the two radiologists was 51% and 63%. Conclusion: Under the conditions of this study, based on the inconsistency of the radiologists’ reports as evidenced by statistical analyses, it was concluded that CBCT imaging is not a reliable diagnostic method for differentiating radicular cysts from granulomas. Surgical biopsy and histopathological evaluation remain the standard procedure for differentiating radicular cysts from granulomas. (J Endod 2010;36:423–428) Key Words Cone beam computed tomography, differentiating lesions, granuloma, radicular cyst T here is no accepted preoperative, nonsurgical method for determining whether a radicular lesion is a cyst or a granuloma. Therefore, there are no outcome studies evaluating the response of radicular cysts to nonsurgical root canal therapy. Biopsy with subsequent histopathological evaluation is the gold standard for identifying a periapical cyst (1–3). Until a reliable preoperative diagnostic method is found, the debate will continue concerning the likelihood of cysts healing after nonsurgical root canal therapy. Previous noninvasive diagnostic attempts such as evaluating periapical radio- graphs (2), contrast media (4), and Papanicolou smears (5) have all been shown to be unreliable. An attempt has been made to use electrophoresis in the differentiation. One study used aspirates of the root canal fluids from 40 teeth and concluded that elec- trophoretic patterns in albumin and globulin may be used for differentiation, but this work has not been reproduced (6). More recently, a study including 12 apical lesions found ultrasound with power Doppler flowmetry to be an accurate nonsurgical method for differentiation and should be further evaluated with a larger sample size (7). Cone beam computed tomography (CBCT) scan has been proposed as a preoper- ative, nonsurgical method for determining the presence of a cyst or a granuloma by measuring ‘‘grayscale value’’ readings on digitized CBCT images (1). In a previous study, 17 periapical radiolucencies were evaluated (with size equal to or greater than 1 cm  1 cm radiographically), and then ‘‘grayscale values’’ were used to interpret CBCT images that distinguished ‘‘solid soft-tissue lesions’’ (suggestive of a granuloma) from those with a lumen (suggestive of a cyst). Their results showed concurrent diag- noses between histopathology and CBCT in 13 of 17 (76%) cases, and it was concluded that ‘‘the CBCT scan may provide a better, more accurate, faster method to differentially diagnosis a solid from a fluid filled lesion.’’ The present study examined an alternative approach to the issue of differentiating cysts from granulomas. Two oral and maxillofacial radiologists independently analyzed CBCT images using the same set of established radiographic criteria (Table 1). Radio- graphic diagnoses were then compared with biopsy reports of 2 oral pathologists who independently evaluated biopsy specimens using the same set of established pathologic criteria (Table 2). The radiologists’ and pathologists’ findings were correlated using receiver operating characteristic (ROC) analysis. In addition, our study modified the previous approach (1) with an increased sample size and the inclusion of smaller peri- apical radiolucencies. CBCT scans have potential in endodontic diagnosis and treatment planning. Our study evaluated its capability for differentiating granulomas from periapical cysts. In From the New York University College of Dentistry, New York, NY, USA. Address requests for reprints to Dr Paul A. Rosenberg, Department of Endodontics, New York University College of Dentistry, 345 East 24th Street, New York, NY 10010-4086. E-mail address: [email protected]. 0099-2399/$0 - see front matter ª 2010 Published by Elsevier Inc. on behalf of American Association of Endodontists. doi:10.1016/j.joen.2009.11.005 Clinical Research JOE — Volume 36, Number 3, March 2010 Histopathology versus CBCT for Differentiating Radicular Cysts from Granulomas 423
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Evaluation of Pathologists (Histopathology) and Radiologists (Cone Beam Computed Tomography)...
Clinical Research
Evaluation of Pathologists (Histopathology) and Radiologists(Cone Beam Computed Tomography) DifferentiatingRadicular Cysts from GranulomasPaul A. Rosenberg, DDS, Jared Frisbie, DDS, Jaehoon Lee, DDS, Kyung Lee, DS,Herbert Frommer, DDS, Shailesh Kottal, DDS, Joan Phelan, DDS, Louis Lin, BDS, DMD, PhD,and Gene Fisch, PhD
Abstract
Introduction: This study investigated the differentiationof radicular cysts from granulomas. Cone beam computedtomography (CBCT) imaging was compared with the ex-isting standard, biopsy and histopathology. Methods:Forty-five patients scheduled for an apicoectomyreceived a CBCT scan of the involved arch. Two oraland maxillofacial radiologists, working independentlyand using the same criteria, categorized the CBCTimages as one of the following: cyst, likely cyst, likelygranuloma, granuloma, or other. After apicoectomies,two oral pathologists, working independently and usingthe same criteria, diagnosed the surgical specimens asone of the following: radicular cyst, granuloma, or other.We examined the following: (1) interrater agreementbetween pathologists as to the biopsy diagnosis, (2) in-terrater agreement between radiologists as to the CBCTdiagnosis, and (3) accuracy of radiologists’ diagnosticassessments using histopathology as the standard.Results: Findings showed strong interrater reliabilitybetween pathologists (k = 0.79, z = 5.46, p < 0.0001)and weak interrater reliability between radiologists (k =0.14, p = not significant). Accuracy (true-positives plustrue-negatives) for the two radiologists was 51% and63%. Conclusion: Under the conditions of this study,based on the inconsistency of the radiologists’ reportsas evidenced by statistical analyses, it was concludedthat CBCT imaging is not a reliable diagnostic methodfor differentiating radicular cysts from granulomas.Surgical biopsy and histopathological evaluation remainthe standard procedure for differentiating radicular cystsfrom granulomas. (J Endod 2010;36:423–428)Key WordsCone beam computed tomography, differentiatinglesions, granuloma, radicular cyst
From the New York University College of Dentistry, New York,Address requests for reprints to Dr Paul A. Rosenberg, Departm
10010-4086. E-mail address: [email protected]/$0 - see front matter
ª 2010 Published by Elsevier Inc. on behalf of American Assocdoi:10.1016/j.joen.2009.11.005
JOE — Volume 36, Number 3, March 2010
There is no accepted preoperative, nonsurgical method for determining whethera radicular lesion is a cyst or a granuloma. Therefore, there are no outcome studies
evaluating the response of radicular cysts to nonsurgical root canal therapy. Biopsy withsubsequent histopathological evaluation is the gold standard for identifying a periapicalcyst (1–3). Until a reliable preoperative diagnostic method is found, the debate willcontinue concerning the likelihood of cysts healing after nonsurgical root canal therapy.
Previous noninvasive diagnostic attempts such as evaluating periapical radio-graphs (2), contrast media (4), and Papanicolou smears (5) have all been shownto be unreliable. An attempt has been made to use electrophoresis in the differentiation.One study used aspirates of the root canal fluids from 40 teeth and concluded that elec-trophoretic patterns in albumin and globulin may be used for differentiation, but thiswork has not been reproduced (6). More recently, a study including 12 apical lesionsfound ultrasound with power Doppler flowmetry to be an accurate nonsurgical methodfor differentiation and should be further evaluated with a larger sample size (7).
Cone beam computed tomography (CBCT) scan has been proposed as a preoper-ative, nonsurgical method for determining the presence of a cyst or a granuloma bymeasuring ‘‘grayscale value’’ readings on digitized CBCT images (1). In a previousstudy, 17 periapical radiolucencies were evaluated (with size equal to or greaterthan 1 cm� 1 cm radiographically), and then ‘‘grayscale values’’ were used to interpretCBCT images that distinguished ‘‘solid soft-tissue lesions’’ (suggestive of a granuloma)from those with a lumen (suggestive of a cyst). Their results showed concurrent diag-noses between histopathology and CBCT in 13 of 17 (76%) cases, and it was concludedthat ‘‘the CBCT scan may provide a better, more accurate, faster method to differentiallydiagnosis a solid from a fluid filled lesion.’’
The present study examined an alternative approach to the issue of differentiatingcysts from granulomas. Two oral and maxillofacial radiologists independently analyzedCBCT images using the same set of established radiographic criteria (Table 1). Radio-graphic diagnoses were then compared with biopsy reports of 2 oral pathologists whoindependently evaluated biopsy specimens using the same set of established pathologiccriteria (Table 2). The radiologists’ and pathologists’ findings were correlated usingreceiver operating characteristic (ROC) analysis. In addition, our study modified theprevious approach (1) with an increased sample size and the inclusion of smaller peri-apical radiolucencies.
CBCT scans have potential in endodontic diagnosis and treatment planning. Ourstudy evaluated its capability for differentiating granulomas from periapical cysts. In
NY, USA.ent of Endodontics, New York University College of Dentistry, 345 East 24th Street, New York, NY
iation of Endodontists.
Histopathology versus CBCT for Differentiating Radicular Cysts from Granulomas 423

TABLE 1. Criteria Used by Radiologists to Evaluate and Diagnose ApicalRadiolucencies
CystWell-defined corticated border with uniform bordersResorption of adjacent tooth rootsDefinite round or oval ‘‘ballooning appearance’’ with an
even expansion of the lesionUniformly radiolucent lumenPerforation of cortical plateDisplacement of adjacent structuresSize greater than 20-mm diameterDisplacement of adjacent tooth rootsMultiple teeth involved periapicallyAssociated with the apex of involved toothFound in maxilla, especially incisors and canines
Likely cystBorder mostly well defined with some areas undefinedMostly circular but not so well-corticated bordersSlight ‘‘ballooning appearance’’ with mostly even expansion
of the lesionMostly radiolucent lumen with some small particulate
radiopacities or internal septaNear perforation of thinning cortical platePossible perforation of cortical plates
Likely granulomaMostly ill-defined noncorticated periphery with some areas
clearly definedLesion centered around region of tooth root other than apexNo perforation of cortical plate
GranulomaIll-defined peripheryLesion starts within apical portion of PDL spaceThe center of the lesion is found at the apex of involved
toothProgressive increase in radiopacity, moving from lumen to
surrounding normal trabecular patternNo perforation of cortical plateNo displacement of adjacent structuresNo resorption of involved teethApical lamina dura lostGradual widening of periodontal membrane space towards
apexOther
Unable to categorize based on presented criteriaFits nonodontogenic diagnosis (lateral periodontal cyst,
ameloblastoma, combination of different lesions, and so on)Has evenly mixed properties of cyst and granuloma
Clinical Research
addition, we added a further analysis comparing interradiologist andinterpathologist reports to assess the reliability of diagnoses fromCBCT images and surgical specimens.
Materials and MethodsForty-five patients referred to New York University College of
Dentistry’s Department of Endodontics and treatment planned forendodontic surgery between February and August 2008 were eligible
TABLE 2. Criteria Used by Pathologists to Evaluate and Diagnose Surgical Specime
Radicular cystTissue composed of fibrous connective tissue and/or granulation t
a combination of both exhibiting either evidence of an epitheliNoncystic inflammatory tissue (granuloma)
Tissue composed of fibrous connective tissue and/or granulation ta combination of both with no evidence of an epithelial lining
OtherTissue composed of only fibrous connective tissue, with no evidenc
epithelial lining (‘apical scar’)An insufficient surgical specimen to make a diagnosis (less than 2Tissue unable to be typed into one of the two above categories
424 Rosenberg et al.
to participate in the study. Inclusion criteria were patients witha minimum age of 18 and a minimum average diameter of the periapicallesion of 5 mm. Exclusion criteria were lesions associated with teethconsidered to have a poor prognosis and any patient classified AmericanSociety of Anesthesiologists III or higher. The protocol was approved bythe New York University Institutional Review Board (#07-390).
Two senior endodontic faculty members were trained in themeasurement of periapical radiolucencies using preoperative periapi-cal radiographs as described by Halse and Molven (8). Twenty deiden-tified, randomly sorted periapical radiographs were used duringcalibration until interexaminer reliability reached a Cohen kappastatistic (9) value of 0.8 (strong agreement) (10). To obtain reproduc-ibility, examiners were tested twice at a 1-month interval, and k wascomputed again in order to determine that the kappa statistic valueof 0.8 had been maintained.
The standard paralleling technique as described by Fava and Dum-mer (11) was used to obtain initial intraoral periapical radiographs. Astandard metric ruler was used with a view box for the measurement ofthe periapical radiolucency. The size of each radiolucency was deter-mined by taking the average of the lesion’s largest dimension and itsextent in the direction perpendicular to the largest dimension (12).After viewing the periapical radiograph independently, each facultyreviewer determined if the lesion was eligible for the study. Only thesamples accepted by both reviewers were used for the study.
After a preliminary clinical and radiographic examination by twosenior endodontic faculty members, the approved subjects receiveda CBCT scan (maxilla, mandible, or both). Before each scan, the unitwas calibrated as per manufacturer’s instructions. The i-CAT CBCTunit (Imaging Sciences International, Inc, Hatfield, PA) was used inthe New York University College of Dentistry Division of Radiology forthis study. It was operated at 120 kVp and 3 to 8 mA. The setting for focalspot was 0.5 mm and the bit depth of the receptor was 14 bit (16,384shades of gray). The detector was a charge-coupled device panel. Allpatients were scanned with the following scanning parameters: 6-cmfield of view, 20 seconds, and 0.4-mm voxels.
Two oral and maxillofacial radiologists independently examinedthe CBCT images for each patient using the XORAN viewing software(Xoran Technologies, Inc, Ann Arbor, MI) under ideal viewing condi-tions. The radiologists independently evaluated CBCT images and wereallowed to manipulate the images using the fullest potential of the three-dimensional viewing software to maximize diagnostic accuracy. Usingthe same set of established criteria for diagnosis (Table 1), the radiol-ogists chose the best diagnosis (out of the five options) for each case.
Apical surgery was performed in the Department of Endodonticsby one of 12 senior residents and overseen by a faculty member.Surgical specimens were obtained as part of the apicoectomy proce-dure. The tissue was processed and stained with hematoxylin and eosin.At least six layers of each surgical specimen were examined. The tissuewas examined independently by two oral pathologists without knowl-edge of the clinical presentation of the patients, surgical observation
ns
issue infiltrated by acute or chronic inflammatory cells oral lining or a cystic lumen lined by epithelium
issue infiltrated by acute or chronic inflammatory cells oror a cystic lumen lined by epithelium
e of any chronic or acute inflammatory cells and no evidence of
mm in greatest diameter)
JOE — Volume 36, Number 3, March 2010
ROC Curve for Radiologist 1 with Pathologist 1
0
0.2
0.4
0.6
0.8
1
0 0.2 0.4 0.6 0.8 1
FP
TP
Radiologist 1 TP / FP rates compared to Pathologist 1 Report
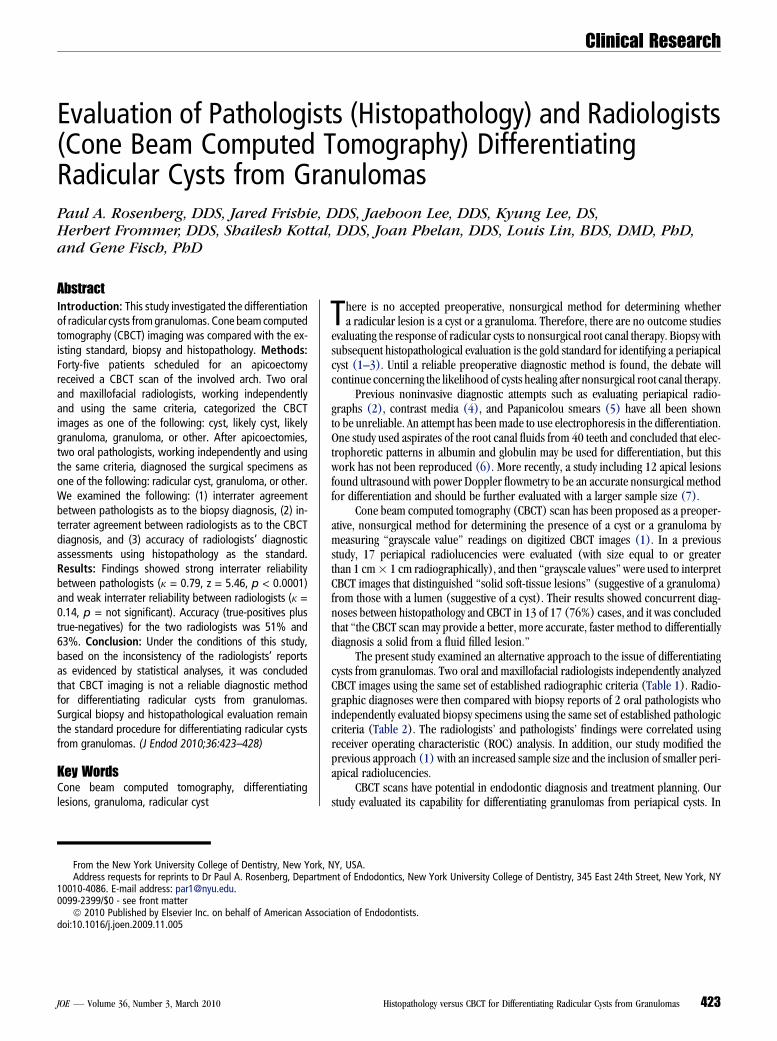
Criterion True Positive (TP) False Positive (FP)
Likely granuloma (likely not cyst)
0.9 0.58
Likely cyst 0.95 0.88 Cyst 0.95 1.0
Figure 1. ROC curve for radiologist 1. The area under the curve) as a propor-tion of the total areas represents the overall accuracy for radiologist 1. Thediagonal line represents chance (50%) accuracy.
ROC Curve for Radiologist 2 with Pathologist 1
0
0.2
0.4
0.6
0.8
1
0 0.2 0.4 0.6 0.8 1
FP
TP
Radiologist 2 TP / FP rates compared to Pathologist 1 Report
Criterion True Positive (TP) False Positive (FP)
Likely granuloma (likely not cyst)
0.14 0.19
Likely cyst 0.67 0.54 Cyst 1.0 0.92
Figure 2. ROC curve for radiologist 2. The area under the curve as a propor-tion of the total areas represents the overall accuracy for radiologist 1. Thediagonal line represents chance (50%) accuracy.
Clinical Research
of the lesions, or CBCT diagnoses. The pathologists were calibratedusing 10 surgical specimens; evaluation criteria are listed in Table 2.The examining oral pathologists independently determined whethertissue represented a radicular cyst or noncystic inflammatory tissue(granuloma) using the listed criteria (Table 2). The data were thencompared with the CBCT diagnoses.
ResultsThree separate analyses were performed: (1) interpathologist, (2)
interradiologist, and (3) radiologist diagnoses compared with thepathologist diagnoses. Fourteen of the 45 cases resulted in a coincidentdiagnosis of all four evaluators (pathologists and radiologists), whereasthe remaining 31 cases showed variance in their diagnoses.
To determine interrater reliability between the two radiologistsand also between the two pathologists, we calculated the Cohen kappa(k). Cohen kappa is a measure of the extent to which two (or more)raters agree on a number of categoric outcomes corrected for chanceagreement. Kappa values range from 0.0 (no agreement) to 1.0 (perfectagreement), with k $ 0.75 denoting excellent reliability (13).
Sensitivity and specificity were used to assess the diagnostic abilityof CBCT scans to differentiate cysts from granulomas. Sensitivity wascalculated as the proportion of true-positive test results (cysts with coin-cident diagnosis by CBCT and biopsy) given the subgroup of patients withthe ‘‘disease’’ (diagnosis of cyst as per biopsy). Specificity was calculatedas the proportion of true-negative results (granulomas with coincidentdiagnosis by CBCT scan and biopsy) in a subgroup of ‘‘disease-free’’subjects (diagnosis of granuloma as per biopsy) (14, 15).
To determine CBCT scan accuracy in diagnostic assessment, weused ROC analysis. In ROC analysis, there are four assessment
JOE — Volume 36, Number 3, March 2010 Histo
outcomes: true-positive, true-negative, false-positive, and false-negative.The assessment of sensitivity is the ability of a diagnostic instrument toidentify a lesion, in this instance, a cyst correctly compared with a ‘‘goldstandard’’(in this instance, the pathologist’s report). It is computed bycalculating the ratio of the true-positives, the number of lesions detectedby the diagnostic instrument, to the total number of lesions identified bythe gold standard. Specificity refers to the ability of a diagnostic instru-ment to detect the absence of a lesion, in this instance, a granulomawhen, in fact, the lesion is not present. It is computed by calculatingthe ratio of true-negatives, in this case, the number of granulomas, de-tected to the total number of granulomas identified by the pathologist.The ROC curve is constructed by plotting the false-positive rate (equal to1� specificity) along the abscissa against the true-positive rate on theordinate. The result is a sequence of paired points connected by linesegments that are plotted from the lowest left-hand corner (0.0, 0.0)to pairs of false-positive, true-positive values until it connects to theuppermost right-hand corner (1.0, 1.0). The area under that curveas a fraction of the total unit square represents the accuracy of the diag-nostic instrument (16). The diagonal line that runs from the lowest left-hand corner (0.0, 0.0) to the uppermost right-hand corner (1.0, 1.0)represents 50% or chance accuracy.
Results indicated that agreement between the two pathologists wasstrong (k = 0.79), and statistically was significantly different from noagreement (z = 5.46, p < 0.0001). However, there was weak agreementbetween radiologists (weighted k = 0.14, p = not significant). In diag-nostic assessment, ROC analysis is used to establish ‘‘sensitivity’’ (theproportion of true-positive cases diagnosed against some gold stan-dard) and ‘‘specificity’’ (the proportion of true-negative cases diag-nosed against some gold standard) with respect to distinct, orderedcriteria. In our study, the criteria were ordered as shown in Table 1,
pathology versus CBCT for Differentiating Radicular Cysts from Granulomas 425
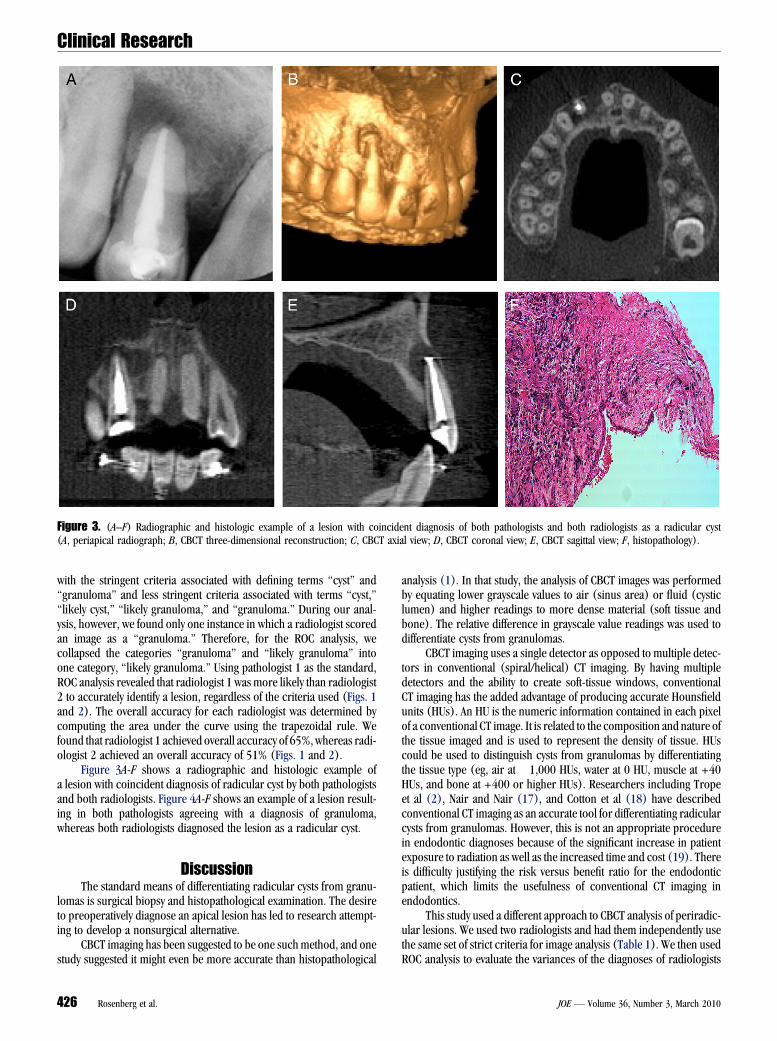
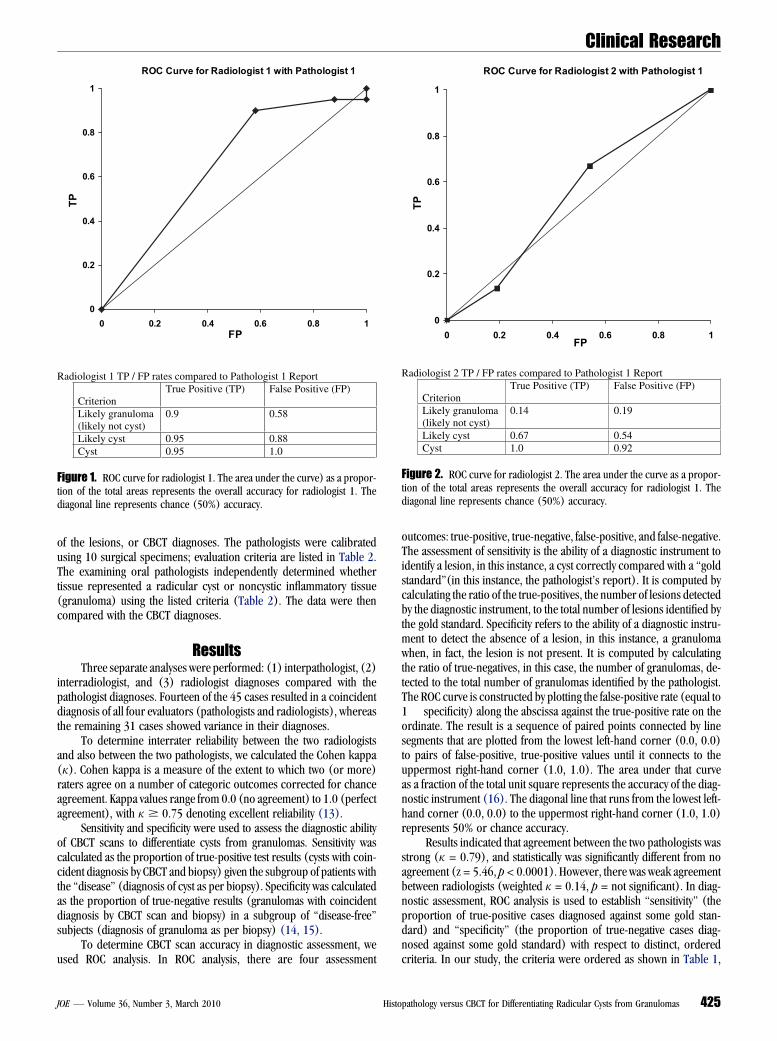
Figure 3. (A–F) Radiographic and histologic example of a lesion with coincident diagnosis of both pathologists and both radiologists as a radicular cyst(A, periapical radiograph; B, CBCT three-dimensional reconstruction; C, CBCT axial view; D, CBCT coronal view; E, CBCT sagittal view; F, histopathology).
Clinical Research
with the stringent criteria associated with defining terms ‘‘cyst’’ and‘‘granuloma’’ and less stringent criteria associated with terms ‘‘cyst,’’‘‘likely cyst,’’ ‘‘likely granuloma,’’ and ‘‘granuloma.’’ During our anal-ysis, however, we found only one instance in which a radiologist scoredan image as a ‘‘granuloma.’’ Therefore, for the ROC analysis, wecollapsed the categories ‘‘granuloma’’ and ‘‘likely granuloma’’ intoone category, ‘‘likely granuloma.’’ Using pathologist 1 as the standard,ROC analysis revealed that radiologist 1 was more likely than radiologist2 to accurately identify a lesion, regardless of the criteria used (Figs. 1and 2). The overall accuracy for each radiologist was determined bycomputing the area under the curve using the trapezoidal rule. Wefound that radiologist 1 achieved overall accuracy of 65%, whereas radi-ologist 2 achieved an overall accuracy of 51% (Figs. 1 and 2).
Figure 3A-F shows a radiographic and histologic example ofa lesion with coincident diagnosis of radicular cyst by both pathologistsand both radiologists. Figure 4A-F shows an example of a lesion result-ing in both pathologists agreeing with a diagnosis of granuloma,whereas both radiologists diagnosed the lesion as a radicular cyst.
DiscussionThe standard means of differentiating radicular cysts from granu-
lomas is surgical biopsy and histopathological examination. The desireto preoperatively diagnose an apical lesion has led to research attempt-ing to develop a nonsurgical alternative.
CBCT imaging has been suggested to be one such method, and onestudy suggested it might even be more accurate than histopathological
426 Rosenberg et al.
analysis (1). In that study, the analysis of CBCT images was performedby equating lower grayscale values to air (sinus area) or fluid (cysticlumen) and higher readings to more dense material (soft tissue andbone). The relative difference in grayscale value readings was used todifferentiate cysts from granulomas.
CBCT imaging uses a single detector as opposed to multiple detec-tors in conventional (spiral/helical) CT imaging. By having multipledetectors and the ability to create soft-tissue windows, conventionalCT imaging has the added advantage of producing accurate Hounsfieldunits (HUs). An HU is the numeric information contained in each pixelof a conventional CT image. It is related to the composition and nature ofthe tissue imaged and is used to represent the density of tissue. HUscould be used to distinguish cysts from granulomas by differentiatingthe tissue type (eg, air at �1,000 HUs, water at 0 HU, muscle at +40HUs, and bone at +400 or higher HUs). Researchers including Tropeet al (2), Nair and Nair (17), and Cotton et al (18) have describedconventional CT imaging as an accurate tool for differentiating radicularcysts from granulomas. However, this is not an appropriate procedurein endodontic diagnoses because of the significant increase in patientexposure to radiation as well as the increased time and cost (19). Thereis difficulty justifying the risk versus benefit ratio for the endodonticpatient, which limits the usefulness of conventional CT imaging inendodontics.
This study used a different approach to CBCT analysis of periradic-ular lesions. We used two radiologists and had them independently usethe same set of strict criteria for image analysis (Table 1). We then usedROC analysis to evaluate the variances of the diagnoses of radiologists
JOE — Volume 36, Number 3, March 2010
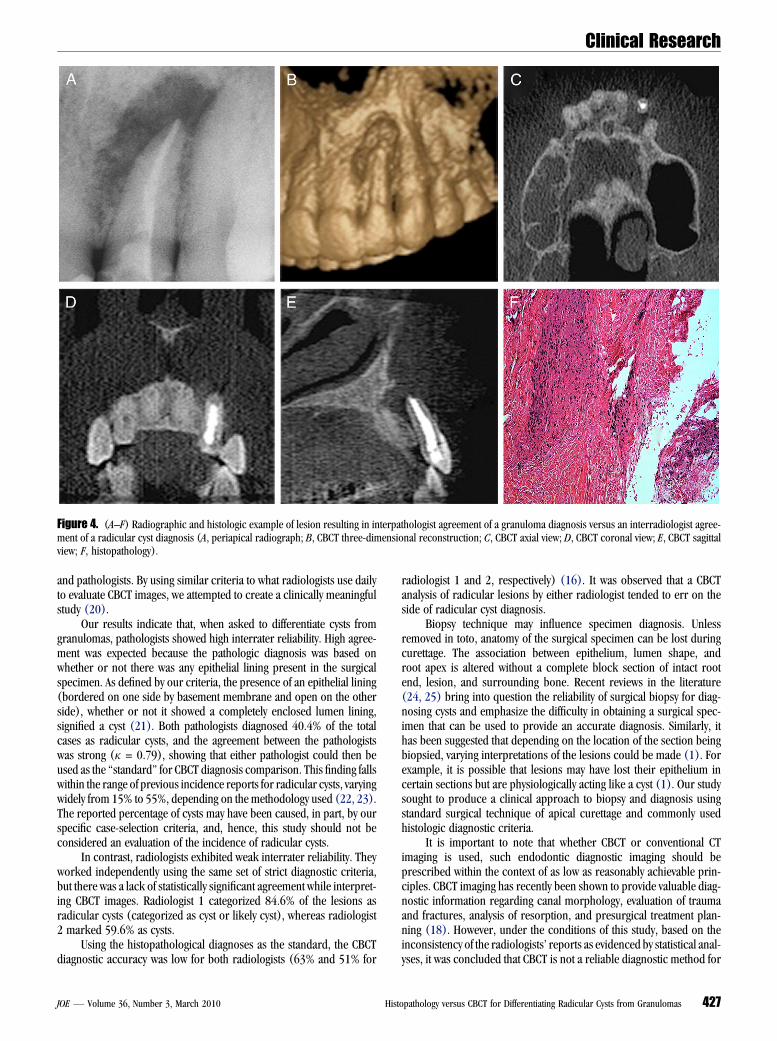
Figure 4. (A–F) Radiographic and histologic example of lesion resulting in interpathologist agreement of a granuloma diagnosis versus an interradiologist agree-ment of a radicular cyst diagnosis (A, periapical radiograph; B, CBCT three-dimensional reconstruction; C, CBCT axial view; D, CBCT coronal view; E, CBCT sagittalview; F, histopathology).
Clinical Research
and pathologists. By using similar criteria to what radiologists use dailyto evaluate CBCT images, we attempted to create a clinically meaningfulstudy (20).
Our results indicate that, when asked to differentiate cysts fromgranulomas, pathologists showed high interrater reliability. High agree-ment was expected because the pathologic diagnosis was based onwhether or not there was any epithelial lining present in the surgicalspecimen. As defined by our criteria, the presence of an epithelial lining(bordered on one side by basement membrane and open on the otherside), whether or not it showed a completely enclosed lumen lining,signified a cyst (21). Both pathologists diagnosed 40.4% of the totalcases as radicular cysts, and the agreement between the pathologistswas strong (k = 0.79), showing that either pathologist could then beused as the ‘‘standard’’ for CBCT diagnosis comparison. This finding fallswithin the range of previous incidence reports for radicular cysts, varyingwidely from 15% to 55%, depending on the methodology used (22, 23).The reported percentage of cysts may have been caused, in part, by ourspecific case-selection criteria, and, hence, this study should not beconsidered an evaluation of the incidence of radicular cysts.
In contrast, radiologists exhibited weak interrater reliability. Theyworked independently using the same set of strict diagnostic criteria,but there was a lack of statistically significant agreement while interpret-ing CBCT images. Radiologist 1 categorized 84.6% of the lesions asradicular cysts (categorized as cyst or likely cyst), whereas radiologist2 marked 59.6% as cysts.
Using the histopathological diagnoses as the standard, the CBCTdiagnostic accuracy was low for both radiologists (63% and 51% for
JOE — Volume 36, Number 3, March 2010 Hist
radiologist 1 and 2, respectively) (16). It was observed that a CBCTanalysis of radicular lesions by either radiologist tended to err on theside of radicular cyst diagnosis.
Biopsy technique may influence specimen diagnosis. Unlessremoved in toto, anatomy of the surgical specimen can be lost duringcurettage. The association between epithelium, lumen shape, androot apex is altered without a complete block section of intact rootend, lesion, and surrounding bone. Recent reviews in the literature(24, 25) bring into question the reliability of surgical biopsy for diag-nosing cysts and emphasize the difficulty in obtaining a surgical spec-imen that can be used to provide an accurate diagnosis. Similarly, ithas been suggested that depending on the location of the section beingbiopsied, varying interpretations of the lesions could be made (1). Forexample, it is possible that lesions may have lost their epithelium incertain sections but are physiologically acting like a cyst (1). Our studysought to produce a clinical approach to biopsy and diagnosis usingstandard surgical technique of apical curettage and commonly usedhistologic diagnostic criteria.
It is important to note that whether CBCT or conventional CTimaging is used, such endodontic diagnostic imaging should beprescribed within the context of as low as reasonably achievable prin-ciples. CBCT imaging has recently been shown to provide valuable diag-nostic information regarding canal morphology, evaluation of traumaand fractures, analysis of resorption, and presurgical treatment plan-ning (18). However, under the conditions of this study, based on theinconsistency of the radiologists’ reports as evidenced by statistical anal-yses, it was concluded that CBCT is not a reliable diagnostic method for
opathology versus CBCT for Differentiating Radicular Cysts from Granulomas 427

Clinical Research
differentiating radicular cysts from granulomas. Surgical biopsy andhistopathological evaluation remain the standard procedure for differ-entiating radicular cysts from granulomas.References1. Simon JH, Enciso R, Malfaz JM, et al. Differential diagnosis of large periapical
lesions using cone-beam computed tomography measurements and biopsy. J Endod2006;32:833–7.
2. Trope M, Pettigrew J, Petras J, et al. Differentiation of radicular cyst and granulomasusing computerized tomography. Endod Dent Traumatol 1989;5:69–72.
3. Huumonen S, Kvist T, Grondahl K, et al. Diagnostic value of computed tomographyin re-treatment of root fillings in maxillary molars. Int Endod J 2006;39:827–33.
4. Cunningham CJ, Penick EC. Use of a roentgenographic contrast medium in thedifferential diagnosis of periapical lesions. Oral Surg Oral Med Oral Pathol 1968;26:96–102.
5. Howell FV, De la Rosa VM. Cytologic evaluation of cystic lesions of the jaws: a newdiagnostic technique. J South Calif Dent Assoc 1968;36:161–6.
6. Morse DR, Patnik JW, Schacterle GR. Electrophoretic differentiation of radicularcysts and granulomas. Oral Surg Oral Med Oral Pathol 1973;35:249–64.
7. Aggarwal V, Logani A, Shah N. The evaluation of computed tomography scans and ultra-sounds in the differential diagnosis of periapical lesions. J Endod 2008;34:1312–5.
8. Halse A, Molven O. A strategy for the diagnosis of periapical pathosis. J Endod 1986;12:534–8.
9. Cohen J. A coefficient of agreement for nominal scales. Educational and Psycholog-ical Measurement 1960;20:37–46.
10. McGinn T, Wyer PC, Newman TB, et al. Tips for learners of evidence-based medicine:3. Measures of observer variability (kappa statistic). CMAJ 2004;171:1369–73.
11. Fava LR, Dummer PM. Periapical radiographic techniques during endodontic diag-nosis and treatment. Int Endod J 1997;30:250–61.
428 Rosenberg et al.
12. Sjogren U, Hagglund B, Sundqvist G, et al. Factors affecting the long-term results ofendodontic treatment. J Endod 1990;16:498–504.
13. Landis JR, Koch GG. The measurement of observer agreement for categorical data.Biometrics 1977;33:159–74.
14. Flahault A, Cadilhac M, Thomas G. Sample size calculation should be performed fordesign accuracy in diagnostic test studies. J Clin Epidemiol 2005;58:859–62.
15. Loong TW. Understanding sensitivity and specificity with the right side of the brain.BMJ 2003;327:716–9.
16. Hanley JA, McNeil BJ. A method of comparing the areas under the receiver operatingcharacteristic curves derived from the same cases. Radiology 1983;148:839–43.
17. Nair MK, Nair UP. Digital and advanced imaging in endodontics: a review. J Endod2007;33:1–6.
18. Cotton TP, Geisler TM, Holden DT, et al. Endodontic applications of cone-beamvolumetric tomography. J Endod 2007;33:1121–32.
19. Ludlow JB, Davies-Ludlow LE, Brooks SL, et al. Dosimetry of 3 CBCT devices for oraland maxillofacial radiology: CB Mercuray, NewTom 3G and i-CAT. DentomaxillofacRadiol 2006;35:219–26.
20. White SC, Pharoah MJ. Oral Radiology, Principles and Interpretation. 5th ed. St.Louis. CV Mosby. 2004.
21. Neville BW, Damm DD, Allen CM, et al. Oral and maxillofacial pathology. 2nd ed.Philadelphia. WB Saunders Co. 2002.
22. Ramachandran Nair PN, Pajarola G, Schroeder HE. Types and incidence of humanperiapical lesions obtained with extracted teeth. Oral Surg Oral Med Oral Pathol OralRadiol Endod 1996;81:93–102.
23. Nair PN. Pathogenesis of apical periodontitis and the causes of endodontic failures.Crit Rev Oral Biol Med 2004;15:348–81.
24. Lin LM, Ricucci D, Lin J, et al. Nonsurgical root canal therapy of large cyst-likeinflammatory periapical lesions and inflammatory apical cysts. J Endod 2009;35:607–15.
25. Lin LM. Proliferation of epithelial cell rests, formation of apical cysts, and regressionof apical cysts after periapical wound healing. J Endod 2007;33:908–16.
JOE — Volume 36, Number 3, March 2010