Esomeprazole: A Review of its Use in the Management of Acid-Related Disorders in the US
36
Esomeprazole A Review of its Use in the Management of Acid-Related Disorders Lesley J. Scott, Christopher J. Dunn, Gordon Mallarkey and Miriam Sharpe Adis International Limited, Auckland, New Zealand Various sections of the manuscript reviewed by: S. Banks, Division of Gastroenterology, Long Island Jewish Medical Center, New York, New York, USA; P. Bytzer, Department of Medicine, Division of Gastroenterology, Glostrup University Hospital, Glostrup, Denmark; C. Florent, Service de Gastro-Enterologie, Hopital Saint-Antoine, Paris, France; L. Lundell, Department of Surgery, University Gothenburg, Sahlgrenska University Hospital, Gothenburg, Sweden; T.C.K. Tham, The Ulster Hospital, Belfast, Northern Ireland; A.B.R. Thomson, Division of Gastroenterology, University of Alberta, Edmonton, Alberta, Canada; G.N.J. Tytgat, Academic Medical Centre, Department of Gastroenterology and Hepatology, University of Amsterdam, Amsterdam, The Netherlands. Contents Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1504 1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1511 2. Pharmacodynamic Properties . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1511 2.1 Mechanism of Action . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1511 2.2 Antisecretory Activity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1512 2.3 Other Effects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1514 3. Pharmacokinetic Properties . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1514 3.1 Healthy Volunteers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1514 3.2 Patients with Gastro-Oesophageal Reflux Disease (GORD) . . . . . . . . . . . . . . . . . . . . 1515 3.3 Special Populations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1516 3.4 Drug Interactions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1516 4. Clinical Efficacy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1517 4.1 GORD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1517 4.1.1 Patients with Erosive Oesophagitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1517 4.1.2 Patients with Symptomatic GORD without Oesophagitis . . . . . . . . . . . . . . . . . . 1522 4.2 Eradication of Helicobacter pylori Infection . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1523 4.2.1 Eradication Rates . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1524 ADIS DRUG EVALUATION Drugs 2002; 62 (10): 1503-1538 0012-6667/02/0010-1503/$30.00/0 © Adis International Limited. All rights reserved. Data Selection Sources: Medical literature published in any language since 1980 on esomeprazole, identified using Medline and EMBASE, supplemented by AdisBase (a proprietary database of Adis International). Additional references were identified from the reference lists of published articles. Bibliographical information, including contributory unpublished data, was also requested from the company developing the drug. Search strategy: Medline search terms were ‘esomeprazole’ or ‘perprazole’ or ‘s-omeprazole. EMBASE search terms were ‘esomeprazole’ or ‘perprazole’. AdisBase search terms were ‘esomeprazole’ or ‘perprazole’ or ‘s-omeprazole’. Searches were last updated 10 Jun 2002. Selection: Studies in patients with gastro-oesophageal reflux disease and Helicobacter pylori infection who received esomeprazole. Inclusion of studies was based mainly on the methods section of the trials. When available, large, well controlled trials with appropriate statistical methodology were preferred. Relevant pharmacodynamic and pharmacokinetic data are also included. Index terms: esomeprazole, proton pump inhibitor, peptic ulcer disease, duodenal ulcer, gastric ulcer, Helicobacter pylori, gastro-oesophageal reflux disease, acid-related dyspepsia, pharmacodynamics, pharmacokinetics, therapeutic use.
Transcript of Esomeprazole: A Review of its Use in the Management of Acid-Related Disorders in the US

EsomeprazoleA Review of its Use in the Management of Acid-Related Disorders
Lesley J. Scott, Christopher J. Dunn, Gordon Mallarkey and Miriam SharpeAdis International Limited, Auckland, New Zealand
Various sections of the manuscript reviewed by:S. Banks, Division of Gastroenterology, Long Island Jewish Medical Center, New York, New York, USA;P. Bytzer, Department of Medicine, Division of Gastroenterology, Glostrup University Hospital, Glostrup,Denmark; C. Florent, Service de Gastro-Enterologie, Hopital Saint-Antoine, Paris, France; L. Lundell,Department of Surgery, University Gothenburg, Sahlgrenska University Hospital, Gothenburg, Sweden;T.C.K. Tham, The Ulster Hospital, Belfast, Northern Ireland; A.B.R. Thomson, Division of Gastroenterology,University of Alberta, Edmonton, Alberta, Canada; G.N.J. Tytgat, Academic Medical Centre, Departmentof Gastroenterology and Hepatology, University of Amsterdam, Amsterdam, The Netherlands.
Contents
Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15041. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15112. Pharmacodynamic Properties . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1511
2.1 Mechanism of Action . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15112.2 Antisecretory Activity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15122.3 Other Effects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1514
3. Pharmacokinetic Properties . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15143.1 Healthy Volunteers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15143.2 Patients with Gastro-Oesophageal Reflux Disease (GORD) . . . . . . . . . . . . . . . . . . . . 15153.3 Special Populations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15163.4 Drug Interactions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1516
4. Clinical Efficacy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15174.1 GORD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1517
4.1.1 Patients with Erosive Oesophagitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15174.1.2 Patients with Symptomatic GORD without Oesophagitis . . . . . . . . . . . . . . . . . . 1522
4.2 Eradication of Helicobacter pylori Infection . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15234.2.1 Eradication Rates . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1524
ADIS DRUG EVALUATION Drugs 2002; 62 (10): 1503-15380012-6667/02/0010-1503/$30.00/0
© Adis International Limited. All rights reserved.
Data Selection
Sources: Medical literature published in any language since 1980 on esomeprazole, identified using Medline and EMBASE,supplemented by AdisBase (a proprietary database of Adis International). Additional references were identified from the reference lists ofpublished articles. Bibliographical information, including contributory unpublished data, was also requested from the company developingthe drug.
Search strategy: Medline search terms were ‘esomeprazole’ or ‘perprazole’ or ‘s-omeprazole. EMBASE search terms were‘esomeprazole’ or ‘perprazole’. AdisBase search terms were ‘esomeprazole’ or ‘perprazole’ or ‘s-omeprazole’. Searches were lastupdated 10 Jun 2002.
Selection: Studies in patients with gastro-oesophageal reflux disease and Helicobacter pylori infection who received esomeprazole.Inclusion of studies was based mainly on the methods section of the trials. When available, large, well controlled trials with appropriatestatistical methodology were preferred. Relevant pharmacodynamic and pharmacokinetic data are also included.
Index terms: esomeprazole, proton pump inhibitor, peptic ulcer disease, duodenal ulcer, gastric ulcer, Helicobacter pylori,gastro-oesophageal reflux disease, acid-related dyspepsia, pharmacodynamics, pharmacokinetics, therapeutic use.

4.2.2 Effects on Ulcer Healing and Symptom Resolution . . . . . . . . . . . . . . . . . . . . . . 15254.3 Pharmacoeconomic Considerations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1526
4.3.1 Reflux Oesophagitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15264.3.2 Symptomatic GORD without Endoscopic Confirmation . . . . . . . . . . . . . . . . . . 15264.3.3 On-Demand Treatment of GORD without Oesophagitis . . . . . . . . . . . . . . . . . . 1526
5. Tolerability . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15275.1 Healing and/or Symptom Resolution Therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . 15275.2 Maintenance Therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1528
6. Dosage and Administration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15297. Place of Esomeprazole in the Management of Acid-Related Disorders . . . . . . . . . . . . . . . 1530
7.1 GORD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15317.2 Eradication of H. pylori Infection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15337.3 Tolerability . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15347.4 Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1535
SummaryAbstract Esomeprazole (S-isomer of omeprazole), the first single optical isomer proton
pump inhibitor, generally provides better acid control than current racemic protonpump inhibitors and has a favourable pharmacokinetic profile relative to om-eprazole.
In a large well designed 8-week trial in patients (n >5000) with erosive oeso-phagitis, esomeprazole recipients achieved significantly higher rates of endo-scopically confirmed healed oesophagitis than those receiving lansoprazole.Respective healed oesophagitis rates with once-daily esomeprazole 40mg orlansoprazole 30mg were 92.6 and 88.8%. Overall, esomeprazole was also betterthan omeprazole, although these differences were not always statistically signif-icance. Ninety-two to 94% of esomeprazole recipients (40mg once daily)achieved healed oesophagitis versus 84 to 90% of omeprazole recipients (20mgonce daily). Esomeprazole was effective across all baseline grades of oesophag-itis; notably, relative to lansoprazole, as baseline severity of disease increased,the difference in rates of healed oesophagitis also increased in favour of esome-prazole. Resolution of heartburn was also significantly better with esomeprazole40mg than with these racemic proton pump inhibitors. Long-term (up to 12months) therapy with esomeprazole effectively maintained healing in these pa-tients.
Once-daily esomeprazole 20 or 40mg for 4 weeks resolved symptoms in pa-tients with symptomatic gastro-oesophageal reflux disease (GORD) withoutoesophagitis. Symptoms were effectively managed in the long-term with symp-tom-driven on-demand esomeprazole (20 or 40mg once daily) .
Eradicating Helicobacter pylori infection is considered pivotal to successfullymanaging duodenal ulcer disease. Seven days’ treatment (twice-daily esome-prazole 20mg plus amoxicillin 1g and clarithromycin 500mg) eradicated H. pyloriin ≥86% of patients (intention-to-treat), a rate that was similar to equivalentomeprazole-based regimens.
Esomeprazole is generally well tolerated, both as monotherapy and in combi-nation with antimicrobial agents, with a tolerability profile similar to that of otherproton pump inhibitors. Few patients discontinued therapy because of treatment-emergent adverse events (<3% of patients), with very few (<1%) drug-relatedserious adverse events reported.
1504 Scott et al.
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

Conclusions: Esomeprazole is an effective, well tolerated treatment for man-aging GORD and for eradicating H. pylori infection in patients with duodenalulcer disease. In 8-week double-blind trials, esomeprazole healed oesophagitisand resolved symptoms in patients with endoscopically confirmed erosive oeso-phagitis and overall, provided better efficacy than omeprazole. Notably, in a large(n >5000 patients) double-blind trial, esomeprazole 40mg provided significantlybetter efficacy than lansoprazole in terms of healing rates and resolution of symp-toms. Long-term therapy with esomeprazole maintained healed oesophagitis inthese patients. Esomeprazole also proved beneficial in patients with symptomaticGORD without oesophagitis. Thus, esomeprazole has emerged as an option forfirst-line therapy in the management of acid-related disorders.
PharmacodynamicProperties
Esomeprazole inhibits the activity of the H+/K+-ATPase enzyme (the protonpump), and thereby reduces secretion of hydrochloric acid by gastric parietalcells.
Superiority of esomeprazole 40mg daily over omeprazole, lansoprazole,rabeprazole and pantoprazole in terms of elevation of intragastric pH has beenshown in a number of randomised, crossover trials (most of which were nonblind)in healthy volunteers and patients with symptoms of gastro-oesophageal refluxdisease (GORD). On the fifth day of treatment intragastric pH was >4 for a mean59.4 to 69.8% of the monitored 24-hour periods in individuals receivingesomeprazole 40mg daily. These percentages were significantly greater thanthose with comparators (43.7 to 62% for esomeprazole 20mg, omeprazole 20 or40mg, rabeprazole 20mg, pantoprazole 40mg, lansoprazole 30mg daily). Simi-larly, esomeprazole 20mg daily was superior to omeprazole 20mg or lansoprazole15mg daily in the maintenance of intragastric pH >4. Higher percentages ofpatients receiving esomeprazole 20 or 40mg compared with recipients of otheragents maintained intragastric pH >4 for periods ranging from at least 8 hours tomore than 16 hours. In one nonblind study in 35 patients with GORD receivingesomeprazole 40mg or rabeprazole 20mg daily, pH was >4 for 23.2 and 11%,respectively, of the first 4 hours after administration of the first dose of studymedication, indicating a more rapid onset of reduction of intragastric pH withesomeprazole.
Esomeprazole has no apparent effect on a variety of endocrine and metabolicfunctions, but the drug increases fasting serum gastrin levels in a dose-relatedfashion.
Pharmacokinetic Profile Esomeprazole is absorbed rapidly after oral administration, with areas under theplasma concentration-time curves (AUCs) increasing in a nonlinear dose-relatedfashion after single doses. Systemic exposure to esomeprazole [as shown by meanAUC extrapolated to infinity (AUC∞)] increases with repeated administration ofthe drug (by 90% with 20mg daily and 159% with 40mg daily relative to day 1after 5 day’s treatment in healthy volunteers). This effect is attributed to reduc-tions in total body clearance and first-pass metabolism with repeated doses. Bind-ing to plasma proteins of esomeprazole (97%) is similar to that seen withomeprazole and other proton pump inhibitors.
Metabolism of esomeprazole is via hepatic cytochrome P450 (CYP) isoen-zymes, chiefly CYP3A4 and CYP2C19, with approximately 80% of each dosebeing excreted as metabolites in the urine. A small proportion of the populationlacks a functional form of the CYP2C19 isoenzyme and are therefore poor me-
Esomeprazole: A Review 1505
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

tabolisers of esomeprazole. AUC data indicate that dosage adjustments are notnecessary in these individuals.
Comparative pharmacokinetic data obtained in patients with GORD showsimilar times to attainment of peak plasma concentrations with esomeprazole andomeprazole (approximately 1 hour). However, after 5 days’ treatment, the geo-metric mean AUC∞ for esomeprazole 20mg was approximately two times higherthan that for omeprazole 20mg daily, whereas that for esomeprazole 40mg dailywas over five times higher than omeprazole 20mg (p < 0.0001 for both differ-ences) in a study in 36 evaluable patients. There was also less interpatient vari-ability in AUC∞ values with esomeprazole than with omeprazole, althoughstatistical significance was not stated for this finding.
Systemic exposure to esomeprazole is not increased sufficiently to warranttolerability concerns in patients with mild to moderate hepatic insufficiency;maximum plasma concentrations increased 28% in 12 patients with mild (Child-Pugh class A) to severe (Child-Pugh class C) hepatic insufficiency. There are noclinically significant gender effects on the drug’s disposition. The potential forinteractions between esomeprazole and other drugs is reported to be low andsimilar to that with omeprazole.
Clinical Efficacy In patients with erosive GORD: In randomised, double-blind, multicentre trialsof 8 weeks’ duration (the usual duration of these trials), esomeprazole effectivelyhealed oesophagitis (primary efficacy endpoint) and resolved heartburn (second-ary endpoint) in patients with GORD. Patients received oral esomeprazole 20 or40mg, lansoprazole 30mg or omeprazole 20mg once daily before breakfast. Pa-tients who showed endoscopically confirmed healed oesophagitis were discon-tinued from studies at 4 weeks.
Overall, esomeprazole was better than omeprazole in terms of endoscopicallyconfirmed healed oesophagitis and resolution of symptoms, although these dif-ferences favouring esomeprazole were not always statistically significant. Nota-bly, in a large (n >5000 patients) well designed trial, significantly more recipientsof esomeprazole 40mg once daily than lansoprazole 30mg once daily showedhealed oesophagitis at 8 weeks (92.6 vs 88.8% of patients; p < 0.001). Similarly,92 to 94% of esomeprazole (40mg once daily) recipients achieved healed oeso-phagitis at 8 weeks compared with 84 to 90% of those receiving omeprazole 20mgdaily. Of these double-blind trials, one evaluated both esomeprazole 20mg and40mg; a significantly higher percentage of patients achieved healed oesophagitisin both the esomeprazole 20 (89.9% of patients; p < 0.05 vs omeprazole) and40mg (94.1%; p < 0.001 vs omeprazole) groups than in the omeprazole 20mggroup (86.9%). Evidence-based analysis using pooled data from two trials con-firmed that esomeprazole was more effective than omeprazole in healing erosiveoesophagitis; 11 patients would need to be treated with esomeprazole 40mg oncedaily rather than omeprazole 20mg once daily to prevent one treatment failure.
The higher response rates with esomeprazole treatment relative to omeprazoleoccurred across all baseline grades of disease severity (based on Los AngelesClassification grades). Furthermore, relative to lansoprazole, as the baseline se-verity of disease increased, the difference in rates of healed oesophagitis alsoincreased in favour of esomeprazole.
Esomeprazole also proved effective in patients with erosive oesophagitis ac-cording to secondary efficacy endpoints (e.g. percentage of heartburn-free daysand nights, and the time to sustained resolution of symptoms). Heartburn resolu-
1506 Scott et al.
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

tion with esomeprazole 40mg was significantly better than that of omeprazole forall secondary efficacy endpoints, with a significantly reduced time to completeresolution of symptoms. Furthermore, esomeprazole recipients experienced sig-nificantly more nights without heartburn relative to lansoprazole, (87.1 vs 85.8%of nights heartburn-free; p ≤ 0.05), with complete resolution of symptoms occur-ring sooner in the esomeprazole group (7 vs 8 days; p ≤ 0.01); there was nobetween-group difference in the number of days without heartburn.
Resolution of symptoms matched healed oesophagitis rates in a post-hoc anal-ysis of pooled data from 8-week randomised, double-blind trials evaluating 4877patients. After 4 weeks’ treatment with esomeprazole 40mg once daily, 83.4 and81% of recipients who had healed oesophagitis were asymptomatic for heartburnand acid regurgitation, respectively, compared with 75.4 and 71.6% of thosereceiving omeprazole 20mg once daily (p < 0.001 for both comparisons).
Maintenance therapy in patients with GORD: Esomeprazole 20 or 40mgonce daily was significantly more effective than placebo in maintaining healing,prolonging the time to recurrence of erosive oesophagitis in two 6-monthrandomised, double-blind, multicentre trials. Healed oesophagitis was main-tained in 79 and 93% (esomeprazole 20mg), 88 and 94% (esomeprazole 40mg),or 29% (placebo) of patients. Subgroup analyses indicated that maintenance ofhealing with esomeprazole treatment was not influenced by gender, age (≥65years vs <65 years of age), initial treatment during the healing phase, time tohealing in this phase (4 vs 8 weeks) or baseline severity of erosive oesophagitis.Similar results were reported in a noncomparative trial of 12 months’ duration.
Although there was no statistically significant difference in the percentage ofpatients who were heartburn-free at 6 months with esomeprazole and placebotreatment, this most likely reflects the fact that only patients with maintainedhealing remained in the study at 6 months.
A significantly higher percentage of esomeprazole (20mg once daily) thanlansoprazole (15mg once daily) recipients remained in remission (primary end-point) at 6 months in a large, randomised, double-blind trial (83 vs 74% of pa-tients; p < 0.001). Esomeprazole recipients showed higher rates of remissionacross all grades of baseline disease severity than lansoprazole-treated patients.Furthermore, significantly more esomeprazole than lansoprazole recipients wereasymptomatic at 6 months [heartburn-free (78 vs 71% of patients), acid regurgi-tation-free (81 vs 72%) and epigastric pain-free (80 vs 75%)].
In patients with symptomatic GORD without oesophagitis: Esomeprazole20 or 40mg once daily for 4 weeks effectively resolved symptoms in patients withsymptomatic GORD without oesophagitis in two randomised double-blind trials.Thirty-three to 42% of patients achieved complete resolution of heartburn (noheartburn during the final 7 days of the 4-week studies) with esomeprazole versus12 and 14% of placebo recipients. Additionally, 63 to 68% of days were heart-burn-free with esomeprazole (20 or 40mg once daily) therapy compared with 36and 46% with placebo. Respective median times to sustained resolution of heart-burn were also significantly shorter in patients receiving esomeprazole (12.1 to17.3 vs 20.8 and 22.3 days).
Symptom-driven on-demand therapy (esomeprazole 20 or 40mg once daily)was effective in the management of patients with symptomatic GORD withouterosive oesophagitis in two 6-month randomised, double-blind, multicentre stud-ies. Log-rank analysis indicated that the time to discontinuation because of un-
Esomeprazole: A Review 1507
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

willingness to continue therapy (primary endpoint) was appreciably longer inthose receiving esomeprazole 20 or 40mg than in placebo recipients (p < 0.0001all comparisons in both studies), with markedly fewer patients having discon-tinued treatment at study end in the esomeprazole than the placebo groups (8 to15% vs 42 and 52% of patients). The vast majority of patients in both treatmentgroups who discontinued treatment did so because of inadequate control of heart-burn.
Eradication of Helicobacter pylori infection: Seven to 10 days’ treatmentwith triple therapy regimens that included esomeprazole (20mg twice daily or40mg once daily) or omeprazole (20mg once daily), plus twice-daily amoxicillin1g and clarithromycin 500mg, effectively eradicated H. pylori infection in pa-tients with duodenal ulcer disease.
In over 400 patients with endoscopically confirmed duodenal ulcers, eradica-tion of H. pylori occurred in 86 to 90% of recipients of triple therapy regimensincluding esomeprazole 20mg twice daily for 7 days in two randomised, double-blind, multicentre trials. These eradication rates were similar to those achievedwith omeprazole-based triple therapy regimens (eradication rate of 88% in bothstudies; intention-to-treat analyses).
As expected, 10 days’ treatment with triple therapy including esomeprazole40mg once daily was significantly (p < 0.001) more effective in eradicating H.pylori infection than 10 days’ dual therapy (esomeprazole plus clarithromycin atthe same dosages) [77 vs 52% of patients; intention-to-treat analysis].
Currently, data evaluating the efficacy of esomeprazole-based triple therapyregimens on ulcer healing are limited. Nevertheless, in a well designed trial, tripletherapy including esomeprazole (20mg twice daily for 1 week) followed by 3weeks’ treatment with placebo was as effective for ulcer healing as a similartwice-daily omeprazole-based triple therapy regimen followed by omeprazole20mg once daily for 3 weeks (91vs 92% of patients experienced ulcer healing;intention-to-treat analysis).
In general, recipients of esomeprazole-based triple therapy regimens showedan improvement in the frequency and severity of epigastric pain and heartburnfrom baseline levels in two double-blind trials. In the largest study, markedlyfewer patients were experiencing epigastric pain (14 vs 96% of patients at base-line) and heartburn (10 vs 66%) after 4 weeks’ treatment (1 week of esome-prazole-based triple therapy, followed by 3 weeks of placebo) than at baseline.Similar symptomatic improvements from baseline were also experienced in thosereceiving omeprazole-based triple therapy for 1 week followed by omeprazole20mg once daily for 3 weeks (epigastric pain experienced by 95% of patients atbaseline vs 15% at 4 weeks; heartburn by 68 vs 5%). These improvements weremaintained in both treatment groups at 8 to 10 weeks’ follow-up.
Pharmacoeconomic considerations: Pharmacoeconomic studies of esome-prazole are currently limited to preliminary cost analyses based on clinical trialresults and/or patient databases.
A decision-analysis model based on pooled data from three 8-week clinicalstudies in 4877 patients with endoscopically confirmed reflux oesophagitisshowed a 14% reduction in direct medical costs with esomeprazole 40mg overomeprazole 20mg daily. The cost saving of £1290 over 8 weeks was increasedto £2064 when treatment failure costs were accounted for. Direct medical costsfor primary care visits, gastroenterologists visits and upper gastrointestinal en-
1508 Scott et al.
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

doscopy were based on 1998 UK values, and those for the acquistion of drugs on2000 values. A further decision-analysis model has shown an apparent savingrelative to omeprazole 20mg daily in direct medical costs from a UK NationalHealth Service perspective when esomeprazole 40mg daily is given to patientswith a diagnosis of GORD without endoscopic confirmation.
Application of results from two 6-month studies in 770 patients receivingon-demand treatment of GORD with esomeprazole 20mg daily or placebo to aMarkov model showed reductions in direct medical costs with esomeprazole of16 and 35%, respectively, relative to intermittent acute 4-week treatment or con-tinuous therapy with omeprazole 20mg daily. UK direct medical costs for primarycare visits, gastroenterologists visits and upper gastrointestinal endoscopy werebased on 1998 values, and those for the acquistion of drugs on 2000 values. Inaddition, an annual cost advantage for esomeprazole 20mg daily over omeprazole10 or 20mg daily has been shown on the basis of UK drug costs, clinical trial dataand drug usage statistics derived from a 1028-patient UK general practicedatabase.
Tolerability Like other proton pump inhibitors, esomeprazole is well tolerated as reported inboth clinical trials and in pooled tolerability data (n = 6682). In two large 8-weekrandomised trials (n = 2405 and 1957), a similar proportion of patients (≈1 to2.6%) receiving esomeprazole 20 or 40mg once daily or omeprazole 20mg oncedaily discontinued treatment due to an adverse event. There was no difference inthe nature or frequency of individual adverse events (1.8 to 8.7% of patients) inthese trials; headache, diarrhoea, nausea, abdominal pain and respiratory infec-tion were most commonly reported. No treatment-related serious adverse eventswere reported with esomeprazole or omeprazole therapy in these studies. Therewere also no clinically relevant changes in laboratory parameters or vital signswith either treatment.
There were no between-group differences in the tolerability profiles ofesomeprazole 40mg once daily or lansoprazole 30mg once daily in a largerandomised, double-blind trial in >5000 patients with erosive oesophagitis. Tenpercent of patients in each treatment group experienced at least one adverse eventconsidered to be drug-related; the most frequently reported adverse events witheither esomeprazole or lansoprazole treatment were headache (5.8 vs 4.5%), di-arrhoea (4.2 vs 4.7%), respiratory infection (2.8 vs 3.8%), abdominal pain (2.9 vs2.9%), flatulence (2.3 vs 2.4%) and nausea (2.1 vs 2.5%). Serious adverse eventsconsidered to be treatment related occurred in 0.7 and 0.5% of patients in theesomeprazole and lansoprazole groups, respectively, with 1.8 and 1.9% of recip-ients discontinuing treatment due to adverse events. There were no clinicallyrelevant changes in laboratory parameters or vital signs in either treatment group.
Triple therapy with esomeprazole plus amoxicillin and clarithromycin for 7or 10 days for the eradication of H. pylori infection was most commonly associ-ated with diarrhoea, taste perversion and abdominal pain according to pooledtolerability data (number of patients not reported). The esomeprazole triple ther-apy regimen was associated with a similar tolerability profile to that of an equiv-alent omeprazole-based regimen.
Maintenance therapy with esomeprazole 20 or 40mg once daily for 6 monthswas generally well tolerated in patients with healed GORD in two randomised,double-blind trials in 318 and 375 patients. The nature of drug-related adverseevents experienced with maintenance treatment was no different from that expe-
Esomeprazole: A Review 1509
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

rienced with 4 to 8 weeks’ treatment. A 12-month noncomparative study in 807patients with healed oesophagitis confirmed that esomeprazole 40mg once dailywas well tolerated.
Patients who received esomeprazole as maintenance therapy remained inrandomised studies for a much longer time than placebo recipients (mean values:116 to 161 vs 59 and 61.5 days). Therefore, direct comparisons of adverse eventincidences were difficult to make. After 1 month of treatment, the incidences ofthe most common adverse events and the proportions of patients who experiencedat least one adverse event were similar in the esomeprazole and placebo groups.Over the 6 months’ duration of these trials, esomeprazole was generally associ-ated with higher rates of discontinuation due to adverse events and higher overallfrequencies of adverse events than placebo, possibly because of the longer treat-ment time with the active drug.
Considerably more patients receiving esomeprazole 20mg as required (up to20 mg/day) than placebo recipients completed a study of symptom-drivenon-demand maintenance therapy in patients without erosive oesophagitis. Moreesomeprazole than placebo recipients experienced adverse events; however, thefrequency of events was similar in the two treatment groups when adjusted forexposure to treatment. Respiratory infection was the most common event in bothtreatment groups.
No enterochromaffin-like cell dysplasia, carcinoids or neoplasia were reportedin pooled tolerability data from noncomparative and randomised studies in 1326patients with healed erosive oesophagitis who received esomeprazole 10, 20 or40 mg/day or placebo for up to 6 or 12 months. Gastric histological scores withboth esomeprazole and placebo fluctuated to a minor extent and there were noconcerns relating to development of atrophic gastritis or clinically significantchanges in enterochromaffin-like cells.
Dosage andAdministration
Dosage recommendations for esomeprazole differ between countries. In the UK,esomeprazole 40mg once daily for 4 to 8 weeks is indicated for the healing oferosive oesophagitis associated with GORD, with a further 4 to 8 weeks at thesame dosage considered if oesophagitis is not healed; the recommended dosagein the US is 20 or 40mg once daily for 4 to 8 weeks, with a further 4 to 8 weeks’treatment considered if oesophagitis is not healed. Esomeprazole 20mg once dailyis recommended in both countries for the maintenance of healed erosive oeso-phagitis. Currently, no controlled studies of >6 months’ duration have been car-ried out; a noncomparative trial of 12 months’ duration has been conducted. Inpatients with symptomatic GORD, esomeprazole 20mg once daily for 4 weeksis recommended in both countries. In the UK, subsequent symptom control canbe achieved using an ‘on-demand’ regimen of 20mg once daily as required.
For the eradication of H. pylori in patients with duodenal ulcer disease, tripletherapy with esomeprazole 20mg twice daily plus twice-daily amoxicillin 1g andclarithromycin 500mg for 7 days is recommended in the UK, whereas in the UStriple therapy consists of esomeprazole 40mg once daily plus amoxicillin 1g twicedaily and clarithromycin 500mg twice daily for 10 days.
Esomeprazole dispersable tablets (multiple unit pellet system) should be swal-lowed whole at least one hour before eating; the pellets may be mixed with applesauce for patients who have difficulty in swallowing. In nursing mothers, a deci-sion should be made whether to discontinue nursing or to discontinue treatment.Although animal studies have shown no evidence of fetal abnormality, there are
1510 Scott et al.
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

no well controlled trials in pregnant women (category B rating); thus, the drugshould be used during pregnancy only if clearly needed. Dosage adjustments arenot necessary in patients who are elderly or those with renal or mild to moderatehepatic impairment. In patients with severe hepatic impairment, the dosage ofesomeprazole should not exceed 20 mg/day. The tolerability and effectiveness ofesomeprazole have not been established in paediatric patients.
Concurrent administration of esomeprazole with warfarin, quinidine, clar-ithromycin or amoxicillin does not produce any clinically significant interactions.Esomeprazole may, however, interfere with the absorption of drugs where gastricpH is an important determinant of bioavailability (e.g. ketoconazole, itra-conazole, digoxin and iron salts). Plasma concentrations of phenytoin should bemonitored when initiating or discontinuing coadministration of esomeprazole.
1. Introduction
Pyridylmethyl benzimidazole sulphides werefirst shown in the early 1970s to inhibit the H+/K+-ATPase enzyme (the proton pump) responsible forthe secretion of hydrochloric acid by gastric pari-etal cells. These agents were subsequently modi-fied to sulphoxides, of which omeprazole was thefirst to be used clinically for the management ofdisease related to excessive gastric acid secretionand activity (reviewed by Thitiphuree and Tal-ley[1]). Since that time, a number of substitutedbenzimidazole proton pump inhibitors have beendeveloped, all of which inhibit gastric acid secre-tion and raise intragastric pH. A detailed review ofomeprazole and its use in Helicobacter pylori in-fection, gastro-oesophageal reflux disease (GORD)and peptic ulcers induced by nonsteroidal anti-in-flammatory drugs (NSAIDs) was published inDrugs in 1998;[2] other agents reviewed in the jour-nal include pantoprazole,[3] rabeprazole[4,5] andlansoprazole.[6-8]
Unlike omeprazole, which is a racemic mixtureof two optical isomers (S- and R-omeprazole),esomeprazole consists of S-omeprazole only (fig-ure 1). This drug is the first proton pump inhibitorto be developed as a single optical isomer; it wasdeveloped to confer advantages over omeprazolein terms of pharmacokinetic characteristics andacid suppression. The pharmacological profile,therapeutic potential and tolerability of esome-prazole have already been summarised briefly inDrugs;[9] this article will review the role of the drug
in the management of patients with GORD and theeradication of H. pylori.
2. Pharmacodynamic Properties
2.1 Mechanism of Action
Like other proton pump inhibitors, esome-prazole is a potent inhibitor of the final commonpathway for hydrochloric acid secretion by gastricparietal cells. The drug is a weak base that is con-centrated in the acidic compartment of the secre-tory canaliculus of the parietal cell where it under-
N
N
S
O
H
N
OCH3
OCH3
CH3H3C
Omeprazole
OCH3
OCH3
CH3H3C
N
N
SN
O
••
Esomeprazole
Fig. 1. Structural formulae of esomeprazole and omeprazole.
Esomeprazole: A Review 1511
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

goes acid-catalysed transformation to a tetracyclicachiral cationic sulphenamide. This then reactswith specific cysteines which results in the inhibi-tion of the H+/K+-ATPase enzyme (see reviews byHuang and Hunt,[10] and Zimmermann[11]). Thebinding of esomeprazole to the proton pump is co-valent and irreversible, producing dosage-depend-ent inhibition with esomeprazole 5 to 40mg dailyin humans.[11,12] The drug has been shown to beoptically stable after administration in humans (seesection 3.1).[13]
2.2 Antisecretory Activity
The extent of mucosal injury and symptoms as-sociated with gastric reflux are dependent on pH.Refluxate with a pH <4 contains active pepsinand is associated with intensification of symp-toms,[14,15] with mucosal healing directly correlat-ing with the proportion of each 24-hour period forwhich the pH of the intragastric compartment isheld above this level.[16] Accordingly, pharmaco-dynamic studies of esomeprazole have focused onthe effect of the drug on intragastric pH.
A number of crossover studies, the majority ofwhich were nonblind, have shown esomeprazole(20 or 40mg daily) to be superior to omepra-zole,[17,18] lansoprazole[19,20] and pantoprazole[21]
in the maintenance of intragastric pH at a level > 4when given orally for 5 days; relative to rabep-razole 10 or 20mg daily, esomeprazole 20mgdaily[22,23] was as effective as either dosage ofrabeprazole whereas esomeprazole 40mg daily[24,25]
was superior to rabeprazole 20mg daily (table I).Superiority of esomeprazole was also shown onday 1 in most studies where this endpoint was eval-uated.[18,20-23,25] These trials were carried out inhealthy volunteers[19,20,22-24] or in patients withsymptoms of GORD,[17,18,21,25] and involved from23 to 115 evaluable individuals. At least 14 days’washout was allowed between treatments in allstudies except one (results presented in a combinedreport[20]) in which this period was stated to be atleast 10 days. The ability of the treatments testedto hold intragastric pH >4 (as shown by placementof transnasal electrodes) was most frequently ex-
pressed in terms of the mean percentage of each24-hour monitoring period with pH >4, and thepercentage of patients maintaining this pH for atleast 12 or 16 hours. Mean 24-hour median pH val-ues were also analysed and reported by some in-vestigators.[17,21,25] All trials assessed statisticalsignificance in terms of the mean difference be-tween treatments for the parameters analysed and,except for two studies (a fully reported double-blind comparison of esomeprazole 20 and 40mgwith omeprazole 20mg daily[17] and a crossoverstudy comparing esomeprazole 40mg with om-eprazole 40mg[18]), all were available as abstractsonly.
On the fifth day of treatment intragastric pH was>4 for a mean 59.4 to 69.8% of the monitored 24-hour periods in individuals receiving esome-prazole 40mg daily (table I).[17,18,20,21,24,25] Thesepercentages were significantly greater than thoseseen with comparators (which ranged from 43.7 to62% for esomeprazole 20mg,[17] omeprazole[17] orrabeprazole 20mg,[24,25] omeprazole[18] or panto-prazole 40mg[21] and lansoprazole 30mg daily[20]).Esomeprazole 40mg daily was similarly superiorto other comparators over the first 24 hours wherethis information was available[18,20,21,25] (table I).
Four comparative trials have evaluated the effi-cacy of esomeprazole 20mg daily in maintainingintragastric pH above a level of 4 in healthyvolunteers[19,22,23] or patients with symptomaticGORD[17] (table I). On the fifth day of treatment,esomeprazole recipients experienced a signifi-cantly higher mean percentage of the 24-hour mon-itoring period with a pH ≥4 than those receiv-ing lansoprazole 15mg daily (50.4 vs 43%; p =0.026).[19] At the same timepoint, esomeprazole20mg daily maintained an intragastric pH level ≥4for a similar percentage of time during the moni-tored 24-hour period as rabeprazole 10mg daily(54.9 vs 48.2%).[22] Moreover, there was no statis-tically significant difference in the percentage oftime intragastric pH was maintained above 4 withesomeprazole 20mg daily or rabeprazole 20mgdaily on day 5 of treatment in another study (56.2vs 62.3% of the 24-hour monitored period).[23] A
1512 Scott et al.
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

Table I. Suppression of intragastric acidity by esomeprazole (ESO) and other proton pump inhibitors. Summary of randomised, crossoverstudies in healthy volunteers and patients with symptoms of gastro-oesophageal reflux disease (GORD). Intragastric pH was monitored for24 hours on day 5 of each treatment period in all studies, and on day 1 where indicated. With the exception of one double-blind study,[17] allof these studies were nonblind
Reference No. and characteristicsof evaluableparticipants
Treatmentregimensa
Mean percentageof 24h period withpH >4
Mean 24hmedian pH
Percentage of participants withintragastric pH >4
for ≥8h for ≥12h for ≥16h
Comparisons with omeprazole (OMP)
Lind et al.[17] 36 with symptoms ofGORD
ESO 20mg 53† 4.1† 76 54 24
ESO 40mg 69.8‡ 4.9‡ 97 92 56
OMP 20mg 43.7 3.6 67 45 14
Röhss et al.[18] 115 with symptoms ofGORD
ESO 40mg Day 1 = 49*** Day 1 = 50 Day 1 = 88
Day 5 = 68*** Day 5 = 16 Day 5 = 55
OMP 40mg Day 1 = 41 Day 1 = 34 Day 1 = 75
Day 5 = 62 Day 5 = 10 Day 5 = 44
Comparisons with lansoprazole (LAN)
Thomson et al.[20]b 48 healthy volunteersc ESO 40mg Day 1 = 57.2** Day 1 = 71 Day 1 = 36
Day 5 = 65.4*** Day 5 = 90 Day 5 = 35
LAN 30mg Day 1 = 51.8 Day 1 = 61 Day 1 = 21
Day 5 = 53 Day 5 = 55 Day 5 = 5
Wilder-Smith et al.[19]b 27 healthy volunteers ESO 20mg 50.4*d 50 23
LAN 15mg 43d 35 15
Comparison with pantoprazole (PAN)
Wilder-Smith et al.[21]b 31 with symptoms ofGORD
ESO 40mg Day 1 = 50*** Day 1 = 3.9*** Day 1 = 39 Day 1 = 26
Day 5 = 66*** Day 5 = 4.7*** Day 5 = 90 Day 5 = 50
PAN 40mg Day 1 = 29 Day 1 = 2.9 Day 1 = 10 Day 1 = 3
Day 5 = 44 Day 5 = 3.7 Day 5 = 30 Day 5 = 10
Comparisons with rabeprazole (RAB)
Baisley et al.[22]b 30 healthy volunteers ESO 20mg Day 1 = 29.9
Day 5 = 54.9
RAB 10mg Day 1 = 30.9
Day 5 = 48.2
Baisley et al.[23]b 24 healthy volunteers ESO 20mg Day 1 = 34
Day 5 = 56.2
RAB 20mg Day 1 = 47.9***
Day 5 = 62.3
Wilder-Smith et al.[24]b 23 healthy volunteers ESO 40mg 61**
RAB 20mg 45.1
Wilder-Smith et al.[25]b 35 with symptoms ofGORD
ESO 40mg Day 1 = 41.5** Day 1 = 3.4**
Day 5 = 59.4*** Day 5 = 4.4***
RAB 20mg Day 1 = 29.4 Day 1 = 2.7
Day 5 = 44.5 Day 5 = 3.5
a All drugs were given orally once daily for 5 days, with a washout period of ≥14 days between treatments (unless stated otherwise).
b Abstract.
c Combined results from two studies. Washout period ≥10 days in one (n = 20).
d pH ≥4.
* p < 0.05, ** p < 0.01, *** p < 0.001 vs comparator; †p < 0.01 vs OMP; ‡p < 0.001 vs OMP and ESO 20mg.
Esomeprazole: A Review 1513
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

double-blind study in patients with symptomaticGORD showed superiority of esomeprazole 20mgdaily over omeprazole 20mg daily in the mainte-nance of intragastric pH >4.[17] The presence of H.pylori in six patients in this study had no statisti-cally or clinically significant effect on results withany treatment. This latter trial also showed a highermean 24-hour median pH value with esomeprazole20mg daily than with omeprazole 20mg daily (4.1vs 3.6; p < 0.01). Similar results for mean 24-hourmedian pH value were also reported for esome-prazole 40mg daily on days 1 and 5 in comparisonswith pantoprazole 40mg[21] and rabeprazole 20mg;[25]
a single-dose study in 21 healthy volunteers alsoindicated that mean 24-hour median pH-valueswere identical for esomeprazole 20mg andlansoprazole 15mg on day 1 (median pH 2.8 forboth treatments).[26]
Higher percentages of esomeprazole than ofcomparator recipients maintained intragastric pHabove 4 for ≥8, ≥12 and ≥16 hours out of 24 hoursin all studies in which this information was re-ported (table I).[17-21,24,25] Trends favouring esome-prazole were consistently evident for this endpoint(no statistical analyses reported in abstracts).
Onset of reduction of intragastric acidity in 35patients with GORD appeared more rapid withesomeprazole 40mg than with rabeprazole 20mgdaily in one of the comparisons.[25] The pH was >4for 23.2 and 11% of the first 4 hours after the firstdose of esomeprazole and rabeprazole (p = 0.006);corresponding group means of median pH valuesfor this period were 2.8 and 2.2 (p = 0.019).
There was no significant difference in the timeto onset of intragastric pH control with esome-prazole or lansoprazole in two randomised, non-blind, crossover, single-dose studies in a total of45 healthy volunteers (both studies reported in asingle abstract).[27] Time taken to achieve an intra-gastric pH of 4 after a single dose of esomperazole40mg or lansoprazole 30mg was 1 hour 22 minutesor 1 hour 29 minutes, respectively; times were alsosimilar in a comparison of esomeprazole 20mgwith lansoprazole 15mg (2 hours 6 minutes vs 1hour 50 minutes).
2.3 Other Effects
Some other pharmacodynamic effects of esomep-razole are detailed in the manufacturer’s productinformation.[12] At dosages of up to 40mg daily forup to 4 weeks, the drug has no apparent effect onthyroid function or carbohydrate metabolism, or oncirculating levels of parathyroid hormone, cortisol,estradiol, testosterone, prolactin, cholecystokininor secretin.
In clinical studies of up to 8 weeks’ duration inapproximately 2700 patients, and of 6 to 12months’ duration in over 1300 patients, esome-prazole increased mean fasting serum gastrin lev-els in a dose-related manner. Increases reached aplateau after 2 to 3 months and returned to baselinelevels within 4 weeks of discontinuation of ther-apy[12] (see also section 5). As reviewed pre-viously, similar increases in gastrin levels havealso been observed with other proton pump inhib-itors.[2-4,7]
3. Pharmacokinetic Properties
The pharmacokinetics of esomeprazole have re-cently been reviewed in detail in Clinical Pharma-cokinetics,[28] and the reader is referred to this ar-ticle for in-depth information. The following is asummary of the pharmacokinetic characteristics ofgreatest clinical interest.
3.1 Healthy Volunteers
Esomeprazole is absorbed rapidly after oral ad-ministration: the peak concentration of the drug inplasma (Cmax) was reached within 0.5 hours of in-gestion of an oral solution containing 20mg andwithin 1 to 3.5 hours of ingestion of 40mg as en-capsulated enteric-coated granules in two studiesin a total of 32 healthy volunteers.[29] Increases insystemic exposure, as shown by areas under theplasma-concentration time curves (AUCs), aredose-related after single doses, increasing in a non-linear fashion.[30] Of major interest, however, is theeffect of repeated administration of esomeprazoleon systemic exposure to the drug. The mean AUCextrapolated to infinity (AUC∞) increased by 90%
1514 Scott et al.
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

and Cmax by 43% relative to day 1 after 5 days’treatment with 20mg daily (as solution) in the twoanalyses in 32 volunteers;[29] mean systemic bio-availability increased from 50 to 68%. This effectwas more pronounced with 40 mg/day, for whichCmax increased by 95% and AUC∞ by 159% overthe same period.
The increase in systemic exposure to esome-prazole after repeated doses is attributed to reduc-tions in total body clearance and first-pass meta-bolism.[28] The above investigations[29] showed theclearance of esomeprazole declined with repeatedadministration. Intravenous doses of 20 or 40mgwere given 5 to 14 days before the first oral doseof esomeprazole, and 1 day after the last dose. Rel-ative to the first dose, mean clearance decreasedby 29% (from 21.7 to 15.5 L/h) and 46% (from 17to 9.2 L/h) after the second 20 and 40mg doses,respectively. Across all treatments, mean plasmaelimination half-life (t1⁄2β ) increased from between0.72 and 0.85 hours to between 0.96 and 1.25hours. The volume of distribution of esomeprazoleat steady state after intravenous administrationwas consistently around 0.25 L/kg.[29]
Similar increases in mean AUC (time not statedin the abstract available) were noted in a study in12 healthy volunteers who received oral solutionsof esomeprazole 5, 10 or 20mg, or omeprazole20mg as encapsulated enteric-coated granules, ina randomised crossover design, once daily for 5days.[28] AUCs increased by 55 and 134% over thisperiod with esomeprazole 10 and 20mg, respec-tively, and by 62% with omeprazole 20mg. TheAUC value for esomeprazole 20mg was 70%higher than that for omeprazole 20mg daily atsteady state.[28]
Esomeprazole is bound to plasma proteins tothe same extent as omeprazole (97%),[12] and to asimilar extent to that of other proton pump inhibi-tors reviewed previously.[3,4,8] The degree of inver-sion to the R-isomer (0.4%)[28] shows that esome-prazole is chirally stable after administration. Thedrug is metabolised extensively in the liver by thecytochrome P 450 (CYP) enzyme system to prod-ucts that lack antisecretory activity. In vitro studies
show that both optical isomers of omeprazole areconverted chiefly to hydroxy and 5-O-desmethylmetabolites by the CYP2C19 isoenzyme, and tothe sulphone by CYP3A4.[31] Approximately 80%of each dose is excreted as metabolites in the urine;the remainder is eliminated as metabolites in thefaeces.[12] The affinity of esomeprazole for theCYP2C19 isoenzyme is approximately ten timesthat for CYP3A4, although the rate at which thehydroxy metabolite is formed is lower, and the rateat which the sulphone and 5-O-desmethyl metabo-lites are formed higher, than with R-omeprazole.The sum of the intrinsic clearance values for for-mation of the three metabolites in vitro from R-om-eprazole was three times that of the S-isomer.[31]
The suggestion that this would be reflected in re-duced clearance and increased AUCs of esomep-razole relative to omeprazole has been borne outby observations in healthy volunteers (see Anders-son et al.[28]) and in patients with GORD (see sec-tion 3.2).[17]
It should be noted that a small proportion of thepopulation (approximately 3% of Caucasians and15% of Asians) do not express a functional formof CYP2C19 and are termed ‘poor metabolisers’.Bioequivalence data for esomeprazole indicateAUC values differ by a factor of less than two be-tween poor metabolisers and the rest of the popu-lation, and dosage reductions are not considerednecessary in these individuals.[28]
Data obtained in 41 healthy volunteers showbioequivalence of esomeprazole when adminis-tered either as the intact dosage form (gelatin cap-sule) as presented for clinical use or as the contentsof the capsule (enteric-coated granules) mixedwith apple sauce.[32]
3.2 Patients with Gastro-OesophagealReflux Disease (GORD)
Pharmacokinetic data from the double-blind,crossover study (reported in section 2.2) in 36evaluable patients with GORD[17] concur with ob-servations in healthy volunteers (section 3.1). Onday 5 of once-daily treatment with capsules con-taining enteric-coated granules, Cmax values for
Esomeprazole: A Review 1515
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)
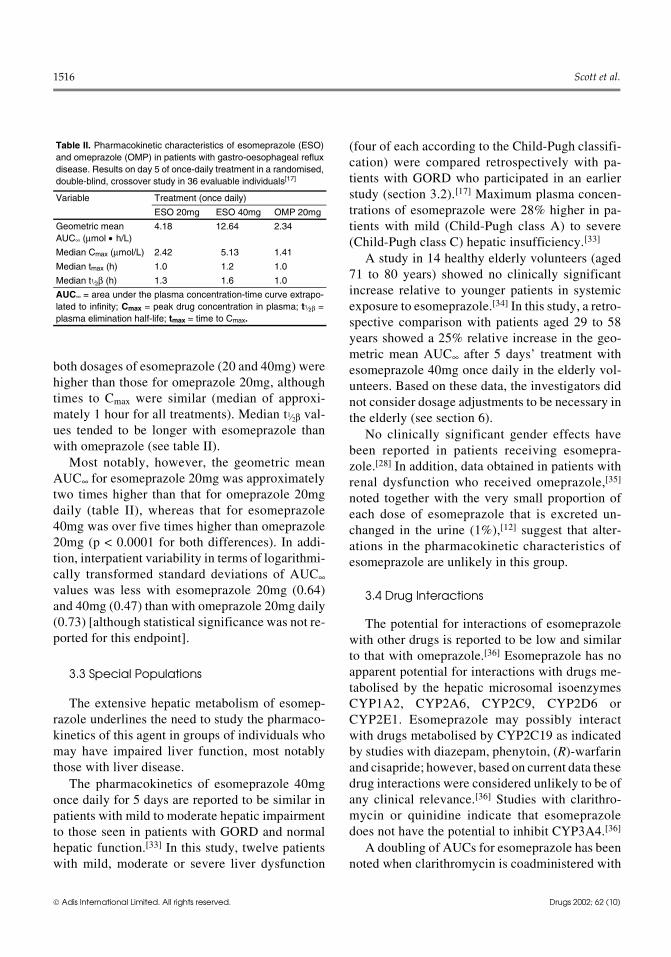
both dosages of esomeprazole (20 and 40mg) werehigher than those for omeprazole 20mg, althoughtimes to Cmax were similar (median of approxi-mately 1 hour for all treatments). Median t1⁄2β val-ues tended to be longer with esomeprazole thanwith omeprazole (see table II).
Most notably, however, the geometric meanAUC∞ for esomeprazole 20mg was approximatelytwo times higher than that for omeprazole 20mgdaily (table II), whereas that for esomeprazole40mg was over five times higher than omeprazole20mg (p < 0.0001 for both differences). In addi-tion, interpatient variability in terms of logarithmi-cally transformed standard deviations of AUC∞values was less with esomeprazole 20mg (0.64)and 40mg (0.47) than with omeprazole 20mg daily(0.73) [although statistical significance was not re-ported for this endpoint].
3.3 Special Populations
The extensive hepatic metabolism of esomep-razole underlines the need to study the pharmaco-kinetics of this agent in groups of individuals whomay have impaired liver function, most notablythose with liver disease.
The pharmacokinetics of esomeprazole 40mgonce daily for 5 days are reported to be similar inpatients with mild to moderate hepatic impairmentto those seen in patients with GORD and normalhepatic function.[33] In this study, twelve patientswith mild, moderate or severe liver dysfunction
(four of each according to the Child-Pugh classifi-cation) were compared retrospectively with pa-tients with GORD who participated in an earlierstudy (section 3.2).[17] Maximum plasma concen-trations of esomeprazole were 28% higher in pa-tients with mild (Child-Pugh class A) to severe(Child-Pugh class C) hepatic insufficiency.[33]
A study in 14 healthy elderly volunteers (aged71 to 80 years) showed no clinically significantincrease relative to younger patients in systemicexposure to esomeprazole.[34] In this study, a retro-spective comparison with patients aged 29 to 58years showed a 25% relative increase in the geo-metric mean AUC∞ after 5 days’ treatment withesomeprazole 40mg once daily in the elderly vol-unteers. Based on these data, the investigators didnot consider dosage adjustments to be necessary inthe elderly (see section 6).
No clinically significant gender effects havebeen reported in patients receiving esomepra-zole.[28] In addition, data obtained in patients withrenal dysfunction who received omeprazole,[35]
noted together with the very small proportion ofeach dose of esomeprazole that is excreted un-changed in the urine (1%),[12] suggest that alter-ations in the pharmacokinetic characteristics ofesomeprazole are unlikely in this group.
3.4 Drug Interactions
The potential for interactions of esomeprazolewith other drugs is reported to be low and similarto that with omeprazole.[36] Esomeprazole has noapparent potential for interactions with drugs me-tabolised by the hepatic microsomal isoenzymesCYP1A2, CYP2A6, CYP2C9, CYP2D6 orCYP2E1. Esomeprazole may possibly interactwith drugs metabolised by CYP2C19 as indicatedby studies with diazepam, phenytoin, (R)-warfarinand cisapride; however, based on current data thesedrug interactions were considered unlikely to be ofany clinical relevance.[36] Studies with clarithro-mycin or quinidine indicate that esomeprazoledoes not have the potential to inhibit CYP3A4.[36]
A doubling of AUCs for esomeprazole has beennoted when clarithromycin is coadministered with
Table II. Pharmacokinetic characteristics of esomeprazole (ESO)and omeprazole (OMP) in patients with gastro-oesophageal refluxdisease. Results on day 5 of once-daily treatment in a randomised,double-blind, crossover study in 36 evaluable individuals[17]
Variable Treatment (once daily)
ESO 20mg ESO 40mg OMP 20mg
Geometric meanAUC∞ (μmol • h/L)
4.18 12.64 2.34
Median Cmax (μmol/L) 2.42 5.13 1.41
Median tmax (h) 1.0 1.2 1.0
Median t1⁄2β (h) 1.3 1.6 1.0
AUC∞ = area under the plasma concentration-time curve extrapo-lated to infinity; Cmax = peak drug concentration in plasma; t1⁄2β =plasma elimination half-life; tmax = time to Cmax.
1516 Scott et al.
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

the drug. This is stated, however, to be unlikely tohave any clinical or tolerability implications.[36]
4. Clinical Efficacy
Several well designed clinical trials, employingboth endoscopic and symptomatic response cri-teria, have compared the efficacy of esomeprazolewith that of other proton pump inhibitors in themanagement of GORD (section 4.1), and in theeradication of H. pylori infection associated withduodenal ulcer disease (section 4.2). The majorityof these large randomised, double-blind, multi-centre trials are fully published,[37-45] although afew are currently only available as abstracts.[46-48]
In addition, a fully published large noncompara-tive trial evaluated 12 months’ maintenance ther-apy in patients with healed oesophagitis.[49] Withinan individual trial, patients in each treatment groupwere well matched in terms of disease severity andother baseline characteristics. All data are for in-tention-to-treat groups unless stated otherwise.
4.1 GORD
The efficacy of esomeprazole for the treatmentof GORD has been evaluated in 4- to 8-week trials(the usual duration for such trials), including alarge (n = 5241), randomised, double-blind, multi-centre trial[40] comparing esomeprazole 40mgonce daily with lansoprazole 30mg once daily. Inaddition, the efficacy of esomeprazole in maintain-ing healing and preventing recurrence of erosiveoesophagitis has been investigated in trials of6[43,44,48] to 12[49] months’ duration.
Clinical endpoints assessed included healing ormaintenance of healing and resolution of symp-toms. Healing or maintenance of healing of ero-sions was determined objectively by endoscopy,with healing rates based on life table analysis,whereas symptom resolution was assessed subjec-tively by investigators and patients based on a five-point scale (0 = none, 4 = severe) for various symp-toms (e.g. frequency and severity of day and nightheartburn, and epigastric pain). Erosive oesophag-itis was graded using the four-grade (A = least se-vere, D = most severe) Los Angeles (LA) Classi-
fication system[50] and was considered healed ifthere were no mucosal breaks as defined by thisgrading system. Resolution of symptoms was de-fined as no heartburn and sustained resolution wasdefined as no heartburn for 7 consecutive days andnights.
Patients (≥18 years of age) eligible for inclusionhad endoscopically investigated GORD; thosewith erosive oesophagitis also had to have hadheartburn for ≥2 of the previous 7 days, whereaspatients with symptomatic GORD (endoscopynegative) had to have had heartburn for ≥4 of theprevious 7 days and for at least 6 months prior tostudy entry. Each individual trial enrolled eitheronly patients with erosive oesophagitis or only pa-tients with symptomatic GORD without oesophag-itis.
Patients with a bleeding disorder or GI bleed-ing, who had undergone gastric and/or oesopha-geal surgery, had signs of severe concomitantdisease [e.g. Zollinger-Ellison syndrome, oesoph-ageal stricture, Barrett’s oesophagus (>3cm insize)], or who received a proton pump inhibitor inthe previous 4 weeks or an H2-receptor antagonistin the previous 2 weeks were excluded.
4.1.1 Patients with Erosive Oesophagitis
Healing and Symptom Resolution TherapyEsomeprazole effectively healed oesophagitis
(primary efficacy endpoint) and resolved heart-burn (secondary endpoint) in patients with GORDin large (n >1900 patients), randomised, double-blind, multicentre trials (table III).
Patients received oral esomeprazole 20 or40mg, lansoprazole 30mg or omeprazole 20mgonce daily before breakfast for 4 to 8 weeks. Pa-tients who showed endoscopically confirmedhealed oesophagitis treatment were discontinuedfrom the study at 4 weeks. In two trials,[41,42] allpatients enrolled were serologically negative forH. pylori infection at study entry and remained inthe intention-to-treat analyses even if they weresubsequently shown to be H. pylori-positive basedon histology; 8[42] and 10%[41] of patients were se-rologically negative but histologically positive forH. pylori. Oesophagitis healing rates were similar
Esomeprazole: A Review 1517
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

in H. pylori-positive and -negative patients. Basedon these results, in the subsequent study,[40] pa-tients were screened for H. pylori at baseline andenrolled regardless of their H. pylori status (15%of intention-to-treat patients were H. pylori-posi-tive).
Overall, esomeprazole treatment was betterthan omeprazole, although this difference in fa-vour of esomeprazole did not always achieve sta-tistical significance.[12,41,42] In two fully publishedrandomised, double-blind trials, significantly (p <0.05 all comparisons) more recipients experiencedhealed oesophagitis at 8 weeks with esomeprazole20 or 40mg once daily than with omeprazole 20mgonce daily (90 to 94% vs 84 to 87% of recipients)[table III].[41,42] Of these trials, one evaluated bothesomeprazole 20 and 40mg; a significantly higherpercentage of patients achieved healed oesophag-itis in both the esomeprazole 20 (89.9% of patients;p < 0.05 vs omeprazole) and 40mg (94.1%; p <0.001 vs omeprazole) groups than in the om-eprazole 20mg group (86.9%) [table III].[41] Atrend favouring esomeprazole was also reported intwo further randomised, double-blind trials (≈1100patients in each trial) for which limited data areavailable in US prescribing information;[12] at 8weeks, rates of healed oesophagitis with esome-
prazole 20 or 40mg once daily were 91 and 92%,respectively, versus 88 and 90% with omeprazole20mg once daily.
Furthermore, a meta-analysis (using a Fixed Ef-fects model) of randomised controlled trials indi-cated esomeprazole 40mg once daily gave higherhealing rates in the treatment of reflux oesophagitisthan omeprazole 20mg once daily after 4 [relativerisk (RR) 1.14; 95% confidence interval (CI) 1.10,1.18] or 8 weeks (RR 1.08, 95% CI 1.05, 1.10),whereas lansoprazole, rabeprazole and panto-prazole showed healing rates similar to those ofomeprazole at the same timepoints.[51]
Evidence-based analysis using pooled datafrom two trials indicated that esomeprazole wasmore effective than omeprazole in healing erosiveoesophagitis.[52] The relative risk reduction foresomeprazole versus omeprazole was 10.2% andabsolute risk reduction 8.7%; thus, to prevent onetreatment failure, 11 patients would need to betreated with esomeprazole 40mg once daily ratherthan omeprazole 20mg once daily.
The higher response rate with esomeprazoletreatment relative to omeprazole occurred acrossall grades of erosive oesophagitis (based on LAClassification grades), although these differencesdid not always reach statistical significance.[41,42]
Table III. Overview of large randomised, double-blind, multicentre, 8-week trials evaluating the efficacy (healing and resolution of symptoms)of esomeprazole (ESO) monotherapy in the management of gastro-oesophageal reflux disease. All data are presented for intention-to-treatgroups
Reference No. ofpts
Treatment regimen(od; 4-8 wks)a
Healing ofoesophagitisb (% pts)
Days withoutHBc (%; mean)
Nights withoutHBc (%; mean)
Time to sustained resolutiond
of HBc (days; median )
Castell et al.[40] 2624 ESO 40mg 92.6*** 72.5 87.1* 7**
2617 LAN 30mg 88.8 70.9 85.8 8
Kahrilas et al.[41] 656 ESO 20mg 89.9† 69.3 83.6† 8
654 ESO 40mg 94.1†† 72.7†† 84.7†† 5††
650 OMP 20mg 86.9 67.1 80.1 9
Richter et al.[42] 1216 ESO 40mg 93.7*** 74.9*** 90.8*** 5***
1209 OMP 20mg 84.2 69.7 87.9 8
a Pts were discontinued from studies at 4 wks if oesophagitis was healed as confirmed by endoscopy.
b Healing defined as normal appearance (absence of mucosal breaks using the Los Angeles Classification Grading system)[50] at wk4 or 8 as assessed by endoscopy. Healing rates were based on life table analysis.
c Based on pt diary records.
d Defined as no HB for seven consecutive days and nights.
HB = heartburn; LAN = lansoprazole; od = once daily; OMP = omeprazole; pt(s) = patient(s); * p ≤ 0.05, ** p ≤ 0.01, *** p < 0.001vs comparator;† p < 0.05, †† p < 0.001 vs OMP.
1518 Scott et al.
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

In one study,[42] significantly more patients acrossall four grades experienced healed oesophagitiswith esomeprazole 40mg than omeprazole 20mgat both 4 and 8 week assessments (p < 0.001 ac-cording to the Cochran-Mantel-Haenszel test).Pooled data (available as an abstract only) from6708 patients participating in US randomised,double-blind, multicentre trials confirmed theseresults (figure 2) [no p values reported in ab-stract].[53]
Furthermore, healed oesophagitis rates weresignificantly (p < 0.001) higher with esomeprazolethan lansoprazole treatment in a large double-blindtrial in more than 5000 patients (table III).[40] At 8weeks, healed oesophagitis had occurred in 92.6%of esomeprazole (40mg once daily) recipients ver-sus 88.8% of those receiving lansoprazole 30mgonce daily in this study.
Notably, esomeprazole treatment effectivelyhealed oesophagitis across all baseline grades ofdisease severity in this large comparative double-blind trial.[40] Furthermore, relative to lans-oprazole, as the baseline severity of disease in-creased, the difference in rates of healedoesophagitis also increased in favour of esomep-razole. Ninety-seven, 92, 88 and 81% of patientswith grade A, B, C or D oesophagitis at baseline,respectively, achieved healed oesophagitis withesomeprazole 40mg daily, whereas the proportionof lansoprazole recipients with healed oesophag-itis decreased to a greater extent as baseline sever-ity of oesophagitis increased (97, 91, 77 and 64%of lansoprazole recipients, respectively) [all val-ues were estimated from a graph]. Hence, therewas an 11% higher healing rate with esomep-razole-treatment in those with grade C disease and
Grade D
Grade C
Grade B
Grade A
0 20 40 60 80 100
(64.1, 83.9)
(77.9, 90.1)
(66.3, 78.6)
(78.7, 88.3)
(88.7, 93.7)
(72.6, 79.5)
(86.8, 92.5)
(91.7, 95)
(86.1, 89.9)
(96, 99)
(95.3, 98)
(93.4, 96.3)
Bas
elin
e se
verit
y of
ero
sive
oes
opha
gitis
(LA
cla
ssifi
catio
n)
ESO 20mg odESO 40mg odOMP 20mg od
Endoscopically-confirmed healed oesophagitis (% patients)
Fig. 2. Effect of baseline severity of erosive oesophagitis on the efficacy of esomeprazole. Pooled data from US randomised,double-blind, multicentre trials in 6708 patients with erosive oesophagitis associated with gastro-oesophageal reflux disease.[53]
Patients were stratified according to the severity of erosive oesophagitis, assessed using the Los Angeles (LA) Classificationsystem[50] [Grades A (mild) to D (severe)], with results reported for intention-to-treat groups. Oesophagitis was considered healed ifthere were no mucosal breaks according to this system, with healing rates based on life table analysis. Patients received once-daily(od) esomeprazole (ESO) 20 (n = 1243) or 40mg (n = 2446), or omeprazole (OMP) 20mg (n = 3019) for 4 to 8 weeks. Numbers inbrackets are the 95% confidence intervals. No p values were reported in the abstract.
Esomeprazole: A Review 1519
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

a 17% higher rate in patients with grade D oeso-phagitis.[40]
Esomeprazole 40mg once daily was also com-pared with lansoprazole 30mg once daily in asmaller (n = 284) randomised, double-blind, multi-centre trial that used a different erosive oesophag-itis grading system (a five-point scale versus thefour-point LA grading scale).[54] In this smallertrial there was no statistical between-group differ-ence in the percentage of patients with healed oeso-phagitis at 8 weeks (healing rates of ≈90% in eachtreatment group). As stated by the authors of thisstudy, it is difficult to make head-to-head compar-isons of these two trials, since they used differentgrading systems for assessing the severity of oeso-phagitis; hence, this study is not tabulated or dis-cussed further.
Esomeprazole also proved effective in patientswith erosive oesophagitis according to secondaryendpoints (e.g. percentage of heartburn-free daysand nights, and time to sustained resolution ofheartburn) [table III].[40-42] Resolution of heartburnwith esomeprazole 40mg was significantly betterthan that of omeprazole 20mg and significantlybetter than or at least as effective as that oflansoprazole (table III). Esomeprazole 40mg sig-nificantly reduced the time to complete resolutionof symptoms relative to omeprazole 20mg[41,42] (p< 0.001 in both studies). In addition, the percentageof days and nights without heartburn were greaterwith esomeprazole 40mg than omeprazole 20mg(p < 0.001 for all comparisons).[41] Compared withlansoprazole, a significantly (p < 0.05) higher per-centage of nights were heartburn-free (87.1 vs85.8% of nights), with sustained resolution ofsymptoms occurring earlier in esomeprazole thanlansoprazole recipients (7 vs 8 days; p ≤ 0.01), butthere was no between-group difference in the num-ber of days that were heartburn-free.[40]
Resolution of symptoms matched healed oeso-phagitis rates in a post-hoc analysis of pooled datafrom 8-week randomised, double-blind trials eval-uating 4877 patients (currently available as ab-stracts only).[55-57] After 4 weeks’ treatment withesomeprazole 40mg once daily, 83.4 and 81% of
recipients who had healed oesophagitis wereasymptomatic for heartburn and acid regurgitation,respectively, compared with 75.4 and 71.6% ofthose receiving omeprazole 20mg once daily (p <0.001 for both comparisons).[55] Furthermore,esomeprazole proved more effective than om-eprazole in preventing nocturnal heartburn [88.1%(95% CI 87.3 to 89%) of nights were heartburn-free with esomeprazole vs 85.1% (95% CI 84.2 to85.9%) with omeprazole].[56] The odds ratio foresomeprazole versus omeprazole in improving theincidence of heartburn was 1.27 (95% CI 1.13 to1.42; p < 0.001).[57] There was a greater probabilityof heartburn resolution in patients with LA Classi-fication grades C or D at baseline than in those withgrades A or B in both treatment groups.[57] Predic-tive probabilities of heartburn resolution withesomeprazole were 0.63 (95% CI 0.60 to 0.66) forpatients with grades C or D disease and 0.55 (95%CI 0.52 to 0.57) for recipients with grades A or Bdisease, whereas respective values for those re-ceiving omeprazole were 0.57 (95% CI 0.54 to0.60) and 0.49 (95% CI 0.46 to 0.51).
Preliminary data comparing the efficacy ofesomeprazole 40mg once daily with that ofpantoprazole 40mg once daily have been reportedin two recently published abstracts;[58,59] the lackof some key trial design details in these abstractpresentations limits discussion of this data.
Maintenance TherapyThe efficacy of esomeprazole 20 or 40mg once
daily in maintaining healing of oesophagitis hasbeen evaluated in two 6-month placebo-controlledtrials.[43,44] Participants had previously receivedesomeprazole or omeprazole for 4 to 8 weeks inclinical trials discussed above. The primary effi-cacy endpoint was the maintenance of healing (as-sessed endoscopically) at 6 months. Althoughthese trials also evaluated treatment with esomep-razole 10mg once daily, these data are not dis-cussed since this dosage is not currently recom-mended (see section 6). Maintenance therapy hasalso been evaluated in 807 patients with healedoesophagitis in a noncomparative trial of 12months’ duration.[49]
1520 Scott et al.
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

In addition, the efficacy of esomeprazole 20mgonce daily versus lansoprazole 15mg once daily(the standard dosage recommended for each agentfor maintenance therapy) has been evaluated in a6-month randomised, double-blind, multicentretrial (available as a poster/abstract).[48] The pri-mary endpoint was the time to recurrence of oeso-phagitis (assessed endoscopically) and/or unwill-ingness to continue due to reflux symptoms(heartburn, epigastric pain and acid regurgitation).All patients received esomeprazole 40mg oncedaily for 4 to 8 weeks during the nonblind healingphase of this trial before randomisation into one ofthe two treatment groups for the 6-month double-blind phase.
Esomeprazole 20 or 40mg once daily was sig-nificantly more effective than placebo in maintain-ing healing in double-blind trials (table IV).[43,44]
Healed oesophagitis was maintained in 79 and93% (esomeprazole 20mg), 88 and 94% (esomep-razole 40mg) or 29% (placebo) of patients.
Esomeprazole also prolonged the time to recur-rence of erosive oesophagitis in these two trials(table IV).[43,44] For example, in the larger study,mean time to recurrence of erosive oesophagitiswas markedly longer with esomeprazole 20 (101days) or 40mg (130) than with placebo (46).[44]
There was a strong association between main-tenance of healing and the absence of heartburn inplacebo-controlled studies.[43,44] For example, inthe larger study,[44] of patients remaining in the
study, 98% of esomeprazole (20 or 40mg) recipi-ents (n = 130 evaluated patients) and 92% of thosereceiving placebo (n = 21) who had no heartburnshowed maintenance of healing. Subgroup analy-ses indicated that maintenance of healing withesomeprazole treatment was not influenced bygender, age (≥65 years vs <65 years of age), initialtreatment during the healing phase of the study,time to healing in this phase (4 vs 8 weeks) or base-line severity of erosive oesophagitis.[43,44]
Although there was no statistically significantdifference in the percentage of patients who wereheartburn-free at 6 months with esomeprazole orplacebo treatment (table IV), this most likely re-flects that only patients with maintained healingremained in the study at 6 months.[43,44] Neverthe-less, at 1 month, an appreciably higher proportionof patients receiving esomeprazole 20 or 40mgwere heartburn-free than recipients of pla-cebo.[43,44] For example, in the larger of the twostudies, 63.7% (58 of 91 patients), 71.3% (62 of87) and 15.5% (13 of 84) of patients in the esome-prazole 20 or 40mg or placebo groups, respec-tively, were heartburn-free (p < 0.001 for both dos-ages of esomeprazole vs placebo).[44]
A significantly higher percentage of esome-prazole (20mg once daily) than lansoprazole(15mg once daily) recipients remained in remis-sion at 6 months in a double-blind trial (83 vs 74%of patients; p < 0.001).[48] Moreover, relative tolansoprazole, a greater proportion of esomeprazole
Table IV. Overview of 6-month randomised, double-blind, multicentre trials evaluating the efficacy of esomeprazole (ESO) administered asmaintenance therapy in patients with healed gastro-oesophageal reflux disease
Reference No. ofpts
Treatmentregimen (od)
Pts with healed oesophagitismaintaineda at 6 months (%)
Mean time to recurrence oferosive oesophagitis (days)
Pts who were heartburn-free at6 months (%) [no. evaluated pts]
Johnson et al.[43] 82 ESO 10mg 57.1* 78 70.5 [NR]
82 ESO 20mg 93.2* 115 72.5 [NR]
77 ESO 40mg 93.6* 163 77.8 [NR]
77 PL 29 34 66.7 [NR]
Vakil et al. [44] 91 ESO 10mg 54.2* 80 66.7 [45]
98 ESO 20mg 78.7* 101 77.8 [63]
92 ESO 40mg 87.9* 130 77.6 [67]
94 PL 29.1 46 52.4 [21]
a Maintenance of healed oesophagitis was defined as normal appearance (absence of mucosal breaks using the Los Angeles Classifica-tion system[50]), as assessed by endoscopy. Healing rates were based on life table analysis.
NR = not reported; od = once daily; PL = placebo; pts = patients; * p < 0.001 vs PL.
Esomeprazole: A Review 1521
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

recipients remained in remission across all gradesof baseline disease severity. In those with baselinedisease severity of grade A or B, 85% of esomep-razole recipients versus 77% of lansoprazole-treated patients remained in remission at 6 months,whereas in those with baseline disease severity ofgrade C or D remission rates were 76 and 59%, re-spectively (p < 0.01 for both comparisons). In addi-tion, significantly more esomeprazole than lan-soprazole recipients were asymptomatic at 6 months[heartburn-free (78 vs 71% of patients; p < 0.01), acidregurgitation-free (81 vs 72%; p < 0.001) and epigas-tric pain-free (80 vs 75%; p < 0.05)] .
The significantly higher percentage of patientsin remission with esomeprazole than lansoprazolewas further illustrated using a management modelof a cohort of patients from two separate trials dis-cussed in this section (an 8-week healing trial con-ducted by Castell et al.[40] and a 6-month mainte-nance study by Lauritsen et al.[48]).[60] Using thismodel, 77% (response rate at 8 weeks × responserate of patients after 6 months in these two trialsi.e. 92.6 × 83% of patients) of patients receiving ahealing regimen of 8 weeks’ esomeprazole 40mgonce daily followed by 6 months’ maintenancetreatment with esomeprazole 20mg once dailywould remain in remission. In contrast, withlansoprazole 30mg once daily for 8 weeks fol-lowed by once-daily lansoprazole 15mg for 6months, 66% (88.8 × 73.9%) of recipients wouldremain in remission.[60] Thus, 11 more esomep-razole than lansoprazole recipients are success-
fully treated for every 100 patients receiving eitheresomeprazole or lansoprazole, which correspondsto a 17% (77–66% = 11%; 11/66 × 100% = 17%)increase in the remission rates with esomeprazoletreatment. Moreover, after 6 months’ treatment inpatients with grade C and D severity of disease,healing was maintained in 65% of esomeprazolerecipients versus 43% of those in the lansoprazolegroup, resulting in a relative increase in remissionrates with esomeprazole compared with lanso-prazole treatment of 50%.
Additionally, esomeprazole 40mg once dailymaintained healed oesophagitis in 93.7 and 89.4%of patients at 6 and 12 months, respectively, in a12-month noncomparative trial.[49] Eighty-twopercent (22 of 27 patients) of recipients who had arecurrence of oesophagitis at 6 months but contin-ued therapy until the end of the trial had endoscop-ically confirmed healed oesophagitis at 12 months.As with the double-blind trials, healing was main-tained irrespective of gender, age, race or initialLA classification.
4.1.2 Patients with SymptomaticGORD without OesophagitisThe efficacy of esomeprazole in patients with
symptomatic GORD without oesophagitis, as con-firmed by endoscopy, has been evaluated in tworandomised, double-blind, multicentre trials (tableV).[47] Esomeprazole 20 or 40mg once daily in themorning for 4 weeks was more effective than pla-cebo according to both primary and secondary ef-ficacy criteria in these trials (reported in a single
Table V. Overview of 4-week randomised, double-blind, multicentre trials evaluating the efficacy of esomeprazole (ESO) in patients withsymptomatic gastro-oesophageal reflux disease without oesophagitis. All data are presented for intention-to-treat groups
Reference No. of pts Treatment (od) Days without HBa (%; mean) Time to sustained resolutionb of HBa (days; mean)
Katz et al.[47]c 121 ESO 20mg 62.7* 17.3*
123 ESO 40mg 62.8* 15.9*
124 PL 46.4 20.8
Katz et al.[47]c 113 ESO 20mg 68* 12.7*
118 ESO 40mg 66.4* 12.1*
118 PL 36.2 22.3
a Based on pts diary cards.
b Defined as no HB for seven consecutive days.
c Two studies reported in the same abstract.
HB = heartburn; od = once daily; PL = placebo; pts = patients; * p < 0.001 vs PL.
1522 Scott et al.
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

abstract).[47] The primary efficacy endpoint wasthe percentage of recipients showing complete res-olution of heartburn (patients with no heartburnduring the final 7 days of the 4-week studies) [fig-ure 3], with 33.3 to 41.6% of patients achievingcomplete resolution with esomeprazole versus11.9 and 13.7% of those in the placebo group (p <0.001 for all comparisons of esomeprazole withplacebo).
Esomeprazole effectively resolved heartburnsymptoms in these patients, with appreciably moreheartburn-free days in the esomeprazole than pla-cebo group (table V).[47] With esomeprazole 20 or40mg once daily 63 to 68% of days were heart-burn-free compared with 36 and 46% with placebotreatment (p < 0.001 for all comparisons). Themean time to sustained resolution of heartburn wasalso significantly shorter with esomeprazole thanplacebo (12.1 to 17.3 vs 20.8 and 22.3 days; p <0.001).
‘On-Demand’ TherapySymptom-driven on-demand therapy in pa-
tients without erosive oesophagitis has been eval-uated in two randomised, double-blind, multi-centre studies (table VI),[45,46] one of which iscurrently available only as an abstract.[46] Patients
enrolled were endoscopy-negative for oesophag-itis following previous short-term treatment withesomeprazole or omeprazole and showed com-plete resolution of heartburn (absence of heartburnduring the last 7 days of the previous 4-week treat-ment period). The primary efficacy endpoint wasthe time to discontinuation of therapy due to un-willingness to continue; the secondary criterionwas the time to discontinuation because of insuffi-cient control of heartburn. Patients received on-demand (as required) therapy with once-daily eso-meprazole 20 or 40mg, or placebo for 6 months.Rescue medication with antacids was also permit-ted.
On-demand therapy proved beneficial accord-ing to both primary and secondary efficacy end-points (table VI).[45,46] Log-rank analysis indicatedthat the time to discontinuation because of un-willingness to continue therapy was appreciablylonger in those receiving esomeprazole 20 or 40mgthan placebo recipients (p < 0.0001 in both stud-ies), with markedly fewer patients having discon-tinued treatment at study end in the esomeprazolethan placebo group (8 to 15% vs 42 and 52% ofpatients) [table VI].[45,46] The major reason for dis-continuation of treatment in both groups was inad-equate control of heartburn (5 to 14% vs 36 and51% of patients discontinued treatment) [table VI].Mean consumption of rescue medication was alsosignificantly (p < 0.0001) higher in placebo thanesomeprazole groups in both studies (mean con-sumption 1.06 to 1.07 tablets vs 0.39 to 0.44 tab-lets) .
4.2 Eradication of Helicobacterpylori Infection
The successful eradication of H. pylori infec-tion has been shown to cure duodenal ulcers andprevent relapse in the majority of patients.[61] Cur-rently, combination therapy with a proton pumpinhibitor plus two antimicrobial drugs given to-gether for 1 to 2 weeks is commonly used for erad-ication of H. pylori infection.
Well designed clinical trials evaluating 7 to 10days’ treatment with triple therapy regimens that
Com
plet
e re
solu
tion
of h
eart
burn
(% o
f pat
ient
s)
45
40
35
30
25
20
15
10
5
0Study 1 Study 2
ESO 20mg odESO 40mg odPL* *
*
*
Fig. 3. Efficacy of esomeprazole (ESO) in patients with symp-tomatic gastro-oesophageal reflux disease. Percentage of pa-tients showing complete resolution of heartburn (no heartburnduring the final 7 days of the study; primary endpoint) in two4-week randomised, double-blind, multicentre trials (reported ina single abstract).[47] 121, 123 and 124 patients received eso-meprazole 20 or 40mg once daily (od) or placebo (PL), respec-tively, in study 1; corresponding patient numbers in study 2 were113, 118 and 118. * p < 0.001 vs PL.
Esomeprazole: A Review 1523
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

included esomeprazole (20mg twice daily or 40mgonce daily) or omeprazole (20mg twice daily), plusamoxicillin (1g twice daily) and clarithromycin(500mg twice daily) are summarised in table VII.Only patients ≥18 years of age with endoscopicallyconfirmed duodenal ulcer disease (at least one ul-cer ≥0.5cm in diameter) or who had a history ofduodenal ulcer disease confirmed by endoscopy orradiology within the previous 5 years were in-cluded. All participants were H. pylori-positive.Patients with a gastric, prepyloric or pyloric ulcer,complications of duodenal ulcer disease (e.g.bleeding or perforation), those with a serious con-comitant disease, and those using NSAIDs, a bis-muth-containing preparation, a proton pump inhib-itor or an antibacterial up to 4 weeks prior to studyentry were excluded.
The primary efficacy endpoint evaluated in allstudies was the H. pylori eradication rate 4[37,39] or4 to 6[38] weeks after completion of triple therapyand was assessed by [13C]-urea breath test,[37-39]
culture[37] and/or histology.[37,38] In addition, ulcerhealing (defined as complete re-epithelialisation ofthe ulcer) was also assessed endoscopically 3 and7 to 9 weeks after completion of triple therapy inone trial.[38] In two[38,39] of the three studies, symp-tom resolution was assessed subjectively by pa-tients using diary records and was based on thefive-point scale described earlier (section 4.1.1).
4.2.1 Eradication RatesIn over 400 patients with endoscopically con-
firmed duodenal ulcer disease, eradication of H.pylori occurred in 86 to 90% of recipients of triple
therapy regimens including esomeprazole 20mgtwice daily for 7 days (table VII).[38,39] These erad-ication rates were similar to those achieved withomeprazole-based triple therapy regimens (eradi-cation rate 88% in both studies). Notably, eradica-tion rates in both treatment groups exceeded theintention-to-treat eradication rate (80%) advocatedin the Maastricht Consensus report[62] and by theAmerican College of Gastroenterology for agentsused to treat H. pylori infection.[63]
As expected, 10 days’ treatment with triple ther-apy including esomeprazole 40mg once daily wassignificantly (p < 0.001) more effective in eradi-cating H. pylori infection than 10 days’ dual ther-apy (esomeprazole plus clarithromycin at the samedosages) in an intention-to-treat analysis (77 vs52% of patients) [table VII].[37] In a smaller study(n = 98) also reported in this paper,[37] the sametriple therapy regimen was more effective thanmonotherapy for 10 days with esomeprazole 40mgonce daily, with eradication of H. pylori occurringin 78 and 4% of recipients, respectively, in inten-tion-to-treat groups (p < 0.001).
Emerging resistance, particularly in the US, toclarithromycin and other antimicrobial agents usedin triple therapy regimens is of increasing concern.Of note, pooled data from the two trials by Laineet al.[37] plus another small (n = 66) study (dualtherapy with the same dosages of esomeprazoleplus clarithromycin or esomeprazole monother-apy; not discussed as this regimen is not currentlyrecommended) reported in the same publication in-dicated that 15% of H. pylori clinical isolates col-
Table VI. Overview of 6-month randomised, double-blind, multicentre trials evaluating the efficacy of esomeprazole (ESO) as ‘on-demand’therapy in patients with gastro-oesophageal reflux disease without erosive oesophagitis
Reference No. of pts Treatment regimen(od prn)
Discontinuation due to unwillingnessto continue therapya (% pts)
Discontinuation of therapy due toinsufficient control of heartburna (% pts)
Talley et al.[45] 170 ESO 20mg 15 14
172 PL 52 51
Talley et al.[46] b 282 ESO 20mg 8 5
293 ESO 40mg 11 9
146 PL 42 36
a At study end.
b Abstract.
od = once daily; PL = placebo; prn = as required; pts = patients.
1524 Scott et al.
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

lected from these patients at baseline were resis-tant to clarithromycin.[37] Resistance levels atbaseline were higher in patients who had pre-viously received H. pylori eradication therapy witha regimen that included clarithromycin than inthose who were clarithromycin treatment-naive atbaseline [61% (14 of 23 patients) vs 12% (52 of422)]. After completion of triple therapy, clar-ithromycin-resistant strains had emerged in 33%(2 of 6 patients) of patients who had clar-ithromycin-susceptible strains of H. pylori at base-line and had failed to eradicate infection, whereasclarithromycin-resistant strains had emerged in85% (23 of 27 patients) of recipients with thesefeatures in the esomeprazole plus clarithromycingroup.
4.2.2 Effects on Ulcer Healing andSymptom ResolutionCurrently, data evaluating the efficacy of
esomeprazole-based triple therapy regimens on ul-cer healing are limited. In a well designed trial,triple therapy including esomeprazole (20mgtwice daily for 1 week) followed by 3 weeks’ treat-ment with placebo was as effective for ulcer heal-ing as a similar twice-daily omeprazole-based tri-ple therapy regimen for 1 week followed byomeprazole 20mg once daily for 3 weeks (91 vs92% of patients experienced ulcer healing; inten-tion-to-treat analysis).[38]
In general, recipients of esomeprazole-tripletherapy regimens experienced a marked improve-ment in the frequency and severity of epigastricpain and heartburn from baseline levels in twodouble-blind trials (see table VII for design de-tails).[38,39] In the larger study, markedly fewer pa-tients were experiencing epigastric pain (14 vs96% of patients at baseline) and heartburn (10 vs66%) after 4 weeks’ treatment (1 week of esome-prazole-based triple therapy followed by 3 weeksof placebo) than at baseline.[38] Similar symptom-atic improvements from baseline to 4 weeks wereseen in the omeprazole group [1 week of om-eprazole-based triple therapy followed by 3 weeksof omeprazole monotherapy (epigastric pain: 95%of patients had symptom at baseline vs 15% of pa-tients after 4 weeks’ treatment; heartburn: 68 vs5%)]. These improvements were maintained inboth treatment groups at 8 to 10 weeks follow-up.All values were estimated from graphs and no sta-tistical data were reported. In addition, at baseline,38 and 36% of patients in the esomeprazole andomeprazole groups, respectively, were experienc-ing severe epigastric pain, whereas after 4 weeks’treatment markedly fewer patients in both groupshad severe epigastric pain (0 and 1% of pa-tients).[38] There was also a decrease from baselinein the proportion of patients experiencing severe
Table VII. Overview of the efficacy of esomeprazole (ESO) in multicentre, randomised, double-blind trials in adult patients with duodenalulcer and confirmed Helicobacter pylori infection. All data are presented for intention-to-treat groups
Reference No. of pts Treatment duration (days) Dosage regimena Eradication rateb (%)
Laine et al.[37] 223 10 ESO 40mg od + AMC 1g bid + CLA 500mg bid 77
215 10 ESO 40mg od + CLA 500mg bid 52
Tulassay et al.[38] 214 7 ESO 20mg + AMC 1g + CLA 500mg; then PLfor 3 wks
86
219 7 OMP 20mg + AMC 1g + CLA 500mg; thenOMP 20mg od for 3 wks
88
Veldhuyzen VanZanten et al.[39]
204 7 ESO 20mg + AMC 1g + CLA 500mg 90
196 7 OMP 20mg + AMC 1g + CLA 500mg 88
a All drugs given orally twice daily unless indicated otherwise.
b Eradication was defined as the absence of H. pylori based on histology,[37-39] culture,[37] and/or urea breath test.[37-39] Eradication rateswere assessed 4[37,39] or 4 to 6 wks after completion of triple therapy.[38]
AMC = amoxicillin; bid = twice daily; CLA = clarithromycin; od = once daily; OMP = omeprazole; PL = placebo; pts = patients; * p < 0.001vs dual therapy.
Esomeprazole: A Review 1525
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

heartburn in both treatment groups (esomeprazole:19 vs 0%; omeprazole: 16 vs 0%).
4.3 Pharmacoeconomic Considerations
The economic importance of upper GI disordersand their management is underlined by the numberof patients who present with the symptoms of thisgroup of disorders each year. Figures from the UKsuggest that the annual prevalence of dyspepsia isover 40%, and that GI disease accounts for 10% ofthe work of general practitioners.[64] The healtheconomic implications of management in primarycare relate mainly to the costs of investigation andtherapy (notably antisecretory drugs), endoscopy,radiology and specialist referral.[64]
Upper GI disorders are also associated withconsiderable impairment of quality of life on awide scale: in the Domestic/International Gastro-enterology Surveillance Study (DIGEST) in 5581respondents from ten countries, the overall rate ofreporting of GI symptoms was 46.4%, which wascompared with an approximate 25% prevalence ofhypertension, asthma and diabetes mellitus.[65] Themost frequently reported symptoms were heart-burn, diarrhoea and postprandial fullness, with 10to 20% of respondents reporting at least one ofthese several times a week. Symptoms were severeor interfered ‘quite a lot’ with daily activities in 7.3and 4.8% of respondents, respectively.[65]
Pharmacoeconomic studies of esomeprazoleare currently limited to direct cost analyses basedon the retrospective study of clinical trial resultsand/or patient databases. Two studies are fullypublished[66,67] and the remainder are available inpreliminary form as abstracts.[68-71]
4.3.1 Reflux OesophagitisPooled data from three 8-week clinical studies
in 4877 patients with reflux oesophagitis showed a14% reduction in direct medical costs with esome-prazole 40mg daily treatment compared with om-eprazole 20mg daily.[66] Data were incorporatedinto a decision-analysis model that considered UKcosts. Direct medical costs for primary care visits,gastroenterologists visits and upper gastrointesti-nal endoscopy were based on 1998 values, and
those for the acquisition of drugs on 2000 values.Healing probabilities were calculated from theclinical trial results, and patient management as-sumptions were based on UK clinical practice. Lifetable estimates of healing rates were 93.4 and86.2% for esomeprazole and omeprazole, respec-tively (p < 0.001), after 8 weeks, with a direct costsaving over the same period of £1290 with esome-prazole over omeprazole. This saving increased to£2064 when the cost of managing treatment failurewas included (treatment failure defined as a patientnot healed as assessed by endoscopy). Similar re-sults were reported when these data were extrapo-lated to include Swedish and Finnish patients.[68]
4.3.2 Symptomatic GORD withoutEndoscopic ConfirmationEsomeprazole 40mg daily showed an apparent
savings over omeprazole 20mg daily in non-en-doscoped GORD in direct medical costs (UK Na-tional Health Service perspective; year of costingnot reported in abstract).[69] Data for the modelwere derived from clinical trials and a UK physi-cian survey. Time with GORD, defined as weekswith symptoms or endoscopic lesions, was used asthe measure of efficacy. The investigation was car-ried out because patients with GORD in the pri-mary care setting usually receive empirical therapybased on symptoms, with no referral for endos-copy.
Time with GORD was 3.3 weeks with esome-prazole and 3.6 weeks with omeprazole, withlower overall direct costs (not detailed) in esome-prazole recipients. This result was sensitive tochanges in drug costs, however. When costs asso-ciated with treatment failure after 8 weeks wereincluded, the cost saving with esomeprazole wasmaintained even when the acquisition cost of om-eprazole was reduced by more than one-third.[69]
4.3.3 On-Demand Treatment of GORDwithout OesophagitisCost advantages of esomeprazole relative to
omeprazole have been reported in three analyses inpatients with GORD without oesophagitis.[67,70,71]
One of these compared on-demand therapy withesomeprazole 20mg daily with intermittent 4-week
1526 Scott et al.
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

acute courses of omeprazole 20mg daily and con-tinuous treatment with the same dosage of om-eprazole (after acute treatment of first relapse).[67]
Relapse probabilities were calculated from the re-sults of two 6-month clinical studies comparingesomeprazole with placebo in 770 patients; patientmanagement assumptions were based on a UKphysician survey, and UK costs applied, in theMarkov model used in this study. Direct medicalcosts for primary care visits, gastroenterologistsvisits and upper gastrointestinal endoscopy werebased on 1998 values, and those for the acquisitionof drugs on 2000 values. On-demand treatmentwith esomeprazole maintained remission in 90%of patients over 6 months, compared with 53% ofplacebo recipients. Direct medical costs were re-duced by 16 and 35% relative to the intermittentand continuous omeprazole treatments, respec-tively.[67] A preliminary report has shown similarresults when the UK survey results were adjustedfor Finland and Sweden on the basis of expert opin-ion and direct medical costs from all three coun-tries were applied to the model.[70]
Further cost-of-treatment data (based on drugcosts alone) have been derived from a primary caredatabase containing information on 1028 om-eprazole-treated patients from approximately 120medical practices in the UK and the two 6-month[45,46] clinical studies of on-demand treat-ment referred to above. Twenty-eight-day costs oftreatment for omeprazole were set at £28.56 for20mg daily and £18.91 for 10mg daily; that foresomeprazole 20mg daily was assumed to be£18.50 (year of costing not reported). Drug usageestimated from the patient database and clinicalstudies showed an annual cost advantage foresomeprazole (figure 4).[71]
5. Tolerability
Esomeprazole 20 or 40 mg/day is generally welltolerated when administered as healing and/orsymptom resolution monotherapy (4 to 8 weeks’duration), maintenance monotherapy (up to oneyear) or in combination with amoxicillin and clar-ithromycin for 7 to 10 days for the eradication of
H. pylori infection. The nature and frequency ofadverse events with esomeprazole were similar tothose experienced with either omeprazole orlansoprazole in well designed 8-week trials.
5.1 Healing and/or SymptomResolution Therapy
In two large 8-week, randomised, double-blindtrials (n = 2405 and 1957), similar percentages ofpatients with erosive oesophagitis who receivedesomeprazole 40 or 20mg or omeprazole 20mgonce daily discontinued treatment because of anadverse event (approximately 1 to 2.6% of pa-tients)[41,42] or experienced an adverse event thatwas considered to be treatment related (15.1 to15.3%).[42] The nature and frequency of adverseevents was also similar in all treatment groups,with the most common (1.8 to 8.7%) being head-ache, diarrhoea, nausea, abdominal pain, respira-tory infection, flatulence and gastritis[41,42] (eventsreported in the larger study are presented in figure5 [42]). No treatment-related serious adverse eventswere reported with esomeprazole or omeprazoletherapy in these studies. There were also no clini-cally relevant changes in laboratory parameters orvital signs with either treatment.
In addition, there were no between-group dif-ferences in the tolerability profiles with esomep-
0
50
100
150
200
250
300
Esomeprazole20mg
Omeprazole10mg
Omeprazole20mg
Ann
ual d
rug
cost
(£)
Fig. 4. Annual cost of treatment with esomeprazole 20mg, om-eprazole 10mg or omeprazole 20mg daily. Drug usage data forpatients with gastro-oesophageal reflux disease without oeso-phagitis were obtained from a UK general practice database(2081 patients) for omeprazole and from two clinical trials foresomeprazole (452 patients).[71] UK drug costs only were in-cluded in the analysis (year of costings not reported in abstract).
Esomeprazole: A Review 1527
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

razole 40mg once daily or lansoprazole 30mg oncedaily in a large randomised, double-blind trial in>5000 patients with erosive oesophagitis.[40] Tenpercent of patients in each treatment group experi-enced at least one adverse event considered to bedrug-related. Reported incidences of adverse eventsin the esomeprazole and lansoprazole groups, respec-tively, were: headache (5.8 vs 4.5%), diarrhoea (4.2vs 4.7%), respiratory infection (2.8 vs 3.8%), abdom-inal pain (2.9 vs 2.9%), flatulence (2.3 vs 2.4%) andnausea (2.1 vs 2.5%). Treatment-related serious ad-verse events occurred in 0.7 and 0.5% of patientsin the esomeprazole and lansoprazole groups, re-spectively, with 1.8 and 1.9% of recipients discon-tinuing treatment due to adverse events. Therewere no clinically relevant changes in laboratoryparameters or vital signs in either treatment group.
In pooled tolerability data from four rando-mised trials reported in the manufacturer’s pre-scribing information for esomeprazole,[12] themost frequently occurring events (>1%) in recipi-ents of esomeprazole 20mg (n = 1240), esomep-razole 40mg (n = 2434) or omeprazole 20mg (n =3008) once daily were headache (5.5, 5.0 and3.8%, respectively) and diarrhoea (no differencebetween incidences; values not reported).
No clinically relevant electrocardiographic ef-fects were reported in 82 healthy volunteers (aged20 to 50 years) who received esomeprazole 40mgonce daily for 5 to 7 days in a pooled analysis ofphase I nonblind studies.[72]
In patients who received triple therapy (esome-prazole plus amoxicillin and clarithromycin) for 7to 10 days for the eradication of H. pylori infection,the most common adverse events were diarrhoea(9.2%), taste perversion (6.6%) and abdominalpain (3.7%), according to pooled tolerability data(number of patients not reported).[12] Adverseevents reported with triple therapy were similar tothose that occurred with either esomeprazole,amoxicillin or clarithromycin alone.[12] In addi-tion, triple therapy was not associated with higherincidences of specific treatment-emergent adverseevents than with esomeprazole alone.[12]
The esomeprazole triple therapy regimen wasassociated with an adverse event profile and fre-quency comparable to that of omeprazole plusamoxicillin and clarithromycin within each ran-domised trial.[38,39] Similar percentages of eso-meprazole and omeprazole recipients reported atleast one adverse event (33 and 29.5%, respec-tively in patients with active duodenal ulcers atbaseline[38] and 58.5 and 54.5% in those with-out[39]). Less than 2% of patients from each studydiscontinued treatment because of adverse events.
5.2 Maintenance Therapy
In two 6-month randomised, double-blind trials(n = 375 and 318), patients who received esome-prazole 10, 20 or 40mg remained in the studies fora much longer time than placebo recipients (meanvalues: 116 to 161 vs 59 and 61.5 days).[43,44]
Therefore, direct comparisons of adverse eventincidences were difficult to make. Over 6 months,esomeprazole was generally associated withhigher rates of discontinuation due to adverseevents (1.3 to 6.5 vs 2.2 and 2.6%)[43,44] and higheroverall frequencies of adverse events (57.1 to 60.9vs 45.7%)[44] than placebo, possibly because of thelonger treatment time with the active drug. How-ever, after 1 month of treatment, the incidences of
0 2 4 6 8
Incidence (% of patients)
Headache
Diarrhoea
Nausea
Abdominalpain
OmeprazoleEsomeprazole
Fig. 5. Tolerability of esomeprazole in an 8-week trial. Compar-ison of adverse events associated with oral esomeprazole 40mgor omeprazole 20mg once daily in 2405 patients with erosiveoesophagitis in a randomised, double-blind, multicentre trial.[42]
1528 Scott et al.
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

the most common adverse events and the propor-tions of patients who experienced at least one ad-verse event were similar in the esomeprazole andplacebo groups in both studies.[43,44] Over the 6-month duration of these trials, the most commonadverse events reported with esomeprazole treat-ment were headache (7.8%), respiratory infection(6.7 or 7.6%), diarrhoea (5.1 or 6.4%), sinusitis(6.3%) and/or flatulence (5.4%).[43,44]
The nature and incidence of adverse events re-ported in a 12-month noncomparative trial (n =807) were similar to those reported in 4- to 8-weektrials.[49] Adverse events related to esomeprazoletreatment for 12 months and reported by >3% ofpatients included diarrhoea, abdominal pain, flat-ulence and headache.
In a study of on-demand maintenance therapyin 341 patients without erosive oesophagitis, con-siderably more patients receiving esomeprazole20mg as required (up to 20 mg/day) completed thestudy than placebo recipients (83 vs 46%).[45] Moreesomeprazole recipients experienced adverseevents (43 vs 27%); however, there was no be-tween-group difference in the frequency of eventswhen data were adjusted for exposure to treatment.Respiratory infection was the most common eventin both treatment groups (esomeprazole 6%, pla-cebo 8%) and one patient from each group with-drew from treatment because of adverse events.
Esomeprazole, like other proton pump inhibi-tors, increases serum gastrin levels (section 2.3).There is some concern that hypergastrinaemia maypromote tissue growth and carcinogenesis (re-viewed by Svoboda[73] and Maton[74]). However,in pooled tolerability data[75] from noncompara-tive[49] and randomised studies[43,44] in a total of1326 patients with healed erosive oesophagitiswho received esomeprazole 10, 20 or 40 mg/dayor placebo for up to 6 or 12 months, no en-terochromaffin-like cell dysplasia, carcinoids orneoplasia were reported; long-term clinical expe-rience is required to confirm these results. Gastrichistological scores in both esomeprazole and pla-cebo recipients fluctuated to a minor extent, andno concerns were raised relating to long-term eso-
meprazole use and atrophic gastritis developmentor clinically significant changes in entero-chromaffin-like cells.[75]
6. Dosage and Administration
Esomeprazole is indicated for the healing andmaintenance of healed erosive oesophagitis asso-ciated with GORD and the treatment of symptom-atic GORD.[12,76] In combination with an appropri-ate antibacterial regimen, esomeprazole is alsoindicated for the eradication of H. pylori infectionin patients with duodenal ulcer disease[12,76] or ahistory of duodenal ulcers within the past 5years.[12] Dosage recommendations for esome-prazole differ from country to country; recommen-dations for the US and the UK are outlined accord-ing to indication in table VIII.
Esomeprazole dispersable tablets [multiple unitpellet system (MUPs)] should be swallowed wholeat least 1 hour before eating. For patients who havedifficulty swallowing, the pellets may be mixedand administered with apple sauce.[32] In nursingmothers, a decision should be made whether to dis-continue nursing or to discontinue treatment. Al-though animal studies have shown no evidence offetal abnormality, there are no well controlled tri-als in pregnant women [US Food and Drug Admin-istration (FDA) category B rating]; thus, the drugshould be used during pregnancy only if clearlyneeded.[12,76] Dosage adjustments are not requiredfor patients who are elderly or have renal or mildto moderate hepatic impairment.[12,33,34,76] In pa-tients with severe hepatic impairment, the dosageof esomeprazole should not exceed 20mg per day(see section 3.3).[12,33,76] The tolerability and effec-tiveness of the drug have not been established inpaediatric patients.[12,36,76]
Coadministration of esomeprazole with pheny-toin, warfarin, quinidine, clarithromycin oramoxicillin does not produce any clinically signif-icant interactions (section 3.4);[12,36] plasma con-centrations of phenytoin should be monitoredwhen initiating or discontinuing coadministrationof esomeprazole.[76] Esomeprazole may interferewith the absorption of drugs where gastric pH is an
Esomeprazole: A Review 1529
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

important determinant of bioavailability, such asketoconazole, digoxin and iron salts. Althoughcoadministration of esomeprazole and diazepamreduced the clearance of diazepam, this interactionis unlikely to be of clinical relevance.
When administering triple therapy for the erad-ication of H. pylori, contraindications and interac-tions for all component drugs including clar-ithromycin and amoxicillin should be considered.
7. Place of Esomeprazole in theManagement of Acid-Related Disorders
Acid-related disorders are common digestivesystem disorders and impose considerable eco-nomic burdens on healthcare systems and societyworldwide.[77] The primary goal in the manage-ment of these disorders is suppression of basal andstimulated gastric acid secretion to alleviate symp-toms, and to allow healing and prevent the recur-rence of ulcers.[78,79] Resolution of symptoms, inturn, is pivotal to improving the patient’s qualityof life and reducing costs associated with acid-re-lated disorders.[78,80-82] Furthermore, reducingacid-induced damage to the oesophagus and othergastrointestinal structures may reduce the risk of
progression to adenocarcinoma and other late com-plications.
Pharmacotherapy is now considered the corner-stone of treatment of acid-related disorders,[78,83,84]
although concurrent changes in lifestyle are alsoadvocated in some guidelines.[83] Although antac-ids and anticholinergic drugs have been used in thepast, improved understanding of the pathophysiol-ogy of acid-related disorders has resulted in thedevelopment of more potent antisecretory agentssuch as the proton pump inhibitors (esomeprazole,omeprazole, lansoprazole, pantoprazole and ra-beprazole). As a class, proton pump inhibitors rep-resent a major advance in the management of acid-related disease, displaying superiority over thehistamine H2-receptor antagonists (e.g. ranitidine,cimetidine) in suppression of basal and stimulatedgastric acid secretion and in the treatment of gastricand duodenal ulcers and GORD.[80,83,85-90] Al-though proton pump inhibitors are generally advo-cated as the treatment of first choice, no individualproton pump inhibitor is recommended over an-other.[83,91]
Esomeprazole is the first proton pump inhibitorto be developed as a single optical isomer (S-iso-mer of omeprazole). This confers pharmacological
Table VIII. Dosage recommendations for oral esomeprazole in adult patients in the US and the UK
Indication UK[76] US[12]
Gastro-oesophageal reflux disease(GORD) with erosive oesophagitis
Healing 40mg od for 4-8 wksa 20 or 40mg od for 4-8 wksa
Maintenance 20mg od in pts with healed erosiveoesophagitisb
20mg od in pts with healed erosiveoesophagitisb
Symptomatic GORD Acute 20mg od for 4 wksc 20mg od for 4 wksd
On-demand 20mg od as required No recommendations
Helicobacter pylori eradication in pts with dudoenal ulcerdiseasee
Triple therapy with esomeprazole20mg plus amoxicillin 1g andclarithromycin 500mg; all agentsadministered bid for 7 days
Triple therapy with esomeprazole40mg od plus amoxicillin 1g bid andclarithromycin 500mg bid for 10days
a If oesophagitis is not healed after 4-8 wks, an additional 4-8 wks’ treatment may be considered.
b Currently, controlled studies of >6 months’ duration have not been carried out; a noncomparative trial of 12 months’ duration has beenconducted[49] (section 4.1.1 and section 5.2).
c If symptoms are unresolved after 4 wks of treatment, further clinical investigations should be carried out.
d If symptoms have not completely resolved after 4 wks, a further 4 wks of treatment may be considered.
e Active disease or a history of disease within the last 5 years.
bid = twice daily; od = once daily; pts = patients.
1530 Scott et al.
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

(see section 2 and 3) advantages to esomeprazoleover omeprazole. In several studies, most of whichwere nonblind crossover trials, esomeprazole atclinically relevant dosages was at least as effectiveas rabeprazole and appreciably better than om-eprazole, lansoprazole or pantoprazole in themaintenance of intragastric pH at a level >4 whengiven for 5 days (see section 2.2). Mucosal healinghas been shown to correlate directly with the pro-portion of each 24-hour period for which the pH ofthe intragastric compartment is held above thislevel. Esomeprazole also demonstrated a faster on-set of action than rabeprazole, which has beenreported to have the fastest onset of action ofthe racemic proton pump inhibitors (i.e. omepra-zole, rabeprazole, lansoprazole and pantopra-zole).[1,11,88,89] In addition, esomeprazole has amore favourable pharmacokinetic profile than om-eprazole, showing higher bioavailability and re-duced interpatient variability (see section 3.2).
These pharmacological advantages are re-flected in the better efficacy of esomeprazole com-pared with lansoprazole or omeprazole (see sec-tion 4.1.1). To date, there are no fully publisheddirect head-to-head comparisons of the clinical ef-ficacy of esomeprazole with rabeprazole orpantoprazole in patients with erosive oesophagitis.
7.1 GORD
GORD is a common chronic, multifactorial dis-order with the potential to cause serious disease,such as Barrett’s oesophagus and ulceration that,in turn, may result in adenocarcinoma.[91] The dis-ease has an estimated incidence of 10 to 40% in thegeneral population;[91-93] however, the true preva-lence of GORD may be considerably higher sincemany patients self-medicate with over-the-counter antacids and never seek medical ad-vice.[77,86,90,94,95] Indeed, heartburn (the most fre-quently occurring symptom) is experienced at leastonce a day by 7% of the US general population,with approximately 40% experiencing heartburn atleast once a month.[92,93,96,97]
Characteristic features of GORD are the pres-ence of reflux symptoms severe enough to cause
impairment of quality of life and/or the presenceof erosive oesophagitis. Forty to 60% of patientshave symptomatic GORD without oesophagitis,with diagnosis based on the presence of symptomsthat typically include heartburn and/or regurgita-tion and in some patients may also include atypicalsymptoms such as asthma, hoarseness and non-cardiac chest pain.[78,83,86] Of note, there is a poorcorrelation between the severity and frequency ofsymptoms associated with GORD and the presenceor severity of erosive oesophagitis.[98-102]
Patients with GORD generally require long-term maintenance therapy; after completion ofsuccessful healing therapy, up to 80% of patientsexperience a recurrence of symptoms and/or oeso-phagitis within 6 to 12 months.[78,84,86,102,103] Pro-ton pump inhibitors have proven the most cost-effective agents for maintenance of healedoesophagitis and are currently the agents of choicein this patient group.[78,79,84,86,91,96] In those withsymptomatic GORD, intermittent or symptom-driven on-demand therapy with either a protonpump inhibitor or an H2-receptor antagonist is rec-ommended for controlling symptoms.[84,91]
Against a background of increasing scrutiny bygovernments and health providers of the costs ofdrug therapy and the high prevalence of gastro-oe-sophageal disorders, it is important to considerdrug expenditure in these patients. Antisecretorymedication constitutes a source of considerable ex-pense for healthcare systems; nevertheless, thetherapeutic benefit associated with this group ofdrugs is beyond doubt, and their cost effectivenessrelative to histamine H2-receptor antagonists in thehealing of reflux oesophagitis and peptic ulcer-ation has been demonstrated (reviewed by Byrneand Murray[104]). Current opinion states that theneed for inclusion of a proton pump inhibitor informularies is beyond doubt; the issue for discus-sion is which to include.[104] Relative acquisitioncosts of proton pump inhibitors vary across coun-tries, and this is likely to be a dominant factor indecisions relating to formulary inclusion. In addi-tion, local licensing arrangements may also needto be considered.
Esomeprazole: A Review 1531
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

Most pharmacoeconomic data relevant to pro-ton pump inhibitors have been derived from stud-ies of omeprazole and (to a lesser extent) lansopra-zole.[104] However, data relevant to esomeprazoleare accumulating, and preliminary reports suggestcost advantages relative to omeprazole in patientswith GORD and those with reflux oesophagitis,although studies are limited to retrospective directcost analyses and modelled scenarios (see section4.3). In light of the promising pharmacodynamic(section 2) and clinical results (section 4) availablefor esomeprazole, prospective pharmacoeconomicstudies are now required to clarify further the placeof the drug relative to other agents of the sameclass. Analyses linking cost to disease outcomes(e.g. cost per episode of reflux avoided) are likelyto be of particular assistance.
Quality-of-life issues should also be consideredwhen assessing the relative merits of agents usedin the management of gastro-oesophageal disor-ders, as these patients have decreased functionalstatus and levels of wellbeing relative to the gen-eral population.[81,82,102,105] Moreover, the impactof GORD on the patient’s quality of life is associ-ated with more absences from work and reducedproductivity relative to the general popula-tion.[106,107] The frequency and severity of heart-burn in patients with GORD has been shown todirectly correlate with impairment of patients’quality of life, regardless of the presence or sever-ity of oesophagitis.[77,102,103,108] Application of ageneral wellbeing instrument and two question-naires specific to gastrointestinal symptomsshowed significant improvements in quality of lifein 146 patients receiving treatment for suspectedpeptic ulcer.[109] Quality-of-life data obtained inpatients receiving esomeprazole are currently notavailable, however, and are therefore awaited withinterest.
Current therapeutic management focuses on al-leviating symptoms and achieving healing, leadingto improvements in patients’ quality of life and po-tentially reducing the subsequent serious conse-quences of prolonged exposure of the oesophagealmucosa to acid. Recent treatment guidelines advo-
cated by the American College of Gastroenterol-ogy[83] and the international multidisciplinaryGenval Workshop Report[108] recommended em-pirical therapy in patients with symptomaticGORD; those who respond to therapy may be pre-sumed to have GORD, whereas further investiga-tions are warranted in those who fail to respond topharmacotherapy. These guidelines recommendantacids and antireflux agents (e.g. histamine H2-receptor antagonists) in combination with lifestylemodifications for the short-term treatment of pa-tients with mild GORD. However, if symptomspersist or are more severe, proton pump inhibitorsare recommended for initial treatment of GORD.According to these guidelines, maintenance ther-apy with a proton pump inhibitor is recommendedin patients with oesophagitis and in those whosesymptoms are refractory to antacids.
Esomeprazole effectively healed oesophagitisand resolved heartburn in patients with GORD (seesection 4.1.1). Overall, esomeprazole was betterthan omeprazole, although differences favouringesomeprazole did not always achieve statisticalsignificance . Of note, in a large (n >5000 patients)well designed 8-week trial, esomeprazole 40mgonce daily was significantly more effective in pro-moting mucosal healing, as confirmed by endos-copy and symptom resolution, than lansoprazole30mg once daily (see section 4.1.1).[40] The differ-ence in rates of healed oesophagitis with esome-prazole versus lansoprazole increased in favour ofesomeprazole as the baseline severity of oesophag-itis increased. This higher response rate withesomeprazole relative to lansoprazole in those withmore severe oesophagitis may be particularly rel-evant in the setting of empirical therapy for GORD,where the underlying disease severity is unknown.The clinical significance of the statistical differ-ences favouring esomeprazole versus lansoprazolewill be best defined by patient responses in thepractice setting.
Esomeprazole also proved effective as mainte-nance therapy. In 6-month double-blind, placebo-controlled trials in patients with healed oesophagitis,esomeprazole 20 or 40mg once daily maintained
1532 Scott et al.
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

healing in 79 to 94% of patients, with >72% ofpatients free from heartburn. Furthermore, esome-prazole 20mg once daily was significantly more ef-fective than lansoprazole 15mg once daily in main-taining remission from oesophagitis and keepingpatients symptom-free at 6 months in a large, dou-ble-blind trial.[48]
In addition, 4-week double-blind trials in pa-tients with symptomatic GORD without oesophag-itis demonstrated that esomeprazole 20 or 40mgonce daily was appreciably more effective thanplacebo in resolving symptoms of GORD (see sec-tion 4.1.2). Symptom-driven on-demand therapyfor 6 months effectively controlled symptoms inthis patient population (see section 4.1.2), al-though on-demand therapy is not currently recom-mended in the US (see section 6). To date, thereare no clinical trials in these patients compar-ing esomeprazole, either as acute treatment oron-demand therapy, with other proton pump inhib-itors.
7.2 Eradication of H. pylori Infection
Research defining the pivotal role of H. pyloriinfection in the pathogenesis of gastric and duode-nal ulcer disease has been central to the successfulmanagement of peptic ulcer disease; approxi-mately 70 and 90% of patients with gastric andduodenal ulcers, respectively, are H. pylori-posi-tive.[110,111] Furthermore, epidemiological evi-dence suggests an association between H. pyloriinfection and the occurrence of distal gastric car-cinoma and gastrin mucosal-associated lymphoidtissue lymphoma.[112,113]
To date, there is no single therapeutic agent thathas been shown to successfully eradicate H. pyloriinfection, with current treatment guidelines rec-ommending triple therapy with an antisecretoryagent (proton pump inhibitor or bismuth-contain-ing compound) plus two antimicrobial agents (ei-ther amoxicillin, clarithromycin, metronidazoleand/or tetracycline).[62,63,85,114-116] Although allproton pump inhibitors have demonstrated anti-bacterial activity in vitro, the exact mechanism in-volved is not yet fully determined. Putative mech-
anisms include the inhibition of H. pylori ureaseenzyme, direct binding to bacterial proteins and/orenhancement of the bioactivity of antimicrobialagents.[88]
Triple therapy consisting of a proton pump in-hibitor plus two antimicrobial agents is now con-sidered the gold standard for eradication of H. py-lori infection, although currently no single tripletherapy regimen is recommended ahead of an-other.[88] American College of Gastroenterologyguidelines[63] and the European HelicobacterPyloriStudy Group (Maastricht Consensus Re-port)[62] advocate that treatment is initiated with atriple therapy regimen that has shown an intention-to-treat eradication rate of ≥80% in clinical trials.Dual therapy including a proton pump inhibitorand an antimicrobial agent is less effective thantriple therapy (60 to 70 vs >80% eradica-tion),[114,117] and hence is no longer recom-mended.[63,114] On the other hand, quadruple ther-apies consisting of a proton pump inhibitor andthree antimicrobial agents have relatively complexdosage regimens which may decrease compli-ance.[85,88] Thus, quadruple therapy is generally re-served for patients who have failed to have H. py-lori eradicated using standard triple therapy.[88] Atpresent, research focuses on the most cost-effec-tive triple therapy regimen, with factors such astolerability, compliance and bacterial resistancepatterns playing a role in determining which regi-men should be used.[63,114]
Of increasing concern is the emergence ofresistance to presently used antimicrobialagents such as clarithromycin and metronida-zole.[111,114,117] Estimates of antimicrobial resis-tance vary but in the US the frequencies of primaryclarithromycin or metronidazole resistance are 6and 3%, respectively.[117] The prevalence of resis-tance developed after eradication of H. pylori (i.e.secondary resistance) is also increasing in theUS.[114] Thus, although at present H. pylori infec-tion is effectively cured via antisecretory and anti-microbial-based triple therapy, research is now fo-cusing on the development of a vaccine to preventH. pylori infection.[117,118]
Esomeprazole: A Review 1533
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

Recommended treatment durations vary be-tween the US and Europe: 1-week triple therapyregimens are commonly used in Europe whereaslower eradication rates with this regimen in theUS have prompted the use of 2-week re-gimens.[85,114,117] Recently, the FDA has approvedthe use of 10 to 14 days’ treatment with tripletherapy including esomeprazole 40mg oncedaily,[119] omeprazole 20mg once daily[114] orlansoprazole 30mg once daily,[114] in combinationwith amoxicillin 1g twice daily and clarithromycin500g twice daily for eradication of H. pylori infec-tion and for prophylaxis of relapse of peptic ulcerin patients with H. pyloriinfection.
Well designed clinical trials have demonstratedthe efficacy of 7- and 10-day triple therapy includ-ing esomeprazole in the eradication of H. pyloriinfection in patients with duodenal ulcer disease(see section 4.2). In two randomised, double-blind,multicentre trials including ≥400 patients, a 7-dayregimen of twice-daily esomeprazole 20mg plusamoxicillin and clarithromycin was as effective incuring H. pylori infection as regimens comprisingomeprazole 20mg twice daily plus the same anti-microbial agents, with eradication rates of ≥86%in all intention-to-treat groups. As expected, a 10-day triple therapy regimen including esomeprazole40mg once daily plus twice daily amoxicillin andclarithromycin was significantly better than a dualtherapy regimen using the same dosages of esome-prazole plus clarithromycin (eradication rate of 77vs 52%; intention-to-treat analysis).
The primary focus of all of these studies was theeradication of H. pylori infection and thus few tri-als measured ulcer healing rates and/or symptomresolution (see section 4.2.2). In a randomised dou-ble-blind trial, triple therapy including esome-prazole 20mg twice daily for 7 days followed by 3weeks’ treatment with placebo was as effective asa similar twice daily omeprazole-based triple ther-apy regimen followed by omeprazole 20mg oncedaily for 3 weeks. Recipients of esomeprazole- oromeprazole-based triple therapy showed markedimprovements from baseline in levels of epigastricpain and heartburn in two well designed trials.
7.3 Tolerability
Esomeprazole (20 or 40 mg/day) was generallywell tolerated in both 8-week and maintenancestudies involving ≈6000 adult patients with GORD(see section 5). The most commonly reported ad-verse events were headache, diarrhoea, nausea, ab-dominal pain and respiratory infection, which oc-curred with an incidence of <9%. Adverse eventsassociated with the long-term administration ofesomeprazole were generally similar to those ob-served with 8 weeks’ treatment. There were no be-tween-group differences in the nature and fre-quency of adverse events reported with eitheresomeprazole or omeprazole treatment.
In addition, the tolerability profiles of esome-prazole 40mg once daily and lansoprazole 30mgonce daily were similar in >5000 patients withGORD in an 8-week well designed trial.[40] Themost frequently reported adverse events wereheadache, diarrhoea, respiratory infection, abdom-inal pain, nausea, flatulence and gastritis, all ofwhich occurred with an incidence of <6%. Therewere no clinically relevant changes in laboratoryparameters or vital signs in either treatment group.Approximately 2% of patients discontinued treat-ment due to adverse events in each group.
Of note, no enterochromaffin-like cell dyspla-sia, carcinoids or neoplasia were reported inpooled data from 1326 patients with healed erosiveoesophagitis who received esomeprazole 10 to 40mg/day for up to 6 or 12 months (see section 5.2).
Esomeprazole-based triple therapy regimens(combined with amoxicillin plus clarithromycin)appear to be well tolerated in adult patients withduodenal ulcer disease (see section 5.1). The mostfrequently reported adverse events were taste per-version, diarrhoea and abdominal pain. Further-more, adverse events associated with triple therapywere reportedly similar to those associated witheither esomeprazole, amoxicillin or clarithromycinalone.[12] Pooled data also indicated that the inci-dence of specific treatment-emergent adverseevents was similar with esomeprazole-based tripletherapy to that of esomeprazole monotherapy.
1534 Scott et al.
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

7.4 Conclusions
In conclusion, esomeprazole is an effective,well tolerated treatment for managing GORD andfor eradicating H. pylori infection in patients withduodenal ulcer disease. In 8-week double-blind tri-als, esomeprazole healed oesophagitis and re-solved symptoms in patients with endoscopicallyconfirmed erosive oesophagitis and, overall, pro-vided better efficacy than omeprazole. Notably, ina large (n >5000 patients) double-blind trial,esomeprazole provided significantly better effi-cacy than lansoprazole in terms of healing ratesand resolution of symptoms. Long-term therapywith esomeprazole maintained healed oesophag-itis in these patients. Esomeprazole also provedbeneficial in patients with symptomatic GORDwithout oesophagitis. Thus, esomeprazole hasemerged as an option for first-line therapy in themanagement of acid-related disorders.
References1. Thitiphuree S, Talley NJ. Esomeprazole, a new proton pump
inhibitor: pharmacological characteristics and clinical effi-cacy. Int J Clin Pract 2000 Oct; 54 (8): 537-41
2. Langtry HD, Wilde MI. Omeprazole: a review of its use inHelicobacter pylori infection, gastro-oesophageal reflux dis-ease and peptic ulcers induced by nonsteroidal anti-inflam-matory drugs. Drugs 1998; 56 (3): 447-86
3. Fitton A, Wiseman L. Pantoprazole: a review of its pharmaco-logical properties and clinical efficacy in the management ofacid-related disorders. Drugs 1996; 51 (3): 460-82
4. Langtry HD, Markham A. Rabeprazole: a review of its use inacid-related gastrointestinal disorders. Drugs 1999 Oct; 58(4): 725-42
5. Carswell CI, Goa KL. Rabeprazole: an update of its use in acid-related disorders. Drugs 2001; 61 (5): 2327-56
6. Spencer CM, Faulds D. Lansoprazole: a reappraisal of its phar-macodynamic and pharmacokinetic properties, and its thera-peutic efficacy in acid-related disorders. Drugs 1994; 48 (3):404-30
7. Langtry HD, Wilde MI. Lansoprazole: an update of its pharma-cological properties and clinical efficacy in the managementof acid-related disorders. Drugs 1997; 54 (3): 473-500
8. Matheson AJ, Jarvis B. Lansoprazole: an update of its place inthe management of acid-related disorders. Drugs 2001; 61(12): 1803-35
9. Spencer CM, Faulds D. Esomeprazole. Drugs 2000 Aug; 60 (2):321-9; discussion 330-1
10. Huang J-Q, Hunt RH. Eradication of Helicobacter pylori infec-tion in the management of patients with dyspepsia and non-ulcer dyspepsia. Yale J Biol Med 1998; 71: 125-33
11. Zimmermann AE. Esomeprazole: a novel proton pump inhibi-tor for the treatment of acid-related disorders. Formulary2000 Nov; 35: 882-93
12. AstraZeneca LP. Nexium (esomeprazole magnesium): delayedrelease capsules. [prescribing information] 2001
13. Hassan-Alin M, Niazi M, Röhss K, et al. Esomeprazole, theS-isomer of omeprazole, is optically stable in humans [ab-stract no. 5697]. Gastroenterology 2000; 118 (4 Suppl. 2):A1244-5
14. Hunt RH. Importance of pH control in the management ofGERD. Arch Intern Med 1999; 159: 649-57
15. Smith JL, Operkun AR, Larkai E, et al. Sensitivity of oesoph-ageal mucosa to pH in gastro-oesophageal reflux disease.Gastroenterology 1989; 96: 683-9
16. Bell NJV, Burget D, Howden CW, et al. Appropriate acid sup-pression for the management of gastro-oesophageal refluxdisease. Digestion 1992; 51 Suppl. 1: 59-67
17. Lind T, Rydberg L, Kylebäck A, et al. Esomeprazole providesimproved acid control versus omeprazole in patients withsymptoms of gastro-oesophageal reflux disease. AlimentPharmacol Ther 2000; 14 (7): 861-7
18. Röhss K, Hasselgren G, Hedenström H. Effect of esomeprazole40mg vs omperazole 40mg on 24-hour intragastric pH in pa-tients with symptoms of gastro-esophageal reflux disease. Di-gest Dis Sci 2002; 47 (5): 954-8
19. Wilder-Smith C, Röhss K, Claar-Nilsson C, et al. Esomeprazole20 mg provides more effective acid control than lansoprazole15 mg [abstract no. P49]. Gut 2000; 47 Suppl. III: A62-3
20. Thomson ABR, Claar-Nilsson C, Hasselgren G, et al. Eso-meprazole 40 mg provides more effective acid control thanlansoprazole 30 mg during single and repeated administration[abstract]. Gut 2000 Dec; 47 Suppl. III: A63
21. Wilder-Smith C, Röhss K, Lundin C, et al. Esomeprazole (E)40 mg provides more effective acid control than pantoprazole(P) 40 mg [abstract no. 352]. Gastroenterology 2000; 118:A22
22. Baisley KJ, Tejura B, Morocutti MD. Rabeprazole 10mg isequivalent to esomeprazole 20mg in control of gastric pH inhealthy volunteers [abstract no. 148]. Am J Gastroenterol2001; 96 (9 Suppl.): S48
23. Baisley KJ, Tejura B, Morocutti A, et al. Rabeprazole 20mg ismore potent than esomeprazole 20mg in control of gastric pHin healthy volunteers [abstract no. 149]. Am J Gastroenterol2001; 96 (9 Suppl.): S48
24. Wilder-Smith C, Röhss K, Claar-Nilsson C, et al. Esomeprazole40 mg provides more effective acid control than rabeprazole20 mg [abstract]. Gut 2000; 47 Suppl. III: A63
25. Wilder-Smith CH, Claar-Nilsson C, Hasselgren G, et al. Eso-meprazole 40mg provides faster and more effective controlthan rabeprazole 20mg in patients with symptoms of GERD[abstract]. Am J Gastroenterol 2001; 96: S45
26. Baxter G, Eriksson K, Nilsson L-G. Lansoprazole 15mg pro-vides as effective acid control as esomeprazole 20mg [ab-stract no. 50]. Scand J Gastroenterol 2001; 34 Suppl. 233: 32
27. Eriksson K, Baxter G, Nilsson L-G. Speed of onset of intragast-ric acid control: lansoprazole and esomeprazole compared[abstract no. 49]. Scand J Gastroenterol 2001; 34 Suppl.233: 32
28. Andersson T, Hassan-Alin M, Hasselgren G, et al. Pharmaco-kinetic studies with esomeprazole, the (S)-isomer of om-eprazole. Clin Pharmacokinet 2001; 40 (6): 411-26
29. Hassan-Alin M, Andersson T, Bredberg E, et al. Pharmacoki-netics of esomeprazole after oral and intravenous administra-tion of single and repeated doses to healthy subjects. Eur JClin Pharmacol 2000 Dec; 56 (9-10): 665-70
30. Andersson T, Bredberg E, Sunzel M, et al. Pharmacokinetics(PK) and effect on pentagastrin stimulated peak acid output
Esomeprazole: A Review 1535
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

(POA) of omeprazole (O) and its 2 optical isomers, S-om-eprazole/ esomeprazole (E) and R-omeprazole (R-O) [ab-stract]. Gastroenterology 2000; 118 (4): A1210
31. Äbelö A, Andersson TB, Antonsson M, et al. Stereoselectivemetabolism of omeprazole by human cytochrome P450 en-zymes. Drug Metab Dispos 2000; 28: 966-72
32. Andersson T, Magner D, Patel J, et al. Esomeprazole 40mgcapsules are bioequivalent when administered intact or as thecontents mixed with apple sauce. Clinical Drug Invest 2001;21 (1): 67-71
33. Sjövall H, Björnsson E, Holmberg J, et al. Pharmacokinetics ofesomeprazole in patients with hepatic impairment. Eur J Gas-troenterol Hepatol 2002; 14: 491-6
34. Hasselgren G, Hassan-Alin M, Andersson T, et al. Pharmaco-kinetic study of esomeprazole in the elderly. Clin Phar-macokinet 2001; 40 (2): 145-50
35. Naesdal J, Andersson T, Bodemar G, et al. Pharmacokinetics of[14C]omeprazole in patients with impaired renal function.Clin Pharmacol Ther 1986; 40 (3): 344-51
36. Andersson T, Hassan-Alin M, Hasselgren G, et al. Drug inter-action studies with esomeprazole, the (S)-isomer of om-eprazole. Clin Pharmacokinet 2001; 40 (7): 523-37
37. Laine L, Fennerty MB, Osato M, et al. Esomeprazole-basedHelicobacter pylori eradication therapy and the effect of an-tibiotic resistance: results of three US multicenter, double-blind trials. Am J Gastroenterol 2000 Dec; 95 (12): 3393-8
38. Tulassay Z, Kryszewski A, Dite P, et al. One week of treatmentwith esomeprazole-based triple therapy eradicates Helicobac-ter pylori and heals patients with duodenal ulcer disease. EurJ Gastroenterol Hepatol 2001; 13: 1457-65
39. Veldhuyzen Van Zanten S, Lauritsen K, Delchier J-C, et al.One-week triple therapy with esomeprazole provides effec-tive eradication of Helicobacter pylori in duodenal ulcer dis-ease. Aliment Pharmacol Ther 2000 Dec; 14 (12): 1605-11
40. Castell DO, Kahrilas PJ, Richter JE, et al. Esomeprazole (40mg)compared with lansoprazole (30mg) in the treatment of ero-sive esophagitis. Am J Gastroenterol 2002; 97 (3): 575-83
41. Kahrilas PJ, Falk GW, Johnson DA, et al. Esomeprazole im-proves healing and symptom resolution as compared with om-eprazole in reflux oesophagitis patients: a randomizedcontrolled trial. Esomeprazole Study Investigators. AlimentPharmacol Ther 2000 Oct; 14 (10): 1249-58
42. Richter JE, Kahrilas PJ, Johanson J, et al. Efficacy and safetyof esomeprazole compared with omeprazole in GERD pa-tients with erosive esophagitis: a randomized controlled trial.Am J Gastroenterol 2001 Mar; 96 (3): 656-65
43. Johnson DA, Benjamin SB, Vakil NB, et al. Esomeprazole oncedaily for 6 months is effective therapy for maintaining healederosive esophagitis and for controlling gastroesophageal re-flux disease symptoms: a randomized, double-blind, placebo-controlled study of efficacy and safety. Am J Gastroenterol2001 Jan; 96 (1): 27-34
44. Vakil NB, Shaker R, Johnson DA, et al. The new proton pumpinhibitor esomeprazole is effective as a maintenance therapyin GERD patients with healed erosive oesophagitis: a 6-month, randomized, double-blind, placebo-controlled studyof efficacy and safety. Aliment Pharmacol Ther 2001 Jul; 15(7): 927-35
45. Talley NJ, Lauritsen K, Tunturi-Hihnala H, et al. Esomeprazole20 mg maintains symptom control in endoscopy-negativegastro-oesophageal reflux disease: a controlled trial of ’on-demand’ therapy for 6 months. Aliment Pharmacol Ther 2001Mar; 15 (3): 347-54
46. Talley NJ, Venables TL, Green JR, et al. Esomeprazole 40mgand 20mg is efficacious in the long-term management of pa-tients with endoscopy-negative GORD: a placebo-controlledtrial of ’on-demand’ therapy for 6 months [abstract/poster].Gastroenterology 2000; 118 (4 Suppl. 2): A658
47. Katz PO, Castell DO, Marino V, et al. Comparison of the newPPI esomeprazole, the S-isomer of omeprazole, vs placebo forthe treatment of symptomatic GERD [abstract no. 49]. Am JGastroenterol 2000 Sep; 95: 2424-5
48. Lauritsen K, Junghard O, Eklund S. Esomeprazole 20mg com-pared with lansoprazole 15mg for maintenance therapy in pa-tients with healed reflux oesophagitis [abstract]. JGastroenterol Hepatol 2002; 17 Suppl.: A1007
49. Maton PN, Vakil NB, Levine JG, et al. Safety and efficacy oflong term esomeprazole therapy in patients with healed ero-sive oesophagitis. Drug Saf 2001; 24 (8): 625-35
50. Lundell LR, Dent J, Bennett JR, et al. Endoscopic assessmentof oesophagitis: clinical and functional correlates and furthervalidation of Los Angeles classification. Gut 1999; 45: 172-80
51. Edwards SJ, Lind T, Lundell L. Systematic review of protonpump inhibitors for the acute treatment of reflux oesophagitis. Aliment Pharmacol Ther 2001; 15 (11): 1729-36
52. Roach AC, Hwang C, Bjorkman DJ. Evidence-based analysisof the benefit of esomeprazole in the treatment of erosiveoesophagitis (EE) [abstract]. Gut 2001; 49 Suppl. III: A2755
53. Vakil NB, Richter JE, Hwang C, et al. Does baseline severityof EE impact healing with esomeprazole? [abstract]. Am JGastroenterol 2000; 95: 2439
54. Howden CW, Ballard II ED, Robieson W. Evidence for thera-peutic equivalence of lansoprazole 30mg and esomeprazole40mg in the treatment of erosive oesophagitis. Clin Drug In-vest 2002; 22: 99-109
55. Johnson DA, Vakil NB, Hwang C, et al. Absence of symptomsin erosive esophagitis patients treated with esomeprazole is ahighly reliable indicator of healing [abstract no. 2237]. Gas-troenterology 2001; 120 Suppl. 1: A439
56. Vakil NB, Katz PO, Hwang C, et al. Nocturnal heartburn is rarein patients with erosive esophagitis treated with esomeprazole[abstract no. 2250]. Gastroenterology 2001; 120 Suppl. 1:A441
57. Maton PN, Vakil NB, Hwang C, et al. The impact of baselineseverity of erosive esophagitis on heartburn resolution in pa-tients treated with esomeprazole or omeprazole [abstract no.2221]. Gastroenterology 2001; 120 Suppl. 1: A435-6
58. Eissele R, Gatz G, Hole U. Equivalent efficacy of pantoprazole40mg and esomeprazole 40mg in patients with GERD [ab-stract no. 137]. Can J Gastroenterol 2002; 16 Suppl. A: 95A
59. Scholten T, Hole U, Gatz G. Similar reduction of symptom loadwithin 4 weeks of treatment with pantoprazole 40mg or eso-meprazole 40mg in patients with moderate to severe GERD[abstract no. 138]. Can J Gastroenterol 2002; 16 Suppl. A: 95A
60. Lind T, Junghard O, Lauritsen K. Esomeprazole and lansop-razole in the management of patients with reflux oesophagitis(RO): combining results from two clinical studies [abstract].J Gastroenterol Hepatol 2002; 17 Suppl.: A1024
61. Dworkin MS, Gold BD, Swerdlow DL. Helicobacter pylori:review of clinical and public health aspects for the practi-tioner. Infect Dis Clin Pract 1999; 8: 137-45
62. Malfertheiner P, et al. Current European concepts in the man-agement of Helicobacter pylori infection: the MaastrichtConsensus Report. The European Helicobacter pylori StudyGroup. Gut 1997; 41: 8-13
1536 Scott et al.
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

63. Howden CW, Hunt RH. Guidelines for the management ofHelicobacter pylori infection. Am J Gastroenterol 1998 Dec;93: 2330-8
64. Jones RH. Clinical economics review: gastrointestinal diseasein primary care. Aliment Pharmacol Ther 1996; 10 (3): 233-9
65. Enck P, Dubois D, Marquis P. Quality of life in patients withupper gastrointestinal symptoms from the Domestic/Interna-tional Gastroenterology Surveillance Study (DIGEST).Scand J Gastroenterol 1999; 231 Suppl.: 48-54
66. Wahlqvist P, Junghard O, Higgins A, et al. Cost effectivenessof esomeprazole compared with omeprazole in the acutetreatment of patients with reflux oesophagitis in the UK.Pharmacoeconomics 2002; 20 (4): 279-87
67. Wahlqvist P, Junghard O, Higgins A, et al. Cost effectivenessof proton pump inhibitors in gastro-oesophageal refluxdisease without oesophagitis: comparison of on-demand eso-meprazole with conventional omeprazole treatment strate-gies. Pharmacoeconomics 2002; 20 (4): 267-77
68. Wahlqvist P. In Finland, Sweden and the UK, esomeprazole iscost-effective compared with omeprazole for the acute treat-ment of patients with reflux oesophagitis [abstract/poster].Value Health 2000; 3: 358
69. Wahlqvist P, Higgins A, Green J. Esomeprazole is cost-effec-tive compared with omeprazole for the acute treatment ofpatients with non-endoscoped GORD in the UK [ab-stract/poster]. Value Health 2000; 3: 360-1
70. Wahlqvist P. In Finland, Sweden and the UK, on demand treat-ment with esomeprazole is cost-effective in patients withGORD without oesophagitis [abstract/poster]. Value Health2000; 3: 360
71. Bate C, Higgins A. On-demand esomeprazole offers value formoney compared with "real-life" maintenance omeprazoletherapy for patients with gastro-oesophageal reflux disease(GORD) without oesophagitis [abstract]. Proceedings of theThird Congress of the European Federation of Internal Med-icine; 2001 May 9-12; Edinburgh, Scotland
72. Hasselgren B, Claar-Nilsson C, Hasselgren G, et al. Studies inhealthy volunteers do not show any electrocardiographiceffects with esomeprazole. Clin Drug Invest 2000; 20 (6):425-31
73. Svoboda AC. Increasing concerns about chronic proton pumpinhibitor use. J Clin Gastroenterol 2001; 33 (1): 3-10
74. Maton PN. Omeprazole. Drug Therapy 1991; 324 (14): 965-7575. Genta RM, Magner DJ, D’Amico D, et al. Safety of long-term
treatment with a new PPI, esomeprazole in GERD patients[abstract no. 326]. Gastroenterology 2000; 118 (4 Suppl. 2):A16
76. AstraZeneca UK Limited. Combined summary of product char-acteristics: nexium 20 and 40mg tablets. 2001
77. Fass R, Fennerty MB, Vakil N. Nonerosive reflux disease: cur-rent concepts and dilemmas. Am J Gastroenterol 2001; 96 (2):303-14
78. Baldi F, Crotta S, Penagini R. Guidelines for the diagnostic andtherapeutic management of patients with gastro-oesophagealreflux disease: a position statement of the Italian Associationof Hospital Gastroenterologists (AIGO), Italian Society ofGastrointestinal Endoscopy (SIED), and Italian Society ofGastroenterology (SIGE). Ital J Gastroenterol Hepatol 1998;30: 107-12
79. Tytgat GNJ. Shortcomings of the first-generation proton pumpinhibitors. Eur J Gastroenterol Hepatol 2001; 13 Suppl. 1:S29-33
80. Robinson M. New-generation proton pump inhibitors: over-coming the limitations of early-generation agents. Eur J Gas-troenterol Hepatol 2001 May; 13 Suppl 1: S43-7
81. Revicki DA, Wood M, Maton PN, et al. The impact of gas-troesophageal reflux disease on health-related quality of life.Am J Med 1998; 104: 252-8
82. Glise H. Quality of life and cost of therapy in reflux disease.Scand J Gastroenterol 1995; 30 Suppl. 210: 38-42
83. De Vault KR, Castell DO. Updated guidelines for the diagnosisand treatment of gastroesophageal reflux disease. Practice Pa-rameters Committee of the American College of Gastroenter-ology. Am J Gastroenterol 1999; 94: 1434-42
84. Kahrilas PJ. Strategies for medical management of reflux dis-ease. Baillieres Clin Gastroenterol 2000 Oct; 15: 775-91
85. Welage LS, Berardi RR. Evaluation of omeprazole, lans-oprazole, pantoprazole, and rabeprazole in the treatment ofacid-related diseases. J Am Pharm Ass 2000; 40 (1): 52-62
86. Galmiche JP, Letessier E, Scarpignato C. Treatment of gastro-oesophageal reflux disease in adults. BMJ 1998; 316: 170-3
87. Berardi RR, Welage LS. Proton pump inhibitors in acid-relateddiseases. Am J Health-Syst Pharm 1998; 55 (1): 2289-98
88. Richardson P, Hawkey CJ, Stack WA. Proton pump inhibitors:pharmacology and rationale for use in gastrointestinal disor-ders. Drugs 1998; 56 (3): 301-35
89. Horn J. The proton pump inhibitors: similarities and differ-ences. Clin Ther 2000; 22 (3): 266-80
90. Bytzer P. On-demand therapy for gastro-oesophageal refluxdisease. Eur J Gastroenterol Hepatol 2001; 13 Suppl. 1: S19-22
91. DiPalma JA. Management of severe gastroesophageal refluxdisease. J Clin Gastroenterol 2001; 32 (1): 19-26
92. Mujica VR, Rao SSC. Recognising atypical manifestations ofGERD: asthma, chest pain, and otolaryngologic disordersmay be due to reflux. Postgrad Med 1999 Jan; 105: 53-66
93. Colin-Jones DG. The role and limitations of H2-receptor antag-onists in the treatment of gastro-oesophageal reflux disease.Aliment Pharmacol Ther 1995; 9 Suppl. 1: 9-14
94. Eisen G. The epidemiology of gastroesophageal reflux disease:what we know and what we need to know. Am J Gastroenterol2001; 96 Suppl.: S16-8
95. Bloom BS, Glise H. What do we know about gastroesophagealreflux disease? Am J Gastroenterol 2001; 96 Suppl.: S1-5
96. Richter JE. Long-term management of gastroesophageal refluxdisease and its complications. Am J Gastroenterol 1997; 92(4): S30-5
97. Kahrilas PJ. Gastroesophageal reflux disease. JAMA 1996; 276(12): 983-8
98. Lind T, Havelund T, Carlsson R, et al. Heartburn without oeso-phagitis: efficacy of omeprazole therapy and features deter-mining therapeutic response. Scand J Gastroenterol 1997; 32:974-9
99. Carlsson R, Dent J, Watts R, et al. Gastro-oesophageal refluxdisease in primary care: an international study of differenttreatment strategies with omeprazole. Euro J GastroenterolHepatol 1997; 10: 119-24
100. Smout APJM. Endoscopy-negative acid reflux disease. Ali-ment Pharmacol Ther 1997; 11 Supl. 1: 81-5
101. Galmiche J-P, Barthelemy P, Hamelin B. Treating the symp-toms of gastro-oesophageal reflux disease: a double-blindcomparison of omeprazole and cisapride. Aliment PharmacolTher 1997; 11: 765-73
102. Holtmann G. Reflux disease: the disorder of the third millen-nium. Eur J Gastroenterol Hepatol 2001; 13 Suppl. 1: S5-11
Esomeprazole: A Review 1537
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)

103. Dent J, Jones R, Kahrilas P, et al. Management of gastro-oe-sophageal reflux disease in general practice. BMJ 2001; 322:344-7
104. Byrne MF, Murray FE. Formulary management of proton pumpinhibitors. Pharmacoeconomics 1999 Sep; 16: 225-46
105. Stewart AL, Greenfield S, Hays RD, et al. Functional status andwell-being of patients with chronic conditions: results fromthe Medical Outcomes Study. JAMA 1989; 262: 907-13
106. Henke CJ, Levin TR, Henning JM, et al. Work loss costs due topeptic ulcer disease and gastroesophageal reflux disease inhealth maintenance organization. Am J Gastroenterol 2000;95: 788-92
107. Wahlqvist P. Symptoms of gastroesophageal reflux disease,perceived productivity, and health-related quality of life. AmJ Gastroenterol 2001; 96 Suppl.: S57-61
108. Dent J, Fendrick AM, Fennerty MB, et al. An evidence-basedappraisal of reflux disease management: the Genval Work-shop Report. Gut 1999; 44 Suppl. 2: S1-16
109. Dimenas E, Glise H, Hallerback B, et al. Quality of life in pa-tients with upper gastrointestinal symptoms. An improvedevaluation of treatment regimens? Scan J Gastroenterol 1993;28 (8): 681-7
110. Hassall E. Peptic ulcer disease and current approaches toHelicobacter pylori. J Pediatr 2001; 138: 462-8
111. Brown LF, Wilson DE. Gastroduodenal ulcers: causes, diagno-sis, prevention and treatment. Comp Ther 1999; 25 (1): 30-8
112. Vakil NB, Go MF. Debating the role of Helicobacter pyloriinfection. Am J Manag Care 2001; 7 Suppl. 1: S27-32
113. Lee J, O’Morain C. Who should be treated for Helicobacterpylori infection? A review of consensus conferences andguidelines. Gastroenterology 1997 Dec; 113 Suppl.: S99-106
114. Go FM, Vakil N. Treatment of Helicobacter pylori infection:gastrointestinal infections. Curr Opin Gastroenterol 1999; 15(1): 72
115. Malfertheiner P. Helicobacter pylori eradication in functionaldyspepsia: new evidence for symptomatic benefit. Eur J Gas-troenterol Hepatol 2001; 13 Suppl. 2: S9-11
116. Bazzoli F. Key points from the revised Maastricht ConsensusReport: the impact on general practice. Eur J GastroenterolHepatol 2001; 13 Suppl. 2: S3-7
117. Hoffman JS, Cave CR. Treatment of Helicobacter pylori. CurrOpin Gastroenterol 2001; 17 (1): 30-4
118. Hoffman JS. Pharmacological therapy of Helicobacter pyloriinfection. Sem Gastroenterol Dis 1997; 8 (3): 156-63
119. Anon. Esomeprazole (nexium). Med Lett Drugs Ther 2001 Apr30; 43 (1103): 36-7
Correspondence: Lesley J. Scott, Adis International Limited,41 Centorian Drive, Private Bag 65901, Mairangi Bay, Auck-land 10, New Zealand.E-mail: [email protected]
1538 Scott et al.
© Adis International Limited. All rights reserved. Drugs 2002; 62 (10)