Episodic and Residual Thought Pathology in Chronic ...
14
394 Episodic and Residual Thought Pathology in Chronic Schizophrenics: Effect of Neuroleptics by Herbert E. Spohn, Lolafaye Coyne, Jan Larson, Frederick Mittleman, Judy Spray, and Kenneth Hayes Abstract We sought to determine the effect of neuroleptic treatment on thought disorder in chronic schizophrenics, using the Thought Disorder Index (TDI). We were able to demonstrate that high levels of thought disorder are found in chronic schizophrenic and schizoaffective patients, while in both bipolar patients and normal controls thought pathology is minimal. Moreover, the TDI appears to be particularly well suited to the characterization of thought disorder in chronic schizophrenics. For total scores on the TDI, we were unable to demonstrate a significant reduction in thought pathology, although it was evident that thought disorder as reflected in the Conceptual Disorgan- ization and Unusual Thought Content subscales of the Brief Psychiatric Rating Scale is signifi- cantly reduced by neuroleptics. In analyses of subscores of the TDI reflecting four levels of severity, we were able to show that more severe forms of thought pathology are normalized by neuroleptics, while less severe pathology is largely unaffected. Our results suggest that neuroleptic treatment reduces thought pathology associated with acute episodes, but that somewhat milder, though still disabling, residual thought pathology persists after clinical remission has been attained. In this report we describe a study designed to assess the relation of neuroleptic treatment to thought disorder or, more precisely, to a measure of thought disorder, the Thought Disorder Index (TDI) (Johnston and Holzman 1979) in chronic schizophrenic inpatients. The rationale for this study is multifold. Notwithstanding recent critiques of thought disorder as a pathognomonic symptom of schizophrenia (Pope and Lipinski 1978; Andreasen 1979b), the phenomenon continues to play an important role in the diagnosis of schizophrenia. If neuroleptic treatment normalizes thought disorder in schizophrenics, or modifies it in some other fashion, the validity of diagnosis in medicated patients is jeopardized. From the vantage point of descriptive psychiatry, therefore, it is of some interest to determine the effects of neuroleptic treatment on thought disorder. The absence of thought disorder symptoms reduced or removed by neuroleptic treatment may "bias" diagnostic judgment. Similarly, treaters of schizophrenic patients, be they behaviorists or psychotherapists, have an interest in knowing to what extent neuroleptics reduce thought pathology that may interfere with treatment. In untreated psychotic patients, acute thought pathology may divert attention from therapeutic interventions. Studies of thought disorder continue to interest investigators concerned with the unraveling of the specific nature of cognitive dysfunction in schizophrenia (Chapman and Chapman 1973). Although the focus of interest has shifted in recent years to exper- imental studies of impairment in the earlier phases of information processing, there continues to be concern with disorders of central processing and with the response or performance side of information processing, i.e., language and communication (Rochester and Martin 1979; Maher 1983). Accord- ingly, an assessment of neuroleptic Reprint requests should be sent to Dr H E Spohn at the Research Department, The Menninger Foundation, Box 829, Topeka, KS 66601 Downloaded from https://academic.oup.com/schizophreniabulletin/article/12/3/394/1865999 by guest on 02 February 2022
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Episodic and Residual Thought Pathology in Chronic ...

394 Episodic and ResidualThought Pathology inChronic Schizophrenics:Effect of Neuroleptics
by Herbert E. Spohn, LolafayeCoyne, Jan Larson, FrederickMittleman, Judy Spray, andKenneth Hayes
Abstract
We sought to determine the effect ofneuroleptic treatment on thoughtdisorder in chronic schizophrenics,using the Thought Disorder Index(TDI). We were able to demonstratethat high levels of thought disorderare found in chronic schizophrenicand schizoaffective patients, while inboth bipolar patients and normalcontrols thought pathology isminimal. Moreover, the TDI appearsto be particularly well suited to thecharacterization of thought disorderin chronic schizophrenics. For totalscores on the TDI, we were unable todemonstrate a significant reduction inthought pathology, although it wasevident that thought disorder asreflected in the Conceptual Disorgan-ization and Unusual ThoughtContent subscales of the BriefPsychiatric Rating Scale is signifi-cantly reduced by neuroleptics. Inanalyses of subscores of the TDIreflecting four levels of severity, wewere able to show that more severeforms of thought pathology arenormalized by neuroleptics, whileless severe pathology is largelyunaffected. Our results suggest thatneuroleptic treatment reduces thoughtpathology associated with acuteepisodes, but that somewhat milder,though still disabling, residualthought pathology persists afterclinical remission has been attained.
In this report we describe a studydesigned to assess the relation ofneuroleptic treatment to thoughtdisorder or, more precisely, to ameasure of thought disorder, theThought Disorder Index (TDI)(Johnston and Holzman 1979) inchronic schizophrenic inpatients. Therationale for this study is multifold.
Notwithstanding recent critiques ofthought disorder as a pathognomonic
symptom of schizophrenia (Pope andLipinski 1978; Andreasen 1979b), thephenomenon continues to play animportant role in the diagnosis ofschizophrenia. If neuroleptictreatment normalizes thoughtdisorder in schizophrenics, ormodifies it in some other fashion, thevalidity of diagnosis in medicatedpatients is jeopardized. From thevantage point of descriptivepsychiatry, therefore, it is of someinterest to determine the effects ofneuroleptic treatment on thoughtdisorder. The absence of thoughtdisorder symptoms reduced orremoved by neuroleptic treatmentmay "bias" diagnostic judgment.Similarly, treaters of schizophrenicpatients, be they behaviorists orpsychotherapists, have an interest inknowing to what extent neurolepticsreduce thought pathology that mayinterfere with treatment. In untreatedpsychotic patients, acute thoughtpathology may divert attention fromtherapeutic interventions.
Studies of thought disordercontinue to interest investigatorsconcerned with the unraveling of thespecific nature of cognitivedysfunction in schizophrenia(Chapman and Chapman 1973).Although the focus of interest hasshifted in recent years to exper-imental studies of impairment in theearlier phases of informationprocessing, there continues to beconcern with disorders of centralprocessing and with the response orperformance side of informationprocessing, i.e., language andcommunication (Rochester andMartin 1979; Maher 1983). Accord-ingly, an assessment of neuroleptic
Reprint requests should be sent toDr H E Spohn at the ResearchDepartment, The Menninger Foundation,Box 829, Topeka, KS 66601
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/3/394/1865999 by guest on 02 February 2022

VOL. 12, NO. 3, 1986 395
effects on thought disorder inmedicated schizophrenics can play aclarifying role, both for studies ofinformation processing as well asstudies of central processing andexpressive behavior.
There is a growing conviction onthe part of investigators concernedwith causation that the identificationof biological markers (Holzman andLevy 1977) and markers of vulner-ability (Nuechterlein and Dawson1984) is a major step in the directionof the elucidation of etiology inschizophrenia. Quite typically,marker studies seek to determine thestate/trait characteristics of behavioridentified as having marker statuspotential. One widely acceptedcriterion for marker status is itspersistence in patients whose clinicalremission has resulted from neuro-leptic treatment. Thus, another majoraim of the present study, andperhaps its theoretically andclinically most interesting one, wasto determine whether thoughtdisorder or aspects of thoughtdisorder merit trait (i.e., marker)status by being manifest as residualsymptoms after a clinical remissionhas been achieved by neuroleptictreatment.
There is a rather small researchliterature that bears on neurolepticeffects on thought disorder. Wereview this literature here in order toshow some of the conceptual andmethodological problems that mustbe addressed in any effort to examineneuroleptic treatment-thoughtdisorder relationships. This researchliterature extends over a period inwhich major changes in theconceptualization and measurementof thought disorder have taken place.Accordingly, we shall also beconcerned with such important recentdevelopments as Andreasen andOlsen's (1982) negative/positivesymptom typology.
In an early and influential study,Orzack, Kornetsky, and Freeman(1967) found that while a pheno-thiazine (carphenazine) normalizedattentional impairment (vigilance),this neuroleptic failed to affect"cognitive" impairment on theWechsler Bellevue Digit SymbolSubstitution Subtest (Wechsler 1944).This finding was in keeping with athen rather widely held view thatphenothiazines were less effective inmodifying cognitive functions inschizophrenics than attentionalfunctions. This hypothesis has sincebeen disconfirmed. Moreover, theDigit Symbol Substitution Test canhardly be considered a valid measureof thought disorder. Nonetheless,there is a much greater volume ofresearch addressed to neuroleptictreatment effects on attention/infor-mation processing than to drugeffects on disorders of centralprocessing and response such asthought disorder, language, andcommunication.
Among the few studies in the latterarea is one by Saretsky (1966), who,in a placebo-controlled design thatemployed measures of "primaryprocess" thinking applied toRorschach protocols, found thatrecently hospitalized chronic schizo-phrenic patients on chlorpromazine"proved to be more capable ofhandling primary process elements"than placebo-treated patients (p.247). Moreover, improvement in thisrespect was positively correlated withclinical improvement, notwith-standing that "degree of thoughtpathology itself is not directlyaffected by drug treatment" (p. 247).
Unlike the study of Orzack,Kornetsky, and Freeman (1967),Saretsky's (1966) investigationattracted very little attention, israther rarely cited, and has not beenreplicated. Three implications of thisstudy are nonetheless of interest. The
expression of thought pathology asmeasured in this study was episodic.That is, on drug treatment, patientsverbalized less thought pathologythan placebo controls, and lessthought pathology than at admissionand before drug treatment. Second,there was some residual thoughtpathology evident even after theachievement of symptomaticremission. Third, there is a hint inSaretsky's data that it was theexpression of thought pathologyrather than thought pathology itselfthat was reduced. This latter findingis consonant with an interpretationthat self-editing processes werestrengthened by neuroleptictreatment.
Two studies (Shimkunas, Gynther,and Smith 1966, 1967) reflect bothconceptual and methodologicalproblems in the determination ofneuroleptic treatment effects onthought disorder. Acutely psychoticchronic schizophrenic patients wereassessed on the Gorham ProverbsTest (Gorham 1956), the WechslerBellevue, and a global severity ratingscale over a 26-week period ofphenothiazine treatment. Placebocontrols were not used in this study,whose central finding was that whilepathology decreased, verbal IQ andproverbs scores did not increase.
Upon determining that theproverbs test scores were morehighly correlated with verbal IQ thanwith psychopathology, Shimkunas,Gynther, and Smith (1967) devisedan autistic response scoring systemthat was highly correlated withpsychopathology. They found asignificant decrease in autisticresponse frequency over the neuro-leptic treatment period.
The results of these two studiesraise a major conceptual issue in themeasurement of thought disorder—namely, that of construct validity.The Gorham Proverbs Test, based on
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/3/394/1865999 by guest on 02 February 2022

396 SCHIZOPHRENIA BULLETIN
Goldstein's (1939) theory of impairedabstracting ability, was found to lackconstruct validity, and the investi-gators were able to demonstrateconstruct validity for their autisticresponse scoring system, whichappeared to be more sensitive toneuroleptic treatment than theconcrete/abstract scoring system usedby Gorham (1956).
There is yet another perspectivethat can be brought to bear on thesetwo studies. It may be that abstractreasoning impairment in chronicschizophrenics is less susceptible toneurolepric normalization thanautistic reasoning. This interpretationsuggests that some forms of thoughtpathology persist after symptomaticremission has been attained and areunaffected by drug treatment.Indeed, Harrow et al. (1972) haveadduced evidence to this effect.
An attempt to replicate thefindings of Shimkunas, Gynther, andSmith (1967) using their autisticresponse scoring system in a placebo-controlled study (Spohn et al. 1977)is instructive with respect tomethodological issues. Spohn et al.(1977) did indeed find that in chronicschizophrenics returned to chlor-promazine treatment after a 6-weekwashout period, frequency of autisticresponses on the Gorham ProverbsTest was substantially reduced. Itcould not be concluded, however,that chlorpromazine specificallyreduced thought disorder of the kindmeasured by the Shimkunas scoringsystem because placebo controlpatients who remained testable afterextended drug withdrawal alsoshowed reduced autistic responses.Two factors combined to producethis counterintuitive finding. Anumber of placebo patients relapsedand therefore proved untestable.Accordingly, their data could not beincluded in drug/placebo
comparisons. Also, there were someindications in the data obtained fromthe placebo patients who remained inremission during the testing periodthat they benefited from practice onrepeated testing with the GorhamProverbs Test, even though threealternate forms of the test were used.
The experience of Spohn et al.(1977) is not an isolated instance ofunrepresentative placebo controls dueto untestability of early relapsingpatients. Payne et al. (1963), in aplacebo-controlled study of theeffects of a phenothiazine (Proke-tazine) on overinclusive thinking inchronic schizophrenics whichproduced negative results, comment:
It must be emphasized that this[testable placebo sample] is notcompletely representative ofchronic schizophrenic patientsbecause of the need to eliminate36% of the originally chosen groupon account of disturbed behavior,[p. 530]
The Payne and Spohn studiespose very serious design andmethodological problems confrontinginvestigators concerned with thedetermination of neuroleptic effectson cognitive dysfunction in generaland thought disorder in particular.The problem is especially acute inplacebo-controlled studies usingwashout and on-placebo periods thatare sufficiently long to permitreduction in neuroleptic control ofpsychotic symptoms. The duration ofsuch periods is not coterminous withthe 10- to 14-day washout requiredfor the near total dissipation of drugsubstance and metabolites from thebody system (Lacoursiere and Spohn1976). It should be added that suchproblems can be mitigated neither byreplacing relapsed placebo controlsnor by estimating scores foruntestable patients.
Perhaps the most successful
demonstration of neuroleptictreatment effects on thought disorderis a study by Hurt, Holzman, andDavis (1983), which used theThought Disorder Index (TDI)(Johnston and Holzman 1979) andinvolved a sample of schizophrenicinpatients with a relatively shorthospitalization experience (80 days).These investigators were able toshow that patients placed onhaloperidol after a flexible 1- to 3-week washout period, and tested oncompletion of washout at 1, 3, 5, 12,and 19 days after washout and atdischarge, steadily reduced the levelof TDI scores (pathological verbal-izations on the Rorschach) and thatthis pattern of TDI reduction wassignificantly congruent with clinicalimprovement as rated on the BriefPsychiatric Rating Scale (BPRS)(Overall and Gorham 1962). Whatmars this otherwise rather convincingdemonstration of TDI sensitivity toneuroleptic treatment is that a notreatment-placebo control group wastested at only two points in the studyperiod—namely, at 5 and 12 daysafter washout—and was not rated onthe BPRS on these two occasions.Therefore, it was not possible toperform the same BPRS-TDI trendanalyses over the total study periodwhich had shown such convincingcongruence in the drug-treated group.If such an analysis had revealed thatan increase or no change in TDIscores over the same assessmentperiod for which treated patient datawere available was paralleled by asimilar pattern of BPRS changes inthe placebo group, it would bepossible to rule out practice effectson the TDI and the effects ofplacebo/expectations and nonsomatictreatments on the BPRS ratings asfactors leading to the kind ofcongruence of improvement on theTDI and BPRS in the haloperidol-treated group.
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/3/394/1865999 by guest on 02 February 2022

VOL. 12, NO. 3, 1988 397
In addition, since the patient groupin the study of Hurt, Holzman, andDavis (1983) is only rather sparselydescribed, it is difficult to determinecomparability of this study to mostof the studies heretofore discussed,all of which involved clearly chronicschizophrenics. On the other hand,unlike most other studies, the Hurtstudy did include normal controlsand was therefore in a position todemonstrate that even at maximumbenefit from neuroleptic treatment,the treated gToup manifested consid-erable residual thought pathology.
Andreasen's (1979a, 1979b)seminal studies of thought, language,and communication disorder inmania, depression, and schizophreniahave an important bearing on studiesof neuroleptic treatment effects onthought disorder in schizophrenia. Ofgreatest relevance in the presentcontext are her findings that withrespect to "Bleulerian" thoughtdisorder, manic and schizophrenicpatients cannot be distinguished and,therefore, that Bleulerian symptomsare not pathognonomic of schizo-phrenia. This finding raises thequestion of specificity of thoughtdisorder to schizophrenia. With theexception of the study of Hurt,Holzman, and Davis (1983), whichused the well-standardized TDI, noneof the other above described investi-gations were concerned with thisissue. Moreover, there isundoubtedly considerable variationwithin this group of studies indiagnostic criteria and reliability intheir application.
Andreasen and Olsen (1982)related Hughlings-Jackson'sdistinction between positive andnegative symptoms to thoughtdisorder in psychosis by identifyingsymptoms such as conceptualdisorganization, delusions, andhallucinations as positive symptoms
and symptoms such as anhedonia,alogia, and amotivation as negativesymptoms. Their recommendationthat these symptom types orcategories be used as diagnostic/classification dimensions has foundrather widespread acceptance. Therelevance of these typologies to thestudy of neuroleptic treatment effectson thought disorder is not quite sosalient as that of the specificity issue.Nonetheless, since there are somedata suggesting that patients charac-terized by negative symptoms are lesssusceptible to neuroleptic treatmentthan patients with positive symptoms(Buchanan et al. 1975), this typologymay have uses in research on neuro-leptic treatment effects.
This critical literature reviewprovides guidance both for theselection of thought disordermeasurement instruments and fordesign and methodology in thedevelopment of a competent study ofneuroleptic treatment effects onthought disorder in chronic schizo-phrenics. More specifically, it is ourview that such instruments should befairly broad-ranging in form andseverity of thought pathologyassessed, that some degree ofconstruct validity should be demon-strable, and that the diagnosticboundaries of its applicability bespecified. In design and method-ology, care should be taken toobviate the loss of relapsed,untestable placebo patients, or statedmore positively, to ensure that theplacebo sample be as representativeof the population as the on-drugsample. Moreover, since repeatedmeasurement is inevitably a factor inthe design of such studies, practiceeffects should be minimized and theschedule of repeated assessments inthe on-drug group should parallelthat in the placebo group. It will beseen below how well these specifi-cations were met in our study.
Methods
Subjects. The core subject sample inthis study comprised 100 chronicschizophrenics who agreed to partici-pate after full disclosure of the natureof their participation and the risksentailed by drug withdrawal. Allpatients were rediagnosed by aproject psychiatrist-social workerteam who used the Schedule forAffective Disorders and Schizo-phrenia-Lifetime Version interviewand the Research Diagnostic Criteria(RDC) (Spitzer, Endicott, and Robins1977). For all subjects, it was deter-mined that they had manifested atherapeutic response to prior neuro-leptic treatment. Patients with ahistory of organicity or substanceabuse were excluded. The averageage of the sample was 32.59 years,and average duration of illness was9.7 years. Average cumulativehospitalization was 6.5 years, andaverage years of education totaled12.58. Twenty-seven percent werefemale patients.
Also recruited to the project were26 RDC-diagnosed schizoaffectivedisorder patients and 25 RDC-diagnosed bipolar (bipolar I)patients, as well as 39 normalcontrols. These diagnosticcomparison groups were involvedonly in data analyses designed todetermine TDI specificity.
Design. The 100 chronic schizo-phrenics were randomized to twoconditions. A group of 36 patientsremained on the active neurolepticthey had received before researchentry throughout a 10-week studyperiod. A second group of 64patients were abruptly withdrawnfrom neuroleptics and placed onplacebo matching in kind and dosethe prewithdrawal neuroleptics theyhad received. No washout was used.
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/3/394/1865999 by guest on 02 February 2022

398 SCHIZOPHRENIA BULLETIN
All patients were tested with anextensive performance test batteryincluding the Rorschach and theWechsler Adult Intelligence Scale(WAIS) in a baseline session beforeexperimental assignment and whilestill fully medicated, and four timesafter experimental assignment at 2-week intervals. Also, on each of thefive occasions of testing, patientswere rated by a psychiatrist on theBPRS and by two research assistantson the Psychologic Rating Scale(King 1954). Testers, raters, projectresearch nurses, patients, andhospital ward staff were unaware ofpatient drug status throughout.
Forty-four patients in the drugwithdrawal condition and fivepatients in the active medicationcondition "relapsed" in the course ofthe 10-week study period. A patientwas considered "relapsed" when bothward staff and project researchnurses, who daily monitored theresearch patient's clinical condition,agreed that the first signs ofsymptom exacerbation were evident.No patient was permitted to undergofull-scale symptom exacerbation. Asubstantial proportion of relapsedpatients were remedicated andcompleted the full five-test-sessionschedule.
For all relapsed patients, dataobtained on the test session closest intime to their relapse were consideredto be largely free of neurolepticmedication effects. Changes in testperformance (other than those thatcould be imputed to practice) in the"relapse" session from testperformance in the preexperimentalassignment baseline session wereregarded as reflecting medicationeffects. Another way of stating thisassumption is to say that deterio-ration in test performance in relapsedpatients was regarded as representingdysfunction normalized or otherwisemodified by neuroleptic treatment.
While reduction in loss of datafrom untestable placebo patients wasan important aim in this design, itseffect was to reverse the roles of on-drug and placebo patients in theconventional, independent groupdrug evaluation design. Patients "ondrug" in the present design served ascontrols for practice and attentioneffects; the drug-withdrawn, on-placebo patients served as experi-mental subjects. Drug withdrawalwas the independent variable and testperformance, the dependent variable.Drug effect hypotheses (i.e., theeffect of neuroleptic treatment onthought disorder) were tested bycontrasting baseline session topostwithdrawal session test changesin control patients (on drug) withthose of experimental subjects (onplacebo/ relapsed).
A critical methodological problemassociated with this unconventionaldesign needs to be addressed.Randomization could not be extendedto the "assignment" of drug-withdrawn patients to relapse andnonrelapse conditions. Factors deter-mining when and whether a givenpatient relapsed could thus not bebrought under experimental controlby randomization. A consequence ofthis in the present study was one ofsignificant dependent variable initiallevel differences among control,relapsed, and nonrelapsed groups.
Of the 44 patients who relapsedduring the 10-week study period, 21did so approximately 2 weeks afterdrug withdrawal, 11 about 4 weeksafter withdrawal, and 12 during theremainder of the study period.Accordingly, 21 patients wereconsidered relapsed in the secondtesting session (session 2), 11 in thethird testing session (session 3), 5 insession 4, and 2 in session 5.Comparisons among these differingduration-to-relapse groups by meansof multivariate analysis of variance
(MANOVA) on BPRS symptomratings scales, demographic andcourse of illness variables indicatedthat these several groups did notdiffer significantly. In the controlgroup, relapse in five patientsoccurred in session 3 (for two) and insession 5 (for three). Drug-withdrawnpatients who were not consideredrelapsed in sessions 2, 3, 4, and 5 diddiffer significantly from controls andrelapsers in these several sessionsprincipally in initial level (session 1)test scores, but on other variables aswell.
That the relapsed patients differedin duration to relapse made possibleseveral independent replicative testsof drug effect hypotheses. We presenttwo such tests in the present report.The first involved data from 21relapsers, 43 drug-withdrawnnonrelapsers, and 36 controls insession 2. The second test, involvingsession 3 data, compares relapsers(13: 11 withdrawn and 2 relapsedcontrols), nonrelapsers (29), controls(33), and 19 patients off drugs insession 2 and remedicated in session3. Including the latter group insession 3 data analyses assuredcomparability of the results ofanalysis of session 2 and session 3data sets because essentially the samegroups of patients were involved inboth analyses.
Tests, Rating Scales, and Scores. TheThought Disorder Index (TDI) isessentially a system for scoringpathological verbalizations on theRorschach test and on the WAIS.Pathological verbalizations areweighted according to four levels ofseverity. "Minimal" severity ofthought pathology (to which a .25weight is assigned) comprises suchresponse characteristics asconcreteness, vagueness, word-finding difficulties, and persever-ation. "Mild" severity (.50) reflects,
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/3/394/1865999 by guest on 02 February 2022

VOL. 12, NO. 3, 1986 399
among others, confused, loose, andfabulized responses. "Moderate"severity (.75) is represented byautistic logic, fluidity, absurdresponses, and confabulations."Maximally severe" responses (1.0)are contaminations, incoherence, andneologisms.
The Rorschach and the WAIS wereadministered in each of the fivesessions by a qualified examiner whoalso administered a series of othertests that will be the subject of subse-quent reports. All 10 cards of theRorschach and four verbal subtestsof the WAIS were administered inthe baseline session (1) and in session3. To mitigate practice effects, anachromatic Rorschach card (I), a redand black card (II), and a chromaticcard (VIII) only were administered insession 2. Also, on these occasions,two verbal subtests of the WAIS(Vocabulary and Similarities) wereadministered. Interrater reliability inscoring using the TDI scoringmanual, among three experiencedclinical psychologists, was found tobe r = .84 at the outset. A singlesenior clinical psychologist memberof that group scored all Rorschachand WAIS protocols subsequently.
TDI scores employed in dataanalysis were (1) the sum of severity-weighted Rorschach verbalizationscorrected by the number ofRorschach responses (TDR) and (2)the sum of weighted responses on theWAIS (TDW). Derived scores used in
data analysis were presence (1) orabsence (0) of one or more patho-logical responses on the Rorschach ateach of the severity levels.
Brief Psychiatric Rating Scale. The 16symptom subscales of the BPRS wereadministered by, for the most part,the same psychiatrist within a timeband of ±24 hours of testing. Inter-rater reliability was established at theoutset at r = .87. Several scoreswere derived from various combi-nations of the BPRS subscales for avariety of purposes in data analysisincluding a total pathology score, aschizophrenic symptom score (themean of ratings on all subscalesreflecting schizophrenic psycho-pathology), a positive/negativesymptom index based on BPRSsubscales: ([Blunted Affect +Emotional Withdrawal]— [Conceptual Disorganization +Unusual Thought Content])/([BluntedAffect and Emotional Withdrawal] +[Conceptual Disorganization andUnusual Thought Content]).
Psychologic Rating Scale. ThePsychologic Rating Scale (King 1954)comprises subscales on which orien-tation to testing, cooperativeness,performance motivation, andattention to instructions in the testsituation were rated by twoexaminers, one of whom observedpatient behavior without awareness
of performance efficiency. Interraterreliability was r = .92. The ratingsof the latter examiner wereconsidered measures of "GeneralDeficit Functioning" and were usedas such in data analyses.
Results
Brief Psychiatric Rating Scale. In aneffort to determine whether patientsconsidered relapsed in session 2 andsession 3 did indeed manifestsymptomatic exacerbation expectedby design, changes in several BPRSscores from session 1 to 2 and from 1to 3 for relapsed patients werecompared with changes in control,nonrelapsed, and remedicatedpatients (in session 3 only) byanalysis of covariance (ANCOVA).Session 1-2 and session 1-3 meanscores for 'Total Pathology" and"Schizophrenic Symptoms" only areshown in table 1. ("Schizophrenic"symptoms represent mean ratings onall those subscales of the BPRS whichclearly reflect psychopathologycharacteristic of schizophrenicpatients.) Because of significantinitial level differences among theseveral groups, initial level served ascovariate in all analyses.
In session 1-2 contrasts, relapsersincreased on all BPRS scores, whileboth controls and nonrelapsedpatients decreased. In multivariateanalysis of covariance (MANCOVA),
Table 1. Brief Psychiatric Rating Scale Total Pathology and schizophrenic symptom group means
Group
Total Pathology Schizophrenic symptoms
S1 S2 S1 S3 Group S1 S2 S1 S3
ControlNonrelapsedRelapsedRemedicated
23.1116.4718.50
21.6915.2122.18
22.8215.6219.6417.53
22.53 Control 1.8113.54 Nonrelapsed 1.2123.51 Relapsed 1.3919.13 Remedicated —
1.721.121.69
1.821.101.591.24
1.82.953
1.891.37
Note.—S1.S2, S3 = session 1, session 2, session 3.
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/3/394/1865999 by guest on 02 February 2022

400 SCHIZOPHRENIA BULLETIN
this pattern of differences in changewas significant for all scores(p< .01).
In session 1-3 contrasts, relapsedpatients as well as remedicatedpatients showed an increase in theseveral BPRS variables, while controlpatients remained at the same level inboth sessions and nonrelapsedpatients decreased somewhat. Again,in MANCOVA, these patterns ofchange differences were found to besignificant (p < .01).
Several inferences may be drawnfrom these findings. Clearly, patientsconsidered relapsed in sessions 2 and3 manifested symptomatic exacer-bation in these sessions. That remedi-cated patients also showed significantBPRS increases in session 3 impliesthat for most of these patientsremedication had not yet regainedsymptomatic control and thattherefore they could be construed tobe in a state of functional relapse.
At the same time, mean increasesin the BPRS variables in relapsed andremedicated patients, whilesignificant, were not substantial, andin the distributions of BPRS scores inthe several comparison groups, therewas some degree of overlap.Accordingly, it must be granted thatrelapsed and remedicated patientswere not in a state of acute, floridexacerbation of symptoms as aconsequence of drug withdrawal.This inference is supported by thefinding that on the Psychologic
Rating Scale—which was construedto reflect general deficitfunctioning—relapsed and remedi-cated subjects in sessions 2 and 3manifested marginally significant(S1-S2, p < .08) or nonsignificantincreases (S1-S3, p < .15) overcontrol and nonrelapsed patients.
These patterns of findings, inessence, imply that the "independentvariable manipulation" aimed at inthe design of the study was attained.Drug withdrawal in a substantialnumber of subjects in sessions 2 and3 had resulted in symptom exacer-bation reflecting some reduction inneuroleptic symptom containment.At the same time, this degree ofsymptom control reduction was notso great as to leave largely impairedthe ability of relapsed and remedi-cated patients to render a scorableperformance on the tests admin-istered in the "relapse" sessions.
Several additional analyses wereperformed with three of the BPRSsubscales: "Conceptual Disorgan-ization," "Hallucinations," and"Unusual Thought Content." Theseanalyses were done because the threesubscales represent measures ofthought disorder independent of theTDI and because they are readilyidentifiable as "positive symptoms"and were used as such in aPositive/Negative Symptom Indexdescribed above. The group means(see table 2) in session 1 for relapsedand remedicated patients were
increased in sessions 2 and 3, whilecontrols and nonrelapsed patientsshowed decreases. ANCOVAindicated that this pattern of changedifferences for all three subscales wassignificant (p < .01). One implicationof this pattern of findings is thatneuroleptic medication tends tonormalize thought pathologyreflected in these BPRS symptomsubscales.
Specificity. In order to determinewhether in the context of the presentstudy, level of thought pathology asmeasured by the TDI was specificallycharacteristic of chronic schizo-phrenics, TDI scores for the latterwere contrasted with TDI scores for26 (RDC) schizoaffective patients and25 (RDC) bipolar patients as well asfor 39 normal controls. Table 3shows mean TDI scores on theRorschach (TDR) and the WAIS(TDW). Because of some departurefrom normality in most of thesedistributions of the raw scores, theywere transformed by Freeman-Tukeytransformations and are shown assuch in table 3. Because of meandifferences among these four groupsin age, sex, and education, thesevariables served as covariates in one-way ANCOVA. The results ofANCOVAs performed both on TDRand TDW scores were virtuallyidentical. Hence, only the TDRanalysis is presented. In ANCOVAcontrast of the four groups, an
Table 2. Group means on subscales of the Brief Psychiatric Rating Scale
Conceptual Disorganization Unusual Thought Content Hallucinations
Group S1 S2 S1 S3 S1 S2 S1 S3 S1 S2 S1 S3
ControlNonrelapsedRelapsedRemedicated
1.83.884
1.70
1
2
.73
.774
.38
1
11
.82
.724
.36
.52
1
12
.83
.724
.95
.08
3.002.002.35
212
.76
.52
.90
3.001.791.591.24
2.83 1.89 1.79 1.79 1.781.23 .907 .745 .621 .4991.93 1.75 2.18 1.90 1.931.42 — — 1.42 1.45
Note —S1, S2, S3 = session 1, session 2, session 3
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/3/394/1865999 by guest on 02 February 2022

VOL. 12, NO. 3, 1986 401
Table 3. Thought Disorder Index group means: Schizophrenics,schizoaffectives, bipolars, and normal controls
Group
SchizophrenicsSchizoaffectivesBipolarsNormals
TDR
Mean
5.925.103.083.47
SD
3.923.032.592.46
TDW
Mean
2.412.291.681.47
SD
1.551.441.02.64
Note.— TDR = sum of severity-weighted Rorechach verbalizations, corrected by number ofRorschach responses. TDW = sum of weighted responses on the Wechsler Adult Intel-ligence Scale.
F >= 20.73, df = 3/179, p < .001was obtained. Orthogonalcomparisons of schizophrenicpatients with schizoaffective patients,and bipolar patients with normalcontrols, were not significant, whileschizophrenic plus schizoaffectivepatients did differ significantly frombipolar patients and normal controls.These results are interpreted asimplying that schizophrenic andschizoaffective patients manifestedsignificantly greater thoughtpathology on the TDR than bipolarpatients and normal controls andthat within neither of these two pairsof groups were there significantdifferences in level of thoughtpathology. More generally speaking,these results suggest that a muchhigher level of thought pathology ischaracteristic not only of schizo-phrenic patients devoid of affectivesymptoms but also schizophrenicswith marked affective symptom-atology than is the case for affectivedisorder patients and normalcontrols.
Two further implications are worthnoting. It comes as something of asurprise, in light of the research liter-ature in this area, that in thoughtpathology schizoaffectives are morelike schizophrenics than affectivedisorder patients. Moreover, it isequally surprising in light of
Andreasen's (1979a) findings ofsimilarities in "Bleulerian" thoughtpathology between schizophrenicsand manic patients that in thepresent data bipolar patients (most ofwhom, to be sure, were not acutelypsychotic) manifest significantlylower thought pathology on the TDIthan schizophrenics. In order toclarify this latter finding, additionalANCOVAs were performed includingonly the three diagnostic groups andcovarying out such nonspecificfactors as general deficit functioning,duration of illness, and premorbidadjustment which were correlatedpositively with TDR in the schizo-phrenics and were greater in thesepatients than in the bipolars.ANCOVA applied to these dataindicated that the differencescontinued to be significant(F = 3.822, df «- 2/141, p < .024),although the removal of the threecovariates "pulled" the adjustedmeans somewhat closer together.This finding provides the first hint inthe present data that the TDImeasures a distinctive form ofthought pathology.
Correlates of TDI. In a further effortto clarify the nature of thoughtpathology measured by the TDI inchronic schizophrenics, it was corre-lated with demographic, symptom,
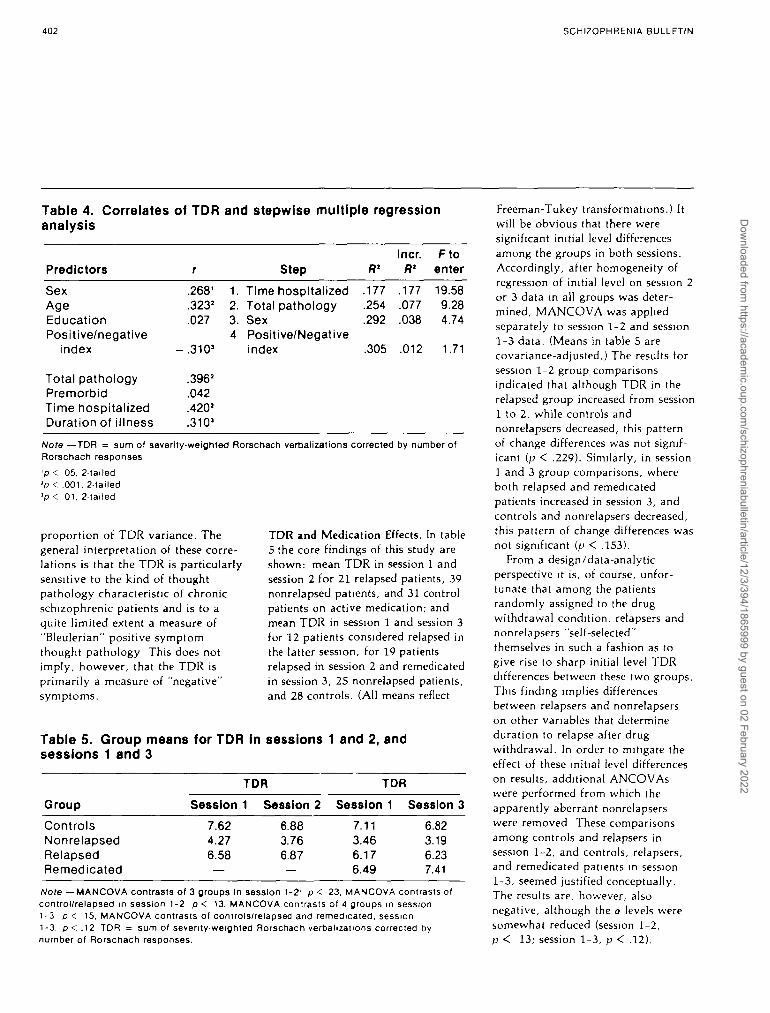
and course of illness variables. Inthese correlations as well as in allsubsequent data analyses, only theTDR was used, largely because itappears to be more sensitive to theelicitation of thought pathology thanthe TDW. Moreover, in the presentas well as all subsequent dataanalyses, the TDR distributions werefound to depart from normality andwere accordingly transformed bymeans of a Freeman-Tukey trans-formation. More specifically, thevariables correlated with TDR weresex, age, education, Total Pathologyon the BPRS, the Positive/NegativeSymptom Index (also BPRS based;see above), premorbid adjustment,duration of illness, and cumulativehospitalization time. Because ofoutlier duration-of-illness scores, alog transformation was applied.These correlations are shown in table4. It will be evident from this tablethat severity of illness and chronicityindices dominate the correlationalpicture. The more severely ill and thelonger the duration of illness andhospitalization, the greater the TDRthought pathology. The negativecorrelation of TDR with thePositive/Negative Symptom Index,which is, of course, strongly corre-lated with Total Pathology, indicatesthat positive symptoms vary directlywith TDR severity.
Stepwise multiple regressionanalysis (also shown in table 4)generally confirms these inferences indemonstrating that length ofhospitalization and severity of illnessmake independent contributions inaccounting for TDR variance, andthat sex (female patients manifestedhigher TDRs) and the Positive/Negative Symptom Index account forabout 30 percent of the TDRvariance. It is of some interest thatthe Positive/Negative SymptomIndex accounts independently ofBPRS Total Pathology for a minimal
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/3/394/1865999 by guest on 02 February 2022
402 SCHIZOPHRENIA BULLETIN
Table 4. Correlates of TDR and stepwise multiple regressionanalysis
Predictors
SexAgeEducationPositive/negative
index
Total pathologyPremorbidTime hospitalizedDuration of illness
r
.2681
.323*
.027
- .310 3
.396'
.042
.420'
.310'
1.2.3.4
Step
Time hospitalizedTotal pathologySexPositive/Negativeindex
.177
.254
.292
.305
Incr.R1
.177
.077
.038
.012
Ftoenter
19.589.284.74
1.71
Note —TDR = sum of severity-weighted Rorschach verbalizations corrected by number ofRorschach responses'p < 05, 2-tailed'p < .001, 2-tailed'p < 01, 2-tailed
proportion of TDR variance. Thegeneral interpretation of these corre-lations is that the TDR is particularlysensitive to the kind of thoughtpathology characteristic of chronicschizophrenic patients and is to aquite limited extent a measure of"Bleulerian" positive symptomthought pathology This does notimply, however, that the TDR isprimarily a measure of "negative"symptoms.
TDR and Medication Effects. In table5 the core findings of this study areshown: mean TDR in session 1 andsession 2 for 21 relapsed patients, 39nonrelapsed patients, and 31 controlpatients on active medication; andmean TDR in session 1 and session 3for 12 patients considered relapsed inthe latter session, for 19 patientsrelapsed in session 2 and remedicatedin session 3, 25 nonrelapsed patients,and 28 controls. (All means reflect
Table 5. Group means for TDR in sessions 1 and 2, andsessions 1 and 3
Group
ControlsNonrelapsedRelapsedRemedicated
Session
7.624.276.58
TDR
1 Session 2
6.883.766.87
Session
7.113.466.176.49
TDR
1 Session 3
6.823.196.237.41
Note —MANCOVA contrasts of 3 groups In session 1-2' p < 23, MANCOVA contrasts ofcontrol/relapsed in session 1-2 p < 13. MANCOVA contrasts of 4 groups in session1-3 p < 15, MANCOVA contrasts of controls/relapsed and remedicated, session1-3. p < .12 TDR = sum of seventy-weighted Rorschach verbalizations corrected bynumber of Rorschach responses.
Freeman-Tukey transformations.) Itwill be obvious that there weresignificant initial level differencesamong the groups in both sessions.Accordingly, after homogeneity ofregression of initial level on session 2or 3 data in all groups was deter-mined, MANCOVA was appliedseparately to session 1-2 and session1-3 data. (Means in table 5 arecovariance-adjusted.) The results forsession 1-2 group comparisonsindicated that although TDR in therelapsed group increased from session1 to 2, while controls andnonrelapsers decreased, this patternof change differences was not signif-icant (p < .229). Similarly, in session1 and 3 group comparisons, whereboth relapsed and remedicatedpatients increased in session 3, andcontrols and nonrelapsers decreased,this pattern of change differences wasnot significant (p < .153).
From a design/data-analyticperspective it is, of course, unfor-tunate that among the patientsrandomly assigned to the drugwithdrawal condition, relapsers andnonrelapsers "self-selected"themselves in such a fashion as togive rise to sharp initial level TDRdifferences between these two groups.This finding implies differencesbetween relapsers and nonrelapserson other variables that determineduration to relapse after drugwithdrawal. In order to mitigate theeffect of these initial level differenceson results, additional ANCOVAswere performed from which theapparently aberrant nonrelapserswere removed These comparisonsamong controls and relapsers insession 1-2, and controls, relapsers,and remedicated patients in session1-3, seemed justified conceptually.The results are, however, alsonegative, although the a levels weresomewhat reduced (session 1-2,p < 13; session 1-3, p < .12).
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/3/394/1865999 by guest on 02 February 2022

VOL. 12, NO. 3, 1986 403
In all these analyses, power suffi-cient to detect anything other thanlarge mean differences was inade-quate. It seems probable that withgreater power the observed meandifferences might have been signif-icant. Even in this eventuality,however, it could not be concludedthat the formal thought pathologymeasured by the TDR is normalizedto more than a minimal extent byneuroleptic treatment in chronicschizophrenics.
These conclusions led us to afurther consideration of the findingsobtained in similar analyses of suchpositive symptom BPRS subscales asConceptual Disorganization andUnusual Thought Content. For bothof these scales (see table 2), with thesame statistical power, the effect waslarge enough to yield significantmean differences with respect topatterns of change among all thecomparison groups in sessions 1-2and sessions 1-3. The directions ofchange differences suggest that theseforms of thought pathology aresubstantially normalized by neuro-leptic medication.
These forms of thought pathologyare moderately correlated with TDR(see table 4), which is, it will berecalled, a composite scorecomprising four levels of thoughtpathology, the more severe of whichare defined in terms similar to thoseof Conceptual Disorganization andUnusual Thought Content. On thebasis of these considerations, weundertook a further set of TDRanalyses in which this summary scorewas decomposed into its severity-weighted constituents. The aim ofthese analyses was to test theprovisional hypothesis that signif-icant change due to relapse wasdemonstrable only for the two mostsevere subscores (see Methodssection) and not for the two lesssevere subscores. A further impli-
cation of this hypothesis is thatneuroleptic treatment selectivelynormalized more severe thoughtpathology while leaving unmodifiedmilder, less severe thought pathologyas characterized by the TDR.
The scores for these analyses werein binary form: 0 = no pathologicalresponses and 1 = ^ 1 pathologicalresponse assigned to each of the fourseverity levels, "minimal" (.25),"mild" (.50), "moderate" (.75), and"severe" (1.0), for all patients. Theproportions of pathological responsesat each level in the prewithdrawalsession (1) for all patients are shownin figure 1. The proportions arebased on responses to all 10Rorschach cards.
It is evident from figure 1 thatminimal and mild thought pathology(reflecting concreteness, vagueness,and perseveration, as well asconfusion, looseness, and fabuli-zations) is represented in substan-tially greater response proportionthan moderate and severe thoughtpathology (reflecting autistic logic,absurd responses, incoherence, andneologisms). This may well explainwhy the Positive/Negative SymptomIndex (comprising, among othersubscales, Conceptual Disorgan-ization and Unusual ThoughtContent) accounted for only a rathersmall proportion of the total TDRvariance.
Table 6 presents proportions ofpresent (1) and absent (0) thoughtpathology for control patients andrelapsed patients at minimal, mild,moderate, and severe levels insessions 1 and 2. For reasons alreadyadduced above, nonrelapsers insession 2 were excluded in theanalysis applied to these data. Table7 shows the same data for controlsand relapsed and remedicatedpatients combined in sessions 1 and3. Combining the latter two groupsseemed justified by the finding that
both groups manifested symptomaticexacerbation in session 3.
Log linear analysis applied to thesedata yielded the following results. Insession 1-2 (table 6) the x1 for theinteraction of group by proportionsof present/absent responses forminimal pathology in session 1 wassignificant {p < .03), indicating thatthe relapsed group showed a smallerproportion of pathological responsesthan the control group. No suchsignificant x' was obtained in session2. The joint x2 for group comparisonof the patterns of proportions in bothsessions 1 and 2, however, was notsignificant. For mild thoughtpathology, neither the within-sessioninteractions with group nor thebetween-session interactions withgroup were significant. It isconcluded from this pattern offindings that neither control norrelapsed patients manifested anincrease in minimal and mild thoughtpathology in session 2. Indeed, ratherthe opposite was true. Both groupsshowed reductions in session 2.
At the moderate and severe levelsof TDR thought pathology, a
Figure 1. Percent thoughtpathology (TDR) at 4 levels ofseverity in session 1
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/3/394/1865999 by guest on 02 February 2022

404 SCHIZOPHRENIA BULLETIN
Table 6. Proportions of present/absent thought pathology by
Group
ControlRelapsed
Minimal (.25)
Session 1 Session 2
Absent Present Absent Present
.54 .46
.67 .34.63 .37.71 .29
Mild
Session 1
(-50)
Session 2
Absent Present Absent Present
.61 .39
.52 .46.74 .26.71 .29
levels of TDR severity
Moderate (.75)
Session 1 Session 2
Absent Present Absent Present
.70
.80.30.20
.74
.57.26.43
in sessions
Severe (1.0)
1-2
Session 1 Session 2
Absent Present Absent Present
.94
.95.06 .94.05 .85
.06
.15
Note. — TDR = sum of severity-weighted Rorschach verbalizations corrected by number ol Rorschach responses.
somewhat different pattern emerges.In session 1, at both moderate andsevere levels, the relapsed patientsmanifest a significantly smallerproportion of thought pathologythan the controls (p < .01). Insession 2, however, this pattern isreversed. Relapsed patients show asignificant increase in proportion ofboth moderate and severe thoughtpathology, while the controls reducethought pathology (p < .01). Thejoint x2 for session by group inter-actions at the moderate level(contrasting patterns of proportionsbetween groups in session 1 andsession 2) is significant (p < 05),while at the severe level, amarginally significant x2 (p < .06) isobtained. It thus appears that whileat the minimal and mild levels signif-icant differences in proportions ofmanifest thought pathology betweencontrols and relapsed subjects withinor between sessions could not bedemonstrated, at the moderate and
severe levels, relapsed patientsrelative to control patients and tothemselves in session 1 showedsignificant increases in proportions ofthought pathology in the session inwhich their relapse was manifest.
A similar pattern of results is seenin session 1-session 3 comparisons ofcontrols, and relapsers and remedi-cated patients combined (see table 7).The x2 for the interaction of groupby proportions of presence/absenceof minimal thought pathology insession 1 and session 3 is significantfor each session (session 1: p < .02;session 3- p < .001). The joint x2
contrasting the patterns of propor-tions between groups in both session1 and session 3 is also significant(p < .02). Inspection of proportionsshown in table 7 for minimalpathology indicates that both insession 1 and session 3 therelapsed/remedicated patientsmanifested less thought pathologythan the controls, although both
groups showed a reduction inpathology in session 3
At the mild level in session 1, thegroup by present/absent proportionsX2 is not significant. In session 3,however, this interaction is signif-icant (p < 002). Moreover, the jointX2 contrasting the proportion patternsamong groups for sessions 1 and 3 ismarginally significant (p < .06). Itappears, therefore, that while bothcontrols and relapsed/remedicatedpatients showed reductions in mildthought pathology, the latter groupdid so to a significantly smallerextent than the former.
At both the moderate and severelevels of thought pathology, adifferent pattern of results obtains.Within-session interactions insessions 1 and 3 are significant(session 1- p < .01; session 3: p< .01), and between-session inter-actions are similarly significant (p< .03). Inspection of table 7 indicatesthat at both moderate and severe
Table 7. Proportions of present/absent thought pathology by levels of TDR severity in sessions 1-3
Minimal (.25) Mild (.50) Moderate (.75) Severe (1.0)
Group
Session 1 Session 3 Session 1 Session 3 Session 1 Session 3 Session 1 Session 3
Absent Present Absent Present Absent Present Absent Present Absent Present Absent Present Absent Present Absent Present
Control .18 .82 .35 .65 .28 .72 .56 .44 .47 .53 .50 .50 .84 .16 .84 .16Relapsed &
remedi-cated .32 .68 .41 .59 .29 .71 .43 .57 61 .39 .35 .65 .87 .13 .80 .20
Note — TDR = sum of severity-weighted Rorschach verbalizations corrected by number of Rorschach responses
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/3/394/1865999 by guest on 02 February 2022

VOL. 12, NO. 3, 1986 405
levels, relapsed/remedicated patientsshow a smaller proportion of patho-logical responses, while in session 3this pattern is reversed; controlsreduce proportions of pathologicalresponses, while these are seen to beincreased over session 1 in therelapsed/remedicated patients. Fromthese results, both in session 1-2 andsession 1-3 tests, the inference isdrawn that neuroleptics tend tonormalize moderate and severethought pathology, while minimaland mild thought pathology islargely unaffected by these drugs.
Discussion
The central finding in this study isthat more severe thought pathologyin chronic schizophrenics, heredefined both by subscales of theBPRS and scoring categories on theTDI, are to some extent normalizedby neuroleptic medication, while lesssevere levels of thought pathology,specifically defined by types ofscoring categories on the TDI, areunmodified by neurolepticmedication. Indeed, it may be saidthat the neuroleptics are not so muchselective in normalizing degree ofseverity of thought pathology as theyare selective in the kind of thoughtpathology that is reduced. Thus, itmay be inferred that vivid, dramatic,gross distortions of reality, delusions,and hallucinations typicallyassociated with an acute episode arereduced and even removed, while akind of disorientation vis-a-visreality, as well as concreteness andlooseness, persists as residual thoughtpathology after a clinical remissionhas been attained by neuroleptictreatment. It remains now to examinethe implications of these findings fordiagnosis of medicated patients, fortreatment and rehabilitation, forexperimental study of thought
disorder, for mechanisms of drugaction, and for thought disorder as atrait in chronic schizophrenia.
From the perspective of descriptivepsychiatry and diagnostic processes,the present findings suggest that thepresenting clinical picture inmedicated chronic schizophrenicpatients will be to some extentdistorted. The probable absence ofAndreasen's "positive symptoms"exemplifies this point. Clinicalpsychologists will identify fewseverely pathological responses onpsychological testing; neuropsychol-ogists may interpret residual thoughtpathology as reflecting mild brain-based cognitive deficit.
In many mental hospitals,psychiatrists, already aware thatmedication may reduce presentingthought disorder in medicated newadmissions, routinely withdraw suchpatients from neuroleptics in order toobtain a "pure" symptomatic andphenomenological picture. Investi-gators concerned with the experi-mental study of thought disorderwould be well advised to do thesame. Indeed, the present findingslend particular force to Chapmanand Chapman's (1973) recom-mendation that experimental studiesof thought disorder should beperformed with drug-free schizo-phrenic patients only. At the sametime, studies of language inmedicated chronic schizophrenics areunlikely to reflect the full range ofcommunication difficulties.
Our findings also have some impli-cations for efforts at therapy andrehabilitation with chronic schizo-phrenic patients. The psychotherapistwill find his medicated chronicschizophrenic patient less distractedby hallucinations and lesspreoccupied by and fixed ondelusions. Thus, the process oftherapy will proceed with asomewhat greater degree of attention
to the immediate realities of thetherapeutic situation.
Behavior therapists and socialskills trainers (Wallace and Boone1984) seeking to rehabilitate or even"habilitate" chronic schizophrenicpatients have long recognized thatsuch efforts are feasible only withmedicated chronic schizophrenics. Atthe same time, it is generally agreedthat social skills training is difficultto generalize and tends not to endurelong beyond even persistent trainingefforts. Perhaps the presentfindings of residual concreteness,perseveration, vagueness, andlooseness in thought processes mayreflect the difficulties that social skillstrainers encounter.
These findings suggest thatremitted chronic patients do notexperience events as connected. Theyhave little confidence in thecontinuity of events and in theirrecurrence under specifiable circum-stances. Their ability to derivemeaning by induction is impaired.Subjectively, they experience realityas fragmentary, disjointed, andunpredictable. Perhaps mostimportant of all, they sense aterrifying disparity between theirability to cope and the multiplechallenges to cope with which familyand community confront them.
The findings of this study leaveunanswered questions regardingspecific mechanisms whereby neuro-leptic medication reduces themanifestation of the more severeaspects of thought pathology. On thebasis of the research literature in thisregard, two hypotheses aresuggested. The drugs may specificallyact on thought pathology such thatthe frequency with which grosslydisordered thinking is inconsciousness reduced or eveneliminated. On the other hand,neuroleptics may not directly affectthought pathology but may
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/3/394/1865999 by guest on 02 February 2022

406 SCHIZOPHRENIA BULLETIN
strengthen the schizophrenic'sawareness of the social inappro-priateness of bizarre ideas and thuspermit the "editing out" of theseideas in communication with suchothers in the present study as theRorschach examiner and the psychi-atrist interviewer. In view of the fact,however, that residual thoughtpathology as defined in the presentstudy entails considerable lack ofcognitive clarity, it seems unlikelythat chronic patients' judgment of thesignificance of interpersonalsituations would lead them to editout all socially inappropriateideation.
Finally, we address issues relatedto the question of whether residualthought pathology can be considereda trait of chronic schizophrenia aswell as further implications of neuro-leptic selectivity in normalizingthought pathology.
Our data satisfy some "trait"criteria but not others. We haveshown that residual thoughtpathology is present both in clinicalremission and in acute episodes. Thisfact satisfies an important criterion.Symptoms or dysfunctions that aremodified or normalized by neuro-leptic treatment clearly do not merittrait status. We have not been able todemonstrate, however, that what hasbeen designated by us as residualthought pathology predates theinitial onset of the illness andwhether it has persisted throughoutthe entire course of illness. Ourfindings, however, should encourageresearch addressed to these issuesbecause it may well lead to theidentification of thought pathologyas a marker of vulnerability inschizophrenia.
There is yet a further speculationthat our findings of neuroleptic selec-tivity encourage. It may well be thatthose symptoms and dysfunctionsthat neuroleptics normalize are
typically nonspecific to the illness. Itis well known that neuroleptics donormalize "positive" symptoms inacute manics. On the other hand,those dysfunctions that neurolepticsdo not normalize, e.g , residualthought pathology, eye trackingdeviance (Holzman and Levy 1977),and skin conductance orientingresponse dysfunction (Bernstein et al.1982), may well be illness-specific.
References
Andreasen, N.C. Thought, language,and communication disorders: I.Clinical assessment, definition ofterms, and evaluation of theirreliability. Archives of GeneralPsychiatry, 36:1315-1321, 1979a.
Andreasen, N.C. Thought, language,and communication disorders: II.Diagnostic significance. Archives ofGeneral Psychiatry, 36:1325-1330,1979b.
Andreasen, N.C, and Olsen, S.Negative v positive schizophrenia.Archives of General Psychiatry,39.789-794, 1982.Bernstein, A.S.; Frith, CD.,Gruzelier, J.H.; Patterson, T.,Straube, E.; Venables, P.H.; andZahn, T.P. An analysis of the skinconductance orienting response insamples of American, British, andGerman schizophrenics. BiologicalPsychology, 14:155-211, 1982.
Buchanan, F.H.; Parton, R.V.;Warren, J W., and Baker, E.P.Double-blind trial of L-dopa inchronic schizophrenia. Australianand New Zealand Journal ofPsychiatry, 9:269-271, 1975.
Chapman, L.J., and Chapman, J.P.Disordered Thought in Schizo-phrenia. New York: Appleton-Century-Crofts, 1973
Goldstein, K. The significance of
special mental tests for diagnosis andprognosis in schizophrenia. AmericanJournal of Psychiatry, 96:575-587,1939.
Gorham, D.R. Use of the proverbstest for differentiating schizophreniafrom normals. Journal of ConsultingPsychology, 20:435-440, 1956.
Harrow, M.; Tucker, G.;Himmelhoch, J.; and Putnam, N., Jr.Schizophrenic "thought disorders"after the acute phase. AmericanJournal of Psychiatry, 128:824-829,1972.Holzman, P.S., and Levy, D.L.Smooth pursuit eye movements andfunctional psychoses: A review.Schizophrenia Bulletin, 3:15-27,1977.
Hurt, S.W.; Holzman, P.S.; andDavis, J.M. Thought disorder—Themeasurement of its changes. Archivesof General Psychiatry, 40:1281-1285,1983.Johnston, M.H., and Holzman, P.S.Assessing Schizophrenic Thinking.Washington: Jossey-Bass, 1979.
King, H.E. Psychomotor Aspects ofMental Disease Cambridge,MA: Harvard University Press,1954.
Lacoursiere, R.B., and Spohn, H.E.How long does chlorpromazine last?Journal of Nervous and MentalDisease, 163:267-275, 1976Maher, B.A. A tentative theory ofschizophrenic utterance. In: Maher,B.A., ed. Progress in ExperimentalPersonality Research. Vol. 12. NewYork: Academic Press, 1983. pp.1-52.
Nuechterlein, K.H., and Dawson,M.E. Information processing andattentional functioning in the devel-opmental course of schizophrenicdisorders. Schizophrenia Bulletin,10:160-203, 1984.Orzack, M.H.; Kornetsky, C; and
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/3/394/1865999 by guest on 02 February 2022

VOL. 12, NO. 3, 1986 407
Freeman, H. The effects of dailyadministration of carphenazine onattention in the schizophrenic patient.Psychopharmacologia, 11:31-38,1967.
Overall, J.E., and Gorham, D.R. TheBrief Psychiatric Rating Scale.Psychological Reports, 10:799-812,1962.
Payne, R.W.; Friedlander, D.;Laverty, S.G.; and Haden, P.Overinclusive thought disorder inchronic schizophrenics and itsresponse to "Proketazine." BritishJournal of Psychiatry, 109:523-530,1963.
Pope, H.G., Jr., and Lipinski, J.F.Diagnosis in schizophrenia and manicillness. Archives of GeneralPsychiatry, 35:811-828, 1978.Rochester, S., and Martin, J.R.Crazy Talk: A Study of theDiscourse of Schizophrenic Speakers.New York: Plenum Press, 1979.
Saretsky, T. Effects of chlor-promazine on primary-processthought manifestations. Journal ofAbnormal Psychology, 71:247-252,1966.
Shimkunas, A.M.; Gynther, M.D.;and Smith, K. Abstracting ability of
schizophrenics before and duringphenothiazine therapy. Archives ofGeneral Psychiatry, 14:79-83, 1966.
Shimkunas, A.M.; Gynther, M.D.;and Smith, K. Schizophrenicresponses to the proverbs test:Abstract, concrete, or autistic.Journal of Abnormal Psychology,72:128-133, 1967.
Spitzer, R.L.; Endicott, ].; andRobins, E. Research DiagnosticCriteria: Rationale and reliability.Archives of General Psychiatry,35:773-782, 1978.
Spohn, H.E.; Lacoursiere, R.B.;Thompson, K.; and Coyne, L.Phenothiazine effects on psycho-logical and psychophysiologicaldysfunction in chronic schizo-phrenics. Archives of GeneralPsychiatry, 34:633-644, 1977.
Wallace, J.C., and Boone, S.E.Cognitive factors in the social skillsof schizophrenic patients:Implications for treatment. In:Spaulding, W.D., and Cole, J.K.,eds. Theories of Schizophrenia:Symposium on Motivation, 1983.Lincoln, NB: University of NebraskaPress, 1984.Wechsler, D. The Measurement of
Adult Intelligence. Baltimore,MD: Williams and Wilkins, 1944.
Acknowledgments
The research reported in this articlewas supported entirely by USPHSResearch Grant MH-32220-01.
The generous collaboration ofpatient participants and helpfulcooperation of staff at the Colmery-CNeil VA Medical Center, Topeka,KS; the Topeka State Hospital; andthe C.F. Menninger MemorialHospital are gratefully acknowl-edged.
The Authors
Herbert E. Spohn, Ph.D., is Director,Research Department; LolafayeCoyne, Ph.D., is Director, StatisticalLaboratory; Jan Larson, M.S.W., isStaff Social Worker; Judy Spray,B.S., is Senior Research Assistant;and Kenneth Hayes, B.A., isResearch Assistant, The MenningerFoundation, Topeka, KS. FrederickMittleman, M.D., is MedicalDirector, Research PsychiatricCenter, Kansas City, MO.
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/12/3/394/1865999 by guest on 02 February 2022