Epidemiology of human leptospirosis in Trinidad and Tobago, 1996–2007: A retrospective study
6
Acta Tropica 112 (2009) 260–265 Contents lists available at ScienceDirect Acta Tropica journal homepage: www.elsevier.com/locate/actatropica Epidemiology of human leptospirosis in Trinidad and Tobago, 1996–2007: A retrospective study Andrea R.M. Mohan a , Anton Cumberbatch b , Abiodun A. Adesiyun c , Dave D. Chadee a,∗ a Department of Life Sciences, The University of The West Indies, St. Augustine, Trinidad and Tobago b Ministry of Health, 63 Park Street, Port of Spain, Trinidad and Tobago c Faculty of Medical Sciences, School of Veterinary Medicine, St. Augustine, Trinidad and Tobago article info Article history: Received 2 June 2009 Received in revised form 2 August 2009 Accepted 5 August 2009 Available online 11 August 2009 Keywords: Leptospirosis Epidemiology Seasonal distribution Age and sex Risk factors Trinidad abstract A retrospective study to describe the epidemiology of human leptospirosis in Trinidad and Tobago during 1996–2007 was conducted. All confirmed cases of leptospirosis was analyzed according to age, sex, sea- sonality and geographic distribution. A total of 278 cases were recorded, with an average annual incidence rate of 1.84 per 100,000 population. Seventy-five percent of the cases occurred during the wet season, with the highest number of cases recorded in November. A positive correlation was found between number of cases and rainfall. Males constituted 80% of all cases, and the overall male:female ratio was 4.6:1. The total case fatality rate was 5.8%, with deaths among males four times more common than in females. Clinical leptospirosis was greatest in the 10–19 age group and lowest in the 0–9 age group. The total prevalence was 22 per 100,000 population, with the highest prevalence 41 per 100,000 recorded in the regional cor- poration of Sangre Grande and the lowest (6 per 100,000) in the city of Port of Spain. The lack of important information and active surveillance showed that the level of awareness of the disease is low in the country. The disease is still under-reported, and is considered to be of significant public health importance. © 2009 Elsevier B.V. All rights reserved. 1. Introduction Leptospirosis is regarded as an emerging zoonosis of global importance (Levett, 2001). It is caused by pathogenic bacte- ria belonging to the genus Leptospira which contains over 230 pathogenic serovars (Pappas and Cascio, 2006). The World Health Organisation (2003) reported the incidence of leptospirosis to range between 0.1 and 1 per 100,000 population per year in tem- perate regions and between 10 and 100 per 100,000 population per year in tropical regions. In both regions, however, leptospirosis is a seasonal disease, with significant peaks occurring during sum- mer or autumn in temperate regions, and in the wet season in the tropics (Levett, 2004). Human infections occur primarily when individuals come in contact directly or indirectly with urine containing viable lep- tospires from rodents, or by ingesting contaminated food or water (WHO, 2003). The clinical manifestations of leptospirosis are extremely varied, ranging from mild ‘flu-like’ symptoms, to dengue-like symptoms such as high fever and severe aches and pains, to very severe such as jaundice and organ failure (Bharti et al., 2003). For this reason, there is a high level of misdiagnosis and/or underreporting of leptospirosis in many countries because ∗ Corresponding author. Tel.: +1 868 662 2002x3740; fax: +1 868 663 5241. E-mail address: [email protected] (D.D. Chadee). the symptoms are very similar to other communicable diseases (Levett, 2001). Regionally, leptospirosis is endemic to many South American and Caribbean countries including Trinidad and Tobago (Szyfres, 1976; Green et al., 1978). In humans, more males contract the dis- ease than females and this may be related to the different types of occupational exposure and daily activities (Plank and Dean, 2000). In Trinidad and Tobago, the prevalence of the disease in the human population was found to be 9% (Everard et al., 1987). However, after the pioneering work of Everard et al. (1985, 1987) no studies have been conducted over the last 20 years to determine the changing epidemiological patterns of this disease in Trinidad and Tobago. This is especially important because many public health workers consider the prevalence of leptospirosis to be higher than 9% as the disease is generally under reported in the country especially as public awareness of the disease is low (Everard et al., 1985). In order to fill this 20-year gap, a retrospective study was con- ducted with two major objectives: to estimate the incidence of leptospirosis, and to determine any changes in the epidemiology of the disease in Trinidad and Tobago. 2. Methodology 2.1. Study area The twin island nation of Trinidad and Tobago is located approx- imately 11 ◦ north latitude, 15 km from the east coast of Venezuela, 0001-706X/$ – see front matter © 2009 Elsevier B.V. All rights reserved. doi:10.1016/j.actatropica.2009.08.007
Transcript of Epidemiology of human leptospirosis in Trinidad and Tobago, 1996–2007: A retrospective study
EA
Aa
b
c
a
ARRAA
KLESART
1
irpOrpyamt
ctwadpea
0d
Acta Tropica 112 (2009) 260–265
Contents lists available at ScienceDirect
Acta Tropica
journa l homepage: www.e lsev ier .com/ locate /ac ta t ropica
pidemiology of human leptospirosis in Trinidad and Tobago, 1996–2007:retrospective study
ndrea R.M. Mohana, Anton Cumberbatchb, Abiodun A. Adesiyunc, Dave D. Chadeea,∗
Department of Life Sciences, The University of The West Indies, St. Augustine, Trinidad and TobagoMinistry of Health, 63 Park Street, Port of Spain, Trinidad and TobagoFaculty of Medical Sciences, School of Veterinary Medicine, St. Augustine, Trinidad and Tobago
r t i c l e i n f o
rticle history:eceived 2 June 2009eceived in revised form 2 August 2009ccepted 5 August 2009vailable online 11 August 2009
a b s t r a c t
A retrospective study to describe the epidemiology of human leptospirosis in Trinidad and Tobago during1996–2007 was conducted. All confirmed cases of leptospirosis was analyzed according to age, sex, sea-sonality and geographic distribution. A total of 278 cases were recorded, with an average annual incidencerate of 1.84 per 100,000 population. Seventy-five percent of the cases occurred during the wet season, withthe highest number of cases recorded in November. A positive correlation was found between number of
eywords:eptospirosispidemiologyeasonal distributionge and sex
cases and rainfall. Males constituted 80% of all cases, and the overall male:female ratio was 4.6:1. The totalcase fatality rate was 5.8%, with deaths among males four times more common than in females. Clinicalleptospirosis was greatest in the 10–19 age group and lowest in the 0–9 age group. The total prevalencewas 22 per 100,000 population, with the highest prevalence 41 per 100,000 recorded in the regional cor-poration of Sangre Grande and the lowest (6 per 100,000) in the city of Port of Spain. The lack of important
rveillrepor
isk factorsrinidad
information and active suThe disease is still under-
. Introduction
Leptospirosis is regarded as an emerging zoonosis of globalmportance (Levett, 2001). It is caused by pathogenic bacte-ia belonging to the genus Leptospira which contains over 230athogenic serovars (Pappas and Cascio, 2006). The World Healthrganisation (2003) reported the incidence of leptospirosis to
ange between 0.1 and 1 per 100,000 population per year in tem-erate regions and between 10 and 100 per 100,000 population perear in tropical regions. In both regions, however, leptospirosis isseasonal disease, with significant peaks occurring during sum-er or autumn in temperate regions, and in the wet season in the
ropics (Levett, 2004).Human infections occur primarily when individuals come in
ontact directly or indirectly with urine containing viable lep-ospires from rodents, or by ingesting contaminated food orater (WHO, 2003). The clinical manifestations of leptospirosis
re extremely varied, ranging from mild ‘flu-like’ symptoms, to
engue-like symptoms such as high fever and severe aches andains, to very severe such as jaundice and organ failure (Bhartit al., 2003). For this reason, there is a high level of misdiagnosisnd/or underreporting of leptospirosis in many countries because∗ Corresponding author. Tel.: +1 868 662 2002x3740; fax: +1 868 663 5241.E-mail address: [email protected] (D.D. Chadee).
001-706X/$ – see front matter © 2009 Elsevier B.V. All rights reserved.oi:10.1016/j.actatropica.2009.08.007
ance showed that the level of awareness of the disease is low in the country.ted, and is considered to be of significant public health importance.
© 2009 Elsevier B.V. All rights reserved.
the symptoms are very similar to other communicable diseases(Levett, 2001).
Regionally, leptospirosis is endemic to many South Americanand Caribbean countries including Trinidad and Tobago (Szyfres,1976; Green et al., 1978). In humans, more males contract the dis-ease than females and this may be related to the different types ofoccupational exposure and daily activities (Plank and Dean, 2000).In Trinidad and Tobago, the prevalence of the disease in the humanpopulation was found to be 9% (Everard et al., 1987). However, afterthe pioneering work of Everard et al. (1985, 1987) no studies havebeen conducted over the last 20 years to determine the changingepidemiological patterns of this disease in Trinidad and Tobago.This is especially important because many public health workersconsider the prevalence of leptospirosis to be higher than 9% asthe disease is generally under reported in the country especially aspublic awareness of the disease is low (Everard et al., 1985).
In order to fill this 20-year gap, a retrospective study was con-ducted with two major objectives: to estimate the incidence ofleptospirosis, and to determine any changes in the epidemiologyof the disease in Trinidad and Tobago.
2. Methodology
2.1. Study area
The twin island nation of Trinidad and Tobago is located approx-imately 11◦ north latitude, 15 km from the east coast of Venezuela,
A.R.M. Mohan et al. / Acta Tropica 112 (2009) 260–265 261
palitie
fGaa(ateawnicfDsrIa
2
Cs3jaEa
2
ofAbc
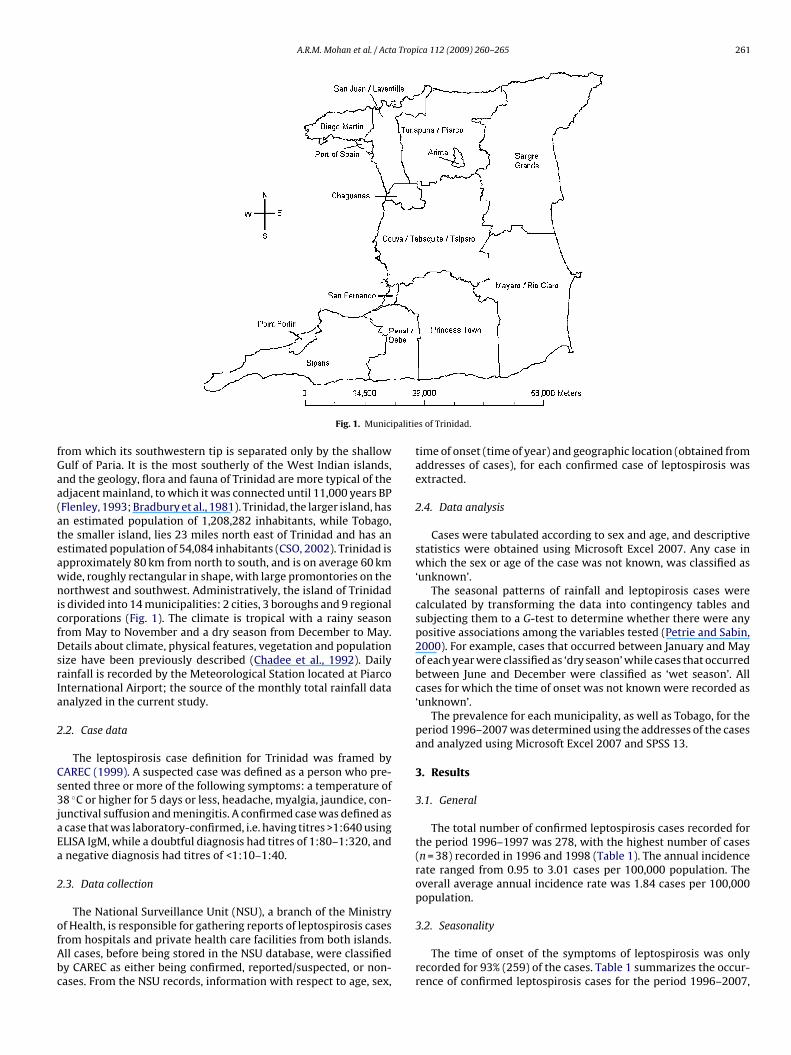
Fig. 1. Munici
rom which its southwestern tip is separated only by the shallowulf of Paria. It is the most southerly of the West Indian islands,nd the geology, flora and fauna of Trinidad are more typical of thedjacent mainland, to which it was connected until 11,000 years BPFlenley, 1993; Bradbury et al., 1981). Trinidad, the larger island, hasn estimated population of 1,208,282 inhabitants, while Tobago,he smaller island, lies 23 miles north east of Trinidad and has anstimated population of 54,084 inhabitants (CSO, 2002). Trinidad ispproximately 80 km from north to south, and is on average 60 kmide, roughly rectangular in shape, with large promontories on theorthwest and southwest. Administratively, the island of Trinidad
s divided into 14 municipalities: 2 cities, 3 boroughs and 9 regionalorporations (Fig. 1). The climate is tropical with a rainy seasonrom May to November and a dry season from December to May.etails about climate, physical features, vegetation and population
ize have been previously described (Chadee et al., 1992). Dailyainfall is recorded by the Meteorological Station located at Piarconternational Airport; the source of the monthly total rainfall datanalyzed in the current study.
.2. Case data
The leptospirosis case definition for Trinidad was framed byAREC (1999). A suspected case was defined as a person who pre-ented three or more of the following symptoms: a temperature of8 ◦C or higher for 5 days or less, headache, myalgia, jaundice, con-
unctival suffusion and meningitis. A confirmed case was defined ascase that was laboratory-confirmed, i.e. having titres >1:640 usingLISA IgM, while a doubtful diagnosis had titres of 1:80–1:320, andnegative diagnosis had titres of <1:10–1:40.
.3. Data collection
The National Surveillance Unit (NSU), a branch of the Ministry
f Health, is responsible for gathering reports of leptospirosis casesrom hospitals and private health care facilities from both islands.ll cases, before being stored in the NSU database, were classifiedy CAREC as either being confirmed, reported/suspected, or non-ases. From the NSU records, information with respect to age, sex,s of Trinidad.
time of onset (time of year) and geographic location (obtained fromaddresses of cases), for each confirmed case of leptospirosis wasextracted.
2.4. Data analysis
Cases were tabulated according to sex and age, and descriptivestatistics were obtained using Microsoft Excel 2007. Any case inwhich the sex or age of the case was not known, was classified as‘unknown’.
The seasonal patterns of rainfall and leptopirosis cases werecalculated by transforming the data into contingency tables andsubjecting them to a G-test to determine whether there were anypositive associations among the variables tested (Petrie and Sabin,2000). For example, cases that occurred between January and Mayof each year were classified as ‘dry season’ while cases that occurredbetween June and December were classified as ‘wet season’. Allcases for which the time of onset was not known were recorded as‘unknown’.
The prevalence for each municipality, as well as Tobago, for theperiod 1996–2007 was determined using the addresses of the casesand analyzed using Microsoft Excel 2007 and SPSS 13.
3. Results
3.1. General
The total number of confirmed leptospirosis cases recorded forthe period 1996–1997 was 278, with the highest number of cases(n = 38) recorded in 1996 and 1998 (Table 1). The annual incidencerate ranged from 0.95 to 3.01 cases per 100,000 population. Theoverall average annual incidence rate was 1.84 cases per 100,000population.
3.2. Seasonality
The time of onset of the symptoms of leptospirosis was onlyrecorded for 93% (259) of the cases. Table 1 summarizes the occur-rence of confirmed leptospirosis cases for the period 1996–2007,

262 A.R.M. Mohan et al. / Acta Tropica 112 (2009) 260–265
Table 1Seasonality and incidence of leptospirosis during the period 1996–2007 in Trinidad and Tobago.
Year Dry Season Wet Season Unknown Total Incidence (per 100,000 population)
1996 4 34 0 38 3.011997 7 5 0 12 0.951998 3 35 0 38 3.011999 8 16 0 24 1.92000 1 18 0 19 1.512001 5 11 0 16 1.272002 6 15 2 23 1.822003 3 12 0 15 1.192004 2 7 3 12 0.952005 5 19 4 28 2.222006 20 10 62007 2 11 4
Total 66 193 19
F(
wobct
congtb
o
group information. The age groups 10–19, 20–29, 30–39 and 40–49
TT
ig. 2. Monthly distribution of confirmed Leptospirosis cases in Trinidad and Tobago1996–2007).
hich showed that significantly more cases (G = 24.7; 1df; P < .0.05)r 75% of all cases occurred in the wet season, May to Novem-er (193 cases), than during the dry season, December to May (66ases). The only year in which the number of cases was greater inhe dry season than the wet season was 2006.
Fig. 2 summarizes the distribution of confirmed leptospirosisases and rainfall by months of the year. The general annual cyclef the disease was as follows: the number of cases declined sig-ificantly (G = 121.5; 4df; P < 0.05) from January to February, thenradually, with the lowest numbers occurring in the months March
o May. From June, the number of cases increased until December,ut not significantly (P > 0.05).The results also showed a lag of 1–2 months between the onsetf the rainy season (heavy rainfall) and peak number of cases
able 2otal number of confirmed male and female leptospirosis cases and deaths for 1996–200
Year Cases
Male (n) Male (%) Female (n) Female (%) Unknown
1996 34 89 4 11 01997 8 67 4 33 01998 28 74 10 26 01999 20 83 4 17 02000 16 84 3 16 02001 13 81 3 19 02002 20 87 3 13 02003 11 73 4 27 02004 10 83 2 17 02005 23 82 5 18 02006 26 72 8 22 22007 13 77 3 18 1
Total 222 78 53 21 3
36 2.8517 1.35
278 Average = 1.84
(Fig. 2)—this feature consistently occurred during the years 1996,1998, 1999, 2002, 2003, 2004, 2005 and 2006. In addition, signifi-cantly more cases of leptospirosis occurred from June to January butwith the greatest number recorded during the month of November(17%; n = 45). In contrast, the lowest percentage of cases occurredduring the months of March to May (3%, n = 7 for each month). Over-all, there was a weak positive association between number of casesand amount of rainfall recorded each month for the entire studyperiod (r = 0.56).
3.3. Sex, age and mortality
Table 2 shows the distribution of cases according to sex for theperiod 1996–2007. Of the 278 confirmed cases, 80% were male(n = 222) while 19% were female (n = 53). The sex of 3 cases wasunknown hence—the numbers not adding up to 278. The meannumber of cases for this 12-year period was 23. For each year, thenumber of males contracting leptospirosis significantly outnum-bered the number of females, with the overall male: female ratiobeing 4.6:1 (P < 0.05).
Among the male cases, the highest percentage occurred in the10–19 age group (25%; n = 51), and the lowest percentage in the0–9 age group (2%; n = 3). However, for the female cases, the high-est percentage occurred in the 30–39 age group (36%; n = 18) andthe lowest percentage in the 0–9 age group (0%; n = 0). Fig. 3 showsthe distribution of cases according to age groups and sex. Datafrom the 12-year study provided only 91% (255 cases) with age
represented the largest sector of the population contracting lep-tospirosis (for both sexes) but with the highest number recordedin the 10–19 group (22%; n = 56). However, there was only a 2% dif-ference between this age group 10–19 and the 20–29 and 30–39
7 in Trinidad and Tobago.
M:F ratio Deaths Case Fatality rate (%)
Total Male Female
38 8.5 5 0 13.212 2.0 0 0 038 2.8 0 0 024 5.0 0 0 019 5.3 2 1 15.816 4.3 0 1 6.323 6.7 0 0 015 2.8 1 0 6.712 5.0 2 0 16.728 4.6 3 0 10.736 3.3 0 1 2.817 4.3 0 0 0
278 4.6 13 3 5.8

A.R.M. Mohan et al. / Acta Trop
Fig. 3. Confirmed leptospirosis cases (male and female) according to age group forthe period 1996–2007 in Trinidad and Tobago.
Table 3Leptospirosis prevalence according to geographic location in Trinidad and Tobagofrom 1996 to 2007.
Municipality Population Total no.of cases
Prevalence/100,000
Port of Spain 49,031 3 6.1San Fernando 55,419 12 21.7Arima 32,278 10 31.0Chaguanas 67,433 13 19.3Point Fortin 19,056 3 15.7Diego Martin 105,720 8 7.6San Juan/Laventille 157,295 20 12.7Tunapuna/Piarco 203,975 45 22.1Sangre Grande 65,680 27 41.1Couva/Tabaquite/Talparo 162,779 55 33.8Princes Town 91,947 16 17.4Mayaro/Rio Claro 32,143 7 21.8Penal/Debe 83,609 13 15.5Siparia 81,917 6 7.3
a1nt(
wfnw
3
oHSb7pp2
4
nitE
Tobago 54,084 2 3.7Unknown 38
Total 1,262,366 278 22.0
ge group (20% of all cases occurred in both these groups). Also,9% of all cases fell within the 40–49 age groups. Thus, there wereo significant differences among these age groups (P > 0.05). In con-rast, the smallest percentage of cases occurred in the 0–9 age groupn = 3).
The total number of deaths that occurred for this 12-year periodas 16 (Table 2). The overall case fatality rate was 5.8%, with death
our times more common in males than females, however, it wasot possible to test for significant differences as the number of casesas very few.
.4. Geographical distribution
For the 12-year period, the majority of confirmed cases (n = 55)ccurred in the corporation of Couva/Tabaquite/Talparo (Table 3).owever, the highest prevalence occurred in the corporation ofangre Grande (41.1 cases per 100,000 people). The smallest num-er of cases and the lowest prevalence occurred in Tobago (n = 3;.3 cases per 100,000 people). In Trinidad, leptospirosis was leastrevalent in the city of Port of Spain (n = 3; 6.1 cases per 100,000opulation). The overall prevalence for Trinidad and Tobago was2 cases per 100,000 people.
. Discussion
It should be noted that epidemic outbreaks of leptospirosis haveever been recorded in Trinidad and Tobago, where the annual
ncidence rate is 1.84 per 100,000 population and is much lowerhan the rates found in many tropical regions. Thailand’s Bureau ofpidemiology (2007) reported an incidence of 5.2 per 100,000 pop-
ica 112 (2009) 260–265 263
ulation. Barbados’ annual incidence rate is around 13.3 per 100,000population (Damude et al., 1979; Everard et al., 1982, 1984), whilethe rate in the Andaman Islands was 50 per 100,000 population(Pappas et al., 2008). However, when data from the present studyare compared with the study carried out by Everard et al. (1989)in Trinidad during the period 1977 to February 1982, the aver-age number of cases per month was similar (2.1 vs 2.2). Possiblereasons for the similar epidemiological pattern are the surveil-lance system adopted (passive) and the underreporting due to alow index of suspicion, which has hardly changed since that time.Interestingly, the average incidence rate reported in the country’sMinistry of Health Annual Statistical Report for 2004–2005 was1.45 per 100,000 population. The small difference between thenumber of laboratory-confirmed cases in that report and in thispresent study can probably be attributed to the time of onset ofsome of these cases (particularly end-of-year cases) and when theywere reported.
The results of this study show that leptospirosis is a seasonal dis-ease in Trinidad and Tobago, with most cases occurring during thelater months of the rainy season. This finding is consistent with theresults from other studies conducted in both temperate and tropicalregions of the world including the Caribbean region (Levett, 2004).Within the Caribbean region leptospirosis studies have shown apositive correlation with the rainy season in Jamaica (Segree et al.,1982), in Barbados (Douglin et al., 1997), in Grenada (Everard et al.,1992), in Guadeloupe (Herrmann-Storck et al., 2005) as well as inTrinidad and Tobago (as found in the current study).
It is noteworthy that in many parts of the world public healthofficials are aware and concerned that heavy rainfall and floodingcan lead to outbreaks of the disease especially in tropical countries(Pappachan et al., 2004; Kupek et al., 2000). During the rainy sea-son the soil remains moist and can lead to the collection of poolsof water in the environment, which allow for a longer survival rateof the leptospires, and ultimately, can lead to an increase in expo-sure to the bacteria by humans. Therefore, the incidence is usuallyconsiderably higher during the wet season with significant out-breaks reported when heavy rainfall and flooding occur (Sarkar etal., 2002). In Trinidad and Tobago, flooding occurs each year and thefrequency of flooding episodes is increasing and this is primarilydue to changing demographic patterns, destruction of ecologicallysensitive areas such as wet lands, deforestation, urbanization andclimate change (Chen et al., 2006). These flooding episodes have notbeen restricted to Trinidad and Tobago but rather have been expe-rienced in Guyana, Suriname, Barbados, Jamaica, Haiti and Cuba(Chen et al., 2006), so the incidence of leptospirosis is expected toincrease significantly in the future.
The results showed that more males contracted leptospirosisthan females (Table 3). Within the Caribbean region similar resultshave been reported in Barbados, Grenada, Jamaica and previouslyin Trinidad (Herrmann-Storck et al., 2005; Everard et al., 1992) butAlston and Broom (1958) reported that males were no more suscep-tible to leptospirosis than females in Guadeloupe. Consequently, itis possible that it may not be the issue of susceptibility but the factthat more males are infected with the disease than females becausethey have jobs or undertake activities that may put them more atrisk of contracting leptospirosis. However, with respect to mortal-ity, results generated in the current study demonstrated that lessthan 19% or 3 cases out of a total of 16 deaths occurred amongfemale patients. In contrast, the results of a similar 12-year studyconducted in Barbados revealed that deaths among females werealmost twice as common as among males (Everard et al., 1995). It
is clear that although, the case fatality rate is low in Trinidad com-pared to that of other tropical countries such as Barbados (Damudeet al., 1979), the rate observed in Trinidad and Tobago, 5.7%, stillfalls within the range of up to 20% recognized by the WHO as thecurrent status throughout the world (WHO, 1999).
2 a Trop
osTtspstie
i2cs2it2tgttbird(iipw
trtit‘ccti
tllihda(w(n
crfisdwlr
64 A.R.M. Mohan et al. / Act
The finding that the majority of cases (both males and females)ccurred between the ages of 10 and 49 suggests that these per-ons are more active than persons who fall outside of this range.he lack of significant differences between the number of males inhe 10–19 age group, and the 20–29, 30–39 and 40–49 age groupsuggest that infection is more due to risk activities rather than occu-ation because most in the 10–19 age group are either in primary orecondary school, or entering university. While people belongingo the 20–29, 30–39 and 40–49 age groups belong to the work-ng class and would theoretically have an increased environmentalxposure over persons in the youngest and oldest age groups.
In a similar study conducted in Barbados during 1968–1974,t was found that the highest percentage of cases occurred in the0–29 age group (Damude et al., 1979), whereas the highest per-entage of cases occurred in the 10–19 age group in this currenttudy. The 22% higher incidence in the 30–39 age group than in the0–29 and the 40–49 age groups for females suggests that females
n the 30–39 age group may be more active in the environmenthan females in the other age groups. However, in Barbados only% of all female cases occurred in this age group (30–39), whilehe largest percentage (25%) occurred in the 50–59 and ≥60 ageroups (Damude et al., 1979). The increase in number of cases fromhe 50–59 to the ≥60 age groups may be due to decreased resis-ance to leptospirosis, as older persons’ immune systems tend toe weaker. In Trinidad (present study), the small number of cases
n the 0–9 and the 50–≥60 age groups, in general, may be due toeduced exposure to risk factors. However, in previous studies con-ucted by Everard and Fraser-Chanpong (1979) and Everard et al.1989) in Trinidad showed 9.5% of children were seropositive, thats, 12 children under the age of 10 tested positive for leptospiralmmunoglobulins; 8 of them being female but they lived in closeroximity to, and were in direct contact with, livestock and thereas an absence of tap-borne water.
Based on the results of the present study it would be incorrecto conclude that the occurrence of leptospirosis is occupationallyelated or due to risk activities solely, since information related tohe cause of leptospirosis among citizens of Trinidad and Tobagos grossly lacking. Information on occupation would have added tohe analysis, as occupation types could be labelled as ‘high risk’,medium risk’ and ‘low risk’ (with respect to level of exposure toertain risk factors, e.g. constant contact with animals, or constantontact with freshwater systems, etc.). It has been shown that lep-ospirosis can occur due to occupation and recreational activitiesn developing countries (CDC, 1997; Bharti et al., 2003).
Data from the present study suggest that there may be no rela-ionship between geographical distribution and the prevalence ofeptospirosis, i.e. there is no urban or rural bias when it comes toeptospirosis prevalence in Trinidad. However, Everard et al. (1985)n a previous study found that the prevalence of leptospirosis wasigher in rural than in urban areas in Trinidad. Studies in largereveloping countries such as Brazil have shown that there has beenrise of leptospirosis prevalence in urban areas due to urban decay
Ko et al., 1999; Sarkar et al., 2002). However, sanitary conditionsithin city areas of Trinidad and Tobago are still relatively good
Focks and Chadee, 1997), and this may be the reason for the smallumber of cases in these urban areas.
While it is still not known if leptospirosis is a disease of signifi-ant public health importance in Trinidad and Tobago, all previouseports suggest that the disease is underreported. Although testingacilities for leptospirosis infections within the various countriesn the Caribbean region have increased, many do not test for
erovars—information that aids in the understanding of the epi-emiology and transmission of the disease to humans. Other factorshich contribute to underreporting is the lack of active surveil-ance and an absence of important information such as occupation,ecreational and daily activities, symptoms experienced due to lep-
ica 112 (2009) 260–265
tospirosis, as well as the socio-economic status of patients—all ofwhich are important for creating awareness among the populationof Trinidad and Tobago. This lack of information is also common tomany other countries that lack the proper diagnostic facilities, andis often frustrating to researchers trying to determine the exact sta-tus of the disease in their respective countries (Hasnain and Ahmed,2004).
The main effect of underreporting in Trinidad and Tobago is thatthe disease will always be given less public health importance thandengue and dengue haemorrhagic fever. This means that certainpublic health issues, for example, rodent control may never be givenpriority by the government. Underreporting thus causes the levelof awareness of the disease to remain low. The effect of increasingawareness and the index of suspicion of leptospirosis can help toincrease the number of cases reported. This was demonstrated inJamaica, where the number of reported cases nearly doubled in ayear after a veterinary conference helped to stimulate awarenessamong clinicians (Segree et al., 1982). It is believed that leptospiro-sis is found wherever it is looked for, and thus, will continue to bea disease of public health importance in Trinidad and Tobago andthe Caribbean region (Vinetz, 2004).
Acknowledgements
Many thanks must be given to Mr. Karmesh Sharma of theMinistry of Health, Dr. Avery Hinds and the staff of the NationalSurveillance Unit for helping with the collection of data for thisstudy. Thanks must also be given to the staff at the MeterologicalOffice of Trinidad and Tobago at Piarco for providing rainfall datawhich helped with part of the analysis in this study.
References
Alston, J.M., Broom, J.C., 1958. Leptospirosis in Man and Animals. E. & S. LivingsoneLtd., Edinburgh and London.
Bharti, A.R., Nally, J.E., Ricaldi, J.N., et al., 2003. Leptospirosis: a zoonotic disease ofglobal importance. Lancet Infect. Dis. 3, 757–771.
Bradbury, J.P., Leyden, B., Salgado-labouriau, M., Lewis Jr., W.M., Schubert, C., Bin-gord, M.W., Frey, D.G., Whitehead, D.R., Weibezahn, F.H., 1981. Late quaternaryhistory of lake Valencia. Science 214, 1299–1305.
Bureau of Epidemiology, 2007. Annual Epidemiological Surveillance Report. Min-istry of Public Health, Thailand.
CAREC, 1999. Selected Diseases Under Surveillance. Public Health Surveillance: ACaribbean Communicable Disease Surveillance Manual For Action. CaribbeanEpidemiology Centre, The Desktop Publishing Unit, Port of Spain, pp. 105–110.
CDC, 1997. Outbreak of leptospirosis among white-water rafters—Costa Rica, 1996.Morb. Mortal. Rep. 46 (25), 577–579.
CSO, 2002. 2000 Population and Housing Census Register. Ministry of Planning andDevelopment, Port of Spain.
Chadee, D.D., Maitre, A.L., Tilluckdharry, C.C., 1992. An outbreak of Plasmodium vivaxmalaria in Trinidad. W. I. Ann. Trop. Med. Parasitol. 86, 583–590.
Chen, A.A., Chadee, D.D., Rawlins, S.C., 2006. Climate Change Impact on Dengue: TheCaribbean Experience. Phoenix Press, Mona Jamaica.
Damude, D.F., Jones, C.J., White, H.St.C., Myers, D.M., 1979. The problem of humanleptospirosis in Barbados. Trans. R. Soc. Trop. Med. Hyg. 73 (2), 169–177.
Douglin, C.P., Jordan, C., Rock, R., Hurley, A., Levett, P.N., 1997. Risk factors for severeleptospirosis in the parish of St. Andrew, Barbados. Emerg. Infect. Dis. 3 (1),78–80.
Everard, C.O.R., Bennett, S., Edwards, C.N., Nicholson, G.D., et al., 1992. An investiga-tion of some risk factors for severe leptospirosis on Barbados. J. Trop. Med. Hyg.95 (1), 13–22.
Everard, C.O.R., Edwards, C.N., Webb, G.B., White, H.St.C., Nicholson, G.D., 1984. Theprevalence of severe leptospirosis among humans on Barbados. Trans. R. Soc.Trop. Med. Hyg. 78, 596–603.
Everard, C.O.R., Edwards, C.N., Everard, J.N., Carrington, D.G., 1995. A twelve-yearstudy of leptospirosis on Barbados. Eur. J. Epidemiol. 11 (3), 311–320.
Everard, C.O.R., Ferdinand, G.A., Butcher, L.V., Everard, J.D., 1989. Leptospirosis inpiggery workers on Trinidad. J. Trop. Med. Hyg. 92 (4), 253–258.
Everard, C.O.R., Fraser-Chanpong, G.M., 1979. Serological evidence of leptospirosis
in Caribbean schoolchildren. Trans. R. Soc. Trop. Med. Hyg. 73 (5), 591–593.Everard, C.O.R., Fraser-Chanpong, G.M., Everard, J.D., 1987. The incidence of severeleptospirosis in Trinidad. Trop. Geogr. Med. 39 (2), 126–132.
Everard, C.O.R., Fraser-Chanpong, G.M., Hayes, R., Bhagwandin, L.J., Butcher, L.V.,1982. A survey of leptospirosis in febrile patients mainly from hospitals andclinics in Trinidad. Trans. R. Soc. Trop. Med. Hyg. 76 (4), 487–492.

a Trop
E
F
F
G
HH
K
K
LL
A.R.M. Mohan et al. / Act
verard, C.O.R., Hayes, R.J., Fraser-Chanpong, G.M., 1985. A serosurvey for leptospiro-sis in Trinidad among urban and rural dwellers and persons occupationally atrisk. Trans. R. Soc. Trop. Med. Hyg. 79 (1), 96–105.
lenley, J.R., 1993. The palaeoecology of Easter Island and its ecological dis-aster. In: Fischer, S.R. (Ed.), Easter Island Studies. Contributions to theHistory of Rapanui in Memory of William T. Mulloy. Oxbow, Oxford,pp. 27–45.
ocks, D.A., Chadee, D.D., 1997. Pupal survey: an epidemiologically significantsurveillance method for Aedes aegypti: an example using data from Trinidad.Am. J. Trop. Med. Hyg. 56, 159–167.
reen, A.E., Sulzer, C.R., Everard, C.O.R., Jones, W.I., 1978. Four new Leptospiraserotypes from Trinidad. W. I. Med. J. 27, 1171–1226.
asnain, S.E., Ahmed, N., 2004. Leptospirosis. Lancet Infect. Dis. 4, 543.errmann-Storck, C., Brioudes, A., Quirin, R., et al., 2005. Retrospective review of
leptospirosis in Guadeloupe, French West Indies 1994–2001. W. I. Med. J. 54 (1),42–46.
o, A.I., Galvao, R.M., Ribeirodourado, C.M., Johnson, W.D., Riley, L.W., 1999. Urbanepidemic of severe leptospirosis in Brazil. Salvador Leptospirosis Study Group.Lancet 354, 820–825.
upek, E., de Sousa, S.F.M.C., de Souza, P.J.M., 2000. The relationship between rainfalland human leptospirosis in Florianopolis, Brazil, 1991–1996. Braz. J. Infect. Dis.4, 131–134.
evett, P.N., 2001. Leptospirosis. Clin. Microbiol. Rev. 14 (2), 296–326.evett, P.N., 2004. Leptospirosis: a forgotten zoonosis? Clin. Appl. Immunol. Rev. 4,
435–448.
ica 112 (2009) 260–265 265
Pappachan, M.J., Sheela, M., Aravindan, K.P., 2004. Relation of rainfall pattern andepidemic leptospirosis in the Indian state of Kerala. J. Epidemiol. Commun.Health 58, 1054–1055.
Pappas, G., Cascio, A., 2006. Optimal treatment of leptospirosis: queries and projec-tions. Int. J. Antimicrob. Agents 28, 491–496.
Pappas, G., Papadimitriou, P., Siozopoulou, V., Christou, L., Akritidis, N., 2008. Theglobalization of leptospirosis: worldwide incidence trends. Int. J. Infect. Dis. 12,351–357.
Petrie, A., Sabin, C., 2000. Medical Statistics at a Glance, 2nd ed. Wiley-Blackwell,United Kingdom.
Plank, R., Dean, D., 2000. Overview of the epidemiology, microbiology, and pathogen-sis of Leptospira spp. in humans. Microbes Infect. 2, 1265–1276.
Sarkar, U., Nascimento, S.F., Barbosa, R., et al., 2002. Population-based case-controlinvestigation of risk factors during an urban epidemic. Am. J. Trop. Med. Hyg. 66(5), 605–610.
Segree, W., Fitz-Henly, M., Rawlins, J., Bowen-Wright, C., 1982. Leptospirosis: areview of the Jamaican experience compared with other Caribbean Territories.W. I. Med. J. 31, 54–56.
Szyfres, B., 1976. Leptospirosis as an animal and public health problem in Latin
America and the Caribbean area. Bol. Sanit. Panam. 81, 110–125.Vinetz, J., 2004. Leptospirosis is everywhere; just have to know what to look for. Buthow? Swiss Med. Wkly. 134, 331–332.
WHO, 1999. Leptospirosis worldwide. Wkly. Epidemiol. Rev. 74, 237–242.WHO, 2003. Human Leptospirosis: Guidance for Diagnosis, Surveillance and Control.
World Health Organization, Malta.